Daily Automated Telephone Assessment and Intervention Improved 1-Month Outcome in Paroled Offenders
19
http://ijo.sagepub.com/ Criminology Therapy and Comparative International Journal of Offender http://ijo.sagepub.com/content/early/2014/03/11/0306624X14526800 The online version of this article can be found at: DOI: 10.1177/0306624X14526800 published online 13 March 2014 Int J Offender Ther Comp Criminol Berglund Claes Andersson, Zoran Vasiljevic, Peter Höglund, Agneta Öjehagen and Mats 1-Month Outcome in Paroled Offenders Daily Automated Telephone Assessment and Intervention Improved Published by: http://www.sagepublications.com can be found at: Criminology International Journal of Offender Therapy and Comparative Additional services and information for http://ijo.sagepub.com/cgi/alerts Email Alerts: http://ijo.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://ijo.sagepub.com/content/early/2014/03/11/0306624X14526800.refs.html Citations: What is This? - Mar 13, 2014 OnlineFirst Version of Record >> at Karolinska Institutets Universitetsbibliotek on March 16, 2014 ijo.sagepub.com Downloaded from at Karolinska Institutets Universitetsbibliotek on March 16, 2014 ijo.sagepub.com Downloaded from
Transcript of Daily Automated Telephone Assessment and Intervention Improved 1-Month Outcome in Paroled Offenders
http://ijo.sagepub.com/Criminology
Therapy and Comparative International Journal of Offender
http://ijo.sagepub.com/content/early/2014/03/11/0306624X14526800The online version of this article can be found at:
DOI: 10.1177/0306624X14526800
published online 13 March 2014Int J Offender Ther Comp CriminolBerglund
Claes Andersson, Zoran Vasiljevic, Peter Höglund, Agneta Öjehagen and Mats1-Month Outcome in Paroled Offenders
Daily Automated Telephone Assessment and Intervention Improved
Published by:
http://www.sagepublications.com
can be found at:CriminologyInternational Journal of Offender Therapy and ComparativeAdditional services and information for
http://ijo.sagepub.com/cgi/alertsEmail Alerts:
http://ijo.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://ijo.sagepub.com/content/early/2014/03/11/0306624X14526800.refs.htmlCitations:
What is This?
- Mar 13, 2014OnlineFirst Version of Record >>
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
International Journal ofOffender Therapy and
Comparative Criminology 1 –18
© The Author(s) 2014Reprints and permissions:
sagepub.com/journalsPermissions.nav DOI: 10.1177/0306624X14526800
ijo.sagepub.com
Article
Daily Automated Telephone Assessment and Intervention Improved 1-Month Outcome in Paroled Offenders
Claes Andersson1, Zoran Vasiljevic1, Peter Höglund2, Agneta Öjehagen2, and Mats Berglund2
AbstractThis randomized trial evaluates whether automated telephony could be used to perform daily assessments in paroled offenders (N = 108) during their first 30 days after leaving prison. All subjects were called daily and answered assessment questions. Based on the content of their daily assessments, subjects in the intervention group received immediate feedback and a recommendation by automated telephony, and their probation officers also received a daily report by email. The outcome variables were analyzed using linear mixed models. The intervention group showed greater improvement than the control group in the summary scores (M = 9.6, 95% confidence interval [CI] = [0.5, 18.7], p = .038), in mental symptoms (M = 4.6, CI = [0.2, 9.0], p = .042), in alcohol drinking (M = 0.8, CI = [0.1, 1.4], p = .031), in drug use (M = 1.0, CI = [0.5, 1.6], p = .000), and in most stressful daily event (M = 1.9, CI = [1.1, 2.7], p = .000). In conclusion, automated telephony may be used to follow up and to give interventions, resulting in reduced stress and drug use, in paroled offenders.
KeywordsInteractive Voice Response (IVR), brief intervention, paroled offenders, stress, mental symptoms, substance use
Introduction
The Prison and Probation Services are responsible for reducing recidivism in con-victed criminals. In Sweden, about 23,000 sentences are passed every year. Of those
1Malmö University, Sweden2Lund University, Sweden
Corresponding Author:Claes Andersson, Department of Criminology, Malmö University, 205 06 Malmö, Sweden. Email: [email protected]
526800 IJOXXX10.1177/0306624X14526800International Journal of Offender Therapy and Comparative CriminologyAndersson et al.research-article2014
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
2 International Journal of Offender Therapy and Comparative Criminology
who have been convicted in some way, about a quarter commit a new crime within 1 year and about half commit a new crime within 3 years (Langan & Levin, 2002; Swedish National Council for Crime Prevention, 2007; Wallman, 2005). Recidivism varies greatly, with the highest rates found in paroled offenders, where about two out of five commit a new crime within 1 year (Swedish National Audit Office, 2004). The risk of committing a new crime or violating the terms of parole is greatest in the first days, weeks, and months after release (National Research Council, 2008).
It is obviously important to develop methods that facilitate the re-entry process. Effective or promising interventions may either reduce the actual rates of recidivism or improve associated variables (National Research Council, 2008; Seiter & Kadela, 2003), where the latter approach is based on the assumption that rehabilitation of basic strengths helps to reduce criminality (Ward, Yates, & Willis, 2012). Variables associ-ated with crime and recidivism in crime have been divided into static risk factors such as criminal history and family background, and dynamic risk factors, which change over time, where acute dynamic factors reflect immediate situations or circumstances and/or immediate emotional states that may change almost instantaneously (Andrews & Bonta, 2010; Zamble & Quinsey, 1997).
In a recent study, the re-entry process was defined as a stressful event, where a sometimes overwhelmingly positive feeling at release was soon followed by events that resulted in difficulties such as substance abuse cravings and practical problems (Phillips & Lindsay, 2011). Stress has been identified as an acute dynamic risk factor for crime and criminal recidivism, both according to classical strain theories (Merton, 1938), and the more recent coping-relapse model of criminal recidivism (Zamble & Quinsey,1997), and in the Risk-Need-Responsibility (RNR) model of correctional assessment (Andrews & Bonta, 2010). Stress is defined as an unspecific reaction, which is activated by either a threat or a demand (Morse, 1998), and that often results in an anxious or depressive emotional response sometimes recognized as the fight-or-flight response, and which is managed through various types of either adaptive or maladaptive coping strategies (Everly & Lating, 2002; Gelder, Harrison, & Cowen, 2006). Substance use and craving for substances has also been defined as an acute dynamic risk factor for criminal recidivism (Andrews & Bonta, 2010), and are often also considered as a common maladaptive strategy to cope with stress (al’Abusi, 2007).
It has been argued that static risk factors are important in designing initial treatment intensity, but that they have no practical value when attempting to direct and monitor the re-entry process. Only dynamic risk factors can be subject to interventions that may result in reduced risk of committing a new crime (Andrews & Bonta, 2010; Hansson & Harris, 2000; Zamble & Quinsey,1997). However, the work of the correc-tional officers is mainly based on static data and not on dynamic data (Jones, Brown, & Zamble, 2010), and their work situation is associated with a significant workload and difficulties in keeping up with their work (Finney, Stergiopoulos, Hensel, Bonato, & Dewa, 2013), which further restricts their ability to monitor daily changes in their clients as well as their possibility to offer appropriate interventions based on these results.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 3
Cognitive relapse prevention is a well-known technique for reducing the likelihood and severity of relapse following the cessation or reduction of problematic behaviors, including substance abuse (Carroll, 1996; Irvin, Bowers, Dunn, & Wang, 1999), depression (Katon et al., 2001), and sexual offending (Barnett, Manderville-Norden, & Rakestrow, 2014). The intervention is designed to strengthen the individual’s ability to handle high-risk situations, such as stressful events that often arise without warning, and where attempts to refrain from a particular behavior are threatened (Witkiewitz & Marlatt, 2004). Brief cognitive interventions, which in the shortest version only include assessment of the targeted behavior and clear and direct feedback that helps the individual to increase risk awareness and to think differently about the problematic behavior, have been used successfully as counselor-supported interventions in the field of substance abuse (Hendershot, Witkiewitz, George, & Marlatt, 2011; White et al., 2010). Automated interventions using pre-programmed computerized scripts and various technologies have also been found to have potential to support behavior change (Kennedy et al., 2012; Webb, Joseph, Yardley, & Michie, 2010).
A possible way to implement the concept of dynamic risk factors in the Prison and Probation Services might be automated telephony, which is a well-established technol-ogy where a central computer is programmed to use pre-programmed scripts in inter-action with the user via their own mobile telephone handset (Corkrey & Parkinson, 2002). This technology has been used to study the interaction mood and behavior (Gee, Coventry, & Birkenhead, 2005), for screening and short interventions (Corkrey, Parkinson, & Bates, 2005), after-care and case management (Hall & Huber, 2000; Lee, Friedman, Cukor, & Ahern, 2003), and to understand and avoid relapse after treatment (Kaminer, Litt, Burke, & Burleson, 2006; Mundt, Moore, & Bean, 2006). As mobile phones are carried and used daily in all kinds of groups in most countries, including in Sweden marginalized groups such as drug users (Hakansson, Isendahl, Wallin, & Berglund, 2011), automated telephony enables assessment and interventions on psy-chosocial factors in everyday life. Furthermore, it could generate reports for the treat-ment provider who can then evaluate treatment results and improve decisions on individual need of care.
Electronic monitoring has been used to reduce recidivism (Bulman, 2010). Recently, automated telephony successfully reduced criminal recidivism in juvenile probation-ers who had completed an extensive cognitive intervention program. The system was used twice daily during the year following treatment, to monitor how well the proba-tioners were accomplishing their goals, and to congratulate them when they were mak-ing progress or to encourage them if they were struggling (Burraston, Bahr, & Cherrington, 2013; Burraston, Cherrington, & Bahr, 2012).
This study investigates whether automated telephony can be used within the Prison and Probation Services to systematically monitor acute dynamic risk factors, including stress, symptoms of anxiety and depression, and use of, as well as craving for, alcohol and drugs in general paroled offenders during 30 consecutive days following proba-tion. The study also investigates the effects of a brief cognitive intervention based on the trend (positive, negative, or no change) for the summary scores of these daily assessments. The intervention includes both an automated immediate feedback and a
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from

4 International Journal of Offender Therapy and Comparative Criminology
recommendation to the paroled offender, and a daily report sent to the probation offi-cer by email; these can be used to evaluate the treatment results and improve decisions on individual need of care.
To the best of our knowledge, this is the first study in general paroled offenders who uses automated telephony to monitor and intervene on the daily development of acute dynamic risk factors associated with criminal recidivism. As the intervention is auto-mated and not person-dependent, it could easily be implemented in the Prison and Probation Service, either as a stand-alone intervention or in combination with other efforts to reduce criminal recidivism.
Method
Study Design
This study was a randomized trial (Altman, 1990; Lewis-Beck, Bryman, & Liao, 2004) using automated telephony in a population of general paroled offenders, who were recruited and allocated to two groups while still in prison. In both groups, acute dynamic risk factors were monitored by daily assessments during 30 consecutive days following probation. In addition to these assessments, parolees in the intervention group received daily feedback, including recommendations based on the results of these assessments, and their correctional officers received a daily report on their cli-ent’s progress. The feedback and the email report were not given to those in the control group, meaning that the feedback and the email report were the only difference between the two groups. For both groups, each call ended with a brief reminder about the next scheduled call.
Organization: The Swedish Prison and Probation Service
The Swedish Prison and Probation Service are divided into six geographic regions. Participants were recruited from a total of 13 open and closed prisons, all of the 9 prisons in the Southern region and 4 of the 6 in the Eastern region. The prisons have about 96% of all available places in these two regions. There was no difference between offenders at the included and excluded prisons. During imprisonment, the participants often serve time at different prisons before being paroled. Prison and pro-bation office are independent, and there is no nesting on parole office and prison. Offenders were paroled to 30 different probation offices out of a total of 34 probation offices in Sweden, 11 out of 12 in the South and East region, and 19 out of 22 in the other four regions. Paroled offenders often change parole office or parole officer. The current study involved 93 probation officers, 49 in the South and East region, and 44 in other regions.
Recruitment
Participants were recruited from the Swedish Prison and Probation Service between December 2009 and August 2010. Eligible participants were all paroled offenders,
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 5
serving both short and extended sentences, leaving prison on probation that included contact with a defined probation officer assigned by the Swedish Prison and Probation Services in the region where the participant lives. It is mandatory procedure to provide supervision of paroled offenders, but without any additional intervention such as intensive supervision with electronic monitoring or in-patient care at a health and rehabilitation clinic. All participants needed to be sufficiently fluent in Swedish, and able to register their own telephone number no later than the date of parole. In Sweden, paroled offenders include sentences of a minimum of 1-month imprisonment.
At each prison, assigned personnel were responsible for identifying all potential offenders about to leave prison on probation, and these offenders were scheduled to take part in regular individual or group meetings with the researcher before they left prison. After giving informed consent to the study, each offender took part in pre-assessments by calling the project’s central computer to register their mobile telephone number and date of probation. In this pre-assessment, they responded to the same questions that were used later in their follow-up calls. Offenders who were willing to participate, but could not provide a mobile telephone number, were given the opportu-nity to complete their registration with a telephone number before the day of parole. When the parole had finally been confirmed and a probation officer assigned by the probation services, the researcher informed each individual probation officer by email about the participation and the study procedures, including email reports for those assigned to the intervention group. This part of the study could not be blinded, because some probation officers were assigned to receive daily reports on their client’s progress.
The report sent to the probation officer did not include any information that could possibly result in any adverse action toward the paroled offender, and the offender was carefully informed about this when agreeing to participate.
All study procedures were approved by the regional research ethics committee, and all participants signed informed consent forms, including information that the partici-pating offender could withdraw consent at any time, and that such withdrawal would result in their assessments being excluded.
Assessment
The central computer was programmed to perform one daily telephone assessment for each participant, starting the day after probation and continuing for 30 consecutive days. The central computer was programmed to perform two attempts to reach the participant every hour between noon and 9.00 p.m.
The first assessment after parole started with a brief reminder of the project, and the last assessment ended by thanking the subject for participation in the study. Assessment procedures were otherwise designed to be very short, thereby minimizing the time consumed for each respondent. For example, all scales were constructed in a standard-ized way, and only a single tap on the telephones keys was needed to respond to each question. Furthermore, there was no need for the responder to listen through the entire question with its response alternatives before responding. As mobile phones are
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from

6 International Journal of Offender Therapy and Comparative Criminology
generally considered to be personal, the calls did not include a confirmation of the respondent’s identity, but personal code had to be given before entering responses.
Pre-assessment at prison and daily assessments during 30 consecutive days after parole involved a total of 21 items. Stress was measured with the Arnetz and Hasson stress questionnaire (AHSS), which involves seven items measuring common indices of stress, such as current health status, quality of sleep, life control, and ability to con-centrate (Andersson, Johnsson, Berglund, & Öjehagen, 2009). In this study, the Cronbach’s alpha coefficient ranged between .76 and .96, compared with .79 in the original study. The eight-item dichotomized version of the Symptoms Check List (SCL-8D; Fink et al., 1995) was used to assess symptoms of anxiety and depression. The Cronbach’s alpha coefficient ranged between .91 and .97, compared with .80 in the original study. Daily reports of craving for alcohol and drugs were assessed by using two items adopted from the Alcohol Urge Questionnaire (Bohn, Krahn, & Staehler, 1995), assessing current urge on a scale ranging from not at all to a large extent. Current use was then assessed by simply asking whether the offender had drunk alcohol or used any drugs the previous day. The respondent then rated the inten-sity of consumption on a scale from zero to very high. Finally, Daily Assessment of Daily Experience (Stone & Neale, 1982) was used, where the participant was asked to make a voice recording, maximum 30 s, about their most stressful daily event, and then rate the severity of this event on a scale ranging from not at all to very severe. In this article, severity but not type of most stressful event is reported. Type of stressful events will be presented in a separate article. SCL-8D was regarded as the primary outcome, and other measures were regarded as secondary outcomes. The reason for this is that the present intervention is primarily aimed at reducing stress, the items included in SCL-8D are well-documented, and the emotions measured by the instru-ment is commonly regarded as a stress response (Everly & Lating, 2002).
All questions used in this study were rated on a 10-digit scale, ranging from 0 (negative) to 9 (positive). This means that a low score was considered as less favorable for all variables, including substance use and substance urges, and that improvements should result in higher scores. With the exception of the rating of most stressful event, the remaining 19 questions were summarized to a total scale ranging from 0 (maxi-mum negative) to 171 points (maximum positive). The total figure was used for feed-back to the paroled offender as well as in reports to the parole officer. The psychometric properties of the total scale have been evaluated, and the Cronbach’s alpha coefficient for the complete scales ranged between .89 and .98.
Randomization
At pre-assessment, the central computer was programmed to generate a 1:1 random allo-cation sequence using a fixed-block size of 10 to ensure balanced study arms. If the paroled offender received feedback, including recommendation, at the end of the first assessment after parole, they knew the group to which they had been assigned. The con-trol group received no such feedback. This means that the study was blinded to all offend-ers until the end of their first assessment after parole, when some of the offenders received a feedback based on their responses; this could not be blinded to the participants.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 7
Intervention
Immediately after the daily assessments, brief feedback was given by the automated telephone system, including a recommendation to the paroled offender. At the same time, an email report was sent to the probation officer responsible for each specific offender, according to the information provided to the probation officer at recruitment.
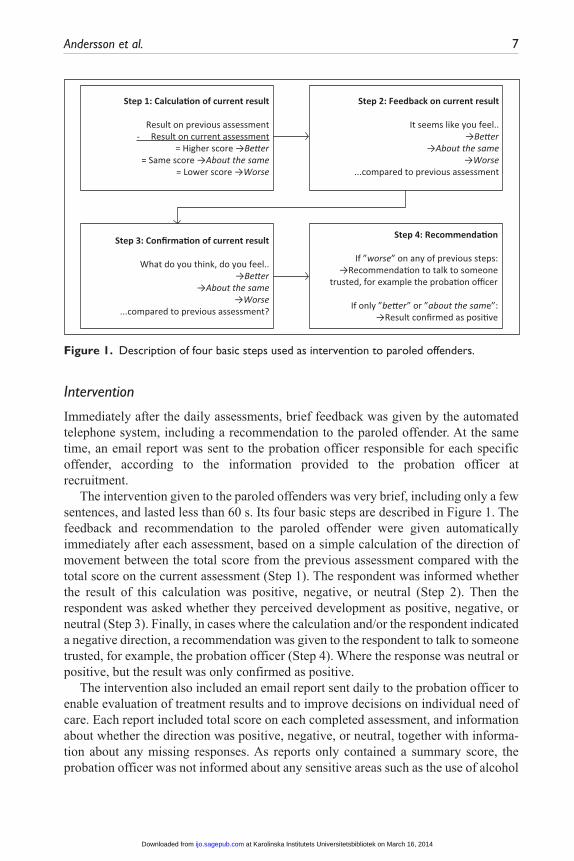
The intervention given to the paroled offenders was very brief, including only a few sentences, and lasted less than 60 s. Its four basic steps are described in Figure 1. The feedback and recommendation to the paroled offender were given automatically immediately after each assessment, based on a simple calculation of the direction of movement between the total score from the previous assessment compared with the total score on the current assessment (Step 1). The respondent was informed whether the result of this calculation was positive, negative, or neutral (Step 2). Then the respondent was asked whether they perceived development as positive, negative, or neutral (Step 3). Finally, in cases where the calculation and/or the respondent indicated a negative direction, a recommendation was given to the respondent to talk to someone trusted, for example, the probation officer (Step 4). Where the response was neutral or positive, but the result was only confirmed as positive.
The intervention also included an email report sent daily to the probation officer to enable evaluation of treatment results and to improve decisions on individual need of care. Each report included total score on each completed assessment, and information about whether the direction was positive, negative, or neutral, together with informa-tion about any missing responses. As reports only contained a summary score, the probation officer was not informed about any sensitive areas such as the use of alcohol
Step 1: Calcula�on of current result
Result on previous assessment- Result on current assessment
= Higher score →Be�er= Same score →About the same
= Lower score →Worse
Step 2: Feedback on current result
It seems like you feel..→Be�er
→About the same→Worse
...compared to previous assessment
Step 3: Confirma�on of current result
What do you think, do you feel..→Be�er
→About the same→Worse
...compared to previous assessment?
Step 4: Recommenda�on
If ”worse” on any of previous steps:→Recommenda�on to talk to someone
trusted, for example the proba�on officer
If only ”be�er” or ”about the same”:→Result confirmed as posi�ve
Figure 1. Description of four basic steps used as intervention to paroled offenders.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from

8 International Journal of Offender Therapy and Comparative Criminology
and drugs. No data were collected on whether the probation officers actually read the daily reports.
Statistical Analysis
SPSS version 20 was used in all the statistical calculations. Descriptive statistics are presented as mean (SD) for continuous variables and as counts for categorical data. The study was randomized, but some subjects withdrew their consent before the inter-vention/control period. Baseline characteristics of subjects who were included and excluded from the final sample, as well of the participating subjects in the intervention group and the control group, were compared using Mann–Whitney tests for continu-ous variables and Fisher’s exact test for categorical variables. The outcome variables were analyzed using repeated measures linear mixed-growth model, where group (intervention vs. control) and day were entered as fixed effects and subjects as random effect (intercept). Treatment of missing data is also included in this program. For repeated measurements, an autocorrelation structure of order 1 was pre-specified, as we used a linear mixed-growth model with repeated measurements over 30 days and with one measurement each day, that is, equidistant measures. Furthermore, partici-pants remember their response from the preceding day. In addition, we expected only small changes from rather high initial values and so we assume a homoskedastic cova-riance structure.
Participants
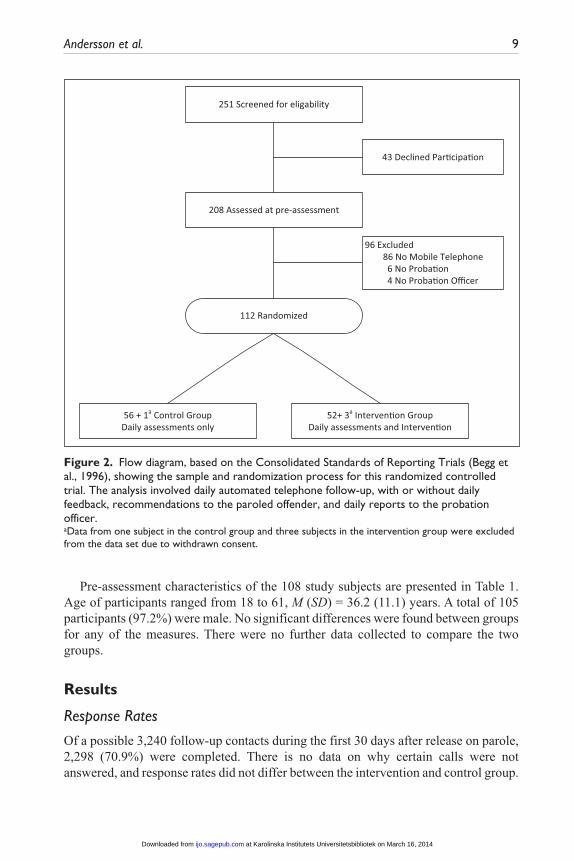
As shown in Figure 2, 251 offenders were screened for eligibility, of which 43 (17%) declined participation, and 208 were assessed at pre-assessment. Attrition analysis was not possible because data were not collected on those who declined participation. However, clients who rejected participation did so when someone else at the same group meeting had already expressed unwillingness to participate. The most common reason cited by clients who did not want to participate was that they wanted to have as little contact as possible with the Prison and Probation Services after their parole.
Ninety-three were excluded for not fulfilling the eligibility criteria. The remaining 112 participants were randomized to two groups: one group has to be simply moni-tored for 30 days after probation, and the other has to be monitored and receive inter-ventions. Four offenders, one in the control group and three in the intervention group, withdrew consent, stating that the monitoring was too intense and therefore experi-enced as an adverse event. These withdrawals were excluded from the data set accord-ing to informed consent approved by the institutional board. The final sample included a data set with 108 paroled offenders.
At pre-assessment, the 93 subjects who were excluded for not fulfilling the eligibil-ity criteria reported less positive scores on the urge to consume drugs item (6.1 ± 3.4 vs. 7.2 ± 2.8, p = .028), on the AHSS scale (37.6 ± 11.9 vs. 40.9 ± 11.7, p = .045), and on the total scale (112.8 ± 30.4 vs. 120.7 ± 31.1, p = .042), compared with the 108 subjects included in the final sample. There was no difference on the other scales, or in age and gender.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 9
Pre-assessment characteristics of the 108 study subjects are presented in Table 1. Age of participants ranged from 18 to 61, M (SD) = 36.2 (11.1) years. A total of 105 participants (97.2%) were male. No significant differences were found between groups for any of the measures. There were no further data collected to compare the two groups.
Results
Response Rates
Of a possible 3,240 follow-up contacts during the first 30 days after release on parole, 2,298 (70.9%) were completed. There is no data on why certain calls were not answered, and response rates did not differ between the intervention and control group.
251 Screened for eligability
208 Assessed at pre-assessment
43 Declined Par�cipa�on
112 Randomized
96 Excluded86 No Mobile Telephone
6 No Proba�on4 No Proba�on Officer
56 + 1a Control GroupDaily assessments only
52+ 3a Interven�on GroupDaily assessments and Interven�on
Figure 2. Flow diagram, based on the Consolidated Standards of Reporting Trials (Begg et al., 1996), showing the sample and randomization process for this randomized controlled trial. The analysis involved daily automated telephone follow-up, with or without daily feedback, recommendations to the paroled offender, and daily reports to the probation officer.aData from one subject in the control group and three subjects in the intervention group were excluded from the data set due to withdrawn consent.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
10 International Journal of Offender Therapy and Comparative Criminology
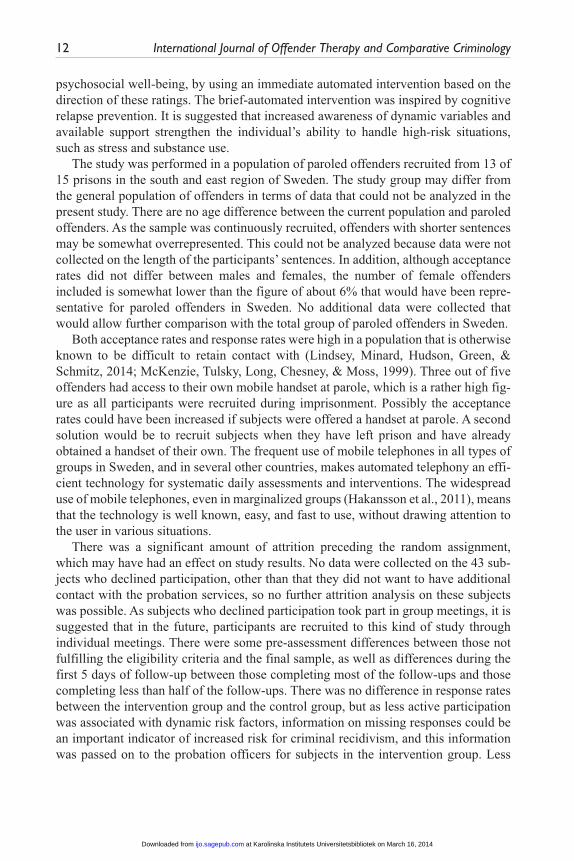
On average, offenders completed 21.3 (SD = 10.4) follow-up interviews after parole. Twenty-eight (25.9%) of the offenders participated in all the follow-up interviews and another 15 (13.9%) offenders completed all but one telephone interview. A total of 79 (73.1%) completed at least half of the telephone follow-ups. These 79 offenders com-pleted on average 27.3 (SD = 3.5) follow-ups, compared with 5.6 (SD = 3.9) in the remaining 29 offenders.
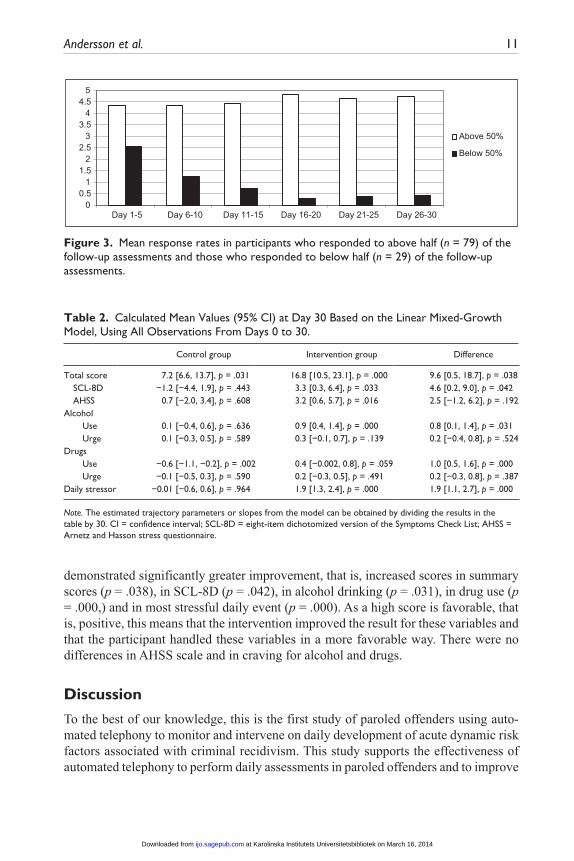
Figure 3 shows mean response rates after parole for those completing more than and less than half of the assessments. The 79 subjects who responded to more than half of the follow-ups had stable high response rates throughout the follow-up period, while mean response rates declined in the other group.
There was no difference between the two groups at pre-assessment, while the 29 individuals who responded to less than half of the follow-ups had less favorable scores. Their lower scores indicated a more negative outcome: the first 5 days after parole for SCL-8D (45.3 ± 19.8 vs. 56.9 ± 15.3, p = .006), alcohol use (5.6 ± 2.8 vs. 7.5 ± 1.7, p = .004), alcohol urge (5.9 ± 3.1 vs. 8.1 ± 1.6, p = .001), drug use (6.5 ± 2.9 vs. 8.1 ± 1.5, p = .002), drug urge (6.1 ± 2.7 vs. 8.0 ± 1.5, p = .001), and on the total scale (112.1 ± 39.2 vs. 136.9 ± 30.4, p = .004) compared with those responding to more than half of the follow-ups. No further data were collected that would allow comparison between the two groups.
Intervention Effect
The predicted mean scores at Day 30 for the control group and for the intervention group are shown in Table 2. Compared with the control group, the intervention group
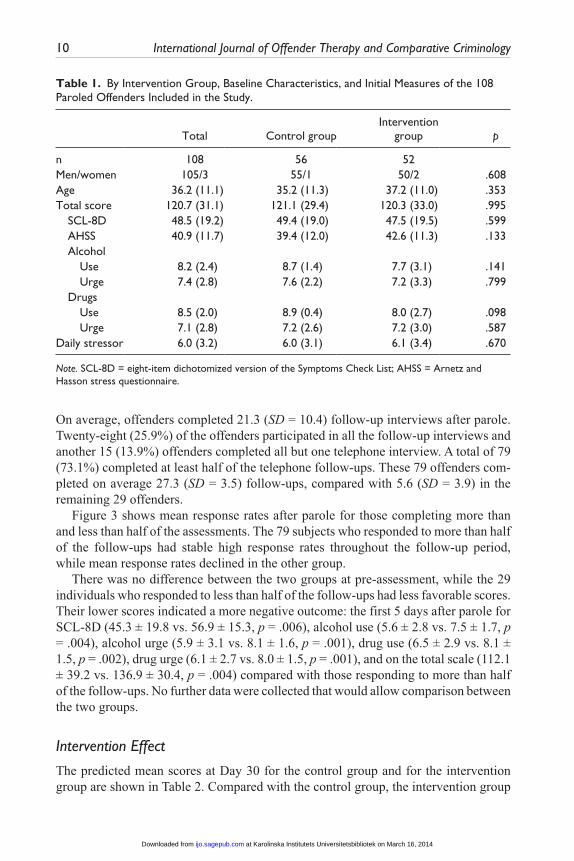
Table 1. By Intervention Group, Baseline Characteristics, and Initial Measures of the 108 Paroled Offenders Included in the Study.
Total Control groupIntervention
group p
n 108 56 52 Men/women 105/3 55/1 50/2 .608Age 36.2 (11.1) 35.2 (11.3) 37.2 (11.0) .353Total score 120.7 (31.1) 121.1 (29.4) 120.3 (33.0) .995 SCL-8D 48.5 (19.2) 49.4 (19.0) 47.5 (19.5) .599 AHSS 40.9 (11.7) 39.4 (12.0) 42.6 (11.3) .133 Alcohol Use 8.2 (2.4) 8.7 (1.4) 7.7 (3.1) .141 Urge 7.4 (2.8) 7.6 (2.2) 7.2 (3.3) .799 Drugs Use 8.5 (2.0) 8.9 (0.4) 8.0 (2.7) .098 Urge 7.1 (2.8) 7.2 (2.6) 7.2 (3.0) .587Daily stressor 6.0 (3.2) 6.0 (3.1) 6.1 (3.4) .670
Note. SCL-8D = eight-item dichotomized version of the Symptoms Check List; AHSS = Arnetz and Hasson stress questionnaire.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 11
demonstrated significantly greater improvement, that is, increased scores in summary scores (p = .038), in SCL-8D (p = .042), in alcohol drinking (p = .031), in drug use (p = .000,) and in most stressful daily event (p = .000). As a high score is favorable, that is, positive, this means that the intervention improved the result for these variables and that the participant handled these variables in a more favorable way. There were no differences in AHSS scale and in craving for alcohol and drugs.
Discussion
To the best of our knowledge, this is the first study of paroled offenders using auto-mated telephony to monitor and intervene on daily development of acute dynamic risk factors associated with criminal recidivism. This study supports the effectiveness of automated telephony to perform daily assessments in paroled offenders and to improve
00.5
11.5
22.5
33.5
44.5
5
Day 1-5 Day 6-10 Day 11-15 Day 16-20 Day 21-25 Day 26-30
Above 50%
Below 50%
Figure 3. Mean response rates in participants who responded to above half (n = 79) of the follow-up assessments and those who responded to below half (n = 29) of the follow-up assessments.
Table 2. Calculated Mean Values (95% CI) at Day 30 Based on the Linear Mixed-Growth Model, Using All Observations From Days 0 to 30.
Control group Intervention group Difference
Total score 7.2 [6.6, 13.7], p = .031 16.8 [10.5, 23.1], p = .000 9.6 [0.5, 18.7], p = .038 SCL-8D −1.2 [−4.4, 1.9], p = .443 3.3 [0.3, 6.4], p = .033 4.6 [0.2, 9.0], p = .042 AHSS 0.7 [−2.0, 3.4], p = .608 3.2 [0.6, 5.7], p = .016 2.5 [−1.2, 6.2], p = .192Alcohol Use 0.1 [−0.4, 0.6], p = .636 0.9 [0.4, 1.4], p = .000 0.8 [0.1, 1.4], p = .031 Urge 0.1 [−0.3, 0.5], p = .589 0.3 [−0.1, 0.7], p = .139 0.2 [−0.4, 0.8], p = .524Drugs Use −0.6 [−1.1, −0.2], p = .002 0.4 [−0.002, 0.8], p = .059 1.0 [0.5, 1.6], p = .000 Urge −0.1 [−0.5, 0.3], p = .590 0.2 [−0.3, 0.5], p = .491 0.2 [−0.3, 0.8], p = .387Daily stressor −0.01 [−0.6, 0.6], p = .964 1.9 [1.3, 2.4], p = .000 1.9 [1.1, 2.7], p = .000
Note. The estimated trajectory parameters or slopes from the model can be obtained by dividing the results in the table by 30. CI = confidence interval; SCL-8D = eight-item dichotomized version of the Symptoms Check List; AHSS = Arnetz and Hasson stress questionnaire.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
12 International Journal of Offender Therapy and Comparative Criminology
psychosocial well-being, by using an immediate automated intervention based on the direction of these ratings. The brief-automated intervention was inspired by cognitive relapse prevention. It is suggested that increased awareness of dynamic variables and available support strengthen the individual’s ability to handle high-risk situations, such as stress and substance use.
The study was performed in a population of paroled offenders recruited from 13 of 15 prisons in the south and east region of Sweden. The study group may differ from the general population of offenders in terms of data that could not be analyzed in the present study. There are no age difference between the current population and paroled offenders. As the sample was continuously recruited, offenders with shorter sentences may be somewhat overrepresented. This could not be analyzed because data were not collected on the length of the participants’ sentences. In addition, although acceptance rates did not differ between males and females, the number of female offenders included is somewhat lower than the figure of about 6% that would have been repre-sentative for paroled offenders in Sweden. No additional data were collected that would allow further comparison with the total group of paroled offenders in Sweden.
Both acceptance rates and response rates were high in a population that is otherwise known to be difficult to retain contact with (Lindsey, Minard, Hudson, Green, & Schmitz, 2014; McKenzie, Tulsky, Long, Chesney, & Moss, 1999). Three out of five offenders had access to their own mobile handset at parole, which is a rather high fig-ure as all participants were recruited during imprisonment. Possibly the acceptance rates could have been increased if subjects were offered a handset at parole. A second solution would be to recruit subjects when they have left prison and have already obtained a handset of their own. The frequent use of mobile telephones in all types of groups in Sweden, and in several other countries, makes automated telephony an effi-cient technology for systematic daily assessments and interventions. The widespread use of mobile telephones, even in marginalized groups (Hakansson et al., 2011), means that the technology is well known, easy, and fast to use, without drawing attention to the user in various situations.
There was a significant amount of attrition preceding the random assignment, which may have had an effect on study results. No data were collected on the 43 sub-jects who declined participation, other than that they did not want to have additional contact with the probation services, so no further attrition analysis on these subjects was possible. As subjects who declined participation took part in group meetings, it is suggested that in the future, participants are recruited to this kind of study through individual meetings. There were some pre-assessment differences between those not fulfilling the eligibility criteria and the final sample, as well as differences during the first 5 days of follow-up between those completing most of the follow-ups and those completing less than half of the follow-ups. There was no difference in response rates between the intervention group and the control group, but as less active participation was associated with dynamic risk factors, information on missing responses could be an important indicator of increased risk for criminal recidivism, and this information was passed on to the probation officers for subjects in the intervention group. Less
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 13
active participation may also be explained by demographic data, length of imprison-ment, and re-arrests or non-planned drug treatments during the follow-up period. These kind of data were not available in the present study.
When data are gathered through different types of surveys, including postal or email questionnaires, it could be argued that answers may have been retrieved from an unintended respondent. As mobile telephones are generally considered to be a per-sonal belonging, and carried by the owner, the risk of collecting data from non-intended persons was considered to be low in the present study. When using Interactive Voice Response (IVR) technology, various kinds of confirmations can be added to secure that each call is answered by the intended person. However, such procedures would increase the length of the survey, and possibly exclude answers from subjects unable to use advanced identification systems, and which would probably lower the response rates.
In this study, questions were asked about the sensitive issue of drug use, which according to Swedish law is criminal. This kind of question could be asked because answers to individual questions were not reported to the Prison and Probation Service. Nothing was included in the reports to the probation officers that could result in any negative consequences for the offenders, who were informed about this on entering the study. This procedure also reduces the risk that offenders in the intervention group underreport use of alcohol and drugs to avoid contact with their probation officer. Even though the summarized reports that were sent to the probation officer, including whether the probation officers took part in the email reports, have not been systemati-cally studied in this analysis, the officer’s work could be made more effective by pro-viding information on the progress of the offenders. This kind of information could be used both as a base for priorities—who are in need and who are not—and as a material used in treatment of the offender. The way in which automated reports affect priorities and the way in which reports can be included in the treatment of offenders are impor-tant issues that could be studied in the future.
A minor adverse event involved five participants (4%), who withdrew their consent due to the perceived over-intensity of follow-up. This indicates that optimal frequency for the assessments still has to be evaluated. A previous study using automated tele-phony in subjects discharged from acute psychiatric inpatient care suggests that fol-low-ups should be made at least twice a week to obtain sufficient response rates (Johansson, Remvall, Malgerud, Lindgren, & Andersson, 2013).
This study does not include a control group with any kind of daily assessment, and which could provide information about the intervention effects in relation to the man-datory treatment provided by the probation services. It is assumed that the daily assess-ments conducted in both groups have a positive effect, supplementing the mandatory treatment that was also provided to both groups. To further evaluate the feasibility of daily follow-ups and interventions, future studies could also include focus groups including both parolees and parole officers.
Even though the dynamic risk factors associated to crime and criminal recidivism are reduced, the study does not assess the effect on actual rates of criminal recidivism. An application to analyze this kind of data for the present sample has been sent to the
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from

14 International Journal of Offender Therapy and Comparative Criminology
Swedish Prison and Probation Services, so hopefully this data can be analyzed and presented in a separate article. The intervention effect on criminal recidivism is also subject to further studies. The results are also limited to the effect in the first month after parole, during which the risk of committing a new crime or violating the terms of parole is greatest, and the durability over a longer period is not assessed. In future studies, not only the effects on psychosocial factors but also the clinical significance of these effects, such as the effect on relapse in crime, should be analyzed over a 12-month period.
The study limitations also include both absence of objective measures and quantity/frequency measures of alcohol and drugs. Future designs could be improved by using validated scales in daily assessments, or by performing complementary assessments using objective measures such as segmental hair analysis. The measures used in this study were selected to give a brief indication of substance use. Each item was designed to be answered in the same way to minimize the time consumed for each respondent. This was similar to the experience in a previous study in university students, where the average length of the assessments was only 29 s for the same number of questions (Andersson, Söderpalm Gordh, & Berglund, 2007). For the convenience of the respon-dents, all scales used in the study corresponded to the 10-numbered keys on the cell phone. Each scale was constructed with a wide range of steps, and both total scores and sub-scores were analyzed. Alcohol and drugs were used by participants in this study, and the reduction in use found is important as the risk of criminal relapse in prisoners with substance abuse is increased by substance use, even when controlling for type and severity of crime and psychiatric problems (Hakansson & Berglund, 2012). Further development of brief measures of alcohol and drug use suitable for daily automated telephone assessments is important in future analysis of the quantity and frequency of substance use.
The most important lessons learned for others who are interested in doing an auto-mated telephony intervention in paroled offender’s concern factors that could improve participation rates. To increase participation rates, individual recruitment should be used, as group meetings were associated with declined participation. Moreover, either a mobile telephone could be offered to those who have no access to a handset of their own or participants could be recruited when the offenders are already on parole and have obtained their own handset. Participants could also be recruited only in cases where probation and a probation officer have been confirmed. A final suggestion con-cerns less frequent follow-ups and/or less frequent reminders on daily follow-ups, as some participants withdrew their consent due to perceived over-intensity.
In spite of the study limitations, the result may have implications for correctional officers who have limited time to follow up and intervene on paroled offenders, even though acute dynamic risk factors are known to be associated with criminal recidi-vism. This study shows that the probation services can monitor and intervene on dynamic risk factors. There was no need to train the users, and the intervention involved no supervision, and may be easily implemented within the Prison and Probation Service as it is not person-dependent and does not demand personnel resources. These kinds of automated systems could probably also be used for
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 15
follow-up of treatment results in specific groups of paroled offenders using other dynamic variables than stress and substance use, such as aggression in relation to domestic violence or other variables associated with antisocial personality patterns. The system could also be used for interventions in other settings relating to psychoso-cial health, such as in treatment of alcohol and drug dependence (Hendershot et al., 2011; White et al., 2010).
In conclusion, automated telephony was found to be an effective technology that could be used with paroled offenders to assess progress and to give interventions to reduce stress and substance use. If the findings could be replicated in future work, implications for paroled offenders and the Prison and Probation Service could be important.
Authors’ Note
The funding organization had no role in the design or conduct of the study, collection, manage-ment, analysis, and interpretation of the data, or in the preparation, review, or approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Swedish Prison and Probation Service awarded to Claes Andersson (Principal Investigator), Agneta Öjehagen, and Mats Berglund.
References
al’Abusi, M. (2007). Stress and addiction: Biological and psychological mechanism. Burlington, MA: Elsevier.
Altman, D. G. (1990). Practical statistics for medical research. Boca Raton, FL: Chapman & Hall.
Andersson, C., Johnsson, K. O., Berglund, M., & Öjehagen, A. (2009). Measurement prop-erties of the Arnetz and Hasson stress questionnaire in Swedish university freshmen. Scandinavian Journal of Public Health, 37, 273-279.
Andersson, C., Söderpalm Gordh, A. H. V., & Berglund, M. (2007). Use of real-time interac-tive voice response in a study of stress and alcohol consumption. Alcoholism: Clinical & Experimental Research, 31, 1908-1912.
Andrews, D. A., & Bonta, J. (2010). The psychology of criminal conduct (5th ed.). New Providence, NJ: Matthew Bender.
Barnett, G. D., Manderville-Norden, R., & Rakestrow, J. (2014). The good lives model or relapse prevention: What works better in facilitating change? Sexual Abuse: A Journal of Research and Treatment, 26, 3-33. doi:10.1177/1079063212474473
Begg, C., Cho, M., & Eeastwood, S. (1996). Improving the quality of reporting of randomized controlled trials: The CONSORT statement. JAMA, 276, 637-639.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from

16 International Journal of Offender Therapy and Comparative Criminology
Bohn, M. J., Krahn, D. D., & Staehler, B. A. (1995). Development and initial validation of a measure of drinking urges in abstinent alcoholics. Alcoholism: Clinical & Experimental Research, 19, 600-606.
Bulman, P. (2010, December). Electronic monitoring reduces recidivism. Corrections Today, 72(6), 72-73.
Burraston, B. O., Bahr, S. J., & Cherrington, D. J. (2013). Reducing juvenile delinquency with automated cell phone calls. International Journal of Offender Therapy and Comparative Criminology. Advance online publication. doi:0306624X13480947
Burraston, B. O., Cherrington, D. J., & Bahr, S. J. (2012). Reducing juvenile recidivism with cognitive training and a cell phone follow-up: An evaluation of the real victory program. International Journal of Offender Therapy and Comparative Criminology, 56, 61-80.
Carroll, K. M. (1996). Relapse prevention as a psychosocial treatment: A review of controlled clinical trials. Experimental and Clinical Psychopharmacology, 4, 46-54.
Corkrey, R., & Parkinson, L. (2002). Interactive voice response: Review of studies 1989-2000. Behavior Research Methods, 34, 342-353.
Corkrey, R., Parkinson, L., & Bates, L. (2005). Pressing the key pad: Trial of a novel approach to health promotion advice. Preventive Medicine, 41, 657-666.
Everly, G. S., Jr., & Lating, J. M. (2002). A clinical guide to the treatment of the human stress response (2nd ed.). New York, NY: Kluwer Academic Publishers.
Fink, P., Jensen, J., Borgquist, L., Brevik, J. L., Dalgard, O. S., Sandager, I., . . .Munk-Jörgensen, P. (1995). Psychiatric morbidity in primary public health care: A Nordic multicentre investigation. Part I: Method and prevalence of psychiatric morbidity. Acta Psychiatrica Scandinavica, 92, 409-418.
Finney, C., Stergiopoulos, E., Hensel, J., Bonato, S., & Dewa, C. S. (2013). Organizational stressors associated with job stress and burnout in correctional officers: A systematic review. BMC Public Health, 13, Article 82.
Gee, P., Coventry, K. R., & Birkenhead, D. (2005). Mood state and gambling: Using mobile telephones to track emotions. British Journal of Psychology, 96, 53-66.
Gelder, M., Harrison, P., & Cowen, P. (2006). Shorter Oxford textbook of psychiatry (5th ed.). Oxford, UK: Oxford University Press.
Hakansson, A., & Berglund, M. (2012). Risk factors for criminal recidivism: A prospective follow-up study in prisoners with substance abuse. BMC Psychiatry, 12(1), Article 111. Retrieved from http://www.biomedcentral.com/1471-244X/12/111
Hakansson, A., Isendahl, P., Wallin, C., & Berglund, M. (2011). Efficacy of mobile telephone contact for follow-up in injecting heroin users. The American Journal of Drug and Alcohol Abuse, 37, 89-92.
Hall, J. A., & Huber, D. L. (2000). Telephone management in substance abuse treatment. Telemedicine and e-Health Journal, 6(4), 401-407.
Hansson, K. R., & Harris, A. J. R. (2000). Where should we intervene? Dynamic predictors of sexual offense recidivism. Criminal Justice and Behavior, 27, 6-35.
Hendershot, C. S., Witkiewitz, K., George, W. H., & Marlatt, G. A. (2011). Relapse prevention for addictive behaviors. Substance Abuse Treatment, Prevention, and Policy, 19(6), Article 17. doi:10.1186/1747-597X-6-17
Irvin, J. E., Bowers, C. A., Dunn, M. E., & Wang, M. C. (1999). Efficacy of relapse prevention: A meta-analytic review. Journal of Consulting and Clinical Psychology, 67, 563-570.
Johansson, B. A., Remvall, S., Malgerud, R., Lindgren, A., & Andersson, C. (2013). Interactive voice response-and automated follow-up technique for adolescents discharged from acute psychiatric inpatient care: A randomized controlled trial. SpringerPlus, 2, Article 146.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from
Andersson et al. 17
Jones, N. J., Brown, S. L., & Zamble, E. (2010). Predicting criminal recidivism in adult male offenders: Researcher versus parole officer assessment of dynamic risk. Criminal Justice and Behavior, 37, 860-882.
Kaminer, Y., Litt, M. D., Burke, R. H., & Burleson, J. A. (2006). An Interactive Voice Response (IVR) system for adolescents with alcohol use disorders: A pilot study. American Journal on Addictions, 15(S1), 122-125.
Katon, W., Rutter, C., Ludman, E. J., Von Korff, M., Lin, E., Simon, G., . . .Unützer, J. (2001). A randomized trial of relapse prevention of depression in primary care. Archives of General Psychiatry, 58, 241-247.
Kennedy, C. M., Powell, J., Payne, T. H., Ainsworth, J., Boyd, A., & Buchan, I. (2012). Active assistance technology for health-related behavior change: An interdisciplinary review. Journal of Medical Internet Research, 14(3), e80.
Langan, P. A., & Levin, D. J. (2002). Recidivism of prisoners released in 1994. Federal Sentencing Reporter, 15, 58-65.
Lee, H., Friedman, M. E., Cukor, P., & Ahern, D. (2003). Interactive Voice Response System (IVRS) in health care services. Nursing Outlook, 51(6), 277-283.
Lewis-Beck, M. S., Bryman, A., & Liao, T. F. (2004). Encyclopedia of social science research methods. Thousand Oaks, CA: SAGE.
Lindsey, J. A., Minard, C. G., Hudson, S., Green, C. E., & Schmitz, J. M. (2014). Using prize-based incentives to enhance daily Interactive Voice Response (IVR) compliance: A feasi-bility study. Journal of Substance Abuse Treatment, 46, 74-77.
McKenzie, M., Tulsky, J. P., Long, H. L., Chesney, M., & Moss, A. (1999). Tracking and follow-up of marginalized populations: A review. Journal of Healthcare for the Poor and Underserved, 10(4), 409-429.
Merton, R.K. (1938). Social structure and anomie. American Sociological Review, 3(5), 672-682.
Morse, D. R. (1998). Confronting existential anxiety: The ultimate stressor. Stress & Medicine, 14, 109-119.
Mundt, J. C., Moore, H. K., & Bean, P. (2006). An interactive voice response program to reduce drinking relapse: A feasibility study. Journal of Substance Abuse Treatment, 30, 21-29.
National Research Council. (2008). Parole, desistance from crime, and community integration (Committee on Community Supervision and Desistance from Crime, Committee on Law and Justice, Division of Behavioral and Social Sciences and Education). Washington, DC: The National Academies Press.
Phillips, L. A., & Lindsay, M. (2011). Prison to society: A mixed methods analysis of coping with reentry. International Journal of Offender Therapy and Comparative Criminology, 55, 136-154.
Seiter, R. P., & Kadela, K. R. (2003). Prisoner reentry: What works, what does not, and what is promising. Crime & Delinquency, 49, 360-388.
Stone, A. A., & Neale, J. M. (1982). Development of a methodology for assessing daily experi-ences. In A. Baum & J. Singer (Eds.), Advances in environmental psychology: Environment and health (Vol. 4, pp. 49-83). New York, NY: Lawrence Erlbaum.
Swedish National Audit Office. (2004). Återfall i brott eller anpassning i samhället – uppföljning av kriminalvårdens klienter [Relapse in crime or adaptation in society—Monitoring the prison service clients], 5, 76.
Swedish National Council for Crime Prevention. (2007). Kriminalstatistik 2006 [Crime Statistics 2006], 20, 267.
Wallman, J. (2005). Unpacking recidivism. Criminology & Public Policy, 4, 479-483.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from

18 International Journal of Offender Therapy and Comparative Criminology
Ward, T., Yates, P. M., & Willis, G. M. (2012). The good lives model and the risk need respon-sivity model: A critical response to Andrews, Bonta, and Wormith (2011). Criminal Justice and Behavior, 39, 94-110.
Webb, T. L., Joseph, J., Yardley, L., & Michie, S. (2010). Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. Journal of Medical Internet Research, 12(1), e4.
White, A., Kavanagh, D., Stallman, H., Klein, B., Kay-Lambkin, F., Proudfoot, J., . . .Young, R. (2010). Online alcohol interventions: A systematic review. Journal of Medical Internet Research, 12(5), e62.
Witkiewitz, K., & Marlatt, A. G. (2004). Relapse prevention for alcohol and drug problems. American Psychologist, 59, 224-235.
Zamble, E., & Quinsey, V. L. (1997). The criminal recidivism process. Cambridge, UK: Cambridge University Press.
at Karolinska Institutets Universitetsbibliotek on March 16, 2014ijo.sagepub.comDownloaded from