
Critical Care Nursing of Infants and Children
28
University of Pennsylvania ScholarlyCommons Miscellaneous Papers Miscellaneous Papers 1-1-2001 Critical Care Nursing of Infants and Children Martha A. Q. Curley University of Pennsylvania, [email protected] Patricia A. Moloney-Harmon e Children's Hospital at Sinai Copyright by the author. Reprinted from Critical Care Nursing of Infants and Children, Martha A.Q. Curley and Patricia A. Moloney-Harmon (Editors), (Philadelphia: W.B. Saunders Co., 2001), 1,128 pages. NOTE: At the time of publication, the author, Martha Curley was affiliated with the Children's Hospital of Boston. Currently, she is a faculty member in the School of Nursing at the University of Pennsylvania. is paper is posted at ScholarlyCommons. hp://repository.upenn.edu/miscellaneous_papers/4 For more information, please contact [email protected].
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Critical Care Nursing of Infants and Children
University of PennsylvaniaScholarlyCommons
Miscellaneous Papers Miscellaneous Papers
1-1-2001
Critical Care Nursing of Infants and ChildrenMartha A. Q. CurleyUniversity of Pennsylvania, [email protected]
Patricia A. Moloney-HarmonThe Children's Hospital at Sinai
Copyright by the author. Reprinted from Critical Care Nursing of Infants and Children, Martha A.Q. Curley and Patricia A. Moloney-Harmon(Editors), (Philadelphia: W.B. Saunders Co., 2001), 1,128 pages.
NOTE: At the time of publication, the author, Martha Curley was affiliated with the Children's Hospital of Boston. Currently, she is a faculty memberin the School of Nursing at the University of Pennsylvania.
This paper is posted at ScholarlyCommons. http://repository.upenn.edu/miscellaneous_papers/4For more information, please contact [email protected].
Please Note: The full version of this book and all of its chapters (below) can be found on ScholarlyCommons (from the University of Pennsylvania) at http://repository.upenn.edu/miscellaneous_papers/4/ Information page in ScholarlyCommons Full book front.pdf - Front Matter, Contributors, Forward, Preface, Acknowledgements, and Contents Chapter 1.pdf - The Essence of Pediatric Critical Care Nursing Chapter 2.pdf - Caring Practices: Providing Developmentally Supportive Care Chapter_3.pdf - Caring Practices: The Impact of the Critical Care Experience on the Family Chapter_4.pdf - Leadership in Pediatric Critical Care Chapter 5.pdf - Facilitation of Learning Chapter_6.pdf - Advocacy and Moral Agency: A Road Map for Navigating Ethical Issues in Pediatric Critical Care Chapter_7.pdf - Tissue Perfusion Chapter 8.pdf - Oxygenation and Ventilation Chapter_9.pdf - Acid Base Balance Chapter 10.pdf - Intracranial Dynamics Chapter 11.pdf - Fluid and Electrolyte Regulation Chapter 12.pdf - Nutrition Support Chapter 13.pdf - Clinical Pharmacology Chapter_14.pdf - Thermal Regulation Chapter_15.pdf - Host Defenses Chapter 16.pdf - Skin Integrity Chapter_17.pdf - Caring Practices: Providing Comfort Chapter 18.pdf - Cardiovascular Critical Care Problems Chapter 19.pdf - Pulmonary Critical Care Problems Chapter 20.pdf - Neurologic Critical Care Problems Chapter 21.pdf - Renal Critical Care Problems Chapter 22.pdf - Gastrointestinal Critical Care Problems Chapter_23.pdf - Endocrine Critical Care Problems Chapter_24.pdf - Hematologic Critical Care Problems Chapter_25.pdf - Oncologic Critical Care Problems Chapter_26.pdf - Organ Transplantation Chapter 27.pdf - Shock Chapter_28.pdf - Trauma Chapter_29.pdf - Thermal Injury Chapter 30.pdf - Toxic Ingestions Chapter_31.pdf - Resuscitation and Transport of Infants and Children back.pdf - Appendices and Index
Toxic IngestionsMaureen A. Madden
COMMON PRINCIPLES OF EMERGENCY AND CRITICAL
CARE MANAGEMENT
ToxidromesIdentification of ToxinThe Unknown ToxinGastrointestinal Decontamination
PHARMACEUTICAL TOXINS
AcetaminophenBarbituratesCarbamazepineClonidineIronTheophyllineCyclic (Tricyclic) Antidepressants
NONPHARMACEUTICAL TOXINS-THE ALCOHOLS
AND DRUGS OF ABUSE
MethanolEthylene GlycolIsopropanolEthanolCocaineHeroinMethadonePhencyclidine
HOUSEHOLD TOXINS
CausticsHydrocarbons
SUMMARY
999
Poisoning continues to be a significant cause of pediatricinjury. Five percent of all accidental childhood deaths
are related to poisoning. Methods of exposure to toxicagents vary, with ingestions accounting for the majority ofexposures. I The 1998 Annual Report of the AmericanAssociation of Poison Control Centers Toxic ExposureSurveillance System reported more than 2 miUion humanexposures to toxins that year. Fifty-three percent of the casesinvolved children younger than 6 years of age. Malespredominated in the ingestions under age 13, whereasteenage cases involved more females. I The majority ofthe 755 fatalities were associated with ingestion andinhalation exposures. Children younger than 6 years accounted for 2.1 % of the fatalities, whereas adolescentsaccounted for 5.9%.
The substances involved most often in human exposureare not the most toxic but the most readily accessible. Someof the more common agents involved in pediatric exposuresare cosmetics, cleaning fluids, analgesics, plants, and coughand cold preparations. Toxic effects do not often occur withthese substances because children usually do not ingestamounts sufficient to produce toxicity.
Other agents ingested less often but that do not requirelarge exposures to produce toxic effects are barbiturates,clonidine, iron, theophylline, antidepressants, alcohols, cocaine, and caustics. The ingestion ofthese substances causesthe greatest percentage of hospitalizations, intensive careunit (rCU) admissions, and fatalities in pediatric poisonings.Table 30-1 compares the most common with the most toxicsubstances ingested.
Characteristics that place children at risk of ingestions differ for various age groups. Toddlers are newlymobile, curious, and anxious to explore their environment through reaching, climbing, and tasting. They arewithout suicidal intent. Usually only one substance is

1000 Part V Multisystem Problems
TABLE 30-1 Most Common Versus MostToxic Agents Ingested
\1;
,from Lilovitz TL, Klein-Schwartz W, Caravali EM el al: 1998
I~ual Report of Ihe American Association of Poison Control
?~.'.:•.'.".'.'.,nlers Toxic Exposure Surveillance Syslem, Am J Emerg Med,1,7:435-487, 1999.r~ost common in pediatric exposures for younger than 6 years'tot age.':~Listed in order of frequency in human exposures.
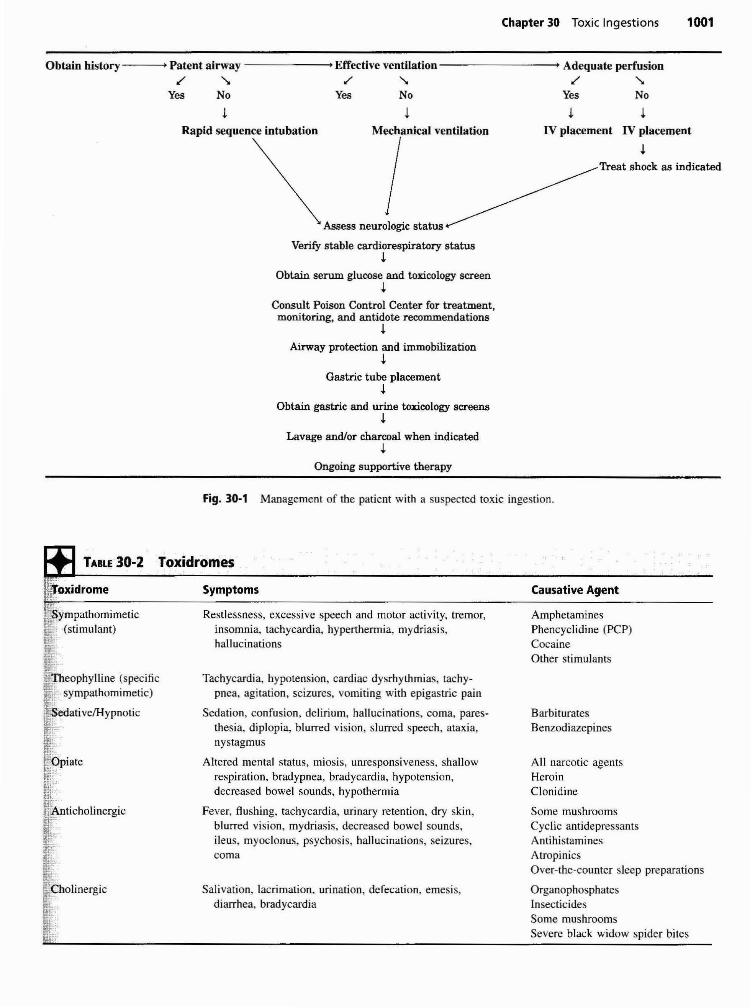
Initial evaluation of the patient in whom a toxic ingestion isknown or suspected includes establishing a patent airway,effective ventilatory pattern, and adequate perfusion. Primary measures to stabilize the patient's condition are basedon the priorities of resuscitation. In the secondary phase ofevaluation, clinical signs that identify the toxin are observed, and appropriate treatment is initiated. Fig. 30-1provides an algorithm for management of the patient with aknown or suspected toxic ingestion.
After initial evaluation and stabilization, the examinationfocuses on the assessment of the central and autonomicnervous system; eye findings; changes in skin, oral, andgastrointestinal (GI) mucosa; and odors. These areas represent the ones most likely affected in toxic syndromes. Theclinical syndromes, called toxidromes, comprise a constellation of signs and symptoms that suggest a specific class ofpoisoning, Toxidromes help identify the toxin so thatappropriate treatment can be initiated in a timely manner.The most common toxidromes are sympathomimetic, theophylline, sedati ve/hypnotic, opiate, anticholinergic, andcholinergic.3-
4 Table 30-2 presents the toxidromes withassociated symptoms and causative agents.
Toxidromes
COMMON PRINCIPLES OF EMERGENCYAND CRITICAL CARE MANAGEMENT
MostToxict
AnalgesicsAntidepressantsStimulants/street drugsCardiovascular drugsSedativeslHypnoticsAlcoholsChemicalsGases and fumesCleaning substancesAnticonvulsantsAsthma therapiesAntihistaminesHydrocarbonsAutomotive productsHormones/Hormone
antagonistsInsecticideslPesticides
rost Common"
~osmetics
"._ '-leaning substancesfi\nalgesics~Iants
IFforeign bodies"Cough/cold preparations~:.ropicals, esticides/lnsecticides~ tamins"'. timicrobials
I[GI preparationsl s/Crafts/Oftice supplies:'" "ydrocarbonsif.: .. .~nlJhlstanunes
!Hormones and hormone,ll:-antagoniststl~-
Identification of Toxin
involved, and the amount ingested tends to be small andnontoxic. Toddlers often present for evaluation soon afteringestion,
An increasing number of significant pediatric exposuresin children younger than 6 years of age involve ingestion ofa grandparent's or other elderly caretaker's medicine. Theseagents, often in sustained-release dosage forms, tend to bemore toxic to children.
Most adolescent ingestions occur in the home and areintentional rather than accidental. They are associated withacademic difficulties, social adjustment problems, failedromances, family issues, or the death of a loved one.Adolescent ingestions commonly involve multiple substances, they are a result of either suicide attempts orsubstance abuse, and commonly a delay occurs betweeningestion and when medical attention is sought.
At present, 65 poison control centers serve 257.5million of the estimated 270.3 million people living inthe United States. I Poison control centers have streamlinedthe most efficient methods of diagnosing and treatingpoisonings. Other significant contributions made by thecenters include education, prevention, research, and legislation, For example, the development of child-resistantcontainers (resulting from the Poison Prevention Act of1970) is credited with significant reduction in morbidity and mortality from accidental ingestions, particularlyaspirin products2
The goal of identification is to determine which patients areat risk for toxic effects. An additional goal is to minimizeintervention for children not at risk for toxic effects becausethe majority of pediatric ingestions result in no harm to thechild.5 For the vast majority of patients, the clinicalcondition rather than the specific ingredients of the ingestiondirects the management. This approach does not precludetreating specific toxins or toxidromes, but rather enforcesthe concept of basic clinical management and resuscitationtechniques.6
A thorough history is obtained, including type andamount of ingestion if known; the possibility of multipleagents; time of ingestion; time of presentation; any historyof vomiting, choking. coughing, or alteration in mentalstatus; and any interventions performed before presentationat the medical facility, Regardless of the history of thesubstance ingested by a child or adolescent, serum and urinetoxicology screens may be necessary to rule out thepossibility of unknown ingestants, Appropriate laboratorystudies include basic serum chemistry studies in symptomatic patients, confirmation of suspected toxins, and thedetermination for the need of specific antidotal therapy. Toxicologic analysis in children is most valuable toidentify serum drug levels, but unexpected findings rarelylead to changes in management.7
•8 Suicide attempts in
clude evaluation for unreported agents, including salicylates and acetaminophen. because most adolescents withsuicidal intent are unreliable when reporting ingested
Chapter 30 Toxic Ingestions 1001
IV placement IV placement
J.Treat shock as indicated
~
Rapid sequence intubation
Obtain history ----+, Patent airway --------+1 Effective ventilation----------+1 Adequate perfusion
.£ '" .£" .£"Yes No Yes No Yes No
~
Mechanical ventilation
IAssess neurologic status
Verify stable cardiorespiratory statusJ.
Obtain serum glucose and toxicology screen~
Consult Poison Control Center for treatment,monitoring, and antidote recommendations
~
Airway protection and immobilization~
Gastric tube placement~
Obtain gastric and urine toxicology screens~
Lavage and/or charcoal when indicated~
Ongoing supportive therapy
Fig. 30·1 Management of the patient with a suspected toxic ingestion.
TABLE 30-2 Toxidromes
Causative Agent
BarbituratesBenzodiazepines
AmphetaminesPhencyclidine (PCP)CocaineOther stimulants
All narcotic agentsHeroinClonidine
Some mushroomsCyclic antidepressantsAntihistaminesAtropinicsOver-the-counter sleep preparations
OrganophosphatesInsecticidesSome mushroomsSevere black widow spider bites
Tachycardia, hypotension, cardiac dysrhythmias, tachypnea, agitation, seizures, vomiting with epigastric pain
Sedation, confusion, delirium, hallucinations, coma, paresthesia, diplopia, hlurred vision, slurred speech, ataxia,nystagmus
Altered mental status, miosis, unresponsiveness, shallowrespiration, bradypnea, bradycardia, hypotension,decreased bowel sounds, hypothermia
Fever, flushing, tachycardia, urinary retention, dry skin,blurred vision, mydriasis, decreased bowel sounds,ileus, myoclonus, psychosis, hallucinations, seizures.coma
Symptoms
Restlessness, excessive speech and motor activity, tremor,insomnia, tachycardia, hyperthermia, mydriasis,hallucinations
Salivation, lacrimation, urination, defecation, emesis,diarrhea, bradycardia
I·" •~iltOXldrome
;,ympathomimetic!iti,. (stimulant)~:I;~eophylline (specificl!iJ. h" )~E sympat omlmelIC
I'li.~.;:.-.:.i::~_yp"mk~4i"
OOi~~iliAn· . h I' .~1:' tIC 0 merglc
IE·~;:"~:..
I-~ bolinergic
F·[
~.

1002 Part V Multisystem Problems
agents. There is limited data and information to distinguishlethal concentrations of certain drugs and toxic substancesin children.5,9.IO
The Unknown ToxinWhen the name or the amount of a poison ingested isunknown, the incident is unwitnessed, or the history isvague, the child is treated as though a harmful substancewas consumed. If elements of the history provided arecontradictory or questionable, it is especially important torule out the possibility of trauma as a cause of the patient'sphysical injuries. Physical assessment focuses on the potential for unreported traumatic injuries, as well as significantdetails related to the ingestion, and a clinical presentationthat suggests a toxidrome. The availability of antidotes suchas naloxone (Narcan), glucose, oxygen, diphenhydramine(Benadryl), physostigmine, digoxin immune Fab (Digibind), methylene blue, deferoxamine, N-acetylcysteine(NAC) (Mucomyst), calcium gluconate, and glucagon isnecessary when the ingestion of a toxic substance is suspected. 10, I J The local poison control center can providedetails regarding the indications and guidelines for use ofthese antidotes, Further emergency and critical care management is guided by the principle of simultaneous stabilization, diagnosis, and treatment.
Further management focuses on GI decontamination.Once the ingestant is correctly identified, the managementcan focus specifically on principles related to that toxin.
Gastrointestinal DecontaminationReducing the life-threatening potential of an ingestedsubstance is an early treatment goal and depends on theeffectiveness of several different treatment modalities.These modalities may include decreasing absorption of thetoxin, altering metabolism, increasing elimination of theingested substance, or administering a specific antidote orother suitable therapy.12
Decreasing AbsorptionGastric Emptying. The best gastric emptying tech
nique to employ depends on clinical status. An individualized approach based on the timing of ingestion, type ofsubstance, and amount of the ingested substance in conjunction with the clinical status will dictate treatment decisions.
Gastric emptying is performed when a benefit is anticipated and one of the following conditions exist: thesubstance does not bind to activated charcoal, it is difficultto remove by gastric lavage (e.g" large pills), the opportunity to use activated charcoal is significantly delayed, or thechild presents within I hour of ingestion with significantcentral nervous system (CNS) symptoms. Gastric emptyinghas limited benefit if attempted more than I hour afteringestion because most toxins have already been absorbedor passed through the pylorus. Ipecac-induced emesis andgastric lavage are two techniques used for gastric emptying.
Ipecac. when recommended, is the agent of choice forforced emesis, Ipecac is very useful in the home for
immediate treatment of accidental ingestions. However, it isno longer favored in the clinical setting because it causessignificant delay in the administration of activated charcoalbecause of prolonged vomiting. Ipecac acts as both a localgastric irritant and a central stimulant, triggering thevomiting center in the reticular formation. The result iscoordinated muscular activity of the stomach and smallintestine, producing emesis, Dosages of 10 ml for infantsolder than 6 months, 15 ml for children 1 to 12 years, and30 ml for children older than 12 years usually produceemesis in 20 minutes. 13
Ipecac is contraindicated in infants younger than 6months of age, with the ingestion of strong caustics (acids oralkalis) or hydrocarbons, and in the presence of neurologicimpairment. Other contraindications are loss of the gagreflex and ingestion of agents likely to cause rapid onset ofCNS depression or seizures (e.g., clonidine, cyclic antidepressants, lindane, cocaine, and isoniazid).
Gastric lavage evacuates the stomach and augmentsdecontamination in the presence of residual toxins. Thesubstance is flushed through a large-bore nasogastric ororogastric tube (28 to 38 Fr) with room temperature fluidsuntil the yield is clear. The tube size required for effectivelavage may be too large for pediatric patients; the largestbore tube, known as an Ewald tube, can be placed only inadolescents, Tracheal intubation precedes lavage for patients in whom the gag reflex is diminished and ability toprotect the airway is compromised to avoid the hazards ofvomiting and subsequent aspiration.
Gastric lavage is no longer considered the standard ofcare in pediatric patients. There is a lack of strong clinicalevidence supporting the efficacy of lavage in improvingoutcomes of poisoned patients. But gastric lavage is stillrecommended if the amount ingested is very large, ifpresentation takes place within I to 2 hours of ingestingagents that delay gastric emptying (e.g., barbiturates,anticholinergic drugs), if sustained-release and insolublecompounds have been ingested, or if the agent is particularlytoxic2
,13,14 Because activated charcoal is very effective, it isgiven at the initiation of the lavage procedure and possiblyrepeated at its conclusion. Gastric lavage is contraindicatedwith caustic and hydrocarbon ingestions.
Activated Charcoal. Activated charcoal reduces absorption of a toxin by binding with it in the GI tract. It is bestadministered by nasogastric or orogastric tube to smallchildren who may refuse to drink it because of its poorpalatability and gritty texture. The commonly recommendeddose of I g/kg may result in undertreatment with pediatricingestions, but alternative recommendations depend onknowledge of the amount ingested. If the amount ingested isknown, a total charcoal dose is administered, determined bya charcoal to ingestant ratio of 10 g: I g, The total volume offluid required to achieve this dose may require division intosmaller aliquots (15 to 25 g) given every I to 2 hours. Theextended dosing regimen may provide for increased efficacyin preventing absorption of sustained-release agents. Whenthe amount of the ingestant is unknown, then a dose ofI g/kg is recommended. Preparations of IS g, 25 g, or 50 gof acti vated charcoal are commercially available. Adminis-

tration of the entire premixed preparation that most closelyapproximates the child's weight is reasonable and oftenmeets or exceeds the recommended I glkg dose.
Activated charcoal binds all organic substances but is noteffective with alcohols and glycols, hydrocarbons, caustics,heavy metals such as lead, mercury, lithium, and arsenic, oragents with rapid onset. 15 Ideally, charcoal is administeredwithin 2 hours of the ingestion. The first dose of activatedcharcoal is most effective in children when combined witha properly dosed cathartic such as sorbitol. Once bound tothe charcoal, sorbitol propels the toxin rapidly through theintestinal tract, decreasing intestinal transit time. Subsequent doses of activated charcoal are administered withoutcathartics to avoid severe diarrhea, fluid shifts, and electrolyte abnormalities, resulting in complications such ashypernatremia and seizures.
The patient's ability to tolerate charcoal varies. Charcoaladministration is usually followed by periods of vomiting, especially when it has been preceded by ipecac orwhen given with sorbitol. It is difficult to determinewhether nausea has subsided in young children who areunable to completely describe physical symptoms. Thepotential hazards of vomiting and aspiration are significantfor patients with diminished ability to protect the airway, and intubation is indicated before administration ofcharcoal.
Priorities for patients who receive charcoal includepositioning in left lateral decubints with the head of the bedelevated, ensuring that suction is readily available to protectthe airway if vomiting occurs, and immobilizing the child tomaintain intravenous patency and the position of the gastrictube. The presence of bowel sounds is assessed beforeadministering charcoal because absent bowel sounds mayindicate development of an ileus or obstruction. Charcoal iscontraindicated in these situations.
Enhancing Elimination. Multiple-dose activatedcharcoal has been shown to enhance elimination of certain agents. This is a separate role for activated charcoalin addition to preventing absorption. Repeated dosinghas been shown to enhance elimination of toxins byinterrupting hepatic recirculation of the ingested drug orits metabolites, adsorbing after initial absorption, oradsorbing tOltins secreted across the gastric membraneinto the bowel lumen by a GI dialysis effect. This role iswell described for several drugs, such as theophylline,phenobarbital, salicylates, carbamazepine, and phenytoin.Drugs in a bound state adsorbed to activated charcoal arenontoxic. 15
Whole Bowel irrigation. Whole bowel irrigation hasemerged as a new modality to augment gastric decontamination, particularly for sustained-release or enteric-coatedpreparations, drug-filled packets, and ingestions not adsorbed to activated charcoal (i.e., heavy metals). A polyethylene glycol-balanced electrolyte solution (Golytely orColyte) hastens the evacuation of substances from the GItract without creating fluid and electrolyte shifts. Theirrigating solution is infused via a nasogastric tube at a rateof 15 to 40 mllkg/hr and continued until the rectal effluentis clear or until radiopaque tOltins disappear or pass into
Chapter 30 TOltic Ingestions 1003
the cecum on a kidney-ureter-bladder film. Whole bowelirrigation is contraindicated with bowel obstruction, perforation, or ileus5
Alkaline Diuresis. Forced diuresis with alkalinizationof urine pH may enhance the removal of toltins that areweak acids via ion trapping. Alkalinization of urine willshift the acid-base equilibrium of weak acids from theuncharged state to ions that do not readily cross cellmembranes. This causes the ions to be trapped in the renaltubular lumen, reducing reabsorption and enhancing excretion. Urinary alkalinization is accomplished by administering intravenous sodium bicarbonate until the urine pHapproaches 7.5. The intravenous solution is infused at a rateof 1.5 to 2 times maintenance volume for the patient tomaintain urine output at a minimum of 2 ml/kg/hr. Alkalinediuresis has been predominately used to enhance elimination of salicylates and phenobarbital.5
.12 This technique is
limited by the risk of intravascular volume depletion andpotential for excessive alkalinization.
Extracorporeal Methods. Extracorporeal methodsof drug removal are useful in certain life-threateningingestions when substantial absorption of the toxin hasalready occurred. Methods of extracorporeal drug removalinclude peritoneal dialysis, hemodialysis, hemoperfusion,and plasmapheresis. The decision to use extracorporealremoval techniques is based on the clinical features of thepoisoning. Dialysis or hemoperfusion is considered whenthe child's condition progressively deteriorates despiteintensive supportive therapy. These techniques are highlyinvasive and have proven to be beneficial with a limitednumber of toxins.
Dialysis eliminates toxic substances by movement ofsolutes across a semipermeable membrane as a result of aconcentration gradient. The effectiveness of peritonealdialysis and hemodialysis depends on the molecular weight,lipid-water solubility, protein-binding properties, time ofingestion, and plasma concentration of the toxin. Peritonealdialysis is far less effective than hemodialysis and is usedonly occasionally in acute ingestions. Hemodialysis hasproven to be effective in enhancing elimination of salicylates, ethylene glycol, methanol, lithium, and isopropanol.!3
Hemoperfusion involves the passage of blood over anadsorbent matrix material of charcoal or resin. Althoughhemoperfusion is preferred over hemodialysis for severaltoxins, hemodialysis is more readily initiated and is oftenused instead. Hypotension and thrombocytopenia are potential complications of hemoperfusion. Plasmapheresis separates harmful substances from the plasma by continuouscentrifugation. Substances that are eliminated best by thismethod have small volumes of distribution and tight plasmaprotein-binding properties.
The sections that follow detail the care of children whohave ingested potentially harmful toxic substances. Pharmaceutical agents include acetaminophen, barbiturates, carbamazepine, c1onidine, iron, theophylline, and cyclic antidepressants. Nonpharmaceutical agents discussed are thealcohols (methanol, ethylene glycol, isopropanol, and ethanol), drugs of abuse (cocaine, heroin, methadone, andphencyclidine [PCP]), and household toxins (caustics and
1004 Part V Multisystem Problems
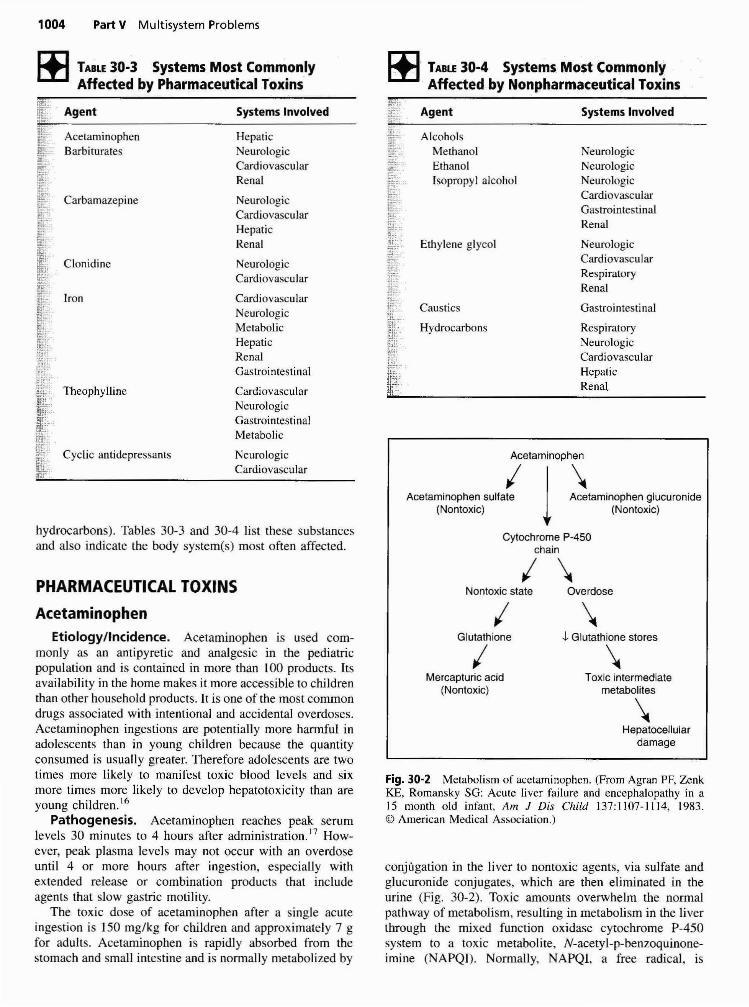
TABLE 30-3 Systems Most CommonlyAffected by Pharmaceutical Toxins
~ TABLE 30·4 Systems Most Commonly. Affected by Nonpharmaceutical Toxins
hydrocarbons). Tables 30-3 and 30-4 list these substancesand also indicate the body system(s) most often affected.
Cytochrome P-450chain
Systems Involved
NeurologicNeurologicNeurologicCardiovascularGastrointestinalRenal
NeurologicCardiovascularRespiratoryRenal
Gastrointestinal
RespiratoryNeurologicCardiovascularHepaticRenal
Ethylene glycol
AlcoholsMethanolEthanolIsopropyl alcohol
Hydrocarbons
Agent
Caustics
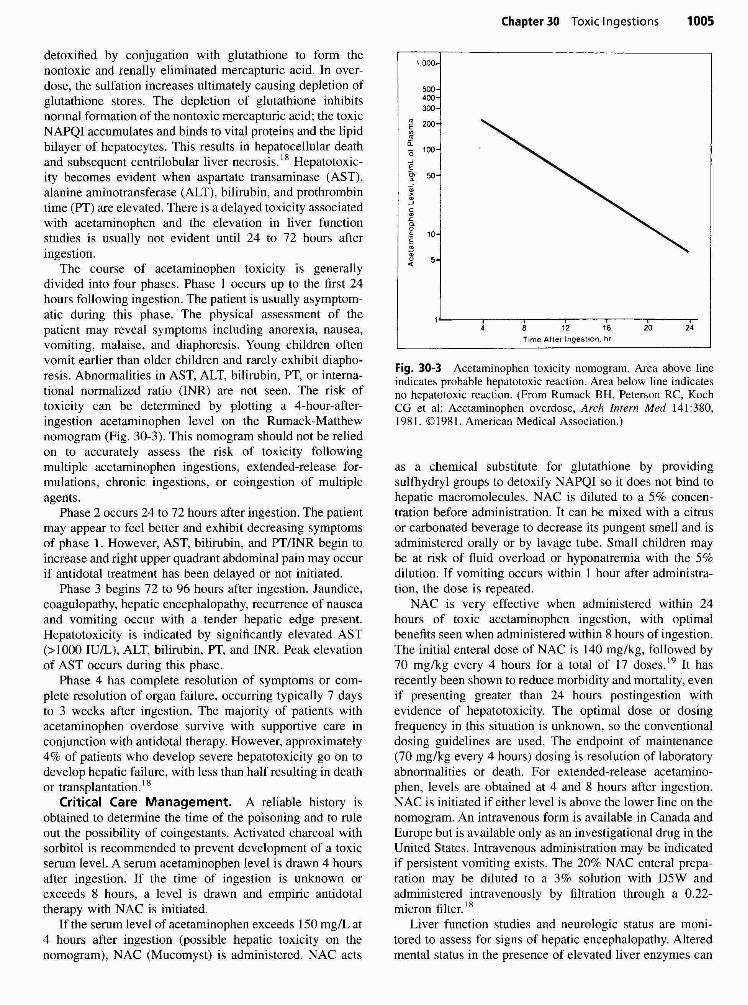
Acetaminophen
Acetaminophen sUlfa{ 1~taminoPhen glucuronide(Nontoxic) (Nontoxic)
Systems Involved
HepaticNeurologicCardiovascularRenal
NeurologicCardiovascularHepaticRenal
NeurologicCardiovascular
CardiovascularNeurologicMetabolicHepaticRenalGastrointestinal
CardiovascularNeurologicGastrointestinalMetabolic
NeurologicCardiovascular
Agent
Iron
AcetaminophenBarbiturates
Carbamazepine
Clonidine
Theophylline
Cyclic antidepressants
I \PHARMACEUTICAL TOXINS Nontoxic state Overdose
Fig. 30·2 Metabolism of acetaminophen. (From Agran PF, ZcnkKE, Romansky SG: Acute liver failure and encephalopathy in a15 month old infant, Am J Dis Child 137:1107-1114,1983.© American Medical Association.)
conjugation in the liver to nontoxic agents, via sulfate andglucuronide conjugates, which are then eliminated in theurine (Fig. 30-2). Toxic amounts overwhelm the normalpathway of metabolism, resulting in metabolism in the liverthrough the mixed function oxidase cytochrome PA50system to a toxic metabolite, N-acetyl-p-benzoquinoneimine (NAPQI). Normally, NAPQI, a free radical, is
Acetaminophen
Etiology/Incidence. Acetaminophen is used commonly as an antipyretic and analgesic in the pediatricpopulation and is contained in more than 100 products. Itsavailability in the home makes it more accessible to childrenthan other household products. It is one of the most commondrugs associated with intentional and accidental overdoses.Acetaminophen ingestions are potentially more harmful inadolescents than in young children because the quantityconsumed is usually greater. Therefore adolescents are twotimes more likely to manifest toxic blood levels and sixmore times more likely to develop hepatotoxicity than areyoung children. 16
Pathogenesis. Acetaminophen reaches peak serumlevels 30 minutes to 4 hours after administration. I? However, peak plasma levels may not occur with an overdoseuntil 4 or more hours after ingestion, especially withextended release or combination products that includeagents that slow gastric motility.
The toxic dose of acetaminophen after a single acuteingestion is 150 mg/kg for children and approximately 7 gfor adults. Acetanlinophen is rapidly absorbed from thestomach and small intestine and is normally metabolized by
IGlutathione
IMercapturic acid
(Nontoxic)
\1 Glutathione stores
\Toxic intermediate
metabolites
\Hepatocellular
damage
Chapter 30 Toxic Ingestions 1005
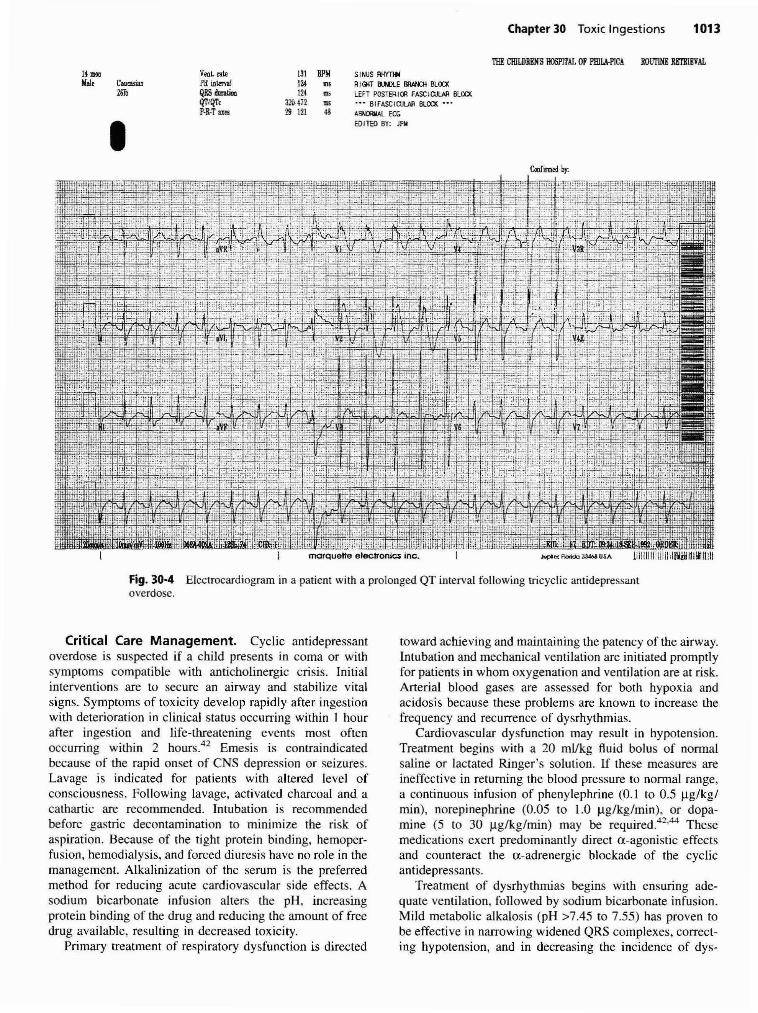
1,000
Fig. 30-3 Acetaminophen toxicity nomogram. Area above lineindicates probable hepatotoxic reaction. Area below line indicatesno hepatotoxic reaction. (From Rumack BH, Peterson RC, KochCG et al: Acetaminophen overdose, Arch Intern Med 141:380,1981. ©1981, American Medical Association.)
as a chemical substitute for glutathione by providingsulfhydryl groups to detoxify NAPQI so it does not bind tohepatic macromolecules. NAC is diluted to a 5% concentration before administration. It can be mixed with a citrusor carbonated beverage to decrease its pungent smell and isadministered orally or by lavage tube. Small children maybe at risk of fluid overload or hyponatremia with the 5%dilution. If vomiting occurs within I hour after administration, the dose is repeated.
NAC is very effective when administered within 24hours of toxic acetaminophen ingestion, with optimalbenefits seen when administered within 8 hours of ingestion.The initial enteral dose of NAC is 140 mg/kg, followed by70 mg/kg every 4 hours for a total of 17 doses19 It hasrecently been shown to reduce morbidity and mortality, evenif presenting greater than 24 hours postingestion withevidence of hepatotoxicity. The optimal dose or dosingfrequency in this situation is unknown, so the conventionaldosing guidelines are used. The endpoint of maintenance(70 mg/kg every 4 hours) dosing is resolution of laboratoryabnormalities or death. For extended-release acetaminophen, levels are obtained at 4 and 8 hours after ingestion.NAC is initiated if either level is above the lower line on thenomogram. An intravenous form is available in Canada andEurope but is available only as an investigational drug in theUnited States. Intravenous administration may be indicatedif persistent vomiting exists. The 20% NAC enteral preparation may be diluted to a 3% solution with D5W andadministered intravenously by filtration through a 0.22micron filter. 18
Liver function studies and neurologic status are monitored to assess for signs of hepatic encephalopathy. Alteredmental status in the presence of elevated liver enzymes can
24201612
Time After Ingestion, hrB
500400300
~ 200
•a:'0 100
E~
~~
-'c~
~
<>gE•ii<t
detoxified by conjugation with glutathione to form thenontoxic and renally eliminated mercapturic acid. In overdose, the sulfation increases ultimately causing depletion ofglutathione stores. The depletion of glutathione inhibitsnormal formation of the nontoxic mercapturic acid; the toxicNAPQI accumulates and binds to vital proteins and the lipidbilayer of hepatocytes. This results in hepatocellular deathand subsequent centrilobular liver necrosis. 18 Hepatotoxicity becomes evident when aspartate transaminase (AST),alanine aminotransferase (ALT), bilirubin, and prothrombintime (PT) are elevated. There is a delayed toxicity associatedwith acetaminophen and the elevation in liver functionstudies is usually not evident until 24 to 72 hours afteringestion.
The course of acetaminophen toxicity is generallydivided into four phases. Phase I occurs up to the first 24hours following ingestion. The patient is usually asymptomatic during this phase. The physical assessment of thepatient may reveal symptoms induding anorexia, nausea,vomiting, malaise, and diaphoresis. Young children oftenvomit earlier than older children and rarely exhibit diaphoresis. Abnormalities in AST, ALT, bilirubin, PT, or international normalized ratio (INR) are not seen. The risk oftoxicity can be determined by plotting a 4-hour-afteringestion acetaminophen level on the Rumack-Matthewnomogram (Fig. 30-3). This nomogram should not be reliedon to accurately assess the risk of toxicity followingmultiple acetaminophen ingestions, extended-release formulations, chronic ingestions, or coingestion of multipleagents.
Phase 2 occurs 24 to 72 hours after ingestion. The patientmay appear to feel better and exhibit decreasing symptomsof phase I. However, AST, bilirubin, and PT/INR begin toincrease and right upper quadrant abdominal pain may occurif antidotal treatment has been delayed or not initiated.
Phase 3 begins 72 to 96 hours after ingestion. Jaundice,coagulopathy, hepatic encephalopathy, recurrence of nauseaand vomiting occur with a tender hepatic edge present.Hepatotoxicity is indicated by significantly elevated AST(>1000 lUlL), ALT, bilirubin, PT, and INR. Peak elevationof AST occurs during this phase.
Phase 4 has complete resolution of symptoms or complete resolution of organ failure, occurring typically 7 daysto 3 weeks after ingestion. The majority of patients withacetaminophen overdose survive with supportive care inconjunction with antidotal therapy. However, approximately4% of patients who develop severe hepatotoxicity go on todevelop hepatic failure, with less than half resulting in deathor transplantation. 18
Critical Care Management. A reliable history isobtained to determine the time of the poisoning and to ruleout the possibility of coingestants. Activated charcoal withsorbitol is recommended to prevent development of a toxicserum level. A serum acetaminophen level is drawn 4 hoursafter ingestion. If the time of ingestion is unknown orexceeds 8 hours, a level is drawn and empiric antidotaltherapy with NAC is initiated.
If the serum level of acetaminophen exceeds 150 mg/L at4 hours after ingestion (possible hepatic toxicity on thenomogram), NAC (Mucomyst) is administered. NAC acts

1006 Part V Multisystem Problems
Barbiturates
progress to hepatic coma and death in severe acetaminopheningestions.
TABLE 30·5 Classification of Barbituratesby Duration of Action
At toxic levels, barbiturates primarily act as depressantsof the CNS and cardiovascular system. The medication,dose, and route of ingestion influence the effect of theoverdose on the child. In addition, children metabolizebarbiturates faster than adults. The initial signs and symptoms of toxicity are slurred speech, ataxia, lethargy,nystagmus, headache, and confusion or coma. As toxicitybecomes more severe, deep tendon and brain stem reflexesmay be depressed, but this usually occurs well afterrespiratory depression occurs. Shock may occur secondaryto medullary depression, peripheral vasodilatation, or diminished myocardial contractility. Other findings mayinclude hypoglycemia, hypothermia, and bullous skin lesions20 The child may demonstrate miosis early, with acommon late presentation of dilated pupils unresponsive tolight. Early deaths occur as a result of respiratory arrest,cardiovascular dysrhythmias, and circulatory collapse,whereas delayed deaths are due to acute renal failure,aspiration pneumonitis, pulmonary edema, and cerebraledema.
Respiratory dysfunction results from depression of therespiratory control centers in the brainstem. The neurogenicdrive to breathe may be obliterated and the mechanismsthat affect respiratory rhythm may be altered. As respiratory depression continues, hypoxemia and hypercarbiadevelop. The cough reflex may be suppressed, and the childmay experience laryngospasm resulting from inhibition ofsmooth muscle activity.
Critical Care Management. Management of a patient with a suspected barbiturate overdose, as with any CNSdepressant, begins with an assessment and stabilization ofthe airway. Once the airway is protected, whether withintubation or an active gag reflex, gastric emptying bylavage can be attempted, followed by administration ofactivated charcoal and a cathartic. If phenobarbital isidentified as the toxic agent, multiple doses of activatedcharcoal may be administered.
If warranted by inadequate gas exchange, the unconscious patient is placed on mechanical ventilation. For thepatient who presents in shock, aggressive intravascularvolume replacement is begun with crystalloid fluid (20mllkg). Assessment for adequate renal function is essential.
Cardiovascular and nervous system dysfunction istreated primarily with supportive care. Temperature is assessed regularly to prevent hypothermia-induced ventricularfibrillation. If the child is hypothermic, the first line oftreatment is to prevent further heat loss.
Respiratory dysfunction is managed by ensuring a patentairway and adequate gas exchange. Assessment of arterialblood gases and serum pH guides intervention. The presenceof aspiration pneumonitis requires treatment with antibiotictherapy.
Cardiovascular dysfunction treatment includes volumereplacement as needed. If volume replacement does notresolve hypotension, continuous infusion of dopamine (I to20 llg/kg/min) or dobutamine (2 to 12 llg/kg/min) may berequired.
With phenobarbital, alkalinization of the urine (maintaining urine pH >7.5) with sodium bicarbonate is helpfulwith excretion. This is best accomplished by intravenous
Hexobarbital
Methohexitalsodium
Ultrashort
Thiopental sodium
Short toIntermediate
Amobarbital
Butabarbitalsodium
Pentobarbitalsodium
Secobarbital
Etiology/Incidence. Barbiturates are a class ofsedative-hypnotic agents and include phenobarbital andpentobarbital. Indications for prescribed use include induction of sleep, sedation, and inhibition of epileptiformactivity. Barbiturates are classified according to theirduration of action: ultrashort, short, intermediate, or longacting (Table 30-5). In this drug class, barbiturates that arehighly lipid soluble have a more rapid onset and a shorterduration of action, as well as a greater degree of hypnoticactivity compared with those that are less lipophilic.Duration of action, however, does not correlate with theserum half-life of these medications.20
CNS effects are related to the brain tissue concentrationof barbiturate. The effect of barbiturates is primarily on theCNS through inhibition of neurotransmission across neuronal and neuroeffector junctions. Therapeutic doses ofbarbiturates do not produce toxic effects unless used incombination with other medications or alcohol. Approximately three times the therapeutic dose of a barbiturate isnecessary to produce the side effects of overdose.
Pathogenesis. Barbiturates have a very narrow therapeutic index (i.e., the difference between an effective doseand a lethal dose is small). Barbiturates are usually takenorally. When taken with liquids, absorption is hastened;when taken with food, absorption is slowed. Serum levelsare only somewhat indicative of toxicity because of thediscrepancy between plasma and brain tissue concentration.Patients most at risk for death are those who are not treateddespite elevated serum levels: greater than or equal to 3mg/dl for short-acting barbiturates, greater than or equal to7 mg/dl for intermediate-acting barbiturates, and greaterthan or equal to 10 mg/dl for long-acting barbiturates? I
Short-acting barbiturates, particularly those with high lipidsolubility, are considered more toxic than the longer-actingforms?O Short-acting agents are absorbed in the smallintestine and transformed in the liver to inactive metabolites,which are excreted predominantly in urine. Phenobarbital, along-acting agent, is only partly metabolized in the liver.
trom Bertino JS. Reed MD: Barbiturate and nonbarbiturate sedative~ 'ypnolic intoxication in children, Pediatr Clio North Am 33:705. 1986.~..

Chapter 30 Toxic Ingestions 1007
1Jl. TABLE 30·6 Stages of· CarbamazepineOverdose With Serum Level andClinical Signs
Clinical Signs
Nystagmus, drowsiness. ataxia
Stupor or coma. abnormalpupillary reaction to light.respiratory depression
Irritability, combativeness,choreiform movements.hallucinations
15-25 Ilg/ml
>25 ~g/ml
Serum Level
ing gastric emptying time. Following acute ingestion, theCNS and cardiovascular systems are the most affected, withsome hepatic and renal system involvement.
Carbamazepine toxicity produces prominent neurologicsigns and symptoms. In mild to moderate toxicity, nystagmus, drowsiness, and ataxia are common24 At higher serumconcentrations, symptoms in children include dystonia,choreoathetosis, seizures, and stupor. Other clinical symptoms of toxicity include nausea, vomiting, respiratorydepression, hypothermia, and coma. The patient's neurologic status may wax and wane following carbamazepineoverdose, with increased absorption in stage 4, when normalperistalsis resumes.
Cardiac conduction delays, dysrhythmias, and hypotension indicate cardiovascular system dysfunction. Theseeffects are the result of the fact that carbamazepine chemicalstructure is similar to that of cyclic antidepressants.
Acute hepatic dysfunction occasionally occurs followingcarbamazepine overdose. Alteration in renal function mayinclude hyponatremia and syndrome of inappropriate antidiuretic hormone (SIADH). These side effects can bepresent with long-term administration of carbamazepine andaggravated by overdose.
Critical Care Management. Upon presentation, assessment of the airway is made and stabilization withintubation is performed, especially if CNS depression ispresent. Emesis is not used with carbamazepine, but gastriclavage may be performed once a secure airway is presentand if the child presents within I hour of ingestion.Multiple-dose activated charcoal is the therapy of choice incarbamazepine overdose. Repeated doses are recommendedbecause the serum half-life of carbamazepine may bereduced by as much as 50% with this therapy, whichdecreases enterohepatic recirculation and increases elimination25 Catharsis is not recommended because of thepotential for increased systemic absorption as a result ofincreased drug distribution throughout the GI tract.26
liii,: I
11Iii'~JII~:;
11
1008 Part V Multisystem Problems
The need for intensive monitoring is anticipated following significant ingestions of carbamazepine. Children aremonitored in the ICU until their condition has remainedstable for 24 hours because of the risk of relapse duringstage 4 with increased reabsorption. Concretions of carbamazepine are suspected when plasma levels rise or themanifestation of symptoms is delayed?3 An abdominalradiograph is performed to confirm this diagnosis, andsurgical intervention with gastrotomy may be necessary.
Neurologic dysfunction with respiratory depression mayrequire tracheal intubation and mechanical ventilation. Thecombative patient is protected from injury. Paradoxicseizures may occur with toxic carbamazepine levels and aretreated with benzodiazepines or phenobarbital. 27
Cardiovascular dysfunction is assessed by ECG monitoring for conduction delays and dysrhythmias and hemodynamic monitoring for hypotension. Hypotension is treatedwith fluid boluses, and if unresponsive to fluid, vasopressorsare initiated.
Alteration in hepatic function is assessed by liverfunction studies. Conventional therapy, including monitoring serum glucose levels and administration of clottingfactors for prolonged clotting time, is recommended forhepatic dysfunction. Carbamazepine can be removed bycharcoal hemoperfusion, but this therapy is reserved forpatients who are not responding to multiple doses ofactivated charcoal or who are clinically worsening evenwith aggressive management.4
At high carbamazepine levels, vasopressin secretion canbe stimulated, leading to fluid retention, SIADH, andhyponatremia. Monitoring of serum electrolytes, particularly sodium and for adequate urinary output, is necessary toidentify SIADH. Treatment with water restriction andsodium supplementation is initiated promptly.
ClonidineEtiology/Incidence. Clonidine is the most com
monly used centrally acting antihypertensive and is nowindicated for migraine headache prophylaxis; attentiondeficit/hyperactivity disorder; Tourette's syndrome; andmanagement of opioid, ethanol, and nicotine withdrawal.Clonidine can cause significant toxicity in children. Clonidine centrally stimulates postsynaptic a-adrenergic receptors, which inhibits sympathetic discharge and producesdecreased peripheral vascular tone, heart rate, stroke volume, and cardiac output. 28 Clonidine also inhibits uptake ofnorepinephrine by neuronal tissues, producing CNS depression. Clonidine is available in 0.1-, 0.2-, and 0.3-mg tabletsand transdermal patches. The transdermal patches contain2.5, 5.0, or 7.5 mg of clonidine and are designed to release0.1, 0.2, or 0.3 mg of clonidine per day over a period of1 week. 29
Pathogenesis. Clonidine is well absorbed from theGl tract, metabolized by the liver, and excreted unchangedprimarily in urine. Its effects are evident 30 to 60 minutesafter ingestion and peak approximately 2 to 3 hoursfollowing oral administration, with effects up to 8 hours.Antihypertensive effects are present for as long as 24 hours
following an oral dose. Overdose in children has beendocumented with as little as a O.I-mg dose or by dermalexposure, mouthing, or ingestion of a transdermal patch. Adiscarded transdermal patch contains enough clonidine toproduce overdose symptoms in a child.
Clonidine overdose invol ves an exaggeration of theclonidine pharmacologic properties primarily affecting theCNS and the cardiovascular systems. The majority ofchildren develop symptoms within 1 hour of a clonidineoverdose. There is no progression or development ofsymptoms or toxic effects more than 4 hours after presentation to the hospital.30
CNS dysfunction mimics narcotic overdose, wheremiosis, coma, and respiratory depression are the hallmarks.Symptoms vary from lethargy, somnolence, stupor, or coma,and are postulated to be from inhibition of the uptake ofnorepinephrine by the neurons, which then blocks noradrenergic activity?] Patients who are severely obtundedmay have decreased ventilatory effort and hypoxia and mayrequire intubation and mechanical ventilation to maintainadequate respiratory effort. Other CNS symptoms includehypothermia, which is attributed to a-adrenergic receptorstimulation of the serotonin-acetylcholine pathways, causing decreased metabolic heat production and increased heatloss?9 Cool, pale skin is presumed to be the result ofvasoconstriction. Hypotonia, hyporeflexia, and irritabilitymay also be seen.
Cardiovascular system dysfunction depends on theplasma level of clonidine. Serum levels of higher than 10 to15 mg/ml stimulate the release of norepinephrine, whichcauses the peripheral a-receptors to vasoconstrict, resultingin transient hypertension. The hypertensive phase is shortlived because clonidine overdose triggers a centrally mediated sympathetic inhibition causing hypotension. Patientswith a serum level lower than 10 mg/ml present withnormotension or hypotension. Sinus bradycardia, a knownside effect, is commonly noted in children with clonidineoverdose?O Conduction abnormalities including first-degreeheart block and second-degree atrioventricular block areseen in both overdose and therapeutic dosing. Patients withunderlying conduction dysfunction and the very young aremost at risk for sinus bradycardia and conduction delays.28
Critical Care Management. If clonidine ingestion issuspected, emesis is contraindicated because of the risk ofrapid CNS and respiratory depression. Activated charcoaladministration with or without prior gastric lavage can beconsidered if instituted early. Gastric lavage has limitedutility because clonidine is rapidly absorbed and patientstypically present following the onset of symptoms.
Appropriate therapy focuses on respiratory and hemodynamic status. Most clonidine overdoses respond well tosupportive measures. If hypotension and shock are present,the child is treated with infusion of 20 ml/kg of intravenousfluid and placed in the Trendelenburg position. If signs ofshock do not resolve with those measures, an infusion ofdopamine (5 to 10 ~g/kg/min) is begun.
Patients usually require supportive and symptomatictreatment in the critical care setting for less than 24 hoursfollowing clonidine overdose. Careful monitoring of vital

Chapter 30 Toxic Ingestions 1009
ljiiFrom Hcnretig FM, Temple AR: Acute iron poisoning in children. ClinIfni> Med 4:579. 1984.
~ TABLE 30-7 Serum Iron Level andPotential Severity of Intoxication
of iron exceeds the total iron-binding capacity. Excess freeiron is directly toxic to the vasculature and leads to therelease of vasoactive substances including serotonin andhistamine. Excess quantities of ferritin lead to vasodilationresulting in increased vascular permeability and fluid loss,with subsequent hypotension and metabolic acidosis.34 Thefree iron is deposited in the liver, spleen, and kidneys. Theseiron deposits cause pathophysiologic changes in the mitochondria, result in free radical formation and lipid peroxidation that contribute to necrosis, cell death, and tissueinjury.4 Metabolic acidosis develops as a result of poisoningof the mitochondria, compromising cellular respiration andproducing lactic acidosis. Serum iron levels peak 2 to 4hours following ingestion, and begin to fall 6 hours afteringestion. Table 30-7 shows the correlation between serumiron levels and toxicity. An iron concentration higher than350 Ilg/dl is indicative of moderate to severe toxicity.35
Pathogenesis. The pathophysiology of iron toxicityis related to the development of metabolic acidosis. Irontoxicity is mediated through both local and systemic effects.Acute iron poisoning in children follows the classic fiveclinical stages of iron toxicity. The initial stage begins from30 minutes after ingestion to no later than 6 hours and is theresult of the corrosive effects of iron on the GI mucosa. Thechild complains of nausea and moderate to severe abdominal pain and presents with vomiting, diarrhea, or GIhemorrhage. Vomitus and stools may be dark gray or blackbecause of the presence of iron. In severe poisoning, thechild may present with hypotension, shock, and coma. If achild presents in coma shortly following an iron ingestion,the prognosis for neurologic recovery is poor.36
The second phase of iron toxicity is described as thelatent stage. The child is asymptomatic, with mild lethargypresent. It is a deceptive period that occurs 6 to 24 hourspostingestion, but this phase may be absent in children withsevere poisoning.
Profound toxicity is evident with patients who progressto the third phase, 12 to 48 hours after ingestion. Shockresults from the free iron, causing venous pooling, whichcreates relative hypovolemia, vasodilatation, and poor
Potential Toxicity
None
Minimal toxicity
Moderate toxicity; chelation usuallynot necessary
Severe toxicity; start chelationimmediately
Potentially lethal; start maximumchelation immediately
500-1000
>1000
<100
100-350
350-500
~tserum Iron Level
Etiology/lncidence. Iron ingestion is one of the morecommon childhood ingestions because of the availability ofiron and iron-containing compounds in the household. Thesimilarity of colors, shapes, and flavorings between multivitamins and other iron-containing products and candymakes them especially enticing to children. Iron supplementation is prescribed for pregnant women, and iron is acommon component in both pediatric and adult multivitamins. Elemental iron is available in combination withgluconate, sulfate, or fumarate salts; each preparation hasvarying amounts of elemental iron. Cases of iron ingestionrarely require intensive care management if toxicity isrecognized and treated promptly. Iron supplements used tobe the leading cause of fatal ingestions in children, but theincidence is now declining. The Food and Drug Administration (FDA) mandates that all iron-containing preparationsdisplay a warning label to inform of potential toxicity forchildren with accidental overdose.
After ingestion in normal doses, 10 to 15 mg of iron isabsorbed daily through the GI tract33 Ferrous iron isabsorbed into the mucosal cells of the duodenum andjejunum and is oxidized to ferric iron, where it is bound toferritin, an iron storage protein. It is then released into theplasma, where it is bound to transferrin, an iron-specificbinding globulin. Iron bound to transferrin is nontoxic.
With acute iron overdose, the total serum concentration
Iron
signs, including temperature, is necessary. Hypothermia istreated with passive rewarming to maintain a normal bodytemperature. Tracheal intubation and mechanical ventilationare instituted if respiratory effort is absent or inadequate tomaintain normal serum oxygen and carbon dioxide levels.Control of the airway protects the child from aspiration andsubsequent respiratory compromise.
Cardiovascular dysfunction treatment is based on thechild's symptoms. Bradycardia associated with cardiovascular compromise is responsive to intravenous atropine(0.10 mg/kg); although repeated doses may be necessarybecause of the long half-life of clonidine.2K
•3o Hypotension
is treated first with volume infusion, and then withdopamine infusion, as described in the initial managementsection. Treatment with a nitroprusside infusion (0.5 to 0.8l.I.g/kg/minute) is instituted for a hypertensive phase only ifend-organ compromise is noted. Dysrhythmias resolve withdecreasing serum clonidine levels and usually do not requiretreatment.
Naloxone (Narcan) is recommended for treatment of allpatients with clonidine overdoses in which CNS, cardiovascular, or respiratory depression is present. 32 Naloxone wasfirst used because of the similarity in clonidine overdosesymptoms to opioid toxicity. The interaction betweenclonidine and opioid receptors is poorly understood, butseveral patients experiencing clonidine overdose haveresponded well to naloxone. The initial naloxone dose is0.0 I mg/kg, and if no response is noted, a repeat dose of 0.1mg/kg is administered. A continuous infusion of naloxonemay be necessary secondary to its short half-life.

1010 Part V Multisystem Problems
cardiac output. Subsequent poor perfusion and ischemiaresults in a worsening metabolic acidosis. An iron-inducedcoagulopathy may cause increased bleeding and exacerbatehypovolemia. Systemic signs of toxicity include lethargy,hyperventilation, hypoglycemia, seizures, and coma.
The fourth stage of iron toxicity consists of hepatic injuryor failure. This may occur 2 to 3 days after severe ironingestion. It is thought to be a direct result of uptake of ironby the liver's reticuloendothelial system. Alterations inglucose metabolism, coagulopathies, and hepatic encephalopathy accompany hepatic failure.
The final stage occurs days to weeks after the ironoverdose and only rarely occurs. The initial gastric insultcan progress to gastric outlet obstruction secondary todevelopment of strictures, stenosis, or scarring.34
Critical Care Management. Toxicity is dependenton the amount of elemental iron ingested. Ingestion of morethan 20 mg/kg of elemental iron produces GI effects;ingestion of more than 60 mg/kg causes systemic toxiceffects; and ingestion more than 250 mg/kg is potentiallylethal. Iron levels may not correlate with amount ingestedand clinical symptoms. Children who ingest greater than 20mg/kg or who are symptomatic, regardless of serum level,need to be treated. Following stabilization of the airway,breathing, and circulation, GI decontamination proceduresare considered. Activated charcoal does not bind to iron andtherefore is not utilized. Gastric emesis may have limitedbenefit in a child who has already vomited several times andmay obscure the severity of toxicity based on GI symptoms.Gastric lavage to remove pills and fragments may beineffective if the tablets are large or several hours haveelapsed since ingestion. If lavage is used, only normal salineor tap water is used. Other compositions, including sodiumbicarbonate, have been studied as lavage solutions. Theyhave not shown any greater benefit, and potential risks withelectrolyte imbalances have limited their utility.34
Whole bowel irrigation has become the standard of carefor severely poisoned patients with large GI burdens of iron.After lavage, an abdominal radiograph is obtained to document the presence of retained iron tablets in the stomach andpylorus. If present, irrigation with polyethylene glycol electrolyte lavage solution (Golytely) enhances stooling whilequickly emptying iron from the GI tract. 37 This solution isinstilled at room temperature into the stomach via nasogastric tube at 250 to 500 ml/hour for children younger than5 years and up to 2 Llhour for adolescents. Whole bowelirrigation continues until diarrhea is produced and the effluent resembles the infusate. If lavage and whole bowel irrigation are unsuccessful in removing intact iron tablets, emergency gastrotomy may be considered35
Chelation therapy, which binds iron into a solublecomplex, is initiated in the emergency department after abaseline urine sample is obtained, with intravenous deferoxamine at a maximum dose of 15 mg/kg/hour for childrenin whom severe intoxication is suspected. The dailymaximum recommended dose is 360 mg/kg/day, with alimit of 6 g. Hypotension may occur with the infusion ofdeferoxamine and may limit the rate of infusion. Deferoxamine combines with iron to form ferrioxamine, which is
excreted by the renal system; it appears that deferoxaminecannot remove iron once bound to transferrin but can chelatefree iron and iron being transported between transferrin andferritin. }}.34 The urine changes to "vin rose," a pink color,shortly after chelation begins. Serum iron levels arefollowed during chelation therapy. Chelation is discontinuedwhen the serum iron level falls below 100 ~.g/dl, the childappears clinically well, the anion-gap acidosis has resolved,and there is no further urine color change.36
Initial laboratory studies include complete blood count(CBC); serum electrolytes including glucose, renal, andhepatic function; blood type and cross-match; total ironbinding time; a serum iron level 2 to 6 hours after ingestion;and coagulation studies. These values help to guide management, especially for the child who is asymptomatic atpresentation. Initial management also includes close monitoring for the known side effects of iron toxicity. Intravenous access is obtained in any child with suspectedmoderate to severe toxicity so that hypotension, metabolicacidosis, hypoglycemia, and blood dyscrasias can be treatedpromptly. Continuous monitoring of the adequacy of thechild's airway, breathing, and circulation, particularly bloodpressure, is necessary.
Patients who manifest clinical signs and symptoms oftoxicity, such as metabolic acidosis, hemodynamic instability, and lethargy, are managed in an ICU and are dischargedonly after 24 hours of clinical stability following therapy.Cardiovascular assessment includes central venous pressuremonitoring to provide a guide to the patient's volume statusand fluid management. Periodic assessment of serumhemoglobin and hematocrit levels is necessary to trackblood loss via the Gl tract. All stools and emesis are testedfor presence of blood. Blood loss via stools or emesis isreplaced. Volume replacement with blood components orother fluids is initiated early in the treatment of hypotension.Intravenous infusion of catecholamines, such as epinephrine(0.2 to 2.0 ~g/kg/min) or dopamine (l to 20 )lg/kg/min),may be required to treat hypotension that is refractory tovolume replacement.
Neurologic dysfunction management is primarily supportive. If the child has inadequate cough or gag reflexes,tracheal intubation is performed and mechanical ventilationinstituted. Acid-base balance is assessed by serial measurement of serum pH and bicarbonate ions. Intravenous sodiumbicarbonate is administered as necessary to treat metabolicacidosis.
Hepatic failure requires assessment and treatment ofhypoglycemia and coagulopathy. Hypoglycemia is treatedwith intravenous infusion of dextrose-containing solutions,the concentrations of which are titrated to maintain theserum glucose level above 80 to 100 mg/dl. Increased PT,partial thromboplastin time (PTT), or clinical signs ofbleeding are treated with infusion of the appropriate clottingfactors.
Renal function is assessed by hourly measurement ofurine output and periodic monitoring of specific gravity,blood urea nitrogen (BUN), and serum creatinine. If acuterenal failure occurs, continuous hemofiltration or hemodialysis can be used to remove ferrioxarnine, as well as other

metabolic end products34 Renal transplantation may benecessary if the renal system does not recover following irontoxicity.
GI dysfunction is monitored by serial assessment ofabdominal girth and tenseness and for the presence of bloodin gastric contents and stool. H2 blockers may be administered to protect the upper GI tract. If GI perforation issuspected, the child requires an exploratory laparotomy toidentify and manage areas of necrosis. Peritonitis is treatedwith appropriate antibiotic therapy. All severe icon overdoses require follow-up several weeks after ingestion toevaluate for GI complications, such as strictures andstenosis, which may require surgical intervention.
TheophyllineEtiology/Incidence. Theophylline is most commonly
used in children as a bronchodilator to relieve bronchospasm associated with asthma. The therapeutic serum levelranges from 10 to 20 mglL. Each 1 mg/kg of theophyllineraises the serum level by 2 mglL. Theophylline is availablein liquid, capsule, tablet, and suspended-release preparations. Maintenance dosages vary with each child based onweight, concentration of the preparation, and extent ofillness. Theophylline toxicity is characterized by serumlevels higher than 20 mglL. Acute toxicity is affected by thetype of preparation ingested, route of exposure, age-relatedclearance rate, and drug and nondrug interactions. The toxiceffects following chronic overdose do not correlate withserum drug levels. Precipitating factors associated withtheophylline overdoses include dosage errors, accidentalingestions, suicide attempts, respiratory tract infections, orerythromycin administration.38
Pathogenesis. Pharmacologic properties of theophylline include CNS stimulation, positive chronotropic andinotropic effects, antagonizing adenosine activity, reductionof peripheral arteriolar resistance, relaxation of bronchialsmooth muscle, inhibition of mast cell degranulation,increase in renal blood flow and glomerular filtration rate,and increases in gastric acid and pepsin secretion. Theseprocesses are accelerated in situations when theophyllinetoxicity occurs. Theophylline toxicity primarily affects theGl tract, CNS, and cardiovascular system.4 The mostcommon symptoms of theophylline toxicity include nauseaand vomiting, tachydysrhythmias, seizures, hypotension,metabolic acidosis, and hypokalemia. Severe toxicity willalso produce hematemesis and bloody diarrhea.
Patients are at risk from the cardiac effects with severeoverdoses secondary to excessive catecholamine stimulationof the myocardium exacerbated by hypokalemia, hypocalcemia, hypophosphatemia, metabolic acidosis, and an increased myocardial oxygen demand. Altered cardiac outputresults from supraventricular dysrhythmias such as sinustachycardia, atrial tachycardia, atrial flutter, and atrialfibrillation. Ventricular dysrhythmias may develop, butsustained dysrhythmias that require prolonged therapy arerare. Serious dysrhythmias occur most often in youngpatients with acute theophylline overdoses when serumlevels exceed 50 Ilg/m1.39 Theophylline's ~2 effects, which
Chapter 30 Toxic Ingestions 1011
reduce peripheral vascular resistance, are responsible forsevere hypotension and reduced myocardial perfusionassociated with toxicity.
CNS disturbances include agitation, headache, confusion, tremulousness, hyperreflexia from cerebral excitation,and seizures. In acute intoxication, seizures are infrequentand are usually focal and brief. Theophylline causes anincrease of cyclic adenosine monophosphate (cAMP) byinhibiting the activity of phosphodiesterase, the enzymeresponsible for metabolizing cAMP. This results in smoothmuscle relaxation, peripheral vasodilation, myocardial stimulation, and CNS excitation.
Other metabolic disorders that may result from theophylline overdose are hyperglycemia from increased gluconeogenesis, and glycogenolysis caused by catecholaminerelease. Hypokalemia occurs early and is the result ofpotassium moving into the cells secondary to hyperglycemia, loss of potassium through vomiting, and the diureticaction of theophylline. All of these may contribute to thecardiac dysrhythmias. 38
Critical Care Management. In severe overdose,gastric lavage and activated charcoal with a cathartic mayboth be used, up to 4 hours after ingestion with regularpreparations and up to 8 to 12 hours after ingestion ofsustained-release preparations. Emesis is not typicallyemployed because of rapid onset of seizures and protractedvomiting caused by toxicity. If vomiting inhibits the instillation of activated charcoal, an antiemetic may be administered because activated charcoal is very effective in reducing serum theophylline levels. For severe intoxication,multiple-dose charcoal has been indicated. Initial laboratorystudies necessary are theophylline level at presentation, followed by repeat levels in 2 to 4 hours, serum electrolytes,glucose, calcium, and baseline coagulation studies. Seizuresare treated with a benzodiazepine followed by phenobarbitalif the seizure does not resolve. It may be necessary to intubate the child and to provide ventilatory support and neuromuscular blockade to help control the seizure activity.38
Priorities include monitoring for cardiac dysrhythmias.The patient's electrolytes are carefully evaluated over timeand rapidly corrected if a dysrhythmia develops. Thesedysrhythmias usually resolve spontaneously as the theophylline level returns to the therapeutic range. If the patient isunstable or not tolerating the dysrhythmia, treatment withlow doses of propranolol (0.02 mg/kg IV) repeated every5 to 10 minutes (with a maximum of 0.1 mg/kg IV) isrecommended4o The desired response to propranolol whentreating hypotension, sinus tachycardia, atrial fibrillation,and rapid ventricular rates is a return to the patient'sbaseline parameters for blood pressure and cardiac rhythm.Esmolol is another effective agent currently under investigation for use with theophylline toxicity38 One case studyreports effective treatment of tachycardia and hypotensionwith administration of intravenous esmolol, an ultra-shortacting ~-blocker, in a 500-llg/kg bolus over I minute,followed· by a 50-llg/kg/min continuous infusion.4
\ Propranolol and other nonselective ~-blockers are used cautiously in asthmatic patients because they may causebronchospasm.

1012 Part V Multisystem Problems
Maintaining seizure precautions and ongoing assessmentof level of consciousness is necessary to limit the degree ofcerebral anoxia caused by seizure activity. Because acorrelation exists between the length of seizure activity andmorbidity and mortality, seizures are controlled as soon aspossible. Lorazepam (0.05 mg/kg TV) is indicated forimmediate cessation of seizure activity and is administered with phenobarbital (10 mg/kg) for continued seizurecontrol.
The effectiveness of antiemetics in theophylline toxicity is variable. Recommendations include the use of metoc10pramide (2 mg/kg TV) or ranitidine (l to 2 mg/kg/dayTV) to control vomiting and increase the tolerance ofcharcoal. Metoclopramide and ondansetron may be morebeneficial because they promote gastric motility and donot lower the seizure threshold. Multidose activatedcharcoal is typically used rather than whole bowel irrigation because of the risk of irrigation decreasing theeffectiveness of the charcoal. However, whole bowelirrigation is beneficial with ingestion of sustained-releasepreparations.
Hemoperfusion is effective at enhancing the eliminationof theophylline and is instituted early in treatment, whenpatients with protracted vomiting do not allow the instillation of charcoal. Indications for hemoperfusion includeunstable hemodynamics, uncontrolled seizures, inability togive charcoal despite antiemetic therapy with persistentelevation in theophylline levels after 6 to 8 hours, extensivehematemesis, serum theophylline levels between 40 and 60~g/ml in chronic overdoses or 90 and I00 ~g/ml in acuteoverdoses.4 In some circumstances, it may be beneficial toperform whole bowel irrigation and charcoal hemoperfusionsimultaneously. The patient is assessed for signs of thrombocytopenia, hypocalcemia, and infection at the catheterinsertion site when hemoperfusion is in progress.
Other interventions include administration of potassium,phosphate, and sodium bicarbonate with subsequent monitoring oflaboratory values to evaluate the resolution of toxiceffects.
Cyclic (Tricyclic) AntidepressantsEtiology/lncidence. The cyclic antidepressants are
the most widely prescribed pharmacologic treatment fordepression in adults and children. Tricyclic antidepressantsare one type of this class of drugs. The cyclic antidepressants can be divided into the first-generation and secondgeneration antidepressants. The first-generation, or tricyclic,antidepressants were developed in the 1960s. The secondgeneration cyclic antidepressants were released during the1980s and I990s to improve the therapeutic index, decreaseside effects and adverse reactions, and reduce the incidenceof serious toxicity. As the mechanisms of action have become more selecti ve, the incidence of cardiac and neurologic toxicity has decreased. In addition to depression, children also are prescribed cyclic antidepressants for treatmentof hyperkinesis, sleep disorders, school phobias, and enuresis. Adults are prescribed cyclic antidepressants for depression, chronic pain, and sleep disorders. The more com-
mon tricyclics include amitriptyline (Elavil), desipramine(Norpramin), imipramine (Tofranil), whereas the secondgeneration antidepressants include amoxapine (Asendin),fluoxetine (Prozac), sertraline (Zoloft), paroxetine (Paxil),and bupropion (Wellbutrin).
Pathogenesis. When ingested, cyclic antidepressantsare initially rapidly absorbed from the GI tract, unlessanticholinergic effects decrease the rate of absorption byslowing GI motility. The drugs have large volumes ofdistribution and are largely protein bound. The drugs bind toproteins at a certain pH, typically a more alkaline pH;therefore acidemia may increase the amount of unbound orfree drug in the pTasma. Serum levels are of little use inoverdose because of the extent of protein binding andvolume of distribution. These drugs are highly lipid soluble,sparingly water soluble and extensively metabolized on thefirst pass through the liver.42 Cyclic antidepressant toxicityprimarily affects the central nervous and cardiovascularsystems accompanied by anticholinergic crisis. Toxicity ismediated by anticholinergic effects, quinidine-like effectson cardiac function, direct a-receptor blockade, and inhibition of catecholamine reuptake in the CNS and peripheralnervous system. A quinidine-like effect is the membranedepressant effect on the myocardium through inhibition ofsodium channels. Symptoms of toxicity develop within 4 to6 hours but may be delayed for up to 24 hours.43
Cyclic antidepressant toxicity may progress rapidly,initially presenting with anticholinergic signs and progressing to lethal dysrhythmias and hypotension. Anticholinergiceffects on the CNS include respiratory depression, agitation,lethargy, hallucinations, hyperthermia, ataxia, choreoathetoid movements, seizures, and coma. Peripheral anticholinergic effects include hypotension, decreased GI motility, dryand flushed skin, urinary retention, sinus tachycardia,mydriasis, and hyperreflexia. 42
,44,45 Seizures occur in 10%to 20% of patients with tricyclic antidepressant overdoseand are most likely to occur in comatose patients46
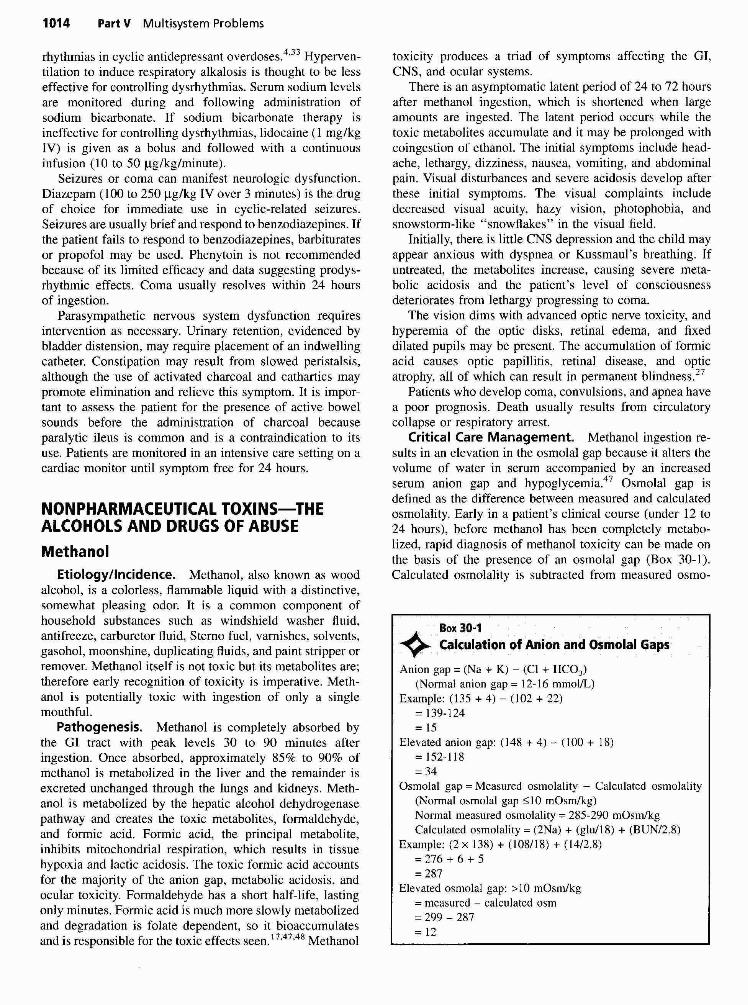
Cardiovascular dysfunction often accompanies cyclicantidepressant overdose because of the increase in thepolarization period. Decreased cardiac output may occur asa result of myocardial depression or dysrhythmias. Cyclicantidepressant's quinidine-like effects slow cardiac conduction and causes myocardial depression, prolonging the PRand QRS interval. These measurements should use thestandard lead for pediatric QRS measurement, the precordiallead Vs' The widened QRS interval provides the bestmeasurement of tricyclic antidepressants, with an interval ofmore than 100 milliseconds seen as evidence of seriousoverdose (Fig. 30-4). Increased repolarization time facilitates ventricular tachycardia, ventricular fibrillation, orasystole.44 Decreased inotropy is evidenced with generalsigns of decreased cardiac output and hypotension.
Seizures and coma with severe overdose dominateneurologic dysfunction. Respiratory failure can occur fromC S depression, seizure-related apnea, upper airway obstruction, or pulmonary edema. Because acidosis increasesthe amount of free drug in the serum, even mild hypoventilation may potentiate dysrhythmias and aggravate the poorinotropic performance of the myocardium.
Chapter 30 Toxic Ingestions 1013
TIlE CllILllRElfS lIOOPlTAL or PHlJA.P1CA ROlITlNE RmIEVAL11_Male CllIlcasian
2iTh
I
VenL ratePR inltM1QRS lim"",QTIQT,P-R-Tues
131 RPM124 ml
121 '"321H12 ...29 \21 48
SlNU$ RHYTI-NRIGHT BlNJlE BRAN:H BLlXXLEFT POSTERIOO FA$CIOJlAR BLCXX••• 8lFASCl0..llAR BlOCK •••A.~!AWAl EGGEDIlS) BY: JPN
Fig. 30-4 Electrocardiogram in a patient with a prolonged QT interval following tricyclic antidepressantoverdose.
Critical Care Management. Cyclic antidepressantoverdose is suspected if a child presents in coma or withsymptoms compatible with anticholinergic crisis. Initialinterventions are to secure an airway and stabilize vitalsigns. Symptoms of toxicity develop rapidly after ingestionwith deterioration in clinical status occurring within I hourafter ingestion and life-threatening events most oftenoccurring within 2 hours.42 Emesis is contraindicatedbecause of the rapid onset of CNS depression or seizures.Lavage is indicated for patients with altered level ofconsciousness. Following lavage, activated charcoal and acathartic are recommended. Intubation is recommendedbefore gastric decontamination to minimize the risk ofaspiration. Because of the tight protein binding, hemoperfusion, hemodialysis, and forced diuresis have no role in themanagement. Alkalinization of the serum is the preferredmethod for reducing acute cardiovascular side effects. Asodium bicarbonate infusion alters the pH, increasingprotein binding of the drug and reducing the amount of freedrug available, resulting in decreased toxicity.
Primary treatment of respiratory dysfunction is directed
toward achieving and maintaining the patency of the airway.Intubation and mechanical ventilation are initiated promptlyfor patients in whom oxygenation and ventilation are at risk.Arterial blood gases are assessed for both hypoxia andacidosis because these problems are known to increase thefrequency and recurrence of dysrhythmias.
Cardiovascular dysfunction may result in hypotension.Treatment begins with a 20 mVkg fluid bolus of normalsaline or lactated Ringer's solution. If these measures areineffective in returning the blood pressure to normal range.a continuous infusion of phenylephrine (0. I to 0.5 /lg/kg/min), norepinephrine (0.05 to 1.0 /lg/kg/min), or dopamine (5 to 30 /lglkg/min) may be required42
.44 These
medications exert predominantly direct a-agonistic effectsand counteract the a-adrenergic blockade of the cyclicantidepressants.
Treatment of dysrhythmias begins with ensuring adequate ventilation, followed by sodium bicarbonate infusion.Mild metabolic alkalosis (pH>7.45 to 7.55) has proven tobe effective in narrowing widened QRS complexes, correcting hypotension, and in decreasing the incidence of dys-
1014 Part V Multisystem Problems
rhythmias in cyclic antidepressant overdoses.4,33 Hyperven
tilation to induce respiratory alkalosis is thought to be lesseffective for controlling dysrhythmias, Serum sodium levelsare monitored during and following administration ofsodium bicarbonate, If sodium bicarbonate therapy isineffective for controlling dysrhythmias, lidocaine (I mg/kgIV) is given as a bolus and followed with a continuousinfusion (10 to 50 Ilg/kg/minute),
Seizures or coma can manifest neurologic dysfunction,Diazepam (100 to 250 Ilg/kg IV over 3 minutes) is the drugof choice for immediate use in cyclic-related seizures,Seizures are usually brief and respond to benzodiazepines, Ifthe patient fails to respond to benzodiazepines, barbituratesor propofol may be used, Phenytoin is not recommendedbecause of its limited efficacy and data suggesting prodysrhythmic effects, Coma usually resolves within 24 hoursof ingestion.
Parasympathetic nervous system dysfunction requiresintervention as necessary, Urinary retention, evidenced bybladder distension, may require placement of an indwellingcatheter, Constipation may result from slowed peristalsis,although the use of activated charcoal and cathartics maypromote elimination and relieve this symptom, It is important to assess the patient for the presence of active bowelsounds before the administration of charcoal becauseparalytic ileus is common and is a contraindication to itsuse. Patients are monitored in an intensive care setting on acardiac monitor until symptom free for 24 hours,
NONPHARMACEUTICAL TOXINS-THEALCOHOLS AND DRUGS OF ABUSE
MethanolEtiology/Incidence. Methanol, also known as wood
alcohol, is a colorless, flammable liquid with a distinctive,somewhat pleasing odor. It is a common component ofhousehold substances such as windshield washer fluid,antifreeze, carburetor fluid, Sterno fuel, varnishes, solvents.gasohol, moonshine, duplicating fluids, and paint stripper orremover. Methanol itself is not toxic but its metabolites are;therefore early recognition of toxicity is imperative. Methanol is potentially toxic with ingestion of only a singlemouthfuL
Pathogenesis. Methanol is completely absorbed bythe GI tract with peak levels 30 to 90 minutes afteringestion, Once absorbed, approximately 85% to 90% ofmethanol is metabolized in the liver and the remainder isexcreted unchanged through the lungs and kidneys, Methanol is metabolized by the hepatic alcohol dehydrogenasepathway and creates the toxic metabolites, formaldehyde,and formic acid. Formic acid, the principal metabolite,inhibits mitochondrial respiration, which results in tissuehypoxia and lactic acidosis. The toxic formic acid accountsfor the majority of the anion gap, metabolic acidosis, andocular toxicity, Formaldehyde has a short half-life, lastingonly minutes, Formic acid is much more slowly metabolizedand degradation is folate dependent, so it bioaccumulatesand is responsible for the toxic effects seen, 17,47.48 Methanol
toxIcity produces a triad of symptoms affecting the GI,CNS, and ocular systems,
There is an asymptomatic latent period of 24 to 72 hoursafter methanol ingestion, which is shortened when largeamounts are ingested. The latent period occurs while thetoxic metabolites accumulate and it may be prolonged withcoingestion of ethanoL The initial symptoms include headache, lethargy, dizziness, nausea, vomiting, and abdominalpain. Visual disturbances and severe acidosis develop afterthese initial symptoms, The visual complaints includedecreased visual acuity, hazy vision, photophobia, andsnowstorm-like "snowflakes" in the visual field.
Initially, there is little CNS depression and the child mayappear anxious with dyspnea or Kussmaul's breathing, Ifuntreated, the metabolites increase, causing severe metabolic acidosis and the patient's level of consciousnessdeteriorates from lethargy progressing to coma,
The vision dims with advanced optic nerve toxicity, andhyperemia of the optic disks, retinal edema, and fixeddilated pupils may be present. The accumulation of formicacid causes optic papillitis, retinal disease, and opticatrophy, all of which can result in permanent blindness.27
Patients who develop coma, convulsions, and apnea havea poor prognosis. Death usually results from circulatorycollapse or respiratory arrest.
Critical Care Management. Methanol ingestion results in an elevation in the osmolal gap because it alters thevolume of water in serum accompanied by an increasedserum anion gap and hypoglycemia.47 Osmolal gap isdefined as the difference between measured and calculatedosmolality. Early in a patient's clinical course (under 12 to24 hours), before methanol has been completely metabolized, rapid diagnosis of methanol toxicity can be made onthe basis of the presence of an osmolal gap (Box 30-1).Calculated osmolality is subtracted from measured osmo-

lality and nonnally does not exceed 10 mOsmlkg. Theelevated osmolal gap gradually resolves as methanol ismetabolized, toxic metabolites fonn, and an anion gapmetabolic acidosis develops48
Under nonnal circumstances, the anion gap is 12 to 16mmollL. An elevated anion gap occurs later in the clinicalcourse of patients with methanol ingestion because ofretention of nonvolatile organic acids. Calculation of theosmolal and anion gap is useful for the initial managementof patients in whom methanol ingestion is suspectedbecause it identifies the presence of hannful substances,therefore eliminating delay in treatment while specificlaboratory levels are awaited. For a patient who is symptomatic, is acidotic, or has a peak level of 20 mg/dl ofmethanol, treatment is initiated with an ethanol infusion.
Patients who appear neurologically impaired are intubated to ensure an adequate airway and effective ventilation.Although the benefits of charcoal administration are unknown in methanol ingestions, charcoal is usually recommended, especially if ingestion of multiple substances issuspected.
Treatment of metabolic acidosis includes correction ofpH and base deficit by administration of sodium bicarbonate. AlLhough acidosis may be reversed, ocular damageassociated with the toxic effects of methanol metabolismoften persists.
Alcohol dehydrogenase has a greater affinity for ethanOlthan methanol, therefore ethanol infusions are used toinhibit methanol metabolism to toxic metabolites of fonnaldehyde and formic acid, which promotes its excretionunchanged by the lungs and kidneys. Ethanol is administered in a 5% to 10% solution intravenously or orally in a20% to 30% solution. A loading dose (7.6 to 10 rnlJkg) isadministered intravenously in 10% dextrose solution over30 minutes. Maintenance dosage is 0.15 ml/kg/hr orally of95% ETOH solution or 1.4 ml/kg/hr intravenously of a 10%ethanol solution, until a serum level of 100 mg/dl isachieved.
Alcohol dehydrogenase inhibitors (ADHs) are generallymaintained until methanol levels are less than 20 mg/dl. TheFDA recently approved fomepizole (4-MP, Antizol) forethylene glycol poisoning, and it is being researched for itsutility with methanol toxicity. Fomepizole has a greateraffinity for alcohol dehydrogenase versus ethanol or methanol and has a better safety profile than ethanol.47 Inaddition, folic acid is being recommended to enhance thefolate-dependent metabolism of fonnic acid. The pediatricdose of sodium folate is I mg/kg every 4 to 6 hours.
Hemodialysis enhances the elimination of methanol andits toxic byproducts and is indicated in patients with a serumlevel of 50 mg/dl, severe metabolic acidosis, ingestion ofmore than 40 ml or in the presence of neurologic or visualdisturbances33
•48 Higher doses of ethanol are required
during hemodialysis because ethanol is easily dialyzed.49
Maintenance doses of 250 to 350 mglkg/hour are requiredto achieve and maintain the necessary serum level.
Patient monitoring includes evaluating arterial bloodgases, blood alcohol level, and serum glucose level to assessthe effectiveness of ethanol administration. Glucose is
Chapter 30 Toxic Ingestions 1015
monitored closely because glycogen stores are depletedrapidly after methanol ingestion. Complications of dialysis,such as infection and hypoglycemia, are recognized andtreated early.
Ethylene GlycolEtiology/Incidence. Ethylene glycol is a colorless,
sweet-tasting liquid with a faint odor found in pennanenttypes of antifreezes and coolants. It is also contained in latexpaint, glass cleaners, stains, dyes, waxes, inks, and a varietyof household cleaners, including floor waxes and polishes,shoe polishes, and surface cleaning solutions. Ethyleneglycol ingestions have been attributed to its bittersweettaste. Ethylene glycol poisonings usually occur as isolatedinstances with children. In adolescents and adults, toxicitycommonly occurs when ethylene glycol is ingested as anethanol substitute.
Pathogenesis. Ethylene glycol is rapidly absorbed,peaking in the bloodstream within I to 4 hours of ingestion.Once absorbed, a significant amount is eliminated by thekidneys; however, renal toxicity is acute and progressive.Once renal compromise is present, almost all of the ethyleneglycol is then metabolized in the liver by alcohol dehydrogenase to glycolaldehyde, glyoxylic acid, oxalic acid, andfonnic acid. As with methanol, the toxicity of ethyleneglycol results from its metabolites. Ethylene glycol producesCNS depression, and its metabolites cause metabolic aniongap acidosis, hypocalcemia, further CNS depression, andtissue damage.48 After a delay of 12 to 24 hours, oxalatecrystals may appear in the urine (when oxalic acid chelatesserum calcium) and is deposited in the tissues, causing acuterenal failure, metabolic acidosis, and cardiac and CNStoxicity. Ingestion of an amount as small as 1.4 to 1.6 mllkgcan be lethal.
Three clinical stages of poisoning have been described.Progression and severity of signs in these stages dependon the ingested dose. Stage I occurs from 1 to 12 hoursafter ingestion and is characterized by nausea, vomiting,metabolic acidosis, oxalate crystalluria, and progressivecentral nervous signs including elation, slurred speech,confusion, nystagmus, depressed deep tendon reflexes,myoclonic jerks, and seizures without the characteristicethanol odor on the breath. Hyperemia of the CNSproduces symptoms of inebriation, such as ataxia, swpor,and coma. A result of calcium oxalate crystal depositionin the leptomeninges, vessel walls, and perivascular spacesis meningoencephalitis.
After the first 12 to 18 hours, tachycardia, tachypnea,mild hypertension, congestive heart failure, cyanosis, andpulmonary edema leading to cardiorespiratory failure characterize the second stage. Myocardial and pulmonarydysfunction occur as a result of accumulation of the toxicintennediate and deposition of calcium oxalate crystals inthe heart and lungs.
The third stage occurs I to 3 days after ingestion and ismarked by flank pain, hematuria, proteinuria, oliguria, acutetubular necrosis, and renal failure. Damage to the renaltubules is thought to be caused by the byproducts glycolal-

1016 Part V Multisystem Problems
dehyde, glycolic, and glyoxylic acid, during ethylene glycolmetabolism.33
Critical Care Management. Ventilatory support, ifneeded, is initiated immediately. Emesis is contraindicatedbecause of the risk for CNS depression. Gastric lavage isindicated for patients presenting within several hours afteringestion of massive amounts or if gastric motility is slowedby another ingestant or coma. Activated charcoal does notbind to ethylene glycol and is not used.
Ethanol administration blocks ethylene glycol metabolism and development of toxic metabolites through alcoholdehydrogenase binding. A loading dose of ethanol is givenwhen there are clinical signs and a history of ethylene glycolingestion, severe or persistent metabolic acidosis, or a bloodethylene glycol level of 25 mg/dl or higher. Ethanol loadingis also recommended for patients who are awaiting ethyleneglycol semm determinations or hemodialysis. The antidote,fomepizole, is a potent inhibitor of ADH and was approvedby the FDA for the treatment of ethylene glycol poisoning.Reports indicate that the intravenous administration offomepizole every 12 hours prevents renal damage andmetabolic abnormalities associated with the metabolism ofethylene glycol to its toxic metabolites.50
In cases when ethylene glycol concentration is higherthan 50 mg/dl or renal failure exists, hemodialysis isrecommended. Thiamine (0.25 to 0.5 mg/kg) and pyridoxine (I to 2 mg/kg) administration are thought to decreaseoxalate production. The prevention of oxalate crystalformation and subsequent deposition in the kidney arebenefits of forced diuresis in the treatment of ethylene glycolintoxication.
Priorities for critical care management include meticulous assessment of intake and output to ensure adequatehydration despite forced diuresis. Care is aimed towardenhancing clearance of ethylene glycol and its metabolites.If hemodialysis is required, care is focused on the maintenance of normal hemodynamics and fluid and electrolytebalance during therapy. Ethanol administration is continueduntil the ethylene glycol level reaches zero.
Close monitoring of blood gas and calcium determinations are necessary for early detection and treatment ofmetabolic acidosis and hypocalcemia. Intravenous sodiumbicarbonate (I to 2 mEq/kg) is indicated because ethyleneglycol is metabolized faster than methanol, resulting in amore profound metabolic acidosis. Calcium chloride (10 to20 mg/kg/dose) is required to reverse the hypocalcemiaeffects of calcium oxalate precipitation in the semm.
IsopropanolEtiology/Incidence. Isopropyl alcohol is a clear,
colorless solution, found in rubbing alcohol, antifreeze, skinlotions, and glass cleaners. Parents may use isopropanol forsponging a child to reduce fever with isolated cases resultingin stupor or coma. Consequently, this practice is stronglydiscouraged.
Pathogenesis. The peak absorption of isopropanoloccurs in about 30 minutes because of rapid GI absorptionwith complete absorption in 2 hours. Isopropanol is a eNSand cardiac depressant. Approximately 20% to 50% of
isopropanol is excreted unchanged by the kidneys. The liveris responsible for about 50% to 80% of isopropanolmetabolism converting it to acetone. The kidneys primarilyexcrete acetone with some excretion through the lungs. Thehalf-life of isopropanol is 4 to 6 hours and that of acetone is16 to 20 hours. Acetone acts as a CNS depressant and theprolonged CNS depression seen with isopropanol ingestionis related in part to the acetone's effect.
Isopropanol toxicity produces CNS effects includingdepression, ataxia, confusion, stupor. and coma. The depression has been described to be 2 to 3 times more profoundthan ethanol ingestions.47 Patients may appear intoxicatedbut do not smell like alcohol; rather they have the fruity odorof acetone. Hyperglycemia, inconsistent pupil size, miosis.and depressed or absent deep tendon reflexes are other eNSmanifestations characteristic of isopropanol toxicity.
As a myocardial depressant, acetone causes alteredcardiac function with profound hypotension and has beennoted to be a poor prognostic sign. Patients may have sinustachycardia but usually no other cardiac dysrhythmias.Impaired GI system function results from the effects ofisopropanol as a local irritant. GI symptoms such asgastritis, abdominal pain, vomiting, and hematemesis usually occur as a result of isopropanol ingestion. Renal tubularnecrosis, myopathy, and hemolytic anemia have also developed after ingestion of isopropanol.
Critical Care Management. Supportive care is theprimary treatment. Airway protection is crucial to preventaspiration should vomiting occur. Emesis is not recommended because of the rapid CNS depression associatedwith isopropanol. Gastric lavage is recommended because itmay limit absorption and helps to decrease the localirritation in the lining of the stomach. Serum isopropylalcohol level confirms and quantitates alcohol level, but theclinical presentation is a better indicator of prognosis.
Therapy for isopropanol ingestion is fairly nonspecific.focusing mostly on general supportive care. Maintainingadequate ventilation and normotension is the primary goal.Care of children with isopropanol toxicity necessitatesclose monitoring for and correction of fluid and electrolyte imbalances. If hypoglycemia develops. the patientwill require adjustment of intravenous glucose infusionsto maintain serum glucose in the normal range of 80 to120 mg/dl.
Hypotension is treated with fluid boluses (20 ml/kg IV)and vasopressor support if needed. Hemodialysis is usedwhen serum isopropyl alcohol levels are greater than 400mg/dl or hypotension is refractory to treatment.
EthanolEtiology/Incidence. Ethanol is found in alcoholic
beverages, perfumes, cologne, cold preparations, aftershave,mouthwash, and antiseptics. Blood ethanol levels less than50 mg/dl can produce mild intoxication in children;however, a lethal dose has been estimated at 3 mg/kgequivalent (e.g., 5 to 10 ounces of mouthwash or I to 2ounces of cologne).4 Ethanol is more likely to be ingestedthan some other substances because these products are useddaily and are usually within reach of young children.

Pathogenesis. Ethanol is rapidly absorbed from thegastric tract, peaking in the serum 30 to 60 minutes afteringestion when the stomach is empty. Absorption is delayedwhen food is present in the stomach and total absorptionmay take up to 6 hours. A total of 90% is metabolized in theliver by alcohol and aldehyde dehydrogenases with someoxidation. The kidney excretes the remainder. Ethanolaffects the reticular activating system, causing direct CNSdepression, decreased motor function, and decreased levelof consciousness. At high concentrations, ethanol is ananesthetic and can cause autonomic dysfunction, hypothermia, and hypotension with subsequent coma and death fromrespiratory depression and cardiovascular collapse.
Ethanol ingestion may be manifested clinically byflushed face, diaphoresis, agitation, or ebullient and loquacious speech resulting from early disinhibition. This mayprogress to ataxia, slurred speech, blurred or double vision,drowsiness, stupor, depression, or coma. Significant intoxication is characterized by the presence of an osmolal gap(see Box 30-1). Ethanol metabolism causes impairedgluconeogenesis during the Krebs cycle. Profound hypoglycemia can ultimately lead to convulsions and coma in thepediatric patient, but the prognosis for children who ingestethanol is generally good.
Critical Care Management. The initial treatment forethanol intoxication involves providing supportive measuressuch as airway protection, oxygen, and monitoring fluids.Emesis is contraindicated because of rapid CNS depression.Gastric lavage may be recommended when the child is seenwithin 30 to 60 minutes after ingestion and CNS depressionis present. Charcoal and forced diuresis are ineffectivebecause the liver is the primary metabolic pathway. Cardiacand respiratory support is necessary in addition to theinitiation of an intravenous infusion of 10% dextrose ifhypoglycemia exists.
Supportive therapy with ongoing monitoring of vitalfunctions until toxic effects subside is the primary focus ofintensive care. Children who ingest ethanol require frequentserum glucose and ethanol determination and assessment forchanges in mental status. Reassuring parents by noting signsof improvement in clinical status is helpful as the childprogresses through the recovery period. The patient needs tobe protected against aspiration. If hypoxia develops, thepatient may require intubation and mechanical ventilation.Intravenous fluids are administered to replace urinary lossesand correct electrolyte imbalance, acidemia, and hypotension. If hypotension is refractory, vasopressors may benecessary. Hypothermia is treated with passive rewarming;and normothermia is the goal. Maintaining seizure precautions is necessary until symptoms of neurologic toxicityabate. If the blood ethanol.level is greater than 300 to 350mg/dl and clinical deterioration progresses despite supportive care, hemodialysis is used4
CocaineEtiology/Incidence. Grown in Peru and Bolivia,
cocaine is an alkaloid that is extracted from the leaves of theErythroxylum coca plant. It is crystallized as hydrochloridesalt. prescribed as a local anesthetic and mucous membrane
Chapter 30 Toxic Ingestions 1017
vasoconstrictor, and used illicitly as a CNS stimulant. Theadulterants with which cocaine is diluted for illicit useinclude local anesthetics, sugars, stimulants, toxins, andinert compounds and may also exert toxic effects51
Cocaine may be injected intravenously, sniffed intranasally, ingested, or applied to the mucous membranes.Cocaine can also be smoked in its free-base form known as"crack." Children may be exposed to cocaine by passivetransmission via the placenta in utero, or in breast milk, orby inhalation of crack vapors.52 Cocaine is well absorbed byall mucous membranes, metabolized by liver esterases andplasma cholinesterase, degraded nonenzymatically, andexcreted in the urine as its primary metabolite, benzoylecgonine. 53 Cocaine levels in blood may be detected withinseveral minutes of ingestion. They peak in J5 to 30 minutesand persist for up to 8 hours.54 Cocaine may be detected inurine within I hour of ingestion or administration andpersists for up to 3 days in children and 5 days in neonatesfollowing exposure.
Pathogenesis. Three systems primarily affected bycocaine's toxic effects are the neurologic system, thecardiovascular system, and the respiratory system. Cocainestimulates the sympathetic nervous system, and an overdoseis especially toxic to the brain and heart. Cocaine stimulatesthe presynaptic release of dopamine, norepinephrine, serotonin, and acetylcholine in the CNS. It alters normalintraneural communication by augmenting the effects of thecatecholamines, norepinephrine, and dopamine. Cocainestimulates the "fight or flight" mechanism, evidenced byclinical signs of stimulation of norepinephrine secretion.Signs and symptoms are dose related, with low dosesproducing euphoria and CNS stimulation and high dosesproducing anxiety, agitation, paranoid delusions, mydriasis,hypertension, hyperthermia, tachycardia, and cardiac dysrhythmias.4 As cocaine continues to stimulate norepinephrine and dopamine release, the cardiovascular and neurologic systems demonstrate progressive stimulation that mayprogress to exhaustion, producing coma and cardiopulmonary arrest.
Cardiovascular dysfunction is first manifested by sinustachycardia or supraventricular dysrhythmias followed byhypertension, peripheral vasoconstriction, ventricular ectopy. and occasionally, ventricular fibrillation or asystole.These signs may occur as a result of the toxic action cocaineexerts on the tissues of the myocardium directly. or becauseof its effect of sensitizing the heart to the actions ofnorepinephrine and dopamine.44 Evidence of a toxic dose isseen when heart rate and blood pressure peak and begin tofall, ventricular dysrhythmias become more frequent, andthe patient begins to show signs of shock with decreasedperipheral perfusion and cyanosis. Progression of signsincludes ventricular fibrillation, circulatory collapse, and anashen appearance before cardiac arrest. Cocaine-inducedcoronary artery vasoconstriction may also cause myocardialischemia or infarction related to increased myocardialoxygen demand and cocaine's thrombogenic potential.53
Neurologic dysfunction begins as the cerebral cortex isstimulated. Dysfunction is further evident with talkativeness, hyperalertness, mydriasis, and nausea and/or vomitingoccurring. As stimulation continues and cocaine affects the

1018 Part V Multisystem Problems
functions of the medulla, the child becomes hyperthermic,develops hyperreflexia, and may have seizures. As the CNSbecomes exhausted, the child becomes comatose withflaccid paralysis.
Tachypnea and increased depth of respiration evidencethe early stimulation phase of the CNS. Later, depression ofthe medullary respiratory center occurs, the child becomesmore dyspneic and may progress to cyanosis and respiratoryfailure. Seizures, or respiratory depression secondary toantiepileptic medications, may also contribute to respiratoryfailure in cocaine toxicity. Cerebral vascular accidents,including subarachnoid hemorrhage, cerebral infarction,transient ischemic attacks, and seizures have been reportedwith cocaine toxicity. Seizures may develop secondary toinfarction or hemorrhage, and the majority are single,generalized, and not associated with any lasting neurologicdeficits53
Critical Care Management. Because cocaine isabsorbed quickly with smoking, snorting, or injection, notreatment can decrease its absorption or enhance its excretion. If cocaine is ingested, GI decontamination may beconsidered after initial stabilization of airway, breathing,and circulation. Initial management of cocaine exposuredepends on the phase at which the patient presents for care.Adequate cardiovascular and respiratory function is ensured. Assessment of cardiovascular function includes heartrate and rhythm, blood pressure, and peripheral perfusion.Respiratory evaluation includes assessment of both respiratory rate and depth, with pulse oximetry or arterial blood gasanalysis as needed. Intravenous access is obtained promptlyand vital signs are monitored frequently. Continuous coretemperature monitoring is initiated to assess for hyperthermia. Emesis is not used, but activated charcoal and acathartic may be given for oral ingestions. Whole bowelirrigation has been used safely to remove packets and crackvials in drug smugglers.
Cardiovascular dysfunction is initially treated with fluidresuscitation. There is significant controversy regarding theuse of antidysrhythmics with cocaine ingestion. The majority of antidysrhythmic agents are contraindicated becausethey exacerbate the problems of coronary artery spasm,ischemia, infarction, and ventricular arrhythmias. A lidocaine bolus (I mg/kg) and continuous infusion (10 to 50!!g/kg/min) may be required to suppress ventricular arrhythmias if no other alternatives are present. Benzodiazepinesslow the heart rate, may have an additive antiarrhythmiceffect, and are added, if not already used, only to offerprotection against the combined proconvulsant effect oflidocaine and cocaine. If unable to determine whether thedysrhythmia is from ischemia or sodium channel blockadewith QRS widening, sodium bicarbonate and benzodiazepines are given first, followed by lidocaine if dysrhythmiaspersist.53 Nitroglycerin may be used to relieve chest painand angina. Severe hypertension resulting from vasoconstriction is best treated with sedatives such as diazepam(40 to 200 !!g/kg IV) or lorazepam (30 !!g/kg/day in threeor four doses intravenously) in an effort to control hypertension, calm the patient, prevent seizures, and decreasehypertonicity. If these measures fail to control hypertension,
a continuous infusion of nitroprusside (0.2 to 10 !!g/kg/min)may be necessary. Pulmonary artery pressure monitoringmay be indicated to estimate the left heart filling pressuresand to guide management.
Use of a tool such as the Glasgow coma scale or thePediatric Coma Scale guides neurologic assessment. Seizures may be treated with diazepam (I ()() to 250 !!g/kg) orlorazepam (50 !!g/kg) given intravenously over 3 minutes.Hyperpyrexia is aggressively treated with cooling blanketsor tepid baths, avoiding shivering, which increases bodytemperature. Respiratory dysfunction management includesmaintenance of a patent airway as the first priority. Oxygenmay be administered to prevent complications of hypoxemia. Intubation is considered if the child is unable tomaintain a patent airway, adequate cough, or gag reflexes; ifseizures compromise respiratory function; or if arterialblood gas analysis demonstrates hypercarbia. Mechanicalventilation may be required to treat respiratory insufficiencyor respiratory failure.
HeroinEtiology/Incidence. Heroin is an illicit semisyn
thetic narcotic agent initially developed as a less-addictingmorphine substitute. It originally gained popularity in the1970s, but now a resurgence of heroin use and abuse hasoccurred in the 1990s. Heroin has become cheaper and morereadily available in the past few years, and a new generationof young heroin users has developed novel patterns ofabuse.
Heroin acts as a pro-drug that allows for rapid CNSabsorption, providing euphoric and toxic effects. All routesof administration rapidly absorb heroin with intravenousheroin at serum peak levels within I minute. Intranasal andintramuscular heroin reach peak levels in 3 to 5 minutes, andsubcutaneous heroin reaches peak levels within 5 to 10minutes. Heroin is seven times more toxic than intravenousmorphine and the route of administration strongly affects thedrug's potential for overdose or death. The majority ofnonfatal and fatal heroin overdoses occur when injectedintravenously.
Pathogenesis. Heroin is highly lipid soluble withrapid and complete uptake into the CNS that produces afeeling of intoxication. Heroin produces opiate intoxicationsyndrome consisting of altered mental status, miosis, andrespiratory depression. It reacts with three types of receptors, mu, kappa, and delta, to produce a wide range ofchanges in the CNS. Initial effects include euphoria,sedation, impaired thinking, miosis, and mild decrease inblood pressure and urinary retention. Toxic ingestionsproduce hypotension, bradycar.dia, depressed respiration,agitation, uncontrolled muscle movements, hallucinations,headache, nausea and vomiting, stupor, coma, seizures, ordeath54
The mu receptors are responsible for most of theanalgesic effects, respiratory depression, delayed GI motility, miosis, and euphoria, whereas kappa agonists, independent of the mu receptors, produce analgesia, respiratorydepression, and dysphoria. Delta receptors work to mediate

spinal analgesia. Centrally mediated respiratory depressionis caused by a direct effect on the brainstem, reducingresponsiveness to carbon dioxide. Respiratory depression isthe dominant symptom and the most common cause of deathin heroin overdose. Heroin crosses the blood-brain barrierwithin 15 to 20 seconds and achieves a high brain level ofboth heroin and its metabolites. In the CNS, heroin isquickly hydrolyzed to a substrate that is metabolized over 20to 30 minutes to morphine. Heroin and its metabolites bothhave significant agonist and analgesic effects on the CNS.Any circulating heroin can be hydrolyzed in the peripheraltissues of the kidneys and liver to morphine. The byproducts of morphine are water soluble and readily excretedin urine and bile55
Critical Care Management. Heroin intoxication isusually witnessed, and identification of the toxin is known.Initial management includes assessment of adequacy ofventilation and airway stability. The majority of patients will present with inadequate respiratory effort andrequire assistance with bag-valve-mask breathing andoxygen delivery. If ingestion of heroin is confinned,parenteral naloxone therapy is initiated. If the patient doesnot respond to naloxone within 10 minutes, or the airwayis unstable, then intubation is performed. If the patient isbreathing well without support, naloxone is not administered, and the patient is observed. Emesis is contraindicated because of rapid absorption of heroin and CNSdepression.
Gastric decontamination with whole bowel irrigation andactivated charcoal is used in cases of body packers or"mules" who attempt to smuggle large numbers of concentrated drug packets by ingesting them. These individuals aretypically asymptomatic but are at risk for delayed andprolonged toxicity from packet rupture. If symptomatic, acontinuous infusion of naloxone can be administered inconjunction with gastric decontamination.
Ongoing management typically consists of supportivecare, primarily of the respiratory system with assistedventilation, until the CNS depressive effects are no longerpresent. In the hypoventilating patient suspected of heroinoverdose, an initial dose of naloxone (0.1 mg/kg) may begiven, followed by a higher dose (maximum 2 mg) if noresponse is seen in 3 to 5 minutes. The short duration ofaction of naloxone may require multiple doses untilrespiratory compromise is no longer present. A chestradiograph is obtained for patients who clinically presentwith a significant cough or poor oxygenation.
Naloxone treatment of heroin overdose is associated withcomplications, including seizures, tachycardia, severe agitation, nausea and vomiting, diaphoresis, and hypertension.Heroin has a I% to 3% associated risk of inducingnoncardiogenic pulmonary edema, whereas naloxone isassociated with a 1.6% rate of complications, includingseizures and arrhythmias.55 Patients with heroin overdoseand respiratory compromise require observation and cardiorespiratory monitoring until cessation of clinical symptoms.Patients are carefully evaluated to rule out coingestion,especially benzodiazepines, which contribute to a muchhigher complication rate.
Chapter 30 Toxic Ingestions 1019
MethadoneEtiology/Incidence. Methadone is a synthetic nar
cotic that is used in the treatment of heroin addiction andwithdrawal. Methadone is unrelated to morphine but issimilar in mu effect. It replaces the illicit substance with alegal, oral, and long-acting agent, but excessive dosing maycause toxicity. Methadone will produce symptoms similar toheroin intoxication and overdose. Children are particularlysusceptible to the effects of methadone overdose, withrespiratory depression and death potentially occurring witha lO-mg dose.
Pathogenesis. Methadone is very lipid soluble andwell absorbed from the GI tract into the blood stream witha long elimination half-life of 15 to 20 hours in children.Methadone is 70% to 90% bound to albumin and plasmaproteins. The oral duration of action is 6 to 8 hours initiallyand 22 to 48 hours after repeated doses. It is hydrolyzed witha fairly extensive metabolism on first pass through the liver.Methadone is excreted in sweat and saliva, and 10% isexcreted unchanged along with metabolites in urine andstool.54
Methadone can produce mild side effects such asdrowsiness, lightheadedness, weakness, euphoria, drymouth, and urinary retention with proper dosing. Symptomsof methadone overdose include marked drowsiness, confusion, tremors, nausea and vomiting, cold and clammy skin,hypotension, hypothermia, bradycardia, miosis, seizures,stupor leading to coma, and severe respiratory depression56
Critical Care Management. Methadone has a slowonset of action and a very long duration of effect. Allpatients who present with methadone toxicity requirehospitalization and monitoring. Initial management consistsof assessment and stabilization of respiratory effort. Intubation is performed for all patients with significant respiratorydepression. If respiratory depression is not immediatelyaddressed, cyanosis, hypoxia, and apnea may develop. Themajor cause of death in methadone toxicity is respiratoryarrest.
Emesis is contraindicated. Activated charcoal maybe worthwhile because gastric motility is slowed bymethadone.
The majority of critical care management is supportive innature. The child may require intubation and mechanicalventilation support until respiratory depression subsides.The patient is initially NPO, and intravenous fluid is givenfor hydration. Naloxone is given intravenously as a continuous infusion, starting with a loading dose (0.005 mg/kg)followed by an infusion of 0.0025 mg/kg/hr, taperinggradually as symptoms resolve to avoid relapse. Hypotension is treated with fluid boluses (20 ml/kg) and if refractorymay require inotropic support.
PhencyclidineEtiology/Incidence. Phencyclidine (PCP) was devel
oped in the 1950s as a dissociative anesthetic-analgesic. Itwas the prototype of a drug combining analgesic andanesthetic actions without respiratory or cardiovasculardepression. PCP produced dysphoric effects and was rapidly

1020 Part V Multisystem Problems
adapted as a street drug after being removed from thepharmaceutical market. PCP is easily and cheaply synthesized from readily obtainable ingredients. It typically usedby polydrug abusers57
PCP can be smoked, snorted, or ingested. [t has a rapidonset of action and may elicit drug-induced psychosis withflashbacks lasting for weeks.
Pathogenesis. PCP is a highly lipid-soluble drug,which is also soluble in water and alcohol. It is metabolizedby the liver to hydroxyl and glucuronide and then excretedin the urine as an inactive complex within 12 hours ofingestion. PCP is thought to block the calcium channelinflux, which results from glutamate binding.
PCP primarily affects the CNS, stimulating a-adrenergicreceptors and potentiating catecholamines. The major effects are psychologic, sympathomimetic, cholinergic, andcerebellar. People may have sharply contrasting responses toPCP. It has profound effects on thinking, alters time perception and sense of reality, affects mood, and may create adreamlike, euphoric, or depressed state. Intoxication withPCP may produce negative effects including disorientation,confusion, anxiety, irritability, paranoid states, hostility, orbeUigerence. Dangerously violent behavior may develop.58
At high doses, PCP abuse may produce nystagmus, hypertension, tachycardia, salivation, flushing, sweating, dizziness, blurred vision, ataxia, and CNS stimulation or depression. The symptoms are quite variable, and children presentwith miosis, choreoathetosis, and seizures more often thanadults.57 The presence of hypertension, abnormal behavior,and miosis in children strongly suggest PCP poisoning.Most fatalities associated with PCP poisoning are related toviolent actions rather than the toxicity of the dose. 19
Critical Care Management. Initial managementconsists of assessing and maintaining adequate respiration,circulation, and thermoregulation. To prevent self-injury. thepatient is safely restrained, using physical and chemicalmethods as necessary. If the patient has a history of recentingestion of PCP, GI decontamination is initiated. Gastriclavage may be performed once the patient's anxiety oragitation is weU controlled. Activated charcoal effectivelyabsorbs PCP and increases its nonrenal clearance. Unlessthere are specific contraindications, sorbitol is administeredwith the activated charcoal. Alkaline diuresis, hemoperfusion, and hemodialysis are not beneficial because of thesubstantial protein binding, high lipid solubility, and limitedrenal excretion of PCP.
The continuation of supportive treatment until resolution of symptoms is the primary treatment. If seizuresoccur, benzodiazepines can be used in addition to treating agitation. Hyperthermia is treated with passive cooling techniques. The patient is kept weU hydrated tolessen the effects of rhabdomyolysis and prevent deposition of pigment in the kidneys, which could lead to renalfailure.
The majority of patients rapidly regain nomlal CNSfunction within several hours of using PCP. However, somepatients may remain comatose or exhibit bizarre behaviorfor days or even weeks after ingesting high doses. Patients
who may have an underlying psychiatric disorder may alsohave symptoms for an extended period.
The major complication of PCP is from injuries related tobehavior, including self-inflicted injuries, injuries fromexceptional physical exertion, or injuries from resistingphysical restraints. Patients who have ingested PCP appearto be unaware of their surroundings and pain because ofPCP's dissociative anesthetic effects.
HOUSEHOLD TOXINS
CausticsEtiology/Incidence. A caustic is a substance that
causes functional and cellular damage on contact with bodysurfaces. The injury results as neutralization of the substance takes place at the expense of the tissues, releasingthermal energy and causing burns. Caustics are classified asstrong acids or alkalis and can be found in most homes. Theincidence of caustic injuries to the esophagus has increasedsignificantly since the use of concentrated liquid alkalinecleansers became popular. In addition, many accidentalchildhood ingestions occur as a result of the substancesbeing placed or stored in easily accessible and familiarcontainers such as milk cartons and soda cans. Commonsources of acid exposure include toilet bowel cleaner,swimming pool products, and battery fluid. Householdsources of alkali agents include drain openers, lye, hairpermanent products, and oven cleaners. The skin, eyes,respiratory tract, and GI tract are all systems affected bycaustic injury. Ingestion of caustics causes the mostlife-threatening and long-term morbidity. 59
The majority of caustic burns to the esophagus are aresult of sodium hydroxide or lye ingestions and most oftenoccur in children younger than 5 years of age.60 Commercialammonia is an alkali that causes ulcers or full-thicknessburns to the esophagus after ingestion and irritation to thelungs or pulmonary edema after inhalation. Toilet bowlcleaners that contain sulfuric, hydrochloric, or phosphoricacid burn the oropharyngeal mucosa and are usually spit outon contact. Detergents and bleach are commonly ingestedby children and produce local irritation without causingnecrosis.
Pathogenesis. Esophageal burns produced by theingestion of caustic agents are classified as first-degreeburns, which produce hyperemia and superficial desquamation; second-degree burns, which result in blisters andshaUow mucosal ulcers; and third-degree burns, whichproduce deeper ulceration into the esophageal muscle. Caustics can affect a variety of regions along theGI tract in addition to the esophagus because of the agents'low surface tension and ability to spread to a largesurface area.
The location of the injury varies but can involve thecricopharyngeal area, impression of the aortic arch and leftbronchus, lower esophageal sphincter, and stomach. Greaterdamage occurs in these locations because the ingested agentmay become stagnant. Granular agents may imbed in the

tissues of the oropharynx or proximal esophagus, whereasliquid agents produce damage along the entire esophagus tothe stomach lining. When the lower esophageal sphincter isinvolved, the resting pressure decreases, causing reflux ofthe agent back and forth between the esophagus andstomach. This is usually followed by violent regurgitation.
Acids produce a coagulating necrosis in the stomach andesophagus, resulting in eschar formation. This limits deeppenetration into the tissue, but leads to metabolic acidosisand pooling of acids in the stomach.
Alkaline agents usually affect the mouth, esophagus, andstomach. However, it is possible to have esophageal burnswithout oral involvement if the agent is swallowed rapidly.The alkali acts as a solvent on the lipoprotein lining, causinga liquefaction necrosis with inflammation and deep penetration into the mucosal, submucosal, and muscular layers ofthe esophagus and stomach. This is followed several dayslater by saponification of mucosal fats and proteins,thrombosis of adjacent blood vessels, cell necrosis, andtissue degeneration. Sloughing develops 4 to 7 days afteringestion when bacteria invade the injured areas. Thedevelopment of strictures can occur anytime between 21 and42 days after exposure61
Critical Care Management. The identity, concentration, pH, and amount of substance ingested are important toascertain. Depending on the severity of injury, the patientmay present with physical findings of impending airwayobstruction. If possible, gentle or fiber-optic intubation ispreferred over blind nasotracheal because of the increasedrisk of soft-tissue perforation. Emesis is contraindicatedbecause of the reexposure to the caustic agent. Gastriclavage is also contraindicated for both acid and alkaliingestions. Large liquid acid ingestions may benefit fromnasogastric suction because pyloric sphincter spasm mayprolong the contact time with the gastric mucosa. Activatedcharcoal is relatively contraindicated because of pooradsorption and endoscopic interference. If the gag reflex isintact, dilution may be beneficial in the ingestion of solid orgranular alkaline material if performed within 30 minutesof ingestion. The child can be given a small amount oftap water (5 ml/kg) to dilute the substance, but the riskof inducing emesis is weighed against the benefit ofdilution. Acids are not diluted with water because ofexcessive heat production. All small children, symptomaticpatients, and those with altered mental status are admittedfor observation and subsequent endoscopy to evaluate theextent of injury.
Hydration accompanied by NPO for 12 to 24 hours untilthe extent of the injuries has been determined is initiated.The child requires close observation for drooling or thepresence of lesions in the oral mucosa, stridor, hoarseness,subcutaneous air, respiratory distress, acute peritonitis, andhematemesis in the early stages of hospitalization. Airwayedema or obstruction may occur up to 48 hours after analkaline exposure, and delayed perforation may occur up to4 days after an acid exposure.
The child who has sustained first-degree bums isassessed for the ability to tolerate liquids and slowly
Chapter 30 Toxic Ingestions 1021
advanced to a regular diet. For children with second-degreeand third-degree bums or evidence of perforation, theadministration of antibiotics and antacids may be indicated. These children may also need parenteral nutritionand an endoscopy 2 to 3 weeks after the ingestion toevaluate the extent of esophageal dysmotility or strictureformation. Repeated esophageal dilations may be requiredif strictures develop.59.61 Long-term sequelae may requiresurgical intervention to repair the severely damagedesophagus.
HydrocarbonsEtiology/lncidence. Fully 60% of all hydrocarbon
exposures involve children and 90% of hydrocarbon-relateddeaths involved children, younger than 5 years of age.Hydrocarbons are defined as all-organic compounds madeof predominately carbon and hydrogen molecules, including those derived from petroleum distillation. Hydrocarbons are classified into four different categories: aliphatics(paraffins), aromatics, alicyclics or cycloparaffins, andhalogenated products. Aliphatic hydrocarbons are found inthe form of petroleum distillates such as furniture polish,lamp oil, lighter fluid, propane, and isobutane. Aromatichydrocarbons, such as benzene, toluene, and xylene, arefound in glues, nail polish, paints, and paint removers.Alicyclic hydrocarbons are otherwise known as turpentine,cyclopropane, and cyclohexane. Halogenated hydrocarbons, such as carbon tetrachloride, chloroform, methylenechloride, Freon, and trichloromethane, are particularlyharmful because they produce various forms of systemictoxicity.
Pathogenesis. The pulmonary system is predominately affected by hydrocarbon ingestion. The CNS, GI,cardiac, and dermatologic systems are also commonlyaffected with rare hematologic, hepatic, and renal effects.Aliphatic hydrocarbons produce minimal systemic toxicitybut may cause pulmonary injury, depending on theirviscosity and ease of aspiration. Alicyclics can producepulmonary aspiration and direct CNS depression. Aromatic and halogenated hydrocarbons can cause cardiacarrhythmias in addition to aspiration and CNS depression(Box 30-2).
The risk of aspiration depends on the viscosity, surfacetension, and volatility of the substance. The lower theviscosity and surface tension and the higher the volatility,the greater the risk of aspiration.62 Products with lowviscosity pose a high aspiration hazard because of thetendency to spread over a large surface area. Chemicalpneumonitis may develop from as little as a few millilitersof a hydrocarbon. Aspiration usually occurs at the time ofingestion or upon emesis. Large amounts of most alicyclicand aromatic hydrocarbons can be tolerated by ingestion ifnot aspirated. Agents that are not aspirated easily but thatcause systemic toxicity (i.e., the halogenated hydrocarbons)induce neurotoxicity. Benzene, in addition, is associatedwith aplastic and acute myeloblastic anemia because of itsability to injure bone marrow.
1022 Part V Multisystem Problems
Box 36-2 ._~ Clinical Manifestations.o.f
. .... Hydrocarbon Ingestion
I. Pulmonary dysfunctionTachypnea, dyspnea, adventitious breath sounds, oxygendesaturation, cyanosis
2. CNS dysfunctionEuphoria, agitation, restlessness, confusion, seizures, coma
3. Cardiovascular dysfunctionVentricular dysrhytbmias (tachycardia, fibrillation)
4. Gastrointestinal dysfunctionOropharyngeal irritation, gastric irritation, vomiting.hematemesis
5. Hepatic dysfunctionElevated liver enzymes, hepatomegaly
6. Renal dysfunctionUrine positive for albumin, cells, casts
The ingestion of a hydrocarbon causes irritation of themouth, pharynx, and gastric mucosa and is usually followedby vomiting. Aspiration of these substances, which are lipidsolvents, leads to hydrocarbon pneumonitis within 12 to 24hours after exposure and is typically accompanied by rapiddevelopment of low-grade fever. 62
Hydrocarbons disrupt surfactant, cause direct injury tothe epithelium and pulmonary capillaries and create bronchospasm, alveolar instability, and collapse resulting inatelectasis and pulmonary edema. Symptoms exhibitedinclude coughing, retractions, grunting, tachypnea, dyspnea,cyanosis, and severe hypoxia. Physical examination ischaracterized by rales on auscultation, rhonchi, wheezing, ordecreased breath sounds. Positive radiographic findings,such as perihilar densities, basilar pneumonitis, atelectasis,and consolidation, have been noted as early as 2 hours afteringestion.63 Other pulmonary complications include pneumatoceles, emphysema, pleural effusion, pneumothorax,pneumomediastinum, and pneumopericardium.
Halogenated and aromatic hydrocarbons are well absorbed by the GI tract and pulmonary system. This enablesthem to cause direct CNS depression resulting in headache,dizziness, ataxia, lethargy, changes in mental status, andseizures. Patients can also exhibit signs of narcosis, inebriation, or coma.4
Inhalation of halogenated hydrocarbons has been knownto cause fatal ventricular dysrhythmias resulting frommyocardial sensitization to catecholamines. The pathophysiologic effect of inhalation of these substances causesincreased ventricular irritability, predisposing the heart toventricular fibrillation.
All hydrocarbons produce symptoms of Gr distressincluding nausea, vomiting, hematemesis, and diarrhea.Absorption varies, depending on the type of hydrocarbon.Aliphatic hydrocarbons have minimal absorption, whereasalicyclic, aromatic, and halogenated hydrocarbons can havesignificant GI absorption.
Halogenated hydrocarbons have been known to producecentrilobular necrosis. Specific types include carbon tetra-
chloride and chloroform, which induce fatty degeneration ofthe liver, resulting in necrosis.64
Many halogenated hydrocarbons that produce hepaticdysfunction also cause renal tubular acidosis. Damageoccurs directly to the proximal tubule and the loop of Henlefrom carbon tetrachloride. This leads to acute renal failurebetween I and 7 days after exposure.64
Critical Care Management. Ingestion of hydrocar-. bons commonly leads to gagging with pulmonary aspi
ration. Aspiration may lead to the rapid development ofchemical pneumonitis and intubation, and mechanicalventilation is initiated quickly, preferably using a cuffedendotracheal tube. Once initial stabilization is achieved,consideration of gastric decontamination is considered.Gastric emptying remains a controversial recommendation.Because the majority of hydrocarbons do not causesystemic toxicity but have significant risk for causingpulmonary injury, emesis and gastric lavage are notrecommended. When there are no contraindications, gastricemptying may be helpful for hydrocarbons that haveinherent toxicity, have been ingested with a toxin, or havebeen used to stabilize a toxin or when a large volumeof hydrocarbon is ingested. Hydrocarbons that haveinherent toxicity include CHAMP: C--camphor, Hhalogenated hydrocarbons, A-aromatic hydrocarbons,M-hydrocarbons associated with metals, and Phydrocarbons associated with pesticides65
Children with a history of hydrocarbon ingestion aremonitored for signs of pulmonary aspiration, includingcoughing, choking, or gagging and oxygen desaturation onpulse oximetry. If these signs are present, a chest radiographis necessary to evaluate potential parenchymal injury.Clothes are removed, copious bathing is done, and eyeirrigation performed if necessary to reduce absorption byother routes.
Admission to the rcu is warranted in children withsevere parenchymal injury and pneumonia. Care of thesepatients includes mechanical ventilation and close attentionto maintenance of a patent airway, effecti ve pulmonarytoilet, and routine monitoring of arterial blood gases untilsymptoms of respiratory compromise subside. Pulmonarydysfunction and radiographic changes detem1ine the degreeof mechanical support required in the acute phase ofparenchymal injury. Severe injuries may require the use ofextracorporeal membrane oxygenation.
SUMMARYChildren who have ingested pharmaceutical or nonpharmaceutical toxins are a critical care nursing challenge inthe emergency department and the ICU. The effects of atoxic ingestion may be systemic, involving many organsystems. Finely tuned collaboration between nurses, physicians, and poison experts is necessary for a positiveoutcome for these patients. Intentional ingestions necessitate the involvement of psychiatry. Accidental ingestionsrequire education and reinforcement by the health careteam for caregivers and children to decrease the probabilityof a reoccurrence.
REFERENCES
Chapter 30 Toxic Ingestions 1023
1. Litovitz TL. Klein-Schwartz W, Caravati EMet al: 1998 Annual Report of the AmericanAssociation of Poison Control Centers ToxicExposure Surveillance System, Am J Emerl{
Med 17:435-487, 1999.2. Liebelt EL. DeAngelis CD: Evolving !rends
and treatment advances in pediatric poisonings. JAMA 282:1113-1115.1999.
3. Aks SE: Toxidromes. In Toxicon, 2000, athttp://toxicon.er.uic.edultoxidro.htm.
4. Rodgers GC. Matayunas NJ: Handbook ofcommon poisonings of children, ed 3, ElkGrove. III. 1994. American Academy ofPediatrics.
5. Bond GR: TI,e poisoned child: evolvingconcepts in care, Emerx Med CIi" North Am13:343-355, 1995.
6. Goldfrank LR, Romenbaum NE. Lewin NAet al: Principles of managing the poisonedpatient or overdosed patient: an overview. InGoldfrank LR, Flomenhaum NE, Lewis NAct al. eds: Coldfrank :~ toxicologic emergen·cies, ed 6, Stamford, Conn, 1998, Appleton &Lange.
7. Belson MG. Simon HK, Sullivan K et al: Theutility of toxicologic analysis in children withsuspected ingestions, Pediatr Emerg Care15:383-387, 1999.
8. Sugarman JM. Rodgers GC. Paul RI: Utilityof loxicology screening in a pediatric emer·gency department, Pediarr Emerg Care 13:194-197, 1997.
9. Hanzlick R: National Association of MedicalExaminers Pediatric Toxicology (Pedtox)Registry Report 3. Case submission summaryand data for acetaminophen, benzene. carboxyhemoglobin. dextromethorphan, ethanol,phenobarbital, and pseudoephedrine, Am JForensic Med Pot/lOl 16:270-277, 1995.
10. Woolf AD, Chrisanthus K: On-site availability of selected antidotes: results of a survey ofMassachusetts hospitals, Am J Emerx Med15:62-66, 1997.
II. Gill F: Pediatric poisonings. In Joy C, ed:PediaIric trauma nursing, Rockville, Md.1989, Aspen Publishers.
12. Prybys KM, Tomassoni AJ: Principles ofpediatric toxicology, Top Emerg Med 18:5672, 1996.
13. Gorelick M: Gastric emptying. In DieckmanR, Fiser D, Selbsl S. eds: PediaTric emergencyand critical care procedures, Sl Louis, 1997.Mosby.
14. Olson KR. Roth B: Update on the management of the patient with overdose, thePedsCCM-Teaching Files, 1997, at http://www.chestnet.org/pcculiesson9-12.htmJ.
15. Lovejoy FH: Childhood poisonings: whatrole for ipecac and charcoal? Comemp Pedi·atr 12:99-108, 1992.
16. Rumack BH: Acetaminophen overdose inchildren and adolescents, Pediotr Clill NorlhAm 33:69/-701, 1986.
17. I. Madsen M: Poisonings, ingestions andovcrdoses, the PedsCCM-Teaching Files.1996, at http://www.peds.umn.eduldivisionslpccmlacp/poison.html.
18. Farrell SE: Toxicity, acetaminophen. In MeFernandez, JT VanDeVoort, MJ Bums et ai,ed: £medicine online medical reference text·
books, 2000, at http://www.emedicine.comlemerg/topic819.htm.
19. Madsen M: Specific toxins. In the PedsCCMTeaching Files. 1996. at http://www.ped.umn.edu/divisions/pccm/teaching/acp/toxin.html.
20. Osborn HH: Barbiturates and other sedativehypnotics. In Goldfrank LR et ai, ed: Goldfrank's toxicologic emergencies, cd 6, Stamford, Conn. 1998. Appleton & Lange.
21. Bertino JS, Reed MD: Barbiturate and nonbarbiturate sedative intoxication in children, Pediatr Clin North Am 33:703-722.1986.
22. Hofert SM: Poisonings. In Sibcny GK.Iannone R. cds: The Harriet Lime ham/bouk.ed 15, St Louis, 2000, Mosby.
23. Doyen S: Carbamazepine. In GoldfrankLR, Flomenbaum NE, Lewin NA, eds:Gold/rallks toxicologic emergencies, cd 6,Stamford, Conn. 1998. Appleton & Lange.
24. Lifshitz M. Gavilov V, Sofer S: Signs andsymptoms of carbamazepine overdose inyoung children. Pedialr Emerg Care 16:2627,2000.
25. Wason S, Baker RC. Carolan Pet al: Carbamazepine overdose-the effects of multipledose activated charcoal, Clin Toxicol 30:3948, 1992.
26. Weaver DF, Camfield P. Fraser A: Massivecarbamazepine overdose: clinical and pharmacologic observations in five episodes. Neurology 38:755-759, 1988.
27. Goldfrank LR, Romenbaum E: Toxie aleohols. In Goldfrank LR, Flomenbaum NE.Lewin NA et al. eds: Goldjrank:fO toxicologicemergellcies, ed 6. Stanlford. Conn. 1998.Appleton & Lange.
28. DeRoos F: Clonidine. In Goldfrank LR,Flomenbaum NE, Lewin NA et aL eds:Gold/rank:f toxicologic emerRellcies, ed 6.Stamford, Conn, 1998, Appleton & Lange.
29. Roberts JR, Zink BI: Clonidine. In HaddadLM. Winchester JF, eds: Clinical management of poisoning and drug vverdoJe, ed 2.Philadelphia, 1990, WB Saunders.
30. Wiley JF II. Wiley CC, Torrey SB et al:Clonidine poisoning in young children, J Pediatr 116:654-658. 1990.
31. Mack RB: C10nidine overdose-kingdom ofthe temporarily infirm, Contemp Pediatrics5:149-154.1988.
32. Lewin NA, Howland MA: Antihypertensiveagents: including beta blockers and calciumchannel blockers. In Goldfrank LR, Flomenbaum NE. Lewin NA et al, eds: Goldfrank:>toxicologic emergencies, ed 4, Norwalk.Conn, 1990, Appleton & Lange.
33. Woolf AD, Berkowitz rD. Liebelt E et al:Poisoning and the critically ill child. lnRogers Me, 00: Texlbook of pediatric intensive care, Baltimore, 1996, Williams &Wilkins.
34. Perrone J: Iron. In Goldfrank LR, Flomenbaum NE, Lewin NA et ai, eds: Goldfrankstoxicologic emergencies, cd 6. Stamford,Conn, 1998. ApplelOn & Lange.
35. Mann KV, Piccioui MA. Spevack TA et al:Management of acute iron overdose. ClinicalPharmacy 8:428-440, 1989.
36. Henretig FM, Temple AR: Acute iron poisoning in children, Clin Lab Med 4:575-586.1984.
37. Everson GW, Bertoccini EJ, O'Leary J: Useof whole bowel irrigation in an infam following iron overdose, Am J ElIlerg Med 9:366369, 1991.
38. Weisman RS: Theophylline. In GoldfrankLR. Romenbaum NE, Lewin NA et aI, eds:Gold/rank's toxicologic emergencies, cd 6,Stamford, Conn, 1998, Appleton & Lange.
39. Gaudreault P, Wason S, Lovejoy Jr. FH: Acutepediatric theophylline overdose: " summaryof 28 cases, J Pediatr 102:474-476. 1983.
40. Gaudreault P. Guay J: Theophylline poisoning: phannacologic considerations and clinical management, Medic:ul Toxicology andArlverse Drug Exposllres 1:169-191,1986.
41. Seneff M et al: Acute theophylline toxicityand the use of esmolol to reverse cardiovascular instability, AmI Emerg Med 19:671-673,1990.
42. Weisman RS: Cyclic antidepressants. InGoldfrank LR. Flomenbaum NE. Lewin NAet ai, eds: Gold/rank '.'I toxicoloXic emergencies, ed 6, Stamford, Conn, 1998, Appleton &Lange.
43. McFee RB, Mofenson HC, Caraccio TR: Anationwide survey of the managemcm ofunintentional low dose tricyclic antidepressant ingestions involving asymptomatic children: implications for the development of anevidenced-based clinical guideline. J TaxieolClin Taxical 38: 15-19, 2000.
44. Bauman LA: Poisoning in the traumatizedpediatric patient, 1m Anesthesial Clini 32:103-121. 1994.
45. Bosse GM, Matyunos NJ: Delayed toxidromes. J Emerg Med 17:679-690, 1999.
46. Braden NJ. Jackson JE, Walson PD: Tricyclicantidepressant overdose, Pediatr Clin NorthAm 33:287-297. 1986.
47. Egland AG, Landry DR: Alcohols. In Bowman JG et aI, ed: Emedicine online medicalreferellce rextbooks, 2000, at http://www.emedicine.eomlemerg/lOpic 19.htm.
48. Dies DF, Guidry SA, McMartin KE et al:Methanol & ethylene glycol intoxication:diagnosis and management, Resident andStaff Physician 43: 12-21, 1997.
49. Jacobsen D, McMartin KE:. Methanol andethylene glycol poisonings: mechanism oftoxicity, clinical course, diagnosis and Irealment, Med Toxicol 1:309-334. 1986.
50. Barceloux DG. Krenzelok EP, Olson K et al:American academy of clinical toxicologypractice guidelines on the treatment of ethylene glycol poisoning. J Toxicol Clin Toxicol37:537-560, 1999.
51. Hollander JE, Hoffman RS: Cocaine. InGoldfrank LR, Flomenbaum NE, Lewin NAet ai, eds: Gold/rank's toxicologic emergencies, ed 6. Stamford. Conn, 1998, Appleton &Lange.
52. Bateman DA, Heagerty MC: Passive freebasecocaine ("crack") inhalation by infants andtoddle"" Am J Dis Child 143:25-27, 1989.
53. Hoffman RS. Hollander JE: Evaluation ofpatients with chest pain after cocaine usc.Critic,,1 Care Clinics 13:809-828, 1997.

1024 Part V Multisystem Problems
54. Nelson LS: Opioids. In Goldfrank LR,Flomenbaum NE, Lewin NA er aI, eds:Goldfrank s toxiculogic emergencieJ. ed 6.Stamford, Conn. 1998, Appleton &Lange.
55. Sporer KA: Acute heroin overdose, AllnIlltern Med 130:584-590, 1999.
56. Presion A: Extract from Ihe methadone brief·ing, ISDD, London, 1996, ar hllp:llwww.drugtext.com.
57. Goldfrank LR, Lewin NA: Phencyclidine. InGoldfrank LR, Flomenbaum NE, Lewin NAet ai, eds: Goldfrank:r toxicologic emergencies, ed 6, Stamford, Conn, 1998, Appleton &Lange.
58. Berger P: Phencyclidine, Enema online Encyclopedia, 2000. at hltp:/lwww.ncbi.nln.nih.gov.encarta.
59. Rao RB, Hoffman RS: Acetaminophen toxicity in an urban county hospital. N Ellg{ J Med338:544-545, 1998.
60. ROlhstein FC: Caustic injuries to the esophagus in children. Pediarr Clin Norrh Am33:665-689, 1986
61. Kardon E: Caustic ingestions. In Kreplick L,VanDeVoot JT, Bums MJ et ai, eds: Emedicine online medical reference textbooks,2000. at hup://www.emedicine.comJemerg/topic86.htm.
62. Henretig FM. Shannon M: Toxicologic emergencies. In Fleisher G, Ludwig S, eds: Texrbook ofemergency medicine. ed 3, Baltimore.1993, Williams & Wilkins.
63. Litovitz TL: The alcohols: ethanol, methanol,isopropanol, ethylene glycol, Pediarr ClinNorrh Am 33:311-323, 1986.
64. Keaton BF: Chlorinaled hydrocarbons. InHaddad LM, Winchester JF, eds: Clinicalmanagement ofpuisoning and drug overdose,ed 2. Philadelphia, 1990, WB Saunders.
65. Shih RD: Hydrocarbons. In GoldfrankLR, Flomenbaum NE. Lewin NA et ai, eds:Gold/rank:') toxicologic emergencies, cd 6,Stamford, Conn, 1998, Appleton & Lange.




















