
Decision to admit in an inner-city psychiatric emergency room: Beyond diagnosis—The psychosocial...
16
DECISION TO ADMIT IN AN INNER-CITY PSYCHIATRIC EMERGENCY ROOM: BEYOND DIAGNOSISJTHE PSYCHOSOCIAL FACTORS Steven Friedman, Ph.D. Donald L. Feinsilver, M.D. Geri W. Davis, Ph.D. Reuben Margolis, Ph.D. OliverJ. David, M.D. Martin Kesselman, M.D. A one week sample of all patients who presented to the psychiatric emergency room of a large general municipal hospial in an inner-city area were studied. Demographic make- up, clinical picture, nature of coping styles, support systems, social, work, and family adjustment were studied as they related to admission status. Diagnosis, psychiatric history, and clinical status predicted admission as well as the nature of the patient's social functioning, coping style, and community supports. The implications of the socio- economics of mental health for treatment planning were discussed. During the past 20 years, the psychiatric emergency room (ER) has become a chief entry point to the mental health delivery system. This is due, largely, to our continuing emphasis on deinstitutionalization and community-based services. Traditionally, studies of psychiatric ER's and their patients have focused mainly on patient variables 1-~ with some -work on therapist variables or the patient-therapist interaction. 7-9 While some positive results on patient variables have emerged they tend to be contradictatory and of timited practical use.l° The psychiatric ER is a unique setting in that the interaction of patient, therapist, community supports and the ER itself will effect treatment planning and dispositional choice.~0,11 At the time of this study Dr. Friedman was Clinical Assistant Professor, Dr. Feinsilver was Chief Resident, Dr. Davis was Clinical Instructor, Dr. Margolis was Associate Professor, Dr. David was Assistant Professor, and Dr. Kesselman was Professor of ClinicaI Psychiatry in the Department of Psychiatry, Kings County Hospital/Downstate Medical Center, Brooklyn, New York. Requests for reprints should be directed to Dr. Friedman, Department of Psychology, Annex 3, Kings County Hospital Center, 451 Clarkson Avenue, Brooklyn, New York, 11203. This research was supported by the Department of Psychiatry at Downstate Medical Center, Eugene B. Feigelson, M.D., Chairman. Ms. Valerie Henkin Geibet of the Scientific Computing Center/Downstate Medical Center provided statistical consultation and Catherine Cozzolino provided assistance in data collection and manuscript preparation. PSYCHIATRICQUARTERLY, 53(4)Winter, 1981 259 0033-2720/81/t600-0259500.95©19Sl HumanSciences Press
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Decision to admit in an inner-city psychiatric emergency room: Beyond diagnosis—The psychosocial...
DECISION TO ADMIT IN AN INNER-CITY PSYCHIATRIC E M E R G E N C Y R O O M : BEYOND D I A G N O S I S J T H E PSYCHOSOCIAL FACTORS
Steven Friedman, Ph.D. Donald L. Feinsilver, M.D.
Geri W. Davis, Ph.D. Reuben Margolis, Ph.D.
OliverJ . David, M.D. Martin Kesselman, M.D.
A one week sample of all patients who presented to the psychiatric emergency room of a large general municipal hospial in an inner-city area were studied. Demographic make- up, clinical picture, nature of coping styles, support systems, social, work, and family adjustment were studied as they related to admission status. Diagnosis, psychiatric history, and clinical status predicted admission as well as the nature of the patient's social functioning, coping style, and community supports. The implications of the socio- economics of mental health for treatment planning were discussed.
During the past 20 years, the psychiatric emergency room (ER) has become a chief entry point to the mental health delivery system. This is due, largely, to our continuing emphasis on deinstitutionalization and community-based services.
Traditionally, studies of psychiatric ER ' s and their patients have focused mainly on patient variables 1-~ with some -work on therapist variables or the patient-therapist interaction. 7-9 While some positive results on patient variables have emerged they tend to be contradictatory and of timited practical use.l° The psychiatric ER is a unique setting in that the interaction of patient, therapist, community supports and the ER itself will effect treatment planning and dispositional choice.~0,11
At the time of this study Dr. Friedman was Clinical Assistant Professor, Dr. Feinsilver was Chief Resident, Dr. Davis was Clinical Instructor, Dr. Margolis was Associate Professor, Dr. David was Assistant Professor, and Dr. Kesselman was Professor of ClinicaI Psychiatry in the Department of Psychiatry, Kings County Hospital/Downstate Medical Center, Brooklyn, New York. Requests for reprints should be directed to Dr. Friedman, Department of Psychology, Annex 3, Kings County Hospital Center, 451 Clarkson Avenue, Brooklyn, New York, 11203. This research was supported by the Department of Psychiatry at Downstate Medical Center, Eugene B. Feigelson, M.D., Chairman. Ms. Valerie Henkin Geibet of the Scientific Computing Center/Downstate Medical Center provided statistical consultation and Catherine Cozzolino provided assistance in data collection and manuscript preparation.
PSYCHIATRIC QUARTERLY, 53(4) Winter, 1981 259 0033-2720/81/t600-0259500.95©19Sl Human Sciences Press
260
PSYCHIATRIC QUARTERLY
As concluded by Gerson and Bassuk 1° in their recent review of ER treatment:
The essential task in the emergency room is to delineate those factors which can be readily translated in a dispositional choice. Keeping this in mind, we need a model aimed at relatively rapid evaluation, containment, and referral of the patient in crisis. Our review of dispositional determinants and our clinical experience indicate that a model integerating an evaluation of both the patient's and the community's adaptive resources and competence and minimizing subtle diagnostic considerations would be of practical use (p. 9).
The purpose of the present study was to examine the pattern of utilization of the psychiatric ER in a large inner-city municipal hospital. This ER, as many throughout the country, is experiencing increasing demands by the community, as well as local, state, and federal regulatory agencies.
The first objective was to programmatically collect demographic, clinical, and dispositional data in order to evaluate and plan the use of the emergency room. Secondly, we attempted to collect information about the patient's support systems and information about the patient's social, work, and community functioning. Thirdly, we attempted to study the patient's typical means of coping with stress and what "help-seeking" behavior they engaged in prior to their arrival to the psychiatric ER. We were also interested in looking at how this behavior effected eventual disposition.
Fourth, we attempted to take a closer look at both homicidal/suicidal ideation and behavior, traditionally part of the legal basis for involuntary hospitalization, and to assess to what extent this was correlated wkh psychiatric hospitalization. Overall, an attempt was made to obtain an understanding of our ER patients, their needs, their support systems within the overall context of their clinical conditions. As noted we hoped to use this information to develop programs and staffing patterns to meet the needs of a large inner-city municipal psychiatric ER which is the gate keeper between large psychiatric hospital systems and the community at large. We hope this information will contribute to the development of the model called for by Gerson & Bassuk 1° for ER treatment.
M E T H O D
Setting
At the time of this study Kings County Psychiatric Hospital, which contains the psychiatric emergency room, was the receiving hospital for psychiatric emergencies for nearly the entire borough of Brooklyn. Our hospital had a catchment area of over two million people. The psychiatric emergency service is fully operational 24 hours a day, seven days a week. Structurally and administratively it is located in its own facilities and accepts referrals from other hospitals and agencies as well as walk-ins.
During weekdays from 9 a.m.-5 p.m. the ER is staffed by 3-4 attending psychiatrists, and occasionally some second-year residents on an ER rotation,
26i
s. FRIEDMAN, et al.
supported by social service, nursing, and clerical staffs. In the evening and on weekends, coverage is provided by first and second-year residents, with supervision by senior residents, and supported by nursing and clerical staffs. There was no social service staff provided on the weekends or evening hours during the time of our study.
Subjects and Procedure
We randomly selected one week in the fall of 1979 to collect data on each and every patient who presented him/herself to the psychiatric ER, 24 hours a day, for the entire week. We had considered taking random samples of patients over a more extended period of time but it was felt that this procedure would unduly interfere with the day-to-day running of one of the busiest psychiatric ERs in the world. The ER was averaging approximately 17,000 patient visits per year resulting in 7,000 admissions. By taking data on every single patient who presented during one randomly selected week it was thought that cooperation from the clerical and clinical staff would be optimal.
As was noted, an attempt was made to collect data on every single patient presenting to the psychiatric ER for one week during October 1979. A total of 264 patients were registered at the receiving desk. Of these, ten patients walked out prior to their being seen by any clinician. An additional ten patients were police prisoners and were admitted directly to the forensic unit. No data was collected on the latter. Six patients were under 16 years old and were referred to the children's walk-in clinic. Excluding these patients from our analysis a total of 238 adult patients were seen. A total of 188 (79% of the total adults) forms were completed by both the clerical and professional staff. There was some information missing on some of the patients but overall we had rather complete data on 188 patients.
Instrument
On coming to the psychiatric ER every patient, following standard pro- cedure, was registered at the reception desk. After the usual registration forms were completed the clerical staff completed the first part of a questionnaire which contained demographic and some historical information. The patient was then seen by a clinician who did a "usual evaluation and workup" . After the eval- uation and treatment plan was completed, the therapist was asked to complete the second half of the questionnaire.* An analysis by age, sex, race, time of evaluation, and decision to admit indicated no significant differences between those patients on whom we were able to obtain complete data and from those patients whom we did not obtain any information. The failure to achieve 100 % completion of the forms was due to several of the clinicians refusing to take part in this voluntary study. We believe, however, that our data is representative of a " typical" one week service load.
*A copy of the questionnaire is available from the authors.

262
PSYCHIATRIC QUARTERLY
RESULTS
Demographics
Table 1 presents the demographic breakdown of our sample and information on how and when they came to our ER. The sample included: slightly more women than men (54.8 % to 45.2 %), a relatively young population (57.4% under 30 years old), and mostly black patients (59.6%) with sizable white (24.5%) and Hispanic (I4.7 %) subgroups. The patients educational level presented in the table shows that 61% of the patients had not completed high school, 14% did obtain a high school diploma, and an additional 14% finished at least one year of post-high school education.
While the greatest number of patients (41.5%) describe themselves as Roman Catholics there are sizable numbers of Southern Baptists (17%) and Fundamental Christians (12.2 %). Roughly 68.6 % of the population were born in the continental U.S. and 27.7 % were born outside the U.S. Of those patients bona in the U.S. 44% were born in Brooklyn and a total of 71% were born within New York state. Patients born in the southern U.S. made up 19% of the U.S. born patients. Of the patients born outside the continental U.S. (N =55), 38% were born in Puerto Rico, 20% in Jamaica, 27% from other Carribean Islands, 7 % from South America, and only 9 % were born outside the Americas (i.e., European).
Table 1 also presents the breakdown of patient 's time of arrival to the ER. As can be seen in the table the greatest number of patients (44.1%) arrive between 4 p.m. and midnight. The next largest number of patients come from 8 a.m. to 4 p.m. (36.2%) and then 12 a.m. to 8 a.m. (19.7%). Walk-ins who came by themselves comprise 26% of our sample. Family, with or without a police escort, accompanied 40% of our patients and 31% of our patients were coerced into coming to our ER without any family present (i.e. police).
Since our ER functions as a receiving hospital (i.e. we receive patients from other hospitals, police) as well as a walk-in clinic, we did some further analysis of how patients come to our hospital. We found a significant interaction of patients means of arrival by the time of day ()C 2 = 14.43, p<.006). Of patients who came alone (N =49) only 16.3% came from 12 a.m. to 8 a.m., 40.8% from 8 a.m. to 4 p.m. , and 42.9% from 4 p.m. to midnight. Similarly, of patients who came with their family (N =76) only 13.2% came from 12 a.m. to 8 a.m., 46.1% from 8 a.m. to 4 p.m. , and 40.8% from 4 p.m. to midnight. However, of patients brought by the police (N = 59), or some other coercive agency, 32.3 % came from 12 a.m. to 8 a.m., only 18.6% from 8 a.m. to 4 p.m. , and 49.2% from 4 p.m. to midnight. A further breakdown of patients arrival by weekday or weekend found no significant differences.
Interestingly, a breakdown of how patients come to our hospital by their ethnic background was significant (?[2 = 15.01, p<.02). We found that of patients who came alone (N =49) only 18.4% were white, 73.5% were black, and 8.2% were Hispanic. Similarly, of patients who came with their family (N = 76) 17.1% were white, 64.5 % were black, and 17.1% were Hispanic. However, of patients who were coerced (N = 59) into coming to our ER 39% were white, 42.4% were black, and 16.9% were Hispanic.

263
S. FRIEDMAN, et al.
TABLE 1
Patient Demographics and Presentation to the ER (N = 188)
Variable N Sample %
Sex: Male 85 45.2 Female 103 54.8
Race: Black 112 59.6 Hispanic 28 14.9 White 46 24.5 Oriental 2 I. i
Age: 16 to 20 31 t6,5 2I to 25 35 t8.6 26 to 30 42 22.3 31 to 35 22 21.8 36 to 50 41 9,0 51 to 79 17
Religion: Southern Baptist 32 17.0 Fundamental Christian 23 12.2 Other Protestant 16 8.5 Catholic 78 41.5 Jewish 12 6.4 Muslim 3 1.6 Other 7 3.7 " N o Rel igion" 12 9.0
Education: 0 to 7 years 20 t 1 7 to 9 years 26 14 9 to tess than 12 68 36 HS or equivalent 26 14 1 year post-HS 16 9 Finished College 6 3 1 year post BA 4 2 No Information 22 12
Country of Origin: Continental United States 129 68.6 Foreign Born 52 27.7 No Information 7 3.7
Means of Arrival to Hospital: Alone 49 26 With Family 76 40 Coercion, No Family 59 31 No Information 4 2
Shift: Midnight-8 a.m. 37 20 8 a.m.-4 p.m. 68 36 4 p.m.-Midnight 83 44
Day: Weekday 129 69 Weekend 59 31
264
PSYCHIATRIC QUARTERLY
PATIENT 'S SUPPORT SYSTEMS AND WORK, FAMILY, AND SOCIAL A D J U S T M E N T
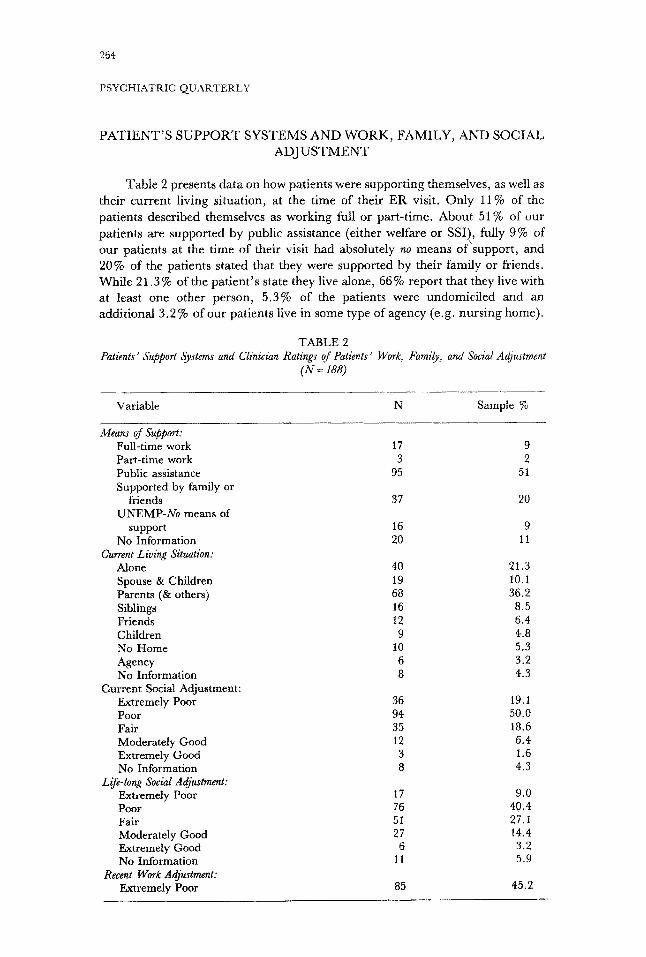
Table 2 presents data on how patients were supporting themselves, as well as their current living situation, at the time of their ER visit. Only 11% of the patients described themselves as working full or part-time. About 51% of our patients are supported by public assistance (either welfare or SSI), fully 9% of our patients at the time of their visit had absolutely no means of support, and 20 % of the patients stated that they were supported by their family or friends. While 21.3 % of the patient's state they live alone, 66 % report that they live with at least one other person, 5.3% of the patients were undomiciled and an additional 3.2 % of our patients live in some type of agency (e.g. nursing home).
TABLE 2 Patients' Support Systems and Clinician Ratings of Patients' Work, Family, and Social Adjustment
(N=188)
Variable N Sample %
Means of Support: Full-time work 17 9 Part-time work 3 2 Public assistance 95 51 Supported by family or
friends 37 20 UNEMP-No means of
support 16 9 No Information 20 11
Current Living Situation: Alone 40 21.3 Spouse & Children 19 10.1 Parents (& others) 68 36.2 Siblings 16 8.5 Friends 12 6.4 Children 9 4.8 No Home 10 5.3 Agency 6 3.2 No Information 8 4.3
Current Social Adjustment: Extremely Poor 36 19.1 Poor 94 50.0 Fair 35 18.6 Moderately Good 12 6.4 Extremely Good 3 1.6 No Information 8 4.3
Life-long Social Adjustment: Extremely Poor 17 9.0 Poor 76 40.4 Fair 51 27.1 Moderately Good 27 14.4 Extremely Good 6 3.2 No Information 11 5.9
Recent Work Adjustment: Extremely Poor 85 45.2

265
S. FRIEDMAN, et ah
TABLE 2, cont. Patients' Support Systems and Clinician Ratings of Patients' Work,
( i V = 188) Family, and Social Adjustment
Variable N Sample % Poor 58 30.9 Fair 21 11.2 Moderately Good 4 2.1 Extremely Good 1 .5 No Information 14 7.4
Life-long Work Adjustment: Extremely Poor 54 28.7 Poor 65 34.6 Fair 29 15.4 Moderately Good 11 5.9 Extremely Good 9 4.8 No Information 20 10.6
Current Family Adjustment: Extremely Poor 36 19.1 Poor 70 37.2 Fair 53 28.2 Moderately Good 11 5.9 Extremely Good 3 1.6 No Information t5 8.0
Life-long Family Adjustment: Extremely Poor 22 11.7 Poor 56 29.8 Fair 65 34.6 Moderately Good 24 t2,8 Extremely Good 5 2.7 No Information 16 8.5
Fully, 45.2 % of the patients had not worked at all in the three months prior to their ER visit and an additional 30.9 % had only "occasional" part-time jobs. Only a total of 2.6% of the patients were described as having "mostly full-time work" . When the patients life-long work adjustment was rated by the clinician, 28.7% were described as "never having worked" and an additional 34.6% of the patients had only "occasional" part-time work. Only 10.7% of the patients presenting to the ER were described as having had mostly full-time work throughout their lives.
Table 2 also contains data on the clinicians global rating on a 1-5 scale, of the patients recent (within the last three months) and life-long social, work, and family adjustment. As shown in the table, 69.1% of the patients were rated as having poor to extremely poor social adjustment within the past three months. Only 8% of the patients were rated as being moderately, or better, socially adjusted during this time period, 49.4% of the patients were rated as having a poor or extremely poor life-long social adjustment, and only 17.6% of the patients were rated as having moderately good, or better, life-long social adjustment.
As shown in the table, 56.3% of the patients were rated as having a poor or extremely poor current family adjustment. In our scale extremely poor family adjustment meant that the family was "totally alienated" and poor family adjustment meant that there were ~'severe" family difficulties (i.e., fighting all the time). Only 8.5 % of the patients were seen as having a moderately good, or
266
PSYCHIATRIC QUARTERLY
better, family adjustment. Ratings of the patient's life-long family adjustment indicate that 41.5 % of the patients were rated as having a poor to extremely poor family adjustment. Only 15.5 % of the patients were seen as having a moderately good to extremely good life-long family adjustment.
Treatment History
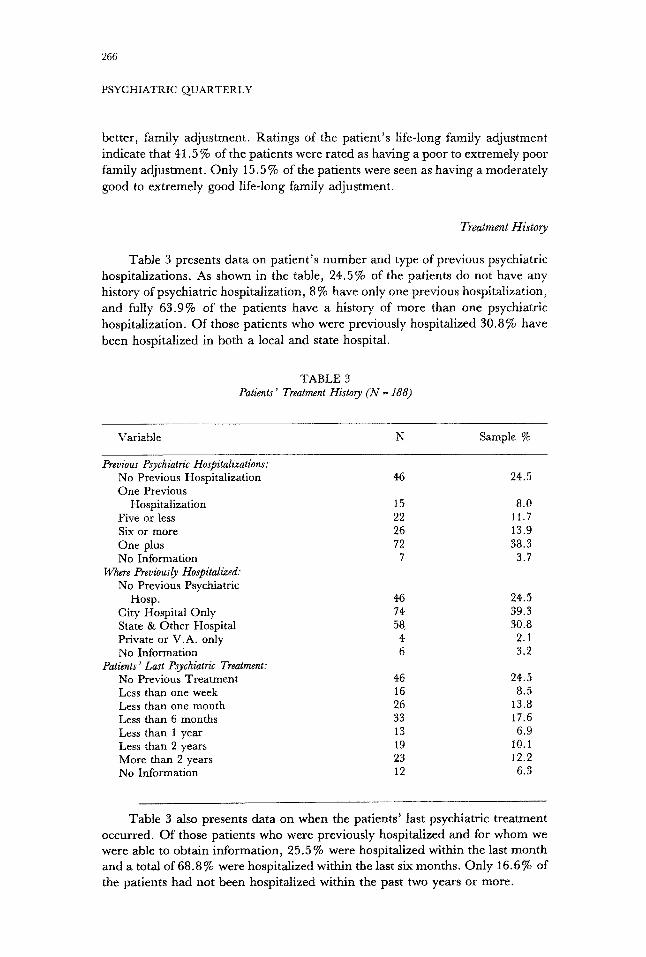
Table 3 presents data on patient's number and type of previous psychiatric hospitalizations. As shown in the table, 24.5% of the patients do not have any history of psychiatric hospitalization, 8 % have only one previous hospitalization, and fully 63.9% of the patients have a history of more than one psychiatric hospitalization. Of those patients who were previously hospitalized 30.8% have been hospitalized in both a local and state hospital.
TABLE 3 Patients' Treatment History ( N = 188)
Variable N Sample %
Previous Psychiatric Hospitalizations: No Previous Hospitalization 46 24.5 One Previous
Hospitalization 15 8.0 Five or less 22 11.7 Six or more 26 13.9 One plus 72 38.3 No Information 7 3.7
Where Previously Hospitalized." No Previous Psychiatric
Hosp. 46 24.5 City Hospital Only 74 39.3 State & Other Hospital 58 30.8 Private or V.A. only 4 2.1 No Information 6 3.2
Patients' Last Psychiatric Treatment: No Previous Treatment 46 24.5 Less than one week 16 8.5 Less than one month 26 13.8 Less than 6 months 33 17.6 Less than 1 year 13 6.9 Less than 2 years 19 10.1 More than 2 years 23 12.2 No Information 12 6.3
Table 3 also presents data on when the patients' last psychiatric treatment occurred. Of those patients who were previously hospitalized and for whom we were able to obtain information, 25.5 % were hospitalized within the last m o n t h and a total of 68.8% were hospitalized within the last six months. Only 16.6% of the patients had not been hospitalized within the past two years or more.
267
s. FRIEDMAN, et al.
Patient's Clinical Status and Coping Strategies
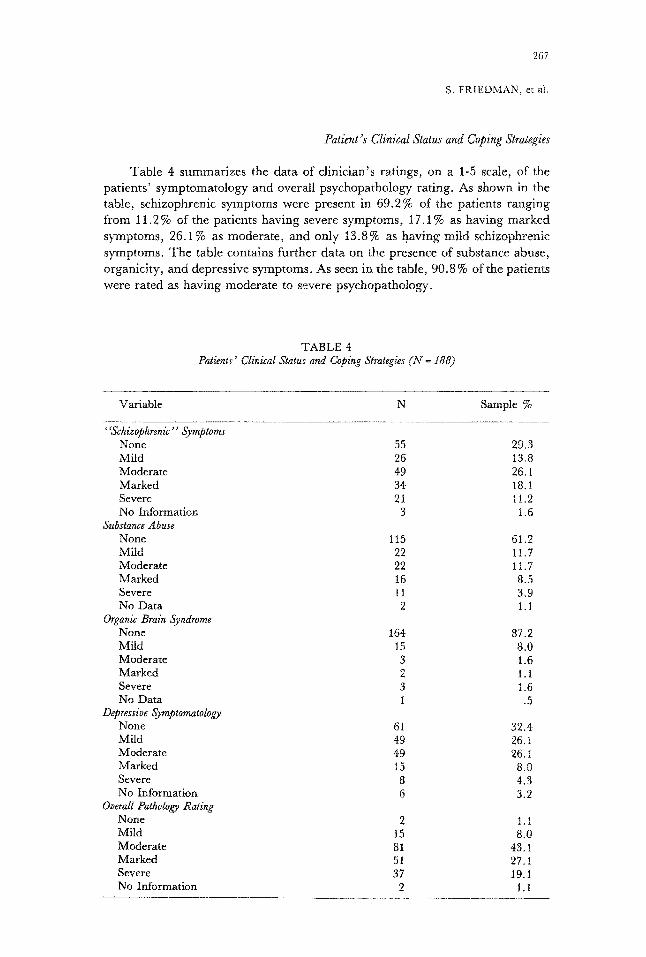
Table 4 summar izes the da ta of c l inic ian 's rat ings, on a 1-5 scale, of the pat ients ' symptomato logy and overall psychopathology rat ing. As shown in the table, schizophrenic symptoms were present in 69.2% of the pat ients ranging from 11.2 % of the pat ients having severe symptoms , 17.1% as having marked symptoms, 26.1% as modera te , and only 13.8% as having mi ld schizophrenic symptoms. The table contains fur ther da ta on the presence of substance abuse, organici ty , and depressive symptoms. As seen in the table, 90.8 % of the patients were ra ted as having modera te to severe psychopathology.
TABLE 4 Patients' Clinical Status and Coping Strategies (iV = ]88)
Variable N Sample %
"Schizophrenic" Symptorm None 55 29.3 Mild 26 13,8 Moderate 49 26.1 Marked 34 18.1 Severe 21 11.2 No Information 3 1.6
Substance Abuse None 115 6t.2 Mild 22 t t. 7 Moderate 22 11.7 Marked 16 8.5 Severe 11 3,9 No Data 2 1.1
Organic Brain Syndrome None 164 87.2 Mild 15 8.0 Moderate 3 1.6 Marked 2 1.1 Severe 3 1.6 No Data t .5
Depressive Symptomatology None 61 32.4 Mild 49 26.1 Moderate 49 26.1 Marked 15 8.0 Severe 8 4.3 No Information 6 3.2
Overall Pathology Rating None 2 t. 1 Mitd 15 8.0 Moderate 81 43.1 Marked 51 27.1 Severe 37 19. i No Information 2 1. i
268
PSYCHIATRIC QUARTERLY
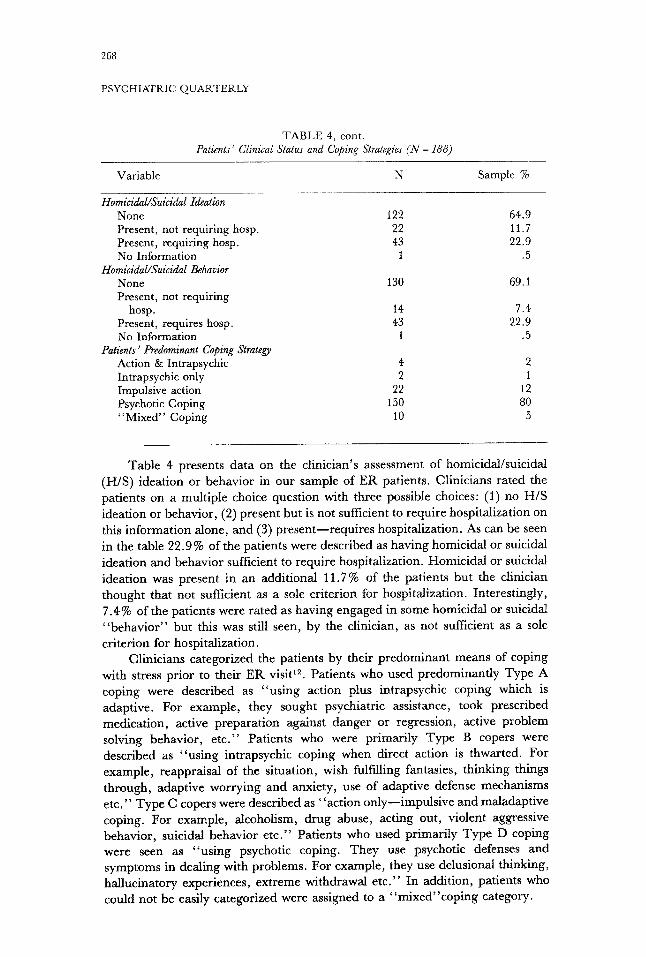
TABLE 4, cont. Patients' Clinical Status and Coping &rategies (iV = 188)
Variable N Sample %
Homicidal~Suicidal Ideation None 122 64.9 Present, not requiring hosp. 22 11.7 Present, requiring hosp. 43 22.9 No Information 1 .5
Homicidal~Suicidal Behavior None 130 69.1 Present, not requiring
hosp. 14 7.4 Present, requires hosp. 43 22.9 No Information 1 .5
Patients' Predominant Coping Strategy Action & Intrapsychic 4 2 Intrapsyehic only 2 1 Impulsive action 22 12 Psychotic Coping 150 80 "Mixed" Coping 10 5
Table 4 presents data on the clinician's assessment of homicidal/suicidal (H/S) ideation or behavior in our sample of ER patients. Clinicians rated the patients on a multiple choice question with three possible choices: (1) no H/S ideation or behavior, (2) present but is not sufficient to require hospitalization on this information alone, and (3) present--requires hospitalization. As can be seen in the table 22.9 % of the patients were described as having homicidal or suicidal ideation and behavior sufficient to require hospitalization. Homicidal or suicidal ideation was present in an additional 11.7% of the patients but the clinician thought that not sufficient as a sole criterion for hospitalization. Interestingly, 7.4% of the patients were rated as having engaged in some homicidal or suicidal "behavior" but this was still seen, by the clinician, as not sufficient as a sole criterion for hospitalization.
Clinicians categorized the patients by their predominant means of coping with stress prior to their ER visit 12. Patients who used predominantly Type A coping were described as "using action plus intrapsychic coping which is adaptive. For example, they sought psychiatric assistance, took prescribed medication, active preparation against danger or regression, active problem solving behavior, etc ." Patients who were primarily Type B copers were described as "using intrapsychic coping when direct action is thwarted. For example, reappraisal of the situation, wish fulfilling fantasies, thinking things through, adaptive worrying and anxiety, use of adaptive defense mechanisms etc." Type Ccopers were described as "action only--impulsive and maladaptive coping. For example, alcoholism, drug abuse, acting out, violent aggressive behavior, suicidal behavior e tc ." Patients who used primarily Type D coping were seen as "using psychotic coping. They use psychotic defenses and symptoms in dealing with problems. For example, they use delusional thinking, hallucinatory experiences, extreme withdrawn etc." In addition, patients who could not be easily categorized were assigned to a "mixed"coping category.
269
S. FRIEDMAN, etal.
As can be seen in Table 4 only 2 % (N = 4) of the patients were seen as using Type A (action and intrapsychic) coping, 1% (N =2) of the patients were described as Type B (intrapsychic only) copers, 12% (N = 22) were described as Type C (impulsive) copers, and fully 80% (N = 150) of the patients were seen as using primarily Type D (psychotic) coping. An additional 5% (N = 10) of the patients were categorized as "mixed" copers.
Clinicians were asked to obtain data on whether the patient made any attempt to "he lp" themselves prior to coming to the ER. It was found that 35.6% of the patients had actively sought "psychiatric assistance" prior to coming to the ER, 22.3% of the patients turned to their "family" for help, 13.8% of the patients took prescribed medication, 12.2% of the patients sought help from "other " professionals (non-mental health), 8 % of the patients turned to their friends, and 5.3% actively sought religious or spiritual help.
The primary diagnosis (ICD-9) of the patients indicated that 28.7% of our patients were diagnosed as schizophrenic paranoid type chronic, t8.1% as schizophrenic chronic undifferentiated, 6.9% as "o the r" schizophrenia, and 10.6% as acute schizophrenic episode. Only 8% of the patients were diagnosed as major affective disorder illness, 5.3% as neurotics, 5.9% as a personality disorder, 1.6% as adjustment reaction, 9.6% with a substance abuse diagnosis, and 3.7 % with Organic Brain Syndrome or Mental Retardation.
Admission Rate
In our sample 59 % of the patients who presented to the ER were admitted. We asked clinicians to explain their decision to admit and to mention the use of possible alternatives to hospitalization which were not present in our ER. Of the patients who were admitted (N = 1 t l ) , 13% were admitted by the clinician because the patient had no residence, 12% were admitted because of a "lack of supportive family," and 6 % were admitted because of need for placement (but not necessarily to a psychiatric hospital). Overall, 31% (N = 34) of the admissions could have been avoided, in the opinion of the admitting clinician, if alternative resources to hospitalization were present.
Predictors of Admission
An analysis of admission rate by sex of the patient, marital status, race, or age of the patient was not significant. The admission rate by shift varied from 50% of patients seen from 8 a.m. to 4 p.m. to a 70.3% admission rate for those patients seen during the 12 a. m. to 8 a.m. shift. The admission rate by time of arrival to the ER approached but was not significant (X 2 =4.43, p<2.10). The admission rate by clinician experience was evaluated. Attendants, who worked from 9 a.m. to 5 p.m. admitted 48.5% of the patients they saw. Residents, who worked all shifts and who carried the entire evening and weekend loads, admitted 61% of the patients they saw. This difference in admission rates approached significance ()~2 = 4.43, p <(. 10).
Admission rate by religious background of the patient was not significant. The admission rates ranged from 46.9% for Southern Baptists (N = 32) to 82.4% for patients who stated that they "had no religion" (N = 12). Similarly, the
270
PSYCHIATRIC QUARTERLY
overall admission rate by the patients living situation was not significant. However, the admission rate ranged from 37.5 % of patients who lived with their siblings (N = 16), to 52.5% of patients who lived by themselves (N =40), 63.2% of patients who lived with their spouse (N = 19), 72.1% of patients who lived with their parents, and 83.3 % of patients who were living in some agency (N = 6).
A breakdown of admission rate by the educational level of the patient was significant (X 2 = 6.0, p <.05). Of those patients who had less than a high school education (N = 114) 53.3% were admitted, as compared to 76.9% of patients with a high school degree (N = 26) and 69.2% of patients (N = 21) who had at least one year of post-high school education.
The breakdown of patients' admission rate by their means of arrival to the hospital was significant (X 2 = 30.12, p <.0001). The admission rate varied from 26.5% of the patients (N =49) who came to the ER alone, 68.4% of patients (N = 76) who were accompanied by their families, and 74.6 % of patients brought by the police or some other coercive agency (N = 59).
We also compared the patients' means of arrival by the clinicians overall rating of psychopathology. This comparison was highly significant (X 2 =23.6, p<.002). Basically, patients who came alone were rated as tess pathological then patients who came with their family or the police.
A breakdown of the admission rate by the patients' previous psychiatric treatment or hospitalization history was highly significant (X 2 =9.59, p<.002; X 2 = 7.85, p<.005). The expected finding was that patients with a history of either psychiatric treatment or hospitalization were more likely to be admitted.
The breakdown of admission rate by the patients' current social or work adjustment were both significant (X 2 =13.43, p<.02; X 2 =11.86, p<.04). The finding was that with decreasing social adjustment there was an increasing admission rate. For example, of patients with an "extremely poor" social adjustment, 69.4% were admitted, while only 16.7% of patients with a moderately good social adjustment were admitted. The trend for admission rates to increase with poorer life-long social adjustment was similar but non- significant. Similarly, with poor recent work and family adjustment there was an increase in the probability of admission. In addition, the pattern for admission rate by the patients' life-long work and family adjustment was similar. Better adjustment was associated with less hospitalization but this finding was non- significant.
A breakdown of admission rate by the patients' previous attempts to help themselves prior to coming to our ER was significant for seeking psychiatric help (X 2 = 4.78, p<.03), turning to "other professionals" (X 2 = 7.57, p <.005), turning to friends (X 2 =3.38, p<.06), and taking prescribed medication (X 2 =4.34, p<.04). For example, of patients who sought psychiatric assistance prior to coming to our ER 47.8% were admitted as compared to an admission rate of 65.3% for those patients who did not seek any psychiatric help. It was not significant for seeking "religious or spiritual help", or for turning to the family
for help. The breakdown of admission rate by the amount of depressive
symptomatology or organic brain syndrome was not significant. However, the breakdown of admission rate by schizophrenic symptomatology was significant
271
S. FRIEDMAN, et al.
(X 2 =47.23, p<.0001). The admission rate ranged from 23.6% of patients who had no schizophrenic symptoms to a 90.5% admission rate for patients with severe schizophrenic symptomatology. The breakdown of admission rate by substance abuse was also significant (X 2 =9.68, p<.05). The admission rate ranged from 50 % of patients with mild substance abuse to 72.7 % of patients with severe substance abuse. Finally, the admission rate by the patients overall pathology was significant (X 2 --33.73, p<.0001). It ranged from only 6.7% of patients with mild symptomatology being admitted to 83.8% of patients with severe psychopathology ratings being admitted.
An analysis of admission rate by the patient's predominant coping style was highly significant (X 2-- 18.12, p<.025). A 65.3% rate of patients who were categorized as basically "psychotic" copers were admitted. In comparison, 40.9% of impulsive or action-oriented copers were admitted, 30% of patients who were rated as "mixed" copers were admitted, and none (N =4) of the patients who used action and intrapsychic coping were admitted.
A breakdown of admission rate by the presence or absence of H/S ideation or behavior was significant (X 2 =30.78, p<.0001). Admission rate ranged from 40.9% of patients who exhibited some homicidal or suicidal ideation (the clinician felt that this information was not sufficient as a sole criterion for hospitalization), to 95.3% of patients whom the clinician felt that the homicidal or suicidal ideation was of sufficient magnitude to warrant admisison. At the same time it is interesting to note that of those patients who did not exhibit any homicidal or suicidal ideation (N =122) or homicidal or suicidal behavior (N =130) 49.2% and 49.7% were admitted (the overwhelming majority as involuntary patients) on some "other basis" besides homicidal/suicidal ideation or behavior.
As expected, the breakdown of admission rate by the primary diagnosis was highly significant (X 2 = 53.12, p<.0001). The admission rate ranged from 90 % of patients with a diagnosis of acute schizophrenic episode, 86.7 % of patients with a major affective illness, 77.8% of chronic schizophrenic, paranoid type, 44.1% of schizophrenics, chronic undifferentiated, 33.3 % of patients with an adjustment reaction or substance abuse diagnosis, 28.6% of organic brain syndrome or mental retardation, 18 % of character disorders, and on!y 10 % of patients with a neurotic diagnosis.
In looking at the family and community resources of patients who were admitted, we found that the patient's means of arrival interacted significantly with the clinicians' rating of alternatives to psychiatric hospitalization (X ~ = 31.7, p<.0001). Of patients who came alone to the hospital and were admitted (N = 18) the admitting clinician felt that 51% of them could have been kept out of the hospital if the patient had " a residence" (N = 6), supportive family (N = 3) or did not require placaement (N = 1) in a non-psychiatric hospital. Of patients who came with their family and were admitted (N = 50) the admitting clinician felt that 84 % needed psychiatric hospitalization in spite of a supportive family. Only 8 % of these patients were seen as needing placement in a non-psychiatric facility and an additional 8 % could have been kept out of the hospital if the family were "more supportive". Patients who were coerced into coming to the hospital a~.d were admitted (N = 39) showed a pattern similar to the patients who came alone.

272
PSYCHIATRIC QUARTERLY
The admitting clinician felt that 38 % of these patients could have been kept out of the hospital if they had a stable residence (N = 8), a supportive family (N = 6), or did not require placement (N = 1) in a non-psychiatric facility.
Further analysis of patients whose family were supportive but felt that they
could not manage the patient out of the hospital showed that these patients exhibited more schizophrenic symptoms (X 2 =53.51, p<.0001) than either patients who came alone or who were coerced into coming to the hospital. Similar findings occurred (X 2 = 33.64, p<.007) when one looked at these patients overall pathology rating. Basically, they were seen as more pathological than patients who came alone to the hospital. The most common primary diagnosis associated with these patients were schizophrenia, chronic paranoid type, schizophrenia chronic undifferentiated type, or acute schizophrenic episode.
DISCUSSION
In this paper the results of a one week survey of all the patients who presented to the psychiatric ER of a large general municipal hospital in an inner- city area were summarized. Various aspects of the patient population were studied to get some idea of demographic makeup, clinical picture, nature of coping styles, support systems, social, work and family adjustment and how they relate to admission rates for this particular sample.
As with other psychiatric ER studies¢.6 the sample contained more women than men, the overwhelming majority of patients were black, a relatively young patient population, and nearly all very poor. However, this patient population contains such a poverty stricken, poorly educated, and frequently out of work group as to be nearly unique. Only 11% of patients have held part or full-time jobs, and over 60% never finished high school. This type of patient population dearly requires, besides psychiatric care, that the essential needs of employment, social support, education, food, and shelter be provided. Until these essentials are met it will clearly affect our ability to provide adequate psychiatric care and the long-term prognosis of our patients?
A large percentage of our patients are born either outside the continental United States or in the southern U.S. These patients, most from rural areas, have different cultural values, beliefs and needs than the American-born inner- city dweller. Serving such a diverse patient population requires that the ER staff be particularly knowledgeable and flexible in working with the different cultural and ethnic groups.
While a substantial proportion of the patients have a history of previous psychiatric hospitalizations, and may be labeled chronic patients, another large percentage (24.5%) have never been psychiatrically hospitalized. Given an almost bi-modal distribution of chronic and "first break" patients, clinical services must be directed towards meeting the different needs of each group.
While many patients come to the hospital alone, and may live alone, over 61% of the patients do have someone they live with. Interestingly, patients who come to our ER with a family member have a higher admission rate than patients who come to our ER alone. This seems to indicate some agenda, sometimes hidden, on the part of the family to help hospitalize the pa t ien tY
273
S. FRIEDMAN, et ak
Our survey indicated that the bulk of the work in our ER is done between 8 a.m. and midnight. In fact, most patients get registered between 2 p .m. -8 p.m. Again having this information is important in deciding if and when to add staff in the ER. While the largest percentage of patients for each shift gets admitted from 12 a .m. -8 a.m. most of these patients are brought by the police and the addition of social service or other staff should have little effect on ihese admissions. However, the addition of a holding area or closer liaison with the police department appears warranted. Based partly on this data we have begun to make changes in the staffing pattern of our ER.
We also found that while a large percentage of the patients do show evidence of homicidal or suicidal ideation and behavior many of these patients do not get admitted. At the same time many patients who do not exhibit any such ideation or behavior are still admitted on some other basis. These patients highlight the fact that while an important part of the traditional/legal basis for the involuntary admission of patients to a psychiatric hospital is " d e a r and present danger to self or others", homicidal and suicidal ideation/behavior are not the sole criterion used by our admitting physicians. This interesting phenomenon needs more study 5,6
As in previous researchg,~l,13admission rates for residents were higher than those of attending psychiatrists. However, this finding was not statistically significant and is potentially biased since attendants worked weekday shifts from 8 a.m. to 4 p.m. while residents tended to do most of their work on evenings, nights and weekends.
Two of the most striking pieces of information collected in our study are the data on the totally inadequate coping styles 12 of our patients and their extremely poor family, work, and social adjustment. Given the severity of their illness and their limited financial and social resources, these patients are under extreme stress. ~* At the same time these patients have very limited means of coping with these problems. In fact we found that when patients do "seek help" prior to coming to the ER the admission rate was decreased. Again, programs which go beyond traditional diagnostic evaluations and treatment are needed to help our patients deal with their everyday stressesJS, I~
We can only speculate that the national policy of deinstitutionatization, while achieving the admirable goal of allowing patients to tive " in the community and in less restrictive environments", has failed in meeting the pressing and diverse needs of psychiatric patients. As our study has highlighted, the chronically ill patients need traditional psychiatric interventions as well as a much broader range of social, economic, and familial interventions. Clearly, our institution at the time of this study was not adequately meeting these needs. One can surmise that similar conditions exist in many other inner-city catchment areas.
Clearly, in our sample, traditional diagnostic and clinical evaluations seem to separate those patients who get admitted from those who do not. At the same time information about the patient 's social functioning, availability of community resources, and the patient 's typical ways of coping with stress also seem to separate those patients who get admitted from those who do not. Obviously, when one begins to plan programmatic changes in a psychiatric hospital and its treatment facilities and programs, data on these social, economic,
274
PSYCHIATRIC QUARTERLY
a n d fami ly sys tems should effect t r e a t m e n t p l a n n i n g . 1° For example , g iven the
e x t r e m e p o v e r t y and lack o f w o r k o u r pa t ien ts face, social and voca t iona l
r ehab i l i t a t ion gea red towards this a r ea b e c o m e s crucial . I n add i t ion , k n o w i n g
that so m a n y pa t ien ts who c o m e wi th the i r famil ies end up be ing a d m i t t e d should
have some b e a r i n g on the way we a p p r o a c h and work wi th these pat ients .
I n s u m m a r y , while o u r sample may- h a v e b e e n b iased towards a v e r y ill,
i m p o v e r i s h e d popu la t i on , the f ind ing tha t the soc io -economics o f m e n t a l hea l th
m u s t be stressed is still v iable . T r a d i t i o n a l d iagnos t ic and t r e a t m e n t
cons ide ra t ions h a v e a p lace in the E R bu t the pa t i en t ' s suppor t systems, cop ing
m e c h a n i s m s , life crises, social a d j u s t m e n t , and the role o f the fami ly and
c o m m u n i t y m u s t be fu r the r s tudied. T h e s e a re i m p o r t a n t var iab les in
m a i n t a i n i n g the m e n t a l hea l th o f pa t ien ts and impacts on the dec is ion r e g a r d i n g
admiss ion .
R E F E R E N C E S
1. Schwartz MD, Errera P: Psychiatric care in a general hospital emergency room: II. Diagnostic features. Arch Gen Psychiat 9:113-121, 1963.
2. Gross HS, Herbert MR, Knatterud GL, Donner L: The effect of race and sex on the variation of diagnosis and disposition in a psychiatric emergency room. J Nerv Ment Dis 148:638-642, 1969.
3. Bauer SF, Balter L: Emergency psychiatric patients in a municipal hospital--Demographic, clinical, and dispositional characteristics. Psychiat Q 45:382-393, 197I.
4. Huffine C, Craig T: Social factors in the utilization of an urban psychiatric emergency service. Arch Gen Psychiat 30:249-255, 1974.
5. Rose SO, Hawkins J: Decision to admit. Arch Gen Psychiat 34:418-421, 1977. 6. Hanson GD, Babigian HM: Reasons for hospitalization from a psychiatric emergency room
service. Psychiat Q3:336-351, 1974. 7. Tischler GL: Decision-making process in the emergency room. Arch Gen P~ychial 14:69-78, 1966. 8. Grosz HJ, Grossman KG: Clinician's response style: A source of variation and bias in clinical
judgments. JAbnorm Psychol 73:207-214, 1968. 9. Streiner DL, Goodman JT, Woodward CA: Correlates of the hospitalization decision: A
replicative study. CanJ Pub Health 66:411-415, 1975. 10. Gerson S, Bassuk E: Psychiatric emergencies: An overview. Am J Psychiat 137:I-11, 1980. 11. Feigelson EB, Davis EB, Mackinnon R, Shands HC, Schwartz CC: The decision to hospitalize.
Arn J Psychiat 135:354-357, 1978. 12. Lazarus RS, Averill JR, Opton EM: The psychology of coping: Issues of research and
assessment. In GV Coelho, D Hamburg, JE Adams (eds): Coping and Adaptation New York, Basic Books, 1974.
13. Meyerson AT, Moss JZ, Belville R, Smith H: Influence of experience on major clinical decisions. Arch Gen Psychiat 36:423-427, 1979.
14. Plutchik R, Hyman I, Conte H, Karasu TB: Medical symptoms and life stresses in psychiatric emergency room patients. JAbnorm Psychol 86:447-449, 1977.
15. Beels CC: Social networks, the family, and the schizophrenic patient: Introduction to the issue. Schiz Bull 4:5t2-521, 1978.
16. Hammer, M, Makiesky-Barrow S, Gutwinth L: Social networks and schizophrenia. Schiz Bull 4:522-545, 1978.




















