Pricing tranches of Collateralize Debt Obligation (CDO) using ...

Do we now have a greater moral obligation to provide better, age-friendly
environments for the promotion of mobility and social interaction?
University of Durham, HPSM MA
Philosophical Issues in Science and Medicine: Summative Essay
Abstract
Aestheticians are taken to have the primary authority of architecture as a realm within philosophy; applying aesthetic theory directly to architecture, in order to ascribe an ‘essence’. It has become apparent that architecture is of wider philosophical interest than originally presumed. As questions arise within the philosophy of medicine as to what factors compromise our biological agency, it is becoming increasingly clear that architectural considerations are relevant to this field of study. The philosophical influence on architecture focuses on the phenomenology of the built environment, and materiality in their sensory aspects. Most of our social activity, living and thriving as human beings happens within the built environment and philosophers of medicine are alert to the ways that space can be incapacitating and cause unnecessary distress, but do not typically focus upon architecture, despite this being a specific concern of ill and disabled persons. This essay argues that there is an apparent need to address the issue of ‘architecturally induced wellness’ within the realm of philosophy, and the built environment can be implemented to promote a fulfilling life, a sense of self and social interaction for the ageing, and allow them to experience a positive sense of wellness through the medium of the built environment.
I declare that this essay is 4552 words long
Anonymous Marking Code: Z0951540 Module Supervisor: Dr. Ian James Kidd
Date of Submission: Easter Term, 15th June 2015 Journal Convention: Ageing and Society
!1

Contents
Introduction………………………………………………………………………..…….……..……3
I: The experience of ageing in urban environments………………………………….…….………..5
I i: Functional Decline ………………………..….……….………….………………7
I ii: A problem with categorising the effects of ageing……………………………….7
II: Beyond bodily needs..………….……………………………………………………..………….11
Conclusion…………………………………………………………………………………………..17
Bibliography……….……………………………………………………………………………..…19
!2

Introduction
We are currently experiencing a shift in the age composition of the world, due to access to better
healthcare and knowledge regarding to the promotion of healthy lifestyles. This will undoubtedly
affect various aspects of society- the way we live, work, how we interact, and, most pertinently, the
environments in which house these activities. It is predicted that by 2030, two-thirds of the world’s
population will be living in cities. Within this focus group, at least a quarter of residents living in
those urban populations will be aged 60+ years, if not more (Phillipson 2011). It can be estimated
that both ageing and growth in urban populations will rapidly increase at a similar rate. This, in the
area of planning at least, has raised the pressing need to address the ostensible “demographic time
bomb” (Harris 2013).
The majority of the current public debate on ageing is characterised by this kind of alarmist
rhetoric, however it can be observed that this exaggerated stance has, at least, positively roused
growing public, policy, and academic interest in ageing populations. Taking this rhetoric into
account, it should be noted that current demographic patterns vary from city to city. Some, like
London, see an overwhelmingly young population, whereas others, including many parts of the
South West, are experiencing a fast-ageing urban population- with more residents entering into their
80s, 90s, or older than ever before (Coughlan 2014).
Whatever the demographic circumstance of cities are now or- in the future; what has become clear
is that older people are still a marginalised age group across urban locations countrywide (Scharf,
Phillipson, Kingston & Smith 2000). Cities are, to many urban planners, imagined to be spaces
constructed for the younger population, with older people atypically incorporated into conventional
masterplanning (Bingham 2014). With this taken into account, we must consider the following
!3

question: Do we have a moral obligation to provide “better”, age-friendly environments for the promotion of mobility and social
interaction?
It is erroneously presumed by many that citizens above the age of 65 are disabled, frail, and non
compos mentis (Altmann 2015). However, the reality is that we are heading towards a future fit, active,
older generation who merely need an adaption their living environments to cope with their slow
reduction in physical, sensory, and, sometimes, mental capacity (Rowles and Bernard 2012). Whilst
governmental action is being taken towards addressing the needs of the sufferers of Alzheimer’s or
Dementia (Social Care, Local Government and Care Partnership Directorate 2014), little seems to
be done in the way of promoting a sense of self, or, indeed, social interaction for the aged, but still
relatively able (Harper 2013).
Despite our increasing comprehension of older adults’ experiences of their environment
phenomenologically, the implementation of these theories are yet to be adequately put into design
practice. Architecture is not solely the practice of making space, but also the transformation into
making meaningful places. We need to appreciate the concept of place-making in order to develop
our understanding on how the built environment is interpreted by the older user. Although we are
becoming more knowledgeable on the effects physical barriers have on mobility and the perception
of space by older adults (Rantakokko, Iwarsson, Mänty, Leinonen & Rantanen 2012) , we are only
in the early stages of confronting the implications this has for the realms of environmental design,
social care, and public policy.
As the environment in which we live is a fundamental aspect of self-actualisation (such that it aides
in the promotion of wellness and allows us to flourish as an individual) it is morally imperative to
provide age-friendly inclusive design, in order to encourage self-actualisation within the ageing
community.
!4

I : The experience of ageing in urban environments
Health is often taken to be a requisite of the Aristotelian ‘good life’ (Macaro 2005) and a necessary
condition for happiness (Boorse 1977). Alas, the question of happiness in old age frequently arises,
yet is insufficiently addressed. Social interaction is an inherent issue in the process of ageing. As their
mobility declines, the elderly citizen finds it more difficult to venture out of the house in order to
engage in everyday activities such as meeting friends, or doing their grocery shopping (Wessels, de
Witte, Jedeloo, van den Heuvel, & van den Heuvel 2004). As their confidence in their ability to walk
fails, so does their confidence to initiate social interaction (Carel 2007). This issue is partially as a
result of unease of leaving their home environment due to the difficulties they face with a built
environment that does not adequately suit their individual needs.
Mobility, for the abled and equally, the impaired, is a fundamental aspect of daily life (Rosenkvist,
Risser, Iwarsson & Ståhl 2010); it is a phenomenological, spatio-temporal engagement between
movement and the environment one engages with. Thus, maintaining this function during the
process of ageing is a crucial aspect in the promotion of an active life and participation within
society (Mollenkoft et al., 2004, Schootman et al., 2006, Shumway-Cook et al. 2002). Similarly,
promoting mobility in public environments is critical, especially when presented with the ‘key facts’-
a common persuasive tool used in public policy. What we gain from these narratives is a description
of the ways in which people approaching old age experience the city in which they live. For
example, fearing the outdoors at certain times of the day , keeping up with the pace of modern 1
life , or a sense of alienation from their surroundings that many of them have lived within for a 2
large majority of their lives.
Around 50% of people aged 75+ fear leaving their homes after dark. 1
41% of those over 65 claim to struggle to keep up with the pace of modern life.2
!5

Despite these ‘key facts’, we seem to be missing the real issue behind these narratives: perhaps the fear
of venturing out has less to do with physical obstructions of a place and more to do with an
emotional disconnection from the place they consider their ‘hometown’ (Handler 2014). The loss of
a spouse could trigger a sense of uncertainty and inhibits the confidence or desire to go out and
socialise, or perhaps it is something related to urban disorder. The lack of care given to street
furniture, paving, issues with graffiti and litter, conjures feelings of insecurity. The lack of care we
put into managing our urban environments may be interpreted, primarily by the older adult, as a
lack of care for their users (Buffel, Phillipson, & Scharf 2012). The place they once considered their
hometown- a place that once held meaning, is now nothing but an unkempt exterior location that
no longer adequately addresses their needs as a service user. We could argue that it is because of
these factors that the ageing service users are suffering from an epistemic injustice- an epistemic loss
as a result of an uneasy, obstructive, and uncared for environment which has led towards a demise
of mobility in the elderly resident.
It is apparent that the world in which the older person dwells is inadequately suited to their specific
needs. The question arises as to whether it is because of this maladaptation that their ‘world’ is
contributing to their inability to cope psychologically. Coupled with difficulties enhanced by
biological dysfunction, it is understandable why so many older people struggle to navigate their
hometowns. Unhappiness with the environments in which we live influences our lives greatly, so
there is no surprise that many ageing service users suffer socially and functionally as a result.
Using this knowledge, how do we adequately address their needs in order to instil happiness, self-
actualisation and a sense of belonging to their immediate environment? Architecturally, we have a
moral obligation to make people feel at home, therefore, using architectural principles such and the
manipulation of space in place-making will allow a means in which to improve the lives of the
ageing person.
!6

I i : Functional biological decline
Functional biological decline is an inevitable consequence of ageing, and multiple health problems
are common in the older population (Karlamangla et al. 2007). The aged generally experience a
gradual decline in physical capacity, manifesting in functional limitations including bending,
kneeling, and maintaining balance (Iwarsson, Ståhl, Löfqvist 2013) . In order to combat these issues,
the use of mobility devices such as walking sticks, zimmer frames, and wheelchairs often play and
important role in daily life in old age. Such devices help older people to remain independent in
everyday activities, feel safe, and participate in society Given the complexity of functional biological 3
decline and dependence on mobility devices, the occurrence of accessibility problems in outdoor
environments and public spaces is evident; indeed, older people often experience usability and safety
problems, when moving in outdoor environments (Shumway-Cook et al. 2002). Consequently, well
designed pedestrian environments and public transportation systems are important requisites for
older people to be able to travel and conduct their everyday activities independently and safely
(Leslie et al. 2005).
In order to come up with efficient solutions to support outdoor mobility in old age, there is a need
for research generating a knowledge base with potential for transfer to practice contacts. The grand
challenge is to increase our understanding in the complexity of the transactional relationship
between person, the environment, and the tasks and activities forming daily life.
I ii: A problem with categorising the effects of ageing
There seems to be a difficulty in defining a category in which the experience of ageing will fit. Most
philosophers seem to divide wellness into health and disease; the experiential feelings of an
see Wressle and Samuelsson 20043
!7

individual that can be used in the application of what constitutes as health and illness. Boorsean
philosophy states that health and disease are ‘and objective matter to be read off biological
facts’ (Boorse 1997) and, whilst this may be the case medically, we cannot say that the experience felt
by one body is an identical experience felt by another. This principle fails to adequately address the
issue of ageing, and cannot be directly applied to the lived experience of the elderly. It can be said
that, whilst not all older adults suffer from illness, a vast majority encounter the same difficulties as
those with health problems- a decline in mobility, or perhaps hardness of hearing and visual ability.
If their environment is ill-suited to their physical needs, then it is inevitable that the aged resident
will reduce their outdoor activity.
Similarly, principles of ontological naturalism would define the process of ageing akin to ‘disease’.
However, there is more to ageing, or indeed, illness, than just a biological dysfunction or failure. We
need to incorporate the social and psychological components of ‘wellness’; an experiential element
in which we can come closer to categorising the process of ageing. It would be more appropriate to
create a new category; one which features an interplay between the lived body and mind alongside
social perceptions associated with ageing- playing a role in how the process of ageing is experienced.
It is a safe assumption that the state of ‘healthiness’ is normality. We can define ‘normalcy’ as a
desirability to either an individual or society in which it is defined. Taking this into consideration,
normativism in this sense could imply that the judgement of what constitutes ‘healthiness’ is a value
judgement with ethical relativism (Boorse 1975). However, normativism manifests itself in a variety
of forms; both as strong or weak normativism. An example of this may be the consideration of
what is considered “desirable”. It may be undesirable that in old age, we are in “poor health” or
disabled, but neither of these are necessarily related to disease. For Marie Jahoda (1958), these
statements adhere with weak normativism: calling a condition ‘healthy’ involves calling it good, and
good conditions satisfy some further descriptive property as well. At present, it would would seem
!8

there is no ‘good’ to the prospect of ageing. If we are to ratify the issue of promoting wellness within
the ageing, we should start by categorising ageing appropriately; by considering ageing, in whatever
state, to be ‘good’ or ‘healthy’. This positive nomenclature should help psychologically increase
wellbeing in the older person- they have exactly the same right to live as many other people living in
the same community setting, and should be given the opportunity to live a self-actualised life; free
from the negative stigma that ageing currently holds.
A phenomenological or metaphysical approach to the subject of ageing, then, may seem more
appropriate, due to the fact it addresses the issue of describing human experience (Cooper 2001). In
practice, phenomenology can be applied to a variety of scenarios: sociological, anthropological,
and, crucially; medical and architectural (Carel 2011). By incorporating phenomenological
principles to practice associated with ageing, we can then discover ways of implementing design to
make engagement with the environment these elderly residents come into contact with (idem.).
However, even this categorisation is not a completely accurate fit. Phenomenology relies somewhat
on an empirical methodology. We cannot truly know what the experience of imposing architecture
and uneven flooring feels to an elderly person- we can only make a “best guess” based on our
experience. The problem here is that many of us are fully mobile; we do not struggle with our gait.
The way to really progress is by employing the suggestions and concerns of all age demographics-
especially those who seem to be forgotten, like the elderly.
We reach an issue insomuch as if we cannot accurately place the subject of ageing as a mode of
identifying what qualifies as being morally imperative within a philosophical medium, then how are
we to comprehend how we can create a better public inclusive design for the aged user to engage
with? The problem with trying to categorise ageing within pre-existing philosophical mediums is
that all of them seem to be fractional. We can categorise and analyse ageing phenomenologically,
biologically and metaphysically, but never reach a true understanding. They tell an incomplete
!9

account as to ‘what it is like’ to be aged; an empirical understanding. We need to strive to create a
new subcategory of phenomenology- the phenomenology of ageing, in order to obtain a full
understanding.
As aforementioned, the elderly demographic is often unaccounted for not only in architecture and
urban planning, but it seems it is a similar scenario within philosophy. If we are to move forward in
incorporating philosophical principles into the realm of architectural planning to promote mobility
and social interaction, we need to understand why this is morally imperative. We need to understand
what is going to help us understand the phenomenology of ageing. Once we understand this, we
need to understand their problems in order to address them. At present, we can only write on a
general level as there is currently little in the way of literature on the importance of architectural
design on wellness. Although this is just an explanatory exercise, it also stresses how pertinent this
issue is becoming in contemporary philosophy of medicine. In order to move forward in making it
possible to promote mobility and wellness within the elderly, then we need to articulate how
philosophy can be applied to architecture specifically in order to gain full understanding.
!10

II: Beyond bodily needs
As previously stated, the focus of this lies in what is beyond the ageing person’s home. For the most
part, older people are more likely to be dissatisfied with their local neighbourhood than they are
with their home environment (Handler 2014). This may be as a result of years of creating a sense of
place within their home; they feel comfortable and able to complete tasks in relative comfort. Here,
we must differentiate what is meant by space and place:
Spaces are locations which, in the Cartesian sense, hold no
meaning to the user.
Places have seen a transformation from being considered a
space, to a process of habitation and life experience. These sites
hold greater to the user and reinforce a sense of community
identity.
A person’s life is a constant interplay of encountering public and private spaces. Over time, these
manifest as places once we impose meaning; as we learn to incorporate the use of these spaces
created for our use (Norberg-Schulz 1980) . We are continually making or remaking place based on
our affiliation with the environment. Identifying with these spaces can either support or constrain
the creation of space. They help sustain and reshape- both positively and negatively- our sense of
identity, and are directly linked to our sense of being or, contrastingly, our sense of being alienated
from society. Although space is still there, the concept of place they have applied to their
neighbourhood community is rapidly diminishing. This may serve as a justification as to why 12%
of all people over the age of 65 feel cut off from society (Age UK 2014). The lack of care in
!11

addressing their specific needs for the promotion of social inclusion and mobility inhibits their
connection with public space.
It can be noted that, thus far, this essay has noted little on the ‘physical fabric’ of the built
environment, but a need to address the age-inclusive urban practice within the architectural
discourse, and how social dynamics are underpinned in people’s everyday lives and experiences of
urban space; especially in areas where social exclusion among the ageing is often experienced more
unevenly.
Age, especially in healthcare architecture is repeatedly referred to as a mounting condition of
decline, dependency and need (TEU 2014). Instead, there is a need to suggest a counter narrative
around age-inclusive environments. We need to look at the primary needs of these older service
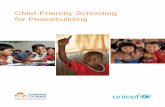
users. The needs of the aged can be seen as a basic inversion of the typical Maslow’s Hierarchy of
Needs: we need to address the higher-level needs before we can become comfortable with the basic-
level needs.
!12

Self-actualisation is a fundamental need which drives all others. In many ways, this is the most basic
need of the elderly. For example, if architecture isn’t sufficiently suited, so that space is no longer
considered a place, then the ageing individual will no longer feel at home in the world. This
encourages a diminishing sense of self-actualisation, and, therefore leads to biological decline. As a
result, basic needs become harder to fulfil. This sets the older person at a hindrance, and leads them
on a downward spiral; trying to cope with all these additional factors makes it harder to promote a
sense of wellbeing.
In order to properly integrate the older person into society, they need to feel as though their voices
have been heard- they are valuable members to society. From there, their self esteem grows and they
develop a sense of belonging in the community in which they live. Should they have difficulties in
their mobility, then they feel comfortable in addressing these issues in order to proceed with
!13
BIOLOGICAL AND PHYSIOLOGICAL NEEDS basic life needs (air, food, drink, shelter, warmth, sleep etc)
SAFETY NEEDS (protection, security, order, law, limits, stability, etc)
SELF ACTUALISATION (personal growth & fulfilment)
ESTEEM NEEDS (achievement, status, responsibility, reputation)
BELONGINGNESS AND LOVE NEEDS (family, affection, relationships, work group, etc)
Maslow’s hierarchy of needs, inverted.

maintaining the higher-level functions; providing themselves with food maintaining their home, etc.
All of these actions connect the older person on a socio-emotional and political level to the urban
environment in which they live.
We can apply the principles of architectural theory in order to ascribe how to create a better
inclusive design for use by older persons.
Space, and, indeed, dwelling within architecture are engagements of thinking between humans, and
how we relate to the environment around us (Denny 2011). In order to understand the basic
principles of design, it is perceived that both space and form need to be understood in order to
create ‘healthy’ and captivating spaces that promote human interaction and mobility within their
environment (Denny, 2014) It is through interaction that we can cultivate and design- to create an
experience through the connection between humankind and architecture. Architecture should be
seen as a a manner of social activity. We thrive within its realm and it enables us to complete a series
of activities.
It is a common misconception that in order to create this connection that high quality aesthetics
need to be implemented. What is forgotten is that there is an intrinsic link between form and space
which ultimately creates experience. Many believe that manipulation of space is the sole creation of
environmental essence, yet this is not the case. As Bruno Zevi (1993) writes:
'...the essence of architecture... does not lie in the material
limitation placed on spatial freedom, but in the way space is
organised into meaningful form through this process of
limitation... the obstructions which determine the perimeter of
possible vision, rather than the 'void' in which this vision is given
play.'
Architecture as Space p30.
!14

For the ageing person, the organisation of space and the subsequent experience gained from their
immediate exterior environment is vital for the promotion of self-actualisation. Twentieth century
phenomenologist and existentialist, Heidegger, questions the concept of creating essence in an
environment by using the architectural principles which he applies to both dwelling and building
(Sharr 2007). Put simply, humans interact with two space typologies; structures such as houses which
we call 'dwelling places', and those such as stadiums, bridges, city centres- heterotopia- which are not
(Heidegger 1971). As part of our expansive human experience, we also rest in the space within the
structures and they enable us to complete our daily activity. Space gives relief. We need it in order to
appreciate the beauty of the architecture as a whole. Essentially, this is what architecture is and is its
principal function; the interaction between space and form are the true essences of creating
architectural experience (Scruton 1979).
Bachelard, a contemporary of Foucault considers space as a phenomenological interrogation of
personal experience. His belief, voiced in ‘The Poetics of Space’, that ‘all really inhabited space bears
the essence of the notion of home’ (Bachelard 1958) is one that all architects should adopt;
especially when designing for an aged demographic. The home bears a sense of intimacy and
evokes memory- a conscious interaction with space and place. The world outside the home,
however, fails to provide the same intimacy. For the home, a strong sense of topophilia is present, 4
yet there rarely is the same environment created, for instance, in city centres. This leaves us with
uninspiring, stressful spaces that inhibit social interaction and the promotion of mobility. A new
essence in age friendly design needs to be implemented- the creation of topophilic spaces that
encourage a sense of wellbeing.
A strong sense of place which often becomes mixed with the sense of cultural identity among certain people 4
and a love of certain aspects of such a place.!15

It is frequently noted that aesthetic forms the true ‘essence’ of architecture. The tactile nature of its
materiality, the intimacy created by manipulation of space, the influence of the senses and the
relationship between interior and exterior all join in union to give the occupant a unique experience
within its realm. This is what the architect dreams of creating; an interaction between humankind
and physical entity (Denny 2014). Whilst there is strong emphasis on the ‘rhetorical’ (the visually
indicated role of architecture), there is little consideration today with the ‘actual’ role of architecture
(Harries 1997); the function of the environment by the user. Although aesthetically pleasing
architectural spaces assist in the creation of place-making, this leaves the architecture as nothing but
a process. Morality, and, consequently, beauty, are remote from the practical need of architecture by
the service user (Tatla 2011).
A problem arises when using the word ‘aesthetic’ in architectural language. There is a frequent
misinterpretation that this should solely apply to the general beauty of built environment; rather
than the experience and essence felt within its presence. This is why the need to develop a
sustainable, safe, and enticing environment should be the primary goal for the architect and urban
designer. These edifices form an integral role in modern society, so it is unfathomable why so many
people are forced to tolerate poor environments: low quality materiality, unkempt public areas, poor
way finding being just a few examples. If the atmosphere created is hostile, then is understandable
why many older people find themselves to be socially excluded from the outside world. The
environments that they were once proud to call their ‘home’ have become alien lands that they fear
entering into (Denny 2014).
!16

Conclusion
This essay has shown that in order to promote self-actualisation, mobility, and a positive sense of
wellbeing, we need to respond to a series of premises. Firstly, it is inevitable that with ageing, comes
a biological decline. However, in order to be well and fully self-actualised, one needs to cope with
their biological state. In order to do this, the creation of meaningful place-making and the
manipulation of space is paramount to promoting a positive sense of wellbeing and self-worth in the
older person. By adjusting the environment in which they live, then they are able to act positively
and lead a fulfilling life- one that they may have once felt was impossible due to the constraints that
the built environment imposed on them. We have a moral obligation to understand that, because we
now have better access to healthcare, that many more people will remain active in their later years.
We have a duty to adapt their immediate outdoor environments in order to cope with their
reduction in physical and sensory needs.
Secondly, we need to understand fully how we can turn public spaces into meaningful places
through age-friendly design. From the phenomenology of illness and disability, we are aware that
environmental factors impact on the wellness of the user. This is perhaps even more apparent in the
older person. Many people have lived in their neighbourhoods for the majority of their lives and are
reluctant to, once again, go through the process of making sense of a new setting in order to
become comfortable and feel safe. As mentioned in this essay, for many elderly users, their
hometowns are becoming more alien to them due to their inability to navigate through the built
environment.
Whilst space is still present, their concept of the place has altered. We have a moral obligation to
make sure that our towns and cities are accessible to a wide variety of age groups, not just the
younger populations. The environment can mean something different for each individual user.
!17

Phenomenologically, a place in which one person may feel safe is not necessarily the same
experience as another. Therefore, what may be good for some- and are conducive to happiness- may
be unfavourable for another. Public place settings are morally responsible for making sure that the
needs of every user are appropriately addressed.
Crucially, we need to understand that architecture and the built environment are resources for
addressing our current issue in the self-actualisation of older persons. We need to, once again, draw
the links between philosophy and architectural theory in order to promote a sense of self, social
interaction, and mobility through the art of making spaces into places.
!18

Bibliography
Bachelard, G. (1958): [1994]. The Poetics of Space. 3rd ed. Boston : Beacon Press. pp.1-245.
Denny, F. (2011). ‘In what ways did Heidegger’s philosophical views on space, on dwelling and on building impact upon his thinking about technology and modernity during the period 1927-1966?’ Unpublished manuscript.
Denny, F. (2014) ‘An Essence in Architecture: Vernacular Solutions to the Humanitarian Issues of the Design for Healthcare’ Unpublished manuscript.
Handler, S. (2014) ‘Actions in an age-friendly landscape’ in: An Age- Friendly Handbook for the Socially Engaged Urban Practitioner Manchester: The University of Manchester Library pp.22-28.
Harries, K. (1997) The Ethical Function of Architecture. Cambridge MA: MIT Press. pp.1-414
Heidegger, M. (1971). "Building Dwelling Thinking." Poetry, Language, Thought. pp.145-61. Print.
S. Iwarsson, Ståhl, A., & Löfqvist, C. (2013) ‘Mobility in Outdoor Environments in Old Age’ in: Rowles, G. G. & Bernard, M. (Eds.) Environmental Gerontology: Making Meaningful Places in Old Age Springer: New York. pp.175-198: 176
Jahoda, M (1958) Current Concepts of Positive Mental Health Basic Books: New York pp.1-152: 76-77.
Norberg-Schulz, C (1980) Genius Loci: Towards a Phenomenology of Architecture. Rizzoli: New York. pp.1-216
Monteau-Ponty, M. (1962) [1945] Phenomenology of Perception New York:Routledge p.137
Phillipson, C. (2011) ‘Developing age-friendly communities: New approaches to growing old in urban communities’ in: I R. Settersten, R. and J. Angel, ‘Handbook of the Sociology of Ageing’ New York: Springer.
Rowles, G. D & Bernard, M. (Eds.) (2012) ‘Preface’ in: Environmental Gerontology: Making Meaningful Places in Old Age New York: Springer Publishing Company. p.xi
Scruton, R. (1979). Has architecture an essence?. In: The Aesthetics of Architecture. New Jersey : Princeton University Press. pp.37-70.
Sharr, A. (2007) ‘Heidegger’s Thinking on Architecture’ in: Heidegger for Architects Oxford:Routledge pp.36-72.
Zevi, B. (1993) Architecture as Space: How to Look at Architecture Da Capo Press Inc: Boston, MA. p.30.
Journal Articles
Boorse, C. (1975) ‘On the Distinction between Disease and Illness’ Philosophy & Public Affairs 5(1) pp.49-68.
Boorse, C (1977) ‘Health as a Theoretical Concept’ Philosophy of Science Vol.44(4) pp.542-573.
Buffel, T. Phillipson, C. and Scharf, T (2012) ‘Ageing in urban environments: Developing ‘age-friendly’ cities’, Critical Social Policy (May 2012), p. 7.
Carel, H. (2007) ‘Can I Be Ill and Happy?’ Philosophia (35) pp.95-110
!19

Carel, H. (2011) ‘Phenomenology and its application in medicine’ Theoretical Medicine and Bioethics 32(1) pp.33-46
Cooper, R. (2001) ‘Disease’ Studies in History and Philosophy of Biological and Biomedical Sciences 33(1) pp.263-282
Handler, S. (2014), ‘A Research and Evaluation Framework for Age-friendly Cities’ UK Urban Ageing Consortium p. 32.
Harper, S. (2013) ‘The Opportunity for “Design to Influence the Ageing Process Itself ’ Population Ageing 6(1) pp.157-59
Harris, K. (2013) Age-friendly societies in our time? A literature review Wood Green Community Services/University of Birmingham p. 1.
Karlamangla, A, Tinetti, M., Guralnik, J., Studenski, S.,Wetle, T., & Reuben, D. (2007) ‘Comorbidity in older adults: Nosology of impairment, diseases, and conditions’ Journal of Gerontology 62A(3) pp.296-300.
Leslie,E., Saelens,B., Frank,L. , Owen, N., Bauman, A., Coffee, N., & Hugo, C. (2005) ‘Residents’ perceptions of walkability attributes in objectively different neighbourhoods: A pilot study’ Health and Place 11(3) pp.227-236.
Mollenkopf, H., Marcelleni, F., Ruoppila, I. , Széman, Z., Tacken M., & Wahl, H-W. (2004) ‘Social and behavioural science perspectives on out-of-home mobility in later-life: Findings from the European project MOBILATE’ European Journal of Ageing 1(1), pp.45-53.
Rantakokko M., Iwarsson, S., Mänty, M., Leinonen, R., & Rantanen, T. (2012). ‘Perceived barriers in the outdoor environment and development of walking difficulties in older people’. Age and Ageing, 41(1), pp. 118-121.
Rosenkvist, J., Risser, R., Iwarsson,S. & Ståhl, A. (2010) ‘Exploring mobility in public environments among people with cognitive functional limitations- challenges and implications for planning’ Mobilities 5(1) pp.131-145.
Social Care, Local Government and Care Partnership Directorate (2014) ‘Closing the gap: priorities for essential change in mental health’
Sylvester, C. (2009) ‘A virtue-based approach to therapeutic recreation practice’ Therapeutic Recreation Journal Vol.43(3) pp.9-25.
Schootman, M., Andresen, E.M., Wolinsky, F.D., Malmstorm, T.K., Miller, J.P. & Miller, D.K. (2006) ‘Neighborhood conditions and risk of incident lower-body functional limitations among middle-aged African Americans’ American Journal of Epidemiology 163(5) pp450-458.
Shumway-Cook, A., Patla, A.E., Stewart, A., Ferrucci, L.,Ciol, M.A., & Guralnik, J.M. (2002) ‘Environmental demands associated with community mobility in older adults with and without disabilities’ Physical Therapy 82(7) pp.670-681
Scharf, T. Phillipson, C., Kingston, P. & Smith, A. (2000) ‘Social exclusion and Older people : Towards a conceptual framework’ Centre for Social Gerontology 6(1) pp.1-23: 11
Tatla, H. (2011) Morality and architecture: evaluation of contemporary architectural practice within the scope of the ontological hermeneutics of Hans-Georg Gadamer. Art, Emotion and Value. 5th Mediterranean Congress of Aesthetics, 2011. 1 (1), pp.1-10.
!20

Wessels, R.D., de Witte, L.P., Jedeloo, S, van den Heuvel, W.P.M., & van den Heuvel, W.J.A. (2004) ‘Effectiveness of provision of outdoor mobility services and devices in the Netherlands’ Clinical Rehabilitation 18(4) pp.371-378
Wressle, E., & Samuelsson, K. (2004) ‘User satisfaction with mobility assistive devices’ Scandinavian Journal of Occupational Therapy 11(3) pp.143-150.
Online
Altmann, R. (2015) ‘Who are you calling old? Let’s ditch ageist stereotypes’ Available: http://www.theguardian.com/society/2015/feb/04/old-ditch-ageist-stereotypes Last accessed: 4th June 2015
Bingham, J. (2014) ‘Elderly being shut out of British cities: Major international study shows biggest age divide in Europe between cities and suburbs’ Available: http://www.telegraph.co.uk/finance/property/retirement/10986304/Elderly-shut-out-of-British-cities.html Last accessed: 4th June 2015.
Coughlan, S. (2014) ‘The town thronged with old people’ Available: http://www.bbc.co.uk/news/magazine-27066299 Last accessed: 4th June 2015.
Other
Feedback from ‘Ageing and the City’ a Learning from Kilburn class held at the Tiny Experimental University at the Tricycle Theatre, London on the 26th April 2014.
TNS Loneliness Omnibus Survey for Age UK (2014)
Further Reading
Carel, H. (2008) Illness: The Cry of the Flesh Durham: Acumen Publishing Limited. pp. ix-168.
Carel, H. & Cooper, R. (eds.) (2013) Health, Illness and Disease: Philosophical Essays Durham: Acumen Publishing Limited. pp.vii-255.
Reed, J., Cook, G., Sullivan, A., and Burridge, C. (2003) ‘Making a move: care-home residents’ experiences of relocation’ in: Ageing & Society 23(1) pp. 225-241.
Kay Toombs, S. (1993) The Meaning of Illness: A Phenomenological Account of the Different Perspectives of Physician and Patient Philosophy and Medicine Series (42) Dordrecht: Kluwer Academic Publishers pp.ix- 159.
!21
Copyright © 2022 FDOKUMEN