Differential Short-Term Memorization for Vocal and Instrumental Rhythms
Upload
independentCategory
view
0download
0
Clinical Neurophysiology 120 (2009) 719–729
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
Cortical sources of resting-state alpha rhythms are abnormal in persistentvegetative state patients
Claudio Babiloni a,b,*, Marco Sarà b, Fabrizio Vecchio c,d, Francesca Pistoia b,e, Fabio Sebastiano f,Paolo Onorati b,g, Giorgio Albertini h, Patrizio Pasqualetti b,c, Giuseppe Cibelli a, Paola Buffo g,Paolo Maria Rossini b,c,i
a Department of Biomedical Sciences, University of Foggia, V.le Pinto 1, 71100 Foggia, Italyb Hospital San Raffaele Cassino, Italyc A.Fa.R., Dip. Neurosci. Osp. FBF, Isola Tiberina, Rome, Italyd IRCCS ‘‘S. Giovanni di Dio-F.B.F.”, Brescia, Italye Department of Internal Medicine and Public Health, University of L’Aquila, L’Aquila, Italyf Epilepsy Surgery Unit, IRCCS, Neuromed Pozzilli, Italyg Department of Physiology and Pharmacology, Università Sapienza, Rome, Italyh IRCCS San Raffaele Pisana, Rome, Italyi Clin. Neurol. University ‘‘Campus Biomedico” Rome, Italy
a r t i c l e i n f o
Article history:Accepted 11 February 2009Available online 18 March 2009
Keywords:ConsciousnessPersistent vegetative state (PVS)Resting-state electroencephalography (EEG)Low-resolution brain electromagneticsource tomography (LORETA)Human cerebral cortex
1388-2457/$36.00 � 2009 International Federation odoi:10.1016/j.clinph.2009.02.157
* Corresponding author. Address: Department of Biof Foggia, V.le Pinto 1, 71100 Foggia, Italy. Tel./fax: +3
E-mail address: [email protected] (C. Babiloni).
a b s t r a c t
Objective: High power of pre-stimulus cortical alpha rhythms (about 8–12 Hz) underlies conscious per-ception in normal subjects. Here we tested the hypothesis that these rhythms are abnormal in persistentvegetative state (PVS) patients, who are awake but not aware of self and environment.Methods: Clinical and resting-state, eyes-closed electroencephalographic (EEG) data were taken from aclinical archive. These data were recorded in 50 PVS subjects (level of cognitive functioning – LCF score:I–II) and in 30 cognitively normal subjects. Rhythms of interest were delta (2–4 Hz), theta (4–8 Hz), alpha1 (8–10.5 Hz), alpha 2 (10.5–13 Hz), beta 1 (13–20 Hz), and beta 2 (20–30 Hz). Cortical sources wereestimated by low-resolution electromagnetic tomography (LORETA). Based on LCF score at 3-monthsfollow-up, PVS patients were retrospectively divided into three groups: 30 subjects who did not recover(NON-REC patients; follow-up LCF: I–II), 8 subjects classified as minimally conscious state patients (MCSpatients; follow-up LCF: III–IV), and 12 subjects who recovered (REC patients; follow-up LCF: V–VIII).Results: Occipital source power of alpha 1 and alpha 2 was high in normal subjects, low in REC patients,and practically null in NON-REC patients. A Cox regression analysis showed that the power of alphasource predicted the rate of the follow up recovery, namely the higher its power, the higher the chanceto recover consciousness. Furthermore, the MCS patients showed intermediate values of occipital alphasource power between REC and NON-REC patients.Conclusions: These results suggest that cortical sources of alpha rhythms are related to the chance ofrecovery at a 3-months follow-up in patients in persistent vegetative state.Significance: Cortical sources of resting alpha rhythms might predict recovery in PVS patients.� 2009 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
1. Introduction
Electroencephalographic (EEG) activity reflects the temporalsynchronization of cortical pyramidal neurons as revealed by thesummation of post-synaptic potentials at their apical dendrites(Pfurtscheller and Lopes da Silva, 1999). These processes of tempo-ral synchronization at theta (about 4–7 Hz) and alpha (about 8–
f Clinical Neurophysiology. Publish
omedical Sciences, University9 0881 711716.
12 Hz) frequencies constitute an important neural substrate forhuman cognition (Klimesch, 1999; Vogt et al., 1998; Klimeschet al., 2001, 2004; Sauseng et al., 2002). Successful encoding ofnew information would depend on the increase of the frontal thetapower, reflecting the functional mode of loops including basal fore-brain, hippocampus, and cerebral cortex (Klimesch, 1999). Later,successful retrieval processes into semantic or episodic long-termmemory would depend on the decrease of posterior alpha power,reflecting the functional mode of loops including basal forebrain,thalamus, and cerebral cortex (Klimesch, 1999). A general rule isas follows: the stronger the pre-stimulus alpha power and its
ed by Elsevier Ireland Ltd. All rights reserved.

720 C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729
power reduction during the stimulus processing, the better thecognitive performance (Neubauer et al., 1995; Klimesch, 1999).
Further studies have demonstrated a strict relationship be-tween ‘‘tonic” cortical EEG rhythms and general cognition alongaging in subjects posed in a resting-state condition. Compared withhealthy elderly (Nold) subjects, Alzheimer’s disease (AD) patientshave been characterized by high power of delta (0–4 Hz) and thetarhythms, and low power of posterior alpha and/or beta (13–30 Hz)rhythms (Dierks et al., 2000; Huang et al., 2000; Ponomareva et al.,2003; Jeong, 2004; Koenig et al., 2005). These EEG abnormalitieswere associated with altered regional cerebral blood flow/metabo-lism and with impaired global cognitive function as evaluated bymini mental state examination (MMSE; Rodriguez et al., 1998,1999; Jeong, 2004). Furthermore, posterior alpha rhythms showeda power decrement in subjects with mild cognitive impairment(MCI) compared with Nold subjects posed in a resting-state condi-tion (Zappoli et al., 1995; Huang et al., 2000; Jelic et al., 2000; Koe-nig et al., 2005; Babiloni et al., 2006a, 2007; Rossini et al., 2007 fora review).
Cortical alpha rhythms also correlate to conscious awareness. Ina previous study (Babiloni et al., 2006b), healthy subjects have re-ceived visuo-spatial stimuli given just at sensory threshold individ-ually defined, and had to verbally report after some seconds if theyconsciously perceived or not those stimuli. Results of that studyshowed that the consciously discriminated stimuli were associatedwith a higher power of alpha rhythms before the stimuli and with agreater reduction of alpha power following the stimuli. Corticalsources of these alpha rhythms were mainly located in occipitaland posterior parietal areas. Another parallel study in healthy sub-jects has shown that interfering repetitive transcranial magneticstimulation (TMS) of the mentioned parietal area at a pre-stimulustime reduced the number of consciously perceived visual stimuli(Babiloni et al., 2007).
Keeping in mind the above data, it can be hypothesized thatcortical alpha rhythms are abnormal in patients with an impair-ment of awareness. Here we tested the hypothesis that cortical al-pha rhythms (i) are markedly reduced in power in patients withpersistent vegetative state (PVS) than in normal control subjectsand (ii) are related to outcome. PVS is a clinical condition of com-plete unawareness of self and environment, accompanied bysleep–wake cycles with either complete or partial preservation ofhypothalamic, brainstem autonomic, and reflex functions (Bernat,2006; Practice Parameters, 1995). The EEG data of the presentstudy were taken by the clinical archive of the Hospital San Raffa-ele Cassino (Cassino, Italy), having some limitations on subjects’clinical, neuroanatomical, and neuropsychological information.However, the study is original, since these EEG data had not beenyet used for the evaluation of cortical sources of resting EEGrhythms.
2. Materials and methods
2.1. Subjects
The present research was performed on archive data of 50 PVSsubjects recruited at Post-Coma Intensive and Rehabilitation CareUnit of San Raffaele Cassino Hospital. In these subjects, the mostcommon causes of PVS were traumatic brain injury (TBI), post an-oxic encephalopathy (PAE), ischemic stroke (IS), intracerebral hem-orrhage (ICH), subarachnoid hemorrhage (SAH). Inclusion criteriarequired sinus rhythm, spontaneous breath and free of any acutecomorbidity. The extension of the brain lesion was visually evalu-ated as low, intermediate, high on structural neuroimages by ex-pert neurologists of the Clinical unit (M.S. and F.P.), since we hadno resources for a computational description of the individual le-sions at this exploratory stage of the research. Exclusion criteria
comprised subjects treated with tricyclic antidepressants, anticho-linergics and drugs decreasing the arousal such as benzodiaze-pines, barbiturates, and neuroleptics. To reduce the inter-subjectsvariability in the topography of brain lesions, we excluded patientswith lesions at brainstem level. All patients were fully evaluated atleast one week after their admission, when the clinical conditionswere relatively stable. Clinical assessment was made by means ofLevels of Cognitive Functioning scale (LCF; Gouvier WD et al.,1987). According to such a scale, the LCF I and II correspond toPVS; the LCF III and IV correspond to minimally conscious state(MCS), with inconsistent but discernible evidence of conscious-ness; the LCF V–VIII correspond to conscious patients with a vari-able level of cognitive impairment. All patients were re-assessed bythe LCF scale about 3 months after the EEG recordings (follow up)whose results are reported in the present study. Based on the fol-low-up LCF values, the patients were divided into three groups. Thefirst group (‘‘NON-REC”) included 30 individuals who became PVSand did not recover at follow up (follow up LCF I–II, 23 males;mean age of 55.5 years ±3 standard error of mean, SEM). The sec-ond group (‘‘REC”) included 12 PVS individuals who recovered atfollow up (follow-up LCF > V, 8 males; mean age of 39.3 years±5.1 SEM). The last group (‘‘MCS”) included 8 PVS subjects classi-fied as minimally conscious state patients at follow up (follow-up LCF III–IV, 3 males, mean age of 53.8 years ±5.4 SEM). This smallgroup of subjects was used to corroborate our working hypothesis.Table 1 shows the basic demographic and clinical characteristics ofthe 50 patients. It should be emphasized that the different etiolo-gies of the PVS were used as covariates in the statistical compari-son of the EEG source activity among the subjects’ groups.
As a control group, 30 cognitively normal subjects (15 males;mean age of 47.1 years ±2.3 SEM) were recruited. The study wasapproved by the Local Institutional Ethics Committee, and com-plies with Good Medical Practice; informed and overt consent ofsubjects’ legal representatives, in line with the Code of Ethics ofthe World Medical Association (Declaration of Helsinki) and thestandards established by the Author’s Institutional Review Boardwere acquired. The use of the data was authorized by means of awritten informed consent of the subjects (controls) or caregivers(PVS patients).
2.2. EEG recordings
EEG data were recorded (cephalic reference; 0.3–70 Hz band-pass; 256 Hz sampling rate; 5 min) in subjects at wakening restingstate (eyes-closed) from 19 electrodes positioned according to theInternational 10–20 system (i.e. Fp1, Fp2, F7, F3, Fz, F4, F8, T3, C3,Cz, C4, T4, T5, P3, Pz, P4, T6, O1, O2). To monitor eye movements,electrooculogram (0.3–70 Hz bandpass) was also collected. TheEEG recordings were performed in the late morning in all subjects.The control subjects were requested to be relaxed and to be en-gaged in no specific mental activity during EEG recording. In orderto keep constant the level of vigilance, an experimenter controlledon-line the subject and the EEG traces to monitor signs of drowsi-ness and sleep onset (increase of ‘‘tonic” theta rhythms, K com-plexes, and sleep spindles; behavior in control subjects). Itshould be remarked that baseline EEG recordings in the patientsof REC, NON-REC, and MCS groups were performed when theywere in the PVS, the sub-division into three groups being retro-spectively performed on the basis of the clinical follow up. The re-corded EEG data were analyzed and fragmented off-line inconsecutive epochs of 2 s. The EEG epochs with ocular, muscular,and other types of artifact were preliminarily identified by a com-puterized automatic procedure. EEG epochs with sporadic blinkingartifacts (less than 10% of the total) were corrected by an autore-gressive method (Moretti et al., 2003). Two independent experi-menters blind to the diagnosis manually confirmed the EEG

Table 1Basic demographic and clinical characteristics of the PVS patients. Abbreviations: M, male; F, female; TBI, traumatic brain injury; PAE, post anoxic encephalopathy; IS, ischemicstroke; ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage; MCS, minimally conscious state.
Subject Gender Age (years) From event to evaluation (days) Cause LCF scale
Baseline 3-Month
Subj 1 F 71 82 TBI II NON-RECSubj 2 F 44 82 SAH I MCSSubj 3 M 31 75 TBI II NON-RECSubj 4 F 65 68 TBI I MCSSubj 5 F 66 65 PAE II NON-RECSubj 6 M 21 65 TBI II MCSSubj 7 M 43 80 PAE II NON-RECSubj 8 M 68 63 PAE II NON-RECSubj 9 M 66 71 PAE II NON-RECSubj 10 M 52 68 ICH II RECSubj 11 M 66 70 INFECTION I NON-RECSubj 12 M 42 98 PAE II NON-RECSubj 13 F 20 44 TBI II RECSubj 14 M 47 32 TBI I NON-RECSubj 15 M 52 67 ICH II RECSubj 16 M 37 45 TBI II NON-RECSubj 17 F 61 48 SAH II MCSSubj 18 F 28 60 PAE II NON-RECSubj 19 M 41 32 TBI II RECSubj 20 M 92 71 IS II NON-RECSubj 21 M 63 82 PAE II NON-RECSubj 22 M 34 32 TBI II NON-RECSubj 23 F 18 43 TBI II RECSubj 24 M 33 56 TBI II RECSubj 25 M 60 82 ICH II NON-RECSubj 26 M 70 41 PAE II NON-RECSubj 27 F 71 73 ICH II NON-RECSubj 28 M 71 41 TBI II NON-RECSubj 29 F 65 54 IS II NON-RECSubj 30 F 17 38 TBI II RECSubj 31 F 40 32 TBI II NON-RECSubj 32 M 73 78 IS II NON-RECSubj 33 M 63 70 ICH I MCSSubj 34 M 74 61 ICH II NON-RECSubj 35 F 68 45 ICH II MCSSubj 36 F 66 67 ICH II RECSubj 37 M 63 98 MENINGIOMA II NON-RECSubj 38 M 48 89 SAH II RECSubj 39 M 44 56 IS II NON-RECSubj 40 F 53 62 TBI II NON-RECSubj 41 M 21 64 TBI II RECSubj 42 F 58 52 CRANIOPHARINGIOMAS II MCSSubj 43 M 38 45 TBI II RECSubj 44 M 66 50 IS II RECSubj 45 M 55 67 TBI I NON-RECSubj 46 M 21 38 TBI II NON-RECSubj 47 M 49 35 PAE II NON-RECSubj 48 M 47 69 ICH II NON-RECSubj 49 M 51 80 PAE II MCSSubj 50 M 56 63 SAH II NON-REC
C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729 721
segments accepted for further analysis. On average, we obtained 98(±10.90 SEM) EEG segments for the Control subjects, 151 EEG seg-ments (±16.43 SEM) for the REC subjects, 143 EEG segments (±7.06SEM) for the NON-REC subjects, and 130 EEG segments (±5.40SEM) for the MCS patients. Each subject was associated to morethan 30 EEG segments, in line with previous EEG studies of thisConsortium (Babiloni et al., 2006c,d).
2.3. Spectral analysis of the EEG data
The digital FFT-based power spectrum analysis (Welch tech-nique, Hanning windowing function, no phase shift) was evaluatedin order to calculate the individual alpha frequency (IAF) peak, de-fined as the frequency associated to the strongest EEG power at theextended alpha range (Klimesch, 1999). Mean IAF peak was 9.8 Hz(±0.2 standard error of mean, SEM) in the Control group. Sincemost of the PVS patients had no clear IAF peaks within the alpha
band (8–12 Hz), we cold not use IAF peak as an anchor point forthe definition of the frequency bands of interest. In line with pre-vious studies (Babiloni et al., 2006c,d). The bands of interest weredelta (2–4 Hz), theta (4–8 Hz), alpha 1 (8–10.5 Hz), alpha 2 (10.5–13 Hz), beta 1 (13–20 Hz), and beta 2 (20–30 Hz).
2.4. Cortical source of EEG rhythms as computed by LORETA
Low-resolution electromagnetic source tomography (LORETA)as provided at http://www.unizh.ch/keyinst/NewLORETA/LORE-TA01.htm was used for the estimation of cortical sources of EEGrhythms (Pascual-Marqui and Michel, 1994; Pascual-Marquiet al., 2002). LORETA is a functional imaging technique belongingto a family of linear inverse solution procedures (Valdès et al.,1998) modeling 3D distributions of EEG sources (Pascual-Marquiet al., 2002). With respect to the dipole modeling of corticalsources, no a priori decision of the dipole position is required by

722 C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729
LORETA procedure. LORETA belongs to the family of linear inversealgorithms like minimum norm solution, weighted minimumnorm solution or weighted resolution optimization (Pascual-Mar-qui et al., 2002; Phillips et al., 2002), and has been successfullyused in recent EEG studies on pathological brain aging using thesame experimental set up (electrode montage, sample frequency,etc.) of the present study (Dierks et al., 2000; Babiloni et al.,2006c,d).
LORETA computes 3D linear solutions (LORETA solutions) forthe EEG inverse problem within a 3-shell spherical head modelincluding scalp, skull, and brain compartments. The brain compart-ment is restricted to the cortical gray matter/hippocampus of ahead model co-registered to the Talairach probability brain atlasand digitized at the Brain Imaging Center of the Montreal Neuro-logical Institute (Talairach and Tournoux, 1988). This compartmentincludes 2394 voxels (7 mm resolution), each voxel containing anequivalent current dipole. Of note, EEG electrode positions werenot co-registered to individual brain source models; unlikely, theofficial LORETA package did not include software to do so and wecould not obtain the digitalization of the electrode position fromour clinical units.
As LORETA solutions is a reference-free method of EEG analysis,one can obtain the same LORETA source distribution for EEG datareferenced to any reference electrode including common average.A normalization of the data was obtained by normalizing the LORE-TA current density at each voxel with the power density averagedacross all frequencies (0.5–45 Hz) and across all 2394 voxels of thebrain volume. After the normalization, the solutions lost the origi-nal physical dimension and were represented by an arbitrary unitscale. This procedure reduced inter-subjects variability and wasused in previous EEG studies (Babiloni et al., 2006d). The generalprocedure fitted the LORETA solutions in a Gaussian distributionand reduced inter-subject variability (Leuchter et al., 1993 andNuwer, 1988). Other methods of normalization using the principalcomponent analysis are effective for estimating the subjective glo-bal factor scale of the EEG data (Hernández et al., 1994). Thesemethods are not available in the LORETA package, so they werenot used in this study.
Solutions of the EEG inverse problem are under-determined andill conditioned when the number of spatial samples (electrodes) islower than that of the unknown samples (current density at eachvoxel). In order to properly address this problem, the corticalLORETA solutions predicting scalp EEG spectral power densitywere regularized to estimate distributed rather than punctualEEG source patterns (Pascual-Marqui and Michel, 1994; Pascual-Marqui et al., 2002). In line with the low spatial resolution of theadopted technique, we used our MATLAB software to collapse thevoxels of LORETA solutions at frontal, central, parietal, occipital,temporal and limbic regions of the brain model coded into Talai-rach space. The Brodmann areas listed in Table 2 formed each ofthese regions of interest (ROIs).
Finally, the main advantage of the regional analysis of LORETAsolutions using an explicit source model co-registered into Talai-
Table 2Brodmann areas included in the cortical regions of interest (ROIs) of the presentstudy. LORETA solutions were collapsed within frontal, central, parietal, occipital,temporal and limbic ROIs.
LORETA Brodmann areas into the regions of interest (ROIs)Frontal 8, 9, 10, 11, 44, 45, 46, 47Central 1, 2, 3, 4, 6Parietal 5, 7, 30, 39, 40, 43Temporal 20, 21, 22, 37, 38, 41, 42Occipital 17, 18, 19Limbic 31, 32, 33, 34, 35, 36
rach space was that our modeling could disentangle rhythms ofcontiguous cortical areas (namely those from the occipital sourcewere disentangled with respect to those of the contiguous parietaland temporal sources etc.).
2.5. Statistical analysis of the LORETA solutions
Statistical analysis was performed by ANOVA using subjects’age and gender as covariates (p < 0.05). Mauchley’s test evaluatedthe sphericity assumption. Correction of the degrees of freedomwas made with the Greenhouse–Geisser procedure. Duncan testwas used for the post-hoc testing (p < 0.05). The ANOVA analysisof the LORETA solutions used the factors Group (control, NON-REC, and REC; independent variable), Band (delta, theta, alpha 1, al-pha 2, beta 1, beta 2), and ROI (frontal, central, parietal, occipital,temporal, limbic). Subjects’ age, gender, etiology, duration sinceonset, days from event to evaluation, causes of PVS, lesion exten-sion, and LCF score at the EEG exam were used as covariates. Spe-cifically, the causes of PVS included traumatic brain injury (TBI),post anoxic encephalopathy (PAE), ischemic stroke (IS), intracere-bral hemorrhage (ICH), and subarachnoid hemorrhage (SAH). Thecategorical variable causes of PVS (6 levels) was recorded to 5(number of levels � 1) dummy variables (coded as absence = 0,presence = 1): such dummy variables were entered as binarycovariates. The working hypothesis would be confirmed by asource pattern of the kind ‘‘control group > REC patients > NON-REC patients” as revealed by post-hoc testing.
The EEG source best fitting the above pattern was used as an in-put for Cox proportional hazard model to test its power in the pre-diction of the recovery of the present PVS patients at follow up. TheLORETA solutions were preliminarily subjected to a double logtransformation. The predictive effects were measured in terms ofHazard Ratio (HR) with the corresponding 95% Confidence Inter-vals (95% CI). Whenever the 95% CI did not include the value 1, asignificant effect was documented with a bilateral alpha error at0.05. After performing Cox regression with each independent var-iable entered as alone (‘‘simple Cox regression”), multiple Coxregression was applied with the following criteria: (i) age and edu-cation were entered as ‘‘forced terms”; (ii) only neurophysiologicalvariables resulted as significant with simple regression analysiswere entered in the multiple regression; and (iii) forward likeli-hood ratio procedure was chosen as a selection method.
3. Results
3.1. Topography of the EEG cortical sources as estimated by LORETA
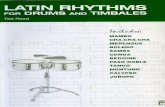
Fig. 1 plots the grand average of the LORETA solutions (i.e. rel-ative power current density at cortical voxels) modeling the dis-tributed EEG cortical sources for delta, theta, alpha 1, alpha 2,beta 1, and beta 2 bands in the normal control group and in theNON-REC and REC patients in PVS. The control group presented al-pha 1 sources with the maximal values of amplitude distributed inparieto-occipital regions. Delta, theta, and alpha 2 sources hadmoderate amplitude values when compared to alpha 1 sources. Fi-nally, beta 1 and beta 2 sources were characterized by lowestamplitude values. Compared to the normal control group, bothgroups of PVS patients showed a decrease in amplitude of alpha1 sources.
3.2. Statistical comparisons of LORETA EEG sources
Fig. 2 shows mean regional normalized LORETA solutions (dis-tributed EEG sources) relative to a statistical ANOVA interaction(F(50,1725) = 3.86; p < 0.00001) among the factors group (control,NON-REC, and REC), Band (delta, theta, alpha 1, alpha 2, beta 1,

Fig. 1. Grand average of low-resolution brain electromagnetic tomography (LORE-TA) solutions (i.e. normalized relative current density at the cortical voxels)modeling the distributed electroencephalographic (EEG) cortical sources for delta,theta, alpha 1, alpha 2, beta 1, beta 2 bands in cognitively normal subjects (control),persistent vegetative state (PVS) patients who recovered at (3-months) follow up(REC), and PVS patients who did not recover at the follow up (NON-REC). The leftside of the maps (top view) corresponds to the left hemisphere. Legend: LORETA,low-resolution brain electromagnetic tomography. Color scale: all power densityestimates were scaled based on the averaged maximum value (i.e. alpha 1 powervalue of occipital region in Control group).
Fig. 2. Regional normalized LORETA solutions (mean across subjects) relative to a statis(control, REC, NON-REC), Band (delta, theta, alpha 1, alpha 2, beta 1, beta 2), and ROIregional normalized LORETA solutions as a dependent variable. Subjects’ age and genderelative power spectra as revealed by a sort of ‘‘virtual” intracranial macro-electrodes locortical region and frequency bands in which LORETA solutions presented statisticall(p < 0.01).
C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729 723
beta 2), and ROI (frontal, central, parietal, occipital, temporal, lim-bic), pointing to a statistical significant difference of posterior al-pha rhythms in the PVS patients when compared with thenormal subjects. In the figure, the LORETA solutions had the shapeof EEG relative power spectra. Notably, profile and magnitude ofthese spectra in the normal control group and in the NON-RECand REC groups of PVS patients differed across various corticalmacro-regions, thus supporting the idea that scalp EEG rhythmsare generated by a distributed pattern of cortical sources. Theplanned post-hoc testing showed that the source pattern of thekind ‘‘control group > REC patients > NON-REC patients” was fittedby the following LORETA solutions: parietal and occipital alpha 1(p < 0.01–0.000001) and alpha 2 (p < 0.01–0.000001) sources. Thenumerical values of Fig. 2 are reported in Table 3 reporting themean values (± SE) of the relative LORETA current density for theControl, NON-REC, and REC groups at the 6 bands (delta, theta, al-pha 1, alpha 2, beta 1, beta 2) and in the 6 ROIs (frontal, central,parietal, occipital, temporal, limbic).
The statistical results showed that occipital alpha 1 and 2sources were the main EEG features distinguishing the PVS pa-tients of the REC vs. NON-REC groups. After a double log transfor-mation, the power distributions of these sources were highlysymmetrical and correlated each other (Pearson test, r = 0.92). Gi-ven the relatively small groups of patients and the risk of alphainflation, we only used one of them (i.e. alpha 1) as an input forthe Cox regression analysis. We preliminarily observed statistical
tical ANOVA interaction (F(50,1725) = 3.86; p < 0.00001) among the factors Group(frontal, central, parietal, occipital, temporal, limbic). This ANOVA design used ther were used as covariates. Regional normalized LORETA solutions modeled the EEGcated on the macrocortical regions of interest. Legend: the rectangle indicates the
y significant LORETA patterns ‘‘control group > REC patients > NON-REC patients”

Table 3Mean values (± SEM) of the relative LORETA current density for the Control, NON-REC, and REC groups at the 6 bands of interest (delta, theta, alpha 1, alpha 2, beta 1, beta 2) andin the 6 ROIs (frontal, central, parietal, occipital, temporal, limbic).
Delta Theta Alpha 1 Alpha 2 Beta 1 Beta 2
Normalized LORETA current density (mean ± standard error of mean)Control groupFrontal 1.80 ± 0.13 1.00 ± 0.10 1.72 ± 0.33 1.02 ± 0.21 0.40 ± 0.05 0.31 ± 0.05Central 1.60 ± 0.13 1.20 ± 0.18 2.51 ± 0.51 1.34 ± 0.35 0.43 ± 0.05 0.27 ± 0.03Parietal 2.09 ± 0.20 1.60 ± 0.22 4.62 ± 0.76 2.03 ± 0.40 0.68 ± 0.06 0.38 ± 0.06Occipital 1.62 ± 0.20 1.19 ± 0.10 3.83 ± 0.71 2.07 ± 0.34 0.61 ± 0.06 0.36 ± 0.07Temporal 2.36 ± 0.22 1.55 ± 0.16 3.77 ± 0.59 2.00 ± 0.33 0.77 ± 0.07 0.52 ± 0.08Limbic 1.44 ± 0.10 0.93 ± 0.07 2.23 ± 0.30 1.18 ± 0.18 0.38 ± 0.03 0.26 ± 0.04
REC patientsFrontal 1.79 ± 0.17 0.74 ± 0.11 0.40 ± 0.07 0.34 ± 0.06 0.28 ± 0.06 0.22 ± 0.06Central 1.50 ± 0.14 0.75 ± 0.15 0.46 ± 0.11 0.38 ± 0.10 0.22 ± 0.04 0.14 ± 0.03Parietal 1.84 ± 0.18 1.07 ± 0.20 0.96 ± 0.23 0.68 ± 0.14 0.33 ± 0.07 0.19 ± 0.04Occipital 1.79 ± 0.18 1.21 ± 0.26 1.41 ± 0.34 0.96 ± 0.22 0.42 ± 0.12 0.25 ± 0.07Temporal 2.26 ± 0.20 1.13 ± 0.16 0.96 ± 0.18 0.76 ± 0.13 0.53 ± 0.18 0.37 ± 0.10Limbic 1.61 ± 0.16 0.80 ± 0.13 0.62 ± 0.12 0.44 ± 0.08 0.24 ± 0.05 0.17 ± 0.04
NON-REC patientsFrontal 2.01 ± 0.14 0.80 ± 0.08 0.35 ± 0.04 0.28 ± 0.05 0.24 ± 0.05 0.25 ± 0.06Central 1.78 ± 0.15 0.80 ± 0.10 0.35 ± 0.05 0.25 ± 0.04 0.19 ± 0.04 0.22 ± 0.08Parietal 1.95 ± 0.16 0.89 ± 0.10 0.39 ± 0.05 0.26 ± 0.03 0.19 ± 0.03 0.49 ± 0.36Occipital 1.97 ± 0.29 0.90 ± 0.17 0.38 ± 0.08 0.26 ± 0.06 0.18 ± 0.04 0.28 ± 0.16Temporal 2.24 ± 0.18 0.98 ± 0.12 0.43 ± 0.05 0.31 ± 0.04 0.27 ± 0.04 0.38 ± 0.16Limbic 1.80 ± 0.14 0.76 ± 0.09 0.30 ± 0.03 0.22 ± 0.03 0.16 ± 0.03 0.16 ± 0.04
724 C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729
effect of age indicating that the lower the age of the PVS patients,the higher the chance to recovery in the whole PVS group(HR = 1.635; p < 0.05). For this reason, the age was considered asconfound in the final model. The Cox regression analysis showedthat the power of occipital alpha 1 sources predicted speed andrate of the follow up recovery across the present PVS patients asa whole group (HR = 1.635; p < 0.05), namely the higher the powerof occipital alpha 1 source, the higher the chance to recover somelevel of consciousness.
3.3. Control analyses
In order to evaluate whether age and relative amount of thesubjects could affect results, we performed a control analysis inwhich each group had the same number of aged-matched subjects.To this aim, the three groups had the following composition: 12normal control subjects (mean age 38.2 ± 3.1 SEM), 12 REC patients(mean age 39.3 ± 5.1 SEM), and 12 NON-REC patients (mean age39.9 ± 2.7 SEM). The ANOVA analysis of the LORETA solutions usedthe factors Group (control, NON-REC, and REC; independent vari-able), Band (delta, theta, alpha 1, alpha 2, beta 1, beta 2), and ROI(frontal, central, parietal, occipital, temporal, limbic). Age and gen-der served as covariates. The results fully confirmed those of themain ANOVA analysis. There was a statistically significant ANOVAinteraction (F(50,825) = 1.395; p < 0.04) among the factors Group,Band, and ROI, pointing to a statistical significant difference inthe PVS patients when compared with the normal subjects. Theplanned post-hoc testing showed that the source pattern of thekind ‘‘Control group > REC patients > NON-REC patients” was fittedby the same regional LORETA solutions of the main ANOVA analy-sis: parietal and occipital alpha 1 (p < 0.0005–0.000001) and alpha2 (p < 0.01–0.000001) sources. As mentioned, PVS patients were di-vided into the NON-REC and REC groups based on the LCF at the 3-months follow-up. Some time after the follow up, 16 ‘‘NON-REC”patients died for several causes (vascular, infective, etc.). To re-move this possible confound, we performed a statistical controlANOVA eliminating these patients; the remaining subjects in-cluded 30 normal control subjects, 14 NON-REC patients, and 12REC patients. The ANOVA analysis of the LORETA solutions usedthe factors Group (control, NON-REC, and REC; independent vari-
able), Band (delta, theta, alpha 1, alpha 2, beta 1, beta 2), and ROI(frontal, central, parietal, occipital, temporal, limbic). Age and gen-der were used as covariates. The results fully confirmed those ofthe main ANOVA analysis. There was a statistical ANOVA interac-tion (F(50,1325) = 2.35; p < 0.00001) among the factors Group,Band, and ROI, pointing to a statistical significant difference inthe PVS patients when compared with the normal subjects. Again,the planned post-hoc testing showed that the source pattern of thekind ‘‘Control group > REC patients > NON-REC” patients was fittedby parietal and occipital alpha 1 (p < 0.01–0.000001) and alpha 2(p < 0.05–0.00005) sources.
One might argue that the results of the present study are biasedby the use of LORETA spherical had volume conductor and sourcespace, which did not take into account the individual brain lesionsof the individual PVS patients. Unlikely, the standard LORETA pack-age does not yet allow to do it. Therefore, this issue was addressedto by a control analysis. To cross-validate the LORETA results, thestatistical analysis was repeated on the EEG spectral power densitycomputed at scalp electrodes. We strictly followed the generalmethodological approach used for the analysis of the LORETA solu-tions. The frequency bands of interest were delta (2–4 Hz), theta(4–8 Hz), alpha 1 (8–10.5 Hz), alpha 2 (10.5–13 Hz), beta 1 (13–20 Hz), and beta 2 (20–30 Hz). The EEG spectral power density ateach electrode was normalized to the EEG spectral power densityaveraged across all frequencies (0.5–45 Hz) and electrodes whichwere grouped in ROIs as follows fro various regions: (i) C3, Czand C4 electrodes for the central region; (ii) F3, Fz and F4 elec-trodes for the frontal; (iii) P3, Pz and P4 electrodes for the parietal;(iv) O1 and O2 electrodes for the occipital; and (v) T3, T4, T5, andT6 for the temporal. Normalized EEG spectral power density wasused as an input for an ANOVA using the factors Group (control,NON-REC, and REC; independent variable), Band (delta, theta, al-pha 1, alpha 2, beta 1, beta 2), and ROI (frontal, central, parietal,occipital, temporal). This ANOVA design showed a statistical inter-action among all factors (F(48,1380) = 4.0; p < 0.00001), pointingto a statistical significant difference of posterior alpha rhythms inthe PVS patients when compared with the normal subjects. Fig. 3shows the profile and magnitude of the EEG spectral power densityrelative to this interaction. This profile confirmed and validatedthat of the regional LORETA solutions. The post-hoc testing

C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729 725
indicated that the pattern of scalp EEG power density ‘‘controlgroup > REC patients > NON-REC patients” was fitted by occipital,parietal, and temporal for both alpha 1 and alpha 2 bands. Overall,the analysis of the scalp EEG spectral power density showed statis-tical effects for alpha 1 and 2 bands not only in parietal and occip-ital areas but also in temporal areas, due to a lower spatialresolution than that obtained by LORETA analysis. Table 4 reportsthe mean values (± SEM) of the normalized, regional spectralpower density for the Control, NON-REC, and REC groups at the 6bands (delta, theta, alpha 1, alpha 2, beta 1, beta 2) and in the 5ROIs (frontal, central, parietal, occipital, temporal).
To corroborate the hypothesis of a relationship between corti-cal alpha rhythms and prognosis in PVS patients, we performed acontrol analysis on the PVS subjects classified as MCS (minimallyconscious state) at the follow up in the mentioned clinical EEG ar-chive. Eight patients passed the inclusion and exclusion criteria ofthe present study (follow-up LCF III–IV, 3 males, mean age of53.8 years ±5.4 SEM). Regional normalized LORETA solutions(distributed EEG sources) were used as an input for a controlANOVA including the factors Group (REC, MCS, and NON-REC;independent variable), Band (alpha 1, alpha 2), and ROI (frontal,central, parietal, occipital, temporal, limbic). Subjects’ age andgender, etiology, and duration since onset were used as covari-ates. This ANOVA design showed a statistical interaction amongall factors (F(10,235) = 2.85; p < 0.0023), pointing to a statistical
Fig. 3. Results of the control data analysis were used as inputs for an ANOVA analysis. Tserved as dependent variables. The ANOVA factors (levels) were group (control, NON-Rcentral, parietal, occipital, temporal). This ANOVA design showed a statistical interactionand magnitude of these spectra in the normal control group and in the NON-REC and RECLOREA solutions, namely that the source pattern of the kind ‘‘control group > REC pati0.000001) and alpha 2 (p < 0.01–0.000001).
significant difference of posterior alpha rhythms in the PVSgroups with different outcome. Fig. 4 shows the profile and mag-nitude of the LORETA solutions relative to this interaction. Theplanned post-hoc testing showed that the source pattern of thekind ‘‘REC patients > MCS patients > NON-REC patients” was fittedby occipital alpha 1 (p < 0.000004–0.000002) source, in line withthe results of the main study.
4. Discussion
In the present retrospective archive study, we tested thehypothesis that cortical alpha rhythms are abnormal in PVS pa-tients, who are awake but not aware of self and environment. Re-sults showed that parietal and occipital source power of low- and/or high-frequency alpha rhythms was high in the normal subjects,low in the REC patients, and practically null in the NON-REC pa-tients. These findings were corroborated by a control analysis ona small group of MCS patients, which showed intermediate ampli-tude of occipital low-frequency alpha sources in these patientswhen compared with the REC and NON-REC patients. Furthermore,a Cox regression analysis showed that the power of the most rep-resentative alpha source (low-frequency, occipital) predicted therate of the follow up recovery, namely the higher its power, thehigher the chance to recover. On the whole, the present resultssuggest that cortical sources of alpha rhythms are related to the
he values (mean across subjects) of the normalized regional spectral power densityEC, and REC), Band (delta, theta, alpha 1, alpha 2, beta 1, beta 2), and ROI (frontal,
(F(40,1380) = 4.0; p < 0.00001) among all the factors. This figure shows the profilegroups of PVS patients. The planned post-hoc testing showed the same results of theents > NON-REC patients” was fitted by the following: occipital alpha 1 (p < 0.01–

Table 4Mean values (± SEM) of the normalized regional spectral power density of the scalp EEG data for the Control, NON-REC, and REC groups at the 6 bands of interest (delta, theta,alpha 1, alpha 2, beta 1, beta 2) and in the 5 ROIs (frontal, central, parietal, occipital, temporal).
Delta Theta Alpha 1 Alpha 2 Beta 1 Beta 2
Normalized EEG power spectrum (mean ± standard error of mean)Control groupFrontal 3.01 ± 0.28 1.95 ± 0.19 3.14 ± 0.41 1.81 ± 0.23 0.59 ± 0.05 0.40 ± 0.05Central 1.44 ± 0.12 1.45 ± 0.24 2.58 ± 0.46 1.94 ± 0.44 0.51 ± 0.05 0.26 ± 0.03Parietal 1.81 ± 0.14 1.82 ± 0.26 4.38 ± 0.69 2.77 ± 0.45 0.63 ± 0.06 0.27 ± 0.04Occipital 2.76 ± 0.36 2.98 ± 0.38 8.41 ± 1.67 4.92 ± 0.80 0.97 ± 0.11 0.49 ± 0.07Temporal 2.28 ± 0.23 1.61 ± 0.12 3.77 ± 0.48 2.35 ± 0.24 0.89 ± 0.07 0.53 ± 0.09
REC patientsFrontal 5.02 ± 0.58 1.75 ± 0.24 1.14 ± 0.19 0.74 ± 0.11 0.40 ± 0.07 0.28 ± 0.07Central 2.02 ± 0.30 1.30 ± 0.23 1.13 ± 0.25 0.75 ± 0.15 0.27 ± 0.05 0.15 ± 0.05Parietal 2.10 ± 0.25 1.44 ± 0.32 1.54 ± 0.36 0.94 ± 0.19 0.29 ± 0.05 0.12 ± 0.02Occipital 2.83 ± 0.26 2.39 ± 0.39 3.70 ± 1.08 2.50 ± 0.86 0.63 ± 0.17 0.32 ± 0.10Temporal 3.99 ± 0.41 2.23 ± 0.31 2.07 ± 0.35 1.51 ± 0.31 0.81 ± 0.25 0.49 ± 0.17
NON-REC patientsFrontal 5.80 ± 0.28 1.91 ± 0.20 0.68 ± 0.07 0.48 ± 0.07 0.37 ± 0.06 0.28 ± 0.06Central 2.72 ± 0.21 1.21 ± 0.15 0.50 ± 0.07 0.30 ± 0.05 0.23 ± 0.06 0.12 ± 0.03Parietal 2.83 ± 0.17 1.24 ± 0.14 0.49 ± 0.06 0.30 ± 0.05 0.21 ± 0.05 0.10 ± 0.03Occipital 3.78 ± 0.44 1.59 ± 0.24 0.64 ± 0.13 0.45 ± 0.13 0.27 ± 0.09 0.14 ± 0.05Temporal 4.38 ± 0.39 1.77 ± 0.22 0.72 ± 0.08 0.46 ± 0.06 0.37 ± 0.07 0.26 ± 0.06
726 C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729
outcome in PVS patients. They also suggest that the use of quanti-tative EEG source analysis can enhance the extraction of informa-tion contents from resting state EEG rhythms in PVS patients,when compared with the standard clinical analysis of these
Fig. 4. Regional normalized LORETA solutions (mean across subjects) relative to a statistiMCS, and NON-REC), Band (alpha 1, alpha 2), and ROI (frontal, central, parietal, occipital, tas a dependent variable. Subjects’ age and gender, etiology, and duration since onset werebands in which LORETA solutions presented statistically significant LORETA patternsminimally conscious state.
rhythms (Kulkarni et al., 2007). However, the present study in-cluded a relatively small number of subjects. This did not allow afurther sub-division of the subject into additional subgroups basedon LCF score and motivates future conclusive pieces of research
cal ANOVA interaction (F(10,235) = 2.85; p < 0.0023) among the factors Group (REC,emporal, limbic). This ANOVA design used the regional normalized LORETA solutionsused as covariates. Legend: the rectangle indicates the cortical region and frequency‘‘REC patients > MCS patients > NON-REC” patients (p < 0.000004). Legend: MCS,

C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729 727
using larger populations, refined clinical scales for the assessmentof residual cognitive functions, and fine patients’ classification inline with recent literature (Leon Carrion et al., 2008).
In the evaluation of the results, a methodological remark shouldbe taken into account, namely the fact that EEG electrode positionswere not co-registered to individual brain source models adaptedto the individual lesions; unlikely, the official LORETA packagedid not include software to do so, and we could not obtain the dig-italization of the electrode position from our clinical units. It is un-likely that this affects the present results, since we used causes ofPVS and lesion extension as covariates in the statistical design. Fur-thermore, LORETA intrinsically produces low spatial resolutionimages of EEG cortical sources, which are relatively insensitive tofine differences in the subjective topography of the brain lesion. Fi-nally, we showed that similar effects of alpha rhythms were ob-served when statistics regarded EEG spectral power densitycomputed at scalp level, with the use of no head or source mathe-matical model. Therefore, the results of the present study motivatefuture investigations with advanced techniques for the assessmentof brain lesion and for the construction of individual head modelfor LORETA analysis. However, LORETA solutions can be consideredas reasonably reliable in the present experimental conditions. In-deed, LORETA has been repeatedly and successfully used fromEEG data collected by 19 electrodes placed according to 10–20 sys-tem like the present study (Anderer et al., 2000, 2003; Cincottiet al., 2004; Isotani et al., 2001; Kawasaki et al., 2004; Laufer andPratt, 2003; Mulert et al., 2001; Veiga et al., 2003; Wintereret al., 2001). Furthermore, it is especially suitable for the study ofcortical sources of resting state EEG rhythms; in these back-groundconditions, brain activity is widely synchronized over cortical man-tle and can be sampled with a relatively low spatial EEG sampling.Finally, LORETA uses an average brain model co-registered to Talai-rach space, which would disentangle the relative functional contri-bution of single cortical lobes in the generation of resting state EEGrhythms in PVS patients. This is a quite rough low-resolution esti-mate, but it solves at least in part the head volume conductor ef-fects that prevent a reliable spatial explanation of scalp EEGrhythms. Resting state EEG rhythms collected at scalp occipitalelectrodes are generated not only from underlying occipital cortexbut also from surrounding cortical regions. As an advantage, LORE-TA has explicit mathematical models accounting for these headvolume conductor effects.
The results of the present study extend several lines of evidenceon the strong implication of cortical alpha rhythms on humanhigher functions. It has been shown that parieto-occipital alpharhythms preceding visuo-spatial stimuli are related to consciousperception (Babiloni et al., 2007). Furthermore, anticipatory alpharhythms have been mainly modulated on the hemisphere contra-lateral to the attended visual stimulus, and the difference of theseanticipatory alpha rhythms between attended and unattendedhemisphere predicted trial-by-trial locus of attention and speedof response to subsequent visual stimuli (Sauseng et al., 2005; Thutet al., 2006). It has been also shown that most intelligent people(high intelligent quotient, IQ) present lowest alpha event-relateddesynchronization (ERD, Pfurtscheller and Lopes da Silva, 1999)during different types of cognitive tasks such as sentence–pictureverification test task (Neubauer et al., 1995), Posner’s letter match-ing test (Neubauer et al., 1999), forward digit span task (Grabneret al., 2004), attention-switching task (Grabner et al., 2004), work-ing memory task (Grabner et al., 2004), and Stankov’s Triplet Num-bers test (Neubauer and Fink, 2003). The same was true in subjectshighly trained for specific skills (‘‘experts”) during the performanceof retrieval short-term memory tasks: alpha ERD was lower in ex-perts than in non-experts (Grabner et al., 2006). Finally, resting-state alpha rhythms have been correlated with attention and gen-eral cognitive skills in aged people (Zappoli et al., 1995; Klimesch,
1999; Huang et al., 2000; Jelic et al., 2000; Doppelmayr et al., 2005;Koenig et al., 2005; Babiloni et al., 2006a).
What is the relationship between PVS and cortical alpharhythms? On one hand, PVS is typically due to severe and wide-spread brain injury, and may reflect a disconnection syndrome ofdifferent cortical networks sub-serving higher functions ratherthan as a dysfunction of a single area or as the consequence of aglobal reduction in cortical metabolism (Laureys, 2005). On theother hand, cortical alpha rhythms are mainly due to basal fore-brain, thalamus, and cortical functional interactions; these interac-tions would facilitate or inhibit the transmission of sensorimotorinformation among subcortical and cortical pathways, and the re-trieval of semantic information from cortical storage (Brunia,1999; Pfurtscheller and Lopes da Silva, 1999; Steriade and Llinas,1988). Within the extended alpha band (8–13 Hz), lower frequen-cies would be associated with global attention–arousal, whereashigher frequencies would be associated with processing of task-specific sensorimotor or semantic information (Klimesch, 1997;Klimesch et al., 1998). Unlikely, alpha frequency peak was hardlyrecognizable in the present PVS patients, and we could just usefixed frequency alpha sub-bands. However, the alterations ofoccipital alpha rhythms occurred across extended frequenciesranging from 8 to 13 Hz, thus both global arousal and task-specificprocesses were involved.
Keeping in mind the above theoretical back-ground, it can bespeculated that among others aspects, PVS includes an impairmentof basal forebrain, thalamus, and cortical interactions as reflectedby oscillations in the alpha range, which would contribute to gen-eral arousal/attention and retrieval of cognitive-motor informa-tion. However, it should be remarked that the present results donot represent a demonstration of a linear causal relationship be-tween abnormal cortical alpha rhythms and higher functionsincluding awareness in PVS patients. Indeed, awareness wouldemerge from quite complex interactions among several cerebralstructures functionally connected with thalamic nuclei and ascen-dant reticular formation (Laureys, 2005). In this respect, neuralnetworks should be regarded as complex cybernetic systems inthe same way as any other natural system. By definition, this kindof complex systems shows a chaotic non-linear behavior as charac-terized by sudden, disproportional, and unpredictable changes(Goldberger et al., 1990; Stam, 2005; Sarà et al., 2008). In prece-dence, it has been reported that, as a consequence of the abovechaotic behavior, several physiological variables including heartrate (HR) and blood pressure show spontaneous fluctuations hav-ing non-linear dynamics. Specifically, non-linear behavior of HRdecreased in severely brain-injured patients with vegetative state,so endorsing the hypothesis that a neural networks derangementmay be responsible for the reduction of neural complexity associ-ated with disorders of consciousness (Sarà et al., 2008).
5. Conclusions
Are cortical alpha rhythms abnormal in PVS patients, who areawake but not aware due to widespread brain injury? We showedthat parietal and occipital source power of alpha rhythms was highin the normal subjects, low in the PVS patients who recoveredsome level of consciousness at (3-months) follow up, and practi-cally null in the PVS patients who did not recover. For illustrativepurposes, a Cox regression analysis confirmed that occipital alphasources predicted the recovery in our relatively small group of PVSpatients. These results suggest that cortical sources of resting alpharhythms are related to the outcome of PVS patients at 3-monthsfollow up. Future perspective research should confirm that corticalsources of resting alpha rhythms might predict recovery in PVSpatients.

728 C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729
Acknowledgements
The research was granted by Tosinvest Sanità and AssociationFatebenefratelli for Research (AFaR). We thank Prof. Fabrizio Eus-ebi for his continuous support. Dr. Paola Buffo participated to thisstudy in the framework of his Ph.D. program at the Doctoral Schoolin Neurophysiology, Department of Physiology and Pharmacology,University of Rome ‘‘Sapienza”.
References
Anderer P, Saletu B, Pascual-Marqui RD. Effect of the 5-HT(1A) partial agonistbuspirone on regional brain electrical activity in man: a functionalneuroimaging study using low-resolution electromagnetic tomography(LORETA). Psychiatry Res 2000;100(2):81–96.
Anderer P, Saletu B, Semlitsch HV, Pascual-Marqui RD. Non-invasive localization ofP300 sources in normal aging and age-associated memory impairment.Neurobiol Aging 2003;24(3):463–79.
Babiloni C, Binetti G, Cassetta E, Dal Forno G, Del Percio C, Ferreri F, et al. Sources ofcortical rhythms change as a function of cognitive impairment in pathologicalaging: a multi-centric study. Clin Neurophysiol 2006a;117(2):252–68.
Babiloni C, Vecchio F, Miriello M, Romani GL, Rossini PM. Visuo-spatialconsciousness and parieto-occipital areas: a high-resolution EEG study. CerebCortex 2006b;16(1):37–46.
Babiloni C, Binetti G, Cassarino A, Dal Forno G, Del Percio C, Ferreri F, et al. Sources ofcortical rhythms in adults during physiological aging: a multi-centric EEGstudy. Hum Brain Mapp 2006c;27(2):162–72.
Babiloni C, Benussi L, Binetti G, Cassetta E, Dal Forno G, Del Percio C, et al.Apolipoprotein E and alpha brain rhythms in mild cognitive impairment: amulticentric EEG study. Ann Neurol 2006d;59(2):323–34.
Babiloni C, Vecchio F, Rossi S, De Capua A, Bartalini S, Ulivelli M, et al. Humanventral parietal cortex plays a functional role on visuospatial attention andprimary consciousness. A repetitive transcranial magnetic stimulation study.Cereb Cortex 2007;17(6):1486–92.
Bernat JL. Chronic disorders of consciousness. Lancet 2006;367(9517):1181–92[Review: Erratum in Lancet 2006;367(9528):2060].
Brunia CH. Neural aspects of anticipatory behavior. Acta Psychol (Amst)1999;101(2–3):213–42 [Review].
Cincotti F, Babiloni C, Miniussi C, Carducci F, Moretti D, Salinari S, et al. EEGdeblurring techniques in a clinical context. Methods Inf Med 2004;43(1):114–7.
Dierks T, Jelic V, Pascual-Marqui RD, Wahlund LO, Julin P, Linden DEJ, et al. Spatialpattern of cerebral glucose metabolism (PET) correlates with localization ofintracerebral EEG-generators in Alzheimer’s disease. Clin Neurophysiol2000;111:1817–24.
Doppelmayr M, Klimesch W, Hödlmoser K, Sauseng P, Gruber W. Intelligencerelated upper alpha desynchronization in a semantic memory task. Brain ResBull 2005;66(2):171–7.
Goldberger AL, Rigney DR, West BJ. Chaos and fractals in human physiology. Sci Am1990;262(2):42–9.
Gouvier WD, Blanton PD, LaPorte KK, Nepomuceno C. Reliability and validity of theDisability Rating Scale and the Levels of Cognitive Functioning Scale inmonitoring recovery from severe head injury. Arch Phys Med Rehabil1987;68:94–7.
Grabner RH, Fink A, Stipacek A, Neuper C, Neubauer AC. Intelligence and workingmemory systems: evidence of neural efficiency in alpha band ERD. Brain ResCogn Brain Res 2004;20(2):212–25.
Grabner RH, Neubauer AC, Stern E. Superior performance and neural efficiency: theimpact of intelligence and expertise. Brain Res Bull 2006;69(4):422–39.
Hernández JL, Valdés P, Biscay R, Virués T, Szava S, Bosch J, et al. A global scale factorin brain topography. Int J Neurosci 1994;76:267–78.
Huang C, Wahlund LO, Dierks T, Julin P, Winblad B, Jelic V. Discrimination ofAlzheimer’s disease and mild cognitive impairment by equivalent EEG sources:a cross-sectional and longitudinal study. Clin Neurophysiol 2000;11:1961–7.
Isotani T, Lehmann D, Pascual-Marqui RD, Kochi K, Wackermann J, Saito N, et al. EEGsource localization and global dimensional complexity in high- and low-hypnotizable subjects: a pilot study. Neuropsychobiology 2001;44(4):192–8.
Jelic V, Johansson SE, Almkvist O, Shigeta M, Julin P, Nordberg A, et al. Quantitativeelectroencephalography in mild cognitive impairment: longitudinal changesand possible prediction of Alzheimer’s disease. Neurobiol Aging2000;21:533–40.
Jeong J. EEG dynamics in patients with Alzheimer’s disease. Clin Neurophysiol2004;115(7):1490–505.
Kawasaki T, Tanaka S, Wang J, Hokama H, Hiramatsu K. Abnormalities of P300cortical current density in unmedicated depressed patients revealed by LORETAanalysis of event-related potentials. Psychiatry Clin Neurosci2004;58(1):68–75.
Klimesch W. EEG-alpha rhythms and memory processes. Int J Psychophysiol1997;26(1–3):319–440 [Review].
Klimesch W. EEG alpha and theta oscillations reflect cognitive and memoryperformance: a review and analysis. Brain Res Rev 1999;29:169–95.
Klimesch W, Doppelmayr M, Russegger H, Pachinger T, Schwaiger J. Induced alphaband power changes in the human EEG and attention. Neurosci Lett1998;244(2):73–6.
Klimesch W, Doppelmayr M, Stadler W, Pollhuber D, Sauseng P, Rohm D. Episodicretrieval is reflected by a process specific increase in humanelectroencephalographic theta activity. Neurosci Lett 2001;13;302(1):49–52.
Klimesch W, Schack B, Schabus M, Doppelmayr M, Gruber W, Sauseng P. Phase-locked alpha and theta oscillations generate the P1–N1 complex and arerelated to memory performance. Brain Res Cogn Brain Res2004;19(3):302–16.
Koenig T, Prichep L, Dierks T, Hubl D, Wahlund LO, John ER, et al. Decreased EEGsynchronization in Alzheimer’s disease and mild cognitive impairment.Neurobiol Aging 2005;26(2):165–71.
Kulkarni VP, Lin K, Benbadis SR. EEG findings in the persistent vegetative state. J ClinNeurophysiol 2007;24(6):433–7.
Laufer I, Pratt H. Evoked potentials to auditory movement sensation in duplexperception. Clin Neurophysiol 2003;114(7):1316–31.
Laureys S. The neural correlate of (un)awareness: lessons from the vegetative state.Trends Cogn Sci 2005;9:556–9.
Leon-Carrion J, Martin-Rodriguez JF, Damas-Lopez J, Barroso y Martin JM,Dominguez-Morales MR. Brain function in the minimally conscious state: aquantitative neurophysiological study. Clin Neurophysiol2008;119(7):1506–14.
Leuchter AF, Cook IA, Newton TF, Dunkin J, Walter DO, Rosenberg Tompson S, et al.Regional differences in brain electrical activity in dementia: use of spectralpower and spectral ratio measures. Electroencephalogr Clin Neurophysiol1993;87:385–93.
Moretti DV, Babiloni F, Carducci F, Cincotti F, Remondini E, Rossini PM, et al.Computerized processing of EEG–EOG–EMG artifacts for multicentric studies inEEG oscillations and event-related potentials. Int J Pshycophysiol2003;47(3):199–216.
Mulert C, Gallinat J, Pascual-Marqui R, Dorn H, Frick K, Schlattmann P, et al. Reducedevent-related current density in the anterior cingulate cortex in schizophrenia.Neuroimage 2001;13(4):589–600.
Neubauer AC, Fink A. Fluid intelligence and neural efficiency: effects of taskcomplexity and sex. Pers Indiv Differ 2003;35:811–27.
Neubauer AC, Freudenthaler HH, Pfurtscheller G. Intelligence and spatio-temporal patterns of event-related desynchronization. Intelligence1995;20:249–67.
Neubauer AC, Sange G, Pfurtscheller G. Psychometric intelligence and event-relateddesynchronization during performance of a letter matching task. revised series.In: Pfurtscheller G, Lopes da Silva FH, editors. Handbook ofelectroencephalography and clinical neurophysiology 1999;vol.6. Amsterdam: Elsevier; 1999. p. 219–31.
Nuwer MR. Quantitative EEG. I: techniques and problems of frequency analysis andtopographic mapping. J Clin Neurophysiol 1988;5:1–43.
Pascual-Marqui RD, Michel CM. LORETA (low resolution brain electromagnetictomography): new authentic 3D functional images of the brain. ISBET NewslettISSN 1994;5:4–8.
Pascual-Marqui RD, Esslen M, Kochi K, Lehmann D. Functional imaging with lowresolution brain electromagnetic tomography (LORETA): a review. MethodsFind Exp Clin Pharmacol 2002;24:91–5.
Pfurtscheller G, Lopes da Silva FH. Event-related EEG/MEG synchronization anddesynchronization: basic principles. Clin Neurophysiol 1999;110(11):1842–57[Review].
Phillips C, Rugg MD, Friston KJ. Systemic regularization of linear inverse solutions ofthe EEG source localization problem. Neuroimage 2002;17:287–301.
Ponomareva NV, Selesneva ND, Jarikov GA. EEG alterations in subjects at highfamilial risk for Alzheimer’s disease. Neuropsychobiology 2003;48(3):152–9.
Rodriguez G, Nobili F, Rocca G, DeCarli F, Gianelli MV, Rosadini G. Quantitativeelectroencephalography and regional Cerebral Blood Flow: discriminantanalysis between Alzheimer’s patients and healthy controls. Dement GeriatrCogn Disord 1998;9:238–74.
Rodriguez G, Copello F, Nobili F, Vitali P, Perego G, Nobili F. EEG spectral profile tostage Alzheimer’s disease. Clin Neurophysiol 1999;110:1831–7.
Rossini PM, Rossi S, Babiloni C, Polich J. Clinical neurophysiology of aging brain:from normal aging to neurodegeneration. Prog Neurobiol 2007;83(6):375–400[Epub 2007 Aug 8, Review].
Sarà M, Sebastiano F, Sacco S, Pistoia F, Onorati P, Albertini G, et al. Heart rate nonlinear dynamics in patients with persistent vegetative state: a preliminaryreport. Brain Inj 2008;22(1):33–7.
Sauseng P, Klimesch W, Gruber W, Doppelmayr M, Stadler W, Schabus M. Theinterplay between theta and alpha oscillations in the humanelectroencephalogram reflects the transfer of information between memorysystems. Neurosci Lett 2002;324(2):121–4.
Sauseng P, Klimesch W, Stadler W, Schabus M, Doppelmayr M, Hanslmayr S, et al. Ashift of visual spatial attention is selectively associated with human EEG alphaactivity. Eur J Neurosci 2005;22(11):2917–26.
Stam CJ. Non linear dynamical analysis of EEG and MEG: review of an emergingfield. Clin Neurophysiol 2005;116:2266–301.
Steriade M, Llinas RR. The functional states of the thalamus and the associatedneuronal interplay. Physiol Rev 1988;68(3):649–742.
Talairach J, Tournoux P. Co-planar stereotaxic atlas of the humanbrain. Stuttgart: Thieme; 1988.
Thut G, Nietzel A, Brandt SA, Pascual-Leone A. Alpha-band electroencephalographicactivity over occipital cortex indexes visuospatial attention bias and predictsvisual target detection. J Neurosci 2006;26:9494–502.

C. Babiloni et al. / Clinical Neurophysiology 120 (2009) 719–729 729
Valdès P, Picton TW, Trujillo N, Bosch J, Aubert E, Riera J. EEG–MEG source imagingwith statistical neuroanatomy. Neuroimage 1998;4:635.
Veiga H, Deslandes A, Cagy M, Fiszman A, Piedade RA, Ribeiro P. Neurocorticalelectrical activity tomography in chronic schizophrenics. Arq Neuropsiquiatr2003;61(3B):712–7. Epub 2003 Oct 28.
Vogt F, Klimesch W, Doppelmayr M. High-frequency components in thealpha band and memory performance. J Clin Neurophysiol1998;15(2):167–72.
Winterer G, Mulert C, Mientus S, Gallinat J, Schlattmann P, Dorn H, et al. P300 andLORETA: comparison of normal subjects and schizophrenic patients. BrainTopogr 2001;13(4):299–313.
Zappoli R, Versari A, Paganini M, Arnetoli G, Muscas GC, Gangemi PF, et al. Brainelectrical activity (quantitative EEG and bit-mapping neurocognitive CNVcomponents), psychometrics and clinical findings in presenile subjects withinitial mild cognitive decline or probable Alzheimer-type dementia. Ital J NeurolSci 1995;16(6):341–76 [Review].
Copyright © 2022 FDOKUMEN