Dimensions of Tribal Health in Sahayadri Region: Assessment and Administration of Health in Tribal...
27
Anurag Shukla (MAD11004) Independent Study on Tribal Health Mentor: Dr Shreelata Rao Seshadri Dimensions of Tribal Health in Sahayadri Region: Assessment and Administration of Health in Tribal Communities living near Chas Kaman Dam
Transcript of Dimensions of Tribal Health in Sahayadri Region: Assessment and Administration of Health in Tribal...
Anurag Shukla
(MAD11004)Independent Study on Tribal
Health
Mentor: Dr Shreelata Rao
Seshadri
Dimensions of TribalHealth in Sahayadri
Region: Assessment andAdministration ofHealth in Tribal
Communities living nearChas Kaman Dam
Abstract
Due to a combination of societal attitudes, varying beliefsystems, and governmental neglect, tribal populationsthroughout India have long been denied basic healthcare. As aresult, gaping disparities in health status of tribals, whencompared to general population living in the same area, areevident. To assess health status of tribal population andtheir access to public and private health care in post-economic reforms and post-NRHM period, 8 week long study wasdone in months of November and December in 2012 among thethree tribal communities i.e. Mahadev Koli, Katkari and Thakurin Rajguru Nagar taluk of Pune district. Data was collected byvisiting each tribal household, conducting individual andfocused group interviews. Panchayat members and local healthadministration also actively participated in the study. Ananalysis of the data collected among the tribals shows thatdespite the fact that rural health infrastructure has improveddrastically in post-NRHM period; there has not been muchimprovement in health status of tribal communities. Theirhabitats are still inaccessible by the road and landlessnessis a common feature among them. Most of the tribals are livingbelow poverty line and don’t spend much on health care. Theyhave common tendency to underreport their illness and amongthem the rate of utilization of public health services is verylow. These tribal communities have high maternal mortality andinfant mortality rates with high prevalence of infectiousdiseases like Dengue fever, Malaria, Pneumonia andTuberculosis. There are historical reasons for their pooreconomic and societal status and their rights and demands havebeen progressively neglected in policy discourses.
Table of ContentsIntroduction.......................................................3Section I: Tribals, their habitat, social and cultural values......4
Section 2 : Perception, access, reporting of ailments and Utilization of Public and Private Health Servies..................11
Section 3: Marginalization of tribals, processes of “Peasantization”and “State Simplification” leading to poverty and Landlessness....14
Conclusion: Mobilization and Creating awareness as answers to tribals inaccessibility to public and private health care.........16
Introduction
The term “tribe” was used by the colonial government in Indiato categorize a large number of groups who did not fit thecategories of ‘caste’ or ‘Hindu’. The term subsumedcommunities very different from one another in terms ofdemographic size, linguistic and cultural traits, ecologicalconditions, material conditions of living, but essentially‘primitive’, ‘backward’ and ‘uncivilized’ in character. Afterindependence, ‘Scheduled Tribe (ST) came to be used to denotetribes which were scheduled as such under the Constitution ofIndia, distinguished from other communities by relativeisolation, cultural distinctiveness and low level ofproduction and subsistence.
Notwithstanding the fact that tribals were given someprivileges and concessions in form of reservations and specialbudgetary provisions, their condition remains abysmal. Theirsocio-economic status, human development index clearly showthat they have not benefitted from the protective measuresprovided by the government since independence. Majority ofthem continue to be marginalized by the process of so calleddevelopment of the last six decade. It is who have borne thecost of industrialization, urbanization, construction of bigdams, mining and quarrying and other development activities.Their health status too remains very poor, even worse off thanSub-Saharan countries. Their general health indicators likeInfant Mortality Rate (IMR), Maternal Mortality Rate (MMR),and Total Fertility Rate (TFR) remain very high in comparisonwith other caste groups and communities.
In State of Maharashtra where tribals constitute 10 per centof total population, their health status signifies a state ofdoomed and distress. Very rarely in any tribal area has anyhealth infrastructure like public health centers, access toservices provided by ANM and ASHA workers? Unsurprisingly, in
absence of any kind of government support for their health,they have very low level of health awareness and minimalexpectation from the government side. They have beensystematically neglected and subjugated in course of policyformation and implementation. They are trapped in viciouscircle of poverty and distress. Despite the fact thatMaharashtra continues to achieve 10 per cent economic growth,their status remains unchanged and in some cases it has beendeteriorated.
This paper is based on survey and field work conducted inRajgurunagar taluk of Puna District in Maharashtra. Paperstudies the health status of tribal population living in theabovementioned region. Study focuses mainly on three tribalgroups: Mahadeo Kolis, Thakars and Katkaris. Field work forthis study was done in six weeks’ time starting on 3rd Novemberand ending in 20th December. Data was collected throughhousehold surveys that included sampling of houses inproportion of 5 to 1 and conducting individual and focusedgroup interviews.
This paper has been divided in four sections. First sectiondoes the task of introducing tribal groups (Mahadeo Kolis,Thakars and Katkaris) living near Chas Kaman dam inRajgurunagar taluka of Pune district and further provides dataon their socio-economic status, occupations, health status,access to different government services (electricity, pipedwater supply) and programs. Second section documents thegeneral attitudes and perceptions of population and officialstowards health services provided by both government andprivate health service providers. This section also providesdetails on the process of policy formation and implementationat local level. Third section explains the processes of ’Statesimplification’ and “peasantization” through which thesetribes were systemically marginalized. This section alsoexplores the status of “landlessness” in tribals and explainshow inequities in land-ownership reproduce inequities in otherhuman development indicators. Forth section sums up the
discussion and further it provides some insights intodevelopment of tribals and their comparatively better accessto public services in States where tribals have alreadyachieved high level of human development (Mijoram, Kerala andTamilnadu).
Section I: Tribals, their habitat, social andcultural values
There are three mountain ranges in Maharashtra known asSahayadri, Satpuda and Gondwana ranges. In total there are 47Scheduled Tribe population groups in the State and majority ofthem are inhabitants of these geographically difficultterrain. Our field work was done in the Sahayadri region whichhas tribal population belonging to Mahadeo Kolis, the Thakarsand the Katkaris. Under scope of this field work, only thosetribal populations were studied that was living under thejurisdiction of Gundelwadi gram Panchayat. Except this, studyalso covered tribal population living near village Darakwadi.
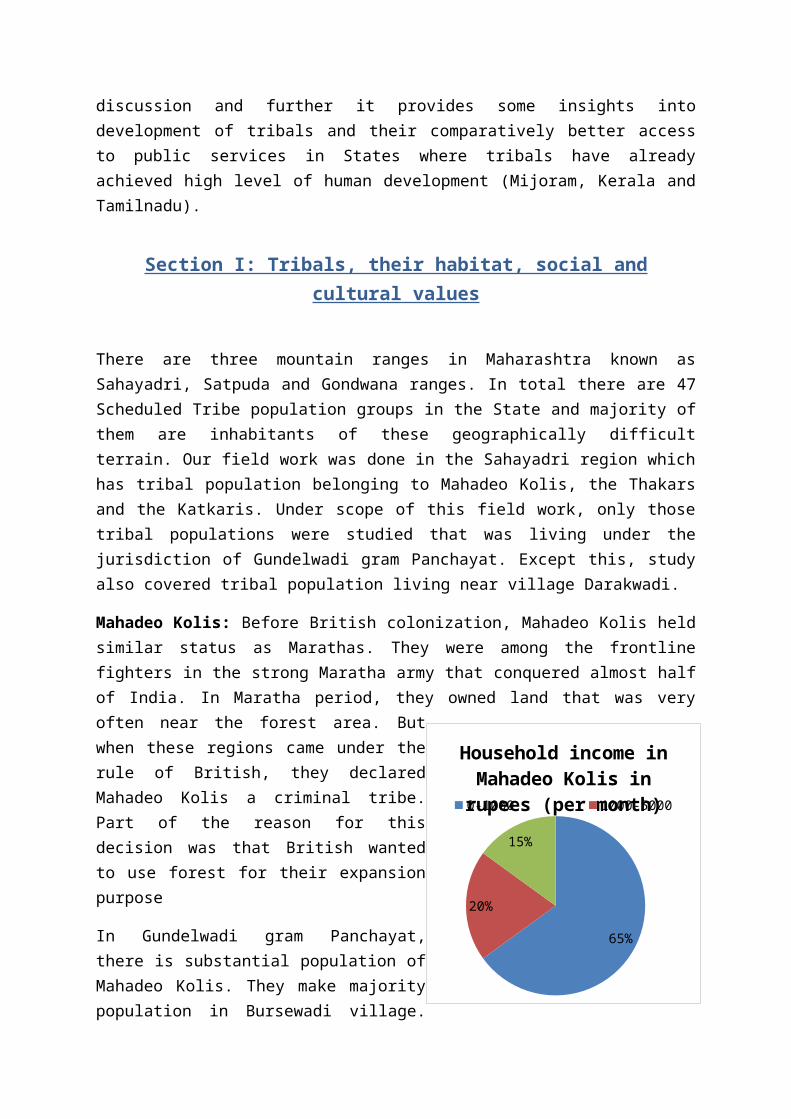
Mahadeo Kolis: Before British colonization, Mahadeo Kolis heldsimilar status as Marathas. They were among the frontlinefighters in the strong Maratha army that conquered almost halfof India. In Maratha period, they owned land that was veryoften near the forest area. Butwhen these regions came under therule of British, they declaredMahadeo Kolis a criminal tribe.Part of the reason for thisdecision was that British wantedto use forest for their expansionpurpose
In Gundelwadi gram Panchayat,there is substantial population ofMahadeo Kolis. They make majoritypopulation in Bursewadi village.
65%
20%
15%
Household income in Mahadeo Kolis in rupees (per month)0-1000 1000-5000
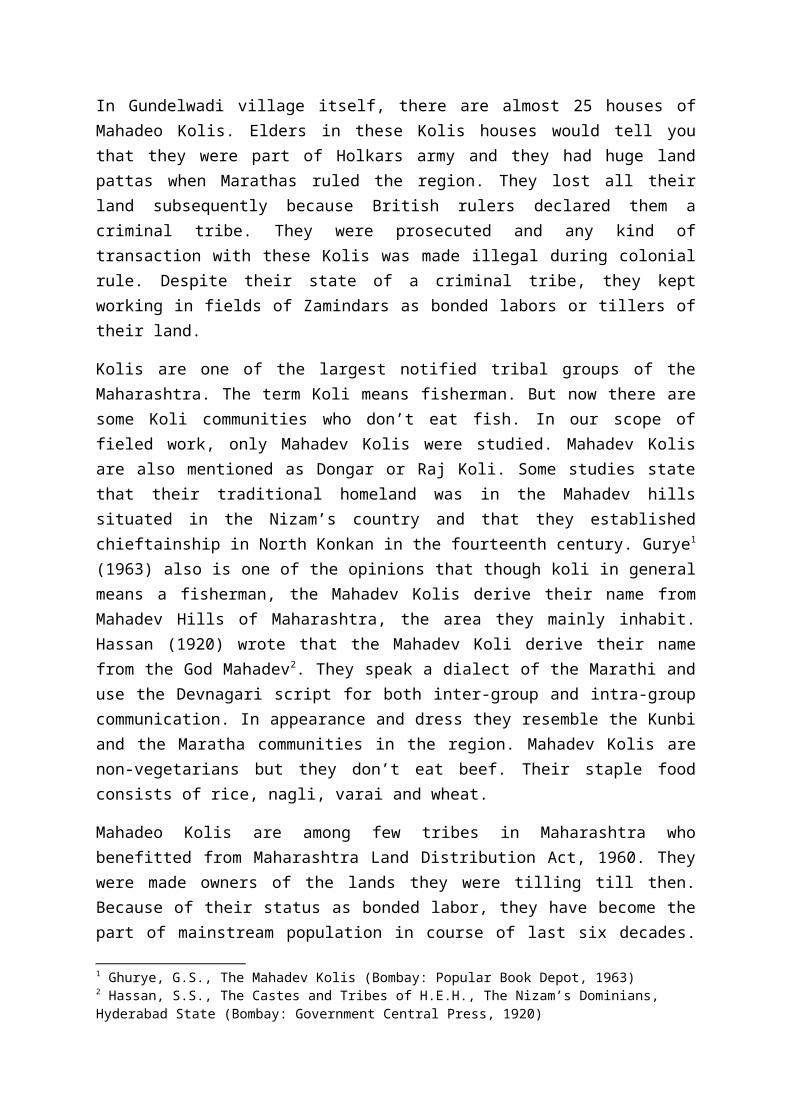
In Gundelwadi village itself, there are almost 25 houses ofMahadeo Kolis. Elders in these Kolis houses would tell youthat they were part of Holkars army and they had huge landpattas when Marathas ruled the region. They lost all theirland subsequently because British rulers declared them acriminal tribe. They were prosecuted and any kind oftransaction with these Kolis was made illegal during colonialrule. Despite their state of a criminal tribe, they keptworking in fields of Zamindars as bonded labors or tillers oftheir land.
Kolis are one of the largest notified tribal groups of theMaharashtra. The term Koli means fisherman. But now there aresome Koli communities who don’t eat fish. In our scope offieled work, only Mahadev Kolis were studied. Mahadev Kolisare also mentioned as Dongar or Raj Koli. Some studies statethat their traditional homeland was in the Mahadev hillssituated in the Nizam’s country and that they establishedchieftainship in North Konkan in the fourteenth century. Gurye1
(1963) also is one of the opinions that though koli in generalmeans a fisherman, the Mahadev Kolis derive their name fromMahadev Hills of Maharashtra, the area they mainly inhabit.Hassan (1920) wrote that the Mahadev Koli derive their namefrom the God Mahadev2. They speak a dialect of the Marathi anduse the Devnagari script for both inter-group and intra-groupcommunication. In appearance and dress they resemble the Kunbiand the Maratha communities in the region. Mahadev Kolis arenon-vegetarians but they don’t eat beef. Their staple foodconsists of rice, nagli, varai and wheat.
Mahadeo Kolis are among few tribes in Maharashtra whobenefitted from Maharashtra Land Distribution Act, 1960. Theywere made owners of the lands they were tilling till then.Because of their status as bonded labor, they have become thepart of mainstream population in course of last six decades.
1 Ghurye, G.S., The Mahadev Kolis (Bombay: Popular Book Depot, 1963)2 Hassan, S.S., The Castes and Tribes of H.E.H., The Nizam’s Dominians, Hyderabad State (Bombay: Government Central Press, 1920)
Their attitudes, habits, cultural traits have become moresimilar to the Marathas than to a tribe. Because of theirmainstream character, they are facing same problems as facedby general population. Mahadeo Kolis are marginal land owners.They have 3 to 5 acre land per household. In their land, theymainly grow Jawar, Bajra, peanuts. Some of them also growcrops like rice, onion and potato. Interestingly, whateverthey grow in their fields is only enough for their
consumption. They don’t save anything that can be categorizedas agriculture income. Their income after selling theiragriculture produce stand at zero as they have to immediatelybuy seeds, fertilizers etc. Women in Mahadeo koli householdwork in the fields and men often go to Mumbai or Pune to earnadditional income to compensate for their other expenditures.In average, men stay in cities for five or six months in ayear and save somewhere around ten thousand to twentythousand. They engaged themselves as construction labors orworkers at small shops. This additional income of ten thousandto twenty thousand take cares of their others need likehealthcare, clothing, expenditure in ceremonies. In case ofany serious calamity, community members help each other byproviding loans. Number of livestock with a household dependson the household income. Some of them who don’t own any landonly have goats as livestock and they sell their milk. Those
036
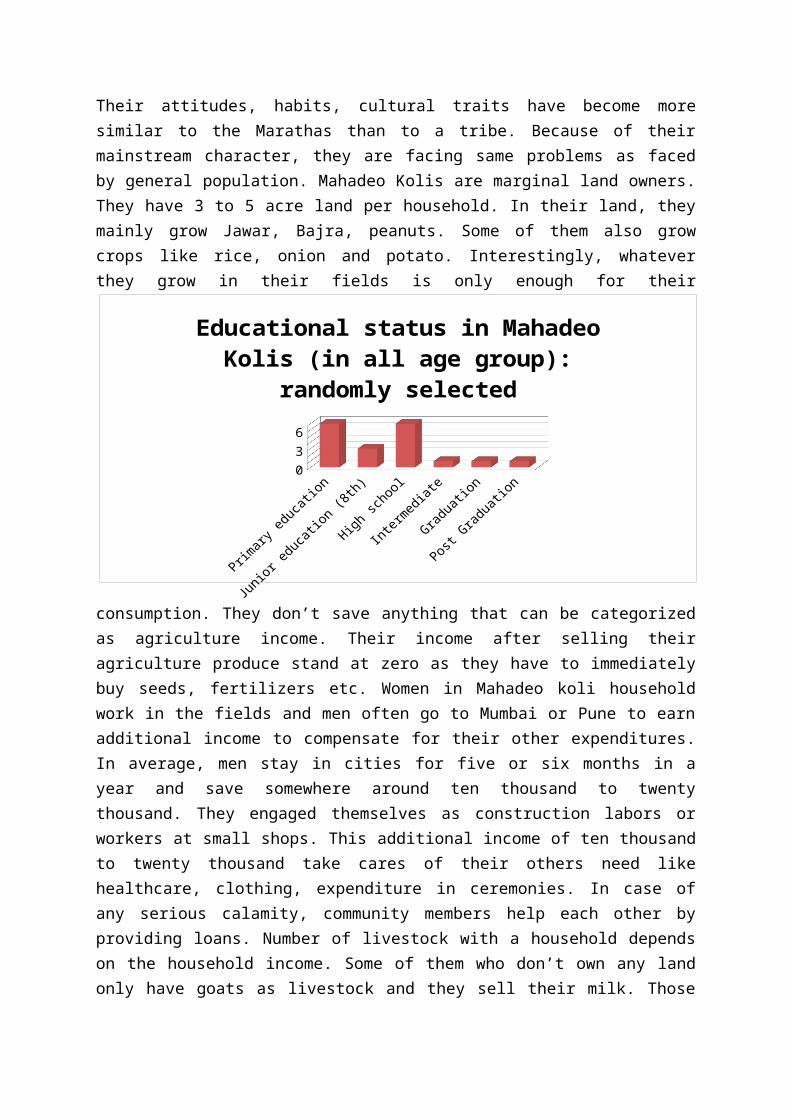
Educational status in Mahadeo Kolis (in all age group):
randomly selected
who own land here have at least one cow and one ox. Livestockmakes important part of their livelihood as they can sell themilk in the nearest dairy in Gundelwadi at 20 per liter. In 20houses surveyed, only two houses had buffaloes. Their incomealso exceeded others.
In Gundelwadi gram Panchayat, almost all villages have primaryschool. Bursewadi and Gundelwadi have junior schools also. If
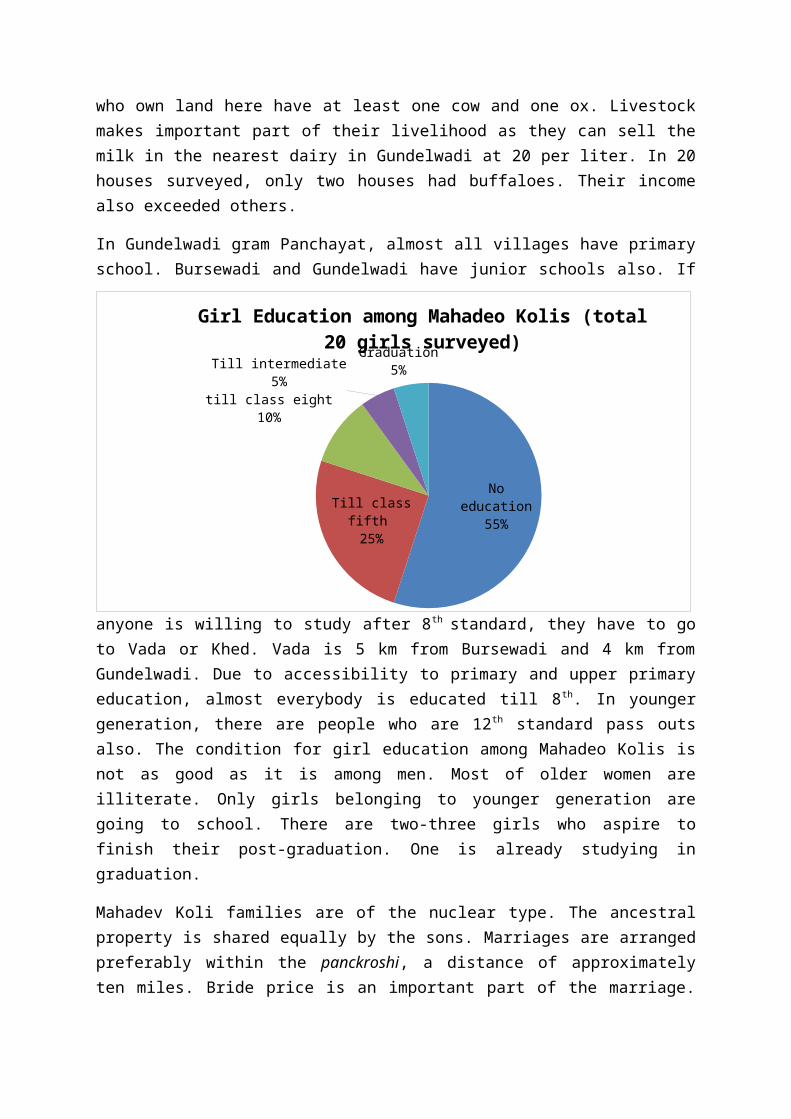
anyone is willing to study after 8th standard, they have to goto Vada or Khed. Vada is 5 km from Bursewadi and 4 km fromGundelwadi. Due to accessibility to primary and upper primaryeducation, almost everybody is educated till 8th. In youngergeneration, there are people who are 12th standard pass outsalso. The condition for girl education among Mahadeo Kolis isnot as good as it is among men. Most of older women areilliterate. Only girls belonging to younger generation aregoing to school. There are two-three girls who aspire tofinish their post-graduation. One is already studying ingraduation.
Mahadev Koli families are of the nuclear type. The ancestralproperty is shared equally by the sons. Marriages are arrangedpreferably within the panckroshi, a distance of approximatelyten miles. Bride price is an important part of the marriage.
No education
55%Till class fifth 25%
till class eight10%
Till intermediate5%
Graduation5%
Girl Education among Mahadeo Kolis (total 20 girls surveyed)
Divorce and remarriage are allowed. Holi is their importantfestival and singing of religious songs (bhajans) is a popularform of recreation.
Koli’s increasing contact with urban centers and regularinteraction with other communities have contributed towardsmodifying traditional patterns of their life and helped themgain wider acceptance in the society.
The health status of the Kolis may be summarized by thefollowing indicators that coincide with self-reports of thegeneral population. Almost All Koli households in Bursewadiand Gundalwadi have toilets. Some families are dependent onpublic toilets built by Panchayat. Waste disposal consists ofseptic tanks. Drainage system was found very poor condition inboth villages. It was particularly very bad where Kolis houseswere situated. For drinking water, these Koli families aredependent on hand-pumps. There is piped water supply but theycomplain that supply water is often very muddy and salty. Theydon’t use it for drinking purpose. It has been noted thatthere have been Typhoid, Malaria and Dengue outbreaks in thesevillages in every 2-3 years of time. This is particularly dueto poor drainage and waste disposal system.
Most Koli women report dizziness and fatigue, which we cantake as an indication of anaemia. Some women are acutelyanaemic. Their diet consists of jawar or bajra roti, greenvegetable curry, lentils and eggs or curd/milk. Most Koliwomen are aware about nutritional advantages of greenvegetables like spinach (palak) or banana but they are notable to take it on daily basis because of economicconstraints.
The Thakars:
Thakars are concentrated in the Thakarwadi village. There are42 houses belonging to this tribe. Thakar people believe that
they are the descendants of the Chittorgarh Rajputs, who lefttheir original home in Rajasthan for this place. The communityunderstudy is divided into two endogamous divisions, Ma Thakarand Ka Thakar. In the course of study, data was collectedamong the Ma Thakar only. These people speak a corrupt form ofMarathi, an Indo-Aryan language, and use the Devnagri script.
Generally the Thakar are short-statured. Unlike other tribalcommunities of the region, they show a tendency towards abroad head shape. These people have a broad facial profilewith a broad nose. They are basically non-vegetarians and arevery fond of dry fish. The meat of wild animal is alsoconsumed. Jowar, rice, nagli and wheat are their staplefoodgrains, consumed with pulses and vegetables. Some of themsmoke beedis, chew loose tobacco and consume liquor.
The Thakar groups, Ka Thakar and Ma Thakar, are divided intoseveral exogamous clans, which are known as arhnam. The clansare Daroda, Mengal, Singpuria, Singwa, Sidh and Wak. Ethoven(1922) identified the above mentioned endogamous divisions andthirty-five exogamous kul, like Sotok, Vagh, Pavar andZugarya3. Cross-cousin marriages are allowed among them. Theage at marriage is fifteen years for girls and eighteen forboys. Marriage alliances are contracted mostly throughnegotiation. Bride price is paid. A necklace and toe-rings aremarriage symbols for Thakar women. Usually monogamy is theform of marriage among them. The women participate in alleconomic and domestic work, including wage earning. Thakarinterdine with the Kolis but not with the Katkaris. It isinteresting that these commensal rules are strictly followedby their women, while their men folk are not very seriousabout it.
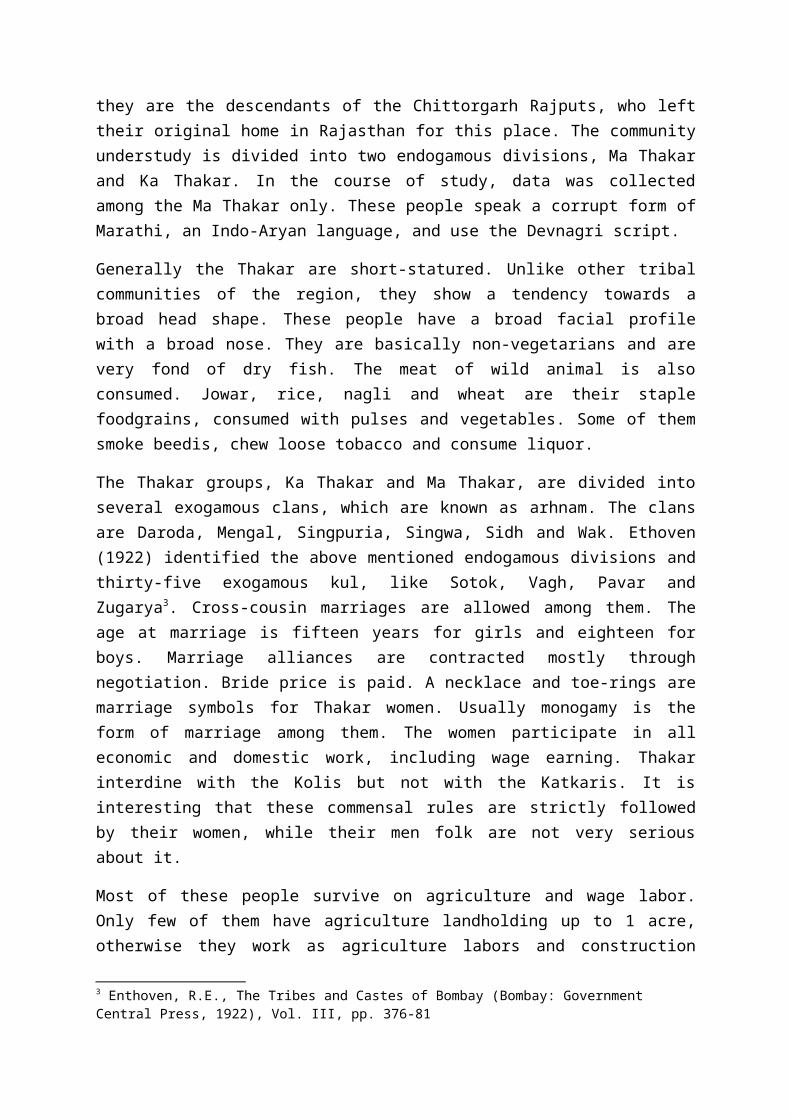
Most of these people survive on agriculture and wage labor.Only few of them have agriculture landholding up to 1 acre,otherwise they work as agriculture labors and construction
3 Enthoven, R.E., The Tribes and Castes of Bombay (Bombay: Government Central Press, 1922), Vol. III, pp. 376-81
labors in towns and cities like Rajgurunagar, Chakan and Pune.Most of the households are very poor. Only one hand-pumpsupplies water for whole of the village.
Figure 1 Occupation wisedistribution among Thakars
Village has oneprimary school with 25children mainly fromvillage. Village hasvery poor record whenit comes to adult
education. Only one girl in whole village was educated tillclass 8. Most of other adult girls are illiterate or drop-outsfrom the primary education. In case of men population, datacollection doesn’t give any different picture. Not one of theadult men had passed 10th standard. Economic constraints andinaccessibility to schools were main reasons behind drop-outs.
Some profiles from Thakarwadi village:
Name: Chhaya Sitaram Bhange
Age: 22 years
Sex: Female
Children: 1 son,
Caste: Thakar
Occupation: Housewife
Landholding: 1 acre
No toilet, No water available at home, depended on hand-pumpwater. When Chhaya was pregnant, she was frequently taken tohospital by her husband. She got regular vaccination by ANM(Auxiliary Nursing Midwife). Her child was underweight at thetime of birth and was diagnosed with Pneumonia. She had to
13
21
53
Agriculture labor Construction laborland holding (1 acre)permanently unemployed
take her child to district hospital but ultimately she had toadmit her in a private hospital. Even after spending 70thousand rupees, her child could not recover properly. She hadto take loan from her relatives and she has not been able torepay the entire amount yet.
Name: Sangeeta Name: Dheerabai Name:Manisha
Age: 30 years Age: 30 yearsAge: 23 years
Caste: Thakar Caste: ThakarCaste: Thakar
Agriculture Laborer Agriculture laborerConstruction laborer
Income: 100/60rs per day 100/60rs per day150rs per day
2 goats as additional income Selling cow milkNil
No toilet No toilet No toilet
No electricity in the house No electricity No electricity
All the women we spoke with had deliveries at home. They tookhelp of dai/aaya. Only Manisha had delivery in hospital andshe did get money from hospital under Janani Suraksha Yojna.Others were not very positive about services provided at thePublic Health Center at Wada. They complained that they didn’tget any injection from the PHC whenever they were bitten aninsect. Nurse didn’t come to their home for regularvaccination and immunization and rarely did they get irontablets from her.
Name: Ishwar Kadle
Age: 22 years
Children: 2
Caste: Thakar
Occupation: Driver, earns 3500rs per month, additional incomecomes from selling lambs and goats they have.
Total no of family members: 6
Land-holding: 3 acre, mainly marsh land
Sends his children to primary school and understands thateducation is essential for survival in this world. At the timeof his wife’s delivery, he took her to Narayangaon PHC anddelivery was done free of cost. He also got the amountstipulated under the Jananai Suraksha Yojna.
The Katkari:
They are also known as Kathodi or Kathodia, they areconcentrated in the Raigad, Pune and Thane districts ofMaharashtra, where their settlements are along the foothillsof the Sahayadri range. The Katkaris are grouped with theKathodi along with other subgroups in order to notifying themas a scheduled tribe in Maharashtra. They speak in the Marathilanguage and use the Devanagri script. Enthoven (1922) hasdescribed the Kathodis or Katkaries as a tribe of catechumakers.
Katkaris are short-statured, round-headed people. They have abroad nasal and facial profile. The incidence of sickle celltrait is comparatively low among them in comparison with othertribal groups of Central and Western India. Katkaris are non-vegetarians who eat pork. Dry fish is eaten regularly by them.Rice, nagli and millet are their staple cereals. Alcoholicdrinks, brewed at home an as well purchased from the weeklymarkets, are consumed. The Katkari females can be easilyindentified by their ornaments, especially ear-rings, tattoomarks on their forehead and arms and the style of wearing thesaree above the knee.
Among the Katkaris, negotiated marriages are convention.Monogamy is the most popular form of marriage, though polygamyis allowed. They pay a bride price and follow the partrilocalrule of residence. The custom of child marriage has beenreplaced by adult marriage. A neckless, green glass banglesand a dot on the forehead are regarded as symbol of marriage.Divorce is permissible and a divorced person is allowed tomarry. The mixed extended type of family is common among them.The sons inherit ancestral property equally. The womenparticipate in whatever small agriculture activities thesetribes do. They contribute in enhancing family’s income byselling seasonal vegetables and forest-produce at weeklymarket.
The traditional occupation of the Katkari was catechu-making.Things like poultry farming have been recently introduced intothe Katkari economy. The Katkaris are mainly Hindus. They havevery rice oral tradition. Their dances are performedaccompanied by folk-songs and percussion instruments.
Their response towards formal education has been very poor.Most of the adult men are drop-out after primary education andwomen are illiterate. There has been some improvement underthe Sarva Shiksha Abhiyaan but Katkaris locality still doesn’thave a government primary school near their habitation. Thereare 21 houses of Katkaris near Darakwadi village. They don’thave any water facility. Toilets are non-existent, and theyare still living in Kachcha houses. Immunization and otherchild-welfare schemes are not well-functioning among theKatkari population. They don’t have access to aaganwadi centreso that they can avail certain child welfare services.
The Katkari habitation near village DarakwadiNo drinking water facility, no toilets, living in Kachchahouses.No access to immunization and child-welfare schemes. Noaaganwadi centre in their localityNo primary school, Most of the girls in the community don’t goto school.
In absence of any residence proof, they can’t avail anyfacilities provided under the public distribution system.Wood collected from forest is their main fuel resource. Theyare still engaged snake-hunting, bird hunting and othertraditional occupations.
Section 2 : Perception, access, reporting of ailmentsand Utilization of Public and Private Health Servies
Broadly understood, access to healthcare services involves theability of patients to use services that (a) they themselvesdesire, (b) experts believe they require. These means are byno means mutually exclusive. A good system of informationflows to the patient and his/her household, a well-functioningreferral system as well as an appropriate understanding of thebenefits of healthcare utilization can create an environmentwhere there is disjoint between what patients desire and whatexpert believe they require.
But that is one of the issues that affect access. The physicalavailability of healthcare professionals and healthcareinfrastructure is another issue. There are demand and supplyside issues, quality, utilization and reporting issues thatone needs to keep in the mind while evaluating accessibilityof public and private health care. If look at the patternamong tribal population about illness reporting, it can beeasily understood that income has positive relationship withreporting of diseases.
The more income a tribal population earn, the more they spendon their health care. It is true for almost all of the socio-economic groups. In a study, Srinivasan and Mohanty (2004)find that STs (49 per cent) and SCs (41 per cent) have a muchhigher proportion of households living under ‘abject poverty’
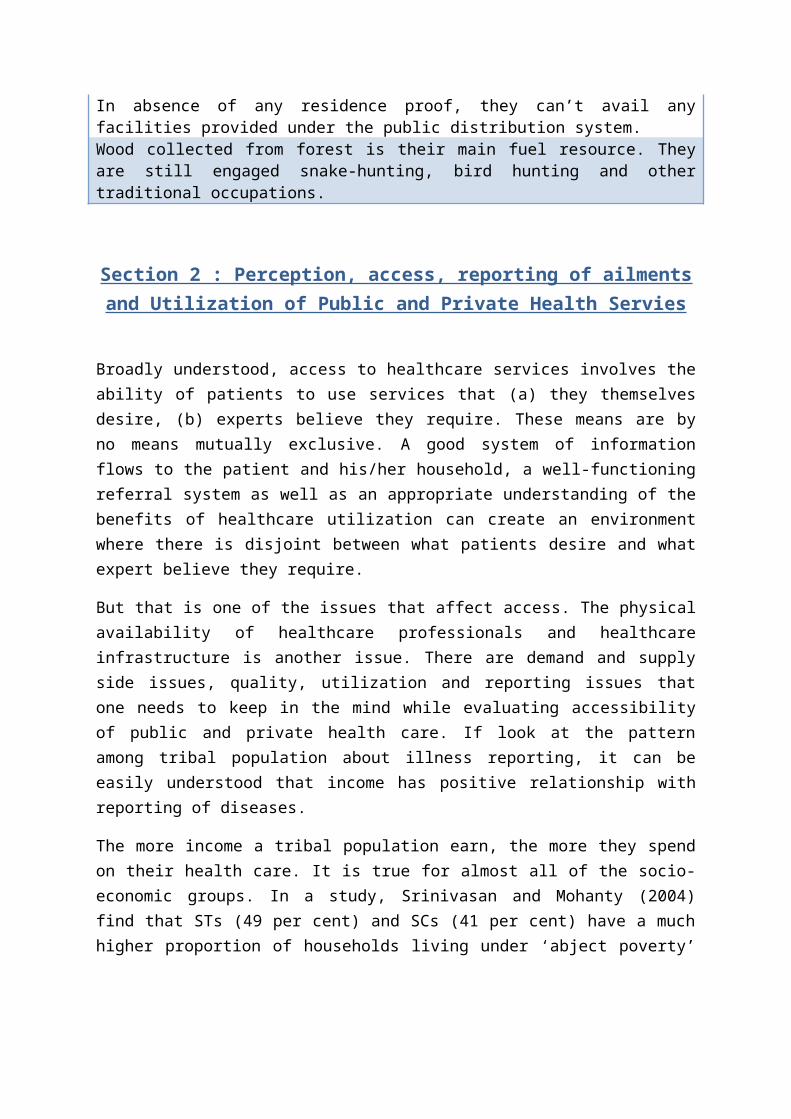
and ‘moderate poverty’4. If we look at prevalence rates acrosssocial groups, while many studies have shown that householdsbelonging to marginalized groups such as the Scheduled Tribe(ST) reveal a much lower utilization of health services andour study among tribal population confirms this trend. Even incase of reporting of ailments, wide gap exists between STs andother social groups. Among men population group, above 45years age group reported most ailments. In case of women,population between age group 20-45 years reported most numbersof ailments, which broadly corresponds to their reproductiveyears.
Overall, women seem to have more health problems than men(though those under 19 years of age report a lower prevalenceof ailments than their male counterparts).
Age Groups (years) Male Female0-9 9.4 8.310-19 4.5 4.420-34 4.4 6.535-44 7.1 10.445-59 11.4 14.360 and above 30.9 31.2Total 8.6 9.7Table 1 Percentage of People Ailing across Age and Gender among tribal population
An analysis of the reasons for untreated ailments providesinsights into the factors that influence accessibility tomedical services. Reasons like physical proximity to healthfacilities, perception and financial constraints are play rolebehind under-utilization of public health care facilities.Also there is a clear trend in tribals towards self-treatingthemselves through herbal medicines or allopathic medicinesbought from a pharmacy. They firmly believe that ailments likeheadache and fever are not serious enough to go to hospitalfor treatment. Women feel embarrassed to share theirreproductive and menstrual problems with a male doctor and in
4 Srinivasan, K and S K Mohanty, 2004, Deprivation of basic amenities by Caste and Religion, Empirical study using NFHS Data, EPW
face of unavailability of lady doctor in hospitals, they haveno choice but to take home treatment.
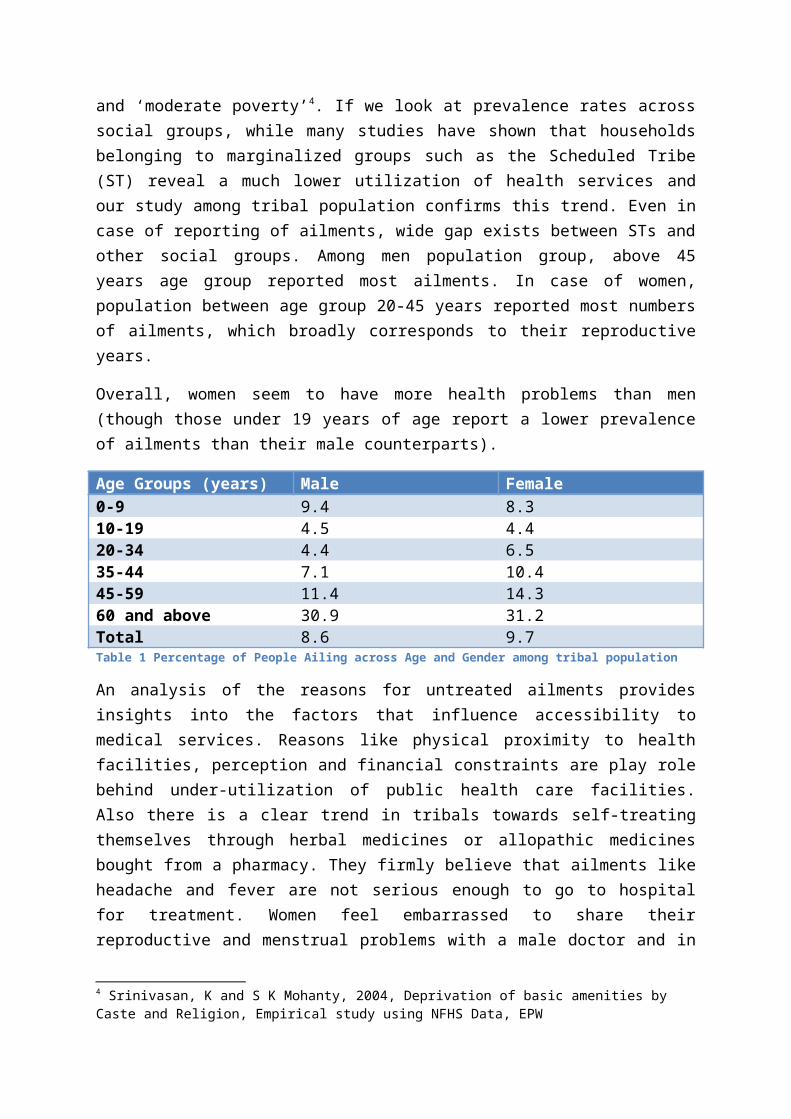
Reason for not seekingtreatment
Percentage
No medical facility in theneighbourhood
10.3
Lack of faith 3.1Long waiting 1.1Financial reasons 29.8Ailments not consideredserious
39.7
Others 16.0Total 100.0Table 2 Reasons for Not Seeking Treatment for a reported Ailment (%)
Tribals habitation near Chas Kaman dam are served by a newlybuilt PHC in village called Wada. Tribal who are still notconnected with the pucca road have comparatively poor accessof hospital and medical services. Tribal households complainthat their houses are often ignored by ANMs and ASHA workers.Their houses are connected to main road only by narrow laneswhich makes almost impossible for any ambulance to enter thesevillages, ANM visits the village once a month only.
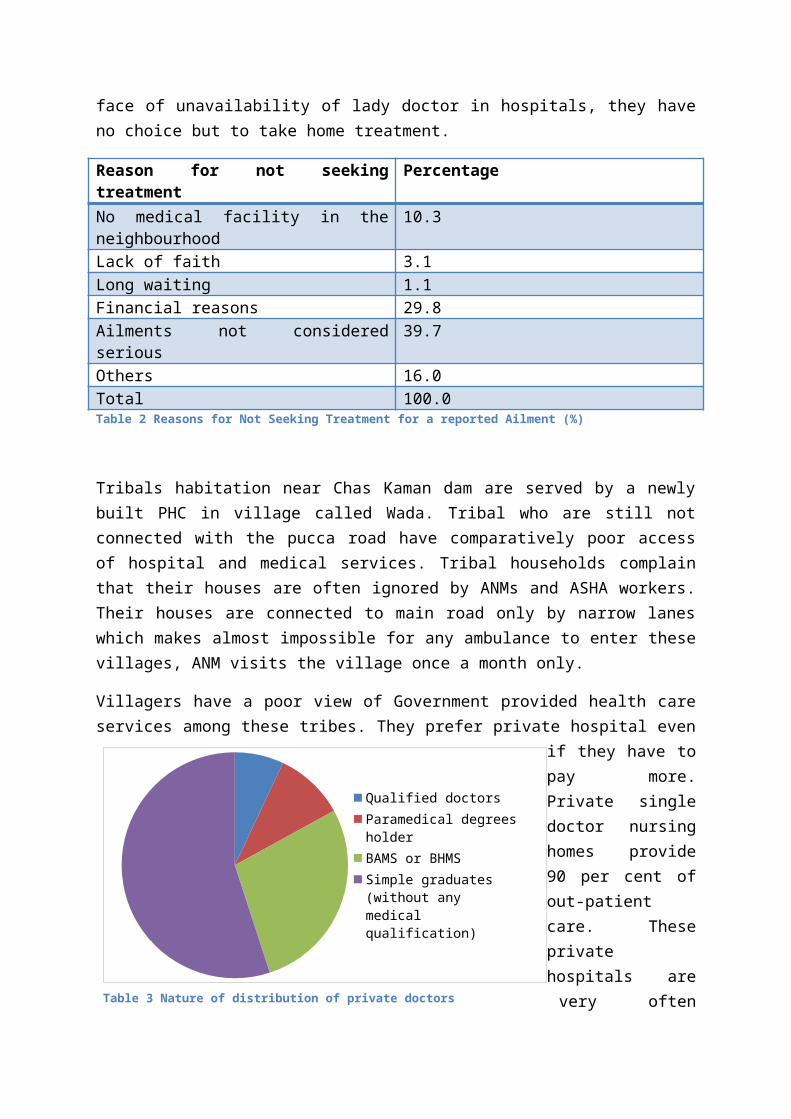
Villagers have a poor view of Government provided health careservices among these tribes. They prefer private hospital even
if they have topay more.Private singledoctor nursinghomes provide90 per cent ofout-patientcare. Theseprivatehospitals arevery oftenTable 3 Nature of distribution of private doctors
Qualified doctorsParamedical degrees holderBAMS or BHMSSimple graduates (without any medical qualification)
operated by non-medical graduates. Most of them don’t have anykind of medical degree or diploma. A bird-eye view of theseprivate hospitals will tell you that only 10 per cent of theseprivate doctors are having MBBS degree. 35 per cent have BAMSor BHMS degrees. 55 per cent of these private doctors don’thave even simple graduate degree. 10 per cent of these privatedoctors are former paramedical employees of some privatehospital. Most of the times, negligence of staffs working ingovernment hospital and their unwelcoming behaviour isresponsible for this poor image.
A quick view of PHC shows sign of human resource constraints.According to NRHM guidelines, there should be 2 or 3 doctorsin a rural PHC. In Wada PHC, there is only one doctor and hetoo has recently joined the hospital. Post of Pharmacist islying vacant since the inception of the hospital. MedicalOfficer Dr Prabandh R. Bhise is an MBBS. Meeting with him wasquite revealing. He spoke on out-patient and in-patientfacilities provided by his PHC. Dr Binse says that hishospital receives mostly accidental cases and cases of snake-bites and insect-bites. In-patient care is available for thesekinds of cases in the PHC. He also talked about policy changesat district level with the change of District Health Officer.Under the new DHO, focus is more on reducing the number of IMRand MMR and safe delivery at hospital. Under previous DHO,central theme of working was family planning. He emphasisedthat after he took over hospital administration, not a case ofmaternal mortality has been reported. Apart from JananiSuraksha Yozna, two other schemes Shardagram Aarogya Sanjivni(started in July 2012) and Paro are serving pregnant women.These two schemes are state-funded. Under Paro scheme, womenare given kit with baby clothes, nappies, soap, powder etc.
According to Medical Officer, tribal women face acute Irondeficiency. This is generally due to lack of Iron Folic acidin their diet. He admits that malnutrition among women andchildren is a big issue and can only be solved by interlinkingit with food-security, financial security in form of job-
guarantee and proper education facilities. He feels thatgovernment should make more serious effort towards removingmalnutrition that is endemic in tribal women and children. Itis ironical that 2/3 of world maternal and infant mortalityhappen in India. PHC has the task of improving health statusin 16 villages. One ANM in rural area shoulders task ofmanaging around 5-6 villages and 2000 population. There havebeen cases where no new appointment was made after theretirement of one medical staff.
There is no government mobile van in PHC here; instead PHC hascontracted 5 private vehicles owners in case of emergencyreferral. In case of hiring these contractual vehicles,villagers have to pay 7rs per km, remaining is paid by thestate government. Villagers complained that these vehiclestake too much time in reaching the spot so that very oftenthey have to arrange their private vehicle.
Institution of ASHA doesn’t seem to function properly. Thereis a need for overhauling the system by intensifying awarenesscampaign of Out-reach health services like ASHA. Only a veryare aware about it. They don’t even seem to know that whatthis ‘ASHA’ is and if there any position of ASHA in theirvillage? Medical officer himself states that although he knowsthat there are 18 ASHAs are working in his jurisdiction but hehas yet met one ASHA worker. He also seemed to upset about theMPW (Multi-purpose Health Worker) lying vacant in his hospitaleven after he has already requested DHO office to fill thesevacancies as soon as possible.
Tribals like drinking home-prepared liquor. This subsequentlycreates other problems. If they don’t get their home madeliquor, they buy it from the market. This is a greatopportunity cost because this money can be spend on improvinghealth and Nutrition or sending girls to schools. Women folkschew tobacco.
Local self-government institutions like Gram Panchayat canplay a significant role here. But Panchayat doesn’t seem to
give the health enough priority it needs. Water and Sanitationinfrastructure in all villages is in very dismal condition.Routine check-up of Aaganwadis is done by the PHC officials.PHC procures medicines from Zila Panchayat office. Samplesfrom water sources are collected and sent to Rural Hospital inKhed. Blood transfusion facility is only available at RuralHospital in Manchar.
Most of the population here is still excluded from any kind ofBank help (in form of loans, grants and saving accounts).Government’s claim of ‘financial inclusion” has not reached tothese unfortunate ones. Hardly any tribal household has thebank account which is now consider necessary for any kind offinancial assistance in forms of loan, grants or subsidies.
Section 3: Marginalization of tribals, processes of“Peasantization” and “State Simplification” leading
to poverty and Landlessness
Poor health status of tribal population is directly linked totheir poverty and destitution. Most the tribals are livingunder or slightly above the Poverty Line as defined bygovernment of India. As different studies and reports haveshown that landlessness and poor educational status are veryoften lead to poor utilization of health services. Reverse isalso true, with increasing household income, people investmore and more in merit goods like health and education. Tribalcommunities, which became impoverished and marginalized due totheir alienation from land and forest, the resources on whichtheir survival has depended, loss of livelihoods, the questionof rights of the adivasis to the natural resources, issuesconcerning conservation and the role of local communities, theresistance of the adivasis to the injustice perpetrated by theState, and the responsibility of the state towards nearly 8per cent of the most vulnerable part of our population. Thissection, with the help of literature available on tribal
affairs, looks into the historical processes and pre and post-colonial policies and regulation that have been responsiblefor marginalization and alienation of tribals.
In his seminal article “Forestry in British and Post-BritishIndia: A Historical Analysis”, Ram Chandra Guha looked at thehistorical process which affected the adivasi communities inthe very fundamental way5. Article unravels the process wherebythrough the introduction of forestry policy, management andlegislation, customary rights of the forest communities havebeen progressively curtailed. Guha argues that three is amarked degree of continuity between the colonial and post-colonial forest policy and management in India. While colonialpolicy was essentially guided by the need for “crucial rawmaterial for imperia interests, such as railways and the worldwars’, in the post-independence times it has been ‘thecommercial and industrial interests’, which have directed theforest policy. In spite of lip-service paid to the needs ofthe forest communities in the policy documents, the forestcommunities have experienced a progressive loss of controlover their habitat.
Extending Guha’s argument, Sanjeeva Kumar sees the protest ofthe Garos as an expression of ‘their dissatisfaction with thecolonial natural resource management based on expropriation-encroachment, reservation on forests, imposition of rent,forced labor and infringement on customs’. Kumar makes a veryimportant point that the traditional and time-tested resourcemanagement systems of tribals were ‘replaced by centralizedadministrative rules and institutions, often alien to land andculture’. ‘These interventions’, he argues, ‘can be seen asthe state’s attempt to arrange the natural resources andpopulace in standard categories that simplified its limitedfunction of taxation and maintenance of law and order’.Although he agrees that there is now greater recognition onthe part of the policy-makers of the need for resource5 Guha Ram Chandra, Forestry in British and Post-British India: A Historical Analysis, Economic and Political Weekly
conservation and people’s participation in the forest-management. But, ‘they are in the danger of becoming justanother top-heavy project of ‘standardization’ and state‘simplification’, bereft of people’s involvement andindigenous knowledge’6.
Ashok Upadhyaya unravels the process of what he calls,peasantization, whereby the adivasis of Thane district, inpresent-day Maharashtra, were transformed from being a part ofa subsistence economy to becoming a part of the rent payingformation as tenants and forced labor during the colonialperiod. They were subsumed into a mode of cultivation ‘wheremonetization marked the whole process of circulation ofcommodities, where payment of revenue in cash was mandatory’7.In absence of any institutional and infrastructural facilitieslike credit and market, protection against alienation, largenumber lost their lands to the non-adivasi moneylender-landlord, who emerged as a powerful figure on the villagescene.
Sad part of the story of alienation for tribals is, Union andState governments did nothing to protect the rights ofvulnerable groups. Data on alienation and restoration oftribal land shows that in Andhra Pradesh, Bihar, Gujarat,Karnataka, Madhya Pradesh and Maharashtra, alienation amongthe tribals is remarkably higher both in terms of area andnumber. In Odisha, land alienation cases have been rejectedand many are pending in the court. The above observations aresupported by two studies conducted in Tamil Nadu in the years1989 and 1998, which show that degree of alienation of triballands to non-tribals, institutions and government departmentshas not reduced at all over this period8. Outright sale,mortgage, leasing out and encroachment are the main forms of
6 Kumar Sanjeeva, State Simplification: Garo Protest in the Late NineteenthCentury and Early Twentieth Century Assam, EPW7 Upadhyaya Ashok K., Peasantization of Adivasis in Thane District, EPW8 Selvarajan E., Alienation of Triba Lands in Tamil Nadu: Panel Data Analysis, EPW
land alienation and indebtedness. The small and marginalfarmers have thereby become landless labors.
This land alienation of tribals is not happening only by non-tribals but State is actively acquiring land from a largenumber of tribal cultivators in the name of environmentprotection. The implementation of the Maharashtra PrivateForests (Acquisition) Act nullifies the benefits that accruedto many of the tenants and the landless laborers through theland reforms legislation.
Now applying findings and learning from these articles, onecan easily conclude that tribals living near Chas Kaman damare also the victims of same historical processes thatmarginalized and alienated the tribals in India. In GramPanchayat of Gundelwadi, adivasis used to collect Minor ForestProduce (MFP) for hills in form medication plants, fuel-woodetc and used to leave their cattle for grazing. But whenBritish government passed its draconian Forest Act, 1878,these forest regions in this area were declared property ofState and banned any kind of activity in the forest regionwithout permission of Forest Department. Later on, post-independence governments assured continuity of colonialpolicies by giving one entire hill range to one privatecompany which prohibited any entry into forests by barricadingand stop-overs. So now those same tribals who used to utilizethis hill-range as a common-property resources are nowdependent on same company for their livelihood.
Conclusion: Mobilization and Creating awareness asanswers to tribals inaccessibility to public and
private health care`
Analysis done in this paper shows that tribals remainunderserved by the present healthcare system. This has been
observed in many respects. Below listed are some insightsemerged from the study done among tribal population livingnear Chas Kaman dam:
i. Tribals have inadequate access to quality healthcare, andthis is particularly true for those tribals who are stillliving forested area and are inaccessible through road.
ii. Physical proximity to facilities and the cost oftreatment are two important determinants of access.
iii. Private healthcare providers predominate in bothinstitutional and non-institutional services.
iv. ‘Unqualified’ practitioners form the bulk of privatepractitioners in the studied region and are the mostaccessible source of treatment for many, especially poortribal households.
v. For tribals, public healthcare services are not alwaysfree. Often, they don’t even have medicines or diagnosticequipment, making it necessary for the patients topurchase the product/services from the market.
vi. There are critical gaps in infrastructure especially withrespect to the presence of healthcare centres and well-trained staff.
vii. Out-reach services provided by Primary Health Centers(PHCs) are inadequate in tribal areas.
viii. They are extremely poor. They are not the part of MahatmaGandhi National Rural Employment Guarantee Act. They workas contract laborers or agriculture laborers.
ix. Water and sanitation infrastructure is very poor intribal inhabited areas.
x. Malnutrition level is very high among tribal children.Most of the tribal women have acute anemia.
xi. Landlessness is a common feature among tribals. Theydon’t have any kind of permanent source of livelihood.
xii. One third of the tribal children especially girls don’tgo to school. There is high dropout rate among tribalgirls when they reach at stage for puberty.
Analysis clearly indicates that there is a need of addressingbasic healthcare demands of tribals. State governments havetribal sub-plans for the development of tribal areas but mostof time money allocated to these plans remains unutilized.This money can be utilized in developing infrastructure intribal areas. There are some critical areas where quick gainsare possible if interventions are designed systematically.These areas are:
i. Serious intervention in reducing infant and maternalmortality rates among tribals through awareness campaignsand providing health infrastructure near to their homes.
ii. Protection against the financial risks of healthproblems. They should be integrated with Employmentschemes.
iii. Enable and empower them to make informed choices onissues that affect their health and healthcare.
iv. Universal provision of a minimum level of high quality,high impact health services, such as immunization, safemotherhood programmes, communicable disease control.Family planning and first referral clinical services intribal areas.
v. Provide them better access to education and nutrition.
States like Kerela, Tami Nadu and Mijoram have donecomparatively well in area of tribal health. In these states,there is not much disparity between health status of tribalpopulation and general population. It has been possible onlythrough sustained attempt to provide them betterinfrastructure and make them aware about their rights, throughmobilization and participation.