
Etiology of community acquired pneumonia among adult patients requiring hospitalization in Taiwan

Eur Arch Otorhinolaryngol (2009) 266:1553–1561
DOI 10.1007/s00405-009-0957-0OTOLOGY
Comparison of acquired cholesteatoma between pediatric and adult patients
Cristina de Carvalho Dornelles · Sady Selaimen da Costa · Luíse Meurer · Letícia Petersen Schmidt Rosito · Andrei Roberto da Silva · Sabrina Lima Alves
Received: 8 April 2008 / Accepted: 10 March 2009 / Published online: 26 March 2009© Springer-Verlag 2009
Abstract The quantiWcation of angiogenesis and metallo-proteinases may be useful in cholesteatoma behaviorassessment as markers of its aggressiveness. The objectiveof this study is to compare markers CD31, MMP2 andMMP9 in pediatric and adult patients. This study is basedon cross-sectional studies of pediatric (·18 years old) andadult groups (¸19 years old). Samples of 120 cholesteato-mas were Wxed in 10% formol, prepared on Wve slides ofeach sample through habitual histological techniques, andnumber of blood vessels (CD31), marking with MMP2 and
MMP9, number of matrix cells and thickness at perimatrixcell were observed. Data were analyzed through SPSSusing Spearman and Mann–Whitney coeYcients. Choleste-atomas were equally distributed: 60 in pediatric patients(11.77 § 3.57 years); 60 in adult patients (38.29 § 14.51years). When correlating the number of blood vessels andmetalloproteinases with perimatrix thickness, we obtainedthe following values: pediatric CD31, 7 (4–11); adultCD31, 4 (0–10) (P = 0.044); pediatric cytoplasmatic MMP2,1 (0–3); adult cytoplasmatic MMP2, 0 (0–1) (P = 0.006);pediatric nuclear MMP2, 0 (0–1); adult nuclear MMP2, 0(0–1) (P = 0.056); pediatric MMP9, 2 (0–4); adult MMP9,0 (0–4) (P = 0.049). In conclusion, pediatric cholesteatomaspresent a more exacerbated inXammatory degree, producemore metalloproteinases, factors that, when combined, couldcharacterize pediatric cholesteatomas as more aggressivethan adult cholesteatomas.
Keywords Perimatrix · InXammation · Cholesteatoma · Angiogenesis · Collagenases
Introduction
Cholesteatomas were deWned by Schuknecht [1] as theaccumulation of scaled keratin inside the middle ear or anypneumatized area in the temporal bone deriving from a ker-atinized squamous epithelium. The annual incidence ofcholesteatoma was about 3 per 100,000 in children and 9.2per 100,000 in adult. There is male predominance, approxi-mately 1.4 times higher in men than in women [2–4].
Acquired cholesteatoma presented three histologicalcomponents: matrix, perimatrix and cystic content [5](Fig. 1). The matrix is a keratinized stratiWed squamous epi-thelium, with four layers that are identical to normal skin.
C. de Carvalho Dornelles (&)Centro de Otite Média do Brasil, Serviço de Otorrinolaringologia, Hospital de Clínicas de Porto Alegre, Rua Ramiro Barcelos, 2350, Zona 19, sala 1922, Porto Alegre CEP: 90003010, Brazile-mail: [email protected]
C. de Carvalho Dornelles · S. S. da CostaOphthalmology and Ear, Nose and Throat Department, Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, Brazil
S. S. da Costa · L. P. S. RositoSurgery Department, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
L. MeurerPathology Department, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
C. de Carvalho Dornelles · L. P. S. RositoEar, Nose and Throat Service, Hospital de Clínicas de Porto Alegre (HCPA), Porto Alegre, Brazil
A. R. da SilvaSUS Jundiaí, São Paulo, Brazil
S. L. AlvesRua Ramiro Barcelos, 2350, sala 1922, São Paulo, Brazil
123

1554 Eur Arch Otorhinolaryngol (2009) 266:1553–1561
The perimatrix is a loose connective tissue, containing col-lagen Wbers, Wbrocytes and inXammatory cells. The cysticcontent is constituted for keratin lamellae and ephitelialdebris [5].
Controversies exist as to whether cholesteatomas behavediVerently in children than in adults. On one hand, Sheehy[6], Tos [7] and Edelstein [8] believe that pediatric choleste-atomas are less expansive, leading to a lower rate of compli-cations. On the other hand, Glasscock [9], Ruah [10], Bujia[11], Palva [12] and SudhoV [13] hold that cholesteatomasoriginating in childhood are more aggressive and have moreextensive growth patterns. Smythe [14] considers pediatriccholesteatomas to be so diVerent from adult cholesteatomasthat they should be considered diVerent diseases.
In this context, Quaranta et al. [15] observed that theperimatrix of pediatric cholesteatomas is richer in mononu-clear inXammatory elements than that of adults. Based onthis Wnding, they suggest that the characteristics of the per-imatrix exert an important role in the pathogenesis of cho-lesteatomas, which could explain diVerences in thebehavior of pediatric and adult cholesteatomas [15].
Histological studies conducted by Dornelles et al. [16–18] identiWed an inverse correlation between the cholestea-toma perimatrix thickness and the patient’s age on the sur-gery date, as well as a direct correlation between thethickness and the histological degree of the inXammation atthe perimatrix. These Wndings suggest that the perimatrix isthicker and has a more exacerbated inXammatory process inpediatric cholesteatomas. It is known that the cholestea-toma growth requires angiogenesis in the perimatrix con-junctive tissue [19]. In these studies [16–18], theinXammatory activity degree of the perimatrix was calcu-lated through semi-quantitative measurements [20]. A moreprecise measurement of the inXammatory activity is the
angiogenesis quantiWcation, which can be performedimmunohistochemically by counting the blood vessels inthe perimatrix, through immunohistochemistry with markerCD31 [21, 22].
The exacerbated inXammatory process in cholesteatomaperimatrix adds more complexity to the chronic otitis mediawith cholesteatoma (COMC), with the bone erosion power,a characteristic that is almost universal of the COMC, oneof the parameters employed to assess its aggressiveness.Bernal-Sprekelsen et al. [23] suggested that metalloprotein-ases (MMPs) could explain part of the invasive anddestructive activities (destruction of ossicles and other partsof the temporal bone) of the ear cholesteatoma. MMPs arerelated to several aspects of tissue growth and invasion andthe stimulation of angiogenesis.
The quantiWcation of angiogenesis and metalloprotein-ases as markers of aggressiveness may be useful in choles-teatoma behavior assessment. Thus, the purpose of thisstudy is to analyze immunohistochemically both matrix andperimatrix of acquired cholesteatomas in children andadults, with markers CD31, MMP2 and MMP9, and corre-late such Wndings with their histological components andthe patient’s age on the surgery date.
Methods
This study was a comparative and contemporaneous cross-sectional analysis, approved by the institution in 2003. Allpatients signed the consent term for the anonymous utiliza-tion of data in scientiWc publications.
Patients were included according to the following crite-ria: (1) diagnosis of chronic otitis media with cholestea-toma; (2) presence of matrix (keratinized stratiWedsquamous epithelium) and perimatrix (loose connectivetissue) in the cholesteatoma sample collected (Fig. 1 is arepresentative cholesteatoma, showing histological compo-nents). Exclusion criteria were as follows: (1) diagnosis ofcongenital cholesteatoma; (2) sample inadequate for immu-nohistochemistry processing. The patients were divided intwo groups, according to their age at the time of surgery(adults if above 18 years old and children until that age).Sixty cholesteatomas were included in each group.
Tissue samples were collected, between May 2003 andMarch 2007, by the operating ENT surgeon, in speciWcssites of the middle ear and mastoid: mesotympanum (overthe bulging of the promontory); the medial wall of the ante-rior epitympanum, the prominence of the lateral semicircu-lar canal. These areas were chosen due to the smoothness ofthe surface making the removal of big pieces of well-con-served matrix and perimatrix possible. Samples of thesesites were thought to probably contain matrix and perima-trix, and have to measure at least 5 mm2. The material was
Fig. 1 Scanned image of the slide, cross-sectional cut of the choleste-atoma, stained with hematoxylin–eosin. The three constituting parts:a perimatrix, b matrix, c cystic content. MagniWcation: £100
123

Eur Arch Otorhinolaryngol (2009) 266:1553–1561 1555
immediately Wxed in 10% formol and processed by usualhistological techniques with inclusion in paraYn.
Five slides of each sample were prepared for morpholog-ical and immunohistochemical analysis. The slides wereanalyzed using a light microscope at 200 powers by twoindependent observers (one, a faculty member of thePathology Department of the Universidade Federal of RioGrande do Sul Medical School, and the other, the Wrstauthor). The slides were “blinded” prior to interpretation.
The Wrst slide was stained with hematoxylin–eosin (HE)(Fig. 2a). After conWrming the presence of matrix and per-imatrix, the following components were evaluated: averagenumber of epithelial cell layers of matrix, presence orabsence of delimiting epithelium, hyperplasia, Wbrosis andgranuloma.
The mean number of matrix cells layers was obtained bycounting cell layers in Wve diVerent Welds of slides. Theaverage value of those was considered for statistic analysis.
After slide evaluation in HE, with histological integrityconWrmation of the samples, the second slide was stainedwith Picrosyrius (Fig. 2b), for the perimatrix thicknessmeasurement. This stain was used for allowing a betterdiVerentiation of the perimatrix than with the HE stain(3A), as Picrosyrius stains the collagen Wbers in dark red,making it easier to delimit the thickness to be measured.The perimatrix thickness was obtained through analysis ofcomputerized images using ImagePro Plus Media Cyber-netics software (Fig. 3). Laminas were examined on alltheir extensions and 20 measurements of perimatrix wereobtained by each cholesteatoma, in order to denote theintrapatients variability. Using the 20 measures of eachperimatrix, we obtained the median, which is the summa-rizing measure for the analysis of perimatrix’s thickness.In cases in which perimatrix was extremely thin, not per-mitting the measurement the thickness was considered aszero.
Fig. 2 Histological image of the cholesteatoma stained with hematoxylin–eosin (a) and Picrosyrius (b): 1, perimatrix; 2, matrix; 3, cystic content. MagniWcation: £100
Fig. 3 Image obtained with ImagePro Plus through thickness measurement technique
123

1556 Eur Arch Otorhinolaryngol (2009) 266:1553–1561
The same cholesteatomas used in the sections with Pic-rosyrius stain were submitted to the immunohistochemistrytechnique employed in the Pathology Service routine,which consists in deparaYnization, rehydration, antigenretrieval, endogenous peroxidase inactivation, and blockingof non-speciWc background staining.
The third slide was prepared for counting the mean num-ber of blood vessels using the primary anti-CD31 antibody(clone JC7OA, Dako Cytomation, Carpinteria, CA, USA).The material was incubated for 12 h, at 4°C and 1:40 dilu-tion, followed by the application of streptavidin–biotin per-oxidase complex (LSAB, Dako) and print processing withdiaminobenzidine tetrahydrochloride (Kit DAB, Dako).
The mean number of blood vessels in the perimatrix(stained by the anti-CD31 antibody reaction) was collectedcontinuously, through the Chalkley count, where a 25-pointgrid is placed onto a scanned image and all points that coin-cide with the marked vessels are counted (Fig. 4). Two toWve images were used, depending on the size of the cho-lesteatomas, and the mean value was obtained with thenumber of counted vessels in each image. The perimatrixareas with evident granulation tissue were avoided in imagecapture. Reading of slides was performed by two indepen-dent observers (one was a student at the Pathology Depart-ment and one was the main researcher), the Wnal variablewas the mean value of all readings performed with eachslide.
In order to evaluate the production of metalloprotein-ases, the last two slides were prepared using anti-MMP2(72 kDa Collagennase IV, Chemicon International, USA)
and anti-MMP9 (clone 9D4.2, Chemicon International,USA) antibodies. Cuts of cholesteatomas were incubatedfor 72 h, at 4°C and 1:40 dilution, followed by the applica-tion of biotin–streptavidin peroxidase complex (LSAB,Dako) and print processing with diaminobenzidine tetrahy-drochloride (Kit DAB, Dako). Immunoreactivity ofmetalloproteinases was observed in the matrix of choleste-atomas, being MMP9 in the cytoplasm of epithelium cellsand MMP2 in the cytoplasm and nucleus.
The intensity of MMP2 and MMP9 colorings wasobserved and the results were expressed as 0, 1, 2 and 3,according to the metalloproteinase coloring intensity(absent, mild, moderate and accentuated, respectively).Besides the coloring evaluation, the percentage of stainedmaterial was also estimated, using a scale ranging from 0(no immunoreactivity) to 100% (all material was stained).Such percentage was dichotomized as follows: 1, percent-ages ranging from 0 to 50%; 2, from 51 to 100%. The Wnalvariable to be statistically analyzed was the product resultof the coloring intensity (0–3) using the multiplying factor(1 or 2) resulting from the percentage of stained material.
Frequency tables were used for descriptive data. Spear-man’s coeYcient was used in the statistical analysis, in thecorrelation of the mean number of blood vessels and thequantiWcation of metalloproteinases with the mean numberof cells in the matrix, the perimatrix thickness and thepatient’s age on the surgery date. The Mann–Whitney testwas used to compare the perimatrix thickness, the meannumber of blood vessels and the quantiWcation of metallo-proteinases between the groups. Fisher’s exact test was
Fig. 4 Image of ImagePro Plus Media Cybernetics software screen, showing Chalkley grid: 1, blood vessel marked that does not coincide with the grid point, 2 point that coincides with blood vessel
123

Eur Arch Otorhinolaryngol (2009) 266:1553–1561 1557
used to compare the presence of delimitating epithelium,hyperplasia, Wbrosis and granuloma between the groups.The analysis was performed through software applicationSPSS 13.0 for Windows. Values of P · 0.05 were consid-ered as statistically signiWcant.
Results
Demographic data
The sample was composed of 120 cholesteatomas, whichwere equally distributed in the pediatric and adult groups.The sample was also equally divided in terms of genre.
The mean § standard deviation of patient’s age on thesurgery date was 24.99 § 16.80 years. The pediatric grouppresented mean age of 11.75 § 3.48 years and the adultgroup presented mean age of 38.02 § 14.31.
As the dates did not present normal distribution, fromthis point, the median and interquartile interval will be pre-sented. By the same fact, all the statistical analysis will becarried out with nonparametric tests.
Histological Wndings
The mean number of cell layers in the matrix ranged from 2to 23, with median value of 6 (5–9). Hyperplasia in thematrix was identiWed in 35% of the cholesteatomas, 14%presented granuloma and 67% presented Wbrosis. The pres-ence of simple cuboidal epithelium, delimitating the perim-atrix in its depth plane, occurred in 20% of the cases.
The variable perimatrix thickness appeared in choleste-atomas from diVerent patients as well as in the materialfrom the same individual. One species in particular pre-sented areas from very delicate thickness to thick parts. Thethickness was 78 �m (34–217), considering the minimumvalue of 0 and the maximum value of 1,269. In sevencases—six adults and one pediatric case—the perimatrixwas extremely thin that it could not be measured, and wasconsidered as 0. Figure 5 shows some representative exam-ples of the variation in the histological composition foundin this sample of acquired cholesteatomas.
When stratiWed in age groups, the histological compo-nents analyzed in this study presented a similar distributionin both groups, except for the perimatrix thickness and thepresence of delimitating epithelium (Table 1).
Immunohistochemical Wndings
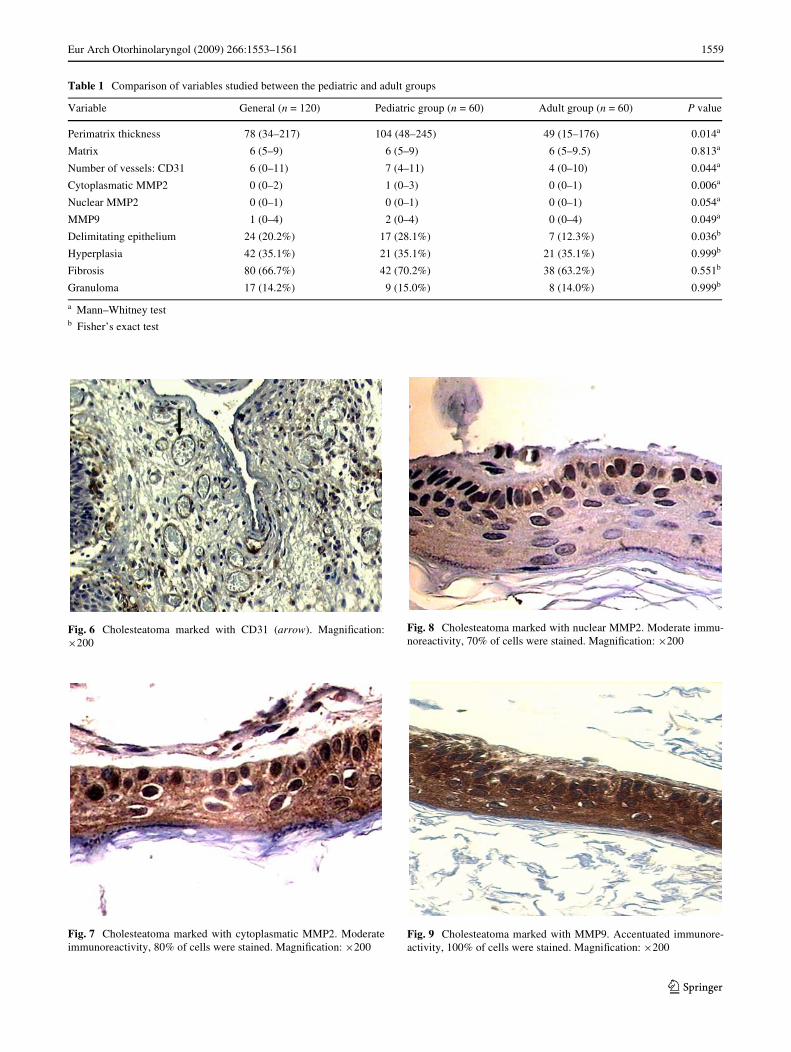
The mean number of blood vessels (Fig. 6) was 6 (0–11). Inthe pediatric group, this number was 7 (4–11) and 4 (0–10)in the adult group.
Cytoplasmatic MMP2 median value (Fig. 7) was 0 (0–1).In the pediatric group, this value was 1 (0–3) and 0 (0–1) inthe adult group.
The results of nuclear MMP2 (Fig. 8) were similar.Median value for the general group: 0 (0–1); in the pediat-ric group, it was 1 (0–1) and 0 (0–1) in the adult group.
MMP9 median value (Fig. 9) was 1 (0–4). In the pediat-ric group, this value was 2 (0–4) and 0 (0–4) in the adultgroup.
When comparing the mean value of blood vessels, thequantity of cytoplasmatic MMP2, nuclear MMP2 andMMP9 between the groups using the Mann–Whitney test,all variables analyzed showed a statistically signiWcantdiVerence.
Table 1 shows the comparison of histological and immu-nohistochemical variables between the pediatric and adultgroups, using Mann–Whitney and Fisher’s exact tests.
When correlating the mean number of blood vessels withthe mean number of metalloproteinases, with the meannumber of cell layers of the matrix and with the perimatrixthickness, strong correlations are found. Besides, an inversecorrelation of cytoplasmatic MMP2 with the patient’s ageon the surgery date was found (Table 2).
Discussion
In a series of studies conducted by our group [16–18] weanalyzed the histological inXammatory degree of the perim-atrix of acquired cholesteatomas, using a semi-quantitativevariable Wnd [16–18] a strong and inverse correlation thepatient’s age on the surgery date with the inXammatory pro-cess, i.e., the younger the patient, the larger the inXamma-tion. In this study, we attempted to enhance the precision ofthis analysis using a quantitative variable resulting from themeasurement through immunohistochemistry, anti-CD31antibody (marker of angiogenesis). With this variable, wefound a statistical diVerence of the angiogenesis betweenthe age groups (pediatric and adult groups) and we notesthat the mean number of blood vessels in the perimatrix ismuch higher in the pediatric group. This Wnding suggeststhat the inXammatory process is more exacerbated in chil-dren, a characteristic that could involve a higher aggres-siveness degree of the cholesteatomas presented by thepediatric group.
Besides the angiogenesis measurement, we also studiedthe metalloproteinases. This enzymes are closely associatedwith pathological absorption of the extra-cellular matrix inchronic inXammatory processes [24]. MMP activity is regu-lated by tissue inhibitor of metalloproteinase (TIMP) andthe interruption of such combination may lead to apathological process. Figure 10 shows the sites of MMP
123

1558 Eur Arch Otorhinolaryngol (2009) 266:1553–1561
production, expression and activity in the cholesteatomas(adapted from Medina and Radomski [25]).
Metalloproteinases are proteolytic enzymes that candegrade components of the connective tissue [24]. In addi-tion, the production of metalloproteinases is induced by theinXammatory process (cholesteatoma when infected possi-bly increases the production of this enzymes) [25].
Our results indicated that the metalloproteinases (cyto-plasmatic MMP2, nuclear MMP2 and MMP9) showedincreased expression in pediatric cholesteatomas. Itshould be noted that cytoplasmatic MMP2 was alsoinversely correlated with the patient’s age on the surgerydate, i.e., the younger the patient, the higher this proteinexpression.
Fig. 5 Representative cholesteatomas of the sample, illustrating theirhistological components: 1, perimatrix; 2, matrix; 3, cystic content.a Epitympanic cholesteatoma from a female patient of 44 years old. Inhistological terms, it presents stratiWed scaly keratinized epithelium,mean number of cell layers: three. Perimatrix is absent. MagniWcation:£200. b Epitympanic cholesteatoma from a male patient of 37 yearsold. In histological terms, it presents stratiWed scaly keratinized epithe-lium, mean number of cell layers: six. Narrow and Wbrotic perimatrix,with rare lymphocytes. Absence of granuloma. MagniWcation: £200.c Mesotympanic cholesteatoma from a female patient of 35 years old.In histological terms, it presents stratiWed scaly keratinized epithelium,mean number of cell layers: four. Very narrow perimatrix, no Wbrosisand no inXammatory inWltrate. MagniWcation: £200. d Mesotympaniccholesteatoma from a male patient of 16 years old. In histological
terms, it presents stratiWed scaly keratinized epithelium, mean numberof cell layers: six. Narrow and delicate perimatrix, no Wbrosis and withlittle inXammatory inWltrate. MagniWcation: £200. e Epitympanic cho-lesteatoma from a female patient of 11 years old. In histological terms,it presents stratiWed scaly keratinized epithelium, mean number of epi-thelial cell layers: 12. The perimatrix presents dense Wbrosis, accentu-ated chronic inXammatory inWltrate and is delimitated in its depthplane by simple cuboidal epithelium. MagniWcation: £50. f Mesotym-panic cholesteatoma from a female patient of 7 years old. In histologi-cal terms, it presents stratiWed scaly keratinized epithelium, meannumber of cell layers: 13. The perimatrix presents mild Wbrosis withaccentuated inXammatory inWltrate and neutrocytic exudation, beingdelimitated in its depth plane by simple cuboidal epithelium. Absenceof granuloma. MagniWcation: £50
123
Eur Arch Otorhinolaryngol (2009) 266:1553–1561 1559
Table 1 Comparison of variables studied between the pediatric and adult groups
a Mann–Whitney testb Fisher’s exact test
Variable General (n = 120) Pediatric group (n = 60) Adult group (n = 60) P value
Perimatrix thickness 78 (34–217) 104 (48–245) 49 (15–176) 0.014a
Matrix 6 (5–9) 6 (5–9) 6 (5–9.5) 0.813a
Number of vessels: CD31 6 (0–11) 7 (4–11) 4 (0–10) 0.044a
Cytoplasmatic MMP2 0 (0–2) 1 (0–3) 0 (0–1) 0.006a
Nuclear MMP2 0 (0–1) 0 (0–1) 0 (0–1) 0.054a
MMP9 1 (0–4) 2 (0–4) 0 (0–4) 0.049a
Delimitating epithelium 24 (20.2%) 17 (28.1%) 7 (12.3%) 0.036b
Hyperplasia 42 (35.1%) 21 (35.1%) 21 (35.1%) 0.999b
Fibrosis 80 (66.7%) 42 (70.2%) 38 (63.2%) 0.551b
Granuloma 17 (14.2%) 9 (15.0%) 8 (14.0%) 0.999b
Fig. 6 Cholesteatoma marked with CD31 (arrow). MagniWcation:£200
Fig. 7 Cholesteatoma marked with cytoplasmatic MMP2. Moderateimmunoreactivity, 80% of cells were stained. MagniWcation: £200
Fig. 8 Cholesteatoma marked with nuclear MMP2. Moderate immu-noreactivity, 70% of cells were stained. MagniWcation: £200
Fig. 9 Cholesteatoma marked with MMP9. Accentuated immunore-activity, 100% of cells were stained. MagniWcation: £200
123

1560 Eur Arch Otorhinolaryngol (2009) 266:1553–1561
We know that MMP2 is a proteolytic enzyme associatedwith the ability to penetrate into and invade adjacent tissues[26]. In normal biological processes, the metalloproteinases
are responsible for the bony tissue homeostase, with higherexpression in inXammatory osteolytic diseases. Based onour results, we can suggest that pediatric cholesteatomas
Table 2 Correlations found when comparing the studied variables
Age, patient’s age on the surgery date (years); thickness, perimatrix thickness (�m); matrix, mean number of cell layers in the matrix; inXammation,histological inXammation degree; CD31, mean number of blood vessels in the perimatrix; c MMP2, reactivity of metalloproteinase 2 in the matrixcell cytoplasm; n MMP2, reactivity of metalloproteinase 2 in matrix cell nucleus; MMP9, reactivity of metalloproteinase 9 in the matrix cell cyto-plasm; Spearman’s correlation coeYcient (P value)
Age Thickness Matrix CD31 c MMP2 n MMP2 MMP9
Age – ¡0.256 (0.008) ¡0.010 (0.919) ¡0.164 (0.160) ¡0.248 (0.027) ¡0.139 (0.180) ¡0.154 (0.173)
Thickness ¡0.256 (0.008) – 0.479 (<0.0001) 0.742 (<0.0001) 0.465 (<0.0001) 0.414 (<0.0001) 0.643 (<0.0001)
Matrix ¡0.010 (0.919) 0.439 (<0.0001) – 0.473 (<0.0001) 0.302 (<0.0001) 0.183 (0.077) 0.300 (0.007)
CD31 ¡0.164 (0.160) 0.742 (<0.0001) 0.473 (<0.0001) – 0.539 (<0.0001) 0.515 (<0.0001) 0.850 (<0.0001)
c MMP2 ¡0.248 (0.027) 0.465 (<0.0001) 0.302 (<0.0001) 0.539 (<0.0001) – 0.908 (<0.0001) 0.664 (<0.0001)
n MMP2 ¡0.139 (0.180) 0.414 (<0.0001) 0.183 (0.077) 0.515 (<0.0001) 0.908 (<0.0001) – 0.548 (<0.0001)
MMP9 ¡0.154 (0.173) 0.643 (<0.0001) 0.300 (0.007) 0.850 (<0.0001) 0.664 (<0.0001) 0.548 (<0.0001) –
Fig. 10 Summary of the diVer-ent cell types that produce MMP and TIMP. The cholesteatoma matrix may initiate the immuno-logical response with the activa-tion of diVerent cells in the perimatrix, such as macro-phages, Wbroblasts and leuko-cytes, releasing cytokines, such as interleukin-1 (IL-1) and the tumoral necrosis factor (TNF-�). The activated immunological cells can also release both MMP and TIMP. Physiological condi-tions may cause unbalanced MMP/TIMP. InXammatory reactions lead to unbalance of MMP in relation to TIMP, which may cause the extra-cellular matrix remodeling
123

Eur Arch Otorhinolaryngol (2009) 266:1553–1561 1561
present a greater potential for bone invasion and erosion, asa result of the higher expression of metalloproteinases andthis aggressiveness is possibly related to a series of bio-chemical process that occur in the perimatrix.
Combining the Wnds this study and the results of our pre-vious studies [16–18], we combine numbers of clues pointto greater aggressiveness of chronic otitis media with cho-lesteatoma in children: the pediatric cholesteatomas presenta thicker perimatrix, a more exacerbated inXammatory pro-cess, a higher degree of angiogenesis and produce moremetalloproteinases than cholesteatomas of adult patients.
Conclusions
The expressions of CD31, cytoplasmatic MMP2, nuclearMMP2 and MMP9 are higher in the pediatric group.
The mean number of blood vessels is strongly correlatedwith the quantity of metalloproteinases, the mean numberof cell layers in the matrix, the perimatrix thickness and thehistological inXammation degree.
Acknowledgments We would like to thank the Pathology and Ear,Nose and Throat Departments of the Hospital de Clínicas de PortoAlegre, for the permission to use their facilities and enable the devel-opment of this project. The Research and Post Graduation Group of theHospital de Clínicas de Porto Alegre (GPPG-HCPA) and the PostGraduation Program in Medical Sciences: Pediatrics Department of theUniversidade Federal do Rio Grande do Sul, for their technical sup-port. The Fundo de Incentivo à Pesquisa e Eventos of the Hospital deClínicas de Porto Alegre (FIPE-HCPA), for the research Wnancing.
ConXict of interest statement The authors did not have a Wnancialrelationship with the organization that sponsored the research.
References
1. Schuknecht HF (1974) The pathology of the ear. Harvard Univer-sity, Cambridge
2. Tos M (1988) Incidence, etiology and pathogenesis of cholestea-toma in children: a long-term study of results. Otol Rhinol Laryn-gol 40:110–117
3. Kemppainen HO, Puhakka HJ, Laippala PJ, Sipila MM, ManninenMP, Karma PH (1999) Epidemiology and etiology of middle earcholesteatoma. Acta Otolaryngol 119:568–572
4. Quantin L, Fernández SC, Moretti J (2002) Congenital cholestea-toma of external auditory canal. Int J Pediatr Otorhinolaryngol62:175–179
5. Lim DJ, Saunders WE (1972) Acquired cholesteatoma: light andelectron microscopic observations. Ann Otol 81:2–12
6. Sheehy JL (1978) Management of cholesteatoma in children. AdvOtorhinolaryngol 23:58–64
7. Tos M (1983) Treatment of cholesteatoma in children: a long-termstudy of results. J Otol 4:189–197
8. Edelstein DR (1989) Acquired cholesteatoma in pediatric agegroup. Otoloraryngol Clin North Am 22(5):955–964
9. Glasscock ME, Dickins JFE, Wiet R (1981) Cholesteatoma in chil-dren. Laryngoscope 91:1743–1753
10. Ruah CB, Schachem PA, Paparella MM, Zelterman D (1992)Mechanisms of retraction pocket formation in the pediatric tym-panic membrane. Arch Otolaryngol Head Neck Surg118(12):1298–1305
11. Bujia J, Holly A, Antoli-Candela F, Tapia MG (1996) Immunobi-ological peculiarities of cholesteatoma in children: quantiWcationof epithelial proliferation by MIB1. Laryngoscope 106(7):865–868
12. Palva A, Karma P, Kärjä J (1997) Cholesteatoma in children. ArchOtolaryngol 103(2):74–77
13. SudhoV H, Dazert S, Gonzales AM, Borkowski G, Park SY, BairdA et al (2000) Angiogenesis and angiogenic growth factors in mid-dle ear cholesteatoma. Am J Otol 21:793–798
14. Smythe JL, Brachman D, Grahm M (1984) Complications of cho-lesteatoma: a report on 1024 cases. In: Swartz JD (ed) Cholesteato-mas of the middle ear. Diagnosis, etiology and complications.Radiol Clin North Am 22:15–34
15. Quaranta A, Resta L, Santangelo A (1986) Otomastoid cholestea-toma in children: histopathological Wndings. Int J Pediatric Otorh-inolaryngol 12(2):121–126
16. Dornelles CD (2004) Colesteatomas Adquiridos: Análise Compar-ativa da Perimatriz entre Pacientes Pediátricos e Adultos [disser-tação]. Porto Alegre, UFRGS
17. Dornelles CD, Costa SS, Meurer L, Schweiger C (2005) Com-paração da espessura da perimatriz, de colesteatomas adquiridos,entre pacientes pediátricos e adultos. Rev Bras ORL 71(6):792–797
18. Dornelles CD, Costa SS, Meurer L, Schweiger C (2006) Descriçãohistológica de colesteatomas adquiridos: comparação entre amo-stras de crianças e de adultos. Rev Bras ORL 72(5):641–648
19. Milewski C (1998) Role of perimatrix Wbroblast in development ofacquire middle ear cholesteatoma. A hypothesis. HNO 46(5):494–501
20. Baak JPA (1991) Manual of quantitative pathology in cancer diag-nosis and prognosis. Springer, New York
21. Meurer L (2003) Densidade microvascular e expressãoimunoistoquímica de p21: associação com sobrevida em pacientessubmetidos à cirurgia por carcinoma epidermóide de esôfago[tese]. Porto Alegre, UFRGS
22. Folkman J (1995) Tumor angiogenesis. In: Mendelson JHP, IsraelMA, Liotta LA (eds) The molecular basis of cancer. WB Saunders,Philadelphia, pp 206–232
23. Bernal-Sprekelsen M, Ebmeyer J, Anonopoulos A, Borkowiski G,SudhoV H (2001) Alteraciones de la membrana basal en el coles-teatoma de oído medio. Acta Otorrinolaringol Esp 52(4):330–335
24. Wilmoth JG, Schultz GS, Antonelli PJ (2003) Tympanic mem-brane metalloproteinase inXammatory response. OtolaryngolHead Neck Surg 129(6):647–654
25. Medina C, Radomski MW (2006) Role of matrix metalloproteinasesin intestinal inXammation. J Pharmacol Exp Ther 318(3):933–938
26. Banerjee AR, James R, Narula AA (1998) Matrix metalloprotein-ase-2 and matrix metalloproteinase-9 in cholesteatoma and deepmeatal skin. Clin Otolaryngol 23(4):345–347
123
Copyright © 2022 FDOKUMEN




















