Development and testing of an instrument to assess nurses’ knowledge, risk perception, health...
11
ORIGINAL ARTICLE Development and testing of an instrument to assess nurses’ knowledge, risk perception, health beliefs and behaviours related to influenza vaccination Jing Zhang, Alison E While and Ian J Norman Aims and objectives. To develop an instrument to measure nurses’ knowledge, risk perception and health beliefs towards influenza and influenza vaccination and their vaccination behaviours and evaluate its construct validity and internal consistency reliability. Background. Although instruments to assess predictors of nurses’ vaccination behaviours have been developed, their validity and reliability have not been reported. Design. Instrument development and initial validity and reliability testing. Methods. The instrument was developed drawing on a literature review and expert consultation and was refined through pilot work. A cross-sectional survey using a revised version of the instrument was conducted among a convenience sample of 520 registered nurses (response rate 77 4%). Cronbach’s alpha coefficient was calculated to determine internal consistency of the sub- scale in the instrument. Principal components analysis with varimax rotation was carried out to evaluate the instrument’s construct validity and examine its internal structure. Results. Cronbach’s alpha coefficients for the three newly developed scales ranged from 0 70–0 76. Principal components analysis produced a good fit and confirmed the internal design of the instrument. In the seasonal influenza knowledge sub-scale four factors explained 44 8% of the total variance; in the H1N1 knowledge sub-scale two factors explained 44 7% of the total variance. Three factors in the risk perception scale contributed 50 5% of the total variance and two factors in the vaccination behaviours scale contributed 62 1% of the total variance. Conclusions. An instrument has been developed to assess nurses’ knowledge, risk perception and health beliefs towards influenza and influenza vaccination and their vaccination behaviours. The instrument was valid and reliable for the setting where it was used. Relevance to clinical practice. This instrument could be used to assess nurses’ knowledge, risk perception, health beliefs towards influenza and influenza vaccination and their vaccination behaviours. The three newly developed scales could also be used independently to measure variables influencing nurses’ vaccination practices. Key words: behaviours, influenza vaccination, instrument development, knowledge, nurses, risk perception Accepted for publication: 26 March 2011 Introduction Influenza is an acute viral infection that spreads easily from person to person. In temperate regions influenza epidemics occur almost annually and have been shown to be associated with short-term increases in severe morbidity and overall mortality (WHO 2009a). Vaccination is commonly recogni- sed as the principal measure for preventing influenza and reducing the impact of epidemics (WHO 2005). High-risk groups are usually targeted for influenza vaccination as well Authors: Jing Zhang, MSc, Associate Professor, Second Military Medical University, School of Nursing, Shanghai, China; Alison E While, PhD, Professor, King’s College London, Florence Nightingale School of Nursing and Midwifery; Ian J Norman, PhD, Professor, King’s College London, Florence Nightingale School of Nursing and Midwifery, London, UK Correspondence: Alison E While, Professor, King’s College London, Florence Nightingale School of Nursing and Midwifery, James Clerk Maxwell Building, 57 Waterloo Road, London SE1 8WA, UK. Telephone: +44 20 7848 3022. E-mail: [email protected] Ó 2012 Blackwell Publishing Ltd Journal of Clinical Nursing, doi: 10.1111/j.1365-2702.2011.03794.x 1
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Development and testing of an instrument to assess nurses’ knowledge, risk perception, health...

ORIGINAL ARTICLE
Development and testing of an instrument to assess nurses’ knowledge,
risk perception, health beliefs and behaviours related to influenza
vaccination
Jing Zhang, Alison E While and Ian J Norman
Aims and objectives. To develop an instrument to measure nurses’ knowledge, risk perception and health beliefs towards influenza
and influenza vaccination and their vaccination behaviours and evaluate its construct validity and internal consistency reliability.
Background. Although instruments to assess predictors of nurses’ vaccination behaviours have been developed, their validity and
reliability have not been reported.
Design. Instrument development and initial validity and reliability testing.
Methods. The instrument was developed drawing on a literature review and expert consultation and was refined through pilot
work. A cross-sectional survey using a revised version of the instrument was conducted among a convenience sample of 520
registered nurses (response rate 77Æ4%). Cronbach’s alpha coefficient was calculated to determine internal consistency of the sub-
scale in the instrument. Principal components analysis with varimax rotation was carried out to evaluate the instrument’s construct
validity and examine its internal structure.
Results. Cronbach’s alpha coefficients for the three newly developed scales ranged from 0Æ70–0Æ76. Principal components analysis
produced a good fit and confirmed the internal design of the instrument. In the seasonal influenza knowledge sub-scale four factors
explained 44Æ8% of the total variance; in the H1N1 knowledge sub-scale two factors explained 44Æ7% of the total variance. Three
factors in the risk perception scale contributed 50Æ5% of the total variance and two factors in the vaccination behaviours scale
contributed 62Æ1% of the total variance.
Conclusions. An instrument has been developed to assess nurses’ knowledge, risk perception and health beliefs towards influenza
and influenza vaccination and their vaccination behaviours. The instrument was valid and reliable for the setting where it was used.
Relevance to clinical practice. This instrument could be used to assess nurses’ knowledge, risk perception, health beliefs towards
influenza and influenza vaccination and their vaccination behaviours. The three newly developed scales could also be used
independently to measure variables influencing nurses’ vaccination practices.
Key words: behaviours, influenza vaccination, instrument development, knowledge, nurses, risk perception
Accepted for publication: 26 March 2011
Introduction
Influenza is an acute viral infection that spreads easily from
person to person. In temperate regions influenza epidemics
occur almost annually and have been shown to be associated
with short-term increases in severe morbidity and overall
mortality (WHO 2009a). Vaccination is commonly recogni-
sed as the principal measure for preventing influenza and
reducing the impact of epidemics (WHO 2005). High-risk
groups are usually targeted for influenza vaccination as well
Authors: Jing Zhang, MSc, Associate Professor, Second Military
Medical University, School of Nursing, Shanghai, China; Alison E
While, PhD, Professor, King’s College London, Florence Nightingale
School of Nursing and Midwifery; Ian J Norman, PhD, Professor,
King’s College London, Florence Nightingale School of Nursing and
Midwifery, London, UK
Correspondence: Alison E While, Professor, King’s College London,
Florence Nightingale School of Nursing and Midwifery, James Clerk
Maxwell Building, 57 Waterloo Road, London SE1 8WA, UK.
Telephone: +44 20 7848 3022.
E-mail: [email protected]
� 2012 Blackwell Publishing Ltd
Journal of Clinical Nursing, doi: 10.1111/j.1365-2702.2011.03794.x 1

as those with regular, frequent contact with high-risk people,
such as healthcare workers (HCWs) (WHO 2000, 2005,
Poland et al. 2005, Centres for Disease Control and Preven-
tion 2007, Straetemans et al. 2007). However, studies have
shown that vaccination rates of HCWs remain suboptimal
worldwide (Harrison & Abbott 2002, Lester et al. 2003,
Abramson & Levi 2008, Blank et al. 2008, Maltezou et al.
2008, Mereckiene et al. 2008) and nurses, although a group
that has the most patient contact, are more reluctant to
receive vaccination compared with other HCWs (Martinello
et al. 2003, Brunton et al. 2005, O’Reilly et al. 2005,
Christini et al. 2007, de Juanes et al. 2007, Livni et al.
2008, Norton et al. 2008, Shahrabani et al. 2009).
Several studies have been conducted to explore the
variables contributing to the uptake or refusal of vaccination
among nurses. A strong association between nurses’ knowl-
edge of influenza and influenza vaccination and their vacci-
nation status has been noted in various surveys (Martinello
et al. 2003, O’Reilly et al. 2005, Willis & Wortley 2007,
Livni et al. 2008, Falomir-Pichastor et al. 2009, Shahrabani
et al. 2009), that is, vaccinated nurses have significantly
higher knowledge scores or are more likely to answer
knowledge questions correctly. Attitudes towards influenza
and vaccination, including the perception of risk related to
influenza or pandemics, have been identified as another major
variable influencing nurses’ decision-making about vaccina-
tion (Campos & Jalaludin 2003, Brunton et al. 2005,
O’Reilly et al. 2005, Chalmers 2006, Tam et al. 2008,
Shahrabani et al. 2009). Several studies have suggested other
predictors associated with nurses’ vaccination including age,
previous vaccination history, professional ethos, group iden-
tification and health motivation (Campos & Jalaludin 2003,
Ofstead et al. 2008, Falomir-Pichastor et al. 2009, Norton
et al. 2008, Shahrabani et al. 2009).
Vaccination campaigns have attempted to improve vacci-
nation rates among HCWs in some local settings but these
campaigns have not always obtained the expected outcomes
among nurses (Harbarth et al. 1998, Sartor et al. 2004,
Ofstead et al. 2008) although others have reported increased
vaccination coverage of HCWs (Bryant et al. 2004, Kuntz
et al. 2008, Ribner et al. 2008, Polgreen et al. 2009). We
hypothesise that this may be due to variables influencing
nurses’ vaccination behaviours that have not been clearly
identified because the instruments used in the above studies
were not systematically developed and tested.
There are few reports detailing rigorously developed
instruments with validity and reliability testing. This paper
describes the development and testing of an instrument (the
King’s Nurses’ Influenza Vaccination Questionnaire) to
measure nurses’ knowledge, risk perception, health beliefs
relating to influenza and influenza vaccination as well as
vaccination behaviours. This instrument could aid the
exploration of variables which influence nurses’ vaccination
decisions so that vaccination campaigns may be evidence-
based.
Background
A literature search revealed 15 different instruments to assess
nurses’ knowledge, attitudes, risk perception, or health
beliefs towards influenza and influenza vaccination. How-
ever, for most of these instruments few details about their
development or validity and reliability testing were reported.
Five instruments were developed as part of surveys.
Martinello et al. (2003) developed a questionnaire to mea-
sure HCWs’ knowledge regarding influenza vaccination and
risk perception about the spread of influenza and used it in a
cross-sectional survey in a US hospital. A self-administered
questionnaire was developed by O’Reilly et al. (2005) to
assess influenza vaccination status, reasons for or against
vaccination, knowledge and attitudes towards influenza
vaccination using a Likert scale for nurses working in elderly
care units from three hospitals in the UK. An Israeli cross-
sectional survey of physicians and nurses used a three-section
questionnaire to assess participants’ occupational data,
knowledge about influenza vaccine and reasons for taking
or not taking a vaccination (Livni et al. 2008). Falomir-
Pichastor et al. (2009) surveyed a large convenience sample
of nurses in Switzerland using a self-developed tool compris-
ing a 11-point scale to assess vaccination status and intention,
reasons for or against vaccination, perceived negative conse-
quences of vaccination, group identification and professional
duties. A short questionnaire was developed by Christini
et al. (2007) to assess vaccination status and intention,
motivating factors for vaccination, degree of contact with
high-risk individuals, perceived risk of side effects of vaccine
and incidence of influenza-like illness among HCWs in two
US hospitals. All these instruments were developed to
measure important aspects of influencing factors underlying
influenza vaccination behaviours among HCWs or nurses,
but the absence of evidence relating to questionnaire devel-
opment and subsequent testing raises questions about their
rigour and wider utility.
Two instruments drew on previous studies. Campos and
Jalaludin (2003) developed a questionnaire to assess the
predictive factors underlying influenza vaccination and beliefs
and knowledge of influenza and vaccine among hospital-
based nurses. The first element of the questionnaire was
modified from a questionnaire originally developed by
Chapman and Coups and used with a large convenience
J Zhang et al.
� 2012 Blackwell Publishing Ltd
2 Journal of Clinical Nursing

sample of healthy adults in US (Chapman & Coups 1999a,b).
However, both original papers and the later paper did not
report details about the questionnaire development and
testing. Another element of the questionnaire sought to
measure Health Belief Model (Becker et al. 2004) variables
drawing on Shahrabani et al.’s (2009) instrument which was
based on the questionnaire of Blue and Valley (2002) with no
evidence of validity and reliability testing. Another instru-
ment drew on a previous survey undertaken in Australia
which had been used to survey HCWs in China (Seale et al.
2010). Again there was no report of instrument testing nor
general translation and back-translation or of a cultural
adjustment phase which is usual when an instrument has
been developed for another context.
Six studies reported a pilot test before the field survey. A
New Zealand version of questionnaires assessing knowledge
and attitudes of general practitioners about influenza vacci-
nation (Brunton et al. 2005) was developed drawing on a
previous study carried out in Australia (Litt et al. 1995). The
questionnaire was pilot tested with a small group before use
in the main study but no details of the pilot testing and
results were reported. Tam et al. (2008) developed a ques-
tionnaire to assess nurses’ experience with SARS, attitudes
towards the avian influenza epidemic and views on influenza
vaccination uptake in Hong Kong. Although a pilot study is
reported, no details were provided. Further, section two of
their questionnaire seeking nurses’ views towards the avian
influenza epidemic was adapted from Imai et al.’s (2005)
study which also did not report testing by the original
researchers. A US survey administered an online question-
naire developed from a literature review and consultation
with experts to collect data about influenza vaccination
history and vaccination intention, reasons for declining
vaccination, knowledge about vaccination and cues to action
amongst nurses (Ofstead et al. 2008). Although it was pilot
tested and revised prior to the main data collection, the
validity and reliability of the questionnaire were not
reported. Several instruments were pilot tested with conve-
nience samples to ensure clarity and ease of administration
(Chalmers 2006, Norton et al. 2008, Clark et al. 2009).
Chalmers (2006) reported pre-testing and piloting of the
questionnaire prior to refinement of its design and content to
increase its reliability, validity and practicability but the pilot
study results were not reported.
We found no valid and reliable instrument that had been
developed to measure nurses’ knowledge, risk perception,
health beliefs, vaccination behaviours and other important
variables. Hence, this study aimed to develop an instrument
and evaluate it for construct validity and internal consistency
reliability.
Method
Aim
The study aimed to develop and test an instrument to
measure nurses’ knowledge, risk perception and behaviour
relating to influenza and influenza vaccination.
Design
A cross-sectional, descriptive instrument development study
was designed. The instrument measuring nurses’ knowledge,
risk perception, health beliefs and behaviours relating to
influenza vaccination was developed and tested using three
steps: (1) Construction of the instrument: an initial draft of the
instrument was developed from the literature review and
expert consultation. The initial draft instrument was reviewed
by experts to assess content validity. (2) Testing for clarity and
feasibility for use: a pilot survey was conducted to test the
clarity and feasibility of the revised instrument in a small
sample of nurses and a revised version of the instrument was
developed. (3) Assessment of validity and reliability: the new
version of the instrument was distributed to a large sample of
nurses to calculate the internal consistency coefficient of the
instrument. The data were also subjected to exploratory factor
analysis to test construct validity.
Ethical considerations
The study was approved by the University’s Research Ethics
Committee. All participation was voluntary, confidential and
anonymous.
Step 1: Construction of the instrument
Key components of the instrument were derived from an
overview of the existing literature about the determinants of
nurses’ influenza vaccination behaviours (Zhang et al. 2010).
These factors and predictors were used to generate a
preliminary list of items for the instrument focusing on the
following areas:
• Demographic data of nurses including gender, age group,
educational qualifications, work place, clinical speciality
and years of registration as a nurse and direct patient
contact.
• Knowledge about influenza and the influenza vaccination.
• Perception of the risk of influenza and pandemics.
• Health beliefs.
• Practices regarding influenza vaccination.
• Reasons for having or not having the influenza vaccination.
Original article Nurses’ influenza vaccination instrument
� 2012 Blackwell Publishing Ltd
Journal of Clinical Nursing 3

The preliminary list of items was discussed with two nurse
experts (co-literature reviewers) who checked whether the
items represented key content. Wording and comprehension
of the items as well as scoring methods were also checked
with the statistician involved in the first step. For each of the
items, experts were asked if the wording was clear, if the item
fitted with the aim of study and if the item was needed. Two
open-items were suggested by the statistician to replace of
original closed items because open items ‘provide forthright
and valuable insights into people’s perceptions of the issues
involved and to get a feel for the words and phrases that they
use’ (Jackson & Furnham 2000, p. 116). Feedback from the
experts resulted in the adjustment of the wording for several
of the items and two open items replaced the closed items.
Changes were introduced and another draft of the instrument
was produced.
Step 2: Testing for clarity and feasibility for use
A pilot study was conducted to ensure that the revised
instrument was clear, understandable and feasible for use in a
sample of nurses. Twelve nurses enrolled in a university
continuing professional development course were invited to
participate in the pilot study. They were asked to complete
the initial draft of the instrument and afterwards they were
asked to provide their comments about problems in com-
pleting it, including whether it was clear and understandable
and also whether the content was complete and relevant
(Polit & Hungler 1993). Only four of those invited agreed to
participate in the pilot study (six declined; two were absent
from the class). They completed the instrument with no item
non-response within 7–15 minutes. The instrument was
considered easy to complete and not long. All items were
considered relevant to the aim of study and no suggestions
were made regarding the exclusion of any items or the
addition of new items. No items were ambiguous or caused
unease. However, suggestions were made regarding the
instrument’s layout so that it would be more compressed
and look shorter. A final version of the instrument was
developed.
The final version comprised six sections, combining open
and closed items to measure nurses’ knowledge, risk percep-
tion towards influenza and the influenza vaccination as well
as their vaccination behaviours:
Section one (30 items): asks nurses to assess true or false
of statements relating to knowledge about influenza and the
influenza vaccination (including 22 items about seasonal
influenza and vaccination and eight items about H1N1 and
vaccination). The correct response to each item was based
on the World Health Organization (WHO) guidelines
(WHO 2000, 2009a,b,c,d). The correct answers for 19
items required a positive response while the other 11 items
required a negative response. We quantified the degree of
knowledge by calculating the knowledge (K) score. The
original K-score was defined as the total number of correct
(either positive or negative) answers to the 30 items; the
maximum possible original K-score was 30. There were
also two sub-scores for knowledge: seasonal knowledge
(SK) score and H1N1 knowledge (HK) score, with the
maximum possible score of 22 and 8 respectively. We also
converted the original scores to a 100% scoring system
where K, SK and HK% with scores ranging from 0–100%
respectively.
Section two (12 items): a four-point Likert scale was used
to assess nurses’ perception of risk towards influenza and
pandemic. We quantified the degree of concept of risk
perception by calculating the risk perception (R) score.
Responses to items were positive except one item (B3_5)
which was needed to be reversed when calculating the R
score. The R-score was defined as the average of the values
ticked for each item (i.e. where 1, strongly disagree; 4,
strongly agree; 0, not decided) with item B3_5 needing to be
reversed before summing. R score is ranging of 0–4.
Section three (18 items): The Multidimensional Health
Locus of Control (MHLC) scale (Wallston 1993) was used to
examine nurses’ beliefs regarding whether his or her health
status is determined by the actions of individuals and if so,
whether the locus of that control is ‘internal’, ‘chance’ or
‘powerful others’. The MHLC is an 18-item, six-point Likert-
type questionnaire including three subscales. The score on
each sub-scale is the sum of the values ticked for each item
(i.e. where 1, strongly disagree and 6, strongly agree). No
items need to be reversed before summing. All of the sub-
scales are independent of one another. The full scale has
acceptable test–retest reliability with coefficients ranging
from r = 0Æ60–0Æ70 and internal consistency with coefficients
ranging from a = 0Æ60–0Æ75 (Wallston 2005).
Section four (nine items): assesses nurses’ practices relating
to seasonal influenza and H1N1 vaccination. Nurses are
asked to indicate whether or not: (1) they had been
vaccinated in the last 12 months; (2) they had recommended
vaccine to their patients in the past; (3) they intend to receive
vaccination in the following year and (4) they intend to
recommend vaccinations to their patients in the future. An
open item also asked about their vaccination practices over
the last five years. Responses to these items constitute the
main dependent variables of the study.
Section five (two open items): reasons for accepting or
refusing vaccination are asked inviting three reasons why
they might (or not) have the vaccination.
J Zhang et al.
� 2012 Blackwell Publishing Ltd
4 Journal of Clinical Nursing

Section six (10 items): demographic and professional data
are sought including gender, age group, educational qualifi-
cations, place of work, speciality, years as a registered nurse
and whether or not they have direct patient contact.
Step 3: Assessment of reliability and construct validity
A survey using the final version of the instrument to test
validity and reliability of the instrument was conducted
among a large convenience sample of qualified nurses
attending university continuing professional development
courses between May–November 2010 using a self-complete
questionnaire. A total 936 qualified nurses attending 39
classes were invited to participate in the survey (some may
have been invited more than once if they attended more than
one class but they were reminded they should only participate
on one occasion). One of the researchers distributed the
information sheets directly to potential participants and
questionnaires if they agreed to participate in the survey. A
freepost addressed envelope was provided to enable all
completed questionnaires to be returned directly to the
researchers. Non-response was not followed up because the
questionnaire completion was anonymous.
All items were designed to contribute to the same under-
lying construct of vaccination and therefore, the Cronbach’s
alpha coefficient was used to determine the internal consis-
tency reliability of sections 1–4 of questionnaire (Dunn
1989). Values of Cronbach’s alpha above 0Æ70 are considered
to be indicative of good internal reliability (consistency)
(Nunally 1978).
Exploratory factor analysis (EFA) was initially performed
to examine the internal structure of the section one (knowl-
edge), two (risk perception) and four (vaccination behav-
iours). Conditions for the adequacy of the factor analysis
were checked first based on: (1) a sample size of a minimum
of 1:5 items to subject ratios for the reliability of the factors
emerging; (2) significant Bartlett’s test of sphericity and (3)
large values of the Kaiser–Meyer–Olkin (KMO). Principal
components analysis and varimax rotation with Kaiser
normalisation were selected for the factor extraction in this
study. The Kaiser’s criterion based on eigenvalues and the
Scree test was used for calculating the factors’ numbers as
well as a subjective evaluation of how meaningfully the items
loaded on factors (Jackson & Furnham 2000, Waston &
Thompson 2006).
Statistical analysis
Statistical analysis was performed using SPSSSPSS 15.0 software
(SPSS Inc., Chicago, IL, USA). Data were first analysed using
descriptive statistics including mean and standard deviation
(SD). Cronbach’s alpha coefficients and factor analysis
(principal component analysis with varimax rotations) was
used to examine which factors of the sections comprised
coherent groups of items (Knapp & Brown 1995).
Results
Descriptive statistics
A total of 520 registered nurses completed the questionnaire
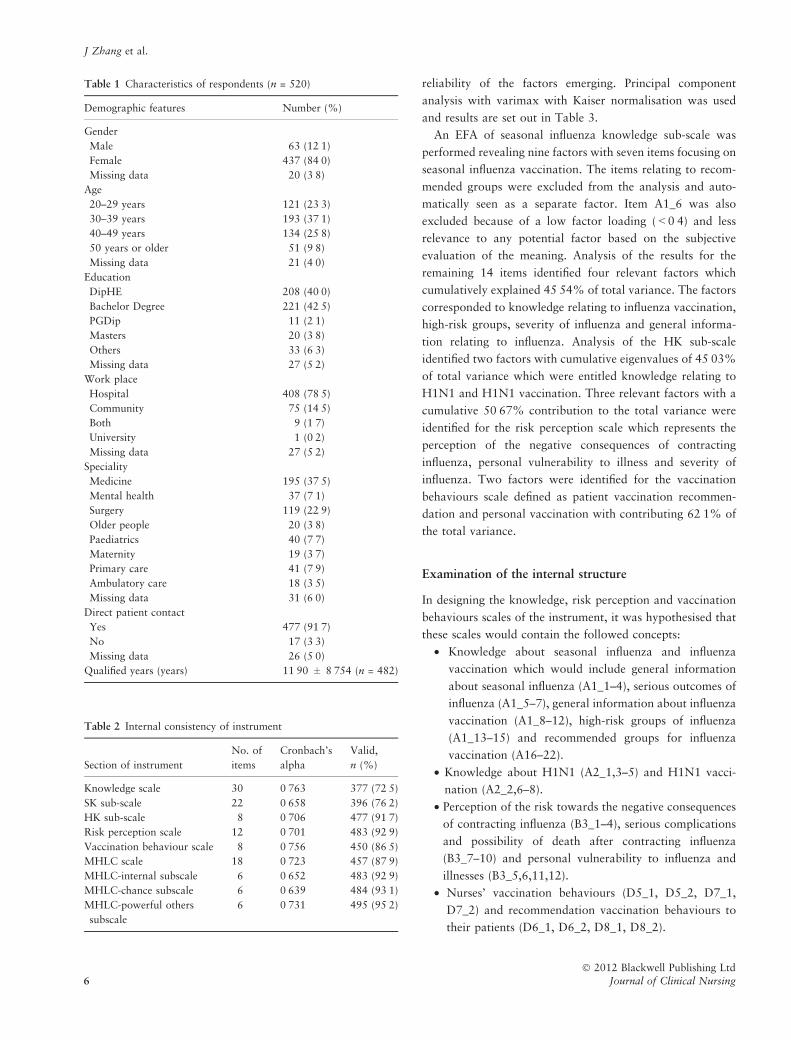
from 672 distributed (77Æ4% response rate). The character-
istics of respondents are summarised in Table 1. Most of the
nurses were female (84Æ0%) and worked in hospitals (79Æ2%)
and 91Æ7% of the sample reported having direct patient
contact. Overall 187 of 506 respondents (37Æ0%) reported
receiving the influenza vaccination in the last 12 months; and
35Æ3% (172 of 487) of the respondents reported receiving the
H1N1 vaccination in 2009.
Reliability
The mean scores for the knowledge and risk perception scales
were: K% 69Æ7 (SD 12Æ26, n = 494); SK%73Æ2 (SD 11Æ73,
n = 503); HK% 59Æ4 (SD 23Æ61, n = 507); and R 2Æ3 (SD
0Æ44, n = 510). Cronbach’s alpha coefficients ranged from
0Æ701–0Æ763 for each scale of instrument with alpha coeffi-
cients of 0Æ639–0Æ731 for the sub-scales of knowledge and
sub-scales of MHLC scale (Table 2). Thus, all scales of the
questionnaire met the internal consistency criterion of at least
0Æ70 for a newly developed instrument (Nunally & Bernstein
1994).
Factor analysis
As the instrument was constructed to comprise six sections
based on an analysis of relevant references, a separate factor
analysis was done on each of the seasonal influenza knowl-
edge, HK, risk perception and vaccination behaviours scales.
For the former three scales, the KMO test values, which
measures the sampling adequacy, were >0Æ60 (0Æ672, 0Æ739
and 0Æ667, respectively) indicating that a factor analysis
could be performed and all the significance values of
Bartlett’s Test of Sphericity were less than 0Æ001 indicating
the suitability of the data for factor analysis. The KMO value
of the vaccination behaviours scale was 0Æ576 with Bartlett’s
p value less than 0Æ001 so that EFA was also performed. The
ratios of sample size to the number of items ranged from
1:18Æ0 (for the seasonal influenza knowledge sub-scale) and
1:59Æ6 (for the vaccination behaviours scale) indicated the
Original article Nurses’ influenza vaccination instrument
� 2012 Blackwell Publishing Ltd
Journal of Clinical Nursing 5
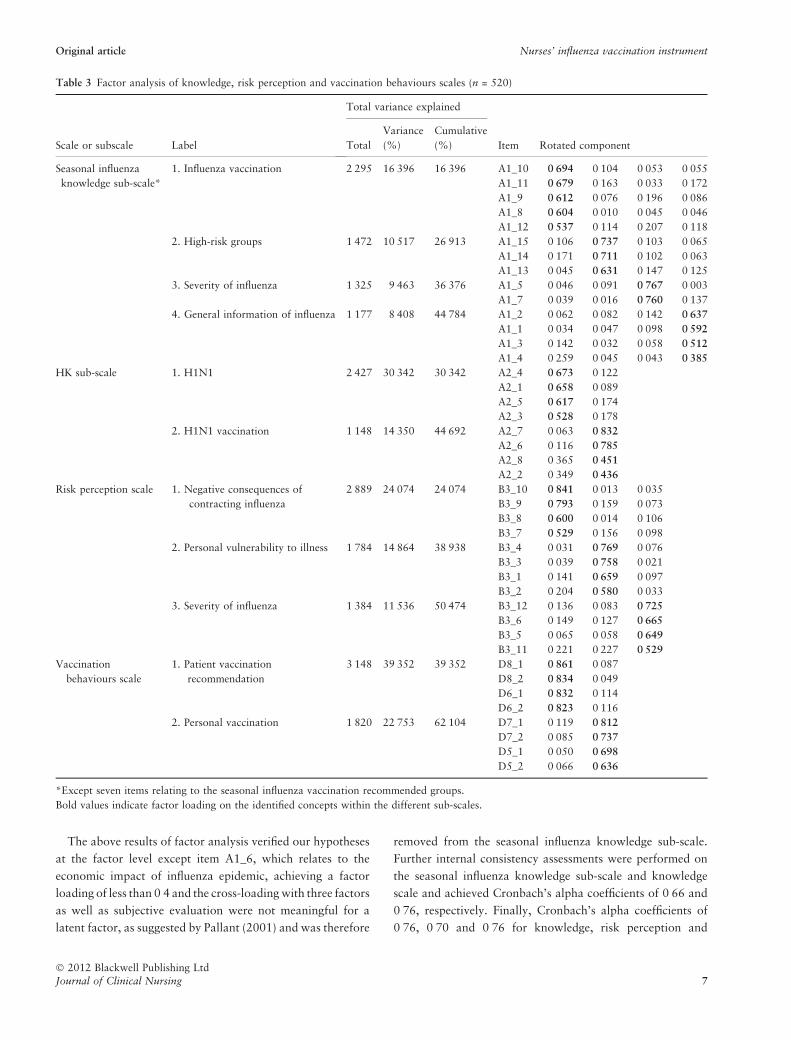
reliability of the factors emerging. Principal component
analysis with varimax with Kaiser normalisation was used
and results are set out in Table 3.
An EFA of seasonal influenza knowledge sub-scale was
performed revealing nine factors with seven items focusing on
seasonal influenza vaccination. The items relating to recom-
mended groups were excluded from the analysis and auto-
matically seen as a separate factor. Item A1_6 was also
excluded because of a low factor loading (<0Æ4) and less
relevance to any potential factor based on the subjective
evaluation of the meaning. Analysis of the results for the
remaining 14 items identified four relevant factors which
cumulatively explained 45Æ54% of total variance. The factors
corresponded to knowledge relating to influenza vaccination,
high-risk groups, severity of influenza and general informa-
tion relating to influenza. Analysis of the HK sub-scale
identified two factors with cumulative eigenvalues of 45Æ03%
of total variance which were entitled knowledge relating to
H1N1 and H1N1 vaccination. Three relevant factors with a
cumulative 50Æ67% contribution to the total variance were
identified for the risk perception scale which represents the
perception of the negative consequences of contracting
influenza, personal vulnerability to illness and severity of
influenza. Two factors were identified for the vaccination
behaviours scale defined as patient vaccination recommen-
dation and personal vaccination with contributing 62Æ1% of
the total variance.
Examination of the internal structure
In designing the knowledge, risk perception and vaccination
behaviours scales of the instrument, it was hypothesised that
these scales would contain the followed concepts:
• Knowledge about seasonal influenza and influenza
vaccination which would include general information
about seasonal influenza (A1_1–4), serious outcomes of
influenza (A1_5–7), general information about influenza
vaccination (A1_8–12), high-risk groups of influenza
(A1_13–15) and recommended groups for influenza
vaccination (A16–22).
• Knowledge about H1N1 (A2_1,3–5) and H1N1 vacci-
nation (A2_2,6–8).
• Perception of the risk towards the negative consequences
of contracting influenza (B3_1–4), serious complications
and possibility of death after contracting influenza
(B3_7–10) and personal vulnerability to influenza and
illnesses (B3_5,6,11,12).
• Nurses’ vaccination behaviours (D5_1, D5_2, D7_1,
D7_2) and recommendation vaccination behaviours to
their patients (D6_1, D6_2, D8_1, D8_2).
Table 2 Internal consistency of instrument
Section of instrument
No. of
items
Cronbach’s
alpha
Valid,
n (%)
Knowledge scale 30 0Æ763 377 (72Æ5)
SK sub-scale 22 0Æ658 396 (76Æ2)
HK sub-scale 8 0Æ706 477 (91Æ7)
Risk perception scale 12 0Æ701 483 (92Æ9)
Vaccination behaviour scale 8 0Æ756 450 (86Æ5)
MHLC scale 18 0Æ723 457 (87Æ9)
MHLC-internal subscale 6 0Æ652 483 (92Æ9)
MHLC-chance subscale 6 0Æ639 484 (93Æ1)
MHLC-powerful others
subscale
6 0Æ731 495 (95Æ2)
Table 1 Characteristics of respondents (n = 520)
Demographic features Number (%)
Gender
Male 63 (12Æ1)
Female 437 (84Æ0)
Missing data 20 (3Æ8)
Age
20–29 years 121 (23Æ3)
30–39 years 193 (37Æ1)
40–49 years 134 (25Æ8)
50 years or older 51 (9Æ8)
Missing data 21 (4Æ0)
Education
DipHE 208 (40Æ0)
Bachelor Degree 221 (42Æ5)
PGDip 11 (2Æ1)
Masters 20 (3Æ8)
Others 33 (6Æ3)
Missing data 27 (5Æ2)
Work place
Hospital 408 (78Æ5)
Community 75 (14Æ5)
Both 9 (1Æ7)
University 1 (0Æ2)
Missing data 27 (5Æ2)
Speciality
Medicine 195 (37Æ5)
Mental health 37 (7Æ1)
Surgery 119 (22Æ9)
Older people 20 (3Æ8)
Paediatrics 40 (7Æ7)
Maternity 19 (3Æ7)
Primary care 41 (7Æ9)
Ambulatory care 18 (3Æ5)
Missing data 31 (6Æ0)
Direct patient contact
Yes 477 (91Æ7)
No 17 (3Æ3)
Missing data 26 (5Æ0)
Qualified years (years) 11Æ90 ± 8Æ754 (n = 482)
J Zhang et al.
� 2012 Blackwell Publishing Ltd
6 Journal of Clinical Nursing
The above results of factor analysis verified our hypotheses
at the factor level except item A1_6, which relates to the
economic impact of influenza epidemic, achieving a factor
loading of less than 0Æ4 and the cross-loading with three factors
as well as subjective evaluation were not meaningful for a
latent factor, as suggested by Pallant (2001) and was therefore
removed from the seasonal influenza knowledge sub-scale.
Further internal consistency assessments were performed on
the seasonal influenza knowledge sub-scale and knowledge
scale and achieved Cronbach’s alpha coefficients of 0Æ66 and
0Æ76, respectively. Finally, Cronbach’s alpha coefficients of
0Æ76, 0Æ70 and 0Æ76 for knowledge, risk perception and
Table 3 Factor analysis of knowledge, risk perception and vaccination behaviours scales (n = 520)
Scale or subscale Label
Total variance explained
Item Rotated componentTotal
Variance
(%)
Cumulative
(%)
Seasonal influenza
knowledge sub-scale*
1. Influenza vaccination 2Æ295 16Æ396 16Æ396 A1_10 0Æ694 0Æ104 0Æ053 �0Æ055
A1_11 0Æ679 0Æ163 �0Æ033 0Æ172
A1_9 0Æ612 0Æ076 0Æ196 �0Æ086
A1_8 0Æ604 �0Æ010 �0Æ045 �0Æ046
A1_12 0Æ537 �0Æ114 0Æ207 0Æ118
2. High-risk groups 1Æ472 10Æ517 26Æ913 A1_15 �0Æ106 0Æ737 0Æ103 �0Æ065
A1_14 0Æ171 0Æ711 �0Æ102 �0Æ063
A1_13 �0Æ045 0Æ631 0Æ147 0Æ125
3. Severity of influenza 1Æ325 9Æ463 36Æ376 A1_5 0Æ046 0Æ091 0Æ767 0Æ003
A1_7 �0Æ039 0Æ016 0Æ760 0Æ137
4. General information of influenza 1Æ177 8Æ408 44Æ784 A1_2 �0Æ062 0Æ082 0Æ142 0Æ637
A1_1 0Æ034 �0Æ047 0Æ098 0Æ592
A1_3 �0Æ142 �0Æ032 �0Æ058 0Æ512
A1_4 0Æ259 �0Æ045 0Æ043 0Æ385
HK sub-scale 1. H1N1 2Æ427 30Æ342 30Æ342 A2_4 0Æ673 0Æ122
A2_1 0Æ658 �0Æ089
A2_5 0Æ617 0Æ174
A2_3 0Æ528 0Æ178
2. H1N1 vaccination 1Æ148 14Æ350 44Æ692 A2_7 0Æ063 0Æ832
A2_6 0Æ116 0Æ785
A2_8 0Æ365 0Æ451
A2_2 0Æ349 0Æ436
Risk perception scale 1. Negative consequences of
contracting influenza
2Æ889 24Æ074 24Æ074 B3_10 0Æ841 �0Æ013 0Æ035
B3_9 0Æ793 0Æ159 0Æ073
B3_8 0Æ600 �0Æ014 0Æ106
B3_7 0Æ529 0Æ156 0Æ098
2. Personal vulnerability to illness 1Æ784 14Æ864 38Æ938 B3_4 �0Æ031 0Æ769 0Æ076
B3_3 �0Æ039 0Æ758 0Æ021
B3_1 0Æ141 0Æ659 0Æ097
B3_2 0Æ204 0Æ580 0Æ033
3. Severity of influenza 1Æ384 11Æ536 50Æ474 B3_12 0Æ136 0Æ083 0Æ725
B3_6 0Æ149 �0Æ127 0Æ665
B3_5 �0Æ065 0Æ058 0Æ649
B3_11 0Æ221 0Æ227 0Æ529
Vaccination
behaviours scale
1. Patient vaccination
recommendation
3Æ148 39Æ352 39Æ352 D8_1 0Æ861 0Æ087
D8_2 0Æ834 0Æ049
D6_1 0Æ832 0Æ114
D6_2 0Æ823 0Æ116
2. Personal vaccination 1Æ820 22Æ753 62Æ104 D7_1 0Æ119 0Æ812
D7_2 0Æ085 0Æ737
D5_1 0Æ050 0Æ698
D5_2 0Æ066 0Æ636
*Except seven items relating to the seasonal influenza vaccination recommended groups.
Bold values indicate factor loading on the identified concepts within the different sub-scales.
Original article Nurses’ influenza vaccination instrument
� 2012 Blackwell Publishing Ltd
Journal of Clinical Nursing 7

vaccination behaviours scales provided evidence of internal
consistency reliability of these scales of the instrument.
Discussion
This study addressed the development of an instrument to
measure nurses’ knowledge, risk perception, health beliefs
towards influenza and influenza vaccination and their vacci-
nation behaviours. It contains six sections, where knowledge,
risk perception and vaccination behaviours scales were newly
developed. The questionnaire items were identified through
review of the literature and initial support was given for
construct validity and internal consistency reliability of each
scale.
To ensure the content validity of the instrument, expert
consultation and the pilot survey were used. There is no
criterion for the optimum number of experts but the
literature recommends that 2–20 are necessary for the content
validity process (NNSDO 2005). This study used two content
experts to review for relevance and clarity of items and the
later results of factor analyses provide evidence that the
experts captured the core content of each scale.
The construct validity analyses indicate a good fit with the
initial design of the newly developed scales of knowledge, risk
perception and vaccination behaviours scales. The knowledge
scale measures how well nurses’ have mastery of the
knowledge related to seasonal influenza and vaccination as
well as H1N1 influenza and vaccination, with the seasonal
influenza knowledge sub-scale including five dimensions (i.e.
knowledge about general information, severity, vaccination,
high-risk groups and vaccination recommended groups) and
the HK sub-scale having two dimensions (i.e. knowledge
related H1N1 and vaccination). The risk perception scale
measures how nurses feel the risk related influenza and
pandemic with three dimensions assessing nurses’ perception
to personal vulnerability to illness, negative consequences of
contracting influenza and severity of influenza respectively.
The vaccination behaviours scale measures nurses’ vaccina-
tion status and intent and vaccination recommendation to
their patients, which are defined as personal vaccination and
patient vaccination recommendation dimensions.
Although there was not an exact match with the initial
design of the seasonal influenza knowledge scale of the
instrument, the results of the factor analysis demonstrate a
relatively strong fit except for one item, i.e. A1_6 (An
epidemic can have an economic impact through lost work-
force productivity and strain on health services). This item
was initially designed together with two other items (A1_5
and A1_7) to assess nurses’ knowledge about the serious
consequences of seasonal influenza but the factor analysis
showed it to have a low factor loading and less relevance to
any potential factor. Double checking of its meaning also
suggested that its focus is on a social impact rather than a
personal level effect, thus this item was excluded from
analysis and the final analysis showed a good fit to the initial
design of this sub-scale.
The MHLC scale (Wallston 1993) was used to examine
nurses’ health locus of control. The Cronbach’s alpha
coefficients of the scale and sub-scale were 0Æ723, 0Æ652,
0Æ639 and 0Æ731, respectively showing an acceptable reliabil-
ity. This is consistent with previous testing for whole scale
with coefficients ranging from 0Æ60–0Æ75 (Wallston 2005)
and indicates that the MHLC is reliable.
Limitations
Several limitations should be kept in mind when interpreting
the results of this study. First, the test survey was conducted
with a convenience sample and therefore the findings may not
be generalisable especially to nurses not working in London
or in hospital medicine or surgery settings as the sample was
not representative of nurses working across care settings or
outside London. The extent of potential bias is unknown,
however, a large sample size with a high response rate offered
relevant valid data for the instrument testing. Further testing
with the recruitment of nurses across care settings and
outside London would provide data relating to bias. Second,
the overall knowledge scores of the participants were
remarkably low especially the HK scores and we are not
sure whether these responses have had some effects on
reliability and validity testing of the instrument. Third, the
instrument was developed as an evaluation measure among
nurses in the UK and is most suitable for this population
because it is specific to the UK healthcare system and wording
customs in British English. This might limit the application of
the instrument to other HCWs groups or nurses in other
countries without further refinement and testing.
Conclusions
This study developed and tested a multi-section instrument
which may be useful as an easy-to-use self-report measure
of nurses’ knowledge, risk perception, health beliefs
towards influenza and influenza vaccination and their
vaccination behaviours. The analyses of reliability and
validity demonstrated the strong psychometric properties of
the three the newly developed scales, namely, the knowl-
edge, risk perception and vaccination behaviours scales.
Further research using this instrument is needed to test the
tool among nurses with varying characteristics and explore
J Zhang et al.
� 2012 Blackwell Publishing Ltd
8 Journal of Clinical Nursing

the links to factors identified in this study and nurses’
vaccination behaviours.
Relevance to clinical practice
We have developed a valid and reliable instrument to assess
nurses’ knowledge, risk perception, health beliefs towards
influenza and influenza vaccination and their vaccination
behaviours. The three newly developed scales could also be
used independently to measure factors influencing nurses’
vaccination practices. The factors identified may help policy
makers and administrators understand the aspects of knowl-
edge and risk perception towards influenza and vaccination
which underpin nurses’ vaccination behaviours.
Acknowledgments
We are grateful to all the study participants and Peter Milligan
(Florence Nightingale School of Nursing and Midwifery,
King’s College London, London, UK) for his statistical advice.
Contributions
Study design: JZ, AEW, IJN; data collection and analysis: JZ,
AEW and manuscript preparation: JZ, AEW, IJN.
Conflict of interest
None declared.
References
Abramson ZH & Levi O (2008) Influenza
vaccination among primary healthcare
workers. Vaccine 26, 2482–2489.
Becker MH, Drachman RH & Kirscht JP
(1974) A new approach to explaining
sick-role behavior in low-income po-
pulations. American Journal of Public
Health 64, 2005–2216.
Blank PR, Schwenkglenks M & Szucs TD
(2008) Influenza vaccination coverage
rates in five European countries during
season 2006/07 and trends over six
consecutive seasons. BMC Public
Health 8, 272.
Blue CL & Valley JM (2002) Predictors of
influenza vaccine: acceptance among
healthy adult workers. AAOHN Jour-
nal 50, 227–235.
Brunton C, Weir R & Jennings L (2005)
Knowledge and attitudes about influ-
enza vaccination amongst general
practitioners, practice nurses and peo-
ple aged 65 and over. The New Zealand
Medical Journal 118, U1434.
Bryant KA, Stover B, Cain L, Levine GL,
Siegel J & Jarvis WR (2004) Improving
influenza immunization rates among
healthcare workers caring for high-risk
pediatric patients. Infection Control and
Hospital Epidemiology 25, 912–917.
Campos W & Jalaludin BB (2003) Predic-
tors of influenza vaccination amongst
Australian nurses. Australian Journal of
Advanced Nursing 20, 19–21.
Centres for Disease Control and Prevention
(2007) Prevention and control of influ-
enza. Recommendations of the Advi-
sory Committee on Immunization
Practices (ACIP). MMWR Recommen-
dations and Reports 56, 1–54.
Chalmers C (2006) Understanding health-
care worker uptake of influenza vacci-
nation: a survey. British Journal of
Infection Control 7, 12.
Chapman GB & Coups EJ (1999a) Time
preferences and preventive health
behaviour: acceptance of the influenza
vaccine. Medical Decision Making 19,
307–314.
Chapman GB & Coups EJ (1999b) Predic-
tors of influenza vaccine acceptance
among healthy adults. Preventive
Medicine 29, 249–262.
Christini AB, Shutt KA & Byers KE (2007)
Influenza vaccination rates and moti-
vators among healthcare worker
groups. Infection Control and Hospital
Epidemiology 28, 171–177.
Clark SJ, Cowan AE & Wortley PM (2009)
Influenza vaccination attitudes and
practices among US registered nurses.
American Journal of Infection Control
37, 551–556.
Dunn G (1989) The Design and Analysis of
Reliability Studies: The Statistical
Evaluation of Measurement Errors.
Oxford University Press, New York.
Falomir-Pichastor JM, Toscani L & Despo-
intes SH (2009) Determinants of flu
vaccination among nurses: the effects of
group identification and professional
responsibility. Applied Psychology: An
International Review 58, 42–58.
Harbarth S, Siegrist CA, Schira JC, Wunderli
W & Pittet D (1998) Influenza immuni-
zation: improving compliance of health-
care workers. Infection Control and
Hospital Epidemiology 19, 337–342.
Harrison J & Abbott P (2002) Vaccination
against influenza: UK health care
workers not on-message. Occupational
Medicine 52, 277–279.
Imai T, Takahashi K, Hoshuyama T,
Hasegawa N, Lim M-K & Koh D
(2005) SARS risk perceptions in
healthcare workers, Japan. Emerging
Infectious Diseases 11, 404–410.
Jackson C & Furnham A (2000) Designing
and Analysing Questionnaires and
Surveys: A Manual for Health Profes-
sionals and Administrators. Whurr
Publishers Ltd, London.
de Juanes JR, de Codes AG, Arrazola MP,
Jaen F, Sanz MI & Gonzalez A (2007)
Influenza vaccination coverage among
hospital personnel over three consecu-
tive vaccination campaigns (2001–
2002 to 2003–2004). Vaccine 25, 201–
204.
Knapp TR & Brown JK (1995) Ten mea-
surement commandments that often
should be broken. Research in Nursing
and Health 18, 465–469.
Kuntz JL, Holley S, Helms CM, Cavanaugh
JE, Vande Berg J, Herwaldt LA &
Polgreen PM (2008) Use of a pandemic
preparedness drill to increase rates of
influenza vaccination among healthcare
workers. Infection Control and Hospi-
tal Epidemiology 29, 111–115.
Lester RT, McGeer A, Tomlinson G &
Detsky AS (2003) Use of, effectiveness
of and attitudes regarding influenza
vaccine among house staff. Infection
Original article Nurses’ influenza vaccination instrument
� 2012 Blackwell Publishing Ltd
Journal of Clinical Nursing 9
Control and Hospital Epidemiology
24, 839–844.
Litt J, Radford A & Lake P (1995) Predic-
tors of vaccination against influenza in
the elderly. 5th National Immunisation
Conference, Sydney.
Livni G, Chodik G, Yaari A, Tirosh N &
Ashkenazi S (2008) Attitudes, knowl-
edge and factors related to acceptance
of influenza vaccine by paediatric
healthcare workers. Journal of Pediatric
Infectious Diseases 3, 111–117.
Maltezou HC, Maragos A, Katerelos P, Pa-
isi A, Karageorgou K, Papadimitriou T
& Pierroutsakos IN (2008) Influenza
vaccination acceptance among health-
care workers: a nationwide survey.
Vaccine 26, 1408–1410.
Martinello RA, Jone L & Topal JE (2003)
Correlation between healthcare work-
ers’ knowledge of influenza vaccine and
vaccine receipt. Infection Control and
Hospital Epidemiology 24, 845–847.
Mereckiene J, Cotter S, Nicoll A, Levy-
Bruhl D, Ferro A, Tridente G, Zanoni
G, Berra P, Salmaso S, O’Flanagan D &
O’Flanagan D (2008) National seasonal
influenza vaccination survey in Europe.
Eurosurveillance 13, 19017.
National Nursing Staff Development Orga-
nization (NNSDO) (2005) Validating
Research Instruments. Available at:
http://www.nnsdo.org/dmdocuments/
ValidatingResearchInstruments.pdf (acc-
essed 3 September 2010).
Norton SP, Scheifele DW, Bettinger JA &
West RM (2008) Influenza vaccination
in paediatric nurses: cross-sectional
study of coverage, refusal and factors in
acceptance. Vaccine 26, 2942–2948.
Nunally JC (1978) Psychometric Theory.
McGraw-Hill, New York.
Nunally JC & Bernstein IH (1994) Psycho-
metric Theory. McGraw-Hill, New
York.
Ofstead CL, Tucker SJ, Beebe TJ & Poland
GA (2008) Influenza vaccination among
registered nurses: information receipt,
knowledge and decision-making at an
institution with a multifaceted educa-
tional program. Infection Control and
Hospital Epidemiology 29, 99–106.
O’Reilly FW, Cran GW & Stevens AB
(2005) Factors affecting influenza vac-
cine uptake among health care workers.
Occupational Medicine 55, 474–479.
Pallant J (2001) SPSS Survival Manual. A
Step by Step Guide to Data Analysis
Using SPSS. Allen & Unwin, Crows
Nest, NSW.
Poland GA, Tosh P & Jacobson RM (2005)
Requiring influenza vaccination for
health care workers: seven truths we
must accept. Vaccine 23, 2251–2255.
Polgreen PM, Polgreen LA, Evans T &
Helms C (2009) A statewide system for
improving influenza vaccination rates
in hospital employees. Infection Con-
trol and Hospital Epidemiology 30,
474–478.
Polit DF & Beck CT (2004) Nursing
Research: Principles and Methods, 7th
edn. Lippincott, New York, NY.
Polit DF & Hungler BP (1993) Nursing
Research. Methods, Appraisal and Uti-
lization, 3rd edn. Lippincott Company,
Philadelphia, Pennsylvania.
Ribner BS, Hall C, Steinberg JP, Bornstein
WA, Chakkalakal R, Emamifar A,
Eichel I, Lee PC, Castellano PZ &
Grossman GD (2008) Use of a manda-
tory declination form in a program for
influenza vaccination of healthcare
workers. Infection Control and Hospi-
tal Epidemiology 29, 302–308.
Sartor C, Tissot-Dupont H, Zandotti C,
Martin F, Roques P & Drancourt M
(2004) Use of a mobile cart influenza
program for vaccination of hospital
employees. Infection Control and Hos-
pital Epidemiology 25, 918–922.
Seale H, Wang Q, Yang P, Dwyer DE,
Wang X, Zhang Y & MacIntyre CR
(2010) Influenza vaccination amongst
hospital health care workers in Beijing.
Occupational Medicine 60, 335–339.
Shahrabani S, Benzion U & Din GY (2009)
Factors affecting nurses’ decision to get
the flu vaccine. The European Journal
of Health Economics 10, 227–231.
Straetemans M, Buchholz U, Reiter S, Haas
W & Krause G (2007) Prioritization
strategies for pandemic influenza vac-
cine in 27 countries of European Union
and the Global Health Security Action
Group: a review. BMC Public Health 7,
236.
Tam DKP, Lee S-S & Lee S (2008) Impact of
severe acute respiratory syndrome and
the perceived avian influenza epidemic
on the increased rate of influenza vac-
cination among nurses in Hong Kong.
Infection Control and Hospital Epide-
miology 29, 256–261.
Wallston KA (1993) Multidimensional
Health Locus of Control (MHLC)
Scales. Available at: http://www.vander
bilt.edu/nursing/kwallston/mhlcscales.
htm (accessed 11 October 2010).
Wallston KA (2005) The validity of the
multidimensional health locus of con-
trol scales. Journal of Health Psychol-
ogy 10, 623–631.
Waston R & Thompson DR (2006) Use of
factor analysis in Journal of Advanced
Nursing: literature review. Journal of
Advanced Nursing 55, 330–341.
Willis BC & Wortley P (2007) Nurses’
attitudes and beliefs about influenza
and the influenza vaccine: a summary
of focus groups in Alabama and Mich-
igan. American Journal of Infection
Control 35, 20–24.
World Health Organization (2000) Influ-
enza Vaccines: Recommendations for
the Use of Inactivated Influenza Vac-
cines and Other Preventive Measures.
Available at: http://www.who.int/doc
store/wer/pdf/2000/wer7535.pdf (accessed
11 October 2010).
World Health Organization (2005) Influ-
enza Vaccines: WHO Position Paper.
Available at: http://www.who.int/wer/
2005/wer8033.pdf (accessed 3 Septem-
ber 2010).
World Health Organization (2009a) WHO
Influenza (Seasonal) Fact Sheet. Avail-
able at: http://www.who.int/mediacen
tre/factsheets/fs211/en (accessed 3 Sep-
tember 2010).
World Health Organization (2009b) Pan-
demic (H1N1) 2009: Frequently Asked
Questions. Available at: http://www.
who.int/csr/disease/swineflu/frequently_
asked_questions/en/index.html (accessed
11 October 2010).
World Health Organization (2009c) Sea-
sonal Influenza Vaccines and Pandemic
(H1N1) 2009. Available at: http://www.
who.int/csr/disease/swineflu/frequently_
asked_questions/vaccine_preparedness/
seasonal_influenza/en/index.html (acces-
sed 11 October 2010).
World Health Organization (2009d) Safety
of Pandemic (H1N1) 2009 Vaccines.
Available at: http://www.who.int/csr/
disease/swineflu/frequently_asked_ques
tions/vaccine_preparedness/safety_appro
val/en/index.html (accessed 11 October
2010).
Zhang J, While AE & Norman IJ (2010)
Knowledge and attitude regarding
influenza vaccination among nurses: a
research review. Vaccine 28, 7207–7214.
J Zhang et al.
� 2012 Blackwell Publishing Ltd
10 Journal of Clinical Nursing

The Journal of Clinical Nursing (JCN) is an international, peer reviewed journal that aims to promote a high standard of
clinically related scholarship which supports the practice and discipline of nursing.
For further information and full author guidelines, please visit JCN on the Wiley Online Library website: http://
wileyonlinelibrary.com/journal/jocn
Reasons to submit your paper to JCN:High-impact forum: one of the world’s most cited nursing journals and with an impact factor of 1Æ228 – ranked 23 of 85
within Thomson Reuters Journal Citation Report (Social Science – Nursing) in 2009.
One of the most read nursing journals in the world: over 1 million articles downloaded online per year and accessible in over
7000 libraries worldwide (including over 4000 in developing countries with free or low cost access).
Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jcnur.
Early View: rapid online publication (with doi for referencing) for accepted articles in final form, and fully citable.
Positive publishing experience: rapid double-blind peer review with constructive feedback.
Online Open: the option to make your article freely and openly accessible to non-subscribers upon publication in Wiley
Online Library, as well as the option to deposit the article in your preferred archive.
Original article Nurses’ influenza vaccination instrument
� 2012 Blackwell Publishing Ltd
Journal of Clinical Nursing 11