
Comprehensive revision of radiology for frCr 2B - AME Books
337
Medical Imaging Case Collections, Series 1: COMPREHENSIVE REVISION OF RADIOLOGY FOR FRCR 2B Richa Arora Quantitative Imaging in Medicine and Surgery Comprehensive Revision of Radiology for FRCR 2B This book is meant for Radiology trainees across the world preparing for their final practical exams, particularly those appearing for ‘Part 2B of Fellowship of the Roy- al College of Radiologists’ examination. It covers all the three components of the exam: long cases, viva cases and Rapid reporting and has more than 300 images with a wide variety of cases often asked in the exam. The book includes cases with all types of imaging modalities (plain radiographs, barium studies, mammograms, Ultrasound, CT, MRI) with particular stress on plain radiographs, as they constitute majority of the exam cases. Thoracic imaging and Musculoskeletal Radiology are also given special emphasis as these cases are more prevalent in the exam and require extra practice. It will prove to be more useful if used as a revision and practice book before the exam after having read the text books. Medical Imaging Case Collections, Series 1 Richa Arora Includes ·Long cases ·Viva cases ·Rapid Reporting COMPREHENSIVE REVISION OF RADIOLOGY FOR FRCR 2B
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Comprehensive revision of radiology for frCr 2B - AME Books
Medical Im
aging Case C
ollections, Series 1:
Co
mp
reh
ensiv
e re
visio
n
of r
ad
iolo
gy
for
frC
r 2B
R
icha Arora
Quantitative Imaging in Medicine and Surgery
Comprehensive Revision of Radiology for FRCR 2B
This book is meant for Radiology trainees across the world preparing for their final practical exams, particularly those appearing for ‘Part 2B of Fellowship of the Roy-al College of Radiologists’ examination. It covers all the three components of the exam: long cases, viva cases and Rapid reporting and has more than 300 images with a wide variety of cases often asked in the exam.
The book includes cases with all types of imaging modalities (plain radiographs, barium studies, mammograms, Ultrasound, CT, MRI) with particular stress on plain radiographs, as they constitute majority of the exam cases. Thoracic imaging and Musculoskeletal Radiology are also given special emphasis as these cases are more prevalent in the exam and require extra practice.
It will prove to be more useful if used as a revision and practice book before the exam after having read the text books.
Medical Imaging Case Collections, Series 1
Richa Arora
Includes ·Long cases·Viva cases·Rapid Reporting
Comprehensive revisionof radiology for frCr 2B

AME Publishing Company
Room 604 6/F Hollywood Center, 77-91 Queen’s road, Sheung Wan, Hong Kong
Information on this title: www.amepc.orgFor more information, contact [email protected]
Copyright © AME Publishing Company. All rights reserved.
This publication is in copyright. Subject to statutory exception and to the provisions of relevant collective licensing agreements, no reproduction of any part may take place without the written permission of AME Publishing Company.
First published 2015Printed in China by AME Publishing Company
Richa Arora
Medical Imaging Case Collections, Series 1:
Comprehensive Revision of Radiology for FRCR 2B
ISBN: 978-988-14027-2-1 Hardback
AME Publishing Company has no responsibility for the persistence or accuracy of URLs for external or third-party internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, accurate or appropriate.
The advice and opinions expressed in this book are solely those of the author and do not necessarily represent the views or practices of AME Publishing Company. No representations are made by AME Publishing Company about the suitability of the information contained in this book, and there is no consent, endorsement or recommendation provided by AME Publishing Company, express or implied, with regard to its contents.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Table of Contents
Preface ............................................................................................................................................................... i
Image contributors ...........................................................................................................................................ii
Dedications .......................................................................................................................................................iii
How to prepare for long cases and oral examination .....................................................................................iv
Section 1—Long cases
Set 1 ................................................................................................................................................................................... 1
Set 2 ................................................................................................................................................................................. 19
Set 3 ................................................................................................................................................................................. 36
Set 4 ................................................................................................................................................................................. 52
Set 5 ................................................................................................................................................................................. 67
Section 2—Oral examinations/viva
Set 1 .................................................................................................................................................................................. 83 Set 2 ................................................................................................................................................................................ 97
Set 3 ................................................................................................................................................................................ 111
Set 4 ................................................................................................................................................................................ 127
Set 5 ............................................................................................................................................................................... 143
Section 3—Rapid reporting
How to prepare for rapid reporting ..............................................................................................................v
Set 1 ................................................................................................................................................................................ 160
Set 2 ................................................................................................................................................................................ 189
Set 3 ................................................................................................................................................................................ 219
Set 4 ................................................................................................................................................................................ 249
Set 5 ................................................................................................................................................................................ 278
Answers of rapid reporting ........................................................................................................................................ 309
Index ............................................................................................................................................................................ 313


i
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Preface
This book is meant for Radiology trainees across the world preparing for their final practical exams, particularly those appearing for ‘Part 2B of Fellowship of The Royal College of Radiologists’ examination. The exam is held in London (autumn & spring), Singapore (spring) and Hong Kong (autumn) and is given by candidates after completing 3 years of training in a recognized university. It has three components: long cases, oral examination and rapid reporting.
The book covers all the three modules and has good collection of cases often given in the exam. Each long case and viva case is described in the same pattern as that of ‘answer booklet of long cases’ of The Royal College. So even viva cases can be used for practice of written test. The case explanation includes description of findings, diagnosis, differential diagnosis, management, important points to remember (concise description of the entity helpful for the oral exam) along with the references. I have tried to include cases with all types of imaging modalities (plain radiographs, barium studies, mammograms, ultrasound, CT, MRI) with particular stress on plain radiographs, as they constitute majority of the exam cases. Thoracic imaging and Musculoskeletal Radiology are also given special emphasis as these cases are generally asked and require more practice.
Five practice tests of ‘rapid reporting’ are also included along with the complete check list of each anatomical area and practical points to prepare for it. I have tried to cover lot many pathologies asked in the rapid reporting, therefore, the number of abnormal films are on the higher side in each set.
Hence the book will prove to be more useful if used as a revision and practice book before the exam after having read the text books.
My sincere wishes for all the examinees!
Richa Arora, MD, FRCR, MMedDepartment of Radiology and Imageology,
Nizam’s Institute of Medical Sciences, Hyderabad, India(Email: [email protected].)
ii
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Images contributed by:
(I) Dr. Richa Arora, MD, FRCR, MMed, Assistant Professor. Department of Radiology and Imageology, Nizam’s Institute of Medical Sciences, Hyderabad, India.
(II) Dr. Shivanand Gamnagatti, Additional Professor. Department of Radiology, All India Institute of Medical Sciences, New Delhi, India.
(III) Dr. Manjunath YC. Consultant Radiologist, Varuni Medical Diagnostics, Kolar, India.(IV) Dr. Smriti Hari, Additional Professor. Department of Radiology, All India Institute of Medical Sciences, New Delhi,
India.(V) Dr. Krithika Rangarajan, Senior Resident. Department of Radiology, All India Institute of Medical Sciences, New
Delhi, India.
iii
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Dedicated to my parents

iv
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
How to prepare for long cases and oral examination
There is no significant difference in the preparation of long cases and viva (as far as knowledge is concerned) except that you require proper time management in the written exam and confidence as that of a consultant for the viva. The purpose of written exam is to test your capability to format a report and of oral exam is to check your communication skills as a consultant in radiology. Moreover, in viva majority of cases are of conventional radiology i.e., plain radiographs, barium studies, intravenous pyelograms etc. where as long cases often have CT and MR images as well.
Long cases test has six cases which are to be done in 60 minutes. It is important to attempt all the cases in order to pass. Therefore, it is advisable to give 8 minutes to each case, so that you can spend last 10 minutes for your doubts. Hence, always practice with your watch. Use ‘bullet points’ instead of long theories for a good score and effective time management. All the cases in this book are written in the same manner as that of answer book template (observations, diagnosis, differential diagnosis and management) of the exam. Use them as practice tests and subsequently check the answers. Important points related to the topic can be revised at the end of each case, which are particularly helpful for the viva.
For a successful oral examination one needs to follow certain tips. Practice as many cases as possible using various books or teaching radiology websites. Practice with some study partner or in groups as it helps to overcome the stress and you can learn many things from their performance. If you get an ‘aunt minnie’ score well with your practiced speech. Listen carefully to the history given by the examiner. Be systematic in your approach while describing findings to all the cases pertaining to each body system. That way you will not miss any finding and will be able to solve any case even those with diagnostic dilemma. Be careful not to miss any life-threatening condition like bowel perforation, pneumothorax or brain herniation etc. Always suggest immediate referral to the concerned clinician for these emergency cases for their prompt treatment. Ask for old films if relevant. Discuss further management in all the cases. Do not panic and presume your failure if you don’t do well in any particular case. You can easily pass if you perform well in subsequent cases.
Section 1—Long cases
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 1
Set 1
Case 1
History
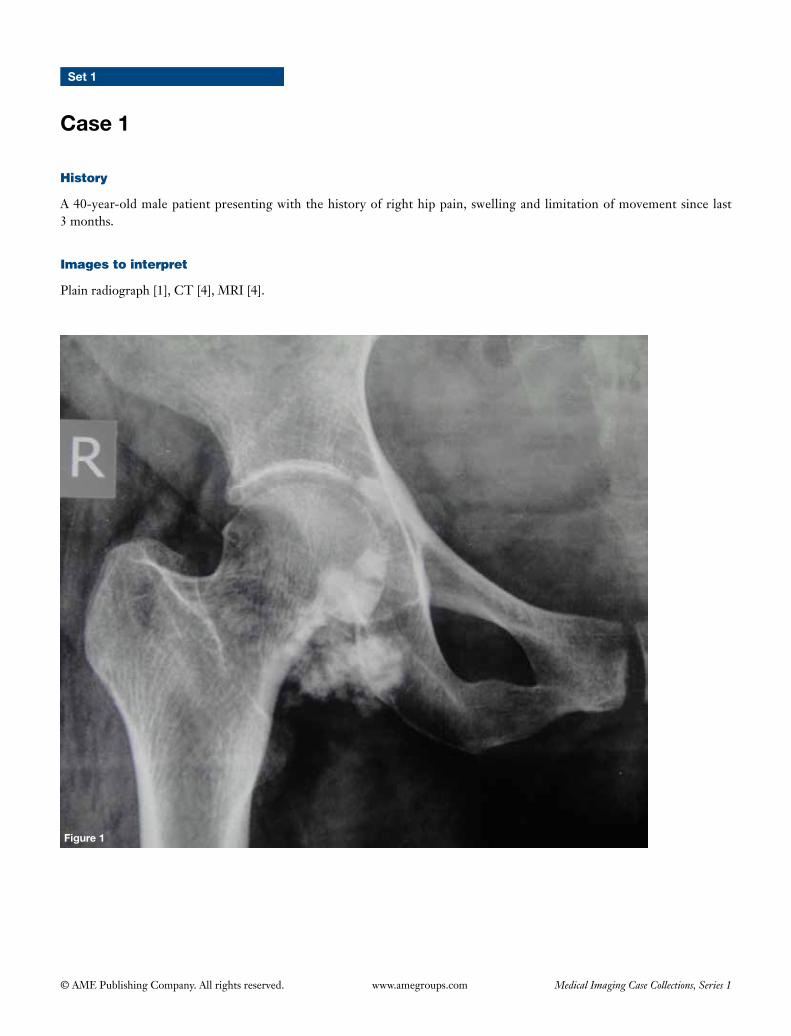
A 40-year-old male patient presenting with the history of right hip pain, swelling and limitation of movement since last 3 months.
Images to interpret
Plain radiograph [1], CT [4], MRI [4].
2
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2
A B
Figure 3
BA
3
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 5
A B
A B
Figure 4
4
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
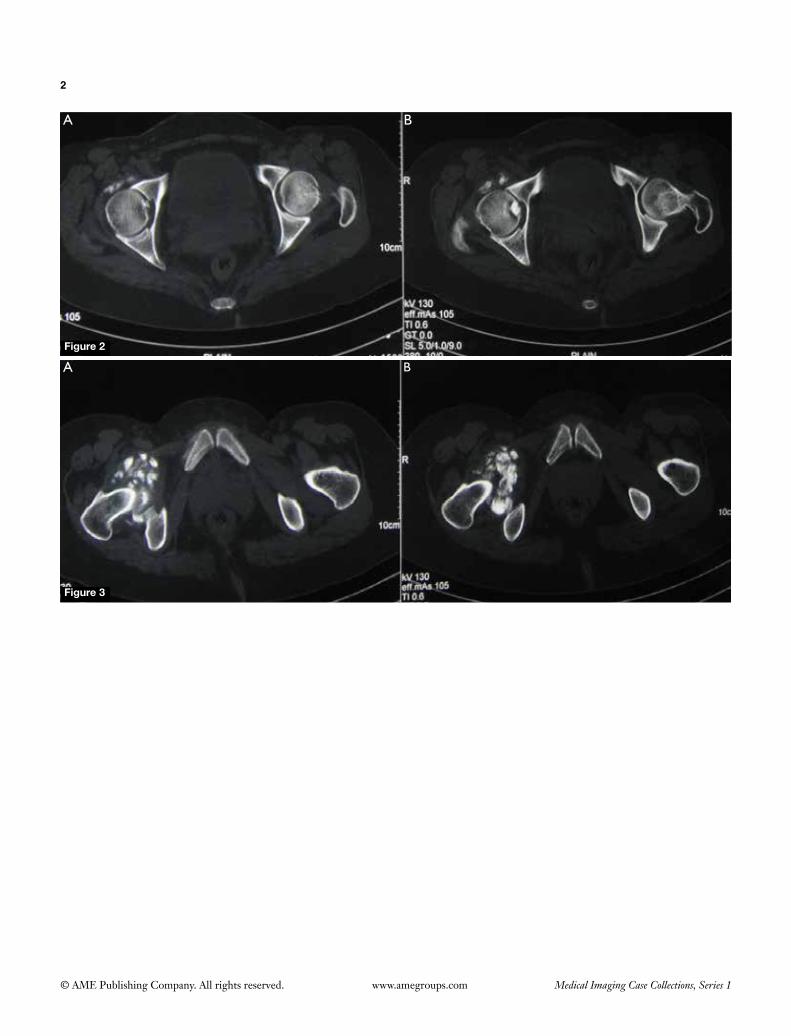
Plain radiograph right hip frontal view (Figure1)
(I) Multiplecalcifiedandossifiedloosebodies(almostofsimilar size) seen overlying right hip joint mainly on the inferior aspect;
(II) Articularmarginsof right femur and acetabulumappear normal with normal intervening joint space and with no evidence of degenerative changes.
Non-contrast CT of both hip joints axial bone window images (Figures 2,3)
(I) CT confirms intraarticular location of the loose bodies;
(II) Left hip joint is normal.
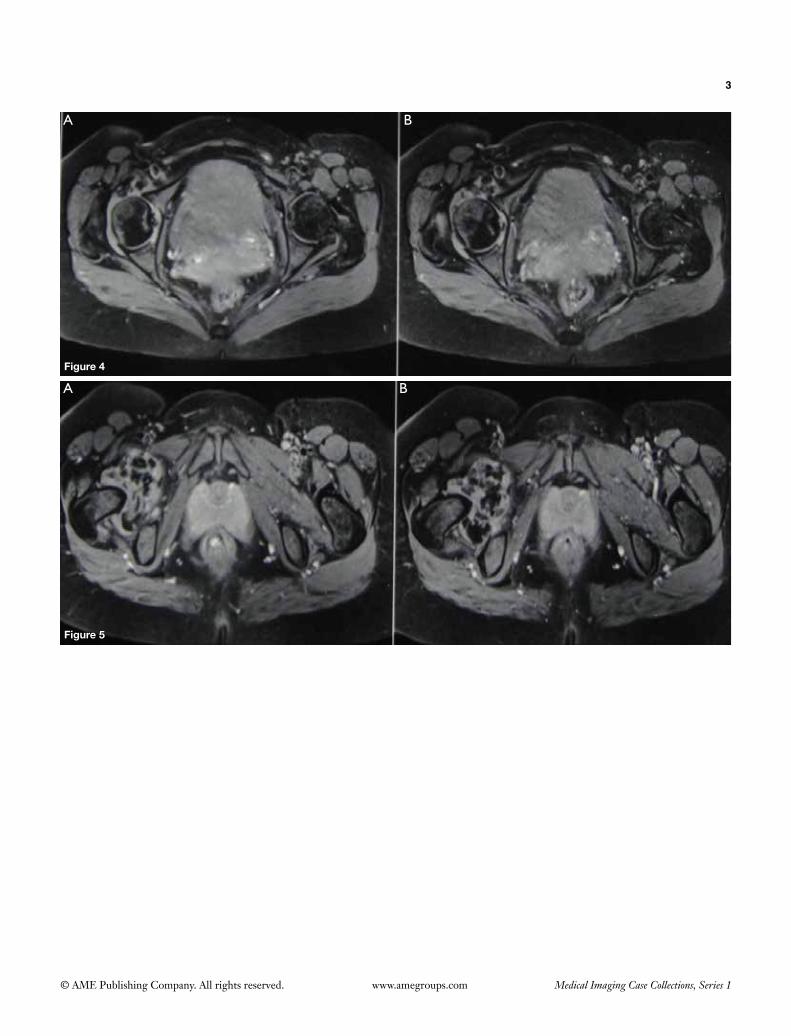
MRI axial gradient recalled echo (GRE) sequence images (Figures 4,5)
(I) MRIconfirmsplainradiographicandCTfindings;(II) LoosebodiesshowingbloomingonGREsequence;(III) There is evidence of synovial proliferation along the
right hip joint with multiple calcified and ossified loosebodiesofuniformsize.Extension intherightiliopsoasandobturatorexternusbursaalsonoted.
Diagnosis
Primary synovial chondromatosis.
Differential diagnosis
Secondary synovial chondromatosis (ruled out as there are noosteoarthriticchangesintherighthipandloosebodiesare of similar size).
Management
Orthopedic referral for the total synovectomy along with removalofchondralbodies.
Important points to remember
• Primary synovial chondromatosis i s a benignmonoarticulardisordercharacterizedbycartilaginousmetaplasia of synovium with the formation of multipleloosebodies,whichundergocalcificationandossification with time. The etiology is still unknown. It most commonly involves joints and less commonly tendonsheathsandbursae(1).
• Itmainlyaffectsmales (M:F:2-4:1)during3rd to 5th decades of life.
• Radiographic features dependon the stage of thedisease.Whenthechondralbodiesareunmineralized,radiographsmaybenormal(30%ofthecases)ormayshow periarticular erosions, widened joint space, soft tissue surrounding the joint. Later, ‘ring and arc’ type chondroid calcificationmaybe seen inmetaplasticsynoviumand loosebodies.Fullyossifiedbodiesofuniformsizeareseeninthe‘burntout’disease.CTishelpful in confirming intraarticular location and early mineralizationofthenodules(1,2).
• MRIfindingsinclude:jointeffusion,synovialproliferationand loosebodies formation.Non-calcifiedchondralbodies(subtypeA)demonstrateintermediatetolowsignalonT1andhighsignalonT2typicalofcartilage.Theyare difficult to differentiate from surrounding fluid and synoviumandcontrastenhancedsequenceshavearoletoshowperipheralenhancement.Calcifiednodules(subtypeB—75%ofcases)showlowsignalonallthesequenceswithbloomingonGREsequences.Ossifiednodules(subtypeC—9%ofthecases)demonstratefattymarrowwithalowsignalrim(1,2).
• Differentials onMR include secondary synovialchondromatosis (occurs due to severe degenerative changes in the joint, affects older age group and loose bodiesare typically less than5 innumberandnon-uniform in size), pigmented villonodular synovitis, synovial hemangioma, amyloid arthropathy and gout (1).
• Complications include: secondary osteoarthritis,secondary chondrosarcoma (rare) (1).
References
1. McKenzieG,RabyN,RitchieD.Apictorialreviewofprimarysynovialosteochondromatosis.EurRadiol2008;18:2662-9.2. MurpheyMD,VidalJA,Fanburg-SmithJC,GajewskiDA.Imagingofsynovialchondromatosiswithradiologic-pathologic
correlation.Radiographics2007;27:1465-88.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
History
A 60-year-old male patient presenting with progressive dyspnoea and weight loss.
Images to interpret
Plain radiograph [1], CT [7].
Figure 1
6
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
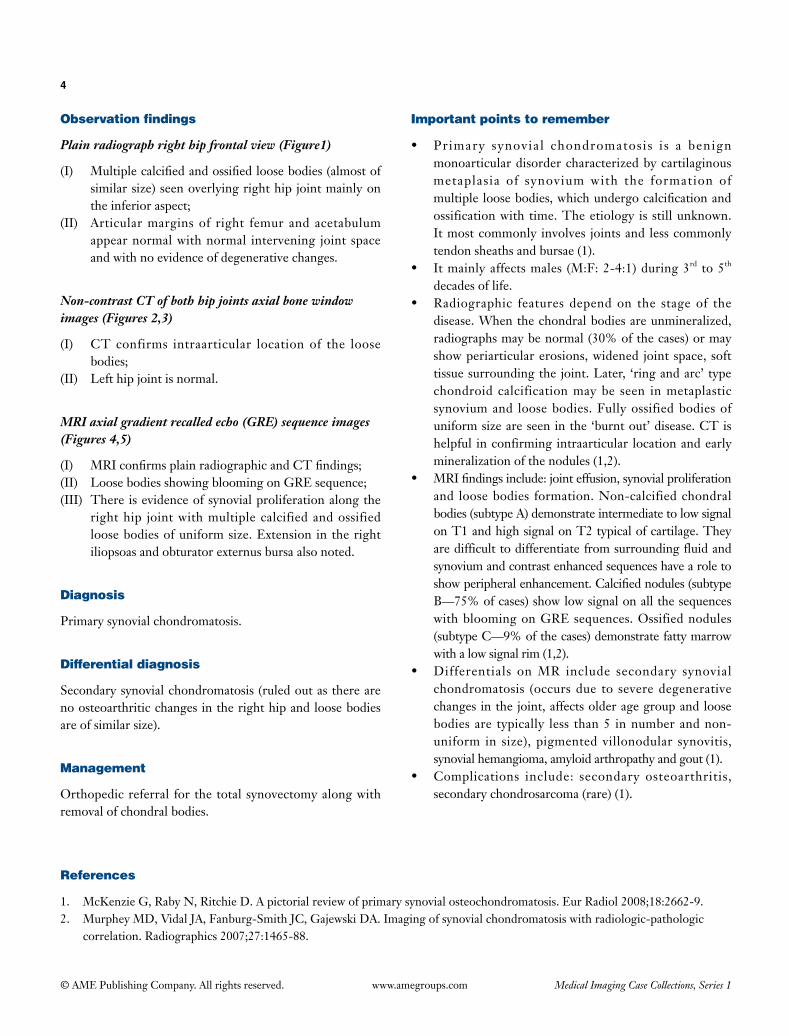
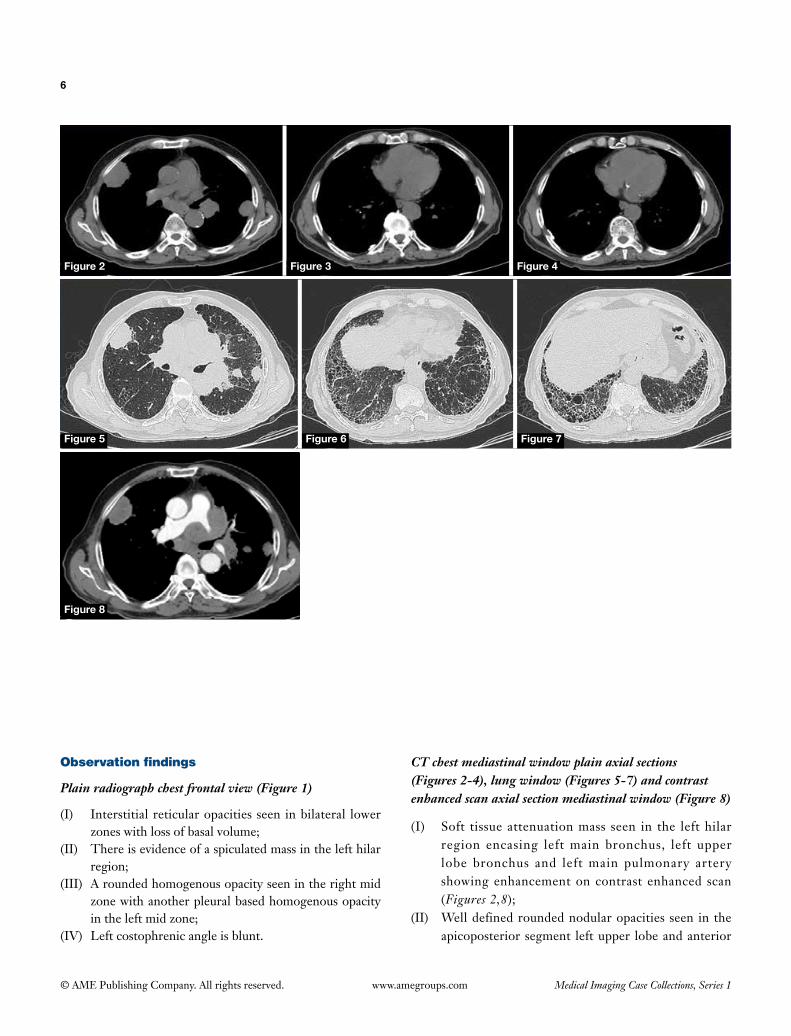
Plain radiograph chest frontal view (Figure 1)
(I) Interstitial reticular opacities seen in bilateral lower zones with loss of basal volume;
(II) There is evidence of a spiculated mass in the left hilar region;
(III) A rounded homogenous opacity seen in the right mid zone with another pleural based homogenous opacity in the left mid zone;
(IV) Left costophrenic angle is blunt.
CT chest mediastinal window plain axial sections (Figures 2-4), lung window (Figures 5-7) and contrast enhanced scan axial section mediastinal window (Figure 8)
(I) Soft tissue attenuation mass seen in the left hilar region encasing left main bronchus, left upper lobe bronchus and left main pulmonary artery showing enhancement on contrast enhanced scan (Figures 2,8);
(II) Well defined rounded nodular opacities seen in the apicoposterior segment left upper lobe and anterior
Figure 2 Figure 4
Figure 5 Figure 6 Figure 7
Figure 8
Figure 3
7
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
segment right upper lobe (Figures 5,8);(III) There is thickening of interlobular and intralobular
septae seen in both lungs predominantly involving subpleural regions and both lower lobes along with honeycombing (Figures 5-7);
(IV) Calcified pleural plaques seen on the right side (Figures 3,4).
Interpretation: basal fibrosis with calcified pleural plaques with bronchogenic carcinoma left lung with metastases in both lungs.
Diagnosis
Asbestosis with asbestos related pleural disease with metastatic bronchogenic carcinoma.
Differential diagnosis
Basal fibrosis due to other causes (collagen vascular diseases, drug related UIP, idiopathic pulmonary fibrosis etc.) with bronchogenic carcinoma.
Management
• Take occupational history of the patient.• Bronchoscopic biopsy of the left hilar mass.• Further metastatic work up for staging of the bronchogenic
carcinoma (to r/o liver, adrenals, bone, brain mets).• Multidisciplinary team discussion and management.
Important points to remember
• Asbestos constitutes group of naturally occurring silicate minerals and heavy asbestos exposure is mainly encountered in men working in the setting of construction, mining or ship/automotive industry (1).
• Asbestos-induced diseases mainly occur in the chest and comprise pleural effusion, pleural plaques, diffuse pleural thickening, rounded atelectasis, asbestosis, malignant
mesothelioma and bronchogenic carcinoma (1).• Benign pleural effusions are the earliest pleural based
manifestation, which often occurs within 10 years of exposure and contain hemorrhagic exudates of mixed cellularity.
• Pleural plaques—most common finding, usually arise from parietal pleura, occur 20-30 years after exposure, often involve posterolateral chest wall between 7th to 10th ribs, diaphragmatic pleura and mediastinal pleura with sparing of apices and costophrenic angles (calcification occurs in 10-15% of the cases) (1).
• Diffuse pleural thickening—less specific, occurs due to thickening and fibrosis of the visceral pleura which fuses with the parietal pleura. Imaging shows diffuse continous sheet like pleural thickening involving costophrenic angles and apices covering at least 25% of the total chest wall on a chest radiograph (50% if unilateral) with thickness of at least 5 mm in at least one of its site (1).
• Asbestosis-diffuse interstitial fibrosis caused by asbestos inhalation with latent period of 20 years or longer. Imaging features—subpleural reticulation with some ground glass opacities mainly in lower lobes with shaggy cardiac silhouette and ill-defined diaphragmatic contours. Honey combing and volume loss seen in advanced stages (1).
• Malignant mesothelioma—occurs with a latency of 35-40 years, strong association with asbestos exposure particularly crocidolite and often involves pleura and peritoneum but can occur in tunica vaginalis and pericardium. Imaging shows nodular pleural thickening of >1 cm, involving mediastinal pleura and fissures often with pleural effusion with contraction of hemithorax. Invasion of chest wall, mediastinum including pericardium & great vessels etc., diaphragm along with metastasis to liver, lung and nodes can occur (1).
• Bronchogenic carcinoma—variable latent period, more than synergistic effect of smoking, either squamous cell or adenocarcinoma (1).
References
1. Roach HD, Davies GJ, Attanoos R, Crane M, Adams H, Phillips S. Asbestos: when the dust settles an imaging review of asbestos-related disease. Radiographics 2002;22 Spec No:S167-84.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
History
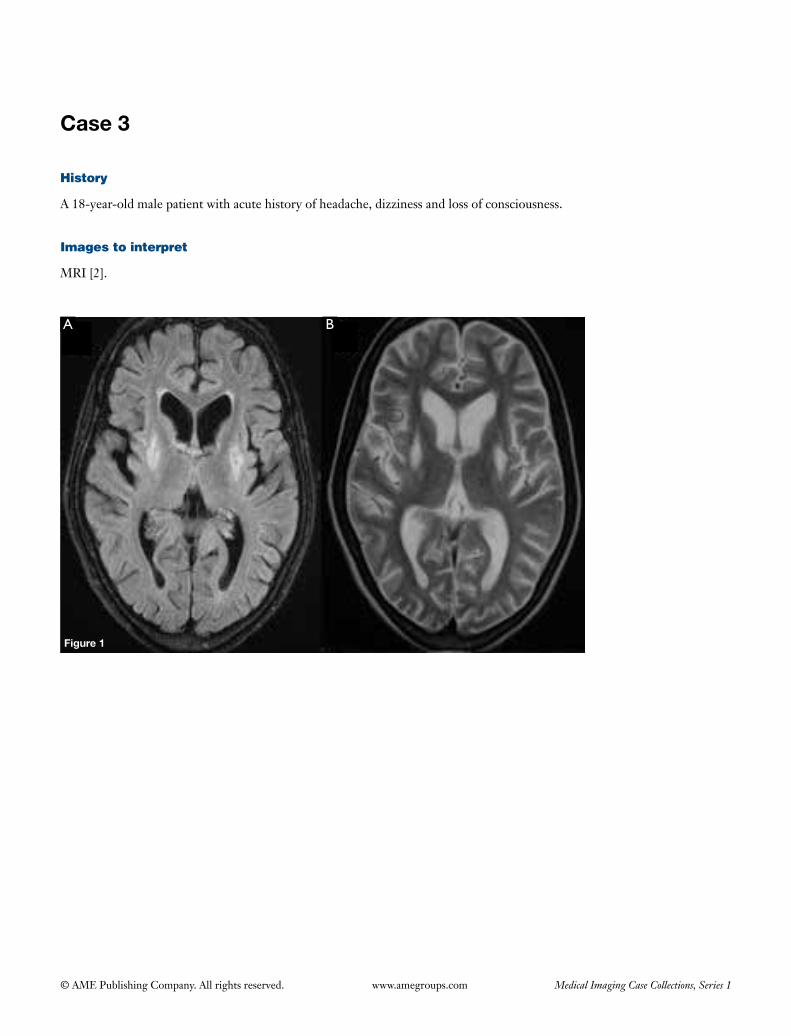
A 18-year-old male patient with acute history of headache, dizziness and loss of consciousness.
Images to interpret
MRI [2].
A B
Figure 1

9
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
MRI axial FLAIR (Figure 1A) and T2 (Figure 1B ) weighted images of the brain at the level of basal ganglia
(I) Symmetric T2 and FLAIR hyperintensities seen in the bilateral globus pallidi with mild collapse (Figure 1A,B);
(II) Rest of the basal ganglia, visualized grey and white matter shows no abnormality.
Diagnosis
Carbon monoxide poisoning.
Differential diagnosis
• Anoxiaduetoothercauses.• Toxicencephalopathies(cyanide/methanol).• Wilsondisease.• Creutzfeldt-Jakobdisease.• Mitochondrialencephalopathy(Leighdisease).
Management
• Takedetailedhistoryofaccidentalorsuicidalpoisoningforconfirmationofdiagnosis.
• Reviewrestof the images alongwith thediffusionweighted images for complete evaluation of grey and white matter.
• Immediatereferraltoneurologistformanagementwith100% oxygen.
Important points to remember
• Carbonmonoxide poisoning is an important andleading cause of accidental poisoning leading to non-cardiogenic pulmonary edema and anoxic-ischemic encephalopathy (1).
• Mechanism of action: binds to heme protein ofhemoglobin forming carboxyhemoglobin reducing oxygen carrying capacity of blood and causing tissue hypoxia; inhibits mitochondrial electron transport enzyme system interrupting oxidative phosphorylation and activates polymorphonuclearleukocytescausinglipidperoxidationin the brain leading to long term sequelae (1).
• Imaging features include:bilateral symmetric lesionsin brain most commonly globus pallidi. Other areas involved include cerebral white matter (often periventricular white matter and centrum semiovale). Occasionally,otherdeepgreymatternucleilikecaudatenucleus, putamen and thalamus are affected, but less so than the globus pallidus. Cases of severe poisoning also have involvement of brainstem, cerebellum, subcortical white matter, corpus callosum, external and internal capsules. The lesions are hypodense on CT, hypointense on T1 (though few areas of hemorrhage can be hyperintense), hyperintense on T2 and FLAIR sequences. Diffusion weighted images can show restricted diffusion due to cytotoxic edema (1).
References
1. LoCP,ChenSY,LeeKW,ChenWL,ChenCY,HsuehCJ,HuangGS.Braininjuryafteracutecarbonmonoxidepoisoning:earlyandlatecomplications.AJRAmJRoentgenol2007;189:W205-11.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
History
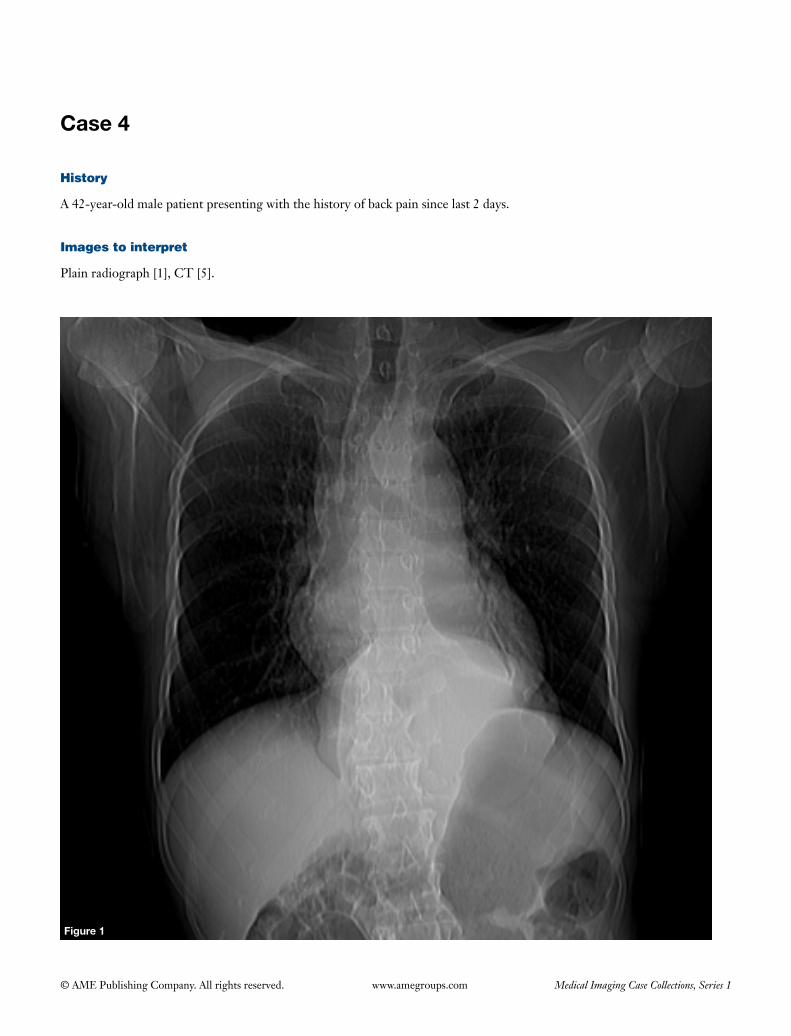
A 42-year-old male patient presenting with the history of back pain since last 2 days.
Images to interpret
Plain radiograph [1], CT [5].
Figure 1
11
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
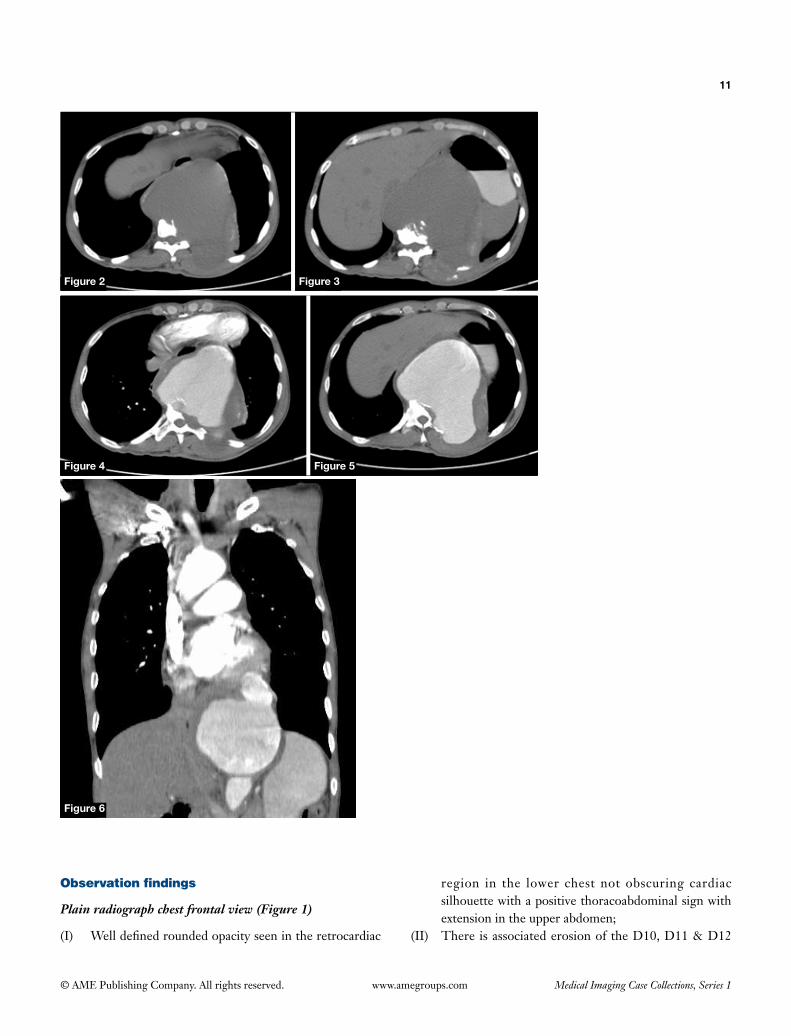
(I) Welldefinedroundedopacityseenintheretrocardiac
region in the lower chest not obscuring cardiacsilhouettewithapositivethoracoabdominalsignwithextensionintheupperabdomen;
(II) There is associated erosion of the D10, D11 & D12
Figure 6
Figure 2 Figure 3
Figure 4 Figure 5

12
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
vertebralbodiesandthe leftpediclesalongwiththeposterior aspect of left 10th and 11thribs(suggestingleftparavertebrallocation).Discspacesarenormal;
(III) Nocalcificationseenintheopacity;(IV) Lungfieldsclear;(V) Nopleuraleffusionseen.
Plain (Figures 2,3) and contrast enhanced CT of chest axial sections (Figures 4,5) and coronal reconstructed image (Figure 6)
(I) There is saccular dilatation of lower thoracicdescending aorta extending in the upper part ofabdominal aorta with a wide neck with peripheral curvilinearcalcificationofthewallandpartialthrombusin it. The posterior aortic wall is closely apposed to the spine (draped aorta sign). The posterolateral wall of the aneurysmontheleftsideisirregularandaneurysmisextendingintheleftposteriorchestwallinvolvingleftparaspinalmusculature;
(II) There is associated erosion of the D10, D11 & D12 vertebralbodiesalongwiththeirleftsidedpedicles&transverseprocessesandposterioraspectof left10th and 11th ribs.
Diagnosis
Containedruptureofdescendingaorticaneurysm.
Differential diagnosis
Aortic dissection.
Management
• Look for theremainingscan forcompleteextentofaneurysmwithinvolvementofsidebranches.
• Urgentreferraltocardiovascularsurgeon.
Important points to remember
• Aortic aneurysm isdefinedaspermanentabnormaldilatation of the aorta more than 50% of its normal diameter.Normaldiameter:ascendingaorta<4cm;descendingthoracicaorta<3cm;abdominalaorta<2cm. Thereforeaortic aneurysmcanbedefinedas aorticdiameter >4 cm in descending thoracic aorta and >3 cm in abdominal aorta.
• Etiology includes: connective tissuedisorders likeMarfan’s syndrome,Ehlers-Danlos syndrome,cysticmedialdegeneration;vasculitis—Takayasu’sarteritis,giant cell arteritis, trauma; infections—syphillis,mycosis; atherosclerosis; non-infective aortitis inseronegative spondyloarthropathies andrheumatoidarthritis;rheumaticfever(1).
• Complications:rupture,aorto-bronchialfistula,aorto-esophageal fistula,distalembolisation,compressionofadjacent structures,vertebralerosion, thromboticocclusionofbranchvessels,infection(1,2).
• Imaging features: rupturedaneurysm—extravasationofcontrast, retroperitonealhematoma,discontinuityof aortic wall, focal discontinuity in continousintimalcalcification, tangentialcalciumsign (intimalcalcificationpoints away fromthevesselwall alongwiththeretroperitonealleakage).Impendingrupture—hyperattenuationcrescentsign(suggestingintramuralhemorrhageorhemorrhagewithin the thrombus),increasedaneurysmsize(diameterof>7cm),increasedgrowthrate(morethanorequalto10mmperyear),low thrombus to lumenratio.Contained rupture—draped aorta sign (as in our case), vertebral bodyerosion (2).
• Treatment is indicatedincasesofrupture/impendingrupture/containedrupture/size>5cminwomenand>5.5cminmenforabdominalaorta;>5cmincasesofMarfan’s syndrome/ifgrowthrateexceeds>1cmperyearandtreatmentoptionsincludeendovascularrepair/opensurgicalrepair(1).
References
1. AgarwalPP,ChughtaiA,MatzingerFR,KazerooniEA.MultidetectorCTofthoracicaorticaneurysms.Radiographics2009;29:537-52.
2. RakitaD,NewatiaA,HinesJJ,SiegelDN,FriedmanB.SpectrumofCTfindingsinruptureandimpendingruptureofabdominalaorticaneurysms.Radiographics2007;27:497-507.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
History
A 66-year-old male patient with history of dysphagia for solids and liquids since last 2 months.
Images to interpret
Barium swallow [1], CT [2].
Figure 1

14
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Barium swallow frontal view (Figure1)
Long segment smooth narrowing seen in the distal esophagus with dilatation and hold up of contrast in the proximal esophagus with irregularity in the region of gastroesophageal junction and cardiac end of the stomach.
Contrast enhanced CT of lower chest axial section mediastinal window at the level of lower esophagus (Figure 2) and sagittal reformatted image (Figure 3)
(I) Concentric wall thickening in the lower esophagus involving gastroesophageal junction with less than 90 degrees of contact with the descending aorta;
(II) The proximal esophagus is mildly dilated.
Diagnosis
Pseudoachalasia.
Differential diagnosis
Achalasia cardia.
Management
• ReviewremainingsectionsofCTforcompleteextentof esophageal carcinoma and metastasis in lungs, adrenals, liver and lymph nodes for staging.
• Multidisciplinaryteamdiscussion.
Important points to remember
• Achalasiacardiaisamotilitydisordercharacterizedbyincomplete relaxation of the lower esophageal sphincter due todegenerationof neurons in theAuerbach’splexus, resulting in weak contractions that are uncoordinatedandnon-propulsivewithabsentprimaryperistalsis (1).
• Imaging findingson contrast swallow:pronouncedtertiary contractions in theearlyphase followedbyfailure of relaxation of lower esophageal sphincter (LES) and dilated esophagus (maximal in the distal esophagus) with short segment smooth tapered narrowing at lower endgivingbirdbeakappearance(1).
• Pseudoachalasia is a type of esophagealmotilitydisorder that mimicks idiopathic achalsia. Its most commoncause is submucosaladenocarcinomaof the
Figure 3Figure 2
15
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
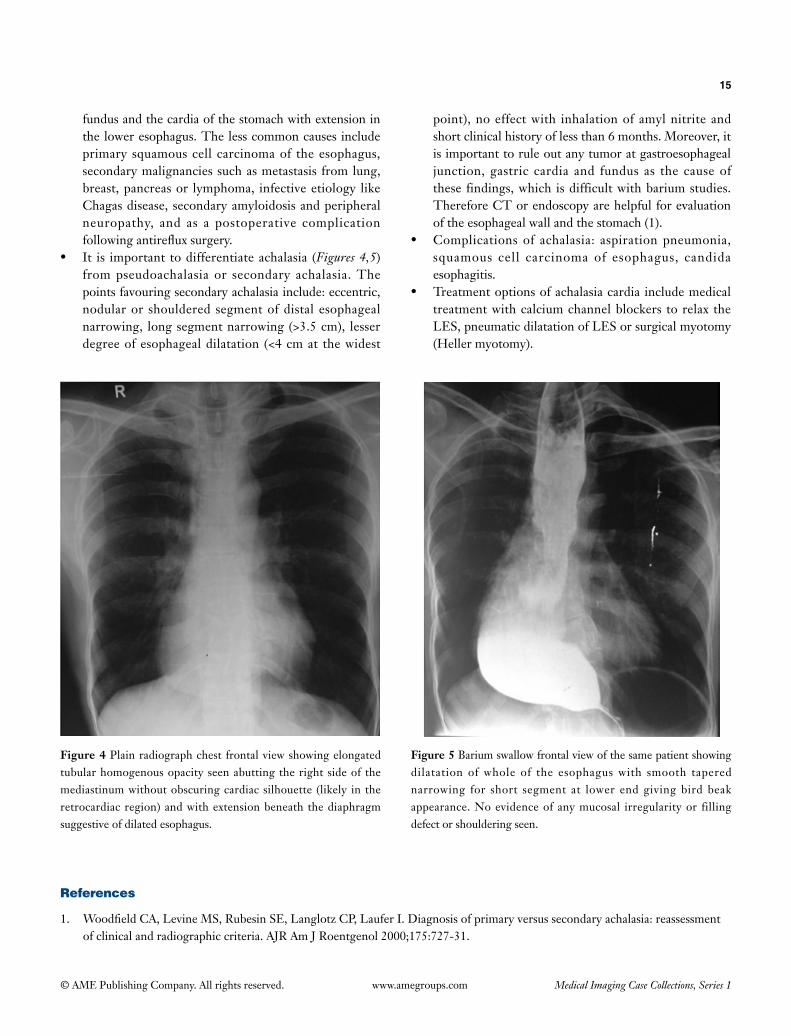
Figure 4 Plain radiograph chest frontal view showing elongated tubularhomogenousopacityseenabuttingtherightsideof themediastinumwithoutobscuringcardiacsilhouette (likely in theretrocardiacregion)andwithextensionbeneaththediaphragmsuggestive of dilated esophagus.
Figure 5 Barium swallow frontal view of the same patient showing dilatation of whole of the esophagus with smooth tapered narrowing for short segment at lower end giving bird beak appearance. No evidence of any mucosal irregularity or filling defect or shouldering seen.
fundus and the cardia of the stomach with extension in the lower esophagus. The less common causes include primary squamous cell carcinoma of the esophagus, secondary malignancies such as metastasis from lung, breast,pancreasor lymphoma, infectiveetiology likeChagas disease, secondary amyloidosis and peripheral neuropathy, and as a postoperative complication followingantirefluxsurgery.
• It is important todifferentiateachalasia (Figures 4,5) from pseudoachalasia or secondary achalasia. The pointsfavouringsecondaryachalasiainclude:eccentric,nodular or shouldered segment of distal esophageal narrowing, long segment narrowing (>3.5 cm), lesser degree of esophageal dilatation (<4 cm at the widest
point), no effect with inhalation of amyl nitrite and shortclinicalhistoryoflessthan6months.Moreover,itis important to rule out any tumor at gastroesophageal junction, gastric cardia and fundus as the cause of these findings,which isdifficultwithbariumstudies.Therefore CT or endoscopy are helpful for evaluation of the esophageal wall and the stomach (1).
• Complicationsof achalasia: aspirationpneumonia,squamous cell carcinoma of esophagus, candida esophagitis.
• Treatmentoptionsofachalasiacardia includemedicaltreatmentwithcalciumchannelblockers torelax theLES, pneumatic dilatation of LES or surgical myotomy (Heller myotomy).
References
1. WoodfieldCA,LevineMS,RubesinSE,LanglotzCP,LauferI.Diagnosisofprimaryversussecondaryachalasia:reassessmentofclinicalandradiographiccriteria.AJRAmJRoentgenol2000;175:727-31.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
History
A 31-year-old female. No history.
Images to interpret
Plain radiograph [1], CT [3].
Figure 1
17
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 4
Figure 3Figure 2
18
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph abdomen supine view (Figure 1)
(I) There is blunting of left costophrenic angle;(II) Mottled gas collection noted in the left renal fossa and
crescentic gas collection in the perinephric region;(III) Left psoas shadow is obscured;(IV) Rest of the radiograph is unremarkable.
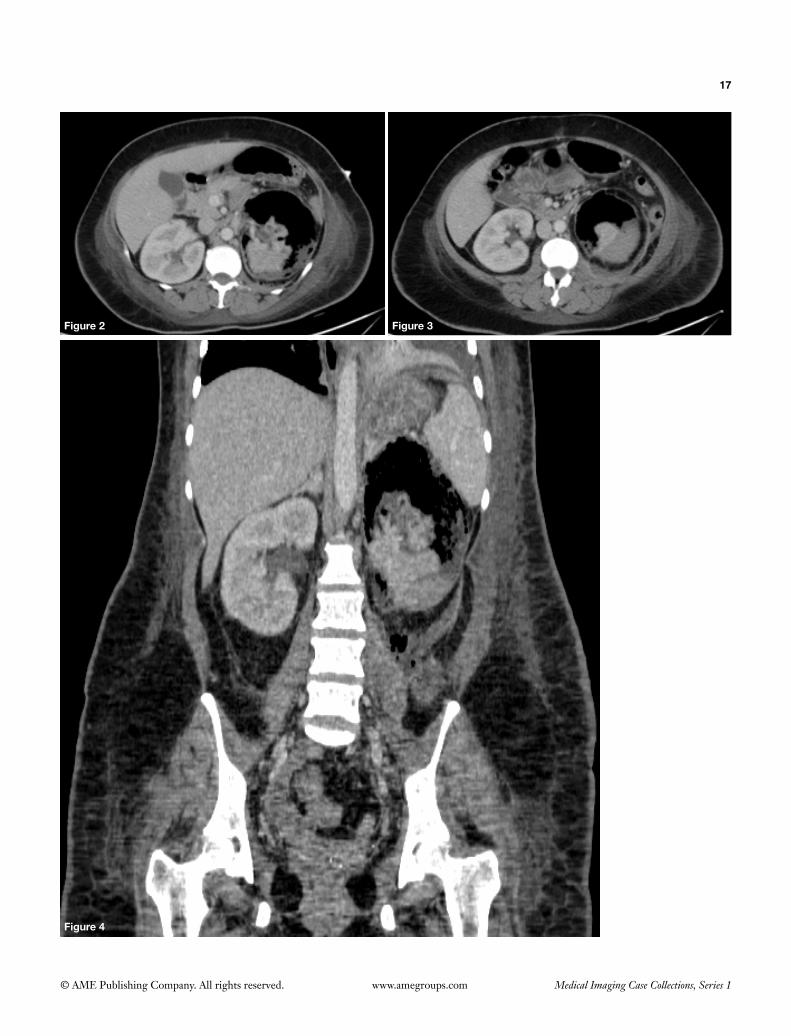
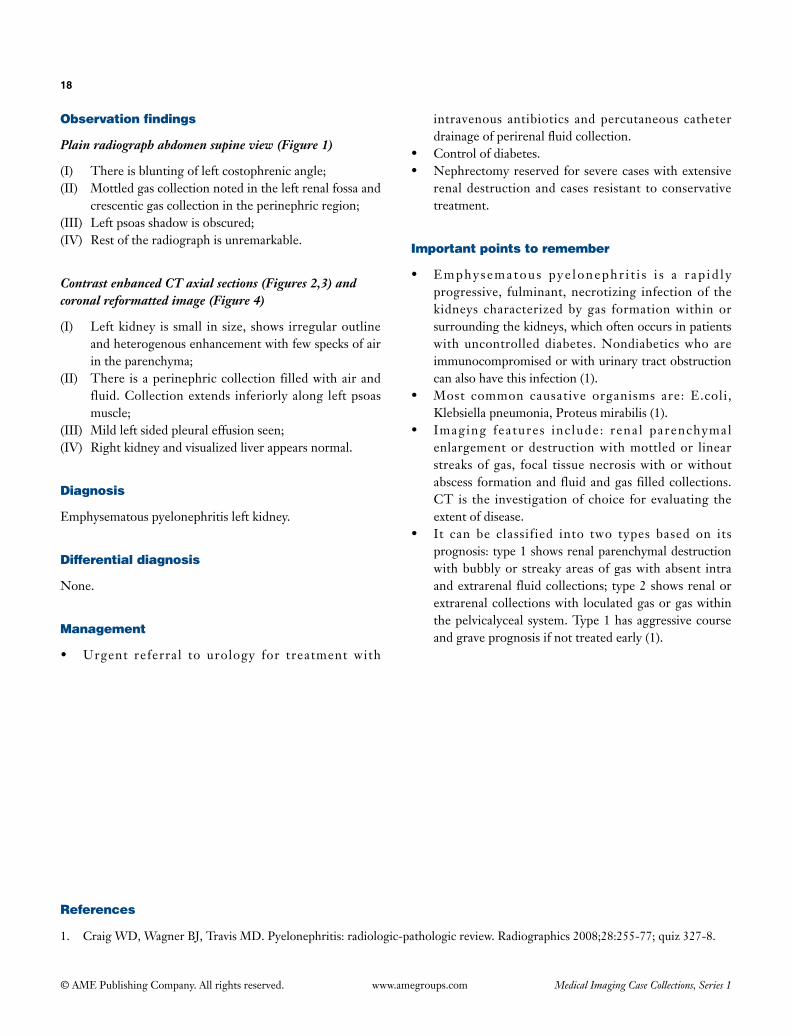
Contrast enhanced CT axial sections (Figures 2,3) and coronal reformatted image (Figure 4)
(I) Left kidney is small in size, shows irregular outline and heterogenous enhancement with few specks of air in the parenchyma;
(II) There is a perinephric collection filled with air and fluid. Collection extends inferiorly along left psoas muscle;
(III) Mild left sided pleural effusion seen;(IV) Right kidney and visualized liver appears normal.
Diagnosis
Emphysematous pyelonephritis left kidney.
Differential diagnosis
None.
Management
• Urgent referral to urology for treatment with
intravenous antibiotics and percutaneous catheter drainageofperirenalfluidcollection.
• Controlofdiabetes.• Nephrectomyreservedforseverecaseswithextensive
renal destruction and cases resistant to conservative treatment.
Important points to remember
• Emphysematous pye lonephr i t i s i s a r ap id l yprogressive, fulminant, necrotizing infection of the kidneys characterized by gas formation within or surrounding the kidneys, which often occurs in patients with uncontrolled diabetes. Nondiabetics who are immunocompromised or with urinary tract obstruction can also have this infection (1).
• Most common causative organisms are: E.coli,Klebsiella pneumonia, Proteus mirabilis (1).
• Imaging features include: renal parenchymalenlargement or destruction with mottled or linear streaks of gas, focal tissue necrosis with or without abscess formation and fluid and gas filled collections. CT is the investigation of choice for evaluating the extent of disease.
• It can be classified into two types based on itsprognosis:type1showsrenalparenchymaldestructionwith bubbly or streaky areas of gas with absent intra and extrarenal fluid collections; type 2 shows renal or extrarenal collections with loculated gas or gas within the pelvicalyceal system. Type 1 has aggressive course and grave prognosis if not treated early (1).
References
1. CraigWD,WagnerBJ,TravisMD.Pyelonephritis:radiologic-pathologicreview.Radiographics2008;28:255-77;quiz327-8.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 2
Case 1
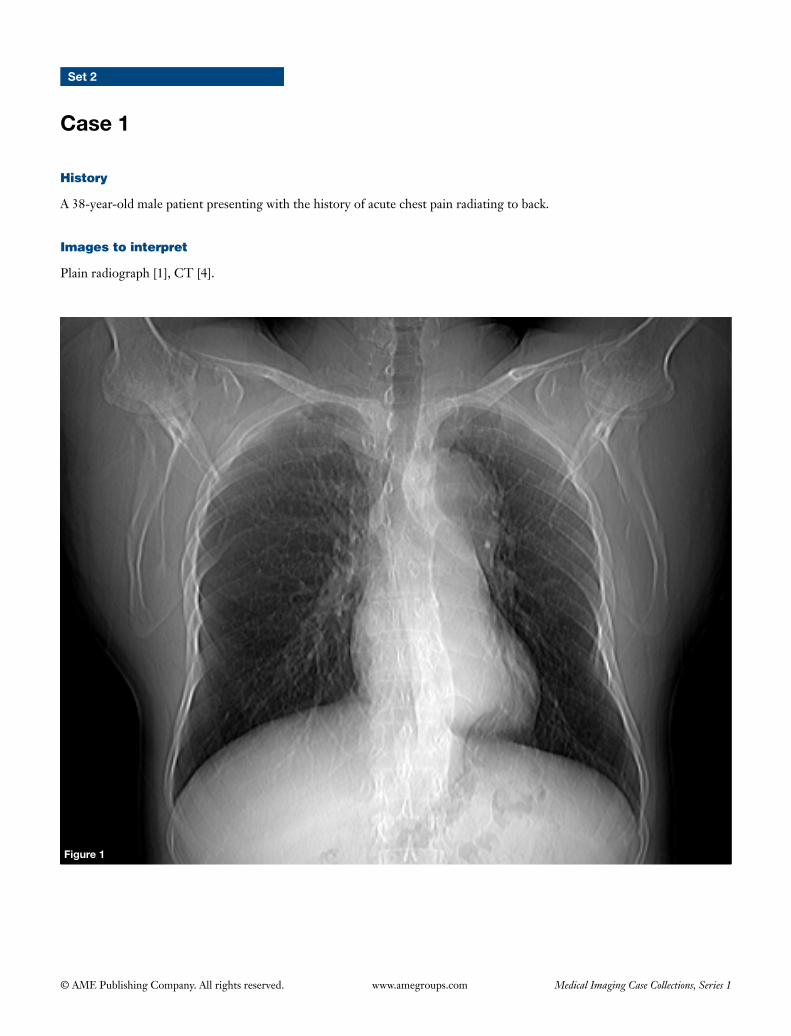
History
A 38-year-old male patient presenting with the history of acute chest pain radiating to back.
Images to interpret
Plain radiograph [1], CT [4].
Figure 1

20
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 5Figure 4
Figure 3Figure 2

21
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Aortic arch and descending aorta are ectatic with slight irregularity of its contour;
(II) Cardiac size is normal;(III) No evidence of pleural effusion seen and lung fields
are clear.
CT aortogram axial images (Figures 2-5)
(I) Thereisevidenceof intimalflapinthedistalpartofaortic arch dividing aorta into two lumens;
(II) It is extending distally in the descending thoracic aorta up to two chambers level;
(III) Medial lumen shows continuity with the proximal part of aortic arch and is smaller than the lateral lumen;
(IV) Lateral lumen is larger (causing dilatation of the aortic arch and descending aorta), shows evidence of partial thrombosis and wedges around the medial lumen giving a ‘beak-sign’;
(V) Ascending aorta is normal;(VI) No evidence of pleural/pericardial effusion seen.
Diagnosis
Aortic dissection (Stanford type A).
Differential diagnosis
None.
Management
• Evaluation of rest of theCT images to look forthe proximal and distal extent of the dissection and involvement of side branches.
• EvaluationofiliacarteriesonCTangiogramtocheckpossibilities of endovascular treatment.
• Endovasculartherapy.• Surgeryincomplicatedcases.
Important points to remember
• Acuteaortic syndromescompriseaorticemergenciesthat include aortic dissection, intramural hematoma, penetrating aortic ulcer, aortic aneurysm leak and traumatic aortic transection (1).
• Aorticdissectionrefers tobloodenteringthemediallayer of the aortic wall through a tear or penetrating ulcer in the intima, forming a second blood filled channel within the wall (2).
• Acute aort ic syndromes and aort ic dissect ionare classified into two subtypes on the basis of Stanford classification (which has replaced DeBakey classification): type A involving ascending aorta and the arch with or without descending aorta; type B with involvement of descending aorta distal to the origin of left subclavian artery (1).
• Themajorpredisposing factors foraorticdissectioninclude: hypertension, atherosclerosis, connective tissue disorders likeMarfan syndromeandEhlers-Danlossyndrome, vasculitis, pregnancy or iatrogenic.
• Itisimportanttodifferentiatetruelumenfromthefalselumen for optimal placement of endovascular graft and stent in the true lumen of aorta and the branch vessels, to prevent end-organ ischemia (3).
• True lumen can best be identified based on itscontinuity with the undissected portion of the aorta. However,indifficultcasesothersignsarehelpful.Thefeatures indicative of true lumen include: smaller cross-sectional area (due to compression by false lumen), outer wall calcification & eccentric flap calcification. The signs of false lumen include: larger cross-sectional area, beak sign, delayed enhancement, thrombus formation, collagenous media remnants (cobweb sign), wrap arounds true lumen in patients with involvement of the aortic arch (3).
References
1. MacuraKJ,CorlFM,FishmanEK,BluemkeDA.Pathogenesisinacuteaorticsyndromes:aorticdissection,intramuralhematoma, and penetrating atherosclerotic aortic ulcer. AJR Am J Roentgenol 2003;181:309-16.
2. SebastiàC,PallisaE,QuirogaS,Alvarez-CastellsA,DominguezR,EvangelistaA.Aorticdissection:diagnosisandfollow-upwith helical CT. Radiographics 1999;19:45-60; quiz 149-50.
3. LePageMA,QuintLE,SonnadSS,DeebGM,WilliamsDM.Aorticdissection:CTfeaturesthatdistinguishtruelumenfromfalse lumen. AJR Am J Roentgenol 2001;177:207-11.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
Figure 1
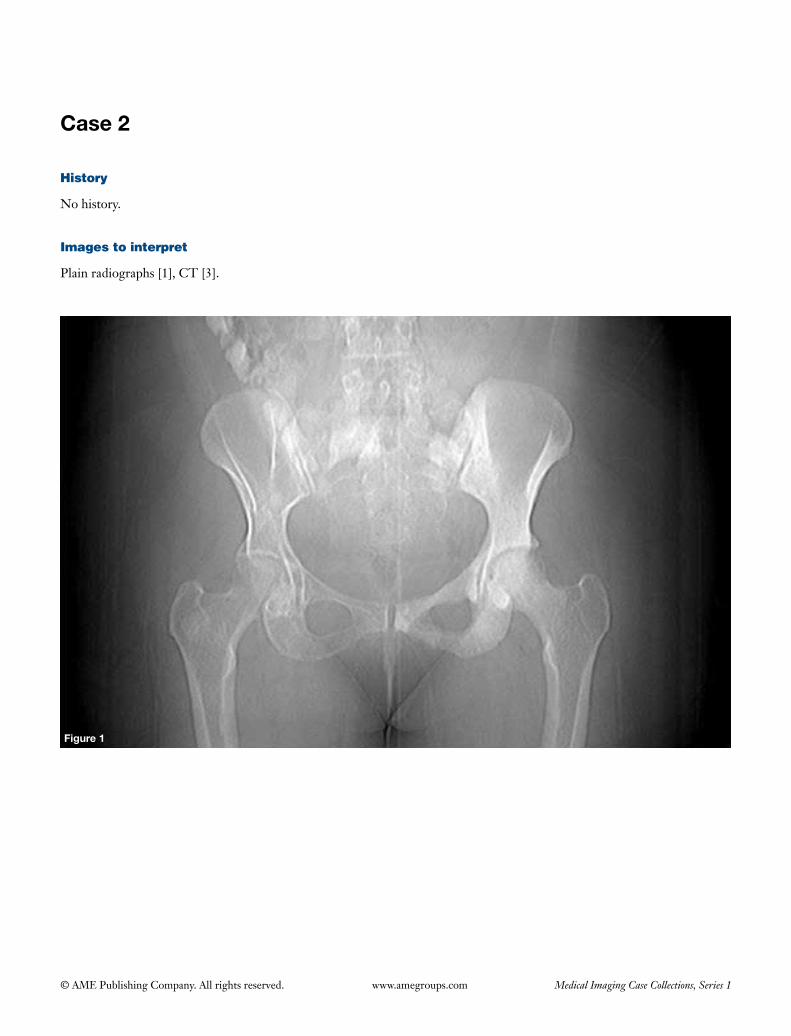
History
No history.
Images to interpret
Plain radiographs [1], CT [3].
23
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 3
Figure 2
Figure 4
24
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph pelvis frontal view (Figure 1)
(I) There is diffuse sclerosis of whole of left hemipelvis involving iliac bone, ischium and pubis with mild bony expansion. Sclerosis of head and neck of left femur also seen;
(II) Few sclerotic foci seen in bilateral sacral ala, right iliac bone, right acetabulum and right proximal femur.
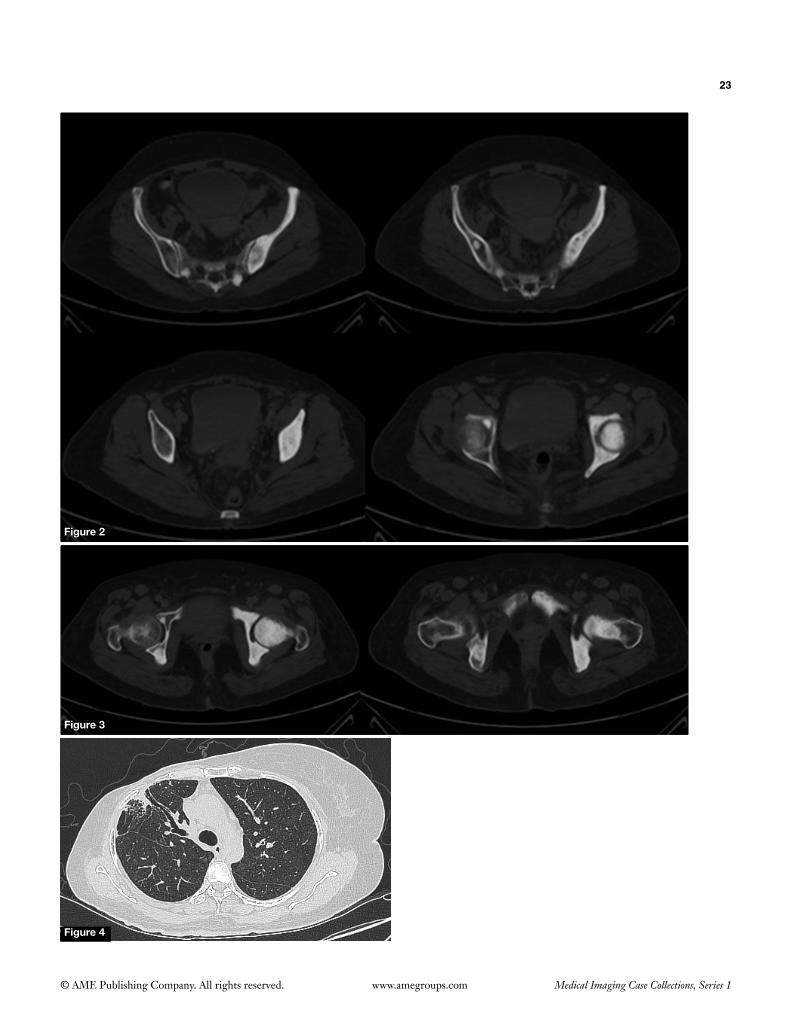
CT pelvis bone window images (Figures 2,3)
CT confirms plain radiographic findings.
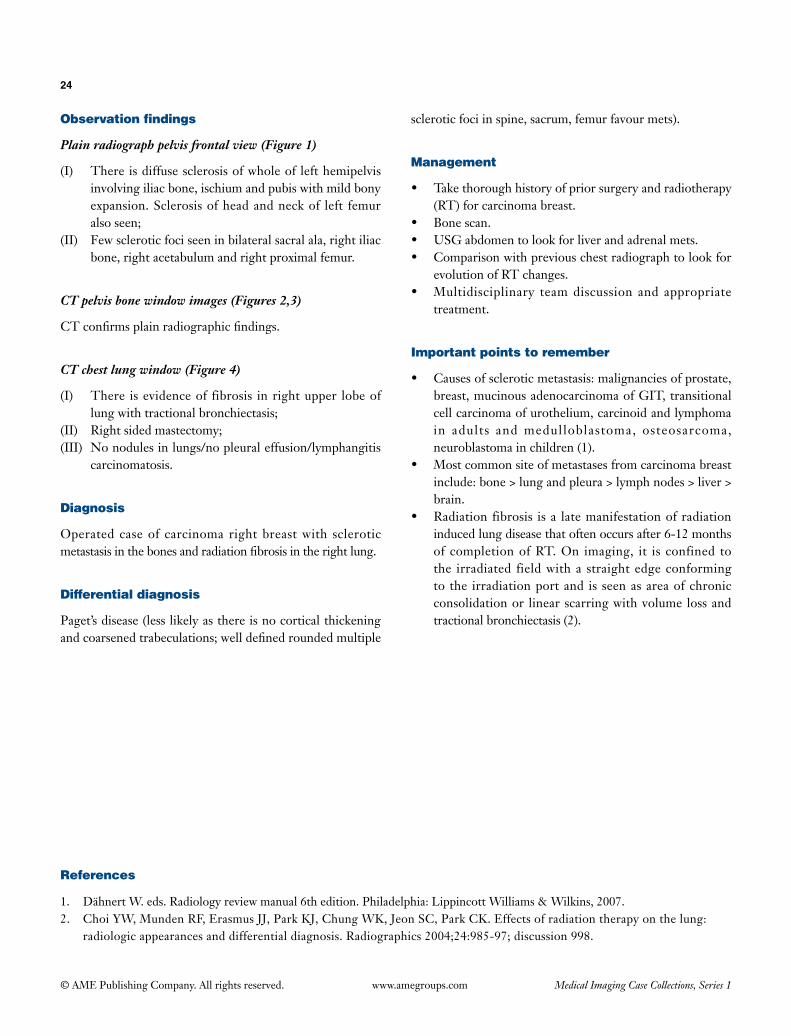
CT chest lung window (Figure 4)
(I) There is evidence of fibrosis in right upper lobe of lung with tractional bronchiectasis;
(II) Right sided mastectomy;(III) No nodules in lungs/no pleural effusion/lymphangitis
carcinomatosis.
Diagnosis
Operated case of carcinoma right breast with sclerotic metastasis in the bones and radiation fibrosis in the right lung.
Differential diagnosis
Paget’s disease (less likely as there is no cortical thickening and coarsened trabeculations; well defined rounded multiple
sclerotic foci in spine, sacrum, femur favour mets).
Management
• Take thorough history of prior surgery and radiotherapy (RT) for carcinoma breast.
• Bone scan.• USG abdomen to look for liver and adrenal mets.• Comparison with previous chest radiograph to look for
evolution of RT changes.• Multidisciplinary team discussion and appropriate
treatment.
Important points to remember
• Causes of sclerotic metastasis: malignancies of prostate, breast, mucinous adenocarcinoma of GIT, transitional cell carcinoma of urothelium, carcinoid and lymphoma in adults and medulloblastoma, osteosarcoma, neuroblastoma in children (1).
• Most common site of metastases from carcinoma breast include: bone > lung and pleura > lymph nodes > liver > brain.
• Radiation fibrosis is a late manifestation of radiation induced lung disease that often occurs after 6-12 months of completion of RT. On imaging, it is confined to the irradiated field with a straight edge conforming to the irradiation port and is seen as area of chronic consolidation or linear scarring with volume loss and tractional bronchiectasis (2).
References
1. Dähnert W. eds. Radiology review manual 6th edition. Philadelphia: Lippincott Williams & Wilkins, 2007.2. Choi YW, Munden RF, Erasmus JJ, Park KJ, Chung WK, Jeon SC, Park CK. Effects of radiation therapy on the lung:
radiologic appearances and differential diagnosis. Radiographics 2004;24:985-97; discussion 998.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
Figure 1
A B
History
A 30-year-old female patient presented with history of pain and swelling above left ankle since last 6 months.
Images to interpret
Plain radiograph [2], MRI [3].

26
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
A B C
Figure 2

27
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Frontal and lateral radiograph of left leg with ankle (Figure 1A,B)
(I) Welldefined,eccentric,expansile,radiolucentlesion,noted in the distal metaphysis of left tibia on the anterolateralaspectwithlongaxisparalleltolongaxisof long bone. Lesion has thin sclerotic rim;
(II) Nomatrixmineralizationseen;(III) Noperiosteal reaction/corticaldestructionor soft
tissuecomponent;(IV) Distal articular surfaceof tibiaandankle jointare
normal;(V) Restofthevisualizedbonesarenormal.
Axial T1, T2 and coronal STIR (Figure 2A, B and C, respectively) images of MRI of the left ankle at the level of distal tibia
(I) MRIconfirmsplainradiographicfindings;(II) Lesion shows isointense signal on T1 weighted
sequenceand veryhighsignalonT2weightedandSTIRsequence.
Diagnosis
Chondromyxoidfibroma.
Differential diagnosis
• Nonossifyingfibroma(occursinyoungeragegroup).• Aneursmalbonecyst (less likelyasageof thepatient
ismore and onMRI, aneurysmal bone cysts are
multiseptatedcysticlesionswithfluid-fluidlevels).• Giantcelltumorandchondroblastoma(predominantly
epiphyseal location).
Management
• Referraltoorthopedicianformanagement.• Enblocresection is thepreferredmodeof treatment
asrecurrenceratesarequitehigh(almost25%)withcurettageandbonegrafting.
Important points to remember
• Chondromyxoidfibromasarerare,benign,cartilaginoustumors (constitute<1%of allbone tumors),whichshowa variable amountof chondroid, fibrous andmyxoidcomponentsonhistopathology.Theageofonset is often 2nd to 3rd decade (1).
• Radiographically, they aregenerally seen as awelldefined, eccentric, lobulated, expansile, radiolucentlesion in the metaphysis of long bones with a sclerotic rim.Theyarecharacteristicallyovoid,with longaxisparallel to longaxisof thehostbone.Septationsareseenin57%ofthecasesandmatrixmineralizationisuncommon(seeninabout12%ofthecases)(1,2).
• MRIfeaturesarenon-specificandlesionsarehypointenseonT1andhyperintenseonT2weightedsequences.Mostof them(approximately70%)demonstrateperipheralnodularenhancement,whilerestshowdiffusehomogenous/heterogenousenhancement.Bonescintigraphyisalsonotspecificandshowsdoughnutsign(increaseduptakeperipherally with photopenic centre) (1,2).
References
1. vanHeerdenJ,VerwayenJC,BamDA.Chondromyxoidfibroma-acaseseriesandradiologicalreview.SAOrthopJ2010;9:61-4.
2. EisenbergRL.Bubblylesionsofbone.AJRAmJRoentgenol2009;193:W79-94.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
History
No history.
Images to interpret
CT [5].
Figure 1
Figure 2
Figure 3
Figure 4

29
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 5
30
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
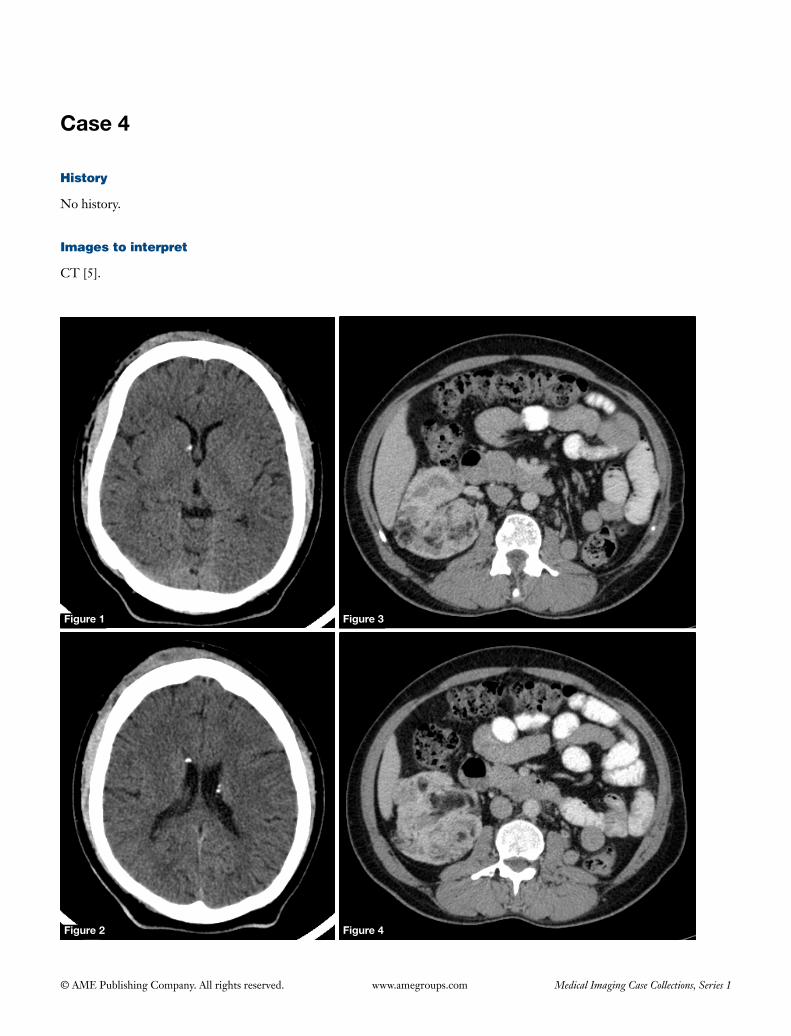
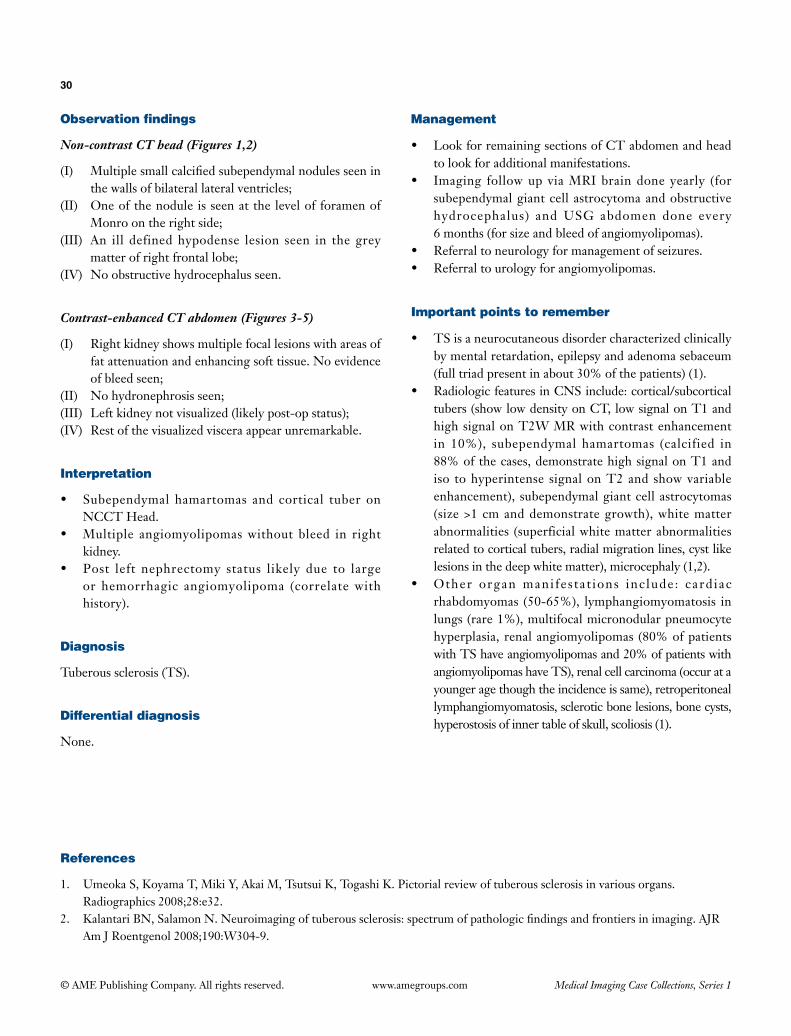
Non-contrast CT head (Figures 1,2)
(I) Multiplesmallcalcifiedsubependymalnodulesseeninthewallsofbilaterallateralventricles;
(II) OneofthenoduleisseenatthelevelofforamenofMonroontherightside;
(III) An ill definedhypodense lesion seen in thegreymatterofrightfrontallobe;
(IV) Noobstructivehydrocephalusseen.
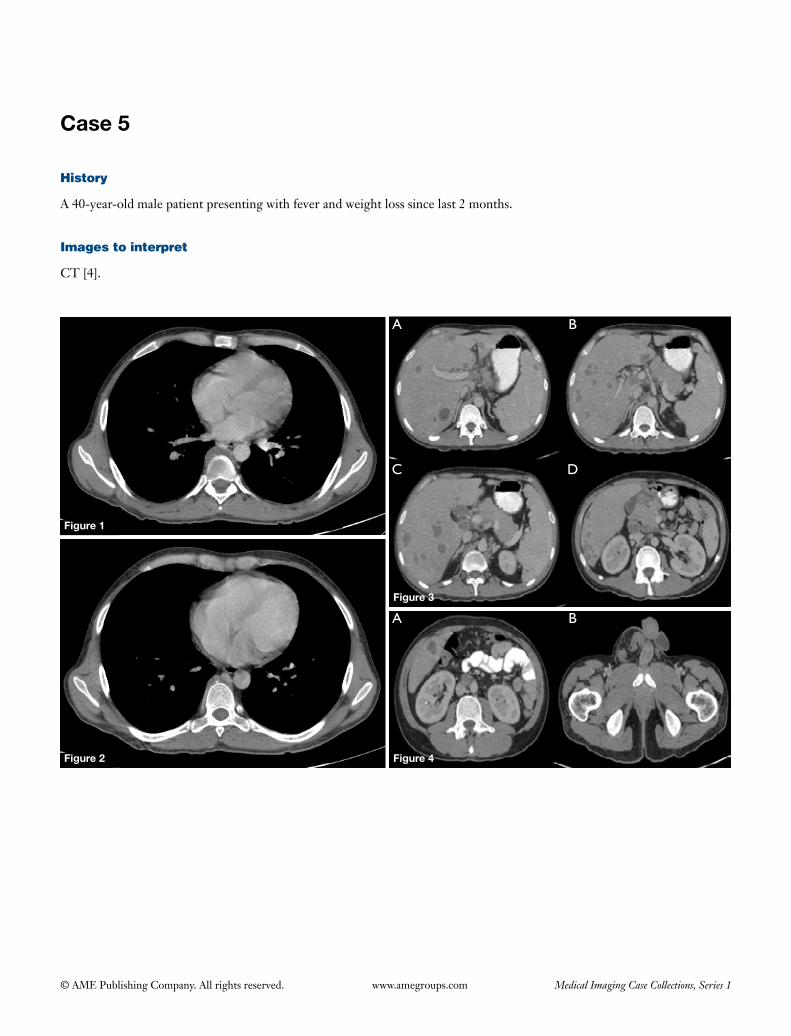
Contrast-enhanced CT abdomen (Figures 3-5)
(I) Rightkidneyshowsmultiplefocallesionswithareasoffatattenuationandenhancingsofttissue.Noevidenceofbleedseen;
(II) Nohydronephrosisseen;(III) Leftkidneynotvisualized(likelypost-opstatus);(IV) Restofthevisualizedvisceraappearunremarkable.
Interpretation
• Subependymal hamartomas and cortical tuber onNCCTHead.
• Multiple angiomyolipomaswithout bleed in rightkidney.
• Post left nephrectomy status likely due to largeor hemorrhagic angiomyolipoma (correlatewithhistory).
Diagnosis
Tuberoussclerosis(TS).
Differential diagnosis
None.
Management
• LookforremainingsectionsofCTabdomenandheadtolookforadditionalmanifestations.
• Imaging followup viaMRIbraindoneyearly (forsubependymalgiantcellastrocytomaandobstructivehydrocephalus) andUSG abdomen done every 6months(forsizeandbleedofangiomyolipomas).
• Referraltoneurologyformanagementofseizures.• Referraltourologyforangiomyolipomas.
Important points to remember
• TSisaneurocutaneousdisordercharacterizedclinicallybymentalretardation,epilepsyandadenomasebaceum(fulltriadpresentinabout30%ofthepatients)(1).
• RadiologicfeaturesinCNSinclude:cortical/subcorticaltubers(showlowdensityonCT,lowsignalonT1andhighsignalonT2WMRwithcontrastenhancementin 10%), subependymal hamartomas (calcified in88%ofthecases,demonstratehighsignalonT1andiso tohyperintense signalonT2and showvariableenhancement), subependymalgiantcellastrocytomas(size>1cmanddemonstrategrowth),whitematterabnormalities (superficialwhitematterabnormalitiesrelatedtocorticaltubers,radialmigrationlines,cystlikelesionsinthedeepwhitematter),microcephaly(1,2).
• Other organ mani fes ta t ions inc lude : card iacrhabdomyomas (50-65%), lymphangiomyomatosis inlungs(rare1%),multifocalmicronodularpneumocytehyperplasia, renalangiomyolipomas (80%ofpatientswithTShaveangiomyolipomasand20%ofpatientswithangiomyolipomashaveTS),renalcellcarcinoma(occuratayoungeragethoughtheincidenceissame),retroperitoneallymphangiomyomatosis,scleroticbonelesions,bonecysts,hyperostosisofinnertableofskull,scoliosis(1).
References
1. UmeokaS,KoyamaT,MikiY,AkaiM,TsutsuiK,TogashiK.Pictorialreviewoftuberoussclerosisinvariousorgans.Radiographics2008;28:e32.
2. KalantariBN,SalamonN.Neuroimagingoftuberoussclerosis:spectrumofpathologicfindingsandfrontiersinimaging.AJRAmJRoentgenol2008;190:W304-9.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
Figure 2
Figure 1
Figure 2
Figure 3
Figure 4
A
A
B
B
C D
History
A 40-year-old male patient presenting with fever and weight loss since last 2 months.
Images to interpret
CT [4].
32
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
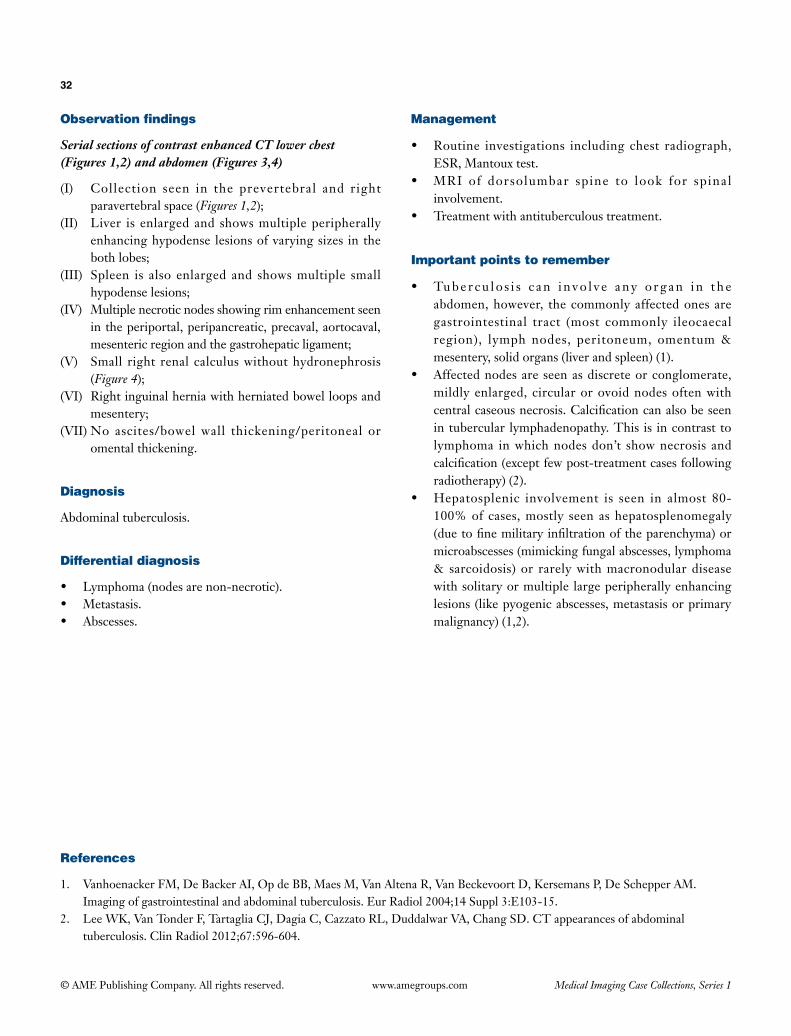
Serial sections of contrast enhanced CT lower chest (Figures 1,2) and abdomen (Figures 3,4)
(I) Collection seen in the prevertebral and right paravertebral space (Figures 1,2);
(II) Liver is enlarged and shows multiple peripherally enhancing hypodense lesions of varying sizes in the both lobes;
(III) Spleen is also enlarged and shows multiple small hypodense lesions;
(IV) Multiple necrotic nodes showing rim enhancement seen in the periportal, peripancreatic, precaval, aortocaval, mesenteric region and the gastrohepatic ligament;
(V) Small right renal calculus without hydronephrosis (Figure 4);
(VI) Right inguinal hernia with herniated bowel loops and mesentery;
(VII) No ascites/bowel wall thickening/peritoneal or omental thickening.
Diagnosis
Abdominal tuberculosis.
Differential diagnosis
• Lymphoma(nodesarenon-necrotic).• Metastasis.• Abscesses.
Management
• Routine investigations including chest radiograph,ESR, Mantoux test.
• MRI of dorsolumbar spine to look for spinalinvolvement.
• Treatmentwithantituberculoustreatment.
Important points to remember
• Tube r cu lo s i s c an i n vo l v e any o rg an i n t h eabdomen, however, the commonly affected ones are gastrointestinal tract (most commonly ileocaecal region), lymph nodes, peritoneum, omentum & mesentery, solid organs (liver and spleen) (1).
• Affectednodesareseenasdiscreteorconglomerate,mildly enlarged, circular or ovoid nodes often with centralcaseousnecrosis.Calcificationcanalsobeseenin tubercular lymphadenopathy. This is in contrast to lymphoma in which nodes don’t show necrosis and calcification(exceptfewpost-treatmentcasesfollowingradiotherapy) (2).
• Hepatosplenic involvement is seen in almost 80-100% of cases, mostly seen as hepatosplenomegaly (duetofinemilitaryinfiltrationoftheparenchyma)ormicroabscesses (mimicking fungal abscesses, lymphoma & sarcoidosis) or rarely with macronodular disease with solitary or multiple large peripherally enhancing lesions (like pyogenic abscesses, metastasis or primary malignancy) (1,2).
References
1. Vanhoenacker FM, De Backer AI, Op de BB, Maes M, Van Altena R, Van Beckevoort D, Kersemans P, De Schepper AM. Imaging of gastrointestinal and abdominal tuberculosis. Eur Radiol 2004;14 Suppl 3:E103-15.
2. Lee WK, Van Tonder F, Tartaglia CJ, Dagia C, Cazzato RL, Duddalwar VA, Chang SD. CT appearances of abdominal tuberculosis. Clin Radiol 2012;67:596-604.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
Figure 1
History
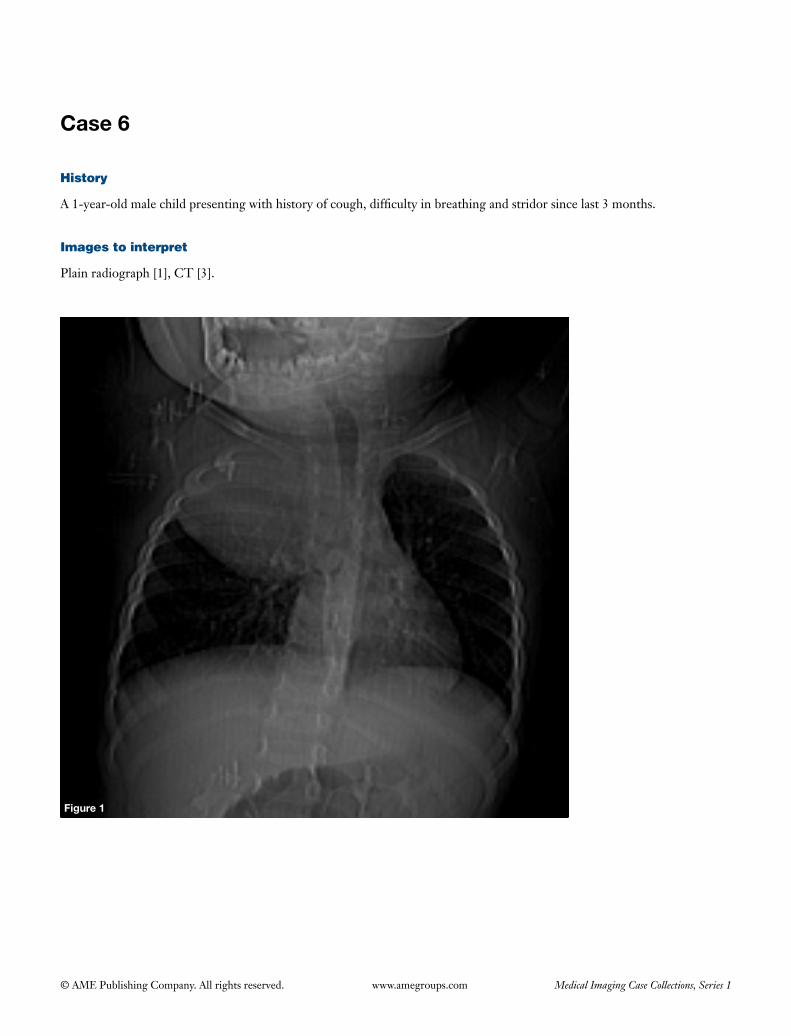
A 1-year-old male child presenting with history of cough, difficulty in breathing and stridor since last 3 months.
Images to interpret
Plain radiograph [1], CT [3].
34
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2 Figure 3
Figure 4
35
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) A homogenous opacity seen in the right upper and mid zone with broad base towards the mediastinum with evidence of calcification in it. The lesion has well defined inferior border, while the superior borders is indistinct. Lesion is extending superiorly in the neck;
(II) There is mass effect on the trachea in the form of compression and displacement towards left side;
(III) No cavitation seen within the mass;(IV) Rest of the lung fields is clear. No pleural effusion;(V) Visualized bones appear normal.
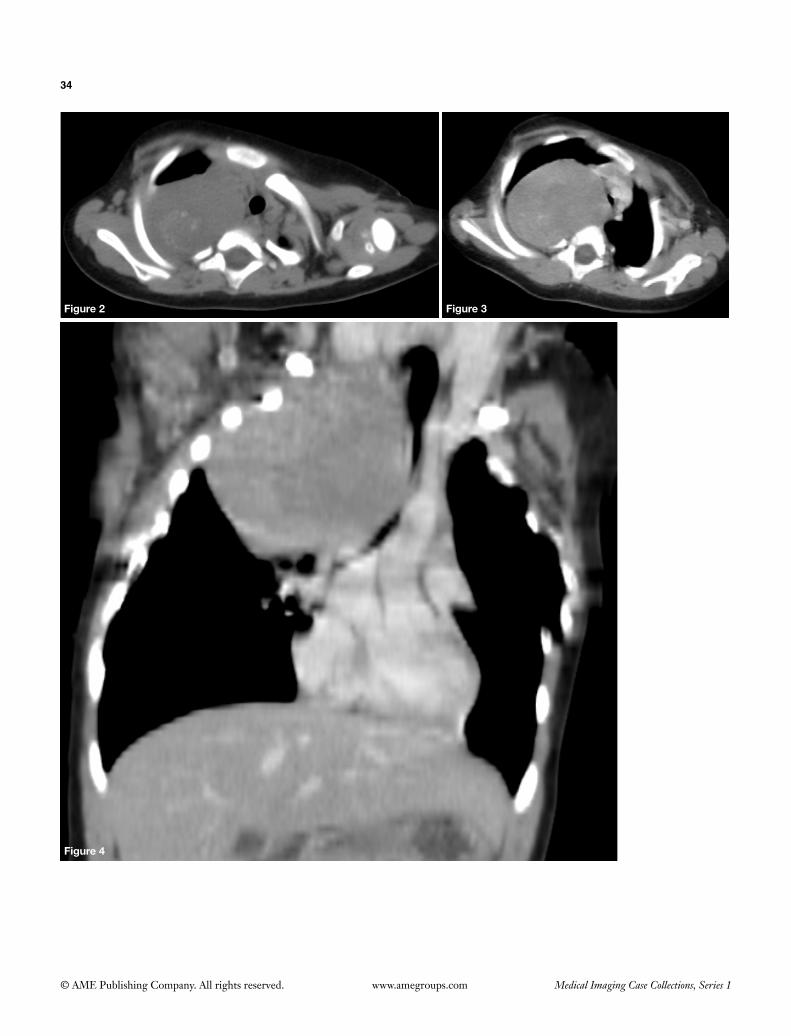
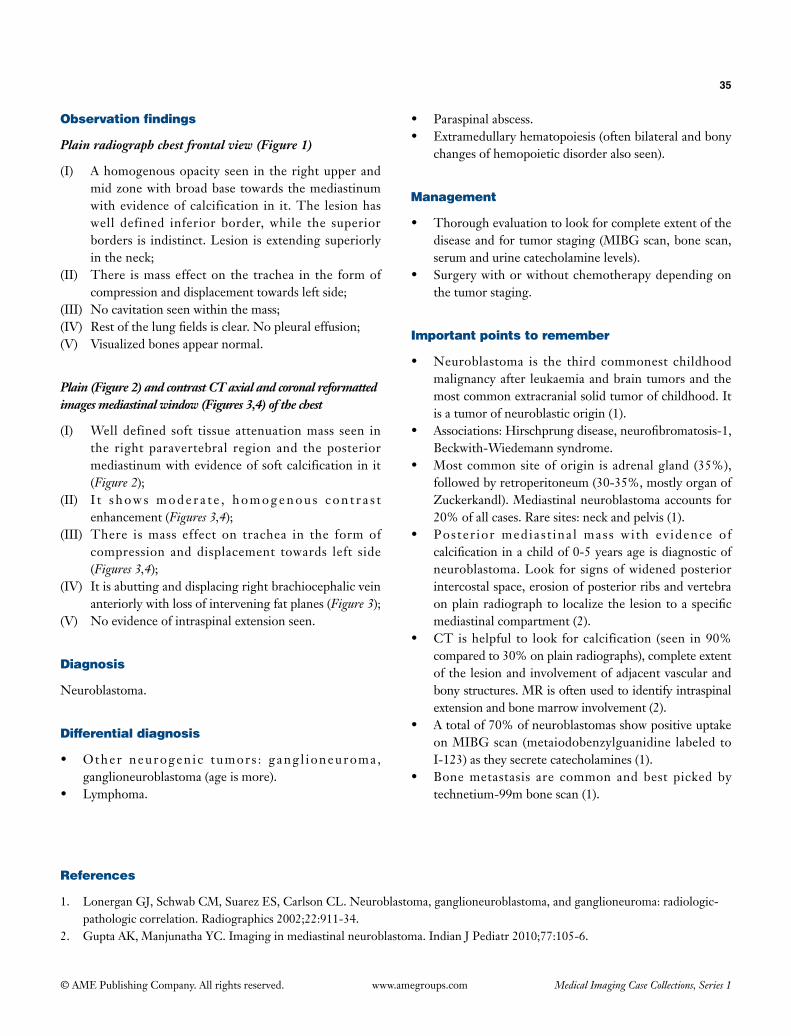
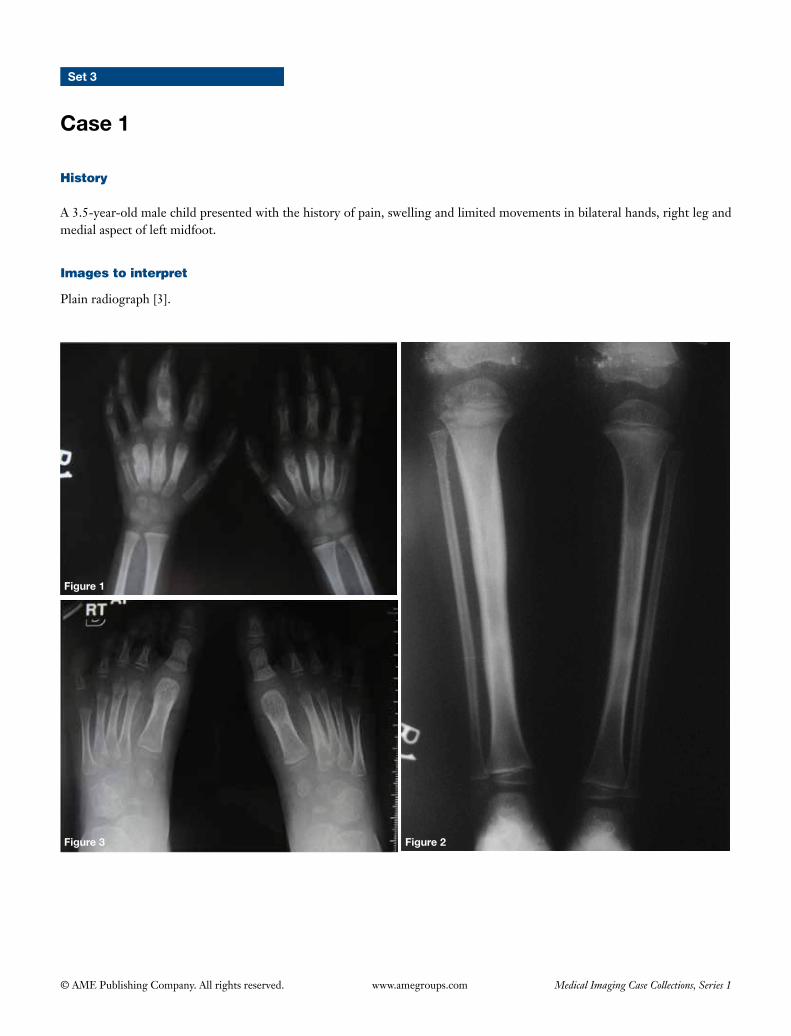
Plain (Figure 2) and contrast CT axial and coronal reformatted images mediastinal window (Figures 3,4) of the chest
(I) Well defined soft tissue attenuation mass seen in the right paravertebral region and the posterior mediastinum with evidence of soft calcification in it (Figure 2);
(II) I t s h o w s m o d e r a t e , h o m o g e n o u s c o n t r a s t enhancement (Figures 3,4);
(III) There is mass effect on trachea in the form of compression and displacement towards left side (Figures 3,4);
(IV) It is abutting and displacing right brachiocephalic vein anteriorly with loss of intervening fat planes (Figure 3);
(V) No evidence of intraspinal extension seen.
Diagnosis
Neuroblastoma.
Differential diagnosis
• Other neurogen ic tumors : gang l ioneuroma , ganglioneuroblastoma (age is more).
• Lymphoma.
• Paraspinal abscess.• Extramedullary hematopoiesis (often bilateral and bony
changes of hemopoietic disorder also seen).
Management
• Thorough evaluation to look for complete extent of the disease and for tumor staging (MIBG scan, bone scan, serum and urine catecholamine levels).
• Surgery with or without chemotherapy depending on the tumor staging.
Important points to remember
• Neuroblastoma is the third commonest childhood malignancy after leukaemia and brain tumors and the most common extracranial solid tumor of childhood. It is a tumor of neuroblastic origin (1).
• Associations: Hirschprung disease, neurofibromatosis-1, Beckwith-Wiedemann syndrome.
• Most common site of origin is adrenal gland (35%), followed by retroperitoneum (30-35%, mostly organ of Zuckerkandl). Mediastinal neuroblastoma accounts for 20% of all cases. Rare sites: neck and pelvis (1).
• Poster ior medias t ina l mass wi th ev idence of calcification in a child of 0-5 years age is diagnostic of neuroblastoma. Look for signs of widened posterior intercostal space, erosion of posterior ribs and vertebra on plain radiograph to localize the lesion to a specific mediastinal compartment (2).
• CT is helpful to look for calcification (seen in 90% compared to 30% on plain radiographs), complete extent of the lesion and involvement of adjacent vascular and bony structures. MR is often used to identify intraspinal extension and bone marrow involvement (2).
• A total of 70% of neuroblastomas show positive uptake on MIBG scan (metaiodobenzylguanidine labeled to I-123) as they secrete catecholamines (1).
• Bone metastasis are common and best picked by technetium-99m bone scan (1).
References
1. Lonergan GJ, Schwab CM, Suarez ES, Carlson CL. Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma: radiologic-pathologic correlation. Radiographics 2002;22:911-34.
2. Gupta AK, Manjunatha YC. Imaging in mediastinal neuroblastoma. Indian J Pediatr 2010;77:105-6.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 3
Case 1
History
A 3.5-year-old male child presented with the history of pain, swelling and limited movements in bilateral hands, right leg and medial aspect of left midfoot.
Images to interpret
Plain radiograph [3].
Figure 2Figure 3
Figure 1
37
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph bilateral hands frontal view (Figure 1)
(I) There is symmetric involvement of second, third and fourth metacarpals and proximal phalanx of middle finger of both hands, which show sclerosis along with periosteal reaction in the metadiaphysis causing bony expansion (R > L side) along with the surrounding soft tissue swelling;
(II) Rest of the bones and joints appear normal.
Plain radiograph both legs with knees and ankles frontal view (Figure 2)
(I) There is sclerosis with cortical thickening and periosteal reaction seen involving diaphysis of right tibia causing bony expansion;
(II) Both knee and ankle joints appear normal.
Plain radiograph both feet frontal view (Figure 3)
(I) There is periosteal reaction noted involving shaft of second metatarsal;
(II) Rest of the visualized bones and joints appear normal.
Diagnosis
Chronic recurrent multifocal osteomyelitis (CRMO).
Differential diagnosis
• Chronic infectious osteomyelitis.• Leukemia/lymphoma.• Ewing’s sarcoma.
Management
• Further evaluation with imaging guided biopsy and culture to establish the diagnosis.
• Referral to pediatric rheumatologist and orthopedician
for further management with non-steroidal anti-inflammatory drugs, steroids methotrexate, colchicines, interferon etc.
Important points to remember
• CRMO is an idiopathic inflammatory disorder of bone characterized by multifocal non-infective bone lesions, a course of exacerbations and remissions and an association with other inflammatory disorders like psoriasis, inflammatory bowel disease and palmoplantar pustulosis (1).
• Skeletal distribution: long tubular bones (lower extremity three times more common than upper extremity) and clavicle; tibia most commonly involved; though lesions can occur through out the skeleton including spine, pelvis, sacroiliac joint, ribs, sternum, scapula, mandible, hands and feet etc. (1).
• Radiographic features include: lytic lesion at metaphysis or metaphyseal equivalent of a bone which develops sclerosis and hyperostosis over time (2).
• Points to favour CRMO over infectious osteomyelitis include: insidious onset with relapsing-remitting course, unusual location like involvement of medial clavicle, bilateral symmetrical lesions, frequent multifocality of disease, absence of abscess, fistula formation or sequestra, lack of response to antibiotics, absence of involvement of intervertebral disc in the spine, coexisting other inflammatory disorders and negative culture results (1,2).
• Role of MR: to further evaluate cases with negative radiographs & with strong clinical suspicion of the entity; whole body MR to look for multifocality of the lesions; for determining the extent of disease; to look for transphyseal involvement; for soft tissue inflammation; periostitis; clinically occult joint effusions; for follow-up of lesions during exacerbations especially when radiographs show profound sclerosis (active areas show hyperintensity on T2 and contrast enhancement) (1).
References
1. Khanna G, Sato TS, Ferguson P. Imaging of chronic recurrent multifocal osteomyelitis. Radiographics 2009;29:1159-77.2. Iyer RS, Thapa MM, Chew FS. Chronic recurrent multifocal osteomyelitis: review. AJR Am J Roentgenol 2011;196(6 Suppl):S87-91.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
Figure 1
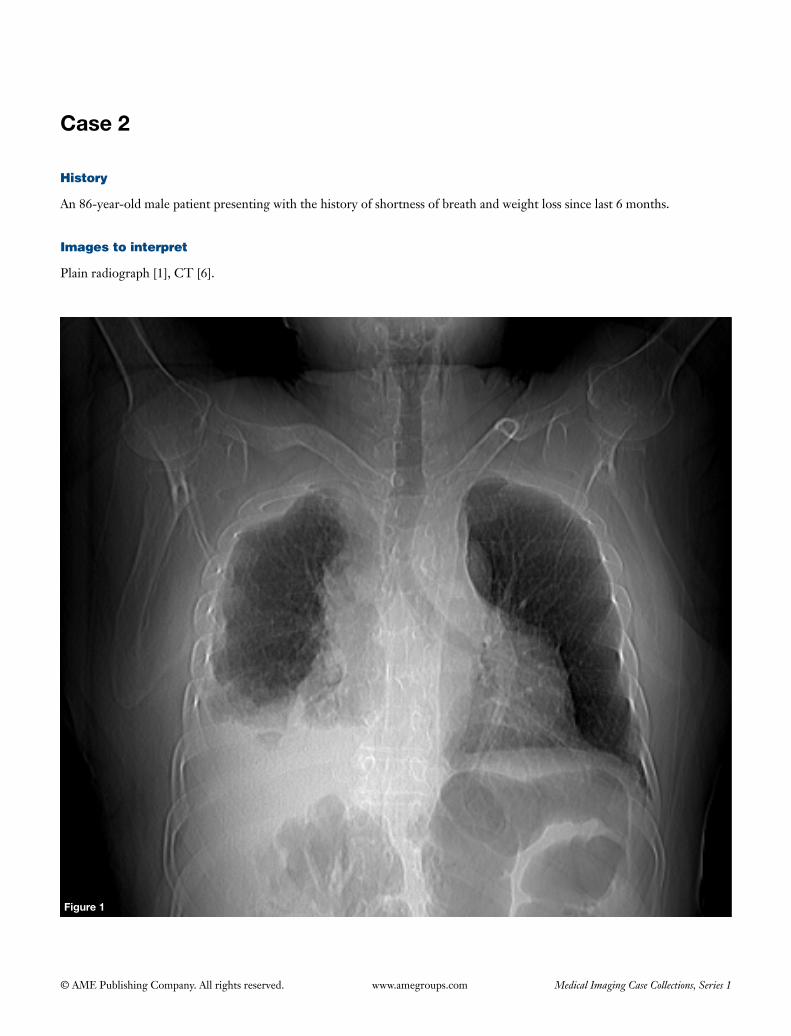
History
An 86-year-old male patient presenting with the history of shortness of breath and weight loss since last 6 months.
Images to interpret
Plain radiograph [1], CT [6].
39
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 4
Figure 6 Figure 7
Figure 2
Figure 3 Figure 4 Figure 5

40
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Nodular pleural thickening seen encasing right lung;(II) Right costophrenic angle is blunt likely due to pleural
effusion;(III) The volume of right lung is decreased;(IV) Mediastinum, visualized bones and left lung appear
normal.
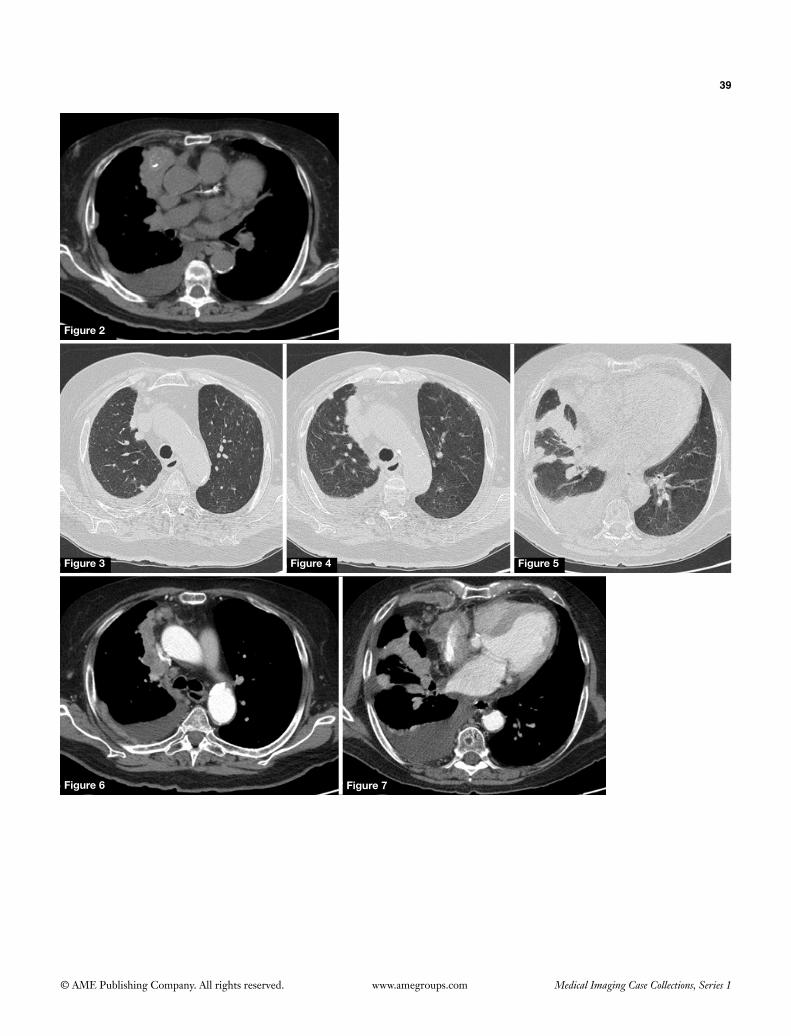
Plain CT chest mediastinal window (Figure 2), lung window (Figures 3-5) and contrast CT mediastinal window (Figures 6,7) axial sections
(I) CTconfirmsradiographicfindings;(II) Enhancing nodular pleural thickening (with evidence
ofcalcification)measuringmorethan1cminthicknessseen encasing right lung [with involvement of mediastinal pleura (Figures 2,6) and along major and minorfissure(Figures 5,7)];
(III) Moderate right sided pleural effusion seen (Figures 6,7);
(IV) There is volume loss of right hemithorax;(V) Few well defined nodules seen involving subpleural
region of right upper lobe of lung (Figures 3,4);(VI) Left lung and pleura are normal.
Diagnosis
Malignant mesothelioma with lung mets.
Differential diagnosis
Metastasis involving right sided pleura and right lung (unlikely as disease is unilateral and there is volume loss of affected hemithorax).
Management
• Takeoccupationalhistory.• ReviewremainingsectionsofCTforevaluatingextent.• Thoroughmetastaticworkup.• Multidisciplinaryteamdiscussion.
Important points to remember
• Nodularpleuralthickening,thicknessmorethan1cm,involvementofmediastinalpleuraandlungfissuresandassociation with the pleural effusion favour malignant pleural thickening.
• Malignantmesotheliomaisahighlymalignanttumor,which usually arises from pleura and is often associated with the history of asbestos exposure (1).
• Involvementofdiaphragm,extrapleural fat, ribsandvital mediastinal structures denote unresectability (1).
• Metastaticpleuraldisease isaclosedifferentialwithwhichdifferentiationisdifficult.Bilateralinvolvement,preserved volume of affected hemithorax, absence of pleural plaques and relevant occupational history are the points which favour metastasis. The common primaries to metastasise to pleura include: lung, breast, ovary, stomach, invasive thymoma and lymphoma (1).
References
1. SurekaB,ThukralBB,MittalMK,MittalA,SinhaM.Radiologicalreviewofpleuraltumors.IndianJRadiolImaging2013;23:313-20.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
Figure 1
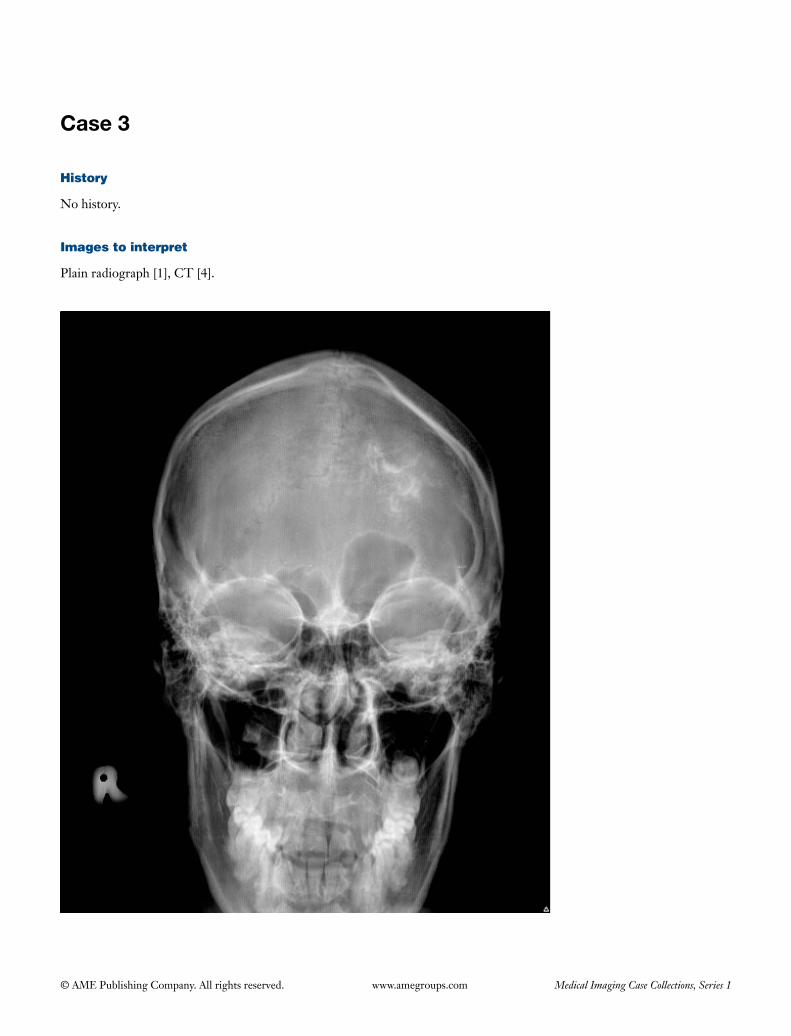
History
No history.
Images to interpret
Plain radiograph [1], CT [4].
42
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 3
Figure 4 Figure 5
A B C
BA
Figure 2
43
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
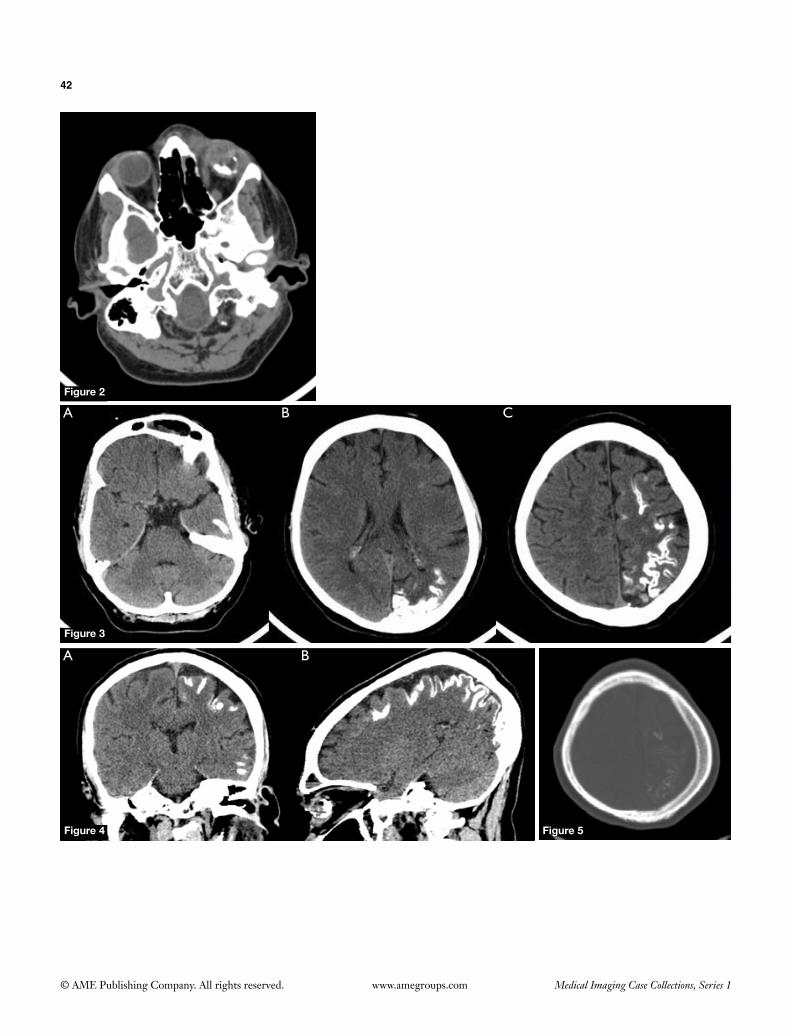
Plain radiograph skull frontal view (Figure 1)
(I) Gyriform calcification overlying left side of cranial vault;
(II) Calvarial thickening and frontal sinus enlargement on the left side.
Axial non-contrast CT of head brain window serial sections (Figures 2,3), coronal & sagittal reformatted images brain window (Figure 4), axial section CT head bone window (Figure 5)
(I) Densecurvilinearcalcificationontheposterioraspectof globe and in the iris involving left eyeball (Figure 2) suggestive of choroidal osteoma;
(II) There is diffuse hemiatrophy of the left cerebral hemisphere more pronounced in the parieto-occipital region (Figures 3,4);
(III) Gyriform calcification seen in the subcortical white matter giving ‘tram-track’ appearance (Figures 3,4).
(IV) There is thickening of the ipsilateral calvarial vault (Figure 5).
(V) Ipsilateral frontal sinus enlargement (Figure 3A) and elevation of the left petrous temporal bone (Figure 4A) seen.
Diagnosis
Sturge-Weber syndrome.
Differential diagnosis
• Cerebralarterio-venousmalformation.• CongenitalTORCHinfection.• Dyke-Davidoff-Masson syndrome (hemi cerebral
atrophy with calvarial changes but no pial angiomas and corticalcalcifications).
Management
• ContrastenhancedMRIforexactextentofleptomeningealangiomatous involvement.
• Neurologyreferralforcontroloftheseizures.• Neurosurgical referral for hemispherectomy in
refractory cases to medical therapy.• Ophthalmologyreferral.
Important points to remember
• Sturge-Weber syndrome (encephalotrigeminalangiomatosis) is a rare, sporadic, neurocutaneous disordercharacterizedbyleptomeningealangiomasandipsilateral port-wine stain (congenital facial cutaneous hemangioma) in the distribution of ophthalmic divison of the trigeminal nerve (1). It is often hemispheric.
• There isabsenceofnormalcorticalvenousdrainagealong with pial angiomas which cause ischaemia of the cortexandwhitematter leading tohemiatrophyanddystrophiccorticalcalcifications.
• Imaging features include: hemi cerebral atrophy(sometimes lobar or bilateral involvement may be seen),tram-trackcorticalandsubcorticalcalcifications,leptomeningealenhancement (appreciatedonMRascalcificationsobscureenhancementonCT),ipsilateralenlargementofchoroidplexus,calvariumandregionalparanasal sinuses (1).
• Associations include: coarctation of aorta andparaganglioma.
• MRspectroscopyshowselevatedcholinewithminimaldecrease in N-acetyl aspartate (1).
References
1. LinDD,BarkerPB,KrautMA,ComiA.EarlycharacteristicsofSturge-WebersyndromeshownbyperfusionMRimagingandprotonMRspectroscopicimaging.AJNRAmJNeuroradiol2003;24:1912-5.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
Figure 1 Figure 2 Figure 3
Figure 4 Figure 5
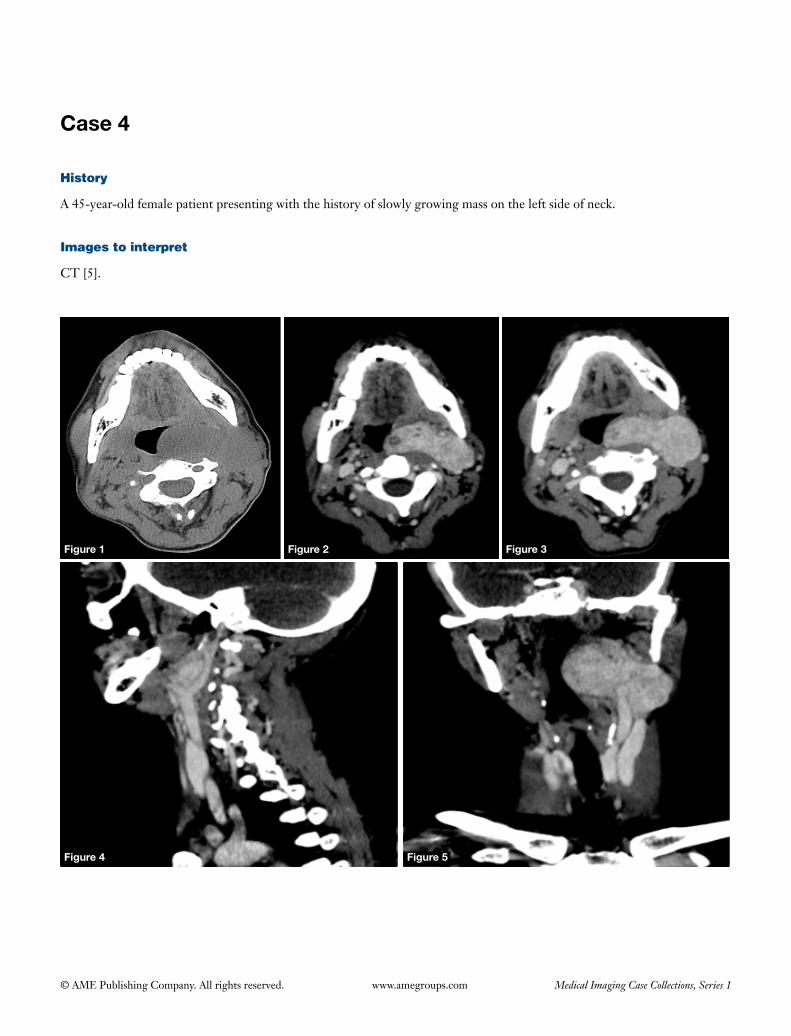
History
A 45-year-old female patient presenting with the history of slowly growing mass on the left side of neck.
Images to interpret
CT [5].
45
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
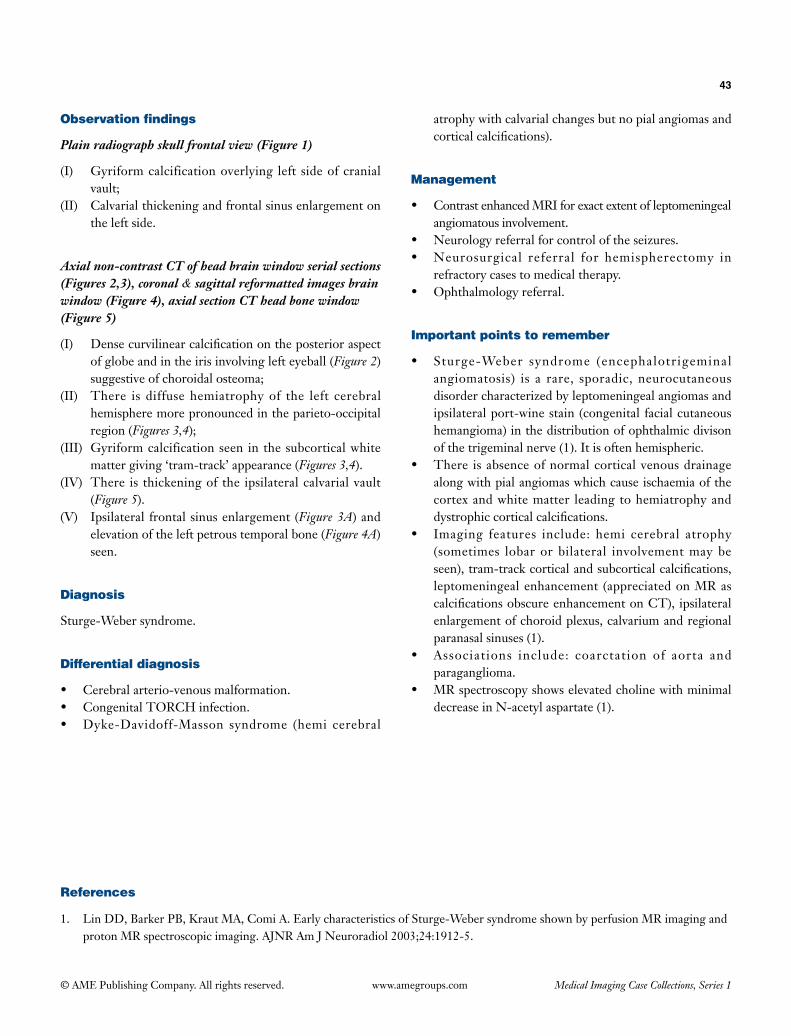
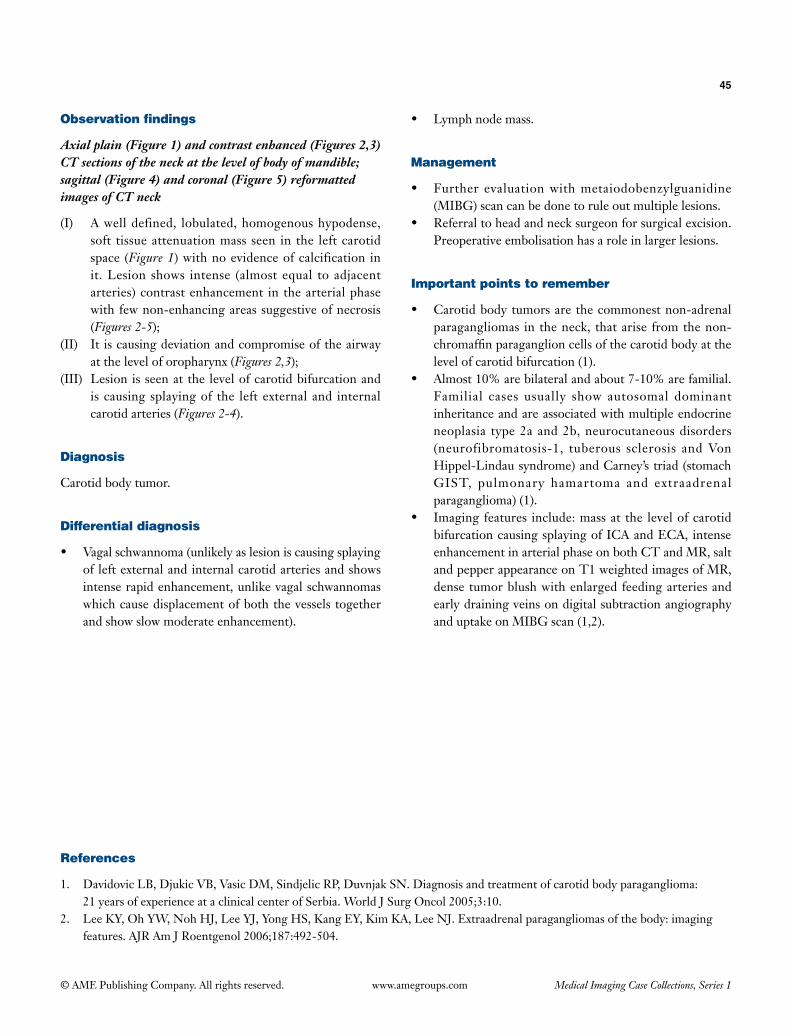
Observation findings
Axial plain (Figure 1) and contrast enhanced (Figures 2,3) CT sections of the neck at the level of body of mandible; sagittal (Figure 4) and coronal (Figure 5) reformatted images of CT neck
(I) A well defined, lobulated, homogenous hypodense, soft tissue attenuation mass seen in the left carotid space (Figure 1) with no evidence of calcification in it. Lesion shows intense (almost equal to adjacent arteries) contrast enhancement in the arterial phase with few non-enhancing areas suggestive of necrosis (Figures 2-5);
(II) It is causing deviation and compromise of the airway at the level of oropharynx (Figures 2,3);
(III) Lesion is seen at the level of carotid bifurcation and is causing splaying of the left external and internal carotid arteries (Figures 2-4).
Diagnosis
Carotid body tumor.
Differential diagnosis
• Vagalschwannoma(unlikelyaslesioniscausingsplayingof left external and internal carotid arteries and shows intense rapid enhancement, unlike vagal schwannomas which cause displacement of both the vessels together and show slow moderate enhancement).
• Lymphnodemass.
Management
• Further evaluationwithmetaiodobenzylguanidine(MIBG) scan can be done to rule out multiple lesions.
• Referraltoheadandnecksurgeonforsurgicalexcision.Preoperative embolisation has a role in larger lesions.
Important points to remember
• Carotidbodytumorsarethecommonestnon-adrenalparagangliomas in the neck, that arise from the non-chromaffinparaganglioncellsofthecarotidbodyatthelevel of carotid bifurcation (1).
• Almost10%arebilateralandabout7-10%arefamilial.Familial cases usually show autosomal dominantinheritance and are associated with multiple endocrine neoplasia type 2a and 2b, neurocutaneous disorders (neurofibromatosis-1, tuberous sclerosis andVonHippel-Lindau syndrome) and Carney’s triad (stomach GIST, pulmonary hamartoma and extraadrenal paraganglioma) (1).
• Imagingfeatures include:massat the levelofcarotidbifurcation causing splaying of ICA and ECA, intense enhancementinarterialphaseonbothCTandMR,saltandpepperappearanceonT1weightedimagesofMR,dense tumor blush with enlarged feeding arteries and early draining veins on digital subtraction angiography and uptake on MIBG scan (1,2).
References
1. DavidovicLB,DjukicVB,VasicDM,SindjelicRP,DuvnjakSN.Diagnosisandtreatmentofcarotidbodyparaganglioma: 21yearsofexperienceataclinicalcenterofSerbia.WorldJSurgOncol2005;3:10.
2. LeeKY,OhYW,NohHJ,LeeYJ,YongHS,KangEY,KimKA,LeeNJ.Extraadrenalparagangliomasofthebody:imagingfeatures.AJRAmJRoentgenol2006;187:492-504.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
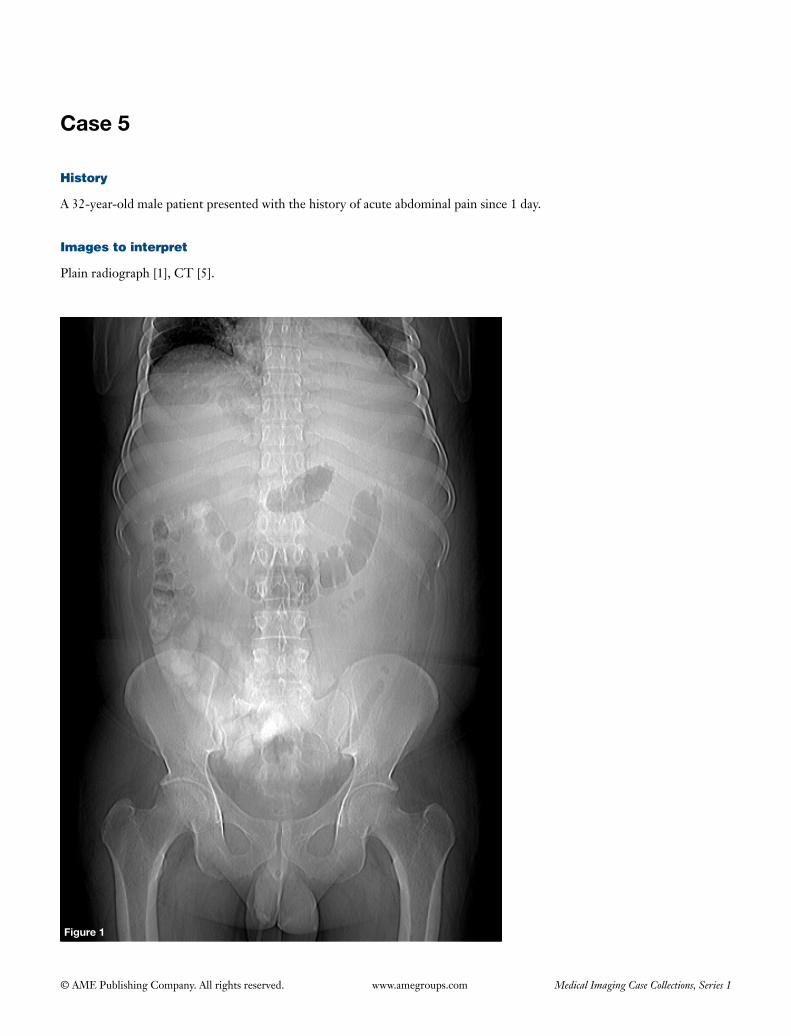
History
A 32-year-old male patient presented with the history of acute abdominal pain since 1 day.
Images to interpret
Plain radiograph [1], CT [5].
Figure 1
47
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2 Figure 3
Figure 4 Figure 5
Figure 6

48
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph abdomen supine (Figure 1)
(I) Mild left sided pleural effusion seen;(II) Left psoas shadow is obscured;(III) Transverse colon is mildly dilated with abrupt marrowing
at the level of splenic flexure (colon cut off sign);(IV) No evidence of gall stones/pneumobilia seen;(V) No free gas seen in peritoneal cavity.
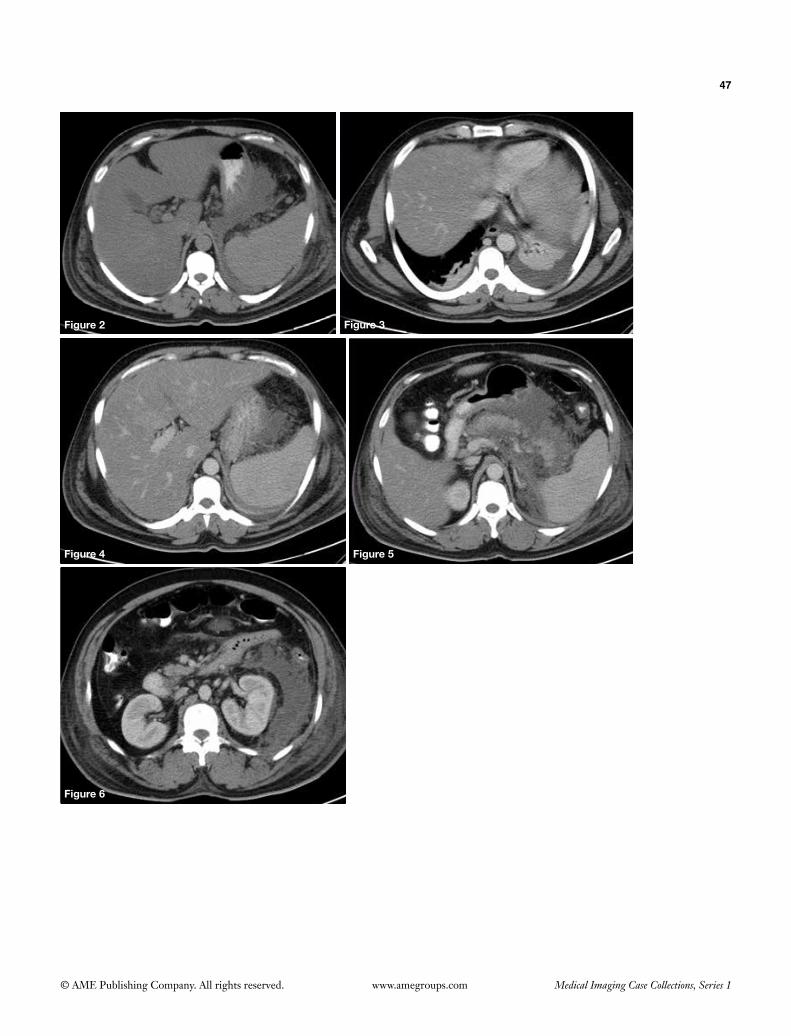
Plain (Figure 2) and contrast enhanced CT (Figures 3-6) axial sections
(I) Mild bilateral (L > R) pleural effusion with subsegmental atelectasis of underlying left lower lobe of lung seen (Figure 3);
(II) Liver shows diffuse low density suggestive of diffuse fatty change (Figures 2,4);
(III) Pancreas is mildly bulky, shows irregular outline with heterogenous enhancement. Gross peripancreatic fluid, oedema and fat stranding seen (Figure 5);
(IV) There is thickening of anterior pararenal fascia and lateral conal fascia seen on the left side (Figure 6).
Diagnosis
Acute oedematous pancreatitis likely due to alcoholism.
Differential diagnosis
None.
Management
• Immediate referral to medical gastroenterology.
• Serum amylase and lipase.
Important points to remember
• Risk factors for pancreatitis include: gall stones, chronic alcohol abuse, penetrating trauma, drugs like steroids, metabolic disorders like hypercalcemia and hyperlipidemia, hereditary pancreatitis, cystic fibrosis, autoimmune pancreatitis, anatomical abnormalities (pancreatic divisum).
• Radiographic features include: gall stones, biliary gas, sentinel loop sign (dilated C loop of duodenum), dilated transverse colon with colon cut off sign, obscuration of left psoas shadow, left pleural effusion, pancreatic calcification (chronic cases) (1). CT features include: pancreatic oedema, indistinct margins, heterogenous enhancement, peripancreatic fat stranding and fluid collections, pleural effusion, fatty liver, gall stones.
• Compl icat ions : f lu id col lect ions , pseudocyst formation, pancreatic abscess, pancreatic necrosis, venous thrombosis (portal and splenic veins), arterial pseudoaneurysm (splenic artery, gastroduodenal artery).
• CT severity index: based on CECT findings and correlates with clinical prognosis. It includes severity of pancreatitis and extent of pancreatic necrosis. Grading of acute pancreatitis: 0, normal pancreas; 1, pancreatic enlargement; 2, peripancreatic inflammation; 3, single peripancreatic fluid collection; 4, two or more fluid collections and/or retroperitoneal air. Pancreatic necrosis: 0, no necrosis; 2, <30% necrosis; 4, 30-50% necrosis; 6, >50% necrosis. Both are added to form CT severity index (2). It is divided into three groups based on morbidity and mortality: 0-3, mild; 4-6, moderate; 7-10, severe.
References
1. Davis S, Parbhoo SP, Gibson MJ. The plain abdominal radiograph in acute pancreatitis. Clin Radiol 1980;31:87-93.2. Balthazar EJ. Acute pancreatitis: assessment of severity with clinical and CT evaluation. Radiology 2002;223:603-13.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
Figure 1
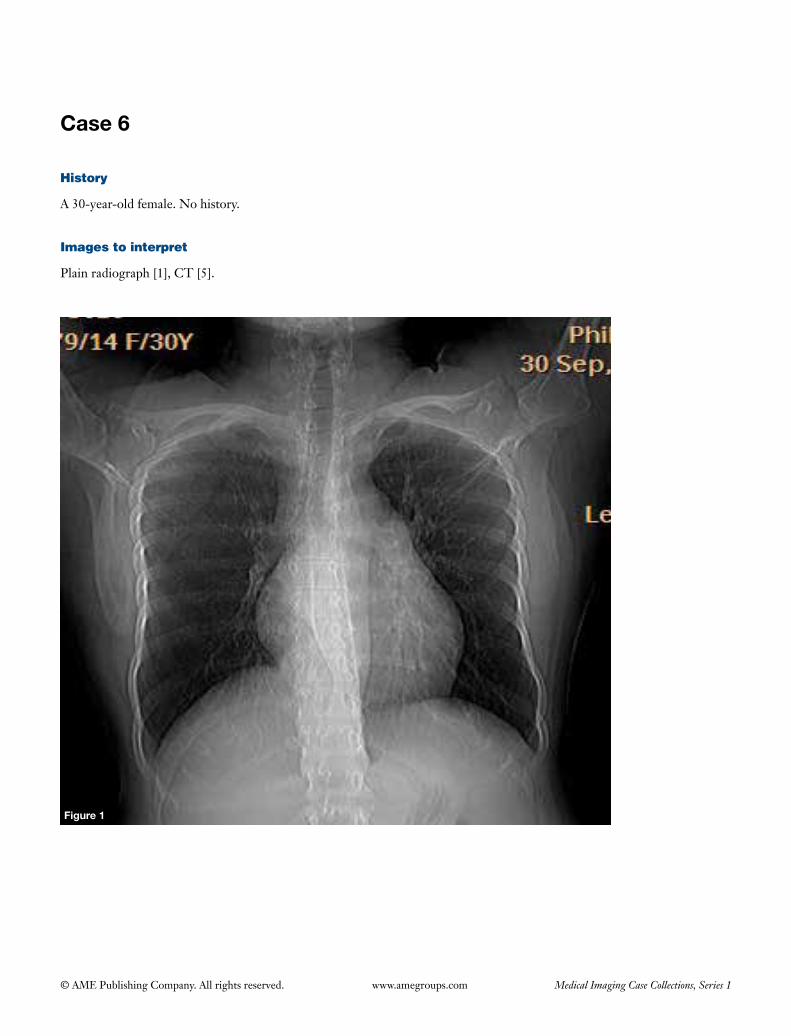
History
A 30-year-old female. No history.
Images to interpret
Plain radiograph [1], CT [5].
50
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
51
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
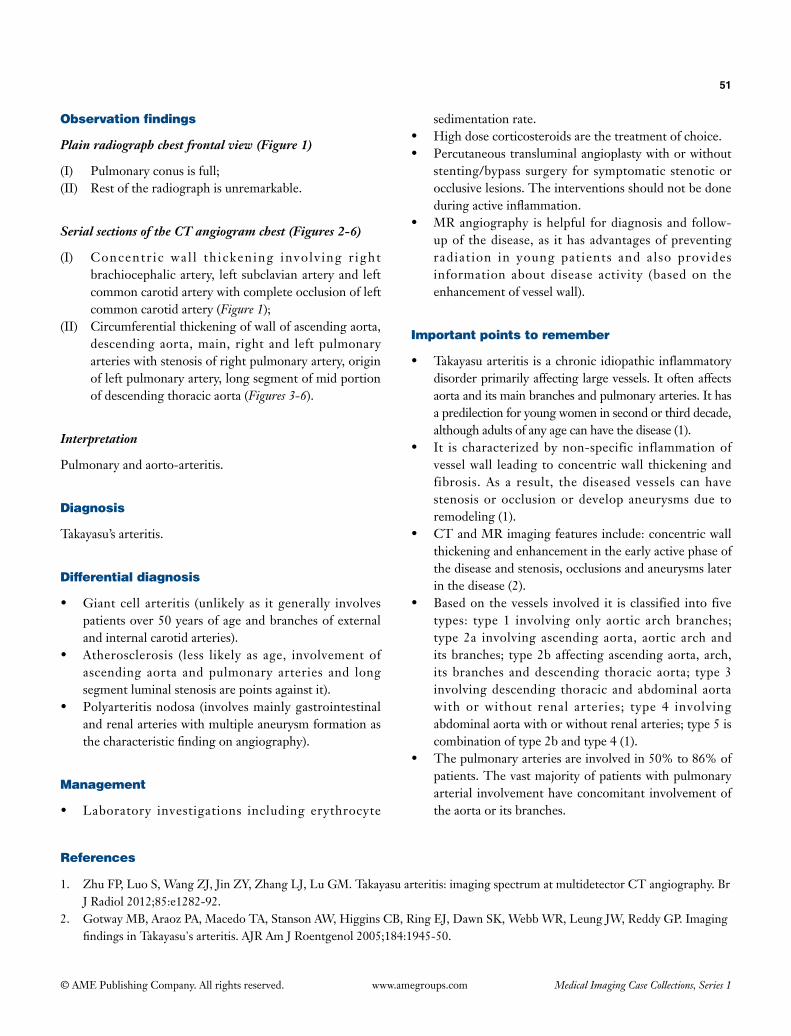
Plain radiograph chest frontal view (Figure 1)
(I) Pulmonary conus is full;(II) Rest of the radiograph is unremarkable.
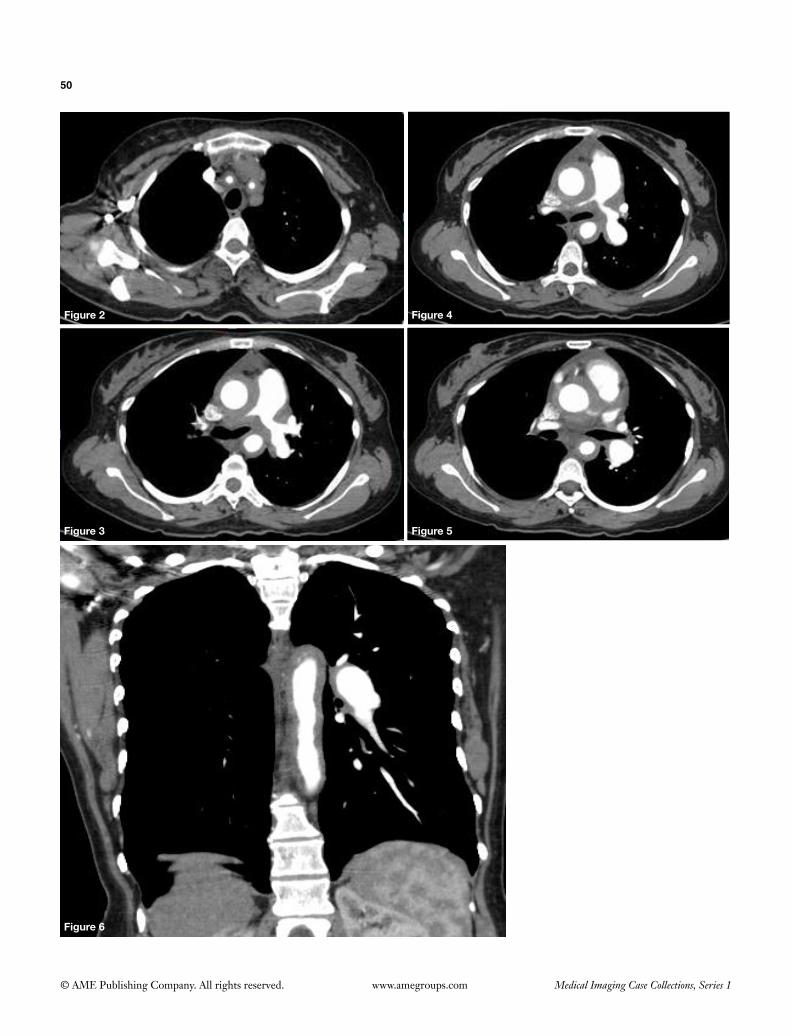
Serial sections of the CT angiogram chest (Figures 2-6)
(I) Concentr ic wal l th ickening involv ing r ight brachiocephalic artery, left subclavian artery and left common carotid artery with complete occlusion of left common carotid artery (Figure 1);
(II) Circumferential thickening of wall of ascending aorta, descending aorta, main, right and left pulmonary arteries with stenosis of right pulmonary artery, origin of left pulmonary artery, long segment of mid portion of descending thoracic aorta (Figures 3-6).
Interpretation
Pulmonary and aorto-arteritis.
Diagnosis
Takayasu’s arteritis.
Differential diagnosis
• Giantcell arteritis (unlikely as itgenerally involvespatients over 50 years of age and branches of external and internal carotid arteries).
• Atherosclerosis (less likely as age, involvement ofascending aorta and pulmonary arteries and long segment luminal stenosis are points against it).
• Polyarteritisnodosa (involvesmainlygastrointestinaland renal arteries with multiple aneurysm formation as thecharacteristicfindingonangiography).
Management
• Laboratory investigations including erythrocyte
sedimentation rate.• Highdosecorticosteroidsarethetreatmentofchoice.• Percutaneoustransluminalangioplastywithorwithout
stenting/bypass surgery for symptomatic stenotic or occlusive lesions. The interventions should not be done duringactiveinflammation.
• MRangiography ishelpful fordiagnosisand follow-up of the disease, as it has advantages of preventing radiation in young patients and also provides information about disease activity (based on the enhancement of vessel wall).
Important points to remember
• Takayasuarteritis isachronicidiopathicinflammatorydisorder primarily affecting large vessels. It often affects aorta and its main branches and pulmonary arteries. It has a predilection for young women in second or third decade, although adults of any age can have the disease (1).
• It is characterizedbynon-specific inflammationofvessel wall leading to concentric wall thickening and fibrosis. As a result, the diseased vessels can have stenosis or occlusion or develop aneurysms due to remodeling (1).
• CTandMRimagingfeaturesinclude:concentricwallthickening and enhancement in the early active phase of the disease and stenosis, occlusions and aneurysms later in the disease (2).
• Basedonthevessels involved it isclassified into fivetypes: type 1 involvingonly aortic archbranches;type 2a involving ascending aorta, aortic arch and its branches; type 2b affecting ascending aorta, arch, its branches and descending thoracic aorta; type 3 involving descending thoracic and abdominal aorta with or without renal arteries; type 4 involving abdominal aorta with or without renal arteries; type 5 is combination of type 2b and type 4 (1).
• Thepulmonaryarteriesareinvolvedin50%to86%ofpatients. The vast majority of patients with pulmonary arterial involvement have concomitant involvement of the aorta or its branches.
References
1. ZhuFP,LuoS,WangZJ,JinZY,ZhangLJ,LuGM.Takayasuarteritis:imagingspectrumatmultidetectorCTangiography.BrJRadiol2012;85:e1282-92.
2. GotwayMB,AraozPA,MacedoTA,StansonAW,HigginsCB,RingEJ,DawnSK,WebbWR,LeungJW,ReddyGP.ImagingfindingsinTakayasu'sarteritis.AJRAmJRoentgenol2005;184:1945-50.
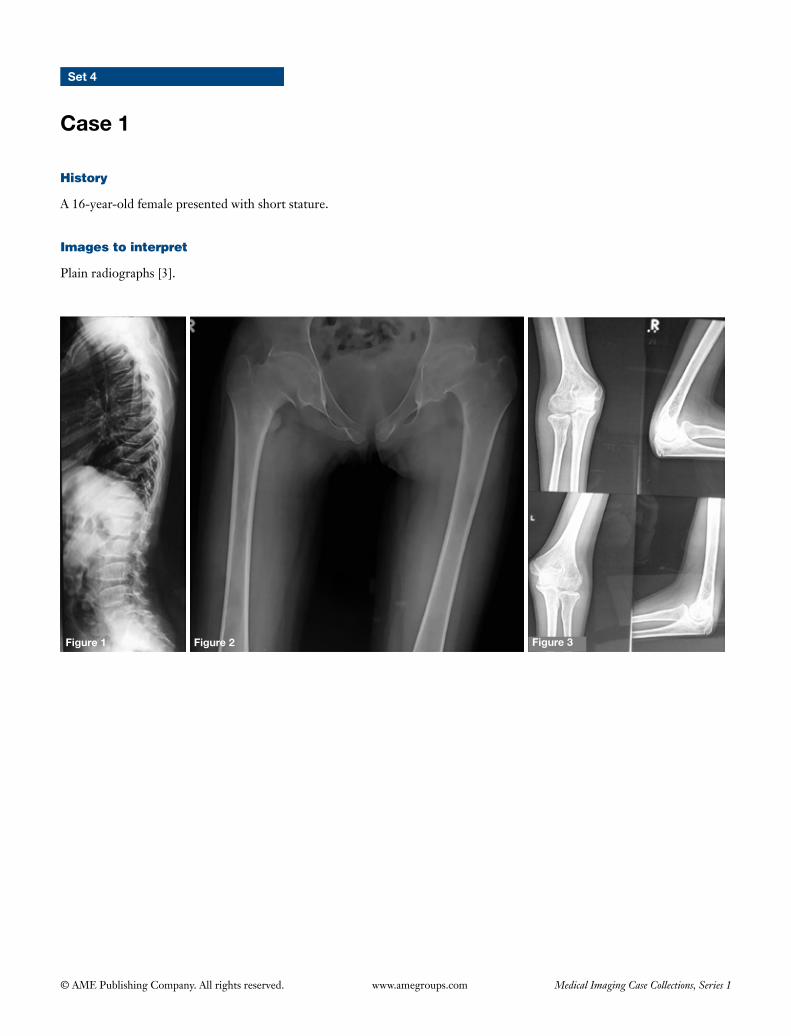
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 4
Case 1
Figure 1 Figure 3Figure 2
History
A 16-year-old female presented with short stature.
Images to interpret
Plain radiographs [3].

53
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Lateral radiograph dorsolumbar spine (Figure 1)
(I) Diffuse platyspondyly with mounds of bone over central and posterior parts of superior and inferior endplates causing hump-shaped vertebra;
(II) Disc spaces are thin.
Frontal radiograph both hip joints (Figure 2)
(I) Flattened dysplastic bilateral femoral heads with irregularity;
(II) Slight reduction of bilateral hip joint space;(III) Theproximalfemoralmetaphysisareflared.
Bilateral elbow (AP & lateral view) (Figure 3)
Flattening with broadening of bilateral radial heads with irregularity of bilateral capitellum.
Diagnosis
Spondyloepiphyseal dysplasia tarda.
Differential diagnosis
• Morquio’sdisease.• Multipleepiphysealdysplasia.
Management
• Geneticcounsellingandfamilyscreening.• Avoidanceofactivitiesthatcauseunduestressonspine
or weight bearing joints.• Surgical intervention (joint replacement or spine
surgery).
Important points to remember
• Spondyloepiphyseal dysplasia tarda is ahereditarychondrodysplasia characterized by disproportionate dwarfism due to involvement of both spine and
epiphysis of long bones, likely due to structural defects in type 2 collagen. It is usually transmitted in X-linked recessive mode though autosomal dominant and recessive transmissions are also reported. It manifests in late childhood or adolescence (compared to spondyloepiphyseal dysplasia congenita that is more severe and is recognized at birth and transmitted in autosomal dominant mode) (1).
• Pathognomonicimagingfeaturesincludeplatyspondylywith mounds of dense bone over central and posterior parts of vertebral end plates causing anterior beaking (in some cases absence of ossification of anterior margins of vertebral end plates causes this appearance), kyphoscoliosis, small iliac wings, flattened and dysplastic epiphysis of long bones (more pronounced in proximal femoral epiphysis) (1).
• Complications include short stature, prematureosteoarthritis and atlantoaxial instability (more common in spondyloepiphyseal dysplasia congenita due to odontoid hypoplasia or os odontoideum).
• Morquio’s disease (Mucopolysaccharidosis type 4)shows similar features but additionally shows central beaking of vertebra with posterior scalloping, normal disc height, proximal metacarpal tapering, coxa valga, genu valgum. It also has cardiac & visceral involvement, cornealcloudingandmetabolicabnormalities.Multipleepiphyseal dysplasia will have absence of spinal involvement (1).
• Platyspondyly (flatteningof vertebralbody) canbegeneralized affecting all vertebrae, some of the vertebral bodies (multiple platyspondyly or anisospondyly) or solitaryvertebra(vertebraplana).Causesofcongenitalplatyspondyly which is generalized or multiple include: thanatophoric dwarfism, osteogenesis imperfecta type 2, Morquio’s syndrome, achondroplas ia ,pseudoachondroplasia, spondyloepiphyseal dysplasia, Kniest syndrome. Vertebra plana causes include: trauma, eosinophilic granuloma, tumors (mets, lymphoma, myeloma), infections including tuberculosis, avascular necrosis (due to steroids/idiopathic), benign lesion like hemangioma.
References
1. Lakhar BN, Raphael R. Spondyloepiphyseal dysplasia: An evaluation of six cases. Indian J Radiol Imaging 2003;13:199-203.
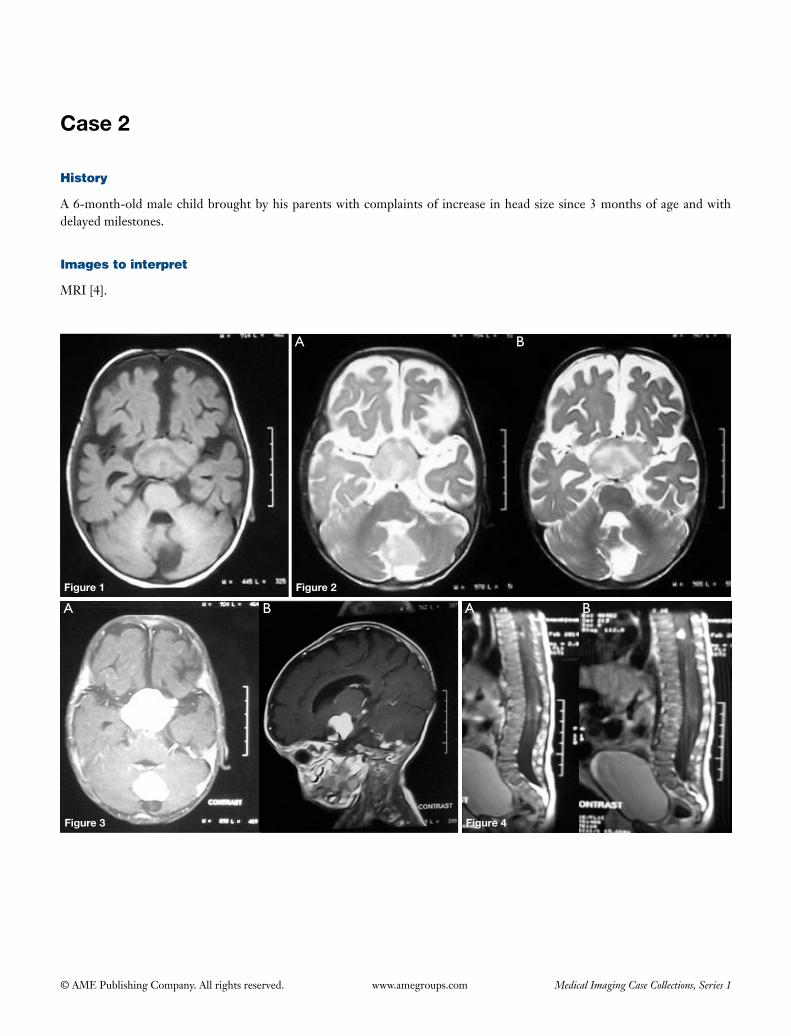
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
Figure 2
Figure 3 Figure 4
Figure 1
A
A A
B
B B
History
A 6-month-old male child brought by his parents with complaints of increase in head size since 3 months of age and with delayed milestones.
Images to interpret
MRI [4].
55
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Axial T1 (Figure 1), T2 (Figure 2), post gad T1 axial and sag (Figure 3) brain images and post gad T1 sagittal dorsolumbar spine (Figure 4) showing
(I) Well defined rounded mass isointense on T1 and T2 weighted sequences noted in suprasellar region encasing optic chiasma, with intense homogenous contrast enhancement (Figures 1-3);
(II) Another solid cystic mass seen involving cerebellar vermis with intense enhancement of solid component with obstructive hydrocephalus due to compression of fourth ventricle (Figures 1-3);
(III) Two small enhancing rounded lesions in intradural extramedullary space at D8 and L1 levels (Figure 4).
Interpretation
Chiasmatic glioma with pilocytic astrocytoma of cerebellar vermis and two neurofibromas in spine.
Diagnosis
Neurofibromatosis-1 (NF1).
Differential diagnosis
None.
Management
• Family screening and genetic counselling.• Educate the patient about the disease and its potential
complications particularly neurofibrosarcoma or malignant peripheral nerve sheath tumors (approximate risk 2-3%).
• Review of remaining images of MRI brain and whole spine screening to assess complete manifestations of the disease.
• Visual assessment.• Follow ups with neurologist and neurosurgeon.• Surgical management.
Important points to remember
• NF1 (von Recklinghausen’s disease) is the most common neurocutaneous disorder with 50% of cases transmitted in autosomal dominant manner. Clinical diagnosis is based on two or more of these criteria: >6 cafe au lait spots, two neurofibromas or one plexiform neurofibroma, optic glioma, characteristic osseous lesion like sphenoid wing dysplasia, two or more iris hamartomas, axillary or inguinal freckling and first degree relative of NF1 (1).
• Important features on imaging include: CNS (optic pathway glioma, hamartomas in basal ganglia and white matter of cerebral hemispheres, pilocytic astrocytomas in brain and spine, neurofibromas, moyamoya disease, dural calcification at vertex, lateral thoracic meningoceles), musculoskeletal (sphenoid wing dysplasia, posterior vertebral scalloping, hypoplasia of posterior elements, kyphoscoliosis, enlarged neural foramina, multiple neurofibromas involving long bones, tibial or ulnar pseudoarthrosis), vascular (renal artery stenosis, coarctation of aorta, pheochromocytoma or paraganglioma), chest (lower lobe fibrosis with upper lobe bullae, corpulmonale, pulmonary artery hypertension), breast (neurofibromatosis of the breast) (1,2).
• NF2 is a rare phakomatosis with multiple CNS tumors [multiple inherited schwannomas (mostly vestibular), meningiomas and ependymomas (MISME)] (2).
References
1. Williams VC, Lucas J, Babcock MA, Gutmann DH, Korf B, Maria BL. Neurofibromatosis type 1 revisited. Pediatrics 2009;123:124-33.
2. Aoki S, Barkovich AJ, Nishimura K, Kjos BO, Machida T, Cogen P, Edwards M, Norman D. Neurofibromatosis types 1 and 2: cranial MR findings. Radiology 1989;172:527-34.
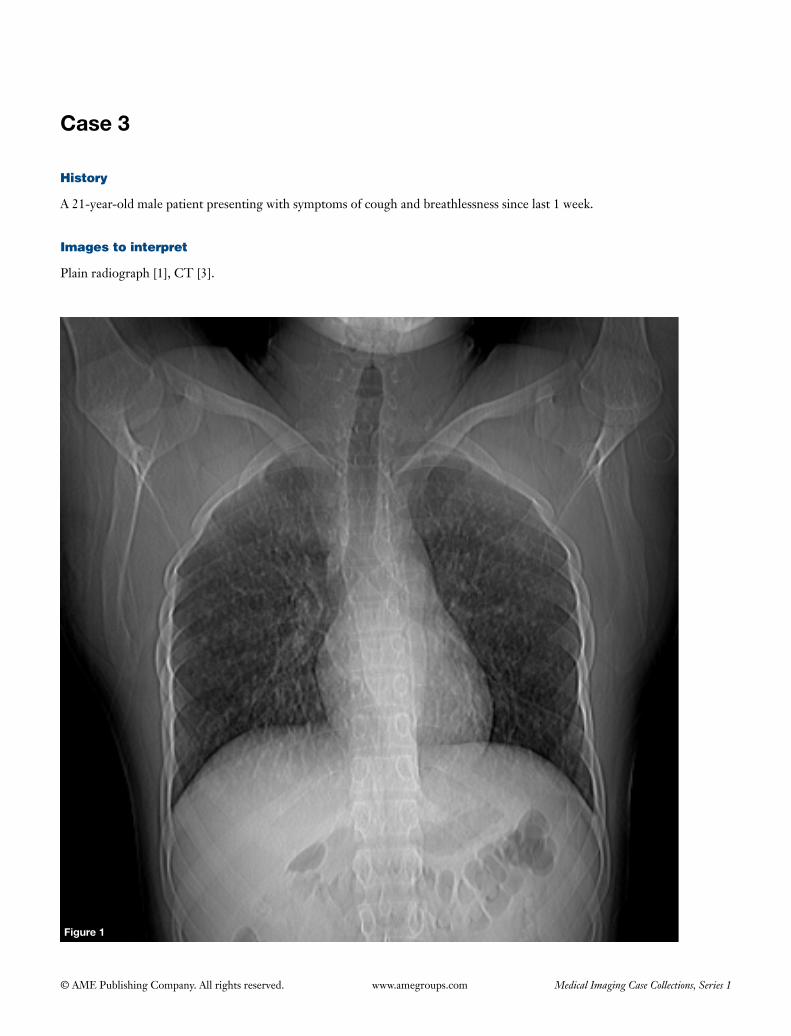
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
Figure 1
History
A 21-year-old male patient presenting with symptoms of cough and breathlessness since last 1 week.
Images to interpret
Plain radiograph [1], CT [3].
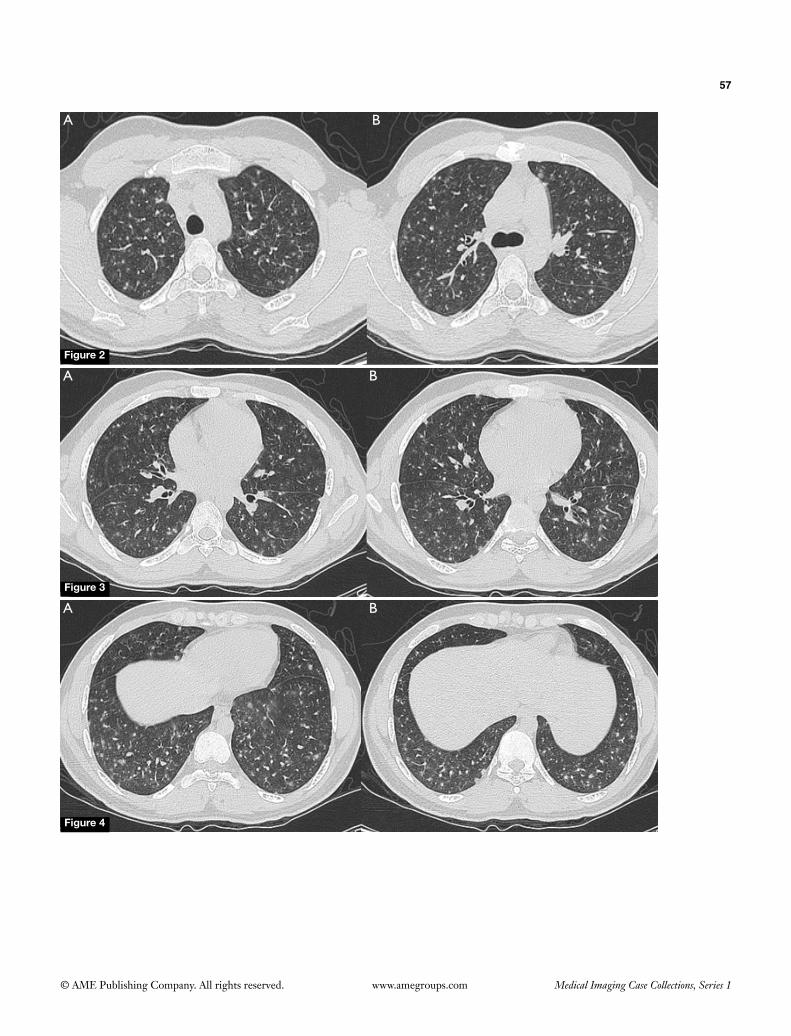
57
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
B
B
A
A
Figure 2
A B
Figure 4
Figure 3
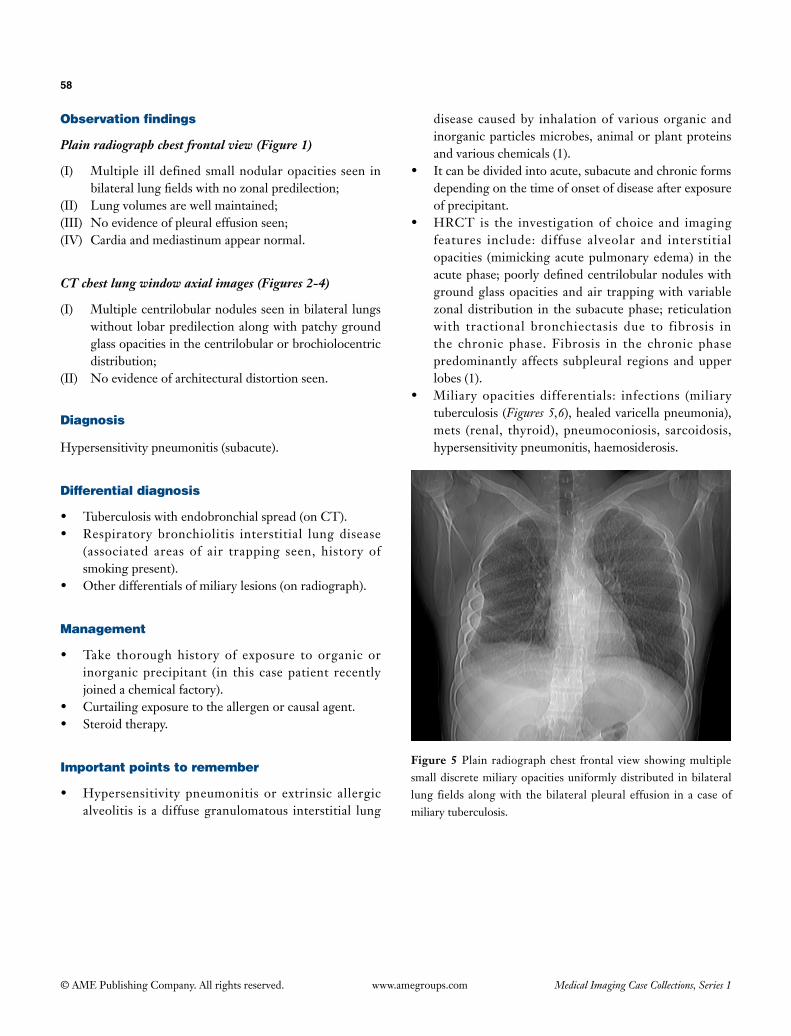
58
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Multiple ill defined small nodular opacities seen in bilateral lung fields with no zonal predilection;
(II) Lung volumes are well maintained;(III) No evidence of pleural effusion seen;(IV) Cardia and mediastinum appear normal.
CT chest lung window axial images (Figures 2-4)
(I) Multiple centrilobular nodules seen in bilateral lungs without lobar predilection along with patchy ground glass opacities in the centrilobular or brochiolocentric distribution;
(II) No evidence of architectural distortion seen.
Diagnosis
Hypersensitivity pneumonitis (subacute).
Differential diagnosis
• Tuberculosis with endobronchial spread (on CT).• Respiratory bronchiolitis interstitial lung disease
(associated areas of air trapping seen, history of smoking present).
• Other differentials of miliary lesions (on radiograph).
Management
• Take thorough history of exposure to organic or inorganic precipitant (in this case patient recently joined a chemical factory).
• Curtailing exposure to the allergen or causal agent.• Steroid therapy.
Important points to remember
• Hypersensitivity pneumonitis or extrinsic allergic alveolitis is a diffuse granulomatous interstitial lung
disease caused by inhalation of various organic and inorganic particles microbes, animal or plant proteins and various chemicals (1).
• It can be divided into acute, subacute and chronic forms depending on the time of onset of disease after exposure of precipitant.
• HRCT is the investigation of choice and imaging features include: diffuse alveolar and interstitial opacities (mimicking acute pulmonary edema) in the acute phase; poorly defined centrilobular nodules with ground glass opacities and air trapping with variable zonal distribution in the subacute phase; reticulation with tractional bronchiectasis due to fibrosis in the chronic phase. Fibrosis in the chronic phase predominantly affects subpleural regions and upper lobes (1).
• Miliary opacities differentials: infections (miliary tuberculosis (Figures 5,6), healed varicella pneumonia), mets (renal, thyroid), pneumoconiosis, sarcoidosis, hypersensitivity pneumonitis, haemosiderosis.
Figure 5 Plain radiograph chest frontal view showing multiple small discrete miliary opacities uniformly distributed in bilateral lung fields along with the bilateral pleural effusion in a case of miliary tuberculosis.

59
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 6 CT chest lung window of the same patient showing multiple small discrete miliary opacities uniformly distributed in bilateral lung fields with bilateral effusion (left > right).
References
1. Silva CI, Churg A, Müller NL. Hypersensitivity pneumonitis: spectrum of high-resolution CT and pathologic findings. AJR Am J Roentgenol 2007;188:334-44.
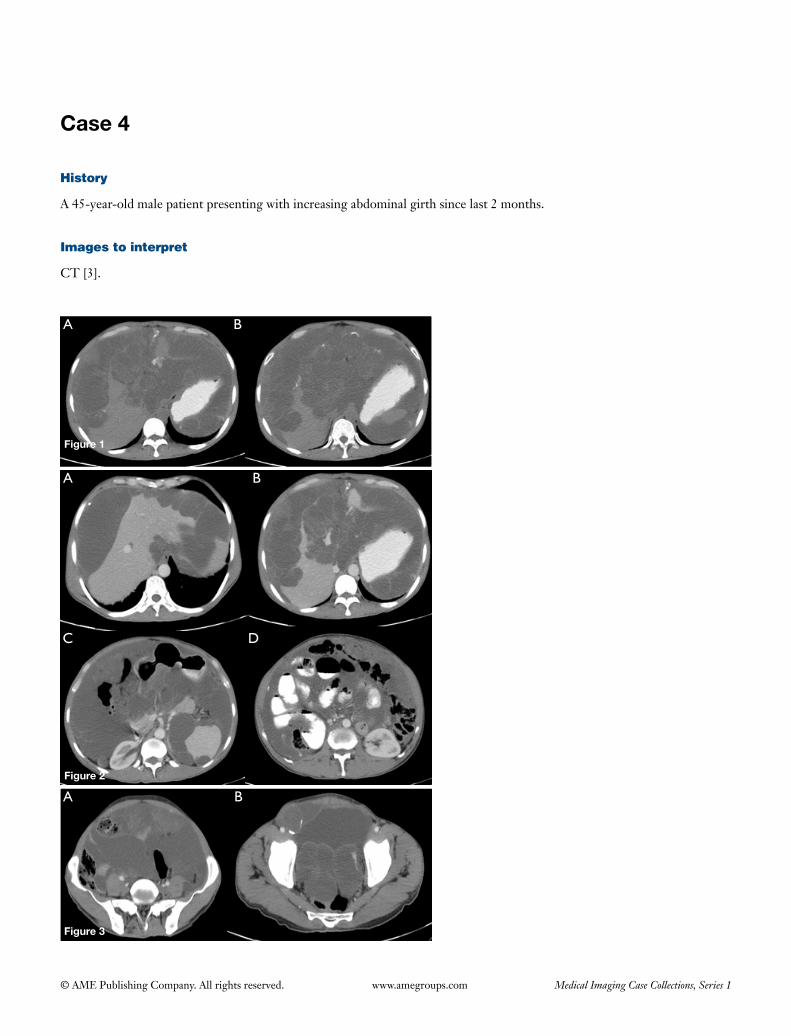
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
A B
B
B
C D
A
A
Figure 2
Figure 1
Figure 3
History
A 45-year-old male patient presenting with increasing abdominal girth since last 2 months.
Images to interpret
CT [3].

61
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Contrast enhanced CT of the abdomen serial sections (Figures 1-3)
(I) Lobulated, low-attenuation, peritoneal implants in both abdomen and pelvis showing rim calcification with gross septated ascites (Figures 1-3);
(II) Scalloping of surface of liver and spleen (Figures 1,2);(III) Gross omental thickening with narrowing of
transverse colon (Figure 2);(IV) Peritoneal implants in pelvis causing indentation of
base of bladder and narrowing of rectum (Figure 3).
Diagnosis
Pseudomyxoma peritonei.
Differential diagnosis
• Peritonealcarcinomatosis.• Peritonealsarcomatosis.
Management
Cytoreductive surgery followed by infusion of intraperitoneal
chemotherapy.
Important points to remember
• Pseudomyxomaperitonei (alsoknownas jellybelly)refers to mucinous implants on the peritoneal surfaces with diffuse collections of gelatinous material in the peritoneal cavity secondary to rupture of a mucinous tumor (most common cause is appendix tumor, others being mucinous tumors of colon, rectum, stomach, pancreas, ovary, urachus and gall bladder) (1,2).
• It has two pathological subtypes with differentprognosis: peritoneal adenomucinosis (primary tumor is benign, generally an adenoma) and peritoneal mucinous carcinoma (primary tumor is malignant or mucinous adenocarcinoma) (2).
• Imaging fea tures inc lude : gross a sc i tes wi th septations and internal non-mobile echoes (on USG), lobulated low attenuation mucinous implants over peritoneal surfaces often with rim calcifications, omental thickening, septated pseudoascites, scalloping of surface of liver & spleen, varying degrees of compression of the visceral organs like bowel, ureter, IVC (on CT) (2,3).
References
1. Sulkin TV, O'Neill H, Amin AI, Moran B. CT in pseudomyxoma peritonei: a review of 17 cases. Clin Radiol 2002;57:608-13.2. Ebrahim ZI, Lockhat ZI, Ismail F. Pseudomyxoma peritonei (PMP)–a rare entity. S Afr J Radiol 2011;15:79-81.3. Devang B, Allen C, Sean C. Pseudomyxoma peritonei. App Radiol 2005;34:6-8.
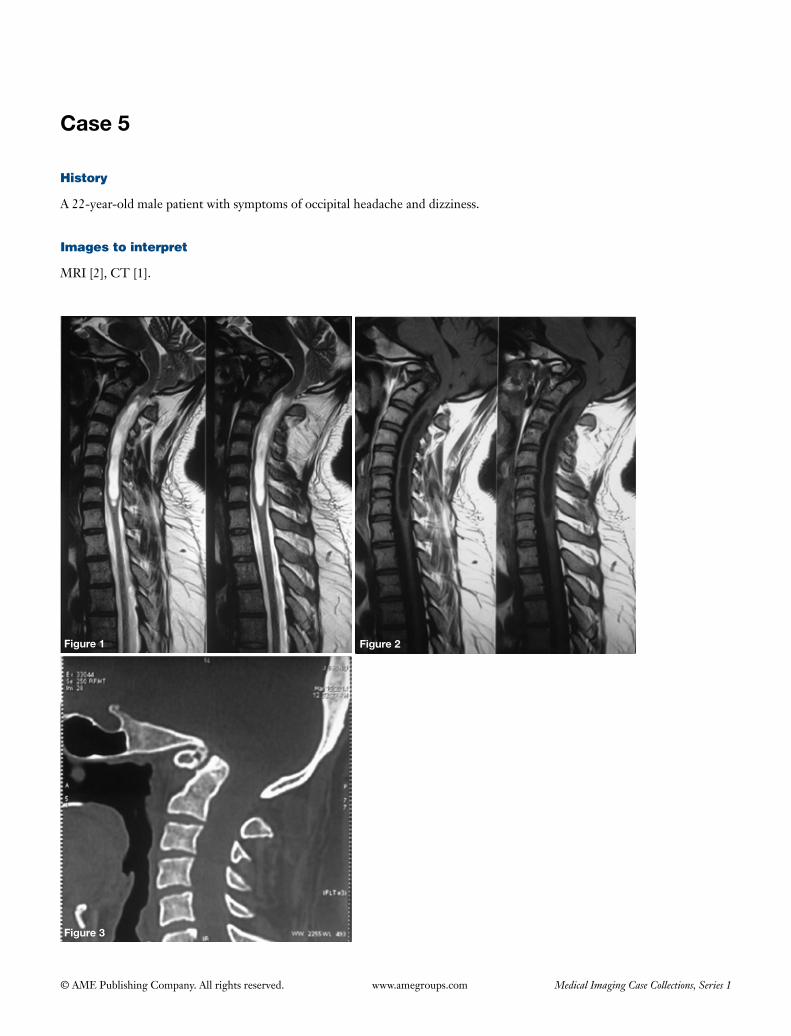
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
Figure 1 Figure 2
Figure 3
History
A 22-year-old male patient with symptoms of occipital headache and dizziness.
Images to interpret
MRI [2], CT [1].

63
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Sagittal T2 and T1 weighted images of cervical spine (Figures 1,2 respectively) and CT cervical spine (Figure 3) showing evidence of
(I) Herniation of cerebellar tonsills;(II) Mass effect on lower medulla, cervicomedullary
junction and upper spinal cord;(III) Syrinx in spinal cord from C2 to C7;(IV) Flattening of base of skull;(V) No evidence of basilar invagination or segmentation
anomalies of cervical spine including block vertebra or atlanto-occipital assimilation (important to mention negative findings which could be associated with the entity).
Diagnosis
Chiari 1 malformation with platybasia.
Differential diagnosis
None.
Management
• Neurosurgicalreferral;• Non-surgical:Patientswithnoneurological signs
referabletoposteriorfossaareavoidedsurgery.Patientsare kept on yearly follow-ups. Non-steroidal anti-inflammatorydrugs(NSAIDS)forsymptomslikeneckpain,headacheanddizziness.Patientshouldbeadvisedto avoid activities that precipitate symptoms like
straining or involving forceful movements like lifting heavy weights or playing football;
• Surgical:Posteriorfossadecompressioninpatientswithfeatures of brainstem compression.
Important points to remember
• Chiari1isthecommonestoutofallchiarimalformationsand is characterized by herniation of peg like cerebellar tonsils more than 5 mm below the foramen magnum. Commonassociations:syringomyeliaandhydrocephalus(both due to abnormal CSF flow dynamics), platybasia, basilar invagination, Sprengel deformity, Crouzon syndrome and Klippel-Feil syndrome (1);
• Chiari2consistsofcaudaldisplacementofcerebellarvermis, medulla and fourth ventricle through the foramen magnum and often associated with lumbosacral myelomeningocele (2);
• Chiari 3 is chiari 2withoccipital orhigh cervicalencephalocele;
• Chiari4iscerebellarhypoplasiawithoutherniationorcaudal displacement;
• Platybasia isflatteningofbaseofskullwithskullbaseanglemorethan143degrees(skullbaseanglecanbecalculated between two lines drawn from nasion to centre of pituitary fossa and another line from later point to anterior border of foramen magnum or basion andnormallyvaries from125-143degrees). Itcanbedue to congenital causes like osteogenesis imperfecta, cleidocranial dysostosis, chiari malformations or acquired causes of skull base softening like rickets, osteomalacia,Paget’sdisease(3).
References
1. ElsterAD,ChenMY.ChiariImalformations:clinicalandradiologicreappraisal.Radiology1992;183:347-53.2. PearceJM.Arnoldchiari,or“CruveilhierclelandChiari”malformation.JNeurolNeurosurgPsychiatry2000;68:13.3. KoenigsbergRA,VakilN,HongTA,HtaikT,FaerberE,MaioranoT,DuaM,FaroS,GonzalesC.Evaluationofplatybasia
withMRimaging.AJNRAmJNeuroradiol2005;26:89-92.
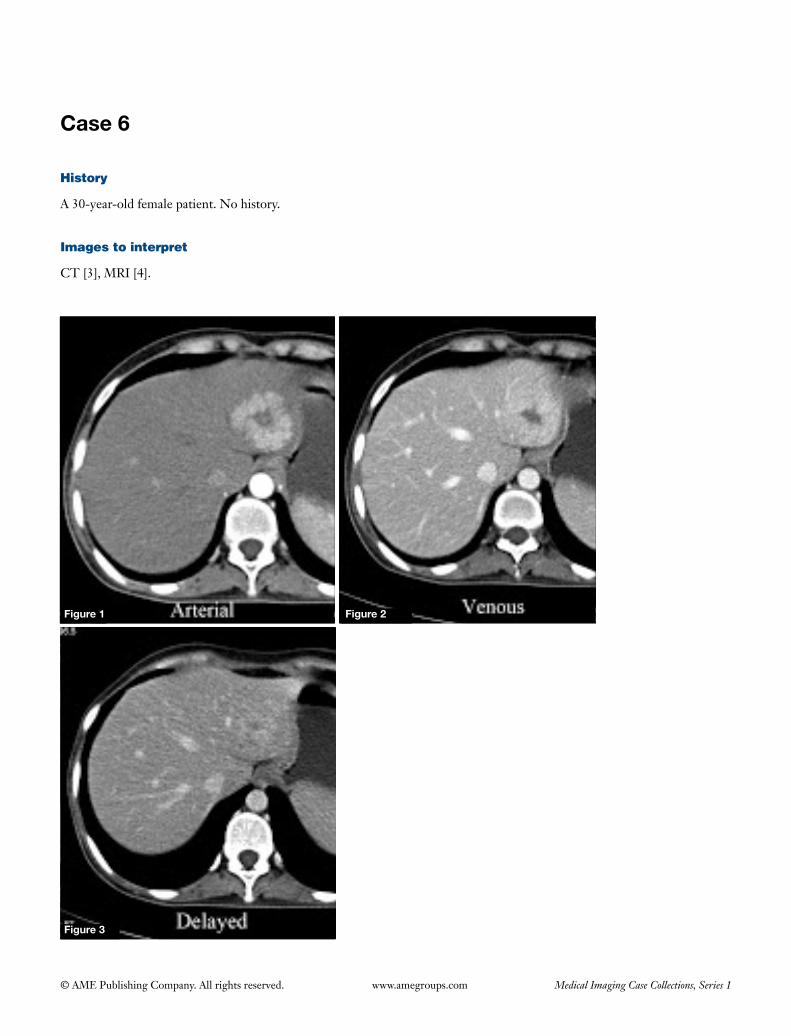
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
History
A 30-year-old female patient. No history.
Images to interpret
CT [3], MRI [4].
Figure 1 Figure 2
Figure 3
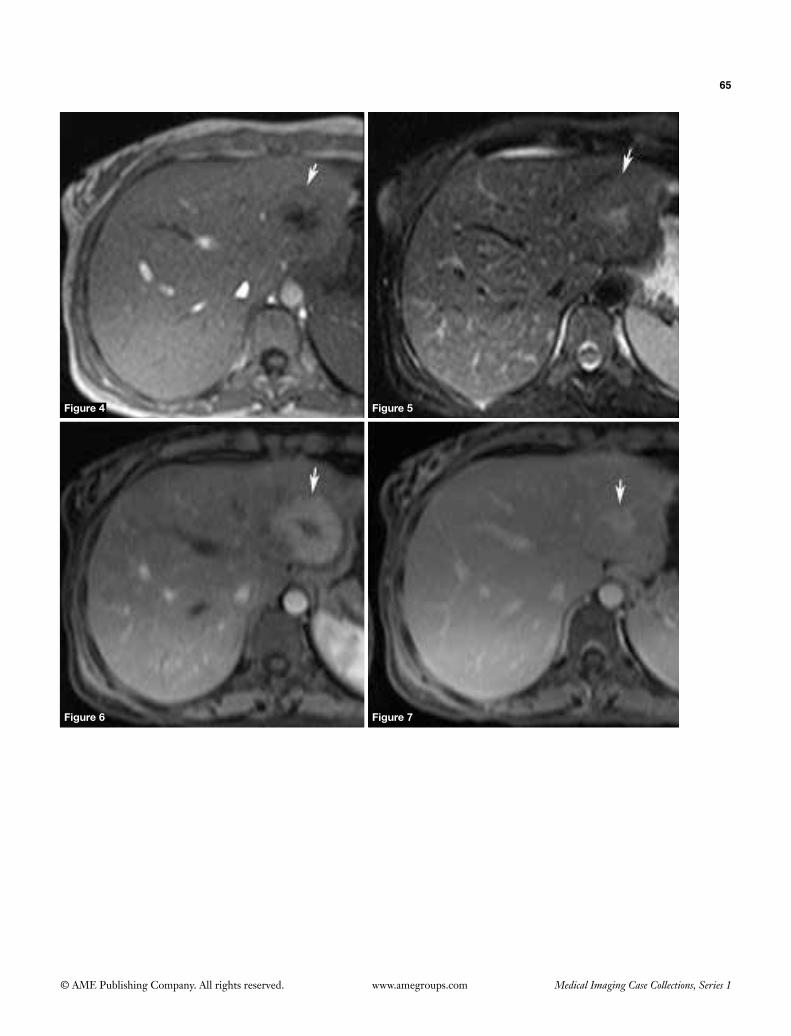
65
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 4 Figure 5
Figure 6 Figure 7

66
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Contrast enhanced CT axial, arterial (Figure 1), portal venous (Figure 2) and delayed (Figure 3) phases
The lesion shows intense enhancement in the arterial phase (Figure 1), partial wash-out in the portal venous phase with lesion slightly hyperattenuating than the adjacent liver (Figure 2) and becomes isoattenuating to the liver in the equilibrium phase with enhancement of the central scar (Figure 3).
MRI axial T1 (Figure 4), T2 (Figure 5), contrast enhanced arterial phase (Figure 6), equilibrium phase (Figure 7) images
(I) Well defined rounded lesion mildly hypointense on T1 (Figure 4), slightly hyperintense on T2 (Figure 5) weighted images seen with a central stellate scar which is hypointense on T1 (Figure 4) and hyperintense on T2 weighted (Figure 5) images;
(II) Lesion shows homogenous, moderate contrast enhancement in arterial phase with non-enhancing scar in centre (Figure 6) and wash-out in the equilibrium phase with enhancement of scar (Figure 7);
(III) Surrounding liver is normal with no evidence of cirrhosis.
Diagnosis
Focal nodular hyperplasia (FNH).
Differential diagnosis
• Hepaticadenoma• Fibrolamellarhepatocellularcarcinoma(HCC).• ConventionalHCC.• Hypervascularmetastasis.
Management
• Asymptomatic,smalllesionsaremanagedconservatively
as the risk of complications like rupture and hemorrhage is very less and they don’t carry any malignant potential.
• Large,symptomatic lesionsor lesionswithdiagnosticdilemma with adenoma or HCC require excision.
Important points to remember
• FNHisabenign,hepatic lesion,oftenseeninyoungwomen, that is thought to arise as a result of hyperplastic response to congenital vascular malformation or vascular injury. These are asymptomatic, mostly detected as an incidental finding on radiological scans done for other reasons (1).
• Theyareoftensolitaryvascularlesions,andcomposedof benign-appearing hepatocytes, Kupffer cells and bile ducts in a normal liver (1,2).
• Imaging featuresof typical lesionsonCTandMRinclude: isoechoic/mildly hypo or hyperechoic on USG, isodense on plain CT, mildly hypointense on T1, mildly hyperintense on T2, homogenous intense enhancement in the arterial phase, partial wash-out with most lesions being isoattenuating or slightly hyperattenuating to the adjacent liver in the portal venous and delayed phase. The scar is hypointense on T1, hyperintense on T2 (compared to fibrolamellar HCC in which scar is hypointense on both T1 and T2W sequences) and shows enhancement in theequilibriumphase.LiverspecificMRIcontrastagents(gadolinium BOPTA and gadolinium-EOB-DTPA) are agents that show some hepatic excretion (thus help in demonstrating functioning hepatic tissue) and show same enhancement pattern as that of conventional extracellular contrast agents in arterial, portal and equilibrium phases. Scans obtained in delayed phase (20 min to 2 h) after administering these agents show persistent uptake in FNH due to presence of functioning hepatocytes (compared to undifferentiated HCC) (1,2).
• FNHshowsuptakeontechnetium99msulphurcolloidscans due to presence of Kupffer cells and this feature is helpful in differentiating these lesions from adenoma, HCC and hepatic mets.
References
1. Hussain SM, Terkivatan T, Zondervan PE, Lanjouw E, de Rave S, Ijzermans JN, de Man RA. Focal nodular hyperplasia: findingsatstate-of-the-artMRimaging,US,CT,andpathologicanalysis.Radiographics2004;24:3-17;discussion18-9.
2. Mortelé KJ, Praet M, Van Vlierberghe H, de Hemptinne B, Zou K, Ros PR. Focal nodular hyperplasia of the liver: detection andcharacterizationwithplainanddynamic-enhancedMRI.AbdomImaging2002;27:700-7.
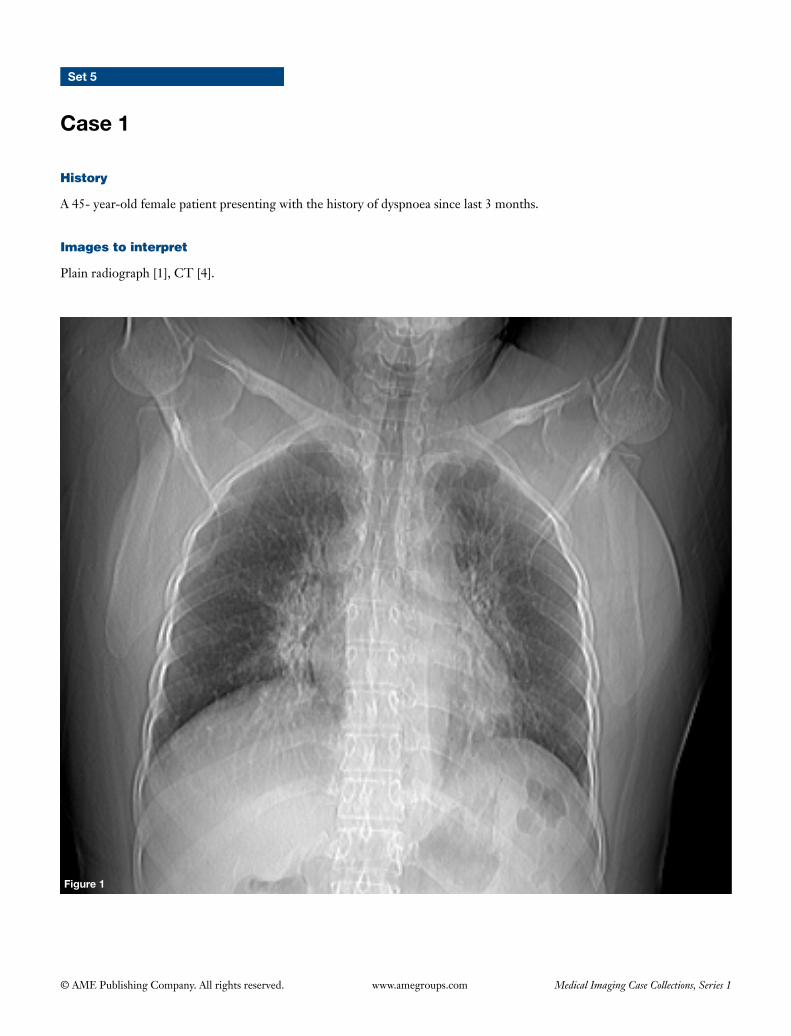
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 5
Case 1
Figure 1
History
A 45- year-old female patient presenting with the history of dyspnoea since last 3 months.
Images to interpret
Plain radiograph [1], CT [4].
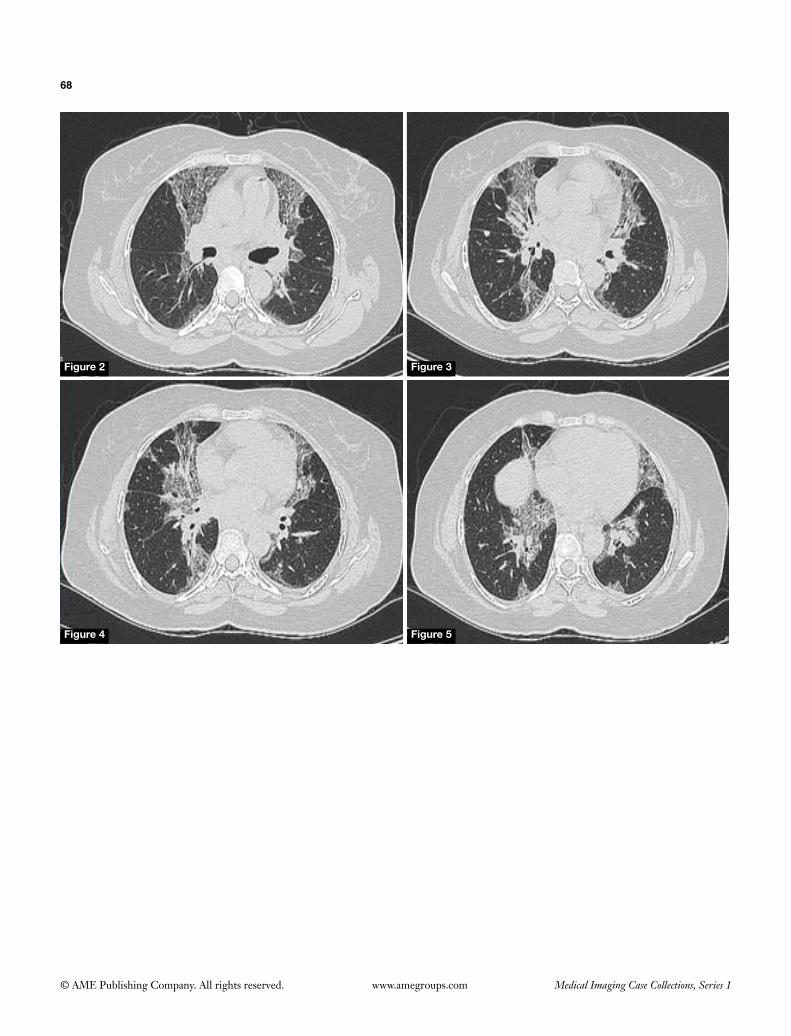
68
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2 Figure 3
Figure 4 Figure 5
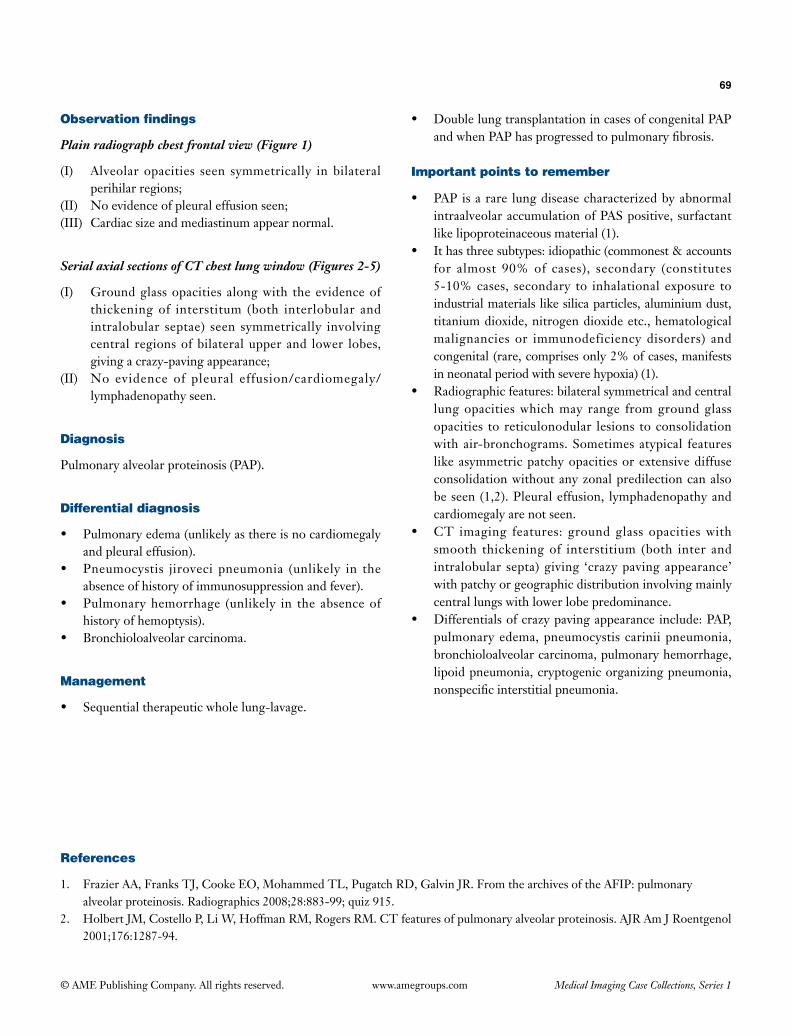
69
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Alveolar opacities seen symmetrically in bilateral perihilar regions;
(II) No evidence of pleural effusion seen;(III) Cardiac size and mediastinum appear normal.
Serial axial sections of CT chest lung window (Figures 2-5)
(I) Ground glass opacities along with the evidence of thickening of interstitum (both interlobular and intralobular septae) seen symmetrically involving central regions of bilateral upper and lower lobes, giving a crazy-paving appearance;
(II) No evidence of pleural effusion/cardiomegaly/lymphadenopathy seen.
Diagnosis
Pulmonary alveolar proteinosis (PAP).
Differential diagnosis
• Pulmonaryedema(unlikelyasthereisnocardiomegalyand pleural effusion).
• Pneumocystis jiroveci pneumonia (unlikely in theabsence of history of immunosuppression and fever).
• Pulmonaryhemorrhage (unlikely in the absenceofhistory of hemoptysis).
• Bronchioloalveolarcarcinoma.
Management
• Sequentialtherapeuticwholelung-lavage.
• DoublelungtransplantationincasesofcongenitalPAPandwhenPAPhasprogressedtopulmonaryfibrosis.
Important points to remember
• PAPisarare lungdiseasecharacterizedbyabnormalintraalveolaraccumulationofPASpositive,surfactantlike lipoproteinaceous material (1).
• Ithasthreesubtypes:idiopathic(commonest&accountsfor almost 90% of cases), secondary (constitutes 5-10% cases, secondary to inhalational exposure to industrial materials like silica particles, aluminium dust, titanium dioxide, nitrogen dioxide etc., hematological malignancies or immunodeficiency disorders) and congenital (rare, comprises only 2% of cases, manifests in neonatal period with severe hypoxia) (1).
• Radiographicfeatures:bilateralsymmetricalandcentrallung opacities which may range from ground glass opacities to reticulonodular lesions to consolidation withair-bronchograms.Sometimesatypical featureslike asymmetric patchy opacities or extensive diffuse consolidation without any zonal predilection can also be seen (1,2). Pleural effusion, lymphadenopathy and cardiomegaly are not seen.
• CT imaging features: groundglass opacitieswithsmooth thickening of interstitium (both inter and intralobular septa) giving ‘crazy paving appearance’ with patchy or geographic distribution involving mainly central lungs with lower lobe predominance.
• Differentialsofcrazypavingappearanceinclude:PAP,pulmonary edema, pneumocystis carinii pneumonia, bronchioloalveolar carcinoma, pulmonary hemorrhage, lipoid pneumonia, cryptogenic organizing pneumonia, nonspecificinterstitialpneumonia.
References
1. FrazierAA,FranksTJ,CookeEO,MohammedTL,PugatchRD,GalvinJR.FromthearchivesoftheAFIP:pulmonaryalveolarproteinosis.Radiographics2008;28:883-99;quiz915.
2. HolbertJM,CostelloP,LiW,HoffmanRM,RogersRM.CTfeaturesofpulmonaryalveolarproteinosis.AJRAmJRoentgenol2001;176:1287-94.
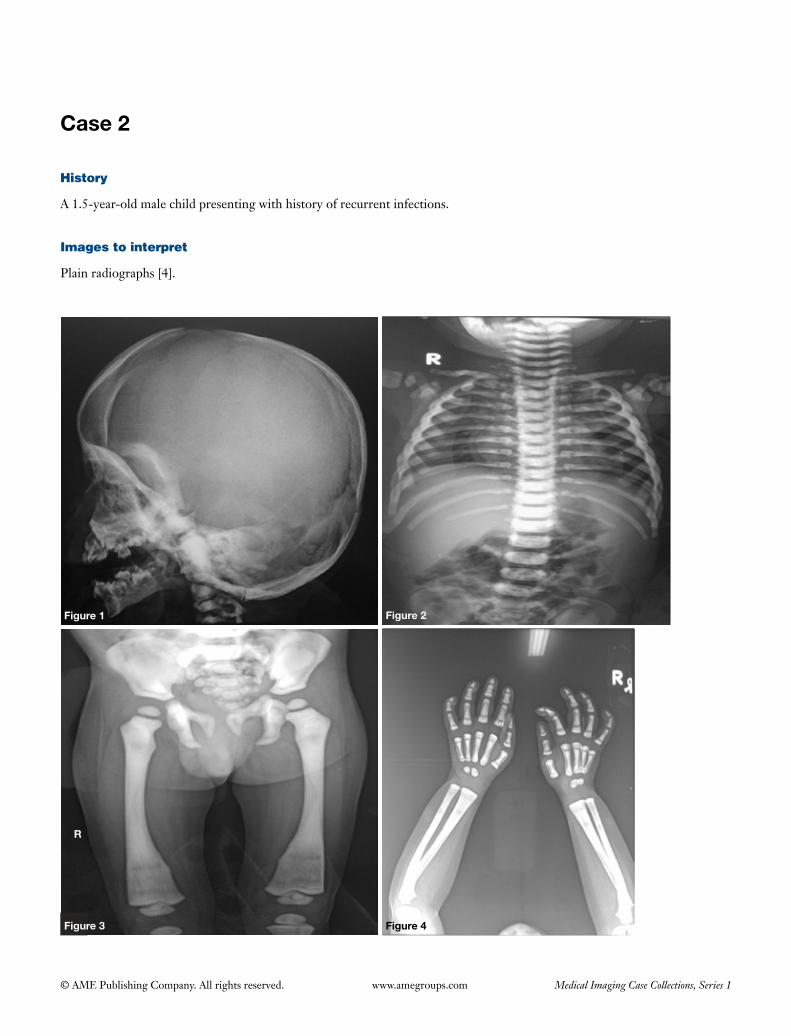
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
History
A 1.5-year-old male child presenting with history of recurrent infections.
Images to interpret
Plain radiographs [4].
Figure 1 Figure 2
Figure 4
R
Figure 3
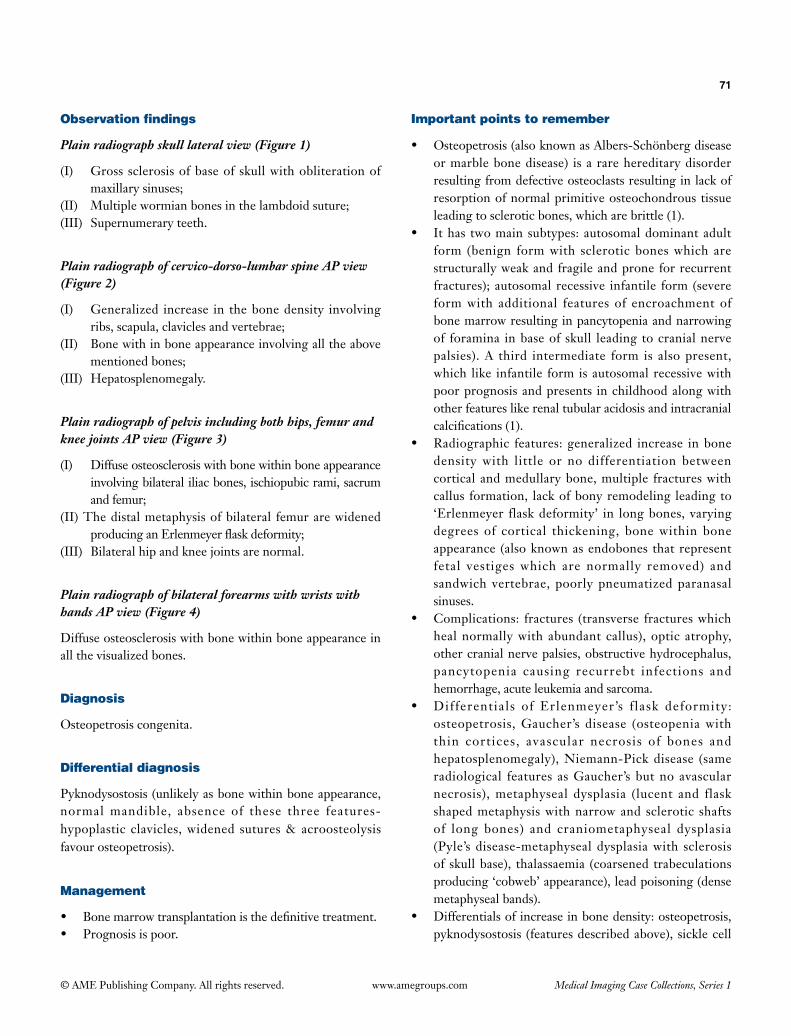
71
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph skull lateral view (Figure 1)
(I) Gross sclerosis of base of skull with obliteration of maxillary sinuses;
(II) Multiple wormian bones in the lambdoid suture;(III) Supernumerary teeth.
Plain radiograph of cervico-dorso-lumbar spine AP view (Figure 2)
(I) Generalized increase in the bone density involving ribs, scapula, clavicles and vertebrae;
(II) Bone with in bone appearance involving all the above mentioned bones;
(III) Hepatosplenomegaly.
Plain radiograph of pelvis including both hips, femur and knee joints AP view (Figure 3)
(I) Diffuse osteosclerosis with bone within bone appearance involving bilateral iliac bones, ischiopubic rami, sacrum and femur;
(II) The distal metaphysis of bilateral femur are widened producing an Erlenmeyer flask deformity;
(III) Bilateral hip and knee joints are normal.
Plain radiograph of bilateral forearms with wrists with hands AP view (Figure 4)
Diffuse osteosclerosis with bone within bone appearance in all the visualized bones.
Diagnosis
Osteopetrosis congenita.
Differential diagnosis
Pyknodysostosis (unlikely as bone within bone appearance, normal mandible, absence of these three features- hypoplastic clavicles, widened sutures & acroosteolysis favour osteopetrosis).
Management
• Bone marrow transplantation is the definitive treatment.• Prognosis is poor.
Important points to remember
• Osteopetrosis (also known as Albers-Schönberg disease or marble bone disease) is a rare hereditary disorder resulting from defective osteoclasts resulting in lack of resorption of normal primitive osteochondrous tissue leading to sclerotic bones, which are brittle (1).
• It has two main subtypes: autosomal dominant adult form (benign form with sclerotic bones which are structurally weak and fragile and prone for recurrent fractures); autosomal recessive infantile form (severe form with additional features of encroachment of bone marrow resulting in pancytopenia and narrowing of foramina in base of skull leading to cranial nerve palsies). A third intermediate form is also present, which like infantile form is autosomal recessive with poor prognosis and presents in childhood along with other features like renal tubular acidosis and intracranial calcifications (1).
• Radiographic features: generalized increase in bone density with little or no differentiation between cortical and medullary bone, multiple fractures with callus formation, lack of bony remodeling leading to ‘Erlenmeyer flask deformity’ in long bones, varying degrees of cortical thickening, bone within bone appearance (also known as endobones that represent fetal vestiges which are normally removed) and sandwich vertebrae, poorly pneumatized paranasal sinuses.
• Complications: fractures (transverse fractures which heal normally with abundant callus), optic atrophy, other cranial nerve palsies, obstructive hydrocephalus, pancytopenia causing recurrebt infections and hemorrhage, acute leukemia and sarcoma.
• Differentials of Erlenmeyer’s f lask deformity: osteopetrosis, Gaucher’s disease (osteopenia with thin cortices, avascular necrosis of bones and hepatosplenomegaly), Niemann-Pick disease (same radiological features as Gaucher’s but no avascular necrosis), metaphyseal dysplasia (lucent and flask shaped metaphysis with narrow and sclerotic shafts of long bones) and craniometaphyseal dysplasia (Pyle’s disease-metaphyseal dysplasia with sclerosis of skull base), thalassaemia (coarsened trabeculations producing ‘cobweb’ appearance), lead poisoning (dense metaphyseal bands).
• Differentials of increase in bone density: osteopetrosis, pyknodysostosis (features described above), sickle cell

72
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
disease (gallstones, splenic atrophy and calcification, avascular necrosis of bones and H-shaped vertebra, renal papillary necrosis), fluorosis (interosseous membrane and ligamentous insertion calcification), rena l os teodys t rophy ( fea tures o f secondary hyperparathyroidism, evidence of haemodialysis line
on chest radiograph or peritoneal dialysis line on abdominal radiograph), sclerotic metastases (evidence of primary malignancy or mets in other organs), myelofibrosis (massive splenomegaly), mastocytosis (splenomegaly, small bowel thickening).
References
1. Phatak SV, Kolwadkar PK, Phatak MS. Osteopetrosis congenita: A case report. Indian J Radiol Imaging 2003;13:387-8.
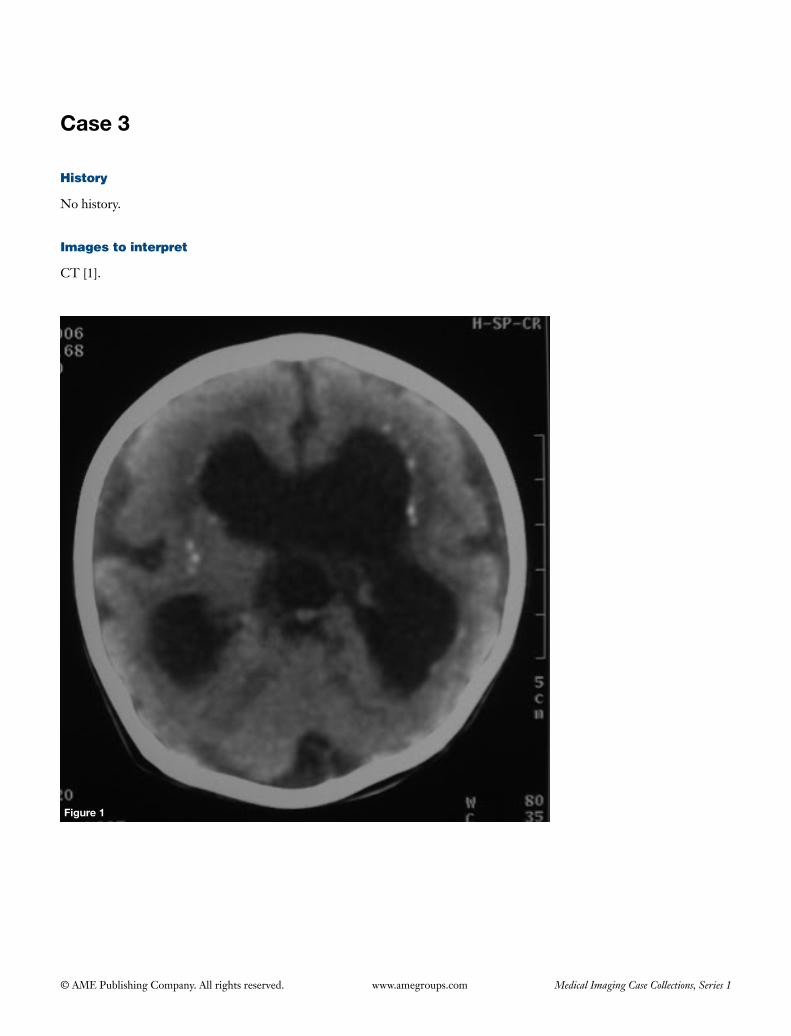
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
History
No history.
Images to interpret
CT [1].
Figure 1

74
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain non-contrast CT head axial section (Figure 1)
(I) Paucity of white matter noted;(II) Dilatation of bilateral lateral and third ventricles with
periventricular ooze;(III) Periventricularcalcificationseen;(IV) Brain surface is smooth with a few poorly formed gyri
and absence of sulcation with a typical ‘figure of 8’ appearance suggestive of lissencephaly.
Diagnosis
Congenital cytomegalovirus infection.
Differential diagnosis
• OtherTORCHinfection.• Tuberoussclerosis.• Congenitallymphocyticchoriomeningitis.
Management
• Serological testsor cultures for virus isolation for
confirmingdiagnosis.• Further examination and investigations for other
systemic manifestations.• Referral topediatrician forsupportive treatmentand
management with ganciclovir.
Important points to remember
• Cytomegalovirus is themost common cause ofcongenital infection affecting about 1% of all l ive births and can be acquired prenatal ly or perinatally (1).
• Mani fes ta t ions inc lude : CNS [microcephaly,periventricular calcifications, ventricular adhesions,hydrocephalus, neuronalmigrational anomalies(includingpachygyriaandlissencephalyasinourcase),whitematter lesions,periventricularcysts,cerebellarhypoplasia,corticalatrophy,lenticulostriatevasculopathy,intracranial hemorrhage], intrauterine growthretardation,prematurity,chorioretinitis,sensorineuralhearingloss,pneumonia,hepatosplenomegaly,hepatitis,fetal intrahepatic calcification, jaundice,petechiae,thrombocytopenia(1,2).
References
1. CeolaAF,AngtuacoTL.UScaseoftheday.Congenitalcytomegalovirusinfection.Radiographics1999;19:1385-7.2. FinkKR,ThapaMM,IshakGE,PruthiS.Neuroimagingofpediatriccentralnervoussystemcytomegalovirusinfection.
Radiographics2010;30:1779-96.
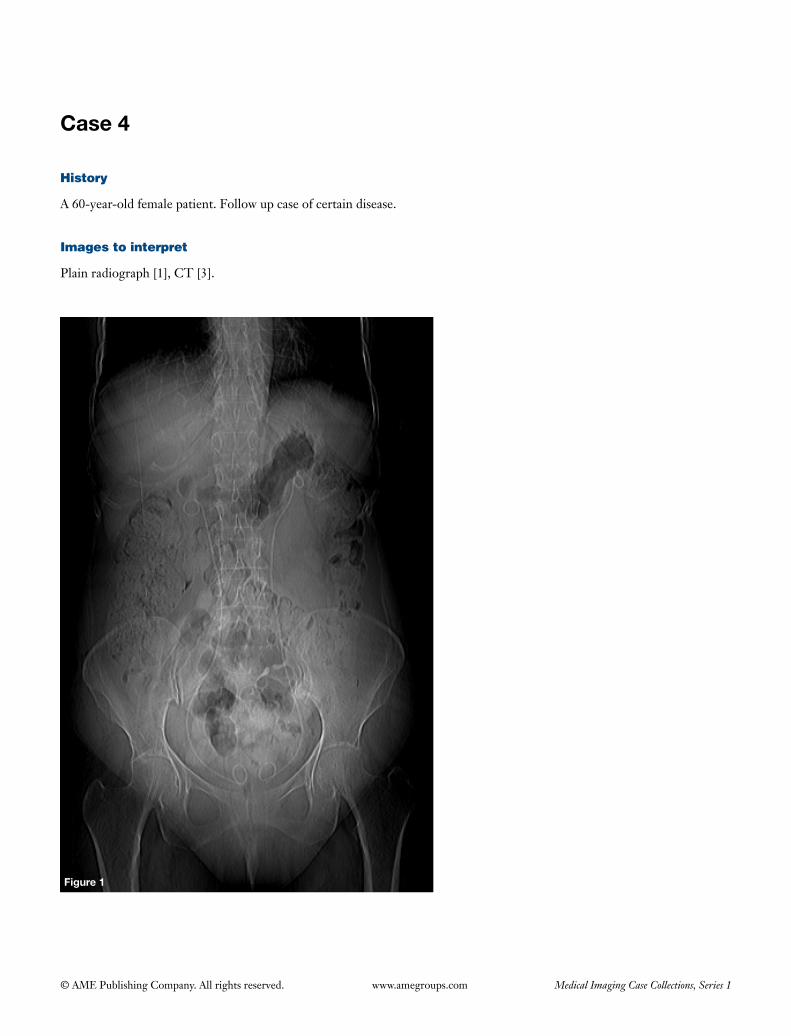
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
Figure 1
History
A 60-year-old female patient. Follow up case of certain disease.
Images to interpret
Plain radiograph [1], CT [3].
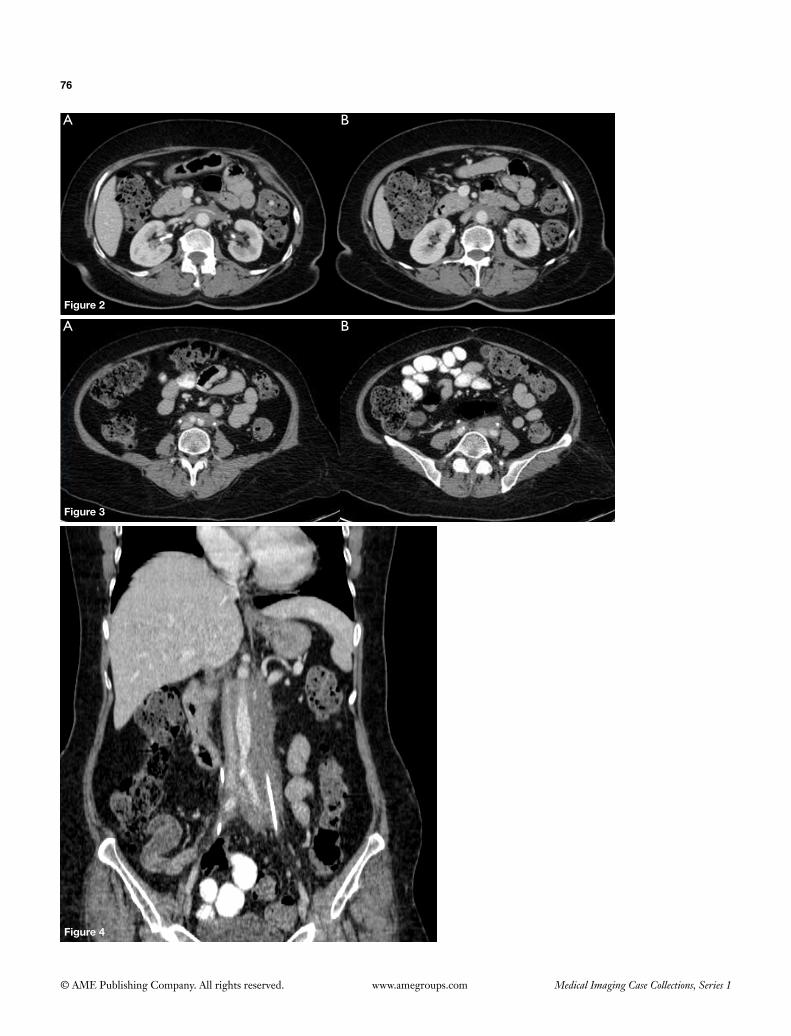
76
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
A
A B
B
Figure 2
Figure 3
Figure 4
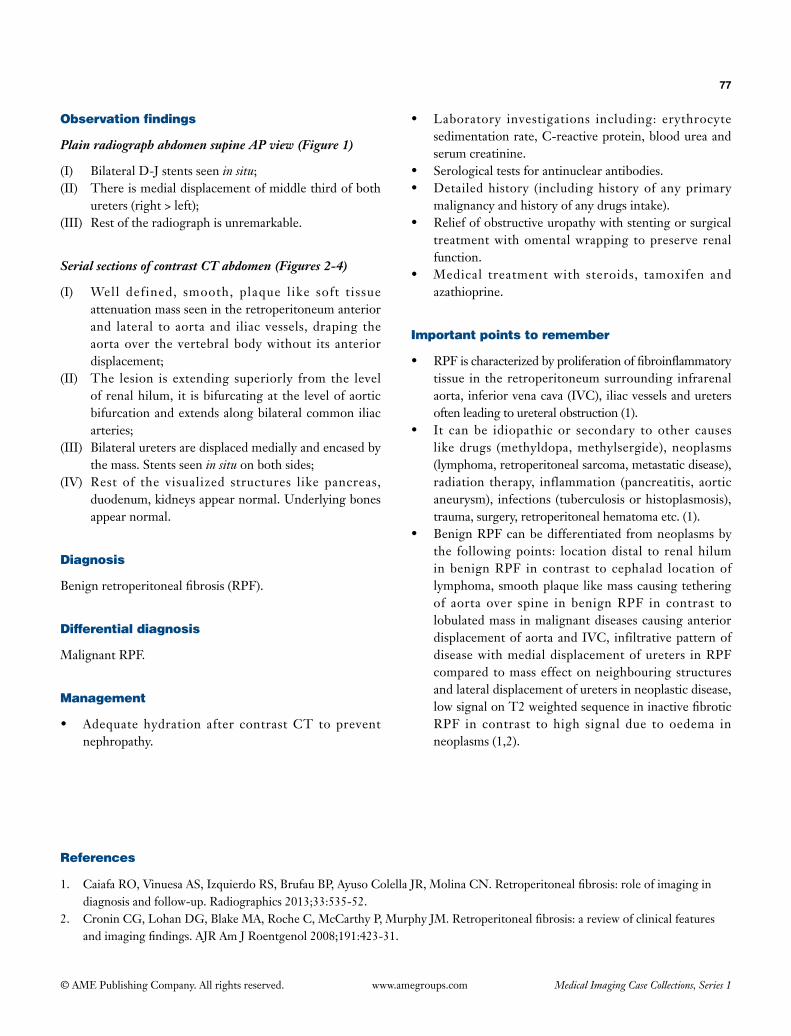
77
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph abdomen supine AP view (Figure 1)
(I) Bilateral D-J stents seen in situ;(II) There is medial displacement of middle third of both
ureters (right > left);(III) Rest of the radiograph is unremarkable.
Serial sections of contrast CT abdomen (Figures 2-4)
(I) Well defined, smooth, plaque like soft tissue attenuation mass seen in the retroperitoneum anterior and lateral to aorta and iliac vessels, draping the aorta over the vertebral body without its anterior displacement;
(II) The lesion is extending superiorly from the level of renal hilum, it is bifurcating at the level of aortic bifurcation and extends along bilateral common iliac arteries;
(III) Bilateral ureters are displaced medially and encased by the mass. Stents seen in situ on both sides;
(IV) Rest of the visualized structures like pancreas, duodenum, kidneys appear normal. Underlying bones appear normal.
Diagnosis
Benign retroperitoneal fibrosis (RPF).
Differential diagnosis
Malignant RPF.
Management
• Adequate hydration after contrast CT to prevent nephropathy.
• Laboratory investigations including: erythrocyte sedimentation rate, C-reactive protein, blood urea and serum creatinine.
• Serological tests for antinuclear antibodies.• Detailed history (including history of any primary
malignancy and history of any drugs intake).• Relief of obstructive uropathy with stenting or surgical
treatment with omental wrapping to preserve renal function.
• Medical treatment with steroids, tamoxifen and azathioprine.
Important points to remember
• RPF is characterized by proliferation of fibroinflammatory tissue in the retroperitoneum surrounding infrarenal aorta, inferior vena cava (IVC), iliac vessels and ureters often leading to ureteral obstruction (1).
• It can be idiopathic or secondary to other causes like drugs (methyldopa, methylsergide), neoplasms (lymphoma, retroperitoneal sarcoma, metastatic disease), radiation therapy, inflammation (pancreatitis, aortic aneurysm), infections (tuberculosis or histoplasmosis), trauma, surgery, retroperitoneal hematoma etc. (1).
• Benign RPF can be differentiated from neoplasms by the following points: location distal to renal hilum in benign RPF in contrast to cephalad location of lymphoma, smooth plaque like mass causing tethering of aorta over spine in benign RPF in contrast to lobulated mass in malignant diseases causing anterior displacement of aorta and IVC, infiltrative pattern of disease with medial displacement of ureters in RPF compared to mass effect on neighbouring structures and lateral displacement of ureters in neoplastic disease, low signal on T2 weighted sequence in inactive fibrotic RPF in contrast to high signal due to oedema in neoplasms (1,2).
References
1. Caiafa RO, Vinuesa AS, Izquierdo RS, Brufau BP, Ayuso Colella JR, Molina CN. Retroperitoneal fibrosis: role of imaging in diagnosis and follow-up. Radiographics 2013;33:535-52.
2. Cronin CG, Lohan DG, Blake MA, Roche C, McCarthy P, Murphy JM. Retroperitoneal fibrosis: a review of clinical features and imaging findings. AJR Am J Roentgenol 2008;191:423-31.
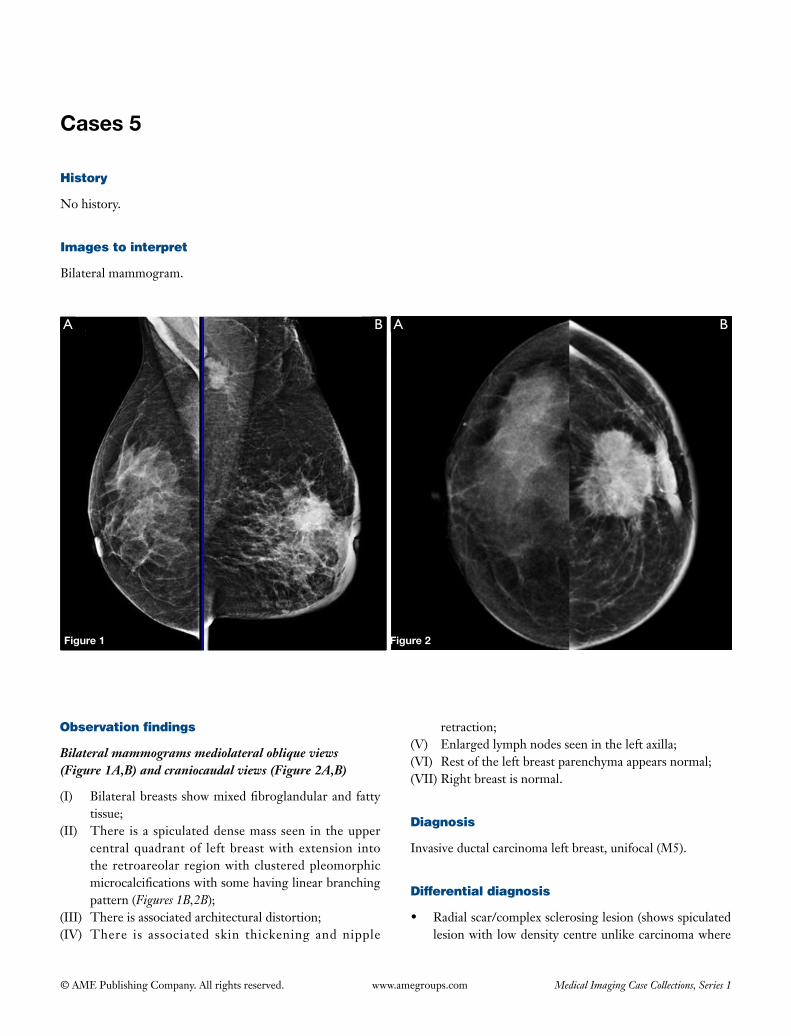
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Cases 5
History
No history.
Images to interpret
Bilateral mammogram.
A B A B
Figure 1 Figure 2
Observation findings
Bilateral mammograms mediolateral oblique views (Figure 1A,B) and craniocaudal views (Figure 2A,B)
(I) Bilateralbreastsshowmixedfibroglandularandfattytissue;
(II) There isa spiculateddensemassseen in theuppercentralquadrantof leftbreastwithextension intotheretroareolarregionwithclusteredpleomorphicmicrocalcificationswithsomehavinglinearbranchingpattern(Figures 1B,2B);
(III) Thereisassociatedarchitecturaldistortion;(IV) There is associated skin thickening and nipple
retraction;(V) Enlargedlymphnodesseenintheleftaxilla;(VI) Restoftheleftbreastparenchymaappearsnormal;(VII)Rightbreastisnormal.
Diagnosis
Invasiveductalcarcinomaleftbreast,unifocal(M5).
Differential diagnosis
• Radialscar/complexsclerosinglesion(showsspiculatedlesionwithlowdensitycentreunlikecarcinomawhere
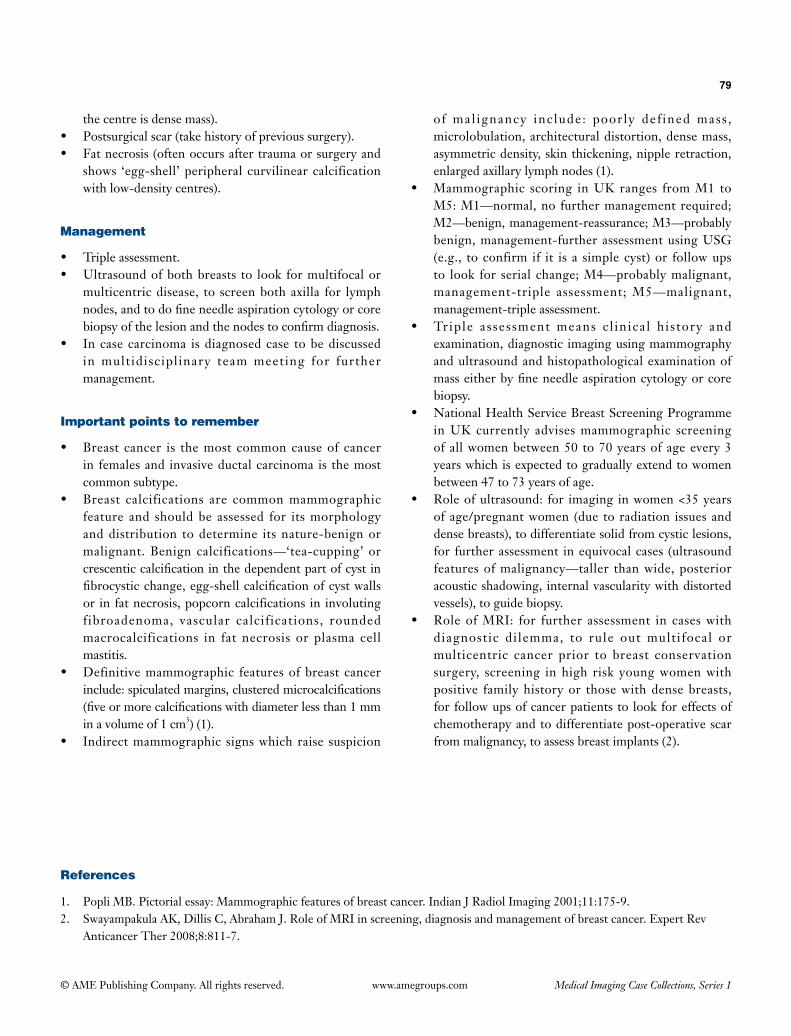
79
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
thecentreisdensemass).• Postsurgicalscar(takehistoryofprevioussurgery).• Fatnecrosis(oftenoccursaftertraumaorsurgeryand
shows ‘egg-shell’peripheralcurvilinearcalcificationwithlow-densitycentres).
Management
• Tripleassessment.• Ultrasoundofbothbreasts to look formultifocalor
multicentricdisease, to screenbothaxilla for lymphnodes,andtodofineneedleaspirationcytologyorcorebiopsyofthelesionandthenodestoconfirmdiagnosis.
• Incasecarcinoma isdiagnosedcase tobediscussedin multidisciplinary teammeeting for furthermanagement.
Important points to remember
• Breast cancer is themost commoncauseof cancerin femalesand invasiveductalcarcinomais themostcommonsubtype.
• Breast calcifications are commonmammographicfeature and shouldbe assessed for itsmorphologyanddistribution todetermine itsnature-benignormalignant.Benign calcifications—‘tea-cupping’orcrescenticcalcificationinthedependentpartofcystinfibrocysticchange,egg-shellcalcificationofcystwallsor infatnecrosis,popcorncalcifications in involutingfibroadenoma, vascular calcifications, roundedmacrocalcifications in fat necrosis or plasma cellmastitis.
• Definitivemammographic featuresofbreast cancerinclude:spiculatedmargins,clusteredmicrocalcifications(fiveormorecalcificationswithdiameterlessthan1mminavolumeof1cm3)(1).
• Indirectmammographic signswhichraise suspicion
of mal ignancy inc lude: poor ly def ined mass ,microlobulation,architecturaldistortion,densemass,asymmetricdensity,skinthickening,nippleretraction,enlargedaxillarylymphnodes(1).
• Mammographic scoring inUKranges fromM1 toM5:M1—normal,no furthermanagementrequired;M2—benign,management-reassurance;M3—probablybenign,management-furtherassessmentusingUSG(e.g., toconfirm if it is a simplecyst)or followupsto look for serial change;M4—probablymalignant,management-triple assessment;M5—malignant,management-tripleassessment.
• Triple assessment means c l inica l his tory andexamination,diagnostic imagingusingmammographyandultrasoundandhistopathologicalexaminationofmasseitherbyfineneedleaspirationcytologyorcorebiopsy.
• NationalHealthServiceBreastScreeningProgrammeinUKcurrently advisesmammographic screeningofallwomenbetween50 to70yearsofageevery3yearswhichisexpectedtograduallyextendtowomenbetween47to73yearsofage.
• Roleofultrasound: for imaging inwomen<35yearsofage/pregnantwomen (due toradiation issuesanddensebreasts),todifferentiatesolidfromcysticlesions,for furtherassessment inequivocalcases (ultrasoundfeaturesofmalignancy—taller thanwide,posterioracousticshadowing, internalvascularitywithdistortedvessels),toguidebiopsy.
• RoleofMRI: for further assessment in caseswithdiagnostic dilemma, to rule out multifocal ormulticentric cancer prior to breast conservationsurgery, screening inhigh risk youngwomenwithpositive familyhistoryor thosewithdensebreasts,forfollowupsofcancerpatientstolookforeffectsofchemotherapyandtodifferentiatepost-operativescarfrommalignancy,toassessbreastimplants(2).
References
1. PopliMB.Pictorialessay:Mammographicfeaturesofbreastcancer.IndianJRadiolImaging2001;11:175-9.2. SwayampakulaAK,DillisC,AbrahamJ.RoleofMRIinscreening,diagnosisandmanagementofbreastcancer.ExpertRev
AnticancerTher2008;8:811-7.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
History
A 40-year-old male patient attended medical fitness test for his job.
Images to interpret
Plain radiograph [1], CT [3].
Figure 1
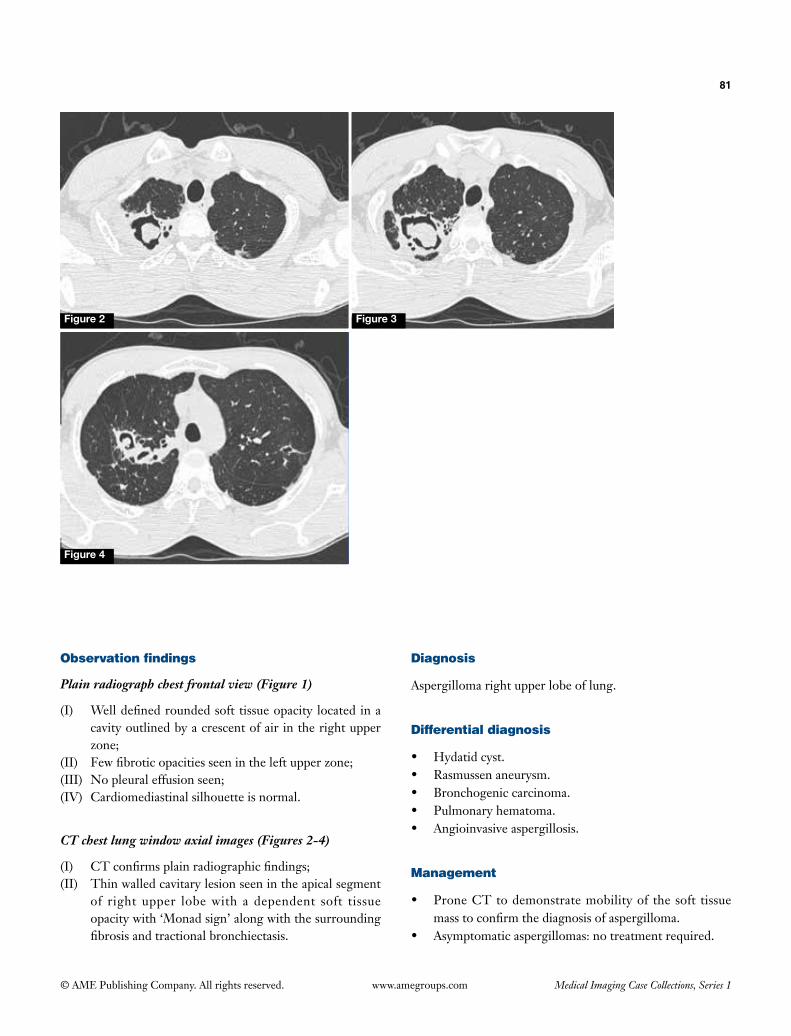
81
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Well defined rounded soft tissue opacity located in a cavity outlined by a crescent of air in the right upper zone;
(II) Few fibrotic opacities seen in the left upper zone;(III) No pleural effusion seen;(IV) Cardiomediastinal silhouette is normal.
CT chest lung window axial images (Figures 2-4)
(I) CT confirms plain radiographic findings;(II) Thin walled cavitary lesion seen in the apical segment
of right upper lobe with a dependent soft tissue opacity with ‘Monad sign’ along with the surrounding fibrosis and tractional bronchiectasis.
Diagnosis
Aspergilloma right upper lobe of lung.
Differential diagnosis
• Hydatid cyst.• Rasmussen aneurysm.• Bronchogenic carcinoma.• Pulmonary hematoma.• Angioinvasive aspergillosis.
Management
• Prone CT to demonstrate mobility of the soft tissue mass to confirm the diagnosis of aspergilloma.
• Asymptomatic aspergillomas: no treatment required.
Figure 2 Figure 3
Figure 4
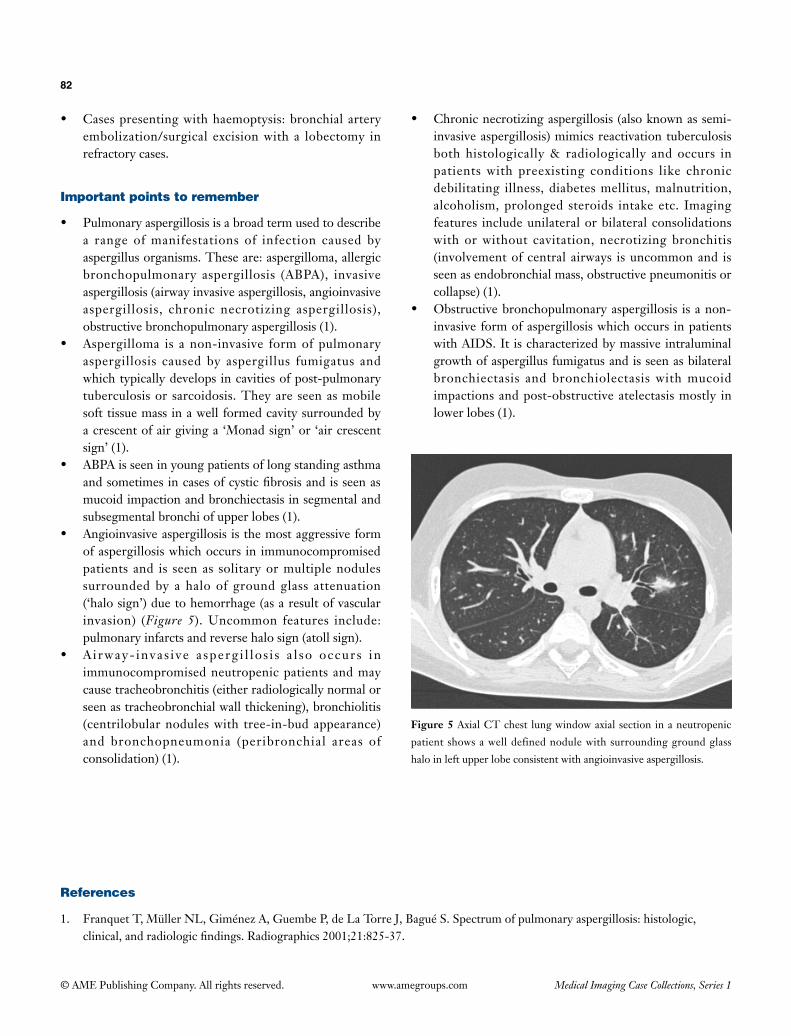
82
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
• Cases presenting with haemoptysis: bronchial artery embolization/surgical excision with a lobectomy in refractory cases.
Important points to remember
• Pulmonary aspergillosis is a broad term used to describe a range of manifestations of infection caused by aspergillus organisms. These are: aspergilloma, allergic bronchopulmonary aspergillosis (ABPA), invasive aspergillosis (airway invasive aspergillosis, angioinvasive aspergillosis, chronic necrotizing aspergillosis), obstructive bronchopulmonary aspergillosis (1).
• Aspergilloma is a non-invasive form of pulmonary aspergillosis caused by aspergillus fumigatus and which typically develops in cavities of post-pulmonary tuberculosis or sarcoidosis. They are seen as mobile soft tissue mass in a well formed cavity surrounded by a crescent of air giving a ‘Monad sign’ or ‘air crescent sign’ (1).
• ABPA is seen in young patients of long standing asthma and sometimes in cases of cystic fibrosis and is seen as mucoid impaction and bronchiectasis in segmental and subsegmental bronchi of upper lobes (1).
• Angioinvasive aspergillosis is the most aggressive form of aspergillosis which occurs in immunocompromised patients and is seen as solitary or multiple nodules surrounded by a halo of ground glass attenuation (‘halo sign’) due to hemorrhage (as a result of vascular invasion) (Figure 5). Uncommon features include: pulmonary infarcts and reverse halo sign (atoll sign).
• A i rway- invas i ve a sperg i l lo s i s a l so occur s in immunocompromised neutropenic patients and may cause tracheobronchitis (either radiologically normal or seen as tracheobronchial wall thickening), bronchiolitis (centrilobular nodules with tree-in-bud appearance) and bronchopneumonia (peribronchial areas of consolidation) (1).
• Chronic necrotizing aspergillosis (also known as semi-invasive aspergillosis) mimics reactivation tuberculosis both histologically & radiologically and occurs in patients with preexisting conditions like chronic debilitating illness, diabetes mellitus, malnutrition, alcoholism, prolonged steroids intake etc. Imaging features include unilateral or bilateral consolidations with or without cavitation, necrotizing bronchitis (involvement of central airways is uncommon and is seen as endobronchial mass, obstructive pneumonitis or collapse) (1).
• Obstructive bronchopulmonary aspergillosis is a non-invasive form of aspergillosis which occurs in patients with AIDS. It is characterized by massive intraluminal growth of aspergillus fumigatus and is seen as bilateral bronchiectasis and bronchiolectasis with mucoid impactions and post-obstructive atelectasis mostly in lower lobes (1).
Figure 5 Axial CT chest lung window axial section in a neutropenic
patient shows a well defined nodule with surrounding ground glass
halo in left upper lobe consistent with angioinvasive aspergillosis.
References
1. Franquet T, Müller NL, Giménez A, Guembe P, de La Torre J, Bagué S. Spectrum of pulmonary aspergillosis: histologic, clinical, and radiologic findings. Radiographics 2001;21:825-37.
Section 2—Oral examinations/viva

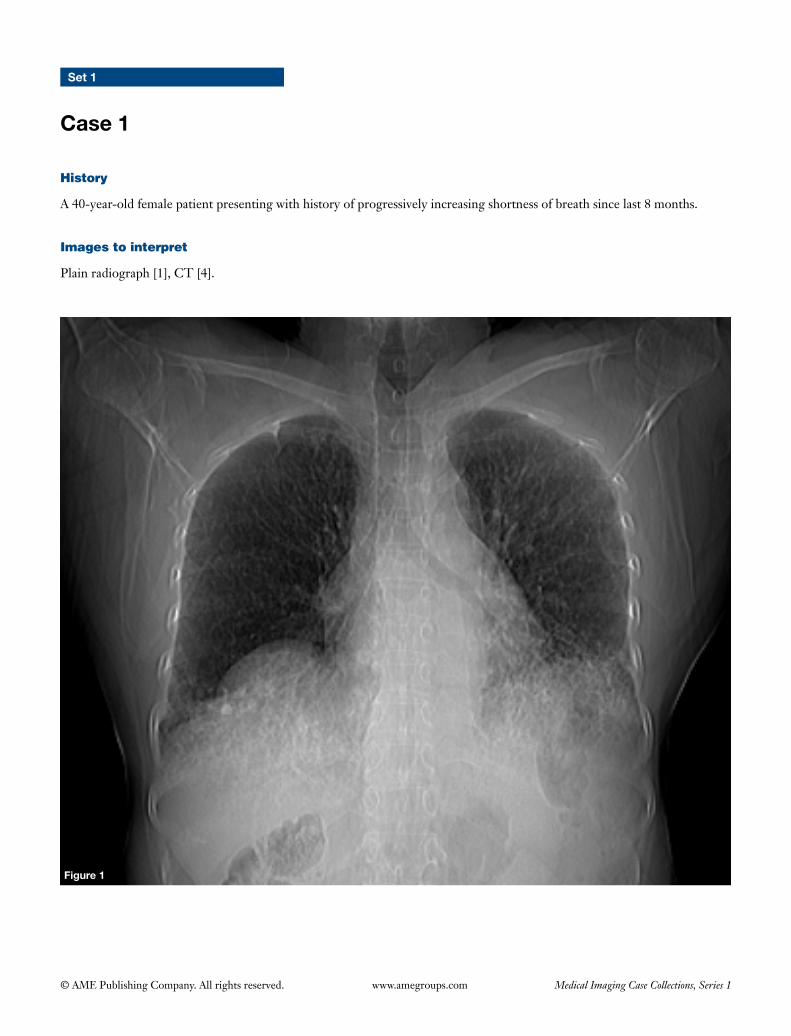
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 1
Case 1
Figure 1
History
A 40-year-old female patient presenting with history of progressively increasing shortness of breath since last 8 months.
Images to interpret
Plain radiograph [1], CT [4].
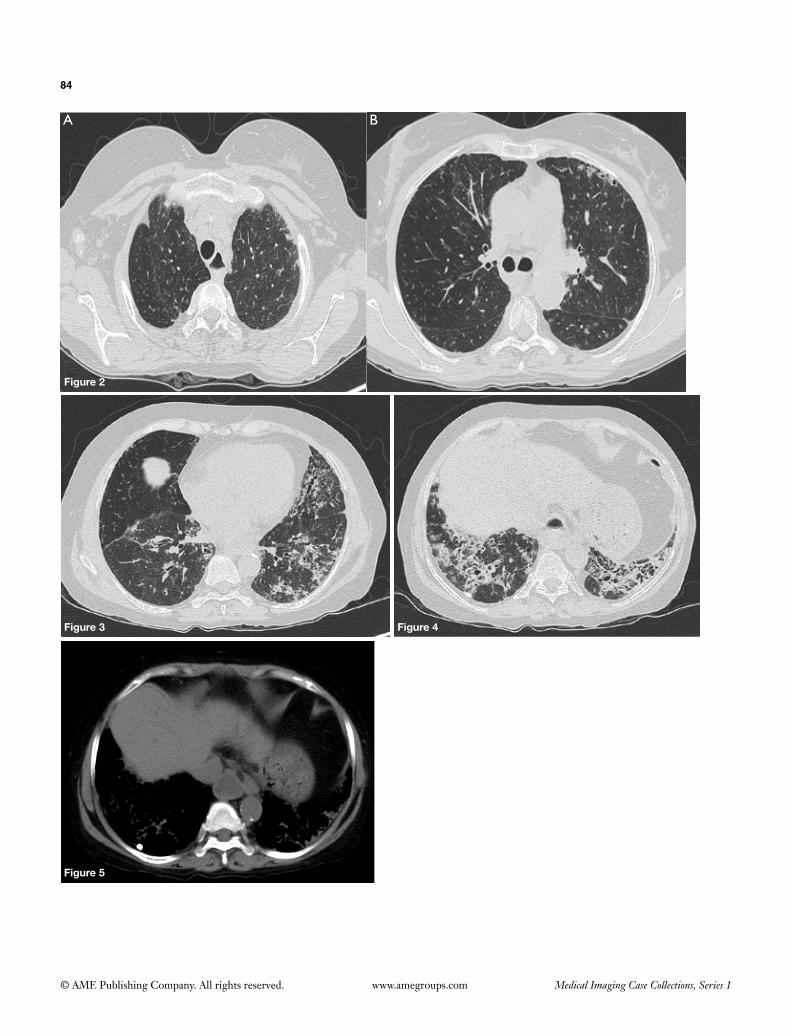
84
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2
Figure 3 Figure 4
Figure 5
A B
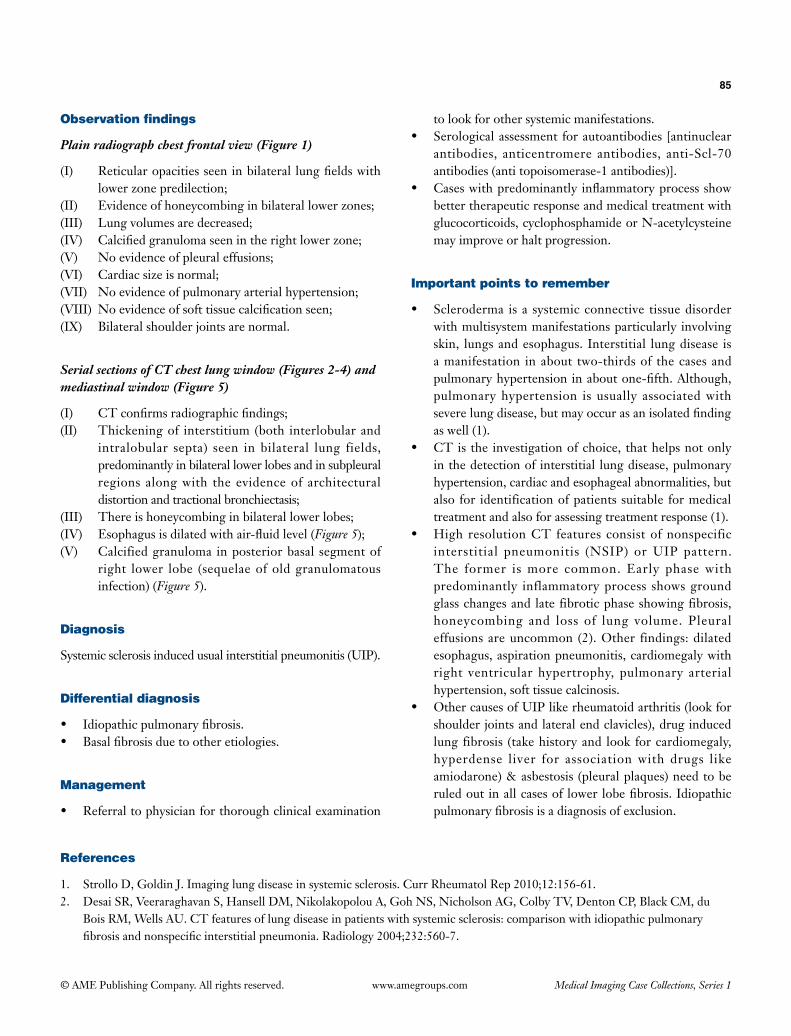
85
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Reticularopacitiesseeninbilateral lungfieldswithlower zone predilection;
(II) Evidence of honeycombing in bilateral lower zones;(III) Lung volumes are decreased;(IV) Calcifiedgranulomaseenintherightlowerzone;(V) No evidence of pleural effusions;(VI) Cardiac size is normal;(VII) No evidence of pulmonary arterial hypertension;(VIII) Noevidenceofsofttissuecalcificationseen;(IX) Bilateral shoulder joints are normal.
Serial sections of CT chest lung window (Figures 2-4) and mediastinal window (Figure 5)
(I) CTconfirmsradiographicfindings;(II) Thickening of interstitium (both interlobular and
intralobular septa) seen in bilateral lung fields, predominantly in bilateral lower lobes and in subpleural regions along with the evidence of architectural distortion and tractional bronchiectasis;
(III) There is honeycombing in bilateral lower lobes;(IV) Esophagusisdilatedwithair-fluidlevel(Figure 5);(V) Calcified granuloma in posterior basal segment of
right lower lobe (sequelae of old granulomatous infection) (Figure 5).
Diagnosis
Systemic sclerosis induced usual interstitial pneumonitis (UIP).
Differential diagnosis
• Idiopathicpulmonaryfibrosis.• Basalfibrosisduetootheretiologies.
Management
• Referraltophysicianforthoroughclinicalexamination
to look for other systemic manifestations.• Serologicalassessmentforautoantibodies [antinuclear
antibodies, anticentromere antibodies, anti-Scl-70 antibodies (anti topoisomerase-1 antibodies)].
• Caseswithpredominantlyinflammatoryprocessshowbetter therapeutic response and medical treatment with glucocorticoids, cyclophosphamide or N-acetylcysteine may improve or halt progression.
Important points to remember
• Scleroderma isa systemicconnective tissuedisorderwith multisystem manifestations particularly involving skin, lungs and esophagus. Interstitial lung disease is a manifestation in about two-thirds of the cases and pulmonaryhypertensioninaboutone-fifth.Although,pulmonary hypertension is usually associated with severelungdisease,butmayoccurasanisolatedfindingas well (1).
• CTisthe investigationofchoice, thathelpsnotonlyin the detection of interstitial lung disease, pulmonary hypertension, cardiac and esophageal abnormalities, but also for identification of patients suitable for medical treatment and also for assessing treatment response (1).
• High resolutionCT features consistofnonspecificinterstitial pneumonitis (NSIP) or UIP pattern. The former is more common. Early phase with predominantly inflammatory process shows ground glass changes and late fibrotic phase showing fibrosis, honeycombing and loss of lung volume. Pleural effusions are uncommon (2). Other findings: dilated esophagus, aspiration pneumonitis, cardiomegaly with right ventricular hypertrophy, pulmonary arterial hypertension, soft tissue calcinosis.
• OthercausesofUIPlikerheumatoidarthritis(lookforshoulder joints and lateral end clavicles), drug induced lung fibrosis (take history and look for cardiomegaly, hyperdense liver for association with drugs like amiodarone) & asbestosis (pleural plaques) need to be ruledoutinallcasesof lowerlobefibrosis.Idiopathicpulmonaryfibrosisisadiagnosisofexclusion.
References
1. Strollo D, Goldin J. Imaging lung disease in systemic sclerosis. Curr Rheumatol Rep 2010;12:156-61.2. DesaiSR,VeeraraghavanS,HansellDM,NikolakopolouA,GohNS,NicholsonAG,ColbyTV,DentonCP,BlackCM,du
BoisRM,WellsAU.CTfeaturesoflungdiseaseinpatientswithsystemicsclerosis:comparisonwithidiopathicpulmonaryfibrosisandnonspecificinterstitialpneumonia.Radiology2004;232:560-7.
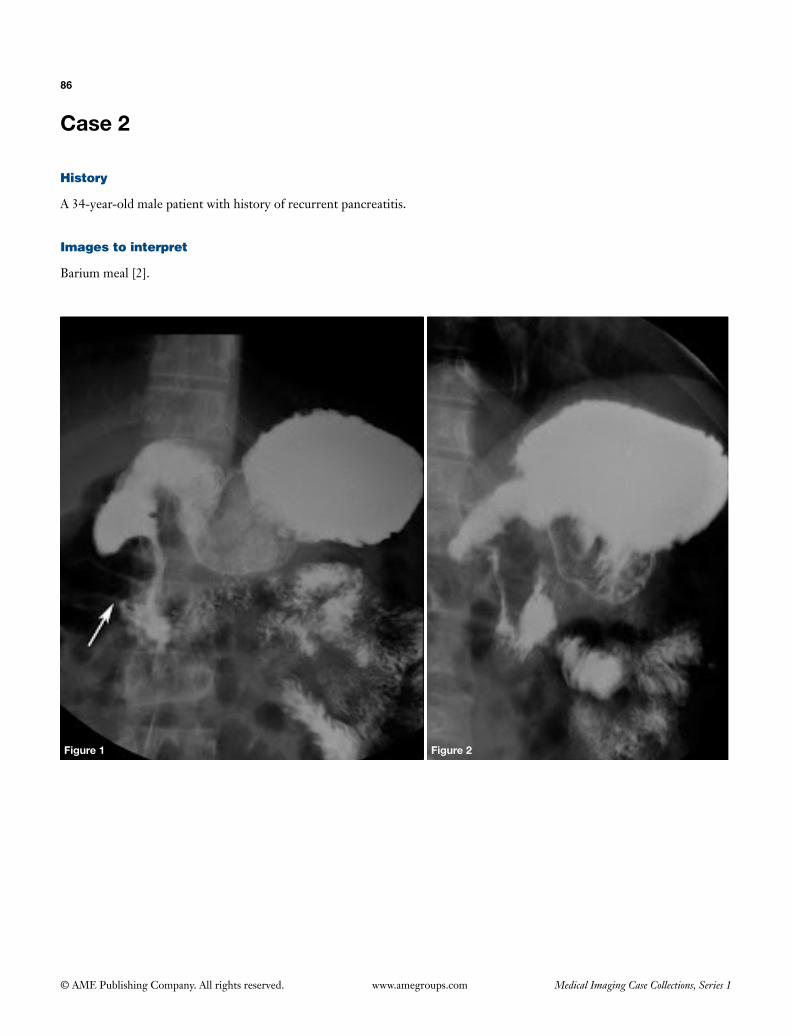
86
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
History
A 34-year-old male patient with history of recurrent pancreatitis.
Images to interpret
Barium meal [2].
Figure 1 Figure 2

87
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Spot images of barium meal (Figures 1,2)
(I) Focal eccentric smooth narrowing seen in the second part of duodenum predominantly involving the lateral wall;
(II) Stomach and rest of the duodenum & small bowel appears normal in course, caliber and outline. There is no widening of the ‘C loop’. Duodenojejunal flexure appears normal.
Diagnosis
Annular pancreas.
Differential diagnosis
• Periampullary edema/malignancy (involves medial wall).
• Duodenal malignancy (causes concentric narrowing with ulceration and shouldering).
Management
• Further work up with CT and MRI to confirm the diagnosis and evaluate ductal anatomy.
• Surgical bypass of the duodenal obstruction with duodenoduodenostomy.
Important points to remember
• Annular pancreas is a rare congenital anomaly in which
pancreas encircles (completely or partially) second part of duodenum and occurs due to failure or incomplete rotation of the ventral bud causing a segment of pancreas encircling the second part of duodenum (1).
• Associations: down syndrome, tracheoesophageal fistula, duodenal atresia, imperforate anus, intraductal papillary mucinous tumor, pancreatic cancer (1).
• Presentation can occur at any age with polyhydramnios during antenatal period, persistent vomiting in neonates and recurrent pancreatitis in adults.
• Complications: pancreatitis, peptic ulcer.• Imaging features include: double bubble sign on plain
radiograph (in neonates); CT and MR both show pancreatic tissue and an annular duct encircling the descending duodenum completely or incompletely with or without duodenal narrowing and proximal dilatation. Associated pancreatitis can also be seen. ERCP and MRCP are further helpful in demonstrating the ductal anatomy. Most cases show annular duct communicating with the main duct (duct of Wirsung). In few cases pancreatic duct drain into accessory pancreatic duct of santorini or directly into the duodenum (1).
• Differentials of narrowing in second part of duodenum on barium studies include: midgut volvulus, duplication cyst, duodenal web, choledochal cyst, pancreatic masses, pancreatic pseudocyst along with the annular pancreas. Duplication cyst, choledochal cyst, pancreatic masses, pancreatic pseudocyst cause widening of the C loop with compression of the medial wall of descending duodenum (2). Midgut volvulus shows additional findings of malrotated bowel configuration with corkscrew sign.
References
1. Sandrasegaran K, Patel A, Fogel EL, Zyromski NJ, Pitt HA. Annular pancreas in adults. AJR Am J Roentgenol 2009;193:455-60.
2. Gupta P, Debi U, Sinha SK, Prasad KK. Upper gastrointestinal barium evaluation of duodenal pathology: A pictorial review. World J Radiol 2014;6:613-8.
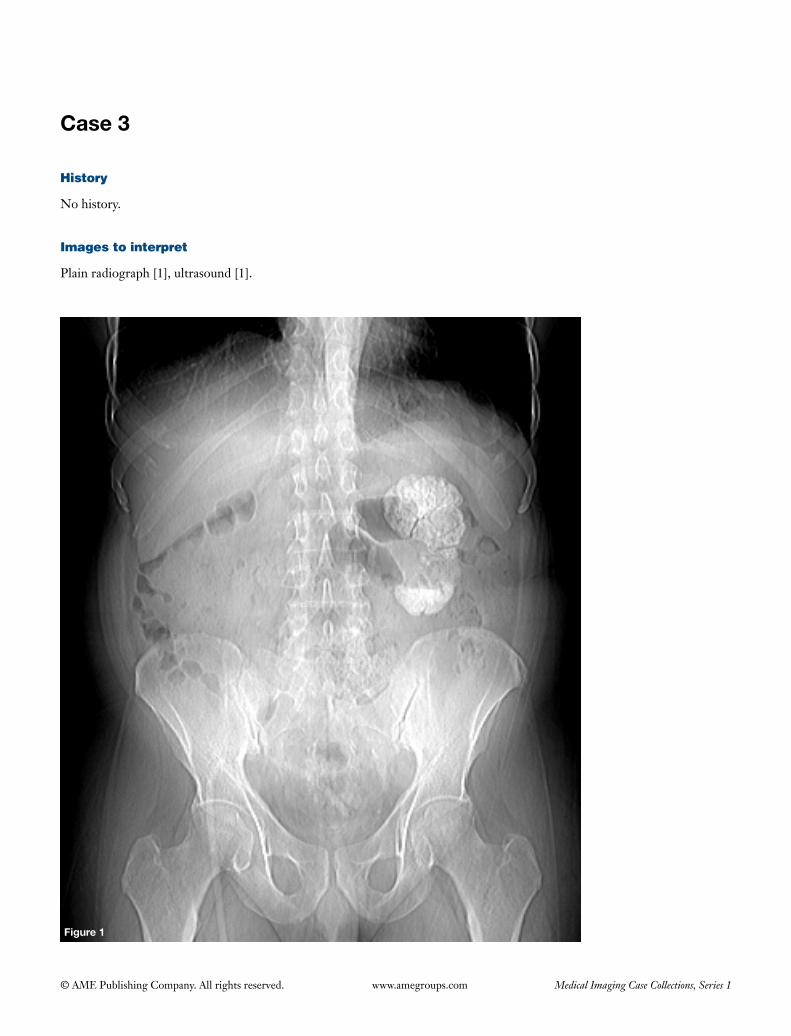
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
History
No history.
Images to interpret
Plain radiograph [1], ultrasound [1].
Figure 1

89
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2

90
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph abdomen frontal view (Figure 1)
(I) Amorphouscalcificationseenoutliningtheentireleftkidney,whichissmallinsize;
(II) Rest of the radiograph is unremarkablewith nocalcificationnoted inrightkidney,bilateraluretersandurinarybladder.
Ultrasound images of both kidneys (Figure 2)
(I) Thereisevidenceofcalcificationnotedinentireleftkidneywithpostacousticshadowingwithnormalcontour;
(II) Leftkidneyissmallinsize;(III) Right kidney appears normal in size, shape and
echotexture.
Diagnosis
Puttykidney[autonephrectomyduetorenal tuberculosis(TB)].
Differential diagnosis
None.
Important points to remember
• GenitourinarytractisthesecondcommonestsiteofTBafterlungs.Almostone-fourthofthesepatientshaveaknownhistoryofpulmonaryTB(1).
• Imaging features include: renal parenchymalcalcificationswhich can be amorphous, granular,curv i l inear or g lobular on p la in radiograph,parenchymal scars, necrotizing papil l i t is withirregularityofthepapillarytips,infundibularstrictures,phantom calyx, hydronephrosis, ureteralmucosalirregularity (saw-toothureter), ureteral strictures,ureteralshortening(pipe-stemureter),reducedbladdercapacity (thimblebladder)on intravenousurography,parenchymalcalcifications, corticalgranulomaswithcaseousor calcifiedmaterial, scars,dilatedcalyces,cortical thinning,urothelial thickeningand fibroticstrictures involving infundibulum, renal pelvis oruretersonCT.Thediseaseisunilateralinabout75%ofthecasesonimaging.Bilateralcasesshowasymmetricinvolvement(1,2).
• Puttykidneyisextensiveparenchymalcalcificationinanautonephrectomizedkidneyandisafeatureofend-stageTB(1).
References
1. GibsonMS,PuckettML,ShellyME.Renaltuberculosis.Radiographics2004;24:251-6.2. MerchantS,BharatiA,MerchantN.Tuberculosisofthegenitourinarysystem-Urinarytracttuberculosis:Renal
tuberculosis-PartII.IndianJRadiolImaging2013;23:64-77.
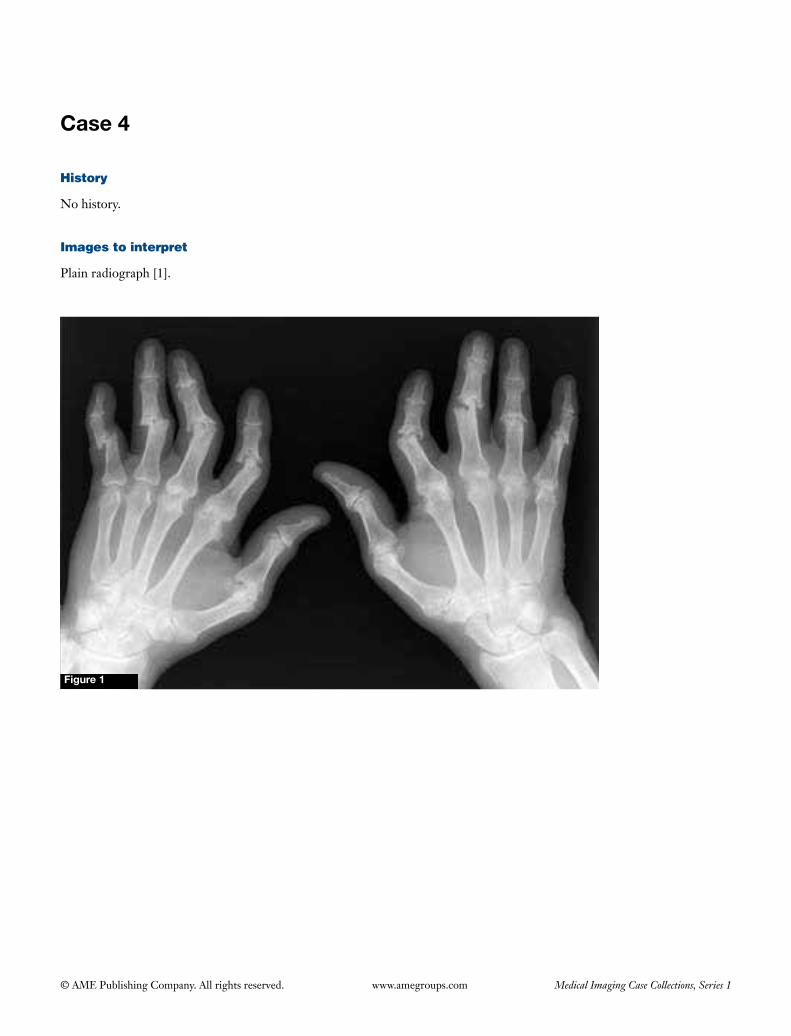
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
History
No history.
Images to interpret
Plain radiograph [1].
Figure 1
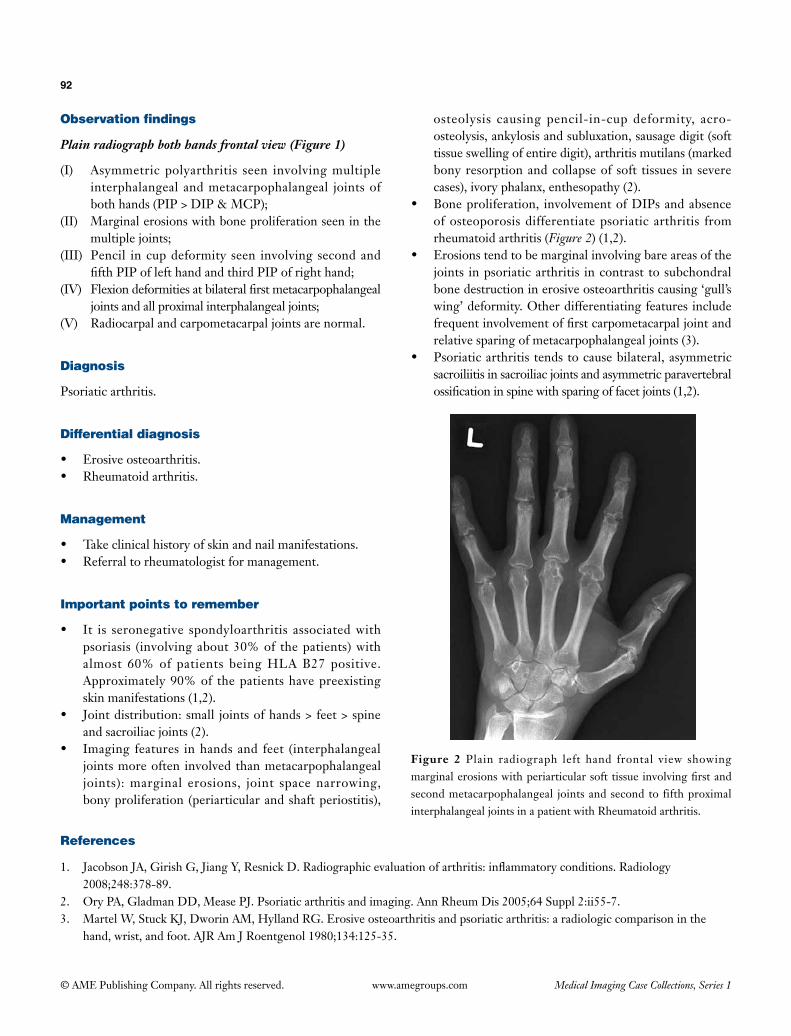
92
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph both hands frontal view (Figure 1)
(I) Asymmetric polyarthritis seen involving multiple interphalangeal and metacarpophalangeal joints of both hands (PIP > DIP & MCP);
(II) Marginal erosions with bone proliferation seen in the multiple joints;
(III) Pencil in cup deformity seen involving second and fifth PIP of left hand and third PIP of right hand;
(IV) Flexion deformities at bilateral first metacarpophalangeal joints and all proximal interphalangeal joints;
(V) Radiocarpal and carpometacarpal joints are normal.
Diagnosis
Psoriatic arthritis.
Differential diagnosis
• Erosive osteoarthritis.• Rheumatoid arthritis.
Management
• Take clinical history of skin and nail manifestations.• Referral to rheumatologist for management.
Important points to remember
• It is seronegative spondyloarthritis associated with psoriasis (involving about 30% of the patients) with almost 60% of patients being HLA B27 positive. Approximately 90% of the patients have preexisting skin manifestations (1,2).
• Joint distribution: small joints of hands > feet > spine and sacroiliac joints (2).
• Imaging features in hands and feet (interphalangeal joints more often involved than metacarpophalangeal joints): marginal erosions, joint space narrowing, bony proliferation (periarticular and shaft periostitis),
osteolysis causing pencil-in-cup deformity, acro-osteolysis, ankylosis and subluxation, sausage digit (soft tissue swelling of entire digit), arthritis mutilans (marked bony resorption and collapse of soft tissues in severe cases), ivory phalanx, enthesopathy (2).
• Bone proliferation, involvement of DIPs and absence of osteoporosis differentiate psoriatic arthritis from rheumatoid arthritis (Figure 2) (1,2).
• Erosions tend to be marginal involving bare areas of the joints in psoriatic arthritis in contrast to subchondral bone destruction in erosive osteoarthritis causing ‘gull’s wing’ deformity. Other differentiating features include frequent involvement of first carpometacarpal joint and relative sparing of metacarpophalangeal joints (3).
• Psoriatic arthritis tends to cause bilateral, asymmetric sacroiliitis in sacroiliac joints and asymmetric paravertebral ossification in spine with sparing of facet joints (1,2).
Figure 2 Plain radiograph left hand frontal view showing marginal erosions with periarticular soft tissue involving first and second metacarpophalangeal joints and second to fifth proximal interphalangeal joints in a patient with Rheumatoid arthritis.
References
1. Jacobson JA, Girish G, Jiang Y, Resnick D. Radiographic evaluation of arthritis: inflammatory conditions. Radiology 2008;248:378-89.
2. Ory PA, Gladman DD, Mease PJ. Psoriatic arthritis and imaging. Ann Rheum Dis 2005;64 Suppl 2:ii55-7.3. Martel W, Stuck KJ, Dworin AM, Hylland RG. Erosive osteoarthritis and psoriatic arthritis: a radiologic comparison in the
hand, wrist, and foot. AJR Am J Roentgenol 1980;134:125-35.
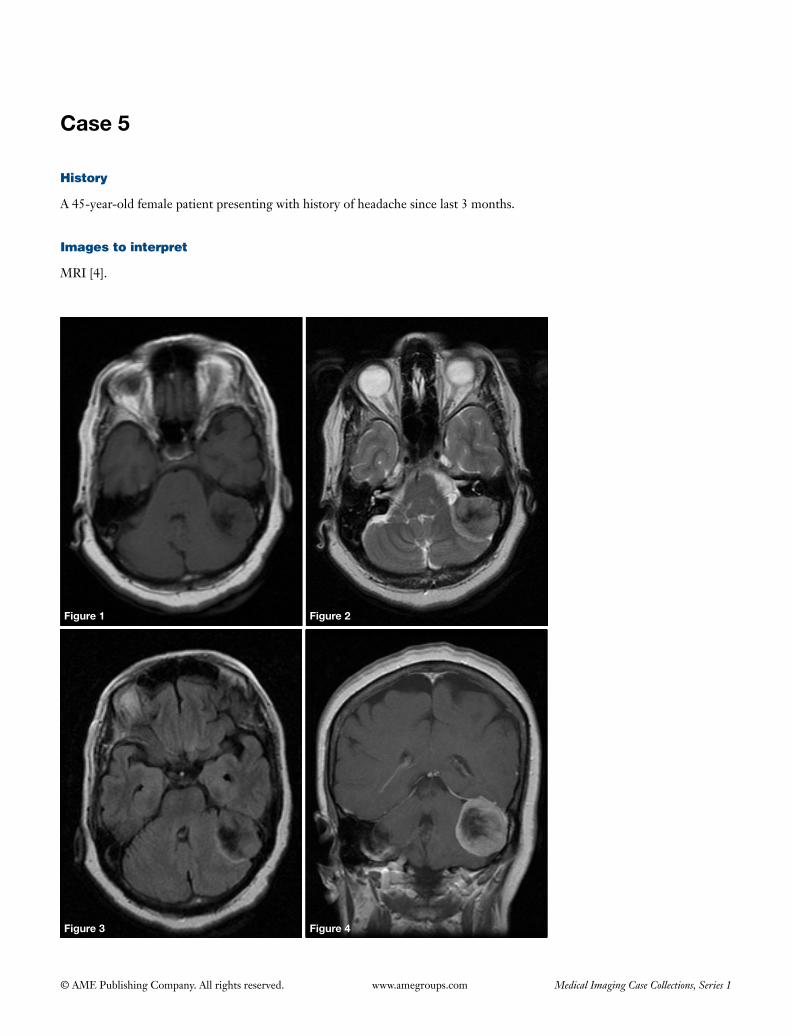
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
Figure 1 Figure 2
Figure 3 Figure 4
History
A 45-year-old female patient presenting with history of headache since last 3 months.
Images to interpret
MRI [4].
94
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
MRI axial T1, T2 and FLAIR sequences (Figures 1, 2 and 3, respectively) and coronal post contrast T1 weighted image (Figure 4)
(I) Well defined, extraaxial, ovoid mass with broad base towards left tentorium seen in left cerebellopontine angle cistern causing its widening;
(II) Lesion is isointense on T1, iso to minimally hyperintense on T2 and FLAIR sequences. Central stellate shaped hypointense area seen on all the sequences (likely due to calcification) (Figures 1-3);
(III) The lesion shows marked homogenous enhancement (except for the calcified area) (Figure 4);
(IV) There is mild perilesional edema and mass effect on the fourth ventricle with early hydrocephalus (Figure 3);
(V) Bilateral internal auditory canals are normal. Left petrous temporal bone is normal (Figure 2);
(VI) Right CP angle cistern is normal.
Diagnosis
Meningioma.
Differential diagnosis
• Schwannoma (check below mentioned points for differentiation).
• Metastasis (age, minimal perilesional edema, absence of history of primary malignancy are features against mets).
Management
• Urgent neurosurgical referral in view of mass effect and early hydrocephalus.
• Review rest of the images to look for other lesions (meningioma, schwannoma and ependymoma to rule
out association with NF2).
Important points to remember
• Meningiomas are the commonest extraaxial neoplasms and most common non-glial primary tumors of the CNS, that arise from the arachnoid cap cells of the meninges (1).
• About 85-90% of them are supratentorial usually involving parasagittal convexity, sphenoid ridge, parasellar region. Infratentorial meningiomas account for 5-10% of the lesions and often seen in the cerebellopontine cistern. Uncommon locations include: orbits, paranasal sinuses, intraventricular and intraosseous (entirely within the calvarium) (2).
• Most of them are benign and typical imaging features include: well circumscribed, homogenous, extraaxial lesions with broad base towards dura, hyperdense on CT and isointense on T1 & iso to minimally hyperintense on T2 weighted sequences, variable restricted diffusion (as these are hypercellular) and show marked homogenous enhancement. Calcification is seen in 20-30% of cases and hyperostosis or lysis of adjacent bone is another associated finding. CSF cleft sign and dural tail sign are other features helpful for the diagnosis (1,2).
• Atypical features include: large meningeal cysts, ring enhancement, metaplastic changes like fatty transformation (2).
• MRS shows elevated alanine, glutamate and choline with decreased NAA and creatine (1).
• Schwannoma is a close differential. The points favouring schwannoma include: hypodense on CT, hyperintense on T2 weighted images on MR, intralesional cystic areas, absence of calcification, hyperostosis & dural tail sign, no obtuse angle with the petrous temporal bone, extension and widening of internal auditory canal.
References
1. Siegelman ES, Mishkin MM, Taveras JM. Past, present, and future of radiology of meningioma. Radiographics 1991;11:899-910.
2. Buetow MP, Buetow PC, Smirniotopoulos JG. Typical, atypical, and misleading features in meningioma. Radiographics 1991;11:1087-106.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
Figure 1 Figure 2
Figure 3 Figure 4
History
No history.
Images to interpret
Plain radiographs [2], CT [2].
96
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph left ankle frontal and lateral view (Figures 1,2)
(I) There is evidence of dorsal talar beak on anterior aspect of talus (Figure 2);
(II) There is posterior continuity of talus and sustentaculum tali giving a ‘C sign’ (Figure 2);
(III) Non-visualization of middle subtalar joint;(IV) Dysmorphic sustentaculum tali with curved undersurface;(V) Tibiotalar joint appears normal.
Coronal reconstructed CT images of left ankle (Figures 3,4)
(I) There is evidence of decreased joint space between middle facet of talus and sustentaculum tali with irregularity of articular surface and mile subchondral sclerosis;
(II) Tibiotalar joint is normal.
Diagnosis
Talocalcaneal coalition (non-osseous type).
Differential diagnosis
None.
Management
Orthopedic referral for surgical resection in symptomatic
cases.
Important points to remember
• Tarsalcoalitionisanabnormalunionbetweentwoormore bones of the mid or hindfoot, which can be bony, cartilaginousorfibrous(1).
• Thetwomostcommonsubtypesofcongenital tarsalcoalitions include: calcaneonavicular and talocalcaneal (ofteninvolvesthemiddlefacet)(1).
• Plainradiographic featuresof talocalcanealcoalitioninclude: dorsal projection from head of talus (dorsal talar beak), C sign (continuous arc between the medial cortex of talus and inferior cortex of sustentaculum tali), dysmorphic sustentaculum tali with curved undersurface,seenonthelateralview(1).
• Characteristicradiographicfeaturesofcalcaneonavicularcoalition include: anteater sign (elongated and broadened anterior process of calcaneus), reverse anteater sign (elongated lateral navicular) and short talar neck, which areseenonthelateralview(1).
• Role ofCT andMR: to confirm the diagnosis inequivocal cases, to differentiate osseous from non-osseous coalition, to depict extent of joint involvement, to look for shape of middle facet joint in cases of talocalcaneal coalition and to look for secondary degenerative changes. MRoffersadvantageofdifferentiating fibrous fromcartilaginous coalition and of depicting bone marrow edema in the adjacent bones. These details are of vital importance during surgical planning (2,3).
References
1. CrimJR,KjeldsbergKM.Radiographicdiagnosisoftarsalcoalition.AJRAmJRoentgenol2004;182:323-8.2. RozanskyA,VarleyE,MoorM,WengerDR,MubarakSJ.Aradiologicclassificationoftalocalcanealcoalitionsbasedon3D
reconstruction.JChildOrthop2010;4:129-35.3. NewmanJS,NewbergAH.Congenitaltarsalcoalition:multimodalityevaluationwithemphasisonCTandMRimaging.
Radiographics2000;20:321-32;quiz526-7,532.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 2
Case 1
A B
Figure 1
History
A 10-year-old male presenting with history of left hip pain since last 1 month.
Images to interpret
Plain radiograph [1], MRI [3].
A B
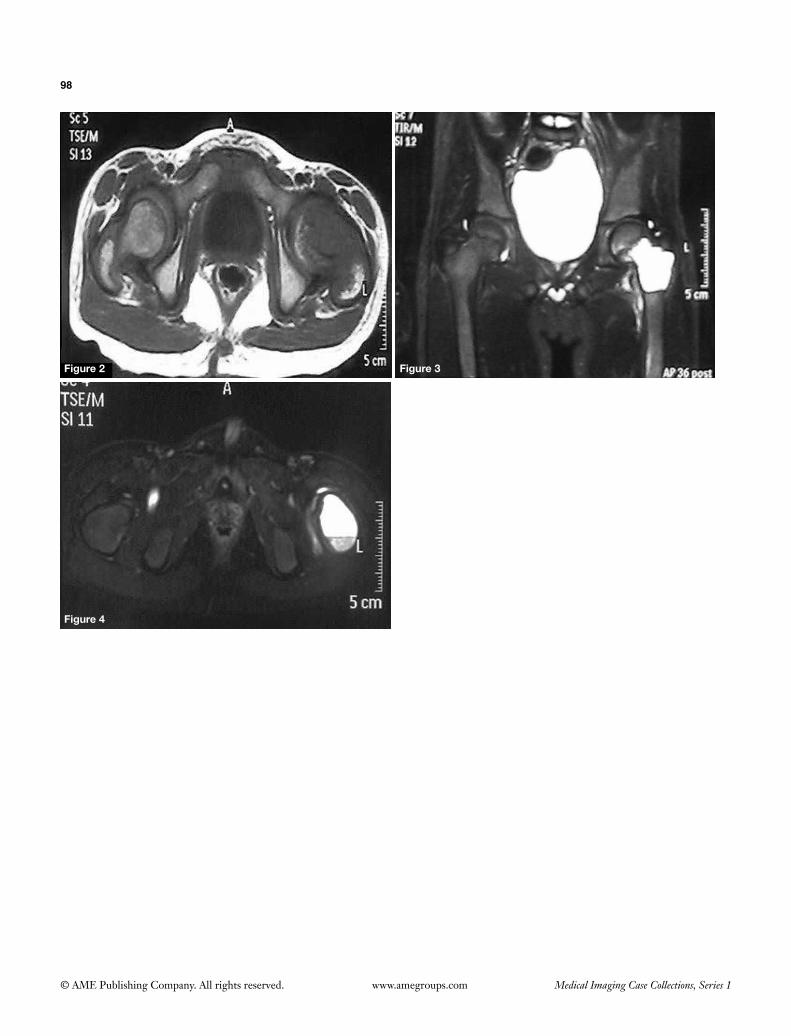
98
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2 Figure 3
Figure 4
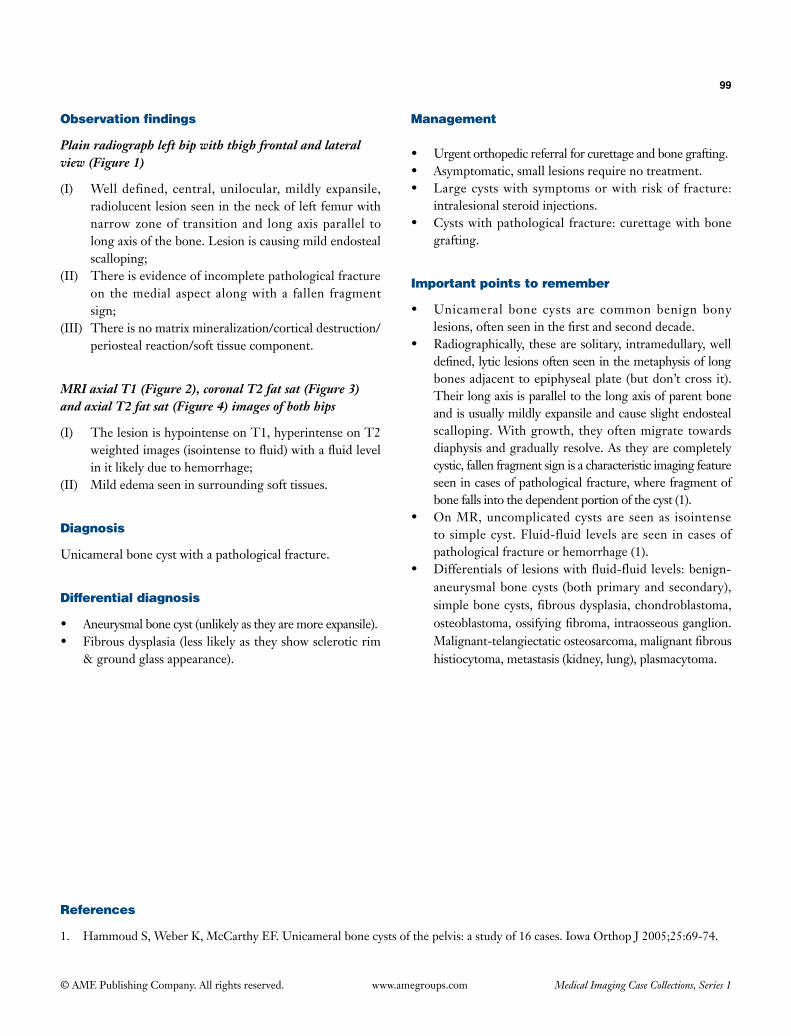
99
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph left hip with thigh frontal and lateral view (Figure 1)
(I) Well defined, central, unilocular, mildly expansile, radiolucent lesion seen in the neck of left femur with narrow zone of transition and long axis parallel to long axis of the bone. Lesion is causing mild endosteal scalloping;
(II) There is evidence of incomplete pathological fracture on the medial aspect along with a fallen fragment sign;
(III) There is no matrix mineralization/cortical destruction/periosteal reaction/soft tissue component.
MRI axial T1 (Figure 2), coronal T2 fat sat (Figure 3) and axial T2 fat sat (Figure 4) images of both hips
(I) The lesion is hypointense on T1, hyperintense on T2 weighted images (isointense to fluid) with a fluid level in it likely due to hemorrhage;
(II) Mild edema seen in surrounding soft tissues.
Diagnosis
Unicameral bone cyst with a pathological fracture.
Differential diagnosis
• Aneurysmal bone cyst (unlikely as they are more expansile).• Fibrous dysplasia (less likely as they show sclerotic rim
& ground glass appearance).
Management
• Urgent orthopedic referral for curettage and bone grafting.• Asymptomatic, small lesions require no treatment.• Large cysts with symptoms or with risk of fracture:
intralesional steroid injections.• Cysts with pathological fracture: curettage with bone
grafting.
Important points to remember
• Unicameral bone cysts are common benign bony lesions, often seen in the first and second decade.
• Radiographically, these are solitary, intramedullary, well defined, lytic lesions often seen in the metaphysis of long bones adjacent to epiphyseal plate (but don’t cross it). Their long axis is parallel to the long axis of parent bone and is usually mildly expansile and cause slight endosteal scalloping. With growth, they often migrate towards diaphysis and gradually resolve. As they are completely cystic, fallen fragment sign is a characteristic imaging feature seen in cases of pathological fracture, where fragment of bone falls into the dependent portion of the cyst (1).
• On MR, uncomplicated cysts are seen as isointense to simple cyst. Fluid-fluid levels are seen in cases of pathological fracture or hemorrhage (1).
• Differentials of lesions with fluid-fluid levels: benign-aneurysmal bone cysts (both primary and secondary), simple bone cysts, fibrous dysplasia, chondroblastoma, osteoblastoma, ossifying fibroma, intraosseous ganglion. Malignant-telangiectatic osteosarcoma, malignant fibrous histiocytoma, metastasis (kidney, lung), plasmacytoma.
References
1. Hammoud S, Weber K, McCarthy EF. Unicameral bone cysts of the pelvis: a study of 16 cases. Iowa Orthop J 2005;25:69-74.
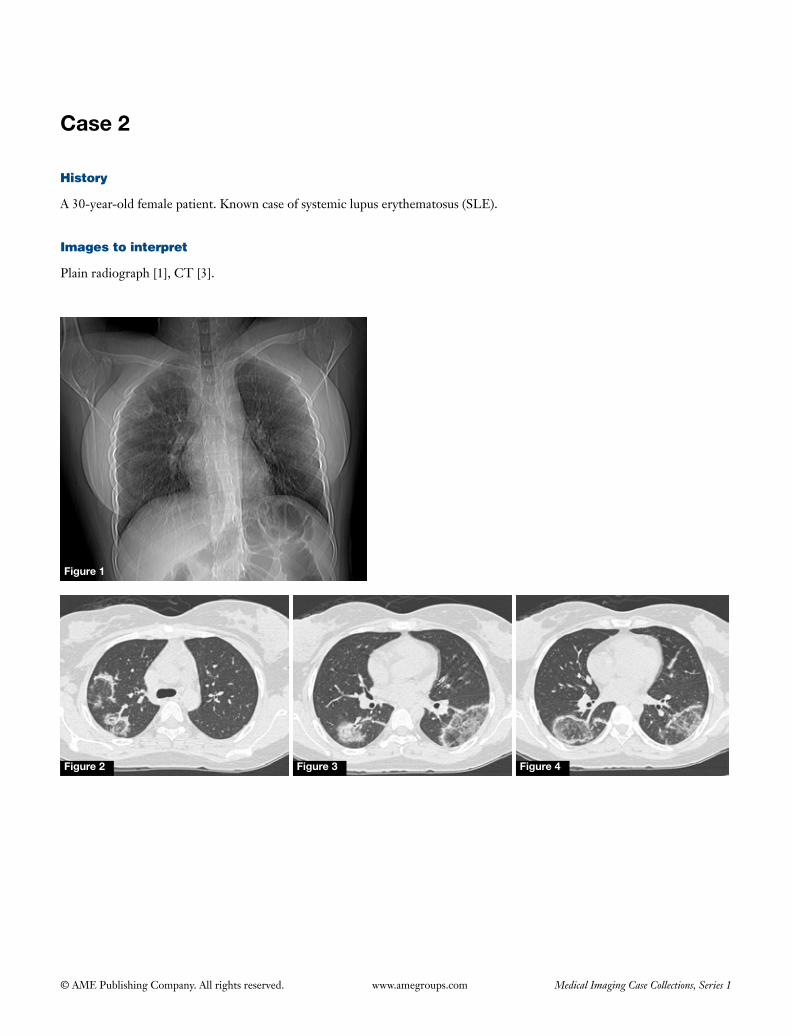
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
History
A 30-year-old female patient. Known case of systemic lupus erythematosus (SLE).
Images to interpret
Plain radiograph [1], CT [3].
Figure 1
Figure 2 Figure 3 Figure 4

101
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Patchy air space opacities seen in right upper zone;(II) Crescentic area of consolidation seen in right upper &
lower and left mid zone;(III) No evidence of pleural effusion seen.
CT chest lung window axial sections (Figures 2-4)
(I) Opacities with central ground glass attenuation with surrounding denser crescentic or ring consolidations (giving reverse halo sign or atoll sign) seen in posterior segment of right upper lobe and apical segment of both lower lobes;
(II) No evidence of mediastinal lymphadenopathy seen.
Diagnosis
SLE induced non-specific interstitial pneumonitis (NSIP).
Differential diagnosis
Cryptogenic organizing pneumonia, infective etiologies (invasive fungal infections, histoplasmosis, blastomycosis, paracoccidiomycosis, tuberculosis (TB), pneumocystis jiroveci pneumonia), NSIP related to collagen vascular diseases (like SLE, rheumatoid arthritis), sarcoidosis, Wegener’s granulomatosis, lymphatoid granulomatosis,
adenocarcinoma, lipoid pneumonia, pulmonary infarcts, post treatment changes (post radiofrequency ablation and after radiotherapy) (1).
Management
• Deta i led h i s tory for symptoms of in fec t ion , immunocompromised state, history of any malignancy & collagen vascular disorders, treatment, ingestion or inhalation of mineral oils etc. should be taken.
• Referral to chest physician for further management.
Important points to remember
• CT halo sign (ground glass opacity surrounding a pulmonary nodule—represents haemorrhage) is seen in infectious diseases [invasive fungal infections (most commonly angioinvasive aspergillosis), septic emboli, TB and mycobacterium avium intracellulare infection of the lungs (less often)], primary lung tumors (most commonly adenocarcinoma, less often—Kaposi sarcoma, squamous cell carcinoma), hemorrhagic metastasis (choriocarcinoma, melanoma, angiosarcoma etc.), Wegener’s granulomatosis, organizing pneumonia, pulmonary endometriosis.
• In reverse halo sign, nodular appearance of ring of consolidation differentiates active granulomatous disease like TB and sarcoidosis from cryptogenic organizing pneumonia (1,2).
References
1. Godoy MC, Viswanathan C, Marchiori E, Truong MT, Benveniste MF, Rossi S, Marom EM. The reversed halo sign: update and differential diagnosis. Br J Radiol 2012;85:1226-35.
2. Marchiori E, Zanetti G, Irion KL, Nobre LF, Hochhegger B, Mançano AD, Escuissato DL. Reversed halo sign in active pulmonary tuberculosis: criteria for differentiation from cryptogenic organizing pneumonia. AJR Am J Roentgenol 2011;197:1324-7.
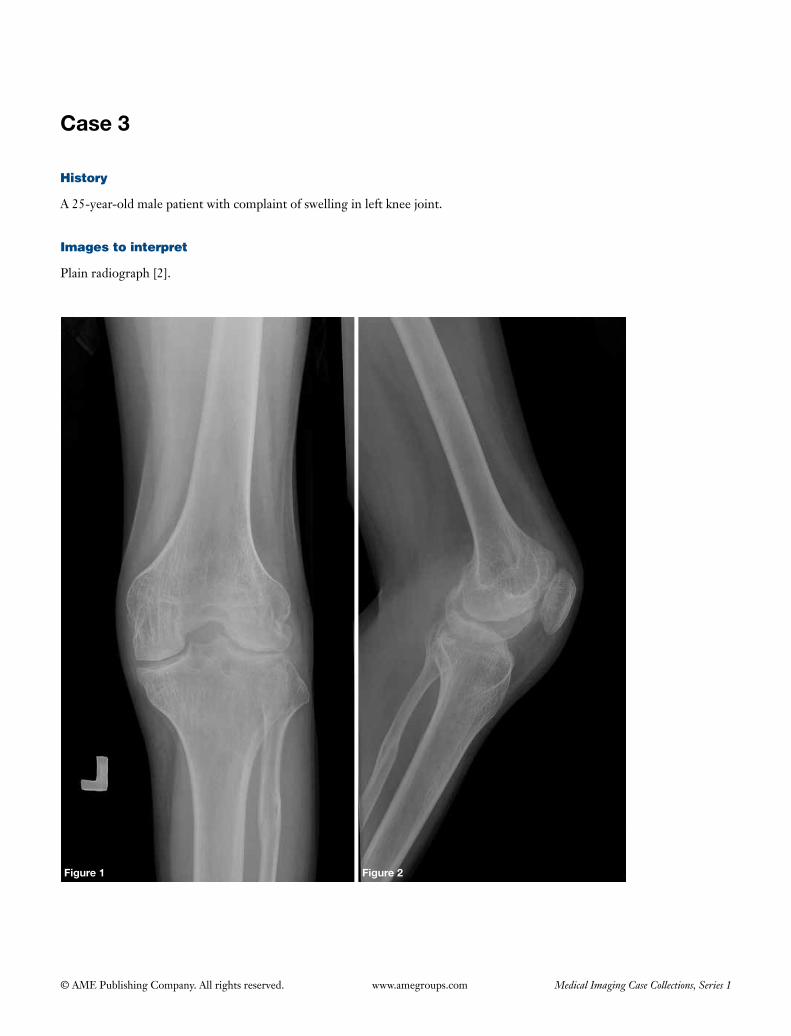
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
History
A 25-year-old male patient with complaint of swelling in left knee joint.
Images to interpret
Plain radiograph [2].
Figure 1 Figure 2
103
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph left knee frontal (Figure 1) and lateral view (Figure 2)
(I) There is evidence of periarticular osteopenia;(II) There is evidence of enlargement of femoral and tibial
condyles with flattened condylar surfaces and mildly reduced joint space with gracile diaphysis;
(III) Widening of intercondylar notch seen;(IV) Squared inferior margin of patella present.
Diagnosis
Hemophilic arthropathy.
Differential diagnosis
Juvenile rheumatoid arthritis (JRA).
Management
• Take clinicalhistoryofbleedingmanifestations indifferent organs.
• CoagulationfactorVIII&IXassays.• Prophylactic factor VIII or IX replacement in
cases presenting early to prevent joint destruction. Synovectomy and radio synarthroses in early hemophilic arthropathy.
• Surgicalarthrodesisorjointreplacementforendstagedisease.
Important points to remember
• Hemophilia is aX-linked recessive disorder thatoccurs due to deficiency of clotting factors VIII (hemophiliaA) and IX (hemophiliaB), bothhaves imilar c l inical presentat ion and radiological manifestations (1).
• Musculoskeletal system is the commonest systeminvolved with bleeding most often in joints followed by soft tissues and bones (hemophilic pseudotumors- intramuscular/intraosseous which can be intramedullary orsubperiosteal)(1,2).
• Jointsinvolvedinclude:knee>ankle>elbow>shoulder>hip(1).
• Radiographic features include: joint ef fus ion(hemarthrosis),epiphysealovergrowth,periarticularosteopenia(duetohyperemia),earlyclosureofphysealplate,secondarydegenerativechanges.Otherfeatures:knee-widenedintercondylarnotch,squaringofpatella,flatteningofcondylarsurface(1,2).
• MRhelps indiagnosis at early stage.MR findingsinclude: synovial hypertrophywith hemosiderindeposition (seen as hypointense foci on T1 and T2 weighted sequences with blooming on gradient echo sequence),haemarthrosis,cartilage lossanderosions(1,2).
• Points to differentiate from JRA: female gender,bilateralsymmetric involvement,andnohemosiderinonMRarepointsthatfavourJRA.
References
1. KerrR.Imagingofmusculoskeletalcomplicationsofhemophilia.SeminMusculoskeletRadiol2003;7:127-36.2. NgWH,ChuWC,ShingMK,LamWW,ChikKW,LiCK,LiCK,LingSC.Roleofimaginginmanagementof
hemophilicpatients.AJRAmJRoentgenol2005;184:1619-23.
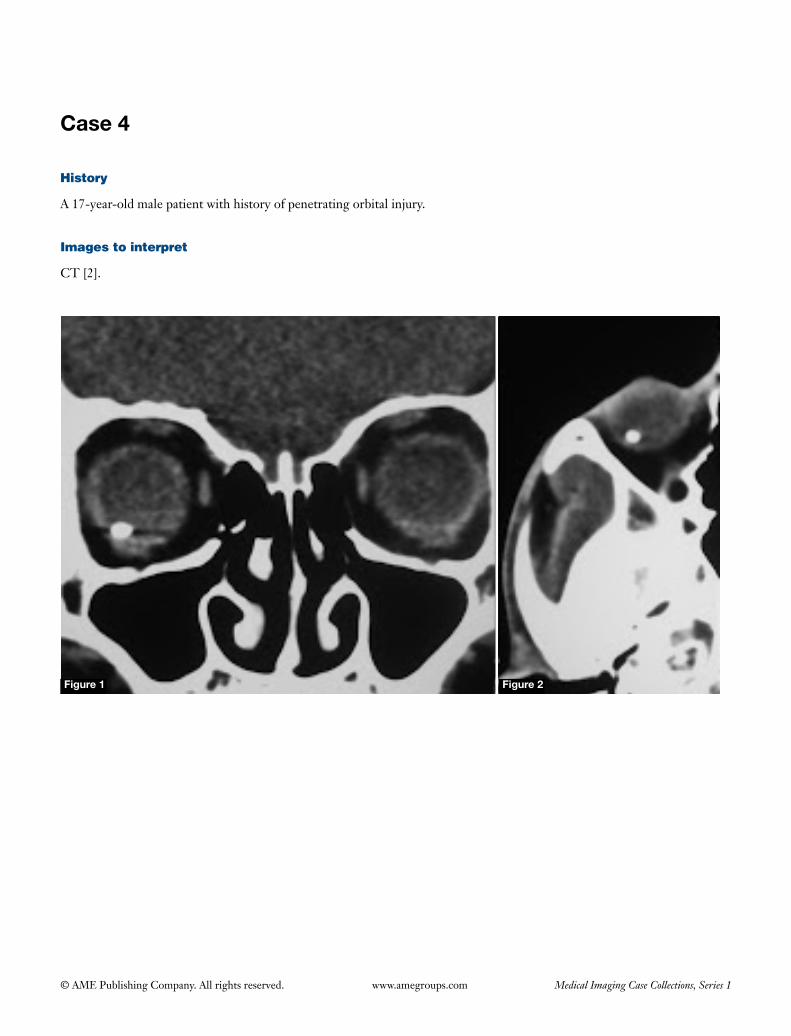
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
History
A 17-year-old male patient with history of penetrating orbital injury.
Images to interpret
CT [2].
Figure 1 Figure 2
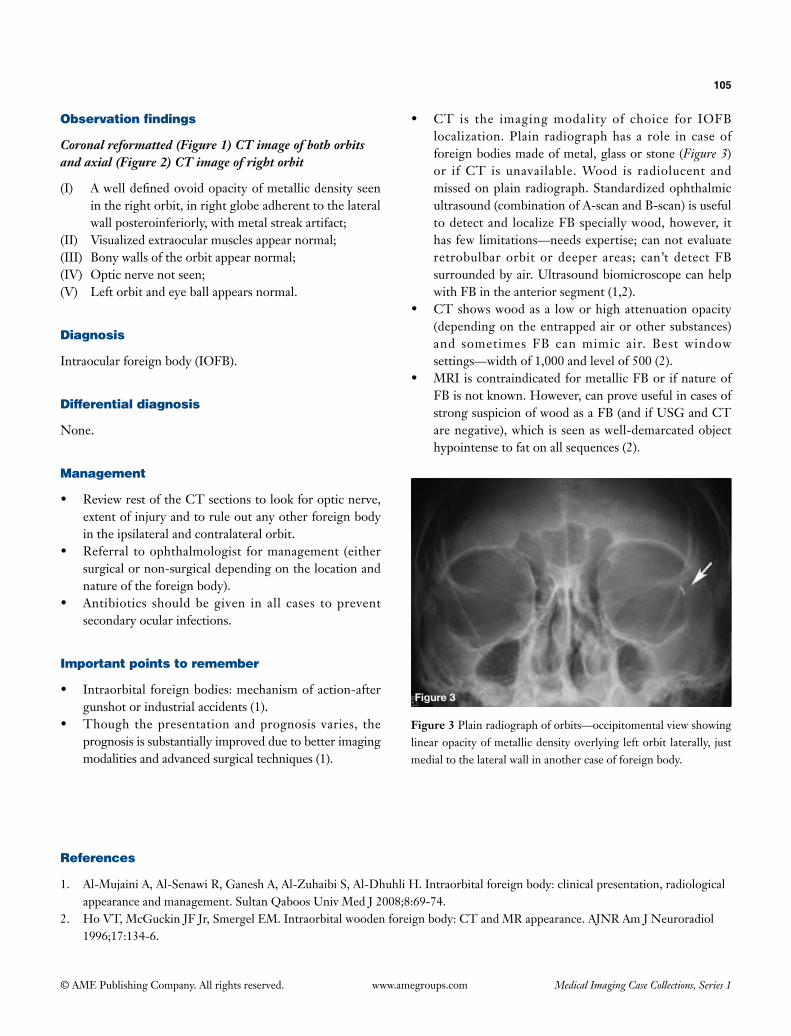
105
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Coronal reformatted (Figure 1) CT image of both orbits and axial (Figure 2) CT image of right orbit
(I) Awelldefinedovoidopacityofmetallicdensityseenin the right orbit, in right globe adherent to the lateral wallposteroinferiorly,withmetalstreakartifact;
(II) Visualizedextraocularmusclesappearnormal;(III) Bonywallsoftheorbitappearnormal;(IV) Opticnervenotseen;(V) Left orbit and eye ball appears normal.
Diagnosis
Intraocularforeignbody(IOFB).
Differential diagnosis
None.
Management
• ReviewrestoftheCTsectionstolookforopticnerve,extent of injury and to rule out any other foreign body intheipsilateralandcontralateralorbit.
• Referral toophthalmologist formanagement (eithersurgicalornon-surgicaldependingonthelocationandnature of the foreign body).
• Antibiotics shouldbegiven in all cases topreventsecondaryocularinfections.
Important points to remember
• Intraorbital foreignbodies:mechanismofaction-aftergunshotorindustrialaccidents(1).
• Though thepresentationandprognosis varies, theprognosisissubstantiallyimprovedduetobetterimagingmodalitiesandadvancedsurgicaltechniques(1).
• CT is the imagingmodality of choice for IOFBlocalization.Plain radiographhas a role in caseofforeign bodies made of metal, glass or stone (Figure 3) or ifCT is unavailable.Wood is radiolucent andmissedonplainradiograph.Standardizedophthalmicultrasound(combinationofA-scanandB-scan)isusefultodetectand localizeFBspeciallywood,however, ithasfewlimitations—needsexpertise;cannotevaluateretrobulbarorbit or deeper areas; can’t detectFBsurroundedbyair.UltrasoundbiomicroscopecanhelpwithFBintheanteriorsegment(1,2).
• CTshowswoodasa loworhighattenuationopacity(dependingontheentrappedairorothersubstances)and sometimes FB canmimic air. Best windowsettings—widthof1,000andlevelof500(2).
• MRIiscontraindicatedformetallicFBorifnatureofFBisnotknown.However,canproveusefulincasesofstrongsuspicionofwoodasaFB(andifUSGandCTarenegative),whichisseenaswell-demarcatedobjecthypointensetofatonallsequences(2).
Figure 3
Figure 3Plainradiographoforbits—occipitomentalviewshowinglinearopacityofmetallicdensityoverlyingleftorbitlaterally, justmedialtothelateralwallinanothercaseofforeignbody.
References
1. Al-MujainiA,Al-SenawiR,GaneshA,Al-ZuhaibiS,Al-DhuhliH.Intraorbitalforeignbody:clinicalpresentation,radiologicalappearanceandmanagement.SultanQaboosUnivMedJ2008;8:69-74.
2. HoVT,McGuckinJFJr,SmergelEM.Intraorbitalwoodenforeignbody:CTandMRappearance.AJNRAmJNeuroradiol1996;17:134-6.
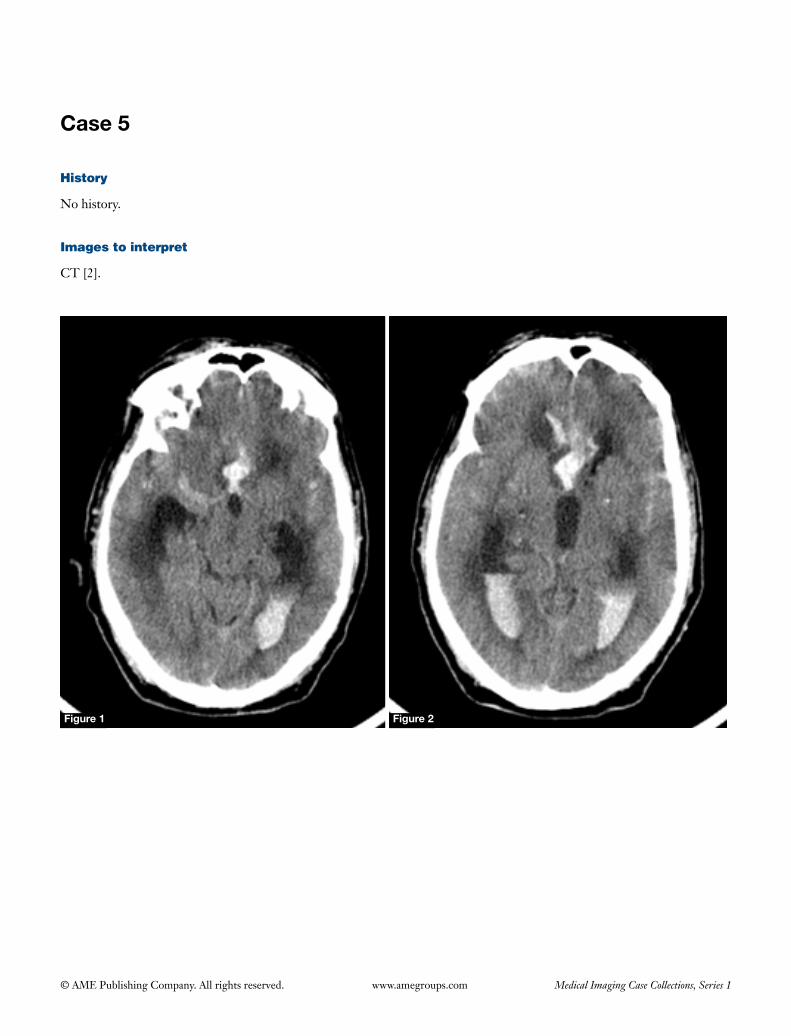
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
History
No history.
Images to interpret
CT [2].
Figure 1 Figure 2
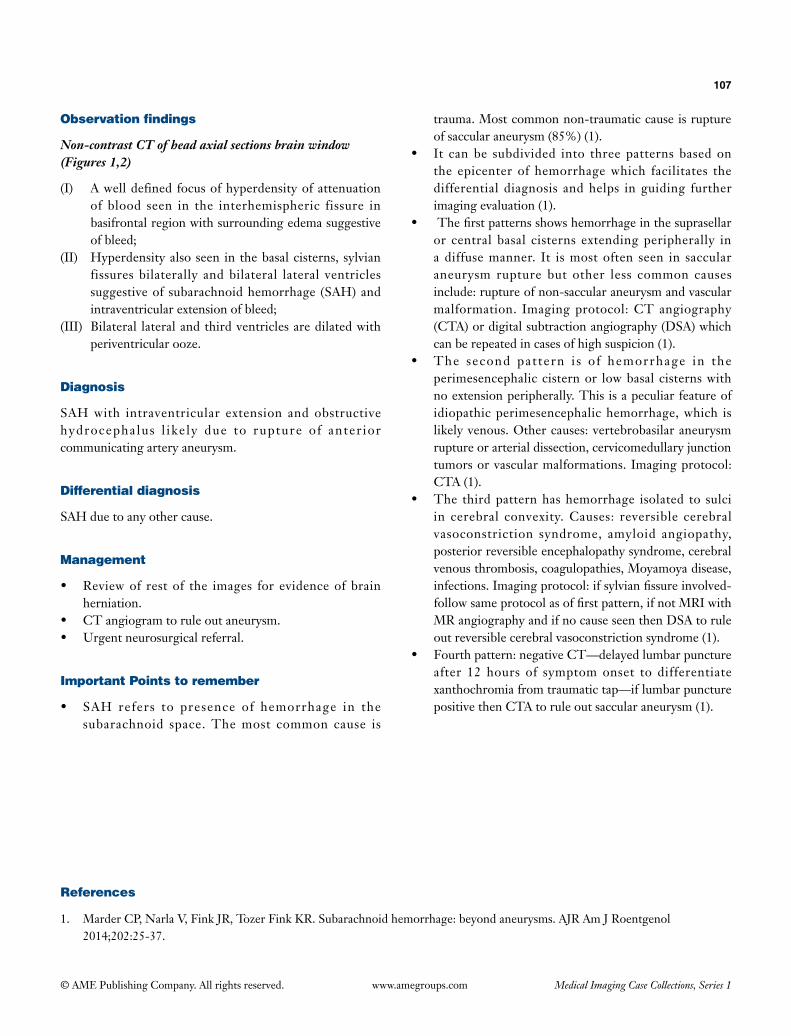
107
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Non-contrast CT of head axial sections brain window (Figures 1,2)
(I) A well defined focus of hyperdensity of attenuation of blood seen in the interhemispheric fissure in basifrontal region with surrounding edema suggestive of bleed;
(II) Hyperdensity also seen in the basal cisterns, sylvian fissures bilaterally and bilateral lateral ventricles suggestive of subarachnoid hemorrhage (SAH) and intraventricular extension of bleed;
(III) Bilateral lateral and third ventricles are dilated with periventricular ooze.
Diagnosis
SAH with intraventricular extension and obstructive hydrocephalus l ike ly due to rupture of anter ior communicating artery aneurysm.
Differential diagnosis
SAH due to any other cause.
Management
• Reviewof restof the images for evidenceofbrainherniation.
• CTangiogramtoruleoutaneurysm.• Urgentneurosurgicalreferral.
Important Points to remember
• SAH refers to presence of hemorrhage in thesubarachnoid space. The most common cause is
trauma. Most common non-traumatic cause is rupture of saccular aneurysm (85%) (1).
• It canbe subdivided into three patterns basedonthe epicenter of hemorrhage which facilitates the differential diagnosis and helps in guiding further imaging evaluation (1).
• Thefirstpatternsshowshemorrhageinthesuprasellaror central basal cisterns extending peripherally in a diffuse manner. It is most often seen in saccular aneurysm rupture but other less common causes include: rupture of non-saccular aneurysm and vascular malformation. Imaging protocol: CT angiography (CTA) or digital subtraction angiography (DSA) which can be repeated in cases of high suspicion (1).
• The second pat tern i s o f hemorrhage in theperimesencephalic cistern or low basal cisterns with no extension peripherally. This is a peculiar feature of idiopathic perimesencephalic hemorrhage, which is likely venous. Other causes: vertebrobasilar aneurysm rupture or arterial dissection, cervicomedullary junction tumors or vascular malformations. Imaging protocol: CTA (1).
• The thirdpatternhashemorrhage isolated to sulciin cerebral convexity. Causes: reversible cerebral vasoconstriction syndrome, amyloid angiopathy, posterior reversible encephalopathy syndrome, cerebral venous thrombosis, coagulopathies, Moyamoya disease, infections.Imagingprotocol:ifsylvianfissureinvolved-followsameprotocolasoffirstpattern,ifnotMRIwithMRangiographyandifnocauseseenthenDSAtoruleout reversible cerebral vasoconstriction syndrome (1).
• Fourthpattern:negativeCT—delayedlumbarpunctureafter 12 hours of symptom onset to differentiate xanthochromiafromtraumatictap—iflumbarpuncturepositive then CTA to rule out saccular aneurysm (1).
References
1. MarderCP,NarlaV,FinkJR,TozerFinkKR.Subarachnoidhemorrhage:beyondaneurysms.AJRAmJRoentgenol2014;202:25-37.
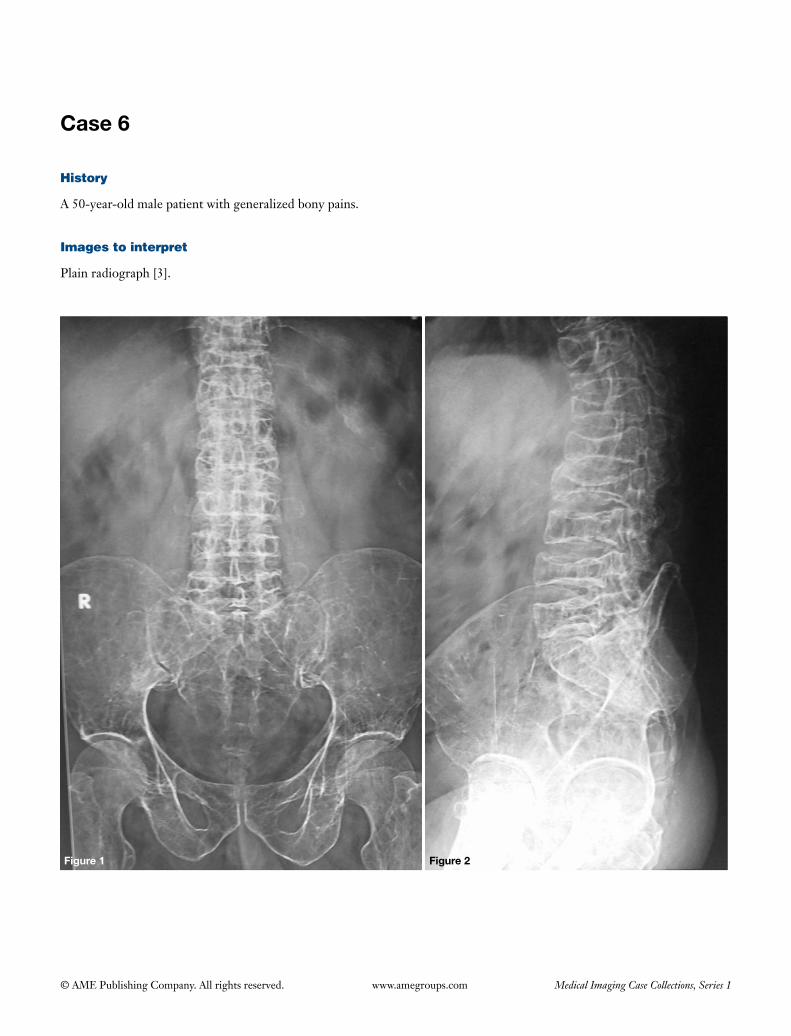
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
History
A 50-year-old male patient with generalized bony pains.
Images to interpret
Plain radiograph [3].
Figure 1 Figure 2
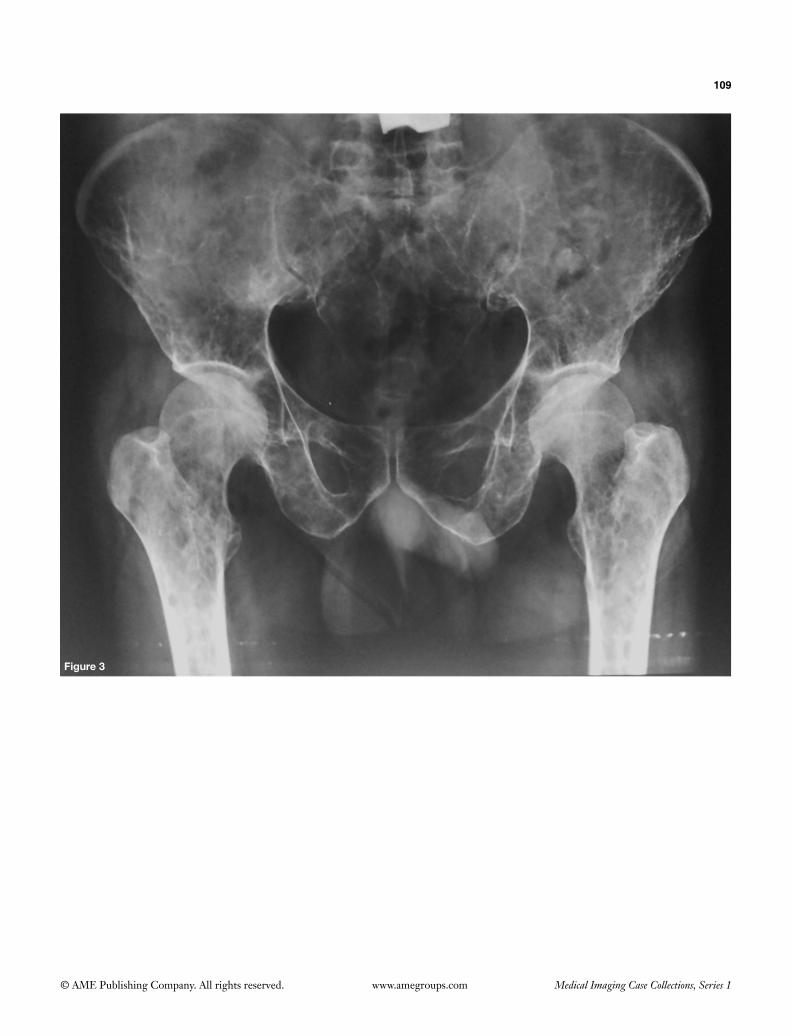
109
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 3

110
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph lumbosacral spine frontal (Figure 1) and lateral view (Figure 2) and pelvis with bilateral hips frontal view (Figure 3)
(I) Generalized osteopenia seen;(II) There is collapse of multiple lumbar and lower dorsal
vertebral bodies;(III) Multiple, discrete, small lytic lesions of uniform size
seen involving spine, sacrum, bilateral pelvic bones and bilateral proximal femur.
Diagnosis
Multiple myeloma.
Differential diagnosis
Metastases.
Management
• Serumelectrophoresis.• UrineevaluationforBenceJonesproteins.• Otherinvestigations:serumcalcium,albuminglobulin
ratio.• SkeletalsurveyorwholebodyMRItolookfordisease
burden.• Orthopedicreferralfortreatment.
Important points to remember
• MultiplemyelomaisaclonalB-lymphocyteneoplasmof terminally differentiated plasma cells and constitutes the most common primary malignant bone neoplasm in adults (1).
• Ithasfourdistinctformsofinvolvement:solitarylesion(plasmacytoma); diffuse skeletal involvementwithmultipledefinedlesions(myelomatosis);diffuseskeletalosteopenia; sclerosing myeloma (1).
• Commonsitesof involvement:vertebrae, ribs, skull,scapula, pelvis, long bones, extraosseous myeloma (rare) (1).
• Radiographicfeaturesinclude:plasmacytoma—solitary,large, expansile, septated, lytic lesion with soap-bubbleappearance;myelomatosis—most lesionsarepurely osteolytic, with discrete margins (punched-out), elliptical, of uniform size, with endosteal scalloping when the lesions are subcortical (especially in long bones);diffuse skeletalosteopenia—predominantlyinvolvesthespinewithoutwelldefinedlyticlesionsandalong with multiple compression fractures; sclerosing myeloma—rare,only3%ofcaseslesionsaresclerotic,often in association with polyneuropathy, organomegaly, endocrinopathy,monoclonalgammopathy,skinchanges(POEMS) syndrome (1). Sclerosis often seenwithfracture or following treatment.
• Points that favourmyeloma overmets include:involvementofmandible,clavicle,distalaxialskeleton,absence of involvement of posterior elements of vertebra, absence of large soft tissue component with bony lesions, cold on bone scan.
• WholebodyMRiscurrentlyrecommendedtoevaluatedisease burden and for staging in addition to plain radiographs in thesepatients.MR imagingpatternsinclude: normalmarrow;micronodular/variegatedpattern; a focal pattern and a diffuse pattern. Typical myeloma lesions show low signal on T1, high signal onT2andSTIRandenhancementongadolinium-enhancedimages.MRandPET-CTarealsohelpfulinevaluating treatment response (2).
References
1. AngtuacoEJ,FassasAB,WalkerR,SethiR,BarlogieB.Multiplemyeloma:clinicalreviewanddiagnosticimaging.Radiology2004;231:11-23.
2. HanrahanCJ,ChristensenCR,CrimJR.CurrentconceptsintheevaluationofmultiplemyelomawithMRimagingandFDGPET/CT.Radiographics2010;30:127-42.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 3
Case 1
History
A 35-year-old male patient (athlete by occupation) with complaints of left leg pain since last 1 month.
Images to interpret
Plain radiograph [1], MRI [2].
Figure 1
A B
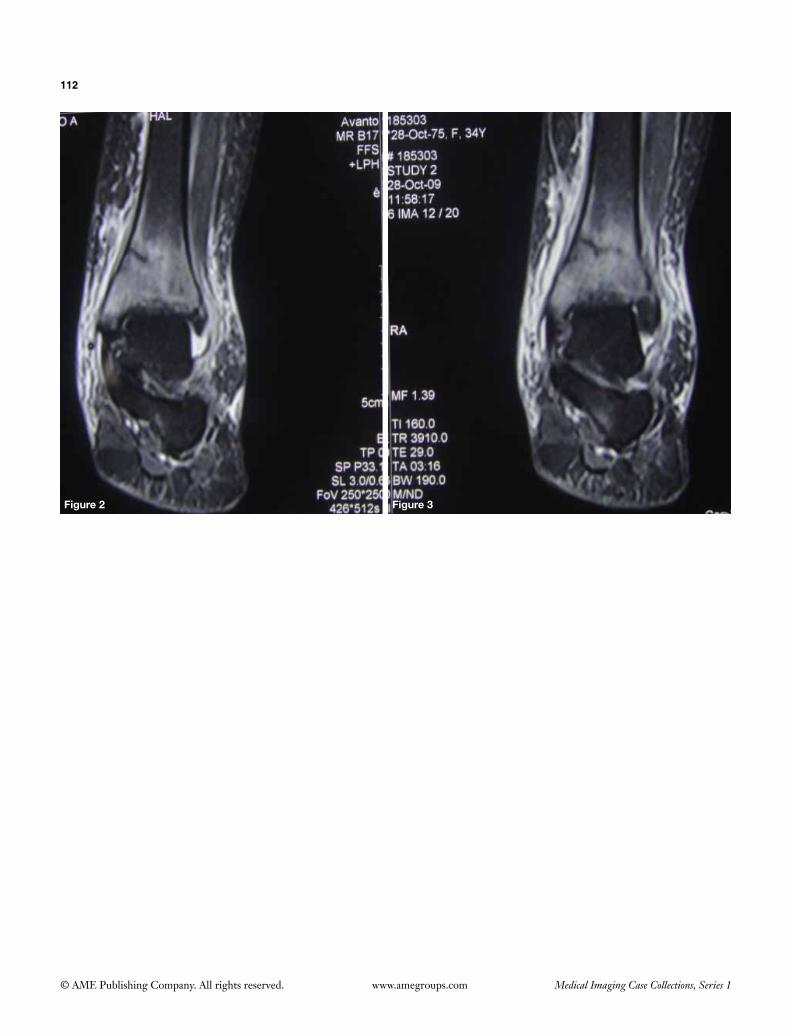
112
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2 Figure 3

113
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph left leg with ankle frontal (Figure 1A) and lateral view (Figure 1B)
(I) A thin, incomplete, linear sclerotic band seen in the distal metaphysis of left tibia perpendicular to the cortex posteromedially;
(II) Mild soft tissue swelling seen in the left lower leg and ankle with blurred fat planes;
(III) Rest of the visualized bones and ankle joint appears normal.
Coronal STIR images of MRI of left leg with ankle (Figures 2,3)
(I) A th in , incomple te , hypo in tense l ine s een perpendicular to cortex of left tibia on medial aspect reaching up to medial cortex with surrounding marrow edema;
(II) Oedema of surrounding skin and subcutaneous tissues seen;
(III) Mild effusion seen in the left ankle joint.
Diagnosis
Fatigue fracture (stress fracture) left tibia.
Differential diagnosis
Osteomyelitis.
Management
Orthopedic referral for conservative management with rest and supplements of calcium and vitamin D and if required
analgesics.
Important points to remember
• Stressfracturesoccurduetomismatchbetweenbonestrength and chronic mechanical stress on the bone. They have two subtypes: fatigue fractures—occur when healthyboneisexposedtorepeatedstress;insufficiencyfractures-occur in weakened bones (1).
• Most common sites for fatigue fractures: tibia,navicular, metatarsals, fibula, femur, pelvis and spine. People in high-intensity training such as athletes and military recruits are predisposed for these fractures (1).
• Insufficiency fracturesoccur incasesofosteoporosis,previous radiation therapy and chemotherapy, chronic renal failure, chronic rheumatological diseases and corticosteroid therapy. Most common sites include: pelvis, sacrum and proximal femoral fractures (1).
• Radiographic features include: scleroticband, solidthick periosteal reaction and endosteal thickening (later stage). Follow up radiograph after 2-3 weeks may reveal initially indistinct fracture. MRI is the modality of choice for cases with suspicion of stress fractures as it hashighestsensitivityandmorespecificitythanabonescan (1).
• MRIisparticularlyusefulforsacralfracturesobscuredon radiographs. Coronal sequences are the most useful to depict characteristic ‘H’ shaped fractures where vertical planes correspond to regions of maximal stress and horizontal fracture to loss of lateral support by parasagittal fractures (produce ‘Honda sign’ on bone scan). Proximal femoral fractures are seen as subtle neck angulation, trabecular angulation and subcapital impaction line (1).
References
1. Jarraya M, Hayashi D, Roemer FW, Crema MD, Diaz L, Conlin J, Marra MD, Jomaah N, Guermazi A. Radiographically occult and subtle fractures: a pictorial review. Radiol Res Pract 2013;2013:370169.
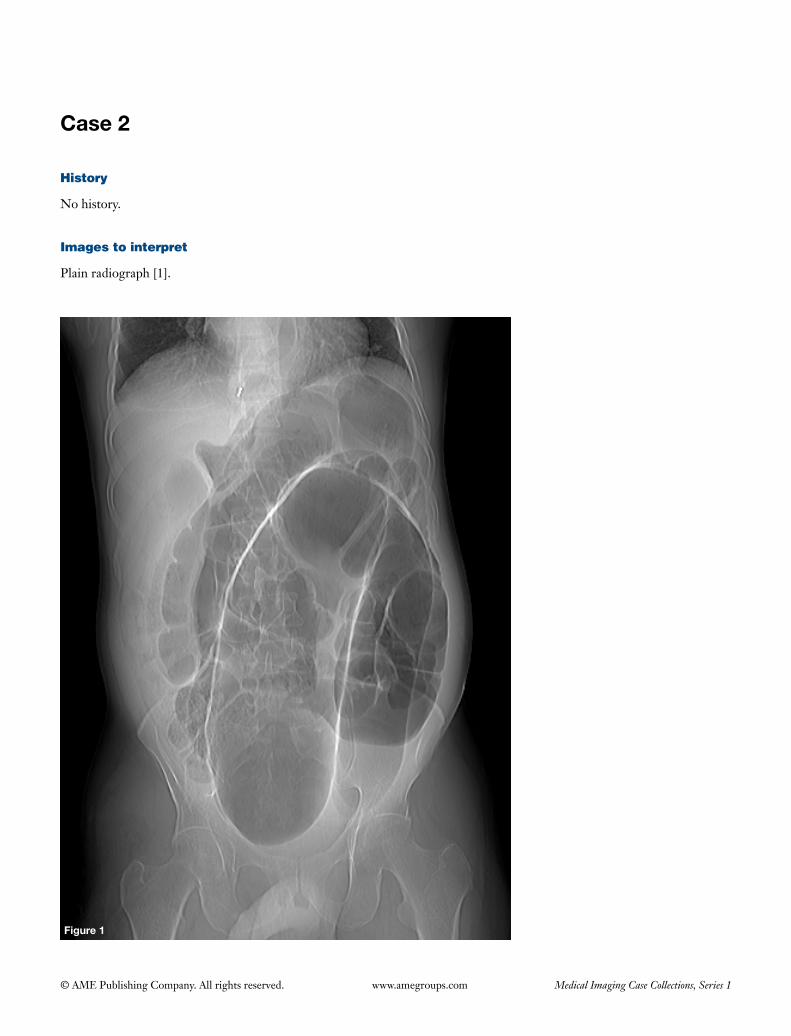
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
History
No history.
Images to interpret
Plain radiograph [1].
Figure 1

115
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph abdomen frontal view (supine position) (Figure 1)
(I) Grossly dilated ‘inverted U shaped’ loop of bowel without haustral markings and with ‘coffee bean sign’ seen in the left hemiabdomen with apex in the left upper quadrant;
(II) Absence of rectal gas;(III) Proximal colonic distension present;(IV) No free gas in the peritoneal cavity;(V) No evidence of pneumatosis intestinalis/portal venous
gas present.
Diagnosis
Sigmoid volvulus causing large bowel obstruction.
Differential diagnosis
• Caecalvolvulus.• Othercausesoflargebowelobstruction.
Management
• Immediategastroenterologyreferralfordecompressionwith barium enema or rectal tube insertion or rigid/flexiblesigmoidoscopyinuncomplicatedcases.
• Cases with features of ischemia or perforation-laparotomy with or without bowel resection.
Important points to remember
• Volvulus is twistingof bowel along itsmesentericattachment site with most common locations being sigmoid colon and cecum. Early correct diagnosis is essential for prompt management to avoid catastrophic consequences.
• Radiographic featuresof sigmoidvolvulus include:distended, ahaustrated, inverted U shaped loop of sigmoid colonwith coffee-bean sign oftenwithfewair-fluid levelswith absent rectal gas andwith
lowerendpointingtopelvis.Othervariable imagingcharacteristics include: apex pointing right upperquadrant (may vary), proximal large bowel obstruction, liver overlap sign, northern exposure sign (distended loop extending cephalad to transverse colon), Frimann Dahl’s sign (three dense lines converging towards site of obstruction) (1).
• Watersolublecontrastenemaorbariumenemashows‘bird-of-prey sign’with abruptly tapered bariumcolumn at the point of volvulus (Figure 2).
• CTshows‘whirlsign’withtwistingofmesenteryandmesenteric vessels along with the radiographic signs. It further helps to rule out complications (bowel ischemia, perforation) (2).
• Pointsdifferentiating sigmoidvolvulus fromcaecalvolvulus include:ahaustrated loopwith fewair fluidlevels with lower end pointing to pelvis (in comparison to haustrated loop in left upper quadrant with no air fluid levels in caecal volvulus). Proximal large bowel obstruction further favours sigmoid volvulus.
Figure 2 Single image of barium enema showing abrupt tapering ofbariumcolumnatthepointoftwistinsigmoidcolon(bird-of-prey sign).
References
1. BurrellHC,BakerDM,WardropP,EvansAJ.Significantplainfilmfindingsinsigmoidvolvulus.ClinRadiol1994;49:317-9.2. VandendriesC,JullèsMC,Boulay-ColettaI,LoriauJ,ZinsM.Diagnosisofcolonicvolvulus:findingsonmultidetectorCT
withthree-dimensionalreconstructions.BrJRadiol2010;83:983-90.
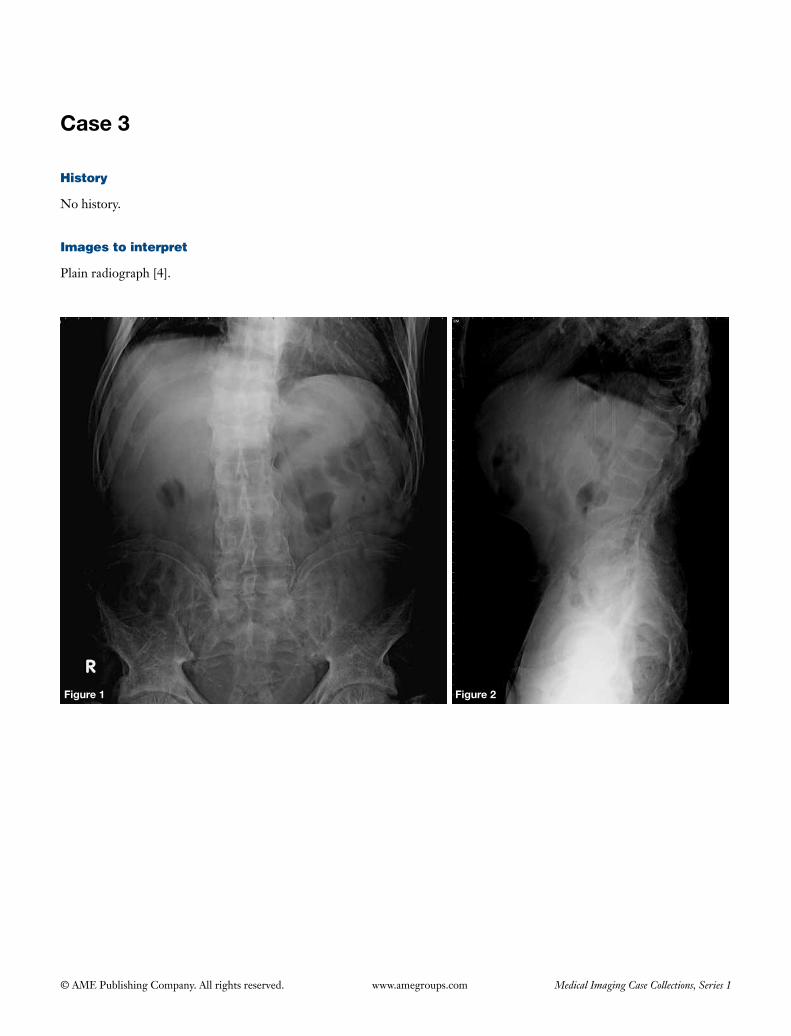
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
History
No history.
Images to interpret
Plain radiograph [4].
Figure 1 Figure 2

117
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 3
Figure 4

118
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph lumbosacral spine frontal (Figure 1) and lateral view (Figure 2)
(I) There is evidence of bilateral symmetric sacroiliitis (Figure 1);
(II) Syndesmophytes noted in the lumbar spine giving bamboo spine appearance (Figure 1);
(III) There is squaring of lumbar vertebra;(IV) Facet joint ankylosis seen in the lumbar spine.
Plain radiograph cervical spine lateral (Figure 3) and frontal view (Figure 4)
(I) Syndesmophytes seen in the cervical spine;(II) Facet joints are normal;(III) Atlantoaxial joint is normal;(IV) Bone density is normal.
Diagnosis
Ankylosing spondylitis.
Differential diagnosis
• Psoriaticarthritis.• Reiter’ssyndrome.• Enteropathicarthritis.
Management
• Referral to rheumatologist for furthermanagement
with nonsteroidal anti-inflammatory drugs and physiotherapy.
• Detailedhistoryandfurther investigationstoruleoutmultisystemic involvement.
Important points to remember
• Ankylosingspondylitis(alsoknownasMarie-Strumpelldisease) is a chronic seronegative spondyloarthropathy (HLA B27 positive in almost 90% of the patients) predominantly affecting spine (causes ankylosis), but also involves sacroiliac joints and other large and small joints (1).
• Radiographic features include:bilateral symmetricsacroiliitis, spinal changes (vertical marginal symmetric syndesmophytes due to ossification of outer annulus fibrosus leading to bamboo spine, erosions at corners ofvertebralbodies-Romanuslesions,reactivesclerosisof these erosions-shiny corner sign, squaring of vertebra, calcification of spinal ligaments, dagger sign-calcification of interspinous ligament, facet joint ankylosis, enthesopathy, fractures with pseudoarthrosis), large joints—hips & knees (bilateral symmetric involvement with uniform joint space narrowing with bony proliferation) (1,2).
• Otherassociations:upper lobe fibrosis in lungswithbullous changes, anterior uveitis, inflammatory bowel disease, aortitis with aortic valve disease (1).
• Psoriatic arthrit is and Reiter’s disease can bedifferentiated by presence of asymmetric sacroiliac joint involvementandasymmetricparavertebralossificationswith relative sparing of the facet joints (1,2).
References
1. BennettDL,OhashiK,El-KhouryGY.Spondyloarthropathies:ankylosingspondylitisandpsoriaticarthritis.RadiolClinNorthAm2004;42:121-34.
2. JacobsonJA,GirishG,JiangY,ResnickD.Radiographicevaluationofarthritis:inflammatoryconditions.Radiology2008;248:378-89.
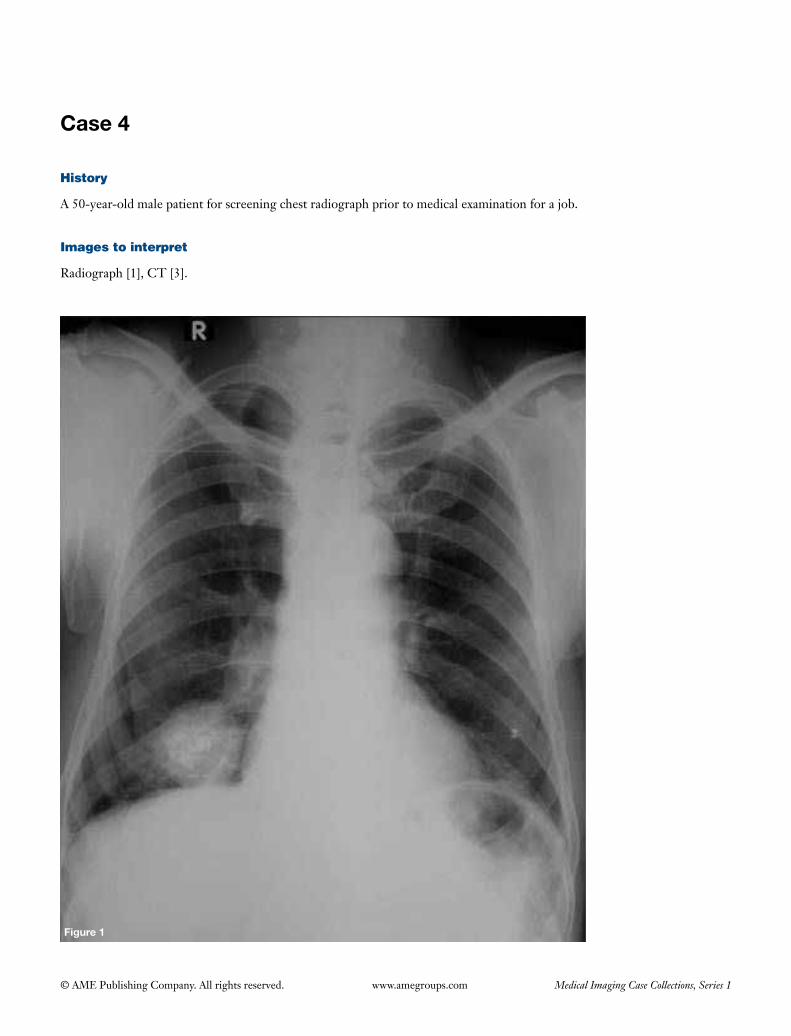
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
Figure 1
History
A 50-year-old male patient for screening chest radiograph prior to medical examination for a job.
Images to interpret
Radiograph [1], CT [3].

120
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 4
Figure 2 Figure 3

121
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Well defined solitary rounded opacity with popcorn calcification seen in right lower zone in right paracardiac region;
(II) No evidence of pleural effusion;(III) Visualized bony structures and soft tissues are normal.
Axial and coronal reformatted plain CT images of chest mediastinal window (Figures 2-4)
(I) CTconfirmsradiographicfindings.Lesionisinrightmiddle lobe;
(II) Few low attenuation areas of attenuation of fat also noted in the lesion (Figures 2,3);
(III) Restoflungfieldsareclear.
Diagnosis
Pulmonary hamartoma.
Differential diagnosis
• Solitarycalcifiedmetastasis (unlikelyas lesionshowsareasoffatdensityspecificforhamartomaandmetsareusually multiple with a history of primary malignancy).
• Bronchial carcinoid (unlikely as typical carcinoidsare usually central, do not contain fat, calcification is eccentricanduncommon,showmarkedhomogenouscontrast enhancement and imaging features of
peripheralpulmonarycarcinoidsarenonspecific).
Management
• Smallperipheral asymtomatichamartomaswithnoatypical features: infrequent followups to look forgrowth.
• Largeendobrochialhamartomasorhamartomawithatypical features: surgical resection.
Important points to remember
• Pulmonaryhamartomasare thecommonestbenignlung tumor and they contain cartilage, connective tissue, muscle, fat and bone in lungs (as they are composed of tissues normally found in the organ of origin) (1).
• Majority of them are small (<4 cm in size) andperipheral (about 90% of cases).
• Intralesional fat is seen in60%of thecases (almostpathognomonicandassessedwithCT)andcalcificationin 20-30%. Cavitation is unusual (2).
• Theygrowslowlywithdoubling timeofmore than 400daysandmalignanttransformationisquiterare.
• Carney’striad(oftenseeninyoungwomen):pulmonaryhamartoma with extra-adrenal paraganglioma and gastricgastrointestinalstromaltumor(GIST)(1).
• Differentials of calcified lungmetastasis include:mets from osteosarcoma, chondrosarcoma, mucinous adenocarcinoma of GIT and breast, papillary carcinoma thyroid, giant cell tumor of bone, synovial sarcoma.
References
1. ThomasJW,StaerkelGA,WhitmanGJ.Pulmonaryhamartoma.AJRAmJRoentgenol1999;172:1643.2. SiegelmanSS,KhouriNF,ScottWWJr,LeoFP,HamperUM,FishmanEK,ZerhouniEA.Pulmonaryhamartoma:CT
findings.Radiology1986;160:313-7.
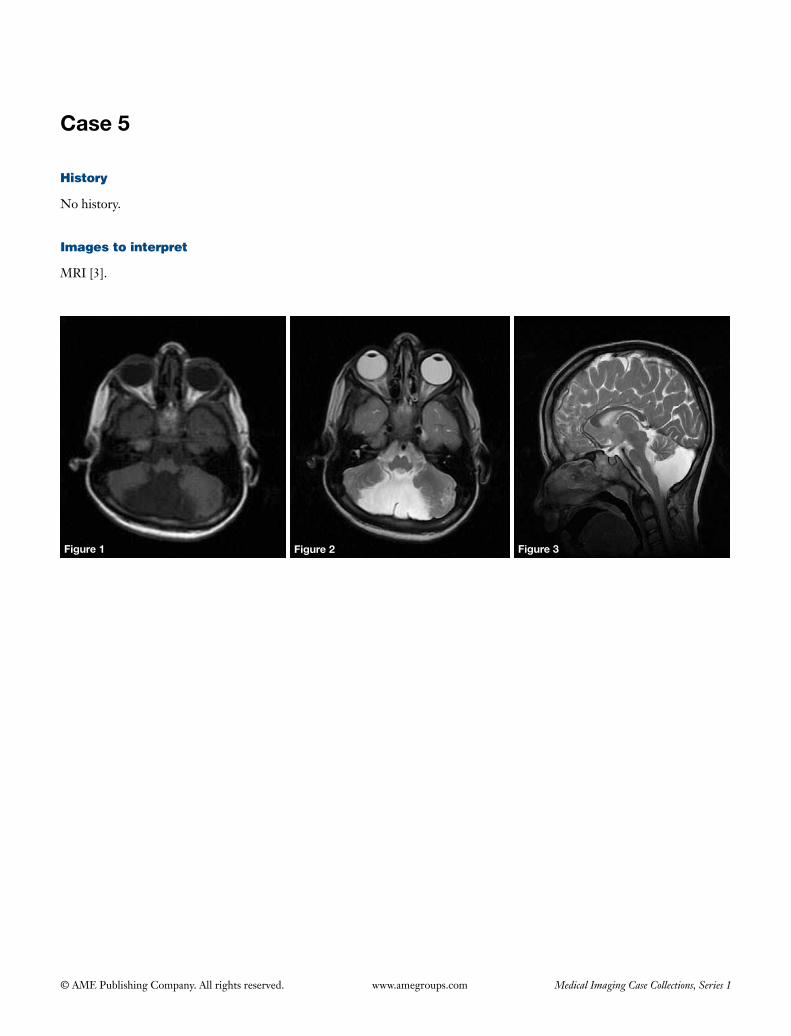
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
Figure 1 Figure 2 Figure 3
History
No history.
Images to interpret
MRI [3].

123
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Axial T1 (Figure 1), axial T2 (Figure 2) and sagittal T2 (Figure 3) weighted images of MRI Brain showing
(I) Posterior fossa cyst that communicates with the fourth ventricle;
(II) Hypoplastic vermis on the inferior aspect;(III) Normal size of the posterior fossa;(IV) No hydrocephalus.
Diagnosis
Dandy walker (DW) variant.
Differential diagnosis
• Arachnoidcyst;• Megacisternamagna.
Management
• Neurosurgicalreferral.• Cystoperitonealshuntingincasesofhydrocephalus.• PoorprognosisincasesofDWmalformation.
References
1. PatelS,BarkovichAJ.Analysisandclassificationofcerebellarmalformations.AJNRAmJNeuroradiol2002;23:1074-87.2. KolliasSS,BallWSJr,PrengerEC.Cysticmalformationsoftheposteriorfossa:differentialdiagnosisclarifiedthrough
embryologicanalysis.Radiographics1993;13:1211-31.
Important points to remember
• DWcontinuumischaracterizedbyposteriorfossacystthatcommunicateswiththefourthventriclealongwiththehypoplasticvermis.ClassicDWmalformationisatthe most severe end of the spectrum and is differentiated from theDWvariantby thepresenceof enlargedposteriorfossawithtorcular-lambdoidinversion(1).
• Most caseshave sporadic inheritance.Obstructivehydrocephalus is common and is due to aqueductal stenosis.OtherassociationsincludeCNSabnormalities(neuronalmigrationalanomalies,agenesisofcorpuscallosum, lipoma of corpus callosum, holoprosencephaly, cerebellarhypoplasia)andotherabnormalities(cardiacanomalies, cleft palate, polydactyly or syndactyly) apart fromtrisomy18and13.
• Mega cisternamagna canbedifferentiated by thepresenceofnormalcerebellarvermisandhemispheres.Arachnoidcyst is anotherdifferential thatmimicksmegacisternamagnaradiologically,butitcausesmasseffectoncerebellum, fourthventricleandsometimesscallopingof innercortexofoccipitalbone.However,theexactdifferentiationbetweenthe two ispossiblewith ventriculogramor cisternogram to show thecommunication ofmega cisternamagnawith theperimedullarysubarachnoidspace(2).

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
Figure 1 Figure 2
History
A 27-year-old female patient presenting with history of pain and swelling in left lower limb since last 1 month.
Images to interpret
Plain radiograph [2], MRI [2].

125
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 3 Figure 4

126
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph thigh with knee frontal and lateral view (Figures 1,2)
(I) Welldefined,solitary,eccentric,expansile,lyticlesionseen in the anterolateral femoral condyle. Lesion is subarticular.Thecortex isdeficienton the lateralaspect with soft tissue component. The zone of transition is narrow without sclerosis;
(II) There is pathological fracture of the articular surface;(III) There is no periosteal reaction;(IV) Opacificationofsuprapatellarbursaalsoseen.
MRI coronal T2 weighted (Figure 3) and sag T1 weighted (Figure 4) images
(I) MRIconfirmsplainradiographfindings;(II) Lesion is isointense on both T1 and T2 weighted
sequences with few hyperintense areas in the center on T2W sequence;
(III) Lesion shows low signal periphery on both the sequences;
(IV) There is high signal marrow edema in the adjacent bone marrow (Figure 3).
Diagnosis
Giant cell tumor (main diagnosis).
Differential diagnosis
Aneurysmal bone cyst (unlikely as age is more, lesion is subarticular,nofluid-fluidlevelsonMR).
Management
• Urgentorthopedicreferral.• Curettageandpackingwithpolymethylmethacrylate
(PMMA)orbonechips,however, therecurrencerateis high.
• Widelocalexcisioncarrieslesschancesofrecurrence.
Important points to remember
• Giant cell tumor is a commonbenign (but locallyaggressive) bone tumor, typical ly seen in theepimetaphyseal locationof longbones.Characteristicradiographic imaging features include: eccentric, expansile,unmineralized,lyticlesioninepimetaphysealregion of long bones with narrow zone of transition and without a sclerotic border in a skeletally mature patient.AggressiveGCTScanshowilldefinedborders.Theoverlyingcortex isoftenthinned&expandedordeficient.Softtissuecomponent,pathologicalfractureand periosteal reaction can also be seen (1).
• OnMRI, the so l id component shows low tointermediate signal on both T1 and T2 weighted sequenceswith low signal periphery.GCTswithsecondaryABCalsoshowfluid-fluidlevels(1).
• MultipleGCTsarerareandoccur incasesofPaget’sdisease.MalignantGCTsoccurin5-10%ofthecases(1).
• Differentialsof lesionswithfluid-fluid levels:benign-aneurysmal bone cysts (both primary and secondary), simplebonecysts,fibrousdysplasia,chondroblastoma,osteoblastoma, ossifying fibroma, intraosseous ganglion. Malignant-telangiectatic osteosarcoma, malignant fibrous histiocytoma, metastasis (kidney, lung), plasmacytoma.
References
1. MurpheyMD,NomikosGC,FlemmingDJ,GannonFH,TempleHT,KransdorfMJ.FromthearchivesofAFIP.Imagingofgiantcelltumorandgiantcellreparativegranulomaofbone:radiologic-pathologiccorrelation.Radiographics2001;21:1283-309.
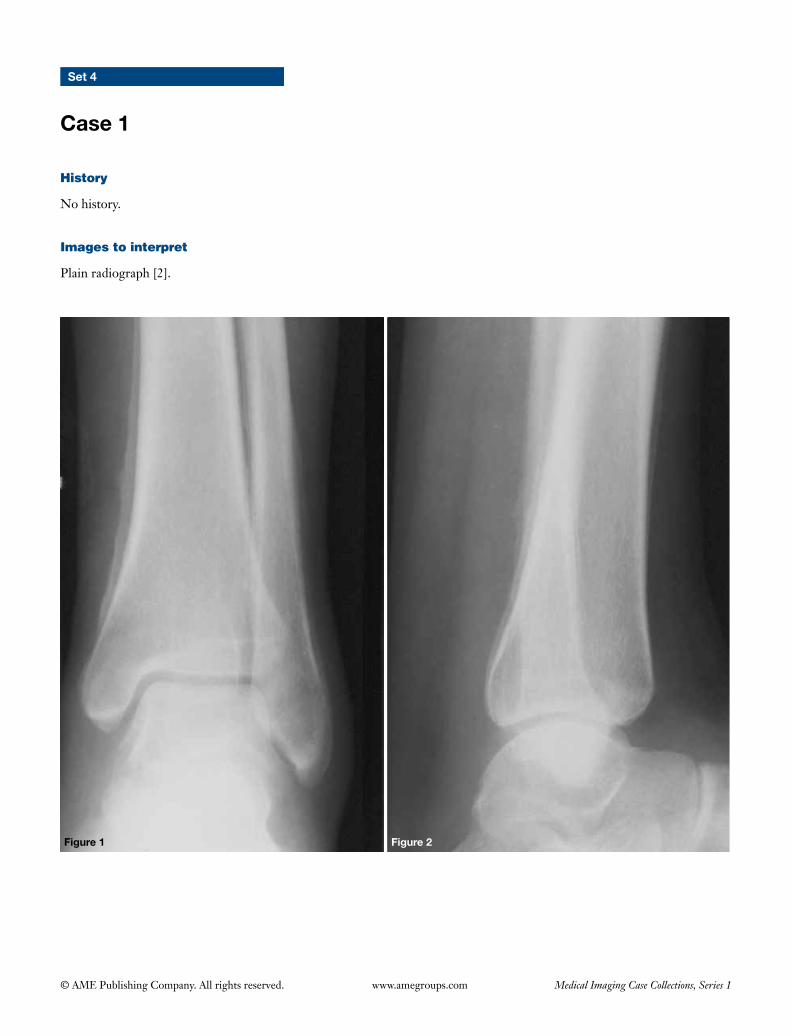
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 4
Case 1
History
No history.
Images to interpret
Plain radiograph [2].
Figure 1 Figure 2

128
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph ankle (marker not given) frontal (Figure 1) and lateral (Figure 2) view
(I) Smooth, linear, uninterrupted periosteal reaction seen over distal metadiaphyseal region of tibia and fibula. Epiphysis are spared;
(II) Ankle joint appears normal.
Diagnosis
Secondary hypertrophic osteoarthropathy.
Differential diagnosis
• Pachydermoperiostosis.• Thyroid acropachy.• Chronic venous insufficiency.
Management
Take radiograph of the contralateral ankle to confirm the diagnosis. Further work up to rule out etiology of hypertrophic osteoarthropathy (HOA) (most importantly chest radiograph).
Important points to remember
• Hypertrophic osteoarthropathy is a syndrome characterized by proliferative periostitis of the long bones associated with oligopolysynovitis and digital clubbing (1).
• The et io logies inc lude: thorac ic pathologies [bronchogenic carcinoma (Figures 3,4), lung abscess, bronchiectasis, pulmonary mets, pleural fibroma and mesothelioma, cyanotic congenital heart disease], primary biliary cirrhosis, inflammatory bowel diseases, celiac disease, Whipple disease, and familial forms (primary HOA).
• Imaging features of secondary HOA include: smooth, bilateral symmetric periosteal reaction involving metadiaphyseal region of the long bones of distal extremities. The periostitis becomes more prominent and multilayered as the disease progresses (1).
• Primary HOA/pachydermoperiostosis is an autosomal dominant, self limiting disorder, which often affects young males and can be differentiated from the secondary HOA by coexistence of periosteal thickening (involving epiphysis along with the metadiaphysis) and cutaneous thickening with absence of any predisposing pathology (1).
• Chronic venous insufficiency often affects lower limbs and is either unilateral or bilateral, asymmetric and phleboliths can be seen.
• Thyroid acropachy often affects hands mainly radial side of thumb and index finger although all phalanges and metacarpals can be involved.
Figure 3
Figure 3 Chest radiograph of the same patient showing right apical mass.
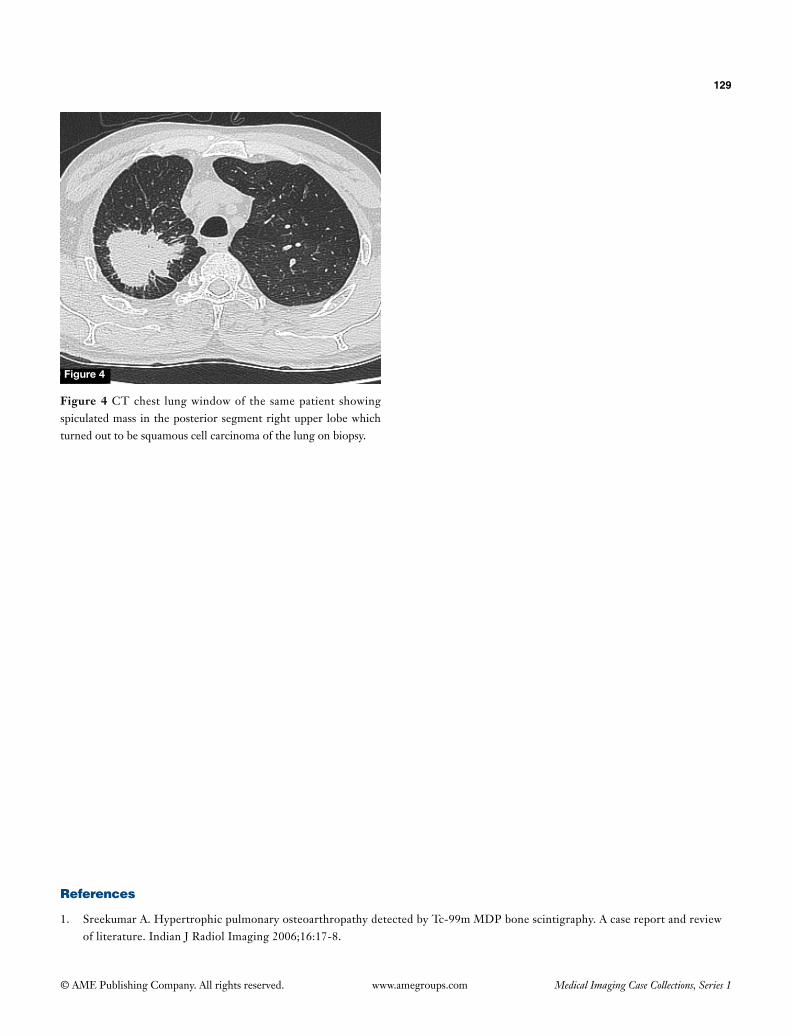
129
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
References
1. Sreekumar A. Hypertrophic pulmonary osteoarthropathy detected by Tc-99m MDP bone scintigraphy. A case report and review of literature. Indian J Radiol Imaging 2006;16:17-8.
Figure 4
Figure 4 CT chest lung window of the same patient showing spiculated mass in the posterior segment right upper lobe which turned out to be squamous cell carcinoma of the lung on biopsy.
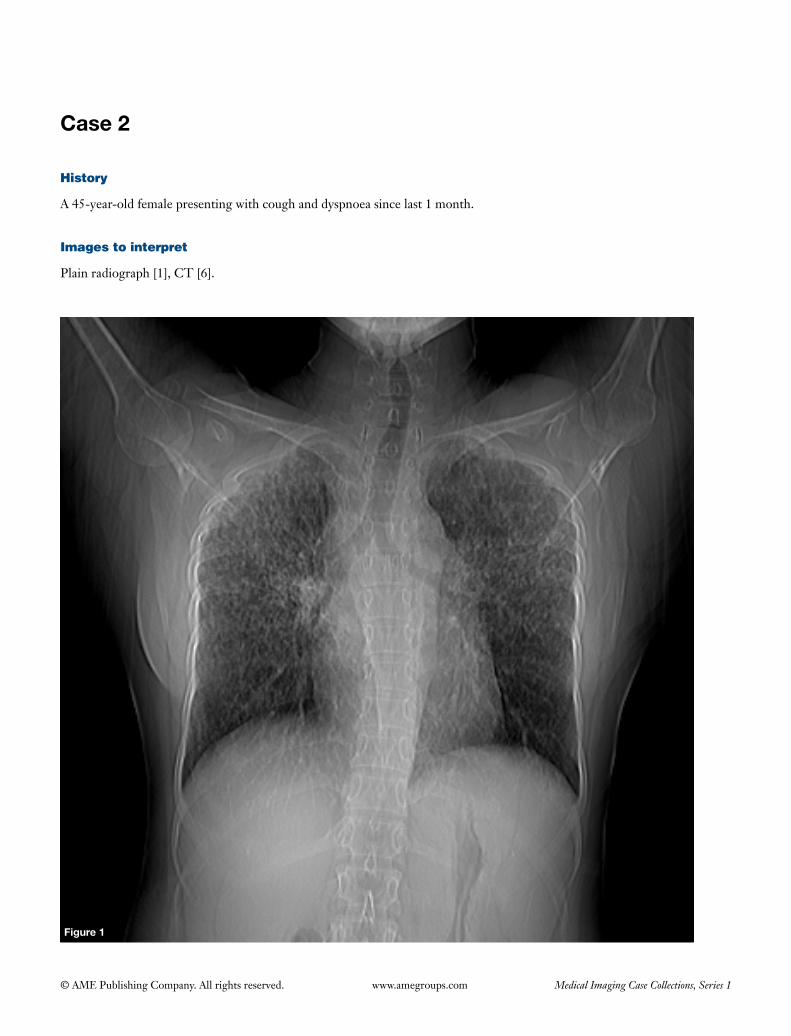
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
History
A 45-year-old female presenting with cough and dyspnoea since last 1 month.
Images to interpret
Plain radiograph [1], CT [6].
Figure 1
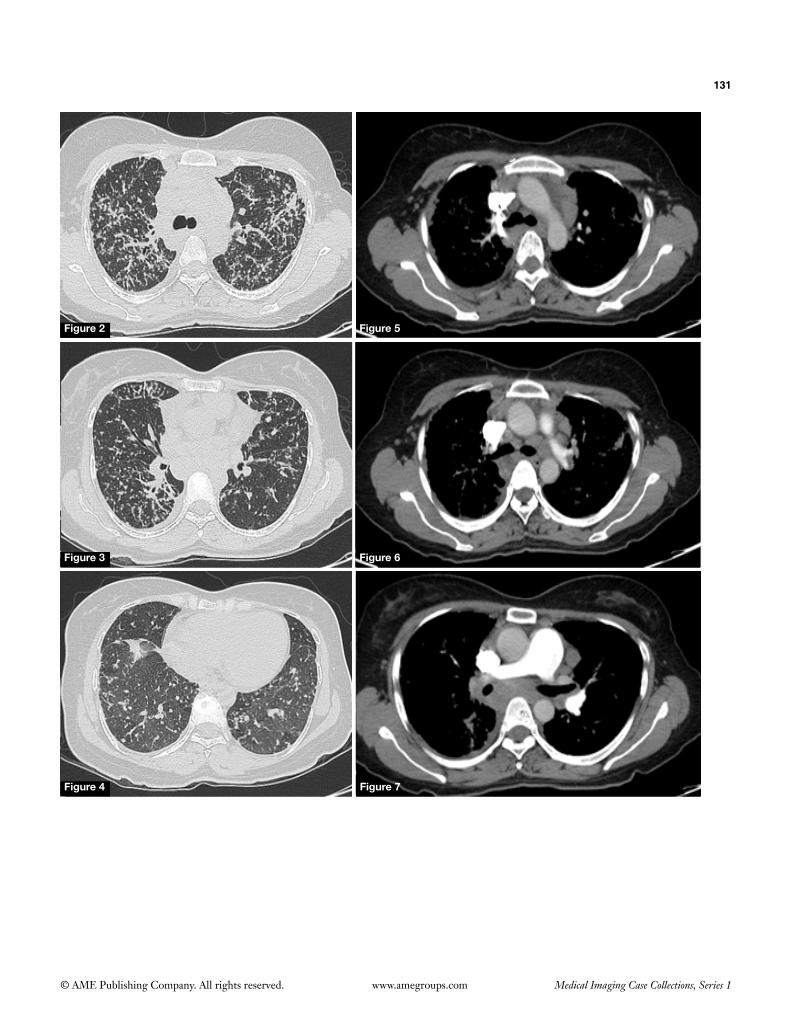
131
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 5
Figure 6
Figure 7Figure 4
Figure 3
Figure 2

132
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Reticulonodularopacitiesseeninbilateral lungfieldsmost pronounced in bilateral upper and mid zones;
(II) Bilateral hilar lymphadenopathy seen;(III) Lung volumes are normal;(IV) No pleural effusion seen.
CECT chest lung window (Figures 2-4) and mediastinal window (Figures 5-7)
(I) Multiple small nodules seen in peribronchovascular and subpleural region (perilymphatic distribution);
(II) Areas of mosaic attenuation in bilateral lower lobes of lungs likely due to small airways disease;
(III) Enlarged homogenous lymph nodes seen in prevascular, precarinal, subcarinal and bilateral hilar regionswithnoevidenceofcalcificationandnecrosis.
Diagnosis
Sarcoidosis (stage 3).
Differential diagnosis
• Lymphangitis carcinomatosis (DDofperilymphaticnodules).
• Lymphoma(DDofperilymphaticnodules).
Management
• Detailedhistoryandclinicalexaminationto lookforextrathoracicmanifestationsofsarcoidosis.
• Serumcalciumandangiotensinconvertingenzyme(ACE) levels.
• Referraltochestphysicianformanagementwithsteroids.
Important points to remember
• Sarcoidosis isanon-caseatinggranulomatousmulti-
system disease of unknown etiology, in which pulmonary and mediastinal manifestations are seen in over 90% of individuals (1).
• Thoracicmanifestations include:bilateralhilar andmediastinal nodal enlargement (garland triad—bilateral hilar and right paratracheal node enlargement) with or withoutegg-shellcalcification,reticulonodularopacitieson radiograph and perilymphatic nodules on HRCT, coalescence of nodules to form ill-defined, peripheral airspace-like opacities which frequently contain air bronchograms-alveolar sarcoidosis (misnomer as it represents interstitial rather than intra-alveolar pathology, sarcoid-galaxysignwhich is seenas largecoalescent nodules surrounded by satellite nodules is part of the same process), upper lobe fibrosis mainly involving posterior segments (2).
• Stagesofpulmonarysarcoidosisonplainradiograph:stage 0—normal; stage 1—hilar/mediastinal nodal enlargement; stage 2—parenchymal disease and nodal enlargement; stage 3—parenchymal disease only; stage 4—pulmonaryfibrosis(2).
• Extrathoracicmanifestations:CNS(pachymeningitisand leptomeningitis, cranial nerve palsies-facial nerve, diabetes insipidus, parenchymal involvement of brain and myelopathy), head and neck (parotitis, ocular involvement-uveitis, cervical lymphadenopathy), musculoskeletalinvolvement(inflammatoryarthralgia,Löfgren syndrome, myopathy, skeletal sarcoidosis which mainly affects hands causing lace like bony destruction/cystic bone lesions/rarely sclerotic bone lesions), cardiomyopathy-arrythmias & heart block, hepatosplenomegaly with or without focal hepatic and splenic lesions, skin (erythema nodosum, lupus pernio) (1).
• Differentialsofeggshellcalcificationof lymphnodesinclude: silicosis, sarcoidosis, lymphoma followingradiotherapy.
• Differentials of bilateral hilar lymphadenopathyinclude:sarcoidosis,lymphoma,tuberculosis.
References
1. Koyama T, Ueda H, Togashi K, Umeoka S, Kataoka M, Nagai S. Radiologic manifestations of sarcoidosis in various organs. Radiographics2004;24:87-104.
2. CriadoE,SánchezM,RamírezJ,ArguisP,deCaraltTM,PereaRJ,XaubetA.Pulmonarysarcoidosis:typicalandatypicalmanifestationsathigh-resolutionCTwithpathologiccorrelation.Radiographics2010;30:1567-86.
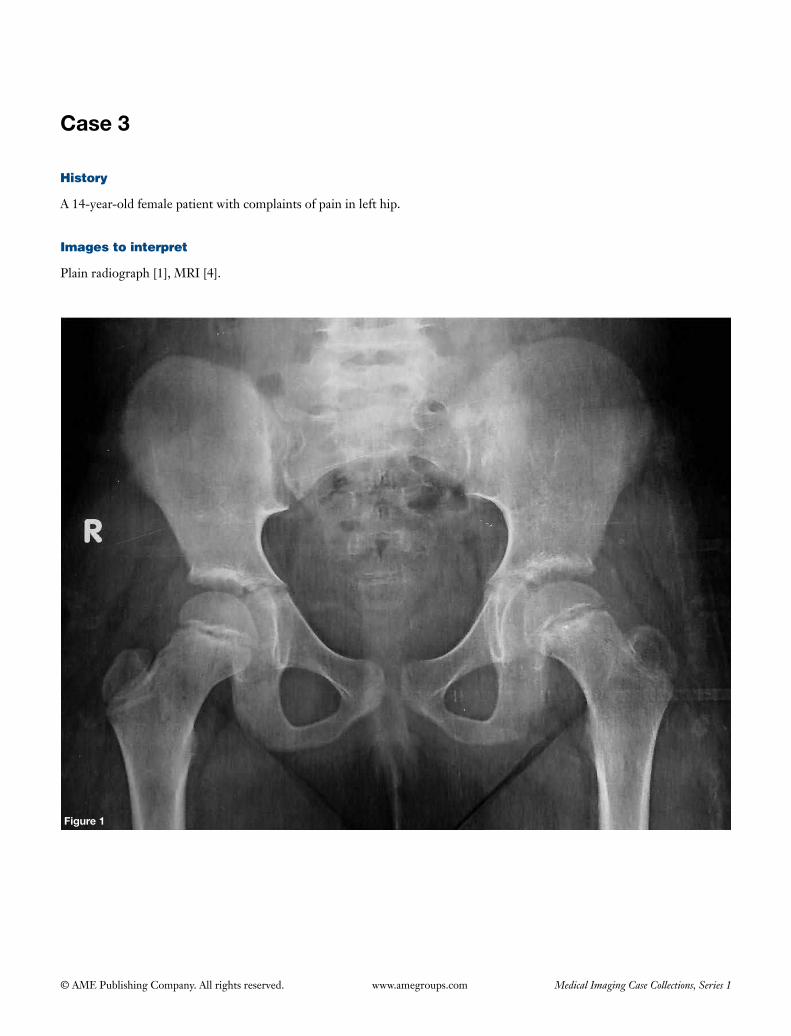
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
History
A 14-year-old female patient with complaints of pain in left hip.
Images to interpret
Plain radiograph [1], MRI [4].
Figure 1
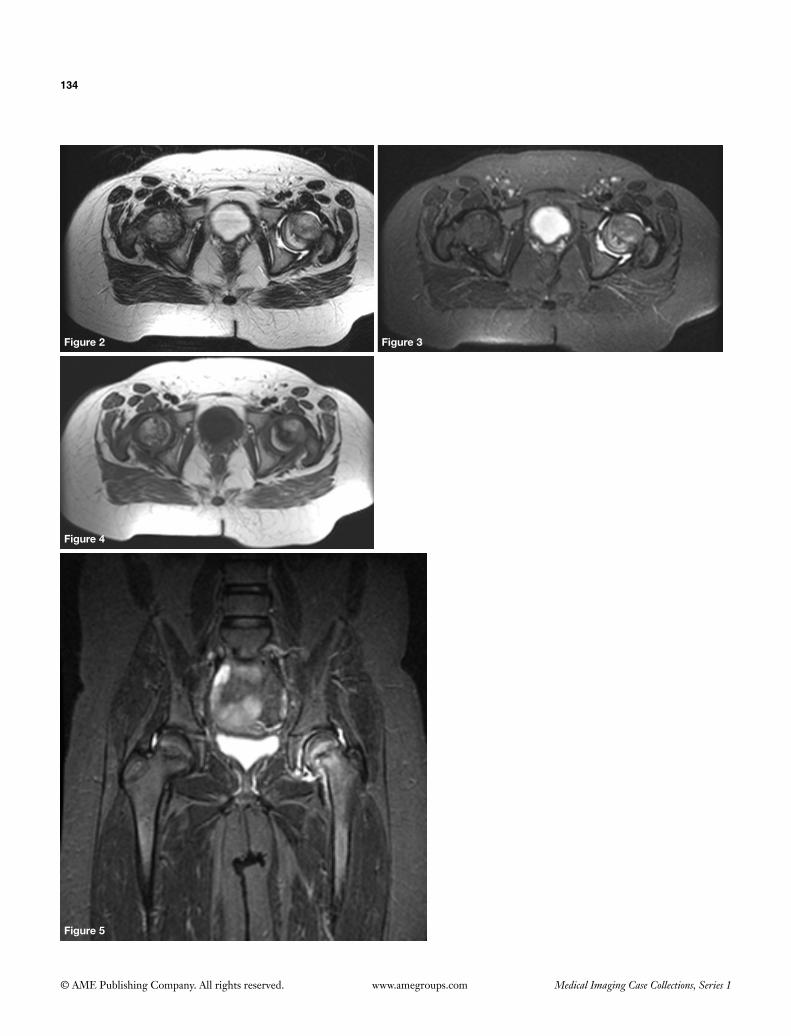
134
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 5
Figure 2 Figure 3
Figure 4
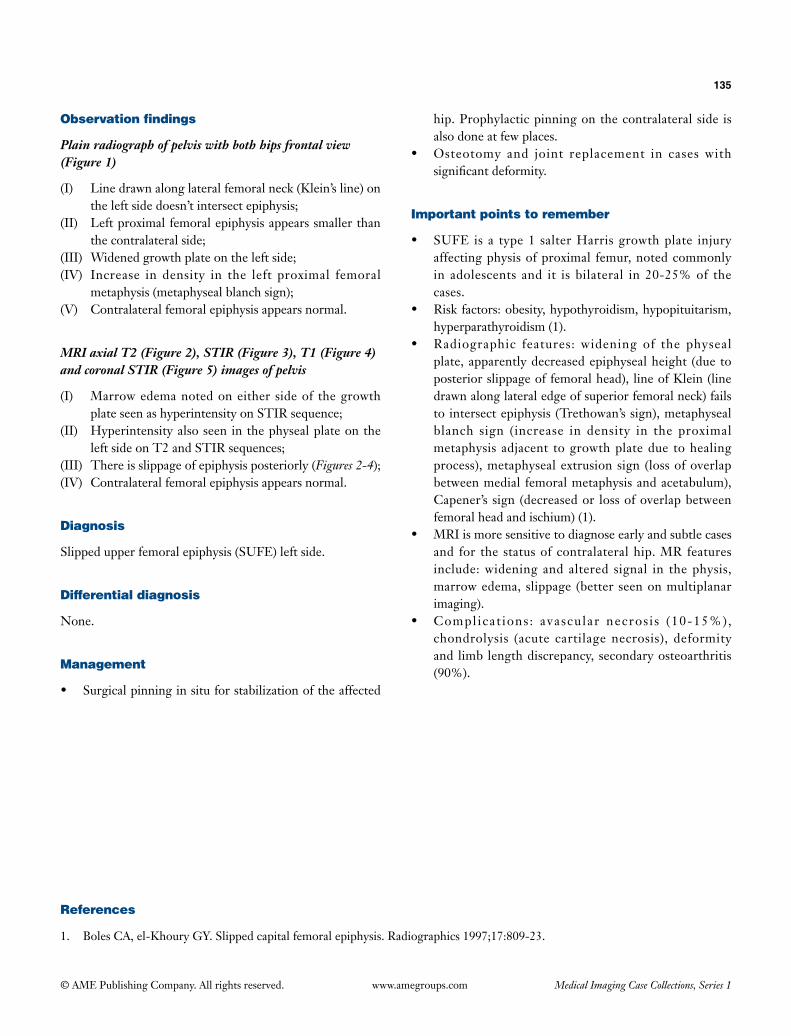
135
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph of pelvis with both hips frontal view (Figure 1)
(I) Line drawn along lateral femoral neck (Klein’s line) on the left side doesn’t intersect epiphysis;
(II) Left proximal femoral epiphysis appears smaller than the contralateral side;
(III) Widened growth plate on the left side;(IV) Increase in density in the left proximal femoral
metaphysis (metaphyseal blanch sign);(V) Contralateral femoral epiphysis appears normal.
MRI axial T2 (Figure 2), STIR (Figure 3), T1 (Figure 4) and coronal STIR (Figure 5) images of pelvis
(I) Marrow edema noted on either side of the growth plate seen as hyperintensity on STIR sequence;
(II) Hyperintensity also seen in the physeal plate on the left side on T2 and STIR sequences;
(III) There is slippage of epiphysis posteriorly (Figures 2-4);(IV) Contralateral femoral epiphysis appears normal.
Diagnosis
Slipped upper femoral epiphysis (SUFE) left side.
Differential diagnosis
None.
Management
• Surgicalpinninginsituforstabilizationoftheaffected
hip. Prophylactic pinning on the contralateral side is also done at few places.
• Osteotomy and joint replacement in cases withsignificantdeformity.
Important points to remember
• SUFE is a type1 salterHarrisgrowthplate injuryaffecting physis of proximal femur, noted commonly in adolescents and it is bilateral in 20-25% of the cases.
• Riskfactors:obesity,hypothyroidism,hypopituitarism,hyperparathyroidism (1).
• Radiographic features: widening of the physealplate, apparently decreased epiphyseal height (due to posterior slippage of femoral head), line of Klein (line drawn along lateral edge of superior femoral neck) fails to intersect epiphysis (Trethowan’s sign), metaphyseal blanch sign (increase in density in the proximal metaphysis adjacent togrowthplatedue tohealingprocess), metaphyseal extrusion sign (loss of overlap between medial femoral metaphysis and acetabulum), Capener’s sign (decreased or loss of overlap between femoral head and ischium) (1).
• MRIismoresensitivetodiagnoseearlyandsubtlecasesand for the status of contralateral hip. MR features include:widening and altered signal in thephysis,marrow edema, slippage (better seen on multiplanar imaging).
• Compl icat ions : avascular necros i s (10-15%),chondrolysis (acute cartilage necrosis), deformity and limb length discrepancy, secondary osteoarthritis (90%).
References
1. BolesCA,el-KhouryGY.Slippedcapitalfemoralepiphysis.Radiographics1997;17:809-23.
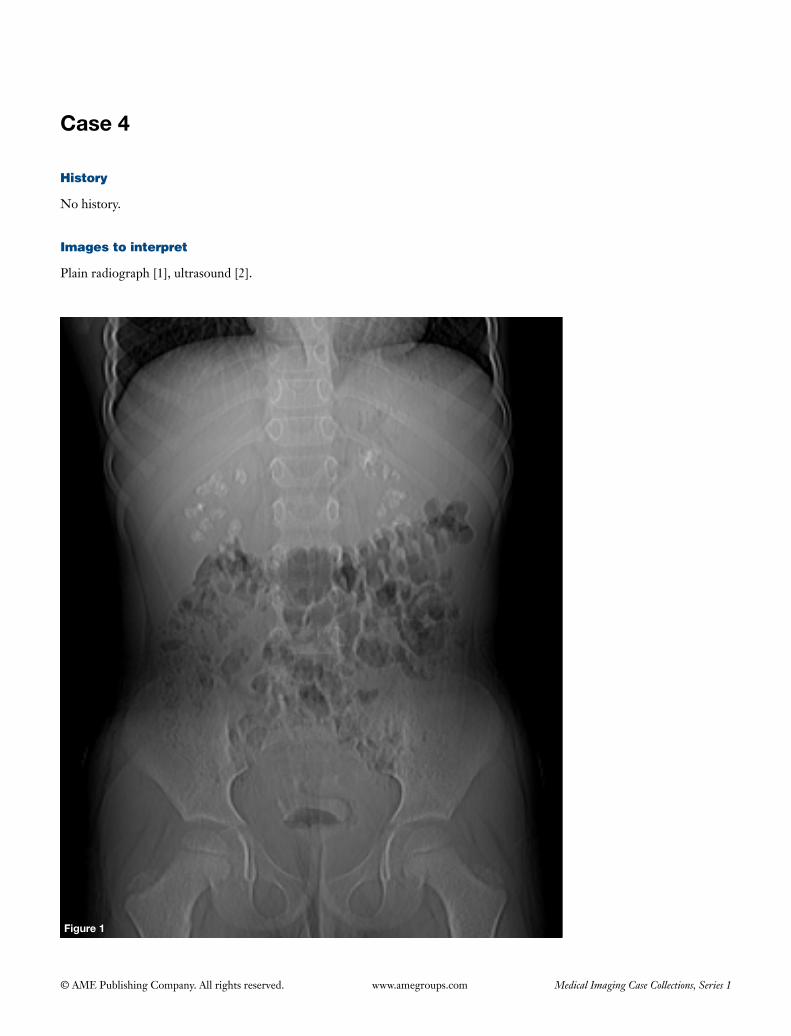
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
History
No history.
Images to interpret
Plain radiograph [1], ultrasound [2].
Figure 1

137
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2 Figure 3
RK LK
138
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph abdomen frontal supine view (Figure 1)
(I) Multiple foci of macroscopic calcifications noted scattered symmetrically in both renal areas in the region of renal medulla;
(II) No other stones seen in the region of bilateral ureters and urinary bladder/no other calcifications seen in the abdomen;
(III) Visualized bones appear normal with no evidence of hyperparathyroidism.
Ultrasound images of both kidneys (Figures 2,3)
(I) Multiple areas of increased echogenicity seen involving all the medullary pyramids of both kidneys;
(II) Renal cortex is normal;(III) No evidence of hydronephrosis seen.
Diagnosis
Medullary nephrocalcinosis.
Differential diagnosis
None.
Management
Further work up to find out the etiology to treat treatable
causes like infection.
Important points to remember
• Medullary nephrocalcinosis is deposition of calcium in the distal convoluted tubules (renal pyramids) in the renal medulla (1,2).
• Causes include: primary hyperparathyroidism (most common cause in adults-causes symmetric medullary nephrocalcinosis); distal renal tubular acidosis (second most common cause in adults and most common in children-causes symmetric medullary nephrocalcinosis), medullary sponge kidney (most common cause of asymmetric medullary nephrocalcinosis) ; hypercalcemia (milk-alkal i syndrome, sarcoidosis, hypervitaminosis D, malignant hypercalcemia due to bone mets, multiple myeloma), idiopathic hypercalciuria, other endocrine causes (hyperthyroidism, Cushing’s syndrome), renal papillary necrosis, infection and hyperoxaluria (causes both cortical and medullary nephrocalcinosis) (1,2).
• Complication—renal failure. Medullary sponge kidney and idiopathic hypercalciuria—best prognosis; hyperoxaluria—worst prognosis.
• Causes of cortical nephrocalcinosis include: renal cortical necrosis due to any cause (sepsis, drugs etc.), chronic glomerulonephritis, Alport syndrome, renal transplant rejection, hyperoxaluria (1,2).
References
1. Dähnert W. eds. Radiology review manual 6th edition. Philadelphia: Lippincott Williams & Wilkins, 2007.2. Dyer RB, Chen MY, Zagoria RJ. Abnormal calcifications in the urinary tract. Radiographics 1998;18:1405-24.
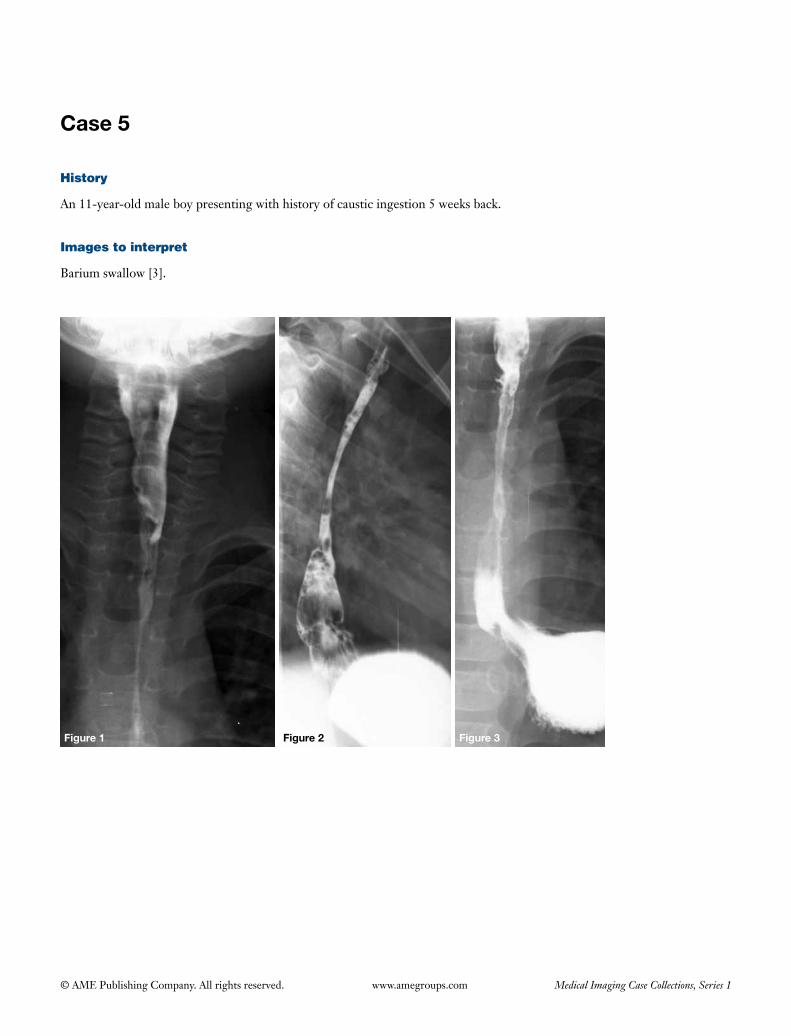
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
Figure 1 Figure 2 Figure 3
History
An 11-year-old male boy presenting with history of caustic ingestion 5 weeks back.
Images to interpret
Barium swallow [3].
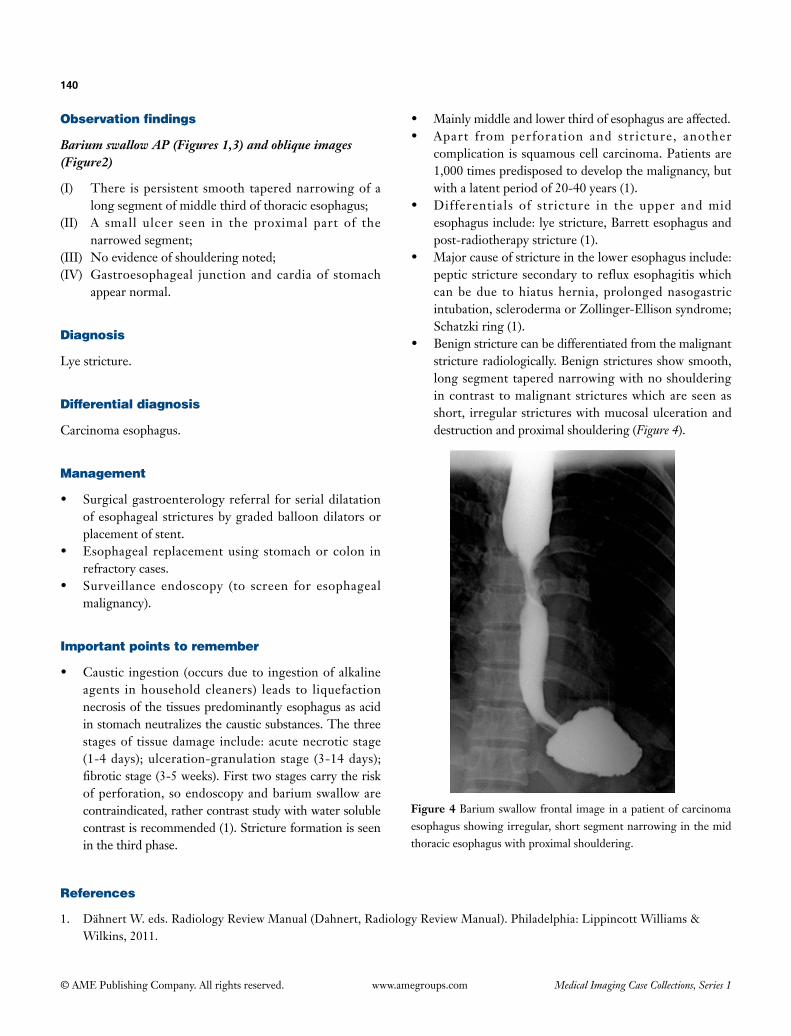
140
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Barium swallow AP (Figures 1,3) and oblique images (Figure2)
(I) There is persistent smooth tapered narrowing of a long segment of middle third of thoracic esophagus;
(II) A small ulcer seen in the proximal part of the narrowed segment;
(III) No evidence of shouldering noted;(IV) Gastroesophageal junction and cardia of stomach
appear normal.
Diagnosis
Lye stricture.
Differential diagnosis
Carcinoma esophagus.
Management
• Surgicalgastroenterologyreferral forserialdilatationof esophageal strictures by graded balloon dilators or placement of stent.
• Esophageal replacementusing stomachorcolon inrefractory cases.
• Surveillance endoscopy (to screen for esophagealmalignancy).
Important points to remember
• Caustic ingestion(occursdueto ingestionofalkalineagents in household cleaners) leads to liquefaction necrosis of the tissues predominantly esophagus as acid in stomach neutralizes the caustic substances. The three stages of tissue damage include: acute necrotic stage (1-4 days); ulceration-granulation stage (3-14 days); fibroticstage(3-5weeks).Firsttwostagescarrytheriskof perforation, so endoscopy and barium swallow are contraindicated, rather contrast study with water soluble contrastisrecommended(1).Strictureformationisseenin the third phase.
• Mainlymiddleandlowerthirdofesophagusareaffected.• Apart from perforation and stricture, another
complication is squamous cell carcinoma. Patients are 1,000 times predisposed to develop the malignancy, but with a latent period of 20-40 years (1).
• Differentials of stricture in the upper andmidesophagus include: lye stricture, Barrett esophagus and post-radiotherapy stricture (1).
• Majorcauseofstrictureintheloweresophagusinclude:peptic stricture secondary to reflux esophagitis which can be due to hiatus hernia, prolonged nasogastric intubation,sclerodermaorZollinger-Ellisonsyndrome;Schatzkiring(1).
• Benignstricturecanbedifferentiatedfromthemalignantstricture radiologically. Benign strictures show smooth, long segment tapered narrowing with no shouldering in contrast to malignant strictures which are seen as short, irregular strictures with mucosal ulceration and destruction and proximal shouldering (Figure 4).
Figure 4 Barium swallow frontal image in a patient of carcinoma esophagus showing irregular, short segment narrowing in the mid thoracic esophagus with proximal shouldering.
References
1. DähnertW.eds.RadiologyReviewManual(Dahnert,RadiologyReviewManual).Philadelphia:LippincottWilliams&Wilkins,2011.
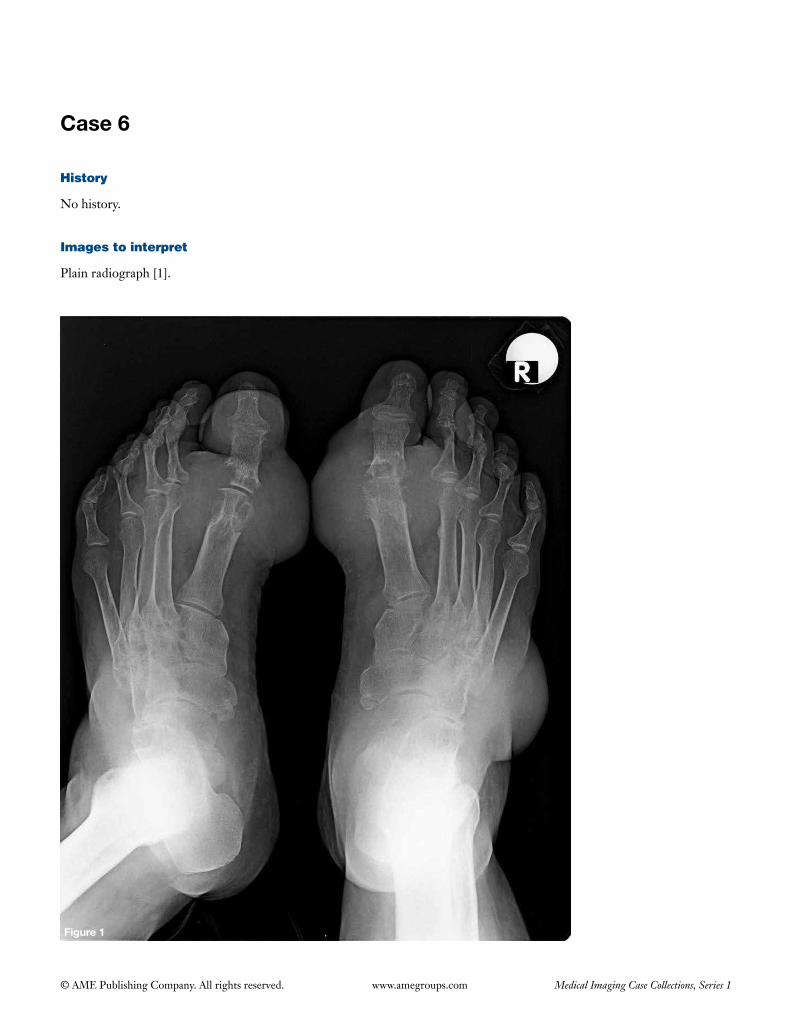
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
History
No history.
Images to interpret
Plain radiograph [1].
Figure 1

142
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph bilateral foot frontal view (Figure 1)
(I) Punched out erosions seen with sclerotic margins and overhanging edges in juxtaarticular location along bilateral first metatarsophalangeal joints;
(II) Gross eccentric periarticular soft tissue swelling seen bilaterally along first metatarsophalangeal joints;
(III) Joint space appears normal;(IV) Diffuse osteopenia seen (likely due to disuse);(V) Rest of the joints appear normal.
Diagnosis
Gout.
Differential diagnosis
None.
Management
• Serum uric acid levels.• Referra l to rheumatologis t for correct ion of
hyperuricemia and further management.
Important points to remember
• Gout occurs due to deposition of monosodium urate crystals in synovial membranes, articular cartilage, ligaments, tendon and bursae often in men above 40 years of age (1).
• It can be idiopathic or secondary to myeloproliferative
disorders, hyperparathyroidism, glycogen storage disorders, chronic renal failure, certain medications like thiazides.
• Location: small joints of hands and feet particularly first metatarsophalangeal joint > elbow, wrist, knee, shoulder, hip, sacroiliac joint, bones, ear pinna, tendons, ligaments, bursa.
• Radiographic features (develop after a long latent period of 6-12 years after hyperuricemia) include: arthropathy (joint effusion; juxtaarticular, punched out erosions with sclerotic margins and overhanging edges; absence of periaricular osteopenia; joint space preservation; chondrocalcinosis), crystal deposition in bones (punched out lytic lesions with sclerotic & overhanging margins with preserved bone density, avascular necrosis particularly of humeral and femoral heads), soft tissue findings (aural calcification; bilateral prepatellar and olecranon bursitis; eccentric, juxtaarticular soft tissue swelling may calcify) (1).
• Ultrasound helps in detecting non-calcified tophi in soft tissues and joints along with the synovitis at early stage. ‘Double contour sign’—urate deposition over most superficial layer of hyaline cartilage is seen as irregular echogenic line producing this sign. Tophus is seen as anechoic halo (fibrovascular zone) surrounding hyperechoic heterogenous center of synovia l proliferation (2).
• MR is more sensitive for early detection of tophi and bone erosions in these patients and for assessment of deeper structures. Tophus is hypointense on T1 and shows heterogenous intermediate to low signal on T2 with enhancement on gadolinium enhanced images (1,2).
References
1. Perez-Ruiz F, Dalbeth N, Urresola A, de Miguel E, Schlesinger N. Imaging of gout: findings and utility. Arthritis Res Ther 2009;11:232.
2. Girish G, Melville DM, Kaeley GS, Brandon CJ, Goyal JR, Jacobson JA, Jamadar DA. Imaging appearances in gout. Arthritis 2013;2013:673401.
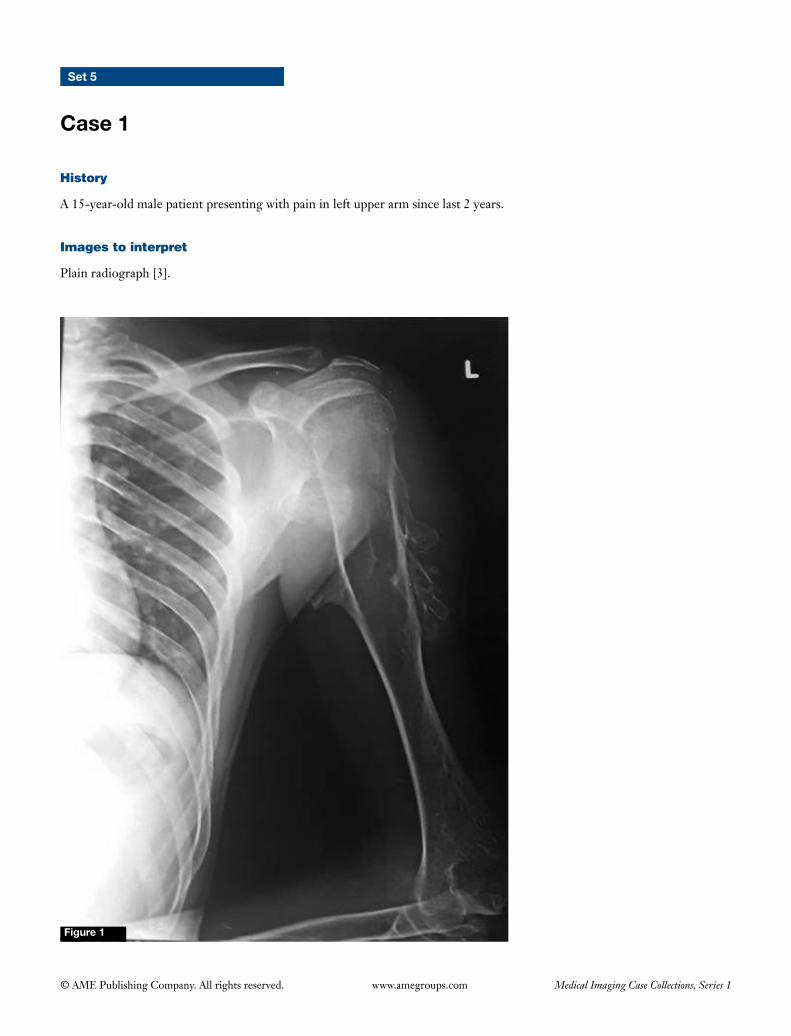
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 5
Case 1
Figure 1
History
A 15-year-old male patient presenting with pain in left upper arm since last 2 years.
Images to interpret
Plain radiograph [3].

144
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 3
Figure 2
A B
BA
145
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph left shoulder with arm frontal view (Figure 1)
(I) Multiple osseous outgrowths seen arising from the proximal metadiaphyseal region of left humerus projecting away from the shoulder joint, with cortex in continuity with the cortex (both from the medial and the lateral cortex);
(II) Another bony outgrowth seen arising from the lateral border of scapula.
Plain radiograph both forearms with wrist frontal and lateral view (Figures 2,3)
(I) Sessile osseous outgrowth also seen in the distal metadiaphyseal region of bilateral ulna with shortened both ulna (left more than the right) with radius longer than the ulna;
(II) Another osteochondroma seen arising from the distal metadiaphysis of right radius;
(III) Mild radial bowing of the left radius noted;(IV) Distal radioulnar joint is widened on the left side;(V) No evidence of pathological fracture, cortical
destruction or soft tissue component noted in any of the lesion.
Interpretation
Multiple osteochondromas with reverse Madelung’s deformity bilaterally.
Diagnosis
Diaphyseal aclasis with reverse Madelung’s deformity (bilaterally).
Differential diagnosis
None.
Management
• Uncomplicatedandasymptomaticosteochondromasdon’t require any treatment except for regular follow ups, due to risk of malignant transformation.
• Multiple surgical options are available for reverseMadelung’s deformity (as it may be painful or due to cosmetic and functional deformity), depending on the symptoms and patient’s choice.
Important points to remember
• Diaphyseal aclasisormultiplehereditary exostosisis an autosomal dominant disorder, characterized by development of multiple osteochondromas.
• Complications include: pathological fracture,compression of neurovascular bundle, bursitis, growth deformities, malignant transformation (up to 25% of patients), cord compression (if arising from posterior elements of vertebra) (1).
• Featuresofmalignanttransformationorchondrosarcomainclude:paininpreviouslyasymptomaticlesion,suddenincrease in size, destruction of cortex with associated soft tissue component, cartilage cap thickness >1.5 cm, destructionofalreadyexistingcalcification(1).
References
1. MurpheyMD,ChoiJJ,KransdorfMJ,FlemmingDJ,GannonFH.Imagingofosteochondroma:variantsandcomplicationswithradiologic-pathologiccorrelation.Radiographics2000;20:1407-34.
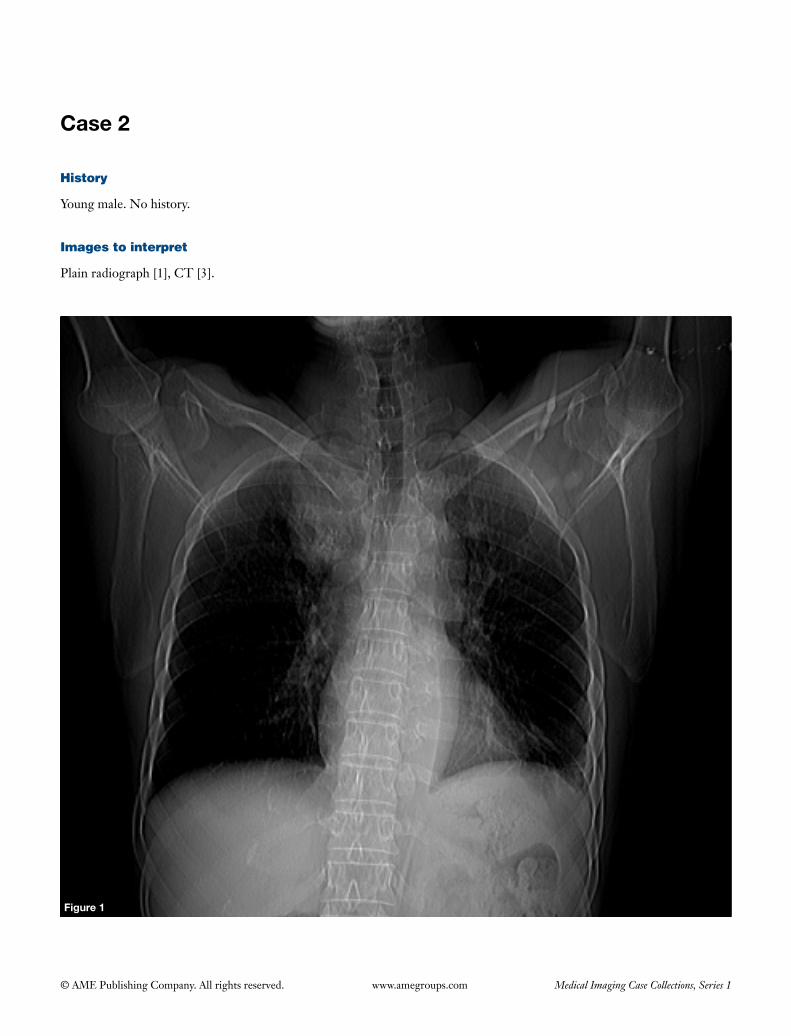
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 2
Figure 1
History
Young male. No history.
Images to interpret
Plain radiograph [1], CT [3].
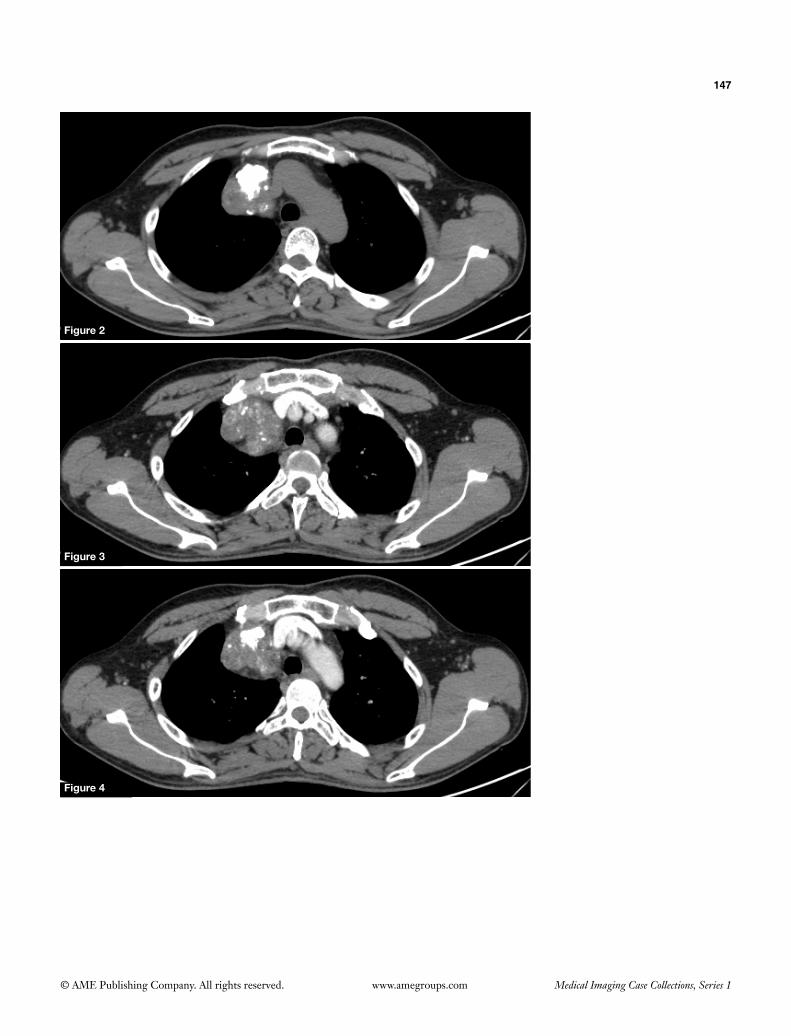
147
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2
Figure 3
Figure 4
148
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph chest frontal view (Figure 1)
(I) Welldefinedhomogenousopacityseeninrightupperzone abutting right side of mediastinum with broad base towards mediastinum and forming right angle with it. The lateral and inferior borders of the lesion arewelldefined;
(II) Themass shows evidence of coarse calcificationinferiorlywithsomeshowingmorphologyoftooth;
(III) Mildleftsidedpleuraleffusionseen;(IV) Calcifiedlymphnodeseeninleftaxilla;(V) Lungfieldsareclear.
Plain (Figure 2) and contrast CT (Figures 3,4) chest axial images mediastinal window
(I) CTconfirmsradiographicfindings;(II) Welldefinedroundedsofttissuedensitymassseenin
anterosuperiormediastinumwithcoarsecalcificationinitandfewareasofattenuationoffat;
(III) Thesofttissuecomponentshowsmildenhancementoncontrastscan;
(IV) Lesion is abutting left brachiocephalic veinwithmaintained fat planes.
Diagnosis
Mediastinal teratoma.
Differential diagnosis
• Thymoma(oftenoccurinthe4th to 5thdecadeof life,calcification isoften curvilinearor amorphous,no
intralesional fat seen).• Lymphoma (don’t show intra les ional fa t and
calcificationexceptinfewpost-treatmentcases).
Management
• USGoftestis.• Serumalphafetoprotein,beta-HCGlevels.• Complete surgical resection is curative inmature
teratoma, while immature teratomas require adjuvant chemotherapy.
Important points to remember
• Mediastinalteratomasarethecommonestextragonadalgermcelltumors(1,2).
• Thesecanbeeithermature teratomasor immatureteratomas based on their level of differentiation. Most arebenign,however,malignant transformationcanoccurineitherofthemwithadenocarcinomamostlyarising frommature teratoma and angiosarcomaor rhabdomyosarcoma complicating immature ones (1).
• Matureteratomasareusuallycystic,whereas,immatureareoftensolid(2).
• Invasionofgreatvessels,myocardium, lung,phrenicnervesuggestmalignancy(2).
• Differentials of lesions in anteriormediastinum:thymoma, teratoma, lymphoma, thyroid masses.
• Thymomahas associationwithmyasthenia gravis(33% of patients with thymoma have myasthenia and 15% of patients with myasthenia have thymoma), hypogammaglobulinemia,pureredcellaplasia,collagenvasculardisorders.
References
1. UenoT,TanakaYO,NagataM,TsunodaH,AnnoI,IshikawaS,KawaiK,ItaiY.Spectrumofgermcelltumors:fromheadtotoe.Radiographics2004;24:387-404.
2. Rosado-de-ChristensonML,TempletonPA,MoranCA.FromthearchivesoftheAFIP.Mediastinalgermcelltumors:radiologicandpathologiccorrelation.Radiographics1992;12:1013-30.
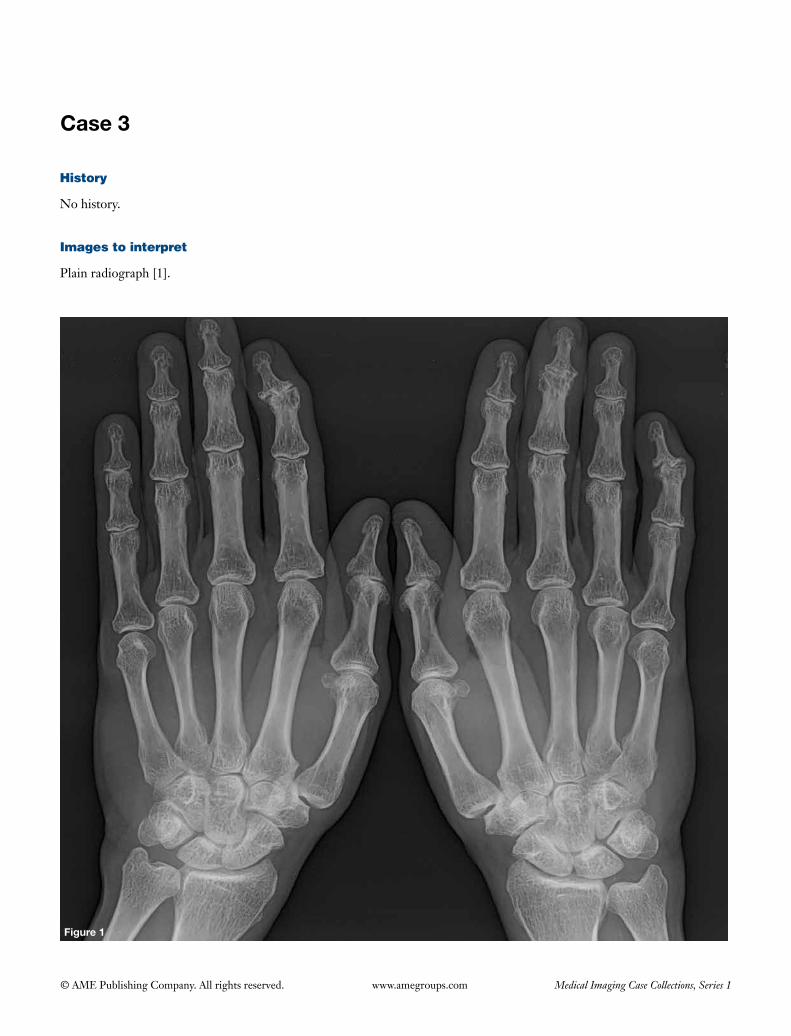
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 3
History
No history.
Images to interpret
Plain radiograph [1].
Figure 1
150
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph both hands frontal view (Figure 1)
(I) Asymmetric arthritis involving distal interphalangeal (DIP) joints of both hands (2nd and 3rd in left hand and 5th in right hand);
(II) Central erosions noted involving above mentioned joints giving ‘gull’s wing’ deformity;
(III) Joint space narrowing and marginal osteophystosis seen in above mentioned locations;
(IV) Rest of the bones and joints appear normal.
Diagnosis
Erosive osteoarthritis.
Differential diagnosis
• Psoriaticarthritis.• Rheumatoidarthritis.
Management
Referral to rheumatologist.
Important points to remember
• Erosiveosteoarthritis isa formofosteoarthritiswithadditionalinflammatorycomponent.
• Joint distribution (similar to osteoarthritis):DIPjoints > proximal interphalangeal (PIP) joints > first carpometacarpal (CPC) joint (1).
• Imagingfeaturesinclude:subchondralerosionscausing‘gull’s wing’ deformity involving two interphalangeal joints, diffuse cartilage space loss, joint ankyloses (1).
• Points thatdifferentiateerosiveosteoarthritis fromrheumatoidarthritis include:involvementofDIPsandtrapezio-metacarpal joint in the former with sparing of metacarpophalangeal joints (unlike latter), central erosions in contrast to marginal erosions in rheumatoid arthritis, absence of osteopenia and periarticular soft tissue swelling in the former (1).
References
1. MartelW,StuckKJ,DworinAM,HyllandRG.Erosiveosteoarthritisandpsoriaticarthritis:aradiologiccomparisoninthehand,wrist,andfoot.AJRAmJRoentgenol1980;134:125-35.
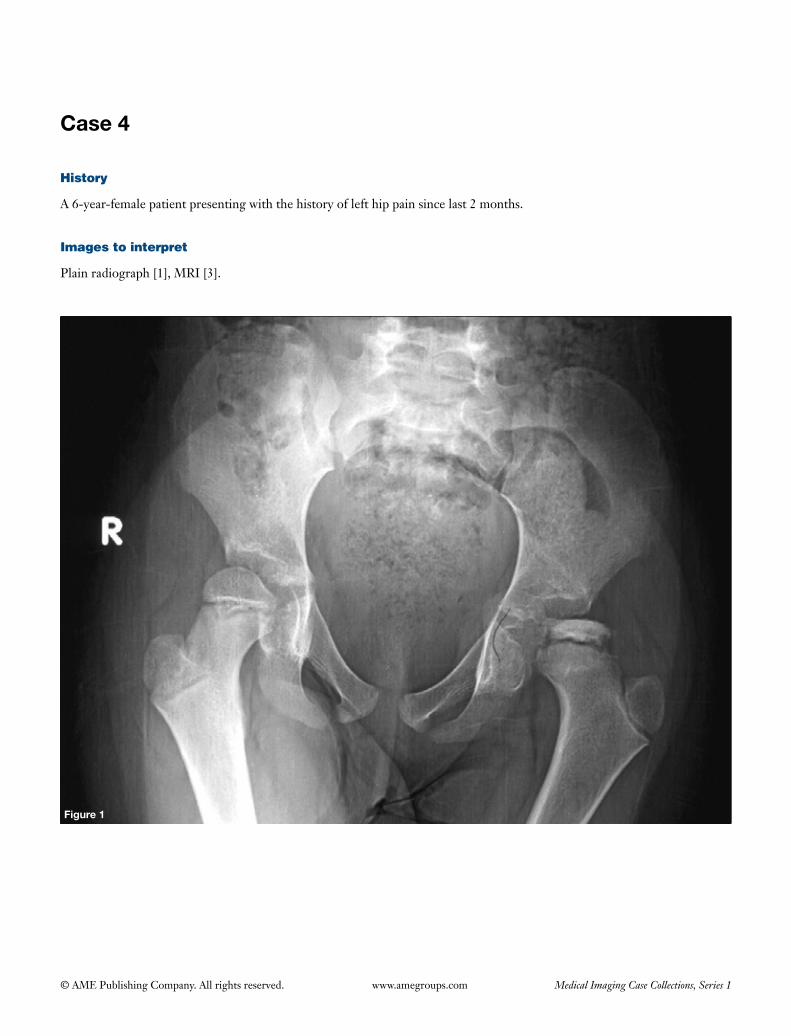
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 4
History
A 6-year-female patient presenting with the history of left hip pain since last 2 months.
Images to interpret
Plain radiograph [1], MRI [3].
Figure 1

152
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2
A B C
Figure 3
Figure 4

153
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph pelvis with bilateral hips frontal view (Figure 1)
(I) There is collapse and sclerosis of left proximal femoral epiphysis with mild irregularity of its contour. Mild radiolucency seen in the proximal metaphysis. Growth plate appears normal;
(II) Displacement of fat planes seen around left hip joint suggestive of effusion;
(III) Right hip joint appears normal.
MRI coronal STIR (Figure 2), axial T1 (Figure 3) and axial T2 fat sat (Figure 4) images
(I) MRIconfirmsradiographicfindings;(II) There is collapse of left proximal femoral epiphysis
with focal hypointense signal in the center of ossific nucleus on all the sequences;
(III) Marrow edema seen in the proximal metadiaphyseal region of left femur;
(IV) Mild effusion seen in the left hip joint;(V) Left acetabulum is normal;(VI) Right hip joint is normal.
Diagnosis
Legg-Calve-Perthes disease left side.
Differential diagnosis
Avascular necrosis due to other causes.
Management
• Orthopedicreferral.• Restwithminimalweight-bearingontheaffectedside.• Bracinginmildercasesorfemoralneckandacetabular
osteotomies in severe cases. The aim of the procedure is to correct femoro-acetabular malalignment.
Important points to remember
• Perthesdisease is idiopathicavascularnecrosisof theproximal femoral epiphysis that usually affects children between2and14yearsofagewithapeakaround5years.
• Itisimportanttolookforthecontralateralfemoralhead
as bilateral involvement is seen in 10-20% of the cases (1).• Radiographicfeaturesinclude:smallsizeandsclerosisof
the femoral head with widening of the medial joint space and radiolucency in the metaphysis in the early phase and fragmentation and subchondral lucency (crescent sign)inthelatephaseonplainradiographwithflatteningand deformity in the advanced burnt out stage (1).
• MRIhasanadvantageoverplainradiographasithelpsnot only in the early diagnosis and ruling out involvement of the contralateral side, but also helps in determining the extent of involvement of femoral head (determines prognosis) and assessing joint congruency in various joint positions, thus helping in guiding management (1,2).
• Othercausesof avascularnecrosis in children like:steroids use, sickle cell disease,Gaucher’s diseaseandleukaemiashouldbeexcludedbeforemakingthediagnosis of Perthes disease (1).
• Imagingfeaturesofsicklecelldiseaseinclude:multiplebone infarcts mainly involving humeral and femoral heads & vertebra [causing H shaped or Lincoln log vertebra due to microvascular endplate infarctions (Figures 5,6)], marrow hyperplasia, osteomyelitis, calcifiedshrunkenspleen,gallstonesandrenalpapillarynecrosis.
Figure 5
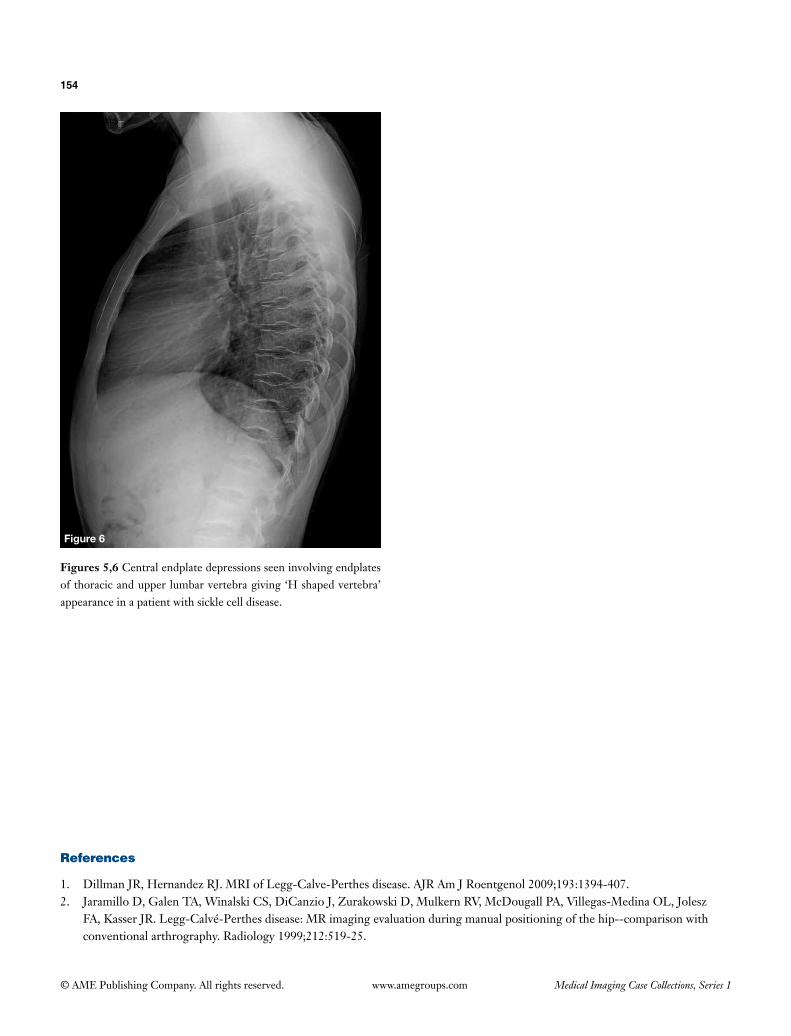
154
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figures 5,6 Central endplate depressions seen involving endplates ofthoracicandupperlumbarvertebragiving‘Hshapedvertebra’appearanceinapatientwithsicklecelldisease.
Figure 6
References
1. DillmanJR,HernandezRJ.MRIofLegg-Calve-Perthesdisease.AJRAmJRoentgenol2009;193:1394-407.2. JaramilloD,GalenTA,WinalskiCS,DiCanzioJ,ZurakowskiD,MulkernRV,McDougallPA,Villegas-MedinaOL,Jolesz
FA,KasserJR.Legg-Calvé-Perthesdisease:MRimagingevaluationduringmanualpositioningofthehip--comparisonwithconventionalarthrography.Radiology1999;212:519-25.
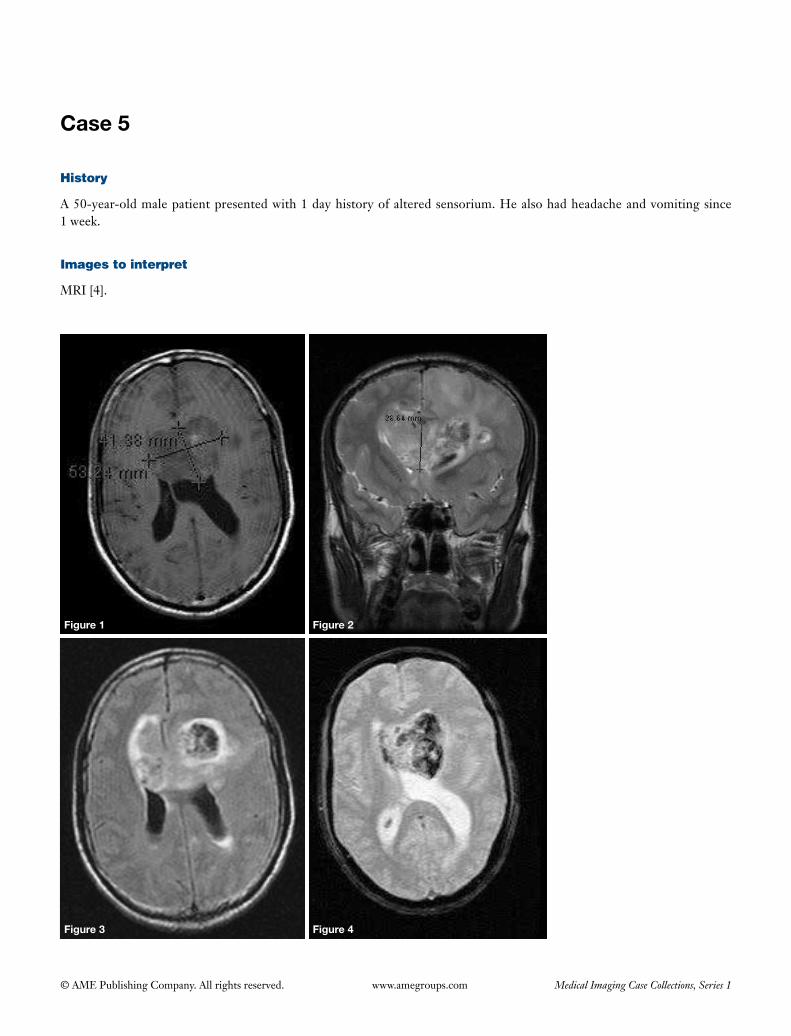
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 5
Figure 1 Figure 2
Figure 3 Figure 4
History
A 50-year-old male patient presented with 1 day history of altered sensorium. He also had headache and vomiting since 1 week.
Images to interpret
MRI [4].
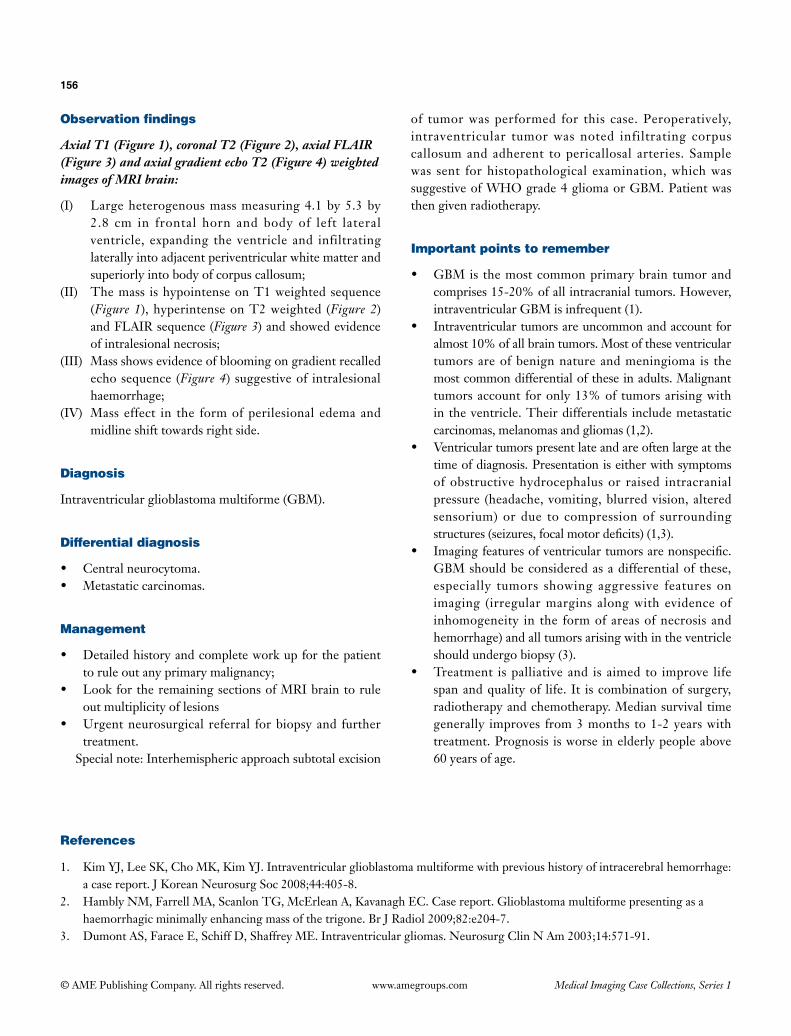
156
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Axial T1 (Figure 1), coronal T2 (Figure 2), axial FLAIR (Figure 3) and axial gradient echo T2 (Figure 4) weighted images of MRI brain:
(I) Large heterogenous mass measuring 4.1 by 5.3 by 2.8 cm in frontal horn and body of left lateral ventricle, expanding the ventricle and infiltrating laterally into adjacent periventricular white matter and superiorly into body of corpus callosum;
(II) The mass is hypointense on T1 weighted sequence (Figure 1), hyperintense on T2 weighted (Figure 2) and FLAIR sequence (Figure 3) and showed evidence of intralesional necrosis;
(III) Mass shows evidence of blooming on gradient recalled echo sequence (Figure 4) suggestive of intralesional haemorrhage;
(IV) Mass effect in the form of perilesional edema and midline shift towards right side.
Diagnosis
Intraventricular glioblastoma multiforme (GBM).
Differential diagnosis
• Centralneurocytoma.• Metastaticcarcinomas.
Management
• Detailedhistoryandcompleteworkupforthepatientto rule out any primary malignancy;
• LookfortheremainingsectionsofMRIbraintoruleout multiplicity of lesions
• Urgentneurosurgical referral forbiopsyand furthertreatment.
Special note: Interhemispheric approach subtotal excision
of tumor was performed for this case. Peroperatively, intraventricular tumor was noted infiltrating corpus callosum and adherent to pericallosal arteries. Sample was sent for histopathological examination, which was suggestive of WHO grade 4 glioma or GBM. Patient was then given radiotherapy.
Important points to remember
• GBMis themostcommonprimarybraintumorandcomprises 15-20% of all intracranial tumors. However, intraventricular GBM is infrequent (1).
• Intraventriculartumorsareuncommonandaccountforalmost 10% of all brain tumors. Most of these ventricular tumors are of benign nature and meningioma is the most common differential of these in adults. Malignant tumors account for only 13% of tumors arising with in the ventricle. Their differentials include metastatic carcinomas, melanomas and gliomas (1,2).
• Ventriculartumorspresentlateandareoftenlargeatthetime of diagnosis. Presentation is either with symptoms of obstructive hydrocephalus or raised intracranial pressure (headache, vomiting, blurred vision, altered sensorium) or due to compression of surrounding structures(seizures,focalmotordeficits)(1,3).
• Imagingfeaturesofventriculartumorsarenonspecific.GBM should be considered as a differential of these, especially tumors showing aggressive features on imaging (irregular margins along with evidence of inhomogeneity in the form of areas of necrosis and hemorrhage) and all tumors arising with in the ventricle should undergo biopsy (3).
• Treatment ispalliativeand is aimed to improve lifespan and quality of life. It is combination of surgery, radiotherapy and chemotherapy. Median survival time generally improves from 3 months to 1-2 years with treatment. Prognosis is worse in elderly people above 60 years of age.
References
1. KimYJ,LeeSK,ChoMK,KimYJ.Intraventricularglioblastomamultiformewithprevioushistoryofintracerebralhemorrhage:a case report. J Korean Neurosurg Soc 2008;44:405-8.
2. HamblyNM,FarrellMA,ScanlonTG,McErleanA,KavanaghEC.Casereport.Glioblastomamultiformepresentingasahaemorrhagic minimally enhancing mass of the trigone. Br J Radiol 2009;82:e204-7.
3. DumontAS,FaraceE,SchiffD,ShaffreyME.Intraventriculargliomas.NeurosurgClinNAm2003;14:571-91.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Case 6
Figure 1
History
A 52-year-old female patient presented with complaints of lump abdomen since last 6 months.
Images to interpret
Plain radiograph [1], CT [3].
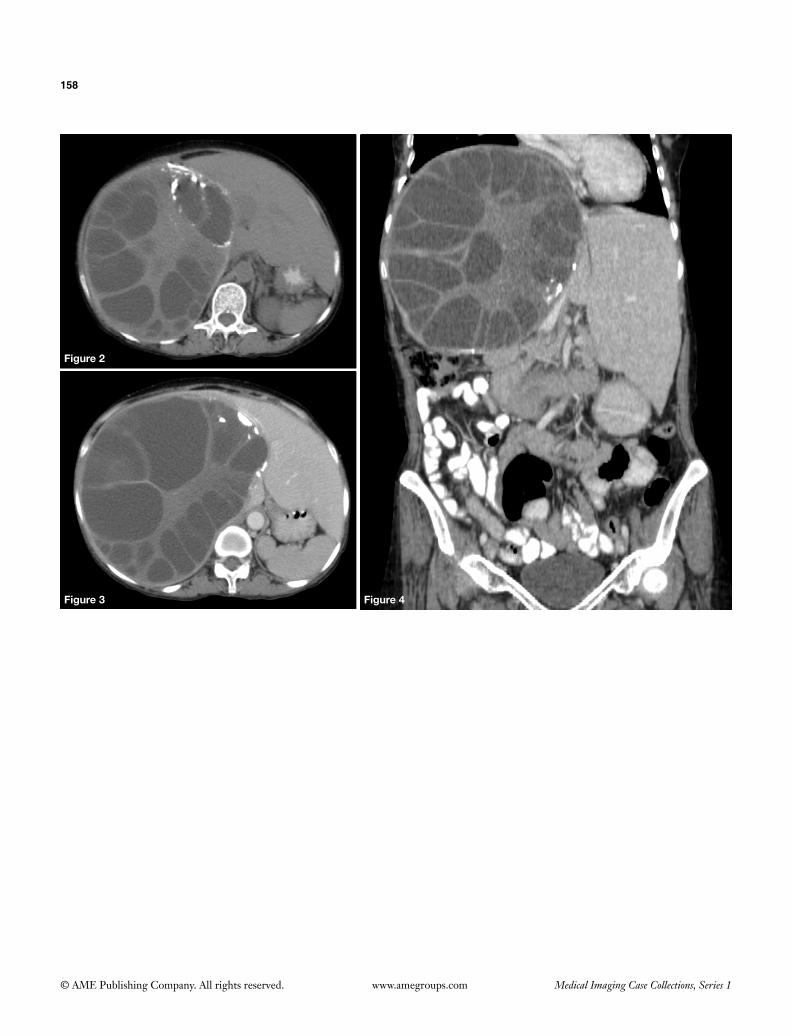
158
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Figure 2
Figure 3 Figure 4
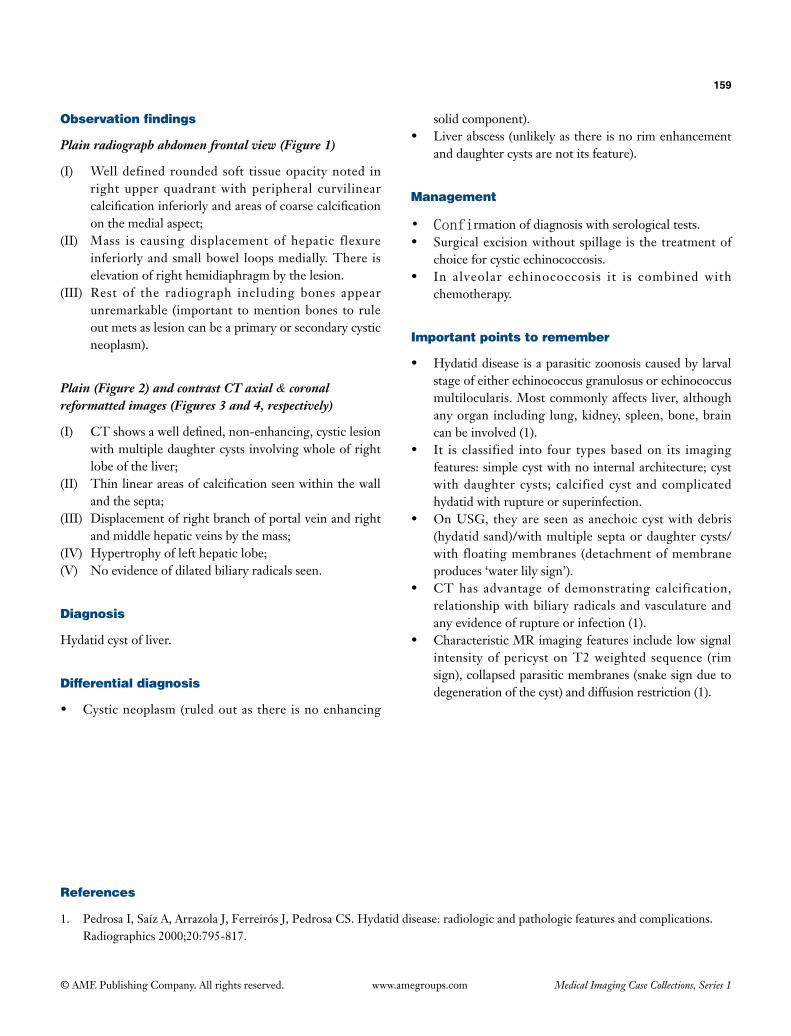
159
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Observation findings
Plain radiograph abdomen frontal view (Figure 1)
(I) Well defined rounded soft tissue opacity noted in right upper quadrant with peripheral curvilinear calcification inferiorly and areas of coarse calcification on the medial aspect;
(II) Mass is causing displacement of hepatic flexure inferiorly and small bowel loops medially. There is elevation of right hemidiaphragm by the lesion.
(III) Rest of the radiograph including bones appear unremarkable (important to mention bones to rule out mets as lesion can be a primary or secondary cystic neoplasm).
Plain (Figure 2) and contrast CT axial & coronal reformatted images (Figures 3 and 4, respectively)
(I) CT shows a well defined, non-enhancing, cystic lesion with multiple daughter cysts involving whole of right lobe of the liver;
(II) Thin linear areas of calcification seen within the wall and the septa;
(III) Displacement of right branch of portal vein and right and middle hepatic veins by the mass;
(IV) Hypertrophy of left hepatic lobe;(V) No evidence of dilated biliary radicals seen.
Diagnosis
Hydatid cyst of liver.
Differential diagnosis
• Cystic neoplasm (ruled out as there is no enhancing
solid component).• Liver abscess (unlikely as there is no rim enhancement
and daughter cysts are not its feature).
Management
• Confirmation of diagnosis with serological tests.• Surgical excision without spillage is the treatment of
choice for cystic echinococcosis.• In alveolar echinococcosis it is combined with
chemotherapy.
Important points to remember
• Hydatid disease is a parasitic zoonosis caused by larval stage of either echinococcus granulosus or echinococcus multilocularis. Most commonly affects liver, although any organ including lung, kidney, spleen, bone, brain can be involved (1).
• It is classified into four types based on its imaging features: simple cyst with no internal architecture; cyst with daughter cysts; calcified cyst and complicated hydatid with rupture or superinfection.
• On USG, they are seen as anechoic cyst with debris (hydatid sand)/with multiple septa or daughter cysts/with floating membranes (detachment of membrane produces ‘water lily sign’).
• CT has advantage of demonstrating calcification, relationship with biliary radicals and vasculature and any evidence of rupture or infection (1).
• Characteristic MR imaging features include low signal intensity of pericyst on T2 weighted sequence (rim sign), collapsed parasitic membranes (snake sign due to degeneration of the cyst) and diffusion restriction (1).
References
1. Pedrosa I, Saíz A, Arrazola J, Ferreirós J, Pedrosa CS. Hydatid disease: radiologic and pathologic features and complications. Radiographics 2000;20:795-817.

Section 3—Rapid reporting

v
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
How to prepare for rapid reporting
Important points
• Theonlykeytoscorewell inrapidreportingistopractice.It increaseslevelofconfidencetopickabnormalitiesandmakesyoufinishthetestin25minutes,givingsomeextratimeforthedoubtfulcases.Alwayspracticewithyourwatch.
• Prepareyourownchecklist foreachanatomicalregionandfollowthesamemethodicalapproachwhilereportingallcaseseverytime.
• Don’tforgettoseecorticesofallthevisualizedbones.• Rememberabnormalitiesareneversubtleandsodon’tovercallnormalfilms.• Youwillbegiven30cases,whicharetobefinishedin35minutes.Theyareamixtureofnormalandabnormalcaseswith
abnormalcasesusuallyrangingfrom13to19.• Anatomicalvariants likecervicalribs,accessoryossicles,segmentationabnormalities,spinabifidaetc.areconsidered
normalinrapidreporting.Degenerativechangesarealsonormal.
Here is the checklist which I have prepared. You can make your own.
Skull
• Fractures.• Sphenoidsinusfluidlevel.• Pneumocranium.• Lyticorsclerotic lesions (as inmultiplemyelomaor
pepperpotskullinhyperparathyroidism).• Pagetsdiseaseorfibrousdysplasia.• Enlargedsella.• Cervical spine fractures including atlantoaxial
dislocation.• Mandibularfracturesandlyticlesions.
Face
• Blowoutfracturesoftheorbit(teardropsign).• Eyebrowsign(orbitalemphysema).• Maxillafracturesandmaxillarysinusairfluidlevels.• Tripodfracturesandzygomaticarchfractures(lookfor
theelephanttrunk).• TracethethreeMcGrigor’slines.• Mandibularfractures.• Temporomandibularjointdislocation.
Cervical spine
• Skullfractures.• Sphenoidsinusfluidlevel.• Enlargedsella.
• Atlantoaxialdislocation.• Fracturesinallthreecolumnsofvertebra.• Subluxationsincludinglockedandperchedfacets(look
foralignment).• Destructionandscleroticlesionsofvertebrainallthree
columns.• Prevertebralsofttissuewidening.• Lunglesionsinvolvingapex.• Pneumothorax.• Clavicleandlesionsofupperribs.• Esophagealforeignbody.
Thoracic spine
• Fractures(checkallthreecolumns).• Destructionorerosionofvertebra.• Scleroticlesionsinvolvingvertebra.• Paraspinalsofttissueorhematoma.• Absentpedicle.• Pathologiesinthelung.
Lumbosacral spine
• Pathologyinthelungbases.• Fractures.• Lyticandscleroticlesionsincludingabsentpedicle.• Parsdefect.• Spondylolisthesis.• Widenedpsoas.• Abdominalaorticaneurysm.• Sacroileitis.
vi
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
• Sacralmassesandsacralinsufficiencyfractures.• Pelvicbonespathology.
Chest
• Checksitus(checkmarkeralso).• Lookformalpositionedlinesandtubes.• Pneumothorax(checkapicesandlookfordeepsulcus
sign).• Pneumomediastinum(continousdiaphragmsign).• Pneumoperitoneum.• Thyroidmass.• Tracheaandparatrachealstripe.• Hilarandmediastinalnodesandmasses.• Silhouettesign.• Pulmonarynodules inall theareas includinghidden
areas (apices, retrocardiac region,hila,beneath thediaphragm).
• Lobarcollapse (checkpositionofhila,diaphragm&trachea).
• Checkallbones for fracturesand lyticandscleroticlesions:(I) Clavicles;(II) Scapula;(III)Humerus;(IV)Shoulderdislocation;(V) Ribs;(VI)Spine.
• Paraspinalmass.
Abdomen
• Pathologyinlungbases.• Pneumoperitoneum(airunderthediaphragm,Rigler’s
sign, rightupperquadrant lucency,visible falciformligament,footballsign).
• Pneumoretroperitoneum(sharpoutliningofkidneysandpsoas).
• Airatotherabnormalsites (pneumatosis intestinalis,portalvenousgas,pneumobilia-ruleoutgallstoneileus).
• Calcifiedaneurysm.• Otherabnormalcalcifications(gallstones,renalcalculi,
appendicolith,chroniccalcificpancreatitis).• Widenedpsoas.• Bowelobstruction.• Inguinalhernia/diaphragmatichernia.• Bones: fractures anddeposits in lower ribs, spine,
sacrumandpelvis.
Pelvis
• Sacroiliacjointsforwideningandsacroileitis.• Pubicdiastasis.• Sacralinsufficiencyfractures.• Subtlepubicramifractures/looserszones.• Avulsion fractures (anterior superior and anterior
inferioriliacsupine,pubicsymphysis,ischialtuberosity,greater&lessertrochanters).
• Pelvicdeposits.• Avascularnecrosisoffemurhead.• Hipdislocation.• Developmentaldysplasiaofhip/Perthesdisease/slipped
capitalfemoralepiphysisinchildren.
Shoulder
• Shoulderdislocation(anterior/posterior/inferior).• Acromioclavicularjointsubluxation/dislocation.• Coracoclaviculardisruption(>1.3cm).• Fracturesofhumerus(humeralhead,greatertuberosity,
humeralneck,shaft).• Ribfractures.• Pneumothorax.• Lunglesions.• Depositsinallbones.
Elbow
• Posteriorfatpadsign.• Supracondylar fractureofhumerus (lookforanterior
humeralline).• Radialhead fractureandradialdislocation (look for
radio-capitellarline).• Fracture ulna with proximal radio-ulnar joint
dislocation(Monteggiafracturedislocation).• Fractureolecranon.• Fracturecoronoidprocessofulna.• Fracturelateralepicondyle.• Avulsionofmedialepicondyle(rememberCRITOE).
Wrist
• Distalradiusfracture(lookfordorsalsmoothsurfaceandradialangleonlateralradiograph).
• Torus/greenstickfracturesinchildren.• Distalradio-ulnardislocation(lookforassociatedradial
fractureasinGalleazifracturedislocation).
vii
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
• Carpalbone fractures (scaphoid-seeonall scaphoidviews,triquetral-lateralview,hamate-obliqueview).
• Scapholunatedissociation(Terry-Thomassign).• Lunate/perilunatedislocations.• Dislocationofbaseof4thand5thmetacarpals.• Erosions.
Hand
• Lookforallthepointsgiveninwrist.• Enchondroma.• Acroosteolysis.• Erosions and lytic lesions (brown tumors,metsof
carcinomalung).• Subtlespiralmetacarpalfractures.• Interphalangealjointdislocation.• Traceeachcortexforfractures.
Knee
• Osteochondraldefect (oftenseenon lateralaspectofmedialfemoralcondyle).
• Lipohaemarthrosis(fatfluidlevel).• Patellarfracturesanddislocation.• Tibial fractures—tibial spine, tibialplateau,Segond
fracture (avulsion fractureon lateralaspectof tibialplateau).
Ankle
• Distalfibularfracture.• Osteochondraldefectontalardome.• Talusfracture(talardomeandtalarneck).• Baseof5thmetatarsal(seenonthelateralview).• Fractureofmedialmalleolus (also look forproximal
fibularfracture—Maisonneuvefracture).• Disruption of anklemortice (widening ofmedial
tibiotalarjoint).• Salter-Harrisfracturesindistaltibiainchildren.• Toddler’sfracture.• Hypertrophicosteoarthropathy.• Focallesions:Brodie’sabscessandmets.• Tarsaldislocation.• Calcaneumfracture(Bohler’sangle,scleroticorlucent
lines).
Foot
• Lookforanklefractures.• Lisfrancfracturedislocation.• Fractures of second and thirdmetatarsals (march
fracture).• Fracturebaseoffifthmetatarsal.• Traceallthecorticesandlookforphalangealfractures.• Erosions.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 1
1.

161
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
2.

162
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
3. 4.
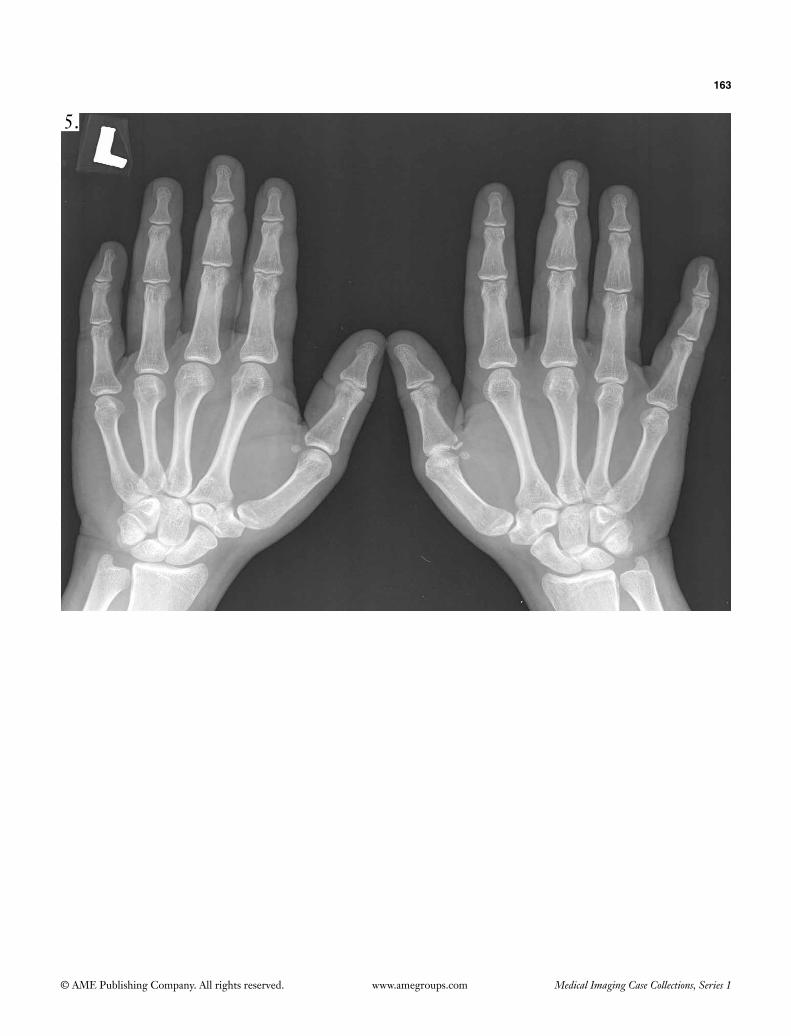
163
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
5.

164
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
6.
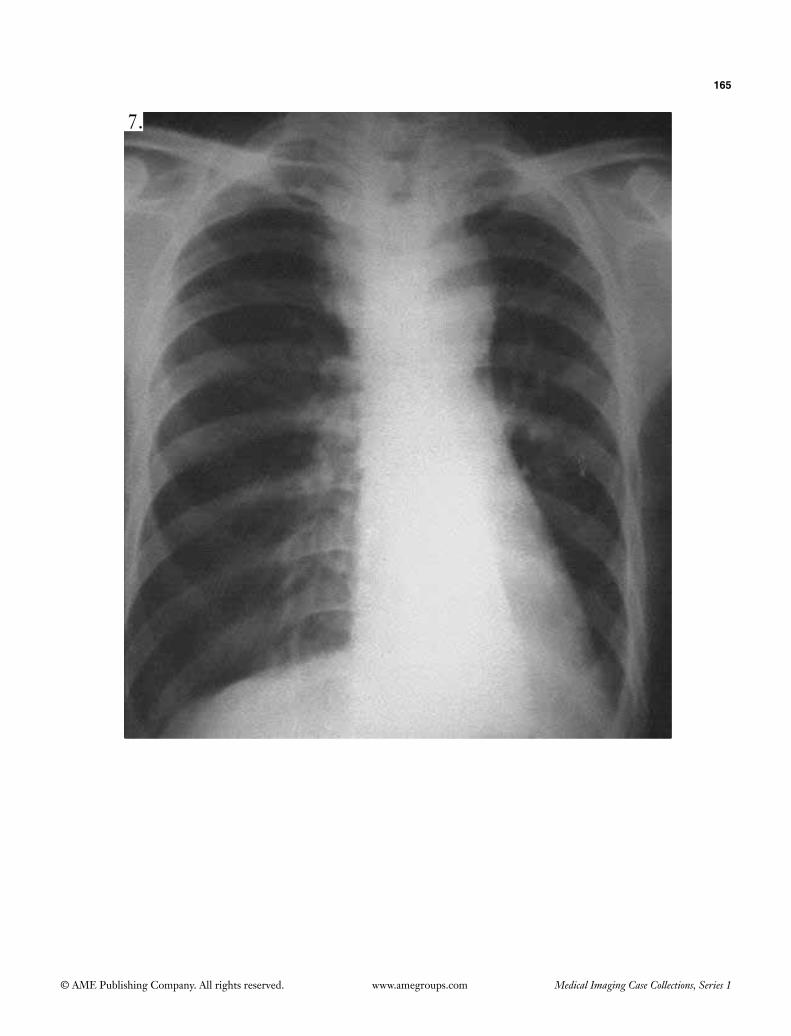
165
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
7.
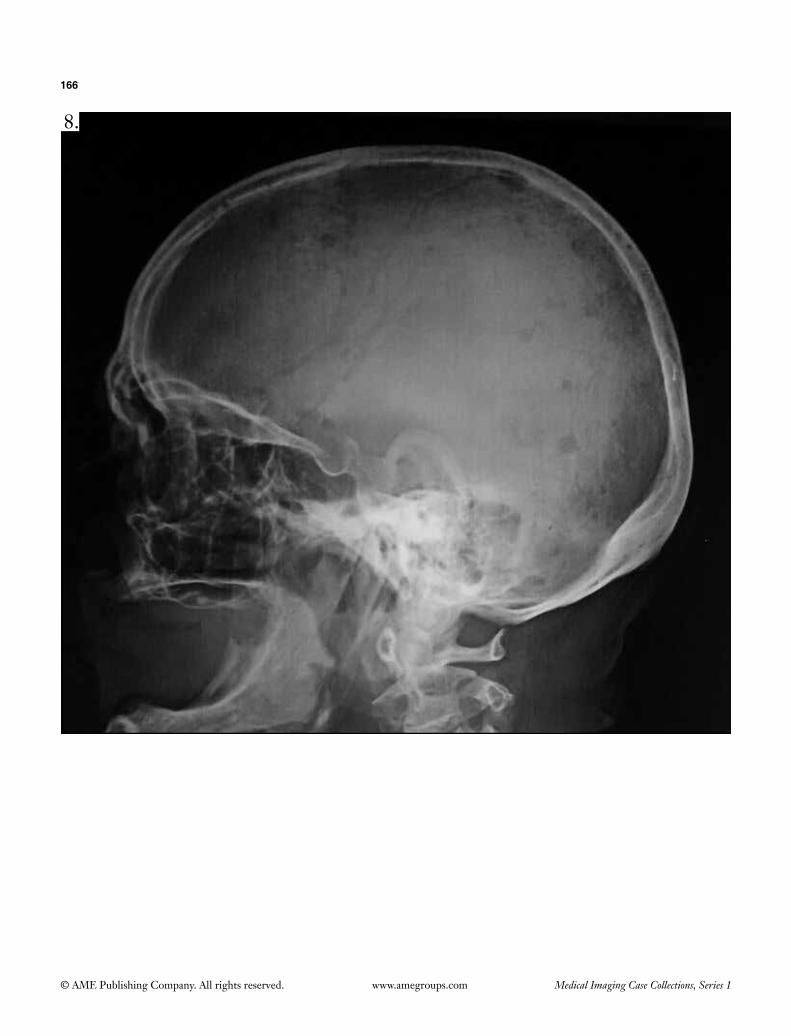
166
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
8.

167
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
9.

168
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
10.
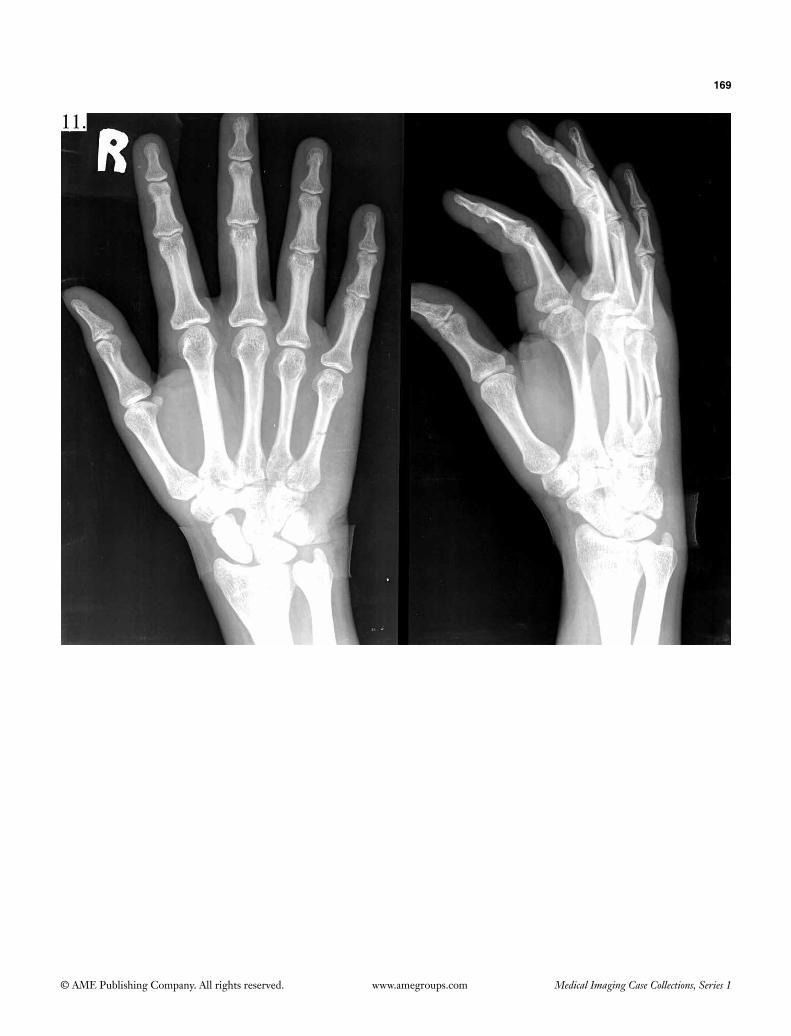
169
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
11.
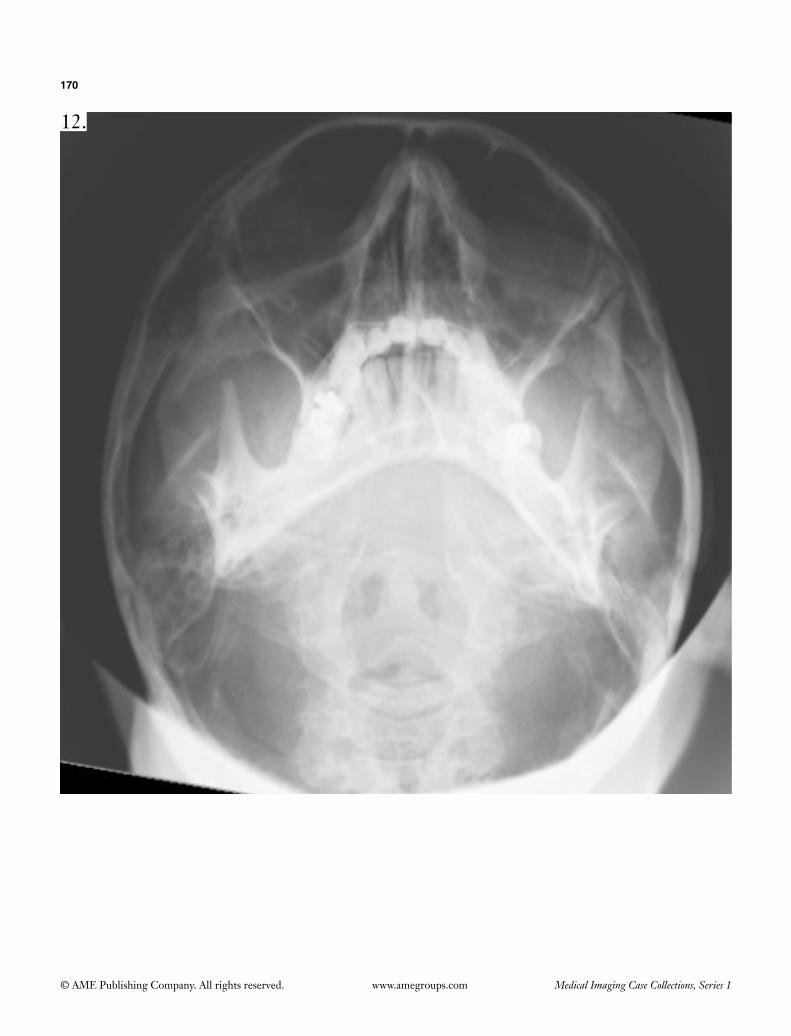
170
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
12.

171
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
13.
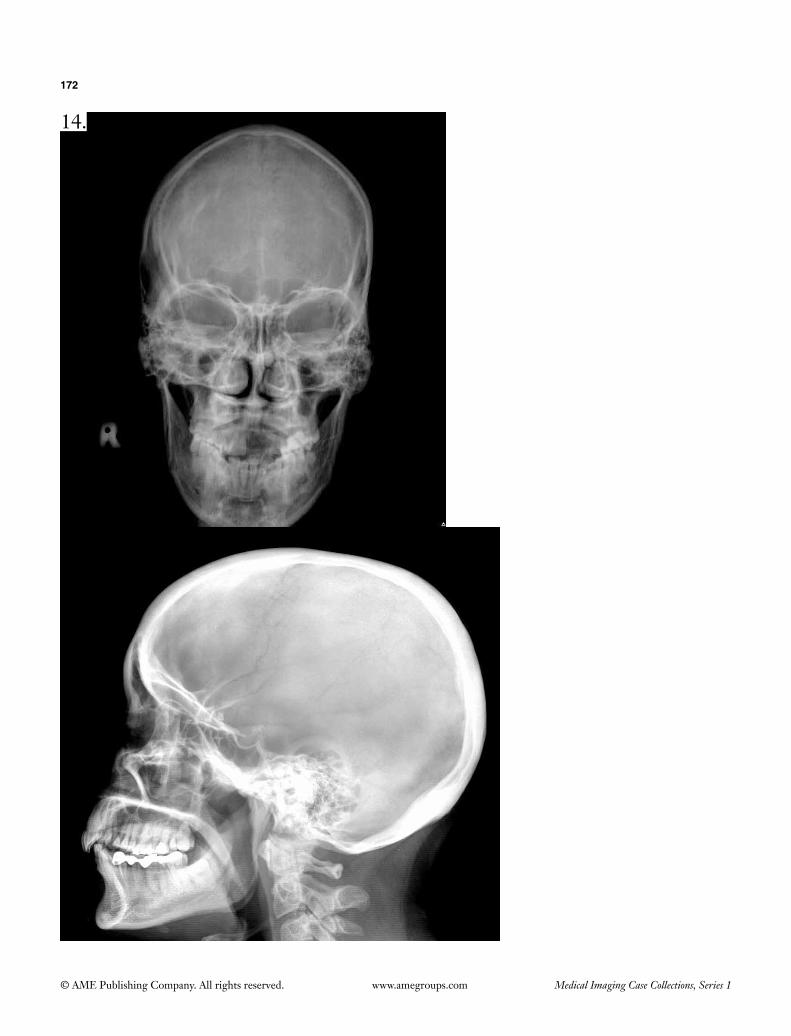
172
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
14.
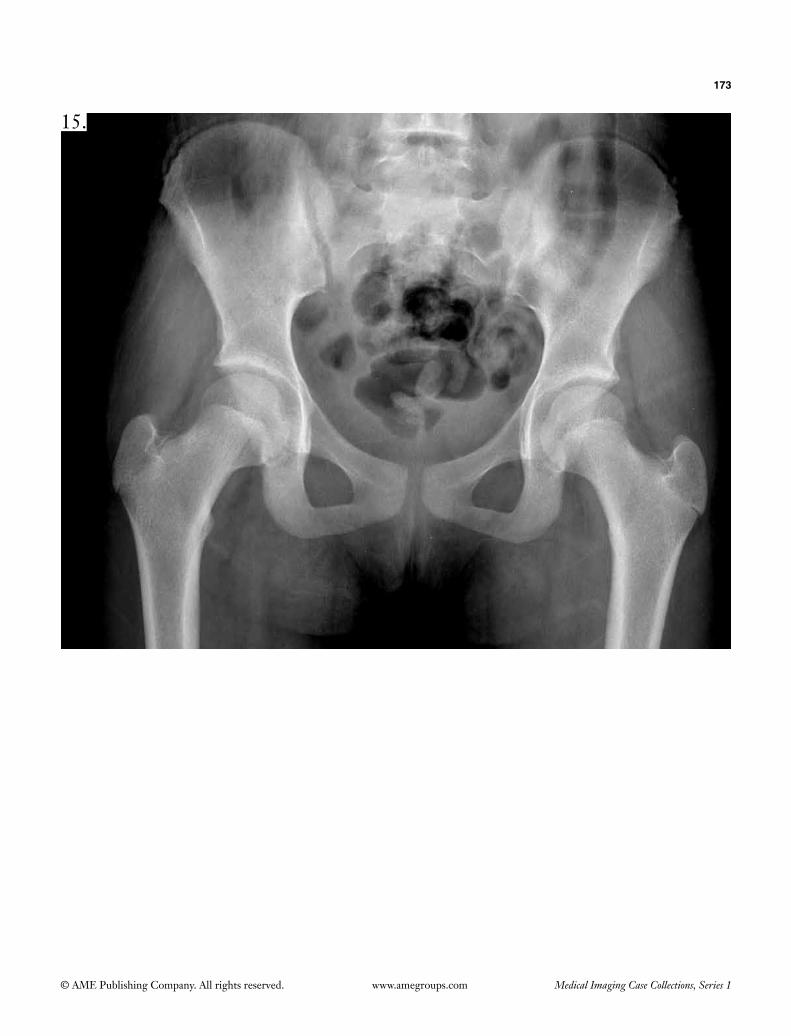
173
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
15.

174
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
16.

175
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
17.

176
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
18.

177
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
19.

178
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
20.

179
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
21.
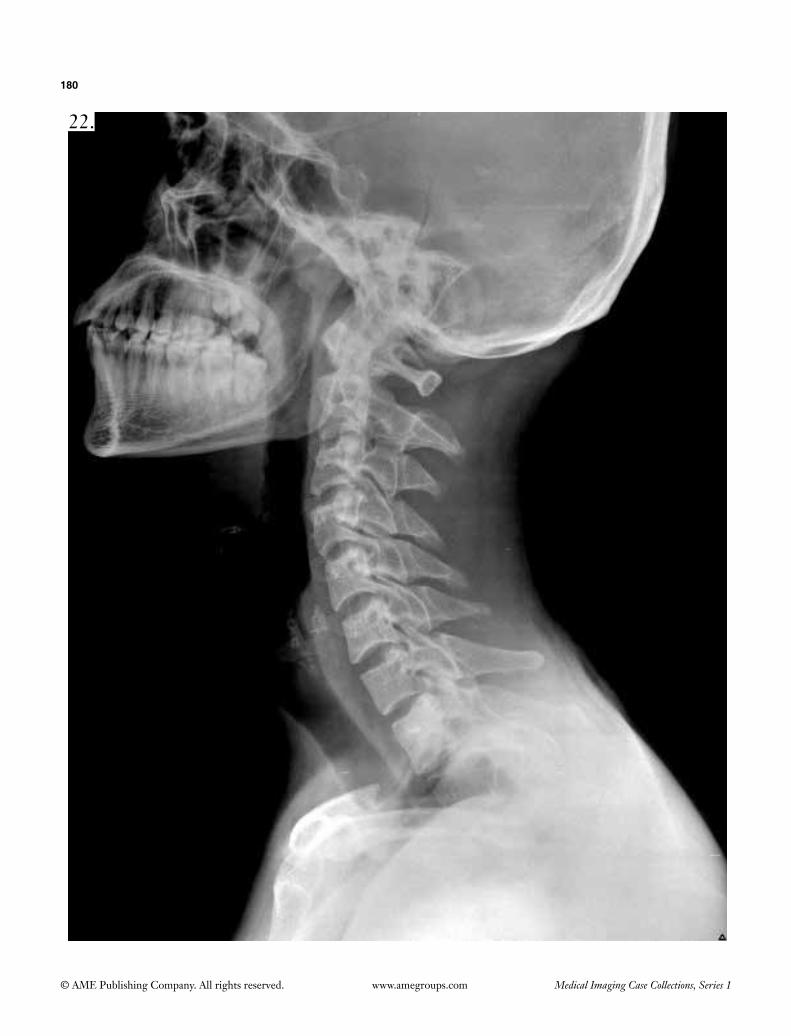
180
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
22.

181
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
23.
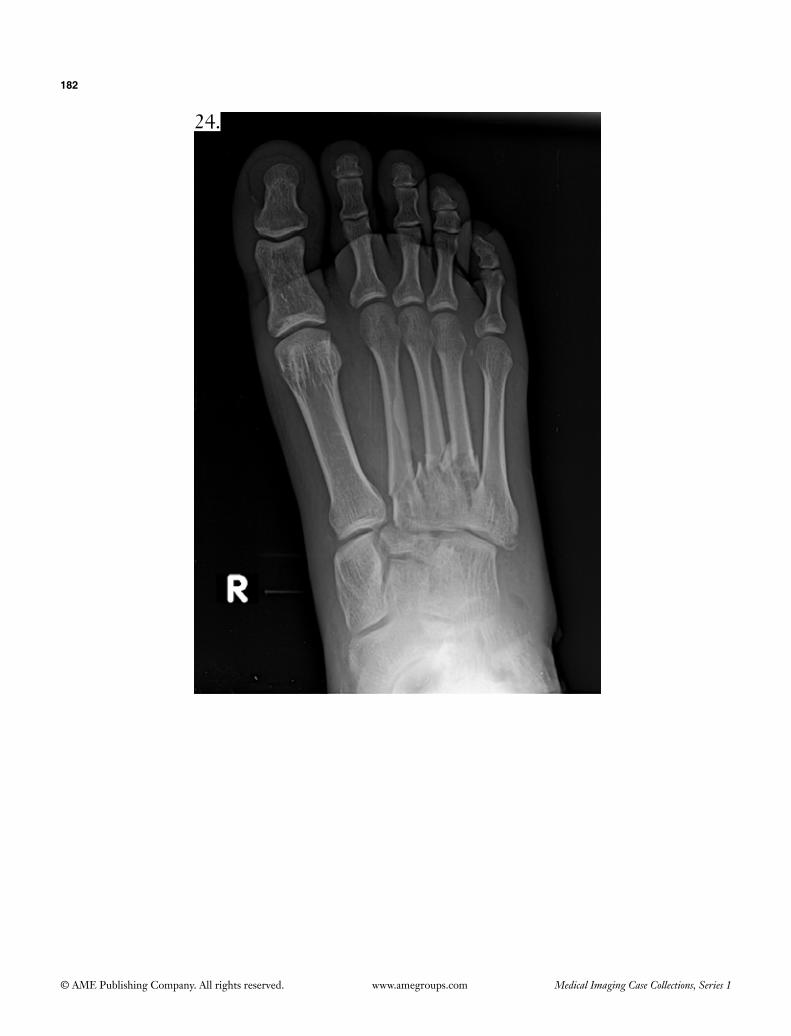
182
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
24.

183
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
25.
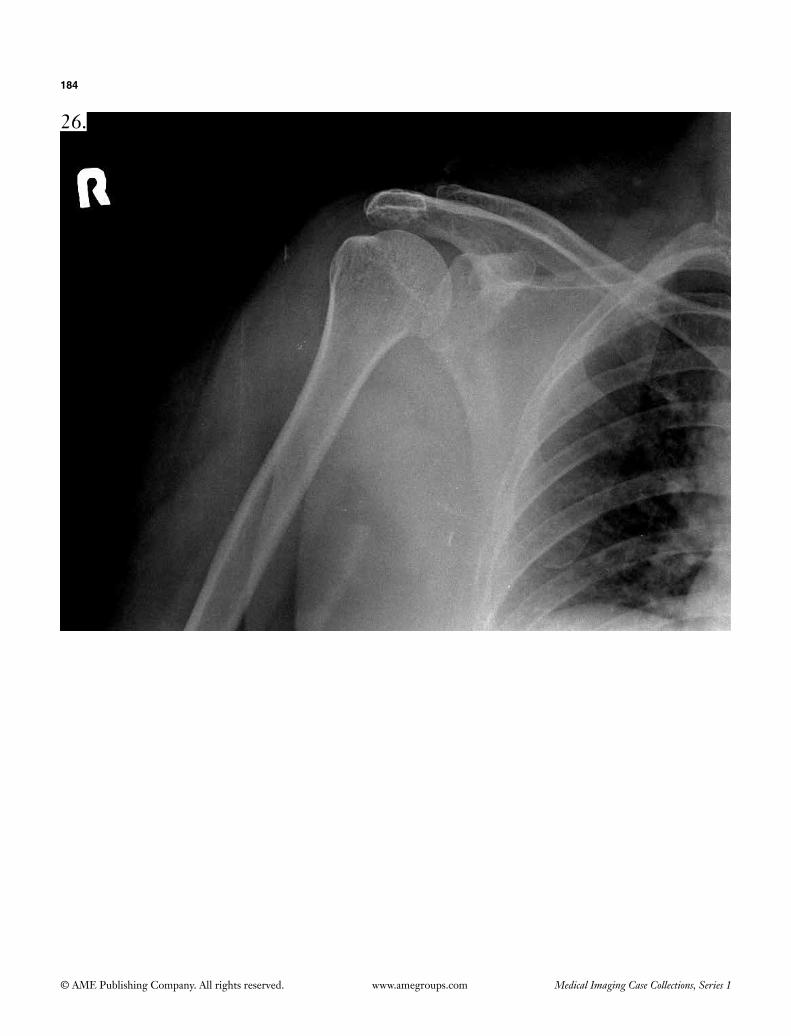
184
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
26.

185
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
27.

186
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
28.

187
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
29.

188
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
30.
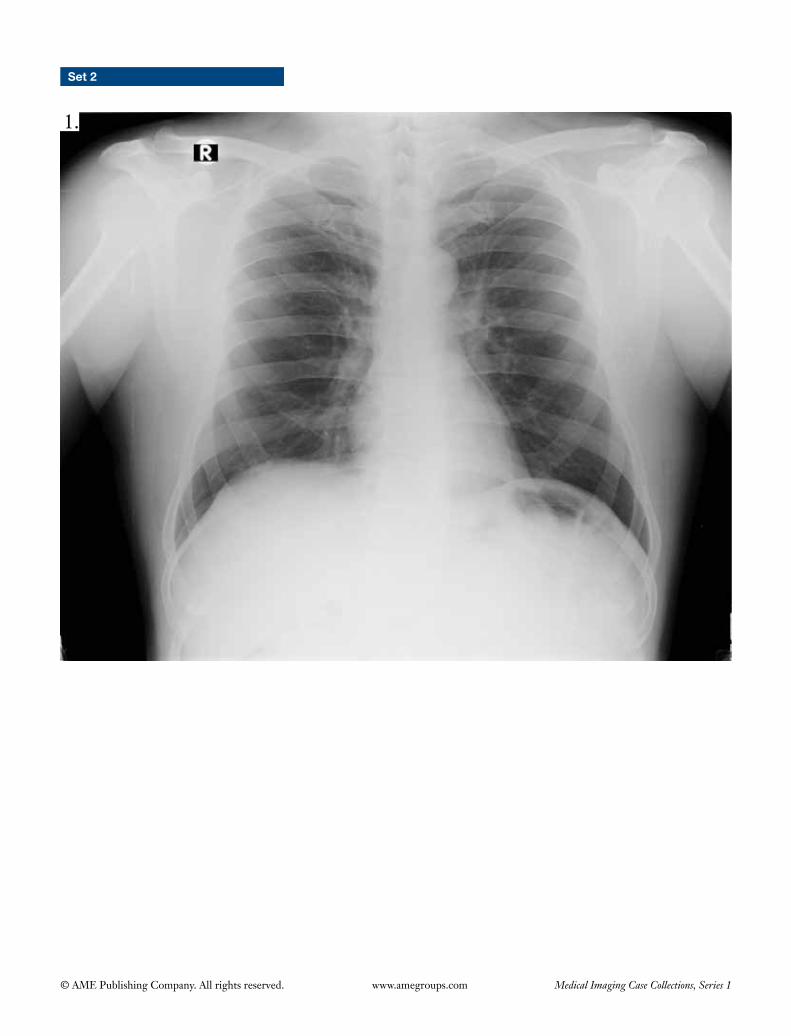
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 2
1.

190
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
2.

191
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
3.

192
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
4.

193
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
5.

194
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
6.

195
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
7.

196
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
8.

197
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
9.

198
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
10.

199
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
11.

200
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
12.

201
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
13.
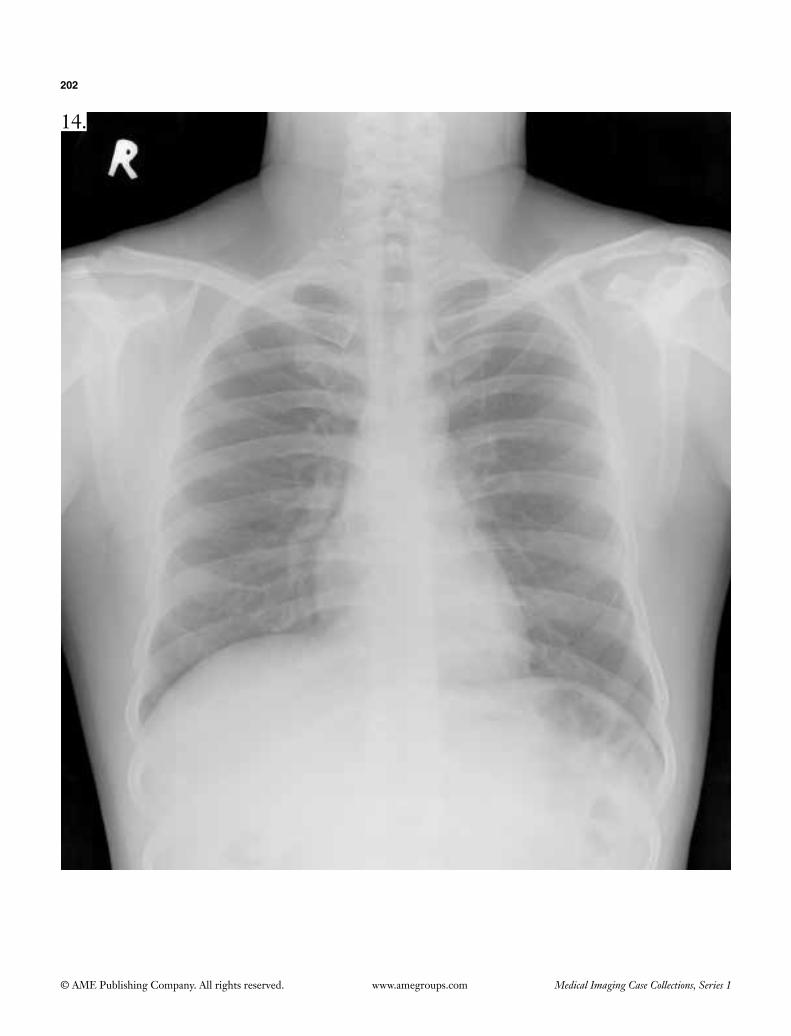
202
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
14.

203
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
15.

204
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
16.

205
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
17.

206
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
18.

207
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
19.

208
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
20.

209
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
21.

210
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
22.

211
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
23.

212
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
24.

213
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
25.

214
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
26.
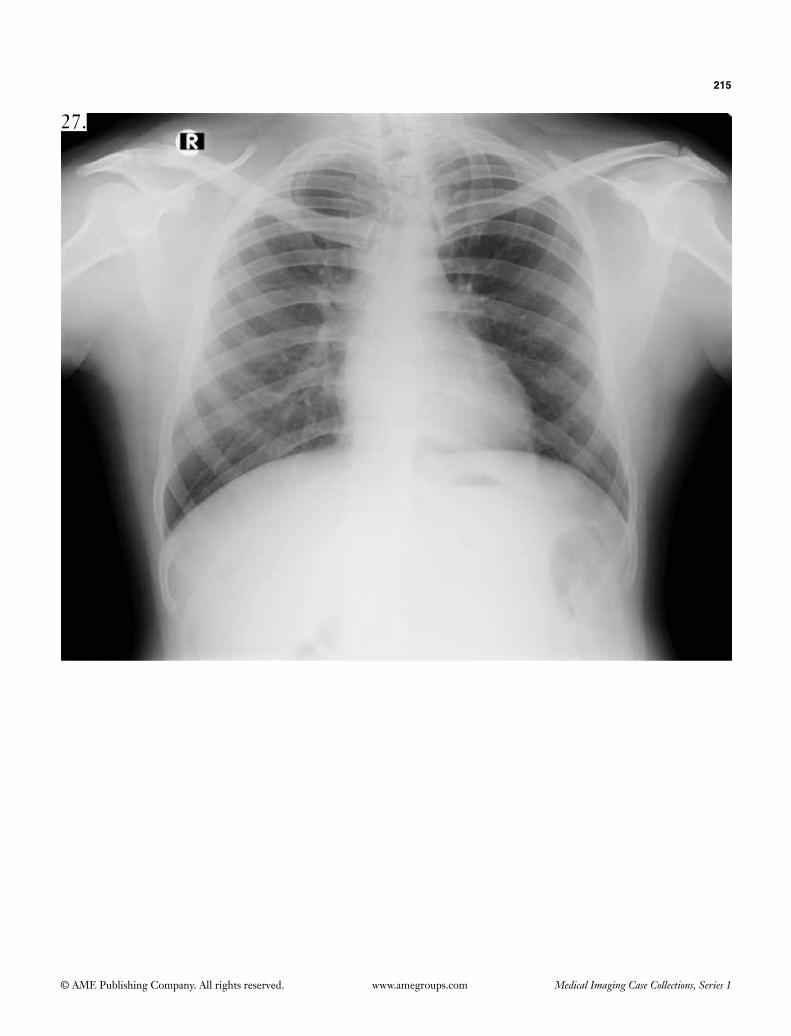
215
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
27.

216
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
28.

217
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
29.

218
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
30.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 3
1.
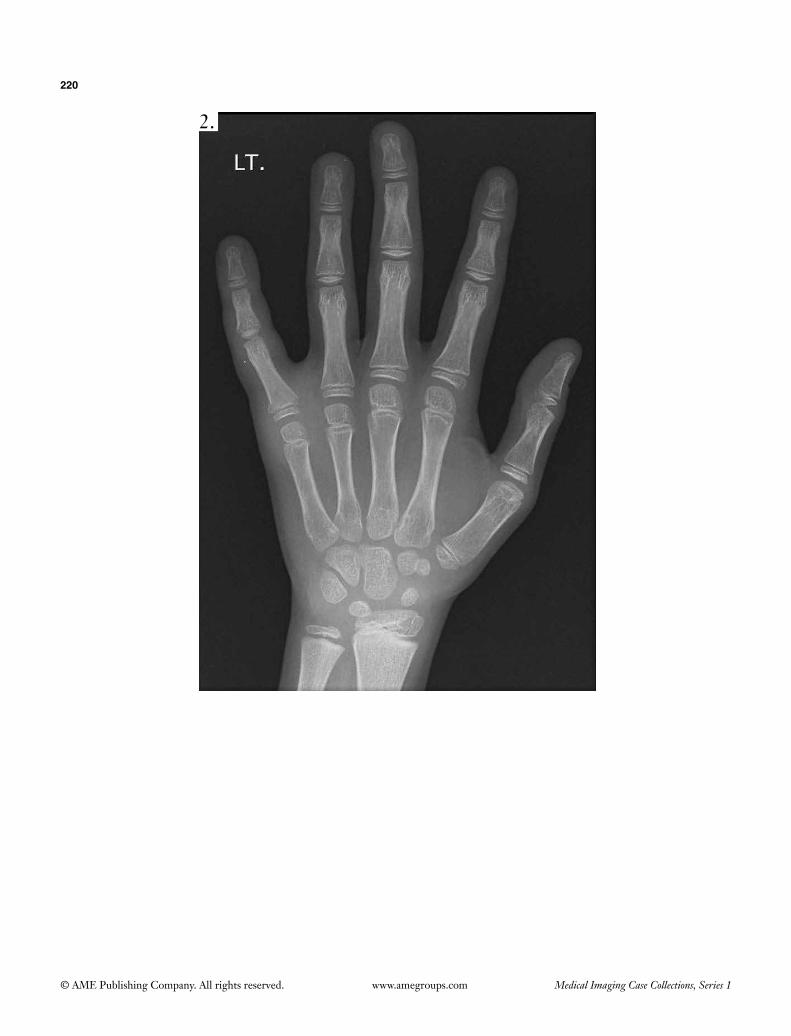
220
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
2.

221
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
3.
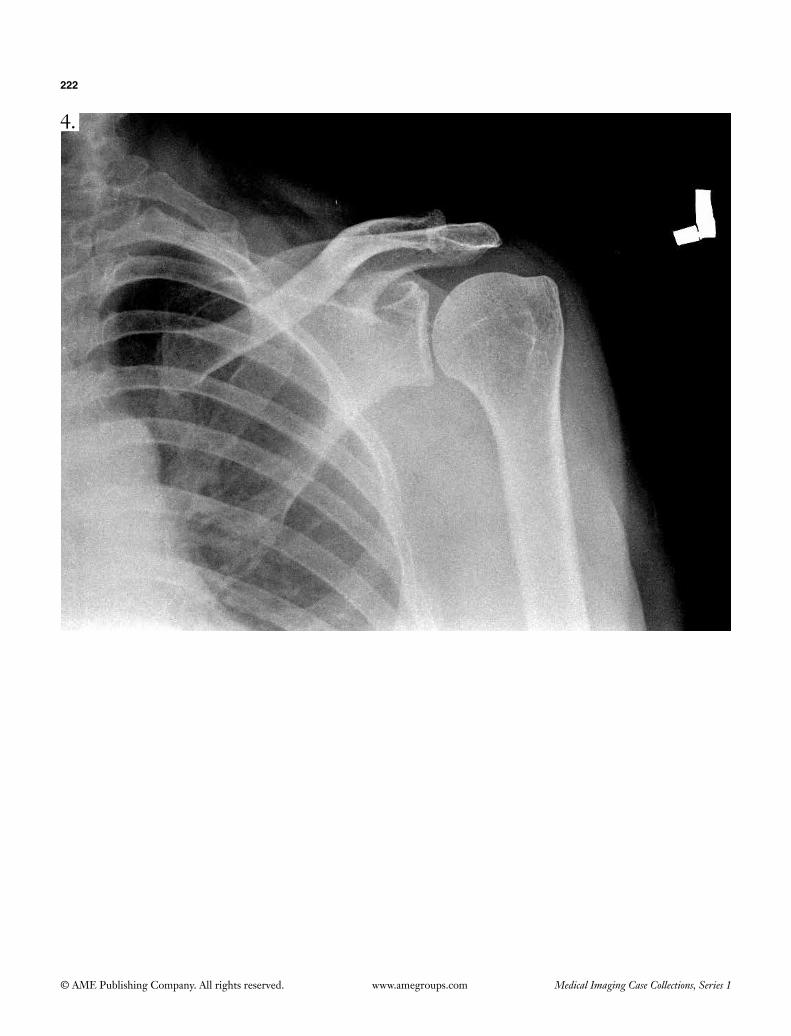
222
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
4.
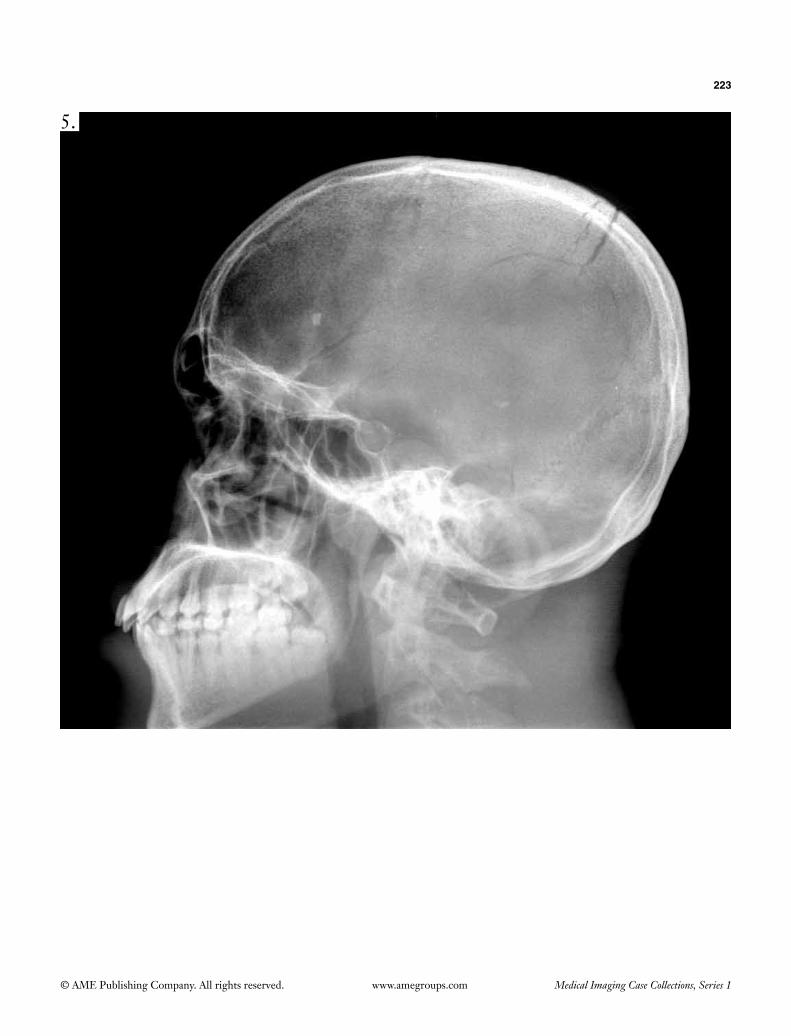
223
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
5.

224
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
6.

225
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
7.

226
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
8.

227
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
9.

228
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
10.

229
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
11.

230
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
12.
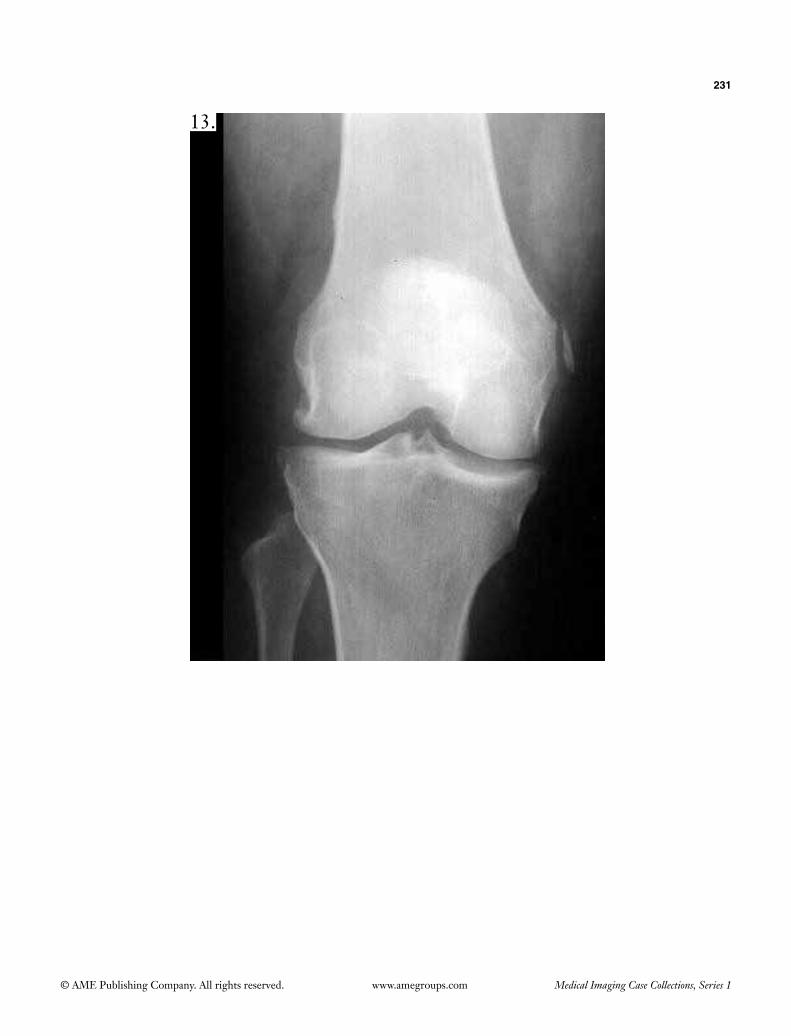
231
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
13.

232
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
14.
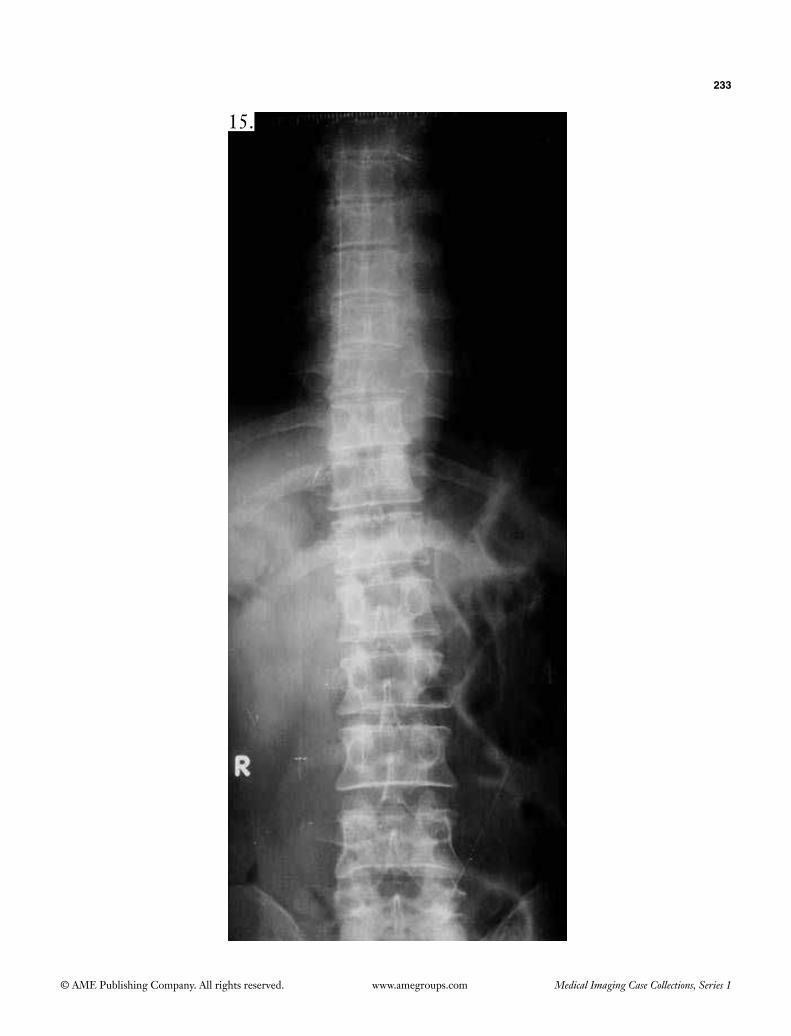
233
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
15.
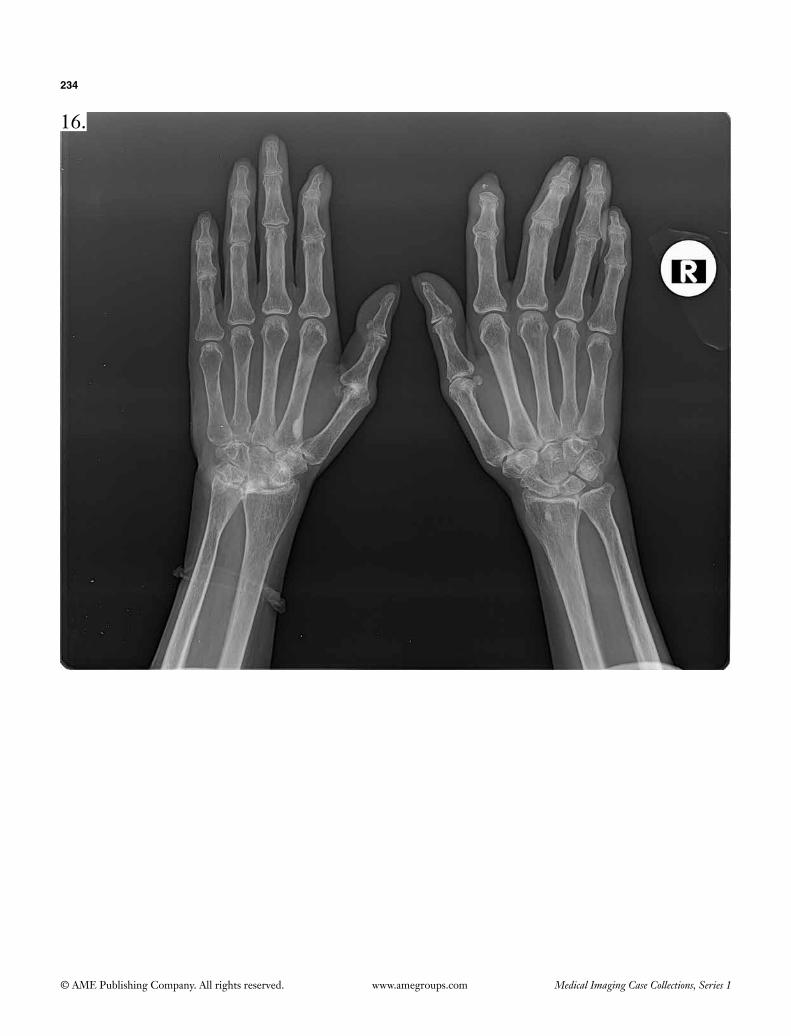
234
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
16.

235
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
17.

236
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
18.

237
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
19.
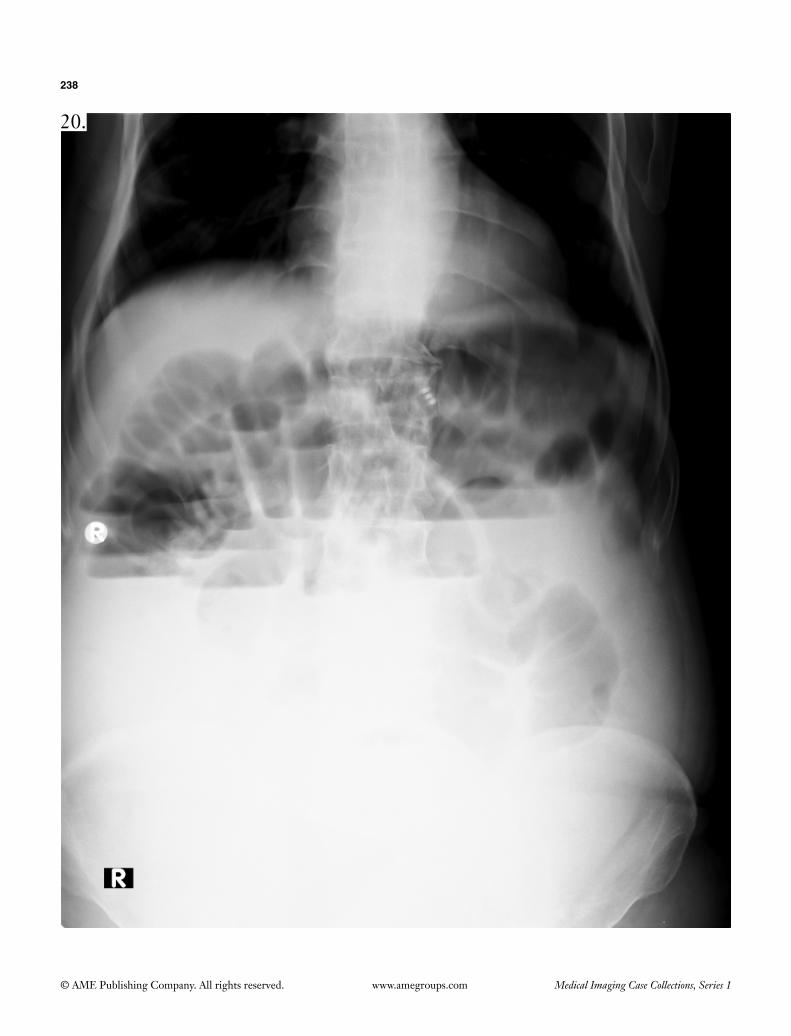
238
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
20.

239
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
21.

240
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
22.
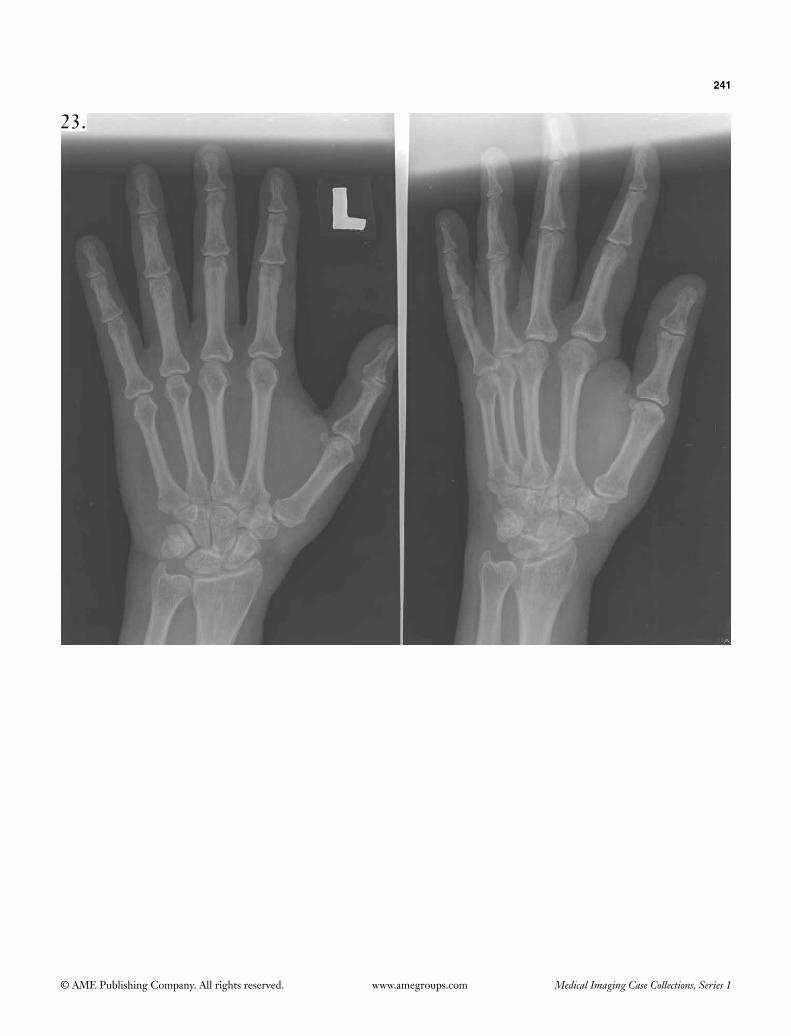
241
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
23.
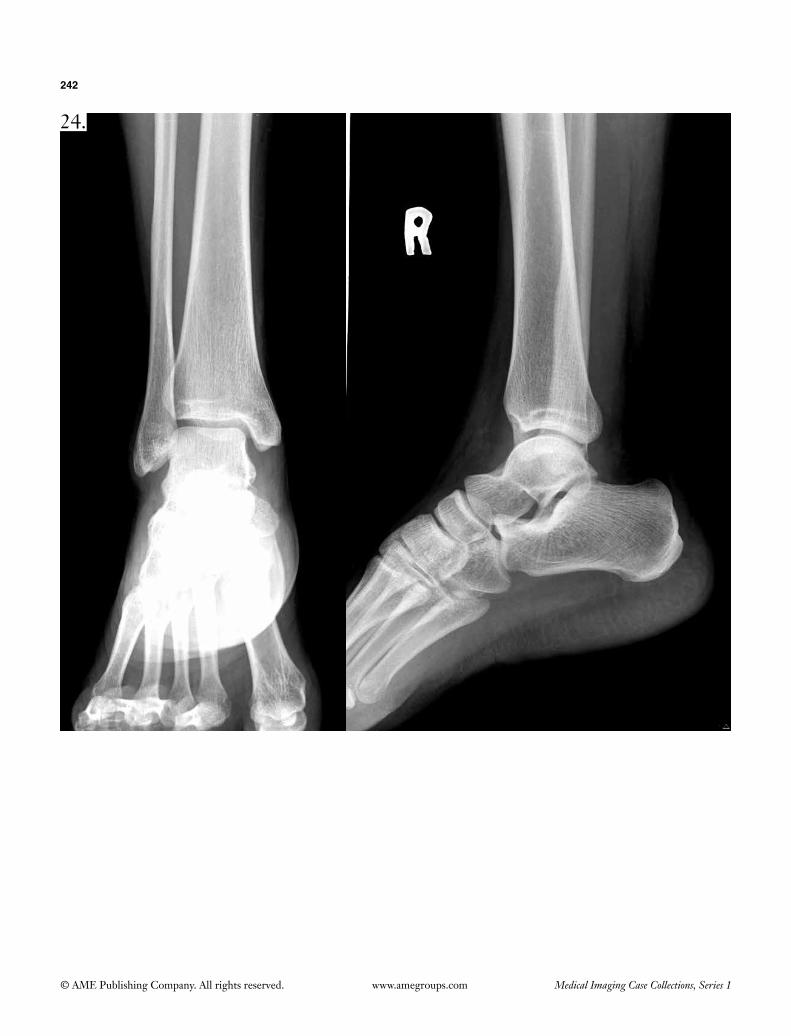
242
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
24.

243
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
25.

244
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
26.

245
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
27.
RIGHT
27.

246
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
28.

247
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
29.

248
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
30.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 4
1.
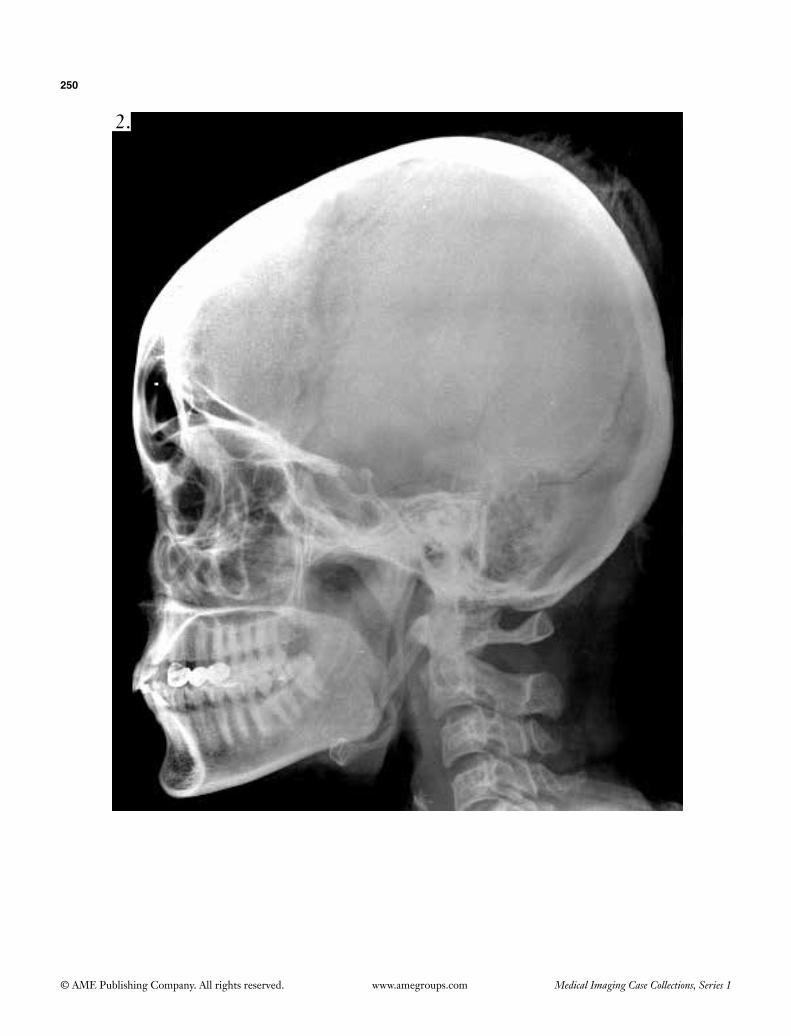
250
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
2.
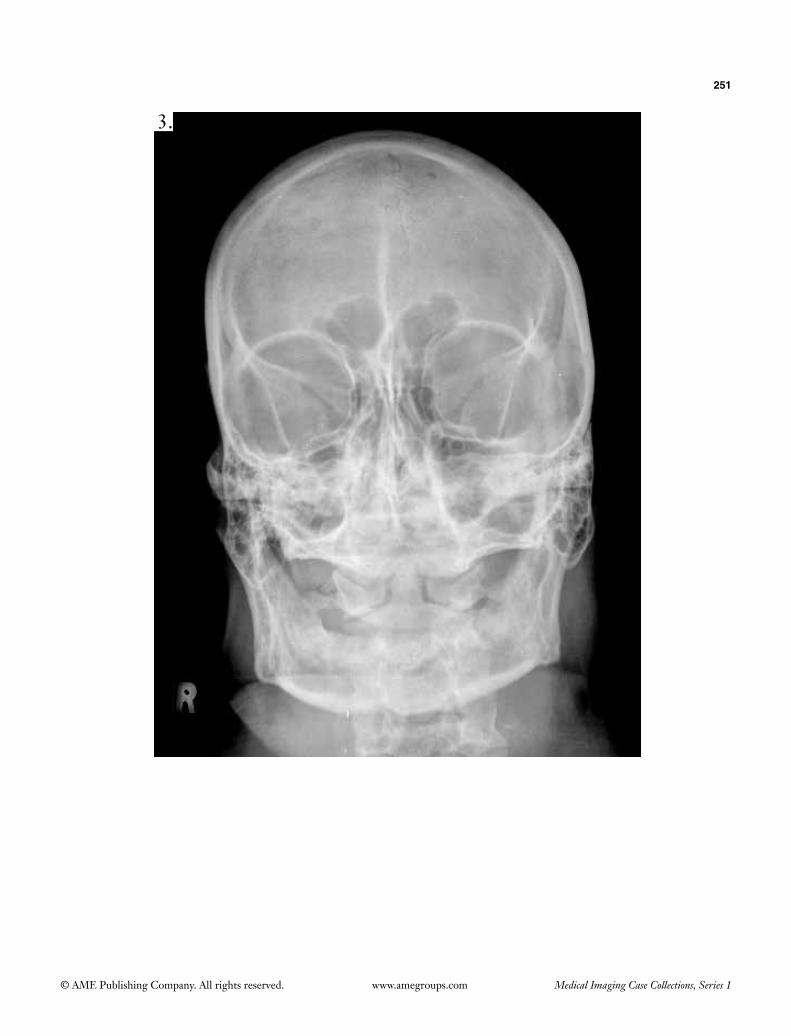
251
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
3.
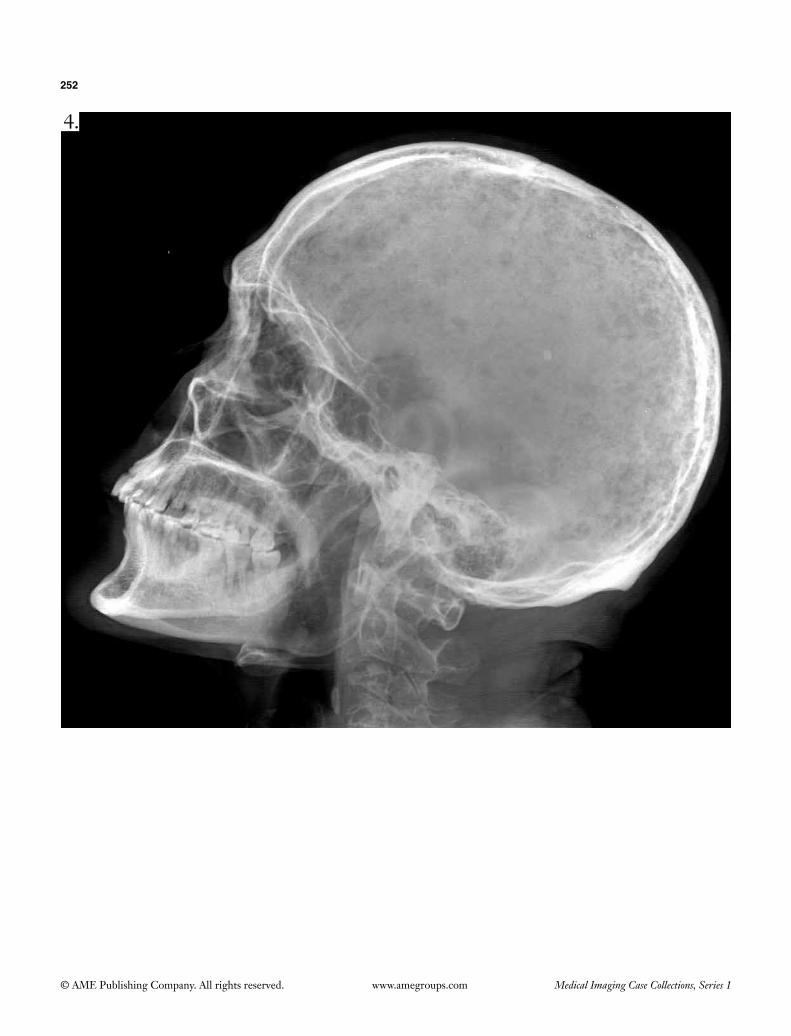
252
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
4.

253
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
5.

254
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
6.

255
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
7.

256
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
8.
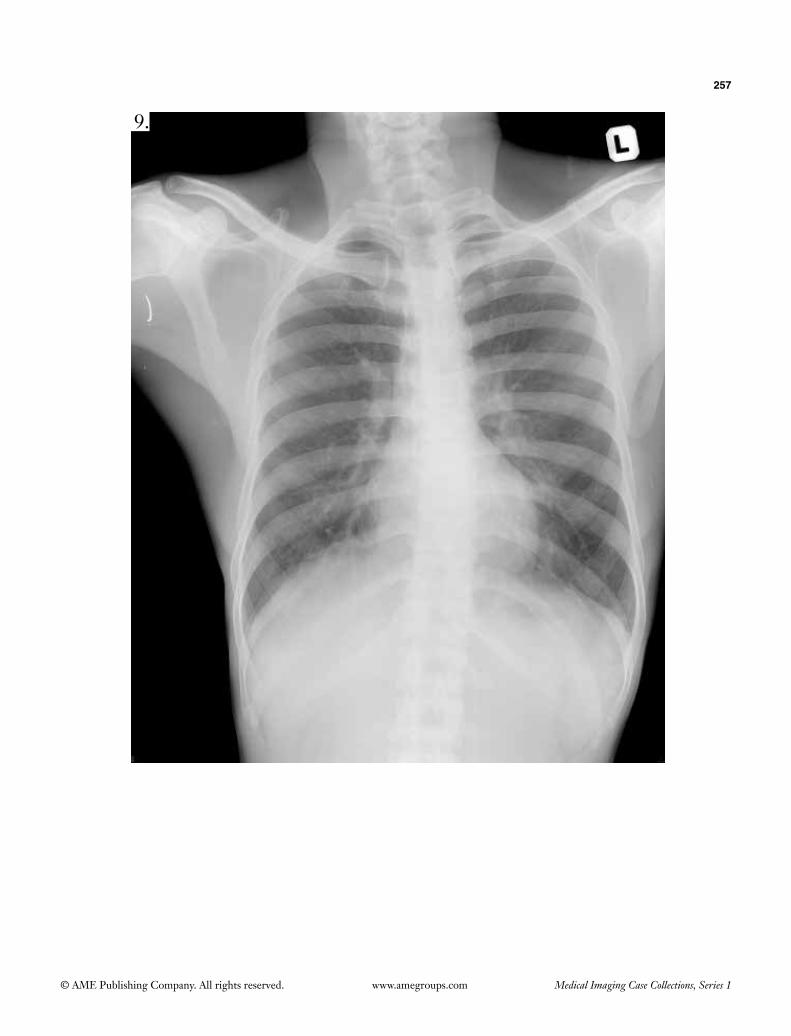
257
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
9.

258
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
10.

259
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
11.

260
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
12.

261
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
13.
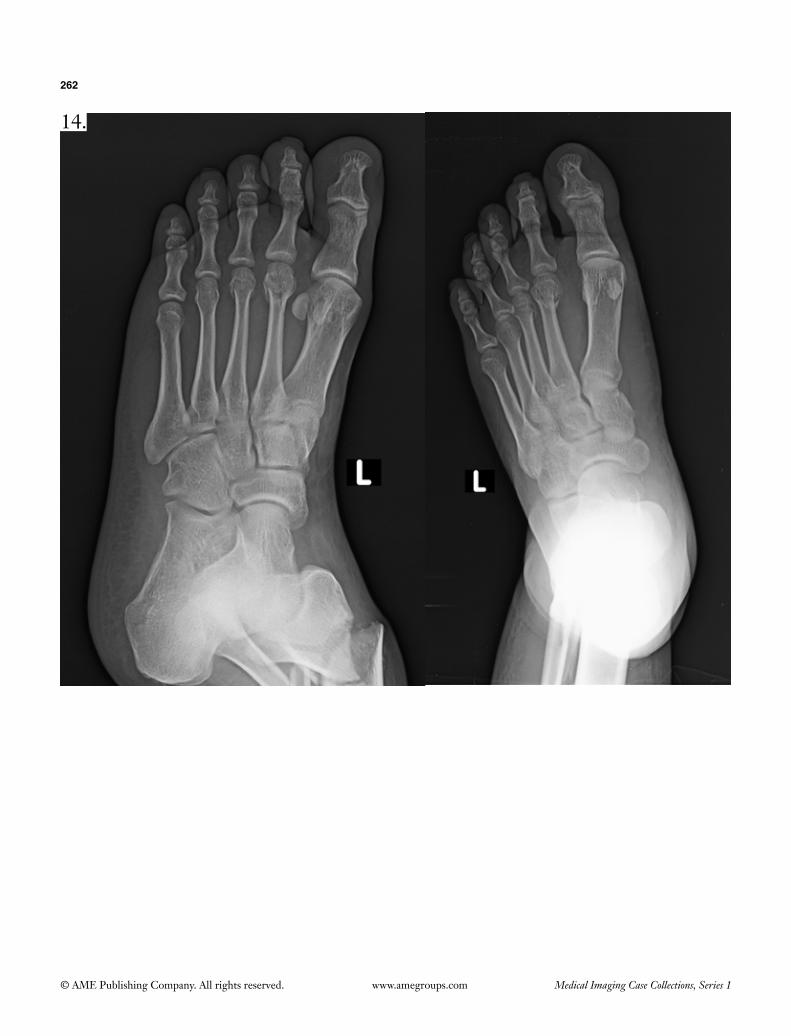
262
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
14.
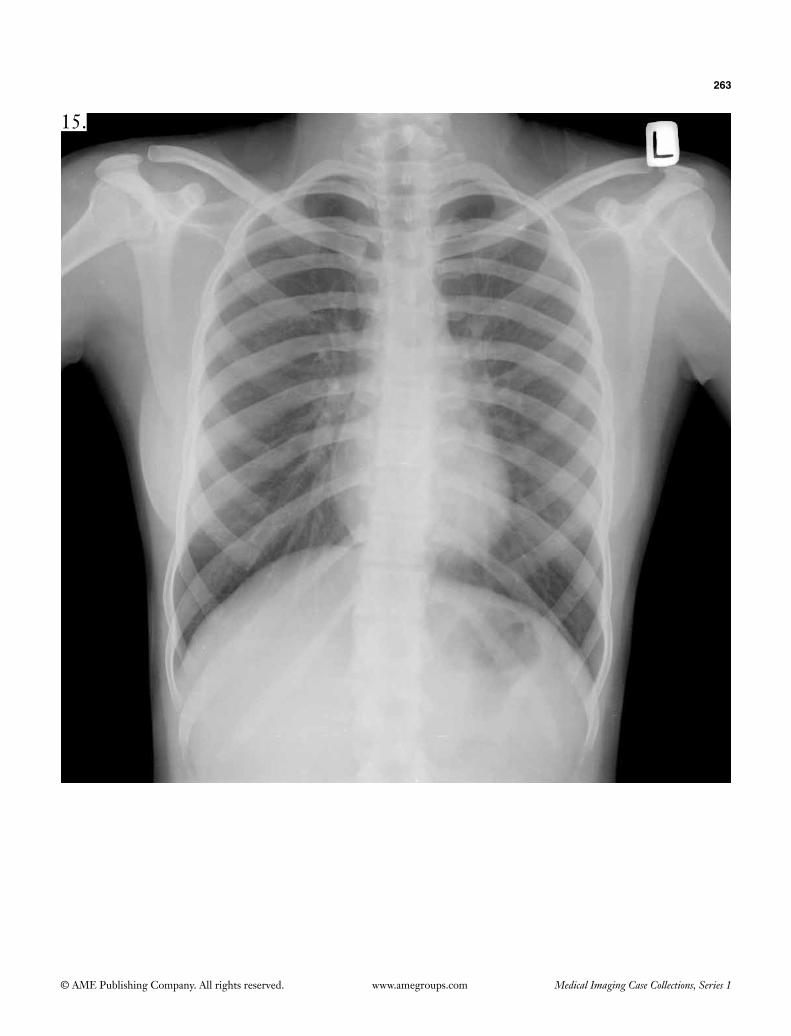
263
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
15.

264
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
16.

265
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
17.

266
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
18.

267
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
19.

268
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
20.

269
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
21.

270
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
22.

271
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
23.

272
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
24. 25.

273
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
26.

274
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
27.

275
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
28.

276
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
29.
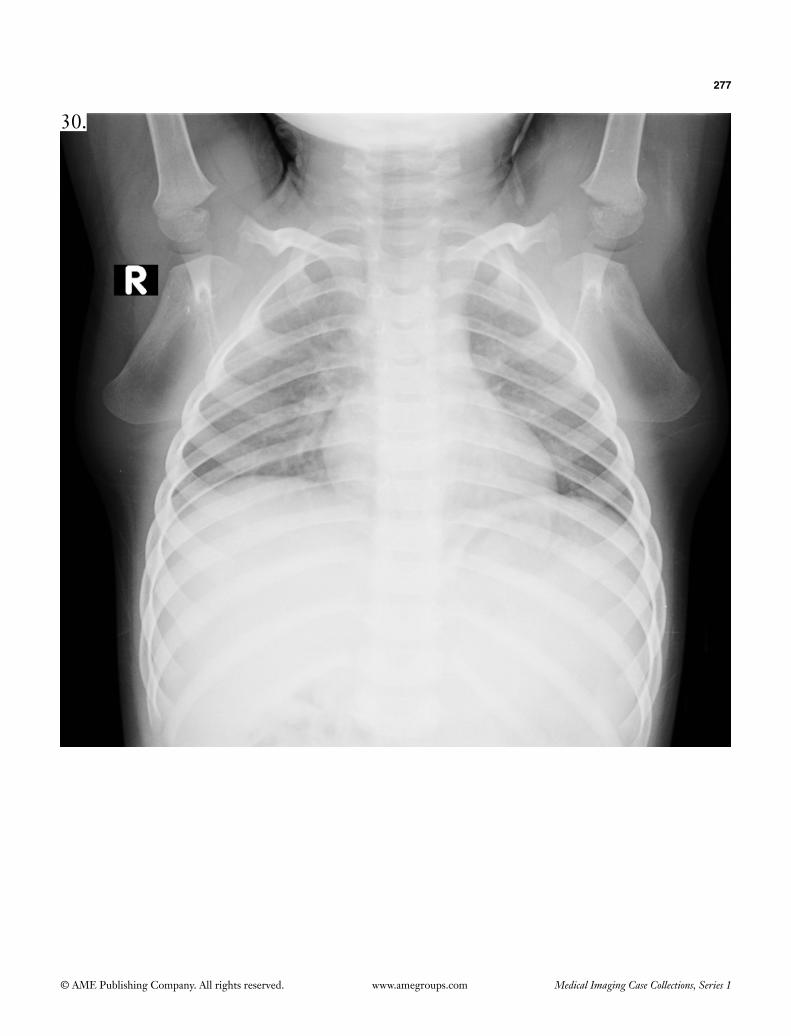
277
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
30.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Set 5
1.

279
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
2.
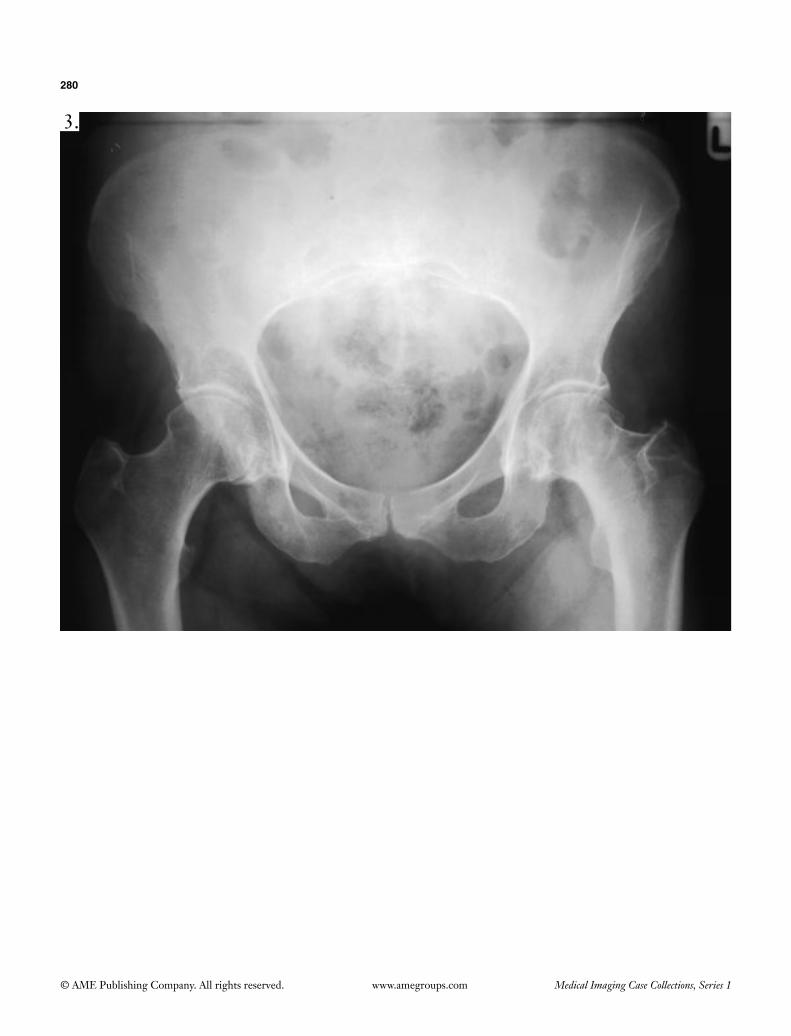
280
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
3.

281
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
4.

282
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
5.

283
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
6.
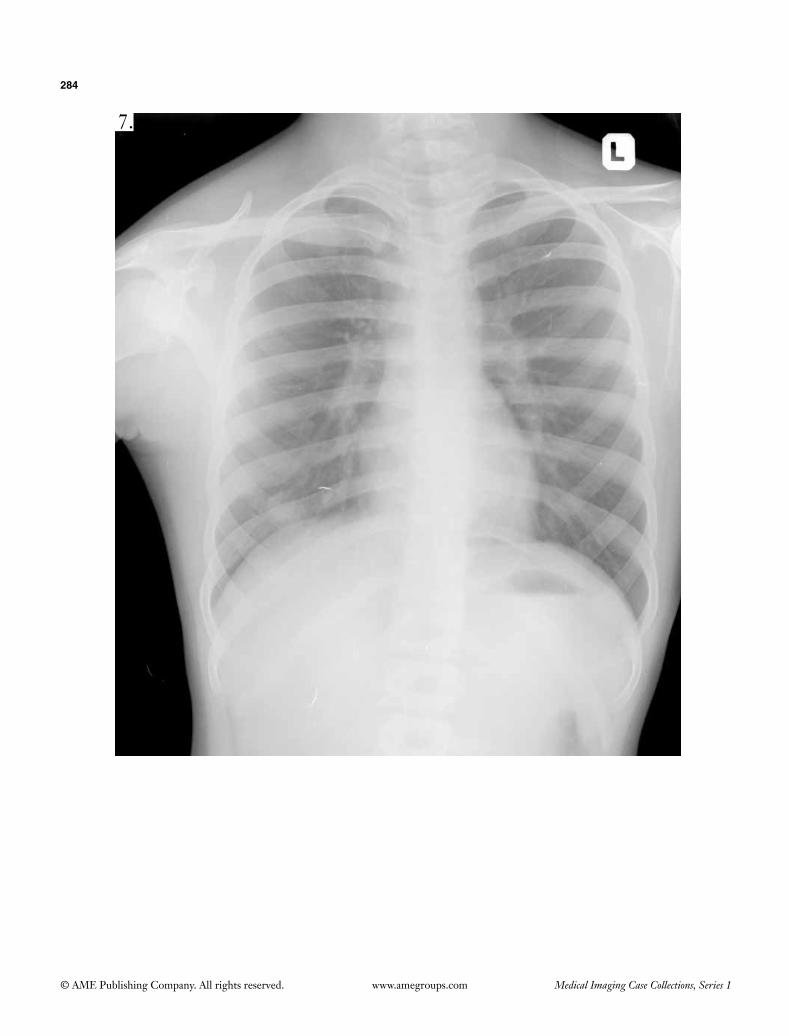
284
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
7.

285
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
8.

286
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
9.

287
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
10.

288
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
11.

289
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
12.

290
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
13.

291
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
14.
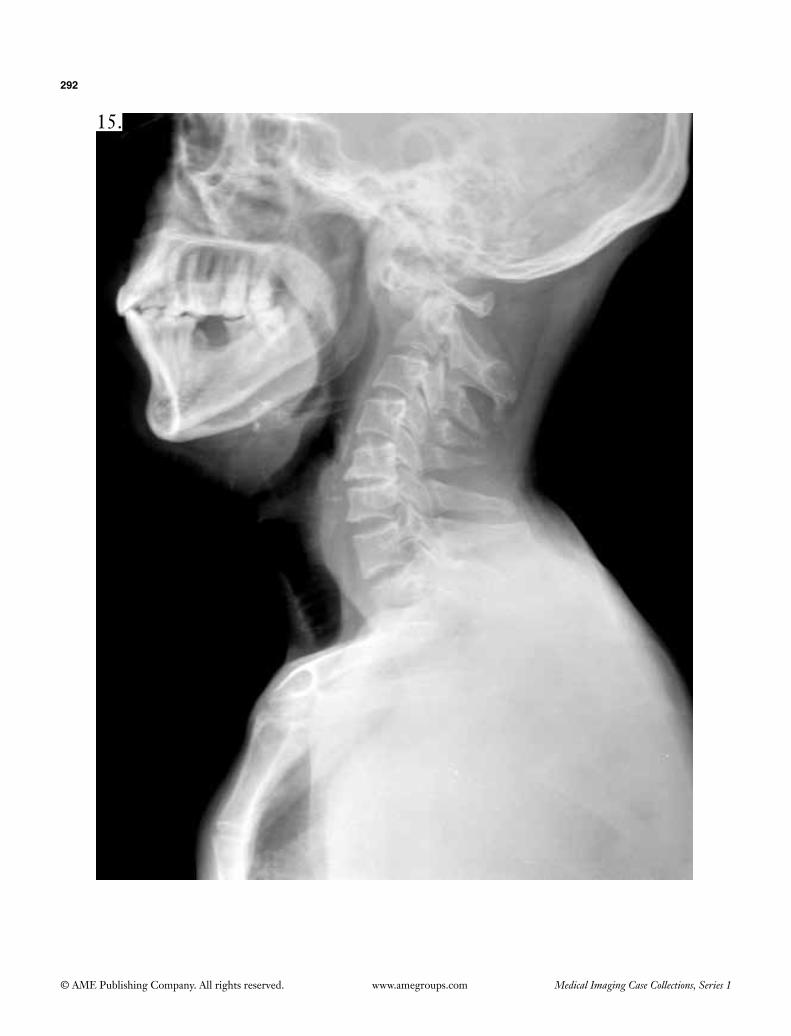
292
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
15.

293
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
16.

294
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
17.

295
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
18.

296
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
19.

297
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
20.
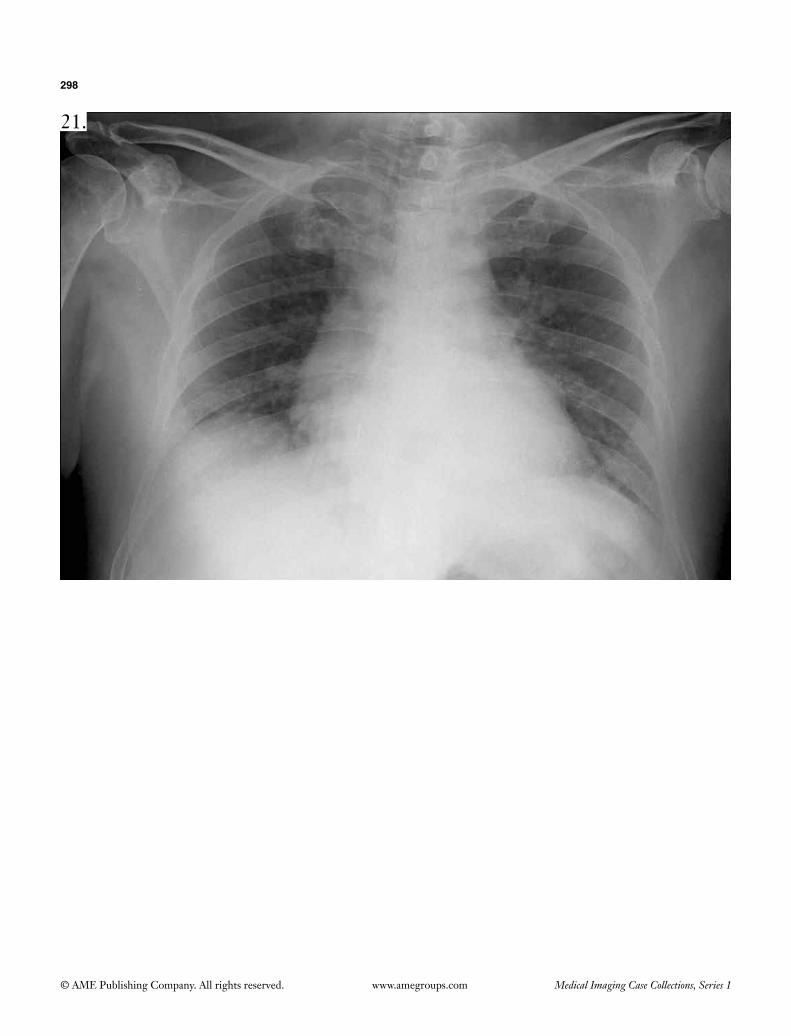
298
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
21.

299
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
22.
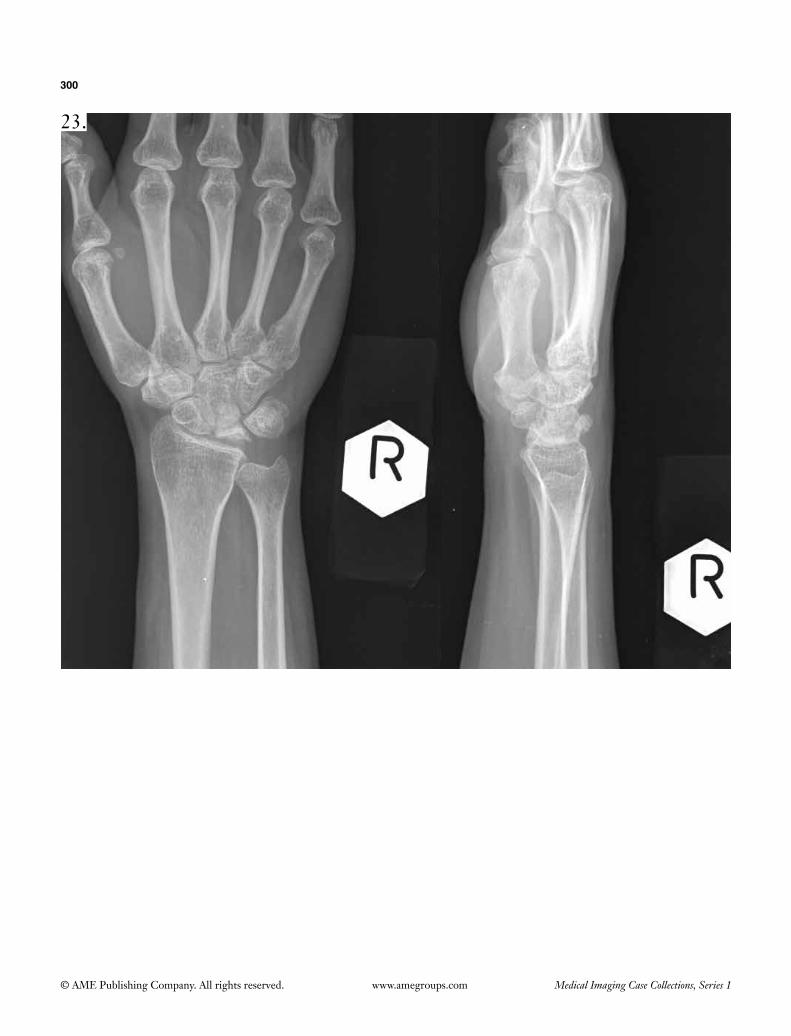
300
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
23.

301
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
24.

302
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
25.

303
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
26.

304
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
27.
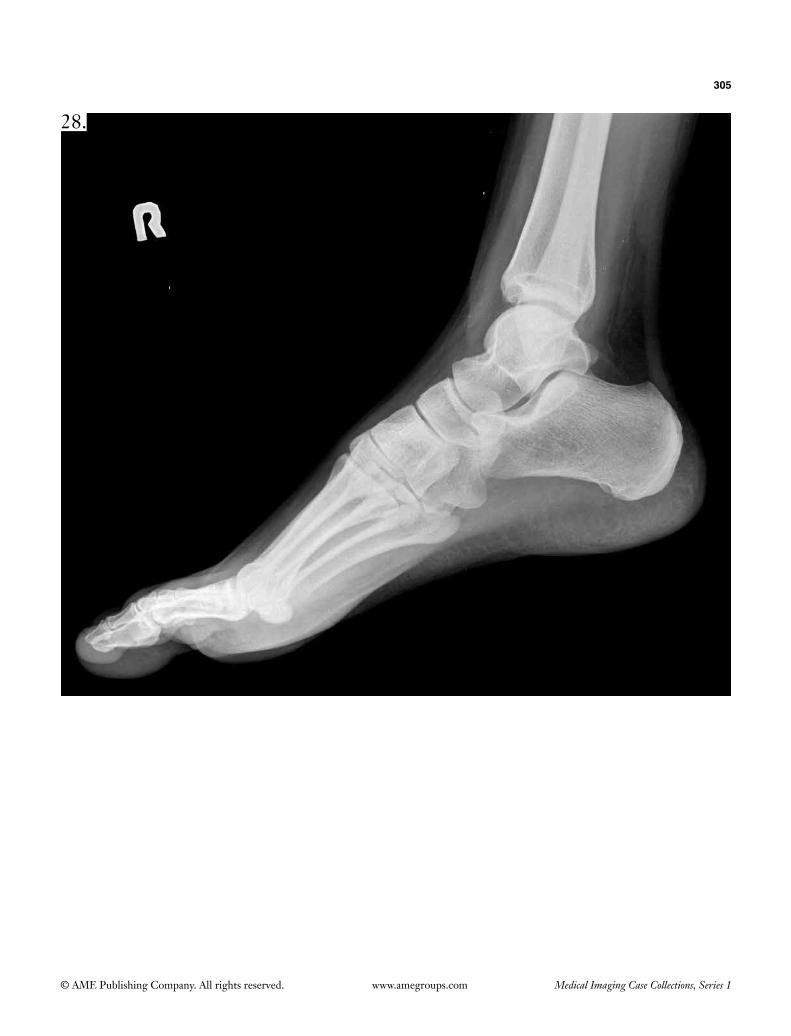
305
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
28.

306
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
29.
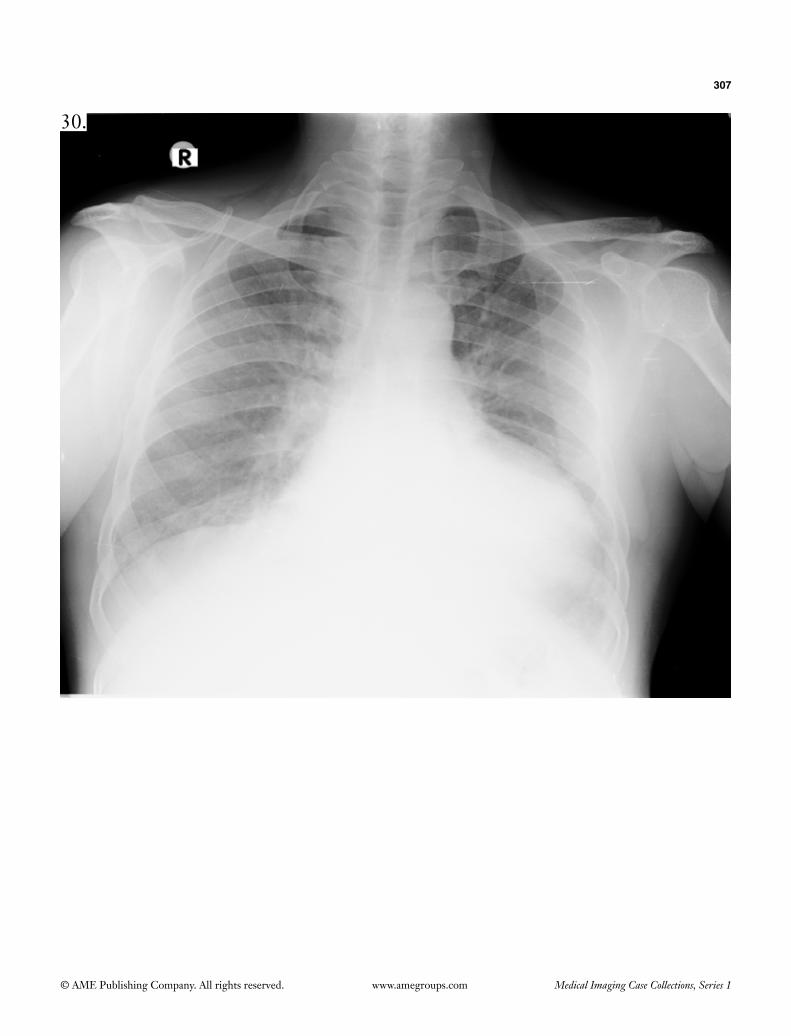
307
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
30.

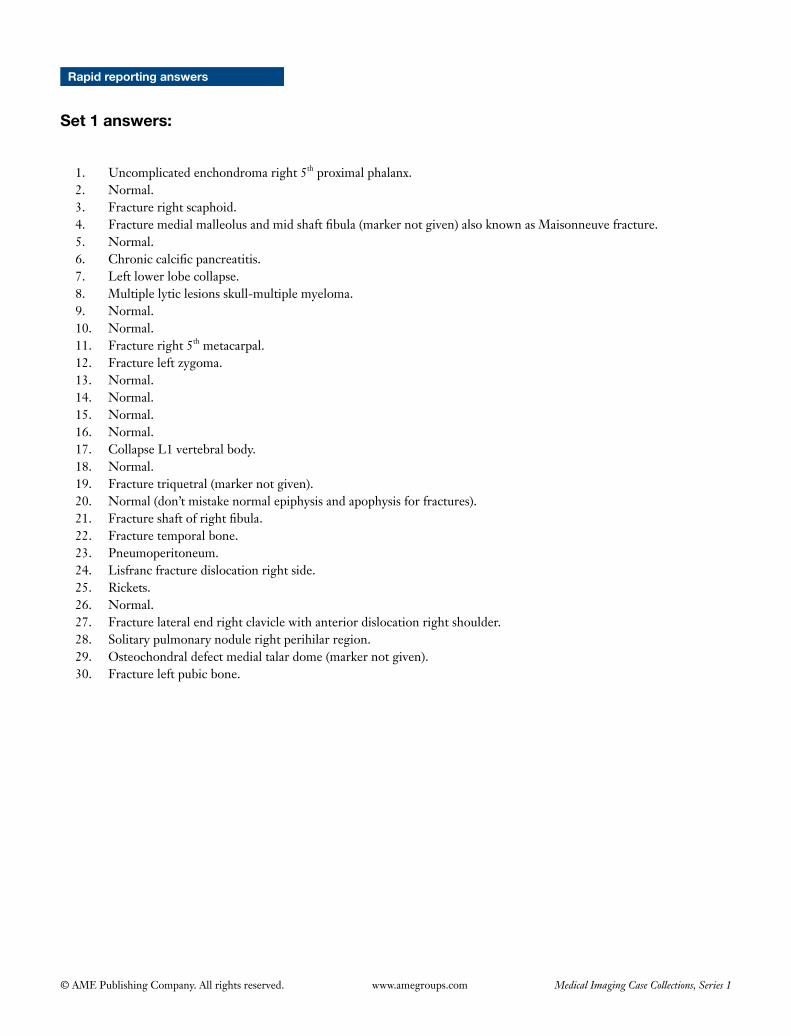
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Rapid reporting answers
Set 1 answers:
1. Uncomplicated enchondroma right 5th proximal phalanx.2. Normal.3. Fracture right scaphoid.4. Fracturemedialmalleolusandmidshaftfibula(markernotgiven)alsoknownasMaisonneuvefracture.5. Normal.6. Chroniccalcificpancreatitis.7. Leftlowerlobecollapse.8. Multiplelyticlesionsskull-multiplemyeloma.9. Normal.10. Normal.11. Fracture right 5th metacarpal.12. Fractureleftzygoma.13. Normal.14. Normal.15. Normal.16. Normal.17. CollapseL1vertebralbody.18. Normal.19. Fracturetriquetral(markernotgiven).20. Normal(don’tmistakenormalepiphysisandapophysisforfractures).21. Fractureshaftofrightfibula.22. Fracturetemporalbone.23. Pneumoperitoneum.24. Lisfranc fracture dislocation right side.25. Rickets.26. Normal.27. Fracturelateralendrightclaviclewithanteriordislocationrightshoulder.28. Solitarypulmonarynodulerightperihilarregion.29. Osteochondraldefectmedialtalardome(markernotgiven).30. Fractureleftpubicbone.
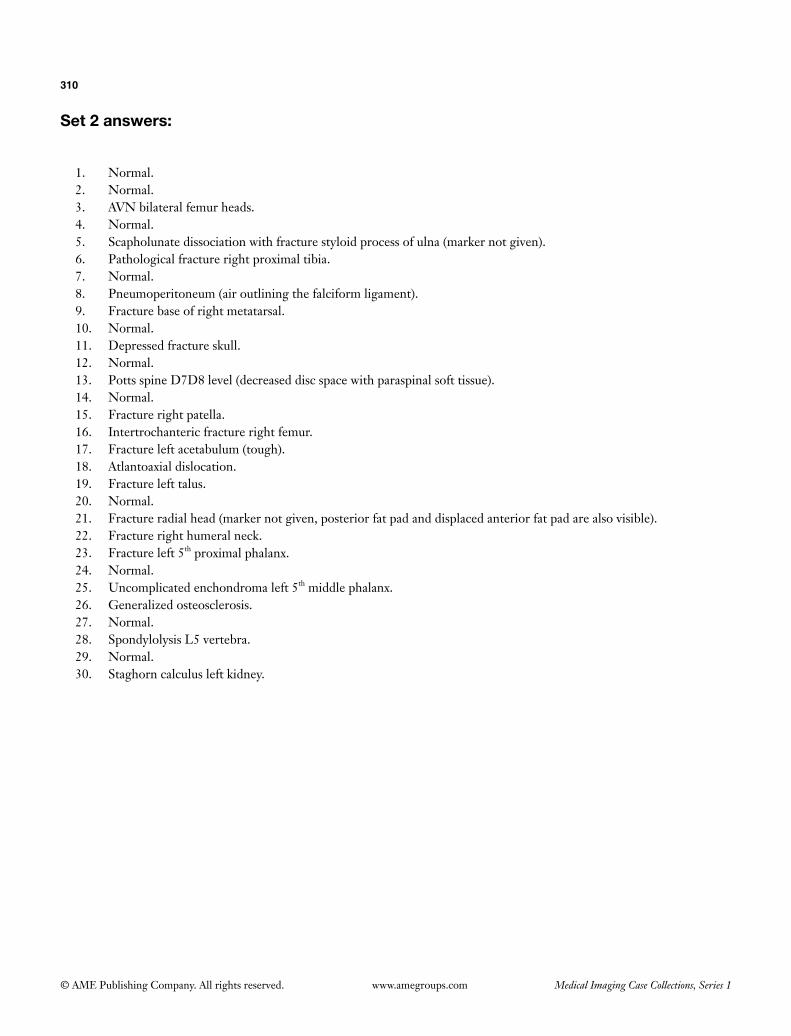
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
310
Set 2 answers:
1. Normal.2. Normal.3. AVN bilateral femur heads.4. Normal.5. Scapholunate dissociation with fracture styloid process of ulna (marker not given).6. Pathological fracture right proximal tibia.7. Normal.8. Pneumoperitoneum (air outlining the falciform ligament).9. Fracture base of right metatarsal.10. Normal.11. Depressed fracture skull.12. Normal.13. Potts spine D7D8 level (decreased disc space with paraspinal soft tissue).14. Normal.15. Fracture right patella.16. Intertrochanteric fracture right femur.17. Fracture left acetabulum (tough).18. Atlantoaxial dislocation.19. Fracture left talus.20. Normal.21. Fracture radial head (marker not given, posterior fat pad and displaced anterior fat pad are also visible).22. Fracture right humeral neck.23. Fracture left 5th proximal phalanx.24. Normal.25. Uncomplicated enchondroma left 5th middle phalanx.26. Generalized osteosclerosis.27. Normal.28. Spondylolysis L5 vertebra.29. Normal.30. Staghorn calculus left kidney.
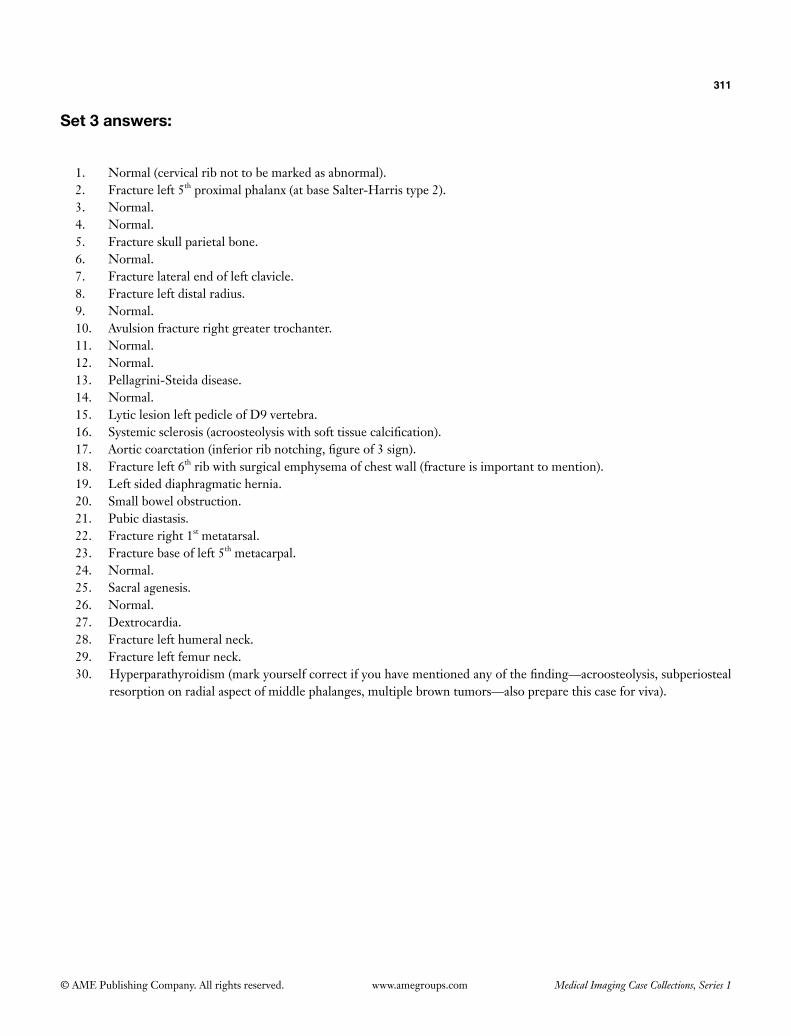
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
311
Set 3 answers:
1. Normal (cervical rib not to be marked as abnormal).2. Fracture left 5th proximal phalanx (at base Salter-Harris type 2).3. Normal.4. Normal.5. Fracture skull parietal bone.6. Normal.7. Fracture lateral end of left clavicle.8. Fracture left distal radius.9. Normal.10. Avulsion fracture right greater trochanter.11. Normal.12. Normal.13. Pellagrini-Steida disease.14. Normal.15. Lytic lesion left pedicle of D9 vertebra.16. Systemicsclerosis(acroosteolysiswithsofttissuecalcification).17. Aorticcoarctation(inferiorribnotching,figureof3sign).18. Fracture left 6th rib with surgical emphysema of chest wall (fracture is important to mention).19. Left sided diaphragmatic hernia.20. Small bowel obstruction.21. Pubic diastasis.22. Fracture right 1st metatarsal.23. Fracture base of left 5th metacarpal.24. Normal.25. Sacral agenesis.26. Normal.27. Dextrocardia.28. Fracture left humeral neck.29. Fracture left femur neck.30. Hyperparathyroidism(markyourselfcorrectifyouhavementionedanyofthefinding—acroosteolysis,subperiosteal
resorptiononradialaspectofmiddlephalanges,multiplebrowntumors—alsopreparethiscaseforviva).
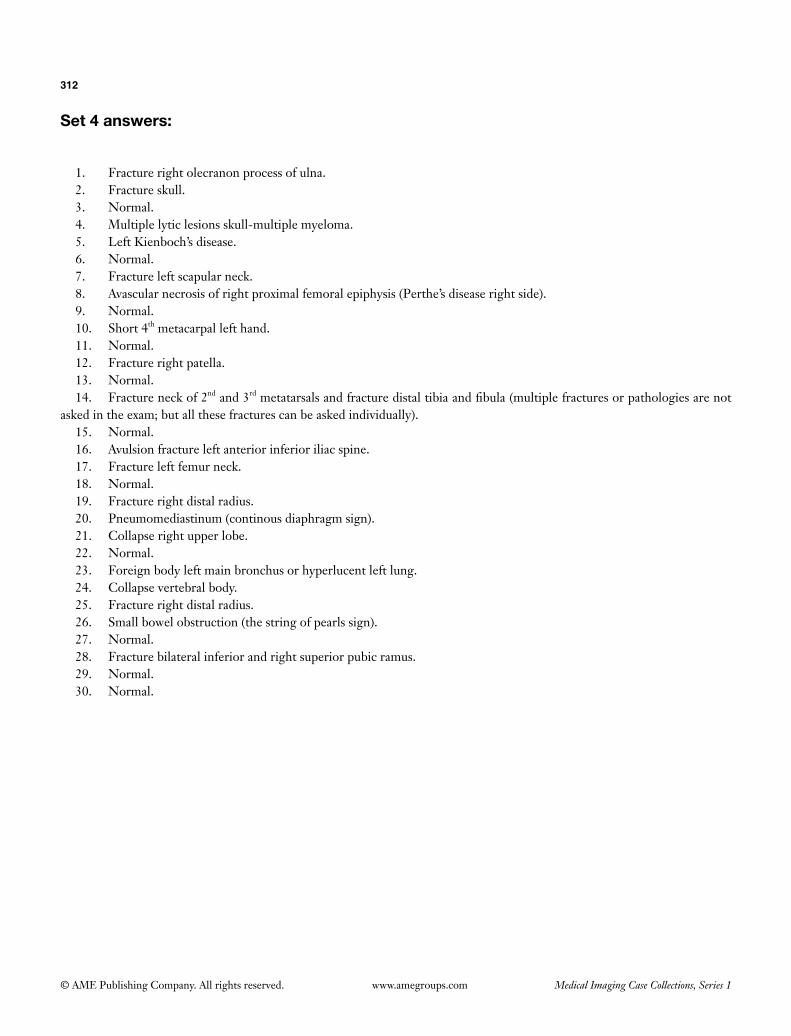
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
312
Set 4 answers:
1. Fracture right olecranon process of ulna.2. Fracture skull.3. Normal.4. Multiple lytic lesions skull-multiple myeloma.5. Left Kienboch’s disease.6. Normal.7. Fracture left scapular neck.8. Avascular necrosis of right proximal femoral epiphysis (Perthe’s disease right side).9. Normal.10. Short 4th metacarpal left hand.11. Normal.12. Fracture right patella.13. Normal.14. Fracture neck of 2nd and 3rd metatarsals and fracture distal tibia and fibula (multiple fractures or pathologies are not
asked in the exam; but all these fractures can be asked individually).15. Normal.16. Avulsion fracture left anterior inferior iliac spine.17. Fracture left femur neck.18. Normal.19. Fracture right distal radius.20. Pneumomediastinum (continous diaphragm sign).21. Collapse right upper lobe.22. Normal.23. Foreign body left main bronchus or hyperlucent left lung.24. Collapse vertebral body.25. Fracture right distal radius.26. Small bowel obstruction (the string of pearls sign).27. Normal.28. Fracture bilateral inferior and right superior pubic ramus.29. Normal.30. Normal.
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
313
Set 5 answers:
1. Collapse right middle lobe of lung.2. Normal.3. Fracture left neck of femur.4. Normal.5. Bilateral slipped capital femoral epiphysis.6. Normal.7. Solitary pulmonary nodule right lower zone.8. Normal.9. Leftsupraspinatuscalcifictendonitis.10. Normal.11. Right bony Bankart lesion.12. Normal.13. Fracture right distal pole of scaphoid.14. Small bowel obstruction.15. Fracture odontoid process.16. Osteochondral defect left medial femoral condyle.17. Normal.18. Fracture L2 vertebra.19. Fracture right calcaneum.20. Fracture neck of right 2nd, 3rd and 4th metatarsals.21. Fracture medial end of right clavicle.22. Fracture neck of right scapula.23. Right Kienboch’s disease.24. Normal.25. Fracture base of left 5th metatarsal.26. Normal.27. Fractureshaftofrightfemur(checkcornerofthefilm).28. Normal.29. Fracture right humeral head.30. Normal.

© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Abdominal tuberculosis—page no. 32Achalasia cardia—page no. 14,15Air crescent sign—page no. 82Albers-Schönberg disease—page no.71Allergic bronchopulmonary aspergillosis—page no. 82Amyloid arthropathy—page no. 4Aneurysmal bone cyst—page no. 27,99,126Angiomyolipoma—page no. 30Ankylosing spondylitis—page no. 118Annular pancreas—page no. 87Anoxia—page no. 9Anteater sign—page no. 96Aortic
aneurysm—page no. 12,21dissection—page no. 12,21
Aorto-arteritis—page no. 51Arachnoid cyst—page no. 123Arnold chiari malformations—page no. 63Arthritis mutilans—page no. 92Asbestos related pleural disease—page no. 7Asbestosis—page no. 7,85Aspergilloma—page no. 81,82Aspergillosis—page no. 81,82,101Atherosclerosis—page no. 12,21,51Atoll sign—page no. 82,101Avascular necrosis—page no. 53,71,142,153Basal fibrosis—page no. 7,85Basilar invagination—page no. 63Beak sign—page no. 21Beckwith wiedemann syndrome—page no. 35Bird beak sign—page no. 14,15Bird-of-prey sign—page no. 115Breast
calcifications—page no. 79carcinoma—page no. 24,78
Bronchial carcinoid—page no. 121Bronchogenic carcinoma—page no. 7,81,128C sign—page no. 96Caecal volvulus—page no. 115Calcified metastasis lung—page no. 121Capener’s sign—page no. 135Carbon monoxide poisoning—page no. 9Carcinoid—page no. 24,121Carcinoma breast—page no. 24Carney’s triad—page no. 45,121Carotid body tumor—page no. 45Caustic ingestion—page no. 140Central neurocytoma—page no. 156
Cerebellar hypoplasia—page no. 63,74,123Chagas disease—page no. 15Chiari malformations—page no. 63Chiasmatic glioma—page no. 55Chondroblastoma—page no. 27,99,126Chondrocalcinosis—page no. 142Chondromyxoid fibroma—page no. 27Chondrosarcoma—page no. 4,121,145Chronic
infectious osteomyelitis—page no. 37recurrent multifocal osteomyelitis (CRMO)—page no. 37
Cobwebappearance—page no. 71sign—page no. 21
Coffee bean sign—page no. 115Colon cut off sign—page no. 48Congenital TORCH infection—page no. 43,74Cortical nephrocalcinosis—page no. 138Crazy paving appearance—page no. 69Crescent sign—page no. 153Creutzfeldt jakob disease—page no. 9Crouzon syndrome—page no. 63CSF cleft sign—page no. 94CT
halo sign—page no. 101severity index—page no. 48
Cytomegalovirus infection—page no. 74Dagger sign—page no. 118Dandy-walker
continuum—page no. 123malformation—page no. 123variant—page no. 123
Diaphyseal aclasis—page no. 145Double
bubble sign—page no. 87contour sign—page no. 142
Doughnut sign—page no. 27Draped aorta sign—page no. 12Drug-induced lung fibrosis—page no. 85Duodenal malignancy—page no. 87Dural tail sign—page no. 94Dyke-davidoff masson syndrome—page no. 43Echinococcosis—page no. 159Egg-shell calcification—page no. 79,132Emphysematous pyelonephritis—page no. 18Encephalotrigeminal angiomatosis—page no. 43Enteropathic arthritis—page no. 118Erlenmeyer’s flask deformity—page no. 71
Index
315
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Erosive osteoarthritis—page no. 92,150Erythema nodosum—page no. 132Esophageal
carcinoma—page no. 14,140stricture—page no. 140
Ewing’s sarcoma—page no. 37Extramedullary hematopoiesis—page no. 35Fallen fragment sign—page no. 99Fatigue fracture—page no. 113Fibrolamellar hepatocellular carcinoma—page no. 66Fibrous dysplasia—page no. 99,126Figure of 8 appearance—page no. 74Fluid-fluid levels—page no. 99,126Focal nodular hyperplasia—page no. 66Frimann Dahl’s sign—page no. 115Ganglioneuroblastoma—page no. 35Ganglioneuroma—page no. 35Giant cell
arteritis—page no. 51tumor—page no. 27,121,126
Glioblastoma multiforme—page no. 156Gout—page no. 4,142Gull’s wing deformity—page no. 92,150Hemophilia—page no. 103Hemophilic arthropathy—page no. 103Hepatic adenoma—page no. 66Hepatocellular carcinoma—page no. 66Hilar lymphadenopathy—page no. 132Hirschprung disease—page no. 35Honda sign—page no. 113H-shaped vertebra—page no. 153,154Hydatid cyst—page no. 81,159Hyperattenuation crescent sign—page no. 12Hyperparathyroidism—page no. 135,138,142Hypersensitivity pneumonitis—page no. 58Hypertrophic osteoarthropathy—page no. 128Hyperuricemia—page no. 142Idiopathic pulmonary fibrosis (IPF)—page no. 85Insufficiency fracture—page no. 113Intraocular foreign body—page no. 105Intraventricular
glioblastoma multiforme—page no. 156tumors—page no. 156
Ivory phalanx—page no. 92Jelly belly—page no. 61Juvenile rheumatoid arthritis (JRA)—page no. 103Klippel-Feil syndrome—page no. 63Legg-calve perthe’s disease—page no. 153
Leigh’s disease—page no. 9Lincoln Log vertebra—page no. 153,154Lissencephaly—page no. 74Liver
abscess—page no. 159overlap sign—page no. 115
Lofgren syndrome—page no. 132Lupus pernio—page no. 132Lye stricture—page no. 140Lymphangiomyomatosis—page no. 30Lymphoma—page no. 32,35,37Madelung’s deformity—page no. 145Malignant mesothelioma—page no. 7,40Mammographic scoring—page no. 79Marble bone disease—page no. 71Medullary
nephrocalcinosis—page no. 138sponge kidney—page no. 138
Mega cisterna magna—page no. 123Meningioma—page no. 55,94,156Metaiodobenzylguanidine (MIBG) scan—page no. 35,45Metaphyseal
blanch sign—page no. 135extrusion sign—page no. 135
Metastasis—page no. 110Military opacities—page no. 58MISME—page no. 55Monad sign—page no. 81,82Morquio’s disease—page no. 53Mucopolysaccharidosis—page no. 53Multiple
epiphyseal dysplasia—page no. 53hereditary exostosis—page no. 145myeloma—page no. 110,138
Myasthenia gravis—page no. 148Myelomatosis—page no. 110Neuroblastoma—page no. 35Neurocutaneous disorder—page no. 30,43,45,55Neurofibroma—page no. 55Neurofibromatosis-1—page no. 35,45,55Neurofibromatosis-2—page no. 55Non-cardiogenic pulmonary edema—page no. 9Nonossifying fibroma—page no. 27Ophthalmic ultrasound—page no. 105Osteochondroma—page no. 145Osteopetrosis—page no. 71Pachydermoperiostosis—page no. 128Pachygyria—page no. 74
316
© AME Publishing Company. All rights reserved. Medical Imaging Case Collections, Series 1www.amegroups.com
Paget’s disease—page no. 24,63,126Pancreatic pseudocyst—page no. 87Pancreatitis—page no. 48,86,87Paraganglioma—page no. 45,121Pencil in cup deformity—page no. 92Periampullary carcinoma—page no. 87Perimesencephalic hemorrhage—page no. 107Peritoneal
adenomucinosis—page no. 61carcinomatosis—page no. 61mucinous carcinoma—page no. 61sarcomatosis—page no. 61
Periventricular calcification—page no. 74Pigmented villonodular synovitis—page no. 4Pilocytic astrocytoma—page no. 55Pipe stem ureter—page no. 90Plasmacytoma—page no. 110,126Platybasia—page no. 63Platyspondyly—page no. 53Pleural
metastasis—page no. 40plaque—page no. 7,40thickening—page no. 7,40
Pneumocystiscarinii pneumonia—page no. 69jiroveci pneumonia—page no. 69,101
POEMS syndrome—page no. 110Polyarteritis nodosa—page no. 51Popcorn calcification—page no. 79,121Port-wine stain—page no. 43Pseudoachalasia—page no. 14,15Pseudomyxoma peritonei—page no. 61Psoriatic arthritis—page no. 92,118,150Pulmonary
alveolar proteinosis—page no. 69edema—page no. 9,58,69hamartoma—page no. 45,121hemorrhage—page no. 69
Putty kidney—page no. 90Pyknodysostosis—page no. 71Radiation fibrosis—page no. 24Reiter’s syndrome—page no. 118Renal
tuberculosis—page no. 90tubular acidosis—page no. 71,138
Respiratory bronchiolitis-interstitial lung disease—page no. 58Retroperitoneal fibrosis—page no. 77Reverse
anteater sign—page no. 96halo sign—page no. 82,101
Rheumatoid arthritis—page no. 12,85,92,101,150Rim sign—page no. 159Romanus lesions—page no. 118Saccular intracranial aneurysm—page no. 107Sarcoidosis—page no. 132,138Sausage digit—page no. 92Saw tooth ureter—page no. 90Schwannoma—page no. 45,55,94Sclerosing myeloma—page no. 110Sclerotic metastasis—page no. 24Secondary achalasia—page no. 15Shiny corner sign—page no. 118Sickle cell disease—page no. 71,153,154Sigmoid volvulus—page no. 115Simple bone cyst—page no. 99,126Slipped capital femoral epiphysis—page no. 135Snake sign—page no. 159Spondyloepiphyseal dysplasia tarda—page no. 53Sprengel deformity—page no. 63Stanford classification—page no. 21Stress fracture—page no. 113Sturge-weber syndrome—page no. 43Subarachnoid hemorrhage—page no. 107Subependymal hamartoma—page no. 30Sulphur colloid scan—page no. 66Synovial chondromatosis—page no. 4Syringomyelia—page no. 63Systemic
lupus erythematosus—page no. 100sclerosis—page no. 85
Takayasu’s arteritis—page no. 51Talocalcaneal coalition—page no. 96Tangential calcium sign—page no. 12Teratoma—page no. 148Thimble bladder—page no. 90Thymoma—page no. 40,148Thyroid acropachy—page no. 128Toxic encephalopathy—page no. 9Trethowan’s sign—page no. 135Tuberculosis—page no. 32,58,90,101,132Tuberous sclerosis—page no. 30,45,74Unicameral bone cyst—page no. 99Usual interstitial pneumonitis (UIP)—page no. 85Vagal schwannoma—page no. 45Vertebra plana—page no. 53Water lily sign—page no. 159Wilson disease—page no. 9


![financial management 2b [bsr2b01, fnm02b2] last assessment ...](https://static.fdokumen.com/doc/165x107/631aa5b5c51d6b41aa04e9e3/financial-management-2b-bsr2b01-fnm02b2-last-assessment-.jpg)

















