Study on Corrective Abrasive Finishing for Workpiece Surface ...
Corrective osteotomies in malunited distal radius fractures:external ®xation as one stage and hemicallotasis procedures
D. Pennig*, T. Gausepohl, K. Mader
Department of Trauma Surgery, Hand and Reconstructive Surgery, St. Vinzenz-Hospital, Merheimer Straûe 221-223, D-50733 Cologne, Germany
Abstract
The correction of distal radius malunion was carried out using a radio-radial ®xator. The two techniques used in 14 caseswere one stage correction or gradual correction by hemicallotasis. The techniques are described and the patients treated were
evaluated. # 2000 Elsevier Science Ltd. All rights reserved.
1. Introduction
Distal radial fractures often result in malunion withincongruency of the radiocarpal and the distal radioul-nar joint, especially after conservative treatment [1].Rotational movement in the forearm depends on thedistal radioulnar joint and the resulting rotatory mala-lignment of the articulating parts of the distal radiusleading to pathological tethering of the radiocarpaland ulnocarpal ligaments and malfunction of the car-pal ligament complex. Aims of correcting maluniteddistal radius fractures include the restoration of thenormal radial angle, the dorsal radial angle, the distalradioulnar joint, radial length and the rotated distalmetaphyseal radius.
Recently, plating has been used considerably for cor-rection of distal radius malunion [2,4,5], using a pal-mar approach usually combined with acorticocancellous bone grafting. Other authors ®xedthis graft with K-wires [6] plus additional casting. Thecorrection of radial length remains challenging, mainlydue to the shortened soft tissue and tendons in thewrist region and the palmar approach itself has itscomplications [5]. Most commonly, malunion results inhyperextension of the wrist with resulting dorsal short-
ening. Therefore correction and plate ®xation with apalmar approach is an indirect procedure.
In order to ease realignment of the distal articulatingfragment of the distal radius, we use extra-articularexternal ®xation (radioradial) mounted dorsally withdistraction and reposition capacities provided bydouble ball joints [3,9±11].
Two general techniques can be applied with thisexternal ®xator: the single-step correction combinedwith corticocancellous bone graft and gradual correc-tion by hemicallotasis [7,8].
2. Operative technique
2.1. Single stage correction with external ®xation
A prerequisite for using external ®xation in correc-tion of the distal radius is a device with distraction ca-pacity with well-de®ned calibration. A double balljoint allows gradual realignment of the distal part ofthe radius in the reposition process. Therefore, we usean external ®xator with two short clamps (one slidingand one distraction±compression module; Ortho®x Srl.Italy, Fig. 1). On the sliding clamp, with in®nitely vari-able adjustment of the position of the ®xator screwsare placed at right angle to the bone long axis usingthe so-called t-clamp (Fig. 1, right). The t-clamp allows
Injury, Int. J. Care Injured 31 (2000) 78±91
0020-1383/00/$ - see front matter # 2000 Elsevier Science Ltd. All rights reserved.
PII: S0020-1383(99 )00266 -1
www.elsevier.com/locate/injury
* Corresponding author.
placement of screws parallel to the joint line from dor-sally.
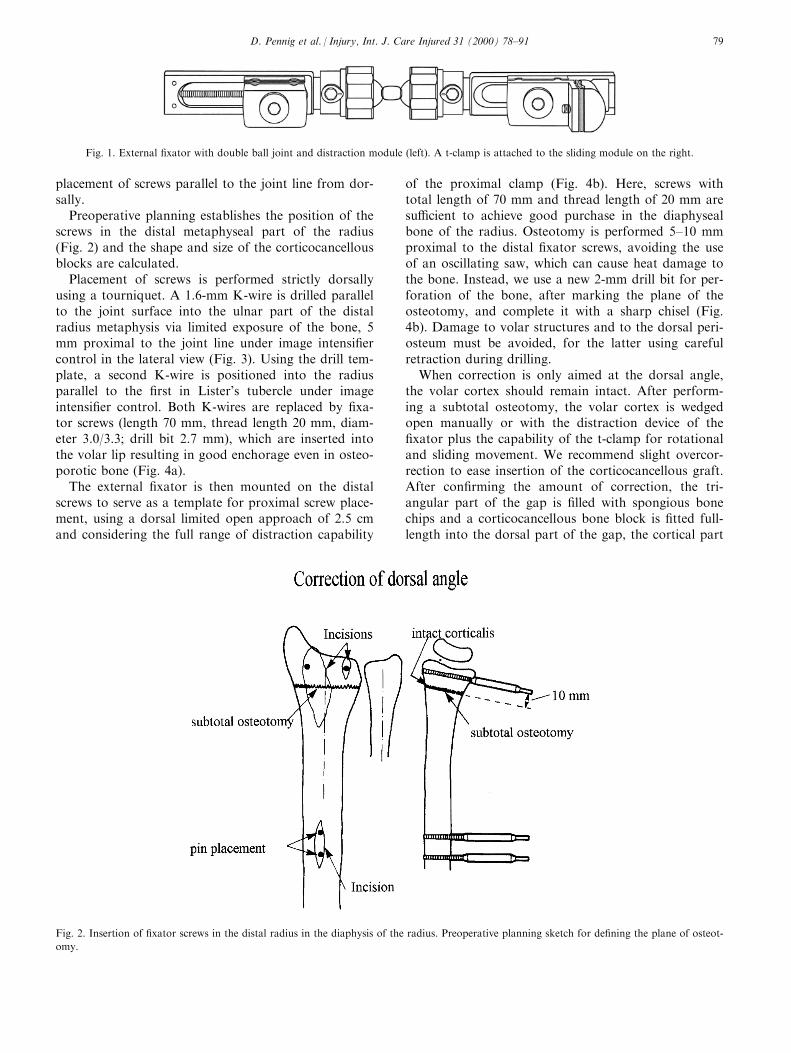
Preoperative planning establishes the position of thescrews in the distal metaphyseal part of the radius(Fig. 2) and the shape and size of the corticocancellousblocks are calculated.
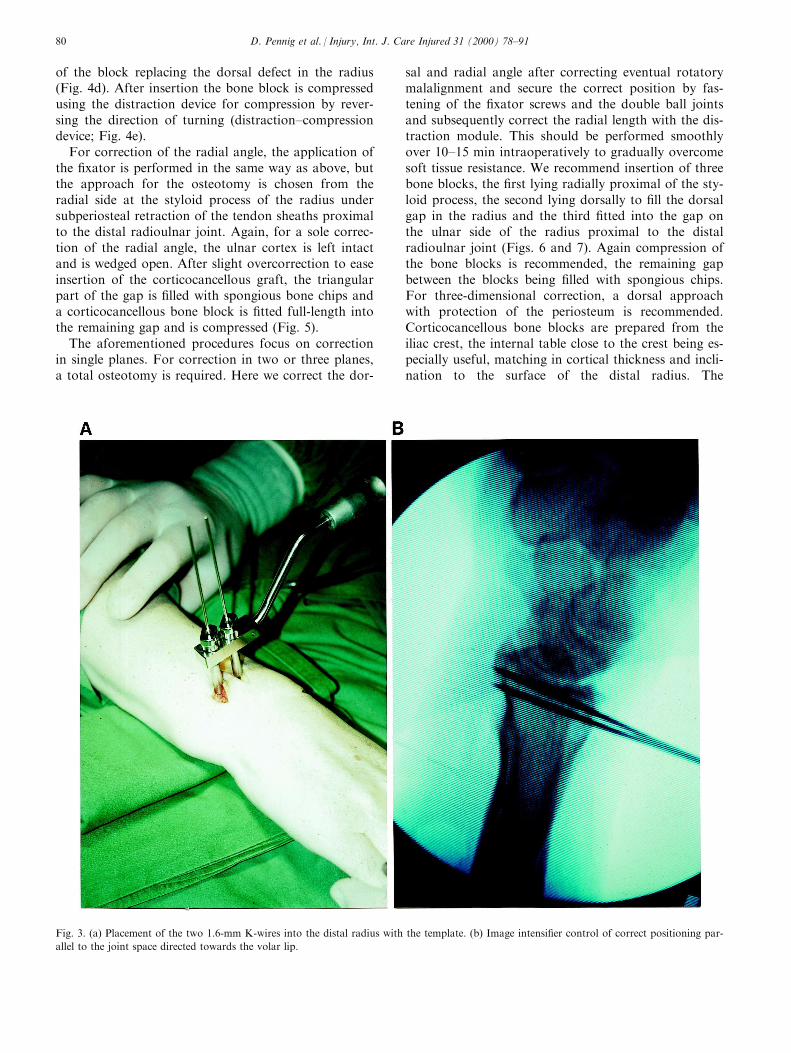
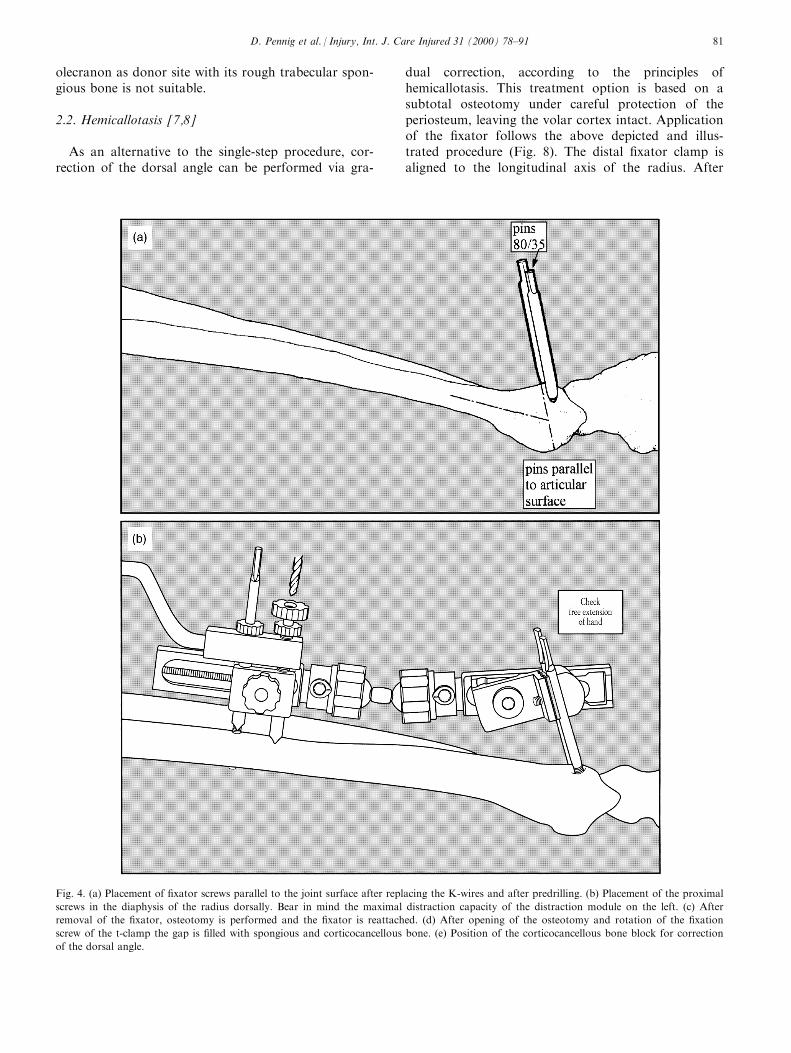
Placement of screws is performed strictly dorsallyusing a tourniquet. A 1.6-mm K-wire is drilled parallelto the joint surface into the ulnar part of the distalradius metaphysis via limited exposure of the bone, 5mm proximal to the joint line under image intensi®ercontrol in the lateral view (Fig. 3). Using the drill tem-plate, a second K-wire is positioned into the radiusparallel to the ®rst in Lister's tubercle under imageintensi®er control. Both K-wires are replaced by ®xa-tor screws (length 70 mm, thread length 20 mm, diam-eter 3.0/3.3; drill bit 2.7 mm), which are inserted intothe volar lip resulting in good enchorage even in osteo-porotic bone (Fig. 4a).
The external ®xator is then mounted on the distalscrews to serve as a template for proximal screw place-ment, using a dorsal limited open approach of 2.5 cmand considering the full range of distraction capability
of the proximal clamp (Fig. 4b). Here, screws withtotal length of 70 mm and thread length of 20 mm aresu�cient to achieve good purchase in the diaphysealbone of the radius. Osteotomy is performed 5±10 mmproximal to the distal ®xator screws, avoiding the useof an oscillating saw, which can cause heat damage tothe bone. Instead, we use a new 2-mm drill bit for per-foration of the bone, after marking the plane of theosteotomy, and complete it with a sharp chisel (Fig.4b). Damage to volar structures and to the dorsal peri-osteum must be avoided, for the latter using carefulretraction during drilling.
When correction is only aimed at the dorsal angle,the volar cortex should remain intact. After perform-ing a subtotal osteotomy, the volar cortex is wedgedopen manually or with the distraction device of the®xator plus the capability of the t-clamp for rotationaland sliding movement. We recommend slight overcor-rection to ease insertion of the corticocancellous graft.After con®rming the amount of correction, the tri-angular part of the gap is ®lled with spongious bonechips and a corticocancellous bone block is ®tted full-length into the dorsal part of the gap, the cortical part
Fig. 1. External ®xator with double ball joint and distraction module (left). A t-clamp is attached to the sliding module on the right.
Fig. 2. Insertion of ®xator screws in the distal radius in the diaphysis of the radius. Preoperative planning sketch for de®ning the plane of osteot-
omy.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±91 79
of the block replacing the dorsal defect in the radius(Fig. 4d). After insertion the bone block is compressedusing the distraction device for compression by rever-sing the direction of turning (distraction±compressiondevice; Fig. 4e).
For correction of the radial angle, the application ofthe ®xator is performed in the same way as above, butthe approach for the osteotomy is chosen from theradial side at the styloid process of the radius undersubperiosteal retraction of the tendon sheaths proximalto the distal radioulnar joint. Again, for a sole correc-tion of the radial angle, the ulnar cortex is left intactand is wedged open. After slight overcorrection to easeinsertion of the corticocancellous graft, the triangularpart of the gap is ®lled with spongious bone chips anda corticocancellous bone block is ®tted full-length intothe remaining gap and is compressed (Fig. 5).
The aforementioned procedures focus on correctionin single planes. For correction in two or three planes,a total osteotomy is required. Here we correct the dor-
sal and radial angle after correcting eventual rotatorymalalignment and secure the correct position by fas-tening of the ®xator screws and the double ball jointsand subsequently correct the radial length with the dis-traction module. This should be performed smoothlyover 10±15 min intraoperatively to gradually overcomesoft tissue resistance. We recommend insertion of threebone blocks, the ®rst lying radially proximal of the sty-loid process, the second lying dorsally to ®ll the dorsalgap in the radius and the third ®tted into the gap onthe ulnar side of the radius proximal to the distalradioulnar joint (Figs. 6 and 7). Again compression ofthe bone blocks is recommended, the remaining gapbetween the blocks being ®lled with spongious chips.For three-dimensional correction, a dorsal approachwith protection of the periosteum is recommended.Corticocancellous bone blocks are prepared from theiliac crest, the internal table close to the crest being es-pecially useful, matching in cortical thickness and incli-nation to the surface of the distal radius. The
Fig. 3. (a) Placement of the two 1.6-mm K-wires into the distal radius with the template. (b) Image intensi®er control of correct positioning par-
allel to the joint space directed towards the volar lip.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±9180
olecranon as donor site with its rough trabecular spon-gious bone is not suitable.
2.2. Hemicallotasis [7,8]
As an alternative to the single-step procedure, cor-rection of the dorsal angle can be performed via gra-
dual correction, according to the principles ofhemicallotasis. This treatment option is based on asubtotal osteotomy under careful protection of theperiosteum, leaving the volar cortex intact. Applicationof the ®xator follows the above depicted and illus-trated procedure (Fig. 8). The distal ®xator clamp isaligned to the longitudinal axis of the radius. After
Fig. 4. (a) Placement of ®xator screws parallel to the joint surface after replacing the K-wires and after predrilling. (b) Placement of the proximal
screws in the diaphysis of the radius dorsally. Bear in mind the maximal distraction capacity of the distraction module on the left. (c) After
removal of the ®xator, osteotomy is performed and the ®xator is reattached. (d) After opening of the osteotomy and rotation of the ®xation
screw of the t-clamp the gap is ®lled with spongious and corticocancellous bone. (e) Position of the corticocancellous bone block for correction
of the dorsal angle.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±91 81
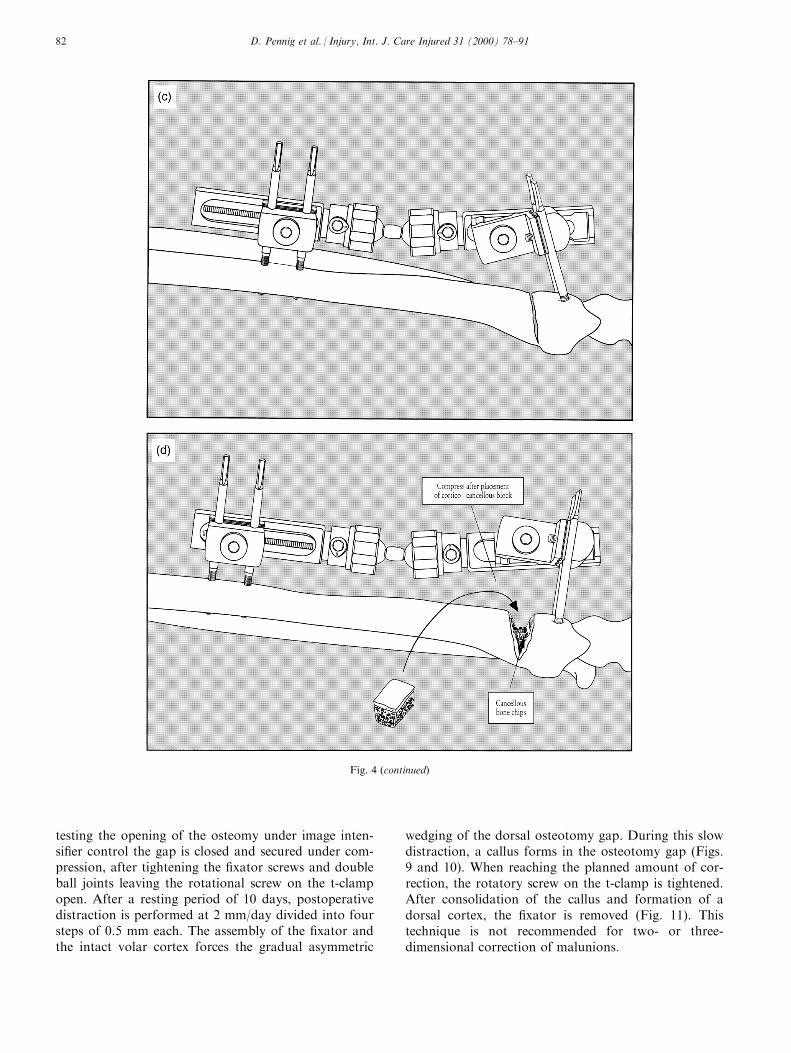
testing the opening of the osteomy under image inten-si®er control the gap is closed and secured under com-pression, after tightening the ®xator screws and doubleball joints leaving the rotational screw on the t-clampopen. After a resting period of 10 days, postoperativedistraction is performed at 2 mm/day divided into foursteps of 0.5 mm each. The assembly of the ®xator andthe intact volar cortex forces the gradual asymmetric
wedging of the dorsal osteotomy gap. During this slowdistraction, a callus forms in the osteotomy gap (Figs.9 and 10). When reaching the planned amount of cor-rection, the rotatory screw on the t-clamp is tightened.After consolidation of the callus and formation of adorsal cortex, the ®xator is removed (Fig. 11). Thistechnique is not recommended for two- or three-dimensional correction of malunions.
Fig. 4 (continued)
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±9182
3. Results
Fourteen patients were treated for malunited distalradius fractures in our department according to theabove presented techniques between 1994 and 1996(age 15±65 years). Eight patients were treated by singlestage correction (all three-dimensional), ®ve by gradual
correction and one 15-year-old patient by asymmetri-cal correction of the growth plate after post-traumaticpartial fusion. In all cases preoperative planned correc-tion was achieved. As complications, we recorded twopin-track infections in two patients in the proximal pingroup, which healed without surgical intervention.There were no neurological impairments and averageremoval of the ®xator was after eight weeks.
4. Discussion
For correction of two- or three-dimensional mal-united distal radius fractures, we routinely use theradioradial external ®xator with double ball joint, t-clamp with sliding and rotatory facility and distrac-tion capacity. After insertion of the distal screwsparallel to the joint surface, the ease of realignmentof the distal fragment of the radius appears advan-tageous. After correcting possible rotatory com-ponents of the fragment, radial and dorsal anglescan be readjusted. Radial shortening can be cor-rected gradually by intraoperative distraction. Bonegaps after osteotomy resulting after correction are®lled with corticocancellous bone blocks. A restingperiod with bracing of the forearm for 72 h post-operatively, paired with constant elevation, is rec-ommended, followed by intensive physiotherapy ofall arcs of motion of the wrist joint. Bone healing
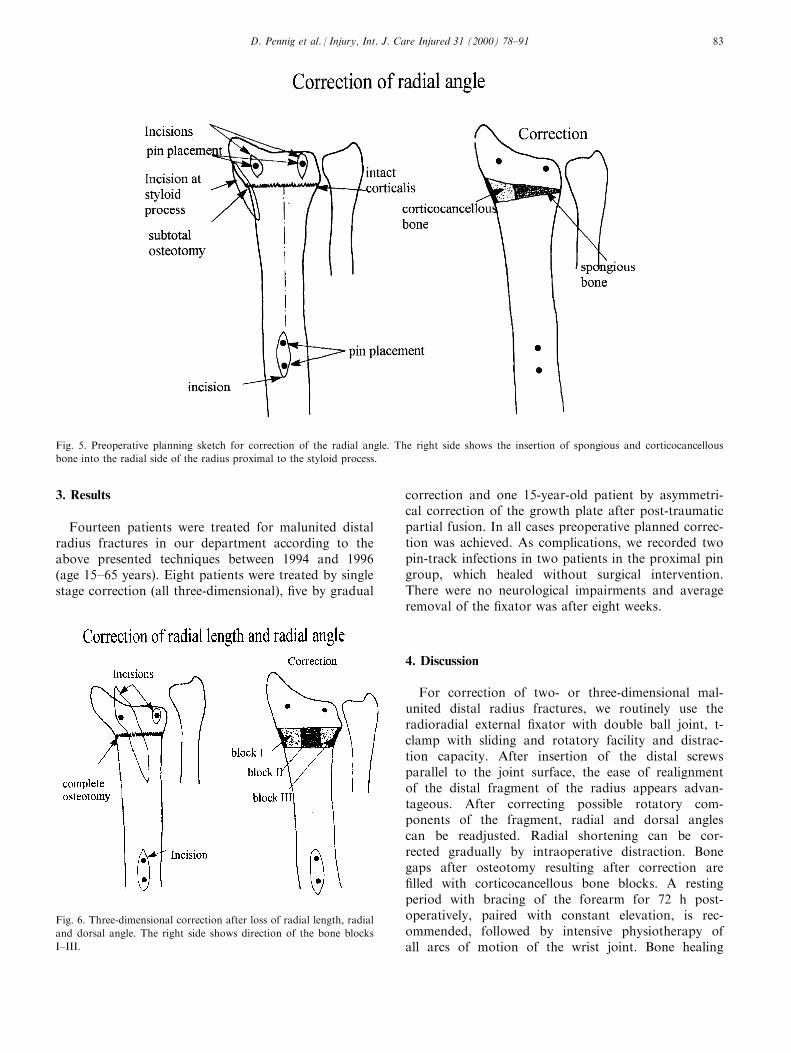
Fig. 5. Preoperative planning sketch for correction of the radial angle. The right side shows the insertion of spongious and corticocancellous
bone into the radial side of the radius proximal to the styloid process.
Fig. 6. Three-dimensional correction after loss of radial length, radial
and dorsal angle. The right side shows direction of the bone blocks
I±III.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±91 83
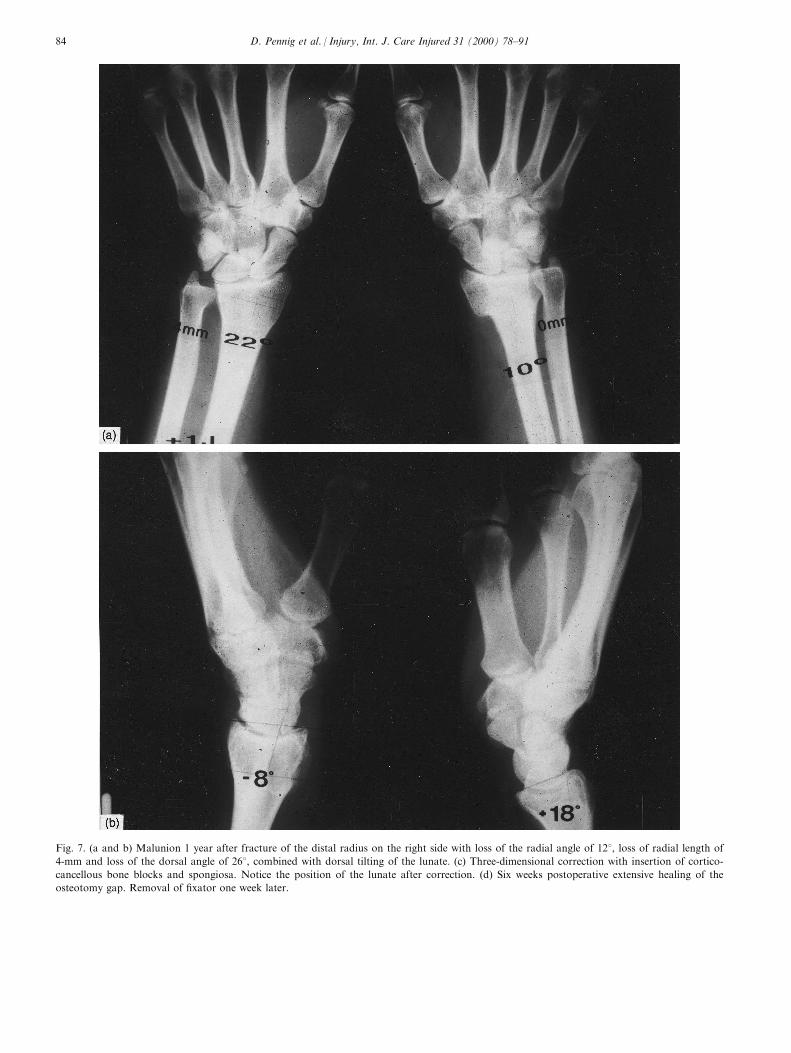
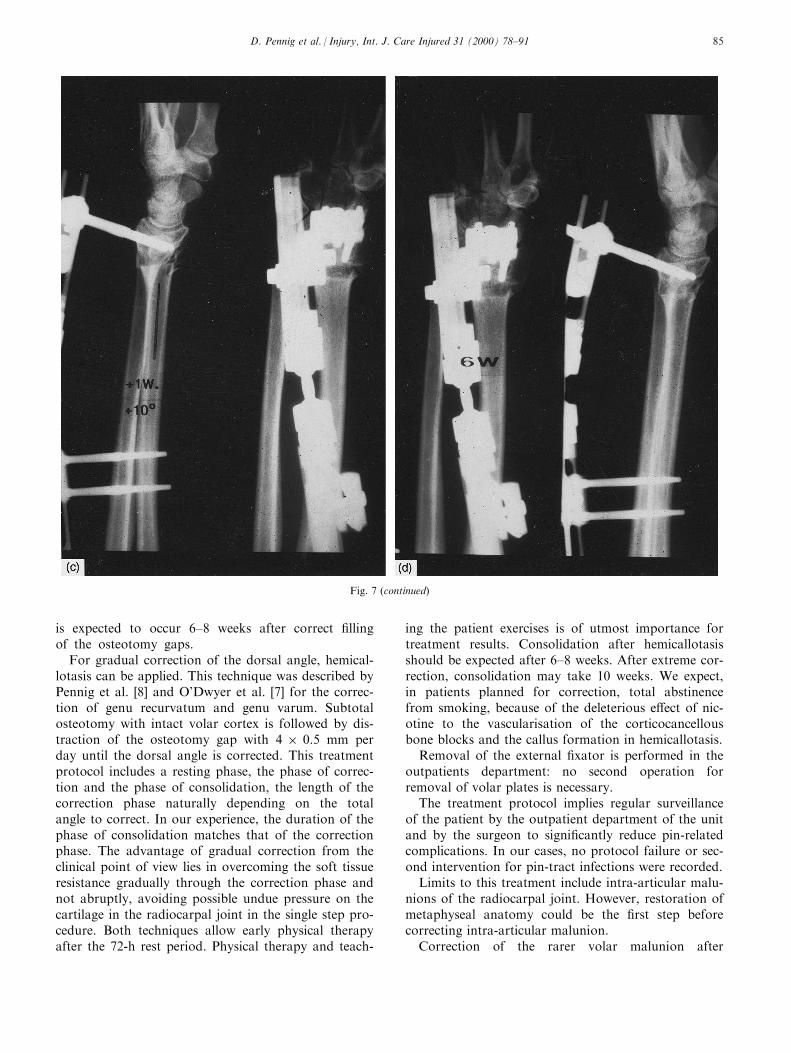
Fig. 7. (a and b) Malunion 1 year after fracture of the distal radius on the right side with loss of the radial angle of 128, loss of radial length of
4-mm and loss of the dorsal angle of 268, combined with dorsal tilting of the lunate. (c) Three-dimensional correction with insertion of cortico-
cancellous bone blocks and spongiosa. Notice the position of the lunate after correction. (d) Six weeks postoperative extensive healing of the
osteotomy gap. Removal of ®xator one week later.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±9184
is expected to occur 6±8 weeks after correct ®llingof the osteotomy gaps.
For gradual correction of the dorsal angle, hemical-lotasis can be applied. This technique was described byPennig et al. [8] and O'Dwyer et al. [7] for the correc-tion of genu recurvatum and genu varum. Subtotalosteotomy with intact volar cortex is followed by dis-traction of the osteotomy gap with 4 � 0.5 mm perday until the dorsal angle is corrected. This treatmentprotocol includes a resting phase, the phase of correc-tion and the phase of consolidation, the length of thecorrection phase naturally depending on the totalangle to correct. In our experience, the duration of thephase of consolidation matches that of the correctionphase. The advantage of gradual correction from theclinical point of view lies in overcoming the soft tissueresistance gradually through the correction phase andnot abruptly, avoiding possible undue pressure on thecartilage in the radiocarpal joint in the single step pro-cedure. Both techniques allow early physical therapyafter the 72-h rest period. Physical therapy and teach-
ing the patient exercises is of utmost importance fortreatment results. Consolidation after hemicallotasisshould be expected after 6±8 weeks. After extreme cor-rection, consolidation may take 10 weeks. We expect,in patients planned for correction, total abstinencefrom smoking, because of the deleterious e�ect of nic-otine to the vascularisation of the corticocancellousbone blocks and the callus formation in hemicallotasis.
Removal of the external ®xator is performed in theoutpatients department: no second operation forremoval of volar plates is necessary.
The treatment protocol implies regular surveillanceof the patient by the outpatient department of the unitand by the surgeon to signi®cantly reduce pin-relatedcomplications. In our cases, no protocol failure or sec-ond intervention for pin-tract infections were recorded.
Limits to this treatment include intra-articular malu-nions of the radiocarpal joint. However, restoration ofmetaphyseal anatomy could be the ®rst step beforecorrecting intra-articular malunion.
Correction of the rarer volar malunion after
Fig. 7 (continued)
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±91 85
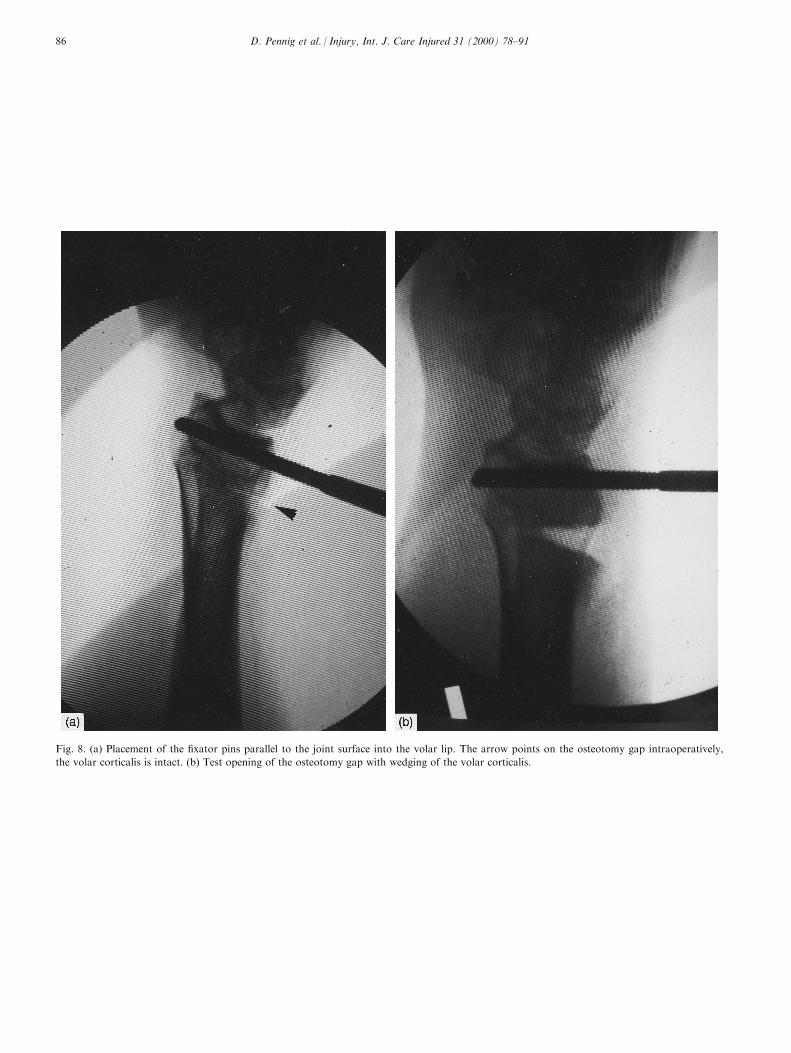
Fig. 8. (a) Placement of the ®xator pins parallel to the joint surface into the volar lip. The arrow points on the osteotomy gap intraoperatively,
the volar corticalis is intact. (b) Test opening of the osteotomy gap with wedging of the volar corticalis.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±9186

Fig. 9. (a) Application of the external ®xator after subtotal osteotomy with intact cortex, dorsal approach. (b) Under distraction (four steps 0.5
mm each per day) the bone gap opens on the dorsal aspect of the radius, while rotation occurs in the screw ®xing the t-clamp. (c) Correction is
completed after achieving the planned position.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±91 87
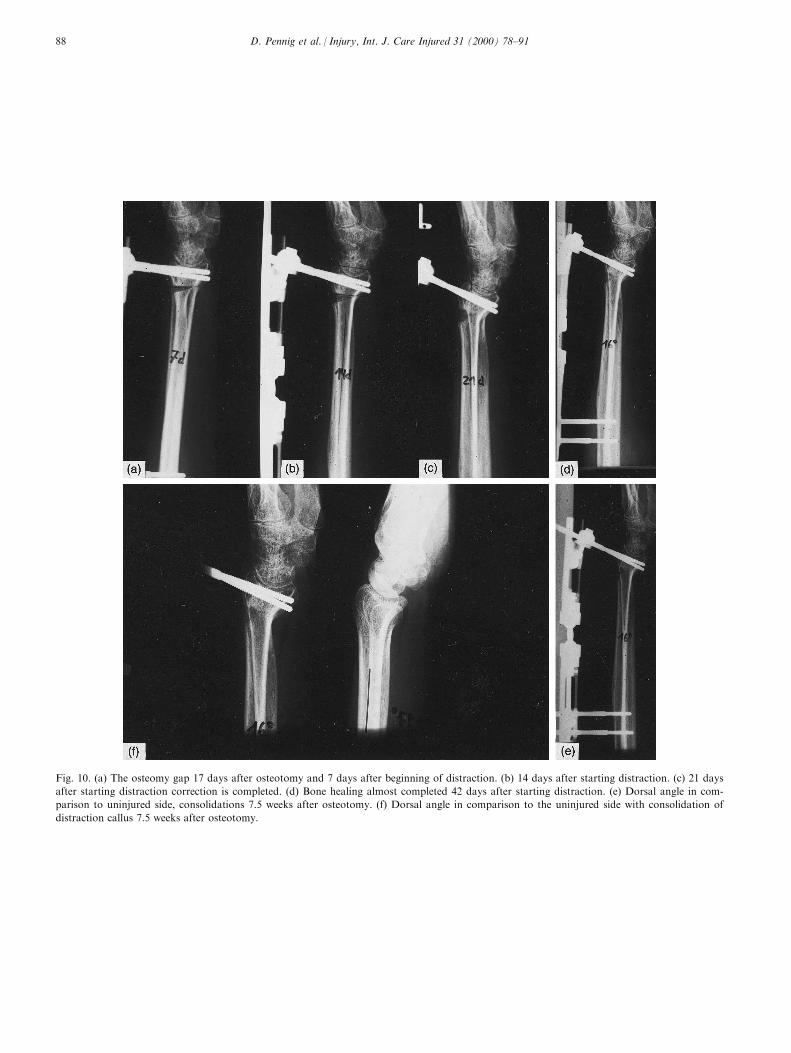
Fig. 10. (a) The osteomy gap 17 days after osteotomy and 7 days after beginning of distraction. (b) 14 days after starting distraction. (c) 21 days
after starting distraction correction is completed. (d) Bone healing almost completed 42 days after starting distraction. (e) Dorsal angle in com-
parison to uninjured side, consolidations 7.5 weeks after osteotomy. (f) Dorsal angle in comparison to the uninjured side with consolidation of
distraction callus 7.5 weeks after osteotomy.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±9188
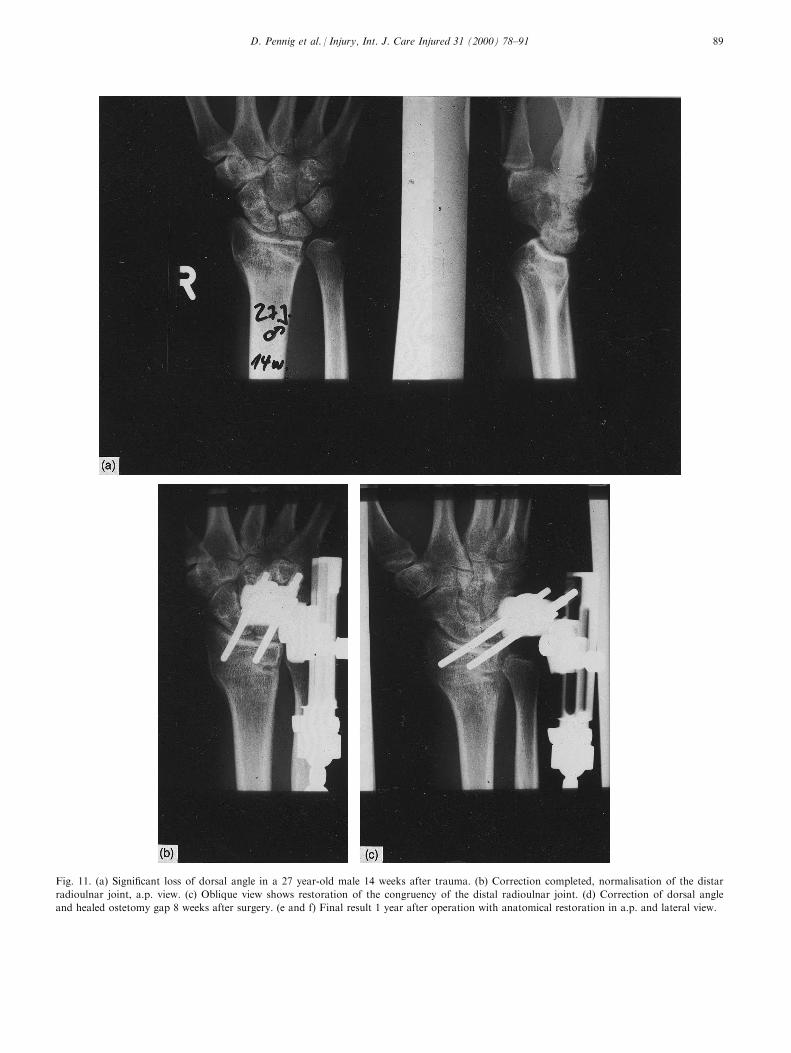
Fig. 11. (a) Signi®cant loss of dorsal angle in a 27 year-old male 14 weeks after trauma. (b) Correction completed, normalisation of the distar
radioulnar joint, a.p. view. (c) Oblique view shows restoration of the congruency of the distal radioulnar joint. (d) Correction of dorsal angle
and healed ostetomy gap 8 weeks after surgery. (e and f) Final result 1 year after operation with anatomical restoration in a.p. and lateral view.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±91 89

Fig. 11 (continued)
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±9190

Smith- or Barton-fractures are not susceptible to thedepicted treatment protocol due to unfavourablebiomechanical surroundings and here we proceed toopen correction with bone block interposition andvolar plating.
With concomitant severe arthritis, we do not rec-ommend this protocol and perform denervation pro-cedures. Patients with severe osteoporosis and poorly-controlled diabetes are also excluded. Naturally,patients with bad compliance are not suitable for cor-rective procedures. Our experiences encourage furtherusage of the double ball joint ®xator for reposition,retention and ®nal treatment of malunited distal radiusfractures.
References
[1] Buck-Gramcko D. Frakturen am distalen Radiusende.
Stuttgart: Hippokrates, 1987.
[2] Fernandez DL. Correction of posttraumatic wrist by osteotomy,
bone grafting and internal ®xation. Journal of Bone and Joint
Surgery (Am) 1982;64:1164.
[3] Klein W, De e W. Erste Erfahrungen mit einem neuen
Handgelenks®xateur zur Behandlung distaler Radiusfrakturen.
Handchirurgie Mikrochirurgie Plastische Chirurgie 1987;24:202.
[4] Lanz U, Kron W. Neue Technik zur Korrktur in Fehlstellung
verheilter distaler Radiusfrakturen. Handchirurgie 1976;8:203.
[5] Lanz U. Korrekturosteotomie nach distalen Radiusfrakturen,
Technick und Ergebnisse. In: Buck-Gramcko D, editor.
Frakturen am Distalen Radiusende. Stuttgart: Hippokrates,
1987. p. 69.
[6] Leung KS, Shen WY, Leung PC, et al. Ligamentotaxis and
bone grafting for comminuted fractures of the distal radius.
Journal of Bone and Joint Surgery (Br) 1989;71:838.
[7] O'Dywer KJ, MacEacher AG, Pennig D. Corrective tibial
osteotomy for genu recurvatum by callus distraction using an
external ®xator. Chirurgia Degli Organi di Movimento
1991;76:355±8.
[8] Pennig D, Baranowski D. Genu recurvatum due to partial
growth arrest in the proximal tibial physis: correction by callus
distraction. Archives of Orthopedic Trauma Surgery
1989;108:119±21.
[9] Pennig D. Dynamic external ®xation of distal radius fractures.
Hand Clinics 1993;9:587±602.
[10] Pennig D, Gausepohl T. Extrarticular and transarticular exter-
nal ®xation with early motion in distal radius fractures and mal-
unions. Orthopedic Surgical Techniques 1995;9:51±65.
[11] Pennig D, Gausepohl T. External ®xation of the wrist. Injury
1996;27:1±15.
D. Pennig et al. / Injury, Int. J. Care Injured 31 (2000) 78±91 91
Copyright © 2022 FDOKUMEN