
Clinical trials update from the American Heart Association 2006: OAT, SALT 1 and 2, MAGIC, ABCD,...
9
Clinical trials update from the American Heart Association meeting: ACORN-CSD, primary care trial of chronic disease management, PEACE, CREATE, SHIELD, A-HeFT, GEMINI, vitamin E meta-analysis, ESCAPE, CARP, and SCD-HeFT cost-effectiveness study Rhidian J. Shelton a , Periaswamy Velavan a , Nikolay P. Nikitin a , Alison P. Coletta a, * , Andrew L. Clark a , Alan S. Rigby a , Nick Freemantle b , John G.F. Cleland a a Department of Cardiology, University of Hull, Castle Hill Hospital, Cottingham, Kingston-upon-Hull HU15 5JQ, UK b Department of Primary Care and General Practice, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK Received 15 November 2004; accepted 23 November 2004 Abstract This article provides information and a commentary on landmark trials presented at the American Heart Association meeting held in November 2004, relevant to the pathophysiology, prevention, and treatment of heart failure. An open trial of the ACORN Cardiac Support Device (CSD) showed encouraging preliminary results in patients with severe heart failure. The PEACE (Prevention of Events with Angiotensin-Converting Enzyme inhibition) study supports data from previous studies showing that ACE inhibitors reduce vascular events in patients at increased risk. The CREATE (clinical trial of metabolic modulation in acute MI treatment evaluation) study of patients with acute myocardial infarction (MI) showed no mortality benefit of a glucose/insulin/potassium regimen, but treatment with reviparin reduced the incidence of death, MI, or stroke. Azimilide was not associated with a significant reduction in shocks, but reduced the shocks or episodes of markedly symptomatic ventricular tachycardia terminated by pacing in the SHIELD (Shock Inhibition Evaluation with Azimilide) study. The addition of isosorbide dinitrate plus hydralazine to standard therapy improved survival in black heart failure patients in the A-HeFT (African– American Heart Failure Trial) study. In an investigation of hypertensive patients with diabetes, carvedilol had fewer adverse effects on diabetic control than metoprolol. A meta-analysis of high-dose vitamin E supplementation suggested an association with increased mortality. The ESCAPE (Evaluation Study of CHF and Pulmonary Artery Catheterisation Effectiveness) study showed no benefit of pulmonary artery catheterisation over clinical management in patients with severe heart failure. Routine prophylactic coronary revascularisation for stable coronary disease prior to major vascular surgery showed no benefit in the CARP (Coronary Artery Revascularization Prophylaxis) study. Analysis of data from SCD-HeFT supports the cost-effectiveness of ICDs in heart failure, although overall cost implications may be prohibitive. D 2004 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. Keywords: ACORN-CSD; Primary care trial of chronic disease management; PEACE; CREATE; SHIELD; A-HeFT; GEMINI; Vitamin E meta-analysis; ESCAPE; CARP; SCD-HeFT cost-effectiveness 1. ACORN Cardiac Support Device (CSD) trial The ACORN CSD is a high-technology fibre mesh that can be wrapped around the heart to provide some external elastic constraint and, therefore, myocardial support in diastole. Theoretically, this could prevent progressive left ventricular dilatation or even reverse it by reducing diastolic myocardial transmural stress [1]. Apart from the obvious risks of surgery and infection, there is a theoretical risk of producing iatrogenic pericardial restriction. The ACORN-CSD trial enrolled 300 patients with heart failure (NYHA II–IV, 6 MWT b150 m) and LVSD (EF 1388-9842/$ - see front matter D 2004 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.ejheart.2004.11.008 * Corresponding author. Tel.: +44 1482 624086; fax: +44 1482 624085. E-mail address: [email protected] (A.P. Coletta). The European Journal of Heart Failure 7 (2005) 127 – 135 www.elsevier.com/locate/heafai by guest on June 12, 2013 http://eurjhf.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Clinical trials update from the American Heart Association 2006: OAT, SALT 1 and 2, MAGIC, ABCD,...

www.elsevier.com/locate/heafai
The European Journal of Heart
Dow
nloaded from
Clinical trials update from the American Heart Association meeting:
ACORN-CSD, primary care trial of chronic disease management,
PEACE, CREATE, SHIELD, A-HeFT, GEMINI, vitamin E meta-analysis,
ESCAPE, CARP, and SCD-HeFT cost-effectiveness study
Rhidian J. Sheltona, Periaswamy Velavana, Nikolay P. Nikitina, Alison P. Colettaa,*,
Andrew L. Clarka, Alan S. Rigbya, Nick Freemantleb, John G.F. Clelanda
aDepartment of Cardiology, University of Hull, Castle Hill Hospital, Cottingham, Kingston-upon-Hull HU15 5JQ, UKbDepartment of Primary Care and General Practice, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK
Received 15 November 2004; accepted 23 November 2004
by guest on June 12, 2013http://eurjhf.oxfordjournals.org/
Abstract
This article provides information and a commentary on landmark trials presented at the American Heart Association meeting held in
November 2004, relevant to the pathophysiology, prevention, and treatment of heart failure. An open trial of the ACORN Cardiac Support
Device (CSD) showed encouraging preliminary results in patients with severe heart failure. The PEACE (Prevention of Events with
Angiotensin-Converting Enzyme inhibition) study supports data from previous studies showing that ACE inhibitors reduce vascular events in
patients at increased risk. The CREATE (clinical trial of metabolic modulation in acute MI treatment evaluation) study of patients with acute
myocardial infarction (MI) showed no mortality benefit of a glucose/insulin/potassium regimen, but treatment with reviparin reduced the
incidence of death, MI, or stroke. Azimilide was not associated with a significant reduction in shocks, but reduced the shocks or episodes of
markedly symptomatic ventricular tachycardia terminated by pacing in the SHIELD (Shock Inhibition Evaluation with Azimilide) study. The
addition of isosorbide dinitrate plus hydralazine to standard therapy improved survival in black heart failure patients in the A-HeFT (African–
American Heart Failure Trial) study. In an investigation of hypertensive patients with diabetes, carvedilol had fewer adverse effects on
diabetic control than metoprolol. A meta-analysis of high-dose vitamin E supplementation suggested an association with increased mortality.
The ESCAPE (Evaluation Study of CHF and Pulmonary Artery Catheterisation Effectiveness) study showed no benefit of pulmonary artery
catheterisation over clinical management in patients with severe heart failure. Routine prophylactic coronary revascularisation for stable
coronary disease prior to major vascular surgery showed no benefit in the CARP (Coronary Artery Revascularization Prophylaxis) study.
Analysis of data from SCD-HeFT supports the cost-effectiveness of ICDs in heart failure, although overall cost implications may be
prohibitive.
D 2004 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
Keywords: ACORN-CSD; Primary care trial of chronic disease management; PEACE; CREATE; SHIELD; A-HeFT; GEMINI; Vitamin E meta-analysis;
ESCAPE; CARP; SCD-HeFT cost-effectiveness
1. ACORN Cardiac Support Device (CSD) trial
The ACORN CSD is a high-technology fibre mesh that
can be wrapped around the heart to provide some external
1388-9842/$ - see front matter D 2004 European Society of Cardiology. Publishe
doi:10.1016/j.ejheart.2004.11.008
* Corresponding author. Tel.: +44 1482 624086; fax: +44 1482
624085.
E-mail address: [email protected] (A.P. Coletta).
elastic constraint and, therefore, myocardial support in
diastole. Theoretically, this could prevent progressive left
ventricular dilatation or even reverse it by reducing diastolic
myocardial transmural stress [1]. Apart from the obvious
risks of surgery and infection, there is a theoretical risk of
producing iatrogenic pericardial restriction.
The ACORN-CSD trial enrolled 300 patients with heart
failure (NYHA II–IV, 6 MWT b150 m) and LVSD (EF
Failure 7 (2005) 127–135
d by Elsevier B.V. All rights reserved.
R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135128
by guest ohttp://eurjhf.oxfordjournals.org/
Dow
nloaded from
b35% and LVEDD N60 mm) who did not require CABG.
Of these, 193 patients were scheduled for mitral valve
surgery for mitral regurgitation. These patients were
randomised to no additional procedure (n=102) or addi-
tional CSD (n=91). A total of 107 patients did not require
mitral surgery and these were randomised to receive (n=57)
or not to receive (n=50) CSD in addition to optimal medical
therapy. The primary endpoint of the trial was a composite
of (a) death, (b) major cardiac procedures (CABG, valve
surgery, LVAD, transplant, or CRT), and (c) worsening
NYHA class.
The patients enrolled had a mean age of 52 years, 55%
were men, only 10% had IHD, mean LVEF was 27.4% (but
many had severe mitral regurgitation), and LVEDD was 72
mm. Over the following year, the ACORN-CSD reduced LV
diastolic volume by about 25 ml more than control
( pb0.01), with some evidence of increasing effect over
time. Trends to improvement in LVEF (3% v 1%) were not
significant. Quality of life scores (Minnesota and SF36)
both improved ( pb0.05 and p=0.015, respectively) but
NYHA class did not. However, the trial was unblinded and
therefore subjective measurements should be treated with
caution. Rehospitalisation and mortality were unaffected,
but major cardiac procedures were reduced and therefore the
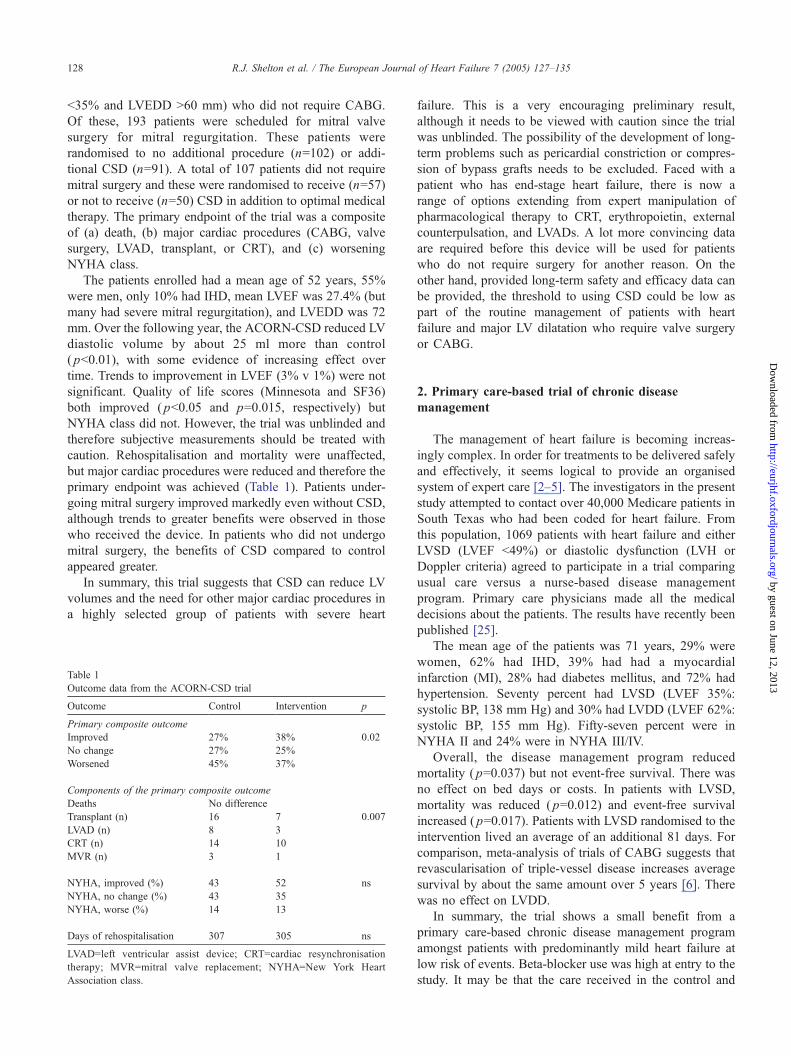
primary endpoint was achieved (Table 1). Patients under-
going mitral surgery improved markedly even without CSD,
although trends to greater benefits were observed in those
who received the device. In patients who did not undergo
mitral surgery, the benefits of CSD compared to control
appeared greater.
In summary, this trial suggests that CSD can reduce LV
volumes and the need for other major cardiac procedures in
a highly selected group of patients with severe heart
Table 1
Outcome data from the ACORN-CSD trial
Outcome Control Intervention p
Primary composite outcome
Improved 27% 38% 0.02
No change 27% 25%
Worsened 45% 37%
Components of the primary composite outcome
Deaths No difference
Transplant (n) 16 7 0.007
LVAD (n) 8 3
CRT (n) 14 10
MVR (n) 3 1
NYHA, improved (%) 43 52 ns
NYHA, no change (%) 43 35
NYHA, worse (%) 14 13
Days of rehospitalisation 307 305 ns
LVAD=left ventricular assist device; CRT=cardiac resynchronisation
therapy; MVR=mitral valve replacement; NYHA=New York Heart
Association class.
failure. This is a very encouraging preliminary result,
although it needs to be viewed with caution since the trial
was unblinded. The possibility of the development of long-
term problems such as pericardial constriction or compres-
sion of bypass grafts needs to be excluded. Faced with a
patient who has end-stage heart failure, there is now a
range of options extending from expert manipulation of
pharmacological therapy to CRT, erythropoietin, external
counterpulsation, and LVADs. A lot more convincing data
are required before this device will be used for patients
who do not require surgery for another reason. On the
other hand, provided long-term safety and efficacy data can
be provided, the threshold to using CSD could be low as
part of the routine management of patients with heart
failure and major LV dilatation who require valve surgery
or CABG.
n June 12, 2013
2. Primary care-based trial of chronic disease
management
The management of heart failure is becoming increas-
ingly complex. In order for treatments to be delivered safely
and effectively, it seems logical to provide an organised
system of expert care [2–5]. The investigators in the present
study attempted to contact over 40,000 Medicare patients in
South Texas who had been coded for heart failure. From
this population, 1069 patients with heart failure and either
LVSD (LVEF b49%) or diastolic dysfunction (LVH or
Doppler criteria) agreed to participate in a trial comparing
usual care versus a nurse-based disease management
program. Primary care physicians made all the medical
decisions about the patients. The results have recently been
published [25].
The mean age of the patients was 71 years, 29% were
women, 62% had IHD, 39% had had a myocardial
infarction (MI), 28% had diabetes mellitus, and 72% had
hypertension. Seventy percent had LVSD (LVEF 35%:
systolic BP, 138 mm Hg) and 30% had LVDD (LVEF 62%:
systolic BP, 155 mm Hg). Fifty-seven percent were in
NYHA II and 24% were in NYHA III/IV.
Overall, the disease management program reduced
mortality ( p=0.037) but not event-free survival. There was
no effect on bed days or costs. In patients with LVSD,
mortality was reduced ( p=0.012) and event-free survival
increased ( p=0.017). Patients with LVSD randomised to the
intervention lived an average of an additional 81 days. For
comparison, meta-analysis of trials of CABG suggests that
revascularisation of triple-vessel disease increases average
survival by about the same amount over 5 years [6]. There
was no effect on LVDD.
In summary, the trial shows a small benefit from a
primary care-based chronic disease management program
amongst patients with predominantly mild heart failure at
low risk of events. Beta-blocker use was high at entry to the
study. It may be that the care received in the control and

R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135 129
intervention groups was rather similar. Other studies have
suggested that specialist care might have increased benefits
further. The data are consistent with other studies that have
shown either a reduction in mortality or in rehospitalisation,
or both [2,3]. The lack of effect in patients with LVDD may
reflect the better prognosis of (and lack of effective
therapies for) this group of patients.
by guest on June 12, 2013http://eurjhf.oxfordjournals.org/
Dow
nloaded from
3. PEACE: Prevention of Events with
Angiotensin-Converting Enzyme inhibition
The results of PEACE have already been reported [7].
Briefly, the study recruited 8290 patients aged N50 years
with proven stable coronary disease in whom a LVEF b40%
or serum creatinine N177 Amol/l had been excluded, and
who had tolerated 2 mg of trandolapril for 2 weeks. Patients
were then randomised to double-blind placebo or trando-
lapril 4 mg/day. The initial intention was to randomise
N14,000 patients with a primary endpoint of death or MI.
Due to poor recruitment, the primary endpoint was
expanded to include coronary revascularisation, and this
increase in event rate allowed a reduction in study size to
8100 patients. The mean follow-up was 4.8 years.
The mean age of the patients was 64 years, 54% had had
a MI, and 17% had diabetes. Ninety percent were receiving
aspirin, 70% lipid-lowering drugs, and 60% beta-blockers.
Seventy-two percent had undergone revascularisation prior
to entry and a further 19% underwent first or repeat
revascularisation during the course of the study.
Trandolapril did not reduce any of the primary or
preplanned secondary outcomes. Overall, there were only
six fewer cardiovascular deaths on trandolapril compared to
placebo. The trial appears resoundingly neutral—but is it
really different from HOPE and EUROPA, trials in which
the ACE inhibitors ramipril and perindopril were shown to
reduce cardiovascular events? The answer is probably not.
The confidence intervals surrounding the modest effects of
ACE inhibitor on the same endpoint in all three trials
overlap. Indeed, for the most robust outcome, all-cause
mortality, the relative benefits in PEACE (11%), EUROPA
(11%), and HOPE (16%) are very similar. Absolute benefits
were also similar but small (0.9%, 0.8%, and 1.8%,
respectively). The HOPE trial did observe a reduction in
revascularisation, where intervention was predominantly
CABG ( p=0.002), an outcome that showed a strong
positive trend in PEACE. On the other hand, revascularisa-
tion was not reduced in EUROPA and revascularisation in
this trial was probably predominantly by PCI, an outcome
on which trandolapril had no effect in PEACE. Had
coronary revascularisation been added to the primary
endpoint of EUROPA, the effects of perindopril would
have been attenuated or lost. Unfortunately, the PEACE trial
has insufficient power to show an effect on outcomes such
as CVS death, MI, or stroke because it included fewer
patients than either EUROPA or HOPE, and also had a
lower annual event rate compared to HOPE (about 2%
compared to about 3%).
In HOPE, for every 1000 patients treated for 5 years,
between 20 and 60 patients would have CVS death, MI, or
stroke prevented. In EUROPA, it would be between 15 and
40, and in PEACE, up to about 20. Of course, this means
that over 90% of patients in each of the trials obtained no
demonstrable benefit. The PEACE study should make us
reconsider the medical philosophy of treating large
numbers of patients for small benefits. Accurate targeting
of highly effective therapy to the individual patient’s needs
should be the goal of modern medicine. PEACE may mark
the beginning of the end of the era of the megatrial.
Although large studies may provide tight confidence
intervals around their result, the clinical relevance of any
intervention that requires a large long-term study to show a
statistical effect must be questioned. In other words, large
studies are only really useful when they are neutral or
when they are stopped early.
However, it is possible that the trials had genuinely
different results. Trandolapril reduced mortality in the
TRACE study and cannot be considered ineffective, but
important differences between ACE inhibitors are possible.
It may be that higher doses are required in the patient group
recruited to PEACE, although the dose of ramipril was only
10 mg/day in HOPE. On the other hand, differences in
treatment or patients may be important. Diabetes was more
common in HOPE, but no benefit in this subgroup was
observed in PEACE. Most of the benefits in HOPE were
confined to the 25% of patients who were not taking aspirin
(Fig. 1). High aspirin use may have accounted for the trend to
lesser benefit observed in EUROPA and PEACE. However,
the rate of death or MI on active treatment in EUROPA and
PEACE was similar despite a much higher rate of
revascularisation in the latter trial. Could it be that the
benefits of revascularisation and ACE inhibitors are also
similar but not additive?
New-onset diabetes mellitus was common in PEACE
(one in eight patients) and almost twice as common as in
HOPE, which can only be partially accounted for by the
higher baseline prevalence of diabetes in HOPE. The high
rate may reflect changing criteria or improved surveillance
for diabetes. The small reduction in the number of patients
developing diabetes on trandolapril in PEACE is a
consistent feature of trials of ACE inhibitors as well as
ARBs. It is not clear whether this reflects a direct effect on
cellular function or an indirect effect mediated through
changes in weight and body composition.
The PEACE study reported that about one in every 25
patients had heart failure as the primary cause of death or
hospitalisation. Extrapolating from epidemiological data and
from the HOPE study, this finding suggests that about three
times as many patients may have exhibited new-onset heart
failure in other ways than was reported, making it potentially
the most common serious CVS event in PEACE. Again, the
consistency between the trials is remarkable.
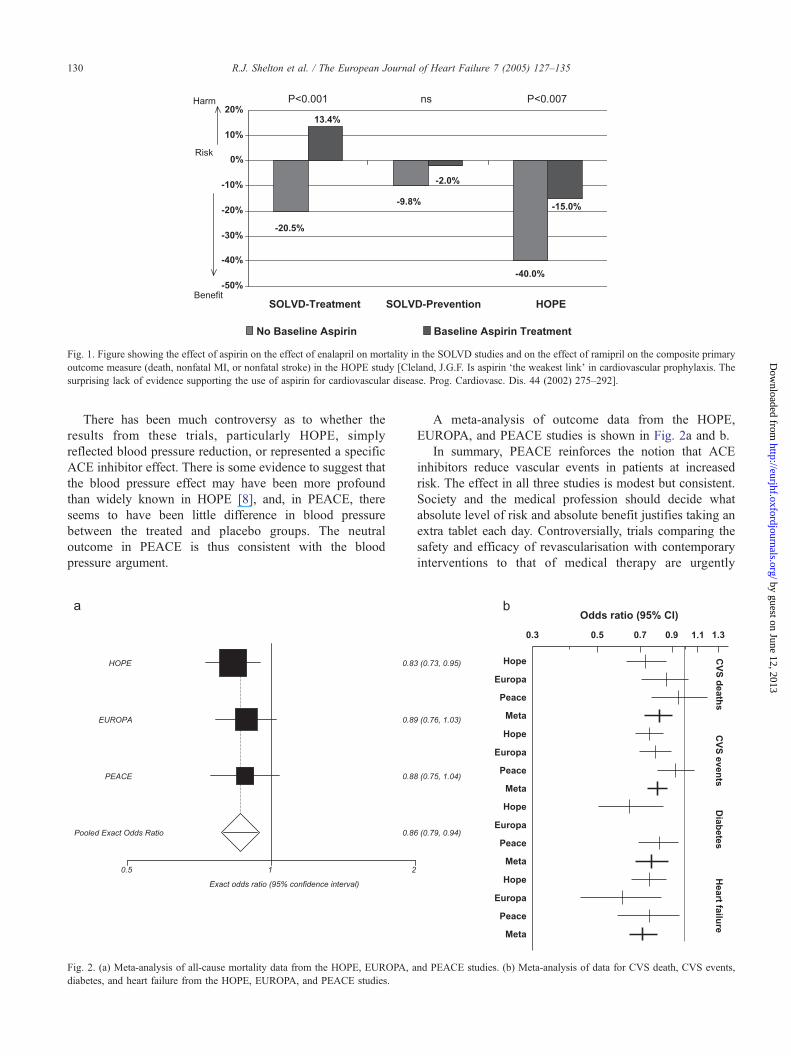
Fig. 1. Figure showing the effect of aspirin on the effect of enalapril on mortality in the SOLVD studies and on the effect of ramipril on the composite primary
outcome measure (death, nonfatal MI, or nonfatal stroke) in the HOPE study [Cleland, J.G.F. Is aspirin dthe weakest linkT in cardiovascular prophylaxis. The
surprising lack of evidence supporting the use of aspirin for cardiovascular disease. Prog. Cardiovasc. Dis. 44 (2002) 275–292].
R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135130
http://eurjhf.oxfordjournals.orgD
ownloaded from
There has been much controversy as to whether the
results from these trials, particularly HOPE, simply
reflected blood pressure reduction, or represented a specific
ACE inhibitor effect. There is some evidence to suggest that
the blood pressure effect may have been more profound
than widely known in HOPE [8], and, in PEACE, there
seems to have been little difference in blood pressure
between the treated and placebo groups. The neutral
outcome in PEACE is thus consistent with the blood
pressure argument.
Fig. 2. (a) Meta-analysis of all-cause mortality data from the HOPE, EUROPA, a
diabetes, and heart failure from the HOPE, EUROPA, and PEACE studies.
A meta-analysis of outcome data from the HOPE,
EUROPA, and PEACE studies is shown in Fig. 2a and b.
In summary, PEACE reinforces the notion that ACE
inhibitors reduce vascular events in patients at increased
risk. The effect in all three studies is modest but consistent.
Society and the medical profession should decide what
absolute level of risk and absolute benefit justifies taking an
extra tablet each day. Controversially, trials comparing the
safety and efficacy of revascularisation with contemporary
interventions to that of medical therapy are urgently
nd PEACE studies. (b) Meta-analysis of data for CVS death, CVS events,
by guest on June 12, 2013/

R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135 131
required since this is an area of medical practice that lacks
an adequate evidence base.
http://D
ownloaded from
4. CREATE: clinical trial of metabolic modulation in
acute MI treatment evaluation
This study of more than 20,000 patients tested two
hypotheses in patients with acute MI. The first hypothesis
was that a glucose/insulin/potassium regimen would reduce
mortality (it did not). Major morbidity was also not reduced
and there were more adverse events. The second hypothesis
was to test the effect of a low-molecular-weight heparin,
reviparin, on 7- and 30-day incidence of death, MI, or
stroke. Reviparin reduced the composite outcome at both
time points, mainly due to an effect on death and MI.
The benefit from reviparin was greater the earlier it was
given. The majority of these patients received thrombolysis
with streptokinase, in whom antithrombotic treatment is
commonly withheld or delayed for several hours (as
compared with patients receiving alteplase/tenecteplase).
CREATE should encourage earlier use of low-molecular-
weight heparin in patients who have received streptokinase.
by guest on June 12, 2013eurjhf.oxfordjournals.org/
5. SHIELD: Shock Inhibition Evaluation with Azimilide
Azimilide is an antiarrhythmic drug with potassium
channel-blocking properties that prolongs the cardiac
action potential and refractory periods and is theoretically
useful for the prevention of VT/VF. This double-blind,
placebo-controlled trial randomised patients (mean LVEF
34%) with an ICD and recent VT or VF to azimilide (at
two dose levels) or placebo and followed them for 1 year.
Azimilide was not associated with a significant reduction
in shocks but did reduce shocks or episodes of markedly
symptomatic VT terminated by pacing (Table 2). Mortal-
ity was not reduced, but cardiovascular hospitalisations,
including those for heart failure, were reduced by the
lower dose. The reduction was either due to fewer ICD
shocks (which may cause myocardial damage) or sup-
pression of supraventricular and ventricular arrhythmias.
There were five patients in the azimilide group and one
patient in the placebo group who developed torsades de
Table 2
Efficacy data from the SHIELD study
Placebo
(n=214)
Azimilide,
75 mg (n=220)
Azimilide,
125 mg (n=199)
p
All-cause shock
Patients 113 (53%) 106 (48%) 91 (46%) ns
Events 613 472 480
Shocks or episodes of markedly symptomatic VT terminated by pacing
Patients 124 (58%) 114 (52%) 100 (50%) 0.005
Events 1459 665 737
pointes. Because the patients had ICDs, they were
protected from the worst effects of this outcome.
6. A-HeFT: African–American Heart Failure Trial
This study has recently been published in the New
England Journal of Medicine [9,10]. Briefly, 1050 African–
American patients with NYHA III/IV heart failure were
randomised to placebo or Bidil (a combination of hydrala-
zine/isosorbide dinitrate) on top of treatment with ACE
inhibitors, beta-blockers, and diuretics. The rationale for this
was the observation that only African–American patients
received benefit with the combination in V-HeFT I [11] and
that dBidilT outperformed enalapril in this subgroup in V-
HeFT II [11]. African–American patients may not have
benefited from enalapril in SOLVD [12], although data on
this latter point are conflicting [13]. However, in neither V-
HeFT trial was there a significant interaction on mortality
between race and treatment (Table 3).
The primary endpoint of the study included death,
hospitalisation, and patient well-being. The study was
stopped early by its DSMB after only 86 deaths had
occurred and only a mean of 10 months of follow-up
accrued due to a 43% reduction in mortality with Bidil. This
is unfortunate since studies stopped early for benefit tend to
overestimate effects, and the number of deaths is not large
enough to convince all observers. However, the result is
encouraging. The use of ACE inhibitors and beta-blockers
other than carvedilol [14] must now be questioned in this
population. Whether Bidil is effective in other racial groups
is presumably the next big question. Data have not so far
provided convincing evidence that either nitrates or
hydralazine used alone adds to the benefits of ACE
inhibition [15].
7. GEMINI: glycemic effects in diabetes mellitus:
carvedilol–metoprolol comparison in hypertensives
This randomised study of 1235 hypertensive patients
suggested that carvedilol (target dose 25 mg, bid; mean
achieved dose 17.5, mg bid) had fewer adverse effects on
insulin sensitivity and diabetes control compared to meto-
prolol tartrate (target dose 200 mg, bid; mean achieved dose
128 mg, bid). There were more problems with bradycardia
in those assigned to metoprolol [16]. It is unclear as to what
extent the difference observed is due to dose or drug,
although its findings are in keeping with other studies in
heart failure [17,18].
8. Vitamin E meta-analysis
This meta-analysis suggested that high-dose vitamin E
supplements were associated with increased mortality,
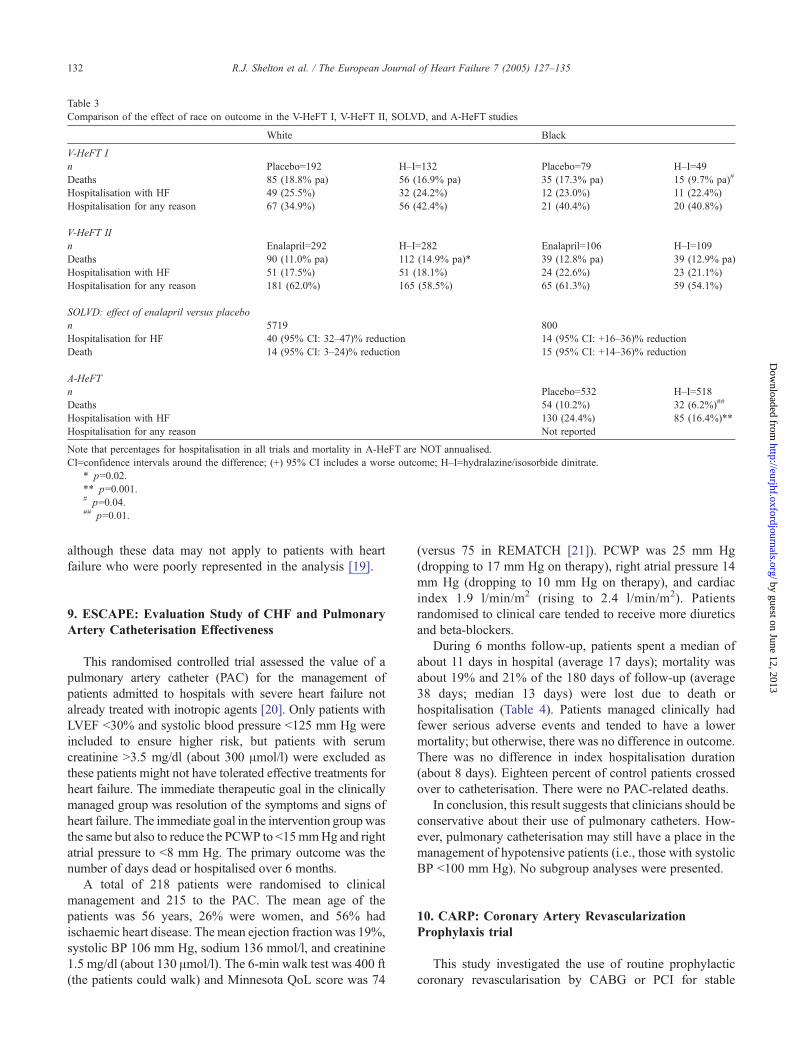
Table 3
Comparison of the effect of race on outcome in the V-HeFT I, V-HeFT II, SOLVD, and A-HeFT studies
White Black
V-HeFT I
n Placebo=192 H–I=132 Placebo=79 H–I=49
Deaths 85 (18.8% pa) 56 (16.9% pa) 35 (17.3% pa) 15 (9.7% pa)#
Hospitalisation with HF 49 (25.5%) 32 (24.2%) 12 (23.0%) 11 (22.4%)
Hospitalisation for any reason 67 (34.9%) 56 (42.4%) 21 (40.4%) 20 (40.8%)
V-HeFT II
n Enalapril=292 H–I=282 Enalapril=106 H–I=109
Deaths 90 (11.0% pa) 112 (14.9% pa)* 39 (12.8% pa) 39 (12.9% pa)
Hospitalisation with HF 51 (17.5%) 51 (18.1%) 24 (22.6%) 23 (21.1%)
Hospitalisation for any reason 181 (62.0%) 165 (58.5%) 65 (61.3%) 59 (54.1%)
SOLVD: effect of enalapril versus placebo
n 5719 800
Hospitalisation for HF 40 (95% CI: 32–47)% reduction 14 (95% CI: +16–36)% reduction
Death 14 (95% CI: 3–24)% reduction 15 (95% CI: +14–36)% reduction
A-HeFT
n Placebo=532 H–I=518
Deaths 54 (10.2%) 32 (6.2%)##
Hospitalisation with HF 130 (24.4%) 85 (16.4%)**
Hospitalisation for any reason Not reported
Note that percentages for hospitalisation in all trials and mortality in A-HeFT are NOT annualised.
CI=confidence intervals around the difference; (+) 95% CI includes a worse outcome; H–I=hydralazine/isosorbide dinitrate.
* p=0.02.
** p=0.001.# p=0.04.## p=0.01.
R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135132
http://eurjhf.oxfordjournals.org/D
ownloaded from
although these data may not apply to patients with heart
failure who were poorly represented in the analysis [19].
by guest on June 12, 2013
9. ESCAPE: Evaluation Study of CHF and Pulmonary
Artery Catheterisation Effectiveness
This randomised controlled trial assessed the value of a
pulmonary artery catheter (PAC) for the management of
patients admitted to hospitals with severe heart failure not
already treated with inotropic agents [20]. Only patients with
LVEF b30% and systolic blood pressure b125 mm Hg were
included to ensure higher risk, but patients with serum
creatinine N3.5 mg/dl (about 300 Amol/l) were excluded as
these patients might not have tolerated effective treatments for
heart failure. The immediate therapeutic goal in the clinically
managed group was resolution of the symptoms and signs of
heart failure. The immediate goal in the intervention groupwas
the same but also to reduce the PCWP to b15mmHg and right
atrial pressure to b8 mm Hg. The primary outcome was the
number of days dead or hospitalised over 6 months.
A total of 218 patients were randomised to clinical
management and 215 to the PAC. The mean age of the
patients was 56 years, 26% were women, and 56% had
ischaemic heart disease. Themean ejection fraction was 19%,
systolic BP 106 mm Hg, sodium 136 mmol/l, and creatinine
1.5 mg/dl (about 130 Amol/l). The 6-min walk test was 400 ft
(the patients could walk) and Minnesota QoL score was 74
(versus 75 in REMATCH [21]). PCWP was 25 mm Hg
(dropping to 17 mm Hg on therapy), right atrial pressure 14
mm Hg (dropping to 10 mm Hg on therapy), and cardiac
index 1.9 l/min/m2 (rising to 2.4 l/min/m2). Patients
randomised to clinical care tended to receive more diuretics
and beta-blockers.
During 6 months follow-up, patients spent a median of
about 11 days in hospital (average 17 days); mortality was
about 19% and 21% of the 180 days of follow-up (average
38 days; median 13 days) were lost due to death or
hospitalisation (Table 4). Patients managed clinically had
fewer serious adverse events and tended to have a lower
mortality; but otherwise, there was no difference in outcome.
There was no difference in index hospitalisation duration
(about 8 days). Eighteen percent of control patients crossed
over to catheterisation. There were no PAC-related deaths.
In conclusion, this result suggests that clinicians should be
conservative about their use of pulmonary catheters. How-
ever, pulmonary catheterisation may still have a place in the
management of hypotensive patients (i.e., those with systolic
BP b100 mm Hg). No subgroup analyses were presented.
10. CARP: Coronary Artery Revascularization
Prophylaxis trial
This study investigated the use of routine prophylactic
coronary revascularisation by CABG or PCI for stable

Table 4
Outcome data from the ESCAPE study
Clinical PAC
Number of patients 218 215
Days dead or hospitalised
(average/median)
36
(20%)/13 (6%)
38
(21%)/13 (6%)
Mortality 17.4% 20.9%
Rehospitalisation (per patient) 2.1 2.1
Days in hospital (average/median) 16 (7%) /11
(6%)
17 (8%)/11
(6%)
Pulmonary complications of PAC (%) 0 1.0
Infected PAC (%) 0 1.9
Antibiotic for infection (%) 9.2 13
Cardiac arrest (%) 2.3 4.2
30-day mortality (%) 5 4.7
PAC=pulmonary artery catheterisation.
R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135 133
by guest on June 12, 2013http://eurjhf.oxfordjournals.org/
Dow
nloaded from
coronary disease prior to major surgery for abdominal aortic
(33%) or peripheral (leg) vascular disease [22,23]. The
primary endpoint was long-term all-cause mortality. The
study was adequately powered for this endpoint. A total of
5859 patients were screened for inclusion and 80% were
excluded mainly because the patient/procedure was consid-
ered to have such a low risk that angiography was not
necessary, or because the vascular surgery was urgent and
had to proceed without delay. A total of 1190 had an
angiogram. This showed no coronary obstruction in only
5%, no revascularisable lesion in 20%, and left main
coronary disease in 8%. These patients were excluded.
Eventually, 510 were randomised. Thirty-five percent of this
group had three-vessel coronary disease, 44% had myocar-
dial perfusion imaging indicating moderate or high risk, and
their mean age was 66 years. Eighty percent of patients were
on a beta-blocker and 50% on a statin. Coronary revascu-
larisation was by percutaneous intervention in 59% of cases
and 41% had CABG. Coronary revascularisation led to
about 7 weeks delay (versus 1–3 weeks in the control group)
in vascular surgery during which 10 patients died.
Perioperative outcome following peripheral vascular
surgery was similar in each group in terms of mortality
and MI. During a median follow-up of 2.7 years, all-cause
mortality was similar in the two groups at about 23%. Only
25% of deaths were from coronary disease in each group
(Table 5).
These data suggest, with few caveats, that routine
preoperative revascularisation for vascular—and probably
by extension of other types—surgery is not warranted.
Preoperative assessment by stress echo or nuclear cardiol-
ogy tests will identify patients at increased risk, but as
Table 5
Outcome data from the CARP study
No revascularisation Revascularisation
n 252 258
30-day mortality (%) 3.4 3.1
Mortality at 2.7 years (%) 23 22
Postoperative MI (%) 14.3 11.6
intervention has not been shown to decrease risk, the value
of such tests should be questioned. However, noninvasive
techniques could have a role in excluding left main coronary
disease. It may be better to focus on the use of beta-blockers
and statins in this setting rather than investigating and
intervening on coronary disease.
11. SCD-HeFT cost-effectiveness study
Governments increasingly use estimates of cost-effec-
tiveness to decide which interventions to adopt. These
calculations should be performed on locally derived data
since costs (mainly salaries) may vary widely. However,
estimates from one country provide a starting point for
others. In the United States and UK, a cost per life year
gained (LYG) of less than US$50,000 is generally consid-
ered cost-effective, whilst costs in excess of US$100,000
would generally be considered cost-ineffective. However,
governments implement many interventions that are not
cost-effective (for instance, air bags in cars or some railway
safety measures, both of which are thought to cost in excess
of 1 million per LYG).
This analysis of the SCD-HeFT trial [24] suggested that
ICDs were fairly cost-effective. The analysis assumed that
the average cost of a simple device with leads but not
implantation costs in the United States was US$17,500
(range US$13,000–23,700) and that the average cost of
5-year management in the control group was about
US$43,000 and in the ICD group was US$62,000 per
patient (Table 6). The primary analysis extrapolated the
within-trial follow-up to lifetime expectation. The median
longevity in the control group was estimated to be 8.4 years,
rising to 10.9 years with an ICD.
On this basis, the calculation suggests that the cost per
life year gained is US$33,000, similar to that estimated for
MADIT II (about US$50,000 per LYG). There was a
powerful interaction between NYHA class and outcome
( p=0.0002). ICDs did not appear effective (and therefore
not cost-effective) in patients who had NYHA III heart
failure. Patients with milder NYHA II heart failure had a
cost of US$26,000 per LYG. If this interaction was ignored
and the benefits were assumed to be the same regardless of
NYHA class, the cost-effectiveness was still higher in
NYHA III patients (US$35,000 vs. US$45,000). If only cost
over the lifetime of the study is considered, the cost rises to
US$77,000 per LYG. If quality-adjusted life years (QALY)
Table 6
Cost of ICD therapy and control in the SCD-HeFT trial
Control (US$) ICD (US$)
Hospital costs 30,691 46,804
Outpatient costs 2863 3745
Pharmacological therapy 8019 9026
Total 43,077 61,967
ICD=implantable cardioverter defibrillator.

R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135134
by guest on June 1http://eurjhf.oxfordjournals.org/
Dow
nloaded from
are considered, then the estimated cost per QALY was about
US$35,000. Analysis of other subgroups including age N65
years, LVEF b30%, and QRS width N120 ms showed little
variation in cost-effectiveness.
Clearly, this analysis suggests that ICDs are cost-effective
by current criteria. Are there any reasons not to implant them
in most patients with low ejection fraction heart failure? In
fact, there are many reasons to be cautious. Firstly, ICDs are
not as cost-effective to implement as ACE inhibitors, beta-
blockers, or spironolactone, nor as cost-effective as some
other measures, such as heart failure nurses or telemonitor-
ing. Implementation rates for these effective, inexpensive
treatments are low. Only once an adequate protocol for the
implementation and monitoring of pharmacological treat-
ment is in place should ICDs be considered. Secondly, new
technologies such as CRT may provide most or all of the
mortality benefits of ICDs at lower cost, whilst also
improving patient symptoms. Thirdly, it is possible that
properly informed patients may decide that they do not want
a device, knowing that more than 90% of recipients will not
benefit from the device over 5 years and that 10–20% of
patients will get inappropriate shocks. Finally, only consid-
ering new cases of heart failure and assuming that only 25%
of patients receive an ICD because the patient has refused the
device or is considered too frail then a regional centre
covering a population of 2 million people will need to
implant about 500 devices per year. Once steady state has
been reached, the excess treatment costs may be about o20
million per year, based on this model. Even though ICDs
might be cost-effective, it is possible that health services will
be unable to afford to implement therapy.
Ultimately, the best solution is to target ICD use more
accurately. Unfortunately, no technology or strategy has
convincingly shown that it can usefully detect who will and
who will not benefit from an ICD.
2, 2013
References
[1] Mann DL, Acker MA, Jessup M, Sabbah HN, Starling RC, Kubo SH,
On behalf of the ACORN Investigators. Rationale, design and
methods for a pivotal randomised clinical trial for the assessment of
a cardiac support device in patients with New York Heart association
Class III–IV heart failure. J Card Fail 2004;10(3):185–92.
[2] Louis AA, Turner T, Gretton M, Baksh A, Cleland JGF. A systematic
review of telemonitoring for the management of heart failure. Eur J
Heart Fail 2003;5:583–90.
[3] Gonseth J, Gullar-Castillon P, Banegas JR, Rodriguez-Artalejo JR.
The effectiveness of disease management programmes in reducing
hospital re-admission in older patients with heart failure: a systematic
review and meta-analysis of published reports. Eur Heart J 2004;
25:1570–95.
[4] Fox KF, Cowie MR, Wood DA, Coates AJ, Poole-Wilson PA, Sutton
GC. A rapid access heart failure clinic provides a prompt diagnosis
and appropriate management of new heart failure presenting in the
community. Eur J Heart Fail 2000;2(423):429.
[5] Wright SP, Walsh H, Ingley KM, Muncaster SA, Gamble GD, Pearl A,
et al. Uptake of self-management strategies in a heart failure
management programme. Eur J Heart Fail 2003;5:371–80.
[6] Yusuf S, Zucker D, Peduzzi P, Fisher LD, Takaro T, Kennedy JW, et
al. Effect of coronary artery bypass graft surgery on survival:
overview of 10 year results from randomised trials by the Coronary
Artery Bypass Graft Surgery Trialists Collaboration. Lancet 1994;
344:563–70.
[7] The PEACE Trial Investigators. Angiotensin converting enzyme
inhibition in stable coronary artery disease. N Engl J Med 2004;
351:2058–68.
[8] Svensson P, de Faire U, Sleight P, Yusuf S, Stergren J. Comparative
effects of ramipril on ambulatory and office blood pressures: a HOPE
substudy. Hypertension 2001;38:e28–32.
[9] Franciosa JA, Taylor AL, Cohn JN, Yancy CW, Ziesche S, Olukotun
A, et al. A-HeFT Investigators. African–American Heart Failure Trial
(A-HeFT): rationale, design and methodology. J Card Fail 2002;
8(3):128–35.
[10] Taylor AL, et al. For the A-HeFT Trial Investigators. Combination
of isosorbide dinitrate and hydralazine in blacks with heart failure.
N Engl J Med 2004;351:2049–57.
[11] Carson P, et al. For the V-HeFT Trial Study Group. Racial differences
in response to therapy for heart failure: analysis of the vasodilator—
heart failure trials. J Card Fail 1999;5(3):178–87.
[12] Exner DV, Dries DL, Domanski MJ, Cohn JN. Lesser response to
ACE inhibitor therapy in black as compared with white patients with
left ventricular dysfunction. N Engl J Med 2001;344:1351–7 [Ref.
ID 5269].
[13] Dries DL, Strong MH, Cooper R, Drazner MH. Efficacy of
angiotensin converting enzyme inhibition in reducing progression
from asymptomatic left ventricular dysfunction to symptomatic
heart failure in black and white patients. J Am Coll Cardiol 2002;
40:311–7.
[14] Yancy CW, et al. For the US Carvedilol Heart Failure Study Group.
Race and the response to adrenergic blockade with carvedilol in
patients with chronic heart failure. N Engl J Med 2001;344:1358–65.
[15] Massie BM, Packer M, Hanlon JT, Combs DT. Hemodynamic
responses to combined therapy with captopril and hydralazine in
patients with severe heart failure. J Am Coll Cardiol 1983;2:338–44.
[16] Bakris GL, et al. For the GEMINI Investigators. Metabolic effects of
carvedilol vs. metoprolol in patients with type 2 diabetes mellitus and
hypertension. JAMA 2004;292(18):2227–36.
[17] Refsgaard J, Thomsen C, Andreassen F, Gotzsche O. Carvedilol does
not alter the insulin sensitivity in patients with congestive heart
failure. Eur J Heart Fail 2002;4:445–53.
[18] Nodari S, Metra M, Cas AD, Cas LD. Efficacy and tolerability of the
long term administration of carvedilol in patients with chronic heart
failure with and without concomitant diabetes mellitus. Eur J Heart
Fail 2003;5:803–9.
[19] Miller ER, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel JL,
Guallar E. Meta-analysis: high dose vitamin E supplementation may
increase all-cause mortality. Ann Intern Med 2004;142 [in press].
[20] Shah MA, et al. For the ESCAPE Investigators. Evaluation study of
congestive heart failure and pulmonary artery catheterisation effec-
tiveness (ESCAPE): design and rationale. Am Heart J 2001;141:
528–35.
[21] Rose EA, et al. For the Randomized Evaluation of Mechanical
Assistance for the Treatment of Congestive Heart Failure
(REMATCH) Study Group. Long-term use of a left ventricular assist
device for end-stage heart failure. N Engl J Med 2001;345(20):
1435–43.
[22] McFalls EO, Ward HB, Krupski WC, Goldman S, Littooy F,
Eagle K, et al. Prophylactic coronary artery revascularisation for
elective vascular surgery: study design. Control Clin Trials 1999;
20:297–308.
[23] Pierpont GL,Mortiz TE, Goldman S, KrupskiWC, Littooy F,WardHB,
et al. Current Opinion on Revascularisation Study Investigators.
Disparate opinions regarding indications for coronary artery revascu-
larisation before elective vascular surgery. Am J Cardiol 2004;
94(9):1124–8.

R.J. Shelton et al. / The European Journal of Heart Failure 7 (2005) 127–135 135
[24] Cleland JGF, Ghosh J, Freemantle N, Kaye GC, Nasir M, Clark AL, et
al. Clinical trials update and cumulative meta-analyses from the
American College of Cardiology: WATCH, SCD-HeFT, DINAMIT,
CASINO, INSPIRE, STRATUS-US, RIO-LIPIDS and cardiac
resynchronisation therapy in heart failure. Eur J Heart Fail 2004;
6:501–8.
[25] Galbreath AD, Krasuski RA, Smith B, Stajdhuhar KC, Kwan MD,
Ellis R, et al. Long-term healthcare and cost outcomes of disease
management in a large randomised community based population with
heart failure. Circulation 2004110 [in press].
by guest on June 12, 2013http://eurjhf.oxfordjournals.org/
Dow
nloaded from




















