
Nr. Surg. 774) 15.10.2020 - Fmi - Facultatea de Matematică și ...

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/authorsrights
Author's personal copy
British Journal of Oral and Maxillofacial Surgery 51 (2013) 922–927
Available online at www.sciencedirect.com
Evaluation of p53 protein as a prognostic factor for oralcancer surgeryTommaso Cutilli a,∗, Pietro Leocata b, Vincenza Dolo c, Emma Altobelli d
a Department of Life, Health & Environmental Sciences, Maxillofacial Surgery Unit, University of L’Aquila, Italyb Pathological Anatomy, University of L’Aquila, Italyc Clinical Pathology, University of L’Aquila, Italyd Medical Statistics and Epidemiology, University of L’Aquila, Italy
Accepted 24 May 2013Available online 20 June 2013
Abstract
We have analysed concentrations of the p53 protein in advanced oral carcinomas immunohistochemically and genetically to detect thepercentage of overexpression of this antioncogene that indicates a high probability of mutation. This would point to it being a useful prognosticfactor, if we consider the importance of the relation between genetic alterations of p53 and poor overall survival. Seventy-five non-consecutivepatients with oral squamous cell carcinoma and metastatic nodes were enrolled if there was homogeneity in histopathological grading (G2)of their tumours, and they were treated according to a multidisciplinary treatment plan. Monoclonal antibodies, extraction of DNA, andamplification of the polymerase chain reaction (PCR) were used for the immunohistochemical and genetic analyses. There was a significantinverse correlation between p53 overexpression and response to chemotherapy and a stronger association between high P53 overexpression(%) and a genetic mutation of p53 (p = 0.0001). More than 50% overexpression indicated a strong probability of genetic mutation. There wasno association between response to chemotherapy and age-groups or TNM classification (p = 0.2), but there was a significant one betweensex and site of tumour (p < 0.001). Three prognostic factors were significantly related to prognosis: site of tumour (p = 0.01), response tochemotherapy (p = 0.002), and immuno p53 (p = 0.0001). A tumour that is characterised by p53 overexpression of more than 50% indicates apoor prognosis.© 2013 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.
Keywords: Oral cancer; Surgery; Multimodal treatment; p53 Status
Introduction
In oral carcinomas the site, size, and advanced stage of thetumour, invaded cervical nodes, extracapsular spread, andundifferentiated malignant tissue are associated with poorprognosis. These classic elements are still considered impor-tant in the planning of treatment and for the evaluation ofprognosis.1–4 Resection is the main treatment, and is oftenincluded in multidisciplinary protocols.5,6
∗ Corresponding author. Tel.: +39 862368558; fax: +39 862368547.E-mail addresses: [email protected] (T. Cutilli),
[email protected] (P. Leocata), [email protected] (V. Dolo),[email protected] (E. Altobelli).
The TNM classification often does not explain the clinicalbehaviour of the tumour, and it is quite common for tumourswith equivalent TNM and homogeneous histopathologicalgrading to evolve differently in terms of natural history,response to treatment, outcome of radical resection, andoverall survival. The answer must be found in the biologi-cal pattern of the tumour, which is closely connected to itsbehaviour (more or less aggression), and that can predict theprognosis. The oncogenetic pattern may therefore provideuseful indications for adequate treatment, and often requiresa multidisciplinary team approach as most patients are elderlywith advanced tumours.7–10
Varying percentages of oncogenes expressed, and theirrelated modified chromosomal sites, have been identified inoral tumours. These include N-ras (5%–10%) and L-myc
0266-4356/$ – see front matter © 2013 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.bjoms.2013.05.150

Author's personal copy
T. Cutilli et al. / British Journal of Oral and Maxillofacial Surgery 51 (2013) 922–927 923
(6%–11%) on chromosome 1; N-myc (4%–38%) on chro-mosome 2; genomic fragile sites on chromosome 3; K-ras(6%–33%) on chromosome 6; Erb-1 (3%–25%) on chromo-some 7; c-myc (5%–40%) on chromosome 8; genomic fragilesites on chromosome 9; genomic fragile sites on chromosome10; H-ras (30%–40%), erb-1, erb-2 (30%), INT-2, Bcl-1,PRAD-1 (60%) on chromosome 11; and K-ras (5%–10%) onchromosome 12. We have also detected appreciable expres-sion of p16, p21, p27, pRb, Ki-67 and p63-alpha, in particularthe delta-N shaped.11–13
However, the most studied oncogene is undoubtedly thep53 suppressor gene (from 4% to 50% expressed), whichis detected on chromosome 17, and today it is evident thatknowledge of the patient’s p53 status is of great impor-tance in the management of oral squamous cell carcinoma(SCC).14–18 In our previous research studies we used a costlybiomolecular analysis (a polymerase chain reaction (PCR)technique for extraction and amplification of DNA), whichshowed that mutations of this genic product were associatedwith a poor response to induction chemotherapy, the outcomeof radical resection, and overall survival.19–24
The current need is to be able to predict the tumour’sresponse to treatment and to define prognosis by usingimmunohistochemical analysis alone without having to resortto such expensive methods. To achieve this we planned astudy to define the value of p53 overexpression that cor-responds to a strong probability of mutation of the tumoursuppressor gene. The importance is that there may be rela-tions between the genetic alterations in p53 and poor overallsurvival. Here we report the results of this study.
Materials and methods
Despite the difficulties associated with complex biomolec-ular analysis and its high cost, we have been able to enrol75 non-consecutive patients with advanced oral SCC whowere treated at the Maxillofacial Surgery Operative Unit ofthe University of L’Aquila, Italy. They were 57 men and18 women (mean age 67, range 57–72 years) who wereselected from a total of 420 patients with oral cancer who wereunder observation from January 1992 to January 2012. Inclu-sion criteria were: homogeneity of histopathological grading(G2); and inclusion in a multidisciplinary treatment plan(neoadjuvant chemotherapy, radical resection, and postop-erative radiotherapy), which was defined by the oncologicalteam. The histopathological analysis was made by the samepathologist. The grading “G2” diagnosis was based on mod-erate cellular differentiation. We enrolled tumours with thesame pathological grading because tumours with differentgrades would give unreliable data about the behaviour of p53.We chose the intermediate grade G2 because we thought wewould get a better biomolecular analysis. The patients wereall smokers.
Induction chemotherapy was given according to thefollowing protocol: cis-diaminedichloroplatinum (CDDP,
20 mg/m2 intravenously on days 1–5) and 5-fluorouracil(5-FU, 1000 mg/m2 continuous infusion, volumetric pump2 ml/hour for 5 days). After 3 cycles of chemotherapytumours were restage clinically and by computed tomography(CT) and magnetic resonance imaging (MRI). Radical exci-sion and neck dissection followed by adjuvant radiotherapycompleted the treatment. To achieve the aim of the research,a monoclonal p53-antibody (DO-7 clone) was used for theimmunohistochemical study. We counted the tumour cells,with or without expression/field, for the assessment. DNAextraction and PCR amplification (175, 181, and 189 p53codons) were used for the genetic biomolecular analysis.
The frequency of p53-related mutations and the frequencyof TNM, p53, and response to chemotherapy were the pro-gnostic factors that were evaluated using the chi square testfor trend. Correlation was done with Spearman’s correlation.
We used survival analysis to describe the overall mortality,and analysis of prognostic factors was by univariate analysis.The product limit method was used to evaluate the probabilityof survival to 12 months in relation to four clinical and geneticvariables. Differences between survival curves were assessedusing the log rank test. Probabilities of less than 0.05 wereaccepted as significant, and statistical tests were done withthe aid of SAS/STAT 9.2, 2nd ed.
Results
There were 18 women (24%) and 57 men (76%), mean (SD)age 66 (6) years and Table 1 shows the distribution of vari-ables.
Among the tumours attached to the gingiva, 9 had p53overexpression, and there was a genetic mutation in 6. Amongthose without mutations (n = 30) response to chemotherapywas 55%–90%, and overall survival 7–21 months. In thosetumours with mutations, the response was 15%–80%, andsurvival 8–21 months.
Of the tumours of the oral floor, all 9 showed pathologicalexpression of p53 and the presence of mutation. The diseaseprogressed in all 9, with survival being 6–8 months.
In tumours of the cheek 3/9 tumours expressed p53 witha genetic mutation. Response to chemotherapy varied from70% to 90%, and overall survival ranged from 15–18 months.If there was a p53 genetic mutation the disease progressed,and overall survival was 8 months. Of the tumours of thetongue all but one showed p53 pathological expression andthey all had a mutation of the p53 gene. In those tumours witha genetic mutation neoadjuvant chemotherapy stabilised thedisease in 4, and it progressed in 7. The remaining one had apartial response, and overall survival was 10–17 months.
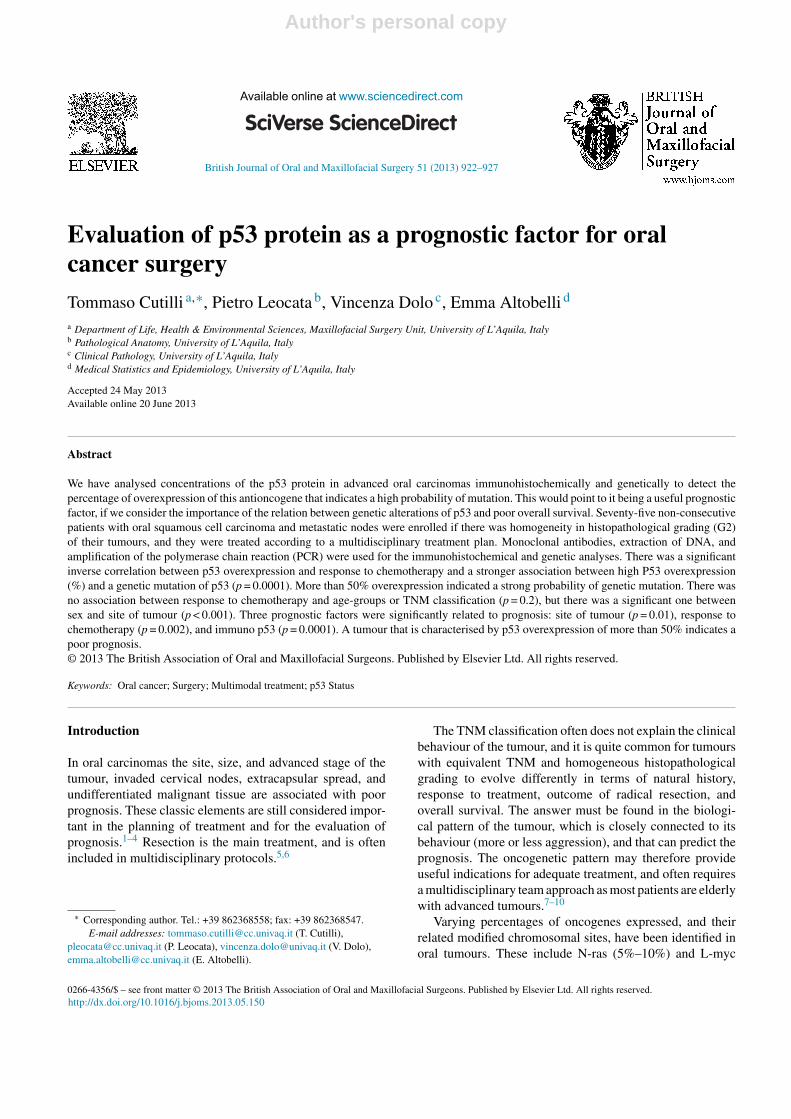
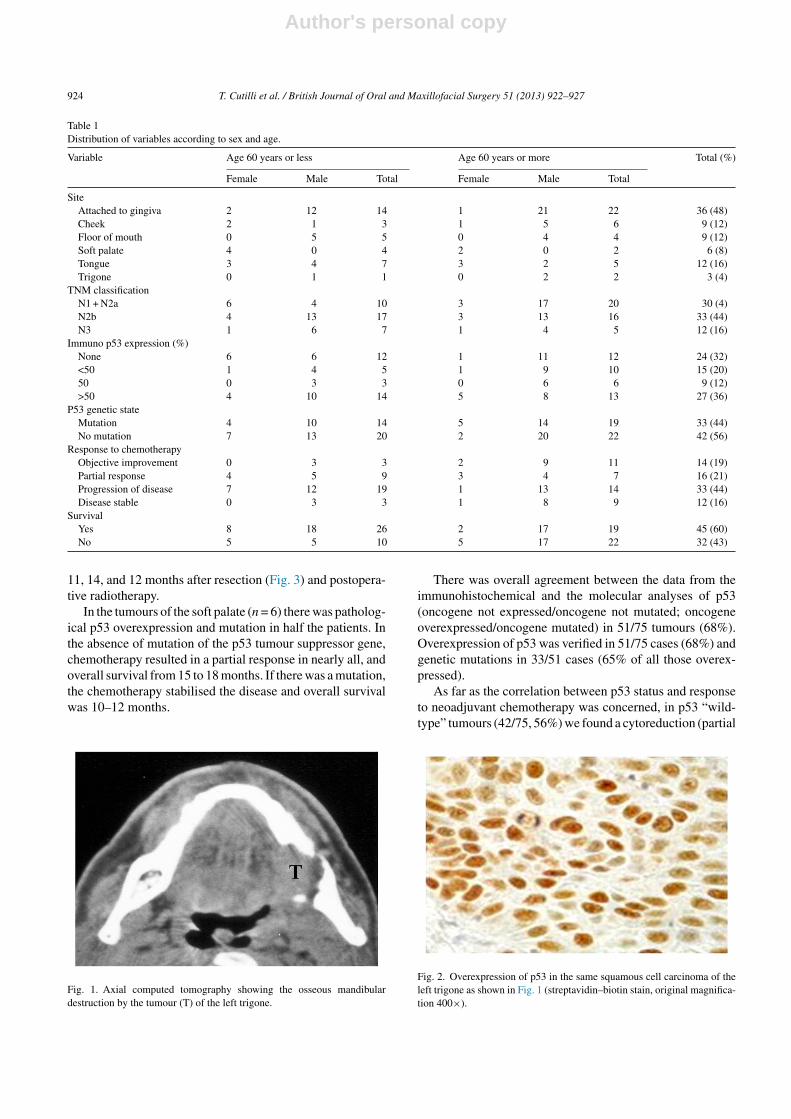
In the tumours of the retromolar trigone (Fig. 1) there waspathological expression of p53 in 1 of the 3 tumours (Fig. 2),and there was also a genetic p53 mutation (Fig. 2.). MRIshowed progression of the disease and overall survival was,
Author's personal copy
924 T. Cutilli et al. / British Journal of Oral and Maxillofacial Surgery 51 (2013) 922–927
Table 1Distribution of variables according to sex and age.
Variable Age 60 years or less Age 60 years or more Total (%)
Female Male Total Female Male Total
SiteAttached to gingiva 2 12 14 1 21 22 36 (48)Cheek 2 1 3 1 5 6 9 (12)Floor of mouth 0 5 5 0 4 4 9 (12)Soft palate 4 0 4 2 0 2 6 (8)Tongue 3 4 7 3 2 5 12 (16)Trigone 0 1 1 0 2 2 3 (4)
TNM classificationN1 + N2a 6 4 10 3 17 20 30 (4)N2b 4 13 17 3 13 16 33 (44)N3 1 6 7 1 4 5 12 (16)
Immuno p53 expression (%)None 6 6 12 1 11 12 24 (32)<50 1 4 5 1 9 10 15 (20)50 0 3 3 0 6 6 9 (12)>50 4 10 14 5 8 13 27 (36)
P53 genetic stateMutation 4 10 14 5 14 19 33 (44)No mutation 7 13 20 2 20 22 42 (56)
Response to chemotherapyObjective improvement 0 3 3 2 9 11 14 (19)Partial response 4 5 9 3 4 7 16 (21)Progression of disease 7 12 19 1 13 14 33 (44)Disease stable 0 3 3 1 8 9 12 (16)
SurvivalYes 8 18 26 2 17 19 45 (60)No 5 5 10 5 17 22 32 (43)
11, 14, and 12 months after resection (Fig. 3) and postopera-tive radiotherapy.
In the tumours of the soft palate (n = 6) there was patholog-ical p53 overexpression and mutation in half the patients. Inthe absence of mutation of the p53 tumour suppressor gene,chemotherapy resulted in a partial response in nearly all, andoverall survival from 15 to 18 months. If there was a mutation,the chemotherapy stabilised the disease and overall survivalwas 10–12 months.
Fig. 1. Axial computed tomography showing the osseous mandibulardestruction by the tumour (T) of the left trigone.
There was overall agreement between the data from theimmunohistochemical and the molecular analyses of p53(oncogene not expressed/oncogene not mutated; oncogeneoverexpressed/oncogene mutated) in 51/75 tumours (68%).Overexpression of p53 was verified in 51/75 cases (68%) andgenetic mutations in 33/51 cases (65% of all those overex-pressed).
As far as the correlation between p53 status and responseto neoadjuvant chemotherapy was concerned, in p53 “wild-type” tumours (42/75, 56%) we found a cytoreduction (partial
Fig. 2. Overexpression of p53 in the same squamous cell carcinoma of theleft trigone as shown in Fig. 1 (streptavidin–biotin stain, original magnifica-tion 400×).

Author's personal copy
T. Cutilli et al. / British Journal of Oral and Maxillofacial Surgery 51 (2013) 922–927 925
Table 2Survival analysis for clinical and genetic variables.
Variable No of patients (n = 75) No of deaths (n = 30) Cumulative probability of 12 months’ survival (%) Log rank test (p)
Site of tumourAttached to gingiva 36 20 85.6 0.01Cheek 9 1 66.7Floor of mouth 9 3 25.9Soft palate 6 2 83.3Tongue 12 4 55.6Trigone 3 0 66.7
TNM classificationN1-N2a 30 15 78.9 0.20N2b 33 10 58.5N3 12 5 41.7
Immuno p53 expression (%)None 24 8 100 0.0001<50 15 10 10050 9 4 22.0>50 27 8 32.0
Response to chemotherapyObjective improvement 14 7 70.1 0.001Partial response 16 5 35.1Progression of disease 33 13 93.9Disease stable 12 5 46.9
response ≥50% of tumoral volume). There was no associa-tion between response to chemotherapy and age group orTNM stage (p = 0.22; p = 0.6). However, we did find a sig-nificant association between sex and the site of the tumour(p < 0.001); we found that 12/14 of tumours attached to thegingiva were in men.
The cumulative survival of the entire group after 38months’ follow-up was 26% (SE 6.4). The results of uni-variate analysis of the prognostic meaning of the mainexplanatory variables are shown in Table 2. The log ranktest indicates that 3 prognostic factors were significantlyrelated to prognosis: site of tumour (p = 0.01), immunop53 (p = 0.0001), response to chemotherapy (p = 0.002)(Figs. 4 and 5). Table 3 shows a relation between immunop53 and genetic p53 (p < 0.0001).
Fig. 3. The surgical specimen (12 × 10 cm).
Finally, we evaluated the following variables using thechi square test for trend: TNM stage, immuno p53 expres-sion, and response to chemotherapy, and found no significantrelations (TMN stage p = 0.35; immunop53 p = 0.18; andresponse to chemotherapy p = 0.77).
In the cases with overexpression of p53 of more than50%, there were mutations in 72.7% of tumours. Howeverthere were 18.2% mutations in the tumours in which thehistopathological expression was lower than 50%. There wassignificant inverse correlation between overexpressed p53and the response to chemotherapy (r = −0.761; p = 0.001).
Discussion
Oncogenetic study is increasingly crucial in the staging ofa tumour, particularly among oral cancers. Classic clinicaland radiological signs, humoral markers, and histopatho-logical grading often do not reflect the natural history andthe behaviour of individual tumours. Biological screeningbased on the study of specific oncogenes and tumour sup-pressor genes give important data by which we can assessthe functional condition of tumour cells, the characteristicsof progression, the tendency to respond to the treatments ornot, the probability of relapse, and global survival.21,25
These elements are important considering that oral SCCare often at an advanced stage when they are diagnosed,and require wide surgical excision and a multidisciplinaryapproach to treatment.
P53 can certainly be correlated with induction andprogression of a tumour and we have found significant evi-dence of correlation between p53 status and prognosis inour previous research studies. They indicated that tumours

Author's personal copy
926 T. Cutilli et al. / British Journal of Oral and Maxillofacial Surgery 51 (2013) 922–927
Fig. 4. Product limit survival estimates: immunop53 expression. FOLLOW = duration of follow-up, and IMMP = immuno p53.
Fig. 5. Product limit survival estimates: response to the chemotherapy. FOLLOW = duration of follow-up, and RES = response to chemotherapy.
characterised by high p53 overexpression are resistant tochemotherapy and have reduced overall survival after sur-gical and adjuvant radiotherapeutic treatment compared withcases in which the oncogene is not overexpressed (p = 0.0005and p = 0.0001).24
Our research addresses the need for improved understand-ing of the prognostic value of p53 in oral SCC. We can verifythat in our group 50% of linked p53-antibodies in histopatho-logical specimens seem to indicate a cut-off point. If there is
more than 50% of oncogene expressed there is a strong prob-ability of genetic mutation, which compromises the gene andits related cellular function.
It is important to emphasise that as our series of patients isnot consecutive, the distribution of the oral neoplastic lesionswas not that found in a normal series.
We studied a group of patients selected on the basis ofhomogeneous histopathological grading. This allowed us togive more importance to these data because we were able to
Table 3Statistical analysis of the relation between the immunohistochemical and the genetic results. Data are number of patients.
Immuno p53 expression (%) No mutation present (n = 42) Mutation present (n = 33) Chi square test for trend
None 24 0 <0.0001<50 15 050 3 6>50 0 27

Author's personal copy
T. Cutilli et al. / British Journal of Oral and Maxillofacial Surgery 51 (2013) 922–927 927
place more emphasis, in individual cases, on the oncogeneticpattern and the specific biological features of neoplastic tissuethat can solve the problems mentioned in the introduction ofthis paper.
These data show particularly that an immunohistochem-ical tumoral pattern characterised by overexpression of p53of more than 50% indicates a poor prognosis. Immunohis-tochemical evaluation of p53 should therefore be includedroutinely in the oncological staging of oral cancers, mostly inadvanced lesions that need multidisciplinary treatment. Theoncogenic pattern supplies important elements for diagnosticand prognostic evaluation, in addition to classic screening.
Conflict of interest
There is not conflict of interest.
References
1. Bankfalvi A, Piffko J. Prognostic and predictive factors in oral cancer:the role of the invasive tumor front. J Oral Pathol Med 2000;29:291–8.
2. Jan JC, Hsu WH, Liu SA, et al. Prognostic factors in patients with buccalsquamous cell carcinoma: 10-year experience. J Oral Maxillofac Surg2011;69:396–404.
3. Liao CT, Huang SF, Chen IH, et al. Outcome analysis of patients withpn2 oral cavity cancer. Ann Surg Oncol 2010;17:1118–26.
4. Holmes JD, Martin RA, Gutta R. Characteristics of head and neck cancerpatients referred to an oral and maxillofacial surgeon in the United Statesfor management. J Oral Maxillofac Surg 2010;68:555–61.
5. Specenier P, Vermorken JB. Advances in the systemic treatment of headand neck cancers: review. Curr Opin Oncol 2010;22:200–5.
6. Jenwitheesuk K, Surakunprapha P, Chowchuen B, et al. Results of mul-tidisciplinary therapy of squamous cell carcinoma of the buccal mucosaat Srinagarind Hospital, Thailand. J Med Assoc Thai 2010;93:1262–7.
7. Pérez-Sayáns M, Somoza-Martín JM, Barros-Angueira F, et al. Geneticand molecular alterations associated with oral squamous cell cancer.Oncol Rep 2009;22:1277–82.
8. Schwartz JL. Biomarkers and molecular epidemiology and chemo-prevention of oral carcinogenesis. Crit Rev Oral Biol Med 2000;11:92–122.
9. Shah NG, Trivedi TI, Tankshali RA, et al. Molecular alterations in oralcarcinogenesis: significant risk predictors in malignant transformationand tumor progression. Int J Biol Markers 2007;22:132–43.
10. Shah NG, Trivedi TI, Tankshali RA, et al. Prognostic significance ofmolecular markers in oral squamous cell carcinoma: a multivariateanalysis. Head Neck 2009;31:1544–56.
11. Shillitoe EJ, May M, Tale V, et al. Genome-wide analysis of oral cancer-early results from the cancer genome anatomy project. Oral Oncol2000;36:8–16.
12. Murugan AK, Munirajan AK, Tsuchida N. Ras oncogenes in oral cancer:the past 20 years. Oral Oncol 2012;48:383–92.
13. Saito T, Nakajima T, Mogi K. Immunohistochemical analysis of cellcycle-associated proteins p16, pRb, p53, p27 and Ki-67 in oral cancerand precancer with special reference to verrucous carcinomas. J OralPathol Med 1999;28:226–32.
14. Sidransky D, Boyle J, Koch W. Molecular screening. Prospects for a newapproach. Arch Otolaryngol Head Neck Surg 1993;119:1187–90.
15. Boyle JO, Hakim J, Koch W, et al. The incidence of p53 muta-tions increases with progression of head and neck cancer. Cancer Res1993;53:4477–80.
16. Jones A. A general review of the p53 gene and oral squamous cell carci-noma. Ann R Australas Coll Dent Surg 1998;14:66–9.
17. Nylander K, Dabelsteen E, Hall PA. The p53 role molecule and its pro-gnostic role in squamous cell carcimonas of the head and neck. J OralPathol Med 2000;29:413–25.
18. Tandon S, Tudur-Smith C, Riley RD, Boyd MT, Jones TM. A systematicreview of p53 as a prognostic factor of survival in squamous cell carci-noma of the four main anatomical subsites of the head and neck. CancerEpidemiol Biomarkers Prev 2010;19:574–87.
19. Cutilli T, Papola F, Corbacelli A. p53 overexpression and mutation,chemoresistance and patient survival in oral and maxillofacial squamouscarcinoma. J Chemother 1997;9:123–4.
20. Cutilli T, Papola F, Di Emidio P, et al. p53 mutation and chemoresistancein oral and maxillofacial squamous cell carcinoma. Role of p53 in the cellcycle control and in the modulating action of chemotherapeutic agents.Minerva Stomatol 1997;46:671–8 (paper in Italian).
21. Cutilli T, Papola F, Di Emidio P, et al. p53 tumor suppressor protein and H-Ras oncogene in maxillofacial tumors: immunohistochemical and geneticinvestigaion, induction chemotherapy response and prognosis evaluation.J Chemother 1998;10:411–7.
22. Cutilli T, Di Emidio P, Papola F, et al. Oromaxillofacial tumours: immuno-histochemical study, genetic analysis and response to chemotherapeutictreatment. In: Paper presented at XXI national congress of Italian societyof surgical oncology.; 1997. Felice Circeo, Italy.
23. Cutilli T, Di Emidio P, Papola F, et al. P53 and H-RAS immunohisto-chemical and genetic investigation in maxillofacial tumours. In: Paperpresented at 22nd meeting of the european study group for cell prolif-eration, 5th congress of the Italian society for basic and applied cellkinetics.; 1997. Rimini, Italy.
24. Cutilli T, Altobelli E, Caniglia L, et al. Relation between p53 and H-rasoverexpression and mutation in maxillofacial tumours. In: Paper pre-sented at V international congress of the European association of surgicalsciences.; 2001. Naples, Italy.
25. Cutilli T, Di Emidio P, Papola F, et al. P53 and H-RAS immunohisto-chemical and genetic investigation in maxillofacial tumours. In: Paperpresented at 22nd meeting of the European study group for cell prolifera-tion, 5th congress of the Italian society for basic and applied cell kinetics.Rimini, Italy; 1997.
Copyright © 2022 FDOKUMEN




















