Differentiation of AD, HD and PD on CVLT (Kramer)
10
Neuropsychology, Volume 3, pp. 111-120 Printed in the UK. All rights reserved. 0894-4105/89 $3.00 + .00 Copyright © 1989 Philadelphia Neuropsychology Society Differentiation of Alzheimer's, Huntington's, and Parkinson's Disease Patients on the Basis of Verbal Learning Characteristics JOEL H. KRAMER University of California, San Francisco School of Medicine San Francisco, California BONNIE E. LEVIN University of Miami School of Medicine Miami, Florida JASON BRANDT Johns Hopkins University School of Medicine Baltimore, Maryland DEAN C. DELIS VA Medical Center San Diego, California University of California, San Diego School of Medicine San Diego, California Abstract This study examined the degree to which patients with dementia could be differentiated on the basis of their verbal learning characteristics. Patients with Parkinson's disease (PD), Huntington's disease (HD), and probable Alzheimer's disease (AD) were administered the California Verbal Learning Test. PD and HD patients were divided into subgroups to control for the severity of overall memory impairment. Discriminant function analysis correctly categorized over 76% of cases. Intrusions, perseverations, and rate of forgetting were the most discriminating variables. Profile differences between HD and PD were sufficiently robust to separate these two groups with reasonable accuracy. These results do not support a simplistic cortical-subcortical dichotomy; rather, individual dementing syndromes have unique patterns of verbal learning performance that are distinct from one another. Keywords: Cortical dementia, subcortical dementia, verbal learning, California. Verbal Learning Test, Alzheimer's disease, Parkinson's disease, Huntington's disease. Address correspondence to: Joel H. Kramer, Psy.D., Memory Clinic & Alzheimer Center, Department of Psychiatry, University of California, San Francisco, 1350 Seventh Avenue, CSBS 228, San Francisco, CA 94143, USA. 111 This document is copyrighted by the American Psychological Association or one of its allied publishers. This article is intended solely for the personal use of the individual user and is not to be disseminated broadly.
-
Upload
johnshopkins -
Category
Documents
-
view
2 -
download
0
Transcript of Differentiation of AD, HD and PD on CVLT (Kramer)

Neuropsychology, Volume 3, pp. 111-120 Printed in the UK. All rights reserved.
0894-4105/89 $3.00 + .00 Copyright © 1989 Philadelphia Neuropsychology Society
Differentiation of Alzheimer's, Huntington's, and Parkinson's Disease Patients on the Basis
of Verbal Learning Characteristics
JOEL H. KRAMER
University of California, San Francisco School of Medicine San Francisco, California
BONNIE E. LEVIN
University of Miami School of Medicine Miami, Florida
JASON BRANDT
Johns Hopkins University School of Medicine Baltimore, Maryland
DEAN C. DELIS
VA Medical Center San Diego, California
University of California, San Diego School of Medicine San Diego, California
Abstract This study examined the degree to which patients with dementia could be differentiated on the basis of their verbal learning characteristics. Patients with Parkinson's disease (PD), Huntington's disease (HD), and probable Alzheimer's disease (AD) were administered the California Verbal Learning Test. PD and HD patients were divided into subgroups to control for the severity of overall memory impairment. Discriminant function analysis correctly categorized over 76% of cases. Intrusions, perseverations, and rate of forgetting were the most discriminating variables. Profile differences between HD and PD were sufficiently robust to separate these two groups with reasonable accuracy. These results do not support a simplistic cortical-subcortical dichotomy; rather, individual dementing syndromes have unique patterns of verbal learning performance that are distinct from one another.
Keywords: Cortical dementia, subcortical dementia, verbal learning, California. Verbal Learning Test, Alzheimer's disease, Parkinson's disease, Huntington's disease.
Address correspondence to: Joel H. Kramer, Psy.D., Memory Clinic & Alzheimer Center, Department of Psychiatry, University of California, San Francisco, 1350 Seventh Avenue, CSBS 228, San Francisco, CA 94143, USA.
111
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

112 J. H. Kramer et al.
Several authors have proposed a distinction between cortical and subcortical dementias (Huber & Paulson, 1985; see reviews by Cummings & Benson, 1984; Whitehouse, 1986). The hallmark feature of cortical dementias is a broad-based decline in cognition involving memory, language, visuospatial ability, calculations, praxis, and gnosis. Neuropathological and neuroirnaging studies indicate significant cortical atrophy and hypometabolism (Jagust, Budinger, & Reed, 1987). Alzheimer's disease (AD) and Pick's disease are typically cited as examples of cortical dementias. The concept of subcortical dementia was introduced in the early 1970s to describe the mental changes accompanying diseases of the brainstem and basal ganglia seen in Huntington's disease (HD) , Parkinson's disease (PD), and progressive supranuclear palsy (Albert, Feldman, & Willis, 1974; McHugh & Folstein, 1973). These dementias have been characterized by memory deficits, psychomotor slowing, and disturbance of mood, with an absence of apraxia, agnosia, or aphasia.
The division of dementias into cortical and subcortical subtypes has been criticized on neuroanatomical grounds (Boller, Mizutoni, Roessmann, & Gambetti, 1980; Hakim & Mathieson, 1979; Tagliavini & Pilleri, 1983; Whitehouse, 1986). It is still possible, however, that the two dementia subtypes can be differentiated on the basis of neuropsychological performance and that such a distinction may be clinically meaningful. A number of investigators have compared subcortically demented patients with cortically demented patients and have found differences in neuropsychological test performance. Huber, Shuttleworth, Paulson, Bellchambers, and Clapp (1986), for example, administered the Mini Mental State Exam (MMSE; Folstein, Folstein, & McHugh, 1975), TrailMaking Test Part A, and measures of language, memory, praxis, visuospatial ability, and depression to AD patients, PD patients, and normal controls. The PD patients were found to have mild impairment of memory and visuospatial ability, intact language and praxis, and clinically significant levels of depression. In contrast, AD patients had language impairment and apraxia in addition to more severe deficits in memory and visuospatial functions. Brandt, Folstein, and Folstein (1988) equated subgroups of HD and AD patients on dementia severity, and investigated whether the two dementias could be differentiated by their pattern of scores on individual MMSE items. Using linear discriminant function analysis, they correctly classified 83 % of the AD cases and 84 % of the HD cases. Importantly, their discriminant function appeared to hold up with a new, albeit small, cross-validation sample.
Studies have also reported different patterns of memory impairment associated with cortical and subcortical dementias. Cummings (1986) characterized subcortical disorders as having predominately recall deficits with improved performance on recognition testing, whereas in cortical dementias, the memory impairment includes both recall and recognition. In support of this distinction, Moss, Albert, Butters, and Payne (1986) found that although AD and HD patients had similar levels of short-delay recall, HD patients showed superior verbal recognition and slower rates of forgetting than AD patients. Tweedy, Langer, and McDowell (1982) reported that PD patients were also partially aided by a recognition format, although they continued to be impaired relative to controls. Differences between cortical and subcortical dementias have also been reported in the rate of intrusion errors (Butters, Granholm, Salmon, Grant, & Wolfe, 1987; Kramer et al., 1988) and the capacity for normal implicit memory, as revealed by semantic priming and motor skill learning (Heindel, Salmon, Shults, Walicke, & Butters, 1989; Shimamura, Salmon, Squires, & Butters, 1987).
Although many performance differences have been found when a cortical dementia has been contrasted with a subcortical dementia, demonstration of such differences is not
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
Verbal Learning in Dementia 113
sufficient to support the validity of a cortical-subcortical distinction. First, it is important to control for the overall severity of the dementia or memory disorder. The validity of some reported differences between dementia subtypes (e.g., Huber et al., 1986) have been called into question because the groups were not equated on overall degree of impairment. Thus, differences in neuropsychological proftles could simply reflect one group being disproportionately more impaired (Mayeux, 1987). Second, it would be important to test several dementia groups. Finding neuropsychological differences between a single cortical dementia and a single subcortical dementia merely establishes that the two diseases are different from one another. To conclude that cortical and subcortical dementias represent meaningful subtypes, it is necessary to show that subcortical syndromes such as PD and HD are more similar to one another, and distinct from cortical dementias such as AD and Pick's disease (Brandt et al., 1988).
The purpose of the present study was to determine the extent to which HD, PD, and AD patients could be discriminated from one another on the basis of their verbal learning characteristics. If subcortical dementias form an identifiable subgroup, then the verbal learning performances of PD and HD patients may be more difficult to discriminate from one another and more easily distinguishable from that of AD patients.
Method
Subjects
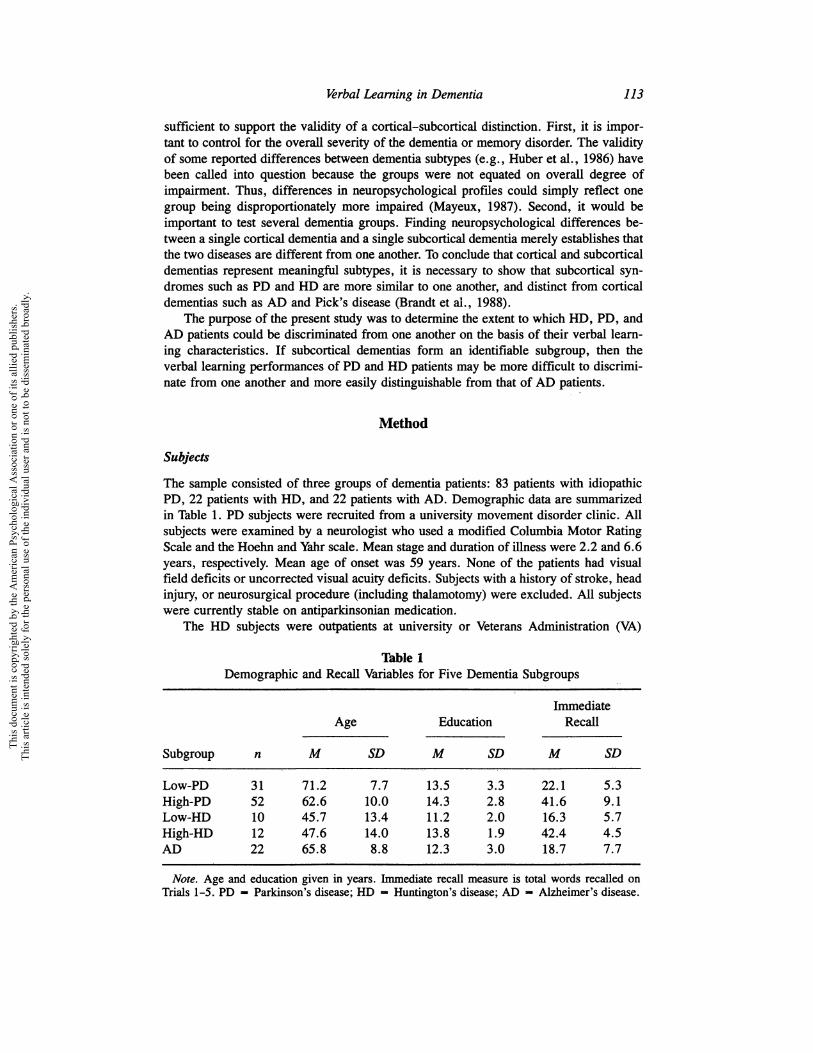
The sample consisted of three groups of dementia patients: 83 patients with idiopathic PD, 22 patients with HD, and 22 patients with AD. Demographic data are summarized in Table 1. PD subjects were recruited from a university movement disorder clinic. All subjects were examined by a neurologist who used a modified Columbia Motor Rating Scale and the Hoehn and Yahr scale. Mean stage and duration of illness were 2.2 and 6.6 years, respectively. Mean age of onset was 59 years. None of the patients had visual field deficits or uncorrected visual acuity deficits. Subjects with a history of stroke, head injury, or neurosurgical procedure (including thalamotomy) were excluded. All subjects were currently stable on antiparkinsonian medication.
The HD subjects were outpatients at university or Veterans Administration (VA)
Thble 1 Demographic and Recall Variables for Five Dementia Subgroups
Immediate Age Education Recall
Subgroup n M SD M SD M SD
Low-PD 31 71.2 7.7 13.5 3.3 22.1 5.3 High-PD 52 62.6 10.0 14.3 2.8 41.6 9.1 Low-HD 10 45.7 13.4 11.2 2.0 16.3 5.7 High-HD 12 47.6 14.0 13.8 1.9 42.4 4.5 AD 22 65.8 8.8 12.3 3.0 18.7 7.7
Note. Age and education given in years. Immediate recall measure is total words recalled on Trials 1-5. PD - Parkinson's disease; HD - Huntington's disease; AD - Alzheimer's disease.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

114 J. H. Kramer et al.
Medical Centers. Diagnosis was made by senior clinicians using standardized procedures (Folstein, Leigh, Parhad, & Folstein, 1986). All patients had choreiform movements and/or impairment of voluntary movement, cognitive and/or psychiatric symptoms, and unambiguous family histories of Huntington's Dise~se.
The AD subjects were patients at VA Medical Centers. They were all clinically diagnosed by an experienced neurologist. All of them met the NINCDS-ADRDA Work Group criteria for clinical diagnosis of probable Alzheimer's disease (McKhann et al., 1984). Medical history, computed tomography (CT) scan, and laboratory workup were used to rule out other causes of cognitive dysfunction.
Procedure
All subjects were administered the California Verbal Learning Test (CVLT; Delis, Kramer, Kaplan, & Ober, 1987) according to standardized procedures. The CVLT consists of five learning trials of a 16-word target list and a single learning trial of an interference list. Following the interference list, memory for the target list is assessed on short-delay free- and cued recall, long-delay (20 min) free and cued recall, and long-delay recognition trials.
Previous research investigating memory disorders in dementia has demonstrated the importance of measuring error types (Fuld, Katzman, Davies, & Terry, 1982; Kramer et al., 1988), learning styles (Ober, Koss, Friedland, & Delis, 1985), encoding (Wilson, Bacon, Fox, & Kazniak, 1983), and retrieval (Tweedy et al., 1982). Accordingly, measures of learning characteristics and error types were also included in the analyses. These measures were frequency and rate of intrusions, perseverations, false positive errors on recognition, rate of acquisition and forgetting, and serial position effects. The total number of words recalled during the five learning trials, which has been shown to correlate highly with composite measures of memory, serves as an index of overall memory functioning (Delis, Cullum, Butters, Cairns, & Prifitera, 1988).
Results
The patient groups were first compared on the total number of words correctly recalled on the five learning trials to determine if there were group differences in overall memory functioning. The AD patients recalled significantly fewer words than the HD and PD patients, F(2, 127) ,... 18.07, p < .0001. No differences were found between the PD and HD groups. To control for overall levels of memory proficiency, the HD and PD samples were divided into subgroups using a cutoff score of 30 words correctly recalled on the five learning trials. This resulted in five groups: 52 high-functioning PD patients (high-PD), 12 high-functioning HD patients (high-HD), 31 low-functioning PD patients (low-PD), 10 low-functioning HD patients (low-HD), and 22 low-functioning patients with AD (see Thble 1). There were no significant differences in recall levels between the two high-functioning groups or among the three low-functioning groups.
A stepwise discriminant function analysis using Wilk's criterion was performed to determine whether the pattern of memory performance could correctly classify the patients into the five groups. The prior probability of group membership was set at .20. Because the HD and PD groups were subdivided on the basis of their immediate recall, levels of recall were excluded from further analyses. Ten variables measuring intrusions, recognition hits and false positives, response bias, perseverative responses, rate of learning, rate of forgetting, interference effects, and percentage of responses from the re-
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
Verbal Learning in Dementia 115
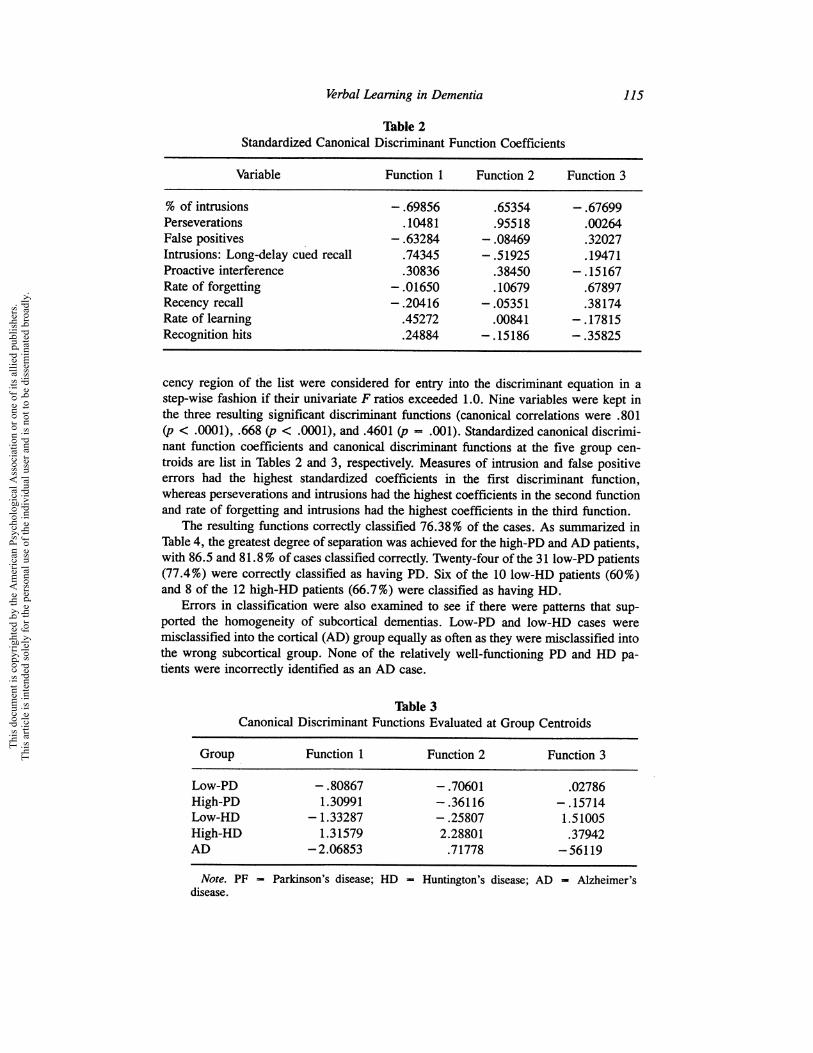
Table 2 Standardized Canonical Discriminant Function Coefficients
Variable Function 1 Function 2 Function 3
% of intrusions -.69856 .65354 -.67699 Perseverations .10481 .95518 .00264 False positives - .63284 - .08469 .32027 Intrusions: Long-delay cued recall .74345 - .51925 .19471 Proactive interference .30836 .38450 -.15167 Rate of forgetting - .01650 .10679 .67897 Recency recall - .20416 -.05351 .38174 Rate of learning .45272 .00841 - .17815 Recognition hits .24884 -.15186 - .35825
cency region of the list were considered for entry into the discriminant equation in a step-wise fashion if their univariate F ratios exceeded 1.0. Nine variables were kept in the three resulting significant discriminant functions (canonical correlations were .801 (p < .0001), .668 (p < .0001), and .4601 (p == .001). Standardized canonical discriminant function coefficients and canonical discriminant functions at the five group centroids are list in Tables 2 and 3, respectively. Measures of intrusion and false positive errors had the highest standardized coefficients in the first discriminant function, whereas perseverations and intrusions had the highest coefficients in the second function and rate of forgetting and intrusions had the highest coefficients in the third function.
The resulting functions correctly classified 76.38 % of the cases. As summarized in Table 4, the greatest degree of separation was achieved for the high-PD and AD patients, with 86.5 and 81.8% of cases classified correctly. Twenty-four of the 311ow-PD patients (77.4%) were correctly classified as having PD. Six of the 10 low-HD patients (60%) and 8 of the 12 high-HD patients (66.7%) were classified as having HD.
Errors in classification were also examined to see if there were patterns that supported the homogeneity of subcortical dementias. Low-PD and low-HD cases were misclassified into the cortical (AD) group equally as often as they were misclassified into the wrong subcortical group. None of the relatively well-functioning PD and HD patients were incorrectly identified as an AD case.
Thble 3 Canonical Discriminant Functions Evaluated at Group Centroids
Group Function 1 Function 2 Function 3
Low-PD - .80867 -.70601 .02786 High-PD 1.30991 - .36116 -.15714 Low-HD -1.33287 - .25807 1.51005 High-HD 1.31579 2.28801 .37942 AD -2.06853 .71778 -56119
Note. PF Parkinson's disease; HD - Huntington's disease; AD - Alzheimer's disease.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
116 J. H. Kramer et al.
Table 4 Classification Results for Five Dementia Subgroups
Predicted Group Membership
Number Low-PD High-PD Low-HD High-HD AD Actual of Group Cases Number % Number % Number % Number % Number %
Low-PD 31 20 64.5 4 12.9 3 9.7 0 .0 4 12.9 High-PD 52 4 7.7 45 86.5 1 1.9 2 3.8 0 .0 Low-HD 10 1 10.0 1 10.0 6 60.0 0 .0 2 20.0 High-HD 12 1 8.3 3 25.0 0 .0 8 66.7 0 .0 AD 22 2 9.1 0 .0 4.5 1 4.5 0 81.8
Note. "Grouped" cases correctly classified - 76.38%. PF Huntington's disease; AD - Alzheimer's disease.
Parkinson's disease; HD -
A multiple-regression analysis was performed to identify which variables were most predictive of diagnosis after accounting for variance due to recall levels. Immediate free recall and variables from the discriminant functions were the predictor variables; diagnosis served as the dependent measure. Immediate free recall was forced into the regression equation first, followed by the remaining variables entered in a stepwise fashion. Two variables were kept in the regression equation, total perseverative responses (F change = 23.8, P < .0001) and percentage of total responses that were intrusions (F change = 8.9, p -< .01).
Because the CVLT's ability to discriminate between the two subcortical groups was of specific interest, a second mUltiple regression was performed using only the PD and HD patients. Immediate free recall was forced into the regression equation first, followed by the remaining variables in a stepwise fashion. Significant increases in R2 resulting from entering total number of perseverations (F change = 39.6, p < .00 1) and the rate of forgetting between the learning trials and short-delay free recall (F change = 6.0, p < .05).
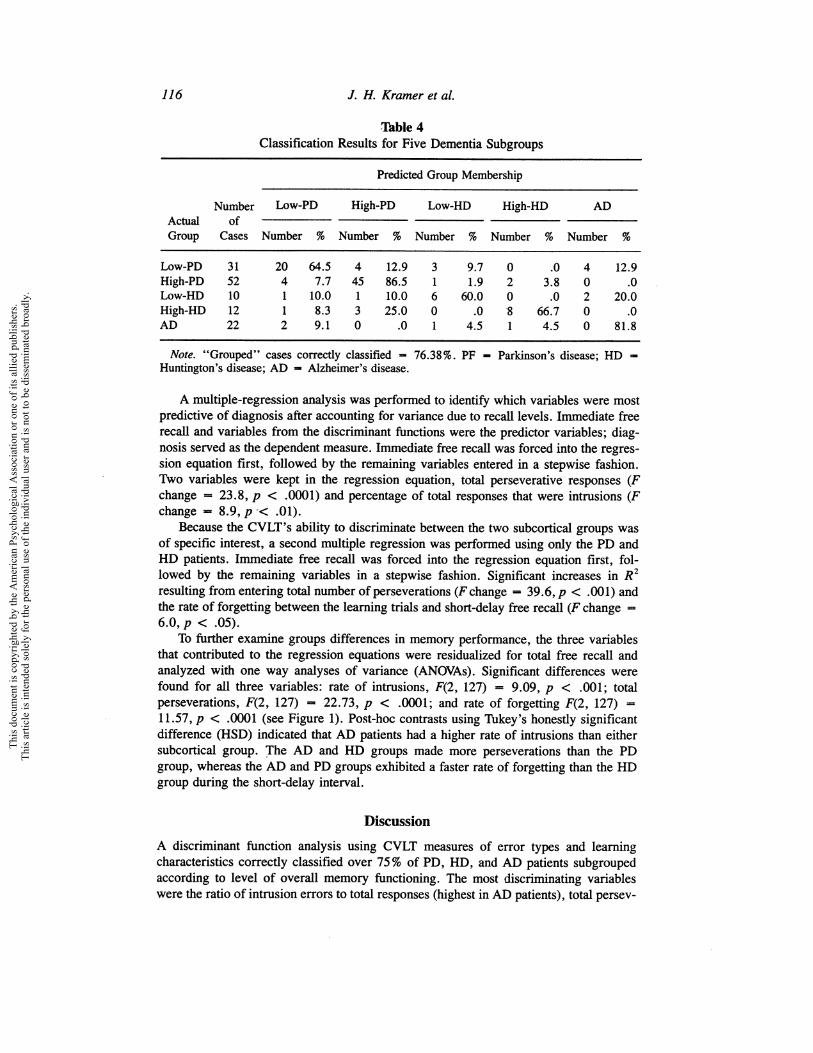
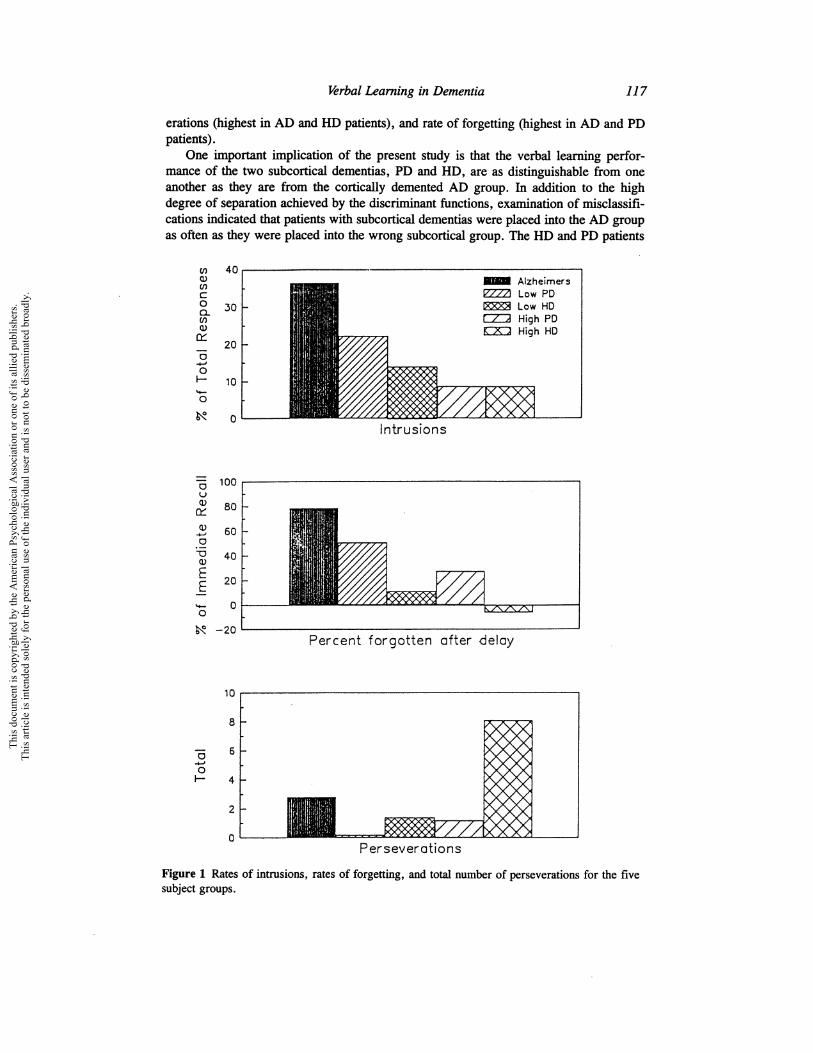
To further examine groups differences in memory performance, the three variables that contributed to the regression equations were residualized for total free recall and analyzed with one way analyses of variance (ANOVAs). Significant differences were found for all three variables: rate of intrusions, F(2, 127) = 9.09, p < .001; total perseverations, F(2, 127) ... 22.73, P < .0001; and rate of forgetting F(2, 127) = 11.57, p < .0001 (see Figure 1). Post-hoc contrasts using Tukey's honestly significant difference (HSD) indicated that AD patients had a higher rate of intrusions than either subcortical group. The AD and HD groups made more perseverations than the PD group, whereas the AD and PD groups exhibited a faster rate of forgetting than the HD group during the short-delay interval.
Discussion
A discriminant function analysis using CVLT measures of error types and learning characteristics correctly classified over 75% of PD, HD, and AD patients subgrouped according to level of overall memory functioning. The most discriminating variables were the ratio of intrusion errors to total responses (highest in AD patients), total persev-
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
Verbal Learning in Dementia 117
erations (highest in AD and HD patients), and rate of forgetting (highest in AD and PD patients).
One important implication of the present study is that the verbal learning performance of the two subcortical dementias, PD and HD, are as distinguishable from one another as they are from the cortically demented AD group. In addition to the high degree of separation achieved by the discriminant functions, examination of misclassifications indicated that patients with subcortical dementias were placed into the AD group as often as they were placed into the wrong subcortical group. The HD and PD patients
CIl 40 Q) - Alzheimers CIl
I2ZZI Low PD c 0 30 ~ Low HD a.
c::::z::::;l High PD CIl Q) CK:) High HD
0:: 20
0 +' 0 I- 10 ..... 0
~ 0 Intrusions
0 100 u Q) 80 0:: Q) 60 ..... 0
u 40 Q)
E 20 E ..... 0 0
~ -20 Percent forgotten after delay
10
8
0 6 +' 0 I- 4
2
0 Perseverations
Figure 1 Rates of intrusions, rates of forgetting, and total number of perseverations for the five subject groups.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

118 J. H. Kramer et al.
differed significantly from one another in the number of perseverations and the rate of forgetting. Our findings are in contrast to the conclusion of Mayeux et al. (1983) that the dementias of AD, HD, and PD are clinically similar, and are consistent with the findings of Goodin and Aminoff (1986) who found evoked potential differences between patients with PD, HD, and AD. Heindel et al. (1989) also reported data inconsistent with the cortical-subcortical distinction. They found different profIles of implicit memory in PD, HD, and AD patients. AD patients had intact motor skill learning and impaired verbal priming, whereas HD patients showed the reverse pattern and PD patients were impaired on both tasks. Thus, our results add to the growing body of evidence indicating that the cortical-subcortical dichotomy may be too simplistic, its utility being limited to more superficial characterizations of dementia SUbtypes.
The finding that AD patients are prone to intrusion errors is in agreement with previous studies (Fuld et al., 1982; Kramer et al., 1988; Wilson et al., 1983). The AD patients made proportionately more intrusion errors than any of the other groups, supporting the hypothesis that intrusions may be characteristic of AD and not simply an attribute of severe dementia. Note, however, that only severely impaired AD patients were included in the study; very mildly impaired AD patients may exhibit a different pattern.
The higher frequency of perseverative errors in the HD patients is consistent with previous reports of perseverations in HD (Josiassen, Curry, & Mancall, 1983). Impaired search and retrieval processes previously reported in HD patients (Brandt, 1985) may also be linked to the tendency of HD patients to repeat previously recalled items on the CVLT. The slower rate of forgetting observed in the HD groups is also consistent with previous research (Moss et al., 1986) .
. It should be stressed that in the regression analyses, overall degree of memory impairment, as measured by levels of immediate free recall, explained a significant proportion of the variance; measures of recognition memory, rate of acquisition, and recency recall did not significantly improve prediction of diagnosis. The finding that recognition memory indices (hits and false positives) were associated with severity level and not specific diagnosis or dementia subtype conflicts with Cummings's (1986) claim that subcortical dementias are distinguishable from cortical dementias by virtue of their enhanced performance on recognition testing. Our results also contrast with those of Moss et al. (1986), who found that although HD and AD patients had equally impaired recognition memory for faces, spatial stimuli, colors, and patterns, HD patients had better verbal recognition memory than AD patients.
It will be important to replicate the results of these discriminant function analyses because some shrinkage in correct classification rates can be anticipated. Also, although the effects of age and education on the variables of interest tend to be minimal, future studies should attempt to reduce differences in age and education between diagnostic groups and subgroups (e.g., high-PD vs. low-PD). Nevertheless, these data support the view that individual dementia syndromes have unique patterns of verbal learning performance that are distinguishable from one another. Butters and his colleagues (Butters, 1985,; Butters, Wolfe, Martone, Granholm, & Cermak, 1986; Heindel et al., 1989) have also shown that reliable differences exist between the memory disorders of HD, Korsakoffs, and AD on laboratory measures of recognition memory. release from proactive interference. rates of forgetting. remote memory, and implicit memory. The present results further indicate that discriminability can be achieved by a single, clinical instrument that is receiving widespread use. The observed differences between the dementias underscore the need for additional investigations of how individual clinical syndromes
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

Verbal Learning in Dementia 119
may have unique properties. The present findings also reinforce Mayeux's (1987) assertion that overall impairment must be controlled for when examining the pattern of deficits amongst different cognitive disorders.
References
Albert, M. L., Feldman, R. G., & WIllis, A. L. (1974). The "subcortical dementia" ofprogressive supranuclear palsy. Journal of Neurology, Neurosurgery, and Psychiatry, 37, 121-130.
Boller, E, Mizutani, T., Roessmann, U., & Gambetti, P. (1980). Parkinson disease, dementia, and Alzheimer disease: clinicopathological correlations. Annals of Neurology, 7, 329-335.
Brandt, J. (1985). Access to knowledge in the dementia of Huntington's disease: Developmental Neuropsychology, 1, 335-348.
Brandt, J., Folstein, S. E., Folstein, M. E (1988). Differential cognitive impairment in Alzheimer's Disease and Huntington's Disease. Archives of Neurology, 23, 555-561.
Butters, N. (1985). Alcoholic Korsakoffs syndrome: Some unresolved issues concerning etiology, neuropathology, and cognitive deficits. Journal of Clinical and Experimental Neuropsychology, 7, 181-210.
Butters, N., Granholm, E., Salmon, D. P., Grant, I., & Wolfe, J. (1987). Episodic and semantic memory: A comparison of amnesic and demented patients. Journal of Clinical and Experimental Neuropsychology, 9, 479-497.
Butters, N., Wolfe, J., Martone, M., Granholm, E., & Cermak, L. S. (1986). Memory disorders associated with Huntington's disease: Verbal recall, recognition and procedural memory. Neuropsychologia, 23, 729-744.
Cummings, J. L. (1986). Subcortical dementia: neuropsychology, neuropsychiatry, and pathophysiology. British Journal of Psychiatry, 149, 682-697.
Cummings, J. L., & Benson, D. F. (1984). Subcortical dementia: Review of an emerging concept. Archives of Neurology, 41, 874-879.
Delis, D. C., Cullum, C. M., Butters, N., Cairns, P., & Prifitera, A. (1988). Wechsler Memory Scale-Revised and the California Verbal Learning Test: Convergence and divergence. The Clinical Neuropsychologist, 2, 188-196.
Delis, D. C., Kramer, J. H., Kaplan, E., & Ober, B. A. (1987). California Verbal Learning Test: Research edition. San Antonio, Psychological Corporation.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). Mini-mental state: A practical method for grading the cognitive state of patient for the clinician. Journal of Psychiatric Research, 12, 189-198.
Folstein, S. E., Leigh, R. J., Parhad, I. M., & Folstein, M. F. (1986). The diagnosis of Huntington's disease. Neurology, 36, 1279-1283.
Fuld, P., Katzman, R., Davies, P., & Terry, R. D. (1982). Intrusions as a sign of Alzheimer dementia: Chemical and pathological verification. Annals of Neurology, 11, 155-159.
Goodin, D. S., & Aminoff, M. J. (1986). Electrophysiological differences between subtypes of dementia. Brain, 109, 11 03-1113.
Hakim, A. M., & Mathieson, G. (1979). Dementia in Parkinson disease: A neuropathologic study. Neurology, 29, 1209-1214.
Heindel, W. C., Salmon, D. P., Shults, C. W., Walicke, P. A., & Butters, N. (1989). Neuropsychological evidence for multiple implicit memory systems: A comparison of Alzheimer's, Huntington's and Parkinson's disease patients. Journal of Neuroscience, 9, 582-587.
Huber, S., & Paulson, G. (1985). The concept of subcortical dementia. American Journal of Psychiatry, 142, 1312-1317.
Huber, S. J., Shuttleworth, E. C., Paulson, G. w., Bellchambers, M. J. G., & Clapp, L. E. (1986). Cortical vs subcortical dementia: Neuropsychological differences. Archives of Neurology, 43, 392-394.
Jagust, W. J., Budinger, T. F., & Reed, B. R. (1987). The diagnosis of dementia with single photon emission tomography. Archives of Neurology, 44, 258-262.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

120 J. H. Kramer et al.
Josiassen, R. C., Curry, I. M., & Mancall, E. L. (1983). Development of neuropsychological deficits in Huntington's disease. Archives of Neurology, 40, 791-796.
Kramer, J. H., Delis, D. C., Blusewicz, M. J., Brandt, J., Ober, B. A., & Strauss, M. (1988). Verbal memory errors in Alzheimer's and Huntington's Dementias. Developmental Neuropsychology, 4, 1-15.
Mayeux, R. (1987). Subcortical dementia. Archives of Neurology, 44, 129-130. Mayeux, R., Stern, Y., Rosen, J., & Benson, D. F. (1983). Is "subcortical dementia" a recogniz
able clinical entity. Annals of Neurology, 14, 278-283. McHugh, P. R., Folstein, M. F. (1973, April). Subcortical dementia. Address to the American
Academy of Neurology, Boston, MA. McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., & Stadlan, E. M. (1984).
Clinical diagnosis of Alzheimer's disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology, 34, 939-944.
Moss, M. B., Albert, M. S., Butters, N., & Payne, M. (1986). Differential patterns of memory loss among patients with Alzheimer's disease, Huntington's disease, and alcoholic Korsakoff's syndrome. Archives of Neurology, 43, 239-246.
Ober, B. A., Koss, E., Friedland, R. P., & Delis, D. C. (1985). Processes of verbal memory failure in Alzheimer's-type dementia. Brain and Cognition, 4, 90-103.
Shimamura, A. P., Salmon, D. P., Squires, L. R., & Butters, N. (1987). Memory dysfunction and word priming in dementia and amnesia. Behavioral Neuroscience, 101, 347-351.
Tagliavini, F., & Pilleri, G. (1983). Neuronal counts in basal nucleus of Meynert in Alzheimer disease and in simple senile dementia. Lancet, 1,469-470.
Tweedy, J. R., Langer, K. G., & McDowell, F. H. (1982). The effect of semantic relations on the memory deficit associated with Parkinson's disease. Journal of Clinical Neuropsychology, 4, 235-247.
Whitehouse, P. J. (1986). The concept of subcortical and cortical dementia: Another look. Annals of Neurology, 19, 1-6.
Wilson, R. S., Bacon, L. D., Fox, J. H., & Kazniak, A. W. (1983). Primary memory and secondary memory in dementia of the Alzheimer's type. Journal of Clinical Neuropsychology, 5,337-344.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.