
Course and Learning Outcome(s) Course and Learning Outcome(s
Upload
khangminh22Category
view
5download
0
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop
Complex Regional Pain Syndrome: Outcome Measures
and Sensory InnovationsTara Packham, OTReg.(Ont), PhD
@TaraLPackham
1
Presenter Disclosure
Presenter: Tara Packham
Relationships with commercial interests:
Grants/Research Support: none relevant to this talk
Speakers Bureau/Honoraria: American Society of Hand Therapists, Canadian Association of Occupational Therapists
Consulting Fees: none
Other: Publications with Elsevier and Springer Nature
This program has received financial support from the Ministry of Health and Long Term Care
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop
Objectives
Measuring what matters
Plasticity in practice
Sensational suggestions
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop

Complex Regional Pain Syndrome
May develop after injury (Type 1: formerly RSD) or be associated with a nerve injury (Type 2: formerly causalgia)
More often seen in upper limb and in women; increasing age and genetics may add to risk profile
(Bruehl, 2015)
Complex Regional Pain Syndrome
May develop after injury (Type 1: formerly RSD) or be associated with a nerve injury (Type 2: formerly causalgia)
More often seen in lower limb and in girls; age and genetics may add to risk profile
(Mesaroli et al, 2019)
Complex Regional Pain Syndrome
CRPS is characterized by disproportionate pain and: swelling and temperature changes
changes in colour and sweating
elevated sensory responses
changes in skin, hair growth, nails
weakness, incoordination, dystonia
changes in cortical representations
psychological features
Regional
not just local
Pain & other symptoms experienced throughout the affected limb
Sensory changes may not follow classic nerve distributions
Some persons will experience neuropathic pain features in other body regions … (Harden et al, 2013)
Pain
unpleasant sensory and emotional perception
Syndrome
a group of symptoms
Complex
mechanisms implicated
Mechanistic cascade (Gierthmühlen et al, 2014)
Increased circulating stress hormones (sensitive/irritable systems)
Focal osteopenia (bone loss)
Consequences of immobilization (muscle loss)
Body perception disturbance (limb feels foreign)
Dystonia (muscle cramps/spasms)
Inflammatory signs (colour, temperature, swelling)
Hyperalgesia, allodynia, spontaneous pain (hypersensitivity)
Kinesiophobia, guarding, altered movement patterns (fear of movement, freezing, motor extinction)
CRPS is NOT Chronic Regional Pain Syndrome because of PLASTICITY
If maladaptive plasticity and altered perception are core to our understanding of the symptom mechanisms…
…then adaptive plasticity (including graded stimuli and response training) should reduce symptoms by normalizing the perceptions
(Moseley & Flor, 2012; Mansour et al, 2014)
Assessment
Patient-reported core outcome measures set for research is in international validation process [COMPACT] (Grieve et al, 2017)
‘Objective’ core measures set for research is in development
** Persons with CRPS gauge recovery relative to pain (Llewellyn et al, 2018)
4 consensus meetings including international scholars, clinicians and patient representatives
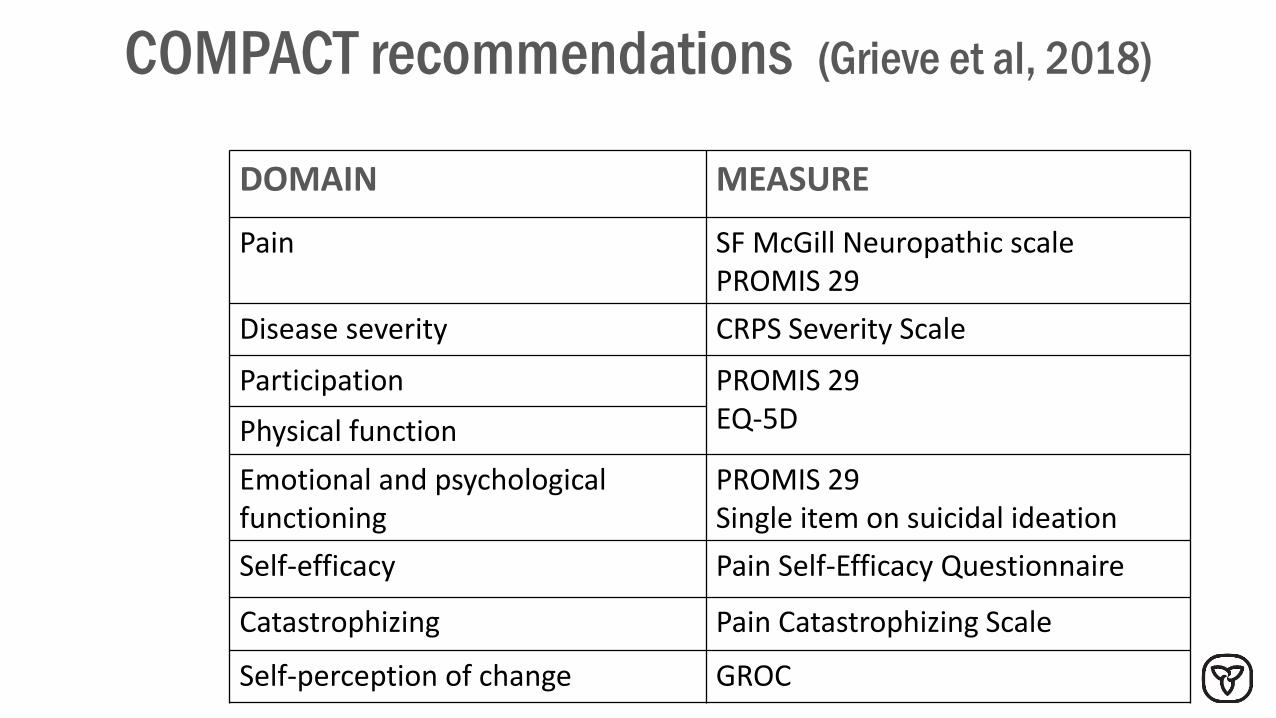
COMPACT recommendations (Grieve et al, 2018)
DOMAIN MEASURE
Pain SF McGill Neuropathic scalePROMIS 29
Disease severity CRPS Severity Scale
Participation PROMIS 29EQ-5DPhysical function
Emotional and psychological functioning
PROMIS 29Single item on suicidal ideation
Self-efficacy Pain Self-Efficacy Questionnaire
Catastrophizing Pain Catastrophizing Scale
Self-perception of change GROC
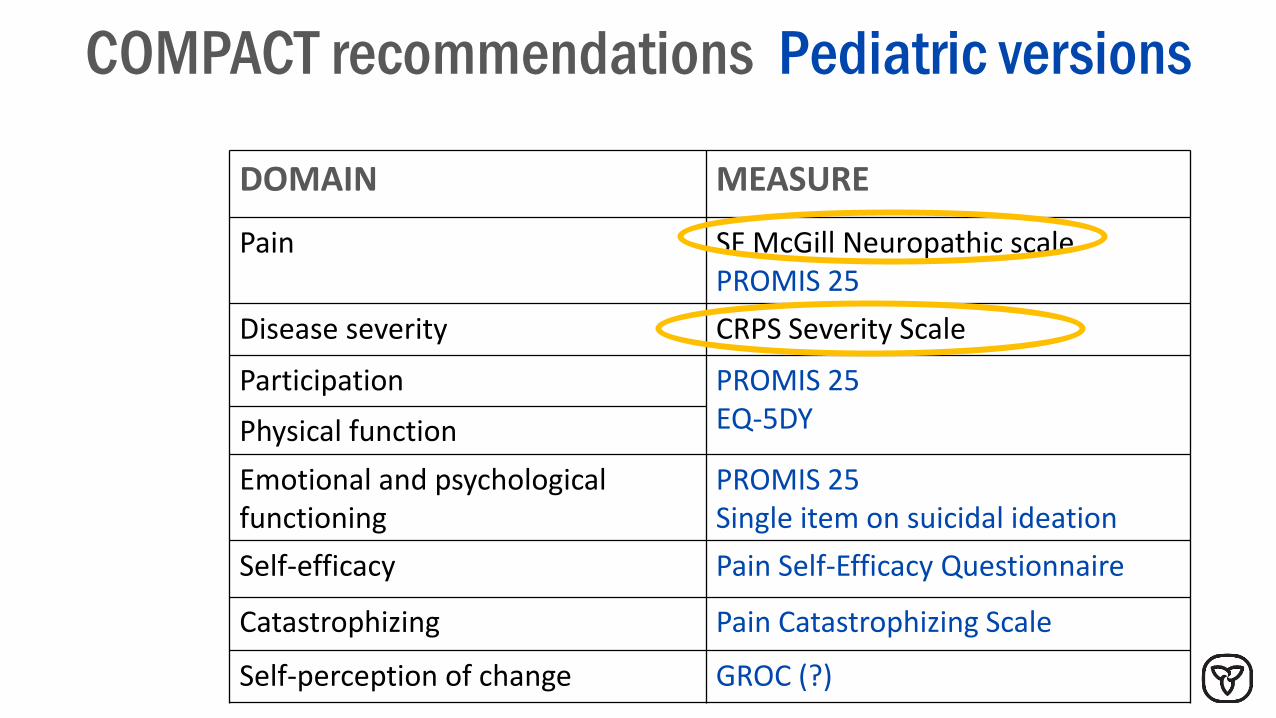
COMPACT recommendations Pediatric versions
DOMAIN MEASURE
Pain SF McGill Neuropathic scalePROMIS 25
Disease severity CRPS Severity Scale
Participation PROMIS 25EQ-5DYPhysical function
Emotional and psychological functioning
PROMIS 25Single item on suicidal ideation
Self-efficacy Pain Self-Efficacy Questionnaire
Catastrophizing Pain Catastrophizing Scale
Self-perception of change GROC (?)
von Baeyer CL. Pain Res Manage 11(3) 2006
‘Describing pain only in terms of its intensity is like describing music only in terms of its loudness.’
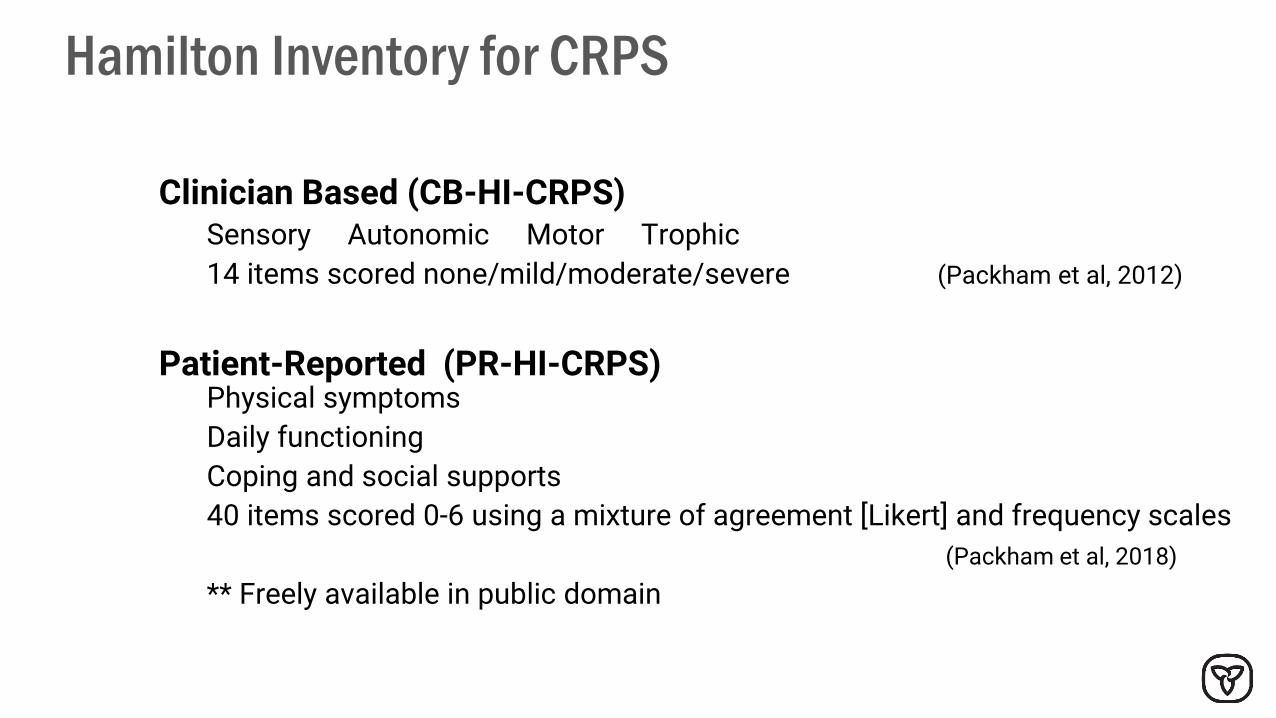
Hamilton Inventory for CRPS
Clinician Based (CB-HI-CRPS)Sensory Autonomic Motor Trophic
14 items scored none/mild/moderate/severe (Packham et al, 2012)
Patient-Reported (PR-HI-CRPS)Physical symptoms
Daily functioning
Coping and social supports
40 items scored 0-6 using a mixture of agreement [Likert] and frequency scales
(Packham et al, 2018)
** Freely available in public domain
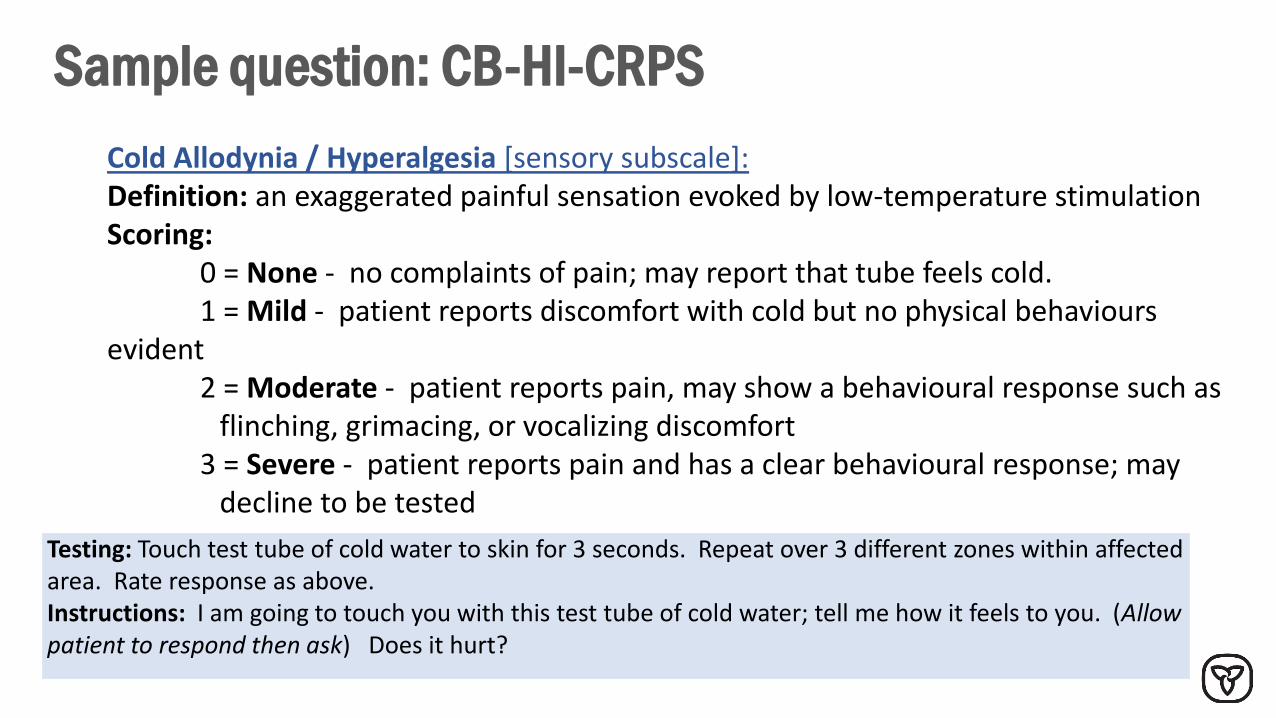
Sample question: CB-HI-CRPS
Testing: Touch test tube of cold water to skin for 3 seconds. Repeat over 3 different zones within affected area. Rate response as above.Instructions: I am going to touch you with this test tube of cold water; tell me how it feels to you. (Allow patient to respond then ask) Does it hurt?
Cold Allodynia / Hyperalgesia [sensory subscale]:Definition: an exaggerated painful sensation evoked by low-temperature stimulation Scoring:
0 = None - no complaints of pain; may report that tube feels cold.1 = Mild - patient reports discomfort with cold but no physical behaviours
evident2 = Moderate - patient reports pain, may show a behavioural response such as
flinching, grimacing, or vocalizing discomfort3 = Severe - patient reports pain and has a clear behavioural response; may
decline to be tested
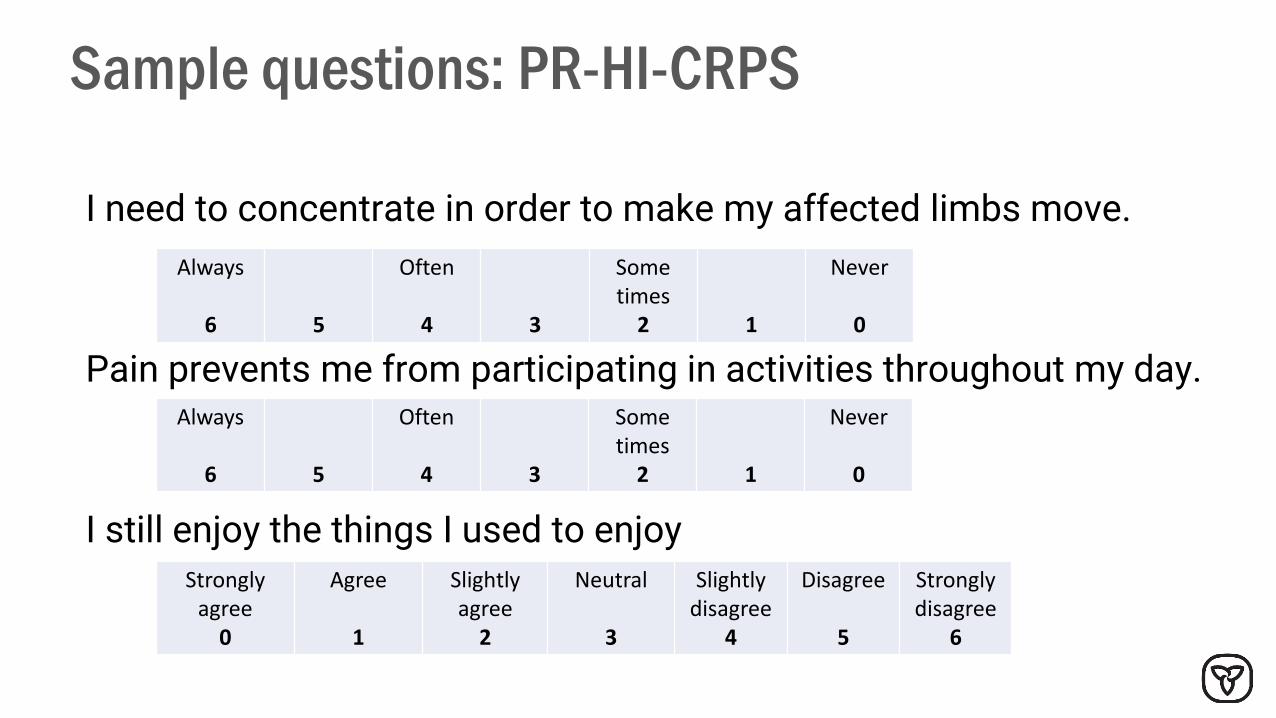
Sample questions: PR-HI-CRPS
I need to concentrate in order to make my affected limbs move.
Pain prevents me from participating in activities throughout my day.
I still enjoy the things I used to enjoy
Always
6 5
Often
4 3
Some times
2 1
Never
0
Always
6 5
Often
4 3
Some times
2 1
Never
0
Strongly agree
0
Agree
1
Slightly agree
2
Neutral
3
Slightlydisagree
4
Disagree
5
Strongly disagree
6
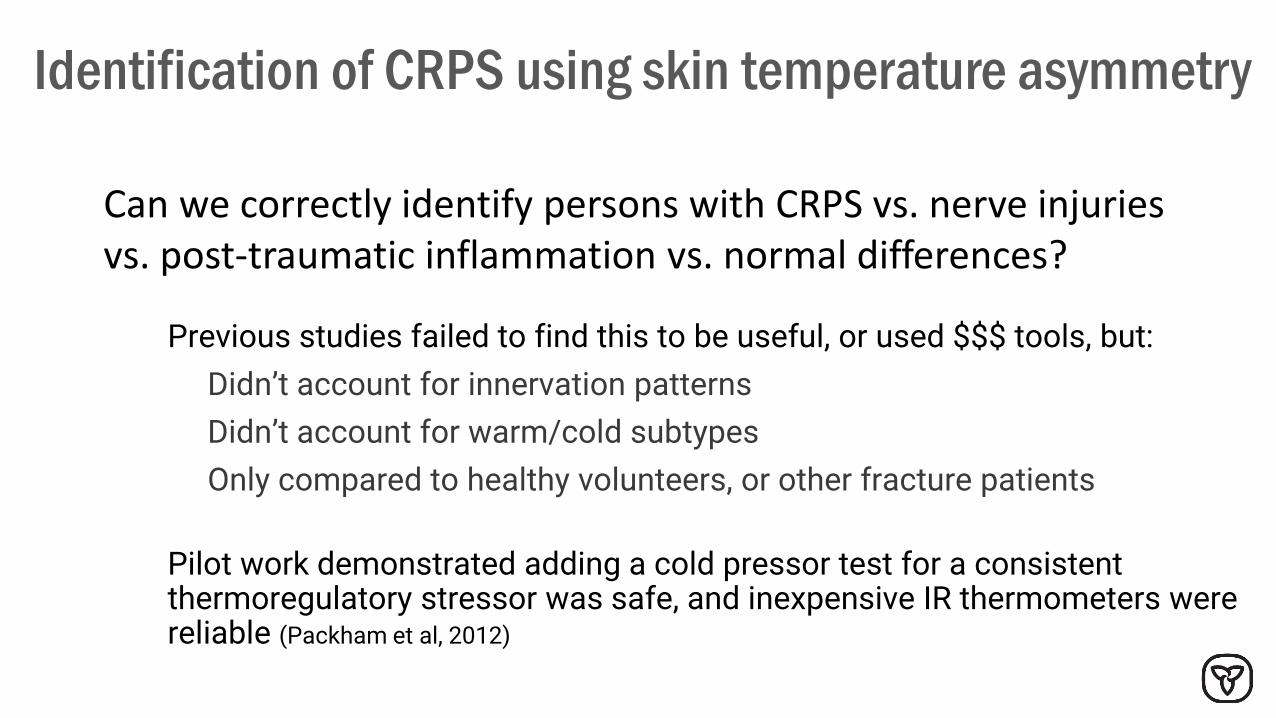
Identification of CRPS using skin temperature asymmetry
Previous studies failed to find this to be useful, or used $$$ tools, but:
Didn’t account for innervation patterns
Didn’t account for warm/cold subtypes
Only compared to healthy volunteers, or other fracture patients
Pilot work demonstrated adding a cold pressor test for a consistent thermoregulatory stressor was safe, and inexpensive IR thermometers were reliable (Packham et al, 2012)
Can we correctly identify persons with CRPS vs. nerve injuries vs. post-traumatic inflammation vs. normal differences?
Copies of the Hamilton Inventories are freely available from [email protected]
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop
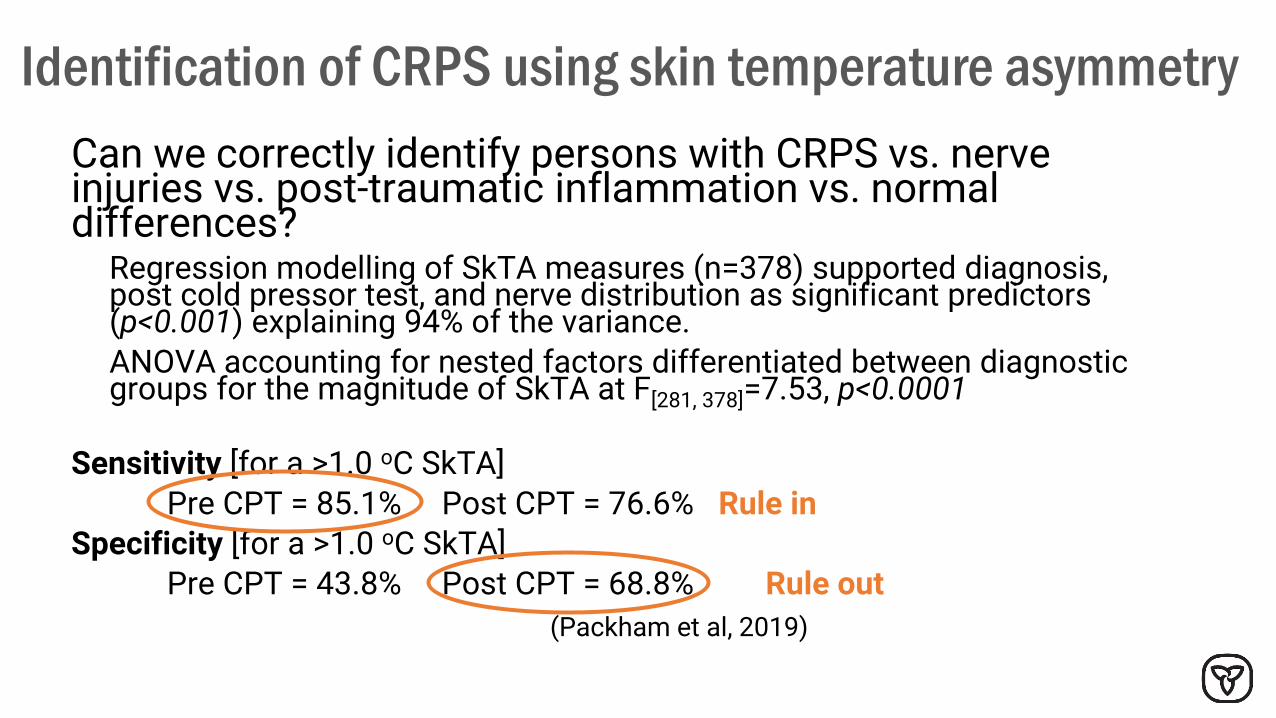
Identification of CRPS using skin temperature asymmetry
Can we correctly identify persons with CRPS vs. nerve injuries vs. post-traumatic inflammation vs. normal differences?
Regression modelling of SkTA measures (n=378) supported diagnosis, post cold pressor test, and nerve distribution as significant predictors (p<0.001) explaining 94% of the variance.
ANOVA accounting for nested factors differentiated between diagnostic groups for the magnitude of SkTA at F[281, 378]=7.53, p<0.0001
Sensitivity [for a >1.0 oC SkTA]
Pre CPT = 85.1% Post CPT = 76.6% Rule in
Specificity [for a >1.0 oC SkTA]
Pre CPT = 43.8% Post CPT = 68.8% Rule out
(Packham et al, 2019)
21
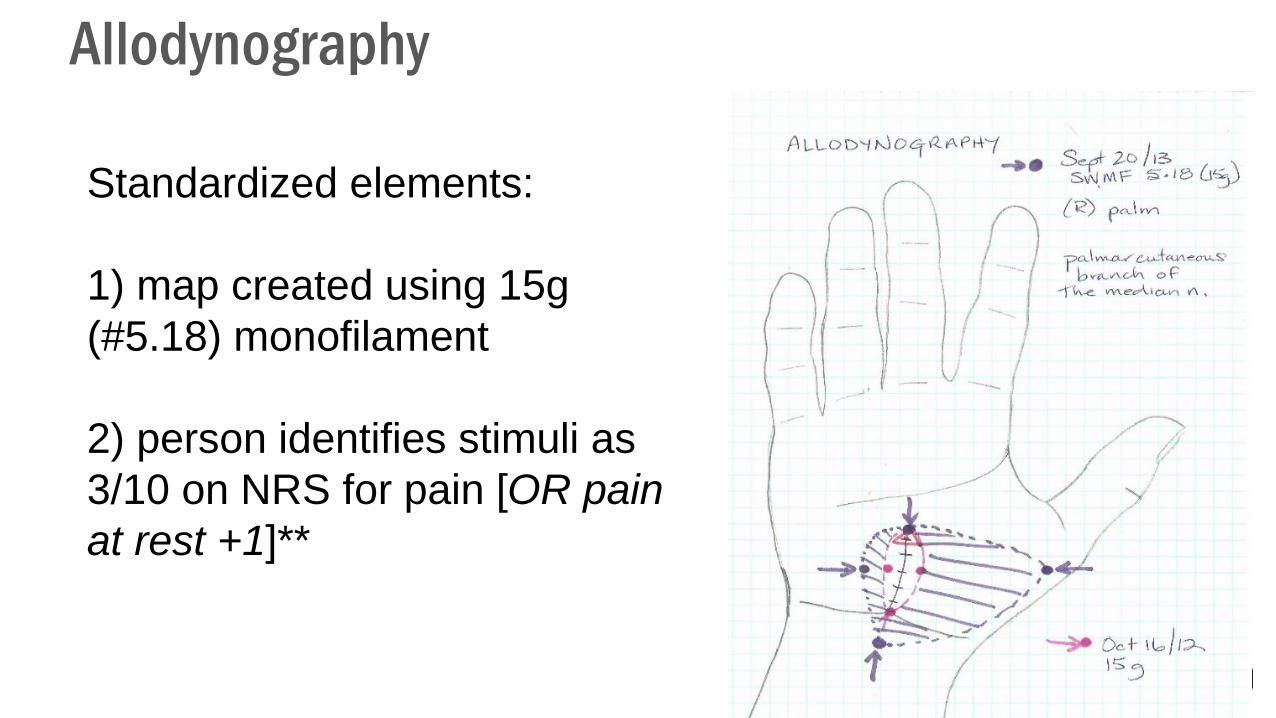
Allodynography
Standardized elements:
1) map created using 15g
(#5.18) monofilament
2) person identifies stimuli as
3/10 on NRS for pain [OR pain
at rest +1]**
22
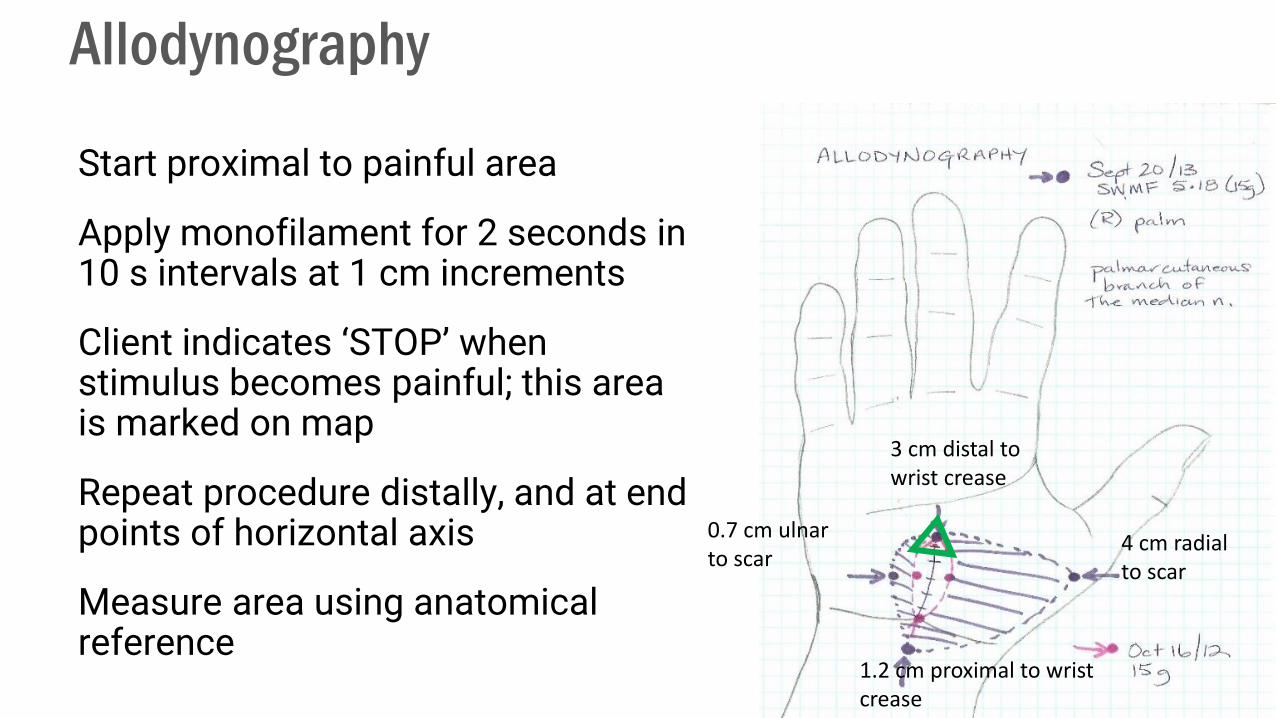
Allodynography
Start proximal to painful area
Apply monofilament for 2 seconds in 10 s intervals at 1 cm increments
Client indicates ‘STOP’ when stimulus becomes painful; this area is marked on map
Repeat procedure distally, and at end points of horizontal axis
Measure area using anatomical reference
1.2 cm proximal to wrist crease
3 cm distal to wrist crease
4 cm radial to scar
0.7 cm ulnar to scar

Reliability of Allodynography
Completed only in consenting participants demonstrating allodynia as defined by a painful response to a static touch with a 15g monofilament
Inter-rater reliability (n=12)ICC 2,1 = 0.97 [95%CI 0.90 - 0.99] single measures
Test-retest reliability (n=10) ICC 2,1 = 0.89 [95%CI=0.59-0.97] single measures
**p<0.001 for both(Packham et al, 2020)

Rainbow Pain Scale
24
Colours represent the severity of allodynia as represented by
the smallest amount of pressure which elicits a painful
response (Spicher et al, 2015; similar to Keizer et al, 2007).
Colour rating Purple Indigo Blue Green Yellow Orange Red
Pressure 15 g 8 g 4g 1.4g 0.6 0.16 0.04
Interpretation Discrete Significant Serious

25
Rainbow Pain Scale
The area tested for the Rainbow pain scale is marked on the allodynography map with a star
‘Colour’ category is also recorded there Rainbow pain
scale: blue ( 4 g)
26
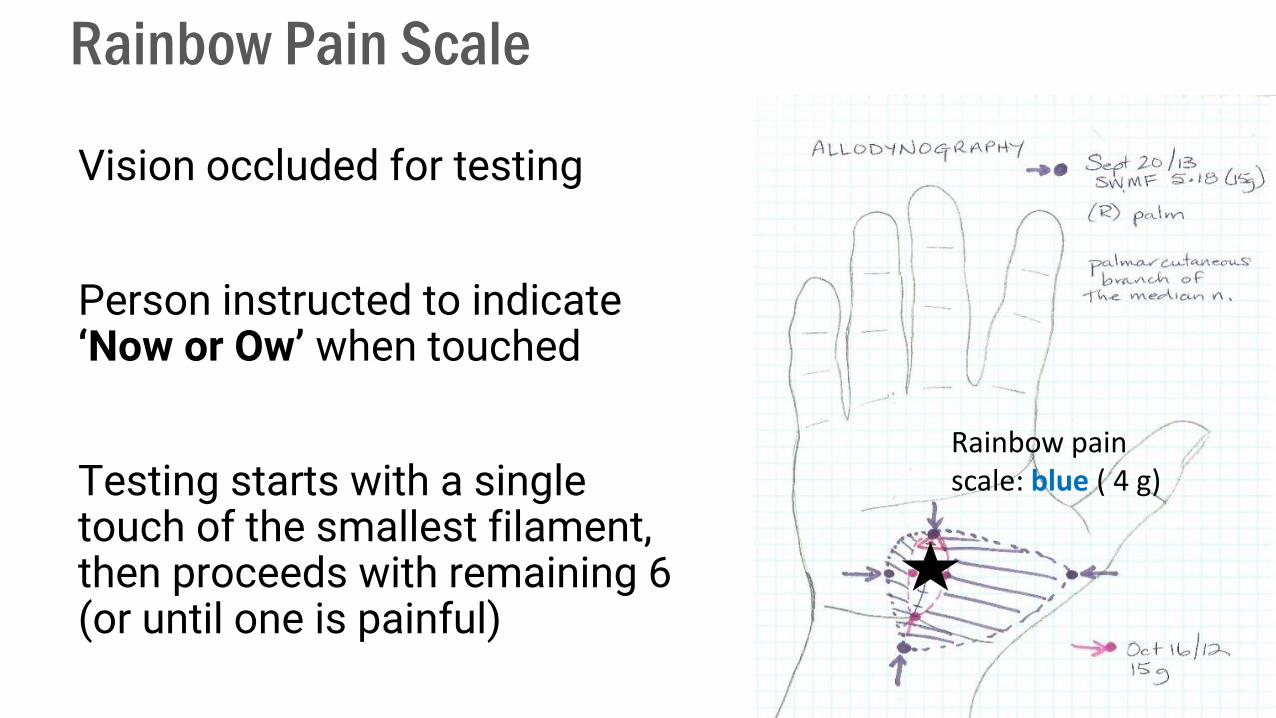
Rainbow Pain Scale
Vision occluded for testing
Person instructed to indicate ‘Now or Ow’ when touched
Testing starts with a single touch of the smallest filament, then proceeds with remaining 6 (or until one is painful)
Rainbow pain scale: blue ( 4 g)
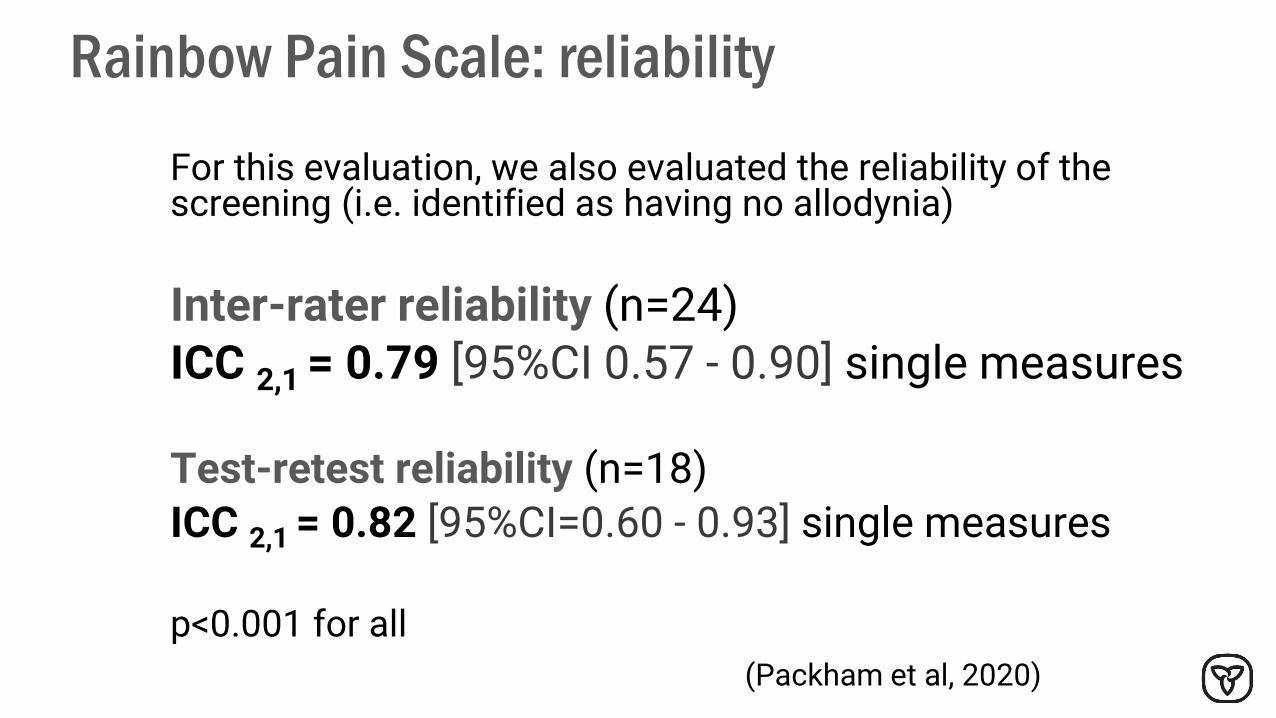
Rainbow Pain Scale: reliability
For this evaluation, we also evaluated the reliability of the screening (i.e. identified as having no allodynia)
Inter-rater reliability (n=24) ICC 2,1 = 0.79 [95%CI 0.57 - 0.90] single measures
Test-retest reliability (n=18)
ICC 2,1 = 0.82 [95%CI=0.60 - 0.93] single measures
p<0.001 for all
(Packham et al, 2020)
Somatosensory Rehabilitation
Conservative treatment for painful somatosensory disorders
Developed by an OT in Switzerland (Claude Spicher); therapists are trained and certified in method through U. of Brussels (CSTP©)
Key principle:
Reduce sensitization through comfortable sensory stimulation and sensory re-education
Basic tenets of the Somatosensory Rehabilitation Method (SRM)
1) Precise evaluation to define the territory that is painful to touch (allodynography & rainbow pain scale)
2) Formation of a plausible neuroanatomical hypothesis of the peripheral nerve branch(es) underlying the painful territory and contributing to peripheral sensitization
3) Avoid reinforcement of the sensitization mechanisms by minimizing evocation of pain by temporarily limiting touch (and consequently functional use) of the painful zone
4) Comfortable somatosensory ‘counter-stimulation’(tactile and/or vibratory) and sensory re-education
(Spicher et al, 2020)
29

Home Program: working zones
Avoid touch and movement in the red zone (thumb and wrist)
Counterstimulation ONLY on the green zone
Sensory re-education starting on the green zone and progressing into the yellow zone but NEVER on the red zone
Always STOP if it is painful
Consider a soft wrist and thumb support if tolerated (minimize intermittent touch)
Example for allodynia in DRSB territory

Distant vibrotactile counterstimulation
Comfortable tactile stimulation 8 times daily for no longer than one minute
Working zone on a non-painful area of skin anatomically related to the painful zone
- as close as you can get, but as far away as you need to be for the signals to be experienced as NORMAL & COMFORTABLE- a proximal cutaneous area of the same branch OR - arising from the same cord of the plexus OR- entering the spinal cord above or below the painful signals
Microfleece, fur, silk, lotion; stroking or rubbing
31

Sensory re-education strategies
Localization
Discrimination Direction of movementBig or smallLetter and shape recognitionHot and coldTextures
Mindful recognition (traditional re-education)
Tailored for maximum independence
NO desensitization! (Moseley et al, 2008; Lewis et al, 2011; Spicher et al, 2015)
32

Typical SRM treatment session
Review of home program – how often, working zone, response
Review of activities and problem-solving for challenges
Demonstration of re-education activities
Modification of home program based on feedback
Monthly re-evaluation of allodynia
33
Complimentary modalities in SRM
Gentle heat or TENS applied to working zone
Nerve glides through working zone
Gentle compression over allodynic territory to permit functional use (compression bandage, splinting, spandex undergarments) to minimize evoked pain from touch
Deep breathing and proximal massage for lymph drainage rather than local massage
Graded motor imagery for those with motor concerns; incorporate proprioceptive retraining in sensory re-education elements
Serial casting or low-load prolonged stretch static progressive splinting instead of PROM or CPM
34
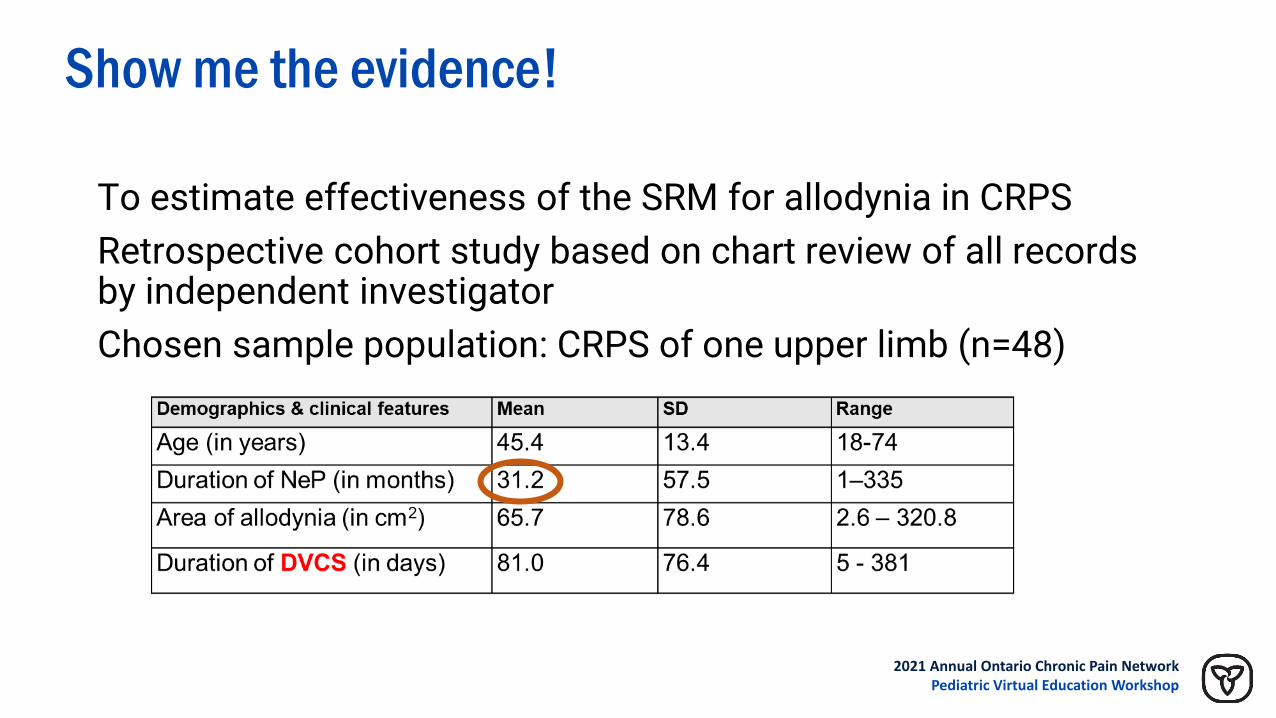
Show me the evidence!
To estimate effectiveness of the SRM for allodynia in CRPS
Retrospective cohort study based on chart review of all records by independent investigator
Chosen sample population: CRPS of one upper limb (n=48)
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop

Pain improves but doesn’t always disappear
Results
Baseline tQDSA (x=51.4, SD=17.1) *n=58 maps from 48 persons
Final tQDSA (x=20.4, SD=20.0) t(57)=13.6, p< 0.001
Final tQDSA for subgroup (58%) who completed full treatment (x=12.3, SD 10.2, range 0-41)
Effect Size (Cohen’s d) = 1.64 *all subjects, accounting for paired samples
QDSA = Questionnaire Douleur St. Antoine
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop
Limitations
No control group
Potential for bias (selection bias, response bias)
No long-term follow-up
Heterogenous severity and duration
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop
Take aways
Validated pediatric evaluations for CRPS symptoms and pain qualia are lacking
‘New’ evaluations to consider:
Skin temperature asymmetry of >1 Co
Allodynography, allodynia severity (rainbow pain scale) using monofilaments
Somatosensory rehabilitation = sensory re-education principles applied in a new framework
2021 Annual Ontario Chronic Pain Network Pediatric Virtual Education Workshop
References
Bruehl S. Complex regional pain syndrome. BMJ. 2015 Jul 29;351:h2730.
Gierthmühlen J, Binder A, Baron R. Mechanism-based treatment in complex regional pain syndromes. Nat Rev Neurol. 2014;10(9):1-11.
Grieve S, Perez RS, Birklein F, Brunner F, Bruehl S, Harden RN, et al. Recommendations for a first Core Outcome Measurement set for complex regional PAin syndrome Clinical sTudies (COMPACT). Pain. 2017;158(6):1083–90.
Harden RN, Maihofner C, Abousaad E, et al. A prospective, multisite, international validation of the Complex Regional Pain Syndrome Severity Score. Pain. 2017;158(8):1430-1436.
Lewis JS, Coales K, Hall J, McCabe CS. “Now you see it, now you do not”: sensory-motor re-education in complex regional pain syndrome. Hand Ther. 2011;16(2):29-38.
Llewellyn A, McCabe CS, Hibberd Y, et al. Are you better? A multi-centre study of patient-defined recovery from Complex Regional Pain Syndrome. Eur J Pain (United Kingdom). 2018;22(3):551–64.
Mansour AR, Farmer MA, Baliki MN, Apkarian AV. Chronic pain: the role of learning and brain plasticity. Restor Neurol Neurosci. 2014;32(1):129–39.
References
Mesaroli G, Ruskin D, Campbell F, et al. Clinical Features of Pediatric Complex Regional Pain Syndrome. Clin J Pain. 2019;35(12):1.
Moseley GL, Flor H. Targeting cortical representations in the treatment of chronic pain: A review. Neurorehabil Neural Repair. 2012;26(6):646-652.
Packham T, Holly J. Mechanism-specific rehabilitation management of complex regional pain syndrome: Proposed recommendations from evidence synthesis. J Hand Ther. 2018;31(1):10-19.
Packham T, Holly J. Therapists’ management of complex regional pain syndrome. In Skirven et al (eds) Rehabilitation of the Hand (8th ed.) Elsevier, 2020.
Packham T, Spicher CJ, MacDermid JC et al. Somatosensory rehabilitation for allodynia in complex regional pain syndrome of the upper limb: A retrospective cohort study. J Hand Ther. 2018;31(1):1-9.
Packham T, MacDermid JC, Henry J, Bain JR. The Hamilton Inventory for Complex Regional Pain Syndrome: A cognitive debriefing study of the clinician-based component. J Hand Ther. 2012;25(1):97-112.
Packham TL, MacDermid JC, Michlovitz SL, Buckley N. Content validation of the Patient-ReportedHamilton Inventory for Complex Regional Pain Syndrome. Can J Occup Ther. 2018. Apr;85(2):99-105.
Packham T, Spicher C, MacDermid J, Quintal I, Buckley N. Evaluating a sensitive issue: reliability of a clinical evaluation for allodynia severity. Somatosensory & Motor Research. 2020 Mar;37(1):22-27.
References
Packham T, Spicher CJ, MacDermid JC, Buckley DN. Allodynography: Reliability of a New Procedure for Objective Clinical Examination of Static Mechanical Allodynia. Pain Medicine.2020; 21(1), 2020, 101–108.
Packham T, MacDermid JC, Bain J, Buckley DN. Cold-pressor stimulated skin temperature asymmetries for the identification of CRPS. Canadian Journal of Pain 2018. 2(1). doi:10.1080/24740527.2018.1504283
Spicher C, Quintal I, Vittaz M. Reeducation Sensitive Des Douleurs Neuropathiques. (3rd ed). Montpellier, France: Sauramps Medical, 2015.
Spicher CJ, Packham TL, Buchet N, Quintal I, Sprumont P. Atlas of cutaneous branch territories for the diagnosis of neuropathic pain [1st ed. English]. Switzerland: Springer Nature. 2020.
Copyright © 2022 FDOKUMEN




















