
Cytogenetic Analysis of 124 Prospectively Ascertained Male Germ Cell Tumors1
8
(CANCER RESEARCH 52. 2285-2291. April 15. 19921 Cytogenetic Analysis of 124 Prospectively Ascertained Male Germ Cell Tumors1 Eduardo Rodriguez,2 Susan Mathew, Victor Reuter, David H. Ilson, George J. Bosl, and R. S. K. Chaganti Laboratory of Cancer Genetics, Sloan-Kettering Institute [E. R., S. M., R. S. K. C.J, and the Departments of Pathology [V. R., R. S. K. C.J and Medicine [G. J. BJ, Memorial Hospital, Memorial Sloan-Kettering Cancer Center, New York, New York 10021 ABSTRACT We report the cytogenetic analysis of 124 adult male germ cell tumors ascertained consecutively at the Memorial Sloan-Kettering Cancer Center between 1988 and 1990. Biopsies from testicular and extragonadal pri mary and metastatic lesions studied included all histológica!subtypes of germ cell tumors and cases of malignant transformation. Nonrandom numerical and structural chromosomal abnormalities including i(12p), the previously described characteristic marker of these tumors, were determined, and their frequency was compared between histológica! subtypes, between gonadal and extragonadal lesions, and between pri mary and transformed lesions. The frequency and copy number of i(12p) were found to be higher in nonseminomas compared with seminomas. Nonrandom sites of chromosome rearrangements associated with specific histologies comprised lp32-36 and 7ql 1.2 in teratomas and Ip22 in yolk sac tumors. Some tumors that underwent malignant differentiation exhib ited chromosome changes previously described to be nonrandomly asso ciated with de novo tumors with the same histológica!characteristics. Cytological evidence of gene amplification in the form of homogeneously staining regions and/or double minutes was detected in 24% of extrago nadal lesions, mainly metastatic tumors, suggesting amplification of a gene(s) associated with metastatic progression of these tumors. While a number of previous small cytogenetic series or individual case reports of germ cell tumors identified several of the features of these tumors reported here, this series comprises analysis of the largest group of tumors ascertained consecutively at a single institution, defines the inci dence of nonrandom abnormalities in tumor subsets, and addresses their biological significance. INTRODUCTION Adult male GCTs3 are a heterogenous group of neoplasms. Their biological properties and responsiveness to chemotherapy make them a model system for the study of differentiation, malignant transformation, and drug sensitivity. GCTs may originate in the testis or at extragonadal sites (mediastinum, retroperitoneum, pineal). Histologically, they comprise two main entities: seminomas, composed of neoplastic germ cells which mimic gametogenesis and act as immature spermatogenic cells; and nonseminomas, composed of embryonic neoplastic germ cells which mimic histogenesis of the early embryo (1). Among nonseminomas, embryonal carcinoma is a pluripotent tumor which may progress along extraembryonic or tropho- blastic lineages to form yolk sac tumor or choriocarcinoma or along the embryonic lineage to form teratoma. Both seminomas and nonseminomas have been suggested to originate from a common precursor cell, carcinoma in situ of the testis, which is the neoplastic counterpart of a gonocyte (2, 3). Individual tumors may present several histologies: when they contain only nonseminomatous components, they are termed mixed GCTs; and when they present seminomatous and nonseminomatous elements, they are termed combined GCTs (4). Occasionally, Received 9/24/91; accepted 2/4/92. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1Supported in part by NIH Research Grant CA-05826. 2To whom requests for reprints should be addressed, at Box 391, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021. 3The abbreviations used are: GCT, germ cell tumor; ERMS, embryonal rhabdomyosarcoma; HSR, homogeneously staining region. teratomatous components of nonseminomatous GCTs undergo malignant differentiation into tumors typically encountered in other organs and tissues such as sarcoma, adenocarcinoma, neuroblastoma, or myeloid leukemia (5-7). Cytogenetic analyses of adult male GCTs have identified i(12p) as a common marker to all histologies and sites, occur ring in over 80% of described cases (8-15). However, recurrent abnormalities other than i(12p) remain to be defined in GCT. We report here the cytogenetic analysis of 124 consecutively ascertained specimens of GCTs derived from 106 patients and representing all described histological subtypes. The tumors studied included testicular and extragonadal presentation of primary as well as metastatic lesions biopsied prior to and after treatment. This series comprises the largest cytogenetic series of GCTs analyzed so far and enabled us to examine the asso ciation between nonrandom chromosome abnormalities and histological and biological features of these tumors. MATERIALS AND METHODS Tumor Ascertainment and Cell Culture. The tumors studied represent a consecutive ascertainment of all GCTs seen at the Memorial Sloan- Kettering Cancer Center between January 1988 and December 1990. A total of 124 specimens from 106 patients were processed for culture and cytogenetic analysis. Upon receipt in the laboratory, each biopsy specimen was finely minced with scalpels into 2- to 3-mm pieces and digested in growth medium containing collagenase II (GIBCO) at a concentration of 200 units/ml for 4 to 16 h. After disaggregation, cells were centrifugea, transferred to fresh medium, and cultured in a 5% CO2 atmosphere at 37°C. The growth medium comprised RPMI 1640 (500 ml), 15% fetal calf serum, 1% 200 m\i L-glutamine, 5 Mg/ml of insulin, 5 ng/ml of transferrin, 5 Mg/ml of sodium satinate, and 50 ng/ ml of penicillin/streptomycin. Tumors were staged according to the criteria of Hendry et al. (16). Diagnostic histopathology was performed according to conventional methods. Information on the clinical status and laboratory data on the patients including serum levels of a-fetopro- tein, human chorionic gonadotropin, and láclatedehydrogenase were obtained at the time of tumor resection. Cytogenetic Analysis. Cells for cytogenetic analysis were harvested following short-term culture (1 to 10 days after seeding of the cells) by conventional methods. Metaphases were accumulated by Colcemid treatment (final concentration, 0.01 to 0.02 Mg/ml) that ranged from 6 to 14 h and stained to reveal Q- or G-banding patterns. Karyotypes were described according to the International System for Human Cy togenetic Nomenclature (17). Clonality was defined by the detection of two cells with the same structural abnormality or nonrandom gain of the same chromosome or three cells with loss of the same chromosome. RESULTS Of the 124 specimens processed for cytogenetic analysis, abnormal clones were found in 65 biopsies from 58 patients; 29 showed normal karyotypes and 30 did not yield dividing cells. Of the 65 specimens with clonal abnormalities, 40 were derived from metastatic lesions, and 25 were from primary tumors; 34 specimens were from patients who underwent chemotherapy, and 31 were from previously untreated patients; 15 specimens were primary extragonadal in origin (in each of these cases, an occult testicular lesion was ruled out by sonog- 2285 Research. on December 5, 2014. © 1992 American Association for Cancer cancerres.aacrjournals.org Downloaded from
Transcript of Cytogenetic Analysis of 124 Prospectively Ascertained Male Germ Cell Tumors1

(CANCER RESEARCH 52. 2285-2291. April 15. 19921
Cytogenetic Analysis of 124 Prospectively Ascertained Male Germ Cell Tumors1
Eduardo Rodriguez,2 Susan Mathew, Victor Reuter, David H. Ilson, George J. Bosl, and R. S. K. Chaganti
Laboratory of Cancer Genetics, Sloan-Kettering Institute [E. R., S. M., R. S. K. C.J, and the Departments of Pathology [V. R., R. S. K. C.J and Medicine [G. J. BJ,Memorial Hospital, Memorial Sloan-Kettering Cancer Center, New York, New York 10021
ABSTRACT
We report the cytogenetic analysis of 124 adult male germ cell tumorsascertained consecutively at the Memorial Sloan-Kettering Cancer Centerbetween 1988 and 1990. Biopsies from testicular and extragonadal primary and metastatic lesions studied included all histológica!subtypes ofgerm cell tumors and cases of malignant transformation. Nonrandomnumerical and structural chromosomal abnormalities including i(12p),the previously described characteristic marker of these tumors, weredetermined, and their frequency was compared between histológica!subtypes, between gonadal and extragonadal lesions, and between primary and transformed lesions. The frequency and copy number of i(12p)were found to be higher in nonseminomas compared with seminomas.Nonrandom sites of chromosome rearrangements associated with specifichistologies comprised lp32-36 and 7ql 1.2 in teratomas and Ip22 in yolksac tumors. Some tumors that underwent malignant differentiation exhibited chromosome changes previously described to be nonrandomly associated with de novo tumors with the same histológica!characteristics.Cytological evidence of gene amplification in the form of homogeneouslystaining regions and/or double minutes was detected in 24% of extragonadal lesions, mainly metastatic tumors, suggesting amplification of agene(s) associated with metastatic progression of these tumors. While anumber of previous small cytogenetic series or individual case reports ofgerm cell tumors identified several of the features of these tumorsreported here, this series comprises analysis of the largest group oftumors ascertained consecutively at a single institution, defines the incidence of nonrandom abnormalities in tumor subsets, and addresses theirbiological significance.
INTRODUCTION
Adult male GCTs3 are a heterogenous group of neoplasms.
Their biological properties and responsiveness to chemotherapymake them a model system for the study of differentiation,malignant transformation, and drug sensitivity. GCTs mayoriginate in the testis or at extragonadal sites (mediastinum,retroperitoneum, pineal). Histologically, they comprise twomain entities: seminomas, composed of neoplastic germ cellswhich mimic gametogenesis and act as immature spermatogeniccells; and nonseminomas, composed of embryonic neoplasticgerm cells which mimic histogenesis of the early embryo (1).Among nonseminomas, embryonal carcinoma is a pluripotenttumor which may progress along extraembryonic or tropho-blastic lineages to form yolk sac tumor or choriocarcinoma oralong the embryonic lineage to form teratoma. Both seminomasand nonseminomas have been suggested to originate from acommon precursor cell, carcinoma in situ of the testis, which isthe neoplastic counterpart of a gonocyte (2, 3). Individualtumors may present several histologies: when they contain onlynonseminomatous components, they are termed mixed GCTs;and when they present seminomatous and nonseminomatouselements, they are termed combined GCTs (4). Occasionally,
Received 9/24/91; accepted 2/4/92.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Supported in part by NIH Research Grant CA-05826.2To whom requests for reprints should be addressed, at Box 391, Memorial
Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021.3The abbreviations used are: GCT, germ cell tumor; ERMS, embryonal
rhabdomyosarcoma; HSR, homogeneously staining region.
teratomatous components of nonseminomatous GCTs undergomalignant differentiation into tumors typically encountered inother organs and tissues such as sarcoma, adenocarcinoma,neuroblastoma, or myeloid leukemia (5-7).
Cytogenetic analyses of adult male GCTs have identifiedi(12p) as a common marker to all histologies and sites, occurring in over 80% of described cases (8-15). However, recurrentabnormalities other than i(12p) remain to be defined in GCT.We report here the cytogenetic analysis of 124 consecutivelyascertained specimens of GCTs derived from 106 patients andrepresenting all described histological subtypes. The tumorsstudied included testicular and extragonadal presentation ofprimary as well as metastatic lesions biopsied prior to and aftertreatment. This series comprises the largest cytogenetic seriesof GCTs analyzed so far and enabled us to examine the association between nonrandom chromosome abnormalities andhistological and biological features of these tumors.
MATERIALS AND METHODS
Tumor Ascertainment and Cell Culture. The tumors studied representa consecutive ascertainment of all GCTs seen at the Memorial Sloan-Kettering Cancer Center between January 1988 and December 1990.A total of 124 specimens from 106 patients were processed for cultureand cytogenetic analysis. Upon receipt in the laboratory, each biopsyspecimen was finely minced with scalpels into 2- to 3-mm pieces anddigested in growth medium containing collagenase II (GIBCO) at aconcentration of 200 units/ml for 4 to 16 h. After disaggregation, cellswere centrifugea, transferred to fresh medium, and cultured in a 5%CO2 atmosphere at 37°C.The growth medium comprised RPMI 1640
(500 ml), 15% fetal calf serum, 1% 200 m\i L-glutamine, 5 Mg/ml ofinsulin, 5 ng/ml of transferrin, 5 Mg/ml of sodium satinate, and 50 ng/ml of penicillin/streptomycin. Tumors were staged according to thecriteria of Hendry et al. (16). Diagnostic histopathology was performedaccording to conventional methods. Information on the clinical statusand laboratory data on the patients including serum levels of a-fetopro-tein, human chorionic gonadotropin, and láclatedehydrogenase wereobtained at the time of tumor resection.
Cytogenetic Analysis. Cells for cytogenetic analysis were harvestedfollowing short-term culture (1 to 10 days after seeding of the cells) byconventional methods. Metaphases were accumulated by Colcemidtreatment (final concentration, 0.01 to 0.02 Mg/ml) that ranged from 6to 14 h and stained to reveal Q- or G-banding patterns. Karyotypeswere described according to the International System for Human Cytogenetic Nomenclature (17). Clonality was defined by the detection oftwo cells with the same structural abnormality or nonrandom gain ofthe same chromosome or three cells with loss of the same chromosome.
RESULTS
Of the 124 specimens processed for cytogenetic analysis,abnormal clones were found in 65 biopsies from 58 patients;29 showed normal karyotypes and 30 did not yield dividingcells. Of the 65 specimens with clonal abnormalities, 40 werederived from metastatic lesions, and 25 were from primarytumors; 34 specimens were from patients who underwentchemotherapy, and 31 were from previously untreated patients;15 specimens were primary extragonadal in origin (in each ofthese cases, an occult testicular lesion was ruled out by sonog-
2285
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

MALE GERM CELL TUMOR CYTOGENETIC ANALYSIS
raphy), and the remaining were of testicular origin. Table 1records the cytogenetic success rate in each of the histologicalsubsets and shows that abnormal clones were less frequentlydetected in seminomas, yolk sac tumors, and mixed tumorscompared with teratomas, embryonal carcinomas, combinedtumors, and tumors exhibiting malignant transformation.
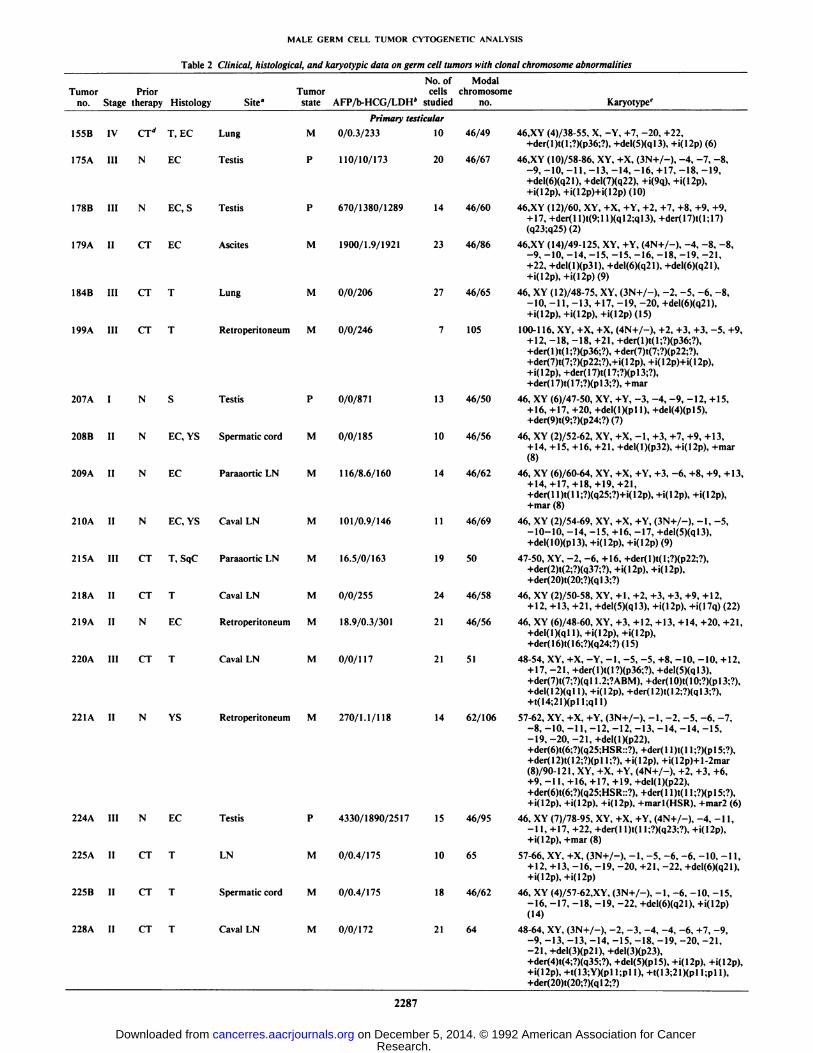
The cytogenetic data on 27 of these specimens with clonalchromosome abnormalities were published by us previously (7,14, 18). Table 2 summarizes the clinical, histological, andkaryotypic data on the remaining 38 specimens with clonalchromosome abnormalities. The karyotypes in general werecharacterized by gains of chromosomes and the presence ofmarker chromosomes. The modal chromosome numbersranged from 46 to 124; one tumor was pseudodiploid, 23tumors were hyperdiploid, 31 tumors were near-triploid, 5tumors were near-tetraploid, and 2 tumors were near-penta-ploid. In an additional 2 tumors, 2 related abnormal clones inthe diploid and tetraploid ranges were detected. Finally, anadditional tumor presented two abnormal clones in the triploidand pentaploid ranges.
The mean of the modal numbers of the short and long armsof chromosomes (including those in structural abnormalitieswhen a complete arm could be identified) was calculated andshown in Fig. 1. Most autosomal arms were in the near-triploidrange except 12p which was overrepresented. In nonseminomasthe X chromosome was represented by more copies (mean,1.66) than the Y chromosome (mean, 1.24), whereas in seminomas the Y chromosome (mean, 1.71) was represented bymore copies than the X chromosome (mean, 1.29). The i(12p)marker, characteristic of germ cell tumors, was observed in 56(86%) tumors; its copy number varied from 1 to 4. Seminomashad an average of 1.2 i(12p) copies per cell which was seen in71% of the specimens. Teratomas and embryonal carcinomashad an average of 2 i(12p)s per cell which was seen in 89% ofthe former and 83% of the latter. Yolk sac tumors had anaverage of 1.4 i(12p) copies per cell which was seen in 100% ofthe specimens. Deletions or translocations affecting the 12ql 1-25 region were observed in 11 specimens from 10 patients, 9 ofthese also having one or more copies of i(12p). The relevantbreakpoints comprised one at 12qll, 3 at 12ql3, 5 at 12ql5,and one each at 12q21, 12q22, 12q24, and 12q25. A total of 9specimens did not exhibit an i(12p). Of these, 6 had abnormalities of chromosome 12 which comprised a del(12q) in one (No.176A), translocations affecting 12p in 2 (Nos. 231A and 251 A),a der(12) chromosome with a translocation affecting both thep and q arms in one (No. 240A), while 2 showed monosomy 12
Table 1 Cytogenetic success rate among the histological subsets of GCT patientsstudied
HistologicalsubsetTeratomaSeminomaEmbryonal
carcinomaYolksactumorChoriocarcinomaMixed
tumorCombinedtumorMalignant
transformationLeukemiaNeuroepitheliomaEmbryonal
rhabdomyosarcomaOthersarcomaSquamouscarcinomaUndifTerentiated
carcinomaNo.
ofpatients125252574185114122No.
ofBiopsies125252594195214122CytogeneticsFailureNormalAbnormal29552700000005970061001000187134264213122
Total 120 124 30 29 65
(Nos. 207A and 249A). The remaining 3 specimens (Nos. 178A,178B, and 238A) from two other patients had no rearrangements affecting chromosome 12; however, 2 specimensexhibited aberrantly banded marker chromosomes of unknownorigin (Nos. 178A and 238A).
Fig. 2 illustrates chromosomal sites involved in clonal rearrangements 3 or more times each, and Figs. 3 and 4 arerepresentative of full karyotypes from an embryonal carcinoma(242A) and a teratoma (231 A). Fig. 5 is an idiogram of thehuman karyotype showing all the breakpoints encountered inthis series according to histology and comparing primary withmetastatic lesions. Some breakpoints were nonrandomly associated (P < 0.05) with certain histologies, e.g., lp32-36 (7 of18 in teratomas compared with one of 32 in the rest of thetumors with single histology); 7qll.2 (3 of 18 in teratomascompared with 0 of 32 in the rest of the tumors with singlehistology); and Ip22 (2 of 4 in yolk sac tumors compared with2 of 48 in the rest of tumors with single histology). We wereable to isolate regions of pure yolk sac and pure teratoma andperform cytogenetic analysis from one patient (No. 235; Table2). The only difference in the karyotype between the two histologies was the presence of a del(l)(p22) in the yolk sac whichwas absent in the teratoma.
Some breakpoints were found only in metastatic lesions, e.g.,10pl3 (4 of 40), 7qll.2 (3 of 40), and 12pll-ql3 (7 of 40).Interestingly, in Patient 159, a 10pl3 rearrangement was seenonly in the metastatic lesion (No. 159B) but not in the primarylesion (No. 159A). Some breakpoints were significantly morefrequent in posttherapy specimens (P < 0.05), e.g., 6q21 (6 of34 posttherapy, one of 31 pretherapy), while other breakpointswere seen only in posttherapy specimens, e.g., Ip36 (6 of 34),7ql3 (3 of 34), and 12qll-13 (5 of 34).
Another finding of interest was cytological evidence of geneamplification in the form of HSRs and/or double minute chromosomes in 6 of the tumors (Nos. 23A, 51D, 74A, 154A, 221 A,240A). An additional, 6 tumors presented aberrantly bandedmarker chromosomes with a repeating banding pattern of unknown origin which may also represent amplification (Nos.76C, 178A, 220A, 238A, 242A, 248A) (Fig. 1). Of these, 8were resected from the retroperitoneum, 3 from lymph nodes,and one from the mediastinum.
In this series, we had the opportunity to study chromosomechanges associated with malignant transformation of GCTs. Atotal of 9 tumors presented with transformed histologies. In 2i(12p)-positive teratomas, we were able to study both the primary and malignant components. In the first case (No. 149), apatient with primary mediastinal teratoma/yolk sac tumor developed an acute nonlymphocytic leukemia 18 mo followingthe initial GCT; the leukemia retained the i(12p) of the primarytumor and, in addition, acquired a del(5)(q 13) (6). In the secondcase (No. 203), a mediastinal GCT comprised discreet segmentsof teratoma and ERMS. Clonal relatedness was demonstratedby the presence of i(12p) in both, and the ERMS in additionacquired a der(2) t(2;?)(q37;?) (7). In an additional case (No.243), only the transformed state was available for cytogeneticanalysis, a neuroepithelioma which exhibited both an i(12p)and a der(l 1) t(l I;?)(q24;?). In addition to the above, 5 mixedtumors (Nos. 159A, 2ISA, 244A, 246A, and 262A) exhibitedmalignant differentiation. In one of these (No. 246A), thetransformation was to ERMS which showed a der(2)t(2;l)(p21;qll) and multiple copies of chromosome 2. In another of these (No. 215A), the transformation was to a squa-
2286
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
MALE GERM CELL TUMOR CVTOGENETIC ANALYSIS
Table 2 Clinical, histological, and karyotypic data on germ cell tumors with donai chromosome abnormalities
Tumor Prior Tumorno. Stage therapy Histology Site"state155B
IV CT¿ T, EC Lung M
175A III N EC TestisPI78B
III N EC, S Testis P
179A II CT EC AscitesM184B
III CT T Lung M
199A III CT T RetroperitoneumM207A
I N S Testis P
208B II N EC, YS Spermatic cord M
209 A II N EC Paraaortic LN MAFP/b-HCG/LDH*No.
ofcells
studiedPrimary
testicular
0/0.3/23310110/10/173
20670/1380/1289
14
1900/1.9/1921230/0/206
27
0/0/24670/0/871
13
0/0/185 10
116/8.6/160 14Modal
chromosomeno.46/49
46/6746/60
46/8646/65
10546/50
46/56
46/62Karyotype'46.XY
(4)/38-55, X, -Y, +7, -20,+22,+der(l)t(l;?)(p36;?),+del(5)(ql3), +i(12p)(6)46.XY
(10J/58-86, XY, +X, (3N+/-). -4, -7, -8,-9, -10, -11, -13, -14, -16, +17, -18, -19,+del(6)(q21). +del(7)(q22), +i(9q),+i(12p).46.XY
(12)/60, XY. +X, +Y, +2. +7, +8, +9, +9,+ 17, +der(ll)t(9;ll)(ql2;ql3), +der( 17)1(1:17)(q23;q25)(2)46.XY
(14)/49-125, XY, +Y, (4N+/-), -4, -8. -8,-9, -10, -14, -15, -15, -16, -18, -19, -21,+22, +del(l)(p31), +del(6)(q21).+del(6)(q21),46.
XY (12)/48-75, XY, (3N+/-), -2, -5, -6.-8,-10,-11, -13, +17, -19, -20, +del(6)(q21),
100-1 16, XY, +X, +X, (4N+/-), +2. +3. +3. -5,+9,+12,-18, -18, +21, +der(l)t(l;?)(p36;?),
+der( 1)t(l ;?)(p36;?), +der(7)t(7;?)(p22;?),+der(7)t(7;?)(p22;?),+i( 12p), +i( 12p)+i( 12p),+i( 12p), +der( 17)t( 17;?)(pl 3;?),+der( 17)t( 17;?)(p 13;?),+mar46,
XY (6)/47-50, XY, +Y, -3, -4, -9, -12, +15,+ 16, +17, +20, +del(l)(pl 1), +del(4)(pl5),
+der(9)t(9;?)(p24;?)(7)46,
XY (2)/52-62, XY, +X, -1, +3, +7, +9.+13.+14, +15, +16, +21, +del(l)(p32), +i(12p), +mar
(8)46,XY (6)/60-64, XY, +X, +Y, +3. -6, +8, +9, +13.
210A II N EC, YS Cavai LN M
2ISA III CT T, SqC Paraaortic LN M
+ 14,+17,+18,+19,+21,+der( 11)t( 11;?)(q25;?)+i( 12p). +i( 12p), +i( 12p),+mar (8)
101/0.9/146 11 46/69 46, XY (2)/54-69, XY,+X.+Y, (3N+/-),-1.-5.-10-10, -14. -15. +16, -17, +del(5)(ql3),+del(10)(pl3), +i(12p), +i(12p) (9)
16.5/0/163 19 50 47-50, XY.-2,-6,+16.+der(l)t(l:?)(p22;?).+der(2)t(2;?)(q37;?), +i+der(20)t(20:?)(ql3;?)
218A II CT T
219A II NEC220A
III CT T
221A II NYS224A
III NEC225A
II CTT225B
II CTT228A
II CT TCavai
LN M 0/0/255 24 46/58 46, XY (2J/50-58, XY. +1, +2, +3, +3, +9, +12,+ 12, +13, +21, +del(5)(ql3), +i(12p), +i(17q)(22)Retroperitoneum
M 18.9/0.3/301 21 46/56 46, XY (6J/48-60. XY, +3. +12, +13. +14, +20,+21,+del(l)(qll),+i(12p). +i(12p),
+der(16)t(16;?)(q24;?)(15)CavaiLN M 0/0/117 21 51 48-54, XY, +X, -Y, -1, -5, -5, +8, -10, -10, +12,
+ 17, -21, +der(l)t(l?)(p36;?). +del(5)(ql3),+der(7)t(7;?)(q 11.2;?ABM). +der( 10)t( 10;?)(p 13;?),+del( 12)(q 11), +i( 12p), +der( 12)t( 12;?)(q 13;?),Retroperitoneum
M 270/1.1/118 14 62/106 57-62, XY, +X, +Y, (3N+/-), -1, -2, -5, -6,-7,-8,-10, -11, -12, -12, -13, -14, -14, -15.
-19, -20, -21,+del(l)(p22),+der(6)t(6;?)(q25;HSR::?), +der( 11)t( 11;?)(p 15;?).+der( 12)t( 12;?)(p 11;?). +i( 12p). +i( 12p)+ 1-2mar(8)/90-121, XY, +X, +Y, (4N+/-), +2, +3, +6,+9, -11, +16, +17, +19, +del(l)(p22),+der(6)t(6;?)(q25;HSR::?), +der( 11)t( 11;?)(p 15;?).+i(12p). +i(12p), +i(12p), +marl(HSR), +mar2(6)Testis
P 4330/1890/2517 15 46/95 46. XY (7)/78-95, XY, +X, +Y, (4N+/-), -4. -11,-1 1, +17, +22, +der(l l)t(l I;?)(q23;?), +i(12p),+i(12p), +mar(8)LN
M 0/0.4/175 10 65 57-66, XY, +X, (3N+/-), -1, -5, -6, -6, -10, -11,+ 12, +13, -16, -19, -20, +21, -22,+del(6)(q21),Spermatic
cord M 0/0.4/175 18 46/62 46, XY (4)/57-62,XY, (3N+/-), -1, -6, -10, -15,-16, -17, -18, -19, -22. +del(6)(q21), +i(12p)
(14)CavaiLN M 0/0/172 21 64 48-64, XY, (3N+/-), -2, -3, -4, -4, -6, +7, -9,
-9, -13, -13. -14, -15, -18, -19, -20, -21.-21, +del(3)(p21), +del(3)(p23),+der(4)t(4;?)(q35;?), +del(5)(pl5). +i(12p),+i(12p).+der(20)t(20;?)(ql2;?)
2287
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

MALE GERM CELL TUMOR CYTOGENETIC ANALYSIS
Table 2 Continued
Tumor Priorno. Stage therapy Histology Site°
No. of ModalTumor cells chromosome
state AFP/b-HCG/LDH* studied no. Karyotype'
229A II CT T Testis
260A 11
261A I
262A I
P ' 1660/0.5/359
23IA II CT T RetrocavaILN M 0/0/188
233A II N EC Testis P 87/55/250
236A l N IT, EC, Testis PYS
238 A II N EC
240A III CT T
242 A II N EC
243A IV CT NE
Retroperitoneum M
Cavai LN
Cloquet LN
M
M
246A II CT T. ERM Retroperitoneum M
247A II N EC Interaortic LN M
248A II N EC Retroperitoneum M
249A III N C
251A I N S
CT T
Testis
Testis
Retroperitoneum M
N S Testis
N T, ERM Testis
235A III CT YS
235B III CT T
Mediastinum M
Mediastinum M
P244A III CT T, EC, YS, MediastinumSAR
365/7/161
0/1/163
Retroperitoneum M 0/0.9/157
0/1.9/167
0/1/373
0/0/150
0/0/170
111/4/134
0/265/202
0/0/160
22/1/197
0/0/272
393/0/194
19 124
21 56
12 46/73
24 66
14 46/56
14 56
24 67
8 76
14 46/60
12 46/48
16 46/63
13 46/48/91
10 46/94
13 46/57
11 46/47
26 55/55
Primar)' mediastinal
24.2/0/192 12 51
24.2/0/192 17 48/49
0/0/399 17 86
90-124. XY, +X, +X, +X, +Y, (4N+/-). +2, +3, +5,+6, +8. +9, +11, +11, +13, +14, +15, +17, +17,+20.+21,+21,+21,+21,+22,+der(l)t(l;?)(p36;?), +del(5)(ql3), +del(6)(q2l),+del(7)(q22), +i(12p). +i(12p). +i(12p). +i(12p),+der(17)(pl3;?),+l-2mar
49-58, XY, +X, +1, +5, +7, -12, +17, +20, +21.-22, +der(l)t(l;?)(p36;?). +del(8)(ql3),+der( 12)t( 12;?) (p 12;?), +der( 12)t( 12;?)(p 13;?).+marl t(l::?::7) (q25::?::ql 1.2)
46.XY (2)/60-90. XY. +X, +Y, (3N+/-). +12, -19,
51-66, XY, +X. +Y, (3N+/-), -4, -5. -9, -10. -13,-18. -19. +i(12p). +i(12p)
46, XY (7)/54-77, XY, +X, +1, +9, +12, +15, -19,+20. +21. +22. +der(7)t(7;?)(q22;?). +marl(ABM),+mar2(ABM)(7)
47-56. XY. +5, +6, +12, -16. +17. +19, +22, +HSR(Iq44). +dcr(8)t(7;8)(ql 1.2;q24). +der(12)(?::pl 1-q24::?), +der(15)t(15;?)(pl I;?),+der(l6)t(16;?)(q24;?)
52-68, XY, +X, (3N+/-). -4, -6, +7, -9. -10. -1 1,+ 13, -15, -16, -17, -19, +i(l2p).+der(16)t(16;?)(q22;?), +i(17q). +mar(ABM)
60-76, XY, +X, (3N+/-), +2. -3, -5. -1 1, -1 1.-15, +21, +21, -22, -22. +der(l 1)1(11;?)(q24;7),+der( 11)t(11;?Xq24:?), +der( 11X?::pl5-q24::7),
+der( 12)t( 1; 12)(q 11;q 13), +dcr( 13)t( 13;?)(p 11;?),+der( 15)t( 15;?)(pl 1:?), +t( 15; 15)(pl 1:pl 1). +marl .+marl
46, XY (10)/52-60, XY, +X, (3N+/-), -1, -5, -6,-7, -8, -9, -10, -14, -14, -15, -15, -16, -17,-19, -19, +del(l)(q25). +der(2)t(2;l)(p21;ql I),+i(12p), +i(12p), +marl (4)
46.XY (7J/47-49, XY, -2, +5, -6. +18, +der(9)t(2;9)(qll;P24). +i(12p)(5)46, XY (41/55-63. XY, (3N+/-), -1, -4. -5, -7, -8.
-9. -10. -11. -15, -18. -22, +del(l)(pl3),+der(4)t(4;?)(q35;?), +i(12p). +marl(ABM), +mar2
(ABM)(12)46, XY (5)/47-50, XY. -12. +17. +del(l)(pl 1).
+del(7)(q21) (3V73-96. XY, +X, +Y, (4N+/-),-12, -15, +mar(5)
46. XY (6)/87-94, XY, +X, +Y, (4N+/-), -6, -6,-9, - 12, +22, +del( 1)(p 11). +del(6)(q 14),+del(6)(q 16), +der( 12)t( 12:?)(p 13;?).
46, XY (2)/53-57, XY, +Y, +4, +12, +13, -16, +21,+del( 1)(p22), +del(6)(q 15). +der(9)t(9;?)(p 11;?),
), +mar(ll)
46, XY (7)/46-48, XY, +18, +i(12p) (4)
52-56. XY. +3, +7. +8. -10, -1 1. +12, +14, +15,+ 17, +20. +del(10)(q24). +del(l I)(q23), +i(I2p)(18)/52-56. XY, +3, +7, +8, -1 1, +12, +14. +15,+ 17, +20. +del(ll)(q23). +i(12p)(8)
46-51, XY, +21, +22, +del(l)(p22), +i(12p),+del(16)(ql2)
45-49, XY, +21. +i(12p) (14)/49, XY, +21, +i(12p),+del(16)(ql2)
48-97.XY,+X,+Y,(4N+/-),-l,-2,+3,-5,-6, -8, +9,-10, -13, -13, -15,-17, -17, -19,+20. +i(l2p).
" Site of tumor sampled for karyotype analysis.* Serum tumor markers at the time of biopsy: AFP. n-fetoprotein (normal. 0 to 40 ng/ml); b-HCG. B-chorionic gonadotropin (normal. 0 to 2 ng/ml); LDH. láclate
dehydrogenase (normal, 60 to 200 units/liter).c Modal karyotypes are presented which are described according to the composite karyotype convention as defined in 1985 (17).''CT, chemotherapy; T, mature teratoma; EC. embryonal carcinoma; M, metastatic: N, none; P, primary; S. seminoma; YS. yolk sac; LN, lymph node; SqC.
squamous carcinoma: ABM, aberrantly banded marker: IT, immature tcratoma: NE, neurocpithelial: ERM. embryonal rhabdomyosarcoma; C, choriocarcinoma;SAR, sarcoma.
2288
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

MALE GERM CELL TUMOR CYTOGENETIC ANALYSIS
5 - nonseminoma
J L J L _1_ I I I L J_1 2 3 4 5 6 7 8 910111213141516171819 20 21 22 x y
ChromosomeFig. 1. Mean modal numbers of short and long arms of each chromosome in
seminomatous and nonseminomatous GCTs (structural abnormalities, when awhole chromosome arm is present are also included).
f
1p36
r-5q13
1p32
P6q21
1p22
Si-7qtt2 7q22
mous carcinoma with embryonic muscle differentiation whichexhibited a der(2) t(2;?)(q37;?).
DISCUSSION
We have performed karyotypic analysis of 124 serially ascertained adult male GCTs representing all histological types andof testicular and extragonadal origin. One or more copies ofi(12p), the characteristic marker of germ cell tumors, werepresent in 86% of these tumors. We have recently shown, byusing fluorescence in situ hybridization with a chromosome 12centromere-specific «-satellite DNA probe and by analysis ofrestriction fragment length polymorphisms of loci on 12q, thatthe most probable mechanism of i(12p) formation is by acentromeric interchange between nonsister chromatids of thehomologs during S or G2 (19).
Greco et al. (20) have shown that a small group of patientswith midline undifferentiated carcinoma respond to cisplatinchemotherapy similar to GCT, suggesting that some of thesetumors indeed are of germ cell origin. We have recently shownthat cytogenetic and/or DNA analysis can assist in the diagnosisof poorly differentiated midline carcinomas and that a subsetof them, indeed, are GCTs (18). In the present series, weencountered three midline carcinomas (Nos. 75A, 176A, 212A),2 with an undifferentiated histology and one with the histologyof seminoma. Two of the three tumors were i(12p) positive,confirming their germ cell origin, while the other exhibited adel(12q).
Although the high incidence of i(12p) in GCTs suggests animportant role for this marker in the biology of these tumors,other rearrangements affecting 12q, in particular deletions andrearrangement breaks involving the region 12ql3-q22, wereidentified by us. Notably, two of the tumors which did notexhibit i(12p) had clones with monosomy 12, and a third onehad a del(12q). Deletions of 12q have also been reported by usin established GCT cell lines (21). Based on these data, we havepreviously suggested loss of a candidate tumor suppressor geneon 12q as the initial genetic change in these tumors (14, 21).
ir9p24
12q13
ir10p13
12q15
ìf'{
11q23
,"
¡(12p)
«*
12p13
¡(13p11
21q11 ABMs
tir
i\
èli13
<»19
Õ v
IH
ÃŒli14
r f20
:Ã10
!15
21 22
i) IH
11
16 17
XX Y
12
li
18
Õ i
ABMFig. 2. Nonrandom breakpoints encountered in GCTs. Each of the breakpointswas found in three or more different patients. Arrows, sites of breakpoints. ABMs, Fig. 3. Representative karyotype from Patient 242A. Arrows, sites of break-aberrantly banded markers found in S different patients. points. *. nonclonal marker.
2289
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

MALE GERM CELL TUMOR CVTOGENETIC ANALYSIS
A K
u<
i)
it13
19
14 15
1 "!
10 11
16 17
•¿�>«
12
if18
20
4* 4
21 22
1Õ •¿�XX Y
Fig. 4. Representative karyotype from Patient 231 A. Arrows, sites of breakpoints. *, nonclonal marker.
Some of the nonrandom rearrangements encountered in thisstudy were associated with certain histologies, suggesting thatthey may affect critical genes involved in differentiation pathways or are responsible for malignant development. Thus, thelp32-36 region has previously been reported as a nonrandomsite of rearrangement in teratomas (12). We confirm thisobservation.
In this series, we have encountered three cases of malignanttransformation of teratomas to distinct histological types inwhich a specific rearrangement frequently found in de novotumors of the same histology was acquired by i(12p)-positiveGCTs: a del 5(ql3) in a case of a leukemic transformation (6);a translocation affecting 2q37 in the ERMS component of amediastinal tumor comprising a discreet, clonally related, teratoma and ERMS (7); and a translocation affecting 1Iq24 in acase of neuroepithelial transformation of a teratoma, a breakpoint which has previously been reported in de novo neuroepi-theliomas (22). In addition to the above, some rearrangementsnoted were predominantly seen in metastatic lesions, such asthose affecting 10pl3 and 12pll-ql3. It is possible that theserearrangements may affect genes the products of which renderthe cells more susceptible to invasion and metastasis.
Cytological evidence of gene amplification in the form ofdouble minute chromosomes and/or HSRs was present in 6specimens. An additional 6 specimens showed aberrantlybanded marker chromosomes, which may also represent geneamplification. All 12 specimens were resected from extrago-nadal sites; 11 were metastatic lesions and one was a primarymediastinal lesion. These data suggest amplification of a gene(s)associated with metastatic progression of GCTs. Hybridizationof DNA from cultured cells of two HSR-bearing tumors with apanel of probes for genes known to be amplified in other tumorsystems did not identify the amplified gene, suggesting amplification of a novel gene(s) (Ref. 14; Footnote 4). Isolation ofthis amplified gene(s) is of considerable interest since it mayshed light on the basis of refractory tumors.
De Jong et al. (23) suggested a model for the initial andsubsequent steps in GCT development based on changes in
4 Unpublished results.
GCT BREAKPOINTSMETASTATIC/PRIMARY
(40) (25)ooo«o
•¿�OOA
OQ®
BtAl
DOS
oSo
« o;lì1
Fig. 5. Ideogram showing breakpoints in GCTs encountered in this study. Onthe left of each chromosome are breakpoints encountered in metastatic specimens.On the right of each chromosome are breakpoints encountered in primaryspecimens. O, teratoma (18); A, embryonal carcinoma (13); D, seminoma (7); ®,mixed with malignant transformation (5); •¿�,mixed (6); •¿�,combined (4); 0, yolksac (4); *, malignant transformation (4); O, choriocarcinoma (2); A, undifferen-tiated carcinoma (2).
ploidy levels in target cells. According to this model, the firststep in the progression of GCTs is polyploidization of a dys-
plastic germ cell precursor, resulting in carcinoma in situ. Aninitial loss of DNA (by nondisjunction) leads to invasive seminoma through which all other types develop. Nonseminomasare suggested to develop by further rapid loss of DNA. However, our data presented here show that not all adult male germcell tumors pass through a polyploidization (tetraploid) stage,since some of them have near-diploid or hyperdiploid chromo
some numbers, which could be better explained by simplenondisjunctional events in diploid cells.
The data presented here are consistent with our model ofGCT origin based on an initial loss of function of a tumorsuppressor gene on 12q. The frequent ras gene mutationsrecently reported in these tumors by us (24) and others (25)may play a role in furthering their proliferative potential. Wehave also identified a number of cytogenetic pathways of malignant progression which include nondisjunction, nonrandomrearrangements affecting specific chromosomal sites, and geneamplification. We also showed that malignant differentiationof teratoma cells to specific histologies may be associated withthe same nonrandom or specific chromosome changes that arefound in de novo tumors of the same histologies. Thus, thestudies reported here present a number of molecularly testablemodels for the understanding of the biology and clinical behavior of these tumors.
ACKNOWLEDGMENTS
We thank Marilyn Evans for help with preparation of the manuscript.2290
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from
MALE GERM CELL TUMOR CYTOGENETIC ANALYSIS
REFERENCES
1. Ulbright, T. M., and Roth, L. M. Recent developments in the pathology ofgerm cell tumors. Semin. Diagn. Pathol., 4: 304-319, 1987.
2. Holstein, A. F., Schuette, B., Becker, H., and Hartmann, M. Morphology ofnormal and malignant germ cells. Int. J. Androl., 10: 1-18, 1987.
3. Skakkebaek, N. I1.., Berthelsen, J. G., Giwercman, A., and Mueller, J.Carcinoma-/n-jiru of the testis: possible origin from gonocytes and precursorof all types of germ cell tumours except spermatocytoma. Int. J. Androl., II):19-28, 1987.
4. Pugh, R. C. B. Combined tumours, in: R. C. B. Pugh (ed.), Pathology of theTestis, pp. 245-258. Oxford: Blackwell, 1976.
5. Ulbright, T. M., Loehrer, P. J., Roth, L. M., Einhorn, L. H., Williams, S.D., and Clark, S. A. The development of non-germ cell malignancies withingerm cell tumors. Cancer (Phila.), 54: 1824-1833, 1984.
6. Chaganti, R. S. K., Ladanyi, M., Samaniego, F., Reuter, V., Jhanwar, S.,and Bosl, G. J. Malignant hematopoietic differentiation of a germ cell tumor.Genes Chromosomes Cancer, /.- 83-87, 1989.
7. Rodriguez, E., Reuter, V. E., Mies, C., Bosl, G. J., and Chaganti, R. S. K.Abnormalities of 2q: a common genetic link between rhabdomyosarcomaand hepatoblastoma. Genes Chromosomes Cancer, 3: 122-127, 1991.
8. Atkin, N. B., and Baker, M. C. Specific chromosome change, i(12p), intesticular tumors? Lancet, 2: 1349, 1982.
9. Atkin, N. B., and Baker, M. C. i(12p): specific chromosomal marker inseminoma and malignant teratoma of the testis? Cancer Genet. Cytogenet.,10:199-204, 1983.
10. Gibas, Z., Prout, G. R., Pontes, J. E., and Sandberg, A. A. Chromosomechanges in germ cell tumors of the testis. Cancer Genet. Cytogenet., 19:245-252, 1986.
11. Castedo, S. M. M. J., De Jong, B., Oosterhuis, J. W., Seruca, R., te Meerman,G. J., Dam, A., and Koops, H. S. Cytogenetic analysis of ten humanseminomas. Cancer Res., 49:439-443, 1989.
12. Castedo, S. M. M. J., de Jong, B., Oosterhuis, J. W., Idenburg, V. J. S.,Seruca, R., Buist, J., te Meerman, G. J., Koops, H. S., Sleijfer, D. T.Chromosomal changes in mature residual teratomas following polychemoth-erapy. Cancer Res., 49: 672-676, 1989.
13. Castedo, S. M. M. J., de Jong, B., Oosterhuis, J. W., Seruca, R., Idenburg,V. J. S., Dam, A., te Meerman, G. J., Koops, H. S., and Sleijfer, D. T.Chromosomal changes in human primary testicular nonseminomatous germcell tumors. Cancer Res., 49: 5696-5701, 1989.
14. Samaniego, F., Rodriguez, E., Houldsworth, J., Murty, V. V. V. S., Ladanyi,
M., Lele, K. P., Chen, Q., Dmitrovsky, E., Geller, N. L., Reuter, V., Jhanwar,S. C., Bosl, G. J., and Chaganti, R. S. K. Cytogenetic and molecular analysisof human male germ cell tumors: chromosome 12 abnormalities and geneamplification. Genes Chromosomes Cancer, /: 289-300, 1990.
15. Bosl, J. G., Dmitrovsky, E., Reuter, V. E., Samaniego, F., Rodriguez, E.,Geller, N. L., and Chaganti, R. S. K. Isochromosome of chromosome 12p: aclinically useful chromosomal marker for male germ cell tumors. J. Nati.Cancer Inst., 18: 1874-1878, 1989.
16. Hendry, W. F., Barrett, A., McElwain, T. J., Wallace, D. M., and Peckham,M. J. The role of surgery in the combined management of métastasesfrommalignant teratomas of testis. Br. J. Urol., 52: 38-44, 1980.
17. Harden, D. G., and Klinger, H. P. (eds.). An International System for HumanCytogenetic Nomenclature. Basel: Karger, 1985.
18. Motzer, R. J., Rodriguez, E., Reuter, V. E., Samaniego, F., Dmitrovsky, E.,Bajorin, D. F., Pfister, D. G., Parsa, N. Z., Chaganti, R. S. K., and Bosl, G.J. Genetic analysis as an aid in diagnosis for patients with midline carcinomasof uncertain histologies. J. Nati. Cancer Inst., S3: 341-346, 1991.
19. Mukherjee, A. B., Murty, V. V. V. S., Rodriguez, E., Reuter, V. E., Bosl, G.J., and Chaganti, R. S. K. Detection and analysis of origin of i(12p), adiagnostic marker of human male germ cell tumors, by fluorescence in situhybridization. Genes Chromosomes Cancer, 3: 300-307, 1991.
20. Greco, F. A., Vaughn, W. K., and Hainsworth, J. D. Advanced poorlydifferentiated carcinoma of unknown primary site: recognition of a treatablesyndrome. Ann. Intern. Med., ¡04:547-553, 1986.
21. Murty, V. V. V. S., Dmitrovsky, E., Bosl, G. J., and Chaganti, R. S. K.Nonrandom chromosome abnormalities in testicular and ovarian germ celltumor cell lines. Cancer Genet. Cytogenet., 50:67-73, 1990.
22. Whang-Peng, J., Triche, T. J., Knutsen, T., Miser, J., Douglass, E. C., andIsrael, M. A. Chromosome translocation in peripheral neuroepithelioma. N.Engl. J. Med., 311: 584-585, 1984.
23. De Jong, B., Oosterhuis, J. W., Castedo, S. M. M. J., Vos, A., and teMeerman, G. J. Pathogenesis of adult testicular germ cell tumors. A cyto-genetic model. Cancer Genet. Cytogenet., 48: 143-167, 1990.
24. Ganguly, S., Murty, V. V. V. S., Samaniego, F., Bosl, G. J., and Chaganti,R. S. K. Detection of preferential NRAS mutations in human male germ celltumors by the polymerase chain reaction. Genes Chromosomes Cancer, 1:228-232, 1989.
25. Bos, J. L. ras oncogene in human cancer: a review. Cancer Res., 49: 4682-4689, 1989.
2291
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from

1992;52:2285-2291. Cancer Res Eduardo Rodriguez, Susan Mathew, Victor Reuter, et al. Germ Cell TumorsCytogenetic Analysis of 124 Prospectively Ascertained Male
Updated version
http://cancerres.aacrjournals.org/content/52/8/2285
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
Research. on December 5, 2014. © 1992 American Association for Cancercancerres.aacrjournals.org Downloaded from




















