Discourse structure differences in lay and professional health communication
26
Discourse structure differences in lay and professional health communication Jennie A. Abrahamson and Victoria L. Rubin Faculty of Information and Media Studies, Language & information Technology Research Lab (LiT.RL), University of Western Ontario, London, Canada Abstract Purpose – In this paper the authors seek to compare lay (consumer) and professional (physician) discourse structures in answers to diabetes-related questions in a public consumer health information website. Design/methodology/approach – Ten consumer and ten physician question threads were aligned. They generated 26 consumer and ten physician answers, constituting a total dataset of 717 discourse units (in sentences or sentence fragments). The authors depart from previous LIS health information behaviour research by utilizing a computational linguistics-based theoretical framework of rhetorical structure theory, which enables research at the pragmatics level of linguistics in terms of the goals and effects of human communication. Findings – The authors reveal differences in discourse organization by identifying prevalent rhetorical relations in each type of discourse. Consumer answers included predominately (66 per cent) presentational rhetorical structure relations, those intended to motivate or otherwise help a user do something (e.g. motivation, concession, and enablement). Physician answers included mainly subject matter relations (64 per cent), intended to inform, or simply transfer information to a user (e.g. elaboration, condition, and interpretation). Research limitations/implications – The findings suggest different communicative goals expressed in lay and professional health information sharing. Consumers appear to be more motivating, or activating, and more polite (linguistically) than physicians in how they share information with consumers online in similar topics in diabetes management. The authors consider whether one source of information encourages adherence to healthy behaviour more effectively than another. Originality/value – Analysing discourse structure – using rhetorical structure theory – is a novel and promising approach in information behaviour research, and one that traverses the lexico-semantic level of linguistic analysis towards pragmatics of language use. Keywords Health information seeking, Information sharing, Provision of information, Information behaviour, Internet discussion groups, Diabetes, Information use, Pragmatic use of language, Information exchange, Internet Paper type Research paper The current issue and full text archive of this journal is available at www.emeraldinsight.com/0022-0418.htm An earlier version of this paper was presented at the 2011 Canadian Association for Information Science conference. The authors wish to thank the Everydayhelth.com forum participants whose publicly available questions and answers illuminate new perspectives on lay and professional health communication. The authors are also grateful for suggestions offered by anonymous reviewers for the CAIS/ACSI 2011 Conference and for Journal of Documentation. The authors thank Tatiana Vashchilko for her help with peer debriefing; her participation was partly funded by the New Research and Scholarly Initiative Award (10-303) awarded to Dr Victoria Rubin. Jennie Abrahamson’s work was supported in part by a Graduate Research Scholarship from the University of Western Ontario. JDOC 68,6 826 Received 27 January 2012 Revised 18 April 2012 Accepted 19 April 2012 Journal of Documentation Vol. 68 No. 6, 2012 pp. 826-851 q Emerald Group Publishing Limited 0022-0418 DOI 10.1108/00220411211277064
Transcript of Discourse structure differences in lay and professional health communication

Discourse structure differences inlay and professional health
communicationJennie A. Abrahamson and Victoria L. Rubin
Faculty of Information and Media Studies,Language & information Technology Research Lab (LiT.RL),
University of Western Ontario, London, Canada
Abstract
Purpose – In this paper the authors seek to compare lay (consumer) and professional (physician)discourse structures in answers to diabetes-related questions in a public consumer health informationwebsite.
Design/methodology/approach – Ten consumer and ten physician question threads were aligned.They generated 26 consumer and ten physician answers, constituting a total dataset of 717 discourseunits (in sentences or sentence fragments). The authors depart from previous LIS health informationbehaviour research by utilizing a computational linguistics-based theoretical framework of rhetoricalstructure theory, which enables research at the pragmatics level of linguistics in terms of the goals andeffects of human communication.
Findings – The authors reveal differences in discourse organization by identifying prevalentrhetorical relations in each type of discourse. Consumer answers included predominately (66 per cent)presentational rhetorical structure relations, those intended to motivate or otherwise help a user dosomething (e.g. motivation, concession, and enablement). Physician answers included mainly subjectmatter relations (64 per cent), intended to inform, or simply transfer information to a user(e.g. elaboration, condition, and interpretation).
Research limitations/implications – The findings suggest different communicative goalsexpressed in lay and professional health information sharing. Consumers appear to be moremotivating, or activating, and more polite (linguistically) than physicians in how they share informationwith consumers online in similar topics in diabetes management. The authors consider whether onesource of information encourages adherence to healthy behaviour more effectively than another.
Originality/value – Analysing discourse structure – using rhetorical structure theory – is a noveland promising approach in information behaviour research, and one that traverses the lexico-semanticlevel of linguistic analysis towards pragmatics of language use.
Keywords Health information seeking, Information sharing, Provision of information,Information behaviour, Internet discussion groups, Diabetes, Information use, Pragmatic use of language,Information exchange, Internet
Paper type Research paper
The current issue and full text archive of this journal is available at
www.emeraldinsight.com/0022-0418.htm
An earlier version of this paper was presented at the 2011 Canadian Association for InformationScience conference.
The authors wish to thank the Everydayhelth.com forum participants whose publicly availablequestions and answers illuminate new perspectives on lay and professional health communication.The authors are also grateful for suggestions offered by anonymous reviewers for the CAIS/ACSI2011 Conference and for Journal of Documentation. The authors thank Tatiana Vashchilko for herhelp with peer debriefing; her participation was partly funded by the New Research and ScholarlyInitiative Award (10-303) awarded to Dr Victoria Rubin. Jennie Abrahamson’s work was supportedin part by a Graduate Research Scholarship from the University of Western Ontario.
JDOC68,6
826
Received 27 January 2012Revised 18 April 2012Accepted 19 April 2012
Journal of DocumentationVol. 68 No. 6, 2012pp. 826-851q Emerald Group Publishing Limited0022-0418DOI 10.1108/00220411211277064

IntroductionResearchers and clinicians have long acknowledged that the majority of health caretakes place in everyday life environments, well beyond the threshold of the formal,clinical health care system (Kleinman et al., 1978). Pursuing health in contemporaryeveryday life is both an opportunity and a challenge. Health information seekers or“consumers”[1], have a variety of sources to choose from when seeking information. Asthe availability and use of online health information continues to grow (Fox, 2011a;Diefenbach et al., 2009), internet resources have become the top health and wellnessinformation source people report choosing in the US (Elkin, 2008). A recent US surveyfound that 80 per cent of internet users seek health information online (Fox, 2011a).Despite the availability and purported interest in health and wellness information,people’s adherence rates for recommended treatment or preventive health careregimens rarely rise above 50 per cent globally (World Health Organization, 2011).
DiMatteo (2004, p. 200) defines adherence as people doing “what their healthprofessionals recommend.” Adherence originates in the clinical setting of the healthcare system, but is enacted by consumers as part of their “mastery of everyday life”(Savolainen, 2008). The current study expands the former biomedically-baseddefinition of adherence to encompass the information and self-care practices peopleengage in to learn how to live with, or prevent chronic disease[2] in their everydaylives. Adherence is particularly important in chronic disease care, where complyingwith prescribed or recommended medication regimens or lifestyle changes (such asdietary practices or physical exercise) often must become lifelong activities to ensurequality or length of life.
Good and Del Vecchio Good have described health care and related discourses asfundamentally “social” activities because, regardless of whether care takes place in aclinical or everyday setting, it is “the product of human beings interacting andcommunicating with one another” (Good and Del Vecchio Good, 1981, p. 187). In thecontemporary online social environment, one in four American internet users livingwith chronic diseases such as high blood pressure, diabetes, heart or lung conditions,or cancer go online to “find others with similar health conditions” (Fox, 2011b, p. 2),and internet discussion forums are among the most popular social media sources theyuse (Sarasohn-Kahn, 2008).
The second most common source Americans seek health information from isphysicians (Elkin, 2008). People turn to physicians or other health professionals for“practical advice in coping with day-to-day health situations” almost as often as theychoose to turn to their peers or significant others (Fox, 2011b, p. 4). Nonetheless,physicians frequently express concern regarding the effects of consumer informationseeking and sharing (Ferguson, 2002). Yet, research has confirmed that participation inonline support groups such as discussion forums can improve health outcomes(Neuhauser and Kreps, 2010). However, little is known about how such improvement isachieved.
This study explores the communication spaces between consumers, and betweenphysicians and consumers interacting via a US-based consumer health informationwebsite. We consider whether one source of information (consumer or physician)encourages adherence to healthy behaviour more effectively than another. This workaddresses recent library and information science (LIS) calls for more research ininformation sharing, use, and effects (Savolainen, 2009). This research also addresses a
Discoursestructure
differences
827

critical need identified in health care and health communication for investigations ofthe impact of consumer-to-consumer communication on medication adherence(Diefenbach et al. (2009) and “what people are doing when they are trying to carryout their (personal health care) regimens” (McCoy, 2009, p. 128). Adherence isessentially a goal-based activity, in which consumers and/or their health careprofessionals (i.e. physicians, nurses, dieticians or physical therapists) identify goalsfor various health behaviours such as taking medication, exercising or making dietarychanges (Christensen, 2004).
We depart from previous LIS health information behaviour research by utilizing acomputational linguistics-based theoretical framework for this study. The framework,rhetorical structure theory (RST), supports studying the goals and effects of humancommunication (Mann and Thompson, 1988). Using RST facilitates research at thepragmatics level of linguistics, which enables the comparison ofconsumer-to-consumer and physician-to-consumer communication in onlinequestion-and-answering diabetes discourses. We accomplish this by first consideringthe context of chronic disease and diabetes, then reviewing adherence and itsrelationship to information sharing, both within health care and the LIS literature. Wethen position our work at the linguistic level of pragmatics, and discuss the empiricalstudy methodology, major findings, and implications.
This work informs consumer-centred health communication and promotion, andcarries theoretical value in LIS due to its contributions to the understanding ofinformation sharing and use, and due to its application of RST methodology toinformation behaviour research.
Literature reviewContext: chronic disease and diabetesChronic diseases account for 60 per cent of deaths worldwide (World HealthOrganization, 2011). As chronic disease rates and associated human and societal costsclimb throughout the world at an alarming pace, it is becoming increasingly urgent tounderstand how to support chronic disease prevention and treatment (World HealthOrganization, 2011).
Approximately one in 13 adults currently has diabetes; this figure is expected togrow to one in ten adults, or 552 million worldwide by 2030 (International DiabetesFederation, 2011). The related annual global health care expenditure for diabetes iscurrently 499 billion in international dollars (ID), a figure anticipated to increase to 654ID in 2030 (International Diabetes Federation, 2011). Living with or preventingdiabetes and other chronic diseases requires information about illness managementand preventive regimens to try to adopt or maintain medication and other treatmentprotocols such as dietary changes and exercise. These lifestyle changes affect theeveryday life of consumers, their family, friends, and coworkers (Hunt and Arar, 2001;Christensen, 2004). The physical consequences of adherence failures in diabetes areserious, and include potentially irreversible damage to eyes, kidneys, and nerves(Vermeire et al., 2005) and a possible 80 per cent increase in risk of death (Elliott, 2009).
Adherence and information sharing in LIS and health care literatureNon-adherence to prescribed treatments has been widely studied as a health careproblem. High non-adherence rates persist and few effective solutions have been found,
JDOC68,6
828

even though several possible causes have been identified such as medication cost,cultural issues including conflicting health beliefs or patient/treatment preferencemismatches, literacy challenges; forgetfulness as well as unsatisfactorypatient-provider communication (Christensen, 2004; Elliott, 2009). Most adherencechallenge assessments focus on patient responsibility or failures, rarely consideringthe role of the physician, or a joint role between patient and physician (Hunt and Arar,2001).
Information sharing and use is a recurrent theme in the adherence literature inhealth care. While physicians often believe that they spend adequate time educatingpatients about various treatments including medications, observational studies revealthat they spend less than one minute discussing new treatment regimens, if that. Evenwhen physicians share health information with patients intended to facilitate patientrecovery or health maintenance, patients frequently report that this information is“confusing” or “inadequate” (Alexander et al., 2006, p. 330).
Few LIS researchers have focused on treatment or medication adherence andinformation sharing. Sligo and Jameson (2000) advocated for adherence research intheir report on New Zealand Pacific Islander immigrant women’s informationbehaviour related to screening recommendations for cervical cancer. Sligo and Jamesonconcluded that further everyday life studies related to adherence and how people’senvironment “structures their capacity to accept and interpret new knowledge is calledfor” (Sligo and Jameson, 2000, p. 860). More recent work has begun to considerinformation use and adherence-related behaviour in chronic disease and healthinformation behaviour studies. In a study of “health information mastering” in aFinnish population, Ek and Widen-Wulff (2008) observed that most health promotioncommunication is predicated on an information transfer model, based on “theassumption that health promoting knowledge and corresponding behaviour areautomatically created as people are subjected to [. . .] information” (p. 74). Ek andWiden-Wulff cautioned that “information is not synonymous with knowledge, neitheris the transformation of knowledge into behaviour a simple linear process” (Ek andWiden-Wulff, 2008, p. 74). Palsdottir considered multiple aspects of how Icelanders’information behaviour and health beliefs are related to preventive health behaviour(Palsdottir, 2008).
Several studies have examined peer-to-peer information seeking and sharing in bothelectronic and offline environments. Oliphant (2010) and Neal and McKenzie (2011)studied the relationship of cognitive authority to information practices among patientsexperiencing depression or endometriosis, respectively. LIS studies on HIV/AIDS havebegun to more directly integrate the study of adherence and information use in theirresearch. Hogan and Palmer (2005) described adherence as an information intensiveactivity. Veinot (2009) highlighted the interplay of health information exchange andemotional support sharing and identified HIV/AIDS information seeking as a socialprocess carried out between people with HIV/AIDs and their friends or family members.Veinot also observed the importance of experiential information to her participants asthey developed “ongoing health management routines” (Veinot, 2010, n.p.).
Ferguson found that consumers identified online patient groups as being more usefulthan health professionals for the majority of health care needs studied (Ferguson, 1999;Fox, 2011b, p. 13). Several researchers have surveyed this environment in studies ofpeer-to-peer information behaviour or advice giving (see, for instance, Savolainen, 2011a;
Discoursestructure
differences
829

Oliphant, 2010; Neal and McKenzie, 2011). Savolainen (2011b) and Kouper (2010) providerecent comprehensive reviews of related work. Kouper states that prior research inadvice giving has focused on “issues of social support [. . .] trust, credibility (with anemphasis on peer-to-peer communication) [. . .] and the linguistic aspects ofprofessional-to-public advice” (Kouper, 2010, pp. 3-5). Kouper studied both thesolicitation and giving of advice amongst participants in a motherhood community blog,with a focus on pragmatic linguistic aspects of expressions of politeness or hedging(e.g. expressions of uncertainty). Savolainen (2011b) compared peer-to-peer informationneeds and information sharing expressed in question and answering in blogs anddiscussion forums for consumers “coping with depression” (p. 2). Savolainen also notesthat prior LIS work in online support communities has focused on peer-to-peer ratherthan physician-to-consumer communication.
Health care researchers have also begun to advocate for studying the social aspectsof diabetes patients’ lives and how patients’ social networks may affect their adherence(e.g. Van Dam et al., 2005). Bissell et al. identify the space between consumers andhealth professionals (such as physicians) as a space where the expertise of both shouldcombine to achieve “mutually agreed goals” (Bissell et al., 2004, p. 851).
Characteristics of lay versus professional health discourseLittle is known about pragmatic differences between lay and professional discourses inhealth communication. It is clear that lay people and health care professionals oftenexpress themselves differently, but the majority of the differences have been attributedto lexico-semantic choices (such as complex medical terms and abbreviations), and forinstance, to physician preference for lengthy words and sentences (Zethsen andAkehave, 2006). However, consumer health vocabulary research finds that consumervocabulary may be more similar than different from health professional vocabulary(Smith and Stavri, 2005). Calling it physician “adaptability” in language use, or “lexicalentrainment” Bromme et al. (2005) found that advanced medical students adapt theirlevel or content of language to the language found in patient questions posed (p. 572).Prior research suggests that “the difference between the lay (consumer) andprofessional (e.g. physician) knowledge base of health and disease is likely to extendbeyond simple term labels, into the underlying concepts that are the basis for (the useof) these terms” (Keselman et al., 2008, p. 496). Patel and Kaufman (1989) suggest thatsuch conceptual level uses may be related to pragmatic versus semantic characteristicsand uses of language in health communication.
Current studyObjectivesThis study analyses and compares consumer and physician answer discourses on apublic consumer health internet portal, and furthers LIS research by incorporating thelevel of pragmatics in linguistic analysis and extending the use of Rhetorical StructureTheory (Mann and Thompson, 1988) to consumer and physician perspectives. Themain linguistic premise in this study is that language is typically used to achievevarious goals in human communication (Bonvillain, 2008). Speakers (or writers)generally convey various information or meaning to those who listen (or read) with agoal in mind. We equate speakers/writers to “information providers or sharers”, andlisteners/readers – to “users” in LIS.
JDOC68,6
830

The pragmatic level of discourse specifically seeks to explain the meaning oflinguistic messages or information in terms of the context of use (Leech and Weisser,2004). Pragmatics facilitates consideration of how each information sharing group useslanguage “to convey desires, beliefs, and intentions” (Bickmore and Giorgino, 2006,p. 557) and to achieve goals, akin to the conveyance of prescribed medication, othertreatment, and lifestyle changes such as diet and exercise in everyday health care andhealth promotion. Successful communication is essential to consumer adherence.
Based on a review of prior consumer health information seeking and use studies aswell as on our preliminary analysis of health forum threads, we hypothesise thatconsumer and physician answers discourses may differ in their pragmatic use oflanguage and in their communicative goals. We posit the following research questions:
(1) What are the general characteristics of physician versus consumer discourses atthe pragmatics level?
(2) How do the consumer and physician discourses differ in their goals for healthcommunication?
Analytical framework: rhetorical structure theoryDeveloped by Mann and Thompson (1988), rhetorical structure theory (RST) has hadtwo principal uses: discourse analysis and automatic text generation, and has beenextensively empirically tested (Taboada and Mann, 2006). In RST each sentence or itspart, called elementary discourse units (EDUs), stands in a certain kind of relation to itssurrounding EDUs in context. For instance, an EDU might elaborate on the statementin the preceding EDU (as in elaboration relation). The overall rhetorical structure ofdiscourse is revealed after each individual relation is identified and labelled.
The basic elements of a standard RST relation are a nucleus – the main point of thetext, which can stand alone as comprehensible, and a satellite – supplementary text thataugments or refers to the nucleus and cannot stand alone. There are two general RSTrelation types: subject matter and presentational. Subject matter relations are primarilydescriptive in nature: they identify or describe situations, problems, solutions, whilepresentational relations have a goal and are intended to precipitate various effects on thereader (Taboada, 2004). Table I lists both types of relations in the first and second column
Subject matter relations Presentational relations Multinuclear relations
Circumstance Antithesis ContrastCondition Background JointElaboration Concession List (structured)Evaluation Enablement SequenceInterpretation EvidenceNon-volitional cause JustifyNon-volitional result MotivationOtherwise RestatementPurpose SummarySolutionhoodVolitional causeVolitional result
Source: Adapted from Mann and Taboada (2010)
Table I.Rhetorical structure
theory relationclassification
Discoursestructure
differences
831

respectively. Some relations, the multinuclear relations, do not contain satellites; theirnuclei are considered comparable in importance (Table I, third column). Table I containsthe total of 25 RST relations used in this study as a codebook for discourse analysis.
Descriptive titles of RST relations such as circumstance or condition, are oftensupplemented with definitions that place certain constraints on the parts of relations(on the nucleus, satellite, or a combination of the two) and further identify an effect onthe reader intended by the writer (Mann and Thompson, 1988). Mann and Thompsondetail the following intended effects of six of the presentational relations on readers:
(1) Motivation – increases desire (to do something).
(2) Antithesis – increases positive regard.
(3) Background – increases ability.
(4) Enablement – increases belief.
(5) Justify – increases acceptance.
(6) Concession – increases positive regard (Mann and Thompson, 1987, p. 18).
Table II illustrates the presentational relation Motivation with an excerpt from ourdataset: the writer urges the reader to action (stated in the nucleus EDU) and providesmotivation in satellite.
An RST analysis is often performed graphically, by connecting and labellingrelations identified in discourse, using a specialized tool or manual approach. Figure 1demonstrates a manual analysis of six EDUs from a physician’s answer to a consumerquestion about blood test recommendations. The physician uses elaboration and jointrelationships to expand on several factors that influence the frequency of blood tests.
MethodologyData sourceThe data for this study were obtained from a freely and publicly available consumerhealth information website, Everydayhealth.com, that hosts both consumer discussion
Name
Constraints on eithersatellite or nucleus(individually)
Constraints on bothnucleus and satellite(together) Intention of writer
Motivation(presentational relation)
On nucleus: nucleus isan action in whichreader is the actor(including accepting anoffer), unrealized withrespect to the context ofnucleus
Comprehendingsatellite increasesreader’s desire toperform action innucleus
Reader’s desire toperform action innucleus is increased
Example 1 (ID: Cons_Ans_4.2.2-3-4-5_P3)
Nucleus [Email me at (address omitted)]Satellite [and I will forward a glycemic index and a boatload of very usefulinformation.The information will explain how to use the table and other meal planninghelp.The information may help you avoid becoming diabetic.]
Table II.Motivation relationdefinition and example
JDOC68,6
832

forums and “ask a physician” sections. On this popular “HON code certified” site,consumers can seek and share information about preventive health care and treatmentfor a variety of health conditions, utilising both professional and peer informationresources, such as blogs, support groups, and a variety of articles written by healtheducators or health care providers. This study utilises the site’s consumer discussionforum for diabetes, described as one of the most popular groups on the site (Alexa.com,2011), as well as the corresponding “ask a professional (physician)” question-answersections for diabetes. Most site users are English speaking, and female; 83 per cent ofusers are from the US. Users typically visit the website from home, report having acollege or “some college” education and belonging to either of the three predominantage groups (in descending order 55-64, 65 þ , and 45-54 years of age) (Alexa.com,2011).
The site supports the consumer information seeking scenario utilised in this study– that of the consumer searching or sharing health information about chronic healthconditions from both laypeople (consumers) and professionals (physicians).
DatasetOur dataset consists of consumer-to-consumer question-answers conceptually alignedwith consumer-to-physician question-answers. Alignment was performed by the firstauthor utilizing content analysis (Krippendorf, 2004) of both questions and answersfound on the consumer discussion forum area and the “ask a professional” areas of thesite during a two-week period in early autumn 2010. Questions from theconsumer-to-consumer section were selected first, their corresponding consumeranswers were identified, captured in vivo and archived for later analysis. Then, movingsequentially through the “ask a professional” diabetes pages of the website,
Figure 1.Sample segment of a
graphical rhetoricalstructure theory analysis
of a physician’s answer
Discoursestructure
differences
833

consumer-to-physician questions were selected and matched withconsumer-to-consumer questions, if they were judged to share common themes, asexemplified in Table III.
The second author reviewed and agreed upon these and similar alignment choices inall cases. Using questions solely for alignment purposes, we focus on the two types ofanswers to matched questions which constitute the consumer and physician discoursesamples for this study. Sample texts, similar to consumer and physician answers inTable III, were analysed within RST framework and compared (pair-wise, within- andacross-group) in terms of their discourse structure and communicative goals.
Analytical framework applicationMann and Thompson based the development of RST on a set of 24 relations, yetemphasised that these relations could be expanded, depending upon research needs, toaccommodate text conditions not identified in their original research. These relationsets function as codebooks, where relation definitions are used to assign relations toanalysed data. As listed in Table I, we used a total of 25 relations: the original 24relations set, the most empirically tested set (Taboada, 2004) plus the relation list (usedhere as structured list) added later by Mann and Thompson (see Mann and Taboada(2010) for complete list of relation definitions).
Example 2a-b. Consumer-to-consumercommunication
Example 2c-d. Physician-to-consumercommunication
2.a. Consumer question“My daughter is 6 years old and was diagnosedwith diabetes this July. Does anyone know ofalterante (sic.) medicine options for her? Herbs,vitamins, massage therapy, homeopathy, etc.”
2.c. Consumer question“I’ve heard a lot of conflicting information aboutusing dietary supplements to help lower myblood glucose levels. What’s the deal? Do any ofthem really work?”
2.b. Consumer answer (excerpt)“At her age she is likely type I. That means thather pancreas is not producing any insulin. Thereare no reliable alternatives to taking insulin. Ihave heard about things like boiling green beansand using the water as a substitute for insulin.But such experiments are risky. It will help yougreatly to find a holistic doctor. Other doctorshave virtually no training in nutrition. Diabetesis a diet based disease. They will addresseverything with pharmaceuticals, which willcause long term damage to her liver.The best thing that you can do for her (type I orII) is to get her off of pro-oxidant foods like highfats, prepared foods (nearly anything in a box orcan), caffeine, sodas or colas, artificialsweeteners except xylitol or stevia, highglycemic index foods, and processed flourproducts . . . ”
2.d. Physician answer (excerpt)“The short answer is, we’re not yet sure . . . someof the studies have shown that Cocinia indic,konjac mannan, and American ginseng canlower glucose levels. Ipomoea batatas,Momordica charantia, nopal, aloe vera,vanadium, Gymnema sylvestre, and fenugreekrequire further investigation to determine theireffect on glucose. Alpha lipoic acid, magnesium,chromium, L-carnitine, and vitamin E have notbeen found to be effective for lowering glucose.As a doctor trained in Western medicine, I’lladmit that my response to you is biased. It relieson evidence from rigorous and replicablescientific research (or lack thereof), and the kindof evidence I’d like to see is not available formany of the dietary supplements. While thisdoesn’t mean that all supplements areineffective, there isn’t sufficient evidence at thistime to recommend their use to lower glucoselevels . . . ”
Table III.Sample consumerquestions and relatedanswers provided by aconsumer and aphysician
JDOC68,6
834

RST analysis proceduresRhetorical structure theory relations from the inventory of 25 (Table I) were assignedvia manual annotation by the first author, following the steps in a classic RST analysis(Mann and Thompson, 1987):
(1) The answers in the dataset are segmented into sentences or clauses:“elementary discourse units,” or EDUs.
(2) RST relations are assigned by looking at EDUs and EDU neighbours, ifrelations are clear.
(3) Larger structural elements are assigned, if applicable.
(4) The analysis is iteratively continued until all text units are analyzed.
(5) Each marked relation is verified to have satisfied nucleus/satellite constraintsand writer intentions/reader effects requirements.
With elementary discourse units identified in the data, frequency counts and percentageoccurrence of relations within each discourse were calculated. To supplement the RSTanalysis, quantitative lexical analyses with the Natural Language Processing Toolkit orNLTK (Bird et al., 2009) were used to compare and report such measures within eachdiscourse group as the overall data size and average sentence length.
Rhetorical structure theory analysis can be applied at various levels of textstructure granularity for the RST relations, from text segments and clausesparagraphs (Taboada, 2004; Taboada and Mann, 2006; Bateman and Delin, 2006),based on research objectives. We used the elementary discourse unit (EDU) as the unitof analysis with which certain complications can arise. For instance, in the physiciandata, structured lists, signalled by either numerical or bulleted headings for listelements, were separated in our procedures into several EDUs constituting a structuredlist. We counted structured lists because we saw them as representing intent (animportant aspect of our research questions) on the physician’s part to presentinformation in a certain way (by list). Though no Structured Lists were found in theconsumer data, some of consumer data included unstructured enumerations, runningin text. For instance, “[. . .] problems such as burning feet, kidney problems, eyeproblems, and other problems [. . .]”(excerpt ID: Cons_Ans_5.4.7_P10)[3]. Suchembedded lists were not separated into separate EDUs due to their noun phrasegranularity, adhering as closely as possible to classic RST analysis, which omits lists.
Study scope, assumptions, and data exclusion criteriaThough RST has been previously used in the analysis of some visual media, the scopeof this study was limited to text found within answers to questions posted indiscussion threads. For instance, we excluded some website content (such as outwardhyperlinks) and imagery (including emoticons). Other exclusions were threadscontaining commercial advertisements, regardless of format, solicitations for finding“friends with diabetes,” or research project recruitments.
The greetings in each post (such as “Hi” or “Dear” (as an opening form of address)and closing signatures (including names at the end of a message, etc.) were deemed tohave no rhetorical relation function regarding text organisation with surrounding text,as per Mann et al. (1992). Instead, these greetings and signatures are simply“conventional properties of the (post)” (p. 24).
Discoursestructure
differences
835

We also assumed that each question is related to its answers, on a meta-level, as aSolutionhood relation (defined as a solution to a problem or question stated or implied)(cf. Abelen et al., 1993). Taking questions for granted we only accounted for frequenciesand distribution of the RST relations found within the body of the answers. Anecessary inclusion criteria was an answer to the original question posed in the thread.
Using our research questions to guide the level of our analysis, we focused onidentifying goals and intentions in each text, which resulted in a pragmatic macro-levelanalysis, in order to attend to the “writer’s overall purpose” (Abelen et al., 1993, p. 339).
Reliability and validity or trustworthiness proceduresIn addition to undertaking careful data collection and archiving procedures, severalmeasures helped to ensure the reliability and validity, or trustworthiness of the presentresearch (Lincoln and Guba, 1985). The first author, who had four months experiencewith RST analysis prior to commencing study data analysis, conducted close andrepeated readings of the data over a period of several weeks. Data and correspondinganalyses were reviewed at least two times to ensure trustworthiness of the primaryanalysis. This afforded immersion in the data, utilizing the constant comparativemethod, as advocated by Lincoln and Guba (1985). A recent investigation of slimmingblogs served as a model for the present study (Savolainen, 2011a). Iterative checks(both within and across analysed texts) were performed to safeguard consistency incoding of the dataset with RST relations
Intracoder reliability agreement of an average of 78 per cent was achieved based onthe 10 per cent of the data (82 per cent agreement for consumer, 70 per cent – forphysician data). The first author re-coded 10 per cent of the final dataset after havingspent several weeks away from the data. Related intracoder consistency measuresincluded checking data for negative case analysis (i.e. when no relations for a particularrelation definition were found). For example, the initial coding of the data identified noMotivation relations for the physicians. Data were therefore reviewed specifically forpossible evidence of Motivation relations. This procedure was repeated for othernegative coding instances, including otherwise, circumstance, structured list, sequence,and contrast in both discourses. Some RST relations such as background and elaborationpresented specific challenges for disambiguation. Close reading of the relation definitionsfor each, re-reading of the data, along with consulting prior RST research and codingmanuals (cf. Mann and Thompson, 1987; Taboada, 2004) facilitated resolution of codingambiguities. A notable difference between the two was resolved: the Background relationwas deemed to explain why or how something described in text exists or occurs, whileelaboration was found to simply provide additional or straightforward descriptiveinformation (describing more what something is, rather than why or how it exists oroperates) (Mann and Taboada, 2010). These observations were incorporated in thecodebook. In addition, another researcher familiar with RST analysis served as a peerdebriefer during the final stages of data analysis.
ResultsDataset characteristics and participant demographicsTwenty pair-wise aligned consumer questions with their corresponding answers werecollected. The dataset includes 26 consumer answers (about three answers per questionon average), and ten physician answers (with a one-to-one questions-to-answers ratio).
JDOC68,6
836

Initially, 13 diabetes consumer-to-consumer discussion threads were collected from thewebsite. Based on our exclusion criteria outlined in Methods, three of these threadswere eliminated. The study was centred on the remaining ten threads, which coveredtopics such as questions related to being new to diabetes, avoiding diabetes throughprevention, how to count carbohydrates, etc. From these ten threads, 41consumer-to-consumer answer posts were originally collected and were reduced tothe final set of consumer-to-consumer answers directly relevant to the originalquestions was 26 postings in total. Some of the excluded posts contained no answers tothe original question at all, discussed tangentially related issues, or started a newembedded thread.
Physician answers were found in the consumer-questions with a physician-answeror “ask a doctor” area. At the time of data gathering the website included 78 physiciananswers to consumer questions (64 for type-two diabetes, and 14 for less commontype-one diabetes). Ten answers from these data were matched with the ten consumeranswers as described in the methodology section above.
Participant demographicsThe consumer answers were contributed by 14 unique authors (two answers on averageper consumer) with 11 single answers and three productive authors. The physiciananswers were contributed by a single, female physician, a diabetes specialist. Limitedparticipant demographics were available (see Table IV), though participants nearlymatched the majority user profile for the Everdayhealth.com website (Alexa.com, 2011).Most of participants reporting their gender were females, aged between (in descendingorder) 55-64; 65 or over; or 45-54 years. Mean participant age was 58 years.
Consumer versus physician discourse distributionsAided by NLTK data processing (Bird et al., 2009), general dataset distributions areshown in Table V by number of characters, words, and elementary discourse units(EDUs). Note the comparability of physician and consumer discourses on almost allmeasures. Particularly interesting is how close the total numbers of words between the
n %
GenderFemale 8 57Male 3 21Unknown 3 21
Age (yrs)18-24 0 025-34 1 735-44 0 045-54 2 1455-64 5 3665 þ 4 29Unknown 2 14Ave: 58
Note: n ¼ 14
Table IV.Consumer participant
demographics
Discoursestructure
differences
837

two discourses are, given the fact that consumer data included 26 answers, whilephysician data included ten answers. The number of consumer EDUs is 129 higherthan their number in the physician data. Consumer discourse is known to be morediffuse, which this difference may reflect. On average, physician EDUs containapproximately two more words per EDU than the consumer EDUs do. This finding isconsistent with known physician preference for lengthy words and/or sentences(Zethsen and Akehave, 2006).
A total of 717 elementary discourse units were identified, including 291 rhetoricalrelations. Table VI demonstrates that the consumer answers contained fewer identifieddiscourse units on average (16.3 as compared to 29.4 – in physicians’ answers), as wellas fewer average rhetorical relations within each answer (6.7 compared to 11.8).
Data measurements Consumer answers Physician answers
Number of characters(excl. spaces) 18,482 17,876Words 4,051 3,494Number of EDUsa 423 294Ave., words per EDU 9.6 11.9Min, words per EDU 3 1Example: shortest EDU “I have both.” [referring to diabetes
or lupus problems]“Congratulations!”
Max, words per EDU 30 34Example: longest EDU “. . . like high fats, prepared foods
(nearly anything in a box or can),caffeine, sodas or colas, artificialsweeteners except xylitol or stevia,high glycemic index foods, andprocessed flour products.” [referringto pro-oxidant foods]
“Here’s why: As your blood glucoserises above the normal level, yourrisk of developing damage in thebody’s small blood vessels, andultimately your risk of a heart attackor stroke, also rises.” [referring toblood sugar level numbers that arenot in the diabetic range]
Note: aEDUs: elementary discourse units (unit of analysis in the dataset)
Table V.Comparative datadescription per type ofanswers
Units of analysis Data types Counts Ave., per question Ave., per answer
Questions Consumers 10 n/a n/aPhysicians 10 n/a n/aCombined 20 n/a n/a
Answers Consumers 26 2.6 n/aPhysicians 10 1.0 n/aCombined 36 1.8 n/a
Elementary discourse units, EDU Consumers 423 42.3 16.3Physicians 294 29.4 29.4Combined 717 35.9 19.9
Rhetorical relations Consumers 173 17.3 6.7Physicians 118 11.8 11.8Combined 291 14.6 8.1
Table VI.Dataset description:collected questions andanswers, identifiedelementary discourseunits, and rhetoricalrelations
JDOC68,6
838

Twenty-four of the 25 relations used were present in the dataset overall. Neither groupused the otherwise relation. Table VII demonstrates the 23 relations used by theconsumers, distinctly missing structured list and otherwise, and 20 relations used byphysicians with five absent – circumstance, otherwise, purpose, joint, and sequence. InTable VII, zeros in consumer and physician answers (highlighted in grey) indicate thecategories that are not present in the corresponding type of answers.
The last column in Table VII (on the right) also depicts the relations distribution,starting from the types of relations that were used more frequently by physicians at thetop, and ending with the relations used more frequently by consumers (at the bottom).The negative numbers indicate that physicians used the rhetorical relations more timesthan the consumers; positive numbers indicate that consumers used more of that relationtypes. For instance, the relation of elaboration (listed first in Table VII), was used 20times less by the consumers than physicians (11 2 31 ¼ 220), while Motivation (listedlast) was used 38 times more by the consumers than physicians (42 2 4 ¼ þ38). Notethat the elaboration with a structured list structure was not found in the consumer data.
No. RST relationsConsumeranswers
Physiciananswers
Absolute differencebetween consumer
and physiciananswers
1 Elaboration 11 31 2202 Evaluation 3 10 273 Condition 7 13 264a Structured list 0 4 244b Elaboration and structured list 0 4 245 Interpretation 3 6 236 Antithesis 3 5 227 Non-volitional result 2 4 228 Solutionhood 3 5 229 Background 11 13 22
10 Volitional cause 1 2 2111a Otherwise 0 0 012 Non-volitional cause 1 1 013 Summary 2 2 014 Restatement 3 2 115 Purpose 2 0 216 Contrast 4 1 317 Volitional result 4 1 318 Circumstance 5 0 519 Joint 5 0 520 Evidence 8 2 621 Sequence 7 0 722 Justify 12 2 1023 Enablement 15 2 1324 Concession 19 4 1525 Motivation 42 4 38
Total: 173 118 Ave. ¼ 2.5
Note: aNeither group (consumers or physicians) used the relation otherwise; Categories on top areused more by physicians, on bottom by consumers
Table VII.Distribution of rhetoricalstructure theory relations
in consumer andphysician answers (per
discourse type), sorted bypair-wise difference
between total identifiedrelations
Discoursestructure
differences
839
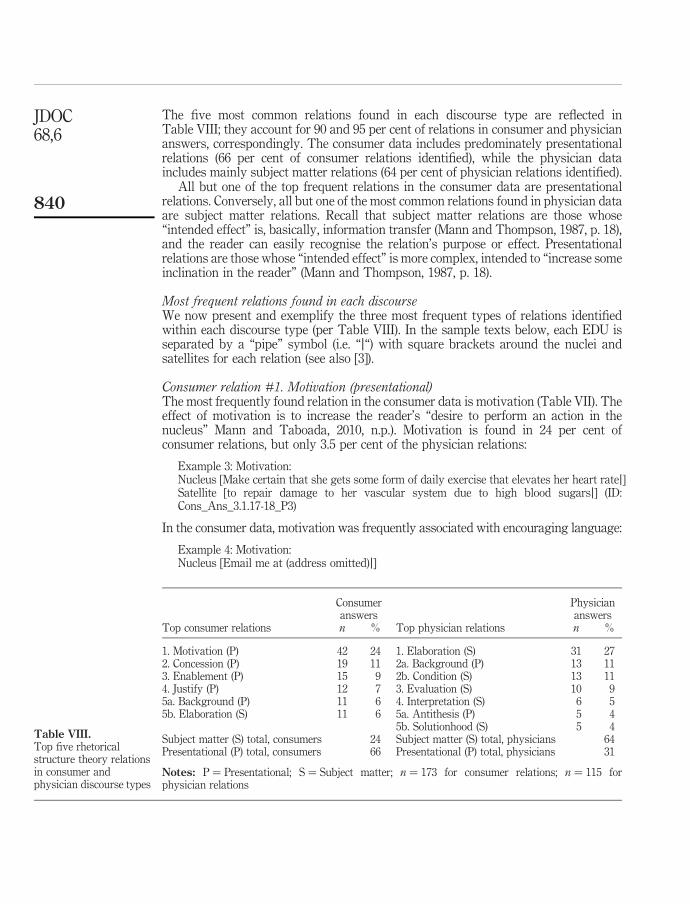
The five most common relations found in each discourse type are reflected inTable VIII; they account for 90 and 95 per cent of relations in consumer and physiciananswers, correspondingly. The consumer data includes predominately presentationalrelations (66 per cent of consumer relations identified), while the physician dataincludes mainly subject matter relations (64 per cent of physician relations identified).
All but one of the top frequent relations in the consumer data are presentationalrelations. Conversely, all but one of the most common relations found in physician dataare subject matter relations. Recall that subject matter relations are those whose“intended effect” is, basically, information transfer (Mann and Thompson, 1987, p. 18),and the reader can easily recognise the relation’s purpose or effect. Presentationalrelations are those whose “intended effect” is more complex, intended to “increase someinclination in the reader” (Mann and Thompson, 1987, p. 18).
Most frequent relations found in each discourseWe now present and exemplify the three most frequent types of relations identifiedwithin each discourse type (per Table VIII). In the sample texts below, each EDU isseparated by a “pipe” symbol (i.e. “j“) with square brackets around the nuclei andsatellites for each relation (see also [3]).
Consumer relation #1. Motivation (presentational)The most frequently found relation in the consumer data is motivation (Table VII). Theeffect of motivation is to increase the reader’s “desire to perform an action in thenucleus” Mann and Taboada, 2010, n.p.). Motivation is found in 24 per cent ofconsumer relations, but only 3.5 per cent of the physician relations:
Example 3: Motivation:Nucleus [Make certain that she gets some form of daily exercise that elevates her heart ratej]Satellite [to repair damage to her vascular system due to high blood sugarsj] (ID:Cons_Ans_3.1.17-18_P3)
In the consumer data, motivation was frequently associated with encouraging language:
Example 4: Motivation:Nucleus [Email me at (address omitted)j]
Consumeranswers
Physiciananswers
Top consumer relations n % Top physician relations n %
1. Motivation (P) 42 24 1. Elaboration (S) 31 272. Concession (P) 19 11 2a. Background (P) 13 113. Enablement (P) 15 9 2b. Condition (S) 13 114. Justify (P) 12 7 3. Evaluation (S) 10 95a. Background (P) 11 6 4. Interpretation (S) 6 55b. Elaboration (S) 11 6 5a. Antithesis (P) 5 4
5b. Solutionhood (S) 5 4Subject matter (S) total, consumers 24 Subject matter (S) total, physicians 64Presentational (P) total, consumers 66 Presentational (P) total, physicians 31
Notes: P ¼ Presentational; S ¼ Subject matter; n ¼ 173 for consumer relations; n ¼ 115 forphysician relations
Table VIII.Top five rhetoricalstructure theory relationsin consumer andphysician discourse types
JDOC68,6
840

Satellite [and I will forward a glycemic index and a boatload of very useful informationjThe information will explain how to use the table and other meal planning help.jThe information may help you avoid becoming diabetic.] (ID:Cons_Ans_4.2.2-3-4-5_P3)
The nucleus above presents a possible action, to email the writer, and the satelliteoffers motivation or encouragement for the reader to do so (that he will share “usefulinformation”).
An example from the physician data encourages or motivates the reader to dosomething (“take control of the disease”). While the overall effect is similar forMotivation relations found in the consumer data, there are subtle differences betweenthe two discourses:
Example 5: Motivation:Satellite [Because diabetes involves something that is so basic to our existence – foodj– it can seem to control our lives.j]Nucleus [But the challenge – and your goal – is to take control of the disease instead.j] (ID:Dr_Ans_7.1.5-6-7)
Note how the physician shows empathy and decreases the distance between herself andher reader in the satellite text by stating how diabetes “can seem to control our lives.” Inthe nucleus, the physician identifies the reader’s goal for them, as “(their) goal,” and thendistances herself further by referring to diabetes abstractly, as “the disease.”
Physician relation #1. Elaboration (subject matter)The most frequently found relation in the physician data is the Elaboration relation (27per cent physician relations; 6 per cent consumer relations, Table VIII). Elaboration’seffect is that the reader “recognises the satellite as providing additional detail for thenucleus [. . .] (also), the reader identifies the element of subject matter for which (the)detail is provided” Mann and Taboada, 2010, n.p.):
Example 6: Elaboration:Nucleus [you can probably prevent the onset of diabetes and other complications,j]Satellite [such as coronary artery disease.j] (ID: Dr_Ans_8.1.17-18)
The reader can easily connect “coronary artery disease” in the satellite as anelaboration of “other complications” referred to in the nucleus.
Consumer relation #2. Concession (presentational)The second most common consumer relation is concession, found in 11 per cent ofconsumer relations and 3.5 per cent of physician relations. The effect of Concession isthat the “reader’s positive regard for (the) nucleus is increased” (Mann and Taboada,2010, n.p.). Concession is also recognised as a relation that exhibits politeness, apragmatic linguistic tool in communication that has the effect of softening theinteraction, and allowing the reader/hearer to “save face” (Taboada, 2004). In example7, the specific effect is to allow the reader to choose among the suggestions the writer isoffering:
Example 7: Concession:Satellite [Maybe your doctor could give you a diet,j]Nucleus [or maybe some good books from the Diabetes Section at the book store can helpj](ID: Cons_Ans_4.1.2-3_P13)
Discoursestructure
differences
841

Physician relation #2a. Background (presentational) and -#2b. Condition (subject matter)Background and condition tie for the second most common physician relations (11percent of physician relations each), while in consumer discourse both are used lessprominently (6 and 4 percent, respectively). The effect of background is the “reader’sability to comprehend (the) nucleus increases” (Mann and Taboada, 2010, n.p.). Inexample 8 the reader is told in the nucleus that “prevention is key.” The function of thesatellite is background information because it tells the reader why prevention is key:
Example 8: Background:Nucleus [Now that you’ve been diagnosed with prediabetes,jprevention is key.j]Satellite [Prediabetes is characterized by either impaired fasting glucose (IFG) or impairedglucose tolerance (IGT).jBoth of these terms refer to the level of sugar in the bloodstream,jand they’re both ways of saying that you have prediabetes.j] (ID: Dr_Ans_8_1_3-4-5-7)
The effect of condition is that the “reader recognizes how the realization of (the) nucleusdepends on the realization of (the) satellite” (Mann and Taboada, 2010, n.p.). Example 9comes from the same answer as the Background Example 8. The nucleus dependsupon the reader having a certain fasting glucose level: “If you have [. . .]” Note that anelaboration relation is embedded in the example below as the parenthetical text in thesatellite “(a test in which [. . .])” decoding for the reader what a fasting glucose level is:
Example 9: Condition:Satellite [If your fasting glucose level (a test in which blood is drawn after six hours withoutfood) is between 100 and 125 mg/dl,j]Nucleus [you have IFG.] (ID: Dr_Ans_8_1_8-9)
Consumer relation #3. Enablement (presentational)Enablement is the third most common consumer relation. It increases the “reader’spotential ability to perform the action in (the) nucleus” (Mann and Taboada, 2010, n.p.).The nucleus in example 10 is part of a larger text that encourages the reader to go tothe website stated in the nucleus, and then tells the reader how to use the website:
Example 10: Enablement:Nucleus [http://www.joslin.harvard.edu/diabetes_information.html.j]Satellite [Then click on the left bar under Joslin Clinical guidelinesjand read the section of the PDF about glucosej](ID: Cons_Ans_6.1.3-4-5_P4)
Physician Relation #3. Evaluation (subject matter)The third most common physician relation is evaluation. The reader can use the text inthe satellite to assess the claim made by the writer in the nucleus with the potentialeffect of strengthening the claim or assigning value to the nucleus statement:
Example 11: Evaluation:Nucleus [The good news is that laboratory studies have determined mechanisms by whichsome dietary supplements might reduce glucose levels,jincluding increasing insulin secretion from the pancreas, decreasing the rate of carbohydrate(glucose, or sugar) absorption from the gut, and speeding the rate of glucose entry into cells.]Satellite [However, many of the studies, which examined the effect of specific dietary supplementson glucose levels, do not meet standards for conclusive trials or have not been replicated.jAs a result, the conclusions from these studies are not sufficient to recommend the use of thesesupplements.] (ID: Dr_Ans_3_1_3-4-5-6)
JDOC68,6
842

DiscussionRST relations and the semantic-pragmatic levels of communicationIn this study, we tentatively connect adherence behaviour with RST relation effects andcall for further empirical tests of the idea. Our findings suggest that consumer answersmay be more effective at facilitating healthy behaviour in fellow consumers thanphysicians, based on considering the “effects” of the most common relations found ineach discourse. The finding that the majority of consumer answer discourse relationswere presentational suggests that the consumer answers may be more able to trigger aresponse action in readers or users of shared information. For example, the significanceof the most prevalent consumer discourse relation, Motivation, is that it representstextual information that may increase the reader’s desire or inclination to perform anaction (Mann and Taboada, 2010), such as a healthy behaviour, like walking.
Other researchers have found that consumers report that finding internet healthinformation lead them to change their behaviour (Neuhauser and Kreps, 2010). Also,there may be a relationship between RST and self-efficacy, a health behaviour theorythat a consumer’s belief in his or her ability to achieve a given goal will result in greatergoal achievement (Bandura, 1997). Increasing people’s self-efficacy can also lead totheir “active participation” and “better disease management” (Allen et al., 2008, p. 107).RST presentational relations, because of their emphasis on increasing readers’ desire,belief, or ability to perform actions, may therefore be useful in increasing self-efficacy.
Mann and Thompson (1988, 1987) suggest that, on the linguistic level, RST subjectmatter relations are mostly semantic (i.e. putting forth a factual level argument, orfulfilling the purpose of information acquisition), whereas the presentational relationsare pragmatic (i.e. contributing to the achievement of a goal, or information use). In LISresearch, connections may be possible between semantic or subject matter relations asexamples of the information transfer model, and pragmatic relations as examples of theconstructionist theoretical approach in LIS (Savolainen, 2008).
Our introductory question about the ability of one source of information to encourageadherence to healthy behaviour more effectively than another (consumer versusphysician) – is partly answered here. The presence of more presentational relations inconsumer discourse than in physician discourse suggests that the consumer discourse ismore goal-oriented than the physician discourse. In other words, laypeople/consumersmay be more effective at inspiring healthy behaviour. In particular, the predominance ofthe Motivation relation in consumer versus physician data (24 per cent versus 3.5 percent) suggests that the consumers are more encouraging of behaviour or actions reflectedin the analysed texts. The second and third most common consumer discourse relationsalso demonstrate that the consumer discourse is more polite due to the frequency of theconcession relation (11 per cent of consumer; 3.5 per cent of physician relations), andmore enabling (in the sense of making actions/decisions more feasible or possible bysupplying means, knowledge or opportunity) due to the enablement relation (9 per centof consumer; 1.7 per cent of physician relations).
The prevalence of elaboration relations in the physician data compared to theconsumer data (27 per cent versus 6 per cent) suggests that the physician discoursecould be more factual. The physician discourse is perhaps more literally informative, inthat it provides more information, though not about how to use or integrate thatinformation into everyday life. This also suggests that the physician discourse is morerooted in the information transfer model of communication than the consumer
Discoursestructure
differences
843

discourse. The prevalence of the condition relation, the second most common physicianrelation compared to findings in the consumer discourse (11 per cent versus 4 per cent)indicates that the physician discourse is more reliant on establishing or sharing factsfor developing or couching (literally, conditioning) arguments or shared information.The frequency of the other second most common physician relation, the backgroundrelation (11 per cent in physician; 6 per cent in consumer data), demonstrate physicianintention to help (or concern about the need to help) consumers comprehend healthinformation.
Hartzler and Pratt’s (2011) recent findings, drawn from comparing patient (lay) andclinician (professional) expertise, appear to corroborate our results regarding theprevalence of pragmatic versus semantic relations in consumer versus physiciandiscourses. Hartzler and Pratt found that patient shared expertise/informationemphasised “actionable advice,” delivered in narrative style, while clinician expertiseemphasised “prescriptive action strategies,” rich in “direct instructions” rather than“personal stories” (n.p.).
The occurrence of structured lists in physician data and their absence in consumerdata may reflect physician training and use of “problem lists” to guide patient care inpractice (Hunter, 1991, p. 84). Physicians generate these lists during patient care anduse them to carry out treatment plans for their patients. These physician findingssignify a more professional approach to communication, with a characteristicemphasis on hedging (couching or qualifying communication), providing facts orevidence, and simplifying health communication (Zethsen and Akehave, 2006).
Value of pragmatics level analysisSituating this and future research at the pragmatics level of linguistics allows us toexamine language use and meaning in context, an important topic within LIS, and ininformation behaviour studies in particular (Courtright, 2007). This approach enabledus to see that presentational (pragmatic) linguistic relations appear to increase readers’desire to act, believe or accept shared information, such as treatment or prevention tips.Subject matter (semantic) linguistic relations emphasise more formal language aspects,and appear less capable of conveying deeper levels of meaning which can lead toaction-oriented use of information (Mann and Thompson, 1988). This work extendsprior health information LIS investigations by focusing more on argument structureand how shared information may affect information use, rather than on the content ortypes of information shared (affective, personal, etc.) in online discourse in particular.
The use of RST for information behaviour research appears to be limited to ourstudy and another study that used RST to develop search templates for users to inputguided searches based on desired relation effects (Vechtomova and Zhang, 2009). Wehave demonstrated that RST offers a new approach to discourse analysis forinformation behaviour and practice studies, and recommend incorporating it in furtherstudies. RST could prove particularly helpful in producing tailored health informationand communication, both online (utilizing computational linguistics or artificialintelligence approaches), and in-person, from a more user-centred perspective than iscurrently the norm (Alpay et al., 2009). RST research involving consumers directly(through in-person interviews) or indirectly (through analysis of consumer texts) mayincrease our understanding of how to improve treatment adherence in diabetes andother chronic diseases.
JDOC68,6
844

Findings regarding the prevalence of linguistic politeness in theconsumer-to-consumer discourse suggest that the scope of further research could beexpanded to compare politeness in lay and professional communication. Such workcould draw on and inform research on practice of reference transactions, andspecifically, on politeness aspects of greeting and closing rituals in informationservices (cf. Park et al., 2010).
ImplicationsOur findings suggest that RST is a helpful theory for studies in the areas of everydaylife information seeking (ELIS) and health information use. McKenzie (2003), Talja andHansen (2006), and Veinot (2009), among others in LIS, have advocated for more such“user-to-user” information behaviour and information retrieval work in everyday liferesearch. In the peer-to-peer information sharing and use domain, RST research seemspromising for the subdomain of lay information mediary behaviour (LIMB)(Abrahamson et al., 2008). Applying RST utilizing the LIMB theoretical framework,which considers how people seek or share information, from or on behalf of others, canfacilitate studying aspects of information seeking and sharing, and communication ingroups such as families and other close-tie, everyday life social networks. Bickmoreand Giorgino (2006) note that such multivocal dialogue is “understudied in bothlinguistics and computational linguistics”, yet such groups can play key roles inadherence (p. 569).
Savolainen’s findings (2011b) that some health bloggers report fewer needs forfactual information and greater needs for opinion or experience-based issue evaluationsupport an argument that consumers prefer a consumer discourse compared to thephysician discourse (see also Veinot, 2010, and Neal and McKenzie, 2011, regardingsuch preferences). However, human communication is a complex act. Physicians andother clinicians have also been found to prefer peer-to-peer communication over otherforms of communication (see, for example, Forsythe et al., 1992). Our findings mayextend beyond the consumer-to-consumer health information sharing domain, andrelate to a more general peer-to-peer discourse or knowledge translation andcommunication model. The prevalence of presentational rhetorical relations,particularly Motivation relations, could apply to discourse among peers of any kind(e.g., lay or professional), not just health information consumers. Confirming thishypothesis is beyond the present study scope, but doing so could provide direction forfuture research which seeks to understand information source roles and the effects ofinformation exchange in knowledge translation and information use across varieddomains.
This study is descriptive in nature, and its results should not be interpretedprescriptively without considering the broader pragmatic situation and the desiredperception. Pin-pointing and detailing discourse structure differences between lay andprofessional language may invite attempts at mimicking, accommodating, andultimately mis-representing a lay or professional identity, especially in onlineenvironments. Keeping both benevolent or malevolent intentions in mind, Rubin (2010)cautions against the adverse effects of intentional deception as it often “rendersinformation unreliable” when detected, and “it ruins trust and credibility” which are“essential to successful communication” or information seeking.
Discoursestructure
differences
845

LimitationsThis work addresses Alpay et al.’s (2009) call for research that can “(bridge) the gapbetween access to information and information understanding” in future consumerhealth information system development. Alpay et al. (2009) describe the future of suchwork as one “shaped by an increase in the aging population, who are prone to chronicconditions and are in need of more involvement in the self-management of their chronicdiseases” (p. 2). While our results reflect such an aging population, they are notgeneralizable, due to small study design and lack of triangulating methodology.However, though our total participants and sample size were limited, participantdemographics (age and gender) reflect average user demographics for the websitestudied.
We did not ask users for direct feedback regarding whether effects observed in RSTrelations yield actual effects they experienced. While RST has been used widely inresearch in multiple domains (Taboada and Mann, 2006), few studies to date haveincorporated participant feedback regarding relations found, with the recent exceptionof Vechtomova and Zhang (2009). This is recommended in future research as a meansfor triangulating results. Findings regarding presentational versus subject matterrelations and possible user effects are compelling, but some users/readers may actuallyprefer the physician answer discourse, precisely for its more descriptive nature. Sinceconsumer-to-consumer discussion forum participants are more likely to be consumerdiscourse-oriented, they represent a possible source of study bias. It will also beimportant in future work to include multiple physician “voices” in the physiciandiscourse. Further related research would be also strengthened by taking a moreinternational approach to explore possible culturally-based or country-specific healthcommunication differences.
ConclusionsThe present study compares lay (consumer) and professional (physician) discourses inhealth information sharing on a consumer health diabetes website. We findpreliminary evidence of differences between discourses at the pragmatics level oflinguistics, using rhetorical structure theory to guide our analysis.
Based on analysed RST definitions, information consumers share, and how theyshare it with other consumers appears to be more motivating, or activating, and morepolite (linguistically) than what, or how physicians share information with consumersonline in similar topics in diabetes management. More research is needed to providemore in-depth and generalizable results.
Living with or preventing chronic disease requires “nearly continuous decisionmaking and adjustments to changing circumstances (or contexts)” by consumers(Wagner et al., 2005). Our results cross the threshold of the health clinic towards“home”, and everyday life environments, where health information is dynamicallyprocessed yet its use is understudied (Mattingly et al., 2011). Such research contributesto our understanding of the process of knowledge translation in health care and otherdomains, where professional information is shared in various settings, yet ultimatelyapplied or used in lay or everyday life environments.
Because RST was employed in prior studies to inform system design via automatictext generation, summarisation, and other algorithmic-based information scienceapplications, the present study can also contribute to future integrated information
JDOC68,6
846

behaviour and information retrieval system research. We hope that such studies caneventually facilitate the design of information systems that draw in a more balancedmanner on both approaches (Jarvelin and Ingwersen, 2004), thus taking user-centredinformation system design to a new level.
Notes
1. The term “consumer(s)” here encompasses both patients who are experiencing illness, andpeople who are well, but seeking or sharing health information for various purposes. Thisterm is controversial, but is commonly used in the health information seeking andinformatics literature. A challenge to such terminology is beyond the scope of this research(cf. Lewis et al., 2005).
2. The US National Center for Health Statistics defines “chronic disease” as “(a disease) lasting3 months or more.” This definition includes cancer when it fits this duration.(MedicineNet.com definition of “chronic disease,” available at: www.medterms.com/script/main/art.asp?articlekey ¼ 33490 (accessed 10 December 2011).
3. Each example carries an identification number from the dataset with consumer answersmarked as “Cons_Ans” and physician as “Dr_Ans”.
References
Abelen, E., Redeker, G. and Thompson, S.A. (1993), “The rhetorical structure of US-Americanand Dutch fund-raising letters”, Text, Vol. 13 No. 3, pp. 323-50.
Abrahamson, J.A., Fisher, K.E., Turner, A.G., Durrance, J.C. and Turner, T.C. (2008),“Lay information mediary behavior uncovered: exploring how nonprofessionals seekhealth information for themselves and others online”, Journal of the Medical LibraryAssociation, Vol. 96 No. 4, pp. 310-23.
Alexa.com (2011), “Website statistics”, available at: www.alexa.com (accessed 10 September2011).
Alexander, S.C., Sleath, B., Golin, C.E. and Kalinowski, C.T. (2006), “Provider-patientcommunication and treatment adherence”, in Bosworth, H.B., Oddone, E.Z. andWeinberger, M. (Eds), Patient Treatment Adherence: Concepts, Interventions, andMeasurement, Lawrence Erlbaum Associates, London, pp. 329-72.
Allen, M., Iezzoni, L.I., Huang, A., Huang, L. and Leveille, S.G. (2008), “Improvingpatient-clinician communication about chronic conditions: description of aninternet-based nurse e-coach intervention”, Nursing Research, Vol. 57 No. 2, pp. 107-12.
Alpay, L., Verhoef, J., Kie, B., Te’eni, D. and Setsloot-Schonk, J.H.M. (2009), “Current challenges inconsumer health informatics: bridging the gap between access to information andinformation understanding”, Biomedical Informatics Insights, Vol. 2 No. 1, pp. 1-10.
Bandura, A. (1997), Self-efficacy: The Exercise of Control, Freeman, New York, NY.
Bateman, J. and Delin, J. (2006), “Rhetorical structure theory”, in Brown, K. (Ed.), Encyclopedia ofLanguage and Linguistics, 2nd ed., Elsevier, Amsterdam, pp. 589-97.
Bickmore, T. and Giorgino, T. (2006), “Health dialog systems for patients and consumers”,Journal of Biomedical Informatics, Vol. 39 No. 5, pp. 556-71.
Bird, S., Ewan, K. and Loper, E. (2009), Natural Language Processing with Python: AnalyzingText with the Natural Language Toolkit, O’Reilly Media, Sebastopol, CA.
Bissell, P., May, C.R. and Noyce, P.R. (2004), “From compliance to concordance: barriers toaccomplishing a re-framed model of health care interactions”, Social Science and Medicine,Vol. 58 No. 4, pp. 851-62.
Discoursestructure
differences
847

Bonvillain, N. (2008), Language, Culture, and Communication: The Meaning of Messages, 5th ed.,Pearson/Prentice Hall, Upper Saddle River, NJ.
Bromme, R., Jucks, R. and Wagner, T. (2005), “How to refer to ‘diabetes’? Language in onlinehealth advice”, Applied Cognitive Psychology, Vol. 19 No. 5, pp. 569-86.
Christensen, A.J. (2004), Patient Adherence to Medical Treatment Regimens: Bridging the GapBetween Behavioral Science and Biomedicine, Yale University Press, New Haven, CT.
Courtright, C. (2007), “Context in information behavior research”, Annual Review of InformationScience and Technology, Vol. 41, pp. 273-306.
DiMatteo, M.R. (2004), “Variations in patients’ adherence to medical recommendations:quantitative review of 50 years of research”, Medical Care, Vol. 42 No. 3, pp. 200-9.
Diefenbach, M., Turner, G., Carpenter, K.M., Sheldon, L.K., Mustian, K.M., Gerend, M.A., Rini, C.,von Wagner, C., Gritz, E.R., McQueen, A., Prayor-Patterson, H.M. and Miller, S.M. (2009),“Cancer and patient-physician communication”, Journal of Health Communication, Vol. 14,pp. 57-65.
Ek, S. and Widen-Wulff, G. (2008), “Information mastering, perceived health and societal status:an empirical study of the Finnish population”, Libri, Vol. 58, pp. 74-81.
Elkin, N. (2008), “How America searches: health and wellness”, available at: www.icrossing.com/sites/default/files/how-america-searches-health-and-wellness.pdf (accessed 10 December2011).
Elliott, R. (2009), “Non-adherence to medicines: not solved but solvable”, Journal of HealthServices Research & Policy, Vol. 14 No. 1, pp. 58-61.
Ferguson, T. (1999), “E-patients prefer egroups to doctors for 10 of 12 aspects of health care”,The Ferguson Report, available at: www.fergusonreport.com/articles/fr039905.htm(accessed 10 December 2011).
Ferguson, T. (2002), “From patients to end users: quality of online patient networks needs moreattention than quality of online health information”, British Medical Journal, Vol. 324No. 7337, pp. 555-6.
Forsythe, D.E., Buchanan, B.G., Osheroff, J.A. and Miller, R.A. (1992), “Expanding the concept ofmedical information: an observational study of physicians’ information needs”, Computersand Biomedical Research, Vol. 25 No. 2, pp. 181-200.
Fox, S. (2011a), “Health topics”, Pew Internet & American Life Project, Washington, DC, availableat: http://pewinternet.org/Reports/2011/HealthTopics.aspx (accessed 12 September 2011).
Fox, S. (2011b), “Peer-to-peer healthcare”, Pew Internet & American Life Project, Washington,DC, available at: http://pewinternet.org/Reports/2011/P2PHealthcare.aspx (accessed12 September 2011).
Good, B.J. and Del Vecchio Good, M. (1981), “The semantics of medical discourse”, in Mendelsohn,E. and Elkana, Y. (Eds), Sciences and Cultures: Anthropological and Historical Studies ofthe Sciences, Reidel, Dordrecht, pp. 177-212.
Hartzler, A. and Pratt, W. (2011), “Managing the personal side of health: how patient expertisediffers from the expertise of clinicians”, Journal of Medical Internet Research, Vol. 13 No. 3,p. e62.
Hogan, T.P. and Palmer, C.L. (2005), “Information preferences and practices among people livingwith HIV/AIDS: results from a nationwide survey”, Journal of the Medical LibraryAssociation, Vol. 93 No. 4, pp. 431-9.
Hunt, L.M. and Arar, N.H. (2001), “An analytical framework for contrasting patient and providerviews of the process of chronic disease management”, Medical Anthropology Quarterly,Vol. 15 No. 3, pp. 347-67.
JDOC68,6
848

Hunter, K.M. (1991), Doctors’ Stories: The Narrative Structure of Medical Knowledge, PrincetonUniversity Press, Princeton, NJ.
International Diabetes Federation (2011), “IDF diabetes atlas”, available at: www.idf.org/diabetesatlas/5e (accessed 28 December 2011).
Jarvelin, K. and Ingwersen, P. (2004), “Information seeking research needs extension towardstasks and technology”, Information Research, Vol. 10 No. 1, paper 212, available at: http://InformationR.net/ir/10-1/paper212.html (accessed 10 September 2011).
Keselman, A., Smith, C.A., Divita, G., Kim, H., Browne, A.C., Leroy, G. and Zeng-Treitler, Q.(2008), “Consumer health concepts that do not map to the UMLS: where do they fit?”,Journal of the American Medical Informatics Association, Vol. 15 No. 4, pp. 496-505.
Kleinman, A., Eisenberg, L. and Good, B. (1978), “Culture, illness, and care: clinical lessons fromanthropologic and cross-cultural research”, Annals of Internal Medicine, Vol. 88 No. 2,pp. 251-8.
Kouper, I. (2010), “The pragmatics of peer advice in a LiveJournal community”,Language@Internet, Vol. 7, article 1, available at: www.languageatinternet.org/articles/2010/2464/Kouper.pdf (accessed 26 December 2011).
Krippendorf, K. (2004), Content Analysis: An Introduction to its Methodology, 2nd ed., SagePublications, Thousand Oaks, CA.
Leech, G. and Weisser, M. (2004), “Pragmatics and dialogue”, in Mitkov, R. (Ed.), The OxfordHandbook of Computational Linguistics, Oxford University Press, London, pp. 136-56.
Lewis, D., Chang, B.L. and Friedman, C.P. (2005), “Consumer health informatics”, in Lewis, D.,Eysenbach, G., Kukafka, R., Stavri, P.Z. and Jimison, H. (Eds), Consumer Health Informatics:Informing Consumers and Improving Health Care, Springer, New York, NY, pp. 1-7.
Lincoln, Y.S. and Guba, E.G. (1985), Naturalistic Inquiry, Sage Publications, Newbury Park, CA.
McCoy, L. (2009), “Time, self, and the medication day: a closer look at the everyday work ofadherence”, Sociology of Health and Illness, Vol. 3 No. 1, pp. 128-46.
McKenzie, P.J. (2003), “A model of information practices in accounts of everyday life informationseeking”, Journal of Documentation, Vol. 59 No. 1, pp. 19-40.
Mann, W.C. and Taboada, M. (2010), “RST definitions”, available at: www.sfu.ca/rst/01intro/definitions.html (accessed 10 December 2011).
Mann, W.C. and Thompson, S.A. (1987), Rhetorical Structure Theory: A Theory of TextOrganization, Information Sciences Institute, Marina Del Ray, CA.
Mann, W.C. and Thompson, S.A. (1988), “Rhetorical structure theory: toward a functional theoryof text organization”, Text, Vol. 8 No. 3, pp. 243-81.
Mann, W.C., Matthiessen, C.M. and Thompson, S.A. (1992), “Rhetorical structure theory and textanalysis”, in Mann, W.C. and Thompson, S.A. (Eds), Discourse Description: DiverseLinguistic Analyses of a Fund-raising Text, John Benjamins, Amsterdam, pp. 39-78.
Mattingly, C., Grøn, L. and Meinert, L. (2011), “Chronic homework in emerging borderlands ofhealthcare”, Culture, Medicine, and Psychiatry, Vol. 35 No. 3, pp. 347-75.
Neal, D.M. and McKenzie, P.J. (2011), “Putting the pieces together: endometriosis blogs, cognitiveauthority, and collaborative information behavior”, Journal of the Medical LibraryAssociation, Vol. 99 No. 2, pp. 127-34.
Neuhauser, L. and Kreps, G.L. (2010), “eHealth communication and behavior change: promiseand performance”, Social Semiotics, Vol. 20 No. 1, pp. 9-27.
Discoursestructure
differences
849

Oliphant, T. (2010), “The information practices of people living with depression: constructingcredibility and authority”, unpublished doctoral dissertation, Faculty of Information& Media Studies, University of Western Ontario, London.
Palsdottir, A. (2008), “Information behavior, health self-efficacy beliefs, and health behavior inIcelanders’ everyday life”, Information Research, Vol. 13 No. 1, paper 334, available at:http://InformationR.net/ir/13-1/paper334.html (accessed 28 December 2011).
Park, J., Li, G. and Burger, A. (2010), “Opening and closing rituals of the virtual reference serviceof the Internet Public Library”, Journal of Documentation, Vol. 66 No. 6, pp. 807-23.
Patel, V.L., Evans, D.A. and Kaufman, D.R. (1989), “A cognitive framework for doctor-patientinteraction”, in Patel, V.L. and Evans, D.A. (Eds), Cognitive Science in Medicine: BiomedicalModeling, MIT Press, Cambridge, MA, pp. 257-312.
Rubin, V.L. (2010), “On deception and deception detection: content analysis ofcomputer-mediated stated beliefs”, Proceedings of the American Society for InformationScience and Technology Annual Meeting: Navigating Streams in an InformationEcosystem, October 22-27, Pittsburgh, PA.
Sarasohn-Kahn, J. (2008), “The wisdom of patients: health care meets online social media”,California Healthcare Foundation, Oakland, CA, available at: www.chcf.org/, /media/MEDIA%20LIBRARY%20Files/PDF/H/PDF%20HealthCareSocialMedia.pdf(accessed 28 December 2011).
Savolainen, R. (2008), Everyday Information Practices: A Social Phenomenological Perspective,Scarecrow Press, Lanham, MD.
Savolainen, R. (2009), “Information use and information processing: comparison ofconceptualizations”, Journal of Documentation, Vol. 65 No. 2, pp. 187-207.
Savolainen, R. (2011a), “Asking and sharing information in the blogosphere: the case of slimmingblogs”, Library & Information Science Research, Vol. 33, pp. 73-9.
Savolainen, R. (2011b), “Requesting and providing information in blogs and internet discussionforums”, Journal of Documentation, Vol. 67 No. 5, pp. 863-86.
Sligo, F.X. and Jameson, A.M. (2000), “The knowledge-behavior gap in the use of healthinformation”, Journal of the American Society for Information Science, Vol. 51 No. 9,pp. 858-69.
Smith, C.A. and Stavri, P.Z. (2005), “Consumer health vocabulary”, in Lewis, D., Eysenbach, G.,Kukafka, R., Stavri, P.Z. and Jimison, H. (Eds), Consumer Health Informatics: InformingConsumers and Improving Health Care, Springer, New York, NY, pp. 122-28.
Taboada, M. (2004), Building Coherence and Cohesion: Task-Oriented Dialogue in English andSpanish, John Benjamins, Amsterdam.
Taboada, M. and Mann, W.C. (2006), “Rhetorical structure theory: looking back and movingahead”, Discourse Studies, Vol. 8 No. 3, pp. 423-59.
Talja, S. and Hansen, P. (2006), “Information sharing”, in Spink, A. and Cole, C. (Eds),New Directions in Human Information Behavior, Springer, New York, NY, pp. 113-34.
Van Dam, H.A., van der Horst, F.G., Knoops, L., Ryckman, R.M., Crebolder, H.F.J.M. and van denBorne, B.H.W. (2005), “Social support in diabetes: a systematic review of controlledintervention studies”, Patient Education and Counseling, Vol. 59 No. 1, pp. 1-12.
Vechtomova, O. and Zhang, H. (2009), “Articulating complex information needs using querytemplates”, Journal of Information Science, Vol. 35 No. 4, pp. 439-52.
Veinot, T.C. (2009), “Interactive acquisition and sharing: understanding the dynamics ofHIV/AIDS information networks”, Journal of the American Society for Information Scienceand Technology, Vol. 60 No. 11, pp. 2313-32.
JDOC68,6
850

Veinot, T.D. (2010), “‘We have a lot of information to share with each other’: understanding thevalue of peer-based health information exchange”, Information Research, Vol. 15 No. 4,paper 452, available at: http://InformationR.net/ir/15-4/paper452.html (accessed 28December 2011).
Vermeire, E., Wens, J., Van Royen, P., Biot, Y., Hearnshaw, H. and Lindenmeyer, A. (2005),“Interventions for improving adherence to treatment recommendations in people with type2 diabetes mellitus”, Cochrane Database Systematic Reviews, Vol. 2005 No. 2, CD003638.
Wagner, E.H., Bennett, S.M., Austin, B.T., Greene, S.M., Schaefer, J.K. and Vonkorff, M.M. (2005),“Finding common ground: patient-centeredness and evidence-based chronic illness care”,Journal of Alternative and Complementary Medicine, Vol. 11, pp. S7-S15, Supplement 1.
World Health Organization (2011), “Global status report on noncommunicable diseases 2010”,available at: www.who.int/nmh/publications/ncd_report_full_en.pdf (accessed28 December 2011).
Zethsen, K.K. and Akehave, I. (2006), “Medical communication: professional-lay”, in Brown, K.(Ed.), Encyclopedia of Language and Linguistics, 2nd ed., Elsevier, Amsterdam, pp. 644-9.
About the authorsJennie A. Abrahamson is a Doctoral Student in Library and Information Science at the Faculty ofInformation and Media Studies, and a member of the Language & information TechnologyResearch Lab (LiT.RL) at the University of Western Ontario, London, Canada. Jennie has anMLIS from the University of Washington iSchool, Seattle, WA, USA. She also earned a Master ofBiomedical Informatics (MBI) from the School of Medicine at Oregon Health and ScienceUniversity, Portland, OR, USA, while completing a US National Institutes of Health/NationalLibrary of Medicine-funded research training fellowship. Jennie’s experience working inacademic and community reference and information services inspires her research interests inhow people seek and use information to solve problems in everyday life, how information affectshealth outcomes, and connecting user- and system-centred research to improve informationsystems. She focuses on interpersonal and secondary information seeking via the study of layinformation mediary behaviour (“LIMB”, or people seeking information from, or on behalf orbecause of others in everyday life). Adjunct interests include integrated research methods, healthinformation seeking, consumer health informatics, information disparities, and social and ethicalaspects of ICT design and use.
Victoria L. Rubin is an Assistant Professor at the Faculty of Information and Media Studiesand the Principal Investigator of the Language & information Technology Research Lab(LiT.RL) at the University of Western Ontario, London, Canada. She received her PhD inInformation Science and Technology in 2006, her MA in Linguistics in 1997 from SyracuseUniversity, NY, USA, and a BA in English, French, and Interpretation from the Kharkiv NationalUniversity, in 1993. Dr Rubin’s research interests are broadly in information organisation andinformation technology. She specializes in information retrieval and natural language processingtechniques that enable analyses of texts to identify, extract, and organize structured knowledge.She investigates complex human behaviours that are, at least partly, expressed throughlanguage such as certainty, emotions, credibility, trust, and deception. The language in each caseexhibits subtle but discernible properties that can be identified and traced computationally. Herlab focuses on modelling these phenomena and developing methodologies for acquiringappropriate and reliable cues for identification, classification and detection, first manually thancomputationally, based on natural language processing and machine learning techniques.Victoria L. Rubin is the corresponding author and can be contacted at: [email protected]
Discoursestructure
differences
851
To purchase reprints of this article please e-mail: [email protected] visit our web site for further details: www.emeraldinsight.com/reprints