Control of Neglected Tropical Diseases in Burundi: Partnerships, Achievements, Challenges, and...
9
Policy Platform Control of Neglected Tropical Diseases in Burundi: Partnerships, Achievements, Challenges, and Lessons Learned after Four Years of Programme Implementation One ´ sime Ndayishimiye 1 , Giuseppina Ortu 2 *, Ricardo J. Soares Magalhaes 3 , Archie Clements 3 , Johan Willems 4 , Jane Whitton 2 , Warren Lancaster 5 , Adrian Hopkins 6 , Alan Fenwick 2 1 Programme National Inte ´gre ´ de lutte contre les Maladies Tropicales Ne ´ glige ´es et la Ce ´cite ´ (PNIMTNC) - Ministe `re de la Sante ´ Publique et de la lutte contre le SIDA, Bujumbura, Burundi, 2 Schistosomiasis Control Initiative - Imperial College, Department of Infectious Disease Epidemiology, London, United Kingdom, 3 University of Queensland, Infectious Disease Epidemiology Unit, School of Population Health, Herston, Queensland, Australia, 4 CBM Regional Office for Central Africa, Parklands, Nairobi, Kenya, 5 END Fund/Geneva Global, London, United Kingdom, 6 Mectizan Donation Programme, Decatur, Georgia, United States of America Introduction Neglected tropical diseases (NTDs) are a group of 17 conditions that together affect over 1,000,000,000 people in the developing world [1]. Nongovernmental organisations (NGOs) and public-private partnerships have joined efforts to place the NTDs in the spotlight, especially the seven that can be treated with an annual dose of safe and effective drugs: trachoma, three soil-transmitted helminthiases (STHs, ascariasis, hookworm infections, and trich- uriasis), lymphatic filariasis (LF), onchocer- ciasis, and schistosomiasis (SCH) [2]. On the wave of this new interest in NTDs, Burundi was selected in 2007 by the Legatum Foundation for financial support for a national NTD programme. Before 2007, Burundi hosted two min- isterial programmes related to treatment of parasitic diseases: the National Pro- gramme for the Control of Transmissible Diseases and Deficiencies (Lutte contre le Maladies Transmissibles et Carentielles [LMTC]), responsible for managing ma- laria, worm infections, and nutrition, and an onchocerciasis control programme (Programme National de Lutte contre l’Onchocercose [PNLO]). The PNLO, supported by the African Programme for Onchocerciasis Control (APOC) [3] and CBM (formerly known as Christian Blind Mission) [4], involved the annual admin- istration of ivermectin (IVM) in ten endemic districts (namely Cibitoke, Bu- banza, Bururi, Rutana, Mpanda, Ru- monge, Matana, Gihofi, Mabayi, and the Kayogoro commune in the Makamba district) via the well-established Commu- nity Directed Treatment with Ivermectin (CDTI) strategy [5]. For other NTDs, such as trachoma and LF, no specific pro- grammes were in place in Burundi at that time. Due to limited funding, the LMTC priori- tised malaria control activities. Nevertheless, distribution of praziquantel (PZQ) in health centres and mebendazole (MBZ) in schools was already happening between 1973 and 1992 in areas considered highly endemic [6,7]. Historical epidemiological data on STHs [8] and a survey performed in 2005 [9] suggested that both Schistosoma mansoni and STH infections were wide- spread, with SCH prevalence varying across provinces (range 0–61%, mean 22%) and the overall prevalence of STHs reaching 59.7%. With the beginning of the civil war in 1993, national prevention and control activities slowed down considerably. De- spite the continued political instability, the Ministry of Health (MoH), with UNICEF and the WHO, introduced an annual Mother and Child Health Week (MCHW) in 2003, during which vaccinations, mi- cronutrients, bed nets, and deworming drugs were distributed. Prior to 2007, trachoma and LF prev- alence had never been thoroughly inves- tigated in Burundi. A few cases of trachoma were suspected among refugees, and there was evidence of cases of elephantiasis, one of the clinical manifes- tations of LF, although they were likely due to podoconiosis [10]. Sparse historical epidemiologic data and the presence of a few early-stage health initiatives (LMTC, PNLO, and MCHW) created an excellent opportunity to roll out an NTD control programme in Burundi. With the specific objectives of defining the popu- lation at risk for each infection and elaborat- ing and implementing a drug treatment strategy targeting the population at risk, the final aspiration was to create a solid frame- work for a sustainable NTD control pro- gramme integrated with the health initiatives already in place that would continue after the end of the donor-funded programme. The present paper provides a critical overview after four years of a programme that started in Burundi in June 2007. Strategies, achievements, challenges, les- sons learned, and future steps for the country, especially in relation to schisto- somiasis and STHs, are discussed. The onchocerciasis programme coordinated by the national programme is not described in this paper. Details on trachoma that have not been reported already by others [11] are presented as part of the ongoing activities of the NTD programme, as well as the mapping results for LF. Assessing the burden of NTDs NTD mapping was an important step for defining the population at risk of infections and for rolling out drug delivery strategies at the national level. In 2007, 20 primary schools in the country were randomly selected to assess Citation: Ndayishimiye O, Ortu G, Soares Magalhaes RJ, Clements A, Willems J, et al. (2014) Control of Neglected Tropical Diseases in Burundi: Partnerships, Achievements, Challenges, and Lessons Learned after Four Years of Programme Implementation. PLoS Negl Trop Dis 8(5): e2684. doi:10.1371/journal.pntd.0002684 Editor: William Evan Secor, Centers for Disease Control and Prevention, United States of America Published May 1, 2014 Copyright: ß 2014 Ndayishimiye et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Funding: The NTD programme in Burundi was supported by the investment group Legatum and Geneva Global. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Competing Interests: The authors have declared that no competing interests exist. * E-mail: [email protected] PLOS Neglected Tropical Diseases | www.plosntds.org 1 May 2014 | Volume 8 | Issue 5 | e2684
Transcript of Control of Neglected Tropical Diseases in Burundi: Partnerships, Achievements, Challenges, and...

Policy Platform
Control of Neglected Tropical Diseases in Burundi:Partnerships, Achievements, Challenges, and LessonsLearned after Four Years of Programme ImplementationOnesime Ndayishimiye1, Giuseppina Ortu2*, Ricardo J. Soares Magalhaes3, Archie Clements3,
Johan Willems4, Jane Whitton2, Warren Lancaster5, Adrian Hopkins6, Alan Fenwick2
1 Programme National Integre de lutte contre les Maladies Tropicales Negligees et la Cecite (PNIMTNC) - Ministere de la Sante Publique et de la lutte contre le SIDA,
Bujumbura, Burundi, 2 Schistosomiasis Control Initiative - Imperial College, Department of Infectious Disease Epidemiology, London, United Kingdom, 3 University of
Queensland, Infectious Disease Epidemiology Unit, School of Population Health, Herston, Queensland, Australia, 4 CBM Regional Office for Central Africa, Parklands,
Nairobi, Kenya, 5 END Fund/Geneva Global, London, United Kingdom, 6 Mectizan Donation Programme, Decatur, Georgia, United States of America
Introduction
Neglected tropical diseases (NTDs) are
a group of 17 conditions that together
affect over 1,000,000,000 people in the
developing world [1]. Nongovernmental
organisations (NGOs) and public-private
partnerships have joined efforts to place
the NTDs in the spotlight, especially the
seven that can be treated with an annual
dose of safe and effective drugs: trachoma,
three soil-transmitted helminthiases (STHs,
ascariasis, hookworm infections, and trich-
uriasis), lymphatic filariasis (LF), onchocer-
ciasis, and schistosomiasis (SCH) [2]. On
the wave of this new interest in NTDs,
Burundi was selected in 2007 by the
Legatum Foundation for financial support
for a national NTD programme.
Before 2007, Burundi hosted two min-
isterial programmes related to treatment of
parasitic diseases: the National Pro-
gramme for the Control of Transmissible
Diseases and Deficiencies (Lutte contre le
Maladies Transmissibles et Carentielles
[LMTC]), responsible for managing ma-
laria, worm infections, and nutrition, and
an onchocerciasis control programme
(Programme National de Lutte contre
l’Onchocercose [PNLO]). The PNLO,
supported by the African Programme for
Onchocerciasis Control (APOC) [3] and
CBM (formerly known as Christian Blind
Mission) [4], involved the annual admin-
istration of ivermectin (IVM) in ten
endemic districts (namely Cibitoke, Bu-
banza, Bururi, Rutana, Mpanda, Ru-
monge, Matana, Gihofi, Mabayi, and the
Kayogoro commune in the Makamba
district) via the well-established Commu-
nity Directed Treatment with Ivermectin
(CDTI) strategy [5]. For other NTDs, such
as trachoma and LF, no specific pro-
grammes were in place in Burundi at that
time.
Due to limited funding, the LMTC priori-
tised malaria control activities. Nevertheless,
distribution of praziquantel (PZQ) in
health centres and mebendazole (MBZ)
in schools was already happening between
1973 and 1992 in areas considered highly
endemic [6,7]. Historical epidemiological
data on STHs [8] and a survey performed
in 2005 [9] suggested that both Schistosoma
mansoni and STH infections were wide-
spread, with SCH prevalence varying
across provinces (range 0–61%, mean
22%) and the overall prevalence of STHs
reaching 59.7%.
With the beginning of the civil war in
1993, national prevention and control
activities slowed down considerably. De-
spite the continued political instability, the
Ministry of Health (MoH), with UNICEF
and the WHO, introduced an annual
Mother and Child Health Week (MCHW)
in 2003, during which vaccinations, mi-
cronutrients, bed nets, and deworming
drugs were distributed.
Prior to 2007, trachoma and LF prev-
alence had never been thoroughly inves-
tigated in Burundi. A few cases of
trachoma were suspected among refugees,
and there was evidence of cases of
elephantiasis, one of the clinical manifes-
tations of LF, although they were likely
due to podoconiosis [10].
Sparse historical epidemiologic data and
the presence of a few early-stage health
initiatives (LMTC, PNLO, and MCHW)
created an excellent opportunity to roll out an
NTD control programme in Burundi. With
the specific objectives of defining the popu-
lation at risk for each infection and elaborat-
ing and implementing a drug treatment
strategy targeting the population at risk, the
final aspiration was to create a solid frame-
work for a sustainable NTD control pro-
gramme integrated with the health initiatives
already in place that would continue after the
end of the donor-funded programme.
The present paper provides a critical
overview after four years of a programme
that started in Burundi in June 2007.
Strategies, achievements, challenges, les-
sons learned, and future steps for the
country, especially in relation to schisto-
somiasis and STHs, are discussed. The
onchocerciasis programme coordinated by
the national programme is not described
in this paper. Details on trachoma that
have not been reported already by others
[11] are presented as part of the ongoing
activities of the NTD programme, as well
as the mapping results for LF.
Assessing the burden of NTDsNTD mapping was an important step
for defining the population at risk of
infections and for rolling out drug delivery
strategies at the national level.
In 2007, 20 primary schools in the
country were randomly selected to assess
Citation: Ndayishimiye O, Ortu G, Soares Magalhaes RJ, Clements A, Willems J, et al. (2014) Control ofNeglected Tropical Diseases in Burundi: Partnerships, Achievements, Challenges, and Lessons Learned afterFour Years of Programme Implementation. PLoS Negl Trop Dis 8(5): e2684. doi:10.1371/journal.pntd.0002684
Editor: William Evan Secor, Centers for Disease Control and Prevention, United States of America
Published May 1, 2014
Copyright: � 2014 Ndayishimiye et al. This is an open-access article distributed under the terms of theCreative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in anymedium, provided the original author and source are credited.
Funding: The NTD programme in Burundi was supported by the investment group Legatum and GenevaGlobal. The funders had no role in study design, data collection and analysis, decision to publish, or preparationof the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
PLOS Neglected Tropical Diseases | www.plosntds.org 1 May 2014 | Volume 8 | Issue 5 | e2684
intestinal schistosomiasis and STHs (using
the Kato-Katz method for diagnosis) [12]
and urinary schistosomiasis (using the
urine filtration method). For LF mapping,
because transmission was known to be
minimal at altitudes over 1,300 m [12,13],
the NTD control programme mapped LF
only in communes situated below
1,500 m. A total of 1,754 adults (aged 15
and above with roughly 100 people per
community for a total of 17 communities)
were tested via the LF immunocromato-
graphic test (ICT) card [14].
Results of the parasitological surveys
confirmed that urinary schistosomiasis and
LF were not endemic in the country,
whereas intestinal schistosomiasis was
highly focalized in areas with close proximity
to water bodies. STHs, particularly hook-
worm, were widely distributed, supporting
a mass drug treatment approach targeting
nearly the whole population [15]. The
enclosed supporting information (Tables
S1, S2, S3) outlines the estimated preva-
lence of worm infections in each commune,
with the corresponding risk category as per
WHO guidelines.
For trachoma, a rapid assessment was
performed [16–18], in which an average
of 50 adults and 50 children aged 1–9
years per community were examined
(n = 2,253 children, n = 1,845 adults). This
survey revealed the presence of active
trachoma in the country and was followed
by a more detailed survey in 2009–2010,
in which 20,659 children were examined
in 11 districts [11]. Results from this
survey demonstrated a prevalence of
children with follicular trachoma (TF)
above 10% in three districts (Buhiga,
Muyinga, and Nyabikere). An extension
of this survey to ten other districts also
showed TF above 10% in the Rutana
district (2013 stakeholders meeting held in
Burundi, unreferenced).
All the data obtained were compiled
and integrated with environmental and
country demographic information to cre-
ate maps predicting areas at risk of
infections (Tables S1, S2, S3) [15] that
were then used for defining drug treatment
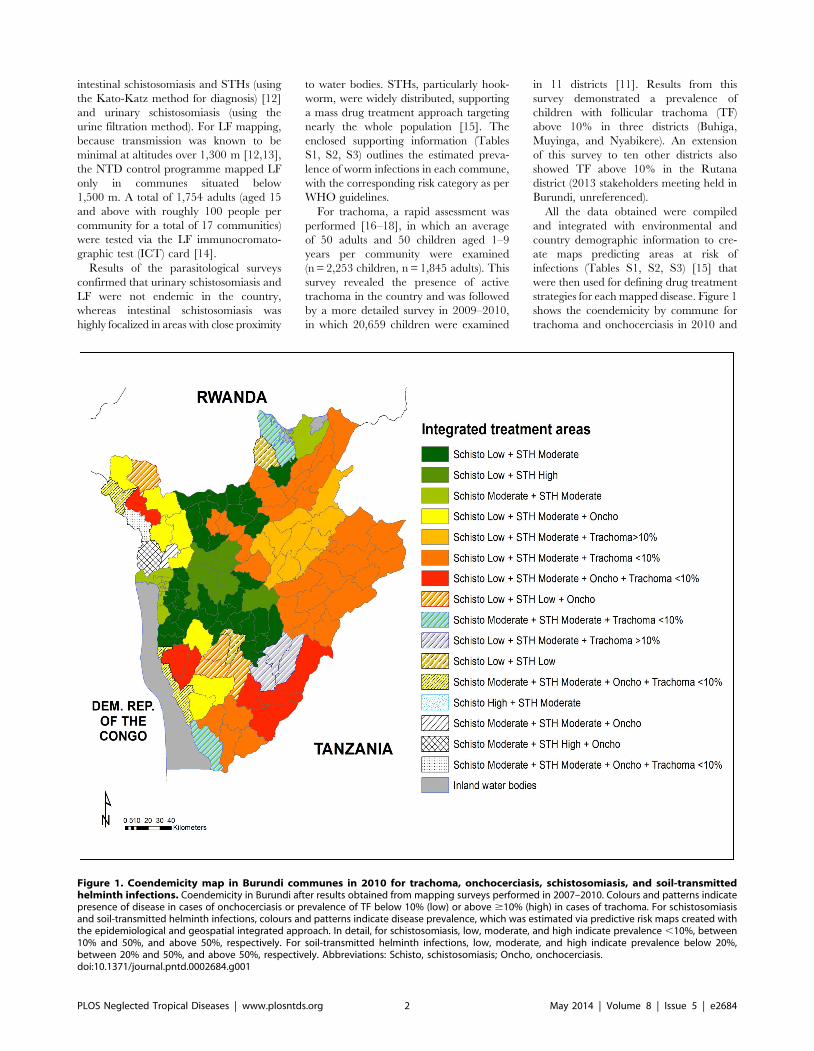
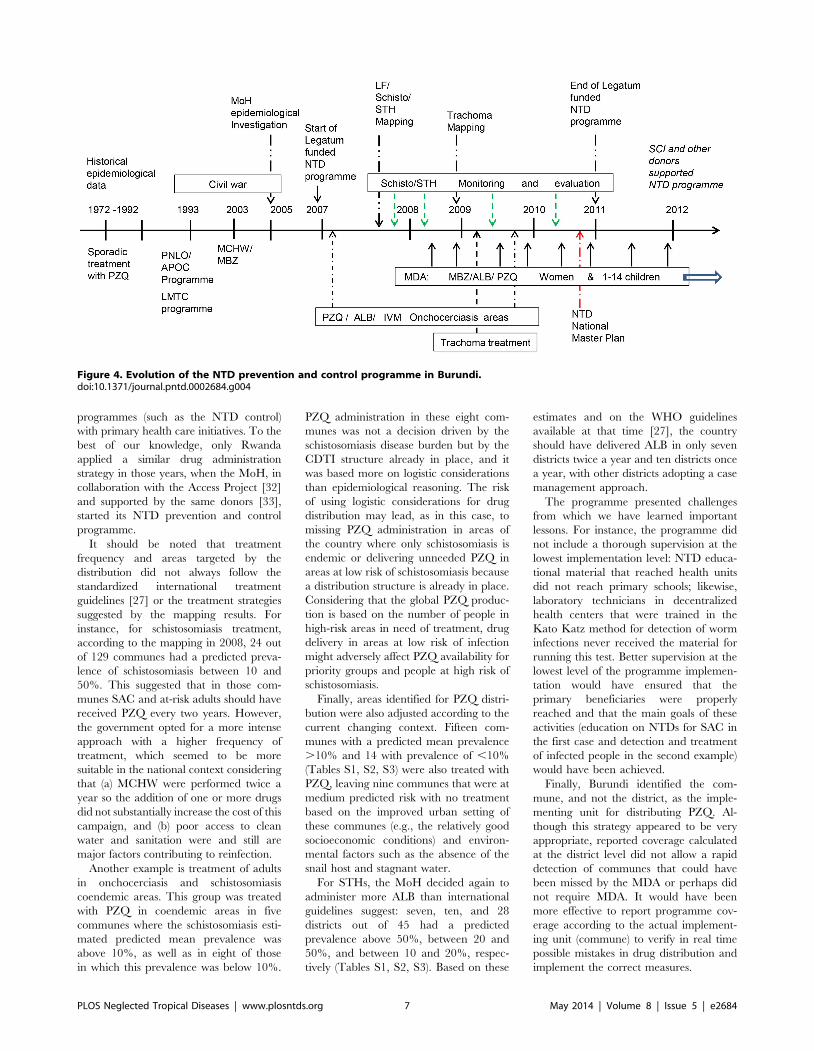
strategies for each mapped disease. Figure 1
shows the coendemicity by commune for
trachoma and onchocerciasis in 2010 and
Figure 1. Coendemicity map in Burundi communes in 2010 for trachoma, onchocerciasis, schistosomiasis, and soil-transmittedhelminth infections. Coendemicity in Burundi after results obtained from mapping surveys performed in 2007–2010. Colours and patterns indicatepresence of disease in cases of onchocerciasis or prevalence of TF below 10% (low) or above $10% (high) in cases of trachoma. For schistosomiasisand soil-transmitted helminth infections, colours and patterns indicate disease prevalence, which was estimated via predictive risk maps created withthe epidemiological and geospatial integrated approach. In detail, for schistosomiasis, low, moderate, and high indicate prevalence ,10%, between10% and 50%, and above 50%, respectively. For soil-transmitted helminth infections, low, moderate, and high indicate prevalence below 20%,between 20% and 50%, and above 50%, respectively. Abbreviations: Schisto, schistosomiasis; Oncho, onchocerciasis.doi:10.1371/journal.pntd.0002684.g001
PLOS Neglected Tropical Diseases | www.plosntds.org 2 May 2014 | Volume 8 | Issue 5 | e2684
the areas estimated at risk of SCH and
STHs as per mapping results finalized in
2008. Areas with predicted prevalence
estimates $10% for SCH, any STH, or
TF were considered at risk of infection.
Based on these results and on the census
performed in 2008 [19], the estimated
population at risk was calculated based on
an annual growth of 1.03%. Children
between 1 and 4 years of age and 5 and
14 years of age and pregnant women
between the ages of 15 and 49 represented
14.2%, 26.7%, and 5.0% of the total
population, respectively, as estimated by
the census. Two thirds of the pregnant
women were assumed to be in the 2nd or
3rd trimester of pregnancy.
Programme implementationPartnerships and leadership. In
2007 the Burundian MoH developed a
national NTD working plan and
partnered with various organisations for
implementation of a four-year programme
(2007–2011) (Figure 2). Funding was
provided by the investment group
Legatum [20] and was channelled
through Geneva Global [21], the
international philanthropy adviser to the
Global Network for NTD Control
(GNNTDC) [22], which acted as the
primary awarder. The Schistosomiasis
Control Initiative (SCI) [23,24], an NGO
which has been running NTD control
programmes in Africa since 2003, used its
expertise to assist the Burundian MoH
NTD control programme in developing
action plans. CBM [4], an international
NGO that works on preventing and curing
disabilities, was subcontracted to assist the
NTD control programme by providing
management support.
The MoH provided 20 civil servants
who constituted the NTD team and office
space. The newly formed NTD group
represented a focal point within the MoH
for consolidating partnerships with other
international organizations. These new
partnerships facilitated donation of drugs
such as MBZ and/or albendazole (ALB)
from Feed the Children International,
UNICEF, and Food for the Hungry.
PZQ was purchased by SCI on behalf of
Geneva Global, whereas a partnership
with the International Trachoma Initiative
led to the donation of azithromycin (AZT).
Drug distribution strategies:
Options and opportunities. In 2007,
the existing CDTI structure had been
established in six districts endemic for
onchocerciasis, in Rutana, Bururi, and
Makamba provinces. In contrast, the
MCHW strategy was a national
campaign, occurring twice per year, in
which vitamin supplementation,
vaccinations, and MBZ were distributed
to preschool-age children at health posts
available throughout the country.
Based on these health structures and the
information on NTD coendemicity ob-
tained via the mapping surveys, the MoH
piloted an integrated drug distribution in
December 2007 in which people in areas
endemic for onchocerciasis, SCH, and
STHs received IVM, PZQ, and ALB.
However, the integrated delivery strategy
that used Community Directed Distribu-
tors (CDDs) had to be reviewed for the
following reasons: (a) distribution of addi-
tional drugs was perceived as an increased
workload by volunteer CDDs; hence,
there was a risk that extra incentives
would be requested for delivering addi-
tional drugs, and (b) the CDTI network
only covered 6 districts at that time,
whereas some drugs, such as ALB, had
to be distributed at the national level. The
creation of a CDTI network for the entire
country was not an option as it would have
taken many years and the population
needed to be treated as soon as possible.
The alternate system that was used in
the country, the MCHW, performed
better in terms of geographic coverage.
However, both drug delivery systems,
CDTI and MCHW, did not have school-
age children (SAC) as the primary target
population in the treatment campaigns.
Children between 5 and 14 years of age
are the most affected by schistosomiasis
and to some extent by STHs, and
alternative strategies had to be designed
to specifically target this population. One
option was to use primary schools as drug
distribution points to ensure that SAC
were treated in schools during treatment
campaigns. For SAC not enrolled in
primary schools, possible options were to
make PZQ and ALB available in health
posts where treatments for children (aged
under 5) were already distributed and to
create extra distribution points in areas in
which health posts were far from villages.
To accomplish these treatment goals, the
Ministry of Health and the Ministry of
Education agreed to endorse PZQ and
ALB administration to children in primary
schools during the MCHW. During the
national campaigns, mobile clinics (‘‘sites
avances’’) were also set up to specifically
target SAC that were not enrolled in
schools and for villages located more than
5 km from health posts.
In 2008, the combination of MCHW,
primary school treatments, and mobile
clinics was embraced as the best-perform-
ing strategy for delivering nationwide
antihelmintic treatments to children 1- to
4-years-old (MBZ), SAC (PZQ and ALB),
and mothers (ALB). In areas endemic for
trachoma, azithromycin and tetracycline
distribution was done through health
workers in villages and in health centres.
Distribution of these drugs was not
integrated with other NTD treatment
campaigns as areas at risk of trachoma
were limited; based on the available
epidemiological data, it seemed that only
one round of treatment was required.
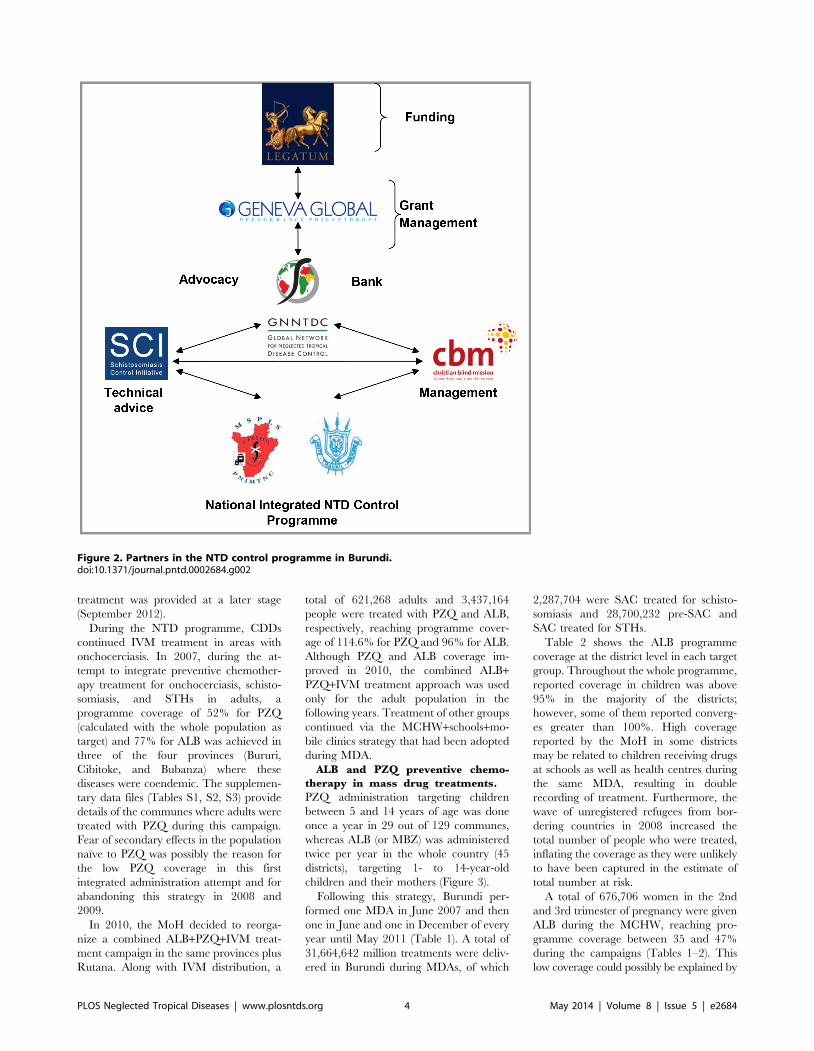
Figure 3 summarizes the delivery strategies
adopted in Burundi during the NTD
programme and their target populations.
Rolling out MCHW, school-based,
and mobile clinic treatment. Imple-
mentation of this innovative strategy
involved several steps: (a) setting up a
committee to engage partners in financing
several activities related to the national
mass drug administration campaign and to
identify potential financial gaps; (b)
training on drug administration proce-
dures; (c) mobilizing the target population
with national media, local leaders (e.g.,
priests and imams), and village chiefs;
(d) dispatching drugs to the district
and commune levels as well as to
schools; (e) launching the mass drug
administration (MDA); (f) supervising
drug distribution activities to monitor
shortages and verify completion of WHO
template treatment forms [25]; and (f)
evaluating the national programme and
geographical drug coverage as per WHO
guidelines [26].
On a daily basis in each district, the
number of people whose treatment was
observed was entered in a database that
was sent to a provincial office and finally
reported to a central office in charge of
combining data from all 45 districts.
Programme managers set an expectation
of reaching 25% coverage on the first day
of the campaign. If coverage was below
this expectation, village chiefs were
alerted and solicited to sensitize the
population.
Trachoma treatment and PZQ,
IVM, and ALB administration in
adults. Treatment for trachoma was
limited to those cases that were found
positive after the rapid assessment
performed in year 2 and the survey
performed in year 3. In year 4, the
programme distributed azithromycin and
tetracycline (TRT) in three of the four
endemic districts (Buhiga, Muyinga, and
Nyabikere) where TF was found above
10%. A total of 668,719 people were
treated, reaching a programme coverage
of 91% (calculated with the whole
population as target) and a geographic
coverage of 75%. For Rutana district,
PLOS Neglected Tropical Diseases | www.plosntds.org 3 May 2014 | Volume 8 | Issue 5 | e2684
treatment was provided at a later stage
(September 2012).
During the NTD programme, CDDs
continued IVM treatment in areas with
onchocerciasis. In 2007, during the at-
tempt to integrate preventive chemother-
apy treatment for onchocerciasis, schisto-
somiasis, and STHs in adults, a
programme coverage of 52% for PZQ
(calculated with the whole population as
target) and 77% for ALB was achieved in
three of the four provinces (Bururi,
Cibitoke, and Bubanza) where these
diseases were coendemic. The supplemen-
tary data files (Tables S1, S2, S3) provide
details of the communes where adults were
treated with PZQ during this campaign.
Fear of secondary effects in the population
naıve to PZQ was possibly the reason for
the low PZQ coverage in this first
integrated administration attempt and for
abandoning this strategy in 2008 and
2009.
In 2010, the MoH decided to reorga-
nize a combined ALB+PZQ+IVM treat-
ment campaign in the same provinces plus
Rutana. Along with IVM distribution, a
total of 621,268 adults and 3,437,164
people were treated with PZQ and ALB,
respectively, reaching programme cover-
age of 114.6% for PZQ and 96% for ALB.
Although PZQ and ALB coverage im-
proved in 2010, the combined ALB+PZQ+IVM treatment approach was used
only for the adult population in the
following years. Treatment of other groups
continued via the MCHW+schools+mo-
bile clinics strategy that had been adopted
during MDA.
ALB and PZQ preventive chemo-
therapy in mass drug treatments.
PZQ administration targeting children
between 5 and 14 years of age was done
once a year in 29 out of 129 communes,
whereas ALB (or MBZ) was administered
twice per year in the whole country (45
districts), targeting 1- to 14-year-old
children and their mothers (Figure 3).
Following this strategy, Burundi per-
formed one MDA in June 2007 and then
one in June and one in December of every
year until May 2011 (Table 1). A total of
31,664,642 million treatments were deliv-
ered in Burundi during MDAs, of which
2,287,704 were SAC treated for schisto-
somiasis and 28,700,232 pre-SAC and
SAC treated for STHs.
Table 2 shows the ALB programme
coverage at the district level in each target
group. Throughout the whole programme,
reported coverage in children was above
95% in the majority of the districts;
however, some of them reported converg-
es greater than 100%. High coverage
reported by the MoH in some districts
may be related to children receiving drugs
at schools as well as health centres during
the same MDA, resulting in double
recording of treatment. Furthermore, the
wave of unregistered refugees from bor-
dering countries in 2008 increased the
total number of people who were treated,
inflating the coverage as they were unlikely
to have been captured in the estimate of
total number at risk.
A total of 676,706 women in the 2nd
and 3rd trimester of pregnancy were given
ALB during the MCHW, reaching pro-
gramme coverage between 35 and 47%
during the campaigns (Tables 1–2). This
low coverage could possibly be explained by
Figure 2. Partners in the NTD control programme in Burundi.doi:10.1371/journal.pntd.0002684.g002
PLOS Neglected Tropical Diseases | www.plosntds.org 4 May 2014 | Volume 8 | Issue 5 | e2684
the fact that during prenatal consultations,
women diagnosed with worm infections
were often advised not to take any drug
during pregnancy. International guidelines
supporting helminth treatment in pregnant
women [27,28] encouraged the government
to offer ALB as a blanket treatment to
pregnant women for free during the
MCHW campaign. However, during this
campaign, women were free to make the
final decision on either taking ALB free of
charge (irrespective of their infection status)
or paying a fee for treatment at the health
centre if infection was found after the
pregnancy was over. Currently the MoH is
looking into new strategies to sensitise
pregnant women to deworming activities.
For PZQ, treatment was limited to 29
communes at risk of infection (Tables S1, S2,
S3). Because treatment decisions were made
at the commune level and the number of
people treated was reported by district, it was
not possible to calculate the geographic
coverage or the programme coverage for
each commune every year. From personal
communications, reported coverage at the
national level for PZQ administration in
school-age children was 87.9%, 92.2%,
114.6%, and 95.9% in MDAs performed in
the years 2008–2011, respectively; however,
it was not clear whether this coverage was
calculated based on the targeted population
at the commune level or at the district level.
Discussion
Opportunities, challenges, andlessons learned
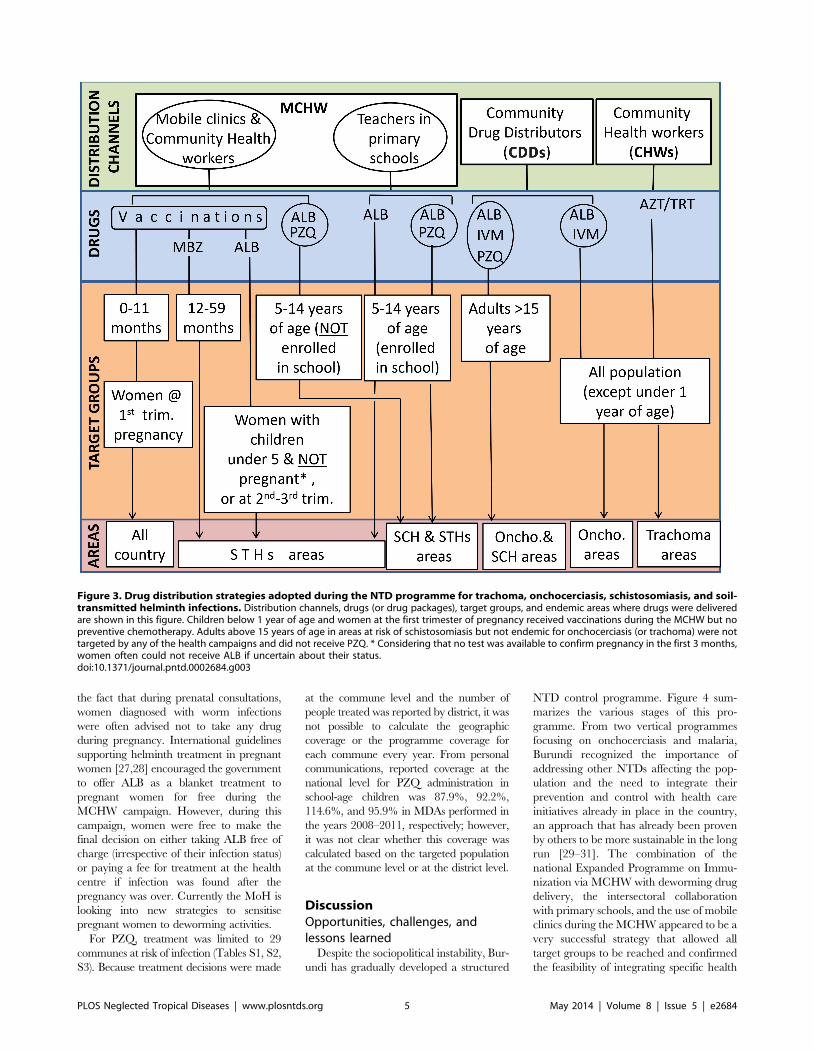
Despite the sociopolitical instability, Bur-
undi has gradually developed a structured
NTD control programme. Figure 4 sum-
marizes the various stages of this pro-
gramme. From two vertical programmes
focusing on onchocerciasis and malaria,
Burundi recognized the importance of
addressing other NTDs affecting the pop-
ulation and the need to integrate their
prevention and control with health care
initiatives already in place in the country,
an approach that has already been proven
by others to be more sustainable in the long
run [29–31]. The combination of the
national Expanded Programme on Immu-
nization via MCHW with deworming drug
delivery, the intersectoral collaboration
with primary schools, and the use of mobile
clinics during the MCHW appeared to be a
very successful strategy that allowed all
target groups to be reached and confirmed
the feasibility of integrating specific health
Figure 3. Drug distribution strategies adopted during the NTD programme for trachoma, onchocerciasis, schistosomiasis, and soil-transmitted helminth infections. Distribution channels, drugs (or drug packages), target groups, and endemic areas where drugs were deliveredare shown in this figure. Children below 1 year of age and women at the first trimester of pregnancy received vaccinations during the MCHW but nopreventive chemotherapy. Adults above 15 years of age in areas at risk of schistosomiasis but not endemic for onchocerciasis (or trachoma) were nottargeted by any of the health campaigns and did not receive PZQ. * Considering that no test was available to confirm pregnancy in the first 3 months,women often could not receive ALB if uncertain about their status.doi:10.1371/journal.pntd.0002684.g003
PLOS Neglected Tropical Diseases | www.plosntds.org 5 May 2014 | Volume 8 | Issue 5 | e2684

Ta
ble
1.
Ind
ivid
ual
str
eat
ed
for
sch
isto
som
iasi
san
dST
Hs
ine
ach
MD
Ain
Bu
run
di.
Ta
rge
tg
rou
p2
00
72
00
8*
20
09
*2
01
02
01
1T
ota
lin
div
idu
als
tre
ate
din
all
MD
As
Jun
eJu
ne
De
cJu
ne
De
cJu
ne
De
cJu
ne
Sch
isto
som
iasi
s(a
ge
gro
up
5–
14
y/o
)
N/A
58
8,2
14
N/A
54
5,9
50
N/A
55
1,7
57
N/A
60
1,7
83
2,2
87
,70
4
ST
Hs
(ag
eg
rou
p1
–4
y/o
)1
,03
7,1
69
99
2,9
81
1,0
58
,03
43
,45
8,0
18
1,0
58
,03
41
,00
5,9
97
3,8
12
,95
81
,16
9,6
69
28
,70
0,2
32
ST
Hs
(ag
eg
rou
p5
–1
4y
/o2
,07
4,1
83
3,1
83
,87
22
,39
3,4
29
2,3
93
,42
92
,51
7,2
75
2,5
45
,18
4
ST
Hs
(pre
gn
an
tw
om
en
—2
nd
/3rd
trim
est
er)
98
,16
91
07
,94
0—
—1
22
,12
41
04
,46
61
23
,36
21
20
,64
56
76
,70
6
To
tal
nu
mb
er
of
ind
ivid
ua
lstr
ea
ted
ea
chy
ea
r
3,2
09
,52
14
,87
3,0
07
3,5
59
,40
34
,00
3,9
68
3,5
73
,58
74
,17
9,4
95
3,9
36
,32
04
,43
7,2
81
31
,66
4,6
42
*In
De
cem
be
r2
00
8an
dJu
ne
20
09
,w
om
en
did
no
tre
ceiv
etr
eat
me
nt.
do
i:10
.13
71
/jo
urn
al.p
ntd
.00
02
68
4.t
00
1
Ta
ble
2.
Pro
gra
mm
eco
vera
ge
for
STH
s.
20
07
a2
00
8b
20
09
b2
01
0c
20
11
d
Ta
rge
tg
rou
pJu
ne
Jun
eD
ec
Jun
eD
ec
Jun
eD
ec
Jun
e
Me
an
SD
Me
an
SD
Me
an
SD
Me
an
SD
Me
an
SD
Me
an
SD
Me
an
SD
Me
an
SD
ST
Hs
(1–
4y
/o)
95
.11
1.4
92
.83
0.0
98
.52
6.6
10
8.0
35
.79
5.6
25
.88
1.8
14
.61
08
.31
6.8
98
.64
1.8
ST
Hs
(5–
14
y/o
)9
8.9
19
.51
60
.04
4.2
11
8.5
30
.51
15
.12
9.6
10
9.1
12
.91
14
.55
1.1
ST
Hs
(pre
gn
an
tw
om
en
—2
nd
/3rd
trim
est
er)
38
.01
3.3
43
.11
8.8
--
--
47
.52
2.3
36
.11
2.5
42
.99
.24
2.0
18
.1
Me
ans
and
stan
dar
dd
evi
atio
ns
(SD
)ar
eca
lcu
late
db
ase
do
nd
istr
ict
pro
gra
mm
eco
vera
ge
rep
ort
ed
by
the
Min
istr
yo
fH
eal
thfo
re
ach
dis
tric
taf
ter
eve
ryM
DA
.P
rog
ram
me
cove
rag
ew
asca
lcu
late
das
the
pro
po
rtio
no
fa
spe
cifi
cg
rou
po
fin
div
idu
als
that
rece
ive
dA
LBo
ver
the
tota
ln
um
be
ro
fin
div
idu
als
wit
hin
that
gro
up
inth
eim
ple
me
nti
ng
un
itd
ee
me
dat
risk
of
STH
infe
ctio
n[2
6].
InD
ece
mb
er
20
08
and
Jun
e2
00
9,
wo
me
nw
ere
no
ttr
eat
ed
.G
eo
gra
ph
icco
vera
ge
for
ALB
was
alw
ays
10
0%
.aIn
20
07
cove
rag
ew
asre
po
rte
db
yp
rovi
nce
(n=
17
).b
Dis
tric
tsN
yab
ike
re,
Gah
om
bo
,B
usi
ni,
and
Vu
mb
id
idn
ot
exi
stas
adm
inis
trat
ive
un
its
in2
00
8–
20
09
(n=
41
).cN
ew
adm
inis
trat
ive
syst
em
incl
ud
ed
45
dis
tric
ts(n
=4
5).
dW
om
en
’sco
vera
ge
was
no
tre
po
rte
din
Jun
e2
01
1fo
rK
ayan
zad
istr
ict.
do
i:10
.13
71
/jo
urn
al.p
ntd
.00
02
68
4.t
00
2
PLOS Neglected Tropical Diseases | www.plosntds.org 6 May 2014 | Volume 8 | Issue 5 | e2684
programmes (such as the NTD control)
with primary health care initiatives. To the
best of our knowledge, only Rwanda
applied a similar drug administration
strategy in those years, when the MoH, in
collaboration with the Access Project [32]
and supported by the same donors [33],
started its NTD prevention and control
programme.
It should be noted that treatment
frequency and areas targeted by the
distribution did not always follow the
standardized international treatment
guidelines [27] or the treatment strategies
suggested by the mapping results. For
instance, for schistosomiasis treatment,
according to the mapping in 2008, 24 out
of 129 communes had a predicted preva-
lence of schistosomiasis between 10 and
50%. This suggested that in those com-
munes SAC and at-risk adults should have
received PZQ every two years. However,
the government opted for a more intense
approach with a higher frequency of
treatment, which seemed to be more
suitable in the national context considering
that (a) MCHW were performed twice a
year so the addition of one or more drugs
did not substantially increase the cost of this
campaign, and (b) poor access to clean
water and sanitation were and still are
major factors contributing to reinfection.
Another example is treatment of adults
in onchocerciasis and schistosomiasis
coendemic areas. This group was treated
with PZQ in coendemic areas in five
communes where the schistosomiasis esti-
mated predicted mean prevalence was
above 10%, as well as in eight of those
in which this prevalence was below 10%.
PZQ administration in these eight com-
munes was not a decision driven by the
schistosomiasis disease burden but by the
CDTI structure already in place, and it
was based more on logistic considerations
than epidemiological reasoning. The risk
of using logistic considerations for drug
distribution may lead, as in this case, to
missing PZQ administration in areas of
the country where only schistosomiasis is
endemic or delivering unneeded PZQ in
areas at low risk of schistosomiasis because
a distribution structure is already in place.
Considering that the global PZQ produc-
tion is based on the number of people in
high-risk areas in need of treatment, drug
delivery in areas at low risk of infection
might adversely affect PZQ availability for
priority groups and people at high risk of
schistosomiasis.
Finally, areas identified for PZQ distri-
bution were also adjusted according to the
current changing context. Fifteen com-
munes with a predicted mean prevalence
.10% and 14 with prevalence of ,10%
(Tables S1, S2, S3) were also treated with
PZQ, leaving nine communes that were at
medium predicted risk with no treatment
based on the improved urban setting of
these communes (e.g., the relatively good
socioeconomic conditions) and environ-
mental factors such as the absence of the
snail host and stagnant water.
For STHs, the MoH decided again to
administer more ALB than international
guidelines suggest: seven, ten, and 28
districts out of 45 had a predicted
prevalence above 50%, between 20 and
50%, and between 10 and 20%, respec-
tively (Tables S1, S2, S3). Based on these
estimates and on the WHO guidelines
available at that time [27], the country
should have delivered ALB in only seven
districts twice a year and ten districts once
a year, with other districts adopting a case
management approach.
The programme presented challenges
from which we have learned important
lessons. For instance, the programme did
not include a thorough supervision at the
lowest implementation level: NTD educa-
tional material that reached health units
did not reach primary schools; likewise,
laboratory technicians in decentralized
health centers that were trained in the
Kato Katz method for detection of worm
infections never received the material for
running this test. Better supervision at the
lowest level of the programme implemen-
tation would have ensured that the
primary beneficiaries were properly
reached and that the main goals of these
activities (education on NTDs for SAC in
the first case and detection and treatment
of infected people in the second example)
would have been achieved.
Finally, Burundi identified the com-
mune, and not the district, as the imple-
menting unit for distributing PZQ. Al-
though this strategy appeared to be very
appropriate, reported coverage calculated
at the district level did not allow a rapid
detection of communes that could have
been missed by the MDA or perhaps did
not require MDA. It would have been
more effective to report programme cov-
erage according to the actual implement-
ing unit (commune) to verify in real time
possible mistakes in drug distribution and
implement the correct measures.
Figure 4. Evolution of the NTD prevention and control programme in Burundi.doi:10.1371/journal.pntd.0002684.g004
PLOS Neglected Tropical Diseases | www.plosntds.org 7 May 2014 | Volume 8 | Issue 5 | e2684

Looking aheadBurundi benefitted greatly from this
NTD programme, which has resulted in
the mapping of the four major NTDs
(schistosomiasis, STHs, LF, and partially
trachoma), delivery of treatments reaching
the population at risk of infections with
good coverage, and a five-year national
plan for NTD prevention and control
endorsed by WHO and validated by the
MoH. The programme has also demon-
strated that the integration of NTD
treatments with other health initiatives,
such as the Expanded Programme of
Immunization and the use of mobile
clinics plus primary schools as additional
distribution sites, is a powerful strategy for
reaching the whole population at risk.
With the current drug donation programs
[34,35] and the continuous financial and
technical support from international
NGOs, especially from UNICEF for the
MCHW campaigns, Burundi is in a
position to complete the mapping of
trachoma in the remaining 24 districts
and to continue MDAs for the major
NTDs affecting the population.
For the sustainability of this NTD
programme and with the final aim of
eliminating these diseases, the initiation of
a multidisciplinary approach involving
other ministries, such as those responsible
for water and sanitation, is paramount. All
these intersectoral initiatives could be
effectively coordinated by the government
to ensure their long-term sustainability.
Coordination and effective management
of intersectoral initiatives could be
achieved by establishing technical groups
within the MoH that would be responsible
for linking specific NTD control needs
with other initiatives relevant to this
programme (e.g., water and sanitation
initiatives). Delegation of these groups for
all technical aspects of the NTD manage-
ment and divulgation of intersectoral work
plans and technical material would be the
next steps to achieve an effective coordi-
nation of multidisciplinary activities.
These steps will imply a shift towards
complete ownership of the NTD pro-
gramme by the MoH.
Meanwhile, effort should be put into the
development of an efficient decentralized
routine surveillance system within the
primary health care structure for effective
case detection, management, and follow-
up care. This step should be taken in
Burundi when disease prevalence has been
reduced and case management replaces
mass drug administration. After initial
technical and financial support from
international stakeholders for building
NTD surveillance capacity, financial com-
mitment of the MoH to maintain this
structure in decentralized areas will ulti-
mately be expected for sustainability of the
NTD prevention, control, and surveillance
program in Burundi.
Supporting Information
Table S1 Burundi administrativeunits in year 2012. Administrative units
in Burundi updated to year 2012 (prov-
inces, districts, and communes).
(XLSX)
Table S2 Estimated risk prevalenceof schistosomiasis in each communeand treatment by commune in 2007–2011. Epidemiological data obtained in
2007 during the mapping were compiled
and integrated with environmental and
country demographic information to obtain
estimated mean prevalence of schistosomi-
asis in each commune. Based on WHO
guidelines (2006), communes were classified
as high, moderate, and low risk of infection.
These data were then used to create maps
predicting areas at risk of schistosomiasis
(see Figure 1). The table also provides
information about praziquantel treatment
and the population targeted in each com-
mune.
(XLSX)
Table S3 Estimated risk preva-lence of soil-transmitted helminthinfections in each district. Epidemio-
logical data obtained in 2007 during the
mapping were compiled and integrated
with environmental and country demo-
graphic information to obtain estimated
mean prevalence of soil-transmitted hel-
minth infections in each district. Based on
WHO guidelines (2006), districts were
classified as high, moderate, and low risk
of infection. These data were then used to
create maps predicting areas at risk of soil-
transmitted helminth infections (see
Figure 1). The table also provides infor-
mation about suggested drug strategies for
each district based on predicted risk and
on WHO guidelines available in 2006.
(XLSX)
Acknowledgments
The authors would like to thank the team of the
Burundian NTD Control programme and its
partners: SCI, CBM, the GNNTDC, and
Geneva Global. Finally, our gratitude is extend-
ed to the health staff, teachers, and communities
without whom this programme could not be
successful.
References
1. World Health Organization (2012) Accelerating
work to overcome the global impact of neglected
tropical diseases—A roadmap for implementa-
tion. Available: http://whqlibdoc.who.int/hq/
2012/WHO_HTM_NTD_2012.1_eng.pdf. Ac-
cessed 1 April 2014.
2. Hotez PJ, Molyneux DH, Fenwick A, Ottesen E,
Ehrlich Sachs S, et al. (2006) Incorporating a
Rapid-Impact Package for Neglected Tropical
Diseases with Programs for HIV/AIDS, Tuber-
culosis, and Malaria. PLoS Med 3: e102.
3. World Health Organization (2014) African Pro-
gramme for Onchocerciasis Control (APOC).
Available: http://www.who.int/blindness/
partnerships/APOC/en/. Accessed 1 April 2014.
4. CBM (2014) CBM – ex Christoffel-Blindmission.
Available: http://www.cbmuk.org.uk/. Accessed
1 April 2014.
5. World Health Organization (2012) African Pro-
gramme for Onchocerciasis Control (APOC)—
Community-directed treatment with ivermectin
(CDTI). Available: http://www.who.int/apoc/
cdti/en/. Accessed 1 April 2014.
6. Engels D, Ndoricimpa J, Gryseels B (1993)
Schistosomiasis mansoni in Burundi: progress in
its control since 1985. Bull World Health Organ
71: 207–214.
7. Engels D, Ndoricimpa J, Nahimana S, Gryseels B
(1994) Control of Schistosoma mansoni and
intestinal helminths: 8-year follow-up of an urban
school programme in Bujumbura, Burundi. Acta
Tropica 58: 127–140.
8. World Health Organzation (2005) Communicable
disease toolkit - Burundi Profile. WHO/CDS/
NTD/DCE/2005.2a. Available: http://www.
who.int/diseasecontrol_emergencies/toolkits/
Burundi_profile_ok.pdf. Accessed 1 April 2014.
9. Dismas B (2005) Rapport d’enquete sur la
situation epidemiologique de la bilharziose dans
les ecoles primaires des provinces endemiques du
Burundi. Burundi: Programme de Lutte contre
les Maladies Transmissibles et Carentielles, Min-
istere de la Sante Publique; Burundi. 44 p.
10. Price EW (1976) Endemic elephantiasis of the
lower legs in Rwanda and Burundi. Trop Geogr
Med 28: 283–290.
11. Ndayishimiye O, Willems J, Manirakiza E, Smith
JL, Gashikanyi R, et al. (2011) Population-based
survey of active trachoma in 11 districts of
Burundi. Ophthalmic Epidemiol 18: 146–149.
12. Gyapong JO, Remme JH (2001) The use of grid
sampling methodology for rapid assessment of the
distribution of bancroftian filariasis. Trans R Soc
Trop Med Hyg 95: 681–686.
13. Gyapong M, Gyapong JO, Owusu-Banahene G
(2001) Community-directed treatment: the way
forward to eliminating lymphatic filariasis as a
public-health problem in Ghana. Ann Trop Med
Parasitol 95: 77–86.
14. World Health Organization (2005) Monitoring
and epidemiological assessment of the pro-
gramme to eliminate lymphatic fi lariasis at
implementation unit level. WHO/CDS/CPE/
CEE/2005.50. Available: http://whqlibdoc.who.
int/hq/2005/who_cds_cpe_cee_2005.50.pdf.
Accessed 1 April 2014.
15. Clements AC, Deville MA, Ndayishimiye O,
Brooker S, Fenwick A (2010) Spatial co-distribu-
tion of neglected tropical diseases in the east
African great lakes region: revisiting the justifica-
tion for integrated control. Trop Med Int Health
15: 198–207.
16. World Health Organization (2001) Guidelines for
rapid assessment for bliding trachoma. WHO/
PBD/GET/00.8. Available: http://www.who.
PLOS Neglected Tropical Diseases | www.plosntds.org 8 May 2014 | Volume 8 | Issue 5 | e2684

int/blindness/TRA-ENGLISH.pdf. Accessed 1
April 2014.17. Thylefors B, Dawson CR, Jones BR, West SK,
Taylor HR (1987) A simple system for the
assessment of trachoma and its complications.Bull World Health Organ 65: 477–483.
18. Jeremiah Ngondi MR, Fiona Matthews, CarolBrayne, Paul Emerson (2009) Trachoma survey
methods: a literature review. Bull World Health
Organ 87: 143–151.19. Ministry of Health, Burundi, Burundi (2010)
Troisieme recensement general de la populationet de l’habitat de 2008. Available: http://www.
paris21.org/sites/default/files/BURUNDI-population-2008.PDF. Accessed 1 April 2014.
20. Legatum Foundation (2014) Legatum Founda-
tion. Available: http://www.legatum.com/foundation. Accessed 1 April 2014.
21. Geneva Global (2012) GENEVA GLOBAL—Performance philanthropy. Available: http://
www.genevaglobal.com/. Accessed 1 April 2014.
22. Sabin Vaccine Institute (2014) GNNTD GlobalNetwork of Neglected Tropical Diseases. Avail-
able: http://www.globalnetwork.org/. Accessed 1April 2014.
23. Fenwick A, Webster JP, Bosque-Oliva E, Blair L,Fleming FM, et al. (2009) The Schistosomiasis
Control Initiative (SCI): rationale, development
and implementation from 2002–2008. Parasitol-
ogy 136: 1719–1730.24. Garba A, Toure S, Dembele R, Boisier P, Tohon
Z, et al. (2009) Present and future schistosomiasis
control activities with support from the Schisto-somiasis Control Initiative in West Africa. Para-
sitology 136: 1731–1737.25. World Health Organization (2011) Helminth
control in school-age children. A guide for
programme managers of control programmes.A v a i l a b l e : h t t p : // w h q l i bd o c . w h o . i n t /
publications/2011/9789241548267_eng.pdf. Ac-cessed 1 April 2014.
26. World Health Organization (2010) Monitoringdrug coverage for preventive chemotherapy.
A v a i l a b l e : h t tp :/ / w h q l ib do c . w h o . i n t /
publications/2010/9789241599993_eng.pdf. Ac-cessed 1 April 2014.
27. World Health Organization (2006) Preventivechemotherapy in human helminthiasis. Available:
http://whqlibdoc.who.int/publications/2006/
9241547103_eng.pdf. Accessed 1 April 2014.28. World Health Organization (1994) Informal
consultation on hookworm infection and anaemiain girls and women. WHO/CTD/SIP/96.1.
Available: http://whqlibdoc.who.int/hq/1996/WHO_CTD_SIP_96.1.pdf. Accessed 1 April
2014.
29. Utzinger J, Raso G, Brooker S, De Savigny D,
Tanner M, et al. (2009) Schistosomiasis andneglected tropical diseases: towards integrated
and sustainable control and a word of caution.
Parasitology 136: 1859–1874.30. Zhang Y, MacArthur C, Mubila L, Baker S
(2010) Control of neglected tropical diseasesneeds a long-term commitment. BMC Med 8: 67.
31. Dembele M, Bamani S, Dembele R, Traore MO,
Goita S, et al. (2012) Implementing preventivechemotherapy through an integrated National
Neglected Tropical Disease Control Program inMali. PLoS Negl Trop Dis 6: e1574.
32. ACCESS (2009) Project Access—Annual Report.Available: http://tap.pmhclients.com/images/
u p l o a d s / p r e s s / A N N U A L _ R E P O R T _
19FEB10b.pdf. Accessed 1 April 2014.33. Ruxin J, Negin J (2012) Removing the neglect from
neglected tropical diseases: the Rwandan experi-ence 2008–2010. Glob Public Health 7: 812–822.
34. Gustavsen KM, Bradley MH, Wright AL (2009)
GlaxoSmithKline and Merck: private-sector col-laboration for the elimination of lymphatic filari-
asis. Ann Trop Med Parasitol 103 Suppl 1: S11–5.35. MerckGroup (2012) Global Health Progress.
Available: http://www.globalhealthprogress.org/programs/merck-praziquante l -donat ion-
program. Accessed 1 April 2014.
PLOS Neglected Tropical Diseases | www.plosntds.org 9 May 2014 | Volume 8 | Issue 5 | e2684