
Developing the readiness to alter sun-protective behaviour questionnaire (RASP-B
13
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Developing the readiness to alter sun-protective behaviour questionnaire (RASP-B

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Developing the readiness to alter sun-protective behaviour questionnaire(RASP-B)
Rohan D. Borschmann a,*, David Cottrell b
a David Goldberg Centre, Room H1.16, Institute of Psychiatry, De Crespigny Park, SE5 8AF, London, United Kingdomb James Cook University, Cairns, Australia
1. Introduction
1.1. Sun-protective behaviour
The dangers associated with regular or prolonged sun exposureare well documented and include premature aging, sunburn and,most seriously, skin cancer [1–3]. Epidemiological evidencesuggests that exposure to sunlight is associated with higher ratesof all major types of skin cancer [4]. Approximately five percent ofnatural sunlight is composed of ultraviolet radiation (UVR), and itis this UVR which can cause skin cancer and other harmful damageto skin [5]. UVB radiation (the section of UVR consisting ofwavelengths between 315 and 280 nm) is extremely effective atcausing biological damage and accounts for approximately 80% ofthe most harmful effects associated with sun exposure, such assunburn and skin cancer. UVA radiation (315–400 nm) contributesthe remaining 20%, resulting in the less harmful effects such aswrinkles and skin discolouration. UVB acts as a carcinogen when it
results in mutations in the DNA structure of skin cells. When thesemutations affect the tumour-suppressive genes sufficiently tointerrupt routine cell cycling, tumours are induced which may goon to form skin cancers [2,6].
Australia has the highest incidence of skin cancer of anycountry in the world and Queensland has the highest incidenceof all Australian states and territories [7]. On average, two out ofevery three Australians will be treated for skin cancer at somestage during their lives [8] and it is estimated that approxi-mately 80 percent of all new cancers diagnosed in Australia areskin cancers [9]. Although the incidence of skin cancer inAustralia has plateaued since 1985, skin cancer still costs theAustralian community more than AUS$300 million (s150million) annually [10–12] as approximately 434,000 peoplereceive treatment [8].
Each year in Queensland alone, over 2000 cases of skin cancerare diagnosed and over 200 deaths are attributed to the disease[13,14]. Incidence is highest in coastal regions (where sunbathingis commonplace) compared with the rural interior and anincreased incidence during the 1960s and 1970s coincided withchanges in fashion and social behaviour that led to young peoplespending more time in the sun with less protective clothing [7].
Cancer Epidemiology 33 (2009) 451–462
A R T I C L E I N F O
Article history:
Accepted 15 September 2009
Keywords:
Stage of change
Sun-protection
Skin cancer
Melanoma
Transtheoretical model
Behaviour change
RASP-B
A B S T R A C T
Background: Australia has the highest incidence of skin cancer of any country in the world, even though
the risk of contracting the disease can be lowered considerably by engaging in appropriate sun-
protective behaviours. We aimed to construct and validate a questionnaire to assess the readiness of a
group of mostly young people to change their levels of sun-protective behaviour by assigning them to a
stage of change based on the transtheoretical model of behaviour change. Method: A sample of 122
undergraduate students in Queensland, Australia completed the readiness to alter sun-protective
behaviour questionnaire (the RASP-B, a 12-item questionnaire about their attitudes toward sun-
protection), in addition to a short questionnaire about their current sun-protective behaviours. Results: A
principal component analysis revealed a clear three-factor structure corresponding to the precontem-
plation, contemplation, and action stages of the transtheoretical model. Participants in the action stage
reported engaging in significantly higher levels of sun-protective behaviour than participants in the
earlier precontemplation and contemplation stages. These behaviours included avoiding exposure to
direct sunlight by wearing long-sleeved clothing and remaining in the shade or indoors. Participants in
the different stages reported no significant differences in the reported frequency of sunscreen use,
although respondents across all three stages reported using sunscreen infrequently. Conclusion: The
RASP-B requires approximately 5 min to complete, can be self-administered and has satisfactory
psychometric properties, and thus has utility in primary health care settings where time and client–
practitioner contact are often limited.
Crown Copyright � 2009 Published by Elsevier Ltd. All rights reserved.
* Corresponding author. Tel.: +44 207 848 5093; fax: +44 207 848 0333.
E-mail address: [email protected] (R.D. Borschmann).
Contents lists available at ScienceDirect
Cancer EpidemiologyThe International Journal of Cancer Epidemiology, Detection, and Prevention
journa l homepage: www.cancerepidemiology.net .
1877-7821/$ – see front matter . Crown Copyright � 2009 Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.canep.2009.09.003

Author's personal copy
It is the behavioural link between sun exposure and skin cancerwhich provides the most promising avenue for decreasing theincidence of skin cancer. The World Health Organization recom-mends several sun-protective behaviours including wearingprotective clothing, staying in the shade, avoiding the sun in themiddle of the day and regularly applying sunscreen when outdoors[15]. Since UVR passes easily through water, swimming in eitherthe sea or open-air pools offers little protection against itsdamaging effects [5]. In light of this, many government healthagencies have targeted behaviour change in terms of sun-protective and sun-avoidance behaviours as the primary meansof mitigating skin cancer deaths [13,12,16,17].
Skin cancer research conducted in several Australian states hascontributed to the development of various community campaigns,the aims of which are to reduce the incidence, morbidity andmortality of skin cancer by changing attitudes and behaviours, aswell as controlling existing disease [12]. For example, each year,the Skin Cancer Foundation of Western Australia spends more thanAUS$1.2 million (s600,000) on research into skin cancer and theprevention campaigns that have stemmed from this research havehelped to change the way individuals living in Western Australiaperceive, and behave in, the sun [17]. This, in turn, has contributedto a reduction in age-standardised rates of skin cancer reportedduring this period [18]. In Queensland, the current state-wide ‘‘SunSafety’’ campaign provides sun-related information to schools,workplaces, health professionals and the general public, andreminds residents that the Queensland sun can inflict the samedamage during winter as it can during summer [16]. Much of thiscampaign specifically addresses people in the 18–30-year-old agegroup. National research has suggested that campaigns such asthese have combined to play an important role in alteringAustralian society’s perceptions of the dangers associated withsun exposure and have contributed to significant reductions in sunexposure in several Australian states [12].
Despite some 30 years of sun-protection promotion campaigns,skin cancer still poses a significant public health risk in the state ofQueensland. Young people, such as university students, may stillbe at an increased risk of developing skin cancer, as many youngpeople associate a suntan with an attractive and healthyappearance [9,19]. They also often have fewer occupationalcommitments and an increased capacity to spend time outdoorsexposed to the sun when compared with average members of theworkforce. As the effects of UVR in causing skin cancer arecumulative, it is anticipated that reducing sun exposure early inthe lifespan would retard the rate of tumour developmentthroughout the lifespan [2]. Assessing university students’ beliefsand behaviours about sun-protection is therefore an importantarea of research.
The continuing high incidence of risk-taking behaviours relatedto sun exposure amongst university-aged individuals [9] suggeststhat more than just informational and scare campaigns arerequired to change behaviours. This is especially true amongstyoung people. One approach is to take into account the currentstate of the individual and target behaviour change messages totheir readiness to accept different types of information.
1.2. The transtheoretical model of behaviour change
The transtheoretical model of behaviour change (hereafterTTM) proposed by Prochaska and DiClemente [20] has gainedwidespread acceptance in the health psychology literature. It hasbeen used effectively in explaining the pattern of acquisition andcessation of a variety of potentially health-compromising beha-viours, including sun exposure [21], smoking [22], excessivealcohol consumption [23], and the misuse of both licit and illicitdrugs [24] (also see [25] for a comprehensive review). The TTM
details six stages of change: precontemplation (not thinking aboutchange), contemplation (seriously considering change), prepara-tion (planning to change in the foreseeable future), action(initiation of overt behaviour change), maintenance (sustainedbehaviour change over at least 6 months), and termination (returnto pre-morbid behaviour, as though never having changed thebehaviour in the first place). It is hypothesised that individualsprogress sequentially through these stages during the process ofreducing or eliminating health-compromising behaviours [26].One of the unique advantages of the TTM is that it addresses thetransitional nature of change and unlike competing theories, doesnot assume any pre-existing level of willingness to change. Thissuggests that even individuals in the precontemplation stage, whoare not concerned about their health-compromising behaviour anddisplay no evidence of a desire for change, can benefit from anintervention tailored specifically for such a population. Suchtargeted interventions assume, however, that the stage of change aperson has reached can be accurately assessed [23].
1.3. Sun-protective behaviour and the TTM
Despite the benefits associated with engaging in sun-protectivebehaviour, there is currently no questionnaire in the literature thataccurately assesses how willing individuals are to change theircurrent levels of sun-protective behaviour. When consideration isgiven to the fact that such a questionnaire could feasibly be used inthe planning and development of effective interventions (and theirsubsequent evaluations), it becomes apparent that this absenceneeds to be addressed. Several studies have attempted to assignindividuals to a stage of change in relation to sun-protectivebehaviour using a variety of methods [21,27–34], though thesestudies have typically contained a number of methodologicallimitations. These limitations include attempting to assess andalter numerous behaviours simultaneously (thereby dedicatingless attention to sun-protective behaviour) [31,35], assigningparticipants to a stage of change on the basis of their responses toonly a small number of questions [21,28,29,36], and utilisingfemale-only samples [27]. In a large descriptive study by Wein-stock and colleagues [34], over 2000 beach goers were individuallyinterviewed regarding their sun-protective behaviours andassigned to stages of change corresponding to the TTM. Theyreported relationships between stages of change and sun-protective behaviours consistent with the TTM. The only limitationof this study is the interview method employed, which is costly andtime consuming as well as being unsuitable for large-scaleinterventions. Finally, several of the aforementioned studies wereconducted in Sweden [21,27–29] and, given the differencesbetween the Swedish and Australian climates, likely sun exposurebehaviours and the perceived risk of skin cancer, it would beinappropriate to generalise the results of such studies to theAustralian population.
Accurately assessing an individual’s current stage of change inrelation to sun-protective behaviour – and providing feedback andeducation in relation to such behaviour – could potentially servethree primary functions; firstly, it may help to increase theindividual’s level of sun-protective behaviour, which woulddecrease their likelihood of contracting skin cancer. Secondly, itmay help to decrease the individual’s level of deliberate sunexposure, further decreasing the risk of contracting skin cancer.Finally, it may contribute to more efficient and effective use of timeallocated to health promotion interventions in primary health caresettings; after all, if the treating health professional is alreadyaware of which stage of change the client is in, an interventiontargeted specifically at that stage could be implemented withmaximum efficiency and minimal delay. When it is considered thatapproximately 40% of at-risk individuals for a particular health-
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462452

Author's personal copy
compromising behaviour are believed to be in each of theprecontemplation and contemplation stages, and that the actionstage is typically the busiest stage in the process of behaviourchange [37], it would be imperative for such a questionnaire toinclude an assessment of these three stages. The aim of the presentstudy was therefore to construct and validate a questionnairedesigned to allocate respondents to either the precontemplation,contemplation or action stages of change in relation to sun-protective behaviour using a sample of university students. Wetargeted this group for two reasons: firstly, they are a particularlyat-risk group because they are most likely to display a range ofhigh-risk sun-related behaviours [38]. Secondly, we sought tovalidate the assignment to stages of change based on ourquestionnaire by looking at the sun-related behaviours eachcategory reported. For this procedure to be sensitive to differencesbetween stages, the sample needs to display a wide range of sun-related behaviours (from tanning through to remaining indoors).Older individuals in Queensland tend to display less variation inbehaviour [38] and thus would make discriminations betweenbehaviours displayed in the various stages more difficult.
2. Materials and methods
2.1. Study population
Participants were recruited from the student population atJames Cook University (JCU), in Far North Queensland, Australia.This was considered to be a group of individuals likely to engage inrisky sun exposure behaviours and therefore a particularlyrelevant group to examine. The sample consisted of 123 under-graduate psychology students, ranging in age from 18 to 44 years(M = 26.8, SD = 10.2). Thirty-four participants (27.6%) were maleand 89 (72.4%) were female. Students viewed a brief presentationabout the study during their psychology tutorial classes beforebeing invited to participate. In an attempt to approximately matchthe sample size of 141 from the Rollnick et al. [23] study, a total of140 students were invited to participate, of which 123 students(88%) agreed. All respondents signed an informed consent formbefore completing the questionnaire in private at their leisure.The study was approved by the JCU Human Ethics Committee(H1590).
2.2. Questionnaire
The RASP-B (see Appendix 1) contains 12 items and is designedto assess which stage of change respondents are in with regard tosun-protective behaviour. These 12 items were adapted to apply tosun-protective behaviour from the Rollnick et al. [23] study of
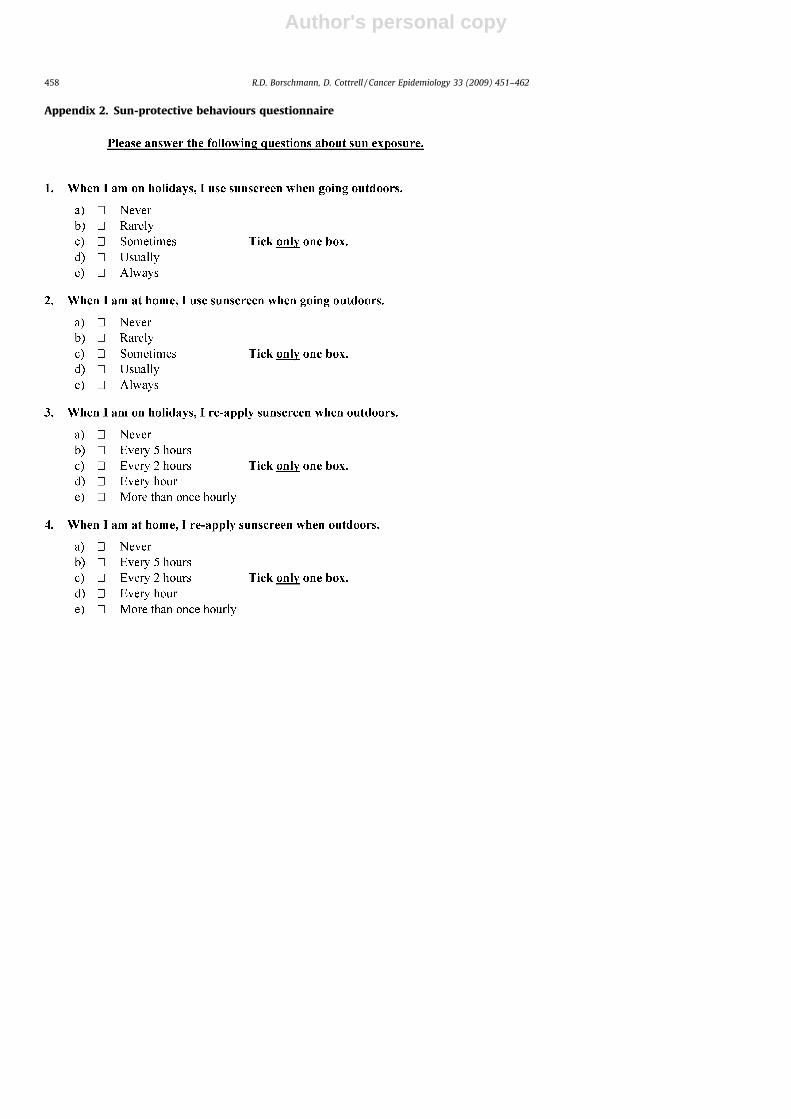
alcohol consumption. Four items refer to each of the precontem-plation, contemplation, and action stages of the TTM. Respondentswere asked to endorse one of five options ranging from ‘‘Stronglyagree’’ to ‘‘Strongly disagree’’ for each of the 12 items. A further 14items were included after the RASP-B (see Appendix 2), assessingrespondents’ current patterns of sun-protective behaviours (suchas avoiding the sun or applying sunscreen), as well as potentiallyhealth-compromising behaviours (such as sunbathing or visiting atanning salon).
3. Results
3.1. Statistical analysis
Only ‘p’ values below .05 were considered statisticallysignificant. Descriptive statistics have been included in the maintext in cases where significant results were found. All analyseswere conducted using SPSS 15.0 for Windows.
3.2. Calculation of scale scores
Responses obtained from the 12 RASP-B items were convertedinto stage scores to represent the extent to which participantscould be assigned to each of the three stages. To calculate thesestage scores, responses to each stage of change item were scored asfollows: ‘‘�2 = Strongly disagree’’, ‘‘�1 = Disagree’’, ‘‘0 = Neitheragree nor disagree’’, ‘‘+1 = Agree’’, and ‘‘+2 = Strongly agree’’. Therewere four statements corresponding to each stage and thereforethe total score for each stage ranged from�8 to +8. One participantobtained a score of zero for each of the three stages (by endorsing‘‘0 = Neither agree nor disagree’’ for all 12 of the stage of changeitems in the questionnaire) and was consequently not assigned toany of the three stages. This participant was excluded from allfurther data analysis and thus the sample was reduced to 122participants.
3.3. Item correlation analysis
In order to establish the extent to which the 12 RASP-B itemswere inter-correlated with each other, a principal componentsanalysis with Varimax rotation was conducted on responses tothese items. This analysis resulted in a clear three-factor structurecorresponding to the precontemplation, contemplation, and actionstages. The first three factors combined to account for 63.4% of thetotal variance observed. Item loadings for these three factors arerepresented in Table 1, along with the total variance explained byeach and the items in the instrument corresponding to each stageof change.
Table 1Item loadings for the first three components extracted from Varimax rotation on the 12 RASP-B items and percentage of variance accounted for by each.
RASP-B items Components
C 26.7% A 24.9% P 12.0%
1 I do not think I spend too much time exposed to the sun. (P) �0.75 �0.03 0.05
2 I am trying to spend less time in the sun than I used to. (A) �0.01 0.75 �0.35
3 I enjoy spending time in the sun, but sometimes I spend too much time in the sun. (C) 0.80 0.24 0.13
4 Sometimes I think I should spend less time in the sun. (C) 0.77 0.27 �0.02
5 It’s a waste of time thinking about how much time I spend in the sun. (P) �0.05 �0.11 0.83
6 I have just recently changed my sun exposure habits. (A) 0.28 0.66 0.31
7 Anyone can talk about wanting to do something about reducing their sun exposure,
but I am actually doing something about it. (A)
�0.25 0.75 �0.20
8 I am at the stage where I should think about spending less time in the sun. (C) 0.37 0.59 �0.23
9 The amount of time I spend in the sun is a problem sometimes. (C) 0.68 0.21 0.08
10 There is no need for me to think about changing my sun exposure habits. (P) �0.61 �0.29 0.38
11 I am actually changing my sun exposure habits right now. (A) 0.27 0.80 �0.04
12 Spending less time in the sun would be pointless for me. (P) �0.46 �0.44 0.50
P, precontemplation; C, contemplation; A, action.
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462 453

Author's personal copy
As shown in Table 1, each item loaded most heavily on the stageof change it was intended to reflect, with the exception of itemeight. This item was included as a contemplation item, although itloaded most heavily on the action stage. This may have occurredbecause participants who had already made behavioural changesbelieved that this statement also applied to them (i.e., ‘‘I am at thestage where I should think about spending less time in the sun [and
therefore I am making some conscious changes.]’’). To facilitatecomparisons with the Rollnick et al. [23] study, this item was left induring subsequent analyses, however its validity is uncertain.
3.4. Internal consistency
To test the internal consistency of the RASP-B, Cronbach’s alphacoefficient was calculated for the three-stage of change scales(each comprising 4-item scores ranging from �2 to +2). Resultswere as follows: precontemplation = .67, contemplation = .72, andaction = .76. Together with the factor analysis this suggests that,within each subscale, the items can confidently be regarded asassessing the same underlying construct.
3.5. Allocation to stage of change
Each participant was assigned to a stage of change based onthe procedure of Rollnick et al. [23]. A total score for each of theprecontemplation, contemplation and action stages for eachparticipant was calculated from their responses to the 12 RASP-B items. In the event that a participants’ total score for twostages was the same, the participant was allocated to the stagefarthest along the continuum (under the rationale that this mustbe assumed to be the farthest point reached in the changeprocess). Using this method, 47 (38.5%) participants wereallocated to the precontemplation stage, 43 (35.2%) to thecontemplation stage, and 32 (26.3%) to the action stage. Thisincluded 10 participants who obtained ties between stages. Theoverall distribution of participants was consistent withthe prediction made by Prochaska [25] that, in any populationfor any health-related behaviour, approximately 40% of peoplewill fall into each of the precontemplation and contemplationstages.
3.6. Stage of change and gender
A Chi-square analysis was performed on the demographic datato determine whether significant differences existed between male
and female participants in relation to their distribution across thestages of change for sun-protective behaviour. Table 2 shows theresults of this analysis. Significant differences were observed in thedistribution of male and female participants across the stages ofchange; x2(2, N = 200) = 8.07, p < .05. Specifically, a higherproportion of female participants were found to be in theprecontemplation stage than males, and a higher proportion ofmale participants were found to be in the action stage thanfemales.
3.7. Sun-avoidance behaviours
Participants were asked to indicate what proportion of timethey actively protected themselves from the sun by applyingsunscreen or avoided direct sunlight during summer by wearinglong-sleeved clothing, by remaining in the shade or by remainingindoors. For each of these four behaviours, participants were askedto endorse one of the following options: ‘‘0 = Never’’, ‘‘1 = Rarely’’,‘‘2 = Sometimes’’, ‘‘3 = Usually’’, ‘‘4 = Always’’. Mean scores werecalculated for participants in the precontemplation, contempla-tion, and action stages for each of the four behaviours and areshown in Table 3.
Four one-way ANOVAs with post hoc comparisons wereconducted and significant differences were found betweenparticipants in the different stages of change for wearinglong-sleeved clothing (F2,119 = 3.97, p < .05), remaining in theshade (F2,119 = 11.04, p < .001), and remaining indoors(F2,119 = 7.77, p < .001). No significant differences were observedin the reported frequency of sunscreen use by respondents inthe different stages (F2,119 = 1.44, p = .241), though it was notedthat respondents across all three stages reported usingsunscreen infrequently. Post hoc Tukey’s HSD comparisonsindicated that participants in the action stage reported ‘‘Wear-ing long-sleeved clothing’’ significantly more often thanparticipants in the contemplation stage (p < .05). No othersignificant differences were observed between the stages inrelation to wearing long-sleeved clothing. Participants in theaction stage also reported ‘‘Remaining in the shade’’ more thanparticipants in the contemplation stage (p < .01). Unexpectedly,participants in the precontemplation stage also reported‘‘Remaining in the shade’’ more than participants in thecontemplation stage (p < .001). The difference between parti-cipants in the precontemplation and action stages was notsignificant. Finally, participants in the action stage reported‘‘Remaining indoors’’ significantly more than participants in thecontemplation stage (p < .001). Participants in the precontem-plation stage also reported ‘‘Remaining Indoors’’ more thanparticipants in the contemplation stage (p < .001). The differ-ence between mean scores obtained by participants in theprecontemplation and action stages was not significant.
4. Discussion
The first aim of the present study was to construct a briefquestionnaire (the RASP-B) to assess stage of change in relation tosun-protective behaviour. A principal components analysis of
Table 2Observed (and expected) frequencies for stages of change by gender.
Precontemplation Contemplation Action Total, n
Observed n (expected n) Observed n (expected n) Observed n (expected n)
Male 7 (13.1) 13 (12) 14 (8.9) 34
Female 40 (33.9) 30 (31) 18 (23.1) 88
Total 47 43 32 122
Table 3Mean scores and standard deviations obtained by participants in the precontem-
plation, contemplation, and action stages of change for the four sun-avoidance
behaviours.
Avoidance behaviour Precontemplation
M (SD)
Contemplation
M (SD)
Action
M (SD)
Applying sunscreen 2.38 (1.13) 2.00 (1.05) 2.34 (1.29)
Long-sleeve clothing 1.79 (1.20) 1.44 (1.05) 2.19 (1.15)
Remaining in the shade 2.79 (0.88) 2.65 (1.15) 3.28 (0.92)
Remaining indoors 2.43 (0.85) 1.95 (0.98) 2.59 (0.67)
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462454

Author's personal copy
RASP-B responses of 122 university students revealed a clearthree-factor structure corresponding to the precontemplation,contemplation, and action stages of the TTM. Taken together, thesethree factors accounted for 63% of the total variance observed inquestionnaire responses, which was similar to the 69% of varianceobserved in the Rollnick et al. [23] study. The Cronbach’s alphacoefficients for the three-stage of change scales ranged from 0.67to 0.76 which were similar to the Cronbach’s alpha coefficientsobserved in the [23] study, which ranged from 0.73 to 0.85. Bothquestionnaires thus appear to have comparable and satisfactorypsychometric properties.
The RASP-B requires approximately 5 min to complete, can beself-administered and has satisfactory psychometric properties;thus, it has utility in primary health care settings, where both timeand client-professional contact are often limited. Our studyexpanded on research published in recent years exploring thevalidity and reliability of questionnaires assessing readiness tochange sun-protective behaviours [21,27]. The RASP-B focuses oncurrent patterns of sun-protective behaviour and a comprehensiveassessment of participants’ readiness to change such behaviour.The brevity of the RASP-B facilitates expedient completion withminimal intrusiveness.
The second aim was to assess the current levels of sun-protective behaviour of a sample of Queensland universitystudents and compare the sun-related behaviours they reportto the stage of change as measured by our questionnaire. Asexpected the group as a whole displayed a wide range of sun-protective behaviours. Results suggested that participants in theaction stage reported engaging in significantly higher levels ofsun-protective behaviour than participants in both the precon-templation and contemplation stages. Participants in the actionstage reported avoiding exposure to direct sunlight significantlymore often than participants in the earlier stages by wearing long-sleeved clothing, by remaining in the shade, or by remainingindoors. The TTM predicts that participants in the action stagetypically engage in more health-protective behaviour thanparticipants in the earlier stages and this prediction wassupported by our results.
Overall, participants reported poor levels of sun-protectivebehaviour. Just one in four participants (25%) reported that theyusually or always applied sunscreen when spending timeoutdoors, whilst almost half (46%) reported that they neverapplied sunscreen when outdoors. This finding was similar toprevious Queensland-based research which reported that lessthan one in three (32.5%) respondents aged 18–24 years reportedwearing sunscreen when outdoors [9]. Patterns such as these areof concern when it is considered that the data were collected in theregion with the world’s highest incidence of skin cancer and thatthe UV radiation index in Cairns averages in the ‘extreme’ rangefor 6 months of the year, only dropping into the ‘high’ range duringmid winter [39]. Given that the sample used in this study (i.e.,young people) are likely to have more time available to spend inthe sun than most and that they have been the target of recentgovernment sun damage mitigation campaigns, it would seemthat the message is falling of deaf ears. This appears to beespecially true of females, who reported sunbathing significantlymore often and applying sunscreen significantly less often thanmales.
Significantly more females than males were found to be in theprecontemplation stage and significantly fewer females were inthe action stage. Similar results have been reported in other studiesin which females have been more likely than males to be in theprecontemplation stage (and less likely to be in the action stage)for sun-protective behaviour [21,28].
One limitation of the present study was that it utilised a non-clinical sample, a majority of which were female. Subsequentstudies may wish to examine the validity of the RASP-B usinggender-matched samples or clinical populations affected by skincancer. While there are undoubtedly age-related changes in sunexposure behaviour, the current study targeted a sample mostlikely to display a wide range of sun-related behaviours in orderto gain the most sensitivity in assessing the validity of the stagesof change questionnaire. While the items on the RASP-B do notcontain any obvious age bias, it is an empirical question as tohow well it distinguishes between stages of change in youngerand older individuals. Nevertheless, when it is considered thatstage-matched behaviour change interventions may be moreeffective than generic interventions, the true value of the RASP-Bmay lie in predicting which intervention is most appropriate foran individual by establishing which stage of change they are in.This may contribute to more efficient use of primary health caretime, shortened intervention completion times and a potentialincrease in overall client health.
5. Conclusions
The RASP-B was developed as a brief questionnaire tomeasure peoples’ sun-protective behaviours and their readinessto change these behaviours. We administered the RASP-B to asample of university students from Queensland and found it tohave acceptable psychometric properties. The patterns ofreported sun-protective behaviours were consistent with thosepredicted based on the transtheoretical model of behaviourchange. As the RASP-B can be self-administered in approxi-mately 5 min, the instrument may be of considerable utilityin primary health care settings across Australia. Wespeculate that behavioural interventions aimed at modifyingsun-protective behaviours will be more successful if they targetindividuals based on their individual readiness to change. TheRASP-B, as described here, will facilitate such targeted inter-ventions.
Conflict of interest
No conflict of interest.
Sources of support
Nil.
Acknowledgements
The authors wish to thank Associate Professor Ricky van derZwan and Dr. Anne Swinbourne for their contributions to earlystages of the study and to previous drafts of this paper.
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462 455

Author's personal copy
Appendix 1. Readiness to alter sun-protective behaviour questionnaire (RASP-B)
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462456

Author's personal copy
Appendix 1 (Continued )
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462 457
Author's personal copy
Appendix 2. Sun-protective behaviours questionnaire
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462458

Author's personal copy
Appendix 2 (Continued )
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462 459

Author's personal copy
Appendix 2 (Continued )
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462460

Author's personal copy
Appendix 2 (Continued )
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462 461
Author's personal copy
References
[1] Arthey S, Clarke V. Suntanning and sun protection: a review of the psycho-logical literature. Soc Sci Med 1995;40(2):265–72.
[2] Kripke M, Ananthaswamy H. Carcinogenesis: ultraviolet radiation. In: Freed-berg I, Eisen A, Wolff K, Austen K, Goldsmith L, Katz S, eds. Fitzpatrick’sdermatology in general medicine. 6th ed., New York: McGraw-Hill, 2003 :371–7.
[3] Rossi J, Blais L, Redding C, Weinstock M. Preventing skin cancer throughbehavior change: implications for interventions. Dermatol Clin 1995;13(3):613–22.
[4] Elwood J, Jopson J. Melanoma and sun exposure: an overview of publishedstudies. Int J Cancer 1997;73:198–203.
[5] Diffey B. What is light? Photodermatol Photoimmunol Photomed 2002;18:68–74.
[6] Hussein M. Ultraviolet radiation and skin cancer: molecular mechanisms. JCutan Pathol 2005;32:191–205.
[7] Smith T. The Queensland Melanoma Project—an exercise in health education.Br Med J 1979;1:253–4.
[8] Cancer Council Australia. Skin cancer facts & figures. Cancer Council website2009. Available from: URL: http://www.cancer.org.au/cancersmartlifestyle/SunSmart/Skincancerfactsandfigures.htm.
[9] Queensland Government. 2005 Sun Safe Survey Report. Queensland, Australia:Queensland Health, Queensland Government; 2005.
[10] Garvin T, Eyles J. Public health responses for skin cancer prevention: the policyframing of sun safety in Australia, Canada and England. Social Sci Med2001;53:1175–89.
[11] Giles G, Armstrong B, Burton R, Staples M, Thursfield V. Has mortality frommelanomas stopped rising in Australia? Analysis of trends between 1934 and1994. Br Med J 1996;312(7039):1121.
[12] Montague M, Borland R, Sinclair C. Slip! Slop! Slap! and SunSmart, 1980–2000: skin cancer control and 20 years of population-based campaigning.Health Educ Behav 2001;28(3):290–305.
[13] Buettner P, Raasch B. Incidence rates of skin cancer in Townsville, Australia. IntJ Cancer 1998;78(5):587–93.
[14] SunSmart. SunSmart. SunSmart website 2003. Available from: URL: http://www.sunsmart.com.au/.
[15] World Health Organization. Global Solar UV Index: A Practical Guide. Geneva:World Health Organization; 2002.
[16] Queensland Government. Skin Cancer. Government website 2009. Availablefrom: URL: http://www.health.qld.gov.au/sunsafety/skin_cancer/default.asp.
[17] The Cancer Council of Western Australia. Research. Cancer Council website2006. Available from: URL: http://www.cancerwa.asn.au/research/.
[18] Slevin T, Clarkson J, English D. Skin cancer control in Western Australia: is itworking and what have we learned? Radiat Prot Dosimetry 2000;91(1–3):303–6.
[19] Miller A, Ashton W, McHoskey J, Gimble. What price attractiveness? Stereo-type and risk factors in suntanning behavior. J Appl Social Psychol1990;20(15):1272–300.
[20] Prochaska J, DiClemente C. Transtheoretical therapy: toward a more inte-grated model of change. Psychother Theory Res Pract 1982;20:161–73.
[21] Kristjansson S, Helgason A, Rosdahl I, Holm L, Ullen H. Readiness to changesun-protective behaviour. Eur J Cancer Prev 2001;10:289–96.
[22] Prochaska J, DiClemente C. Toward a comprehensive model of change. In:Miller W, Heather N, eds. Treating addictive behaviours. New York: Plenum,1986.
[23] Rollnick S, Heather N, Gold R, Hall W. Development of a short ‘readiness tochange’ questionnaire for use in brief, opportunistic interventions amongexcessive drinkers. Br J Addict 1992;87:743–54.
[24] Sutton S. Can ‘stages of change’ provide guidance in the treatment of addic-tion?: a critical examination of Prochaska & DiClemente’s model. In: EdwardsG, Dare E, eds. Psychotherapy, psychological treatments and the addictions.Cambridge: University Press, 1996: 189–205.
[25] Prochaska J. Strong and weak principles for progressing from precontempla-tion to action on the basis of twelve problem behaviors. Health Psychol1994;13(1):47–51.
[26] Velicier W, Hughes S, Fava J, Prochaska J. An empirical typology of subjectswithin stages of change. Addict Behav 1995;20(3):299–320.
[27] Branstrom R, Kristjansson S, Ullen H, Brandberg Y. Stability of questionnaireitems measuring behaviours, attitudes and stages of change related to sunexposure. Melanoma Res 2002;12:513–9.
[28] Kristjansson S, Branstrom R, Ullen H, Helgason A. Transtheoretical model:investigation of adolescents’ sunbathing behaviour. Eur J Cancer Prev2003;12(6):501–8.
[29] Kristjansson S, Ullen H, Helgason A. The importance of assessing readiness tochange sun-protection behaviours: a population-based study. Eur J Cancer2004;40:2773–80.
[30] Maddock J, Redding C, Rossi J, Weinstock M. Development and validation of anappearance motivation attitudes scale for sun protection. Psychol Health2005;20(6):775–88.
[31] Prochaska J, Velicier W, Redding C, Rossi J, Goldstein M, DePue J, et al. Stage-based expert systems to guide a population of primary care patients to quitsmoking, eat healthier, prevent skin cancer, and receive regular mammo-grams. Prev Med 2005;41:406–16.
[32] Rossi J, Blais L, Weinstock M. The Rhode Island sun smart project: skin cancerprevention reaches the beaches. Am J Public Health 1994;84(4):672–4.
[33] Weinstock M, Rossi J, Redding C, Maddock J, Cottrell S. Sun protectionbehaviors and stages of change for the primary prevention of skin cancersamong beachgoers in southeastern New England. Ann Behav Med2000;22:286–93.
[34] Weinstock M, Rossi J, Redding C, Maddock J. Randomized controlled commu-nity trial of the efficacy of a multicomponent stage-matched intervention toincrease sun protection among beachgoers. Prev Med 2002;35:584–92.
[35] Prochaska J, Velicier W, Rossi J, Redding C, Greene G, Rossi S, et al. Multiple riskexpert systems interventions: impact of simultaneous stage-matched expertsystems interventions for smoking, high-fat diet, and sun exposure in apopulation of parents. Health Psychol 2004;23(5):503–16.
[36] Pagoto S, McChargue D, Fuqua R. Effects of a multicomponent intervention onmotivation and subprotection behaviors among midwestern beachgoers.Health Psychol 2003;22(4):429–33.
[37] Prochaska J, DiClemente C. Stages and processes of self-change of smoking:toward an integrative model of change. J Consult Clin Psychol 1983;51:390–5.
[38] Queensland Health, 2005 Sun Safe Survey Report. Queensland, Australia:Queensland Health, Queensland Government; 2005.
[39] Bureau of Meteorology. Average monthly UV index. Government website2009. Available from: URL: http://www.bom.gov.au/jsp/ncc/climate_averages/uv-index/index.jsp?period=mar#maps.
R.D. Borschmann, D. Cottrell / Cancer Epidemiology 33 (2009) 451–462462




















