
DEPUY SHAPES ROBOTICS STRATEGY AROUND PATIENT
62
In Vivo pharma intelligence ❚ informa JULY/AUGUST 2018 invivo.pharmaintelligence.informa.com vol. 36 ❚ no. 07 Cancer Vaccines: Is There A Future Beyond Trial And Error? Exclusive Interview: Novo’s Sørensen Reflects On CEO Years And Tasks Ahead For Industry NASH: Flying The Plane While Building It BY ASHLEY YEO DEPUY SHAPES ROBOTICS STRATEGY AROUND PATIENT
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of DEPUY SHAPES ROBOTICS STRATEGY AROUND PATIENT

In Vivopharma intelligence ❚ informa
JULY/AUGUST 2018invivo.pharmaintelligence.informa.com
vol. 36 ❚ no. 07
Cancer Vaccines: Is There A Future Beyond
Trial And Error?
Exclusive Interview: Novo’s Sørensen Reflects On CEO
Years And Tasks Ahead For Industry
NASH: Flying The Plane While
Building It
BY ASHLEY YEO
DEPUY SHAPES ROBOTICS STRATEGY AROUND PATIENT

PAGE BLANK INTENTIONALLY

©2016 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 1
CONTENTS ❚invivo.pharm
aintelligence.informa.com
July/August 2018In Vivo
Pharma intelligence |
STRATEGIC INSIGHTS FOR LIFE SCIENCES DECISION-MAKERS
In VivoPharma intelligence |
1 4 Cancer Vaccines: Is There A Future Beyond Trial And Error?WILLIAM LOONEY
Strong foundational research in immunology and some promising early-phase trial results have so far failed to expedite the validation of vaccines to treat cancer. In Vivo examines biopharma’s enduring optimism about the future of cancer vaccinology, including a closer look at one company’s platform to tackle the incurable malignancies that beset the mother of all organs: the human brain.
32 Back To The Future: Novo’s Sørensen Reflects On CEO Years And Tasks Ahead For IndustryLUCIE ELLIS
Lars Rebien Sørensen scrutinizes the pharmaceutical industry and shares with In Vivo his vision for the future of the Novo Nordisk Foundation. With 16 years as CEO of Novo Nordisk under his belt, as well as many more years in leadership roles at the Danish company, Sørensen reflects on the past and gives his predictions for the future of the innovative drug development sector.
2 6 Regenerative Medicine Is Here: New Payment Models Key To Patient AccessFRANCESCA COOK, TED SLOCOMB AND
MICHAEL WERNER
Potentially curative regenerative medicine therapies are no longer theoretical, but instead have become reality. As more and more gene, cell and tissue-based therapies reach the market, the need for payment solutions is becoming more pressing. The Alliance for Regenerative Medicine has consulted with payers and other stakeholders to consider the barriers to alternative payment models and look at possible solutions. 3 6
STRATEGIC INSIGHTS FOR LIFE SCIENCES DECISION-MAKERS
ORPHAN MEDICINES: AVERTING PRICE DEBACLES AND WINNING PAYER SUPPORT
SPONSORED BY: SYNEOS HEALTH
As coverage and reimbursement landscapes change, drug developers must assess how health care systems will handle the incoming wave of treatments for rare diseases that often carry a high list price, and they should prepare for restrictive practices that pass more of the costs along to patients.
2 0
NASH: Flying The Plane While Building ItAMAMA SADIQ, ILIYANA P. ATANASOVA
AND KATHERINE J. FRANKLIN
Drug development for nonalcoholic steatohepatitis (NASH), a form of liver disease, is a game of incomplete information: pipeline evolution is occurring in parallel with continued efforts to better understand and manage the disease. To date, no therapy for patients with NASH has been approved and consequences of the condition can be severe, including cirrhosis and hepatocellular carcinoma.
❚ Ortho Demand Pull: DePuy Synthes Shaping Digital And Robotic Surgery Strategy Around Patient NeedsAshley Yeo
Johnson & Johnson’s DePuy Synthes orthopedic business has taken a measured view of digital and robotic capabilities, rather than acquiring assets that perhaps do not fully meet its strategic needs. For the business’ global R&D head Euan Thomson, any new technology must augment the group’s abilities to drive meaningful outcomes.
8 COV E R

2 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ CONTENTSin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
In VivoPharma intelligence | July/August 2018
Vacations are calling, the smell of barbeque smoke is in the air, summer is upon us… but there has been no rest for the In Vivo team. For this July and August combined issue, we are exploring a num-ber of topics including the changes coming to the orthopedic surgery market, which is being pro-pelled by the rise of robotics. This edition’s cover story, from Ashley Yeo, focuses on Johnson & Johnson’s DePuy Synthes and its watch and wait strategy for digital and robotics in-vestment. DePuy Synthes has been biding its time, assessing critical areas to place its cash in robotics and building a system it believes puts the patient
at the center of the technology. Further exploring the world of orthopedic sur-gery, In Vivo has looked at the strategies being tested by implants manufacturer Corin Orthopedics Holdings and the robotics specialist Intuitive Surgical Inc. Intuitive’s da Vinci technology has blazed a trail for robotic-assisted minimally-invasive surgery in five specialties: gynecologic surgery, urological surgery, gen-eral surgery, cardiothoracic surgery, and head and neck surgery. For these exclu-sive online articles visit invivo.pharmaintelligence.informa.com.
Also included in the summer issue is an exclusive interview with Novo Nordisk’s former CEO of more than a decade, Lars Rebien Sørensen. He discusses his new roles as chair of the Novo Nordisk Foundation and chair of Novo Holdings, the lessons he learnt from many years leading a top innovative pharma company and the foundation’s new five-year grant strategy.
Meanwhile, In Vivo’s William Looney explores the progress of cancer vaccines in the clinic. The big question that still remains in the field of oncological vaccine development is which of the many immunologically driven platform approaches has the best chance of producing breakthrough results for waiting cancer pa-tients? Immunomic Therapeutics Inc.’s CEO Dr. Bill Hearl talks about the com-pany’s cancer vaccine development pipeline and its journey to bring the technology from the bench to the clinic.
❚ From The EditorDEPARTMENTS
AROUND THE INDUSTRY 4 Personalization And Digital Are
Pushing IVDs Onto The Health Care High Ground ASHLEY YEO
6 Record-Breaking First Half For Start-Ups Raising Cash In Europe MIKE WARD
40 ON THE MOVERecent executive appointments in the life sciences industry REGINA PALESKI
44 DEAL-MAKINGDeals Shaping The Medical Industry, June 2018 THE STRATEGIC TRANSACTIONS TEAM
LUCIE ELLIS
❚ Intuitive Sets Pace In A Robotics Segment Where Ortho Players Are Finding Their Feet ASHLEY YEO
❚ The Personal Touch: Ortho Implants Challenger Corin Creates Its Own Value Pathway ASHLEY YEO
❚ Deals In Depth, May 2018 AMANDA MICKLUS
In Vivo: Always Online FirstRelevant and exclusive online-only content at your fingertips 24/7.
Full access to our 35-year archive.
Access your subscription by visiting: invivo.pharmaintelligence.informa.com and log in.
Don’t have an online user account? Quickly and easily create one by clicking on the “Create your account” link at the top of the page.
Contact: [email protected] or call: (888) 670-8900 or +1 (908) 748-1221 for additional information.
All stock images in this publication courtesy of www.shutterstock.com unless otherwise stated.
/invivo@invivo/invivo
EXCLUSIVE ONLINE CONTENTinvivo.pharmaintelligence.informa.com

©2016 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 3
CONTENTS ❚invivo.pharm
aintelligence.informa.com
❚ Up-Front
With 16 years as CEO of diabetes giant
Novo Nordisk under his belt, as well as
many more years in leadership roles at
the Danish company, Lars Rebien
Sørensen reflects on the past and gives
his predictions for the future of the
innovative drug development sector.
Page 32
Patient access to transformative regenerative medicines will be hindered if health care systems are not prepared for the implications of such medical innovation – an analysis from Alliance for Regenerative Medicine explores payment and reimbursement issues. Page 26
“ If a therapeutic vaccine platform is to succeed, you must be able to mobilize all these beneficial actors for a single-minded assault on the cancer,” says Dr. Catherine Wu, leader in cancer vaccine research. Page 14
Strategic partnerships and cross-collaboration between biopharma, diagnostic companies, academic centers and regulatory agencies may serve as a catalyst to accelerated development in nonalcohlic steatohepatitis. Experts from strategy consultancy Clarion explore the NASH clinical pipeline. Page 20
“We now have a relentless focus
on automation and bringing
technologies to health care systems that
add value, and are not just marketing tools.”
Dr. Euan Thomson, global R&D head for
Johnson & Johnson’s DePuy Synthes
business, discusses the company’s
patient-centric approach
to robotics. Page 8
SNAPSHOTS FROM JULY/AUGUST'S CONTENT

4 | In Vivo | July/August 2018 invivo.pharmamedtechbi.cominvi
vo.p
harm
aint
ellig
ence
.info
rma.
com
❚ Around The Industry
Personalization And Digital Are Pushing IVDs Onto The Health Care High Ground In vitro diagnostics champions like the UK's Sir John Bell are no longer the exception. He is not the first to talk up the vital contribution of diagnostic medicine to modern heath care. He won't be the last, but his public figure status and importance to life sciences in the UK give his words resonance. (Also see "World In Motion – The Shape Of The New Health Care Technology Ecosystem In 2022" - In Vivo, June 2018.) Others have doubtless said it better, but perhaps not more succinctly than his recent soundbite on the ABHI's news portal that simply said that therapy cannot work to its best without diagnostic medicine. That, and digital medicine, are the future of heath care.
Jesús Rueda Rodriguez, director for international affairs at MedTech Europe, elucidates on the theme. Speaking to In Vivo, Rueda said that diagnostic in-formation is becoming more relevant to patients in a more direct way. Formerly the IVDs regulatory affairs director at EDMA (European Diagnostic Manufactur-ers Association), Rueda said two things have made a major difference in the way diagnostics are perceived and used.
One is the generation of increasing vol-umes of personalized information that are helping patients get the right treatments at the right time. For that, the right diagnosis of the patient's condition is vital. There has been a lot of investment in genetics and in collecting information over time from patients. "We now have more results, and because of better analysis, we are getting more out of those results," he says. Ten years ago, genetic testing was a mystery to much of the public, but now, gene tests are more routine, better accepted and more frequently requested. The information de-rived from them is making a big difference in the diagnosis and treatment of patients.
COMMUNICATION OF RESULTS HAS REVOLUTIONIZED PERCEPTIONSAnd the second is a consequence of the realization that "diagnostics" is not just a lab concept, but is available to everyone as a general tool: the sector has become much better at communicating diagnostic test results. "The way that results are now being delivered means that people
are really understanding the value of di-agnostics." Take for example BRCA1 and breast cancer – the information seems pragmatic, less esoteric, not necessarily needing specialist knowledge, says Rue-da. In short, everything is much clearer.
Three trends have converged to pro-duce this perceptibly upbeat message. And although Rueda confesses to being a hard-wired optimist, it's a compelling enough scenario that he describes.
First of all, industry recognized the problem and began to use more data and do more studies to validate the results, thereby building more confidence in these results. Next, the physicians themselves are understanding and using the results much more often, to the extent that test-ing has become more routine medical practice, not just a one-off request.
And thirdly, there is no ignoring the cultural phenomenon of diagnostic test-ing on the patient side. High-profile news items about celebrities undergoing tests has surely played a part here, helping people to relate to tests better. The result is that diagnostics is suddenly no longer the province of doctors alone; it is a world where easy-to-obtain test results can be provided via apps that explain matters in a detailed, yet simple way. "The fact that people are more involved is a driving lot of the change," he notes.
Faster results are another element. As-says are moving out of the lab and to the bedside or to the physician's office. Much faster turnaround means patients do not
have to wait days to get their results. In the past, their interest may have waned as the momentum dropped, but that is less so in 2018.
IS INVESTMENT INCREASING AS A RESULT?The IVDs space of the medtech industry has always been rich territory for R&D and innovation, Rueda claims, partly be-cause of its close links to biotech. There has always been strong investment in the sector, and that is accelerating, given the increasing opportunities and the broader acceptance of the technologies. It comes from both the private and public sectors. But because of the investment culture in Europe, it is not always as easy in Europe as it is in the US, which has more appetite for risk-taking.
Those more resource-intensive diag-nostic procedures can attract significantly more funding than previously. However, the traditional route to market, whereby a start-up would develop an idea from a lab or university into a straightforward, low-cost test, still exists. Rueda predicts that the commodity test segment side will continue to be stable.
As to point-of-care, it has yet to find its right position within health care systems. "There's no doubt that POC has huge growth potential, but maybe we are not quite there yet in delivering the solutions that people are comfortable with." The UK's
JESÚS RUEDA RODRÍGUEZ

©2017 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 5
AROUND THE INDUSTRY ❚invivo.pharm
aintelligence.informa.com
BIVDA industry association recently voiced the same sentiments. (Also see "IVDs Are Hitting An Adoption 'Glass Ceiling' While A £7Bn UK Opportunity Goes Begging" - Medtech Insight, June 17, 2018.)
Rueda is sure that IVD start-ups will continue to be picked up and developed by larger companies, but that there will also be new and interesting models of how to deliver health care, where there is much innovation ongoing that will benefit the IVDs sector. "The past system of silos and separate cost centers is starting to change, and that will definitely benefit diagnostics in the long run," says Rueda, observing that Germany, France, the UK, Spain and the Netherlands were leading the way on this in Europe.
Digital will drive part of the change in the IVDs sector. There is much more invest-ment in this area, but stakeholders are still working on getting the right mix and defining how to use the technologies and make use of the information derived. "Apps require people that use them to interact with them, and we are still working on that 'experiment' on a huge scale," says Rueda. "It's the holy grail of health care and no one has the answer just yet." Elsewhere, some companies are already seeing themselves as service providers rather than as merely providers of tests. The major groups are all eyeing the opportunities here, and are po-sitioning themselves differently. "Nobody expects health care to be the same in 10 years' time."
Overall, the climate for acceptance of diagnostics has improved markedly. "We're starting to find better pathways to really show clinicians the value of IVDs, and patients want to be aware of the op-tions, and that will increase the use of IVDs." The eternal conundrum for IVDs is that these relatively low-cost tests do not share fully in the benefits they bring further along the care pathway. Pilots are said to be ongoing to demonstrate the value of diagnostics to the whole health care system.
IVDR: SHORT–TERM PAIN FOR LONG TERM QUALITY GAINThe EU 28 is a market of some €10–11 billion for IVDs, representing 10% of the wider EU medtech market. It is growing, albeit not dramatically at present, but there are fears that this growth could be
trimmed, and the quality and volume of innovation ahead reduced, as a result of the forthcoming EU In Vitro Diagnostics Regulation (IVDR). "We're going to see a shift in innovation, and the IVDR will certainly have an effect," says Rueda. One change is that more upfront data will be required on some tests, meaning they will be better validated and better studied.
This will be a cost to manufacturers, but on the flip side, it would help uptake over the longer term, given that the products are now better backed up by claims. Some IVD technologies will be made obsolete by IVDR, perhaps the older tests that are inex-pensive but perhaps do not perform quite as well as some others. Obsolescence will not be a huge issue, maybe resulting in the loss of a few percent of the current range, Rueda believes. And while the IVDR will increase time to market, the products will be of better quality and show better performance.
"While there will not be a significant shortfall in product availability, I am concerned about rare disease therapies – those products with low market vol-umes that require a very high threshold of evidence," says Rueda. There are ways around the problem. Rueda notes that tests use basically similar platforms, and so a lot of information could be useful across several tests, meaning not all tests would need to be done from scratch. In addition, there is the prospect of public or European Commission funding to support such products.
NB NUMBER NOT INDICTIVE OF COVERAGENotified bodies (NBs) serving the EU IVDs market could halve in number. Current indications are that just 11 notified bod-ies have signaled that they will continue auditing the EU IVD sector, come May 26, 2022. This has given rise to fears about capacity and market coverage, but in Rueda's view, there is a need to look more deeply. "The number of NBs is a terrible metric by which to measure the IVDR. Much better is to look at the number of actual auditors."
These 11 probably cover 80% to 90% of the market, and many of the remaining NBs would be niche, he explaines. The big question is, will they be ready? There is a lot of work to do, as 80% to 90% of IVDs
will now need full NB oversight, as the old system of self-certification or listing in annex 1 or 2 of the IVDD (IVD Directive) is phased out. There are consequently major fears over the readiness of the system.
However, IVDs have two more years than devices to prepare, and Rueda ob-serves that IVD companies, right now, are not particularly stressed. He foresees the usual last-minute scramble, but es-sentially considers it manageable, to the extent that the extra two years (to May 2024) of "soft" transition available for manufacturers to keep their IVDD registrations in place is unlikely to be heavily used. This would only apply to the 10% or so IVDs that were required to undergo NB auditing under the IVDD. As such, it won't be a major game changer in the IVDs field. "The IVDs industry is not over-worried so far, and the message is essentially positive," says Rueda. But Europe does have its hurdles. The problem for manufacturers is the sheer number of different systems, and that value is looked at differently across Europe. "You have to show it over and over again, but this is an area where we want to develop a model for easier assessment, and the European Commission is reportedly trying to develop a solution to that."
BREXIT NOT A TOP CONCERN FOR IVDS INDUSTRYBrexit will cause short-term disruption for the next two to three years to the wider European IVDs sector in areas such as shipping products, for instance. But it will be managed, by and large, ac-cording to Rueda, who instead sees the top three challenges for European IVDs manufacturers as:• Access to markets:
ensuring new technology is adopted • Innovation:
finding the "right" innovation • Visibility of IVDs:
getting health systems and clinicians to engage with IVDs
In spite of these challenges, and the IVDR, the EU IVDs sector is in a good phase right now, and it does not necessarily take an "optimist by nature" like MTE's Rueda to see that this is a valid assessment. IV005355
ASHLEY YEO [email protected]

6 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ AROUND THE INDUSTRYin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
Record-Breaking First Half For Start-Ups Raising Cash In Europe
Europe’s biotech start-up environment has been boosted by prominent venture capital groups launching new funds, and this investor enthusiasm looks to be sustainable. As the second half of 2018 got underway, Abingworth, which announced it had raised $315 million for its 12th fund ABV VII, said it intends to allocate about 50% of that sum in Europe, while Forbion, which announced a first close of Forbion IV at €275 million, is earmarking up to 80% of its money for European opportunities.
These two closings add to other prominent new fund launches by European venture capitalists during 2018. In Febru-ary, Andera Partners (formerly Edmond de Rothschild Investment Partners) closed its BioDiscovery 5 fund at €345 million, with an expectation that 70% of the capital will be put to work in European companies; two-thirds of which will be invested in biotech with the remainder in medtech. In April, Sofinnova Partners launched Sofinnova Crossover I with €275 million ($321 million), above the original first-close target of €250 million, with an expectation that 80% of the money will be allocated to European opportunities.
Speaking to European venture capital-ists, it is clear there is a growing demand to invest in European biotechs that are considered more attractive than their US counterparts. In the US, there is a huge amount of cash looking for opportunities, which means that investors are finding they need to offer higher and higher valu-ations to participate in rounds. In Europe, there is less competition for investments and so valuations are not as frothy.
In the first half of this year, European biotechs raised just over $1.6 billion from venture and private capital sources, which represents just under 14% of the total amount raised globally over the same time period. Interestingly, Europe’s share of start-up financing was higher highlight-ing the enthusiasm for investors to create businesses underpinned by research from world-class institutions, or around under-resourced or deprioritized assets out of pharma companies.
European biotechs raising seed, series A and series B money from venture and private capital sources secured just under $1.1 billion, about 20% of the global total. In contrast, in 2017, European biotechs
raised $1.25 billion – about 17% of the global take – in seed, series A and series B rounds. Indeed, the sum raised in the first six months of 2018 is the most ever raised for early-stage financing in any half-year period. US start-ups during the same period raised just over $4.4 billion.
A major trend is the increased fervour for European biotechs from US investors either directly participating in company fundraising or through participation as lim-ited partners in new venture capital funds.
BioNTech AG topped the European list, raising $270 million in a series A round at the start of the year. Europe’s largest private biotech company, with more than 750 employees, has ambitions to be a fully integrated biopharmaceutical company. It already has four mRNA-derived clinical programs in place and expects to broaden its clinical activity in the next 18 months across its whole portfolio. Originally backed by the Strüngmann family office, BioNTech was able to broaden its share-holder base in the series A round with new investors including Redmile Group, which led the round, Janus Henderson Investors, Invus, and Fidelity.
The UK continues to dominate European biotech start-up activity with five of the
top 10 financings in the first half. Oxford Nanopore Technologies Ltd., the Oxford-based developer of portable nanopore analysis devices, topped the British list when it raised £100 million ($133 million) with backing from global investors includ-ing GIC (Singapore), CCB International (CCBI, China), Hostplus (Australia), as well as its existing investors. The company will use the funds to support the next phase of commercial development as well as expanding its suite of nanopore analysis devices. (Also see "Oxford Nanopore Hits £1.5bn Valuation With Latest £100m Round" - Medtech Insight, March 22, 2018.)
Freeline Therapeutics Ltd., a London-based clinical-stage company focused on treatment of chronic systemic diseases with liver targeted adeno-associated virus (AAV) gene therapy, secured more than £88 million of new capital in a series B financing round led by Syncona, which committed £85 million with the remainder coming from the UCL Technology Fund (UCL TF). Both these investors participated in the £34.8 million series A round in 2015. Freeline will use the funds to drive its lead-ing programs in hemophilia B and Fabry disease through clinical development, and the cash will enable Freeline to further enhance its manufacturing and analytics capabilities. (Also see "Venture Funding Deals: I-Mab Is The Mega-Round Leader With $220m Series C" - Scrip, July 5, 2018.)
US investors flocked to take the op-portunity to back the British pharma-focused artificial intelligence company BenevolentAI as it raised $115 million from new and existing investors at a pre-money valuation of $2 billion. While not specifically identifying most of its back-ers, the company said the majority of the investors are from the US. The balance of raised funds came from existing investors, including Woodford Investment Manage-ment. The sum raised was the largest to date for a pharma-focused AI business. Since 2013, the company has raised more than $200 million.
Cambridge, UK-based Crescendo Biologics Ltd. also reached out to non-
BioNTech topped
the European list,
raising $270 million
in a series A round
at the start of 2018

©2017 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 7
AROUND THE INDUSTRY ❚invivo.pharm
aintelligence.informa.com
European investors as China’s Quan Capi-tal participated in the $70 million series B round that was led by new investor Andera Partners and included existing investors Sofinnova Partners, IP Group, EMBL and Takeda Ventures. The company, which raised $28.6 million in a 2013 series A round led by Imperial Innovations Group, is developing Humabodies, small antigen-binding proteins composed of human im-munoglobulin heavy chain variable region fragments generated in mice. The com-pany is preparing to enter the clinic with lead cancer candidate CB307, a bispecific T-cell engager targeting prostate-specific membrane antigen. (Also see "Crescendo Raises $70m In Largest European Biotech Series B Of Year" - Scrip, April 30, 2018.)
Slipping in at 10th place in the Eu-ropean early-stage fundraising table is Brighton, UK-based Enterprise Therapeu-tics Ltd., which is developing preclinical programs targeting two ion channels to treat diseases including cystic fibrosis, chronic obstructive pulmonary disease and asthma. Enterprise was also able to attract a major US investor as a co-lead for its £29 million series B round. US group Versant Ventures co-led the round with Novartis Venture Fund; the pair joined ad-ditional new investor Forbion and existing investors Epidarex Capital and IP Group.
Gosselies, Belgium-based oncology firm iTeos Therapeutics SA raised $75 mil-lion in an oversubscribed series B round led by US investor MPM Capital, which
invested more than half the total. Ad-ditional new investors HBM Partners and 6 Dimensions Capital participated in the round alongside all the company’s previ-ous investors. The immuno-oncology fo-cused company plans to use the new funds to move its lead program, EOS100850, an adenosine A2A antagonist, into the clinic this year, and it will progress a second asset, EOS884448, an anti-TIGT antibody, into the clinic in 2019.
Dublin-based Sublimity Therapeutics Ltd. (formerly Sigmoid Pharma Ltd.), a spe-cialty pharmaceutical company focused on the treatment of ulcerative colitis, managed to get third place in the European rankings after it completed a $64 million financing to further the development of STI-0529 for the treatment of moderate to severe ulcer-ative colitis. The financing was co-led by US investors OrbiMed and Longitude Capital, with participation from HBM Healthcare Investments.
US investor Orbimed, one of the big-gest backers of global biotech, also led the €40 million series B round raised by Enyo Pharma SAS, a Lyon, France-based clinical-stage biopharma developing an FXR agonist (EYP001) as its lead program, targeting both chronic hepatitis B and NASH. Joining Orbimed were new inves-tors Andera and BpiFrance Large Venture and existing investors Sofinnova Private Capital VII, Morningside Venture Invest-ments, InnoBIo and Inserm Transfert. The company closed a series A round at
€22 million in 2016. The new funds will be used to finance the two first Phase II clinical trials of EYP001.
Aarhus, Denmark-based NMD Pharma AS, which is focused on neuromuscular disorders, raised €38 million in a se-ries A round led by new investor INKEF Capital. The financing was supported by Roche Venture Fund, also a new inves-tor, and existing investors Novo Seeds and Lundbeckfonden Emerge, which had previously participated in the 2016 seed round alongside Capnova. Still at the pre-clinical stage, NMD Pharma is developing small molecule inhibitors of the CIC-1 ion channel that have the potential to treat rare neuromuscular disorders and acute hospital care indications where there are neuromuscular transmission deficits.
While European biotech entrepreneurs have probably never had it so good, there are two potential clouds on the horizon. First, is the impact the UK’s exit might have on the ability to tap into European VC sources, which tend to have a more gener-ous allocation for EU-domiciled companies compared with non-EU opportunities. Second, European companies still need to look across the Atlantic and tap into the deep pools of capital that exist stateside. The sight of Europe’s most promising start-ups heading to NASDAQ can be expected to continue for some time. IV005373
MIKE [email protected]
Exhibit 1
Top European Early-Stage Bioscience Financings H1 2018
COMPANY LOCATION FOCUS ROUND AMOUNT RAISED BioNTech AG Mainz, Germany Oncology A $270M
Oxford Nanopore Technologies Ltd. Oxford, UK Analytical devices Not disclosed £100M
Freeline Therapeutics Ltd. London, UK Gene therapy B £88M
Benevolent AI London, UK AI-driven drug discovery Not disclosed $115M
iTeos Therapeutics SA Gosselies, Belgium Immuno-oncology B $75M
Crescendo Biologics Ltd. Cambridge, UK Humabodies B $70M
Sublimity Therapeutics Ltd. Dublin, Ireland Inflammation Not disclosed $64M
Enyo Pharma SAS Lyon, France Liver diseases B €40M
NMD Pharma AS Aarhus, Denmark Neuromuscular disorders A €38M
Enterprise Therapeutics Ltd. Brighton, UK Respiratory diseases B £29M
SOURCE: In Vivo

8 | In Vivo | July/August 2018 pharmamedtechbi.com
❚ REVIEWING ROBOTICS
Shut
ters
tock
: Cop
yrig
ht In
fo
DePuy Synthes Shaping Digital And Robotic Surgery Strategy Around Patient Needs
DePuy Synthes has laid the foundations for its orthopedic robotic offering, and has thoughtfully pulled the elements together to craft what it sees as the optimum package for surgeons and patients.
Its vision puts patients in a more central role. Orthopedics is about mobility, and mobility determines lifestyle, says DePuy Synthes, which plans to address real-world outcomes as they are viewed by patients.
So what? The consensus is that the big players in ortho will each have a robot by the end of this year, but how central robotics should be to such a mature surgery is a moot point – and DePuy Synthes has an answer to that.
BY ASHLEY YEO
ORTHO DEMAND PULL:

©2017 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 9
REVIEWING ROBOTICS ❚invivo.pharm
aintelligence.informa.com
Is DePuy Synthes late to the digital and robotics party? New technologies, tools and capabilities regularly emerge and become either central or peripheral to health care, and the wheels of medtech busi-ness turn regardless. That
seems to be the attitude at orthopedics giant DePuy Synthes, which in recent months has identified and acted on its own considered plan to maximize value for patients and users with a selective approach to technology integration.
Euan Thomson, PhD, global R&D head for Johnson & Johnson’s DePuy Synthes business, believes that his group has developed a platform for a solid digital strategy, centered around brand-based technology solutions. It draws in robotics, imaging and digital education systems, as well as products and services that interact directly with patients. Thomson spoke to In Vivo about the company’s plans.
In Vivo: In digital health care, the pic-ture is becoming clearer and the needs better defined. While some companies set their stalls out early, others ad-opted a watch and wait policy. It seems DePuy Synthes is in the latter camp.
Euan Thomson: In an environment focused on technology solutions such as robotics, we are targeting the use of tech-nology to drive outcomes. This includes robotics, and the company’s February
2018 acquisition of Orthotaxy SAS, a privately held developer of software-enabled surgery technologies, including a differentiated robotic-assisted surgery solution, fits in here. But our vision is much broader than that. Orthopedics is a mature field, and while companies have been investing in this space for many years, there are still gaps and potential for improvement in outcomes. In back surgery, for example, we still see cases of 20–40% failure rates. Also, 20% of patients are still dissatisfied with their total knee replacements, and we know that outcomes vary among centers, both in terms of productivity and clinical outcomes: surgeons who perform greater numbers of a given surgery tend to lean towards better outcomes. Our analysis shows that what drives outcomes is more than just the technology, implants and instrumentation. So we use the need to drive outcomes as a starting point.
What does drive those outcomes in the orthopedic arena, seen from DePuy Synthes’ angle?
We think there are three pools of activ-ity that drive outcomes. The first is cer-tainly technology, and as a company we always aim for the best possible implant quality and instrumentation. Surgical techniques also make a difference. And then the patients themselves can make a difference. Patients can influence out-comes from the point of patient selection and patient preparedness, in areas such
as body mass index (BMI) and lifestyle habits (smoking, alcohol consump-tion), which can also influence time to recovery. Our feeling is that all three pools of activity must be addressed. So taking a step back, we think that the role of robotic technology is to support the two areas that are not addressed by the implant and instrumentation technolo-gies. Firstly, it is an attempt across the board to address human factors relating to surgical techniques. Robots are there to improve the manual dexterity of the surgeon and move toward more consis-tent and potentially better outcomes. And secondly, we’ve designed what we call Digital Surgery, for the entire continuum of care, which both includes and goes beyond robotics to monitor pa-tients, help physicians with pre-surgery patient assessments and guide patients through rehab. And outside the operating room, there are other technologies that can help maintain optimum standards of care during the operative procedure, which include surgery standardization technologies like that of the SPI (Surgical Process Institute), as an example.
The purchase of SPI predated Or-thotaxy. How does it fit into the plan?
SPI provides a digital checklist that guides not just the surgeon but the whole team through surgical procedures. Surgeons who use the same OR team con-sistently tend to achieve better outcomes – regardless of who is on the team. By
JOHNSON & JOHNSON’S DEPUY SYNTHES ORTHOPEDIC BUSINESS HAS TAKEN A MEASURED
VIEW OF DIGITAL AND ROBOTIC CAPABILITIES, RATHER THAN ACQUIRING ASSETS THAT
PERHAPS DO NOT FULLY MEET ITS STRATEGIC NEEDS. FOR THE BUSINESS’ GLOBAL R&D
HEAD EUAN THOMSON, ANY NEW TECHNOLOGY MUST AUGMENT THE GROUP’S ABILITIES
TO DRIVE MEANINGFUL OUTCOMES.

10 | In Vivo | July/August 2018 pharmamedtechbi.cominvi
vo.p
harm
aint
ellig
ence
.info
rma.
com
❚ REVIEWING ROBOTICS
doing the right thing at the right time, they are supporting the surgeon who is thus also able to do the right thing at the right time, meaning that efficiency and clinical outcomes will be optimized. And it supports our strategic vision, which is not simply to chase the latest and brightest technologies, but rather to use technology to drive, improve and optimize outcomes.
At what point did DePuy Synthes fully adopt the outcomes and value-based approach to patient care, and what were the catalysts for that change in thinking?
It’s been an evolution, and the ideas have been solidifying over several years, but in the past year or so we’ve really rolled up our sleeves on this. I have two roles – leading R&D for DePuy Synthes and also co-leading R&D for all of John-son & Johnson Medical Devices, par-ticularly in digital technologies. Our R&D organization is setting up a dedicated digital technologies team to address all areas – this is the team that is building the Orthotaxy robotics system. We also have partnerships and internal builds in place to address patient monitoring – those individuals will coordinate that activity within and for SPI, and for other solutions such as C-SATS, a University of Washington spin-out that uses technol-ogy to facilitate performance reviews for surgeons, which we acquired recently. That company does a review of video gathered in the OR, for educational pur-poses. They segment it into stages, crowd source a review of each video segment and give feedback to the surgeon on dif-ferences in what’s observed in the videos compared with standard-of-care type vid-eos. They have started with laparoscopy. The idea is that feedback is used by the surgeon as learning as they go along. It’s part of the same digital and robotics initiative, which has all come together within the last 12 months.
Some orthopedics stakeholders view robotics as cumbersome and not fast enough, but now that DePuy Synthes’ strategy is coming together, how is Orthotaxy different?
We took our time looking at robotics. It’s a field where it is arguably very easy
to succeed – robots appeal to patients’ needs and very often, robotics are ac-quired on the back of a tick-box mentality. They are marketed to the outside world as guaranteeing improvement of procedure quality. I’m not convinced by that. What we were looking for in robotics was some-thing that really would move the needle in terms of outcomes, without interrupt-ing workflow or adding to the complexity of a procedure. We see large, cumbersome systems in the million-dollar range that have to be wheeled in the OR for each pro-cedure, get in the surgeon’s way and very often require support from a dedicated team to enable the surgeon to operate it. We didn’t want to go in that direction. When we found the Orthotaxy system, we believe we saw a very different type of robot – a platform, rather than a sys-tem. (Also see “J&J Adds To Robotic Focus With French Firm Acquisition” - Medtech Insight, February 22, 2018.) It is a small, almost portable system that can be lifted by the surgeon, maneuvered into position and held there with a support arm. It has a navigation component, which refreshes images 300 times a second and automati-cally adjusts position to compensate for motions by the surgeon or the patient. The concept can be applied to different techniques: in the field of total knee replacement, the end effector is a guide system that is continually adjusting the guide block, with the surgeon remaining in control and using the saw through the guide block. The surgeon is doing the cut, but the accuracy is being controlled by the robotic alignment assisted by the continuously updating Orthotaxy system. In spine procedures, the saw guide block would be replaced with a drill guide component – the system refreshed in the same way for, say pedicle screws, to continuously guide alignment. It’s a modular concept. It doesn’t get in the way of workflows. We’ve found it easy to use, intuitive and extremely accurate. This is what we feel is the future.
Is keeping the surgeon in control of the orthopedic procedure, rather than be-ing led by the robotic technology, a key element of the DePuy Synthes offering?
This is a total orthopedics platform. The difference between this and other platforms is that the technology doesn’t
dominate the whole procedure, so you’re not doing a robotic procedure, but a procedure that includes robotics. There could be segments of any procedure – hip, shoulder, etc. – that would incor-porate robotics. But the capabilities of the easy-to-move-around, versatile and modular technology from Orthotaxy give it huge potential. One of our guiding principles is that surgeons should have their own workflow, and the robot should fit into that. We believe that procedures incorporating the Orthotaxy system will be faster than others. I don’t think any other systems can make that claim. We also believe that this is a unique platform, and that when we bring it to market, it will significantly disrupt the existing robotics platforms. So our vision for implementation is that robotics is one piece of the answer. We’re aiming for a 2020 “market ready” for this technol-ogy, for one or more procedures, which is pretty ambitious, but we feel achiev-able. By the time we get there, we want to have operating rooms ready to receive it and for other digital technologies that we already have – like SPI – to also be in place. SPI has already defined a proce-dure to ensure the team uses the robotic platform in the optimum way.
What are the remaining parts of the puzzle DePuy Synthes needs to com-plete a holistic digital orthopedic of-fering in the operating room?
We have big initiatives around patient engagement and monitoring. Patients are strong influencers on outcomes. Most of the outcome measures we use today are surgical outcome measures that the surgeons can visualize from the data pre-sented to them. But there is a broader vi-sion that includes the patient perception of outcome. Patients are looking for “hu-man things” – day-to-day functions like being able to move without discomfort. These are elements that drive outcomes in their minds, not parameters such as radiographic healing. Today, the indus-try is only very loosely connected with that, and there is room for improvement there. Orthopedics is about mobility, and mobility determines lifestyle. We have to get inside mobility and lifestyle to under-stand the success or failure of a procedure from a patient’s perspective. And also to

©2017 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 11
REVIEWING ROBOTICS ❚invivo.pharm
aintelligence.informa.com
think about real-world outcomes as they are viewed by patients. Our initiative to find ways of quantifying and monitoring such things is at an early stage, but we can use the existing connected digital platform, Johnson & Johnson Health Partner [currently available in the US], which taps into patients’ motivations and their underlying drive to get and stay healthy as they recover from knee, hip or weight loss surgery. Or help them prepare physically, mentally and emotionally for surgery and their customized, real-time care that becomes personalized over time. This in turn helps us gather infor-mation about outcomes, and we aim to supplement it by using automated ways of assessing lifestyle and motion.
In EMEA, as part of the CareAdvantage value-based approach, the company offers the Care4Today patient pathway solution (also see “The Tailor Will See You Now – J&J’s EMEA VP Explains Total Care Partnership For Hospital Systems” - In Vivo, February 2018). This includes the Orthopedic Program that provides hospitals and patients with resources to ensure consistent, coordinated care while supporting patients to take control of their own treatment and recovery. Patients, for the most part, want to do the right thing; where we can make a difference is in acknowledging that the “right thing” tends to be personalized, rather than generic. For example, helping them to understand the fundamental im-portance of adhering to their post-surgery rehabilitation protocol can really make a difference in terms of outcomes.
The role as a provider of technol-ogy has changed and companies like DePuy Synthes are now offering more of a package of services.
That’s what we’re moving toward. All the basic elements are in place today: this is no pipe dream or future vision, as we already have a continuum and are now working on enhancing that. We have Health Partner for monitoring patients (set up for the US in November 2017), Care4Today, used by the European team and a software planning system that can calculate the optimum cutting angle for a knee replacement. We have SPI for guiding the team and organizing the workflow, to ensure efficient and ef-
fective team flow during the procedure itself, and post care monitoring. We be-lieve Orthotaxy will be a game-changer, as we believe it is a truly different con-cept in that it is a modular system that integrates itself with the workflow and maintains and improves the quality of the procedure. We’re focused on ortho-pedics, but this digital surgery concept applies to all surgery in different ways. Outcomes and the broad-based ap-proach is what is guiding DePuy Synthes right now. But looking forward five to 10 years, we will be integrated much more into the Internet of Things (IoT) world, and the sensing of patients’ lifestyles becomes more based on passive sen-sors that we use in our everyday life, as opposed to active sensors, like apps and wearables. Many household items will ultimately be a sensor of some sort, observing behaviors and piecing together information that can help build a picture of a person’s well-being, diet, work patterns, exercise routines, and, in fact, all things that have an impact on health care. That will help us un-derstand what makes the difference in terms of outcomes, over time, and across all surgeries. In the OR, other technolo-gies will come to bear, even though we are not convinced that they are ready to be used for anything other than educa-tion yet. Virtual reality and augmented reality will find their way into the OR, but there are a number of steps needed before they can safely add value.
On the theme of value, can you define what value digital and robotic offer-ings like yours will bring to providers?
SPI has evidence to show that its tech-nology significantly reduces OR times and can increase the capacity of the OR, which is clearly a driver in the public and private sectors, simply by making sure that the right equipment is in the room before the procedure starts. And the OR team follows an optimized workflow. It’s a system that provides a learning tool: as the team goes through each step of the procedure, it can be analyzed to see where optimization is both possible and needed. This system sits on the same data platform as another system that monitors patients and tracks how fast each patient returns to full mobility, and
To underline what
drives our strategy,
our technologies
today are a platform
into which robotics
fit – our ambition is
to explain that to
the world.
– Dr. Euan Thomson,
DePuy Synthes Global
Head R&D

12 | In Vivo | July/August 2018 pharmamedtechbi.cominvi
vo.p
harm
aint
ellig
ence
.info
rma.
com
❚ REVIEWING ROBOTICS
there is the ability to link the two. It is the beginnings of a vast data platform across all procedures, and that’s where the new insights, AI and machine learning come into play, as we transition from effective monitoring and analysis into an environ-ment where we can give more real-time guidance about procedures.
Will non-digital technologies also be able to play into this environment?
We now have a relentless focus on automation and bringing technologies to health care systems that add value, and are not just marketing tools. The ME1000 Surgical Impacter [currently only available in the US, and later in
other countries] that we recently acquired from Medical Enterprises Distribution is a classic example of a great technology that automates steps in joint replacement and aims to increase efficiency and accuracy while reducing surgeon fatigue. There is potential to combine the ME1000 and robotic technologies that could reduce the time for performing some surgical procedures by up to 30%, clearly adding value to both the patient and our health care customers. As Johnson & Johnson is the largest health care group in the world, we have access to a huge network of clin-ics. In this era of intelligent solutions and data gathering, we find ourselves in a strong position and able to differentiate
ourselves from any of our competitors. In my mind, it’s time-to-data, which means time-to-insight. It is important for us to keep focused, get these technologies to market and make sure we bring them together in an intelligent way so that they optimize care. If we do that, we’ll be in an almost unassailable position.
It seems that DePuy Synthes has found the angle it wishes to exploit in the digitally enabled and robotic OR spaces of the future.
We’ve identified our role and strategy in the digital space, and our strategy is well evolved. Our robotics fit into the digitization of the surgical process. But
❚DEPUY SYNTHES’ MEASURED PATH TO BUILDING A DIGITAL SURGERY CAPABILITY
Bringing together the various assets and capabilities of Johnson & Johnson’s DePuy Synthes orthopedic division will be a challenge, but it is one that global head of R&D Euan Thomson, PhD, relishes, especially now that the key elements have been brought into the group.
The key “game-changer” for orthopedics, as Thomson de-scribed in an interview with In Vivo, was the February 2018 purchase of Orthotaxy SAS’ robotic-assisted solution that will bring a next-generation robotics technology to market.
With that acquisition, the company will continue the devel-opment of the differentiated robotic-assisted tool first for total and partial knee replacement, and later for multiple ortho-pedic surgery procedures, such as spinal fusion surgery. The terms were not disclosed, but the purchase was significant in terms of giving DePuy Synthes the central technology it needed to participate in orthopedic robotic surgery, bearing in mind Stryker Corp.’s Mako, Smith & Nephew PLC’s Navio surgical system (from Blue Belt Technologies Inc.) and Zimmer Biomet Holdings Inc.’s ongoing work on its Rosa platform. The X-ray based Rosa is scheduled for limited launch in the second half of 2018, the company having completed a fully functional demo for knee application. In spine, Medtronic and Israel-based Mazor Robotics Ltd entered into a strategic agreement in May 2016.
TARGETING PERSONALIZED ORTHOPEDIC PATIENT CAREDePuy Synthes’ idea is to use it as part of a holistic approach to orthopedic surgery across the episode of care to enhance surgi-cal efficiency, promote better clinical outcomes and increase patient satisfaction. Orthotaxy’s technology will be a critical part of a complete solution that uses enabling technologies to personalize orthopedic patient care, optimize surgery, and bring value to customers and patients, says DePuy Synthes.
The platform enables the use of innovative solutions, which include surgical planning software and patient-specific sur-gical guides. In turn, surgeons can plan implant placements on preoperative CT or MRI images. The system also includes guides designed to fit patients’ anatomies, help insert surgi-cal instruments, and perform surgery in accordance with a planned strategy.
Orthotaxy, a simplified joint-stock company, was founded by Stéphane Lavallée, a robotics entrepreneur, and is based in La Tronche, Grenoble. Its R&D is now being done by a “distributed effort,” says Thomson, but the Orthotaxy R&D team stays in France, while DePuy Synthes has also started to build up the team in the US to support its work.
The surgical procedures and release timings are not being disclosed, but as Jefferies equity research managing director Ray Denhoy tells In Vivo, DePuy Synthes now has “a dog in the fight” in orthopedic robotics.
In a period of intense focus on building out its robotic capa-bility, DePuy Synthes kept the momentum going with the mid-April 2018 acquisition of C-SATS (Crowd-Sourced Assessment of Technical Skills), a Seattle, WA-based start-up that uses technology to facilitate performance reviews for surgeons.
Founded in 2014 and spun out of the University of Wash-ington, C-SATS has built a cloud-based performance manage-ment system that evaluates surgeons and helps improve their skills. It uses operating room cameras to record a surgeon’s performance, and is seen as a scalable platform powered by data capture, analytics and artificial intelligence.
C-SATS’ technology will be integrated into the Johnson & Johnson Institute education and training platform. It will enable J&J to partner with health care systems in a differenti-ated way and change how surgeons learn by allowing them to anonymously receive input on actual cases to improve their

©2017 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 13
REVIEWING ROBOTICS ❚invivo.pharm
aintelligence.informa.com
technical skills. The notion goes that internal peer reviews can be open to bias. C-SATS’ CEO is Derek Streat.
Predating both of these and helping to build out the horizons for both what is possible and what is DePuy Synthes’ preferred route in robotic assisted surgery was the October 2017 purchase by Johnson & Johnson Medical GmbH of Germany-based software company Surgical Process Institute (SPI). SPI specializes in the standardization and digitalization of surgical workflows in the operating room, and provides innovative software solutions to improve pa-tient outcomes and OR efficiency by reducing variability in surgical procedures.
Thomson’s view is that successful surgery is dependent not only on surgeon performance, but also on many steps during a procedure with diverse surgical teams that have to work seamlessly together.
SPI stole a march on the competition with its Surgical
Procedure Manager (SPM) proprietary software solution, which standardizes surgery by translating the whole surgical experience into a detailed, step-by-step checklist that follows best-in-class standards. Gunter Trojandt is managing direc-tor of SPI. The group’s technology is available in the EMEA region, with full worldwide availability targeted for 2019.
These digital capabilities were acquired within an intense seven-month period from October 2017 to April 2018. Two and a half years earlier, in March 2015, Johnson & Johnson and Google set up the joint venture for development of a next-generation surgical robotic system, which in Decem-ber 2015 was named Verb Surgical. Verb Surgical CEO Scott Huennekens shares Thomson’s assertion that robots should be just part of a platform for digital surgery, among many other factors.IV005368
� Hips � Knees
� Trauma
� Spine & Other
DePuy Synthes
Sales In 2017 ($m) Except Where Indicated
� Hips � Knees
� Trauma & Extremities
� Sports Medicine
� Arthroscopic Tech
Smith & Nephew
� Hips � Knees
� Trauma & Extremities
� Spine � Neurotech
� Other Ortho
Stryker
� Hips � Knees
� Surgical, Extremities, Trauma
� Spine & CMF
� Dental � Other
Zimmer Biomet
� Spine
Medtronic Spine Sales
3,725
2,616
1,523
1,394 1,303
1,595 1,709
759
2,737 2,668
1,879
1,478
751
1,423
321419
599615
627
495
984
337(Fiscal 2018 $m)
there are always ways of improving, as technology evolves. Looking to Verb Surgical, its value is that it cuts across all J&J’s medical devices. (Also see “Exec Chat: How Verb Surgical Will Deliver On Surgery 4.0” - Medtech Insight, Novo-vember 14, 2017.) It has made significant progress over recent years, and our job is to make sure we can synchronize it with other tools like C-SATS, SPI and our broader surgical vision. So, when we bring a best-in-class surgical robot to the market, it’s in a best-in-class system that optimizes outcomes. Right now, the priority is to communicate to the orthopedic market, but our vision goes beyond robotics. For us, it’s a relent-
less focus on outcomes, clinical benefit and optimizing value for patients. To underline what drives our strategy, our technologies today are a platform into which robotics fit. Our ambition is to ex-plain that to the world, and get partners to engage with us on that journey. We’ve had some strong responses so far. IV005367
Comments: Email the author: [email protected]
Intuitive Sets Pace In A Robotics Segment Where Ortho Players
Are Finding Their Feet
Patients are keen on new technologies, but Jefferies Healthcare equity analyst Raj Denhoy, says it is not a done deal for health care robotics just yet.
https://bit.ly/2mEC8Uq
READ MORE ONLINE

14 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ ONCOLOGY INNOVATIONin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
The arrival of immunotherapy as a fourth weapon in the armamentarium against cancer – following on the traditional mainstays of surgery, chemo-therapy and radiation – has brought fresh attention to the role that vaccines can play in stimulating the body’s natural defenses against the abnormal cell growth that leads to malignancies. Vaccines are currently in limited
use to prevent viral-based cancers like HPV, but the real promise lies in their potential in treating and fighting recurrence for patients already diagnosed with the disease. And industry interest in this platform is mounting, as evidenced by the nearly 400 therapeutic vaccine trials for cancers reported from industry, academia and govern-ment through the clinicaltrials.gov website.
Vaccinology as a tool to treat cancer is not a new concept. Vaccines complement the immune response and have broad appeal because of their ease of administration and lack of significant side effects. Research dating back to the early 1950s proved a higher incidence of malignant tumors in mice that presented with a weak or compromised im-mune system compared to those with a normal immune response. This was buttressed by detection of an inherent “immunological surveillance mechanism,” whereby the immune system can be stimulated to recall prior invasive cell activity to better target and enhance the potency of its response to a new tumor threat.
It was not lost on researchers that this is precisely what a vaccine does in inducing immunity against a much wider circle of pathogens. The problem in cancer, however, is the complexity and heterogenicity of cancer cell expression, whose very raison d’etre is to suppress immunity while also making it hard to identify a single uniform pathway to activate the immune system against a growing tumor. Because cancer cells evolve from a patient’s own healthy cells – and much is still unknown about that process –
Cancer Vaccines: Is There A Future Beyond Trial And Error?
Strong foundational research in immunology and some promising early phase trial results have so far failed to expedite the validation of vaccines to treat cancer. In Vivo examines biopharma’s enduring optimism about the future of cancer vaccinology, including a closer look at one company’s platform to tackle the incurable malignancies that beset the mother of all organs: the human brain.
BY WILLIAM LOONEY
A substantive academic presence in cancer vaccines research makes for more candor in highlighting the challenges of fighting the adaptive heterogeneity of cancer’s defense mechanisms – and to do so on a uniquely personalized basis.
Immunomic Therapeutics Inc. is an example of how biotech has leveraged ties to academia, resulting in a novel nucleic acid vaccine platform, UNITE, that holds promise against hard to treat cancers like glioblastoma.
So what? The big question - which no one yet has the answer to - is which of the many immunologic vaccine approaches has the best chance of producing breakthrough results. Clinical evidence is still scant, as most relevant trials are in Phase I.

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 15
ONCOLOGY INNOVATION ❚invivo.pharm
aintelligence.informa.com
they have a leg up in escaping detection. And the antigens that signal the presence of a malignancy to the immune system’s frontline of T-cells are multiple, diverse and endlessly adaptable. This reduces the ability of the T-cells to consistently carry out their task to recognize, bind and destroy.
Dr. Catherine Wu, a leader in cancer vaccine research with affiliations to the Dana-Farber Cancer Institute (DFCI), the Broad Institute and Harvard Medical School, notes that researchers face com-plexities in designing even the simplest vaccines – but the challenge has been compounded in applying the process to cancers. Says Wu, “a lot of juggling is involved in identifying the specific antigen to target, figuring the optimal way to deliver the vaccine and selecting an appropriate immuno-stimulatory adjuvant, while all the time working around the negative immuno-resistance space that tumors create around them, allowing malignant cells to proliferate unchecked.”
However, Wu and many other cancer researchers interviewed by In Vivo be-lieve that the fallow period in vaccines discovery may finally be coming to an end, for two reasons. The first is improved understanding of how to target a critical immunologic defense mechanism, the PD-1 checkpoint blockade, that attaches and neutralizes a crucial protein that can-cer cells rely on to confuse and counter at-tacks from the immune system’s “helper” T-cells. This led, in 2014, to FDA approval of the first two drugs – Keytruda (pembro-luzimab) and Opdivo (nivolumab) – in a new therapy class known as checkpoint inhibitors. These genetically advanced biologic drugs are designed to dismantle the cancer cell defense and allow T-cells to recognize and unleash their payloads on cancer cells.
The second is the steady expansion over the past decade in the ability to sequence the genetic profile of an indi-vidual patient, including accurate map-ping of cancerous growths and tumor samples, rapidly and at much lower cost. “This has opened the door to us finding better antigens to target, reducing what has been a major barrier to the design of vaccines that could be efficacious against an individual’s specific disease profile,”
said Wu. “It’s confirmatory of the promise of personalized medicine because, with sequencing, we can systematically iden-tify the mutations that make each cancer case unique and provide a computational assessment of which mutations have the most potential in stimulating an individu-al immune response.” Combined, the ad-vances have revived the entire innovative industry’s interest in the immunologic potential of therapeutic cancer vaccines, with sequencing reinforced by the wider understanding of cancer’s underlying biology through the checkpoint blockade therapy response.
Dr. Wu’s optimism is not misplaced, given that her own work on therapeutic vaccines conducted at Dana-Farber has shown promise in boosting immune response in post-surgical melanoma patients deemed to be at high risk of relapse. In a July 2017 paper published in Nature, her team from DFCI and the Broad Institute revealed results of a Phase I proof-of-principle trial on a neo-antigen based vaccine, NeoVax, in a small cohort of six melanoma patients. Four of the six evidenced expanded regular neo-antigen specific T-cell populations along with a broader repertoire of new T-cell specifications, resulting in enhanced
tumor control leading to no recurrence of melanoma 25 months after vaccination. The other two study patients with recur-rent melanoma received the anti-PD-1 checkpoint inhibitor pembroluzimab, in addition to NeoVax, resulting in complete tumor regression.
“The study confirms the merits of much of what we hope to gain from a therapeu-tic cancer vaccine, which is the ability to stimulate beneficial sub-types of T-cells that can work collaboratively to eliminate tumors,” Wu said. “If a therapeutic vac-cine platform is to succeed, you must be able to mobilize all these beneficial actors for a single-minded assault on the cancer.”
Wu’s group at DFCI will continue to em-phasize small path-finding foundational research initiatives, including a study now commencing to improve predictive computational algorithms that can bet-ter identify neo-antigens most likely to generate an escalating immune system response. “As an academic, we are well-positioned to test hypotheses and learn the deep biology and mechanisms under-lying effective human immune responses. We expect our data to help guide drug developers toward the most efficacious vaccine platform, one with maximum potency and minimal side effects. Im-munotherapy as a treatment modality in cancer has now come of age. With so much activity in this space it mandates academia and industry to partner and work even more closely together.”
The important thing is that money continues to flow toward cancer vaccine therapeutics, which benefits as a side-bar to the sustained R&D frenzy around immuno-oncology in general. The VC community remains bullish on long-term prospects for cancer vaccines – more importantly, so too does big pharma, which has inked a number of collabora-tion deals with leading-edge biotechs like Advaxis Inc. (with Amgen Inc.), Moderna Therapeutics LLC (Merck & Co. Inc.), BioNTech AG (Roche/Genen-tech), CureVac AG (Eli Lilly & Co.), Neon Therapeutics Inc. (Bristol-Myers Squibb Co.) and Transgene (Merck Serono SA). An In Vivo round-up of clinical trials (see Exhibit 1) at the active recruiting stage indicates the extent of such contacts, along with evidence that the trial process
It’s hard to beat the potential of therapeutic cancer vaccines – a personalized treatment that is sustainable and efficacious over time, with minimal side effects and relative ease of administration.
Les Funtleyder

16 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ ONCOLOGY INNOVATIONin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
overall is nascent. With most studies at Phase I, sponsors are unlikely to be able to deliver meaningful data that resonates with patients, regulators – and payers – until well into the next decade.
Yet the underlying science is so prom-ising, the payoff – if and when it occurs – should be enough to satiate the pessi-mists. “It’s hard to beat the potential of therapeutic cancer vaccines – a person-alized treatment that is sustainable and
efficacious over time, with minimal side effects and relative ease of administra-tion,” said Les Funtleyder, health care portfolio manager for E Squared Capital Management and a member of In Vivo’s Editorial Advisory Board.
Building A Vaccines Business: The Calculus Of Chance Given the long legacy of failure in tar-geting vaccines as a treatment pathway
for cancer, it is important to underscore how new science, entrepreneurial drive, and unconventional, cross-disciplinary partnerships are contributing to current clinical progress in this field. A case in point is Immunomic Therapeutics, a privately held start-up founded in 2005 and focused on gene-based antigen vac-cines against hard to treat cancers like glioblastoma. That it exists today is due to an informal encounter several decades
Exhibit 1. Therapeutic Cancer Vaccines In Active Clinical Trials
TITLE INDICATION/PHASE COMPLETION DATEAdvaxis with Amgen
Expressing personalized tumor antigens study Metastatic colon cancer, metastatic head and neck cancer, metastatic NSCLC/Phase I
September 2020
Advaxis with Merck & Co.
ADXS3 1-142 alone and in combination with Pembrolizumab (MK-3475) in patients with prostate cancer KEYNOTE-046
Prostate cancer/Phase II December 2019
AstraZeneca Adjuvant PVX-410 vaccine and Durvalumab in Stage II/III triple-negative breast cancer
Breast Cancer/Phase I August 2022
Bioven Europe Safety & efficacy of EGF vaccine in Stage IV Biomarker Positive Wild-Type EGF-R NSCLC
NSCLC/Phase III March 2020
BioNTech with Genentech
PCV RO7198457 as single agent and in combination with Atezolizumab in patients with locally advanced or metastatic tumors
Various solid cancers/Phase I October 2020
Bristol-Myers Squibb
Neo-antigen DNA vaccine with Nivolumab/Ipilimumab and PROSTVAC in metastatic hormone-sensitive prostate cancer
Metastatic, hormone-sensitive prostate cancer/Phase I
August 2023
Bristol-Myers Squibb
CRS-207, Nivolumab, and Ipilimumab, with or without GVAX pancreas vaccine in patients with pancreatic cancer
Pancreatic cancer/Phase II October 2019
CureVac Intratumoral CV8102 in cMEL, cSCC, hnSCC and ACC
Melanoma, Squamous cell skin carcinoma, Squamous cell and carcinoma of head and neck, Adenoid cystic carcinoma/Phase I
December 2019
CureVac Combination immuno-therapy and mRNA vaccine in NSCLC
Metastatic NSCLC/Phase I and II December 2024
Genentech/Roche Atezolizumab in combination with a personalized vaccine in urothelial cancer
Urothelial, bladder cancer/Phase I April 2020
Immunomic Therapeutics
Vaccine therapy for newly diagnosed Glioblastoma multiforme
Glioblastoma multiforme, malignant Glioma, Grade IV Astrocytoma/Phase II
June 2024
Inovio Pharmaceuticals
Vaccine + Durvalumab in Human Papilloma Virus (HPV) cancers
HPV, male and female genital organs/Phase II
January 2021
MabVax Therapeutics
177Lu human monoclonal antibody 5B1 (MVT-1075) in combination with a blocking dose of MVT-5873 as radioimmunotherapy
Pancreatic carcinoma tumors that express CA 19-9/Phase I
December 2019
Medimmune Neoantigen DNA vaccine alone vs. neoantigen DNA vaccine plus Durvalumab in triple negative breast cancer following standard of care therapy
Triple negative breast cancer/Phase I
March 2021

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 17
ONCOLOGY INNOVATION ❚invivo.pharm
aintelligence.informa.com
ago between its founder and CEO, Dr. Bill Hearl, a bench scientist, inventor and early biotech entrepreneur, and Dr. Tom August, a professor of pharmacology and molecular science at the Johns-Hopkins Medical School.
At the time, the two were among around 10 researchers interested in ways genetic immunotherapy could mobilize powerful antigen-presenting cells against invasive pathogens like viruses and allergens or
even cancerous tumors. Hearl, in an in-terview with In Vivo, said “We were both drawn to the fact that cell-based antigens and antibodies were not being effectively sequenced and deployed to attack these invasive threats – a lost opportunity in im-munization. What was needed was a spe-cialized, ‘professional’ antigen-presenting cellular cohort to amplify the response to an invasive threat by teaching ‘amateur’ (i.e. helper) immune cells to improve their
disease targeting and containment capa-bilities. This concentrated set of weaponry could form the basis for a more structured, sustainable and safe immune response in the individual patient.”
As it turned out, August had already established a pathway toward this goal through his Johns-Hopkins research on protein structures, which in 1985 led to the discovery of the lysosome-associated membrane protein (LAMP).
Exhibit 1. Therapeutic Cancer Vaccines In Active Clinical Trials
TITLE INDICATION/PHASE COMPLETION DATEMerck & Co. PVX-410 vaccine plus Pembrolizumab in HLA-A2+
metastatic triple negative breast cancerTriple negative breast cancer, metastatic breast cancer/Phase I
December 2024
Moderna Therapeutics with Merck & Co.
Safety, tolerability and immunogenicity of mRNA-4157 alone in subjects with re-selected solid tumors and in combination with Pembrolizumab in subjects with un-reselectable solid tumors
Solid tumors/Phase I March 2020
NantBioScience Quilt-2.025 NANT neoepitope yeast vaccine (YE-NEO-001): Adjuvant immunotherapy using a personalized neoepitope – based vaccine to induce T-cell responses in subjects with previously treated cancers
Colorectal cancer, triple-negative breast cancer, head and neck squamous cell carcinoma, melanoma, NSCLC, pancreatic cancer, liver cancer, hormone receptive positive tumor/Phase I
December 2020
Neon Therapeutics
Personalized neoantigen cancer vaccine with and without low-dose cyclophosphamide in treatment-naive asymptomatic patients with IGHV unmutated chronic lymphocytic leukemia
Lymphocytic leukemia/Phase I September 2023
Neon Therapeutics with Merck & Co.
Personal cancer vaccine (NEO-PV-01) with Pembrolizumab and chemotherapy for lung cancer
Lung cancer, NSCLC/Phase I February 2021
Neon Therapeutics with Bristol-Myers Squibb Co.
Personal cancer vaccine (NEO-PV-01) with Nivolumab for melanoma, lung or bladder cancer
Urinary and bladder cancer, melanoma, NSCLC, lung cancer/Phase I
December 2020
Pfizer Evaluate escalating doses of a vaccine-based immunotherapy regimen for prostate cancer
Prostatic neoplasms/Phase I March 2021
Sotio PPF Group DCVAC/OvCa added to first line carboplatin and paclitaxel in newly diagnosed epithelial ovarian carcinoma
Ovarian epithelial cancer/Phase II December 2023
Transgene with Merck KGaA
TG4001 and Avelumab in HPV16 positive R/M cancers and expansion cohort to oropharyngeal SCCHN
Head and neck squamous cell carcinoma (SCCHN), HPV positive oropharyngeal squamous cell carcinoma, HPV-related carcinoma/Phase Ib and II
May 2021
Transgene with Bristol-Myers Squibb
Efficacy and safety of first-line chemotherapy combined with TG4010 and Nivolumab in patients with advanced non-squamous NSCLC
NSCLC/Phase II May 2020
SOURCES: Trialtrove; clinicaltrials.gov

18 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ ONCOLOGY INNOVATIONin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
LAMP is a class of proteins with unique properties that facilitate the delivery of gatekeeper antigens to optimize the antibody response in fighting invaders. “When I looked at what Tom August had in LAMP, a light literally went on in my head. I realized this platform could help direct the histocompatibility complex of task-oriented, antigen-presenting cells – such as dendritic, macrophage and endothelial cells – to activate the immune system’s front-line of T-cells to identify and dispatch a malignantly transformed regular somatic cell, eliminating it as a threat to normal cells. LAMP has the potential to use the body’s natural bio-chemistry to help develop a complete immune response, aided by simplified vaccine design and delivery.”
August’s breakthrough thesis was com-pelling enough for Hearl to invite him to co-found a company together to pursue work on a new class of vaccine thera-pies, all driven by the LAMP platform. Hearl believed the greatest potential for this technology lay in oncology, a view reinforced by the discovery that LAMP had already been evaluated in studies in HPV at Johns Hopkins University and in clinical studies on several cancers – pros-tate, melanoma, acute myeloid leukemia and glioblastoma – conducted at Duke University, Emory University and by a research team at Brussels University in Belgium. It turned out that August had shared his LAMP research with them and several other academic labs but by 2005 had stopped promoting the work and lost touch with the recipients.
Nevertheless, according to Hearl, the fact that some of the research had been peer-reviewed and published demonstrated the clinical versatility of LAMP in address-ing not only cancer, but a wide variety of other conditions demanding an immune response, including potentially lucrative applications against common environmen-tal and food allergies. There was another lead-in from studies August conducted in his own lab at Johns-Hopkins on the HIV virus and pest-borne flavivirus infections like dengue and yellow fever. In all such cases, vaccines were the obvious and most efficacious delivery vehicle.
The first thing the new company did was to secure intellectual property rights in 2006 to August’s platform under the
trademark LAMP-Vax. To raise money, Hearl orchestrated an early sub-licensing deal for the LAMP-Vax platform with Geron Corp., a clinical-stage drug de-veloper applying LAMP-Vax to treatment for hematologic malignancies. “I have always believed that oncology held the most promise under the LAMP-Vax plat-form,” Hearl notes, “but the stumbling block was we lacked the means to raise the large sums of money required to do clinical studies in cancer. Hence we launched the new company by looking back to allergy vaccines, whose develop-ment costs were very inexpensive in com-parison to cancer yet still presented us with an attractive market opportunity.”
Immunomic progressed its work on allergens, resulting in an investigational vaccine to treat various tree pollens, including cupressus japonica, the most common tree-borne allergen in Japan. The efforts culminated in two licenses, including a landmark agreement in 2015 with Japan’s Astellas Pharma Inc., in which Immunomic granted Astellas global commercial rights to any product for human allergy diseases derived from the LAMP-Vax platform. Under terms of the deal, Immunomic received a $300 million up-front payment from Astellas as well as a 10% royalty on net sales of all future Astellas medicines for these dis-eases, including a Phase I trial program on peanut allergy. Most important, in addition to giving Immunomic access to a predictable revenue stream to fund future research, the company kept ownership rights to the LAMP-Vax platform for other disease applications – including cancer immunotherapy vaccines.
Hearl emphasizes the relationship with Astellas continues, with Immunomic retaining responsibility for manufacture of the Japanese red cedar pollen product now owned by Astellas. It also can receive another $55 million in milestone pay-ments from Astellas under the original deal. “We value it as an additional reve-nue-producing resource for Immunomic going forward, one that fuels our work in oncology and which most other early-stage biotech innovators don’t have.”
Clearly, the LAMP technology remains the centerpiece of Immunomic’s value proposition to the provider community, investors and patients. The emphasis,
however, has changed, from the early work in allergy to embrace therapeutic vaccines in immuno-oncology, and in-volving new science, patents, and other complementary tools and methods. “We are tackling much more, at the enter-prise level, in terms of our capacity to apply new knowledge and expertise,” says Hearl.
To reflect this evolution, the company has repositioned the LAMP platform under a new descriptive acronym called UNITE – the Universal Intracellular Targeted Expres-sion platform -- which management sees as an appropriate marker for Immunomic’s move to capture the immune-oncology vaccine space. “UNITE correctly describes what the company has built over the past decade, and signifies our move beyond the original LAMP design to a combination of intracellular and molecular biology meth-ods for enhanced MHC-II presentation, along with potent adjuvant and delivery technologies that result in a unified and complete immune system response. That’s why we now call it UNITE.”
Immunomic’s current agenda centers on development of a vaccine for newly diagnosed glioblastoma based on the UNITE platform. The other priority is building and growing a pipeline around other virally driven and neo-antigen based cancers.
The company is supporting a Phase II 150-patient trial – known as ATTAC-II – conducted by researchers from the University of Florida and Duke University (with funding from the National Cancer Institute) to determine if its investiga-tional dendritic cell vaccine (pp65+LAMP DC) is effective for treatment of glioblas-toma, when administered with standard of care chemotherapy and radiation. The randomized, blinded and placebo-controlled study intends to show that the vaccine will increase the effectiveness of the powerful immune-boosting dendritic cell by helping it educate those “helper” immune and cytotoxic T-cells to attack and neutralize the brain malignancy. In other words, by giving the pp65+LAMP DC vaccine as a shot under the skin, the immune system could be activated in a full-blown attack on the malignant tumor cells, while leaving normal cells alone.
“This is a long-term exercise, dating as far back as 2006, to establish the clini-

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 19
ONCOLOGY INNOVATION ❚invivo.pharm
aintelligence.informa.com
cal merits of our platform in advancing gene-based vaccine therapy against hard-to-treat cancers like glioblastoma,” said Immunomic’s SVP for R&D Dr. Teri Heiland in an interview with In Vivo. In addition to its academic partners at the University of Florida and Duke, Im-munomic has ties to small commercial partners like Annias Immunothera-peutics Inc., from which Immunomic obtained certain IP rights to enhance the LAMP-Vax platform. Heiland relates that the Duke researchers, in an earlier study dubbed ATTAC, demonstrated that a dendritic vaccine built around the proprietary LAMP-Vax platform, when combined with radiation and che-motherapy, could prolong survival for newly diagnosed glioblastoma patients. “While the ATTAC-II study seeks to es-tablish proof of concept for the dendritic cell-based immunotherapy approach in the clinic, my R&D team has developed an upgraded, direct nucleic acid based version of the vaccine that we plan to translate directly into clinical trials later in 2019,” Heiland said. Meanwhile, Hearl and Heiland expect a readout of prelimi-nary data from ATTAC-II in 2020 or 2021, with a final result due in 2024. There are also plans to launch another company-sponsored clinical study later this year designed to support proof-of-concept for the pp65+LAMP DC vaccine and validate the approach to manufacturing and com-mercialization.
From Many, One?Hearl is not worried about that lengthy timeline to commercialization of his principal asset, contending that everyone in the therapeutic cancer vaccine space shares an awareness of the extent of the scientific challenge. “It’s a function of resources – where I believe we are com-petitive with the rest of the trade – and the ability to differentiate in producing a genuine treatment advance, beyond the lab,” he says. While numerous other biotechs are involved in vaccine-based research directed at brain malignan-cies, Hearl insists the UNITE platform is precedent-setting because it engages all four standard elements of the immune response, including expedited activation of “helper” T-cells necessary to produce a prolonged attack on a cancerous growth.
“Solving for cancer from an immune system approach absolutely requires that global response, which in our asset is reinforced because UNITE supports delivery of an additional, upgraded cy-totoxic payload.”
In addition, UNITE mimics a key at-tribute of the standard vaccine – an immunological “memory.” This enables the immune system to recognize and ad-dress successive waves of malignant cell invaders, in much the same way that a tetanus shot can stop a pathogen intro-duced when you step on a nail, years after it was administered. “UNITE technology will know what the relevant antigen looks like and activate the T-cells to respond directly. It’s a very important piece of the puzzle – you want that strong initial wave of attack to shrink and disappear the tumor, but it’s also critical to have that immunological memory so that, if and when the cancer reappears, the immune system will quickly crank up without having to initiate an entire new course of treatment. It amounts to an ongoing enhanced process of immune system monitoring, although Hearl admits this is the also the intent behind other thera-peutic cancer vaccines being tested by competitors. “With the UNITE platform, the pieces of that puzzle just fit together better, in our view.”
UNITE is agnostic in terms of the dis-tinction that researchers sometimes make between DNA vaccines and those based on mRNA. “We are not constrained by the format of the nucleic acid – UNITE allows us to pursue any format we choose,” responds Hearl. “In fact, the vaccine we are currently testing for glioblastoma is an mRNA treatment.” The conclusion he drew was that Immunomic had the capability to compete – or partner – with any of the big players in cancer vaccine, including the segment’s acknowledged leader, Moderna Therapeutics, which focuses on the mRNA approach. “Each of our competitors, which, in addition to Moderna, must include our fellow pub-licly-traded biotechs Inovio, BioNTech, and Cure Vac, have had some biologic success,” Hearl notes. “In my view, this gives the entire science behind immuno-logic vaccines credibility and validation. Of course, we’d like to see them using our UNITE technology to stimulate the
best possible immune system response. But ultimately what’s most important for patients and society is to have that success in multiple areas – there are no boundaries on disease.”
Immunomic claims that early studies reliant on the platform showed signifi-cant improvement in survival compared to the normal 20-month course of glio-blastoma in patients, post diagnosis. While the small study population and focus on early stage cancer renders this research preliminary by nature, it nevertheless piqued Hearl’s interest in making glioblastoma the company’s first venture in the cancer vaccine space. In addition to the obvious medical need, Immunomic believes that a vaccine workable against glioblastoma – cancers of the brain are among the most difficult to treat – could serve as a model for addressing many other types of cancer going forward. “We intend to use this project to develop a strategy to identify what particular type of antigens might fit UNITE best, which is the essential step in expanding our anti-cancer portfolio beyond glioblastoma.” As CEO, Hearl has set this as a priority for the company over the next 12 to 24 months.
Overall, Immunomic is confident it inhabits some of the most fertile terrain in the expanding landscape of immuno-on-cology, with FDA approval of several ef-fective, personalized therapeutic cancer vaccines projected as a probability within the next decade. Hearl was particularly excited by the potential of vaccines in conjunction with combination therapies involving the many new checkpoint inhibitor drugs now becoming avail-able to clinicians. “There will be a next wave of checkpoint inhibitor drugs for use in combination with treatment vac-cines – thoughtful, individually tailored combinations of therapies that boost the capacity of the immune system to educate itself in finding and killing tumor cells,” he says. “We can finally say goodbye to the past of throwing everything against the wall and just seeing what sticks. Can-cer vaccines will be a real business – and a boon for patients.” IV005362
Comments: Email the author: [email protected]

20 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DISEASE ANALYSISin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
Nonalcoholic fatty liver disease (NAFLD) is a silent epidemic of the western world, reported to affect a quarter of the US population. Prevalence of this condition has exploded in the last two decades and continues to grow worldwide, triggered by a surge in obesity and other related risk factors. Despite the high prevalence and recent interest in the space, NAFLD is
still an emerging therapeutic area with incomplete scientific understanding and an evolving clinical care paradigm. Fortunately, the academic, medical and biopharma communities are actively engaged in addressing this emerging public health issue.
However, it is important to note that NAFLD represents a spectrum of disorders, en-compassing a broad range of severities. The milder form of the disease, nonalcoholic fatty liver (NAFL), accounts for the majority of NAFLD patients, with a prevalence of approximately 65 million in the US. As the name suggests, nonalcoholic fatty liver is characterized by steatosis, or excessive fat in the liver. Accumulated fat, in combina-tion with other factors such as insulin resistance, subjects the liver to metabolic and oxidative stress, triggering inflammation.
This inflammation marks the transition from NAFL to the more severe form of the disease, NASH, which affects approximately 15 million people in the US. In a 2017 BMC Medicine article, scientists described NASH as metabolic poisoning due to liver overload with glucose and fat. If the disease is not controlled at this stage, injured liver cells start dying and, in turn, switch on wound-healing processes to replace dead hepatocytes. However, if the underlying causes of NASH are not removed, natural repair mechanisms become dysregulated and lead to tissue scaring known as fibrosis, which can ultimately lead to complete loss of liver function (see Exhibit 1).
Given the lack of approved therapies, clinical management of NAFL and NASH relies
Nonalcoholic Steatohepatitis: Flying The Plane While Building It
Drug development for nonalcoholic steatohepatitis (NASH), a form of liver disease, is a game of incomplete information: pipeline evolution is occurring in parallel with continued efforts to better understand and manage the disease. To date, no therapy for patients with NASH has been approved and consequences of the condition can be severe, including cirrhosis and hepatocellular carcinoma.
BY AMAMA SADIQ, ILIYANA P. ATANASOVA AND KATHERINE J. FRANKLIN
Despite prolonged and costly development with many unique challenges, NASH research and development is attracting significant investment.
Efforts of developers currently pioneering the first wave of late-stage trials and continued investments in the understanding of the disease will drive the field forward.
So what? Strategic partnerships and cross-collaboration between biopharma, diagnostic companies, academic centers, and regulatory agencies may serve as a catalyst to accelerated development.

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 21
DISEASE ANALYSIS ❚invivo.pharm
aintelligence.informa.com
on diet and exercise, but is associated with poor compliance. Although asymp-tomatic in the early stages, patients are at risk for progression to serious complica-tions such as cirrhosis, liver failure, and hepatocellular carcinoma. In fact, NASH is projected to become the lead cause of liver transplant in the US by 2020.
Given the high prevalence and po-tentially severe consequences of the disease, NASH represents a substantial unmet medical need and a significant burden on healthcare systems. As a result, NASH has recently garnered tremendous interest and investment from the biopharmaceutical industry. Hundreds of pharma companies are engaged in the space, addressing the disease from numerous angles: dozens of mechanisms of action, hundreds of clinical trials, and thousands of patients are currently involved in building out this emerging therapeutic area (see Exhibit 2).
Even the most conservative analysts expect NASH to grow into a multi-billion-dollar opportunity. But devel-opers interested in capitalizing on this opportunity in the short-term are faced with significant roadblocks. The field is in its infancy – partly understood patho-physiology and natural history coupled with lack of non-invasive diagnostic/prognostic tools stand in the way of suc-cessful clinical development.
NASH Patients Not One Size Fits AllNASH is a complex disorder, character-ized by multiple distinct patient phe-notypes that have different outcomes and timelines of progression. This het-erogeneity poses a challenge to clinical development as the natural history of the disorder is not completely understood. Longitudinal studies demonstrate that only 10% to 20% of NASH patients end up with major liver complications such as cirrhosis or liver-related death. Dr. Raza Malik, assistant professor of medicine at Harvard Medical School and director of the Liver Failure Program at Beth Israel Deaconess Medical Center in Boston, ex-plained that figuring out how to identify the patients at risk was important not just for drug development but ultimately for clinical practice. “We need to know who is at risk for dire consequences to decide who to treat,” he noted.
Currently, researchers and physicians are unsure what differentiates the minor-ity of NASH patients who go on to develop serious liver complications from those who do not. Existing evidence suggests that the fibrosis stage is the strongest pre-dictor of liver transplantation and liver-related mortality. Severity of liver fibrosis (stage) in NASH is measured on a scale ranging from F0 to F4, where F0 denotes no fibrosis and F4 is the most severe stage known as cirrhosis. In the absence of
alternative markers for risk-stratification, this known correlation between fibrosis severity and long-term outcomes has focused clinical development on NASH patients with fibrosis rather than with earlier disease. But the interpatient vari-ability does not stop here; even fibrotic patients follow a heterogeneous course. Recent studies have highlighted that patients tend to fall into roughly three equal groups – progressors, regressors, and those with stable disease (see Exhibit 3). Rates of fibrosis progression also vary considerably – while on average it takes seven to 10 years for fibrosis to worsen by one stage, a fraction of patients prog-ress much more rapidly, stepping from no fibrosis to cirrhosis in as little as five years, as noted inthe 2015 paper Fibrosis Progression in Nonalcoholic Fatty Liver versus Nonalcoholic Steatohepatitis: A Systematic Review and Meta-analysis of Paired-Biopsy Studies.
Heterogeneity in the underlying etiol-ogy of NASH is likely one of the key fac-tors behind this diversity in prognosis and rate of progression. The current hypothesis is that NASH develops due to the interplay of distinct influences, including genetic predisposition and risk factors such as obesity, metabolic syn-drome (a cluster of abnormalities, such as hypertension, high blood sugar, and excess fat around the waist, leading to predisposition to cardiovascular disease
ObesityT2D
DyslipidemiaOther factors
Cirrhosis
Scar tissuereplaces livercells
~1-3M
Hepatocellularcarcinoma
Cancer
~70-200K
~80M people with NAFLD
}NASH
Fat plusinflammation,scarring
~15MUS prevalence
Fatty liver/NAFL
Fat accumulationonly
~65MUS prevalence
Exhibit 1Disease Progression And Epidemiology Of NAFLD
SOURCES: Willams et al., Gastroenterology 2011; Cohen et al., Science 2011; de Alwis et al., J of Hepatol 2008; Clarion Analysis
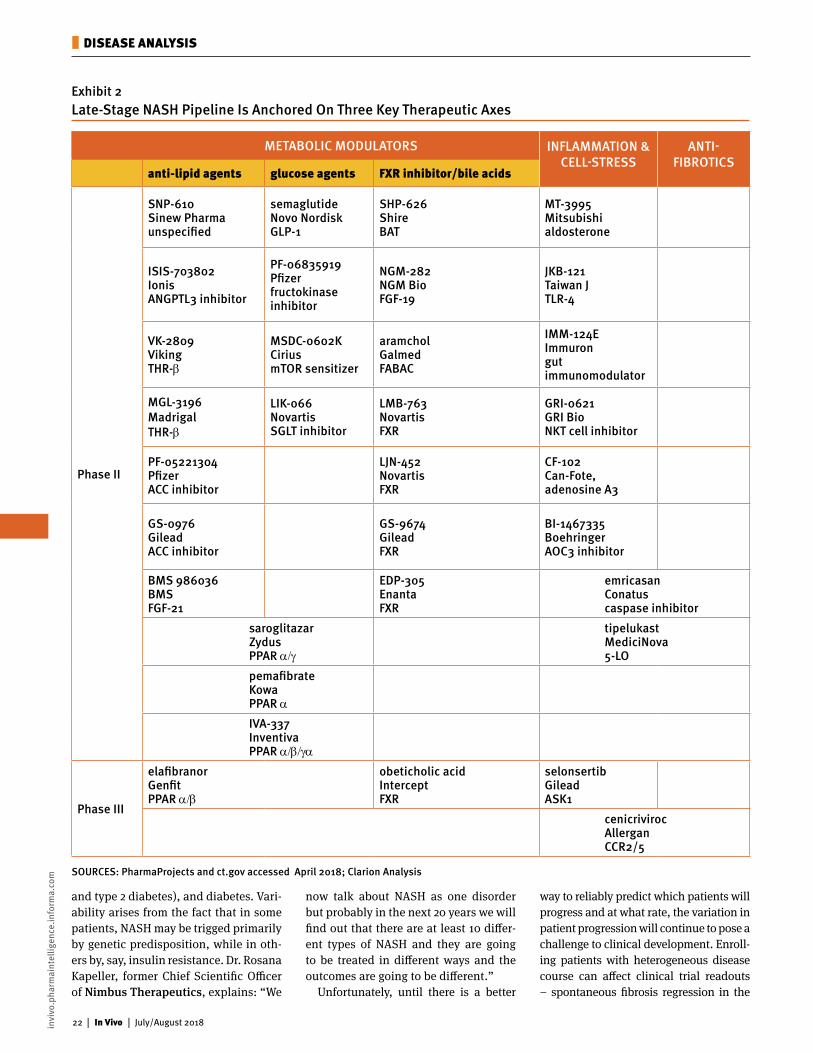
22 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DISEASE ANALYSISin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
and type 2 diabetes), and diabetes. Vari-ability arises from the fact that in some patients, NASH may be trigged primarily by genetic predisposition, while in oth-ers by, say, insulin resistance. Dr. Rosana Kapeller, former Chief Scientific Officer of Nimbus Therapeutics, explains: “We
now talk about NASH as one disorder but probably in the next 20 years we will find out that there are at least 10 differ-ent types of NASH and they are going to be treated in different ways and the outcomes are going to be different.”
Unfortunately, until there is a better
way to reliably predict which patients will progress and at what rate, the variation in patient progression will continue to pose a challenge to clinical development. Enroll-ing patients with heterogeneous disease course can affect clinical trial readouts – spontaneous fibrosis regression in the
Exhibit 2Late-Stage NASH Pipeline Is Anchored On Three Key Therapeutic Axes
SOURCES: PharmaProjects and ct.gov accessed April 2018; Clarion Analysis
METABOLIC MODULATORS INFLAMMATION & CELL-STRESS
ANTI- FIBROTICS
anti-lipid agents glucose agents FXR inhibitor/bile acids
Phase II
SNP-610 Sinew Pharma unspecified
semaglutideNovo Nordisk GLP-1
SHP-626 Shire BAT
MT-3995 Mitsubishi aldosterone
ISIS-703802 Ionis ANGPTL3 inhibitor
PF-06835919 Pfizer fructokinase inhibitor
NGM-282 NGM Bio FGF-19
JKB-121 Taiwan J TLR-4
VK-2809 Viking THR-β
MSDC-0602K Cirius mTOR sensitizer
aramchol Galmed FABAC
IMM-124E Immuron gut immunomodulator
MGL-3196 Madrigal THR-β
LIK-066Novartis SGLT inhibitor
LMB-763 Novartis FXR
GRI-0621 GRI Bio NKT cell inhibitor
PF-05221304 Pfizer ACC inhibitor
LJN-452 Novartis FXR
CF-102 Can-Fote, adenosine A3
GS-0976 Gilead ACC inhibitor
GS-9674 Gilead FXR
BI-1467335 Boehringer AOC3 inhibitor
BMS 986036 BMS FGF-21
EDP-305 Enanta FXR
emricasan Conatus caspase inhibitor
saroglitazar Zydus PPAR α/γ
tipelukast MediciNova 5-LO
pemafibrate Kowa PPAR α
IVA-337 Inventiva PPAR α/β/γα
Phase III
elafibranor Genfit PPAR α/β
obeticholic acid Intercept FXR
selonsertib Gilead ASK1
cenicriviroc Allergan CCR2/5

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 23
DISEASE ANALYSIS ❚invivo.pharm
aintelligence.informa.com
placebo arm of a study could obscure thera-peutic efficacy due to high placebo effects.
To fill the knowledge gaps around the natural history of NASH more expedi-tiously, drug developers can partner with academic institutions to conduct longitu-dinal observational studies. A real world example from a therapeutic area where this approach has made an impact is the Framingham Heart study – a multigenera-tional, observational study to understand cardiovascular disease. The study started in 1945, sparked by the death of US Presi-dent Franklin D. Roosevelt due to a heart condition. At the time, little was known about the causes of heart disease, so, in order to further understand the condition, President Harry Truman signed the Na-tional Heart Act allocating half a million dollars for research in the area. Interest-ingly, what was meant to be a 20-year epidemiological heart study continues to this day and has been critical in advanc-ing understanding of the disease and continues to guide clinical development.
Developers are currently making ef-forts to study NASH natural history in pivotal trials by, for example, enrolling a small number of patients with milder disease purely for exploratory purposes. Pooling data from all of the ongoing clini-cal trials will undoubtedly advance the understanding of how NASH develops and progresses. These learnings can be supplemented by sponsoring academic studies to study the real-world hetero-geneity of the disease, outside of the controlled environment of clinical trials.
The Case For Combination TreatmentNASH is not only heterogeneous in terms of its root causes but also in terms of the biological mechanisms driving progression – a complexity that must be accounted for when selecting a therapeutic approach. The progression of NASH is affected by a multitude of biological pathways that could be pursued as potential therapeutic targets. “Our understanding of the underly-ing pathophysiology is still evolving,” says Dr. Malik, “we know which pathways are involved but we don’t know the hierarchy of the pathways and their relative contribu-tions.” It is this biologic complexity, and the unanswered questions surrounding it, that likely explains the development of a large volume of pipeline agents with remarkably diverse targets.
Dr. Kapeller explains that “current in-vestigational approaches target three key axes – fat, inflammation, and fibrosis.” Some drugs aim to resolve metabolic issues, such as excess fat or insulin resis-tance, others target inflammation, and still others aim to chew up fibrotic scars. As NASH is complex and multifactorial, Dr. Kapeller anticipates that a single thera-peutic target will not be able to effectively manage NASH in all patients but she is hopeful that the ultimate solution to the disorder lies in combination approaches. According to Dr. Kapeller, “Targeting fi-brosis is not enough; I think you definitely need to target all three underlying mecha-nisms – fat, inflammation and fibrosis. We don’t know yet which approach is going to
be the most effective but I think you might have to hit all three axes equally.”
Indeed, the monotherapies in develop-ment are not effective in all patients. In trials, 10% to 20% of patients on placebo are responders compared to 30% to 50% of patients on investigational compounds – in other words, the drugs benefit only about a third of participants. Scientists have not been surprised by these modest results and have interpreted them as evi-dence that several underlying processes contribute in varying amounts to the over-all disease progression. The hope is that combining compounds targeting multiple pathways in the progression of NASH will offer improved efficacy to more patients.
Prime Time For Combos?Combination approaches were a central topic at the 2nd annual NASH Summit held in Boston, MA, in April 2018. While many are united behind the vision of combina-tion treatment as the ultimate solution to NASH, there are mixed views on whether it is timely to take investigational combos into the clinic. Those in favor of immediate pursuit cite the modest efficacy observed in ongoing trials as key motivation. More cau-tious developers believe the understanding of NASH biology is currently insufficient to support rational design of combina-tions, and warn that repeat trial failures may jeopardize the ability to justify future trials for the entire field. With the excep-tion of ongoing activity in oncology, it is generally unusual to be exploring combi-nation approaches before either asset has demonstrated efficacy as a monotherapy. Advancing combinations of investigational agents is inherently more exploratory than combining approved drugs. Complexity arises from having to predict drug-drug interactions, including resultant toxicity and synergistic therapeutic effects, from limited safety and efficacy data.
However, skepticism may be quelled as soon as the first Phase II combination trials read out in a year or so. Compelling evidence that combinations outperform monotherapy in preclinical studies is emerging from multiple developers. Furthermore, the first-in-human test of a combo approach completed earlier this year; Gilead Sciences Inc. reported a positive efficacy signal from a proof-of-concept study of several combination
Exhibit 3Nash Patients Experience Variable Disease Progression
Note: Data based on longitudinal study of 96 NASH pts with mean follow-up of 3.2 yrsSOURCES: Adams LA, J Hepatol. 2005
In the absence of e�ective treatment, NASH patients experience:
~35%Progressive Fibrosis
~35%Stable Fibrosis
~30%Fibrosis Regression

24 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DISEASE ANALYSISin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
treatments in NASH and intends to de-velop them further.
Premature or not, pursuit of combina-tion therapies is likely here to stay. In addition to Gilead, Pfizer Inc. is plan-ning to test combinations independently, while Novartis AG and Allergan PLC just kicked-off the first cross-company collaboration trial. It may be timely for other developers to reflect on how to best navigate a space that is already shifting focus to combinations. Dedicating re-sources to cracking the NASH riddle is an important consideration for accelerating development. Focus could range from in vitro organ systems with human tissue to help generate more precise rationale for how to combine treatments to precision medicine approaches for identification of the right treatment for the right patient. On the strategic front, exploring suitable cross-company partnerships to combine compounds with complementary mecha-nisms of actions that best address the underlying complexity of the disorder is of significant importance.
Considerations For Clinical Trial DesignTesting in the right patient population is critical to success. Numerous clinical trials are currently underway despite the challenges outlined above. Dr. Kapeller advises that “selecting the right patient population is key to successful clinical development,” given the significant het-erogeneity of clinical outcomes and thera-peutic needs across patient segments. From a strategic perspective, biopharma would ideally pursue the opportunity that combines the highest clinical unmet need with the lowest developmental hurdles.
Some practicing hepatologists propose that the ideal approach to NASH would be to intervene relatively early, in patients with F1 or F2 fibrosis, to prevent pro-gression to more advanced disease. The concern is that “if you try to intervene in F3 or F4, you may have missed the boat on these patients,” says Dr. Malik. In fact, “for a long time, companies were focusing on F1 and F2,” explains Dr. Ka-peller, but as NASH is a slow-progressing disorder “it was taking too long to show therapeutic effect.” As a result, the FDA and the EMA started advising developers to focus on F2 and above, given the higher
likelihood of these patients progress-ing to serious liver events sooner. “You can’t do clinical trials for 20 years,” says Kapeller. Targeting advanced disease al-lows us to demonstrate efficacy in more practical time-frames providing some much-needed cost relief.
Currently, developers can pursue two distinct pathways to FDA or EMA approval (see Exhibit 4). One approach is accelerated/conditional approval, based on reasonably accepted surrogate endpoints in moderate-severe disease (NASH F2-F3). This approach requires post-approval studies to demonstrate that the surrogates translate to clinically meaningful benefit. The other option is a standard approval, based on hard clinical outcomes in compensated cirrhosis. Both options have their own unique consider-ations and deciding which path to pursue should be primarily guided by the mecha-nism of action of the drug that is being assessed. While potentially a shorter path to market, accelerated approval based on novel surrogate biomarkers leaves room for payers to place significant restrictions on product utilization until definite ap-proval is obtained. Pursuing standard approval in compensated cirrhosis is equally risky as the patient population is much sicker and harder to manage. Furthermore, demonstrating efficacy in cirrhosis likely requires a therapeutic approach with strong anti-fibrotic effect.
Keeping tabs on co-morbid condi-tions. While a regulatory pathway for approval of NASH treatments has been established, clinical success remains uncertain. Beyond ensuring that tri-als enroll patients in the right stage of disease progression, developers must also be mindful of the fact that NASH frequently co-exists with comorbid con-ditions such as obesity, type 2 diabetes and cardiovascular disease. Each of these conditions is associated with its own set of clinical complications, which may affect outcomes in clinical trials. In some cases, the comorbid condition may actually be a stronger driver of risk and mortality than NASH. “The endpoints have to reflect the patient population that you are assessing your drug on,” advises Dr. Malik. He explains that “in patients with obesity and mild NASH, morbid-ity and mortality will be primarily from
While a regulatory
pathway for approval
of NASH treatments
has been established,
clinical success
remains uncertain.
Beyond ensuring that
trials enroll patients
in the right stage of
disease progression,
developers must also
be mindful of
comorbid conditions
such as obesity,
type 2 diabetes
and cardiovascular
disease.

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 25
DISEASE ANALYSIS ❚invivo.pharm
aintelligence.informa.com
diabetes, CVD, and stroke, and assessing liver-related mortality in those patients is inappropriate.”
While the field has shifted focus onto patients with advanced disease who are at the highest risk of liver-related mor-tality, early trial readouts are starting to show that even patients with increased risk of liver events have elevated cardio-vascular risk with their obesity, which could still taint trial outcomes. “Trials need to be very carefully developed to make sure you are selecting the right patient population to demonstrate a liver outcome,” concludes Dr. Malik.
The high frequency of co-morbid con-ditions in NASH patients also impacts the safety profile required for approval of a potential NASH therapy. For example, as more than a third of NASH patients suc-cumb to cardiovascular events, regula-tors require that NASH drugs are at least neutral in terms of cardiovascular risk. Pivotal trials are expected to demonstrate no sign of elevated CVD risk, which has to be confirmed by large post-approval safety studies.
Non-Invasive Biomarkers NeededThe lack of non-invasive biomarkers for diagnosis, risk stratification and treat-ment monitoring of NASH is one of the key hurdles facing the field. Currently, liver biopsy is the only accepted approach for diagnosis and assessment of response in trials. However, biopsy is invasive, carries risk of hospitalization and mortal-
ity, and is prone to sampling error and high inter-observer variability. Various alternative approaches are in develop-ment but none are ready for prime time yet. Reliable methods for quantification of fat and fibrosis are starting to emerge but detecting inflammation remains an unsolved challenge. “We need tools that allow us to distinguish steatosis (simple fat) from steatohepatitis (fat with inflam-mation),” says Dr. Malik.
Ongoing innovation in the diagnostics space has the potential to accelerate drug development and ultimately reshape how patients are managed. However, adopting new biomarkers in clinical trials requires substantial efforts and investment to validate the reliability of these biomark-ers as surrogate endpoints. In an effort to address one of the biggest challenges in the field, developers are currently inte-grating exploratory markers as secondary endpoints in Phase II and Phase III stud-ies. The field has also seen the formation of two multi-stakeholder consortia, LIT-MUS and NIMBLE, aimed at accelerating validation of non-invasive markers by sharing resources and patient samples. A collaboration between European bio-pharma and academic entities, LITMUS is overseen by the Brussels-based Innova-tive Medicines Initiative. NIMBIL is the North American counterpart, supported by the NIH.
A biopharma company can further their position in the field by investing in develop-ing and validating innovative diagnostic
techniques to improve on current limita-tions of biopsy and facilitate easier trial recruitment. At the very least, it is strate-gically important to surveil development in non-invasive markers and endpoints to adopt the latest innovations in trial design.
The Rest Is UnwrittenIt is clear that the story of NASH is just starting to be written and that the ulti-mate NASH therapeutic is still some years in the making. Dr. Malik explains, “This is a young condition, the pathophysiology is evolving, drug development is evolv-ing; we have to be patient and we will identify the answer hopefully in the next decade or two.” While current patients are not adequately managed by diet and lifestyle modifications, typically due to issues with compliance, the evidence that these interventions can alter the course of the disease is perceived as encourag-ing proof that the condition is reversible.
The continued efforts of academic, clinical, biotech and biopharma com-munities will drive the field forward and bring the field closer to a solution. How-ever, building a complex therapeutic area from the ground up requires substantial investment, time and cross-collaboration between all relevant stakeholders to ac-celerate development. IV005370
Amama Sadiq, MD, MPH, is a Medical Director and Engagement Manager at Clarion, a life sciences strategy consul-tancy located in Boston, MA. She can be reached at [email protected]. Iliyana P. Atanasova, PhD, and Kath-erine J Franklin are Consultants at Clarion.
[Editor’s note: In February 2018, Clarion partnered with MassBio to co-host a panel on NASH. The event brought together a diverse group of esteemed NASH thought-leaders, blending medical, commercial, and health economics viewpoints. The content of this article reports on some of the issues discussed by the panel. Clarion thanks MassBio for this collaboration and the panelists Raza Malik, MD, Rosana Kapeller, MD, PhD, and Jagpreet Chhat-wal, PhD, for their perspectives, as well as Thomas J. Murtagh, a Founder and Managing Director at Clarion, for his sup-port and many contributions.]
Exhibit 4Two Potential Regulatory Pathways Exist For Investigational Drugs
De�nite Approval
Anti-NASH DrugNASH with F2-F3
Clinical OutcomesConditional approval
Follow-up studies with clinical outcomes
Reasonably likely surrogate endpoints
Anti-�brotic DrugCompensated Cirrhosis

26 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ MARKET ACCESS DISRUPTION in
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
Many regenerative medicines seek to provide a transformative and long-lasting effect with a single treatment, potentially enabling a shift from a focus on chronic therapy to possible cures. Patient access to these transformative therapies will be hindered, however, if the health care system is not prepared for the implications of such medical innovation.
The current system is organized around paying for chronic interventions based on episodes of care rather than based on value and patient outcomes. The political and payer uproar associated with the launch of Gilead Sciences Inc.’s Sovaldi (sofosbuvir) for hepatitis C in 2013 illustrates how the transformative clinical impact of a product is not always sufficient to ensure patient access post-launch, and that short-term payer budget considerations play a significant role in public and private payer decision-making. (Also see “Cost Pushback Limiting Hepatitis C Drug Utilization” - Pink Sheet, June 20, 2016.)
To ensure access to regenerative medicines, key stakeholders – including developers, public and private payers, health care providers, patient advocacy groups and policy makers – must work together to optimize and modernize the health care system to en-sure the benefit from these new, transformative products can be realized. The Alliance for Regenerative Medicine (ARM), a global, multi-stakeholder organization dedicated to the advancement of gene and cell therapies, is concerned about reimbursement issues and has reached out to payers and other stakeholders. Here we review legal barriers to gene and cell therapy adoption and present several US-focused, market-based and policy solutions to overcome reimbursement challenges.
Regenerative Medicine Is Here: New Payment Models Key To Patient Access
Potentially curative regenerative medicine therapies are no longer theoretical, but instead have become reality. As more and more gene, cell and tissue-based therapies reach the market, the need for payment solutions is becoming more pressing. The Alliance for Regenerative Medicine has consulted with payers and other stakeholders to consider the barriers to alternative payment models and look at possible solutions.
BY FRANCESCA COOK, TED SLOCOMB AND MICHAEL WERNER
More and more regenerative medicines are reaching the market, but the payment solutions are not yet in place.
Patient access to these transformative therapies will be hindered if the health care system is not prepared for the implications of such medical innovation.
Payers are consistently concerned about the limited data available and long-term effects of regenerative medicines, as well as the affordability and budget impact of one-time treatments.
So what? Ensuring sustainable access requires both market-based solutions and action by governments, insurers and manufacturers. Demonstration projects are needed.

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 27
MARKET ACCESS DISRUPTION ❚invivo.pharm
aintelligence.informa.com
Curative Gene And Cell Therapies Require Unique ThinkingRegenerative medicines can address the underlying cause of disease, providing a persistent impact after one administra-tion. Such curative therapies are therefore uniquely valuable, whether that value is measured in saved lives, improvements in health-related quality of life, savings to the health care system due to averted costs associated with chronic disease manage-ment, or the broader impact to society as individuals and caregivers can more fully contribute to economies. Exhibit 1 summarizes the ways in which potentially curative regenerative medicines are dif-ferent from conventional therapies and chronic disease management.
High expectations for durable, and transformative therapies are tempered, however, by concerns that the treatment cost could overwhelm the health care sys-tem as new therapies become available. If paid for as drugs are today, the cost of regenerative medicines intended to be ad-ministered once or only a few times would be incurred up front and could present a financing challenge for some insurers. Associated savings, however, will accrue over a longer period of time.
For rare diseases, common targets of gene and cell therapies, there are fewer pa-tients and often higher annual treatment costs. Currently, chronic therapies for rare diseases, such as enzyme replacement therapies, often cost $300,000 to $800,000 per year – many millions of dollars over the lifetime of a patient – but the costs are spread out over time, thereby reducing any one-time budget expense. Regenerative medicines offer the potential to move from
chronic treatments to potentially one-time treatments, both transforming the lives of patients and in some cases significantly reducing lifetime treatment costs.
Potential ChallengesRecent experience from the first gene and cell therapies approved in Europe suggests that turning the promising science of regenerative medicine into sustainably successful business models will not be easy:
• uniQure NV’s Glybera (alipogene tiparvovec), a gene therapy approved by the European Medicines Agency (EMA) in 2012, was the first and only therapy for an orphan lipid disorder lipoprotein lipase deficiency and was priced at €1 million. Only four patients were treated in Germany before uniQure withdrew the product from the market in 2017, citing significant investments and low patient demand. (Also see “White Flag Raised: UniQure Gives Up On Glybera, But Not Gene Therapies” - Scrip, April 21 , 2017.)
• GlaxoSmithKline PLC’s Strimvelis, the first ex vivo gene therapy, received EMA approval in 2016 to treat ADA-SCID
Exhibit 1.Summary Of Unique Attributes Of Many Gene And Cell Therapies And Their Implications
SOURCE: Alliance for Regenerative Medicine
Curative potential• High clinical and economic value• Potential for surge adoption at approval
− Targeting underlying biology− Dramatic magnitude of effect− Impact on quantity and quality of life
• Technical uncertainty• Need for specialized centers of excellence• High cost of goods• Need for new and specialized codes
Product complexity− Viral manufacturing− Specific route-of-administration− Autologous cell processing
Gene And Cell Therapy Attributes Market Introduction Implications
• Higher one-time price• Long-term clinical uncertainty at approval• Potential inability to switch to alternative therapies
“One and done”− Single or acute administration vs. chronic− Repeat administration may not be feasible− Irreversible procedure
This is the third part of an annual re-view of issues facing the regenerative medicine field by the Alliance for Re-generative Medicine. The first article considered the prospects for curative therapies and potential barriers to adoption, and the second looked at the need for new payment models.
Curative Regenerative Medicines: Preparing Health Care Systems For The Coming Wave, November 15, 2016
New Payment And Financing Models For Curative Regenerative Medicines, July 24, 2017

28 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ MARKET ACCESS DISRUPTION in
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
and was priced at £600,000. As of June 2018, five patients have been treated, following a total of 13 referrals received to date, with more patients scheduled for 2018. This is in line with GSK’s pro-jections, according to the incidence of ADA-SCID across Europe (about 15 pa-tients diagnosed per year). GSK divested its rare disease gene therapy assets, in-cluding Strimvelis, selling the portfolio to Orchard Therapeutics in April 2018. (Also see “Orchard To Use Divested GSK Rare Disease Gene Therapies To Grow Globally” - Scrip, April 12, 2018.)
Private and public payers, for their part, appear to be cautiously optimistic about the coming wave of gene and cell therapies, based on favorable public comments and direct engagement with ARM and its mem-ber companies. They intuitively under-stand that these therapies represent unique value propositions as compared with more traditional biopharmaceuticals. However, payers also consistently articulate concerns that broadly fall into two categories:
• Uncertainty: regenerative medicines are still relatively new, and there re-mains considerable uncertainty around their long-term efficacy and safety. In addition, many gene and cell therapies are targeting first approvals in orphan indications via small clinical trials or single-arm studies, and therefore lack traditional, statistical data on the magnitude and duration of the treatment effect at the time of launch. While regulators often agree that small single-arm studies are acceptable for ultra rare indications, the limited data this provides sometimes translates into undesirable unpredictability for payers regarding how many patients will need such therapies, what proportion of pa-tients will respond, how long the effect will last and how much long-term value will ultimately be realized.
• Affordability: many initial cell and gene therapies will target rare diseases, and, given the number of therapies under
development, insurers are concerned they may face a portfolio of new one-time therapies for patients that could collectively strain health plan budgets – already a source of concern. Additionally, for regenerative medicines that target larger, more prevalent diseases, payers may need to plan for a surge in use to durably treat (and potentially cure) an existing prevalent population – with learnings from the Sovaldi instance.
New Payment Models Being TestedAgainst this backdrop, both innovators and payers increasingly are accepting that new models for reimbursement and financing may be needed to support adoption of the wide range of gene and cell therapies. Indeed, several multi-stakeholder efforts are exploring such arrangements. These consortia include the Biotechnology Innovation Organiza-tion (BIO), the New Drug Development Paradigms (NEWDIGS) initiative at MIT, the
As of mid-year 2018, there were more than 950 regenerative medicine therapies in clinical trials, of which more than 90 are in Phase III. In addition, according to the MIT NEWDIGS consortium FoCUS Project (Financing and Reimbursement of Cures in the US), around 39 gene therapies will be approved by the end of 2022. Product candidates in development address diseases involving almost every major organ system, from ultra-orphan neurodegenerative diseases like adrenoleuko-dystrophy, to highly prevalent public health concerns such as several forms of cancer, congestive heart failure and diabetes, ailments that affect tens of millions of patients worldwide.
The US FDA has recognized the need to accelerate regenera-tive therapies. In November 2017, FDA commissioner Scott Gottlieb noted the “transformative promise” of these tech-nologies and said this potential is the reason the FDA is “so committed to encouraging and supporting innovation in this field.” Gottlieb has continued to look for ways to facilitate development of regenerative medicines. (Also see “Gottlieb On Gene Therapies: ‘Very Seductive’ To Think About Acceler-ated Approval Pathway” - Pink Sheet, May 7, 2018.)
The FDA has awarded Breakthrough Therapy Designation to more than 20 regenerative medicine product candidates, to date. And more than 20 product candidates have received Regenerative
Medicine Advanced Therapy (RMAT) designation, a regenerative medicine-specific accelerated approval program created under the 21st Century Cures Act that acknowledges and incorporates the unique attributes of gene and cell therapies and enables enhanced interaction opportunities with the agency.
Two autologous chimeric antigen receptor T-cell (CAR-T) products, Novartis AG’s Kymriah for critically ill children with refractory or relapsing acute lymphoblastic leukemia and Yes-carta (axicabtagene ciloleucel), Kite Pharma Inc.’s therapy for adults with relapsed or refractory large B-cell lymphoma, were approved by the FDA in August and October of 2017, respec-tively. In May 2018, the FDA approved Kymriah for a second indication, the treatment of adult patients with relapsed or refractory large B-cell lymphoma. These technologies are prime examples of the promise of regenerative technolo-gies, achieving dramatic and durable cures. In addition, in December 2017, the FDA approved the first adeno-associated virus (AAV) in vivo gene therapy – Spark Therapeutics Inc.’s Luxturna (voretigene neparvovec-rzyl) for the treatment of patients with vision loss due to confirmed bilallelic RPE65 mutation-associated retinal dystrophy.
Other gene and cell therapies for conditions as diverse as spinal muscular atrophy, hemophilia A and inherited retinal disease have also recently delivered promising clinical data and are poised for regulatory approvals in the next few years.IV005372
❚WHERE DOES THE FIELD OF REGENERATIVE MEDICINE STAND?

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 29
MARKET ACCESS DISRUPTION ❚invivo.pharm
aintelligence.informa.com
Institute for Clinical and Economic Review (ICER), the American Society of Gene and Cell Therapy (ASGCT), and the Margolis Center for Health Policy at Duke University.
The Centers for Medicare and Medicaid Services (CMS) has also highlighted the need to revisit payment models for innova-tive, high-cost, high-value therapies, in-cluding regenerative medicines. Novartis AG launched Kymriah (tisagenlecleucel) in August 2017 with an outcomes-based con-tract agreement already in place with CMS, which said at the time it was committed to “identify[ing] and alleviat[ing] regula-tory barriers [to new payment models] in Medicare and Medicaid.” The agency has continued to look for new ways to handle CAR-T reimbursement.
There is a growing consensus among stakeholders that reimbursement models that enable payers to make their payments over time and/or enable payment tied to the therapy performance may be appro-priate for regenerative medicines, as they facilitate patient access to new therapies quickly while enabling payers to manage their overall budget impact and limit risk if the therapy does not perform as expected. The most common reimbursement models discussed in this context are annuity and pay-for-performance models:
• Annuity models: under an annuity or installment payment model, first raised as a potential option by Jim Wilson et al. in a 2014 Nature Biotech article, payments would be spread over a pre-determined time period. This model recognizes the long-term therapeutic durability of single-administration cell and gene therapies, matches the payment to the multiyear benefit and minimizes large up-front or annual costs for payers.
• Pay-for-performance models: in a performance - or outcomes-based pay-ment system, the reimbursement for a treatment would be adjusted based on whether a pre-specified health outcome is achieved. There are many variations of this value-based model. It could be implemented through discounts on fu-ture payments, indication-based pricing, rebates or even outcomes-based money-back guarantees. This model shares risk between the innovator and the payer.
While annuity payments are a relatively new concept, outcomes-based contracting models have been fairly common in the single-payer systems of Europe and are on the rise in the US. Several US biophar-maceutical companies currently do offer money-back guarantees if performance-
based metrics are not met for certain chronic therapies, including Merck & Co. Inc. for Januvia (sitagliptin) and Janumet (metformin and sitagliptin) for diabetes, Novartis for its heart failure drug Entresto (sacubitril/valsartan), and Regeneron Pharmaceuticals Inc./Sanofi and Amgen Inc. for their PCSK9 inhibitors for dyslip-idemia and secondary prevention of major adverse cardiovascular events.
Finding Acceptance For New Payment ModelsSeveral implementation barriers must be overcome for either annuity models or pay-for-performance models to become a widespread reality. These barriers can be logistical, legal or regulatory. Importantly, many of these implementation barriers are not unique to regenerative medicines and are already being actively discussed in the context of pay-for-performance arrange-ments for existing products. For example:
Medicaid Best Price: manufacturers must report pricing data for drug therapies to the federal government to ensure that the US government, certain health care provid-ers and state governments always receive the “best price” possible for these products under the Medicaid program. The Medicaid best price rule may inhibit manufacturers
Alternative Reimbursement Models
Barriers Solutions
Best Price
AKS
Communication
Payment Over Time
Portability
• Demonstration waivers• Federal legislation
• USG demo waivers• OIG guidance• Safe Harbor
• FDA/CMS early engagement
• USG demo waivers• CMMI guidance• Federal legislation
• Commercial contracting changes• Annuity fund• Federal legislation
Exhibit 2.Alternative Payment Model Barriers And Solutions
SOURCE: Alliance for Regenerative Medicine

30 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ MARKET ACCESS DISRUPTION in
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
from tying price to outcomes.Alternate payment methods, such as
annuities or pay-for-performance agree-ments that include paybacks or rebates, could artificially lower the price by which the government will calculate pricing or rebates. This situation raises the question of how to report the price of a treatment whose true price will not be known until after performance is determined.
Potential Solutions:1. CMS has the authority to address this is-sue through several mechanisms, includ-ing informal discussions with manufactur-ers, formal guidance, or demonstration waivers, which can be approved to test changes in payment methods for Medicare and Medicaid. Individual innovators or industry groups on behalf of manufactur-ers can seek guidance from CMS on how to develop performance-based arrangements without triggering unwarranted rebates and/or how to secure such demonstra-tion waivers. This solution would hinge, in part, on CMS being able to provide this guidance in a timely manner and ensure confidentiality of the information stake-holders provide to the agency as part of the guidance process. 2. Legislation may be necessary and ap-propriate to codify the types of payment arrangements that can be exempt from best price requirements.
Anti-Kickback Statute (AKS): the AKS prohibits the payment or receipt of any remuneration for the referral of items or services reimbursable by federal health care programs. Violators are subject to civil and criminal penalties, as well as the exclusion from participation in federal and state health care programs. Outcomes-based payments introduce new financial arrangements between innovators, payers and providers and have the potential to fall afoul of the AKS if they are perceived to impermissibly create incentives for the adoption of one product over another or for increased use of services or products billed to Medicare or Medicaid. The risks associated with potential violations of the AKS can be a barrier to broad adoption of alternative payment models.
Potential Solutions:1. The Office of the Inspector General (OIG) enforces compliance with the AKS
and will be instrumental in overcoming AKS-related payment barriers by provid-ing clarification on whether alternative payment models are covered under ex-isting “safe harbors,” or by establishing new safe harbors specifically designed to enable alternative payment mechanisms. (Also see “US FDA Extends Payor Commu-nications Safe Harbor To Off-Label Uses” - Pink Sheet, June 12, 2018.)2. CMS may be able to use its authority to conduct demonstration projects and coordinate with the OIG to protect such arrangements under the AKS in order to test new payment models.
If health care system stakeholders address barriers of the kind described above to the implementation of pay-for-performance models for more traditional therapies, the benefits of these changes may also then accrue to innovative regen-erative medicines.
However, gene and cell therapy inno-vators will still face other implementa-tion barriers to new payment models that are more unique to the durable impact of regenerative and other transforma-tive medicines. The idea of annuities or pay-for-performance arrangements under which payers reimburse innovators for the value of a regenerative medicine that accrues over years or even decades after the original administration introduces two fundamental issues:
Payments Over Time: government pay-ers (Medicare and Medicaid) generally require payment at the time of treatment. Under generally accepted accounting rules for financial reporting, an annuity payment model could require insurers to recognize the entire cost of the treatment at the time the therapy was administered, even though full payment has not yet been made. This could cause issues in adopting such a payment model, espe-cially for government insurers.
Potential Solutions:1. Pursue guidance from CMS to ensure that proposed amortized and annuity payment models could allow for the rec-ognition of costs over time until the total amount is gradually paid down.2. Pursue demonstration waivers with CMS, as described earlier.3. Pursue exploration of innovative models via the Center for Medicare and
Both innovators
and payers
increasingly are
accepting that new
models for
reimbursement and
financing may be
needed to support
adoption of the wide
range of gene and
cell therapies.

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 31
MARKET ACCESS DISRUPTION ❚invivo.pharm
aintelligence.informa.com
Medicaid Innovation (CMMI), which was created to develop and test new payment and service delivery models. 4. Federal legislation to eliminate state-to-state variability that may create chal-lenges for the implementation of alterna-tive payment models.
Portability: a major challenge in enact-ing an annuity payment model involving payment over many years is the issue of portability of obligations related to such payments as patients move from one plan to another. Especially in the US, patient movement across health plans is common and there is no specific statu-tory or regulatory provision that requires one payer to continue making payments associated with the contract between an-other payer and a product manufacturer. Therefore, if an insurer enters into an annuity or performance-based arrange-ment intended to span several years, the insurer could be forced to continue pay-ments for an individual who is no longer a member, while another insurer reaps the long-term clinical and cost benefit of the curative therapy.
Potential Solutions:1. Insurers and manufacturers work together and with state insurance regula-tors to identify and implement policies that can support alternative payment mechanisms. For example, insurance contracting changes could be made to allow annuity contracts to follow patients if they switch plans, enabling the transfer of any financial commitment. 2. Create arrangements (e.g, via developer-sponsored patient data registries) that allow original insurers to continue to gain access to relevant patient outcomes data for their former members so that they can continue to make payments or discontinue as appropriate, based on product perfor-mance against the original contract.
3. Create an annuity fund, funded by in-surers, to cover out years should patients switch plans. This option transfers the burden of monitoring patients and tracking health care outcomes to a third party who would manage and administer the fund.
One or more of these contracting changes could be piloted at the state level, while federal legislation is pursued to enable consistency across the country.
Addressing Payer Financing And Patient Access Are Key To AdoptionIn addition to new reimbursement mod-els to pay for gene and cell therapies, employing financing mechanisms, such as reinsurance, stop loss or risk pools, adapted for high-value treatments, also are necessary to give insurers time to determine and accommodate any budget-ary impact of these new therapies, which may introduce higher costs in the near term but generate patient value and cost offsets over the medium to long term. Likewise, new tools may be needed to facilitate patient access to regenerative medicine products. Patients are in-creasingly facing higher out-of-pocket costs due to increased deductibles, co-insurance and premiums for their care, which could impact affordability for patients. Additionally, some gene and cell therapies target rare genetic diseases that are treated at specialty centers across the country. Travel and lodging associated with accessing these specialty centers are often not covered by insurance, limiting access to those who can pay.
ARM and its affiliates are working both independently and in collabora-tion with others to support initiatives to address payer financing and patient access issues. These activities include engagement directly with government and commercial payers and regulatory
bodies on value-based payment options and the establishment of a foundation focused on education and patient access.
Finding a path forward requires both market-based solutions and action by the federal and state governments, insurers and manufacturers. No one entity can achieve these changes on its own, nor will every solution be ideally suited to each new therapy or circumstance.
As with all medical technologies, regenerative medicines will have to dem-onstrate significant and durable clinical benefit and economic value supported by strong data to ensure successful adop-tion and potential price premiums. The goal of the payment models described here is to build an early platform that allows innovators, payers, providers and patients to successfully engage around new gene and cell therapies during the initial period of potential uncertainty and patient demand.
Multi-disciplinary efforts involving all groups need to continue to critically assess such models, and to initiate dem-onstration pilots, where appropriate. ARM and its member organizations will continue to do such work in collabora-tion with others to help pave the way for regenerative medicines to deliver on their transformative promise to patients, to the health care system and to society. IV005371
Francesca Cook, PhD, REGENXBIO, [email protected]; Ted Slocomb, Audentes Therapeutics, [email protected]; Michael Werner, Alliance for Regenerative Medicine, Holland & Knight LLP, [email protected]; Ted Haack, LatticePoint Consulting, [email protected]; Donald Han, Pfizer, [email protected]; Faraz Ali, REGENXBIO, [email protected]
LET’S GET SOCIAL@INVIVOnow
In VivoPharma intelligence |

32 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ EXECUTIVE INSIGHTin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
Lars Rebien Sørensen, a Novo Nordisk AS veteran who was CEO of the dia-betes giant from 2000 to 2016, became chair of Novo Holdings in July 2018 and was also appointed chair of the board of the Novo Nordisk Foundation. He reveals his vision for the future of Novo Holdings and discusses the challenges of moving from the C-suite to chairship roles.
Sørensen joined Novo Nordisk in 1982, beginning his career in enzyme market-ing. He was later appointed a member of corporate management and was given the special responsibility for health care in 1994. He obtained his master’s degree in forestry from the Royal Veterinary and Agricultural University in Denmark in 1981, and a bachelor of science degree in international economics from the Copenhagen Business School in 1983.
Sørensen joined the boards of the Novo Nordisk Foundation and Novo Holdings in March 2017 and was elected vice-chair of the foundation in March 2018. He succeeded Sten Scheibye, who departed both boards on July 1, as chair of both the foundation and Novo Holdings. Sørensen will focus on implementing the foundation’s new five-year strategy for 2018 to 2023.
Under this five-year strategy, the Novo Nordisk Foundation has three main goals: • To enable Novo Nordisk AS and Novozymes AS to reach world-class business results • To develop knowledge-based environments in which innovative people can carry
out research and translate discoveries into new treatments and solutions • To inspire and enable children and young people to learn
Back To The Future: Novo’s Sørensen Reflects On CEO Years And Tasks Ahead For Industry
Lars Rebien Sørensen scrutinizes the pharmaceutical industry and shares with In Vivo his vision for the future of the Novo Nordisk Foundation. With 16 years as CEO of Novo Nordisk under his belt, as well as many more years in leadership roles at the Danish company, Sørensen reflects on the past and gives his predictions for the future of the innovative drug development sector.
BY LUCIE ELLIS
As the new chair of the Novo Nordisk Foundation and Novo Holdings, Sørensen discusses his five-year strategy for progress.
Novo Nordisk’s ex-CEO also highlights his best bit of advice for future leaders of the sector.
So what? Having stepped back from the pharma industry, Sørensen is uniquely positioned to discuss the trials and tribulations already causing a stir, and the events most likely to disrupt the industry in the near future.
LARS REBIEN SØRENSEN

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 33
EXECUTIVE INSIGHT ❚invivo.pharm
aintelligence.informa.com
Scheibye will be a tough act to follow. Under his watch, the foundation’s annual payouts grew from DKK687 million ($106 million) in 2013 to DKK1.3 billion in 2017. In the same period, the total assets of Novo Holdings grew from DKK201 billion in 2013 to DKK358 billion at the end of 2017. However, under its five-year strategy and Sørensen’s leadership, the founda-tion expects its annual grant investments to reach DKK5 billion in 2023.
The Novo Nordisk Foundation is an independent Danish foundation with corporate interests. It has two key objec-tives: to provide a stable basis for the commercial and research activities of the companies in the Novo Group; and to support scientific, humanitarian, and social causes. Novo Holdings is a Danish, private, limited liability company wholly owned by the Novo Nordisk Foundation. It is the holding company of the Novo Group, comprising Novo Nordisk, No-vozymes, and NNIT, and it manages the foundation’s assets.
Having stepped back from the pharma-ceutical industry, Sørensen is in a prime position to reflect on his time as a leader within the sector, highlighting the issues on the horizon for big pharma and also his tips and tricks learnt from more than a decade as CEO of a top 20 drug developer.
In Vivo: What drew you to these new positions at the Novo Foundation and Novo Holdings?
Lars Rebien Sørensen: It is most likely because of my tenure with Novo Nordisk, where I’ve worked for 35 years. This gave me the opportunity to join the Novo Nord-isk Foundation, which owns about 27% of the equity and controls 70% of the votes of Novo Nordisk. It enabled me to get a board seat on the foundation, and I’m now in a position where I will be taking over the chairship of the foundation. With the role as chair of the foundation comes also the chairship of Novo Holdings, which is an investment company that we have created to hold all the assets, reinvest and ensure that the foundation can live up to its phil-anthropic obligations.
So, wearing both hats, what are your immediate goals as you move into these new roles?
Firstly, it is a huge privilege. During my tenure as a working executive and an employee of Novo Nordisk I took part in the business of creating value, now I’m getting the opportunity to look through the barrier as benefits are being funneled back into society at large. Looking at investments that will create, hopefully, a vibrant bioscience ecosystem in Den-mark, perhaps even broader within spe-cific areas. So, it’s a huge, huge privilege and obligation to have.
My goals are focused specifically on the next five years. We have a statutory retirement limit of 70, so I have about five or six years to make an impact together with my colleagues on the board. It is only during the recent five to seven years that the foundation has been able to ac-cumulate wealth and dividends from the operating companies, and it is starting to make a very significant impact in the biotech and life science environment in Denmark and abroad. My role is to ensure that we continue the very successful pe-riod that we’ve been going through under
the leadership of the previous chair. It is going to be a tall order; of course, we have more financial firepower but the circum-stances are likely to be more challenging because of the macro-economic situation that we’re facing now as opposed to what we faced during the last five to 10 years.
Along those lines, what kind of chal-lenges are you expecting and prepar-ing for?
I think it is going to be interesting for us to see if we can find long-term invest-ments where we believe we can generate value. We have as a mandate to invest in very early, even seed money, in starting up or topping up biotech and life science companies in Denmark and Scandinavia. We can find ways of doing that but it is not going to necessarily provide a return. It is more of a philanthropic exercise where we hope to build an ecosystem that Denmark will benefit from. More difficult, though, are the larger financial invest-ments where we are competing to some extent with the venture capital and the general capital players. For life science investments right now, asset values are extraordinarily high. And given the flush of capital available and low interest rates, we have to be very, very careful in select-ing investments where we have insight or experience that we can bring to bear in developing some of these companies or being part owners of these companies.
The foundation’s five-year strategy – could you talk a bit about the salient points of this plan?
If you look back five years, and even longer, the primary focus of the founda-tion’s philanthropic activities and (in those years) relatively modest financial activities was undertaken by Novo Hold-ings. The financial group was focused on seeing if it could develop an ecosystem around metabolism and science, which was directly linked to the commercial interests of the operating companies. Now, with a new strategy, we are recog-nizing that the foundation in its capacity for grants and supporting science has become so large that we need to, and we can, expand our areas of interest. I see this involving natural sciences and including sustainable scientific or technological activities, so that we see
❚NOVO NORDISK FOUNDATION’S GRANT FOCUS AREAS
• Biomedical and health science research and applications
• Patient-centered and research-based care
• Life science research and industrial applications promoting sustainability
• Natural and technical science research and interdisciplinarity
• Education, outreach and innovation
• Social, humanitarian and development aid

34 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ EXECUTIVE INSIGHTin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
research expanding to create a more sustainable society.
If we were to only funnel our phil-anthropic activities into one area, say metabolism, we would probably have a diminishing return in terms of innova-tion and new knowledge than if we were looking more broadly. In the past we were very adamant that our activities should have a societal health benefit and we sought to do that through biomedical research. Now you can easily argue that this can be done through combining bio-informatics with biomedical research and also perhaps diagnostics like genomics. We can combine different disciplines to get better outcomes from the resources we are spending. So, I think in a way you could say that we are diversifying our
areas of interest but it’s also, perhaps, even an acknowledgment that the real breakthroughs will come from cross-disciplinary projects and science.
When you talk about revenue-generat-ing new assets, what are you looking for here?
Approximately 25% of the assets under management by the foundation is what is being dealt with by Novo Holdings – the other 75% is being held as equity in Novo Nordisk or in Novozymes, and we are not in a position to do anything with that ownership other than remain stable owners for the future. So, it’s the 25% of the assets, which equates to some DKK 100 billion, that we have an obligation to try to reinvest. This is being invested all the way from entrepreneurial idea generation and seed money, through to first companies with first rounds of financing, and also venture capital base enterprises and even listed companies. In the future it’s of course our obligation to try to identify, based also on risk as-sessment, companies where we can take a long-term position. Also, if there are to be financial circumstances in the near-term future, which will become more difficult for these companies to finance themselves to create real companies and jobs, and value for society.
What are you expecting to be the big-gest differences between being CEO of a company like Novo Nordisk and being chair of a foundation group?
There is one very important distinction between being a CEO and being a chair-man of any organization, as a CEO you usually have an enormous ability to make your views heard and to make decisions. In a foundation it is more of a collegiate approach. We as the board of the founda-tion use our tools and experiences for the betterment of the enterprise that we are engaged in. This role is quite different from being an executive, so for me per-sonally this is going to be an interesting experience because I’ve primarily been an executive all my life.
Then there are also several similarities because the way we operated at Novo Nordisk was as a collegiate. For example, the entire leadership team of the company was employed directly by the board and
so in that sense you could say it’s not that different. As a chair I need to see if I can recruit some of the best talent in device and medical technology, as well as biosci-ence and finance. Then use those talents to make sure that we’ve made the right decision. But it’s not my ideas, it’s our joint agreed ideas that will be promoted.
What key learnings from your many years at Novo Nordisk do you still carry with you today and find yourself using?
I really enjoyed all my years with Novo Nordisk but what really kept me going, if you will, was the curiosity and the excite-ment about science. I’ve marveled over time at the capabilities of our scientists. We took a narrow perspective in the area of metabolism, diabetes and related dis-orders. We had a very, very in-depth un-derstanding of the science in the area that we were engaged in, and this contributed to many of us, it motivated many of us.
For me personally, being able to apply my curiosity or explore in broader areas than what I used to work in is exciting. It’s just fascinating. And having worked 35 years for the company, it is of course an obligation for me to ensure that the values that have been created by the company and its employees are also put to good use for the betterment of the stakeholders of the existing company.
Having stepped away from an ex-ecutive role, is there one myth about working within the pharmaceutical industry that you are keen to set straight?
The pharmaceutical industry has a public reputation that is sadly not where it should be. I think the pharma-ceutical industry is doing a phenomenal job, and is doing things for the general public and society that cannot be under estimated. However, due to a number of controversial reasons – for example animal testing, human trials, financial/personal financial gain, etc. – it has not gotten the reputation, unfortunately, it deserves in society and that saddens me in some ways. This is something for the current leaders of the pharmaceutical industry to work on, not me; but I will support any work in that regard that they may undertake.
I really enjoyed all
my years with Novo
Nordisk but what
really kept me going,
if you will, was the
curiosity and the
excitement about
science. I’ve
marveled over time
at the capabilities of
our scientists.
Lars Rebien Sørensen

©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 35
EXECUTIVE INSIGHT ❚invivo.pharm
aintelligence.informa.com
Talking of future leaders, what’s the best bit of advice you were given as a CEO that you would pass on?
That’s a tough one. The one thing that we agreed on, the team and I, when I took over 17 years ago at Novo Nordisk, was that we needed to find out who the customer was. We decided that the patient was the customer and if you look at it that way, then of course your relationship with the medical profession changes somewhat. The doctors are not our customers, even though they write the prescriptions, but they are our part-ners in ensuring that the patient gets the proper treatment. I would say to anyone working in the pharmaceutical industry, make sure that you work in the interest of the patient.
And then you have to adopt your strate-gies. Some of those strategies can be quite difficult to deal with, because, say for instance, intellectual property rights are the protection of innovation and pricing of new innovations, and how do you make those available for those that have not the financial means or insurance. Those are difficult decisions but at the end of the day, if you’re not living up to the expectations of the consumer, the patient, then you end up in a difficult position.
Are there aspects of the CEO role you will miss?
Not really. During my time as an ex-ecutive at Novo Nordisk, I think I made more than 100 quarterly announcements because I was part of the leadership team before I became CEO. So, I miss the people that I dealt with during all those years, but the job itself, it’s hugely demanding and I don’t miss the job. How-ever, I have been blessed in the sense that I’m able to continue working with science and health in a less strenuous way you could say. I am excited to be heading a philanthropic organization that largely gives back to society.
Looking ahead, what are your predic-tions for the pharmaceutical sector?
It’s very clear that there are some commercial challenges in relationship to the biggest market in the world, the US market. The old systems for distri-bution of drugs and health insurance plans are not functional in the sense that distribution schemes do not allow all the patients to have clear transparency of the pricing and get access to the drugs that they can afford or they need. That is then challenging for the general global business model of the pharmaceutical industry in that the US has traditionally been the engine of innovation. Not that innovation is not taking place anywhere else but that the US has got the financial
capacity to fund innovations, which are then rolled out subsequently in Europe and elsewhere – to just put it simply. So, the current discussion in the US about the commercial model and the willingness to finance innovation in the US, I think is a fundamental one which is a challenge for the industry. This must be dealt with very diligently and carefully by the leaders of the pharmaceutical industry in the US because it has global ramifications.
Then I think of course in terms of sci-ence, there are some very, very disturbing areas that need attention; neurological sciences, dementia and Alzheimer’s, and others are causing an enormous societal toll and it seems like we’re having less and less scientific endeavor to try to find fundamental ways of dealing with these diseases. Alzheimer’s, for instance, is an area where there’s no real significant progress to my understanding.
Then there’s another area where we’re finding a way to do something in the foundation; we’ve just announced a $150 million investment or commit-ment into developing new antibiotics. Developing a new set of antibiotics is going to be crucial. The assessment is that by 2050 there will be more deaths from infections than if you take cancer, HIV/AIDS, malaria and tuberculosis altogether, so infectious diseases are going to be a huge issue for our children and our grandchildren. And the business model of developing such new concepts is flawed for many reasons, therefore nobody wants to invest in it. So, we are taking it upon ourselves to support that. Antibiotic development is an area where foundations like ours may have to step in and do some of the fundamental work to develop new concepts. IV005360
Comments: Email the author: [email protected]
BREAKDOWN: Novo Holdings And
Its Investments
Established in 1999, Novo Holdings is a Danish private
limited liability company wholly owned by the Novo
Nordisk Foundation.
https://bit.ly/2KSA4H1
READ MORE ONLINE
Phot
o: N
ews
Ãres
und
- Joh
an W
essm
an
LET’S GET SOCIAL@INVIVOnow
In VivoPharma intelligence |

T H O U G H T L E A D E R S H I P I N A S S O C I A T I O N W I T H S Y N E O S H E A L T H
After months of withering scrutiny over pricing, orphan drug developers must have breathed sighs of relief when they read President Trump’s “Blueprint to Lower Drug Prices.” Released in May, the document makes no mention of rare diseases, and in 39 pages the phrase “orphan drugs” appears just once. Many of the proposals in the Blueprint tackle discounts and rebates that
arise mainly when there are multiple therapies to treat non-rare conditions. Dodged bullets aside, however, the market access environment for orphan drugs is
changing quickly in ways that will not reward complacency. With orphan-designated therapies projected to make up one-fifth of global prescription drug sales by 20241, payers are steeling themselves for a wave of treatments with high list prices.
The US Food & Drug Administration (FDA) is making moves to approve orphan drugs using smaller, efficient development programs—action that is feeding the surge of new rare disease drugs. But “approvable” to regulators doesn’t mean payers will provide unfettered access. In fact, patients with rare diseases are already facing a number of
Orphan Medicines: Averting Price Debacles And Winning Payer SupportBY MEG ALEXANDER AND SUSAN SUPONCIC, PHD
As coverage and reimbursement landscapes change, drug developers must assess how healthcare systems will handle the incoming wave of treatments for rare diseases that often carry a high list price, and they should prepare for restrictive practices that pass more of the costs along to patients. Developers can speed orphan medicines to patients through better communication of value to payers and other stakeholders.
36 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
T H O U G H T L E A D E R S H I P I N A S S O C I A T I O N W I T H S Y N E O S H E A L T H
coverage and reimbursement hurdles that seem poised to in-tensify in coming years. The good news: developers can mitigate some of these obstacles by wisely investing time and money during clinical development to substantiate the value of the new drugs and accurately communicate this information on the runway to commercialization.
Among restrictive tools and practices, co-pay accumulator pro-grams have drawn criticism from patient organizations because the value of co-pay cards and other assistance cannot be applied to patient deductibles or out-of-pocket maximums—leaving patients exposed to more of the cost.2 Already, close to one-fifth of self-funded employer plans may be us-ing such programs, and the number could rise to 50 percent by the end of the year, analysts predict.3
Other practices that may be on the rise include prior authorizations applied in expansive ways to restrict coverage well beyond subsets of patients who were excluded from clinical trials, and delays in coverage decisions by health insurers that have the impact of rationing care. Admittedly, reviewing new drugs takes time. This is especially true when acceler-ated regulatory reviews leave payers with less time to prepare and limited evidence to help them manage uncertainty. Still, coverage delays that can stretch to half a year put an undue burden on patients who rely on “fast start” or bridge programs the developers craft to make drugs available during the gap.
Misaligned PerspectivesThe restrictive practices highlighted are not intended to be combative, even though some drug developers see them as blows across the bow. The practices often arise from misalignments in perception of a medicine’s value—which is always in the eyes of the beholder. Insurers, phar-macy benefit managers and employers apply restrictions to products when they do not have enough information on the benefits and durability of response to justify the cost.
Small developers, in particular, often miss precious opportunities to plan for and provide the education and evidence payers require at key junctures in the development process. With limited re-sources, these companies sometimes focus on communicating potential value to investors and regulators. But, in today’s increasingly price-sensitive and restrictive
environment, it is important to learn how payers, prescribers and patients define value too. Developers must be able to substanti-ate and communicate in metrics and language each group un-derstands—and not to wait until the drug is approaching launch.
Outreach to payers requires particular forethought. Early in the development process, orphan drug developers should be gathering evidence payers will find compelling. This ranges from data on disease prevalence, the number of patients who might be in the payer’s plan and the costs for hospitalizations and co-morbidities in the absence of a new medication, to the impact on payers’ budgets and how the drug will reduce cost
burdens to yield savings. By 18 months to a year before approval, the drug developer should be finalizing this information and figuring out how to document and tell a persuasive story.
The Payer’s ViewEvidence of this sort takes time to devel-op. Health economics outcomes research (HEOR) can help, and can be especially persuasive when validated by institu-tions the payers trust. By publishing and presenting this evidence throughout development and commercialization, de-velopers can build a peer-reviewed story of the disease burden and its economic consequences.
James T. Kenney, RPh, MBA, Manager of Specialty and Pharmacy Contracts at Harvard Pilgrim Health Care, says seeing this information before a drug clears FDA review can make a big difference on coverage decisions and timelines.
“If we’re budgeting 12-18 months in advance, it’s nice to know what’s coming so we can put it into our budget models,” Kenney told us in a recent interview. With orphan drugs on an accelerated pathway, the best time may be when the manufac-turer emerges from Phase II, while there’s still a chance to build specific outcome measures into the testing. “That would help us evaluate the drug and figure out how to use it, which is the real spirit of cooperation and collaboration,” he says. “Then, instead of coverage decisions coming six months after launch, maybe we could shorten the timeframe and identify appropriate patients earlier and allow faster access to these agents.”
Some of the communications Kenney describes are constrained by the FDA’s guidance on Section 114 of the 1997 FDA Modernization Act (FDAMA 114).
Early in the development
process, developers
should be gathering
evidence payers will find
compelling, including
data on disease
prevalence and the
number of patients who
might be in the
payer’s plan.
©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 37
T H O U G H T L E A D E R S H I P I N A S S O C I A T I O N W I T H S Y N E O S H E A L T H
As President-Elect of the Academy of Managed Care Pharmacy, Kenney is one of many industry executives—payers and pharma companies alike—who wish to see Congress ease the rules and free up necessary communications.
The Patient ViewA true multidimensional approach must also take stock of how patients and prescribing physicians get information and respond to news. Consider, for example, a small biotech company whose treatment for a genetic disorder has reduced hospitalizations to zero in a trial lasting 18 months. Enthusiasm gets the best of the company’s chief executive. In an earnings call with analysts and media, he discloses an internal proposal to price the drug at $500,000 per treatment.
A decade ago, an earnings call like this might have had few consequences other than raising spirits on Wall Street. Today, messages from a CEO to investors are instantly propagated across a network of highly engaged patients.
Furthermore, suppose that in this call the CEO makes no mention of patient assistance programs or any positive feed-back from health plans—a serious mistake. Instead of winning the support of patients, the pricing message aimed at investors triggers despair in people who now fear they can never afford the drug. Patient groups are activated as critics when they might have been allies of the developer. These groups may now be less likely to assist the developer in charting the natural history of the condition, building registries, recruiting patients in trials, and making a case for the value of the drug.
The most serious consequence of missteps is delaying and diminishing the prospects of access to a new drug. “People for-get that being a patient is full-time job,” explains Jen Horonjeff, PhD, CEO and founder of Savvy Cooperative, an organization that seeks to strengthen partnerships between patients and drug developers. Poor communications among stakeholders “is wildly detrimental to patients gaining access,” Horonjeff said in an interview. “It’s the patient that gets hurt in the end.”
Lack of access is especially cruel at a time when science is delivering mind-spinning advances in atomic-level molecular analysis, DNA engineering and related progress in gene- and cell-therapies. That is why developers and payers alike must find solutions to ensure access while preserving the viability of multiple, co-existing business models in a free-market healthcare environment. When conversations about value are grounded in evidence that is gathered, validated, and communicated with high levels of confidence, solutions will be within reach.
References:
[1] EvaluatePharma. (2018, May 25). Worldwide Orphan Drug Sales are Forecast to Grow at a CAGR of 11.3% from 2018 to 2024, Double the Rate Forecast for the Non-Orphan Drug Market [Press release]. Retrieved from www.evaluategroup.com
[2] Franklin, E. (2018, April 16). Copay Accumulator Programs: What’s at Stake for Patients? Retrieved from www.cancersupportcommunity.org
[3] Silverman, E. (2018, April 18). Which drug makers are most vulnerable to a new cost-shifting maneuver? Retrieved from www.statnews.com
© 2018 by Informa Business Intelligence, Inc., an Informa company. All rights reserved. No part of this publication may be reproduced in any form or incorporated into any information retrieval system without the written permission of the copyright owner.
About The Authors:
Meg Alexander, Managing Director of the reputation & risk management practice at Syneos Health, formerly INC Research/inVentiv Health, helps enhance and protect the reputations of life sciences businesses and their leaders, especially regarding issues related to recalls, compassionate use, lawsuits, pricing debates, contaminants and activist attacks. Susan Suponcic, Ph.D., Managing Director of the pricing and market access practice area at Syneos Health Consulting, assists life-sciences clients with strategic initiatives to optimize, substantiate and capture the value of their innovations across dynamic and demanding global market access environments.
To read more about key factors shaping the U.S. market landscape for rare diseases, download the free full report at www.syneoshealthcommunications.com/orphandrugvalue
38 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com

T H O U G H T L E A D E R S H I P I N A S S O C I A T I O N W I T H S Y N E O S H E A L T H
©2018 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 39
1. Match patient populations of interest with qualified investigators for faster, more successful clinical trials.
2. Get insight into diseased population size to drive country, site and experienced investigator selections for maximum feasibility and rapid decision-making.
SitetrovePharma intelligence | informa
Select clinical trial sites withpinpoint accuracy.
Los Angeles, USA8 Site Locations
London, UK3 Site Locations
Rome, Italy1 Site Location
New York, USA4 Site Locations
Tokyo, JAPAN12 Site Locations
Coverage 70+specific patient segments
US, Japan, France, Italy, Spain,Germany and United Kingdom
Visit https://goo.gl/LmnHrR to find out more.
SelectSmarter
to Sitetrove
NEW

40 | In Vivo | July/August 2018
❚ ON THE MOVEin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
❚ On the MoveRecent executive appointments in the life sciences industry
❚ HOWARD LEVINCMO, RenalGuard Solutions
❚ ELIOT FORSTERChairman, Avacta Group
❚ JOHN CELEBIPresident & CEO
Sensei Biotherapeutics
❚ RICHARD BRUDNICKCBO & Head, Strategy
Codiak BioSciences
❚ DAVID ARKOWITZCFO, Flexion TherapeuticsCOMPANY CHANGES
AMELIO, Steven To: Stimwave LLC, CFO (Jun) From: Paradigm Spine LLC, CFO Phone: 800-965-5134
ARKOWITZ, David To: Flexion Therapeutics Inc.,
CFO (May) From: Visterra Inc., COO & CFO Phone: 781-305-7777
AZELBY, Robert W. To: Alder BioPharmaceuticals Inc.,
Pres. & CEO (Jun) From: Juno Therapeutics Inc.,
EVP, Chief Commercial Officer Phone: 425-205-2900
BRATKOVICH, Lisa To: ChromaDex Corp.,
Chief Mktg. Officer (Jun) From: Direct Upside Group,
CEO & Principal Phone: 949-419-0288
BRUDNICK, Richard To: Codiak BioSciences Inc.,
CBO & Head, Strategy (Jun) From: Bioverativ Inc.,
EVP, Bus. Dev. & Alliance Mgmt. Phone: 617-949-4100
CAGNONI, Pablo J., MD To: Rubius Therapeutics Inc.,
CEO (Jun) From: Tizona Therapeutics Inc.,
Pres. & CEO Phone: 617-679-9600
CELEBI, John To: Sensei Biotherapeutics Inc.,
Pres. & CEO (May) From: X4 Pharmaceuticals Inc., COO Phone: 240-243-8000
DALLAS, Jayson, MD To: Aimmune Therapeutics Inc.,
Pres. & CEO (Jun) From: Ultragenyx Pharmaceuticals Inc.,
Chief Commercial Officer Phone: 650-614-5220
DATT, Joe, MD To: Imara Inc., SVP, Clinical Dev. (May) From: Orchard Therapeutics,
Global Head, Medical Affairs & Clinical Dev., Immunology Franchise Lead
Phone: 617-231-6021
DITONNO, Anthony A. To: Tenax Therapeutics Inc., CEO (Jun) From: Avantis Medical Systems Inc., CEO Phone: 919-855-2100
EPPERLY, Melissa To: PsiOxus Therapeutics Ltd.,
CFO (Jun) From: R-Pharm US LLC,
CFO & Head, Bus. Dev. Phone: +44-1235-835328
FARNAM, John To: Kura Oncology Inc., COO (Jun) From: Receptos Inc., VP, Bus. Ops. Phone: 858-500-8880
FLEURY, Gerald To: Paragon Bioservices Inc., CFO (Jun) From: Pharmaceuticals International Inc.,
CFO Phone: 410-975-4050
FRIEND, David, PhD To: Dare Bioscience Inc., CSO (Jun) From: Evofem Biosciences Inc., CSO Phone: 858-926-7655

July/August 2018 | In Vivo | 41
ON THE MOVE ❚invivo.pharm
aintelligence.informa.com
❚ JERI THOMASSVP, Commercial
Liquidia Technologies
❚ TERRY PIZZIECEO, Horizon Discovery Group
❚ SIDDHARTH PARULKARHead, Global Clinical Operations
Imara
❚ RICHARD MARSHALLCMO, Galecto Biotech
❚ JEANNE MAGRAMCSO, Quentis Therapeutics
GROCH, Brian To: Acasti Pharma Inc., Chief
Commercial Officer (Jun) From: Veru Inc., EVP,
Chief Commercial Officer Phone: 450-686-4555
HENDERSON, Molly To: Advaxis Inc., CFO (Jun) From: Cedar Cliff LLC, Consultant Phone: 609-452-9813
JAROSZ, Mary, RPh To: Dare Bioscience Inc.,
Global Head, Regulatory Affairs (Jun) From: Evofem Biosciences Inc.,
SVP, Regulatory Affairs & Quality Assurance
Phone: 858-926-7655
KIMURA, Alan, MD, PhD To: Enzyvant Sciences Ltd., CMO (Jun) From: SutroVax Inc., CMO Phone: 617-704-9385
KOPPIKAR, Utpal To: Atara Biotherapeutics Inc.,
CFO (Jun) From: Gilead Sciences Inc.,
VP, Corp. & Ops. Finance Phone: 650-278-8930
KRUM, Kaila To: AxoGen Inc., VP, Investor Relations
& Corp. Dev. (Jun) From: William Blair, Equity Research
Analyst, Medical Technology Phone: 386-462-6800
LACHMAN, Avihai To: Dune Medical Devices Inc.,
VP, R&D (Jun) From: Gilat Satellite Networks,
Dir., Antennas & Defense R&D Phone: 484-320-7536
LEVIN, Howard R., MD To: RenalGuard Solutions Inc.,
CMO (May) From: Coridea LLC,
Managing Partner, Pres. & CSO Phone: 508-541-8800
MAGRAM, Jeanne, PhD To: Quentis Therapeutics Inc.,
CSO (May) From: Northern Biologics Inc., CSO Phone: 646-440-9249
MARSHALL, Richard, MD, PhD To: Galecto Biotech AB, CMO (May) From: GlaxoSmithKline PLC,
VP, Head, Fibrosis & Lung Injury Discovery Performance Unit
Phone: +45-70-70-52-10
MCCARTNEY, Michael To: Cancer Genetics Inc.,
Chief Commercial Officer (Jun) From: SciKon Innovation Inc., CEO Phone: 201-528-9200
MOSCATO, JR., Robert C. To: Marina Biotech Inc., CEO (Jun) From: Cerecor Inc., Pres. & CEO Phone: 425-908-3600
PARULKAR, Siddharth To: Imara Inc., Head,
Global Clinical Operations (May) From: FujiFilm Pharmaco. Ltd.,
Global Program Mgr. Phone: 617-231-6021
PERRY, Gregory To: Finch Therapeutics Group Inc.,
CFO (Jun) From: Kala Pharmaceuticals Inc.,
Audit Committee Chairman Phone: 617-229-6499
RODINO-KLAPAC, Louise, PhD To: Sarepta Therapeutics Inc.,
VP, Gene Therapy (Jun) From: Myonexus Therapeutics Inc., CSO Phone: 617-274-4000
RUSSELL, Kerry, MD To: resTorbio Inc.,
VP, Clinical Dev. (Jun) From: Novartis Institutes for Biomedical
Research, Dir. & Senior Translational Med. Expert, Cardiovascular Div.
Phone: 617-482-2333

42 | In Vivo | July/August 2018
❚ ON THE MOVEin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
SATO, Aaron, PhD To: Twist Bioscience Corp.,
CSO, Pharma (Jun) From: LakePharma, CSO Phone: 408-410-0105
SHOU, Yaping, MD, PhD To: Trillium Therapeutics Inc.,
CMO (Jun) From: Takeda Oncology,
Exec. Medical Dir. Phone: 416-595-0627
SNOW, David P. To: Eloxx Pharmaceuticals Ltd.,
CBO (Jun) From: Radius Health Inc.,
Chief Commercial Officer Phone: +972-8-8505664
STARK, Matthew, PhD To: Cardiac Dimensions Inc., VP,
Clinical & Regulatory Affairs (May) From: Terumo Aortic, VP,
Clinical & Regulatory Affairs Phone: 425-605-5900
THIENEL, Ulrich, MD, PhD To: Finch Therapeutics Group Inc.,
CMO (Jun) From: RRD International LLC,
Chief Dev. & Medical Officer Phone: 617-229-6499
THOMAS, Jeri To: Liquidia Technologies Inc.,
SVP, Commercial (May) From: Harrison & Star,
SVP, Strategic Group Planning Phone: 919-328-4400
THORBURN, Jim To: Twist Bioscience Corp., CFO (Jun) From: Televerde, Chief Sales Officer Phone: 408-410-0105
TRAIL, Pamela A., PhD To: Molecular Partners AG, CSO (Jun) From: Regeneron Pharmaceuticals Inc.,
VP, Oncology Strategy & Program Direction
Phone: +41-44-755-7700
VARADAN, Anand To: Karyopharm Therapeutics Inc.,
EVP, Chief Commercial Officer (Jun) From: Ignition Insights LLC, Pres. Phone: 617-658-0600
WALDMAN, Adam To: TG Therapeutics Inc.,
Chief Commercial Officer (Jun) From: Celgene Corp., Head,
US Hematology-Oncology Mktg. Phone: 212-554-4484
WANG, Christina To: Athenex Inc., VP, Clinical Ops. &
Corp. Dev., Asia Pacific (Jun) From: Consultant Phone: 716-427-2950
WILLIAMS, Greg, PhD To: Eloxx Pharmaceuticals Ltd.,
COO (Jun) From: Radius Health Inc.,
Chief Dev. Officer Phone: +972-8-8505664
YODER, Bob To: Trevena Inc., VP,
Sales & Commercial Ops. (Jun) From: Orexigen Therapeutics Inc.,
SVP, Head, Global Commercial Ops., Alliance Mgmt. & IT
Phone: 610-354-8840
YORK, Michael B. To: PhaseBio Pharmaceuticals Inc.,
VP, Corp. Dev. & Commercial Strategy (Jun)
From: Orexigen Therapeutics Inc., VP, Global Bus. Dev. & Alliance Mgmt.
Phone: 610-981-6500
DIRECTORS
DALY, Richard J. To: Opiant Pharmaceuticals Inc.,
Director (Jun) Phone: 424-252-4756
DEESE, Willie To: G1 Therapeutics Inc., Director (Jun) Phone: 919-213-9835
FALBERG, Kathryn To: Tricida Inc., Director (Jun) Phone: 415-429-7800
FORSTER, Eliot To: Avacta Group PLC, Chairman (Jun) Phone: +44-844-414-0452
FREEMAN, Kevin D. To: Galectin Therapeutics Inc.,
Vice Chairman (Jun) Phone: 678-620-3186
JACOBS, Irwin To: Biological Dynamics Inc.,
Director (Apr) Phone: 858-558-8295
KLIBANSKI, Anne, MD To: Albireo Pharma Inc., Director (Jun) Phone: 857-254-5555
LEE, Thai To: Sonde Health Inc., Director (Jun) Phone: 617-456-0982
MOODY, Trevor To: Cardiac Dimensions Inc.,
Director (May) Phone: 425-605-5900
MUNOZ, Alain, MD To: OxThera AB, Director (Jun) Phone: +46-8-660-02-23
OKEY, Stephanie To: Albireo Pharma Inc., Director (Jun) Phone: 857-254-5555
SCHWALM, Cynthia To: G1 Therapeutics Inc., Director (Jun) Phone: 919-213-9835
UIHLEIN, Richard E. To: Galectin Therapeutics Inc.,
Chairman (Jun) Phone: 678-620-3186
July/August 2018 | In Vivo | 43
ON THE MOVE ❚invivo.pharm
aintelligence.informa.com
WYGOD, Martin J. To: Biological Dynamics Inc.,
Director (Apr) Phone: 858-558-8295
ADVISORS
BEUTLER, Bruce, MD To: Batu Biologics Inc.,
Scientific Advisor (Jun) Phone: 213-359-3179
HOPPIN, Jack, PhD To: biOasis Technologies Inc.,
Scientific Advisor (Jun) Phone: 604-295-7014
O’CONNOR, Sue, PhD To: biOasis Technologies Inc.,
Scientific Advisor (Jun) Phone: 604-295-7014
SALTARELLI, Mario, MD, PhD To: biOasis Technologies Inc.,
Scientific Advisor (Jun) Phone: 604-295-7014
PROMOTIONS
JARRETT, Jennifer To: Arcus Biosciences Inc., COO (Jun) From: CBO & CFO Phone: 510-694-6200
LOWRY, Michael W. To: Owens & Minor Inc.,
Chief Accounting Officer (Jun) From: Corp. Controller Phone: 804-723-7000
PIZZIE, Terry To: Horizon Discovery Group PLC,
CEO (May) From: Head, Commercial Ops. Phone: +44-1223-655-580
SHLEVIN, Harold H., PhD To: Galectin Therapeutics Inc.,
CEO (Jul) From: COO Phone: 678-620-3186
RESIGNATIONS
MEIER, Richard A. From: Owens & Minor Inc.,
EVP, CFO (Jun) Phone: 804-723-7000
MOHAN, Pankaj, PhD From: Oncobiologics Inc.,
Chairman & CEO (Jun) Phone: 609-619-3990
OAKLEY, Andrew From: Sosei Group Corp.,
EVP, CFO (Jun) Phone: +81-3-5210-3290
advertise with us and take your business to the next level.
Christopher Keeling +44 203 377 3183 [email protected] Customer Care: +1 888-670-8900 (USA)
In VivoPharma intelligence |

44 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
Derived from Strategic Transactions, Informa’s premium source for tracking life sciences deal activity, the Deal-Making column is a survey of recent health care transactions listed by relevant industry segment – In Vitro Diagnostics, Medical Devices, Pharmaceuticals, and Research, Analytical Equipment and Supplies – and then categorized by type – Acquisition, Alliance, or Financing.
Strategic Transactions is updated daily with in-depth deal analysis, structural and financial terms, and links to SEC-filed contracts.
For information about access please contact Customer Care at 800-332-2181 or [email protected]
�❚ Deal-MakingCovering deals made June 2018
❚ IN VITRO DIAGNOSTICSMergers & AcquisitionsBio-Techne pays $250mm plus earn-outs to buy Exosome Diagnostics
After three years, Roche gains full ownership of Foundation Medicine for $2.4bn
AlliancesJanssen Pharmaceutica grants Saladax exclusive rights to diagnostics-related patents
FinancingsExact Sciences grosses $202.4mm through upsized notes offering
❚ MEDICAL DEVICESMergers & AcquisitionsAcelity acquires Crawford Healthcare
Halyard Health acquires sports medicine-focused device company CoolSystems for $65mm
CoreLink buys Expanding Orthopedics
Advanced Sterilization Products to be acquired by Fortive for $2.7bn in cash
Novartis to spin off Alcon eye care unit as independent company in deal worth up to $5bn
Philips to buy EPD in deal potentially worth over €460mm
AlliancesThermi settles litigation with Viveve; gets rights to patent
Fresenius licenses Humacyte’s Humacyl acellular vessel; makes $150mm investment
MDS Pharm licenses Israeli rights to NanoVibronix’s PainShield and WoundShield ultrasound devices
FinancingsApollo Endosurgery nets $22.26mm via FOPO
Avita Medical commences $A16mm private placement
Neurology-focused nVNS device company electroCore nets $72.5mm in IPO
Haemonetics enters $700mm loan agreement
K2M sells $65mm in debt
Neuronetics nets $100mm in IPO
Medical device company PAVmed nets $9.5mm in rights offering
Latest follow-on grosses $58mm for PolarityTE
Senseonics nets $149.3mm via FOPO
❚ PHARMACEUTICALSMergers & AcquisitionsAkebia and Keryx to merge in $1.3bn stock-for-stock agreement
AMAG divests its Cord Blood Registry division to GI Partners for $530mm
GI Partners acquires donor sperm and egg bank California Cryobank, plans to combine with CBR
Nutriband signs LOI to acquire Carmel Biosciences
AlliancesMerck and 4D pharma enter trial collaboration for solid cancers
E-Scape gets global rights to preclinical compounds from AbbVie
Aerpio grants Gossamer rights to IBD program
Akero gets Phase I NASH compound from Amgen
BridgeBio gets rights to Alexion’s ALXN1101
Alexion, Complement co-develop CP010 for neurodegenerative disorders; Alexion has option to acquire company
Alvogen licenses CEE, Russian, and CIS rights to Theramex’s women’s health products
Amarin gets rights to Mochida IP
Biogen gets option to TMS’s Phase II stroke candidate
CStone gains rights to Blueprint’s cancer candidates
NeuroVive licenses BridgeBio rights to LHON program
Celgene options neuro candidates from Skyhawk; pays $60mm up front
Cipla to market Lilly’s Basaglar in India
Menarini Asia-Pacific gets certain Asian rights to Daiichi Sankyo’s Lixiana
Gilead and Hookipa team up for HIV/HBV vaccine development
Wize grants HPGC Medical rights to LO2A eye drops in China
Shionogi gets global rights to Hsiri compounds
RedHill gets exclusive US co-promotion rights to Napo’s Mytesi
Kramer buys Janssen’s Nizoral anti-dandruff shampoo
Kallyope, Novo Nordisk collaborate on development of obesity and diabetes therapies
TG Therapeutics and Novimmune partner to develop B-cell cancer therapy
Genentech signs microbiome deal around IBD with Microbiotica
Axovant gains worldwide license to Oxford BioMedica’s OXB102 gene therapy candidate for PD
Sanofi Pasteur partners with Translate Bio for infectious disease vaccines
Upsher-Smith gets US rights to six ophthalmic/otic products
Underskin licenses seven Sonoma hypochlorous acid dermatology formulations
TerSera gets US, Canadian rights to Tesaro’s Varubi
Yakult Honsha licenses Japanese duvelisib rights from Verastem
FinancingsADMA Biologics nets $37.6mm via FOPO
Aerpio nets $42.3mm via FOPO

invivo.pharmaintelligence.inform
a.com
©2016 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 45
DEAL-MAKING ❚
❚ IN VITRO DIAGNOSTICS
Mergers & Acquisitions
BIO-TECHNE CORP.Exosome Diagnostics Inc.Bio-Techne Corp. will pay $250mm to acquire privately held biofluid-based di-agnostics firm Exosome Diagnostics Inc. The deal also includes up to $325mm in earn-outs based on achievement of certain EBITDA targets in 2020 and 2022. (Jun.)The company’s founding scientist and CSO Dr. Johan Skog discovered that exosomes (messengers released by living cells) contain nucleic acids including DNA and RNA which can be used for diagnostic pur-poses. The company’s first marketed test, ExoDx Prostate(IntelliScore) (EPI), extracts exosomes from the urine of men with high-grade prostate cancer to detect three unique biomarkers indicative of the aggres-siveness of the disease. This noninvasive method aids in treatment planning for patients with an ambiguous PSA test result. Exosome also launched ExoDx Lung(ALK), a qPCR-based assay that detects five EML4-ALK fusions in plasma of patients with non-small cell lung cancer. (In development, the company has ExoDx Lung(T790M) and ExoDx Lung(EGFR), to detect the presence of T790M and EGFR mutations and aid in therapeutic decision-making for lung cancer patients.) The acquisition is highly complementary to Bio-Techne’s molecular pathology business Advanced Cellular Diagnostics, which offers single-cell-level detection and monitoring of single RNA molecules with its RNAscope RNA in situ hy-bridization platform. Exosome was founded in 2008 and raised close to $95mm through three venture rounds. Investors in the firm include NGN Capital, Forbion Capital, Arcus Ventures, Tiger Partners, and CD Ventures, among others. The company will operate as a subsidiary of Bio-Techne. Investment Banks/Advisors: Moelis & Co. (Exosome Diagnostics Inc.)
ROCHEFoundation Medicine Inc.Roche acquired the remaining 43% stake of publicly traded tumor genomic profiling company Foundation Medicine Inc. (FMI) that it didn’t already own for $2.4bn on a fully diluted basis (total company value of $5.3bn on a fully diluted basis). Roche
Neurology-focused Aptinyx nets $109.5mm in IPO
Autolus’s Nasdaq IPO nets $139.5mm
Gene therapy start-up AVROBIO nets $106.6mm in IPO
Eidos goes public netting $113.5mm
Catabasis nets $39.5mm via FOPO
Registered direct offering nets $20mm for Compugen
Crinetics seeks to go public
Deciphera funds clinical work with $185.9mm public offering
Entera Bio nets $10.3mm in IPO in the US
Forty Seven files for IPO
Galmed nets $70.5mm through public offering
Heron Therapeutics nets $194.7mm in FOPO
Public offering nets $162.9mm for ImmunoGen
Immunomedics nets $260.4mm through public offering
Intrexon offers $200mm of its convertible senior notes
Kadmon nets $106.4mm in concurrent public and registered direct offerings
Kezar’s initial public offering nets $80.2mm
Kura Oncology nets $65mm through public offering
Liquidia files for IPO
Madrigal nets $282.7mm via FOPO
Initial public offering nets $93mm for Magenta Therapeutics
Matinas nets $7.4mm in public offering
Gene therapy start-up MeiraGTx nets $80.2mm in Nasdaq IPO
Mirati nets $115.8mm through public offering
Neon Therapeutics nets $93mm through initial public offering
ObsEva SA nets $68.7mm in FOPO
Public offering nets $8.3mm for Oncolytics Biotech
OptiNose nets $60.1mm via FOPO
Pharnext secures €20.5mm in debt financing; receives first €11.5mm tranche this month
Rhythm nets $163.7mm via FOPO
Axovant raises $25mm in PIPE to support licensing of OXB102 from Oxford BioMedica
Soligenix nets $7.6mm in public offering
TapImmune aims for $70mm PIPE concurrent with closing of merger
Generics company Teligent secures $25mm senior term loan
Theratechnologies nets $55.2mm in bought deal financing
MRNA company Translate Bio nets $113mm in IPO
Tricida’s initial public offering nets $206.7mm
Public offering nets $16.7mm for Trovagene
Vascular Biogenics nets $14.4mm through registered direct offering
Verastem grosses $43mm through private placement
Dermatology-focused Verrica nets $80.2mm in IPO
Viking nets $72.6mm via FOPO
Xeris netted $91.4mm via IPO
Zafgen nets $64.9mm via FOPO
Public offering nets $91.9mm for Zymeworks

46 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
paid $137 in cash per share, a 34% pre-mium. (Jun.)Roche has had a relationship with FMI since 2012, when Roche Venture Fund participat-ed in FMI’s Series B round totaling $56mm. For a $1.03bn investment, Roche acquired approximately 57% of FMI in 2015; concur-rently, the companies also established a clinical and commercial collaboration, joining forces to inform development of combination drugs, novel targets, and companion diagnostics using genomic pro-filing tests. Roche put more money behind FMI in 2016-2017, providing a $200mm credit facility. Since selling its majority ownership to Roche, FMI has remained a publicly traded entity--it completed an IPO in 2013--and under the terms of their new transaction, FMI will continue to operate in-dependently and autonomously (although it’s not clear if the company will cease trad-ing its shares publicly). Within the last year, Roche has been adding to its molecular diagnostics and personalized medicines capabilities--the deal with FMI builds on that and follows acquisitions of Ignyta for $1.7bn and Flatiron Health for $1.9bn. Through its products and services, FMI pro-vides comprehensive genomic profiling for individuals to guide their cancer care. The company performs analyses on solid (using its FoundationOne assay) and hematologi-cal (FoundationOne Heme) tumors, and that information is later used to make informed decisions in clinical practice (Roche has ex-clusive ex-US rights to both tests). FMI says it has profiled more than 180k patients to date (the FoundationCore platform, where these genomic profiles are stored, is being built out into a broader product through partnerships, including one with Flatiron Health). Newer products in its portfolio include FoundationACT, which performs a liquid biopsy to screen for circulating tumor DNA; FoundationFocus, a companion diagnostic for Clovis Oncology’s ovarian cancer drug Rubraca; and FoundationOne CDx (F1CDx), a broad companion diagnostic that can identify the most likely responders to one of 17 targeted therapies for several solid tumor types including non-small cell lung cancer, melanoma, colorectal cancer, ovarian cancer, or breast cancer. FMI also works with industry players and has over 30 biopharma partners including BMS, Novartis, and Pfizer. At the end of Q1 2018, FMI had $60.3mm cash on hand. Its last twelve months of revenue totaled $179.4mm Investment Banks/Advisors: Citigroup Inc. (Roche); Goldman Sachs & Co. (Foundation Medicine Inc.)
Alliances
JOHNSON & JOHNSONJANSSEN PHARMACEUTICA NVSALADAX BIOMEDICAL INC.Janssen Pharmaceutica NV licensed Sal-adax Biomedical Inc. exclusive worldwide
rights to patents related to diagnostics for determining antipsychotic drug levels. (Jun.)The agreement is important because about 40-60% of patients don’t take their antipsychotic medications as prescribed and their doctors are unable to track ad-herence. Therefore the psychiatrists don’t know whether treatment is ineffective due to adherence or lack of the drug efficacy. Saladax seeks to create tests that provide those doctors with information needed to make effective decisions regarding patient treatment. The company currently offers the MyCare psychiatry blood tests that measure the levels of medication that patients are receiving and can help en-able physicians to personalize a treatment plan. Two out of the six tests are cleared in Europe while the remaining four should be cleared in Q3 of this year. Saladax plans to file applications for regulatory approval starting this month. The agree-ment positions Saladax as a leader in the antipsychotic drug testing space.
Financings
EXACT SCIENCES CORP.Exact Sciences Corp. (markets the Colo-guard noninvasive stool DNA-based test for colorectal cancer) grossed $202.4mm through an upsized offering of $190mm aggregate principal amount of its 1% se-nior notes due 2025. The offering is fully fungible and will form a single series with the $690mm aggregate principal amount of notes that Exact issued in January; similar to that offering, the current notes convert to common at a rate of 13.2569 shares per $1k, or $75.43. (Exact’s shares averaged $57.48 at the time of the sale.) (Jun.)Investment Banks/Advisors: Bank of America Merrill Lynch
❚ MEDICAL DEVICES
Mergers & Acquisitions
ACELITY LP INC.CRAWFORD HEALTHCARE LTD.Acelity LP Inc. acquired Crawford Health-care Ltd., a UK-based firm developing skin and wound care products and diagnostics. Financial details were not disclosed. (Jun.)Crawford was formed in 1996 and of-fers skin care lines including SunSense sunscreens, QV emollient cleansers and moisturizers, SilDerm scar therapy, and Zindaclin for acne. Acelity is most interested in its wound care products, noting that the firm’s offerings will greatly complement its own line of advanced wound dressings (AWD). Crawford’s wound products include KerraContact sil-ver dressing, KerraFoam absorbent foam dressing, KerraPro pressure ulcer pads, and KerraCel caboxmethyl cellulose gell-
ing fiber dressing. Crawford’s CEO Richard Anderson will remain at the company’s helm during an initial transition period.
CORELINK LLCEXPANDING ORTHOPEDICS INC.CoreLink LLC acquired fellow closely held spinal device maker Expanding Orthope-dics Inc. (EOI) for an undisclosed sum. (Jun.)EOI offers the FLXfit expandable articu-lated interbody fusion device, which is used together with supplemental fixation to provide structural stability following total or partial discectomy. Its FLXfit 15 is a titanium TLIF interbody device that’s compatible with minimally invasive sur-gery. Both products are FDA approved. The company is also working on the XPED pedicle screw system for spinal fusion sur-gery. It is designed to offer immobilization and stabilization of spinal segments as an adjunct to spinal fusion of the thoracic, lumbar, and/or sacral spine. The device is not cleared for sale in the US. EOI’s devices are complementary to CoreLink’s own interbody fusion devices and pedicle screws. Following the acquisition, Core-Link plans to provide enhanced support for current FLXfit and FLXfit 15 users and create system upgrades for a full com-mercial relaunch set for Q3 2018.
FORTIVE CORP.JOHNSON & JOHNSONEthicon Inc.Advanced Sterilization ProductsFortive Corp. has made a binding offer to acquire Johnson & Johnson’s closely held Advanced Sterilization Products (ASP) for $2.7bn in cash and $0.1bn of retained net receivables. (Jun.)ASP is a division of Ethicon and offers prod-ucts for hospital-acquired infection preven-tion. Specific products including the STER-RAD system, which uses low-temperature hydrogen peroxide gas plasma technology to efficiently and effectively sterilize a wide range of instruments. The company also provides high-level disinfection products including the ENDOCLENS and EVOTECH systems for endoscope reprocessing and cleaning, CIDEZYME detergent, and CIDEX disinfectant. Its products are tough on microorganisms but gentle on endoscopes and other medical devices. In 2017, ASP generated revenue of $775mm. Fortive says the acquisition provides entry into the growing medical sterilization and disinfection market, and is aligned with the firm’s focus on assisting its customers with driving better safety, compliance, and efficiency in critical workflows. Investment Banks/Advisors: Goldman Sachs & Co. (Fortive Corp.)
NOVARTIS AGAlcon Inc.After considering various other options, Novartis AG decided to spin off the

Recognising the best in the globalgenerics and biosimilars industries.
Cocktail Reception & Awards PresentationTuesday, 9 October 2018Palacio Municipal de CongresosMadrid, Spain
Sponsor, Enter, Join us!Find out more about sponsoring or entering
an Award and joining us on the night.
Visit: www.pharmaintelligence.informa.com/ggbaEmail: [email protected] | Call: +44 (0) 1564 777 550
Presented by
In association with
Sponsored by
JN1113 GGB Awards 2018 Advert USA4.indd 1 2018/05/25 10:14

48 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
device-focused parts of its Alcon Inc. eye care division into a separate independent company so the former can focus on its pharma business. (Jun.)The spin-off plan is essentially a share buy-back program worth up to $5bn. Novartis will fund the transaction with the proceeds it received earlier this year after divest-ing to GSK its 36.5% ownership stake in their 2014 consumer health joint venture. Novartis paid $52bn to acquire Alcon from Nestle, first buying a 25% stake in 2008 (for $11bn) and later exercising its option for the remainder of the company in 2010 (paying an additional $41bn). Alcon is made up of three ophthalmologic-focused businesses: surgical, vision care, and pharmaceuticals. The surgical unit has a portfolio of technolo-gies and devices for cataract, retinal, glau-coma, and refractive surgeries; intraocular lenses to treat cataracts and refractive er-rors such as presbyopia and astigmatism; and disposables, including viscoelastics, surgical solutions, and surgical packs, for cataract and vitreoretinal surgery. The vi-sion care division offers a range of contact lenses (daily disposable, monthly replace-ment, and color-enhancing) and lens care products (solutions to clean, rinse, and disinfect contact lenses; rewetting drops; and a daily protein remover) and includes the integrated Ciba Vision brand. In the past years, these two subsidiaries have faced difficulties in growth but in the second half of last year started to see an improvement, thanks to investment by Novartis. Novartis will retain Alcon’s ophthalmology pharma-ceuticals business (which had 2017 sales of $4.6bn), and its pipeline that includes the potential blockbuster brolucizumab (RTH258), now in Phase III for age-related macular degeneration and diabetic macu-lar edema. When the spin-off is completed (expected by the end of 2019), the result will be a new Switzerland-based eye care devices company (listed on both the Swiss and the New York stock exchanges)--led by Alcon’s current COO David Endicott as CEO and Mike Ball (presently Alcon’s CEO) as chairman--with more than 20k employees worldwide and an estimated $7bn in sales.
ROYAL PHILIPS ELECTRONICS NVPhilips HealthcareEPD SOLUTIONS LTD.Royal Philips’ Philips Healthcare is acquir-ing closely held cardiac device maker EPD Solutions Ltd. for €250mm ($292mm) and potentially €210mm ($246mm) more in earn-outs. (Jun.)Based in the British Virgin Islands, EPD was founded by seasoned inventor and entre-preneur Shlomo Ben-Haim, MD, who found-ed many successful device and biomedical firms, including Biosense Webster, which was acquired by Johnson & Johnson for over $400mm. Following the acquisition by Philips, EPD and its employees will become
part of its image-guided therapy business. EPD has developed a cardiac imaging and navigation system, which received the CE Mark in February. The platform combines algorithms and single-use electromagnetic sensors to create a detailed 3D image of the heart during cardiac arrhythmia ablation procedures. EPD has submitted a 510(k) application which is under FDA review. The company hopes that being a part of Philips will allow it to reduce procedure costs and improve efficacy while simpli-fying navigation and treatment. Philips plans to combine EPD’s product with its own systems, including the Azurion next-generation image-guided therapy. Philips’ current image-guided therapy portfolio is used in vascular surgery, angioplasty, and peripheral vascular interventions. With EPD under its belt, it will now address the over €2bn market for image-guided cardiac arrhythmia treatments.
Alliances
ALMIRALL SAThermiVIVEVE MEDICAL INC.As a result of ongoing patent litigation stemming from Viveve Medical Inc.’s 2016 claim against Thermi (now part of Almirall SA) that the latter infringed its patented technology without consent, Viveve grant-ed Thermi a non-exclusive, non-transfer-able license to the IP. In return, Viveve will receive a monetary payment and on-going royalties. The IP in question, US patent No. 8,961,511 (assigned to Viveve), relates to a vaginal remodeling device and the heating/cooling method used to deliver energy to tighten targeted tissues. The technology is incorporated in the current version of Thermi’s ThermiVa temperature controlled radiofrequency energy system, which is indicated in the US, Brazil, and China for dermatological and general electrocoagu-lation and hemostasis surgical procedures and in Europe for electrocoagulation of soft tissues for vulvovaginal laxity. (Jun.)
FRESENIUS SE & CO. KGAAFresenius Medical Care AG & Co. KGAAHUMACYTE INC.Humacyte Inc. granted Fresenius Medical Care AG & Co. KGAA exclusive global rights to commercialize the Humacyl human acellular vessel (HAV). (Jun.)Humacyl is in Phase III trials in the US and Europe. The bioengineered human tissue-based blood vessel is intended to provide vascular access for end-stage renal disease patients on hemodialysis who are not candidates for other options including fis-tulas, grafts, and central venous catheters. Humacyl offers enhancements over those synthetic options including lower risk of infection and other complications. Frese-nius, which is one of the world’s largest dialysis providers, made a $150mm equity
investment in Humacyte under terms of the deal, and now holds a 19% stake.
MDS PHARM LTD.NANOVIBRONIX INC.NanoVibronix Inc. granted MDS Pharm Ltd. an exclusive license to market and distribute its PainShield and WoundShield ultrasound devices in Israel. (Jun.)Incorporating NanoVibronix’s patented low intensity surface acoustic wave (SAW) technology, PainShield and WoundShield are portable handheld ultrasound devices for use by the patient in-home. Both CE-marked devices consist of a reusable driver unit coupled with a disposable patch containing a therapeutic transduc-er, which delivers a localized ultrasound effect to a targeted area. The drug-free PainShield (also FDA approved) provides relief from acute and chronic nerve, mus-cle, joint, and soft tissue pain related to trigeminal neuralgia (a condition caused by nerve compression that interferes with pain pathways). The WoundShield acceler-ates wound healing and facilitates tissue regeneration by increasing capillary perfu-sion and tissue oxygenation. It also has a configuration for topical drug delivery. MDS already has a broad portfolio of drug-free pain management devices, incorpo-rating platforms such as electrotherapy, ultrasound, phototherapy, and TENS, to treat a variety of pain types. Through its established Israeli distribution channels, MDS is an ideal partner for NanoVibronix, enabling the US company to penetrate various markets in that territory, including health care providers, retail pharmacies, and direct-to-consumer online shops.
Financings
APOLLO ENDOSURGERY INC.Apollo Endosurgery Inc. (minimally inva-sive devices for bariatric and gastrointesti-nal procedures) netted $22.26mm through a follow-on public offering of 4.31mm com-mon shares (including full exercise of the overallotment) at $5.50 each. (Jun.)Investment Banks/Advisors: Craig-Hallum Inc.
AVITA MEDICAL LTD.Avita Medical Ltd. (regenerative medicine) raised $A12.8mm ($10.2mm) through the first tranche of a $A16mm private place-ment. Institutional and sophisticated investors purchased 255.5mm shares at A$0.05 (even with the market), and will buy a further 65mm shares following a general meeting in July. Proceeds will support US launch of the RECELL autologous epidermis regeneration device once approved by the FDA (anticipated later this year). (Jun.)
HAEMONETICS CORP.Haemonetics Corp. (blood management devices and services) entered into a

invivo.pharmaintelligence.inform
a.com
©2016 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 49
DEAL-MAKING ❚
$700mm loan agreement, which includes a $350mm unsecured term loan and a $350mm senior unsecured revolving credit facility. Both loans bear interest at an annual rate of LIBOR plus 1.25% and are due in 2023. Proceeds will be used to re-pay an existing $254mm senior unsecured term loan due June 2019. (Jun.)Investment Banks/Advisors: Citigroup Inc.; Citizens Bank NA; JP Morgan Chase & Co.
K2M GROUP HOLDINGS INC.Spinal device maker K2M Group Holdings Inc. sold $65mm (net $61.8mm) in 3% convertible senior notes due 2025 to quali-fied institutional buyers. The notes will pay interest semi-annually in cash on June 30 and December 30, beginning December 30, 2018. They will convert based on an initial rate of 35.2930 common shares per $1k principal amount (equivalent to $28.33; the stock was averaging $23.26). K2M will use $18mm of the proceeds to repay bor-rowings under a revolving credit facility and the remaining funds will be used for general corporate purposes. (Jun.)
NEURONETICS INC.Neuronetics Inc. (neurostimulation device to treat psychiatric and neurological dis-orders) netted $100mm in its initial public offering of 6.325mm shares (including the overallotment) at $17.00. The company originally planned to sell 5mm shares at a $14-16 range. (Jun.)Investment Banks/Advisors: BTIG LLC; Canaccord Genuity Inc.; JMP Securities LLC; Piper Jaffray & Co.; William Blair & Co.
PAVMED INC.PAVmed Inc. (medical devices) netted $9.5mm in an oversubscribed rights offering of 9mm units at $1.15 per unit. Each unit consists of one common share and one Series Z warrant to purchase an additional common share at a strike price of $1.60 (expires April 30, 2024). PAVmed’s lead products address carpal tunnel syndrome (CarpX), precancerous conditions of the esophagus (EsoCheck), vascular access (PortIO) and pediatric ear infections (DisappEAR). (Jun.)Investment Banks/Advisors: Dawson James Securities Inc.; Maxim Group LLC
POLARITYTE INC.PolarityTE Inc. (regenerative tissue prod-ucts and biomaterials) grossed $58mm through a public offering of 2.45mm com-mon shares (including the overallotment) at $23.65. The offering comes just two months after PolarityTE raised $35mm through a separate FOPO. Proceeds will support R&D work and future regulatory/commercialization activities. (Jun.)Investment Banks/Advisors: Cantor Fitzgerald & Co.
SENSEONICS HOLDINGS INC.Senseonics Holdings Inc. (developer of the Eversense implantable continuous glucose monitoring system for diabetics) netted $149.3mm through the follow-on offering of 38.1mm common shares (including full exercise of the overallotment) at $3.9263 each. The company will use the funds to com-mercialize Eversense in the US and for R&D of future configurations of the device. (Jun.)Investment Banks/Advisors: BTIG LLC
❚ PHARMACEUTICALS
Mergers & Acquisitions
AKEBIA THERAPEUTICS INC.KERYX BIOPHARMACEUTICALS INC.Kidney disease drug developers Akebia Therapeutics Inc. and Keryx Biopharma-ceuticals Inc. have agreed to merge in a deal worth $1.3bn. Keryx shareholders will receive 0.37433 common shares of Akebia for each Keryx share held, resulting in an implied ownership of 49.4% Akebia/50.6% Keryx on a fully diluted basis. (Jun.)The combined company will take Akebia’s name and be headed by Akebia’s current CEO John Butler (who, up until late last year, also served as Keryx’s chairman). Keryx brings to the table its marketed drug Au-ryxia (ferric citrate), which is indicated for hyperphosphatemia in dialysis-dependent chronic kidney disease patients and iron deficiency anemia in non-dialysis depen-dent CKD patients. Akebia adds its vada-dustat, a Phase III oral hypoxia-inducible factor prolyl hydroxylase inhibitor (HIF-PHI) for CKD-related anemia. Together, the firms will be able to present to renal disease specialists an all-oral treatment approach and help stave off competition from rivals including FibroGen and GlaxoSmithKline, which both have late-stage HIF projects approaching market approval. Sharehold-ers from both Keryx and Akebia support the business combination; the Baupost Group, a 21.4% stakeholder in Keryx, has agreed to convert its outstanding convert-ible notes into Keryx common prior to closing. Investment Banks/Advisors: MTS Health Partners; Perella Weinberg Partners (Keryx Biopharmaceuticals Inc.); Evercore Partners; JP Morgan Chase & Co. (Akebia Therapeutics Inc.)
AMAG PHARMACEUTICALS INC.Cord Blood Registry Inc.Private equity firm GI Partners agreed to acquire AMAG Pharmaceuticals Inc.’s Cord Blood Registry Inc. (CBR) unit, a newborn stem cell banking company. (Jun.)GI Partners will pay $530mm in cash for the business, which accounts for about 19% of AMAG’s 2017 revenues. Back in June 2015, AMAG bought CBR from PE firm GTCR (which had owned it since 2012) for
$700mm. Founded in 1992, CBR provides direct-to-consumer services related to the collection, processing, cryopreservation, and storage of umbilical cord blood taken immediately after birth. The company of-fers families these services to preserve newborn stem cells for potential future use in transplant medicine to treat certain cancers and blood, immune, and meta-bolic disorders. At the end of 2017, CBR stored approximately 700k umbilical cord blood and cord tissue units isolated from newborn umbilical cords, which CBR says accounts for approximately 40% of all privately stored cord blood and cord tissue units in the US. Additionally, through col-laborations with academia and research in-stitutions, the company incorporates stem cells in regenerative medicine research and FDA-regulated clinical trials. GI Partners plans to merge CBR with donor sperm and egg bank California Cryobank, which GI concurrently acquired from Longitude Capital and NovaQuest Capital. California Cryobank provides frozen donor sperm, frozen donor egg, reproductive tissue stor-age, and cord blood banking services. The combined new entity will create a provider of expanded stem cell storage and repro-ductive tissue services. The divestiture offers AMAG the ability to focus on its drug development efforts in maternal and women’s health, anemia management, and cancer supportive care. AMAG will use the proceeds from the current sale to pay off the remaining $475mm in principal from its 7.875% senior notes due 2023, which the company received as part of an $850mm loan in 2015 to help finance the simultaneous purchase of CBR at that time. Investment Banks/Advisors: Perella Wein-berg Partners (AMAG Pharmaceuticals Inc.)
CALIFORNIA CRYOBANK INC.Private equity firm GI Partners agreed to acquire privately held donor sperm and egg bank California Cryobank Inc. (CCB) from healthcare investors Longitude Capi-tal and NovaQuest Capital. (Jun.)Founded in 1977, CCB provides donor sperm and egg services and reproductive tissue storage for use in future in vitro fertiliza-tion procedures through its reproductive division. Sperm and egg donors undergo a rigorous qualification process as well as extensive medical testing and genetic screening to guarantee the most successful insemination and fertilization and embryo transfer procedures. In December 2016, CCB acquired Donor Egg Bank USA, expand-ing its frozen donor egg banking capabili-ties with egg freezing technology capable of producing success rates comparable to traditional fresh donor egg programs. CCB also has a stem cell division, FamilyCord, which offers cord blood banking services. GI plans to combine CCB with newborn stem cell collection and banking company Cord Blood Registry, which GI concurrently

50 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
acquired from AMAG Pharmaceuticals for $530mm. The new merged entity will bring together the complementary businesses to create a single company specializing in umbilical cord blood and tissue collec-tion and storage and reproductive tissue services, which will serve approximately 600k families in 30 countries.
NUTRIBAND INC.CARMEL BIOSCIENCES INC.Nutriband Inc. signed a letter of intent to acquire closely held Carmel Biosciences Inc. for $3.8mm in stock (issuing 450k restricted common shares). (Jun.)Founded in 2011, Carmel is focused on therapies for cardiovascular and metabolic diseases. It’s working on both liquid refor-mulations of existing drugs and new chemi-cal entities. After receiving FDA approval in December 2017, Carmel’s Prexxartan became the only available oral liquid dos-age form of valsartan in the US. The drug is an angiotensin receptor blocker for treating hypertension in people six years and older. Prexxartan is also indicated for heart failure and stable left ventricular failure or left ven-tricular dysfunction following myocardial infarction. Carmel’s NCEs include CAR208 for central nervous system disorders, INV144 for hypertension, and INV404 for atherosclerosis. Nutriband’s focus is on transdermal and topical technologies.
Alliances
4D PHARMA PLCMERCK & CO. INC.Merck & Co. Inc. and 4D pharma PLC agreed to work together on a trial col-laboration evaluating the combination of Merck’s Keytruda (pembrolizumab) with 4D’s MRx0518 for solid tumors. (Jun.)Preclinical MRx0518 is 4D’s lead candi-date developed with live biotherapeutic products from the human gut microbiome. Preclinical studies have shown reduc-tion in tumor size (with in vivo models) and increased necrotic area surrounding tumor cells. Merck’s Keytruda, a PD-1 antagonist, is marketed for melanoma, NSCLC, Hodgkin’s lymphoma, and head and neck, bladder, stomach, esophageal, and colorectal cancers. It is also awaiting approval for diffuse large B-cell lymphoma and cervical cancer, and is in trials for a number of other solid and blood cancers. The partners will conduct a Phase I trial to study safety, tolerability, and initial benefit of the MRx0518/Keytruda combination in patients with renal, bladder, melanoma, and non-small cell lung cancer who have progressed on prior PD-1 inhibitor therapy.
ABBVIE INC.E-SCAPE BIO INC.AbbVie Inc. licensed E-Scape Bio Inc. worldwide rights to small-molecule selec-tive S1P5 receptor agonists for treating
central nervous system-related lysosomal storage disorders. (Jun.)AbbVie receives an undisclosed up-front cash payment, sales royalties, and gets an equity stake in E-Scape. AbbVie will also nominate an observer to the E-Scape board. The licensed candidates are in late-preclin-ical studies and E-Scape will commence IND preparatory work with an IND filing expected in 2019. S1P5 receptor agonists can reduce the synthesis of metabolites that become highly toxic in the brain and cause lysosomal storage disorders. The newly licensed compounds join E-Scape’s pipeline which includes programs aimed at Parkinson’s and Alzheimer’s diseases.
AERPIO PHARMACEUTICALS INC.GOSSAMER BIO INC.In a deal potentially worth up to $420mm, Aerpio Pharmaceuticals Inc. licensed Gossamer Bio Inc. exclusive global rights to develop and commercialize AKB4924 and related compounds for inflammatory bowel diseases including ulcerative colitis and Crohn’s disease. (Jun.)Gossamer paid Aerpio $20mm up front and could shell out $55mm in development milestones, up to $85mm in regulatory milestones, and up to $260mm in sales milestones with respect to the first licensed product for each of the first two initial indica-tions. Aerpio could also receive sales royal-ties in the high-single-digit to mid-teens (Strategic Transactions assumes 9-16%). Gossamer is obligated to develop and com-mercialize therapies in at least the US, two major European countries, and Japan for at least one of the initial indications. The companies will create a joint committee to oversee development and manufacturing activities. AKB4924 is a hypoxia-inducible factor-1 alpha (HIF-1 alpha) stabilizer that Gossamer renamed as GB004. The com-pound is currently in Phase I for IBD and has potential to have a better efficacy and safety profile and once-daily oral route of adminis-tration compared to current IBD therapies. Gossamer was launched early this year by former Receptos executives and raised $100mm with seed/Series A financing.
AKERO THERAPEUTICS INC.AMGEN INC.Amgen Inc. licensed newly formed Akero Therapeutics Inc. exclusive worldwide rights to its Phase I nonalcoholic steato-hepatitis (NASH) compound AKR001. (Jun.)Akero concurrently raised $65mm in Se-ries A financing to advance the compound into Phase II trials. Specific terms of the licensing agreement were not disclosed. AKR001 is a long-acting fibroblast growth factor 21 (FGF21) analog designed to regu-late metabolism and signaling throughout the body including the liver, reduce liver fat, and suppress inflammation and fibro-sis. There are no FDA-approved drugs for
NASH. Akero plans to evaluate the therapy for other metabolic diseases.
ALEXION PHARMACEUTICALS INC.BRIDGEBIO PHARMAOrigin BiosciencesBridgeBio Pharma acquired from Alexion Pharmaceuticals Inc. ALXN1101 (cyclic pyranopterin monophosphate) for mo-lybdenum cofactor deficiency (MoCD) Type A. (Jun.)Alexion is eligible for development and sales milestones. BridgeBio has launched a new subsidiary, Origin Biosciences, to develop and commercialize ALXN1101. The compound is in Phase III as an enzyme replacement therapy for MoCD, an ultra-rare autosomal recessive inborn error of metabolism caused by a mutation in the MOCS1 gene. The condition causes severe neurological deterioration and usually leads to death in newborns within weeks or months. ALXN1101 was discovered by Orphatec and Alexion got rights to the candidate in early 2011. It has break-through therapy designation from the FDA. BridgeBio has committed sufficient resources to Origin so that it can continue clinical trials, gain regulatory approval, and commercialize the therapy.
ALEXION PHARMACEUTICALS INC.COMPLEMENT PHARMAAlexion Pharmaceuticals Inc. and Comple-ment Pharma are collaborating on the development of Complement’s CP010 for neurodegenerative disorders. (Jun.)Alexion will provide up to €14mm ($16.5mm) in development milestones for the length of the agreement, which runs through Phase Ib development. Comple-ment will conduct preclinical and Phase I studies and retains manufacturing rights for CP010. Alexion has the option to acquire Complement during the agreement term. CP010 is a preclinical humanized mono-clonal antibody that binds to and inhibits the activity of the C6 complement (a protein encoded by the C6 gene), which is mainly synthesized in the liver. Inhibiting C6 pre-vents membrane attack complex--an end-product of complement pathway activation that mediates cellular injury, but is also known to play a role in neurodegeneration--from forming on the surface of pathogen cell membranes in the peripheral or central nervous system. Complement was founded as Regenesance in 2009, but in late 2017 changed its name. Complement’s C6 complement inhibition platform, invented by a team led by company CSO Frank Baas, MD, PhD, and CEO Robert Jan Lamers, MSc, is based on locked-nucleic-acid (LNA) tech-nology. Preclinical evidence suggests that blocking complement activation delays nerve degeneration and may accelerate nerve regeneration. The company plans to initially develop CP010 for acute nerve damage, such as traumatic brain injury or

Entry and General Enquiries:Natalie Cornwell
Tel: +44 (0) 7827 993 776 | Email: [email protected]
Sponsorship and Table Booking Enquiries:Christopher Keeling
Tel: +44 (0) 20 3377 3183 | Email: [email protected]
Scrip Awards 2018
The 14th AnnualScrip Awards
Book your table
28 November 2018 | The Hilton on Park Lane, London, UK
www.scripawards.com2018
Sponsored by Headline Sponsor
JN1238 Scrip Awards 2018 Book your Table Advert US A4.indd 1 2018/07/02 18:36

52 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
Guillain-Barre syndrome, and believes its discoveries could result in potential thera-pies for multiple sclerosis. ALS, or myas-thenia gravis. Complement will benefit from Alexion’s expertise in rare diseases and extensive research in complement biology.
ALVOGEN INC.THERAMEX Alvogen Inc. in-licensed exclusive sales, promotion, and marketing rights to cer-tain Theramex women’s health products within Russia, Central and Eastern Europe, and some Commonwealth of Independent States (CIS) countries. (Jun.)In addition to Russia, territories covered under the agreement are Kazakhstan, Ukraine, Estonia, Latvia, Lithuania, Bosnia and Herzegovina, Bulgaria, Croatia, Czech Republic, Hungary, Macedonia, Serbia, and Slovenia. The deal includes marketed bone health brands Alpha D3 (alfacalcidol) and Actonel (risedronate sodium); certain products from Theramex’s oral contracep-tive portfolio; and candidates from Thera-mex’s development pipeline. Theramex says the marketed products generated $13.5mm in 2017 net revenues, and the pipeline compounds will enable additional potential growth. Late last year, private equity firm CVC Capital Partners acquired the portfolio of Theramex’s assets from Teva; the new company is headquartered in London and sells across 50 European, African, Asia-Pacific, and Latin American countries branded and branded generic products focused on women’s health, specifically contraception, fertility, meno-pause, and osteoporosis. The current deal, in which Alvogen will provide its existing sales and marketing network cov-ering more than 20 CEE markets through 450 sales representatives, strengthens Theramex’s sales efforts in the CEE region and also complements Alvogen’s current women’s health offerings.
AMARIN CORP. PLCMOCHIDA PHARMACEUTICAL CO. LTD.Mochida Pharmaceutical Co. Ltd. granted Amarin Corp. PLC exclusive rights to certain intellectual property for use in de-veloping and commercializing products in the US and certain other territories. (Jun.)The IP is based on the omega-3 acid eicosapentaenoic acid (EPA). Mochida and Amarin are both specializing in the development of EPA therapies for patients at risk for cardiovascular disease. Amarin successfully developed and currently markets Vascepa (icosapent ethyl), the only FDA-approved prescription pure EPA drug. Vascepa is sold as an adjunct to diet for reducing triglyceride levels in adults with hypertriglyceridemia. Amarin is con-ducting the REDUCE-IT cardiovascular out-comes study for the drug and anticipates top-line data before the end of Q3 2018.
BIOGEN INC.TMS CO. LTD.Biogen Inc. received the exclusive option to acquire TMS’s Phase II acute ischemic stroke (AIS) candidate TMS007. (Jun.)Biogen will pay TMS $4mm up-front for the option. It would shell out another $18mm should it pick up the option, in addition to up to $335mm in development and com-mercial milestones plus sales royalties. TMS007 is a plasminogen activator with a unique mechanism of action that can break down blood clots and block inflammation at the site of the clot. Biogen believes the candidate could offer a better therapeu-tic option for AIS patients than current thrombolytic agents. The compound is complementary to Biogen’s Phase III-ready BIIB093 (glibenclamide), also for stroke.
BLUEPRINT MEDICINES CORP.CSTONE PHARMACEUTICALS CO. LTD.Blueprint Medicine Corp. granted CStone Pharmaceuticals Co. Ltd. exclusive rights to develop and sell three of its cancer can-didates (as monotherapies or combination regimens) in Mainland China, Hong Kong, Macau, and Taiwan. (Jun.)Included in the deal are avapritinib (BLU285), a KIT/PDGFR alpha inhibitor in Phase III for gastrointestinal stromal tumors and Phase I for advanced systemic mastocytosis; BLU554, an FGFR4 inhibitor in Phase I for hepatocellular carcinoma; and BLU667, an RET tyrosine kinase in-hibitor in Phase I for thyroid and non-small cell lung cancers. CStone paid $40mm up front and is responsible for $118.5mm in development and regulatory milestones, $227.5mm in sales milestones, and royal-ties ranging from the mid-teens to low-twenties. (Strategic Transactions estimates 14-23%.) CStone will lead all development and commercialization activities in its terri-tories. Also included in the deal is the joint development of a combo candidate using BLU554 together with CStone’s anti-PD-L1 immunotherapy CS1001, which is in Phase I lymphoma studies. The partners will evalu-ate the combination in proof-of-concept trials as a potential first-line treatment for hepatocellular carcinoma.
BRIDGEBIO PHARMAFortify TherapeuticsNEUROVIVE PHARMACEUTICAL ABNeuroVive Pharmaceutical AB licensed BridgeBio Pharma exclusive rights to develop its NVP015 program for Leber’s hereditary optic neuropathy (LHON). (Jun.)BridgeBio has launched Fortify Therapeu-tics to develop selected lead compounds from the NVP015 succinate prodrug program for the localized treatment of LHON. BridgeBio has committed $20mm in financing to the new subsidiary. The licensing agreement is valued at $60mm, consisting of research funding and mile-
stone payments, plus single-digit royalties. LHON is a rare inherited form of vision loss caused by mitochondrial DNA mutations. The NVP015 prodrugs can potentially treat the disease by bypassing the dysfunctional metabolic pathway, thus providing an alternate source of energy to the retinal cells. Santhera’s Raxone is currently the only available therapy for LHON. NeuroVive also has NVP015 in preclinical development for ischemia, cerebral heart failure, and mi-tochondrial disease; these indications are not part of the deal. BridgeBio recently ac-quired Alexion Pharmaceuticals’ ALXN1101 (cyclic pyranopterin monophosphate) for molybdenum cofactor deficiency.
CELGENE CORP.SKYHAWK THERAPEUTICS INC.Celgene Corp. and Skyhawk Therapeu-tics partnered to discover and develop neurological disease candidates using Skyhawk’s RNA expression correction technology. The deal occurred concurrent with Skyhawk’s $40mm Series A round, in which Celgene was also an investor. (Jun.)Under terms of the five-year deal, Celgene gets an exclusive option to license global rights to up to five candidates discovered with the STAR* (Small molecule Therapies for Alternative splicing in RNA) platform. Skyhawk designed STAR* to develop candi-dates that can correct an RNA splicing defect called exon skipping, which results in RNA mutations that cause diseases including cancer and neurological conditions. Celgene paid $60mm up front and could hand over additional license fees, milestones, and roy-alties. Potential indications under the deal include amyotrophic lateral sclerosis, Hun-tington’s disease, and others. This is not the first interaction for Celgene and Skyhawk’s executives. Skyhawk’s co-founder and CEO Bill Haney is also the co-founder and CEO of Dragonfly Therapeutics, an immuno-oncology firm that also shares office space with Skyhawk. In June 2017, Celgene paid $33mm up front for an exclusive option to license global rights to up to four of Dragon-fly’s I/O projects.
CIPLA LTD.ELI LILLY & CO.Eli Lilly & Co. granted Cipla Ltd. rights to market and sell the diabetes therapy Basaglar (insulin glargine injection) in India. (Jun.)Basaglar, distributed in a prefilled pen for once-daily dosing, treats Type I and Type II diabetes. Cipla plans to commence commercialization by the end of this year; the drug was approved in India through the biosimilar pathway. The deal is the second in the diabetes space for Cipla this year. In May, it licensed exclusive rights to market MannKind’s Afrezza, an inhaled insulin drug/device combo also indicated for Type I and Type II diabetes.

invivo.pharmaintelligence.inform
a.com
©2016 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 53
DEAL-MAKING ❚
DAIICHI SANKYO CO. LTD.MENARINI GROUPMenarini Asia-Pacific Holdings Pte. Ltd.Under a multi-year agreement, Daiichi Sankyo Co. Ltd. licensed Menarini Asia-Pacific Holdings Pte. Ltd. exclusive rights to commercialize its cardiovascular drug Lixiana (edoxaban) in the Philippines, Malaysia, and Singapore. (Jun.)Lixiana is an oral once-daily direct factor Xa inhibitor for thrombosis and stroke preven-tion in patients with atrial fibrillation. The anticoagulant is not yet approved in the li-censed Asian territories. It is marketed in the US as Savaysa. Under a 2016 tie-up, Merck sells the drug in various European countries.
GILEAD SCIENCES INC.HOOKIPA BIOTECH AGGilead Sciences Inc. licensed exclusive rights to two arenavirus-based immuno-therapy technologies from Hookipa Bio-tech AG, which it will use to develop vac-cines for HIV and hepatitis B virus. (Jun.)Gilead pays $10mm up front, up to $400mm in development, regulatory, and commercialization milestones, and sales royalties. It gains rights to the TheraT at-tenuated replicating virus, used to elicit potent T-cell responses, and the Vaxwave nonreplicating lymphocytic choriomeningi-
tis virus-based platform, which is designed to enter and activate dendritic cells to fight infectious diseases. The partners will jointly research potential therapeutics, which will be manufactured by Hookipa and developed by Gilead. Gilead first showed public interest in Hookipa and its technologies through the smaller biotech’s Series C venture round late last year. Gilead joined HBM Partners, Hillhouse Capital, Sirona Capital, and an undisclosed US public investment fund as new investors in the company’s $59.5mm Series C round. (Returning investors had also participated.)
HARBIN PHARMACEUTICAL GROUP CO. LTD.
HPGC Medical Co. Ltd.CAN-FITE BIOPHARMA LTD.Wize Pharma Inc.Wize Pharma Inc. licensed Harbin Phar-maceutical Group’s HPGC Medical Co. Ltd. exclusive rights to distribute the ophthalmic LO2A eye drops in China. (Jun.)LO2A is indicated for ophthalmological conditions, including dry eye syndrome (DES), conjunctivochalasis (CCH), and Sjögren’s syndrome. HPGC will obtain regulatory approval for LO2A in China, and pay for costs tied to clinical trials and registration fees. HPGC will purchase mini-mum quantities of LO2A from Wize, which
estimates that sales of the drug in China will be between $22.5mm-$40mm in the five years following approval (expected over the next 18 months).
HSIRI THERAPEUTICS INC.SHIONOGI & CO. LTD.Hsiri Therapeutics Inc. licensed Shionogi & Co. Ltd. exclusive worldwide rights to develop, manufacture, and commercial-ize compounds aimed at non-tuberculous mycobacterial (NTM) diseases and tuber-culosis (TB). (Jun.)Hsiri will receive an up-front payment, de-velopment milestones, and sales royalties. With their unique mechanism of action, the licensed candidates are expected to be more effective at treating mycobacterial infections than current medicines. There is currently a great need for multidrug-resis-tant TB therapies, especially in developed countries. Under the agreement, Shionogi will capitalize on its expertise in small-molecule R&D in the antibacterial space.
JAGUAR HEALTH INC.Napo Pharmaceuticals Inc. REDHILL BIOPHARMA LTD.Napo Pharmaceuticals Inc. licensed RedHill Biopharma Ltd. exclusive rights to co-promote Mytesi (crofelemer) 125mg delayed-release tablets in the US. (Jun.)
CitelinePharma intelligence |
Built by experts.Made for expertsAnalyze clinical trialintelligence your way with thenext generation of Citeline.
Visit pharmaintelligence.informa.com/nextgeneration to learn more.

54 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
Mytesi is the only FDA-approved anti-diarrhe-al agent for noninfectious diarrhea in adults with HIV/AIDS on antiretroviral therapy. The prescription drug is designed to act locally in the gastrointestinal tract to normalize water flow. Mytesi will join RedHill’s US gastro-intestinal product portfolio consisting of Donnatal for irritable bowel syndrome and acute enterocolitis, esomeprazole strontium delayed-release capsules for gastroesopha-geal reflux disease, and EnteraGam for diar-rhea. Under separate previous agreements, Napo had licensed Glenmark and Salix rights to crofelemer however both deals were later terminated because Napo said the firms breached the agreement by stalling the drug’s development.
JOHNSON & JOHNSONJanssen Pharmaceutica NVKRAMER LABORATORIES INC.Janssen Pharmaceutica NV sold Kramer Laboratories Inc. its Nizoral (ketocon-azole) antidandruff shampoo brand. (Jun.)Financial terms of the deal were not disclosed. The product is sold in North America and Latin America and has been around for more than 25 years. Kramer adds Nizoral to its extensive OTC portfolio led by Fungi-Nail Toe & Foot for treating finger and toe fungus.
KALLYOPE INC.NOVO NORDISK ASKallyope Inc. and Novo Nordisk AS are teaming up to discover and develop peptide therapeutics to treat obesity and diabetes. (Jun.)Novo Nordisk will pay Kallyope money up front plus research funding. In return, it has the option to license exclusive global rights to up to six therapeutics resulting from the collaboration. Kallyope will also receive a license fee upon Novo Nordisk’s option exercise, in addition to development and sales milestones and royalties. Both firms will conduct in vitro and in vivo vali-dation studies, after which Novo Nordisk--should it exercise the option--would take over preclinical and clinical development, manufacturing, and commercialization. The gut’s microbiome contains millions of neurons that transport metabolic and nutritional messages to the brain, linking the two in a biochemical signaling network called the gut-brain axis. Kallyope has created a platform that uses sequencing, genetics, circuit mapping, neural imaging, and bioinformatics technologies to unlock the underlying biology of the gut-brain axis signals and how they might influence behavior. The collaboration will capitalize on Kallyope’s IP and Novo Nordisk’s expertise in the development of peptide therapeutics.
NOVIMMUNE SATG THERAPEUTICS INC.Novimmune SA and TG Therapeutics Inc. teamed up to further develop Novim-
mune’s anti-CD47/anti-CD19 bispecific antibody NI1701, which has been renamed TG1801. TG holds an exclusive option to license the project, which the partners will initially jointly develop for B-cell ma-lignancies. (Jun.)TG issued $3mm of its shares up front and could pay up to $185mm in development, regulatory, and sales milestones, plus high-single to low-double-digit royalties. (Strategic Transactions estimates 7-29%.) TG is responsible for clinical development costs through the end of Phase II, and then the pair will share remaining R&D and com-mercialization expenses. TG1801 is a fully-human IgG1 antibody that was designed based on Novimmune’s kappa-lambda body bispecific format. Clinical trials are ex-pected by early 2019. The candidate marks the third targeted immunotherapy in TG’s pipeline, which the company notes have the potential to be combined into effective non-chemotherapy options for a variety of B-cell tumors including chronic lymphocytic leukemia and non-Hodgkin’s lymphoma.
ROCHEGenentech Inc.MICROBIOTICA LTD.Roche’s Genentech Inc. received options to license from Microbiotica Ltd. biomark-ers, targets, and drug candidates in the microbiome area for inflammatory bowel disease (IBD). (Jun.)The deal is Roche’s second recent partner-ship focused on the microbiome, following a tie-up with Lodo last month to find natural drugs in the soil microbiome. Roche was also an early investor in Second Genome, having participated in the biotech’s 2016 Series B which totaled $51mm. In the cur-rent multi-year agreement, Microbiotica is responsible for screening patient samples from Genentech’s IBD clinical trials to identify microbiome biomarker signatures of drug response, IBD targets, and live bacterial therapeutics. Genentech will pay an up-front fee plus up to $534mm in re-search, development, and commercializa-tion milestones, as well as sales royalties. Potentially part of the analysis that Micro-biotica will perform on Roche/Genentech’s IBD pipeline are four candidates in active development, the most advanced of which is Phase III etrolizumab, an alpha4-beta7 integrin antagonist for Crohn’s disease and ulcerative colitis. Roche is also collaborat-ing with Boehringer Ingelheim on locked nucleic acid oglionucleotides for IBD un-der a 2017 alliance. Microbiotica, a 2016 Wellcome Trust Sanger Institute spin-off, has a precision metagenomics microbiome platform that can culture, characterize, and phenotype the majority of a patient’s gut bacteria. Using artificial intelligence tech-nologies, it can identify gut bacteria that is tied to disease phenotypes. The company maintains a microbiota culture collection
and reference genome database for analy-sis and conducting studies. Internally, Microbiotica is working on microbiome candidates for IBD, immuno-oncology, and Clostridium difficile.
ROIVANT SCIENCES GMBHAxovant Sciences Ltd.OXFORD BIOMEDICA PLCAxovant Sciences Ltd. licensed exclusive worldwide rights to Oxford BioMedica PLC’s OXB102, an in vivo lentiviral vec-tor gene therapy, designed to increase dopamine production and reduce motor fluctuations in Parkinson’s disease (PD). Axovant’s license includes rights to the compound in all indications. (Jun.)Axovant will pay $30mm up front (includ-ing a $5mm pre-payment for manufactur-ing activities); up to $55mm in specified development milestones; regulatory and sales milestones up to $757.5mm; plus tired royalties of 7-10% (based on net sales goals ranging from a low of under $1bn to a high of greater than or equal to $4bn). In addition, Axovant will reimburse OBM for the cost as-sociated with up to six full-time employees that OBM will provide to assist with clinical development. OBM is responsible for com-mercial supply and GMP manufacturing. Axovant’s parent company Roivant Sciences is providing the company with $25mm in financing to help fund the transaction. Axov-ant funds all clinical development costs and manufacturing process development and scale-up activities. OXB102, which Axovant has renamed AXO-Lenti-PD, is a re-engi-neered version of OBM’s predecessor gene therapy construct ProSavin (OXB101), which uses OBM’s LentiVector system to deliver directly to the striatum in the brain three genes that encode enzymes responsible for dopamine synthesis: TH (tyrosine hydroxy-lase; converts tyrosine to levodopa), CH1 (GTP-cyclohydrolase 1; synthesizes a critical cofactor in tyrosine hydroxylase activity), and AADC (aromatic amino acid decarboxyl-ase; converts levodopa to dopamine). These three genes reprogram cells that normally do not produce dopamine into cells capable of manufacturing and secreting dopamine. OBM’s LentiVector technology enables the delivery of the genetic material into target cells, with long-lasting gene expression and no known toxicity or adverse immune reactions. AXO-Lenti-PD, currently in pre-clinical studies, is being developed as a more potent formulation of ProSavin with increased transgenic expression, delivering the TAADC, TH, and CH1 genes in a different payload configuration. Results of a Phase I/II study evaluating multiple dosages of ProSavin in advanced PD (first initiated in 2007) demonstrated significant motor im-provements without serious adverse effects in patients who received a one-time admin-istration throughout four years of long-term follow up. Based on this previously gener-ated ProSavin data that clinically validates

invivo.pharmaintelligence.inform
a.com
©2016 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 55
DEAL-MAKING ❚
the mechanism of action, Axovant believes proof-of-concept has been established for the second-generation AXO-Lenti-PD candi-date. Axovant expects to begin a Phase I/II dose escalation trial to assess safety, toler-ability, biomarkers, and other measures of motor function of AXO-Lenti-PD by the end of this year. The deal leverages Axovant’s expertise in neurologic disorders and pro-vides OBM with a partner that can rapidly advance AXO-Lenti-PD to market.
SANOFISanofi PasteurTRANSLATE BIOSanofi Pasteur has teamed up with Translate Bio to develop and sell mRNA vaccines for up to five infectious disease targets. (Jun.)Throughout the initial three-year term, the partners will work together on R&D activi-ties, which will be funded by Sanofi. Trans-late Bio gets $45mm up front, up to $805mm in development, regulatory, and sales mile-stones, and royalties. Sanofi could also pay option exercise fees should the company choose to explore additional pathogen tar-gets. Translate’s mRNA therapeutic platform (MRT; licensed from Shire in 2016) creates mRNA that encodes functional proteins for delivery to target cells in an effort to restore or augment protein function and treat or prevent disease. Translate will manufacture clinical supply and receive payments from Sanofi under a separate agreement. The col-laboration helps Translate expand uses of its technology beyond diseases it is currently studying, including cystic fibrosis and or-nithine transcarbamylase (OTC) deficiency. The tie-up is the second for Sanofi in the mRNA space; it penned a deal with BioNTech in 2015 through which BioNTech is using its mRNA platform to discover up to five cancer immunotherapies for the Big Pharma.
SAWAI PHARMACEUTICAL CO. LTD.Upsher-Smith Laboratories LLCAn undisclosed pharmaceutical company licensed Upsher-Smith Laboratories LLC exclusive rights to market and distribute six ophthalmic and otic ANDA products in the US. (Jun.)The unnamed partner will develop and manufacture the products for Upsher-Smith. The specific drugs were not disclosed, however, they generated com-bined sales of over $1.6bn for the twelve months ending March 2018. Upsher-Smith will register the products with the FDA and upon approval the firm will sell them under its own label. The deal allows Upsher-Smith to expand its generics pipeline.
SONOMA PHARMACEUTICALS INC.NC GROUPEMS SAUnderskin Farmaceutica Ltda.Under a five-year renewable agreement, Brazil’s largest pharmaceutical company
EMS SA, through its Underskin Farmaceu-tica Ltda. unit (U.SK Dermatology; both owned by diversified pharma company NC Group), in-licensed exclusive Brazilian distribution and marketing rights to four Sonoma Pharmaceuticals Inc. prescrip-tion hypochlorous acid (HOCl)-based der-matology products, which include seven formulations incorporating Sonoma’s Microcyn technology. (Jun.)The products included in the deal are Gramacyn hydrogel and liquid for acne (Gramaderm in the US); Celacyn scar treat-ment (Epicyn in the US); Pediacyn spray and gel for atopic dermatitis; and Lasercyn spray and hydrogel for skin cleansing fol-lowing cosmetic procedures. Oxychlorine compounds are produced by the body’s innate immune system in response to infection. One such compound, HOCl, is a broad spectrum antimicrobial agent--which acts against bacteria, viruses, and fungi--and an oxidizing agent that can react with many types of molecules, and is possibly involved in processes such as inhibition of glucose oxidation and DNA replication, depletion of adenine nucleotides, and pro-tein unfolding and aggregation. Sonoma’s Microcyn technology produces electrically charged liquids and gels containing an HOCl solution, which promotes natural debridement and healing. In the royalty-free agreement, EMS agreed to minimum annual purchase amounts of $100k in year one; $250k in year two; $500k in year three; $750k in year four; and $1mm in the fifth year. Sonoma will manufacture the products using the Microcyn chemistry in its Mexico facility. U.SK Dermatology will sell the products, which were all approved in Brazil in October 2017 (all have previ-ously received regulatory clearance or have been launched in other territories), through its 70 direct sales representatives in Brazil, the second-largest dermatology market worldwide. U.SK plans to launch three of the formulations (Gramacyn in both hydro-gel and liquid forms and Celacyn) in Brazil in late summer 2018. The deal provides Sonoma with strong growth internation-ally. The addition of Sonoma’s products complements U.SK Dermatology’s existing dermocosmetic portfolio, which includes anti-aging and skin revitalizing lines.
TERSERA THERAPEUTICS LLCTESARO INC.Tesaro Inc. has licensed TerSera rights to sell the oral and intravenous formula-tions of Varubi (rolapitant) in the US and Canada. (Jun.)Tesaro retains rights to the product outside North America, where it is sold as Varuby. The drug was approved in 2015 for che-motherapy-induced nausea and vomiting. Tesaro received $35mm up front and will get another $5mm eighteen months after deal closing. TerSera will also shell out milestone
payments as follows: $10mm each time the marketing approval for a new indication of rolapitant is granted in the US, and $10mm when net sales of a reformulated version of IV rolapitant reach or exceed $50mm in a calendar year. Tesaro is also eligible for 20% royalties when sales of the IV product reach or exceed $100mm in a twelve-month period. Tesaro got exclusive global rights to rolapitant from Opko Health in late 2010. That deal including an up-front payment of $6mm to Tesaro plus up to $115mm in regu-latory and sales milestones plus double-digit tiered royalties. The current deal allows Tesaro to focus on its oncology drug Zejula.
VERASTEM INC.YAKULT HONSHA CO. LTD.Verastem Inc. granted Yakult Honsha Co. Ltd. exclusive rights to develop and sell duvelisib, a PI3K delta/PI3K gamma inhibitor, in Japan for all cancer indica-tions. (Jun.)Yakult Honsha paid $10mm up front and could hand over up to an additional $90mm in development and commercialization milestones, plus double-digit royalties. Verastem filed an NDA with the FDA for full approval of the candidate for relapsed or refractory chronic lymphocytic/small lymphocytic lymphoma (CLL/SLL), and accelerated approval for relapsed or re-fractory follicular lymphoma (FL). Yakult Honsha plans to focus its initial work on those indications, but also plans to expand to additional cancers including peripheral T-cell lymphoma and diffuse large B-cell lymphoma. The company adds duvelisib to its portfolio of oncology drugs including Elplat (oxaliplatin) for colorectal cancer, and Campto (irinotecan) for solid and blood cancers including lymphoma and breast, colorectal, ovarian, stomach, lung, pancreatic, and squamous cell carcinoma.
Financings
ADMA BIOLOGICS INC.ADMA Biologics Inc. (plasma-based thera-pies for treating primary immune deficiency disease (PIDD) and infectious diseases) netted $37.6mm through the follow-on sale of 8.37mm common shares priced at $4.78. The company will use some of the proceeds to submit the prior approval supplement for and relaunch Bivigam for primary humoral immunodeficiency and to resubmit the BLA for RI002 for PIDD. (Jun.)Investment Banks/Advisors: Chardan Capital Markets; Oppenheimer & Co. Inc.; Raymond James & Associates Inc.
AERPIO PHARMACEUTICALS INC.Ocular disease-focused Aerpio Pharma-ceuticals Inc. netted $42.3mm through the follow-on offering of 11.7mm common shares at $3.85 each. The company con-currently announced it has uplisted to the Nasdaq market; it had been trading on the

56 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
OTC. Aerpio also just granted Gossamer Bio exclusive rights to develop and com-mercialize its IBD candidate AKB4924 and related compounds. (Jun.)Investment Banks/Advisors: Guggenheim Partners LLC; HC Wainwright & Co.; Nation-al Securities Corp.; Needham & Co. Inc.
APTINYX INC.Aptinyx Inc. (CNS disorder drug discovery and development) netted $109.5mm in its upsized initial public offering of 7.4mm shares (including the overallotment) at $16. The company originally anticipated selling 5.33mm shares at a $14-16 range. (Jun.)Investment Banks/Advisors: BMO Finan-cial Group; Cowen & Co. LLC; JP Morgan & Co.; Leerink Partners LLC
AUTOLUS LTD.Autolus Ltd. (T-cell immunotherapies for cancer) netted $139.5mm through its public offering of 8.8mm American Depositary Shares at $17 on the Nasdaq Global Ex-change. (Each ADS represents one ordinary share.) The company originally intended to sell 7.8mm ADSs at a range of $15-17. (Jun.)Investment Banks/Advisors: Goldman Sachs & Co.; Jefferies & Co. Inc.; Wells Fargo Securities LLC; William Blair & Co.
AVROBIO INC.AVROBIO Inc. (cell and gene therapies for rare diseases) netted $106.6mm in its up-sized initial public offering of 6mm shares (including the overallotment) at $19. The company originally anticipated selling 4.4mm shares at a $16-18 range. (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; Morgan Stanley & Co.; Wedbush PacGrow Life Sciences; Wells Fargo Se-curities LLC
BRIDGEBIO PHARMAEIDOS THERAPEUTICS INC.Rare disease-focused Eidos Therapeutics Inc. netted $113.5mm through an initial public offering of 7.19mm common shares (including full exercise of the overallot-ment) priced at $17 each, the high end of its intended range. (Jun.)Investment Banks/Advisors: Bank of America Merrill Lynch; Barclays Bank PLC; JP Morgan & Co. (Eidos Therapeutics Inc.)
CATABASIS PHARMACEUTICALS INC.Catabasis Pharmaceuticals Inc. (drug discovery for multiple diseases) netted $39.5mm via a follow-on offering of 42mm units at $1. Each unit consists of one common share and a five-year warrant to purchase one share at an exercise price of $1.20. The company will use some of the proceeds to fund an upcoming Phase III trial of edasalonexent for Duchenne muscular dystrophy. (Jun.)Investment Banks/Advisors: Oppen-heimer & Co. Inc.
COMPUGEN LTD.Compugen Ltd. netted $20mm through a registered direct offering of 5.3mm ordinary shares at $3.95 (a 4% premium). Investors also received five-year warrants to purchase 4.3mm shares at $4.74. JMP Securities was the placement agent. The company is devel-oping cancer immunotherapies and treat-ments for autoimmune diseases, and will use the proceeds to support ongoing preclinical and clinical work. In April, Compugen penned a $210mm deal with MedImmune for the development of bispecific and multi-specific antibody therapies for cancer. (Jun.)Investment Banks/Advisors: JMP Securi-ties LLC
CRINETICS PHARMACEUTICALS INC.Crinetics Pharmaceuticals Inc. (develop-ing therapies for endocrine disorders) has filed for its initial public offering. (Jun.)Investment Banks/Advisors: JP Morgan & Co.; Leerink Partners LLC; Piper Jaffray & Co.
DECIPHERA PHARMACEUTICALS INC.Oncology drug development company Deciphera Pharmaceuticals Inc. netted $185.9mm through its first public offering since its September 2017 IPO. The company sold 4.9mm common shares (including the overallotment) at $40, and intends to use the majority of the proceeds ($100mm) to fund continued development of lead candi-date DCC2618, which is in Phase III trials as a fourth-line treatment for gastrointestinal stromal tumors (GIST) and earlier trials for additional advanced cancers. (Jun.)Investment Banks/Advisors: Canaccord Genuity Inc.; JMP Securities LLC; JP Mor-gan Chase & Co.; Nomura Securities Inter-national Inc.; Piper Jaffray & Co.; Raymond James & Associates Inc.
ENTERA BIO LTD.Israel-based Entera Bio Ltd. has netted $10.3mm through its US initial public offering of 1.4mm ordinary shares at $8 each. The company also issued warrants to purchase up to 700k ordinary shares. (Jun.)Investment Banks/Advisors: Joseph Gun-nar & Co.; Maxim Group LLC
FORTY SEVEN INC.Immuno-oncology company Forty Seven Inc. filed for its initial public offering. The company plans to sell 6.7mm common shares for between $14-16 apiece. (Jun.)Investment Banks/Advisors: BTIG LLC; Canaccord Genuity Inc.; Credit Suisse Group; Morgan Stanley & Co.; Oppen-heimer & Co. Inc.
GALMED PHARMACEUTICALS LTD.Galmed Pharmaceuticals Ltd. (Israeli biotech developing treatments for liver dis-eases) netted $70.5mm through the public sale of 5mm ordinary shares at $15. Pro-ceeds will support continued development
of Aramchol, a stearoyl-CoA desaturase (SCD1) inhibitor in Phase III for nonalcoholic steatohepatitis, and will also go towards business development activities. (Jun.)Investment Banks/Advisors: Cantor Fitzgerald & Co.; Maxim Group LLC; Raymond James & Associates Inc.; Roth Capital Partners; Stifel Nicolaus & Co. Inc.; SunTrust Banks Inc.
HERON THERAPEUTICS INC.Heron Therapeutics Inc. (Biochronomer polymer-based drug delivery system) netted $194.7mm in a follow-on public of-fering of 5mm shares of common stock at $39.50. The company plans to use the pro-ceeds from the offering for the commercial launch of HTX011 (fixed-dose combination of bupivacaine/meloxicam for postopera-tive pain); the continued commercializa-tion of chemotherapy-induced nausea and vomiting therapies Sustol (granisetron injection) and Cinvanti (aprepitant); and to fund ongoing and future clinical and preclinical trials. (Jun.)Investment Banks/Advisors: Jefferies & Co. Inc.
IMMUNOGEN INC.ImmunoGen Inc. (antibody-drug conju-gates for cancer) netted $162.9mm through a public offering of 15.75mm common shares (including the overallotment) at $11. (The company originally filed to sell 12mm shares.) Proceeds will support R&D, clinical, regulatory, and commercialization activities. Its lead candidate mirvetuximab soravtansine is an ADC in Phase III for platinum-resistant ovarian cancer. (Jun.)Investment Banks/Advisors: Canaccord Genuity Inc.; Cowen & Co. LLC; Goldman Sachs & Co.; HC Wainwright & Co.; JP Morgan Chase & Co.
IMMUNOMEDICS INC.Immunomedics Inc. (monoclonal anti-body-based therapies for cancer and autoimmune diseases) netted $260.4mm through a public offering of 11.5mm shares at $24. Funds will support continued development of lead antibody-drug con-jugate sacituzumab govitecan (Phase II for metastatic triple-negative breast cancer and other metastatic solid tumors), and will also be put towards manufacturing process improvements. (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; Jefferies & Co. Inc.; Morgan Stanley & Co.; Wells Fargo Securities LLC
INTREXON CORP.Intrexon Corp. (synthetic biology for drug discovery) netted $194.5mm through a public offering of $200mm of its 3.5% senior notes due 2023. The notes convert to common at a rate of 58.662 per $1k principal amount, or $17.05 per share. (The company’s stock averaged $15.98 at the time of the offering.) Intrexon concurrently

Are you looking to reach and do business with senior decision makers in pharma and medtech?
To fi nd out how our team can help visit:https://pharmaintelligence.informa.com/marketing-services
We offer a range of marketing opportunities whether you are looking to:• Raise brand awareness• Produce content marketing/thought leadership content• Generate leads• Engage directly with potential clients as well as cementing existing relationships
JN723 Marketing Services Advert.indd 1 2017/11/13 6:08 PM

58 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
priced an offering of 7.5mm common shares at $13.37; the company will loan the shares to JP Morgan Securities through a share borrowing arrangement. Intrexon will not re-ceive any proceeds from that offering. (Jun.)Investment Banks/Advisors: JP Morgan Chase & Co.
KADMON CORP. LLCKadmon Corp. LLC, aka Kadmon Holdings Inc., inflammatory and fibrotic diseases) netted $106.4mm in concurrent financ-ings. In a follow-on public offering, it sold 30.7mm common shares (including full exercise of the over-allotment option) at $3.30 for $95.1mm in proceeds. In the registered direct offering, in which exist-ing investors Vivo Capital, Perceptive Advisors, and Acuta Capital joined new backers Invesco, Venrock, and EcoR1, the company sold 1.4mm shares to the institutional buyers off the existing shelf registration with the sale of the remaining 2.3mm shares expected to close by the end of June, for total net proceeds of $11.3mm. Kadmon plans to use the offering proceeds for preclinical and clinical development of its pipeline, including pursuing regulatory approval for KD025 for cGVHD (chronic graft versus host disease). (Jun.)Investment Banks/Advisors: HC Wain-wright & Co.; Jefferies & Co. Inc.
KEZAR LIFE SCIENCES INC.Kezar Life Sciences Inc. (autoimmune dis-ease and cancer therapies) netted $80.2mm through its initial public offering of 5.75mm common shares (including the overallotment) at $15. (The company had planned to sell 4.67mm shares at a range of $14-16.) (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; Jefferies & Co. Inc.; Wells Fargo Securities LLC; William Blair & Co.
KURA ONCOLOGY INC.Kura Oncology Inc. (precision cancer medicines) netted $65mm through a public offering of 4mm common shares at $16.75. Proceeds will support preclinical and clini-cal development activities, including work on lead candidate tipifarnib, which is in proof-of-concept studies for HRAS-mutant head and neck cancer, peripheral T-lym-phoma, myelodysplastic syndromes, and chronic myelomonocytic leukemia. (Jun.)Investment Banks/Advisors: Leerink Partners LLC
LIQUIDIA TECHNOLOGIES INC.Liquidia Technologies Inc. (particle engi-neering platform for drug development) filed for its initial public offering. (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; Jefferies & Co. Inc.; Needham & Co. Inc.; Wedbush PacGrow Life Sciences
MADRIGAL PHARMACEUTICALS INC.Madrigal Pharmaceuticals Inc. (develop-ing therapies for cardiovascular, metabol-
ic, and liver diseases) netted $282.7mm through the follow-on public offering of 983,607 common shares at $305 each. Stockholders sold an additional 363,625 shares. (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; Goldman Sachs & Co.; HC Wainwright & Co.; JMP Securities LLC; Roth Capital Partners
MAGENTA THERAPEUTICS INC.Magenta Therapeutics Inc. (curative stem cell transplantation) netted $93mm through its initial public offering of 6.67mm common shares at $15, the mid-point of its anticipated range. (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; Goldman Sachs & Co.; JP Morgan Chase & Co.; Wedbush PacGrow Life Sciences
MATINAS BIOPHARMA HOLDINGS INC.Matinas BioPharma Holdings Inc. (lipid nano-crystals technology) netted $7.4mm through the public offering of 8k Series B convertible preferred shares at $1k. The shares convert into 16mm common shares at $0.50 each. The company will use some of the funds for pipeline development. Ma-tinas is preparing to move lead compound MAT2203 into Phase II for preventing fungal infections in patients with acute lymphoblastic leukemia. (Jun.)Investment Banks/Advisors: ThinkEquity Partners LLC
MEIRAGTX HOLDINGS PLCIn its initial public offering on the Nas-daq Exchange, MeiraGTx Holdings PLC (developing AAV gene therapies) netted $80.2mm through the sale of 5.75mm shares (including the overallotment) at $15, the midpoint of its anticipated range. (Jun.)Investment Banks/Advisors: Bank of America Merrill Lynch; Barclays Bank PLC; Chardan Capital Markets; Evercore Partners
MIRATI THERAPEUTICS INC.Mirati Therapeutics Inc. (targeted oncol-ogy) netted $115.8mm through its latest public offering. The company sold 2.75mm common shares at $38.85, and also issued 421,650 pre-funded warrants at $38.849. Some of the proceeds will support contin-ued development of sitravatinib (Phase I/II for bladder and non-small cell lung cancers) and mocetinostat (Phase II for NSCLC), and also MRTX849 (in preclinical studies for NSCLC and colorectal cancer). (Jun.)Investment Banks/Advisors: Barclays Bank PLC; Cowen & Co. LLC; HC Wainwright & Co.; Oppenheimer & Co. Inc.; SunTrust Banks Inc.
NEON THERAPEUTICS INC.Neon Therapeutics Inc. (immuno-oncolo-gy) netted $93mm through its initial public offering of 6.25mm common shares at $16 (the midpoint of the company’s intended range). (Jun.)
Investment Banks/Advisors: Bank of Ameri-ca Merrill Lynch; Mizuho Bank Ltd.; Morgan Stanley & Co.; Oppenheimer & Co. Inc.
OBSEVA SAObsEva SA (woman’s reproductive health therapeutics development) netted $68.7mm through a public offering of 4.75mm shares at $15.39. The company will use the proceeds to advance its cur-rent in-licensed pipeline--which includes linzagolix (OBE2109; for endometriosis and uterine fibroids), nolasiban (OBE001; for improving embryo implantation in assisted reproductive technology (ART) or IVF procedures), and OBE022 (for pre-term labor)--and further invest in pre-commercial activities for those oral candidates. ObsEva concurrently reported it had achieved both primary and second-ary endpoints in a Phase IIb trial of a 75mg dose of its oral GnRH receptor antagonist linzagolix in the endometriosis-associated pain indication; a Phase III trial design studying two additional dosages is ex-pected to start by the end of the year. (Jun.)Investment Banks/Advisors: Credit Suisse Group; HC Wainwright & Co.; JP Morgan & Co.; Jefferies & Co. Inc.; Wedbush PacGrow Life Sciences
ONCOLYTICS BIOTECH INC.Oncolytics Biotech Inc. netted $8.3mm through a public offering of 1.5mm com-mon shares (including the overallotment) at $5.83. The company is developing an intravenously delivered immuno-oncolytic virus Reolysin (pelareorep), and will use the offering proceeds to continue devel-oping the candidate in combination with checkpoint inhibitors (including Merck’s Keytruda for pancreatic cancer). (Jun.)
OPTINOSE INC.In its first financing since going public, OptiNose Inc. (focused on the ear, nose and throat and allergy space) netted $60.1mm through the follow-on offering of 2.88mm common shares (including full exercise of the overallotment) at $22.25 each. Stockholders also sold 2.5mm shares at the same price. The company will use some of the proceeds to commercialize its Xhance nasal spray for nasal polyps and to further develop Xhance as a treatment for chronic sinusitis. (Jun.)Investment Banks/Advisors: BMO Finan-cial Group; Cantor Fitzgerald & Co.; Jef-feries & Co. Inc.; Piper Jaffray & Co.; RBC Capital Markets
PHARNEXT SAPharnext SA (Pleotherapy drug repur-posing platform) secured €20.5mm ($24.1mm) in debt funding consisting of a €20mm bond loan with IPF Partners and up to €500k in convertible securities from Yorkville Advisors in the form convertible bonds with a maturity date of one year following issuance. (Jun.)

invivo.pharmaintelligence.inform
a.com
©2016 Informa Business Information, Inc., an Informa company July/August 2018 | In Vivo | 59
DEAL-MAKING ❚
RHYTHM PHARMACEUTICALS INC.In its first financing since going public, Rhythm Pharmaceuticals Inc. (therapies for rare genetic disorders of obesity) netted $163.7mm through a follow-on offering of 6.59mm common shares (in-cluding full exercise of the overallotment) priced at $26.42. The company will use the proceeds to bring its lead compound setmelanotide through Phase III trials for pro-opiomelanocortin (POMC) deficiency obesity, leptin receptor (LepR) deficiency obesity, Bardet-Biedl syndrome, and Alström syndrome and to prepare the regulatory filings in those indications; for clinical development of setmelanotide for POMC heterozygous deficiency obesity and POMC epigenetic disorders and to develop a once-weekly formulation of the compound; to expand the diagnosis of ge-netic obesity, including genetic sequenc-ing of patients from targeted populations and ongoing genotyping and genetic epidemiology studies; and for preclini-cal studies of the Prader-Willi syndrome candidate RM853, which the company licensed from Takeda in April. (Jun.)Investment Banks/Advisors: Bank of America Merrill Lynch; Cowen & Co. LLC; Morgan Stanley & Co.; Needham & Co. Inc.
ROIVANT SCIENCES GMBHAxovant Sciences Ltd.Axovant Sciences Ltd. grossed $25mm through the private sale of 14.3mm common shares at $1.75 (a 17% premium) to parent Roivant Sciences. The company will use the proceeds to support development of OXB102, which Axovant in-licensed from Ox-ford BioMedica in a concurrent agreement worth up to $842.5mm. The preclinical gene therapy candidate, which Axovant renamed AXO-Lenti-PD, is an in vivo lentiviral vector designed to increase dopamine production and reduce motor fluctuations in Parkin-son’s disease patients. (Jun.)
SOLIGENIX INC.Soligenix Inc. (rare diseases) netted $7.6mm in an underwritten public offering of 7.8mm common shares and warrants to purchase 3.1mm common shares at a com-bined price of $1.03. The warrants have an initial exercise price of $2.25 and expire 42 months from issuance. The company plans to use the proceeds to fund its pivotal Phase III trial of SGX301 for cutaneous T-cell lym-phoma and Phase III trial of SGX942 for oral mucositis in head and neck cancer. (Jun.)
TAPIMMUNE INC.TapImmune Inc. (cancer immunothera-pies) priced a private placement of 17.5mm common shares at $4 apiece, for gross proceeds of $70mm. Piper Jaffray and Nomura are the placement agents. Completion of the financing is contingent upon the closing of TapImmune’s merger with Marker Therapeutics. New Enterprise
Associates will lead and will be joined by Aisling Capital, Perceptive Advisors, and others. The combined entity plans to use the proceeds to advance T-cell vaccine candidate in clinical trials and expand operational and clinical facilities. (Jun.)Investment Banks/Advisors: Nomura Secu-rities International Inc.; Piper Jaffray & Co.
TELIGENT INC.Teligent Inc. (generic drugs) secured a $25mm senior term loan from existing shareholder Highbridge Capital Manage-ment. The loan has an original discount of 2.5%, matures on June 1, 2021, and generally bears interest at LIBOR + 9% (subject to 2% LIBOR floor). The company drew down $15mm at close, with the re-maining $10mm available within 45 days. An additional $50mm may be made avail-able through a separate facility if needed. Teligent plans to use the money to fund product launches related to approvals and to improve its capital structure. (Jun.)Investment Banks/Advisors: Cantor Fitzgerald & Co.
THERATECHNOLOGIES INC.Infectious disease-focused Theratech-nologies Inc. netted $55.2mm (including full exercise of the overallotment) in a bought deal financing of five-year 5.75% convertible unsecured senior notes that are payable semi-annually on June 30 and December 31 of each year, commencing on December 31, 2018. The company will use most of the proceeds to fund obliga-tions due under the termination of a 2008 agreement with EMD Serono in which Theratechnologies regained all rights to tesamorelin (Egrifta). The remaining funds will support commercialization of the HIV drug Trogarzo in Europe and other countries, as well as working capital. (Jun.)Investment Banks/Advisors: CIBC World Markets Corp.; Canaccord Genuity Inc.; Echelon Wealth Partners; Mackie Research Capital Corporation ; National Bank Finan-cial Corp.; RBC Capital Markets
TRANSLATE BIOTranslate Bio Inc. (messenger RNA) netted $113mm in its initial public of-fering of 9.35mm common shares at $13 (midpoint of range) on the Nasdaq. The company had previously announced terms of 7.7mm common shares between $12 and $14 per share. Prior to filing to go public, Translate raised over $75mm in two venture rounds. (Jun.)Investment Banks/Advisors: Citigroup Inc.; Evercore Partners; Leerink Partners LLC
TRICIDA INC.Renal disease drug developer Tricida Inc. netted $206.7mm through its initial pub-lic offering of 11.7mm common shares at $19. (The company initially planned to sell 10.3mm shares at a range of $16-18.) The
IPO is the largest for a US biopharma com-pany since the beginning of 2018. (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; Goldman Sachs & Co.; JP Morgan Chase & Co.
TROVAGENE INC.Trovagene Inc. (precision oncology thera-peutics) netted $16.7mm through its latest public offering. The company sold 9.14mm common shares at $1 (netting $8.5mm), and 8,860 Series B preferred shares at $1k (net $8.2mm). Investors also received five-year warrants to purchase an additional 18mm common at $1.10. Torvagene’s lead candidate is PCM075, a Polo-like kinase 1 (PLK1) selective ATP competitive inhibi-tor, and is in Phase I and Phase II trials for advanced or metastatic solid tumors, acute myeloid leukemia, and metastatic castration-resistant prostate cancer. (Preclinical studies are also underway for NHL, lung cancer, and triple-negative breast cancer.) (Jun.)Investment Banks/Advisors: ThinkEquity Partners LLC
VASCULAR BIOGENICS LTD.Vascular Biogenics Ltd. (also known as VBL Therapeutics; cancer drug develop-ment) netted $14.4mm through a regis-tered direct offering of 5.9mm common shares at $2.625, a slight discount to the market average. Investors also received short-term warrants (expiring January 6, 2020) to purchase 2.95mm shares at $2.51, and long-term four-year warrants to purchase 2.95mm shares at $3. HC Wainwright was the placement agent. Proceeds will support ongoing clinical development. (Jun.)Investment Banks/Advisors: HC Wain-wright & Co.
VERASTEM INC.Verastem Inc. (developing therapies that modulate the tumor microenvironment) grossed $43mm through the private sale of 7.17mm common shares at $6 (a 7% premium) to funds managed by Consonance Capital. Proceeds will sup-port commercialization of lead candidate duvelisib pending anticipated regulatory approval for follicular lymphoma and chronic lymphocytic leukemia. (The FDA accepted the NDA for priority review in April.) Earlier this month, Verastem granted Yakult Honsha exclusive rights to sell duvelisib in Japan. (Jun.)
VERRICA PHARMACEUTICALS INC.Verrica Pharmaceuticals Inc. (topical treat-ments for skin diseases) netted $80.2mm in its initial public offering of 5mm shares (including the overallotment) at $15, the midpoint of its anticipated range. (Jun.)Investment Banks/Advisors: Bank of America Merrill Lynch; Cowen & Co. LLC; Jefferies & Co. Inc.

60 | In Vivo | July/August 2018 invivo.pharmamedtechbi.com
❚ DEAL-MAKINGin
vivo
.pha
rmai
ntel
ligen
ce.in
form
a.co
m
In VivoPharma intelligence |
IN VIVO: [ISSN 2160-9861] is published monthly, except for the combined July/August issue, by Informa Business Intelligence, Inc., 605 Third Avenue, Floor 20-22, New York, NY 10158.
US Toll-Free: +1 888 670 8900 | US Toll: +1 908 547 2200 | UK & Europe: +44 (20) 337 73737
Australia: +61 2 8705 6907 | Japan: +81 3 6273 4260
Office of publication, The Sheridan Group, 66 Peter Parley Row, Berlin, CT 06037. Postmaster: Send address changes to Informa Business Intelligence, 605 Third Avenue,
Floor 20-22, New York, NY 10158.
© 2018 by Informa Business Intelligence, Inc., an Informa company.
All rights reserved.
No part of this publication may be reproduced in any form or incorporated into any information retrieval system without the written permission of the copyright owner.
editorsLucie Ellis
Managing Editor
William Looney Pharma Editor
Ashley Yeo Medtech Editor
Amanda Micklus Principal Analyst
Andrea Charles Editor Custom Content
Regina Paleski Contributing Editor
research managerSteven Muntner
deals analystsBeth Detuzzi, Deanna Kamienski
Maureen Riordan
design supervisorGayle Rembold Furbert
senior designerJanet Haniak
designersJean Marie Smith, Paul Wilkinson
head of editorial ops (pharma) Karen Coleman
head of contentMike Ward
advertisingChristopher Keeling
subscriptionsDan Simmons, Ewan Ritchie
Shinbo Hidenaga
managing directorPhil Jarvis
editorial office605 Third Avenue, Floor 20-22
New York, NY 10017invivo.pharmaintelligence.informa.com
customer [email protected]
editorial advisory boardBrian Chapman
ZS Associates, Partner
Benjamin Comer PwC, Senior Manager
Health Research Institute
Don Creighton ICON
Global Head of Pricing & Market Access
Deborah Dunsire, MD XTuit Pharmaceuticals
President & CEO
Les Funtleyder E Squared Capital Management Health Care Portfolio Manager
Terry Hisey Deloitte, Senior Principal,
Life Science & Health Care Practice
Ken Kaitin, PhD Director, Tufts Center for the Study of Drug Development
Barbara Lopez Kunz DIA, Global Chief Executive
Ellen Licking EY, Senior Analyst
Global Life Sciences
Julie Locklear Managing Partner, Genesis Research
Roger Longman Real Endpoints, CEO
Dan McIntyre Publick House, Partner
Michael Ringel, PhD BCG
Senior Partner & Managing Director
Kenneth Schultz, MD Halozyme, Vice President of Innovation,
Strategy & Business Development
Jack Wong Baxter Healthcare
Head of Regulatory Affairs, APAC
Nadim Yared CVRx, President & CEO
VIKING THERAPEUTICS INC.In its second FOPO in four months, Viking Therapeutics Inc. (developing therapies for metabolic and endocrine disorders) netted $72.6mm through a follow-on public offering of 8.6mm common shares (including full exercise of the overal-lotment) at $9 each. The company will use some of the proceeds for ongoing development of Phase II VK2809 for lipid disorders, Phase II VK5211 to improve lean body mass and muscle and bone strength in patients who’ve had non-elective hip fracture surgery, and preclinical VK0214 for adrenoleukodystrophy. (Jun.)Investment Banks/Advisors: Maxim Group LLC; Roth Capital Partners; SunTrust Banks Inc.; William Blair & Co.
XERIS PHARMACEUTICALS INC.Drug delivery firm Xeris Pharmaceuticals Inc. netted $91.4mm in its upsized initial public offering of 6.56mm common shares (including full exercise of the overallot-ment) at $15, the middle of its intended range. (Jun.)Investment Banks/Advisors: Jefferies & Co. Inc.; Leerink Partners LLC; Mizuho Bank Ltd.; RBC Capital Markets
ZAFGEN INC.Zafgen Inc. (therapies for complex meta-bolic diseases) netted $64.9mm through a follow-on public offering of 9.2mm common shares (including full exercise of the overallotment) at $7.50 each. The company will use some of the proceeds for ongoing development of preclinical ZGN1258 for Prader-Willi syndrome and Phase II ZGN1061 for diabetes. It will also study the potential liver effects of ZGN1061 in NASH and develop an early preclinical-stage orally active MetAP2 inhibitor for liver-specific metabolic disease. (Jun.)Investment Banks/Advisors: Cowen & Co. LLC; JMP Securities LLC; Piper Jaffray & Co.; Wedbush PacGrow Life Sciences
ZYMEWORKS INC.Zymeworks Inc. (multifunctional bio-therapeutics for cancer) netted $91.9mm through a public offering of 6.2mm com-mon shares (including the overallotment) at $15.75. The company plans to use about $50mm of the proceeds to support development of Phase I ZW25 as a single and combo agent for gastroesophageal, breast, and colorectal cancers and other HER2-expressing tumors. Funds will also go towards ZW49 (antibody-drug conjugate in early studies for HER2-expressing cancers), and other preclinical projects. (Jun.)Investment Banks/Advisors: Citigroup Inc.; Paradigm Capital Inc.; Raymond James & Associates Inc.; Wells Fargo Securities LLC




















