Contributions of Music to aging adults' quality of life
19
Journal of Music Therapy, XLVII (3), 2010, 264-281 © 2010 by the American Music Therapy Association Contributions of Music to Aging Adults' Quality of Life Carme Solé, PhD Melissa Mercadal-Brotons, PhD, MT-BC Sofia Gallego, PhD Mariangels Riera, PhD Universität Ramon LIull Barcelona The purpose of this study was: (a) To evaluate and to compare the impact of three music programs (choir, music appreciation and preventive music therapy sessions) on the quality of life of healthy older adults, and (b) to identify the motivations and the difficulties that seniors encounter when participating in activities of this type, in order to come up with recommendations and strategies for the design of appropriate programs for older adults. A pre-posttest quasi- experimental design without equivalent control group was used in this project The sample included 83 persons over 65 years of age. The data collection was carried out through an ad hoc questionnaire that included the four aspects of the construct of quality of life (physical health, subjective health, psychological well-being and interpersonal relations), a questionnaire on motivation and another on satisfaction about the program. This questionnaire on quality of life was administered twice: at the beginning of the programs (pretest) and at the end (posttest). The results of this study indicate that the participants perceived improvements in some aspects of their quality of life. In addition, the main reasons which motivate participation in these musical activities are to broaden the social network and to acquire new knowledge. The results are discussed in the light of the challenges of active and satisfactory aging. This research was stipported by a grant from Obra Social Caixa de Sabadell awarded to CREDEFl (Croup de Recerca en Envelliment: Desenvolupament, Formació i Intervenció—Research group on Aging: Development, Education and intervention)
Transcript of Contributions of Music to aging adults' quality of life

Journal of Music Therapy, XLVII (3), 2010, 264-281© 2010 by the American Music Therapy Association
Contributions of Music to Aging Adults'Quality of Life
Carme Solé, PhDMelissa Mercadal-Brotons, PhD, MT-BCSofia Gallego, PhDMariangels Riera, PhD
Universität Ramon LIullBarcelona
The purpose of this study was: (a) To evaluate and tocompare the impact of three music programs (choir, musicappreciation and preventive music therapy sessions) on thequality of life of healthy older adults, and (b) to identify themotivations and the difficulties that seniors encounter whenparticipating in activities of this type, in order to come upwith recommendations and strategies for the design ofappropriate programs for older adults. A pre-posttest quasi-experimental design without equivalent control group wasused in this project The sample included 83 persons over65 years of age. The data collection was carried out throughan ad hoc questionnaire that included the four aspects of theconstruct of quality of life (physical health, subjective health,psychological well-being and interpersonal relations), aquestionnaire on motivation and another on satisfactionabout the program. This questionnaire on quality of life wasadministered twice: at the beginning of the programs(pretest) and at the end (posttest). The results of this studyindicate that the participants perceived improvements insome aspects of their quality of life. In addition, the mainreasons which motivate participation in these musicalactivities are to broaden the social network and to acquirenew knowledge. The results are discussed in the light of thechallenges of active and satisfactory aging.
This research was stipported by a grant from Obra Social Caixa de Sabadellawarded to CREDEFl (Croup de Recerca en Envelliment: Desenvolupament,Formació i Intervenció—Research group on Aging: Development, Education andintervention)

Vol. XLVII, No. 3, Fall 2010 265
The presence of older people in the developed world, and inmany developing countries, is increasing rapidly (United Nations,2007). The United Nations projects that by 2050, 79% of thepopulation aged 60 years or over, amounting to nearly 1.6 billionwill reside in those countries. However, the size of the elderlypopulation and the speed of population aging vaiy across regions.Europe has the highest proportion of people aged 65 atid older(16%), but the older population is growing fastest in severalcountries in East and Southeast Asia (The National Institute onAging, 2007).
Today, in Spain the number of people older than 65 represents16,6% of the population, and the population projections of theUnited Nations for the year 2050 indicate that this countiy will bethird in the world with older people reaching 34,1% of thepopulation, after Japan (35.9%) and Italy (35.5%) {InformePersonas Mayores Imserso, 2004). This noticeable increase in peopleolder than 65 accentuates the need to establish actions andprograms to contribute to their quality of life. In this sense, manycountries, including Spain, are working towards promoting anactive and satisfactory aging process.
Active aging is defined as "the process of optimizing theopportunities for physical, cognitive, and social wellbeingthroughout life with the objective of increasing a healthy lifeexpectancy, productivity and quality of life in older age" (OMS,2002, p. 12). It is important to offer this population not only thepossibility to remain physically active, but also the opportunity toparticipate in social, economic, cultural, spiritual, and civicactivities throughout later life.
Another irnportant concept is that of satisfactory or successfulaging. Rowe and Kahn (1997) indicate that although there is nofixed pattern of sticcessftil aging, the following characteristicstend to be involved:
1. A low probability of suffering diseases and disabilitiesassociated with aging (health and ability).
2. A high level of physical and cognitive functioning. An activeimplication and commitment towards life. The development ofa specific set of activities.
Successful aging, as Rowe and Kahn (1997) explain, can berelated to two types of basic activities:
266 Journal of Music Therapy
1. Social activities, which are those activities that are able tomaintain pleasant interpersonal relations, and therefore,facilitate a socially healthy and independent life style.
2. Productive activities, which are those that are similarly capableof contributing to the maintenance of social life or personalgrowth. In this category, educational activities are important.
With regard to the educational activities, recent studies indicatethat older people can learn new things, and do them well(Mehrota, 2003). To be active and be part of social activities has apositive impact on the wellbeing of older people, particularly at atime of their lives when they are exposed to a number of loses(professional role—retirement, changes in social circles, loss ofspouses ...). The relationship with other people is a goodpredictor of wellbeing and quality of life.
Quality of life is understood as a multidimensional concept,consisting of the same dimensions for all people. It isinfluenced by environmental and personal factors and theirinteraction, and it is improved through self-determination,resources, inclusion and goals in life. Several authors havetheorized and written on the concept of quality of life. Shalockand Verdugo (2002) indicate that quality of life is a conceptthat refiects a person's desired life conditions in relation toeight basic needs which represent the nucleus of each person'slife dimensions: emotional wellbeing, interpersonal relations,material wellbeing, personal development, physical wellbeing,self-determination, social inclusion, and rights. In this study thefocus will be on four of the dimensions of quality of life:physical health, subjective health, emotional wellbeing andinterpersonal relations.
In 1978 the Spanish Cultural Ministry, having become aware ofthe need to promote continuing education for older people,initiated the program of Aules de la Tercera Edat (ATE) (SeniorsUniversity Programs). These programs are aimed towards peopleolder than 55 and intend to respond to their cultural demands,and their wish to improve knowledge and keep up to date(Manheimer, 2002; Manheimer & Moskow-Mackenzie, 1995).Thus, the programs serve as elements of social transformation andas a means of preserving dignity and improving their quality oflife. They intend to act in two directions:
Vol. XLVII, No. 3, Fall 2010 267
1. Cultural. They intend to generate individual and communitycapacity to live better and to have a more productive andcreative leisure time.
2. Social. The main objective is to give older people the possibilityto become integrated in groups; to promote their participationand recognition in the social task, and to collaborate with thoseinstitutions which carry out research on older people.
These classrooms for older people become meeting points,spaces for dialogue, participation, and education through recrea-tional, educational, and cultural activities These classrooms forolder people become meeting points, spaces for dialogue,participation, and education through recreational, educational,and cultural activities (Jams & Walker, 1997). Older people havethe opportunity to expand and enrich their interpersonal relations,to participate in the management and promotion of culture.
Aging is accompanied by a decline in functioning, at thephysiological and psychological level. One of the consequencesthat many older people have to face as they age is an increase insocial isolation. Providing an environment that maximizes andprolongs functioning and promotes independence and well-beingfor as long as possible is recommended for this age group (Onishiet al., 2006).
There is ample literature reporting on the itnportance andbenefits of music for older adults (Cohen, Bailey, & Nilsson, 2002;McCaffrey, 2008; Prickett, 2000; Ruud, 1997). Listening to musicappears to be rated as a very pleasant experience by older adultssince it promotes relaxation, decreases anxiety and distractspeople from unpleasant experiences (Cutshall et al., 2007). Thecontributions of music to the quality of life and to life satisfactionof older people have been a topic of interest for researchers forsome time (Vanderak, Newman, & Bell, 1983). Coffman (2002)reports that music activities (both passive and active) can affectolder adults' perceptions of their quality of life, placing a strongvalue on the non-musical dimensions of being involved in musicactivities such as physieal, psyehological and social aspects. Musicappears to be a source of entertainment, an activity that allowsolder people to interact with others and share aspects of their life,and gives them an opportunity to connect with a sense ofspirituality (Hays & Minichiello, 2005).
268 Journal of Music Therapy
Research up to the present time highlights some of the generalbenefits of music with older adults and supports its inclusion intheir lives. However, some aspects still remain unanswered. Thepurpose of this study was: (a) To evaluate and to compare theimpact of three music programs (choir, music appreciation andpreventive music therapy sessions) on four dimensions of thequality of life of healthy older adults, and (b) to identify themotivations and the difficulties that seniors encounter whenparticipating in activities of this type, in order to come up withrecommendations and strategies for the design of appropriateprograms for older adults.
Secondary objectives included:
1. To learn about the social-demographic profile of older adultsthat participated in the three different music programs.
2. To evaluate the level of satisfaction with the different programs.
Method
Subjects
A total of 83 people who enrolled in one of three different typesof music activities in the Barcelona area participated in the study.The music activities included ran from October to June(approximately an academic year) and were the following: choir(n = 52), music appreciation class (w = 19), and a preventivemusic therapy program (PMTP) (n = 12). The mean age for theparticipants was of 72.6 years {SD = 6.91), and 83.13% (n = 69)were women and 16.87% (n = 14) were men. The participantshad to meet the following criteria to be included in the project:(a) to live at home, (b) to maintain an independent life, and (c)not to have any major cognitive impairment.
Participants were recruited from a variety of senior centers fromthe Barcelona area that offer different educational, recreationaland cultural activities for older adults. The subjects were enrolledin one of the three music programs: choir, music appreciation orpreventive music therapy.
Instruments
Quality of life was evaluated twice: (a) during the first month ofthe activity (pretest), and 2 weeks before the end of the activity(posttest). The instruments used to collect the data included:
Vol. XLVII, No. 3, Fall 2010 269
1. A researcher-designed questionnaire (Villar et al., 2006) tocollect subjects' demographic information and their reasonsfor enrolling in the different programs. The section onmotivation to participate in the program included 23 itemsgrouped in four main factors: cognitive, social, family related,evasive (avoidance of present problematic situations). Thisquestionnaire included a Likert scale (1-4) and was adminis-tered only in the pretest.
2. Questionnaire on Quality of Life (combination of standardizedtests and researcher-designed questionnaire). This question-naire included four components of this construct: physicalhealth, subjective health, psychological well-being, and inter-personal relations. In order to measure the participant'sphysical health, the questionnaire included items related todays of hospitalization or days of required rest in bed or athome in the last year, and also qtiestions on activities of dailyliving (ADL). With regard to subjective and comparativehealth, subjects had to respond to questions related to theirgeneral health, and its comparison with the health of otherpeople.
In order to measure psychological well-being, a subscale of theCUBRECAVI Quality of Life questionnaire (Fernadez-Ballesteros &Zamairón, 1996) was used in addition to the Rosenberg's self concepttest (Rosenberg, 1965), and the Yesavage depression scale(Yesavage et al, 1982). The Philadelphia Geriatric Scale (PCC)(Lawton, 1975) was used to evaluate life satisfaction. The PCC hasbeen validated and standardized with the Spanish population byStock, Okun, and Gómez (1994).
3. The interpersonal relations factor was measured through aresearcher-designed questionnaire that included five questionsin which the participants had to specify how often theyparticipated in different programs or if they were part ofspecific organizations for older adults.
4. At the posttest, besides the Quality of Life scales, participantsalso filled out a researcher-designed questionnaire to evaluatetheir perception of change in their lives in regards to physicalhealth, self-satisfaction, family relations, activity, friendships,life enjoyment and feelings of usefulness. Participants alsofilled out a questionnaire to evaluate their level of satisfaction
270 Journal of Music Therapy
with different components of the programs: teachers, con-cepts, timing, participation, relationship with other partici-pants, equipment, organization of the program, and overallsatisfaction. In addition, the participants had to evaluate thedifficulties they had encountered to access the chosen musicprogram.
Procedure
The different music activities had the following characteristics:
1. Choir for older adults. Participants in this activity met once aweek to prepare a repertoire of songs to be performed in aconcert. The aim was totally recreational while people acquireand practice some music abilities.
2. Music appreciation class. Participants enrolled in this activitymet once a week to learn basic music concepts. The aim wasprimarily educational.
3. Preventive music therapy. Participants in this activity receivedmusic therapy once a week to work on and practice functionalskills at the physical, cognitive, and social-emotional levelsthrough music. It had a preventive focus, promoting themaintenance of functions by practicing and rehearsing themthrough music activities.
Participants' assistance was monitored by the professionals thatconducted the music activities, in order to assure continuity andregularity in the' activity.
A pre-posttest quasi-experimental design without equivalentcontrol group was used in this project. After having establishedinitial contact with the people in charge of the different programsand obtaining their permission, the researchers explained theaims of the project to the potential participants. Generalinstructions on how to fill out the questionnaires were givensome time before the beginning of a class. Then, the question-naires that were to be filled-in individually were handed out to theparticipants, assuring them that their participation was totallyvoluntary. The following week, the researchers went back to theclassrooms to pick up the completed questionnaires. This sameprocedure was repeated at the end of the program 8 months later.A total of 27 posttest questionnaires were not returned (choir =
Vol. XLVII, No. 3, Fall 2010 271
12, music appreciation class = 10, preventive music therapyprogram = 5).
Results
Descriptive Analyses
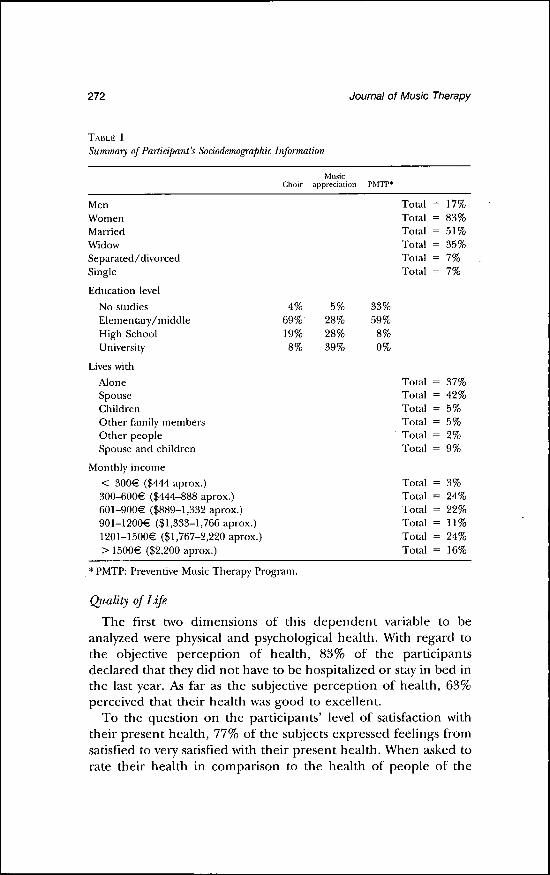
Data were analyzed by the Statistical Package for the SocialSciences (SPSS) 17.0 by an independent statistician. The finalsample included 83 subjects, although the initial sample included101. Table 1 shows a summary of the subjects' socio-demographicinformation. According to these results, the percentage of women(83%) that participated in music activities within the populationof older adults was much higher than men (17%). Likewise, thepercentages of people who were married (51%) or widowed(35%) were higher than those who were single (7%) or divorced(7%).
In general, the educational level of the participants in this studyis of primary/elementary school. However, the participants in themusic appreciation class have a more diverse educational levelthan the participants in the other two music programs.
With regard to the people with whom these subjects live, it canbe observed that living with the spouse (42%) is more commonthan living alone or with other family members in this group ofsubjects.
Regarding monthly income, considering quantities higher than900€ ($1,332 approx.) per month, more participants in thechoral activity had higher incomes (67%) than those in the musicappreciation class (63%) or the PMTP (17%).
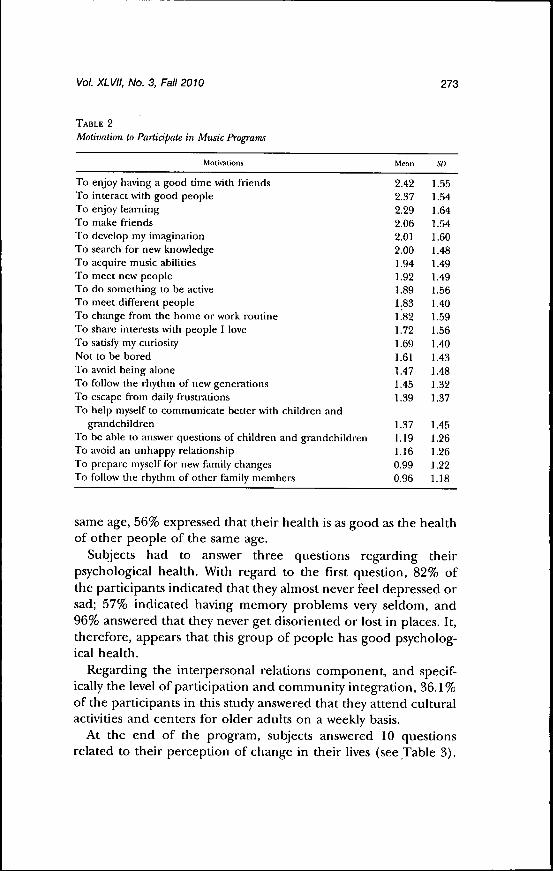
Another portion of the questionnaire that was analyzeddescriptively was the portion on reasons why participants enrolledin these three different types of music activities (see Table 2). Thetype of motivation that the participants rated most were socialreasons ("to have a good time with friends," "be amongst pleasantpeople," and "to make friends") and cognitive reasotis ("to enjoylearning," "to develop my imagination," "to look for newknowledge") as the main motives for participadtig in theseactivities. The lowest ratings referred to family related motives("to follow the rhythm of other family members," "to preparemyself for new family changes," "to be able to answer questions tochildren and grandchildren.").
272 Joumal of Music Therapy
TABLE 1
Summary of Participant's Sododemographic Information
ChoirMvisic
appreciation PMTP*
MenWomenMarriedWidowSeparated/divorcedSingle
Education levelNo studiesElementary/middleHigh SchoolUniversity
Lives withAloneSpouseChildrenOther family membersOther peopleSpotise and children
Monthly income< 300€ ($444 aprox.)300-600€ ($444-888 aprox.)601-900€ ($889-1,332 aprox.)901-1200€ ($1,333-1,766 aprox.)1201-1500€ ($1,767-2,220 aprox.)> 1500€ ($2,200 aprox.)
19%
5%28%28%39%
33%59%
8%0%
TotalTotalTotalTotalTotalTotal
= 179?
= 839?
= 519?
= 359?
= 7%
= 7%
TotalTotalTotalTotalTotalTotal
TotalTotalTotalTotalTotalTotal
= 37%
= 5%
22%11%24%
* PMTP: Prevendve Music Therapy Program.
Quality of Life
The first two dimensions of this dependent variable to beanalyzed were physical and psychological health. With regard tothe objective perception of health, 83% of the participantsdeclared that they did not have to be hospitalized or stay in bed inthe last year. As far as the subjective perception of health, 63%perceived that their health was good to excellent.
To the question on the participants' level of satisfaction withtheir present health, 77% of the subjects expressed feelings fromsatisfied to very satisfied with their present health. When asked torate their health in comparison to the health of people of the
Vol. XLVII, No. 3, Fall 2010 273
TABLE 2
Motivation to Participate in Music Programs
Motivations Mean St)
To enjoy having a good time with friendsTo interact with good peopleTo enjoy learningTo make friendsTo develop my imaginationTo search for new knowledgeTo acquire music abilitiesTo meet new peopleTo do something to be activeTo meet different peopleTo change from the home or work routineTo share interests with people I loveTo satisfy my ctiriosityNot to be boredTo avoid being aloneTo follow the rhythm of new generationsTo escape from daily frustrationsTo help myself to communicate better with children and
grandchildrenTo be able to answer qtiestions of children and grandchildrenTo avoid an unhappy relationshipTo prepare myself for new family changesTo follow the rhythm of other family members
same age, 56% expressed that their health is as good as the healthof other people of the same age.
Subjects had to answer three questions regarding theirpsychological health. With regard to the first question, 82% ofthe participants indicated that they almost never feel depressed orsad; 57% indicated having memory problems very seldom, and96% answered that they never get disoriented or lost in places. It,therefore, appears that this group of people has good psycholog-ical health.
Regarding the interpersonal relations component, and specif-ically the level of participation and community integration, 36.1%of the participants in this study answered that they attend culturalactivities and centers for older adults on a weekly basis.
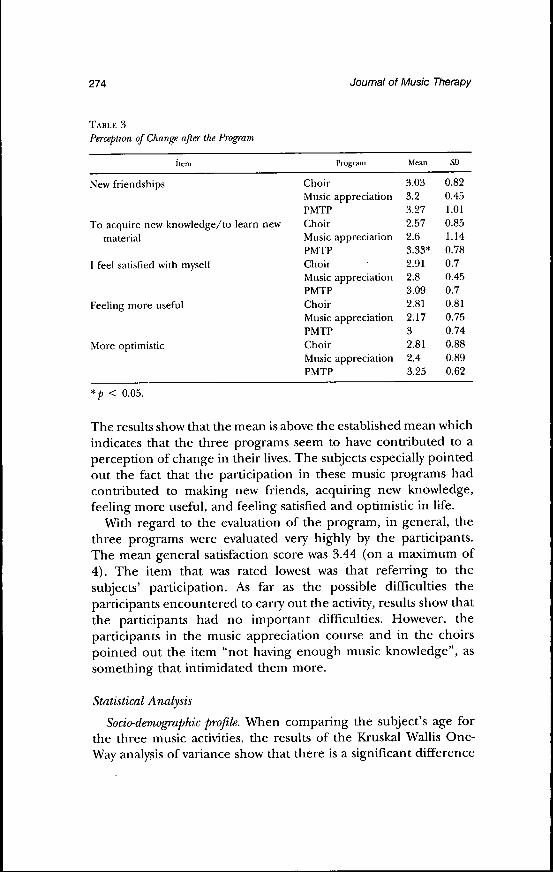
At the end of the program, subjects answered 10 questionsrelated to their perception of change in their lives (see Table 3).
2.422.372.292.062.012.001.941.921.891.831.821.721.691.611.471.451.39
1.371.191.160.990.96
1.551.541.641.541.601.481.491.491.56.40.59
1.56.40.43.48.32.37
.45
.26
.26
.22
.18
274 Journal of Music Therapy
TABLE 3
Perception of Change after the Program
Program Mean
New friendships
To acquire new knowledge/to learnmaterial
I feel satisfied with myself
Eeeling more useful
More optimistic
Choir 3.03 0.82Music appreciation 3.2 0.45PMTP 3.27 1.01
new Choir 2.57 0.85Music appreciation 2.6 1.14PMTP 3.33* 0.78Choir 2.91 0.7Music appreciation 2.8 0.45PMTP 3.09 0.7Choir 2.81 0.81Music appreciation 2.17 0.75PMTP 3 0.74Choir 2.81 0.88Music appreciation 2.4 0.89PMTP 3.25 0.62
*p < 0.05.
The results show that the mean is above the established mean whichindicates that the three programs seem to have contributed to aperception of change in their lives. The subjects especially pointedout the fact that the participation in these music programs hadcontributed to making new friends, acquiring new knowledge,feeling more useful, and feeling satisfied and optimistic in life.
With regard to the evaluation of the program, in general, thethree programs were evaluated very highly by the participants.The mean general satisfaction score was 5.44 (on a maximum of4). The item that was rated lowest was that referring to thesubjects' participation. As far as the possible difficulties theparticipants encountered to carry out the activity, results show thatthe participants had no important difficulties. However, theparticipants in the music appreciation course and in the choirspointed out the item "not having enough music knowledge", assomething that intimidated them more.
Statistical Analysis
Sodo-demographic profile. When comparing the subject's age forthe three music activities, the results of the Kruskal Wallis One-Way analysis of variance show that there is a significant difference
Vol. XLVII, No. 3, Fall 2010 275
TABLE 4
Pre and Posttest Mean Scores and Standard Deviations of the Standardized Scales
Test
Depression PretestDepression PosttestSelf-concept PretestSelf-concept PosttestLife Satisfaction PretestLife Satisfaction Posttest
Mean
45.0443.46*25.8426.3542.3043.84
SI)
10.146.925.464.908.378.37
*A decrease in mean score of the Depression Scale, means an improvement indepression from pre to posttest. The scores of the other two scales show animprovement (higher scores) from pre to posttest.
between the age of the participants in the PMTP and the age ofthe choral groups, the subjects in the PMPT being older thanthose in the choral groups {H = 6.84, df = 2, p < 0.05).
With regard to marital status, there is a significant differencebetween the number of married people in the choral group andin the PMTP (x'̂ = 12.57, df = 2, p < 0.01). There were moremarried people in the choral groups than in the PMTP.
Quality of Life
Pretest. When comparing the answers among subjects in the threemusic activities to the questions related to physical healthperception, results show that there are more participants in thePMTP that perceive their health from good to excellent (x^ =7.03, df = 2,p< 0.05).
From the three questions evaluated with regard to thepsychological health, the question that presents significantdifferences among the three music activities is that referringto "feeling depressed, sad, anxious ....", which seem to affectmore the participants of the PMTP {H = 8.92, df = 2, p <0.05).
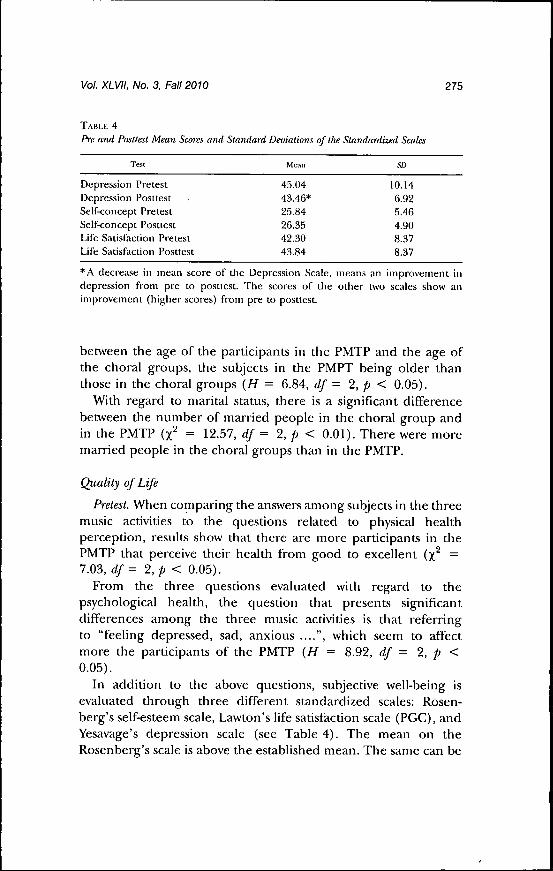
In addition to the above questions, subjective well-being isevaluated through three different standardized scales: Rosen-berg's self-esteem scale, Lawton's life satisfaction scale (PGC), andYesavage's depression scale (see Table 4). The mean on theRosenberg's scale is above the established mean. The same can be

276 Journal of Music Therapy
observed with the Lawton's scores. It is important to mention thatonly the question "You feel less useful as you get older", wasscored slightly below the mean by the participants in this study.Regarding the depression scale, according to the results, it can bestated that there are no symptoms of depression among thesubjects in this study. In addition, the results of the t Tests forrepeated measures show no significant differences between thepretest and the posttest scores for the Rosenberg's self-esteem test(i = -.70, df = 48, p = .49), the Yesavage's depression scale(t = 1.14, df = 51, p = .26) and the Lawton's life satisfactionscale [t = -1.19, df = 49, p = .24).
At the posttest, in the questions related to perceived change intheir lives because of their participation in the three differentmusic programs, the participants in the PMTP score higher inthe item "It helps me to learn new material" (H = 6.46, df = 2,p <.O5).
Conclusions
Everybody is able to learn throughout life, and everybodyshould have the opportunity to keep their knowledge up to date,or to acquire new knowledge. In this project, the focus has beenon musical activities, specifically music appreciation classes, choralgroups and preventive music therapy programs. The impact ofmusic on the quality of life of older adults has been studied,specifically on four aspects of this construct: physical wellbeing(physical health, subjective health), psychological/emotionalwellbeing and interpersonal relations.
One important aspect to highlight is the difference in numberof participants among the three different music activities. Choralsinging is an activity which culturally imbedded, particularlyamong older people, and is offered in the majority of leisurecenter for the aged. On the other hand, music appreciation andpreventive music therapy programs are newer and uncommon,which may explain why they attract less participation.
According to the objectives addressed, the following conclu-sions can be drawn:
Objective 1. To learn about the socio-demographic profile ofolder adults who participate in three musical programs (adultchoirs, music appreciation courses and preventive music therapyprograms).
Vol. XLVII, No. 3, Fall 2010 277
With regard to age, genre and marital status, it is important topoint out that the studied sample has the following profile: retiredpeople and mainly married women. These results are similar tothose of previous studies where the majority of people that areinvolved in educational activities are also married women (Villaret al., 2006, 2007).
As far as the level of education is concerned, this sampleincludes people with an elementary level of studies. Percentagesindicate that very few people have university studies or no studiesat all. In this case, the results are not in concordance with previousstudies in which the participants have a high level of studies.Perhaps one explanation is the fact that previous studies weredone in different settings and with people that attended universityprograms and not cultural programs which are offered from civicand senior centers. Another explanation is the fact that music is avery inclusive and familiar type of activity, easily adaptable todifferent levels of education and functioning. Therefore, theeducation level of the participants is not as important (Davis,Gfeller, & Thaut, 2000).
Regarding the economic variable, the results show that themean level of monthly income is between 900-1200€ ($1,332-1,766, approx.). The differences in income among the partiei-pants in the different programs are not signifieant although theincome of the people involved in choral groups is slighdy higher,and the income level of the participants in the PMTP is notablylow. The fact that all the participants in the PMTP belong to thesame city area (a low-income area) may have affected theseresults.
Objective 2. To identify the motivations of older adults to getinvolved in music activities. The main conclusion that can bereached from the results is that there is no single motive forparticipating in a music program, although some reasons appearto be more important than others. According to the quantitativemeasures, the main reasons for which older adults enroll in musicprograms (choir, music appreciation course or PMPT) are: (a) thepossibility to meet new people and to create new friendships. Thatis, the social component is one of the main reasons thatencourage older adults to enroll in activities; and (b) the needto learn more about music (cognitive component). A consider-able number of people expressed their interest in music.

278 Journal of Music Therapy
especially the participants in the music appreciation course inwhich the sessions take a more theoretical approach.
On the other hand, the types of motivation that are lessimportant to enroll in these different programs are family related.It appears that these people do not have the need to be a part of amusic activity as a form of evasion or as a means of being a part ofan activity that simply fills out their time. Those involved in thechoral groups also expressed the fact that they enjoy singing.
Objective 3. To learn about the level of satisfaction with thedifferent programs and to identify the difficulties or barriers thatthey encounter to do them. It can be concluded that, accordingto the data, the participants rated the three programs very highly.All the different aspects evaluated (teachers, content, timededicated, relationship among participants, space and organiza-tion of the activity) were rated very positively. The componentthat was rated lowest was the subjects' participation (less initiative,less implication, not to take the activity seriously enough). Ingeneral, this perception is equal in all three programs. It appearsthat the majority of participants would like to see moreimplication of their peers in the music activities. The fact thatall these activities take place in civic and senior centers (leisurecenters which are less demanding in terms of performance andimplication), does not encourage students' implication, unlikewhat can be observed in seniors university programs whereattendance and implication are monitored very closely, with themotivator being intellectual enlightenment. The activities evalu-ated in this study are possibly seen more as recreational ratherthan formal activities.
At the qualitative level (open questions), the participants pointout that the best component of the activity is the fact that theyenjoy music very much, and the comradeship that these activitiesgenerate. Regarding aspects about the programs to be improved,they named their participation, as has been mentioned inprevious studies (Hays & Minichiello, 2005).
Difficulties and barriers that the participants come across whencarrying out these activities are, in general, not very relevant. Theonly aspect in which significant differences have been observed is"not to have enough music knowledge", especially in theprogram of music appreciation and choral groups. It is evidentthat more music knowledge is helpful to get more out of the
Vol. XLVII, No. 3, Fall 2010 279
activity although this is not an essential requirement toparticipate in it.
Objective 4. To identify potential changes in quality of life. Oneof the main objectives of this study was to observe and to evaluateif the participation of healthy older adults in three different musicprograms (choral, music appreciation, & PMTP) contributed totheir quality of life. According to the results, it can be stated thatthere are no substantial changes in quality of life between thepretest and the posttest scores. It is important to mention thataccording to the scores of the different subscales, it can beobserved that the initial scores of the different aspects involved inthe quality of life were already very high. This implies that themargin for change was small. That is to say, the subjects thatparticipated in this study already had a good quality of life beforeinitiating any of the music programs. What can be said, though, isthat participating in these programs helped to maintain it.Despite these results, the participants' subjective perception wasthat being involved in these programs improved some compo-nents of their quality of life, especially in social relations (morefriends) and in personal development.
To conclude, it is emphasized that this study is a first step thathas allowed us to gather preliminary data which needs to bereplicated in the future with more systematic studies and withlarger and more varied samples. In addition, the authors see theneed to add semi-structured interviews in future projects in orderto give the participants the possibility to express the changes theyperceive as a consequence of participating in music activities. Thestandardized tests might not pick up these more subtle perceivedchanges, especially in the emotional/affective area.
In general, as has been mentioned in previous studies (Cutshallet al, 2007; McCaffrey, 2008), the results of this project also pointout that being involved in music activities contributes positively toa more active and satisfactory aging process.
Quality of Life is an area that has not been very extensivelyaddressed in the geriatric arena in the music therapy field. Musictherapists have been more concerned about looking at how musicexperiences can improve abilities in specific functional areas. It isimportant to address Quality of Life and to study how music andmusic therapy can contribute to the maintenance and improve-ment of this variable, from a preventive as well as a therapeutic
280 Journal of Music Therapy
sense. Music therapists often work with populations where it isdifficult to foresee specific improvements because of the nature ofthe illness they have. However, music therapy can contribute tothe maintenance of Quality of Life until the end.
ReferencesCoffman, D. (2002). Music and quality of life in older adults. Psychomusicologf, 18,
76-88.Cohen, A., Bailey, B., & Nilsson, T. (2002). The importance of music to seniors.
Psychomusicology, 18, 89-102.Cutshall, S. M., Fenske, L. L., Kelly, R. F., Phillips, B. R., Sundt, T. M., & Bauer,
B. R. (2007). Creation of a healing program at an academic medical center.Complementary Therapies in Clinical Practice, 13, 217-223.
Davis, W., Gfeller, K, & Thaut, M. (2000). Introducción a la Musicoterapia:Teoría y Práctica. Barcelona: Editorial Boileau.
Fernández-Ballesteros, R., & Zamarrón, M. D. (1996). El Cuestionario Breve deCalidad de Vida (CUBRECAVI). En calidad de vida en la vejez en distintoscontextos. Madrid: IMSERSO.
Hays, T., & Minichiello, V. (2005). The contribution of music to quality of life inolder people: An Australian qualitative study. Aging and Society, 25, 261-278.
Imserso. (2004). Las personas mayors en España. Informe 2004. Imserso.Jarvis, P., & Walker, J. (1997). When the process becomes the product. Summer
universities for seniors. Education and Ageing, 12, 60-68.Lawton, M. P. (1975). The Philadelphia Geriatric Center Morale Scale: A revision.
Joumal of Gerontology, 30, 85-89.McCaffrey, R. (2008). Music listening: Its effects in creating a healing environment.
Joumal of Psychosocial Nursing, 46(10), 39-45.Manheimer, R. J., & Moskow-Mackenzie, D. (1995). Transforming older adult
education: An emerging paradigm from a nationwide study. EducationalGerontology, 21(6), 613-632.
Manheimer, R. J. (2002). La educación para mayores en los Estados Unidos:Tendencias y programas de desarrollo. En W.AA., Los modelos marco deprogramas—universitarios para Mayores. Alicante; Universidad Permanentede Alicante, 111-121.
Mehrota, C. M. (2003). In defense of offering educational programs for olderadults. Educational Gerontology, 29, 645-655.
Organización Mundial de la Salud. (2002). Envejecimiento activo. Un marcopolítico. Revista Española de Ceriatría y Gerontología, 37(2), 74—105.
Onishi, J., Masuda, Y., Suzuki, Y, Gotoh, T., Kawamura, T., & Iguchi, A. (2006).The pleasurable recreational activities among community-dwelling olderadults. Archives of Gerontology and Geriatrics, 43, 147-155.
Prickett, C. A. (2000). Music therapy for older people: Research comes of ageacross two decades. In C. Furman (Ed.), Effectiveness of music therapy frrocedures:Documentation of research and clinical practice (pp. 297-322). Silver Spring, MD:American Music Therapy Association.
Rosenberg, M. (1965). Sodety and the adolescent self-image. Princeton, NJ: PrincetonUniversity Press.
Vol. XLVII, No. 3, Fall 2010 281
Rowe, J, W,, & Kahn, R. L. (1997). Successful aging. The Cerontologist, 37, 443-440.Ruttd, E. (1997). Music and the quality of life. Nordic Journal of Music Therapy, 6(2),
86-97.Schalock, R., & Vet dugo. M, (2002/2005). The concept of quality of life in human
.services: A handbook for human service practitiotiers. Washington, D.G.:American Association on Mental Retatdation {Trad. Cast. M. A. Verdugo y C.Jimaro. Calidad de vida. Manual para profesionales de ta salud, educación y serviciossociales. Madrid: Alianza).
Stock, W. A., Okun, M. A., & Gómez, J, (1994). Subjective well-being measures:Reliability and validity among Spanish elders. Intemational Joumal of Aging andHuman Development, 38, 221-235.
The National Institute on Aging. (2007). Research Highlights in the Demography and£i:ono»iicsq/'/lgjng-. tJRLhttp://www.prb,org/pdf07/NIAGrossnationalResearch,pdf
United Nations. (2007), World Economic and Sodal Survey 2007. Development in an/igKing-WorfdOuiimew. URLhttp://www.un.org/esa/policy/wess/wess2007ftles/overviewlanguages/overview_eng,pdf
Vanderak, S., Newman, L, & Bell, S. (1983). The effects of tnusic participation onqtiality of life of the elderly. Music Therapy, 5(1), 71-81.
Villar, F., Pinazo, S., Triado, G., Solé, G., Montoro, J., & Geldrán, M, (2006).Evaluación de programas universitarios para mayores: Motivaciones, dificultadesy contribuáones a la calidad de vida. Informe para el IMSERSO no publicado.
Villar, F., Pinazo, S., Triado, G., Solé, G,, Montoro, J,, & Geldrán, M, (2007).Seguimiento longitudinal de la evaluación de programas universitarios parapersonas mayores. Informe para el IMSERSO no pttblicado.
Yesavage, J, A,, Brink, T, L., Rose, T, L,, Lum, O., Httang, V., & Adey, M., et al.(1982). Development and validation of a geriatric depression screening scale:A preliminary report. Joumal of Psychiatry Research, 1, 37-49.
Copyright of Journal of Music Therapy is the property of American Music Therapy Association, Inc. and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.