
Depressive symptoms in the last days of life of patients with cancer: a nationwide retrospective...
10
Depressive symptoms in the last days of life of patients with cancer: a nationwide retrospective mortality study Elene Janberidze, 1,2 Sandra Martins Pereira, 3 Marianne Jensen Hjermstad, 1,4 Anne Kari Knudsen, 1,2 Stein Kaasa, 1,2 Agnes van der Heide, 5 Bregje Onwuteaka-Philipsen, 3 on behalf of EURO IMPACT For numbered affiliations see end of article. Correspondence to Dr Elene Janberidze, European Palliative Care Research Centre, Department of Cancer Research and Molecular Medicine, Faculty of Medicine, Norwegian University of Science and Technology (NTNU), Kunnskapssenteret 4. etg., St. Olavs Hospital, Trondheim N-7006 Norway; [email protected] Received 16 May 2014 Revised 13 October 2014 Accepted 19 December 2014 To cite: Janberidze E, Pereira SM, Hjermstad MJ, et al. BMJ Supportive & Palliative Care Published Online First: [ please include Day Month Year] doi:10.1136/ bmjspcare-2014-000722 ABSTRACT Objectives Depressive symptoms are common in patients with cancer and tend to increase as death approaches. The study aims were to examine the prevalence of depressive symptoms in patients with cancer in their final 24 h, and their association with other symptoms, sociodemographic and care characteristics. Methods A stratified sample of deaths was drawn by Statistics Netherlands. Questionnaires on patient and care characteristics were sent to the physicians (N=6860) who signed the death certificates (response rate 77.8%). Adult patients with cancer with non-sudden death were included (n=1363). Symptoms during the final 24 h of life were assessed on a 1–5 scale and categorised as 1=no, 2–3=mild/moderate and 4–5=severe/very severe. Results Depressive symptoms were registered in 37.6% of the patients. Patients aged 80 years or more had a reduced risk of having mild/ moderate depressive symptoms compared with those aged 17–65 years (OR 0.70; 95% CI 0.50 to 0.99). Elderly care physicians were more likely to assess patients with severe/very severe depressive symptoms than patients with no depressive symptoms (OR 4.18; 95% CI 1.48 to 11.76). Involvement of pain specialists/palliative care consultants and psychiatrists/psychologists was associated with more ratings of severe/very severe depressive symptoms. Fatigue and confusion were significantly associated with mild/moderate depressive symptoms and anxiety with severe/very severe symptoms. Conclusions More than one-third of the patients were categorised with depressive symptoms during the last 24 h of life. We recommend greater awareness of depression earlier in the disease trajectory to improve care. INTRODUCTION Prevalence rates of depression and anxiety in patients with long-term physical disor- ders are about 25–30%. 1 Also, in patients with advanced cancer, depressive symp- toms are commonly experienced. 2 The reported prevalence rates in this patient population vary considerably from 2% to 56% depending on the assessment method used. 3 Self-reporting of subjective symp- toms in patients with cancer is generally considered as the ‘gold standard’ of assess- ment. 4 However, in the last days of life, compliance with self-report measures vary dramatically 5 since many patients may have multiple concurrent symptoms and a high symptom burden, 6 for example, con- fusion, communication difficulties, and/or physical and cognitive disability. 7 Thus, in this phase, ratings of patients’ symptoms by healthcare providers and/or their next of kin may be a feasible solution. Proxy ratings of this kind are reported to be rea- sonably adequate. 8 The benefits of the proxy ratings may outweigh the limitations when studying groups that would other- wise be excluded from studies. 8–10 Different sociodemographic character- istics and symptoms have been identified as being associated with depression in popu- lations with cancer. Those characteristics include younger age, 11 female gender, 12 marital status 13 and certain cancer diagno- ses such as breast 14 and pancreatic cancer. 15 Most patients with cancer have several symptoms during their disease tra- jectory with fatigue, pain and dyspnoea being among the most common, 6 leading to an impaired quality of life. 16 Many of these somatic symptoms may overlap with Research Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722 1 group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Depressive symptoms in the last days of life of patients with cancer: a nationwide retrospective...
Depressive symptoms in the lastdays of life of patients with cancer:a nationwide retrospectivemortality study
Elene Janberidze,1,2 Sandra Martins Pereira,3 Marianne Jensen Hjermstad,1,4
Anne Kari Knudsen,1,2 Stein Kaasa,1,2 Agnes van der Heide,5
Bregje Onwuteaka-Philipsen,3 on behalf of EURO IMPACT
For numbered affiliations seeend of article.
Correspondence toDr Elene Janberidze, EuropeanPalliative Care Research Centre,Department of Cancer Researchand Molecular Medicine, Facultyof Medicine, NorwegianUniversity of Science andTechnology (NTNU),Kunnskapssenteret 4. etg.,St. Olavs Hospital,Trondheim N-7006 Norway;[email protected]
Received 16 May 2014Revised 13 October 2014Accepted 19 December 2014
To cite: Janberidze E,Pereira SM, Hjermstad MJ,et al. BMJ Supportive &Palliative Care Published OnlineFirst: [please include DayMonth Year] doi:10.1136/bmjspcare-2014-000722
ABSTRACTObjectives Depressive symptoms are commonin patients with cancer and tend to increase asdeath approaches. The study aims were toexamine the prevalence of depressive symptomsin patients with cancer in their final 24 h, andtheir association with other symptoms,sociodemographic and care characteristics.Methods A stratified sample of deaths wasdrawn by Statistics Netherlands. Questionnaireson patient and care characteristics were sent tothe physicians (N=6860) who signed the deathcertificates (response rate 77.8%). Adult patientswith cancer with non-sudden death wereincluded (n=1363). Symptoms during the final24 h of life were assessed on a 1–5 scale andcategorised as 1=no, 2–3=mild/moderate and4–5=severe/very severe.Results Depressive symptoms were registered in37.6% of the patients. Patients aged 80 years ormore had a reduced risk of having mild/moderate depressive symptoms compared withthose aged 17–65 years (OR 0.70; 95% CI 0.50to 0.99). Elderly care physicians were more likelyto assess patients with severe/very severedepressive symptoms than patients with nodepressive symptoms (OR 4.18; 95% CI 1.48 to11.76). Involvement of pain specialists/palliativecare consultants and psychiatrists/psychologistswas associated with more ratings of severe/verysevere depressive symptoms. Fatigue andconfusion were significantly associated withmild/moderate depressive symptoms and anxietywith severe/very severe symptoms.Conclusions More than one-third of thepatients were categorised with depressivesymptoms during the last 24 h of life.We recommend greater awareness ofdepression earlier in the disease trajectory toimprove care.
INTRODUCTIONPrevalence rates of depression and anxietyin patients with long-term physical disor-ders are about 25–30%.1 Also, in patientswith advanced cancer, depressive symp-toms are commonly experienced.2 Thereported prevalence rates in this patientpopulation vary considerably from 2% to56% depending on the assessment methodused.3 Self-reporting of subjective symp-toms in patients with cancer is generallyconsidered as the ‘gold standard’ of assess-ment.4 However, in the last days of life,compliance with self-report measures varydramatically5 since many patients mayhave multiple concurrent symptoms and ahigh symptom burden,6 for example, con-fusion, communication difficulties, and/orphysical and cognitive disability.7 Thus, inthis phase, ratings of patients’ symptomsby healthcare providers and/or their nextof kin may be a feasible solution. Proxyratings of this kind are reported to be rea-sonably adequate.8 The benefits of theproxy ratings may outweigh the limitationswhen studying groups that would other-wise be excluded from studies.8–10
Different sociodemographic character-istics and symptoms have been identified asbeing associated with depression in popu-lations with cancer. Those characteristicsinclude younger age,11 female gender,12
marital status13 and certain cancer diagno-ses such as breast14 and pancreaticcancer.15 Most patients with cancer haveseveral symptoms during their disease tra-jectory with fatigue, pain and dyspnoeabeing among the most common,6 leadingto an impaired quality of life.16 Many ofthese somatic symptoms may overlap with
Research
Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722 1
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from

the nine symptoms included in the diagnostic criteria ofdepression in the Diagnostic and Statistical Manual ofMental Disorders (DSM) V,17 for example, fatigue.18
The present study makes use of survey data from alarge nationwide retrospective death certificate studyfrom the Netherlands conducted in 2005,19 whichexamines different aspects of end-of-life practice. Dataon depression and other symptoms prior to deathwere registered by the attending physicians retrospect-ively, and were used to address the following researchquestions:1. What was the prevalence of depressive symptoms in
patients with cancer in the final 24 h of life based onreports from the attending physician?
2. Were there any associations between depressive symp-toms as reported by physicians and the patients’sociodemographic characteristics and characteristicsof care?
3. Were there any associations between depressive symp-toms and the following common symptoms: pain, vomit-ing, fatigue, dyspnoea, confusion and anxiety?
METHODSStudy designA nationwide retrospective death certificate study wasperformed in 2005 analogous to three previously con-ducted studies.20–22 A stratified sample of deaths wasdrawn by Statistics Netherlands (http://www.cbs.nl)which receives death certificates of all deaths in thecountry. Depending on the cause of death registered onthe death certificate, the death was assigned to one offive strata (1–5). Patients with instant death (eg, car acci-dent) were assigned to stratum 1. Cases from stratum 1did not receive any assistance from a physician prior todeath. Consequently, questionnaires were not sent, butthe cases were retained in the sample. All other deathswere assigned to strata 2–5, with each stratum having ahigher likelihood of having a medical end-of-life deci-sion preceding death.19 The final sample contained halfof the cases in stratum 5, 25% of the cases in stratum 4,12.5% of those in stratum 3, 8.3% of those in stratum2, and all cases in stratum 1 corresponding with the pre-vious publication.19 Patients with cancer registered asthe cause of death were included in stratum 4.For all sampled deaths, a questionnaire was mailed
to the physicians who had signed the death certificate,with a letter including the name and date of birth ofthe diseased person. This information allowed physi-cians to identify the patient and to retrieve relevantinformation from the patient’s medical record.According to Dutch legislation, there was no need forethical committee approval.19
PopulationOf 6860 questionnaires mailed, 5342 were returned,giving a response rate of 77.8%. For the present ana-lysis, cases were excluded if (1) the physicians hadtheir very first contact with the patient after the
patient’s death (n=848), (2) the patient died suddenlyor unexpectedly according to the physician (n=635),(3) the patient was younger than 17 years old(n=121), (4) the cause of death was other than cancer(n=1508) and if (5) the patient was unconscious inthe last days of life (n=709). This resulted in a sampleof 1521 patients, with missing information on depres-sive symptoms in 10.4% (n=158). Thus, the finalstudy population consisted of 1363 cases.
MeasuresA four-page questionnaire was completed 1–2 monthsafter the patient’s death. It included information oncare received by the patient, such as the medical spe-cialty of the attending physician, and whether otherhealthcare providers were involved in the care of thepatient in the last month of life (eg, pain specialist).The prevalence and intensity of the following symp-toms were rated by the physician who signed thedeath certificate: depression, pain, vomiting, fatigue,dyspnoea, confusion and anxiety in the final 24 hbefore death. Symptom intensity was registered on arating scale ranging from 1=no symptoms to 5=verysevere symptoms.Sociodemographic characteristics (eg, gender, age at
death, marital status, place of death) and underlyingcause of death were captured from the death certificates,which were linked to the questionnaires received.
Statistical analysisIn this study, the scale used for rating symptom inten-sity was categorised as 1=no, 2=mild, 3=moderate,4=severe and 5=very severe, and further recodedinto three groups: 1=no, 2–3=mild/moderate and4–5=severe/very severe. Sociodemographic character-istics, care characteristics and patients’ physician-reported symptoms were chosen as independentvariables based on the existing literature.6 11–13
Intensity of depressive symptoms was defined as thedependent variable divided into three categories: no(reference), mild/moderate and severe/very severe.The following analyses were performed:
1. The association between independent and dependentvariables was analysed using the χ2 test (p<0.05).Weighted percentages were applied to adjust for differ-ences in the percentages of deaths sampled from each ofthe five strata, and differences in response rates in rela-tion to the age, sex, marital status, region of residenceand cause of death of the patients. After adjustment, thepercentages were extrapolated to cover a 12-monthperiod to reflect all deaths in the Netherlands in 2005.As a result of this weighting procedure, the percentagespresented cannot be derived from the absolute numberspresented.
2. Multinomial logistic regression analyses were used tofurther study the association between independent anddependent variables. No weighting procedure wasapplied. In the first step of this analysis, all independent
Research
2 Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from
variables that showed a significant association with thedependent variable were entered into the model, exceptfor place of death. This variable was left out from theanalysis because of its high correlation with the medicalspecialty of the attending physician. Using a backwardsstepwise approach, variables were excluded until the laststep of the analysis in which only variables with a statis-tical significance (p<0.05) remained in the model.Results are presented in terms of p values and ORs
along with 95% CIs. All of the statistical analyseswere performed with IBM SPSS Statistics V.19.0 forWindows (IBM Corporation, Armonk, New York,USA).
RESULTSPatient characteristics and prevalence of depressivesymptomsSeventy-two per cent of the patients were 65 years orabove, 43% were female and more than 50% of the
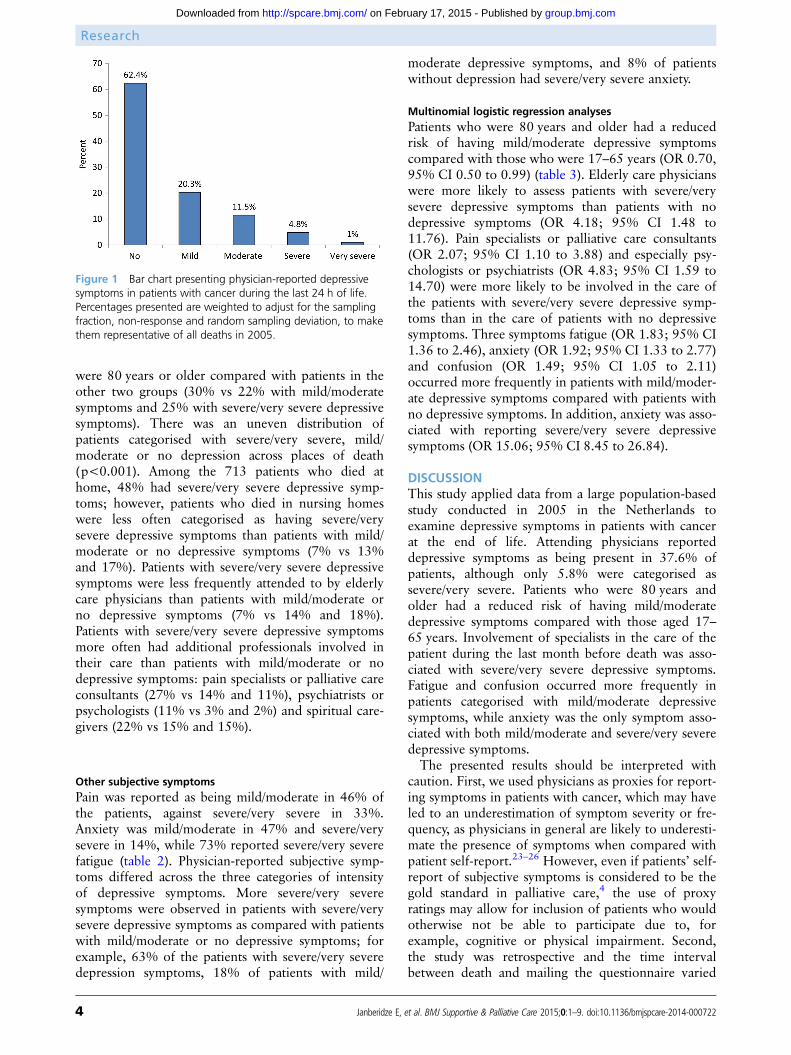
patients were married. Forty-eight per cent died athome, 24% in hospital, 15% in nursing homes and6% in residential homes. General practitionersattended to 60% of the patients before or at the timeof death (table 1). The overall prevalence of depres-sive symptoms in the last 24 h of life was 37.6%,including 31.8% with mild/moderate symptoms and5.8% with severe/very severe depressive symptoms(figure 1).
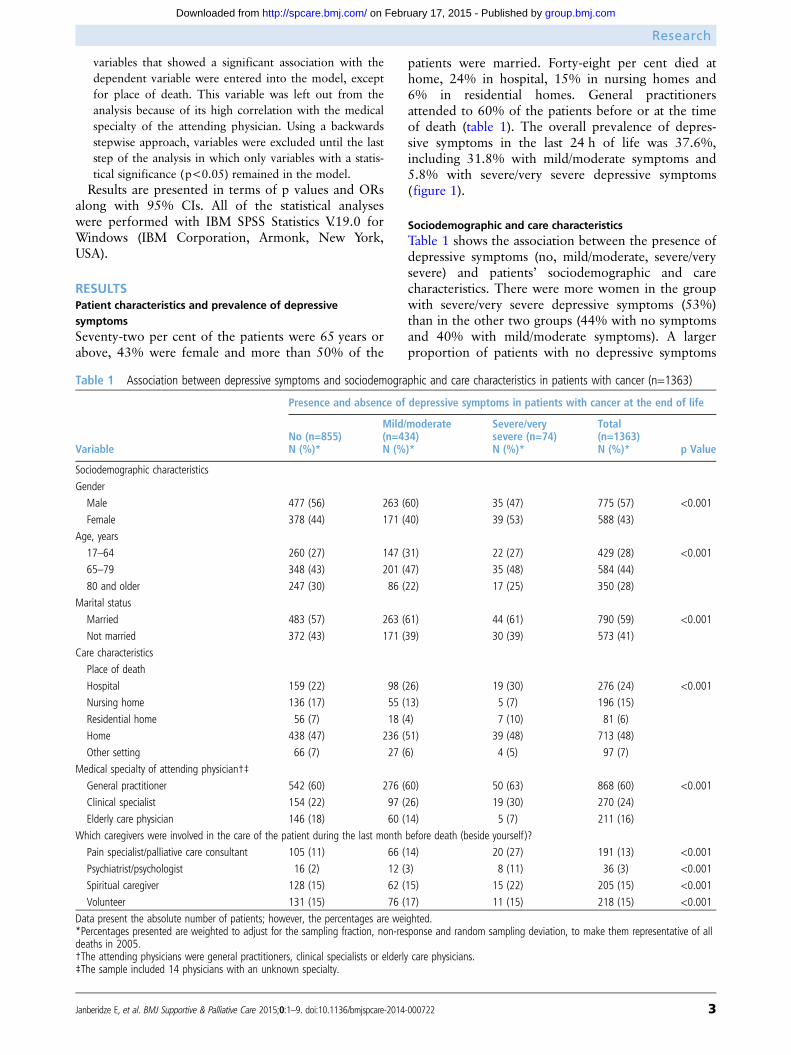
Sociodemographic and care characteristicsTable 1 shows the association between the presence ofdepressive symptoms (no, mild/moderate, severe/verysevere) and patients’ sociodemographic and carecharacteristics. There were more women in the groupwith severe/very severe depressive symptoms (53%)than in the other two groups (44% with no symptomsand 40% with mild/moderate symptoms). A largerproportion of patients with no depressive symptoms
Table 1 Association between depressive symptoms and sociodemographic and care characteristics in patients with cancer (n=1363)
Variable
Presence and absence of depressive symptoms in patients with cancer at the end of life
No (n=855)N (%)*
Mild/moderate(n=434)N (%)*
Severe/verysevere (n=74)N (%)*
Total(n=1363)N (%)* p Value
Sociodemographic characteristics
Gender
Male 477 (56) 263 (60) 35 (47) 775 (57) <0.001
Female 378 (44) 171 (40) 39 (53) 588 (43)
Age, years
17–64 260 (27) 147 (31) 22 (27) 429 (28) <0.001
65–79 348 (43) 201 (47) 35 (48) 584 (44)
80 and older 247 (30) 86 (22) 17 (25) 350 (28)
Marital status
Married 483 (57) 263 (61) 44 (61) 790 (59) <0.001
Not married 372 (43) 171 (39) 30 (39) 573 (41)
Care characteristics
Place of death
Hospital 159 (22) 98 (26) 19 (30) 276 (24) <0.001
Nursing home 136 (17) 55 (13) 5 (7) 196 (15)
Residential home 56 (7) 18 (4) 7 (10) 81 (6)
Home 438 (47) 236 (51) 39 (48) 713 (48)
Other setting 66 (7) 27 (6) 4 (5) 97 (7)
Medical specialty of attending physician†‡
General practitioner 542 (60) 276 (60) 50 (63) 868 (60) <0.001
Clinical specialist 154 (22) 97 (26) 19 (30) 270 (24)
Elderly care physician 146 (18) 60 (14) 5 (7) 211 (16)
Which caregivers were involved in the care of the patient during the last month before death (beside yourself )?
Pain specialist/palliative care consultant 105 (11) 66 (14) 20 (27) 191 (13) <0.001
Psychiatrist/psychologist 16 (2) 12 (3) 8 (11) 36 (3) <0.001
Spiritual caregiver 128 (15) 62 (15) 15 (22) 205 (15) <0.001
Volunteer 131 (15) 76 (17) 11 (15) 218 (15) <0.001
Data present the absolute number of patients; however, the percentages are weighted.*Percentages presented are weighted to adjust for the sampling fraction, non-response and random sampling deviation, to make them representative of alldeaths in 2005.†The attending physicians were general practitioners, clinical specialists or elderly care physicians.‡The sample included 14 physicians with an unknown specialty.
Research
Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722 3
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from
were 80 years or older compared with patients in theother two groups (30% vs 22% with mild/moderatesymptoms and 25% with severe/very severe depressivesymptoms). There was an uneven distribution ofpatients categorised with severe/very severe, mild/moderate or no depression across places of death(p<0.001). Among the 713 patients who died athome, 48% had severe/very severe depressive symp-toms; however, patients who died in nursing homeswere less often categorised as having severe/verysevere depressive symptoms than patients with mild/moderate or no depressive symptoms (7% vs 13%and 17%). Patients with severe/very severe depressivesymptoms were less frequently attended to by elderlycare physicians than patients with mild/moderate orno depressive symptoms (7% vs 14% and 18%).Patients with severe/very severe depressive symptomsmore often had additional professionals involved intheir care than patients with mild/moderate or nodepressive symptoms: pain specialists or palliative careconsultants (27% vs 14% and 11%), psychiatrists orpsychologists (11% vs 3% and 2%) and spiritual care-givers (22% vs 15% and 15%).
Other subjective symptomsPain was reported as being mild/moderate in 46% ofthe patients, against severe/very severe in 33%.Anxiety was mild/moderate in 47% and severe/verysevere in 14%, while 73% reported severe/very severefatigue (table 2). Physician-reported subjective symp-toms differed across the three categories of intensityof depressive symptoms. More severe/very severesymptoms were observed in patients with severe/verysevere depressive symptoms as compared with patientswith mild/moderate or no depressive symptoms; forexample, 63% of the patients with severe/very severedepression symptoms, 18% of patients with mild/
moderate depressive symptoms, and 8% of patientswithout depression had severe/very severe anxiety.
Multinomial logistic regression analysesPatients who were 80 years and older had a reducedrisk of having mild/moderate depressive symptomscompared with those who were 17–65 years (OR 0.70,95% CI 0.50 to 0.99) (table 3). Elderly care physicianswere more likely to assess patients with severe/verysevere depressive symptoms than patients with nodepressive symptoms (OR 4.18; 95% CI 1.48 to11.76). Pain specialists or palliative care consultants(OR 2.07; 95% CI 1.10 to 3.88) and especially psy-chologists or psychiatrists (OR 4.83; 95% CI 1.59 to14.70) were more likely to be involved in the care ofthe patients with severe/very severe depressive symp-toms than in the care of patients with no depressivesymptoms. Three symptoms fatigue (OR 1.83; 95% CI1.36 to 2.46), anxiety (OR 1.92; 95% CI 1.33 to 2.77)and confusion (OR 1.49; 95% CI 1.05 to 2.11)occurred more frequently in patients with mild/moder-ate depressive symptoms compared with patients withno depressive symptoms. In addition, anxiety was asso-ciated with reporting severe/very severe depressivesymptoms (OR 15.06; 95% CI 8.45 to 26.84).
DISCUSSIONThis study applied data from a large population-basedstudy conducted in 2005 in the Netherlands toexamine depressive symptoms in patients with cancerat the end of life. Attending physicians reporteddepressive symptoms as being present in 37.6% ofpatients, although only 5.8% were categorised assevere/very severe. Patients who were 80 years andolder had a reduced risk of having mild/moderatedepressive symptoms compared with those aged 17–65 years. Involvement of specialists in the care of thepatient during the last month before death was asso-ciated with severe/very severe depressive symptoms.Fatigue and confusion occurred more frequently inpatients categorised with mild/moderate depressivesymptoms, while anxiety was the only symptom asso-ciated with both mild/moderate and severe/very severedepressive symptoms.The presented results should be interpreted with
caution. First, we used physicians as proxies for report-ing symptoms in patients with cancer, which may haveled to an underestimation of symptom severity or fre-quency, as physicians in general are likely to underesti-mate the presence of symptoms when compared withpatient self-report.23–26 However, even if patients’ self-report of subjective symptoms is considered to be thegold standard in palliative care,4 the use of proxyratings may allow for inclusion of patients who wouldotherwise not be able to participate due to, forexample, cognitive or physical impairment. Second,the study was retrospective and the time intervalbetween death and mailing the questionnaire varied
Figure 1 Bar chart presenting physician-reported depressivesymptoms in patients with cancer during the last 24 h of life.Percentages presented are weighted to adjust for the samplingfraction, non-response and random sampling deviation, to makethem representative of all deaths in 2005.
Research
4 Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from

between 1 and 2 months, which may have caused arecall error. Missing data on depressive symptoms(10.4%) probably illustrate some difficulties that physi-cians may have had in assessing depression or recallinginformation and could engender bias. However, owingto the large sample size, there are data on depressivesymptoms in 1363 patients, which increases the reli-ability. Furthermore, the major group of attending phy-sicians included general practitioners (60%) who hadbeen the patients’ family doctors for several years.Thus, they did not only sign the death certificates orattend patients during the last days of life but were alsofamiliar with the patient and relatives. Third, no stan-dardised measure with validated cut-off scores wasused for reporting, and the physicians were not askedif they assessed depression with any formal tools in thelast 24 h before death. We also lack information on theuse of medication such as antidepressants, other psy-chotropic drugs and opioids which may have led tofatigue, confusion or development of other distressingsymptoms at the end of life. However, from otherstudies, we know that antidepressants are often pre-scribed close to death and in fact so late that the
therapeutic effects may be questionable.27 28 Detailedregistration of interventions for depressive symptoms,duration of receiving antidepressant medication, infor-mation of when depression was first identified and dur-ation of depressive symptoms would have been givenimportant information about depression and treatmentoutcomes; however, this was beyond the scope of thedeath certificate study. No control group was includedas the primary aim of the study was to describe theexisting practice of end-of-life care in the Netherlands.The major strength of this study is related to the
sample size including 1363 patients with cancer at theend of life. The study included information onpatients extracted from the death certificates in theNetherlands, and involved different care settingsacross the country, making the results representativeof the entire cancer population in the Netherlands.Furthermore, the response to the questionnaire washigh (77.8%).
Prevalence rates of depressive symptomsIn general, a comparison of prevalence rates is chal-lenging partly due to the different study designs,
Table 2 Association between depressive symptoms and other symptoms in patients during the last 24 h before death (n=1363)
Symptoms (missing)
Presence and absence of depressive symptoms in patients with cancer at the end of life
No (n=855)N (%)*
Mild/moderate(n=434)N (%)*
Severe/verysevere (n=74)N (%)*
Total(n=1363)N (%)* p Value
Pain (12%)
No pain 199 (25) 66 (16) 9 (14) 274 (21) <0.001
Mild/moderate pain 388 (45) 29 (40) 627 (46)
Severe/very severe pain 265 (30) 155 (35) 35 (46) 455 (33)
Vomiting (13%)
No vomiting 629 (76) 64 (64) 38 (52) 931 (71) <0.001
Mild/moderate vomiting 147 (16) 119 (27) 21 (31) 287 (20)
Severe/very severe vomiting 73 (8) 21 (9) 12 (17) 127 (9)
Fatigue (12%)
No fatigue 65 (9) 6 (2) 2 (3) 73 (6) <0.001
Mild/moderate fatigue 189 (24) 70 (17) 11 (16) 270 (21)
Severe/very severe fatigue 590 (67) 354 (81) 61 (81) 1005 (73)
Dyspnoea (12%)
No dyspnoea 325 (38) 104 (23) 16 (20) 445 (32) <0.001
Mild/moderate dyspnoea 266 (31) 188 (43) 28 (38) 482 (35)
Severe/very severe dyspnoea 259 (31) 139 (34) 30 (42) 428(33)
Confusion (12%)
No confusion 510 (58) 122 (26) 14 (17) 646 (46) <0.001
Mild/moderate confusion 248 (30) 233 (55) 36 (51) 517 (39)
Severe/very severe confusion 94 (12) 76 (19) 23 (32) 193 (15)
Anxiety (11%)
No anxiety 470 (54) 73 (16) 2 (2) 545 (39) <0.001
Mild/moderate anxiety 311 (38) 283 (66) 26 (35) 620 (47)
Severe/very severe anxiety 72 (8) 75 (18) 46 (63) 193 (14)
Data present the absolute number of patients; however, the percentages are weighted.*Percentages presented are weighted to adjust for the sampling fraction, non-response and random sampling deviation, to make them representative of alldeaths in 2005.
Research
Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722 5
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from

inclusion of patients with different survival time, anduse of different assessment or reporting methods (eg,self-report vs diagnostic tools or proxy ratings). A pre-vious study from the Netherlands examined primarycare patients with cancer at a median of 15 weeksbefore death.29 Depressed mood was reported bygeneral practitioners using a scale from 1 (notdepressed) to 5 (very depressed). According to acut-off score of 2, the prevalence rate for depressivesymptoms was 14%, which corresponds with ourresults (17%) when using the same threshold.Diagnosing depression is challenging, especially in
patients with other somatic illnesses where symptomssuch as fatigue can be related to the cancer, its treat-ment or interpreted as a sign of depression accordingto the DSM-V criteria.17 Unsystematic assessment ofsymptoms,30 lack of communication skills31 and insuffi-cient training of healthcare providers to recognisedepressive symptoms at the end of life could be themost important explanations.32 The attending
physicians reporting the present data were not specific-ally trained to identify depression at the end of life, orto distinguish this from, for example, fatigue or latestage infirmity. On the other hand, initiation of psycho-logical interventions near the end of life may some-times be thought to be too late or symptoms could beregarded as a normal part of the dying process.33
Sociodemographic and care characteristicsOur results regarding age were inconclusive andcannot confirm results from other studies showing thatyounger age may be associated with depression.11 Theassociation between severe/very severe depressivesymptoms and elderly care physicians might partly beexplained by the fact that patients in need of specialistcare have a higher symptom burden than patients notrequiring specialist care.34 Furthermore, specialists areexpected to have more experience with patients havingcomplex conditions and may thus identify patientswith cancer with depressive symptoms more easily
Table 3 Variables associated with depressive symptoms in multinomial logistic regression analyses (N=1363)
Presence and absence of depressive symptoms in patients with cancer at the end of life
VariableMild/moderate (n=434)OR (95% CI) p Value
Severe/very severe (n=74)OR (95% CI) p Value
Age
17–64 1.00 1.00
65–79 1.09 (0.83 to 1.44) 0.530 0.55 (0.84 to 2.89) 0.162
80 and older 0.70 (0.50 to 0.99) 0.043 1.52 (0.71 to 3.22) 0.277
Medical specialty of attending physician*
General practitioner 1.00 1.00
Clinical specialist 1.30 (0.96 to 1.76) 0.095 1.16 (0.62 to 2.18) 0.641
Elderly care physician 1.13 (0.78 to 1.62) 0.517 4.18 (1.48 to 11.76) 0.007
Which caregivers were involved in the care of the patient during the last month before death (beside yourself )?
Pain specialist/palliative care consultant
No 1.00 1.00
Yes 1.16 (0.82 to 1.64) 0.412 2.07 (1.10 to 3.88) 0.023
Psychiatrist/psychologist
No 1.00 1.00
Yes 1.37 (0.59 to 3.21) 0.467 4.83 (1.59 to 14.70) 0.006
Symptoms during the last 24 h before death
Fatigue
No 1.00 1.00
Yes 1.83 (1.36 to 2.46) <0.001 1.46 (0.73 to 2.91) 0.282
Anxiety
No 1.00 1.00
Yes 1.92 (1.33 to 2.77) <0.001 15.06 (8.45 to 26.84) <0.001
Confusion
No 1.00 1.00
Yes 1.49 (1.05 to 2.11) 0.025 1.48 (0.79 to 2.79) 0.223
No weighting procedure was conducted during multinomial logistic regression analysis. Bold numbers represent ORs and 95% CIs showing statisticallysignificant difference (ORs differs significantly from 1.00) between the categories of mild/moderate or severe/very severe depressive symptoms comparedwith the group with no depressive symptoms (reference category).The variables not reaching statistical significance in multinomial logistic regression were: spiritual caregiver involved in the care of the patient for the lastmonth before death, patients’ marital status, volunteer involved in the care of the patients for the last month before death, physical symptoms such aspain, vomiting, dyspnoea and patients’ gender.*The attending physicians were general practitioners, clinical specialists or elderly care physicians.
Research
6 Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from

than general practitioners would.35 Additional profes-sional caregivers besides the responsible physicianinvolved in the management of patients with cancer inthe last month before death (eg, pain specialist) appearto facilitate more precise patient identification in needof symptom treatment. Specialists in general may tendto systematically assess and be able to diagnose thepatients with complex conditions. However, our datashowed that additional specialists were involved onlyin a minor group of the patient cohort.
SymptomsPatients with advanced cancer often experience symp-toms that are coexisting and interdependent, espe-cially when facing the end of life.6 36 37 Studies showan association between uncontrolled physical symp-toms, such as pain, and depression,38 39 but the caus-ality of this relationship is unclear.38 In this study, thepatients were reported to have a relatively highsymptom burden in the last 24 h of life; for example,79% of the patients had pain (46% reported as mod-erate and 33% as severe). In the univariate analyses,an association between pain and depressive symptomswas observed. However, unexpectedly, no such associ-ation was found in the multinomial logistic regression.In this study, there was an association betweeninvolvement of pain specialists in patient treatmentand severe depressive symptoms. This may indicatethat patients with depressive symptoms have acomplex symptomatology and may need a multidiscip-linary palliative care approach. Data on the actualpain treatment were not available.Fatigue is known to be more frequent and severe
among depressed than non-depressed patients.40
Diagnosis of depression according to the DSM-V cri-teria17 is established if five of nine criteria symptoms arepresent, with fatigue or loss of energy being one ofthese. Our data showed that 73% of the patients wereexperiencing severe/very severe fatigue in the final 24 hbefore death. Healthcare providers may have inter-preted fatigue as part of the dying process, a sign ofdepression, or something that may have contributed tothe development of depression in patients with bothsymptoms. In addition, anxiety was the only variableassociated with both mild/moderate and severe/verysevere depressive symptoms. This could be explained bythe interdependent nature of those two conditions.37
The seemingly high prevalence of symptoms in thisstudy, and of depressive symptoms in particular,points to a need to increase awareness of thoroughsymptom assessment throughout the cancer diseasetrajectory. According to the WHO’s revised definitionof palliative care,41early integration of palliative carein the management of patients with cancer is recom-mended.42 Introducing palliative care early to thepatients with its systematic approach to symptomassessment increases the awareness and attention tosymptoms at an earlier stage and results in better
symptom control and quality of life, also at the end oflife.42–46 For example, in the well-known study byTemel et al,42 patients with non-small cell lung cancerwho were randomised to palliative care had signifi-cantly fewer depressive symptoms than those in thestandard group.
CONCLUSIONSThis study showed that more than one-third ofpatients with cancer were rated as having mild/moder-ate to severe/very severe depressive symptoms by theattending physicians during the last 24 h of life.Multiple symptoms, and especially depressive symp-toms, in patients with cancer at the end of life still callfor special attention. Improved knowledge amonghealthcare providers about assessment, classificationand treatment of depression and depressive symptomsin patients with advanced cancer would be importantto optimise cancer patient care throughout the diseasetrajectory.
Author affiliations1European Palliative Care Research Centre (PRC),Department of Cancer Research and MolecularMedicine, Faculty of Medicine, Norwegian Universityof Science and Technology (NTNU), Trondheim,Norway2Department of Oncology, St. Olavs Hospital,Trondheim University Hospital, Trondheim, Norway3Department of Public and Occupational Health, VUUniversity Medical Center, and EMGO+ Institutefor Health and Care Research, VUmc ExpertiseCenter for Palliative Care, Amsterdam, Netherlands4Regional Centre for Excellence in Palliative Care,South Eastern Norway, Oslo University Hospital,Oslo, Norway5Department of Public Health, Erasmus MedicalCenter, Rotterdam, The Netherlands
Acknowledgements The authors thank the following EUROIMPACT collaborators for their contribution.
Collaborators This article is part of the European Intersectorialand Multidisciplinary Palliative Care Research Training (EUROIMPACT). EURO IMPACT is funded by the European UnionSeventh Framework Programme (FP7/2007–2013, under grantagreement n° [264697]). EURO IMPACTaims to develop amultidisciplinary, multi-professional and inter-sectorialeducational and research training framework for palliative careresearch in Europe. EURO IMPACT is coordinated by ProfessorLuc Deliens, Professor Lieve Van den Block, Zeger De Groote,Joachim Cohen and Koen Pardon of the End-of-Life CareResearch Group, Ghent University & Vrije Universiteit Brussel,Brussels, Belgium. Other partners are: Anneke Francke, LucDeliens and Roeline Pasman, VU University Medical Center,EMGO Institute for health and care research, Amsterdam, TheNetherlands; Richard Harding and Irene J Higginson, King’sCollege London, Cicely Saunders Institute, London, and CicelySaunders International, London; and Sarah Brearley and SheilaPayne, International Observatory on End-of-Life Care,Lancaster University, Lancaster, UK; Augusto Caraceni, EAPCResearch Network, Trondheim, Norway; and FondazioneIRCCS Istituto Nazionale dei Tumori, Milan, Italy, and GuidoMiccinesi, Cancer Research and Prevention Institute, Florence,
Research
Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722 7
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from

Italy; Sophie Pautex, EUGMS European Union GeriatricMedicine Society, Geneva, Switzerland; Karen Linden, SpringerScience and Business Media, Houten, The Netherlands.
Contributors BO-P and AVDH were responsible for the studyconcept and devised the questionnaire. Statistics Netherlandsmade the stratification analysis. EJ led the statistical analysis andwriting of the paper; all co-authors commented on the draftand agree on the final content.
Funding This study was funded by the NetherlandsOrganisation for Health Research and Development (ZonMw),grant number 1151.0001, and the VU University MedicalCenter, EMGO Institute for Health and Care Research,Department of General Practice & Elderly Care medicine, andthe Department of Public and Occupational Health,Amsterdam, The Netherlands.
Competing interests None.
Provenance and peer review Not commissioned; externallypeer reviewed.
Data sharing statement EJ, BOP and AVDH have access to thefull data set.
REFERENCES1 Cimpean D, Drake RE. Treating co-morbid chronic medical
conditions and anxiety/depression. Epidemiol Psychiatric Sci2011;20:141–50.
2 Hotopf M, Chidgey J, Addington-Hall J, et al. Depression inadvanced disease: a systematic review part 1. Prevalence andcase finding. Palliat Med 2002;16:81–97.
3 Janberidze E, Hjermstad MJ, Haugen DF, et al. How arepatient populations characterized in studies investigatingdepression in advanced cancer? Results from a systematicliterature review. J Pain Symptom Manage 2014;48:678–98.
4 Sneeuw KC, Aaronson NK, Sprangers MA, et al. Comparisonof patient and proxy EORTC QLQ-C30 ratings in assessing thequality of life of cancer patients. J Clin Epidemiol1998;51:617–31.
5 Hui D, Glitza I, Chisholm G, et al. Attrition rates, reasons, andpredictive factors in supportive care and palliative oncologyclinical trials. Cancer 2013;119:1098–105.
6 Laugsand EA, Kaasa S, de Conno F, et al. Intensity andtreatment of symptoms in 3,030 palliative care patients:a cross-sectional survey of the EAPC Research Network. JOpioid Manag 2009;5:11–21.
7 Kurita GP, Sjogren P, Ekholm O, et al. Prevalence andpredictors of cognitive dysfunction in opioid-treated patientswith cancer: a multinational study. J Clin Oncol2011;29:1297–303.
8 Sneeuw KC, Sprangers MA, Aaronson NK. The role of healthcare providers and significant others in evaluating the qualityof life of patients with chronic disease. J Clin Epidemiol2002;55:1130–43.
9 Klepstad P, Hjermstad MJ. Are all patients that count includedin palliative care studies? BMJ Support Palliat Care2013;3:292–3.
10 Stone PC, Gwilliam B, Keeley V, et al. Factors affectingrecruitment to an observational multicentre palliative carestudy. BMJ Support Palliat Care 2013;3:318–23.
11 Lo C, Lin J, Gagliese L, et al. Age and depression in patientswith metastatic cancer: the protective effects of attachmentsecurity and spiritual wellbeing. Ageing Soc 2010;30:325–36.
12 Strong V, Waters R, Hibberd C, et al. Emotional distress incancer patients: the Edinburgh Cancer Centre symptom study.Br J Cancer 2007;96:868–74.
13 Schlegel RJ, Manning MA, Molix LA, et al. Predictors ofdepressive symptoms among breast cancer patientsduring the first year post diagnosis. Psychol Health2012;27:277–93.
14 Zabora J, Brintzenhofeszoc K, Curbow B, et al. The prevalenceof psychological distress by cancer site. Psychooncology2001;10:19–28.
15 Mayr M, Schmid RM. Pancreatic cancer and depression: mythand truth. BMC Cancer 2010;10:569.
16 Zoega S, Fridriksdottir N, Sigurdardottir V, et al. Pain andother symptoms and their relationship to quality of life incancer patients on opioids. Qual Life Res 2013;22:1273–80.
17 American Psychiatric Association. DSM-5 task force. Diagnosticand statistical manual of mental disorders: DSM-5. 5th edn.Washington DC: American Psychiatric Association, 2013.
18 Wang XS. Pathophysiology of cancer-related fatigue. Clin JOncol Nurs 2008;12(5 Suppl):11–20.
19 van der Heide A, Onwuteaka-Philipsen BD, Rurup ML, et al.End-of-life practices in the Netherlands under the EuthanasiaAct. N Engl J Med 2007;356:1957–65.
20 Van Der Maas PJ, Van Delden JJ, Pijnenborg L, et al.Euthanasia and other medical decisions concerning the end oflife. Lancet 1991;338:669–74.
21 Onwuteaka-Philipsen BD, van der Heide A, Koper D, et al.Euthanasia and other end-of-life decisions in the Netherlandsin 1990, 1995, and 2001. Lancet 2003;362:395–9.
22 van der Maas PJ, van der Wal G, Haverkate I, et al.Euthanasia, physician-assisted suicide, and other medicalpractices involving the end of life in the Netherlands,1990–1995. N Engl J Med 1996;335:1699–705.
23 Xiao C, Polomano R, Bruner DW. Comparison betweenpatient-reported and clinician-observed symptoms in oncology.Cancer Nurs 2013;36:E1–16.
24 Kutner JS, Kassner CT, Nowels DE. Symptom burden at theend of life: hospice providers’ perceptions. J Pain SymptomManage 2001;21:473–80.
25 Stromgren AS, Groenvold M, Pedersen L, et al. Does themedical record cover the symptoms experienced by cancerpatients receiving palliative care? A comparison of the recordand patient self-rating. J Pain Symptom Manage2001;21:189–96.
26 Laugsand EA, Sprangers MA, Bjordal K, et al. Health careproviders underestimate symptom intensities of cancer patients:a multicenter European study. Health Qual Life Outcomes2010;8:104.
27 Ng CG, Boks MP, Smeets HM, et al. Prescription patterns forpsychotropic drugs in cancer patients; a large population studyin the Netherlands. Psychooncology 2013;22:762–7.
28 Shimizu K, Akechi T, Shimamoto M, et al. Can psychiatricintervention improve major depression in very near end-of-lifecancer patients? Palliat Support Care 2007;5:3–9.
29 Ruijs CD, Kerkhof AJ, van der Wal G, et al. Depression andexplicit requests for euthanasia in end-of-life cancer patients inprimary care in the Netherlands: a longitudinal, prospectivestudy. Fam Pract 2011;28:393–9.
30 Mitchell AJ. New developments in the detection and treatmentof depression in cancer settings. Prog Neurol Psychiatry2011;15:12–20.
31 Noorani NH, Montagnini M. Recognizing depression inpalliative care patients. J Palliat Med 2007;10:458–64.
32 Mellor D, McCabe MP, Davison TE, et al. Barriers to thedetection and management of depression by palliative careprofessional carers among their patients: perspectives from
Research
8 Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from
professional carers and patients’ family members. Am J HospPalliat Care 2013;30:12–20.
33 Periyakoil VS, Hallenbeck J. Identifying and managingpreparatory grief and depression at the end of life. Am FamPhysician 2002;65:883–90.
34 Quill TE, Abernethy AP. Generalist plus specialist palliative care—creating a more sustainable model. N Engl J Med2013;368:1173–5.
35 Koopmans RT, Lavrijsen JC, Hoek JF, et al. Dutch elderly carephysician: a new generation of nursing home physicianspecialists. J Am Geriatr Soc 2010;58:1807–9.
36 Kroenke K, Theobald D, Wu J, et al. The association ofdepression and pain with health-related quality of life,disability, and health care use in cancer patients. J PainSymptom Manage 2010;40:327–41.
37 O’Connor M, White K, Kristjanson LJ, et al. The prevalenceof anxiety and depression in palliative care patients with cancerin Western Australia and New South Wales. Med J Aust2010;193(5 Suppl):S44–7.
38 Laird BJ, Boyd AC, Colvin LA, et al. Are cancer pain anddepression interdependent? A systematic review.Psychooncology 2009;18:459–64.
39 Mystakidou K, Tsilika E, Parpa E, et al. Psychological distressof patients with advanced cancer: influence and contribution
of pain severity and pain interference. Cancer Nurs2006;29:400–5.
40 Kroenke K, Zhong X, Theobald D, et al. Somatic symptoms inpatients with cancer experiencing pain or depression:prevalence, disability, and health care use. Arch Intern Med2010;170:1686–94.
41 World Health Organization. National cancer controlprogrammes: Policies and managerial guidelines. SecondaryNational cancer control programmes: policies and managerialguidelines. 2002. http://www.who.int/cancer/publications/nccp2002/en/index.html
42 Temel JS, Greer JA, Muzikansky A, et al. Early palliative carefor patients with metastatic non-small-cell lung cancer. N EnglJ Med 2010;363:733–42.
43 Zimmermann C, Swami N, Krzyzanowska M, et al. Earlypalliative care for patients with advanced cancer: a cluster-randomised controlled trial. Lancet 2014;383:1721–30.
44 Hui D, Kim SH, Roquemore J, et al. Impact of timing andsetting of palliative care referral on quality of end-of-life carein cancer patients. Cancer 2014;120:1743–9.
45 Barton MK. Early outpatient referral to palliative care servicesimproves end-of-life care. CA Cancer J Clin 2014;64:223–4.
46 Saarto T. Palliative care and oncology: the case for earlyintegration. EJPC 2014;21:109.
Research
Janberidze E, et al. BMJ Supportive & Palliative Care 2015;0:1–9. doi:10.1136/bmjspcare-2014-000722 9
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from

retrospective mortality studyof patients with cancer: a nationwide Depressive symptoms in the last days of life
Onwuteaka-PhilipsenAnne Kari Knudsen, Stein Kaasa, Agnes van der Heide and Bregje Elene Janberidze, Sandra Martins Pereira, Marianne Jensen Hjermstad,
published online February 9, 2015BMJ Support Palliat Care
22http://spcare.bmj.com/content/early/2015/02/09/bmjspcare-2014-0007Updated information and services can be found at:
These include:
References
#BIBL22http://spcare.bmj.com/content/early/2015/02/09/bmjspcare-2014-0007This article cites 43 articles, 6 of which you can access for free at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on February 17, 2015 - Published by http://spcare.bmj.com/Downloaded from




















