
Diarrheal Disease - USAID
230
Implementing Diarrheal Disease Control Programs The PRITECH Experience Edited by Karen White and Eileen Hanlon Management Sciences for Health Academy for Educational Development 1993
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Diarrheal Disease - USAID

ImplementingDiarrheal DiseaseControl ProgramsThe PRITECH Experience
Edited by Karen White and Eileen Hanlon
Management Sciences for HealthAcademy for Educational Development
1993

PRITECH (fechnologies for Primary HealthCare), sponsoredby the U.S. Agencyfor International Development, is a consortium of experienced, internationally known organizations led by Management Sciences fer Health. Subcontractorsinclude the Academy for Educational Development, the Johns HopkinsUniversity School of Hygiene and Public Health, the Program for AppropriateTechnology in Health, the Centre for Development and Population Activities,and Creative Associates International. PRITECH assists developing countriesto implement national diarrheal disease control programs and related activities, often as part of integrated programs of maternal and child health.
This document was funded by the Agency for International Development undercontract #DPE-5969-Z-00-7064-00, project #936-5969.
This book represents the opinions of the authors and does not represent A.I.D.policies or opinions.
This publication may be reproduced ifcredit is properly given. Suggested citation: K. White and E. Hanlon (eds.), "Implementing Diarrheal Disease ControlPrograms: The PRITECH Experience," M.1nagement Sciences for HealthPRITECH Project, Arlington, VA, 1993.ISBN 0-913723-30-4
Design by: Gerald Quinn
Production by: Cesar Caminero, Communications Development, Inc.
Printed on recycled paper.
ii

CONTENTS
Introduction: The PRITECH Experienceby Glenn O. Patterson and FRITECH staff .. ~ 1
Is the PRITfCI Field Mechanism a Model for the Future?A View from the Fieldby Robin Waite Steinwand 9
The Complexity of Health Communications 35
The Ciclopc Innovations in Rural Communication:Reaching the Unreachable Villages in Mexicoby Selene Alvarez L and Peter L Spain 37
zambian Popular Theater Dramatizes Diarrhea Treatmentand Preventionby Paul J. Freund and Benedict Phiri 43
Collaborating for Effective Health Communicationin Cameroonby Robin Waite Steinwand and Hugh Waters 51
Posters, Flyers, and Flipcharts:Usc of Health Education Materials in the Sahelby Elizabeth Herman and Suzanne Prysor-Jones 67
"We Couldn't Have Asked for More!"Lessons Learned in Information Disseminationby Karen White and lisa Dipko 79
Training and the OJIality of Care 95
Integrating Diarrhea Control Traininginto Nursing School Curricula in the Sahelby Suzanne Prysor-Jones 97
Successful Diarrheal Disease Training:Lessons from Cameroonby Robin Waite Steinwand and Ndeso Sylvester Atanga 107
linking Training and Performance: An Evaluationof Diarrhea Case Management Training in the Philippinesby Lawrence J. Casazza and Scott Endsley 123
iii

0IWns of the Ugandan National Diarrhea Training Unit:Steps in the Processby Lawrence J. Casazza 131
Cholera Control Activities in Guyanaand the Role of Training Workshopsby David A. Sack. and C. James Hospcdalcs 149
Improving ORS Supply and Distribution in the Philippinesby David Alt 161
Tapping the Potential of the Private Sector 177
Enlisting the Commercial Sector in Public Healthby Camille Saadc 179
Mobilizing the Private Sector for Public Health in IndollCliaby Lucia Fcrraz-Tabor 193
The Commercialization of ORSin zambia: Problems, Progress, and Prospectsby Paul J. Freund 207
The PRITECH-PROCOSI Collaboration:Working with a PVO Consortium in Boliviaby Ana Maria Aguilar and Peter L. Spain 217
Collaborating with Nongovcmmental Organizationsin Kenyaby Karm E. Blyth 227
iv

INTRODUCTION: THE PRITECH EXPERIENCE
The development of an inexpensive, safe, and effec- Glenn o. Patterson is
tive oral rehydration solution (ORS) revolutionized the tht Projcrl Dircrlor.
management of diarrhea in developing countries. Thissimple technology greatly expanded access to life-savingtherapy for cholera and other dehydrating diarrheas. Itformed the basis for the establishment of diarrheal dis-ease control (COD) programs in more than 100 develop-ing countries throughout the world.
The development of ORS, however, was only thebeg.... Jling of the story. To reach its life-saving potential,O1"S had to be imported or manufactured, packaged,financed, and distnbuted. Health workers had to betrained and supervised in the use of ORS. National policies had to be developed and negotiated. The populationhad to be alerted to the availability of ORS throughappropriate communication channels. Other aspects ofdiarrhea case management-such as the initial homemanagement of diarrhea, indications for referral to ahealth facility, effective feeding recommendations, theappropriate use of antibiotics, and the management ofcomplications-had to be defined. Systems had to be created to manage these tasks, to address problems, and tomonitor and evaluate progress. These activities comprisethe essence of the PRITECH experience.
The PRITECH experience thus refers to a ten-yeareffort to initiate, develop, and support diarrheal diseasecontrol efforts in countries suffering high rates of diarrheal morbidity and mortality. The lessuns learnedinclude successes and failures, challenges and obstacles.The relevance of these lessons extends far beyond the fieldof COD. It is hoped that by documenting them, this volume will facilitate a variety of other disease controlefforts.
Wheit IS PRITECH?
A.LO. initiated the five-year PRITECH (Technologiesfor Primary Health Care) Project in 1983 as a means ofimplementing oral rehydration therapy, one of its twinengines for improving child survival in developing countries (the other engine being immunizations). PRITECH II,the second five-year project, ran from 1988 to 1993. TheOffice of Health in ALO.'s Bureau for Research and
INTRODUCTION: THE PRITECH EXPERIENCE 1

Dcvdopment financed part of the $36 million bu ..~ d forPRITEOI ll. USAID field missions financed the n ....nainingshare through buy-ins for country-specific programs.
During the life of the project, PRITECH operatedtwenty-seven country and regional programs in Africa,Asia, and Latin America. Typically, PRlTECH organized aproject design team that worked with the local USAIDmission and the public health authorities in the countryto plan a multi-year program of assistance. The assistance usually included development or refinement of anational plan of action, implementation of a trainingprogram, initiation of communication activities. financing and coordination of consultant services, and supportofoperations re5edI'Ch. During the second halfof the project, PRlTECH also provided considerable technical inputto help parastatal companies produce ORS and to encourage local commercial production. Resident representatives worked directly with national COD teams to implement country programs. PRITECH also establishedregional offices in Senegal and Cameroon to provide additional support to country programs in the Sahel and inEastern and Southern Africa. Another regional office wasestablished in Honduras to facilitate activities in CentralAmerica.
The project was carried out under the leadership ofManagement Sciences for Health in collaboration withthe Academy for i.ducational Development, the JohnsHopkins University School of Hygiene and Public Health,the Program for Appropriate Technology in Health, theCentre for Development and Population Activities, andCreative Associates International. In all of its work,PRITECH has collaborated closely with the World HealthOrganization, UNICEF, and other public and privatedonors, at both the headquarters level and within individual countries.
Lpssons Lei.1rnecl
Some of the many lessons learned from ten years ofimplementing diarrheal disease control programs aredocumented in this volume. The opening paper discusses the country representative as a mechanism for building capacity within countries and for implementing programs. The first group of papers describes a variety ofmethods, some unconventional, for communicatingmessages about the prevention and home management
2 INTRODUCTION: THE PRITECH EXPERIENCE

of diarrhea. It also includes a dcsaiption of PRITECH'scxtrcmdypopular information dissemination effort. Thesecond section describes a series of prcscrvice and inscrvice programs to train health workers to provide effective case management of diarrhea. Collaboration withnongovernmental organizations and commcrciaJ. companies is the subject of the last section and rcprcscnts thearea in which PRITECH bas done the most innovativework.
These papers, most of which dcscn'bc individualcountry experiences, capture only a fraction of thelessons learned through the PRITECH experience. A number of more gcncrallessons emerge from the combined.experience of the twenty-three country programs:
Systematic training is effective in changing healthworker behavior.
The diarrhea case management approach has established. new standards for the treatment ofsick. children inhealth facilities. Health workers no longer respond to amother's complaint ofdiarrhea with a prescription alone,nordo they recommend withholdir~food and fluids during diarrhea. Although health facility surveys show thatpcrfonnancc is far from ideal, taking a history and conducting a physical exam is now the norm throughout theworld.
COD programs are effective In reducing deaths dueto dehydration.
Prior to the introduction ofORS, health facilities wereoften inundated with children requiring intravenoustherapy for diarrhea-induced dehydration. Now, severely dehydrated children arc rarely SCC11. This is probablybecause caregivers arc administering fluids and seekinghdp early in the course of the illness.
Continued feeding during diarrhea and nutritioncounseUng are critical components of diarrheacase management.
Cardully conducted studies have conclusivdyshown that continued feeding during diarrhea not onlycauses no hano, but is actually therapeutic in decreasingthe severity and duration of the diarrhea. In many settings, the prevalence of malnutrition among childrenpresenting to health facilities with diarrhea is very high.
INTRODUCTION: THE PRlTECH EXPERIENCE 3

4
These facts emphasize the importance of nutritionassessment and counseling during these encounters.
The commcrdal private sector can be a valuableally in ina-easing the availability of OKS and inspreading case management messages.
Although public programs have increased the availability of DRS in health facilities, a large untapped market of other consumers still exists worldwide-a marketthat is ripe for increased corporate action. The commercial private sector can complement COO efforts by making DRS a common household item. PRITECH hasacquired substantial experience in enlisting the marketing strengths of the private sector in DRS pr<,duction andsales and in promoting preventive measU1'es such ashandwashing and breastfeeding.
Operations research can be effectively integratedinto COO program activities.
When provided with technical assistance with studydesign and with analysis, national COO programs areboth interested in and able to conduct studies to answerimportant prograIIllnatic questions. Operations researchsupported by PRITECH includes studies of the distribution and use of health education materials, research todevelop culturally appropriate feeding recommendationsfor children with diarrhea, evaluations of the effectiveness of training, investigations into the etiology ofdysentery, and aSSf:ssments of caregivers' performancein preparing sugar-salt solution.
Enthusiastic and committed individuals make adifference in the success of COO efforts.
Many of the successes of the PRITECH Project can beattributed to the commitment of individuals: the diarrhea treatment unit director who created a model training and outreach program, the dynamic program manager who effectively elicited and coordinated supportfrom a varidy of funding agencies, the respected university professor who mobilized support of pediatricians inhis country. An important goal of any disease controleffort must be to identify, nurture, and support theseenthusiastic individuals.
INTRODUCTION: THE PRITECH EXPERIENCE

Although COD programs have made great strides inthe fidds of training, communications, marketing, management, and research, the tasks that lie ahead are at leastas t:haIlcnging as those completed. The PRITECH cxpcriC11CC has idmtified a number of issues that will be keyduring the next tm years of COD efforts.
More effective strategies for encouraging swtamed behavior change among caregivers andhealth workers must be implemented.
Awarmcss of and knowledge about appropriate casemanagcmmt practices are not sufficient to achieve sustained behavior change. Health care workers and caregivers must perceive that these new practices arc of personal benefit to them, and an advantage over eurrmtpractices. COD programs must therefore pay increasedattmtion to understanding what m.:>tivatcs caregiversand health care workers, to presenting recommendedpractices in ways that appeal to their needs, and to supporting and reinforcing desired changes.
CDD programs must compete with other diseasecontrol initiatives in an atmosphere of dwindlingresources.
Although childhood diarrheal deaths have bem drastically reduced, it is estimated that 3 millionchildren continue to die annually from diarrheal diseases. Gains thathave been achieved will be lost if support is withdrawn.In order to maintain interest and funding, programsmust systematically demonstrate their effectivmess andpursue ways of integrating activities with other programs.
Cholera control efforts must be channeled throughnational COD programs In ways that support andstrengthen ongoing COD efforts.
Although more childrm die from non-cholera diarrhea in one day than die ofcholera in one year, there is afCc1J' that the rcsurgmce of cholera in Africa and theAmericas will distract attention and funds from CODprograms. Cholera control committees have been created outside of the national COD programs, often withhigher political status, and sometimes without the participation of the COD program personnel. When appro-
INTRODUCTION: THE PRlTECH EXPERIENCE 5

6
priate, COD programs should usc the higher profile ofthecholera program to upgrade their own programs and tobroadm their contacts inside and outside the ministry ofhealth. I.ikcwisc, cholera control efforts should takeadvantage ofexisting channels and mechanisms for CODtraining and communications, while at the same timestrcngthming COD programs.
Integration and decentralization should not bepursued as goals in themselves, but evaluated asstrategies for achieving public health objectives.
Many ministries ofhealth and donors have expressedinterest in integrating COD programs with other programs such as those for the control of measles, malaria,nutrition, and acute respiratory infections. Althoughthere is clearly a good rationale for doing so, integrationitself will not solve chronic problems of suboptimaltraining, inadequate budgets, poor supervision, and difficult logistics. Before large investments arc put intorevising training materials and reorganizing ministries,some key issues regarding integration must be addressed:What precisely is meant by "integration"? What is thebest mixture of child survival programs to be integrated? Is integrated training efficient and effective? Whichprogram components are most amenable to integration?At which levels of the health system does integrationwork?
Similarly, donors and national COD programs havesought to extend the reach ofCOD efforts through dccmtralization of COD program activities to regional or dis.:.triet levels. PRITECH cxpcrimce suggests that, for dccmtralization to promote the achievement of public healthgoals, the following requirements must be met: 1)involvemmt of peripheral COD staff in the developmmtand dissemination of the national COD policy; 2) institutionalized mechanisms for communication betweendiffermt levels and well-defined assigned responsibilities;3) a carefully planned strategy to decentralize trainingand ensure supervision; 4) standardized policies andtools; 5) availability of sufficient resources to the locallevel; and 6) continued and regular supervision by central staff to provide leadership and consistency.
INTRODUCTION: THE PRlTECH EXPEIUENCE

Collaboration with other actors and -allies'" mustbe pursued to expand the reach of the public sector.
These collaborators might include traditional healers, nongovernm.mtal organizations, schools, and com"mcrcial companies.
Service delivery must be adapted to meet the needsof urban populations and other high-risk groups.
Urban slums, refugee camps, and war-stricken areasall contain childrm at high risk for diarrheal diseases.There is still much to learn about effectively reachinghigh-risk populations in a sustainable way. How can aCOD program communicate with households about oralrehydration therapy? How can programs reduce the burdm of disease in overcrowded areas whm governmentresources for mviromnmtal improvements are limitedand populations are growing at an exponential rate?
Oear and comprehensive protocols for the management of dysentery and persistent diarrheamust be implemented.
As programs to promote the availability and usc ofORS achieve success, the number of children dying fromdiarrhea-induced dehydration has dramaticallydecreased. Deaths from other causes of diarrhea-relatedmortality-specifically dysentery and persistent diarrhea-have not been proportionately reduced. Therefore,in some areas, dysentery and persistent diarrhea accountfor roughly 30 to SO percent of diarrhea-associateddeaths in children under age five. Reducing these deathswill be an important challenge for COD programs incoming years.
INTRODUCTION: THE PIU'l'ECH EXPERIENCE 7

IS THE PRITECH COUNTRY REPRESENTATIVEMECHANISM A MODEL FOR THE FUTURE?A VIEW FROM THE FIELD
Minutes from the 1992 meeting of the TechnicalAdvisory Group on diarrheal disease control call attention to the enonnous success of &e country representative mechanism in the PRITEOi Project. (The group ischaired by AI.O.'s Office of Health with representativesfrom UNICEF, the World Bank, the World Health Organization, several universities, and nongovcmmentalorganizations who work in child survival.) The firstpoint listed on which the advisory group reached consensus refers to this success:
PRITECH's use of long-term advisors in developingcountries has been remarkably effective in tenns ofsuccessful program implementation and cost-cffcctivcness. The advisors have developed relationshipswith the local ministries of health, coordinateddonor resources in the COO field, and helped toestablish national health policy. Despite the heavyadministrative burden of establishing and sustaining such long-term programs, the approach meritscontinuation.
Robin Waite Steinwand was theCameroon CountryRqnsmtativc.
L•
BdC!\fjIOllllcl , ..
Long-tenn technical advisors, or cvuntry representatives, are not unique to the PRITECH Project nor arethey the sole answer to increasing the success of development assistance projects. Also, the maintenance of afull-time representative of a single project in-countryentails a considerable cost. Nevertheless, the PRITEOiProject has demonstrated considerable success in the useofresident technical advisors (country representatives) toaid the development of strong national control of diarrheal disease programs.
This paper, written from the perspective of a formercountry representative, looks at the evolution of thecountry representative role. It also identifies the characteristics that have contrib,"ted to the success of thismodel. The paper's purpose is to encourage discussionand consideration of the model for Oeler assistance projects of its kind.
• COUNTRYREPRESENTATlVE MECHANISM
!"revfo'~CJ Pa~e BlaDk9

10
HlsTORICAL CONTEXT
When the PRITECH Project was conccivtd, there wasno intent to place long-term staff in the fidel. Oral rehydration therapy was a proven technology, and it waswiddy believed that countries would require only shortterm consultants from the United States and abroad toimplement programs to promote oral rehydration. Someof the earliest project support was to national CDD programs in the Sahd, where a regional office fidded shortterm consultants in response to country requests. A needwas soon identified, however, to have individuals incountry who could assist the national COD programwith day-to-day follow-up ofplanned activities. Inkeeping with project philosophy to avoid costly in-countryadvisors and a budget that did not include funds for longterm advisors, and to minimize the compensation gapbetween national program staffs and expatriate technical advisors, the first country representatives wererecruited locally for organizational rather than technicalskills. In short, these representatives cost the project lessthan high-profile health professionals and were backedup with strong technical support from a growing regional office.
The success of the Sahd mood brought an increasing realization that money invested in a full-time presence reaped program rewards worth replicating. As thePRITEOI Project expanded into other countries andregions of the world, representatives were identified andhired (mostly locally) with more public health and program management expertise than before, sometimesbecause of availability in-country, sometimes by specific country request. Soon the range of skills and skill levels of the representatives was as varied as the countriesin which they worked. Country programs with full-timetechnical assistance generally progressed more quickly,and funding expanded to permit this important enhancement to the project.
THE PRITECH MANAGEMENT MODEL
Discussion of the PRITEOI country representativemust include the framework within which a representative operates. As a centrally-funded A.I.D. project,PRITECH has a Washington, D.C.-based headquarterswith administrative as well as technical staff. Together
THE COUNTRY REPRESENTATIVE MECHANISM

with regional staffs in Africa and Central America, theyoversee and support country representatives in Africa,Asia, and Central and South America.
Sustained programs-national COD programs thatreceive substantiallong-tcrm support from PRITECHhave country representatives. Intermittent programsreceive only sporadic assistance, sometimes as a first steptoward a fully sustained program. They have no representative and thus are not discussed here.
All country representatives with the PRITECH Projectreceive strong technical and administrative backup fromregional and headquarters staff, but depending on theregion and the particular needs of the country program,there are different management structures for their support. In general, these can be divided into two categories,described below.
COUNTRY REPREsENTATIVEWITH REGIONAL OFFICE SUPERVISION
Two regional offices in Africa support country programs: the Sahel Regional Office, and the Central, Eastand Southern Africa Office. A third, in Central America,handles primarily region-wide programs.
Sahel Regional OfficeThis regional management mood has been quite suc
cessful in meeting the needs of the country programs. Itincludes a regional technical support office with its ownbudget and has representatives in most operational countries. Key characteristics are:• The regional staff consists of senior managers and
technical specialists recruited mostly from within theregion, which strengthens local resources andstrengthens PRITECH's relationships with countries.
• Routine, frequent country visits are budgeted and programmed. Trouble-shooting visits can occur as needed; short trips for specific needs are more feasible.(Travd of technical staff from headquarters reql:.ireslonger trips, planned carefully in advance.)
• Regular staff dcvdopmcnt, such as participation inWorld Health Organization (WHO) orientation ortraining courses, is programmed into a regional budget and plans.
• The regional staffcan facilitate good cross-fertilizationamong countries through visits of country rcpresen-
THE COUNTRY REPRESENTATIVE MECHANISM 11

tatives and their colleagues to other countries in theregion and sharing of problems and solutions byregional staffwith countries in similar circumstances.
• The region draws on a pool of regular consultants tosupplement skills of regional staff when needed.
Central, East, and Southern AfricaUntil recently, only a few of the sustained country
programs have had representatives, while most countryprograms were intermittent programs, supported byvisits as deemed necessary from a regional programmanager. Since there has been only one person in theregional office, countries have depended on a combination ofheadquarters staff, the regional person and a bankof outside consultants for technical support.
Country Representative with no Regional OfficeFor the most part, country programs in this catego
ry have been larger countries in South Asia and Africawith greater in-country technical resources. Their country representatives have been more senior and more technically expert in diarrheal disease control. They tend tobe more autonomous, receiving some technical support,but primarily administrative and financial support fromheadquarters.
St l('lHjtlls of the COlillt ry Rl'prt~Sl\llt(ltlVC!Ml~chlllW)1ll
PRITECH's country representatives have been successful for a number of reasons, some of which are characteristic of long-term advisors in general. Bilateralhealth projects and private voluntary organizations havefor years used a full-time project representative in-country. With the right combination ofpersonalities, this person can greatl} facilitate communications among partiesinvolved in the project area, act as a catalyst, and provideimportant continuity often lacking whea relying solelyon short-term technical assistance.
Some qualities particular to the PRITECH countryrepresentative mechanism, though perhaps not unique,have largely contributed to making this mechanism anoutstanding success of the PRITECH Project. Theseinclude flexibility in funding, strong technical support,an emphasis on building relationships and sustainability, and a mandate to facilitate donor coordination. (Seegeneric position description in Box 1.)
12 THE COUNTRY REPRESENTATIVE MECHANISM

13
THE REPRESENTATIVE AS CATALYST
Full-time presence in countryNot enough C"'ClIl be said of the value of having a pro
ject,representative in place who can build a relationshipof trust with the country program staff, whose role it isto gently nudge policymakerc; to concentrate on CODissues and to follow thrm..:c;h with plans. Although diarrhea is usually among the top priority diseases in a country, a well thought-out action plan may become derailedwhile ministry of health officials deal with other press-
Box 1. Position Description
Title: Country representative
Reports to: Senior program manager
Overall responsibilities:The country representative manages, lmder the direction of the senior program manager, PRITECH's resources for canying out "sustained" countryprograms. The country representative coordinates with lISAID and otherdonors that support the program. The country representative reports to thePRITECH Project director about the progress of the country program.
Specific responsibilities:• Assists the national COO program manager to implement the national plan,providing staff assistance to help organize and administer program activities.• Manage PRITECH activities in accordance with the PRITECH program planand the annual implementation plan. Prepare drafts of the implementationplan and subsequent revisions.• Administer PRITECH funds in accordance with AI.O.'s contract requirements and the contractor's financial management procedures.• Identify program implementation problems and bring them to the attention of the senior program manager and PRITECH Project director.• Prepare regular reports as indicated by PRITECH, including periodic fieldnotes addressed to the PRITECH Project director.• Coordinate with other donors that support the Imtional COD program, andkeep PRITECH's spon'lor (usually lISAIO, or perhaps UNICEF) informedabout the status of program activities.• Facilitate the work of PRITECH consultants, including preparation ofscopesof work and arranging administrative support.
Qpalifications:• Experience working in the country, preferably with health services programs.• Fluency in the language used by the government.• Strong rrumagerial, organizational, and administrative skills.• Training or work experience as an expert in a technical area of COO desirable.• Social science research skills will be important where PRITECH responsibilities include operations research and surveys.
THE COUNTRY REPRESENTATIVE MECHANISM

14
ing health issues, throwing off activities scheduledmonths in advance. Likewise, ministries of health areoften short on support personnel and well-planned activities can fail to happen for lack of follow-up on small butimportant details. There is no substitute for a person whocan help to follow through with small details that requiretime and energy and an understanding of the issues.
Country representatives help the COO team wheremost needed, from the mundane to the highly technical.Their role is not highly defined, so they have been able torespond to changing nat~onal needs in a very timelymanner. This flexibility has !;;o:atly enhanced the level oftrust that develops between the representative and hostcountry officials.
The country representative has also provided important program continuity at times of major personnelchanges within a ministry of health. As an outsider, theTl'Presentative has been able to serve as a bridge betweenthe old and new appointees, with less vulnerability tosuspicions and tensions that often accompany majorshakeups than the host country program staff. This hasbeen true in Cameroon, zambia, Pakistan, Mali, andNiger, among others.
Funding flexibilityPerhaps more than any other characteristic, the abil
ity to disburse funds in a flexible manner has enhancedthe representatives' effectiveness, credibility, and trust.Unlike many project representatives, PRITECH representatives can use country program funds to support localcosts at short notice, if necessary.
This mechanism has given country representatives acertain influence over program direction that donorswith fixed budget line items seldom have. Likewise, therepresentative is able to support creative directions of theministry of health that might otherwise get lost in thefunding process; to advance funds for crucial activitiesbudgeted by major donors when their funds were late inarriving; and to recognize and respond to immediateunforeseen needs of the program. A full-time representative is well-placed to judge the most appropriatemoments to use funds to support real program needs andwhen to hold off and let program managers work outsolutions of their own. All PRITECH financial support, ofcourse, must be within the budget allocations and coun-
THE COUNTRY REPRESENTATIVE MECHANISM

try program strategy and annual workplan approved byPRrrECH headquarters and the A.LD. project officer.
Local recruitment 8r.'d familiarity with countryWhat began out ofbudgetary necessity has proved a
source of great wealth to the PRITECH Project. Mostcountry representatives have been recruited locally.While previous in-country experience is neither a prerequisite to nor a guarantee of success in that country,local recruitment can result in identifying a country representative who has already established professionalcredIbility with the ministry of health and other healthpoHcyrnakers and donors. This also allows the ministryof health to participate more fully in the selection anddecisionmaking process. This selection process overallhas produced a diverse international group of countryrepresentatives--a rich mixture of skills and nationalities. The representative fOWld in-country may be animpartial outsider, able to avoid involvement in ministrypolitics, yet known to key players through past experience with other projects in-country. Ironically, the mostly expatriate COWltry representatives have often been saidto provide Ucontinuity" to ministries of health in whichstaffing and structural changes are frequent.
The country representative in zambia, for example,has been called a unational treasure" for his longstandingrole in health planning. Before joining PRITECH, heworked with the National University of zambia for fiveyears and helped establish a national community healthresearch unit and national primary health care development committees. As the new government in Z..mbia hasembarked on major health policy reforms, the representative has helped to shape those reforms. His intimateunderstanding of the new policy directions has greatlyenhanced his ability to act as a spokesman in Washington, D.C., for these changes, which is all the more usefulfor a COWltry program whose A.LD. support is entirelyfrom central funds.
With previous knowledge of the country and a flexible role, the PRlTECH representative has been able toadapt the PRITECH COO agenda to facilitate achievementof overall program objectives in the light of changinghost-COWltry conditions and personnel.
THE COUNTRY REPRESENTATIVE MECHANISM 15

16
In-c:ounby support of short-term technical assistance
Th~ presence of a country represmtative has madean mormous difference in the effectivmess of short-termconsultants to the COO programs. The representative isin a position to recognize early and respond to ministryof health needs for outside technical assistance. The representative can help ministry staff to better define thetype ofassistance they need, and provides a link to available resources through the network of contacts with theregional and home offictS as well as with the multinational donors. Similarly, the country represmtative canassist th~ ministry with adequate preparation for a consultant, and can oversee and help assure follow-up to thevisit. The country representative can also help the ministry to assure appropriate representation of host country nationals on technical assistance and evaluationteams. This further strmgthms the possibility of appropriate follow-up when the Itexperts" have gone home.
PRITECH generally uses its own regional or headquarters staff, plus a core of familiar consultants, forshort-term technical assistance. These are people withwhom country represmtatives have easy contact so thatquestions about follow-up or further information needscan be communicated. Very often, the same consultant(s) return several times to the same country.Through this system, the needs of the host country aremore readily met and their confidence in the consultanthas been successfully established.
Support from PRITECHlWasbingtonThe ability of the PRITECH country represmtatives
to provide a broad range of support to national COO programs has bem made possible by the very strong network of technical support as well as financial and administrative back-up which the project offers. PRITECH'stechnical experts work in concert with WHO's COO andAcute Respiratory Infection Programme staff in Geneva;oftm PRITECH works under the auspices of WHO whmimplementing activities in countries. It is this in-housesupport, backed by the technical weight and guidelinesof WHO, which has so enhanced the representatives'credibility.
THE COUNTRY REPRESErlrATIVE MECHANISM

Tedmical expertiseCmmtry representatives are buttressed technically
by a strong network of experts in many areas of diarrheal disease management. The project has in-housetechnical expertise in diarrhea case managemmt, communications and training, operations research, supervision and evaluation, breastfeeding, project managemmt,and private sector oral rehydration salt production andmarketing: A broader range of specialists can be accessedthrough PRITEOI's subcontractors. Through regularsupervision and support visits, a regional technical officer or headquarters staff assigned to the country program can help the cmmtry represmtative and nationalCOO team to assess progress or specific program needs.When there is a difficult decision to make or an unpopular judgmmt on use of funds, this outside person canintervene rather than hinder the representative's relationship with colleagues in-country.
Visits by technical support people (from headquarters, the Sahel Regional Office, or PRITECH's consultantbank) are programmed according to the country program's needs and plans. Because these people work withmany country programs, they facilitate sharing of experiences and program materials across countries.
The PRITECH Information Cmter located at headquarters provides an excellmt resource, sharing the latest technical information as well as infonnation aboutother country programs and materials produced. Theexistence of an in-house infonnation collection and dissemination center not only lessens tum-around time oninformation requests by representatives for the countryprogram, but also provides the represmtatives withappropriate technical material for activities related totreatment providers, }X>licymakers, and oral rehydrationsalt producers. Scientific papers and the timely technicalreviews in the Technical Literature Update on Diarrhea canhelp convince doubting physicians of the benefits of oralrehydration therapy. In countries where up-to-dateinformation is hard to find, the ability to present pertinent documents or to put potential collaborators onPRrrECH's mailing list for technical publications heightens the representative's credIbility on COD substantially.When the Indonesian country representative wanted toconvince a multinational corporation to promote soapfor handwashing to prevmt diarrhea, for instance, sheused sup}x>rting research from the Infonnation Center.
THE COUNTRY REPRESENTATIVE MECHANISM 17

]
18
Fidd notes and other communicationsCmmtry representatives keep regional and head
quarters staff abreast of country program activities andplans through standardized documentation of programexperiences (monthly field notes) as well as telephonecontact when needed. Both are two-way communications. Response to the field notes from headquarters hasplayed an invaluable part in supporting the work of thecountry reprcsmtatives and improving the ability offieldstaff and technical support staff to communicate. Individual members of the technical or administrative teamsread and respond to issues raised with which they canhelp. When the Cameroon representative wrote in herfield notes of initial plans to develop a local mothers'pamphlet on oral rehydration therapy, for instance, theTcchnical Unit immediately sent out samples of othersfrom around the world. Less formal telephone communications with a supervisor provide technical feedback,moral support, and the opportunity to discuss programoptions and issues as needed by the country representative.
Field notes arc copied to COO program managers andUSAIO missions, in addition to PRITECH staff, to document agreements on program plans.
PROMOTION AND FACILITATIONOF COMMUNICATIONS
Communications within the Ministry of HealthWith a primary task to strengthen program man
agement, the country representative frequently encourages and helps colleagues to recognize the importance ofteamwork. As an outsider, usually based in a ministryofhealth office, the country representative can more easily make the first attempt to bring another branch intothe COD planning process. The national COD coordinator may be too junior within the ministry hierarchy totake the initiative to link up other services with the CODprogram or for other reasons may not have pursued theadvantages of integrated programming. Country representatives have quite successfully helped COD programsto extend their planning sphere to include offices ofhealth mucation, maternal and child health, research andplanning, and nutrition.
In the Sahel countries, for example, PRITECH has frequently helped bring COD program managers to work
THE COUNTRY REPRESENTATIVE MECHANISM

with staff of the health education unit; health educationstaff receive training in materials production which thmbenefits all programs.
Communications between the Ministry of Healthand USAID
The PRITEOI representative is oftm based in theministry of health complex, but since PRITECH isfinanced byAI.D., the rcpresmtative is perceived as having some of the authority ofan A.I.D. employee. At thesame time, he or she is seen as having a very detailedunderstanding of ministry programs and problems.Much morc than chiefs of bilateral assistance projects,the country representative is perceived as a helpful broker for the interests of the host government ministry andAI.D. The ministry of health has a representative theycan trust to interpret their programming directions andrequests for assistance and who, with perhaps years ofexperience in country, has developed an intimate understanding of ministry policies IUld goals.
likewise, USAID, whose health sector is increasingly understaffed due to budgetary constraints, can turn tosomeone who works closely with the ministry and is fluent in the national language, and who, being bound byUS government rcguIations for management of funds,can help to interpret those regulations to ministry officiaIs. The representative is also in a good position to findappropriate opportunities to remind ministry officials oftheir commitments to the donors. At the same time, thercprcscntative, through regular written reports and frequent informal visits to USAID, serves as a CDD technical advisor to USAID.
In Pakistan, for instance, where the COD programwas heavily funded by USAID, the PRITECH representative played a crucial role in facilitating communicationsby organizing meetings and providing the governmentand USAID with regular memos and briefings onPRITEOI's and each others' activities. She also promotedand facilitated visits to health centers and project sites byUSAID and by visiting dignitaries such as a US Congressional delegation arrd commcrciaI sector representatives.
Communications with USAlD and A.I.D./WashlngtonCompared to projects with only short-term techni
cal assistance, the PRrrECH country representative greatly reduces the management burdm on AI.D. The repre-
THE COUNTRY REPRESENTATIVE MECHANISM 19

20
sentative helps the national program staff keep theUSAID mission abreast of project issue; as they arise.When short-tmn technical assistance is needed, thecmmtry representative lays the groundwork and assuresfollow up. In Washington, the PRITECH central officebandies nCCtSsary arrangements, usually for its own inhouse staffor frequently used consultants.
Through country technical support visits and country representative communications, the PRITECH regional and headquarters staffs maintain an in-depth understanding ofpolicy directions and program activities. TheAI.D. project officer for the PRITECH Project in Washington meets frequently with headquarters staff, supplementing the program information received fromAI.D.'s country misf.ion. In this way, PRITECH's centraloffice and the AI.D. project officer remain abreast of project activities and can actively promote the project andalert their colleagues at WHO and UNICEF headquartersabout emerging problems in countries that need coordinated action. By extension, the national COO programhas a strong international forum for publidzing its programs and its needs. Ukewise, notable successes can bequickly communicated.
Communications among donorsThe generic job description for a PRITECH country
representative specifies that the representative will fadlitate the coordination of donor activities in COD. Manybroader health projects overlap with COD activities, so inpractice country repK$entatives have fadlitated information sharing for man}! primary health care activities.The perception of the PRITECH representative as moreneutral than someof the major donors enhances the ability to initiate coordination. When the country representative has been in country for some time, personal relationships allow himlher to talk about issues that maynot be discussed in official meetings. 'fllis may help to initiate coordination that was lacking or to diffuse misunderstandings early on. Also, in many countries, thenational COD coordinator is required by ministry ofhealth protocol to follow the hierarchy in order to makecontactwith donor agendes. Through informal contacts,the representative isable to keep donors abreast of important ministry activities in COD and thereby decrease thepossibility of misunderstandings as well as keep COD inthe donors' minds between the important formal min-
THE COUNTRY REPRESENTATIVE MECHANISM
istry contacts. This infonnal network has bem especially important in cmmtries where no fonnal COD coordinating lxxfy has been established.
The country representative uses this coordinationrole to mobilize donor support for the COD programbefore fonnal negotiations begin or for special needswithin a budget period. In several countries PRITECH hassuccessfully garnered the involvement of the private sector in the national COD program. The country representative can more easily approach the private commercialsector and smooth over any fear that discussions withgavcmment will lead to increased regulation of theirbusiness.
In one country, the country representative becameaware through infonnal discussions that a major donorplanned to circumvent communications with the ministry on its five-year funding plan. The representativewas able to apply subtle outside pressure to reintroducerealistic ministry participation in the process.
Coordination with other A.J.D. projectsThe anmtry representative has frequently hdped
USAIDand the ministryofhealth to coordinate COD activities with other AI.D centrally-funded projects, many ofwhich have no full-time representation in country.
It is inherent to the PRmCH rp.presentative's role tohelp the COD program coordinate with bilateral healthprojects to insure integration into global primary healthcare.
Although the country representative mood has successfullyenhanced the PRrrECH Project's ability to support national COD programs around the world, a fewkey issues have recurred throughout the life of the project which bear analysis here. As increasingly projectsengage full-time technical assistance, it is hoped that thelessons of the PRrrECH Project will help other projectsmake informed decisions.
STRONO PREsENCE VERSUS THE RIsKOF DEPENDENCY
The primary goals of PRlTECH's country representatives have been to help bolster the COO program in its
THE COUNTRY REPRESENTATIVE MECHANISM 21

22
initial stages and to help the ministry of health to develop the managerial capacity to sustain the program in thelong term. In itself this implies a dilemma, since longterm donor and ministry commitment to the programmay depend heavily on early success.
The country representative has been an importantfactor in keeping the COD program on target, often helping with unforeseen necessities common to a young program. While the need may have arisen as a result ofinadequate planning, a good representative can effectivelydistinguish between immediate, unforeseen needs andthose that should be better planned pr can wait forplanned funds to come through. With time, managerialskills are strengthened so that fewer and fewer situationsrequire quick-fix funding or intervention. The representative, having established credibility and the trust ofministry personnel, can more readily take a hard line onfunding when necessary. Nevertheless, the dangeralways exists that the representative will become tooinvolved, too interested in immediate results to standback and allow program personnel to confront managerial decisions. Ifso, the project risks creating a dependency on the representative's timely interventions. The flexibility so important to the representative and newprogram's success can, if misapplied, hinder the program's long-term sustainability.
Country representatives must dedicate themselves tofostering good managerial habits such as long- andshort-term planning and regular meetings with interested parties. They must daily assess and make judgmentsas to the amount of involvement to take, never usurpingthe host country staff's ownership ofboth program successes and disappointments. The goal is to move gradually from a role of active collaborator to outside technical advisor as the program becomes more firmly plantedin the ministl1' priorities and budget.
RECOMMENl)ATIONS
Both recrui~ent and supervision of country representatives m~~ stress the importance of building sustainability over the rteed to achieve quickprogram growth and success.
It is incumbent on the project, once a representativeis hired to assure slhe does not lose sight of the ultimategoal-a sustainable COD program with strong manage-
THE COUNTRY REPRESENTATIVE MECHANISM

mmt and only sporadic outside assistance. This is anongoing process from orimtation through supervisionand performance reviews.• RLcruitmmt. Selection of a country represmtative
should favor an individual who can maintain theproper pcrspcctive and balance over more technicalqualifications. Good judgmmt, maturity, sensitivity,and humility should figure prominently among applicant qualifications.
• Orientation. A solid orimtation for every employeeshouldclearly emphasize the project's position on sustainability. This might include case studies of difficultsituations encountered by past representatives.
• Supervision and personnel evaluation. Because there isoftm a fine line betwcm sustainability and programachievement, frequent contacts by supervisory personnel from the region and headquarters are necessaryto give the representative an outside clear perspective.Regular perfonnance reviews should include the developmmt of annual workplans, which have the representative address the issue of sustainability versusdependency.
The donor (OSMD) and pro;ect supervisors mustacknowledge that good proj«t management andsustainabllity will not be achieved overnight.
They must not value immediate results to the detriment of consensus-building and the creation of broadnational support for the program.
ExPATRIATE VERSUS HOST COUNTRY NATIONALREPREsENTATIVE
Without a doubt, anyone involved in internationalhealth has debated this issue for years and PRITECH is noexception. PRITECH has chosen to hire primarily expatriates already living in the country of service. There aresome cxceptions-cxpatriates hired from outside thecooperating country and host country or cooperatingcountry nationals. Flexibility has been a key factor, taking into account the wishes ofministry ofhealth officialsas well as availability of appropriat.-: candidates in country. In many cases, PRITECH has bem fortunate to findan individual living in the country and looking for workwho has public health and management experience inother countries as well.
THE COUNTRY REPRESENTATIVE MECHANISM 23

24
The advantages of an expatriate are many. Slhearrives as an impartial outsider, with no political attachment in country. Not duty bound to a local patronagesystem, the expatriate can spend less time denying favorsand can more easily make unpopular decisions. Someonewho has had previous experience with the US govcmment budgetary process can talk more easily with donorsand the USAID mission. If the person has in-countryexperience, he may have established professional credibility with local officials and have a greater understanding of the politics of business in that country. With abasic familiarity of the culture, a locally hired expatriatealso tends to realize more readily the limitations of hisknowledge of the culture. In a large multicultural country, a country national from one region of the countrymay have difficulty admitting to gaps in knowledge ofother regions.
On the other hand, country nationals bring a heightened sensitivity to process to thejob. Keenly aware of thecultural norms and fluent in one or several of the locallanguages, they can involve the right people and understand how not to offend others. However, the compensation package of a country national representative raises myriad problems. If compensated as otherrepresentatives, particularly in a country with few private voluntary organizations and generally low wages,their work can be blocked by abundant jealousy amongless well-paid ministry counterparts. Compensation at alevel commensurate with other nationals but differentfrom representatives in other countries can lead to strainwith the project.
One argument for hiring country nationals as project technical advisors is the need to build local resources.PRITECH has attempted a different approach, in the SahelRegional Office, which has been very successful. Most ofthe staff of the regional office is from the region. Theirknowledge of the region enhances their work and working relationships as technical support people, withoutmany of the hindrances of working in a managerial andadvisory role in their own country. As regional staff,they can avoid the issue of nongovernmental organization salary versus ministry of health salary levels.
Ideally, a conscientious expatriate representative willseek the national COD staff's technical knowledge anddepth of understanding of the problems to complementhis own understanding and perspective. As the program
THE COUNTRY REPRESENTATIVE MECHAMSM

gains strength, it should be far easier for an expatriateadvisor to work himself out of a job than for someonefrom the country who is more emotionally attached. Theexpatriate representative can achieve little, however,without dedicated colleagues-national counterparts.
RECOMMENDATIONS
In general, an expatriate can assume the role ofoutside technical consultant (country representative role) with more success and fewer problemsthan a country national.
If an expatriate can be identified who has alreadyestablished professional cred1bility in country, this hasadditional benefits for the project. If a project plans notto hire country nationals as representatives, this shouldbe stated policy with a clear justification.
A project should have a well-defined and publicized recruitment and hiring policy.
Such a policy details all aspects of the compensationpackage and which categories of individuals have accessto them (country nationals, third country nationals, andUS nationals hired locally, and so on).
Encourage the hiring of local talent and expertise.Local personnel should be recruited when hiring a
representative for a nearby country with a new program, and to staff regional offices and as regular consultants whenever possible.
DECENTRALIZATION VERSUS STRONG TECHNICALAND ADMINISTRATIVE OVERSIGHT
The PRITECH Project is relatively decentralized. Itscountry representatives exercise a great deal of latitudein making judgments about the technical content of theproject, in developing relationships with the ministry ofhealth and other partners, and in defining project direction based on ministry programming needs. This latitude, or flexibility, has contributed to more responsiveproject assistance.
Ironically, effective decentralization is possible onlythrough strong technical and administrative supportfrom the central staff to the representative, their decisionmaker in the field. Frustration ofcentral or field staff
THE COUNTRY REPRESENTATIVE MECHANISM 25
26
has sometimes resulted from lapses in the central systemof support to the field or in communications to and fromthe field.
Some key elements of the support system wereimplemented only as the proj"'d: grew, sometimes aftercostly errors had demonstrated a clear need for them. Forexample, improved financial orientation is gainingmomentum because country representatives not welltrained in accounting would submit confusing financialrecords or make transactions requiring much time andfield visits to correct. For better technical orientation, inthe second phase of the project, new country representatives began participating in a WHO course on COD, giving representatives an early familiarity with the technical jargon and policy directions of ministry of healthpersonnel.
Other components of the central support system,such as headquarters to field communications, startedout on firm footing, but have fluctuated over the life ofthe project. Headquarters staff provided excellent andtimely feedback on all field notes until staff changes andother issues at the central level usurped important timefor this task. Feedback became sporadic and the countryrepresentatives more isolated.
As discussed earlier, the technical resources availableto PRITECH representatives greatly extend both the depthand breadth of technical expertise they bring to theIl..1tiOnal COD program. However, as the project hasgroiVD, it has become increasingly difficult to schedule avisit by the appropriate centrally located technical personat the time most needed. PRITECH's Sahel Regional Office,with its own cadre of specialists, has demonstrated theability to respond more expediently to the country programs that it serves. Because of the lack of funding, thishas not been repIicated for other regions that are geographically far from headquarters.
The project has also experienced occasional difficultiesamong its tiers (headquarters, region, country representative). For example, technical staff who have the advantage of stronger technical skills and a multinational perspective may question a national policy decision whichdoes not seem to concur with international guidelines,though the country representative may defend it as a wellthought-out exception to the guidelines. The regionaloffice may insist on being the conduit for all official communications between headquarters and the country rep-
THE COUNTRY REPRESENTATIVE MECHANISM
•

rescntative, though this can add significant delays if theregional supervisor bas a heavy travel schedule.
RECOMMENDATIONS
Every effort should be made to provide strong central support necessary to enhance and maintaineffective decentralization.
All support-strong technical backup, financial, andadministrative support, and good field to headquarterscommunications-should be with the primary goal ofassuring the full participation of country program staffin the successful development of their COD programs.
Strong technical backup:• Standardize technical orientation for all new country
representatives to include preservice technical briefingsby central staffand early participation in a WHO CODcourse.
• Provide strong support to representatives by technicalresource people (1) in response to needs expressed bythe country program; and (2) through informationupdates distributed to keep the field abreast of currentinternational policy directions. To facilitate the bestuse of technical resources, country representativesshould receive a directory of technical resource peopleand areas of specialization.
• The Sahel Regional Office model for technical supporthas been very effective. To the extent other regions andprojects could benefit, resources should be committedto replicate this experience.
• Information requests must be responded to quickly.PRITECH's Information C~nter has institutionalizedthe capability of rapid and thorough response to allinformation needs related to COD, as well as documentation and sharing of country program experiences. This model or a centralized variation for several projects in a similar field, merits furtherimplemmtation.
Financial and administrative support:All new country representatives should receive rig
orous orientation on contract and A.I.D regulations,company policies, and project financial managementfrom the outset, with early follow-up visits as necessary.It is especially important that a country representative
THE COUNTRY REPRESENTATIVE MECHANISM 27
28
whose job it is to advise the ministry of health on program management have a sound command of financialand reporting requirements for the project.
QocumentatioD and good communications:• Standardize field reports and provide rapid construc
tive response to monthly reports. Docummtation ofproject experiences is one of the greatest missing elemmts in good projects, but timely feedback is probably the greatest incmtive for field staff to devote timeto documenting those experiences. Field reports shouldhave a standardized format, streamlined so as to posethe least burdm to people whose primary role is providing on-site technical support.
• Response to field notes is essmtial and should not besubject to other pressures on headquarters staff.Important clemmts of cmtral feedback to reportsinclude: (1) acknowledgment of communicationswithin short interval; (2) positive nature of response;(3) sharing of experiences (programming dilemmasand solutions); and (4) rapid response by technicalunit and information center to information needsexpressed in reports.
• Field notes (from country represmtative to headquarters) should be copied to all interested parties (CODprogram staff, the USAID health officer, the countryrepresentative's supervisor). The goal is candid reporting that can serve further discussion on programdevelopment. Issues requiring discretionary treatmentshould be handled separately.
• Both country representatives and supervisory staffshould assure that there is adequate communicationon program direction and issues through regularsupervisory visits and informal telephone or other
.communications.
COST OF LONG-TERM COUNTRY REPRESENTATIVES
The introduction to this paper refers to a quote fromthe 1992 Technical Advisory Group report that "the useof long-term advisors...has been remarkably effective interms of successful program implemmtation and costeffectiveness." [emphasis added] There is substantial evidence that the country representatives have been generally effective. But their cost has varied considerably overthe life of the project and no systematic cost-benefit
THE COUNTRY REPRESENTATIVE MECHANISM

analysis of long-term country representatives versus aseries ofshort-term consultants has been conducted. Projects and those who fund them clearly must consider thetrade-offs.
Early in the project, country representatives werehired locally and received few of the benefits contained intheAI.D. Handbook for Contractors. Roughly, the average annual cost for a single country representative on atwo-year contract was less than $50,000 during the firstphase of the project. Today country representatives havea diversity of technical backgrounds (including physicians) and receive the standard benefits package allowedby A.I.D. Exact figures were not available, but someA.I.D. projects budget $200,000 to $275,000 a year tocover a family of four at the high end of the salary scale.
In addition, any consideration of the cost of a resident technical advisor must factor in the expense of thesupport network that so enhances hislher work. Theproject paid an average of $370,000 a year over a sevenyear period for staff salaries and benefits of the SahelRegional Office ($600,000 in a year when full benefitswere in effect), an office that supports five to six countries (four with country representatives). Nevertheless,the existence of technical support in the region allows forless costly and more timely consultancies to the individual programs. (An average one-month consultancy fromthe United States costs $15-20,000, allowing for perdiem, travel, salary, and other expenses.)
On top of the substantial cost to the project of a resident representative, the full benefits package presents thecompany managing the project with an administrativeburden, requiring yet more support staff to oversee itsproper implementation. The growing diversity of overseas staff adds another layer of complexity. Box 2 showsthe number of administrative details that must beaddressed prior to placing a staff member in the field.
Do the significant advantages of full-time countryrepresentatives outweigh the heavy financial cost andmanagement burden of maintaining and supportingthem in the field? The benefits package is the same appliedto all US government employees or US contractors overseas; salary and benefits packages for private voluntaryorganizations, corporations, and international organizations differ almost on a par with their diverse philosophies and fiscal situations. Originally developed to luretechnical experts overseas and to compensate them for
THE COUNTRY REPRESENTATIVE MECHANISM 29

Box2. Employment checklist
10Name CouDtry
UJl.c:wz. 'J1Ibd ClIlUI&IJ CoqIIntIDgCllIUIdrJor..sdla& DatJaaal DallaaalAD....,..
Job .....IICbi Y Y YJobsmtiJIg y y yRNllme y y yA.LD. toDD 1420 Y Y YRafelmllldid(1IDI1 CIDdldate CIDIJ) Y Y YA.LD. pmJlCt ame.r IppravaJa:
Jobdl.;.~ y Y YIIUnltlw traval Y yt ytarK, tam. aDd DIgOtlatkms Y Y YT"~ Y Y YOdmtauaa traftl y yt yt
A.LD. amtrac:tiDg amCi IppronIa:IDmalaJur y Y YFldenlllWdlDum l ·1117watnr Y Y Y
TeDDl at IaigDIDeDt Ippmed Y y Y ~,
IIeDe1lt8 pIaD eDrl:lllmeat Y Y YDINc\ depoIIIt IUtborlzatlaD Y ya yaAmmll pelfonDlDl» ClbjllCttv. Y Y YPJogram UalDlDg Y Y Y
0......""""'"A.LD.~ ame.r IppravaJa:
TrIVIIID aDd froID pelt Y Y YBduCllUaDal travel:
TQ aDd froID us IdIool y Y N/ATQ aDd froID IIdIool outaldlt us y y N/A
RUtrlVll y y N/AHome1M.travel Y Y N/A
UD. CDIItraetlDgamCi IpprovU:Saluy1Dcr...r y y yHIred outaIde US Y Y YSblppIDg trom outIIde US Y Y YStorage OUUIde US Y Y Y8111pDcttlpa:allnltit1taDaJIIidIUS Y y y8111pDcttl~nltit1taDQ1lIIdeUS y y y110m tbID 2 WHU orieDtItJDD or tralDlDg Y Y Y
USAID IDIaIaD ClClIICUmDCM:Pemoa Y Y YIDmalaJur N y4 y4PIJIDIDt In US doUm N Y YTrIVIIID poal' y y yNumber ctwolt mumper"'__Number ctwolt ell,.per"'__Are IppllaDcea pmvtdltd?Colt ct UvIDg quutersLilt ct recognized boUd.,.III -=tIOOl bcXId mquirld?AJIowIDcM:
Pole dlfrerenUal N Y N/APole N y N/ASlJppleIMbtIl paR N y N/ATemporIrJ IodgIDg N y N/A
30 THE COUNTRY REPRESENTATIVE MECHANISM
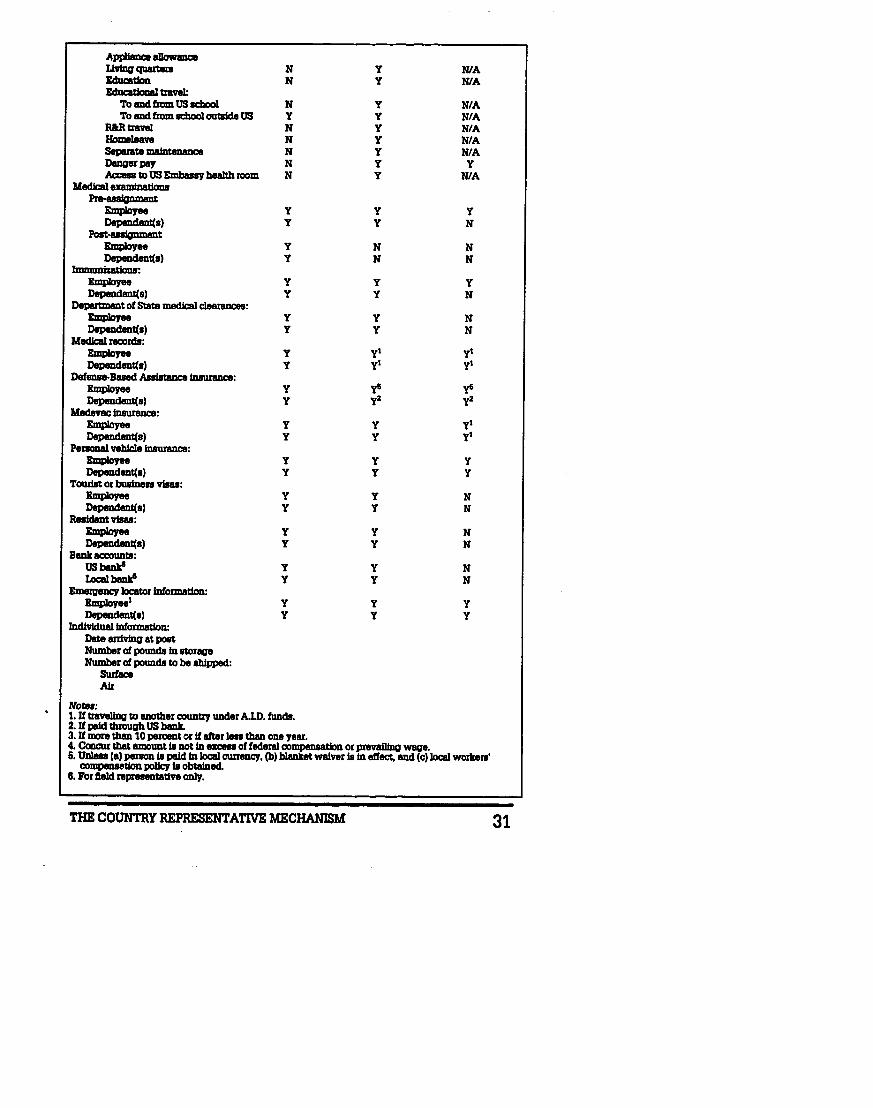
AppIlaDce 8DowIDceUviIlg qIWtEs H y NlAEdncadoD H y NlAEdncadoDaJ travel:
To III1d flam US ICbool H Y N/ATo III1d flam scbool outside US Y Y N/A
lWltmve1 H Y N/AHomeJeave H Y N/ASeparate mabtteneDce N y N/ADaDgerpay H y yAa:ess to US Embassy b8a1th room H Y N/A
Medlcal uamlnatlonsPrlHnlgmnent
Employee Y Y YDependent(s) y Y N
Post-uslgnmentEmployee y H NDependent(s) y H N
ImmuDizRtinns~
Employee y y y~s) Y Y N
Depmment of State medlcal c:le8mDces:Employee y y NDependent(s) Y Y N
Medlcal records:Employee y yl ylDependllDt(s) Y yl yl
DefflD8ltoBased AsslstaDce 1DsurBDce:Employee y yts y6Dependent(s) Y y2 y2
Medev8c 1DsurBDce:Employee y y ylDependent(s) y Y yl
PemoDal vehIcJe iDsuraDce:Employee y y yDependent(s) Y Y Y
TowlBt or buliDess visas:Employee y y NDependent(s) Y Y N
ResideDt visas:Employee y y NDependent(s) Y Y N
BlIDk IICCOUDts:usbllDk' y y NLocalbank' y y N
Emergency locator IDformatioD:lmpIoyeel y Y YDependent(s) Y Y Y
IDd1vIduallDfonnatlon:Date anivtng at postNumber of pounds In storaqeNumber of pounds to be shipped:
SurfaceAir
Notel:1. If traveIlng to lIIIOther country under A.lD. funds.2. Ifpaid tbrough US b8nJL3. If more than 10 percent or If after less than ODe year.4. Ccmcur tbat amount Is not In ezcess of feder8l compensation or preval1lDQ waqe.6. UDIea (8) person Is pe1d In Joc::al cuuency, (b) b1aDket waiver Is In effect, and (e) Joc::al workers'
CllJIII)8IIDtion poUcy Is obtained.8. For lIe1d representative only.
THE COUNTRY REPRESENTATIVE MECHANISM 31

32
dangerous or hardship living situations, distance fromhome and family, higher cost of living, and so forth,some parts of the package may no longer be relevant ornecessary in the 1990s to attract appropriate personnel.
To change the remuneration system for one projectwould achieve little and hurt that project. If the argument is accepted that the country representative mechanism can significantly enhance program success andshould be replicated, then in the face of shrinking aidfunding it will be incumbent on donors and contractorsto review and revise the system across the board.
RECOMMENDATIONS
Long-term technical advisors (country representatives) can be an important component of successfuldevelopment assistance and should be budgeted intomajor project proposals similar to the PRITECH Project.
A.I.D. should consider convening representatives ofgroups working in development overseas to study inearnest and propose a revised standard benefits packagethat better reflects circumstances today (availability ofpersonnel, Iiving conditions and requirements, ease oftravel, and so forth).
A revised package should place less strain on overallproject funds and allow for the widespread use of country representatives in future projects.
A project should have written criteria for determining eligibility for each part of the benefit package.
These standards should reflect the overall development philosophy of the funding organizations and thediverse make-up ofcurrent technical staff. Job applicantsshould be informed of the criteria before being hired.
THE COUNTRY REPRESENTATIVE MECHANISM

- .- .
r-r
T Jlllt-T
:: :=~:::~- ...
I

THE CO:MPLEXITY OF HEALTH COMMUNICATIONS
~municators used to think that communica
tion was a one-way street, deserted but for them.. was the buDet theory of communication,
w en communicators were confident that if the messagewent out (whether spokm or written or broadcast), theaudiCllCe would hear the message, understand it, and adupon it. When oral rehydration salts were being introduced into the developing world in the carly 1980s, therewas still a good deal of this innocent confidcncc-that themiraculous effects oforal rehydration saltswould instantly convince people to seck it out and usc it for every caseof diarrhea. This is a simplification, but only a slight one.
But an innovation is rarely played out on a blank.slate. Rather, an innovation usually involves the introduction of a new produd or technology into a well-trodmarketplace. Just because oral rehydration was new didnot mean that people had not been dealing with diarrheabefore. Indeed, there existed well-cntrcnched diarrheathcrapics-both traditional and Westcrn-that peoplewere already using, for reasons that made sense to them.
Thus, people do not do things without reason. Whilehealth messages try to get people to change their behavior, people already have good reasons for doing whatthey are doing. To get them to change, we need to givethem better reasons. We need to make change rewarding, remembering that the status quo is already rewarding to some degree.
The following papers show that the communicationprocess is a marvdously VIbrant affair. PRITECH's experience in health communications has extended acrossmany countries, addressed many audiences, and usedmany methods. The papers in this section demonstratethe importance of the following dements in a healthcommunication intervention.
USE OF ALTERNATIVE CHANNELS
Most national programs for the control of diarrhealdisease have relied on traditional information and communication channels of the ministry of health system to distribute their educational materials. As the Cameroon andSahd papers show, however, public health workers arc notusing or distributing materials to the best advantage.
THE COMPLEXITY OF HEALTH COMMUNICATIONS
Previous Paqe DIal tl,.
35

36
In addition, many people do not usc governmenthealth centers. In response to these problems, PRITECHfound alternative ways to distribute educational matcriaIsto mothers. These channels included the usc ofvillagemarkets in ruraI Mexico, usc of popular theater in peri-urbanareas in Zambia, and the use of nongovernmental groupsto distribute health education materials in Cameroon.
PARTICIPATION
Not only is participatory learning a good theoreticalapproach, people like it. People like to have their own cultural forms used, like the Zambian popular theater or theMexican lottery games, and people like to choose from aselection of information that they can use, as they dofrom information products offered by the PRITECH andORANA information centers. People also like to be listened to and be taken seriously, a fact that must be considered in any successful implementation effort.
TARGETING SPECIFIC AUDIENCES
Addressing health education interventions to smaller,homogeneous groups is often more manageable and moresuccessful. The messages and materials can be developedto suit the needs of a target group. And communities athigher risk of diarrheal disease can be reached directly, tohelp encourage better care among families that are mostlikely to experience the illness. For example, the Ciclopegroup worked in rural Mexican villages where many parents do not have access to health care services. And thepopular theater groups of zambia traveled through periurban areas, which other health programs had neglected.
REsEARCH AND MONITORING
listening is a basic communication skill, and in thepublic health communication setting, listening is done in asystematic way, called research. Research is simply systematic listening, and is the first step in the communicationprocess. The studies from the Sahel and Cameroon demonstrate the value of and need for research and evaluation.
The days of one-way communication streets probably never really existed. Today's effective communicatorknows that the work is more interesting than that, andleads to so many more opportunities.
THE COMPLEXITY OF HEALTH COMMUNICATIONS

THE ClCLOPE INNOVATIONSIN RURAL COMMUNICATION:REACHING THE UNREACHABLE VILLAGES IN MEXICO
Nobody knows how many small villages there are inMexico, but there are tens of thousands of hamlets withfewer than SOO inhabitants scattered throughout thecountry. For the national health secretary, trying to provide health services broadly and equitably, these manytiny settlements offer unique challenges. People in vill!\ges are at particularly high risk for disease, due to theirisolation, their lack of education, their limited diets, theirlack of access to services, and often their lack of Spanishfluency. And for women, who care for children whenthey are sick, all these disadvantages are compounded bygender. The health secretary, responsible for the world'slargest city as well as thouSands of small towns, has toseek creative solutions to the needs of th~e numerousbut far-flung rural peoples.
In January 1990, the Mexican health secretary askedPRITECH to help him to do just that. PRITECH had beenworking with the national diarrheal disease control program for several years by then, training Ministry ofHealth staff, in a cascade design intended to reach out torural areas. However, all the constraints that make ruralpeople high-risk in the first place had been conspiring todilute training efforts as information diffused from themain towns. To reach beyond these constraints,PRITECH had to come up with a fresh strategy, a truerural communication strategy.
PRITECH enlisted a local consulting group, the Ciclope group. Ciclope had done research with rural indigenous people, specifically in terms of their diarrheal treatment practices, and had developed training strategies towork with them. With a unique track record in medicaland anthropological research among indigenous people,Ciclope enjoyed entree to those communities.
COllsll<lll1ls to ORT Proll1otIon in Rlirdl Ar('ilS
For this first effort, Ciclope focused on two states,Hidalgo and Veracruz, for eight months through December 1991. The infant mortality rate due to diarrhealdehydration remains high in both Hidalgo and Veracruz.In Hidalgo, for 1984, the rate was 647 cases per 100,000
THE CICLOPE INNOVATIONS IN RURAL COMMUNICATION
Sdmc Alvarez L. isdirector of the CiclopcGroup, and Pder L.Spain was a PRITECHSenior Program 0ffi-cer.
37

38
childrm under age one and 689 cases per 100,000 children ages one to five years old.1 For Veracruz, in 1987,the rate of deaths due to diarrhea was 340 deaths per100,000 children under age one and 49 deaths per100,000 children ages one to five.1
In both states, these deaths occur mainly among therural population. Peasants and indigenous peoples of themost distant and scattered communities are the groupsthat contribute most to these infant-mortality rates. Inan analysis of infant and preschool mortality done on the1980 population census, Ciclope had earlier determinedwhich municipalities had the highest infant and childmortality rates in Hidalgo and Veracruz. Moreover, inHidalgo, death records were studied in the civil registriesof a sample of those municipalities identified by the Ciclope analysis of the 1980 census. Records that mentioneddehydration as a primary cause of death for childrenunder five were cross-tabulated with the communitieswhere those deaths occurred. What Ciclope had foundwas this: the number of deaths from dehydrationincreased in direct relation with the distance of the communities from the municipal center (county seat) wherethe civil registries are located.3
Ciclope conducted the same analysis for Veracruz.There, Ciclope found that the majority of the deaths werein areas where seasonal agriculture is practiced, areaswhere there is mainly an indigenous population.· ForVeracruz, however, the health secretariat had determinedthat the areas just outside the principal cities were theareas of greatest diarrheal incidence.'
Most of these deaths are preventable with oral rehydration therapy (ORT). But, in these regions, ORT promotion is hindered by lack of pcrsonnd, lack of access,lack of health-system infrastructure, and the low educationallevd of this population.' Another important consideration for ORT promotion in Hidalgo and Veracruz isthat ORT use is very low in both states, according to anational study done by the federal health secretariat. InHidalgo, 14 percent of diarrhea cases were treated withORT, while in Veracruz the figure was 4 percenU
The specter of cholera had further heightened thepopulation's interest in diarrheal disease control, and Ciclope reported that their ability to reach out to the peoplein their own milieu found an eager acccptance that theyhad not anticipated. To meet the need for information,
THE COMPLEXITY OF HEALTH COMMUNICATIONS

PRITECH supplied cholera materials from the PanAmerican Health Organization to the Ciclopc team.
Rt1dCl1lllCj tilt, RIll it!· PllJ)lIldftlJll TllloUrlll Mclrket Ev~mt:-i
To reduce the cases of infant and prcschoo1 dehydration due to diarrhea among the rural and indigenouspopulations of these two Mexican states, Ciclope decidedto implement, on a state-wide level, the methods validated in their research study AtAn education/communication campaign in rural indigenous communities for thepromotion of ORT," carried out during its education/communication campaign in Parts of Hidalgo from1987to 1990. The approach was to use familiar mediaradio, comic books, face-to-face training of health auxiliaries-in fresh ways, along with presentations atregional markets to bring messages of diarrhea prevention and management to rural people.
The Ciclope team first trained rural health auxiliariesin proPer diarrhea management, and then followed themup in their own communities, offering supervision andguidance for their encounters with village women. Inteaching health auxiliaries about correct diarrh::3 casemanagement, Ciclope employed a clever teaching toola gourd with a face Painted to resemble a baby, withholes and other adjusbnents made to illustrate theprocess arid effects of diarrheal dehydration. The aimwas to draw out the mothers to explain their situationand to adapt new information to it.
In implementing this strategy, Ciclope has movedaway from the top-down teaching approach to one thatrecognizes the abilities of the learner and, indeed, theessential active role of the learner in her/his own educa-
Number of rural health auxiliaries and supervisors trained and numberof training courses given, by state
Hidalgo Veracruz Courses given
Total(total=2t)
AuxiIiarics AuxiIiarics Supavius trained HiJaIgo VcracrozMay 18 6 22 5 51 1 2June 25 3 54 9 91 2 2July 26 4 23 5 58 2 0August 26 6 21 4 57 2 2September 9 6 20 6 41 1 1October 18 5 21 5 49 1 1November 35 6 22 6 56 1 1December 25 3 20 4 46 1 1Total 182 39 203 44 449 11 10
THE CICLOPE INNOVATIONS IN RURAL COMMUNICATION 39

S1wppm could takt homt 4 comic bookdepictirw the same story presented at themarIcet.
40
tion. Ciclope training-whether for health workers,through media, or in the markets-is always participatc.ry, with lots ofgames and exercises that put the learners and teachers into roles quite different from those normally found in a Mexican classroom.
But the keystone of the Ciclope approach was themarket days. Ciclope could not go personally to womenin their viIIages, but market days draw these hard-toreach women together like a magnet, every week. Markets are unique, personal media.
After their training the auxiliaries took part in themarket-day events, which were announced ahead of timeon the radio to alert the region. All during the month ofmarket-day events, the local radio also featured dramasabout diarrhea management, produced in dramatic fashion by professionals, and featuring an entertaining"poetic" answer-man format.
At each market event, the level of energy projectedby Ciclope staff and the retrained health workers had tocompete with the bustle of the market's competingattractions. Wedged beside produce vendors and competing with tapes of ranchero music, Ciclope unfurled their
banners, and hawked their ownwares with a popular Mexicanbingo-like lottery game, completewith prizes to winners and participants, to attract people to the boothand hold them with entertaining
, education (or educational entertainment). It worked: rural people,especially women, came, stayed,won prizes, and went awayhappy-and, we hope, a bit moresavvy about caring for their children with diarrhea.
The learning consisted of ashort tlipchart presentation about adramatic case of diarrhea in whicha little boy is rescued from dehydration and possible death. by a
. mother's proper use of ORT. Themtertainment consisted of the lottery game, the answers to which
came from the tlip-chart presentation. Thus, mtertainmmt reinforcededucation, and the repetition of the
THE COMPLEXITY OF HEALTH COMMUNICATIONS

ORT information was not lost on participants in thegame nor on the many spectators who crowded aroundthroughout the day-including, eventually, some produce vendors and tape salesmen. Thefli~was distributed in comic-book form after the presentation.
In all, 93 market events took place, with the lotterybeing staged 1,251 times. Those who played the lotterytotaled 11,681, with another 7,500 (estimated) personslooking on. Over 15,000 comic books were given out atthe markets, along with over 22,000 packets of oralrehydration salts.
The colorfulJlipchart tells the storyofa mother treating her child with oral dehydrationthuapy.
)Il1PdCt. uf t1j(~ R11Il,t1 C()lllllllllllc<~t 1011 SUilt c~qy
To evaluate the program, interviews were doneacross all the markets with lottery participants and withpeople who had not taken part in the lottery. 1he result:the Ciclopc booth has provided major learning gains forparticipants. While labor intensive, this approach hasshown that it can reach rural, indigenous women, whoare so critical to the health oftheir high-riskchildren, andfor whom market day is their regular contact with theoutside world.
•THE CICLOPE INNOVATIONS IN RURAL COMMUNICATION 41

Furthermore, the federal health secretariat is actively developing plans to broaden the Ciclope approach intoother Mexican states.
In reviewing the overall Ciclope approach and itsimpact, most impressive was the use of multiple channels that were brought to bear on the education of therural womenand their health care providers. Though wemay cite the market events as a clever innovation, thischannel was fully integrated with other more conventional channels like training and mass media. That theintervention was not restricted to one or another intervention, with all the strengths and weaknesses of thatone method, represents an exciting portrayal of the Ciclope methodvis-A-vis this very hard-ta-reach populationof women.
In addition, drawing these women out to speak andexchange ideas in full participatory fashion, even to criticize Ciclope's ideas in a constructive and secure fashion,is a major accomplishment that will serve them in otherways besides their seeking of health care. Most stirringis to see rural women awaken to their potential, toemerge from the timidity that has been a part of theirculture for so long. Bringing them out so that theybecome informed and perceptive health care consumersgoes well beyond the scope of traditional health education. Now convinced of their own power to deal withtheir children's illnesses in certain definite respects, theyare no longer totally dependent on either traditionalindigenous healers or traditional Western medicine.
Notes:1 PIannlng Unit of the Coordinated 5avlca, HIdalgo State, Sm'dariat for Health, 1984.2 EpIdan101ogy Dlrutorate, CoordInattd Strvk:a, Vtracruz State, 1987.3 S. Alvaru, ·Child Survival and ORT In MaIco,· UNAM, 1989.4 Tmth GmmII Cmsus or Pmplc and Homes, 1980. Vtraa'\lZ State, vol. 30, Mcxfoo, 1984., National Congras on Gostromttl"Ology, Xalape, VtrlIa'UZ, Mcxioo, 1990.6 S. Alvaru, ·Child Swvlval and ORT in MaIco,· UNAM, 1989.7 '"Diarrhea Mortality, Morbidity, and TrtatmmtS~ for McxilXl,· Gtntral DIrutorate for Epidaniology, Health 5urdariat, MaIco, 1986.
••
•
42 THE COMPLEXITY OF HEALTH COMMUNICATIONS

ZAMBIANPOPULARTHEATERDRAMATlZESDIARRHEA TREATMENT AND PREVENTION
WhmPRITECHbeganworkinzambiain 1986, therewere few health education materials available on diarrhea and oral rehydration therapy. Nor was there anactive social campaign to promote the local oral rehydration salts, Madzi-a-Moyo. The parastatal companyproducing Madzi-a-Moyo complained that the productwas not being aggressively promoted. The parastatal hadvery limited resources either for distribution or advertising and depended on the Ministry to fulfill these functions.
Paul J. Freund is thePRmCH zambiaCountry Rcprcsmtativc. and BmtdictPhiri is the Imdcr ofthe MaIozo TheatreGroup.
The Maloza Theater Group performs.
To address this problem the PRITECH representativeorganized a health education and social mobilizationcommittee as a subcommittee of the national control ofdiarrheal diseases (COD) coordinating committee. Thesubcommittee, chaired by the Ministry's health education specialist, included representatives from the WorldHealth Organization and PRITECH, and specialists in theareas of nutrition, primary health care, and media. Thesubcommittee's mandate was to outline a COD healtheducation strategy and workplan. The emphasis was ondeveloping cost-effective ways to promote oral rehydration therapy to the community, to increase awareness bydecisionmakers, and to sensitizejournalists to child-survival issues.
ZAMBIAN POPULAR THEATER 43

Why Use Popular Theater?Popular theater is commonly defined as a people's theater speaking to the common man in his language, and dealing with problems of dira:t relevance to hissituation. It is termed -popular" btcause it involves the whole community, notjust small groups or specific social classes. Popular theater can be an effective toolin development programs because it can be used as:·.Entertainmmt. Popular theater can attract and hold the interest of large num-~~~~ .• An oral medium. It can involve the poorest groups and classes who are oftm left
out of devdopmmt activities because of their illiteracy.• A dramatic rrpresentation of local problems. Popular theater provides a codification of reality that can be used by the participants in analyzing their situation.• Collective apression and a communal activity. It creates the context for cooperative rather than individual thinking and action. t
One of the most import?.nt and useful aspects of popular theater is its dramatization of local situations and problems. Popular theater allows people to viewthemselves and their situation in new ways. 1bis cxpcrimce spurs people to discuss their problems and to offer suggestions on what can be done about them.Popular theater is not an md in itself but serves as a catalyst for education andaction. It is a medium of social transformation and a way of making art sociallyrdevant.
1 R. Kidd and M. Byram. 1978. "Popular Thratre and participation in Dcvdopmcnt: Thn:e BotswanaCase Studks." Bosde Tshwaraganang Publications 3. Univasity College of Botswana, Gabarone.
Us lllg POjJulEl I' Thea tel'
The PRITECH representative had previous experiencein using a popular theatergroup in a World Health Organization project on alcohol abuse, and he believed thatthis approach would be effective in promoting oral rehydration therapy. In view of the high costs of radio andtelevision spots and the fact that only 20 percent of zambians own a radio--and even fewer a television-itseemed appropriate to find a solution that was cost-effective, culturally appropriate, community-based, and ableto reach large numbers ofpeople. The use ofpopular theater seemed to satisfy all of these requirements.
A THREE-MONTH 1'RIAL
The subcommittee agreed to implement the methodon a trial basis. Two popular theater groups-the Bakayaand the Maloza-agreed to work full-time on the project.Both had previous experience performing plays on socialissues such as youth unemployment, alcohol abuse, andnutrition.
Each of the groups was asked to develop a short play(twenty to thirty minutes) on the theme of diarrhea and
44 THE COMPLEXITY OF HEALTH COMMUNICATIONS

to include messages on the use of oral rehydration salts,breastfeeding, continued feeding, and the use ofother fluids during diarrhea. The play was also intended to promote the use ofMadzi-a-Moyo. The groups were provided with literature on the national COD program,diarrhea, oral rehydration salts, and related issues.
After three weeks the submitted scripts werereviewed by members of the health education subcommittee and revisions suggested. Each group was thenrequested to present the play for the committee members. The performances, which included singing anddancing, were presented in the local language (Nyanja)and lasted approximately thirty-five to forty-five minutes. After a few more changes suggested by the subcommittee, arrangements were made to draw up a performance schedule for each group.
With formal letters of mtroduction from the Ministry ofHealth, the groups traveled to local communities.Each group performed six times a week, covering fortydifferent peri-urban, high-density compounds in Lusaka. The schedule was arranged sothat the two groups would not beperforming at the same time in thesame compound.
The groups were responsiblefor advertising performance timesand locations within the communities. The Maloza group precededeach performance with a door-todoor campaign informing house- .holds that a play on Madzi-a-Moyowould be held. If the householdmembers could not attend, theywere given a brief description oforal rehydration salts. One memberof the group was costumed in a traditional Makishi mask (used duringinitiation ceremonies) and wasknown as Mr. Madzi-a-Moyo.
The Bakaya group preferredmore extensive singing and drumming to attract an audience for theirplays. The basic structure of the playsby each group was similar: one grouppresented a child getting diarrheathrough poor sanitation and hygiene, Mr. Madzi-a-M~.
ZAMBIAN POPULAR THEATER 45

46
tbm visiting the health center and receiving instructions onuse of oral rehydration salts; the other group focused onbottlefeeding as one of the causes of diarrhea.
The groups were also asked to keep a journal torecord the results of audience discussions and numbersof people attending the performances. Each group followed the performances with discussions with the audience. The performances were held in a variety of placesincluding community halls, market places, outside clinics, work sites, schools, and along busy roadsides. Eachgroup was periodically visited by subcommittee members to monitor their perfonnance, to correct misinformation, and to suggest revisions in their technique.
By the end of a three-month period, the two groupshad succeeded in reaching an estimated 80,000 people,predominantly women and children. Many local political leaders expressed their appreciation for the groups'perfonnances, and clinic staff wrote letters praising theirwork. One of the perfonnances of the Maloza group wasrecorded and broadcast several times on local-languageradio programs. The evaluation by the subcommitteeand the self-assessment by the groups' leaders were verypositive and both felt that the approach was an excellentway to disseminate health education messages and toraise awareness of oral rehydration therapy.
After completion of the first round of performancesthe theater groups concentrated on expanding theirrepertoire, refining their techniques, organizing trainingfor other groups in Lusaka and other provinces, and perfonning for various events (such as national health daysand agricultural shows). Following the success and positive response to the initial three months of performances, Maloza was chosen to carry out another roundof perfonnances. The second period began in 1988 andincluded more emphasis on the proper mixing of oralrehydration salts, the importance of continued feedingduring and after diarrheal episodes, and illness prevention. The subcommittee reviewed and refined the newplays, and asked the theater group to work more closely with community and health workers in the performing areas.
SPREADING THE MESSAGE
One of the concerns of the subcommittee was howto use popular theater to spread the message beyond the
THE COMPLEXITY OF HEALTH COMMUNICATIONS

Lusaka urbanarea. 11le subcommitteedecided to buildoncarlier work by the Department of Cultural Services,which bad promoted the formation of theater groups inlocal districts to present plays on agricultural development and youth Wlemployment. Because many of theselocal theater groups were either from secondary schoolsor working closely with schools, the subcommitteedecided to target teachers interested in drama. UNICEFagreed to sponsor two workshops for drama teachers,which allowed them to share ideas about popular theater, receive instruction from theater artists and Ministryof Health personnel, and to carry out practical work innearby villages. The teachers then returned to theirrespective schools and began teaching their own groupsthe health education plays they bad learned, or creatednewones basedon the infonnation and ideas shared during the workshops.
THE CHOLERA PLAYS
zambia had experienced periodic cholera outbreaksbetween 1978 and 1988 that were confined to the northern regions of the country. But in 1990, cholera quicklyspread to five provinces-resulting in over 2,OOC .ases and144 deaths-marking the beginning of an l;.-iJl"nlic thathas persisted to the present day. The fact that cholera hadaffected urban areas and resulted in a high death rateprompted the Ministry of Health to put into place variousmeasures, including a national cholera surveillance committee, to organize logistics and coordinate and monitordonor support. Cholera treatment centers were set up,health workers were called from other areas to assist, andthe social mobilization campaign was intensified.
Soon after the cholera outbreak of 1990 hit Lusaka,the PRrrECH representative and the Maloza group leaderdiscussed the possibility of using popular theater tospread cholera awareness and prevention messages.Unfortunately, due to the banning of all social gatherings and school closings, the group was unable to perfonn. Nevertheless, the Maloza group leader took the initiative to organize a workshop to assist other theatergroups to develop plays on cholera. Technical supportwas provided by the health education unit, COD program staff, and PRITECH. Seven theater groups took partin the workshop, which included discussions and practice in script development and performance techniques.
ZAMBIAN POPULAR THEATER 47

IllllJdCI.
48
Each group developed plays on various health messages,such as hygiene, control and prevention ofcholera, waterstorage, handwashing, food hygiene, and the importanceof going to the clinic early when cholera is suspected.
The Maloza theater group restarted work in urbanLusaka in March 1991. During the most recent outbreakin Lusaka (October 1992 to March 1993), the theatergroups have continued their involvement in choleraactivities. The Maloza group has focused on developingmore effective ways to. mobilize community actiongroups. They have also worked with schools, in collaboration with UNICEF, to improve hygiene and sanitationpractices. Inaddition, the Maloza cholera play was filmedby the zambia National Broadcasting Corporation andhas been broadcast periodically since November 1992.
Finally, the Maloza group performed for a video oncholera filmed by the Educational Trust for the Environment, sponsored by the World Health Organization. Thevideo, which focuses on positive responses to a choleraepidemic, will be shown to policymakers worldwide.
The usefulness ofpopular theater has more than fulfilled expectations. The groups have not only succeededin raising awareness of oral rehydration therapy in thegeneral community in urban Lusaka, but they have alsotrained drama teachers and theater groups throughoutthe country. The theater groups have also promptedcommunity participation and community actionthrough their efforts.
This includes the formation oflocal cholera committees and community efforts to clean their environment.The theater groups have sensitized politicians, locallcaders, and the media through their participation in localcommunity events.
Moreover, the success of the Maloza group hasinspired others to form theater for development groups,which have developed and performed plays on health anddevelopment issues. The rapid spread of the use of popular theater by other programs and organizations since1986 confirms the value and potential of the approach todisseminate health education and development messages.The use of popular theater for health education caughton quickly and other programs within the Ministry ofHealth (such as AIDS, nutrition, and maternal and child
THE COMPLEXITY OF HEALTH COMMUNICATIONS

health), and nongovcmmental organizations (NORAD,UNICEF, YWCA, Rotary dub) began using the: groupsfor their programs.
The benefit to the COD program has been veryimportant both in terms of raising awareness of oralrehydration therapy in the early stage of the COO program and for the promotion of related issues (such asbreastfeeding, nutrition, immunization, and water andsanitation). Raising awareness of or:u rehydration saltshas led to their increased use, as confirmed by staff in periurban Lusaka clinics.
L(~SSOI1S Learned
Popular theater is a cost-effective, culturallyappropriate way to reach large numbers of people.
Ithas broad implications for COO as well as for otherdevelopment programs, particularly those intended toreach the community and instigate community action.First, in contrast to the $30,000 spent on posters andleaflets, the total expenditure: for two popular theatergroups to work full-time for three months cost less than$5,000. Second, the approach is obviously preferable toimposed programs, which often do not lead to community participation. Popular theater can be adapted to different situations and nontraditionals locations (such asbus stops, markets, and schools), and performances canbe revised to keep them informative and entertaining.
Popular theater does not replace other health education techniques.
The use of popular theater is not an end in itself andit is important to distinguish between informing andeducating. While popular theater may succeed in raisingawareness, it is not entirely appropriate to provide education on proper mixing of oral rehydration salts, or todeliver detailed health education messages.
Popular theater should be used in conjunction withother efforts. For example, theater groups can increasetheir effectiveness if they work with clinic staffby eitherperforming at clinics as part of the clinics' health education program or by having clinic staff attend and participate in audience discussions. Finally, the audio- andvideotaping of popular theater performances can extendthe impact of popular theater considerably.
ZAMBIAN POPULAR THEATER 49

50
Popular theater is partidpatory.A major advantage of popular theater is that it
involves the community as an audience and creates genuine communication between health care workers andthe community. It is not top-down propaganda; insteadit allows free expression that enables the community toanalyze its problems and to develop ways ofdealing withthem. The popular theater approach can easily incorporate audience dialogue to correct popular misconceptionsand to gauge how well the message was received.
The success of popular theater has led to its sustainabllity.
The number of organizations and programs usingpopular theater to deliver health education messages andto promote community action has increased considerably over the years. The popular theater groups are currently in the process of forming their own associationthat will strengthen their ability to respond to Ministryof Health and donor requests and to organize trainingactivities.
THE COMPLEXITY OF HEALTH COMMUNICATIONS

COLLABORATING FOR EF'F'ECTIVE HEALTHCOMMUNICATION IN CAMEROON
Infonnation, education, and communications activities have figured prominently in the evolution ofCameroon's national program for the control of diarrheal diseases (COD). In 1989, prior to launching thecommunications component of the national COD program, Ministry of Health officials mapped out an ambitious program intended to overcome many of the difficulties previously encountered with communicationsactivities in Cameroon and elsewhere.
Multisectoral collaboration was the major emphasisof the first annual communications campaign for COD,launched in 1990, and of the subsequent annual campaigns. The COD program initially took the lead in organizing a wide-ranging coalition at me national level,including representatives of other ministries and members of the press, dedicated to raising public awareness ofthe treatment and dangers of childhood diarrhea. Strongcontacts were established between national- and provincial-level health education representatives, and collaborative COD activities were organized with nongovernmental organizations, community development agents,and community-based religious groups.
The CDD program and PRITECH developed a series ofhigh-quality print materials on the treatment ofdiarrheafor the campaigns. These materials were developed afterconducting studies to determine culturally appropriatemessages. The materials were also extensively pretested.The COD program also emphasized timely evaluation ofthe distribution strategies used and of the materialsthemselves.
This paper chronicles the efforts of the national CODprogram and PRITECH to promote and ensure multisectoral collaboration for CDD communication activities,including the unique advantages and difficulties that thisapproach presented.
O('VC!Uj)lllq il Strilteqy. ,
The national CDD program was launched in 1987,with the production of the country's first five-year planfor the control of diarrheal diseases. Although the program initially emphasized training of key health profes-
HEALTH COMMUNICATION IN CAMEROON
Robin Waite Steinwand and HughWaters are both former Cameroon C0untry Representatives.
51

LUTTONSCONTRE LA DIARRHEE !
...
MateIials Produced by the Cameroonian CDD ProgramProgram Logo
Provincial health educatorsreturned home from the healthcommunication workshop withthree designs for a national pr0gram logo, which each was tofield test in hislher province.Comments received from thepretesting indicated one omission: failure to define the ultimate message of the logo iTtadvance hampered interpretation ofpretest results. Nevertheless, the entire process of involving a multiscctoral group in thedesign and pretesting of the logoproved an cxcdlent experience.
The resulting logo, chosenfinally by national programstaff as best representing themessage of good home management of diarrhea, was printedon stickers for wide distnbutionfor general promotional purposes. It also appears on all printmaterials. Logo tee shirts wereprinted for distn1nltion toimportant collaborators and toMinistry of Health personnel, aswell as for futurl use as prizes
m;~~;ful negotiations by the LET'S FIGHT DIARRHOEA ICOD team with a regionalmatchbox producer resulted in L- -.I
the production of over 1 million matchboxes with the COD logo, with no production or marketing fee. These matchboxes were di"ltributed or sold throughouta vast marketing area, encompassing all of CamcrOO>1 and neighboring Chad andthe Central African Republic.Health Care Calendar
In 1989, PRITECH, the COD program, other services of the Ministry of Health,and other donors worked with the health education service to produce an annual primary health care calendar. Each month deals with a specific health topic,suggesting a theme for htalth education sessions throughout the month. October, a peak month for diarrheal illness, is reserved for the messages from the CODprogram.MixIng Flyer
Pending studies to determine the safety and efficacy of traditional home solutions, national policymakers decided to emphasize the use of oral rehydrationsolution during diarrhea. Therefore, the first flyer designed for use by child caretakers provided accurate mixing and administration instructions for standardone-liter oral rehydration salt packets. The Atelier de Mat&icl Audiovisuel andthe Ministry's health education service assisted with design of the Oyer, whichwas then extensively pretested by the service. The CDD program produced a total
52 THE COMPLEXITY OF HEALTH COMMUNICATIONS

ram.... NdoMI de Lutte
DIARRHEE
DIARRHEE?
QUE DOlT-ON FAIREA LA MAISON CONTRELES DANGERS DE LA
SUIVRELES 4 REGLES O'OR
of 120,000 flyers for distribution tohealth facilities along with oral rehydration salt packets. Instructions forhealth workers onhow to use the flyerwere also prepared, stipulating thateach mother would receive one flyerwith two packets of oral rehydrationsalts for home use.Home Treatmmt Flyer
The national COD program,PRITEOi, the Atelier de MatbidAudiovisud, and the health educationservice produced a second flyer describing four rules ofhome management ofdiarrhea:• Continue breastfccding• Continue feeding• Give plenty of fluids (expressed ingeneral terms)• Seek care at a health center in case ofdanger signs.
One hundred and twenty-five thousand copies of the flyer, plus instructions for health workers, were distnbuted through a combination of publichealth channels and other community-based groups.Reprint of Posters
A three-poster set dCSO'lbing treatment in health facilities was the firstproduct devdoped by the COD program. After three years of use, theCOD program revised and reprintedthe poster series. Revisions to the firsttwo posters took into account suggestions from users and the director of theCOD training program. The thirdposter now more accuratdy paraUdsthe mothers' flyer for home treatment,and reflects revisions in WHO policy.nus second printing produced enoughposters to place one set in every healthfacility in the country. '---------------'
In acknowledgment of the cultural and linguistic diversity of Cameroon, theflyers and posters were produced in three versions:• A French version with appropriate illustrations for northern Cameroon• A French version with appropriate illustrations for southern Cameroon• An English version with appropriate illustrations for southern Cameroon.
sionals, the strategy docummt also defined a criticalhealth communication component for parmt educationfor home case management of childhood diarrhea.
HEALTH COMMUNICATION IN CAMEROON 53

54
The program's early preoccupation with improvingdiarrhea case management by health professionalsthrough training reflected the conviction that good homemanagement behaviors, including timely referral, wouldonlybe achieved and sustained with the support ofhealthcare providers.
Thus the first print materials produced by the program in 1988 were a three-poster series for clinic andhospital staff on the evaluation and treatment of diarrheal dehydration. An adaptation of the World HealthOrganization (WHO) evaluation and treatment chart,they were designed, tested and producedby the COO program and the Atelier de Matmel Audiovisuel (a nongovernmental health education organization). Althoughthe posters primarily described treatment in the healthcenter, one poster guided the health worker in teachingmothers about home management.
Only at the end of the first program year did the COOprogram begin preparation for health education activities. Working in collaboration with the Ministry ofHealth's health education service, the program undertook a national qualitative (that is, focus group) studyof cultural beliefs, attitudes, and practices regardingchildhood diarrhea. The study examined six differentsociocultural areas across Cameroon.
In a workshop at the conclusion of the study, COOprogram staff met with national- and provincial-levelhealth educators, representatives of other Ministry ofHealth services, and collaborating ministries to finalizenational and regional conclusions. They also drafted recommendations for ,policy and future action using thefocus group study results. Pending an opportunity tostudy the safety and effectiveness of the many homesolutions identified in the study, the group decided thatonly water and oral rehydration salts would be promoted for use in diarrhea episodes.
A PRITECH assessment of the national COO program, conducted in March 1989, praised the focus groupstudy as a foundation for developing appropriate healthmessages and recommended that communication activities proceed without further delay. However, the assessment team agreed with the program's decision to beginhealth communication training before a communications effort. The PRITECH team proposed that a national workshop be held to produce "a detailed national communications strategy for COO and operations plans to
THE COMPLEXITY OF HEALTH COMMUNICATIONS

implement the strategy ur.der the leadership of the healtheducation service and the COD team."1
With tacit agreement from the health education service, the COD program staffand PRITECH held a ten-dayintensive communication planning workshop in Junc1989. This was a multisectoral workshop: in attendancewere ten health education service staff; two nationallevel staff; the provincial health educator f;om eachprovince; staff from the nutrition, hygiene and sanitation, and l-r"mary health care services of the Ministry ofHealth; and representatives from CARE, the Atelier deMatmcl Audiovisuel, the national radio and televisionstations, and the Ministries ofAgriculture and Women'sAffairs.
Participants of the workshop were enthusiasticabout the resulting preliminary communication strategy, which built on the recommendations from the focusgroup research and incorporated the strengths ,Jf multisectoral collaboration. In addition to the strat.ogy, thegroup developed and began pretesting models for anational program logo. For many, this was a fit.' experience with pretesting materials.
The communication strategy laid the base for anational COD campaign in six phases, with distinct messages for each phase according to the diarrhea season.Provincial activities were to parallel the national mediacampaign, and print materials were produced and distributed to support the mass media through interpersonal communication. (See the box for a description ofthe materials produced.)
Problems With the NntlOlwl Campcllgn I ,
Most of the COD program's health communicationactivities were carried out in collaboration with othergovernment offices or organizations. Although theseactivities were successful, difficulties within the Ministryof Health and in keeping the collaborators interestedslowed progress. The principal barriers were insufficientfinancing, competition from better funded public healthprograms, and a generally weak health education service.
The national communication campaign for diarrhealdisease control was scheduled to be launched by the minister of health in October 1989, just prior to the peakdiarrhea season. But a number of circumstances intervened to delay the acmallaunch date by four months,
HEALTH COMMUNICATION IN CAMEROON 55

.. 56
until late February 1990. This delay not only affected thetimeliness of the messages, but eroded much of theenthusiasm of the multisectoral group and confusedprovincial health ~ucato~ •. ~" were attempting to follow the initial calendar without support from the ccptrallevel.
ORGANlZATIONAL CHANGES
Shortly after the communication workshop, theMinistry of Health was completely reorganized, placingthe COD program and the health education service undertwo separate directorates. The working relationshipbetween these two services, which had previously beenbased on informal understandings, succumbed to perceived turf battles in the new structure, without formalwritten documentation of the working relationship anddivision of responsibilities. The I~ngthy process of fillingnew IX'sitions delayed resolution of the problem. Furthermore, the already limited COD staff members had tospend most of their time covering unfilled positions, andthe PRITECH representative temporarily and un.wittingly became the primary spokesperson for diarrheal disease. Ministry leadership became too mired in the reorganization and appointment process to provide theoversight necessary for an undertEiking as crucial as ayear-long media campaign.
A COALITION IN JEOPARDY
Concerned about the seriousness of these difficulties,the Minister of Health delayed his support for the campaign. As the official launch date was delayed severaltimes, partners in the campaign, perceiving ambiguity ofthe leadership toward diarrheal disease control, waveredin their support.
This perceived lack of leadership within the Ministryof Health for the COD communication campaign contributed to decreased interest on the part of potential collaborators and the loss of potential human and financialresources to other Ministry programs. Sensing a changein Ministry priorities, a new UNICEF medical officer proposed a shift in UNICEF funding from COD to the vaccination program, with ultimately negative effects for theCOD program. Multisectoral members of the COD coali-
THE COMPLEXITY OF HEALTH COMMUNICATIONS

tion began to lose interest as the campaign appeared lessand less important to the Ministry of Health.
A related problem was competition among donorfinanced disease control programs for the attention ofkey Ministry of Health personnel and the media. TheAIDS control program, for example, became increasingiy important in Cameroon and was well-financed byWHO and other donors. Both Ministry of Health personnel and members of the media were inclined toincrease their involvement with the AIDS program, partly due to the lure of overseas travel opportunities andseminars paying handsome. per diems. The COD program, with comparatively insignificant external financing, successfully relied on strong personal working relationships with key collaborators. However, the COOprogram also had difficulty in achieving recognition andobtaining radio air time (ostensibly free for public healthprograms) as appropriate given the importance of diarrheal diseases in Cameroon.
Ironically, all of the above problems with the CODcommunication campaign called attention to the direneed for COD staff. By the' time the campaign waslaunched, not one but two people were appointed towork full-time for the national COD program.
INADEQUATE SuPPLY OF ORAL REHYDRATIONSALTS
As the programmed campaign launch dateapproached, the COD team learned that a large order fororal rehydration salt packets, scheduled to arrive beforethe campaign, was never placed due to financial d.ifficulties at the national pharmaceutical parastatal. The uncertain supply threw into question a previously firm policyto promote oral rehydration salts instead of locally available home solutions.
INADEQUATE DISTRIBUTIONAND USE OF EDUCATIONAL MATERIALS
Anecdotal evidence and observations by supervisorssuggested that traditional methods for the distribution ofhealth education materials (from the national level downthrough several tiers of the health system to health centers) frequently resulted in materials being stockpiled inan interim warehouse. Inadequate storage conditions,
HEALTH COMMUNICATION IN CAMEROON 57
with the risk of rodent and climatic damage, seriouslydamaged materials before they reached their target audi-ence.
During supervisory visits prior to preparing thecommunication strategy, the national COD teamencountered health center personnel complaining of alack of health education tools while several old educational flipcharts sat dust-covered and out-of-reach in thecenter. Furthermore, supervisors observed that in oneon-one consultations with mothers of small children,health workers rarely made use of available visual aids.
Thus, in developing its communication strategy, thenational COD team decided to emphasize better end-useof materials in two ways:• Testing and evaluating new distribution approaches,
including the use of non-health sectors to reach thepopulation, and
• I:.nhancing communication skills of health and outreach workers who explain and distnbute health education materials.
()"f'!< ()IIIII1Cj tll\~ PIl)I)I{~111C; •
Som~ of the key problems related to the first CODcommunication campaign were resolved in later campaigns. New approaches, such as distnbution of flyersthrough alternative channels, were employed to addressexisting problems.
The 1990-1991 and the 1992-1993 campaigns reiterated the different messages that had been designed forthe first campaign. The messages were slightly revisedand distributed to health education staff at the centraland provinciallcvels as well as to newspaper and radiorepresentatives. The friction between the Ministrydepartments containing the COD program and the healtheducation service was resolved when a formal, writtenagreement was signed authorizing one of the key servicestaff to work nearly full-time with the COD program.
The contributions ofthis service staffmember, and thenew COD staffadded in 1990, enabled individual planningsessions with health education representatives innearly allof the provinces. Increased personnel working with theCOD program permitted new initiatives, including negotiations with a private company for the widespread distribution ofmatchboxes containing the COD logo. Additionally, the service became morc involved in the devdopment
58 THE COMPLEXITY OF HEALTH COMMUNICATIONS
........~'~ .~~'f : ~~.... ~

and pretesting of educational materials for the COD program, particularly th( flyers.
Despite the strength of these personal contacts, andthe importance of COD communication initiatives at theprovincial level and in pilot areas, the national campaignsnever achieved the high profile and visibility that hadbem envisioned at the outset of the COD communicationstrategy.
NEW DISTRIBUTION APPROACHES
The first flyer prcduced by the national COD program, discussing proper preparation of oral rehydrationsalts, was distnbuted almost exclusively through Ministry of Health channels to public health facilities, whereit was intmded to be given to mothers. However, severebottlenecks in the Ministry system and a lack of clarityas to the purpose of the flyer combined to reduce thepotential effectiveness of this important educational tool.
Distribution of the second flyer, on home treatmentofdiarrhea, was designed to avoid bottlenecks in theMinistry of Health distribution system and involve otherpotential distribution agents to supplement distributionthrough the official health system. In addition to controlled distribution through health centers in certainparts of the country, three pilot zones were targeted forintensive distnbution of the flyer. In each zone, themethod of distribution was different, enabling eventualcomparison of the effectiveness of the methods used. Thefollowing are the provinces and distnbution methodsused:• The Extreme North Province, through community
based health centers supported by CARE,• The littoral Province, through the Ministry of Agri
culture's community development agents,• The Northwest Province, through community-based
religious groups.In the Littoral and Northwest Provinces, the COD
program and PRITECH organized short seminars withthe dis~buting organizations, discussing technicalpoints related to diarrhea case management and helpingwith the development of specific plans for distnbution ofthe flyer. During the seminars, emphasis was placed onthe importance of providing personal counseling tomothers receiving the flyer.
HEALTH COMMUNICATION IN CAMEROON 59

IMPROVING USE OF MATERIALS
To hdp health workers make the best use of visualmaterials distributed by the COD program for qualityhealth education, the program implemented the following three-pronged approach:
Active involvement of provindal educatorsPrior to the 1989 communications planning work
shop, the health education service appointed a healtheducator in each province to organize and supervise theservice's activities and to oversee materials distribution.These provincial health education representatives participated in the formulation of the communication strategy and messages, in pretesting materials, and in organizing local efforts for multisectoral distribution. TheCDO team took advantage of a family pIanning workshop to present and explain the mixing flyer to these representatives before its distribution.
Technical trainingThe COD clinical management course was revised to
highlight good health worker-patient communicationsas an essential part of correct case management. Available print materials are now presented and used duringtraining.
Instructions for print materialsThe COO program devdoped detailed instruction
sheets for health and outreach workers to be used witheach flyer. These sheets explain how to use and distribute the flyers and provide a more detailed explanation ofthe technical content of the messages.
Widespread communication activities for diarrhealdisease have been undertaken for a re1ativdy short timein Cameroon. While significant data are available concerning awareness of the dangers and treatment ofchildhood diarrhea, some caution should be used in interpreting the influence of the COD program on such awareness.
The messages emphasized by the COD program'sprint materials and radio spots have been those of effective home treatment for ,iliarrhea: giving liquids (includ-
60 THE COMPLEXlTY OF HEALTH COMMUNICATIONS

ing oral rehydration salts), feeding, brcastfecding, andrecognizing danger signs of dehydration.
A WHO household survey conducted in twoprovinces in 1991 indicates that, in general, theCameroonian population is well aware of the importanceof these measures.2 Although the survey showed a lowoverall use rate of oral rehydration salts (only 5 percentof mothers treating a diarrheal episode in the last twenty-four hours administered oral rehydration salts), rateswere high for continued giving ofliquids during diarrheaepisodes (88 percent ofcaregivers), continued feeding (76percent of caregivers), and ct'ntinued breastfeeding (99percent of breastfeeding mothers). Thirty-seven percentofcaregivers demonstrated knowledge ofall four criteriafor referral to a health facility. Another 1991 surveyshowed that, nationally, 18 percent of caregivers hadgiven oral rehydration salts during a diarrheal episodewithin the last two weeks.3
The evaluation of specific health education effortshas been more conclusive. A health facilities survey in1991 sought to identify the percentage of health workers giving correct advice to carctakers-a key emphasisduring COD training ofhealth workers.4 Fifty-seven percent of health workers interviewed provided effectiveadvice concerning the importance of increased fluids intreating diarrhea; 71 percent provided advice concerningthe preparation of oral rehydration solution.
In 1992, a study of the home treatment flyer and itsdistnbution was carried out in those pilot areas wherethe flyer had been distnbuted. The study showed promising results: 12 percent of caregivers randomly interviewed had received a copy of the flyer; of these, 79 percent had kept it. Sixty-four percent of the flyer'srecipients referred to it when their children subsequently had diarrhea. These results lend credibility to theexperimental approaches used by the COD program todistribute the flyer...
The home treatment flyer study shows the importance ofcounseling in the distnbution of print matcria1s.Mothers who received the flyer and mothers who merely saw it at a health facility showed similar levels ofunderstanding of the message when counseling from thehealth workers was controlled for. In light of this finding, it might be more practical and less expensive to printa more durable educational aide, perhaps printed on loosecardboard and laminated in plastic. However, other fac-
HEALTH COMMUNICATION IN CAMEROON 61

tors should also be considered, including the intangiblepsychological value of providing health workers andother distributing agents with matcriaIs to distribute tothe caregivers. These matcriaIs have a perceived value inthe eyes of individuals receiving them, thereby enhancing the credibility and the professional satisfaction of thedistributors.
Radio, television, and ncw5pllper contnoutions to thecommunication efforts have been strong at times, butsporadic. Typically, newspaper and television coveragehas resulted from individual initiatives or spcciaI eventsand has not had a regular, institutionaIized character.Radio messages have been broadcast with regularity onfive of the ten provincial radio stations, and sporadicalIyby the national radio station. Support from the press ofCOD has only come about through individual-interventions on bchaIf of the COD program-the sustainednationwide coalition that was originally anticipated bythe program never took root.
Ll'SSOllS Ll'dllll'c1
COLLABORATION
From the beginning, the national COD program haspursued a multiscctoral approach to its communicationcomponent. Collaborative relationships with other government services, sectors, donors, and nongovernmentalorganizations can strengthen and enhance the reach of acommunications effort. However, the following pointsshould be addressed in developing and sustaining collaborative relationships for health communications:
The program must have strong commitment andsupport from the Ministry of Health and fromdonors.
The broader the collaborative network, the moreauthority-and financial resources-will be needed tomaintain it.
The Ministry of Health must buDd and support astrong health education service.
Strengthening the service should not be a splinteredeffort by each program or donor-supported project. Theservice should have clear written guidelines for workingwith and meeting the health education needs of the
62 THE COMPLEXITY OF HEALTH COMMUNICATIONS

diverse programs and projects of the Ministry of Health.Successfulmultiscctoral collaboration in communicationrequires a positive collaborative relationship between thelead program (such as COD) and a strong health education service.
other mhUstries and sectors offer varied channelsand reach different audiences.
Collaboration with other sectors, such as agriculture, community development, and women's affairs, canenhance a program's ability to get its messages andmaterials to previously neglected population groups.Similarly, nongovernmental organizations (religiousand community groups, volunteer organizations) pr0vide new outreach channels that usually have fewerbureaucratic and political constraints.
Personal collaborative relationships at the lowerlevels can be valuable.
Provincial personnel should be used to organize localmultisectoral efforts. Personal relationships at thispcripherallcvcl can be more easily translated into sustainable working arrangements. This is particularly truein working with the media to provide ostensibly free coverage for national health programs. Health workers, too,canbe consideredprimary collaborators in passing essential messages about home treabnent. However, to do so,they must receive improved training in health eduCationand interpersonal communications.
PREPARATION AND FOLLOW-UP
A successful communications effort necessitatescareful planning as well as policy statements and messages that accuratdy reflect local realities to the extentpossible. The timing of a communication initiativeshould balance the need for sufficient planning andresearch with the need to move forward with the education of child caretakers and creation of demand for thekind of diarrhea management health workers are beingtrained to provide. The Cameroon experience demonstrates the importance of the following prerequisites tolaunching a communications campaign:
HEALTH COMMUNICATION IN CAMEROON 63

Cl>llCIIISI()11S
64
Prior to a communication effort, the COD programshould develop and publish national policy guidelines.
Existence ofa policy will assure consistency betweenhealth education messages and the information transmitted to health workers in training. Studies should beplanned to seek information still needed to define morespecific policies, such as choice and exact preparation ofhome solutions.
Formative research, such as the focus group stud- .les, aids in the development of culturally appropriate messages.
At the provincial and peripherallcvels, messages tailored to local practices can enhance program credIbility.
COD program personnel must ensure adequatesupplies.
All supplies defined in policy as a part of the program (packets of oral rehydration salts, containers formixing, and so forth) must exist in adequate quantitywhere needed before launching a communication effort.Though this may imply prior resolution of a systemicproblem within the health system (such as a drug distribution network), the credibility of the COD program andviability of the communication effort will depend on it.
Where a large collaborative effort is planned, aUcollaborating partners should participate in strategy and message development.
The pre-existence offirm policy helps the program tomaintain control over the process and final planningproducts.
A well-organized national communication effortwill only succeed through extensive follow-up withaU partners responsible for Its implementation.
This implies the need for sufficient cure staff (in theCOD program and the health education service) from theoutset.
This paper underlines the complications and difficulties associated with a government-led nationwide communication program with multiple partners. The
THE COMPLEXITY OF HEALTH COMMUNICATIONS
Cameroon COD communication campaigns lackedimportant elements necessary for success. These elements included dynamic support from the leadership inthe Ministry ofHealth and sustained long-term funding.
Nevertheless, the Cameroon COD program has beenable to acllieve a considerable amount in the area ofhealth education. A conscientious and thoroughapproach to the development of print materials has produced culturally appropriate and effective materials thatwill continue to be used by the program well after thecompletion of the PRITEOI Project.
Strong interpersonal contacts between the COD pro.gram and individual members of the press have producedpositive if not constant newspaper and radio contributions to COD. Similar contacts with health educators atthe provincial level, and with representatives of nongovernmental organizations, have led to a wide range ofsuccessful pilot activities for health communications,and have reached a significant portion of the population.
Nota:1 Agma PrIns, Owona Essomba Rmr, Ndao S. Atanga, and othm, "PRITECH II Assasmmt:Cameroon National Control of Dlarrhtal DiKasa Program," ArlIngton,VA, ManlIgemmt Sdcnas forHmlth PRrrECH Project, STP-012-CA, 1989.2 WHO, "Enqufte sur Is morbidltl rt Is prise m charge des cas de cfiarrhlc," ArUngton, VA, Managemmt Sdcnas for Health PRrrECH l'rt!Iect, RAD-067-eA, August 1992.3 MartIn Ballpe, MldanI Fotso, and Bernard 1lat'mc,I!nqultldlmographlqut Itdt Ia1ItJ, Cal.1l!/'OUn1991, Columbia, MD: Macro Intanatlonallnc, Da:cmba 1992.4 Moussa CoulIbaliy, "Etude de Is prise m charge des au de dlarrhle dana les formations sanltalrcs desI'roYincelI du Uttoral rt du Sud au Cameroun,· ArIIngton,VA, ManlIgemmt Sdmas for HealthPRrrECH 1'rt!Iect, RAD-056-CA and U'C-Q32-CA, March 1993.
HEALTH COMMUNICATION IN CAMEROON 65

POSTERS, FLYERS, AND FLIPCHARTS:USE OF HEALTH EDUCATION MATERIALSIN THE SAHEL
PRITEOI has provided technical and managementassistance in the establishment and implementation ofnational diarrheal disease control (COD) programs in theSahel region of Africa since the early 1980s. The firstCOD action plans developed by the ministries of healthin Niger (1984), Mali, Mauritania, and Senegal (1985)concentrated on training health workers in case management and on developing communication strategies topromote appropriate household management of diarrhea. This represented the first systematic effort in thesecountries to coordinate the practices of and advice givenby health workers with public health messages promoted through the mass media and other communicationchannels.
PRITECH assisted the COD program and health education staff in each country to identify culturally appropriate strategies and messages to promote recommendedpractices at the household level. The available literaturewas reviewed and focus group research carried outamong different ethnic groups in each country. This initial research was conducted with mothers ofyoung children, older women, and other local experts (includinghealth workers) in the treatment of sick children.
COD program and health education staff, in some. cases in collaboration with a national COD committee,determined the type of educational materials that weredeveloped. The decision was based on examples fromother COO programs, previous experience with educational materials within the country, and the COD program's communication goals. All four countries chose todevelop radio and television spots as well as printed materials.
Printed materials developed for face-to-face communication included:• Home-care flyers illustrating the preparation of oral
rehydration salts and other recommended practices. Itwas intended that these "memory aides" would beexplained and distnbuted to mothers by health staff,village health workers, traditional birth attendants,and educators from other sectors. .
Elizabeth Hcnnan i5 aTechnical Officer. andSuzanne Prysor-Joncswas the Senior Pr0gram Manager, SahdRegional 0fIia.
POSTERS~YERS,AND FLIPCHA\T2
rrmODSl'age Blank67

• illustrated booklets to be kept by health staff, villagehealth workers, and school teachers and used forteaching about diarrhea prevention, dehydration,feeding during and after diarrhea, and the preparationof oral rehydration salts or sugar-salt solution.
• A flipchart comprised of the same pictures as the illustrated booklet (Niger only). This was for use duringgroup education sessions in health facilities.
• A poster depicting a mother administering oral rehydration therapy (oral rehydration salts or sugar-saltsolution, according to the country's policy) andincluding the same pictorial instructions as the homecare flyer.
All printed materials used national languages(approximately five per country). They were pretested bythe COD and health education staff using focus groupdiscussions or interviews with mothers, village healthworkers, traditional birth attendants, and health staff.
The Mali COD program organized a campaign tolaunch the communication activities. This c:onsisted of anational song contest, coordir..ated teaching activities in allthe schools in Bamako, and radio and television spots. Theother countries introduced activities more gradually.
Printed materials were to be included in the decentralized training of health and other workers in eachcountry. Photocopies of draft materials were providedfor initial sessions for which final versions were not yetavailable. The training was designed to include instruction on the use of the face-to-face educational materials.Role plays were recommended but not always carried outin practice.
The printed materials were distributed throughoutthe public health system. Each regional and district director was responsible for assuring that the materialsreached all levels of the health sector as well as schoolteachers, literacy workers, and other developmentagents. The materials were packed with a note explaining the purpose and intended user for each type.
Initial training and communication or health education activities were evaluated in a number of ways.Household surveys of knowledge, attitude, and practices(KAP) related to diarrheal diseases showed that the activities had made a considerable impact on mothers' aware-
68 THE COMPLEXITY OF HEALTH COMMUNICATIONS

ness and use of oral. rehydration therapy. The percentageof mothers using oral rehydration therapy to treat arecent diarrheal episode has increased to between 24 percent (Senegal) and 40 percent (Mali ar..d Mauritania),compared with less than 7 percent before the activities ofthe national COD programs. The KAP studies alsoshowed that more than 60 percent of mothers withknowledge of oral rehydration therapy had gained itirnm contacts with health staff. Changes in other behaviors i"eIated to the household management of diarrhea,such as feeding and giving adequate amounts of fluids,were negligIole.
Unfortunately, the results of subsequent healthfacility surveys suggested a problem with the use of theface-ta-face communication materials produced and distributed by the national COO programs. Observationsmade at the time of COD supervisory visits confirmedthat the COD program materials were not displayed inmany health facilities, and they were rarely, if ever,referred to during interactions with mothers and othercaregivers. Outreach activities also required improvement as rehydration therapy knowledge and rates ofusevaried considerably between towns with health facilitiesand villages without them.
The reasons for the underuse of COO health education materials and ways ofimproving the situation were,however, not evident. Did the problem lie with the materials themselves? Were the formats or the content inappropriate? Were the materials too complex or too bulky
POSTERS, FLYERS, AND FLIPCHARTS 69

for easy uce? Alternatively, was the problem one of distn'bution and management? Were the materials reachingthe health facilities? Ifso, had they been distn'buted to thewrong people and simply locked away in closets? Werethere administrative or organizational barriers to the useof educational materials? Did the existing attitudes ofhealth workers or their supervisors discourage their use?
The answers to these questions would have important implications for the national COD programs. Without understanding the reasons for underuse of the materials, it was impossible to know what measures to taketo address it. After the initial set of materials had beendistributed, programs had to decide whether to simplyreprint the materials as initially developed, to revisethem, or to abandon the idea of supplying print materials to health facilities.
Given that the problem of underuse of COD healtheducation materials appeared to be common throughoutmany countries in the region, PRITEOI's Sahel RegionalOffice proposed to coordinate a series of brief investigations into the reasons behind this situation. A researchproposal was developed by a West African social scientist in coordination with PRITECH regional and headquarters staff. It was subsequently adapted and implemented by COD programs in four countries in the region.
I11V('st Iqatlllfj the RellSOI1~ for Ul~(l(!lllSe' : .
STUDY DESIGN
A standard survey format was used tC' conduct interviews with health care and social service workers in theirplaces of work. The methodology employed open-endedinterviews and direct observations. An observation guideWM used to record the kinds of educational materialsavailabl~ in health facilities and to document interactionsbetween health workers and patients with diarrhea (ortheir caregivers).
Studies were cond:.lcted in four Sahel countries.Fifty-seven health facilities were visited in Mauritania(19), Mali (9), Nig,·~ (12), and Senegal (35). The healthfacilities were selected to include all levels (from thenational referral hospital to local health posts) in bothurban and rural areas. In two of the studiC!l, private faciliti:s were represented as well as public fac:Uities.
70 THE COMPLEXITY OF HEALTH COMMUNICATIONS

'.
One hundred and seventy-three health care andsociaI service workers were interviewed individually: 43in Mauritania, 31 in Mali, 32 in Niger, and 67 in Senegal. The workers were well disbibuted in terms of age,gender, and number of years in service.
The study observed and inquired about the use of alltypes of educational materials including those prodncedby other programs or interventions. It also sought toverify reported education.1.l actWities by reviewing facilities' schedules aud p.crnity reports.
STUDY RESUL'tS
Availability of materials within health facilitiesThe most common type ofeducational material found
in all the facilities visited was the poster. Flyers, tlipcharts,and items for demonstration were less frequently encountered. Unfortunatdy, two of the researchers noted that theposters were not always easily visible to patients or theircaregivers, and appeared to be positioned as decorationsrather than as teaching aids. The investigators in Mauritania and in Niger noted a large number and variety ofmaterials promoting pharmaceutical products.
With a few exceptions in Malil and Niger,:J most of thehospitals visited, particularly the large referral hospitalsand teaching facilities, lacked significant educationalmaterials and activities. This is ofparticular note since thehospitals are generally located in the national or regionalcapitals and are easily accessible to the dism"bution centers. Hospitals with diarrhea treatment units and feedingrehabilitation units were more likdy to have materials inthose settings.
In Senegal, the availability of posters and other printmaterials in lower-Ievd health faCilities was quite good.J
Demonstration materials (for mbdni oral rehydrationsalts and for family plal1ning) w~'- Jim(ted to the maternal and child health centers. b Mauritania, posters onCDD, immunizations, family p1anring, and hygiene wereavailable in 15 of 19 facilities visited. In Niger and Mali theavailability was quite variable among facilities. The availability was n",t a function of rural versus urban locationof the health fa.cility, nor of the accessibility of the facility.
Thus, the distribution system, although not ideal,did not appear to be a major factor in the underusr. ofeducational materials. In fact, m..my of the facilities that
POSTERS, FLYERS, AND FLIPCHARTS 71
l-

.J
72
had no materials displayed were found to have themstored away and forgotten in closets.
Attitudes toward health educationWhen asked directly, all the health workers inter
viewed acknowledged the importance ofhealth educationand the usefulness ofhealth education materials. Furtherquestioning, however, revealed less favorable attitudes.In Mauritania, for example, only five of the forty-threeworkers interviewed identified health education as anessential activity to which they accorded more time thanother activities. Four of those were lower-level healthauxiliaries. Most of the health workers felt that healtheducation was not an important part of their own jobsfor a variety of reasons.
The twenty-five physicians interviewed in the fourstudies all attributed their nonuse of health educationmaterials to lack of time. Both physicians and nursesplaced priority on the activities of consultation, prescription, and treatment. Although they reported providingverbal instructions to patients at the time of consultation,obStiVatioIlS suggested that this was seldom the case.
Although midwives reported playing an active role inhealth education and expressed interest in obtaining morematerials and training, they ·,....(1"e unwilling to identifythemselves as health educators. Paramedical workersincluding public health agents and ·''.iociaI action personnel" were the most motivated and available to providehealth education. But they received little training in healtheducation techniques and seldom had acces" to educational materials.
Thus, althoughalmost all of the health workers interviewed acknowledged the importance of health education,in practice these activities appeared to be assigned to individuals at the bottom of the health worker hierarchy. Theindividuals assigned to "do" health education were unlikely to be the ones sent for in-service training. They werealso the individuals least likely to have the authority tomake decisions or to set priorities within health facili~es.
The location of health education activitiesIn all four studies hospital staff consistently
expressed the attitude that there is a lack of time forhealth education in a referral setting in which the mostseriously iII cases are managed. The low use of educational materials was also att:ibuted to the absence of
THE COMPLEXITY OF HEALTH COMMUNICATIONS
....
materials and Jack of interest in education on the part ofthe senior and technical staff. Similarly, health educationactivities were not established in the health centers andwere not reflected in routine work schedules and plans.
Throughout the Sahel, the maternal and child healthcenter is considered the optimal site for health education.Most have educational materials and rooms or spacesadaptable for group sessions. Indeed, the group educationsession, occurring before consultations, is the most common form ofhealth education. Most centers post a schedule of presentations on topics such as family planning,nutrition, immunizations, and diarrheal disease control.Ironically, however, printed health education materialsare seldom referred to during these sessions. There is evena question as to whether all the scheduled sessions actually take place. For example, one researcher noted the factthat health education group sessions are usually scheduled at 8:00 or 8:30 in the morning, while health workers do not usually report until 9:00 a.m.·
In other health facilities, health education activities arereported to be "informal." None of the studies, however,found cvideru:e that individual counselling takes place. Thereasons given to explain this deficiency included the lackof training in education and communication, the lack ofmaterials, the Jack of time, an underlying attitude thateducational efforts are ineffective in changing behavior,and internal management problems regarding the storageof materials.
It appears, therefore, tllat just as health workers tendto delegate health educationactivities to the individuals whoare lowest in the health worker hierarchy, health facilitiesalso tend toshirk their responsibility for theseactivities, delegating them primarily to the maternal and child healthcenters. Although health education activities and materialsare visible in these centers, the place ofhealth education stillappears to be marginal to other curative activities. Healtheducation seems to be viewed as an activity that is separatefrom case management and that is somewhat of a luxurythat can be dispensed with when time and resources areshort. There is little understanding that health educationdeals not only with public health and prevention, but is alsoan integral part of good case management.
Attitudes toward and understanding of materialsQuestioning about the specific health education
materials available in facilities revealed that the quality
POSTERS, FLYERS, AND FLlPCHARTS 73

74
and cultural appropriateness of the materials did notappear to be a problem. There were many recommendations to diversify the type of materials provided. It wasnoted that posters, the most common type, must be limited to one or two messages. Flipcharts, flyers, and audiovisual equipment would be helpful in providing a morecomprehensive presentation ofa topic. Health workers inurban areas were particularly anxious to have access tomovies and videos.
It is questionable, however, whether this is a positiverecommendation as most hoped that audiovisual materials would "free them" from the responsibility of providing health education and allow them to tend to moreimportant duties.
Although testing mothers' comprehension of education materials was not part of the study design, th~
investigators in Mauritania conducted brief interviewswith seven mothers who brol'ght their children to healthfacilities for consultations. They found that only two ofthe mothers could correctly interpret a poster distributedby the COD program. This questions the utility ofposters that are distnbuted to be simply pasted on thewalls of health facilities.
Training in health educationSpecific training in health education was extremely
limited. Senegal was the only country in which any of theinterviewees had received special training in health education techniques and in the use of health education materials. The training, however, had been limited to regionalhealth officers and to senior health education personnel.
A proportion ofhealth workers inall four countries hadreceived some form of training in health education in thecontext of courses organized by programs (such as COD,AIDS, family planning). The researchers' assessment of theeffectiveness of that training varied. The study in Mali concluded that the nurses who had received training in healtheducation and who had received some educational materialsdid not use the materialsb'~use of their preoccupationwithcurative care. In Mauritania, however, the researchers concluded that health education training had greatly improvedthe attitudes and performance of those trained.
Most of the health workers interviewed expressedinterest in receiving training in health education techniques. The interest was particularly strong among"social action" personnel and public health personnel.
THE COMPLEXITY OF HEALTH COMMUNICATIONS

[Jsll1q r lll~ Rpsults of the Il1veStlC!atlon . '.
Prior to conducting the studies on the distributionand use ofhealth education materials, the COO programsin the Sahel had planned to reprint materials on thehousehold management of diarrhea, and to develop others on oral rchydrittion salts, hygiene, and nutrition. Itwas decided, as a result of the findings, to proceed morecautiously before undertaking another round of massproduction and distnoution. The COD programs decidedto join with other programs and projects to attempt toimprove health education activities within the countries.
Meetings were held with health education staff andwith regional COD and health education supervisors todiscuss the research findings and to explore possible solutions to the problems identified. In Mali and Senegal,these meetings coincided with the start-up of HealthComproject' activities. As a result, training in interpersonalcommunication skills became a focus of the Ministry ofHealth and HealthCom workplans. In Niger, Senegal, andBurkina Faso, increased emphasis was placed on healtheducation techniques and the use of educational materials in subsequent training-of-trainers workshops anddecentralized training sponsored by the COD programs.
To support these efforts to improve health educationskills, PRITECH's Sahel office modified the manuals usedfor the training-of-trainers sessions and for inseMcetraining to strengthen the health education componentand to include role-plays involving the use of educational materials. The modules for usc by nursing schools inthe region were similarly modified.
In Mali and Niger, local production of oral rehydration salts began after completion of the research. Theresults of the studies influenced the decision to printfewer materials for the general public and to producemore materials for prescribers and drug sales persons.Radio and television sl'Ots were developed as before.
Ethnographic research and household trials on feeding during and after diarrhea are being conducted in several countries in the region. The results of these studieswill be used to develop counselling cards and other materials related to child nutrition. When introducing thesematerials, the emphasis will be placed on training healthworkers to use the materials to help them counsel effectively.
POSTERS, FLYERS, AND FLIPCHARTS 75

Finally, the results of the studies have inspired othercountries to critically evaluate the effectiveness of materials developed by the COD programs. For example, theCDD program of Cameroon recently completed a studyof two home care flyers that were to be distributed tomothers through the public health system and throughcommunity organizations. The program studied caregivers' recognition of the flyers, the availability of flyersin households, knowledge about the content of the flyers, and influence of the flyers on reported behavior.
Lessons Learned .
When COD programs were initiated in the Sahel, itwas assumed that making appropriate educational materials available to health staff and other educators wouldensure widespread and effective education and counsellingon oral rehydration therapy. The results of the four studies summarized in this paper caused serious questioningof this assumption and pointed to problems with healtheducation activities in general. It is now recognized thatthe provision of high quality materials is necessary butnot sufficient for improving health education.
The problem is not limited to the COO program butrelates to the undervaluing of, and perhaps the perceivedineffectiveness of, health education activities. This problemof attitude and priorities is too often reflected in the limited budgets and low status afforded to health educationdepartments and programs. The value placed on healtheducation must be reflected by its position within the ministry and communicated to health workers at all levels.
The importance of health education can be communicated and reinforced in a number of ways:• Training in use of education materials must be part of
health worker preservice and inservice training. It isnecessary that the training include very basic conceptssuch as showing the pictures to the individual who isto be educated, and following the script of the materials. Training must include demonstration of, practiceof, and appropriate feedback on communication techniques.
• Health education materials and activities must be integrated into the routines of hospitals and other acutecare facilities as these are' the training sites for uppcrlevel health workers. If health education continues tobe ignored in these settings, not only will the patients
76 THE COMPLEXITY OF HEALTH COMMUNICATIONS

suffer, but students will have no models for incorporating health education into case management. It isimportant to stress that health education is not onlya preventive measure, but is part of good case management. Educational materials, when used properly,can increase patient understanding, improve compliance, save time and improve outcome.
• Senior-level health workers and supervisors must betrained in how to teach, supervise, and support the useof educational materials. This may require a redefinition of theirjob descriptions to include the distrIbutionof materials and the encouragement of health education activities through supervision and monitoring.
• Training in appropriate techniques and in the use ofmaterials should be provided to those health and community workers most actively involved in health education. This will clearly require collaboration withother health programs and other sectors.
The studies also point to the need for more carefulevaluation of the use and effectiveness of different typesof materials. For example, the results suggested thatposters, although the most common type ofmaterial, areused as decorations and seldom explained to patients orcaregivers. Simple follow-up studies are needed to determine whether counseling cards, flyers, and other materials that can be easily used in face-ta-face communication are more useful and effective.
It is generally felt that printed materials are still lacking in health facilities at all levels in the Sahel and thatmore are needed. There is now, however, a greater understanding that the appropriate use of educational materials is not automatic and that there is no short-cut toimproving health worker motivation and skills. Resolving the problems will require considerable time andresources and must take place systematically throughthe concerted effort of different national programs supported by donors and nongovernmental organizations.
Notes:1 Makanc Kane. ·Utilization du matbid lducatif par lea agmts de santt au Mali." Arllngton,VA,Managtmmt ScitllCtS for Htalth PRITECH Project, RAD 024-SA, July 1990.2 Mamadou Smc. "Utilisation du matbid tducatlt'danJ 10 structures de santt au Nigu.·Arlington.VA, Managtmmt Scimces for Htalth PRITECH Project, RAD 024-SA, Dtctmbu 1990.3 Mamadou Sme and Mbaye Diop, "Utilisation du matmd lducatif par ItS pmonnds soc:io-sanitairesau 5enegaI." Managtmmt Sciences for Health PRITECH Project, RAD 02S-SA, Septtmbtr 1991.4 Sldy Baldy Kane and Moussa Fan. "Etude sur l'utUization du matbid lducatif par 10 personnds desantt m Mauritanie." ArUngton. VA, Managtmmt ScIences for Htalth PRITECH Prqject, RAD 024-SA,August 1991., Communication and Marketing for Child Survival. or HealthCom. Is a prtlject managed by theAcadtmy for Educational Dcvdopmmt for A.J.D. The project aim, to Incrtalle the Impact of health andchUd survival programs through Improved communication and social marketing activities.
POSTERS, FLYERS, AND FLIPCHARTS 77

WE COULDN'T HAVE ASKED FOR MORE!LESSONS LEARNED IN INFORMATIONDISSEMINATION
Tile Need for Health InformatlOll
For many people in the developing world, informationis a scarce and precious commodity. Unlike their counterparts in industrialized countries, who are often hardpressed to keep up with the literature, health practitioners and policymakers in developing countries often makedecisions without the benefit of the most up-to-date information. Health workers in rural Tanzania, for instance,stated that they could not adequately perform their dutiesbecause of their academic and professional isolation andthe lack ofaccess to libraries near their workplaces, amongother factors.! Similarly, a survey found that doctors andclinical officers in Zimbabwe felt isolated, with no meansof improving their professional skills.2 The majority ofsuch health workers have no access to current information whatsoever, despite the fact that information is critical to the success of health programs.
Even in urban areas, libraries in medical schools andhospitals can rarely afford more than a handful of coreprofessional journals, much less the online databases,research reports, and monographs commonly found inUS libraries. Most libraries lack the forejgn currency topay for foreign journal subscriptions, and donor agencies are reluctant to fund recurrent costs.
Opportunities for continuing education throughtraining courses may also be few and far between. Evenofficials responsible for setting health policy and implementing primary health care programs in ministries ofhealth have limited access to information or training.Information is such a valuable commodity that somepolicymakers hide reports and articles away in theirdesks or at home, convinced that information, rare as itis, represents power and should not be shared.
Karm White is theInformation Managerlind U5a Dipko WIIS
an Information Specialist.
Information clearinghouses are one vehicle for meeting the pressing need for information on the part ofhealth workers and others. A clearinghouse is a special-
WE COULDN'T HAVE ASKED FOR MOREl 79
Previous Page Blanl!

ized information dissemination center that collectsinformation on one topic, repackages and synthesizes it,and distributes it to a target audience. It is different froma herary in several ways. First, while heraries mainlyserve clients who visit in person, clearinghouses mainlyserve clients by mail or phone, often receiving no visitors at all. Second, while hbraries collect information ona broad range of topics, clearinghouses usually limittheir acquisitions to one field, such as diabetes or cancer.Finally, clearinghouses emphasize outreach, or dissemination, of infonnation.
The PRITECH Information Center collects information about diarrheal disease control and other relatedhealth interventions and disseminates it to health practitioners and policymakers worldwide.' The collectionconsists mainly of publishedjoumal articles, documentsfrom the World Health Organization (WHO) and otherdonor agencies, and reports generated by the PRITECHProject. The Information Center helps increase awareness of the proper treatment of diarrhea and management of programs for the control of diarrheal diseases(COD) through the following mechanisms:
RESPONSE TO INFORMATIONREQUESTS
Through its database and accessto online data bases, the Information Center responds to about 1,500requests a year, primarily fromhealth professionals in the developing world. The database, consistingofmore than 6,000 documents, canbe searched by author, title, subject,source, language, and country. TheCenter can provide computer printouts of citations on a particulartopic or copies of the documentsthemselves. The Center also pro-duces an annotated bibliography
each year which lists the entire collection; copies of thecollection's documents can be requested at no cost.
What Do Clients Ask For?• A phannacrotical company in Mexico asked whether ORS containingglycine was more effective than DRSwith glucose. The Information Centersent articles that demonstrated that itwas not.• The COD program manager inMadagascar asked for examples ofCOD policies from other countries.The Center sent policies from severalother French-speaking countries.• The director of primary health careprograms in northern Peru requestedmaterials on cholera prevention. TheCenter sent the WHO Guidelines forCholera Control, as well as articles onbrcastrccding, hygiene, and immunization.
80 THE COMPLEXITY OF HEALTH COMMUNICATIONS

MONTHLY ACQUISITIONS LIsT
Before they can request copies of specific documents,people must know that they exist. The Information Center has several current awareness tools-mechanisms forkeeping people up-to-date on the most current literaturein their field. The first of these is the MonthlyAcquisitionsList, an annotated list of key child survival articles thatreaders can order at no cost. The Center sends the list tomore than 350 policymakers and project implementers.Readers include the overseas offices of private voluntaryorganizations, COD program managers, overseas information centers, and health officers at USAID missions.Another current awareness tool is the Technical LiteratureUpdate on Diarrhea.
TECHNICAL L1TERATURE UPDATE ON DIARRHEA(TLV)
Since 1985, PRITECH has distributed the nu, abimonthly publication that reviews articles on diarrhealdisease control and related interventions, such as breastfeeding promotion and nutrition programs. Each issuefeatures abstracts of published articles on a particulartopic or issue, such as sustainability of health projects or___________________••1OC _
WE COULDN'T HAVE ASKED FOR MOREl 81

the role of traditional healers in COO programs.PRITECH's technical editor then provides expert commentary on the articles, explaining how they are relevantto health practitioners and policymakers involved withchild survival programs. Readers can ask for copies of thearticles reviewed, or for bound copies ofnuback issues.The nu is available in English, French, and Spanish tomore than 17,000 readers throughout the world. ThePRITECH Information Center distributes the English andSpanish versions, while the Office de Recherches sur l'Alimentation et la Nutrition Africaines (ORANA) distributesthe French. The most popular TLU issue to date was aspecial issue on cholera, produced in response to the LatinAmerican cholera epidemic of Spring 1991.
DOCUMENTING PRITECH's COUNTRY PROGRAMEXPERIENCES
Since the Information Center is part of a project thatimplements COO programs overseas, it serves as theinstitutional memory of PRITECH, as well as a clearinghouse of technical documents. This is accomplishedthrough two mecha~lisms:maintaining the project's central files, and producing reports on PRITECH programexperiences in developing countries. Without a documentation effort, PRITECH's experiences in helping tomanage COO programs would be lost. The InformationCenter publishes a quarterly highlights report, whichdocuments the project's progress on a quarterly basis; aseries of country program profiles, which describePRITECH activities in country programs; and a series ofoccasional papers, which provide useful "lessons learned"in COO program implementation.
Target AudIences .
The PRITECH Information Center currently servestwo distinct groups of people: child survival policymakers and project implementers; and health practitionerssuch as physicians, nurses, and community healthworkers. However, the Center's target audiences haveevolved over time. In 1983, the Information Center targeted a small group of users to receive information products, including health officers at USAIO missions, technical officers at AI.O./Washington, PRITECH staff, andmanagers of COO programs in developing countries.
82 THE COMPLEXITY OF HEALTH COMMUNICATIONS

Later, when the project acquired long-term country representatives stationed in developing countries, theybecame yet another user group.
For country representatives, the Center could provideaccess to technical information as well as serve a crossfertilization function. Since many of the representativeshad no contact with each other, they could not learnfrom each other's successes or failures. The Center identified reports, forms, and audiovisual materials producedby PRITECH field offices that could be shared with theothers. Country representatives also used articles in leading medical journals, such as the New England Journal ofMedicine and The Lancet, to convince developing countryphysicians that oral rehydration therapy is endorsed bythe US medical establishment. A country representativein an Asian country used technical articles from theInformation Center to convince manufacturers of oralrehydration salts to promote continued feeding andbreastfeeding along with the salts, as they wouldimprove its efficacy.
As the Information Center mandate and the range ofproject publications expanded, the Center attempted toreach additional groups. In 1989, for instance, the Center decided to translate the nu into French and Spanish,which enabled the project to reach health professionals inLatin America and French-speaking African countries.Since then, the Center has successfully targeted the following groups:• Health practitioners, such as physicians, nurses, and
community health workers, in developing countries.In 1988 and in 1992, the Information Center conducted readers' surveys of the1lU. Although the mainpurpose of the surveys was to determine the usefulness of the 1lU, the surveys also asked the readers tosupply names of other individuals and organizationsthat would benefit from receiving the nu. In 1992,readers generously provided some 4,000 names inresponse. Word of mouth was another mechanism bywhich many health workers learned about the Information Center; they mentioned having seen aPRITECH publication on the desk of a colleague.PRITECH has reached many additional health practitioners by distributing publications at national andinternational health conferences. Health workers indeveloping countries now make up fully 25 percent ofthe Information Center's clients.
WE COULDN'T HAVE ASKED FOR MOREl 83

• Fifld ojJi.ces of the private voluntary organizations registered withA.I.D. working in the area ofchild survival.The field offices of such organizations as CARE andSave the Children are staffed largely by countrynationals who are implementing projects in maternaland child health, nutrition, COD, and immunization.They constitute one of PRlTECH's most enthusiasticgroups of information consumers. In 1989, privatevoluntary organizations made up just 3 percent ofPRITEOi'sinformationrequests; today, they make up15 percent.
• Medkal schools in sub-Saharan Africa. In 1991, theAmericanAssociation for the Advancement of Scie:lcecontacted 100 African medical schools and researchorganizations on PRlTECH's behalf through its journal distribution program. As a result, many organizations have asked to receive the nu on a regularbasis.
The current mix of Information Center clients isshown in figure 1.
From the beginning, the Information Center has alsotargeted health information centers in developing countries to help them expand their collections. One of theseis the ORANA Information Center on Child Survival inDakar, Senegal.
Coll,tl)lHiltIOIl Wit il Uw ORANA' IllforlllrltlOll Cl~Ilt.Cl
Fisurt 1. Users of the PRlTECH InfonnationCenttr,1992
Misc:dlancous12"
A.1.D.andmissions
10f6
84
Donon
3"
In 1985, PRITECH contractedORANA in Dakar, Senegal, to createa regional information center focusing on COD to respond to the needsof Francophone African countries.Because of PRITEOi's involvement·in the national health systems ofseveral Sahelian countries, PRlTEOicould assess information needs atdifferent levels and identify ways ofreaching health policymakers andpractitioners with COD materials.
The ORANA Information Centeron Child Survival maintains stronglinks to the PRITECH/Sahel Regional
Office in Dakar and to the PRITEOi Information Center.The Sahel Regional Office provides technical guidance tothe ORANA Information Center and publishes docu-
THE COMPLEXITY OF HEALTH COMMUNICATIONS
•

..
ments incollaboration with ORANA. The PRITECH Information Center maintains an exchange relationship withORANA, contributing substantiPUy to ORANA's collection of technical articles on child survival topics.
Like the PRITECH Information Center, ORANA distributes acquisitions lists and sends them to a mailing listof 850 decisionmakers in ministries of health and international organizations; teachers, students, and horariesin schools of health; researchers; and journalists in lh-:Francophone Africa.. region who are concerned withchild sumval issues. ORANA also distributes the Frenchversion of PRITECH's nu.
In addition, ORANA translates and distnoutes fulltext technical documents that are deemed to be of specialimportance to those working in the COD area jn Africa.To dab:, about twenty such documents have been distributed on topics such as the relation between diarrheaand nutrition, improved weaning practices, and management of dysentery cases. ORANA has also publishedcompilations of technical documents originally published in French.
Since 1985, ORANA has produced a number of keypublications in the diarrheal disease field in collaborationwith the PRITECH Sahel Regional Office. These publications are particularly noteworthy because they focus onstudies, statistics, or health education materials that havebeen developed in Africa. ORANA has taken advantage ofits location in West Africa to devdop a collection rich in
20
lS
10
S
3.5
~16'7
I le,.'7
.2~+---If----......----t---+-----I1988 1989 1990 1991
Fiscal year1992
Figure 2. Number of11.U rtaders (in U",v.sands;,
__________,.fto..,nJI'lt..,.¥"'.,'.~~~.~ _
WE COULDN'T HAVE .ASlCED' f,(;il. b.CPUi 85

,.
African documents, su("~. as theses in the CDD field frommedical schools in francophone Africa.
The ORANA Infonnation Center has made a specialeffort to reach out to regional medical and nursing schoollibraries. Periodically, the Center identifies a particularlyuseful document, such as an up-to-date training manual on diarrhea from the World Health Organization, andrequests a sufficient numb~ of copies from the publisher to send each school {numbering about ninety) a set.Between 1985 and 1991, three such groups of documents were sent to these schools, for a total of forty-twodocuments each. Distnbution of the mini-librariesenables professors and students in a variety of hcalthrelated fields to have access to th~ newest informationabout diarrheal disease, nutrition, and vitamin A.
IlllPlict Oil Users . '.
One of the best indicators of success in informationdissemination is growth in the number of requests. Figures 2 and 3 show that the mailing list of the TLU andthe number of requests handled each year have growntremendously since 1989, when the Center began keeping statistics. In addition, many information requestscome "---om repeat customers, who have been so pleasedwith the information received the first time that theyhave returned for more.
..Ii
Comments from Readers• The manager ofa child survival project in Malawi writes that "sincePRITECH started to send me documents.••my work has bem made easier to carry on. 1 have at least somematerial to refer to when making decisions."• A nurse in Nigeria writes, "I am verygrateful for the slides and audiocassette smt to me...especially now thatwe are ~appling with an outbreak ofcholera m this arr.a. The materials arevcrv bdpful in our health educationaCtivities...• A doctor in Kathmandu writes that"receiving the n.U would hdp theregional offices and myself to deal withthe severe diarrhea problems weface...In countries like Laos or Nepal, itis almost impossible to find a goodmedical h'brary."
READER'S SURVEYS
In 1992, PRITECH conducted asurvey to determine how readersuse the TLU. Eight percent (or 822)of those contacted by mail returnedthe survey. Forty-six percent of therespondents reported that readingthe TLU has changed the way theyteach by keeping them updated withthe latest scientific infonnation.Many reported using the TLU as areference for preparation of lecturesand as reading material for students. Similarly, 43 percent ofrespondents stated that the TLU haschanged the way they manage diarrheal disease cases. In general,
86 THE COMPLEXITY OF HEALTH COMMUNICATIONS

respondents reported that their use of antidiarrhealdrugs, unnecessary anhbiotics and intravenous therapyhad decreased, while their commibnent to oral rehydration salts and promotion of brcastfeeding and feedingduring diarrhea increased.
Requests
Fisure 3. Number ofrequests handled by the PRITECH Information Center
That same year, the Information Center conducted asurvey to determine how readers use the Monthly Acquisitions List and with whom they share it. Twenty percent of those contacted by mail returned the survey. Virtually all of the respondents, which include USAIO healthofficers, COO program managers, private voluntaryorganizations working on child survival, and overseas·information centers, reported that the Monthly Acquisitions List was effective in keeping them current on COOtopics. For example, the director of the Office of Population and Family Health of USAID/Amman commentedthat "the PRITECHAcquisitions List is excc11ent and keepsme up to date on COD."
The majority found the list to be wc11-formatted andeasy to use. Two-thirds reported that they share the listwith colleagues and national counterparts; of these, onethird share the list with seven or more people. The fieldoffices of private voluntary organizations were particu-
WE COULDN'T HAVE ASKED FOR MOREl 87

]I:
larly enthusiastic about the service, since they have limited access to child survival articles. A program officer atProject Concern International commented that nthePRITEOI Acquisitions List has been a fabulous, efficientresource and has improved the technical quality of ourwork.n
IMPACT OF THE OHANA INFORMATION CENTER
A recent readers' survey conducted by ORANArevealed that for almost SO percent of respondents, theORANA Infonnation Center was their only source ofinformation in the COO field. In addition, as an Africanorganization, ORANA has more credibility among otherAfrican organizations than would a US-based organization. Certainly, other African organizations have dispIafed a degree of willingness to share resources thatmight not have been the case with American- or European-based organizations.
In collaboration with the PRITECH Sahel RegionalOffice, ORANA has produced several documents that areuniquely West African: a bibliography of documentswritten by Africans or about Africa on diarrheal diseasesand related issues; a bibliography of theses collected fromuniversities and schools of health in Francophone Africa;a guide to COO health education materials fromAfrica;and a statistical manual on the epidemiology ofdiarrheal diseases and the impact ofCOO programs in theSahel.
Lessons LC<lrllCcI . .
Demand for information among developing country health professionals is insatiable.
The growing volume of information requests (andrepeat requests) from developing country health professionals has shown that demand for infonnation is notbeing met elsewhere. Health professionals desperatelyneed infonnation that will help them manage diarrhealdisease cases and train other health workers, and have little access to information in-country. For most healthpractitioners and policymakers in developing countries,access to current awareness tools, such as bibliographies,is not enough. In fact, bibliographies may only tantalizeand frustrate developing country readers, who have nohope of obtaining the documents listed. Free document
88 THE COMPLEXITY OF HEALTH COMMUNICATIONS

delivery to support current awareness tools is thereforeessential. The A.I.D. Office of Health approved increasesin the Information Center's budget over the years thatallowed the Center to cover the costs of photocopyingand postage for document delivery. Without free document delivery, the Center's effectiveness would have beencrippled.
BuDding up a clientele overseas takes years.Originally, the Information Center had few clients in
developing countries. Several factors changed this situation. First, the installation of field representatives inmany developing countries provided the Center with agroup of enthusiastic promoters of PRITECH products.Several field representatives volunteered to distributehundreds of copies of the nu in their respective countries, or set up small information centers within ministries of health. Second, the Information Center adopteda proactive strategy of identifying and disseminatingdocuments of interest to particular target audiences.When the cholera epidemic began in Latin America, forinstance, the Center developed an information packageconsisting of documents on cholera treatment and prevention and sent it to health officers at USAID missions.The Center also attended international and regionalhealth conferences to publicize its services. In addition,many health practitior••rs learned about the Centerthrough word of mouth.
Demand is greatest among project implementersfor practical, rather than technical, information.
An analysis of the documents that project implementers (such as the field offices of private voluntaryorganizations) request has shown that they are mostinterested in project evaluations, practical, "how-to"articles about establishing successful child survival progr3IIlS, and the like, rather than technical articles on epidemiology of diarrheal diseases. Every effort should bemade to identify and disseminate such material.
A project information center should disseminateinformation about the project, as well as technicalinformation.
While disseminating up-to-date technical information has increased the knowledge and skills of manyhealth practitioners, the Center plays an equally valuable
WE COULDN'T HAVE ASICED FOR MOREl 89

90
role in documenting the experiences of PRITECH countryprograms. As mentioned earlier, demand for practicalinformation about the success and failure of child survival programs is extremely high. Without documentation of current program efforts, implementing agenciesare doomed to repeat the mistakes of the past.
Reaching overseas h1Jraries and information services is particularly important, since these institutions reach hundreds of developing countrynationals.
The ORANA Information Center, for example,receives a good proportion of all its documents fromPRITECH. These documents are in turn sent out to anaudience of850 policymakers in the health field throughout francophone Africa. The PRITECH Information Center also sends documents to child survival informationcenters in Uganda, Pakistan, the Philippines, Indonesia,GuatcmaIa, and Bangladesh. Another important usergroup is mcdicallibraries in developing countries. During 1991, the Center focused on reaching more studentsin medical and uursing schools, who will use the information they receive from PRITECH to benefit theirpatients throughout their medical careers.
The idea ofa regional information center that spedalizes in collecting regional information and indistributing information to the countries in thatregion is a viabl~ one.
The constant level of demand for ORANA's productsdemonstrates the need for COD information amongAfrican policymakers and health professionals. In addition, establishment of the ORANA Information Centerhas built local capacity in the areas of information andpublication management. Furthermore, translation,printing, and document distribution at the regional levelis both a feasible and effective use of resources.
The relationship between the PRITECH Sahel Regional Office and the ORANA Information Center has beenmutually beneficial. From ORANA's point of view, theInformation Center has benefitted from the technicalguidance that the Sahel Regional Office has offered indevelopment of matcriaIs, such as a chart on the pathophysiology of diarrhea and the health education manual. On the regional office's side, the Information Centerhas provided the office with a convenient and effective
THE COMPLEXITY OF HEALTH COMMUNICATIONS

mechanism for production and distribution of importanttechnical products. Both organizations have gained.
Exchange relationships are very helpful in buildinga collection.
Early in its history, the Information Center established relationships with the other A.I.D.-funded healthinformation centers in the United States, as well as withoverseas institutions such as the Instituto de Nutricionde Centro America y Panama in Guatemala, the International Centre for Diarrhoeal Disease Research,Bangladesh, and the Appropriate Health Resources andTechnologies Action Group in England. Other information centers can not only supply copies of hard-toacquire documents, they can offer advice in mailing listand publication development. Collaboration onjoint projects is another possibility. PRITECH and AHRTAG arccurrently planning to produce a diarrheal disease information directory together.
It would be useful if A.I.D. required compab"blesoftware systems for all A.I.D.-funded informationcenters.
The A.I.D. Office of Health currently funds manyinformation centers both in the United States and overseas. A.I.D. does not, however, specify which kind ofsoftware a new information center should use, eventhough it encourages information centers to exchangedocuments and collaborate. The fact that each contractor may have a different software system prevents contractors from communicating by modem and being ableto search each other's collections. It also makes collaboration on projects, such as joint bibliographies, or sharing mailing lists, more difficult.
Information dissemination is rewarding~In contrast to development interventions that may
take years to mature, positive feedback from informationdissemination is often immediate. Readers frequentlywrite by return mail to express their satisfaction with thematerials. As the director ofa Nigerian healthclinic wroterecently, "We couldn't have asked for morel"
NotES:1 wnson Lmdlta and Shd!a O'Sullivan, "FIndIngs of a Rcsoun:e Centre Nmis Assessment Surveyundertaken In the Continuing Education ZOnal Centres, Tanzania," London, AHRTAG, 1991.2 Helga Patrlklos, "Getting Information to Health Workers," Health Pollq and Planning, vol. 4, no. 3,1989, pp. 257-260.
WE COULDN'T HAVE ASKED FOR MOREl 91
~~;;_: t!.~'y ..~;'~~'1:~~-~
r-
[--<--

TRAINING AND THE QUALITY OF CARE
~e goal of training in the area ofdiarrheal diseasesis to change the behavior of health workers so
that they will provide high-quality health services to children in need. This means training healthworkers to assess diarrheal episodes and treat patientsaccording to the World Health Organization (WHO)guidelines. It also means the retraining of health workers to use anbbiotics only in cases ofdysentery or choleraand to discontinue all use of antidiarrheal drugs.
Training objectives not only apply to clinical activities, but to the supervision of health workers as well, tosustain performance after training and continuallyupdate skills.
During the first few years of the project, PRITECH'stechnical input for training activities was limited to thedesign and support of medical education activities.PRITECH depended on WHO to d(\'elop guidelines for inservice case management and supervisory training programs. In turn, PRITECH funded many WHO coursesthrough PRITECH country programs.
But as national control of diarrheal disease (COD)programs developed and matured, COD managersbecame increasingly interested in evaluating the effectiveness of their training activities and in ways to updatethe cc·ntent as well as training methods. The developmentof training efforts in Uganda, Cameroon, and the Sahelfrom the "need3 assessment" stage to the incorporationof COD issues into routine training programs are tracedby Prysor-Jones, Steinwand, and Casazza in the following papers. All three point to the need to involve the usersearly in curriculum development and the importance ofparticipatory learning and practical experience in addition to didactic lectures.
But the quality of the health workers' performance isrelated to other factors too. Casazza and Endsley document this lesson in their paper on training in the Philippines. Other factors found to affect the success of traininginclude the quality of internal supervision and the availability of a Hcritical massH of other trained workers working in the same facility. In another paper set in the Philippines, Alt descn"bes the development ofan ordering systemfor oral rehydration salts that greatly improved the avail-
NURSING SCHOOL CURRICULA IN THE SAHEL
Prerious Page Blank95

96
ability of sufficient supplies, a prerequisite to case management.
Finally, COD training must be responsive to changing clinicaland programmatic needs. The recent outbreak.of cholera in the Americas stimulated the development ofrelevant case management training for clinicians in theCaribbean. In another paper, Sack and Hospedalesdescnbe the regional clinical case management courseoffered by the Caribbean Epidemiology Center and howit affected cholera case management in Guyana.
PRITECH's experience and other reviews of healthworker performance after training in case managementand supervision highlight the following issues that stillneed to be addressed:• Integration of COD training into the basic and inser
vice training of nurses and doctors to meet newlyemerging clinical needs, such as cholera.
• Design and implementation of national COD trainingstrategies that decentralize and integrate training, andprovide follow-up support to trainees.
• Identification of training gaps and weaknesses in theevaluation of the training itself, to improve trainingactivities continually.
• Design of methods to assess training and health worker performance, identifying those elements in additionto current training practices that are obstacles toimplementation of the training.
At this point, those involved in COD training are learning to frame the questions related to measuring trainingoutcomes better. It is hoped that this will lead to a greaterreturn on investment, better training techniques, andimproved quality of care. But much work remains to bedone; methodologies need simplification and refinementand content requires revision. Moreover, the process fordeveloping these solutions within the context of a national COD program is a major challenge. All national CODprograms as well as the technical assistance agencies supporting them should direct their energies to these points.
The lessons learned from diarrheal disease controlefforts can have broad application to other child survivaltraining activities such as acute respiratory infections,immunizations, and nutrition education. We hope: thatthe experience gained in these COD training efforts willfind application in the design of new, more integratedcurricula as well as in a broader view of training as anintegral part of any health intervention.
TRAINING AND THE aUAIJTY OF CARE

INTEGRATING DIARRHEA CONTROL TRAININGINTO NURSING SCHOOL CURRICULA IN THE SAHEL
PRITECH established the Sahel Regional Office in1985 to provide sustained supervision and follow-up tocountries in the Sahel region that requested PRITECHassistance. Technical and managerial assistance in thedevelopment and implementation of national diarrhealdisease control (COD) programs for six Sahelian countries-Burkina Faso, The Gambia, Mali, Mauritania,Niger, and Senegal-is provided by three regional officersbased in Dakar.
The Neecl for Preservice Training
In the Sahel, as elsewhere, nurses working at thecommunity level are frequently in charge of managinghealth centers and supervising health workers. Acceptance and effective use of oral rehydration therapy in thenational health service ultimately depends on the nurses. The strategies for reaching nurses and other healthprofessionals with information on oral rehydration therapy include preservice training (at the nursing or medical school level) and inservice training (retraining healthprofessionals through workshops or seminars after theyhave entered practice). Reaching health professionals atthe preservice level is a more cost-effective strategy.However, nursing school curricula in the mid-1980s inthe Sahel did not cover information on oral rehydrationtherapy. Changing curricula in the schools of nursing
.has therefore become an important element of PRITECH'sstrategy in the Sahel.
Suzanne Prysor-Joneswas Senior ProgramManager. SahelRegional Offict.
Development and Follow-up of r:rursing School Modules
In 1986, Dr. Suzanne Prysor-Jones, PRITECHregional director for the Sahel, and Dr. Diego Buriot,World Health Organization (WHO)/AFRO DiarrhoealDisease Programme coordinator, developed a plan forrevising curricula at schools of nursing in the Sahel.WHO/AFRO provided about 50 percent of the fundingrequired, including the time and travel costs of an advisor and all the costs pertaining to two regional workshops. PRITECH contributed the time ofDr. Prysor-Jonesand Dr. Adama Kone of the Sahel office, as well as the
NURSING SCHOOL CURRICULA IN THE SAHEL 97

98
printing costs of the training modules developed.PRlTECH has also covered the cost of following up on theuse of the modules by working with twenty-one nursing schools in the region.
It was agreed that a set of competency-based modules of intermediate level (that is, for workers between
the community-health level andphysicians) would be appropriatefor preservice training, and thatschools of nursing in five countriesshould be approached to participatein the curriculum development andapplication. The five countries initially involved were Mali, Niger,Senegal, Mauritania, and BurkinaFaso. In all but the latter, PRITECHwas already involved with nationalCOD programs. .
After a series of discussions onform and content among WHO/Brazzaville, WHO/Sub-Region I,PRITECH, national COD coordinators, and training school authorities, a small team formed, composedof PRITECHISahel staff and a WHOconsultant resident in Dakar.
Although the WHO Control of Diarrhoeal Disease Programme had developed a training course for healthworkers,l it was not specifically aimed toward nursingstudents. The team used the WHO materials as a starting point, adapting them for the Sahel region and revising them to build nursing skills. The team developed afirst draft of the following booklets:
Module t. Epidemiological Overview and ClinicalConceptsModule 2. The Treatment and Prevention of Diarrhoeal DiseaseModule 2. Appendix: CholeraModule 3. Application of Health Education Techniques to Diarrhoeal Disease Control ProgramsModule 4. Elements of a National Program to Combat Diarrhoeal DiseasesField Training WorkbookTeacher's Guide
Modules 1 to 4 are used in the classroom, while thetraining workbook is used during practicums.
TRAINING AND THE QUAIJTY OF CARE

An important element of the development of themodules was the participation of key personnel at thenursing schools themselves. During the summer of1986, the PRITECH/WHO team visited eleven schools inMali, Niger, Burkina Faso, Mauritania, and Senegal todiscuss the current teaching of COO, introduce the ideaof the modules, and propose an outline of their content.Later, PRITECH and WHO invited two representativesfrom each school and the national COO coordinator fromeach participating country to attend a workshop to discuss the first draft of the modules in detail. Ouring thefirst half of 1987, \lmO and PRITECH revised the modules following the workshop recommendations andcomments from WHO/Geneva, WHOlBrazzaville, andPRITECH advisors. By August 1987, 6,000 copies of themodules had been printed in French.
The next step involved a second visit to the elevenschools to discuss integration of the new modules intothe school curriculum. Many schools have large classes,which make group activities more difficult. PRITECHcontinued to communicate with the schools through visits and phone calls after use of the modules had begun,to encourage use and help them overcome integrationproblems.
Several characteristics made the modules useable inthe different Sahel countries. First, the francophonecountries have similar school systems, making integration strategies and material to be covered similar acrossthe Sahel. Second, educational materials from the national COO programs from each country were integratedinto the modules. Finally, drawings showing scenes andpeoples from the region were used to illustrate the booklets.
In 1988, an Arabic version of the modules becameavailable, and in 1989, the English translation was printed specifically for nursing schools in The Gambia. Overthe next few years, ten more schools expressed interestin incorporating the modules into their curricula, bringing the total count to twenty-one.
The modules are now being used in sixteen of thetwenty-one schools in the six Sahel countries in whichPRITECH works. The active involvement of the nationalCOO programs has been an important factor both inadopting and in following up on the modules. The CODprograms in Mali, Niger, Burkina Faso, Mauritania, and
,..The GambiaJ1ave played important roles in ensuring the
NURSING SCHOOL CURRICULA IN THE SAHEL 99
.~.

continued adoption of the modules. In Senegal, which didnot have an active COD program from 1986 to 1992, theadoption rate has been poor.
The PRITECH Sahel Regional Office has attempted tofollow up on the schC'ols during visits to the differentCOD programs. These visits have commonly served as astimulus for COD programs to become more involvedwith the training schools.
Illlp~t1of the Nursing SGl100~ ModUles t
No systematic evaluation of the modules has takenplace to date. Such an evaluation would probably showconsiderable variability in results. Encounters withrecent graduates during a health-facility survey, carriedout in late 1990 by the Ministry of Health and PRITECHin Burkina Faso, showed that some graduates had a goodlevel ofknowledge and practice, whereas others (from thesame school) were poor in both.] The apparent conclusion is that teaching and learning have been uneven.However, there are several indications that the moduleshave made a positive impact on nurse training and havealso provided a possible model for other public healthprograms.
First, use of the modules has resulted in the allocation of more time to COD issues in all participating nursing schools. According to information collected duringthe initial visits to the schools, COD issues, includinghygiene and cholera, were previously allocated a maximum of eight to ten hours of teaching time. By currentestimates, schools now average at least thirty hours ofCOD training, not including workbook use duringpracticums.
Second, informal interviews with teachers and students have revealed considerable satisfaction with themodules. The modules have been characterized by students in Mali as "easy to follow," "clearly and conciselypresented," "good for reference," and "different (positively) from the frequent lecture and note-taking system."Similarly, teachers have tended to have few criticisms ofthe modules as far as form and content are concerned.
Third, the existence of the modules h:~.5 facilitatedcommunication links between national COD programsand training schools, providing a possible model for otherpriority public health programs. In all six countries, the
100 TRAINING AND THE QUALITY OF CARE

modules provided the COD programs with the first occasion for approaching the training schools.
COD program coordinators often found to their surprise that teachers had very little awareness of thenational COD program and its implications for the tasksthat would be demanded of the students in the field following their training. The coordinators also found thateducation materials developed or used by the COD programs (such as local liter containers, posters, flyers, andbooklets) were usually not available for teaching. CODprograms have, on the whole, followed up by providingeducational materials and other assistance.
Finally, the modules have generated considerableinterest from countries outside the region. The COD program in Chad, for instance, intends to introduce the modules in its nurse training school. The COD program in theComoros has requested twenty-one sets. And, districtmedical officers in Burkina Faso have requested largenumbers of modules to be used for inservice training.This prompted the development in 1988 or an inservicetraining manual, Manuel de recyclage, based on the modules, using the same format and content.
This inservice manual is more concise than the teaching modules and is published in loose-leaf form, so thatit can be easily updated or changed to fit national program needs. So far, the manual has been widely used inBurkina Faso and in Niger. The COD programs in Nigerand Senegal have reprinted their own versions of themanual. It has also been adapted for Mauritania and usedthere on a small scale.
Common Problems Encountered
Schools have difficulty finding suffident time in thecurriculum to teach all of the modules.
Directors tend to complain that the modules take uptoo much time in the curriculum, though most have managed to accommodate them in one way or another. Module 3, for instance, which is on educational techniques forCOD, is often taught in health education classes.
Some of the auxiliary-level, two-year trainingcourses do not use Modules 3 and 4. In fact, some of thelearning objectives of Module 3 and most of the objectives of Module 4 are designed mainly for state registerednurse-level training.
NURSING SCHOOL CURRICULA IN THE SAHEL 101

102
The pedagogical ability of the teaching staff isquite uneven in many of the schools and refreshercourses within the schools have been diffimlt toorganize.
Many of the teachers in the schools are wcll-qualified and arc quite at home with participatory teachingmethods and use of materials such as the COO modules.The part-time teachers have not always benefited fromthe same level of training in pedagogy, and even some ofthe permanent staff require refresher training.
In almost all of the schools, there are enough skillsamong the permanent teaching staff to ensure adequaterefresher training of their colleagues and part-time staff.This is not easy to organize, however, and assistancefrom outsiders would probably help. One problem is theexpectation that workshops will provide per diems tocover daily expenses, a request that most donors cannotfulfill when the activity takes place in the nonnal workplace.
Many of the teaching staff require training in COOpolicy and case management.
Many of the teachers have only a sketchy knowledgeof COO program issues and ORT case management practices. As COD programs organize more inscrvice trainingcourses, it would be beneficial to include them as participants.
The teaching of the modules by part-time staffjeopardizes the sustainabllity ')f the modules'teaching.
The modulfs are usually taught by pennanentschool staff, with the help of part-time staff, such as apediatrician. But when the teaching has been done entirely by a part-time teacher, the use of the modules was discontinued.when the teacher concerned terminated hisinvolvement with the school.
Some of the obstacles to improvements in teachingmethods are ftnancial.
Several schools have complained of difficulties doingsome of the practical exercises in the community or inhealth services (outside of practicums) because of lack oftransportation. Others have found some creative solutions to this. Means of transport to prepare the staff atrural practicum sites and to follow up the students dur-
TRAINING AND THE QUALITY OF CARE

ing their practicums is a problem cited by almost all ofthe schools.
Student practicums are often ill-prepared andbarely supervised.
Most nursing students in the Sahel must fulfill a oneto three-month practicum r~quirement in order to graduate. However, students tend to be used mainly as extrahands for miscellaneous routine activities, which limitstheir opportunities for learning new skills. Most schoolsdo not have clear guidelines for the practicums (exceptfor schools using the COO field training module). Sometimes there are learning objectives, but these are nottranslated systematically into specific learning activities.The Field Training Workbook is thus a big departure inmethodology.
A PRITECH visit to a sample of nursing studentsfrom Dakar during their rural practicum showed considerable variation among students. About 50 percentwere using the Field Training Workbook, but the exercises requiring case follnw-up, community work, andgroup education sessions tended not to be done. The other50 percent were completely absorbed by the routineactivities of the centers to which they had been assigned.The Senegal school does do a preparatory visit to thehealth centers, so recommendations for better preparation of the resident health staff during this visit weremade to the school.
Case management is p()(,r in some of the healthfacilities where students do their urban and ruralprarticums.
It is usually difficult, if not impossible, for teachersfrom the schools to intervene in the case managementpractices of the health services where the students areplaced. It is not always possible to choose services withgood case management practices as practicum sites, asthere are many students to place and relatively few services willing to accommodate them.
The national COO programs have a key role to playhere in working to upgrade case management practice ingeneral, to ensure that there will be some consistencybetween what the students see in the field and what theyhave learned in school. PRITECH is assisting with theestablishment of oral rehydration units in most of thecountries, and practices are slowly improving.
NURSING SCHOOL CURRICULA IN THE SAHEL 103

Lessons Learned .
Partidpation of schools in the development of themodules was a motivating factor in their subsequent use.
Nine of the eleven schools that participated in thedevelopment of the modules are in fact using them. Oneof the participating schools not using them did use themin the past but, because of personnel changes, discontinued their use. The other school not using them has hada complete change of personnel.
For those schools not involved in developing themodules, a workshop to introduce them can be useful. Athree-day workshop on teaching methodology and someCOO content was organized in The Gambia for teachersfrom the four training schools in May 1989, once themodules had been translated into English. Two of thefour schools are now using the modules and a third hasasked the national COO program for assistance in theiruse.
In the new school in Ouayaguiya, Burkina Faso, aworkshop seems to have been unnecessary; the modulesare being used there without one. Some of the teachersalready had experience with them elsewhere, and a pediatrician who has long championed the cause oforal rehydration therapy teaches in the school.
The active involvement of the national CDD program is a key factor in adopting the modules.
As mentioned above, the COO programs in Mali,Niger, Mauritania, and The Gambia have played animportant role in ensuring adoption of the modules. Theinvolvement of each COO program is also necessary foreffective problem-solving after initial adoption.
The certified nurses' school in Bamako, for example,was distributing the modules to students without actually teaching them. The teachers seemed to have difficulty with their integration and teaching. Since the twoother schools in Bamako were already using them quitewell, the Mali COO program arranged for a teacher fromone of these schools to provide assistance. This wasapparently well-received by all, and the modules are nowintegrated into the curriculum.
104 TRAINING AND THE aUAIJTY OF CARE

The intervention ofan outside agency is often necessary to support the follow-up efforts of the CODprogram.
The nursing school systems are often not under theMinistry of Health. Thus, national COD programs maynot always have adequate authority or leverage toencourage new teachings. In some countries, COD program staff prefer to have the participation of PRITECHpersonnel when contacts with the schools are made. Theschools are usually fairly autonomous and the presenceof an outsider, working on a regional basis, gives a certain legitimacy and weight to the intervention and cancircumvent sensitivities. This has been the case particularly in Mali and Mauritania.
In the absence of a structured CDD program (as inSenegal and in Burkina Faso until late 1990), PRITECHhas been alone in working with the schools. This is definitely a sub-optimal situation; the success in changingcurricula comes with the strength of cooperationbetween the national COD programs and PRITECH.
It is possible to introduce COD teaching modulesinto a curriculum that is not run on a modularbasis.
Sixty-six percent of the schools contacted are nowusing the COD modules. All but one of them have spreadthe COD modules throughout the curriculum, usuallyover a two-year period. Only one school has run a weeklong seminar to go through all of the modules at one time.
Having enough sets of training materials availablefor teachers and students alike is an importantmotivating factor for the introduction of new content.
Students and teachers expressed appreciation thateveryone concerned has a set. This allows students toprepare by themselves outside the classroom, and to keepthe modules as reference materials.
Although the provision of modules for all studentsrequires resources and organization, the cost of a set ofmodules at the time was only US$6.00 (6,000 sets wereprinted in French to last through 1992). The English version cost US$14.00 per set (only 600 copies were made,for The Gambia). The Arabic version has only been photocopied so far, because final corrections of the languagehave not yet been submitted by the Mauritanian school.
NURSING SCHOOL CURRICULA IN THE SAHEL 105
".

The modules seem to be quite usable in an Englishschool system, judging by the Gambian experience.
Although Gambian school officials did not participate in the drafting of the modules and Gambian schoolsarc based on the British system, the state registered andstate enrolled nursing schools adopted the modules withlittle apparent difficulty. Workshops were conducted tointroduce the modules to the school staff.
Improvements in teaching methods r~ considerable follow-up.
As with attempts to change behavior in any setting,steady and periodic follow-up is required to improveteaching methods. School authorities in Mauritania, forexample, agreed in January 1990 that a meeting onteaching the CDD modules should be held with all thepermanent and part-time staff and the national CDDprogram. It took another PRITECH visit to the school inMay, several proddings from the CDD coordinator, indirect messages from Dakar, and a change of directorshipat the school before the meeting finally took place.
Notes:1 Control of Diarrhoeal DiMast Programme. ManllBf"l"lt of the Patimt with Diarrhota: Suptn'i5orySlciU6. Geneva: WHO, 1987rtv. 1990.2 Burkina Paso Health Pacilities Survry 1990.
106 TRAINING AND THE QUAUTY OF CARE

SUCCESSFUL DIARRHEAL DISEASE TRAINING:LESSONS FROM CAMEROON
The foundation for the current national control ofdiarrheal diseases (COD) program in Cameroon wasestablished in early 1987 during a national conference onoral rehydration therapy. Prior to this conference, diarrhea treatment in Cameroon was haphazard. Medicalpersonnel treated most diarrheas with medications andintravenous therapy, even though most cases could havebenefited from simple oral rehydration therapy (CRT).While most of these practitioners had heard of CRT, fewcould describe the technique of application. Researchprior to the conference showed that morbidity and mortality from diarrhea in children under age five constituted a serious threat to health (half of all deaths were as::odated with diarrhea), but there was little indication thathealth authorities took this threat seriously.
The conference brought diarrhea to the attention ofhealth planners and providers. Representatives frommany sectors and all provinces in Cameroon debated andrecommended treatment policies and goals and strategiesfor the achievement of good case management and diarrhea prevention. Though atljustments have been made tomeet the evolving needs and realities of the health caresystem in Cameroon, the principles established at theconference remain the foundation of the COD program.Not surprisingly, it was decided that training would playa major role in establishing universal good diarrhea care.
The conference participants outlined a basic "trickledown" approach to training that has undergone onlyminor modifications since 1987. According to the trickledown strategy, the program would first seek to train themost influential group of health care providers-physicians in charge of preventive medicine, pediatric services,and maternal and child health services at the national andprovincial levels. Unless these people fully accepted andpracticed "good case management" including CRT, anyothers trained might soon abandon their own use ofORT. These doctors would in tum train nurses and otherdoctors at the provincial level, who would train divisional staff and so on through to the health center personnel at the periphery and the ultimate health careproviders-the parents.
LESSONS FROM CAMEROON
Robin Waitt Steinwand was thePRITECH CameroonCaunby Representative and NdesoSylvester Atanga isthe Provincial QUa ofScvice for Statisticsand Epidemio-logy inthe Cameroon Minisby of Health.
107

With a structural reorganization in late 1989, theMinistry of Health, in collaboration with several donororganizations, began an expansion of primary healthcare coverage known as "the reorientation of primaryhealth care." Based on the Bamako Initiative, thisapproach emphasizes community involvement, costrecovery, integrated primary care, and supervision ofhealth care activities within a health district. Implicationsfor the CDO program are a more concrete framework fortraining and supervision of activities, and a system forbdter management of essential program supplies (oralrehydration salts and education and demonstrationmaterials). It has also meant that the COO program hasmoved gradually from its initial status as a developing("vertical") program to its integration into a functioningprimary health care system. Similarly, the training program has been adapted to meet the needs of the system.
DIfficulties wltU Ea.rly Trall1ll1g
The first national course trained thirty physicians,and the participants returned to their posts, apparentlyenthusiastic. However, after several months, conversations with field personnel and visits to the field showedthat these physicians were neither practicing ORT nortraining others. Cartons of oral rehydration salts hadbeen forgotten about in provincial warehouses; intravenous therapy was still routinely used in hospitals; andchildren with diarrhea were sent home from health centers with no treatment other than a prescription-themother having received no counseling for home treatment.
While maintaining the essential focus of the trainingstrategy, program personnel undertook a careful analysis of field realities and barriers to success. Over the nexteighteen months they designed, tested, and revised a successful training program and complemented this withnon-training program support. That process and someof the successful innovations are described below.
The failure of the initial training program to have thedesired multiplier effect was attributed to four problems:• Trained personnel returned to work in health facilities
that had no materials for oral rehydration. Manyworkers also believed :hat this important new technology (ORT) required the establishment of an ORT"unit"; when space or personnel constraints prohibit-
108 TRAINING AND THE QUAUTY OF CARE

c • the opening of a separate room for ORT, the therapy was quickly abandoned.
• Although workers trained in the first clinical coursewere all medical professionals with a high level oftechnical knowledge, most possessed few, ifany, skillsfor organizing or conducting effective participatorytraining. They also had no training model or coursedesign, no teaching materials, and no funds for train-ing.
• Most participants were not actually aware of whatspecific follow-up was expected of them.
• In light of all of the above, the workers perceived thatORT was not a priority of the Ministry of Health.
Irnplementmg the Solution
TARGETED ACTION
Having identified these problems, the national COOprogram team r,~spondedwith the following actions:
Elaboration and wide dissemination of a nationalCDD program strategy statement
By compiling a concise document detailing nationalpolicy and program strategy, which was signed by theminister of health, ministry officials were finally able toconvey the importance of good case management anddiarrhea prevention. The training section of this document clearly described the trickle-down strategy fortraining health personnel with annual targets and designated responsibilities. The COO program leaders sensed aneed to give the training increased visibility and credibility, and the minister appointed a high-level and esteemedpediatrician as the COO training coordinator.
Provision of health facilities with basic equipmentand materials for ORT
The minimum of materials considered essential forproviding and demonstrating to parents good case management was supplied to all major health facilities (hospitals and maternal and child health clinics). As the program continues, materials are also provided to healthcenters with trained personnel or to centers that havedemonstrated earnest efforts to implement program policy. The importance of assuring trained personnel an
LESSONS FROM CAMEROON 109

110
uninterrupted supply .. : rehydration salts also cannot beoverstated.
The program eventually redefined ORT "unit" to ORT"comer," meaning adequate space for treatment andcounseling. Larger (training) units, like provincial hospitals, are strongly encouraged to mirror an actual treatment setting with an emphasis on minimizing materialneeds.
Training of trainersIn order to establish a pool of trainers at the nation
al and provincial levels, the program organized threetraining-of-trainers courses: one for national-level clinical (pediatrics, and maternal and child health centers) andMinistry of Health program personnel, and two forprovincial supcrvisors-both doctors and nurses (oneeach for French speakers and English speakers).
Development of training modulesDuring the training of trainers, participants devel
oped a detailed task analysis for diarrheal disease controlactivities (good case management and prevention) at thehealth center. This task analysis provided the basis forthe development of clinical training modules. WorldHealth Organization (WHO) guidelines and trainingmaterials, as well as materials from several other countries, were gleaned to develop modules best suited toCameroon's realities.
The modules consist of a trainer's guide and traineehandouts. The trainer's guide for each session includes:• Session objectives,• Approximate time for session,• Materials (trainee handouts and trainer handouts,
which provide additional technical information for thetrainer),
• Learning activities (step-by-step descriptions of activities for participatory learning).
The trainee handouts constitute a packet of usefulreference material for the health worker upon return tohis work site.
The modules were tested during several trainingcourses over an eighteen-month period. Modificationswere made after each course based on evaluations andfeedback by trainers and trainees.
TRAINING AND THE QUAIJTY OF CARE

KEY CHARACTERISTICS OF THE TRA1NINaSTRATEGY
As the new training strategy was developed and tested, scvcra1 ideas, detailed below, were implemented in anattempt to address difficulties that had been identifiedeither in previous training in Cameroon or in other countries. Some are characteristic of general trends in training worldwide (such as participatory training, integrated primary health care, use of local educational materialsand workplans). Others, though perhaps not unique toCameroon, are unusual and have worked quite well(such as provincial training teams, strong emphasis oncommunications and use of local terminology, teamapproach, role plays ofspecific difficulties encounteredbytrained personnel).
Creating a pool of skilled trainers in eachprovince. Trainers skilled in partidpatory training canbe a valuable asset to all health programs. The COO program trained several key health professionals at theprovincial level whose job entails training and supervision (as mentioned above in the training of trainers).Many of these people have developed into skilled trainers, demonstrating their usefulness for COD training,and now can effectively train health workers in otheraspects of primary health care. Program personnel havebuilt in an incentive system in that someone identifiedwith strong training skills from one province can be usedto assist with a course in another province. This personcan then serve as a model for less experienced trainers.
Result: Because workers initially trained as trainersare also in charge of other provincial primary care programs, many have bem used as trainers for the immunization program, AIDS, health education, and so forth.This pool of trainers at the provincial level thus enhancesthe governmmt's efforts at integrating primary care andhas two distinct advantages for the COD program overthe use of a national training team.
First, the program can train a large pool of personnel in a relatively short period of time and at a reasonable cost, because neither trainers nor trainees need totravel far from their work site, and several training sessions can be held concurrently in different provinces. Second, by virtue of this system, the supervisees are oftentrained by their supervisor who is already convinced ofthe efficacy of good case management.
LESSONS FROM CAMEROON 111

112
Training health personnel from different categories as a team. To the extent possible, doctors andnurses are trained togcther-thcir skills and experiencescomplement each other in training as in the treatmentsetting.
Result: The depth of information desired or understood by different levels ofpractitioners during the training poses some difficulties, which trainers have tried tosurmount by making additional literature available tothose who want more detail. In general, however, thissystem has produced excellent teamwork, and evidenceduring training sessions ofa great deal ofmutual respect.
Supervisory visits to posts where the team has beentrained have shown generally very good leadership fromthe physician in charge of implementing COO goals.
Using participatory training instead of moredogmatic training methods. The clinical trainingassumes that the participants are health professionalswith substantial knowledge and experience workingwith children with diarrhea and related illness and withtheir parents. It seeks to build on these experiences andallows the participant to discover for himself the value ofthe treatment and prevention strategies promoted by theMinistry of Health and WHO. Role plays, active discussion, team exercises (group work), and especially supervised hands-on experience all encourage self-discovery.
Result: In general we observed very active participation from all participants in a training session. The endof course evaluations have mostly praised the "activelearning" parts of training.
Promotion of integrated primary health carethroughout training. Though there are specific treatment protocols for diarrhe... that must be mastered by thehealth worker, it is important that the trainee understand the interrelationship of illnesses. (Physicians reluctant to embrace ORT have commonly cited the danger ofoverlooking related illness.) Health workers are encouraged throughout the course to use every patient contactto assess nutritional problems, verify and improve vaccination status, identify other infections, and provideappropriate counseling for continued health (breastfeeding, nutrition and weaning, child spacing, hygiene, andso on). A skills checklist for hands-on practice assessesthe trainee's ability to consider all aspects of the child'shealth (see Box 1).
TRAINING AND THE aUAUTY OF CARE

As the Ministry of Health moves to implement thereorientation of primary health care through health districts, the COD program has adapted its training materials accordingly, targeting the health district supervisorsfor early training-the chief medical officer and the primary health care coordinator. The revised materialsinclude new sections on community involvement forCOD and on managing COD activities at the health district level, as well as the topics of nutrition and cholera.A streamlined version of the course (three days ratherthan five) has also been produced-intended to be used ina one-week integrated primary care training coveringother interventions, such as immunizations or malaria.
Result: Although trainees have improved markedlyin their attention to the whole patient during training,the results of a recent training evaluation indicate thatthis skill is still weak in practice (see page 115). However, the overall reorientation to further emphasize integrated management ofcare is intended to remedy this situation.
Box 1. Supervisory Skills Checklist for Hands-onPractice
. Evaluation• Evaluate the degree of dehydration• Evaluate other signs for related illness• Select appropriate treatmentTreatment• Determine the quantity of oral rehydration solution to begiven• Determine the duration of treatment• Administer treatment him(her)self first• Teach the mother to administer the treatmentAdvice to be given to the mother• Advice on breastfeeding• Advice about liquids• Advice about nutrition• Advice on the danger signs (when to seek referral)• Advice about what to do for future episodes of diarrhea• Advice on difficulties that may be encountered during theadministration of ORSCommunication with the mother• Facilitate dialogue with the mother• Reassure the mother• Ask open-ended questions• Ask questions to verify comprehensionOilier problems• Verify vaccination and nutritional statusIi Correct referral if necessary
LESSONS FROM CAMEROON 113

114
Participants plan the training follow-up. To becertain that trained personnel clearly understand theirrole in assuring good case management and diarrhea prevention activities after training, each participant preparesa three-month plan for follow-up, which he presents onthe last day to colleagues and trainers for critique andfeedback.
Result: The presentations and critiques have provided a lively end to training sessions and indicate that agreat deal of thought is given to follow-up. In the revisedtraining, participants present as a district team. A copyof the workplan is submitted to provincial supervisors.Trainees are visited by national or provincial staff within the three-month period after training and the plan isconsulted, though the degree to which it is emphasizedin follow-up varies.
The order of topics in training reflects programpriorities. Because improved health worker-parentcommunication figures prominently in program goals,counseling (form and content) is covered in detail earlyin the course.
WHO's treatment plans A and B, which comprisemost of all diarrhea cases that a health worker will see,are taught at the beginning of the course. Plan C, for thetreatment of severe diarrhea, is presented near the end ofthe course, once the trainee has gained full confidence incorrect management of the majority of cases. In thisway, plan C can be taught in the detail it requires, andthe mastery of plans A and Bis not clouded by the morecomplex equations for intravenous and oral solutionsthat plan C entails. (See Box 2.)
Result: There has been much resistance to this orderof topics among trainers who previously took an ORTcourse with the traditional clustering of topics (physiology; evaluation and treatment plans A, B, C, and medicines all together and in the beginning of training). Butonce trainers are convinced, the trainees seem to respondwell, giving the desired priority and energy to such earlytopics as counseling-the key component of treatment ofplan A cases (no apparent dehydration) in the healthfacility.
Emphasis is placed on improved communications.Good case management begins at home. Thus,
health workers are encouraged to use center-based treatment as a tool for convincing parents of the efficacy of
TRAINING AND THE QUAUTY OF CARE

EVALUAnON OF DEHYDRATIONPLANA PLANS PLANC
GENERAL CONDlTlON GoocI, .... "Re.t..... Intt.bIcI"EYES ~ SUnken
TEARS "'"-'t Abient
TONGUE AND MOUTH IIoIItTHIRST NomIII "Thirsty"
SKIN PINCH Returns "Return. slowly"
NO SIGNS OF... _201___•
CHOOSE DEHYDRATION..........._,-_.:
MODERATEPLAN DEHYDRATION
+ +USE TREATllENf WEIGH THE PATIENT
AND USETREATMENT
PLANA PLANS
ORT and training them in its application. In addition toverifying clinical skills, the checklist for hands-on practice e:;sesses communications skills-such as listening,asking open (not leading) questions, and confirming parents' understanding of instructions for home care.
Result: When there are actual cases for hands-onpractice during training, the existence of communications skills on a checklist has helped to maintain theimportance of those skills. However, there has been achronic problem of too few actual cases for thoroughhands-on practice by all trainees.
Participants are encouraged to use local terminologyand beliefs for improved communication. Ca.:ie studiesand classroom examples teach and encourage the use oflocal terminology when communicating with mothersabout diarrhea and its symptoms. The program conducted qualitative research to identify tenninology andtraditional beliefs about diarrhea, and these results havebeen written up for the health workers, including localvocabulary lists. case studies from WHO's modules weremodified to reflect beliefs and include local terms foundduring the research.
LESSONS FROM CAMEROON 115

116
Throughout the training, participants are encouraged. to improve communication through better awareness of traditions and to:• Encourage positive traditions,• Discourage only':larmfu1 traditional practices• Leave alone those tlvAt are neither useful nor hannful.
Result: As trainh.g progresses, participants begin totalk with greater ease about local beliefs and their ownadherence to some. Two recent studies (a health facilitysurvey and a study of educational materials) have notspecifically looked at whether there is any long-termimpact of this approach. At the very least, however, thereis empirical evidence of a much improved. attitude during training toward communicating with mothers usingtheir own terms and belief framework.
Role plays help anticipate challenges after training.
Participants are selected for key role plays of difficult situations that trained personnel have frequentlyencountered when they return to their post:• Presenting a three-month workplan to his local supervi
sor and convincing same of value and importance ofORT.
• Convincing a colleague not to prescribe antidiarrhealdrugs.
• Convincing a mother not to abandon'breastfeeding during child's diarrheal episode.
The other participants critique their colleagues' roleplay and offer some ideas for confronting these difficulties.
Result: These role plays have helped many participants to solidify their beliefs and prepare to be challengedabout them. In addition, they help the trainers identifypoints of uncertainty and lack of conviction among participants before the last day of training.
Visual materials prepared in Cameroon are usedwhenever possible as models.
All communication or health-education materialsproduced for the Cameroon program are used in someway during the training. Through clinical training withthe posters, communications training with the flyers,and their combined use in hands-on work, trainers candemonstrate the usefulness of locally produced information materials and increase health worker awareness of
TRAINING AND THE QUALITY OF CARE

their availability. Also, posters and flyers are distnbutedthrough training (although not exclusively).
Result: No evaluation has been conducted of theimpact of training on the use of information and educational materials during counseling, though a health facilities survey found a high percentage of trained personnel(92 percent) used appropriate tools for counseling(demonstrations or print materials). Pending the abilityof program perl'Onnel to do specific training in counseling ar, {use ofmatt.."ials, the use of these materials inclinical trcuning sets an t:Xcellent example.
Impact of the Tra l)ing
The PRITECH Project assisted the Ministry of Health tocarry out a health facilities survey' in June 1991 as part ofanevaluationof the COD program at the end of its first five yearsof operation. The survey helped to assess the ability of healthworkers to manage diarrhea cases effectively according to thenational COD program guidelines. As one objective of the survey was to evaluate the clinical training to date, evaluatorscompared personnel who had been trained by the COD program with those who had not participated in a CDD course.
Although there were too few actual diarrhea cases topermit any conclusive comparison of trained and"untrained" personnel through direct observation, theresults of the interviews with personnel indicated consistently better knowledge of good diarrhea case managementamong those trained by the program. Trained personnel correctly cited the criteria for evaluating a case of diarrhea in 72percent of respondents versus 54 percent of untrained personnel. For assessment of dehydration, 81 percent of thosetrained responded correctly versus 62 percent, and 44 percent of trained personnel correctly calculate<! four treatmentregimens against 25 percent of those not trained.
Regarding the improper use of medicines, a habit thetraining program has tried very hard to break, 91 percent ofuntrained personnel were found to prescnbe antidiarrhealdrugs compared with 61 percent of trained personnel.
Survey results also demonstrated better awareness oftrained personnel concerning counseling methods and content, though the overall results in the area of communications are not yet as satisfying. For example, only 33 percentof trained personnel correctly cited all four pieces of adviceon home treatment (versus 19 percent for untrained peJrsonnel): fluids, feeding, breastfeeding and danger signs.
LESSONS FROM CAMEROON 117

118
Since mothers are the primary care providers for diarrhea,their own -training- by health personnel throughimproved communications cannot be overemphasized.
The cvaluaf.on results also demonstrate clearly theimportance of other program support to trained pcrsonnd, in addition to training. Some examples include:
ORS SUPPLIES AND SUPPLY MANAGEMENT
Personnel whl'J have good theoretical knowledge ofthe treatment of patients with moderate or severe dehydration are nevertheless unable to adhere to the correcttreatment without the necessary oral rehydration saltpackets and intravenous solutions. Thirty-six percent ofall health facilities surveyed were without oral rehydration salts at the time of the evaluation.
HEALTH EDUCATION AND COMMUNICATIONSUPPLIES
Enhanced training in counseling techniques is onlyas good as the ability of the health personnel to apply thetechniques (for example, use of visual materials whilegiving individual health education). The diarrhea treatment chart was seen in 47 percent of facilities visited during the evaluation. Brochures for mothers on ORS preparation were available in only 6 percent of the facilities,whereas those for diarrhea treatment and prevention,printed more recently and distributed through community extension sources, were found in 21 percent.
OTHER MATERIALS FOR ORT AND NUTRITION
Personnd are encouraged to demonstrate the preparation of ORS to mothers of children with diarrhea andothers. However, the health facility survey found that inonly 33 percent of observed cases was demonstrationused as an education technique. This result could in partbe due to the fact that only 28 percent of centers inventoried had the materials necessary for a demonstration.Similarly, all childrm with diarrhea should be weighedand their growth charted, both for the purposes of determining treatmmt quantities and for assessing risk formalnutrition, recurring diarrhea, and so forth. Fortythree percent of facilities were without child scales.
TRAINING AND THE QUALITY OF CARE

WIDELY DISSEMINATED NATIONAL POLICY
The usc of antidiarrheal medicines remains unacceptably high, both in theory (when interviewed) and inpractice, despite strong messages during training thatthese medicines are strictly contraindicatect This misusemight only be successfully curtailed when importationpolicies reflect ministry standard treatment policies.
SuPERVISION
Once trained, it is essential that skills be reinforced bysupervisors who understand their support role. Only onethird of health workers interviewed had received at leastone supervisory visit in the previous twelve months.
In summary, experience and research have shownthat the Cameroon COO training program has been highly successful. The central-level COO staff has worked
Lessons Learned
with people at all levels and in several branches of healthto develop a training program appropriate to the country's specific needs and in keeping with new directions inhealth policy. The process will continue as evaluationspoint to other needs. The COO reorientation trainingcourse has now taken place in four provinces in close collaboration with the donor organizations working withthose provinces and the Ministry of Health. The CODtraining approach has been seen as a model for other vertical programs seeking to become integrated into the newhealth care system.
Two major dilemmas have been confronted in thisprogram for which there are no easy answers. There aretrade-offs which each country must assess in light of itsown priorities.
Trickle-down training versus complete controlover training of aU personnel.
A key element of this training program remains theidea that district-level supervisors, trained directly by theCOO program, in turn train the health-center-level personnel within their districts. Essentially this means relinquishing control over the quality of training received bythe health-center personnel. The Cameroon programmade this choice for reasons of economic necessity and
LESSONS FROM CAMEROON 119

120
in order to train as many people as quickly as possibleafter a core group of field personnel were trained (that is,convinced of the essentials of good case management).For the original core of trainers to train all health personnel would take too many years and would leave thetrainers unable to perform other important support tothose trained (for example, supervision and supply management). Also, it was deemed necessary to spread thework quickly so that those trained would not becomediscouraged as the only disciples of a new treatment andabandon it. However, with the trick1e-down trainingapproach, the selection of the first layer of trainees ineach district is ofcritical importance. Unless extreme careis taken in the selection of these original participants,they cannot be counted on to train others reliably.
Thus, the program has identified several qualitiesthat should be sought when selecting participants:• Leadership sk.ills,• Individual initiative,• Good communications sk.ills,• Dynamic character,• Discipline,• Good social skills,• Academic qualifications.
Beyond identification of these qualifications, the fieldsupervisor sending the candidates for training must bemade to understand the rationale for the selectionprocess. Alternatively, CDO program staff can selecttrainees during supervisory visits or operational studieslike the health facilities survey. Ideally, all candidates(future trainers) will be individuals who will not onlytrain and inspire others in the field, but will be capable ofmobilizing the community to participate in good homemanagement of diarrhea.
COD training versus integrated primary healthcare training.
This is perhaps the most debated issue in training designtoday and there are trade-offs to both approaches. TheCameroon program has successfully used both approachesin an attempt to balance of the needs of the COD programand the need to conform to the country's health policydevelopment. Early in the program, when many in themedical community staunchly opposed oral rehydrationfor the management ofdiarrhea, a five-day in-depth course
TRAINING AND THE aUAIJTY OF CARE

with plenty of time to observe actual cases was essential tobring key physicians and nurses around Integrated primary health care training simply would not have been effective for the COD program.
However, three years into the program, several hundred people bad been trained and the health facility surveyresults showed that 93 percent of diarrhea cases observedwere presaibed ORT (either oral rehydration salts or sugarsalt solution), though most of those cases were treated bypeople not yet trained A certain level of acceptance in themedical community had been achieved Thus, at a point inwhich ORT was generally becoming more accepted for casemanagement, the Ministry of Health began a strong pushto integrate and decentralize primary health care services.The gradual change to a shortened training program integrated with other components ofprimary health care couldnow occur without impeding the program's ability toachieve its goals. To reinforce its training within the integrated health center concept, COD program staffhave compiled a health center manual highlighting good case management and communications activities from the fulltraining materials.
In summary, some important elements of theCameroon training remained critical to its success, whetherasa verticalprogram or as part ofintegratedprimary healthcare. Prior to training, the Ministry ofHealth must developclear policy guidelines and disseminate these guidelinesthrough directives to health personnel and public healtheducation. During the actual training, the use of skilled(trained) trainers, local language and appropriate in-country examples, guided hands-on practice, a variety ofparticipatory activities drawing on the trainees' experiences, andclear reiteration of the program's policies and priorities (forexample, good communications, integrated health care) areall very effective. Good training is only as good as the follow-up and support received by the health worker. Thus,supervision within three months of training which refersto an action plan prepared by the trainee is critical, as iseffective management of other program components: supply management, evaluation, and communications.
Nota:1 MouS8ll CouIlbaly. "Etud, tit la priM trI charsr da cas tit dialThit dM6ltsjimnlltionl sanltalrts daprIItIinIa du littoral It du IIlId IW Call1tl'Ollll." Arlington, VA, Managemmt Sciences for Health PRITECH~,RAD-OS6-CAand LPC-032-cA, March 1993.
LESSONS FROM CAMEROON 121

LINKING 'l'RAINING AND PERFORMANCE:AN EVALUATION OF DIARRHEA CASEMANAGEMENT TRAINING IN THE PHn..IPPINES
This paper presents tbe methods and results of a collaborative evaluation of the training efforts of the Philippines national control of diarrheal diseases program. Itrepresents the combined effort of participants from thePRITECH Project, Quality Assurance Project, the Divisionof Control of Diarrheal and Acute Respiratory DiseasesProgramme of the World Health Organization (WHO),and most importantly, the diarrheal diseases program ofthe phllippines Department of Health. This evaluationattempted to link results obtained from assessment ofactual training courses in diarrheal case managementwith evaluation of the subsequent performance of thehealth worker in the field.
This evaluation design was innovative in tworespects: it attempted to measure not only acquiredknowledge but also acquired skills of health workersthrough use of simulated cases, and it attempted to linkdocumented skills attainment during training with actual performance in a health facility. Moreover, it attempted to identify factors beyond training that may affect thequality of case management in health care settings.
Since the establishment of WHO's Programme forControl of Diarrhoeal Diseases in 1980, considerableprogress has been achieved in reducing mortality due toacute dehydration. Today, more than 125 national diarrheal disease control programs are active worldwide. Acornerstone of these efforts is the training of healthworkers in correct case management of diarrhea in children. WHO has produced and distributed standardizedtraining materials for different levels of health workers,including a comprehensive curriculum for diarrheatraining units. Diarrhea training units are publicly funded centers for training trainers and health workers indiarrheal case management. They are usually located inhealth facilities that see large numbers of diarrhea cases,to allow sufficient hands-on training.
Tile N('('d for EVillllilt/Ol1
The Philippines national program for diarrheal diseases control has been one of the global leaders in pro-
UlwrmcC J. Casazzaand SCott Endsley artTechnical 0fIim's.
TRAIrWG IN ~PHDJPPINF.h
rreV10US raga El~l1k123

motion of oral rehydration therapy. Since the establishment of the Nationalllhydration, Treatment, and Training Centre in Manila in 1985, the national program hashad an active, national-level training program in diarrheal case management training. There are now threenational diarrhea training units as well as seven regional diarrhea training units. Despite these intensive training efforts, evidence from supervisory visits indicatedthat case management by health workers might not beas good as expected.
The Philippines Department of Health requested thatthe PRITECH Project conduct an evaluation of the diarrhea training units. To meet this request, PRITECH collaborated with the WHO, the Quality Assurance Project,and the Philippin~ diarrheal disease control program.Together, they designed and implemented a two-phaseevaluation: first to assess the quality of training in diarrhea training units (Part A), and then to assess the performance of graduates upon return to their home facility (Part B). Part A was conducted in September 1991 andPart B in January and February 1992.
Methodology .
The fundamental premise of training is that goodtraining produces skilled health workers upon graduation who are capable of performing adequate case management rpon return to their health facility. Case management is the clinical assessment, treatment, andcounseling for children with diarrhea.
But two questions arise from this training premise.Does the actual training, which follows the prescribed curriculum, lead to skilled graduates? And how are the workers' skills affected by a variety of extrinsic factors uponreturn to the health facility? This last question can beschematically represented in the behavior model shown infigure 1. This model proposes that there are both intrinsicand extrinsic factors that have an impact on the qualityof diarrhea case management. Furthermore, these factorsmay precede or result from the case-management performance.
The evaluation design was comprised of two parts.The instruments designed to collect information for theevaluation are shown in Table 1. The two columns on theleft were applied in Part A, the one on the right to Part B.
124 TRAINING AND THE QUAIJTY OF CARE

Factors affectingcase management performance
Figure 1.
Tc1ble 1. Instruments used tocollect evaluation dataPart A PartSObservation Casechecklists observation
• Practicals • Health worker• Case interview
presentations • Supervisor• Class exercises interview• Planning • Case
sessions simulation• Director • Facility
interview inventory• Trainee
valuation• Written exam• Facilitator
evaluations• Case
simulations
The two national-level diarrheatraining units that were chosen forPart A of the evaluation had muchexperience using WHO's trainingunit curriculum. The quality of thetraining was assessed using detailedstandardized course observationsand participant questionnaires. Thelevel of knowledge and skill of eachtrainee was assessed through written pre- and post-tests, instructorevaluations, exercises in action pkmdevelopment, and case simulations.The simulation exercises included aseries of five standardized case simulations designed to measureassessment, treatment, and counseling skills.
In Part B, a modified version of the WHOHealth Facility Surveyl was used to examinethe quality of case management in the healthfacility, as well as to identify intrinsic andextrinsic factors that may have an impact onthe quality of performance. Some of the factors identified are listed in Box 1.
When selecting health facilities for Part B,attempts were made to identify facilities inwhich a graduate who had been trained since1990, using a curriculum similar to thatobserved during Part A, could be located. Thesurvey ofthe health facilities included the observation of health workers managing actual
TRAINING IN THE PHILIPPINES
Box 1. FactorsAffecting HealthWorker PerformanceFormal trainingExternal supervisionInternal supervisionTraining cove-agelnservice trainingFacility equipmentInformation resourcesFacility proceduresHealth worker satisfactionRewards and punishments
125

Rt~S111ts
126
childhood diarrhea cases, interviews with health workersand their supervisors, another standardized case-management simulation, and an invmtory of materials and suJrplies related to diarrhea case management. The case simulation exercise was a composite of four of the five casesimulations used in Part A.
During Part A, groups of thirteen to fifteen participantswere observed and tested during training courses at twonational diarrhea training units. Both courses were judgedto be -adequate" in terms ofcontent and methods of instruction, although one diarrhea training unit course had too fewpatients available for practical training.
It was determined from written pre- and post-teststhat all participants improved their knowledge in casemanagement and diarrhea prevention. Participants of thetwo courses differed, however, in the adequacy of theapplied knowledge demonstrated during the case simulations. Performance in clinical assessment and treatmentwas judged satisfactory for trainees in the course withmore exposure to hands-on practicals, but was weaker fortrainees who were in the course with fewer patients. In thelatter, more time was available for additionallcctures androle plays about communicating with mothers. So,trainees in this course demonstrated better counselingskills in simulations. The evaluation shows that it is difficult to replace experience and confidence gained in managing actual cases with any other training method. Theresults of the case simulations strongly suggest that thebetter skills in assessment and management of diarrheaare associated with more extensive practical experiencewith patients.
Action plans, specifying training and service modifications to be made upon ,"eturn to the home !acility, weredevdoped by trainees as Jmrt of the diarrhea training unitcurriculum. Part A fouml that the designs ofaction planswere well-devdoped in both diarrhea training units. Thiswas confirmed during Pl\rt B, when nearly all (91 percent) of the training unit graduates reported having beenable to implement some or all of their action plans.
During Part B, seventeen hcaith facilities in fiveregions were visited. One hundred and devm healthworkers were interviewed, and 106 of these participatedin the case simulations. Forty-two actual cases ofdiarrhea
TRAINING AND THE QUAUTY OF CARE

Box 2. Key CharacteristicsofPanBHealth facilities (17 visited)80 percent were hospitals (60 percentregional or provincial)76 percent had trained departmentheads100 percent had ORT units30 percent (five) had diarrhea trainingunits41 percent had adequate drug supplies64 percent had adequate ORS supplies41 percent were adequatd}. equipped82 percent had adequate IV supplies75 percent had adequate staffingHealth workers (111 interviewed)86 percent were female71 percent were physicians69 percent had previous experience75 percent were fonnally trained (ofwhich 67 percent at a diarrhea trainingunit)70 percent routinely treated childrenwith diarrhea83 percent had trained other workers20 to 25 percent were satisfied withspace and equipment40 percent were satisfied with theirsupervision5 percent prescribed antidiarrheals
were observed being managed, thirty of these being managed by health workers who had also been interviewedand givm the case simulation. But only elevm of thetwmty-sevm health workers trained in Part A were evaluated in Part B, thus pointing out the logistical complexity of following up a specific subsarnple of traineesobserved during a givm training course. Box 2 summarizes some of the key characteristics of the health facilitiesvisited and the health workers interviewed.
The key findings to note in Box 2 were that all of thefacilities had ORT units, and that three-quarters of pediatric dcpartmmt heads responsible for these units hadbem trained in diarrhea case managemmt, as were threequarters of the medical staff reporting to the dcpartmmtheads. But only a fourth of these facilities were judged tobe adequate in the areas of basic ORT equipmmt, ORSsupplies, staffing, and staff motivation.
The health workers' diarrhea case managemmt wasexcellmt, regardless of their previous training (see Table 2). Sixty to80 percmt of health workers performed adequately on assessmmtand treatmmt of cases, based onknowledge testing, case observation,and case simulation. Counselingperformance was considerablyweaker. The lack. of significant differences bctwem groups of workers(that is, those trained at diarrheatraining units and those not) wasinterpreted as reflecting the extmsive in-house training (or "echotraining"). Sixty-seven percent saidthat they had organized formal echotraining upon return from the training unit; 83 percent said that theyhad givm training to another worker, formally or informally.
Beyond training itself, otherfactors that were found to affectcase management performance significantly included: practicums intraining, internal supervision, andadequate training coverage (definedas more than SO percent of the
TRAINING IN THE PHILIPPINES 127

Table 2. Percentage of doctors showingadequate case management
Doctorswbo DoctOl'5 who didSkill trained at diarrhea not train at. . unit . . unit
Actual casesHistory 69 46Clinical 62 69Treatmmt 100 85Counsclin~ 8 15Simulated casesHistory 74 80Clinical 72 80Treatmmt 69 80Counseling 26 15
health workers that see children with diarrhea havingbeen trained).
As can be seen in Figure 2, adequate practical experience in assessment, treatment, and counseling duringtraining is significantly associated with better performance in the health facility. This reinforces the strong,underlying tenet of the WHO training unit curricula,which is that participants learn by doing.
An unexpected finding from Part Bwas that internal,but not external, supervision was associated withimprovement in case management. The external supervision system for diarrheal disease control in the Philippines is focused on supervising health facilities asopposed to health workers' performance. Upgrading ofhealth worker skills is seen as a function of departmentheads and others trained in case management. Performance levels were highest in facilities in which there werea majority of health workers who had been trained andin which echo training was occurring.
LE~SS()nS Learned
This evaluation attempted to link. training with performance. Even in the Philippines, which has relativelygood record-keeping, it was difficult to follow upprospectively graduates of the diarrhea training unitcourses observed during Part A. However, retrospectivedata on training were gathered through interviews,which, coupled with course evaluations, may allownational program managers to draw conclusions regard-
128 TRAINING AND THE QUAIJTY OF CARE

ing the impact of training on perfonnance. As independent activities, course evaluation and perfonnance evaluation are both important functions that national programs can use to improve training and to identifypossible interventions to improve and sustain performance in health facilities. The following are some of thelessons learned from .' :s exercise.
Case management skill
6O+------::--;::s:,"""""'---11----------__�
5O+------------1r-:=........="""""'='~f-----__1
4O+-----------iI----------__1
30+------:--------11----------__1
20 +--------...---~"""_::l----------__1
10 +-------------.;~:::.....--=::---=::!--------1
Docton who felt they hadadequate praeticum
S1d1l
• History
o ClIDicaJlIII8l18ment
• Treatment
A Homecaaemanagement
Y Counseling
Note: Adequale pr8CtIcum _ deIllIed u maDlQiDo IIlI8alll one cue with IUpervlslon ad feedblck.
Figure 2. Case simulation performance, by quality ofpracticum
Health worker performance is influenced by internal supervision.
It is intriguing to note that this limited evaluationshowed that the internal training and support activities ofhealth facilities-in contrast to facility supplies and external activities, such as supervision-make a difference inthe quality of performance. Internal supervision in thiscontext consists of the presence of an immediate supervisor who occasionally observes the worker treat cases anda knowledgeable resource person available for consultation on a complicated case. The development of distancelearning materials and a training curriculum for smallhealth facilities could improve this in-house learning.
TRAINING IN THE PHILIPPINES 129

Case simulation exercises for diarrhea case-management training warrant further development.
Given the finding that one of the two diarrhea trainingunit courses had difficulty finding sufficient numbers ofpatients for practical experience, case simulations-both asa training approach and as an evaluative approach-needfurther development. This evaluation was not a good validation of simulation because the levels of actual case performance were so high. A different sampling strategy forhealth facilities would allow wider variance in performance,and would possibly permitvalidation ofsimulationas a substitute for observation. Simulations as a training approachhave been successfully used in other interventions, such aslactation management training and training for the management of acute respiratory infections.
The methodology developed for this strategy haspotential future applications for training, evaluation, and supervision.
The potential future applications of this evaluationmethodology are summarized in Box 3. The methods usedin Part A could be standardized to provide a mechanism formonitoring and evaluating case-management trainingcourses at all levels. In this way, course organizers can evaluate their own programs and then improve components for
,...-----------, which deficiencies are found. The methods used inBox 3., Future Part B could, in a revised form, be used for moni-Applications toring and evaluating the performance of workersTraining evaluation during supervision, periodic health facility sur-Course assessments d fi d '!\ edifiedPeriodic external evalua- veys, an ocuse program revtews.. mtions (training and pro- form ofPart Bhas been recently used in the focusedgram reviews) program reviews in Kenya and Cameroon. Final-Perfonnance cvaluation ly, based on the C]; : '~rience of the Philippines train-Skills competency testing ing evaluation. WHO is currently revising theHealth facility surveys health facility survey protocol to address moreSupervision comprehensively those factors that have an impactProgram reviews tr . .Training reviews on alIUng.
New and improved ways are needed to evalu-ate training of health workers systematically in developingcountries, and to monitor and evaluate their performancein their work settings. As we continue to identify andaddress the factors that contribute to the quality of performance, it will become possible to design more appropriateinterventions to improve health services.
Notts:I WHO Programmt for tht Control of Diarrhotal Dista5ts, Htallh Facilily Survty Manual: DialThoraCast Managtrllellt, CDD/SER/90.1, Gtntva, World Htalth Organization, 1990.
130 TRAINING AND THE QUALITY OF CARE

ORIGINS OF THE UGANDAN NATIONAL DIARRHEATRAINING UNIT: STEPS IN THE PROCESSI.· I .J'.' 1< Illl I \. I'. I :.1
The Ugandan Ministry of Health started a nationalcontrol of diarrheal diseases (COD) program in 1984 asone of the child survival programs working toward thegoal ofprimary health care for all. Initially, the programwas directed primarily at diarrheal case management athealth centers and was linked operationally with theexpanded program in immunization. In addition to promoting oral rehydration therapy in health units and hospitals, the program recently expanded to reach the community level using the health inspectorate personnel.Organizationally, the national COD program is a part ofthe maternal and child health division, which alsoincludcs immunizations, family planning, and nutrition.
The national COD program is in a continuousproccss of adaptation as it adjusts to the newly evolvingorder of the Ministry of Health and the Government ofUganda. Several emerging national and Ministry directions are helping to shape the thinking for the COD program. Thcse include:• A national emphasis on decentralized budgeting, plan
ning, and implementation of government-sponsoredactivitics.
• A focus on the districts (thirty-nine in total) as the keyunit of decentralization.
• A Ministry of Health emphasis on integrated priInmyhealth care, with a concomitant and growing emphasis on collaborative planning and implementationbetween the Ministry's functional (that is, training,health education, and planning) an~ disease-specific(such as COD, immunizations, or AIDS) departments.
The PRITECH Project's activities in Uganda are currently focused in the following areas:• Development of a health personnel training strategy
centered on the creation of a national-level diarrheatraining unit (DlU),
• Development of a strategy for the training of traditional healers,
• Development of an inservice training strategy for thehealth inspectorate,
• Promotion of commercial oral rehydration salt production,
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT
Lawrmcc J. Casazzais a Tcchnical Offiar.
131

• Development of planning and management capacitywithin the national COD program,
• Input into diarrheal disease control by nongovernmental organizations.This paper tracks the progress that was made
between March 1990 and July 1992 in establishing thenational DTIl. During this period, Dr. Casazza, PRlTECHtechnical officer, made seven trips to Uganda to assistwith the DTU effort. The continuous work done by theteam made up of staff from the national COD program,Mulago Hospital, and the pediatrics department of theMakerere University School of Medicine-with supportfrom the local UNICEF office and Sjoerd Postma,PRlTECH's country representative in Uganda-was theessential element that contributed to the success of thiseffort.
~
Diarrhea training units, or DTUs, are publicly funded centers for training both future trainers and healthworkers in diarrheal case management. They are usually located in health facilities that see large numbers ofdiarrheal cases, to provide adequate hands-on practiceduring training. PRlTECH assisted a Ugandan team in theestablishment of a national DTU at Mulago Hospital.This process involved eight steps:• Preliminary planning stage,• Planning the physical set-up of the DTU,• Assessing the training needs through a health facility
survey,• Collaborating with lactation management training,• Developing an overall training strategy to include the
follow-up of trainees,• Developing a curriculum,• Pretesting the curriculum,• Continually revising and updating the curriculum,• Formal opening of the national DTU.
Except for the last two steps, which continue on intothe future, they correspond with the trips by PRITECHstaff to Uganda to provide the team with technical assistance as it engaged in the activities to move the oru initiative ahead.
stalJl1shment of the NatlOna DTU at Mulago Hospital _
132 TRAINING AND THE QUAIJTY OF CARE

RATIONALE FOR A DTU
The Ministry of Health's national COO program haslong recognized the need to establish a D1U associatedwith Makerere University's Mulago Hospital in Kampala. The hospital, which serves a large pediatric population of in-patients and out-patients, has lacked a facility to pursue diarrheal disease training and researchobjectives. For the purpose of this paper, the oro function as a training institution is highlighted.
The training-related purpose of the OlU is to trainmedical officers, interns, residents, and medical and nursing students in correct case management ofdiarrheal disease. This training also includes modules to providetrainees with instruction to become coo trainers whenthey return to their home facilities. Finally, the OlU staffplans to be involved with follow-up of the trainees'progress in the field.
MOVING FROM IDEAS TO ACTION
The original plan for establishing a OlU in Ugandastipulated that the World Health Organization (WHO)would take the lead in its development. However, inMarch 1990, the WHO country representative and Dr.
Official opening of the Child Survival Training Unit, May 1993.
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 133

Fred Musonge, the national COO program manager,agreed that the technical assistance responsibility for theOTII effort would be transferred to PRITECH. WHOwould provide technical training materials as needed, andWHOlBrazzaville agreed to supply additional trainingmaterials. The local UNICEF and USAID offices agreed tosupport this arrangement as well.
Mulago Hospital had already designated a locationon its compound for the OTII. Drs. George Zirembuziand Elizabeth Kiboneka, from the Makerere University'smedical school pediatrics department and Mulago Hospital staff, indicated their willingness to serve as the OTIIdirectors. Together they brought strong technical and
,....------------..., managerial leadership to the OTIIBox 1. Prelimjnary PIan for the effort. While the steps outlined inEstablishment of the Diarrhea the initial implementation plan wereTraining Unit purposely comprehensive (Box 1),Facility preparation they proved somewhat overwhelm-• Site selection ing to the Ugandan team, because• Hosrital approval they had many other teaching and• Facility remodeling clinical obligations in addition to the• Equipmmt procuremmt• 1.lbrary establishmmt OTU planning tasks. Furthermore,Training preparation PRITECH had no continuous repre-• D'IU staff training sentation in Uganda at that time• Curriculum preparation that would assist them with this• CU.r.riculum finalization effort. However, continuous dia-• Development of training schedules logue with Dr. Musonge throughfor:
• Medical studmts letter and telephone kept the• Housestaff momentum alive. Also, the team• Nursing students greatly benefited from the back-• District hospital staff d t hni al un ti £<• Maternal and child health staff groun ec C orma on or-• District health officers warded by PRITECH's Information
Training activities Center, which eventually formed the• Selection of additional instructors nucleus of the future OTU library.• Procurement of supplies Simultaneously, the role of the• Reproduction of training materials future OTU was being incorporated• Lodging arrangements into the five-year national COO• Implemmtation of training courses plan. According to the plan, the OTURoutine services was envisioned to be a key element• Referral system design in the COO training strategy and• Record system design• Design of reporting system for would figure prominently in thenational program and hospital plan's two main themes: decentral• Preparation and production of forms ization ofCOO responsibilities to theEvaluation district level and increased emphasis• Health facility survey on preventive efforts in diarrheal• Follow-up survey disease control.
134 TRAINING AND THE QUAIJTY OF CARE

By May 1990, the DTII directors bad prepared a draftproposal for the OTU including floor plan, furniture, andequipment list for the unit, which they shared with the
Ministry, UNICEF, and USAID. Three importantdecisions were made at this time:• WHO would fund and provide technical assistance for
a baseline national health facility survey scheduled forFebruary 1991.
• UNICEF, while supportive of the DTII concept, wouldprovide funds for the site remodeling only after theteam bad demonstrated their commitment with theinstitution of diarrheal case management services.
• Mulago IIospital administrators would officiallyassign the proposed OTU site to the master plan forthe rehabilitation of Mulago Hospital, being finalizedwith the World Bank.
The site of the proposed OTU was ideally located inthe old Mulago complex with easy access to the mainpediatric out-patient triage facility where several hundred children are screened daily. It shared a building withthe social pediatric ward, thus linking the unit to a homevisiting program for those cases with complicating socialproblems.
.LrnooNGTaMmNGTOP~O~CE
In February 1991, Or. Jeanne Newman (QualityAssurance Project), Dr. Judith Graeff (HealthCom Project), and Dr. Casazza of PRITECH traveled to Uganda.Before departing, they formulated a conceptual framework linking the OTU training to the performance of thehealth worker after exposure to the course. This framework, shown in Box 2, calls for a follow-up system ofsupport and supervision for the trainees, primarily at thehealth facility level. This activity connects ~he trainingprogram to an evaluation and supervisory function useful for management purposes as well as for identifyingnew training needs. Implied in this framework is theimportance of supplementing the training in diarrheacase management with training in the areas of supervision, communications, and inservice or on-the-job training. This approach was presented by the consultants anddiscussed with the COO program director and futureOTIl faculty members.
The national COO training strategy therefore adopted a comprehensive conceptual framework that included
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 135

Box 2. Conceptual Framework of the Impact ofDiP..rrheaTraining on Health Worker Performance
supervisory and support activities directed to the districtlevel to ensure that the trained workers would indeed beable to perform as trained upon returning to their homefacilities. This concept would come into full play onlywhen the training program had involved decentralization of the courses to the district levels. This change willbe phased in after June 1993, following the first training-of-trainers course for district-level health teams.
ROLE OF THE HEALTH FACILITY SURVEY
The WHO Health Facility Survey of Diarrhoea CaseManagement was carried out in February and March1991. The objectives of the survey, identified by thenational COD program, were: 1) to assess the quality of
136 TRAINING AND THE aUAIJTY OF CARE

Box 3. Results of the HealthFacility SUrvey• Oral rehydration salts were used frequentlyand were in adequate supply.• Mothers knew good home-care practices.• Health workers' assessment of diarrhea was inadequate.• Inappropriate treatment was selectedfor children with some dehydration.• Children with severe dehydrationwere not treated according to nationalpolicy.• Anhbiotics were overused, althoughantidiarrheals were rarely used.• Counseling for mothers was inadequate.
diarrhea case management in health facilities where supplies for an oral rehydration comer had already beendelivered, and 2) to identify strengths and weaknessesthat could be enhanced or improved through training orbetter facility support.
Dr. Musonge decided that the surveyors for the healthfacility survey should be largely comprised of future D1Ufaculty members, thus providing them with first-handexposure to the clinical problems and staffing constraintsin the districts. This proved to be a major formative decision, as it anticipated the future role of the DTU facultyas support and supervisors to the field trainees.
On completion of the survey data collection, thesame team proceeded to data analysis with technicalassistance from WHO, UNICEF, andPRITECH. The results are summarized in Box 3. This exercise provedinvaluable in sensitizing the participants to the real difficulties thatfuture DTU trainees would face inimplementing their acquired training in the field. Also, drawing fromtheir field exposure to actual clinicalconditions, they were convinced ofthe need to incorporate a strongemphasis on nutrition into the DTUtraining and to link. their effortswith breastfeeding promotion.
With the completion of thehealth facility survey, the teamresponsible for the DTU curriculum development decidedthat, based on the needs assessment provided by the surveydata, they needed more than a minor adaptation ofexistingcase management training materials. Rather, the situationwarranted a major effort to redesign the participants' training materials as well as those needed for the training oftrainers. Dr. Musonge decided that a group composed ofthose who had taken part in the survey as well as additionaltechnical specialists in nutrition, obstetrics, training, andcurriculum development issues would hold a three-dayworkshop to design a curriculum outline.
DEVELOPING THE CURRICULUM
The group concluded that a modular approachwould be the most practical one for the OTU curriculum
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 137

138
because it is the most flexlole in responding to the needsof the various categories of workers to be addressed intraining and the particular skills required in their respective job descriptions. Additional modules could also beadded as called for by the on-going training evaluationor to accommodate any posSlole expansion of the DTU'sfunction in the future.
For each of the five modules named below, the possible audience was identified together with a draft list ofsubjects to be covered. Also, the specific performance andtraining objec:tives, resource materials, suggested teaching activitiC:i, and evaluation methods to be included inthe module were defined. The modules are:
Module t. Understanding Diarrhea (an overview oftechnical concepts and epidemiologic information)
Module 2. Diarrhea Case Management (muchmore detailed technical instruction with hands-on practice)
Module 3. Communication Skills (general conceptsfor effective communication and counseling)
Module 4. Supervisory Skills (general descriptionof app.roaches to supervision activities)
Module S. Training Skills (guidelines with exercises for training of trainers).
The latter three modules, while using COO situationsas illustrations, would be adaptable to other training programs such as the control of respiratory infections andbreastfeeding promotion.
In the process, the members of the team learned howdifficult and tedious curriculum development is toaccomplish. Although most of them were experienceduniversity-level teachers, they had never undertaken theentire process, beginning with a needs assessment andfollowing it through to the development and testing ofthe final materials.
COLLABORATION WITH THE LACTATIONMANAGEMENT CLINIC
The first discussions concerning collaboration withthe newly established lactation management clinic tookplace with Dr. Mukasa, the clinic's director, in May1990. Dr. Mukasa had recently returned from a trainingcourse at Wellstart1 (San Diego), under PRITECH auspices, along with five others who received basic trainingin order to establish lactation promotion activities at both
TRAINING AND THE QUAIJTY OF CARE

Mulago and Mbarbara hospitals. The Ugandan Wellstartassociates proposed to link. the development of theirtraining curriculum to that of the DlU. This was a logical choice as the -generic" modules (Modules 3,4, and5) could be shared. The D1U staff also wished to incorporate brcastfceding promotion and instruction in lactation management into the D1U course. Therefore twoadditional modules were added to the list:
Module 6. Understanding Brcastfeeding (an overview of technical information on breastfecding and lactation)
Module 7. Ladation Management (more comprehensive technical training with practical instruction).
Once again, in April 1992, Dr. Musonge gathered acompetent, hard-working group of technical personstogether, most of them veterans from the August 1991workshop in Jinja, where the modular outlines had beendrafted. This time he was assisted in preparation by hiscompetent staff and by Sjoerd Postma, who had beenhired by PRITECH in October 1991 as its full-time representative in Uganda. Mr. Postma's presence greatly facilitated the in-country follow-up of progress as well ascoordination with other donors and the PRITECH officein Washington.
Mary Kroeger, a nurse-midwife from Wellstart, alsocame to assist with developing the two breastfeedingmodules. After five days of work in small groupsassigned to the various modules, the team emerged withconsiderable detail on content, teaching activities, andspecific resource materials for all seven modules. Training mate:ials were derived from several WHO resources,the extensive COO and nutrition literature, and breastfeeding references-all greatly contributing to the draftproduct.
Even with the modules developed, however, therewas still no clear idea how they would be used in actualtraining. The team hoped that this would be clarified during their pretesting. Nor had the team yet devised a training implementation schedule, although it was envisionedthat eventually On! training would be decentralized tothe district level with the national Dn! staff serving asfacilitators to the local trainers who had completed atraining-of-trainers course at the national OlU.
By this time, the On! had been operational for threemonths as a service provider for pediatric diarrhea casescoming into Mulago Hospital. But a brief assessment of
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 139
140
the health workers' performance pointed up the need toupgrade the standard of care as soon as possible. Exceptfor the three faculty members who had received casemanagement training several years before at variousinternational COD training centers, there were no adequately trained D1U personnel in Uganda. In fact, thecurriculum development process additionally provided anecessary update of skills and knowledge to staff whohad received previous COD training.
TRAooNa-OF-TRA!NERs COURSE
The DnI team decided that the modules were readyfor pretesting in July 1992. But in order to speed up thedevelopment process, the pretesting was incorporatedinto a training-of-trainers course. While this was not theideal situation, there were significant numbers of "new"participants (all were future DTU trainers and resourcepersons) who had not been involved in the earlier curriculum development steps and whose direct input wasimportant to the finished product. Now they would have"hands-on" practice with the full content of the course.Financial support for the training came fromUNICEF/Uganda, and WHO sponsored the participationof Dr. Hans Troeddson, WHO representative from Zambia, as an experienced course facilitator together with Dr.Casazza, sponsored by PRITECH.
The participants included twenty-five trainees, withthree coming from Mbarbara University Hospital, wherea second lactation management clinic and DTU areplanned. The Mulago Hospital participants included theDTU nurses and their senior nursing officer, the medicalofficer in-charge, and a team of supervisory pediatricians. A clinical nutritionist, a health educator, a health
. visitor, an obstetrician, and a nurse tutor, together withnursing officers assigned to lactation management atMulago Hospital, rounded out the multi-disciplinarygroup selected as future trainers and resource persons.
During the ten-day course, the group workedthrough all seven modules developed in the earlier workshop. They decided to focus the course on Modules 1 and2 dealing with diarrhea case management and Modules6 and 7 for lactation management training. The threegeneric modules would be interspersed throughout thecourse at appropriate times. The diarrhea case management training materials consisted of selected WHO train-
TRAJNINQ AND THE QUALITY OF CARE

Mrs. Jmrina Mutabazi presenting at the trainin,g-of-trainers course.
ing materials with additional updated hand-outs fromthe literature. The lactation management componentrelied heavily onWdlstart training materials. Finally, thegroup agreed that the products for the course would bethe revised training Modules 1 through 7, and the 199293 oru training plan of action.
The general approach to the didactic training activities was as follows: the person responsible for the module presented its learning objectives in their prescribedorder using all the preselected training materials andhand-outs; after the presentation of each learning objective, the audience provided feed-back to the presenter onthe adequacy and clarity of the technical material as wellas on the training methods employed. The speaker's useof audiovisual equipment was also critiqued.
Using the evaluation checklists, Dr. Casazza recorded his observations of the various learning activities, aswell as a summary of the group's remarks. At the end ofeach week, the key faculty members for both diarrheacase management and lactation management, togetherwith the PRITECH country representative and consultants, convened for a thorough review of the week'sactivities.
In general, the modules required only minor revisionsand reorganization. It became evident that Modules 1,2,6, and 7 were the core modules for diarrhea case management and lactation management training; Modules 3, 4,
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 141
]
142
and 5 were important as references to be read by the participants who would incorporate the concepts presented inthem within the context of the core modules.
This was especially true for the subject areas of training and communication skills.
Dr. Ezra Teri, a UNICEF health education consultantto the Ministry of Health, was helpful in clarifying theessential elements in Modules 3 and 5 dealing with training and communication skills. These modules were readas homework the night before their presentation; thentheir salient points were discussed as they related to COOand breastfeeding training and clinical service. The participants' enthusiasm for more detailed instructions onhow to improve lectures, demonstrations, andgroup discussions markedly increased as they became more awareof the importance of the methodological aspects of training to their effectiveness as teachers.
Module 4 on supervisory skills was only briefly presented as the content was seen to be more relevant to asupervisory skills course for the relevant participants,but the interpersonal skills used in supervising personnelwere practiced as they are related to training skills aswell. This module could serve as a useful conceptualintroductory building block to follow-up training insupervisory skills.
Corresponding with the presentation order of thecore modules, hands-on practice sessions for both breastfeeding and COO were carried out at Mulago Hospital,except for one side trip to nearby Rubaga Hospital to visita busy oral rehydration comer there. When the regularcourses are offered in the future, the goal will be to dedicate about 50 percent of the total agenda time to practical training.
There was ample opportunity for all the participantsto have sufficient exposure to a variety of clinical problems associated with pregnant and postpartum mothersat the prenatal clinic at Mulago and the outpatient lactation management clinic, respectively. But the overcrowded space for these out-patient services made it difficult to accommodate the trainees. Furthermore, mostof the common breastfeeding problems encountered bypost-partum mothers can be adequately demonstratedon the ward.
The newly remodeled OnI was the site for the COOpracticals and case presentations; it easily accommodated the busy patient flow along with the added trainees
TRAINING AND THE QUAIJTY OF CARE
and facilitators. During the training course the DTU initiated feeding of the patients together with rehydration;this will become a routine activity for the unit.
One of the most significant accomplishments of thetraining of trainers was the design and pretesting of anew OTU case management form to be used for all casespresenting to the unit. The form incorporates data collection for many of the risk factors associated with diarrheal disease in infants and toddlers as presented in thedidactic portion of the training. These factors includenutritional and dietary assessment and immunizationstatus. Furthermore, it links the information collected inthe history-taking with the relevant preventive messagesto be stressed in the counselling activity. Finally, it forcesthe health worker to conduct a thorough investigationof the whole child by responding to each and every question on the one-page form, thus promoting a degree ofquality assurance to the interaction.
The training-of-trainers participants used a draftversion of this form throughout the course and contributed helpful suggestions for its revision, which wereincorporated immediately. It was agreed that this formwould be used routinely in the OTII after its finalizationand the data collected would be analyzed regularly by Dr.Charles Mugero and the oru pediatricians.
F'uTtmE ACTIVITIES
The group reached a consensus that in the futurethere could be separate courses for CDO and lactationmanagement, but regardless of which emphasis thecourse presents, all courses will contain elements ofmodules 1, 2, 6, and 7. Depending on the roles and functionsof the health workers to be trained, the specific courseagenda can be designed to include those selected learningobjectives chosen from the four core modules that bestreflect the course objective. For example, only nursingand medical school tutors would be possible candidatesfor all objectives ofall modules, while pediatricians mightfind modules 1 and 6 redundant in view of their previous education. Modules 3, 4, and 5 would be included asappropriate for the audience.
Finally, the group agreed that the next training activities would build on the training of trainers to address theneeds of: (1) the newly assigned, yet untrained OTUstaff; (2) other relevant Mulago Hospital staff, especial-
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 143

ly those in the pediatric department; (3) OTU staff withmajor organizational and programmatic responsibilities;(4) the district-level teams who would later decentralizethe COO and lactation management training; and (5)principal tutors of training schools. Health workers whohad been involved in this training of trainers would becalled upon to participate in these training activities tofurther refine the modules and their own teaching skills.The funding for these future activities would be forthcoming from WHO, UNICEF, USAIO, and the Ministryof Health.
Impact of the DTU
The DTU team agreed that there should be no outcome evaluation of the DTU efforts for at least the firstsix months. During this period, a series ofcourses will beconducted with the dual objectives of: (1) training healthcare workers and (2) refining the training skills of thetrainers. An exchange of trainers with the national OTUin zambia is also scheduled.
By the end of 1992, two additional courses had beenconductedby the trainers, thus training fifty-two doctors,midwives, and nurses from Mulago and Mbarara hospitals. Two more courses are planned for the near future.After each course, the trainers showed keen interest inevaluating the knowledge and skills acquired by the participants as well as improving their own skills in assessing these changes. The modules will be finalized in rnid1993, incorporating comments from the course trainersand participants. So far, there has not been any supervision or support activity undertaken by OTU faculty,because the participants were comprised of faculty and ...staff from the two hospitals that will function as DTUs.The decentralization of training and the follow-up super-visory and support activity will begin in June 1993.
Both the Ugandan government and UNICEF/Uganda are looking to the DTU and its team of trainers tofunction as a potential platform for a national case management training center. Additional disease-specific modules will be developed for this purpose in order tostrengthen the quality of case management applied toother major killers in the under-five population, namely, acute respiratory infections and malaria. With the
144 TRAINING AND THE aUAUTY OF CARE

WHO case management protocol available for respiratory infections, this could be the next step for the OlU.
As a spin-off effect of the establishment of the OTU,its staff can now make a stronger case for facilities to beprovided by Mulago Hospital in support of the OlUactivities. These include a hostel for the trainees, regulardrug supplies, and food from the central kitchen for OTUcases.
Finally, while UNICEF assisted in the development ofthe structural improvement of the facility, PRITECH provided computer equipment for word processing and caseload monitoring, equipment for producing trainingmaterials, and minor kitchen items. The OTU (presentlycalled the Child Survival Training Unit) now functionsregularly on a twenty-four-hour basis with an averageof thirty patients seen daily. Many are complicated caseswith malnutrition, acute respiratory infections, or suspected AIDS, thus contributing to a greater number ofmoderately and severely dehydrated cases.
Lessons Learned
Training should be linked with a supervision andsupport system to be effective.
A major challenge to health training efforts is todevelop courses that are relevant to the needs of theworkers and the clients that they serve. As more emphasis is given to assessing the quality of these trainingefforts, the measure of success hinges more on the measurement of competency developed in carrying out newskills and changed behavior in both the health workersand the caretakers (mothers). The behavioral changemeasurements become the focus for the monitoring andevaluation of the training efforts. Thus, the follow-up ofthe trainees and the clients they serve can be an informational source for the entire program. Through a support and supervisory role assigned to the trainers(already the OTU faculty is primed for this from theexperience of the health facility survey), other elementsin addition to current COO training practices can be identified as obstacles to implementation of the trainingreceived. This follow-up step provides feedback to thoseinvolved with logistics, administration, and eventuallyplanning for the overall project.
While the implementation of the support and supervision concept has not been fully worked out for the pro-
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 145
,.
146
gram at this time, the concept proved to be a strengthening element in unifying the donors and the diverse participants from the university and ministry ranks behindthe rationale for the olu.
Curriculum development is a key activity aroundwhich "national ownership" ofa CDD training program can be established.
Through the steps involved in the process of developing a curriculum, the olu faculty became intimatelyfamiliar with the needs of the health workers and theclinical conditions they treat. This process began with a"needs assessment" accomplished with the health facility survey. The actual curriculum preparation phase followed, which required interdisciplinary collaboration toaddress the technical content as well as the methodological issues. Most importantly, it will include a supervisory and support activity that ties the training component into the overall strategic planning and evaluationactivities of the program once the training becomesdecentralized.
A specific case management protocol provides acore for a clinical service delivery program.
WHO deserves much credit for the development andpromotion of its case management protocol for diarrhealdisease. Lending its name to the protocol gives it credibility among clinical experts in the medical field globally. But more importantly, the protocol provides theneeded technical guidance for specific diagnostic, treatment, and counselling activities essential to handlingpatients presenting with the illness. For cases ofdiarrhealdisease, the diagnostic and treatment procedures that theprotocol advocates are more simple and cost-effectivethan the practices currently in place. In Uganda, the curriculum embraced all the assessment, treatment, andcounseling principles of the protocol while giving it thespecificity needed to make it nationally appropriate. Furthermore, it sets standards of care that can be translatedinto indicators for measuring not only the quality ofcaregiven by the health workers but the training theyreceived as well. As WHO develops new protocols for usein management of the sick child, the experience gained byOTIl staff and faculty can be expanded to address theseclinical situations as well.
TRAINING AND THEOTJ~ OF CARE
This uprocess development" approach is time-consuming.
The time expended from the initial discussions withthe national COO program leaders until the testing of themodules was approximately two-and-a-haH years.Although some of this time was spent in site acquisitionand remodeling, it is conceivable that this period wouldhave been shorter if the available WHO materials hadbeen directly adopted for courses. It remains to be seenjust what long-term effects this process has had on theprofessional development of the trainers and the qualityand sustainability of their work in the future. No doubtthere will be revisions added to the course content as aresult of feed-back from the trainees; the modules aredesigned to accommodate such updating as well as newsubjects as needed.
Curriculum development requires adequate technical assistance inputs.
By expanding the scope of the technical content toinclude breastfeeding, communications, training, andsupervision, the need for additional technical expertiseexpanded to include both local and internationalresources. This brought together professional resourcesthat, if isolated by subject area (such as breastfeedingpromotion or diarrheal contro!), would not have had theopportunity to interact and develop the integrated curriculum. Another example is the assistance of an expertfrom the Ministry of Education in addressing issues ofgeneral curriculum development. His guidance wasessential for adherence to national educational standardsrequired before introducing a new curriculum into government and university training programs.
Multi-donor involvement is essential from early onfor successful completion and sustainability of theeffort.
The DTU program represents the combined efforts ofWHO, UNICEF, PRITECH and USAIO, the Ministry ofHealth, Makerere University School of Medicine, Wellstart, and the Quality Assurance and HealthCom projects. In addition, a World Bank-sponsored team wasinvolved in the decision on the OTU site. The persistentadvocacy for the DTU by the COO program was key tothis complex coordination of donors. Also, the PRITECHresident representative assisted greatly in this effort.
THE UGANDAN NATIONAL DIARRHEA TRAINING UNIT 147

With the anticipated phase-out of PRITECH funding inmid-1993, it was esscntialforits long-tmn survival thatthis dfort have multiple agencies interested and alreadyinvolved. The probability of the DlU's continuing activities and its sustainability for the future have been established at this time because of the extensive investment infunding and effort that each organization has contnbuted so far.
Notes:1 Wdbtart San Diego IJK:tatlon Program educates health professlonab from dcvdoplng counbiesabout lactation management.
148 TRAINING AND THE QUAIJTY OF CARE

CHOLERA CONTROL ACTMTIES IN GUYANAAND THE ROLE OF TRAINING WORKSHOPS
Box 1. Objectives of theCARECIPRITECH TrainingSessions on Cholera Control• To sensitize health care workers tothe signs of cholera,• To keep health care workers alert tooutbreaks,• To mabIe participants to provideappropriate and cost-effccive manage·mcnt of cholera cases,• To equip participants with tcchr~cal
materials for training other healt!. careproviders,• To plan for follow-on trainir.g byparticipants in their respective (ountries.
In response to the cholera epidemic that began in Peruin 1991, the Caribbean Epidemiology Center (CAREC)developed a plan to assure adequate preparations amongits member countries for possible cholera outbreaks.CAREC, a regional office of the World Health Organization, helps to prevent, control, and eliminate disease inthe Caribbean, and to promote health. As part of thecholera preparedness effort, CAREC and the PRITECHProject jointly sponsored a two-day training session inclinical case management in Georgetown, Guyana forhealth professionals from Guyana and Suriname in May1992.1 Later, PRITECH and CAREC sponsored a regionalworkshop in clinical case management in Port-of-Spain,Trinidad. Two physicians from Guyana attended theworkshop: Dr. Haydock Wilson, the chief medical officerfor the Guyana Ministry of Health, and Dr. Leslie R. Persaad, the chief medical officer of the Guyana Sugar Corporation. At the time of the training sessions, cholera hadnot appeared in any of the CAREC countries except forBelize.
Subsequently, cholera spreadfrom Venezuela to Guyana inNovember 1992 (about six monthsafter the workshop). Dr. JamesHospedales, an epidemiologist withCAREC, was called in as an epidemiological consultant immediately after cholera was detected.Since then, about 600 cases haveoccurred with several deaths.
In April 1993, PRITECH sentDr. HospedaIes, who directed theTrinidad workshop, and Dr. DavidSack of PRITECH, who had assistedat the workshop, to Guyana for afollow-up visit. The purpose of the visit was to evaluatecholera control activites in Guyana and to describe therole that CAREC and the CAREC/PRITECH workshopplayed in assisting with the cholera control program andon second-generation case management training. Thispaper evaluates the role the training provided in enhanc-
CHOLERA CONTROL ACTMTIES IN GUYANA
David A. SacIt is aPRrrEOi TechnicalOffiar and C. JamesHospcdaJes is Epidemiologist at theCan"bbean EpidemiologyCcntcr.
149
'"

ing the ability of the medical staff to control the choleraepidemic in Guyana.
Cholera Preparedness III Guyana·
Bordered by Venezuela, Suriname, and Brazil, on thenortheast coast of South America, Guyana has an areaof 83,000 square miles and is divided into ten administrative regions. Cholera has occurred in the three regionsmost proximate to Venezuela. Of the total population of750,000, most live along the coastal areas. Several racialgroups exist, reflecting Guyana's colonial past: East Indians, African, Chinese, Amerindian, and whites. TheAmerindians tend to live in the remote areas and havepoorer hygiene and sanitation conditions.
...-------------.., The coastal area where mostBox 2. Cholera-Related Events people live is a riverain area (GuyanaRelevant for Guyana means land of rivers). Flooding is• Appearance of cholera in Peru (Jan- common during the wet season, anduary 1991) much of the land is below sea level.;~~g~~~~= With estuaries, there is a shellfish1992) industry and exports, and an• CAREClPRITECH workshop at increased risk of cholera, especiallyCAREC (June 1992) of the endemic form. Other tropical• Appearance of cholera in Venezuela diseases comm ~,! in Guyana includeadjacent to Guyana (August 1992) malaria (mosth !'.fialciparum), Ban-• Enhanced surveillance and training 1
in regions adjacent to Venezuela, croftianfilariasi.s, and recently AIDS.development of Wilson-Beard cholera With the appearance of choleracots and Wilson cholera straw in Peru and its spread to other South(August-November,1992) American countries, it became• Appearance of first cases in Guyana apparent that Guyana would even(November 1992)• Case-control study of cholera, joint tually become affected. The spreadproject between Ministry of Health from Peru continued to Ecuador,and CAREC (November 1992) Colombia, Venezuela, and finally to• Consultancy by Hosp~es(CAREC) Guyana. Factors that increase theand Sack (PRITECH) (April 1993) cholera risk for Guyana include (1)
its low-lying riverain area and estuaries, where manypeople rely on fishing and shellfish; (2) traditionalhygiene and water behaviors practiced by many of thepeople; and (3) many remote areas where access tocholera treatment is difficult. Drinking water directlyfrom the river is common, even without a water container to store water briefly, and the toilets used are frequently a bush. The Amerindian population are at especially high risk because they have retained thesetraditional practices, and have a preponderance of blood
150 TRAINING AND THE QUAIJTY OF CARE

group 0, which makes them an especially high riskgroUp.1 Being remote both geographically as well associally, they are also at higher risk of death should theybecome ill.
When cholera was recognized in neighboringVenezuela in August 1992, surveillance was intensifiedin the adjoining regions of Guyana. Dr. Wilson of theMinistry of Health led the way in this effort, visiting thehospitals and health centers, to insure that ea1'ly caseswould be recognized and reported immediately to theMinistry. Furthermore, supplies and logistics needed forcholera case management were organized, and healtheducation efforts directed at drinking boiled or treatedwater and cooking fish and shellfish were intensified. OnNovember 5, a case was described that appeared clinically to be cholera and was subsequently confirmed bacteriologically. The Ministry of Health responded immediately to the case description by sending teams of doctorsand nurses from Georgetown, including Dr. Wilson, tothe cholera-infected area. Though a few of the earlypatients died, most survived and the overall case fatalityrate has been less than 2 percent. During the early epidemic, the Ministry of Health also rotated about fortydoctors and nurses from other parts of the country to thecholera-affected area to provide them with clinical experience with management of cases.
By April 1993, the numbers of cases had droppedconsiderably, though two cholera deaths among threecases in a village occurred during the month of March.The cases are illustrative of many of the constraints incontrolling cholera in developing countries includingGuyana.
The first case was an Amerindian man who developed acute diarrhea on March 3 and was treated withoral rehydration salts in the village. He recovered by thenext day, but by then his wife developed severe diarrhea.She was treated by the headman of the village with localmedicines plus Lomotil, but was not taken to the healthcenter, did not receive rehydration, and later died onMarch S. The headman who had treated the wife developed abdominal discomfort two days later, followed bysevere diarrhea on the night of March 9. The next morning he was taken to the health center, where he was seenby the health assistant. He was given one liter of intravenous fluid and appeared to revive, but again becamedehydrated and died that day. A fecal specimen from the
CHOLERA CONTROL ACTIVITIES IN GUYANA 151
headman was cultured and was positive for V. choloae01 but specimens were not obtained from the others inthis cluster. Drinking water for the village was from thecreek.and was used directly without boiling. Tetracyclineprophylaxis was given to the villagers.
Since the authors were not present during this cluster of cases, one must be careful in making judgments;however, this experience points to several aspects ofcholera case management that went wrong. The firstcase, though it fit the description, was not recognized tobe cholera. When the wife became ill, her illness also wasnot recognized and she was not taken to the health center. Instead, inappropriate antidiarrheal and traditionalmedicines were used. Why the husband, but not the wife,received oral rehydration salts was not known. Finally,the headman was taken to the health center where facilities were available to give appropriate rehydration.Unfortunately, the health assistant was not sufficientlyknowledgeable or experienced to give adequate amountsof fluids to rehydrate and maintain hydration. These factors were further compounded by the occurrence of thecluster within a traditional society where water and sanitary practices are unhygienic, where access to care ispoor, and where use of ineffective treatments may prevent use of effective rehydration. Better training of thehealth assistant should have prevented the headman'sdeath, but better information and communications wereneeded for the first two cases.
Impilct of the Trallling .
The authors traveled to Georgetown inApril 1993 todetermine if the training activities carried out previouslyhad had an impact on case management in Guyana. Theymet with key individuals in the Ministry of Health, thePublic Hospital, Georgetown, including the cholera treatment ward, the emergency ward, and the laboratory;and visited one of the trainees who had come to CAREC.At the Public Hospital, Georgetown, nurses who hadworked in the epidemics and had been trained by Dr. Wilson (a CAREC trainee) were interviewed. Physicians in theemergency ward, who were caring for an adult patientwith severe diarrhea, were also interviewed.
It was not possible in the short time available todevelop or test any formal instruments to determine theimpact of the training; however, the interviews were use-
152 TRAINING AND THE QUALITY OF CARE

ful in gaining a perception of the role the training playedin the national response to cholera.
The CAREC workshop on clinical case managementin Georgetown was well attended; however, many of thekey persons (especially from the Public Hospital, Georgetown) could not be present and a second session had tobe planned. The workshop thus attempted to reach themaximum number of people, but not a highly selectedgroup. On the other hand, the regional workshop inTrinidad only allowed two participants from Guyana.The two persons chosen were very appropriate: the firstlater became the key Ministry of Health clinician in thefield when cholera spread to Guyana and became wellknown for his successful efforts there. The other participant was the chief medical officer for the sugar company, the largest industry in the country. Hence, key decision makers from both public and private medical carewere represented at the CAREC workshop.
USEFULNESS OF THE 1'RAINING
The training was felt to have accomplished severalgoals. First, it raised awareness in the medical community of the threat of cholera and initiated a process of dealing with it in a more realistic fashion. Stories ofcholera asit affected Peru had the potential of creating unrealisticfears, and the workshops improved understanding of thedisease in a manner that allowed participants to plan constructively for its control. Second, the CAREC regionalworkshop facilitated the personal development of two keypersons who would provide leadership to the national program. Working within the Ministry ofHealth, Dr. Wilsonorganized the surveillance in the regions close toVenezuela, organized the logistics for case management,and prepared the medical staffin the area to deal with casesshould they appear. When cholera did appear, he returnedto the cholera-affected area, assisted with case management, and trained others. In addition to training the staffin the immediate area, he trained staff from other parts ofthe country to prepare them to treat cases if cholera wereto break out in their regions.
Dr. Persaad, the chief medical officer of the GuyanaSugar Corporation, was the other CAREC trainee. Thesugar corporation employs 22,000 workers in eightestates located in four regions, and provides medical benefits to the employees and families, totalling 120,000
CHOLERA CONTROL ACTMTIES IN GUYANA 153

154
beneficiaries. Since the CAREC workshop, Dr. Persaadhas: (1) held a one-day cholera workshop for his medicalstaff using the materials provided at the workshop; (2)insured that each of his estates have the supplies andmedicines for treatment of patients (cholera cots, rehydration fluids/supplies, tetracycline); and (3) formed acholera control committee for the sugar corporation,which has since evolved into a health and safety committee. The sugar corporation has a central medical facility near Georgetown and health centers in each of theestates, most equipped with ambulances.
In addition, the CAREC regional workshop resultedin secondary training within Guyana, and the trainingmaterials from Trinidad were used in this training. Dr.Persaad carried out a formal workshop using the training materials with the staffof the sugar corporation, andDr. Wilson was· the primary trainer for the Ministry ofHealth, training the hospital and health center personnelin the cholera-affected areas as well as training nurses atthe Public Hospital, Georgetown, and doctors and nurses from other regions of Guyana. Based on interviewswith the nurses at the Public Hospital, these staff had anexcellent grasp of the concepts of cholera management,of the need for rapid rehydration, and of the appropriateuse of oral rehydration therapy.
INNOVATIONS IN CASE MANAGEMENT
The training also provided a fundamental understanding of cholera treatment that led to innovations bythe Ministry of Health. For example, cholera cots areusually made from army cots by cutting a hole in themiddle. Unfortunately, the army cots in Guyana have athird leg in the position where the hole should be, preventing effective use of these cots. Because of a shortageof funds, Dr. Wilson and Mr. Beard designed a very inexpensive cholera cot out of locally available materials.
The Wilson-Beard cholera cot uses two long 2" by 2"boards and two plastic fertilizer bags to make a stretcher, and the stretcher fits into a locally made frame. Thefertilizer bags are placed with a small gap between them,the gap serving as the hole in the normal cholera cot. TheWilson-Beard cot had several advantages. It was economical, as it uses locally available materials. The plas-
, tic fertilizer bags could easily be cleaned and soaked indisinfectant after use, and could be discarded when worn
TRAINING AND THE QUAUTY OF CARE

The Wilson-Beard cholera cot.
out. The stretcher was transportable and could be usedto carry patients some distance (not possible with standard cholera cots). Development of the cot addressed apractical problem of case management, and solved it in arational and creative manner.
A second innovation was the "Wilson straw" foradministering oral rehydration solution. Being shortstaffed, a medical team from the peripheral hospital recognized that it would be difficult to administer oral rehydration solution and to measure the amount of solutiondrunk by the patient, as well as the amount of stoolpassed. They solved this problem by using leftover intravenous fluid bottles as pitchers for oral rehydration solution, and placing old plastic intravenous tubing into thebottle as a long straw. With the bottles on tables slightly higher than the beds, patients could suck on the strawand drink oral rehydration solution with little effort, andthe volumes could easily be monitored by the nurses.
These two examples demonstrate the application ofappropriate solutions to practical problems being facedwith case management, using the standard principles ofcholera therapy learned during the workshops.
CHOLERA TRAINING AS A BOOSTTO DEVELOPMENT OF REGIONAL RESOURCES
One aspect of any training is that the trainer is alsothe learner. In this regard the professionals at CAREC-
CHOLERA CONTROL ACTMTIES IN GUYANA 155

156
who were experienced in epidemiology, microbiology,and nursing, but had not previously dealt with cholerabecame the regional experts and the primary consultantswhen cholera appeared. The fact that CAREC was calledand that Dr. HospcdaIes came to Guyana within the firstfew days of the first case in Guyana provides evidence ofthe confidence in this resource. The cooperation of theMinistry of Health with his consultations, and the success of the case control studies he carried out is furtherevidence of the importance of building up this type ofregional capability.J
CHOLERA AS AN ENTREE TO OTHER PuBucHEALTH ACTIVITIES
Cholera was a stimulus for initiating other usefulactivities. Examples include improved communicationbetween sanitationand health staff, and upgrading of thelaboratory.
At the Guyana Sugar Corporation, Dr. Persaad organized a cholera coordination committee after returningfrom the CAREC workshop. The goal of the committeewas to identify preventive interventions that coulddecrease the risk of cholera on the estates. Both medicaland engineering staff were included on the committee.Surveys of the estates were carried out to identify riskfactors for cholera. During the initial phase of the committee's work, several defects were detected dealing withwater and sanitation, and plans are underway to correctthese. During this process, other problems were detectedin addition to the threat of cholera, and the committeehas evolved into a health and safety committee to addressthe wider scope of issues. The new committee will continue to address the broader needs of the community, butcholera was the stimulus for the improved intersectoralcommunication.
The microbiology laboratory had fallen into a lowstate ofpreparedness during the preceding decade. Located on the grounds of the Public Hospital, Georgetown, ithad nearly ceased to function, and the roof was literallyfalling in. The lab had fallen into such a state of disrepairthat although typhoid fever is a serious problem inGuyana, the causative organism could not be isolated.With the threat of cholera, however, resources are againbeing put into the laboratory. Some equipment is beingpurchased, and a microbiologist has been recruited to
TRAINING AND THE aUAUTY OF CARE

upgrade the lab. This should benefit cholera controlefforts, as well as the control of other bacterial diseasesin Guyana.
DEFICIENCIES IN THE 1'RAINING
Training in cholera management was carried outwithout an overall training strategy. While many persons were trained in case management, it was not clearthat all of the appropriate staff had been trained. Forexample, physicians in the emergency ward at the Public Hospital, Georgetown, where cases were most likelyto present in the capital city, were skeptical ofcorrect casemanagement and were not aware of many of theresources for management of cases. Physicians appearedto be quite independent in their approach, and plans toimprove morale as well as case management are needed.
Second, the training was carried out with no handson experience, since cases were not available during thetraining session. Without practical experience, thetrainees were not able to become proficient in proper casemanagement during the training session. The assumption in carrying out the training without the practicalaspects was that physicians would quickly learn how toapply their knowledge when they do begin seeingpatients, that is, there would be a rapid and correct learning curve because of the training. Without the training,wrong practices would develop and later training wouldbe more difficult. Despite the lack of hands-on training,however, the experience in Guyana shows that the accelerated learning did occur.
A third deficiency of the training was that it did notprepare the Ministry of Health to deal with the press.This was not a goal of the training so its failure in thisregard is not unexpected. The press was very interestedin the appearance ofcholera, and was insistent on knowing as much as possible very rapidly. The Ministry ofHealth attempted to provide the information, but wanted to be sure that the information was correct before itwas released. Because confirmation of cholera cases frequently requires a few days, the ministry was in theuncomfortable position of appearing to be withholdinginformation during the time it took to confirm cases.While not a priority for training workshops, a strategyfor educating the press about cholera was needed. Clearly the press can provide a service to the community by
CHOLERA CONTROL ACTIVITIES IN GUYANA 157
..
,.
-

•
educating them about risk factors, purifying water, andso forth, and can advise them to seek medical care ifsymptoms develop. However, the press can also createpanic in an attempt to sensationaIize the news aboutcholera.
Lessons "Learned . I "
The regional training model worked well in~uyanaand should be replicated elsewhere.
Because the training was conducted through theregional center at CAREC, it established an availableresource for assistance when cholera appeared. In thecontext of the Caribbean region, this was a most effective strategy. Training limited to national programswould have been much less effective, and would not haveled to the development of sustainable expertise in theregion. Participants in the CAREC training were recognized as experts in cholera manage"Uent and control inGuyana. This recognitio7"! facilitated the plans for cholerasurveillance, established cholera coni. )1 leadership in thefield, and helped to provide an organized response to theproblem. Confidence in the trainees appeared to be a factor in the confident approach taken by the Ministry ofHealth in dealing with the epidemic. The CAREC trainingsuccessfully raised the level of awareness within themedical community. Previously, cholera was known tobe a dreaded disease, associated with fear and panic. Withthe training, cholera was highlighted, but it was alsounderstood to be a problem that could be controlled.
Training should be one element in an overallcholera preparedness strategy.
The CAREC training was one part of the overallcholera control strategy. Clearly, the Ministry of Healthofficials, the Pan American Health Organization (ofwhich CAREC is a part), and many others spent considerable time in managing the various aspects of thecholera control effort, and the training provided was seenas part of this overall response.
Good training should equip partidpants with theability to improvise, to respond to local conditions.
The CAREC training provided an understanding ofthe principles of rehydration upon which cost effectiveinnovations could be made, as illustrated by the Wilson-
•
158 TRAINING AND THE QUAIJTY OF CARE

Beard bed and the WJ1son oral rehydration so.utionstraw.
More physicians and nurses should have beentrained prior to the epidemic.
Further training should be conducted within anoverall training strategy, however, to insure that criticalstaff who are most likely to manage cases are the onesreceiving the training, and that the training is part of anoverall plan for upgrading case management of choleraand diarrhea patients.
Training using a facility with cases to providehands-on training would have made the trainingmore relevant and would have further acceleratedthe learning curve.
Simulations can partially compensate for the lack ofhands-on training; however, simulations do not providethe experience for the trainee to gain confidence. Onestrategy to provide hands-on training has been to sendtrainees to an international training site, such as theInternational Centre for Diarrhoeal Disease Research,Bangladesh. While excellent experience can be gained, thecosts of sending trainees abroad prevents such trainingfor many participants.
Another strategy that can be used within a countryis to send medical staff from unaffected areas to choleraaffected areas. This strategy has been used in Guyana.This type of training, while useful, is not adequate forhigh-level training of medical leaders, as it fails to provide an academic environment.
A final strategy, which has not yet been attempted,is to establish a regional training center in South America in an area where cholera cases and highly qualifiedstaff can be found-providing both an excellent academic environment and practical hands-on experience forappropriate case management. Such a regional trainingcenter would also allow training in Spanish.
Training materials specifically designed for use bythe trainees would have been helpful.
Trainees were given extensive printed documentsfrom WHO and audiovisual materials from the US Centers for Disease Control and Prevention, all ofwhich wereuseful, but were not given a packaged course specifically for second generation trainees. It would require much
CHOLERA CONTROL ACTIVITIES IN GUYANA 159

additional work and a knowledge ofwhich level ofhealthpersonnel would be reached in secondary training, however, to develop such a course.
In summary, the CARECIPRITECH training accomplished its goals and contnbuted to the national choleracontrol program. Through appropriate case management, most deaths were averted, and cost-effective innovations were effectively developed and used by the dedicated physicians and nurses in Guyana.
Nota:1 F. Davachi, "Cholera Case Managemmt for Hralth Care ProvIders, Training Conference InGuyana,"Arlington, VA, Management Sdcnas for Hralth. PRITECH PrqjKt, ACP-022-GY. 1992.~ The blood group of the Amcrlndlan population In Guyana has r.,t been determined, but other native§roups In South Amcrlca have hem all110lt cxduslvdy blood group o.
J. Hospcdala. T. llWan, and R. Cummings, "A Case Control Study ofCholera Outbreak InGuyana:CAREC Survci11ancc Report, vol. 18, NovembcrlDcambcr 1992, pp. 81-86.
160 TRAINING AND THE QUAIJTY OF CARE

IMPROVING ORS SUPPLY AND DISTRIBUTIONIN THE PHILIPPINESI", 11, 1\ 1,1 \ It
The Philippines is a nation of 7,000 islands, with amonsoon-type rainy season during which typhoons arefrequent. The Department of Health in the Philippines isstructured in fourteen regional health offices, sixty cityhealth offices, seventy-five provincial health offices, and276 district health offices. There are approximately 600hospitals, 2,100 rural health units and 1,000 barangay(village) health stations in the Department of Health system.
Lack of an ORS Ordering System
These geographic features and the complex administrative structure, combined with difficulties in oral rehydration salts (ORS) supply at the national level, wereamong the factors contributing to an undersupply andmaldistribution of ORS in the Department of Health system. A PRlTECH evaluation of the Department's controlof diarrheal diseases (COD) program in September 1988reported that there were stockouts and an undersupplyof ORS in some areas and an oversupply in others. Fieldvisits by COD program staff also found an insufficientand irregular supply, with some facilities being completely out of ORS and others having more than a oneyear supply.
During these visits it was observed that there was noreliable system in place for'determining the amount ofORS each facility should receive. As they received ORS,higher officials in the administrative chain would simplyallocate it to the next lower-level facility, usually givingeach facility the same amount. While in a few instancesthere were attempts to allocate based on the populationof the catchment areas of the facilities receiving the ORS,this was basically a "push" system, with the receivingfacilities passively waiting for ORS to be given, or onlyrequesting ORS when they ran out or nearly ran out ofstock. A number of problems common to the overallDepartment of Health logistics system-for example,inadequate warehousing, lack of transport, and lack of alogistic information system, were also observed to beadversely affecting the ORS supply.
David A1t was thePhilippines CountryRcprcsa1tative.
IMPROVING ORS SUPPLY AND DISTRIBUTION IN Tm: PI:J1' ·...,PMB 101

The problem of undersupply of ORS at the nationallevel was related to a deterioration in the Department ofHealth's ORS production facility and a series of delaysand other problems in importing ORS from donors. Bylate 1989 the Department had awarded a contract to aPhilippine drug manufacturer for the production ofOresol, the Department's brand ofORS. These shipmentswere received on schedule and in sufficient quantity,thereby ending the problem of chronic shortage of supply at the national level.
The overall problems in the system, such as warehousing, transport, and the information system, are tobe addressed in a World Bank-funded project beginningin 1991. The PRITECH-assisted study leading up to theWorld Bank effort recommended that the physical movement ofdrugs and medical supplies be from three national hub warehouses directly to the district health officelevel. This should reduce the backtracking of suppliesand the additional warehousing and handling of suppliesat the regional and provincial levels. The orders for drugsand supplies and the notifications that orders have beensent will still be sent through the provincial and regionallevcls.
While these problems were being addressed, the CODprogram also undertook to develop and implement asimple, rational system for determining how much ORSeach facility should stock, and for knowing when to reorder and how much to order. Surveys of ORS supplywere undertaken in 1989 and again in 1990, and showeda very encouraging improvement in ORS supply at alllevels. The following section describes the ORS orderingsystem and explains how the system was developed andimplemented.
Tile PhlllPPllWS OrclE!r1I1Cj Systl~lll
OBJECTIVES
The Philippines ORS ordering system has three majorobjectives:• To minimize the number of times when facilities run
outofORS,• To minimize the number of situations where ORS
reaches its expiration date without being dispensed,and
162 TRAINING AND THE QUAJJTY OF CARE

• To achieve the above two objectives with the leastamount of capital tied up in DRS invmtory.
ORS SuPPLY P1PELINE
The DRS supply pipeline is designed to ensure asteady flow of DRS from the supplier to the Departmentof Health's central office and from there to the Department's field units.
An DRS authorized stock. level is set for each facilityin the Department system. The authorized stock level isbased on the diarrhea caseload of the facility, and isexpressed in terms of months of supply.
Box 1 is a diagram of the DRS supply pipeline. Onthe diagram the "months of supply" is expressed as arange, such as one to three months, with the higher ofthe two numbers being the authorized supply level. Thelower number is the number of months' supply that thestock. level is likely to drop to at the end of a peak diarrhea season month, when DRS is being consumed rapidly. For example, during peak season, a normal threemonths' supply might be used twice as fast, so that afterone month, two months' supply has been used, and onlyone month's supply remains.
Larger amounts (months of supply) of DRS are keptat the district and city levels than at the regional andprovincial levels. This is done so that the ORS is kept closest to the level at which it will be used. The pipeline isalso designed this way because many regional andprovincial offices do not have proper storage space forlarge amounts of DRS and other medicines.
The regional and provincial offices act as "passthrough" facilities only. When the quarterly ORS supply is received at these levels, it is quickly (within abouttwo weeks) sent to the next lower levels, based on therequests from those levels. The regional and provincialoffices retain as a "buffer" an ORS supply sufficient forone month's use for the mtire regional or provincialcatchment area.
When diarrhea outbreaks occur, the DRS stock levels at the district and city offices should be sufficient tocope with them. If an area still needs DRS on an emergency basis, it can request it from a neighboring city ordistrict office, or from the provincial or regional onemonth buffer stock.
------------------,._------IMPROVING ORS SUPPLY AND DISTRIBUTION IN THE PHILIPPINES 163

o -1111l11lh IUPPY of OIlS
(2-i 1IIll8) - tile IIUIIlber of IIIOIIlIIs ORS 8IIIW wID be • utile l'adIIty(q) - quart8dy reordeIlDg(m) -1IIOIllhIy I80IdeIlDg
Box 1. ORS Supply Pipeline
SlIppIIer
! Specialty r-r-rIMiDistry 0::0 ) HDspitals L...L-l-J
I lq) c::I:I:l• (2-6 mos) 12-6 DIllS)
. D )RegiaDalbospital cr=I:JT (1-4 DIllS) 1m) (1-3 DIllS)
__-+) City health olfi:e cr=I:J~ City bospital r-r-r-llq) 1m) LLLJcr=I:J 11-3mos)
(2-6 DIllS) ~~~0Il1m) 11-3mos)
ProvincialD Provincial hospital r-r-r--1(q) --~) 1m) L-.l..........L11-4mos) (1-3 DIllS)
) Citybea1tholfi:e cr=I:J Citybo 'tal r-r-r-llq) ~ lm)8Pl LLLJ
cr=I:J 11-3mos)
(2-6 DIllS) ~Bamn&r~OIl1m) (1-3 mos)
DistrIct cr=I:J~ Districtbospital cr=I:Jlq) cr=I:J (m) 11-3 mos)~ (2-6mos)
Ruralhea1th~unit L...-..L-.L....(m) (1-3 mos)
~~uaer::Dstation(m) (1-31008)
Because diarrhea is a very seasonal disease, theauthorized stock level for direct-service facilities (hospitals, rural health units and barangay health stations) isset at three months. This means that at the end of themonth in the non-peak diarrhea season these facilitieswould be expected to have a balance of about a twomonth supply of ORS. At the end of the month in thepeak diarrhea season, the balance on hand in these facilities would be near a one-month supply of ORS.
164 TRAINING AND THE QUALITY OF CARE
CALCULATING AUTHORIZED STOCK LEvELs
Health facilities calculate their authorized ORS stock,levels only once a year. This calculation is nonnally donein the early part of the fourth quarter ofeach year to prepare for the coming year.
The top half of Box 2 is the fonn used by ba.angayhealth stations, rural health units and district, provincial, and regional hospitals for calculating their authorized stock levels. The following are explanatory notes onthefonn:
Line 1. If the calculation is being done prior to the endof the calendar year, the number ofcases entered herecan be for the most recent twelve consecutive monthsfor which figures are available.Line2. Two packets are used per diarrhea episode as anaverage ORS consumption figure for field health facilities. Large provincial and regional hospitals which seea larger portion of dehydrated cases should use a figure of four packets on line two.Line 3. The COO staff at the regional and provinciallevels, in consultation with their field units, determinethe percentage increase or decrease to be used in linethree. The expected increase or decrease is affected byactivities such as training of new health workers inCOD, establishing new ORS providers, promotionalactivities, and so forth.Line 4. This is the facility's estimate of the amount ofORS that it will give to other organizations and practitioners for use with their patients.Line 7. The authorized stock level for direct-servicefacilities is three times the average monthly projecteduse.In calculating the authorized stock level for district
and city offices, the diarrhea caseload figure used on line1 is the consolidated figure for all cases scen at facilitieswithin the district or city office catchment area. On line7 the figure from line 6 is multiplied by six, since districtand city officers are authorized a six-month stock level.In all other respects, the calculation for district and cityoffices is the same as for direct-service facilities.
Similarly, the calculation for regional and provincialoffices uses the same fonnula, except that on line 7 thefigure from line 6 is multipliedby four, since regional andprovincial offices have a four-month authorized stocklevel.
IMPROVING ORS SUPPLY AND DISTRIBUTION IN THE PHILIPPINES 165

Box2.Calculating your authorized ORS stock level for 1991
Name offacllily Type _
Location Prepared by _
UwdclpaIItyIClty DIaulct 1'Iu'rIDclI
1. DiaIrbea cases of all aoes seen or reported In 1990
2. Multiply line 1 by 2 packets
3. Multiply I1De 2 by (the upected pert'8J1tage IDcrease ordec:rease In cases for 1991) _
4. Expec:ted numbers of ORS packets to be diatrIJ:luted toprivate c1InIcs, l101IgOVeIDJI1ental organ1zatkms. etc.. In 1991
6. Add lines 2, 3, and 4
8. Divide line 6 by 12 months (-average monWy ORS usage)
7. Multiply line 8 by 3 (-authorized ORS stoeJt level)
Reordering ORS in a monthly basis
•
Authorb:ecl BaJanceat Amount Amount1I0Dtb Itoc:IE Ine1 time of order co order Date rec:e1Yecl Date Remarb
J8J1U8IYFebruary
Martb
April
May
.Jun&
July
August
S8ptember
October
November
December
Once the authorized stock level is calculated for afacility, it is used for placing orders for ORS throughoutthe year.
ORDERING ORS
This ORS ordering system is a "pull" system. Theamount of ORS sent each month or quarter from onelevel to the next lower ievel is based on the amount
166 TRAINING AND THE QUAIJTY OF CARE
requested from the lower level. No ORS is sent automatically from one level to the next.
From the nationallevd through the district level, theordering dates are coordinated so that each level ordersits ORS in time to receive the orderjust prior to receivingthe ORS orders from the facilities in the level below it.The following is the schedule for placing ORS orders:• Barangays order ORS in the last week of each month.• Rural health units and hospitals order ORS in the first
week of each month.• Districts and cities order ORS from the province at the
beginning of January, April, July, and October.• The provinces order ORS from the regions in the mid
dle of March, June, September, and December.• The regions send their quarterly ORS requests to the
COD national office by radio message at the end ofFebruary, May, August, and November.
• The Department of Health's central office ships ORS tothe regions during the first two weeks ofMarch, June,September, and December.
The bottom half of the form in Box 2 used for calculating the facility's authorized stock level is used to calculate the amount of DRS to order. The form is used fora one-year period. If the facility is re-ordcring on a quarterly basis, there is one line for each of the four quarters.This form is retained by the facility, and ifproperly filledout provides a running record of the DRS supply situation in the facility, which can be easily monitored bysupervisors.
To calculate the amount to order, the health workerat the facility writes the authorized stock level from line7 in column 1 on the form.
She then does a physical count of DRS on hand andwrites that number in column 2, NBalance of Order."
She then subtracts the balance at time of order (column 2) from the authorized stock level (column 1). Theresult is the amount to order (column 3). If the numberin column 3 is a negative number it means the facilityhas more DRS than it is authorized to have; the workerdoes not place an order if the number in column 3 is anegative number. If the number is positive the healthworker shows the calculation to the COD coordinator atthe next higher level and requests that amount of DRS.For the rural health unit and above, a standard government requisition and issue voucher is completed.
IMPROVING OBS SUPPLY AND DISTRIBUTION IN THE PHILIPPINES 167
..

Once the health facility receives the ORS, the healthworker enters the amount received and date received incolumn 4.
At all higher levels, the procedure for ordering is thesame as that descn"bcd above, with the exception that theordering is done quarterly.
Each facility keeps a folder with its COD records init. This form for calculating the authorized stock leveland for calculating the amount to order each time is keptin the folder. In addition, each facility keeps a copy of theform for each facility which orders from it, and updatesthis copy each time an ORS order is received and sent. Forexample, a rural health unit, in addition to its own form,should have updated copies for all the barangay healthstations that order from it.
\
ExCEPTIONS TO AUTHORIZED STOCK LEVELAND FREQUENCY OF ORDERING
In some regions, there are provinces, districts, andrural health units that cannot be easily reached in therainy season. These locations with limited access areusually in the mountains or on remote islands. In thesecases, the facilities are given a larger authorized stocklevel than shown on the forms. They also order less frequently than quarterly or monthly. The Department ofHealth's COD program staff, in the central office, assistthe field units inadapting the ordering forms so they canbe used for these spccialsituations.
D(~Vt~ lop lllq aile! Supple"lllcll t 111g the Syste III
TESTING THE SYsTEM
The PRITECH and WHO resident COD advisors prepared an original version of the ordering system andintroduced it to the regional COD coordinators at a meeting in February 1989. It was agreed at this meeting thateach region would test the new system for three to sixmonths in one district. The regions were given a formatfor reporting their experiences in implementing the system. In addition to these reports the PRITECH advisorand the COD administrative officer visited the test districts in four regions. As a result of the reports (from tenregions only as the other four were not able to do the
168 TRAINING AND THE QUAUTY OF CARE

pilot test) and field observations, the following actionswere taken:• The formula for calculating the ORS authorized stock
level was simplified by eliminating a calculation forwastage.
• The amount of ORS to be held at the regional andprovincia1levels was reduced. It was determined thatthey should act as "pass through" facilities, sendingmost of the ORS they receive almost immediately tothe next lower levels.
• The authorized stock level for direct-service facilities(hospitals, rural health units, and barangay health stations) was originally set at two months, and was tobe doubled for the peak season and reduced after thepeak season. This decision caused confusion. The stocklevel was consequently raised to three months forthese facilities, which is sufficient for both low seasonand peak season.
• Written directions, in the form of a training module,were prepared for the system.
• The two forms for calculating the authorized stocklevel and the amount of ORS to order were combinedinto a single form which can be used for a whole year.
• It was agreed that higher authorized stock levels andless frequent ordering periods could be used dependingon special circumstances in various places.
All of the regions visited were eager to expand thesystem to the whole region.
IMPLEMENTING THE REvIsED SYsTEM
The new, revised ORS ordering system was introduced to the regional COD coordinators at a nationalmeeting in October 1989. Because the ordering systemhad not been reviewed and approved by the Departmentof Health executive committee, its implementation in thefield was not mandatory. It was agreed at the meetingthat the COD coordinators from each region would discuss the system with their regional technical staff andregional director and determine to what extent the system would be implemented. All regions implemented thesystem in at least some of their provinces.
Field monitoring visits to eleven of the fourteenregions during 1990 revealed that implementation of thesystem was going very slowly, and that it was not beingimplemented as extensively and as well as had been
IMPROVING ORS SUPPLY AND DISTRIBUTION IN THE PHILIPPINES 169

170
expected. The main reason for this was that district,provincial, and regional staff were preoccupied with ahost ofinitiatives mandated by the central office. Insomecases, the training and orientation to the new system wasnot done until near the end of the second quarter of 1990.
A number of specific problems were observed duringthe field visit, including:• Most regions had not ordered enough ORS to fill the
pipeline at the start of implementation of the system.They were to have placed this "special order" to fill thepipelines based on their estimates of how much ORSwas in the system at various levels. As a result, ordersfor ORS from lower levels in the system could not befilled completely by the higher levels. This situationwas very frustrating to those trying to implement thesystem correctly.
• The regions had not reproduced enough copies of theform for calculating authorized stock levels and theamounts to order, even though each region had beengiven a set of stencils for this purpose by the nationalCOO office. As a result, many facilities were found tohave no forms, to be using the wrong forms, or to beusing handwritten forms.
• Key people at the district level sometimes missed theorientation to the system because of their involvementin other activititS. This fact resulted in the system notbeing implemented in those districts or in being incorrectly implemented.
• In some cases the quality of the second-level trainingand orientation to the system had not been sufficient,resulting in confusion about the system among nurses and midwives.
• Many provincial health offices were mixing their ORSstock. with that of the nearby districts, which use thesame warehouse. This practice resulted in their placing smaller orders to the region than they should have.A similar problem was observed between the districtsand rural health units.
• Large provincial regional hospitals were using three tofour packets of ORS per case, resulting in the authorized stock. levels arrived at by the formula (whichassumed two packets per case) being too low.
• Some facilities with a three-month authorized stocklevel were dividing the stock level by three before filling in column 1 of the form, because they thoughtthey should just order what they needed for one
TRAINING AND THE aUAUTY OF CARE

month. This action seemed to have come from theirearlier experience when they would be out of or nearly out of ORS before asking for more.
• Some facilities were counting only diarrhea case... inchildren under five when filling out line 1 of the calculation for authorized stock level, apparently becauseof the Maternal and Child Health Service's focus on theunder-five target group. The result was too low anauthorized stock level.
• Lack of transportation resulted in facilities receivingless ORS than they ordered and in receiving it late.
As a result of these visits, the regional COO coordinators pledged to' give more time to monitoring the ORSsystem, with special attention being given to the problems listed above. All regions found to have insufficientORS for the initial filling of the pipeline placed very largespecial orders to correct the situation.
The field visits by the national COO office staff tomonitor the implementation of the ORS ordering systemwere made more effective by the use of a checklist formonitoring implementation of the system. During thevisits, various field staff were taught how to use thechecklist. The monitoring checklist appears as Box 3.
ImpClct of the System
The first nationwide ORS supply survey was conducted in February 1989. It covered 1,203 health facilities in sixty-eight of the seventy-five provinces of thePhilippines. Forty percent, or 486 of the facilities surveyed, were found to be Nat risk," meaning they had noORS in stock, had only expired ORS in stock, less than aone-month supply ofORS (barangays, rural health units,cities, and hospitals), or less than a three-month supplyof ORS (regions, provinces, districts). In some provinces,as many as 88 percent of the surveyed facilities were Natrisk."
The overriding problem revealed by the survey wasa shortage of ORS supply in many facilities. The exception to this general finding was the city health offices.Forty percent of them hAd more than a six-month supply of ORS, and only 11 percent had less than a onemonth supply.
In July 1990, a second nationwide ORS supply survey of 1,205 health facilities was undertaken. In spite ofthe slow start in implementing the system, the survey
IMPROVING ORS SUPPLY AND DISTRIBUTION IN THE PHILIPPINES 171

showed that in those regions and provinces where theCOD coordinators were able to introduce the new DRSordering system and closely supervise its implementation there were marked improvements in the DRS supply situation.
In the 1990 survey, only 6 percent of the facilitieswere out of DRS on the day of the survey, compared to14 percent in 1989. In addition, a total of 25 percent of
Box 3. DRS Monitoring Checklist
Facility ----------- Date ----------
Use this checklist when monitoring whether a facility is correctly using the newORS ordering scheme. Use the back of the sheet for any additional notes.
YES NO
1. Does the facility have the ORS calculation and ordering form?
2. Is it the correct form for the facility?
3. Did the facility correctly calculate its authorized stock level?(If no, note on the bC\ck of this page what they did wrong.)What is the facility's authorized level?
4. Did the facility place its order(s) at the correct time?(If no, note on the back of this page what they did wrong.)
6. When they ordered, d:d they calculate the correct amount toordeI?(If no, note on the back of this page what they did wrong.)
6. Did the fa::ility received the amount of ORS it ordered?(If no, note on the back of this page why they did nOl)
7. If the facility received more or less than ordered, is there acomment in the remarks column as to why this happened?
8. How much ORS does the facility have on hand (do a physicalcount)ORSonhand-
9. Is this less thar. a one month suppli?(If yes, note the reasons for this on the back of this page.)
10. Does the facility keep an ORS stock card?
11. Dnes the balance stated in the stock cardmatch the actual balance on hand from physical count?
12. Will the ORS reach its expiration date before it is consumed?
13. If the facility been monitored is an IPHO, DHO or RHU does ithave copies of the ORS calculation and ordering form for eachofthe facilities belowit,le., tile IPHO has forms for each DHO,DHO has forros for each RHU, RHO has forms for each BHS?(If not. note the reason for this in the back of this page.)
172 TRAINING AND THE QUAIJTY OF CARE

the facilities were "at risk" compared to 40 percent "atrisk" in 1989.
All regions except two showed declines in the percentage of "at risk" facilities. The two most improvedregions, in terms of reduction in percentage of "at risk"facilities, went from 1989 figures of S6 percent and 48percent to 1990 figures of 13 percent and 10 percent,respectively.
One region showed an increase in fcOicilities "at risk"from 1989 (23 percent) to 1990 (33 percent). This regionwas implementing the ORS on<'_nng system in only oneof its seven provinces. That provi.."1ce had no facilities "atrisk."
In the 1989 survey, forty-eight out of sixty-eightprovinces surveyed (71 percent) had some facilitieswhich were out of ORS. In the 1990 survey this haddropped to thirty out of sixty-eight provinces (44 percent).
Lessons Learned
Ensure that there is plenty of ORS available at thenational level prior to launching a new orderingsystem.
This might be as much as a one-year supply if thepipeline is fairly empty. It is extremely frustrating to fieldpersonnel to introduce a system and then not be able tofill the orders. The problem in this case was the fact thata special order of 3.9 million packets of ORS from USAIDand UNICEF that was supposed to have been availablewas found to be mislabeled. It took some time for thisproblem to be corrected and as a result, the central officecould not fill the orders from the field.
Prepare a simple set ofclear instru~tionsand related training materials at the outset.
Because the pilot test was launchrd C"1 very shortnotice, the instructions were only verbal. The only written materials were the forms.
Conduct the first pUot tests in fewer regions, andexpand to only three full regions after the revisions.
Monitor these three regions much mere closely thanit was possible to do for the full fourteen regions. Expand
IMPROVING ORS SUPPLY AND DISTRIBUTION IN THE PHILIPPINES 173

174
to all the regions only after working out the problemsencountered in this expanded trial.
Involve a regular Department of Health employeefrom the central office in the development andimplementation of the system.
The assigned counterpart, the administrative officer,was a contract employee whose services ended at thesame time as those of the PRITECH advisor.
Explain clearly to the regional eDD coordinatorsthe need to fill the supply pipeline at the outset.
A large special order of ORS at the beginning enablesregional offices to fill the orders from the districts andcities. This need was not emphasized enough during theOctober 1989 training season.
Emphasize more clearly to the regions the importance of their providing sufficient copies of theordering forms for all levels in the system.
Expecting provincial and district levels to r~type thesample forms "n stencils proved to be a si6nificant bottleneck to implementation.
TRAINING AND THE aUAUTY OF CARE

-=---
T_" -"_"~,, .......... =-.. -

TAPPING THE POTENTIAL OF THE PRIVATE SECTOR
-ae first two sections of this volume dcscnbe successful collaborative relationships with min
istries of health in public sector programs for thecontrol of diarrheal disease (COD). By contrast, this section covers PRlTEOI's experiences in engaging the private sector in COD activities. Data from developing countries demonstrate that the private sector, includingprivate physicans, pharmacists, retailers, mission hospitals, and traditional healers, is the health care provider offirst choice in many countries. A study in rural India, forinstance, found that 83 percent ofmothers consultedprivate practitioners for their children with diarrhea, whileonly 7.5 percent visited public health centers.!
The commercial sector, including pharmaceuticalcompanies and consumer goods companies, is obviouslya very important part of the private sector, yet nationalCOD programs t.ave had little or no experience in working with it. PRITEOI believes that the commercial sectorshould playa role in every COD program. PRITEOI hasdeveloped an approach for using commercial sectorstrengths to increase the availability of oral rehydrationsalts and health education regarding correct diarrhealdisease management. The commercial sector can beenlisted to participate in the COD effort, to promote, sell,and distribute CRS packets and to provide informationabout home management and prevention of diarrhealdisease to a broad segment of the population.
In Pakistan, PRITEOI pioneered interventions thatdraw upon social marketing experience and that rely primarily upon the private sector to finance its own CDOmarketing effort.2 The work in Pakistan succeeded inmobilizing the commercial sector to replace the publicsector as the main channel of delivering ORS to consumers. The model developed in Pakistan has been successfully applied in Indonesia, Kenya, and Mexico. Thepapers by Camille Saade, Lucia Ferraz-Tabor, and PaulFreund descnbe the PRITEOI approach to collaboratingwith the commercial sector and some of the lessonslearned.
Nongovernmental organizations are another important part of the private sector. In Bolivia, the USAID mission helped establish a coordinating group of child survival private voluntary organizations. Ana Maria
TAPPING THE;~TENTIAL OF THE PRIVATE SEQ:I;<;\R k 177Previous PagerJl~n

Aguilar and Peter Spain dcscnbe PRITECH's assistance tothis group in the paper in this volume. In addition,PRITECH and the Centre for Development and PopulationActivities conducted a workshop for Anglophone Africannongovernmental organizations (NGOs) to extend theircommunity-based COD activities. In her paper on working with NGOs in Kmya, Karen Blyth describes howPRITECH followed up on the workshop with KmyanNGOs.
PRITECH has also conducted research on the attitudesand practices of traditional healers regarding diarrhealdisease management, and has explored the possibilities offruitful collaboration between national COD programsand healers.3 An initiative to train healers to collaborateeffectively with the biomedical establishment in Ugandawill be written up in a future PRITECH occasional paper.
One of the greatest upcoming challenges for the CODfield is identifying new ways of reaching the nongovernmental health sector, particularly private practitioners and pharmacists. For it is only when COD programs take advantage of the full complement ofresources in the public and private sectors that substantial progress in saving children's lives can be made.
Nota:1 Indian Markd Ratan:h BU1't8u, "KAP Study on DIarrhoea: ASummary Report,· report prtpaml forUNICEF, IMRBIHV/40326, 1988.:I See LucIa Fcrraz-Tabor and WWlam Jansen II Farglns New PlI1't1Imhlps: PIUTECH', PakUtan~, Arlington, VA, Managmlmt Sdmcu for Health PRITECH I'rt!lect, 1991.3 See Paul Fmmd, "Traditional Healm and DIarrhea: Raulls c:l a Ra:mt Survq in zambia," paperpramted at the Amalean Public Health Assodatlon annual medlng, ChIcago, October 22-26, 1989;and Janice Hogle and Agma PrIns, "ProspectI for Collaborating with Traditional Healm In AfrIca,"ArlIngton, VA, Managemmt Sdmcu for Health, PRITECH Project, 1992.
178 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

ENLISTING THE COMMERCIAL SECTORIN PUBLIC HEALTH
The vast majority of control of diarrheal disease(COD) activities around the world have been organizedwithinand continue to be implemented by the public sector. That the global COD effort was structured in such afashion is not surprising, because it followed conventional devdopmmt models and used traditional publicsector health networks. The public sector approach hasrealized considerable progress in certain areas, such asincreasing public awareness of oral rehydration therapy(ORT) and effective use ofORT within public health facilities.1 Statistics from many countries show that publicknowledge and awareness of ORT exceed 80 percent.
Camille Saade is aSocial Marketing Specialist.
LllllltCltlOllS of P~1IJI1C Sector CDD Efforts , .
India·*
CommWII'Y'Family
Philippines*
COIIIJIIWIl'Y' TradltlODll1Family Heal..
Pbarmac:l8ta1"
Where mothers go for treatment ofchildrm.with diarrhea.
Public sector-only approachesare, however, constrained by twobasic shortcomings. First, such public sector programs have structurallimitations in extending COD services to the general populace. Thefigures show, for instance, thatonly a small percentage of people inIndia or the Philippines consult public sector health personnd for childhood diarrheal disease.
A very disturbing statistic thatcommonly emerges from devdopingcountries is the consistently lowrates of actual use of oral rehydration salts (ORS) in households duringdiarrheal episodes. Even in countrieswith general awareness levels ofORSover 80 percent, household ORS userates are often considerably lower.According to the World Health Organization, ORS use rates do not exceed21 percent.2 A significant gapbetween ORS awareness and useclearly has emerged throughout thedevdoping world.
ENLISTING THE COMMERCIAL SECTOR 179

One reason that ORS use is so low is that currentglobal demand is not fully met by supply. A commonlimitation of public sector health systems is the regularsupply and distribution of needed medical supplies to allhealth facilities. This is particularly true for facilities atthe primary health care level.
Second, public sector programs suffer from limitations in long-term sustainability. Such programs requireregular infusions of financial support from governmentsand donors. COD programs that strive to reach 100 pc .cent of the population need large quantities of financialresources over long periods of time to be fully successful. The strain of sustaining these endeavors over timecould be eased considerably if substantial COD serviceswere undertaken by the private sector on a self-financing, commercial basis. By allocating human, material,and financial resources to cost-effective production andmarketing activities, private companies could help fill thegap between total consumer demand and what was currently produced by the public sector.
In several countries, experience has shown that thecommercial sector can provide useful information onORT and scll ORS at prices sufficient to provide the differmt links in the distribution chain with a profit incentive. Yet these prices are affordable to significant portionsof the population. The long-term sustainable availability of ORS has been accomplished with the commercialsector's own funds, investing the major part of thefinances required to launch ORS, and minimizing donorand host country financing.
If the full benefit of ORT and other diarrheal diseasemanagement practices is to be realized, other sectors providing primary health care services must also be enlistedto be active users and promoters of such practices. Thecommercial sector is one group that can be engaged toparticipate in the effort to promote, scll, and distribute .ORS packets, as well as to provide information regardinghome management of diarrheal diseases to a broad segment of the population.
PRITI-':CH'L, C()llllllt'l cldl St'cfo! Illlt lilllV('
To address the limitations of a public sector-onlyapproach, PRITECH embarked on an initiative to involvethe commercial sector more widely in public health interventions. Specifically, PRITECH aimed to (1) complement
180 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

PRITECH's MethodologyTo encourage the private sector to participate in COD activities, PRITECH:• Assesses the current commercialmarket and the potential for increasedcommercial sales (including marketresearch).• Identifies promising commercial sector players that can realize that potential.• Designs a national ORS plan in coordination with the national COD program.• Approaches targeted commercialfirms and seeks their involvement,both in terms of market potential andpossible contributions to national public health objectives.• Provides technical assistance in marketing according to each company'scapacities and resources.• Monitors and evaluates the publichealth impact of COD activities undertaken by commercial firms.
the ongoing efforts of the national COD program; (2)promote oral rehydration therapy, rather thanjust DRS;(3) develop a sustainable marketing model; (4) maximizeDRS marketing potential, acting on both demand andsupply; and (5) help prevent diarrheal incidence throughbreastfeeding and handwashing promotion.
PRITECH's STRATEGY
The criteria used to sdect suitable candidate countriesfor DRS commercialization activities included: (1) countries with a commitment to and a policy endorsing theuse of DRS as a home treatment remedy; (2) countrieswhere privatization is a well-established approach supported by the government; (3) countries with a welldeveloped commercial sector; (4) countries with a sizeable consumer market potentialwhere DRS can be considered anover-the-counter product, availablewithout prescription; and (5) countries in which the USAID missionsupported the commercializationeffort.
PRITECH typically followed amethodology developed and refinedthrough experience working withthe commercial sector. The methodology began with a rapid assessment of the DRS market situationand the attitudes and practices ofconsumers, health providers, suppliers, and manufacturers. PRITECHthen identified DRS needs, marketand environmental constraints andopportunities, and the most suitableplayers for each market segment.Potential companies were not limited to the pharmaceutical industry,as food and beverage companies offer a much wider distribution channel.
Findings from these assessments formed the basis ofa preliminary DRS plan that incorporated the nationalCDD program objectives. PRITECH attempted to achievethese objectives by developing strategies ensuring thebest market coverage. In collaboration with the CDD pro-
ENLISTING THE COMMERCIAL SECTOR 181

gram and donor agencies, PRITECH selected and initiatedthe approach to the targeted companies. .
PRITECH attached great importance to careful preparation of a presentation to the companies' decisionmak.ers. PRITECH devdoped a brochure-"Good Health, Goodr--,...-------------, Business"-targeted to commercial
companies that was used in the initial approach to decisionmakers. Inen- - some countries, PRITECH made its
: (J) .. :~ initial presentation to a group of:w-- companies; in others, presentations:·z.-·:- were made individually. Presenta(jj- tion of ORS market opportunities
was tailored to each company's...ffi strengths. In addition, PRITECH. - strived to demonstrate that publicC health objectives could represento .. business opportunities. Typically,o - the solicited companies made their(!). own marketing assessments and
.. GoOD-HEALTH -....... ~:;?:ty:=~:~o~:~ c;=~~worked with the company as earlyin the planning process as possible.
Technical assistance offered byPRITECH aimed at strengthening the capacity of the companies in areas as varied as good manufacturing practices,quality control, market research, marketing planning,communication strategy, and material development.Throughout, PRITEal provided continuous guidance toensure that the communication message was in line withthe national COD policy. PRITECH monitored the implementation of the ORS launch campaign and worked withthe companies, the COD program, andcollaborating agencies in evaluating the impact of the intervention accordingto indicators incorporated into the companies' objectives.
COLLABORATION IN SPECIFIC COUNTRIES
Honduras. The high awareness of oral rehydrationtherapy generated by a mass media campaign and thesubsequent demand for ORS were not being met by asupply of a readily available, affordable ORS. In the private sector, only high-priced imported ORS was sold inpharmacies. The govcmrnent felt there was a need for an
182 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

ORS product accessible to the large rural population mostin need of it.
In 1988, a PRITECH marketing expert worked withthe HealthCom Project J to identify and assist a pharmaceutical manufacturer to develop the ORS that the Ministry of Health wanted. An introductory marketing planwas developedjointly with the selected producer, Quimifar, in an effort to increase popular access to ORS. Themarketing approach adopted by the company included asegmented marketing strategy that began with Hidrosol,a low-priced "popular" product, to be distributed in ruraldrug outlets and grocery stores. A higher-priced brand,distnouted exclusively to pharmacies and promoted onlyto doctors, was expected to follow soon after the launchof the popular brand. The government agreed to continue mass advertising for the Ministry of Health's ORSbrand, Utrosol, which generated a beneficial spin-offeffect on the demand for the "popular" commercialbrand, Hidrosol.Indonesia. The fielding of a PRITECH rcp~{..;mtative inIndonesia in 1991 facilitated the expansion of Indonesia'sORS production and marketing. Assistance has been provided to several ORS producers to optimize their marketpotential, expand distribution networks, and ensureaccuracy of the promotional messages. A major consumer goods company was successfully enlisted tolaunch a generic handwashing campaign, along with thepromotion of its soap, to prevent diarrhea.4
Jordan. The main local ORS producer, Al-Hikma,became disenchanted with the sales performance of itsORS despite the mass media campaign funded byUNICEF. In 1989, PRITECH provided short-term technical assistance that helped Al-Hikma revitalize the marketing of its ORS. This was accomplished by refocusingthe company's ORS marketing strategy on its usual target audience-physicians and pharmacists-using thecompany's main marketing resource: its own detailingforce. PRITECH helped develop the marketing plan andthe detailing material. Now ORS is part of the company'sregular d~tailing program.Kenya. Due to the 1990 change in government regulations regarding the standard ORS packet size, half of theORS producers dropped out of the market. In 1991, totalproduction and importation of ORS was about 5 millionpackets, mostly purchased by donor agencies and distributed by the government. With donor agencies
ENUSnNaTHECO~C~SECTOR-
183

184
increasingly reluctant to continue the free supply ofORS,the government wanted to share the burden of supplying and distributing ORS with the commercial sector.
PRITECH assessed the market potential andresearched the interest and ability of current and formerORS producers to mass market ORS nationwide. Onecompany, Sterling-Health, stood out among the othersfor its advantageous capacities in production, qualitycontrol, mass distn"bution, and advertising. In coordination with UNICEF, PRITECH worked to persuade Sterling-Health to re-enter the ORS market. A marketresearch study demonstrated to the company that therewas an untapped market, especially in the rural areas,where Sterling-Health has a leading edge. Poolingresources from UNICEF, PRITECH, and Sterling-Health,an exhaustive marketing campaign was designed andadvertising concepts pretested. The company is marshalling its resources to meet the anticipated launch ofthe new ORS brand in July 1993. In addition, PRITECHhas worked with a major soap-producing company inEast Africa to incorporate handwashing messages in itssoap promotion campaign.Madagascar. In 1988, UNICEF established a productionline, Odiva, with an annual capacity of 1 million ORSpackets within the government drug distribution facility. UNICEF also supplied the facility with enough freeraw material for the estimated production of the firsttwo years. To date, most of the Odiva packets have beenchannelled through the public health system, whichabsorbed only 300,000 to 500,000 packets a year. In1992, with some promotion efforts, the private sectorpurchased 100,000 packets for sale in pharmacies andnongovernmental health facilities. However, the proceeds from the commercial sales to the private sectorwere not sufficient to provide Odiva with the financialreturns needed to recover the operating costs of its production.
As part of the new policy towards privatization, thegovernment now wants to shift Odiva production to theprivate sector. In late 1992, PRITECH assessed the commercial market, identified potential players, and developed options that would allow the government to attractthe commercial sector, while gradually phasing-outfrom ORS production. The option selected by the government consists of first implementing an intensive promotional campaign aimed at generating ORS demand
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

from both retailers and consumers, in order to prime themarket and make it more attractive to potential partners.Mall and Niger. Prior to 1989, ORS was not availableoutside ofpublic distribution channels in Mali and Niger.In 1989 and 1990, PRITEOI provided training and technical assistance to develop commercial marketing capacity within the parastatal pharmaceutical companies thatproduce ORS. This new marketing function has allowedthe parastatals to distribute and promote their ORS moreeffectively within the small but growing private sector.Areas of marketing assistance included planning, marketresearch, distribution, promotion, merchandising, andsales training.Mexico. Despite significant progress in ORT awareness,there are large unmet ORS needs mainly among middleand low-income groups in rural areas. ORS sales in theprivate sector were dominated by high-priced liquidbrands, available mostly in pharmacies in the urbanareas. There were no ORS packets in the rural retail outlets. Of the local ORS packet manufacturers who produced for the government tender, none had the capacityto market ORS in any significant way.
PRITEOI undertookan exhaustive market analysis toidentify potential ORS marketers that could reach theunder-served rural areas. In order to measure the marketpotential and highlight its attractiveness to potentialmarketers, PRITEOI conducted three market researchstudies on consumers' and shopkeepers' attitudes towardORS and on ORS price sensitivity. Results of the studieswere presented to selected companies, which in turn madetheir ownassessments. This led to a short list of two companies that PRITECH is encouraging to produce ORS.Pakistan. In Pakistan, PRITECH found a huge ORS production capacity among seven ORS producers, yet latentdemand from households was not being met. Over aneighteen-month period, PRITECH helped to develop anational ORS marketing plan (involving seven ORS manufacturers) that identified key issues for harnessing bothgovernment and private sector resources in a nationalCOD effort. PRITECH forged a partnership between thegovernment and the private sector that created incentivesfor outreach distribution and synergistic advertisingefforts. The government agreed to accelerate generic ORSadvertising, while the companies, through promotion oftheir own brands, capitalized on the existing awarenessand translated it into product sales. PRITECH stimulated
E~nNGTHECO~~SECTOR 185

186
ORS producers to increase their marketing efforts byupgrading their marketing and selling skills throughtraining workshops. It provided individual technicalassistance to the partner companies, helping each onedevelop a specific marketing plan and a promotion campaign according to its resources.'zambia. ORS supply, including local ORS productionand imported donations, was insufficient to meet annual demand, which was estimated at 8 million packets. In1991, a local subsidiary of Cadbury-Schweppes, a beverage company with a wide distnoution network, produced and launched Cresa, an orange-flavored brand ofORS. Being unfamiliar with marketing health products,the company requested and received assistance fromPRITECH on how best to utilize its nationwide consumergoods distribution network to market ORS packets effectively. PRITECH helped develop an appropriate marketing plan and identified the need to implement good manufacturing practices and quality control standards.6
REGIONAL APPROACH
Because the market structure of individual Asiancountries was similar but progress in ORS marketingacross the region was uneven, PRITECH conducted aregional workshop for selected ORS manufacturers inAsia called "Expanding ORS Marketing to New Horizons." The conference, which was the first internationalORS marketing workshop of its kind, brought togethersenior executives from Asian pharmaceutical companiesthat produce ORS to discuss current issues and newdevelopments in ORS marketing. Marketing executivesfrom sixteen companies from India, Indonesia, Pakistan,the Philippines, Sri lanka, and Thailand, representing 15percent of estimated worldwide ORS production, attended the workshop.
The workshop's objective was to exchange ideas andexperiences on new strategies aimed at expanding ORSbeyond the usual urban areas. The participants made themost of this unique opportunity by discussing genuineproblems, experiences, and ideas with their corporatepeers. Many acquired new skills and techniques such asdevelopment of rural marketing strategies, while othersfine-tuned their existing marketing plans and strategies.Other participants came away assured that their marke~g strategies were correct. The participants left the
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR
(-
•
,

meeting with rencwed mthusiasm and a commitment toincrease the usc of oral rehydration therapy throughimproved marketing of ORS.7
I lll~ ) (Ict... . U .". • '.
STJSTAINAB:tLITY
The principal benefit of I'RlTECH's social marketingapproach is that th.: commerLll sector ectivities under-
, taken will be self-sustainable in the future. PRlTECH hasnot subsidized any product costs or promotion costsexcept in rare specific cases where initial co-funding isappropriate: The project stimulated companies to investin new or expanded ORS marketing efforts using theirown rCfources, ha.."Ilessing theif existing marketing andsales capabilities, and reaping the benefits of increasedsales. PRlTECH's ar!,roach has aimed at identifying market opportunities and developing strategies jointly withthe companies to exploit these opportunities in the mostcost-effective way possible according to each company'sresources. The momentum generated by PRlTECH ismaintained by individual companies and fueled by continued interest from the major donor agencies.
PROMOTION OF aRT, RATHER THAN ORS ALONE
Since the PRITECH commcrciaI sector initiativebegan, the trend toward treating diarrhea with oral rehydration therapy has accelerated in many countries wherePRITECH has worked. The companies that have collaborated with PRITECH now promote the correct hometreatment for diarrhea, including continued feeding andbreastfeeding, instead ofjust their ORS brand. Often theirpromotion also includes preventive measures such a.;
hygiene practices and continued breastfeeding.
EASING OF REGULATORY CONSTRAINTS
In countries where ORS distnoution was limited byregulations to pharmacies only, PRITECH lobbied thedrug regulatory authority to remove the product fromthe restrictive drug list. ORS can now be found in groceryshops ir~ n:.any rural areas where there i.e; no pharmacy.
PRITECH also acted to eliminate disin:entives fo!' ORSmanufacturing by requesdng a ta.~ ,x~mpt-j.;m on_____________....·..'.~· ..""· ..........-'....·I'I.l. .._ ..• __
ENLISTING THE COMMERCIAL SECTO!.·1 187

imported ingredients and packaging material from thegovernment finance authorities. This exemption allowedthe ORS manufacturers to produce at a lesser cost, thusfreeing additional funds for distribution and promotionexpenses.
In addition, PRITECH worked closely with nationalCOD programs to restrict the availability and usc ofantidiarrheal drugs, especially for JXodiatric use. Antidiarrheal drugs arc useless for treating most childhood diarrhea and can be dangerous as well. Many countries havebanned the use of these drugs in government health facilities; some have also extended the ban to sales by thecommercial sector.
ExpANDING ORS AVAILABILITY THROUGHALTERNATIVE DISTRIBUTION CHANNELS
Most ORS manufacturers are pharmaceutical companies used to distrIbuting their drugs through pharmacies. However, pharmacies arc seldom located in ruralareas, where the need for ORS is considerable. PRITECHhas been working with current manufacturers to broaden their distribution networks and to identify additionaldistrIbution sy.;tems that increase the availability of ORSthrough a wide range of retail outlets. In some instances,PRlTECH acted as a broker between an ORS manufacturer and a consumer goods company to foster a partnership aimed at broadening the distribution and thus theavailability of ORS to those who need it.
Ll~SS()J1S LCitrt1cd "
We need to enlist the commercial sector.The commercial sector is an established force in
health care services. Increasingly, with the privatizationtrend as a means to alleviate the burden from the publicsector, the commercial sector is assuming a larger shareof health care delivery.
The commercial sector needs guidance.If left alone, the commercial sector could potentially
conflict with the public health policy. Even among wellintentioned ORS producers, promotion of a commercialORS brand was often incorrect, promoting conflictingpractices. Examples abound of ORS promotional material that advised the withdrawal of food during diarrhea,
-,-------------------------188 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

recommended use of specific infant formulas and bottlefeeding, or legitimized the usc of antidiarrhcals throughcopromotion with ORS.
Private sector involvement can take many shapes.With appropriate guidance, the private sector can be
involved not only in marketing of products, but also inhealth education and promotion of preventive measures.
We can motivate the commerdal sector throughdifferent means.
There are several ways to motivate commercial companies to get involved in controlling diarrheal disease.Although profit is a major motivating factor, it is not theonly one. Enhancing the company image is another powerful motivation, especially with well-established companies. Marketing and helping disseminate a life-savingproduct for children such as DRS reflects well on thecompany image. Many decisionmakers are increasinglysensitive to the social environment and want to play therole of good corporate citizens in their communities.Recognition of these good deeds by international organizations or associations can reinforce such behaviors.
A catalyst such as PRITECH is necessary.To leverage the strengths of the current and poten
tial players, a catalyst, understanding the systems andmotivation of each, is needed to sensitize, guide, steer,and mobilize the different resources in a synergistic way.PRITECH has found that a contributing factor for successin mobilizing the commercial sector is the presence of amotivated resident advisor who can provide follow-up toshort-term technical assistance and keep the targetedcompanies interested.
We should ensure the support of opinion leadersand other influentials.
The support of leading physicians and national medical and pediatric associations can be invaluable inencouraging physicians to prescnbe DRS.
The image of OKS must be upgraded.Identification of ORS as a public health product has
hindered commercialization. Because of the way inwhich ORS was introduced to most developing countries,DRS quickly became identified as a public sector product
ENLISTING THE COMMERCIAL SECTOR 189
190
by the commercial pharmaceutical market. Prospectivemanufacturers were given exact specifications by theministry of health or the donor organizations for producing ORS. They then bid on tenders to produce theamounts of ORS needed to operate government programs. Many firms that produced ORS in the developingworld therefore did not have the same product controlover ORS as they would over a product in their regularproduct line. Essentially, marketing and distributiondecisions for DRS rested in the hands of the public sector.Attempts to mold the image of ORS in the minds of consumers through the mass media also lay in the domainof the public sector.
Competition from antidiarrheal drugs should beaddressed.
Current market profiles indicate that commercialORS faces stiff competition from antidiarrhcals, antibiotics, motility inhibitors, and intestinal adsorbents.Many of these products hold leading positions within themarketplaces of developing countries.
Most prescriptions for diarrhea cases include at leastone antidiarrheal and one antibacterial. Some prescriptions also include DRS, but few consist only of DRS.When they write prescriptions for diarrhea, privatehealth care professionals may well be influencedby prodl:.ct image (the more medicinal and technically advancedthe better), and by their own perceptions ofwhat patientsexpect (specialized drugs and stopping the diarrhea). Regulatory measures restricting the use of antidiarrheals inchildren should go in tandem with an educational efforton the benefits of ORT.
In addition, anhbiotics and antidiarrheals are commonly sold at a retail price level considerably higher thanthat of DRS, but which consumers seem willing to pay.The potential profit margin differential between antidiarrheals and DRS favors the former. Another advantageantidiarrheals enjoy is the control and flexibility thatmanufacturers have in deciding the course of productlife. The formulation, package design, brand name, andproduct image are all variables over which the manufacturers can exercise control. Greater freedom to respondflexibly to market forces is valued by commercial firms.
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

Companies should not be denied the use of theirmarketing tools for OKS.
In a competitive environment, companies thrive byidentifying a market segment and then increasing theirmarket share b this segment. This technique is calledsegmentation and targeting. A company can choose tocompete in one or in several segments, basing its decisionon its own resources and on the market needs. Once thesegments have been targeted, the company allocates itsresources to the four major elements of the marketingmix: product, price, place, and promotion (the four "P"s),balancing each ingredient according to the marketresponse. ORS should benefit from the application ofthese marketing tools, if it is to stand any chance of success, and not be controlled in its presentation, price, distnbution, and promotion.
Companies should be allowed to differentiate theirproducts.
This is particularly true for over-the-counter pharmaceuticals in which some technical edge (such as theclassic "new and improved" claim) can be used to advantage over the competition and win the allegiance of theconsumer. The standard, low-tech image that ORS hasacquired hampers the ability of commercial ORS suppliers to employ this differential marketing technique. Todifferentiate their ORS brand and ••1ake it more attractive,some manufacturers ofcommercial ORS have added colorand flavorings to the ORS ingredients. Others have toyedwith the size, packaging, or presentation form. However, very few have had any coherent product strategy.
The continuing low retail price allowed for commerdal OKS constitutes a real marketing constraint.
Conventional marketing guidelines for setting pricesfor consumer products suggest that prices should domore thanjust cover production and packaging costs. Inaddition, price-setting must take into account the priceof competing products as well as what price levels maydo to product image in the minds of consumers (thehigher the price, the better the quality; the lower theprice, the lower the quality). Price is often perceived byhealth planners to be a barrier to ORS use by the poor;thus, price controls serve to keep ORS inexpensive.
ENLISTING THE COMMERCIAL SECTOR 191

Consequently, the greatest potential for making ORScommercially viable in this low-profit environment is toachieve high-volume unit sales. Achieving such highvolume sales is not likely in many developing countriesif retail sales are limited to phannacies and drug selleroutlets. Higher volume unit sales might be possible ifconsumer ORS were distributed and made available as anover-the-counter product in consumer goods shops thatsell common, everyday products like matches, soap, oraspirin.
One element of consumer demand for diarrhealproducts is the desire ofcaretakers to stop or shorten the diarrheal episode in children.
Suppliers of commercial antidiarrheal products try,in part, to meet that consumer demand. Indeed, stoppingdiarrhea is a major criterion ofconsumers in their assessment of the efficacy of diarrheal products. To date, ORShas been unable to meet this aspect ofconsumer demand.Attempts have been made to convince consumers thatORS is effective and that they should not expect diarrheaepisodes to be shorten",d. Nevertheless, the consumerdemand to stop or shorten diarrheal episodes appears toremain a significant unsatisfied need in many developingas well as developed countries. There is a need for product development and research where the public and private sectors can collaborate, for instance by acceleratingthe research on cereal-based ORS and on other treatmentalternatives that have the potential for satisfying thisdemand.
Notes:1 aRT amslJts of fluid replaammt, continum breastfmling, and fmling.2 World Health Organl-zatlon, -Programme for Control of Diarrhoeal DiseaKs Eighth ProgrammeReport, 1990-1991,- Gmeva: WHO, 1992.3 Communication and Marketing for Child Survival, a project sponsored by A.I.D., managm by theAaldemy for Educational Devdopmmt.4 LucIa perraz-Tabor, -Mobilizing the PrIvate Sedor for Publk Health In Indonesia,- In this volume.s See LucIa Pmaz-Tabor and WIlliam Jansen II, l'orifnB New Partnrr-sh/p6: PRmCH's PakUtan ExptrftII«, ArUngton,VA. Managemmt SdenctS for Health, PRITECH Project, 1991.6 See Paul J. Freund, --xbe Commerdallzation ofoRS In Zambia: Problems, Progras, and Prospects,- Inthis volume.7 See Camille Saade and Holly Tucker, 8tyDnd 1'harrrw:ID: New Pmp«tfvcs In ORS Markttins, ArUngton,VA. Managemmt Sciences for Health, PRITECH Project, 1993.
192 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

MOBU,IZING THE PRIVATE SECTORFOR PUBLIC HEALTH IN INDONESIA!I\ I, It 1.1 I (' I' 1.11'1 ,! ..
Despite progress made by the national control ofdiarrheal disease (COD) program, diarrhea still accountsfor about 130,000 deaths ofchildren under five each yearin Indonesia. l The potential of the private sector, particularly commercial companies, to reduce these deaths hasbeen relatively untapped to date. Sales of oral rehydration salts (ORS) are low compared to those of harmfulantidiarrheal drugs, and access to ORS through commercial sales outlets is limited.
In collaboration with the Indonesian Ministry ofHealth and USAIO/Jakarta, the PRITECH Project developed a program to tap the potential of Indonesia'sdynamic commercial sector. The program was designedto complement the government's efforts to reduce childhood mortality and morbidity due to diarrhea by developing and implementing a sustainable approach throughthe commercial sector.
PRITECH wanted to make the private sector activitiesas self-sufficient as possible, by motivating commercialfirms to invest the bulk of all capital required for thecommercialization of ORS. Self-sufficiency would optimize the chances for post-program continuation andminimize the possibility of fostering donor dependence.The project also intended to develop a replicable approachfor maximizing the role of the private sector in diarrhealdisease control and other public health programs in moreadvanced developing countries like Indonesia.
Lack of COll1merclrl! St~ctor Promotion of ORS
Since 1980, Indonesia's COD program has distributed ORS and accompanying promotional and educational messages through its provincial health departments. By 1991, ORS was well known amongIndonesians, but commercial sales of the product werevery low. While ORS was available through public healthcenters, over 30 percent of the ORS available in the public sector was purchased by UNICEF, which plans to stopproviding ORS 'nationwide in Indonesia in 1994. Thus,the public supply of ORS will be reduced, which, coupledwith the lack of commercially available ORS, will have anegative impact on the treatment of diarrhea in the
MOBILIZING THE PRIVATE SECTOR IN INDONESIA
Lucia Faraz-Tabor isthe Indonesia Country Rcprcscntativc andis the former PakistanCountry Rcprcscntativc.
193

194
home. Low sales were ciue to several factors: the lack ofORS promotion by its producers, unavailability of ORSin retail shops, and the negative image ofORS on the partof the public.
SuPPLY FACTORS
Prior to the collaborative effort among the commercial sector, the government, and PRITECH, pharmaceutical companies had been very effective in promoting otherproducts (some of them potentially harmful, such asantidiarrheal drugs and infant formula) but did not putany resources or effort into the promotion of ORS. Producers did not allocate funds for promotion of ORS nordid they detail-that is, have their salespeople explain theuse and i1l1portance of-oRS to physicians or other dispensers. Most ORS producers interviewed by this writerprior to the initiation of PRITECH's effort stated that ORSwas a "low-tech" product for low-income people. Theydid not believe that ORS was worthy of investment ofmoney, energy, or time because "ORS is the responsibility of the government, not a commercial product."
Although there were twenty-seven companieslicensed to produce ORS, only seven companies actuallyproduced it. Commercial sales of ORS were estimated tobe about 1,050,000 packets annually; however, morethan two-thirds of commercial production was sold tothe government or UNICEF. Companies believed thatthere was no commercial market for ORS and that thegovernment alone could meet the public need for it. Overall, ORS represented a small percentage of sales by thecompanies producing it: under 5 percent and, in mostcases, less than 1 percent of their total sales. Thus, ORSwas one of the lowest priority products for the existingproducers.
In general, ORS producers were not promoting ORS,except on rare occasions; a few producers, for instance,detailed ORS in limited areas during cholera outbreaks.The very few promotional materials some producers hadwere either old, of very limited availability, unused, orlimited to promoting the company's ORS brand. No ORSproducer used printed or point-of-sale materials to promoteORS.
In addition, ORS producers did not promote breastfeeding and feeding with ORS, which are critical elementsin the correct treatment of diarrhea. This omission rep-
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

resented amissed opportunity to disseminate information about correct case management to physicians andparents.
Although ORS is a general public drug, meaning thatit could be sold in all sales outlets, it was actually available almost exclusively in pharmaceutical outlets. Aretail survey showed that only 7 percent of small shopssold ORS.1 Yet most Indonesians purchased goods fromthese small shops. Thus, access to this life-saving product was limited to a very small segment of the population. On the other hand, antidiarrheal drugs and anbbiotics sold well and seemed to be easily available even insmall shops, despite the fact that they cost more thanORS and, in some cases, were supposed to be sold by prescription only.
DEMAND FACTORS
As in most countries, DRS in Indonesia is positionedas a low-cost, low-tech product for low-income peoplea market positioning that may have defeated any effortsto promote it. This "only-for-the-poor" and "just-sugarsalt" image seemed to undermine potential interest inORS. In consequence, pharmaceutical companies manufactured ORS mostly for government tender, few physicians prescribed it, and few parents bought it. Data ondrug prescriptions and use showed that antidiarrhealdrugs and antibiotics were prescribed and used far morefrequently than DRS. Parents did spend money to treattheir children with diarrhea-but little for DRS.
The low-income positioning also resulted in very fewupper-class mothers using DRS.J And because the poorer classes want the best for their children and associate"the best" with products purchased by the upper classes,the poor families may have been discouraged from usingORS. Finally, the low-income positioning may alsoexplain the lack of "clout" of ORS with physicians, whoseldom prescribed it.
FtllSlllCj IlltCI(~St. 111 ORS
The results from the situation analysis highlightedareas for improvement, as well as conditions for effectivechange.
MOBILIZING THE PRIVATE SECTOR IN INDONESIA 195
•

196
CONDmONS FOR CHANGE
Before deciding to collaborate with the commercialsector, PRITECH determined that the necessary conditions for change were present. These conditions includedthe size of the potential DRS market, adequate demand,and adequate production capacity.
Potential market for OKSIn Indonesia, there is a potentially enormous market
for DRS. According to government data, the incidence ofdiarrhea ranges between 120 and 360 cases per 1,000people per year, and 60 to 70 percent of cases occuramong children under age five, who have an average oftwo diarrhea episodes per year. The theoretical marketfor DRS could be as large as 197 million liters of ORS, or98S million packets (200 mI).
In addition, the government had recently banned allantimotility and most antidiarrheal drugs, leaving a vacuum in the market. If the ORS producers worked quickly enough, they could take advantage of the vacuum bypositioning oral rehydration treatment as the first-linetreatment for children with diarrhea.
UNICEF's withdrawal from tendering DRS for thegovernment would also increase the potential commercial market for DRS.
DemandAwareness of OraUt, the public-sector brand of ORS,
seemed to be very high. The national survey conductedby the Ministry of Health in 1990 showed 80 percentawareness.• A recent survey in Jakarta showed evenhigher awareness: 97 percent of all classes and 100 percent of the highest income classes had heard of ORS.'Actual use in the community, however, was substantially lower. According to the national survey, the percentage of those who had ever used ORS ranged from 16percent in the less-developed provinces to 2S percent inthe most developed provinces, with an average of 20 percent. The Jakarta survey showed higher use rates: 6Spercent of those surveyed said they had used DRS. Thelowest use rates were for mothers in the wealthiestincome group, of whom only 30 percent had ever usedDRS, followed by the poorest group, with 50 percent.About 70 percent of all other classes used ORS.
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

A survey of shopkeepers in retail shops, drugstores,and pharmacies in Jakarta was also conducted.6
Although most shopkeepers recommended drugs ratherthan DRS for diarrhea in general, when the question wasnarrowed to children with diarrhea, over 90 percentmentioned DRS, compared with about SS percent whomentioned drugs. However, qualitative research byresearchers, posing as mothers who actually asked forrecommendations for diarrhea for their children, showedmuch higher recommendations of antidiarrheal drugsand anbbiotics. At any rate, 9S percent of shopkeepersstated that DRS was a popular product. This figure indicates that there was at least some demand for DRS thathad not been met, probably because it was not availablein outlets most frequently used by consumers.
Adequate production capacityIndonesia has a thriving commercial sector that suc
cessfully reaches a large portion of the population withconsumer products and traditional and prescriptionmedicines. There was enough production capacity in thecountry-over 70 percent of it in the commercial sector-to meet the potential demand for DRS.
Previous collaborative effortsBy 1992, the national COO program had already
conducted social marketing campaigns for DRS, in onecase in collaboration with P.T. Pharos, an DRS producer.These efforts demonstrated that the private sector waswilling to participate and could be enlisted to contributeto social campaigns in Indonesia. For instance, a USAIOproject with the Ministry of Health used social marketing to increase access to DRS in demonstration areas inWest Java. This project combined a massive generic massmedia campaign with interpersonal efforts by government health teams and a commercial DRS producer.UNICEF had also conducted distribution efforts,although they did not include commercial companies.
Recent efforts to stimulate the demand for DRSincluded a mass media campaign about or.'~ rehydrationtherapy conducted by the Indonesian advertising counciland the Program for Appropiate Technology in Health incollaboration with the private sector. In this campaign,advertising agencies developed television spots, marketresearch companies pretested them, and television and
MOBILIZING THE PRIVATE SECTOR IN INDONESIA 197

198
radio stations contnbuted free air time. PRITECH saw thepotential of continuing and increasing this effort.
.AREAs FOR IMPROVEMENT
Expanding distributionMost ORS producers had one or more distnbutors,
who limited their distribution to pharmacies, renderingORS difficult to obtain in retail stores. Several factorscontributed to the lack of availability of ORS outsidepharmacies. First, small shops often obtained drugs suchas ORS from drugstores, instead of from wholesalers,which may make the product more expensive. Adding tothe lack of interest in ORS, the length of the distributionpipeline made it difficult for companies to monitor product distribution. Thus, they could not answer questionsabout the type, number, or locations of outlets wheretheir ORS was distnbuted.
The low availability of ORS in retail outlets and thehigh awareness of the product as well as the statementby shopkeepers that ORS was a popular product, supported the hypothesis that the lack of availability of ORSwas a key factor in the low rates of ORS use. PRITECHused this information to motivate ORS producers tobroaden their distnbution networks.
Promoting corred case management of diarrheaImproving the quality of care of children with diar
rhea was even more important than making ORS accessible to parents who needed it. To date, the most effectivecontinuing drug education of physicians had come fromthe detailers of drug companies who introduced andexplained to doctors how to use their products. Thus, oneof the most cost-effective approaches to improve casemanagement was to convince ORS producers to includemessages about breastfeeding and feeding when detailingtheir brand of ORS.
To accomplish this, PRITECH summarized researchthat showed that, when given with breastmilk. or food(particularly starches), ORS reduced stool output morethan any drug currently in the market. The researchfindings stimulated ORS producers to explore the possibility of positioning ORS with breast milk and food.
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

PRITECH liS Catillyst, •
To expand the distnoution of DRS and pn>mote thecase management of diarrhea, PRITECH developed a program to work with commercial companies to:• Increase ORS production and sales by the commercial
sector, broadening distribution of ORS from mostlyphannaceutical to consumer outlets;
• Motivate ORS producers and marketers to promotebreastfeeding and food along with ORS; and
• Promote at least one preventive strategy, such ashandwashing, through the commercial sector.
COORDINATION WITH COMMERCIAL COMPANIES
PRITECH approached commercial companies withthe ORS survey research, to convince them of the opportunities and benefits offered by the ORS market. The project emphasized the substantial gap between awarenessand use, which could be turned into demand. PRITECHalso emphasized ORS distribution as one of the key areasin which to concentrate.
PRITECH acted as a catalyst for helping private companies begin promotion. Specific activities undertaken byPRITECI-T. included:• Promoting interaction among private sector compa
nies and groups and between public and private sectors through meetings, seminars, workshops and frequent informal contacts.
• Maintaining a continual flow of information to keep allORS producers updated on relevant technical and marketing information.
• Disseminating results of market research to the private sector to provide information that enabled ORSmarketers to refine, improve, or change marketingapproaches.
• Initiating and facilitating working relationshipsbetween professional associations-particularly themedical association-and ORS and soap producers andmarketers.
• Working with interested companies to develop ageneric plan for marketing ORS in Indonesia, including promotion of oral rehydration therapy.
• Providing technical assistance to producers and marketers with brand-specific marketing plans and pro-
MOBILIZING THE PRIVATE SECTOR IN INDONESIA 199

,
200
motion of ORS and other products related to diarrhea,such as soaps for handwashing.
• Mobilizing private sector resources to support promotion of the government's key objectives for theCOO program, particularly oral rehydration therapyand preventive measures (such as handwashing andbreastfeeding). This effort built upon the existing collaborative effort between the Ministry of Health andlocal or international nongovernmental organizations.
MARKETING WORKSHOPS
The first, and perhaps most important, activity ofthe project was ajoint seminar with the Indonesian drugregulatory agency and the Ministry of Health. A positiverelationship with the drug regulatory agency is one ofthe highest priorities of the pharmaceutical industry. Inaddition, the national COD program manager urged DRSproducers to join the national effort.
In July 1992, PRITECH/Washington held a marketing conference for Asian ORS producers in Singapore,which several Indonesian firms attended.7 The conference, which was the first international ORS marketingworkshop of its kind, brought together senior executivesfrom Asian pharmaceutical companies that produce ORSto discuss current issues and new developments in DRSmarketing. It provided a forum for the cross-fertilizationof marketing ideas among the participating companies.Several companies presented successful marketingstrategies they had used for reaching rural populations,traditionally the hardest population to reach with DRS.Others displayed innovative ORS advertising materialsaimed at physicians, pharmacists, shopkeepers, and consumers.
Participants learned from each other's experiencesthat DRS 'can be a profitable product, and that it is desirable to work in partnership with the government andnonprofit sectors to promote public health objectives.
Later that month, PRITECHllndonesia conducted anAdvanced Marketing Workshop for ORS producers inIndonesia. The purpose of the workshop was to enhancethe capabilities of ORS producers t\> increase ORS production, broaden distrIbution, and promote oral rehydration therapy. Participants included marketing directors of several ORS manufacturing firms, as well as
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR
•

representatives from the drug regulatory agency, thenational COD program, WHO, .md UNICEF.
The workshop began with .' series of presentationsthat updated the participating companies on currentdiarrhea treatment guidelines and the activities of thegovernment and major donors in promoting oral rehydration therapy. The workshop's highlight, however,consisted of a participatory exercise in which the participants developed a strategic marketing plan for ORS in asimulated case study emulating the market situation inIndonesia. Samples of marketing materials from othercountries were also available to provide examples ofproven techniques that the Indonesians could try.
By the end of the workshops, participants appearedto agree that the ORS market held considerable promisefor their companies and were motivated to increase ORSmarketing activity. In addition, the workshop offered thecompanies the opportunity to network with each other,the government, and other agencies and to explore waysof complementing the government's COD efforts.
COLLABORATION WITH THE INDONESIAN MEDICALAssOCIATION
Most doctors in Indonesia belong to the Indonesianmedical association, which is, next to detailing, the onlyvehicle for reaching private practitioners nationwide inIndonesia. The association has chapters thoughoutIndonesia that meet once a month. It also sponsors seminars and training for its members for which participantsare given credits. Early in the program, PRITECHobtained the commitment of the association to add management of diarrhea to its training programs. The association also agreed to collaborate with PRITECH and several other private sector groups on a generichandwashing campaign. Other planned activities includedevelopment of a training video and module on diarrhealdisease treatment to be used by the association's chapters, circulation of posters and desk reference materialsfor physicians through the association's publication, andpublication of Dialogue on Diarrhoea with partial fundingby commercial firms and PRITECH.
MOBILIZING THE PRIVATE SECTOR IN INDONESIA 201

HANDWASHING CAMPAIGN
PRITECH initiated a collaborative effort to promotehandwashing with Unilever(Indonesia's major soap producer), Untas AdvertisingAgency, the Indonesian medical association, and theadvertising council. To convince Unilever to promotesoap for handwashing, thePRITECH field representativeoffered international studiesand local market researchdemonstrating that washing
./ hands with soap could reducethe incidence of diarrhea by as
II.,. .. much as 30 percent. The localmarket research showed that90 percent washed hands with
Ingat! Cucilah Tangan Sabalurn Makan. soap after eating, but fewer-ur-..........._- than 10 percent used soap
IKATAN DOKTER INDONESIA---- Lifebuoy before eating. With a 50 per-Handwashing campaign poster. cent share of the soap market
in Indonesia, Unilever hadmuch to gain financially from sponsoring a generic handwashing campaign aimed at increasing the use of soap.PRITECH's role was to initiate the effort and to serve as amember of the team that developed the campaign.
The handwashing campaign, funded by Unilever, isunderway. A corporate advertisement about Lifebuoysoap for handwashing is being telecast and paid for byUnilcver. In addition, a public service announcementabout handwashing to prevent diarrhea was telecast inMay 1993. The advertising council has obtained freemedia placement on the three television stations.
A handwashing poster for school children developed incollaboration with the Indonesian medical association wasdistributed to schools throughout Indonesia and is beingused as part of a health education effort in 1,000 schoolsin Jakarta by a local foundation, the Yayasan KusumaBuana. A poster for physicians was distributedby the medical association to its members through its chapters. Radiospots are expected to be broadcast in mid-1993.
202 TAPPING THE POTENTIAL OF THE PR1VATE SECTOR

IIl1j)clCt of the Progrlllll ,
Although the program began just one year ago,PRITEOI has seen the short-term effects, includingincreased ORS sales and sustair.able collaboration amonglocal institutions. For the first time, the Indonesian CODannual plan includes ccmmercial sector activities.PRITECH has successful1y obtained support for privateincluding commercial-sector activities from three keydepartments within the Ministry of Health: the nationalCOD program, the drug regulatory agency, and the community health education unit. All three have supportedand participated in the PRITEQI-initiatcd activities.PRITEOI is perceived as a resource by relevant departments within the Ministry ofHealth, which have requested PRITEQI's collaboration in numerous activities.
Most of the efforts focused on motivating ORS andsoap producers to use their own resources to promoteORS, brcastfecding and food, and soap for handwashingto prevent diseases, particularly diarrhea. PRITEOI'swork with commercial companies also shows encouraging results. Thus far, several ORS producers have begunto increase or show willingness to allocate additionalresources to ORS production, distribution, or promotion.Although PRITEOI cannot claim that sales increases aresolely due to the PRITECH effort, sales of ORS haveshown an increase. Unit (standard 200 mI) salesincreased by 20 percent, from 6,926,300 packets in 1991to 8,285,200 in 1992. Values increased by 26 percent,from 1,244,700 to 1,565,9JO rupiahs. The market shareof ORS in the diarrheal drug market also increased from9 percent in 1991 to 12 percent in 1992.
In addition, several ORS producers have agreed topromote ORS along with breast milk and food, andtwo-Abbott and P.T. Pharos-have begun promotionwith key messages developed by PRITECH. Also,PRITECH formed a private sector partnership to developand sponsor the handwashing campaign.
Another critical component of the PRITECH effortwas an increase in the generic promotion of oral rehydration therapy and handwashing. This was one of thebest ways of convincing ORS and soap producers toinvest in brand-specific promotion. Once producers realized that generic promotion would increase generaldemand for a product, they were more likely to increaseefforts to promote their own brands.
MOBILIZING THE PRIVATE SECTOR IN INDONESIA 203
.'

However, it was the Ministry of Health that broughtthese groups together. During a national meeting to discuss the national COD plan, the head of the contagiousdiseases unit ofthe Ministry ofHealth (under which diarrheal disease faIls) suggested. that PRlTECH initiate amulti-sectoral group, including the commercial sector,to work on diarrheal diseases. DRS producers participat-ing in a commercial sector marketing seminar had made it.
a similar suggestion. Thus, with governmental and pri-vate sector support, PRITECH started. the group.
UNICEF thought ofa name for thegroup: Ke1ompok Kerjasama. untuk l'rormsi. Anak Sehat (Working Group for Pr0motion ofChild Health). Members include representatives ofthe government, private and commercial finns, nongovernmental organizations, and international agencies. Duringthe first meeting, participants made presentations of theiractivities related. to diarrheal diseases. They focused on sharing information about who is doing what and providing aforum for government/private sector interaction. Thegrouphas formed. subgroups to work on various activities.
Lessons Le,ullecl ~
The PRITECH strategy of enlisting the commercialsector to promote DRS was tested and implemented inPakistan.' PRITECH's experience in developing thisapproach in Pakistan and replicating it in Indonesia leadsto the following conclusions.
It would be possible to replicate this model successfully in countries where the following conditions are met:• Existence of an active commercial sector,• A competitive environment consisting of multiple DRS
producers,• Presence of commercial soap producers,• Fairly high public awareness of DRS (at least 50 per
cent),• Insufficient government supplies of DRS, leading to
the need. to find alternative methods of obtaining anddistributing DRS.
For the model to work, the following groups mustbe involved from the beginning:
The government. The critical importance of government involvement cannot be overemphasized. Perhaps
204 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

PRITECH's most important role has been that of liaisonbetween the government and commercial sectors. Thecontribution PRITECH made was the linkage, coordination, and opening of dialogue between the governmentand commercial sectors. Commercial companies dependon the government to a large extent; the government canmake or break. a pharmaceutical company through regulations. The most important part of the government asfar as the phannaceutical industry is concerned is thedrug regulatory agency. It is critical to involve the drugagency from the beginning of the effort.
Commercial firms are also interested in supportingthe COD and health education divisions of the govcmment, which are in charge of policy and communication,including the mass media. The government must be highly involved initially and gradually decrease its involvement as the commercial sector interest and commitmentincreases. Government commitment to commercial sector involvement in ORS production, distribution, andpromotion increases the support of the commercial sector and ensures supportive policies and regulations,including those that will ultimately reduce governmentinvolvement in ORS purchase and distribution.
Medical and pediatric associations. Pharmaceuticalcompanies are usually willing to invest a lot of time,money, and effort to please these groups. If the medicalassociation in the country emphatically endorses oralrehydration therapy, calls on producers to detail ORS tophysicians, and collaborates in meetings and seminars,pharmaceutical companies will have .: strong incentiveto promote ORS.
The World Health Organization and UNICEF. WHOand UNICEF support is very important to the success ofORS commercial efforts. Strong support for ORS byhighly respected organizations such as WHO andUNICEF motivate a company to produce and market ORSas well.
Groups that can promote oral rehydration therapy.Well-developed and appealing generic, particularly massmedia, promotion of oral rehydration therapy by thecommunication or health education department of thegovernment, UNICEF, advertising associations, or similar groups, can motivate ORS producers to invest in ORSpromotion efforts. It is easier to convert existing awareness into demand for the product than to start fromscratch.
MOBILIZING THE PRIVATE SECTOR IN INDONESIA 205

Opinion kadus in the medical community. Support andprescription by leading physicians are very importantand should not be neglected. Often health promoters inthe public sector miss an opportunity by bypassing thedoctor and going directly to the community. All drugsthat are household drugs (such as aspirin) were, andoften still are, widely prescribed by physicians. It isthrough prescriptions that drugs acquire credIbility withphysicians, pharmacist". shopkeepers, and consumers.
The image of OKS must be improved.If ORS is to become attractive to the commercial sec
tor and to consumers, its image needs to be changed. Inmost countries ORS has been positioned as sugdI'-saltpowder, a low-tech home medicine, most often used bypoor village mothers to treat malnourished, dehydratedbabies. ORS should be positioned as a modern, scientific,and doctor-recommended drug.
The work of the pubHc and commerdal sectors canbe complementary.
The best government-sponsored public health campaigns are developed by advertising and marketing agencies under contract with the government and by nonprofit groups such as advertising councils. ORSproducers can be convinced that it is in their best interest to promote ORS correctly along with breast milk andfood. The advantage of the commercial sector is that itcan reach segments that the government cannot reach.
As countries develop, the role of governmentsbecomes one of managing resources to accomplish public health objectives in the most efficient manner. Mosthealth care costs such as ORS, can be borne by membersof society who can afford them. Government is then leftwith the task and obligation of dispensing free healthcare, including ORS, to the poorest segment of the population.
Nota:I Dilta from Dql8rtmm Kamtatan, P2M.2 SW'YfY Restardt indonesia data.3 SW'YfY Ratareh indonesia data.• Dilta from DqIIrtmm Kesdtatan, P2M., SW'YfY Restardt indonesia data.6 SW'YfY Restardt Indonesia data for PAnt.7 Camille Sa8dt and Hony Tucker. Bqrlnd Phlll'llUJria: film Prrsp«tl_ in ORS Marlcding. ManagernmtSciences for Health PRITECH~. 1993.s Por more information about PRJTECH's Pakilltan efforts, lift Lucia Perraz-Tabor and William H.JllIIKrt n, POfBlnB NM Partnfrshipa: PRITECH's Palcian bpeimce, Arlington,VA, Managemmt Sciena,forHealthPRITECH~,1991.
206 TAPPING THE POTENTIAL OF TIlE PRlVATE SECTOR

COMl\mRCIALIZATION OF ORS IN ZAMBIA:PROBLEMS, PROGRESS, AND PROSPECTS
, I, . I , :, I I I I, • I ", I
The zambian national control of diarrheal diseases(COD) program began in 1986 with the appointment ofa COD program manager, deputy program manager,COD secretariat, and establishment of a National CODCoordinating Committee. PRITECH also began involvement in zambia in 1986 with the appointment of a fulltime representative. The range ofCOD program activitiesincludes policy, planning, training, supervision, educational materials and social mobilization, production anddistnbution of oral rehydration salts, program monitoring and evaluation, and program integration.
Significant progress has been made in each of themajor COD program components in spite of severe economic constraints, shortages of personnel, lack of transport, drought, and epidemics of cholera and dysentery.
Since the beginning of the COD program, provisionof oral rehydration s.:llts (ORS) and promotion of oralrehydration therapy have been high-priority goals. In1986, the Ministry of Health made an important policydecision by banning the use of antidiarrheals in the publie health sector. However, anlidiarrheals are still available from retail chemists and compete with ORS. At thesame time, the COD program began intensive efforts toincret1se awareness of ORS and oral rehydration therapythrough production of educational materials, radio andtelevision spots, and popular theater performances. Anextensive training program to improve case managementof diarrhea was also developed. In 1989, the COD program identified the establishment of oral rehydrationcorners' in all health centers throughout the country asa priority. Since that time kits for oral rehydration therapy corners have been distributed, and training activitiescontinued. Given these priorities and goals it is crucialthat ORS always be available and widely distributed.
Although it is likely that user fees and communityfinancing schemes will be implemented under the newgovernment's health policy reforms, ORS will probablycontinue to be distributed free ofcharge to the public sector. Even if cost-recovery mechanisms are implemented,however, the government will have to explore as manyalternatives as possible to ensure the effective distribution of drugs and delivery of services. One such alterna-
COMMERCIALIZATION OF ORB IN ZAMBIA
Paul J. Freund is thrzambia Country~rtJImtativr.
207

tive is the encouragement of private sector enterprises tobecome involved in the manufacture of essential drugs,including ORS.
The availability and effective distnoution of DRS isan essential component of any CDD prognm. In orderfor other COD intervention efforts to hav~ maximumimpact, ORS must be readily availabie without stockouts. However, ORS availability and distribution remainproblematic issues in the Zambia CDD program. Thereare two main problems: first, the supply ofORS is insuf5cient; second, it is not sustainable.
DEMAND
The estimated theoretical annual demand for ORS is8.1 million packets based on results of the 1986 national COD baseline survey, which found that the nwnber ofepisodes of diarrhea was 5.1 per child under age five(multiplied by 1.6 million children under age five). Thisfigure assumes a negligible use of sugar-salt solution, asteady diarrhea incidence rate, and only one packet perepisode, rather than the recommended two packets perchild per episode.
The current use rate per month is 200 packets inrural health centers, 300 to 500 in urban clinics, 1,000in district hospitals, and 5,000 in central or specialty hospitals. Use by community health workers has been verylow-50 packets a month-due to insufficient suppliesat rural health centers, which supply community healthworkers.
SUPPLY
There are several sources of ORS in zambia, including outside donors, parastatal companies, and nongovernmental organizations. The most important sourcehas been outside donors. UNICEF has supplied an averageof 500,000 packets a year of ORS since 1984 and hasgradually increased supplies to 750,000 to meet choleraepidemic needs and drought-affected area requirements.In addition, since 1985, the Swedish and Dutch governments have been supplying ORS in essential drug kits toall forty-five rural districts in zambia, which provides
208 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

Japproximately 55 percent of zambia's total essentialdrug requirement.
The second source of DRS supply comes from aparastatal company, General Pharmaceuticals Limited,established in 1985. Gmeral Pharmaceuticals producesthe Madzi-a-Moyo brand of DRS and intravenous fluidsfor the Ministry of Health. The company has had numerous production problems occasioned by a lack of foreignexchange to purchase raw materials. UNICEF andPRITECH have provided free raw materials to GmeralPharmaceuticals, as well as packaging m~lerials andadvertising support. The company's production capacity has bern low, averaging 1 million packets pcr year. Inaddition, even with donated raw materials the ex-fadory price per packet was higher than imported supplies.General Pharmaceuticals is currently up for sale as partof the new government's privatization policy and maywell be sold to a private pharmaceutical firm.
Medical Stores Limited is a parastatal that purchases, stores, and distributes drugs for the Ministry ofHealth. It is a modern, efficient operation with sufficienttransport available to ensure adequate distribution ofdrugs. Medical Stores has purchased DRS from GeneralPharmaceuticals when .1 competitive price has beenagreed upon; however, due to the higher cost of Madzia-Mayo, Medical Stores has tended to rely on importedsupplies. Because the essential drugs program covers therural districts, Medical Stores only provides for the urbanline-of-rail towns and cities, including district hospitals,provincial and central hospitals, and the UniversityTeaching Hospital in Lusaka. Medical Stores also distributes drug kits that contain ORS to urban clinics and district hospitals, albeit in far fewer quantities than therequired amounts.
Smaller amounts of ORS available to the public sector come from such sources as the Red Cross, LutheranWorld Federation, the Jaycees, the Young Women'sChristian Association, and donations from variouschurch-mission organizations. The total amount fromthese sources averages less than half a million packetsannually.
El1CUllJ dCl111-<1 PIIVClI (' ORS PIOc!lIU'1 S
Because of the difficulties experienced by public sector suppliers and the impending termination of donor-
COMMERCIALIZATION OF ORS IN ZAMBIA 209

ASSOCIAno WITH DIARRHOEA.
FOR TREATME"T Of OEHYDf\ATIO..
Oresa promotional poster.
TRY lEWORANGE
FLAVOURED
supported projects, :. is important that the private sectorplaya larger role in DRS supply and distnbution. Theprospects for private sector production are good, giventhe new government's privatization policy; three privatecompanies have recently entered or plan to enter the DRSmarket.
The first private sector company to make DRS inzambia was Intcrchem, which produced a one-liter foilpacket in 1987. Interchem production was low, averaging 300,000 packets per year, and was largely sold to thecopper mine-operated hospitals and retail chemists.
...---------------, Intcrchem received technical sup-port from the Program for Appr:>priate Technology in Health to helpdevelop marketing and promotionalmatcriaIs and was geared to launcha campaign for DRS when its production equipment broke down in1989. Since that time, Interchemhas been attempting to repair theequipment without success. However, the company has recentlyreceived approval from its board ofdirectors to purchase new equipment, and plans to resume DRS production later in 1993.
A second company is CadburySchweppcs, a soft drink manufacturer that operates under franchisefrom Cadbury London. Cadbury'sinvolvement in DRS came aboutthrough a personal experience of thegeneral manager, whose owndaughter had a bout of diarrhea.
The daughter had been offered Madzi-a-Moyo DRS andhad refused to drink it until orange juice was added. Theexperience led the general manager to pursue the idea ofproducing an orange-flavored DRS. He had been trainedas a chemist and believed that the company had the technical capacity to produce DRS using existing equipment.He therefore had discussions with the director of Pharmaceutical Services and the chairman of the Food andDrugs Board regarding the formulation. The Food andDrugs Board initially had reservations regarding the flavoring but eventually approved the DRS as a general saleproduct that can be sold in non-pharmacy outlets. The
210 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR
general manager had also contacted pediatricians at theUniversity Teaching Hospital to carry out an acceptability study of the product by children with diarrheaattending the diarrhea training unit.
Cadbury Schweppes decided to call its new ORS"Oresa." The 250 mI packet size conformed to the recommended World Health Organization (WHO) formulation, with the addition of orange flavoring and colorin~.
The company developed a logo and some advertisingmaterials, mostly posters and banners. Up until the timethe product appeared on the market, neither the national COD program nor PRITECH was directly involved.However, as soon as Oresa appeared in retail pharmacies,the PRITECH representative notified the COD programmanager and contacted Cadbury Schweppes.
The COD program expressed concern over the 250 mlpacket size, which might present confusion as to propermixing because the COD program was promoting oneliter packets. There was also the concern that users wouldpurchase only one or two packets (500 mI) believing itwould be sufficient for treatment.
The issue of orange flavoring was discussed in ameeting with the CDD program, WHO, PRITECH, andUNICEF, who agreed that it did not compromise programpolicy as long the WHO-recommended formula ingredients were used. The PRITECH representative then discussed the Oresa possibilities with the assistant directorof medical services and the permanent secretary in theMinistry of Health. Both agreed that Oresa had advantages in that it used mostly locally available ingredients(sodium chloride, sucrose, and sodium bicarbonate),which would conserve foreign exchange. They also likedthe idea of the wide distribution network available toCadbury, which would make ORS more available inremote areas.
Cadbury cuntinued discussions with the Ministry ofHealth and decided to ask the minister of state for healthto launch the product officially in September 1991. Thelaunching took place and was well attended by the Ministry of Health, private physicians, pharmacists, WHO,UNICEF, and PRITECH.
In October, the PRITECH representative suggested toCadbury the possibility ofusing social marketing expertsto assist Cadbury in assessing the current market, todetermine the market potential and outline a marketingcampaign.
COMMERCIALIZATION OF ORB IN ZAMBIA 211
..

212
In January 1992, two PRITECH marketing specialists arrived in zambia to assist Cadbury's staff to develop a marketing plan. They discussed the possibilitiesregarding Cadbury's resourCb and suggested strategiesfor promotion of the product. However, they also raisedconcerns about the production and quality control procedures of Oresa. They recommended independent testing to verify the quality <.'f the product. In addition, theyvisited other private pharmaceutical cOITiparJ~ to discuss their plans for ORS production.
In April, PRITECH received the quality test results ofa sample of Oresa packets sent for testing. Unfortunately, six of the eight packets tested failed the quality control test. The results indicated that there was a problemboth in terms of mixing (composition) and filling(weight>. Although the packets were not dangerous ortoxic, there was a serious quality control problem thatrequired immediate action. The results of the tests wereshared with the Cadbury general manager and managing director by the PRITECH representative, and bothmanagers agreed to look at the matter seriously and takesteps to rectify the problem. The managing directoragreed that further production should stop. A survey ofavailable stock in retail pharmacies revealed that most ofthe Oresa packets had already been sold. The recommendations discussed with the managing director includedthe purchase of new mixing and dispensing equipment,batch numbering, quarantining of manufactured stockwith sample testing, monitoring of the productionprocess, and a clean environment. The possibility ofusing the well-equipped Medical Stores laboratory forquality control was also discussed.
Cadbury's management was generally appreciative ofthe technical advice in spite of the results and was seriousabout implementing the necessary changes. The managing director had already obtained a stamping machine forbatch numbering and had obtained brochures on newmixing and filling machines. Moreover, he suggested thatthe ORS operation be relocated at Cadbury's Copperbeltplant where more space was available.
While the initial enthusiasm for Cadbury's involvement in ORS manufacture has been dampened by the poorquality control results, the technical problems can besolved. If Cadbury can provide a new manufacturing areawith new machines, close monitoring, good quality control, and training of workers then they should be encour-
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

aged to continue. The problems that they have experiencedhave come about because they did not seek technical advicebefore beginning production and had no previous experience in manufacturing a pharmaceutical product.
Clearly, Cadbury saw a market need for a flavoredORS. And judging by the 200,000 packets they sold inthe first few months of marketing, there is a sizeablemarket potential am~ng retailers, private physicians, andhealth facilities operated by mines. However, if Cadburyis serious about marketing ORS, they will have to abideby good manufacturing practices and institute strictquality control procedures.
Gamma, another private pharmaceutical companythat currently manufactures a wide range of products,plans to begin producing a one-liter orange-tlavored ORSin early 1993. The company is constructing new stateof-the-art buildings on its Copperbelt-based facility andhas already placed orders for the ORS equipment.Gamma has well-equipped laboratories and the necessary experience and personnel to ensure a high-qualityproduct. The company already sells pharmaceuticals tothe mines and private physicians throughout the country, as well as exporting to neighboring countries.
Impact \ -
Encouragement of private sector initiatives is a recentdevelopment in Zambia, beginning with the advent of anew government in October 1991. The avowed policy ofthe Movement for Multi Party Democracy was to liberalize the economy, privatize parastatal companies, andallow free market forces to reign. Although it is too earlyto judge the impact of these changes the government hasmoved quickly to remove all impediments to investment.In the health sector, the Ministry of Health has liberalizeddrug tender procedures, allowing Interchem to bid for andwin an open tender to supply community health workerkits (including ORS). The removal of restrictive drugimport regulations and the 100 percent foreign exchangeretention scheme has encouraged local pharmaceuticalfirms to begin manufacturing more drugs. Moreover, themore open, competitive, and enabling environment has ledto more advertising by private sector companies.
Another measure of impact is the consumer demandof Oresa during the time that it was on the market. Thisdemand has kept other producers' interest in ORS pro-
COMMERCIALIZATION OF ORS IN ZAMBIA 213
duction alive. Interchem and Gamma have both purchasedORS equipment and plan production by mid-1993.
Finally, the experience with Cadbury has meant thatthe COO progrC'm will playa more active role in collaborating with the private sector.
Lessons Le?-rrJed .
The experience with General Pharmaceuticals hasdemonstrated the importance of having a enDprogram in place that is actively promoting OKSbefore establishing local production.
The issue of the standardized 750 ml size versus oneliter size packet has created serious problems for the COOprogram since 1986. A recent household case management survey found that 30 percent of the errors in mixing ORS were due to mixing a one-liter packet in a 750ml bottle.
The decision to produce 750 ml packets was based oninadequate research before a COO program was in place.
There is it potential market for other OKS productsin Zambia.
Sales of the flavored, higher-priced CadburySchweppes ORS demonstrate this potential. Even incountries where people have little disposable income, amarket exists for a variety of ORS products.
Actual and potential private sector producersshould be assisted with technical advice and marketing to ensure that messages to consumers areconsistent with enD program goals.
The COO program staff now regularly monitors theactivities of potential producers, such as Gamma andInterchem, to offer technical assistance. These evaluations are discussed at essential drug task force meetings.
A food manufacturing firm may be able to distribute and promote a pharmaceutical product likeOKS, but may not be appropriate to produce sucha product.
Despite the advantages Cadbury Schweppes mayenjoy in terms of wide distribution network and advertising, it is not simply a matter of adapting or converting a food production line to ORS. If food manufacturerswish to produce ORS, they need to provide a clean envi-
214 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

rooment, follow good manufacturing practices, andinstitute strict quality control procedures.
One of the dangers of a more liberalized economyand import regulations is the importation of useless and irrational drugs, including antidiarrheals.
The Ministry of Health is concerned with the quality of drugs imported and has set up testing proceduresfor these drugs. The number of local manufacturers hasincreased and there are already new antidiarrheal mixtures appearing in retail shops. This situation should bemonitored closely. The COO program has plans to workwith the National Pharmaceutical Association and theZambia Pediatric Association to eliminate or restrictantidiarrheals from the market.
Future Prospects
The prospects for continued private sector involvement in ORS are promising, given the present government's steps to liberalize tender procedures and otherrestrictive legislation. The potential market for privatesector producers is also good, particularly if they followgood manufacturing practices and implement strictquality control procedures that will enable them to sellto the public sector as well. Encouraging private sectorproducers will reduce the drain on scarce foreignexchange for imported drugs. Private producers also havebudgets that allow for the promotion and advertising oftheir products, a luxury that the public sector does notenjoy. Private sector promotion ofORS should benefit theCOO program, which depends on the widespread awareness and promotion of ORS.
At the same time, the COO program Will continue tofind ways to improve ORS distribution in the publichealth system. The program will explore alternative distribution networks and expand the range of ORSproviders through improving supply to communityhealth workers and using traditional healers to promoteoral rehydration therapy and ORS.
The new emphasis on the private sector in Zambiapresents challenging and exciting possibilities for theCOO program.
NotC5:1An oral rehydration comer is a sptcial area in a health facility that is arranged for provhling oralrehydration therapy. Aconveniently located and adequately equipptd corner will help staff to managedehydrated cases more easily.
COMMERCIALIZATION OF ORS IN ZAMBIA 215

THE PRITECH-PROCOSI COLLABORATION:WORKING WITH A PVO CONSORTIUM IN BOLIVIA
In August 1985, PRITEOi in:tiatcd activities inBolivia. The PRlTECH mandate was ·to provide technicalassistance to a nationwide child survival education projectimplemmtedby a national privatevoluntary organization(pvO)-Caritas Boliviana. The joint AI.D.;.Washingtonand USAID/La paz project aimed to reduce infant andchild mortality by introducing oral rehydration therapyand child-growth monitoring to the members of 1,800rural mothers' clubs.
The PRITEOi team in Bolivia provided technicalassistance to Caritas Bolivians and assumed additionalimplemmtation and funding responsibilities. In 1988,the final year of the PRITEOi I Project, PRITEOi expanded activities by providing technical support to a varietyof USAID-funded international PVOs with child survival projects.
Coincident with the conclusion of the originalPRITECH commitments to Caritas Boliviana in 1988,USAID/La Paz established a coordinating group forAI.D.-funded PVOs working in child survival programs in Bolivia. The purpose of this consortium wasto avoid duplication of services and to make the greatest use ofall resources available to child survival PVOs.
As a way to build on the gains that PRITECH hadmade up to 1988 and as a way to channel resources tothe new consortium, PRITECH offered to provide the services of our experienced Bolivian staff to the group. ThePRITEOi library and librarian had already been incorporated into the consortium, with aU costs covered by theconsortium. PRITEOi then proposed that Doctora AnaMaria Aguilar, its Bclivian technical medical consultant,and Licmciada Susana Barrera, its Bolivian educationalconsultant, join the consortium as technical resourcepersons, but employed with PRITECH funds. Thisarrangemmt allowed the previous PRITECH investmentin Bolivia to be carried forward with evm broader impactthan was :'i,')ssible working with one PVO alone (CaritasBoliviana) md fit in effectively with the new consortiumto support child survival activities more widely inBolivia. The consortium was also to be coordinating itsefforts with those of the Ministry of Health.
THE PlUTECH·PROCOSI COLLABORATION
Previous Page Blank
Ana Maria Aguilar isthe Bolivia CountryRqlrtscntativt, andPeter L Spain was aSenior OperationsOfficer.
A',.,The PROCOSIlogo
217
Thus from 1988 to 1991, PRITEOI provided technical assistance to the consortium of A.I.D.-funded PVOsworking in health in Bolivia. This consortium was calledthe Programa de Coordinacion en Supcrvivmcia Infantil(pROCOSI), and members included CARE, Project Concern, Save the Children, Andean Rural Health Care, Mealsfor Millions, Caritas Boliviana, Freedom from Hunger,Catholic Relief Services, Plan International, and ProjectEsperanza. Because of the constraints within the Ministry of Health in Bolivia, PVOs plly an important rolein the delivery of health services, in l~any areas not justsupplementing Ministry of Health efforts but taking onthe principal burden of health care delivery.
Tile Need for ASSlStClllCt: III Dli.1Jrllelll Disease COlltrol
PRITEOI's goals were:• To assist PROCOSI in developing activities and mate
rials that would better coordinate the child survivalprograms of its various PVO members and enhancethe technical appropriateness and effectiveness of themembers;
• To assist individual PVO members of PROCOSI todevelop effective and comprehensive child survivalprograms and activities, particularly in the area ofdiarrheal disease control; .md to assist PROCOSI andits members to make of their child survival activitiesand materials consistent with those of the Ministry ofHealth;
• To support limited but focused research of villagewomen by PVOs to increase the understanding of thereasons that deter women from adopting recommended practices for the control of diarrheal disease.We were especially interested in learning how to closethe knowledge and practices gap-the failure ofmothers who know about recommended diarrheal diseasecontrol practices to adopt those practices.
PRITEOI also proposed to make available to PROCOSI up to three months of external technical assistanceannually. The consortium was encouraged to makerequests for assistance through USAID/La Paz.
Thus, Dra. Aguilar and tic. Barrera became part ofthe PROCOSI executive secretariat. As a pediatrician, Dra.Aguilar provided guidance to PVO members on allaspects ofchild survival, while putting emphr.sis on diarrheal disease control. tic. Barrera, a communicator and
218 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

educator, worked with PVO members on the development of educational materials, ensuring their technicalquality through collaboration with the PRITECH pediatrician and ensuring that all materials were developed onthe basis of community research and pretesting. A keyrole of the communicator was to standardize messages,so that mothers would not be confused by variations inmessage content among member PVOs. Both PRITECHprofessionals provided technical review of requests forsubgrants that came from members to the consortium.
At the outset of the PRITECH-PROCOSI collaboration, V.-a. Aguilar completed a review of all of the PVOs'diarrheal disease activities. She found that all had diarrheal dise~sc control among their priorities, and all werecommitted to the norms published by the government(conforming with the guidelines of the World HealthOrganization). But, in fact, applied programs werescarce, few people were trained in proper case management, and little had been done to train health workers orto communicate with mothers. Medical recordkecpingwas also weak. A few PVOs had rehydration units, thebest of which were run by Plan International in the cityof Sucre, where about thirty units were in operation.
In sum, the PVOs were committed to the control ofdiarrheal distast, but in practice had few robust activities and limited vision for this priority. They were doingsome things in diarrheal disease control, but for the mostpart their efforts were weak and constrained by lack .oftrained staff. They worked in an integrated fashion, uniting efforts on several child survival interventions, butwith little technical guidance. The review recommendeda workshop to identify and shore up weak areas of diarrheal control programs.
P!()VI<llllq it VISIO!l
PRITECH has given PROCOSI a comprehensive capacity in relation to diarrhea control activities. UsingPRITECH technical assistance, PROCOSI has been able tooffer its members support in training, supervision, information services, and the development of educationalmaterials.
Training activities were the most needed and themost numerous, and comprised the concrete implementation of national and World Health Organization poli-
THE PRlTECH·PROCOSI COLLABORATION 219

Box 1. PROCOSI TrainingActivities Assisted by PRITECH• A diarrhea training module for fiddpromoters, in collaboration ·~·.rith CARE.• A seminar to review the technicalaspects of child survival with all thePVOs.• On-site training for PVO staff aboutcase managemmt of diarrhea.• A course to retrain Caritas Bolivianafidd staffand mothers' clubs about diarrhea, with emphasis on areas ofdifficulty in comprehmsion and practice.• A follow-up plan for five dioceses, tosupport and reinforce the fidd staff intheir use of educational material, incollaboration with Caritas Boliviana.• Training and retraining courses inchild survival, for nurse's aides andrural health promoters, in collaborationwith the Oruro Health District and Pr0ject Concern.• Courses in integrated child health atthe La paz Childrm's Hospital.• A vmture into formal education withSave the Childrm, in the schools ofInquisivi Province, to validate a healthcurriculwn on diarrhea managcmmtand prevention.• A retraining course for nurse's aids onfeeding during and after diarrhea, inVillamontes-Yacuita, with Project Espcranza.
220
cies for diarrhea control. Theseactivities are described in Box 1.
Training without subsequentsupervision can quickly lose itsimpact. PRITECH's medical consultant worked from within PROCOSI to strengthen field supervision and to ensure that trainingmarked the beginning of a relationship with a supervisor. Thisincluded regular technical supervision of PROCOSI projects, workshop follow-up, and field visitsspecifically directed to members'diarrhea programs.
The educational materialscomponent of diarrhea trainingwas the full-time concern ofPRITECH's educational consultant, beginning with a workshopon the production of educationalmaterials about diarrhea. Held inSanta Cruz, with participation bystaff from three health districts,six diocesan Caritas Bolivianaoffices, Project Esperanza, and theAndean Rural Health Care, theworkshop produced two games
and a thirteen-page flipchart. Subsequent productsincluded a redesigned user's guide for the Caritas Boliviana diarrheal control flipchart; implementation of theeducational material "Windows of Health" (messagesabout oral rehydration therapy and diarrhea prevention), in concert with the growth monitoring programof the Ministry of Health; and development and testingofa new "Road to Health" card with CARE. As part of theeducational radio project of Project Esperanza, PRITECHdeveloped diarrheal control messages for radio dramasand produced other broadcasts in support of child s~vival.
The PROCOSI Documentation Center, while notstaffed by PRlTECH consultants, represents the institutionalization ofan earlier PRITECH initiative; the center'sactivities have become a major part ofPROCOSI's servicesto its members and to other organizations working in
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

Box 2. PReCOSIDocumentation CenterActivities• Published annotated btbliographiesof the consortium's hbrary ho1dings,dealing with diarrhea, brcastfccding,and immunizations. A second volumeon diarrhea was also published.• Distnbuted a btbliography and documents sent from PRITECH's Information Center to the PVOs and otherinterested parties. The PROCOSIDocumentation Center likens its rolewithin Bolivia to the role of the PRITECH Information Center globally.• Published, with Caritas Boliviana,the educational material needed for theProyect:o Mcjoramimto Infantil.(PRITECH also assisted this project: during PRITECH's first phase in Bolivia.)
child survival. Some of the center'sactivities are presented in Box 2.
Ora. Aguilar continued heractive participation in COfAlMA,the corebrcastfceding group, whosemembers were sent for h'aining byA.I.D. to Wcllstart (San Diego) in1988. COfALMA's membersinclude influential staff memberswithin major Bolivian hospitals aswell as the Ministry of Health.Using this background and callingupon her COfAlMA colleagues,Dra. Aguilar was able to carry outvarious activities with the PVOsabout brcastfecding, emphasizingits role in preventing diarrhea.
Inaddition, as an example of thelinks that PRITECH has been able tomaintain throughout the Bolivian health community,Dra. Aguilar-in collaboration with the bilateral community, child health projects, and with the support andguidance of the PRITECH technical unit-has undertaken a study of persistent diarrhea among children presenting with diarrhea at the La paz Children's Hospital.Further, Lie. Barrera collaborated with the A.LD. Nutrition Communication Project on the production of avideo, called ICommuniquemonos yal, I for training community health workers on how to counsel mothers during growth monitoring sessions. This video followed asimple theme, based on Talking to Mothers about Diarrhea,2 but very much needed to animate these frequentbut often frustrating encounters by mothers with thehealth system.
Discussions were held with the Ministry of Education for an intervention with children through the formal education system. 'That effort was found to be aduplication of work being done through the radio education project, which incorporates correct diarrhea information into the school curriculum.
In addition to the activities listed above, many othercaIIs on PRITECH were made for services, including collaboration on a video on acute respiratory infections;training workshops in communication methods for thePVOS; the development of a flyer, video, and manual on
THE PRlTECH·PROCOSI COLLABORATION 221

222
Chagas disease; and the supervision of other materialsproduction for the PVOs.
During PRITEOi's work with PROCOSI, severaldevdopments warrant mention:• The cxecut:W( !.t<:~tary of PROCOSI resigned follow
ing an outside ~\lationof the consortium that wascxtrcmdy aitica1 of its management omd accounting.A new executive secretary, hired shortlythereafter, stayed on for two years, but ""as also dismissed. Finally, a third executive secretary wasinstalled. All this was indicative of the growing painsofan organization like PROCOSI, an amalgam involving many independent agencies that are learning towork together.
• The Ministry of Health and the La paz Children's Hospital have occasionally sought assistance from thePRITECH physician. The job description, approved atthe start by all parties, was flexible enough to respondto limited requests and, indeed, recognized the value oflinks between the PVOs and the public sector.PRITECH's role as a linkamong institutions has earnedlasting respect.
• The individual PVOs have not developed strong diarrhea-focused programs; rather, like the Ministry ofHealth, their emphasis has been on integrated programs, touching on several aspects of child survival.Within this context, however, PRITECH still has beenable to contribute.
In 1990, an A.I.D. evaluation was carried out toreview PROCOSI because its initial funding was comingto an end. The first operational program grant was toexpire at the end of July 1991, and A.I.D. needed guidance on whether PROCOSI should be continued. The evaluators gave high marks to the technical inputs by PROCOSI, including the PRITECH staff, calling them "skillful,qualified employees." But the evaluation cited manymajor dements of PROCOSI for modification, and recommended that the technical assistance provided byPRITECH be funded directly by PROCOSI under its anticipated new grant from USAlD. The evaluators concluded that the differences in salaries and benefits betweenPROCOSI and PRITECHIBolivia staff were disruptive andneeded to be diminated.
The implication of this recommendation was thatPRITECH would no longer provide technical assistance toPROCOSI. PROCOSI made direct offers of employment to
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

PRlTECH's Susana Barnra and CaritasBoliviana's Cornelio Ballesteros participatein a ccmfmnt:t on health tducation in theAmericas.
both advisc.rs, asking them tobecome PROCOSI staff by October1991, or to conclude their service toPROCOSI. The communicationadviser chose to stay on, while thepediatrician chose to conclude herPROCOSI work. However, Ora.Aguilar remained with PRITECH,providing tcchnical assistance to theMinistry ofHealth (cspccialIy for itscholera program) and other institutions.
Exemplary of PRITECH'srespected role within PROCOSI andamong the PVOs was the requestthat lie. Barrera be one of the evaluators on the team from CatholicRelief Services that evaluated theCaritas Mejoramiento Infantil Project in the altiplano and valleyregions of the country. 'Ibis projectwas carried on with PRITECH tcchnical assistance, andthere had at times been strains between Caritas Bolivianaand PRrrECH. But the two tcchnical PRITECH staff haveearned the respect of the PVOs with their seriousness,professionalism, and perseverance.
Although they were physically within the PROCOSIoffices and formal members of the PROCOSI staff, thePRITECH technical staff also represented a link. with theMinistry of Health programs, based on previous andongoing relationships with those programs. As the technical resource within PROCOSI, PRITECH was able toensure technical quality control and to diffuse the experience of individual PVOs among their colleagues; PVOshave been traditionally quite independent, without regular interchange on technical matters.
The public-private links for which PRlTECH is largely responsible in the Bolivian health sector arc veryunusual and very desirable to maintain. In a resourcepoor country like Bolivia, such collaboration means thatthe resources that arc available will be used according tostandard policies and that duplication and turf battlesbetween the public and private sectors will be minimal.
THE PlUTECH·PROCOSl COLLABORATION 223

Apart from its technical input, PRlTEOi representeda way for the PROCCSI members to relate to each othertechnically and to rclatl: to the Ministry of Health bothtcchnicallyand operationally.
Recognizing the reality of the integrated programs inBolivia and the reality of the diarrhea focus of thePRITEOI contract, PRITECHlWashington urged Ora.Aguilar and lic. Barrera to involve themselves in substantive diarrheal activities each month and report thoseactivities in detail. At the same time, PRITEOI urgedthem to contnbute in other child survival areas as theycould, to promote the integral programs of which theyare a part.
PRITECH found that the PVO consortium was auseful vehicle for its technical assistance.
The growing pains of the organization, documentedin the evaluation, are being dealt with, and the awardingof the second operational program grant representsUSAID's endorsement of the progress to date. The desireto standardize staffing, thereby eliminating PRITECH'stechnical assistance role, may be the best for PROCOSI inthe long run, if they can maintain in-house technicalability.
Because of prior links established by PRITEOI staffwith the Ministry of Health and other health agencies,the PRITECH connection within PROCOSI gave PROCOSIentree among these groups as well. The non-PROCOSIstatus of the PRITECH team allowed them greater flexibility in dealing with these other groups, to the advantage of all parties.
It should not be assumed that PVOs want international technical assistance.
PRITECH had budgeted $120,000 for additional outside technical assistance. PROCOSI's members did notmake use of outside technical assistance; at least, none ofthem made any call on the budgeted funds. Perhapsbecause this assistance would have come from outsidethe country, the PVO directors felt uncomfortable withspending for international assistance (even though it wasnot their money); they tend to be more grassroots-oriented and relate less to international consultants. As aresult, the money for technical assistance went unspent.
224 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

DedsionmaJdng in a consortium can be slow anddifficult.
As an organization, PROCOSI was slow to make decisions or to communicate with outside institutions suchas PRITEOi. PROCOSI let its first executive secretary gobecause he acted too independently, in the view of theexecutive committee. Therefore, the second secretary wasreluctant to speak for the group-as indeed, he was notauthorized to do---and the group found it difficult todevelop consensus promptly, ifat all. With ten members,each with a tradition of independence, decisionmakingwas a very dchbcrate process.
While working among the ten members of the consortium had its complexity, it has since been observedthat status as PRITEOi employees actually affordedgreater flexibility than did PROCOSI staff status.
Notes:I A booklet about the developmmt of this training vidro Is available from the Aaldemy for Educational Devdopmmt Nutrition Communication Prqject, 1255 23rd Street NW, Washington, OC 20037.2 TlIlktna to Mothrrs //bout DfIurlItlI Is a booklet written by PRITECH for health workers. Its purpose isto guide health workers to become dfectivl: communicators whm dealing with mothers and theirchlJdrm In a clinical setting, In reaJgnition ci the unique opportunity for teaching that this mrounteraffords and the wldesJllUd miscommunication that actually does oa:ur in many, if not most, clinicalsettings. TaWns to Mothm //bout DfIurlIa is available in Spanish and English from the PRITECH Information Cmter, the Pan Amulcan Health Organization's Special Programme for Maternal and ChildHtlIlth and Population, and the World Health Organization's Programme for Control of D1arrhOtllIDistases.
THE PRITECH-PROCOSI COLLABORATION 225

COLLABORATING WITH NONGOVERNMENTALORGANIZATIONS IN KENYAI, ! 'I" , ',1 :!:
In Kmya, few caretakers know about the importanceof early home treatmmt of diarrhea. Diarrheal diseasescontinue to be a leading cause ofchildhood morbidityandmortality. The principal role of the national control ofdiarrheal disease (COD) program in the Ministry ofHealth is to support the public sector through government health facilities and outreach activities. The publicsector, however, has never possessed the resources necessary to reach all caretakers. Therefore, COD programswill have limited access to the total population inKmya-and limited impact on morbidity and mortality-as long as their activities target only public healthsector services.
In Kenya, over 40 percent of health care is providedby nongovernmental organizations, or NGOs. Yet theyhave only indirectly benefited from donor assistance inthe control of diarrheal diseases. Although some NGOhealth care workers have completed training programson diarrhea management, the majority of the NGO andmission (or church-based) hospital staff have not beentrained in good clinical case management.
The NGO health care community needs to update itsknowledge of and practices for the prevention and management of diarrheal diseases at all staff levels. NGO andmission hospital workers need to be trained in diarrheamanagement to improve their hospital practices. Veryfew mission hospitals have established oral rehydrationcomers! in their maternal and child out-patient clinics orin their pediatric wards. NGO and mission hospitals oftenhave crowded pediatric wards where health workers tmdto use intravenous therapy for dehydrated patimts evenwhen it is not necessary. Many NGO hospital providersneed skills on how to better advise caretakers about homecase management. The NGO health care community alsohas a wide network of community health care workerswho would benefit from skills training in oral rehydration therapy.
The Kenya Catholic Secretariat (KCS) and the Christian Association of Kenya (CfIAK), the two largest NGOhealth care providers, togetht'I' provide 75 percent ofNGO health care services. A third NGO, Aga Khan HealthServices, has played a leading role in community-based
Karen E. Blyth is CUTrmtly the Madagascar Counby Rcpnscntam and was theKenya Counby Representative.
227

health care projects in Mombasa and Kisumu, wherediarrhea remains a leading cause of childhood morbidityand mortality. In 1992, PRITEOI/Kmya approachedthese three major NGOs to discuss ways to collaborate inorder to improve diarrhea management in their healthfacilities and home case management in their communities.
Dt~Vl)I()Plllq ll'St!,ltCqy fOl NGOs,ill
PRITEOI's overall strategy for Kmya aims to develop additional channels to promote improved diarrheamanagement in health care facilities and in the home.Strengthening the CDO capabilities of NGOs accomplishes this aim, while building on the existing commitmentof community-based NGOs to prevent diarrhea and topromote home case management in their communities.This effort, in turn, complements and reinforces achievements in the public health sector.
PHAsE I: RAIsING AWARENESS
After the workshop, PRITECH/Kenya began working with theKmyan workshop participantsfrom KCS, CHAK, and Aga KhanHealth Services in the development
PHAsE ll: DESIGNING THE NGOlNmATIVE
In March 1992, PRITECH, in collaboration with theCentre for Development and Population Activities(CEDPA),2 sponsored a regional workshop entitled.,Extending COO Services through Community-based
NGOs" in Nairobi. More than twenty-five participants from twelveNGOs in eight Anglophone Africancountries attended, including KCS,CHAK, and Aga Khan Health Services from Kenya. The workshopgenerated tremendous interest andheightened recognition that diarrheal diseases are still a leading causeof high childhood morbidity andmortality rates in Africa.
Goals of the PRITECH NGOInitiative• Enable a cadre of diarrheal diseasetrainers within the NGO or churchhealth community in Kmya to carryout good diarrhea clinical case management and community outreachtraining for health workers.• Train 10 to 15 percent of NGO mission hospital health workers in fourprovinces in good clinical case management of diarrheal diseases toimprove their hospital diarrhea management practices.• Train twenty community outreachhealth professionals from the NGO orchurch community in the areas ofhome case management and prevention of diarrheal diseases in order toeducate child caretakers in their ruralcommunities.
228 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

of the NGO initiative. Together they developed a diarrheamanagcmOlt training strategy for the hospital staff ofl<CS and OIAK (discussed below). They also developed acommunity outreach strategy for home case managemOlt and the prevOltion of diarrhea. The Aga KhanHealth Services wrote a proposal Oltitled "ImprovingDiarrhea Home Case Management," which was subsequOltly funded by CEDPA The purpose of the Aga KhanHealth Services proposal was to pilot-test a home casemanagemOlt educational strategy within Aga Khan'sPrimary Health Care Project in Mombasa.
In addition, PRlTECH/Kcnya contacted the Missionfor EssOltial Drugs (MEDS), which supplies mission hospitals with essential drugs. Until 1991, MEnS did nothave oral rehydration salts on its essential drug list butwould deliver oral rehydration salts to mission hospitalsonly when spccialIy ordered. Most mission hospitalswere "making their own oral rehydration solution andpromoting sugar-salt solution for home treatment. Theywere not maintaining a stock of packets oforal rehydration salts for discharged patients, who may have neededto continue the treatment at home. PRITECH believedthat if MEDS were persuaded to supply oral rehydrationsalts routinely to mission hospitals, then the hospitalswould be much more likely to keep rehydration salts instock and dispense them more b"bcrally.
PHAsE ill: CREATING A PROJECT PLAN
PRITECHlKmya created a project plan for the NGOinitiative. Due to a shortfall of PRITECH funds in 1992,the original project plan was modified and jointly funded by PRITECH, UNlCEFlKenya, and CEDPA. The WorldHealth Organization (WHO) supplied materials for thetraining programs. The NGO initiative builds upon theexpertise and resources of the Ministry of Health's CODprogram, which will help the NGO health care community upgrade their diarrhea management practices.
The plan outlined several strategies to reach the project goals:• Modify the public sector's diarrhea clinical manage
ment training to meet the needs of the NGO and mission hospitals.
• Train a core cadre of NGO and mission hospital workers in diarrhea managemOlt, home case managemmt,and the prevention of diarrheal diseases.
COLLABORATING WITH NGOS IN KENYA-
229

• Trainapproximatdy eighty NGO and mission healthpersonnd in clinical management of diarrheal diseases, using existing public sector oral rehydrationtraining units or provincial diarrheal training units.
• Identify four NGO health facilities with sufficientresources to build and staff their own diarrhea training units for training staff in the future.
• Develop a simple health facility monitoring tool thatthe NGO and mission trainers and supervisors couldusc to monitor progress in improved case management.
• Train approximatdy twenty hospital and community outreach workers in home case management andprevention of diarrhea.
Illlp!<'IlH:IlTII1Cj tlw NGO Illltl<n.lvl~ ,
The strategies resulted in a host of activities. As ofDecember 1992, some of the activities had already beenimplemented, while others were in the planning stage.
REvIsION OF THE NATIONAL 1'RAINING PROGRAM
Prior to beginning the NGO COO initiative, it wasimportant to address the key recommendations fromrecent evaluations of the national COO program's training courscs.3 As the national COD training team was incharge of conducting the diarrhea management trainingcourses fer the NGO health care community, it wasessenCdl to upgrade their skills as course facilitators. Thenational COD program requested assistance fromWHO/Geneva to enhance the program's training strategy and benefit the NGO health care community.
WHO trained the Ministry facilitators, coordinated anational training-of-trainers course on clinical management of diarrheal diseases, and assisted the national CODprogram to revise the three-day operational course intoa five-day diarrhea management course. The trainingof-trainers course was for Ministry pcrsonnd from fourprovinces who: (1) were physicians, clinical officers, ornurse or matrons; (2) were experienced in treating diarrhea patients, including both dehydrated and complicated cases; (3) had previously attended a clinical management course sponsored by the national COD program;and (4) had past training experience or a strong desire tobe a trainer.
230 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

In collaboration with PR1TECH and WHO, thenational COD program organized the second nationaltraining-of-trainers course on clinical management ofdiarrheal diseases, which followed WHO standard procedures.4 During the last day of the course, the participantsprepared a draft plan of action and training schedule fortraining activities in their respective districts. As a resultof the facilitators' briefing and training course, a sampleagenda for a five-day diarrhea management course wasdeveloped, which will be sent as a guide to all Ministryof Health district trainers. It will also be sent to prospective NGO hospital CDD trainers.
The greatest benefit gained from WHO's training offacilitators was that the national CDD training team wasevenbetterprepared to conduct future MinistryofHealthand NGO diarrhea me"JB'j4'!tlent training-of-trainerscourses.
A first step in the NGO initiative was for the national CDD program to assess the current NGO hospital andoutreach diarrhea management practices before a training strategy could be developed. A CDD health facilitymonitoring tool was used to assess current hospital diarrhea management practices in order to highlight problem areas in the training programs. The monitoring toolcould also be used as an internal self-assessment tool byNGOstaff.
Because ofCHAK's busy schedule, PRITECH began byfirst working with KCS in 1992 and followed with CHAKin 1993. A core staff comprised of members from thenational COO program, PRITECH, and KCS thet~fore carried out a CDO training needs assessment in westernKenya in August 1992. The objectives of the trainingassessment were to:• Assess the knowledge, attitudes, and practices in diar
rhea management of the NGO hospitals anli the community outreach programs,
• Identify one NGO facility per province that could bedeveloped as a future diarrhea training unit for clinical management training,
• Identify from these facilities potential participants forNGO diarrheal management training-of-trainerscourses. These participants would then serve as future
COLLABORATING WITH NGOS IN ICENYA 231

232
trainers at their hospitals to ensure good hospital diarrhea management practices.
TRAINING OF NGO 1'RAINERs
Following a hospital assessment of the mission hospitals, training-of-trainers workshops on diarrhea management were planned. The goal of the workshops wasto develop a cadre of COO trainers, within the missioncommunity, who would be capable ofcarrying out goodCOO clinical case management training for health workers at their respective hospitals. The projected outcome ofthe workshop would be the establishment of oral rehydration comers, good diarrhea management practices,and adequate counseling to mothers on home case managcm:nt. The five-day workshop curriculum usedWrlO"S diarrhea management training-of-traincrscourse and was facilitated by the staff of the nationalCOO program.
SUPERVISORY FOLLOW-UP VISITS
The health facility monitoring tool that was used bythe national COO program to assess mission hospital andoutreach diarrhea management practices was also usedby the national COO program and NGO supervisory staff
CDD program staffm«t: with the nurse-in-charge of the MisikhuCatholic Mission Hospital.
TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

to monitor the progress of each mission hospital inimproved case management. Supervisory visits tookplace from two to three months after the training-oftrainers workshops. A full day was spent by the supervisory team with each mission hospital and their respective staffs, visiting their newly established oralrehydration comers, and monitoring and strengtheningimprovements milde in case management. Problemsexperienced by mission staff were discussed togetherwith the national COD program team.
This was an essential step in the process. Followingthe first monitoring and supervisory visit, routine follow-up is essential to motivate mission hospital staffwho are faced with erratic supply of oral rehydrationsalts, overcrowding in pediatric wards, and colleagueswho arc rductant to accept updated case managementpractices.
CLINICAL MANAGEMENT TRAINING WORKSHOPS
The NGO trainers, once trained, plan to deliver clinical case management workshops to their hospital staffthrough 1993. Primary outcomes from this inscrvicehospital clinical management training will be improvedhospital diarrhea management practices and the establishment of an oral rehydration unit at the maternal andchild clinic or the pediatric ward. The NGO trainers areidentifying government hospital facilities where oralrehydration units are already in place, to be used for casemanagement practicums in the NGO trainings.
COMMUNITY OUTREACH AND PREvENTIONWORKSHOP
CEDPA, through PRITECH, is supporting and monitoring the Aga Khan Health Mombasa Primary HealthCare Project to improve diarrhea home case managementin Mtaa Location, Kwale District. The goal of this operations research project is to reduce diarrhea morbidity andmortality in Mtaa through a community-based healtheducation program that promotes the three primarymessages of home case management of diarrhea: givemore fluids, increase feeding, and refer the child to ahealth center if the child is still sick.
The study aims for two main outcomes. First, thestudy plans to increase the proportion of mothers and
COLLABORATING WITH NGOS IN KENYA 233

carctak.crs who are capable ofpracticing home case management of diarrhea. The second objective is to increasethe number of health workers in Mtaa with skills tocounsel caretakers ofchildrm with diarrhea to reduce themorbidity and mortality rates due to diarrhea in Mtaa.
11111J.lC t ()f til!' NGO Illltl.l!l'.'!'
As the NGO initiative is only in its infancy stage, itis premature to draw conclusive statements regardingthe impact of the solution to the problem addressed.
One notable improvement, however, has been thedecision, made in 1992, by the MEDS to include oralrehydration salts on their essential drug list. MEDS is alsorequesting a significantly greater stock supply fromUNICEF. This indicates that NGO and mission hospitalsare convinced that they should maintain a steady supplyof oral rehydration salts packets for out-patient homemanagement use.
Another achievement has been greater understanding on the part of the NGO health care community as towhy the Ministry's national program does not recommend that health care institutions promote sugar-saltsolution. Inaccurate measurements and poor mixingtechniques have resulted in unacccptably high failurerates for sugar-salt solution preparation.
The NGO mission hospital staffhas also shown commitment and eagcmess to review their current hospitalpractices ofdiarrhea management and seeks hdp inmaking recommended improvements in order to reach WHOstandards. NGO hospitals are not only committed toserving their populations with the best possible services,but are activdy seeking mechanisms and practices thatwill reduce their overall operational and managementcosts in this inflationary period in Kmya.
Oral rehydration comers are now established andoperating at the ~orityof NGO mission hospitals thatparticipated in the NGO training of trainers. Some NGOmission hospital staffs reduced patient casdoads in pediatric wards in a three-month period after establishingoral rehydration comers.
As a result of the PRITECH NGO initiative, missionhospitals and community outreach projects have redoubled their efforts to reduce the morbidity and mortalityrates of diarrhea in children under age five.
234 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR

Ll;SSOIlS Ll'illlwcI . , .
Collaborative efforts can raise health worker andcaretaker knowledge of case management ofdiarrhea.
Because PRITEOIIKmya was restricted to workingwith the public sector until the last year of the project,the opportunity to work with the NGO health carc community was almost lost. This active nctwork of healthservices reaches an important proportion of the population and is an important channel to reaching healthworkers and patients. PRITECH would have had muchgreater impact on diarrhea management had it beguncollaborating with NGOs in t 987 when it began operating in Kenya. Similarly, thc NGO health care community would have greatly benefited from a longer span ofcollaboration with PRITECH.
Unfortunately, PRITECHlKenya missed an important opportunity to work with NGO community outreach n~tworks in raising the knowledgc of rural parentsand caretake&~.More emphasis must be given to the dissemination of important messages regarding preventionand home case management of diarrhea in the future.Donors need to implement strategies that will reach ruralcommunities more effectively to raise knowledge andimprove practices about oral rehydration therapy.
NGOs must be carefully chosen.PRITECH used the following guidelines in selecting
the NGOs that would participate in the NGO program:(1) ability to meet PRITECH objectives, (2) eagerness ofthe NGO to update information, and (3) potential for sustainability.
NGOs can be easier to work with than public programs.
Mission hospitals in Kenya attract staff who arecxtemely dedicated and share a common goal of servingtheir communities. They are better staffed, betterequipped, and use more creative ways than governmenthospitals to sustain activities and seek financial support.NGOs can be easier to work with as their bureaucracy isless cumbersome. Furthermore, they are more flexible,and they are skillful at sustaining their hospitals in acost-effective manner.
COLLABORATING WITH NGOS IN KENYA 235
The skills and expertise of the Ministry of Health'sCDD program should be used for training the NGOhealth care community.
The Ministry is a valuable resource for health personnel trained and skilled in diarrhea case management.These skills need to be disseminated throughout theentire Kenyan health care system, not kept solely within the public health system. This is most importantbecause the Ministry has limitcrl access to the entireKenyan population. Public health irr'pact will be multiplied if the skills resident within the Ministry are sharedwith the NGO community and thus to the larger population of Kenya. In 1993 and beyond, the national program, in collaboration with UNICEF and WHO, willensure that the NGO health care community is providedwith high-quality training and updated technical guidance in good diarrhea management practices.
Supervision and monitoring of trained staff mustbe included in the implementation plan.
Routine monitoring and supervisory visits by thenational COD progrlUT. and NGO supervisory staff areessential in motivating and problem-solving with themission hospital staff.
Oral rehydration salts must be available in NGOfacilities before establishing a program.
In the case of Kenya, all mission hospitals made theirown oral rehydration salts and some hospitals had a supply from donors or purchased through MEDS.
NotfS:I An oral rdlydration lXJl'l1Cf is an area ofa dinic set aside for treating children with oral rdlydrationsolution and for counsdlng famny members about how to care for their sick child.2 CEDPA, a subcontractor the PRITECH Project, is dedicated to improving the managerial skills ofdevdoplng CXlUntry proffSsionals In health and population. .3 See, for example, Sc:ott Endsley and Agma Prins,-Kmya focused Programme Review, Phase 11,MJngton, VA, Managemmt Sdmc:es for Health PRJTECH Project, ECP-011-KE, October 1992.4 World Health Organization, Guldd1nfJ for Conducting TraInlng Courses at Health Centers and SmallHospitals, CDDISERl90.2 rev.1, Geneva, 1992. .
I
236 TAPPING THE POTENTIAL OF THE PRIVATE SECTOR




















