Conference Report: 15th - Khon Kaen University
348
Conference Report: 15 th KVAC, 2014 Sustainable Development on One Health Table of Contents Background 2 Conference Hosts & Venue 2 Conference Committee 3 Conference Program 7 Lists of Participants 9 Oral Presentation 40 Poster Presentation 43 Evaluation Results of the Conference 46 Budget Summary 48 Activities (Pictures) 49 ANNEX (Conference Proceeding) 61 1
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Conference Report: 15th - Khon Kaen University

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Table of Contents
Background 2
Conference Hosts & Venue 2
Conference Committee 3
Conference Program 7
Lists of Participants 9
Oral Presentation 40
Poster Presentation 43
Evaluation Results of the Conference 46
Budget Summary 48
Activities (Pictures) 49
ANNEX (Conference Proceeding) 61
1

International Conference Sustainable Development on One Health
CONFERENCE REPORT 15th KKU Veterinary Annual International Conference (KVAC) 24-25 April 2014 Pullman Hotel, Khon Kaen, THAILAND
Organized by Faculty of Veterinary Medicine
Khon Kaen University

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Background
Human and animal health is currently affected from changes of balance between
environment and pathogens. The changes of balance in nature may cause transmission of
diseases to human and animals or between human and animals. In addition, incidences of
many emerging infectious diseases have different patterns and adaptation from the former
ones. These make the prevention and control of diseases more sophisticated and need
collaboration between professional disciplines to solve the problems. Therefore all countries in
ASEAN agreed to collaborate to build the One Health project together, and exchanges of
knowledge in new technology, communication skills, and academics are necessary to reach the
goal.
The 15th VMKKU annual international conference on “Sustainable Development on ONE
Health” aims to provide and present information/knowledge to all delegates the current major
issues eq. emerging & re-emerging diseases, zoonosis and to build a linkage capacity between
researchers, academic professors and other people in various disciplines which will build
cooperation networks among all delegates in the future.
Hosts
1. Faculty of Veterinary Medicine, Khon Kaen University, Thailand
2. Cummings School of Veterinary Medicine, Tufts University, USA
3. US Agency for International Development (USAID)
Venue: Pullman Hotel, Khon Kaen, Thailand
Date: April 24-25, 2014
Registration Fee
Delegate Until March 31, 2014 After March 31, 2014 Student 1,500 Baht 2,000 Baht
Thai delegate 2,500 Baht 3,000 Baht
International delegate 2,500 Baht (US$ 85) 3,000 Baht (US$ 100)
2
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
The 15th KVAC Committee Scientific Advisory Committee
1. President of Khon Kaen University
2. Dean of the Faculty of Veterinary Medicine, Khon Kean University
Organizing Committee
1. Assoc.Prof.Dr.Somboon Sangmaneedet Chairman
2. Assoc.Prof.Chuchat Kamollerd
3. Asst.Prof.Dr.Sarthorn Porntrakulpipat
4. Asst.Prof.Ekkachai Pattarapanwichien
5. Asst.Prof.Dr.Prapaporn Tungthanathanich
6. Asst.Prof.Dr.Sirikachorn Tangkawattana
7. Asst.Prof.Dr.Kwankate Kanistanon
8. Asst.Prof.Dr.Jatesada Jiwakanon
9. Asst.Prof.Dr.Weerapol Taweenan
10. Asst.Prof.Dr.Naruepon Kampa
11. Asst.Prof.Arayaporn Macotpet
12. Asst.Prof.Chaiwat Charatsaeng
13. Miss Ancharin Ounthaisong
14. Mrs.Sombat Saengpol
Scientific Committee
1. Asst.Prof.Dr.Kwankate Kanistanon Chairman
2. Assoc.Prof.Dr.Fanan Suksawat
3. Assoc.Prof.Dr.Bongkot Noppon
4. Asst.Prof.Dr.Peerapol Sukon
5. Asst.Prof.Dr.Sirikachorn Tangkawattana
6. Asst.Prof.Dr.Weerapol Taweenan
7. Asst.Prof.Dr.Sarthorn Porntrakulpipat
3
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
8. Asst.Prof.Dr.Chaiyapas Thamrongyoswittayakul
9. Asst.Prof.Dr.Sompoth Weerakhun
10. Asst.Prof.Dr.Ranee Singh
11. Dr.Tawatchai Pohuang
12. Miss Numfa Fungbun
13. Mrs.Suthida Chanlun
Information Committee
1. Asst.Prof.Dr.Jatesada Jiwakanon Chairman
2. Asst.Prof.Dr.Weerapol Taweenan
3. Asst.Prof.Dr.Suchat Wattanachai
4. Mr.Pitakpong Maneerattanarungroj
5. Mr.Pongchai Muennoy
6. Mr.Chalermpan Sirabutra
7. Miss Chanida Chainn
8. Mr.Yanyong Wangprecha
9. Miss Ratana Daosawa
10. Mrs.Bunserm Somboon
11. Mrs.Prayoon Khamtat
12. Mrs.Prisna Vichatham
13. Mrs.Wan Buajan
14. Mrs.Prapatson Thihta
15. Miss Ancharin Ounthaisong
Treasurer Committee
1. Assoc.Prof.Chuchat Kamollerd Chairman
2. Mrs.Phatchareeya Konchan
3. Mrs.Suthathip Wattanachai
4. Miss Wichayanun Kanla
5. Mr.Weera Suparuk
4

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Exhibition committee
1. Asst.Prof.Dr.Naruepon Kampa Chairman
2. Mr.Somphong Hoisang
3. Miss Sarocha Permsub
4. Miss Meena Visungrae
5. Miss Tanit Ariyakong
6. Mrs.Promporn Tongtieum
7. Miss Jitrapon Suanbun
8. Miss Pailin Simmalee
9. Miss Parinda Namkoksi
Banquet committee
1. Asst.Prof.Dr.Prapaporn Tungthanathanich Chairman
2. Assoc.Prof.Dr.Bongkot Noppon
3. Asst.Prof.Varaporn Sukolapong
4. Mrs.Nusara Suwannachot
5. Mrs.Yupadee Charoensawang
Registration committee
1. Asst.Prof.Arayaporn Macotpet Chairman
2. Miss Suphannika Pnutthachalee
3. Miss Chuleephorn Praha
4. Miss Narishra Lertchaisathapon
5. Miss Sarocha Permsub
6. Miss Kavintra Iranoy
7. Mrs.Sudarat Buatuan
8. Miss Pailin Simmalee
9. Miss Jitrapon Suanbun
10. Miss Supavadi Sriputorn
11. Mrs.Sombat Saengpol
5

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Ceremony and Reception committee
1. Asst.Prof.Dr.Sirikachorn Tangkawattana Chairman
2. Assoc.Prof.Dr.Fanan Suksawat
3. Asst.Prof.Dr.Sarthorn Porntrakulpipat
4. Asst.Prof.Dr.Weerapol Taweenan
5. Asst.Prof.Dr.Kochakorn Direksin
6. Asst.Prof.Dr.Ranee Singh
7. Asst.Prof.Dr.Aran Chanlun
8. Dr.Trasida Ployngam
9. Mrs.Nusara Suwannachot
10. Mr.Sithiporn Kapbualoi
11. Miss Jongkolwan Chansombat
Transportation committee
1. Asst.Prof.Chaiwat Charatsaeng Chairman
2. Mrs.Yupadee Jaroensawang
3. Mr.Amporn Krisornsri
4. Mr.Pongpan Pongsapung
Evaluation committee
1. Asst.Prof.Ekkachai Pattarapanwichien Chairman
2. Mr.Samai Kengkan
3. Mrs.Aranya Sirikraiwan
4. Miss Nathapop Sechang
5. Mrs.Aoythip Subso
6

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
7

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
8

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
List of participants
Honorary Guests
Weerachai Kosuwon
Sivapong sungpradit
Suwicha kasemsuwan
Jaturong Jariyanoravisse
Ammuay Totarin
Notpadol Vorathongchai
Theerachai Wongcharoo
Silthum Wara-Aswapati
Manvika pholpark
Prayut Sriviroj
Somsak Pitaksanurath
Nuchawana Luanganggoon
Sauwanan Bumrerraj
Wongwiwat Tassaneeyakul
Speakers
Dr.Michael Kosoy
Dr.Suwit Somponpun
Dr.Flavie Goutard
Dr.Sakdid Anulomsombat
Dr.Fumihiko Sano
Dr.Serge Morand
Dr.Viginia T Rentko
Dr.Supaporn Wacharapluesadee
Dr.Sanipa Suradhat
Dr.Taweesak Songserm
9

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Dr.Narong Kitpanit
Dr.Narudee Kashemsant
Dr.Nongyao Kasatpibal
Dr.Romziah Sidik
Dr.Eric Brum
Dr.Pierre Echaubard
Mr.Pichai Jirawattanapon
Mr.Annop Suriyasomboon
Dr.Sompoth Weerakun
Dr.Sunpetch Angkititrakul
Miss.Arayaporn Macotpet
Mr.Ekkachai Pattarapanwichien
Mrs.Nithiwadee Lertittikul
Mr.Eakkasit Barameechaithanan
Mr.Mongkol Prongcharoen
Thai delegates (KKU Alumni)
Amornrat Sasiphonganun
Suksant Chanprasert
Wipasiri Amornwittayawech
Jaturon Ponrach
Netchanok Jiwakanon
Rutch Khattiya
Tanawat Sopispornmongkil
Torpong Prasertsang
Apinya Suebprom
Chumpon Ukot
Dilok Aunpomma
10

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Pichet Tongpan
Prasert Wongnak
Ratchapon Suebprom
Changgrit Niyomtong
Donruethai Sreta
Ekkawit Natumploy
Karuna Kuntaramongkol
Manasak Sudching
Nikorn Muabkhunthod
Nopphadon Sombunret
Prayuth Kusolrat
Sirirat Suwannarong
Sukanya Leethongdee
Taweesak Bungsri
Wanida Loida
Warasit Chaiyasing
Wutthichai Suknuek
Anone Thuangsanthia
Anothai Phaetkit
Budsaba Thammapol
Sompong Wongma
Supan Paidong
Supranee Dermpun
Tharadorn Jitjuk
Wasan Ruche
Wichaporn Lerdweeraphon
Weerapat Phengpa
Apichai Poonchai
11

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Chatree Chumnandee
Jakkapat Prachachit
Jarturon Kasipun
Kittipong Jundeekrayom
Kriangkrai Thongkorn
Panwipa Detrat
Ruttachuk Rungsiwiwut
Sudthidol Piyadeatsoontorn
Sumonchat Sangpanya
Theerapong Racharoen
Chatchay Moangphukeaw
Apichai Jaiharn
Borpit Kotphuwiang
Panithan Sirisathit
Piya Srisathaporn
Sutheeraphoj Thong-in
Wipawadee Phathomrapeepong
Kesanee Khusrithepprathan
Amornrat Patcharinwittaya
Anupong Chantarasakha
Chatchai Sarachai
Ekkpol Upala
Jamikorn Wongkalasin
Kingkarn Boonsaya seeyo
Kittikhun Ratanaponsean
Komsan Makphol
Nathawut Seeyo
Noppadon Buddhthai
12

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Pakorn Sawatsing
Pathompong Sawattanakul
Supab Vorakrut
Sutthidet Tenissara
Wasinsala Salaphol
Boonchai Singthong
Chanyaporn Kwangrut
Janchai Aroonyadech
Kitsana Phonsawai
Kongrit Hemburut
Kwanhatai Rotjanakomet
Natnada Kheawsanam
Nattakarn Khuruphan
Panyawat Saikang
Supachai Sripai
Thammarath Horaprom
Wannasiri Waidab
Warachanan Saengpandee
Wiyada Prirdprao
Kanutpisit Kwangrut
Silapakit Boonpo
Weerapat phengpa
Apinya Chumnangul
Chanika Khusawangwong
Chayanon Chompoosan
Chootima Suwor
Chutcharee Niyamosot
Kanchana Pantaamat
13
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Phennarin Doungmala
Naovarat Kampoosiri
Naphatraphee Chanthee
Narathip Vorawattanatham
Narudee Chumpol
Nichapa Sansurin
Orawan Kumjam
Pornthip Tongsuk
Ranong Sripiphat
Ruamporn Ownthum
Sarinee Putkean
Sineenart Sakamula
Siriporn Putchutara
Sumitta Thongprapa
Suvaluk Seesupa
Thawatchai Sojunda
Treenet Phangsiangsa
Virinthita Praphakorn
Waravut Charernreun
Borwornlak Sankong
Yaowarase Chot-on
Aksarapa Kumnurdrut
Amornrut Sawating
Chanwit Mutarporn
Darin Khorprasertsuke
Decha Khotsombat
Jetnipatcha Chaimuang
Karunrat Sakultarn
14
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Mintra Charoenwatana
Nantakarn Sri-pui
Nunthida Phothin
Napaporn Khemphet
Nattavut Phomnikorn
Omjit Pantuprom
Prach Tatong
Pumin Sumamarn
Sirikorn Mamkliang
Sutharat Sriboonrueng
Sutthiwat Chapanya
Thitiwong Phu-Oap
Warut Sakultarn
Adundache Bungwai
Angkana Konpoodphraw
Apirat Thongyam
Kamonchanok Soipet
Nathatai Wanachalerm
Nopparat Bhavabhutanon
Oracha Ritisit
Piyathida Lunthaisong
Piyawat Polwiengtham
Sukpunya Butphom
Arnusa Juntacud
Catthareeya Sukwan
Chatchalerm Lerttham
Jirapa Boontoe
Jurairat Chueachun
15

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Katwadee Kotphuwiang
Kitisak Wiboonaut
Kullaya Chuntakul
Monthon Tungsitchanakun
Prayad Srikotr
Panasarun Lertsatchayarn
Pramot Phuangchomphoo
Rattanaporn Khongchaiyaphum
Sudawan Chuenpreecha
Sukanya Athirote
Sureeporn Chidchua
Worawut Bowonnimit
Adithep Konputtar
Arthit Prakunee
Nantharaporn kumtan
Pradit Peetanonchai
Phattaraphong Konglam
Pornploy Thongjurai
Samart Onsongchan
Theerakul Nilnont
Wansane Toanan
Amornrat Durongphongtorm
Anuwat Amatachaya
Chatanun Eamudomkarn
Chompunoot Wangboon
Kanokwan Konyanee
Kittikant Muksombat
Nattaya Watwiengkam
16

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Opal Pitaksakulrat
Pitchaya Matchimakul
Pongphol Pongthisong
Pratana Yongsakulchai
Sirirat Phomjareet
Titima Sangmo
Wanida Leesirikul
Angkapun Rungsai
Benchamoporn Dongkham
Charinya Pimson
Lalada Waenwong
Namfon Phoasalee
Napaporn Wiratthikowit
Nuntaphorn Mongmai
Parisa Keeratikulapas
Pichet Seating
Pimsuda suwannasaeng
Ponjun Butchaingam
Raksawan Deenonpoe
Rubkhwan Nganwai
Setthakit Chitsanoor
Siriluck Phanjanya
Sirisawad Chansri
Tanagorn Pintapagung
Tanut Sriputtarin
Thanyakorn Chalalai
Thitikum Pudkamchot
Wanwisa Jamikorn
17

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Wilasinee Srisanyong
Wisit Panpanit
Chayanon chompoosan
Aphisit Sakunsong
Aphinya Wijarn
Ard-ong Onwan
Bunnada Siriporn
Cherdpong Phupolphan
Chinwiwat Piamsakun
Itnarin Mongkon
Kanissarinn Sakundech
Lakkhana Rotchanakusol
Montira Yossapol
Nattapong Chaipunha
Nongyao pinyosri
Nuttee Saowadee
Pacharee Toondee
Pailin Jinagool
Pakphum Panopas
Panida Pongvittayanon
Peerachart Juntako
Rucksak Rucksaken
Ruttikan Woralar
Tarid Purisotayo
Thiryu Somphabutr
Tula Danchanchai
Yada Charoensin
Prachya Engkhaninun
18

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Ackanerut Kaewsai
Ajchareeya Lekkrathoke
Atchara Poopuak
Attapon Prajanang
Chanokchon Sethawongsin
Chirasak Promnin
Chotika Siriwalailuk
Jatuporn Arunprai
Jirapt Arunorat
Jongjaroen Maksuwan
Ketchanok Seanplum
Kittira Sarasamak
Kraiwat Chawong
Kulcharee Raksaboon
Lomfang Insawang
Maneenard Choodetwattana
Nasara Thanaviratananich
Nisarat Jitpiromsri
Nitipat Khumhirun
Nuttathida Ruengsrithanyakij
Pawarat Chancharoen
Pranpreya kummee
Premwadee Ninsoam
Rachanida Yingdon
Saisroy Songprasert
Sarit Singhutsatit
Siri Kitjaritaphum
Thanaporn Asawapattanakul
19
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Thantip Rungsang
Thongchai That-injun
Wanee Wattanasuthipong
Wichchayen Arechwichai
Yanyong Pivpong
Kallayanee Santhong
Anisara Singmang
Art Sawangwong
Chatchai Duangtawan
Chonlaya Prabwongsa
Kamonrat Tangtragoon
Kamonrat Phosuwan
Kanograt Sukchalerm
Khomkrich Surithet
Manoon Joomsila
Pachaapun Srijun
Pakawat Tawornpanich
Parimaporn Palagrai
Pariyanon Kantha
Parkorn Boonterng
Phitchaya Saenubol
Pimchanok thonglon
Piti Pata
Pongpreecha Malaluang
Preechakorn Panwiset
Puttida Roimanee
Rattaphon Tong-aram
Samart Srimongkon
20

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Sathita Patjanasoontorn
Sirilak Chanta-utsa
Sunanta Sukkhapat
Thiti Srikongpan
Wasupon Chatan
Watchara Muenpoh
Yadfon Phonthongchisawat
Yanisa Singhapong
Yupadee Kotamee
Yuwadee Phimsri
Jutanun Laomanotham
Alisara Sinsorn
Chutima Chuntarakot
Dheera Kongkaen
Kirawat Chantarasena
Krai Kaisaeng
Napassanan Chayantanatinnakorn
Navissara Wongni
Neti Danchanchai
Pajaree Homkhaw
Paksiree Saranaruk
Patchariya Laobannue
Patinya Patikae
Paweena Phatan
Piyawat Sriprasit
Rawikan Inchuai
Satawat Tuksawalabudt
Sawanya Saengchan
21

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Sirintra Pokapanich
Songkaid Upontain
Sukhonthip Khueangchaingkhwang
Supawadee Liangchaisiri
Tharathorn Laophakdee
Thassanee Wedchapan
Thatsna Poonsirinawin
Thitiwit Noinamtieng
Tirapat Klaengkratok
Wittawat Wechtaisong
Wachirapong Kaewbooddee
Warasorn Praseartkulchai
Waranya kanhachon
Warapong Samala
Wacharapol Promsut
Watcharapol Suyapoh
Worakan Boonhoh
Phuncharat Nilsuwan
Thanyapawn Chantarujikaaong
Adjima Boonchuen
Chotimon Seesan
Ekanun vuwong
Goragod Labarom
Jakkarin Jinarat
Jintana soommart
Kritjit Phannithi
Leeyakorn Nonthadi
Narakorn benjanan
22

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Notthasuong Suttipattananggul
Pattarakitti Nernchut
Paween Srirari
Phirawich Sa-ardta
Phongwarit Sirikanchanawong
Pinyada Promna
Pongpanot Tangkijchote
Ponlakrit Charoenchanikran
Raksakoon Srikrainoon
Ruxpon Dejkong
Sarocha Luangchan
Siwayu Rattanakanokchai
Sukanda Haoharn
Sunissa Siriroj
Supaporn Boonkwang
Waraporn Saeng-Authai
Wigunya Mongkoljit
Woraphong Rungphueng
Natapol Pumipuntu
Rittichai pilachai
Cooperative Education
Duangkhamol suraruangchai
Nattha Pothiard
Kesanee Khusrithepprathan
Sirikul Suntararak
Watcharapong
Suriyakul Na Ayuthaya
23

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Thanunporn Tunburintip
Chanika Bamrungpakdee
Chavin chaisongkram
Chatchawan jaisaard
Nicharat Sawatipun
Jutamas Chavalit
Noppadol nooncomewong
Souphinthong saymanyvong
Company
Weera Suksap
Apichart sapsiripaiboon
Kuntera Wunprapa
Thana Wichachai
Kemchompoo atikhanpak
Trin nakkhatnathwan
Adisorn Chatsuphap
Rachaya Karnjanaakkaradech
Kanchit Anudechakul
Neti Chansanitsri
Krissada Chanasophon
Sumonnachat Sang
Noppadon Woratongchai
Winai Jarabrum
Winai Jarabran
Tanakrit Ardtaweekul
Yingsa Suraseang
Neti Junsanitsir
24

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Klahan Sritongtuam
Kheemchompu Atthikanyaphak
Nutjaree Saejueng
Puachmongkol Apaengpan
Jitsupa Wuttikornwipak
Maneenard Choodechwattana
Kritsana Janpeng
Pipat Apichanangkul
Kritnarin Boonmeepitak
Channimit Thumnoo
Narongrit Sattrapai
Pichai Lorsilathong
Rattapol Horsin
Sunruthai Tuntitawatchaikun
Chaichan Woranitat
Natanut Sopon
Patraporn Sriputachote
Worathida Sangrat
Kittiya Morarai
Busyamas Saiviseth
Satityot Suntornsatitpimol
Preeyachat Kongapirak
Gusumaporn Duangpratum
Thawatchai Sojunda
Kritsadin Boonmeepitak
Somnuk Wonginjan
Pramote Tannwat
Jakrit Prasert
25

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Adul Tongsima
Jaruwan Chaitrikan
Natthawut Limpitaporn
Pornchai Amornwittayavej
Rattaya Vachirodom
Taksaorn Chumnansilp
Sirichai Tejrungchaikul
Apinya Muadmuang
Songwut Pratitung
Danai Sroysuk
Pratummard Aksorn
Achinee Rooncharoen
Rochana Somsri
Namthip Aiumsungnoen
Chadaporn Sirisakulwong
Phudith Jitnamkorn
Thanapon Nernsiri
Jantamart Anekkarnjananon
Natakorn Duanghatsadee
Vipasinee Chaisinghan
NiTima Tatiyapiradee
Pakorn Joontrakul
Garantarat Triyasorasai
Jinttanakarn Jongjailan
Paholyut Soranate
Suchatchaya Thanabavorndit
Sunanta Yathikul
Chaiya Pontri
26

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Surachai Vechurai
Panprapai Wanglah
Nut Sawadrath
Chatwalee Boonthum
Udom Chinvanicharoen
Karnchana Mungmeesri
Pakphum Kietjanon
Sittipol Rittiyoong
Kritsana Sanmano
Sathaporn Anarmat
Dusit Laohasinarong
Wilas Wiboonsirikul
Chaiyong Kritsanakriangkrai
Pradit Dookruk
Teeraparb Aroonpairoj
Veeradej Goroskanapong
Suksama Narattanakorn
Sujate Cheumchom
Jarupat Saichat
Suwanaporn Srichaiyorak
Cherdsak Yatpin
Prenaphan weraphan
Ariyaporn Sripun
27

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Faculty Staffs
Arinee Chatchawanchonteera
Ekkachai Pattarapanwichien
Jaruwan Kampa
Nusara Suwannachot
Prapan Kaenjampa
Ruangthong Kitcharoenpunya
Sirikachorn Tangkawattana
Somboon Sangmaneedet
Surasit Auanpromma
Suthida Chanlun
Sutisak Nopwinyoowong
Thanakarn Nasri
Varaporn Sukolapong
Weerapol Taweenan
Suphattra Jitimanee
Aran Chanlun
Arayaporn Macotpet
Chaiyapas Thamrongyoswittayakul
Fanan Suksawat
Jatesada Jiwakanon
Kanit Chukanhom
Kanlaya Chuachan
Kochakorn Direksin
Manassanan Borisutpeth
Pimchanok Suwannathada
Sarthorn Porntrakulpipat
Sompoth Weerakhun
28

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Tawatchai Pohuang
Trasida Ployngam
Adisak Sangkaew
Chaiwat Jarassaeng
Duangdaun Kaenkangploo
Naruepon Kampa
Pongrat Jaisil
Pongthorn Suwannathada
Prayong Saengsriruang
Preenun Jitasombuti
Saksiri Sirisathien
Sarawut Sringam
Suchat Wattanachai
Suneerat Aiumlamai
Suphannika Phutthachalee
Suvaluk Srisupa
Bongkot Noppon
Chaiyaporn Soikum
Nillapan Vongsahai
Piyawat Saipan
Prapansak Chaveerach
Pirat Sornplang
Narisorn Na-Ngam
Sunpetch Angkititrakul
Pinsaw Kromratanaphorn
Seri Kang-air
Chuchat Kamollerd
Panchompoo Muanglai
29

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Peerapol Sukon
Phuttipong Pongpan
Prasarn Tangkawattana
Preeyaporn Surachon
Saijai Kongpechr
Suwit Uopasai
Geerasak Thiratanaboon
Kwankate Kanistanon
Prapaporn Tungthanathanich
Patchanee Sringam
Pisit Suwannachot
Jareerat Aiemsaard
Korawuth Punareewattana
Ranee Singh
Awirut Wichaiwong
Chalermkwan Nonthakotr
Chuleephorn Praha
Eakkasit Barameechaithanun
Jeerasak Khlongkhlaoe
Karn Yongvanit
Kawintra Aiyaranoi
Meena Wisungre
Narichsara Lertchaisathaporn
Nitaya Boonbal
Nitiwadee Leritthikul
Pattaraanong Bupata
Peerapat Deesuk
Pithai Kanbutra
30

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Piyasak Wipoosak
Rawinnipa Weerakaittikun
Sarocha Permsab
Somphong Hoisang
Thanakorn Srirat
Sombat Saengpol
Ancharin Aounthaisong
Pitakpong Maneeratrungroj
Yanyong Wangpreecha
Chalermpun Sirabutr
Chanida Chainn
Pachareeya Konchan
Sutathip Wattanachai
Weera Suparak
Vichayanun Kanla
Thanit Ariyakong
Pairin Simalee
Parinda Namkoksri
Yupadee Charoensawang
Sudarat Buatuan
Jittraporn Suanboon
Supawadee Sriphutorn
Sittiporn Karbbualoi
Samai Kangkan
Aranya Sirikaiwan
Nathapob Sae-chang
Aoithip Supso
Punorn Raksanit
31

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Supanee Poonon
Pongoun Pongsapang
Delegate
Natenapha Kledjeen
Somsiri Indramanee
Worawit Waraadsawapati
Satis Pholpark
Usa Naksakul
Sompong Juntaharn
Apirom Charoenchai
Visit Funchim
Sirinapa Srikam
Patharee Jenchangkol
Phukphon Munglue
Waleemas Jairak
Tippayaporn Nonkookhetkhong
Kongkiat Kraisutthikarn
Wanlop Likitsuntonwong
Pradtana Meedech
Xin Huo
Virya Hour
Bunthon Chea
Sudarat Damrongwatanapokin
Titiwut Panyanon
Sathaporn Anarmat
Chumporn Sankwa
Blumibhcuh Srimongkol
32
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Sirisak Angsupakorn
Kiattisak Pimpsong
Faculty of Agriculture, National University of Loas, Nabong Campus
Bountang Sisouphon
Latsamy Soulivongsa
Khao Keonam
Thipphakone Lacksivy
Khonesavanh Phomvixay
Souksavath Tansouphanh
Phonesavanh Phommasone
Ekaphod Chanhda
Khaothong Souliyaphom
Somsanith Kanharath
Bounmark Phouttaphone
Sitthasone Xaymountry
Athid Syhakhung
Douang Oy Inmeeboun
Ketsapha Chanthason
Anousith Many
Syfong Maniboun
Bounsoung Theplakhone
Chanhpheng Sisouphonyalath
Ladsajuck Phanomsouk
Phetthanouxay Sythavixay
Khampheng Lee
Thongsy Lao
Sonexay Sengthala
33
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Somdy Khamphanh
Amphone Keosengthong
Khamphai Sengngam
Ed Phengsombath
Khaikham Tonglongxiong
Phonepasert Manivong
Kethsana Inthavong
Meedao Syxomphou
Bouachanh Chanthalath
Songkane Vilaysayaveth
Phonemany Xaysamone
Bounhome Saiyasan
Tennapha Chanthalangsy
Vienta Phengmixai
Phonemany Hounglaty
Choummala Vanmanivong
Khitsamay Donephachan
Bouxay Kammany
Southsaychay Phaythoun
Lamphaen Pannouvong
Malaphone Silaphet
Graduate Students
Banphen Keomoungkhoun
Chittraporn yeanpet
Khampasong ninasopha
Nam Nguyen Hoai
Nawarat Pha-obnga
34

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Ninh Le Ngoc
Noppadol nooncomewong
Noppadon Somphol
Piya sereerak
Somphanh Bounyavong
Sujira Thammawung
Thet Naing aye
Pongsatorn Tuchpramuk
Akkarapat Butsurin
Undergraduate students
Karnsuda Wijitphan
Karnchanok Saengpaeng
Katsara Wichasan
Threetip Mityodwong
Tarinee Pongprom
Netsai Chamnit
Prapasara Potchimplee
Pattamaporn Kongphan
Peeraya Chumponwomg
Puttachad Jinjio
Parin Khianman
Yaowapa Thonkhaw
Raksarat Sakulrak
Rangsiyaporn Naiyanet
Rattiya Panphoom
Wichaya Thomas
Naphat Rungroj
35

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Sornkrit Rakpanit
Saknarin Yoshpunya
Sitanon Khachainchat
Sujitta Pumtong
Phimda Khotbanthao
Onjira Chaopong
Arunee Bupasiri
Jittree Jessadapagorn
Tidaratt Sittisak
Satit Wattanasinpisal
Apinya Tantanasakun
Kamonchanok Phongsamsuan
Kittisak Patchaikotha
Chanida Nindee
Chortip Sajjaviriya
Nattawipa Suwannasaeng
Nattawut Sereesongsaeng
Nunthaporn Keawkamthong
Nantawan Jantakul
Prapussorn Jongmeesuk
Prechaya Sripakdee
Piyachart Jitplodprong
Phitchayoot Srisuriyachai
Mattawan Kamnerdlom
Rungdarun Budpeng
Saiwaroon Siriwong
Seksun Charoenjaruwong
Hutsathorn Jamsri
36
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Suparat Sangwipasnapaporn
Krittika Promma-Eng
Kitima Sinsawad
Kuncharee Prakalung
Khannamthong Phunnoi
Juthaporn Piamwaree
Juthamuk Ruengsorn
Thanipat Boonsanong
Thapanon Voraphan
Nattaphon Suchaniwat
Nattawut Thongdee
Tayasorn Suwan
Tanu Taekitpattana
Tunyaporn Tangtagool
Thareerat Phatthong
Namthip Savetprasatn
Nissa Mututanont
Pornchanit Tanticharoenviroj
Patthanun Jitlerd
Piroonporn Dechma
Pattaraporn Pakdeedindan
Yanyong Werawatakul
Yaowapa Tuangtananan
Wanida Kiatjarernseree
Wararak Phannoy
Witan Kaewkhiew
Satatam Noo-Aium
Saran Thipkositkun
37

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Supapit Kanthawat
Syriam Sooksawasdi Na Ayudhya
Sujittra Thaipradist
Sutiwat Chumsang
Sutisa Choosing
Supaporn Saeteaw
Tharathip Pumrachut
Suvijuk Phuantong
Ariya Ittarat
Arthit Ngamchuen
Arthit Sriart
Areeya Korzem
Kanyapatch Bootsriphum
Natcha Monchaivanakit
Natcha Thabunruang
Nontawit Yochai
Nubdao Wongkongdech
Nipat Pitoonpong
Nutjaree Rungrut
Preedee Worraditsakulchai
Mantana Thavikul
Sarawut Butkun
Kanchana Suksompian
Jariya Chaykaew
Thipsuda Huadwongsa
Thana Pengkasame
Anchisa Chaipreedaporn
Sasikarn Montri
38

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Suphang Uttamo
Chotika Tessrimuang
Bunyamon Sapmanee
Parames Uthakum
Category of Participants’ Nationality
1. Thai 7. Canada
2. Lao PDR 8. Australia
3. Vietnam 9. China
4. Philippines 10. USA
5. Indonesia 11. Germany
6. Myanmar
39

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Summary of Oral and Poster Presentations
Oral Presentation
1. Influence of feeding patterns on subclinical laminitis in lactating cows of smallholder dairy
farms in Thailand
Rittichai Pilachai, J. Th. Schonewille, C. Thamrongyoswittayakul, S. Aiumlamai, C.
Wachirapakorn, H. Everts and W. H. Hendriks
2. Subclinical mastitis and associated risk factors in dairy cows in Udon Thani of Thailand
Rittichai Pilachai, Pranpreya Kummee and Sudawan Chuenpreecha
3. The effect of sub-acute ruminal acidosis challenge on inflammatory response and hoof pain
in dairy heifers
Suvaluk Seesupa, Chalong Wachirapakorn and Suneerat Aiumlamai
4. Critical processes of knowledge management for reduction of somatic cell count in bulk milk
of smallholder dairy farms
Aran Chanlun, Chaiyapas Thamrongyoswittayakul, Suthida Chanlun, Pitaya Papirom,
Manassanan Borisuthpetch and Pithai Kanbutra
5. Optimal period for detection of bacterial contamination in milk using resazurin reduction test
Nattaphon Suchaniwat, Thana Pengkasame, Nubdao Wongkongdech, and Aran Chanlun
6. Comparison of Antibacterial Activities of Clausena wallichii Oliv’s and Clausena lansium
Skeels’s extracts against Staphylococcus aureus causing Mastitis in Cattle
Nissa Mututanont, Khannamthong Phunnoi, Wanida Kiatcharoenseree, Noppadol Sompol,
Jinda Wangboonskul and Arinee Chatchawanchontheera
7. Progesterone concentrations of dairy cows following post insemination Crestar® and GnRH
treatments during summer
Khampasong Ninnasopha, Saksiri Sirisatien, Niran Junkou, Suvaluk Seesupa,
Phuangphaka Sadee and Suneerat Aiumlamai
8. Polyvinyl Alcohol (PVA) Concentrations as the Ice Blocker on Viability of Vitrification Bovine
Oocytes
Chatree Chumnandee and Saksiri Sirisathein
40

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
9. Effect of Bovine Viral Diarrhea virus infection on herd’s fertility of dairy heifers in
Northeastern Thailand
Theerakul Nilnont, Suneerat Aiumlamai, Kwankate Kanistanon and Jaruwan Kampa
10. Expression profile of rabies nucleoprotein, phosphoprotein, and glycoprotein genes in
furious and paralytic rabies of canine origin
Wanlop Likitsuntonwong, Akanitt Jittmittraphap, Veera Tepsumethano, Supaporn
Wacharapluesadee, Thiravat Hemachudha and Shanop Shuangshoti
11. Rabbit Model of Right Ventricular Hypertrophy Induced by Pulmonary Artery Banding
Pradtana Meedech, Nakkawee Saengklub, Vudhiporn Limprasut, Sarinee Kalandakanond-
Thongsong, Anusak Kijtawornrat and Somporn Techangamsuwan4
12. Effect of low intensity laser therapy on healing of rabbit tibial defects: an evaluation based
on Cone beam computed tomography
Nguyen Hoai Nam, Naruepon Kampa, Peerapol Sukon, Pongsathorn Tuchpramuk, Pipop
Sutthiprapaporn and Pornpop Rattana-arpha
13. Effects of L-carnitine on Blood urea nitrogen in Fancy carp (Cyprinus carpio)
Naratip Pudsadee, Dilok Wongsathien and Rutch Khattiya
14. Monitoring of Influenza A Viruses in a Live Bird Market in Thailand by Using the Sentinel
Bird Model
Waleemas Jairak, Kirana Noradechanon, Supassama Chaiyawong, Duangduean
Prakairungnamthip, Nutthawan Nonthabenjawan, Aunyaratana Thontiravong and Alongkorn
Amonsin
15. In Vitro Screening of Lactic Acid Bacteria Isolated from Muscovy Duck Ceca for Their
Potentially Probiotic Properties
Chuchat Kamollerd, Preeyaporn Surachon, Panchompoo Maunglai, Wilailak Siripornadulsil
and Peerapol Sukon
16. Effects of galangal (Alpinia galanga) ethanolic extracts against caecal coccidiosis caused
by Eimeria tenella in broilers
Somphanh Bounyavong, Somboon Sangmaneedet, Gun Rungpiriyadej, Supitcha
Settavakin, Napat Hirunsirapat, Weerapol Taweenan, Peerapol Sukon and Jareerat
Aiemsaard
41
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
17. Effect and concentration of Roselle (Hibiscus sabdariffa) calyces extract on blood glucose,
insulin, triglyceride and cholesterol levels in induced hyperglycemic cats
Ranee Singh
18. Dose-comparison trial of praziquantel against feline opisthorchiasis in human endemic areas
Piya Sereerak, Sirikachorn Tangkawattana and Banchob Sripa
19. Detection of Babesia, Ehrlichia and Hepatozoon in Domestic Dogs Using Microscopy
Examination and PCR Techniques in Prakou Villages Phalub District, Khon Kaen
Threetip Mityodwong, Prapasara Potchimplee, Parin Khianman, Somboon Sangmaneedet
and Thidarut Boonmars
20. Survey of upper respiratory tract of Thoroughbred racing horses in Northeastern Thailand
using an Endoscope
Tidaratt Sittisak, Kitima Sinsawat, Pornchanit Tanticharoenviroj and Suphannika
Phutthachalee
42

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Poster Presentation
1. Efficacy of Betel Vine Extract against Staphylococcus aureus Causing Bovine Mastitis
Karnsuda Wijitphan, Phimda Khotbantha, Phaphatsanant Phongsarmsuan and Jareerat
Aimsaard
2. The Effects of Aflatoxin B1 and Yeast (Saccharomyces cerevisiae) Supplementation in
Dairy Cow Feed on Rumen Fermentation by In vitro Gas Production Technique
Piroonporn Dechma, Supaporn Saeteaw, Natcha Monchaivanakit, Chittraporn Yeanpet and
Chaiyapas Thamrongyoswittayakul
3. Effect of Different Levels of Rubber Seed Kernel in Total Mixed Ration for Dairy Cow on in
vitro Fermentation using Gas Production Technique
Nawarat Pha-obnga, Chalong Wachirapakorn and Suneerat Aiumlamai
4. Reproductive Performance of Dairy Cattle in Northeast Thailand
Waranya Kanhachon, Nitima Tatiyaapiradee, Alisra Sinsorn, Amnuay Thotharin, Suvaluk
Srisupa and Suneerat Aiumlamai
5. Progesterone Profiles in Ovulation Induction by Long Time Insertion of CIDR®-B with Low
Dose eCG and TAI with hCG in Anoestrus in Beef Cattle
Chaiwat Jarassaeng, Saksiri Sirisathien, Adisak Sangkaew, Sarawut Sri-ngam Pongthorn,
Suwannathada, Suneerat Aiumlama, Suvaluk Seesupa, Chatchai Suebkom, and
Phuangphaka Sadee
6. Low Dose of eCG and Fixed-time Artificial Insemination with hCG in Ovulation Induction
Program in Beef Cattle
Chaiwat Jarassaeng, Saksiri Sirisathien, Adisak Sangkaew, Sarawut Sri-ngam, Pongthorn
Suwannathada, Suneerat Aiumlamai, Suvaluk Seesupa, Chatchai Suebkom and
Phuangphaka Sadee
7. Comparisons of the Efficiency of Synchronizing the Estrus Cycle with Two Intramuscular or
Intravulvo Submucosal Injections of Cloprostenol in Mixed Native Breed Goat
Sarawut Sringam, Kamonthep Chaisawat and Piyawat Sombutkiripaiboon
8. Full-length Coding Sequence Analysis of the Genome Segments A and B of Infectious
Bursal Disease Virus from Northeastern, Thailand
43
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Tawatchai Pohuang, Kingkarn Sarachu and Kanlaya Chuachan
9. Effects of Limnophila aromatic Merr. Crude Extracts on the Growth Inhibition of Salmonella
Tarinee Pongprom, Peeraya Chumponwong, Nunthaporn Kaewkamthong and Bongkot
Noppon
10. Quantification of Total Bacterial Counts and Enterobacteriaceae Loads during the Chicken
Slaughtering Process
Tayasorn Suwan, Saran Thipkositkun, Arthi Sri-art, Apiradee Sopa, Prapansak Chaveerach
and Bongkot Noppon
11. Efficiency of Acetic Acid Solution to Salmonella Enteritidis
Juthaporn Piamwaree, Nattawut Thongdee, Vitan Kaewkhiew and Sunpetch Angkititrakul
12. Antimicrobial Resistance among Escherichia coli Isolated from Chicken and Pig
Pranpreya Kummee, Kaewkamon Khongmak, Prasert Namchai, Wanwisa Satsomnuek,
Rittichai Pilachai and Sudawan Chuenpreecha
13. Prevalence of Salmonella spp. in the Slaughtering Process at the Local Slaughterhouse in
Khon Kaen
Raksarat Sakulrak, Thanipat Boonsanong, Tharathip Pumrachat, Prapansak Chaveerach
and Bongkot Noppon
14. Effects of Herbal Supplementations on Growth Performance, Feed Utilization, and
Hematological Indices of Nile tilapia (Oreochromis niloticus)
Nitchanakul Klaisok, Rungnapa Poomjan, Korakan Pharadee, Sumalee Seemabut, Suchaya
Wiriyakarun, Chutima Maneekulsaub, Namfon Saisee, Prakit Samakkha and Phukphon
Munglue
15. Intensity of Metacercariae in Cyprinidae Fish in Five Districts from Khon Kaen and Nong
Bua Lamphu Provinces
Sornkrit Rakpanit, Nuttawut Sereesongsaeng, Yanyong Werawatakul, Surasit Auanpromma
and Prapan Kaenjampa
16. Case Report: Unicornuate Uterus in a Thai Domestic Cat
Somphong Hoisang, Panisara Kunkitti, Arayapon Macotpet, and Ekkachai
Pattarapanwichien
44

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
17. Acaricidal Properties of the Essential Oil of Syzygium aromaticum (Clove Oil) against
Brown Dog Tick (Rhipicephalus sanguineus)
Wichaya Thomas, Saknarin Yoshpunya, Hutsathorn Jamsri, Jareerat Aimsaard and
Weerapol Taweenan
18. Serum and Tissue Malondialdehyde Levels in Canine Mammary Cancer
Arayaporn Macotpet, Satatam Noo-aium, Suvijuk Phountong, Sarawut Butkun, Ekkachai
Pattarapanwichien, Sarocha Permsub and Rawinnipa Weerakaittikun
19. Gastro-duodenal Mucormycosis in a Dog: A Case Report
Chalermkwan Nonthakotr, Piyasak Wipoosak, Pongrat Jaisil, Arayaporn Macotpet and
Ekkachai Pattarapanwichien
20. Prevalence of Opisthorchis viverrini in Dogs and Cats in Villages Surrounding Ubolrat Dam
in Five Districts of Khon Kaen Province and Nong Bua Lam Phu Province
Naphat Rungroj, Onjira Chaopong, Prapussorn Jongmeesuk and Surasit Aunpromma
21. Analysis of E-cadherin Expression and PCNA in Feline Mammary Carcinomas Using
Tissue Microarray Technique
Siripitch Sithiyuno, Adjima Boonchuen, Chotimon Seesan, Suwit Balthaisong, Prasarn
Tangkawattana, Anudep Rungsipipat, and Sirikachorn Tangkawattana
22. Apoptosis of Neurons and Inflammatory Cells in the Central Nervous System of Canine
Rabies
Sirinapa Srikam, Preecha Ruangvejvorachai, Veera Tepsumethanon and Shanop
Shuangshoti
23. Gastro-duodenal Cysticercosis in Cat: A Case Report
Chuleephorn Praha, Nittaya Boonban, Arayaporn Macotpet and Ekkachai
Pattarapanwichien
24. Effect of Azadirachin on Terminating Eggs and Lavae of Rhipicephalus sanguineus
Natcha Thaboonruang, Nutjaree Rungrat, Pattaraporn Pakdeedindan and Ranee Singh
25. Prevalence of Gastrointestinal Helminthes in House Rats in 4 Districts of Khon Kaen
Province
Satit Wattanasinpisal, Nattawipa Suwannasaeng, Parames Uthakum, Wansane Toanan and
Somboon Sangmaneedet
45

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
26. Bacteriophages Selection from Nature and Environment in order to Study the Efficacy for
Burkholderia pseudomallei prophylaxis, treatment and control in infected mice and
environment
Pittaya Papirom and Narisorn Na-ngam
27. The potential uses of avermectin derivatives for anti-Trichinella spiralis in mice
Sutiwat Chumsang, Thareerat Phatthong and Somboon Sangmaneedet
Evaluation Results of the Conference
Total number of Feedback = 250
1. How did you hear about the conference?
Sources Percentage
Website 28.0
Magazine 1.2
Leaflet 1.2
Friend 25.6
Facebook 14.4
Others (alumni, USAID, Invitation) 29.6
Total 100.0
2. What were the key factors influencing your decision to attend?
Objectives Percentage
Speaker 20.8
Content 50.8
Meet Friend 10.0
CE Score 11.6
Venue 3.8
Others 3.0
Total 100.0
46

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
3. How would you rate the organization of the conference?
Grading Percentage
Excellence 22.0
Very good 54.4
Good 22.0
Satisfactory 1.6
Need Improvement 0.0
4. How would you rate the overall of conference?
Grading Percentage
Excellence 26.0
Very good 50.8
Good 21.6
Satisfactory 1.6
Need Improvement 0.00
5. How would you rate the reception of conference?
Grading Percentage
Excellence 25.2
Very good 51.6
Good 22.0
Satisfactory 1.2
Need Improvement 0.0
47
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Budget Summary
No. Items Cost (Baht)
1 Lunch, dinner, coffee break, conference rooms 674,000.00
2 Materials and wage cost for advertisement, displays, proceeding 140,780.17
3 Conference bags 173,000.00
4 Accommodations for invited speakers 51,000.00
5 Travel fares for invited speakers 135,705.00
6 Speaker compensation 38,000.00
7 Speaker reception 13,195.00
Total 1,225,680.17
48

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Activities
Registration
49

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
50

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
MOU Ceremony
51

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Opening Ceremony
52

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
53

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
54

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Presentation
55

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Nabong Students (LAO PDR)
56

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
57

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Presentation Awards
58

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
59
Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
Corporate Activities
60

Conference Report: 15th KVAC, 2014 Sustainable Development on One Health
ANNEX
Conference Proceeding
61
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
The 15th Khon Kaen Veterinary Annual International Conference 2014
“Sustainable Development on ONE Health”
24-25 April 2014
Pullman Hotel, Khon Kaen, Thailand
PROCEEDING
Organized by Faculty of Veterinary Medicine, Khon Kaen University, Thailand
Edited by Kwankate Kanistanon
Ranee Singh
Weerapol Taweenan
Suthida Chanlun
Printed by Khon Kaen Printing Co., Ltd.
64-66 Ruenrom Road
Amphoe Muang, Khon Kaen 40000
Tel. +66 4322 1938
ISBN 978-616-223-369-2
The 15th Khon Kaen Veterinary Annual International Conference 2014 (15th KVAC, Khon Kaen, Thailand) “Sustainable Development on ONE Health”, April 24th -25th , 2014 / Organized by Faculty of Veterinary Medicine, Khon Kaen University, Thailand.
Abstracts and full-text papers of all oral and poster presentation published in The 15th Khon Kaen Veterinary Annual International Conference 2014: “Sustainable Development on ONE Health” proceeding passed a peer review process by the scientific committee of the conference. Proceeding did not require all authors of a research paper to sign the letter of submission, nor do they impose an order on the list of authors. Submission to the conference is obtained by scientific committee meaning that all the listed authors have agreed all of the contents. The corresponding (submitting) author is responsible for having ensured that this agreement has been reached, and for managing all communication between the committee and all co-authors, before and after publication. Each author is responsible for the content and accuracy of the entire manuscript.
©2014 The Faculty of Veterinary Medicine, Khon Kaen University
ISBN 978-616-223-369-2

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
The 15th Khon Kaen Veterinary Annual International Conference 2014
“Sustainable Development on ONE Health”
24-25 April 2014
Pullman Hotel, Khon Kaen, Thailand
PROCEEDING
Organized by Faculty of Veterinary Medicine, Khon Kaen University, Thailand
Edited by Kwankate Kanistanon
Ranee Singh
Weerapol Taweenan
Suthida Chanlun
Printed by Khon Kaen Printing Co., Ltd.
64-66 Ruenrom Road
Amphoe Muang, Khon Kaen 40000
Tel. +66 4322 1938
ISBN 978-616-223-369-2
The 15th Khon Kaen Veterinary Annual International Conference 2014 (15th KVAC, Khon Kaen, Thailand) “Sustainable Development on ONE Health”, April 24th -25th , 2014 / Organized by Faculty of Veterinary Medicine, Khon Kaen University, Thailand.
Abstracts and full-text papers of all oral and poster presentation published in The 15th Khon Kaen Veterinary Annual International Conference 2014: “Sustainable Development on ONE Health” proceeding passed a peer review process by the scientific committee of the conference. Proceeding did not require all authors of a research paper to sign the letter of submission, nor do they impose an order on the list of authors. Submission to the conference is obtained by scientific committee meaning that all the listed authors have agreed all of the contents. The corresponding (submitting) author is responsible for having ensured that this agreement has been reached, and for managing all communication between the committee and all co-authors, before and after publication. Each author is responsible for the content and accuracy of the entire manuscript.
©2014 The Faculty of Veterinary Medicine, Khon Kaen University
ISBN 978-616-223-369-2

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
Contents
Welcome
Committees
General Information
Scientific Program
Invited Speakers
Speaker’s Notes
Oral Presentation
Poster Presentation
Welcome Message from the President of Khon Kaen University
Dear Distinguished Delegates, I am very pleased to warmly welcome you to Khon Kaen and to the International Conference on “Sustainable Development on One Health” being held on 24-25 April 2014. This conference is hosted by the Faculty of Veterinary Medicine, Khon Kaen University. The year 2014 is a very special moment for Khon Kaen University to celebrate the KKU 50th anniversary of devotion to society, and Khon Kaen Veterinary Annual International Conference (KVAC) is one of our highlight celebrating activities. To achieve success in One Health goal, everyone needs to develop the sustainable strategies and applications targeting in improve the well-being of humans, animals, and ecosystems. I hope that this conference could build the strength of One Health Knowledge and connection among delegates by sharing experience and learning with each other. I would like to thanks the VMKKU, USAID, Tufts University and all the delegates in making this conference successful.
Warmest regards
Associate Professor Dr.Kittichai Trirattanasirichai President of Khon Kaen University, Thailand
1
23
111
185

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
Contents
Welcome
Committees
General Information
Scientific Program
Invited Speakers
Speaker’s Notes
Oral Presentation
Poster Presentation
Welcome Message from the President of Khon Kaen University
Dear Distinguished Delegates, I am very pleased to warmly welcome you to Khon Kaen and to the International Conference on “Sustainable Development on One Health” being held on 24-25 April 2014. This conference is hosted by the Faculty of Veterinary Medicine, Khon Kaen University. The year 2014 is a very special moment for Khon Kaen University to celebrate the KKU 50th anniversary of devotion to society, and Khon Kaen Veterinary Annual International Conference (KVAC) is one of our highlight celebrating activities. To achieve success in One Health goal, everyone needs to develop the sustainable strategies and applications targeting in improve the well-being of humans, animals, and ecosystems. I hope that this conference could build the strength of One Health Knowledge and connection among delegates by sharing experience and learning with each other. I would like to thanks the VMKKU, USAID, Tufts University and all the delegates in making this conference successful.
Warmest regards
Associate Professor Dr.Kittichai Trirattanasirichai President of Khon Kaen University, Thailand

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
Welcome Message from the Dean, Faculty of Veterinary Medicine, KKU
It is a great honor for the Faculty of Veterinary Medicine, Khon Kaen University, Thailand to host the annual conference, the 15th KVAC: Sustainable Development on One Health. The conference is held at Pullman Hotel, Khon Kaen, Thailand on 24-25 April 2014 to celebrate the KKU’s 50 years of social devotion and VM KKU’s 28 years of the animal health hub for community. This conference aims to provide updated information and knowledge to all delegates on the current major issues eq. emerging zoonotic diseases, SEAOHUN networking for one health, sustainable development on one health, human-animal-ecosystems interface and food safety. The small animal care is also discussed to share experiences with the participants. These topics are contributed to aware broad aspects which currently influencing human and animal health. Let me take this opportunity to welcome my dear veterinary and scientific colleagues, co-hosts, supporting agencies to actively participate, share, learn and engage in the KVAC2014 conference. We all look forward to seeing the collaboration in academic and friendship to support the sustainable development on one health. On behalf of the Dean of Faculty of Veterinary Medicine, Khon Kaen University, I would like to express my appreciation and sincere gratitude to the co-host, USAID and Tufts University and to all agencies which supported the KVAC 2014. We also welcome a great number of VM-KKU alumni to attend the conference and to celebrate 50 years of KKU. I would like to thanks all the sponsors who support and make this conference success in this year. With warm regards,
Associate Professor Dr.Suneerat Aiumlamai Dean, Faculty of Veterinary Medicine Khon Kaen University, Thailand
Welcome Message from Chairman of the 14th KVAC
Khon Kaen, April 2014
Dear Distinguished Delegates, It is my great honor to welcome you to the 15th Khon Kaen Veterinary International Annual Conference, 2014. This year is very special as it is the 50th anniversary of devoting to society of Khon Kaen University. According to AEC’s activity schedule, the 2014 conference is come early than the former years. The conference is hosted by the Faculty of Veterinary Medicine, Khon Kaen University with contribution from Tufts University and US Agency for International Development (USAID). The conference focuses on many interesting issues of sustainable development on One Health, including small animals and livestock medicine, and infectious diseases. I would like to thanks all committees, speakers, sponsors, co-hosts and all delegates who support and contribute to the successful of the conference. I also would like to take this opportunity to welcome home for the VM-KKU alumni, and thanks all for their social devotion. Best Regards,
Associate Professor Dr.Somboon Sangmaneedet Chairman of the 15th KVAC Conference

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
Welcome Message from the Dean, Faculty of Veterinary Medicine, KKU
It is a great honor for the Faculty of Veterinary Medicine, Khon Kaen University, Thailand to host the annual conference, the 15th KVAC: Sustainable Development on One Health. The conference is held at Pullman Hotel, Khon Kaen, Thailand on 24-25 April 2014 to celebrate the KKU’s 50 years of social devotion and VM KKU’s 28 years of the animal health hub for community. This conference aims to provide updated information and knowledge to all delegates on the current major issues eq. emerging zoonotic diseases, SEAOHUN networking for one health, sustainable development on one health, human-animal-ecosystems interface and food safety. The small animal care is also discussed to share experiences with the participants. These topics are contributed to aware broad aspects which currently influencing human and animal health. Let me take this opportunity to welcome my dear veterinary and scientific colleagues, co-hosts, supporting agencies to actively participate, share, learn and engage in the KVAC2014 conference. We all look forward to seeing the collaboration in academic and friendship to support the sustainable development on one health. On behalf of the Dean of Faculty of Veterinary Medicine, Khon Kaen University, I would like to express my appreciation and sincere gratitude to the co-host, USAID and Tufts University and to all agencies which supported the KVAC 2014. We also welcome a great number of VM-KKU alumni to attend the conference and to celebrate 50 years of KKU. I would like to thanks all the sponsors who support and make this conference success in this year. With warm regards,
Associate Professor Dr.Suneerat Aiumlamai Dean, Faculty of Veterinary Medicine Khon Kaen University, Thailand
Welcome Message from Chairman of the 14th KVAC
Khon Kaen, April 2014
Dear Distinguished Delegates, It is my great honor to welcome you to the 15th Khon Kaen Veterinary International Annual Conference, 2014. This year is very special as it is the 50th anniversary of devoting to society of Khon Kaen University. According to AEC’s activity schedule, the 2014 conference is come early than the former years. The conference is hosted by the Faculty of Veterinary Medicine, Khon Kaen University with contribution from Tufts University and US Agency for International Development (USAID). The conference focuses on many interesting issues of sustainable development on One Health, including small animals and livestock medicine, and infectious diseases. I would like to thanks all committees, speakers, sponsors, co-hosts and all delegates who support and contribute to the successful of the conference. I also would like to take this opportunity to welcome home for the VM-KKU alumni, and thanks all for their social devotion. Best Regards,
Associate Professor Dr.Somboon Sangmaneedet Chairman of the 15th KVAC Conference

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
Message from Scientific Committee Chairman
Welcome to the proceeding of the 15th annual scientific conference organized by the Faculty of Veterinary Medicine at Khon Kaen University. This year, the conference has been scheduled earlier than usual due to the change of semester agenda in all universities in Thailand. This year we also received research articles from authors outside Khon Kaen University for poster or oral presentation more than ever. I think this is a sign showing that the KVAC conference has become more publicly well-known. For the authors whose articles are not included in the presentation this year, I hope that you will give us a chance to consider your new articles in the next coming years. Finally, I must apologize all the authors for such an urgent revision we requested and I am very grateful for those who give us a chance to serve you better in the future.
Assistant Professor Dr. Kwankate Kanistanon Chairman, Scientific Committee
The 15th KVAC Committee
Scientific Advisory Committee 1. President of Khon Kaen University 2. Dean of the Faculty of Veterinary Medicine, Khon Kean University
Organizing Committee
1. Assoc.Prof.Dr.Somboon Sangmaneedet Chairman 2. Assoc.Prof.Chuchat Kamollerd 3. Asst.Prof.Dr.Sarthorn Porntrakulpipat 4. Asst.Prof.Ekkachai Pattarapanwichien 5. Asst.Prof.Dr.Prapaporn Tungthanathanich 6. Asst.Prof.Dr.Sirikachorn Tangkawattana 7. Asst.Prof.Dr.Kwankate Kanistanon 8. Asst.Prof.Dr.Jatesada Jiwakanon 9. Asst.Prof.Dr.Weerapol Taweenan 10. Asst.Prof.Dr.Naruepon Kampa 11. Asst.Prof.Arayaporn Macotpet 12. Asst.Prof.Chaiwat Charatsaeng 13. Miss Ancharin Ounthaisong 14. Mrs.Sombat Saengpol
Scientific Committee
1. Asst.Prof.Dr.Kwankate Kanistanon Chairman 2. Assoc.Prof.Dr.Fanan Suksawat 3. Assoc.Prof.Dr.Bongkot Noppon 4. Asst.Prof.Dr.Peerapol Sukon 5. Asst.Prof.Dr.Sirikachorn Tangkawattana 6. Asst.Prof.Dr.Weerapol Taweenan 7. Asst.Prof.Dr.Sarthorn Porntrakulpipat 8. Asst.Prof.Dr.Chaiyapas Thamrongyoswittayakul 9. Asst.Prof.Dr.Sompoth Weerakhun 10. Asst.Prof.Dr.Ranee Singh 11. Dr.Tawatchai Pohuang 12. Miss Numfa Fungbun 13. Mrs.Suthida Chanlun
Information Committee
1. Asst.Prof.Dr.Jatesada Jiwakanon Chairman 2. Asst.Prof.Dr.Weerapol Taweenan 3. Asst.Prof.Dr.Suchat Wattanachai 4. Mr.Pitakpong Maneerattanarungroj 5. Mr.Pongchai Muennoy 6. Mr.Chalermpan Sirabutra 7. Miss Chanida Chainn 8. Mr.Yanyong Wangprecha 9. Miss Ratana Daosawa

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
Message from Scientific Committee Chairman
Welcome to the proceeding of the 15th annual scientific conference organized by the Faculty of Veterinary Medicine at Khon Kaen University. This year, the conference has been scheduled earlier than usual due to the change of semester agenda in all universities in Thailand. This year we also received research articles from authors outside Khon Kaen University for poster or oral presentation more than ever. I think this is a sign showing that the KVAC conference has become more publicly well-known. For the authors whose articles are not included in the presentation this year, I hope that you will give us a chance to consider your new articles in the next coming years. Finally, I must apologize all the authors for such an urgent revision we requested and I am very grateful for those who give us a chance to serve you better in the future.
Assistant Professor Dr. Kwankate Kanistanon Chairman, Scientific Committee
The 15th KVAC Committee
Scientific Advisory Committee 1. President of Khon Kaen University 2. Dean of the Faculty of Veterinary Medicine, Khon Kean University
Organizing Committee
1. Assoc.Prof.Dr.Somboon Sangmaneedet Chairman 2. Assoc.Prof.Chuchat Kamollerd 3. Asst.Prof.Dr.Sarthorn Porntrakulpipat 4. Asst.Prof.Ekkachai Pattarapanwichien 5. Asst.Prof.Dr.Prapaporn Tungthanathanich 6. Asst.Prof.Dr.Sirikachorn Tangkawattana 7. Asst.Prof.Dr.Kwankate Kanistanon 8. Asst.Prof.Dr.Jatesada Jiwakanon 9. Asst.Prof.Dr.Weerapol Taweenan 10. Asst.Prof.Dr.Naruepon Kampa 11. Asst.Prof.Arayaporn Macotpet 12. Asst.Prof.Chaiwat Charatsaeng 13. Miss Ancharin Ounthaisong 14. Mrs.Sombat Saengpol
Scientific Committee
1. Asst.Prof.Dr.Kwankate Kanistanon Chairman 2. Assoc.Prof.Dr.Fanan Suksawat 3. Assoc.Prof.Dr.Bongkot Noppon 4. Asst.Prof.Dr.Peerapol Sukon 5. Asst.Prof.Dr.Sirikachorn Tangkawattana 6. Asst.Prof.Dr.Weerapol Taweenan 7. Asst.Prof.Dr.Sarthorn Porntrakulpipat 8. Asst.Prof.Dr.Chaiyapas Thamrongyoswittayakul 9. Asst.Prof.Dr.Sompoth Weerakhun 10. Asst.Prof.Dr.Ranee Singh 11. Dr.Tawatchai Pohuang 12. Miss Numfa Fungbun 13. Mrs.Suthida Chanlun
Information Committee
1. Asst.Prof.Dr.Jatesada Jiwakanon Chairman 2. Asst.Prof.Dr.Weerapol Taweenan 3. Asst.Prof.Dr.Suchat Wattanachai 4. Mr.Pitakpong Maneerattanarungroj 5. Mr.Pongchai Muennoy 6. Mr.Chalermpan Sirabutra 7. Miss Chanida Chainn 8. Mr.Yanyong Wangprecha 9. Miss Ratana Daosawa
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
10. Mrs.Bunserm Somboon 11. Mrs.Prayoon Khamtat 12. Mrs.Prisna Vichatham 13. Mrs.Wan Buajan 14. Mrs.Prapatson Thihta 15. Miss Ancharin Ounthaisong
Treasurer Committee
1. Assoc.Prof.Chuchat Kamollerd Chairman 2. Mrs.Phatchareeya Konchan 3. Mrs.Suthathip Wattanachai 4. Miss Wichayanun Kanla 5. Mr.Weera Suparuk
Exhibition committee
1. Asst.Prof.Dr.Naruepon Kampa Chairman 2. Mr.Somphong Hoisang 3. Miss Sarocha Permsub 4. Miss Meena Visungrae 5. Miss Tanit Ariyakong 6. Mrs.Promporn Tongtieum 7. Miss Jitrapon Suanbun 8. Miss Pailin Simmalee 9. Miss Parinda Namkoksi
Banquet committee
1. Asst.Prof.Dr.Prapaporn Tungthanathanich Chairman 2. Assoc.Prof.Dr.Bongkot Noppon 3. Asst.Prof.Varaporn Sukolapong 4. Mrs.Nusara Suwannachot 5. Mrs.Yupadee Charoensawang
Registration committee
1. Asst.Prof.Arayaporn Macotpet Chairman 2. Miss Suphannika Pnutthachalee 3. Miss Chuleephorn Praha 4. Miss Narishra Lertchaisathapon 5. Miss Sarocha Permsub 6. Miss Kavintra Iranoy 7. Mrs.Sudarat Buatuan 8. Miss Pailin Simmalee 9. Miss Jitrapon Suanbun 10. Miss Supavadi Sriputorn 11. Mrs.Sombat Saengpol
Ceremony and Reception committee 1. Asst.Prof.Dr.Sirikachorn Tangkawattana Chairman 2. Assoc.Prof.Dr.Fanan Suksawat 3. Asst.Prof.Dr.Sarthorn Porntrakulpipat 4. Asst.Prof.Dr.Weerapol Taweenan 5. Asst.Prof.Dr.Kochakorn Direksin 6. Asst.Prof.Dr.Ranee Singh 7. Asst.Prof.Dr.Aran Chanlun 8. Dr.Trasida Ployngam 9. Mrs.Nusara Suwannachot 10. Mr.Sithiporn Kapbualoi 11. Miss Jongkolwan Chansombat
Transportation committee 1. Asst.Prof.Chaiwat Charatsaeng Chairman 2. Mrs.Yupadee Jaroensawang 3. Mr.Amporn Krisornsri 4. Mr.Pongpan Pongsapung
Evaluation committee
1. Asst.Prof.Ekkachai Pattarapanwichien Chairman 2. Mr.Samai Kengkan 3. Mrs.Aranya Sirikraiwan 4. Miss Nathapop Sechang 5. Mrs.Aoythip Subso
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
10. Mrs.Bunserm Somboon 11. Mrs.Prayoon Khamtat 12. Mrs.Prisna Vichatham 13. Mrs.Wan Buajan 14. Mrs.Prapatson Thihta 15. Miss Ancharin Ounthaisong
Treasurer Committee
1. Assoc.Prof.Chuchat Kamollerd Chairman 2. Mrs.Phatchareeya Konchan 3. Mrs.Suthathip Wattanachai 4. Miss Wichayanun Kanla 5. Mr.Weera Suparuk
Exhibition committee
1. Asst.Prof.Dr.Naruepon Kampa Chairman 2. Mr.Somphong Hoisang 3. Miss Sarocha Permsub 4. Miss Meena Visungrae 5. Miss Tanit Ariyakong 6. Mrs.Promporn Tongtieum 7. Miss Jitrapon Suanbun 8. Miss Pailin Simmalee 9. Miss Parinda Namkoksi
Banquet committee
1. Asst.Prof.Dr.Prapaporn Tungthanathanich Chairman 2. Assoc.Prof.Dr.Bongkot Noppon 3. Asst.Prof.Varaporn Sukolapong 4. Mrs.Nusara Suwannachot 5. Mrs.Yupadee Charoensawang
Registration committee
1. Asst.Prof.Arayaporn Macotpet Chairman 2. Miss Suphannika Pnutthachalee 3. Miss Chuleephorn Praha 4. Miss Narishra Lertchaisathapon 5. Miss Sarocha Permsub 6. Miss Kavintra Iranoy 7. Mrs.Sudarat Buatuan 8. Miss Pailin Simmalee 9. Miss Jitrapon Suanbun 10. Miss Supavadi Sriputorn 11. Mrs.Sombat Saengpol
Ceremony and Reception committee 1. Asst.Prof.Dr.Sirikachorn Tangkawattana Chairman 2. Assoc.Prof.Dr.Fanan Suksawat 3. Asst.Prof.Dr.Sarthorn Porntrakulpipat 4. Asst.Prof.Dr.Weerapol Taweenan 5. Asst.Prof.Dr.Kochakorn Direksin 6. Asst.Prof.Dr.Ranee Singh 7. Asst.Prof.Dr.Aran Chanlun 8. Dr.Trasida Ployngam 9. Mrs.Nusara Suwannachot 10. Mr.Sithiporn Kapbualoi 11. Miss Jongkolwan Chansombat
Transportation committee 1. Asst.Prof.Chaiwat Charatsaeng Chairman 2. Mrs.Yupadee Jaroensawang 3. Mr.Amporn Krisornsri 4. Mr.Pongpan Pongsapung
Evaluation committee
1. Asst.Prof.Ekkachai Pattarapanwichien Chairman 2. Mr.Samai Kengkan 3. Mrs.Aranya Sirikraiwan 4. Miss Nathapop Sechang 5. Mrs.Aoythip Subso

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
General Information
Registration and Information desk- on the 2th floor of Pullman Hotel Opening Hours Thursday 24th April 2014 08.00-16.00 Friday 25th April 2014 08.00-16.00 Conference Website: http://kvac.kku.ac.th
Conference Venue Pullman Hotel
9-9 Prachasumran Rd. Muang, Khon Kaen, 40000
Phone: +66 (43) 322 155 Website: http://pullmanhotels.com
Program Materials
Your conference kit provided at registration counter will contain the conference program and proceeding CD and souvenir.
Identification Badges
Please wear your identification badge at all times while you are attending the conference.
Official Language
The official language of the conference is English.
Onsite Conference Services
Onsite internet counter and computer access will be provided as a complimentary for all participants. Photocopying, fax, and telephone services will be provided to participants on commercial basis.
Coffee/Tea
Coffee, tea and refreshment are included in the registration fee of participants and will be available throughout the conference at the assigned area during the breaks.
Lunch
Lunches are included in the registration fee of participants. Lunches will be served at 12.00-13.00
Liability and Insurance
The Organizing Committee will not assure any responsibility for damages or injuries to person or property during the conference. It is recommended that participants should arrange their own personal travel and health insurance.
Speaker-Ready Desk
On the 2th floor of Pullman Hotel, we arrange a room for speakers to prepare their presentation. A desk for loading speaker’s presentation is in front of the room and is available from 07.45-16.00.
Instruction for presenters
Poster
The posters are grouped by session and number. The number corresponds to the number in the abstract book. Poster should be displayed from Thursday 24th April, 08.30 hours until Friday 25th April, 16.00 hours. Posters should be mounted with double sided tape only which will be provided. Assistance and material for mounting the posters will be available, at the information desk. The authors of posters are expected to be available for answering questions during the poster session, coffee break time, Thursday.
Oral presentations
Time for your presentation is in the detailed of Oral presentation schedule in this proceeding.
The conference language is English. The time schedule is tight and chairman will be strict on time, so please keep to the time allocated for you; 12 minutes talk and 3 minutes for question and discussion. If you aim at 10 minutes talk, you will be on the safe side.
Power point presentation should be downloaded on the computer in Speaker-Ready Desk from 07.45-16.00. The operative system of the computer in the lecture rooms is Window 7. Please make sure that your presentation is compatible. It is not allowed to use individual computers for presentation.
If you wish to provide your presentation after the conference by showing it on our official webpage, please inform our staff at the Speaker-Ready room about your decision. And if you do not want to, the files of your presentation will be deleted after the conference. However, please let us know your decision on your presentation day.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
General Information
Registration and Information desk- on the 2th floor of Pullman Hotel Opening Hours Thursday 24th April 2014 08.00-16.00 Friday 25th April 2014 08.00-16.00 Conference Website: http://kvac.kku.ac.th
Conference Venue Pullman Hotel
9-9 Prachasumran Rd. Muang, Khon Kaen, 40000
Phone: +66 (43) 322 155 Website: http://pullmanhotels.com
Program Materials
Your conference kit provided at registration counter will contain the conference program and proceeding CD and souvenir.
Identification Badges
Please wear your identification badge at all times while you are attending the conference.
Official Language
The official language of the conference is English.
Onsite Conference Services
Onsite internet counter and computer access will be provided as a complimentary for all participants. Photocopying, fax, and telephone services will be provided to participants on commercial basis.
Coffee/Tea
Coffee, tea and refreshment are included in the registration fee of participants and will be available throughout the conference at the assigned area during the breaks.
Lunch
Lunches are included in the registration fee of participants. Lunches will be served at 12.00-13.00
Liability and Insurance
The Organizing Committee will not assure any responsibility for damages or injuries to person or property during the conference. It is recommended that participants should arrange their own personal travel and health insurance.
Speaker-Ready Desk
On the 2th floor of Pullman Hotel, we arrange a room for speakers to prepare their presentation. A desk for loading speaker’s presentation is in front of the room and is available from 07.45-16.00.
Instruction for presenters
Poster
The posters are grouped by session and number. The number corresponds to the number in the abstract book. Poster should be displayed from Thursday 24th April, 08.30 hours until Friday 25th April, 16.00 hours. Posters should be mounted with double sided tape only which will be provided. Assistance and material for mounting the posters will be available, at the information desk. The authors of posters are expected to be available for answering questions during the poster session, coffee break time, Thursday.
Oral presentations
Time for your presentation is in the detailed of Oral presentation schedule in this proceeding.
The conference language is English. The time schedule is tight and chairman will be strict on time, so please keep to the time allocated for you; 12 minutes talk and 3 minutes for question and discussion. If you aim at 10 minutes talk, you will be on the safe side.
Power point presentation should be downloaded on the computer in Speaker-Ready Desk from 07.45-16.00. The operative system of the computer in the lecture rooms is Window 7. Please make sure that your presentation is compatible. It is not allowed to use individual computers for presentation.
If you wish to provide your presentation after the conference by showing it on our official webpage, please inform our staff at the Speaker-Ready room about your decision. And if you do not want to, the files of your presentation will be deleted after the conference. However, please let us know your decision on your presentation day.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
15th Khon Kaen Veterinary Annual International Conference (15th KVAC) “Sustainable Development on ONE Health”
24-25 April 2014, Pullman Hotel, Khon Kaen
24 April 2014
Time
Orchid Ballroom 1 ONE Health
Livestock & Infectious Diseases (Eng)
Orchid Ballroom 2 Small Animal Medicine
(Thai)
Orchid Ballroom 3 Scientific Presentation
08.00-09.30 am Registration / Opening ceremony
09.30-10.30 am Emerging Zoonotic Diseases: Global and Local Perspectives (Dr.Michael Kosoy, CDC)
10.30-11.30 am SEAOHUN : Networking to Promote ONE Health in Southeast Asia (Dr.Suwit Somponpun, USAID)
11.30-01.00 pm Lunch
01.00-03.00 pm
Sustainable Development on ONE Health
(01.00-02.00 pm) Common Canine Tumors I (Arayaporn Macotpet, KKU) Moderator: Dr.Fanan Suksawat
Oral Scientific Presentation (Eng)
The ONE Health Surveillance on Nipah virus in Thailand (Dr.Supaporn Wacharapluesadee, CU)
Emerging Influenza in Asia: The Current Situation (Dr.Taweesak Songserm, KU)
Sustainable ONE Health Research in SEA (Dr.Flavie Goutard, CIRAD)
(02.00-03.00 pm) Common Canine Tumors II (Ekkachai Pattarapanwichien, KKU) Moderator: Dr.Fanan Suksawat
Impacts of Biodiversity & Land Use Changes on Zoonotic Infectious Diseases in Southeast Asia (Dr.Serge Morand)
Coffee Break (served) / Poster Symposium
03.00-04.00 pm
Panel Discussion: Sustainable Development on ONE Health Moderator: Dr.Sirikachorn Tangkawattana
Clinical Management of Canine Seborrhea (Dr.Narong Kitpanit) Moderator: Dr.Fanan Suksawat
Oral Scientific Presentation (Eng)
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
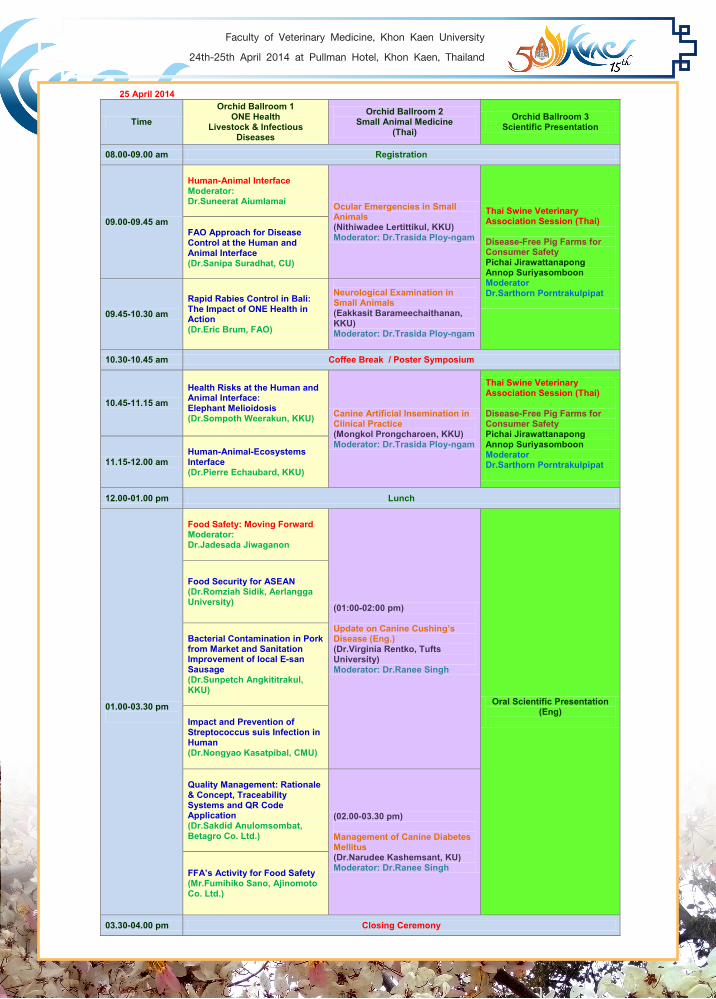
25 April 2014
Time
Orchid Ballroom 1 ONE Health
Livestock & Infectious Diseases
Orchid Ballroom 2 Small Animal Medicine
(Thai)
Orchid Ballroom 3 Scientific Presentation
08.00-09.00 am Registration
09.00-09.45 am
Human-Animal Interface Moderator: Dr.Suneerat Aiumlamai Ocular Emergencies in Small
Animals (Nithiwadee Lertittikul, KKU) Moderator: Dr.Trasida Ploy-ngam
Thai Swine Veterinary Association Session (Thai) Disease-Free Pig Farms for Consumer Safety Pichai Jirawattanapong Annop Suriyasomboon Moderator Dr.Sarthorn Porntrakulpipat
FAO Approach for Disease Control at the Human and Animal Interface (Dr.Sanipa Suradhat, CU)
09.45-10.30 am
Rapid Rabies Control in Bali: The Impact of ONE Health in Action (Dr.Eric Brum, FAO)
Neurological Examination in Small Animals (Eakkasit Barameechaithanan, KKU) Moderator: Dr.Trasida Ploy-ngam
10.30-10.45 am Coffee Break / Poster Symposium
10.45-11.15 am
Health Risks at the Human and Animal Interface: Elephant Melioidosis (Dr.Sompoth Weerakun, KKU)
Canine Artificial Insemination in Clinical Practice (Mongkol Prongcharoen, KKU) Moderator: Dr.Trasida Ploy-ngam
Thai Swine Veterinary Association Session (Thai) Disease-Free Pig Farms for Consumer Safety Pichai Jirawattanapong Annop Suriyasomboon Moderator Dr.Sarthorn Porntrakulpipat
11.15-12.00 am
Human-Animal-Ecosystems Interface (Dr.Pierre Echaubard, KKU)
12.00-01.00 pm Lunch
01.00-03.30 pm
Food Safety: Moving Forward Moderator: Dr.Jadesada Jiwaganon
(01:00-02:00 pm) Update on Canine Cushing’s Disease (Eng.) (Dr.Virginia Rentko, Tufts University) Moderator: Dr.Ranee Singh
Oral Scientific Presentation (Eng)
Food Security for ASEAN (Dr.Romziah Sidik, Aerlangga University)
Bacterial Contamination in Pork from Market and Sanitation Improvement of local E-san Sausage (Dr.Sunpetch Angkititrakul, KKU) Impact and Prevention of Streptococcus suis Infection in Human (Dr.Nongyao Kasatpibal, CMU) Quality Management: Rationale & Concept, Traceability Systems and QR Code Application (Dr.Sakdid Anulomsombat, Betagro Co. Ltd.)
(02.00-03.30 pm) Management of Canine Diabetes Mellitus (Dr.Narudee Kashemsant, KU) Moderator: Dr.Ranee Singh
FFA’s Activity for Food Safety (Mr.Fumihiko Sano, Ajinomoto Co. Ltd.)
03.30-04.00 pm Closing Ceremony
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand
Invited Speaker

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 1
Dr. Michael Y. Kosoy, Ph.D. AREA OF EXPERTISE: Ecology, epidemiology, and microbiology of zoonotic infectious diseases, including hantaviruses, arenaviruses, tick-borne encephalitis, plague, tularemia, and bartonellosis. EDUCATION: Mechnikov Odessa State University, Ukraine, Biology, M.S. 1978 Gamaleya Institute of Epidemiology and Microbiology, Russia, Epidemiology, Ph.D. 1987 PROFESSIONAL HISTORY: 2007– Present, Laboratory Chief, Division of Vector-Borne Diseases, CDC 2009 – Present, Global Disease Detection Technical Support Corps Member, CDC 1999-2006, Research Biologist, Division of Vector-Borne Diseases, CDC 1994-1999, Research Fellow, Division of Viral and Rickettsial Diseases, CDC 1991-1993, Director, Laboratory of Epizootiology and Ecological Pathology of Animals 1979-1993, Research Biologist and Team Leader, Institute of Epidemiology and Microbiology MEMBERSHIP IN PROFESSIONAL SOCIETIES: American Society of Tropical Medicine and Hygiene; American Society for Microbiology; International Conference on Diseases in Nature Communicable to Man (past president) INTERNATIONAL ACTIVITIES Canada (2003-2006); Georgia (country) (2011-2014); Guatemala (2010-2014); Japan (2006-2009); Kazakhstan (1999-2003, 2010-2012); Kenya (2008-2011); Kosovo (2000); Thailand (2003-2014); Vietnam (2007-2014); Russia (2003-2006); Republic of Congo (1995), P. R. China (1999-2013) HONORS:
U.S. Department of Health and Human Services Secretary’s Award for Extraordinary and Outstanding Team Effort in Mounting a Response to the Ebola Hemorrhagic Fever Epidemic (1996).
Secretary’s Award for Distinguished Service (2003). PUBLICATIONS: More than 130 publications

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health2
Dr. Suwit Somponpun, Ph.D. Dr. Suwit Somponpun is a biomedical researcher with over 15 years of translational research experience behind him. An alumnus of Mahidol University, he graduated with a Bachelor’s degree in pharmacy in 1996 before completing PhD in biomedical science from Edinburgh University where he was engaged in multidisciplinary research training in Neuroendocrinology. In 2000, he relocated to the U.S. and took up a postdoctoral position at the Chicago Medical School where he continued with his research into the role of steroids in hypothalamic neurons. He subsequently moved to the University of Colorado Health Sciences Center, the NIH in Bethesda, and Tripler Army Medical Center in Honolulu. In 2009, he joined and was appointed tenure track assistant professor in the Department of Anatomy, Biochemistry and Physiology at the University of Hawaii, School of Medicine where he remained a faculty member and contributed to the preclinical teaching until 2011 when he relocated back to Thailand. Upon his return and until very recently, he served as Senior Research Scientist in the Department of Veterinary Medicine at Armed Forces Research Institute of Medical Sciences (AFRIMS) where he led the nonhuman primate research effort across multitudes of diseases, including Malaria, HIV and Dengue fever. He currently serves as Program Manager for the SEAOHUN Foundation and is working to develop comprehensive strategies for capacity building for the Foundation and to provide support for the network universities across SEA.
Dr. Supaporn Wacharapluesadee, Ph.D
EXPERIENCES : June 1994 – February 1997 Biochemical Technician, Department of Entomology, AFRIMS; March 1997– August 1997 Researcher on cancer research, Department of Immunology, Chulaporn Research Instiute; September 1997 – September 2000 Medical technologist, The HIV/AIDS Collaboration Thai-US, Thailand October 2000 – Present
Laboratory Chief, Neuroscience Center for Research and Development & WHO Collaborating Center for Research and Training on Viral Zoonoses, Faculty of Medicine, Chulalongkorn University
PUBLICATIONS: 1. Saraya A, Mahavihakanont A, Shuangshoti S, Sittidetboripat N, Deesudchit T, Callahan M,
Wacharapluesadee S, Wilde H, Hemachudha T. Autoimmune causes of encephalitis syndrome in Thailand: prospective study of 103 patients. BMC Neurol. 2013 Oct 20;13(1):150
2. Wacharapluesadee S, Sintunawa C, Kaewpom T, Khongnomnan K, Olival KJ, Epstein JH, Rodpan A, Sangsri P, Intarut N, Chindamporn A, Suksawa K, Hemachudha T. Group C betacoronavirus in bat guano fertilizer, Thailand. Emerg Infect Dis. 2013 Aug;19(8).
3. Drexler JF, Corman VM, Müller MA, Lukashev AN, Gmyl A, Coutard B, Adam A, Ritz D, Leijten LM, van Riel D, Kallies R, Klose SM, Gloza-Rausch F, Binger T, Annan A, Adu-Sarkodie Y, Oppong S, Bourgarel M, Rupp D, Hoffmann B, Schlegel M, Kümmerer BM, Krüger DH, Schmidt-Chanasit J, Setién AA, Cottontail VM, Hemachudha T, Wacharapluesadee S, Osterrieder K, Bartenschlager R, Matthee S, Beer M, Kuiken T, Reusken C, Leroy EM, Ulrich RG, Drosten C. Evidence for novel hepaciviruses in rodents. PLoS Pathog. 2013 Jun;9(6):e1003438.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 3
Dr. Suwit Somponpun, Ph.D. Dr. Suwit Somponpun is a biomedical researcher with over 15 years of translational research experience behind him. An alumnus of Mahidol University, he graduated with a Bachelor’s degree in pharmacy in 1996 before completing PhD in biomedical science from Edinburgh University where he was engaged in multidisciplinary research training in Neuroendocrinology. In 2000, he relocated to the U.S. and took up a postdoctoral position at the Chicago Medical School where he continued with his research into the role of steroids in hypothalamic neurons. He subsequently moved to the University of Colorado Health Sciences Center, the NIH in Bethesda, and Tripler Army Medical Center in Honolulu. In 2009, he joined and was appointed tenure track assistant professor in the Department of Anatomy, Biochemistry and Physiology at the University of Hawaii, School of Medicine where he remained a faculty member and contributed to the preclinical teaching until 2011 when he relocated back to Thailand. Upon his return and until very recently, he served as Senior Research Scientist in the Department of Veterinary Medicine at Armed Forces Research Institute of Medical Sciences (AFRIMS) where he led the nonhuman primate research effort across multitudes of diseases, including Malaria, HIV and Dengue fever. He currently serves as Program Manager for the SEAOHUN Foundation and is working to develop comprehensive strategies for capacity building for the Foundation and to provide support for the network universities across SEA.
Dr. Supaporn Wacharapluesadee, Ph.D
EXPERIENCES : June 1994 – February 1997 Biochemical Technician, Department of Entomology, AFRIMS; March 1997– August 1997 Researcher on cancer research, Department of Immunology, Chulaporn Research Instiute; September 1997 – September 2000 Medical technologist, The HIV/AIDS Collaboration Thai-US, Thailand October 2000 – Present
Laboratory Chief, Neuroscience Center for Research and Development & WHO Collaborating Center for Research and Training on Viral Zoonoses, Faculty of Medicine, Chulalongkorn University
PUBLICATIONS: 1. Saraya A, Mahavihakanont A, Shuangshoti S, Sittidetboripat N, Deesudchit T, Callahan M,
Wacharapluesadee S, Wilde H, Hemachudha T. Autoimmune causes of encephalitis syndrome in Thailand: prospective study of 103 patients. BMC Neurol. 2013 Oct 20;13(1):150
2. Wacharapluesadee S, Sintunawa C, Kaewpom T, Khongnomnan K, Olival KJ, Epstein JH, Rodpan A, Sangsri P, Intarut N, Chindamporn A, Suksawa K, Hemachudha T. Group C betacoronavirus in bat guano fertilizer, Thailand. Emerg Infect Dis. 2013 Aug;19(8).
3. Drexler JF, Corman VM, Müller MA, Lukashev AN, Gmyl A, Coutard B, Adam A, Ritz D, Leijten LM, van Riel D, Kallies R, Klose SM, Gloza-Rausch F, Binger T, Annan A, Adu-Sarkodie Y, Oppong S, Bourgarel M, Rupp D, Hoffmann B, Schlegel M, Kümmerer BM, Krüger DH, Schmidt-Chanasit J, Setién AA, Cottontail VM, Hemachudha T, Wacharapluesadee S, Osterrieder K, Bartenschlager R, Matthee S, Beer M, Kuiken T, Reusken C, Leroy EM, Ulrich RG, Drosten C. Evidence for novel hepaciviruses in rodents. PLoS Pathog. 2013 Jun;9(6):e1003438.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health4
4. Breed AC, Meers J, Sendow I, Bossart KN, Barr JA, Smith I, Wacharapluesadee S, Wang L, Field HE. The Distribution of Henipaviruses in Southeast Asia and Australasia: Is Wallace's Line a Barrier to Nipah Virus? PLoS One. 2013 Apr 24;8(4):e61316. doi: 10.1371
5. Hemachudha T, Ugolini G, Sungkarat W, Laothamatas J, Shuangshoti S, Wacharapluesadee S. Human Rabies: neuropathogenesis, diagnosis and management. Lancet Neurology. May 2013. 498-513.
6. Shuangshoti S, Thepa N, Phukpattaranont P, Jittmittraphap A, Intarut N, Tepsumethanon V, Wacharapluesadee S, Thorner PS, Hemachudha T. Reduced viral burden in paralytic compared to furious canine rabies is associated with prominent inflammation at the brainstem level. BMC Vet Res. 2013 Feb 14;9(1):31
7. Virojanapirom P, Khawplod P, Sawangvaree A, Wacharapluesadee S, Hemachudha T, Yamada K, Morimoto K, Nishizono A. Molecular analysis of the mutational effects of Thai street rabies virus with increased virulence in mice after passages in the BHK cell line. Arch Virol. 2012 Nov;157(11):2201-5.
8. Wilde H, Hemachudha T, Wacharapluesadee S, Lumlertdacha B, Tepsumethanon V. Rabies in Asia: The Classical Zoonosis. Curr Top Microbiol Immunol. 2012 Jun 8
9. Wacharapluesadee S, Tepsumethanon V, Supavonwong P, Kaewpom T, Intarut N, Hemachudha T. Detection of rabies viral RNA by TaqMan real-time RT-PCR using non-neural specimens from dogs infected with rabies virus. J Virol Methods. 2012 Sep;184(1-2):109-12.
10. Wilde H, Wacharapluesadee S, Hemachudha T. Currently approved post-exposure rabies prophylaxis regimens. Travel Med Infect Dis. 2012 May 10.
11. Pasutharnchat N, Wacharapluesadee S, Hemachudha T. Clinical manifestations of acetylcholine receptor antibody positive and negative myasthenia gravis. J Med Assoc Thai. 2012 Mar;95(3):313-9.
12. Thanomsridetchai N, Singhto N, Tepsumethanon V, Shuangshoti S, Wacharapluesadee S, Sinchaikul S, Chen ST, Hemachudha T, Thongboonkerd V. Comprehensive proteome analysis of hippocampus, brainstem, and spinal cord from paralytic and furious dogs naturally infected with rabies. J Proteome Res. 2011 Nov 4;10(11):4911-24.
13. Wacharapluesadee S, Phumesin P, Supavonwong P, Khawplod P, Intarut N, Hemachudha T.Comparative detection of rabies RNA by NASBA, real-time PCR and conventional PCR. J Virol Methods. 2011 Aug;175(2):278-82.
14. Dacheux L, Wacharapluesadee S, Hemachudha T, Meslin FX, Buchy P, Reynes JM, Bourhy H. More Accurate Insight into the Incidence of Human Rabies in Developing Countries through Validated Laboratory Techniques. PLoS Negl Trop Dis. 2010 Nov 30;4(11):e765.
15. Tenzin, Wacharapluesadee S, Denduangboripant J, Dhand NK, Dorji R, Tshering D, Rinzin K, Raika V, Dahal N, Ward MP. Rabies virus strains circulating in Bhutan: implications for control. Epidemiol Infect. 2010 Nov 26:1-6.
16. Saraya A, Wacharapluesadee S, Khawplod P, Tepsumethanon S, Briggs D, Asawavichienjinda T, Hemachudha T. A preliminary study of chemo- and cytokine responses in rabies vaccine recipients of intradermal and intramuscular regimens. Vaccine. 2010 May 12.
17. Wacharapluesadee S, Hemachudha T. Ante- and post-mortem diagnosis of rabies using nucleic acid-amplification tests. Expert Rev Mol Diagn. 2010 Mar;10(2):207-18.
18. Shantavasinkul P, Tantawichien T, Wacharapluesadee S, Jeamanukoolkit A, Udomchaisakul P, Chattranukulchai P, Wongsaroj P, Khawplod P, Wilde H, Hemachudha T. Failure of rabies postexposure prophylaxis in patients presenting with unusual manifestations. Clin Infect Dis. 2010 Jan 1;50(1):77-9.
19. Wacharapluesadee S, Boongird B, Wanghongsa S, Ratanasetyuth N, Supavonwong P, Saengsen D, Gongal G. N., Hemachudha T. A Longitudinal Study of the Prevalence of Nipah Virus in Pteropus lylei Bats in Thailand: evidence for seasonal preference in disease transmission. Vector Borne Zoonotic Dis. 2010 Mar;10(2):183-90.
20. Wilde H, Wacharapluesadee S, Hemachudha T and Tepsumethanon V. Rabies. In: Kris Heggenhougen and Stella Quah, editors International Encyclopedia of Public Health, Vol 5. San Diego: Academic Press; 2008. pp. 463-470.
21. Wacharapluesadee S, Sutipanya J, Damrongwatanapokin S, Phumesin P, Chamnanpood P, Leowijuk C, Hemachudha T. Development of a TaqMan real-time RT-PCR assay for the detection of rabies virus.J Virol Methods. 2008 Aug;151(2):317-20.
22. Laothamatas J, Wacharapluesadee S, Lumlertdacha B, Ampawong S, Tepsumethanon V, Shuangshoti S, Phumesin P, Asavaphatiboon S, Worapruekjaru L, Avihingsanon Y, Israsena N, Lafon M, Wilde H, Hemachudha T.Furious and paralytic rabies of canine origin: neuroimaging with virological and cytokine studies.J Neurovirol. 2008 Apr;14(2):119-29.
23. Wacharapluesadee S, Hemachudha T. Duplex nested RT-PCR for detection of Nipah virus RNA from urine specimens of bats. J Virol Methods. 2007 Apr;141(1):97-101.
24. Hemachudha T, Wacharapluesadee S, Laothamatas J, Wilde H. Rabies. Curr Neurol Neurosci Rep. 2006 Nov;6(6):460-8. Review.
25. Hemachudha T, Sunsaneewitayakul B, Desudchit T, Suankratay C, Sittipunt C, Wacharapluesadee S, Khawplod P, Wilde H, Jackson AC. Failure of therapeutic coma and ketamine for therapy of human rabies. J Neurovirol. 2006 Oct;12(5):407-9.
26. Wacharapluesadee S, Boongird K, Wanghongsa S, Phumesin P, Hemachudha T. Drinking bat blood may be hazardous to your health.Clin Infect Dis. 2006;43:269

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 5
4. Breed AC, Meers J, Sendow I, Bossart KN, Barr JA, Smith I, Wacharapluesadee S, Wang L, Field HE. The Distribution of Henipaviruses in Southeast Asia and Australasia: Is Wallace's Line a Barrier to Nipah Virus? PLoS One. 2013 Apr 24;8(4):e61316. doi: 10.1371
5. Hemachudha T, Ugolini G, Sungkarat W, Laothamatas J, Shuangshoti S, Wacharapluesadee S. Human Rabies: neuropathogenesis, diagnosis and management. Lancet Neurology. May 2013. 498-513.
6. Shuangshoti S, Thepa N, Phukpattaranont P, Jittmittraphap A, Intarut N, Tepsumethanon V, Wacharapluesadee S, Thorner PS, Hemachudha T. Reduced viral burden in paralytic compared to furious canine rabies is associated with prominent inflammation at the brainstem level. BMC Vet Res. 2013 Feb 14;9(1):31
7. Virojanapirom P, Khawplod P, Sawangvaree A, Wacharapluesadee S, Hemachudha T, Yamada K, Morimoto K, Nishizono A. Molecular analysis of the mutational effects of Thai street rabies virus with increased virulence in mice after passages in the BHK cell line. Arch Virol. 2012 Nov;157(11):2201-5.
8. Wilde H, Hemachudha T, Wacharapluesadee S, Lumlertdacha B, Tepsumethanon V. Rabies in Asia: The Classical Zoonosis. Curr Top Microbiol Immunol. 2012 Jun 8
9. Wacharapluesadee S, Tepsumethanon V, Supavonwong P, Kaewpom T, Intarut N, Hemachudha T. Detection of rabies viral RNA by TaqMan real-time RT-PCR using non-neural specimens from dogs infected with rabies virus. J Virol Methods. 2012 Sep;184(1-2):109-12.
10. Wilde H, Wacharapluesadee S, Hemachudha T. Currently approved post-exposure rabies prophylaxis regimens. Travel Med Infect Dis. 2012 May 10.
11. Pasutharnchat N, Wacharapluesadee S, Hemachudha T. Clinical manifestations of acetylcholine receptor antibody positive and negative myasthenia gravis. J Med Assoc Thai. 2012 Mar;95(3):313-9.
12. Thanomsridetchai N, Singhto N, Tepsumethanon V, Shuangshoti S, Wacharapluesadee S, Sinchaikul S, Chen ST, Hemachudha T, Thongboonkerd V. Comprehensive proteome analysis of hippocampus, brainstem, and spinal cord from paralytic and furious dogs naturally infected with rabies. J Proteome Res. 2011 Nov 4;10(11):4911-24.
13. Wacharapluesadee S, Phumesin P, Supavonwong P, Khawplod P, Intarut N, Hemachudha T.Comparative detection of rabies RNA by NASBA, real-time PCR and conventional PCR. J Virol Methods. 2011 Aug;175(2):278-82.
14. Dacheux L, Wacharapluesadee S, Hemachudha T, Meslin FX, Buchy P, Reynes JM, Bourhy H. More Accurate Insight into the Incidence of Human Rabies in Developing Countries through Validated Laboratory Techniques. PLoS Negl Trop Dis. 2010 Nov 30;4(11):e765.
15. Tenzin, Wacharapluesadee S, Denduangboripant J, Dhand NK, Dorji R, Tshering D, Rinzin K, Raika V, Dahal N, Ward MP. Rabies virus strains circulating in Bhutan: implications for control. Epidemiol Infect. 2010 Nov 26:1-6.
16. Saraya A, Wacharapluesadee S, Khawplod P, Tepsumethanon S, Briggs D, Asawavichienjinda T, Hemachudha T. A preliminary study of chemo- and cytokine responses in rabies vaccine recipients of intradermal and intramuscular regimens. Vaccine. 2010 May 12.
17. Wacharapluesadee S, Hemachudha T. Ante- and post-mortem diagnosis of rabies using nucleic acid-amplification tests. Expert Rev Mol Diagn. 2010 Mar;10(2):207-18.
18. Shantavasinkul P, Tantawichien T, Wacharapluesadee S, Jeamanukoolkit A, Udomchaisakul P, Chattranukulchai P, Wongsaroj P, Khawplod P, Wilde H, Hemachudha T. Failure of rabies postexposure prophylaxis in patients presenting with unusual manifestations. Clin Infect Dis. 2010 Jan 1;50(1):77-9.
19. Wacharapluesadee S, Boongird B, Wanghongsa S, Ratanasetyuth N, Supavonwong P, Saengsen D, Gongal G. N., Hemachudha T. A Longitudinal Study of the Prevalence of Nipah Virus in Pteropus lylei Bats in Thailand: evidence for seasonal preference in disease transmission. Vector Borne Zoonotic Dis. 2010 Mar;10(2):183-90.
20. Wilde H, Wacharapluesadee S, Hemachudha T and Tepsumethanon V. Rabies. In: Kris Heggenhougen and Stella Quah, editors International Encyclopedia of Public Health, Vol 5. San Diego: Academic Press; 2008. pp. 463-470.
21. Wacharapluesadee S, Sutipanya J, Damrongwatanapokin S, Phumesin P, Chamnanpood P, Leowijuk C, Hemachudha T. Development of a TaqMan real-time RT-PCR assay for the detection of rabies virus.J Virol Methods. 2008 Aug;151(2):317-20.
22. Laothamatas J, Wacharapluesadee S, Lumlertdacha B, Ampawong S, Tepsumethanon V, Shuangshoti S, Phumesin P, Asavaphatiboon S, Worapruekjaru L, Avihingsanon Y, Israsena N, Lafon M, Wilde H, Hemachudha T.Furious and paralytic rabies of canine origin: neuroimaging with virological and cytokine studies.J Neurovirol. 2008 Apr;14(2):119-29.
23. Wacharapluesadee S, Hemachudha T. Duplex nested RT-PCR for detection of Nipah virus RNA from urine specimens of bats. J Virol Methods. 2007 Apr;141(1):97-101.
24. Hemachudha T, Wacharapluesadee S, Laothamatas J, Wilde H. Rabies. Curr Neurol Neurosci Rep. 2006 Nov;6(6):460-8. Review.
25. Hemachudha T, Sunsaneewitayakul B, Desudchit T, Suankratay C, Sittipunt C, Wacharapluesadee S, Khawplod P, Wilde H, Jackson AC. Failure of therapeutic coma and ketamine for therapy of human rabies. J Neurovirol. 2006 Oct;12(5):407-9.
26. Wacharapluesadee S, Boongird K, Wanghongsa S, Phumesin P, Hemachudha T. Drinking bat blood may be hazardous to your health.Clin Infect Dis. 2006;43:269

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health6
27. Wacharapluesadee S, Ruangvejvorachai P, Hemachudha T. A simple method for detection of rabies viral sequences in 16-year old archival brain specimens with one-week fixation in formalin. J Virol Methods. 2006;134:267-71.
28. Wacharapluesadee S, Lumlertdacha B, Boongird K, Wanghongsa S, Chanhome L, Rollin P, Stockton P, Rupprecht CE, Ksiazek TG, Hemachudha T. Bat Nipah virus, Thailand. Emerg Infect Dis. 2005; 11:1949-51.
29. Lumlertdacha B, Wacharapluesadee S, Denduangboripant J, Ruankaew N, Hoonsuwan W, Puanghat A, Sakarasaeranee P, Briggs D, Hemachudha T. Complex genetic structure of the rabies virus in Bangkok and its surrounding provinces, Thailand: implications for canine rabies control. Trans R Soc Trop Med Hyg. 2006;100:276-81.
30. Juntrakul S, Ruangvejvorachai P, Shuangshoti S, Wacharapluesadee S, Hemachudha T. Mechanisms of escape phenomenon of spinal cord and brainstem in human rabies. BMC Infect Dis. 2005; 5:104.
31. Lumlertdacha B, Wacharapluesadee S, Chanhome L, Hemachudha T. Bat lyssavirus in Thailand. J Med Assoc Thai. 2005; 88:1011-4.
32. Wacharapluesadee S, Hemachudha T. Rabies diagnosis in human. J Med Assoc Thai. 2005; 88:859-66.
33. Sintunawa J, Wacharapluesadee S, Wilde H, Hemachudha T. Paradigm shift in rabies control. J Med Assoc Thailand 2004; 87:1530-8.
34. Lumlertdacha B, Boongird K, Wanghongsa S, Wacharapluesadee S, Chanhome L, Khawplod P, Hemachudha T, Kuzmin I, Rupprecht CE. Survey for Bat Lyssaviruses in Thailand. Emerg Infect Dis 2005; 11:232-236.
35. Hemachudha T, Wacharapluesadee S, Mitrabhakdi E, Wilde H, Morimoto K, Lewis RA. Pathophysiology of human paralytic rabies. J Neurovirol 2005:11:93-100.
36. Hemachudha T, Wacharapluesadee S. Ante mortem diagnosis of human rabies. Clin Infect Dis 2004: 39:1085-6.
37. Suja MS, Mahadevan A, Sundaram C, Mani J, Chandrashekhar Sagar B, Hemachudha T, Wacharapluesadee S, Denduangboripant J, Madhusudana SN, Shankar SK. Rabies encephalitis following fox bite. Histological and Immunohistochemical evaluation of lesions caused by virus. Clin Neuropathol. 2004; 23:271-6.
38. Sitprija V, Sriarron C, Lumlertdaecha B, Phumesin P, Khawplod P, Wacharapluesadee S, Wilde H, Hemachudha T. Does contact with urine and blood of a rabies infected dog represent rabies risk? Clin Infect Dis 2003:37:1399-400.
39. Hemachudha T, Wacharapluesadee S, Lumlertdaecha B, Orciari LA, Rupprecht CE, La-ongpant M, Juntrakul S, Denduangboripant J . Sequence analysis of rabies virus in humans exhibiting furious or paralytic rabies. J Infect Dis 2003:188:960-6.
40. Hemachudha T, Sunsaneewitayakul B, Mitrabhakdi E, Suankratay C, Laothamathas J, Wacharapluesadee S, Khawplod P, Wilde H. Paralytic complications following intravenous rabies immune globulin treatment in a patient with furious rabies. Int J Infect Dis 2003:7:76-7
41. Wacharapluesadee S, Phumesin P, Hemachudha T. Dried brain spot in the diagnosis of human and animal rabies. Clin Infect Dis 2003; 36: 674-5.
42. Wacharapluesadee S, Hemachudha T.Urine as a source of rabies RNA detaction in the diagnosis of human rabies. Clinical Infectious Dieases. 2002; 34:874-5.
43. Hemachudha T, Mitrabhakdi E, Wacharapluesadee S. Clinical features of human encephalitic and paralytic rabies. Rabies control in Asia. John Libbey
44. Wacharapluesadee S, Hemachudha T. Rapid diagnosis of human rabies using nucleic acid sequence based amplification. Lancet 2001;358:892-93.Eurotext, Paris 2001; 10-19.
Book’s chapter 1. Wilde H, Hemachudha T, Wacharapluesadee S. Rabies chapter. Tropical Diseases in Travalers. Blackwell.2009. 2. Wilde H, Wacharapluesadee S, Hemachudha T, Tepsumethanon V. Rabies.International Encyclopedia of Public Health. Editor HK Heggenhaugen. Academic Press. San Diego, Cal. 2008 3. Hemachudha T, Mitrabhakdi E, Wacharapluesadee S. Clinical features of human encephalitic and paralytic rabies. Rabies control in Asia. John Libbey Eurotext, Paris 2001, 10-18.
Address
WHO Collaborating Centre for Research and Training on Viral Zoonoses Faculty of Medicine, Chulalongkorn University Patumwan, Bangkok 10330, Thailand Tel:(662) 256 4000, ext 3561 Fax:(662) 652 3122, Email: [email protected]

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 7
27. Wacharapluesadee S, Ruangvejvorachai P, Hemachudha T. A simple method for detection of rabies viral sequences in 16-year old archival brain specimens with one-week fixation in formalin. J Virol Methods. 2006;134:267-71.
28. Wacharapluesadee S, Lumlertdacha B, Boongird K, Wanghongsa S, Chanhome L, Rollin P, Stockton P, Rupprecht CE, Ksiazek TG, Hemachudha T. Bat Nipah virus, Thailand. Emerg Infect Dis. 2005; 11:1949-51.
29. Lumlertdacha B, Wacharapluesadee S, Denduangboripant J, Ruankaew N, Hoonsuwan W, Puanghat A, Sakarasaeranee P, Briggs D, Hemachudha T. Complex genetic structure of the rabies virus in Bangkok and its surrounding provinces, Thailand: implications for canine rabies control. Trans R Soc Trop Med Hyg. 2006;100:276-81.
30. Juntrakul S, Ruangvejvorachai P, Shuangshoti S, Wacharapluesadee S, Hemachudha T. Mechanisms of escape phenomenon of spinal cord and brainstem in human rabies. BMC Infect Dis. 2005; 5:104.
31. Lumlertdacha B, Wacharapluesadee S, Chanhome L, Hemachudha T. Bat lyssavirus in Thailand. J Med Assoc Thai. 2005; 88:1011-4.
32. Wacharapluesadee S, Hemachudha T. Rabies diagnosis in human. J Med Assoc Thai. 2005; 88:859-66.
33. Sintunawa J, Wacharapluesadee S, Wilde H, Hemachudha T. Paradigm shift in rabies control. J Med Assoc Thailand 2004; 87:1530-8.
34. Lumlertdacha B, Boongird K, Wanghongsa S, Wacharapluesadee S, Chanhome L, Khawplod P, Hemachudha T, Kuzmin I, Rupprecht CE. Survey for Bat Lyssaviruses in Thailand. Emerg Infect Dis 2005; 11:232-236.
35. Hemachudha T, Wacharapluesadee S, Mitrabhakdi E, Wilde H, Morimoto K, Lewis RA. Pathophysiology of human paralytic rabies. J Neurovirol 2005:11:93-100.
36. Hemachudha T, Wacharapluesadee S. Ante mortem diagnosis of human rabies. Clin Infect Dis 2004: 39:1085-6.
37. Suja MS, Mahadevan A, Sundaram C, Mani J, Chandrashekhar Sagar B, Hemachudha T, Wacharapluesadee S, Denduangboripant J, Madhusudana SN, Shankar SK. Rabies encephalitis following fox bite. Histological and Immunohistochemical evaluation of lesions caused by virus. Clin Neuropathol. 2004; 23:271-6.
38. Sitprija V, Sriarron C, Lumlertdaecha B, Phumesin P, Khawplod P, Wacharapluesadee S, Wilde H, Hemachudha T. Does contact with urine and blood of a rabies infected dog represent rabies risk? Clin Infect Dis 2003:37:1399-400.
39. Hemachudha T, Wacharapluesadee S, Lumlertdaecha B, Orciari LA, Rupprecht CE, La-ongpant M, Juntrakul S, Denduangboripant J . Sequence analysis of rabies virus in humans exhibiting furious or paralytic rabies. J Infect Dis 2003:188:960-6.
40. Hemachudha T, Sunsaneewitayakul B, Mitrabhakdi E, Suankratay C, Laothamathas J, Wacharapluesadee S, Khawplod P, Wilde H. Paralytic complications following intravenous rabies immune globulin treatment in a patient with furious rabies. Int J Infect Dis 2003:7:76-7
41. Wacharapluesadee S, Phumesin P, Hemachudha T. Dried brain spot in the diagnosis of human and animal rabies. Clin Infect Dis 2003; 36: 674-5.
42. Wacharapluesadee S, Hemachudha T.Urine as a source of rabies RNA detaction in the diagnosis of human rabies. Clinical Infectious Dieases. 2002; 34:874-5.
43. Hemachudha T, Mitrabhakdi E, Wacharapluesadee S. Clinical features of human encephalitic and paralytic rabies. Rabies control in Asia. John Libbey
44. Wacharapluesadee S, Hemachudha T. Rapid diagnosis of human rabies using nucleic acid sequence based amplification. Lancet 2001;358:892-93.Eurotext, Paris 2001; 10-19.
Book’s chapter 1. Wilde H, Hemachudha T, Wacharapluesadee S. Rabies chapter. Tropical Diseases in Travalers. Blackwell.2009. 2. Wilde H, Wacharapluesadee S, Hemachudha T, Tepsumethanon V. Rabies.International Encyclopedia of Public Health. Editor HK Heggenhaugen. Academic Press. San Diego, Cal. 2008 3. Hemachudha T, Mitrabhakdi E, Wacharapluesadee S. Clinical features of human encephalitic and paralytic rabies. Rabies control in Asia. John Libbey Eurotext, Paris 2001, 10-18.
Address
WHO Collaborating Centre for Research and Training on Viral Zoonoses Faculty of Medicine, Chulalongkorn University Patumwan, Bangkok 10330, Thailand Tel:(662) 256 4000, ext 3561 Fax:(662) 652 3122, Email: [email protected]

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health8
Dr. Flavie Luce Goutard
Organisation: CIRAD Current job title: Researcher epidemiologist
Dr Flavie Goutard is a veterinarian specialised in applied epidemiology. She works for CIRAD since 2005 within the research unit AGIRs. She has 15 years of experience in the field of infectious diseases epidemiology in tropical countries, working mainly on the development of adapted surveillance and control strategies for animal diseases in rural settings. She worked as an international consultant for the FAO and OIE in the development of training course in epidemiology. Her recent research focus on participatory epidemiology, evaluation of surveillance, risk assessment and on the ways to improve zoonotic diseases detection with risk-based methodology. She is actually adjunct professor at Kasetsart University, Bangkok, Thailand, coordinating the creation of a new Master Program in One Health field.
Dr. Serge MORAND, PhD, DR1 CNRS
Serge Morand is interested in evolutionary ecology of host-parasite interactions and population ecology of parasites and pathogens. Field parasitologist, he is concerned at the role of biodiversity as risks and insurance for zoonotic emerging infectious diseases. He is conducting several projects on the impacts of global changes (climate, land use, biodiversity loss) on the links between biodiversity and health in Southeast Asia, using rodent-borne diseases as a model. Serge Morand is member of the scientific board of the French Research Foundation for Biodiversity (FRB). Address: Centre Christophe Mérieux, CIRAD-AGIRs, Vientiane, Lao PDR Adjunct Professor: Department of Helminthology, Faculty of Tropical Medicine, Mahidol University Education: Ms.Sc Thesis, 1983, University of Rennes 1 (France) Ph.D. Thesis, 1988 University of Rennes 1 (France) Royal Society Fellow, 1995, Department of Zoology, University of Oxford (UK) Current projects in Southeast Asia 2012-2015 Project ANR BiodivHealthSEA “Local impacts and perceptions of global changes: health, biodiversity and zoonoses in Southeast Asia” (Coordinator) www.biodivhealthsea.org 2008-2012: Project ANR CERoPath
www.ceropath.org 2013-2014 Project AFD-CNRS PathoDivSEA “Pathogen diversity in Southeast Asia” Scientific production >300 refereed papers in international journals, 33 book chapters, 10 books Last books in press: Morand S, Krasnov, Tim Littlewood T (eds) (2014) Parasite diversity and diversification: evolutionary ecology meets phylogenetics. Cambridge University Press (in press) Morand S, Dujardin J-P, Lefait-Rollin R, Apiwathnasorn C (eds) (2014) Socio-ecological dimensions of Infectious Diseases. Springer Singapore (in prep)

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 9
Dr. Flavie Luce Goutard
Organisation: CIRAD Current job title: Researcher epidemiologist
Dr Flavie Goutard is a veterinarian specialised in applied epidemiology. She works for CIRAD since 2005 within the research unit AGIRs. She has 15 years of experience in the field of infectious diseases epidemiology in tropical countries, working mainly on the development of adapted surveillance and control strategies for animal diseases in rural settings. She worked as an international consultant for the FAO and OIE in the development of training course in epidemiology. Her recent research focus on participatory epidemiology, evaluation of surveillance, risk assessment and on the ways to improve zoonotic diseases detection with risk-based methodology. She is actually adjunct professor at Kasetsart University, Bangkok, Thailand, coordinating the creation of a new Master Program in One Health field.
Dr. Serge MORAND, PhD, DR1 CNRS
Serge Morand is interested in evolutionary ecology of host-parasite interactions and population ecology of parasites and pathogens. Field parasitologist, he is concerned at the role of biodiversity as risks and insurance for zoonotic emerging infectious diseases. He is conducting several projects on the impacts of global changes (climate, land use, biodiversity loss) on the links between biodiversity and health in Southeast Asia, using rodent-borne diseases as a model. Serge Morand is member of the scientific board of the French Research Foundation for Biodiversity (FRB). Address: Centre Christophe Mérieux, CIRAD-AGIRs, Vientiane, Lao PDR Adjunct Professor: Department of Helminthology, Faculty of Tropical Medicine, Mahidol University Education: Ms.Sc Thesis, 1983, University of Rennes 1 (France) Ph.D. Thesis, 1988 University of Rennes 1 (France) Royal Society Fellow, 1995, Department of Zoology, University of Oxford (UK) Current projects in Southeast Asia 2012-2015 Project ANR BiodivHealthSEA “Local impacts and perceptions of global changes: health, biodiversity and zoonoses in Southeast Asia” (Coordinator) www.biodivhealthsea.org 2008-2012: Project ANR CERoPath
www.ceropath.org 2013-2014 Project AFD-CNRS PathoDivSEA “Pathogen diversity in Southeast Asia” Scientific production >300 refereed papers in international journals, 33 book chapters, 10 books Last books in press: Morand S, Krasnov, Tim Littlewood T (eds) (2014) Parasite diversity and diversification: evolutionary ecology meets phylogenetics. Cambridge University Press (in press) Morand S, Dujardin J-P, Lefait-Rollin R, Apiwathnasorn C (eds) (2014) Socio-ecological dimensions of Infectious Diseases. Springer Singapore (in prep)

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health10
Assoc. Prof. Dr. Narong Kitpanit, Ph.D.
Dr.Narong Kitpanit was graduated the degree of Doctor of Veterinary Medicine in 1965. He obtained Post-graduate Diploma in Animal Science from the University of Copanhagen in 1974 and PhD. degree in Animal Science from the Tokyo University of Agriculture in 1980. Dr.Kitpanit was engaged in teaching career at Khonkaen University where he had Contributed to established the Faculty of Veterinary Medicine in 1986. He has long been involved in small animal practice and his main interest in Dermatology. He had published the guide book in small animal clinical practice and practical dermatology. He was often invited from Technical conferences to share his past experiences. In 1998, he was honoured the award as the Veterinary Practitioner of the Year from the Veterinary practitioner Association of Thailand. Dr.Narong Kitpanit is currently the Director of Suanluang Animal Hospital in Bangkok.
Assoc. Prof. Dr. Sanipa Suradhat, Ph.D.
Assoc. Prof. Dr. Sanipa is a Thai veterinarian with a DVM degree from Chulalongkorn University, Thailand, and a PhD from the Department of Veterinary Microbiology, University of Saskatchewan, Saskatoon, Canada. She is currently an Associate Professor at the Department of Veterinary Microbiology and an Associate Dean for Policy and Planning Affairs at the Faculty of Veterinary Science, Chulalongkorn University. Dr. Sanipa’s research interest include the fields of immunology and vaccinology. She has also been involved in research activities related to emerging infectious viral diseases in animals and served as the executive committee at the Chulalongkorn University Center of Excellence in Emerging Infectious Diseases in Animals (CU-EIDAs). Since 2012, Dr. Sanipa has joined the Regional Support Unit at the Emergency Center for Transboundary Animal Diseases, Food and Agriculture Organization of the United Nations for Asia and the Pacific (FAO-ECTAD-RAP) as the Regional Laboratory Network Coordinator, supporting development of diagnostic capacity in Asia in partnership with WHO, OIE, ASEAN and a number of countries in South and Southeast Asia.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 11
Assoc. Prof. Dr. Narong Kitpanit, Ph.D.
Dr.Narong Kitpanit was graduated the degree of Doctor of Veterinary Medicine in 1965. He obtained Post-graduate Diploma in Animal Science from the University of Copanhagen in 1974 and PhD. degree in Animal Science from the Tokyo University of Agriculture in 1980. Dr.Kitpanit was engaged in teaching career at Khonkaen University where he had Contributed to established the Faculty of Veterinary Medicine in 1986. He has long been involved in small animal practice and his main interest in Dermatology. He had published the guide book in small animal clinical practice and practical dermatology. He was often invited from Technical conferences to share his past experiences. In 1998, he was honoured the award as the Veterinary Practitioner of the Year from the Veterinary practitioner Association of Thailand. Dr.Narong Kitpanit is currently the Director of Suanluang Animal Hospital in Bangkok.
Assoc. Prof. Dr. Sanipa Suradhat, Ph.D.
Assoc. Prof. Dr. Sanipa is a Thai veterinarian with a DVM degree from Chulalongkorn University, Thailand, and a PhD from the Department of Veterinary Microbiology, University of Saskatchewan, Saskatoon, Canada. She is currently an Associate Professor at the Department of Veterinary Microbiology and an Associate Dean for Policy and Planning Affairs at the Faculty of Veterinary Science, Chulalongkorn University. Dr. Sanipa’s research interest include the fields of immunology and vaccinology. She has also been involved in research activities related to emerging infectious viral diseases in animals and served as the executive committee at the Chulalongkorn University Center of Excellence in Emerging Infectious Diseases in Animals (CU-EIDAs). Since 2012, Dr. Sanipa has joined the Regional Support Unit at the Emergency Center for Transboundary Animal Diseases, Food and Agriculture Organization of the United Nations for Asia and the Pacific (FAO-ECTAD-RAP) as the Regional Laboratory Network Coordinator, supporting development of diagnostic capacity in Asia in partnership with WHO, OIE, ASEAN and a number of countries in South and Southeast Asia.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health12
Dr. Pierre Echaubard
I am using host-parasite interactions as a model system to investigate evolutionary and ecological mechanisms. The questions I am particularly interested in are local adaptation, the evolution of virulence and resistance/tolerance and more recently the link between community processes, host-parasite coevolutionary dynamics and disease transmission. I use a wide variety of conceptual framework and methodologies ranging from population genetics, life history evolution, coevolution theory and evolutionary epidemiology and design both lab and field experiments to address my research questions. While focusing mainly on theoretical aspects of host-pathogens coevolutionary dynamics, I’m also eager to promote the dialogue between basic and applied research in disease ecology through collaborations with conservation and public health authorities. My current research focuses on understanding the eco-evolutionary determinants of Opistorchis viverrini transmission in rural northeastern Thailand, and to provide novel conceptual perspectives to delineate sustainable strategies of disease control.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 13
Dr. Pierre Echaubard
I am using host-parasite interactions as a model system to investigate evolutionary and ecological mechanisms. The questions I am particularly interested in are local adaptation, the evolution of virulence and resistance/tolerance and more recently the link between community processes, host-parasite coevolutionary dynamics and disease transmission. I use a wide variety of conceptual framework and methodologies ranging from population genetics, life history evolution, coevolution theory and evolutionary epidemiology and design both lab and field experiments to address my research questions. While focusing mainly on theoretical aspects of host-pathogens coevolutionary dynamics, I’m also eager to promote the dialogue between basic and applied research in disease ecology through collaborations with conservation and public health authorities. My current research focuses on understanding the eco-evolutionary determinants of Opistorchis viverrini transmission in rural northeastern Thailand, and to provide novel conceptual perspectives to delineate sustainable strategies of disease control.
Eakkasit Barameechaithanan, DVM Veterinary Practitioner Veterinary Teaching Hospital Faculty of Veterinary Medicine Khon Kaen University Education: DVM 2007, Mahanakorn University of Technology, Thailand

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health14
Prof. Romziah Sidik, Ph.D. DVM.
Department of Animal Husbandry Graduate School of Faculty of Veterinary Medicine Airlangga University ACADEMIC DEGREES: DVM. 1978 Airlangga University (Faculty of Veterinary Medicine) Ph.D. 1987 University Putra Malaysia (Faculty of Veterinary Medicine and Animal Science) PROFESSIONAL APPOINTMENTS: 1978 - 1990 Lecturer, Faculty of Veterinary Medicine, Airlangga University 1990 - 2005 Associate Professor, Faculty of Veterinary Medicine, Airlangga University 2005 - up to now Professor, of Faculty of Veterinary Medicine, Airlangga University EXPERIENCES: 2005 - 2010 Dean, Faculty of Veterinary Medicine, Airlangga University 2010 - up to now Dean, Faculty of Veterinary Medicine, Airlangga University 2010 - 2013 Secretary of Indonesian Veterinary School Association (IVSA) 2010 - 2013 Vice President of Southeast Asian Veterinary Schools Association(SEAVSA) 2012 - up to now President of Asian Veterinary Schools Association (AAVS) RESEARCH INTERESTS:
Animal Nutrition
Animal Production
Animal Health
Animal Welfare
Asst. Prof. Dr. Nongyao Kasatpibal, RN, MNS, PhD.
Faculty of Nursing, Chiang Mai University Muang, Chiang Mai 50200, Thailand E-mail: [email protected] Assistant Professor Dr. Nongyao Kasatpibal obtained her Bachelor of Science in Nursing and Midwifery degree in 1988 from Faculty of Nursing, Chiang Mai University. In 1997, she graduated with a Master's degree in nursing specializing as an infection control nurse from Faculty of Nursing, Chiang Mai University. She completed her PhD in Epidemiology from Faculty of Medicine, Prince of Songkla University in 2006.
In 2007, WHO invited her to work as a WHO Temporary Adviser in Prevention Infection for the Global Patient Safety Challenge "Safe Surgery, Saves Lives" from 2007 to 2009.
From 2009 to present, she has been the Committee for the National Seminar on Infection Control, Thailand (Research Affairs)
In 2009, she got an international award, The Society for Healthcare Epidemiology of America (SHEA) International Ambassador Program Award.
From 2011 to present, she has had an opportunity to be a sub-committee to develop the Thai National Guidelines in Infection Control.
In 2013, she was a co-author of One Health Course and One Health Module Facilitator Guide, organized by USAID.
From 2013 to present, she is also a principal investigator and organizer of the 1) Trans-disciplinary Capacity Building of THOHUN and VOHUN for Streptococcus suis Infection Prevention: Training of the Trainers, and 2) Development of Training Program & Educational Materials for Prevention of Streptococcus suis Infection.
In summary, Dr. Nongyao has involved in a global movement to endeavor the aspect of infection prevention and control.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 15
Prof. Romziah Sidik, Ph.D. DVM.
Department of Animal Husbandry Graduate School of Faculty of Veterinary Medicine Airlangga University ACADEMIC DEGREES: DVM. 1978 Airlangga University (Faculty of Veterinary Medicine) Ph.D. 1987 University Putra Malaysia (Faculty of Veterinary Medicine and Animal Science) PROFESSIONAL APPOINTMENTS: 1978 - 1990 Lecturer, Faculty of Veterinary Medicine, Airlangga University 1990 - 2005 Associate Professor, Faculty of Veterinary Medicine, Airlangga University 2005 - up to now Professor, of Faculty of Veterinary Medicine, Airlangga University EXPERIENCES: 2005 - 2010 Dean, Faculty of Veterinary Medicine, Airlangga University 2010 - up to now Dean, Faculty of Veterinary Medicine, Airlangga University 2010 - 2013 Secretary of Indonesian Veterinary School Association (IVSA) 2010 - 2013 Vice President of Southeast Asian Veterinary Schools Association(SEAVSA) 2012 - up to now President of Asian Veterinary Schools Association (AAVS) RESEARCH INTERESTS:
Animal Nutrition
Animal Production
Animal Health
Animal Welfare
Asst. Prof. Dr. Nongyao Kasatpibal, RN, MNS, PhD.
Faculty of Nursing, Chiang Mai University Muang, Chiang Mai 50200, Thailand E-mail: [email protected] Assistant Professor Dr. Nongyao Kasatpibal obtained her Bachelor of Science in Nursing and Midwifery degree in 1988 from Faculty of Nursing, Chiang Mai University. In 1997, she graduated with a Master's degree in nursing specializing as an infection control nurse from Faculty of Nursing, Chiang Mai University. She completed her PhD in Epidemiology from Faculty of Medicine, Prince of Songkla University in 2006.
In 2007, WHO invited her to work as a WHO Temporary Adviser in Prevention Infection for the Global Patient Safety Challenge "Safe Surgery, Saves Lives" from 2007 to 2009.
From 2009 to present, she has been the Committee for the National Seminar on Infection Control, Thailand (Research Affairs)
In 2009, she got an international award, The Society for Healthcare Epidemiology of America (SHEA) International Ambassador Program Award.
From 2011 to present, she has had an opportunity to be a sub-committee to develop the Thai National Guidelines in Infection Control.
In 2013, she was a co-author of One Health Course and One Health Module Facilitator Guide, organized by USAID.
From 2013 to present, she is also a principal investigator and organizer of the 1) Trans-disciplinary Capacity Building of THOHUN and VOHUN for Streptococcus suis Infection Prevention: Training of the Trainers, and 2) Development of Training Program & Educational Materials for Prevention of Streptococcus suis Infection.
In summary, Dr. Nongyao has involved in a global movement to endeavor the aspect of infection prevention and control.
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health16
Sakdid Anulomsombat
Senior Specialist, Betagro Group
Sakdid Anulomsombat educations are Doctor of Veterinary Medicine and Master’s degree in Science, Veterinary Public Health at Chulalongkorn University. After graduated, I started my profession as a Vet Practitioner at Thonglor Small Animal Hospital and later as a Quality Assurance Manager with the World leader airline catering, LSG Sky Chefs, Lufthansa in Thailand. In 2003, I joined the work at Betagro as an Assistant Manager, Food safety & Quality Assurance Office. My responsibilities were implementing, developing, auditing and training of food safety and quality assurance systems such as Good Agricultural Practice, Good Manufacturing Practice, HACCP for poultry, swine and food business. At the present, I have worked as a senior specialist at CEO office since February 2014. My hobbies are travelling, gardening and biking.
Mr. Fumihiko Sano
FFA’s Activity for Food Safety, Ajinomoto Frozen Foods Co. Mr. Sano received his Master of Engineering from Tokyo Institute of Technology in 1999. He entered Ajinomoto Co., Food Research Institute in 1999. From 2008, he works at Ajinomoto Frozen Foods (Thailand). Current position is the General Manager of Thai Division Laboratory, R&D Center.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 17
Sakdid Anulomsombat
Senior Specialist, Betagro Group
Sakdid Anulomsombat educations are Doctor of Veterinary Medicine and Master’s degree in Science, Veterinary Public Health at Chulalongkorn University. After graduated, I started my profession as a Vet Practitioner at Thonglor Small Animal Hospital and later as a Quality Assurance Manager with the World leader airline catering, LSG Sky Chefs, Lufthansa in Thailand. In 2003, I joined the work at Betagro as an Assistant Manager, Food safety & Quality Assurance Office. My responsibilities were implementing, developing, auditing and training of food safety and quality assurance systems such as Good Agricultural Practice, Good Manufacturing Practice, HACCP for poultry, swine and food business. At the present, I have worked as a senior specialist at CEO office since February 2014. My hobbies are travelling, gardening and biking.
Mr. Fumihiko Sano
FFA’s Activity for Food Safety, Ajinomoto Frozen Foods Co. Mr. Sano received his Master of Engineering from Tokyo Institute of Technology in 1999. He entered Ajinomoto Co., Food Research Institute in 1999. From 2008, he works at Ajinomoto Frozen Foods (Thailand). Current position is the General Manager of Thai Division Laboratory, R&D Center.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health18
Dr. Virginia Rentko, VMD DACVIM
Name and degrees Virginia Rentko, VMD DACVIM
Place of Birth or Citizenship Philadelphia, PA
Present Business Address 200 Westboto Rd North Grafton MA 01536
Undergraduate Education (College) Bachelor of Arts, 1981, Biology cum laude: Boston University
Advanced Degree(s) VMD - 1987, University of Pennyslvania MS - Zoology, 1983, The Ohio State University Thesis: Characterization of Type I Phosphodiesterase activity from the brush-border membrane of the rat tapeworm, Hymenolepis dimunita.
Board Certification Diplomate, American College of Veterinary Internal Medicine
Present Title/Position 1) Medical Director, Tufts Cummings School Veterinary Medicine, Foster Hospital for
Small Animals and Hospital for Large Animals 2) Clinical Associate Professor
Professional Positions Hospital Director, Tufts Veterinary Emergency Treatment and Specialties, 2009-2011 Vice President, Preclinical Research, Biopure Corporation, 2001-2008 Vice President, Veterinary Medicine, Biopure Corporation, 1998-2001 Director, Veterinary Medicine, Biopure Corporation, 1991-1998 Residency Internal Medicine, Tufts University, 1988-1991 Internship University of Pennsylvania, 1987-1988
Administrative Positions 1. Chair, Biopure IACUC Committee, 1992-2002 2. Executive Director, Association of Veterinary Hematology and Transfusion Medicine,
2000-2004 3. Executive Committee Member, Biopure Corporate Strategic Planning, 2000-2008 4. Dean’s Council, 2011- present 5. Executive Faculty Board, 2011-present 6. ACVIM Education and Research Committee, 2012- present 7. Ad hoc Communications Committee (2012-present) 8. Provost’s Strategic Planning Committee on Entrepreneurship and Innovation (2013) 9. Executive Committee Member, Veterinary Management Group (Equine Academic
Hospitals) 2013-present Professional Society Membership
Massachusetts Veterinary Medical Association American Veterinary Medical Association American College of Veterinary Internal Medicine Association of Veterinary Hematology and Transfusion Medicine
Honors and Other Distinction
Student-awarded, Outstanding Small Animal Medicine Resident Award, 1990 Committees 1. Outside University
1. Chair, Biopure IACUC Committee, 1992-2002 2. Executive Director, Association of Veterinary Hematology and Transfusion Medicine, 2000-2004 3. Executive Committee Member, Biopure Corporate Strategic Planning, 2000-2008 4. Education and Research Committee, American College of Veterinary Internal Medicine, 2012-2015. 5. Executive Committee Member, Veterinary Management Group (Equine Academic Hospitals) 2013-present
Editorial Review (Journals): Vet Pharm Therap, ad hoc reviewer (2005-2009) 4-5/yr] Vet Technician; ad hoc reviewer (2005-present) [4-5/yr]
2. Within University
Executive Faculty Board 2011- present Dean’s Council 2011- present Provost’s Strategic Planning Entrepreneurship and Innovation Working Group, 2012
Research Interests (Past and Present) Hemoglobin based oxygen carrying solutions
Hematology, Red cell disorders Small animal internal medicine

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 19
Dr. Virginia Rentko, VMD DACVIM
Name and degrees Virginia Rentko, VMD DACVIM
Place of Birth or Citizenship Philadelphia, PA
Present Business Address 200 Westboto Rd North Grafton MA 01536
Undergraduate Education (College) Bachelor of Arts, 1981, Biology cum laude: Boston University
Advanced Degree(s) VMD - 1987, University of Pennyslvania MS - Zoology, 1983, The Ohio State University Thesis: Characterization of Type I Phosphodiesterase activity from the brush-border membrane of the rat tapeworm, Hymenolepis dimunita.
Board Certification Diplomate, American College of Veterinary Internal Medicine
Present Title/Position 1) Medical Director, Tufts Cummings School Veterinary Medicine, Foster Hospital for
Small Animals and Hospital for Large Animals 2) Clinical Associate Professor
Professional Positions Hospital Director, Tufts Veterinary Emergency Treatment and Specialties, 2009-2011 Vice President, Preclinical Research, Biopure Corporation, 2001-2008 Vice President, Veterinary Medicine, Biopure Corporation, 1998-2001 Director, Veterinary Medicine, Biopure Corporation, 1991-1998 Residency Internal Medicine, Tufts University, 1988-1991 Internship University of Pennsylvania, 1987-1988
Administrative Positions 1. Chair, Biopure IACUC Committee, 1992-2002 2. Executive Director, Association of Veterinary Hematology and Transfusion Medicine,
2000-2004 3. Executive Committee Member, Biopure Corporate Strategic Planning, 2000-2008 4. Dean’s Council, 2011- present 5. Executive Faculty Board, 2011-present 6. ACVIM Education and Research Committee, 2012- present 7. Ad hoc Communications Committee (2012-present) 8. Provost’s Strategic Planning Committee on Entrepreneurship and Innovation (2013) 9. Executive Committee Member, Veterinary Management Group (Equine Academic
Hospitals) 2013-present Professional Society Membership
Massachusetts Veterinary Medical Association American Veterinary Medical Association American College of Veterinary Internal Medicine Association of Veterinary Hematology and Transfusion Medicine
Honors and Other Distinction
Student-awarded, Outstanding Small Animal Medicine Resident Award, 1990 Committees 1. Outside University
1. Chair, Biopure IACUC Committee, 1992-2002 2. Executive Director, Association of Veterinary Hematology and Transfusion Medicine, 2000-2004 3. Executive Committee Member, Biopure Corporate Strategic Planning, 2000-2008 4. Education and Research Committee, American College of Veterinary Internal Medicine, 2012-2015. 5. Executive Committee Member, Veterinary Management Group (Equine Academic Hospitals) 2013-present
Editorial Review (Journals): Vet Pharm Therap, ad hoc reviewer (2005-2009) 4-5/yr] Vet Technician; ad hoc reviewer (2005-present) [4-5/yr]
2. Within University
Executive Faculty Board 2011- present Dean’s Council 2011- present Provost’s Strategic Planning Entrepreneurship and Innovation Working Group, 2012
Research Interests (Past and Present) Hemoglobin based oxygen carrying solutions
Hematology, Red cell disorders Small animal internal medicine

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health20

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 21
Speaker’s Notes

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health22

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 23
Emerging Zoonotic Diseases: Global and Local perspectives
Michael Kosoy Division of Vector-Borne Diseases,
National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention (CDC), Fort Collins, Colorado USA
The current situation in studies of zoonotic infectious diseases can be characterized by two trends. The first is exponential progress in the development of new methods for identifying and studying zoonoses resulting in a rapidly increasing number of new publications. The second is a growing worldwide microbial threat made evident in the appearance of novel zoonotic diseases and the extensive spread of pathogens not considered dangerous in previous decades. There are many factors contributing to both trends. In the keynote I wish to emphasize an underlying phenomenon of increasing disconnection between the accruing body of information about zoonotic pathogens, infected animals, influence of environmental factors on epidemic processes, and our limited understanding of infectious processes. The concept of emergence was developed as a central element of the scientific paradigm that generally is called as “science of complexity”. Emergence refers to how manifestation at a larger scale arises from the detailed structure and relationships at a detail scale. It was not accidentally that very soon after introduction of this concept of emergence into general science it found an application in the description of infectious diseases. The infectious diseases represent very complex systems. The key event in the emergence of most infectious diseases is a change in host–parasite ecology. However, any parasitic system exists in the natural or anthropogenically modified environment that provides more complexities and making a prediction of the trends in developing infectious diseases much harder. Commonly investigators detect infected animals in a particular area, and microbial agents are identified in laboratories according to accepted criteria, but after that we try to estimate the increased risk of the distribution and prevalence of some diseases for an extensive territory, potentially on global scale. We might consider details that are important from the perspective of public health or veterinary medicine, for example emphasizing the number of human or animal cases. This is important, but a simplification of the parameters that characterize such a complex system as infectious diseases may mask emergent properties. While the importance of emerging diseases is obvious and this term is very widely used in scientific literature and in the media, a selection of different criteria for defining emerging infectious could be challenging. For the convenience purpose, "emerging" infectious diseases are often defined as infections that have newly

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health24
appeared in a population or have existed but are rapidly increasing in incidence or geographic range. The factors for emerging zoonotic diseases can relate to transitions in genetic structure of pathogens; introduction of pathogens to new areas; increased concentration of people and animals within a particular territory; increased contact between animals and people; increased a number of immunocompromised individuals; movement of animals at different scales; and environmental changes caused by natural trends, like climate, or as the direct results of human activities; and many other factors. Besides, an increased number of cases and recognition of diseases as zoonotic in origin can relate to the discovery of new organisms that could not be previously recognized because of the progress in diagnostic methodologies. Despite awareness that disease emergence may be related to ecological change, new studies should analyze the underlying environmental drivers of the dynamics of disease emergence at different scales as ecological change and disease emergence are often mediated through complex and large-scale processes that cannot be explained by traditional approaches to use simplified definitions of pathogens and hosts and reducing complexity of ecological factors. A new model of investigation requires a dynamic shift of perspectives in the ‘simplicity-complexity’ dimension: from virulence factors to multi-sided descriptions of the pathogens; from particular microbes to wide microbial communities; from clinical manifestations to a variety of infectious patterns; from findings of infectious agents to defining a natural focus of the infection as a self-regulated system; from single factors affecting host-parasite relations to the complex ecological context. Various aspects of interactions between hosts, vectors, pathogens, and environmental niches will be discussed.
SEAOHUN – Networking for One Health in South East Asia
Dr. Suwit Somponpun Program Manager, SEAOHUN Foundation
One Health is a concept defined as “the collaborative effort of multiple disciplines working locally, nationally and globally to address critical challenges and attain optimal health for people, domestic and wild animals and the environment”. A One Health approach to responding to outbreaks of emerging infectious diseases, and zoonoses in particular, has been endorsed by three global bodies, FAO, WHO and OIE. Following on from successful programs to respond to regional epidemics of Highly Pathogenic Avian Influenza in poultry, which also threatened the health of people, and in response to an increase in the number of emerging infectious disease threats worldwide, USAID launched the Emerging Pandemic Threats (EPT) Program in 2009. One of the four components of this program, RESPOND, was tasked with providing capacity building assistance to national and regional governments and institutions in SEA. A significant outcome of the RESPOND project was the establishment of SEAOHUN, the South East Asia One Health University Network, and allied country-level networks, INDOHUN, MyOHUN, THOHUN and VOHUN, in Indonesia, Malaysia, Thailand and Vietnam, respectively. The stimulus for the creation of SEAOHUN was a belief that to embed the One Health philosophy in the future leaders of agencies responding to new disease threats, an understanding and acceptance of the principles involved should be emphasized to a young age group, with university students being the most obvious target. The aim of promoting and facilitating the teaching of One Health and the competencies required for One Health is the creation of a ‘new student species’, who upon graduating will become advocates and strong supporters of the necessity for multiple disciplines to work together to combat emerging disease threats. This presentation will outline the establishment and structure of SEAOHUN, the platform activities and strategies undertaken in the first two years of the Network and the future directions for Network members under USAID’s newly proposed Emerging Pandemic Threats 2 program.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 25
SEAOHUN – Networking for One Health in South East Asia
Dr. Suwit Somponpun Program Manager, SEAOHUN Foundation
One Health is a concept defined as “the collaborative effort of multiple disciplines working locally, nationally and globally to address critical challenges and attain optimal health for people, domestic and wild animals and the environment”. A One Health approach to responding to outbreaks of emerging infectious diseases, and zoonoses in particular, has been endorsed by three global bodies, FAO, WHO and OIE. Following on from successful programs to respond to regional epidemics of Highly Pathogenic Avian Influenza in poultry, which also threatened the health of people, and in response to an increase in the number of emerging infectious disease threats worldwide, USAID launched the Emerging Pandemic Threats (EPT) Program in 2009. One of the four components of this program, RESPOND, was tasked with providing capacity building assistance to national and regional governments and institutions in SEA. A significant outcome of the RESPOND project was the establishment of SEAOHUN, the South East Asia One Health University Network, and allied country-level networks, INDOHUN, MyOHUN, THOHUN and VOHUN, in Indonesia, Malaysia, Thailand and Vietnam, respectively. The stimulus for the creation of SEAOHUN was a belief that to embed the One Health philosophy in the future leaders of agencies responding to new disease threats, an understanding and acceptance of the principles involved should be emphasized to a young age group, with university students being the most obvious target. The aim of promoting and facilitating the teaching of One Health and the competencies required for One Health is the creation of a ‘new student species’, who upon graduating will become advocates and strong supporters of the necessity for multiple disciplines to work together to combat emerging disease threats. This presentation will outline the establishment and structure of SEAOHUN, the platform activities and strategies undertaken in the first two years of the Network and the future directions for Network members under USAID’s newly proposed Emerging Pandemic Threats 2 program.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health26
The ONE Health Surveillance on Nipah virus in Thailand
Supaporn Wacharapluesadee1* Prateep Duengkae2 Patarapol Maneeorn3 Sanipa Suradhat4 Rachod Tantilertcharoen4 Chirapol Sintunawa5
Abhinbhen Saraya1 Michael V Callahan6 Pierre Rollin7 Henry Wilde1 and Thiravat Hemachudha1
1WHO-CC for Research and Training on Viral Zoonoses, Faculty of Medicine, Chulalongkorn University Bangkok, 2Faculty of Forestry, Kasetsart University, Bangkok,
3Department of National Parks, Wildlife and Plant Conservation, Ministry of Natural Resources and Environment,
4Center of Excellence in Emerging Infectious Diseases in Animals, Faculty of Veterinary Science, Chulalongkorn University (CU-EIDAs),
5Faculty of Faculty of Environment and Resource Studies, Mahodol University, 6Division of Infectious Diseases Massachusetts General Hospital Harvard Medical School
Boston, Massachusetts, 7 Centers for Disease Control and Prevention, Atlanta, Georgia, USA *Corresponding author:
Supaporn Wacharapluesadee, PhD WHO Collaborating Centre for Research and Training on Viral Zoonoses,
Faculty of Medicine, Chulalongkorn University, Bangkok, 10330, Thailand Tel: (662) 256 4000 ext: 3561, Fax: (662) 652 3122
E-mail address: [email protected]
Nipah virus (NiV) infection is a newly emerging zoonosis that causes severe disease in both animals and humans. Fruit bats of the genus Pteropus are the natural reservoir (Yob et al., 2001; Halpin et al. 2011; Yadav et al. 2012). Thailand borders Malaysia where NiV outbreaks were documented in 1998. Since the initial outbreak of NiV encephalitis in Malaysian abattoir pig workers in 1998 (Chua et al., 2000), there have been more than 25 human outbreaks in India and Bangladesh. The outbreaks in Bangladesh have occurred almost every year since 2001 and tended to be seasonal (Luby et al., 2009; Lo et al., 2012). Humans develop disease from having contact with virus contaminated tissues from infected pigs (Malaysia) (Chua, 2003) or otherwise by drinking bat-contaminated fresh date palm sap (Bangladesh) (Luby et al., 2006). Human-to-human transmission poses a serious threat and has been only documented in Bangladesh (Gurley et al., 2007). Thailand harbors at least 20 million bats with at least 138 species. There are four species of bats of the genus Pteropus, the NiV natural reservoir, roosting in Thailand (P. lylei, P.hypomelanus, P.vampyrus and P.intermedius). Surveys of NiV infection in Thai bats is being conducted since 2002. Three species of Pteropus bats; P. lylei, P.hypomelanus, and P.vampyrus, have been demonstrated to be infected by NiV (Wacharapluesadee et al., 2005). To date there has been no report of pig or human cases of NiV infection in Thailand.
Although NiV infection has been found mainly in 3 species of Pteropus bats, P. lylei is dominant reservoir in Thailand due to its population size (>30,000 bats) and distribution. Its habitat is closer to humans compared to the other two Pteropus species. Seasonal prevalence of NiV transmission in P. lylei has been shown during April-May (Wacharapluesadee et al., 2010). Genetic characterization of NiV found in P. lylei in Thailand, based on 357 base pairs of nucleoprotein gene, indicated 2 existing genotypes: Bangladesh- and Malaysian- like (Wacharapluesadee and Hemachudha, 2007). Although both strains are co-circulating, the Bangladesh-like genotype dominates in P.lylei bat populations (Wacharapluesadee et al., 2013) One health approach in tackling emerging infectious diseases originated from wildlife is mandatory. This requires collaboration among people in different fields of animal and human diseases. This study seeks to demonstrate that a "One Health" approach to disease surveillance can help investigators gain insight into epidemiologic factors influencing disease transmission and thus help public health authorities to implement effective control of zoonotic diseases originating from wildlife. The community based public education and participation is considered as effective prevention measures. The study site was Chonburi province where NiV is endemic in fruit-eating bats, (P.lylei) (Wacharapluesadee et al., 2010). Assessing the risk of Nipah virus emergence at the high risk areas, has been conducted in villagers, pigs, and bats at the areas where NiV infection has been demonstrated in bats. Villagers living among NiV-positive bat colonies were evaluated for high-risk behaviors, for recent cases of encephalitis and underwent serology screening for NiV exposure. Pig’s blood samples from these two farms were collected and tested for NiV IgG antibody. Bats were trapped monthly at two commercial pig farms. The study was done in parallel with studies of NiV transmission within local bat colonies. Blood, saliva and urine was collected from each bat for further investigation. Community risk assessment was carried out by testing for NiV IgG antibody from blood of villagers at Chonburi province, living near the temple with NiV infected bats and by behavioral investigation. Evaluation of basic knowledge on EID was conducted by using questionnaires. Villagers were educated and trained to be aware of this disease. Blood samples were assayed for NiV antibody using an indirect ELISA for IgG antibodies against NiV-infected cell lysate. Positive criteria for NiV infection was a dilution ≥1:400. This study found no positive NiV serologies and no cases of encephalitis for the preceding annum among the 418 villagers who were evaluated.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 27
Although NiV infection has been found mainly in 3 species of Pteropus bats, P. lylei is dominant reservoir in Thailand due to its population size (>30,000 bats) and distribution. Its habitat is closer to humans compared to the other two Pteropus species. Seasonal prevalence of NiV transmission in P. lylei has been shown during April-May (Wacharapluesadee et al., 2010). Genetic characterization of NiV found in P. lylei in Thailand, based on 357 base pairs of nucleoprotein gene, indicated 2 existing genotypes: Bangladesh- and Malaysian- like (Wacharapluesadee and Hemachudha, 2007). Although both strains are co-circulating, the Bangladesh-like genotype dominates in P.lylei bat populations (Wacharapluesadee et al., 2013) One health approach in tackling emerging infectious diseases originated from wildlife is mandatory. This requires collaboration among people in different fields of animal and human diseases. This study seeks to demonstrate that a "One Health" approach to disease surveillance can help investigators gain insight into epidemiologic factors influencing disease transmission and thus help public health authorities to implement effective control of zoonotic diseases originating from wildlife. The community based public education and participation is considered as effective prevention measures. The study site was Chonburi province where NiV is endemic in fruit-eating bats, (P.lylei) (Wacharapluesadee et al., 2010). Assessing the risk of Nipah virus emergence at the high risk areas, has been conducted in villagers, pigs, and bats at the areas where NiV infection has been demonstrated in bats. Villagers living among NiV-positive bat colonies were evaluated for high-risk behaviors, for recent cases of encephalitis and underwent serology screening for NiV exposure. Pig’s blood samples from these two farms were collected and tested for NiV IgG antibody. Bats were trapped monthly at two commercial pig farms. The study was done in parallel with studies of NiV transmission within local bat colonies. Blood, saliva and urine was collected from each bat for further investigation. Community risk assessment was carried out by testing for NiV IgG antibody from blood of villagers at Chonburi province, living near the temple with NiV infected bats and by behavioral investigation. Evaluation of basic knowledge on EID was conducted by using questionnaires. Villagers were educated and trained to be aware of this disease. Blood samples were assayed for NiV antibody using an indirect ELISA for IgG antibodies against NiV-infected cell lysate. Positive criteria for NiV infection was a dilution ≥1:400. This study found no positive NiV serologies and no cases of encephalitis for the preceding annum among the 418 villagers who were evaluated.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health28
An integrated educational module was designed and used. Training of village health volunteers (VHV) to gain insight into basic practices helping in investigation of uncommon symptoms was carried out. The rapid response and reporting system from local to a referral hospital, King Chulalongkorn Memorial Hospital, was established. By providing basic knowledge and a simple but practical reporting system, an effective investigation process by the local community was initiated. This also established a network for monitoring before a future outbreak could spread. It was found that a grassroots movement was a powerful tool to drive the One Health concept to sustainability.
Figure. Process of community risk assessment and education in this study. Risk of NiV transmission from bats to pigs was assessed at two pig farms in Chonburi province, central Thailand, within 5 km of a bat roost where NiV infection had previously been demonstrated. During January-December 2012, blood samples were collected from 246 randomly-selected pigs throughout the year. All pigs tested negative for NiV IgG. Although there was no evidence of NiV infection in pigs, NiV-infected bats near pig farms pose a potential risk of NiV transmission to pigs. Measures to prevent contact between pigs and bats or bat body fluids are warranted. Bats were trapped monthly at two pig farms and the roost. Blood, saliva and urine were collected from each bat. Blood samples were tested for anti-NiV IgG using ELISA; bat saliva and urine were tested for viral RNA by PCR. The overall seroprevalence of NiV IgG in bats was 10.2% with limited seasonal variation. NiV RNA was found in the saliva of P. lylei bats trapped at one pig farm in May and July and bats trapped at the roost in March and April. The finding of NiV infected bats at the pig farms raises concern of possible NiV transmission to pigs. Although there were no evidence of NiV infection in pigs in the same study, measures to prevent bats
from coming into contact with pigs and avoidance of feeding pigs with partially eaten fruits must be actively promoted. Inter-sectoral cooperation among wildlife-animal-human sectors assists in recognition and response to emergence of NiV outbreak in Thailand. This study successfully demonstrates the viability of the transboundary "One Health" approach. Establishment of alert system and promotion of awareness at the level of rural villages is a second key success for this "One Health" initiative. The ultimate goal of the whole process cannot be achieved without public recognition and willingness, otherwise this cannot be sustainable. Policy makers must value this as an opportunity in strengthening public health infrastructure. Acknowledgements: We acknowledge active support from the Thai Red Cross Society, Chulalongkorn University, Department of Livestock Development, Department of National Parks Wildlife and Plant Conservation, Department of Disease Control, Centers for Disease Control and Prevention, Atlanta, Georgia, USA, Food and Agriculture Organization of the United Nations (FAO), and the enthusiastic help of our villagers. Financial supports came from the Thailand Research Fund (RDG5420089), the Ratchadaphiseksomphot Endowment Fund of Chulalongkorn University (RES560530148-HR), the "Research Chair Grant" National Science and Technology Development Agency (NSTDA), Thailand, and by the US Naval Health Research Center BAA-10-93 under Cooperative Agreement Number W911NF-11-2-0041. Ethic approval was obtained from the Institution Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand. References Chua KB, Bellini WJ, Rota PA, Harcourt BH, Tamin A, Lam SK, et al. (2000). Nipah
virus: a recently emergent deadly paramyxovirus. Science, 288:1432-1435. Chua KB. (2003). Nipah virus outbreak in Malaysia. J Clin Virol, 26: 265-275. Gurley ES, Montgomery JM, Hossain MJ, Bell M, Azad AK, Islam MR, et al. (2007). Person-to-person transmission of Nipah virus in a Bangladeshi community. Emerg Infect Dis,13: 1031-1037. Halpin K, Hyatt AD, Fogarty R, Middleton D, Bingham J, Epstein JH, et al. (2011).
Pteropid bats are confirmed as the reservoir hosts of henipaviruses: a comprehensive experimental study of virus transmission. Am J Trop Med Hyg, 85: 946-951.
Lo MK, Lowe L, Hummel KB, Sazzad HM, Gurley ES, Hossain MJ, et al. (2012). Characterization of Nipah virus from outbreaks in Bangladesh, 2008-2010. Emerg Infect Dis, 18: 248-255.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 29
from coming into contact with pigs and avoidance of feeding pigs with partially eaten fruits must be actively promoted. Inter-sectoral cooperation among wildlife-animal-human sectors assists in recognition and response to emergence of NiV outbreak in Thailand. This study successfully demonstrates the viability of the transboundary "One Health" approach. Establishment of alert system and promotion of awareness at the level of rural villages is a second key success for this "One Health" initiative. The ultimate goal of the whole process cannot be achieved without public recognition and willingness, otherwise this cannot be sustainable. Policy makers must value this as an opportunity in strengthening public health infrastructure. Acknowledgements: We acknowledge active support from the Thai Red Cross Society, Chulalongkorn University, Department of Livestock Development, Department of National Parks Wildlife and Plant Conservation, Department of Disease Control, Centers for Disease Control and Prevention, Atlanta, Georgia, USA, Food and Agriculture Organization of the United Nations (FAO), and the enthusiastic help of our villagers. Financial supports came from the Thailand Research Fund (RDG5420089), the Ratchadaphiseksomphot Endowment Fund of Chulalongkorn University (RES560530148-HR), the "Research Chair Grant" National Science and Technology Development Agency (NSTDA), Thailand, and by the US Naval Health Research Center BAA-10-93 under Cooperative Agreement Number W911NF-11-2-0041. Ethic approval was obtained from the Institution Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand. References Chua KB, Bellini WJ, Rota PA, Harcourt BH, Tamin A, Lam SK, et al. (2000). Nipah
virus: a recently emergent deadly paramyxovirus. Science, 288:1432-1435. Chua KB. (2003). Nipah virus outbreak in Malaysia. J Clin Virol, 26: 265-275. Gurley ES, Montgomery JM, Hossain MJ, Bell M, Azad AK, Islam MR, et al. (2007). Person-to-person transmission of Nipah virus in a Bangladeshi community. Emerg Infect Dis,13: 1031-1037. Halpin K, Hyatt AD, Fogarty R, Middleton D, Bingham J, Epstein JH, et al. (2011).
Pteropid bats are confirmed as the reservoir hosts of henipaviruses: a comprehensive experimental study of virus transmission. Am J Trop Med Hyg, 85: 946-951.
Lo MK, Lowe L, Hummel KB, Sazzad HM, Gurley ES, Hossain MJ, et al. (2012). Characterization of Nipah virus from outbreaks in Bangladesh, 2008-2010. Emerg Infect Dis, 18: 248-255.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health30
Luby SP, Rahman M, Hossain MJ, Blum LS, Husain MM, Gurley E, et al. (2006). Foodborne transmission of Nipah virus, Bangladesh. Emerg Infect Dis, 12: 1888-1894.
Luby SP, Hossain MJ, Gurley ES, Ahmed BN, Banu S, Khan SU, et al. (2009). Recurrent zoonotic transmission of Nipah virus into humans, Bangladesh, 2001-2007. Emerg Infect Dis, 15: 1229-1235.
Wacharapluesadee S, Lumlertdacha B, Boongird K, Wanghongsa S, Chanhome L, Rollin P, et al. (2005). Bat Nipah virus, Thailand. Emerg Infect Dis, 11: 1949-1951.
Wacharapluesadee S, Hemachudha T. (2007). Duplex nested RT-PCR for detection of Nipah virus RNA from urine specimens of bats. J Virol Methods, 141: 97-101. Wacharapluesadee S, Boongird K, Wanghongsa S, Ratanasetyuth N, Supavonwong P,
Saengsen D, et al. (2010). A Longitudinal Study of the Prevalence of Nipah Virus in Pteropus lylei Bats in Thailand: Evidence for Seasonal Preference in Disease Transmission. Vector Borne Zoonotic Dis, 10: 183-190.
Wacharapluesadee S, Ngamprasertwong T, Kaewpom T, Kattong P, Rodpana A, Wanghongsa S, et al. (2013) Genetic characterization of Nipah virus from Thai fruit bats (Pteropus lylei). Asian Biomedicine, 7: 813-819.
Yadav PD, Raut CG, Shete AM, Mishra AC, Towner JS, Nichol ST, et al. (2012). Detection of Nipah Virus RNA in Fruit Bat (Pteropus giganteus) from India. Am J Trop Med Hyg, 87: 576-578.
Yob JM, Field H, Rashdi AM, Morrissy C, van der Heide B, Rota P, et al. (2001). Nipah virus infection in bats (order Chiroptera) in peninsular Malaysia. Emerg Infect Dis, 7: 439-441.
Sustainable One Health Research in Southeast Asia
Goutard F.L.1 Binot A.1 Cappelle J.1 Duboz R.1 Morand S.1 Peyre M.1
Roger F. 1 and GREASE Regional Network partners 1Cirad, AGIRs Research Unit, France
ABSTRACT Zoonotic diseases cause 2.2 million deaths and 2.4 billion cases of human illness every year throughout the world. They are concentrated in low and middle-income countries in Asia and Africa, but the whole world is at risk of a potential pandemic. To combat these diseases, the international organisations are promoting the One Health concept, which is aimed at jointly addressing human health, animal health and the environment. However, the implementation of this approach is encountering numerous technical, scientific and institutional difficulties. Research will facilitate this implementation. This is shown by the interdisciplinary research conducted in SE Asia, associating methods used in the fields of human health and animal health, as well as the different stakeholders within these sectors. The promising findings of this research are helping to define the content of the concept and prefigure the management of the One Health initiative.
The One Health concept is difficult to implement: researchers, public authorities and operators are often locked into their own discipline or field of action.
Modelling and human and social sciences, which study socio-ecosystems as a whole, facilitate sectoral integration.
Participatory approaches are being implemented as alternative or complementary methods.
Corresponding author: Dr François Roger Cirad AGIRs, Montpellier 34398, France Faculty of Veterinary Medicine, Kasetsart University, Bangkok 10900, Thailand [email protected]

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 31
Sustainable One Health Research in Southeast Asia
Goutard F.L.1 Binot A.1 Cappelle J.1 Duboz R.1 Morand S.1 Peyre M.1
Roger F. 1 and GREASE Regional Network partners 1Cirad, AGIRs Research Unit, France
ABSTRACT Zoonotic diseases cause 2.2 million deaths and 2.4 billion cases of human illness every year throughout the world. They are concentrated in low and middle-income countries in Asia and Africa, but the whole world is at risk of a potential pandemic. To combat these diseases, the international organisations are promoting the One Health concept, which is aimed at jointly addressing human health, animal health and the environment. However, the implementation of this approach is encountering numerous technical, scientific and institutional difficulties. Research will facilitate this implementation. This is shown by the interdisciplinary research conducted in SE Asia, associating methods used in the fields of human health and animal health, as well as the different stakeholders within these sectors. The promising findings of this research are helping to define the content of the concept and prefigure the management of the One Health initiative.
The One Health concept is difficult to implement: researchers, public authorities and operators are often locked into their own discipline or field of action.
Modelling and human and social sciences, which study socio-ecosystems as a whole, facilitate sectoral integration.
Participatory approaches are being implemented as alternative or complementary methods.
Corresponding author: Dr François Roger Cirad AGIRs, Montpellier 34398, France Faculty of Veterinary Medicine, Kasetsart University, Bangkok 10900, Thailand [email protected]

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health32
Zoonotic diseases, which can be transmitted from domestic and wild animals to humans as well as from humans to animals, cause 2.2 million deaths and 2.4 billion cases of human illness every year in the world. They represent 60% of human infectious diseases and 75% of emerging diseases (ILRI, 2012). Many zoonoses are concentrated in low- or middle-income countries in Africa and Asia (Bordier and Roger, 2013), but the risk of pandemic exists at the global level: a new virus strain of influenza, for example, could emerge from an animal and be transmitted to humans; or a virus hosted by animals such as bats or rodents could be transmitted to humans. It is therefore important to target high-risk countries. The international organisations are promoting the One Health concept. This concept is well suited to countries with limited resources (Atlas, 2013) for combating zoonoses as well as exclusively animal diseases with potentially serious indirect consequences for human health and the economy. Launched in 2008, the One Health initiative is based on the following premise: in an interconnected world that is undergoing considerable climate and environmental change, human, animal and environmental health are inextricably linked. It advocates interdisciplinary research, public health programmes that are common to humans and animals, and health training and education (Zinsstag et al., 2005). However, the One Health concept is difficult to implement: researchers, public authorities and operators are often locked into their own discipline or field of action, whether intellectually or institutionally. Research can act as a facilitator, as shown by the work of CIRAD’s AGIRs research unit and its partners throughout the regional Network GREASE (Management of Emerging Epidemiological Risks in Southeast Asia). This research focuses on the following areas in Southeast Asia: the ecology of pathogens borne by small mammals (bats and rodents); the epidemiology of diseases, such as influenza and the optimisation of monitoring and surveillance systems. This research implements the recommendations of the One Health concept: connecting several disciplines (epidemiology, ecology, microbiology, parasitology and, more recently, human and social science); combining methods used in both animal and human health; associating stakeholders from both sectors; and setting up training programmes. In Southeast Asia, parasitologists from human and veterinary medicine are identifying rodent-borne pathogens that are transmissible to humans (Herbreteau et al., 2012); and ecologists and geographers are studying their environment. But isolating a parasite or a virus in a bat or a rodent does not necessarily mean that this pathogen will emerge in humans and cause an epidemic. Modelling studies, including probabilistic risk assessment, associating human medicine, veterinary medicine and environmental science are identifying the dangers at the human-animal interface and proposing preventive measures.
New research questions are emerging, which require the contribution of ecology and human and social science: for example, the role of the environment on health, whether positive (ecosystem services for disease regulation) or negative (biodiversity loss, environmental degradation, and exposure of humans and domestic animals to new pathogens), (Morand et al., 2014). Ecology and human and social science will need to be systematically associated in the study of zoonoses in order to accurately describe the impact and perception of diseases, to understand behaviour that facilitates their transmission, and to compare “before and after” and “here and elsewhere” situations. Health geography will also have a key role to play in One Health research. Indeed, this scientific field provides new frameworks by mobilising other disciplines from life science and human and social science. These disciplines, which study social ecosystems as a whole, also help to bring the different sectors closer together. The intersectoral approach is another characteristic of One Health research. To create links between veterinary medicine and human medicine, epidemiology acts as a catalyst (Tarantola et al., 2014) as well as modelling (Collineau et al., 2013) including companion modelling (Barreteau et al., 2014). Its goal is the same whatever the sector: better understanding diseases in their systemic dimension in order to target monitoring and surveillance and thereby improve health. The methods used are also the same: studying humans and animals under real conditions of exposure to biological, behavioural and environmental factors so as to identify those which influence health and diseases, using biostatistics and modelling. In Southeast Asia, this discipline has made it possible to study the epidemiological system for influenza without being restricted to either that of animals or that of humans. Research has shown that certain influenza viruses affecting humans or birds, especially the pandemic influenza virus (H1N1pdm), are transmitted from humans to pigs, and then to other pigs (Trevennec et al., 2009; Rith et al., 2012). Since this animal can host human and avian viruses and recombine them, it could be the source of new highly pathogenic strains of influenza that are transmissible between human beings. Research associating veterinary epidemiologists and virologists and epidemiologists from the medical sector is beginning in order to improve detection systems for potentially pandemic strains in pig farms (Netrabukkana et al., 2014). Surveillance systems are another vector for intersectoral synergies. Methods of disease monitoring and surveillance are being developed based on analysis and modelling of the ecology of pathogens or of epidemiological systems in time and space. In this sector too, research practices may be useful in implementing the One Health concept, provided they are assessed. In Cambodia, for example, a project to

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 33
New research questions are emerging, which require the contribution of ecology and human and social science: for example, the role of the environment on health, whether positive (ecosystem services for disease regulation) or negative (biodiversity loss, environmental degradation, and exposure of humans and domestic animals to new pathogens), (Morand et al., 2014). Ecology and human and social science will need to be systematically associated in the study of zoonoses in order to accurately describe the impact and perception of diseases, to understand behaviour that facilitates their transmission, and to compare “before and after” and “here and elsewhere” situations. Health geography will also have a key role to play in One Health research. Indeed, this scientific field provides new frameworks by mobilising other disciplines from life science and human and social science. These disciplines, which study social ecosystems as a whole, also help to bring the different sectors closer together. The intersectoral approach is another characteristic of One Health research. To create links between veterinary medicine and human medicine, epidemiology acts as a catalyst (Tarantola et al., 2014) as well as modelling (Collineau et al., 2013) including companion modelling (Barreteau et al., 2014). Its goal is the same whatever the sector: better understanding diseases in their systemic dimension in order to target monitoring and surveillance and thereby improve health. The methods used are also the same: studying humans and animals under real conditions of exposure to biological, behavioural and environmental factors so as to identify those which influence health and diseases, using biostatistics and modelling. In Southeast Asia, this discipline has made it possible to study the epidemiological system for influenza without being restricted to either that of animals or that of humans. Research has shown that certain influenza viruses affecting humans or birds, especially the pandemic influenza virus (H1N1pdm), are transmitted from humans to pigs, and then to other pigs (Trevennec et al., 2009; Rith et al., 2012). Since this animal can host human and avian viruses and recombine them, it could be the source of new highly pathogenic strains of influenza that are transmissible between human beings. Research associating veterinary epidemiologists and virologists and epidemiologists from the medical sector is beginning in order to improve detection systems for potentially pandemic strains in pig farms (Netrabukkana et al., 2014). Surveillance systems are another vector for intersectoral synergies. Methods of disease monitoring and surveillance are being developed based on analysis and modelling of the ecology of pathogens or of epidemiological systems in time and space. In this sector too, research practices may be useful in implementing the One Health concept, provided they are assessed. In Cambodia, for example, a project to

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health34
monitor influenza viruses in animals and humans associates researchers (epidemiologists, virologists) and sectors (veterinary and medical), with the aim of pooling the resources available to human health services and livestock services, and of enhancing the efficiency of surveillance systems (Goutard et al., 2012). To offset the shortcomings of classical surveillance systems, which require considerable human and financial resources, participatory approaches are being implemented as alternative or complementary methods (Calba et al., 2014). These approaches have been experimented to apprehend the social costs and benefits of zoonotic disease surveillance systems, often not considered within an evaluation process as difficult to measure (Delabouglise et al., 2012). The social constraints linked to the implementation of zoonotic disease management programs at local level are keys to ensure efficacy and sustainability of those programs (Delabouglise et al., 2013). Integration of social, economic and epidemiological issues needs be considered during the design phase of any disease management program. This remains true when merging animal and public health issues. In Southeast Asia, a new network, SEA-PREID (Participatory Research on Emerging Infectious Diseases in Southeast Asia: http://penaph.net/seapreid/), is fostering participatory epidemiology in order to optimise surveillance systems. It integrates different disciplines and sectors, and brings together livestock farmers, decision-makers and scientists. Associations between sectors and between stakeholders need to be strengthened in order to combat zoonotic diseases. Control methods must also be optimised. In Cambodia, for example, veterinary and medical doctors are working on rabies (Ponsich et al., 2012), a major zoonosis in Southeast Asia. In order to reduce the number and consequences of bites to humans, they are attempting to enhance methods to control canine populations in rural areas and to decentralise health care facilities. Not only do the research practices forge links between researchers from different disciplines and stakeholders from various sectors, but they also help to develop networks, monitoring centres, platforms and training programmes, which disseminate the principles of the One Health concept and facilitate its implementation and governance. In Southeast Asia, five academic and veterinary research establishments have worked along with CIRAD to create a research network in animal health and veterinary public health, GREASE. By fostering synergies and sharing skills at the regional level, GREASE aims to improve the management of risks associated with transboundary and emerging diseases. Close links with the ‘Institut Pasteur’ network, a key promoter and actor of the One Health initiative, are developing the connection with human health.
Certificate and in-house training courses are another tool, helping to build capacities and encouraging partnerships. Professional training is given to physicians by veterinarians. CIRAD’s veterinarians are thus training Chinese public health workers in the methods and principles of risk analysis. They take the methods used by veterinarians, such as decision trees, and adapt them to the needs of human public health. They study methods for the quantitative assessment of surveillance networks in animal health and human health, which can be adapted to future intersectoral systems for monitoring zoonotic diseases. In 2015, a new international “One Health” master program named “InterRisk: Assessment and management of health risks at the human, animal and ecosystem interface” will be opened in Thailand. This master is organized jointly by Kasetsart University (Bangkok, Thailand), the Institut National Polytechnique de Toulouse (France) and CIRAD (International Center in Agricultural Research for Development, France). This master’s curriculum has been designed to fit the key competencies identified during a regional web-survey carried out in 2011 across members of international organizations, academic, public and private sectors in SEA. Some modules will also be opened to professionals engaged in a continuing education program, with the possibility of e-learning courses. Double accreditation from French and Thai universities will ensure education quality and diploma validity (Paul et al., 2013). Efforts to educate students in a “One Health” perspective and at a regional scale will be made, by making veterinary, medical and biosciences students work together on real cross-country problems. Also, special attention will be given during the courses to community-based participatory actions. Innovative pedagogical tools (active learning, real case problem-solving, field visits, and computer-based modules) will be promoted. Through teachings and internships, students will interact with professionals from the private agricultural sector, international organisations, governmental agencies, NGOs and research institutes. The master will initiate the creation of professional social networks at a regional level. In a context of trade globalization and climate change, “InterRisk” graduates will be able to conceptualise and design holistic programs integrating epidemiological, ecological, and socio-economic approaches to tailor public health and animal diseases control policy decisions to the actual SEA situation. Towards one public health? Whether assessing the risks of emergence of a new human disease originating in wild or domestic animals, studying or controlling existing zoonoses, or coordinating sectors and stakeholders, research shows that it is possible and valuable to work together in a One Health perspective, and that these partnerships are prefiguring the application of this concept. So why not use just one

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 35
Certificate and in-house training courses are another tool, helping to build capacities and encouraging partnerships. Professional training is given to physicians by veterinarians. CIRAD’s veterinarians are thus training Chinese public health workers in the methods and principles of risk analysis. They take the methods used by veterinarians, such as decision trees, and adapt them to the needs of human public health. They study methods for the quantitative assessment of surveillance networks in animal health and human health, which can be adapted to future intersectoral systems for monitoring zoonotic diseases. In 2015, a new international “One Health” master program named “InterRisk: Assessment and management of health risks at the human, animal and ecosystem interface” will be opened in Thailand. This master is organized jointly by Kasetsart University (Bangkok, Thailand), the Institut National Polytechnique de Toulouse (France) and CIRAD (International Center in Agricultural Research for Development, France). This master’s curriculum has been designed to fit the key competencies identified during a regional web-survey carried out in 2011 across members of international organizations, academic, public and private sectors in SEA. Some modules will also be opened to professionals engaged in a continuing education program, with the possibility of e-learning courses. Double accreditation from French and Thai universities will ensure education quality and diploma validity (Paul et al., 2013). Efforts to educate students in a “One Health” perspective and at a regional scale will be made, by making veterinary, medical and biosciences students work together on real cross-country problems. Also, special attention will be given during the courses to community-based participatory actions. Innovative pedagogical tools (active learning, real case problem-solving, field visits, and computer-based modules) will be promoted. Through teachings and internships, students will interact with professionals from the private agricultural sector, international organisations, governmental agencies, NGOs and research institutes. The master will initiate the creation of professional social networks at a regional level. In a context of trade globalization and climate change, “InterRisk” graduates will be able to conceptualise and design holistic programs integrating epidemiological, ecological, and socio-economic approaches to tailor public health and animal diseases control policy decisions to the actual SEA situation. Towards one public health? Whether assessing the risks of emergence of a new human disease originating in wild or domestic animals, studying or controlling existing zoonoses, or coordinating sectors and stakeholders, research shows that it is possible and valuable to work together in a One Health perspective, and that these partnerships are prefiguring the application of this concept. So why not use just one

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health36
term: “public health”? Public health refers to the prevention of disease and the well-being of human societies. Veterinary public health covers actions concerning animals and their products aimed at protecting, preserving and improving human health and well-being. The One Health concept is working to achieve this. ACKNOWLEDGMENT This research was conducted within the framework of the GREASE network (http://www.grease-network.org. It associated the following partners: Institut Pasteur International Network, IRD, CNRS, INP-ENVT (France); EpiX Analytics (United States); Royal Veterinary College (University of London, United Kingdom); Murdoch University (Australia); University of Hong Kong (China). Several international agencies (FAO, OIE, WHO, ILRI) took part in the research; they have an important role to play in the implementation of One Health. CIRAD researchers and PhD students (ecologists, veterinary epidemiologists and an anthropologist) are from from the AGIRs research unit (Animal and Integrated Risk Management, http://ur-agirs.cirad.fr); socio-economists from the MOISA research unit (Markets, Organisations, Institutions and Stakeholder Strategies, http://umr-moisa.cirad.fr/ ); Parasitologists from InterTryp (Host-Vector-Parasites Interactions in Trypanosomidae infections, http://umr-intertryp.cirad.fr). REFERENCES: Atlas RM (2013). One Health: Its Origins and Future. Curr Top Microbiol Immunol. 365:1-13. Barreteau, O., Bousquet, F., Étienne, M., Souchère, V., & d’Aquino, P. (2014).
Companion modelling: a method of adaptive and participatory research. In Companion Modelling (pp. 13-40). Springer Netherlands
Bordier, M., & Roger, F. (2013). Zoonoses in South-East Asia: a regional burden, a global threat. Animal Health Research Reviews, 14(01), 40-67 Calba, C., Ponsich, A., Nam, S., Collineau, L., Min, S., Thonnat, J., & Goutard, F. L.
(2014). Development of a participatory tool for the evaluation of Village Animal Health Workers in Cambodia. Acta Trop. Feb 25;134C:17-28
Collineau, L., Duboz, R., Paul, M., Peyre, M., Goutard, F., Holl, S., Roger, F. (2013). Application of loop analysis for the qualitative assessment of surveillance and control in veterinary epidemiology. Emerg Themes Epidemiol. 13;10(1):7
Delabouglise A, Antoine-Moussiaux N, Phan DT, Nguyen TT, Dao CD, Dao TH, Pham TTH, Vu DT, Nguyen VK, Binot A, F, Roger F, Peyre M. 2012. Methodological framework for a participatory approach to evaluate the socio-economic factors impairing the efficacy of animal health surveillance systems. 13th ISVEE conference, Maastricht, Netherlands, August 20-24.
Delabouglise A, Antoine-Moussiaux N, Phan DT, Dao CD, Nguyen TT, Pham TTH, Truong DB, Le TH, Kasemsuwan S, Binot A, Roger F, Peyre M. 2013. Impact of social and economical constraints on the performances of Highly Pathogenic Avian Influenza surveillance systems in Vietnam and Thailand. Options for the Control of Influenza VIII, Cape Town, South Africa, 5-10 Sep 2013
Goutard, F., Ponsich, A., Ly, S., Holl, D., Allal, L., Dab, W., Roger, F., Stärk, K.D.C. (2012). “One Health” approach to quantitatively compare human and animal surveillance systems for avian influenza H5N1 in Cambodia. International Symposium on Veterinary Epidemiology and Economics (ISVEE), Maastricht, Netherlands, 20-24 August. Wageningen Academic Publishers
Herbreteau, V., Bordes, F., Jittapalapong, S., Supputamongkol, Y., Morand, S. (2012). Rodent-borne diseases in Thailand: targeting rodent carriers and risky habitats. Infection Ecology and Epidemiology 2: 18637 - http://dx.doi.org/10.3402/iee.v2i0.18637
ILRI. (2012). Mapping of poverty and likely zoonoses hotspots. Zoonoses Project 4. Report to Department for International Development, UK. ILRI, Nairobi, Kenya. 119 pp.
Morand, S., Jittapalapong, S., Suputtamongkol, Y., Abdullah, M. T., and Huan, T. B. (2014). Infectious Diseases and Their Outbreaks in Asia-Pacific: Biodiversity and Its Regulation Loss Matter. PloS one, 9(2), e90032.
Netrabukkana, P., Cappelle, J., Trevennec, C., Roger, F., Goutard, F., Buchy, P., Robertson I., Fenwick, S. (2014). Epidemiological Analysis of Influenza A Infection in Cambodian Pigs and Recommendations for Surveillance Strategies. Transboundary and emerging diseases. doi: 10.1111/tbed.12204
Paul, M. C., Rukkwamsuk, T., Tulayakul, P., Suprasert, A., Roger, F., Bertagnoli, S., and Goutard, F. L. (2013). InterRisk: an International One Health Master Program in Southeast Asia. ICERI2013 Proceedings, 3089-3098
Peyre, M., Zahhaf, A., Figuié, M., Binot, A., Bonnet, P., Goutard, F., Roger, F. (2011). Socioeconomical evaluation of surveillance systems for emerging animal diseases: merging veterinary and public health issues. First International One Health Congress, Melbourne, Australia, 14‐16 February. EcoHealth 7, S8–S170
Ponsich, A., Goutard, F., Sorn, S., Tarantola, A., (2012). A 6-months descriptive study of dog bites in rural Cambodia. Int J Infect Dis 2012; 16S1:57.027. Rith, S., Netrabukkana, P., Sorn, S., Mumford, E., Mey, C., Holl, D., Goutard, F.,
Bunthin, Y., Fenwick, S., Robertson, I., Roger, F., Buchy, P. (2012). Serologic evidence of human influenza virus infections in swine populations, Cambodia. Influenza Other Respi Viruses. 30 May. DOI:10.1111/j.1750-2659.2012.00382.x.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 37
Delabouglise A, Antoine-Moussiaux N, Phan DT, Dao CD, Nguyen TT, Pham TTH, Truong DB, Le TH, Kasemsuwan S, Binot A, Roger F, Peyre M. 2013. Impact of social and economical constraints on the performances of Highly Pathogenic Avian Influenza surveillance systems in Vietnam and Thailand. Options for the Control of Influenza VIII, Cape Town, South Africa, 5-10 Sep 2013
Goutard, F., Ponsich, A., Ly, S., Holl, D., Allal, L., Dab, W., Roger, F., Stärk, K.D.C. (2012). “One Health” approach to quantitatively compare human and animal surveillance systems for avian influenza H5N1 in Cambodia. International Symposium on Veterinary Epidemiology and Economics (ISVEE), Maastricht, Netherlands, 20-24 August. Wageningen Academic Publishers
Herbreteau, V., Bordes, F., Jittapalapong, S., Supputamongkol, Y., Morand, S. (2012). Rodent-borne diseases in Thailand: targeting rodent carriers and risky habitats. Infection Ecology and Epidemiology 2: 18637 - http://dx.doi.org/10.3402/iee.v2i0.18637
ILRI. (2012). Mapping of poverty and likely zoonoses hotspots. Zoonoses Project 4. Report to Department for International Development, UK. ILRI, Nairobi, Kenya. 119 pp.
Morand, S., Jittapalapong, S., Suputtamongkol, Y., Abdullah, M. T., and Huan, T. B. (2014). Infectious Diseases and Their Outbreaks in Asia-Pacific: Biodiversity and Its Regulation Loss Matter. PloS one, 9(2), e90032.
Netrabukkana, P., Cappelle, J., Trevennec, C., Roger, F., Goutard, F., Buchy, P., Robertson I., Fenwick, S. (2014). Epidemiological Analysis of Influenza A Infection in Cambodian Pigs and Recommendations for Surveillance Strategies. Transboundary and emerging diseases. doi: 10.1111/tbed.12204
Paul, M. C., Rukkwamsuk, T., Tulayakul, P., Suprasert, A., Roger, F., Bertagnoli, S., and Goutard, F. L. (2013). InterRisk: an International One Health Master Program in Southeast Asia. ICERI2013 Proceedings, 3089-3098
Peyre, M., Zahhaf, A., Figuié, M., Binot, A., Bonnet, P., Goutard, F., Roger, F. (2011). Socioeconomical evaluation of surveillance systems for emerging animal diseases: merging veterinary and public health issues. First International One Health Congress, Melbourne, Australia, 14‐16 February. EcoHealth 7, S8–S170
Ponsich, A., Goutard, F., Sorn, S., Tarantola, A., (2012). A 6-months descriptive study of dog bites in rural Cambodia. Int J Infect Dis 2012; 16S1:57.027. Rith, S., Netrabukkana, P., Sorn, S., Mumford, E., Mey, C., Holl, D., Goutard, F.,
Bunthin, Y., Fenwick, S., Robertson, I., Roger, F., Buchy, P. (2012). Serologic evidence of human influenza virus infections in swine populations, Cambodia. Influenza Other Respi Viruses. 30 May. DOI:10.1111/j.1750-2659.2012.00382.x.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health38
Tarantola, A., Goutard, F., Newton, P., de Lamballerie, X., Lortholary, O., Cappelle, J., and Buchy, P. (2014). Estimating the Burden of Japanese Encephalitis Virus and Other Encephalitides in Countries of the Mekong Region. PLOS Neglected Tropical Diseases, 8(1), e2533.
Trevennec, K., Leger, L., Lyazrhi, F., Baudon, E., Cheung, C.Y., Roger, F., Peiris, M., Garcia, J.-M. (2011). Transmission of pandemic influenza H1N1 (2009) in Vietnamese swine in 2009-2010. Influenza Other Respi Viruses. 30 Dec. DOI: 10.1111/j.1750-2659.2011.00324.x.
Zinsstag, J., Schelling, E., Wyss, K., Mahamat, M.B. (2005) Potential of cooperation between human and animal health to strengthen health systems. Lancet. 366 (9503): 2142-5.
Impacts of Biodiversity and Land Use Changes on Zoonotic Infectious Diseases in Southeast Asia
Serge Morand
(CNRS-CIRAD, Centre d’Infectiologie Christophe Mérieux du Laos, Vientiane, Lao PDR)
Numerous parasitic and infectious diseases are emerging, re-emerging or causing recurrent outbreaks in Southeast-Asia, a hot spot of both infectious disease emergence and biodiversity at threat. Here, we present ongoing results on the potential effects of global change, biodiversity and land use on the epidemiology and diversity of infectious diseases, focusing on zoonotic diseases (and more specifically rodent-borne diseases), from regional to local scales.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 39
Impacts of Biodiversity and Land Use Changes on Zoonotic Infectious Diseases in Southeast Asia
Serge Morand
(CNRS-CIRAD, Centre d’Infectiologie Christophe Mérieux du Laos, Vientiane, Lao PDR)
Numerous parasitic and infectious diseases are emerging, re-emerging or causing recurrent outbreaks in Southeast-Asia, a hot spot of both infectious disease emergence and biodiversity at threat. Here, we present ongoing results on the potential effects of global change, biodiversity and land use on the epidemiology and diversity of infectious diseases, focusing on zoonotic diseases (and more specifically rodent-borne diseases), from regional to local scales.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health40
Clinical management of canine seborrhea
Narong Kitpanit E.mail [email protected]
Suanluang animal hospital, 267 Chalermprakiat R.9 Nongborn, Pravet, Bangkok 10250 Tel. 02-7262258, FAX. 02-7263476
Seborrhea is a skin disorder that causes scale formation, excessive greasiness of the skin and hair coat and sometimes lead to a secondary infection of the skin. Common forms may include seborrhea sicca, seborrhea oleosa and seborrheic dermatitis. Etiologically, seborrhea is classified into primary and secondary types.
Canine primary seborrhea, the most common primary type is an inherited disorder of epidermal proliferation. The breeds most commonly afflicted include American Cocker Spaniel, English Springer Spaniel and other breeds. The basal cells in dogs with seborrhea are hyper productive and the renewal time is also decreased. The calculated epidermal renewal time was approximately 9 days as compared with 22 days in normal dogs. The epidermis, the hair follicle infundibulum and sebaceous glands are all hyper proliferation, but the hair root matrix is normal. The clinical signs may varies from dog to dog as a dull hair coat with excessive scale, greasy malodorous skin and seberrheic dermatitis are common in most cases. Hyperkeratosis of footpads and nasal planum may be seen in some dogs. Pruritis may or may not be present. These dogs are prone to Staphylococcus and Malassezia secondary infections.
Canine secondary seborrhea are those caused by external or internal insult that alters the epidermal proliferation. In most instances, inflammations, infections, hormonal imbalance, nutritional factors, environmental factors and any diseases can cause secondary seborrhea. (e.g., hypersensitivity, bacterial infections, parasitic infections, dermatophytosis, sex hormone imbalance, hypothyroidism, hyperadrenocorticism, deficiency or excessive nutrients, maldigestion, malabsorption and etc.) Management of canine primary seborrhea Primary seborrhea is incurable but treatable. Therapy is directed towards controlling the clinical signs, following regimens should be considered.
Ensure good nutrition
Hair coat clipped
Control of secondary infections and ectoparasites
Control of ceruminous otitis externa
Topical therapy : shampoo and emollients are extremely helpful
Systemic therapy
Topical management of scaly seborrhea Intense bathing 1-3 times a week is required in scaly seborrheic dogs, until the skin condition is improved (approximately 2-3 weeks) then the bathing frequency should be decreased to once weekly or as needed for maintenance regimen (every 1-2 weeks). Over bathing especially with dry seborrheic dog can result in increasing scaling The response of bathing in long hair dog is dramatically improved if the coat is clipped. For mildly to moderately scaly seborrhea, moisturizing hypoallergenic shampoo (e.g., colloidal oatmeal etc.) 1-2 times a week may be useful. And oral EFA supplementation (EPA 40-80 mg/kg/d) may be beneficial. For more severely scaly seborrhea, antiseborrheic shampoo, a sulfur and salicylic acid shampoo bathing 2-3 times a week is best. These dogs are also beneficial from daily spray with 50-75% propylene glycol or 5% lactic acid. Coconut oil or baby oil soaking and rinse is also helpful. Oral EFA supplementation is also beneficial. For hyperkeratosis of footpads, this can be difficult to manage however, daily soaking with 50% propylene glycol may be useful. Topical management of oily seborrhea In dogs with oily seborrhea, need shampoos that contain strong degreasing action with potent antibacterial activities because these dogs are prone to bacterial and yeast infections, therefore systemic treatment with appropriate antibiotics and antifungal agents to control secondary infections are strongly recommended. However, all strong degreasing agents can disrupt the epidermal barrier and increase tranepidermal water loss, with resultant worsening of the seborrhea and after bath rinse can prevent this, but it may make the dog too greasy. For dogs with mildly to moderately greasy skin, mild degreasing shampoo are recommended e.g., sulfur and salicylic acid shampoo, mild tar, ethyl lactate shampoo (mild degreasing property) For dogs with severely greasing skin are often bathed with potent degreasing shampoo e.g., benzoyl peroxide shampoo, selenium sulfide (Selsun 1%), tar etc. Topical management for seborrheic dermatitis. As mentioned before, these dogs are prone to bacterial and Malassezia infections. Any secondary skin infections should be treated with both topical and systemic therapies. Systemic periodic retreatment or long term therapy may be needed
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 41
Topical management of scaly seborrhea Intense bathing 1-3 times a week is required in scaly seborrheic dogs, until the skin condition is improved (approximately 2-3 weeks) then the bathing frequency should be decreased to once weekly or as needed for maintenance regimen (every 1-2 weeks). Over bathing especially with dry seborrheic dog can result in increasing scaling The response of bathing in long hair dog is dramatically improved if the coat is clipped. For mildly to moderately scaly seborrhea, moisturizing hypoallergenic shampoo (e.g., colloidal oatmeal etc.) 1-2 times a week may be useful. And oral EFA supplementation (EPA 40-80 mg/kg/d) may be beneficial. For more severely scaly seborrhea, antiseborrheic shampoo, a sulfur and salicylic acid shampoo bathing 2-3 times a week is best. These dogs are also beneficial from daily spray with 50-75% propylene glycol or 5% lactic acid. Coconut oil or baby oil soaking and rinse is also helpful. Oral EFA supplementation is also beneficial. For hyperkeratosis of footpads, this can be difficult to manage however, daily soaking with 50% propylene glycol may be useful. Topical management of oily seborrhea In dogs with oily seborrhea, need shampoos that contain strong degreasing action with potent antibacterial activities because these dogs are prone to bacterial and yeast infections, therefore systemic treatment with appropriate antibiotics and antifungal agents to control secondary infections are strongly recommended. However, all strong degreasing agents can disrupt the epidermal barrier and increase tranepidermal water loss, with resultant worsening of the seborrhea and after bath rinse can prevent this, but it may make the dog too greasy. For dogs with mildly to moderately greasy skin, mild degreasing shampoo are recommended e.g., sulfur and salicylic acid shampoo, mild tar, ethyl lactate shampoo (mild degreasing property) For dogs with severely greasing skin are often bathed with potent degreasing shampoo e.g., benzoyl peroxide shampoo, selenium sulfide (Selsun 1%), tar etc. Topical management for seborrheic dermatitis. As mentioned before, these dogs are prone to bacterial and Malassezia infections. Any secondary skin infections should be treated with both topical and systemic therapies. Systemic periodic retreatment or long term therapy may be needed

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health42
because these dogs are usually susceptible to recurring infection. Topical treatment with antibacterial and antifungal shampoo are stongly recommended. The following agents should be considered.
Antibacterial shampoo : chlorhexidine, ethyl lactate, benzoyl peroxide, povidone iodine shampoo.
Antifungal shampoo : chlorhexidine, ketoconazole, miconazole, povidone iodine.
Antibacterial and antifungal shampoo : chlorhexidine, povidone iodine, chlorhexidine + miconazole, chlorhexidine + ketoconazole
Systemic therapy of canine primary seborrhea
Secondary bacterial infection should be treated with appropriate antibiotics. Periodic retreatment or long-term therapy (low-dose, pulse therapy) may be needed because these dogs are susceptible to recurring infection. Cephalexin is commonly first choice in dog, but amoxy - clavulanate may be alternated
Retinoic acids have been used extensively in seborrheic dogs with varying results. Isotretinoin 1-2 mg/kg po. sid. to remission, then tapered to qod. or one week on - one week off, or Acitretin 0.5-1 mg/kg po. sid. may be helpful in some dogs.
Oral essential fatty acids supplementation may be helpful as an adjunct therapy (EPA 40-80 mg/kg/po. sid. )
Vitamin A 500-1,000 1U/kg po. sid.
Calcitriol (D3) 0.01 mcg/kg (10 ng/kg) po. sid. may be helpful in some cases. Calcitriol can decrease cell proliferation.
Prednisolone are not generally recommended. However, for dogs with severely pruritis, treatment with corticosteroids may be helpful
Management of canine secondary seborrhea The aim of treatment in secondary seborrhea is to correct its underlying causes. With this treatment the seborrheicic signs are usually resolved in 30-60 day. However, in chronic cases, a complete response may be longer. Because these dogs prone to Staphylococcus and Malassezia secondary infections, appropriate treatment of secondary infections and correction of the underlying causes can result in rapid improvement. The topical agents used in primary seborrhea are also used in correction secondary seborrhea but treatment protocols are less intensed.
Causes of secondary seborrhea in dog (Medleau and Hnilica,2006)
Infectious: Pyoderma, Dermatophytosis, Malasezzia dermatitis, Leishmaniasis.
Allergic: Flea allergy dermatitis, Atopy, Food hypersensitivity, Contact dermatitis.
Endocrine: Hypothyroidism, Hyperadrenocorticism, Sex hormone imbalance, Diabetes mellitus.
Parasitic: Demodicosis, Scabies, Cheyletiellosis, Pediculosis, Otodectes spp.
Nutritional: Vitamin A-responsive dermatosis, Zinc-responsive dermatosis, Dietary imbalance.
Immune-mediated: Pemphigus foliaceus, Pemphigus erythematosus, Discoid lupus erythematosus, Systemic lupus erythematosus, Cutaneous drug reaction, Sebaceous adenitis.
Metabolic: Malabsorption/maldigestion, Superficial necrolytic dermatitis.
Neoplastic: Cutaneous epitheliotropic lymphoma. Bibliography Medleau,L.and Hnilica,K.(2006).Small Animal Dermatology.2nd ed. In Keratinization and seborrheic disorders.pp295-326.Saunders,Elsevier. Scott,D.,Miller, Jr., W. and Griffin,C.(2001). Muller and kirk’s Small Animal
Dermatology. 6th ed. In Keratinization defects. pp1025-1053. W.B. Saunders company.
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 43
Causes of secondary seborrhea in dog (Medleau and Hnilica,2006)
Infectious: Pyoderma, Dermatophytosis, Malasezzia dermatitis, Leishmaniasis.
Allergic: Flea allergy dermatitis, Atopy, Food hypersensitivity, Contact dermatitis.
Endocrine: Hypothyroidism, Hyperadrenocorticism, Sex hormone imbalance, Diabetes mellitus.
Parasitic: Demodicosis, Scabies, Cheyletiellosis, Pediculosis, Otodectes spp.
Nutritional: Vitamin A-responsive dermatosis, Zinc-responsive dermatosis, Dietary imbalance.
Immune-mediated: Pemphigus foliaceus, Pemphigus erythematosus, Discoid lupus erythematosus, Systemic lupus erythematosus, Cutaneous drug reaction, Sebaceous adenitis.
Metabolic: Malabsorption/maldigestion, Superficial necrolytic dermatitis.
Neoplastic: Cutaneous epitheliotropic lymphoma. Bibliography Medleau,L.and Hnilica,K.(2006).Small Animal Dermatology.2nd ed. In Keratinization and seborrheic disorders.pp295-326.Saunders,Elsevier. Scott,D.,Miller, Jr., W. and Griffin,C.(2001). Muller and kirk’s Small Animal
Dermatology. 6th ed. In Keratinization defects. pp1025-1053. W.B. Saunders company.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health44
FAO APPROACH FOR DISEASE CONTROL AT THE HUMAN AND ANIMAL INTERFACE: LABORATORY PERSPECTIVES
1
S. Suradhat2 W. Kalpravidh K. Wongsthapornchai R. Morales T. Sothyra A. Rangkuti and S. Morzaria
Emergency Center for Transboundary Animal Diseases (ECTAD), Food and Agriculture Organization, Regional Office for Asia and the Pacific (FAO-RAP), Bangkok, Thailand
FAO's mission is “To help build a food-secure world for present and future generations”, assuring that people have regular access to high-quality food to lead active and healthy lives. Our mandate is to improve nutrition, increase agricultural productivity, raise the standard of living in rural populations and contribute to global economic growth. Presently, the world has faced a major challenge of emergence and spread of high impact infectious diseases (EIDs) affecting animal production and public health. Livestock sector developments in the Asia-Pacific region are creating a fertile ground for the emergence of animal diseases, some of which may have zoonotic potential resulting in critical impacts on livestock productivity, and public health issues. Having recognized the importance of emerging and endemic zoonotic and food-borne diseases, FAO has been involved in global and regional efforts to diminish the risk and minimize their potential impacts. With the overall goal of ensuring food security and safety, improving the livelihoods of farming communities and promoting animal health and public well-being, FAO has been focusing on development of capacities related to veterinary services on disease control to promote their governance in disease control and emergency response in accordance to the international standards. In addition, assistance has been given to the member countries to develop rational and targeted control program for specific diseases through scientific information derived from field surveillance, disease intelligence and strategic research. FAO also promotes wide-ranging collaboration across sectors and disciplines to address a broader range of drivers of zoonotic diseases. In particular, FAO in partnership with OIE and WHO continue to support the strengthening of existing animal and public health surveillance, prevention and preparedness, and response systems at the country, regional and international levels.
1 Part of this article was presented at APHCA-OIE Workshop, 24-25 September 2013, Thimphu, Bhutan.
2 Present address: Faculty of Veterinary Science, Chulalongkorn University, Bangkok 10330, Thailand, [email protected].
Regional Capacity Building and Networking Program There are four levels of capacity development in FAO’s Corporate Strategy: individual, organizational, sector/network and enabling environment levels. At individual level, people can be trained to increase their knowledge and skills. The organizational capacity can be strengthened by improving structures, mechanisms and procedures and will enable the skilled human resources to utilize their knowledge to perform their services. A network can be formed among the organizations within and among the sectors to share their experiences and resources. Within the network, the coherent policies and strategies of the organizations and sectors are required with good coordination and this would enable to form policies and institutional framework with high-level commitment resulting in a higher scale of development impact. However, aiming at higher level would take longer time and more resources. Following such strategy, FAO has been systematically building the national and regional capacities of the three main technical components, laboratory, epidemiology and risk determination and risk mitigation, to support zoonotic disease control. The capacity building and networking program is supported by various sources of funding (development partners and FAO) for country and regional projects related to zoonotic and food-borne diseases control. In this lecture, the work on strengthening of the veterinary diagnostic services will be used as an example of FAO’s key effort on capacity development.
Support in Planning and Policy
Development and Coordination
Capacity Building and Networking

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 45
Regional Capacity Building and Networking Program There are four levels of capacity development in FAO’s Corporate Strategy: individual, organizational, sector/network and enabling environment levels. At individual level, people can be trained to increase their knowledge and skills. The organizational capacity can be strengthened by improving structures, mechanisms and procedures and will enable the skilled human resources to utilize their knowledge to perform their services. A network can be formed among the organizations within and among the sectors to share their experiences and resources. Within the network, the coherent policies and strategies of the organizations and sectors are required with good coordination and this would enable to form policies and institutional framework with high-level commitment resulting in a higher scale of development impact. However, aiming at higher level would take longer time and more resources. Following such strategy, FAO has been systematically building the national and regional capacities of the three main technical components, laboratory, epidemiology and risk determination and risk mitigation, to support zoonotic disease control. The capacity building and networking program is supported by various sources of funding (development partners and FAO) for country and regional projects related to zoonotic and food-borne diseases control. In this lecture, the work on strengthening of the veterinary diagnostic services will be used as an example of FAO’s key effort on capacity development.
Support in Planning and Policy
Development and Coordination
Capacity Building and Networking

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health46
Laboratory Capacity Building and Networking Program Utilizing programmatic approach, FAO has provided assistance to strengthen quality veterinary diagnostic services among the national veterinary and partner laboratories. FAO’s laboratory capacity development program for the Regional Laboratory Network (RLN) laboratory members aims to assist the national veterinary diagnostic laboratories in fulfilling their roles and responsibilities related to diagnosis and reporting of the occurrence of the animal and/or potentially zoonotic diseases in a reliable and timely manner. Four technical components are focused including: strengthening of diagnostic capacity, assuring the quality of laboratory services, improving laboratory biosafety facilitating laboratory networking at national and regional levels. The implemented activities focused on laboratory capacity assessments, regional and in-country trainings and workshops, provision of equipment, reagents and supplies, the Regional Quality Assurance (QA) program, the Regional Biosafety Program and Regional Laboratory Networking events. Currently, there are 31 laboratories (national diagnostic and allied laboratories) from 11 countries in Southeast Asia and South Asia regions participated in the capacity development program. The implemented technical areas of each laboratory may be varied depending on the geographical region and the responsibility of the laboratories. In some cases, customized technical assistance programs were provided to the laboratories with specific needs. The major source of findings for the laboratory capacity development during the past few years are USAID-Emerging Pandemic Threat (EPT)-IDENTIFY and the EU-Highly Pathogenic Emerging Diseases (HPED) programs. The Regional Quality Assurance Program Laboratory Quality Assurance (QA) is one of the strategic goals of the ASEAN-endorsed Regional Strategic Framework for Laboratory Capacity Building and Networking. The key objective of the program is to assure the quality of diagnostic services carried out by the member laboratories of the Regional Laboratory Network (RLN). The program is conducted through collaborations with several partners including Australian Animal Health Laboratory (AAHL), OIE, Regional Leading/Reference
laboratories, and relevant partners. A 4-step approach for the Regional QA Program includes 1) regional trainings on diagnosis of the selected priority diseases and laboratory QA; 2) regional proficiency testing (PT) activities; 3) backstopping missions by the international laboratory experts to provide assistance in rectifying problems based on the PT results; and 4) advocacy for support to enhance and sustain the laboratory QA program at the participating laboratories. The 6 targeted diseases of the current Regional QA program, including 2 zoonotic diseases, are Avian Influenza A, Newcastle Disease (ND), Rabies, African Swine Fever (ASF), Classical Swine Fever (CSF), and Porcine Reproductive and Respiratory Syndrome Virus (PRRS). The Regional QA program significant improves the diagnostic capacity in the region. Through these activities, the member laboratories in the regional network were able to harmonize and improve the test sensitivity to a satisfactory level. Not only ensuring the quality of ongoing diagnostic services, the program has been proven critically of value, in the face of emerging Influenza A (H7N9) virus, when the regional laboratory network mechanisms and diagnostic protocols can be efficiently implemented at the member laboratories with better confidence in quality services. Regional Biosafety Program Since 2010, FAO has been conducting a biosafety enhancement program for national veterinary laboratories in countries of South and Southeast Asia. The activities include biosafety risk assessment, development of biosafety standard operation protocols (SOPs) and regional and in-country trainings, and annual biosafety cabinet (BSC) certification and servicing. The results of the regional biosafety activities were reported back to the relevant regional laboratory network meetings to update network members on the progress of the program and to advocate for support related to laboratory biosafety management from the relevant laboratory authorities and stakeholders. The Regional Biosafety Program has been very well received among the network laboratories. During the past few years, the numbers of laboratories which participated and received the benefit from the program has remarkably expanded. In 2013, 29 laboratories from 10 countries had enrolled in the program. Strengthening of regional and international laboratory networks FAO encourages and supports the countries to establish the national laboratory network and also to participate in the regional network. The aims of such networking are to implement the regional quality assurance and biosafety improvement programs as well as to share experience and resources among the network members. To mentor the laboratories in the region, an expert group has been formed consisting of experts from international reference laboratories for the target diseases to provide technical advisory to the network members. The importance of quality assurance program and laboratory biosafety system has been advocated to
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 47
laboratories, and relevant partners. A 4-step approach for the Regional QA Program includes 1) regional trainings on diagnosis of the selected priority diseases and laboratory QA; 2) regional proficiency testing (PT) activities; 3) backstopping missions by the international laboratory experts to provide assistance in rectifying problems based on the PT results; and 4) advocacy for support to enhance and sustain the laboratory QA program at the participating laboratories. The 6 targeted diseases of the current Regional QA program, including 2 zoonotic diseases, are Avian Influenza A, Newcastle Disease (ND), Rabies, African Swine Fever (ASF), Classical Swine Fever (CSF), and Porcine Reproductive and Respiratory Syndrome Virus (PRRS). The Regional QA program significant improves the diagnostic capacity in the region. Through these activities, the member laboratories in the regional network were able to harmonize and improve the test sensitivity to a satisfactory level. Not only ensuring the quality of ongoing diagnostic services, the program has been proven critically of value, in the face of emerging Influenza A (H7N9) virus, when the regional laboratory network mechanisms and diagnostic protocols can be efficiently implemented at the member laboratories with better confidence in quality services. Regional Biosafety Program Since 2010, FAO has been conducting a biosafety enhancement program for national veterinary laboratories in countries of South and Southeast Asia. The activities include biosafety risk assessment, development of biosafety standard operation protocols (SOPs) and regional and in-country trainings, and annual biosafety cabinet (BSC) certification and servicing. The results of the regional biosafety activities were reported back to the relevant regional laboratory network meetings to update network members on the progress of the program and to advocate for support related to laboratory biosafety management from the relevant laboratory authorities and stakeholders. The Regional Biosafety Program has been very well received among the network laboratories. During the past few years, the numbers of laboratories which participated and received the benefit from the program has remarkably expanded. In 2013, 29 laboratories from 10 countries had enrolled in the program. Strengthening of regional and international laboratory networks FAO encourages and supports the countries to establish the national laboratory network and also to participate in the regional network. The aims of such networking are to implement the regional quality assurance and biosafety improvement programs as well as to share experience and resources among the network members. To mentor the laboratories in the region, an expert group has been formed consisting of experts from international reference laboratories for the target diseases to provide technical advisory to the network members. The importance of quality assurance program and laboratory biosafety system has been advocated to

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health48
the laboratory director level at the Laboratory Director Forum jointly organized by FAO and OIE for their support to participate in the program and for the longer term carry out this on a routine basis. Support in planning and policy development and coordination Regional strategic framework for laboratory capacity building and networking For the longer-term impact, building capacity at the institutional level is required. FAO has been working with other international partners including OIE, experts from regional and international leading laboratories that have relevant work in the region to develop regional strategic framework for laboratory development. This is to ensure that the efforts in capacity building in the field of laboratory are carried out in a sustainable way and address needs of the countries and the region. In Southeast Asia, the establishment and endorsement by ASEAN of the “Regional strategic framework for laboratory capacity building and networking (Laboratory Framework)” in August 2012 represents a full engagement of the key regional stakeholder in supporting sustainable quality laboratory services across the region and has a significant impact on the regional preparedness against the newly emerging pathogens. The ASEAN Sectoral Working Group on Livestock (ASWGL)’s endorsement conveys a strong political commitment and expresses ownership and accountability of ASEAN on the achievement of the Laboratory Framework and the implementation thereof. The Laboratory Directors’ Forum provides a venue for discussion of issues related to
the national veterinary diagnostic laboratories, make strategic recommendations on these issues and act as a coordinating platform to promote laboratory quality services, collaboration and networking among the member national veterinary diagnostic laboratories within the RLN. In May 2013, the Laboratory Director
Forum has been recognized as the ASEAN ad-hoc laboratory focal group for animal health laboratory. The recognition of the Laboratory Directors’ Forum followed the
endorsement of the Laboratory Framework and marked the first time in ASEAN history to institutionalize a group dedicated to animal health laboratory issues. The Forum is mandated to support the implementation and monitoring of the Lab Framework, and to provide advices to relevant ASEAN sectoral bodies on related subject matters. In October 2013, the ASEAN Laboratory Directors’ Forum (ALDF) was held, for the first time, in closed consultation with ASEAN secretariat, convened the directors of the national veterinary laboratories and of the leading/reference laboratories from the ASEAN Member States. The ALDF Meeting discussed and agreed on the Terms of Reference (TOR) and Plan of Actions for 2013-2014 to be submitted to the 22nd ASWGL Meeting for consideration and approval. Establishment of ASEAN Coordination Centre for Animal Health and Zoonosis (ACCAHZ) Noting the continuing threats of TADs and zoonoses, AMS recognises the need for each AMS to build up its capacities and capabilities, as well as the need for a comprehensive, integrated, and concerted regional coordination mechanism (RCM) to deal with Transboundary animal diseases and zoonoses. In 2011, ASEAN Ministers endorsed the Comprehensive Proposal for the Establishment of the Regional Coordination Mechanism on Animal Health and Zoonoses (RCM) and later named as the ASEAN Coordination Centre for Animal Health and Zoonosis (ACCAHZ). An ad hoc group consisting of relevant officers from each member country was appointed as the Preparatory Committee (PrepCom) to be responsible to develop the Terms of Reference of the Center and to develop necessary instruments and frameworks to ensure a fully functioning and sustaining ACCAHZ. The ASEAN Regional Support Unit (RSU) was formed in 2010, as an interim coordination of ACCAHZ. The ASEAN RSU is currently funded by the Food and Agriculture Organization of the United Nations (FAO) through the European Union Highly Pathogenic Emerging and Re-emerging Diseases Programme (EU-HPED). The ASEAN RSU comprises of ASEAN technical experts in the fields of laboratory and epidemiology who provide not only the technical inputs to the regional capacity building program but also provide their coordination roles among member countries, ASEAN Secretariat and relevant bodies to ensure a sustainable capacity to deal with animal and zoonotic diseases. The operations of ASEAN RSU and their outcomes have exemplified the benefits of ACCAHZ, and testify to the continuation of these achievements when ACCAHZ becomes operational. Tripartite FAO-OIE-WHO Collaboration FAO-OIE-WHO continue to collaborate and coordinate global activities to address health risks at the animal-human-ecosystems interfaces particularly where a disease has the potential to impact on a large numbers of people and animals. This inter-

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 49
endorsement of the Laboratory Framework and marked the first time in ASEAN history to institutionalize a group dedicated to animal health laboratory issues. The Forum is mandated to support the implementation and monitoring of the Lab Framework, and to provide advices to relevant ASEAN sectoral bodies on related subject matters. In October 2013, the ASEAN Laboratory Directors’ Forum (ALDF) was held, for the first time, in closed consultation with ASEAN secretariat, convened the directors of the national veterinary laboratories and of the leading/reference laboratories from the ASEAN Member States. The ALDF Meeting discussed and agreed on the Terms of Reference (TOR) and Plan of Actions for 2013-2014 to be submitted to the 22nd ASWGL Meeting for consideration and approval. Establishment of ASEAN Coordination Centre for Animal Health and Zoonosis (ACCAHZ) Noting the continuing threats of TADs and zoonoses, AMS recognises the need for each AMS to build up its capacities and capabilities, as well as the need for a comprehensive, integrated, and concerted regional coordination mechanism (RCM) to deal with Transboundary animal diseases and zoonoses. In 2011, ASEAN Ministers endorsed the Comprehensive Proposal for the Establishment of the Regional Coordination Mechanism on Animal Health and Zoonoses (RCM) and later named as the ASEAN Coordination Centre for Animal Health and Zoonosis (ACCAHZ). An ad hoc group consisting of relevant officers from each member country was appointed as the Preparatory Committee (PrepCom) to be responsible to develop the Terms of Reference of the Center and to develop necessary instruments and frameworks to ensure a fully functioning and sustaining ACCAHZ. The ASEAN Regional Support Unit (RSU) was formed in 2010, as an interim coordination of ACCAHZ. The ASEAN RSU is currently funded by the Food and Agriculture Organization of the United Nations (FAO) through the European Union Highly Pathogenic Emerging and Re-emerging Diseases Programme (EU-HPED). The ASEAN RSU comprises of ASEAN technical experts in the fields of laboratory and epidemiology who provide not only the technical inputs to the regional capacity building program but also provide their coordination roles among member countries, ASEAN Secretariat and relevant bodies to ensure a sustainable capacity to deal with animal and zoonotic diseases. The operations of ASEAN RSU and their outcomes have exemplified the benefits of ACCAHZ, and testify to the continuation of these achievements when ACCAHZ becomes operational. Tripartite FAO-OIE-WHO Collaboration FAO-OIE-WHO continue to collaborate and coordinate global activities to address health risks at the animal-human-ecosystems interfaces particularly where a disease has the potential to impact on a large numbers of people and animals. This inter-

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health50
sectoral and multi-disciplinary approach is considered crucial to addressing the complex problem of zoonoses and other emerging infectious diseases. FAO is committed to the One Health approach to address emerging and re-emerging infectious animal and zoonotic diseases, which impact negatively on people’s wellbeing, safety and livelihoods. FAO, in collaboration with OIE and WHO as well as other international partners, has supported the coordination and several joint activities between animal and public health sectors at country, regional and global levels for disease specific activities. One Health Events such as symposia, meetings, planning, etc. have been jointly organized with the government authorities and the Tripartites in several member countries. The Tripartite members have taken turn in organizing the “Regional Workshop on Collaboration between Human-Animal Health Sectors on Zoonoses Prevention and Control for Asia” since 2010 and the fourth workshop will be organized in November 2013. The workshop aims to bring together authorities from relevant sectors, animal, human and wildlife health, to discuss the coordination mechanisms that can be implemented at the country level to improve multi-sectoral collaboration in managing emerging infectious diseases. Avian influenza, rabies and antimicrobial resistance have been identified as priority health problems that the coordination mechanisms can be applied to. Support to the prevention and control of specific zoonotic diseases FAO also supports several disease-specific programs, related to prevention and control of key zoonotic diseases in Asia, including Avian Influenza, Rabies, Nipah, Brucellosis and Anthrax. The disease specific program encompasses several components including disease surveillance and control, planning and policy development, cross-border collaboration, partner coordination, laboratory and epidemiology capacity building, value chain analysis, outbreak investigation, risk assessment etc.
Impacts, challenges and ways forward While it is recognized that country capacities in dealing with specific zoonotic diseases particularly avian influenza have been improved, it is expected that the countries would be able to apply such capacities to other emerging infectious and transboundary animal diseases. Various challenges to achieve this expectation include the limited number of human resources with proper skills. More importantly, political commitment from the government to ensure career path of human resources who have been trained, and to develop the national strategies related to animal health/disease control so financial resources can be in place to sustain activities in longer term. These challenges have even made it more difficult to apply/adapt to the changing environments or future emerging threats. FAO has made efforts to address the challenges in sustaining the investment that has been made by employing concurrently building capacity at institutional level including strategic planning and system development at national and regional levels. In addition, FAO continues to advocate to the decision makers of the member countries on such challenges that require their commitment and proactive involvement. However, the fact that national financial resources are limited in several developing countries, advocacy needs to be made to developmental partners to continue to support those countries to deal with the key emerging zoonotic and transboundary diseases of the global concerns.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 51
Impacts, challenges and ways forward While it is recognized that country capacities in dealing with specific zoonotic diseases particularly avian influenza have been improved, it is expected that the countries would be able to apply such capacities to other emerging infectious and transboundary animal diseases. Various challenges to achieve this expectation include the limited number of human resources with proper skills. More importantly, political commitment from the government to ensure career path of human resources who have been trained, and to develop the national strategies related to animal health/disease control so financial resources can be in place to sustain activities in longer term. These challenges have even made it more difficult to apply/adapt to the changing environments or future emerging threats. FAO has made efforts to address the challenges in sustaining the investment that has been made by employing concurrently building capacity at institutional level including strategic planning and system development at national and regional levels. In addition, FAO continues to advocate to the decision makers of the member countries on such challenges that require their commitment and proactive involvement. However, the fact that national financial resources are limited in several developing countries, advocacy needs to be made to developmental partners to continue to support those countries to deal with the key emerging zoonotic and transboundary diseases of the global concerns.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health52
Health Risks at the Human and Animal Interface: Elephant Melioidosis
Asst. Prof. Sompoth Weerakhun, DVM., PhD Department of Medicine, Faculty of Veterinary Medicine,
Khonkaen University, Khonkaen 40002, Thailand Corresponding author: [email protected]
Elephant is the one of most interested and important animals, cause impressive enormous size, intelligent, tame, playful, and longevity. Captive or domesticated elephants were human used for many purposes such as for war that found historical war elephants in many countries of Asia, ceremonial purposes, forestry working, transport, circus, and zoo. Elephants rapidly decline, Asian elephant (Elephas maximus) in Thailand and might the other countries nearby are typically decreasing of number found since 1900, that domesticated elephants are declined from 100,000 animals to about 2,500 animals now. The number decreasing of them is very critical and awareness, thus there must protected from any conditions that harmful population such as environment, nutrition, management, and diseases. Many conditions escape for unknown until now, we need investigation and perform the team and standard methods. Melioidosis is the most common harmful disease in human and several animals in endemic area, many people killed yearly, and loss of huge economic. However, there are no studied and reported in elephants that also same environmental risk for melioidosis. Burkholderia pseudomallei is a facultative intracellular gram-negative bacillus that causes the disease melioidosis. Melioidosis has recognized as an important public health problem in endemic area of Southeast Asia and Northern Australia, typically remaining between the latitudes of 20˚N and 20˚S, first case was reported at Myanmar in 1911, as a glanders-like condition, that 38 cases killed (Whitmore and Krishnaswami, 1912). It has also been recognized as a potential global threat in the realm of bioterrorism (Category B, Centers for Disease Control, U.S). Several reports have provided reviews of the known distribution such as Australia, Papua New Guinea, Thailand, Malaysia, Loa People’s Democratic Republic, Cambodia, Taiwan and China that already environmental studied (Cheng and Currie, 2005). Moreover, the disease was found in sub-Saharan Africa, Central and South America and the Caribbean (Cheng and Currie, 2005). Although, this pathogen has excellent studied in the parts of the world detailed above, many area of the world simply lack of the diagnostic capabilities and investigation. Thus, the distribution of the disease is really still poorly understood. B. pseudomallei can be isolated from soil and water in the endemic areas that it was believed in relate to increasing the level of human and animal patient due to melioidosis. However, remain unknown how it is disseminated in the environment, what environmental factors limit its geographic ranges, and
what environmental risk factors are important associated increases the disease. The presence of the pathogen in environment has been associated with land use that the presence of animals; domestic or livestock or native wild species has been associated with positive soil samples (Kaestli et al., 2009). Pathogen also was possibly environmental contaminated by bird’s defecation, but rare (Kaestli et al., 2009). Some reports described positive samples were isolated from area around creek with high water content or in close to grass land, so animals can be infected and dispersal though grazing (Kaestli et al., 2009). However, some factors have been found promoting persistence and growth of this bacterium, such as higher aeration (O2) and nitrogen content, watering, and lower pH (5.0-6.0) (Kaestli et al., 2009). Clay soil associated with oxidized iron was related to the presence of B. pseudomallei (Kaestli et al., 2007; Kaestli et al., 2009). Sandy soil has also been reported to allow the bacterium move freely with the flow of water and therefore increase contact and infect the human and animals during the rainy season (Choy et al., 2000; Cheng and Currie, 2005). Water bores has also believed as a source of Burkholderia pseudomallei with soft, acidic, low salinity and higher iron contented in water (Draper et al., 2010). However, B. pseudomallei has been found to well survive in other conditions (Pumpuang et al., 2011). B. pseudomallei is highly pathogenic for human and animals, with high morbidity and mortality rate in endemic areas. The incidence for melioidosis has been reported as highest in Northern Australia (50.2/100,000) that range from 5.4 to 50.2 per 100,000 people (Parameswaran et al., 2012). Thailand has also reported with the high incidence about 4.4 cases per 100,000 people or 2,000 to 3,000 cases yearly range from 4.4 to 21.3 cases per 100,000 people. In addition, it has been reported 0.19/100,000 in Taiwan, 1.7/100,000 in Singapore, and 4.3 to 16.35/100,000 in Malaysia (Soffler, 2012). The typical high incidences of bacteremic melioidosis patient were studied in Northern Australia (Currie et al., 2010) and Thailand (Limmathurotsakul et al., 2010) as 50 to 55% of melioidosis patient, similar other country of Southeast Asia. Singapore used to report highest as 90.9%, but more recently reported as 50.4% (Soffler, 2012). Taiwan presented the higher incidence range of bacteremia as 75 to 81.1% that was associated with an outbreak of cases following Typhoon Haitang in July of 2005 (Soffler, 2012). The relation in wet season to the outbreak of melioidosis has been studied, that found unusually heavy rain, strong wind and flash flooding in early 2004 preceded a cluster of melioidosis cases that associated increasing pneumonia patient and mortality rate (Soffler, 2012). In Australia, it was reported as many as 81% of melioidosis patient that presented during rainy season (Currie et al., 2010). The intensity of rainfall (≥125 mm 14 days prior to presentation) has been significantly correlated as an independently risk factor for pneumonia, septic shock and death in Australia (Currie and Jacups, 2003). It was believed that the bacterium can be freely move toward the surface when the

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 53
what environmental risk factors are important associated increases the disease. The presence of the pathogen in environment has been associated with land use that the presence of animals; domestic or livestock or native wild species has been associated with positive soil samples (Kaestli et al., 2009). Pathogen also was possibly environmental contaminated by bird’s defecation, but rare (Kaestli et al., 2009). Some reports described positive samples were isolated from area around creek with high water content or in close to grass land, so animals can be infected and dispersal though grazing (Kaestli et al., 2009). However, some factors have been found promoting persistence and growth of this bacterium, such as higher aeration (O2) and nitrogen content, watering, and lower pH (5.0-6.0) (Kaestli et al., 2009). Clay soil associated with oxidized iron was related to the presence of B. pseudomallei (Kaestli et al., 2007; Kaestli et al., 2009). Sandy soil has also been reported to allow the bacterium move freely with the flow of water and therefore increase contact and infect the human and animals during the rainy season (Choy et al., 2000; Cheng and Currie, 2005). Water bores has also believed as a source of Burkholderia pseudomallei with soft, acidic, low salinity and higher iron contented in water (Draper et al., 2010). However, B. pseudomallei has been found to well survive in other conditions (Pumpuang et al., 2011). B. pseudomallei is highly pathogenic for human and animals, with high morbidity and mortality rate in endemic areas. The incidence for melioidosis has been reported as highest in Northern Australia (50.2/100,000) that range from 5.4 to 50.2 per 100,000 people (Parameswaran et al., 2012). Thailand has also reported with the high incidence about 4.4 cases per 100,000 people or 2,000 to 3,000 cases yearly range from 4.4 to 21.3 cases per 100,000 people. In addition, it has been reported 0.19/100,000 in Taiwan, 1.7/100,000 in Singapore, and 4.3 to 16.35/100,000 in Malaysia (Soffler, 2012). The typical high incidences of bacteremic melioidosis patient were studied in Northern Australia (Currie et al., 2010) and Thailand (Limmathurotsakul et al., 2010) as 50 to 55% of melioidosis patient, similar other country of Southeast Asia. Singapore used to report highest as 90.9%, but more recently reported as 50.4% (Soffler, 2012). Taiwan presented the higher incidence range of bacteremia as 75 to 81.1% that was associated with an outbreak of cases following Typhoon Haitang in July of 2005 (Soffler, 2012). The relation in wet season to the outbreak of melioidosis has been studied, that found unusually heavy rain, strong wind and flash flooding in early 2004 preceded a cluster of melioidosis cases that associated increasing pneumonia patient and mortality rate (Soffler, 2012). In Australia, it was reported as many as 81% of melioidosis patient that presented during rainy season (Currie et al., 2010). The intensity of rainfall (≥125 mm 14 days prior to presentation) has been significantly correlated as an independently risk factor for pneumonia, septic shock and death in Australia (Currie and Jacups, 2003). It was believed that the bacterium can be freely move toward the surface when the

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health54
rainfall and flow with the water, then increasing contact with human and animals by direct contraction and aerosol. However, some largest studied of Thailand reported as a significant negative correlation with rainfall (Limmathurotsakul et al., 2010). The patients due to melioidosis were retrospective and prospective studied that showed the amount of patient with soil exposure. The disease was associated with rice farming, the amount of melioidosis patients were rice farmer in Vietnam, Cambodia and Thailand as 69.4 to 84.9% (Suputtamongkol et al., 1994; Suputtamongkol et al., 1999; Soffler, 2012). The correlation of disease to soil exposure was studied in other occupations that higher level of soil exposure, the results showed that they were also risk for melioidosis and death (Soffler, 2012). Moreover, contaminated drinking water without treat with boiled was increase risk of acquiring melioidosis for 2.5 times (Limmathurotsakul et al., 2012). B. pseudomallei can also be isolated from blood, eyes, wound, pus, sputum, vaginal swabs, milk, urine, and feces (Soffler, 2012). It is typically infected by the route of percutaneous inoculation, inhalation, ingestion, sexual transmission, transplacental, and zoonotic transmission (Soffler, 2012). Three cases of suspected zoonotic transmission have been described from Australia (Choy et al., 2000). Milk from infected goats has cultured positive, zoonotic transmission of melioidosis through infected milk has been a serious concern in endemic areas (Choy et al., 2000). It is also contaminated to environment by urine, feces, exudates or carcasses that leading to human exposure and infection. The clinical signs of melioidosis is multi-organs involved, depend on the organs defected. The incubation period is variable that almost acute 2 to 3 days only (Dance et al., 1989), but some documents reviewed more chronic and long term for year to several decades (Soffler, 2012). There is no typical presentation of disease that sometime called ‘remarkable imitator’. However, there is patterns of disease and manifestation of melioidosis that is more common than others. Pulmonary melioidosis is recognized as the most common presentation and most common cause of fatal community-acquired septicemic pneumonia (Dance et al., 1989; Suputtamongkol et al., 1994). Hepatic and splenic granulomatous and abscessation are more frequently found in Thai patients (Maude et al., 2012). Thus, clinical signs in pneumonia often include fever, cough, dyspnea, thoracic pain, hemoptysis, and leukocytosis (Soffler, 2012). Septicemic melioidosis is also most common that half of patients are displayed septic shock. Animal melioidosis show most common of chronic that develop numerous foci in internal organs, thus animals present no typical signs, multiorgan dysfunction, septic shock and death (Soffler, 2012). Melioidosis in Thailand were almost studied in human, firstly reported in 1955 by Jittivej et al. (Limmathurotsakul et al., 2013). The reports of melioidosis in Thailand were only three cases between 1955 to 1964 due to lack of investigation and
diagnostic capacities. Then in 1985, increasing reports of melioidosis and high mortality was retrospective studied that found 595 patients with high fatality as 90% of septicemic melioidosis patients (134/154) (Limmathurotsakul et al., 2013). Recently, there are more than 2,500 culture-confirmed melioidosis in Thailand each year and as the world’s highest. The patients about 57.4% of melioidosis were septicemia that high fatality as 80 to 90%. The absolutely diagnose and treat can typically help decreasing, but 40% of septicemic melioidosis cases still died. Therefore, it is estimated that more than 1,000 people died (Limmathurotsakul et al., 2013). Since 2007 until 2013, the number of patient was reported as 920 cases (8 died), 1,350 cases (11 died), 3,920 cases (12 died), and 1,735 cases (2 died) in 2007, 2009, 2011, and 2013 (between Jan to Aug), respectively (Limmathurotsakul et al., 2013). The incidence of melioidosis showed significantly highly endemic in Northeast Thailand compared other parts of Thailand as 8 to 10 times (Leelarasamee et al., 1996; Vuddahakul et al., 1999), whereas Central, North and South Thailand were lower and similar number as 13 to 18 cases per 100,000 people (Vuddahakul et al., 1999). The bacterium were also isolated from soil compared the part, the data showed that Northeast Thailand was also highest incidence (20%) or 2 to 4 times compared other parts (4-6%) (Vuddahakul et al., 1999; Wuthieknun et al., 1995), and the number of colony (cfu.) from soil was the most highest (230 cfu./ml.) as 20 times compared other parts of Thailand (10 cfu./ml.) (Smith et al., 1995; Wuthieknun et al., 1995). Burkholderia pseudomallei infection is the second most common cause of community-acquired bacteremia in Northeast Thailand (19.3%), compared Escherichia coli (23.1%) and Staphylococcus aureus (8.2%) (Limmathurotsakul et al., 2013). Melioidosis in Northeast Thailand caused people death equal tuberculosis, but higher than other common infectious diseases such as dengue, measles, and leptospirosis (Limmathurotsakul et al., 2013). The average cost per fatal case of melioidosis was around $14,500. Therefore, it could be estimated that at least $14,500,000 (฿435,000,000) economic burden in Thailand (Bhengsri et al., 2013).
The animal melioidosis was well reported in Australia, the native animals and livestock such as camel, alpaca, goat and sheep were high susceptible for the disease (Choy et al., 2000). Dog and cat were firstly reported affected by melioidosis in 1932 by Stanton and Fletcher (Soffler, 2012). Several animals have been reported for infection of B. pseudomallei such as horse, mule, cattle, buffalo, pig, dog, cat, deer, kangaroo, koala, crocodile, dolphin, wallaby, panda, gorilla, monkey, langur, zebra, rabbit, penguin, and parrot (Chen and Currie, 2005; Sprague and Neubauer, 2004). Elephant kept in Thailand were also detected the antibody for melioidosis (Punchoopet et al., 2012). Seroprevalence of animal melioidosis using indirect haemagglutination test (IHA) has been established that sensitivity and specificity as 90% and 71%, respectively at cut-off 1:160 (Chailert et al., 2004), common used for screening melioidosis in the endemic area. Melioidosis antibody of cattle in the

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 55
diagnostic capacities. Then in 1985, increasing reports of melioidosis and high mortality was retrospective studied that found 595 patients with high fatality as 90% of septicemic melioidosis patients (134/154) (Limmathurotsakul et al., 2013). Recently, there are more than 2,500 culture-confirmed melioidosis in Thailand each year and as the world’s highest. The patients about 57.4% of melioidosis were septicemia that high fatality as 80 to 90%. The absolutely diagnose and treat can typically help decreasing, but 40% of septicemic melioidosis cases still died. Therefore, it is estimated that more than 1,000 people died (Limmathurotsakul et al., 2013). Since 2007 until 2013, the number of patient was reported as 920 cases (8 died), 1,350 cases (11 died), 3,920 cases (12 died), and 1,735 cases (2 died) in 2007, 2009, 2011, and 2013 (between Jan to Aug), respectively (Limmathurotsakul et al., 2013). The incidence of melioidosis showed significantly highly endemic in Northeast Thailand compared other parts of Thailand as 8 to 10 times (Leelarasamee et al., 1996; Vuddahakul et al., 1999), whereas Central, North and South Thailand were lower and similar number as 13 to 18 cases per 100,000 people (Vuddahakul et al., 1999). The bacterium were also isolated from soil compared the part, the data showed that Northeast Thailand was also highest incidence (20%) or 2 to 4 times compared other parts (4-6%) (Vuddahakul et al., 1999; Wuthieknun et al., 1995), and the number of colony (cfu.) from soil was the most highest (230 cfu./ml.) as 20 times compared other parts of Thailand (10 cfu./ml.) (Smith et al., 1995; Wuthieknun et al., 1995). Burkholderia pseudomallei infection is the second most common cause of community-acquired bacteremia in Northeast Thailand (19.3%), compared Escherichia coli (23.1%) and Staphylococcus aureus (8.2%) (Limmathurotsakul et al., 2013). Melioidosis in Northeast Thailand caused people death equal tuberculosis, but higher than other common infectious diseases such as dengue, measles, and leptospirosis (Limmathurotsakul et al., 2013). The average cost per fatal case of melioidosis was around $14,500. Therefore, it could be estimated that at least $14,500,000 (฿435,000,000) economic burden in Thailand (Bhengsri et al., 2013).
The animal melioidosis was well reported in Australia, the native animals and livestock such as camel, alpaca, goat and sheep were high susceptible for the disease (Choy et al., 2000). Dog and cat were firstly reported affected by melioidosis in 1932 by Stanton and Fletcher (Soffler, 2012). Several animals have been reported for infection of B. pseudomallei such as horse, mule, cattle, buffalo, pig, dog, cat, deer, kangaroo, koala, crocodile, dolphin, wallaby, panda, gorilla, monkey, langur, zebra, rabbit, penguin, and parrot (Chen and Currie, 2005; Sprague and Neubauer, 2004). Elephant kept in Thailand were also detected the antibody for melioidosis (Punchoopet et al., 2012). Seroprevalence of animal melioidosis using indirect haemagglutination test (IHA) has been established that sensitivity and specificity as 90% and 71%, respectively at cut-off 1:160 (Chailert et al., 2004), common used for screening melioidosis in the endemic area. Melioidosis antibody of cattle in the

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health56
North Thailand was detected that in Chiang Mai Province and Chiang Rai Province presented 0.4% (Srikitjakarn et al., 2002) and 1.45% (Tiwananthakorn et al., 2003), respectively. Goat and sheep in the South Thailand presented 0.5% (Thongnoon et al., 2001). Cattle kept in upper part of Northeast Thailand presented 4.97% (Thongpan et al., 2006), whereas beef, dairy cow and buffalo in lower part presented 9.56%, 1.02% and 0.76%, respectively and accumulated total as 9.44% (Wongnak and Thecho, 2010). There were 49 livestock animals died, collected from East and South Thailand since 2006 to 2010, and then were culture-confirmed melioidosis. Goat was highest incidence compared with pig and cattle. (Limmathurotsakul et al., 2012). Positive bacterial cultured was presented in wildlife such as deer, crocodile, monkey and camel (Intharasri et al., 2004; Thongpan et al., 2006; Wongnak and Thecho, 2010; Srikawkheaw and Lawhavinit, 2010). This data showed all environmental part of Thailand might risk for melioidosis.
Seroprevalence of melioidosis in elephants all part of Thailand, 485 animals was investigated in 2010 through 2011 by indirect haemagglutination test. This was first report that established for melioidosis in Asian elephant. The results described that Asian elephant in Thailand were high antibody titer for Burkholderia pseudomallei, as 25.36% (123/485), and also reported that Northeast Thailand was the most incidences as 50.65% (39/77) and significantly differed from other parts (p<0.05), followed by East, South, Central and North as 24.18% (44/182), 21.95% (9/41), 19.01% (23/121) and 12.5% (8/56), respectively at cut-off 1:160 (Punchoopet et al., 2012). ). Although, they displayed higher titer cut-off (1:160) compared with other domestic animals (cattle, goat, sheep, pig, deer) in endemic area (18 Provinces) as only 1.6 to 2% of seroprevalence (Intharasri et al., 2004; Srikawkheaw and Lawhavinit, 2010), the elephants did not show any clinical signs or subclinical, that found in native animal species, and also in human on the endemic area. The researchers plan to do more for investigation and using other gold standard methods confirmed. Although, no publication reported of elephant melioidosis using culture-confirmed, one death case was suspected melioidosis in elephant with granulomatous lesion. The author also detected one case of camel infected and culture-confirmed, it displayed granulomatous on lung, spleen, kidney, liver, peritoneum and multiorgans. In addition, the incidence of animal melioidosis showed also significantly highly endemic in Northeast compared other parts of Thailand. Animal melioidosis has also been described in several animals in Thailand, which parallels in human and also associated with environment. We believed that several animals and amount number infected for B. pseudomallei and must intensive investigated and performed microbiological facilities such as bacterial culture and PCR.
Recently, elephants of two countries nearby Maekong River; Surin Province, Thailand, and Sayabouly Province, Loa People’s Democratic Republic, are planned to melioidosis investigation. Health status of elephants will observed and recorded, and provide screening serum antibody detection of melioidosis by indirect haemagglutination test, bacterial culture-confirmed from trunk swab, sputum, urine, feces, and blood, and also might provide PCR for DNA or RNA identification. Environment risks are also bacterial culture detected by soil, water, feeds (grass or hays), and animals defecation. References: Bhengsri, S., Lertiendumrong, J., Baggett, H.C., et al. (2013). Economic burden of
bacteremic melioidosis in Eastern and Northeastern, Thailand. Am. J. Trop. Med. Hyg., 89(2): 369-373.
Chailert, S., Sriar-rarmrungrueng, T., Porntong, W. and Tomanakan, K. (2004). Seroepidemiology and serodiagnosis of melioidosis in Khonkaen using Burkhoderia pseudomallei antigen by Passive Hemagglutination Agglutination (PHA). Khonkaen Hospital Medical J., 28(2): 120-126.
Cheng, A.C. and Currie, B.J. (2005). Melioidosis: Epidemiology, pathophysiology, and management. Clin. Microbiol. Rev., 18(2): 383-416.
Choy, J.L., Mayo, M., Jamaat, A. and Currie, B.J. (2000). Animal melioidosis in Australia. Acta. Tropica., 153-158.
Currie, B.J. and Jacups, S.P. (2003). Intensity of rainfall and severity of melioidosis. Australia. Emerging. Infect. Dis., 9: 1538-1542.
Currie, B.J., Ward, L. and Cheng, A.C. (2010). The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS. Negl. Trop. Dis., 4: e900.
Dance, D.A., Davis, T.M.E., Wattanagoom, Y., Chaowakul, W., Saiphan, P., Looareesuwan, S., Wuthienun, V. and White, N.J. (1989). Acute suppurative parotitis caused by Pseudomonas pseudomallei in children. J. Infect. Dis., 159: 654-660.
Draper, A.D., Mayo, M., Harrington, G., Karp, D., Yinfoo, D., et al. (2010). Association of the melioidosis agent Burkhoderia pseudomallei with water parameters in rural water supplies in northern Australia. Appl. Environ. Microbiol., 76: 5305-5307.
Intharasri, N., Thammasart, S. and Ekkatathr, M. (2004). Seroprevalence of melioidosis in livestock. National Institute of Animal Health, The 19th Livestock Annual Conference 2004. 26-30 May 2004. (in Thai)
Kaestli, M., Mayo, M., Harrington, G., Watt, F.,Hill, J., et al. (2007). Sensitive and specific molecular detection of Burkhoderia pseudomallei, the causative agent of melioidosis, in the soil of tropical northern Australia. Appl. Environ. Microbiol., 73: 6891-6897.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 57
Recently, elephants of two countries nearby Maekong River; Surin Province, Thailand, and Sayabouly Province, Loa People’s Democratic Republic, are planned to melioidosis investigation. Health status of elephants will observed and recorded, and provide screening serum antibody detection of melioidosis by indirect haemagglutination test, bacterial culture-confirmed from trunk swab, sputum, urine, feces, and blood, and also might provide PCR for DNA or RNA identification. Environment risks are also bacterial culture detected by soil, water, feeds (grass or hays), and animals defecation. References: Bhengsri, S., Lertiendumrong, J., Baggett, H.C., et al. (2013). Economic burden of
bacteremic melioidosis in Eastern and Northeastern, Thailand. Am. J. Trop. Med. Hyg., 89(2): 369-373.
Chailert, S., Sriar-rarmrungrueng, T., Porntong, W. and Tomanakan, K. (2004). Seroepidemiology and serodiagnosis of melioidosis in Khonkaen using Burkhoderia pseudomallei antigen by Passive Hemagglutination Agglutination (PHA). Khonkaen Hospital Medical J., 28(2): 120-126.
Cheng, A.C. and Currie, B.J. (2005). Melioidosis: Epidemiology, pathophysiology, and management. Clin. Microbiol. Rev., 18(2): 383-416.
Choy, J.L., Mayo, M., Jamaat, A. and Currie, B.J. (2000). Animal melioidosis in Australia. Acta. Tropica., 153-158.
Currie, B.J. and Jacups, S.P. (2003). Intensity of rainfall and severity of melioidosis. Australia. Emerging. Infect. Dis., 9: 1538-1542.
Currie, B.J., Ward, L. and Cheng, A.C. (2010). The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS. Negl. Trop. Dis., 4: e900.
Dance, D.A., Davis, T.M.E., Wattanagoom, Y., Chaowakul, W., Saiphan, P., Looareesuwan, S., Wuthienun, V. and White, N.J. (1989). Acute suppurative parotitis caused by Pseudomonas pseudomallei in children. J. Infect. Dis., 159: 654-660.
Draper, A.D., Mayo, M., Harrington, G., Karp, D., Yinfoo, D., et al. (2010). Association of the melioidosis agent Burkhoderia pseudomallei with water parameters in rural water supplies in northern Australia. Appl. Environ. Microbiol., 76: 5305-5307.
Intharasri, N., Thammasart, S. and Ekkatathr, M. (2004). Seroprevalence of melioidosis in livestock. National Institute of Animal Health, The 19th Livestock Annual Conference 2004. 26-30 May 2004. (in Thai)
Kaestli, M., Mayo, M., Harrington, G., Watt, F.,Hill, J., et al. (2007). Sensitive and specific molecular detection of Burkhoderia pseudomallei, the causative agent of melioidosis, in the soil of tropical northern Australia. Appl. Environ. Microbiol., 73: 6891-6897.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health58
Kaestli, M., Mayo, M., Harrington, G., Ward, L., Watt, F., et al. (2009). Landscape changes influence the occurrence of melioidosis bacterium Burkhoderia pseudomallei in soil in northern Australia. PLoS. Negl. Trop. Dis., 3: e364.
Leelarasamee, A., Trakulsomboon, S and Kusum, M. (1996). Geographical distribution and rate of positive culture for Burkhoderia pseudomallei in Thailand. Skin and deep tissue infection: a revisited. Bangkok, Medical media., 203-204.
Limmathurotsakul, D., Wongratanacheewin, S., Teerawattanasook, N., Wongsuvan, G., Chaisuksant, S., et al. (2010). Increasing incidence of human melioidosis in Northeast Thailand. Am. J. Trop. Med. Hyg., 82(6): 1113-1117.
Limmathurotsakul, D., Thammasart, S., Warrasuth, N., et al. (2012). Melioidosis in animals, Thailand, 2006-2010. Emerg. Infect. Dis., 18(2): 325-327.
Limmathurotsakul, D. (2013). Summary of current situation of melioidosis in Thailand. In Quick summary document for Ministry of Public Health Thailand. pp 10. Ministry of Public Health Thailand.
Maude, R.R., Vatcharapreechasakul, T., Ariyaprasert, P., Maude, R.J., Hongsuwan, M., et al. (2012). Prospective observational study of the frequency and features of intra-abdominal abscesses in patients with melioidosis in northeast Thailand. Trans. R. Soc. Trop. Med. Hyg., 106: 629-631.
Parameswaran, U., Baird, R.W., Ward, L.M., Currie, B.J. (2012). Melioidosis at Royal Darwin Hospital in the big 2009-2010 wet season: comparison with the proceeding 20 years. Med. J. Aus., 196:345-348.
Pumpuang, A., Chantratita, N., Wikraphat, C., Saiprom, N., Day, N.P., et al. (2011). Survival of Burkhoderia pseudomallei in distilled water for 16 years. Trans. R. Soc. Trop. Med. Hyg., 105: 598-600.
Punchoopet, P., Weerakhun, S., Sukon, P., Charoenpunt, P., Yindee, M. (2012). Seroprevalence of Burkhoderia pseudomallei in Asian elephants in Thailand by indirect hemagglutination test. KKU. Vet. J., 22(2): 132-140.
Smith, M.D., Wuthiekanum, V., Walsh, A.L. and White, N.J. (1995). Quantitative recovery of Burkhoderia pseudomallei from soil in Thailand. Trans. R. Soc. Trop. Med. Hyg., 89: 488-490.
Soffler, C. (2012). The development and characterization of caprine infection models of melioidosis. In Partial fulfillment of the requirements for the degree of Doctor of Philosophy. pp 169. Colorado State University.
Sprague, L.D. and Neubauer, H. (2004). Melioidosis in animals: A review on epizootiology, diagnosis and clinical presentation. J. Vet. Med., 51: 305-320.
Srikawkheaw, N. and Lawhavinit, O.A. (2010). The study of the detection of IgG antibody against Burkhoderia pseudomallei by ELISA and Indirect Haemagglutination Test. [Online]. Available from: http://anchan.lib.ku.ac.th/agnet/bitstream/123456789/542/1/KC 4603014.pdf. 15/12/2010.
Srikitjakarn, L., Sirimalaisuwan, A., Khattiya, R., Krueasukhon, K and Mekaprateep, M. (2002). Seroprevalence of melioidosis in dairy cattle in Chiang Mai Province, northern Thailand. Southeast Asian. J. Trop. Med. Public. Health., 33(4): 739-741.
Suputtamongkol, Y., Hall, A.J., Dance, D.A., Chaowakul, W., Rajchanuvong, A., et al. (1994). The epidemiology of melioidosis in Ubon Ratchatani, northeast Thailand. Int. J. Epidemiol., 23: 1082-1090.
Suputtamongkol, Y., Chaowakul, W., Chetchotisakd, P., Lertpatanasuwun, N., Intaranongpai, S., et al. (1999). Clin. Infect. Dis., 29: 408-413.
Tiwananthakorn, W., Saksaghawong, C., Krueasukhon, K., Sankwan, C., Chanachai, K and Pimgham, K. (2003). Seroprevalence of melioidosis using indirect hemagglutination antibody technique in dairy cows in Chiang Rai Province, Thailand. In The 11th International symposium of the world association of veterinary laboratory diagnosticians and OIE seminar on biotechnology, November 9-13, 2003.
Thongnoon, P., Chumek, P. and Aowchareon, B. (2001). Seroprevalence of Burkholderia pseudomallei infection of goat and sheep in Livestock Office of area 9. Thai. Vet. J. 11(3): 20-26. (in Thai)
Thongpan, P., Jongkajornpong, L. and Chareonchai, A. (2006). Seroprevalence of melioidosis of dairy and beef in Livestocks Office of area 4 Khonkaen. Thai-NIAH eJournal. _:64-76. (in Thai)
Vuddahakul, V., Yharavichikul, P., Na-Ngam, N., Jitsurong, S., Kunthawa, B., Noimay, P., Bimla, A. and Thamlikitkul, V. (1999). Epidemiology of Burkhoderia pseudomallei in Thailand. Am. J. Trop. Med. Hyg., 60(3): 458-461.
Whitmore, A. and Krishnaswami, C.S. (1912). An account of the discovery of a hitherto underscribed infective disease occurring among the population of Rangoon. Indian. Med. Gaz., 47: 262-267.
Wongnak, P. and Thecho, S. (2010). Seroprevalence of melioidosis, paratuberculosis and brucellosis of large animals in lower area of northern east Thailand. Available from: http://www.dld.go.th/pvlo_yst/webfile/research/research01.pdf. 22/11/2553 (in Thai)
Wuthieknun, V., Smith, M.D., Dance, D.A. and White, N.J. (1995). Isolation of Pseudomonas pseudomallei from soil in north-eastern Thailand. Trans. R. Soc. Trop. Med. Hyg., 89: 41-43.
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 59
Srikitjakarn, L., Sirimalaisuwan, A., Khattiya, R., Krueasukhon, K and Mekaprateep, M. (2002). Seroprevalence of melioidosis in dairy cattle in Chiang Mai Province, northern Thailand. Southeast Asian. J. Trop. Med. Public. Health., 33(4): 739-741.
Suputtamongkol, Y., Hall, A.J., Dance, D.A., Chaowakul, W., Rajchanuvong, A., et al. (1994). The epidemiology of melioidosis in Ubon Ratchatani, northeast Thailand. Int. J. Epidemiol., 23: 1082-1090.
Suputtamongkol, Y., Chaowakul, W., Chetchotisakd, P., Lertpatanasuwun, N., Intaranongpai, S., et al. (1999). Clin. Infect. Dis., 29: 408-413.
Tiwananthakorn, W., Saksaghawong, C., Krueasukhon, K., Sankwan, C., Chanachai, K and Pimgham, K. (2003). Seroprevalence of melioidosis using indirect hemagglutination antibody technique in dairy cows in Chiang Rai Province, Thailand. In The 11th International symposium of the world association of veterinary laboratory diagnosticians and OIE seminar on biotechnology, November 9-13, 2003.
Thongnoon, P., Chumek, P. and Aowchareon, B. (2001). Seroprevalence of Burkholderia pseudomallei infection of goat and sheep in Livestock Office of area 9. Thai. Vet. J. 11(3): 20-26. (in Thai)
Thongpan, P., Jongkajornpong, L. and Chareonchai, A. (2006). Seroprevalence of melioidosis of dairy and beef in Livestocks Office of area 4 Khonkaen. Thai-NIAH eJournal. _:64-76. (in Thai)
Vuddahakul, V., Yharavichikul, P., Na-Ngam, N., Jitsurong, S., Kunthawa, B., Noimay, P., Bimla, A. and Thamlikitkul, V. (1999). Epidemiology of Burkhoderia pseudomallei in Thailand. Am. J. Trop. Med. Hyg., 60(3): 458-461.
Whitmore, A. and Krishnaswami, C.S. (1912). An account of the discovery of a hitherto underscribed infective disease occurring among the population of Rangoon. Indian. Med. Gaz., 47: 262-267.
Wongnak, P. and Thecho, S. (2010). Seroprevalence of melioidosis, paratuberculosis and brucellosis of large animals in lower area of northern east Thailand. Available from: http://www.dld.go.th/pvlo_yst/webfile/research/research01.pdf. 22/11/2553 (in Thai)
Wuthieknun, V., Smith, M.D., Dance, D.A. and White, N.J. (1995). Isolation of Pseudomonas pseudomallei from soil in north-eastern Thailand. Trans. R. Soc. Trop. Med. Hyg., 89: 41-43.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health60
"HEALTH RISKS AT THE HUMAN-ANIMAL-ECOSYSTEM INTERFACE"
Eco-evolutionary perspectives on infectious diseases: scaling-up causal inference to understand biocomplexity in host-parasite relationships
Pierre Echaubard
Biology Department, Laurentian University, Ontario, Canada & Tropical Disease Research laboratory, Khon Kaen University Thailand
1- Ecosystem perspectives in H-P interactions: an eco-evolutionary justification Host-parasite (H-P) relationships are fundamentally embedded and can be perceived as functional nested complex systems: the parasite behaves as a system within its host, itself a system, nested within an ecological community, another system, nested itself in a larger ecosystem and so on (Horwitz and Wilcox 2005). Each system (from the parasite to the ecosystem) maintains its internal order by importing available energy/matter from and exporting wastes back into their host environments. The biological and physical dynamics of each system operates on vastly different scales and the broad causal mechanisms by which change arises on one scale are modulated by dominant mechanisms operating at higher or lower scales. As such, determinants of disease are connected to each other through synergies along a spatio-temporal continuum which eventually parallels a functional eco-evolutionary gradient where intimate coevolutionary processes between the host and the parasite are contingent upon broad scale ecological and environmental processes. In essence H-P relationships are thus eco-evolutionary entities. Practically, this functional definition of H-P systems emphasizes the context-dependent nature of infection outcomes and the dynamism of the very nature of the relationship between the host and its parasite: H-P relationships may switch from being apparently benign to detrimental in response to host condition or through strategic expression aimed at enhancing transmission (Renaud and de Meeüs 1991; Brown, Schmid-Hempel, and Schmid-Hempel 2003). The environment within which the interaction takes place and the scales at which the emergent mechanism occur need therefore to be accounted if we want to understand disease severity and periodicity. Ultimately this definition justifies the need to envision diseases from an ecosystem perspective and to carefully consider spatial and temporal scales of occurrence of disease determinants if we want to implement comprehensive research and delineate sustainable strategies of disease control (Galvani 2003).
2- Ecosystem change and Health: an illustration Beyond the conceptual evidence, many examples of the emergence and spread of infectious or parasitic diseases support the relevance of using an eco-evolutionary framework and an ecosystem perspective for the understanding of disease dynamics. The epidemics of infectious or parasitic diseases, such as lyme disease or shistosomiasis represent striking illustrations of cascading effects where landuse changes disrupt ecological functioning and alter host distribution, abundance and life-history which ultimately lead to the modification of coevolutionary processes and patterns of parasite virulence. For example, a key element in the re-emergence of schistosomiasis is the increasing number of habitats that are becoming favourable to the different snail species that are suitable intermediate hosts for the parasite (Constantin de Magny et al. 2008). Snails are abundant in rice fields and water reservoirs. Thus areas set aside for fish farms (e.g., Lake Nasser in Africa) have greatly increased the parasite’s transmission, and consequently human morbidity and mortality in the region. Changes in trophic webs due to the introduction of new species have also facilitated the increase in snail populations that are responsible for the transmission of schistosomiasis. For example, Lake Victoria in East Africa has hosted a great diversity of cichlid fish for several thousand years, and this exceptional diversity has led to spectacular specializations in several fish species. In particular, several cichlids have adapted to feed exclusively on mollusks, thus regulating their populations and keeping their densities low enough to slow down the transmission of the parasite to humans. However, the Nile perch, Lates niloticus was introduced to stimulate the local economy around Lake Victoria (Constantin de Magny et al. 2008) most often to the detriment of diversity of native cichlids species in turn leading to an explosion of mollusk populations. The increase in the human population seeking to take advantage of the new local economy, linked to fishing thus generated new centres for the transmission of schistosomiasis (Ogutu-Ohwayo 1990). This example, one among many others, highlight the complexity of the causal pathway leading to variation in disease outcomes and underlines the critical need of an ecosystemic approach to understand infectious disease dynamics in general and helminthiases in particular (Arya et al. 2009).
3- A novel eco-evolutionary framework for the understanding of Opisthorchis
viverrini transmission and delineating sustainable strategies for its control. Liver fluke infection caused by Opisthorchis viverrini (Ov) and related species is a major public health problem in Asia and Eastern Europe. Currently, more than 600 million people are at risk of infection with these trematodes (Keiser and Utzinger 2005). O. viverrini is endemic in Southeast Asian countries, including Thailand, Lao People’s Democratic Republic, Vietnam, and Cambodia (Sripa et al. 2007). Due to

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 61
2- Ecosystem change and Health: an illustration Beyond the conceptual evidence, many examples of the emergence and spread of infectious or parasitic diseases support the relevance of using an eco-evolutionary framework and an ecosystem perspective for the understanding of disease dynamics. The epidemics of infectious or parasitic diseases, such as lyme disease or shistosomiasis represent striking illustrations of cascading effects where landuse changes disrupt ecological functioning and alter host distribution, abundance and life-history which ultimately lead to the modification of coevolutionary processes and patterns of parasite virulence. For example, a key element in the re-emergence of schistosomiasis is the increasing number of habitats that are becoming favourable to the different snail species that are suitable intermediate hosts for the parasite (Constantin de Magny et al. 2008). Snails are abundant in rice fields and water reservoirs. Thus areas set aside for fish farms (e.g., Lake Nasser in Africa) have greatly increased the parasite’s transmission, and consequently human morbidity and mortality in the region. Changes in trophic webs due to the introduction of new species have also facilitated the increase in snail populations that are responsible for the transmission of schistosomiasis. For example, Lake Victoria in East Africa has hosted a great diversity of cichlid fish for several thousand years, and this exceptional diversity has led to spectacular specializations in several fish species. In particular, several cichlids have adapted to feed exclusively on mollusks, thus regulating their populations and keeping their densities low enough to slow down the transmission of the parasite to humans. However, the Nile perch, Lates niloticus was introduced to stimulate the local economy around Lake Victoria (Constantin de Magny et al. 2008) most often to the detriment of diversity of native cichlids species in turn leading to an explosion of mollusk populations. The increase in the human population seeking to take advantage of the new local economy, linked to fishing thus generated new centres for the transmission of schistosomiasis (Ogutu-Ohwayo 1990). This example, one among many others, highlight the complexity of the causal pathway leading to variation in disease outcomes and underlines the critical need of an ecosystemic approach to understand infectious disease dynamics in general and helminthiases in particular (Arya et al. 2009).
3- A novel eco-evolutionary framework for the understanding of Opisthorchis
viverrini transmission and delineating sustainable strategies for its control. Liver fluke infection caused by Opisthorchis viverrini (Ov) and related species is a major public health problem in Asia and Eastern Europe. Currently, more than 600 million people are at risk of infection with these trematodes (Keiser and Utzinger 2005). O. viverrini is endemic in Southeast Asian countries, including Thailand, Lao People’s Democratic Republic, Vietnam, and Cambodia (Sripa et al. 2007). Due to

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health62
poor sanitation practices and inadequate sewerage infrastructure, people infected with O. viverrini pass parasite eggs in their faeces and into natural water reservoirs, where the parasite eggs are eaten by the first intermediate host: snails of the genus Bithynia. After hatching, free swimming cercariae are released from the infected snails and locate their next intermediate host, cyprinoid fishes. Once in the fish, the cercaria encysts in the fins, skin, and muscles, and become metacercariae. The metacercariae are infective to humans and other fish-eating mammals upon ingestion of raw or undercooked fish and in turn the parasite’s life cycle is completed (Sripa et al. 2007). Until recently, most of the research on Opisthorchiasis was conducted to assess direct causation of disease spread and severity where proximate genetic, cellular and immunological mechanisms at the individual host level have been investigated in a vacuum. While this fundamental knowledge has been critical to delineate immediate short term remediation plans, it remains insufficient to define sustainable control strategies because this approach cannot integrate the extreme complexity of Ov transmission determinants across temporal and spatial scales. Aware of the necessity to incorporate environmental components to our understanding of Ov transmission dynamics, the research community started relatively recently to go out the lab and collect data on environmental variation and how it related to intermediate host distribution and abundance. However, to date the knowledge acquired still remains fragmentary and observed trends are unclear at best. The main reasons for this seems to be the absence of a cohesive and operational socio-ecological conceptual framework, capable of incorporating eco-evolutionary determinants occurring at various spatial and temporal scales and offering methodologies prompt to capture the extent of their variability. Numerous aspects of Opisthorchiasis indicate the strong context-dependency of its transmission dynamics and advocate the use of an ecosystem approach for its understanding. In particular, evidence suggests that agricultural practices and the intensification and modernization of rice farming, may boost Ov infection at the village/settlement level. For example, water parameters such as salinity and high amounts of faecal pollution correlate with the relative abundance of Bithynia snails and may be related to infection prevalence (Suwannatrai et al. 2011; Kaewkes et al. 2012). We however don’t know how and to what extent water quality and landscape architecture affect snails community through the alteration of ecological interactions and to what extent it favors the proliferation of Bithynia to the detriment of other species in certain area of intense humanization. It appears therefore critical to investigate how the patterns of ecological regulation of Bithynia populations are modulated by landuse practices and to document potential dilution or amplification effects of Ov transmission in snails communities (Begon 2008). Furthermore, recent broad scale investigations of Bithynia and Ov genetic variability indicate the occurrence of several potential cryptic species of Bithynia and several putative
strains of Ov that seemed to have coevolved in the same geographic areas (Kiatsopit et al. 2013; Saijuntha et al. 2007; Andrews, Sithithaworn, and Petney 2008). While further research is needed in this direction, the conclusions of these studies strongly suggest that genotypic interactions between specific Bithynia “cryptic species” and Ov strains may lead to different infection and transmission success depending on which Ov strain infects which Bithynia host. The importance of such evolutionary processes and there consequences for Bithynia susceptibility and Ov transmission success has been largely ignored until now. Current research on Ov need therefore to incorporate both ecological and evolutionary processes into a cohesive and operational conceptual framework in order to capture the range of direct and indirect determinants of disease transmission among intermediate hosts. Concomitantly, it is critical to approach the human component of the transmission dynamics from a similarly holistic perspective and to acknowledge the synergies among social and ecological components in determining disease prevalence, intensity and spread. Ultimately, disease biologists from all disciplines need to work together more effectively to integrate knowledge of the functioning of socio-ecological systems with knowledge of pathogens, cells, tissues and immune systems and to develop effective management strategies based upon this integration (Keesing, Ostfeld, and Eviner 2008).
Literature cited Andrews, Ross H., Paiboon Sithithaworn, and Trevor N. Petney. 2008. “Opisthorchis
Viverrini: An Underestimated Parasite in World Health.” Trends in Parasitology 24 (11): 497–501.
Arya, N, J Howard, S Isaacs, M L Mcallister, S Murphy, D Rapport, and D Waltner-Toews. 2009. “Time for an Ecosystem Approach to Public Health? Lessons from Two Infectious Disease Outbreaks in Canada.” Global Public Health 4 (1): 31–49.
Begon, Michael. 2008. “Effects of Host Diversity on Disease Dynamics.” In Infectious Disease Ecology: Effects of Ecosystems on Disease and of Disease on Ecosystems, Ostfeld, R. S., Keesing, F., Eviner, V. T. Prnceton, New Jersey, USA: Princeton University Press.
Brown, Mark J. F., Regula Schmid-Hempel, and Paul Schmid-Hempel. 2003. “Strong Context-Dependent Virulence in a Host–parasite System: Reconciling Genetic Evidence with Theory.” Journal of Animal Ecology 72 (6): 994–1002.
Constantin de Magny, Guillaume, François Renaud, Patrick Durand, and Jean-François Guégan. 2008. “Health Ecology: A New Tool, the Macroscope.” In , Thomas F., Renaud F., Gueguan J.-F., 129–48. Oxford University Press.
Galvani, Alison P. 2003. “Epidemiology Meets Evolutionary Ecology.” Trends in Ecology & Evolution 18 (3): 132–39.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 63
strains of Ov that seemed to have coevolved in the same geographic areas (Kiatsopit et al. 2013; Saijuntha et al. 2007; Andrews, Sithithaworn, and Petney 2008). While further research is needed in this direction, the conclusions of these studies strongly suggest that genotypic interactions between specific Bithynia “cryptic species” and Ov strains may lead to different infection and transmission success depending on which Ov strain infects which Bithynia host. The importance of such evolutionary processes and there consequences for Bithynia susceptibility and Ov transmission success has been largely ignored until now. Current research on Ov need therefore to incorporate both ecological and evolutionary processes into a cohesive and operational conceptual framework in order to capture the range of direct and indirect determinants of disease transmission among intermediate hosts. Concomitantly, it is critical to approach the human component of the transmission dynamics from a similarly holistic perspective and to acknowledge the synergies among social and ecological components in determining disease prevalence, intensity and spread. Ultimately, disease biologists from all disciplines need to work together more effectively to integrate knowledge of the functioning of socio-ecological systems with knowledge of pathogens, cells, tissues and immune systems and to develop effective management strategies based upon this integration (Keesing, Ostfeld, and Eviner 2008).
Literature cited Andrews, Ross H., Paiboon Sithithaworn, and Trevor N. Petney. 2008. “Opisthorchis
Viverrini: An Underestimated Parasite in World Health.” Trends in Parasitology 24 (11): 497–501.
Arya, N, J Howard, S Isaacs, M L Mcallister, S Murphy, D Rapport, and D Waltner-Toews. 2009. “Time for an Ecosystem Approach to Public Health? Lessons from Two Infectious Disease Outbreaks in Canada.” Global Public Health 4 (1): 31–49.
Begon, Michael. 2008. “Effects of Host Diversity on Disease Dynamics.” In Infectious Disease Ecology: Effects of Ecosystems on Disease and of Disease on Ecosystems, Ostfeld, R. S., Keesing, F., Eviner, V. T. Prnceton, New Jersey, USA: Princeton University Press.
Brown, Mark J. F., Regula Schmid-Hempel, and Paul Schmid-Hempel. 2003. “Strong Context-Dependent Virulence in a Host–parasite System: Reconciling Genetic Evidence with Theory.” Journal of Animal Ecology 72 (6): 994–1002.
Constantin de Magny, Guillaume, François Renaud, Patrick Durand, and Jean-François Guégan. 2008. “Health Ecology: A New Tool, the Macroscope.” In , Thomas F., Renaud F., Gueguan J.-F., 129–48. Oxford University Press.
Galvani, Alison P. 2003. “Epidemiology Meets Evolutionary Ecology.” Trends in Ecology & Evolution 18 (3): 132–39.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health64
Horwitz, Pierre, and Bruce A Wilcox. 2005. “Parasites, Ecosystems and Sustainability: An Ecological and Complex Systems Perspective.” International Journal for Parasitology 35 (7): 725–32.
Kaewkes, Wanlop, Sasithorn Kaewkes, Smarn Tesana, Thewarach Laha, and Banchob Sripa. 2012. “Fecal Bacterial Contamination in Natural Water Reservoirs as an Indicator of Seasonal Infection by Opisthorchis Viverrini in Snail Intermediate Hosts.” Parasitology International 61 (1): 49–51.
Keesing, Felicia, Richard S. Ostfeld, and Valerie T. Eviner. 2008. “Introduction.” In Infectious Disease Ecology: Effects of Ecosystems on Disease and of Disease on Ecosystems, Ostfeld, R. S., Keesing, F., Eviner, V. T., 1–5. Princeton, New Jersey, USA: Princeton University Press.
Keiser, Jennifer, and Jürg Utzinger. 2005. “Emerging Foodborne Trematodiasis.” Emerging Infectious Diseases 11 (10): 1507–14.
Kiatsopit, Nadda, Paiboon Sithithaworn, Weerachai Saijuntha, Trevor N. Petney, and Ross H. Andrews. 2013. “Opisthorchis Viverrini: Implications of the Systematics of First Intermediate Hosts, Bithynia Snail Species in Thailand and Lao PDR.” Infection, Genetics and Evolution 14 (March): 313–19.
Ogutu-Ohwayo, Richard. 1990. “The Decline of the Native Fishes of Lakes Victoria and Kyoga (East Africa) and the Impact of Introduced Species, Especially the Nile Perch, Lates Niloticus, and the Nile Tilapia, Oreochromis Niloticus.” Environmental Biology of Fishes 27 (2): 81–96.
Renaud, F., and T. de Meeüs. 1991. “A Simple Model of Host-Parasite Evolutionary Relationships. Parasitism: Compromise or Conflict?” Journal of Theoretical Biology 152 (3): 319–27.
Saijuntha, Weerachai, Paiboon Sithithaworn, Sopit Wongkham, Thewarach Laha, Vichit Pipitgool, Smarn Tesana, Neil B. Chilton, Trevor N. Petney, and Ross H. Andrews. 2007. “Evidence of a Species Complex within the Food-Borne Trematode Opisthorchis Viverrini and Possible Co-Evolution with Their First Intermediate Hosts.” International Journal for Parasitology 37 (6): 695–703.
Sripa, Banchob, Sasithorn Kaewkes, Paiboon Sithithaworn, Eimorn Mairiang, Thewarach Laha, Michael Smout, Chawalit Pairojkul, Vajaraphongsa Bhudhisawasdi, Smarn Tesana, and Bandit Thinkamrop. 2007. “Liver Fluke Induces Cholangiocarcinoma.” PLoS Medicine 4 (7): e201.
Suwannatrai, Apiporn, Kulwadee Suwannatrai, Surat Haruay, Supawadee Piratae, Chalida Thammasiri, Panita Khampoosa, Jutharat Kulsantiwong, et al. 2011. “Effect of Soil Surface Salt on the Density and Distribution of the Snail Bithynia Siamensis Goniomphalos in Northeast Thailand.” Geospatial Health 5 (2): 183–90.
Ocular Emergencies
Nithiwadee Lertittikul Veterinary Teaching Hospital,
Faculty of Veterinary Medicine, Khonkaen University, Khon Kaen 40002, Thailand
Proptosis Proptosis is displacement of the eyeball out of the eye socket.This problem can occur following trauma to the head region. It is most common in brachycephalic dog. Breed predisposed include: brachycephalic dog: pug, shihTzu, Pekingese. They have large eyelid opening, and to shallow orbit. This allows the globe to be easily displace. Prognosis is more common problem. But the dog breed with long nose and eye deep to the bony socket (dolichocephalic dog). Proptosis is rare and uncommon for the bone of face (skull) and jaw to be fractured. Cause : Trauma to face and head - fighting, hit by car, head trauma : Manual to restraint (pulling on the skin over the head)
Fully to examination To examination of the eye: PLR, periorbital tissue, optic nerve, extraocular muscles, hyphema Emergency management for proptosis 1) Replace the globe as soon as possible to prevent severe corneal damage and keep
the eye moist with Pretroleum jelly or antibiotic ointment. 2) Carefully examine the patient for systemic injuries. When the patient is stable,
induce general anesthesia 3) When eyelid get trapped behind the prolapsed globe. To reposition the eyeball
necessary to perform a lateral canthotomy to provide more exposure.Suture or spey hook can be use to pull the eyelids forward as the globe is gently pushed back into the eye socket.
4) Apply lubricant Antibiotic ointment to allow the globe to be easily 5) Sutured are pre-place in the upper and lower eyelids by temporary tarsorrhaphy
suture three or four simple interrupted or horizontal mattress suture of 3/0 or 4/0 nylon
6) suture should enter and exit at the eyelids margin and not on the conjunctival surface so as to prevent suture rubbing on the cornea.
7) Topical atropine and antibiotic are indicated to prevent uveitis

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 65
Ocular Emergencies
Nithiwadee Lertittikul Veterinary Teaching Hospital,
Faculty of Veterinary Medicine, Khonkaen University, Khon Kaen 40002, Thailand
Proptosis Proptosis is displacement of the eyeball out of the eye socket.This problem can occur following trauma to the head region. It is most common in brachycephalic dog. Breed predisposed include: brachycephalic dog: pug, shihTzu, Pekingese. They have large eyelid opening, and to shallow orbit. This allows the globe to be easily displace. Prognosis is more common problem. But the dog breed with long nose and eye deep to the bony socket (dolichocephalic dog). Proptosis is rare and uncommon for the bone of face (skull) and jaw to be fractured. Cause : Trauma to face and head - fighting, hit by car, head trauma : Manual to restraint (pulling on the skin over the head)
Fully to examination To examination of the eye: PLR, periorbital tissue, optic nerve, extraocular muscles, hyphema Emergency management for proptosis 1) Replace the globe as soon as possible to prevent severe corneal damage and keep
the eye moist with Pretroleum jelly or antibiotic ointment. 2) Carefully examine the patient for systemic injuries. When the patient is stable,
induce general anesthesia 3) When eyelid get trapped behind the prolapsed globe. To reposition the eyeball
necessary to perform a lateral canthotomy to provide more exposure.Suture or spey hook can be use to pull the eyelids forward as the globe is gently pushed back into the eye socket.
4) Apply lubricant Antibiotic ointment to allow the globe to be easily 5) Sutured are pre-place in the upper and lower eyelids by temporary tarsorrhaphy
suture three or four simple interrupted or horizontal mattress suture of 3/0 or 4/0 nylon
6) suture should enter and exit at the eyelids margin and not on the conjunctival surface so as to prevent suture rubbing on the cornea.
7) Topical atropine and antibiotic are indicated to prevent uveitis

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health66
8) Give corticosteroid 0.1-0.2mg/kg to control secondary uveitis and systemic steroid may be use to treatment optic neuritis to present.
9) Aviod use to NSAIDs when the dog to present hyphema 10)The tarsorrhaphy is left in place for 10-21 day Beware: exposure keratitis after the suture have been remove. Complication: Keratoconjunctivitis sicca and ulceration secondary to exposure are common in the postoperative. : Lateral strabismus and exposure keratitis “Further necessary to Surgery’’….Permanent partial tarsorrhaphy. Prognosis : Examine the eye 1) Most of the extraocular muscles (median and ventral rectus muscle) have been
ruptured, complete avulsion of three or more muscle the prognosis is poor, 2) Hyphema because it is usually associated with severe damage to the uvea tract. Prognosis is poor. If to present total hyphema, usually enucleation 3) Corneal or sclera rupture (the shape of globe is abnormal) because end up with
phthisis bulbi if left. Prognosis poor. 4) Pupillary light reflex (PLR) : A constirctied pupil suggests that at least the optic nerve is intact.
: A dilated pupil non-responsive indicates probable damage to the optic nerve or oculomotor nerve, pupil carries the poorest prognosis.
5) Breed : Breed with deep set eye (dolichocephalic dog) that are present with a globe
prolapsed have a much poorer prognosis than brachycephalic breed.
David J. Maggs, 2013
Acute glaucoma Acute glaucoma to present painful, red eyes (episcleral congestion) and blue eyes (diffuse corneal oedema). Vision is often impaired or absent. The pupil is unresponsive and semidilated. It is characterized by an increase intraocular pressure (IOP in dog normal 14-24 mmHg and cat normal 12-26 mmHg) Breeds predisposed: Bassets, Cocker Spaniels (English and American Cocker), Poodles, Chihuahua, Border Collie. Causes: Primary glaucoma occurs without other eye disease being present. Primary glaucoma is thought to arise from an inherent abnormality with the aqueous humour outflow system, and includes pectinate ligament dysplasia (goniodysgenesis) and is present in both eyes. Clinical Signs: 1) Red eye : deep perilimbal hyperemia (episcleral vessel congestion) 2) Blue eye : corneal edema 3) Pupil : non-responsive or mid dilated 4) Other signs : Pain = Blepharospasm, epiphora, Vission loss (Vision+/-, Dazzle +/-) Tomometry------IOP>25 mmHg Note:
- IOP=60-90 mmHg, the retina can survive for hours rather than day in dog - 3 day duration, IOP < 50 mmHg, 18% had vision return in a short term - Vision may return as long as 2weeks after hypertensive treatment, so there is
no hurry to enucleation. Emergency Treatment: The Primary aim of the treatment of acute glaucoma is the rapid reduction of IOP to within a safe target rang (≤20 mmHg)
Treatment for Acute Glaucoma 1) Topical PGF Derivatives (Prostaglandin analogues) : latanoprost, travoprost, bimatoprost to reduce IOP by increase the outflow
of aqueous from uveoscleral junction. : Drug of choice to treatment acute primary glaucoma. : 1 to 2 Drop to reduce IOP within 15-30 min, and recheck IOP in 1-2 hr (Maximun effect at 2 hr.) : IOP reduce to continued with prostaglandin q 12 hr. until IOP ≤ 20 mmHg : For primary glaucoma due to miotic effect : No effect in cat

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 67
Acute glaucoma Acute glaucoma to present painful, red eyes (episcleral congestion) and blue eyes (diffuse corneal oedema). Vision is often impaired or absent. The pupil is unresponsive and semidilated. It is characterized by an increase intraocular pressure (IOP in dog normal 14-24 mmHg and cat normal 12-26 mmHg) Breeds predisposed: Bassets, Cocker Spaniels (English and American Cocker), Poodles, Chihuahua, Border Collie. Causes: Primary glaucoma occurs without other eye disease being present. Primary glaucoma is thought to arise from an inherent abnormality with the aqueous humour outflow system, and includes pectinate ligament dysplasia (goniodysgenesis) and is present in both eyes. Clinical Signs: 1) Red eye : deep perilimbal hyperemia (episcleral vessel congestion) 2) Blue eye : corneal edema 3) Pupil : non-responsive or mid dilated 4) Other signs : Pain = Blepharospasm, epiphora, Vission loss (Vision+/-, Dazzle +/-) Tomometry------IOP>25 mmHg Note:
- IOP=60-90 mmHg, the retina can survive for hours rather than day in dog - 3 day duration, IOP < 50 mmHg, 18% had vision return in a short term - Vision may return as long as 2weeks after hypertensive treatment, so there is
no hurry to enucleation. Emergency Treatment: The Primary aim of the treatment of acute glaucoma is the rapid reduction of IOP to within a safe target rang (≤20 mmHg)
Treatment for Acute Glaucoma 1) Topical PGF Derivatives (Prostaglandin analogues) : latanoprost, travoprost, bimatoprost to reduce IOP by increase the outflow
of aqueous from uveoscleral junction. : Drug of choice to treatment acute primary glaucoma. : 1 to 2 Drop to reduce IOP within 15-30 min, and recheck IOP in 1-2 hr (Maximun effect at 2 hr.) : IOP reduce to continued with prostaglandin q 12 hr. until IOP ≤ 20 mmHg : For primary glaucoma due to miotic effect : No effect in cat

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health68
2) Osmotic diuretic : pull fluid from both aqueous humor and the vitreous : Mannital 1-1.5 g/kg IV (5-7.5 ml/kg of 20% solution over 15-25 min. Decrease IOP for 6 hrs, occasionally, for 2-3 day and water should be restricted for first 2-4 hrs. : Glycerin 1-2 g/kg orally.
Monitor hydration carefully and not be used in CHF or renal failure Can be repeated 2-3 time at 6-12 hrs
3) Carbonic anhydrase inhibitor : Methazolamide or dichlorphenamide : 2.2-4.4mg/kg orally q 8-12 hrs. : Acetazolamide (Diamox) 5-10 mg/kg orally q 8-12 mg/kg.
4) Prophylactic Therapy : Pilocarpine 2% eyes drop every 10 min for 30 min, then every 8-12 hrs. : Timoloi 0.5% bid.
5) Oral therapy : Norvasc (Amlodopine) 0.1-0.2 mg/kg once daily. This drug is a calcium channel blocker that used to treat high blood pressure. It has been found to have a protective effect for blood flow to optic nerve. : Prednisolone 1-2 mg/kg orally. The anti-inflammatory effect are protective ischaemia induced by the acute IOP increase.
David J. Maggs, 2013
Snake spit venom The Venom of all snake and scorpions act as a strong irritant in the eye. Direct ocular contract the Snake spit venom must be first aid treatment immediated. Cobra Venom is yellow, slightly acid. So include protein and non-protein (toxin, enzyme). Clinical sign : Severe Ocularpain, epiphora, immediate blepharospasm : Chemosis and corneal edema : Severe Keratitiatis : Uveitis and Corneal abrasion Treatment : Should be irrigated with water or saline irrigated immediately : Atropine eye drop dilate the pupil to prevent pain from spasm the ciliary muscle : Apply an antibiotic prevent infection : IV corticosteroid : +/- Antibiotic systemic : Collar ‘’’’’’’’’’’’’’’’’Aviod corticosteroid topical are contraindicated in all case of corneal ulceration and any corneal wound’’’’’’’’’’’’’’’’’’’ REFERENCES Gelatt KN, Brooks DE. The canine glaucoma. In; Veterinary Ophthalmology, 3rd edn. (ed. Gelatt KN) Lippincott/Williams & Wikins Baltimore, ‘1999’,701-754. Robin S. Ocular Emergencies. Distance Education Program. Ophthalmology : MModulez, The University of Sydney, 2013; 86-88, 105-110. David J.M., Paul E.M., Ron O. 2013. Slatter’s Fundamentals of Veterinary Ophthalmology 4th Edition. Saunders Elsevier. St.Louis, Missouri, 506p. Heidi F., Elaine H., 2011. Small Animal Ophthalmology : what’s your diagnosis. WILEY-BLACKWELL,.IOWA. pp.105-111.
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 69
Snake spit venom The Venom of all snake and scorpions act as a strong irritant in the eye. Direct ocular contract the Snake spit venom must be first aid treatment immediated. Cobra Venom is yellow, slightly acid. So include protein and non-protein (toxin, enzyme). Clinical sign : Severe Ocularpain, epiphora, immediate blepharospasm : Chemosis and corneal edema : Severe Keratitiatis : Uveitis and Corneal abrasion Treatment : Should be irrigated with water or saline irrigated immediately : Atropine eye drop dilate the pupil to prevent pain from spasm the ciliary muscle : Apply an antibiotic prevent infection : IV corticosteroid : +/- Antibiotic systemic : Collar ‘’’’’’’’’’’’’’’’’Aviod corticosteroid topical are contraindicated in all case of corneal ulceration and any corneal wound’’’’’’’’’’’’’’’’’’’ REFERENCES Gelatt KN, Brooks DE. The canine glaucoma. In; Veterinary Ophthalmology, 3rd edn. (ed. Gelatt KN) Lippincott/Williams & Wikins Baltimore, ‘1999’,701-754. Robin S. Ocular Emergencies. Distance Education Program. Ophthalmology : MModulez, The University of Sydney, 2013; 86-88, 105-110. David J.M., Paul E.M., Ron O. 2013. Slatter’s Fundamentals of Veterinary Ophthalmology 4th Edition. Saunders Elsevier. St.Louis, Missouri, 506p. Heidi F., Elaine H., 2011. Small Animal Ophthalmology : what’s your diagnosis. WILEY-BLACKWELL,.IOWA. pp.105-111.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health70
Neurological Examination in small animal
Eakkasit Barameechaithanan Veterinary Teaching Hospital,
Faculty of Veterinary Medicine, Khonkaen University, Khon Kaen 40002, Thailand
The neurologic examination is usually described as a complicated process that is wholly separate from the physical examination. In reality, much of the neurologic examination is done as a routine part of the physical examination. The examiner needs only to be aware of what is being observed. The addition of a few extra steps completes the examination. A brief description of integration of the neurologic examination with the physical examination of a small animal patient is presented as an example. This is followed by detailed discussion of each of the components. The process of completing the neurologic examination differs depending on the examiner’s routine in a physical examination. Aims of the neurological examination
1. Confirm the problem is caused by a lesion in the nervous system 2. Localize the lesion in the nervous system 3. Determine the cause and estimate the severity in nervous system 4. Estimate the prognosis
History taking and signalment The species, breed, age and sex of the patient may provide important clues to the diagnosis. Although few diagnoses can be positively ruled in or out the basis of the signalment, many diseases are more or less likely to occur among certain groups of animals. The prevalence of some disease varies greatly among species and breeds. Many infectious diseases are species specific such as canine distemper, feline infectious peritonitis and equine protozoal encephalomyelitis. Known inherited diseases must be considered, especially in cases involving multiple offspring of the same litter or lineage. The appendix lists many of the disease with a species or breed predilection. Young animals are more likely to have congenital and inherited disorders and infectious diseases. Older animals are more likely to have degenerative and neoplastic diseases. Although these criteria are not absolute, the probability is much greater that a 8-year-old brachycephalic dog experiencing seizures will have a neoplasm of the central nervous system (CNS) rather than a congenital anomaly. In the preliminary assessment, and sometimes in the final assessment, a diagnosis is an ordering of probabilities.
Components of the neurological examination 1. Observation - during every physical examination, should observe the animal’s
mental status, posture and movement. The animal should be allowed to move around the examination room or in an open area while the history is being taken. The examiner can obtain a general impression of the animal’s level of consciousness and behavior its response to environmental stimuli or to people. Observe mental status, posture, gait.
2. Palpation - after observation and history taking have been assessed, the physical
examination is initiated. Careful palpation of the musculoskeletal and integumentary systems should be performed at one time or on a regional basis in conjunction with other parts of the examination. Comparison of one side with the other for symmetry is best done as one step in the examination.
3. Postural Reactions - the complex responses that maintain an animal’s normal,
upright position are known as postural reactions. If an animal’s weight is shifted from one side to the other, from front to rear or from rear to front, the increased load on the supporting limbs requires increased tone in the extensor muscles to keep the limb from collapsing. Part of the adjustment in tone is accomplished through spinal reflexes, but for the changes to be smooth and coordinated, the sensory and motor systems of the brain must be involved. Abnormalities of complex reactions do not provide precise localize because lesions in any one of several areas of the nervous system may affect the reaction. The assessment of postural reactions is an important part of the neurologic examination. Minimal deficits in the function of a key component such as the cerebrum may cause significant alterations in postural reactions that are not detected when one observes the gait. Two major types of postural reactions are used. The first consists of hopping, wheelbarrowing and extensor postural thrust; these require movement of the limb to correct for displacement of the body and differ only in which limbs are tested. Weight bearing occurs, and so weakness has a significant impact on the performance of the reaction. The second type includes proprioceptive positioning and placing; these usually are performed with some support of the animal’s weight. Therefore weakness has less influence on performance. Both types of reactions are useful. Because the pathways for the postural reactions are similar, interpretation is essentially the same for all reactions. The following postural reactions are listed in a sequence convenient for performing an examination, hopping and proprioceptive positioning reactions should be tested. If they are normal, abnormalities are unlikely to be found in the other reactions.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 71
Components of the neurological examination 1. Observation - during every physical examination, should observe the animal’s
mental status, posture and movement. The animal should be allowed to move around the examination room or in an open area while the history is being taken. The examiner can obtain a general impression of the animal’s level of consciousness and behavior its response to environmental stimuli or to people. Observe mental status, posture, gait.
2. Palpation - after observation and history taking have been assessed, the physical
examination is initiated. Careful palpation of the musculoskeletal and integumentary systems should be performed at one time or on a regional basis in conjunction with other parts of the examination. Comparison of one side with the other for symmetry is best done as one step in the examination.
3. Postural Reactions - the complex responses that maintain an animal’s normal,
upright position are known as postural reactions. If an animal’s weight is shifted from one side to the other, from front to rear or from rear to front, the increased load on the supporting limbs requires increased tone in the extensor muscles to keep the limb from collapsing. Part of the adjustment in tone is accomplished through spinal reflexes, but for the changes to be smooth and coordinated, the sensory and motor systems of the brain must be involved. Abnormalities of complex reactions do not provide precise localize because lesions in any one of several areas of the nervous system may affect the reaction. The assessment of postural reactions is an important part of the neurologic examination. Minimal deficits in the function of a key component such as the cerebrum may cause significant alterations in postural reactions that are not detected when one observes the gait. Two major types of postural reactions are used. The first consists of hopping, wheelbarrowing and extensor postural thrust; these require movement of the limb to correct for displacement of the body and differ only in which limbs are tested. Weight bearing occurs, and so weakness has a significant impact on the performance of the reaction. The second type includes proprioceptive positioning and placing; these usually are performed with some support of the animal’s weight. Therefore weakness has less influence on performance. Both types of reactions are useful. Because the pathways for the postural reactions are similar, interpretation is essentially the same for all reactions. The following postural reactions are listed in a sequence convenient for performing an examination, hopping and proprioceptive positioning reactions should be tested. If they are normal, abnormalities are unlikely to be found in the other reactions.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health72
4. Spinal Reflexes - examination of the spinal reflexes tests the integrity of the sensory and motor components of the reflex arc and the influence of descending motor pathways on the reflex. Absence or depression of a reflex indicates complete or partial loss of either sensory or motor (LMN) components of the reflex; a normal reaction indicates that both sensory and motor components are intact; and exaggerated response indicates an abnormality in the motor pathways (UMN) that normally have an inhibitory influence on the reflex or a deficit that results in paresis of the antagonistic muscles is present. The examination should be performed with the animal in lateral recumbency. Muscle tone, previously evaluated with the animal in a standing position, should be evaluated again at this time. The pelvic limbs are tested first. Passive manipucially in the extensor muscles. Spreading the toes with slight pressure on the footpads elicits the extensor thrust reflex. The myotatic (stretch) reflexes then are evaluated. Routinely, only the patellar (knee jerk or quadriceps) reflex is tested. The cranial tibial and gastrocnemius muscles can also be evaluated, but the reflexes are more difficult to elicit and quantify. Next, the flexor reflex is tested by gently pinching the toes. To maintain cooperation of the patient, the examiner should apply the mildest stimulus that elicits a response. If flexion is induced by touching the foot, one need not crush the toe with a hemostat. The most predictable myotatic reflex in the thoracic limb is elicited when the extensor carpi radialis muscle (tendons over the carpus in large animals) is struck, producing a slight extension of the carpus. The triceps and biceps reflexes are difficult to elicit and evaluate in many normal animals. After examining the limbs on one side, the veterinarian turns the animal and examines the opposite limbs. With the exception of the flexor reflex, thoracic limb reflexes are inconsistenly elicited even in normal animals. The perineal reflex is a contraction of the anal sphincter in response to a touch, a pinprick, or a pinch in the perineal area. Flexion of the tail may occur simultaneously.
5. Cranial Nerves - examination of the cranial nerves(CN) is an important part,
especially when disease of the brain is suspected. An abnormality of a CN constitutes evidence of a specific, localized area of disease not provided by postural reactions. The CN examination is not difficult, and the most commonly affected CNs can be evaluated quickly. The majority of the evaluation of CN is done through testing reflexes. Two assessments differ and are denoted by the term “response”: the menace response and response to noxious stimulation of the nasal mucosa. The term response is used to specifically imply that the response observed to the stimulus requires normal forebrain function. This is in contradistinction to other cranial nerve reflexes, which analogous to spinal reflexes, only need normal functional integrity of a specific segment of the brainstem to be normal. Detection of any abnormalities on the screening
examination may be followed by a more complete examination to define the abnormality further.
6. Sensation – the sensory examination provides information relative to the
anatomic location and severity of the lesion. At this point in the neurologic examination, sensation has been tested by assessment of the CNs, spinal reflexes and proprioceptive positioning. Sensory modalities still to be tested include hyperesthesia, superficial pain and deep pain from the limbs and the trunk.
References Michael D. Lorenz, Joan R. Coates, Marc Kent. 2011. Handbook of veterinary
neurology. Fifth edition. Elsevier Saunders. Missouri. pp. 3-35. Simon R. Platt, Natasha J. Olby. 2004. BSVA Manual of Canine and Feline Neurology.
Third edition. British Small Veterinary Association. Gloucester. pp. 3-23.
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 73
examination may be followed by a more complete examination to define the abnormality further.
6. Sensation – the sensory examination provides information relative to the
anatomic location and severity of the lesion. At this point in the neurologic examination, sensation has been tested by assessment of the CNs, spinal reflexes and proprioceptive positioning. Sensory modalities still to be tested include hyperesthesia, superficial pain and deep pain from the limbs and the trunk.
References Michael D. Lorenz, Joan R. Coates, Marc Kent. 2011. Handbook of veterinary
neurology. Fifth edition. Elsevier Saunders. Missouri. pp. 3-35. Simon R. Platt, Natasha J. Olby. 2004. BSVA Manual of Canine and Feline Neurology.
Third edition. British Small Veterinary Association. Gloucester. pp. 3-23.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health74
FOOD SECURITY FOR ASSOCIATION OF SOUTHEAST ASIAN NATION
Romziah Sidik, 2014
Professor in Department of Animal Husbandry, Faculty of Veterinary Medicine of Airlangga University,
Surabaya-Indonesia. Humans need some adequate food to maintain their life and survival with healthy conditions and their good intelligence development. The security it means over the next meal is essential. Therefore, since 1996 by World Summit defined food security as “when people at all times have access to sufficient, safe, nutritious food to maintain a healthy and active life”, (ADB, 2013). According to World Bank, food security is defined as the availability and affordability to food to all the citizens of a country, with the essential elements being the availability of food and the ability to acquire it. World Health Organization (WHO) mentions about three pillars of food security:
1. Food availability covers the supply, it is provided by food production and technology, inventory, efficiency of supply chains, and local and international trade.
2. Food access, it means the ability to obtain adequate quantities of food, the purchasing power needed, adequate delivery mechanism, which include social nets.
3. Food utilization, depend on the need to meet dietary needs and cultural preferences.
Many factors due to food security, likes: the changes of food consumption and production with drive for global food sustainability, and its force by: the population growth, changes of demographics, any economic rises with the impact on structural transformation economically, social, and culturally holds the important consequences for the global food system.
It was predicted that global population will increased about 56%, it around 2.6 billion increasing of global population during year 2010 to 2050. The Asia – Pacific increase one to third of increasing global population, and it about 804. 48 million increasing the population with 71% will be in South Asia, and 189.48 million in ASEAN (Figure 1).
2564.48
804.48
189.43
World
South Asia
ASEAN
Figure1. Prediction of The World Population numbers (million) on 2010 - 2050.
Source: ADB (2013)
Based on the economic condition, it is followed by increasing the region Gross Domestic Production (GDP) from 7.6% during 1990 to 2010 to exceed about 3.4% from global average. ADB (2011) predicted that developing Asia will account for more than half of global GDP on 2050, and the cereal demand more than 60% demand in developing world will come from South and East Asia region in year 2030. By increasing income and population will impact on regional and global food systems as well.
Rapid industrialization and urbanization, with the region transformation will impact on the growing competition and overexploitation of natural resources will increasing constrict the region’s ability to produce some foods. Increasing the used petroleum products has the secondary effects on food prices due to increased the cost of energy and fertilizers, however some agricultural production have been diverted to bio-fuel production.
Climate change be impacted the availability of agricultural resources and the sustainable of food security. Severe floods and droughts as seen as the impact of climate change in some vulnerable countries as well as the increasing temperature in the region will impacts on reducing crop productivity. The climate change not only impact on the sustainable agriculture productions, also it had been impacted on livestock and fisheries productions. Rice is the large portion of daily caloric intake in Asia and Pacific (see Figure 2); therefore the economic growth and industrialization are crucial in many Asia economies, also its economic and political on market intervention by government is need it.
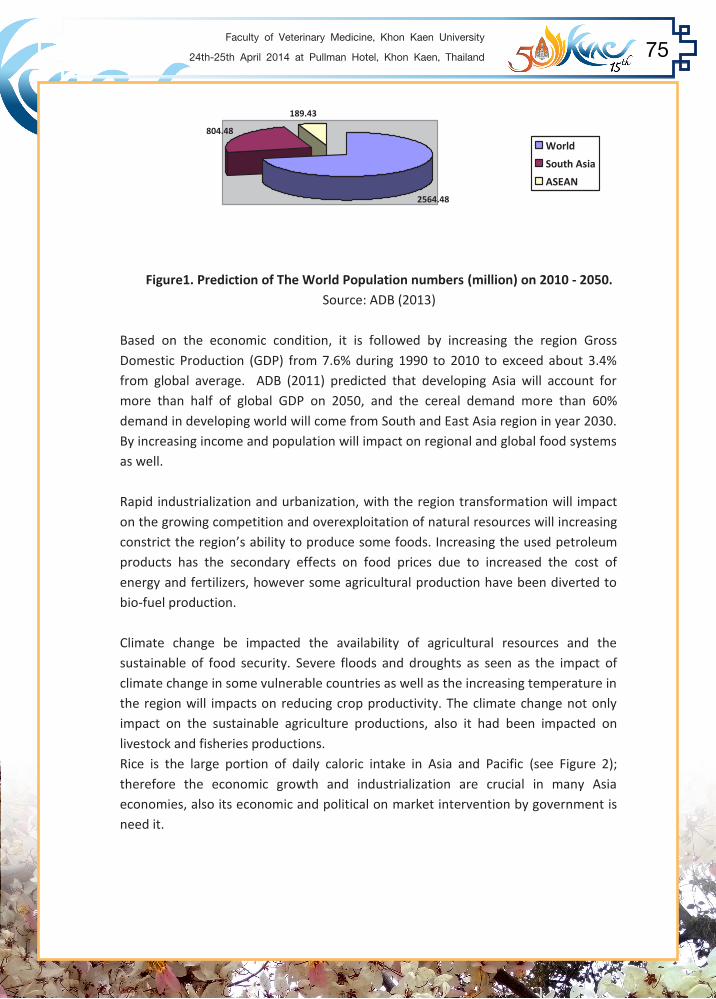
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 75
2564.48
804.48
189.43
World
South Asia
ASEAN
Figure1. Prediction of The World Population numbers (million) on 2010 - 2050.
Source: ADB (2013)
Based on the economic condition, it is followed by increasing the region Gross Domestic Production (GDP) from 7.6% during 1990 to 2010 to exceed about 3.4% from global average. ADB (2011) predicted that developing Asia will account for more than half of global GDP on 2050, and the cereal demand more than 60% demand in developing world will come from South and East Asia region in year 2030. By increasing income and population will impact on regional and global food systems as well.
Rapid industrialization and urbanization, with the region transformation will impact on the growing competition and overexploitation of natural resources will increasing constrict the region’s ability to produce some foods. Increasing the used petroleum products has the secondary effects on food prices due to increased the cost of energy and fertilizers, however some agricultural production have been diverted to bio-fuel production.
Climate change be impacted the availability of agricultural resources and the sustainable of food security. Severe floods and droughts as seen as the impact of climate change in some vulnerable countries as well as the increasing temperature in the region will impacts on reducing crop productivity. The climate change not only impact on the sustainable agriculture productions, also it had been impacted on livestock and fisheries productions. Rice is the large portion of daily caloric intake in Asia and Pacific (see Figure 2); therefore the economic growth and industrialization are crucial in many Asia economies, also its economic and political on market intervention by government is need it.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health76
537
2816
0
500
1000
1500
2000
2500
3000
Average Rice Consumption(kCal/Capita/Day)
Average Total Food Consumption(kCal/Capita/Day)
Average Share of Rice in Total FoodConsumption (%)
Average RiceConsumption(kCal/Capita/Day)
537
Average Total FoodConsumption(kCal/Capita/Day)
2816
Average Share of Ricein Total FoodConsumption (%)
19.1
Figure 2. Rice consumption, caloric intake, and percentage of calories
from rice on 2007-2009 (Source: ADB 2013).
Figure 2 showed the average rice consumption about 537 Kcal/capital/day or 19.1% average share of rice in total food consumption which about 2816 Kcal/capital/day. Based on the pattern and respect to food security, the ASEAN member countries were classified into three sub groups: 1. Singapore and Brunei is the countries with made up of the relatively food secure countries. 2. The countries with contribute on a declining share in GDP, employment and International trade of agriculture sector, such as Malaysia, Indonesia, Thailand, and Philippines, except Vietnam, 3. The countries with economic transition with require special attention, include: Cambodia, Lao PDR and Myanmar. Seven priority areas of cooperation for strengthening food security in ASEAN region, includes: facilitating and promoting intra and extra ASEAN trade in agriculture, fishery, and forestry products; technology generation and transfer; private sector involvement and investment among others; some action sector programs were endorses by policy coordination, research, technology transfer, production, marketing, investment and promotion. These programs be supported to AFTA (ASEAN Free Trade Area), reported by Bello, A.L. (2004).
The dynamic of livestock sector globally be changed, currently in the developing countries is rapidly increasing demand for livestock products. However in developed countries, it was stagnant on demand of livestock products, but it was increased in production system, efficiency and sustainable environment. The factors that influence on changed of livestock product demand are: human population growth; income growth and urbanization; production level in different livestock systems, development of science and technology, increasing population numbers of livestock (Thornton, P.K. 2010). Therefore, currently the increasing productions of livestock sector have share about 33% of agricultural GDP.
269.08
322.75
53.67 40.9
108.18 119.77
11.59
80
160.9202.98
42.08 32
0
50
100
150
200
250
300
350
2010 2020 Quantity,million
CurrentKg/person
World
Developed
Developing
Figure 3. Meat Consumption (poultry, beef and pork) in year 2010 to 2020 (million MT)
Source: Roppa, L. ( 2012)
Based on: OCDE-FAO Agriculture Outlook 2011-2020 ( 2011), figure 3 showed increasing meat consumption which include poultry, beef and pork in the world, developed and developing countries on 2010 and predicted to 2020. The quantity of meat consumption was increase about four times in the developing countries compared to developed countries. Currently, the average meat consumption annually by each person is 80.0 kg/person in developed countries, and about 32.0 kg/person in developing countries. Even the meat consumption/person still high in developed countries, but it was known that livestock products need by developing countries increase faster as well as the growth of livestock systems.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 77
The dynamic of livestock sector globally be changed, currently in the developing countries is rapidly increasing demand for livestock products. However in developed countries, it was stagnant on demand of livestock products, but it was increased in production system, efficiency and sustainable environment. The factors that influence on changed of livestock product demand are: human population growth; income growth and urbanization; production level in different livestock systems, development of science and technology, increasing population numbers of livestock (Thornton, P.K. 2010). Therefore, currently the increasing productions of livestock sector have share about 33% of agricultural GDP.
269.08
322.75
53.67 40.9
108.18 119.77
11.59
80
160.9202.98
42.08 32
0
50
100
150
200
250
300
350
2010 2020 Quantity,million
CurrentKg/person
World
Developed
Developing
Figure 3. Meat Consumption (poultry, beef and pork) in year 2010 to 2020 (million MT)
Source: Roppa, L. ( 2012)
Based on: OCDE-FAO Agriculture Outlook 2011-2020 ( 2011), figure 3 showed increasing meat consumption which include poultry, beef and pork in the world, developed and developing countries on 2010 and predicted to 2020. The quantity of meat consumption was increase about four times in the developing countries compared to developed countries. Currently, the average meat consumption annually by each person is 80.0 kg/person in developed countries, and about 32.0 kg/person in developing countries. Even the meat consumption/person still high in developed countries, but it was known that livestock products need by developing countries increase faster as well as the growth of livestock systems.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health78
270.41
111.37
159.04
46.28
323.83
123.77
200.05
57.31 53.4212.4
41.0111 19.711.125.723.8
0
50
100
150
200
250
300
350
2010 (Million T)2020 (Million T) Quantity(Million T)
%
World
Developed
Developing
Latin America
Figure 4. Meat Production growth 2010 - 2020: 19,7% Source: Roppa, L. (2012)
Figure 4 reflex about the growth of meat production from 2010 to 2020 which increase around 19.7% in the world. Predicted meat production growth in the developing countries is to 25.7%, however in the developed countries only 11.1%. It’s really any stagnant on livestock growth in the developed countries (OCDE-FAO, 2011).
15,514,2
9,4
1,8
16,6 16
9,6
2
0
2468
1012
141618
2010 2020
Pork
Poultry
Beef
Sheep
Figure 5. Predicted of Meat Consumption (kg/person/year) based on Species, Year 2010 to 2020. Source: Roppa, L. ( 2012)
Based on: OCDE-FAO Agriculture Outlook 2011-2020 which reported by ROPPA (2012), the quantity of meat consumption by species in the world varied. During 2010 consumption of pork, poultry, beef, and sheep about 15.5 kg/person/y; 14.2 kg/person/y; 9.4 kg/person/y; and 1.8 kg/person/y, respectively. So, totally meet consumption is 40.9 kg/person/y. Predicted meat consumption by species to 2020 about 16.6 kg/person/y of pork, 16.0 kg/person/y of poultry, 9.6 kg/person/y of beef and 2 kg/person/y of sheep, and totally 44.2 kg/person/y. Almost meat of pork and
poultry were higher consumed by human, than followed by beef meat and sheep. Predicted meat consumption by species to 2020 showed any increasing each type of meat with round about 7.1%; 12.6%; 2.1%; and 11.1% of pork, poultry, beef and sheep meat, respectively (Figure 5). Totally of meat consumption from 2010 to 2020 increased about 8.1%. Based on figure 4, the meat production growth from 2010 to 2020 be increased about 19.7%, it means the available meat production from 2010 to 2020 will be covered as food security in the world. Over recent decades, Indonesia’s food security situation has improved considerably. And the prevalence of malnutrition has decreased significantly. Indonesia is the fourth country with high population in the world, currently the population number about 250 million people. By predicted of population number to 2025 Indonesia’s population growth to 280 million, it be impact on food supply and demand. The Indonesian government instigated a food self sufficiency policy by National Food Law in 2012, with the target of meeting 90% of the national food needs on 2015 be supplied by domestic production (ADB, 2013). Since 2005 up to now the average meat consumption in Indonesia is 2.1 kg/capita/y as well as predicted to 2015. In 2010 meat consumption demand is 526 ton with meat production about 223.332 ton, it deficit 303.532 ton , it about 57.61%. By predicted to 2015 the meat consumption demand 560.456 ton and meat production be 226.883 ton, with deficit about 333.573 ton, which is equal to 40.48% (DGI, 2013). In Indonesia since 2010 the average milk consumption per person is 6.5 kg/y, with milk demand 1549.60 ton/y, however milk production only 567.465 ton, and it was deficit about 982.135 ton ( 63.38%). The milk product have been deficit again about 63.17% when it be predicted year to 2015 , even milk consumption per person still 6.5 kg/y, and milk demand is 1648.40 ton with milk production level is 607.187 ton. It seen that milk product slightly increase, but by increasing number of population makes milk production is not sufficient in each year. By the condition, Indonesia need milk and meat be supplied by the other country or it should be imported of meat and or yearling cattle and milk. Based on government policy, it is should be reduced the amount of imported animal food products to meet sufficient food demand and productions. The livestock systems and technology could be promoted as a driver of change, which include three main factor: breeding and genetic engineering, nutrition, and disease control. Now, the question is how the strategies to improve and increase livestock products related to meet food security?

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 79
poultry were higher consumed by human, than followed by beef meat and sheep. Predicted meat consumption by species to 2020 showed any increasing each type of meat with round about 7.1%; 12.6%; 2.1%; and 11.1% of pork, poultry, beef and sheep meat, respectively (Figure 5). Totally of meat consumption from 2010 to 2020 increased about 8.1%. Based on figure 4, the meat production growth from 2010 to 2020 be increased about 19.7%, it means the available meat production from 2010 to 2020 will be covered as food security in the world. Over recent decades, Indonesia’s food security situation has improved considerably. And the prevalence of malnutrition has decreased significantly. Indonesia is the fourth country with high population in the world, currently the population number about 250 million people. By predicted of population number to 2025 Indonesia’s population growth to 280 million, it be impact on food supply and demand. The Indonesian government instigated a food self sufficiency policy by National Food Law in 2012, with the target of meeting 90% of the national food needs on 2015 be supplied by domestic production (ADB, 2013). Since 2005 up to now the average meat consumption in Indonesia is 2.1 kg/capita/y as well as predicted to 2015. In 2010 meat consumption demand is 526 ton with meat production about 223.332 ton, it deficit 303.532 ton , it about 57.61%. By predicted to 2015 the meat consumption demand 560.456 ton and meat production be 226.883 ton, with deficit about 333.573 ton, which is equal to 40.48% (DGI, 2013). In Indonesia since 2010 the average milk consumption per person is 6.5 kg/y, with milk demand 1549.60 ton/y, however milk production only 567.465 ton, and it was deficit about 982.135 ton ( 63.38%). The milk product have been deficit again about 63.17% when it be predicted year to 2015 , even milk consumption per person still 6.5 kg/y, and milk demand is 1648.40 ton with milk production level is 607.187 ton. It seen that milk product slightly increase, but by increasing number of population makes milk production is not sufficient in each year. By the condition, Indonesia need milk and meat be supplied by the other country or it should be imported of meat and or yearling cattle and milk. Based on government policy, it is should be reduced the amount of imported animal food products to meet sufficient food demand and productions. The livestock systems and technology could be promoted as a driver of change, which include three main factor: breeding and genetic engineering, nutrition, and disease control. Now, the question is how the strategies to improve and increase livestock products related to meet food security?
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health80
Impact and Prevention of Streptococcus suis Infection
Nongyao Kasatpibal, PhD Introduction Streptococcus suis (S. suis) infection is an emerging zoonotic pathogen in human. Since the first documented human S. suis case was reported from Denmark in 1968, the numbers of human cases have been significantly increased in several countries. It has become recognized as an important life-threaten zoonotic disease for human when a large outbreak of S. suis infection occurred in Sichuan province, China in 2005, associated with 215 cases (66 laboratory confirmed, 149 probable) and 39 deaths. A review article in 2007 found that 409 human S. suis cases were reported worldwide and increased to more than 700 cases in 2009. In the literature, human S. suis infections were most often reported from Southeast Asia including China (332 cases), Vietnam (293 cases), and Thailand (118 cases). Other cases were reported in Europe such as The Netherlands (41 cases), United Kingdom (15 cases), and Denmark (12 cases). In Thailand, the first human S. suis case was reported in 1987. A literature revealed that most cases were reported from the northern region. During 1999-2000, a cluster of 10 fatal cases of S. suis infection was reported from Lamphun province. Between May 2000 and December 2002, 41 culture confirmed S. suis infection at Chiang Mai University Hospital, a referral hospital in Northern Thailand; the number of cases admitted to this hospital were 10, 11, and 20 per year, respectively (average 1 case per month). The cumulative cases in Chiang Mai University Hospital from 2000 to 2013 were 164 cases. Over the past few years, several outbreaks of human S. suis infection were reported. In 2007, an outbreak occurred in Phayao province, which involved 23 cases. One year later, a large outbreak was reported from Chiang Mai and Lamphun associated with 44 cases. In 2010, reported 23 cases including five deaths in Phetchabun province and 31 human cases were confirmed, with a case fatality of 16.1% , a population-based study in Phayao province.
Pathogen S. suis is a gram-positive, facultative an- aerobic coccus that easily grown on blood agar. Identification is based on biochemical reactions and capsular serotyping. Based on agglutination with a panel of antiserum samples, 35 different S. suis serovars can be identified. The most common causative pathogens in human were serotype 2 for 165 cases (92.2%) and serotype 14 for 12 cases (6.7%).
The strategies for achieving food security by some research and development the issues, includes (ADB, 2013):
1. Ensuring the sustainability of global food systems by improving the efficiency of food production and delivery, and also maximizing the benefits of international trade.
2. Reducing poverty and vulnerability to food insecurity, to ensure the ability to purchase sufficient and nutritious food. Reducing price impact on real incomes of poor house holds, providing social safety nets for supporting economic growth. To change the number of poverty by four factors, such as: improving incomes, food prices, non food prices, and change in population.
3. Establishing risk management system and tools. 4. To change the number of poverty by four factors, such as: improving incomes,
food prices, non food prices, and change in population. References Asia Developed Bank, 2013. Food Security in Asia and Pacific.
Publication No. RPT 135 848 - 2. Bello, A.L. (2004). Ensuring Food Security – A Case Study for ASEAN Integration.
Asian J. Agric. And Development., Vol 2. Nos. 1&2. Directorate General Livestock Services of Indonesia, 2013. Statistic of Livestock
Production in Indonesia. Roppa, L. 2012. Global Meat Production Towards 2020.
ROPPA Consulting. Thornton, P.K. 2010. Livestock Production: Recent trends, Future Prospect. Phil. Trans. R. Soc. B. (2010) 365. 2853-2867.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 81
Impact and Prevention of Streptococcus suis Infection
Nongyao Kasatpibal, PhD Introduction Streptococcus suis (S. suis) infection is an emerging zoonotic pathogen in human. Since the first documented human S. suis case was reported from Denmark in 1968, the numbers of human cases have been significantly increased in several countries. It has become recognized as an important life-threaten zoonotic disease for human when a large outbreak of S. suis infection occurred in Sichuan province, China in 2005, associated with 215 cases (66 laboratory confirmed, 149 probable) and 39 deaths. A review article in 2007 found that 409 human S. suis cases were reported worldwide and increased to more than 700 cases in 2009. In the literature, human S. suis infections were most often reported from Southeast Asia including China (332 cases), Vietnam (293 cases), and Thailand (118 cases). Other cases were reported in Europe such as The Netherlands (41 cases), United Kingdom (15 cases), and Denmark (12 cases). In Thailand, the first human S. suis case was reported in 1987. A literature revealed that most cases were reported from the northern region. During 1999-2000, a cluster of 10 fatal cases of S. suis infection was reported from Lamphun province. Between May 2000 and December 2002, 41 culture confirmed S. suis infection at Chiang Mai University Hospital, a referral hospital in Northern Thailand; the number of cases admitted to this hospital were 10, 11, and 20 per year, respectively (average 1 case per month). The cumulative cases in Chiang Mai University Hospital from 2000 to 2013 were 164 cases. Over the past few years, several outbreaks of human S. suis infection were reported. In 2007, an outbreak occurred in Phayao province, which involved 23 cases. One year later, a large outbreak was reported from Chiang Mai and Lamphun associated with 44 cases. In 2010, reported 23 cases including five deaths in Phetchabun province and 31 human cases were confirmed, with a case fatality of 16.1% , a population-based study in Phayao province.
Pathogen S. suis is a gram-positive, facultative an- aerobic coccus that easily grown on blood agar. Identification is based on biochemical reactions and capsular serotyping. Based on agglutination with a panel of antiserum samples, 35 different S. suis serovars can be identified. The most common causative pathogens in human were serotype 2 for 165 cases (92.2%) and serotype 14 for 12 cases (6.7%).

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health82
S. suis type 2 can survive in dust, manure, and pig carcasses for days or even months under optimal conditions. It can survive for 10 min at 60 °C, 2 h at 50 °C, and 6 weeks in carcasses at 10 °C. This organism can survive for 1 month in dust at 0 °C and for over 3 months in faces, whereas at 25 °C, it can survive for 24 h in dust and for 8 days in faces.
Transmission S. suis is transmitted to humans through close or direct contact with infected pigs and pork products. People in direct contact with pigs (e.g., pig farmers, abattoir workers, persons transporting pork, meat inspectors and butchers) are usually infected through the skin injuries. Inoculation through cuts and sores in the skin are assumed to be associated with a short incubation time. The pathogen also enters the body via mucosal membranes of the eye, mouth or nose. However, most cases reported from Thailand and Vietnam transmitted through eating raw pork, pig fresh blood, or under-cooked pork. Currently, there is no evidence of human-to-human transmission. Predisposing factors Human S. suis infections are most often reported from countries where pig-rearing is common. It’s higher in males than females (male-to-female patient ratio = 3.5:1.0 to 6.5:1.0) and most cases aged 47–55 years. Most outbreaks are related to preceding epizootics, and occur among people with direct contact with infected pigs. The major risk factors identified from a large outbreak in China included slaughtering a sick pig (OR = 11.9; 95% CI, 3.4–42.8) or handling the carcass of a pig that had died from unknown causes (OR = 3.0; 95% CI, 1.0–8.8). Several studied reported that an important risk factor of S. suis infection is occupational exposure including pig breeder/farmer, butcher/abattoir, slaughterer, meat transporter, meat processing veterinarian and cook. In developed countries, the annual risk of developing S. suis meningitis among abattoir workers and pig breeders has been estimated to be 3.0 cases per 100,000 population whereas the risk is 1.2 cases per 100,000 population for butchers. The studies from Hong Kong and Vietnam reported that contact with contaminated pork and individuals who were unaware of any exposure to pork were risk factors of infections. S. suis was isolated from 6.1% of raw pork meat from 3 of the 6 wet markets in Hong Kong, it is likely that, besides occupational exposure, processing or consuming uncooked or under-cooked pork products is also a risk factor for infection. A study from Thailand reported that 62.5% of cases had a past history of the consumption of raw pork and/or pig fresh blood, and 25% contact with pig products. A case-control study from Vietnam has identified risk factors related to S. suis bacterial meningitis were eating high risk dishes, including such dishes as undercooked pig blood and pig intestine (OR = 4.44; 95%CI, 2.15–9.15), occupations related to pigs (OR = 5.52; 95%CI, 1.49–20.39), and exposures to pigs or pork in the
presence of skin injuries (OR = 15.96; 95%CI, 2.97–85.72) comparing to community control. Splenectomy, and to a lesser extent, alcoholism, diabetes mellitus, cancer, have been suggested as important predisposing factors for development of serious S. suis infection. The fatality rate for S suis infection after splenectomy seems to be approximately 80%. It has even been suggested that individuals who have had splenectomies should be excluded from the meat trade or pig farms. Incubation period The incubation period ranges from a few hours (in case of direct entry of the pathogen into blood via skin wounds) to three weeks, with the average being 2 days. Clinical features The most commons clinical manifestations of S. suis infections are meningitis and sepsis; hearing loss is a frequent complication. 1. Meningitis is the most common presentation and the symptoms are severe
headache, high fever (> 38 °C) and vomiting. 2. S. suis can also be associated with other systemic complications such as sepsis,
pneumonia, arthritis, endocarditis and streptococcal toxic shock-like syndrome (STSS). In severe cases, skin bleeding ranging from petechial to extensive ecchymosis is also common.
3. Profound deafness and other cranial nerve abnormalities, such as vestibular impairment, are the most commonly (more than 50% of cases) reported neurological sequelae of the disease.
4. Case fatality rates with S. suis meningitis range between 2.6 to 63% among patients with accompanying septic shock.
A study in Thailand have shown that the clinical manifestations included infective endocarditis, meningitis, sepsis, spondylodiscitis, and endophthalmitis in 16, 13, 10, 1, and 1 patients, respectively. The overall mortality rate was 19.5%.
Figure 1. Streptococcus suis infection in Thailand: distribution and pathogenesis
(Emerg Infect Dis 2011).

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 83
presence of skin injuries (OR = 15.96; 95%CI, 2.97–85.72) comparing to community control. Splenectomy, and to a lesser extent, alcoholism, diabetes mellitus, cancer, have been suggested as important predisposing factors for development of serious S. suis infection. The fatality rate for S suis infection after splenectomy seems to be approximately 80%. It has even been suggested that individuals who have had splenectomies should be excluded from the meat trade or pig farms. Incubation period The incubation period ranges from a few hours (in case of direct entry of the pathogen into blood via skin wounds) to three weeks, with the average being 2 days. Clinical features The most commons clinical manifestations of S. suis infections are meningitis and sepsis; hearing loss is a frequent complication. 1. Meningitis is the most common presentation and the symptoms are severe
headache, high fever (> 38 °C) and vomiting. 2. S. suis can also be associated with other systemic complications such as sepsis,
pneumonia, arthritis, endocarditis and streptococcal toxic shock-like syndrome (STSS). In severe cases, skin bleeding ranging from petechial to extensive ecchymosis is also common.
3. Profound deafness and other cranial nerve abnormalities, such as vestibular impairment, are the most commonly (more than 50% of cases) reported neurological sequelae of the disease.
4. Case fatality rates with S. suis meningitis range between 2.6 to 63% among patients with accompanying septic shock.
A study in Thailand have shown that the clinical manifestations included infective endocarditis, meningitis, sepsis, spondylodiscitis, and endophthalmitis in 16, 13, 10, 1, and 1 patients, respectively. The overall mortality rate was 19.5%.
Figure 1. Streptococcus suis infection in Thailand: distribution and pathogenesis
(Emerg Infect Dis 2011).

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health84
Diagnosis Presumptive diagnosis of S. suis infections in human is based on clinical signs and symptoms, and past history that closed contact to infected pig or pork. Confirmation of infection must be achieved by isolation of infectious agent. 1. Isolation and identification of the pathogen from blood samples, cerebrospinal
fluid, or from joint fluid is the gold standard for diagnosing S. suis infection. 2. The pathogen may be misidentified with other streptococcus species unless the
microbiologist and the clinician are aware of the disease since many laboratories do not routinely specialty α-hemolytic streptococci.
3. In Asia, molecular techniques of detection, like polymerase chain reaction (PCR), improved the rate of pathogen detection.
Management and care The S. suis isolate was highly susceptible to the antibiotics used for treatment, and the patient responded very well and recovered rapidly after treatment. Twenty percent of cases will recovery within 1-12 months. 1. S. suis is sensible to a wide range of antibiotics, including penicillins and
cephalosporins. Therefore, intravenous penicillin G has been a successful treatment in most cases. At least two relapses have been reported after 2 and 4 weeks of treatment; therefore, treatment should be applied for a relatively long period of time (at least 6 weeks). Ampicillin and chloramphenicol, sometimes combined with an aminoglycoside, may also be used. Hearing loss and vestibular disturbances are frequently observed sequelae unrelated to the antibiotic.
2. For less severe cases, single-drug with penicillin or ceftriazone is commonly used. In more severe cases, multiple antibiotics are usually given.
Caring is also very important for S. suis infection patients because good caring can increase the speed of recovery or to make the patient more comfortable from their condition. It ensures relationships between healthcare personnel and patients and their families (a crucial element to life), it is the expression of sympathy and it motivates patients to do the things they can do. The goal of treatment and care is patient health, a state of complete physical, mental (spiritual), and social well -being, and not merely the absence of disease or infirmity. Caring for the well-being of patient is therefore vital. For example, in case of hearing loss, healthcare personnel (HCP) should inform the speaker about patient’s hearing problem before starting a conversation, take a seat nearby the patient in quiet place, turn towards the source of light, so that the patient is visible for speech reading, teach the patient to practice to anticipate vocabulary used in usual conversations, and remove visual obstructions that cover the lips of HCP such as mask. In addition, HCP should repeat the conversation (part
of the message, key word, or full message) when the conversation is not understood, speak slower for speech reading, speak louder, rephrase, and spell the word that is not understood. Providing hearing aid to the patient is also important.
In brief, holistic care should be applied for S. suis cases. This is a system of comprehensive or total patient care that considers the physical, emotional, social, economic, and spiritual needs of the person; his or her response to illness; and the effect of the illness on the ability to meet self-care needs. Impact The impact of S. suis infection is not only physical damage but also mental (spiritual) and social impairment. 1. Health impacts including physical mental (spiritual) and social: S. suis infection is
one of the leading causes of death, reduce quality of life, disability, depression, and suicide. Hearing loss and vestibular impairment are frequently observed sequelae after S. suis meningitis. Hearing loss results in communication problems including difficulty in hearing soft to very loud sounds, depending on the degree of hearing loss. They may hear speech, but may have difficulty in identifying what is spoken. The infection can lead to paralysis affecting to self-care deficit (hygiene, toileting, moving, eat) in some patients. Physical health impairment may affect to social impacts such as changing role or relationship breakdown in the family or society. Some long-term cases have signs and symptoms of depression. It can also lead to commit suicide.
2. Economic impacts: On the level of the household, S. suis infection results in both the loss of income and increased medical expenses/spending on healthcare by the household. The income effects of this lead to spending reduction as well as a substitution effect away from social and towards healthcare and service spending. Some patients loss their jobs resulting in decreasing family income.
Prevention 1. Avoid consumption of raw or partially cooked pork, especially in endemic
countries and when there are outbreaks on swine farms. 2. Consistent use of personal protective equipment (PPE) such as gloves and boots,
and hand washing are likely to prevent most occupational infection among people who handle live pigs and carcasses, such as pig farmers, slaughterhouse workers and veterinarians.
3. There is no human vaccine against S. suis infection.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 85
of the message, key word, or full message) when the conversation is not understood, speak slower for speech reading, speak louder, rephrase, and spell the word that is not understood. Providing hearing aid to the patient is also important.
In brief, holistic care should be applied for S. suis cases. This is a system of comprehensive or total patient care that considers the physical, emotional, social, economic, and spiritual needs of the person; his or her response to illness; and the effect of the illness on the ability to meet self-care needs. Impact The impact of S. suis infection is not only physical damage but also mental (spiritual) and social impairment. 1. Health impacts including physical mental (spiritual) and social: S. suis infection is
one of the leading causes of death, reduce quality of life, disability, depression, and suicide. Hearing loss and vestibular impairment are frequently observed sequelae after S. suis meningitis. Hearing loss results in communication problems including difficulty in hearing soft to very loud sounds, depending on the degree of hearing loss. They may hear speech, but may have difficulty in identifying what is spoken. The infection can lead to paralysis affecting to self-care deficit (hygiene, toileting, moving, eat) in some patients. Physical health impairment may affect to social impacts such as changing role or relationship breakdown in the family or society. Some long-term cases have signs and symptoms of depression. It can also lead to commit suicide.
2. Economic impacts: On the level of the household, S. suis infection results in both the loss of income and increased medical expenses/spending on healthcare by the household. The income effects of this lead to spending reduction as well as a substitution effect away from social and towards healthcare and service spending. Some patients loss their jobs resulting in decreasing family income.
Prevention 1. Avoid consumption of raw or partially cooked pork, especially in endemic
countries and when there are outbreaks on swine farms. 2. Consistent use of personal protective equipment (PPE) such as gloves and boots,
and hand washing are likely to prevent most occupational infection among people who handle live pigs and carcasses, such as pig farmers, slaughterhouse workers and veterinarians.
3. There is no human vaccine against S. suis infection.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health86
Lesson learned in prevention of S. suis infection using one health concept According to my experience, One Health concept is a key to success in strengthen capacity building and developing training program and educational materials for prevention of S. suis infection. The One Health has been defined as "the collaborative effort of multiple disciplines - working locally, nationally, and globally - to attain optimal health for people, animals and the environment." During the three workshops of S. suis infection prevention that conducting between October 2013 and March 2014, One Health concept was apply. I realize that a practical program of collaboration and tools were needed to address the scientific, policy and social questions raised by trans-disciplinary. The participants in these workshops included medical doctors, nurses, veterinarians, epidemiologists, laboratory personnel, social science and communication personnel, local authority personnel, community healthcare personnel, and health sciences students. They came from multi-sectors such as Chiang Mai University, Mahidol University, Kasetsart University, Khon Kaen University, Chulalongkorn University, Bureau of Epidemiology, Department of Livestock Development (DLD) in Chiang Mai, Lamphun and Phayao, Chiang Mai Provincial Public Health Office, EcoHealth-OneHealth Resource Centre, Chiang Mai University, Jomthong Hospital, and Health Promotion Hospitals and District Municipal Offices in Chiang Mai and Phayao. In the first workshop, there were six participants (medical doctor, veterinarians, and university instructors) from the university in Vietnam because S. suis infection is also a major problem in Vietnam.
Key success factors from the workshops 1. Collaboration and trans-disciplinary approach are effective strategies for
developing strategic plan for prevention and control zoonotic disease such as S. suis infection.
2. Building good relationship and collaboration among healthcare professions should lead to reducing the incidence of S. suis infeciton.
3. Really interesting in the meeting issue and having expertise in that area can lead to effective participation, sharing knowledge and experience, and achieve the meeting goals..
4. The outputs and outcomes from the workshop including prevention of S. suis infeciton manual, VDO, posters, stickers, and spot will benefit to participants, communities, countries and global health.
5. Productivity of the workshop results from speakers, moderators, facilitators, and participants.
“We can make a difference in prevention of S. suis infection.”
Take home messages Coming together is a beginning. Keeping together is progress. Working together is success.
- Henry Ford Bibliography 1. Arends N, Hartwig M, Rudolphy M, Zanen HC. Carrier rate of Streptococcus suis
capsular type 2 in palatine tonsils of slaughtered pigs. J. Clin. Microbiol 1984;20(5): 945-7.
2. Balkany TJ, Gantz BJ. Medical and surgical considerations in cochlear implantation. In: Cummings C, Flint LA, editors. Otolaryngology: Head & neck surgery volume 4 (4th ed.). Philadelphia: Elsevier Mosby, 2005, 3637-49.
3. Choi SM, Cho BH, Choi KH, et al. Meningitis caused by Streptococcus suis: case report and review of the literature. J Clin Neurol. 2012;8(1):79-82.
4. Clifton-Hadley FA, Enright MR. Factors affecting the survival of Streptococcus suis type 2. Vet Rec 1984; 114(24): 584–86.
5. Fongcom A, Pruksakorn S, Netsirisawan P, Pongprasert R, Onsibud P. Streptococcus suis infection: a prospective study in northern Thailand. Southeast Asian J Trop Med Public Health. 2009 May; 40(3): 511-7.
6. Gallagher F. Streptococcus suis infection and splenectomy. Lancet. 2001; 357(9262):1129-30.
7. Ho DT, Le TP, Wolbers M, Cao QT, Nguyen VM, et al. Risk factors of Streptococcus suis infection in Vietnam. A case-control study. PLoS One. 2011 Mar 8; 6(3): e17604.
8. Huang YT, Teng LJ, Ho SW, Hsueh PR. Streptococcus suis infection. J Microbiol Immunol Infect 2005; 38(5): 306-13.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 87
“We can make a difference in prevention of S. suis infection.”
Take home messages Coming together is a beginning. Keeping together is progress. Working together is success.
- Henry Ford Bibliography 1. Arends N, Hartwig M, Rudolphy M, Zanen HC. Carrier rate of Streptococcus suis
capsular type 2 in palatine tonsils of slaughtered pigs. J. Clin. Microbiol 1984;20(5): 945-7.
2. Balkany TJ, Gantz BJ. Medical and surgical considerations in cochlear implantation. In: Cummings C, Flint LA, editors. Otolaryngology: Head & neck surgery volume 4 (4th ed.). Philadelphia: Elsevier Mosby, 2005, 3637-49.
3. Choi SM, Cho BH, Choi KH, et al. Meningitis caused by Streptococcus suis: case report and review of the literature. J Clin Neurol. 2012;8(1):79-82.
4. Clifton-Hadley FA, Enright MR. Factors affecting the survival of Streptococcus suis type 2. Vet Rec 1984; 114(24): 584–86.
5. Fongcom A, Pruksakorn S, Netsirisawan P, Pongprasert R, Onsibud P. Streptococcus suis infection: a prospective study in northern Thailand. Southeast Asian J Trop Med Public Health. 2009 May; 40(3): 511-7.
6. Gallagher F. Streptococcus suis infection and splenectomy. Lancet. 2001; 357(9262):1129-30.
7. Ho DT, Le TP, Wolbers M, Cao QT, Nguyen VM, et al. Risk factors of Streptococcus suis infection in Vietnam. A case-control study. PLoS One. 2011 Mar 8; 6(3): e17604.
8. Huang YT, Teng LJ, Ho SW, Hsueh PR. Streptococcus suis infection. J Microbiol Immunol Infect 2005; 38(5): 306-13.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health88
9. Isaradisaikul S, Navacharoen N, Haprasertpong C, Kangsanarak J, Panyathong R. Causes and time-course of vertigo in an ear, nose, and throat clinic. Eur Arch Otorhinolaryngol. 2010 Dec; 267(12): 1837-41. Epub 2010 Jan 22.
10. Kasatpibal N. Epidemiology, pathogenesis and management of Streptococcus suis infection in human. Trans-disciplinary Capacity Building of THOHUN and VOHUN for Streptococcus suis Infection Prevention: Training of the Trainers Workshop. Organized by Faculty of Nursing, Chiang Mai University, Thailand, 61-61 October 3162, Lotus Pang Suan Keaw Hotel, Chiang Mai, Thailand.
11. Kay R, Cheng AF, Tse CY. Streptococcus suis infection in Hong Kong. QJM 1995; 88(1): 39-47.
12. Kerdsin A, Oishi K, Sripakdee S, et al. Clonal dissemination of human isolates of Streptococcus suis serotype 14 in Thailand. J Med Microbiol. 2009 Nov; 58(Pt 11): 1508-13. Epub 2009 Aug 6.
13. Kerdssin A, Dejsirilert S, Puangpatra e al. Genotypic profile of Streptococcus suis serotype 2 and clinical features of infectron I humans, Thailand. Emerg Infect Dis. 2011 May: 17(5): 835-42.
14. Laohapensang K, Rutherford RB, Arworn S. Mycotic abdominal aortic aneurysm due to Streptococcus suis: a case4 report. Surg Infect (Larchmt). 2010 Apr; 11(2): 179-81.
15. Leelarasamee A, Nilakul C, Tien-Grim S, Srifuengfung S, Susaengrat W. Streptococcus suis toxic-shock syndrome and meningitis. J Med Assoc Thai. 1997 Jan; 80(1): 63-8.
16. Lun ZR, Wang Q P, Chen XG, Li AX, Zhu XQ. Streptococcus suis: an emerging zoonotic pathogen. Lancet Infect Dis 2007; 7(3): 201-9.
17. Lütticken R, Temme N, Hahn E, Bartelheimer EW. Meningitis caused by Streptococcus suis: case report and review of the literature. Infection. 1986;14(4):181-5.
18. Mai NT, Hoa NT, Nga TV, et al. Streptococcus suis meningitis in adults in Vietnam. Clin Infect Dis. 2008 Mar 1; 46(5): 659-67.
19. Navacharoen N, Chantharochavong C, Hanprasertpong C, Kangsanarak J, Lekagul. Hearing and vestibular loss in Streptococcus suis infection form swine and traditional raw pork exposure in northern Thailand. S.JLO 20209; 123(8): 857-62.
20. Navacharoen N. Epidemiology, pathogenesis and management of Streptococcus suis infection in human. Trans-disciplinary Capacity Building of THOHUN and VOHUN for Streptococcus suis Infection Prevention: Training of the Trainers Workshop. Organized by Faculty of Nursing, Chiang Mai University, Thailand, 61-61 October 3162, Lotus Pang Suan Keaw Hotel, Chiang Mai, Thailand.
21. Nghia HD, Tu le TP, Wolbers M, et al. Risk factors of Streptococcus suis infection in Vietnam. A case-control study. PLoS One. 2011 Mar 8;6(3):e17604.
22. Padungtod P, Tharavichitkul P, Janya S et al. Incidence and presence of virulence of virulence factors of Streptococcus suis infection in slaughtered pigs for Chiang Mai, Thailand. Southeast Asian J Trop Med Public Health. 2010 Nov; 41(6): 1454-61.
23. Phuapradit P, Boongird P, Boonyakarnkul S, Niramarnsakul S, Ponglikitmongkol S, Vorachit M, et al. Meningitis caused by Streptococcus suis. Intern Med 1987; 3(3): 120-2.
24. Staats JJ, Feder I, Okwumabua O, Chengappa MM. Streptococcus suis: past and present. Veterinary Research Communication 1997; 21 (6), 381-407a.
25. Tang J, Wang C, Feng Y, Yang W, Song H, Chen Z, et al. Streptococcal toxic shock syndrome causes by Streptococcus suis serotype 2. PLoS Med 2006; 3(5): e151.
26. Tee LH, Chee NWC. Vestibular rehabilitation for the Dizzy Patient. Ann Acad Med Singapore 2005; 34(4): 289-94.
27. van de Beek D, de3 Gans J, McIntyre P, Prasad K. Corticosteroids for acute bacterial meningitis. Cocharane Database of Systematic Reviews 2007, Issue 1. Art. No.: CD004405. DOI: 10.1002/14651858.CD004405.pub2
28. Watkins EJ, Brooksby P, Schweiger MS, Enright SM. Septicaemia in a pig-farm worker. Lancet. 2001;357(9249):38.
29. Wertheim HF, Nghia HD, Taylor W, Schultsz C. Streptococcus suis: an emerging human pathogen. Clin Infect Dis. 2009 Mar 1;48(5):617-25.
30. Woo J, Li EK. Streptococcus suis meningitis requires prolonged treatment with penicillin. Infection. 1987; 15(2):129-30.
31. Yu H, Jing H, Chen Z, Zheng H, Zhu X, Wang H, et al. Human Streptococcus suis outbreak, Sichuan, China. Emerg Infect Dis 2006; 12(6): 914-20.
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 89
23. Phuapradit P, Boongird P, Boonyakarnkul S, Niramarnsakul S, Ponglikitmongkol S, Vorachit M, et al. Meningitis caused by Streptococcus suis. Intern Med 1987; 3(3): 120-2.
24. Staats JJ, Feder I, Okwumabua O, Chengappa MM. Streptococcus suis: past and present. Veterinary Research Communication 1997; 21 (6), 381-407a.
25. Tang J, Wang C, Feng Y, Yang W, Song H, Chen Z, et al. Streptococcal toxic shock syndrome causes by Streptococcus suis serotype 2. PLoS Med 2006; 3(5): e151.
26. Tee LH, Chee NWC. Vestibular rehabilitation for the Dizzy Patient. Ann Acad Med Singapore 2005; 34(4): 289-94.
27. van de Beek D, de3 Gans J, McIntyre P, Prasad K. Corticosteroids for acute bacterial meningitis. Cocharane Database of Systematic Reviews 2007, Issue 1. Art. No.: CD004405. DOI: 10.1002/14651858.CD004405.pub2
28. Watkins EJ, Brooksby P, Schweiger MS, Enright SM. Septicaemia in a pig-farm worker. Lancet. 2001;357(9249):38.
29. Wertheim HF, Nghia HD, Taylor W, Schultsz C. Streptococcus suis: an emerging human pathogen. Clin Infect Dis. 2009 Mar 1;48(5):617-25.
30. Woo J, Li EK. Streptococcus suis meningitis requires prolonged treatment with penicillin. Infection. 1987; 15(2):129-30.
31. Yu H, Jing H, Chen Z, Zheng H, Zhu X, Wang H, et al. Human Streptococcus suis outbreak, Sichuan, China. Emerg Infect Dis 2006; 12(6): 914-20.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health90
Quality Management Rationale & Concept Traceability systems and QR Code Application
Dr. Sakdid Anulomsombat
Senior Specialist Betagro Group
Betagro Group is one of the Thailand's leaders in the integrated agricultural businesses covering animal feed, livestock, animal health products as well as the excellent quality food products for export and domestic distribution. Under the corporate vision “Quality for Life”, the Group is committed to meet the different needs and to develop the food safety system for consumers because only good quality food is suitable for good quality living. To ensure the food safety, it is necessary to establish an effective quality assurance system to monitor, control and examine the entire manufacturing process from sourcing, production, processing, distribution and market at every step into one single value chain. In 2009, Betagro Group has initiated Betagro Quality Management (BQM) to standardize its quality assurance system in order to manage and improve safety and quality throughout the entire product supply chain. With careful and continuous implementation, the BQM operates around the clock every day. For this reason it’s also known as “BQM 24/7”. Together with BQM 24/7, the Betagro e-Traceability was also introduced making Betagro Group the very first company in Thailand’ s livestock and food industry to introduce such system allowing consumer to be completely confident in the quality of food products produced by Betagro.
BQM 24/7 is an outstanding, pioneering initiative that enhances the implementation of quality management and food safety standards across the supply chain. With BQM 24/7, the entire process is strictly monitored and controlled around the clock to ensure it meets all international quality and safety standards as well as customer requirements.
Five key elements of BQM 24/7 include Food Quality, Food Safety, Animal Welfare, Service Excellence and Corporate Social Responsibility. At Betagro, all five elements must be followed to ensure full compliance with all international standards and able to be traced 24 hours a day, 7 days a week.
Element 1: Food Quality Betagro is focusing on delivering products of best quality to customers. This is driven by our extensive R&D which is run by a dedicated team of specialists to ensure the products and services live up to customer expectations. Element 2: Food Safety Betagro’s food products are meticulously inspected at all stages of production to make sure they are free from chemical residues, germs, contaminants, and anything that can be health-threatening. Instead of being fully dependent on external compliance audit, Betagro has successfully developed processes and procedures for internal audit and detailed assessment of real-time food safety monitoring across the supply chain. In addition, all of our farms, factories and facilities are continuously evaluated to ensure full compliance with required safety, health and environmental regulations.
Element 3: Animal Welfare
By taking steps to improve the way we are care for and handle animals, Betagro continues to create sustainable commercial farming systems with a focus on animal welfare. Our animal welfare practices are always driven by the latest available scientific research, advice from respected animal welfare experts and potential environmental and food safety implications. Each facility in our supply chain is operated in a way that aligns with these guidelines.
Element 4: Service Excellence The commitment to building a good relationship with customers continues to be at the core of Betagro’s strategy. The relationship between Betagro and its customers is not merely of seller and buyer, but of partners to whom Betagro offers the best possible products and services to help make quality for life.
Element 5: Corporate Social Responsibility At Betagro, it is the ‘golden rule’ that business operations are guided by social responsibility. For over 45 years of business, staff at all levels have been treated fairly and honestly possible impacts to the environment have been decisively managed and minimized; and the sustainability of local communities in areas where Betagro farms and factories are located has been supported through a series of social spirited activities which are meant to improve the quality of life of everyone involved.
By striving to maintain our leading position in terms of quality, business ethics and
ability to keep up with the changing market environment, we offer the best possible products and services to help make the life of our partners and customers better.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 91
Element 1: Food Quality Betagro is focusing on delivering products of best quality to customers. This is driven by our extensive R&D which is run by a dedicated team of specialists to ensure the products and services live up to customer expectations. Element 2: Food Safety Betagro’s food products are meticulously inspected at all stages of production to make sure they are free from chemical residues, germs, contaminants, and anything that can be health-threatening. Instead of being fully dependent on external compliance audit, Betagro has successfully developed processes and procedures for internal audit and detailed assessment of real-time food safety monitoring across the supply chain. In addition, all of our farms, factories and facilities are continuously evaluated to ensure full compliance with required safety, health and environmental regulations.
Element 3: Animal Welfare
By taking steps to improve the way we are care for and handle animals, Betagro continues to create sustainable commercial farming systems with a focus on animal welfare. Our animal welfare practices are always driven by the latest available scientific research, advice from respected animal welfare experts and potential environmental and food safety implications. Each facility in our supply chain is operated in a way that aligns with these guidelines.
Element 4: Service Excellence The commitment to building a good relationship with customers continues to be at the core of Betagro’s strategy. The relationship between Betagro and its customers is not merely of seller and buyer, but of partners to whom Betagro offers the best possible products and services to help make quality for life.
Element 5: Corporate Social Responsibility At Betagro, it is the ‘golden rule’ that business operations are guided by social responsibility. For over 45 years of business, staff at all levels have been treated fairly and honestly possible impacts to the environment have been decisively managed and minimized; and the sustainability of local communities in areas where Betagro farms and factories are located has been supported through a series of social spirited activities which are meant to improve the quality of life of everyone involved.
By striving to maintain our leading position in terms of quality, business ethics and
ability to keep up with the changing market environment, we offer the best possible products and services to help make the life of our partners and customers better.
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health92
e-Traceability: State of the Art Reverse Tracking System by Betagro Modern production technology and agricultural industrial operations are important
factors that push Betagro Group to the nation's a leading company which produces safe and high quality food products. The group adheres seriously to their continuous commitment for high quality and food safety through quality oriented working system and production processes. Manufacturing standard, clean and safe products for customers has been the main goal of Betagro Group for the past 45 years. Betagro Products have earned customers’ confidence and trust due to their standards as well as strictly-monitored manufacturing process. Betagro Group has introduced traceability system to its operations and continued to improve the system until present that the customers can trace their products online with e- Traceability system. Customers can trace important information and origin of products throughout production processes from farm, processed food factory until cooked food factory. Both domestic and international customers can self-check the product themselves.
Domestic customers focus on origin and safety of the products. Information is
retrieved from Betagro Group main database system with data from all production processes administered and managed by assigned staff.
International customers focus on maintaining and managing security system to prevent defects and faults in operation. Betagro Group deploys authority mechanism by providing each customer with username and password where each user has different level of access right to information.
The latest development from Betagro Group is the introduction of Manufacturing Information Technology to monitor all areas of production and to increase speed of work. Betagro is the first and the only company in Thailand using QR Code technology for product traceability in the whole supply chain.
The company introduces QR Code System which allows customers to scan the products quickly and conveniently with their mobile phones. Customers can also trace products via Bangkok-based website at http://www.thaitrace.net Betagro Group supports the government agencies to submit related information to this web site. International importers or customers can check products via a web specifically created for reverse tracking at http://www.clickspyonme.com
Betagro Group’s reverse tracking system has already been in operation. The company is well aware of the importance of food safety and is committed to continuously lifting food safety bars to reduce any problem and increase customers’ confidence to choose products and services from Betagro Group. “To achieve the goal of delivering safe food with premium quality to consumers requires the application of integrity and efficiency throughout the entire system. Every stage, from beginning to end is interconnected so that any single stage cannot be ignored. Importantly, it is essential that all Betagro staff at all levels adhere to our Core Value, Mission and Vision with their collaborative efforts to drive our common goal - Quality for Life”
Vanus Taepaisitphongse Chief Executive Officer
Betagro Group

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 93
The company introduces QR Code System which allows customers to scan the products quickly and conveniently with their mobile phones. Customers can also trace products via Bangkok-based website at http://www.thaitrace.net Betagro Group supports the government agencies to submit related information to this web site. International importers or customers can check products via a web specifically created for reverse tracking at http://www.clickspyonme.com
Betagro Group’s reverse tracking system has already been in operation. The company is well aware of the importance of food safety and is committed to continuously lifting food safety bars to reduce any problem and increase customers’ confidence to choose products and services from Betagro Group. “To achieve the goal of delivering safe food with premium quality to consumers requires the application of integrity and efficiency throughout the entire system. Every stage, from beginning to end is interconnected so that any single stage cannot be ignored. Importantly, it is essential that all Betagro staff at all levels adhere to our Core Value, Mission and Vision with their collaborative efforts to drive our common goal - Quality for Life”
Vanus Taepaisitphongse Chief Executive Officer
Betagro Group

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health94
Update on Canine Cushing’s Disease
Virginia Rentko, VMD, DACVIM Tufts University Cummings School of Veterinary Medicine
Clinical Signs The diagnosis of canine hyperadrenocorticism (HAC) should be based on clinical signs and a history which may include one or more of the most common clinical manifestations or less common signs like ligament laxity and resultant lameness. (Table 1) (Behrend et al, 2013) Some dogs with pituitary dependent hyperadrenocorticism develop a macroadenoma which may cause anorexia, obtundation, and changes in behavior. Sometimes dogs with an adrenal tumor (AT) may show signs of abdominal pain and/or retroperitoneal hemorrhage and anemia. (Lang, et al, 2011) Testing for HAC should be pursued if an adrenal tumor is noted on abdominal imaging for another reason. Table 1. Common clinical signs in dogs
Common Less Common Uncommon
Polydipsia Lethargy Thromboembolism Polyuria Hyperpigmentation Ligament rupture Polyphagia Comedones Facial nerve palsy Panting Thin skin Pseudomyotonia Abdominal distention Poor hair regrowth Testicular atrophy Endocrine alopecia Urine leakage Persistent anestrus Hepatomegaly Insulin-resistant
diabetes mellitus
Muscle weakness Systemic hypertension
From: Behrend, J Vet Int Med 27 (6):1292-1304, 2013 Laboratory Testing Laboratory results of a complete blood count, blood biochemistry, urinalysis, urine protein:creatinine ratio and blood pressure usually suggest HAC. Common laboratory findings are noted in Table 2. However, the lack of laboratory abnormalities does not rule out the diagnosis. Similarly the finding of normally sized adrenal glands on abdominal ultrasound does not rule out HAC.
Table 2. Common laboratory abnormalities in dogs
CBC Serum Biochemistry Panel Urinalysis
Neutrophilic leukocytosis
Increased alkaline phosphatase
Specific gravity ≤1.018-1.020
Lymphopenia Increased alanine aminotransferase
Proteinuria
Eosinopenia Hypercholesterolemia Indicators of urinary tract infection
Thrombocytosis Hypertriglyceridemia Mild erythrocytosis Hyperglycemia
CBC, complete blood count. From: Behrend, J Vet Int Med 27 (6):1292-1304, 2013 Diagnosis is made on the basis on increased cortisol production or decreased sensitivity of the hypothalamic-pituitary-adrenal axis to negative feedback to glucocorticoid challenge. Screening tests include the low dose dexamethasone suppression (LDDS) test, urinary corticoid:creatinine ratio (UCCR) and adrenocorticotrophic (ACTH) stimulation test. If clinical signs are suggestive of HAC and one screening test is negative, a second screening test should be performed. Discordant test results sometime confound the diagnosis. Several scenarios create uncertainty of the diagnosis, e.g., pursuing biochemistry abnormalities with endocrine testing when clinical signs are absent, ruling out diagnosis because adrenal glands are normally sized or biochemistry tests are normal, or solely relying on the ACTH stimulation test. Increased serum alkaline phosphatase (ALP) An increased APL activity is not diagnostic for HAC. In the absence of compatible clinical signs, other causes increased APL should be investigated. A single increase in ALP is not a reason to test for HAC. Urine Cortisol:Creatinine Ratio (UCCR) Urine for UCCR testing should be collected at home first thing in the morning for two consecutive days to avoid stress-induced cortisol secretion when urine is collected at the hospital. Home collection of urine in dogs with suspected HAC results in this test having 99% sensitivity and 77% specificity. (Rinjberk, 1988) Dexamethasone Suppression Testing The low dose dexamethasone suppression (LDDS) test is the gold standard screening test. Dexamethasone causes rapid and prolonged suppression of cortisol secretion. In dogs with AT, cortisol secretion is not suppressed by any dose of dexamethasone. In dogs with PDH, a low dose of dexamethasone (0.01mg/kg) will not suppress
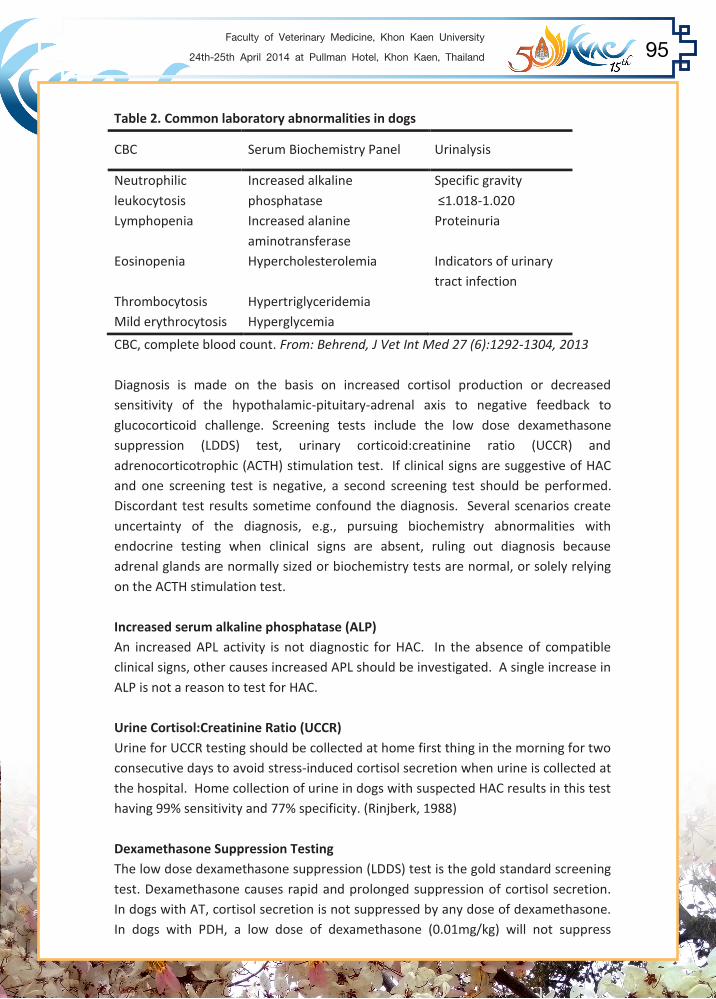
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 95
Table 2. Common laboratory abnormalities in dogs
CBC Serum Biochemistry Panel Urinalysis
Neutrophilic leukocytosis
Increased alkaline phosphatase
Specific gravity ≤1.018-1.020
Lymphopenia Increased alanine aminotransferase
Proteinuria
Eosinopenia Hypercholesterolemia Indicators of urinary tract infection
Thrombocytosis Hypertriglyceridemia Mild erythrocytosis Hyperglycemia
CBC, complete blood count. From: Behrend, J Vet Int Med 27 (6):1292-1304, 2013 Diagnosis is made on the basis on increased cortisol production or decreased sensitivity of the hypothalamic-pituitary-adrenal axis to negative feedback to glucocorticoid challenge. Screening tests include the low dose dexamethasone suppression (LDDS) test, urinary corticoid:creatinine ratio (UCCR) and adrenocorticotrophic (ACTH) stimulation test. If clinical signs are suggestive of HAC and one screening test is negative, a second screening test should be performed. Discordant test results sometime confound the diagnosis. Several scenarios create uncertainty of the diagnosis, e.g., pursuing biochemistry abnormalities with endocrine testing when clinical signs are absent, ruling out diagnosis because adrenal glands are normally sized or biochemistry tests are normal, or solely relying on the ACTH stimulation test. Increased serum alkaline phosphatase (ALP) An increased APL activity is not diagnostic for HAC. In the absence of compatible clinical signs, other causes increased APL should be investigated. A single increase in ALP is not a reason to test for HAC. Urine Cortisol:Creatinine Ratio (UCCR) Urine for UCCR testing should be collected at home first thing in the morning for two consecutive days to avoid stress-induced cortisol secretion when urine is collected at the hospital. Home collection of urine in dogs with suspected HAC results in this test having 99% sensitivity and 77% specificity. (Rinjberk, 1988) Dexamethasone Suppression Testing The low dose dexamethasone suppression (LDDS) test is the gold standard screening test. Dexamethasone causes rapid and prolonged suppression of cortisol secretion. In dogs with AT, cortisol secretion is not suppressed by any dose of dexamethasone. In dogs with PDH, a low dose of dexamethasone (0.01mg/kg) will not suppress

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health96
cortisol release. However, in 75% of dogs with PDH, a higher dose (0.1 mg/kg) will cause a decrease in cortisol concentration. This test can be misleading also. It can be falsely positive with concurrent illness or stress and 25% of dogs with PDH will not have suppression of cortisol concentrations. ACTH Stimulation Test The ACTH stimulation test is a useful test for screening iatrogenic HAC or for monitoring treatment but it too can be misleading when used as a screening test for spontaneous HAC. It has low sensitivity for detecting PDH (approximately 80%) and AT (approximately 57%). (Rinjberk, 1988). Sample handling is important for accurate test results. A recent consensus statement by the American College of Veterinary Internal Medicine recommended that samples for cortisol testing (either serum or plasma) be centrifuged within one hour of collection and refrigerated for up to 24 hours or frozen for longer at -20°C. Urine samples can be stored at 4°C for up to 4 days or at -20°C for >5 days. Samples should be shipped overnight to the laboratory (Behrend, 2013) Endogenous ACTH concentration Endogenous ACTH concentration is the most accurate test to differentiate PDH from AT. The test requires a specialized assay and it can have low sensitivity. ACTH is labile; plasma proteases degrade ACTH unless the sample is rapidly cooled. (Rodriguez Pineiro, 2009) Imaging Radiographs may show abdominal distension, hepatomegaly, and possible mineralization of the pulmonary structures, subcutaneous tissue and adrenal gland. Ultrasound can be used to determine the size of the adrenal glands. Width of the adrenal gland >4 cm is suggestive of malignancy. (Hoerauf, 1999) Occult HAC A dog which appears to have HAC based on history, clinical signs and laboratory findings but has screening test results (LDDS test, UCCR) within the reference range is considered to have “occult HAC.” Treatment Following a diagnosis of hyperadrenocorticism, a decision is needed as to whether to treat the dog medically and if so with what medication. The two most commonly used drugs are mitotane, an adrenocorticolytic compound and trilostane, a competitive 3β-hydroxysteroid dehydrogenase inhibitor. Other drugs include ketoconazole, L-deprenyl, and aminogluthemide. Surgery is indicated for treatment of adrenal tumors. Medical treatment is indicated if clinical signs are advanced. If
changes in blood chemistry led to testing and clinical signs are few, delayed treatment with reassessment may be indicated. However, if certain clinical signs such as systemic hypertension, proteinuria, severe muscle weakness or high blood glucose (diabetes mellitus) are present, medical treatment should be instituted. Recurrent urinary tract infection in a dog with HAC is a reason to pursue treatment. (Forrester SD, 1999) Mitotane Mitotane acts directly on the adrenal cortex causing necrosis, particularly in the zona reticularis. It is fat soluble and has better absorption when given with food. The most common side effects of the drug are gastrointestinal including nausea, vomiting and diarrhea. Discontinuation of the drug usually resolves the signs and Mitotane can be reintroduced at a lower dose successfully. Mitotane is administered as a loading dose of 25-50 mg/kg per day for 5-10 days typically. It is followed by the same dose divided over a week, given to maintain cortisol suppression. Home instructions to monitor food and water intake and observation of any gastrointestinal signs are important. Clinical signs and testing for adrenal suppression are used determine the length of the induction period. Monitoring is best by use of an adrenocorticotropic hormone (ACTH) test. The ACTH test is also used to distinguish adverse effects of Mitotane (hypoadrenocorticism) vs. desired effect of treatment. (Figure 1)
From: Reine N, Topics in Compan An Med 27:25-30, 2012 Adrenal function should be tested within 7-14 days of the induction period, independent of clinical signs. If adrenal suppression is not obtained, the loading dose should continue with weekly testing. UCCR has been used for monitoring; although the test is not as specific as the ACTH stimulation test. If signs of toxicity occur, treatment with daily prednisone (0.3-0.5 mg/kg) can be instituted.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 97
changes in blood chemistry led to testing and clinical signs are few, delayed treatment with reassessment may be indicated. However, if certain clinical signs such as systemic hypertension, proteinuria, severe muscle weakness or high blood glucose (diabetes mellitus) are present, medical treatment should be instituted. Recurrent urinary tract infection in a dog with HAC is a reason to pursue treatment. (Forrester SD, 1999) Mitotane Mitotane acts directly on the adrenal cortex causing necrosis, particularly in the zona reticularis. It is fat soluble and has better absorption when given with food. The most common side effects of the drug are gastrointestinal including nausea, vomiting and diarrhea. Discontinuation of the drug usually resolves the signs and Mitotane can be reintroduced at a lower dose successfully. Mitotane is administered as a loading dose of 25-50 mg/kg per day for 5-10 days typically. It is followed by the same dose divided over a week, given to maintain cortisol suppression. Home instructions to monitor food and water intake and observation of any gastrointestinal signs are important. Clinical signs and testing for adrenal suppression are used determine the length of the induction period. Monitoring is best by use of an adrenocorticotropic hormone (ACTH) test. The ACTH test is also used to distinguish adverse effects of Mitotane (hypoadrenocorticism) vs. desired effect of treatment. (Figure 1)
From: Reine N, Topics in Compan An Med 27:25-30, 2012 Adrenal function should be tested within 7-14 days of the induction period, independent of clinical signs. If adrenal suppression is not obtained, the loading dose should continue with weekly testing. UCCR has been used for monitoring; although the test is not as specific as the ACTH stimulation test. If signs of toxicity occur, treatment with daily prednisone (0.3-0.5 mg/kg) can be instituted.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health98
Prednisone should be withheld for 24 hours prior to ACTH stimulation testing to avoid falsely increased cortisol results. Once a dog has reached the maintenance phase of treatment and clinical signs are stable, ACTH stimulation testing is recommended every 4-6 months. A blood chemistry and urinalysis done at this interval may also provide information to suggest a relapse such as an increase is serum alkaline phosphatase activity or proteinuria or active urine sediment, respectively. If a relapse occurs, a repeated loading period should be started followed by a maintenance dose which is 30%-50% higher than the original one. Trilostane Trilostane is a steroid analog which reversibly inhibits 3β-hyroxysteroid dehydrogenase, blocking the production of cortisol and corticosterone. Trilostane is absorbed from the gastrointestinal tract, with an enhanced rate and extent of absorption when given with food. The dosage rate is 2-6 mg/kg. Initial dosing should start at the low end of the this range, once daily in the morning. Side effects are few; lethargy and loss of appetite are the most common early in the treatment course. They appear reversible with discontinuation of the drug. A blood biochemistry, urinalysis and ACTH stimulation test are monitoring tests to be conducted 10-14 days, 4 weeks and 12 weeks following initiation of treatment. It is important to perform the ACTH stimulation test 4-6 hours post dosing, considering the duration of effect of trilostane. Testing outside of this window could result in misinterpretation of an increased cortisol concentration and inappropriate modification of the dose. For dogs for which the clinical signs are not controlled with once daily dosing, twice daily dosing can be considered. Trilostane is well tolerated twice daily and an overall lower daily dose is usually effective. Changes in dose are not uncommon in dogs beyond 12 weeks of treatment. An ACTH stimulation test is recommended every three months. Although polyuria and polydipsia may respond quickly to treatment, clinical signs such as hair loss, pot-bellied appearance and hyperpigmentation are slower to respond, usually taking up to six months or more. Mitotane vs. Trilostane Median survival times are similar, 708 days for mitotane and 662 days for trilostane. Older age at the time of diagnosis correlates to a shorter survival. (Barker, 2005) One other difference worth noting between treatment with either drug is the ultrasound findings of the adrenal gland. Following treatment with mitotane, the size of the adrenal gland shrinks. In contrast with treatment with trilostane, the adrenal gland’s size increases and its echogenicity may become more heterogenous. (Mantis, 2003)
Overall, the response to treatment with either drug is good. Relapses are common as is the need for adjustment of dosing. Successful treatment requires and an attentive clinician and a dedicated pet owner. Excellent communication is also needed to conduct the required monitoring and set the expectations of the pet owner. References Barker EN, Campbell S, Tebb AJ, Neiger R, Herrtage ME, Reid SWJ, Ramsey IK. A comparison of the survical times of dogs treated with Mitotane vs. Trilostane for pituitary dependent hyperadrenocorticism. J Vet Int Med 19:810-815, 2005. Behrend EN, Kooistra HS, Nelson R, Reusch CE, and Scott-Moncreiff JC. . Diagnosis of Spontaneous Canine Hyperadrenocorticism: 2012 ACVIM Consensus Statement (Small Animal). J Vet Int Med 27 (6):1292-1304, 2013 Forrester SD, Troy GC, Dalton MN, Huffman JW, and Holtzman G. Retrospective evaluation of urinary tract infection in 42 dogs with hyperadrenocorticism or diabetes mellitus or both. J Vet Int Med13:557-560, 1999. Hoerauf A, Reusch C. Ultrasonographic characteristics of both adrenal glands in 15 dogs with functional adrenocortical tumors. J Am Anim Hosp Assoc 35:193- 199, 1999. Lang JM, Schertel E, Kennedy S, Wilson D, Barnhart M, and Danielson B. Elective and emergency surgical management of adrenal gland tumors: 60 cases (1999- 2006). J Am Anim Hosp Assoc 47:428-435, 2011. Mantis P, Lamb CR, Witt AL and Neiger R. Changes in ultrasonographic appearance of adrenal glands in dogs with pituitary-dependent hyperadrenocorticism treated with trilostane. Vet Radiol Ultrasound 44:682-685, 2003. Reine N. Medical management of pituitary-dependent hyperadrenocorticism: Mitotane versus Trilostane. Topics in Compan An Med 27:25-30, 2012. Rijnberk A, van Wess A, Mol JA. Assessment of the two tests for the diagnosis of canine hyperadrenocorticism. Vet Rec 122:178-180, 1988. Rodriguez Pineiro MI, Benchekroum G, de Fornel-Thibaud P, Maurey-Guenec C, Garnier F, Rosenberg D. Accuracy of an adrenocorticotropic hormone (ACTH) immunoluminometric assay for differentiating ACTH-dependent from ACTH- independent hyperadrenocorticism in dogs. J Vet Int Med 23:850-855, 2009.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 99
Overall, the response to treatment with either drug is good. Relapses are common as is the need for adjustment of dosing. Successful treatment requires and an attentive clinician and a dedicated pet owner. Excellent communication is also needed to conduct the required monitoring and set the expectations of the pet owner. References Barker EN, Campbell S, Tebb AJ, Neiger R, Herrtage ME, Reid SWJ, Ramsey IK. A comparison of the survical times of dogs treated with Mitotane vs. Trilostane for pituitary dependent hyperadrenocorticism. J Vet Int Med 19:810-815, 2005. Behrend EN, Kooistra HS, Nelson R, Reusch CE, and Scott-Moncreiff JC. . Diagnosis of Spontaneous Canine Hyperadrenocorticism: 2012 ACVIM Consensus Statement (Small Animal). J Vet Int Med 27 (6):1292-1304, 2013 Forrester SD, Troy GC, Dalton MN, Huffman JW, and Holtzman G. Retrospective evaluation of urinary tract infection in 42 dogs with hyperadrenocorticism or diabetes mellitus or both. J Vet Int Med13:557-560, 1999. Hoerauf A, Reusch C. Ultrasonographic characteristics of both adrenal glands in 15 dogs with functional adrenocortical tumors. J Am Anim Hosp Assoc 35:193- 199, 1999. Lang JM, Schertel E, Kennedy S, Wilson D, Barnhart M, and Danielson B. Elective and emergency surgical management of adrenal gland tumors: 60 cases (1999- 2006). J Am Anim Hosp Assoc 47:428-435, 2011. Mantis P, Lamb CR, Witt AL and Neiger R. Changes in ultrasonographic appearance of adrenal glands in dogs with pituitary-dependent hyperadrenocorticism treated with trilostane. Vet Radiol Ultrasound 44:682-685, 2003. Reine N. Medical management of pituitary-dependent hyperadrenocorticism: Mitotane versus Trilostane. Topics in Compan An Med 27:25-30, 2012. Rijnberk A, van Wess A, Mol JA. Assessment of the two tests for the diagnosis of canine hyperadrenocorticism. Vet Rec 122:178-180, 1988. Rodriguez Pineiro MI, Benchekroum G, de Fornel-Thibaud P, Maurey-Guenec C, Garnier F, Rosenberg D. Accuracy of an adrenocorticotropic hormone (ACTH) immunoluminometric assay for differentiating ACTH-dependent from ACTH- independent hyperadrenocorticism in dogs. J Vet Int Med 23:850-855, 2009.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health100
Management of canine diabetes mellitus; how fast you can get the initial insulin dose
Narudee Kashemsant, DVM, PhD.
Faculty of Veterinary Medicine, Kasetsart University, 50 Pahonyothin Road, Ladyao, Chatuchak Bangkok 10900.
Tel (fax): +6625797538, [email protected]
Among the global changes of lifestyle, not only owner but pets are also affected. Although pet balanced diets are commercially available, some owners still fed their pets home cooked diet. Hence, it is prone to be unbalanced. whenever pet owners changed their lifestyle to be westernized, either high fat or high carbohydrate food were always introduced to their pets. As a result, pets become obese, thereafter, adipocytes start to release proinflammatory cytokines which led pets' health to various diseases such as hyperlipidaemia, cancer, renal disease, hepatic disease, insulin resistance as well as diabetes mellitus. All these diseases are well recognized to be high burden-low quality of life diseases. Diabetes mellitus; comparison among noncommunicable diseases, is concerned to be the fourth causes of human death nowadays (Heron 2013). Along their illness, diabetic patients suffered from disease complications many times. It was displayed that the patients declined their happiness soon after they were diagnosed. It is not only do they reduce their happiness because of the illness, but the augmentation of their economic healthcare. Based on the information reported (Chatterjee S, 2011., Deerochanawong C, 2013.), the total illness cost of Thai diabetic patients was estimated about 28000 Baht/year (16.7% of average annual income of Thai people). It is implied a huge economic burden for the patient's families to deal with. Additionally, this economic burden would likely to be much higher in the cases of complicated diabetes. It was predicted that the cost of diabetes with complication must be 232% higher depend on type of that complication. Comparing to human diabetes, it was suggested that this economic burden could also occurred to the diabetic pet's owner so that to avoid the unnecessary cost happened, the success client communication should be performed. As soon as pets were diagnosed as being diabetic patients, owners have to be explained three important categories as follows; - the necessity of the cooperation between veterinarians and owner toward to the patients including the basic of disease, the differences between human diabetes and pet diabetes and the differences between dog and cat diabetic
- disease followed up plan glucose curve the important of type of meal, portion of meal and timing of meal the important of type of insulin, volume of insulin and timing of insulin follow up protocol - the danger of disease complication and critical condition of disease The necessity of the cooperation between veterinarians and owner toward to the patients The aims of the information conferment with the owner that vets should focus on are to what will go on and to affect their life in the future. It is recommended to follow the owner's and patients' lifestyle. This is well documented to decrease owner's frustration, despondency, and increase owner's cooperation, thereby, reduce their burden respectively. The owner supposes to know the basic of diabetes such as the synchronization between insulin and glucose (from the nutrient), factors influencing insulin function, disease concurrent, complication. Additionally, the differences between human and small animal diabetes and between dog and cat diabetes since many owners could misunderstand from the wrong information they have been educated by social network. The details are as follows; Most nutrients animals got during their meal ultimately convert to glucose during their metabolism (polysaccharide in carbohydrate metabolism, glucogenic amino acid in protein metabolism and glycerol in lipid metabolism), however, the rate of conversion is various. It is therefore that the fast the conversion, the increase the insulin required. Fortunately, this reaction does not interfere insulin function. In contrast in stimulation of insulin release, hyperlipidaemia as well as hormone increasing fatty acid level influences the insulin function. Although their influences are not similar, nonetheless, they could make the pancreatic beta cell end up with apoptosis if their influences are high or prolong. Some factors influencing the insulin function not through the interfering effect of high fatty acid on insulin function, but itself interferes insulin-receptor interaction or insulin signalling transduction. These factors include pancreatitis, pyometra, and dehydration. Based on this knowledge, information should be simplified for the owner to understand in order to increase the cooperative between the veterinarian and pet owners. The owner also have to be concerned about the critical sign of this disease, what to do and not to do during that period. It is important for the sick pets to have a long survival time. At present, owners like to compare disease characteristics occurred in their pet with in human, so that the similarity and differences of the disease in various points of view should inform to reconcile with the owner. In summary, conversation made as soon as

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 101
- disease followed up plan glucose curve the important of type of meal, portion of meal and timing of meal the important of type of insulin, volume of insulin and timing of insulin follow up protocol - the danger of disease complication and critical condition of disease The necessity of the cooperation between veterinarians and owner toward to the patients The aims of the information conferment with the owner that vets should focus on are to what will go on and to affect their life in the future. It is recommended to follow the owner's and patients' lifestyle. This is well documented to decrease owner's frustration, despondency, and increase owner's cooperation, thereby, reduce their burden respectively. The owner supposes to know the basic of diabetes such as the synchronization between insulin and glucose (from the nutrient), factors influencing insulin function, disease concurrent, complication. Additionally, the differences between human and small animal diabetes and between dog and cat diabetes since many owners could misunderstand from the wrong information they have been educated by social network. The details are as follows; Most nutrients animals got during their meal ultimately convert to glucose during their metabolism (polysaccharide in carbohydrate metabolism, glucogenic amino acid in protein metabolism and glycerol in lipid metabolism), however, the rate of conversion is various. It is therefore that the fast the conversion, the increase the insulin required. Fortunately, this reaction does not interfere insulin function. In contrast in stimulation of insulin release, hyperlipidaemia as well as hormone increasing fatty acid level influences the insulin function. Although their influences are not similar, nonetheless, they could make the pancreatic beta cell end up with apoptosis if their influences are high or prolong. Some factors influencing the insulin function not through the interfering effect of high fatty acid on insulin function, but itself interferes insulin-receptor interaction or insulin signalling transduction. These factors include pancreatitis, pyometra, and dehydration. Based on this knowledge, information should be simplified for the owner to understand in order to increase the cooperative between the veterinarian and pet owners. The owner also have to be concerned about the critical sign of this disease, what to do and not to do during that period. It is important for the sick pets to have a long survival time. At present, owners like to compare disease characteristics occurred in their pet with in human, so that the similarity and differences of the disease in various points of view should inform to reconcile with the owner. In summary, conversation made as soon as

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health102
diagnosis done focus on factors influencing on glucose level and exogenous insulin function as well as owner daily activity that can match to the time they need to provide to their pets. Disease followed up plan Glucose curve In commercial market, many kinds of insulin are available (fig 1) for being selected properly during various condition. To the author's point of view, first administration of insulin should not start before the conversation done and the hydration was already corrected. This suggestion is quite differences comparing to the protocol documented in another part of the world (Rijnberk, A, 2010 ). Since the newly diagnosed diabetes in Thai veterinary community always came with either other clinical signs or severe dehydration. To avoid the influences of hyperosmolarity on glucose level, fluid replacement need to be performed 4-6 hours before starting insulin injection.
Figure 1: Illustration of various insulin type and their characteristics The advantage and disadvantage between types of insulin preparation. The short acting insulin preparation is excellent during the patients' critical period or under the complication such as acute pancreatitis, infection or diabetic ketoacidosis (Rijnberk, A, 2010) since it did not required any changes before being utilized. However, short acting insulin preparation could make owner more burden to take care the patients since it needs to be given at least three times a day. The intermediate acting insulin ; both human insulin synthetic NPH or 30:70 porcine Lente preparation, are the routine insulin used in most practices. It is convenience since it only has to be administered every 12 hours after meal. The type of insulin
preparation cannot be given intravenously (Martin GJ, 2001) so it is not insulin of choice during the critical condition of patients with complication. The long acting insulin preparation designed for human diabetes called, Glargine or Detemir, can be wonderful for diabetic cats fed ad libitum. This preparation does not have the peak effect such that hypoglycemia is unlikely to occurred. the disadvantage of this preparation was displayed the less capability to diminish the high level of insulin or in the hyperosmolar diabetic patients. Prior to do glucose curve, the understanding the synchronization among food digestion, glucose level and hormone interaction should be advised. Normal digestion of small animal is between 60-90 minute. It is therefore that the peak effect of insulin preparation used should act in the same time as that period of nutrient load. Additionally, the relation between glucose level and insulin function also based on the amount and type of both insulin and meal animal fed. Hence it is suggested that type, amount and timing of meal owner wishing to feed their pets as well as the timing, type (and quality) and amount of insulin patients got should be consistent, thereby, glucose curve performed can be interpreted. Glucose curve Theoretically, glucose curve should be done while the patients had already been stabilized and start to have their own appetite. Beside than that regular insulin should be used while stabilizing patient's condition and treating concurrent disease. In the diabetic patients without complication, glucose curve can be done as soon as diagnosed. After client communication carried out, pets were hospitalized and hydration was already corrected. fasting glucose was performed before meal and insulin were introduced. Most practices in Thailand recommended intermediate insulin preparation to the owner which should be given immediately after meal. In contrast, if long acting insulin preparation was prescribed, insulin administration should be performed at least two hours prior to meal feeding. the glucose curve protocol is as follows;
• Hospitalize • Follow pet owner’s normal regime. insulin , meal and exercise routine. • Take a blood sample prior to and after insulin injection • Take a blood sample for 24 hours or at least until the concentration has
crossed back above the renal threshold: • Blood glucose concentrations are measured and plotted against time to
produce a blood glucose curve • Administer the insulin soon after meal is done.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 103
preparation cannot be given intravenously (Martin GJ, 2001) so it is not insulin of choice during the critical condition of patients with complication. The long acting insulin preparation designed for human diabetes called, Glargine or Detemir, can be wonderful for diabetic cats fed ad libitum. This preparation does not have the peak effect such that hypoglycemia is unlikely to occurred. the disadvantage of this preparation was displayed the less capability to diminish the high level of insulin or in the hyperosmolar diabetic patients. Prior to do glucose curve, the understanding the synchronization among food digestion, glucose level and hormone interaction should be advised. Normal digestion of small animal is between 60-90 minute. It is therefore that the peak effect of insulin preparation used should act in the same time as that period of nutrient load. Additionally, the relation between glucose level and insulin function also based on the amount and type of both insulin and meal animal fed. Hence it is suggested that type, amount and timing of meal owner wishing to feed their pets as well as the timing, type (and quality) and amount of insulin patients got should be consistent, thereby, glucose curve performed can be interpreted. Glucose curve Theoretically, glucose curve should be done while the patients had already been stabilized and start to have their own appetite. Beside than that regular insulin should be used while stabilizing patient's condition and treating concurrent disease. In the diabetic patients without complication, glucose curve can be done as soon as diagnosed. After client communication carried out, pets were hospitalized and hydration was already corrected. fasting glucose was performed before meal and insulin were introduced. Most practices in Thailand recommended intermediate insulin preparation to the owner which should be given immediately after meal. In contrast, if long acting insulin preparation was prescribed, insulin administration should be performed at least two hours prior to meal feeding. the glucose curve protocol is as follows;
• Hospitalize • Follow pet owner’s normal regime. insulin , meal and exercise routine. • Take a blood sample prior to and after insulin injection • Take a blood sample for 24 hours or at least until the concentration has
crossed back above the renal threshold: • Blood glucose concentrations are measured and plotted against time to
produce a blood glucose curve • Administer the insulin soon after meal is done.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health104
• Take a blood sample every two (to four) hours, o if possible for 24 hours but at least until the concentration has
crossed back above the renal threshold: o More frequent blood sampling (e.g. hourly) may o be required if Somogyi effect is suspected and o difficult to identify. o Be careful not to take too many large blood samples in small dogs and
cats. o Blood glucose concentrations are measured and plotted against time
to produce a blood glucose curve Figure 2: Glucose curve A) showing time interval for blood collection, blood collection supposed to be done in the consistent interval , and done at nadir time B) Illustration displayed the glucose level against time after insulin administered at 8:00 am
During glucose curve carried out, four questions need to be answered in order to get the success interpretation 1. Does glucose decline too fast? It is recommended that glucose should not decrease more than 50mg/dl /hour ( 20-30mg/dl/hour is recommended) 2. What is glucose level at the nadir point? Is it in the acceptable range? 3. At the nadir point, is it at the nadir time as well? 4. How is over all glucose curve? Do most points are in acceptable range?
Fig 3: Illustrated showing the questions leading to glucose curve interpretation If the answers at any points are not as expected, stop doing glucose curve, fix the problem and then start new glucose curve on the day after. Comparing to dogs, cats are much harder to control diabetes since they are prone to be in stress induced hyperglycemia so that level of fructosamine is necessary to take into account for diagnosis. Transient hyperglycemia induced by stress cannot led to high body fructosamine but stress induced in animals admitted for days is long enough to increase fructosamine level. Therefore it is suggested to do glucose curve at home (if possible) in the cat patients.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 105
During glucose curve carried out, four questions need to be answered in order to get the success interpretation 1. Does glucose decline too fast? It is recommended that glucose should not decrease more than 50mg/dl /hour ( 20-30mg/dl/hour is recommended) 2. What is glucose level at the nadir point? Is it in the acceptable range? 3. At the nadir point, is it at the nadir time as well? 4. How is over all glucose curve? Do most points are in acceptable range?
Fig 3: Illustrated showing the questions leading to glucose curve interpretation If the answers at any points are not as expected, stop doing glucose curve, fix the problem and then start new glucose curve on the day after. Comparing to dogs, cats are much harder to control diabetes since they are prone to be in stress induced hyperglycemia so that level of fructosamine is necessary to take into account for diagnosis. Transient hyperglycemia induced by stress cannot led to high body fructosamine but stress induced in animals admitted for days is long enough to increase fructosamine level. Therefore it is suggested to do glucose curve at home (if possible) in the cat patients.
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health106
Short term follow up protocol After getting the initial insulin dose, a short term follow up must be scheduled. Some dogs and cats might be faced with hypoglycemia condition then they do not need insulin injection for a while. It is called honeymoon period (using in the dog's case) or diabetic remission (using in a cat's case). it is because exogenous insulin given help exhausted pancreas recovered and started to synthesize its own mature insulin. Thereby, these endogenous insulin will add up into the patients' circulations then induce the hypoglycemic condition. It is recommended that the owner should concern and enable to recognize clinical signs of hypoglycemic condition, if any, stop administering insulin and bring their pets for hospital visit. Most dogs get into this period for a few days, while cats sometimes are having this diabetic remission for months or years. In this case owners are advised to keep checking their pet's urine for glucose before going back to treatment protocol. One of the key success in diabetic pet's care is the technical aspects taught to the owner. Owner should be able to mix the insulin well and correctly, to draw insulin into syringe without air bubble as well as to administered insulin to their pet with the corrected route and dose Long term follow up protocol The aims of treatment are to eliminate the clinical signs of diabetes mellitus and prevent its complications (both hypoglycemia and critical condition; DKA and hyperosmolar hyperglycemic syndrome), thereby enabling the animal to have a good quality of life. It is not necessary to maintain normal blood glucose levels, as is the aim in humans (Rijnberk, A, 2010). If dogs and cats are doing well, enable to maintain their body weight, no present signs of PU/PD and polyphagia, it is meant that the healthcare protocol is likely to be success. Fructosamine level can be checked to confirm the evident of hyperglycaemia during the past 3-4 weeks. Routine visit can be scheduled every 3-4 months with the owner's observation for diabetic recurrent signs. The examination includes assessment of the owner’s observations of symptoms, measurement of body weight, and measurement of blood glucose and fructosamine concentrations. The presence or absence of polyuria, polydipsia, polyphagia, lethargy, and weight loss are used to assess the quality of metabolic control. Some patients have a hard time to figure out the appropriate dose. If symptoms persist in spite of insulin therapy, the following stepwise approach (Rijnberk, A, 2010) can be used. First step. If the initial workup and treatment is corrected then increase the dose of lente insulin every five to seven days until it reaches 1.0–1.5 U/kg twice daily.
Second step. Confirm that the insulin used by owner is not outdated, has not been diluted, frozen, or heated, and is mixed correctly before being drawn into the syringe by observing the owner’s method of mixing, drawing up, and injecting the insulin. Review the diet and exercise regimen. Third step. Perform a serial blood glucose curve to determine whether there may be a Somogyi effect or short duration of insulin effect. Blood glucose should be measured under the stress free condition every 1–2 h for at least 12 h. Fourth step. If no explanation for the problem has been identified, diseases causing insulin resistance should be considered. The danger of disease complication and critical condition of disease Owner is recommended to report any changes since it can influence insulin function and lead to diabetic critical complication. If any changes was left without any concern, it will soon be either a metabolic acidosis (called diabetic ketoacidosis) leading to multi-organ failure or hyperosmolar hyperglycemic syndrome leading to renal shutdown without acidosis. Inaddition to fluid replace ment at least a few hours prior to insulin administration. Insulin of choice during this period is short acting insulin administered intramuscular route or continuous rate infusion. In summary, the key success to achieve the initial insulin dosage is step by step as follow;
1. client communication to make more clients' understanding about the disease, factor influencing insulin release and function, patients' signs in disease complication.
2. correction of patients' hydration status 3. treating or stabilizing the underlying cause 4. during the period above, short acting is recommended every three to six hours.
5. whenever the patient can be back on food, glucose curve with the daily insulin should be performed.
6. to have clients' cooperation, glucose curve should be plan under the clients and patient's lifestyle with the consistency of type/portion/timing of meal and type/volume/timing of insulin
7. interpretation of glucose curve should be carried out at any point of glucose collection with these four following questions; 1. Does glucose decline too fast? It is recommended that glucose should not
decrease more than 50mg/dl /hour ( 20-30mg/dl/hour is recommended) 2. What is glucose level at the nadir point? Is it in the acceptable range? 3. At the nadir point, is it at the nadir time as well? 4. How is over all glucose curve? Do most points are in acceptable range?

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 107
Second step. Confirm that the insulin used by owner is not outdated, has not been diluted, frozen, or heated, and is mixed correctly before being drawn into the syringe by observing the owner’s method of mixing, drawing up, and injecting the insulin. Review the diet and exercise regimen. Third step. Perform a serial blood glucose curve to determine whether there may be a Somogyi effect or short duration of insulin effect. Blood glucose should be measured under the stress free condition every 1–2 h for at least 12 h. Fourth step. If no explanation for the problem has been identified, diseases causing insulin resistance should be considered. The danger of disease complication and critical condition of disease Owner is recommended to report any changes since it can influence insulin function and lead to diabetic critical complication. If any changes was left without any concern, it will soon be either a metabolic acidosis (called diabetic ketoacidosis) leading to multi-organ failure or hyperosmolar hyperglycemic syndrome leading to renal shutdown without acidosis. Inaddition to fluid replace ment at least a few hours prior to insulin administration. Insulin of choice during this period is short acting insulin administered intramuscular route or continuous rate infusion. In summary, the key success to achieve the initial insulin dosage is step by step as follow;
1. client communication to make more clients' understanding about the disease, factor influencing insulin release and function, patients' signs in disease complication.
2. correction of patients' hydration status 3. treating or stabilizing the underlying cause 4. during the period above, short acting is recommended every three to six hours.
5. whenever the patient can be back on food, glucose curve with the daily insulin should be performed.
6. to have clients' cooperation, glucose curve should be plan under the clients and patient's lifestyle with the consistency of type/portion/timing of meal and type/volume/timing of insulin
7. interpretation of glucose curve should be carried out at any point of glucose collection with these four following questions; 1. Does glucose decline too fast? It is recommended that glucose should not
decrease more than 50mg/dl /hour ( 20-30mg/dl/hour is recommended) 2. What is glucose level at the nadir point? Is it in the acceptable range? 3. At the nadir point, is it at the nadir time as well? 4. How is over all glucose curve? Do most points are in acceptable range?

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health108
If any of these questions receive the unexpected answers, glucose curve should be given up. Maintain fluid replacement and stabilize the patients' hydration. Start new glucose curve whenever the effect of previous insulin has already faded away.
8. concern all changes that occur in patient's condition to avoid the critical disease complication.
if there is some change of the patient's signs, short acting insulin should be used while vets try to treat this concurrent disease
9. Whenever high dose insulin has already been administered to patient, but the uncontrolled glucose is still displayed. The concurrent disease that influence insulin release and function must be figured out. References Chatterjee S, Riewpaiboon A, Piyauthakit P, Riewpaiboon W, Boupaijit K, Panpuwong N, Archavanuntagul V. 2011. Cost of diabetes and its complications in Thailand: a complete picture of economic burden. Health Soc Care Community.;19(3):289-98.
Deerochanawong C, Ferrario A. 2013 Diabetes management in Thailand: a literature review of the burden, costs, and outcomes. Global Health.;9:11
Heron M, 2013 National Vital Statistics Reports,;62,(6)
Martin GJ, Rand JS. 2001 Pharmacology of a 40 IU/ml porcine lente insulin preparation in diabetic cats: findings during the first week and after 5 or 9 weeks of therapy. J Feline Med Surg.;3(1):23-30. Rijnberk, A., Kooistra, H. S. 2010 Clinical Endocrinology of dogs and cats. An Illustrated text. Schlutersche Verlagsgesellschaft mbH & Co. Hannover.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 109
Oral Presentation

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health110
Influence of Feeding Patterns on Subclinical Laminitis in Lactating Cows of Smallholder Dairy Farms in Thailand
R. Pilachai1* J. Th. Schonewille2 C. Thamrongyoswittayakul3
S. Aiumlamai3 C. Wachirapakorn4 H. Everts2 and W. H. Hendriks2 1Program in Veterinary Technology, Faculty of Technology,
Udon Thani Rajabhat University, Udon Thani 41000, Thailand. 2Animal Nutrition Division, Department of Farm Animal Health,
Faculty of Veterinary Medicine, Utrecht University, Utrecht, The Netherlands. 3Faculty of Veterinary Medicine, 4Department of Animal Science,
Faculty of Agriculture,Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Background - Nutrition is an important risk factor for laminitis in dairy cows. However, it is not known whether the typical Thai feeding conditions predispose cows to laminitis.
Objective - To evaluate the importance of dietary crude protein (CP) content, dietary neutral detergent fiber (NDF) content and feeding regime as well as other factors related to management and demographics on the occurrence of (subclinical) laminitis under practical Thai feeding conditions.
Materials and Methods - Hemorrhage of the white line and the sole, sole ulcer and white-line fissure of all four claws of milking cows (n=119) on 25 farms (selected based on the occurrence of lameness) were macroscopically assessed to calculate the prevalence of subclinical laminitis (SCL) on each farm. The prevalence data were categorized into a low and high SCL prevalence farm using medians and standard deviation. Data were collected on farm characteristics, feed and feeding management, floor type and hoof care. Dry matter intake was assessed on each farm and feed ingredients collected and analyzed for dry matter (DM), CP and NDF.
Results - Twelve out of the 25 farms had a prevalence of SCL above 25%. Mean SCL prevalence was 64.0% and 15.3% for the farms with or without a previous lameness, respectively. No significant differences were found for farm characteristics such as herd size, number of milking cows, parity and body condition score between farms with a low (<25%) or a high prevalence (> 25%) of SCL. Percentages of DM and CP content of the rations did not differ, whereas mean NDF content in the ration was significantly higher (P<0.001) in the low compared to the high prevalence farms. Multiple regression analysis of the data showed that a low NDF ration (R2=0.631; P<0.001) and/or in combination with the separate feeding of roughage and concentrate (R2=0.585; P=0.016) was associated with a high SCL prevalence.
Conclusion - It is suggested that mixing concentrate with a substantial part of the roughage is an important strategy to prevent SCL in smallholder dairy farms under Thai feeding conditions. In addition, the dietary NDF content but not the dietary CP level is associated with SCL prevalence in dairy cows under Thai feeding conditions.
Keywords: Nutrition, Risk factor, Laminitis, Dairy cow

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 111
Influence of Feeding Patterns on Subclinical Laminitis in Lactating Cows of Smallholder Dairy Farms in Thailand
R. Pilachai1* J. Th. Schonewille2 C. Thamrongyoswittayakul3
S. Aiumlamai3 C. Wachirapakorn4 H. Everts2 and W. H. Hendriks2 1Program in Veterinary Technology, Faculty of Technology,
Udon Thani Rajabhat University, Udon Thani 41000, Thailand. 2Animal Nutrition Division, Department of Farm Animal Health,
Faculty of Veterinary Medicine, Utrecht University, Utrecht, The Netherlands. 3Faculty of Veterinary Medicine, 4Department of Animal Science,
Faculty of Agriculture,Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Background - Nutrition is an important risk factor for laminitis in dairy cows. However, it is not known whether the typical Thai feeding conditions predispose cows to laminitis.
Objective - To evaluate the importance of dietary crude protein (CP) content, dietary neutral detergent fiber (NDF) content and feeding regime as well as other factors related to management and demographics on the occurrence of (subclinical) laminitis under practical Thai feeding conditions.
Materials and Methods - Hemorrhage of the white line and the sole, sole ulcer and white-line fissure of all four claws of milking cows (n=119) on 25 farms (selected based on the occurrence of lameness) were macroscopically assessed to calculate the prevalence of subclinical laminitis (SCL) on each farm. The prevalence data were categorized into a low and high SCL prevalence farm using medians and standard deviation. Data were collected on farm characteristics, feed and feeding management, floor type and hoof care. Dry matter intake was assessed on each farm and feed ingredients collected and analyzed for dry matter (DM), CP and NDF.
Results - Twelve out of the 25 farms had a prevalence of SCL above 25%. Mean SCL prevalence was 64.0% and 15.3% for the farms with or without a previous lameness, respectively. No significant differences were found for farm characteristics such as herd size, number of milking cows, parity and body condition score between farms with a low (<25%) or a high prevalence (> 25%) of SCL. Percentages of DM and CP content of the rations did not differ, whereas mean NDF content in the ration was significantly higher (P<0.001) in the low compared to the high prevalence farms. Multiple regression analysis of the data showed that a low NDF ration (R2=0.631; P<0.001) and/or in combination with the separate feeding of roughage and concentrate (R2=0.585; P=0.016) was associated with a high SCL prevalence.
Conclusion - It is suggested that mixing concentrate with a substantial part of the roughage is an important strategy to prevent SCL in smallholder dairy farms under Thai feeding conditions. In addition, the dietary NDF content but not the dietary CP level is associated with SCL prevalence in dairy cows under Thai feeding conditions.
Keywords: Nutrition, Risk factor, Laminitis, Dairy cow

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health112
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Subclinical Mastitis and Associated Risk Factors in Dairy Cows in Udon Thani of Thailand
Rittichai Pilachai1 Pranpreya Kummee1 and Sudawan Chuenpreecha1*
1Program in Veterinary Technology, Faculty of Technology, Udon Thani Rajabhat University, Udon Thani 41000, Thailand.
*Corresponding author
Background - Subclinical mastitis (SCM) is a major health problem of the dairy industry in Thailand. Many predisposing factors are related to the occurrence of SCM in dairy cows. However, the SCM-potentially related factors have not been extensively documented in Udon Thani of Thailand.
Objective - To determine the prevalence of SCM and associated risk factors in lactating cows during March, 2012 and September, 2013 in a cross-sectional study.
Materials and Methods - Ninety five herds, out of the 180 dairy farms located in Udon Thani were investigated 1,304 lactating cows were screened to determine the prevalence of SCM using California Mastitis Test. Prevalence of SCM was calculated as a proportion of the affected cows related to the number of selected cows on each farm. Data were categorized as a low and high prevalence of SCM farm using the lowest and highest quintile of the total population. A questionnaire regarding farm characteristics, farm management and milking process was collected. Logistic regression was performed to identify the important factors for SCM.
Results - The prevalence of SCM in lactating cows in Udon Thani province was 30.2%. The univariable model revealed that milking machine only (OR=5.20, 95% CI=1.48-18.33), no washing milking unite every milking (OR=3.33, 95% CI=1.04-10.59), using udder towels for more than one cow (OR=5.39, 95% CI=1.45-20.01), unregulated post-milking teat dip (OR=6.16, 95% CI=1.74-21.84), history of mastitis reported (OR=4.14, 95% CI=1.23-13.89), and number of lactating cow per farm (<11) (OR=4.90, 95% CI=1.45-16.55) were related to the prevalence of SCM (P<0.1). However, the final model of logistic regression, a history of mastitis reported (OR=8.19, p=0.007) and unregulated postmilking teat dip (OR=11.33, p=0.002), were significantly associated with the prevalence of SCM and explained 39.2% of the variation in SCM prevalence between farms.
Conclusion - Farm with a history of chronic- or subclinical- mastitis in combination with improper milking process, unregulated post-milking teat dip was associated with the high SCM prevalence in lactating cows, which is of concerns in controlling the disease.
Keywords: Risk factor, Subclinical mastitis, Lactating cow

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 113
Subclinical Mastitis and Associated Risk Factors in Dairy Cows in Udon Thani of Thailand
Rittichai Pilachai1 Pranpreya Kummee1 and Sudawan Chuenpreecha1*
1Program in Veterinary Technology, Faculty of Technology, Udon Thani Rajabhat University, Udon Thani 41000, Thailand.
*Corresponding author
Background - Subclinical mastitis (SCM) is a major health problem of the dairy industry in Thailand. Many predisposing factors are related to the occurrence of SCM in dairy cows. However, the SCM-potentially related factors have not been extensively documented in Udon Thani of Thailand.
Objective - To determine the prevalence of SCM and associated risk factors in lactating cows during March, 2012 and September, 2013 in a cross-sectional study.
Materials and Methods - Ninety five herds, out of the 180 dairy farms located in Udon Thani were investigated 1,304 lactating cows were screened to determine the prevalence of SCM using California Mastitis Test. Prevalence of SCM was calculated as a proportion of the affected cows related to the number of selected cows on each farm. Data were categorized as a low and high prevalence of SCM farm using the lowest and highest quintile of the total population. A questionnaire regarding farm characteristics, farm management and milking process was collected. Logistic regression was performed to identify the important factors for SCM.
Results - The prevalence of SCM in lactating cows in Udon Thani province was 30.2%. The univariable model revealed that milking machine only (OR=5.20, 95% CI=1.48-18.33), no washing milking unite every milking (OR=3.33, 95% CI=1.04-10.59), using udder towels for more than one cow (OR=5.39, 95% CI=1.45-20.01), unregulated post-milking teat dip (OR=6.16, 95% CI=1.74-21.84), history of mastitis reported (OR=4.14, 95% CI=1.23-13.89), and number of lactating cow per farm (<11) (OR=4.90, 95% CI=1.45-16.55) were related to the prevalence of SCM (P<0.1). However, the final model of logistic regression, a history of mastitis reported (OR=8.19, p=0.007) and unregulated postmilking teat dip (OR=11.33, p=0.002), were significantly associated with the prevalence of SCM and explained 39.2% of the variation in SCM prevalence between farms.
Conclusion - Farm with a history of chronic- or subclinical- mastitis in combination with improper milking process, unregulated post-milking teat dip was associated with the high SCM prevalence in lactating cows, which is of concerns in controlling the disease.
Keywords: Risk factor, Subclinical mastitis, Lactating cow

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health114
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
The Effect of Sub-acute Ruminal Acidosis Challenge on Inflammatory Response and Hoof Pain in Dairy Heifers
Suvaluk Seesupa1 Chalong Wachirapakorn2 and Suneerat Aiumlamai3*
1Graduate Student, Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, 2Department of Animal Science, Faculty of Agriculture,
3Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Overconsumption of concentrate has been hypothesized as an important predisposing factor of hoof pain or laminitis in cattle. Recent studies demonstrated that rapidly fermentable carbohydrate can induce sub-acute ruminal acidosis (SARA) and triggers the rise of acute phase protein response in dairy cattle. However, the association between SARA, inflammatory response, and hoof pain have not been investigated in dairy cattle of Thailand. Objective - To investigate the effect of SARA challenge on inflammatory response and hoof pain in dairy heifers. Materials and Methods - The completely randomize study was assigned with 12 crossbred Holstein-Friesian heifers with an average age and body weight at 14.3±0.3 months and 300.3±14.5 kg, respectively. SARA was challenged in six heifers by overfeeding of concentrate (46% of ground cassava chip, approximately 8 kg DM/day) with limited amount of roughage for 8 days. Other six heifers were served as a control group fed by farm’s concentrate diet with roughage ad libitum. During treatment period (8 days) ruminal fluid was collected by vacuum aspiration via the esophago-stomach tube at 0, 3 and 6 h after morning feeding and 20 ml of blood sample were collected from the jugular vein at 0 and 6 h after morning feeding. Hoof pain, a clinical sign of laminitis, was tested by hoof-tester grasping over the sole of claw on forelimbs. The positive reactions of hoof pain were accepted when the heifer presented both of fasciculation in triceps muscle and attempted to withdraw the leg. Ruminal fluid samples were immediately measured for pH. Heifers were considered as SARA when postprandial rumen pH was below 6.0 (the threshold value) in each day. Lipopolysaccharide-binding protein (LBP), an acute phase proteins, was measured by ELISA technique to ensure the inflammatory response. The data were analysed by Repeated measurement linear mixed model performed under XTMIXED command of STATA version 12.0. Results - In the SARA group, mean of postprandial rumen pH was lower than 6.0 from days 5 to 8 of treatment period and significantly lower (p<0.05) than the control group. The LBP (mg/ml) of the SARA group were significantly higher (p< 0.05) than those from the control group (0 h = 8.50 vs 2.86, and 6 h = 9.61 vs 2.93). Moreover, the LBP in the SARA group were significantly higher (p<0.05) than the control group from days 3 to 8. All heifers in SARA group showed positive pain reaction with hoof testing on days 5 to 8 of the treatment period and the daily proportion of positive hooves were 16.7, 33.3, 75.0 and 83.3%, respectively. No positive pain reaction was detected in the control. Conclusion - SARA challenge by overfeeding of concentrate activated inflammatory response which expressed as elevating LBP and resulted in the occurrence of hoof pain.
Keywords: Sub-acute ruminal acidosis, Hoof pain, Inflammatory response, Heifer

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 115
The Effect of Sub-acute Ruminal Acidosis Challenge on Inflammatory Response and Hoof Pain in Dairy Heifers
Suvaluk Seesupa1 Chalong Wachirapakorn2 and Suneerat Aiumlamai3*
1Graduate Student, Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, 2Department of Animal Science, Faculty of Agriculture,
3Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Overconsumption of concentrate has been hypothesized as an important predisposing factor of hoof pain or laminitis in cattle. Recent studies demonstrated that rapidly fermentable carbohydrate can induce sub-acute ruminal acidosis (SARA) and triggers the rise of acute phase protein response in dairy cattle. However, the association between SARA, inflammatory response, and hoof pain have not been investigated in dairy cattle of Thailand. Objective - To investigate the effect of SARA challenge on inflammatory response and hoof pain in dairy heifers. Materials and Methods - The completely randomize study was assigned with 12 crossbred Holstein-Friesian heifers with an average age and body weight at 14.3±0.3 months and 300.3±14.5 kg, respectively. SARA was challenged in six heifers by overfeeding of concentrate (46% of ground cassava chip, approximately 8 kg DM/day) with limited amount of roughage for 8 days. Other six heifers were served as a control group fed by farm’s concentrate diet with roughage ad libitum. During treatment period (8 days) ruminal fluid was collected by vacuum aspiration via the esophago-stomach tube at 0, 3 and 6 h after morning feeding and 20 ml of blood sample were collected from the jugular vein at 0 and 6 h after morning feeding. Hoof pain, a clinical sign of laminitis, was tested by hoof-tester grasping over the sole of claw on forelimbs. The positive reactions of hoof pain were accepted when the heifer presented both of fasciculation in triceps muscle and attempted to withdraw the leg. Ruminal fluid samples were immediately measured for pH. Heifers were considered as SARA when postprandial rumen pH was below 6.0 (the threshold value) in each day. Lipopolysaccharide-binding protein (LBP), an acute phase proteins, was measured by ELISA technique to ensure the inflammatory response. The data were analysed by Repeated measurement linear mixed model performed under XTMIXED command of STATA version 12.0. Results - In the SARA group, mean of postprandial rumen pH was lower than 6.0 from days 5 to 8 of treatment period and significantly lower (p<0.05) than the control group. The LBP (mg/ml) of the SARA group were significantly higher (p< 0.05) than those from the control group (0 h = 8.50 vs 2.86, and 6 h = 9.61 vs 2.93). Moreover, the LBP in the SARA group were significantly higher (p<0.05) than the control group from days 3 to 8. All heifers in SARA group showed positive pain reaction with hoof testing on days 5 to 8 of the treatment period and the daily proportion of positive hooves were 16.7, 33.3, 75.0 and 83.3%, respectively. No positive pain reaction was detected in the control. Conclusion - SARA challenge by overfeeding of concentrate activated inflammatory response which expressed as elevating LBP and resulted in the occurrence of hoof pain.
Keywords: Sub-acute ruminal acidosis, Hoof pain, Inflammatory response, Heifer

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health116
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Critical Processes of Knowledge Management for Reduction of Somatic Cell Count in Bulk Milk of Smallholder Dairy Farms
Aran Chanlun1* Chaiyapas Thamrongyoswittayakul 1 Suthida Chanlun2
Pitaya Papirom2 Manassanan Borisuthpetch1 and Pithai Kanbutra3 1Department of Medicine, 2Department of Pathobiology, 3Veterinary Teaching Hospital,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author E-mail address: [email protected]
Background - Bovine mastitis causes substantially economic losses in dairy industry worldwide. Somatic cell count (SCC) in bulk milk has been used as the most reliable indicator of udder health status of milking cow in dairy herds. Objective - To demonstrate the efficiency of knowledge managements for decreasing SCC in bulk milk of smallholder dairy farms at the milk collection center. Materials and Methods - The study was carried out at Khon Kaen dairy cooperatives, Khon Kaen province of Thailand during June-September, 2013. The critical processes of knowledge management were established including setup the cut-off value of bulk milk SCC, reform workflow for cooperatives’ personnel, knowledge or information exchanges. The total of 6 seminars at 2 weeks apart were systemically designed and organized for different target groups, i.e. quality control personnel, extension staff, and dairy farmers. Bulk milk SCC was randomly monitored at both morning and afternoon milking times throughout the study. Milk samples of all milk-cans from dairy farms was tested at the milk collection center before pooling into the cooling tank. Presence of SCC in milk samples were manually estimated using California mastitis test (CMT) as a screening tool and Delaval™ cell counter was also used as the confirmatory test when the CMT score ≥2. If SCC was ≥1,000,000 cells per mL, whole milk can was then rejected together with recommendation document. In addition, the extension staff either called the farmers or visited the farms during the same day to investigate the causes. Data was analysed to develop the suitable content for the next seminar. Dairy farmers and cooperatives’ staffs were subjectively invited to attend and contribute to discussion at the seminars. Each seminar comprised of both theoretical and practical activities for sharing the knowledge and experiences related to the situation. Results - There was a trend of significant decrease in bulk milk SCC in the cooling tank of the cooperatives after establishing all the critical processes. Furthermore, when the SCC level of 200,000 cells per mL was considered as the cut-off value, the proportion of dairy herds with low bulk milk SCC at the end of the study was significantly (P<0.05) higher than that of the start. Conclusion - Knowledge management is the most important steps for reduction of bulk milk SCC of dairy herds. However, the critical processes to accomplish the better quality of milk need not only the implementation of the reliable tests but also the effective communication among the stakeholders, i.e. dairy farmers, cooperatives’ staff and extension personnel.
Keywords: Knowledge, Management, Bulk milk, Somatic cell count, Dairy Farms

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 117
Critical Processes of Knowledge Management for Reduction of Somatic Cell Count in Bulk Milk of Smallholder Dairy Farms
Aran Chanlun1* Chaiyapas Thamrongyoswittayakul 1 Suthida Chanlun2
Pitaya Papirom2 Manassanan Borisuthpetch1 and Pithai Kanbutra3 1Department of Medicine, 2Department of Pathobiology, 3Veterinary Teaching Hospital,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author E-mail address: [email protected]
Background - Bovine mastitis causes substantially economic losses in dairy industry worldwide. Somatic cell count (SCC) in bulk milk has been used as the most reliable indicator of udder health status of milking cow in dairy herds. Objective - To demonstrate the efficiency of knowledge managements for decreasing SCC in bulk milk of smallholder dairy farms at the milk collection center. Materials and Methods - The study was carried out at Khon Kaen dairy cooperatives, Khon Kaen province of Thailand during June-September, 2013. The critical processes of knowledge management were established including setup the cut-off value of bulk milk SCC, reform workflow for cooperatives’ personnel, knowledge or information exchanges. The total of 6 seminars at 2 weeks apart were systemically designed and organized for different target groups, i.e. quality control personnel, extension staff, and dairy farmers. Bulk milk SCC was randomly monitored at both morning and afternoon milking times throughout the study. Milk samples of all milk-cans from dairy farms was tested at the milk collection center before pooling into the cooling tank. Presence of SCC in milk samples were manually estimated using California mastitis test (CMT) as a screening tool and Delaval™ cell counter was also used as the confirmatory test when the CMT score ≥2. If SCC was ≥1,000,000 cells per mL, whole milk can was then rejected together with recommendation document. In addition, the extension staff either called the farmers or visited the farms during the same day to investigate the causes. Data was analysed to develop the suitable content for the next seminar. Dairy farmers and cooperatives’ staffs were subjectively invited to attend and contribute to discussion at the seminars. Each seminar comprised of both theoretical and practical activities for sharing the knowledge and experiences related to the situation. Results - There was a trend of significant decrease in bulk milk SCC in the cooling tank of the cooperatives after establishing all the critical processes. Furthermore, when the SCC level of 200,000 cells per mL was considered as the cut-off value, the proportion of dairy herds with low bulk milk SCC at the end of the study was significantly (P<0.05) higher than that of the start. Conclusion - Knowledge management is the most important steps for reduction of bulk milk SCC of dairy herds. However, the critical processes to accomplish the better quality of milk need not only the implementation of the reliable tests but also the effective communication among the stakeholders, i.e. dairy farmers, cooperatives’ staff and extension personnel.
Keywords: Knowledge, Management, Bulk milk, Somatic cell count, Dairy Farms

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health118
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Optimal Period for Detection of Bacterial Contamination in Milk using Resazurin Reduction Test
Nattaphon Suchaniwat1 Thana Pengkasame1 Nubdao Wongkongdech1 and Aran Chanlun2*
1Fifth Year Veterinary Student, 2Department of Medicine, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author E-mail address: [email protected]
Objective - To determine the optimal period for discrimination of bacterial contamination in milk at the milk collection center using the resazurin reduction test.
Materials and Methods - Twenty-seven bulk milk samples were aseptically collected at the milk collection center of Khon Kaen dairy cooperatives, Khon Kaen province of Thailand during January and February, 2014. Each milk sample was tested for presence of bacterial contamination using the resazurin reduction test (RRT), methylene blue reduction test (MBRT), total bacterial count (TBC), coliform count (CC) and Escherichia coli count (EC). Color changes of RRT and MBRT were observed and recorded at the interval of 5 and 10 minutes, respectively. The color changes of RRT were divided into 4 groups; blue-mauve, mauve, mauve-pink, and pink. MBRT was used as the reference test indicating cleanliness of milk. Milk cleanliness according to MBRT results were categorized into 3 groups; excellent, moderate, poor. TBC, CC and EC were obtained using the AOAC approved method (3M PetrifilmTM) following the manufacture’s instruction. Pearson correlation was used to test between the duration of RRT and MBRT.
Results - There was highly statistical correlation (P<0.01, 0.7≤r≤0.8) between RRT and MBRT. Milk which classified into poor cleanliness, mean of the period of color change to blue-mauve, mauve, mauve-pink, and pink were 22, 31, 42 and 56 minutes, respectively. In addition, TBC and CC of milk of poor cleanliness are also higher than that of the acceptable level and coliforms is the dominating bacteria contaminating in milk causing poor cleanliness.
Conclusion - RRT can be used as an effective screening test for improving quality of milk at the milk collection center. Color changes of RRT can be applied as an indicator for discrimination of the different cleanliness of milk.
Keywords: Milk quality, Resazurin reduction test, Bacteria

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 119
Optimal Period for Detection of Bacterial Contamination in Milk using Resazurin Reduction Test
Nattaphon Suchaniwat1 Thana Pengkasame1 Nubdao Wongkongdech1 and Aran Chanlun2*
1Fifth Year Veterinary Student, 2Department of Medicine, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author E-mail address: [email protected]
Objective - To determine the optimal period for discrimination of bacterial contamination in milk at the milk collection center using the resazurin reduction test.
Materials and Methods - Twenty-seven bulk milk samples were aseptically collected at the milk collection center of Khon Kaen dairy cooperatives, Khon Kaen province of Thailand during January and February, 2014. Each milk sample was tested for presence of bacterial contamination using the resazurin reduction test (RRT), methylene blue reduction test (MBRT), total bacterial count (TBC), coliform count (CC) and Escherichia coli count (EC). Color changes of RRT and MBRT were observed and recorded at the interval of 5 and 10 minutes, respectively. The color changes of RRT were divided into 4 groups; blue-mauve, mauve, mauve-pink, and pink. MBRT was used as the reference test indicating cleanliness of milk. Milk cleanliness according to MBRT results were categorized into 3 groups; excellent, moderate, poor. TBC, CC and EC were obtained using the AOAC approved method (3M PetrifilmTM) following the manufacture’s instruction. Pearson correlation was used to test between the duration of RRT and MBRT.
Results - There was highly statistical correlation (P<0.01, 0.7≤r≤0.8) between RRT and MBRT. Milk which classified into poor cleanliness, mean of the period of color change to blue-mauve, mauve, mauve-pink, and pink were 22, 31, 42 and 56 minutes, respectively. In addition, TBC and CC of milk of poor cleanliness are also higher than that of the acceptable level and coliforms is the dominating bacteria contaminating in milk causing poor cleanliness.
Conclusion - RRT can be used as an effective screening test for improving quality of milk at the milk collection center. Color changes of RRT can be applied as an indicator for discrimination of the different cleanliness of milk.
Keywords: Milk quality, Resazurin reduction test, Bacteria

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health120
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
A Comparison of Antibacterial Activities of Clausena wallichii Oliv’s and Clausena lansium Skeels’s Extracts against
Staphylococcus aureus causing Mastitis in Cattle
Nissa Mututanont1 Khannamthong Phunnoi1 Wanida Kiatcharoenseree1 Noppadol Sompol2 Jinda Wangboonskul3 and Arinee Chatchawanchontheera4*
1Fifth Year Veterinary Student, 2Graduate Student, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
3Faculty of Pharmacy, Thamasat University, Pathumthani 12120, Thailand. 4Department of Pathobiology, Faculty of Veterinary Medicine,
Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Background - Mastitis is an endemic disease in dairy cows and causes major loss to the dairy milk industry. The treatment for mastitis includes using antibiotics that are expensive and may pass into the milk. Studies have shown that extracts from Clausena wallichii Oliv and Clausena lansium Skeels possess antimicrobial activity, antiviral activity and anti-inflammatory activity as well.
Objective - To compare the antibacterial effects of C. walchii Oliv and C. lansium Skeels extracts against Staphylococcus aureus in milk samples from cows with subclinical mastitis.
Materials and Methods - Ethanol herbal extracts from leaf stalks and roots of C. wallichii Oliv and leaf stalks, roots, and trunks of C. lansium Skeels were tested against ten isolates of S. aureus isolated from cows with subclinical mastitis and determined their inhibitory and bactericidal effects by Microdilution broth method.
Results and Conclusion - All extracts had antibacterial activities against S. aureus. The minimum inhibition concentrations of extracts from root and leaf stalks from C. wallichii Oliv; and trunk, roots and leaf stalk from C. lansium Skeels are 0.09, 0.36, 0.21, 0.22, 0.25 milligrams per milliliters; and the minimum bactericidal concentrations are 0.09, 0.18, 0.42, 1.74, 0.12 milligrams per milliliters; respectively. Keywords: Antibacterial activities, Clausena wallichii Oliv, Clausena lansium, Staphylococcus aureus, Mastitis

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 121
A Comparison of Antibacterial Activities of Clausena wallichii Oliv’s and Clausena lansium Skeels’s Extracts against
Staphylococcus aureus causing Mastitis in Cattle
Nissa Mututanont1 Khannamthong Phunnoi1 Wanida Kiatcharoenseree1 Noppadol Sompol2 Jinda Wangboonskul3 and Arinee Chatchawanchontheera4*
1Fifth Year Veterinary Student, 2Graduate Student, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
3Faculty of Pharmacy, Thamasat University, Pathumthani 12120, Thailand. 4Department of Pathobiology, Faculty of Veterinary Medicine,
Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Background - Mastitis is an endemic disease in dairy cows and causes major loss to the dairy milk industry. The treatment for mastitis includes using antibiotics that are expensive and may pass into the milk. Studies have shown that extracts from Clausena wallichii Oliv and Clausena lansium Skeels possess antimicrobial activity, antiviral activity and anti-inflammatory activity as well.
Objective - To compare the antibacterial effects of C. walchii Oliv and C. lansium Skeels extracts against Staphylococcus aureus in milk samples from cows with subclinical mastitis.
Materials and Methods - Ethanol herbal extracts from leaf stalks and roots of C. wallichii Oliv and leaf stalks, roots, and trunks of C. lansium Skeels were tested against ten isolates of S. aureus isolated from cows with subclinical mastitis and determined their inhibitory and bactericidal effects by Microdilution broth method.
Results and Conclusion - All extracts had antibacterial activities against S. aureus. The minimum inhibition concentrations of extracts from root and leaf stalks from C. wallichii Oliv; and trunk, roots and leaf stalk from C. lansium Skeels are 0.09, 0.36, 0.21, 0.22, 0.25 milligrams per milliliters; and the minimum bactericidal concentrations are 0.09, 0.18, 0.42, 1.74, 0.12 milligrams per milliliters; respectively. Keywords: Antibacterial activities, Clausena wallichii Oliv, Clausena lansium, Staphylococcus aureus, Mastitis

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health122
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Progesterone Concentrations of Dairy Cows Following Post Insemination Crestar® and GnRH Treatments during Summer
Khampasong Ninnasopha1 Saksiri Sirisatien2 Niran Junkoup3
Suvaluk Seesupa2 Phuangphaka Sadee4 and Suneerat Aiumlamai2* 1Graduate Student, 2Department of Surgery and Theriogenology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. 3Khumjareon Dairy Co-operative, Khonburi District, Nakhon Ratchhasima 30250, Thailand.
4Department of Medicine Srinagarind Hospital, Clinical immunology unit, Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - It is hypothesized that heat stress during summer may cause progesterone insufficiency in early pregnancy resulting in embryonic loss. Supplementation of progesterone might increase circulating progesterone concentration and also pregnancy rate.
Objective - To determine the effect of supplementation of exogenous progesterone and gonadotropin-releasing hormone (GnRH) injection after artificial insemination (AI) on progesterone concentrations of dairy cows during summer.
Materials and Methods - Sixty crossbred (93%Holstein- Friesian) lactating cows were included in the study from April to September 2013 in a commercial dairy farm at Nakhonratchasima province, Thailand. The experimental cows were in average age of 3.2±0.7 years, lactation number 1.32±0.47, days in milk 75±36, body condition score 2.76±0.21 and milk yielding 18.75±4.75 kg per day. Cows were visually monitored for standing oestrus and were inseminated at approximately 13.9±3.2 h after the onset of oestrus by two veterinarians using frozen semen from two bulls. The day of AI was considered as day 0. The cows were randomly allocated to three groups (20 cows per group): (i) exogenous progesterone supplementation group, cows received an ear implant containing 3 mg of norgestomet (Crestar®, Intervet International b.v. Boxmeer, The Netherlands) for 14 days (day 5 to day 19) without injection of norgestomet and estradiol valerate (ii) GnRH group, cows received an injection of 50 mcg of lecrielin acetate (Dalmarelin®, FATRO S.P.A. Industrial Pharmaceutical Veterinarian and Bologna, Italy) on day 5 after AI; (iii) control group, 5 ml of physiological saline (placebo) was injected to the cows on day 5 after AI. The ambient temperature and relative humidity (RH) were recorded 3 times/day inside the housing for temperature humidity index (THI) calculation.
Results - The ambient temperature, RH, and THI were 30.1±2.3 °C, 70.8±7.3% and 81.02±2.38, respectively. The average daily THI was above 72 throughout the study period. Moreover 62% of average THI (115 days/183 days) values were higher than 80 which were concerned as moderate stress condition for dairy cows. The progesterone concentrations of cows in Crestar®, GnRH, and a control group on day 12 and day 19 were 8.53± 4.16, 8.31±3.16, 6.29±2.32 (p=0.07) and 4.15±5.45, 7.25±6.92, 6.12±5.22 (p=0.25) ng/ml, respectively. The treated groups had a tendency of higher progesterone concentrations than the control group on day 12.
Conclusion - Progesterone Crestar® and GnRH treatments post AI during summer had no effect on serum progesterone concentrations in dairy cows.
Keywords: GnRH, Progesterone, Dairy cows, Summer

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 123
Progesterone Concentrations of Dairy Cows Following Post Insemination Crestar® and GnRH Treatments during Summer
Khampasong Ninnasopha1 Saksiri Sirisatien2 Niran Junkoup3
Suvaluk Seesupa2 Phuangphaka Sadee4 and Suneerat Aiumlamai2* 1Graduate Student, 2Department of Surgery and Theriogenology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. 3Khumjareon Dairy Co-operative, Khonburi District, Nakhon Ratchhasima 30250, Thailand.
4Department of Medicine Srinagarind Hospital, Clinical immunology unit, Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - It is hypothesized that heat stress during summer may cause progesterone insufficiency in early pregnancy resulting in embryonic loss. Supplementation of progesterone might increase circulating progesterone concentration and also pregnancy rate.
Objective - To determine the effect of supplementation of exogenous progesterone and gonadotropin-releasing hormone (GnRH) injection after artificial insemination (AI) on progesterone concentrations of dairy cows during summer.
Materials and Methods - Sixty crossbred (93%Holstein- Friesian) lactating cows were included in the study from April to September 2013 in a commercial dairy farm at Nakhonratchasima province, Thailand. The experimental cows were in average age of 3.2±0.7 years, lactation number 1.32±0.47, days in milk 75±36, body condition score 2.76±0.21 and milk yielding 18.75±4.75 kg per day. Cows were visually monitored for standing oestrus and were inseminated at approximately 13.9±3.2 h after the onset of oestrus by two veterinarians using frozen semen from two bulls. The day of AI was considered as day 0. The cows were randomly allocated to three groups (20 cows per group): (i) exogenous progesterone supplementation group, cows received an ear implant containing 3 mg of norgestomet (Crestar®, Intervet International b.v. Boxmeer, The Netherlands) for 14 days (day 5 to day 19) without injection of norgestomet and estradiol valerate (ii) GnRH group, cows received an injection of 50 mcg of lecrielin acetate (Dalmarelin®, FATRO S.P.A. Industrial Pharmaceutical Veterinarian and Bologna, Italy) on day 5 after AI; (iii) control group, 5 ml of physiological saline (placebo) was injected to the cows on day 5 after AI. The ambient temperature and relative humidity (RH) were recorded 3 times/day inside the housing for temperature humidity index (THI) calculation.
Results - The ambient temperature, RH, and THI were 30.1±2.3 °C, 70.8±7.3% and 81.02±2.38, respectively. The average daily THI was above 72 throughout the study period. Moreover 62% of average THI (115 days/183 days) values were higher than 80 which were concerned as moderate stress condition for dairy cows. The progesterone concentrations of cows in Crestar®, GnRH, and a control group on day 12 and day 19 were 8.53± 4.16, 8.31±3.16, 6.29±2.32 (p=0.07) and 4.15±5.45, 7.25±6.92, 6.12±5.22 (p=0.25) ng/ml, respectively. The treated groups had a tendency of higher progesterone concentrations than the control group on day 12.
Conclusion - Progesterone Crestar® and GnRH treatments post AI during summer had no effect on serum progesterone concentrations in dairy cows.
Keywords: GnRH, Progesterone, Dairy cows, Summer

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health124
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Polyvinyl Alcohol (PVA) Concentrations as the Ice Blocker on Viability of Vitrification Bovine Oocytes
Chatree Chumnandee1 and Saksiri Sirisathein2* 1Ph.D.Student in Interdisciplinary Veterinary Science,
2Deparment of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. Corresponding author: E-mail: [email protected]
Objective - To examine the putative effect of polyvinyl alcohol (PVA) (molecular weight 9,000-10,000 Da) as the ice blocking agent for vitrification of bovine oocytes. Materials and Methods - The cumulus oocyte complexes (COCs) was in vitro matured in TCM-199 with Earle’s salt at 38.6 ℃, 5.0% CO2 for 22 hours. Experiment 1, the matured oocytes were vitrified in 15.0% ethylene glycol (EG)+15.0% dimethyl sulfoxide (DMSO) with two different concentrations of PVA (0.1% PVA and 1.0% PVA) and without PVA (control). Experiment 2, the matured oocytes were vitrified in 20.0% EG+20.0% DMSO with two concentrations of PVA (the same as experiment 1). After that, the vitrified oocytes were thawed and assessed for viability by fluorescein diacetate (FDA) staining. Results - In Experiment 1, the total viability of vitrified oocytes in 15.0% EG+15.0% DMSO were not different among the supplemented with 0.1% PVA, 1.0% PVA, and control group (72.9, 75.0 and 70.0%, respectively). In Experiment 2, the total viability of vitrified oocytes in 20.0% EG+20.0% DMSO supplemented with 0.1% PVA and 1.0% PVA was not different when compared with that of the control group (78.6, 70.5 and 63.1%, respectively). Conclusion - PVA supplementation had no effect on the viability of vitrified-thawed oocytes.
Keywords: Bovine oocyte, Polyvinyl alcohol, Ice blocker, Vitrification

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 125
Polyvinyl Alcohol (PVA) Concentrations as the Ice Blocker on Viability of Vitrification Bovine Oocytes
Chatree Chumnandee1 and Saksiri Sirisathein2* 1Ph.D.Student in Interdisciplinary Veterinary Science,
2Deparment of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. Corresponding author: E-mail: [email protected]
Objective - To examine the putative effect of polyvinyl alcohol (PVA) (molecular weight 9,000-10,000 Da) as the ice blocking agent for vitrification of bovine oocytes. Materials and Methods - The cumulus oocyte complexes (COCs) was in vitro matured in TCM-199 with Earle’s salt at 38.6 ℃, 5.0% CO2 for 22 hours. Experiment 1, the matured oocytes were vitrified in 15.0% ethylene glycol (EG)+15.0% dimethyl sulfoxide (DMSO) with two different concentrations of PVA (0.1% PVA and 1.0% PVA) and without PVA (control). Experiment 2, the matured oocytes were vitrified in 20.0% EG+20.0% DMSO with two concentrations of PVA (the same as experiment 1). After that, the vitrified oocytes were thawed and assessed for viability by fluorescein diacetate (FDA) staining. Results - In Experiment 1, the total viability of vitrified oocytes in 15.0% EG+15.0% DMSO were not different among the supplemented with 0.1% PVA, 1.0% PVA, and control group (72.9, 75.0 and 70.0%, respectively). In Experiment 2, the total viability of vitrified oocytes in 20.0% EG+20.0% DMSO supplemented with 0.1% PVA and 1.0% PVA was not different when compared with that of the control group (78.6, 70.5 and 63.1%, respectively). Conclusion - PVA supplementation had no effect on the viability of vitrified-thawed oocytes.
Keywords: Bovine oocyte, Polyvinyl alcohol, Ice blocker, Vitrification
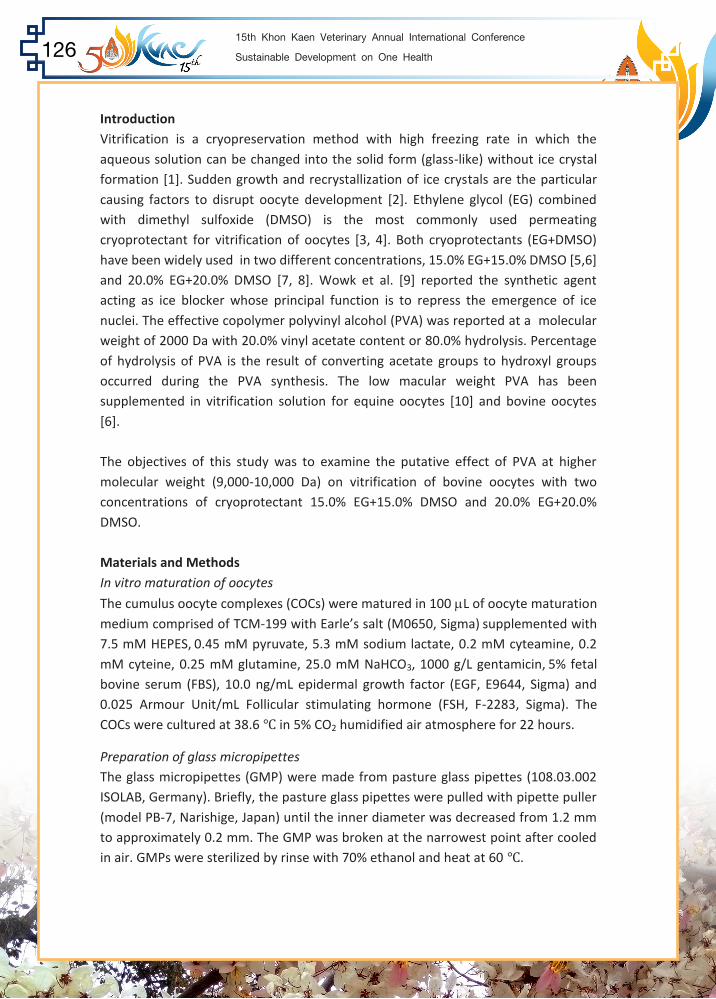
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health126
Introduction Vitrification is a cryopreservation method with high freezing rate in which the aqueous solution can be changed into the solid form (glass-like) without ice crystal formation [1]. Sudden growth and recrystallization of ice crystals are the particular causing factors to disrupt oocyte development [2]. Ethylene glycol (EG) combined with dimethyl sulfoxide (DMSO) is the most commonly used permeating cryoprotectant for vitrification of oocytes [3, 4]. Both cryoprotectants (EG+DMSO) have been widely used in two different concentrations, 15.0% EG+15.0% DMSO [5,6] and 20.0% EG+20.0% DMSO [7, 8]. Wowk et al. [9] reported the synthetic agent acting as ice blocker whose principal function is to repress the emergence of ice nuclei. The effective copolymer polyvinyl alcohol (PVA) was reported at a molecular weight of 2000 Da with 20.0% vinyl acetate content or 80.0% hydrolysis. Percentage of hydrolysis of PVA is the result of converting acetate groups to hydroxyl groups occurred during the PVA synthesis. The low macular weight PVA has been supplemented in vitrification solution for equine oocytes [10] and bovine oocytes [6]. The objectives of this study was to examine the putative effect of PVA at higher molecular weight (9,000-10,000 Da) on vitrification of bovine oocytes with two concentrations of cryoprotectant 15.0% EG+15.0% DMSO and 20.0% EG+20.0% DMSO. Materials and Methods In vitro maturation of oocytes
The cumulus oocyte complexes (COCs) were matured in 100 L of oocyte maturation medium comprised of TCM-199 with Earle’s salt (M0650, Sigma) supplemented with 7.5 mM HEPES, 0.45 mM pyruvate, 5.3 mM sodium lactate, 0.2 mM cyteamine, 0.2 mM cyteine, 0.25 mM glutamine, 25.0 mM NaHCO3, 1000 g/L gentamicin, 5% fetal bovine serum (FBS), 10.0 ng/mL epidermal growth factor (EGF, E9644, Sigma) and 0.025 Armour Unit/mL Follicular stimulating hormone (FSH, F-2283, Sigma). The COCs were cultured at 38.6 ℃ in 5% CO2 humidified air atmosphere for 22 hours.
Preparation of glass micropipettes The glass micropipettes (GMP) were made from pasture glass pipettes (108.03.002 ISOLAB, Germany). Briefly, the pasture glass pipettes were pulled with pipette puller (model PB-7, Narishige, Japan) until the inner diameter was decreased from 1.2 mm to approximately 0.2 mm. The GMP was broken at the narrowest point after cooled in air. GMPs were sterilized by rinse with 70% ethanol and heat at 60 ℃.
Vitrification and thawing of oocytes TCM-199 and 20.0% FBS (final concentration) was need as basal medium for vitrification. The vitrification solution (VS) was prepared by adding ethylene glycol (EG, 03750, Fluka) and dimethyl sulfoxide (DMSO, 23500.260, VWR, BDH Prolabo) into basal medium. The equilibration process of oocytes was perform at room temperature.
Experiment 1, the matured oocytes were placed into vitrification solution 1 (VS1)(7.5% EG+7.5% DMSO) for 2 minutes. Subsequently, the oocytes were placed into vitrification solution 2 (VS2)(15.0% EG+15.0% DMSO and 0.5 M sucrose) with two different concentrations of PVA (0.1%PVA and 1.0%PVA) and without PVA (control) for 12-25 seconds.
Experiment 2, the matured oocytes were placed into VS1 (10.0% EG+10.0% DMSO) for 2 minutes. Subsequently, the oocytes were placed into VS2 (20.0% EG+20.0% DMSO and 0.5 M sucrose) with two different concentrations of PVA (the same as experiment 1) for 12-25 seconds.
The oocytes were loaded into the tip of GMP by capillary effect and immediately immersed into liquid nitrogen. The GMP was inserted into 0.5 mL semen straw as a cab cover and stored from 1 hour to 1 week. Thawing was performed at 38 ℃ by placing the tip of GMP into thawing solution 1 (basal medium and 0.26 M sucrose) for 20 seconds and then, softly expelled into medium to complete 1 minute. After that, the oocytes were placed into thawing solution 2 (basal medium and 0.13 M sucrose) for 2 minutes. Oocytes were then washed in TCM-199 medium and placed into oocyte maturation medium to complete maturation by culturing for 1 hour.
Evaluation of viability of oocytes The vitrified-thawed oocytes were assessed for viability based on esterase enzymatic activity by fluorescein diacetate (FDA, F7378, Sigma) staining as described by Shi et al. [11] with some modifications. Briefly, the oocytes were incubated with pronase for 4 minutes to remove zona pellucida. Subsequently, the oocytes were incubated
with 2.5 g/mL FDA for 5 minutes. Thereafter, the oocytes were placed on slides and covered with glass upon 4 points of vaseline. The oocytes were observed under fluorescent microscope (Carlzeiss Jena, Jenalumar, Germany). High fluorescent staining indicated high viability, low fluorescent staining indicated low viability, and colorless indicated non-viable oocytes.
Statistical analysis
Data were analyzed by Chi-square test (2-test). The p-value of statistical significance was set at p<0.05.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 127
Vitrification and thawing of oocytes TCM-199 and 20.0% FBS (final concentration) was need as basal medium for vitrification. The vitrification solution (VS) was prepared by adding ethylene glycol (EG, 03750, Fluka) and dimethyl sulfoxide (DMSO, 23500.260, VWR, BDH Prolabo) into basal medium. The equilibration process of oocytes was perform at room temperature.
Experiment 1, the matured oocytes were placed into vitrification solution 1 (VS1)(7.5% EG+7.5% DMSO) for 2 minutes. Subsequently, the oocytes were placed into vitrification solution 2 (VS2)(15.0% EG+15.0% DMSO and 0.5 M sucrose) with two different concentrations of PVA (0.1%PVA and 1.0%PVA) and without PVA (control) for 12-25 seconds.
Experiment 2, the matured oocytes were placed into VS1 (10.0% EG+10.0% DMSO) for 2 minutes. Subsequently, the oocytes were placed into VS2 (20.0% EG+20.0% DMSO and 0.5 M sucrose) with two different concentrations of PVA (the same as experiment 1) for 12-25 seconds.
The oocytes were loaded into the tip of GMP by capillary effect and immediately immersed into liquid nitrogen. The GMP was inserted into 0.5 mL semen straw as a cab cover and stored from 1 hour to 1 week. Thawing was performed at 38 ℃ by placing the tip of GMP into thawing solution 1 (basal medium and 0.26 M sucrose) for 20 seconds and then, softly expelled into medium to complete 1 minute. After that, the oocytes were placed into thawing solution 2 (basal medium and 0.13 M sucrose) for 2 minutes. Oocytes were then washed in TCM-199 medium and placed into oocyte maturation medium to complete maturation by culturing for 1 hour.
Evaluation of viability of oocytes The vitrified-thawed oocytes were assessed for viability based on esterase enzymatic activity by fluorescein diacetate (FDA, F7378, Sigma) staining as described by Shi et al. [11] with some modifications. Briefly, the oocytes were incubated with pronase for 4 minutes to remove zona pellucida. Subsequently, the oocytes were incubated
with 2.5 g/mL FDA for 5 minutes. Thereafter, the oocytes were placed on slides and covered with glass upon 4 points of vaseline. The oocytes were observed under fluorescent microscope (Carlzeiss Jena, Jenalumar, Germany). High fluorescent staining indicated high viability, low fluorescent staining indicated low viability, and colorless indicated non-viable oocytes.
Statistical analysis
Data were analyzed by Chi-square test (2-test). The p-value of statistical significance was set at p<0.05.
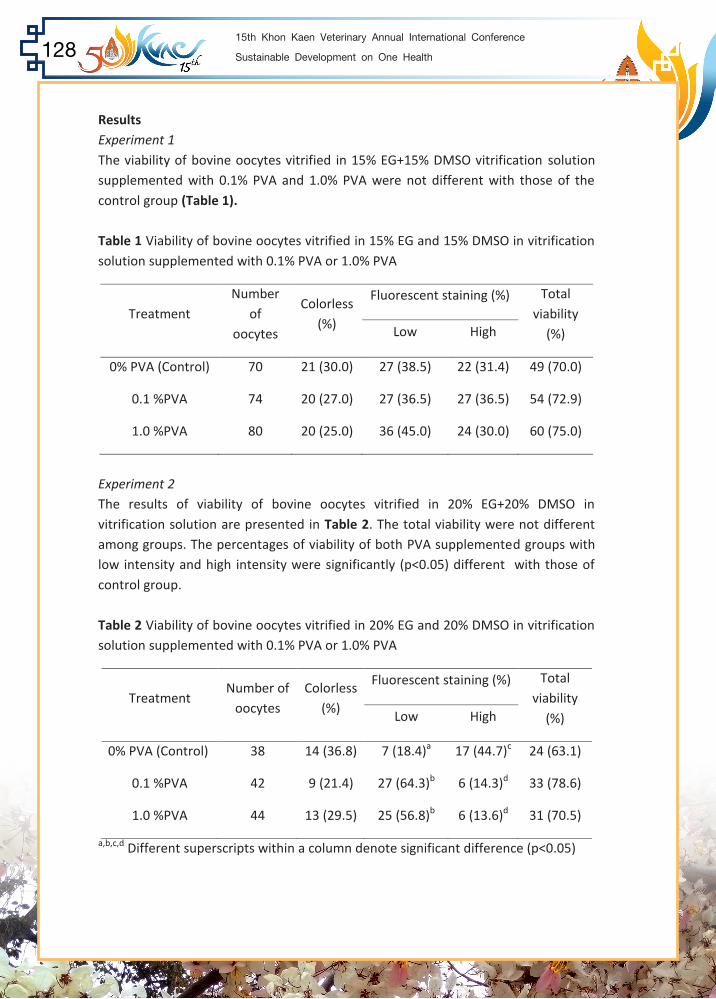
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health128
Results Experiment 1 The viability of bovine oocytes vitrified in 15% EG+15% DMSO vitrification solution supplemented with 0.1% PVA and 1.0% PVA were not different with those of the control group (Table 1). Table 1 Viability of bovine oocytes vitrified in 15% EG and 15% DMSO in vitrification solution supplemented with 0.1% PVA or 1.0% PVA
Treatment Number
of oocytes
Colorless (%)
Fluorescent staining (%) Total viability
(%) Low High
0% PVA (Control) 70 21 (30.0) 27 (38.5) 22 (31.4) 49 (70.0)
0.1 %PVA 74 20 (27.0) 27 (36.5) 27 (36.5) 54 (72.9)
1.0 %PVA 80 20 (25.0) 36 (45.0) 24 (30.0) 60 (75.0)
Experiment 2 The results of viability of bovine oocytes vitrified in 20% EG+20% DMSO in vitrification solution are presented in Table 2. The total viability were not different among groups. The percentages of viability of both PVA supplemented groups with low intensity and high intensity were significantly (p<0.05) different with those of control group. Table 2 Viability of bovine oocytes vitrified in 20% EG and 20% DMSO in vitrification solution supplemented with 0.1% PVA or 1.0% PVA
Treatment Number of
oocytes Colorless
(%)
Fluorescent staining (%) Total viability
(%) Low High
0% PVA (Control) 38 14 (36.8) 7 (18.4)a 17 (44.7)c 24 (63.1)
0.1 %PVA 42 9 (21.4) 27 (64.3)b 6 (14.3)d 33 (78.6)
1.0 %PVA 44 13 (29.5) 25 (56.8)b 6 (13.6)d 31 (70.5)
a,b,c,d Different superscripts within a column denote significant difference (p<0.05)
Discussion In the present study, the results demonstrated that PVA supplementation in both experiments had no effect on total viability when compared with that of control. In experiment 1, the percentages of oocytes with high fluorescent staining were not different among groups. In experiment 2, on the other hand, the oocytes of high fluorescent staining in control group were significant (p<0.05) higher than those of 0.1% PVA and 1.0% PVA groups (44.7, 14.3, and 13.6, respectively). However, it remains unclear whether the difference between high and low fluorescent staining could have the biological consequences. The purpose of using combination of cryoprotectants is to allow the addition of each cryoprotectant with minimized concentration which could reduce intracellular toxicity [11, 12]. Chain et al. [5] reported that the percentages of survival rate of vitrified oocytes in 15.0% EG+15.0% DMSO were 91.8±6.7%. In addition, the study of different concentrations of cryoprotectants by Checura and Seidel Jr. [13] showed that the percentages of cleaved oocytes were not different between 10.0% EG +10.0% DMSO (57.3±4.9%) and 20.0% EG+20.0% DMSO (50.7±5.1%). Similarly, the study by Vajta et al. [3] reported that the cleavage rates of vitrified oocytes were not different between 16.5% EG+16.5% DMSO (47.0%) and 20.0% EG+20.0% DMSO (50.0%). Likewise, present study showed that the total viability of vitrified oocytes in 15.0% EG+15.0% DMSO (average around 72.6%) was not different when compared with those of vitrified oocytes in 20.0% EG+20.0% DMSO (average around 70.7%). The action of PVA is to catch on to the surface of newly formed ice crystals and block any additional supplementary water molecules in the area of growth. The improvement in ice crystal inhibition was achieved by using low molecular weight PVA [9]. According to the results of Zhou et al. [6], it has been demonstrated that the survival rates of vitrified oocytes in 1.0% PVA (low molecular weight PVA; 2,000 Da) supplemented in vitrification solution was 88.4%. On the other hand, Veira et al. [7] reported that the maturation rates of vitrified oocytes in 0.1% of high molecular weight PVA (30,000-70,000 Da) supplemented in vitrification solution was 60.2%. This study showed that the total viability of vitrified oocytes in 0.1% and 1.0% of high molecular weight PVA (9,000-10,000 Da) supplemented in vitrification solution (average around 74.3%) was comparable with previous reports. The results of this study indicated that PVA supplementation had no clear effect on the viability of vitrified oocytes. However, the viability determined by the fluorescent staining is not sufficient to evaluate the developmental competence. Therefore, further study is needed to determine its effect on development of vitrified oocytes.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 129
Discussion In the present study, the results demonstrated that PVA supplementation in both experiments had no effect on total viability when compared with that of control. In experiment 1, the percentages of oocytes with high fluorescent staining were not different among groups. In experiment 2, on the other hand, the oocytes of high fluorescent staining in control group were significant (p<0.05) higher than those of 0.1% PVA and 1.0% PVA groups (44.7, 14.3, and 13.6, respectively). However, it remains unclear whether the difference between high and low fluorescent staining could have the biological consequences. The purpose of using combination of cryoprotectants is to allow the addition of each cryoprotectant with minimized concentration which could reduce intracellular toxicity [11, 12]. Chain et al. [5] reported that the percentages of survival rate of vitrified oocytes in 15.0% EG+15.0% DMSO were 91.8±6.7%. In addition, the study of different concentrations of cryoprotectants by Checura and Seidel Jr. [13] showed that the percentages of cleaved oocytes were not different between 10.0% EG +10.0% DMSO (57.3±4.9%) and 20.0% EG+20.0% DMSO (50.7±5.1%). Similarly, the study by Vajta et al. [3] reported that the cleavage rates of vitrified oocytes were not different between 16.5% EG+16.5% DMSO (47.0%) and 20.0% EG+20.0% DMSO (50.0%). Likewise, present study showed that the total viability of vitrified oocytes in 15.0% EG+15.0% DMSO (average around 72.6%) was not different when compared with those of vitrified oocytes in 20.0% EG+20.0% DMSO (average around 70.7%). The action of PVA is to catch on to the surface of newly formed ice crystals and block any additional supplementary water molecules in the area of growth. The improvement in ice crystal inhibition was achieved by using low molecular weight PVA [9]. According to the results of Zhou et al. [6], it has been demonstrated that the survival rates of vitrified oocytes in 1.0% PVA (low molecular weight PVA; 2,000 Da) supplemented in vitrification solution was 88.4%. On the other hand, Veira et al. [7] reported that the maturation rates of vitrified oocytes in 0.1% of high molecular weight PVA (30,000-70,000 Da) supplemented in vitrification solution was 60.2%. This study showed that the total viability of vitrified oocytes in 0.1% and 1.0% of high molecular weight PVA (9,000-10,000 Da) supplemented in vitrification solution (average around 74.3%) was comparable with previous reports. The results of this study indicated that PVA supplementation had no clear effect on the viability of vitrified oocytes. However, the viability determined by the fluorescent staining is not sufficient to evaluate the developmental competence. Therefore, further study is needed to determine its effect on development of vitrified oocytes.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health130
Acknowledgement This work was supported by Office of the Higher Education Commission
References 1. Rall WF, Fahy GM. Ice-free cryopreservation of mouse embryos at -196 degrees C
by vitrification. Nature. 1985;313(6003):573-575. (abstract). 2. Fahy GM, Wowk B, Wu J, Paynter S. Improved vitrification solutions based on the
predictability of vitrification solution toxicity. Cryobiology. 2004;48(1):22-35. 3. Vajta G, Holm P, Kuwayama M, Booth PJ, Jacobsen H, Greve T, et al. Open Pulled
Straw (OPS) vitrification: a new way to reduce cryoinjuries of bovine ova and embryos. Mol Reprod Dev. 1998;51(1):53-58.
4. Prentice-Biensch JR, Singh J, Mapletoft RJ, Anzar M. Vitrification of immature bovine cumulus-oocyte complexes: effects of cryoprotectants, the vitrification procedure and warming time on cleavage and embryo development. Reprod Biol and Endocrin. 2012;10:73.
5. Chian RC, Kuwayama M, Tan L, Tan J, Kato O, Nagai T. High survival rate of bovine oocytes matured in vitro following vitrification. J Reprod Dev. 2004;50(6):685- 696.
6. Zhou XL, Al Naib A, Sun DW, Lonergan P. Bovine oocyte vitrification using the Cryotop method: effect of cumulus cells and vitrification protocol on survival and subsequent development. Cryobiology. 2010;61(1):66-72.
7. Vieira AD, Forell F, Feltrin C, Rodrigues JL. Calves born after direct transfer of Vitrified bovine in vitro-produced blastocysts derived from vitrified immature oocytes. Reprod Domest Anim. 2008;43(3):314-318.
8. Diez C, Duque P, Gomez E, Hidalgo CO, Tamargo C, Rodriguez A, et al. Bovine oocyte vitrification before or after meiotic arrest: effects on ultrastructure and developmental ability. Theriogenology. 2005;64(2):317-333.
9. Wowk B, Leitl E, Rasch CM, Mesbah-Karimi N, Harris SB, Fahy GM. Vitrification enhancement by synthetic ice blocking agents. Cryobiology. 2000;40(3):228- 236.
10. de Leon PM, Campos VF, Corcini CD, Santos EC, Rambo G, Lucia T, Jr., et al. Cryopreservation of immature equine oocytes, comparing a solid surface vitrification process with open pulled straws and the use of a synthetic ice blocker. Theriogenology. 2012;77(1):21-27.
11. Shi WQ, Zhu SE, Zhang D, Wang WH, Tang GL, Hou YP, et al. Improved development by Taxol pretreatment after vitrification of in vitro matured porcine oocytes. Reproduction. 2006;131(4):795-804.
12. He X, Park EY, Fowler A, Yarmush ML, Toner M. Vitrification by ultra-fast cooling at a low concentration of cryoprotectants in a quartz micro-capillary: a study
using murine embryonic stem cells. Cryobiology. 2008;56(3):223-32. 13. Checura CM, Seidel GE, Jr. Effect of macromolecules in solutions for vitrification
of mature bovine oocytes. Theriogenology. 2007;67(5):919-930.
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 131
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health132
Effect of Bovine Viral Diarrhea Virus infection on Herd’s Fertility of Dairy Heifers in Northeastern Thailand
Theerakul Nilnont1 Suneerat Aiumlamai1
Kwankate Kanistanon1 and Jaruwan Kampa1*
1Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Background - Bovine Viral diarrhea virus (BVDV) is distributed worldwide and causes substantial economic loss in cattle production including the adverse reproductive performance. During the past 2 decades, the studies on prevalence of BVDV infection in dairy cattle were carried out in various part of Thailand, indicating widespread and endemic infection. Although active BVDV infection can lower fertility performance in dairy cows, field studies of the effect of BVDV infection on heifer reproductive performance are less documented.
Objective - To investigate the effects of BVDV-active infection on the reproductive performance of dairy heifers.
Materials and Methods - During March- April 2011, bulk tank milk samples from 933 herds in 9 milk collection centers were collected and tested for antibody against BVDV by indirect ELISA kits (SVANOVIR® biotech, AB). The herds were classified into 4 different classes according to presence of seropositive and virus-carrying animals in the herds; class 0 (BVDV-free), class 1 and 2 (recent or historic infection, respectively) and class 3 (BVDV-active infection). Heifer’s reproductive data of class 0 and class 3 herds were analyzed for difference between class 0 and class 3 herds. The reproductive indices of each dairy heifer (age at first service; AFS, age at conception; AC, age at first calving; AFC, number of service per conception; SPC and conception rate; CR) of class 0 and class 3 herds (81 herds each class) were used indicator of herd performance. For statistical analysis, univariate binary logistic regression was used and the reproductive indices were categorized to binomial variable based on the expected heifer reproductive values of Thailand.
Results - It was indicated the significantly negative effect of BVDV-active infection on heifer fertility. Median of AFS, AC and AFC (month) of heifer in class 3 herds (24.19, 26.13 and 35.63) was higher (p <0.05) than the class 0 herd (22.10, 24.56 and 34.15), with OR=4.97, 3.04 and 2.99, respectively. However, conception rate of heifer in class 0 and class 3 herds were not different (48.7% vs 47.1%, respectively).
Conclusion - This report suggested that BVDV-active infection is one of the most considerable factors that could influence the reproductive efficiency of replacement heifer. This evidence does not only cause a primary loss due to the first production by the affected heifers but also may lead to an unnecessary cull-out which causes substantial loss to the farmers.
Keywords: BVDV, Active infection, Heifer reproductive performance, Northeastern, Thailand

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 133
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health134
Expression Profile of Rabies Nucleoprotein, Phosphoprotein, and Glycoprotein Genes in Furious and Paralytic Rabies of Canine Origin
Wanlop Likitsuntonwong1 Akanitt Jittmittraphap1 Veera Tepsumethanon2
Supaporn Wacharapluesadee1,3 Thiravat Hemachudha1,3 and Shanop Shuangshoti1,4,5*
1WHO Collaborating Center for Research and Training on Viral Zoonoses, Bangkok, Thailand. 2Queen Saovabha Memorial Institute, Bangkok, Thailand.
3Department of Medicine, 4Department of Pathology, 5Chulalongkorn GenePRO Center Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
*Corresponding author
Background - The pathogenesis of encephalic (furious) and paralytic (dumb) rabies remains to be elucidated. Studies in dogs at the early stage of disease have revealed differences between the two clinical subtypes in terms of neuroimaging, inflammatory response, and viral burden.
Objective - To determine the expression profile of rabies genes (N, P and G) in the different clinical forms of Rabies from canine origin. Materials and Methods - In this study, expression levels of rabies nucleoprotein (N), phosphoprotein (P) and glycoprotein (G) genes were assessed in 6 rabid dogs at the early stage of disease, 3 of each clinical form. The CNS region studied included frontal lobe, hippocampus, pons, and spinal cord (thoracic and sacral levels). Results - The expression levels of rabies genes were generally higher in furious as compared to paralytic rabies in almost all regions. This is particularly true for the P gene that was highly expressed in the brain and pons of furious dogs. Conclusion - Different expressions of the rabies genes were observed between furious and paralytic rabies. The higher expression level of P gene in the brain and brainstem of furious rabies might be associated with less inflammation and the more rapid viral dissemination as compared to the paralytic counterpart. Keywords: Rabies, Dog, Furious, Paralytic, Gene expression, Interferon
Introduction Rabies is an important zoonosis that causes up to 70,000 human deaths worldwide per annum (1). Currently, there is no effective treatment for patients once neurological signs have developed (2). The disease is caused by a non-segmented negative sense RNA rabies virus (RABV) (3, 4). Transmission of rabies to humans or animals is by exposure to saliva of infected animals (5-7). Encephalic (furious) and paralytic (dumb) are the two divergent forms of rabies in dogs, cats, skunks, and human (3). The mechanism contributing to the distinct clinical
forms of rabies is not yet fully understood. A rabid dog transmitted rabies virus to two patients, one patient with the furious form and the other with paralytic rabies, suggesting different host immune responses (8). Switching from encephalitic to paralytic rabies has also been reported in a patient, following administration of high-dose rabies immunoglobulin (9).
In recent studies of canine rabies at the early stage of disease, brainstem inflammation was more prominent in paralytic dogs and was found to be inversely correlated with the viral burden in the brain (1). Interleukin-1 beta (IL1ß) and
interferon-gamma (IFN) were found exclusively in the brains of paralytic dogs (10). The findings suggest that the immune response plays an important role in slowing down the viral spreading into the brain of paralytic dogs (1). Lesser amounts of RABV in the brain of paralytic rabies is also associated with longer survival time as compared to the furious counterpart (1). Since the furious and paralytic rabies at the early stage of disease are different in several aspects, namely the inflammatory response and extent of viral burden (1,3), this study was conducted to determine the expression profile of rabies genes (N, P and G) in the different clinical forms. Materials and Methods Animals and specimen collection Animals enrolled for the study were stray dogs quarantined at the Queen Saovabha Memorial Institute (QSMI), Bangkok, Thailand. The animals were carefully observed by a veterinarian [VT] experienced in rabies. After the animals had developed clinical signs of rabies, saliva was collected for the rabies test using nucleic acid sequence-based amplification (NASBA) technique (11). All dogs were categorized into furious or paralytic subtypes; animals with ambiguous signs were excluded from the study. To observe the early changes in the clinical course, six rabid dogs (3 of each clinical form) were sacrificed immediately; and the frontal lobes, hippocampus, pons, thoracic (T) spinal cords, and sacral (S) spinal cords were collected for further analysis.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 135
Introduction Rabies is an important zoonosis that causes up to 70,000 human deaths worldwide per annum (1). Currently, there is no effective treatment for patients once neurological signs have developed (2). The disease is caused by a non-segmented negative sense RNA rabies virus (RABV) (3, 4). Transmission of rabies to humans or animals is by exposure to saliva of infected animals (5-7). Encephalic (furious) and paralytic (dumb) are the two divergent forms of rabies in dogs, cats, skunks, and human (3). The mechanism contributing to the distinct clinical
forms of rabies is not yet fully understood. A rabid dog transmitted rabies virus to two patients, one patient with the furious form and the other with paralytic rabies, suggesting different host immune responses (8). Switching from encephalitic to paralytic rabies has also been reported in a patient, following administration of high-dose rabies immunoglobulin (9).
In recent studies of canine rabies at the early stage of disease, brainstem inflammation was more prominent in paralytic dogs and was found to be inversely correlated with the viral burden in the brain (1). Interleukin-1 beta (IL1ß) and
interferon-gamma (IFN) were found exclusively in the brains of paralytic dogs (10). The findings suggest that the immune response plays an important role in slowing down the viral spreading into the brain of paralytic dogs (1). Lesser amounts of RABV in the brain of paralytic rabies is also associated with longer survival time as compared to the furious counterpart (1). Since the furious and paralytic rabies at the early stage of disease are different in several aspects, namely the inflammatory response and extent of viral burden (1,3), this study was conducted to determine the expression profile of rabies genes (N, P and G) in the different clinical forms. Materials and Methods Animals and specimen collection Animals enrolled for the study were stray dogs quarantined at the Queen Saovabha Memorial Institute (QSMI), Bangkok, Thailand. The animals were carefully observed by a veterinarian [VT] experienced in rabies. After the animals had developed clinical signs of rabies, saliva was collected for the rabies test using nucleic acid sequence-based amplification (NASBA) technique (11). All dogs were categorized into furious or paralytic subtypes; animals with ambiguous signs were excluded from the study. To observe the early changes in the clinical course, six rabid dogs (3 of each clinical form) were sacrificed immediately; and the frontal lobes, hippocampus, pons, thoracic (T) spinal cords, and sacral (S) spinal cords were collected for further analysis.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health136
RNA extraction RNA was extracted from all samples by the RNeasy lipid tissue mini kit (Qiagen), according to the manufacturers protocol. Once extracted, the RNA concentration was measured by Nanodrop 1000 spectrophotometer (Thermo Fisher Scientific Bioscience Inc.). 500 ng of RNA from each sample was converted to cDNA by Superscript III Reverse Transcriptase (RT) (Invitrogen). Primers Primers for the nucleoprotein (N) gene and the canine GAPDH were modified from the previous study (12). Primers for glycoprotein (G) and phosphoprotein (P) genes were designed by the Primer Blast web base tool, using rabies virus in the NCBI database (accession numbers JN786878.1, JN786877.1, EU086158.1, EU086157.1, HQ232301.1, AY257983.1, AY257982.1, AY257980.1, AF401285.1, HQ166186.1, EU293111.1, GQ303558.1, GQ303557.1, and AB052666); both primers were checked for secondary structure by the Primer3 web base tool. Specificity of all primers was assessed by RT-PCR, visualized for non-specific amplification on ethidium bromide-stained agarose gel. Sequences of all primers are shown in Table 1. Table 1. Details for primers used in rabies gene expression profiles
Target gene
Primer Sequence References
N
RV_N_SYBR_F 5’-TAT TGC TGC ATG TGC
TCC TC 3' 12
RV_N_SYBR_R 5’-TCA TCT GCC AGT GCT
ACG TC-3'
P
RV_P_SYBR_F 5'-CAA ACC GTG GAG GAA
ATC A-3' In house designed
RV_P_SYBR_R 5'-TGC AGA CCA TTC GAG
AGC-3'
G
RV_G_SYBR_F 5'-TAG ATG CAC TGG AGT
CTA TC-3' In house designed
RV_G_SYBR_R 5'- AGC ATC AGC CTC CAT
CAA G-3'
GAPDH
Dog_GAPDH_sh_SYBR_F 5'-GGA GAA AGC TGC CAA
ATA TG-3' 13
Dog_GAPDH_sh_SYBR_R 5'-TGG AAC ATG TAC ACC
ATG TAG-3'
Construction of positive control plasmid Using the primers listed above and Phusion flash mastermix (Thermo Fisher Scientific Bioscience Inc.), RT-PCRs were performed to increase templates of the N, P, G, and canine GAPDH genes. Positive plasmids for each gene were constructed by inserting the PCR products into the pGEM T-Easy vector (Promega). All positive controls were
diluted to 103 to 108, and were used to create the standard curves.
Table 2. Details for primers used in the construction of the positive control
Target gene
Primer Sequence References
N
21g 5’-ATG TAA CAC CTC TAC AAT G 3'
14, 15
CN4 5’-GGA TTG AC(AG) AAG ATC TTG
CTC AT-3'
P
RabPfor 5'-TTA CTT CTC CGG TGA (GA)AC
(GA)AG GAG-3' 14
RabPrev 5'-GAG G(GA)T TTT TGA GTG TCC
TC(GA) TC-3'
G
RabG1.5a 5'-AGA CCT GTG GAT TTG TGG ACG
A-3' 14
Gseq5R 5'- ACC GTT GGT CAC TGG AGC TGC
TAG-3'
GAPDH
GAPDH_F 5'-TCC AGT ATG ATT CTA CCC ACG-3'
In house design
GAPDH_R 5'-TTG TCA TAC CAG GAA ATG AGC-
3'
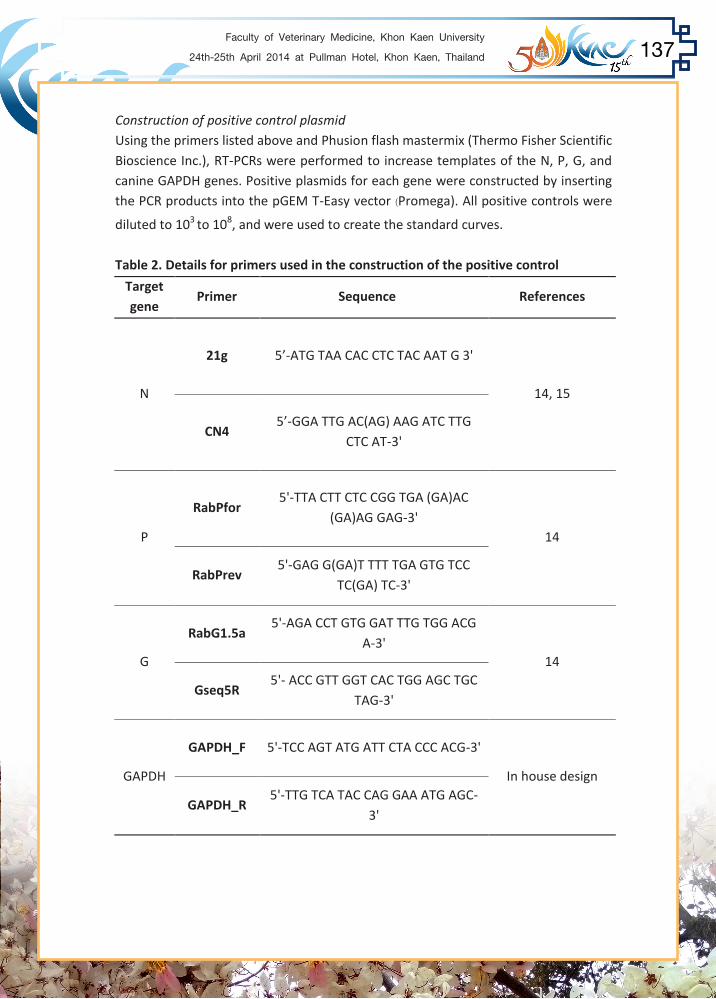
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 137
Construction of positive control plasmid Using the primers listed above and Phusion flash mastermix (Thermo Fisher Scientific Bioscience Inc.), RT-PCRs were performed to increase templates of the N, P, G, and canine GAPDH genes. Positive plasmids for each gene were constructed by inserting the PCR products into the pGEM T-Easy vector (Promega). All positive controls were
diluted to 103 to 108, and were used to create the standard curves.
Table 2. Details for primers used in the construction of the positive control
Target gene
Primer Sequence References
N
21g 5’-ATG TAA CAC CTC TAC AAT G 3'
14, 15
CN4 5’-GGA TTG AC(AG) AAG ATC TTG
CTC AT-3'
P
RabPfor 5'-TTA CTT CTC CGG TGA (GA)AC
(GA)AG GAG-3' 14
RabPrev 5'-GAG G(GA)T TTT TGA GTG TCC
TC(GA) TC-3'
G
RabG1.5a 5'-AGA CCT GTG GAT TTG TGG ACG
A-3' 14
Gseq5R 5'- ACC GTT GGT CAC TGG AGC TGC
TAG-3'
GAPDH
GAPDH_F 5'-TCC AGT ATG ATT CTA CCC ACG-3'
In house design
GAPDH_R 5'-TTG TCA TAC CAG GAA ATG AGC-
3'

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health138
Measurement of rabies genes and canine GAPDH expression level The expression levels of N, P, and G genes were measured by the RT-qPCR technique with SYBR select mastermix (Applied bio system) and the 7500 fast real-time PCR machine (Applied bio system). For each gene, the copy number was calculated by triplicate control plasmid concentrations. To reduce the variation of RNA quality and the efficiency of the reverse transcriptase step among samples, all expression data were normalized with the expression level of canine GAPDH of each sample. Data analysis The expression levels of rabies genes (N, P, G) were compared within each clinical subgroup for the different anatomical regions, and between the clinical subgroups comparing the same anatomical regions, using the unpaired T-test for a two-tailed test (SPSS software version17.0, SPSS Inc.). Results Expression of rabies genes in furious rabies The expression levels of rabies genes in order from greatest to least were as follows: S cord, T cord, brainstem, hippocampus, and frontal lobe. Expression of rabies genes in paralytic rabies The gene expression level was highest in the T cord, followed by the S cord, brainstem, hippocampus, and frontal lobes. Expression of rabies genes between different clinical subtypes Significantly higher expression level of P gene was observed in the furious as compared to the paralytic dogs in all CNS regions examined, except for the thoracic cord (Table 3). Expression of the G gene in the pons and sacral cords, as well as the N gene in the frontal lobes and sacral cords, was also significantly higher in furious canines. Table 3. Comparison of rabies genes between paralytic and furious canine rabies.
S cord T cord Pons Hippocampus Frontal lobe
N gene
P gene
G gene
No difference in gene expression between paralytic and furious groups.
Furious group shows higher gene expression than paralytic group.
Furious group shows lower gene expression than paralytic group.
Discussion RABV contributes to two distinct clinical subtypes, furious (encephalitis) and dumb (paralytic), in dogs and humans (3). Not until recently have differences been identified between the clinical forms at the early stage of rabies infection. Host immune responses and inflammation at the brainstem level have been found to be associated with reduced viral burden in the brain and longer survival times in the paralytic as compared to the furious rabies (1, 10). The current study is the first to evaluate rabies genes in canines in different CNS regions of both clinical manifestations. In parallel with the RABV antigen distribution (1), the expression levels of rabies genes were highest in the spinal cord, followed by the pons and cerebrum. Several studies have shown that rabies N, P and G genes could modulate the host immune response (3, 17, 18, 19). In this cohort, the high expression level of P gene in the early stage furious canines in the brain and pons is of particular interest since this might explain the lesser inflammatory response noted previously in the same dogs (1, 10). A study has shown that the regions containing the self-association domain and the C-terminal region on the P might be associated with IFN sensitivity (20). The phosphoprotein could reduce host immunity by inhibiting host IFN response via prevention of IRF3 phosphorylation and STAT2 translocation (17, 18, 21). The role of IFN in the outcome of rabies is further supported by the shorter survival of type I IFN (α/ß) receptor-deficient mice as compared to the wild-type mice (21). It has also been suggested that the prolonged survival in paralytic as compared to furious rabies is associated with more inflammation and less viral burden (3). In conclusion, the higher expression level of phosphoprotein gene in the furious type might be associated with the lesser extent of immune response and rapid viral spreading into the brain, as compared to the paralytic rabies. Acknowledgments This study was supported by the Research Chair Grant, the National Science and Technology Development Agency (NSTDA), Thailand; the Higher Education Research Promotion and National Research University Project of Thailand, Office of the Higher Education Commission (HR1160A); and Integrated Innovation Academic Center: IIAC, Chulalongkorn University Centenary Academic Development Project.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 139
Discussion RABV contributes to two distinct clinical subtypes, furious (encephalitis) and dumb (paralytic), in dogs and humans (3). Not until recently have differences been identified between the clinical forms at the early stage of rabies infection. Host immune responses and inflammation at the brainstem level have been found to be associated with reduced viral burden in the brain and longer survival times in the paralytic as compared to the furious rabies (1, 10). The current study is the first to evaluate rabies genes in canines in different CNS regions of both clinical manifestations. In parallel with the RABV antigen distribution (1), the expression levels of rabies genes were highest in the spinal cord, followed by the pons and cerebrum. Several studies have shown that rabies N, P and G genes could modulate the host immune response (3, 17, 18, 19). In this cohort, the high expression level of P gene in the early stage furious canines in the brain and pons is of particular interest since this might explain the lesser inflammatory response noted previously in the same dogs (1, 10). A study has shown that the regions containing the self-association domain and the C-terminal region on the P might be associated with IFN sensitivity (20). The phosphoprotein could reduce host immunity by inhibiting host IFN response via prevention of IRF3 phosphorylation and STAT2 translocation (17, 18, 21). The role of IFN in the outcome of rabies is further supported by the shorter survival of type I IFN (α/ß) receptor-deficient mice as compared to the wild-type mice (21). It has also been suggested that the prolonged survival in paralytic as compared to furious rabies is associated with more inflammation and less viral burden (3). In conclusion, the higher expression level of phosphoprotein gene in the furious type might be associated with the lesser extent of immune response and rapid viral spreading into the brain, as compared to the paralytic rabies. Acknowledgments This study was supported by the Research Chair Grant, the National Science and Technology Development Agency (NSTDA), Thailand; the Higher Education Research Promotion and National Research University Project of Thailand, Office of the Higher Education Commission (HR1160A); and Integrated Innovation Academic Center: IIAC, Chulalongkorn University Centenary Academic Development Project.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health140
References 1. Shuangshoti S, Thepa N, Phukpattaranont P, Jittmittraphap A, Intarut N, Tepsumethanon V, Wacharapluesadee S, Thorner PS, Hemachudha T. Reduced viral burden in paralytic compared to furious canine rabies is associated with prominent inflammation at the brainstem level. BMC Vet Res 2013; 14: 31. 2. Hemachudha T, Sunsaneewitayakul B, Desudchit T, Suankratay C, Sittipunt C, Wacharapluesadee S, Khawpold P, Wilde H, Jackson, AC. Failure of therapeutic coma and ketamine for therapy of human rabies. J Neurovirol 2006; 12: 407-9. 3. Hemachudha T, Ugolini G, Wacharapluesadee S, Sungkarat W, Shuangshoti S, Laothamatas J. Human rabies: neuropathogenesis, diagnosis and management. Lancet Neuro 2013; 12: 498-513. 4. Wunner WH. Rabies virus. In: Jackson A, Wunner HW, editors. Rabies. London: Academic Press; 2007. p.23-6. 5. Charlton KM, Casey GA. Experimental oral and nasal transmission of rabies virus in mice. Can J Comp Med 1979; 43: 10-5. 6. Winkler WG, Fashinell TR, Leffingwell L, Howard P, Conomy JP. Airborne rabies transmission in a laboratory worker. JAMA 1973; 226: 1219-1221. 7. Hemachudha T, Wacharapluesadee S, Laothamatas J. Rabies. Curr Neurol Neurosci 2006; 6: 460-8. 8. Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol 2002; 1: 101-9. 9. Hemachudha T, Sunsaneewitayakul B, Mitrabhakdi E, Suankratay C, Laothamatas
J, Wacharapluesadee S, Khawpold P, Wilde H. Paralytic complications following intravenous rabies immune globulin treatment in a patient with furious rabies. Int J Infect Dis 2003; 7: 76-7.
10. Laothamatas J, Wacharapluesadee S, Lumlertdacha B, Ampawong S, Tepsumethanon V, Shuangshoti S, Phumesin P, Asavaphatiboon S, Worapruekjaru L, Avihingsanon Y, Israsena N, Lafon M, Wilde H, Hemachudha T. Furious and paralytic rabies of canine origin: Neuroimaging with virological and cytokine studies. J Neurovirol 2008; 14: 119-29.
11. Wacharapluesedee S, Hemachudha T. Nucleic-acid sequence based amplification in rapid diagnosis of rabies. Lancet 2001; 358: 892-3.
12. Wacharapluesedee S, Sutipanya J, Damrongwatanapokin S, Phumesin P, Chamnanpood P, Leowijuk C, Hemachudha T. Development of TaqMan real- time RT-PCR assay for the detection of rabies virus. J Virol Methods 2008; 151: 317-20.
13. Thanomsridetchai N. Expression of specific protein(s) in brain, brainstem and spinal cord of rabies infected dogs [PhD thesis]. Bangkok, Thailand: Chulalongkorn University; 2010.
14. Virojanapirom P. BHK-cell adapted canine rabies virus variance: mutation in intergenic phosphoprotein and matrix protein gene non-coding region may confer higher neurovirulence in adult mice [PhD thesis]. Bangkok, Thailand: Chulalongkorn University; 2011 15. Fahl WD, Carnieli PJr, Castilho JG, Carrieri ML, Kotait I, Iamamoto K, Oliveira RN, Brandão, PE. Desmodus rotundus and Artibeus spp. Bats might present distinct rabies virus lineages. Braz J Infect Dis 2012; 16: 545-551. 16. Laothamatas J, Hemacudha T, Mitrabhakdi E, Wannakrairot P, Tulayadaechanont
S. MR imaging in human rabies. AJNR Am J Neuroradiol 2003; 24: 1102-9. 17. Brzózka K, Finke S, and Conzelmann KK. Inhibition of interferon signaling by
rabies virus phosphoprotein P: activation-dependent binding of STAT1 and STAT2. J Virol 2006; 80: 2675-83.
18. Schnell MJ,, McGettigan JP, Wirblich C, Papaneri A. The cell biology of rabies virus: using stealth to reach the brain. Nat Rev Microbiol 2010; 8: 51-61.
19. Masatani T, Ito N, Shimizu K, Ito Y, Nakagawa K, Abe M, Yamaoka S, Suqiyama M. Amino acid at positions 273 and 394 in rabies virus nucleoprotein are important for both evasion of host RIG-I mediated antiviral response and pathogenicity. Virus Res 2011; 155: 168-74. 20. Niu X, Tang L, Tseggai T, Guo Y, Fu ZF. Wild-type rabies virus phosphoprotein is associated with viral sensitivity to type I interferon treatment. Arch Virol 2013; 158: 2297-305. 21. Chopy D, Detje CN, Lafage M, Kalinke U, Lafon, M. The type I interferon response bridles rabies virus infection and reduce pathogenicity. J Neurovirol 2011; 17: 353-67.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 141
13. Thanomsridetchai N. Expression of specific protein(s) in brain, brainstem and spinal cord of rabies infected dogs [PhD thesis]. Bangkok, Thailand: Chulalongkorn University; 2010.
14. Virojanapirom P. BHK-cell adapted canine rabies virus variance: mutation in intergenic phosphoprotein and matrix protein gene non-coding region may confer higher neurovirulence in adult mice [PhD thesis]. Bangkok, Thailand: Chulalongkorn University; 2011 15. Fahl WD, Carnieli PJr, Castilho JG, Carrieri ML, Kotait I, Iamamoto K, Oliveira RN, Brandão, PE. Desmodus rotundus and Artibeus spp. Bats might present distinct rabies virus lineages. Braz J Infect Dis 2012; 16: 545-551. 16. Laothamatas J, Hemacudha T, Mitrabhakdi E, Wannakrairot P, Tulayadaechanont
S. MR imaging in human rabies. AJNR Am J Neuroradiol 2003; 24: 1102-9. 17. Brzózka K, Finke S, and Conzelmann KK. Inhibition of interferon signaling by
rabies virus phosphoprotein P: activation-dependent binding of STAT1 and STAT2. J Virol 2006; 80: 2675-83.
18. Schnell MJ,, McGettigan JP, Wirblich C, Papaneri A. The cell biology of rabies virus: using stealth to reach the brain. Nat Rev Microbiol 2010; 8: 51-61.
19. Masatani T, Ito N, Shimizu K, Ito Y, Nakagawa K, Abe M, Yamaoka S, Suqiyama M. Amino acid at positions 273 and 394 in rabies virus nucleoprotein are important for both evasion of host RIG-I mediated antiviral response and pathogenicity. Virus Res 2011; 155: 168-74. 20. Niu X, Tang L, Tseggai T, Guo Y, Fu ZF. Wild-type rabies virus phosphoprotein is associated with viral sensitivity to type I interferon treatment. Arch Virol 2013; 158: 2297-305. 21. Chopy D, Detje CN, Lafage M, Kalinke U, Lafon, M. The type I interferon response bridles rabies virus infection and reduce pathogenicity. J Neurovirol 2011; 17: 353-67.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health142
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Rabbit Model of Right Ventricular Hypertrophy Induced by Pulmonary Artery Banding
Pradtana Meedech1 Nakkawee Saengklub2 Vudhiporn Limprasutr2
Sarinee Kalandakanond-Thongsong2,3 Anusak Kijtawornrat2,3,* and Somporn Techangamsuwan4
1Interdisciplinary Program of Physiology, Graduate School, 2Department of Physiology, Faculty of Veterinary Science,
3Research study and testing of drug’s effect related to cardiovascular system in laboratory animal research clusters, 4Department of Pathology, Faculty of Veterinary Science,
Chulalongkorn University, Bangkok 10330, Thailand. *Corresponding author: [email protected]
Objective - The aim of this study was to characterize a rabbit model of RVH induced by pressure overload due to narrowing of the pulmonary artery. Materials and Methods - New Zealand White rabbits (n=10) were divided into 2 groups: sham operated (SHAM, n=5) and pulmonary artery banding (PAB, n=5). PAB was induced by narrowing the pulmonary artery. Twenty weeks after surgery, hemodynamic, cardiac function, and electrocardiograms were obtained from PAB compared with SHAM. After measurement, rabbits were sacrificed to collect ventricular myocardium for histopathological analysis. Results - After 20 weeks, the % HW to BW ratio of whole heart and right ventricle (RV) and right ventricular free wall thickness were significantly increased in PAB when compared with those in SHAM. PAB had a significant electrical remodeling as demonstrated by lengthening of QT and QTc(F) intervals. PAB also had a significant functional remodeling verified by a decreased contractility index and lengthened time constant of relaxation of RV. Conclusion - The rabbit with PAB demonstrates cardiac remodelling as well as diastolic and systolic dysfunction. Keywords: Cardiac, Hypertrophy, Rabbit, Remodelling, Right ventricle
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 143
Rabbit Model of Right Ventricular Hypertrophy Induced by Pulmonary Artery Banding
Pradtana Meedech1 Nakkawee Saengklub2 Vudhiporn Limprasutr2
Sarinee Kalandakanond-Thongsong2,3 Anusak Kijtawornrat2,3,* and Somporn Techangamsuwan4
1Interdisciplinary Program of Physiology, Graduate School, 2Department of Physiology, Faculty of Veterinary Science,
3Research study and testing of drug’s effect related to cardiovascular system in laboratory animal research clusters, 4Department of Pathology, Faculty of Veterinary Science,
Chulalongkorn University, Bangkok 10330, Thailand. *Corresponding author: [email protected]
Objective - The aim of this study was to characterize a rabbit model of RVH induced by pressure overload due to narrowing of the pulmonary artery. Materials and Methods - New Zealand White rabbits (n=10) were divided into 2 groups: sham operated (SHAM, n=5) and pulmonary artery banding (PAB, n=5). PAB was induced by narrowing the pulmonary artery. Twenty weeks after surgery, hemodynamic, cardiac function, and electrocardiograms were obtained from PAB compared with SHAM. After measurement, rabbits were sacrificed to collect ventricular myocardium for histopathological analysis. Results - After 20 weeks, the % HW to BW ratio of whole heart and right ventricle (RV) and right ventricular free wall thickness were significantly increased in PAB when compared with those in SHAM. PAB had a significant electrical remodeling as demonstrated by lengthening of QT and QTc(F) intervals. PAB also had a significant functional remodeling verified by a decreased contractility index and lengthened time constant of relaxation of RV. Conclusion - The rabbit with PAB demonstrates cardiac remodelling as well as diastolic and systolic dysfunction. Keywords: Cardiac, Hypertrophy, Rabbit, Remodelling, Right ventricle
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health144
Introduction Animal models are useful for several aspects including investigation of disease mechanisms, new therapeutic paradigms, and vaccine development. The rabbit model of right ventricular hypertrophy (RVH) is one of the animal models that has been used extensively for studying the pathophysiology of right ventricular hypertrophy in humans as well as model for arrhythmia screening in drug safety evaluation [1,2]. The pathological condition of RVH may result from pulmonary artery stenosis (PS), tetralogy of Fallot, pulmonary artery hypertension (PAH), essential hypertension or pulmonary diseases [3]. A consequence of an increase in ventricular mass is the development of diastolic and systolic dysfunction, right heart failure, and sudden cardiac death [4,5]. In patients with RVH due to PAH, remodeling of right ventricle resulted in increased heterogeneity of ventricular action potential duration, a substrate for reentry arrhythmia [6]. In animal models of ventricular hypertrophy, Panyasing and colleagues [1] have shown that rabbits with RVH tended to develop the long QT syndrome and torsade de pointes in response to delayed rectifier potassium channel blockers infusion when compared to left ventricular hypertrophy and biventricular hypertrophy. The present study was designed to characterize a rabbit model of RVH induced by pressure overload due to narrowing of the pulmonary artery. Materials and Methods Animals: Adult male New Zealand White rabbits, weighing between 2.3 and 2.9 kg, were used in this study. All procedures were approved by Faculty of Veterinary Science Animal Care and Use Committee, Chulalongkorn University. The rabbits were randomly divided into two groups: sham-operated group (SHAM, n = 5) or pulmonary artery banding group (PAB, n = 5). Details of the surgical procedure were previously described by Panyasing and colleagues (2010). The pulmonary artery was constricted to approximately 3.2 mm at the origin of the vessel so that it was about 50% narrowed. Rabbits in the SHAM group were anesthetized and operated as in PAB group except for the banding of pulmonary artery. Assessments of cardiac function and electrophysiology: After 20 weeks, animals were anesthetized as previously described. The bipolar transthoracic electrocardiograms (ECG) were obtained. A cut-down technique was performed on the right internal carotid artery and the right jugular vein. For the right internal carotid artery, a 2 Fr micromanometer catheter was inserted and placed at the level of aortic arch to measure aortic pressure (AoP). For the right jugular vein, another 2-Fr Millar catheter was inserted into the right atrium to obtain
right atrial pressure (RAP). The right ventricular pressure (RVP) was recorded by advancing the catheter into the right ventricle. Measurement of heart weight and ventricular free wall thickness: At the end of the experiment, all rabbits were euthanized with 200 mg/kg pentobarbital sodium while they were under general anesthesia. The heart was collected, rinsed with physiologic normal saline, patted dry and weighed. The right ventricular free wall thickness was measured at the level of the head of papillary muscle. Weights of atria, left and right ventricle were also collected. Histomorphological study: The heart tissues were fixed with 10% formaldehyde buffer for at least 48 hours. A 3 µm serial section was taken from each ventricle and stained with hematoxylin and eosin (H&E stain), Masson trichrome stain, or Periodic acid-Schiff (PAS) stain. All sections from both groups of rabbits were evaluated by an experienced pathologist. Statistical analysis: All data are presented as mean ± SEM. Parameters of electrophysiology, hemodynamics, and cardiac function were compared between groups at 20 weeks after surgery by using the Student’s unpaired t-test. A probability value of p < 0.05 was considered to be significant. Results In general, a total of 11 rabbits in the banding group were anesthetized and underwent open chest surgery. One rabbit in the pulmonary artery banding group died at the end of procedure due to pneumothorax. Therefore, the success rate of this procedure was 90.9 percent. All surviving rabbits did not show any sign of congestive heart failure during the study period (20 weeks). The parameters of ECG were compared between the SHAM and PAB groups after 20 weeks of surgery (Table 1). In response to chronic pressure overload produced by narrowing of the pulmonary artery, the QT and QTc intervals were significantly lengthened (p<0.05). Chronic pressure overload did not alter RR, PQ, or QRS intervals. The mean arterial blood pressure (MBP) in the PAB group was increased significantly 22.5% (p<0.05) whereas the mean RAP in PAB rabbits tended to increase when compared to SHAM (Table 2). End diastolic pressure (EDP) of the RV was 2.37 times higher in PAB than that in SHAM. End systolic pressure (ESP) of RV was 1.67 times

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 145
right atrial pressure (RAP). The right ventricular pressure (RVP) was recorded by advancing the catheter into the right ventricle. Measurement of heart weight and ventricular free wall thickness: At the end of the experiment, all rabbits were euthanized with 200 mg/kg pentobarbital sodium while they were under general anesthesia. The heart was collected, rinsed with physiologic normal saline, patted dry and weighed. The right ventricular free wall thickness was measured at the level of the head of papillary muscle. Weights of atria, left and right ventricle were also collected. Histomorphological study: The heart tissues were fixed with 10% formaldehyde buffer for at least 48 hours. A 3 µm serial section was taken from each ventricle and stained with hematoxylin and eosin (H&E stain), Masson trichrome stain, or Periodic acid-Schiff (PAS) stain. All sections from both groups of rabbits were evaluated by an experienced pathologist. Statistical analysis: All data are presented as mean ± SEM. Parameters of electrophysiology, hemodynamics, and cardiac function were compared between groups at 20 weeks after surgery by using the Student’s unpaired t-test. A probability value of p < 0.05 was considered to be significant. Results In general, a total of 11 rabbits in the banding group were anesthetized and underwent open chest surgery. One rabbit in the pulmonary artery banding group died at the end of procedure due to pneumothorax. Therefore, the success rate of this procedure was 90.9 percent. All surviving rabbits did not show any sign of congestive heart failure during the study period (20 weeks). The parameters of ECG were compared between the SHAM and PAB groups after 20 weeks of surgery (Table 1). In response to chronic pressure overload produced by narrowing of the pulmonary artery, the QT and QTc intervals were significantly lengthened (p<0.05). Chronic pressure overload did not alter RR, PQ, or QRS intervals. The mean arterial blood pressure (MBP) in the PAB group was increased significantly 22.5% (p<0.05) whereas the mean RAP in PAB rabbits tended to increase when compared to SHAM (Table 2). End diastolic pressure (EDP) of the RV was 2.37 times higher in PAB than that in SHAM. End systolic pressure (ESP) of RV was 1.67 times

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health146
significantly higher in PAB than those in SHAM. The contractility index of the RV was significantly decreased (-39.30%) in PAB rabbits when compared to SHAM rabbits (p<0.05). The time constant of RV isovolumetric relaxation or Tau of the right ventricle for PAB rabbits tended to increase (26.04%, p = 0.1). Anatomical remodeling was determined by assessment of the heart weight/body weight ratio, ventricular free wall thickness, and morphological changes. The %HW/BW in PAB rabbits were increased significantly (p<0.05) for the whole heart (16.66%) and for right ventricle (74.19%) when compared to SHAM rabbits. The right ventricular free wall thickness in PAB were increased significantly (p<0.01) 31.23% when compared with SHAM. The cardiac myocytes of right ventricle appeared to be similar in size in both groups as observed with H&E stains. A Periodic acid-Schiff (PAS) stain, however, demonstrated a marked positive glycogen-magenta in color, (Fig. 1A-B) in rabbits with PAB compared to SHAM rabbits. Moreover, a Masson’s trichrome stain showed marked fibroblast proliferation (blue color, Fig. 1C-D) in PAB rabbits compared with SHAM rabbits. Discussion and conclusion In the present study, PAB induced RVH and causes repolarization remodeling (increased QT and QTc intervals). It has been demonstrated previously that electrical remodeling especially in the right ventricle is the proximate cause of some arrhythmias [7-9]. At 20 weeks after surgery, the contraction of the right ventricle was significantly decreased as suggested by the contractility index. Recent studies in anesthetized guinea pigs and dogs demonstrated that contractility index is reliable for assessment of inotropic state of the heart than dP/dtmax [10]. The relaxation of the right ventricle of rabbit with RVH also decreased significantly as assessed by Tau. The decrease in both myocardial contraction and relaxation after pulmonary banding suggested that RVH in rabbits possesses systolic and diastolic dysfunction. These results are in accordance with previous study in infant rabbits in which the cardiac function was impaired beginning at 3 weeks after surgery [11]. Narrowing of pulmonary artery as used in this study was adjusted to approximately 50 percent of the diameter of the pulmonary artery. This process gradually produces pressure-overload to the right ventricle as the rabbits grew. In the current study, the morphological remodeling was confirmed by a significant increase of %HW/BW ratio of the right ventricle and the whole heart as well as the thickening of right ventricular free wall. The histopathological results of right ventricle demonstrated a
tendency for an increase of fibrous tissue and glycogen replacement of the dead cardiac myocytes in PAB rabbits when compared with SHAM rabbits. These results are consistent with previous studies in infant rabbits and adult rats which demonstrated that pulmonary artery banding induced pressure-overload, right ventricular hypertrophy, and apoptosis of the myocytes beginning at 4 weeks after banding and suggested that the apoptosis may lead to myocardial dysfunction [11-14]. Conclusions
Overall results of this study indicated that rabbits with PAB for 20 weeks developed right ventricular hypertrophy as suggested by electrical, functional, and anatomical remodeling. The electrical remodeling included prolongation of repolarization while the functional remodeling included impaired right and left ventricular function. The anatomical remodeling included thickening of right ventricular free wall, an increased %HW/BW ratio, a marked positive PAS staining, and marked fibroblast proliferation.
Acknowledgement
This study was supported by the 90th
Anniversary of Chulalongkorn University Fund (Ratchadaphiseksomphot Endowment Fund), QTest Labs, LLC, and Ratchadaphisek Sompot endowment fund from Chulalongkorn University (Special Task Force for Activating Research (GSTAR 56-008-31-001). References 1. Panyasing Y, Kijtawornrat A, Rio DC, Carnes C, Hamlin RL. Uni- or bi-ventricular hypertrophy and susceptibility to drug-induced torsades de pointes. J Pharm Toxicol Methods. 2010; 62:148-56. 2. Varian KD, Kijtawornrat A, Gupta SC, Torres CA, Monasky MM, Hiranandani N, et
al. Impairment of diastolic function by lack of frequency-dependent myofiament desensitization rabbit right ventricular hypertrophy. Circ Heart Fail. 2009; 2(5): 472-81.
3. Haddad F, Hunt AS, Rosenthal ND. Right ventricular function in cardiovascular disease, part I anatomy, physiology, aging, and functional assessment of right ventricle. Am J Physiol-Heart Circ Physiol. 2008; 117: 1436-48. 4. Gan CT, Holverda S, Marcus JT, Paulus WJ, Marques KM, Bronzwaer JG, et al. Right ventricular diastolic dysfunction and the acute effects of sildenafil. Chest.
2007; 132: 11-7.
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 147
tendency for an increase of fibrous tissue and glycogen replacement of the dead cardiac myocytes in PAB rabbits when compared with SHAM rabbits. These results are consistent with previous studies in infant rabbits and adult rats which demonstrated that pulmonary artery banding induced pressure-overload, right ventricular hypertrophy, and apoptosis of the myocytes beginning at 4 weeks after banding and suggested that the apoptosis may lead to myocardial dysfunction [11-14]. Conclusions
Overall results of this study indicated that rabbits with PAB for 20 weeks developed right ventricular hypertrophy as suggested by electrical, functional, and anatomical remodeling. The electrical remodeling included prolongation of repolarization while the functional remodeling included impaired right and left ventricular function. The anatomical remodeling included thickening of right ventricular free wall, an increased %HW/BW ratio, a marked positive PAS staining, and marked fibroblast proliferation.
Acknowledgement
This study was supported by the 90th
Anniversary of Chulalongkorn University Fund (Ratchadaphiseksomphot Endowment Fund), QTest Labs, LLC, and Ratchadaphisek Sompot endowment fund from Chulalongkorn University (Special Task Force for Activating Research (GSTAR 56-008-31-001). References 1. Panyasing Y, Kijtawornrat A, Rio DC, Carnes C, Hamlin RL. Uni- or bi-ventricular hypertrophy and susceptibility to drug-induced torsades de pointes. J Pharm Toxicol Methods. 2010; 62:148-56. 2. Varian KD, Kijtawornrat A, Gupta SC, Torres CA, Monasky MM, Hiranandani N, et
al. Impairment of diastolic function by lack of frequency-dependent myofiament desensitization rabbit right ventricular hypertrophy. Circ Heart Fail. 2009; 2(5): 472-81.
3. Haddad F, Hunt AS, Rosenthal ND. Right ventricular function in cardiovascular disease, part I anatomy, physiology, aging, and functional assessment of right ventricle. Am J Physiol-Heart Circ Physiol. 2008; 117: 1436-48. 4. Gan CT, Holverda S, Marcus JT, Paulus WJ, Marques KM, Bronzwaer JG, et al. Right ventricular diastolic dysfunction and the acute effects of sildenafil. Chest.
2007; 132: 11-7.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health148
5. Piao L, Fang YH, Cadete VJ, Wietholt C, Urboniene D, Toth PT, et al. The inhibition of pyruvate dehydrogenase kinase improves impaired cardiac function and
electrical remodeling in two models of right ventricular hypertrophy: resuscitating the hibernating right ventricle. J Mol Med. 2010; 88: 47-60.
7. Henkens IR, Scherptong RW, Kralingen KW. Pulmonary hypertension: the role of the electrocardiogram. Netherlands Heart J. 2008; 16: 250-4.
8. Benoist D, Stones R, Drinkhill M, Bernus O, White E. Arrhythmogenic substrate in hearts of rats with monocrotaline-induced pulmonary hypertension and right
ventricular hypertrophy. Am J Physiol-Heart Circ Physiol. 2011; 300: H2230-7. 9. Umar S, Lee JH, de Lange E, Iorga A, Partow-Navid R, Bapat A, et al. Spontaneous ventricular fibrillation in right ventricular failure secondary to chronic
pulmonary hypertension. Circ Arrhythmia Electrophysiol. 2012; 5:181-90. 10. Tanaka Y, Takase B, Yao T. Right ventricular electrical remodeling and arrhythmogenic substrate in rat pulmonary hypertension. Am J Resp Cell Mol Biol. 2013; 49: 426-36. 11. Kijtawornrat A, Ueyama Y, del Rio C, Sawangkoon S, Buranakarl C, Chaiyabutr N,
et al. Test of the usefulness of a paradigm to identify potential cardiovascular liabilities of four test articles with varying pharmacological properties in
anesthetized guinea pigs. Toxicol Sci. 2014; 137: 458-468. 12. Minegishi S, Kitahori K, Murakami A, Ono M. Mechanism of pressure-overload
right ventricular hypertrophy in infant rabbits. Int Heart J. 2011; 52: 56-60. 13. Ikeda S, Hamada M, Hiwada K. Cardiomyocyte apoptosis with enhanced
Expression of P53 and Bax in right ventricle after pulmonary arterial banding. Life Sci. 1999; 65: 925-33.
14. Teiger E, Than VD, Richard L, Wisnewsky C, Tea BS, Gaboury L, et al. Apoptosis in pressure overload-induced heart hypertrophy in the rat. J Clin Invest. 1996;
97: 2891-7. 15. Braun MU, Szalai P, Strasser RH, Borst MM. Right ventricular hypertrophy and apoptosis after pulmonary artery banding: regulation of PKC isozymes.
Cardiovasc Res. 2003; 59: 658-67.
Table 1 A comparison of electrical remodelling of the right ventricle in sham operated rabbits (SHAM) and pulmonary artery banded (PAB) rabbits. Values are presented as mean ± SEM. Each point was calculated from 1 minute data recording from anesthetized rabbits. *p<0.05 compared with SHAM by using Student unpaired t-test. QTc = corrected QT interval for heart rate by Fridericia formula; ms = milliseconds.
Parameters SHAM PAB RR (ms) 195.1 ± 2.8 227.9 ± 12.9 PQ (ms) 63.4 ± 2.6 66.8 ± 3.8 QRS (ms) 49.3 ± 2.5 54.6 ± 1.9 QT (ms) 128.8 ± 4.0 162.9 ± 5.8* QTc (ms) 222.0 ± 6.4 267.2 ± 7.4*
Table 2 Hemodynamic and cardiac function in sham operated rabbits (SHAM) and pulmonary artery banded (PAB) rabbits. Values are presented as mean ± SEM. Each point was calculated from 1 minute data recording from anesthetized rabbits. *p<0.05 and **p<0.01 compared with SHAM by using Student unpaired t-test. MBP = mean arterial blood pressure; RAP = mean right atrial pressure; EDP = end diastolic pressure; ESP = end systolic pressure; CI = contractility index (the maximal rate of rise of the ventricular pressure divided by the ventricular pressure at that point); Tau = the relaxation time constant; RV = right ventricle; mmHg = millimeter of mercury; ms = milliseconds
Parameters SHAM PAB
MBP (mmHg) 54.6 ± 3.6 66.9 ± 2.7* RAP (mmHg) 3.7 ± 1.6 6.3 ± 2.0 EDPRV (mmHg) 2.9 ± 1.8 6.9 ± 1.4* ESPRV (mmHg) 21.1 ± 2.32 35.3 ± 0.5** CIRV 76.6 ± 17.7 46.5 ± 4.8* TauRV (ms) 19.2 ± 4.8 24.2 ± 1.9

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 149
Table 1 A comparison of electrical remodelling of the right ventricle in sham operated rabbits (SHAM) and pulmonary artery banded (PAB) rabbits. Values are presented as mean ± SEM. Each point was calculated from 1 minute data recording from anesthetized rabbits. *p<0.05 compared with SHAM by using Student unpaired t-test. QTc = corrected QT interval for heart rate by Fridericia formula; ms = milliseconds.
Parameters SHAM PAB RR (ms) 195.1 ± 2.8 227.9 ± 12.9 PQ (ms) 63.4 ± 2.6 66.8 ± 3.8 QRS (ms) 49.3 ± 2.5 54.6 ± 1.9 QT (ms) 128.8 ± 4.0 162.9 ± 5.8* QTc (ms) 222.0 ± 6.4 267.2 ± 7.4*
Table 2 Hemodynamic and cardiac function in sham operated rabbits (SHAM) and pulmonary artery banded (PAB) rabbits. Values are presented as mean ± SEM. Each point was calculated from 1 minute data recording from anesthetized rabbits. *p<0.05 and **p<0.01 compared with SHAM by using Student unpaired t-test. MBP = mean arterial blood pressure; RAP = mean right atrial pressure; EDP = end diastolic pressure; ESP = end systolic pressure; CI = contractility index (the maximal rate of rise of the ventricular pressure divided by the ventricular pressure at that point); Tau = the relaxation time constant; RV = right ventricle; mmHg = millimeter of mercury; ms = milliseconds
Parameters SHAM PAB
MBP (mmHg) 54.6 ± 3.6 66.9 ± 2.7* RAP (mmHg) 3.7 ± 1.6 6.3 ± 2.0 EDPRV (mmHg) 2.9 ± 1.8 6.9 ± 1.4* ESPRV (mmHg) 21.1 ± 2.32 35.3 ± 0.5** CIRV 76.6 ± 17.7 46.5 ± 4.8* TauRV (ms) 19.2 ± 4.8 24.2 ± 1.9

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health150
SHAM PAB
(A) (B)
(C) (D) Figure 1. Histopathological section of right ventricular free wall stained with periodic acid-Schiff (A,B) and Masson’s trichrome (C,D) in sham operated (SHAM) and pulmonary artery banding (PAB) rabbits. 400x; scale bar = 100 µM. Notice that the right ventricular myocytes appeared to be similar in size for both PAB and SHAM. In the PAB group, the PAS and Masson’s trichrome stain demonstrated glycogen deposits (magenta color) and fibroblast proliferation (blue color).

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 151
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health152
Effect of Low Intensity Laser Therapy on Healing of Rabbit Tibial Defects: an Evaluation Based on Cone Beam Computed Tomography
Nguyen Hoai Nam1,2* Naruepon Kampa1 Peerapol Sukon1
Pongsathorn Tuchpramuk1 Pipop Sutthiprapaporn3 and Pornpop Rattana-arpha3 1Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
2Faculty of Veterinary Medicine, Hanoi University of Agriculture, Vietnam. 3Faculty of Dentistry, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Bone fracture deserves as important issue since it causes multiple problems to patients and society. The low intensity laser therapy is a new approach applied for many purposes in medical field, including orthopedics. It has been documented that this phototherapy stimulates the production of cell’s energy resulting in cell mitosis. This therapy can enhance the osteoblastic activity, increase the mineralization of osteoblasts and improve the viability of osteocytes, as consequence, the bone repair process is up-regulated.
Objective - To investigate effects of low intensity laser therapy on the bone repair process of rabbit tibial defects.
Materials and Methods - Eighteen male New Zealand White rabbits aged 7 months were enrolled. Under general anesthesia, round defects sized 3.5 mm were created with a spinning bur on the medial site of tibial crests of both hind-legs. Defected legs were then randomly arranged into 3 groups; group A was treated with a diode laser (830nm, 200mW, 4J/cm2, continuous wave, 8 sessions with 48h interval and first session was at 24h after surgery), group B was treated with the same protocol but a higher dose of 20J/cm2 was applied, and group C was treated as sham control (BTL-5000, Hungary). Nine rabbits were sacrificed at 3rd week and the other half were sacrificed at 6th week. The bone healing was evaluated by using Cone beam computed tomography (CBCT). Each defect was assessed in a series of 12 slices with 300µm thickness for each based on a 7-point grading system combining thickness and density of newly formed bone tissue. The assessment was conducted by three assessors. Then, inter-observer and intra-observer reliabilities were calculated. The difference in bone healing results among groups was analyzed by using Mixed model ANOVA in which treatments and rabbits were fixed and random factors, respectively. All statistical analyses were carried out with an alpha value of 0.05 in SPSS program (IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp).
Results - Low intensity laser therapy failed to stimulate bone healing throughout the course of the present experiment. At 3rd week post-operation, the mean points of groups A, B, C were 5.7, 5.6 and 5.4, respectively, with no significant difference among the three groups (P=0.8). At 6th week after surgery a similar finding was demonstrated. The mean point of group A reached to 6.1 while those of group B and C were 5.8. The statistical comparison resulted in non-significance (P=0.53).
Conclusion - By radiological evaluation, we did not detect any significant effect of low intensity laser therapy on healing of rabbit tibial defects.
Keywords: Bone healing, CBCT, Low intensity laser therapy
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 153
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health154
Effects of L-carnitine on Blood Urea Nitrogen in Fancy Carp (Cyprinus carpio)
Naratip Pudsadee1 Dilok Wongsathien1 and Rutch Khattiya1*
1Department of Food Animal Clinic, Faculty of Veterinary Medicine, Chiangmai University, Chiangmai 50100, Thailand.
*Corresponding author
Objective - To determine the effects of L-carnitine on Blood urea nitrogen (BUN) in Fancy carp (Cyprinus carpio).
Materials and Methods - Sixty juvenile carp were exposed to toxic levels of ammonia at a concentration of 0.02 ppm for 4 weeks. Fish were randomly fed with commercial pellets with L-carnitine at different concentrations of 0, 150, 300 and 600 mg/kg of feed. Blood samples were randomly collected from 3 fishes in each group every week.
Results - The non-L-carnitine supplement group did not show different BUN levels in all weeks. In addition, BUN in the L-carnitine supplement groups do not show significant differences to the non-L-carnitine supplement group (P >0.05).
Conclusion - L-carnitine does not significantly change BUN level in fancy carp after exposed to long-term ammonia at 0.02 ppm.
Keywords: L-carnitine, Blood Urea Nitrogen (BUN), Ammonia toxicity, Fancy carp
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 155
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health156
Monitoring of Influenza A Viruses in a Live Bird Market in Thailand by Using the Sentinel Bird Model
Waleemas Jairak1 Kirana Noradechanon1 Supassama Chaiyawong1
Duangduean Prakairungnamthip2 Nutthawan Nonthabenjawan1 Aunyaratana Thontiravong2 and Alongkorn Amonsin1*
1Faculty of Veterinary Science, 2Department of Veterinary Microbiology, Chulalongkorn University, Bangkok 10330, Thailand.
*Corresponding author Email: [email protected]
Objective - To monitor influenza A virus (IAV) in a Live Bird Market (LBM) in Thailand by using a sentinel bird model. Materials and Methods - From November 2010 through February 2011, the sentinel setting was conducted for influenza A virus (IAV) monitoring in a LBM in Phitsanulok. This LBM has many bird species from different sources. Twenty 14-day-old barbary muscovy ducks (Cairina moschata) were IAV antibodies free were used as the sentinel birds. This sentinel birds were monitored for IAV infection and immunological responses for 10 weeks. In total, 368 swab samples and 183 blood samples were tested for the presence of IAVs and IAV specific antibodies by isolation in embryonated chicken eggs and by blocking NP-ELISA test, respectively. Results - In the serological results, the sentinel ducks were firstly detected the presence of antibodies against IAV at 3 days post placing and then disappeared after 14 days post placement. All positive NP-ELISA samples (n=11) were negative for HI test by H5, H7and H10 antigens. However, no IAV was isolated from theses sentinel birds. Conclusion - These results indicate the possibility of IAV transmission among poultry in the LBM and the effectiveness of the sentinel bird system for IAVs monitoring in the LBM. Keywords: Influenza A virus, Live bird market, Monitoring, Sentinel bird
Introduction Live bird markets (LBMs) have been determined as a potential source of avian influenza viruses because several poultry species from different sources and ages are commonly intermingled [2]. Several subtypes of influenza A virus (IAV) have been isolated in LBMs, including highly pathogenic avian influenza (HPAI) strains and low pathogenic avian influenza (LPAI) viruses [3, 7]. In addition, several studies have suggested that exposure to LBMs or direct contact with freshly slaughtered poultry in LBMs might be a major risk factor for human infection with IAVs especially HPAI H5N1 and novel avian influenza H7N9 [5, 11]. Since the HPAI H5N1 outbreak 2005, LBMs were often selected for surveillance of IAV. The monitoring of IAV in LBMs usually collects samples from live poultry, bird meats and environments [1, 10]. However, information on sentinel bird monitoring in LBMs is limited. This study established a sentinel bird model in a LBM in Thailand. The results can provide information about the effectiveness of a sentinel model for IAV monitoring in a LBM.
Materials and methods Live bird market selection: A LBM in Phitsanulok province of northern Thailand was selected for the sentinel bird setting (Figure1). Several avian species, including Khaki Campbell duck (Anas platyrhynchos), Muscovy duck (Cairina moschata) and Chicken (Gallus gallus domesticus) from different sources were present in this LBM.
Figure1. Phitsanulok province in Thailand was selected for sentinel setting in a live bird market. Sentinel birds: Twenty 14-day-old 20 barbary muscovy ducks (Cairina muschata) were IAV antibodies free were used as the sentinel birds. The ducks was shared the environment with the market poultry such as the pond where receives drain water from the slaughter site and the workers in the LBM.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 157
Introduction Live bird markets (LBMs) have been determined as a potential source of avian influenza viruses because several poultry species from different sources and ages are commonly intermingled [2]. Several subtypes of influenza A virus (IAV) have been isolated in LBMs, including highly pathogenic avian influenza (HPAI) strains and low pathogenic avian influenza (LPAI) viruses [3, 7]. In addition, several studies have suggested that exposure to LBMs or direct contact with freshly slaughtered poultry in LBMs might be a major risk factor for human infection with IAVs especially HPAI H5N1 and novel avian influenza H7N9 [5, 11]. Since the HPAI H5N1 outbreak 2005, LBMs were often selected for surveillance of IAV. The monitoring of IAV in LBMs usually collects samples from live poultry, bird meats and environments [1, 10]. However, information on sentinel bird monitoring in LBMs is limited. This study established a sentinel bird model in a LBM in Thailand. The results can provide information about the effectiveness of a sentinel model for IAV monitoring in a LBM.
Materials and methods Live bird market selection: A LBM in Phitsanulok province of northern Thailand was selected for the sentinel bird setting (Figure1). Several avian species, including Khaki Campbell duck (Anas platyrhynchos), Muscovy duck (Cairina moschata) and Chicken (Gallus gallus domesticus) from different sources were present in this LBM.
Figure1. Phitsanulok province in Thailand was selected for sentinel setting in a live bird market. Sentinel birds: Twenty 14-day-old 20 barbary muscovy ducks (Cairina muschata) were IAV antibodies free were used as the sentinel birds. The ducks was shared the environment with the market poultry such as the pond where receives drain water from the slaughter site and the workers in the LBM.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health158
Collect sample 1 3 5 7 14 21 28 42 56 70
Nov 2010 Dec
Jan Feb 2011 Month
Days post placing
Sample collection: Oropharyngeal swabs, cloacal swabs and blood samples were collected from individual sentinel birds at designated times during November 2010-Febuary 2011 (Figure 2). Oropharyngeal and cloacal swabs were collected by using sterile polyester tip swabs (Puritan®, USA). The swabs were placed in 2 ml of viral transport media (Brain Heart Infusion, BactoTM BD diagnostics, USA) and kept on ice during transportation until they were stored at -80◦c at the laboratory within 24
hours. Blood samples were collected from the jugular veins of sentinel birds; 2 ml without blood anticoagulant. Blood samples were kept on ice during transportation and sera were collected immediately upon arrival. The sera were then stored at -20°c until tested.
Figure2. Sample collection dates of the sentinel birds.
Serological test: Sera were tested for antibodies against influenza A virus with a commercial blocking NP-ELISA kit (FlockChek® AI MultiS-Screen diagnostic kit, IDEXX). For interpretation, the sera with a signal to noise (S/N) value ≤ 0.6 were considered positive. The positive NP-ELISA sera were then subjected to the HI test against H5, H7 and H10 avian influenza viruses [8]. Virus isolation and identification: The embryonated chicken egg inoculation was used as viral isolation for the swab samples [8]. After incubation at 37 ◦c for 72 hours,
the allantoic fluid were collected and tested for haemagglutination (HA) activity by using chicken red blood cells. The positive HA test samples were subjected to RNA extraction (Nucleospin® viral RNA mini kit, Macherey-Nagel, Germany) and then were tested for the M gene using real-time RT-PCR for confirm IAVs infection [9]. Results Serological Study: In total, 183 blood samples were collected from the sentinel ducks from November 2010 to February 2011. At 3 days post placing, 4 out of 19 birds had antibodies against the NP protein of IAVs. Then, 6 out of 18 birds showed seropositive at 7 days post placing as the highest number of seropositive ducks in this study. All birds were seronegative after 21 days post placing (Figure 3). All positive NP-ELISA samples (n=11) were seronegative for avian influenza H5, H7 and H10 viruses by the HI test.
Days after ducks placing Figure3. Serological results by NP-ELISA of nine seropositive sentinel birds during November 2010 to February 2011. Influenza A virus study: During 10 weeks monitoring in sentinel ducks in a LBM, oropharyngeal swabs (n=184) and cloacal swabs (n=184) were collected from the sentinel ducks. All of the swab samples were subjected to viral isolation by egg inoculation. The results showed 0.02% (6/368) of the allantoic fluid samples were positive for HA test. The HA positive swab samples were found since 28 days until 70 days post placing. All HA positive samples, however, were negative by real-time RT-PCR as M gene primer. Discussions and Conclusions Generally, ducks can be detected with influenza immunity as early as 7 days after exposure for the IAVs [6]. In this study, 4 out of 19 sentinel ducks had developed antibodies against IAVs as early as 3 days after placement in the LBM. From the results of a previous study, it can be implied that the immune response of four sentinel ducks at 3 days in this study probably came from the virus exposure before being placed in the LBM. The seropositive ducks from days 7 to 14 after placing were most likely affected by exposure to the influenza A virus in the LBM. Due to the limited IAV subtypes used in our HI test, the anti-HA specific antibodies could not be identified. These results indicated the chance possibility of IAV circulation in this LBM even though no viral shedding was detected from the sentinel ducks in this monitoring. Our results indicated that the sentinel bird could be an effective model for monitor the status of IAVs in a LBM especially by serological study. The sentinel system, however, should be conducted in the study environment over one year to increase the probability of influenza A virus detection [4]. This information will help improve prevention and control program of influenza A virus in LBMs.
No. of positive ELISA
Inverted ELISA
S/N ratio

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 159
Days after ducks placing Figure3. Serological results by NP-ELISA of nine seropositive sentinel birds during November 2010 to February 2011. Influenza A virus study: During 10 weeks monitoring in sentinel ducks in a LBM, oropharyngeal swabs (n=184) and cloacal swabs (n=184) were collected from the sentinel ducks. All of the swab samples were subjected to viral isolation by egg inoculation. The results showed 0.02% (6/368) of the allantoic fluid samples were positive for HA test. The HA positive swab samples were found since 28 days until 70 days post placing. All HA positive samples, however, were negative by real-time RT-PCR as M gene primer. Discussions and Conclusions Generally, ducks can be detected with influenza immunity as early as 7 days after exposure for the IAVs [6]. In this study, 4 out of 19 sentinel ducks had developed antibodies against IAVs as early as 3 days after placement in the LBM. From the results of a previous study, it can be implied that the immune response of four sentinel ducks at 3 days in this study probably came from the virus exposure before being placed in the LBM. The seropositive ducks from days 7 to 14 after placing were most likely affected by exposure to the influenza A virus in the LBM. Due to the limited IAV subtypes used in our HI test, the anti-HA specific antibodies could not be identified. These results indicated the chance possibility of IAV circulation in this LBM even though no viral shedding was detected from the sentinel ducks in this monitoring. Our results indicated that the sentinel bird could be an effective model for monitor the status of IAVs in a LBM especially by serological study. The sentinel system, however, should be conducted in the study environment over one year to increase the probability of influenza A virus detection [4]. This information will help improve prevention and control program of influenza A virus in LBMs.
No. of positive ELISA
Inverted ELISA
S/N ratio

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health160
Acknowledgements We would like to thank all staff of Center of Excellent for Emerging and Re-emerging Infectious Disease, Chulalongkorn University for advice and laboratory works. References 1. Amonsin A, Choatrakol C, Lapkuntod J, Tantilertcharoen R, Thanawongnuwech R,
Suradhat S, et al. Influenza virus (H5N1) in live bird markets and food markets, Thailand. Emerg Infect Dis. 2008;14(11):1739-1742.
2. Cardona C, Yee K, Carpenter T. Are live bird markets reservoirs of avian influenza? Poult Sci. 2009;88(4):856-859. 3. Choi YK, Seo SH, Kim JA, Webster RG. Avian influenza viruses in Korean live poultry markets and their pathogenic potential. J Virol. 2005;332:529-537 4. Globig A, Baumer A, Revilla-Fernandez S, Beer M, Wodak E, Fink M, et al. Ducks as sentinels for avian influenza in wild birds. Emerg Infect Dis. 2009;15(10):1633- 1636. 5. Han J, Jin M, Zhang P, Liu J, Wang L, Wen D, et al. Epidemiological link between exposure to poultry and all influenza A (H7N9) confirmed case in Huzhou city, China, March to May 2013. Euro Surveill. 2013;18(20). 6. Jourdain E, Gunnarsson G, Wahlgren J, Margalef NL, Brojer C, Sahlin S, et al. Influenza virus in a natural host, the mallard: experiment infection data. PLoS One. 2010;5(1):e8935 7. Nguyen DC, Uyeki TM, Jadhao S, Maines T, Shaw M, Matsuoka Y, et al. Isolation
and characterization of avian influenza viruses, including highly pathogenic H5N1, from poultry in live bird markets in Hanoi, Vietnam, in 2001. J Virol.
2005;79(7):4201-4212. 8. OIE (World Organisation for Animal Health). Avian Influenza. In: Manual of Diagnostic Tests and Vaccines for Terrestrial Animals. Vol.1. 7th ed. Paris: World Organisation for Animal Health; 2012. p.436-454. 9. Spackman E, Senne DA, Myers TJ, Bulaga LL, Garber LP, Perdue ML, et al. Development of a real-time reverse transcriptase PCR assay for type A influenza virus and the avian H5 and H7 hemagglutinin subtypes. J Clin Microbiol. 2002; 40(9):3256–3260. 10. Wisedchanwet T, Wongphatcharachai M, Boonyapisitsopa S, Bunpapong N,
Jairak W, Kitikoon P, et al. Influenza A surveillance in live-bird markets: First report of influenza A virus subtype H4N6, H4N9, and H10N3 in Thailand. Avian Dis. 2011;55(4):593-602.
11. Yu H, Feng Z, Zhang X, Xiang N, Huai Y, Zhou L, et al. Human influenza A (H5N1) cases, urban areas of People's Republic of China, 2005-2006. Emerg Infect Dis. 2007;13(7):1061-1064.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 161
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health162
In Vitro Screening of Lactic Acid Bacteria Isolated from Muscovy Duck Ceca for Their Potentially Probiotic Properties
Chuchat Kamollerd1* Preeyaporn Surachon1 Panchompoo Maunglai1
Wilailak Siripornadulsil2 and Peerapol Sukon1,3 1Department of Anatomy, Faculty of Veterinary Medicine, 2Department of Microbiology,
Faculty of Science, 3Research Group for Preventive Technology in Livestock, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Lactic acid bacteria (LAB) are the most common types of microbes as probiotics and remain under extensive investigations.
Objective - To select, by in vitro screening, the LAB strains isolated from Muscovy duck ceca for their potentially probiotic properties.
Materials and methods - The cecal contents were collected aseptically from 5 healthy adult Muscovy ducks and then were grown in de Man Rogosa and Sharpe broth. For the first step of screening, the bacterial colonies were randomly selected, purified, and tested for LAB properties by gram staining, morphology and catalase tests.
Results - Fifty LAB isolates were selected. For the second step of screening, 50 selected isolates were tested for growth inhibition against Salmonella Enteritidis by using agar well diffusion method. Of these 50 isolates, 11 isolates showing the inhibition zone of 10 millimeters or greater were chosen for further screening. For the third step of screening, the 11 selected isolates were tested for acid resistance at pH 2.5 and 3.0. Of 11 isolates, the result showed that the MD5-2 isolate was well tolerated from such tests. The MD5-2 isolate was tested further for growth inhibition against S. Enteritidis by co-culture technique for 2, 4, 6 and 24 hours. The result showed that this isolate was able to survive. When the MD5-2 isolate was tested for antibiotic sensitivity, it was susceptible to penicillin and nitrofurantoin. This isolate was identified by full 16S rDNA sequencing method and it was found that this bacteria was Lactobacillus reuteri. Therefore, this bacterial strain was called as Lactobacillus reuteri MD5-2.
Conclusion - This study indicated that Lactobacillus reuteri MD5-2 may be potentially probiotic strain for further in vivo investigation.
Keywords: Muscovy ducks, Probiotics, Lactic acid bacteria (LAB), Lactobacillus reuteri, Salmonella Enteritidis

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 163
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health164
Effects of Galangal (Alpinia galanga) Ethanolic Extracts against Caecal Coccidiosis caused by Eimeria tenella in Broilers
Somphanh Bounyavong1 Somboon Sangmaneedet2 Gun Rungpiriyadej3 Supitcha Settavakin3 Napat Hirunsirapat3 Weerapol Taweenan2
Peerapol Sukon4 and Jareerat Aimsaard5
1Graduate Student, 2Department of Pathobiology, 3Undergraduate Student, 4Department of Anatomy, 5Department of Pharmacology and Toxicology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. * Corresponding author E-mail address: [email protected]
Objective - To evaluate the anticoccidial efficacy of galangal (Alpinia galanga) ethanolic extracts against caecal coccidiosis caused by Eimeria tenella in broilers. Materials and Methods - One hundred 20 days old broilers (Ross 308), mixed sexes, were randomly assigned into 5 treatment groups (n = 20/group) as positive control (I), galangal ethanolic extracts at 25 (II), 50 (III), 75 (IV) mg/kg body weight and 25 ppm Toltrazuril (V). Broilers in all groups were orally inoculated with 25,000 of E. tenella sporulated oocysts at 20 days old; the body weight gain and caecal lesion scores parameters were assessed. Results - Galangal ethanolic extract was effective against E. tenella infection. Concentrations of 50 and 75 mg/kg per day in 3 consecutive days can significantly (p<0.05) increase average daily gain when compared to positive control. Once infected, it took 5 days for the animals to show clinical signs of mild depression, brown loose faeces and decrease caecal lesion scored in comparison to infected control group. However, the lowest average caecal lesion score was found in chickens treated with Toltrazuril. Conclusion - The study demonstrates that extract of A. galanga could improve weight gain and have a tendency to diminish the severity in caecum of broilers infected with E. tenella. It is suggested that the maximum potential of galangal in medicine and pharmaceutical applications should be explored in further research. Keywords: Caecal coccidiosis, Eimeria tenella, Alpiania galanga, Ethanolic extract, Broiler
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 165
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health166
Effect and Concentration of Roselle (Hibiscus sabdariffa) Calyces Extract on Blood Glucose, Insulin, Triglyceride and Cholesterol Levels
in Induced Hyperglycemic Cats
Ranee Singh1*
Department of Pharmacology and Toxicology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author e-mail: [email protected]
Objectives - [1] To determine the minimal concentration of roselle extract that has efficiency in lowering blood glucose, insulin, triglyceride and cholesterol in hyperglycemic cats, and [2] To compare blood glucose, triglyceride, cholesterol and blood urea nitrogen (BUN) between animals with and without roselle (Hibiscus sabdariffa) extract feeding.
Materials and Methods - Fifteen non-obese, mixed-breed, adult, and clinically healthy cats were used in this study. Following consumption of a controlled diet for 2 weeks, venous blood was collected to determine the baseline of blood glucose. Then cats were randomly separated into 5 groups. Each group had 3 cats. Group 1 received a controlled diet throughout the experiment. Groups 2-5 received high carbohydrate diets (carbohydrate 51% ME) for 2 weeks to induce hyperglycemia. After that, group 2 continued to receive a high carbohydrate diet for 5 weeks while groups 3 and 4 received a high carbohydrate diet with a roselle dosages of 0.1 or 1g/kg BW/day and group 5 a carbose (alpha glucosidase inhibitor) of 25 mg/cat once daily. An intravenous glucose tolerance test (IVGTT) was performed after the 4th week in all groups and fasting blood glucose (FBG) levels were collected to measure triglycerides, cholesterol and BUN. Then blood sample were collected over 24 hours at -5 min, 30 min, 1, 2, 3, 4, 6, 8, 11, 14, 18 and 24 hr in the 5th week. The glucose and insulin values were used to calculate HOMA-IR and HOMA-β (%). The values of blood glucose from the IVGTT and 24 hr test were used to calculate area under the curve (AUC) to compare groups.
Results - The IVGTT tests showed the AUC glucose between cats that received control diets were significantly lower than those receiving the high carbohydrate diets (p<0.05). Similarly, the AUC glucose levels of groups 3 and 4 were significantly lower than group 2 (180.6±25.8, 178.5±10.9 and 270.1±19.1). For the results of glucose from the 24 hours test, the AUC glucose of group 1 was significantly (p<0.05) lower than the AUC glucose of group 2. The AUC glucose was significantly different between groups 2 and 5 (p<0.05). From the results of the HOMA-IR, group 1 (0.1±0.0) was significantly lower than group 2 (0.44±0.08) whereas the results of HOMA- β (%) showed groups 1, 3 and group 5 were 0.27±0.04, 0.13±0.02 and 0.22±0.0 were significantly lower (p<0.05) than group 2 (0.82±0.22). In addition, there was a trend for roselle extract to have a lowering effect on cholesterol, triglyceride and BUN levels when compared to group 2.
Conclusion - The results indicated that the roselle can reduce blood glucose in hyperglycemic cats by reducing insulin resistance. H. sabdariffa extract may be used as alternative medicine in type 2- diabetic cats.
Keywords: Roselle, Triglyceride, Cholesterol, Blood glucose, Insulin resistance

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 167
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health168
Dose-comparison Trial of Praziquantel against Feline Opisthorchiasis in Human Endemic Areas
Piya Sereerak1 Sirikachorn Tangkawattana2,3,4* Banchob Sripa3,4*
1Graduate Student, Department of Medicine, 2Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002,Thailand.
3WHO Collaborating Centre for Research and Control of Opisthorchiasis (Southeast Asian Liver Fluke Disease), Tropical Disease Research Laboratory, Department of Pathology,
Faculty of Medicine, 4Liver Fluke and Cholangiocarcinoma Research Center, Khon Kaen University, Khon Kaen 40002, Thailand.
*co-correspondence: [email protected], [email protected]
Background - Opisthorchiasis, caused by Opisthorchis viverrini (O. viverrini) is a major public health problem in Southeast Asia, especially Thailand. Unsuccessful eradication of the disease is probably from the parasite can persistently reside in animal reservoir hosts especially dogs and cats. Praziquantel (PZQ) is the drug of choice for opisthorchiasis control in both humans and animals; however, there has no specific dose for O. viverrini treatment in cats. Objective - To study the effective dose of praziquantel for feline opisthorchiasis. Materials and Methods - Twenty-eight infected male and female cats from endemic areas in Khon Kaen and Mahasarakram provinces were systematically selected and divided into 2 groups. Dose-comparison trial was conducted to determine 2 single doses of PZQ, 25 and 40 mg/kg respectively (n=14 each group). Intensity of infection was determined by formalin-ether concentration technique (FECT) method. Hematology, blood-chemistry and urinalysis were performed to evaluate animal health status. Results - Thirty days after treatment O. viverrini cure rates and egg reduction rates of 25 mg group were 85.71%, 100% and 40 mg group were 98.04% and 100% respectively. Conclusion - Our study suggests that the effective dose of PZQ is 40 mg/kg for feline opisthorchiasis treatment. Keywords: Feline opisthorchiasis, Praziquantel, Dose, Cure rate, Egg reduction rate
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 169
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health170
Detection of Babesia, Ehrlichia and Hepatozoon in Domestic Dogs Using Microscopy Examination and PCR Techniques in
Prakou Villages Phalub District, Khon Kaen
Threetip Mityodwong1 Prapasara Potchimplee1 Parin Khianman1 Somboon Sangmaneedet2* and Thidarut Boonmars3
1Fifth Year Veterinary Student, 2Department of Pathobiology, Faculty of Veterinary Medicine, 3Department of Parasitology, Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Objective - To determine the prevalence of tick-borne pathogens in domestic dogs by microscopy and PCR techniques. Materials and Methods - A total of 103 EDTA blood samples were collected from domestic dogs in Khon Kaen province, Thailand, in March 2013. Microscopic observation using Giemsa staining and molecular diagnosis using conventional polymerase chain reaction (PCR) were performed. Results - Thirty-nine (37.86%) out of 103 dogs were positive for DNA of tick-borne pathogens. Of the 103 animals, 33.98% was positive for a single infection with Babesia spp., using microscopy; whereas 36.89% was positive using PCR technique. Co-infection with Babesia spp. and E. canis was observed in 0.97%. Conclusion - Both microscopic and PCR diagnostic techniques were useful for tick-borne pathogen detection. PCR was more effective. The present study suggests that diagnosis by PCR technique has high sensitivity and specificity for Babesia spp. and Ehrlichia spp. and for detection of DNA of Babesia spp., E. canis and H. canis from EDTA blood specimens.
Keywords: Ticks, Blood parasite, Babesia, Hepatozoon, Ehrlichia, Domestic dogs, Khon Kaen, Thailand

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 171
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health172
Survey of Upper Respiratory Tract of Thoroughbred Racing Horses in Northeastern Thailand using an Endoscope
Tidaratt Sittisak1 Kitima Sinsawat1
Pornchanit Tanticharoenviroj1 and Suphannika Phutthachalee2*
1Fifth Year Veterinary Student, 2Department of Surgery and Theriogenology, Faculty of Veterinary Medicine , Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Objective - Survey of upper respiratory disorders in Thoroughbred racing horses in northeastern part of Thailand. Materials and Methods - Physical examination of racing horses was performed. The owners were asked to get the horses at canter until they panted. Immediately after the canter was finished, the horse was examined using an endoscope. Results - Total number of horses in this survey was 44. Thirty-eight horses (86.36%) had upper respiratory disorders. The disorders were categorized as idiopathic laryngeal hemiplegia (ILH) in 23 horses (60.53%), pharyngeal lymphoid hyperplasia
(PLH) in 18 horses (47.37%), rhinitis in 7 horses (18.42%), pharyngitis in 6 horses (15.79%), dorsal displacement of the soft palate (DDSP) in 4 horses (10.53%), guttural
pouch empyema in 3 horses (7.89%), epiglottic entrapment in 2 horses (5.26%), nasal
polyp in 1 horse (2.63%) and epiglottitis in 1 horse (2.63%). Some horses might have
more than 1 syndrome of the upper respiratory disorders. In addition, age of horses had significant association with PLH (P<0.01). Other factors
such as sex and height did not relate to any of the syndromes (P>0.05). Keywords : Upper respiratory disorders, Racing horses, Endoscope
Introduction Horse racing is a competition of horses’ speed that only horses with healthy respiratory system can have excellent performance. However, morbidity of upper respiratory tract is a common cause to decrease performance of Thoroughbred racing horses world wide [1]. Upper respiratory tract examination is often done by using endoscopy and it should be done before purchasing horses. Three common causes of upper respiratory obstruction syndrome are idiopathic laryngeal hemiplegia (ILH), dorsal displacement of the soft palate (DDSP) and epiglottic entrapment. They affect upper respiratory tract stenosis then ventilation is decreased. Finally horses have exercise intolerance and poor performance [2]. This study detected the previously mentioned syndrome and also phalyngeal lymphoid hyperplasia (PLH), guttural pouch empyema and nasal polyp. The symptoms affect health of horses adversely but the horses usually show no clinical signs. Endoscopy can detect the early stages of abnormalities before the owners can notice [3]. There has never been a report of prevalence of upper respiratory obstruction syndromes in horses in Thailand. So, the objective of this study is to survey the upper respiratory tract disorders in Thoroughbred racing horses in Northeastern Thailand. Material and methods Animals Thoroughbred racing horses regardless of gender and age that came to Khon Kaen University-Veterinary Teaching Hospital and the Horsepital Korat during January to December, 2013 were included in the study. Study design History taking, weighing and height measuring (KRUUSE, Denmark) were performed in every horse before physical examination by veterinarians. The horses were then get to the canter for five minutes or until the horses were tired (increased respiration rate and panting). Immediately, the veterinarian examined the horses using an endoscope’s brand - Pentax EPM-300P, Japan (Figure 2) and recorded the data. Diagnosis of respiratory tract syndromes and grading the severity of ILH and PLH (Table 2 and 3) were done by only one veterinarian.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 173
Introduction Horse racing is a competition of horses’ speed that only horses with healthy respiratory system can have excellent performance. However, morbidity of upper respiratory tract is a common cause to decrease performance of Thoroughbred racing horses world wide [1]. Upper respiratory tract examination is often done by using endoscopy and it should be done before purchasing horses. Three common causes of upper respiratory obstruction syndrome are idiopathic laryngeal hemiplegia (ILH), dorsal displacement of the soft palate (DDSP) and epiglottic entrapment. They affect upper respiratory tract stenosis then ventilation is decreased. Finally horses have exercise intolerance and poor performance [2]. This study detected the previously mentioned syndrome and also phalyngeal lymphoid hyperplasia (PLH), guttural pouch empyema and nasal polyp. The symptoms affect health of horses adversely but the horses usually show no clinical signs. Endoscopy can detect the early stages of abnormalities before the owners can notice [3]. There has never been a report of prevalence of upper respiratory obstruction syndromes in horses in Thailand. So, the objective of this study is to survey the upper respiratory tract disorders in Thoroughbred racing horses in Northeastern Thailand. Material and methods Animals Thoroughbred racing horses regardless of gender and age that came to Khon Kaen University-Veterinary Teaching Hospital and the Horsepital Korat during January to December, 2013 were included in the study. Study design History taking, weighing and height measuring (KRUUSE, Denmark) were performed in every horse before physical examination by veterinarians. The horses were then get to the canter for five minutes or until the horses were tired (increased respiration rate and panting). Immediately, the veterinarian examined the horses using an endoscope’s brand - Pentax EPM-300P, Japan (Figure 2) and recorded the data. Diagnosis of respiratory tract syndromes and grading the severity of ILH and PLH (Table 2 and 3) were done by only one veterinarian.
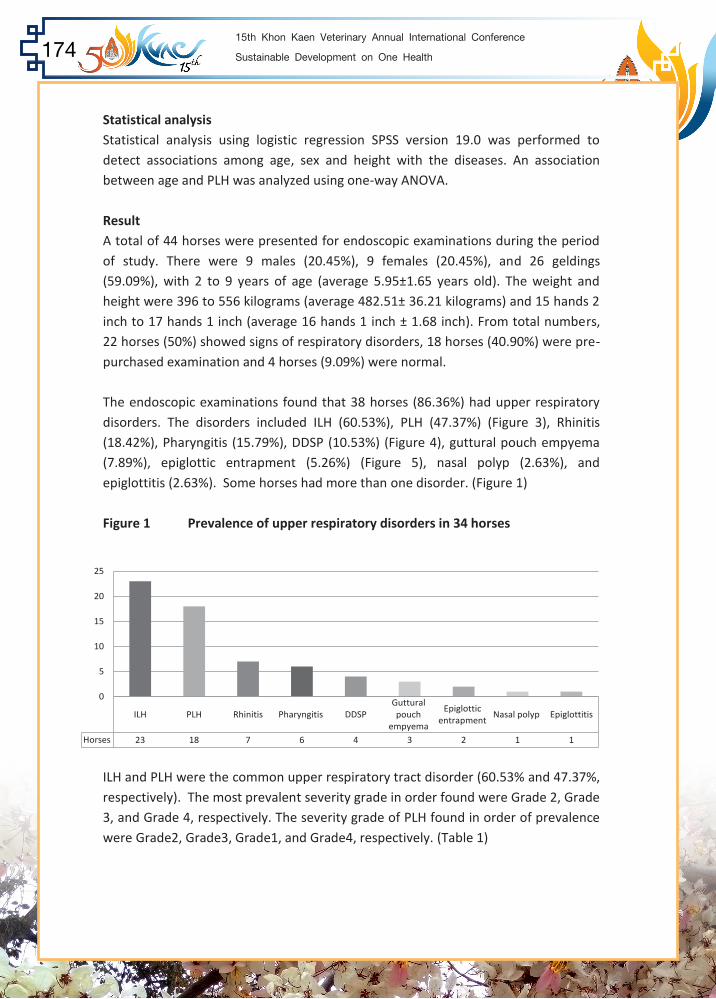
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health174
Statistical analysis Statistical analysis using logistic regression SPSS version 19.0 was performed to detect associations among age, sex and height with the diseases. An association between age and PLH was analyzed using one-way ANOVA. Result A total of 44 horses were presented for endoscopic examinations during the period of study. There were 9 males (20.45%), 9 females (20.45%), and 26 geldings (59.09%), with 2 to 9 years of age (average 5.95±1.65 years old). The weight and height were 396 to 556 kilograms (average 482.51± 36.21 kilograms) and 15 hands 2 inch to 17 hands 1 inch (average 16 hands 1 inch ± 1.68 inch). From total numbers, 22 horses (50%) showed signs of respiratory disorders, 18 horses (40.90%) were pre-purchased examination and 4 horses (9.09%) were normal. The endoscopic examinations found that 38 horses (86.36%) had upper respiratory disorders. The disorders included ILH (60.53%), PLH (47.37%) (Figure 3), Rhinitis (18.42%), Pharyngitis (15.79%), DDSP (10.53%) (Figure 4), guttural pouch empyema (7.89%), epiglottic entrapment (5.26%) (Figure 5), nasal polyp (2.63%), and epiglottitis (2.63%). Some horses had more than one disorder. (Figure 1)
Figure 1 Prevalence of upper respiratory disorders in 34 horses
ILH and PLH were the common upper respiratory tract disorder (60.53% and 47.37%, respectively). The most prevalent severity grade in order found were Grade 2, Grade 3, and Grade 4, respectively. The severity grade of PLH found in order of prevalence were Grade2, Grade3, Grade1, and Grade4, respectively. (Table 1)
ILH PLH Rhinitis Pharyngitis DDSPGuttural pouch
empyema
Epiglottic entrapment
Nasal polyp Epiglottitis
Horses 23 18 7 6 4 3 2 1 1
0
5
10
15
20
25
Table 1 Number of horses by grade of Left laryngeal hemiplegia and Pharyngeal lymphoid hyperplasia
Disease Severity Number %
Left laryngeal hemiplegia
(23 Horses)
Grade 2
Grade 3
Grade 4
13
7
3
56.52
30.43
13.04
Pharyngeal lymphoid
hyperplasia
(18 Horse)
Grade 1
Grade 2
Grade 3
Grade 4
1
9
7
1
5.56
50.00
38.89
5.56
The analysis of relationship among the factors (age, sex, height and weight) showed no statistical correlation with the occurrence of upper airway obstruction syndrome (P>0.05). However, we found that age was associated with PLH (P<0.01). The younger horses showed PLH more common than the older horses. The mean age of horses with PLH was between 3 to 4 years. Discussion The result found that prevalence of ILH was 60.53% ; which was consistent with the study of Pothiappan et al., 2011 [3], but was inconsistent with the study of Brown et al.,2005 that found a less prevalence [7]. This may be due to difference of location because Brown et al., 2005 [7] examined Thoroughbred racehorses in Australia, where the standard of competition is higher than Thailand. In this study, the horses with ILH were affected only at the left side of arythenoid cartilage (Left laryngeal hemiplegia) which was consistent with Pothiappan et al., 2011 [3] and Brown et al., 2005 [7]. The left arytenoid cartilage is the most common side affected (up to 95%) [8]. Laryngeal hemiplegia was observed in horses 3 to 8 years of age (average 6.29±1.45 years old) in this study. Kannegieter and Dore, 1995 reported that horses in the age range of 2 to 7 years old were commonly affected [9]. While Dixon et al., 2002 reported that the age range of 2 to 15 years old was common [10]. The analysis of the relationship among factors (age, sex, height and weight) showed no statistical correlation with the occurrence of upper airway obstruction syndrome (P> 0.05). This was consistent with the study of Anderson et al., 1997. Which reported that age and sex were not correlated with ILH [11]. Brakenhoff et al., 2006 reported that age,
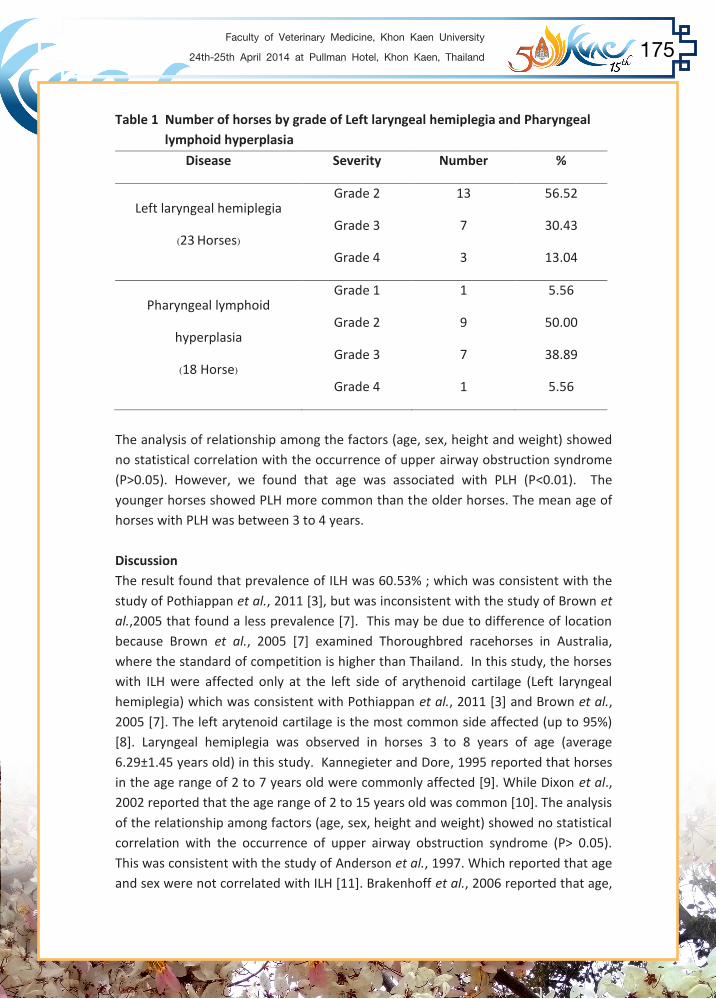
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 175
Table 1 Number of horses by grade of Left laryngeal hemiplegia and Pharyngeal lymphoid hyperplasia
Disease Severity Number %
Left laryngeal hemiplegia
(23 Horses)
Grade 2
Grade 3
Grade 4
13
7
3
56.52
30.43
13.04
Pharyngeal lymphoid
hyperplasia
(18 Horse)
Grade 1
Grade 2
Grade 3
Grade 4
1
9
7
1
5.56
50.00
38.89
5.56
The analysis of relationship among the factors (age, sex, height and weight) showed no statistical correlation with the occurrence of upper airway obstruction syndrome (P>0.05). However, we found that age was associated with PLH (P<0.01). The younger horses showed PLH more common than the older horses. The mean age of horses with PLH was between 3 to 4 years. Discussion The result found that prevalence of ILH was 60.53% ; which was consistent with the study of Pothiappan et al., 2011 [3], but was inconsistent with the study of Brown et al.,2005 that found a less prevalence [7]. This may be due to difference of location because Brown et al., 2005 [7] examined Thoroughbred racehorses in Australia, where the standard of competition is higher than Thailand. In this study, the horses with ILH were affected only at the left side of arythenoid cartilage (Left laryngeal hemiplegia) which was consistent with Pothiappan et al., 2011 [3] and Brown et al., 2005 [7]. The left arytenoid cartilage is the most common side affected (up to 95%) [8]. Laryngeal hemiplegia was observed in horses 3 to 8 years of age (average 6.29±1.45 years old) in this study. Kannegieter and Dore, 1995 reported that horses in the age range of 2 to 7 years old were commonly affected [9]. While Dixon et al., 2002 reported that the age range of 2 to 15 years old was common [10]. The analysis of the relationship among factors (age, sex, height and weight) showed no statistical correlation with the occurrence of upper airway obstruction syndrome (P> 0.05). This was consistent with the study of Anderson et al., 1997. Which reported that age and sex were not correlated with ILH [11]. Brakenhoff et al., 2006 reported that age,

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health176
weight, and sex were not correlated with ILH [12]. However, this was inconsistent with the study of Pothiappan et al., 2011 which discovered that male horses were at higher risk than female horses [3]. PLH tends to affect racing horses 2 to 3 years of age [13]. This study found that affected horses aged 2 to 8 years old with the mean age at 4.94±1.73 years. It might due to a long transportation that affected horses in this study. Younger age of horses was significantly (P<0.01) associated with this syndrome. The mean age of the horses in young group was 4.94±0.36 years old. It was reported that more virulent, symptoms was more prevalent in younger horses [14]. Rhinitis and pharyngitis were affected in horses 3 to 8 years of age, the mean age was 6.15±1.68 years. The diseases usually were found with others syndromes especially horses that had long transportation. Five horses form 11 horses (45.45%) had rhinitis or pharyngitis that had a long trip before. DDSP was found in 4 horses (12.12%), which was consistent with Pothiappan et al.,
2011 that found DDSP at 10% [3]. The horses were 2 to 8 years of age, the mean was 6±2.71 years. Parente et al., 2002 reported that DDSP was found in horses 3 to 4 years old [15]. The horses had respiratory noise and exercise intolerance which agreed with the study of Dorothy M. Ainsworth, 2014 [16]. Guttural pouch empyema was detected mostly in young horses [17]. This study was found the disorder in 6 to 7 years old horses. Epiglottic entrapment was found in 2 horses. Long time of epiglottic entrapment might cause ulcer of epiglottis [18]. In this study, 2 horses had ulcer of epiglottis and epiglottic entrapment. Nasal polyp and epiglottitis were uncommon and were detected in only 1 horse for each syndrome. This report shows trend of upper respiratory syndromes in thoroughbred racing horses that live in northeastern part of Thailand. The owners should aware of importance of racing horses’ respiratory examination before selection of the horses for racing. Acknowledgements The authors gratefully acknowledge the extensive support of Khon Kaen University-Veterinary Teaching Hospital, The Horsepital Korat and participating trainers and owners.
References 1. Holcombe S. and Ducharme N. Abnormality of the upper airway. In. Equine. Sports Med Sur. 2004;559-598 2. Davenport-Goodall CLM and Parente E.J. . Disorders of the larynx. Vet Clin N Am Equine Practice. 2003;19:169-187. 3. Pothiappan P. et al. Incidence of upper respiratory affections associated poor performance in horses. Tamilnadu J Vet Anim Sci. 2011;7(3):123-125. 4. Parente EJ. Treatment and Prognosis for laryngeal hemiplegia. Kennett .
University of Pennsylvania [internet]. 2011 [updated 2011; cited 2013 Jul 12] Available from:
http://www.fvmace.org/49th_Ocala_Equine_Conference/Laryngeal%20hemi plegia.html. 5. Rakestraw P. et al. Arythenoid cartilage movement in resting and exercising
horses. Vet Sur. 1991;20:3-17. 6. Baker GJ. Diseases of pharynx and larynx. In : Robinson NE. Current therapy in equine medicine. : Saunders; 1987 p.607-612. 7. Brown JA. et al. Prevalence of pharyngeal and laryngeal abnormalities in Thoroughbreds racing in Australia, and their association with performance. Equine Vet J. 2005;37(5): 397-401. 8. American college of veterinary surgeons . Laryngeal Hemiplegia in Horses.
American college of veterinary surgeons [internet]. 2013 [updated 2013; cited 2013 Jul 13]; Available from:
https://www.acvs.org/large-animal/laryngeal-hemiplegia. 9. Kannegieter NJ. And Dore ML. Endoscopy of the upper respiratory tract during
track during treadmill exercises a clinical study of 100 horses. Aust Vet J., 1995;72: 101-107.
10. Dixon PM. et al. Clinical and endoscopic evidence of progression in 152 cases of equine recurrent laryngeal neuropathy (RLN). Equine Vet J., 2002;34: 29-34. 11. Anderson BH., Kannegieter NJ. and Goulden BE. Endoscopic observations on laryngeal symmetry and movements in young racing horses. New Zeal Vet J.,
1997;45(5): 188-192. 12. Brakenhoff JE et al. Prevalence of Laryngeal Disease in a Large Population of Competition Draft Horses. AAEP PROCEEDINGS . 2006;52:318-319. 13. Gore T., Gore P. and Giffin JM. Pharyngeal lymphoid hyperplasia. Horses owner’s veterinary handbook 3rd edition : Hoboken, New Jersey; 2008 p.297. 14. Saulez MN. and Gummow B. Prevalence of pharyngeal, laryngeal and tracheal disorders in thoroughbred racehorses, and effect on performance. Vet Rec.
2009;165: 431-435.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 177
References 1. Holcombe S. and Ducharme N. Abnormality of the upper airway. In. Equine. Sports Med Sur. 2004;559-598 2. Davenport-Goodall CLM and Parente E.J. . Disorders of the larynx. Vet Clin N Am Equine Practice. 2003;19:169-187. 3. Pothiappan P. et al. Incidence of upper respiratory affections associated poor performance in horses. Tamilnadu J Vet Anim Sci. 2011;7(3):123-125. 4. Parente EJ. Treatment and Prognosis for laryngeal hemiplegia. Kennett .
University of Pennsylvania [internet]. 2011 [updated 2011; cited 2013 Jul 12] Available from:
http://www.fvmace.org/49th_Ocala_Equine_Conference/Laryngeal%20hemi plegia.html. 5. Rakestraw P. et al. Arythenoid cartilage movement in resting and exercising
horses. Vet Sur. 1991;20:3-17. 6. Baker GJ. Diseases of pharynx and larynx. In : Robinson NE. Current therapy in equine medicine. : Saunders; 1987 p.607-612. 7. Brown JA. et al. Prevalence of pharyngeal and laryngeal abnormalities in Thoroughbreds racing in Australia, and their association with performance. Equine Vet J. 2005;37(5): 397-401. 8. American college of veterinary surgeons . Laryngeal Hemiplegia in Horses.
American college of veterinary surgeons [internet]. 2013 [updated 2013; cited 2013 Jul 13]; Available from:
https://www.acvs.org/large-animal/laryngeal-hemiplegia. 9. Kannegieter NJ. And Dore ML. Endoscopy of the upper respiratory tract during
track during treadmill exercises a clinical study of 100 horses. Aust Vet J., 1995;72: 101-107.
10. Dixon PM. et al. Clinical and endoscopic evidence of progression in 152 cases of equine recurrent laryngeal neuropathy (RLN). Equine Vet J., 2002;34: 29-34. 11. Anderson BH., Kannegieter NJ. and Goulden BE. Endoscopic observations on laryngeal symmetry and movements in young racing horses. New Zeal Vet J.,
1997;45(5): 188-192. 12. Brakenhoff JE et al. Prevalence of Laryngeal Disease in a Large Population of Competition Draft Horses. AAEP PROCEEDINGS . 2006;52:318-319. 13. Gore T., Gore P. and Giffin JM. Pharyngeal lymphoid hyperplasia. Horses owner’s veterinary handbook 3rd edition : Hoboken, New Jersey; 2008 p.297. 14. Saulez MN. and Gummow B. Prevalence of pharyngeal, laryngeal and tracheal disorders in thoroughbred racehorses, and effect on performance. Vet Rec.
2009;165: 431-435.
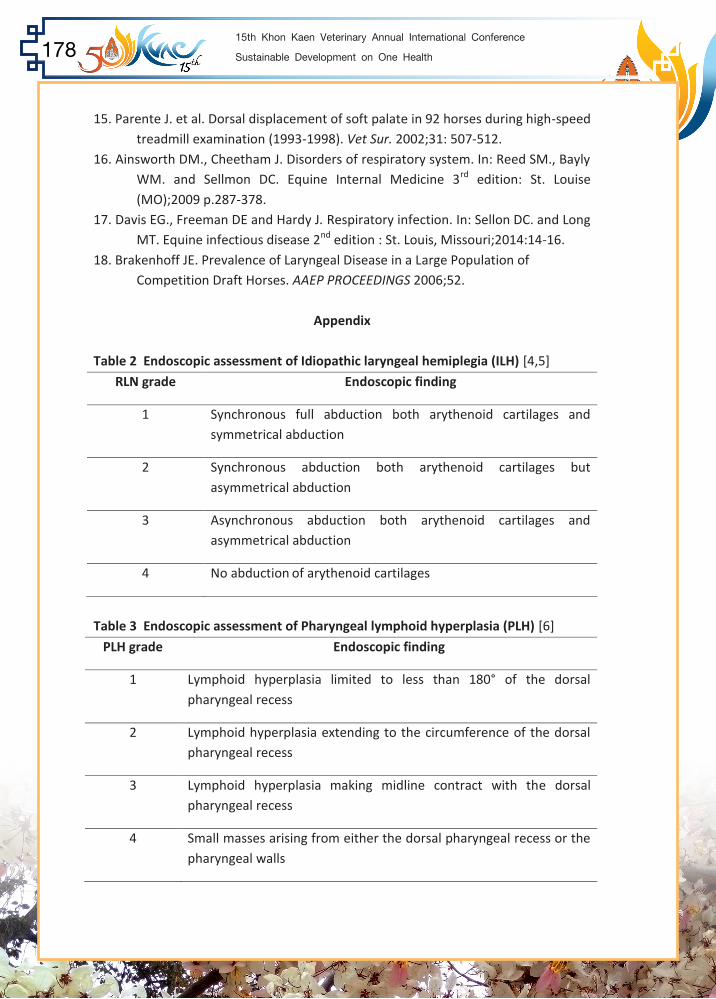
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health178
15. Parente J. et al. Dorsal displacement of soft palate in 92 horses during high-speed treadmill examination (1993-1998). Vet Sur. 2002;31: 507-512. 16. Ainsworth DM., Cheetham J. Disorders of respiratory system. In: Reed SM., Bayly WM. and Sellmon DC. Equine Internal Medicine 3rd edition: St. Louise (MO);2009 p.287-378. 17. Davis EG., Freeman DE and Hardy J. Respiratory infection. In: Sellon DC. and Long MT. Equine infectious disease 2nd edition : St. Louis, Missouri;2014:14-16. 18. Brakenhoff JE. Prevalence of Laryngeal Disease in a Large Population of
Competition Draft Horses. AAEP PROCEEDINGS 2006;52.
Appendix Table 2 Endoscopic assessment of Idiopathic laryngeal hemiplegia (ILH) [4,5]
RLN grade Endoscopic finding
1 Synchronous full abduction both arythenoid cartilages and symmetrical abduction
2 Synchronous abduction both arythenoid cartilages but asymmetrical abduction
3 Asynchronous abduction both arythenoid cartilages and asymmetrical abduction
4 No abduction of arythenoid cartilages
Table 3 Endoscopic assessment of Pharyngeal lymphoid hyperplasia (PLH) [6]
PLH grade Endoscopic finding
1 Lymphoid hyperplasia limited to less than 180° of the dorsal pharyngeal recess
2 Lymphoid hyperplasia extending to the circumference of the dorsal pharyngeal recess
3 Lymphoid hyperplasia making midline contract with the dorsal pharyngeal recess
4 Small masses arising from either the dorsal pharyngeal recess or the pharyngeal walls
Figure 2 Endoscopic examination
Figure 3 Grade 2 of idiopathic laryngeal hemiplegia with grade 2 of pharyngeal lymphoid hyperplasia

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 179
Figure 2 Endoscopic examination
Figure 3 Grade 2 of idiopathic laryngeal hemiplegia with grade 2 of pharyngeal lymphoid hyperplasia

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health180
Figure 4 Dorsal displacement of the soft palate (DDSP)
Figure 5 Epiglottic entrapment with ulcer at aryepiglootic fold

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 181
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health182

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 183
Poster Presentation

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health184
Efficacy of Betel Vine Extract against Staphylococcus aureus Causing Bovine Mastitis
Karnsuda Wijitphan1 Phimda Khotbanthao1
Phaphatsanant Phongsarmsuan1 and Jareerat Aimsaard2* 1Fifth Year Veterinary Student, 2Department of Pharmacology and Toxicology,
Faculty of Veterinary Medicine, KhonKaen University, Khon Kaen 40002, Thailand. *Corresponding author
Objective - To detetmine the efficacy of betel vine extract against Stapphylococcus aureus causing bovine mastitis Materials and Methods - Herbal used in this study was betel vine (Piper betle L.). Betel vine leaves were extracted with 95% ethanol. The tested organisms were 15 samples of Staphylococcus aureus isolated from bovine mastitis and 1 S. aureus DMST 12853. The antibacterial evaluation using disk diffusion and broth microdilution, Gentamicin serves as positive control. Statistical analysis of results was performed by one way analysis of variance (ANOVA) with significance at p value < 0.05. Results - The study revealed that the inhibition zone of 15% betel vine ethanolic extract was 16.0 millimeters, which had no significant difference with positive control (p>0.05). The minimum inhibitory concentration (MIC) and minimum bactericidal inhibition (MBC) of betel vine extract were 0.31%, while the MIC and MBC of gentamicin were 0.00625 and 0.025%, respectively. Conclusion - 15% betel vine ethanolic extract showed the sensitivity to S. aureus causing bovine mastitis. In this study, The MIC and MBC of betel vine ethanolic extract determined less potent antimicrobial agents than the positive control (gentamicin), however the extract was shown to be bacteriostatic at low concentration. Keywords: Crude extract, Betel vine, Bovine mastits, Staphylococcus aureus

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 185
Efficacy of Betel Vine Extract against Staphylococcus aureus Causing Bovine Mastitis
Karnsuda Wijitphan1 Phimda Khotbanthao1
Phaphatsanant Phongsarmsuan1 and Jareerat Aimsaard2* 1Fifth Year Veterinary Student, 2Department of Pharmacology and Toxicology,
Faculty of Veterinary Medicine, KhonKaen University, Khon Kaen 40002, Thailand. *Corresponding author
Objective - To detetmine the efficacy of betel vine extract against Stapphylococcus aureus causing bovine mastitis Materials and Methods - Herbal used in this study was betel vine (Piper betle L.). Betel vine leaves were extracted with 95% ethanol. The tested organisms were 15 samples of Staphylococcus aureus isolated from bovine mastitis and 1 S. aureus DMST 12853. The antibacterial evaluation using disk diffusion and broth microdilution, Gentamicin serves as positive control. Statistical analysis of results was performed by one way analysis of variance (ANOVA) with significance at p value < 0.05. Results - The study revealed that the inhibition zone of 15% betel vine ethanolic extract was 16.0 millimeters, which had no significant difference with positive control (p>0.05). The minimum inhibitory concentration (MIC) and minimum bactericidal inhibition (MBC) of betel vine extract were 0.31%, while the MIC and MBC of gentamicin were 0.00625 and 0.025%, respectively. Conclusion - 15% betel vine ethanolic extract showed the sensitivity to S. aureus causing bovine mastitis. In this study, The MIC and MBC of betel vine ethanolic extract determined less potent antimicrobial agents than the positive control (gentamicin), however the extract was shown to be bacteriostatic at low concentration. Keywords: Crude extract, Betel vine, Bovine mastits, Staphylococcus aureus

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health186
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
The Effects of Aflatoxin B1 and Yeast (Saccharomyces cerevisiae) Supplementation in Dairy Cow Feed on Rumen Fermentation
by In itro Gas Production Technique
Piroonporn Dechma1 Supaporn Saeteaw1 Natcha Monchaivanakit1 Chittraporn Yeanpet2 and Chaiyapas Thamrongyoswittayakul3*
1Fifth Year Veterinary Student, 2Graduate Student, 3Department of Medicine, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author E-mail: [email protected]
Introduction - Contamination of aflatoxin B1 in dairy cow feed has become a major concern for nutritional management and can be easily occur during improper processes, particularly in high humidity storage. Therefore, strategies have been investigated to remove aflatoxin B1 from dairy feedstuffs. Apparently, the biological aspect is considered as one of the most promising approaches for aflatoxin B1 control using yeast (Saccharomyces cerevisiae).
Objective - To determine the effect of aflatoxin B1 and/or the yeast supplementation in dairy cow feed on rumen fermentation and rumen ecology using in vitro gas production technique.
Materials and methods - The experiment was designed in 2×3 factorial in a completely randomized design with 2 factors. Factor A was aflatoxin B1 at 0, 200 ppb and factor B was the yeast at 0, 2, 4 g/kg of feed.
Results - The highest gas production was found in the yeast supplementation at 4 g/kg of feed. In contrast, the gas production was lowest in feed containing 200-ppb aflatoxin B1. However, aflatoxin B1 and the yeast had an irrelevant effect on gas production in rumen fluid. Total gas production was directly associated with the rumen microbial population. After a 4 h incubation, the bacterial population in feed with 200-ppb aflatoxin B1 was lower than in feed without aflatoxin B1 (p<0.05). In addition, bacterial and protozoa population were highest in feed supplemented with the yeast at 4 g/kg (p<0.05) at 4 h incubation. However, aflatoxin B1 had no effect on protozoa population in yeast-supplemented feed at 4 g/kg (p<0.05).
Conclusion - Aflatoxin B1 in dairy cow feed had negative effect on rumen fermentation while the yeast supplementation in feed improved rumen fermentation and rumen ecology. Keywords: Aflatoxin B1, Yeast, Rumen fermentation, in vitro gas production, Feed, Dairy cow
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 187
The Effects of Aflatoxin B1 and Yeast (Saccharomyces cerevisiae) Supplementation in Dairy Cow Feed on Rumen Fermentation
by In itro Gas Production Technique
Piroonporn Dechma1 Supaporn Saeteaw1 Natcha Monchaivanakit1 Chittraporn Yeanpet2 and Chaiyapas Thamrongyoswittayakul3*
1Fifth Year Veterinary Student, 2Graduate Student, 3Department of Medicine, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author E-mail: [email protected]
Introduction - Contamination of aflatoxin B1 in dairy cow feed has become a major concern for nutritional management and can be easily occur during improper processes, particularly in high humidity storage. Therefore, strategies have been investigated to remove aflatoxin B1 from dairy feedstuffs. Apparently, the biological aspect is considered as one of the most promising approaches for aflatoxin B1 control using yeast (Saccharomyces cerevisiae).
Objective - To determine the effect of aflatoxin B1 and/or the yeast supplementation in dairy cow feed on rumen fermentation and rumen ecology using in vitro gas production technique.
Materials and methods - The experiment was designed in 2×3 factorial in a completely randomized design with 2 factors. Factor A was aflatoxin B1 at 0, 200 ppb and factor B was the yeast at 0, 2, 4 g/kg of feed.
Results - The highest gas production was found in the yeast supplementation at 4 g/kg of feed. In contrast, the gas production was lowest in feed containing 200-ppb aflatoxin B1. However, aflatoxin B1 and the yeast had an irrelevant effect on gas production in rumen fluid. Total gas production was directly associated with the rumen microbial population. After a 4 h incubation, the bacterial population in feed with 200-ppb aflatoxin B1 was lower than in feed without aflatoxin B1 (p<0.05). In addition, bacterial and protozoa population were highest in feed supplemented with the yeast at 4 g/kg (p<0.05) at 4 h incubation. However, aflatoxin B1 had no effect on protozoa population in yeast-supplemented feed at 4 g/kg (p<0.05).
Conclusion - Aflatoxin B1 in dairy cow feed had negative effect on rumen fermentation while the yeast supplementation in feed improved rumen fermentation and rumen ecology. Keywords: Aflatoxin B1, Yeast, Rumen fermentation, in vitro gas production, Feed, Dairy cow

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health188
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Effect of Different Levels of Rubber Seed Kernel in Total Mixed Ration for Dairy Cow on in vitro Fermentation using Gas Production Technique
Nawarat Pha-obnga1 Chalong Wachirapakorn2 and Suneerat Aiumlamai3*
1Graduate Student of Ph.D.Program in Interdisciplinary Veterinary Science, 2Department of Animal Science, Faculty of Agriculture, 3Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Rubber seed as a waste product from rubber plantation contains a rich source of fat, especially linoleic and linolenic acids that have positively influenced on reproductive performance in dairy cows. However, there is no record of the rubber seed kernel (RSK) usage in dairy cow rations.
Objective - To determine the fermentation characteristics of total mixed ration (TMR) containing different levels of rubber seed kernel (RSK) using a gas production technique.
Materials and Methods - Rubber seeds were shelled and sun dried for 12 days to reduce hydrocyanic acid and used in TMR at 0, 6.8, 13.6, 20.4 and 27.2 %. The experimental dietary treatments were formulated as isonitrogenous with concentrate to roughage (rice straw) ratio at 60:40. Samples were dried and ground to pass a 2-mm sieve. Each serum bottle contained 200 mg of dietary treatment (in triplicate/treatment). Pooled rumen fluid from three dairy cows was used as inoculums. The bottle filled with 30 ml of rumen fluid and buffer was incubated at
39C. In vitro dry matter digestibility (IVDMD), in vitro organic matter digestibility (IVOMD), ammonia nitrogen (NH3-N) and metabolizable energy (ME) were measured. The data were analyzed by analysis of variance in a completely randomized design and Duncan’s new multiple range test (SPSS Statistics, 17.0).
Results - Gas production characteristics were significant differences among treatments (at 96 h, p<0.01). Gas production at 96 h increased with increasing RSK levels from 0 to 13.6 % in TMR which was significantly higher (p<0.01) than the other levels for all measured parameters. IVDMD at 48 h, IVOMD at 24 and 48 h increased linearly (p<0.05) with increasing RSK level from 0 to 13.6 % in TMR while increasing RSK level above 13.6 % resulted in decreased digestibility of DM and OM (p<0.05). NH3-N concentration was significantly different (p<0.05) among dietary treatments at 24 h. However, the ME was decreased as RSK level was increased.
Conclusion - This study indicated that RSK could be used in ranges from 0 to 13.6 % in TMR and suitable to use as feed for dairy cows.
Keywords: Rubber seed kernel, in vitro fermentation, Gas production technique

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 189
Effect of Different Levels of Rubber Seed Kernel in Total Mixed Ration for Dairy Cow on in vitro Fermentation using Gas Production Technique
Nawarat Pha-obnga1 Chalong Wachirapakorn2 and Suneerat Aiumlamai3*
1Graduate Student of Ph.D.Program in Interdisciplinary Veterinary Science, 2Department of Animal Science, Faculty of Agriculture, 3Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Rubber seed as a waste product from rubber plantation contains a rich source of fat, especially linoleic and linolenic acids that have positively influenced on reproductive performance in dairy cows. However, there is no record of the rubber seed kernel (RSK) usage in dairy cow rations.
Objective - To determine the fermentation characteristics of total mixed ration (TMR) containing different levels of rubber seed kernel (RSK) using a gas production technique.
Materials and Methods - Rubber seeds were shelled and sun dried for 12 days to reduce hydrocyanic acid and used in TMR at 0, 6.8, 13.6, 20.4 and 27.2 %. The experimental dietary treatments were formulated as isonitrogenous with concentrate to roughage (rice straw) ratio at 60:40. Samples were dried and ground to pass a 2-mm sieve. Each serum bottle contained 200 mg of dietary treatment (in triplicate/treatment). Pooled rumen fluid from three dairy cows was used as inoculums. The bottle filled with 30 ml of rumen fluid and buffer was incubated at
39C. In vitro dry matter digestibility (IVDMD), in vitro organic matter digestibility (IVOMD), ammonia nitrogen (NH3-N) and metabolizable energy (ME) were measured. The data were analyzed by analysis of variance in a completely randomized design and Duncan’s new multiple range test (SPSS Statistics, 17.0).
Results - Gas production characteristics were significant differences among treatments (at 96 h, p<0.01). Gas production at 96 h increased with increasing RSK levels from 0 to 13.6 % in TMR which was significantly higher (p<0.01) than the other levels for all measured parameters. IVDMD at 48 h, IVOMD at 24 and 48 h increased linearly (p<0.05) with increasing RSK level from 0 to 13.6 % in TMR while increasing RSK level above 13.6 % resulted in decreased digestibility of DM and OM (p<0.05). NH3-N concentration was significantly different (p<0.05) among dietary treatments at 24 h. However, the ME was decreased as RSK level was increased.
Conclusion - This study indicated that RSK could be used in ranges from 0 to 13.6 % in TMR and suitable to use as feed for dairy cows.
Keywords: Rubber seed kernel, in vitro fermentation, Gas production technique

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health190
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Reproductive Performance of Dairy Cattle in Northeast Thailand
Waranya Kanhachon1 Nitima Tatiyaapiradee1 Alisra Sinsorn1 Amnuay Thotharin2 Suvaluk Srisupa3 and Suneerat Aiumlamai3*
1Fifth Year Veterinary Student, 3Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
2Dairy Farming Promotion Organization of Thailand, Northeastern Branch, Khon Kaen 40260, Thailand.
*corresponding author
Objective - To investigate the reproductive performance of dairy cattle in Northeast Thailand.
Materials and Methods - Ninety six out of 601 farms (15%) in Northeast Thailand (four milk collecting centres at Khon Kaen and three milk collecting centres at Udonthani) were investigated for reproductive performance during 2011-2012. A total of 1,218 crossbred Holstein-Friesian dairy cattle were included in the study. Individual breeding performance data were analyzed using one way analysis of variance and t-test.
Results - Age at first calving (months), calving interval (days), calving to first service (days), calving to conception (days) and service per conception (times) were 35.2±11.2, 470.6±97.2, 87.0 ±35.0, 123.7±59.1, and 2.0±1.3, respectively. Breed of cattle showed a tendency to affect fertility. The calving to first service (days) for >93.0%, 87.5-93.0% and <87.5% of Holstein-Friesian blood group were 137.9±66.1, 122.9±62.4 and 129.3±66.0 (p-value = 0.07), respectively. Better fertility was significantly shown in the cows with higher lactation number. Calving to conception (days) of cows in lactation number >4, 2-3 and 1 were 120.7±56.9, 123.2±61.0 and 142.2±72.7 (p-value<0.01), respectively.
Conclusion - The results demonstrated that fertility of heifers and first lactating cows are needed to be improved.
Keywords: Dairy cattle, Calving interval, Age at first calving, Northeast, Thailand

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 191
Reproductive Performance of Dairy Cattle in Northeast Thailand
Waranya Kanhachon1 Nitima Tatiyaapiradee1 Alisra Sinsorn1 Amnuay Thotharin2 Suvaluk Srisupa3 and Suneerat Aiumlamai3*
1Fifth Year Veterinary Student, 3Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
2Dairy Farming Promotion Organization of Thailand, Northeastern Branch, Khon Kaen 40260, Thailand.
*corresponding author
Objective - To investigate the reproductive performance of dairy cattle in Northeast Thailand.
Materials and Methods - Ninety six out of 601 farms (15%) in Northeast Thailand (four milk collecting centres at Khon Kaen and three milk collecting centres at Udonthani) were investigated for reproductive performance during 2011-2012. A total of 1,218 crossbred Holstein-Friesian dairy cattle were included in the study. Individual breeding performance data were analyzed using one way analysis of variance and t-test.
Results - Age at first calving (months), calving interval (days), calving to first service (days), calving to conception (days) and service per conception (times) were 35.2±11.2, 470.6±97.2, 87.0 ±35.0, 123.7±59.1, and 2.0±1.3, respectively. Breed of cattle showed a tendency to affect fertility. The calving to first service (days) for >93.0%, 87.5-93.0% and <87.5% of Holstein-Friesian blood group were 137.9±66.1, 122.9±62.4 and 129.3±66.0 (p-value = 0.07), respectively. Better fertility was significantly shown in the cows with higher lactation number. Calving to conception (days) of cows in lactation number >4, 2-3 and 1 were 120.7±56.9, 123.2±61.0 and 142.2±72.7 (p-value<0.01), respectively.
Conclusion - The results demonstrated that fertility of heifers and first lactating cows are needed to be improved.
Keywords: Dairy cattle, Calving interval, Age at first calving, Northeast, Thailand

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health192
Introduction Thai dairy farming has been carried on over 50 years and was initially run as a smallholder dairy farming system. Crossbred Holstein-Friesian cattle were raised under tropical conditions. Reproduction is a vital factor in determining the efficiency of animal production, at best a cow should produce a single calf per year. The reproductive performance of dairy cattle in Thailand was lower than that targeted for dairy cattle in general, days open, conception rates and age of first calving were 140-200 days, 20-60% and 30-32 months, respectively (1, 2, 3). The measurement of reproductive efficiency could determine the factors affecting reproductive performance in the area. The objective of present study was to evaluate the reproductive performance of Holstein-Friesian crossbred dairy cattle and effects of breed and lactation on fertility. Materials and Methods Crossbred Holstein-Friesian cattle from 15% of dairy farms from four milk collecting centres at Khon Kaen and three milk collecting centres at Udonthani (96 out of 601 farms) were investigated during 2011-2012. A total of 1,218 dairy cattle were included in the study, and the breeding records of individual cattle were analyzed for reproductive performance. The data were analyzed for age at first calving, calving interval, calving to fist service, calving to conception, and service per conception using descriptive statistic. Effects of breed and lactation number on reproductive performance were analyzed using one way analysis of variance and t-test. Results and Discussion Goals of dairy farming is productivity include both milk quality and reproductive efficiency. The reproductive performance of dairy cattle in Northeast Thailand was shown in Table 1, and the effects of breed and lactation number on reproductive performance were showed in Table 2 and 3. Reproductive performance in this area was poorer than the target of dairy cattle (3, 4, 5). The results suggested that fertility in heifers and first lactation cows need to be improved. Breed of cattle showed a tendency affecting fertility. Cows which had higher lactation number showed significant better fertility. The pure breed of imported bull (semen) was not recommended for insemination in the area which seemed to be under improper management. It is clear that reproductive efficiency of cattle in this area is needed to be improved.
Several factors affect fertility in dairy cattle in Thailand, including nutrition deficiency, improper feeding management, reproductive disease, heat stress, inappropriate artificial insemination and herd health services. Studies have shown that during the hot and humid season, in which the temperature and humidity index (THI) was higher than 75, that the conception rate significantly decreased. In addition, the presence of brucellosis, leptospirosis, ureaplamosis, IBR, BVD, neosporosis as well as blood parasites have been reported in several studies in dairy cattle in Thailand. These could affect health, fertility and production (1, 6). Farmers have to take better care in farm and feeding management to improve fertility of dairy cows in this area. Application on herd health and production management program by dairy extension and veterinarians should be practiced (3, 4, 5). Reproductive records need to be analyzed regularly to update situation of dairying and the information must be used for improvement plan in the future. Therefore, farm visit by veterinarians and extension staffs regularly need to practice for better fertility and production. Acknowledgement This study was supported by Faculty of Veterinary Medicine, Khon Kaen University, Thailand. A special thank to the Dairy Farming Promotion Organization of Thailand, Northeastern Branch, Khon Kaen, Thailand for providing the records of dairy cattle used in the study. References 1. Aiumlamai, S., Kreausukon, K. and Wongnen, N. 2012. Dairy Production and the Marketing System in Thailand. In Proceedings of a Symposium held at the 15th AAAP Congress, Bangkok, Thailand. November 29, 2012.p 57-67. 2. Dairy Farming Promotion Organization of Thailand (D.P.O.). 2014. DPO Sire & Dam Summary 2014. Department of Research and Development Institute. D.P.O. Ministry of Agricultural and Cooperatives, Saraburi, Thailand. 74 p. 3. Aiumlamai, S. 2010. Cattle production and the important of reproductive
efficiency. In: Reproduction in Cattle. Aiumlamai, S. KhonKaen Print. Khon Kaen pp. 395- 451.
4. Brand, A., Noordhuizen, J.P.T.M. and Schukken, Y.H. 1996. Herd Health and
Production Management in Dairy Practice. Wageningen Pers Publ. Wageningen. 543 p. 5. Noakes, D.E., Parkinson, T. J. and England, G.C.W. 2001. Veterinary control of herd fertility. In: Arthur’s Veterinary Reproduction and Obstetrics. Eight ed. Noakes, D.E., Parkinson, T.J., England, G.C.W. and Arthur, G.H. (eds) W.B. Sauders Company Ltd., Philadelphia. pp.511-556.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 193
Several factors affect fertility in dairy cattle in Thailand, including nutrition deficiency, improper feeding management, reproductive disease, heat stress, inappropriate artificial insemination and herd health services. Studies have shown that during the hot and humid season, in which the temperature and humidity index (THI) was higher than 75, that the conception rate significantly decreased. In addition, the presence of brucellosis, leptospirosis, ureaplamosis, IBR, BVD, neosporosis as well as blood parasites have been reported in several studies in dairy cattle in Thailand. These could affect health, fertility and production (1, 6). Farmers have to take better care in farm and feeding management to improve fertility of dairy cows in this area. Application on herd health and production management program by dairy extension and veterinarians should be practiced (3, 4, 5). Reproductive records need to be analyzed regularly to update situation of dairying and the information must be used for improvement plan in the future. Therefore, farm visit by veterinarians and extension staffs regularly need to practice for better fertility and production. Acknowledgement This study was supported by Faculty of Veterinary Medicine, Khon Kaen University, Thailand. A special thank to the Dairy Farming Promotion Organization of Thailand, Northeastern Branch, Khon Kaen, Thailand for providing the records of dairy cattle used in the study. References 1. Aiumlamai, S., Kreausukon, K. and Wongnen, N. 2012. Dairy Production and the Marketing System in Thailand. In Proceedings of a Symposium held at the 15th AAAP Congress, Bangkok, Thailand. November 29, 2012.p 57-67. 2. Dairy Farming Promotion Organization of Thailand (D.P.O.). 2014. DPO Sire & Dam Summary 2014. Department of Research and Development Institute. D.P.O. Ministry of Agricultural and Cooperatives, Saraburi, Thailand. 74 p. 3. Aiumlamai, S. 2010. Cattle production and the important of reproductive
efficiency. In: Reproduction in Cattle. Aiumlamai, S. KhonKaen Print. Khon Kaen pp. 395- 451.
4. Brand, A., Noordhuizen, J.P.T.M. and Schukken, Y.H. 1996. Herd Health and
Production Management in Dairy Practice. Wageningen Pers Publ. Wageningen. 543 p. 5. Noakes, D.E., Parkinson, T. J. and England, G.C.W. 2001. Veterinary control of herd fertility. In: Arthur’s Veterinary Reproduction and Obstetrics. Eight ed. Noakes, D.E., Parkinson, T.J., England, G.C.W. and Arthur, G.H. (eds) W.B. Sauders Company Ltd., Philadelphia. pp.511-556.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health194
6. Aiumlamai, S. 2010. Dairy herd health, feeding and milk quality in Thailand. In Proceedings: 13th Association of Institutes for Tropical Veterinary Medicine (AITVM) Conference. August 23-26, 2010. Bangkok, Thailand. pp. 214-216.
Table 1 Reproductive performances of crossbred Holstein-Friesian cows in Northeast Thailand.
n Mean S.D. Median Mode Minimum Maximum Target Value* Age at first calving 179 35.2 11.2 32.2 26.4 21.5 86.7 < 27 (months) Calving interval 493 470.6 97.2 430.0 379.0 365.0 729.0 < 365 (days) Calving to first service 545 87.0 35.0 82.0 63.0 22.0 190.0 < 60 (days) Calving to conception 545 123.7 59.1 112.5 82.0 22.0 318.0 < 85 (days) Service per conception 564 2.0 1.3 2.0 1.0 1.0 7.0 < 1.5 (times) *Auimlamai, 2010
Table 2 Effect of breed on reproductive performances of crossbred Holstein-Friesian cows in Northeast Thailand. Breed % HF (n) calving interval calving to first calving to service/conception
service conception days days days times (mean±S.D.) (mean±S.D.) (mean±S.D.) (mean±S.D.) <87.5% (167) 459.7±97.6 86.8±35.1 129.3±66.0 2.1±1.3 87.5-93.0%(346) 472.7±95.0 85.1±32.8 122.9±62.4 1.9±1.2 >93.0% (195) 478.1±94.0 90.1±36.1 137.9±66.1 2.1±1.2 p-value 0.278 0.370 0.073 0.092
Table 3 Effect of lactation number on reproductive performances of crossbred Holstein-Friesian cows in Northeast Thailand. Lactation calving interval calving to first calving to service/conception Number (n) service conception days days days times (mean±S.D.) (mean±S.D.) (mean±S.D.) (mean±S.D.) 1 (180) 0 90.6±35.7 142.2±72.7a 2.2±1.4 2-3 (299) 474.8±96.4 85.4±32.6 123.2±61.0b,c 1.9±1.2 >4 (227) 465.5±94.3 84.3±36.1 120.7±56.9c 1.9±1.1 p-value 0.248 0.204 0.003 0.119 a, b, c group with different superscripts are significantly different at p<0.05

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 195
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health196
Progesterone Profiles in Ovulation Induction by Long Time Insertion of CIDR®-B with Low Dose eCG and TAI
with hCG in Anoestrus in Beef Cattle
Chaiwat Jarassaeng1* Saksiri Sirisathien1 Adisak Sangkaew1 Sarawut Sri-ngam1 Pongthorn Suwannathada1 Suneerat Aiumlamai1 Suvaluk Seesupa1
Chatchai Suebkom2 and Phuangphaka Sadee3 1Department of Surgery and Theriogenology, Faculty of Veterinary Medicine,
Khon Kaen University, Khon Kaen 40002, Thailand. 2Khon Kaen Artificial Insemination and Biotechnology Center, Khon Kaen 40000, Thailand.
3Clinical immunology, Department of Medicine Srinagarind Hospital, Faculty of Medicine, Khonkaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Objective - To study the progesterone profiles in ovulation induction program by CIDR®-B and low dose eCG following fixed-time artificial insemination (TAI) with hCG in anoestrus beef cattle.
Materials and Methods - Ten crossbred Brahman with more than 150 days postpartum were introduced to the experiment. The oestrus observation was made by 3 times a day. The rectal palpation and ultra-sonography were determined and measured the ovary once week. All beef cattle were not shown oestrus behaviour and the ovary were not shown change of follicle and no evidence of corpus luteum for 2 months. The CIDR®-B device was inserted intravaginally for 14 days and injected with 300 IU of eCG in removal day. Anoestrus cattle were inseminated with TAI at 72 hours later and injected with 1,500 IU of hCG, and then were inseminated again in 96 hours after removal device. The blood samples were collected in 7 days before experiment, insertion day, 7 days after insertion days, removal days, TAI day for progesterone assays. The progesterone levels were measured by radioimmunoassay.
Results -The average levels of blood progesterone were 0.46, 0.55, 3.95, 1.73, 0.37 ng/ml at -7, 0, 7, 14, AI days respectively.
Conclusion - The result was indicated this ovulation protocol could induct ovulation in anoestrus beef cattle.
Keywords: Progesterone, Ovulation induction, Beef cattle

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 197
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health198
Low Dose of eCG and Fixed-time Artificial Insemination with hCG in Ovulation Induction Program in Beef Cattle
Chaiwat Jarassaeng1* Saksiri Sirisathien1 Adisak Sangkaew1 Sarawut Sri-ngam1
Pongthorn Suwannathada1 Suneerat Aiumlamai1 Suvaluk Seesupa1 Chatchai Suebkom2 and Phuangphaka Sadee3
1Department of Surgery and Theriogenology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
2Khon Kaen Artificial Insemination and Biotechnology Center, Khon Kaen 40000, Thailand. 3Clinical immunology, Department of Medicine Srinagarind Hospital,
Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Objective - To study the efficiency of a ovulation induction by CIDR®-B and low dose eCG following fixed-time artificial insemination (TAI) with hCG and in beef cattle.
Materials and Methods - Fourteen crossbred Brahman with more than 120 days postpartum were introduced to the experiment. The oestrus observation was made by 3 times a day. All beef cattle were not shown oestrus behaviour for 2 months. The CIDR®-B device was inserted intravaginally for 8 days and injected with 300 IU of eCG in removal day. All cattle were inseminated with TAI at 72 hours later and injected with 1,500 IU of hCG. The blood samples were collected in insertion day, TAI day and 23 days post TAI for progesterone assays. The pregnancy diagnosis was done by progesterone level in 23 days post-AI and 28 days with ultrasound machine and 60 days by rectal palpation.
Results - Ovulation induction was successfully ovulated in all cattle. The pregnancy rate was 71 % (10/14) in 23, 28 and 60 days post-artificial insemination.
Conclusion - The hormone protocol and TAI was used and increasing the numbers of insemination and pregnancy rate in anoestrus beef cattle.
Keywords: eCG, hCG, Fixed time-AI, Beef cattle
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 199
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health200
Comparisons of the Efficiency of Synchronizing the Estrus Cycle with Two Intramuscular or Intravulvo Submucosal
Injections of Cloprostenol in Mixed Native Breed Goat
Sarawut Sringam1* Kamonthep Chaisawat1 and Piyawat Sombutkiripaiboon1 1Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Objective - To reduce the cost of hormonal treatment for estrus synchronization in mixed native goat breed by comparing between a two Intramuscular and intravulvo-submucosal injections of cloprostenol.
Materials and Methods - In this experiment, 10 multiparous does were randomly assigned to 2 groups. Animals in each group received either 1) intramuscular injection of 62.5 µg cloprostenol (CLO) (IM group), or 2) intravulvo-submucosal injection of 31.25 µg CLO (IVSM group), 10 days apart.
Results - Four out of 5 does (80%) in IM group and all of does in IVSM group exhibited the signs of estrus. Interval from the second CLO injection to estrus were 42.0±13.9 and 54.0±18.0 h for does in IM and IVSM groups, respectively (P>0.05). After natural breeding, the fertility rates were 60% (3 out of 5) in both groups.
Conclusion - This study emphasizes that estrus synchronization cost in mixed native breed goat can be reduced by using cloprostenol injection via IVSM route. Keywords: Estrus synchronization, Goat, Cloprostenol, Intravulvo submucosal injection

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 201
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health202
Full-length Coding Sequence Analysis of the Genome Segments A and B of Infectious Bursal Disease Virus from Northeastern, Thailand
Tawatchai Pohuang1* Kingkarn Sarachu1 and Kanlaya Chuachan1
1Department of Medicine, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Infectious bursal disease virus (IBDV) causes immunosuppression in chickens with distinctive bursal lesions and may induce clinical disease with high mortality. Genomic sequence information is essential to understand the epidemiology of antigenically and/or pathogenically variable IBDV strains.
Objective - To determine the full-length coding sequence of the segments A and B of a recent Thai IBDV designated as SK53 and KK54.
Materials and Methods - Nucleotide sequencing and alignment of the segments A and B of a recent Thai IBDV designated as SK53 and KK54, and followed by phylogenetic analysis.
Results and Discussion - After the nucleotide sequence alignment, SK53 was closely related with very virulent IBDV strain HLJ-0504 isolated in China with the similarity of the segments A and B of 99.5% and 99.4%, respectively. For the KK54, the segment A had the highest similarity of 99.1% with the HPR-2 isolate from the United States, but the segment B was highly similar (99.3%) to the 9109 isolate from the United States. The results of deduced amino acid sequence alignment showed that VP5 of SK53 was 100% identical with the strain HLJ-0504 whereas that of KK54 was 100% identical with the isolate 9109 and also with the classical strain Irwin Moulthrop. VP2, VP4 and VP3 of SK53 were also highly similar (99.8%) to those of the strain HLJ-0504, VP2, VP4 and VP3 of KK54 were highly (98.6%) similar to those of the HPR-2 isolate and Irwin Moulthrop. VP1 of SK53 was 100% identical with that of the strain HLJ-0504, and that of KK54 was 98.8% indentity with that of the 9109 isolate from the United States.
Conclusion - These results indicate that, at the present, at least two types of IBDV are circulating in the northeast, Thailand. Keywords: Infectious bursal disease virus, Coding sequence, Phylogenetic analysis
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 203
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health204
Effects of Limnophila aromatic Merr. Crude Extracts on the Growth Inhibition of Salmonella
Tarinee Pongprom1 Peeraya Chumponwong1
Nunthaporn Kaewkamthong1 and Bongkot Noppon2* 1Fifth Year Veterinary Student, 2Department of Veterinary Public Health,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Objective - To study the effect of various concentrations of Limnophila aromatic Merr. crude extracts on the inhibition effect of Salmonella isolates from patients in the hospital and water from chicken farms. Materials and Methods - The dry and fresh Limnophila aromatic Merr. extracts were tested using agar well diffusion technique onto Muller Hinton Agar (Oxoid, UK) on 33 isolates of Salmonella spp. i.e. 16 isolates from patients, 16 isolates from water and 1 isolate of Salmonella Enteritidis. Inocula of both types of Salmonella isolates were standardized to 0.5 McFarland, and used in the growth inhibition study. Results - The 4 concentrations of crude extract (3.33, 6.66, 9.99, and 13.2%, w/v) have significant effect on salmonella isolates from both patients and water at p = 0.04, each. When compared between each concentration of the crude extracts, there was no significant difference of the inhibitory zone diameter at p = 0.12 and 0.06, respectively. Conclusion - Limnophila crude extracts can inhibit Salmonella isolates from patients, and water from the chicken farm. However, there was no significant difference at each concentration. Keywords: Growth inhibition, Limnophila aromatic Merr., Salmonella

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 205
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health206
Quantification of Total Bacterial Counts and Enterobacteriaceae Loads during the Chicken Slaughtering Process
Tayasorn Suwan1 Saran Thipkositkun1 Arthi Sri-art1 Apiradee Sopa2
Prapansak Chaveerach2 and Bongkot Noppon2* 1Fifth Year Veterinary Student, 2Department of Veterinary Public Health,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author E-mail: [email protected]
Objective - To determine total bacterial and enterobacteriaceae counts at all steps of the chicken slaughtering process. Materials and Methods - Totally, 234 samples were collected from 39 sample types at the chicken slaughterhouse in Khon Kaen province, Thailand. Total bacterial counts (TBC) were conducted according to AOAC (1990) protocol. Enterobacteriaceae counts (EC) were also employed followed the ISO21528-2:2004. Statistical analysis was done by SPSS statistics, version 22.0. Results - There was no significant different (p>0.05) of TBC both before and after the slaughter process. Most steps were not significantly different (p>0.05) in the TBC, except for the trimming knife and drip water from chiller before and after the operation (p<0.05). EC before and after process were significantly different (p<0.05). EC showed that all steps were not significantly differed (p> 0.05), however, knife and drip water from the rubber fingers of the mechanical pucker were significantly different (p<0.05), both. Statistic indicated a positive correlation (r = 0.6) between TBC and EC, both before and after the slaughter operation. TBC and EC after process among chicken meats were significant difference (p<0.05). There were no significant different (p<0.05) of chicken products both for TBC and EC loads compared with standard. Conclusion - TBC/EC of after process samples were significantly higher from that of standard. In chicken products, TBC was slightly higher than that of standards while EC was lower than standard. This indicated that slaughtering process reduced EC but may not be the case for TBC. Keywords: Chicken, Enterobacteriaceae count, Meat hygiene, Slaughtering process, Total bacterial count

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 207
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health208
Efficiency of Acetic Acid Solution to Salmonella Enteritidis
Juthaporn Piamwaree1 Nattawut Thongdee1 Vitan Kaewkhiew1 and Sunpetch Angkititrakul2*
1Fifth Year Veterinary Student, 2Department of Veterinary Public Health, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Intorduction - Salmonella Enteritidis is a foodborne pathogen which causes food poisoning and it also causes gastrointestinal diseases. The bacteria are usually found in meat and meat products such as beef, pork, chicken meat and egg. Objective - To determine the efficacy of acetic acid from vinegar to inhibit S. Enteritidis contaminated in the meat. Materials and Methods - The concentrations of acetic acid are 1%, 2%, 3%, 4% and 5%, respectively and times for inhibit are 1, 5, 10, 15, 20, 30, 40 and 50 minutes, respectively. Results - The acetic acid from vinegar can fully inhibit of S. Enteritidis were 1%, 2%, 3%, 4% and 5% at 30, 20, 10, 1 and 1 minute, respectively. However, 1% vinegar can inhibit S. Enteritidis in meat contaminated at 40 minutes. Conclusion - Prevention and control of any factors leading to Salmonella contamination in meat and meat products should be beneficial for the good health of consumers. Keywords: Acetic acid, Salmonella Enteritidis
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 209
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health210
Antimicrobial Resistance among Escherichia coli Isolated from Chicken and Pig
Pranpreya Kummee1* Kaewkamon Khongmak1 Prasert Namchai1
Wanwisa Satsomnuek2 Rittichai Pilachai1 and Sudawan Chuenpreecha1 1Program in Veterinary Technology, Faculty of Technology, UdonThani Rajabhat University,
Udon Thani 41000, Thailand. 2National Institute of Animal Health, Thailand. *Corresponding author
Background - Recently, antimicrobial resistant is an important public health problem worldwide including Thailand as a result of overuse of antibiotic. Chicken and pig are frequently contaminated with Escherichia (E) coli, and often resistant to different antimicrobial agents.
Objective - To investigate the antimicrobial resistant and susceptibility of E. coli isolated from chicken and pig.
Materials and Methods - The agar dilution method was employed to assess the sensitivity of 100 E. coli isolates (90 from chickens and 10 from pigs) to 9 antimicrobials according to the Clinical and Laboratory Standards Institute.
Results - It was revealed that 53.3% of E. coli isolated from both chickens and pigs were resistant to all antimicrobial agents used in this study. E. coli isolated from chicken were most sensitive to colistin (all isolates), ciprofloxacin and gentamicin (94.4% and 77.8% of isolates, respectively), whereas the highest rate of resistance was observed to ceftazidim, ampicilin and tetracycline (88.9%, 67.8% and 65.6% of isolates, respectively). E. coli isolates from pigs were most sensitive to ciprofloxacin (90% of isolates) and 60% of the isolates were against to colistin, gentamicin and nalidixic. The most resistant was observed to ceftazidime and tetracycline (all isolates) and ampicilin (90% of isolates).
Conclusion - E. coli isolates from chickens and pigs were resistant to a variety of antimicrobial agents particularly ceftazidime, ampicilin and tetracycline. However, colistin, ciprofloxacin and gentamicin were the most effective antimicrobial agents against all E. coli stains. Keywords: Antimicrobial susceptibility testing, Escherichia coli, Chicken, Pig

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 211
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health212
Prevalence of Salmonella spp. in the Slaughtering Process at the Local Slaughterhouse in Khon Kaen
Raksarat Sakulrak1 Thanipat Boonsanong1 Tharathip Pumrachat1
Prapansak Chaveerach2 and Bongkot Noppon2*
1Fifth Year Veterinary Student, 2Department of Veterinary Public Health, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Objective - The purpose of this study is to determine the prevalence of Salmonella spp. contamination during the slaughtering process at a local slaughterhouse in Khon Kaen province during December, 2555 to November, 2556. Materials and Methods - In total, 1,030 samples were collected from the slaughtering process, once a month for 12 months. This included samples from both before and after each operational step throughout the study. There were 90 cloacal swabs, 30 carton liners, 69 scalding waters, 91 drip waters from defeathering process, 330 samples of surfaces and small equipments at the evisceration step, 72 water samples from the washing-chilling steps, 318 water samples from trimming-cutting steps, and 30 samples of poultry products (breast, thigh, fillets, whole carcass, sausages, chicken balls, chicken bite, and steamed chicken). Isolation of Salmonella spp. was conducted using ISO 6579:20021/AMD 1:2007 protocol. Results - It was noted that the prevalence of Salmonella spp. was 33.0, 27.8, 27.6% at the eviscerating, washing-chilling, and trimming-cutting steps, respectively. However, the highest Salmonella spp. prevalence was found among the used evisceration devices after removed the viscera, used chop boards, and used conveyor belt at 53.3 (16/30), 46.6 (14/30), and 43.3% (23/60), respectively. Conclusion - The contamination of Salmonella spp. in the local slaughterhouse was high and at all steps. Therefore, proper disinfection is of high concern at the evisceration process. Keywords: Chicken, Prevalence, Salmonella spp., Slaughterhouse

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 213
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health214
Effects of Herbal Supplementations on Growth Performance, Feed Utilization, and Hematological Indices of Nile tilapia (Oreochromis niloticus)
Nitchanakul Klaisok1 Rungnapa Poomjan1 Korakan Pharadee1 Sumalee Seemabut1 Suchaya Wiriyakarun1 Chutima Maneekulsaub1
Namfon Saisee1 Prakit Samakkha1 and Phukphon Munglue1* 1Program of Biology, Faculty of Science, Ubon Ratchathani Rajabhat University,
Ubon Ratchathani 34000, Thailand. *Corresponding author
Background - The use of herbal plants has been conducted for the treatment of various ailments since the ancient civilizations, but their uses in fish culture are still limited. Plant-based feed supplementation may provide the elements or compounds that would enhance fish growth and feed utilization. Nelumbo nucifera and Nymphaea pubescens have been reported to have antidiarrheal, antimicrobial, anti-inflammatory, antioxidant and immunomodulatory activities. However, their uses in fish culture as immunostimulants or growth promoters are still limited.
Objective - To investigate the effects of N. nucifera and N. pubescens extracts on growth performance, feed utilization and hematological indices of Nile tilapia (Oreochromis niloticus).
Materials and Methods - The samples of N. nucifera leaves, N. pubescens leaves and N. nucifera peduncles were extracted by using 70% ethanol. One hundred fingerlings were divided into 5 groups: each consisting of 20 fishes. In a feeding trail of 60 days, Group 1-4, fish were fed diets containing 0% (control) or 1% of N. nucifera leaf extract, N. pubescens leaf extract or N. nucifera peduncle, respectively. Group 5 received 0.05% of oxytetracycline and served as a positive control group. Fish were fed two times a day for 60 days.
Results - The diets supplemented with the plant extracts significantly increased fish growth, red blood cells and white blood cells over the control diet (p <0.05). The efficiency of feed was also significant when fish received diets supplemented with 1% of the medicinal plant extracts (p<0.05). In addition, there were no significant changes in the cumulative mortality of the fish fed with the plant extract compared to the control and positive control groups (p >0.05), suggesting that the medicinal herb additives had no toxic effect. The main chemical compounds found in N. nucifera and N. pubescens are steroids, triterpenoids, flavonoids, glycosides and polyphenols, which can improve immunity, growth performance and feed utilization in aquatic animals. In addition, betulinic acid, a triterpenoid found in N. nucifera, possesses several pharmacological properties including anti-tumor and anti-inflammatory. Recent work has indicated that Nymphaea leaf meal produced a significant increase in growth performance and survival rate in common carp, Cyprinus carpio. Taken together, based on dietary supplementations with N. nucifera and N. pubescens extracts in Nile tilapia observed in this present study, their mechanisms of action might be attributed to active ingredients including flavonoids, glycosides, triterpenoids and polyphenols. In addition, the plant extracts did not produce treatment-related signs of toxicity in any of the animals during experimental periods, suggesting that the plant extracts are apparently safe.
Conclusion - It was indicated that N. nucifera and N. pubescens extracts might be used as a natural feed additive in fish diets to enhance fish growth, feed utilization and immunological function. This study also supports the use of N. nucifera and N. pubescens for value added agricultural products. Keywords: Nelumbo nucifera, Nymphaea pubescens, Nile tilapia, Growth performance, Feed utilization, Hematological indices
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 215
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health216
Intensity of Metacercariae in Cyprinidae Fish in Five Districts from Khon Kaen and Nong Bua Lamphu Provinces
Sornkrit Rakpanit1* Nuttawut Sereesongsaeng1 Yanyong Werawatakul1
Surasit Auanpromma2 and Prapan Kaenjampa2
1Fifth Year Veterinary Student, 2Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author Email: [email protected]
Background - Opisthorchiasis, caused by the liver fluke (Opisthorchis viverrini) infection are important public health problem in Thailand, especially Northeast of Thailand. The liver fluke infection in human and animal occurs by eating traditional raw or uncooked fish products. Haplorchiasis caused by trematode Haplorchis spp. Infection, had pathological changes in the small intestine, including mucosal ulceration, mucosal and submucosal hemorrhage, villi atrophy, chronic inflammation of small intestine, and fibrosis of submucosa layer.
Objective - To survey the intensity of metacercaria in the Cyprinidae fish, living surround the Ubolrat dam, Nonsang District, Sriboonruang District of Nongbua Lamphu Province and Nong Rua District, Nong Na Kham District, Ubolrat District of Khon Kaen Province.
Materials and Methods - Between June and November 2556, Cyprinidae fish were sampled 10 times with 5 kilogram each. Fishes were categorized as a necklace of white fish (Henicorhynchus siamensis), Saitan timid fish (Cyclocheilichthys repasson), Thai silver barb (Puntius gonionotus), Saitan red eye fish (Cyclocheilichthys apogon). The muscular tissues were performed by pepsin digestion technique to quantitatively examine the O. viverrini and Haplochis spp. Metacercaria in the fish.
Results - Haplochis spp. metacercaria were found with maximum intensity at Ban Non Sa Wang (0.27 metacercaria per one gram of fish). However, O. viverrini metacercaria was not found in this study.
Conclusion - Only Haplochis spp. Metacercaria in Cyprinidae Fish was found with maximum intensity at Ban Non Sa Wang in this study. Keywords: Trematode, Haplochis spp., Intensity, Cyprinidae fish, Metacercaria

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 217
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health218
Case Report: Unicornuate Uterus in a Thai Domestic Cat
Somphong Hoisang1* Panisara Kunkitti2 Arayapon Macotpet3 and Ekkachai Pattarapanwichien4
1Veterinary Teaching Hospital, 2Department of Surgery and Theriogenology,
3Department of Medicine, 4Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author E-mail address: [email protected]
Case Description - A 6-year-old female Thai Domestic Cat was brought to KKU Veterinary Teaching Hospital for an ovariohysterectomy. Only the left uterine horn and ovary were removed while the right side of uterine horn and ovary could not be found during the first operation. Four years later, the cat came back to the hospital with signs of estrous.
Clinical Findings - The cat was healthy with no signs of any abnormality. Ultrasonography examination found follicular-like at right side of abdominal cavity.
Treatment and Outcome - Exploratory laparotomy revealed right ovary and oviduct, whereas the uterine tube was disappeared. Therefore, the ovary and oviduct were removed. After the second operating, the cat appeared normal and never returned to estrus.
Clinical Relevant - Only a few reports of unicornuate uterus in cats have been recorded. For suspected cases, veterinarians should provide initial treatment by taking history and physical examination. Exploratory laparotomy and sterilization is useful for congenital abnormality cases. Keywords: Unicornuate uterus, Ovary, Cat
Introduction Unicornuate uterus in cat is a congenital disorder caused by defect of Mullerian ducts development of the embryo [1-3]. Only one of the Mullerian ducts is developed. The defect is regarded as a recessive characteristic [4]. The same defect can also cause other abnormalities such as segmental aplasia of the uterine horn, segmental aplasia of the uterine body, and abnormalities of both uterus and kidney. The abnormalities in humans and animals have been reported [5]. Etiology of the abnormality is not verified. One hypothesis is the genetic disorder. There was a report of a woman with defect of Mullerian ducts development that the abnormal karyotypes was found at only 8% [2]. This is consistent with a report by Reichman et al [6], in which the abnormality was unlikely to associate with genetic transmission within the family. In addition, some medications may induce the abnormality, thalidomide and diethylstilbestrol (non-steriodal estrogen) for example [2]. It is difficult to estimate the incidence rate of unicornuate uterus due to no appearance of or unspecific clinical signs. Some reports show that it can be found in 0.001-10% in humans and in some reports, the incidence can reach 8-10% [2]. In animals, there was a report in sheep that it accounts for 3.3% of the total abnormalities of the reproductive system [4]. Objective of this case report is to describe the finding of unicornuate uterus, which is a rare abnormality of reproductive system, in a cat. The information can be helpful for making a decision for diagnosis, clinical prognosis, and treatment of similar abnormality in other animals. The knowledge can be used for informing the owners and further studies as well. History of the case A female, native, Thai Domestic Cat aged 6 years and weighted 3.4 kilograms was taken to the Animal Teaching Hospital at the Faculty of Veterinary Medicine, Khon Kaen University due to signs of estrus. The cat was neutered 4 years previously. The owner informed that the veterinarian who performed the operation found only the left uterine horn and ovary, while the right uterine horn and ovary were missing Therefore, only the left uterine horn and ovary were removed in that operation. The veterinarian informed the owner to observe signs of estrus in the cat and bring the cat back again if the signs appeared. Physical examination showed that the cat was alert and healthy. Ultrasonography examination found a follicular cyst at the right ovary. Exploratory laparotomy using intramuscular injections of 0.04 mg/kg atropine sulphate and 0.2 mg/kg

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 219
Introduction Unicornuate uterus in cat is a congenital disorder caused by defect of Mullerian ducts development of the embryo [1-3]. Only one of the Mullerian ducts is developed. The defect is regarded as a recessive characteristic [4]. The same defect can also cause other abnormalities such as segmental aplasia of the uterine horn, segmental aplasia of the uterine body, and abnormalities of both uterus and kidney. The abnormalities in humans and animals have been reported [5]. Etiology of the abnormality is not verified. One hypothesis is the genetic disorder. There was a report of a woman with defect of Mullerian ducts development that the abnormal karyotypes was found at only 8% [2]. This is consistent with a report by Reichman et al [6], in which the abnormality was unlikely to associate with genetic transmission within the family. In addition, some medications may induce the abnormality, thalidomide and diethylstilbestrol (non-steriodal estrogen) for example [2]. It is difficult to estimate the incidence rate of unicornuate uterus due to no appearance of or unspecific clinical signs. Some reports show that it can be found in 0.001-10% in humans and in some reports, the incidence can reach 8-10% [2]. In animals, there was a report in sheep that it accounts for 3.3% of the total abnormalities of the reproductive system [4]. Objective of this case report is to describe the finding of unicornuate uterus, which is a rare abnormality of reproductive system, in a cat. The information can be helpful for making a decision for diagnosis, clinical prognosis, and treatment of similar abnormality in other animals. The knowledge can be used for informing the owners and further studies as well. History of the case A female, native, Thai Domestic Cat aged 6 years and weighted 3.4 kilograms was taken to the Animal Teaching Hospital at the Faculty of Veterinary Medicine, Khon Kaen University due to signs of estrus. The cat was neutered 4 years previously. The owner informed that the veterinarian who performed the operation found only the left uterine horn and ovary, while the right uterine horn and ovary were missing Therefore, only the left uterine horn and ovary were removed in that operation. The veterinarian informed the owner to observe signs of estrus in the cat and bring the cat back again if the signs appeared. Physical examination showed that the cat was alert and healthy. Ultrasonography examination found a follicular cyst at the right ovary. Exploratory laparotomy using intramuscular injections of 0.04 mg/kg atropine sulphate and 0.2 mg/kg

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health220
acepromazine maleate and an intravenous injection of 25 mg/kg cefazolin prior to the operation was performed. General anesthesia was induced by 10mg/kg Ketamine intravenously. Endotracheal tube was inserted to maintain the general anesthesia with Isoflurane from a semi-closed system anesthetic vaporizer. The cat was in dorsal recumbency position. Sterilization technique was applied for the abdominal laparotomy. The operation revealed a follicle-like mass attached to the intestine mesentery. Connected to the mass is a uterine horn-like duct approximately 2 centimeters long. The end of the duct was not connected to any organs. The mass, along with the duct, was removed. After the operation, the cat received Cephalexin for 7 consecutive days. The signs of estrus have never returned after the operation. Pathological Findings A gross pathological examination found that the mass was ovoid-like shape with a small cyst inside that looked like a follicle. A 2-centimeter duct was adjacent to the mass attached to adipose tissue in the abdomen (Figure 1).
Figure 1. Right ovary (white arrow) and right uterine horn of the cat (dark arrow) The histopathological examination of the right ovary showed various sizes of follicles and corpus luteum (Figure 2). Examination of the duct showed that it was the oviduct, of which the ampulla was engorged with blood. The high and folded polyp of mucous tissue and thickening of muscular layer were also found in the oviduct (Figure 3).
Figure 2. Tertiary follicle (TF), primary follicles (PF) and corpus luteum (CL) can be seen in this ovarian cortex. (bar scale = 1000 µm)
Figure 3. This ampulla of the oviduct was congested (white arrow) with highly folded mucosa (dark arrow) and relatively thick muscularis.(bar scale = 1000 µm) Discussion and Conclusion Uterus is developed from the merging of left and right mullerian ducts in the early embryo stage. The unicornuate uterus is caused by defect of one of the ducts partially or completely. The partial defect of the duct results in undeveloped or atrophy of a uterine horn. The complete defect of the duct results in hemiuterus. Ovary is developed from urogenital ridge. In case of mullerian ducts or urogenital ridge abnormal development, hemiuterus and be found with abnoemality of urinary
CL PF
PF
TF

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 221
Figure 2. Tertiary follicle (TF), primary follicles (PF) and corpus luteum (CL) can be seen in this ovarian cortex. (bar scale = 1000 µm)
Figure 3. This ampulla of the oviduct was congested (white arrow) with highly folded mucosa (dark arrow) and relatively thick muscularis.(bar scale = 1000 µm) Discussion and Conclusion Uterus is developed from the merging of left and right mullerian ducts in the early embryo stage. The unicornuate uterus is caused by defect of one of the ducts partially or completely. The partial defect of the duct results in undeveloped or atrophy of a uterine horn. The complete defect of the duct results in hemiuterus. Ovary is developed from urogenital ridge. In case of mullerian ducts or urogenital ridge abnormal development, hemiuterus and be found with abnoemality of urinary
CL PF
PF
TF

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health222
tract of the same side. The defect concurrently found in both systems was as high as 31% and most of the incidences occur at the kidney [6]. Clinical signs of unicornuate uterus are not apparent and not specific. In humans, there were reports of abortion at 43.8% [2], missing menstruation cycle, abdominal pain, early delivery, and infertility [1]. The chance of survival of the infants is only 29.2%, 43.0% for preterm delivery, and 4% for ectopic delivery. The gestation probability is reduced by 33.0% and the risk of infertility is 23.7%. These are results from the reduction of uterine muscle, defect of circulatory system development or the obstruction of circulatory system that supplies the uterus causing insufficient blood supply of the embryo during early gestation [6]. A report in sheep mentions hydrometra as one of the clinical signs; however the gestation is not disrupted since the other ovary still functions. Therefore, some animals can show signs of estrus [4]. Reduced chance of conception and small litter size are reported in dogs [8]. Diagnosis of unicornuate uterus needs more than one diagnostic tool; for example, laparoscopy together with hysteroscopy. Ultrasonography is highly specific to this abnormality (85-92%) and the accuracy is 44% depending on the position of the animals, experience of veterinarians, and the equipments. The magnetic resonance imaging (MRI) is very specific (96-100%) and more accurate compared to other diagnostic methods [2]. Abdominal laparotomy is another diagnostic method that is a good choice for confirmation [6]. Injection of contrast material into the oviduct has been proved that it not appropriate in dogs [8]. Ovariohysterectomy is recommended for the treatment of this abnormality. References 1. Perrotin, F., Bertrand, J. and Body, G. 1999. Laparoscopic surgery of unicornuate
uterus: Case raport. Hum Reprod. 14(4): 931-933.
2. Ribeiro, S.C., Tormena, R.A., Peterson, T.V., Gonzales, M.O., Serrano, P.G., Almeida, J.A.M. and Baracat, E.C. 2009. Mullerian duct anomalies: review of current management. Sao Paulo Med J. 127(2): 92-6.
3. Engmann, L., Schmidt, D., Nulsen, J., Maier, D. and Benadiva, D. 2004. An unusual anatomic variation of a unicornuate uterus with normal external uterine morphology. Fertil.Steril. 82(4): 950-953.
4. Smith, K.C., Long, S.E. and Parkinson, T.J. 1995. Congenital abnormalities of the ovine paramesonephric ducts. Br. Vet. J. 151(4): 443-452.
5. Goo, M.J., Williams, B.H., Hong, I.H., Park, J.K., Yang, H.J., Yuan, D.W., Lee, H.R., Hong, K.S., Ki, M.R. and Jeong, K.S. 2009. Multiple urogenital abnormalities in a Persian cat: Case raport. J Feline Med Surg. 11(2): 153-155.
6. Reichman, D., Laufer, M. and Robinson, M. 2009. Pregnancy outcomes in unicornuate uteri: a review. Fertil. Steril. 91(5) : 1886-1894.
7. Oppelt, P., von Have, M. Paulsen, M., Strissel, P.L., Strick, R., Brucker, S., Wallwiener, D. and Beckmann, M.W. 2007. Female genital malformations and their associated abnormalities. Fertil Steril. 87(2): 335-342.
8. Guvenc K., Toydemir F.S., Sontas H.B., Senunver A. 2006. A Cocker Spaniel bitch with uterus unicornis (unilateral cornual agenesis). J. Fac. Vet. Med. Istanbul Univ. 32(3): 69-73.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 223
5. Goo, M.J., Williams, B.H., Hong, I.H., Park, J.K., Yang, H.J., Yuan, D.W., Lee, H.R., Hong, K.S., Ki, M.R. and Jeong, K.S. 2009. Multiple urogenital abnormalities in a Persian cat: Case raport. J Feline Med Surg. 11(2): 153-155.
6. Reichman, D., Laufer, M. and Robinson, M. 2009. Pregnancy outcomes in unicornuate uteri: a review. Fertil. Steril. 91(5) : 1886-1894.
7. Oppelt, P., von Have, M. Paulsen, M., Strissel, P.L., Strick, R., Brucker, S., Wallwiener, D. and Beckmann, M.W. 2007. Female genital malformations and their associated abnormalities. Fertil Steril. 87(2): 335-342.
8. Guvenc K., Toydemir F.S., Sontas H.B., Senunver A. 2006. A Cocker Spaniel bitch with uterus unicornis (unilateral cornual agenesis). J. Fac. Vet. Med. Istanbul Univ. 32(3): 69-73.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health224
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Acaricidal Properties of the Essential Oil of Syzygium aromaticum (Clove Oil) against Brown Dog Tick (Rhipicephalus sanguineus)
Wichaya Thomas1 Saknarin Yoshpunya1 Hutsathorn Jamsri1
Jareerat Aimsaard1 and Weerapol Taweenan1* 1Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Objective - to study the appropriate concentration and efficiency of clove oil solution for eliminating brown dog tick (Rhipicephalus sanguineus). Materials and Methods - 144 adult brown dog ticks were collected from a number of dogs and divided into 3 groups, 48 ticks per group. The 48 ticks were incubated for 24 hours at 28-35oC and 60-80% relative humidity. Then, the ticks were equally divided into 6 treatment groups by randomization. The experiments were performed by dropping the treatment solutions including 2.5%, 5%, 10% and 15% clove oil, absolute alcohol and pyrethroid-based commercial acaricide, respectively. Ticks in each group were dropped with treatment solutions for 30 seconds before cleaned and incubated for 24 hours. The results were observed after second incubation. Results - The results after the second incubation showed that 10% and 15% clove oil extracts gave the best results with 91.7% mortality rate, which was significantly different from the mortality rate in the commercial acaricide group, 41.7%. Furthermore, the negative control, 99% alcohol, gave 8.3% mortality rate, which was significantly different from 10% clove oil extract. This indicated that 99% alcohol might not have or have small acaricidal effect against brown dog ticks. Conclusion - This study illustrated that the essential oil of Syzygium aromaticum (Clove oil) at suitable concentration may have acaricidal efficiency against brown dog ticks when compared to commercial acaricidal agents in terms of activated duration and response. However, the safety and adaptation for further use of this essential oil should be considered in the future investigation.
Keywords: Acaricide, Syzygium aromaticum, Clove oil, Rhipicephalus sanguineus

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 225
Acaricidal Properties of the Essential Oil of Syzygium aromaticum (Clove Oil) against Brown Dog Tick (Rhipicephalus sanguineus)
Wichaya Thomas1 Saknarin Yoshpunya1 Hutsathorn Jamsri1
Jareerat Aimsaard1 and Weerapol Taweenan1* 1Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Objective - to study the appropriate concentration and efficiency of clove oil solution for eliminating brown dog tick (Rhipicephalus sanguineus). Materials and Methods - 144 adult brown dog ticks were collected from a number of dogs and divided into 3 groups, 48 ticks per group. The 48 ticks were incubated for 24 hours at 28-35oC and 60-80% relative humidity. Then, the ticks were equally divided into 6 treatment groups by randomization. The experiments were performed by dropping the treatment solutions including 2.5%, 5%, 10% and 15% clove oil, absolute alcohol and pyrethroid-based commercial acaricide, respectively. Ticks in each group were dropped with treatment solutions for 30 seconds before cleaned and incubated for 24 hours. The results were observed after second incubation. Results - The results after the second incubation showed that 10% and 15% clove oil extracts gave the best results with 91.7% mortality rate, which was significantly different from the mortality rate in the commercial acaricide group, 41.7%. Furthermore, the negative control, 99% alcohol, gave 8.3% mortality rate, which was significantly different from 10% clove oil extract. This indicated that 99% alcohol might not have or have small acaricidal effect against brown dog ticks. Conclusion - This study illustrated that the essential oil of Syzygium aromaticum (Clove oil) at suitable concentration may have acaricidal efficiency against brown dog ticks when compared to commercial acaricidal agents in terms of activated duration and response. However, the safety and adaptation for further use of this essential oil should be considered in the future investigation.
Keywords: Acaricide, Syzygium aromaticum, Clove oil, Rhipicephalus sanguineus
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health226
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Serum and Tissue Malondialdehyde Levels in Canine Mammary Cancer
Arayaporn Macotpet1* Satatam Noo-aium1 Suvijuk Phountong1 Sarawut Butkun1 Ekkachai Pattarapanwichien2 Sarocha Permsub3
and Rawinnipa Weerakaittikun3 1Department of Medicine, 2Department of Pathobiology, 3Veterinary Teaching Hospital,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Introduction - Oxidative stress affects biologically to human and animals, leading to cell degeneration and death, and play a significant role in the pathogenesis of cancer. Several retrospective studies have reported that serum malondialdehyde levels were higher in cancerous human and dogs.
Objective - To assess oxidative stress in canine mammary cancer by measuring malondialdehyde levels in serum and tissue samples.
Materials and Methods - Nine dogs diagnosed as canine mammary cancer were recruited in the study. The malondialdehyde levels in serum and tissues were determined by Thiobarbituric acid reactive substance assay and analyzed by Pearson’s correlation analysis.
Results - From nine dogs, it was shown that mean levels of malondialdehyde in serum and tissue were 5.94±0.60 and 1.22±0.37 μmol/L, respectively. The levels of malondialdehyde in serum and tissue were not significantly correlated (r=0.4, p>0.05).
Conclusion - The serum malondialdehyde levels may be a suitable parameter to assess the oxidative stress condition in canine mammary cancer.
Keywords: Malondialdehyde, Mammary cancer, Canine

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 227
Serum and Tissue Malondialdehyde Levels in Canine Mammary Cancer
Arayaporn Macotpet1* Satatam Noo-aium1 Suvijuk Phountong1 Sarawut Butkun1 Ekkachai Pattarapanwichien2 Sarocha Permsub3
and Rawinnipa Weerakaittikun3 1Department of Medicine, 2Department of Pathobiology, 3Veterinary Teaching Hospital,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Introduction - Oxidative stress affects biologically to human and animals, leading to cell degeneration and death, and play a significant role in the pathogenesis of cancer. Several retrospective studies have reported that serum malondialdehyde levels were higher in cancerous human and dogs.
Objective - To assess oxidative stress in canine mammary cancer by measuring malondialdehyde levels in serum and tissue samples.
Materials and Methods - Nine dogs diagnosed as canine mammary cancer were recruited in the study. The malondialdehyde levels in serum and tissues were determined by Thiobarbituric acid reactive substance assay and analyzed by Pearson’s correlation analysis.
Results - From nine dogs, it was shown that mean levels of malondialdehyde in serum and tissue were 5.94±0.60 and 1.22±0.37 μmol/L, respectively. The levels of malondialdehyde in serum and tissue were not significantly correlated (r=0.4, p>0.05).
Conclusion - The serum malondialdehyde levels may be a suitable parameter to assess the oxidative stress condition in canine mammary cancer.
Keywords: Malondialdehyde, Mammary cancer, Canine
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health228
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Gastro-duodenal Mucormycosis in a Dog : A Case Report
Chalermkwan Nonthakotr1* Piyasak Wipoosak1 Pongrat Jaisil2 Arayaporn Macotpet3 and Ekkachai Pattarapanwichien4
1Veterinary Teaching Hospital, 2Department of Surgery and Theriogenology, 3Department of Medicine, 4Department of Pathobiology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Case Descriptio - A one-year-old female Thai Bangkaew was presented at Veterinary
Teaching Hospital, Khon Kaen University for long lasting periodic hematemesis associated with emaciation and unresponsive to antimicrobial treatment.
Clinical Examination and Findings - The abdominal ultrasonography was performed and revealed gastric dilatation and excessive gastric juice associated with proximal duodenum enlargement and hypomotility. Contrast radiography (barium series) indicated hypomotility of gastrointestinal tract. The blood sample was collected. Hematology and biochemical parameters showed mild anemia, leukocytosis, and neutrophilia. A SNAP® cPL (Canine pancrease-specific lipase) test was positive. Treatment and Outcome - Gastric outflow obstruction was suspected. Exploratory laparotomy was performed in order to assess the abnormality of gastrointestinal tract. During operation, severe inflammation, thickening in pylorus and cranial duodenum was found causing a narrowing of gastric outflow. A partial gastro-duodenectomy and anastomosis was performed and tissue biopsy was collected. Histopathology reported Mucormycosis. Accordingly, antimicrobials (cephalexin) in combination of antifungal (itraconazole) were given postoperatively for four weeks. The dog had a good response to treatment with no sign of vomiting and abdominal cramp.
Clinical Relevant and Conclusion - Mucormycosis is any fungal infection caused by Rhizopus and Mucor species which was rare in dog. It is an extremely rare disease in animals and the prognosis is very poor. It could be found in several organ including pulmonary, cutaneous, rhinocerebral, and gastrointestinal tract. However, sugical removal of the lesion followed by antifungal treatment could be helpful in this case.
Keywords: Mucormycosis, gastrointestinal tract, dog

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 229
Gastro-duodenal Mucormycosis in a Dog : A Case Report
Chalermkwan Nonthakotr1* Piyasak Wipoosak1 Pongrat Jaisil2 Arayaporn Macotpet3 and Ekkachai Pattarapanwichien4
1Veterinary Teaching Hospital, 2Department of Surgery and Theriogenology, 3Department of Medicine, 4Department of Pathobiology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Case Descriptio - A one-year-old female Thai Bangkaew was presented at Veterinary
Teaching Hospital, Khon Kaen University for long lasting periodic hematemesis associated with emaciation and unresponsive to antimicrobial treatment.
Clinical Examination and Findings - The abdominal ultrasonography was performed and revealed gastric dilatation and excessive gastric juice associated with proximal duodenum enlargement and hypomotility. Contrast radiography (barium series) indicated hypomotility of gastrointestinal tract. The blood sample was collected. Hematology and biochemical parameters showed mild anemia, leukocytosis, and neutrophilia. A SNAP® cPL (Canine pancrease-specific lipase) test was positive. Treatment and Outcome - Gastric outflow obstruction was suspected. Exploratory laparotomy was performed in order to assess the abnormality of gastrointestinal tract. During operation, severe inflammation, thickening in pylorus and cranial duodenum was found causing a narrowing of gastric outflow. A partial gastro-duodenectomy and anastomosis was performed and tissue biopsy was collected. Histopathology reported Mucormycosis. Accordingly, antimicrobials (cephalexin) in combination of antifungal (itraconazole) were given postoperatively for four weeks. The dog had a good response to treatment with no sign of vomiting and abdominal cramp.
Clinical Relevant and Conclusion - Mucormycosis is any fungal infection caused by Rhizopus and Mucor species which was rare in dog. It is an extremely rare disease in animals and the prognosis is very poor. It could be found in several organ including pulmonary, cutaneous, rhinocerebral, and gastrointestinal tract. However, sugical removal of the lesion followed by antifungal treatment could be helpful in this case.
Keywords: Mucormycosis, gastrointestinal tract, dog

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health230
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Prevalence of Opisthorchis viverrini in Dogs and Cats in Villages Surrounding Ubolrat Dam in Five Districts of Khon Kaen Province and
Nong Bua Lam Phu Province
Naphat Rungroj1* Onjira Chaopong1 Prapussorn Jongmeesuk1 and Surasit Aunpromma2
1Fifth Year Veterinary Student, 2Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Opisthorchiasis is caused by Opisthorchis viverrini. It is caused of bile duct obstruction, jaundice, pathological change of hepatic and cholangiocarcinoma in human. Dogs and cats are important reservoir hosts of O. viverrini and spread out to environment.
Objective - To survey O. viverrini infection in dogs and cats in Nongnakam district, Nong Rua district and Ubolrat district of Khon Kaen province and Non Sang district and Si Bun Rueang district of Nong Bua Lam Phu province in villages surrounding Ubolrat Dam.
Materials and Methods - Quantitative formalin-ether concentration technique was performed to determine the O. viverrini eggs in feces collected from the targeted dogs and cats.
Results - Cats had much higher prevalence (40 out of 150, 26.67%) than dogs (1 out of 655, 0.15%). In this study, O. viverrini infection in dogs (0.15%) and cats (26.67%) were lower than in infected dogs (0.37%) and cats (35.51%) in villages of Chi river basin, Khon Kaen province, respectively.
Conclusion - The prevalence of O. viverrini infection in cat was higher especially in the villages located near the Chi river basin, Khon Kaen province Keywords: Prevalence, Opisthorchis viverrini, Dog, Cat, Khon Kaen Province, Nong Bua Lam Phu Province

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 231
Prevalence of Opisthorchis viverrini in Dogs and Cats in Villages Surrounding Ubolrat Dam in Five Districts of Khon Kaen Province and
Nong Bua Lam Phu Province
Naphat Rungroj1* Onjira Chaopong1 Prapussorn Jongmeesuk1 and Surasit Aunpromma2
1Fifth Year Veterinary Student, 2Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Background - Opisthorchiasis is caused by Opisthorchis viverrini. It is caused of bile duct obstruction, jaundice, pathological change of hepatic and cholangiocarcinoma in human. Dogs and cats are important reservoir hosts of O. viverrini and spread out to environment.
Objective - To survey O. viverrini infection in dogs and cats in Nongnakam district, Nong Rua district and Ubolrat district of Khon Kaen province and Non Sang district and Si Bun Rueang district of Nong Bua Lam Phu province in villages surrounding Ubolrat Dam.
Materials and Methods - Quantitative formalin-ether concentration technique was performed to determine the O. viverrini eggs in feces collected from the targeted dogs and cats.
Results - Cats had much higher prevalence (40 out of 150, 26.67%) than dogs (1 out of 655, 0.15%). In this study, O. viverrini infection in dogs (0.15%) and cats (26.67%) were lower than in infected dogs (0.37%) and cats (35.51%) in villages of Chi river basin, Khon Kaen province, respectively.
Conclusion - The prevalence of O. viverrini infection in cat was higher especially in the villages located near the Chi river basin, Khon Kaen province Keywords: Prevalence, Opisthorchis viverrini, Dog, Cat, Khon Kaen Province, Nong Bua Lam Phu Province
15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health232
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Analysis of E-cadherin Expression and PCNA in Feline Mammary Carcinomas Using Tissue Microarray Technique
Siripitch Sithiyuno1 Adjima Boonchuen1 Chotimon Seesan1 Suwit Balthaisong2,3 Prasarn Tangkawattana1 Anudep Rungsipipat4 and Sirikachorn Tangkawattana1,3*
1Faculty of Veterinary Medicine, 2Faculty of Medicine, 3Tropical Disease Research Laboratory, Khon Kaen University, Khon Kaen 40002, Thailand.
4Faculty of Veterinary Science, Chulalongkorn University, Bangkok, Thailand. *Corresponding author Email address: [email protected]
Objective - To investigate the expression of E-cadherin in the feline mammary carcinomas (FMCs) by using tissue microarray technique. Materials and Methods - Regarding, 48 FMCs were graded following WHO tumor classification for feline mammary tumors. After the histopathological screening, construction of tumor microarray was performed by using “TMA Eazy” module with tissue core of 1.5 mm in diameter. Avidin-biotin complex immunohistochemistry was used for revealing the expression of E-cadherin. Percentage of PCNA and semi-quantitative grading of E-cadherin positive cells were reported. One-way analysis of variance (ANOVA) and chi-square or Fisher’s exact test was performed. The statistical significance was considered at the level of 95% confidence. Results and Discussion - All FMCs were epithelial type in origin of which was simple tubular adenocarcinoma (TAC) (54.17%, 26/48), papillary adenocarcinoma (PA) (10.42%, 5/48), cribriform carcinoma (CC) (14.58%, 7/48) and solid carcinoma (SC) (20.83%, 10/48). PCNA index of TAC, PA, CC, and SC were 55.21±19.99, 53.93±26.53, 35.82±21.19, and 47.29±27.55, respectively. Membranous E-cadherin expressed in all tumor types but did not correlate with their histological classification. E-cadherin grade gradually increased with PCNA index and nuclear grade indicates its involvement with cell proliferation and nuclear differentiation. Moreover, TMA is a high-throughput tool for the work with paraffin embedded tissue with less time and cost.
Keywords: Feline mammary carcinoma, Immunohistochemistry, E-cadherin, Tissue microarray

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 233
Analysis of E-cadherin Expression and PCNA in Feline Mammary Carcinomas Using Tissue Microarray Technique
Siripitch Sithiyuno1 Adjima Boonchuen1 Chotimon Seesan1 Suwit Balthaisong2,3 Prasarn Tangkawattana1 Anudep Rungsipipat4 and Sirikachorn Tangkawattana1,3*
1Faculty of Veterinary Medicine, 2Faculty of Medicine, 3Tropical Disease Research Laboratory, Khon Kaen University, Khon Kaen 40002, Thailand.
4Faculty of Veterinary Science, Chulalongkorn University, Bangkok, Thailand. *Corresponding author Email address: [email protected]
Objective - To investigate the expression of E-cadherin in the feline mammary carcinomas (FMCs) by using tissue microarray technique. Materials and Methods - Regarding, 48 FMCs were graded following WHO tumor classification for feline mammary tumors. After the histopathological screening, construction of tumor microarray was performed by using “TMA Eazy” module with tissue core of 1.5 mm in diameter. Avidin-biotin complex immunohistochemistry was used for revealing the expression of E-cadherin. Percentage of PCNA and semi-quantitative grading of E-cadherin positive cells were reported. One-way analysis of variance (ANOVA) and chi-square or Fisher’s exact test was performed. The statistical significance was considered at the level of 95% confidence. Results and Discussion - All FMCs were epithelial type in origin of which was simple tubular adenocarcinoma (TAC) (54.17%, 26/48), papillary adenocarcinoma (PA) (10.42%, 5/48), cribriform carcinoma (CC) (14.58%, 7/48) and solid carcinoma (SC) (20.83%, 10/48). PCNA index of TAC, PA, CC, and SC were 55.21±19.99, 53.93±26.53, 35.82±21.19, and 47.29±27.55, respectively. Membranous E-cadherin expressed in all tumor types but did not correlate with their histological classification. E-cadherin grade gradually increased with PCNA index and nuclear grade indicates its involvement with cell proliferation and nuclear differentiation. Moreover, TMA is a high-throughput tool for the work with paraffin embedded tissue with less time and cost.
Keywords: Feline mammary carcinoma, Immunohistochemistry, E-cadherin, Tissue microarray

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health234
Introduction Feline mammary carcinoma (FMC) is one of the life-threatening tumors in cats. Its incidence is the third common feline neoplasm [1]. Lymphatic metastasis occurs in regional lymph node and lung [2]. The prognosis depends on tumor size, metastasis at the first detection and surgical outcome [3]. Moreover, grading from histological changes and proliferation markers, as well as other tumor markers, i.e. cell cycle proteins, oncogenes and tumor suppressor genes, could be helpful for the diagnosis and prognosis of FMC [4, 5]. E-cadherin is a transmembrane protein found in epithelial and myoepithelial cells. It plays important roles in cell adhesion and functions as a tumor suppressor gene. In malignant cells, the abnormally uncontrolled growth and dysfunction of protein was found [6, 7]. Only one report describes decreased expression of E-cadherin in feline mammary tumor [8]. This study aims to investigate the expression of E-cadherin in feline mammary carcinoma by the tissue microarray technique. Materials and Methods Tumor sample: Forty-eight feline mammary carcinomas were collected from the Department of Veterinary Pathology, Faculty of Veterinary Science, Chulalongkorn University during 2005-2009. The samples were routinely processed for H&E slides and graded following WHO tumor classification for feline mammary tumors [8]. Construction of tumor microarray: After the histopathological screening, representative areas from donor blocks were punched and manually constructed for the TMA blocks, the “TMA Eazy”, a modified module of Dr. Banchob Sripa of Khon Kean University, Thailand. The tissue core was 1.5 mm in diameter. Each sample was performed in triplicate. Immunohistochemistry: Avidin-biotin complex immunohistochemistry was applied to detect the expression of E-cadherin. Primary antibodies used in this study were monoclonal rabbit anti E-cadherin antibody (clone EP700Y; Roche, Roche Diagnostics, Switzerland) and monoclonal mouse anti-PCNA antibody (Cell Signaling, USA). In addition, human breast cancer and tonsil were used as the positive control. Evaluation: Percentage of PCNA and semi-quantitative grading of E-cadherin positive cells were reported. One-way analysis of variance (ANOVA) and chi-square or Fisher’s exact test was performed. The statistical significance was considered at the level of 95% confidence.
Results and Discussion All FMCs were proven to be epithelial type in origin by our colleagues (Dr. A. Rungsipipat). Majority of FMCs was the simple tubular adenocarcinoma (TAC=54.17%, 26/48). Other FMCs were papillary adenocarcinoma (PAC 10.42%, 5/48), cribriform carcinoma (CC=14.58%, 7/48) and solid carcinoma (SC=20.83%, 10/48). PCNA index of TAC, PA, CC, and SC were 55.21±19.99, 53.93±26.53, 35.82±21.19, and 47.29±27.55, respectively. Membranous staining of E-cadherin was found in all types of FMC but without any correlation with the histological classification. However, gradual increases of E-cadherin grade were in concordance with higher PCNA index and nuclear grade. This suggests that proliferation expression of E-cadherin would probably involve in cell proliferation and nuclear differentiation. In addition, TMA is a useful high-throughput tool for archived paraffin embedding tissue. It saves time and cost.
Figure 1. A) A tissue microarray core with H&E staining (4x), B) with immunostaining (4x), C) Positive control using human breast cancer (10x), and
D) E-cadherin positive cells in FMC (20x)

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 235
Results and Discussion All FMCs were proven to be epithelial type in origin by our colleagues (Dr. A. Rungsipipat). Majority of FMCs was the simple tubular adenocarcinoma (TAC=54.17%, 26/48). Other FMCs were papillary adenocarcinoma (PAC 10.42%, 5/48), cribriform carcinoma (CC=14.58%, 7/48) and solid carcinoma (SC=20.83%, 10/48). PCNA index of TAC, PA, CC, and SC were 55.21±19.99, 53.93±26.53, 35.82±21.19, and 47.29±27.55, respectively. Membranous staining of E-cadherin was found in all types of FMC but without any correlation with the histological classification. However, gradual increases of E-cadherin grade were in concordance with higher PCNA index and nuclear grade. This suggests that proliferation expression of E-cadherin would probably involve in cell proliferation and nuclear differentiation. In addition, TMA is a useful high-throughput tool for archived paraffin embedding tissue. It saves time and cost.
Figure 1. A) A tissue microarray core with H&E staining (4x), B) with immunostaining (4x), C) Positive control using human breast cancer (10x), and
D) E-cadherin positive cells in FMC (20x)

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health236
Acknowledgements We would like to thank to Dr. Banchob Sripa for his TMA Eazy module and TDR Laboratory for the immunoworks. The work was partially supported by the Students’ special problem grants year 2013 of the Faculty of Veterinary Medicine, Khon Kaen University. References [1] Jodi R.V., Sherry L.M., Baljit S. and Elemir S. 2002. Feline mammary
adenocarcinoma: tumor size as a prognostic indicator. Can. Vet. J. 43: 33-37. [2] Misdorp W., 2002. Tumors of the Mammary Gland. In: Meuten D.J. (Ed.), Tumors
in Domestic Animals. Blackwell, Oxford, pp. 575-606. [3] Rutteman G.R. Withrow S.J., MacEwen E.G., 2001. Tumors of the mammary
gland. In: Withrow, S.J., MacEwen, E.G. (Eds.), Small Animal Clinical Oncology. W.B. Saunders Company, Philadelphia, pp. 455-477.
[4] Dias Pereira P., Carvalheira J., Gartner F., 2004. Cell proliferation in feline normal, hyperplastic and neoplastic mammary tissue – an immunohistochemical study. Veterinary Journal 168, 180-185.
[5] Preziosi R., Sarli G., Benazzi C., Mandrioli L., Marcato P.S., 2002. Multiparametric survival analysis of histological stage and proliferative activity in feline mammary carcinomas. Research in Veterinary Science 73, 53-60.
[6] Pereira PD and Grtner F. Expression of E-cadherin in normal, hyperplastic and neoplastic feline mammary tissue. Veterinary Record. 2003;153: 297-302.
[7] Knudsen KA and Wheelock MJ. Cadherins and the Mammary Gland. Journal of Cellular Biochemistry. 2005;95: 488-496.
[8] Zappulli V, De Cecco S, Trez D, Caliari D, Aresu L, Castagnaro M. 2012. Immunohistochemical expression of E-cadherin and β-catenin in feline mammary tumours. J Comp Pathol. 147(2-3):161-70.
[9] Hampe and Misdorp. 1974. Tumour and dysplasias of the mammary gland. In: Bull World Health Organ. 50(1-2):1-6.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 237
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health238
Apoptosis of Neurons and Inflammatory Cells in the Central Nervous System of Canine Rabies
Sirinapa Srikam1* Preecha Ruangvejvorachai1
Veera Tepsumethanon2 and Shanop Shuangshoti1,3
1Department of Pathology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand. 2Queen Saovabha Memorial Institute, Bangkok, Thailand.
3WHO Collaborating Center for Research and Training on Viral Zoonoses, Bangkok, Thailand. *Corresponding author
Background - Rabies encephalitis is a fatal infectious disease that is often neglected. The pathogenesis of encephalitic (furious) and paralytic (dumb) rabies, the two distinct clinical subtypesof rabies in dogs and humans, is not fully understood. Earlier studies in human at the late stage of disease or at postmortem did not show differences between the two forms. In contrast, recent studies at the early stage of rabies infection in dogs have demonstrated differences in terms of neuroimaging (more disturbance in paralytic rabies), inflammatory response (more pronounced in paralytic rabies), and viral burden (more virus in furious dogs). These findings imply that differences between the furious and paralytic rabies are present only at the early stage of infection. Apoptosis plays an important role as a defensive mechanism in eliminating virus-infected cells. While attenuated strains of rabies virus induce apoptosis of neurons, the wild-type (virulent) virus produces apoptosis of inflammatory cells. Most of the studies were, however, performed at the terminal stage of infection. Objective - To determine whether there are differences in the pattern of apoptosis between furious and paralytic rabies at the early stage of disease. Materials and Methods - Seventeen rabid dogs were studied, including the early stage of furious (N=5) and paralytic (N=6) rabies, and the terminal stage of rabies (3 of each clinical forms). For all cases, apoptosis was evaluated by TUNEL technique on the frontal lobe, hippocampus, brainstem, and spinal cord. Results - TUNEL-positive neurons and inflammatory cells were detected at the brainstem(most prominent) and spinal cord, and they were found exclusively at the early stage of infection. These TUNEL-positive cells were more abundant in the paralytic as compared to furious rabies. Conclusions - Neuronal apoptosis does occur in natural rabies infection but it is observed only at the early stage of disease. Prominent apoptosis of neurons in the brainstem level at the early stage of paralytic rabies might impede viral propagation into the brain and explains the longer survival time in paralytic as compared to furious rabies.
Keywords: Rabies, Canine rabies, Furious, Paralytic, Apoptosis
Introduction Rabies is a fatal zoonosis that causes up to 70,000 human deaths in 2011 [1-3]. The disease is caused by a non-segmented negative sense RNA virus that belongs to Rhabdoviridae family [4]. Exposure to saliva of infected animals, particularly dogs, is an important route of transmission to human [5, 6]. Encephalitis (furious) and paralytic (dumb) are the two distinct clinical subtypes of rabies in humans and dogs, the pathogenesis of which remain incompletely understood. In human, the furious to paralytic ratio is approximately 3:1 [7]. Patients with paralytic rabies patients tend to live longer (11 days) than the furious form (5.7 days) [8, 9]. Earlier postmortem study of rabies in human did not show difference in the CNS (central nervous system) between the 2 clinical forms, with regard to distribution of rabies viral antigen and inflammation that was generally mild [10]. There was also no difference noted by magnetic resonance imaging (MRI) studies [11]. Studies in rabid dogs at the early stage of infection have, however, shown otherwise. Structural damage of the brainstem in paralytic rabies due to inflammation was found to be associated with lesser extent of viral burden as compared to the furious subtype [12, 13]. In addition, interleukin-1 beta and interferon-gamma were found exclusively in the paralytic dog brains [12]. All of these findings indicate that, at the early stage of rabies encephalitis, furious and paralytic rabies are different in several aspects, and that the differences are no longer present at the terminal stage of disease. Apoptosis of inflammatory cells is well-known in rabies but neuronal apoptosis is generally absent in the natural infection [14-16]. However, most of the studies were performed at the terminal stage of infection (postmortem). Since it has been shown that furious and paralytic rabies differ at the early not the late stage of illness, apoptotic pattern may also be different. Materials and Methods Sample collection Natural infected rabid dogs quarantine in Queen Saovabha Memorial Institute (QSMI), Bangkok, Thailand, were subjects for the experiment. These animals were categorized to furious group and paralytic group by aveterinarian experienced in rabies [VT], and the rabies diagnosis was confirmed by nucleic acid sequence-based amplification (NASBA) technique [17]. Rabid dogs sacrificed immediately after rabies diagnosis were classified as “Early” group while those observed until death were in the “Late” group. Dogs enrolled for the study included 8 furious (5 early and 3 late) and 9 paralytic (6 early and 3 late) rabies. For each case, frontal lobe, hippocampus, brainstem and spinal cord were removed and fixed in 10% neutral formalin, routinely processed, and embedded paraffin wax.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 239
Introduction Rabies is a fatal zoonosis that causes up to 70,000 human deaths in 2011 [1-3]. The disease is caused by a non-segmented negative sense RNA virus that belongs to Rhabdoviridae family [4]. Exposure to saliva of infected animals, particularly dogs, is an important route of transmission to human [5, 6]. Encephalitis (furious) and paralytic (dumb) are the two distinct clinical subtypes of rabies in humans and dogs, the pathogenesis of which remain incompletely understood. In human, the furious to paralytic ratio is approximately 3:1 [7]. Patients with paralytic rabies patients tend to live longer (11 days) than the furious form (5.7 days) [8, 9]. Earlier postmortem study of rabies in human did not show difference in the CNS (central nervous system) between the 2 clinical forms, with regard to distribution of rabies viral antigen and inflammation that was generally mild [10]. There was also no difference noted by magnetic resonance imaging (MRI) studies [11]. Studies in rabid dogs at the early stage of infection have, however, shown otherwise. Structural damage of the brainstem in paralytic rabies due to inflammation was found to be associated with lesser extent of viral burden as compared to the furious subtype [12, 13]. In addition, interleukin-1 beta and interferon-gamma were found exclusively in the paralytic dog brains [12]. All of these findings indicate that, at the early stage of rabies encephalitis, furious and paralytic rabies are different in several aspects, and that the differences are no longer present at the terminal stage of disease. Apoptosis of inflammatory cells is well-known in rabies but neuronal apoptosis is generally absent in the natural infection [14-16]. However, most of the studies were performed at the terminal stage of infection (postmortem). Since it has been shown that furious and paralytic rabies differ at the early not the late stage of illness, apoptotic pattern may also be different. Materials and Methods Sample collection Natural infected rabid dogs quarantine in Queen Saovabha Memorial Institute (QSMI), Bangkok, Thailand, were subjects for the experiment. These animals were categorized to furious group and paralytic group by aveterinarian experienced in rabies [VT], and the rabies diagnosis was confirmed by nucleic acid sequence-based amplification (NASBA) technique [17]. Rabid dogs sacrificed immediately after rabies diagnosis were classified as “Early” group while those observed until death were in the “Late” group. Dogs enrolled for the study included 8 furious (5 early and 3 late) and 9 paralytic (6 early and 3 late) rabies. For each case, frontal lobe, hippocampus, brainstem and spinal cord were removed and fixed in 10% neutral formalin, routinely processed, and embedded paraffin wax.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health240
Detection of apoptosis Terminal deoxynculeotidyl transferased UTP nick end labeling (TUNEL) were performed in all samples to detect apoptotic cells, using ApopTaq plus peroxidase in situ apoptosis detection kit (Milipore). Lymphoid tissue in tonsil served as positive control in all stained sections. The number of TUNEL positive neurons was semi-quantitatively scored on a scale 0 to 4+ scale from none to most abundant on the followings: 0 = negative, 1+ = 1 – 25%, 2+ = 26 – 50%,3+ = 51 – 75%, and 4+ = 76 – 100 %. Results TUNEL-positive neurons were observed in the brainstem and spinal cord only at the early stage of infection (Table 1). The positive neurons were more prominent in paralytic as compared to furious rabies (Figure 1). TUNEL-positive inflammatory cells were also found, corresponding to the degree of inflammation in the CNS regions examined. No TUNEL-positive neuron was observed at the terminal stage of both clinical forms. Table1. Neuronal apoptosis in canine furious and paralytic rabies
TUNEL-Positive Neurons
CNS Regions
Frontal Hippocampus Brainstem C-T L-S
Furious Early 1 0 0 1+ NA NA
2 0 0 1+ NA NA
3 0 0 2+ 1+ 2+
4 0 0 1+ 0 1+
5 0 0 0 NA NA
Late
6 0 0 0 0 0
7 0 0 0 0 0
8 0 0 0 0 0
Paralytic Early 1 0 0 4+ 2+ 3+
2 0 0 3+ 2+ 2+
3 0 0 4+ NA NA
4 0 0 3+ 0 0
5 0 0 1+ NA NA
6 0 0 3+ NA NA
Late 7 0 NA 0 0 0
8 0 0 0 0 0
9 0 0 0 0 0
C = Cervical cord, T = Thoracic cord, L = Lumbar cord, S = Sacral cord, NA = Not available
Figure 1. Neuronal apoptosis in canine rabies. In addition to TUNEL-positive inflammatory cells, TUNEL-positive neurons are noted in the brainstem at the early stage of rabies infection. The TUNEL-expressing neurons are more abundant in paralytic (A) as compared to furious (B) rabies. (TUNEL stain, original magnification x 400). Discussion Rabies in dogs and humans can manifest as furious (encephalitis) and dumb (paralytic) forms [8, 9]. Recent studies at the early stage of disease have shown that more pronounced inflammation, particularly at the brainstem level and cytokine production in paralytic rabies are associated with less viral burden in the brain [12, 13]. Apoptosis prevents dissemination of viruses within the host, and plays important role as a defensive mechanism in eliminating virus-infected cells [18, 19]. In rabies, apoptosis that occurs in inflammatory cells via up regulation of Fas ligand (FasL), on the other hand, promotes viral spreading [20]. Neurons are the major cellular population in the CNS infected by rabies virus. If neuronal apoptosis occurs, it will reduce viral dissemination. However, apoptosis of neuron does not actually take place in animals infected with street (wild-type) rabies virus [15, 16], with few exceptions [21]. This is contract to the infection with laboratory strains of rabies virus that is known to induce inflammation and neuronal apoptosis [16, 22]. Since paralytic and furious rabies are different at the early stage of disease and the former is characterized by less viral burden and prominent brainstem inflammation, we hypothesized whether neuronal apoptosis might play role at the early course of disease. Our demonstration of neuronal apoptosis, particularly at the brainstem level, of naturally-infected dogs with paralytic rabies supports the hypothesis. Similar to most of the previous postmortem studies [15, 16], no neuronal apoptosis was observed in all of our cases in the late group. Apoptosis of inflammation noted in our cases is in line with the previous reports [13].
A B

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 241
Figure 1. Neuronal apoptosis in canine rabies. In addition to TUNEL-positive inflammatory cells, TUNEL-positive neurons are noted in the brainstem at the early stage of rabies infection. The TUNEL-expressing neurons are more abundant in paralytic (A) as compared to furious (B) rabies. (TUNEL stain, original magnification x 400). Discussion Rabies in dogs and humans can manifest as furious (encephalitis) and dumb (paralytic) forms [8, 9]. Recent studies at the early stage of disease have shown that more pronounced inflammation, particularly at the brainstem level and cytokine production in paralytic rabies are associated with less viral burden in the brain [12, 13]. Apoptosis prevents dissemination of viruses within the host, and plays important role as a defensive mechanism in eliminating virus-infected cells [18, 19]. In rabies, apoptosis that occurs in inflammatory cells via up regulation of Fas ligand (FasL), on the other hand, promotes viral spreading [20]. Neurons are the major cellular population in the CNS infected by rabies virus. If neuronal apoptosis occurs, it will reduce viral dissemination. However, apoptosis of neuron does not actually take place in animals infected with street (wild-type) rabies virus [15, 16], with few exceptions [21]. This is contract to the infection with laboratory strains of rabies virus that is known to induce inflammation and neuronal apoptosis [16, 22]. Since paralytic and furious rabies are different at the early stage of disease and the former is characterized by less viral burden and prominent brainstem inflammation, we hypothesized whether neuronal apoptosis might play role at the early course of disease. Our demonstration of neuronal apoptosis, particularly at the brainstem level, of naturally-infected dogs with paralytic rabies supports the hypothesis. Similar to most of the previous postmortem studies [15, 16], no neuronal apoptosis was observed in all of our cases in the late group. Apoptosis of inflammation noted in our cases is in line with the previous reports [13].
A B

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health242
Conclusions Prominent neuronal apoptosis has been demonstrated in the brainstem of naturally-infected dogs with paralytic rabies. The apoptosis of brainstem neurons might impede viral propagation into the brain, and explain the longer survival time in paralytic as compared to furious rabies. References 1. Rupprecht CE, Hanlon CA, Hemachudha T: Rabies re-examined. Lancet Infect Dis
2002; 2 : 327–343. 2. Chuxnum T, Choomkasian P. Epidemiology of Human Rabies in Thailand.
B.E.2546-2550 (2003-2007 AD). Tren Res Sci Technol; 2: 71-75. 3. Global Alliance for Rabies Control. http://www.rabiescontrol.net. 4. Laothamatas J, Hemachudha T, Mitrabhakdi E, Wannakrairot P,
Tulayadachanont S. MR imaging in human rabies. Am J Neuroradiol 2003; 24: 1102-1109.
5. Winkler WG, Fashinell TR, Leffingwell L, Howard P, Conomy JP. Airborne rabies transmission in a laboratory worker. JAMA 1973; 226: 1219-1221.
6. HemachudhaT,Wacharapluesadee S, LaothamatasJ,Wilde H. Rabies. Curr Neurol Neurosci 2006; 6: 460–468.
7. Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol 2002; 1: 101-109.
8. Mitrabhakdi E, Shuangshoti S, Wannakrairot P, Lewis RA, Susuki K, Laothamatas J, Hemachudha T: Difference in neuropathogeneticmechanisms in human furious and paralytic rabies. J Neurol Sci 2005; 238: 3–10.
9. Hemachudha T, Wacharapluesadee S, Mitrabhakdi E, Wilde H, Morimoto K, Lewis RA. Pathophysiology of human paralytic rabies. J Neurovirol 2005; 11: 93–100.
10. Tirawatnpong S, Hemachudha T, Manutsathit S, Shuangshoti S, Phanthumchinda K, Phanuphak P. Regional distribution of rabies viral antigen in central nervous system of human encephalitic and paralytic rabies. J Neurol Sci 1989; 92(1): 91-99.
11. Laothamatas J, Hemachudha T, Mitrabhakdi E, Wannakrairot P, Tulayadaechanont S. MR imaging in human rabies. AJNR Am J Neuroradiol 2003; 24: 1102–1109.
12. Laothamatas J, Wacharapluesadee S, Lumlertdacha B, Ampawong S, Tepsumethanon V, Shuangshoti S, Phumesin P, Asavaphatiboon S, Worapruekjaru L, Avihingsanon Y, et al. Furious and paralytic rabies of canine origin: neuroimaging with virological and cytokine studies. J Neurovirol 2008; 14: 119–129.
13. Shuangshoti S, Thepa N, Phukpattaranont P, Jittmittraphap A, Intarut N, Tepsumethanon V, Wacharapluesadee S, Thorner PS, Hemachudha T. Reduced viral burden in paralytic compared to furious canine rabies is associated with prominent inflammation at the brainstem level. BMC Vet Res 2013; 14: 31.
14. Jackson AC, Randle E, Lawrance G, and Rossiter JP. Neuronal apoptosis does not play an important role in human rabies encephalitis. J Neurovirol 2008; 14(5): 368–375.
15. Suja MS, Mahadevan A, Madhusudhana SN, Vijayasarathi SK, and Shankar SK. Neuroanatomical mapping of rabies nucleocapsid viral antigen distribution and apoptosis in pathogenesis in street dog rabies-an immunohistochemical study. Clin Neuropathol 2009; 28(2): 113–124.
16. Suja MS, Mahadevan A, Madhusudana SN, Shankar SK. Role of apoptosis in rabies viral encephalitis: a comparative study in mice, canine, and human brain with a review of literature. Patholog Res Int 2011; 2011: 374286.
17. Wacharapluesadee S, Hemachudha T. Nucleic-acid sequence based amplification in the rapid diagnosis of rabies. Lancet 2001; 358: 892–893.
18. Dietzschold B, Morimoto K, Hooper DC. Mechanisms of virus-induced neuronal damage and the clearance of viruses from the CNS. Curr Top Microbiol Immunol 2001; 253: 145–155.
19. Yan X, Mohankumar PS, Dietzschold B, Schnell MJ, Fu ZF. The rabies virus glycoprotein determines the distribution of different rabies virus strains in the brain. J. Neurovirol 2002; 8(4): 345–352.
20. Baloul L, Camelo S, Lafon M. Up-regulation of Fas ligand (FasL) in the central nervous system: a mechanism of immune invasion by rabies virus. J Neurovirol 2004; 10(6): 372-382.
21. Adle-Biassette H, Bourhy H, Gisselbrecht M et al. Rabies encephalitis in a patient with AIDS: a clinicopathological study. Acta Neuropathologica 1996; 92(4): 415–420.
22. Yan X, Prosniak M, Curtis M. T et al. Silver-haired bat rabies virus variant does not induce apoptosis in the brain of experimentally infected mice. J Neurovirol 2001; 6: 518–527.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 243
13. Shuangshoti S, Thepa N, Phukpattaranont P, Jittmittraphap A, Intarut N, Tepsumethanon V, Wacharapluesadee S, Thorner PS, Hemachudha T. Reduced viral burden in paralytic compared to furious canine rabies is associated with prominent inflammation at the brainstem level. BMC Vet Res 2013; 14: 31.
14. Jackson AC, Randle E, Lawrance G, and Rossiter JP. Neuronal apoptosis does not play an important role in human rabies encephalitis. J Neurovirol 2008; 14(5): 368–375.
15. Suja MS, Mahadevan A, Madhusudhana SN, Vijayasarathi SK, and Shankar SK. Neuroanatomical mapping of rabies nucleocapsid viral antigen distribution and apoptosis in pathogenesis in street dog rabies-an immunohistochemical study. Clin Neuropathol 2009; 28(2): 113–124.
16. Suja MS, Mahadevan A, Madhusudana SN, Shankar SK. Role of apoptosis in rabies viral encephalitis: a comparative study in mice, canine, and human brain with a review of literature. Patholog Res Int 2011; 2011: 374286.
17. Wacharapluesadee S, Hemachudha T. Nucleic-acid sequence based amplification in the rapid diagnosis of rabies. Lancet 2001; 358: 892–893.
18. Dietzschold B, Morimoto K, Hooper DC. Mechanisms of virus-induced neuronal damage and the clearance of viruses from the CNS. Curr Top Microbiol Immunol 2001; 253: 145–155.
19. Yan X, Mohankumar PS, Dietzschold B, Schnell MJ, Fu ZF. The rabies virus glycoprotein determines the distribution of different rabies virus strains in the brain. J. Neurovirol 2002; 8(4): 345–352.
20. Baloul L, Camelo S, Lafon M. Up-regulation of Fas ligand (FasL) in the central nervous system: a mechanism of immune invasion by rabies virus. J Neurovirol 2004; 10(6): 372-382.
21. Adle-Biassette H, Bourhy H, Gisselbrecht M et al. Rabies encephalitis in a patient with AIDS: a clinicopathological study. Acta Neuropathologica 1996; 92(4): 415–420.
22. Yan X, Prosniak M, Curtis M. T et al. Silver-haired bat rabies virus variant does not induce apoptosis in the brain of experimentally infected mice. J Neurovirol 2001; 6: 518–527.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health244
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Gastro-duodenal Cysticercosis in Cat: A Case Report
Chuleephorn Praha1* Nittaya Boonban1
Arayaporn Macotpet2 and Ekkachai Pattarapanwichien3
1Veterinary Teaching Hospital, 2Department of Medicine, 3Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Case Description - A 2-year old, female spayed domestic Thai cat was presented at The Veterinary Teaching Hospital, Khon Kaen University with weight loss, anorexia and vomiting. Two months earlier, a cat was found a palpable abdominal mass by the owner.
Clinical Examination and Findings - The defecation and urination were normal. On physical examination, a large palpably abdominal mass was found. The radiology and ultrasonography were performed and revealed hallow mass in cranial to mid-abdomen with peristalsis.
Treatment and Outcome - A surgical exploratory laparotomy showed an enlarged stomach and a thickened gastric wall. The tissue biopsy was done. Cysticercosis was confirmed by histopathology. Cysticercosis is a parasitic infection caused by larval cysts of the Taenia spp..
Clinical Relevant - Currently praziquantel has been recommended for the treatment. Steroids are also used for reducing effects of the cysts on host tissues. Keywords: Cysticercosis, Gastrointestinal tract, Cat

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 245
Gastro-duodenal Cysticercosis in Cat: A Case Report
Chuleephorn Praha1* Nittaya Boonban1
Arayaporn Macotpet2 and Ekkachai Pattarapanwichien3
1Veterinary Teaching Hospital, 2Department of Medicine, 3Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*Corresponding author
Case Description - A 2-year old, female spayed domestic Thai cat was presented at The Veterinary Teaching Hospital, Khon Kaen University with weight loss, anorexia and vomiting. Two months earlier, a cat was found a palpable abdominal mass by the owner.
Clinical Examination and Findings - The defecation and urination were normal. On physical examination, a large palpably abdominal mass was found. The radiology and ultrasonography were performed and revealed hallow mass in cranial to mid-abdomen with peristalsis.
Treatment and Outcome - A surgical exploratory laparotomy showed an enlarged stomach and a thickened gastric wall. The tissue biopsy was done. Cysticercosis was confirmed by histopathology. Cysticercosis is a parasitic infection caused by larval cysts of the Taenia spp..
Clinical Relevant - Currently praziquantel has been recommended for the treatment. Steroids are also used for reducing effects of the cysts on host tissues. Keywords: Cysticercosis, Gastrointestinal tract, Cat

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health246
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Effect of Azadirachin on Terminating Eggs and Lavae of Rhipicephalus sanguineus
Natcha Thaboonruang1 Nutjaree Rungrat1
Pattaraporn Pakdeedindan1 and Ranee Singh2* 1Fifth Year Veterinary Student, 2Department of Phamacology and Toxicology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *corresponding author e-mail: [email protected]
Background - Brown dog ticks (Rhipicephalus sanguineus) are the most widespread and well recognized as a vector of zoonotic diseases such as Rickettsia rickettsii, R. conorii, Ehrlichia canis and many more. Currently, brown dog ticks are considered as urban pests due to their high levels of infestation and ability to parasitize other hosts including humans. Eradication of ticks is principally carried out using chemical products which are prepared in different forms such as shampoo, powder, topical, injection and oral drugs. Most of these products cause high levels of residues that are host intoxicants in animals as well as in humans. These products also caused the resistant development in ticks. Recently, there are many studies of alternative methods of tick control by using plant extraction substances that can replace the chemicals used. Neem is one compound among these plants whose main active ingredient is azadirachin that has been shown to have acaricide and insecticide properties.
Objective - To investigate the efficiency of an alcohol extract of neem at concentrations of 1%, 5% and 10% that would inhibit tick egg hatching and terminate immature ticks.
Materials and Methods - Neem leaves whose main active ingredient is an activator (azadirachin) were extracted by 50% ethyl alcohol. The substance was prepared to be concentrated at 1%, 5%, 10%. Bayticol® 6% and distilled water were used as positive and negative controls. Each substance was put into petri dishes containing 50 tick eggs. Each petri dish contained a 50 mL dose of each substance times 5 replications. The petri dishes were then kept at room temperature to observe. Data were recorded as number of eggs hatching and death rate of immature hatched ticks for the duration of 2 weeks.
Results - Neem extract at 5% and 10% concentration could inhibit 55% and 78%, respectively, of egg hatching of the ticks. Only 10% of the neem extract, however, could inhibit 50% of the immature ticks, which was comparable to Bayticol®.
Conclusion - Neem extract is effective in eliminating ticks by inhibiting the egg hatch and terminating immature ticks. Neem extract acts in a dose dependent manner in terminating immature ticks and inhibiting tick eggs hatching. Neem extract has a potential as a new alternative to be used in controlling ectoparasites which is also of benefit to the environment as it has low toxicity.
Keywords: Neem extracts, Azadirachtin, Rhipicephalus sanguineus, Dog(s), Brown dog tick

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 247
Effect of Azadirachin on Terminating Eggs and Lavae of Rhipicephalus sanguineus
Natcha Thaboonruang1 Nutjaree Rungrat1
Pattaraporn Pakdeedindan1 and Ranee Singh2* 1Fifth Year Veterinary Student, 2Department of Phamacology and Toxicology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *corresponding author e-mail: [email protected]
Background - Brown dog ticks (Rhipicephalus sanguineus) are the most widespread and well recognized as a vector of zoonotic diseases such as Rickettsia rickettsii, R. conorii, Ehrlichia canis and many more. Currently, brown dog ticks are considered as urban pests due to their high levels of infestation and ability to parasitize other hosts including humans. Eradication of ticks is principally carried out using chemical products which are prepared in different forms such as shampoo, powder, topical, injection and oral drugs. Most of these products cause high levels of residues that are host intoxicants in animals as well as in humans. These products also caused the resistant development in ticks. Recently, there are many studies of alternative methods of tick control by using plant extraction substances that can replace the chemicals used. Neem is one compound among these plants whose main active ingredient is azadirachin that has been shown to have acaricide and insecticide properties.
Objective - To investigate the efficiency of an alcohol extract of neem at concentrations of 1%, 5% and 10% that would inhibit tick egg hatching and terminate immature ticks.
Materials and Methods - Neem leaves whose main active ingredient is an activator (azadirachin) were extracted by 50% ethyl alcohol. The substance was prepared to be concentrated at 1%, 5%, 10%. Bayticol® 6% and distilled water were used as positive and negative controls. Each substance was put into petri dishes containing 50 tick eggs. Each petri dish contained a 50 mL dose of each substance times 5 replications. The petri dishes were then kept at room temperature to observe. Data were recorded as number of eggs hatching and death rate of immature hatched ticks for the duration of 2 weeks.
Results - Neem extract at 5% and 10% concentration could inhibit 55% and 78%, respectively, of egg hatching of the ticks. Only 10% of the neem extract, however, could inhibit 50% of the immature ticks, which was comparable to Bayticol®.
Conclusion - Neem extract is effective in eliminating ticks by inhibiting the egg hatch and terminating immature ticks. Neem extract acts in a dose dependent manner in terminating immature ticks and inhibiting tick eggs hatching. Neem extract has a potential as a new alternative to be used in controlling ectoparasites which is also of benefit to the environment as it has low toxicity.
Keywords: Neem extracts, Azadirachtin, Rhipicephalus sanguineus, Dog(s), Brown dog tick

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health248
Introduction Brown dog ticks (R. sanguineus) are the most widespread and well recognized as a vector of zoonotic diseases such as R. rickettsii, R. conorii, E. canis and many more [1]. Currently, brown dog ticks are considered as urban pests due to their high levels of infestation and their ability to parasitize other hosts including human. Eradication of ticks principally uses chemical products which are prepared in different forms such as shampoo, powder, topical, injection and oral drugs [2]. For instance, the topical chemical drug in which the main active substance is Fipronil, can cause irritation of the exposed area, hair loss and if dogs lick the exposed area, can have side effects eg. salivation. Ivermectin injection is easier to use in animals that are difficult to restrain, however, the side effects and contraindications of using this drug in some breeds of dogs, eg. Collies, and Old English Sheep dogs and this compound cannot be used in dogs less than 6 weeks of age. Most of these products cause high levels of residues that are host intoxicants in animals as well as in humans. It can also cause the development of resistance in ticks [3]. Recently, there are many studies of alternative methods of tick control by using plant extract substances that can replace the chemicals used. Neem is one among these plants extracts whose main active ingredient is azadirachin that has shown to have acaricide and insecticide properties [4]. There are few studies of neem extract that has effect on fertility and survival of larvae when tested in R. sanguineus. Thus, this study aims to investigate the efficiency of an alcohol extract of neem at concentrations of 1%, 5% and 10% that could inhibit tick egg hatching and terminate immature ticks that may be useful to apply in the future.
Materials and Methods Extraction The neem leaves were washed and slices into small pieces, then put into a tray by spreading them in a thin layer. The leaves were dried in the incubator at 55oC and left in the incubator for 18-20 hours. Then the dried leaves were crushed and used. The neem alcohol extract was prepared in the laboratory by using crushed dried leaves mixed with 50% ethyl alcohol and stirred well. This mixture was stored in a jar with the cover sealed with paraffin for 3 days. After this period, the extract was filtered and evaporated in an evaporator. The final product was in powder form which was used to prepare dilutions of 1%, 5% and 10%. Experiments in Petri dishes For the egg hatching test, 0-6 hr-old R. sanguineus eggs were used. Five replicate petri dishes were used for treated and positive and negative control samples. The
tick eggs were placed in each petri dish with 50 eggs per plate. In treatment samples an aliquot of 50 µL of neem extract compound preparation with concentrations at 1%, 5% and 10% were pipetted on to the base of the petri dishes. The solutions were distributed thoroughly on each treated dish. Controls consisted of Bayticol® as the positive control and sterile water as the negative control. After that the petri dishes were sealed with paraffin and placed at room temperature. The results were observed and recorded for 2 weeks. Hatched tick eggs were counted every day after treatment. Statistical analysis Data were compared between the groups by using one-way ANOVA and Post-Hoc tests (Multiple comparisons). The statistical significance was considered at the level of 95% confidence. All the data results were represented as mean ± SD. Results and Discussion From the results, 5% and 10% neem extract had efficiency in the elimination of ticks, which can inhibit 55% and 78% egg hatching (Table 1). Only 10% of neem extract, however, can inhibit 50% of the immature ticks, which was comparable to Baytricol® (Table 1). Table 1 Mean ± SD percentages of hatched tick eggs and dead larvae in replicate petri dishes loaded with 50 eggs each after treatment with various concentrations of neem which was extracted by ethyl alcohol in comparison with positive and negative controls.
Substances % Egg hatching (mean±SD)
% Death of larvae (mean±SD)
1% neem extract 100 ± 0.00a 0.00 ± 0.00a
5% neem extract 45.20±7.82b 0.00 ± 0.00a
10% neem extract 22.20 ±15.00c 49.20± 33.41b
Sterile water 92.00 ±11.31a 0.00 ± 0.00a
6% Bayticol® 36.00±22.84b,c 58.81± 27.46b
The negative control was sterile water and the positive control was 6% Baytricol. P< 0.05 for statistical significant between groups (a, b, c). Effective tick control requires suppression of egg and larval production and also elimination of adults. Azadirachin may effectively control ticks [5-7]. The results of

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 249
tick eggs were placed in each petri dish with 50 eggs per plate. In treatment samples an aliquot of 50 µL of neem extract compound preparation with concentrations at 1%, 5% and 10% were pipetted on to the base of the petri dishes. The solutions were distributed thoroughly on each treated dish. Controls consisted of Bayticol® as the positive control and sterile water as the negative control. After that the petri dishes were sealed with paraffin and placed at room temperature. The results were observed and recorded for 2 weeks. Hatched tick eggs were counted every day after treatment. Statistical analysis Data were compared between the groups by using one-way ANOVA and Post-Hoc tests (Multiple comparisons). The statistical significance was considered at the level of 95% confidence. All the data results were represented as mean ± SD. Results and Discussion From the results, 5% and 10% neem extract had efficiency in the elimination of ticks, which can inhibit 55% and 78% egg hatching (Table 1). Only 10% of neem extract, however, can inhibit 50% of the immature ticks, which was comparable to Baytricol® (Table 1). Table 1 Mean ± SD percentages of hatched tick eggs and dead larvae in replicate petri dishes loaded with 50 eggs each after treatment with various concentrations of neem which was extracted by ethyl alcohol in comparison with positive and negative controls.
Substances % Egg hatching (mean±SD)
% Death of larvae (mean±SD)
1% neem extract 100 ± 0.00a 0.00 ± 0.00a
5% neem extract 45.20±7.82b 0.00 ± 0.00a
10% neem extract 22.20 ±15.00c 49.20± 33.41b
Sterile water 92.00 ±11.31a 0.00 ± 0.00a
6% Bayticol® 36.00±22.84b,c 58.81± 27.46b
The negative control was sterile water and the positive control was 6% Baytricol. P< 0.05 for statistical significant between groups (a, b, c). Effective tick control requires suppression of egg and larval production and also elimination of adults. Azadirachin may effectively control ticks [5-7]. The results of

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health250
this study showed the neem leaves extract effectively inhibited egg hatch, however, the concentration of 10% was the minimum dose needed to terminate the tick larvae which is comparable to the commonly used chemical (Bayticol®) in that 64% can inhibit egg hatch and 60% can kill the larvae. Recently, the study by Denardi et al. [1] reported that the aqueous extracts of neem caused the changes in cells of the reproductive system of R. sanguineus especially in the oocytes which also support the current results.
In conclusion, neem extracts are effective in eliminating ticks by inhibiting egg hatch and terminating immature ticks. The results showed that the neem extract acts in a dose dependent manner in terminating immature ticks and inhibit tick egg hatching. Neem extract has the potential as a new alternative in controlling ectoparasites which also may have a benefit to the environment as it has low toxicity. Acknowledgements We would like to thank Dr. Jareerat Aium-saad for her assistance and guidance for the neem extract processes. References 1. Denardi, S.E., Bechara, G.H., de Oliveira, P.R., Camargo-Mathias, M.I., 2010. Azadirachta indica A. Juss (neem) induced morphological changes on oocytes of Rhipicephalus sanguineus (Latreille, 1806) (Acari: Ixodidae) tick females. Exp Parasitol 126, 462-470. 2. Centers for Disease control and prevention. 2012. Life cycle of hard ticks that
spread disease.Online Resources, Inc. [cited 2013 June 25]. 3. Mulla, M.S., Su, T., 1999. Activity and biological effects of neem products against arthropods of medical and veterinary importance. J Am Mosq Control Assoc
15, 133-152. 4. Nation Research Council, 1992. Neem, A tree for solving global problems. National Academy Press, Washington DC, p. 108. 5. Giglioti, R., Forim, M.R., Oliveira, H.N., Chagas, A.C.S., Ferrezini, J., Brito, L.G., Falcoski, T.O.R.S., Albuquerque, L.G., Oliveira, M.C.S., 2011. In vitro acaricidal activity of neem (Azadirachta indica) seed extracts with known azadirachtin concentrations against Rhipicephalus microplus. Vet Parasitol 181, 309-315. 6. Guerrini, V.H., Kriticos, C.M., 1998. Effects of azadirachtin on Ctenocephlides felis
in the dog and the cat. Vet Parasitol 74, 289-297. 7. Landau, S.Y., Provenza, F.D., Gardner, D.R., Pfister, J.A., Knoppel, E.L., Peterson, C., 2009. Neem tree (Azadirachta indica Juss.) extract as a feed additive against the American dog tick (Dermacentor variabilis) in sheep (Ovis aries). Vet
Parasitol 165, 311-317.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 251
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health252
Prevalence of Gastrointestinal Helminthes in House Rats in 4 Districts of Khon Kaen Province
Satit Wattanasinpisal1 Nattawipa Suwannasaeng1 Parames Uthakum1
Wansane Toanan2 and Somboon Sangmaneedet3* 1Fifth Year Veterinary Student, 2Graduate Student, 3Department of Pathobiology,
Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *corresponding author
Objective - To evaluate the prevalence of parasites in gastrointestinal tract of house rats, parasitological surveys were carried out in four districts; Ban Fang, Chum Phae, Manchakhiri, and Phu-Pha-Man of Khon Kaen province. Materials and Methods - House rats in communities were examined for types and species of parasites. Rats were captured from four districts in Khon Kaen province by using cages with bait. The rats were euthanized and necropsied to explore visceral organs and digestive tracts for any dwelling parasites. Digestive contents and feces were examined for parasite’s eggs by modified formalin acetate sedimentation technique. Results - It was indicated that 41.79% rats were infected with at least one type of parasites. The parasites most found in order were Hymenolepis diminuta (21.64%), Strongyloides spp. (10.45%), Capillaria spp. (3.73%), Physaloptera spp. (3.73%) and Hymenolepis nana (2.24%), respectively. Hymenolepis diminuta had the highest prevalence in Ban Fang (50%), Chum Phae (45.65%), Manchakhiri (33.33%) and Phu-Pha-Man (28.0%). In addition, Hymenolepis diminuta had the highest number of eggs per gram feces indicating that people in the community had a higher risk to get H. diminuta directly from rats or contaminated environment than other parasites. Statistical analysis revealed that prevalence of parasitized rats in four districts was not different. Conclusion - Therefore, house rat remains a capable reservoir transmitting parasites to humans in the community. Keywords: Prevalence, Gastrointestinal helminthes, House rat, Khon Kaen
Introduction Rats normally live in poor sanitary areas of the community. These rats are reservoirs of many diseases that are capable of being transmitted directly or indirectly to human [1]. Digestive tract of rat is habitat for many helminthes such as Heterakis sp., Mastophorusmuris, Nippostrongylus brasiliensis, Hymenolepis nana, Hymenolepis diminuta and Taenia spp. [2-9]. The helminthes in intestine will release eggs which will contaminate feces and remain in environment or in the rat carcass. Thus, people in the poor sanitary community could accidentally get these eggs from contaminated environment. The rat helminthes can cause disease and harm to human. Hymenolepis diminuta, a rat tapeworm, has man as an accidental host whom infected from eating infective stage called cysticercoid in cockroach or rat flea. The infected person will show clinical signs of itching, abdominal discomfort, anorexia, weight loss and diarrhea. [10] Hymenolepis nana, a dwarf tapeworm, can cause disease and damage to human same as H. diminuta. Hymenolepis spp. frequently causes listlessness, diarrhea, abdominal discomfort, itching of nose and anus in infected children [11]. Strongyloides spp. is a threadworm nematode causing severe disease to infected person. Human are infected with threadworm by ingestion of infective eggs or larvae, or by skin penetration. The threadworm infected person especially in immune-suppressed patient will show clinical signs of abdominal discomfort, diarrhea, malabsorption, hyper-infection, septicemia, nervous signs and finally death [12]. Capillaria hepatica is another nematode living in rat’s intestine and causes abdominal discomfort, weight loss, anorexia, fever, hepatitis, ascites and bile duct stone in patient [13]. Prevalence of parasitic infection in human of each location differs depending on life styles and geography. Khon Kaen is a large city with dense population in the Northeast Thailand. Its area is about 10,885 square kilometers which many areas are agricultural parts, therefore suitable for rodents especially rat to live and reproduce. Incidence of human liver fluke in the Northeast is highest in Thailand due to eating behavior of local people who customarily eat uncooked food. In addition, no hand washing before meal or after toileting may be factors causing people have a risk of getting an infection from the rodents. Presently, there is no information of prevalence of intestinal parasitic infection in rat living in the house or nearby the communities. To evaluate the prevalence of intestinal parasitic infection in house rat and a risk of people to get parasitic infection, this study aims to examine prevalence and types of parasites in rats, and species that could be transferred to human. Results of the study will be useful for

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 253
Introduction Rats normally live in poor sanitary areas of the community. These rats are reservoirs of many diseases that are capable of being transmitted directly or indirectly to human [1]. Digestive tract of rat is habitat for many helminthes such as Heterakis sp., Mastophorusmuris, Nippostrongylus brasiliensis, Hymenolepis nana, Hymenolepis diminuta and Taenia spp. [2-9]. The helminthes in intestine will release eggs which will contaminate feces and remain in environment or in the rat carcass. Thus, people in the poor sanitary community could accidentally get these eggs from contaminated environment. The rat helminthes can cause disease and harm to human. Hymenolepis diminuta, a rat tapeworm, has man as an accidental host whom infected from eating infective stage called cysticercoid in cockroach or rat flea. The infected person will show clinical signs of itching, abdominal discomfort, anorexia, weight loss and diarrhea. [10] Hymenolepis nana, a dwarf tapeworm, can cause disease and damage to human same as H. diminuta. Hymenolepis spp. frequently causes listlessness, diarrhea, abdominal discomfort, itching of nose and anus in infected children [11]. Strongyloides spp. is a threadworm nematode causing severe disease to infected person. Human are infected with threadworm by ingestion of infective eggs or larvae, or by skin penetration. The threadworm infected person especially in immune-suppressed patient will show clinical signs of abdominal discomfort, diarrhea, malabsorption, hyper-infection, septicemia, nervous signs and finally death [12]. Capillaria hepatica is another nematode living in rat’s intestine and causes abdominal discomfort, weight loss, anorexia, fever, hepatitis, ascites and bile duct stone in patient [13]. Prevalence of parasitic infection in human of each location differs depending on life styles and geography. Khon Kaen is a large city with dense population in the Northeast Thailand. Its area is about 10,885 square kilometers which many areas are agricultural parts, therefore suitable for rodents especially rat to live and reproduce. Incidence of human liver fluke in the Northeast is highest in Thailand due to eating behavior of local people who customarily eat uncooked food. In addition, no hand washing before meal or after toileting may be factors causing people have a risk of getting an infection from the rodents. Presently, there is no information of prevalence of intestinal parasitic infection in rat living in the house or nearby the communities. To evaluate the prevalence of intestinal parasitic infection in house rat and a risk of people to get parasitic infection, this study aims to examine prevalence and types of parasites in rats, and species that could be transferred to human. Results of the study will be useful for

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health254
epidemiology awareness, management of community sanitation, and elimination of risk factors to get parasites from house rats. Materials and Methods Parasitological surveys were carried out in house rats in four districts of Khon Kaen. Rats were captured by using 80 wired cages with bait per village, and numbers of rats in Ban Fang, Chum Phae, Manchakhiri, and Phu-Pha-Man were 42, 21, 46 and 25, respectively. The rats were euthanized and necropsied to explore visceral organs and digestive tracts for any dwelling parasites. Digestive contents and feces were collected and examined for parasite’s eggs by modified formalin acetate sedimentation technique, and to evaluate a density of parasites in rat, numbers of eggs of each parasite were examined per gram feces. Results The overall prevalence of parasitic infection in rats of all four districts was 41.79% (56/134). Prevalence of parasitic infection in Ban Fang, Chum Phae, Manchakhiri, and Phu-Pha-Man were 50% (21/42), 45.65% (21/46), 33.33% (7/21) and 28% (7/25), respectively. Prevalence of parasitic infection in rats of 4 districts were compared and statistically analyzed by Pearson Chi-Square Test. There was no difference (p=0.26) of prevalence of infected rats captured from 4 districts (Table 1). Table 1. Prevalence of parasitic infection in rats in Ban Fang, Chum Phae, Manchakhiri, and Phu-Pha-Man
Infection
Number of rat
Total Ban Fang Chum Phae Manchakhiri Phu-Pha-Man
Parasitic infection
No parasitic infection
Total
21
21
42
21
25
46
7
14
21
7
18
25
56 (41.79%)
78 (58.21%)
134 (100%)
Parasites found in rats’ intestines were shown in Figure 1-5. The overall prevalence of infection in rats according to parasite species: Hymenolepis diminuta, Strongyloides spp., Capillaria spp., Physaloptera spp. and Hymenolepis nana were 21.64% (29/134), 10.45% (14/134), 3.73% (5/134), 3.73% (5/134) and 2.24% (3/134), respectively (Table 2).
Figure 1: Hymenolepis diminuta Figure 2: Hymenolepis nana Figure 3: Strongyloides spp.
Figure 4: Capillaria spp. Figure 5: Physaloptera spp.
Table 2. Prevalence of parasitic infection in 4 districts according to parasite species
Parasite species Number of infected rats
Total Ban Fang Chum Phae Manchakhiri Phu-Pha-Man
Hymenolepis diminuta 11 11 5 2 29 (21.64%)
Hymenolepis nana 3 0 0 0 3 (2.24%)
Strongyloides spp. 5 3 2 4 14 (10.45%)
Capillaria spp. 1 3 0 1 5 (3.73%)
Physaloptera spp. 1 4 0 0 5 (3.73%)
Total infected rats 21 7 21 7 56
Number of rats (n) 42 21 46 25 134
Number of parasite’s eggs found in feces was examined and evaluated as eggs per gram of feces (EPG). Means of EPG of Hymenolepis diminuta, Hymenolepis nana, Strongyloides spp., Capillaria spp., and Physaloptera spp. from all four districts were 1,545 (n=29), 740 (n=3), 1,075 (n=14), 280 (n=5) and 416 (n=5), respectively.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 255
Figure 1: Hymenolepis diminuta Figure 2: Hymenolepis nana Figure 3: Strongyloides spp.
Figure 4: Capillaria spp. Figure 5: Physaloptera spp.
Table 2. Prevalence of parasitic infection in 4 districts according to parasite species
Parasite species Number of infected rats
Total Ban Fang Chum Phae Manchakhiri Phu-Pha-Man
Hymenolepis diminuta 11 11 5 2 29 (21.64%)
Hymenolepis nana 3 0 0 0 3 (2.24%)
Strongyloides spp. 5 3 2 4 14 (10.45%)
Capillaria spp. 1 3 0 1 5 (3.73%)
Physaloptera spp. 1 4 0 0 5 (3.73%)
Total infected rats 21 7 21 7 56
Number of rats (n) 42 21 46 25 134
Number of parasite’s eggs found in feces was examined and evaluated as eggs per gram of feces (EPG). Means of EPG of Hymenolepis diminuta, Hymenolepis nana, Strongyloides spp., Capillaria spp., and Physaloptera spp. from all four districts were 1,545 (n=29), 740 (n=3), 1,075 (n=14), 280 (n=5) and 416 (n=5), respectively.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health256
Discussion and Conclusion The overall prevalence of rats infected with intestinal parasites in 4 districts was 41.79%. Prevalence of infection in rats ranging from highest to lowest was follows: Ban Fang (50%), Chum Phae (45.7%), Manchakhiri (33.3%) and Phu-Pha-Man (28%). Hymenolepis diminuta was the species most found with the highest EPG from all 4 districts of Khon Kaen. Therefore, rats have a chance to disperse eggs of H. diminuta contaminating in environment higher than other parasites. People in the communities also have more chance to be infected with H. diminuta compared to others. The study indicated that H. diminuta had the highest overall prevalence which was corresponded to result that H. diminuta was most found in 4 districts in Khon Kaen. Hymenolepis diminuta also was reported at 15% of 138 rats living in the bad sanitary areas of Bangkok. Highly infection of H. diminuta in human, especially children can cause enteritis, diarrhea, vomiting and dizziness from toxic substances released from the parasite. Eggs of H. diminuta are resistant to chemical and desiccation, therefore they can survive in the environment for a long time.
Strongyloides spp. is harmful to human who gets an infection from eating egg or larvae or from skin penetration. The parasite causes hyperinfection, parasitemia, nervous signs and death in immune-suppressive patient. Human gets infection of Capillaria spp. from fecal oral route. In severe case, patient will show clinical signs of abdominal discomfort, weight loss, anorexia and high fever due to hepatitis, or ascites. Infection and pathogenesis of H. nana are the same as those causes by H. diminuta. Although parasitic infections in rats of all four districts are not different, the overall prevalence of infection in rats is very high (41.79%). Therefore, rats are important reservoirs for zoonotic helminthiasis, and people in the communities have a risk to accidentally get an infection from parasites inhabiting in house rats. Education and good sanitation are needed to reduce that risk and to improve a quality of life in the community. Acknowledgement We thank Dr.Korawuth Punareewattana and Dr.Peerapol Sukon for their assistance and guidance in working on the research. References 1. Suebsaoe, W and Hanrin, W. Control of rodent (rat) causing problems in public health. [internet]
http://www.elearning.msu.ac.th/opencourse/0709%20307/unit5_2_1.html 2. Sangmaneedet, S. Veterinary Helminthology [internet]. Department of
Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University. http://vet.kku.ac.th/pathology/somboon/DOGhelminth/222.html
3. Mafiana CF, Osho MB and Sam-Wobo S. Gastrointestinal helminth parasites of the black rat (Rattus rattus) in Abeokuta, southwest Nigeria [Internet]. J Helminthol; 1997 [cited 2013 Mar 1].
Available from: http://www.ncbi.nlm.nih.gov/pubmed/9705679 4. Cecelia A. Waugh et al. Population distribution and zoonotic potential of gastrointestinal helminths of wild rats Rattusrattus and R. norvegicus from Jamaica [Internet]. Journal of Parasitology; 2006 [cited2013 May 25]. http://www.journalofparasitology.org/doi/pdf/10.1645/GE-795R1.1 5. Saksirisampant, W. and Paonibol, J. Hymenolepis nana and Hymenolepis diminuta. [internet]. Department of Parasitology, Faculty of Medicine, Chulalongkorn University. http://www.cai.md.chula.ac.th/lesson/lesson 4812/index.html 6. Siti N Mohd Zain, Jerzy M Behnke and John W Lewis. Helminth communities from two urban rat populations in Kuala Lumpur, Malaysia [Internet]. University of Malaya; 2012 [cited 2013 May 25].
Available from: http://www.researchgate.net/publication/221684413_ Helminth_communities_from_two_urban_rat_populations_in_Kuala_Lumpur _Malaysia
7. Stanley H. Abadie. The life cycle of Strongyloidesratti [Internet]. Journal of Parasitology; 1963 [cited 2013 May 25].
Available from:http://www.jstor.org/stable/3275991 8. Center for Food Security and Public Health, College of Veterinary Medicine, Iowa State University. Taenia Infections [Internet]. Iowa State University; 2005 [cited 2013 May 25].
Available from: http://www.cfsph.iastate.edu/Factsheets/pdfs/taenia.pdf 9. Paramasvaran, S.et al. Endo-parasite fauna of rodents caught in five wet markets
in Kuala Lumpur and its potential zoonotic implications [Internet]. Tropical Biomedicine; 2009 [cited 2013 May 25].
Available from:http://www.msptm.org/files/67_-_72_Paramasvaran_S.pdf 10. Patamia, I. Cappello, E. Castellano-Chiodo, D. Greco, F. Nigro, L. Cacopardo, B. A Human Case of Hymenolepis diminuta in a Child from Eastern Sicily. Korean J Parasitol. 2010 Jun; 48(2): 167-169. 11. Chero, J. Saito, M. Bustos, J. Blanco, E. Gonzalvez, G. Garcia, H. Hymenolepis nana infection: symptoms and response to nitazoxanide in field conditions. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2007
February; 101(2): 203-205. 12. Gill, G. Bell, D. Strongyloides stercoralis infection in former Far East prisoners of war. Br Med J. 1979 September 8; 2(6190): 572–574. 13. Li, C., H. Yang, Y. Wang. Capillaria hepatica in China. World Journal
Gastroenterology, 2010; 16: 698-702.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 257
3. Mafiana CF, Osho MB and Sam-Wobo S. Gastrointestinal helminth parasites of the black rat (Rattus rattus) in Abeokuta, southwest Nigeria [Internet]. J Helminthol; 1997 [cited 2013 Mar 1].
Available from: http://www.ncbi.nlm.nih.gov/pubmed/9705679 4. Cecelia A. Waugh et al. Population distribution and zoonotic potential of gastrointestinal helminths of wild rats Rattusrattus and R. norvegicus from Jamaica [Internet]. Journal of Parasitology; 2006 [cited2013 May 25]. http://www.journalofparasitology.org/doi/pdf/10.1645/GE-795R1.1 5. Saksirisampant, W. and Paonibol, J. Hymenolepis nana and Hymenolepis diminuta. [internet]. Department of Parasitology, Faculty of Medicine, Chulalongkorn University. http://www.cai.md.chula.ac.th/lesson/lesson 4812/index.html 6. Siti N Mohd Zain, Jerzy M Behnke and John W Lewis. Helminth communities from two urban rat populations in Kuala Lumpur, Malaysia [Internet]. University of Malaya; 2012 [cited 2013 May 25].
Available from: http://www.researchgate.net/publication/221684413_ Helminth_communities_from_two_urban_rat_populations_in_Kuala_Lumpur _Malaysia
7. Stanley H. Abadie. The life cycle of Strongyloidesratti [Internet]. Journal of Parasitology; 1963 [cited 2013 May 25].
Available from:http://www.jstor.org/stable/3275991 8. Center for Food Security and Public Health, College of Veterinary Medicine, Iowa State University. Taenia Infections [Internet]. Iowa State University; 2005 [cited 2013 May 25].
Available from: http://www.cfsph.iastate.edu/Factsheets/pdfs/taenia.pdf 9. Paramasvaran, S.et al. Endo-parasite fauna of rodents caught in five wet markets
in Kuala Lumpur and its potential zoonotic implications [Internet]. Tropical Biomedicine; 2009 [cited 2013 May 25].
Available from:http://www.msptm.org/files/67_-_72_Paramasvaran_S.pdf 10. Patamia, I. Cappello, E. Castellano-Chiodo, D. Greco, F. Nigro, L. Cacopardo, B. A Human Case of Hymenolepis diminuta in a Child from Eastern Sicily. Korean J Parasitol. 2010 Jun; 48(2): 167-169. 11. Chero, J. Saito, M. Bustos, J. Blanco, E. Gonzalvez, G. Garcia, H. Hymenolepis nana infection: symptoms and response to nitazoxanide in field conditions. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2007
February; 101(2): 203-205. 12. Gill, G. Bell, D. Strongyloides stercoralis infection in former Far East prisoners of war. Br Med J. 1979 September 8; 2(6190): 572–574. 13. Li, C., H. Yang, Y. Wang. Capillaria hepatica in China. World Journal
Gastroenterology, 2010; 16: 698-702.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health258
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
Bacteriophages Selection from Nature and Environment in order to Study the Efficacy for Burkholderia pseudomallei prophylaxis,
treatment and control in infected mice and environment
Pittaya Papirom1* and Narisorn Na-ngam1
1Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Objective - To isolate and assess the efficacy of bacteriophage for the prophylaxis and treatment of Burkholderia pseudomallei 576a in infected mice as well as infected sterile soil and water. Results - The mortality rate at the age of 1, 2 and 3 weeks old mice was 0, 2, and 0%, respectively. Control group of mice was given neither bacterium nor phages showed the mortality rate of 0%, each. The group of mice given merely bacterium noted the 0, 6, and 2% mortality, respectively. B. pseudomallei 576a was identified in all blood samples of euthanized mice, except blood samples from mice treated with phage. This indicated that the environmental isolated phage significantly (p<0.05) reduced the mortality rate of the infected mice. Moreover, the isolated phage was inoculated into sterile soil and water at 0, 1, 2, and 3 weeks old mice and the bacterium isolation rate was 10, 4, 2, and 1 samples for each particular week. While phages were isolated from 7, 8, 6, and 3 samples, respectively. This also indicated that the environmental isolated phage showed a significant reduction (p<0.05) of the bacterium in inoculated soil and water. In addition, mice with phage therapy were in good health and phages were also found in their blood samples. The mobility rate of phage treated group of mice at 1, 2, and 3 weeks was at 0, 20, and 10%, respectively and the mortality rate was 0, 20, and 0%, respectively. Of which were lower than the non-phage infected mice. The mobility rate of the non-phage infected mice was at 0, 60, and 20%; and the mortality rate was at 0, 50, and 30%, respectively. Conclusion - Phage was non-toxic in mice and obvious advantage was found compared to the non - phage infected control. Phages significantly reduced (p<0.05) the mortality and mobility of infected mice than the non - phage control group. Keywords: Bacteriophage, Phage, Burkholderia pseudomallei, Melioidosis

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 259
Bacteriophages Selection from Nature and Environment in order to Study the Efficacy for Burkholderia pseudomallei prophylaxis,
treatment and control in infected mice and environment
Pittaya Papirom1* and Narisorn Na-ngam1
1Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand. *Corresponding author
Objective - To isolate and assess the efficacy of bacteriophage for the prophylaxis and treatment of Burkholderia pseudomallei 576a in infected mice as well as infected sterile soil and water. Results - The mortality rate at the age of 1, 2 and 3 weeks old mice was 0, 2, and 0%, respectively. Control group of mice was given neither bacterium nor phages showed the mortality rate of 0%, each. The group of mice given merely bacterium noted the 0, 6, and 2% mortality, respectively. B. pseudomallei 576a was identified in all blood samples of euthanized mice, except blood samples from mice treated with phage. This indicated that the environmental isolated phage significantly (p<0.05) reduced the mortality rate of the infected mice. Moreover, the isolated phage was inoculated into sterile soil and water at 0, 1, 2, and 3 weeks old mice and the bacterium isolation rate was 10, 4, 2, and 1 samples for each particular week. While phages were isolated from 7, 8, 6, and 3 samples, respectively. This also indicated that the environmental isolated phage showed a significant reduction (p<0.05) of the bacterium in inoculated soil and water. In addition, mice with phage therapy were in good health and phages were also found in their blood samples. The mobility rate of phage treated group of mice at 1, 2, and 3 weeks was at 0, 20, and 10%, respectively and the mortality rate was 0, 20, and 0%, respectively. Of which were lower than the non-phage infected mice. The mobility rate of the non-phage infected mice was at 0, 60, and 20%; and the mortality rate was at 0, 50, and 30%, respectively. Conclusion - Phage was non-toxic in mice and obvious advantage was found compared to the non - phage infected control. Phages significantly reduced (p<0.05) the mortality and mobility of infected mice than the non - phage control group. Keywords: Bacteriophage, Phage, Burkholderia pseudomallei, Melioidosis

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health260
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
The potential uses of avermectin derivatives for anti-Trichinella spiralis in mice
Sutiwat Chumsang1* Thareerat Phatthong1 and Somboon Sangmaneedet2
1Fifth Year Veterinary Student, 2Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*corresponding author E-mail: [email protected], [email protected]
Objective - To examine the effectiveness of avermectin derivatives, selamectin and moxidectin, applied on the skin of mice against first infective stage of Trichinella spiralis in muscle. Materials and Methods - Thirty mice age 2 months were raised in the wire cages. Each mouse was infected by ingesting 15 larvae of first infective stage of T. spiralis, Mae Hong Son strain raised at Department of Parasitology, Faculty of Veterinary Medicine, Khon Kaen University. The infected mice were then kept for 30 days and separated to 3 groups containing 10 mice each. The first group is control; the second and third groups are treated with a local spot of commercial product, selamectin and moxidectin, respectively. Mice were euthanized 14 days later and Trichinella larvae in the muscle were carried out by the standard pepsin digestion method. Number of the lived larvae after digestion were examined and compared to evaluate the effectiveness of the drugs. Data were statistically analyzed by non-parametric test, Kruskal-Wallis Test and Mann-Whitney U test at p<0.05 with SPSS statistic software version 22. Results - The results showed that mice in the control group and those treated with selamectin had average numbers of lived larvae in muscle 20.70 and 17.05, respectively (p>0.05). Mice in group treated with moxidectin had an average number of lived larvae in muscle 8.75 which was significantly decreased (p<0.05) comparing to those groups. Conclusion - This study reveals that moxidectin can kill and reduces the number of lived first stage larvae of Trichinella spiralaris in muscle after a single application on the skin.
Keywords: Avermectin, Trichinella spiralis
Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 261
The potential uses of avermectin derivatives for anti-Trichinella spiralis in mice
Sutiwat Chumsang1* Thareerat Phatthong1 and Somboon Sangmaneedet2
1Fifth Year Veterinary Student, 2Department of Pathobiology, Faculty of Veterinary Medicine, Khon Kaen University, Khon Kaen 40002, Thailand.
*corresponding author E-mail: [email protected], [email protected]
Objective - To examine the effectiveness of avermectin derivatives, selamectin and moxidectin, applied on the skin of mice against first infective stage of Trichinella spiralis in muscle. Materials and Methods - Thirty mice age 2 months were raised in the wire cages. Each mouse was infected by ingesting 15 larvae of first infective stage of T. spiralis, Mae Hong Son strain raised at Department of Parasitology, Faculty of Veterinary Medicine, Khon Kaen University. The infected mice were then kept for 30 days and separated to 3 groups containing 10 mice each. The first group is control; the second and third groups are treated with a local spot of commercial product, selamectin and moxidectin, respectively. Mice were euthanized 14 days later and Trichinella larvae in the muscle were carried out by the standard pepsin digestion method. Number of the lived larvae after digestion were examined and compared to evaluate the effectiveness of the drugs. Data were statistically analyzed by non-parametric test, Kruskal-Wallis Test and Mann-Whitney U test at p<0.05 with SPSS statistic software version 22. Results - The results showed that mice in the control group and those treated with selamectin had average numbers of lived larvae in muscle 20.70 and 17.05, respectively (p>0.05). Mice in group treated with moxidectin had an average number of lived larvae in muscle 8.75 which was significantly decreased (p<0.05) comparing to those groups. Conclusion - This study reveals that moxidectin can kill and reduces the number of lived first stage larvae of Trichinella spiralaris in muscle after a single application on the skin.
Keywords: Avermectin, Trichinella spiralis

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health262
Introduction Trichinosis is a zoonosis of mammals such as pig, dog, cat, mouse and wildlife. The disease is caused by Trichinella spp., a round worm which adult living in intestine and infective larva found as dormant stage in muscle. The infected animals normally will not show any clinical signs except in case of heavy infection. An infected patient shows clinical signs of fever, muscle pain, headache, skin rash and itching, hard body movement, and some cases may have conjunctivitis depending on number of ingested larvae [2, 3]. Trichinosis is worldwide distributed, it was first reported in Thailand at Mae-Sareng District, Mae-Hong-Sorn Province in 1962 [1]. The disease sporadically occurs especially in the North where hill-tribe people raise their pigs under poor sanitary environment. In addition, transmission of the disease is also normally found in people who have contaminated raw meat or un-cooked food. Currently, three identified species of Trichinella causing disease in patients are Trichinella spiralis, T. pseudospiralis and T. papuae. Incidence of Trichinosis in Thailand was frequently reported in many locations where people ate un-cooked meat of wild pigs [4]. Treatment of Trichinosis in mild cases is by administration of anthelminthic drugs such as albendazlole or mebendazole which are effective on adult parasites during the enteric or intestinal phase. In contrast, infective stage of Trichinella in muscle is hardly to cure and time consuming. Therefore, this study aims to evaluate an efficacy of avermectin derivatives, moxidectin and selamectin, in treatment of infective larvae living in muscle. The avermectin derivatives have been reported of their highly effectiveness on many nematodes. New features, spot-on or pour-on, of these derivatives have been produced for a tropical application providing convenience for users. The avermectin derivatives act on increasing of gamma amino butyric acid (GABA) at presynaptic neurons. Once GABA released, it inhibits neurotransmitter substance and block stimulation at the post-synaptic of nematodes’ or arthropods’ muscle [5]. The hypothesis of this study is that Trichinella is nematode therefore avermectin derivatives should inhibit or kill the Trichinella larvae inside muscle cells. Materials and Methods First stage larvae of Trichinella spiralis from muscle of mice raised at animal unit of Parasitology Department, Faculty of Medicine, Khon Kaen University were harvested by digestion method. Each mouse, totally 30 mice, ages 60 days were orally inoculated with 15 larvae. The infected mice were randomized into 3 experimental groups with 10 mice per group.
Group 1 is a positive control group orally infected with Trichinella larvae, no treatment. Group 2 is a 30 mg/kg pour-on selamectin treated group. Group 3 is a 0.1 ml pour-on moxidectin treated group. All animals were consequently raised for next 30 days after inoculation, and then were euthanized. Only lived larvae of Trichinella digested from muscle of all mice were examined, enumerated and statistically analyzed by non-parametric test, Kruskal-Wallis Test and Mann-Whitney U test at p<0.05 with SPSS statistic software version 22. Results Average number of lived larvae of treatment groups versus the control was shown in Table 1. Number of lived larvae from each mouse was counted for 5 times. Average numbers of lived Trichinella’s larvae of all 3 experiment groups recovered from the digestion method were significant difference (p>0.05). Selamectin yielded average numbers of lived larvae (20.70) not differed from the control group (17.05). Treatment with moxidectin decreased significant average number of lived larvae (8.75) compared to the other groups (p<0.05). Table 1. Average numbers of lived Trichinella’s larvae of mice in control group, selamectin and moxidectin treated groups.
Mouse no. Control group Selamectin treated group
Moxidectin treated group
1 137.00 491.00 2.20 2 147.00 2.00 0.00 3 3.50 0.00 0.00 4 3.00 100.00 0.40 5 9.20 4.00 2.60 6 0.00 5.40 1.20 7 13.00 20.20 4.00 8 570.00 14.60 1.40 9 21.60 12.40 1.20
10 307.00 0.00 4.00
Conclusion Moxidectin is the most effectiveness in killing the first stage larvae of Trichinella spiralis inhabit in muscle. Administration of moxidectin by spot-on is very convenient, however it may not be applicable in large animals. It is suggested that the optimal dosage of moxidectin should be evaluated to get the highest result.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 263
Group 1 is a positive control group orally infected with Trichinella larvae, no treatment. Group 2 is a 30 mg/kg pour-on selamectin treated group. Group 3 is a 0.1 ml pour-on moxidectin treated group. All animals were consequently raised for next 30 days after inoculation, and then were euthanized. Only lived larvae of Trichinella digested from muscle of all mice were examined, enumerated and statistically analyzed by non-parametric test, Kruskal-Wallis Test and Mann-Whitney U test at p<0.05 with SPSS statistic software version 22. Results Average number of lived larvae of treatment groups versus the control was shown in Table 1. Number of lived larvae from each mouse was counted for 5 times. Average numbers of lived Trichinella’s larvae of all 3 experiment groups recovered from the digestion method were significant difference (p>0.05). Selamectin yielded average numbers of lived larvae (20.70) not differed from the control group (17.05). Treatment with moxidectin decreased significant average number of lived larvae (8.75) compared to the other groups (p<0.05). Table 1. Average numbers of lived Trichinella’s larvae of mice in control group, selamectin and moxidectin treated groups.
Mouse no. Control group Selamectin treated group
Moxidectin treated group
1 137.00 491.00 2.20 2 147.00 2.00 0.00 3 3.50 0.00 0.00 4 3.00 100.00 0.40 5 9.20 4.00 2.60 6 0.00 5.40 1.20 7 13.00 20.20 4.00 8 570.00 14.60 1.40 9 21.60 12.40 1.20
10 307.00 0.00 4.00
Conclusion Moxidectin is the most effectiveness in killing the first stage larvae of Trichinella spiralis inhabit in muscle. Administration of moxidectin by spot-on is very convenient, however it may not be applicable in large animals. It is suggested that the optimal dosage of moxidectin should be evaluated to get the highest result.

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health264
Acknowledgement We would like to thanks Department of Parasitology, Faculty of Medicine, Khon Kaen University for providing Trichinella spiralis, and also all the staffs who advised techniques in inoculation. References 1. Buntanom, Prachum and Naowarat, Akanee. 1962. Outbreak of Trichinosis in Mae-
Sareng District, Mae-Hong-Sorn Province. J Public Health, 33(3) : 302-308.
2. Chaichanapoonpol, Ittipon. 2002. Trichinellosis. First Edition. Northern Research
and Diagnostic Center. 3. Gottstein, B., Pozio, E., Nöckler, K. Epidemiology, Diagnosis, Treatment, and
Control of Trichinellosis. Clin Microbiol Reviews. 2009 January; 22(1): 127-145
4. Kusolsuk, T., Rojekittikhun, W. Trichinellosis in Thailand: Epidemiology, Prevention and Control. J Trop Med Parasitol. 2009: 32:35-43. 5. Plumb C. Selamectin. Plumb’s Veterinary Drug Handbook. 2011 (7): 911-912.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 265
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................
......................................................................................................................................................................................................................................................................

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health266
Peer Review Committee
1. James A. Will*, DVM, PhD, PhD Hon Emeritus Professor 2. Bongkot Noppon** BSc, MPH, M.Phil, PhD
Associate Professor 3. Chaiyapas Thamrongyoswittayakul** DVM, MS, PhD
Assistant Professor 4. Ranee Singh** DVM, MSc, PhD
Assistant Professor
*University of Wisconsin-Madison, USA. **Faculty of Veterinary Medicine, Khon Kaen University, Thailand.

Faculty of Veterinary Medicine, Khon Kaen University
24th-25th April 2014 at Pullman Hotel, Khon Kaen, Thailand 267

15th Khon Kaen Veterinary Annual International Conference
Sustainable Development on One Health268