
Contesting patriotic identities: A study of literary counter
Contesting Rape Narratives: Medicalisation and the Trauma
Model of Victimhood
This dissertation is submitted for the degree of Master of Philosophy at the University of Cambridge Centre for Gender Studies.
Constance Flude, Wolfson College Supervisor: Dr. Elizabeth Foyster
Word Count: 19,996 15th July 2015
2
Table of Contents: PREFACE LIST OF ABBREVIATIONS INTRODUCTION……………………………………………………………………6
The scope of the problem Definitions
CHAPTER 1: RESEARCH AND METHODOLOGY…………………………….8
Methodological justification Methodology Historical Method Modern Method
CHAPTER TWO: MEDICALISING THE RAPE VICTIM…………………….17
Medicalisation
Sex and Medicine in the 19th Century Rape and medicalisation
Medical Jurisprudence and Raped Women in the 19th Century Legitimate forms of speech
Rape in the Courtroom Social Scripts in the Courtroom
Competing Discourses
Hysteria Fallen Women and Corrective Reform
CHAPTER THREE: SHIFTING EPISTEMES, THE CREATION OF THE MODERN RAPE VICTIM………………………………………………………..33
Modern history
‘Breaking the Silence’ Modern Discourses
Culture of Wellness The pathologisation of victims of rape
3
Trauma model The Neurobiological Trauma model
The Expansiveness of the Trauma Model Suppression of an alternative model
CHAPTER FOUR: IMPACT OF THE INCITEMENT TO SPEAK………….46
Incitement to speak: Confessional Society
Talking as healing Talking as potentially harmful Repetition Compulsion
Coming to terms with the labels
Labelling experience ‘Victim’ – ‘Survivor’ Diagnostic Labels
CHAPTER FIVE: WHO DO SUCH CONSTRUCTIONS SERVE?.....................64
The PTSD Brain Procrustean model of therapy Who do labels serve? Market driven model of health
CHAPTER SIX: PERFORMING ILLNESS IDENTITIES……………………..74 CONCLUSION……………………………………………………………………...79 BIBLIOGRAPHY………………………………………………………………..…83 APPENDIX ONE – List of Interviews……………………………………………108 APPENDIX TWO – Participant Consent Form…………………………………109 APPENDIX THREE – Victim, Survivor, Thriver Chart……………………….110 APPENDIX FOUR – Examples of Diagnostic Criteria Tests…………………..112 APPENDIX FIVE – Example of Presenting PTSD as a Physical Ailment……117 APPENDIX SIX – Eby et al. Table of women who attribute physical symptoms to sexual assault………………………………………………………………….118
4
Preface:
This is the result of my own work and includes nothing that is the outcome of work
done in collaboration except where specifically indicated in the text. This dissertation does not exceed the word limit for the respective degree committee.
Constance Flude
5
LIST OF ABBREVIATIONS:
• PTSD: Post traumatic Stress Disorder
• C-PTSD: Chronic/Complex PTSD
• DID: Dissociative Identity Disorder
• RCC: Rape Crisis Centre
• SV: Sexual Violence
• SARC: Sexual Health Referral Centre
• T: Therapist
• CFS: Chronic Fatigue Syndrome
6
INTRODUCTION
Rape is seen as one of the most profoundly damaging and traumatising acts of
violence that can be done to a woman in modern western society. 1 For many, this
form of ‘intimate terrorism’ (Johnson & Ferraro 2000:949) represents a fate worse
than death. The self that exists post-assault is a tainted shadow, whose memory
‘haunts the conscious and unconscious’ perennially threatening to resurface whenever
‘something triggers a reliving of the traumatic event’ (Brison 2002:X). Yet, this truth
has a history (Vucetic 2011:1299). This research attempts to deconstruct unquestioned
connotations and assumptions about the nature of rape victimhood that denote the
conditions of possibility, or prognostic future, of a woman who has been raped
(Deutsch 2007:107).
Using an explicitly Foucauldian framework (delineated in chapter one) I will analyse
the processes through which the ‘rape victim’—in its current morphology—has come
to be culturally identifiable, by locating the discursive shifts in history that have made
this understanding of victimhood, and its corollary with medical understandings of
‘ill-health’, possible. This ‘history of the present’ will isolate the different scenes in
history through which rape victimhood has come to be rendered intelligible to modern
society (Vucetic 2011:1302).
Chapter two will analyse trends in the 19th century, where attempts to create a
typology of rapeable and rapacious bodies brought both the rape victim and the rapist
under the inspecting dominion of the medical profession. The creation of the rape 1 The sample demographic of this research are classified according to biological sex—I.e. I am studying female rape victims. However, the types of identities associated with this form of rape victimhood are gendered. Given that violence ‘marks and makes bodies’, an analysis of women’s accounts of rape, ‘demonstrates that gender is embodied’, that the ‘body’ and the ‘category of woman’ are not simply biological givens (Baily 2001:111). Changes in material reality, of identity categories and corporeality have implications for ‘gendered identity’ that I do not have time to attend to in more than passing detail in this thesis, though what I depict is necessarily gendered.
7
victim as an object of knowledge afforded a new ‘speaking position’ to women who
had ‘fallen owing to violence’ where, through the courtroom, they were given
‘legitimated speech’ in order to articulate their claims of injury. Chapter two also
details how the moral reform movement for ‘fallen’ women can be seen as the
beginnings of a movement towards creating a therapeutic community, stressing the
transformative potential for ‘morally ruined women’.
Chapter three delineates the shifting epistemes between the 19th century
conception of rape, and the modern ‘survivor’ movement associated with second-
wave feminism in the 1970s, and the ways these have shaped modern understandings
of trauma. This chapter explores how the claim of injury normalised the trauma model
of rape and created discourse which pathologised rape victimhood on the one hand,
whilst stressing the moral responsibility for the women ‘to be better than well’ on the
other.
Chapter four explores the modern construction of rape victimhood and how
this impacts on upon the lives of rape victims. It details the construction of the
‘confessing modern subject’ that propounds an understanding that talking about
harms is always cathartic. This chapter is concerned with identity labels and how the
women come to understand and incorporate the labels into their ‘affected identity’.
Chapter five explores the implications of this discourse on the material reality
of these women, and asks the fundamental question: whom do these discourses serve?
In each of these epochs, the rape victim and rape victimhood is made thinkable within
the confines of social, medical and legal establishments, which proffers the victims
specific socio-political and cultural forms of ‘legitimate speech’, and in turn is
‘performed’ by the women (Bourke 2010:7).

8
CHAPTER ONE: RESEARCH AND METHODOLOGY
The scope of the problem
It is estimated that around 18% of all adult women in western society are victims of
actual or attempted rape (Kilpatrick & Acierno 2003:123;Najdowski & Ullman
2009:43). As many as 1 in 10 women will experience some form of sexual
victimisation in their lifetime (Anderson & Doherty 2008:12; Mason & Lodrick
2013:29). According to some studies as many 95% of female rape victims will be
diagnosed with PTSD—highlighting the extent to which rape is seen to be decidedly
pathological (Hauck et al 2007:83). It is therefore pivotal that the discourses that
present such bleak prognostic futures for nearly one-fifth of the adult female
population is problematised.
Definitions
In this thesis, I follow Joanna Bourke in defining rape, not in legalistic terms2 but on
the simple principle that rape is any non-consensual sex ‘act called such by a
participant’ (Bourke 2007:9). This definition is a ‘heuristic device’; it does not
prescribe the ‘correct’ definition or stand as adjudicator over the veracity of claims
(Ibid:10). Instead, such a definition affords the people involved agency over how to
define their understanding of what rape constitutes.
It is important to recognise that not all rapes are the same, sexual violence
occurs on a spectrum of severity from ritualised torture to a grey borderland between
consent/lack of consent. However, I do not wish to make claims as to how
2 Legally rape is defined in the UK under the Sexual Offenses Act 2003, as: ‘(1) A person (A) commits an offence if – (a) he intentionally penetrates the vagina, anus or mouth of another person (B) with his penis, (b) B does not consent to the penetration, and (c) A does not reasonably believe that B consents.
9
traumatising these different experiences are, rather it is the meaning that the women
ascribe to the event that is the determining factor in how it affects them.
Though I will interchangeably use the terms ‘rape victim’ or ‘survivor’3, I do
so only with the following caveat. Such terms are value-laden and serve to both
‘enable and constrain the lived experiences of women’ (Ronai in Lamb 1999:139).
Although many researchers claim to eschew moral judgement in their use of such
terms, the same people often state that ‘many victims are survivors’ (Bourke 2007:7).
This is highly problematic. Literally speaking any woman who is raped, and survives
the event is a ‘survivor’. However, in this conceptualisation, ‘survivor’ asserts a moral
position that is reserved for those who have consciously recoded their identities from
abject victim to empowered survivor (Naples 2003:163).4 The most pertinent issue
with the terms ‘rape victim’ and ‘survivor’ is that they connote an identity position. I
strongly oppose the conflation of an act of violence with an identity position, as I
believe this discursively imposes an ontological reality onto the women that may be
harmful to their sense of selves and future lives (Taylor 2009b:13).5
Unquestioned use of such identity categories is a theft of agency over self-
definition. Within any discussion of the effects of rape and the identity associated
with rape victimhood, the women are not simply passive recipients of a discourse that
dictates the states and shapes of their lives. I do not want to problematically oppose
agency and victimhood as though they are monolithic positions associated with power 3 Though I do use the terms rape victim and survivor interchangeably (because of the inescapability of such terminology), I would prefer to always use ‘victim of rape’ which formulates rape as an act rather than an identity position upon the women under study. 4 I draw upon Judith Butler’s understanding of the abject as a subject position that is ‘unlivable’ or ‘uninhabitable’, but is nevertheless a subject position ‘densely populated’ by those who are excluded from the status of normativity, but are required in discourse to demarcate the domain of the normative subject (Butler 1993:3). 5 Running through this discussion is the idea that sexual violence is ‘constitutive of subjectivity’ (Shepherd 2007:248). The violent act of rape, ‘marks and makes bodies’ (D’Cruze & Rao 2004:503) insofar as both the rape victim and the rapist are brought-into-being by being defined by the act.

10
and powerlessness (Wood 2000:7). Following P. Jackson, I argue that it is the
(self)conceptualisation of identity, agency and lived experience of victims of rape,
that shapes the ontology of rape victimhood (in Yanow & Schwartz-Shea 2013:274).
Methodological justification
Though there is an abundance of academic work on sexual assault that covers a wide
range of themes, most research reifies the idea that rape is profoundly traumatic
(Cahill 2000:43). To suggest otherwise is seen to diminish and ‘grossly
underestimate the psychological and physical trauma’ associated with rape
(Hengehold 1991:94). Poststructuralist theories tend not to be used in sexual violence
research because people feel that destabilising the standpoint, or identity categories
through which people articulate their lived experiences co-opts the voices of
‘survivors’ and robs them of an essential experience and claims pertaining to the
reality of their suffering (Mohanty & Martin 2006:85). However, to suggest that rape
victimhood is not pre-discursively real and that people are directed through normative
prescriptions to a vocabulary and identity position of suffering which are only
possible within our current episteme is not the same as diminishing the reality of a
persons’ suffering. Rather, the deconstruction of a preconceived notion is both
affirmation of the reality as it stands and a radical undoing; allowing for new
possibilities and constructions to arise. Precisely because the act is imbued with such
immense symbolic potential, it is important not to shy away from ‘controversial
topics’.
The main challenge for feminist ethics is ‘how to deal with the tension
between care for the suffering of individuals and concern for issues of power and
oppression’ (N.Martin2001:438). Therefore, my choice in adopting a poststructuralist

11
methodology is predicated upon my ontological presupposition that material reality is
created through discourse and my feminist politic that requires ‘evaluating’ and
‘dismantling’ oppressive structures of thought. Through a feminist-Foucauldian
approach to sexual trauma, I hope to present an understanding of rape victimhood that
neither medicalises, pathologises nor trivialises victimisation, and allows for new
conceptions of rape to be put forward.
Methodology
In constructing a genealogy of rape, I aim to make the past (and present)
representations of—and symbolic meanings attached to—rape, visible, in order to
render them ‘susceptible to critique’ and illuminate ‘taken-for-granted beliefs’ (Fraser
& Gordon 1994:311). Foucault (in Bouchard 1977:139-40) argues against the
assumption that ‘words keep their meaning’, or that ‘ideas retain their logic’. Instead,
he contends that it is important to ‘isolate the different scenes’ in the genealogical
deconstruction of a term or notion, where it has been ‘engaged in different roles’. In
so doing, one is able to look at how some thoughts and ideas linger within our
intellectual and social histories—shaping what is thinkable and knowable within a
given context—but also how ideas radically change and adapt. This highlights the
representational and contingent nature of knowledge, and will allow me to challenge
the status of truth associated with modern constructions of rape victimhood (Foucault
1972:127).
Inhered in Foucault’s conception of ‘regimes of truth’ are pivotal insights into
the ways in which discursive practices, ‘encode, construct, [and] authorise… an
aspirational and often didactic model of human identity’ (Hawthorne 2006:16). In this
view, the terms used to describe social life systematically form the ‘object of which
12
they speak’, powerfully constituting the a priori ‘assumptions, expectations and
explanations’ that govern social life (Baxter 2003:7). Following Foucault, what is
found at the ‘historical beginning’ of term is not the ‘inviolable identity of their
origin; it is the dissension of other things. It is disparity’ (Foucault in Bouchard
1977:140). In this light, rape victimhood has no essential meaning prior to or outside
of discourse, rather ‘truth’ is ‘the sort of error that cannot be refuted because it was
hardened into an unalterable form in the long baking process of history’ (Ibid:144).
Therefore, the construction of a genealogy is predicated on the understanding that
experience of—and meanings attached to—rape, are historically constituted, and
embedded within ‘overlapping networks of relations’ that spatially and temporally
shift (Somers 1994:607).
Vucetic (2011:1300) advances the idea that a genealogy must offer ‘episodes’
in order to ‘perioditise the history of an object of study’, such episodes must be
narrated through examples ‘which are themselves reconstructed in a discourse
analysis’ of an array of historical documents. A genealogy is both an analytical tool
for socio-political research (to write the ‘political histories of truth’), but it is also an
attempt to ‘open the intellectual and political space for resistance to the dominant
regimes of truth’ (Vucetic 2011:1298). Genealogy therefore draws upon two levels of
existence: one that is of a particular historical moment where material reality is lived
(ontological); and the second theoretical, where one attempts to understand from
where we came and where we are going (epistemological) (Shoemaker 2008:13).
Therefore, to destabilise rhetorical commonplaces, a genealogical discourse analysis
must rely upon a ‘comparative method’ (Vucetic 2011:1301).
Historical Method
13
A critical history is intended to enable us to ‘think against the present’ to disturb and
fragment the ‘mundane and quotidian roots of that which claims lofty nobility’ (Rose
1996:41). In order to isolate the given historical constellations of conditions that have
made the current understanding of rape victimhood appear natural, I have adopted the
method of a ‘textual ethnography’ (Jackson in Yanow & Schwartz-Shea 2013:274). A
textual ethnography is a disciplined reading where one engages in ‘observation’ of the
textual records in order to isolate the themes in the history of legitimation struggles
(Ibid:276). Once the themes became identifiable, I conducted a discourse analysis to
understand the processes through which meaning is made in order to understand how
the meanings attached to rape victimhood were deployed in the past, and how these
are continuous/discontinuous with modern day constructions.
During the episodes in history isolated for this research, there were struggles
over the recodification of social phenomena. Such struggles ‘leave a residue in the
form of laws, social practices, and ideologies’ creating assumptions that are ‘so
pervasive’ that they are rarely questioned (Rubin 2011:146). Through an analysis of
sources—such as court sessions, police reports and medical jurisprudence books from
both national and regional archives—I have been able to access the construction of
19th century rape victimhood.
Though most documents were ‘almost exclusively written by men’ (Taylor
2009b:23), through the ruptures, ‘accidents’ and ‘minute deviations’ (Foucault in
Brouchard 1977:146) contained in their pages, an ‘episodic, fragmentary and
contingent’ narrative of women’s social identities becomes accessible (D’Cruze
1998:9). In this way, although the texts are ‘multi-authored’, one can see glimpses of
the tropes and forms of the legitimated types of speech and identity afforded to female

14
rape victims which have rendered visible the ‘actual and possible forms of social
organisation’ and identity as they were linguistically produced and contested
(Weedon 1997:21). Although I primarily focus on sources from the UK, 19th century
medical jurisprudence books were circulated across the Atlantic and most modern
research papers draw on both UK and US sources, despite the different contexts in
which they were deployed.
Modern Method
In order to account for the modern subjectification of the rape victim, I have—as with
the critical history—conducted a discourse analysis of a plethora of sources. I
analysed a number of online ‘survivor’ forums, in order to provide ‘voices’ of
survivors in relation to their experience that I might otherwise not have been able to
access through interviews. All the information used in this research was taken from
the public domain and I have therefore used the online aliases of the forums’ users.
Without membership, no one from the general public could gather details on the users
other than comments which are freely available online. Given that these spaces are
multinational, it has been impossible to isolate different countries for the purpose of
this study.6 Therefore, although this research is more nuanced towards the discursive
regimes of the UK (and US), the term ‘western’ is more appropriate to the
transnational nature of this research, particularly given that medical knowledge is
presented as ‘objective’ and universal, rather than ‘cultural’—and is disseminated on
this basis7. In drawing upon the comments in the online forums, I hope to provide a
6 Within an increasingly globalised world, knowledge and identities are constituted through increasingly connected and interdependent discursive and material regimes’ (Mohanty2003: 521). 7 All the research papers on medical models of rape and trauma are from various countries across the western world, and despite ‘scientific’ differences, they rarely attend to cultural understandings of rape. Instead, rape victimhood is presented in universalised terms and my research therefore attends to the universalisation of rape victimhood
15
representation of ‘survivors’ voices that details their ‘coming-into-being’ as rape
victims (Stern 2006:183).
For the primary data sample, I conducted qualitative interviews of eight
professionals whose work relates to the provision of therapeutic services for rape
victims8. I asked open-ended questions, first finding out the particularities of their
personal experiences of working with rape victims and then focusing on the themes in
my research in a ‘non-directive’ way. I also interviewed three ‘survivors’ and
attended a ‘survivors workshop’9. I conducted semi-structured, qualitative interviews,
asking open (and not leading) questions. I chose this method of data collection
because it offers access to ‘people’s ideas, thoughts and memories in their own words
rather than in the words of the researcher’ (Reinharz 1992:19).
In all of my interviews, I attempted to be ‘engaged but non-obtrusive’ (Eingal in
Bondi 2002:232). All participants signed an informed consent form before the
interview was conducted (see appendix 2), except in the case of the ‘survivors
workshop’ where all the participants were informed that I was there within my
research capacity. I did not record the ‘survivors workshop’ but after I left, noted the
aspects that stood out. Following the workshop, I spoke in more depth with one
8 Duncan McLean, Clinical Pyschologist & Psychoanalyst; Zoe Lodrick, Sexualised Trauma Psychotherapist; Nicc Seccombe, Mental Health services manager; Jacqui Campui Peterborough Rape Crisis Centre; Rachel Matheson SARC; L. Grillo respiratory physiotherapist, NHS; and one woman who founded an organisation for ‘survivors’ providing help and counseling for gynecological and sexual problems who has been anonymised because I accessed the survivors workshop through her organization. This anonymisation has been discussed with my supervisor. (See Appendix 1 for details of interviews) 9 The survivors workshop was attended by around 30 people and was a day of discussions and activities where people were encouraged to talk about their experiences in an open and friendly space. I accessed the workshop through an organisation, which will remain anonymous (as discussed with my supervisor) in order to protect the identities of anyone involved who might be quoted in this thesis. I have cited 4 participants from the workshop in this study and have listed them as (survivor(S) 1 workshop), (S2 workshop 2015) etc.
16
woman (S2) about her experience of the event. She was aware that I would quote her
in my thesis and signed a consent form.
The three ‘survivors’ interviewed for this project had over 10 years time lapse
between the rape and the point of interview and each of them worked in some
capacity, with women who have been raped. In the first instance, I ‘accessed’ these
women through their professional roles so I did not have a ‘gate keeper’ present
during the semi-structured one-to-one interviews. I have anonymised these interviews,
and will not provide details of the organisations, as I want to draw upon the insights
of these women in their ‘survivor’ rather than professional capacity.
To interview people, particularly when dealing with personal experiences such
as the aftermath of a rape, is to ask them to ‘open themselves up to the researchers
questions’, therefore protection of their identities is of utmost importance (Bingley in
Bondi 2002:2009). Interviewing such women afforded me an insight into the
‘narrative voice and the biographical structure’ of people who have personal
experience of rape, but who also work within the therapeutic and research sector and
therefore are doubly positioned ‘between the categories of insider and outsider’
(Eingal in Bondi 2002:232). This allowed for a ‘double hermeneutic’ where they were
able to talk of the aftermath of their experiences with statutory services from their
position as ‘survivor’ and reflect critically upon this from their position ‘within’
service provision (Ibid). This also allowed for richer comparative insight when
looking at the voices of ‘survivors’ within the online forums.
In conducting both the professional interviews and interviews with survivors,
despite differing degrees of critical appraisal of discourses, all responses were to some
extent coded within an already established discourse. Most respondents, to differing
17
extents constructed rape as always traumatic and used medicalised terminologies or
models to refer to victimhood. As with all narratives, the interviews must be viewed
as ‘meaning-constructing’; spoken accounts must therefore be seen as ‘inscribing’ and
creative of material reality (Stern 2006:184).
CHAPTER TWO: MEDICALISING THE RAPE VICTIM
Medicalisation
Medicalisation denotes a process through which nonmedical problems come to be
defined by, and understood through a medical lens, ‘usually in terms of illness or
disorder’ (Conrad 1992:209). The ‘dominion, influence and supervision’ of the
medical profession (Zola 1983:295) was inaugurated during the 19th century, 10 when
doctors and psychologists began to describe and classify pathologies that had
previously ‘remained below the threshold of the visible and expressible’ (Foucault
1973:xii). Thus, it was within the ‘new epistemological space’ of 19th century medical
science (Ramazanoglu & Holland 2002:26), that the medical gaze fixed, ‘isolated and
animated’ objects of knowledge (Foucault 1973:45).
This ‘mode of revelation’ (Heidegger 1977:13), of bringing-something-into-
existence by defining and rendering knowable, ‘certain behaviours, persons and
things’ (Conrad & Schneider 1980:8), is one of the most ‘committed forms’ of social
control, precisely because categorising humans and human behaviours is productive
of and re-produced by the very subjects under surveillance (Pastor 1978:382). The
subject of ‘the gaze’ is thus effected through its perception (Crossley 1993:411), and
10 I use the term ‘19th century’ to refer to the period in which the broad social processes of medicalisation of rape victimhood took place, however it is near impossible to isolate epistemic changes to specific historical dates and the views and constructions of rape at the beginning of the 19th century were radically different from those at the end. However, the period of focus is mostly from around 1860 onwards, although source material ranges from as early as 1814 to as late as the 1930s.
18
through an ‘infolding of an ‘exterior’ to constitute an ‘inside’’, comes not only to
know itself as an object of knowledge but to re-produce—through the ‘internalised
technologies of the self’ (Martin 2005:56)—the prescribed behaviours, characteristics
and tropes associated with such medicalised identities (Venn 2002:30).
Foucault argued that this ‘informationalisation of bodies’ (Wilcox 2014:3)
forged a new alliance between things and words, ‘enabling one to see and to say’
(Foucault 1973:xii). The medical gaze is an ‘active perceptual system’ (Haraway
1988:582) with the power to isolate and classify the ‘forms’ and ‘deformations’ of
certain bodies, behaviours and characteristics (Foucault 1979:136), by visually
‘proving’ their existence (Fielding 1996:176;Stafford 1991:1). This ‘panoptic power’
is a tool for organising and orienting living matter, with the power to designate some
bodies and some things as marginal, and some as normative (Foucault 1980:144-5).
The gaze is therefore ‘the eye that knows and decides, the eye that governs’ (Foucault
1973:108).
Sex and Medicine in the 19th Century
Foucault argued that by the 19th century, the development of understandings of
‘demography’ transformed the ‘social body’ from a ‘jurido-political metaphor’ into a
‘field for medical intervention’ (Foucault 1978:6-7). This fundamentally transformed
the technologies and rationalities of political power, where the state was increasingly
called upon to ensure the ‘welfare’ and ‘normality’ of its citizenry (Rose 1996:48).
Medicine functioned as a ‘public hygiene’ that promised to eliminate ‘defective
individuals’ and ‘bastardised populations’ not only through surveillance and
disciplining techniques, but also through moral self-regulation imposed upon and
reproduced by individuals (Foucault 1979:54). Here, the doctor and the psychologist
19
became a technician to heal the societal body, as well as the individual soul (Foucault
1978:7). This moralising arm of medical science was essential to the developing idea
that sexual behaviours (outside of monogamous heterosexuality) were expressions of
disease or pathology (Hart & Welling 2002:897; Cryle & Downing 2009:2).
Rape and medicalisation
In The History of Sexuality (1979), Foucault argues that sexuality became the locus of
identity during the 19th century. During this time, the sexual act came to be seen as a
way of being11. Following Foucault’s theorisation in Discipline and Punish (1975),
one could argue that the rapist and the rape victim are twice defined, once by the act
(done by, or done to them) and second by the identity position this confers upon them
(Taylor 2009b:13). Forging such characters as ‘objects of knowledge’ with the
intrinsic identities of ‘the rapist’ and ‘the rape victim,’ inculcates and imbues such
identity positions with psychological discourses that ‘categorise[s], observe[s] and
refashion[s]’ the very souls of the subjects (Ibid:8,1).
The construction of the ‘rape victim’ is intimately tied to the quest to establish
rape as a sexual deviancy committed by a small minority of men (Porter 1986:235).
Recognition that sexual violence against women was commonplace would have
required society to address the normativity of a rapacious masculine sexuality. During
the 19th century however, it was still a perfectly acceptable idea that a ‘proper’ lady
would not consent ‘without some force’ (Beck 1825:57). Havelock Ellis’ writings
constructed violent male sexuality as a ‘biological necessity’ because female 11 Though Foucault argues that sexuality is the locus of identity, I would complicate this further. Though sexuality was afforded far more importance during the 19th century, it was certainly not the sole marker of identity. Sexuality and sexual identity were also deeply reliant upon the class formations within the UK—particularly when looking at the typologies of the ‘legitimate’ rape victim (who was mostly a hard working, moralistic, working class woman; rather than a drunk, brawling lewd character.) I will attend to class considerations with more detail in the section of ‘legitimate forms of speech’
20
resistance to intercourse was a ‘natural’ part of the heterosexual mating-game and
‘functioned to increase male arousal’ (Anderson & Doherty 2008:6)12. Therefore, in
order to distance masculine sexuality from recognising itself as violent, the idea that
rape was committed by a small number of determined perverts meant that character
assessments of both the rapist and the raped woman were needed in order to ascertain
guilt (Whitlock 1999:424). Due to the desire to see rapists as a minority, the legal and
medical institutions systematically favoured the idea that most victims were at least
partially deserving of being raped.
Medical Jurisprudence and Raped Women in the 19th Century
The development of a ‘medico-legal’ understanding of rape in the courtroom
sanctioned public speech about rape and women’s bodies within the masculinised
space of the courtroom (S.Robertson 1998:348). The body on display encompassed a
‘constellation’ of gendered discourses concerning ‘disorderly female sexuality’ and
respectability (D’Cruze 1998:144). The raped body was therefore called upon to bear
witness to the crime and in doing so, the woman’s character, integrity and reputation
were put on trial.
Medical writing of the time delineates the areas of ‘expertise’ that doctors
provided in the courtroom space. Doctors claimed the ability to preside over and give
evidence in three areas deemed constituting of guilt: 1) physical struggle, 2) signs of
rape and 3) character of the rape victim. Out of these discourses women were able to
publically express the effects of rape in terms of ‘physical and economic ruin’
12 Such understandings still have bearing on modern constructions of sexuality. Nicola Gavey (2005) argues that this version of heterosexuality, and the idea that women must be, on some level, ‘coaxed’ into sexual submission forms the heterosexual norms that operate as a ‘cultural scaffold for rape’. Furthermore, Lunbeck argues that it is due to this ingrained understanding of male sexual aggressiveness that means that it is ‘sometimes difficult for women to draw a firm line between abuse on the one hand, and consensual sexual activity on the other’ (Lunbeck cited in Showalter 1997:52)
21
(Bourke 2012:16) which provided ‘sexual scripts’ to articulate legitimated grievances
(S.Jackson 1978:30). Such legitimated types of speech encouraged women to deploy
their bodies as evidence of injury: The Ipswich Journal (4th-Dec-1880) for example,
detailed a case where a mother presented her daughter’s bloodied and torn
undergarments as evidence that the rape had taken place.
In a visually oriented culture, where seeing was believing, it is perhaps unsurprising
that doctors came to the legal system with the perspective that rape was a physical
struggle (S.Robertson 1998:348). Rape was the ‘unlawful and carnal knowledge of a
woman by force and against her will: A ravishment of the body and violent
deflowering’ (Paris & Fontblanque 1832:416 emphasis added). There was great
concern during this period over the probability that a rape could be ‘consummated on
a grown female in good health’ (Beck 1823:8). Though it was understood that rape
could be attempted, the ‘entire coition’ of a respectable woman was deemed
‘impossible’, for a woman ‘always possesses sufficient power, by drawing back her
limbs, and by the force of her hands, to prevent the insertion of the penis’ (Farr
1814:41-2). Furthermore, there were many medical jurists who believed that the
vagina acted like a vibrating sword-scabbard providing an ‘effectual power of
resistance’ against rape13 (Thomson 1936:449). Tied up in this discourse were notions
of chastity, respectability and virginity, which were given visual and anatomical
credence through discussions of ‘pure’ and ‘impure’ gynaecology14.
13 The scabbard metaphor depicted the vagina as self-closing at the point of physical attack, as long as the woman did not on some level consent to the sex. 14 For examples see Farr 1814:142; Beck &Beck 1838:147; Paris & Fonblanque 1823:417

22
The identification and interpretation of the ‘signs’ of rape drew upon the
valorised position of the chaste female in Victorian ideals15. Only an innocent virginal
female could (legitimately) be raped against her will, while women who ‘had known’
a man were tarnished with sexual experience and had less legitimacy to claim sexual
grievance16. The underlying idea was that ‘if a (respectable) man had a ‘right’ to a
woman with an ‘unstained name’, it followed that a name-stain would be utterly
devastating to any women who hoped to occupy a respectable niche in society’
(Friedman 2002:1097).
Vickery argues that 19th century advice books provided ‘chapter and verse’ on
how a respectable woman should behave (1993:383). This constructed a ‘particularly
crippling ideology of virtuous femininity’ from which literature regarding rape
victims could draw (Ibid). A virgin’s vagina, for example, was described as ‘small
and endued with a light rose colour’ with ‘hymen intact’ (Farr 1814:44). Such
sensitive descriptions show the reverence for virginity. The woman ‘who has
accustomed herself to venereal habits’, on the other hand—and thus ‘useless to be
believed upon a deposition for a rape’—has lips which are ‘flaccid and distended’ due
to ‘constant friction’ (Ibid:46). Here, it is not clear whether the ‘hymen is wanting’ or
the woman’s moral stature. Doctors asserted that marks of violence would be visible
on the genitals and body following a rape. Marks such as ‘ an inflamed vulva, a
lacerated or ruptured hymen, vaginal discharge’, bruises, scratches, blood and semen,
were taken as corroborating (though not outright) evidence that a rape had taken place
(S.Robertson 1998:364). 15 This was actually enshrined in the law as rape was defined as ‘…ravishment of the body and a violent deflowering’ (Paris & Fontblanque:1832:416 emphasis added). This clearly depicts rape in terms of a theft of the euphemistic ‘flower’. 16 Furthermore, the idea that a married woman could be raped is not spoken about at all—the split is instead between undeserving virgin and deserving whore. This bias was so ingrained that it was not until 1991 that the UK made marital rape an offense.
23
The physician’s statement in the case of 14-year-old Sarah Stevens in 1880,
notes: ‘ I found the front and lower portion of the chimes covered in dried blood and
stains… The internal parts were dilated and bore evidence of having been recently
penetrated…[yet he states that] there was no evidence of violence whatever’ and adds
‘ the girl is as well developed as some women 20 years old would be’ (CRIM
1/11/3)17. What becomes clear here is that ‘signs’ of ‘legitimate’ or ‘illegitimate’
violence were read in accordance with normative value judgements based on
character assessments (Clark 1983:17). The statement that the girl is ‘well developed
enough’ to pass as someone more sexually mature, depicts her as consenting-upon-
the-basis-of-her-appearance. In the margins of the police report taken by the
constable, the girl is reported to have whispered that her assailant ‘fucked’ her, whilst
her own sister describes her as ‘young and idiotic’18. When put together, this amounts
to a character assassination that dismisses her claims of rape by suggesting that she
had consented to the sexual intercourse either on account of her stupidity, her sexual
maturity, or the lack of respectability shown in her coarse language. Thus, it becomes
clear that the visible signs of rape did not ‘go very far towards proving rape, for they
may arise also after consent is given’ (Smith 1908:222).
Wharton and Stilles forcefully argued (1855:336:emphasis added) that each
rape case brought before the court should be judged ‘according to the correspondence
of the injury received with the woman’s narrative, and her character for modesty and
17 The idea that a girl is deserving of rapacious masculine attention on account of ‘looking old enough’ is still prevalent in modern society. In 2013, for example, Judge Nigel Peters claimed that he had ‘taken into account’ that the girl ‘looked and behaved’ a ‘little bit older’ than her 13 years. He also claimed that the girl was predatory and had ‘egged’ the 41-year-old perpetrator on. The man therefore only received a suspended sentence for luring the girl to his house, getting her to strip and perform a sex act on him (Doyle 2013). 18 ‘Idiotic’ could be a reference to the girl having learning difficulties or some form of mental retardation as this was the terminology used at the time to refer to such conditions, however, I could find no further information to confirm this in the case file.
24
veracity’. The assessment of a woman’s character, and thus the ‘veracity’ of her
claims, also intersected with class sensibilities (Bourke 2010:29). Some medical
jurists expected less physical resistance from ‘refined’ middle- and upper-class
women as they were less ‘accustomed to roughness’. The working classes on the
other hand, more attuned to the struggles of hardened life, could ‘give as good as they
got’ and were therefore required to offer more proof of their physical attempts to stop
the attack (Kerr 1935:164).
Legitimate forms of speech
The process of medicalising rape defined and codified the discourses detailing what
rape constituted and whom rape happened to—at least in an institutional setting19.
These hegemonic definitions define and prescribe acceptable discourses and
narratives and are therefore disciplinary. In other words, the authorised discourses are
devices of meaning production that encourage the subject to internalise and embody
‘vocabularies, norms and systems of judgement’ as a way of knowing themselves
(Rose in Hall&Du Gay130-135). Authorised discourses thus form part of the
ontological narratives that allow the individual to access their own self-definition
(Somers 1994:614).
Throughout the 19th century, the meanings of ‘social danger and moral truth’
played out in the courtroom (Mort 2006:108). Ewick & Silbey (1995:209) argue that
the scripted narrative is ‘nowhere more developed’ than in the courtroom where all
participants engage in ‘the telling of tales’ (Donovan 2005:62). Prior to the
popularisation of the ‘psy’ disciplines the local courts and the police ‘were the chief
19 ‘ Whom rape happened to’ means the discursively produced position of the ‘legitimate victim of rape’, rather than the woman who may have actually been raped but not believed within the institutional setting. Therefore, it is a mediated social reality, rather than a literal one that is being referring to.

25
institutional means’ by which women could legitimately speak about their experience
of sexual assault (D’Cruze 1998:13). Thus, rape trials offer insight into the workings
of the criminal justice system and its ‘gender-based moral evaluations’ (Donovan
2005:61), as well as insight into the ways in which women themselves spoke of their
experiences (Conley 1986:519).
Rape in the Courtroom
Rape was rarely prosecuted because ‘giving way to passion’ was seen as the natural
or inevitable activity of bachelors, and the unfortunate (but excusable) vice of married
men (Conley 1986:535; Vigarello 2001:27). The onus for self-preservation thus fell
upon the women (Bryson in Tomaselli & Porter 1986:152-4). If assaulted whilst
outside of ‘proper’ supervision, they would be taken to be a ‘bad woman’ (Walkowitz
1998:1) and therefore considered guilty of provoking the crime.
The Maidstone & Kentish Journal (M&K Jrnl) (26th-Sep-1863) reported that a
man was acquitted despite the jury believing that the rape took place, because ‘she
had acted foolishly in going with the prisoner through the gardens’20. The criminality
of rape was more socially understandable to an all-male jury if the violence involved
was enough to constitute a bodily assault, and often it was due to this that charges of
‘rape’ were reduced to indecent assault in order to secure conviction. Caroline Conley
(1986:521) analysed all cases of rape and assaults in Kent during the 19th century and
20 Such sentiments were oft repeated in the sources I examined at the National Archives in Kew: CRIM 1/543; HO/47/75; CRIM 1/25/1, CRIM 1/8/7 and CRIM 1/8/8 in particular all detail cases where the women are obviously having to continually and repeatedly justify why they were in a position at all –i.e. alone—to be attacked. In the case of R. Footer (CRIM 1/25/1), the woman is subject to three written statements where she is repeatedly asked about why she was in a park alone with a gentleman. It is only when the same attacker, accosts a respectable gentleman and his lady-friend that the case is taken forward and the initial testimony believed.
26
found that the conviction rate of rape trials was 40% in comparison to 85% of other
assault-related felonies21.
The lesser charges of indecent assault and attempted rape tended to be used
when middle-class men were indicted and the evidence too compelling to be
outrightly dismissed (Conley 1986:523). Conley contends that 81% of the cases
examined where the men had a rank above a soldier or labourer were tried under the
lesser charges. A case was dismissed in 1872 because the justice could not be
persuaded to believe that a ‘respectable’ father would rape a domestic servant (M&K
Jrnl 9th-Dec-1872). Conley found that in all but two of the cases involving the rape of
domestic servants by their employers, the employers were ‘off with a fine’
(1986:525). On the other side of this, every case Conley examines where the victim
was identified as a ‘lady’ went to trial and an overwhelming 87% of these cases
returned with convictions for either rape or indecent assault (Conley 1986:530). This
rate dropped to only 10% if the woman was a drunk or prostitute (Ibid). It was not
simply the attackers on trial22. Women thus had to carefully navigate and modify their
characters in the courtroom in order to be seen as legitimate victims of a crime.
Social Scripts in the Courtroom
Social scripts are a means through which ‘values are made coherent’ in particular
contexts and situations (Holquist 1990:137). For the women involved in rape trials in
the 19th century, the very fact of speaking out about sexual and physical assault ‘put 21 Rape law is still weighted in favour of the perpetrators today, as only 5% of rape cases in the UK end in conviction (Bourke 2007:xii). This is particularly shocking given that only an estimated 12-18% of women actually report to the police (Monk & Jones 2014:55; Stanko 1985:37). 22 The court transcripts and police reports actually paint a picture where it was the woman’s character that was primarily on trial rather than that of the mans. In nearly every police report I read at the National Archives, the women give protracted statements where they are subjected to intense questioning regarding the experience, whereas the statements of the accused tend simply to refute the charge. In one case, the only words the accused says in his official statement is ‘I did not do it. I know nothing of this’ (CRIM 1/11/3).
27
their character in jeopardy’. They therefore had to ‘mind the story’ and characterise
themselves as one who had been unjustifiably wronged (D’Cruze 1998:160; 154).
Their position in court was thus inherently contradictory and dangerous. On the one
hand, they could ‘draw upon metaphors of pollution’ in order to explicate the violent
loss of reputation, but in so doing, they also brought their bodies into legal, medical
and public purview where it could be represented as over-sexualised, contaminating
and monstrous (Cook 2012:484). It was therefore crucial that the women play into the
socially scripted, and accepted, typologies of sexual assault narratives.
The most commonly accepted narratives were of an outdoor attack by a
stranger, witnessed by another person (in order to corroborate the woman’s
testimony). The women also used similar vocabularies when describing the attacks,
using phrasing like ‘laid on’, ‘had connexion’ and ‘exposed his persons’ (CRIM
1/13/5; HO/47/75 62; CRIM 1/8/8), as well as repeatedly indicating that they ‘did not
lie down on my own will, the prisoner forced me down. I screamed out but no one
was then about’ (CRIM1/25/1).
Narratives that are emplotted within normative discourses, generate ‘cultural
expectations’ of what should follow (Somers 1994:404). For these stories to be
culturally intelligible to the jurors, the women had to follow such codified scripts in
order to be considered legitimately ‘wronged’. Such narratives are therefore examples
of ‘multiple authorships, whose composition resulted out of precisely located
intersections of power relations and purposes’ (D’Cruze 1998:152). Furthermore,
such ontological narratives necessarily shape the language through which the women
came to understand—and thus directly affected the material reality of—their own
experiences.
28
The effect rape had on women in the 19th century was therefore predicated
upon, and determined by, medicalised, courtroom and wider social narratives around
‘fallen women’. The idea that rape could result in a woman’s life being ‘despaired of’
was framed in moralistic terms over the irreparable damage to her loss of honour
(London & Sporting Chronical 1856:17; Chaddocks in Hamilton & Godkin1861:544).
Recognition of the power of rape to bring about ‘social death’ is indicated through the
fact that women cried out ‘murder!’ rather than ‘rape!’ to get attention (Bourke
2012:14): ‘I endeavoured to cry out murder but… I could not be heard’, ‘he has
murdered me, he has ruined me forever’ (Wakely 1810:5,11).
Competing Discourses
Up until the 1860s, trauma referred to bodily injury (Cardyn in Micale & Lerner
2001:179). Although there was recognition that fear provoked ‘troubling memories’,
there was no formal medical theory of the propensity of terror to cause psychological
wounding (Van der Kolk et al. 1996:47). During the 1860s, Erichsen developed an
understanding of the ‘trauma syndrome’ people developed after being in railway
accidents, and attributed the ‘distress or shock’ they felt to a ‘concussion of the spine’
(Leys 2000:3). Out of this growing body of research it came to be widely accepted
that the ‘emotion of fear alone was sufficient to inflict severe shock on the nervous
system’ (Page 1883:162).
By the 1890s, the meaning of ‘trauma’ had shifted from a physical injury, to
an ‘emotional or psychological factor’ (Prince 1897:614). Bourke argues that
although there was growing understanding that heightened emotional states were
pathogenic across an array of ‘bad events’, this was not applied to rape victims until a
century later in the 1960s (Bourke 2012:1). Certainly at this stage, trauma and

29
traumatisation had not become the natural or inevitable consequences of sexual abuse,
but if one were to look at gendered disorders of mood, such as extreme melancholy or
hysteria, one could find examples that recognised the propensity of rape to cause
psychological wounding. Freud states that ‘at the bottom of every case of hysteria
there are one or more occurrences of premature sexual experience’ (1962:13).
Hysteria
Sexual assault was seen to produce ‘violent hysterics’ in women (Kentish Express:
20th-Jan-1863). Ogston explicitly links hysteria to rape when he asserts that hysteria
could arise ‘from terror or shame’ associated with sexual assault, though admittedly,
he asserts that the ‘profound hysteric coma’ only lasts ‘some hours’ (1878:119). Such
understandings paved the way for the after-effects of sexual trauma to be categorised
in a taxonomy of disordered mental health (Leys 2000:4).
While a diagnosis of hysteria afforded the women recognition of their
suffering, it also exposed them to challenges against the veracity of their claims. One
of the main ‘proofs’ of hysteria in a woman was ‘a propensity to throw about
accusations of sexual immodesty’ (Bourke2010:33). In a case of a woman ‘found
dying’ after being gang raped, Beck and Beck assert that she was in a ‘paroxysm of
hysteria’ and was therefore an ‘imposter’ (1838:148). It was often the case that when
a patient referenced her rape as the cause of a psychiatric ailment, it was taken as
proof of her insanity rather than proof of what she had experienced (Bourke 2012:4).
Furthermore, many doctors and psychiatrists actually believed that hysteric women,
‘addicted to this delectable vice of pathologic accusation’, were harbouring under a
peculiar sexual perversion (Robinson 1828:307-329). Thus, the medical profession
succeeded in fusing non-normative femininity, rape and ‘madness’ together creating a
30
pathologised (and gendered) understanding of what rape can and does do to a woman
(Cryle & Downing 2009:24;Theriot 1993:24).
Females were cast as insane when they ‘transcended the norms of their own
sex’ (Houston 2002:320), therefore any woman displaying behaviours outside of the
strictly policed and narrowly defined ‘norms’ were pathologised in terms of mental
disorder (Figlio 1978:176). In this vein, hysteria was a ‘diagnostic gesture’, a social
role ‘uncomfortably inhabited by suffering women’ and a didactic warning about the
dangers of ‘engaging in ‘unfeminine’ behaviour’ (Briggs 2000:247). It is important to
note here, that by virtue of being raped, women also become inculcated within a
taxonomy of sexual perversions that again adds to their overall depiction as
dysfunctional and disordered creatures.
Fallen Women and Corrective Reform
The Victorian convention that a ‘fallen’ woman’s life was irreparably broken
(Auberback 1980:30) and ‘compelled to suffer the pollution her soul abhors’ (Bartley
1815:40) was subject to contestation though religious philanthropy. Attempts to
debunk the myth of ‘the fallen woman’ subverted her identity to that of the victim,
fallen prey to economic and personal hardship (Melosh 1995:1756-7). Though sin
was seen to cause ‘irrevocable’ damage (Sanford 1892:122), it was also propagated
within certain social movements that women could ‘do penance for their past sins and
purge themselves of their moral contagion’ (Walkowitz 1991:221).
Penitentiaries, as well as some Salvation Army workhouses explicitly
accepted women and girls ‘who ha[d] fallen owing to violence’ (Sister Clare 1873:9),
31
and though to be pitied as victims, they were nevertheless still viewed as ‘sexually
tainted by virtue of the act done to them’ (L. Jackson 2000:107). 23 The need for
repentance combined medical and religious discourses with the institutional policy
that stressed the need for cure and reform (Ruiz 2011:125). The scourge of tainted
sexuality had to be excised through (physical and moral) cleansing, in order to save
the soul (Englehardt 2007:139-142).24 In this way, the penitentiaries offering places to
raped or fallen women can be seen as a nascent therapeutic community, where the
penitents were seen as patients being treated (Mumm 1996:533).
Such institutions attempted to transform the women from morally ruined and
socially dead into respectable and spiritual women (Mumm 1996:527). The women
were therefore encouraged to ‘blot out the memory’ of their abuse so that all
‘remembrance of the iniquity’ may be eliminated (Booth 1916:331). The importance
of ‘forgetting’ for this model of conversion and redemption was twofold: firstly,
forgetting allowed the woman to distance herself from the sexual knowledge that had
marked her initial ruin, and second, it was only through this unburdening from sin that
the women could find a place in heaven (Walker 1991:124).
From this, we can trace the constellation of forces and social processes that came
together during the late 19th and early 20th centuries that are intrinsic to modern day
conceptions of rape victimhood. First, the process of medicalisation privileged
23 Though the reform and penitents movements were primarily focused upon prostitution, there are explicit references to them accepting women who had ‘fallen owing to violence’ particularly in the Salvation Army. What I am trying to explain, is not necessarily that the number of women who had been raped were necessarily statistically prevalent in these places (though I am sure they were), it is that tainted sexuality came to be subjected to ‘corrective’, and ‘transformative’ treatments. This bears many resemblances to the modern day stress on personal transformation of an affected sexual identity (i.e. rape victimhood). 24 The idea of needing to ‘wash away’ the stain of sexuality, that sexuality outside of monogamy was ‘contaminating’, could be said to contribute to modern discourses where raped women feel ‘disgust, feelings of dirtiness and urges to wash’ following a traumatic event (Badour et al. 2013:155). This is so pervasive that in one study conducted by Fairbrother & Ranchman (2004), up to 70% of repondents reported immediate desire to wash following a sexual assault.
32
sexuality as the locus of identity, and encouraged doctors to pathologise deviant
sexualities. By creating the subject position of ‘the rapist’, the rape victim was
inadvertently created in opposition. The rape victim therefore became an object of
knowledge and was subjected to the inspecting gaze of the medical profession which
then created an authorised discourse about what a real rape victim looked like,
shrouding rape victimhood in ‘objective science’.
This medicalisation of victimhood began to see psychological understandings
of trauma gain credibility towards the end of the 19th century, transforming the
understandings of rape from the social (external) to the psychological (internal)
(Bourke 2012:17). This established rape as an attack upon a woman’s sexual identity,
with the power to create a ‘psychic wound’ and violation of ‘self’ which is a
profoundly modern conception. Furthermore, rape victims were afforded legitimised
types of speech within the courtroom, which gave such women the opportunity to
speak about their experiences, albeit through a normative lens. Such discourses
offered didactic models of victimhood with the power to materially alter the way a
woman defined and understood their own identity and experiences.
Contemporaneously, the corrective reform movements subverted the
understanding that a woman’s fall is a kind of social death, by stressing the
transformative and redemptive potential of repentance. Such institutionalised
narratives about personal transformation precede the ‘survivor movement’. Both
movements could be said to promote a therapeutic process where the self is
transformed from abject, corrupted victim into redeemed survivor, though the stress
on remembering, associated with the ‘survivor’ movement is starkly contrasted to the
practice of ‘forgetting’ in the penitents movement (L.Jackson 2000:115).
33
CHAPTER THREE: SHIFTING EPISTEMES
Certain formulations and wider social processes in the 19th century provided the
‘conditions of possibility’ for modern conceptualisations of rape victimhood
(Foucault 1973:xxi-xxii). Such history has significant resemblance with the modern
‘regimes of truth’ (Foucault 1972: 127). First although different discursive
productions of rape would have produced different material experiences of trauma
(Pollock in Mieke2005:187), both historic and modern constructions involve a
permanent loss that is differentially represented as a kind of ‘social death’
(Taylor2009b:23). Secondly, socially scripted narratives of rape are only seen as
socially legitimate if they prescribe to certain tropes. For example, the legitimacy of a
claim of rape is still predicated upon the assessment of character, behaviour and
‘respectability’25, and stories of rape are still more likely to be ‘acceptable’ if it
involves a physical struggle with a stranger.26 Moreoever, rape is only tangible and
thus authentic when it inflicts a visual or visualisable mark. The veracity of claims of
rape in modern society are predicated upon the wounds—whether visible or
invisible—that the woman are able to lay claim to.
Modern history
During the late 19th and early 20th centuries women had no social discourse or
‘collective narrative’ through which to articulate their personal grievances to wider
25 For example, a 2005 Amnesty International survey found that of the 1095 respondents, 22% believed that a woman was wholly or partially responsible for being raped, this increased to 26% if the woman was wearing ‘revealing clothing’, 30% if the woman was drunk, and 37% if the woman had failed to say no clearly enough (cited in Anderson & Doherty 2008:3). 26 The case of Ione Wells is a case in point about this (Evans 2015). Her story of being violently attacked received a huge amount of media attention because she effectively ‘fought off’ her attacker and was not, in the end raped. As an Oxford student coming to her familial home at nighttime she was seen as a ‘respectable’ and ‘undeserving’ victim, rather than a ‘drunk’, ‘immoral’ woman who put herself in a position of danger. In our interview, Zoe Lodrick and I discussed this case and she said ‘it makes me sad when I hear of Ione Wells being so widely spoken about…I’m thinking, how is this narrative going to affect the girls who didn’t fight back’.

34
society (Richardson 1990:128), unless through the limited—and often mediated—
opportunities offered by the courtroom (Brownmiller 1975:xi-xiii). Emphasis placed
on bodily wounding and ‘fight off’ an assailant meant that only a highly scripted
discourse on rape could be articulated. In stark contrast, due to the increasing
popularisation of psychology throughout the 20th century, by the 1970s, researchers
had moved towards a trauma model of rape that viewed the consequences of sexual
violence in predominantly psychological, rather than physiological terms.
The ‘psy’-doctrine that all human beings have an ‘inner domain’ which is
‘structured by the interaction of biographical experience’—with theorised or
hypothesised laws or processes—changed the ontology of western metaphysics (Rose
in Hall & Du Gay 1996:129). Psychology offered the vocabulary and regulatory
techniques through which the interiorised individual could be accessed and governed
(Rose 1996:103). Here, psychology is a mechanism through which the human
condition is constituted by rendering one’s inner life remarkable (Rose 1996:54). Yet,
this ‘remarkability’ is dependent upon an inducement to speak one’s inner self, as
well as the interpersonal power relations (doctor-patient, questioner-speaker)
necessitated by such confessions of the soul (Davis & Manderson 2014:8). This
‘incitement to discourse’ has radically altered the way in which society conceives of
and speaks about rape and rape victimhood (Taylor 2009a:70).
One of the pitfalls of ‘speaking out’ about one’s experiences of sexual
violence is that confession confers an identity position on that person. ‘Narrated
memories’ are foundational (Brison 2002:30). The past is not ‘simply there’; it is
actively reproduced when articulated: ‘the fissure that opens up between experiencing
an event and remembering it in representation is unavoidable’ (Huyssen 1995:3).
35
‘Breaking the Silence’
Second-wave feminism precipitated a ‘radical shift’ in the way that rape was
understood by society, including the ideas that: any man could be a rapist, any woman
could be raped and that rape could occur in a variety of forms (including marital or
acquaintance rape) (Chasteen 2010:107; Plummer 1995). It was during this period
that feminists and trauma theorists alike argued that rape produced the same effects in
women as war did in men, providing a powerful narrative of the chronic
psychological distress caused by sexual violence (Freedman 2006:106). 27 The trauma
narrative can be seen as an attempt to validate and authenticate the political claim of
injury relating to the impact that gendered violence had on women’s lives (Donovan
2005:70). Through the distinctly second-wave feminist project of consciousness-
raising, women started speaking publically about their experiences of sexual assault,
creating ‘survivor discourse’.
‘Survivor discourse’ propounded the political message that sexual violence
against women could no longer be institutionally ignored (Bumiller 2008:13). This
discourse formulated the rape victim as a subject of care rather than an object of
knowledge (Haaken in Lamb 1999:16). For example, archival documents of the
Metropolitan Police in the early 1960s detail how, following intense lobbying by the
National Women’s Council, the Police instituted the requirement for women doctors
to conduct the ‘intimate examinations’ of rape victims (MEPO2/10401). These
documents reveal the processes through which the rape victim came to be
institutionally accepted as a traumatised individual, culminating in the creation of
grass-roots rape crisis centres (RCCs) and helplines, and extended into the
27 For examples see Burgess & Holmstrom 1974; Kilpatrick et al. 1981; Stanko 1985; Kelly 1988; Katz 1984; Brown 1995.
36
institutional practices of the medical and legal professions (Zuspan 1974:145; Bourke
2012:5). Such institutionalisation led to the creation of national ‘codes of ethics’, and
frameworks for helping women through their recovery process. This challenged the
most damaging aspects of the social stigmas attached to rape (Caretta 2011:18).
The early grassroots RCCs understood rape as an expression of a violent
gender war against women (Bumiller 2008:3). This model encouraged women to
confess their experiences of abuse ‘in the name of persuading society as to its reality
as a rape culture’ (Herberle 1996:64), leading many feminists to reify and enshrine
the notion that collective space to grieve the wounds of the gender war were not only
useful socially, but therapeutic (Roestone Collective 2014):
‘I wanted to found a national women’s rape museum… a public space where
women who were survivors could come and grieve the collective pain of other
women who were raped’ (Gage 1992:6)
The model of rape associated with second-wave feminism is indebted to the
constitution of the confessing modern subject, whose inner turmoil must be
articulated, not only to heal the self, but also to heal society. According to Davis,
1971 is the ‘watershed year’ in the emergence of rape as a social problem. The first
‘speak outs’, where women told their stories of abuse were held, reclaim the night
marches took place, and Germaine Greer conducted the first television interview with
a rape victim, on ABC-TV (in Patterson 2002:108). The political necessity of
speaking out—or ‘having voice’—has permanently changed the sexual violence
agenda (Lamb 1999:127). The idea that ‘to speak and to be heard’ is to have privilege
and agency over one’s life, while to remain silent or to be silenced, is oppressive and
37
victimising (Ahrens 2006:263) provided the women’s movement with powerful
justification for the elevation of ‘stories from survivors’ (Lamb 1999:128).
In so doing the ‘new definition of the victim person-category’ was instituted,
providing a collective discourse from which women could speak (Best 1999:95; Davis
in Patterson 2002:121). This model individualised the suffering and encouraged
women to view their experiences in terms of ‘victim’ or ‘survivor’ identities. It also
inadvertently imposed value judgements on speaking (read: voice) and not-speaking
(read: silence) through the articulation of the ‘victim’ and ‘survivor’ labels, where the
‘survivor’ label was valorised for the strength of having ‘the courage-to-heal’
associated with ‘speaking’ out and ‘owning’ ones experiences (Haaken in Lamb
1999:16), while the ‘victim’ was categorised as the silenced, weak and traumatised
other (Naples 2003:163).
In order to collectively politicise rape and suffering, (Cole 2007:12), the
movement required exposing ‘bodies in pain’, as well as ‘dramatising the moral
degradation’ that women suffered (Cole 2007:13) in order to form a politic based
upon the claim of injury (Hanhardt 2013:8). This marks the continuing importance of
‘bodily signs, marks and private parts’ required by wider society to validate women’s
experiences of sexual violence as authentic (S.Robertson 1998:388). It also, through
the ‘language of heightening’28, sensationalised sexual violence by making rape and
the traumatisation of victims ever more visible and imbued with more symbolic
potential to destroy (Scarry 1990:869). Such language of heightening has assigned to
rape and sexual violence a special sign of mental pathology and ‘glorified scandal’
(Foucault 1965:70). 28 The language of heightening is where ‘the meaning is continually lifted out and made more visible through a continuous sequence of clarifications’ (Scarry 1990:869)
38
Furthermore, the ascendancy of an increasingly professionalised language to
detail sexual trauma, as well as the increasing co-optation of responses to rape by the
state (Bevacqua 2000:115), meant that eligibility for services was increasingly linked
to the women’s status as traumatised victims of rape and ‘their ability to recognise
their problems in medical or psychological terms’ (Bumiller 2008:13). A politic of
‘sympathy’—where identities are fashioned around suffering and injuries are
converted into ‘cultural capital’—tends to preserve the status quo (Puar 2011:151).
The sensationalisation of rape discourses and prominence afforded to trauma models
has imbued society with a bias: ‘it is the degree of suffering (not the grotesqueness of
the injustice) that speaks of the wrongness of the assault’ (Armstrong 1996:300).
Therefore, attention has shifted from structural inequalities that render women more
susceptible to violent attacks, to that of an individual exercise of self help (Cole
2007:138).
Such collective narratives of traumatisation and survivorship favoured the
trope of recovery and personal transformation by privileging the voices of empowered
survivors. In turn, this created a movement that required ‘recovery’ from pathology
and ‘closed off alternative stories’ and conceptualisations of rape victimhood (Davis
in Patterson 2002:122). Therefore, the survivors movement was complicit in
discourses that oppressively cast victims of rape in monolithic model suffering and,
rather than cure society of its rape culture, came instead to facilitate the growth of an
extensive recovery movement (Naples 2003:167).
By the 1980s, neoliberal politics and the increasing prominence of the medicalised
model of victimhood depoliticised the survivors movement, shifting the focus of anti-
violence campaigns from communal critiques of structural violence to individualised
39
articulations of personal injury (Duggan 2012:Ch.2). The ascendency of
institutionalised and professional expertise has led to the development of a large
professional apparatus that presents sexual violence as ‘chronic yet treatable problem’
(Bumiller 2008:13). Marcus (in Butler & Scott 1992:387) argues that in conflating the
act of rape with irrevocable personal injury, the second-wave anti-rape movement
accepted rather than rejected a metaphysical status of rape that it can ‘only be feared’
or legally or medically repaired.
Rather than asserting ‘survivors stories’ as the basis of collective organising
against rapacious masculinity, the medicalised model of victimhood instead favoured
individualised and apolitical narratives of ‘recovery’ and personal transformation
(Ovenden 2012:950). The medicalised model of victimhood constitutes victims of rape
as a persistently vulnerable demographic, living in a perpetual state of ‘prognosis (Jain
2007:79). The reification of the trauma model of rape increases the potential of the act
to cause traumatisation in women who have been raped. Contemporaneous to the
construction of rape as always already traumatising, the pervasive culture of wellness
in western ontology has imbued modern society with a tension between capability and
debility, which impacts on the lives of victims of rape (Thackhuk 2011:156).
Modern Discourses
Culture of Wellness
As a result of the 19th century moral reform movements—where the moral imperative
of sanitation, nutrition and family health was promulgated—modern western society
has inherited and extended a ‘culture of wellness’ (Clark et al. 2003:172). The
melding together of the two distinct processes of medicalisation (where the ‘moral
turns into the medical’) and healthicisation (‘where health turns into the moral’)
40
(Conrad 1992:223), has imbued western ontology with a tension between the removal
of personal responsibility (to medical professionals) on the one hand, and the
imposition of unrelenting responsibility to be ‘better than well’ on the other (Puar
2009:167).
The construction of the body and self as never well enough provides an alibi
‘for the translation of sensation and affect into symptom’ (Puar 2009:167), as well as
ensuring the ‘continual enlargement of the domain of the therapeutic’ (Sunder-Rajan
2006:144). This process produces an increasing aversion to, and fear of, suffering
(May 2011:84)—which becomes increasingly pathologised and subjected to
‘corrective treatment’.
Out of this milieu, health itself can be seen as a ‘side effect of successful
normativity’ (Berlant 2007:765). Yet, these discourses rely upon the ‘spurious
binarisation’ of ‘bodily capability and bodily debility’ (Puar 2011:149) therefore, rape
victims who reside in the ‘zone of uninhabitability’ as abject subjects (Butler 1993:3)
bear the brunt of the two competing discourses of healthicisation and medicalisation.
The first puts the responsibility upon them to be ‘better than well’—to be empowered
survivors—whilst the second takes away their powers of self-definition and
pathologises them as mentally abject, rape victims.
The pathologisation of victims of rape
This idea that victims of rape are mentally wounded implicitly ties social constructions
of rape victimhood with mental illness, where their behaviours and identities are read
as ‘irrational, disordered, impaired and frightening’ (Nicki 2001:87). By pathologising
rape victims, both the state and nongovernmental actors are able to advance an
understanding of sexual violence that subsumes complex, unpredictable and
41
uncontrollable life experiences into a predictable set of symptoms (Bumiller 2008:74).
This functions to make sexual violence ‘treatable’, because the woman is required to
assume the responsibility of ‘recovery’, rather than socially and politically ‘treating’
the sex offenders and addressing the realities of western societies rape culture
(Herberle 1996:64)29.
The establishment of certainty around identifiable pathologies is not based
upon ‘the completely observed individuality’ of a persons symptomatology, but is
instead based upon the ‘completely scanned multiplicity of individual fact’ (Foucault
1973:124). This privileges convergent symptoms over divergence; it is easier to
‘treat’, ‘rehabilitate’ and cure’ if there is uniformity, universality and neat
categorisation30.
Trauma model
The trauma paradigm of rape which was first depicted by Burgess and Holmstrom
(1974) as ‘Rape Trauma Syndrome’ (RTS)—and bears many similarities to PTSD—
has infused the vernacular lexicon with medicalised understandings of trauma and the
traumatising impact of rape (Eby et al. 1995:564). This model has become so infused
and normalised within social understandings, that assumptions about the hypothetical
29 This perpetuates victim support models and does not address the complex realities of why women are raped and how to reduce such sexual violence. Privileging such models also leads to funding deficits in research of treatments and therapies of potential and actual sex offenders. For example, the NSPCC used to have a hotline available for people who were worried they were going to commit a sexual offence against a child, but funding for this and similar projects has been cut. The only available projects now focus on people who have already offended within the carceral system to try to stop them recidivating (Lodrick 2015b). The taboo nature of providing sympathy and preventative therapy for people prior to them committing an act means instead that the ‘corrective machinery’ of the state is wielded only after the offense is committed and with minimal success – because by virtue of being labelled as ‘rapist’, the offenders become bound to the identity and therefore are increasingly likely to reoffend. 30 Not to mention the fact that it is easier to ‘treat’ victims of rape than it is to cure society of its rape culture.
42
aftermath of rape are indistinguishable from the medicalised model of trauma (Gavey
& Schmidt 2011:451).
Marecek describes this lexicon for speaking about sexual violence and
subsequent ‘narrative framework for explaining’ the ‘problems’ women develop
following an assault, as ‘trauma talk’ (in Lamb 1999:158). In this conceptualisation,
trauma talk ‘refers to the system of terms, metaphors and models of representation’
that are presented as natural fact when speaking about rape victimhood used by
feminist researchers, mental health professionals, the mass media and wider society
alike (Ibid:158-9). Such medicalised and ‘scientific’ approaches to trauma have
‘tremendous appeal’ to those who work with victims of sexual violence because it
provides an ‘objective’ understanding of the harm caused by such victimisation, that
doesn’t hold rape victims responsible, or ‘to blame for… their own victimisation’
(Gilfus 1999:1240).
Rather, the symptoms of trauma are described in biological or biopsychosocial
terms which lifts the effects of rape out of the hands of the victims (and arguably into
the hands of an expert):
‘She gave me the scientific reason behind my anxiety, panic and PTSD. Seemed
a strange thing to talk about, but I felt it was beneficial’ (Sarretta 2015)
If the 1970s saw the institutionalisation and normalisation of the trauma model of
rape, current conceptions have extended the naturalness of such discourses and
extended the unassailability of this model by locating trauma in the physical make up
of the brain. Although the trauma model of rape is intended to help victims feel as
though they are responding ‘normally’ to traumatic stimuli, there are also aspects of
43
this model that are ‘pathologising, exclusionary and decontextualising’ (Gilfus
1999:1239).
The Neurobiological Trauma model
Modern accounts of psychological trauma are articulated through the physical
componentry of the brain (Corzolino 2002:71). The stress hormones activated in the
amygdala through the traumatic event are seen to ‘alter psychobiology, personal
adjustment and systems of meaning’ (Bloom in Giardiano et al. 2003:405). According
to Lodrick, when a traumatic event occurs ‘terror overwhelms higher brain
functioning’ (2007:4) meaning that the trauma is encoded in the ‘implicit, right hand
side of the brain’ which is fragmentary and emotional rather than in the left hand side
of the brain which is ‘explicit and analytical’ (Lodrick 2015a). Furthermore, during
the assault itself the amygdala regulates the bodies ‘fight, flight, [or] freeze’ response
(Lodrick 2007:4). The freeze response, which is said to occur in somewhere between
37% and 52% of rape victims (Gola et al. 2012:214; Moor et al. 2013:1054) is a
dissociative survival mechanism which enables people to ‘endure experiences that are
at the moment beyond endurable’ (P.Levine 1997:138).
However, such dissociative survival strategies are said to bode badly for
‘future psychological and physical wellbeing,’ as the memories of the trauma are
more likely to be encoded in the emotive right hand side of the brain which is harder
to rationally appraise once the traumatic experience has ended (Giesbrecht &
Merckelbach 2009:338). This encoding in the right hand side of the brain is argued to
be the reason why people experience psychological symptoms post-trauma: ‘traumatic
symptomatology has, at its foundation, a lack of sufficient neural integration’
(Lodrick 2007:9; Herman 1992:28). It is this lack of ‘neural integration’ that is said

44
to cause ‘traumatised people [to] lead traumatic and traumatising lives’ (Van der Kolk
& McFarlane 1996:11).
The Expansiveness of the Trauma Model
The trauma model of rape creates a psychologised ‘rhetorical commonplace’ where the
notion that rape forecasts a devastating array of damage is ‘recognised, characterised
and then standardised’ (O’Malley in Barry et al. 1996:189). Rape is nearly always
depicted as exceptionally traumatic (Petrak 2002:1; Bargelow 2014:118). It is seen to
damage the women ‘for the rest of their lives’ (Matheson interview), affecting the way
they ‘think, learn and remember’ and well as how they feel about themselves, others
and the world (Bloom in Gardiano et al 2003:405)
‘…when he raped me, part of me died. I can’t get over that. I can’t forget, it’s
not possible. Yes, I have learned to live without that part of me’ (Guest_* 2002d)
The trauma model of rape represents not only a comprehensive neurobiological and
‘biopsychosocial’ account of the effects of rape, but it actually represents an all-
encompassing model that is seen to profoundly alter all facets of human experience
and identity irreparably. Not only is this enshrined in medical and professional
discourses, but is infused in wider social narratives as well.31
In the DSM-IV, traumatic experiences can be anything ranging from ‘violent
personal assault’, ‘natural or manmade disasters’, ‘or being diagnosed with a life
threatening illness’ (APA 1994:424). Grouping such experiences into the ‘same
cognitive category’ is highly problematic (Fine 2007:27), as they will tend to receive
the same ‘treatment’ despite being tangibly different (Degloma 2009:113). This 31 For example, Chasteen’s (2010:124-5) research found that all female respondents believed that rape involved permanent damage and destruction of the physical and emotional self, with respondents repeatedly asserting that ‘rape takes something away from you that you can never get back’.
45
creates a culture of ‘abstraction, objectification’, where all victims of rape have
certain attributes, behaviours and identities foisted upon them in a kind of ‘mandated
normativity’ (Stahl 2013:53).
In establishing ‘regimes of truth’ traumatised victimhood is universalised,
abstracted, decontextualized and ultimately, ahistorical. This obscures the socio-
political reality of rape and trauma, as it does not look at ‘the source of the injury or
the social and cultural context of victimisation’ (Gilfus 1999:1242). In universalising
the trauma model, race, gender and class differences are effaced (Daniels 1994:231).
Traumatic injury does not randomly affect people, but is ostensibly more likely to
occur in particular groups: ‘Wounds adhere differently to different people’ (Jain
2006:58). Abstracted models of trauma are said to be gender neutral, yet women are
diagnosed with PTSD at a rate of 2:1 in comparison to men and the length of time they
suffer from symptoms of PTSD is up to four times longer than men (Norris et al. in
Kimerling 2002:3-6). Though it is difficult to extricate pre-trauma gender scripts from
post-trauma memory, it is quite possible that the disparities found in PTSD rates
between men and women are a result of socio-psychological scripts that always
already predispose women to embody and perform post-trauma symptoms that match
diagnostic criteria (Tolin & Foa in Kimerling 2002:349).
Moreover, the idea that rape is not necessarily traumatising tends not to be
asserted for fear of ‘the political dangers of misrepresentation’ (Gavey in Lamb
1999:70). Survivors’ accounts that refute the trauma model are often suppressed and
countered with aspersions to a kind of false-consciousness; that even if rape victims
do not immediately experience psychological symptoms, such symptoms will occur
46
‘after a latency period of months or years following the trauma’ (Koss et al.
1987:169).
CHAPTER FOUR: THE EFFECT OF DISCOURSES ON THE WOMEN
Incitement to Speak: Confessional Society
In Madness and Civilisation, Foucault argues that Freud ‘abolished silence,’ by
inciting his patients to reveal and describe their madness, as though the very act of
revelation in and of itself could lead to a clinical cure for their ailments (1965:275).
The ‘psy’-disciplines have popularised the idea that ‘bottling things up’ (S1 workshop
2015) is maladaptive, whilst ‘getting things off your chest’ is liberating, despite the
fact that Freud later rejected the efficacy of this ‘talking cure’ realising that it could
‘repeat rather than heal trauma’ (Taylor 2009a:70).
The idea that simply talking about something is necessarily curative is
disciplinary insofar as it compels people to explain themselves in a way that
‘discursively fixes their identities’ to the pathology they wish to be cured of
(Ibid:119). This mechanism extends beyond the therapeutic realm. Modern western
society requires its subjects to realise and become their authentic selves, yet to know
oneself requires ‘self-examination, explanation of oneself, [and] revelation of what
one is’ (Foucault 1978:2) before one can truly bear ‘special witness to the truth of
individual personality’ (Brooks 2001:18). Therefore, confessional subjectivity
encourages people to put themselves into words, even if this is damaging
(Shuttleworth 2012:643).
The compulsion to confess has been internalised as a result of ‘infolding’ the
‘exterior’ compulsion, and has guaranteed confession as an intuition of the modern
47
soul (Venn in Patterson 2002:30). The normalcy of this intuition is ensured by the
self-perpetuating understanding that we are repressed, and that the only cure to such
repression is to confess. Western society constantly calls for ‘breaking the silence
over sexual assault’, yet we have been officially ‘breaking’ this ‘silence’ for over 45
years.
Taylor argues the belief that we ‘cannot speak about it’ allows us to feel ‘we
are achieving something important both psychologically and politically’ in the
process of speaking out (2009a:74). For Foucault (1979), the claim that confession is
difficult, that it is an achievement to confess provides the very excuse to confess in
the first place.
This mechanism of truth-production anchors identity to the attention received
in, and the pleasure derived from, the telling of oneself. In turn, the subject is ‘fixed
by the gaze, isolated and animated by the attention’ it receives (Foucault 1979:44-5).
Therefore, for Foucault, the issue is that this hermeneutic of the self is an effect of
power, and rather than revealing an essential or authentic self, confession instead
reveals a disciplined self (Taylor 2009a:78). As such, both the supposed ‘resistance’
to confess and the gratification derived from confessing are erroneously experienced
as the achievement of personal freedom (Foucault 1979:60).
Talking as healing
The cyclic ‘lure of the confessional’ produces a social narrative around rape that
firstly assumes that ‘confessing’ is invariably cathartic and secondly perpetually
requires survivors to ‘reveal’ their experiences (Warner 2002:120) on the basis that
‘we don’t tell enough stories of abuse’ (Burrows 2015).
48
‘I want to be able to say everything I want to say and put it out in the universe in
hopes of healing and bringing closure. I’m not sure where the best place to do
that is. I have come so far but it always seems like there are things that keep me
back’ (Love2013)
The idea that ‘recognition’ in and of itself has curative powers compels acts of self-
disclosure (Joinson 2001:178) and becomes self-perpetuating through the idea that
revelation is a personal achievement:
‘The word [rape] is really hard to get out…Just last week I was telling some
friends of my partner’s and it was really difficult. I got it out though, and I was
proud of myself’ (Guest_* 2001c).
In a psychological case study of how to ‘treat’ rape and trauma, Papaikonomou
(2014:213) encourages therapists to ask their clients to provide a detailed retelling of
the event, asking questions such as ‘‘what was the worst moment for you?’’ As long as
the client remains in their ‘window of tolerance’ (Siegal 1999:523), talking is said to
aid the rape victim assign the trauma to the past, as narrativising the traumatic
experience increases the integration among neural networks (Lodrick 2007:13)32.
Therefore, the need for confession is guaranteed in the presentation of traumatic
memories being coded in the right hand side of the brain and the need for such
memories to be re-encoded in the ‘realm of processed thought’ (Papaikonomou
2014:213).
32 Window of tolerance refers to a state where the client is not over-aroused by the emotive content of the interview such that they still possess the ‘integrative brain functioning’ necessary to be able to appropriately consign the trauma from the left to the right hand side of the brain (Lodrick 2007:13). In order to help keep the client in the window of tolerance, Lodrick asserts it is necessary to ‘ensure the cortical and hippocampal functioning remains available to client. If functioning appears to be significantly impaired ask the client simple cortical questions like: ‘how many fingers am I holding up?’, ‘what colour is that lamp?’… keep the questions simple and observable’ (Ibid).
49
Without re-encoding such memories, victims are thus said to be ‘cut off from
language, deprived of the power of words, trapped in speechless terror’ (Bloom in
Giardiano et al. 2003:422). Therefore, if a woman chooses not to speak of the event,
she is said to ‘bury’ or ‘repress’ her emotions, which is taken to be a maladaptive
coping strategy, pathologised and argued to cause ‘long-term struggles with
depression or PTSD’ (Clarke & Griffin 2008:201). However, the idea that ‘turning off
your emotions’ (Interview 4) is necessarily harmful fails to recognise dissociative
coping strategies as meaningful or natural, let alone as potentially helpful (Warner
2001:30).
‘It happened to me a week ago…when Monday came around (I was expecting to
have nightmares or something and nothing happened) ….I guess what I am trying
to say is that I didn’t feel like a ‘victim’’ (Samealdo 2006)
‘It came as a surprise to me that as time passed I still felt little to nothing about the
rape. I was increasingly bewildered at the odd numbness surrounding the entire
incident. I would check up on it every so often in my mind’ (Survivor cited in
Bargelow 2014:130).
Numbness in the aftermath of trauma is a perfectly logical strategy for self-
preservation, yet both women appear to feel like they should be feeling traumatised.
The disciplinary powers of such discourses culminated in both women actively
seeking to ‘conduct their own conduct’ in accordance with the ideal-type of
victimisation.
In the neurological trauma lexicon, victims of sexual violence ‘protect
themselves against the overwhelming exposure of threatening stimuli by inhibiting
information processing’ (Giesbrecht & Merckelbach 2009:337). However, the trope of
denial is drawn upon to mark rational responses to the rape in pathological terms: she
50
is either lying or in denial (Gavey & Schmidt 2011:443). Ultimately, in pathologising
women’s survival strategies as inherently self-destructive, women's actual ‘attempts at
self-preservation are discredited’ and their need to utilise narrative strategies to
overcome the trauma are ‘paradoxically reinforced’ (Warner 2001:126).
There is widespread recognition that ‘debriefment’ following trauma
significantly increases the likelihood of a person developing PTSD (Chivers-Wilson
2006:116). Further, it is widely accepted that traumatised individuals tend to
traumatically re-enact and repeat their own traumatisation. That there is a ‘valid’ and
‘invalid’ way of talking to rape victims about their experiences—one that is likely to
‘retraumatise’ and one that is likely to aid the person assign the trauma to the past—
presents a troubling picture, highlighting the difficult terrain that survivors have to
navigate.
Talking as potentially harmful
Many ‘survivors’ welcome opportunities to speak out about their experiences because
they have adopted the oft-repeated mantra that ‘telling is freeing’ (Guest_* 2002b).
However, when this claim is questioned further, a far more complex picture emerges:
‘Talking helps me. Before I go I’m a wreck and sick but after I’ve done it, I feel
strong. In less than two hours, I’m talking with a reporter from a newspaper. I’m
in the mess part right now. But after it’s out, I know I’ll feel wonderful’ (Guest _ *
2002a).
Here, although the aftermath of revelation is seen to invoke feelings of strength, the
act of telling is prefaced by intense emotional discomfort. This indicates that in reality
51
telling ‘your story’ is not simply about healing the self, but is bound to the validation
or attention received through the act of telling:
‘The telling of the story itself is totally pointless and potentially harmful without
some relational holding of it…in terms of support networks, in how it is received
and responded to’ (Lodrick 2015a).
In revealing their experiences of rape to somebody, the listener is put in a
position of ‘response-ability’ with the potential to alter the relationship between
themselves and the teller at the point of revelation (Davis & Manderson 2014:156).
This situates the listener in a position of power, insofar as they are faced with a choice,
of ‘whether or not, and how to respond’ (Ibid). During our interview, McClean said
that he found the incitement to speak problematic:
‘...it becomes a spectacle…revealing something about yourself that Is very
painful and personal in a public forum…because actually the response you are
expecting from someone when you reveal something like that is somebody who
is really going to pay attention to your pain and is not just for public
consumption’ (McClean 2015)
Therefore, in ‘confessing’ their experiences of rape, rather than simply revealing
something about the self in order to ‘heal’, the rape victims actually enter into a social
relationship where they hand their most personal and vulnerable experiences over to
somebody else who may or may not respond appropriately:
‘I think… after all these years, it’s not to much the fact that I was raped that hurts
me, it’s the fact that people who I loved, like my friends and my parents,
responded in such negligent ways’ (Interview 2 2015).
According to one study, up to three-quarters of rape victims receive negative reactions
from their informal social support network (Campell et al. 2001). When such
52
validation is lacking this could damage both the victims self-definition and their trust
within their surrounding environment (Bargh et al. 2002:34)
During a group ‘survivor’ session I attended, one woman attempted to hand
out postcards, but was stopped by staff because they thought that the material could
be ‘triggering’ to others in the group. When I spoke to her about it later she said:
‘I felt that there was an invitation to offer something and I thought: here is what I
have to offer. It took courage—every time I put my poems out there, or I put a
tweet out there, or I put my postcards out there… which are basically my naked
soul—it takes a bit of a gasp in and… a leap of faith each time. I mean it takes
something from you. It’s not something I find easy to do, and when [the staff]
took them out, I just went into a place of shame, like there was something wrong
about what I was offering, that it was seen as inappropriate and not to be trusted’
(S2 workshop 2015).
This highlights the extraordinary amount of trust afforded to strangers to sensitively
respond to the outpouring of ‘naked soul’. Particularly within the ‘survivor
movement’ where people group together on the basis of commonality, there is the
‘illusion of support, the illusion that you are surrounded by a whole movement’ who
understand and care for each other (Lodrick 2015a). However, in sharing their most
vulnerable moments, survivors may reassert rather than challenge their vulnerability:
‘The only thing I ever regret when looking back is telling certain people ‘I was
raped’ …I told a teacher at my college about what had happened to me. I don’t
really know why I said anything, I think I just wanted people to know I wasn’t
crazy…and the only remark she made was about the fact that I’d been drinking
that night…as though it was somehow my fault’ (Interview 2 2015).
53
The propensity of negative responses to cause psychological suffering in rape victims
is becoming an area of increasing interest to researchers. Research into how rape
myth acceptance (Baugher et al. 2010:2039; Frese et al. 2004:156), cognitive
distortions33 (Iverson et al. 2015:49) and counterfactual thinking34 (Branscombe et al
2010:267) increase the likelihood that a rape victim will suffer from PTSD and re-
traumatisation, highlights growing acceptance that meaning ascription can negatively
impact upon the victims sense of wellbeing and long-term prognosis. Therefore, if
responses to sexual violence re-impose harmful thinking, the strategy of speaking out
about suffering does not necessarily achieve healing and can actually ‘enact a
‘secondary victimisation’ where the initial trauma is repeated (Campell & Raja
1999:261).
Repetition Compulsion
Van der Kolk (1989:389) argues that traumatised individuals tend to ‘expose
themselves, seemingly compulsively’ to the traumatic retelling or reliving of their
experiences. Due to this ‘repetition compulsion’ traumatised individuals rarely ‘gain
mastery’ over their life experiences and instead, repeatedly cycle behaviours and
cognitions that accentuate the trauma and traumatic sequelae (Lodrick 2007:10). The
online forums are quite literally, riddled with examples of traumatic re-enactments: ‘I
keep coming back over and over again to where I was molested… I can’t stop talking
about it; I’m never done’ (Setrain 2010).
One survivor, when talking of her ‘obsessive’ compulsion to search for
triggering material commented that it is ‘almost like I want to suffer’ (Minute 2010). 33 An example of a cognitive distortion is the idea that ‘bad things happen to bad people’ therefore, because a bad thing happened to me, I must have deserved to be raped. 34 An example of counterfactual thinking is imagining alternative outcomes: if I had not drunk so much alcohol, I would have avoided passing out in the bedroom where I was raped.

54
Another admits: ‘ even though sometimes it hurts I still trigger myself on purpose’
(Anonymouse09 2010). This could be argued to be why so many survivors construct
their lives following their assault as being in a kind of ‘stasis, waiting for life to begin
again’ (Interview 2 2015) or permanently ‘stuck’ in a cycle of depression:
‘When you just keep telling your story over and over… you are just stuck. I cried
and I cried about everything and only felt depression and grief… I was a broken
record’ (Guest_* 2002c).
COMING TO TERMS WITH THE LABELS
In the 21st century, the Internet has become the platform par excellence of self-
expression because, through the ‘intermediation of screens and pseudonyms’
(Reingold in Joinson 2001:178), it offers a kind of liminal space ‘betwixt and
between’ ordinary social interaction, and the ‘hyperpersonal’ interaction afforded by
Internet anonymity (Turner 1967; Walther 1996:3).
It has been shown that people are much more likely to reveal intimate personal
details about themselves to both known and unknown users over the internet (Rice et
al. in Joinson et al. 2007: 10):‘I will be more truthful in my answers here then if I
were to do them alone at home’ (Guest_* 2001a). Internet platforms offer ‘safe’
spaces where rape victims can express their experiences:
‘While I can write those words [‘I was raped’] in a safe space, like here… I don’t
believe I shall ever verbally utter them; not in relation to me’ (Guest_* 2001b).
Furthermore, such online spaces tend to be pools of information, not only providing a
deluge of educational resources and articles about the impact of sexual violence, but
also spaces where symptoms and feelings are discussed and encoded as ‘normal’
(Segal 2009:355-361):
55
‘I’m still navigating my survivor identity… I repeat my story to myself to better
understand who I am and where I’m going. Beyond self-reflection, some helpful
ways to negotiate this process might be connecting online… Reading educational
resources about sexual violence helped me begin articulating and contextualising
my complex emotions’ (Kuo 2015).
Although such spaces aid victims of violence to ‘understand’, ‘articulate’ and
‘contextualise’ their experiences, inevitably it also encourages the women to inherit
the common ‘themes, structures, characters and images’ associated with the
symptomatology of rape victimhood (Showalter 1997:6).
People are ‘extremely suggestible’ (Scheff 1974:450) and the comparison of
one’s inner self to didactic victim-models leads to a ‘more efficient regulation and
normalisation’ of victim-identity through the production of ‘self policing subjects’
(McNay 1992: 87). Experience and identity are linguistic: ‘all of us come to be who
we are (however ephemeral, multiple, and changing) by being located or locating
ourselves (usually unconsciously) in social narratives rarely of our own making’
(Somers 1994:606).
Language is a ‘social practice’ (Marecek in Lamb 1999:159), an assemblage
or technology through which people can access and understand their sense of self and
of being in the world (Potter in Richardson 1996:126). It follows that rape victimhood
is not only ‘scripted’; it also scripts (Marcus cited in Hersford 1999:195). Elaine
Scarry argues that the very act of naming an ‘interior’ event causes ‘an immediate
mental somersault out of the body [and] into external social circumstances’ (1988:16).
‘By labelling it rape straight away I think I hurt myself more somehow…I feel
more damaged by calling it rape than by calling it something awful that happened’
(Baily 2009).
56
Therefore not only is the victim of rape subjected through the act of violence, but her
subjectivity ‘continues to acquire validity and sense through fidelity to’ the violent act
(Calcagno 2009:35).
Labelling experience
Disclosing ones experience and labelling it in a narrative is ‘deeply temporalising’
(Davis & Manderson 2014:161). The act of telling, discursively constitutes an identity
prior to the assault, in opposition to an identity post-assault. This dissociates a
person’s present sense of self from their past self in an artificial way, and could be
argued to be a contributing factor in why rape is seen to simultaneously enact an
‘irreparable loss of past- self’ and create ‘a new identity’ (Lodrick 2015a).
‘Rape victim: I’ve had my ups and downs but I’m kind of getting back to normal
now, whatever that is’…
Counsellor: ‘and that really is difficult because it really is a new normal and you
have to adjust your life and everything that you knew before according to who
you are now.’ (White Buffalo Calf Woman Society 2013)
Homi Bhabha wrote that ‘no name is yours until you speak it’ (cited in Sonntag
2011:223). Through the ‘rituals of storytelling’, women who have been raped come
out of the closet and become rape ‘victims’, or ‘survivors’ (Haaken in Lamb 1999:13).
This naming exercise is required if the survivor is to ‘own’ their experiences and
become empowered. One ‘survivor’ I interviewed described herself as ‘just out and
proud’ (Participant 3 survivor workshop).
This naming exercise is not only a kind of ‘linguistic citation of norms’
(Hollywood in Armour & St.Ville 2006:253), but is a signifying act that encourages
the rape victims to express their identities in terms of the regulatory ideals of
57
traumatised victimhood (Butler 1993:1-2). In this sense, labelling oneself a ‘victim’ or
‘survivor’ is a moment in the ‘dialectic of identity’ (Ronai in Lamb 1999:156) where
self-identity is given value in sense-structures.
‘Victim’ – ‘Survivor’
Labelling yourself or your experiences is not value-neutral. The terms ‘victim’ and
‘survivor’ are already imbued with a priori meanings. A survivor I interviewed said
that she hates the victim-label because people ‘instantly assume you must be weak,
fragile or vulnerable—as though you need to be tiptoed around’. On the other hand,
she disliked ‘survivor’ because it is an ‘inescapable identity—you will always be a
survivor of rape, but victimhood can be transcended’ (Interview 3 2015).
Some women outrightly rejected the labels saying that they don’t ‘walk
around with an S for ‘Survivor’’ on their ‘sleeve’ (Tilted 2003); but some feel that the
‘level of healing’ implied by ‘survival’ isn’t something they will ‘ever accomplish’ or
‘achieve’ (Magdalene 2003; Lora 2003). What becomes clear is that the ‘survivor’
label is very often experienced as being out of reach and reserved for those who have
‘self-consciously redefined their relationship to the experience from one of ‘victim’ to
that of ‘survivor’ (Naples 2003:163).
The values ascribed to each label are continually reinforced in the online
forums where the women list their behaviours against ‘victim’ or ‘survivor’ checklists
(See Appendix 3). For example, Calliehere (2010) was told by her therapist that she
was ‘showing a lot of victim behaviour’. As this behaviour had been ‘diagnosed’ by a
person in a position of (therapeutic) authority, the woman searched the Internet to
educate herself and then compared her character traits to ‘victim’ and ‘survivor’

58
behaviours. In giving credence to the idea, the material likelihood that her behaviours
would be associated with the normative tropes of victimhood were reinforced.
Marking one’s behaviours and feelings against a checklist—mimics the
diagnostic process for a host of mental health diagnoses, such as PTSD and Anxiety
disorders (See Appendix 4). It is indicative of how the inspecting gaze of the clinician
encourages survivors—through the internalised technologies to the self (Martin
2005:56)—to conduct their own conduct in line with medicalised models.
Furthermore, her choice to disseminate this material to others in the space of the
online forum increased the likelihood that they would then come to construct their
own behaviours through this colonising lens:
‘Thanks for sharing! I am sad to say that I am mostly in the victim category as
wellLLLL’ (Wishinguponastar 2010).
This example is representative of one way in which the act of naming and labelling
self and experience can anchor victims of rape to stigmatised identities that can be
‘more painful and debilitating’ than the act of rape itself (Thackuk 2011:141).
The need to name ones experiences of sexual violence to oneself as a way of
assimilating experience into identity often becomes confused by the array of
discourses that incite the survivors to reveal themselves:
‘…this probably seems tiny, but for me it was huge—I… told the nurse to add
‘CSA’ [Child Sexual Abuse] to my medical history. So it’s there!... Going to trust
the doctor…to help me’(Orangeblossom 2014).
In revealing her history as a matter of clinical relevance, not only will
‘Orangeblossom's’ other ailments and complaints be viewed ‘through the coloured
lens of her diagnosis’ (Harris cited in Morrow 2002:7), but she also assumes the
59
‘subject position’ of an abuse victim, which elevates this aspect of her identity to one
of centrality and limits the types of ‘truth’ she can reveal in relation to her traumatic
experiences (Weedon1997:116). Truths allowed in such discourse are the ‘therapeutic
truths of harm’, of ‘symptomatology, survivorship, [and] lifelong suffering’ (Lamb
1999:129).
‘When people know you were raped they just see you as a victim like your entire
personality is taken away, as though all you are is a victim and then they expect
you to be really vulnerable and they are surprised if you are not. Its like they can
only see you as fragile’ (Interview 3 2015).
There are many ways to victimise people, one particularly insidious way is to
‘convince them’ and treat them as though they are victims (Gavey in Lamb 1999:62).
Diagnostic Labels
Modern society increasingly constructs the aftereffects of rape through references to
diagnostic labels. PTSD is one of the most prevalent with research indicating that
between 50% and 95% of women will develop PTSD following an attack (Caretta
2011:7). In addition, sexual violence is increasingly linked to acute pathologies such
as DID (Brand 2012) and borderline personality disorder (Becker 1997), as well as to
a range of comorbidities such as recurrent depression (Kilpatrick et al.1985), eating
disorders (Bordo 1993), chronic pain conditions (Barker 2002) and sexual dysfunction
(Berlo & Esink 2010).
Labels can aid ‘survivors’ in understanding the ‘confounding and confusing’
symptoms they experience. Particularly in the most severe cases of DID35, people are
35 During our interview, Zoe Lodrick used the example a case where her client had called to take out car insurance but found that whilst in a dissociative state she had insured her car with three separate
60
able to ‘put words’ to symptoms and situations that make ‘no sense unless they have
some context’ (Lodrick 2015a). A diagnosis, wraps rational understanding and
medical terminology around what can be very overwhelming and frightening
symptoms—this effectively helps the person to contain the symptoms under the
diagnosis rather than psychosomatically experiencing new ones (Duncan Interview)36.
That being said, labels can be extremely damaging:
‘This business with labels is really just bullshit that avoids the point, and causes
endless cycles of distress and stigma for patients. I’ve been through the psychiatric
mill. They didn’t help me—they loaded me down with incorrect diagnoses and a
boatload of inappropriate heavy-duty pscyh meds, while completely missing and
dismissing two physical illnesses’ (Hellothere 2014).
Not only do mental health labels stigmatise an already vulnerable demographic, it
further reinforces the permanence of their victimhood. Once labels are given, they are
not easily transcended and usually require a professional to remove them:
‘I went back to therapy temporarily… to have my diagnosis updated formally.
Well today, after about five months of therapy, my therapist decided that I am
done. So no more PTSD or DID. My new diagnoses are now: major depression in
full remission. DID in full remission, [and] anxiety disorder’ (Buckaroobanzai
2014).
The discursive permanence of formal diagnosis intersects with wider trends in mental
health advocacy groups who campaign for mental ill-health to be recognised as a
insurers. Furthermore, in an article for Vice Magazine an anonymous writer details the time his girlfriend totally dissociated from her body and couldn’t recognise who he was, believing instead that he was trying to hold her captive (Anonymous 2015). 36 To explain this further, Duncan McClean (2015) told me a story of a client he had worked with, who after smoking very strong marijuana found himself experiencing auditory and visual hallucinations. In receiving a ‘label’—that it was a temporary state of anxiety—he was able to understanding that he was not ‘going mad’ and would not be like this forever. Therefore, the containment of his symptoms within a diagnosis reduced the anxiety experienced regarding the symptoms as well as anxiety over his prognostic future.
61
physical rather than psychological disease (see appendix 5). ‘Buckaroobanzai’ had to
go back to therapy to ‘remove’ her diagnosis, and understands her mental health
diagnoses to be in ‘remission’. In drawing upon the physiological understanding of
remission—that of a ‘temporary or permanent decrease’ in the manifestations of a
disease, she codifies the diagnosis, not as totally healed but as ever present with latent
potential.
Furthermore, people tend to feel a great deal of anxiety around their
diagnoses; they are not simply value-neutral labels but carry the weight of prognostic
futurity and social stigma (Puar 2009:167):
‘I have fibromyalgia and C-PTSD! Two extremely distressing illnesses!!!!…how
do you explain to someone who’s never experienced it and who doesn’t have
flashbacks and amnesia disease that I have—so how can my significant other
comprehend that even if their mother was dying in a hospital that night I COULD
NOT BE THERE’ (Obliterated 2014)
A formal diagnosis can also make rape victims feel more abnormal or isolated, as
their experience becomes less translatable and out-of-reach to their surrounding
support network who, for example, could perhaps empathise with feelings of
depression, but have no access to understandings of complex traumatic diagnoses.
This is often why people with formal diagnoses turn to the internet.
In a recent study, White and Horvitz (2008:1) found that people who utilised
the Internet to access information about health were highly susceptible to an
‘unfounded escalation of concerns about common symptomatology’. Searches for
symptoms and shared experiences are one of the mainstays of the online survivor
62
forums. In response to a forum post by ‘Apache’ (2006) on RTS, which explains the
prognosis, the symptoms and ‘stages’ of the syndrome, one woman commented:
‘I was raped seven years ago…and it is still affecting my daily life. If one can
call it ‘life’!! Recently I was diagnosed with Borderline Personality Disorders
and Emotional Attachment Syndrome, both of which are also a result of the
attack, in my view… I would like to hear from anyone who knows anything
about this condition too—Is it something I will get over?’ (Littleme 2007).
This highlights the extent to which online forums act as a conduit through which the
medicalised jargon and symptomatologies are learned and understood. The online
forums are therefore a place where the diagnostic labels are encoded and assimilated
into the identity of the rape victims that concretises the diagnosis as an identity label.
While there is explicit ambiguity over the terms ‘victim’ and ‘survivor’ in the
online forums, there is an absence of ambiguity over formal medical or psychiatric
diagnosis. Instead, the women refer to their diagnoses such as PTSD or DID, in very
certain and often fatalistic ways. The women talk about their diagnostic labels in a
way that ascribes the disease rather than themselves agency over their lives:
‘…because of my multiple personality disorder, I saw a cupcake and cried for
four hours’ (S3 workshop 2015).
‘I’ve been thinking about goals for 2015, but I feel so limited. I have C-PTSD,
recurrent depression so coping emotionally is hard’ (Hiding fox 2015)
‘My attacks of PTSD are fuck horrible’ (Louise 2003)
The ascription of agency to the diagnosis could be seen as a reaction to healthicisation
of identity where the ‘survivor’ mantle increasingly connotes ‘assuming personal
63
responsibility’ over self-management and contributes to the overall stress the women
feel in the aftermath of the assault (Cole 2007:139):
‘It is really hard to take responsibility for fixing all of the problems that are caused
by being victimised especially because SV and its aftermath makes you feel so
powerless’ (Lis 2003).
On the one hand, a formal diagnosis removes the victim’s culpability in their own
traumatisation, but on the other it places the onus for transformation and self-
management in the hands of the sufferer, by seeing symptomatology as the domain of
individual pathology rather than as a socially determined and culturally bound disease
(Gross & Graham-Bermann 2006:394). However, this also evacuates the victims
control over their own diagnosis:
‘Labels become a way of not having to think about themselves or their difficulties
any further. My patients would say, ‘my doctor says I have manic depressive
illness’ and I would say ‘ok, what does that feel like?’ and they would say, ‘well
you should know, you’re a psychiatrist’…. it becomes a closure and a stop to
dealing with things…’ (McClean 2015).
In this way, a diagnosis of PTSD can represent one of the ‘worst thieves of agency’
because by virtue of its expert nature, this effectively takes the ‘remedy’ out of the
hands of the sufferer (Lamb 1999:111):
‘I have been ‘labelled’ with a disorder… and all my T does is talk about that, I
feel like I’m in a sea drowning yelling ‘help me’ and she is standing on a cliff
near by reading symptoms and asking me ‘on a scale of 1-10…’blah blah’
(Tornpieces 2014).
64
This is particularly problematic given that the criteria for anxiety disorders and
diagnoses like PTSD tend to be incredibly expansive, vague and therefore, applicable
to many in the general population who have not been ‘traumatised’.37
The trend towards the increasing use of diagnostic categories is particularly
problematic because diagnostic labels are increasingly used not only to capture ‘a
small pathological minority, but almost all of us’ (Rose 2006:466). There is an
increasing multitude of conditions on the borders of normality that are diagnosed as
mental pathology. This ‘diagnostic creep’ of the expansive use of psychiatric
diagnosis means that conditions that encompass a spectrum of severity from normal to
severe become monolithically diagnosed as pathological (Conrad 1992:221).
The vague and elastic nature of rape-related psychiatric diagnoses lends itself
to self-diagnosis as every woman (probably even women who have never been raped)
can see something of her own experience within them’ meaning that an ever-
increasing proportion of rape victims will receive formal diagnosis (Chisler &
Johston-Robeldo in Ballou & Brown 2002:177). Labels therefore ‘concretise’ that
which is not concrete.38 This is especially harmful given the trend towards ascribing
biomedical and physical fixity to psychological disorders.
37 See Appendix 3 for example of PTSD and Anxiety Disorder checklist (Carretta 2011: 174). 38 As an aside, this is also particularly problematic when untrained individuals start to deploy diagnostic labels in official settings. Without wanting to give too much credence to a throw away comment – during my interview with Rachel Matheson who worked in a managing position at a SARC as well as a volunteer counsellor, she said: ‘ I love DID, I really do. Its just the most fascinating illness and the people who have it are so lovely’. She then went on to describe a case of a young boy whom she had counselled and she said ‘ I knew it as soon as I saw him that he had it [DID], you could tell because he spoke about being at school and it was his confident persona whilst in the therapy room he was withdrawn and angry’. Though I cannot make comment as to the particulars of this case, I just want to highlight my shock that a person who has some degree of expert authority within the therapeutic setting, but has received no formal training in psychotherapy—and who actively ‘loves’ the diagnosis of DID—is diagnosing people as suffering from this disorder. This shows how easily and the extent to which people come to attribute mental pathology to rape victims. However, who does the diagnosis serve? Is it the expert’s desire and excitement at diagnosing, or, the rape victim being diagnosed?
65
CHAPTER FIVE: WHO DO SUCH CONSTRUCTIONS SERVE?
The PTSD Brain
In the neurobiological account of personhood, mental pathology is the consequence of
a visually identifiable abnormality (Rose 2007:192). In appealing to the physical
nature of neuro-pathology, the new truth technologies of modern biological
psychology appeals to ‘western culture’s affinity for visual proof’ (Thackuk
2011:149). In visually confirming an abnormality within the brain, the stigma
associated with mental illness (and blame attached to mentally ill people) is said to be
reduced in the sense that it renders behaviours which are often misunderstood by
society as more intelligible (Ibid:151). Illustrating pathologies through their particular
molecular materiality changes ontology; ‘different practices and locales embody and
enjoin different senses of selfhood’ and discursively create qualitatively different
material realities (Rose 2007:222).
For example, from a psychological perspective depression is generally
attributed to negative thought cycles, genetic predisposition and low self-esteem
(Horvitz &Wakefield 2007). However, in the biopsychological or neurobiological
‘style of thought’ (Rose in Ericson 2003:412), depression can be visualised and
evidenced as a ‘deficit in monoamine neurotransmitters’ such as norepinephrine and
serotonin (To, Zepf & Woods 2005:102). Neuroimaging is thus pictorially creative of
‘different kinds of brains’ that in turn produces ‘different kinds of minds’ (Dumit
2003:37), as well as different kinds of ‘treatment’.
Even though such ‘diseases of the mind’ are a matter of representation
(Theriot 1993:3) and given meaning through ‘value-judgements’ (Boyd 2000:10), this
kind of biological psychiatry produces ‘operative’ images that have a ‘reality making

66
function’ (Layne 2003:41). The biomedical model of the brain establishes what counts
as an explanation and how this can be ‘treated’—fundamentally altering the way that
people perceive their own subjectivity (Rose 2007:192). The idea that it is possible to
advance a ‘value-free’, objective understanding of mental illness that exists prior to,
and independent of power, simply isn’t the case (Thackhuk 2011:149). By locating
trauma in the structures of the brain, the potentiality of rape to cause permanent and
irrecoverable damage to a persons identity is linguistically (as opposed to biologically)
consolidated.
The PTSD brain is a striking example of the ways that neurobiological psychiatry has
changed the ontological status of rape victimhood. Though it is understood by experts
that PTSD does not necessarily permanently affect the brain and that PTSD is
‘treatable’ (Lodrick 2015a), there is a wealth of misinformation on the Internet (Segal
2009:355):
‘I thought of myself as tainted, like I was going to be scarred permanently by what
happened to me. And when I started researching my PTSD diagnosis there was all
of this stuff on the internet about the effects it has on the brain… it was really
scary… like, not only did I feel tainted but that my brain was actually tainted too’
(Interview 2 2015)
Cerebral atrophy, which is associated with the neurological image of the PTSD brain
(see Fig 1) describes the process where brain tissues ‘shrink’. The visceral mental
imagery evoked by such descriptions, particularly for the average layperson, who
would not know whether such changes are permanent or what areas of the brain tend
to be affected by certain diseases, is almost apocalyptic.
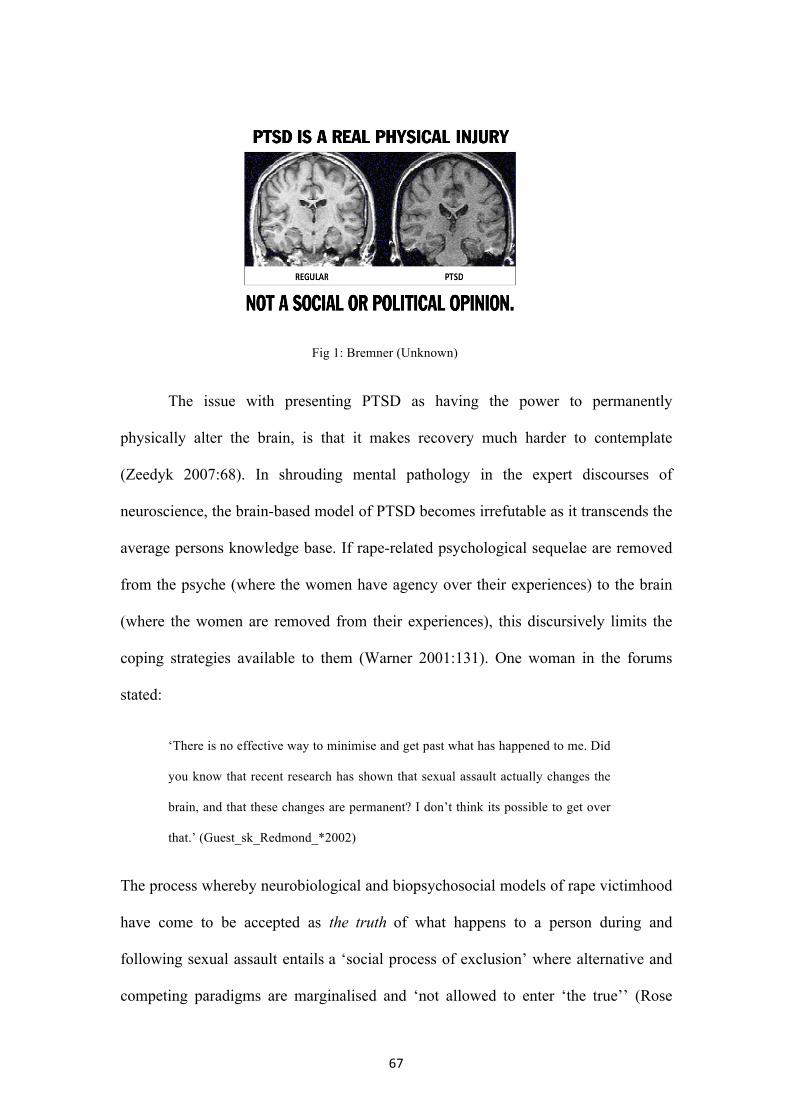
67
Fig 1: Bremner (Unknown)
The issue with presenting PTSD as having the power to permanently
physically alter the brain, is that it makes recovery much harder to contemplate
(Zeedyk 2007:68). In shrouding mental pathology in the expert discourses of
neuroscience, the brain-based model of PTSD becomes irrefutable as it transcends the
average persons knowledge base. If rape-related psychological sequelae are removed
from the psyche (where the women have agency over their experiences) to the brain
(where the women are removed from their experiences), this discursively limits the
coping strategies available to them (Warner 2001:131). One woman in the forums
stated:
‘There is no effective way to minimise and get past what has happened to me. Did
you know that recent research has shown that sexual assault actually changes the
brain, and that these changes are permanent? I don’t think its possible to get over
that.’ (Guest_sk_Redmond_*2002)
The process whereby neurobiological and biopsychosocial models of rape victimhood
have come to be accepted as the truth of what happens to a person during and
following sexual assault entails a ‘social process of exclusion’ where alternative and
competing paradigms are marginalised and ‘not allowed to enter ‘the true’’ (Rose
68
1996:55). In likening the mental pathology of a rape victim to a physical disorder, it is
reconceptualised as something that is beyond the ‘individual’s voluntary control’
(Thackuk 2011:149). In so doing, rape victims are discursively encouraged to
understand their emotions through a physical lens, thereby increasing the likelihood
that they develop other physical conditions.
Though I do not seek to challenge the scientific validity of neurobiological
accounts of trauma, the wholesale adoption of such models needs to be questioned and
problematised. Such accounts have acquired a kind of mythic ascendancy where the
synonymity between rape, trauma and irreparable neurological damage becomes a
‘master signifier authorising and reproducing’ a socially constituted world-view of
what rape does to a person, as well as delineating who is professionally capable of
‘curing’ the rape victims of their continuing traumatic distress (McCutcheon
2002:192).
The assumption that professional treatment for rape victims represents an
‘unqualified good’, presumes that the women will be better off when experts can
correctly recognise their symptoms and treat them accordingly (Bumiller 2008:64).
However, the very idea that
‘…you can diagnose people with mental disorders…,and as though by virtue of
that diagnosis, you can instantly access what the treatment should be and deliver
it, and that is all that is needed ‘to get better’’ (McLean Interview).
presents a mechanistic and rigid model of ‘treatment’. Crucially, this model gives the
clinician defining powers over what constitutes ‘successful recovery’ (Garden
2010:72).
69
Such definitive powers mean that it is the professional who ‘educates’ the
women about their own, subjective, experience of trauma. In this way, therapists
could potentially harm the victims’ self-developed coping strategies (Gavey &
Schmidt 2011:451). Though this is of course not always the case, there is the potential
to do symbolic violence to the victims’ self-assessment. Gavey and Schmidt
(2011:451), contend that given that one of the especially damaging elements of rape is
the ‘forcible taking of control’, a response that on some level ‘mimics that dynamic,
albeit from an ostensibly caring and sympathetic position’ is nonetheless,
problematic.
Procrustean model of therapy
The potential to cause such harm is more pronounced in institutions where services
are tailored specifically for rape victims, such as SARCs or RCCs because they are
more likely to subject the women to an ‘almost colonising interpretative lens’ (Gavey
in Elliot 2008:242):
‘…a lot of organisations that help people with sexual trauma have some sort of
model in their mind before they’ve met them, and so rather than going ‘we have
this individual who is suffering from this, therefore this is how we should treat
it’. They already have a model of what that person might be feeling like and
treat accordingly… people tend to push their ideology’ (McClean 2015).
The integration of institutional care through interagency programmes such as RCCs,
the police, and primary care services does allow for more uniformity in the treatment
of rape victims—and, given that rape myths and victim-blaming is still pervasive,
means that rape victims will generally be received in a sensitive way (Eogan et al
2013:55). However, institutionalisation has also expanded the reach of the normative
70
models of rape victimhood and associated psychological sequelae (S.Levine
2012:409).
A number of the women I spoke to viewed their experiences of RCCs
negatively, as they felt that ‘they had to be the victim’ in order to access the support
they required (Interview 3 2015). One survivor said this of her experience with a
RCC:
‘I was trying to talk to the therapist about the good things in my life, like what
I’d been doing with friends and she just kept bringing me back to the rape and to
the negative things I was experiencing. I mean, in fairness, at the time I probably
was in need of that therapy because I was convinced I was being followed but at
the same time, she made me fill in all these questionnaires about how anxious I
was and then she told me I had PTSD and anxiety disorder… and I just think at
the time, I just wanted to move on even if that meant pretending that everything
was ok for a while… and then after all of that effort in making me talk about
what had happened to me, my 10 sessions were over and I was just kind of left
on my own to try and put the pieces back together’ (Interview 2 2015).
Here, the ‘survivors’ control over her ‘recovery’ was, at least to some degree, taken
away through the denigration of her coping strategy as being a maladaptive
expression of a psychiatric diagnoses. Through the therapeutic process, the survivor
was thereby inculcated into the mandated normativity of traumatic victimhood, firstly
through the incitement to speak about her experiences negatively and secondly by
encouraging her to define her experiences against the diagnostic criteria of PTSD and
Anxiety disorder. When speaking to another woman of her experiences of such
therapies, she commented that
71
‘…squashing people into boxes and giving them 6 sessions… It’s the absolute
antithesis of everything I’ve ever found helpful in my recovery—which is that
spaciousness and being met with expression and not necessarily having clear
stories or boxes for things to fit within… not some expectation of how you should
be…not by changing individuals’ (Interview 1 2015).
It follows that institutional and therapeutic experiences can be experienced as a
‘continuation of a process of victimisation’, particularly if victims (and their
resilience, or coping strategies) are ‘muted’ by the professionals they come into
contact with, or if they are forced into a procrustean model of victimhood and therapy
that doesn’t suit their particular needs (Robson 2011:264). As evidenced, the quality
of therapy varies dramatically from therapist to therapist and institution to institution:
there are ‘RCCs and there are RCCs, just like there are SARCs and there are rooms in
hospitals with SARC written above the door’ (Lodrick 2015b).
Whom do labels serve?
Given that diagnostic labels have the propensity to add to the damage done to the rape
victims’ chances of recovery and long-term prognostic future, it is important to
question whom such diagnostic labels serve. Diagnostic labels are not only ‘much
more useful to researchers’ (as they demarcate the demographic who have to be
classified in order to be studied,) but labels also more readily serve the purpose of
mental health managers than they do victims of violence.
‘I don’t like labels and pigeon-holes but the doctors do. It’s a shame they can’t just
listen to people for the individuals they are and not need a label before they decide
to listen on their own terms only… diagnosis, pigeon-holes and labels aren’t what
is important’ (Bronte 2011).
72
The marketisation of healthcare means that increasing pressure is put upon
service providers to provide quantifiable and measurable outcomes. Particularly
outside of the statutory services, the outcomes of treatment must be costed in order for
the organisations to continue operating (Interview 4). In putting people in arbitrary
boxes, managers can provide ‘effective treatment’, such as 10 therapy sessions for a
rape victim or the prescription of anti-depressants for someone experiencing a
depressive episode. Labelling allows managers and stakeholders to target limited
resources to the most needed areas (Marshall 2012:339).
Market driven model
Nikolas Rose (2007:11) asserts that medicine and medical treatment has been
reshaped by ‘intense capitalisation’. The increasing demands for ‘normalcy’ and the
moralising drive for optimal ‘well-being’ fosters market demand for and consumer
base of ‘products, procedures and drugs’ that will ‘cure’ an increasingly array of
‘abnormalities’ (Farrell & Cacchioni 2012:329). Marketised model of mental health
treats patients a ‘commercial commodity’ where they are measured against pre-set
criteria, and the ‘success’ of the treatment is measured against an abstracted market
model of health (McClean 2015).
The requirement of providing ‘outcomes’ can be particularly damaging. Jacqui
Campui, at the RCC in Peterborough, alluded to the fact that they had had to become
‘more strong’ with state-funding bodies and decided not to provide outcomes such as
‘who has stopped claiming benefits and gone back to work’ because of the treatment
they received at the RCC (Campui interview). In their annual report, the Women and
Girls Network (WGN) (2011:5) actually estimated what violence against women
costs British society each year. Every adult rape is said to cost ‘£96,000 in its
73
emotional and physical impact on the victims, lost economic output due to
convalescence, treatment costs to health services and costs incurred in the criminal
justice system’, costing society a total of £37.6bn each year.
Furthermore, they go on to provide a breakdown of the ‘total value created by
the WGNs’ therapeutic programme; apparently for every ‘£1 invested in WGN, £5 of
social value is generated to clients, their families, wider society and the state’ (WGN
2011:16). In reducing the ‘outcomes’ of women’s lives to the ‘value-added’
financially to society is revealing of who organisations are increasingly accountable to
(i.e. donors).
The problem with donor-accountability is that services are increasingly drawn
upon to provide detailed reports of their service-users, as well as providing better
outcomes for less. This is arguably why there is an increasing number of mental
illness diagnoses (as it provides information) which are said to be ‘treatable’ in the
provided ’10 sessions of therapy’.
PTSD makes sexual assault treatable insofar as donors or insurance companies
(in the case of the US) are more likely to pay out for diagnosed disorders than they are
for ‘stress’ (Lamb 1999:111). The increasing use of diagnostic categories as a way of
accessing much needed funding, as well as the concomitant need to ‘treat’ disorders
efficiently could perhaps be a contributing factor in why between 1990-2000 there
was a 126% increase in the psychiatric drug market in the European Union and 638%
increase in the US (Rose 2006:470). One survivor comments:
‘My psychiatrist thinks I do not need [my therapist] anymore because she ‘cured’
me with a new anti-depressant’ (Lionesscub 2014a)
74
In the age of austerity where funding is limited, it often means that people are
unable to access services. Though some people can afford private treatment the
majority cannot
‘…so these women have plucked up the courage to come to us (RCC), and we
have to tell them that there is a big waiting list and we try to accommodate that as
best we can, but they are often left coping alone’ (Campui interview).
Lengthy waiting times encourage triage assessment where rape victims are more
likely to be seen quickly if they present as particularly traumatised. This means that
‘eligibility and priority for services’ is predicated upon and increasingly linked to the
women’s status as abject victims and their ability to articulate their problems in the
institutionally intelligible model of traumatised victimhood (Bumiller 2008:13).
CHAPTER SIX: PERFORMING ILLNESS IDENTITIES
Framing experiences of rape and the aftermath in terms of the lived experience of
symptoms encourages rape victims to self identify with, and disclose as identity, an
illness narrative (Shapiro 2011:68). The requirement of an illness narrative as a means
of validating their experience is a technology of presencing, it renders their emotions
and somatic pains intelligible to wider society (Jain 2007:78). In presenting their
‘condition’ as being physically debilitating and highlighting their suffering and plight,
the women try to explain their unexplainable symptoms (Barker 2002:282):
‘The FOG you speak of is so real. I tell my family that the song ‘I’m not crazy,
I’m just a little unwell’ is for me… when I wake up feeling so ill, I am so afraid it
may continue and I will never get out of bed. On days like this, I can hardly type…
when the memories come again of my pain it adds so much to the discomfort also’
(Patches 2011).
75
While this may garner support and reduce social stigmas associated with abuse-
related psychological and somatic sequelae, it also encourages the women to
increasingly view all emotions through a physiological lens, which cultivates an
understanding of psychological and physical distress as inextricably linked. Many
‘survivors’ in the online forums recognise that their physical symptoms get worse
when they emotionally relive their abuse:
‘I have fibro that gets worse when my PTSD is acting up so I do believe there is a
link to abuse’ (Darlingluck 2011)
‘That evening I was experiencing an intense pain flare, with the backache, the
headache, feet pain, the dizziness… AND, I was experiencing intense emotional
distress and despair as I’d worked that afternoon with my T, stretching way past
my emotional limits’ (Obliterated 2014)
This physicality is damaging to the long-term prognosis of the women as it marks
transitory emotional stages with discursive permanence that shapes the material
reality these women live out. Furthermore, it has been found that the perceived
severity of the assault is linked to expressions of somatic symptomatology, as the
more life events are perceived as undesirable, the more likely they are to influence
stress levels, thereby influencing somatic distress (Rynd 1988:155-9). They
perennially inhabit their illness identities and ‘perform’ the tropes associated with
traumatised victimhood:
‘The psychiatrist from hell… said that I ‘had been in therapy and sick for so long
that I have no idea what it is to be well’ (Lionnesscub 2014b).
Ultimately, the conversion of emotional turmoil and pain into the
‘camouflaged but culturally acceptable languages of bodily illness’ (Showalter in
76
Boyd 2000:10) means that rape victims are more likely to attribute their physical
symptoms to the rape:
‘I have cerebral palsy and severe bipolar disorder. Neither of those would have
been what they are without the abuse’ (Silentstar 2008).
That Silentstar attributes cerebral palsy—a neurological condition that can occur ‘if
the brain develops abnormally or is damaged before, during or shortly after birth’
(NHS Choices 2015)—in some way, to the sexual violence she experienced,
highlights the expansive ways in which rape and sexual violence achieve ‘master
status’ and foundational centrality to the lives of the women (Becker in Link et al.
1991:303). Everything comes to be coded as being a result of the abuse.
In their study on sexual violence and incidences of physical pain, Eby et al.
(1995) found that 99% of their respondents who had been raped reported at least one
physical health symptom. The most common symptoms were low energy (88%), sleep
problems (77%) and headaches (77%) (Ibid:569) (see appendix 6 for table). The study
found of the 68% of women who reported chronic fatigue, 65% of the women
attributed such symptomatology to the rapes they had experienced.
In viewing experiences of sexual violence as causally linked to physical
symptoms, victims of rape appeal to wider society to validate their suffering. Physical
symptoms are more intelligible to wider society because they are more likely to be
communal (Thackhuk 2011). For example, I spoke to a respiratory physiotherapist
who reported treating a sizeable number of abuse victims for what had been
diagnosed as ‘chronic asthma’ but that she felt was more likely the result of
misdiagnosed panic attacks or anxiety (Grillo 2014). The women who were being
treated had pushed for physiological diagnosis rather than psychological as they felt
77
this better explained their symptomatology. One woman I spoke to at a ‘survivors’
workshop explained that she kept going to A&E because she had ‘muscles that were
too tight around her heart’, yet it later transpired that what she was describing was an
anxiety induced panic attack. She had taken what doctors had explained to her about
panic attacks and reformed their explanations to lend physical credence to her
suffering (S4 workshop 2015 ).
Giving physical tangibility to their symptomatology is a ‘tactical and
persuasive’ move where rape victims seek to ‘recruit’ and ‘convince’ the listener of
the ‘truth of their self account’ (Kokanovich & Philip in Davis & Manderson
2014:58). However, any attempt to tell the truth of oneself is limited by ‘speakability’
(Butler 2005:121); the account that the subject gives of its experience is always
already structured by its ‘relationship to culture, language and moral frameworks’
(Kokanovich & Philip in Davis & Manderson 2014:59). Inevitably such disclosure
comes at a cost. Following Foucault (2001) Butler argues that the ‘price of telling is
always the suspension of a critical relation to the truth regime in which one lives’
(2005:131).
Disclosing ones psychological distress through aspersions to physical
tangibility is a form of self-subjection to regulatory regimes and a highly complex
social performance (Butler in Garry & Pearsall 1996:372). Therefore, when validation
of rape-related sequelae is tethered to the physical tangibility of traumatisation, rape
victims are more likely to be statistically prevalent in cases of contested illnesses such
as Fibromyalgia (Barker 2011), CFS (Dickson et al. 2007; Seccombe 2015), chronic
pain conditions (Dumit 2006) and Borderline personality disorder (Koehne et al
2012). This is because the ‘body believes in what it plays at’ (Bourdieu cited in Butler
78
1997:154). Through the ‘words, acts and gestures’ that link psychological distress to
physiological symptomatology within the ‘affected’ rape-victim identity, the women
are not only discursively constituted by the internalised norms of that psychosomatic
victimhood, but come to ‘perform’ and embody their illness identities. 39
This is not to deny the scientific research that details the way in which stress
hormones impact ‘negatively upon the body’ and immune system, producing short
term and long term physical consequences’ (Bloom in Giardiano et al. 2003:425). A
lot of the women in the forums complain of weakened immune systems:
‘Mybody/brain seems to be breaking down, lately—catching colds frequently,
sleeping way too much (10+ hours a day), poor eating habits, feeling hopeless’
(Blackbird86 2012).
Yet, the difference between ascribing such immune-responses to an innate experience
associated with rape, or whether these physiological symptoms are the result of
feeling victimised, performing—and then becoming—the victim is the difference
between inescapable victimhood, or one that can be transcended. Recognising such
psychosomatic symptoms is not to deny their reality, but recognition of the ‘inherent
duality of mind and body’ and the propensity of language and discourse to construct
reality (Webster in Ballou & Brown 2002:162). The symptoms experienced by the
women undoubtedly have devastating consequences on their self definition and their
39 For example, discourses surrounding sexual violence assert that rape has a detrimental affect on women’s sexuality: ‘ rape locates and mortifies the genitals that it violates’ (Grand 2003:322). This inculcates the women through regulatory regimes into believing that they will experience issues sexually and therefore creates subjective experiences of such conditions: Eby et al. (1995:564) reported that two of the most frequently cited issues rape victims experience are that of painful intercourse (72%) and vaginal pain (63%). However, Berlo & Esink (2010:236) in their meta-analysis of all studies researching sexuality after sexual assault found that the victimised and nonvictimised groups of women did not differ in the frequency of ‘oral sex, sexual intercourse, anal intercourse, masturbation or orgasms’, but the victimised group ‘reported less satisfaction’ than the nonvictimised group. This shows that the physiological response during sex remains unaffected by rape but the perception of sexual stimuli as ‘anxiety provoking’.
79
lives (Showalter 1997:128), but what lies behind such conditions is the very idea of
‘what constitutes a real illness, what doesn’t and what we do to make something real’
(Wessely 1993:338).
I am in no way trying to ‘minimise’ (Sister 2003) or ‘deny the reality’
(Guest_* 2003) of the pain that someone has suffered, nor take away from them what
they view as an essential and foundational aspect to their identity. Self-expression
constructs ‘the durable properties of a character’ (Ricœr 1991:195); it is productive of
material reality. Therefore, even though there is no essential or pre-discursive reality
to the trauma and traumatic sequelae of rape—as it is created in language—this does
not diminish the reality of the trauma and pain produced through discourse and
experienced by the women.
Conclusion
A constellation of forces and devices of meaning production have ‘invented, refined’,
‘stabilised’ (Rose in Hall & Du Gay 1996:130), and disseminated the modern models
of rape and rape victimhood. In providing a critical history of the present, I have
traced the processes of medicalisation in the 19th century that forged both the rapist
and the rape victim as objects of knowledge. This ‘act of seeing’ (Foucault 1963), or
of inspecting bodies, brought-into-being the rape victim, actively creative this identity
in discourse. This social ‘thinkability’ afforded rape victims legitimate types of
speech (within circumscribed settings) to articulate their claim of injury.
Medicalisation has to be set within the complex interplay of competing and
contradictory discourses around rape and rape victimhood, as well as understandings
of gender, madness, trauma, and pathology. Competing discourses at the time
constructed disorderly femininity in terms of mental ill-health and the reform
80
movement can be seen as a nascent therapeutic community, aiming to transform the
abject, corrupted victim into redeemed survivor. These narratives of transformation
fed into the ‘breaking the silence movement’, the stress on remembering, associated
with the ‘survivor’ movement is starkly contrasted to the practice of ‘forgetting’ in the
penitents movement (L.Jackson 2000:115).
The 1970s model of sexual trauma encouraged women to speak publically of
the ‘inner truth’ of their experiences based upon the psychologised understanding that
confession is cathartic and political, but the movement required exposing ‘bodies in
pain’. This dramatised, sensationalised and depoliticised ‘the moral degradation’ that
the women suffered. Increasing stress on ‘recovery’ required rape victims to be ‘better
than well’, whilst taking away their powers of self-definition by pathologising them
as mentally abject and simultaneously magnifying the discursive construction of rape
as always already traumatising. The model of rape-as-trauma represents an all-
encompassing model that is seen to profoundly alter all facets of human experience
and identity irreparably.
I have argued that people are extremely suggestible and the comparison of one’s inner
self to didactic victim-models (both formal and informal labels, behaviours and
symptoms) leads to a more efficient regulation of victim-identity through the
production of ‘self policing subjects’ (McNay 1992: 87). The women become rape
‘victims’ by ‘telling’ and ‘living’ the story of their experience (Andrews et al
2000:78). By assuming the ‘subject position’ of an abuse victim, this aspect of their
identity is afforded foundational centrality and limits the types of truth the women can
reveal in relation to their traumatic experiences (Weedon1997:116).

81
Furthermore, by locating trauma in the structures of the brain, the potentiality
of rape to cause permanent and irrecoverable damage to a persons identity is
linguistically (as opposed to biologically) consolidated. Coping strategies are socially
located practices, and if rape-related psychological sequelae are removed from the
psyche to the brain, the coping strategies available to the rape victims are taken out of
their control, instead giving the clinician defining powers over what constitutes
‘healing’ (Garden 2010:72).
Framing experiences of rape in terms of symptoms encourages rape victims to self
identify with, disclose as identity, and perform an illness narrative (Shapiro 2011:68).
Adopting the ‘sick-role’ increases the material likelihood that the women will ‘feel’ a
range of other symptoms. Through the ‘words, acts and gestures’ that link
psychological distress to physiological symptomatology within the ‘affected’ rape-
victim identity, the women are not only discursively constituted by the internalised
norms of that psychosomatic victimhood, but come to ‘perform’ and embody their
illness identities. Modern medical models of rape victimhood therefore represent
assjeuttisment (subjectification) in ‘both senses of the word’ (Foucault 1979:81).
Fundamentally, what I am trying to argue is not that these conditions don’t
objectively exist, or that they are not experienced physically but rather that because
victimhood is always already invested with medical meaning that far out strips any
real medical basis the victims can only understand any psychological or physiological
pain they may feel through this very particular lens. This creates a prognosis for the
future of these women that is particularly grim.
Not only have they been raped, not only have they got to evaluate themselves
in terms of survivor or victim behaviour, or experience complex psychological

82
trauma; but they also have to cope and navigate scientific and pseudo-scientific
accounts of their diagnoses.
Rape victimhood thus achieves ‘master status’ (Becker in Link et al.
1991:303), where everything comes to be coded as being a result of the abuse, so that
every facet of identity and experience can be read in accordance with and in reaction
to rape victimhood. Furthermore, this is compounded because as a sexual act, rape
victimhood is an identity: one can be traumatised by a violent act and come to terms
with the randomness of violence, but it is incredibly difficult to overcome an identity.
Therefore, ‘before we speak we need to look at where the incitement to speak
originates, what relations of power and domination may exist between those who
incite and those whoa re asked to speak, as well as to whom the disclosure is directed’
(Alcoff & Gray 1993:284).
Through discourse, the ontology of the rape victim is materialised and women become
bound to a ‘spoiled identity’ (Goffman 1986). It is therefore fundamentally important
that we deconstruct rape victimhood to present an understanding of rape victimhood
that neither medicalises, pathologises nor trivialises victimisation, and allows for new
conceptions of rape to be put forward.
83
BIBLIOGRAPHY
Ackerly, b., Stern, m. & True, J. (2006) Feminist Methodologies for International Relations, (Cambridge: Cambridge University Press).
Ahrens, C. (2006) ‘Being Silenced: The Impact of Negative Social Reactions on the Disclosure of Rape’ in American Journal of Community Psychology, 38:2, pp. 263-274.
Alcoff, L. & Gray, L. (1993) ‘Survivor Discourse: Transgression or Recuperation?’ in Signs, 18:2, pp. 260-290.
Anderson, I. & Doherty, K. (2008) Accounting for Rape: Psychology, Feminism and Discourse Analysis in the Study of Sexual Violence, (London, New York: Routledge).
Anonymous (2015) ‘The Night my Girlfriend Dissociated and Forgot Who I Was’ [Online Article] in Vice Magazine, 4th March 2015, Available at: http://www.vice.com/en_uk/read/the-night-my-girlfriend-forgot-who-i-was-944 [Accessed 30th June 2015]
Anonymouse09 (2010) ‘Why do I seek out Triggers?’ [forum] 18th June 2010, Available at: http://www.aftersilence.org/forum/index.php?showtopic=76746 [Accessed 17th March 2015]
Andrews. M., Sclater, S., Squire, C. & Treacher, A. (eds.) (2000) Lines of narrative: Psychosocial Perspectives. Routledge studies in memory and Narrative, (London: Routledge).
APA (1994) Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. (Washington: American Psychology Association).
Apache (2006) ‘PTSD-RTS (Rape Trauma Syndrome)’ [forum] 5th December 2006, Available at: http://www.psychforums.com/rape-trauma/topic16032.html [Accessed 26th February 2015].
Armour, E. & Ville, S. (2006) Bodily Citations: Religion and Judith Butler. (New York, Sussex: Columbia University Press).
Armstrong, L. (1996) ‘In the footsteps of Doctor Freud and down the proverbial garden path’ in Feminism and Psychology,6, p. 298-303.
Auerbach, N. (1980) ‘The Rise of the Fallen Woman’ in Nineteenth-Century Fiction, 35:1, pp. 29-52.
Badour, C., Feldner, M., Babson, K., Blumenthal. H. & Dutton, C. (2013) ‘Disgust, mental contamination, and posttraumatic stress: Unique relations following sexual versus non-sexual assault’ in Journal of Anxiety Disorders, 27, pp. 155-162.

84
Bailey, L. (2001) ‘Gender Shows: First-Time Mothers and Embodied Selves’ in Gender and Society, 15:1, pp. 110-129.
Baily (2009) ‘Who deserves to be here?’ [Forum] 21st September 2009 Available at: http://pandys.org/forums/index.php?showtopic=38182&page=1 [accessed 1st June 2015]
Baines, B. (1998) ‘Effacing Rape in Early Modern Representation’ in ELH, 65:1, pp. 69-98.
Ballou, M. & Brown, L. (2002) Rethinking Mental health and Disorder: Feminist Perspectives, (New York: The Guildford Press).
Bargelow, P. (2014) ‘Numbing After Rape, and Depth of Therapy’ in American Journal of Pyschotherapy, 68:1, pp. 117-139.
Bargh, J., McKenna, K. & Fitzsimons, G. (2002) ‘Can you See the Real Me? Activation and Expression of the “True Self” on the Internet’ in Journal of Social Issues, 58:1, pp. 33-48.
Barker, K. (2002) ‘Self-Help Literature and the Making of an Illness Identity: The case of Fibromyalgia Syndrome’ in Social Problems, 49:3, pp. 279-300.
Barker, K. (2011) ‘Listening to Lyrica: Contested illnesses and pharmaceutical determinism’ in Social Science & Medicine, 73:6, pp. 833-42.
Barry, A., Osborne, T. & Rose, N. (Eds.) (1996) Foucault and Political Reason (London: UCL Press).
Bartley, O. (1815) A Treatise on Forensic Medicine or Medical Jurisprudence. (Bristol: Barry and Son)
Baugher, S., Elhai, J., Monroe, J. & Gray, M. (2010) ‘Rape Myth Acceptance, Sexual Trauma History, and Posttraumatic Stress Disorder’ in Journal of Interpersonal Violence, 25:11, pp. 2036-2053.
Baxter. J. (2003) Positioning Gender in Discourse: A feminist methodology (London: Palgrave MacMillan).
Beck, T. (1823) Elements of Medical Jurisprudence (Albany, New York)
Beck, T. (1825) Elements Of Medical Jurisprudence (London)
Beck, T. & Beck,J. (1838) Elements of Medical Jurisprudence, 6th ed. (Philadelphia).
Becker, D. (1997) Through the looking glass: women and borderline personality disorder ( Boulder: Westview press).
Berlant, L. (2007) ‘Slow Death (Sovereignty, Obesity, Lateral Agency)’ in Critical Inquiry, 33, pp. 754-780.
85
Berlo, W. & Ensink, B. (2012) ‘Problems with Sexuality after Sexual Assault’ in Annual Review of Sex Research, 11:1, pp.235-257.
Best, J. (1999) Random Violence: How We Talk about New Crimes and New Victims. (Berkeley: University of California Press).
Bevacqua, M. (2000) Rape on the public agenda: Feminism and the politics of sexual assault, (Boston, London: Northeastern University Press)
Bingley, A. (2002) ‘ Research Ethics in Practice in L. Bondi. ed., pp. 208-222.
Blackbird86 (2012) ‘Always Sick’ [Forum] 3rd July 2012, Available at: http://pandys.org/forums/index.phpshowtopic=208150&hl=%2Bchronic+%2Bfatigue [Accessed 28th March 2015]
Bloom, S. (2003)‘Understanding the Impact of Sexual Assault: The Nature of Traumatic Experience’ in A. Giardino, E. Datner, & J. Asher Eds., pp. 405-432.
Bondi, L. (ed) (2002) Subjectivities, Knowledges, and Feminist Geographies: The Subjects and Ethics of Social Research. (Oxford, New York: Rownman and Littlefield).
Booth, W. (1916) Orders and Regulations for Officers of the Women’s Social Work of the Salvation Army (London: Salvation Army)
Bordo, S. (2003) Unbearable Weight: Feminism, Western Culture, and the Body, (London, Berkeley: University of California Press).
Bouke, J. (2007) Rape: A History from 1860 to the Present (Virago: London)
Bourke, J. (2012) ‘ Sexual Violence, Bodily Pain, and Trauma: A History’ in Theory, Culture, Society, 29:3, pp. 25-31.
Boyd, K. (2000) ‘Disease, Illness, Sickness, Health, Healing and Wholeness: exploring some elusive concepts’ in Journal of Medical Ethics, 26, pp. 9-17.
Briggs, L. (2000) ‘ The Race of Hysteria: “Overcivilisation” and the “Savage” Woman in late 19th Century Obstetrics and Gynecology’ in American Quarterly, 52:2, pp. 246-273.
Brand, B. (2012) ‘What We Know and What We Need to Learn About the Treatment of Dissociative Disorders’ in Journal of Trauma & Dissociation, 13:4,pp. 387-396.
Branscombe, N., Wohl, M., Owen, S., Allison, J. & N’gbala, A. (2010) ‘ Counterfactual Thinking, Blame Assignment and Well-Being in Rape Victims’ in Basic and Applied Social Psychology, 25:4, pp. 265-273.
Braun, W. & McCutcheon, R. (eds) (2009) Guide to the Study of Religion. (London, New York: Continuum).
86
Bremner, J. (Unknown) ‘The Invisible Epidemic: Post traumatic stress disorder, memory and the brain’ [image & reprinted article] Available at: http://www.pandys.org/articles/invisibleepidemic.html [Accessed online 12th February 2015]
Brison, S. (2002) Aftermath: Violence and the Remaking of a Self, (Princetown, Oxford: Princetown University Press).
Bronte (2011) ‘Chronic Fatigue’ [Forum] 21st January 2011, Available at: http://pandys.org/forums/index.php?showtopic=166221&hl=%2Bchronic+%2Bfatigue [Accessed 12th February 2015].
Brooks, P. (2001) Troubling Confessions: Speaking guilt in law and literature (Chicago, London: Chicago University Press).
Brownmiller, S. (1975) Against Our Will: Men, Women and Rape (New York, London: Bantam Books).
Brouchard, D. (ed) (1977) Language, Counter-Memory, Practice: Selected Essays and Interviews, (Oxford: Basil Blackwell).
Brown, W. (1995) States of Injury: Power and Freedom in Late Modernity (Princeton: Princeton University Press).
Bryson, N. (1986) ‘Two Narratives of Rape in the Visual Arts: Lucretia and the Sabine Women’ in S Tomaselli & R. Porter Eds, pp. 152-173.
Buckaroobanzai (2014) ‘Diagnostic Update’ [Forum] 7th September 2014, Available at: http://www.isurvive.org/forum/viewtopic.php?f=20&t=5843 [Accessed 13th April 2014].
Bumiller, K. (2008) In an Abusive State: How Neoliberalism Appropriated the Feminist Movement Against Sexual Vioelnce, (Durham, London: Duke University Press).
Burgess, A. & Holmstrom, L. (1974) ‘Rape trauma syndrome’ in American Journal of Psychiatry, 131:9, pp. 981-986
Burrows, N. (2015) ’10 Things No One Ever Told You About Life After Sexual Abuse’ in Buzzfeed, http://www.buzzfeed.com/drninab/10-things-no-one-ever-told-you-about-life-after-se-rwj1
Butler, J. (1990) Gender Trouble. (New York, London: Routledge)
Butler, J. & Scott, J. (eds.) (1992) Feminists Theorise the Political ( New York, London: Routledge).
Butler, J. (1993) Bodies that Matter: On the discursive limits of “Sex”, (London, New York: Routledge).
Butler, J. (1996) ‘Imitation and Gender Insubordination’ in Garry & Pearsall Eds., pp. 371-387

87
Butler, J. (1997) Excitable Speech: A Politics of Performance, (London, New York:Routledge).
Butler, J. (2005) Giving an Account of Oneself (New York, London: Fordham University Press).
Cahill, A. (2000) ‘Foucault, Rape, and the Construction of the Feminine Body’ in Hypatia, 15:1, pp. 43-63.
Calcagno, A. (2009) ‘ Foucault and Derrida: The Question of Empowering and Disempowering the Author’’ in Human Studies, 32:1, pp. 33-51.
Calliehere (2010) ‘From Victim, to Survivor, to Thriver’ [Forum] 6th May 2010, Available at: http://www.aftersilence.org/forum/index.php?showtopic=74971 [Accessed 24th April 2015]
Campell, R. & Raja, S. (1999) ‘Secondary Victimization of Rape Victims: Insights from mental health professionals who treat survivors of violence’ in Violence and Victims, 14:3, pp. 261-275.
Campui, J. (2015) Interivew, interviewed by Constance Flude, 16th May 2015 at Race Crisis Peterborough.
Cardyn, L. (2001) ‘The Construction of Female Sexual Trauma in Turn-of-the-Century American Mental Medicine’ in M. Micale & P. Lerner eds., pp. 172-204.
Caretta, C. (2011) ‘Rape Trauma: A Study of Preferred Rape Disclosure Methods and Factors Influencing Psychological Outcomes in Rape Victims’ PhD Thesis, submitted to the faculty of the Graduate School of Vanderbilt University in Nursing Science. Available at: http://etd.library.vanderbilt.edu/available/etd-11112011-114023/unrestricted/CarrieCarrettaFinalDissertationNov311.pdf [ accessed 23rd May 2015]
Charteris, F. (1828) The Remarkable Trial for Rape of the Infamous Colonel Chartres, (London: Smith).
Chasteen,A. (2010) ‘Constructing Rape: Feminism, Change and Women’s Everyday Understandings of Sexual Assault’ in Sociological Spectrum, 21:2, pp. 101-139.
Chivers-Wilson, K. (2006) ‘Sexual Assault and Posttraumatic stress disorder” A review of the biological, psychological and sociological factors and treatments’ in MJM, 9:2, pp. 111-120.
Chrisler, J. & Johston-Robledo, I. (2002) ‘ Raging Hormones? Feminist Perspectives on Premenstrual Syndrome and Postpartum Depression’ in M. Ballou & L. Brown, Eds., pp. 174-197.
Conrad, P. (1992) ‘Medicalization and Social Control’ in Annual Review of Sociology, 18, pp. 209-232.
88
Clark, A. (1983) ‘ Rape Or Seduction? A Controversy Over Sexual Violence In The 19th Century’ in London feminist group (ed) the sexual dynamics of history (London: Pluto 1983.
Clarke, A., Shim,K., Mamo, L., Fosket, R., & Fishman, J. (2003) ‘Biomedicalization: Technoscientific transformations of health, illness and U.S. biomedicine’ in American Sociological Review, 68:2, pp. 161 – 194.
Clarke, L. & Griffin, M.. (2008) ‘Body Image and Aging: Older women and the embodiment of trauma’ in Women’s Studies International Forum, 31, pp. 200-208
Conley, C. (1986) ‘Rape and Justice in Victorian England’ in Victorian Studies, 29:4, pp. 519-536.
Cole. A. (2007) The Cult of true Victimhood: From the War on Welfare to the War on Terror (Stanford: Stanford University Press).
Conrad, P. (1975) ‘The Discovery of hyperkinesis: notes on the medicalisation of deviant behaviour’ in Social Problems, 23, pp. 12-21.
Conrad, P. & Schneider, J. (1980) Deviance and Medicalisation: From Badness to Sickness. (St. Louis: Milbank).
Conrad, P. (1992) ‘Medicalization and Social Control’ in Annual Review of Sociology, 18, pp. 209-232.
Cozolino, L (2002) The Neuroscience of Psychotherapy: Building and rebuilding the human brain, (New York, London: Norton).
CRIM 1/11/3 (1880) Case of Sarah Stevens and C. Gregor, National Archives Kew.
CRIM 1/13/5 (1884) Case of Matilda Townsend and Albert Lawson, National Archives, Kew.
CRIM 1/25/1 (1886) Case of Richard Footer and Elizabeth Mullins, National Archives Kew.
CRIM 1/543 (1931) Case of John Youd, National Archives Kew.
CRIM 1/63/9 (1900) Case of William Baily, National Archives Kew.
CRIM 1/8/7 (1880) Case of William Burrows, National Archives Kew.
CRIM 1/8/8 (1880) Case of Richard Cheeseman and Clara Cheeseman, National Archives Kew.
Crossley, N. (1993) ‘The politics of the gaze: Between Foucualt and Merleau-Ponty’ in Human Studies, 16:399-419.
89
Cryle, P. & Downing L. (2009) ‘Feminine Sexual Pathologies’ in Journal of the History of Sexuality, 18:1, pp. 1-7.
Currie, D. & Raoul, V. (1992) Anatomy of Gender: Women’s Struggle for the Body (Ottawa: Carleton University Press).
Daniels, J. (1994) ‘Exclusion and Emphasis Reframed as a Matter of Ethics’ in Ethics & Behaviour, 4, pp. 229-335.
Darlingluck (2011) ‘Fibromyalgia’ [forum] 16th December 2011, Available at: http://pandys.org/forums/index.phpshowtopic=159085&hl=%2Bchronic+%2Bfatigue#entry1543240 [Accessed 12th February 2015]
Davis, J. (2002) ‘Social Movements and Strategic Narratives: Creating the Sexual Abuse Survivor Account’ in W. Patterson ed, pp. 107-125
Davis, M. & Manderson, L. (Eds) (2014) Disclosure in Health and Illness (London, New York: Routledge).
D’Cruze, S. (1998) Crimes of Outrage: Sex, Violence and Victorian Working Women (London, Manchester: UCL Press).
D’Cruze, S. & Rao, A. (2004) ‘Violence and the vulnerabilities of gender’ in Gender and History, 16:3, pp. 495–512.
Degloma, T. (2009) ‘Expanding Trauma through Space and Time: Mapping the Rhetorical Strategies of Trauma Carrier Groups’ in Social Psycholgoy Quarterly, 72:2, pp. 105-122.
De Man, P. (1984) The Rhetoric of Romanticism (New York: Columbia University Press).
Deutsch, F. (2007) ‘Undoing Gender’ in Gender & Society, 21:1, pp. 106-127.
Dickson, A., Knussen, C. & Flowers, P. (2007) ‘Stigma and the delegitimation of experience: An interpretative phenomenological analysis of people living with chronic fatigue syndrome, in Psychology and Health, 22:7, pp. 851-67.
Donovan, B. (2005) ‘Gender Inequality and Criminal Seduction: Prosecution Sexual Coercion in the Early-20th Century’ in Law & Social Inquiry, 30:1, pp. 61-88.
Doyle, J. (2013) ‘Paedophile freed after judge said victim was ‘sexual predator’ STILL poses risk to children, says his OWN lawyer’ [online article] in Daily Mail Online, 7th August 2013, Available at: http://www.dailymail.co.uk/news/article-2385766/Paedophile-Neil-Wilsons-lawyer-says-sexual-predator-STILL-poses-risk-children.html [Accessed 5th July 2015].
Duggan, L. (2012) Twilight of Equality?: Neoliberalism, Cultural Politics and the Attack on Democracy, (London: Beacon Press).

90
Dumit, J. (2003) ‘Is it me or my brain? Depression and neuroscientific facts’ in Journal of Medical Humanities 24:1, pp. 35–47.
Dumit, J. (2006) ‘Illnesses you have to fight to get: Facts as forces in uncertain emergent illnesses’ in Social Science & Medicine, 62:3,pp. 577-90.
Eby, K., Campbell, J., Sullivan, C., & Davidson, W. (1995) ‘Health effects of experiences of sexual violence for women with abusive partners’ in Health Care for Women international, 16:6: pp. 563-576.
Einagel, V. (2002) ‘ Telling Stories, Making Selves’ in L, Bondi eds., pp. 223-235.
Elliott, C. (2008) Global Empowerment Of Women: Responses To Globalization And Politicized Religions, (New York, London: Routledge)
Englehardt, M. (2007) ‘Seeds of Discontent: Dancing Manias and Medical Inquiry in 19th Century British Literature and Culture’ in Victorian Literature and Culture, 35:1, pp. 135-156.
Eogan, M., McHugh, A. & Holohan, M. (2013) ‘The role of the sexual assault centre’ in Best Practice & Research Clinical Obstetrics and Gynaecology, 27, pp. 47-58.
Ericson, R. (ed) (2003) Risk and Morality, (Toronto: University of Toronto Press)
Erikson, P. (2011) ‘ Sexuality, Medical Anthropology, and Public Health’ in M. Singer & P. Erikson eds, pp. 271- 287.
Evans, M. (2015) ‘Ione Wells: Attacker sentenced to 12 months in custody’ [online article] 6th May 2015 in The Telegraph Online, Available at: http://www.telegraph.co.uk/news/uknews/crime/11585708/Ione-Wells-Attacker-sentenced-to-12-months-in-custody.html [Accessed 9th July 2015]
Ewick, P. & Silbey, S. (1995) ‘Subversive Stories and Hegemonic Tales: Toward a Sociology Of Narrative’ in Law and Society Review, 29, pp. 197-226.
Fairbrother, N. & Rachman, S. (2004) ‘Feelings of mental pollution subsequent to sexual assault’ in Behaviour Research and Therapy, 42, pp. 173–189.
Farr, S. (1814) Elements of Medical Jurisprudence: or a succinct or compendious description of such tokens in the human body as are requisite to determine the Judgement of a coroner, and courts of law, in the cases of divorce, rape, murder etc, to which are added, directions for preserving the public health, 2nd edition (London: J. Callow).
Farrell, J. & Cacchioni, T. (2012) ‘The Medicalization of Women’s Sexual Pain’ in The Journal of Sex Research, 49:4, pp. 328-336.

91
Ferguson, S. (2014) ‘Inspiration Porn: why we need to stop tokenising survivors’ [online article], Available at: http://everydayfeminism.com/2014/10/survivor-stories/ [Accessed online 28th May 2015].
Fielding, H. (1996) ‘Grounding Agency In Depth: The Implications Of Merleau-Ponty’s Thought For The Politics Of Feminism’ in Human Studies, 19. Pp. 175-184
Figlio, K. (1978) ‘Chlorosis and Chronic Disease in 19th Century Britain: The Social Constitution of Somatic Illness in a Capitalist Society’ in Social History, 3:2, pp. 167-97.
Fine, G. (2007) ‘The Construction of Historical Equivalence: Weighing the Red and Brown Scares’ in Symbolic Interaction 30, pp. 27-39.
Foucault, M. ([1965]1988) Madness and Civilization: A History of Insanity in the Age of Reason (New York: Random House).
Foucault, M. (1972) The Archaeology of Knowledge, trans. A. Sheridan Smith, (London: Tavistock)
Foucault, M. (1973) Birth of the Clinic: An Archaeology Of Medical Perception, trans. A.M. Sheridan (London, New York: Routledge)
Foucault, M. (1975) Discipline and Punish: The Birth of the Prison. (New York, London: Vintage).
Foucault, M. (1977) ‘Nietzsche, Genealogy, History’ in D. Bouchard Ed, trans. D Bouchard & S. Simon, pp. 139-164.
Foucault, M. (1978) ‘ About the Concept of the “Dangerous Individual” in 19th
Century Legal Psychiatry’ trans., A. Baudot & J. Couchman, in International Journal of Law and Psychiatry, 1, pp. 1-18.
Foucault, M. (1979) The History of Sexuality: Volume 1, An Introduction, trans. R. Hurley (London: Penguin Books).
Foucault, M. (1980) Power/Knowledge: Selected Interviews and other writings, 1972-1977, ed C. Gordon (London: Pantheon).
Foucault, M. (2001) Fearless Speech, trans. & ed. J. Pearsons, (Los Angeles, London: Semiotexte)
Fraser, N. & Gordon, L. (1994) ‘A Genealogy of Dependency: Tracing a Keywork of the U.S. Welfare State’ in Signs, 19:2, pp. 309-336.
Freedman, K. (2006) ‘The Epistemological Significance of Psychic Trauma’ in Hypatia, 21:2, pp. 104-125.
92
Freud, S. (1962) ‘The Aetiology of Hysteria’ in Standard edition, vol 3. (London: Hogarth Press).
Frese, B., Moya, M. & Megías, J. (2004) ‘Social Perception of Rape: How Rape Myth Acceptance Modulates the Inlfuence of Situational Factors’ in Journal of Interpersonal Violence, 19:2, pp. 143-161.
Friedman, L. (2002) ‘Name Robbers: Privacy, Blackmail, and Assorted Matters in Legal History’ in Hofstra Law Review, 30, pp. 1093-1132.
Gage, C. (1992) ‘The Women’s Rape Museum’ in Off Our Backs, 22:1, pp. 6-9.
Garden, R. (2010) ‘ Disability and narrative: new directions for medicine and the medical humanities’ in Journal of Medical Humanities, 36, pp. 70-74.
Garry, A. & Pearsall, M. (Eds.) (1996) Women, Knowledge, and Reality: Explorations in Feminist Philosophy, (London:Routledge).
Gavey, N. (1999) ’”I Wasn’t Raped, but…”: Revisiting Definitional Problems in Sexual Victimisation’ in S. Lamb (Ed), pp. 57-81.
Gavey, N. (2005) Just Sex? The Cultural Scaffolding of Rape, (London: Routledge).
Gavey, N. (2008) ‘Rape, trauma, and meaning’ in C. M. Elliott ed., pp. 233-246
Gavey, N. & Schmidt, J. (2011) ‘”Trauma of Rape” Discouse: A Double-Edged Template for Understandings of the Impact of Rape?’ in Violence Against Women, 17:4, pp. 433-456.
Giardino, A., Datner, E. & Asher, J. (Eds) (2003) From Sexual Assault: Victimization Across the Lifespan, (Missouri: GW Medical Publishing).
Giesbrecht, T. & Merckelbach, H. (2009) ‘Betrayal trauma theory of dissociative experiences: Stroop and directed forgetting findings’ in The American Journal of Psychology, 122:3, pp. 337-348
Gilfus, M. (1999) ‘The Price of the Ticket: A Survivor-Centered Appraisal of Trauma Theory’ in Violence Against Women, 5:11,pp. 1238-1257.
Goffman, E. (1986). Stigma: Notes on the management of spoiled identity (New York, London:Touchstone).
Gola, H., Engler, H., Schauer, M., Adenauer, H., Riether, C., Kolassa, S., Elbert, T. & Kolassa, I. (2012) ‘Victims of rape show increased cortisol responses to trauma reminders: A stufy in individuals with war- and torture-related PTSD’ in Pscyhoneuroendocrinology, 37, pp. 213-220.
Grand, S. (2003) ‘Unsexed and Ungendered Bodies: The Violated Self’ Studies in Gender and Sexuality, 4:4, pp. 313-341.
93
Gross, M. & Graham-Bermann, A. (2006) ‘Gender, Categories, and Science-as-Usual: A critical reading of Gender and PTSD’ in Violence Against Women, 12:4, pp. 393-406.
Grillo, L. (2014) Interview, interviewed by Constance Flude, 22nd December 2014 [Phone Interview].
Guest_* (2001a) “The Effects: How did it change my life?” [Forum] 18th May 2001, Available at: http://pandys.org/forums/index.php?showtopic=2986 [accessed 18th February 2015]
Guest_* (2001b) ‘”Arr-ay-pee-ee”…spell and say’ [forum] 27th October 2001, Available at: http://pandys.org/forums/index.php?showtopic=2987 [ accessed 2nd February 2015]
Guest_* (2001c) ‘”Arr-ay-pee-ee”…spell and say’ [forum] 30th August 2001, Available at: http://pandys.org/forums/index.php?showtopic=2987 [ accessed 2nd February 2015]
Guest_* (2002a) ‘Telling your story vs. learning to cope’ [forum] 18th June 2002 Available at: http://pandys.org/forums/index.php?showtopic=3000 [Accessed 28th January 2015].
Guest_* (2002b) ‘Telling your story vs. learning to cope’ [forum] 19th June 2002 Available at: http://pandys.org/forums/index.php?showtopic=3000 [Accessed 28th January 2015]
Guest_* (2002c) ‘Telling your story vs. learning to cope’ [forum] 20th June 2002 Available at: http://pandys.org/forums/index.php?showtopic=3000 [Accessed 28th January 2015]
Guest _* (2002d) ‘”Get Over it”’ [forum] 27th June 2002, Available at: http://pandys.org/forums/index.php?showtopic=2997&page=2 [Accessed 2nd March 2015]
Guest _* (2003) ‘”Get Over it”’ [forum] 12th July 2003, Available at: http://pandys.org/forums/index.php?showtopic=2997&page=2 [Accessed 2nd March 2015]
Guest_sk_Redmond_* (2002) ‘ Get Over It’ [Forum] 28th June 2002, Available at: http://pandys.org/forums/index.php?showtopic=2997&page=2 [Accessed 28th March 2015].
Haaken, J. (1999) ‘ Heretical Texts: The Courage to Heal and the Incest Survivor Movement’ in S. Lamb ed., pp. 13-41.
Hall, S. & Du Gay, P. (1996) Questions of Cultural Identity (London: Sage).
Hamilton, A. & Godkin, L. (ed) (1900) A System of LegalMedicine. 2nd ed.. Vol. 2. (New York: E.B. Treat and Co.)
94
Hanhardt, C. (2013) Safe Space: Gay Neighbourhood History and the Politics of Violence (New York: Duke University Press)
Haraway, D. (1988) ‘Situated Knowledges: The Science Question in Feminism and the Privilege of Partial Perspective’ in Feminist Studies, 14:3, pp.575-599.
Hart, G. & Wellings, K. (2002) ‘ Sexual Behaviour and its Medicalisation: In Sickness and in Health’ in British Medical Journal, 324:7342, pp. 896-900.
Hauck, S., Schestatsky, S., Terra, L., Kruel, L. & Ceitlin, L. (2007) ‘Parental bonding and emotional response to trauma: A study of Rape Victims’ in Psychotherapy Research,, 17:1, pp. 83-90.
Hawthorne, S (2006) Origins, Genealogies, and the Politics of Identity: Towards a Feminist Philosophy of Myth. PhD Thesis, University of London. http:eprints.soas.ac.uk/archive/00000144/.
Heidegger, M. (1977) The Question of Technology and Other Essays, trans. W. Lovitt (New York: Harper and Row).
Hellothere (2014) ‘I feel Labelled; I’m Afraid to do Anything’ [Forum] 12th October 2014, available at http://pandys.org/forums/index.php?showtopic=253938&page=2&hl=%2Bmedical+%2Bproblems#entry2143126 [Accessed 18th December 2014]
Hengehold, L. (1994) ‘An Immodest Proposal: Foucault, Hysterization, And The "Second Rape"’ in Hypatia, 9:3, pp. 88-107.
Hengehold, L (2011) ‘When Safety Becomes a Duty: Gender, Loneliness, and Citizenship for Urban Women’ in Women’s Studies Quarterly, 39:1/2, pp. 48-69.
Heberle, R. (1996) ‘Deconstructive Strategies and the Movement against Sexual Violence’ in Hypatia, 11:4, pp. 63-76.
Herman, J. (1992) Trauma and Recovery (New York: Basic Books).
Hersford, W. (1999) ‘Reading rape Stories: Material Rhetoric and the Trauma of Representation’ in College English, 62:2, pp. 192-221.
Hidingfox (2015) ‘Fighting Physical and Mental Illness Alone’ [Forum] 2nd January 2015, Available at: http://pandys.org/forums/index.phpshowtopic=259915&hl=%2Bchronic+%2Bfatigue [Accessed 27th March 2015]
HO/47/75 (1810) ‘Rex Against John Noden’, National Archives, Kew.
Holquist, M. (1990) Dialogism: Bakhtin and his world I (London: Routledge).
95
Horwtiz, A. & Wakefield, J. (eds.) (2007) The Loss of Sadness: How Psychiatry Transformed Normal Sorrow into Depressive Disorder, (New York, Oxford: Oxford University Press).
Houston, R. (2002) ‘Madness and Gender in the Long Eighteenth Century’ in Social History, 27:3, pp. 309-326.
Huyssen, A. (1995) Twilight Memories: Marking Time in a Culture of Amnesia, (New York, London: Routledge).
Iverson, K., King, M., Cunningham, K. & Resick, P. (2015) ‘Rape survivors’ trauma-related beliefs before and after Cognitive processing therapy: Associations with PTSD and depression symptoms’ in Behaviour Research and Therapy, , 66, pp. 49.55.
Jackson, S. (1978) ‘The Social context of rape: sexual scripts and motivation’ in Women’s Studies International Quarterly, 1, pp. 30.
Jackson, L. (2000) ‘’Singing Birds as well as Soap Suds’: The Salvation Army’s Work with Sexually Abused Girls in Edwardian England’ in Gender and History, 12:1, pp. 107-126.
Jackson, P. (2013) ‘Making Sense of Making Sense: Configurational Analysis and the Double Hermeneutic’ in D. Yanow & P. Schwatz-Shea eds, pp. 267-283
Jain, S. (2006) Injury: The Politics of Product Design and Safety Law in the United States (Princeton, Oxford: Princeton University Press).
Jain, S. (2007) ‘Living in Prognosis: Toward an Elegiac Politics’ in Representations, 98:1, pp. 77-92.
Joinson, A. (2001) ‘Self-disclosure in computer-mediated communication: The role fo self-awareness and visual anonymity’ in European Journal of Social Psychology,’ 31, pp. 177-192.
Joinson, A., McKenna, K., Postmes, T., Reips, U. (eds.) (2007) The Oxford Handbook of Internet Psychology, (Oxford: Oxford University Press)
Jolly, R. (2011) ‘Witnessing Embodiment: Trauma, Narrative and Theory at the Limit in Field Research and in the Classroom’ in Australian Feminist Studies, 26:69, pp. 297-317
John Bull and Britannia (1856) Untitled (Saturday 1st November 1856)
Johnson, M. & Ferraro, K. (2000) ‘Research on Domestiv Violence in the 1990s’; marriage distubrances’ in journal of marriage and family 62:4 pp. 948-963
Katz, J. (1984) No Fairy Godmothers, No Magic Wands : The Healing Process After Rape. (Saratoga, London: R.& E).

96
Kelly, L. (1988) Surviving Sexual Violence, (Minneapolis : University of Minnesota Press).
Kentish Express (1863) ‘Untitled’ (20th January 1863)
Kerr, D. (1935) Forensic Medicine (London)
Kilpatrick, D. Resick,P. &. Veronen, L. (1981) ‘Effects of a Rape Experience: A Longitudinal Study’, in Journal of Social Issues 37, pp. 105–22.
Kilpatrick, D., Veronen, L., Best, C. (1985) Factors predicting psychological distress among rape victims (New York: Brunner)
Kilpatrick, D. & Acierno, R. (2003) ‘Mental Health Needs of Crime Victims: Epidemiology and Outcomes’ in Journal of Traumatic Stress, 16:2, pp. 119-132.
Kimerling, R., Ouimette, P. & Wolfe, J. (2002) Gender and PTSD (New York: Guilford).
Koehne, K., Hamilton, B., Sands, N. & Humpheries, C. (2012) ‘Working around a contested diagnosis: Borderline Personality Disorder in adolescence, in Health, 17, pp. 37-56.
Kokanovic, R. & Philip, B. (2014) ‘Emotional Talk: Depression, Diagnosis and Disclosure’ in M. Davis & L. Manderson Eds., pp. 56-71.
Koss, M. Gidycz, C. & Wisniewski, N. (1987) ‘The Scope of Rape: Incidence and prevalence of sexual aggression and victimization in a national sample of higher education students’ in Journal of Consulting and Clinical Psychology, 55, pp. 162-170.
Krause, E., DeRosa, R., ,& Roth, S. (2002) ‘Gender, trauma themes, and PTSD: Narratives of male and female survivors’ in R. Kimerling, P. Ouimette, & J. Wolfe (eds), pp. 349-381
Krause, N. (2005). ‘Traumatic events and meaning in life: Exploring variations in three age cohorts’ in Ageing & Society, 25:4, 501−524.
Kuo, R. (2015) ‘6 Things to Navigate While Coming Out as a Survivor of Sexual Violence’ [online article] Available at: http://everydayfeminism.com/2015/01/coming-out-to-self-as-survivor/ [Accessed 23rd January 2015].
Lamb, S. (Ed) (1999) New Versions of Victims: Feminists Stuggle with the Concept, (New York, London: New York University Press).
Layne, L. (2003) Motherhood lost: A feminist account of pregnancy loss in America (New York,London: Routledge).
97
Levine, P. (1997) Waking the Tiger: Healing Trauma, (Berkley: North Atlantic Books).
Levine, S. (2012) ‘Dancing with Science, Ideology and Technique’ in Journal of Sex Research, 49:4, pp. 408-409.
Leys, R. (2000) Trauma: A Genealogy (Chicago, London: The University of Chicago Press).
Link, B., Mirotznik,J.& Cullen. F. (1991) ‘The effectiveness of stigma coping
orientations: Can negative consequences of mental illness labelling be avoided? Journal of Health and Social Behavior, 32:3, pp. 302–20.
Lionesscub (2014a) ‘How long should T Last For? [forum] 30th November 2014, Available at:
http://pandys.org/forums/index.php?showtopic=258179&hl=%2Bmedical+%2Bproblems#entry2154646, [Accessed 11th January 2015]
Lionesscub (2014b) ‘How long should T Last For? [forum] 2nd December 2014, Available at:
http://pandys.org/forums/index.php?showtopic=258179&hl=%2Bmedical+%2Bproblems#entry2154646, [Accessed 11th January 2015]
Lionnesscub (2014) ‘I feel Labelled; I’m Afraid to do Anything’ [Forum] 14th November 2014, available at http://pandys.org/forums/index.php?showtopic=253938&page=2&hl=%2Bmedical+%2Bproblems#entry2143126 [Accessed 18th December 2014]
Lis (2003) ‘On being a victim…’ [forum] 12th November 2003, Available at: http://pandys.org/forums/index.php?showtopic=6649 [Accessed 24th April 2015]
Littleme (2007) ‘PTSD-RTS (Rape Trauma Syndrome)’ [forum] 17th June 2007, Available at: http://www.psychforums.com/rape-trauma/topic16032.html [Accessed 26th February 2015].
Lodrick, Z. (2007) ‘Psychological Trauma – What Every Trauma Worker Should Know’ in The British Journal of Psychotherapy Integration, 4:2, pp. 1-19.
Lodrick, Z. (2015a) Interview, interviewed by Constance Flude [Phone Interview] on 19th May 2015.
Lodrick, Z. (2015b) Lecture at Fitzwilliam College, Cambridge, 26th April 2015.
98
London and Sporting Chronicle (1851) ‘Bell Life’ (Sunday 2nd March 1851)
London and Sporting Chronicle (1856) ‘Bells Life’ (November 15th 1856)
Lora (2003) ‘On being a victim…’ [forum] 12th November 2003, Available at: http://pandys.org/forums/index.php?showtopic=6649 [Accessed 24th April 2015]
Louise (2003) ‘On being a victim…’ [forum] 13th November 2003, Available at: http://pandys.org/forums/index.php?showtopic=6649 [Accessed 24th April 2015]
Love2013 (2013) ‘Hoping to bring closure’ [forum] 22nd October 2013, available at: http://pandys.org/forums/index.phpshowtopic=236350&hl=%2Bchronic+%2Bfatigue[accessed 28th January 2015]
Magdalene (2003) ‘On being a victim…’ [forum] 12th November 2003, Available at: http://pandys.org/forums/index.php?showtopic=6649 [Accessed 24th April 2015]
Maidstone & Kentish Journal (1863) ‘Untitled’ (26th September 1863).
Maidstone & Kentish Journal (1865) ‘Untitled’ (25th December 1865).
Maidstone & Kentish Journal (1872) ‘Untitled’ (9th December 1872).
Marecek, J. (1999) ‘Trauma Talk in Feminist Clinical Practice’ in S. Lamb Ed., pp. 158-182
Marcus, S. (1992) ‘Fighting Bodies, fighting words: A theory and politics of rape prevention’ in J. Butler & J. Scott (eds.), pp. 385-403.
Martin, N. (2001) ‘Feminist bioethics and psychiatry’ in Journal of Medicine and Philosophy, 26:4, pp. 431–41.
Martin, K. (2003) ‘Giving Birth like a Girl’ in Gender and Society, 17:1, pp. 54-72.
Mattheson, R. (2015) Interview, interviewed by Constance Flude 16th May 2015 at Rape Crisis Peterborough.
May. S. (ed.) (2011) Nietzsche’s On the Genealogy of Morality, (Cambridge, New York: Cambridge University Press).
Meyburgh, T. (2006) ‘The Body Remembers: Body Mapping and Narratives of Physical Trauma’ MA thesis, University of Pretoria.
Mason, F. & Lodrick, Z. (2013) ‘Psychological consequences of sexual assault’ in Best Practice & Research Clinical Obstetrics and Gynaecology , 27, pp. 27-37.
McCutcheon, R. (2009) ‘Myth’ in Braun & McCutcheon eds, pp. 190-208.
99
McNay, L. (1992) Foucault and Feminism (Cambridge: Polity Press).
Melosh, B. (1995) ‘Review’ in The Journal of American History, 81:4, pp. 1756-1757.
MEPO 2/10401 (1962) ‘Report Dealing with Suggested Ammendment of G.O. in Connection with the Medical Examination of the Victims of Sexual and Unnatural Offenses’, National Archives Kew.
Micale, M. & Lerner, P. (2001) Traumatic Pasts: History, Psychiatry and Trauma in the Modern Age, 1870-1930 (London: Cambridge University Press)
Mieke, B. (ed) (2005) The Artemisia files: Artemisia Gentileschi for feminists and other thinking people, (Chicago: University of Chicago Press).
Minute (2010) ‘ Why do I seek out Triggers?’ [forum] 17th June 2010, Available at: http://www.aftersilence.org/forum/index.php?showtopic=76746 [Accessed 17th March 2015]
Mohanty, C. (2003) ‘”Under Western Eyes” Revisited: Feminist Solidarity through Anticaptalist Stuggles’ in Signs, 28:2, pp. 499-535.
Mohanty, C. (with Martin, B.) (2006) Feminism without Borders: Decolonizing Theory, Practicing Solidarity. (London: Duke University Press).
Monk, L. & Jones, A. (2014) ‘ Alcohol consumption as a risk factor for sexual assault: A retrospective analysis’ in Journal of Forensic and Legal Medicine, 23, pp.55-61
Moor, A., Ben-Meir, E., Golan-Shapira, D. & Farchi, M. (2013) ‘Rape: A Trauma of Paralyzing Dehumanization’ in Journal of Aggression, Maltreatment & Trauma, 22:10, pp. 1051-1069.
Morrow, M. (2002) ‘Violence and trauma in the lives of women with serious mental illness: Current practices in service provision’ report for the British Columbia Centre of Excellence for Women’s Health. [online report] Available at: http://bccewh.bc.ca/wp-content/uploads/2012/05/2002_Violence-and-Trauma-in-the-Lives-of-Women-with-Mental-Illness.pdf [Accessed 27thMarch 2015].
Mort, F. (2006) ‘Scandalous Events: Metropolitan Culture and Moral Change in Post-Second World War London’ in Representations, 93:1, pp. 106-137.
Mumm, S. (1996) ‘”Not Worse than Other Girls”: The Convent-Based Rehabilitation of Fallen Women in Victorian Britain’ in Journal of Social History, 29:3, pp. 527-546.
Najdowski, C. & Ullman, S. (2009) ‘PTSD Symptoms and Self-Rated Recovery Among Adult Sexual Assault Survivors: The Effects of Traumatic Life Events and Psychological Variables’ in Psychology of Women Quarterly, 33, p. 43-53.

100
Naples, N. (2003) Feminism and Method: Ethnography, Discourse Analysis, and Activist Research (London: Routledge)
NHS Choices (2015) ‘Cerebral Palsy’ [Website] Available at: http://www.nhs.uk/Conditions/Cerebral-palsy/Pages/Introduction.aspx [Accessed 4th July 2015].
Nicki, A. (2001) ‘The Abused Mind: Feminist Theory, Psychiatric Disability and Trauma’ in Hypatia, 16:4, pp. 80-104.
Norris, F., Foster, J., &Weisshaar, D. (2002) ‘The epidemiology of sex differences in PTSD across developmental, societal, and research contexts’ in R. Kimerling, P. Ouimette,&J.Wolfe (eds.), pp. 3-42.
Obliterated (2014) ‘Fibromyalgia + C-PTSC = I am too tired to do for you, for real’ [Forum] 10th April 2014, Available at: http://pandys.org/forums/index.phpshowtopic=244982&hl=%2Bchronic+%2Bfatigue [Accessed 25th March 2015]
Ogston, F. (1878) Lectures on Medical Jurisprudence (London).
O’Malley, P. (1996) ‘Risk and Responsibility’ in Barry, Osborne & Rose Eds., pp. 189-207.
Orangeblossom (2014) ‘Labels’ [online forum] 26th November 2014, Available at: http://www.isurvive.org/forum/viewtopic.php?f=20&t=6079 [accessed 18th December 2014]
Ovenden, G. (2012) ‘Young women’s management of victim and survivor identities’ in Culture, Health & Sexuality: An International Journal for Research, Intervention and Care, 14:8, pp. 941-954.
Page, H. (1883) Injuries of the Spine and Spinal Cord Without Apparent Mechanical Lesion, and Nervous Shock, in Their Surgical and Medico-Legal Aspects. (London: J. & A. Churchill).
Papaikonomou, M. (2014) ‘Rape and Trauma: A Case Study of a Journey of Recovery’ in Psychology in Africa, 19:2, pp. 213-216.
Paris, J. & Fonblanque, J. (1823) Medical Jurisprudence, vol 1 (London: W. Phillips).
Pastor, P. (1978) ‘Mobilization in Public Drunkenness Control: A comparison of legal and medical approaches’ in Social Problems, 25, pp. 373-84.
Patterson, W.(ed) (2002) Strategic Narrative: New Perspectives on the Power of Personal and Cultural Stories, (Cambridge: Harvard University Press).
Petrak, J. (2002) ‘Rape: History, myths, and realit’, in J. Petrak & B. Hedge (eds), pp. 1-18.
101
Petral, J. & Hedge, B.. (2002) The trauma of sexual assault: Treatment, prevention and practice, (New York: John Wiley)
Pollock, G. (2005) ‘Feminist dilemmas with the art/life problem’ in B. Mieke ed, pp. 169-206.
Potter, J. (1996) ‘Discourse Analysis and Constructionist Approaches: Theoretical Background’ in J. Richardson (ed.), pp. 125-140.
Porter, R. (1986) ‘Rape: Does it have a historical meaning?’ in S.Tomaselli & R. Porter eds., pp. 216-36.
Plummer, K. (1995) Telling Sexual Stories: Power, Change and Social Worlds, (New York,London: Routledge).
Prince, M. (1987) Traumatic Neuroses. (Philadelphia:Lea Brothers and Co).
Puar, J. (2009) ‘ Prognosis time: Towards a geopolitics of affect, debility and capacity’ in Women ad Performance: A journal of feminist theory, 19:2, pp. 161-172.
Puar, J. (2011) ‘Coda: The Cost of Getting Better. Suicide, Sensation, Switchpoints’ in GLQ: A Journal of Lesbian and Gay Studies, pp. 149-158.
Puppe, G. (1894) A Medico-Legal Study of Rape (New York).
Quéniart, A. (1992) ‘Risky Business: Medical Definitions of Pregnancy’ in D. Currie & V. Raoul eds., pp. 161-175.
Ramazanoglu, C. & Holland, J. (2002) Feminist Methodology: Challenges and Choices. (London, New Dehli: SAGE publications)
Reinharz, S. (1992) Social Research Methods: Feminist Perspectives, (London: Oxford University Press).
Rice, R., Shepherd, A., Dutton, W. & Katz,J. (2007) ‘The Internet, Digital Divides and Social Interaction: A comparative analysis and surveys in the US and Britain’ in A. Joinson et al. eds., pp. 7-31.
Ricœr, P. (1991) From Text to Action: Essays in Hermeneutics, trans. K.Blaney & J. Thompson, (Illinois: Northwestern University Press)
Richardson, l. (1990) ‘Narrative And Sociology’ in Journal Of Contemporary Ethnogoraphy 19, pp. 116-35
Richardson, J. (ed.) (1996) Handbook of Qualitative Research Methods, (Leicester: BPS Books).
Robertson, R. (1992) Globalization: Social theory and Global Culture (London: SAGE publications).

102
Robertson, S. (1998) ‘Signs, Marks, and Private Parts: Doctors, Legal discourses, and Evidence of Rape in the United States, 1823-1930. In Journal of the History of Sexuality, 8:3, pp. 345-388
Robinson, W. (1928) America’s Sex and Marriage Problems: Based on Thirty Years Practice and Study (New York).
Robson, R. (2011) ‘Refusing Safety: The Feminist Struggle to be Revolutionary’ in Women’s Studies Quarterly, 39:1/2, pp. 262-269.
Roestone Collective (2014) ‘Safe Space: Towards a Reconceptualization’ in Antipode, 46:5, pp. 1345-1365.
Ronai, C. (1999) ‘In the Line of Sight at Public Eye: In Search of a Victim’ in S. Lamb Ed., pp. 139-157.
Rose, N. (1996) Inventing Ourselves: Psychology, Power and Personhood, (Cambridge: Cambridge University Press).
Rose, N. (1996) ‘Identity, Genealogy, History’ in S. Hall & Du Gay, P. eds, pp. 128-150.
Rose, N. (2006) ‘Disorders Without Borders? The Expanding Scope of Psychiatric Practice’ in BioSocieties, 1, pp. 465-484.
Rose, N. (2003) ‘The neurochemcial self and its anomalies’ in R. Ericson, (ed) pp. 407-37.
Rose. N. (2007) The Politics of Life Itself: Biomedicine, Power and Subjectivity in the Twenty-First Century, (Princetown, Oxford: Princetown University press).
Rubin, G. (2011) Deviations: The Gayle Rubin Reader (London: Duke University Press).
Ruiz, M. (2011) ‘ Gender Policy, the London Lock Asylum Committee (1836-1842)and the Asylum Regulations for 1840’ in Atlantis, 33:2, pp. 123-136.
Rynd.N (1988) ‘Incidence of Psychometric Symptoms in Rape Victims’ in The Journal of Sex Research, 24, pp. 155-161.
Sanford, M. (1892) ‘Rescue Work Among Fallen Women’ in The North Amerian Review, 154:422, pp. 119-122.
Samealdo (2006) ‘Who deserves to be here?’ [Forum] 16th June 2006 Available at: http://pandys.org/forums/index.php?showtopic=38182&page=1 [accessed 1st June 2015]
Saretta (2015) ‘TW T Session 4 – Cortisol vs Compassion’ [Forum] 11th February 2015, available at http://pandys.org/forums/index.php?app=blog&module=display§ion=blog&blogid=5351&showentry=56744 [accessed on 16th February 2015]

103
Scarry, E. (1988) The Body in Pain: the Making and Unmaking of the World, (Oxford: Oxford University Press).
Scarry, E. (1990) ‘ Consent and the Body: Injury, Departure, and Desire’ in New Literary History, 21:4, pp. 867-896.
Scheff, T. (1974) ‘The Labelling Theory of Mental Illness’ in American Sociological Review, 39:3, pp. 444-452.
Segal, J. (2012) ‘The Sexualization of the Medical’ in Journal of Sex Research, 49:4, pp. 369-378.
Segal, J. (2009) ‘Internet Health and the 21st-Century Patient: A Rhetorical View’ in Written Communication, 26:4, pp. 351-369.
Setrain (2010) ‘ Why do I seek out Triggers?’ [forum] 17th June 2010, Available at: http://www.aftersilence.org/forum/index.php?showtopic=76746 [Accessed 17th March 2015].
Shapiro, J. (2011) ‘Illness narratives: reliability, authenticity and the empathic witness’ in Journal of Medical Humanities, 37:2, pp. 68-71
Shepherd, L. (2007) ‘‘Victims, Perpetrators and Actors’ Revisited: Exploring the Potential for a Feminist Reconceptualisation of (International) Security and (Gender) Violence’ in BJPIR,9, pp 239-256
Shoemaker, M. (2008) Genealogy, From Foucault Nietzsche to Foucault: Tracing the History of the Present (Berlin: Saarbrüken)
Showalter, E. (1997) Hystories: Hysterical Epidemics and Modern Culture (London, New York: Columbia University Press).
Shuttleworth, S. (2012) ‘Spiritual Pathology: Priests, Physicians, and The Way of All’ in Victorian Studies, 54:4, pp. 625-653.
Siegal, D. (1999) The Developing Mind: How relationships and the brain interact to shape who we are, (New York: The Guildford Press).
Silentstar (2008) ‘Get Over It’ [Forum] 17th August 2008, Available at: http://pandys.org/forums/index.php?showtopic=2997&page=5 [ Accessed 28th March 2015]
Singer, M. & Erikson, P. (2011) A Companion to Medical Anthropology, (London: Blackwell Publishing).
Sister (2003) ‘”Get Over it”’ [forum] 1st September 2003, Available at: http://pandys.org/forums/index.php?showtopic=2997&page=2 [Accessed 2nd March 2015]
104
Sister Anne Clare's Book (1873) K/AC/1, "The Mother of Penitents and Some of Her Children": Penitentiary Work in the Church of England, CSMVW Archives
Smith, F. (1908) Lectures on Medical Jurisprudence and Toxicology as Delivered at London Hospital, 1900, 2d ed. (London).
Somers, M (1994) ‘The Narrative Constitution Of Identity: A Relational And Network Approach’ in Theory and Society, 23, pp. 605-649.
Sonntag, M. (2011) ‘No Place to Live: The Uninhabitable Body’ in Studies in Gender and Sexuality, 12:3, pp. 221-231.
Stafford, B. (1991) Body of criticism: Imaging the unseen in Enlightenment art and medicine. (Cambridge, MA: The MIT Press).
Stahl, D. (2013) ‘Living into the imagined body: how the diagnostic image confronts the lived body’ in Medical Humanities, 39, pp. 53-58.
Stanko, E. (1985) Intimate Intrusions: women’s experience of male violence (London: Routledge)
Stern, M. (2006) ‘Racism, sexism, classism and much more: reading security-identity in marginalised sites’ in B. Ackerly, M. Stern &J J. True eds., pp. 174-197.
Stocker, S. (2001) ‘Problems of Embodiment and Problematic Embodiment’ in Hypatia, 16:3, pp. 30-55.
Sunder-Rajan, K. (2006) Biocapital: The constitution of postgenomic life. (Durham: Duke University Press).
Taylor, C. (2009a) The Culture of Confession from Augustine to Foucault: A Genealogy of the ‘Confessing Animal (New York, Oxon: Routledge).
Taylor, C. (2009b) ‘Foucault, Feminism, and Sex Crimes’ in Hypatia, 24:4, pp1-25.
Thackhuk, A. (2011) ‘Stigma and the politics of biomedical models of mental illness’ in International Journal of Feminist Approaches to Bioethics, 4:1, pp. 140-163.
Theriot, N. (1993) ‘Women's Voices in Nineteenth-Century Medical Discourse: A Step toward Deconstructing Science’ in Signs 19:1, pp.1-31.
Tilted (2003) ‘On being a victim…’ [forum] 12th November 2003, Available at: http://pandys.org/forums/index.php?showtopic=6649 [Accessed 24th April 2015]
The Times (1828) ‘Crownside’ (18th August 1828).
Thomson, A.. (1936) ‘Lectures on Medical Jurisprudence’ in The Lancet, Sat 24th Deceember 1836, pp 449- 454.
105
Tolin, D. & Foa, E. (2002) ‘Gender and PTSD: A cognitive model’ in R. Kimerling, P. Ouimette, & J.Wolfe (eds.), pp. 76-97).
To, S., Zepf, R.& Woods. A. (2005) ‘The symptoms, neurobiology, and current pharmacological treatment of depressions’ in Journal of Neuroscience Nursing 37:2, pp. 102-7.
Tomaselli, S. & Porter, R. (Eds) (1986) Rape: An Historical and Social Enquiry. (Oxford, New York: Basil Blackwell).
Tornpieces (2014) ‘I feel Labelled; I’m Afraid to do Anything’ [Forum] 18th November 2014, available at http://pandys.org/forums/index.php?showtopic=253938&page=2&hl=%2Bmedical+%2Bproblems#entry2143126 [Accessed 18th December 2014]
Turner, V. (1967) The Forest of Symbols: Aspects of Ndembu Ritual, (Ithaca: Cornell University Press)
Van Der Kolk, B. (1989) ‘The Compulsion To Repeat The Trauma: Re-Enactment, Revictimisation And Masochism’ In Psychiatric Clinics Of North America, 12:2, Pp. 289-411
Van Der Kolk, B., Mcfarlane, A. & Weiseth, L. (1996) Traumatic Stress: The Effects Of Overwhelming Experience Of Mind , Body, And Society’ (New York, London: Guilford Press).
Venn, C. (2002) ‘Narrative Identity, Subject Formation, And the Transfiguration of Subjects’ in W. Patterson ed, pp. 29-50
Vickery, A. (1993) ‘Golden Age to Separate Spheres? A Review of the Categories and Chronology of English Women’s History’ in Historical Journal 36, 383-414.
Vigarello, G. (2001) Histoire du viol: XVI-XX, [History of Rape] (Paris: Seuil).
Vucetic, S. (2011) ‘Genealogy as a research tool in International Relations’ in Review of International Studies, 37:3, pp.1295-1312.
Wakely, C. (1810) ‘Trial of Charles Wakely for a Rape on Mrs. Rebecca Fay’ (New York: McCarty and White).
Waldby, C. (2000) The Invisible human project: informatics bodies and posthuman medicine (London: Routledge).
Walker, P. (1991) ‘“Pulling the Devil’s Kingdom Down”: Gender and Popular Culture in the Salvation Army 1865–1895’ (PhD thesis, Rutgers University).
Walkowitz, J. (1991) City Of Dreadful Delight. Narratives Of Sexual Danger In Late Victorian London, (London: Virago Press)
106
Walkowitz, J. (1998) ‘Going Public: Shopping, Street Harassment, and Streetwalking in Late Victorian London’ in Representations, 62, pp. 1-30.
Walther, J. (1996) ‘Computer-mediated communication: Impersonal, interpersonal, and hyperpersonal interaction’ in Communication Research, 23, pp. 3-43
Warner, S. (2001) ‘Disrupting Identity Through Visible Therapy: A Feminist Post-Structuralist Approach to Working with Women Who have Experienced Child Sexual Abuse’ in Feminist Review, 68, pp. 115-139
Webster, D. (2002) ‘Somatoform and Pain Disorders’ in M. Ballou & L. Brown Eds., pp. 145-173.
Weedon, C. (1997) Feminist practice and Poststructuralist theory, (Cambridge: Blackwell).
Wessely, S. (1993) Chronic Fatigue Syndrome (London: Wiley)
Wharton, F. & Moreton S. (1855) A Treatise on Medical Jurisprudence (Philadelphia).
White Buffalo Calf Woman Society (2013) ‘Break the Silence’ [youtube video] Available at: https://www.youtube.com/watch?v=lpzGVBapKNs[accessed 23rd March 2015].
White, R., & Horvitz, E. (2008). Cyberchondria: Studies of the escalation of medical concerns in Web search. Microsoft Research. Available at http://research.microsoft.com/apps/pubs/default.aspx?id=76529 [ accessed 4th May 2015]
Whitlock, T. (1999) ‘Gender, Medicine, and Consumer Culture in Victorian England: Creating the Kleptomaniac’ in Albion: A Quarterley Concerned with British Studies, 31:3, pp. 413-437.
Wilcox, L. (2015) Bodies of Violence: Theorising Embodied Subjects in International Relations (Oxford: Oxford University Press).
Wishinuponastar (2010) ‘From Victim, to Survivor, to Thriver’ [Forum] 6th May 2010, Available at: http://www.aftersilence.org/forum/index.php?showtopic=74971 [Accessed 24th April 2015]
Women's Resource Center (2011) Women and Girls Network. The WGN Empowerment Model: redressing negative individidual and social impacts of genderd violence through holistic counselling, accessed online 20th November 2014. http//www.wgn.org.uk/images/2011/Reports/WGN%20SROI%20Report%202011.pdf?phpMyAdmin=3c29b1c1cb4db76acb880b548eb6c339&phpMyAdmin=0840c86857f8e66a33666e36d82aa19e

107
Wood, E. (2000) ‘Working in the fantasy factory: the attention hypothesis and the enacting of masculine power in strip clubs’ Journal of Contemporary Ethnography, 29, pp. 5-31.
Yanow, D. & Schwartz-Shea, P. (eds) (2013) Interpretation and Method: Empirical Research Methods and the Interpretative Turn, (London, New York: M.E.Sharpe).
Zeedyk, S. (2007) ‘ The Science of Rape: (Mis)Constructions of Women’s Trauma in Evolutionary Theory’ in Feminist Review, 86, pp. 67-88.
Zola, K. (1983) Socio-Medical Inquiries, (Philadelphia: Temple University Press).
Zuspan F. (1974) ‘Alleged Rape: An Invitational Symposium’ in The Journal of Reproductive Medicine, 12:4, pp. 133-152.

108
APPENDIX ONE: LIST OF INTERVIEWS
Campui, J. (2015) Interivew, interviewed by Constance Flude, 16th May 2015 at Race Crisis Peterborough.
Grillo, L. (2014) Interview, interviewed by Constance Flude, 22nd December 2014 [Phone Interview].
Interview 1 (2015) Anonymised ‘survivor’ interview, interviewed by Constance Flude on 18th May 2015, [Phone Interview]
Interview 2 (2015) Anonymised ‘survivor’ interview, interviewed by Constance Flude on 17th April 2015, at Wellcome Collection, London.
Interview 3 (2015) Anonymised ‘survivor’ interview, Interviewed by Constance Flude on 23rd April at The Breakfast Club, London.
Interview 4 (2015) Anonymised ‘professional’ Interview, interviewed by Constance Flude on 9th May 2015.
Lodrick, Z. (2015a) Interview, interviewed by Constance Flude [Phone Interview] on 19th May 2015.
Mattheson, R. (2015) Interview, interviewed by Constance Flude 16th May 2015 at Rape Crisis Peterborough.
McClean, D. (2015) Interview, Interviewed by Constance Flude on 1st May 2015 at Boulanger Matin (Stroud Green Road, London N4).
Seccombe, N. (2015) Interview, interviewed by Constance Flude on 8th April 2015, [Phone interview].
Survivor 1 (S1) (2015) Anonymised ‘survivor’ cited from ‘Survivors workshop’, recorded by Constance Flude on 9th May 2015.
Survivor 2 (S2) (2015) Anonymised ‘survivor’ cited from ‘Survivors workshop’, recorded by Constance Flude on 9th May 2015.
Survivor 3 (S3) (2015) Anonymised ‘survivor’ cited from ‘Survivors workshop’, recorded by Constance Flude on 9th May 2015.
Survivor 4 (S4) (2015) Anonymised ‘survivor’ cited from ‘Survivors workshop’, recorded by Constance Flude on 9th May 2015.

109
APPENDIX 2: INFORMED CONSENT FORM
Participant Consent Form and Information Sheet
I am required to give you this information and get your signed consent prior to interviewing you, in order to meet the ethical standards prescribed by the University of Cambridge. Please read this consent document carefully before you decide to whether to participate in this study.
Purpose of the research study: This research project aims to look effects that sexual trauma has on women's lives. Looking specifically at the ways that the medical, psychiatric and social institutions set up to aid women through overcoming such trauma, help these women come to terms with what has happened to them.
Who is conducting the study: My name is Connie. I am currently a research student at the University of Cambridge. I have previously conducted research and interviews with women who have been sexually assaulted in Cambodia and Thailand and have researched and worked with vulnerable children and their families in Uganda.
What you will be asked to do in the study: During the interview, I will ask you questions about your experience of the services on offer to victims of rape and your understanding of the difficulties they face. The interview is, in part, predesigned and in part, based upon the discussion on the day. The predesigned questions have passed an ethics review by the University of Cambridge.
Recording: The interview will be recorded on an audio device. If you wish not to be recorded please let me know at the beginning of the interview and I will take written notes instead. If at any point during the interview you wish the recording equipment to be turned off—either permanently or temporarily—I will do so without hesitation.
Anonymity: All of the information you disclose will remain completely anonymous, unless you choose to waiver this anonymity. I will retain in a protected file, the signed copy of this consent form until such a time as my supervisor agrees it can be deleted. The signed form will then be disposed of safely where no one will see that it is signed.
If you agree to participate in this study please sign below. Thank you.
Agreement: I have read the procedure described above. I voluntarily agree to participate in the interview and I have received a copy of this description. I understand that this interview will be audio recorded and consent to this unless otherwise stated. Furthermore, I understand that what I say during the interview may be quoted in the written thesis produced as a result for this research.
Name (Printed) ___________________________________________
Signature: ________________________________________
Date: _________________
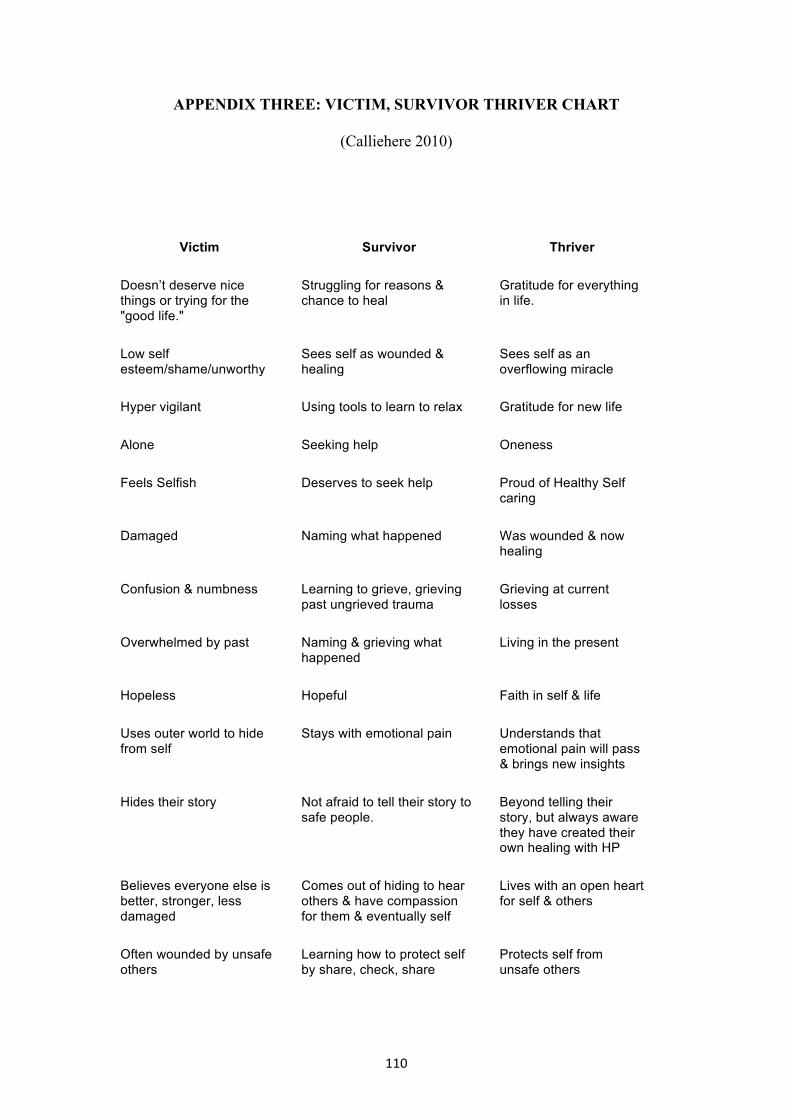
110
APPENDIX THREE: VICTIM, SURVIVOR THRIVER CHART
(Calliehere 2010)
Victim Survivor Thriver
Doesn’t deserve nice things or trying for the "good life."
Struggling for reasons & chance to heal
Gratitude for everything in life.
Low self esteem/shame/unworthy
Sees self as wounded & healing
Sees self as an overflowing miracle
Hyper vigilant Using tools to learn to relax Gratitude for new life
Alone Seeking help Oneness
Feels Selfish Deserves to seek help Proud of Healthy Self caring
Damaged Naming what happened Was wounded & now healing
Confusion & numbness Learning to grieve, grieving past ungrieved trauma
Grieving at current losses
Overwhelmed by past Naming & grieving what happened
Living in the present
Hopeless Hopeful Faith in self & life
Uses outer world to hide from self
Stays with emotional pain Understands that emotional pain will pass & brings new insights
Hides their story Not afraid to tell their story to safe people.
Beyond telling their story, but always aware they have created their own healing with HP
Believes everyone else is better, stronger, less damaged
Comes out of hiding to hear others & have compassion for them & eventually self
Lives with an open heart for self & others
Often wounded by unsafe others
Learning how to protect self by share, check, share
Protects self from unsafe others
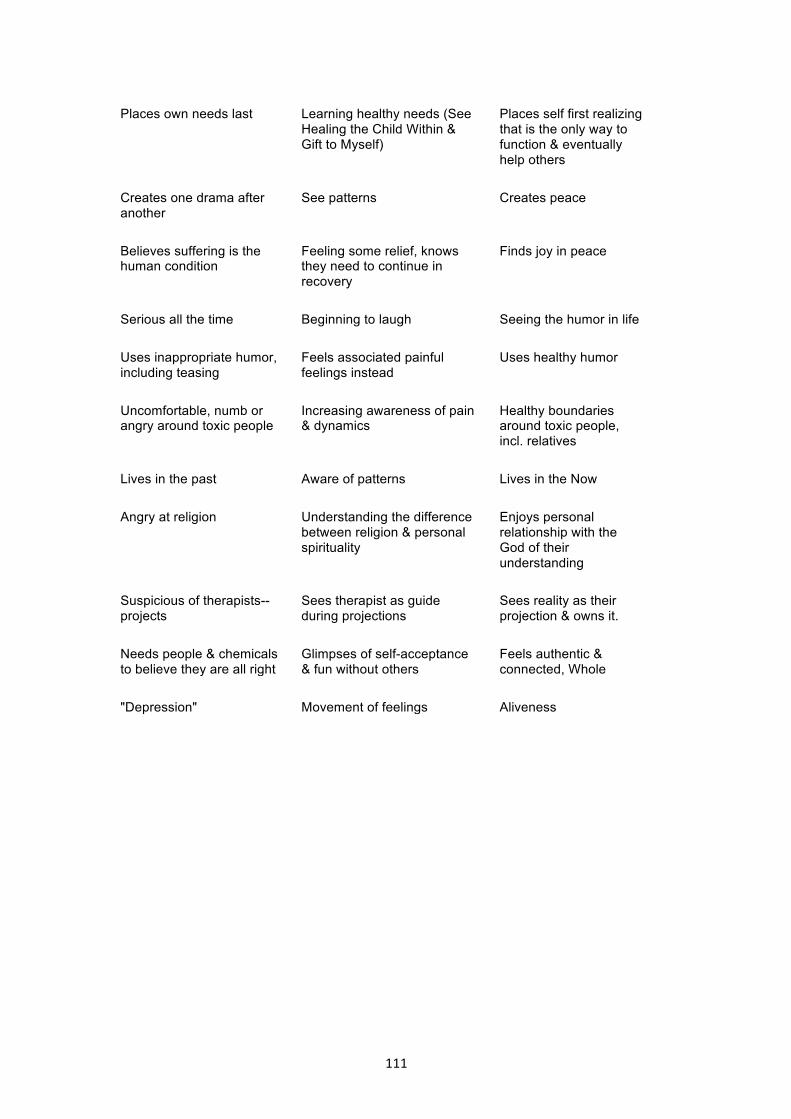
111
Places own needs last Learning healthy needs (See Healing the Child Within & Gift to Myself)
Places self first realizing that is the only way to function & eventually help others
Creates one drama after another
See patterns Creates peace
Believes suffering is the human condition
Feeling some relief, knows they need to continue in recovery
Finds joy in peace
Serious all the time Beginning to laugh Seeing the humor in life
Uses inappropriate humor, including teasing
Feels associated painful feelings instead
Uses healthy humor
Uncomfortable, numb or angry around toxic people
Increasing awareness of pain & dynamics
Healthy boundaries around toxic people, incl. relatives
Lives in the past Aware of patterns Lives in the Now
Angry at religion Understanding the difference between religion & personal spirituality
Enjoys personal relationship with the God of their understanding
Suspicious of therapists-- projects
Sees therapist as guide during projections
Sees reality as their projection & owns it.
Needs people & chemicals to believe they are all right
Glimpses of self-acceptance & fun without others
Feels authentic & connected, Whole
"Depression" Movement of feelings Aliveness
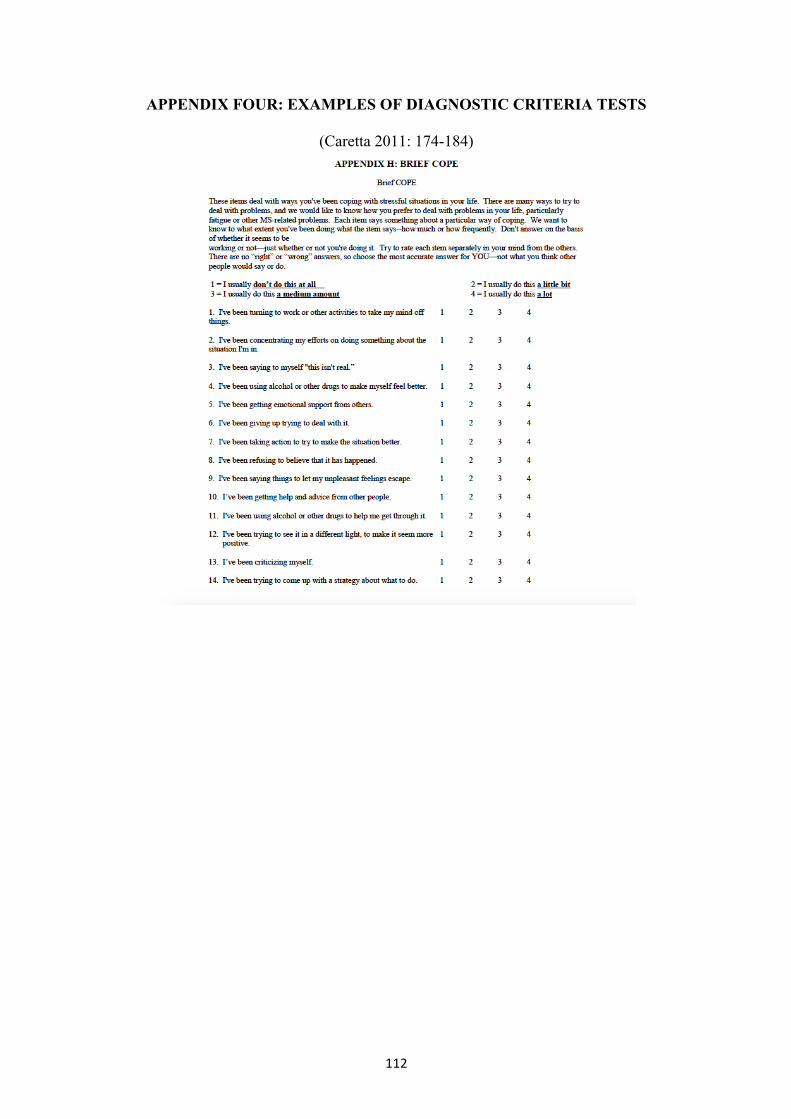
112
APPENDIX FOUR: EXAMPLES OF DIAGNOSTIC CRITERIA TESTS
(Caretta 2011: 174-184)

113
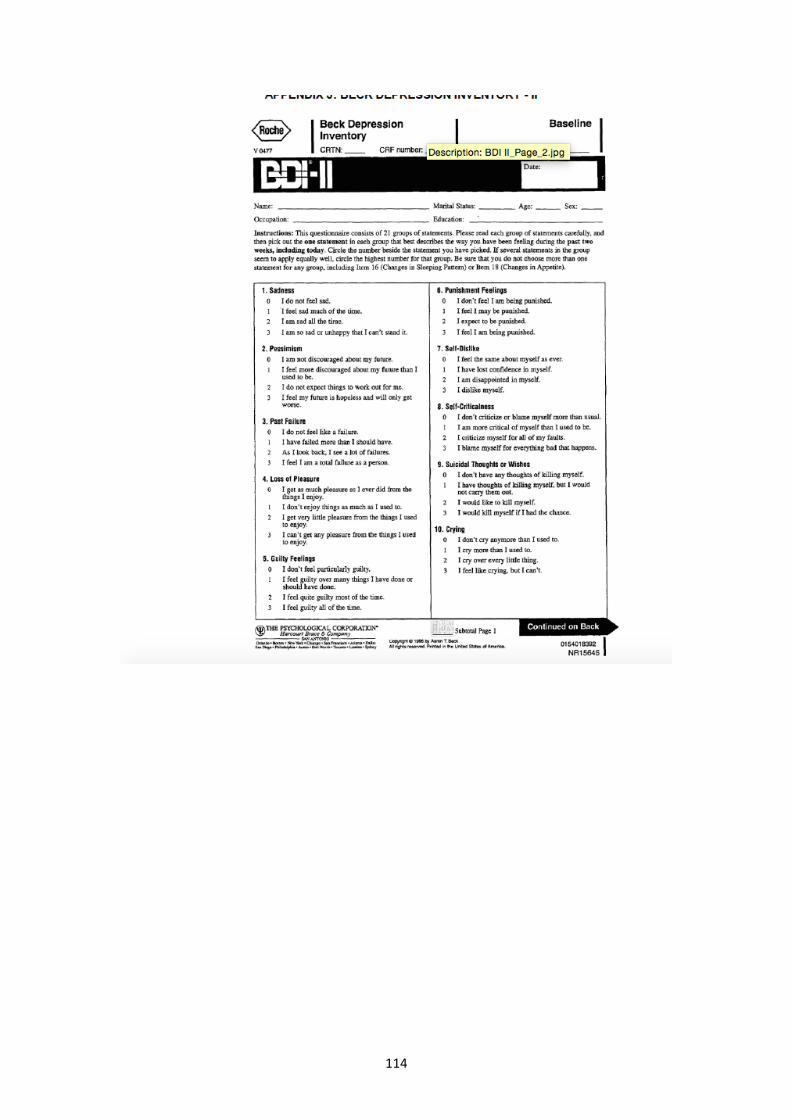
114

115
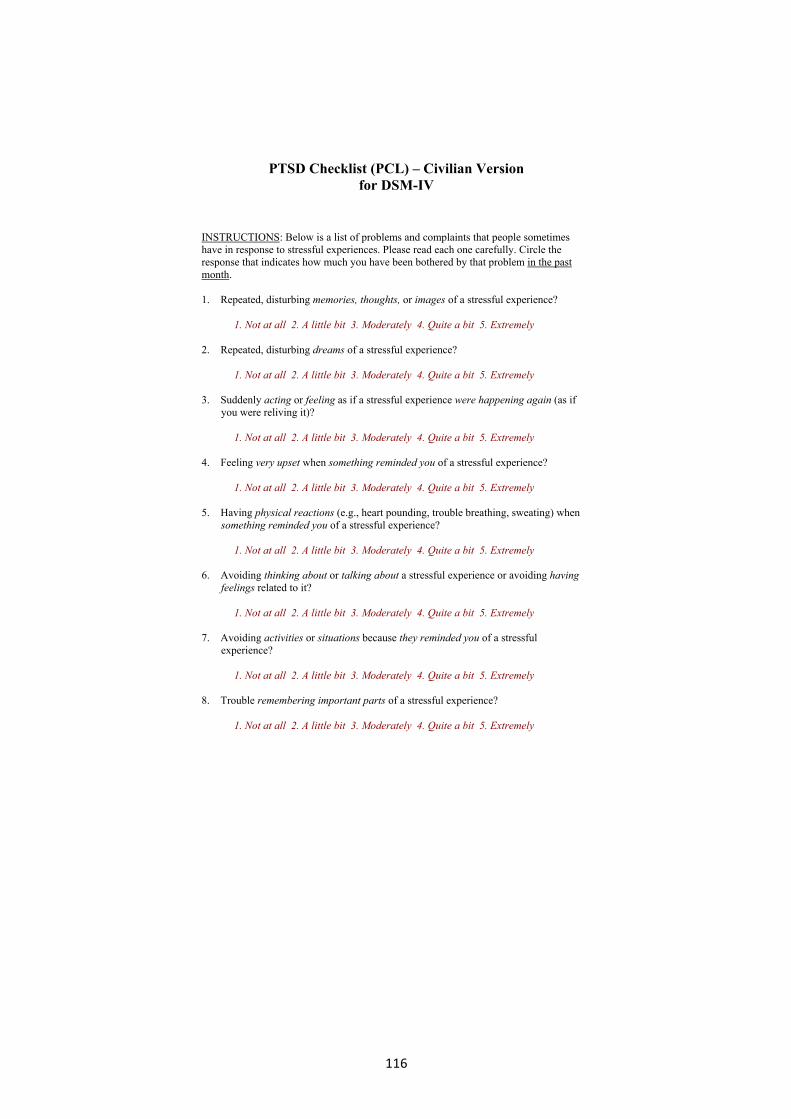
116
PTSD Checklist (PCL) – Civilian Version for DSM-IV
INSTRUCTIONS: Below is a list of problems and complaints that people sometimes have in response to stressful experiences. Please read each one carefully. Circle the response that indicates how much you have been bothered by that problem in the past month.
1. Repeated, disturbing memories, thoughts, or images of a stressful experience?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
2. Repeated, disturbing dreams of a stressful experience?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
3. Suddenly acting or feeling as if a stressful experience were happening again (as if you were reliving it)?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
4. Feeling very upset when something reminded you of a stressful experience?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
5. Having physical reactions (e.g., heart pounding, trouble breathing, sweating) when something reminded you of a stressful experience?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
6. Avoiding thinking about or talking about a stressful experience or avoiding having feelings related to it?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
7. Avoiding activities or situations because they reminded you of a stressful experience?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
8. Trouble remembering important parts of a stressful experience?
1. Not at all 2. A little bit 3. Moderately 4. Quite a bit 5. Extremely
117
APPENDIX FIVE: EXAMPLE OF PRESENTING PTSD AS A PHYSICAL AILMENT
(www.healingfromcomplextraumaandptsd.wordpress.com 2015)
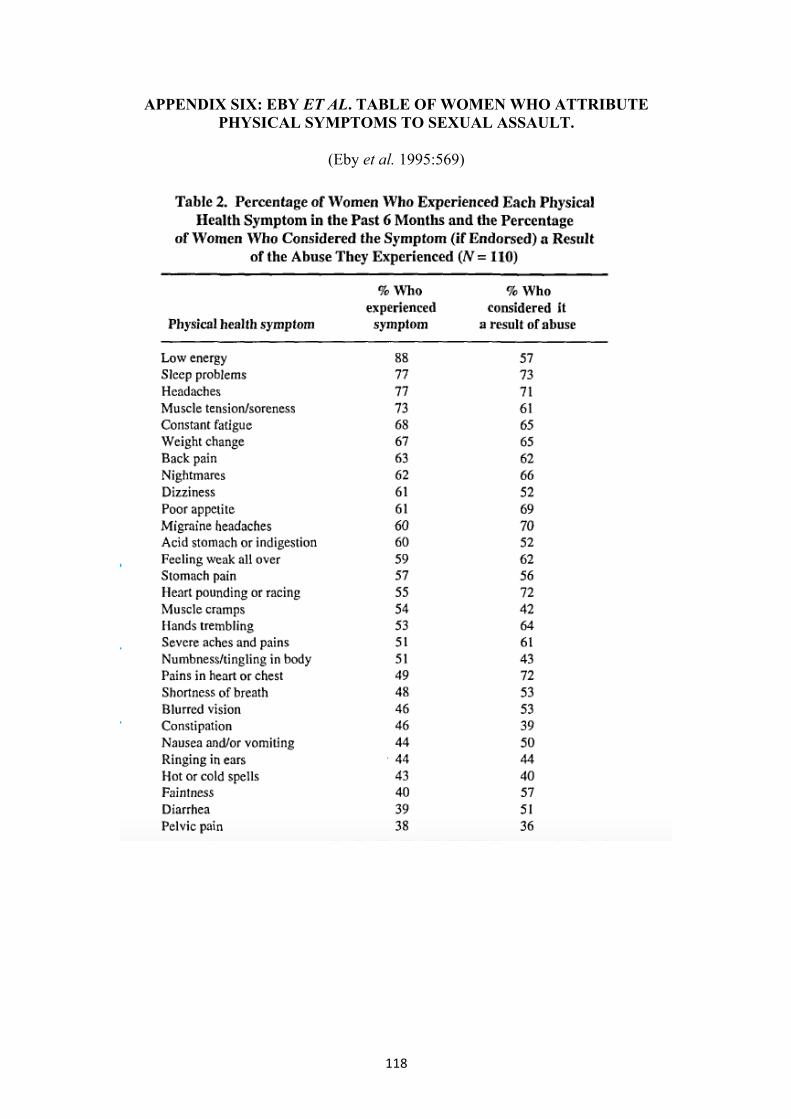
118
APPENDIX SIX: EBY ET AL. TABLE OF WOMEN WHO ATTRIBUTE PHYSICAL SYMPTOMS TO SEXUAL ASSAULT.
(Eby et al. 1995:569)
Copyright © 2022 FDOKUMEN




















