Dental phenomics: advancing genotype to phenotype correlations in craniofacial research.
14
Dental phenomics: advancing genotype to phenotype correlations in craniofacial research R Yong,* S Ranjitkar,* GC Townsend,* RN Smith,† AR Evans,‡ TE Hughes,* D Lekkas,* AH Brook*§ *School of Dentistry, The University of Adelaide, South Australia, Australia. †School of Dentistry, The University of Liverpool, United Kingdom. ‡School of Biological Sciences, Monash University, Melbourne, Victoria, Australia. §School of Dentistry, Queen Mary University of London, United Kingdom. ABSTRACT The field of dental phenomics provides many opportunities to elucidate the roles of genetic, epigenetic and environmen- tal factors in craniofacial development. To date, research findings have helped to clarify the pathogenesis of many condi- tions, aiding diagnosis and clinical management. This paper provides an overview of dental phenomics research in some commonly encountered oral diseases in everyday clinical practice, as well as research relating to craniofacial growth and development. Clinically, advances in cariology and periodontology have led to better diagnostic capabilities and treat- ment provision. In the study of growth and development, important information regarding the varying clinical presenta- tion and pathogenesis of many disorders is now apparent through the accurate quantification of phenotypes. Improvements in two-dimensional (2D) and three-dimensional (3D) imaging and analytical techniques have allowed for accurate dental phenotyping, and efforts are ongoing to apply these in vitro techniques to the in vivo setting. The field of dental phenomics represents an exciting avenue that links research findings to practical application, and collaboration between researcher and clinicians will help advance the field further. Keywords: Dentistry, genetics, epigenetics, phenomics, morphometrics. Abbreviations and acronyms: CL/P = cleft lip and/or palate; CPP-ACP = casein phosphopeptide-amorphous calcium phosphate. DP = digital photography; EDI = Enamel Defects Index; GIS = geographic information system; n-HAp = nano-hydroxyapatite; OPC = orientation patch count; OPCR = orientation patch count rotated; QLF = quantitative light-induced fluorescence; SMMCI = solitary maxillary median central incisor. INTRODUCTION The Human Genome Project has led to major advances in genomics and revealed new frontiers for research and collaboration. 1 However, genetic input alone does not determine all phenotypic traits; rather, the final phenotype of an organism is established via the dynamic interactions between genetic, epigenetic and environmental factors. In dental development, these interactions account for variations in tooth num- ber, size, shape and mineralization within and between species. 2 Advances in phenotyping are crucial in elucidating the roles of these factors, 3–6 and the interactions between them, as well as to further understand the development of the dentition as a Complex Adaptive System. 7 Phenomics is defined as ‘the acquisition of high- dimensional phenotypic data on an organism-wide scale’ 6 and has progressed significantly in various fields over the past decade. Studies of phenotypic traits in human diseases, such as neuropsychiatric syn- dromes 8 and cardiovascular complications, 9 have pro- vided pre-symptomatic biomarkers and insights into disease risk factors. Further understanding of disease pathology and future treatment trends has also been gained via animal modelling of human diseases. 10,11 Plant phenomic research has improved both food quantity and quality by identifying desirable pheno- types and their corresponding genotypes. 12,13 ‘Dental phenomics’ was proposed initially as a new field for quantification of phenotypic variations in the dentition, 14 and it has evolved to encompass other craniofacial structures relevant to the field of den- tistry. The human dentition provides a valuable data- set, as individual teeth have varying developmental time frames. The complex development of each tooth 34 © 2014 Australian Dental Association Australian Dental Journal 2014; 59:(1 Suppl): 34–47 doi: 10.1111/adj.12156 Australian Dental Journal The official journal of the Australian Dental Association
Transcript of Dental phenomics: advancing genotype to phenotype correlations in craniofacial research.
Dental phenomics: advancing genotype to phenotypecorrelations in craniofacial research
R Yong,* S Ranjitkar,* GC Townsend,* RN Smith,† AR Evans,‡ TE Hughes,*D Lekkas,* AH Brook*§
*School of Dentistry, The University of Adelaide, South Australia, Australia.†School of Dentistry, The University of Liverpool, United Kingdom.‡School of Biological Sciences, Monash University, Melbourne, Victoria, Australia.§School of Dentistry, Queen Mary University of London, United Kingdom.
ABSTRACT
The field of dental phenomics provides many opportunities to elucidate the roles of genetic, epigenetic and environmen-tal factors in craniofacial development. To date, research findings have helped to clarify the pathogenesis of many condi-tions, aiding diagnosis and clinical management. This paper provides an overview of dental phenomics research in somecommonly encountered oral diseases in everyday clinical practice, as well as research relating to craniofacial growth anddevelopment. Clinically, advances in cariology and periodontology have led to better diagnostic capabilities and treat-ment provision. In the study of growth and development, important information regarding the varying clinical presenta-tion and pathogenesis of many disorders is now apparent through the accurate quantification of phenotypes.Improvements in two-dimensional (2D) and three-dimensional (3D) imaging and analytical techniques have allowed foraccurate dental phenotyping, and efforts are ongoing to apply these in vitro techniques to the in vivo setting. The fieldof dental phenomics represents an exciting avenue that links research findings to practical application, and collaborationbetween researcher and clinicians will help advance the field further.
Keywords: Dentistry, genetics, epigenetics, phenomics, morphometrics.
Abbreviations and acronyms: CL/P = cleft lip and/or palate; CPP-ACP = casein phosphopeptide-amorphous calcium phosphate.DP = digital photography; EDI = Enamel Defects Index; GIS = geographic information system; n-HAp = nano-hydroxyapatite; OPC =orientation patch count; OPCR = orientation patch count rotated; QLF = quantitative light-induced fluorescence; SMMCI = solitarymaxillary median central incisor.
INTRODUCTION
The Human Genome Project has led to majoradvances in genomics and revealed new frontiers forresearch and collaboration.1 However, genetic inputalone does not determine all phenotypic traits; rather,the final phenotype of an organism is established viathe dynamic interactions between genetic, epigeneticand environmental factors. In dental development,these interactions account for variations in tooth num-ber, size, shape and mineralization within andbetween species.2 Advances in phenotyping are crucialin elucidating the roles of these factors,3–6 and theinteractions between them, as well as to furtherunderstand the development of the dentition as aComplex Adaptive System.7
Phenomics is defined as ‘the acquisition of high-dimensional phenotypic data on an organism-wide
scale’6 and has progressed significantly in variousfields over the past decade. Studies of phenotypictraits in human diseases, such as neuropsychiatric syn-dromes8 and cardiovascular complications,9 have pro-vided pre-symptomatic biomarkers and insights intodisease risk factors. Further understanding of diseasepathology and future treatment trends has also beengained via animal modelling of human diseases.10,11
Plant phenomic research has improved both foodquantity and quality by identifying desirable pheno-types and their corresponding genotypes.12,13
‘Dental phenomics’ was proposed initially as a newfield for quantification of phenotypic variations in thedentition,14 and it has evolved to encompass othercraniofacial structures relevant to the field of den-tistry. The human dentition provides a valuable data-set, as individual teeth have varying developmentaltime frames. The complex development of each tooth
34 © 2014 Australian Dental Association
Australian Dental Journal 2014; 59:(1 Suppl): 34–47
doi: 10.1111/adj.12156
Australian Dental JournalThe official journal of the Australian Dental Association

occurs over several years, while the development ofthe whole human dentition extends, on average, fromthe sixth week in utero to 20 years of age. The teethand jaw bones are resistant to degradation and pro-vide an accessible record of development to highlightthe effects of developmental or pathological events atspecific times. Hence, advances in measuring dentalphenotypes can enhance the genotype-phenotype cor-relation15 to identify contributing factors to observedvariations. Clinically, accurate quantification ofchanges in dental tissues can guide diagnosis andtreatment provision, illustrating the relevance ofdental phenomics to clinical practice.In addition, dental phenomics is applicable to both
dental anthropology and forensic odontology. Sophis-ticated imaging and analytical techniques serve asimportant adjuncts to crime scene investigation andvictim identification. Morphometric analysis of toothdimensions16 and the human mandible17 have pro-vided useful information relating to sexual dimor-phism from skeletal remains. In archaeologicalstudies, three-dimensional (3D) comparisons of humanand great ape craniofacial morphology have providedinsight into evolutionary changes that account for thedistinct differences between species.18 Assessment ofenamel hypoplasia from skeletal remains has also beenused to assess health in the past.19
The aims of this paper are to evaluate approachesused to quantify dental phenotypes and to highlightadvances and future opportunities in key researchareas, together with their clinical relevance. Althoughnew technologies are being applied to phenotyping inmany areas of dental research and practice, thisreview focuses on phenotyping of common oral dis-eases, including dental caries and periodontal disease,as well as craniofacial development.
APPROACHES TO PHENOTYPING
In dental phenomics, a decision to carry out eitherextensive or intensive phenotyping is made based onthe research question. Extensive phenotyping involvesmeasuring a small number of parameters in a largenumber of specimens or individuals,20 while intensivephenotyping measures a large number of parameters ina limited number of specimens.21 A comparison usingexamples of both methods is presented in Table 1.During the development of analytical methods, accu-racy (the closeness of measured values to the truevalue) and precision (the closeness of repeated mea-surements of the same quantity) are essential compo-nents to consider.22 In addition, the methods should bevalid, i.e. the obtained measurements should providean accurate representation of what is intended forassessment. Figure 1 provides a visual representationof the concepts of accuracy, precision and validity.
PHENOTYPING AND ORAL DISEASES
Cariology
Dental caries is one of the most prevalent chronic dis-eases worldwide,23 with its prevention, diagnosis andtreatment comprising a major component of everydayclinical practice. Over the years, an enhanced under-standing of caries aetiology and the application ofminimal intervention principles has revolutionized car-ies management.24,25 The ability to accurately quan-tify caries is of great importance in diagnosing andmonitoring lesions, while also assessing the effective-ness of prescribed intervention.
Caries assessment
Several techniques that rely on the principles of lighttransmission, absorption and scattering have been
Table 1. Examples of extensive and intensivephenotyping
Extensive phenotyping Intensive phenotyping
In one study, alarge number of individuals(n = 134) was examined toidentify the effects of a singlecontributing factor(intrauterinehormone effect)on a small number ofparameters (toothdimensions).20
In another study, a smaller numberof samples (5 from each subgroupof differing genetic make-up) wasutilized to study the specific rolesof certain genes (Amelx andEnam). Each sample wasexamined for a number ofparameters, such as tooth colour,surface whiteness and jawdimensions.21
Scenario 1 Scenario 2
Scenario 4
Scenario 3
Fig. 1 Precision, accuracy and validity (adapted from Harris andSmith22). The bull’s eyes on the ‘red’ dart boards represent the intendedcharacteristic to be tested. The yellow crosses/darts represent the resultsobtained. Scenario 1 demonstrates both low precision and low accuracy.Scenario 2 demonstrates high precision, but low accuracy. Scenario 3demonstrates both high precision and high accuracy. Lastly, scenario 4demonstrates high precision and accuracy, but poor validity as the dartshave completely missed the red board (hitting the purple board instead),thus the method used does not inform on the parameters of interest.
© 2014 Australian Dental Association 35
Dental phenomics in craniofacial research

described to indicate changes in the mineral content ofteeth. The use of quantitative light-induced fluores-cence (QLF) for caries detection26,27 and monitoring28
has shown good validity and may direct a ‘non-restor-ative’ approach to caries management. Currently, no‘actual’ clinical value has been established to indicatean active lesion, but comparison between initial recordswith subsequent readings can be used to suggest thatthis is occurring. A change in fluorescence indicates theprogression of a lesion and may help to justify the needfor restorative intervention. Digital photography (DP)has also been used to assess carious lesions.29,30 Thistechnology may be feasible for surgeries that alreadypossess photographic devices. However, variations inlighting conditions, surface reflection and tooth posi-tion can alter the image properties, thus complicatingthe assessment of a lesion. In addition, difficulty hasalso been reported in comparing two images of thesame tooth at different time points,30,31 indicating theneed for stringent standardization. In a recent study,the absence of glare and reduced variability associatedwith QLF indicated that it is a preferable technique incaries assessment compared to DP.31
In vitro, micro-CT techniques have been employedto quantify changes in the mineral content of toothstructure.32 This technique has been used to quantita-tively evaluate the efficacy of preventive and restor-ative intervention. The use of casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) withsodium fluoride (CPP-ACPF) was found to promotehigher levels of remineralization of enamel when com-pared to the use of CPP-ACP alone.33 In carious den-tine, an increase in radiopacity due to mineraldeposition from the overlying glass ionomer cementjustifies a ‘minimally invasive’ approach to caries man-agement.34 An increase in remineralization potentialby nano-hydroxyapatite (n-HAp) containing tooth-paste when compared to fluoride containing tooth-paste has also been demonstrated using micro-CTtechnology.35 These examples demonstrate howadvances in dental phenomics can reaffirm or directvarious treatment modalities based on stringent evalu-ative protocols.
Caries heritability
Patterns of caries distribution have been used as phe-notypes to further clarify the multifactorial nature ofdental caries.36 Data on familial history and geneticmarkers were obtained and the authors noted cariespatterns in the mandibular canines and premolars asbeing strongly heritable, suggesting a genetic aetiol-ogy.36 The authors concluded that the use of cariesdistribution provides better risk assessment comparedto traditional DMFS/ DMFT indices as it takes intoaccount the site specific nature of caries risk.
Periodontology
The periodontal tissues demonstrate varying responsesto disease risk factors and dental treatment (periodon-tal, restorative and surgical). Hence, this represents acritical consideration during treatment planning. Phe-nomic research is commonly carried out at both theclinical (visible) and cellular (microscopic) levels tounderstand the dynamic nature of the periodontaltissues.
Biotype assessment
Clinically, gingival tissue phenotypes can be classifiedas ‘thin’ or ‘thick’ biotypes, based on the width andthickness of gingival tissue as well as tooth form.37
The ‘thin’ biotype has been associated with anincreased risk of recession, as a result of orthodontictooth movement38 and restorative treatment. In addi-tion, tissue characteristics around an implant are criti-cal to maintain long-term aesthetics.39,40 Hence,different methods have been proposed to quantifyvariations in gingival tissues. Previously, the use of anultrasonic device was deemed a non-invasive41,42 andreproducible43 way to characterize gingival tissues.However, care must be taken to maintain the positionof the transducer probe to ensure an accurate readingis obtained.Another simple method to discriminate thin from
thick gingivae is based on the transparency of theperiodontal probe through the gingival margin.44 Thismethod involves placing a periodontal probe into thegingival sulcus and assigning a score based on the visi-bility of the probe through the gingival tissue. Whilethis technique is non-invasive and cost-effective, it isprone to errors from visual inspection, potentiallyleading to aesthetic complications following surgicaland/or restorative therapy.45 Hence, a more accuratemethod to clinically assess variations in gingival tis-sues is required to ensure thorough preoperative plan-ning. In addition, identification of genetic factors thatinfluence these variations will help to explain the phe-notypic features of gingival cells (i.e. cell populations,differentiation capacity and immunomodulatory prop-erties)46 and advance tissue engineering research(please refer to the paper by Han and colleagues47 inthis issue for further discussion on this topic).
Risk assessment
At the cellular level, variations in periodontal liga-ment cell48 and fibroblast phenotypes49 have providedinsight into tissue responses to both normal and path-ological processes. Various risk factors have also beenestablished for periodontal disease. For example, acomparison between monozygotic and dizygotic
36 © 2014 Australian Dental Association
R Yong et al.

twins50 yielded a heritability estimate of 50% foradult periodontitis, which remained stable despiteadjustments to behavioural variables such as smoking.Other studies reveal variations in T-cell phenotypes51
and genetic polymorphism,52 reinforcing the notionthat periodontal disease is the consequence of com-plex interactions between host and environmentalfactors.53,54 Ultimately, such information helps todirect the profession in risk assessment and treatmentprovision.
PHENOTYPING AND CRANIOFACIALDEVELOPMENT
Tooth morphology: size and shape
Traditional techniques for studying dental morphologyhave been observational, including the development ofnon-continuous indices, classifications and manualmeasurements of linear dimensions, i.e. mesio-distaland bucco-lingual crown dimensions. While the use ofindices and classifications can have satisfactory levelsof intra-operator reproducibility,55 variations betweenobservers may exist with this approach. In addition,linear measurements only provide limited informationconcerning structures of complex forms, i.e. tooth/
arch/facial shape. More sophisticated analytical tech-niques are needed to overcome these limitations. Newmeasurement techniques56–58 can provide accurate andreliable information for additional parameters regard-ing the size, shape, structure and colour of teeth. Con-current assessment of linear measurements, curvedsurfaces and the superimposition of images allows forthe accurate description and quantification of varia-tions among individuals.
Two-dimensional digital imaging
Two-dimensional (2D) digital imaging represents animportant addition to the analysis of dental morphol-ogy. Studies relating to tooth dimensions have mea-sured the phenotype of specific genetic contributionsto odontogenesis. For example, in cases of hypodon-tia, a reduction in crown dimensions in patients withPAX9 mutation suggests a major role of this gene inodontogenesis.59 On the other hand, larger tooth sizedimensions have been observed in individuals withsupernumerary teeth, suggesting a common factorwhich influences both the dental anomaly and theoverall dentition.60,61 A summary of 2D imagingmethodology is provided in Table 2 to highlight theadvantages and limitations of this approach and serve
Table 2. Summary of 2D digital imaging techniques (applicable to the study of both dental morphology andenamel defects)
2D imaging (in vitro)
Equipment Advantages Limitations
An adjustable stand to mountstudy models OR a singletooth holderStandardized lightingA scaleA digital cameraPolarizing capacity
Fixed positioning/reproducible imagingwith calibrationAble to assess a variety of dimensions59
The specimens are not damagedDigital images can be stored andreinvestigated in other locations forcomparison between different studies94
Ability to take polarized images toenhance opacity imaging byremoval of reflection.
Careful calibration of the digital camerais required as settings and imagepresentation can alter colour and surfacecharacteristics of the specimen surfaceLight reflection from surface can altervisual properties – thus, manipulation ofillumination is critical in studyingtooth surfaces94
The samples need to be re-positionedwhen different surfaces are studied
2D imaging (in vivo)
Equipment Advantages Limitations
Mobile digital imaging apparatusincluding a frame to support a digitalcamera and lighting, which facilitatesprecise positioning of camera, lightsand patient (and/or tooth)Semi-automatic software calibrationAdjustable scale for image calibrationPolarization facility
The patient’s head is placed on a purposebuilt chin rest for alignment. An adjustablescale may be moved into the plane of theimage facilitating multiple positioning forvariation in size of both patient head and/or toothThe unit can be used in the field, as thecomponents of the unit can be easily dismantled,transported and reassembledSoftware facilitates calibrated colour imagesspecific to the ambient lighting conditionsand digital camera performance in relationto fixed absolute whiteness, lightness,and colour shift valuesPolarization facilitates opacityimaging without reflections
Requires careful calibration of imagingtechnique and softwareAdjustment of inbuilt lighting is alsocritical, especially when assessingdifferences in colourLimited application for posteriorteeth imaging
© 2014 Australian Dental Association 37
Dental phenomics in craniofacial research

as a basis for future research development. This tech-nique is not only applicable to the assessment ofdental morphology alone, but also useful for a widerange of clinical and research purposes.
Three-dimensional imaging
Methods for 3D imaging of dental morphology beganin the 1960s. Scanning modalities such as stereopho-togrammetry,62–64 the Optocom65 and the ReflexMetrograph66 were used for the assessment of teeth,dental casts and facial features. However, the imple-mentation of these early techniques was extremelytime-consuming, lacked measurement accuracy andshowed substantial inter-operator variability. Earlycomputer technology also had limited analytical andstorage capabilities, thus hampering the widespreadapplication of 3D imaging techniques. The advent oflaser scanning and computer-aided tomography hasovercome these shortcomings, resulting in theincreased use of 3D technology.Generally, the 3D equipment consists of an image
acquisition scanner connected to appropriate com-puter software. Sufficient scanning resolution isimportant to ensure image definition, while the appro-priate software must be able to clean, align and mergethe separate images or models accurately. Analysis ofthe acquired images enables measurement of variousdimensions to quantify variations in size and shapewith a high degree of accuracy and reliability.67–72
Figure 2 provides an example of surface area andangular measurements that are possible with the useof 3D imaging.In one study, scanned 3D models were ‘mapped’
against mathematical grids to objectively quantify theeffects of MSX-1 genetic mutation on tooth morphol-ogy in patients with hypodontia.73 The authors notedvariations in central incisor size, suggesting the role ofdifferent signalling pathways and the genes involvedin odontogenesis. The data on dental morphology can
also supplement clinical examination74,75 and radio-graphic records74,75 to clarify the genetic, epigeneticand environmental factors involved in dental agenesis.Future research involving dental agenesis, both in syn-dromic and non-syndromic forms, will help identifyspecific contributing factors to the condition.76 It iscommon to detect alterations in tooth number andsize in syndromes such as ectodermal dysplasia, sug-gesting the pleiotropic nature of genes during cranio-facial development.77 Information obtained fromvarious studies will also be applicable to the emergingfields of tooth bioengineering and regenerative dentalmedicine.78
Superimposition
2D and 3D morphometric analysis of shape can pro-vide valuable insights into genetic and environmentalcontributions to observed variations between speci-mens. Generally, each specimen is represented by therelative positions of morphological landmarks thatcan be located to establish one-to-one correspondenceamong all tested specimens. This can be particularlychallenging during the comparison of objects of dis-similar size, position and orientation. Hence, the useof Procrustes superimposition removes these differ-ences and is at the core of geometric morphomet-rics,79–81 and this approach has been applied toinvestigate tooth shape.82 Essentially, landmarks wereestablished on 2D images of teeth, and a linear modelwas generated for superimposition to compare thevariations in tooth shape between individuals. Whilethe results showed some promise, the authors high-lighted challenges such as inconsistencies in orienta-tion82 and landmark establishment on curvedsurfaces,83 both resulting in low inter-operator reli-ability and potential inaccuracies in data analysis.On the other hand, the assessment of a solitary
maxillary median central incisor (SMMCI) using theProcrustes analysis demonstrated good validity whenmeasuring symmetry within a single tooth.84 SMMCImay be related to holoprosencephaly, which affectsmidline structures. The premature fusion of the dentallamina from both sides of the maxilla results in a soli-tary incisor. As this tooth represents the distal halvesof both upper central incisors, it demonstrates a highdegree of symmetry.84 Therefore, if a highly symmet-rical lone central incisor is noted, referral to a geneti-cist may be warranted,85 i.e. once factors such astraumatic loss and impaction have been accountedfor.The use of 3D images can supplement the informa-
tion provided via 2D superimposition alone. Smithet al.86 developed a method for 3D superimpositionto form a comparable interface between non-similarobjects (Fig. 3). This approach demonstrated good
96.793396.7933
Area 43.9631
Area 43.9631
Fig. 2 3D model of a study model, demonstrating the angle between thebuccal and palatal cusp tips (to indicate cuspal inclination) of the upperleft first premolar and the occlusal surface area of the upper left secondpremolar. The picture on the right is an enlarged view of the area of
interest.
38 © 2014 Australian Dental Association
R Yong et al.

reliability but the authors highlighted potential chal-lenges with handling 3D images, i.e. the images arenot ‘fixed’ and the orientation of the images can be asource of error. Hence, research to establish a proto-col is ongoing to reduce possible analytical problemsduring image comparison. A study utilizing an elasticstyle of registration (similar mathematically to the dif-fusion approach used by Smith et al.86) has shownincreased sensitivity when comparing 3D datasets.87
These techniques have been shown to be more reliablein establishing differences during the superimpositionof non-identical objects, when compared to the best-fit model, and future application to analysis of dentalstructures is warranted.
Complexity
A relatively new method for quantifying morphologi-cal variation is dental complexity.58 The objective ofthis method is to quantitatively characterize variationin morphology that cannot be captured using linearmeasurements or landmarks. Using a 3D model of thetooth surface, geographic information systems (GIS)algorithms calculate the orientation or aspect of eachpoint on the surface as one of eight cardinal direc-tions, e.g. north, north-east. Contiguous surface pointsthat face the same direction are grouped into a patch,and the total number of patches over the surface isthe ‘orientation patch count’ (OPC). This calculationcan be repeated to give values that are independent ofrotation in the x,y plane, which is then called ‘orienta-tion patch count rotated’ (OPCR).88 Figure 4 illus-trates the ability of OPC to characterize finedifferences in shape – the higher morphological com-plexity of the tooth on the left is quantified as anOPCR of 51.9 compared to 47.5 for the other. While
this method has largely been used to investigate grossdifferences in dental morphology among animal spe-cies,58,89,90 it can also be used to show the contribu-tion of the dentino-enamel junction to outer enamelsurface complexity91 and shows promise as an addi-tional measure of dental phenomics.
Tooth structure: enamel
Two-dimensional digital imaging
Enamel defects present a range of clinical appear-ances, so accurate description and recording are criti-cal for diagnostic purposes as well as aetiologicalstudies. Various indices have been developed in thepast, but each has its limitations.92 The EnamelDefects Index (EDI) was developed based on threecore components, i.e. hypoplasia, opacity and post-eruptive breakdown,93 with each scored on a binaryyes/no basis. The index can be expanded in line withthe specific aims of a study, while still allowing forinter-study comparisons, as the same core componentsare used for data collection and analysis. It is alsoeasy to apply and has shown good validity and repro-ducibility.93,94 In one study, altered enamel character-istics (i.e. demarcated opacities) and surfacetopography were assessed to clarify the role of specificgenes in amelogenesis. It was noted that Amelx andEnam gene mutations in Amelogenesis Imperfecta inexperimental mice were associated with alteredenamel structure and mineralization.21 These subtlechanges have been associated with an increased riskof post-eruptive breakdown,94 demonstrating how
Diffusion registration of upper 1st molars frommonozygotic co-twins
Colour coded distance / differenceoutputs between the two 1st molars
Fig. 3 3D synetic superimposition of upper permanent first molars in apair of monozygotic twins demonstrating differences in shape and surfacearea. Despite monozygotic twins sharing the same genetic information,
the differences indicate that other confounding factors are involved in thefinal tooth morphology.
Height
Orientation
54.5
3.5
2.5
1.5
0.50
1
2
3
4
47.551.9
Fig. 4 Topography maps (top) and orientation maps (bottom) of perma-nent lower right first molars from two different individuals. Each modelis illustrated with orientation patches when first orientation is at 0º, withthe OPCR score at bottom right, demonstrating the differing complexityof the occlusal surfaces between the individuals. Scale bars = 1 mm;
height in mm.
© 2014 Australian Dental Association 39
Dental phenomics in craniofacial research
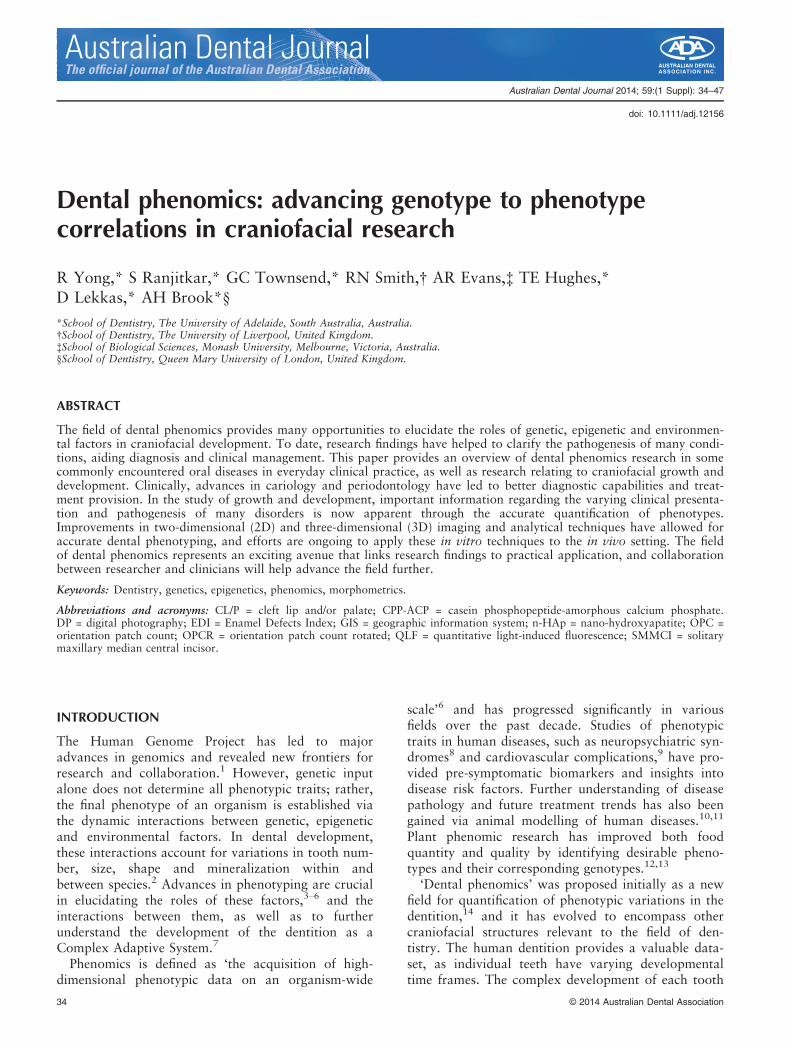
visual changes of the enamel structure are ultimatelylinked to structural integrity. This information is criti-cal for clinicians to establish caries risk and preventivecare for affected patients. In addition, alterations inmandibular morphology have also been attributed toAmelx gene mutations in mice, suggesting amelo-genin’s role as a multifunctional protein in the devel-opment of craniofacial features.21 This associationwarrants further clarification in humans and, if pres-ent, orthodontic assessment may be required as partof the overall management plan. Readers are referredto the paper by Seow95 in this special issue for a morein-depth discussion of developmental defects ofenamel and dentine.Figure 5 provides an example on how 2D imaging
helps to quantify the defects in enamel (from a studymodel), while Fig. 6 demonstrates how polarizedimages clearly demarcate enamel opacities for accu-rate image analysis.
Facial morphology
The study of facial morphology is particularly impor-tant in the fields of orthodontics96 and craniofacialgrowth and development.97 Traditional techniques todiscern morphological features of interest involvedcomparing hand tracings from radiographs96 or 2Dphotographs,97 or combining 2D images to form a 3Drepresentation.63,98 While these methods have pro-vided the building blocks to understand variations infacial morphology, they carry a risk of operator error,along with limited opportunity for analysis. Hence,3D assessment of facial morphology representsanother exciting field of research.
Three-dimensional imaging
Initial images may be obtained via CT imaging, MRIscans,99 laser scanning,100,101 or photogrammetricdevices. Photogrammetric devices provide a non-invasive and faster alternative when compared tothe other imaging techniques and thus they are thefavoured option for image acquisition.102 During theimage acquisition process, several images are obtainedand these need to be merged to form the final facialimage. Hence, appropriate software is utilized togenerate tens of thousands of corresponding pointsbased on certain predetermined landmarks, e.g. theeyes and the corners of the mouth (a technique knownas the dense surface model).103 The generated pointsare subsequently used to align and merge the obtainedscans, resulting in a final image that accurately repli-cates the facial contour and topography.The use of 3D imaging techniques has aided in clar-
ifying the roles of key genes in the development offacial features. In 2012, collaborative efforts by theInternational Visible Trait Genetics (VisiGen) Consor-tium identified five candidate genes (PRDM16, PAX3,TP63, C5orf50 and COL17A) that influence facial
Digital 2D image of an upper incisordemonstrating enamel hypoplasia
Subsequent defects isolated for areameasurement
Fig. 5 Digital 2D image of hypoplastic lesions on an upper incisor(from a study model) compiled with image analysis of the surface
defects.
(a) (b)
(c)
Fig. 6 Demonstration of 2D imaging of opacities under standard illumi-nation (a), polarized illumination (b) and measurement area output from
polarized digital images (c).
40 © 2014 Australian Dental Association
R Yong et al.

phenotypes in individuals of European ancestry viathe comparison of facial morphological landmarks.100
Among the five mentioned genes, PAX 3 showed themost correlation statistically to influence facial mor-phology. In another study, the effects of PAX3 vari-ants to nasion prominence and position wasdemonstrated, further detailing the role this gene playsin facial development.99
In cases of facial dysmorphism, the final image iscompared to ‘references’ to quantify the noted varia-tions104 and this may assist in clarifying the impact ofunderlying genetic influences.105 For example, subtlechanges in facial and nasal shape were noted inpatients with Wolf–Hirschhorn syndrome. This infor-mation clarified how the mutation resulted in varyingclinical presentations of patients.105 In addition, facialmorphometric analysis allows for the assessment ofdisease progression106 and is a non-invasive methodto assess the efficacy of therapeutic intervention bycomparing facial dimensions before and after ther-apy.107 Future research will involve the exploration ofnormal facial variation within different age, genderand ethnic groups. The use of this technology for dis-ease diagnosis, monitoring, pre-surgical assessmentand review of medical intervention (postoperative sur-gical and/or drug therapy) demonstrates its potentialfor a wide range of applications.108–110
Cleft lip and/or palate
Ultrasonography
Another important field of phenomic research hasbeen the study of cleft lip and/or palate (CL/P). Inrecent years, phenotyping of CL/P has expandedunderstanding of the clinical spectrum of the defor-mity, with microform clefts being the mildest form.Subtle clinical presentations such as a small lip oralveolar arch defect can be easily missed,111 andcareful characterization of defects has providedinsight into varying clinical presentations. Clinicalexamination alone fails to detect subepithelialchanges in ‘non-visible’ cases of cleft lip. Ultrasonog-raphy has been used to demonstrate defects in theorbicularis oris muscle in non CL/P relatives of indi-viduals with obvious CL/P,112 highlighting linksbetween certain genetic mutations with non-visible(submucosal) changes in microforms of cleft lip.113
These findings add to the known aetiological factorsof CL/P,114,115 while also improving clinical detec-tion of the more subtle forms. In future, the use ofultrasonography for ‘at-risk’ patients, i.e. relatives ofpatients with obvious CL/P may help to detect minorforms of CL/P. This will reduce the risk of under-diagnosis and help to ascertain the risk of familialinheritance.
COMPUTER MODELLING OF GENOTYPE-PHENOTYPE CORRELATIONS
Once the links between variable phenotypes and theirrespective contributing factors are established, a cohe-sive genotype to phenotype (cG-P) model can be con-structed.6 An accurate model serves as a predictivetool for phenotypic changes when influencing parame-ters are altered and this information is useful in botheducation and future research.Examples of dental cG-P models have been
described.116–119 Tooth cusp patterns have beenaltered by manipulating a targeted signalling pro-tein.116,118 In two other papers, the authors providein-depth discussions of the parameters used to formu-late their models.117,119 The first model117 was termedthe ‘morphodynamic model’ as it was able to repro-duce the morphology of all intermediate stages oftooth development, while also considering the varia-tions in different species. However, this model consid-ered the effects of genetic input alone as the causalfactor for the final observed trait, ignoring the role ofother factors such as epigenetic and environmentalinfluences. Later, the authors built on their earlierwork to include cellular parameters in their secondmodel to more closely resemble the effects of varyingfactors on tooth morphology.119 In a recent paper,the model has been used to explore the adaptive nat-ure of teeth to evolutionary challenges.120
To date, generated cG-P models are only able topredict the morphology of the dentino-enamel junc-tion, but not the outer enamel surface or root anat-omy. As they do not simulate mineralization, thisprevents the investigation of the shape of mineralizedstructures such as enamel. Despite these limitations,the present developments provide the building blocksfor more sophisticated models in the future. The con-structed models should improve the predictive accu-racy, ease of use and enable the completevisualization of tooth structure in relation to alteredgenetic, epigenetic and environmental influences.
FUTURE DIRECTIONS
Advances in research methodology and data acquisi-tion bring analytical challenges. Currently, most phe-notypes are described by either using quantitative(i.e. measurement) or categorical (i.e. the presence orabsence of a particular trait) data. However, in somecases, the answer may lie between two points or cat-egories, leading to the loss of useful information dueto the continuous nature of most phenotypes. Theapplication of state-of-the-art analytical techniquesutilized in other disciplines, including evolutionarybiology121,122 and materials science,123–134 may pro-vide valuable approaches to further characterize the
© 2014 Australian Dental Association 41
Dental phenomics in craniofacial research
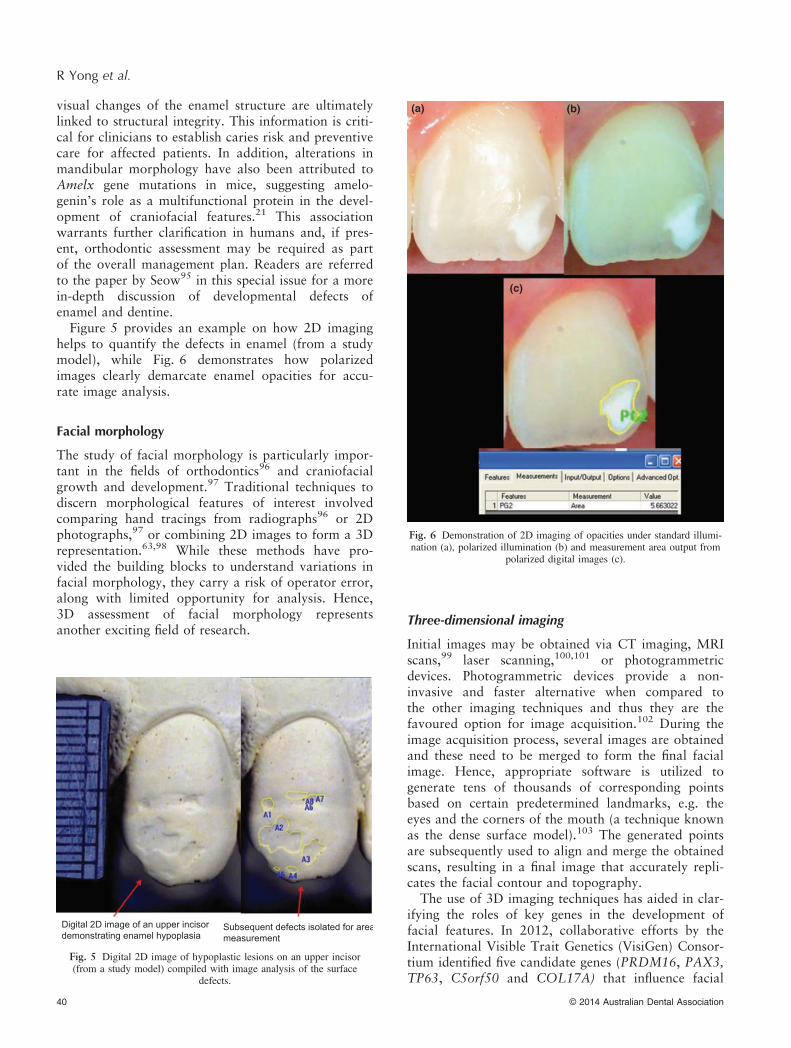
Table 3. Examples of techniques for detailed characterization of structural analysis, mechanical testing and chem-ical composition of teeth in dental phenomic studies. Non-destructive techniques that allow longitudinal changesin the properties of teeth to be assessed, in response to external factors (such as tooth demineralization), haveadvantages over analytical techniques that alter the tooth surface as a result of surface coating and extensivesample preparation. The techniques outlined here are limited to in vitro applications at present, but future tech-nological advancement could enable in vivo applications
Technique Applications Surface/sub-surfaceassessment
Longitudinalassessment
Samplepreparation
Key limitations
Structural analysisMicro computedtomography(micro-CT)
3D quantitative and qualitativeassessment of surfacetopography and sub-surfacefeatures (e.g. DEJ and pulpchamber) by using 3Dreconstructions(Resolution = 5–50 lm)
Surface +sub-surface
+ None Prolonged scanningand data processing
ConfocalMicroscope (CM)
3D qualitative and quantitativeassessment of surface topographyon 3D reconstructions; moreefficient than SEM and atomicforce microscopy (Resolution =1–2 lm)
Surface + None Unable to analysespecimens inhydrated conditions(e.g. in water storage)
Scanning ElectronMicroscopy (SEM)
2D qualitative assessmentof surface topography;can provide limitedinformation on chemicalcomposition (Resolution =2–4 nm)
Surface -(no polishingor sectioning)
Carbon/goldcoating
Unable to conductlongitudinalassessment on theoriginal surfacewithout polishingoff carbon/goldcoating
Environmental ScanningElectron Microscopy(ESEM)
2D quantitative assessmentof surface topography;can provide data onchemical composition(Resolution = 1–2 lm)
Surface + None Reduced resolutioncompared with SEM
Mechanical propertiesNanohardness testing Quantitative assessment of
surface hardness/porosity;provides data on elasticmodulus and deformationbehaviour (Indentation tipradii range from micronsto nanometers)
Surface + shallowsub-surface
+ Highly polished,flat samples
Nanoscratch testing Quantitative assessmentof tribological (wear) properties;provides data on coefficientof friction and surface roughness(Indentation tip radii range frommicrons to nanometers)
Surface + shallowsubsurface
+ Highly polished,flat samples
Scratches cannotbe superimposedbefore and aftertreatment
Chemical compositionEnergy Dispersive X-raySpectroscopy (EDXS)3
Quantitative and qualitativesurface elemental analysis (withatomic number >3), usuallyin combination with SEM(detection limit of 0.1–0.5%wt)or transmission electronmicroscopy (detection limitof 0.01–0.1%wt)
Surface - Carbon/goldcoatingNo additionalpreparation forqualitativeanalysis; flatand polishedfor quantitativeanalysis
Lacks sensitivity fortrace elementanalysis
Time of flightSecondary IonMass Spectrometry(Tof-SIMS)
Semi-quantitative chemicalcharacterization of thetooth surface in the formof organic and inorganicmass spectral data(has high sensitivity inparts per billion for entireelements in the periodic tablefrom 1–2 nm of the surface)
Surface + Highly polished,flat samples
Highly timeconsuming andprone tocontamination (i.e.requires ultra-cleanenvironment forsample processing)
42 © 2014 Australian Dental Association
R Yong et al.

properties of bioceramic materials, such as enameland dentine, from the atomic to macro-scale. Forexample, a combined assessment of structuralanalysis, mechanical properties and chemical compo-sition of teeth will unravel the effects of develop-mental influences on the structure and function ofteeth.135–140 These techniques are summarized inTable 3.The development of more sophisticated analytical
methods will be critical to further develop accuratephenotype quantification. At present, many of thetechniques described are limited to in vitro use, withthe exception of 2D imaging for the assessment oftooth colour,56 enamel defects,57 gingival health141
and plaque scores.142 Efforts to make other in vitrotechniques applicable to the clinical setting are ongo-ing and represent a key area for both researchers andclinicians. In future, one aim is to develop analyticaltechniques to accurately assess variations of toothmorphology and surface characteristics in the dentalchair. This will improve the speed of data acquisitionand enable clinicians to quickly characterize variationsor defects present, and provide appropriate advice andtreatment for affected patients.Dental phenomics presents many exciting opportu-
nities. The use of twin models helps determine thecause of variations seen in dentofacial structures andoral health.143 Cross species data-sharing using animalmodels continues to unravel the impact of mutationsin the human dentition.21,144 Collaboration betweenvarious centres of excellence will be important toadvance the field. The International CollaboratingNetwork in Oro-facial Genetics and Developmentaims to promote international collaboration145 by thesharing of expertise and data. Fragmented scientificresearch in the past, using independent samples andnon-standardized analytical techniques, represents amissed opportunity to enable inter-study comparison.While widespread integrative studies will requiremuch effort, the potential gains for doing so willgreatly benefit understanding of human biology. Clini-cians can also play a crucial role in gathering accuratephenotypic data for analysis, thus actively participat-
ing in ongoing research projects in their respectivefields of interest.
CONCLUSIONS
The craniofacial structures present important biomar-kers for certain diseases and genetic mutations, pro-viding many clues regarding growth and development.Research findings inform the profession of bothnormal and abnormal variations, while also directingtreatment provision. In addition, the significance ofaccurate phenotyping methods to dental anthropologyand forensic odontology has been established.New imaging techniques allow for the preservation
of studied specimens by reducing wear and tear dueto manual handling. The measurements obtained alsoproduce comparable or better reliability when com-pared to manual methods. Furthermore, additionalparameters such as curved surfaces, surface topogra-phy and colour differences can now be assessed accu-rately. These new parameters clarify variations seen inthe craniofacial complex and are relevant to both theclinical and research environment. In clinical practice,the detection of altered dental tissues and submucosalchanges aid recognition of disease and disorders todirect future treatment plans.Dental phenomics helps to increase the yield
obtained from aetiological studies and bridges the gapbetween the research environment and practical appli-cation. Future development in the field of dental phe-nomics will provide many exciting opportunities tounravel the mysteries behind variations in both healthand disease.
ACKNOWLEDGEMENTS
We wish to acknowledge the National Health andMedical Research Council of Australia and the Aus-tralian Dental Research Foundation for supportingvarious ongoing research projects. We also thank DrAtika Ashar from Universiti Kebangsaan Malaysia forthe provision of Fig. 2 and advice on 3D analyticalsoftware.
Table 3. Continued
Technique Applications Surface/sub-surfaceassessment
Longitudinalassessment
Samplepreparation
Key limitations
X-ray PhotoelectronSpectroscopy (XPS)
Quantitative chemicalcharacterization of thetooth surface (as atomicpercentages) using both high-and low-resolution spectra(Spatial resolution <10 lm)
Surface + Highly polished,flat samples
Highly timeconsuming andprone tocontamination(i.e. requires anultra-cleanenvironment forsample processing)
© 2014 Australian Dental Association 43
Dental phenomics in craniofacial research
DISCLOSURE STATEMENT
The authors have no conflicts of interest to declare.
REFERENCES
1. National Human Genome Research Institute. Internationalconsortium completes Human Genome Project: all goalsachieved; new vision for genome research unveiled. 2003.URL: ‘http://www.genome.gov/11006929’. Accessed 15 April2013.
2. Brook AH. Multilevel complex interactions between genetic,epigenetic and environmental factors in the aetiology ofanomalies of dental development. Arch Oral Biol 2009;54S:S3–S17.
3. Frazer KA, Murray SS, Schork NJ, Topol EJ. Human geneticvariation and its contribution to complex traits. Nat RevGenet 2009;10:241–251.
4. Lanktree MB, Hassell RG, Lahiry P, Hegele RA. Phenomics:expanding the role of clinical evaluation in genomic studies.J Investig Med 2010;58:700–706.
5. Bilder RM, Sabb FW, Cannon TD, et al. Phenomics: the sys-tematic study of phenotypes on a genome-wide scale. Neuro-science 2009;164:30–42.
6. Houle D, Govindaraju DR, Omholt S. Phenomics: the nextchallenge. Nat Rev Genet 2010;11:855–866.
7. Brook AH, Brook O’Donnell MD. Modelling the complexityof the dentition. In: Townsend G, Kanazawa E, Takayama H,eds. New directions in dental anthropology. Adelaide: Univer-sity of Adelaide Press, 2012:1–9.
8. Bilder RM, Sabb FW, Parker DS, et al. Cognitive ontologiesfor neuropsychiatric phenomics research. Cogn Neuropsychia-try 2009;14:419–450.
9. Hegele RA. Phenomics, lipodystrophy, and the metabolic syn-drome. Trends Cardiovasc Med 2004;14:133–137.
10. Schofield PN, Sundberg JP, Hoehndorf R, Gkoutos GV. Newapproaches to the representation and analysis of phenotypeknowledge in human diseases and their animal models. BriefFunct Genomics 2011;10:258–265.
11. Meehan TF, Carr CJ, Jay JJ, Bult CJ, Chesler EJ, Blake JA.Autism candidate genes via mouse phenomics. J BiomedInform 2011;44S:S5–11.
12. Tester M, Langridge P. Breeding technologies to increase cropproduction in a changing world. Science 2010;327:818–822.
13. Furbank RT, Tester M. Phenomics-technologies to relieve thephenotyping bottleneck. Trends Plant Sci 2011;16:635–644.
14. Townsend G, Bockmann M, Hughes T, Mihailidis S, Seow S,Brook A. New approaches to dental anthropology based onthe study of twins. In: Townsend G, Kanazawa F, TakayamaH, eds. New directions in dental anthropology: para-digms, methodologies and outcomes. Adelaide: University ofAdelaide Press, 2012:10–21.
15. Shaffer JR, Feingold E, Marazita ML. Genome-wide associa-tion studies: prospects and challenges for oral health. J DentRes 2012;91:637–641.
16. Acharya AB, Mainali S. Sex discrimination potential of buc-colingual and mesiodistal tooth dimensions. J Forensic Sci2008;53:790–792.
17. Coquerelle M, Bookstein FL, Braga J, Halazonetis DJ, WeberGW, Mitteroecker P. Sexual dimorphism of the human man-dible and its association with dental development. Am J PhysAnthropol 2011;145:192–202.
18. Mitteroecker P, Gunz P, Bernhard M, Schaefer K, BooksteinFL. Comparison of cranial ontogenetic trajectories amonggreat apes and humans. J Hum Evol 2004;46:679–698.
19. Hassett BR. Evaluating sources of variation in the identifica-tion of linear hypoplastic defects of enamel: a new quantifiedmethod. J Archaeol Sci 2012;39:560–565.
20. Ribeiro DC, Brook AH, Hughes TE, Sampson WJ, TownsendGC. Intrauterine hormone effects on tooth dimensions. J DentRes 2013;92:425–431.
21. Coxon TL, Brook AH, Barron MJ, Smith RN. Phenotype-genotype correlations in mouse models of amelogenesis im-perfecta caused by Amelx and Enam mutations. Cells TissuesOrgans 2012;196:420–430.
22. Harris EF, Smith RN. Accounting for measurement error: acritical but often overlooked process. Arch Oral Biol2009;54S:S107–S117.
23. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet2007;369:51–59.
24. Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimalintervention dentistry – a review. Int Dent J 2000;50:1–12.
25. Kaidonis JA, Skinner VJ, Lekkas D, Winning TA, TownsendGC. Reorientating dental curricula to reflect a minimallyinvasive dentistry approach for patient-centred management.Aust Dent J 2013;58:(1 Suppl):70–75.
26. Souza JF, Boldieri T, Diniz MB, Rodrigues JA, Lussi A,Cordeiro RCL. Traditional and novel methods for occlusalcaries detection: performance on primary teeth. Lasers MedSci 2013;28:287–295.
27. Diniz MB, Boldieri T, Rodrigues JA, Santos-Pinto L, Lussi A,Cordeiro RCL. The performance of conventional and fluores-cence-based methods for occlusal caries detection: an in vivostudy with histologic validation. J Am Dent Assoc2012;143:339–350.
28. Ferreira Zandon�a A, Ando M, Gomez GF, et al. Longitudinalanalyses of early lesions by fluorescence: an observationalstudy. J Dent Res 2013;92:S84–S89.
29. Iijima Y. Early detection of white spot lesions with digitalcamera and remineralization therapy. Aust Dent J2008;53:274–280.
30. Willmot DR, Benson PE, Pender N, Brook AH. Reproducibil-ity of quantitative measurement of white enamel deminerali-sation by image analysis. Caries Res 2000;34:175–181.
31. Cochrane NJ, Walker GD, Manton DJ, Reynolds EC. Com-parison of quantitative light-induced fluorescence, digitalphotography and transverse microradiography for quantifica-tion of enamel remineralization. Aust Dent J 2012;57:271–276.
32. Cochrane NJ, Anderson P, Davis GR, Adams GG, StaceyMA, Reynolds EC. An x-ray microtomographic study of natu-ral white-spot enamel lesions. J Dent Res 2012;91:185–191.
33. Hamba H, Nikaido T, Inoue G, Sadr A, Tagami J. Effects ofCPP-ACP with sodium fluoride on inhibition of bovineenamel demineralization: a quantitative assessment usingmicro-computed tomography. J Dent 2011;39:405–413.
34. Davis GR, Evershed ANZ, Mills D. Quantitative high con-trast X-ray microtomography for dental research. J Dent2013;41:475–482.
35. Tschoppe P, Zandim DL, Martus P, Kielbassa AM. Enameland dentine remineralization by nano-hydroxyapatite tooth-pastes. J Dent 2011;39:430–437.
36. Shaffer JR, Feingold E, Wang X, et al. Heritable patterns oftooth decay in the permanent dentition: principal componentsand factor analyses. BMC Oral Health 2012;12:7–16.
37. Olsson M, Lindhe J. Periodontal characteristics in individualswith varying form of the upper central incisors. J Clin Period-ontol 1991;18:78–82.
38. Yared KFG, Zenobio EG, Pacheco W. Periodontal status ofmandibular central incisors after orthodontic proclination inadults. Am J Orthod Dentofacial Orthop 2006;130:6.e1–8.
44 © 2014 Australian Dental Association
R Yong et al.

39. Lee A, Fu JH, Wang HL. Soft tissue biotype affects implantsuccess. Implant Dent 2011;20:e38–47.
40. Nisapakultorn K, Suphanantachat S, Silkosessak O, Rattan-amongkolgul S. Factors affecting soft tissue level around ante-rior maxillary single-tooth implants. Clin Oral Implants Res2010;21:662–670.
41. M€uller H-P, Eger T. Gingival phenotypes in young maleadults. J Clin Periodontol 1997;24:65–71.
42. M€uller H-P, Eger T. Masticatory mucosa and periodontalphenotype: a review. Int J Periodontics Restorative Dent2002;22:172–183.
43. Eger T, M€uller HP, Heinecke A. Ultrasonic determination ofgingival thickness. J Clin Periodontol 1996;23:839–845.
44. De Rouck T, Eghbali R, Collys K, De Bruyn H, Cosyn J. Thegingival biotype revisited: transparency of the periodontalprobe through the gingival margin as a method to discriminatethin from thick gingiva. J Clin Periodontol 2009;36:428–433.
45. Eghbali A, De Rouck T, De Bruyn H, Cosyn J. The gingivalbiotype assessed by experienced and inexperienced clinicians.J Clin Periodontol 2009;36:958–963.
46. Fournier BP, Larjava H, Hakkinen L. Gingiva as a source ofstem cells with therapeutic potential. Stem Cells Dev2013;22:3157–3177.
47. Han J, Menicanin D, Gronthos S, Bartold PM. Stem cells, tis-sue engineering and periodontal regeneration. Aust Dent J2013;doi:10.1111/adj.12100 [Epub ahead of print].
48. Lekic P, Rojas J, Birek C, Tenenbaum H, McCulloch CAG.Phenotypic comparison of periodontal ligament cells in vivoand in vitro. J Periodontal Res 2001;36:71–79.
49. Hinz B. Matrix mechanics and regulation of the fibroblastphenotype. Periodontol 2000 2013;63:14–28.
50. Michalowicz BS, Diehl SR, Gunsolley JC, et al. Evidence of asubstantial genetic basis for risk of adult periodontitis. J Peri-odontol 2000;71:1699–1707.
51. Taubman MA, Stoufl ED, Ebersole JL, Smith DJ. Phenotypicstudies of cells from periodontal disease tissues. J PeriodontalRes 1984;19:587–590.
52. McDevitt MJ, Wang H-Y, Knobelman C, et al. Interleukin-1genetic association with periodontitis in clinical practice.J Periodontol 2000;71:156–163.
53. Nares S. The genetic relationship to periodontal disease. Peri-odontol 2000 2003:36–49.
54. Bartold PM, Van Dyke TE. Periodontitis: a host-mediated dis-ruption of microbial homeostasis. Unlearning learned con-cepts. Periodontol 2000 2013;62:203–217.
55. Brook AH. Variables and criteria in prevalence studies ofdental anomalies of number, form and size. Community DentOral Epidemiol 1975;3:288–293.
56. Guan YH, Lath DL, Lilley TH, Willmot DR, Marlow I,Brook AH. The measurement of tooth whiteness by imageanalysis and spectrophotometry: a comparison. J Oral Reha-bil 2005;32:7–15.
57. Brook AH, Smith RN, Elcock C, Al-Sharood M, Shah A,Karmo M. The measurement of tooth morphology: develop-ment and validation of a new image analysis technique. In:Mayhall JT, Heikkinen T, eds. Dental Morphology 1998.Oulu, Finland: Oulu University Press, 1999: 380–387.
58. Evans AR, Wilson GP, Fortelius M, Jernvall J. High-level sim-ilarity of dentitions in carnivorans and rodents. Nature2007;445:78–81.
59. Brook AH, Elcock C, Aggarwal M, et al. Tooth dimensionsin hypodontia with a known PAX9 mutation. Arch Oral Biol2009;54S:S57–S62.
60. Brook AH, Griffin RC, Smith RN, et al. Tooth size patternsin patients with hypodontia and supernumerary teeth. ArchOral Biol 2009;54S:S63–S70.
61. Khalaf K, Smith RN, Elcock C, Brook AH. Multiple crownsize variables of the upper incisors in patients with supernu-merary teeth compared with controls. Arch Oral Biol2009;54S:S71–S78.
62. Berkowitz S, Pruzansky S. Stereophotogrammetry of sericalcasts of cleft palate. Angle Orthod 1968;38:136–149.
63. Savara BS. Applications of photogrammetry for quantitativestudy of tooth and face morphology. Am J Phys Anthropol1965;23:427–434.
64. Berkowitz S. Stereophotogrammetric analysis of casts of nor-mal and abnormal palates. Am J Orthod 1971;60:1–18.
65. Van der Linden FPGM, Boersma H, Zelders T, Peters KA,Raaben JH. Three-dimensional analysis of dental casts bymeans of the Optocom. J Dent Res 1972;51:1100.
66. Takada K, Lowe AA, DeCou R. Operational performance ofthe Reflex Metrograph and its applicability to the three-dimensional analysis of dental casts. Am J Orthod1983;83:195–199.
67. Smith R, Zaitoun H, Coxon T, et al. Defining new dentalphenotypes using 3-D image analysis to enhance discrimina-tion and insights into biological processes. Arch Oral Biol2009;54S:S118–S125.
68. Ashar A, Hughes T, James H, Kaidonis J, Khamis F, Town-send G. Dental crown and arch size in Europeans and Austra-lian Aboriginals. In: Townsend G, Kanazawa E, TakayamaH, eds. New directions in dental anthropology: paradigms,methodologies and outcomes. Adelaide: University of Adela-ide Press, 2012:65–80.
69. El-Zanaty HM, El-Beialy AR, Abou El-Ezz AM, Attia KH,El-Bialy AR, Mostafa YA. Three-dimensional dental measure-ments: an alternative to plaster models. Am J Orthod Dento-facial Orthop 2010;137:259–265.
70. Bootvong K, Liu Z, McGrath C, et al. Virtual model analysisas an alternative approach to plaster model analysis: reliabil-ity and validity. Eur J Orthod 2010;32:589–595.
71. Bell A, Ayoub AF. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models.J Orthod 2003;30:219–223.
72. Santoro M, Galkin S, Teredesai M, Nicolay OF, CangialosiTJ. Comparison of measurements made on digital and plastermodels. Am J Orthod Dentofacial Orthop 2003;124:101–105.
73. Creton M, van den Boogaard MJ, Maal T, et al. Three-dimensional analysis of tooth dimensions in the MSX1-missense mutation. Clin Oral Investig 2013;17:1437–1445.
74. Swinnen S, Bailleul-Forestier I, Arte S, Nieminen P, DevriendtK, Carels C. Investigating the etiology of multiple tooth agen-esis in three sisters with severe oligodontia. Orthod CraniofacRes 2008;11:24–31.
75. Cr�eton M, Cune MS, de Putter C, Ruijter JM, Kuijpers-Jagtman AM. Dentofacial characteristics of patients with hyp-odontia. Clin Oral Investig 2010;14:467–477.
76. De Coster PJ, Marks LA, Martens LC, Huysseune A. Dentalagenesis: genetic and clinical perspectives. J Oral Pathol Med2009;38:1–17.
77. Lexner MO, Bardow A, Hertz JM, Nielsen LA, Kreiborg S.Anomalies of tooth formation in hypohidrotic ectodermaldysplasia. Int J Paediatr Dent 2007;17:10–18.
78. Kapadia H, Mues G, D’Souza R. Genes affecting tooth mor-phogenesis. Orthod Craniofac Res 2007;10:237–244.
79. Goodall C. Procrustes methods in the statistical analysis ofshape. J Roy Statist Soc Ser B 1991;53:285–339.
80. Bookstein FL. Landmark methods for forms without land-marks: localizing group differences in outline shape. Proceed-ings of the Workshop on Mathematical Methods inBiomedical Image Analysis, 1996:279–289.
© 2014 Australian Dental Association 45
Dental phenomics in craniofacial research

81. Rohlf FJ, Slice D. Extensions of the Procrustes method for theoptimal superimposition of landmarks. Syst Biol 1990;39:40–59.
82. Robinson DL, Blackwell PG, Stillman EC, Brook AH. PlanarProcrustes analysis of tooth shape. Arch Oral Biol2001;46:191–199.
83. Robinson DL, Blackwell PG, Stillman EC, Brook AH. Impactof landmark reliability on the planar Procrustes analysis oftooth shape. Arch Oral Biol 2002;47:545–554.
84. DiBiase AT, Elcock C, Smith RN, Brook AH. A new tech-nique for symmetry determination in tooth morphology usingimage analysis: application in the diagnosis of solitary maxil-lary median central incisor. Arch Oral Biol 2006;51:870–875.
85. DiBiase AT, Cobourne MT. Beware the solitary maxillarymedian central incisor. J Orthod 2008;35:16–19.
86. Smith RN, Townsend G, Chen K, Brook A. Synetic superim-position of dental 3D data: application in twin studies. FrontOral Biol 2009;13:142–147.
87. Geng X, Christensen GE, Gu H, Ross TJ, Yang Y. Implicitreference-based group-wise image registration and its applica-tion to structural and functional MRI. Neuroimage 2009;47:1341–1351.
88. Wilson GP, Evans AR, Corfe IJ, Smits PD, Fortelius M,Jernvall J. Adaptive radiation of multituberculates before theextinction of dinosaurs. Nature 2012;483:457–460.
89. Boyer DM, Evans AR, Jernvall J. Evidence of dietary differen-tiation among late Paleocene-early Eocene plesiadapids (mam-malia, primates). Am J Phys Anthropol 2010;142:194–210.
90. Godfrey LR, Winchester JM, King SJ, Boyer DM, Jernvall J.Dental topography indicates ecological contraction of lemurcommunities. Am J Phys Anthropol 2012;148:215–227.
91. Skinner MM, Evans AR, Smith T, et al. Contributions ofenamel-dentine junction shape and enamel deposition to pri-mate molar crown complexity. Am J Phys Anthropol2010;142:157–163.
92. Clarkson J. Review of terminology, classifications, and indicesof developmental defects of enamel. Adv Dent Res1989;3:104–109.
93. Brook AH, Elcock C, Hallonsten AL, et al. The developmentof a new index to measure enamel defects. In: Brook AH, ed.Dental morphology. Sheffield: Sheffield Academic Press, 2001:59–66.
94. Smith RN, Elcock C, Abdellatif A, B€ackman B, Russell JM,Brook AH. Enamel defects in extracted and exfoliated teethfrom patients with Amelogenesis Imperfecta, measured usingthe extended enamel defects index and image analysis. ArchOral Biol 2009;54S:S86–S92.
95. Seow WK. Developmental defects of enamel and dentine:challenges for basic science research and clinical management.Aust Dent J 2013; doi:10.1111/adj.12104 [Epub ahead ofprint].
96. Siriwat PP, Jarabak JR. Malocclusion and facial morphologyis there a relationship? Angle Orthod 1985;55:127–138.
97. Brown T, Townsend GC, Richards LC, Travan GR, Pinker-ton SK. Facial symmetry and mirror imaging in South Austra-lian twins. In: Brown T, Molnar S, eds. Craniofacialvariations in Pacific populations. Adelaide: Anthropology andGenetics Laboratory, The University of Adelaide, 1992:79–98.
98. Ras F, Habets LLMH, van Ginkel FC, Prahl-Andersen B.Quantification of facial morphology using stereophotogram-metry – demonstration of a new concept. J Dent1996;24:369–374.
99. Liu F, van der Lijn F, Schurmann C, et al. A genome-wideassociation study identifies five loci influencing facialmorphology in Europeans. PLoS Genet 2012;8:e1002932.doi:10/1371/journal.pgen.1002932.
100. Paternoster L, Zhurov AI, Toma AM, et al. Genome-wideassociation study of three-dimensional facial morphologyidentifies a variant in PAX3 associated with nasion position.Am J Hum Gen 2012;90:478–485.
101. Kau CH, Richmond S, Zhurov AI, et al. Reliability of mea-suring facial morphology with a 3-dimensional laser scanningsystem. Am J Orthod Dentofacial Orthop 2005;128:424–430.
102. Hammond P, Hutton TJ, Allanson JE, et al. 3D analysis offacial morphology. Am J Med Genet 2004;126:339–348.
103. Hutton TJ, Buxton BF, Hammond P. Dense surface point dis-tribution models of the face. IEEE Workshop on Mathemati-cal Methods in Biomedical Image Analysis. Kauai, Hawaii,2001:153–160.
104. Hammond P, Suttie M. Large-scale objective phenotyping of3D facial morphology. Hum Mutat 2012;33:817–825.
105. Hammond P, Hannes F, Suttie M, et al. Fine-grained facialphenotype-genotype analysis in Wolf-Hirschhorn syndrome.Eur J Hum Genet 2012;20:33–40.
106. Kung S, Walters M, Claes P, Goldblatt J, Souef P, BaynamG. A dysmorphometric analysis to investigate facial pheno-typic signatures as a foundation for non-invasive monitoringof lysosomal storage disorders. J Inherit Metab Dis Reports2012;8:31–39.
107. Baynam GS, Walters M, Dawkins H, Bellgard M, HalbertAR, Claes P. Objective monitoring of mTOR inhibitor ther-apy by three-dimensional facial analysis. Twin Res HumGenet 2013;16:840–844.
108. Baynam G, Walters M, Claes P, et al. The facial evolution:looking backward and moving forward. Hum Mutat2013;34:14–22.
109. Walters M, Claes P, Kakulas E, Clement JG. Robust andregional 3D facial asymmetry assessment in hemimandibularhyperplasia and hemimandibular elongation anomalies. Int JOral Maxillofac Surg 2013;42:36–42.
110. Claes P, Walters M, Clement J. Improved facial outcomeassessment using a 3D anthropometric mask. Int J Oral Max-illofac Surg 2012;41:324–330.
111. Kim EK, Khang SK, Lee TJ, Kim TG. Clinical features of themicroform cleft lip and the ultrastructural characteristics of theorbicularis oris muscle. Cleft Palate Craniofac J 2010;47:297–302.
112. Marazita ML. Subclinical features in non-syndromic cleft lipwith or without cleft palate (CL/P): review of the evidencethat subepithelial orbicularis oris muscle defects are part ofan expanded phenotype for CL/P. Orthod Craniofacial Res2007;10:82–87.
113. Suzuki S, Marazita ML, Cooper ME, et al. Mutations inBMP4 are associated with subepithelial, microform, and overtcleft lip. Am J Hum Gen 2009;84:406–411.
114. Dixon MJ, Marazita ML, Beaty TH, Murray JC. Cleft lipand palate: understanding genetic and environmental influ-ences. Nat Rev Genet 2011;12:167–178.
115. Marazita ML. The evolution of human genetic studies of cleftlip and cleft palate. Annu Rev Genomics Hum Genet2012;13:263–283.
116. Kangas AT, Evans AR, Thesleff I, Jernvall J. Nonindepen-dence of mammalian dental characters. Nature2004;432:211–214.
117. Salazar-Ciudad I, Jernvall J. A gene network model account-ing for development and evolution of mammalian teeth. ProcNat Acad Sci USA 2002;99:8116–8120.
118. Kassai Y, Munne P, Hotta Y, et al. Regulation of mammaliantooth cusp patterning by ectodin. Science 2005;309:2067–2070.
119. Salazar-Ciudad I, Jernvall J. A computational model of teethand the developmental origins of morphological variation.Nature 2010;464:583–586.
46 © 2014 Australian Dental Association
R Yong et al.
120. Salazar-Ciudad I, Marin-Riera M. Adaptive dynamics underdevelopment-based genotype-phenotype maps. Nature2013;497:361–364.
121. Ungar PS, Krueger KL, Blumenschine RJ, Njau J, Scott RS.Dental microwear texture analysis of hominins recovered bythe Olduvai Landscape Paleoanthropology Project, 1995–2007. J Hum Evol 2012;63:429–437.
122. Ungar PS, Brown CA, Bergstrom TS, Walker A. Quantifica-tion of dental microwear by tandem scanning confocalmicroscopy and scale-sensitive fractal analyses. Scanning2003;25:185–193.
123. He LH, Swain MV. Enamel – a ‘metallic-like’ deformablebiocomposite. J Dent 2007;35:431–437.
124. Losic D, Short K, Mitchell JG, Lal R, Voelcker NH. AFMnanoindentations of diatom biosilica surfaces. Langmuir2007;23:5014–5021.
125. Balter V, Reynard B. Secondary ionization mass spectrometryimaging of dilute stable strontium labeling in dentin andenamel. Bone 2008;42:229–234.
126. Xie Z, Swain M, Munroe P, Hoffman M. On the criticalparameters that regulate the deformation behaviour of toothenamel. Biomaterials 2008;29:2697–2703.
127. Xie Z, Kilpatrick N, Swain M, Munroe P, Hoffman M. Trans-mission electron microscope characterisation of molar-incisor-hypomineralisation. J Mater Sci Mater Med 2008;19:3187–3192.
128. Ang SF, Bortel EL, Swain MV, Klocke A, Schneider GA. Size-dependent elastic/inelastic behavior of enamel over millimeterand nanometer length scales. Biomaterials 2010;31:1955–1963.
129. Huang TTY, He L-H, Darendeliler MA, Swain MV. Correla-tion of mineral density and elastic modulus of natural enamelwhite spot lesions using X-ray microtomography and nanoin-dentation. Acta Biomaterialia 2010;6:4553–4559.
130. Jacobs TDB, Carpick RW. Nanoscale wear as a stress-assistedchemical reaction. Nat Nano 2013;8:108–112.
131. De Menezes Oliveira MAH, Torres CP, Gomes-Silva JM, etal. Microstructure and mineral composition of dental enamelof permanent and deciduous teeth. Microsc Res Tech2010;73:572–577.
132. University of South Australia. Ian Wark Research Institute Sci-entific Services. 2013. URL: ‘http://w3.unisa.edu.au/iwri/scien-tificservices/sciservicesbook.pdf’. Accessed 26 October 2013.
133. Adelaide Microscopy. Instrumentation. 2013. URL: ‘https://www.adelaide.edu.au/microscopy/instrumentation/’. Accessed8 November 2013.
134. Australian Microscopy and Microanalysis Research Facility.MyScope: training for advance research. 2013. URL:‘http://www.ammrf.org.au/myscope/analysis/eds/’. Accessed 8November 2013.
135. Anderson PJ, Yong R, Surman TL, Rajion ZA, Ranjitkar S.Application of three-dimensional computed tomography incraniofacial clinical practice and research. Aust Dent J 2014;doi: 10.1111/adj.12154 [Epub ahead of print].
136. Ungar P. Materials science: strong teeth, strong seeds. Nature2008;452:703–705.
137. Ranjitkar S, Kaidonis J, Hall C, Marino V, Richards L.Emerging techniques for the analysis of tooth wear. In:Townsend G, Kanazawa E, Takayama H, eds. New direc-tions in dental anthropology. Adelaide: Adelaide UniversityPress, 2012:123–137.
138. Loch C, Grando LJ, Kieser JA, Sim~oes-Lopes PC. Dentalpathology in dolphins (Cetacea: Delphinidae) from the south-ern coast of Brazil. Dis Aquat Organ 2011;94:225–234.
139. Loch C, Swain MV, van Vuuren LJ, Kieser JA, Fordyce RE.Mechanical properties of dental tissues in dolphins (Cetacea:Delphinoidea and Inioidea). Arch Oral Biol 2013;58:773–779.
140. Loch C, Grando LJ, Schwass DR, Kieser JA, Fordyce RE,Sim~oes-Lopes PC. Dental erosion in South Atlantic dolphins(Cetacea: Delphinidae): a macro and microscopic approach.Mar Mammal Sci 2013;29:338–347.
141. Smith RN, Lath DL, Rawlinson A, Karmo M, Brook AH. Gin-gival inflammation assessment by image analysis: measurementand validation. Int J Dent Hyg 2008;6:137–142.
142. Smith RN, Brook AH, Elcock C. The quantification of dentalplaque using an image analysis system: reliability and valida-tion. J Clin Periodontol 2001;28:1158–1162.
143. Hughes T, Bockmann M, Mihailidis S, et al. Genetic, epige-netic, and environmental influences on dentofacial structuresand oral health: ongoing studies of Australian twins and theirfamilies. Twin Res Hum Genet 2013;16:43–51.
144. Nakatomi M, Hovorakova M, Gritli-Linde A, et al. Evc regu-lates a symmetrical response to Shh signaling in molar devel-opment. J Dent Res 2013;92:222–228.
145. Townsend G, Alvesalo L, Brook A. Variation in the humandentition: some past advances and future opportunities.J Dent Res 2008;87:802–805.
Address for correspondence:Dr Robin Yong
School of DentistryThe University of Adelaide
Adelaide SA 5005Australia
Email: [email protected]
© 2014 Australian Dental Association 47
Dental phenomics in craniofacial research