Does the speech of Turkish-speaking phonologically disordered children differ from that of children...
14
Does the speech of Turkish-speaking phonologically disordered children differ from that of children speaking other languages? SEYHUN TOPBAS ¸ Anadolu University, Turkey (Received 10 July 2004; accepted 10 November 2004) Abstract How phonological disorders should be categorized in Turkish children remained vague for a long period of time due to a lack of normative studies. This paper reports the phonological systems of 70 phonologically disordered children, aged 4;0–8;0, in comparison with the results of a normative study of 665 Turkish-speaking children, aged 1;3–8;0. The current focus is on two aspects of development, mainly the differences between disordered and normal consonant acquisition and phonological error patterns from both longitudinal and cross-sectional data. The second concern of the paper is to sub- classify phonological disorders as proposed in the existing literature by examining the applicability of these proposals to Turkish, a typologically different language. It has been indicated that similar developmental trends occur across languages but consonant acquisition is more rapid and developmental errors are more predictable in Turkish. There is evidence for ambient language influence. Mostly, the sub-classifications of phonological disorders are valid for Turkish-speaking children with apparent saliency to language. Keywords: Phonological disorders, phonological acquisition, classification, cross-linguistic, Turkish Introduction Phonological development and disorders is still an intriguing area for cross-linguistic comparisons. Cross-phonologic studies on language acquisition suggest that there are only broad developmental patterns that can be described as universal. So the idea that children are sensitive to the ambient language is not new. Children’s phonological inventories are not similar within and across languages, rather the similarity is observed on core features (Ingram, 2004). These findings are important for less researched languages as in the case of Turkish, in which assessments for impaired language are compared according to children acquiring other languages. Some cross-phonologic studies of English, German, Potunghua, and Cantonese implied that children learning languages other than English may well use similar strategies of structural and systemic simplifications, but the way in which those strategies were Correspondence: Seyhun Topbas ¸, Anadolu University, Centre for Speech and Language Disorders, Yunusemre Campus, 26470 Eskisehir, Turkey. Tel/Fax: +90 222 335 2337. E-mail: [email protected] Clinical Linguistics & Phonetics, Sept–Oct 2006; 20(7–8): 509–522 ISSN 0269-9206 print/ISSN 1464-5076 online # 2006 Informa UK Ltd. DOI: 10.1080/02699200500266331 Clin Linguist Phon Downloaded from informahealthcare.com by Anadolu Univ. on 09/24/12 For personal use only.
Transcript of Does the speech of Turkish-speaking phonologically disordered children differ from that of children...
Does the speech of Turkish-speaking phonologicallydisordered children differ from that of children speaking
other languages?
SEYHUN TOPBAS
Anadolu University, Turkey
(Received 10 July 2004; accepted 10 November 2004)
AbstractHow phonological disorders should be categorized in Turkish children remained vague for a longperiod of time due to a lack of normative studies. This paper reports the phonological systems of 70phonologically disordered children, aged 4;0–8;0, in comparison with the results of a normative studyof 665 Turkish-speaking children, aged 1;3–8;0. The current focus is on two aspects of development,mainly the differences between disordered and normal consonant acquisition and phonological errorpatterns from both longitudinal and cross-sectional data. The second concern of the paper is to sub-classify phonological disorders as proposed in the existing literature by examining the applicability ofthese proposals to Turkish, a typologically different language. It has been indicated that similardevelopmental trends occur across languages but consonant acquisition is more rapid anddevelopmental errors are more predictable in Turkish. There is evidence for ambient languageinfluence. Mostly, the sub-classifications of phonological disorders are valid for Turkish-speakingchildren with apparent saliency to language.
Keywords: Phonological disorders, phonological acquisition, classification, cross-linguistic, Turkish
Introduction
Phonological development and disorders is still an intriguing area for cross-linguistic
comparisons. Cross-phonologic studies on language acquisition suggest that there are only
broad developmental patterns that can be described as universal. So the idea that children
are sensitive to the ambient language is not new. Children’s phonological inventories are
not similar within and across languages, rather the similarity is observed on core features
(Ingram, 2004). These findings are important for less researched languages as in the case of
Turkish, in which assessments for impaired language are compared according to children
acquiring other languages.
Some cross-phonologic studies of English, German, Potunghua, and Cantonese implied
that children learning languages other than English may well use similar strategies of
structural and systemic simplifications, but the way in which those strategies were
Correspondence: Seyhun Topbas, Anadolu University, Centre for Speech and Language Disorders, Yunusemre Campus, 26470
Eskisehir, Turkey. Tel/Fax: +90 222 335 2337. E-mail: [email protected]
Clinical Linguistics & Phonetics, Sept–Oct 2006; 20(7–8): 509–522
ISSN 0269-9206 print/ISSN 1464-5076 online # 2006 Informa UK Ltd.
DOI: 10.1080/02699200500266331
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.

implemented in terms of realization rules might vary according to the phonetic and
phonological structure of the language being learned (Dodd, 1995; Fox and Dodd, 2001;
So and Dodd, 1995; Hua and Dodd; 2000). However, such studies are few and there is a
need for descriptions in other languages. This will eventually allow the evaluation of
universal classification systems of phonological disorders, and which measures should be
taken into account as the effect of the ambient phonology on disorders.
Classifying sub-groups of children, although widely recognized (Shriberg &
Kwiatkowski, 1982), is controversial. In reviewing the literature Fox and Dodd (2001)
discussed the issue of classifying speech disorders. They summarized that basically medical-
etiological, clinical-inferential/linguistic perspective and psycholinguistic approaches are
widely used in evaluations. Taking into account the advantages and disadvantages of such
approaches, Bradford and Dodd (1996) combined clinical-inferential/linguistic perspective
and psycholinguistic approaches and proposed a four-way classification system based on
the surface error patterns: articulation disorder, delayed phonological development,
deviant-consistent phonological disorder, and deviant-inconsistent phonological disorder.
Using this sub-classification, Goldstein (1996) analysed 20 phonologically disordered
Spanish-speaking Puerto-Rican children; So and Dodd (1995) analysed 17 phonologically
disordered Cantonese-speaking children; Topbas and Konrot (1998) analysed ten
phonologically disordered Turkish-speaking children, Hua and Dodd (2000) analysed 33
phonologically disordered Potunghua-speaking children; and Fox and Dodd (2001)
analysed 110 phonologically disordered German-speaking children, and they all found
support for the proposed sub-classification, although there were minor differences. All
these studies have concluded that although the sub-classification may fit different
languages, which error patterns should be considered unusual or inconsistent and used
as criteria for assessment varies from one language to another.
Bearing in the mind that whether a child should be considered disordered or non-
disordered should be assessed in relation to the normal patterns of the ambient language,
there was a need for normative studies in Turkish. Turkish is one of those languages in
which some aspects of universal and language specific variability have been demonstrated
by applying either a process based (Topbas, 1997; Topbas & Konrot, 1998) or relational
based approach (Topbas & Dincer, 2002). However, only a small number of subjects have
been presented. So, due to lack of normative studies, it remained vague for a long period of
time which error patterns should be considered unusual (and used as criteria for
assessment), and how phonological disorders should be categorized in Turkish children.
It is basically this question that the author would like to answer with data from a large
scale normative study in comparison with phonologically disordered children. Special
emphasis will be given to sub-classifying the disorders as a preliminary analysis to aid
further studies in Turkish. By doing so, evidence will be presented about specific and
universal aspects of variability, and concerning the validity of classification systems for
speech disorders, thereby enabling the results to be compared with existing literature in
other languages.
Brief review of Turkish phonology
Turkish belongs to the Altaic group of language families, and the basic word order is
subject-object-verb (SOV). Its agglutinating nature allows both derivational and inflec-
tional suffixes added to roots leading to long strings of words. The orthography assigns
letters to 21 consonants /p, b, m, n, t, d, ts, dz, k, g, X, f, v, h, s, z, s, z, l, , j/ and eight
510 S. Topbas
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.

vowels /i, Y, y, (O), 2 (a), E, %, 3/ and word-final clusters are restricted to sonorant/
fricative+non-continuant (stop, affricate) i.e., /rk, rt, rp, nk, nt, nc, sk, st, lk, lp/. Word-
initial liquids are borrowings. The allophonic variations of /k, g/ are ruled phonologically
where before back vowels [k, g] occur and before front vowels [c, ]. The controversial ‘‘g’’
or ‘‘soft-g’’, the voiced velar fricative, [X], gave way to lengthening of the previous vowel in
syllable-final position and post-vocalically; in syllable-initial position it does not occur. /v/
has an allophone in intervocalic and final positions: a frictionless continuant [u]. /l/ is
velarized [ ], when it occurs with a tautosyllabic back vowel and palatalized [l] when it
occurs with a tautosyllabic front vowel. The alveolar flap / / is treated as a liquid in general
as its allophonic variations are not context dependent in Turkish: [ , , ]. One main
phonological constraint is the word-final devoicing of voiced non-continuants /b, d, g, dz/where they alternate to /p, t, k, ts/. Other allophonic variations are vowel and consonant
harmony. It is a syllable-timed language, having almost equal duration on syllables. Stress
appears to be on the final syllable although there are exceptions.
Phonological acquisition in Turkish
Although there have not been many studies, different aspects of acquisition have been
studied in normal and disordered Turkish children recently by Topbas, 1988, 1994, 1996,
1997, 2004a; Acarlar & Ege, 1996; Ketrez, 1997; Topbas & Konrot, 1998; Topbas &
Kopkallı-Yavuz, 1998; Kopkallı-Yavuz & Topbas, 2000; Topbas & Dincer, 2002; Yavas &
Topbas, 2004. (For detailed information reader can refer to Topbas and Yavas, 2006.)
According to this research, Turkish children tend to acquire the phonology of their
language very rapidly, with the exception of / / and clusters, following similar paths
observed in other languages (Ingram, 2004). Evidence for language specific aspects has also
been derived from error patterns and from the early suppression of unique phonological
rules of Turkish. Table I and Table II present summaries of acquisition of Turkish
phonology from the normative sample (Topbas & Yavas, 2006).
As can be seen from Table I, by age 3;6 all the sounds seemed to be established at syllable
initial and syllable final positions. Among the very early sounds established by 90% of
children between the ages 13–15 months were labial plosives, alveolar plosives, velar
plosive, nasals and the glide /j/. The order of acquisition can be summarized as
stops.nasals.affricates.glides/liquids.fricatives.flap. The voiced fricative /z/, the glottal
fricative /h/ and the flap / / and its allophonic variations emerged at around 2;6 but only
stabilized at around 4;0 years of age. Among the clusters nasal+stops /nk/ appeared earlier
than flap+stops / t, k/ and liquid+stops /lp/. Although the liquids seemed to occur in
children’s speech much earlier they were subject to deletion when they occurred in clusters.
Table II shows the percentage of children in each age group who used these processes in
at least four words. The most frequently observed processes are summarized in the table.
Most of the processes were suppressed between the ages of 3;6, and 4;0 at the latest. If 10%
of the children used the same error pattern, it was considered as a process. The error
patterns were high around two years of age, which might be due to the increased vocabulary
use at this age. Reduplication, SI voicing, and fronting are among the earliest to be
suppressed. Word final devoicing was observed for /z/ only. Assimilatory substitutions,
although observed with high frequency, both progressively and regressively, disappear
early. The few error patterns observed after age four were liquid deviation and cluster
reduction.
Phonological disorder in Turkish speakers 511
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
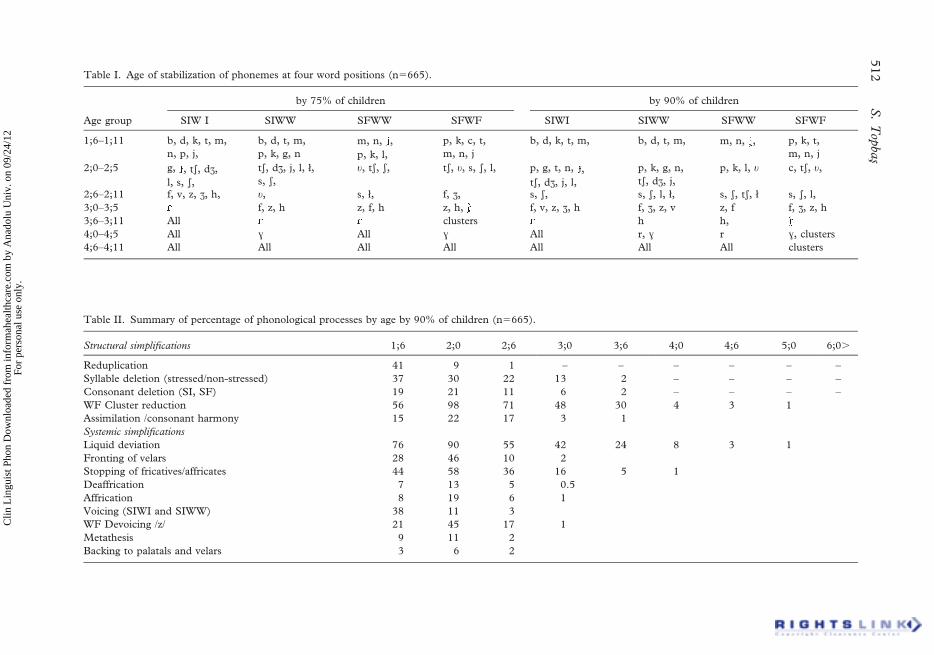
Table I. Age of stabilization of phonemes at four word positions (n5665).
Age group
by 75% of children by 90% of children
SIW I SIWW SFWW SFWF SIWI SIWW SFWW SFWF
1;6–1;11 b, d, k, t, m,
n, p, j,
b, d, t, m,
p, k, g, n
m, n, ,
p, k, l,
p, k, c, t,
m, n, j
b, d, k, t, m, b, d, t, m, m, n, , p, k, t,
m, n, j
2;0–2;5 g, , ts, dz,
l, s, s,
ts, dz, j, l, ł,
s, s,
u, ts, s, ts, u, s, s, l, p, g, t, n, ,
ts, dz, j, l,
p, k, g, n,
ts, dz, j,
p, k, l, u c, ts, u,
2;6–2;11 f, v, z, z, h, u, s, ł, f, z, s, s, s, s, l, ł, s, s, ts, ł s, s, l,
3;0–3;5 f, z, h z, f, h z, h, f, v, z, z, h f, z, z, v z, f f, z, z, h
3;6–3;11 All clusters h h,
4;0–4;5 All X All X All r, X r X, clusters
4;6–4;11 All All All All All All All clusters
Table II. Summary of percentage of phonological processes by age by 90% of children (n5665).
Structural simplifications 1;6 2;0 2;6 3;0 3;6 4;0 4;6 5;0 6;0.
Reduplication 41 9 1 – – – – – –
Syllable deletion (stressed/non-stressed) 37 30 22 13 2 – – – –
Consonant deletion (SI, SF) 19 21 11 6 2 – – – –
WF Cluster reduction 56 98 71 48 30 4 3 1
Assimilation /consonant harmony 15 22 17 3 1
Systemic simplifications
Liquid deviation 76 90 55 42 24 8 3 1
Fronting of velars 28 46 10 2
Stopping of fricatives/affricates 44 58 36 16 5 1
Deaffrication 7 13 5 0.5
Affrication 8 19 6 1
Voicing (SIWI and SIWW) 38 11 3
WF Devoicing /z/ 21 45 17 1
Metathesis 9 11 2
Backing to palatals and velars 3 6 2
512
S.
Top
bas
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
Method
Participants
Seventy monolingual Turkish-speaking children, aged 4;0–8;0 years, participated. They
were diagnosed either at faculty hospitals or other clinics as speech disordered and referred
to Anadolu University, DILKOM (Education, Research and Training Centre for Speech
and Language Disorders) for detailed assessment and therapy. The author, who is a
speech-language pathologist, had assessed them as phonologically and/or articulation
disordered. A laryngologist and a paediatric neurologist also examined the children. No
definable audiological or specific cognitive problems were found. Children with articulation
disorders due to organic etiologies such as cleft palate were not included in the study. The
receptive and expressive language of the children was tested as age appropriate on the
Peabody Picture Vocabulary test (Turkish version). Children with mild expressive delay
were also included since phonological disorders often co-exist with developmental language
delay. None of the children had had any phonological intervention at the time of the
assessment.
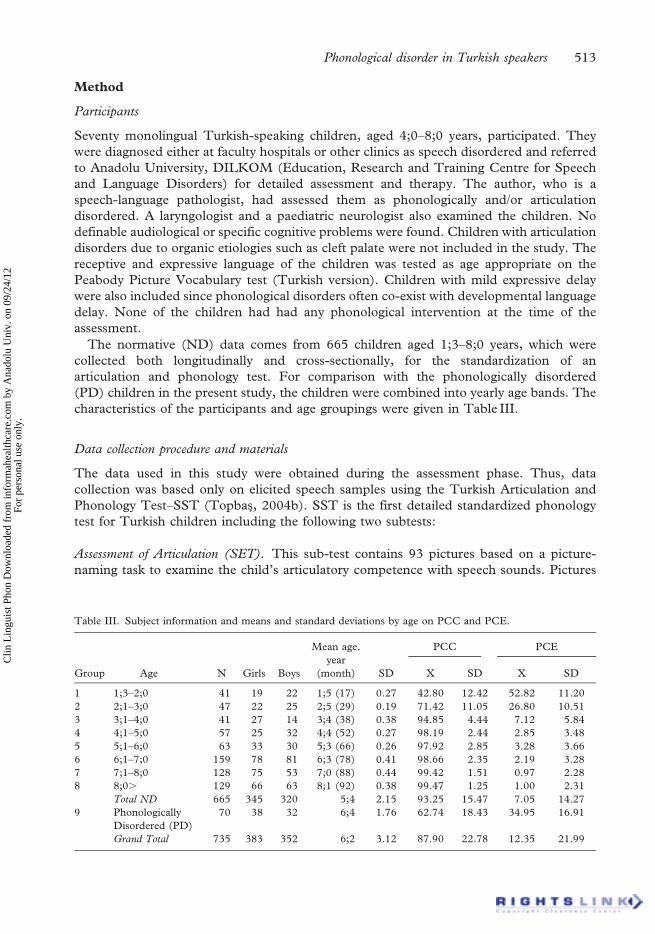
The normative (ND) data comes from 665 children aged 1;3–8;0 years, which were
collected both longitudinally and cross-sectionally, for the standardization of an
articulation and phonology test. For comparison with the phonologically disordered
(PD) children in the present study, the children were combined into yearly age bands. The
characteristics of the participants and age groupings were given in Table III.
Data collection procedure and materials
The data used in this study were obtained during the assessment phase. Thus, data
collection was based only on elicited speech samples using the Turkish Articulation and
Phonology Test–SST (Topbas, 2004b). SST is the first detailed standardized phonology
test for Turkish children including the following two subtests:
Assessment of Articulation (SET). This sub-test contains 93 pictures based on a picture-
naming task to examine the child’s articulatory competence with speech sounds. Pictures
Table III. Subject information and means and standard deviations by age on PCC and PCE.
Group Age N Girls Boys
Mean age.
year
(month) SD
PCC PCE
X SD X SD
1 1;3–2;0 41 19 22 1;5 (17) 0.27 42.80 12.42 52.82 11.20
2 2;1–3;0 47 22 25 2;5 (29) 0.19 71.42 11.05 26.80 10.51
3 3;1–4;0 41 27 14 3;4 (38) 0.38 94.85 4.44 7.12 5.84
4 4;1–5;0 57 25 32 4;4 (52) 0.27 98.19 2.44 2.85 3.48
5 5;1–6;0 63 33 30 5;3 (66) 0.26 97.92 2.85 3.28 3.66
6 6;1–7;0 159 78 81 6;3 (78) 0.41 98.66 2.35 2.19 3.28
7 7;1–8;0 128 75 53 7;0 (88) 0.44 99.42 1.51 0.97 2.28
8 8;0. 129 66 63 8;1 (92) 0.38 99.47 1.25 1.00 2.31
Total ND 665 345 320 5;4 2.15 93.25 15.47 7.05 14.27
9 Phonologically
Disordered (PD)
70 38 32 6;4 1.76 62.74 18.43 34.95 16.91
Grand Total 735 383 352 6;2 3.12 87.90 22.78 12.35 21.99
Phonological disorder in Turkish speakers 513
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
were mostly nouns, and basic colour terms known by young children. The children were
asked to say the target word pictured. If the child failed to produce the item, an imitated
response was expected.
Phonological Analysis Sub-test (SAT). This test is based on phonological process analysis. It
contains 13 pictures of thematic compositions to elicit expressive language sample in
continuous speech. The pictures were appropriate culturally for spontaneous data
collection based on narration, dialogues and conversation. The children were asked to
describe the picture. They were prompted as ‘‘Can you describe what is happening here?
What happened? What do you see in this picture?’’ A conversation was maintained by
questions in relation to the pictures such as ‘‘When is your birthday? Do you also give
parties? Who/what is this? Where does the ambulance go? Did you see an accident?’’ The
words in the test were chosen to provide a representative sample of Turkish phonology.
In SST each phoneme occurred in the following positions:
Syllable-initial word-initial (SIWI) pil (battery)
Syllable-initial within-word (SIWW) intervocalic ka-pı (door)
-C, C- post-consonantal kar-puz (watermelon)
Syllable-final within-word (SFWW)
-C, C- pre-consonantal sap-ka (hat)
Syllable-final word-final (SFWF) top (ball)
Word-final Clusters Turk (Turkish)
The assessments lasted about 1 hour. The recordings were done by speech-language
pathology trainees in a specially designed phoniatrics speech laboratory and recorded on
Sony MZ-R70 Mini-disc digital recorders with a Shure SM48 microphone.
Data analysis procedure
Transcription reliability. The transcriptions of the data were first transcribed by consensus
using IPA and PRDS symbols by MSc students in speech pathology and then by four
speech pathology graduate research assistants who were well trained in phonetic and
phonological analysis. Lastly the reliability analysis was computed by inter-rater reliability
analysis of the first author with the four assistants (91%). This was done on random
sampling of 10 mini-discs. In each disc there were four children’s data. So a total of 40
children’s speech was used for transcription reliability. Then inter-transcribers reliability
correlation coefficient measure was computed among all by Cronbach Alpha as
alpha5.8293 (Hotelling’s T-squared5252.21, F5124.27, sig .000).
Analysis measures. Overall data analysis was done through the forms that were developed
for the SST test. For the present research the transcription of each child’s data were
scanned for the following measures:
Percentage of consonants correct (PCC). In the articulation sub test of the SST test each
phoneme occurred at least four times (except /b, d, g, dz/ since they do not occur word
finally) and in the phonological analysis subtest several times. A phoneme was accepted as
stable if it occurred correctly in at least two different syllable positions of three different
words of the four opportunities. Imitated responses were not analysed. The formula
514 S. Topbas
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
proposed by Shriberg and Kwiatkowski (1982) was used to compute the production
percentages: correct production of consonants divided by target attempts X 100.
Percentage of consonants in error (PCE). PCE was calculated from the phonology subtest
based on spontaneous speech in order to show the variability found in continuous speech. It
is the number of times consonants (deletions and substitutions) were produced in error
divided by the total number of consonants X 100.
Error patterns as percentage of phonological processes (PPP). A detailed analysis was done
through the assessment forms of the phonology sub-test in spontaneous language sampling.
For each child, a process had to be used in at least three different words and used by at least
10% of the children. The percentage of occurrence of processes was computed by the
adapting the formula above. Then, the data were classified according to normative data as
persisting, unusual and variable/inconsistent patterns. For the disordered data a sub-
classification of errors due to severity levels was added to the analysis. Besides descriptive
statistics, a MANOVA, multiple regression and discriminant analysis were used to verify
the age, and gender effects in comparison with disordered development as well as sub-
classifying the error patterns.
Results
Quantitative analysis of performance in phonemic accuracy by age and gender
The means and standard deviations of phonologically disordered children (PD) compared
to normally developing children (ND) according to age, gender and on two measures, per
cent consonants correct (PCC) and consonants in error (PCE) scores can be seen in
Table III. As can be noted, the performance of the PD group was considerably lower on
PCC measures compared to the ND children at all ages and was high in PCE as expected.
Comparison of age and gender effect by MANOVA showed significant age effect in two
measures (PCC F8, 7265827.083, p,.000, R25.994; PCE F8, 7265738.697, p,.000,
R25.918), and post-hoc Tukey HSD analysis showed differences between Group 1, 2 and
all the other groups but no significant differences were found between Group 3 and 4, 5, 6,
7, 8 and 9. This might mean that consonants are produced correctly at around 3;0 years of
age, and that there is not much change after that. No significant difference was found
between the first and second ND group and PD group, which might be interpreted that PD
children’s performance is similar to that of 2;0–3;0 year olds.
As for gender, there seemed no differences between the two gender groups of PD and
ND children at all age groups, on PCC and PCE measures as shown by MANOVA results
(gender: boys vs. girls X conditions: nine groups: PCC F7, 7175.224 p..636; PCE F7,
7175.423 p..516). The gender effect for phonologically disordered children was further
analysed separately by independent samples t-test for PCC and PCE measures but no
significant gender difference was found (PCC t51.345 p..183 and PCE521.355
p..181). A summary of regression analysis by age groups of ND and PD children
suggested that the PCC scores of the PD children were significantly lower than the ND
children (r25.922 F56608.46 p,.000). Figure 1 gives a summary of the PCC of ND and
PD children on each phoneme by age. The most difficult and missing sounds for PD
children were fricatives and liquids, and flap / / which are the latest sounds acquired by the
ND children. Moreover, although the velars were acquired early in ND children they were
subject to error in PD children.
Phonological disorder in Turkish speakers 515
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.

Phonological production accuracy
Phonological error patterns. The normative data showed that although almost all the
phonemes were acquired earlier and articulated correctly in the picture-naming task, error
patterns were observed in the spontaneous speech of the ND children. In the normative
study, these error patterns were defined as structural and systemic phonological processes
by descriptive statistics. These error patterns were obvious in the PD children’s speech as
well. General overview of the results suggests that most of the PD children behave as
younger ND children.
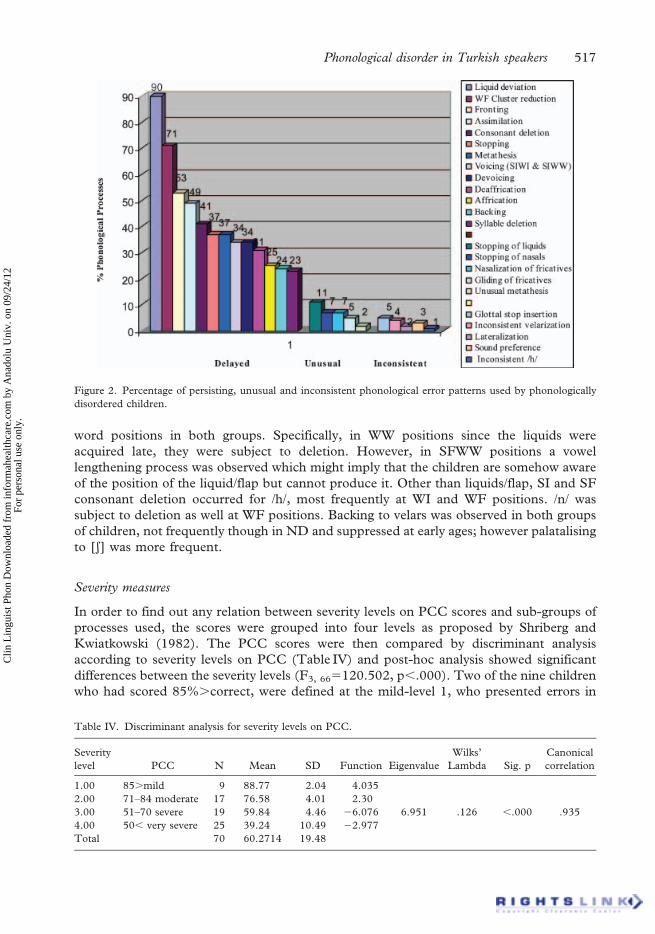
Sub-classification of phonological disorders. The error patterns of PD children were very
variable compared to ND children, some of which were identified as delayed error patterns
typical of ND but were used with high frequency and were not suppressed at the expected
age. The error patterns used by PD children are subdivided into the following categories as
illustrated in Figure 2.
1. The processes that are commonly used among ND children, but which were not
suppressed at around the expected age and which were still used after the age of 5;0,
were grouped under persisting normal processes as described by Grunwell (1985)
and Dodd (1993).
2. The processes that are rarely used or not used among ND children and that were
somehow consistent were grouped as unusual processes. This group showed a
disordered development (Leonard, 1985; Dodd, 1993). Consistency in this study
means that the error patterns can be explained or interpreted systematically by rules.
3. The processes that were not used among ND children, or that were found to be very
idiosyncratic and variable were grouped as inconsistent/variable processes. This
group showed a disordered development as well and the error patterns were very
inconsistent. Inconsistency in this study means that the error patterns cannot be
explained or interpreted systematically by rules but defined in someway and which
cause high unintelligibility. For example, a phoneme can be substituted for different
targets elsewhere.
The delayed error patterns were the ones used by 90% of ND children. They were much
more predictable when compared with children’s error patterns that use unusual and
idiosyncratic patterns. When compared with the normative data, liquid deviation is high in
both ND and PD groups. Consonant deletion was high with respect to SI and SF within
Figure 1. PCC for each consonant by the normative and phonologically disordered group (n5735).
516 S. Topbas
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
word positions in both groups. Specifically, in WW positions since the liquids were
acquired late, they were subject to deletion. However, in SFWW positions a vowel
lengthening process was observed which might imply that the children are somehow aware
of the position of the liquid/flap but cannot produce it. Other than liquids/flap, SI and SF
consonant deletion occurred for /h/, most frequently at WI and WF positions. /n/ was
subject to deletion as well at WF positions. Backing to velars was observed in both groups
of children, not frequently though in ND and suppressed at early ages; however palatalising
to [s] was more frequent.
Severity measures
In order to find out any relation between severity levels on PCC scores and sub-groups of
processes used, the scores were grouped into four levels as proposed by Shriberg and
Kwiatkowski (1982). The PCC scores were then compared by discriminant analysis
according to severity levels on PCC (Table IV) and post-hoc analysis showed significant
differences between the severity levels (F3, 665120.502, p,.000). Two of the nine children
who had scored 85%.correct, were defined at the mild-level 1, who presented errors in
Figure 2. Percentage of persisting, unusual and inconsistent phonological error patterns used by phonologically
disordered children.
Table IV. Discriminant analysis for severity levels on PCC.
Severity
level PCC N Mean SD Function Eigenvalue
Wilks’
Lambda Sig. p
Canonical
correlation
1.00 85.mild 9 88.77 2.04 4.035
2.00 71–84 moderate 17 76.58 4.01 2.30
3.00 51–70 severe 19 59.84 4.46 26.076 6.951 .126 ,.000 .935
4.00 50, very severe 25 39.24 10.49 22.977
Total 70 60.2714 19.48
Phonological disorder in Turkish speakers 517
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
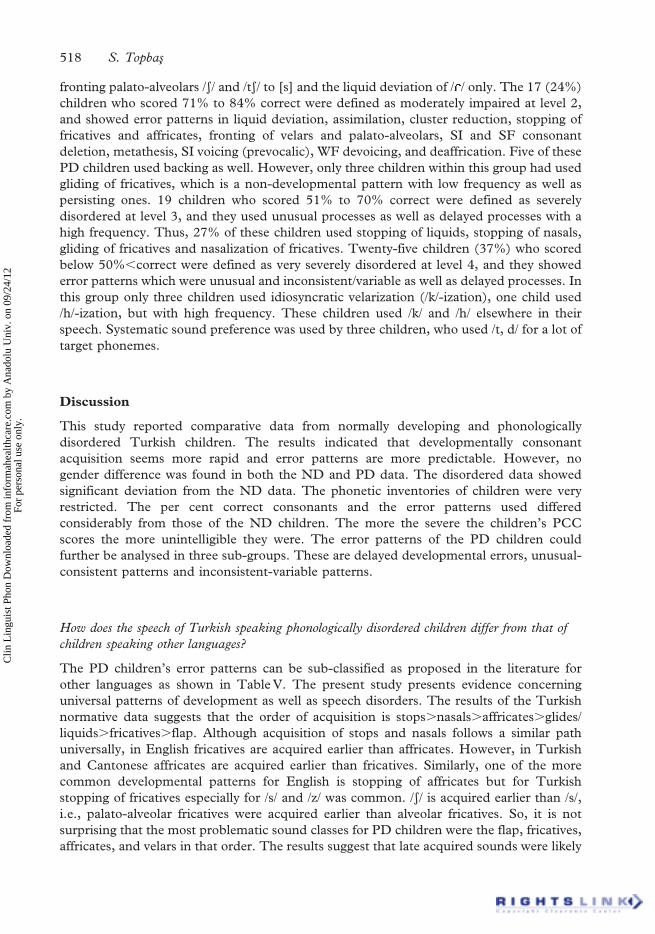
fronting palato-alveolars /s/ and /ts/ to [s] and the liquid deviation of / / only. The 17 (24%)
children who scored 71% to 84% correct were defined as moderately impaired at level 2,
and showed error patterns in liquid deviation, assimilation, cluster reduction, stopping of
fricatives and affricates, fronting of velars and palato-alveolars, SI and SF consonant
deletion, metathesis, SI voicing (prevocalic), WF devoicing, and deaffrication. Five of these
PD children used backing as well. However, only three children within this group had used
gliding of fricatives, which is a non-developmental pattern with low frequency as well as
persisting ones. 19 children who scored 51% to 70% correct were defined as severely
disordered at level 3, and they used unusual processes as well as delayed processes with a
high frequency. Thus, 27% of these children used stopping of liquids, stopping of nasals,
gliding of fricatives and nasalization of fricatives. Twenty-five children (37%) who scored
below 50%,correct were defined as very severely disordered at level 4, and they showed
error patterns which were unusual and inconsistent/variable as well as delayed processes. In
this group only three children used idiosyncratic velarization (/k/-ization), one child used
/h/-ization, but with high frequency. These children used /k/ and /h/ elsewhere in their
speech. Systematic sound preference was used by three children, who used /t, d/ for a lot of
target phonemes.
Discussion
This study reported comparative data from normally developing and phonologically
disordered Turkish children. The results indicated that developmentally consonant
acquisition seems more rapid and error patterns are more predictable. However, no
gender difference was found in both the ND and PD data. The disordered data showed
significant deviation from the ND data. The phonetic inventories of children were very
restricted. The per cent correct consonants and the error patterns used differed
considerably from those of the ND children. The more the severe the children’s PCC
scores the more unintelligible they were. The error patterns of the PD children could
further be analysed in three sub-groups. These are delayed developmental errors, unusual-
consistent patterns and inconsistent-variable patterns.
How does the speech of Turkish speaking phonologically disordered children differ from that of
children speaking other languages?
The PD children’s error patterns can be sub-classified as proposed in the literature for
other languages as shown in Table V. The present study presents evidence concerning
universal patterns of development as well as speech disorders. The results of the Turkish
normative data suggests that the order of acquisition is stops.nasals.affricates.glides/
liquids.fricatives.flap. Although acquisition of stops and nasals follows a similar path
universally, in English fricatives are acquired earlier than affricates. However, in Turkish
and Cantonese affricates are acquired earlier than fricatives. Similarly, one of the more
common developmental patterns for English is stopping of affricates but for Turkish
stopping of fricatives especially for /s/ and /z/ was common. /s/ is acquired earlier than /s/,
i.e., palato-alveolar fricatives were acquired earlier than alveolar fricatives. So, it is not
surprising that the most problematic sound classes for PD children were the flap, fricatives,
affricates, and velars in that order. The results suggest that late acquired sounds were likely
518 S. Topbas
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
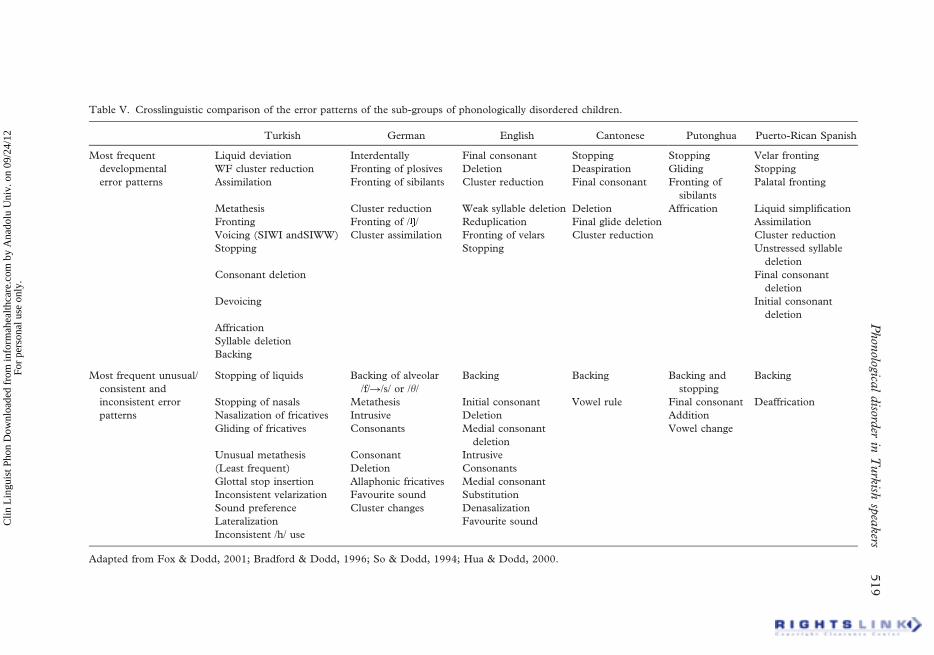
Table V. Crosslinguistic comparison of the error patterns of the sub-groups of phonologically disordered children.
Turkish German English Cantonese Putonghua Puerto-Rican Spanish
Most frequent
developmental
error patterns
Liquid deviation Interdentally Final consonant Stopping Stopping Velar fronting
WF cluster reduction Fronting of plosives Deletion Deaspiration Gliding Stopping
Assimilation Fronting of sibilants Cluster reduction Final consonant Fronting of
sibilants
Palatal fronting
Metathesis Cluster reduction Weak syllable deletion Deletion Affrication Liquid simplification
Fronting Fronting of / / Reduplication Final glide deletion Assimilation
Voicing (SIWI andSIWW) Cluster assimilation Fronting of velars Cluster reduction Cluster reduction
Stopping Stopping Unstressed syllable
deletion
Consonant deletion Final consonant
deletion
Devoicing Initial consonant
deletion
Affrication
Syllable deletion
Backing
Most frequent unusual/
consistent and
inconsistent error
patterns
Stopping of liquids Backing of alveolar
/f/R/s/ or /h/
Backing Backing Backing and
stopping
Backing
Stopping of nasals Metathesis Initial consonant Vowel rule Final consonant Deaffrication
Nasalization of fricatives Intrusive Deletion Addition
Gliding of fricatives Consonants Medial consonant
deletion
Vowel change
Unusual metathesis Consonant Intrusive
(Least frequent) Deletion Consonants
Glottal stop insertion Allaphonic fricatives Medial consonant
Inconsistent velarization Favourite sound Substitution
Sound preference Cluster changes Denasalization
Lateralization Favourite sound
Inconsistent /h/ use
Adapted from Fox & Dodd, 2001; Bradford & Dodd, 1996; So & Dodd, 1994; Hua & Dodd, 2000.
Phon
ological
disord
erin
Turk
ishsp
eakers
519
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
to be problematic, whereas the highest mastery level was for stops, nasals, the glide and the
liquid /l/ and a moderate level for affricates.
When the severity levels are taken into account, it can be inferred that the children falling
into severity level 1 can be considered as showing delayed developmental processes. The
children in the second level also used delayed developmental processes but their frequency
was much higher and the children’s phonetic inventories were greatly restricted. Thus, a
total of 26 children, 37% in this study might be labelled as belonging to a delayed group.
Nineteen children who scored between 50–75% correct used unusual but consistent
processes as well as persisting ones. These children were labelled as being in the unusual
sub-group. Thirty-five per cent of children who scored below 50% showed error patterns
including delayed, unusual and variable, and were very unintelligible. These results are
compatible with the results of Fox and Dodd’s (2001) study of German, Bradford and
Dodd’s (1996) investigation of English, So and Dodd’s (1994) work in Cantonese, Hua
and Dodd’s (2000) and Hua’s (2002) research in Potunghua, and Goldstein’s (1996) study
of Spanish. Yavas and Lamprecht (1988) reported that two of the four phonologically
disordered children they analysed used unusual rules, whereas the other two used persisting
ones. Although there are shared error patterns among languages, there are differences as
well. For example, backing or metathesis is reported as a non-developmental process for
languages other than Turkish. While final consonant deletion is reported for other
languages, in Turkish deletions both post- and pre-consonantal within word were more
frequent. The liquids and the flap were subject to deletion in these positions in both ND
and PD children. Delayed error patterns were typical of normal children but were used with
high frequency, and support the literature that the difference between these groups was
quantitative in nature rather than qualitative (Hua & Dodd, 2000). In this study, children
who fell into this category also used persisting patterns more frequently than ND. Thus, we
can infer that the delayed PD children are sensitive to the structure of their native language
just as the ND children. The analysis covered the general descriptive aspects of the above
categories, to show the necessity of such sub-classifications, which have been reported for
ten subjects in a preliminary analysis as well (Kopkallı-Yavuz & Topbas, 1998). Further
analysis of qualitative aspects may capture more information regarding the similarities and
differences among languages, in a detailed future study. Nevertheless, it can be inferred
that the most frequent error patterns are dependent on the phonological structure of the
language. Although universal tendencies exist, the ambient language effect is apparent in all
languages. Some error types are observed as being very unusual and inconsistent for
Turkish. This might be reflected in the severity of speech errors. Any hypothesis underlying
deficits in these children will be vague for the present aim of this study, and will thus need
further research. However, since the age of the PD children was older than the ND,
classifying the error patterns in terms of surface errors has implications for clinical
treatment provision.
Acknowledgement
The author expresses her gratitude to our research assistants Bulent Togram and Barıs
Dincer and our graduate MSc Speech-Language Pathology students for their assistance in
data collection and transcription. This research has been aided by a grant from Anadolu
University Research Foundation project no. 006 and the Turkish Ministry of Education,
Department of Speech Disorders. Special thanks are due to the anonymous reviewer.
520 S. Topbas
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.
References
Acarlar, F., & Ege, P. (1996). Turkce kazanımda kullanılan fonolojik sureclerin incelenmesi. (Phonological
processes in the acquisition of Turkish). Turk Psikoloji Dergisi, 38, 35–43.
Bradford, & Dodd, B. J. (1996). Do all speech disordered children have motor deficits? Clinical Linguistics and
Phonetics, 10, 77–101.
Dodd, B. (1993). Speech disordered children. In G. Blanken, H. Dittmann, H. Grimm, J. Marshall, & C. W.
Wallesch (Eds.), Linguistic disorders and pathologies (pp. 825–834). Berlin: De Gruyter.
Fox, A. V., & Dodd, B. (2001). Phonologically disordered German-speaking children. American Journal of Speech-
Language Pathology, 10, 291–304.
Goldstein, B. (1996). Error groups in Spanish-speaking children with phonological disorders. In T. W. Powell
(Ed.), Pathologies of speech and language: Contributions of clinical phonetics and linguistics (pp. 171–177). New
Orleans, LA: ICPLA.
Grunwell, P. (1985). Phonological assessment of child speech (PACS). Dorset: NFER-Nelson.
Hua, Z. (2002). Phonological Development in Specific Contexts: Studies of Chinese-speaking Children (pp. 106–120).
Clevedon: Multilingual Matters.
Hua, Z., & Dodd, B. J. (2000). Putonghua (modern Standard Chinese)-speaking children with speech disorders.
Clinical Linguistics and Phonetics, 14, 165–191.
Ingram, D. (2004). Phonological acquisition from a cross-linguistic perspective. Paper presented at ICPLA10, 26–
29 February, University of Louisiana, Lafayette.
Ketrez, F. N. (1997). Bir cocugun dil edinimi surecinde ses aktarımı. (The process of metathesis in the phonology
of a child acquiring Turkish) XIth Linguistics Symposium, 22–23 May, Middle East Technical University,
Ankara.
Kopkall1-Yavuz, H., & Topbas, S. (1998). Phonological processes of Turkish phonologically disordered children:
Language specific or universal? In W. Ziegler, & K. Deger (Eds.), Clinical Phonetics and Linguistics (pp. 88–97).
London: Whurr Publishers.
Kopkall1-Yavuz, H., & Topbas, S. (2000). Children’s preferences in early phonological acquisition: How does it
reflect sensitivity to the ambient language? In A. Goksel, & C. Kerslake (Eds.), Studies on Turkish and Turkic
languages. Harrassowitz Verlag: Wiesbaden.
Leonard, L. B. (1985). Unusual and subtle phonological behaviour in the speech of phonologically disordered
children. Journal of Speech and Hearing Disorders, 50, 4–13.
Shriberg, L. D., & Kwiatkowski, J. (1982). Phonological disorders I: A diagnostic classifiction system. Journal of
Speech and Hearing Disorders, 4, 226–241.
So, L. K. H., & Dodd, B. J. (1994). Phonologically disordered Cantonese-speaking children. Clinical Linguistics
and Phonetics, 8, 235–255.
So, L. K. H., & Dodd, B. J. (1995). The acquisition of phonology by Cantonese-speaking children. Journal of Child
Language, 22, 473–495.
Topbas, S. (1988). The frequency effect and the acquisition of /k, t, ts/ sounds in Turkish. Unpublished thesis,
City University, London.
Topbas, S. (1994). Konusma sorunlu cocukların sesbilgisel cozumleme yontemi ile degerlendirilmesi.
(Phonological analysis of speech disordered children). Unpublished doctoral thesis (pp. 150–250), Anadolu
Universitesi, Eskisehir.
Topbas, S. (1996). Sesbilgisi acısından dil edinimi (Language acquisition. A phonological approach). Dilbilim
Arastırmaları, 4, 118–128. Ankara: Hitit Yay.
Topbas, S. (1997). Turkish children’s phonological acquisition: Implications for phonological disorders. European
Journal of Disorders of Communication, 32, 377–397.
Topbas, S. (2004a). Does the phonology of Turkish-speaking children differ from children learning other
languages. Paper presented at ICPLA 10, 26–29 February, University of Louisiana, Lafayette.
Topbas, S. (2004b). Turkce Sesletim-Sesbilgisi Testi (Turkish Articulation and Phonology Test). Ankara: Milli
Egitim Yayınevi.
Topbas, S. (in press). A Turkish Perspective on communicative disorders. Logopedics Phoniatrics Vocology.
Topbas, S., & Dincer, B. (2002). Universal and language specific aspects of variability in phonological patterns.
IASCL-SRCLD Conference, 16–21 July, University of Wisconsin, Madison.
Topbas, S., & Konrot, A. (1998). Variability in phonological disorders: Can we search for systematicity? Evidence
from Turkish-speaking children. In W. Ziegler, & K. Deger (Eds.), Clinical Phonetics and Linguistics (pp. 79–87).
London: Whurr Publishers.
Topbas, S., & Kopkall1-Yavuz, H. (1998). The onset of a linguistic system: Is there evidence from the acquisition
of final devoicing in Turkish? In A. Sorace, C. Heycock, & R. Shillcock (Eds.), Proceedings of the GALA
Phonological disorder in Turkish speakers 521
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.

Congress (Generative Approaches to Language Acquisition Conference) (pp. 284–289). Edinburgh:
Edinburgh University Press.
Topbas, S., & Yavas, M. (2006). Phonological acquisition and disorders in Turkish. In Z. Hua, & B. Dodd (Eds.),
Phonological development and disorders in Turkish: A multilingual perspective (pp. 233–264). Clevedon: Multi-
lingual Matters.
Yavas, M., & Lamprecht, R. (1988). Processes and intelligibility in disordered phonology. Clinical Linguistics and
Phonetics, 2, 329–345.
Yavas, M., & Topbas, S. (2004). Liquid development in Turkish: Salience vs. frequency. Journal of Multilingual
Communication Disorders, 2, 110–123.
522 Phonological disorder in Turkish speakers
Clin
Lin
guis
t Pho
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y A
nado
lu U
niv.
on
09/2
4/12
For
pers
onal
use
onl
y.