The Case for Cultural Competency in Psychotherapeutic Interventions
Upload
khangminh22Category
view
3download
0
Client factors associated with
psychotherapeutic process and outcome:
A concept analysis
A thesis submitted to the University of Manchester
for the degree of Doctorate in Counselling Psychology (D.Couns.Psych.)
in the Faculty of Humanities
2018
Caroline Vermes
School of Environment, Education and Development

2 of 271
Contents Abstract ......................................................................................................................................................... 6
Declaration .................................................................................................................................................... 7
Copyright ....................................................................................................................................................... 7
Acknowledgements ....................................................................................................................................... 8
Dedication ..................................................................................................................................................... 9
The Author .................................................................................................................................................... 9
CHAPTER 1: INTRODUCTION ....................................................................................................................... 10
1.1 Chapter overview .................................................................................................................................. 10
1.2 Study problem ....................................................................................................................................... 11
1.3 Why concept analysis ............................................................................................................................ 16
1.4 Study purpose and questions ............................................................................................................... 21
1.5 Key terms .............................................................................................................................................. 25
Concepts ................................................................................................................................................. 25
Psychotherapy......................................................................................................................................... 27
Causal syntax in psychotherapy .............................................................................................................. 29
Outcome ................................................................................................................................................. 34
1.6 Study structure ...................................................................................................................................... 37
CHAPTER 2: LITERATURE REVIEW ............................................................................................................... 41
2.1 Chapter overview .................................................................................................................................. 41
2.2 Common factors theory ........................................................................................................................ 41
2.3 Client factors ......................................................................................................................................... 47
2.4 Therapeutic alliance .............................................................................................................................. 58
2.5 Change process theory.......................................................................................................................... 60
CHAPTER 3: METHODOLOGY ...................................................................................................................... 64
3.1 Chapter overview .................................................................................................................................. 64
3.2 Critical realism and theoretical assumptions ........................................................................................ 65
3.3 Muted group epistemology .................................................................................................................. 69
3.4 Concept analysis design ........................................................................................................................ 73
3.5 Participant recruitment and data collection ......................................................................................... 80
3.6 Participant data extraction ................................................................................................................... 88
3.7 Participant data interpretation ............................................................................................................. 93

3 of 271
3.8 Research data collection ..................................................................................................................... 104
3.9 Research data extraction .................................................................................................................... 110
3.10 Research data interpretation ............................................................................................................ 110
3.11 Combining participant and research frameworks ............................................................................ 116
3.12 Rigour ................................................................................................................................................ 121
3.13 Ethics ................................................................................................................................................. 123
CHAPTER 4: RESULTS ................................................................................................................................. 127
4.1 Chapter overview ................................................................................................................................ 127
4.2 Helpful client factors ........................................................................................................................... 127
Stage A: Problem recognition ............................................................................................................... 129
Stage B: From other-focussed to self-focussed commitment to change ............................................. 130
Stage C: New social connections fuel change ....................................................................................... 136
Stage D: Reflective and exploratory learning ....................................................................................... 139
Summary of key findings: Helpful client factors ................................................................................... 146
4.3 Unhelpful client factors ....................................................................................................................... 147
Stage A Non-change: Problem-maintaining social environment .......................................................... 149
Stage B Non-change: No commitment to change ................................................................................ 150
Stage C Non-change: No new connections ........................................................................................... 153
Stage D Non-change: Resource-depletion cycle ................................................................................... 154
Summary of key findings: Unhelpful client factors ............................................................................... 158
CHAPTER 5: DISCUSSION ........................................................................................................................... 160
5.1 Chapter overview ................................................................................................................................ 160
5.2 Study question 1: Factors salient to participants ............................................................................... 161
5.3 Study question 2: Client factors in psychotherapy research .............................................................. 161
5.4 Study question 3: Key components of the reconstructed concept .................................................... 162
5.5 Study question 4: Concept utility for counselling psychology theory ................................................ 165
5.6 Domain ................................................................................................................................................ 178
5.7 Fecundity ............................................................................................................................................. 178
5.8 Differentiation ..................................................................................................................................... 179
5.9 Resonance ........................................................................................................................................... 179
5.10 Consistency ....................................................................................................................................... 184
5.11 Operationalisation ............................................................................................................................ 185
5.12 Recommendation for further study .................................................................................................. 185

4 of 271
5.13 Study limitations ............................................................................................................................... 187
CHAPTER 6: CONCLUSION ......................................................................................................................... 191
6.1 Contributions to knowledge ............................................................................................................... 191
6.2 Closing remarks: Results in relation to aims ....................................................................................... 194
REFERENCES .............................................................................................................................................. 196
APPENDICES .............................................................................................................................................. 226
Appendix 1: Database search screenshots ............................................................................................... 226
Appendix 2: Primary study inclusion criteria ............................................................................................ 228
Appendix 3: 49 studies extracted from 14 reviews/analyses ................................................................... 230
Appendix 4: Research data extraction spreadsheet ................................................................................. 231
Appendix 5: Quality control exclusion criteria .......................................................................................... 233
Appendix 6: Tests, variants and causal syntax chart for moderators ....................................................... 234
Appendix 7: Tests, variants and causal syntax chart for mediators ......................................................... 237
Appendix 8: Tests and causal syntax chart for predictors ........................................................................ 241
Appendix 9: Participant recruitment poster ............................................................................................. 243
Appendix 10: Participant information sheet ............................................................................................. 244
Appendix 11: Interview schedule.............................................................................................................. 246
Appendix 12: Participant consent form .................................................................................................... 247
Appendix 13: Transcript portion ............................................................................................................... 248
Appendix 14: Transcription considerations .............................................................................................. 250
Appendix 15: Interview summaries .......................................................................................................... 253
Appendix 16: Entire interview data spreadsheet ..................................................................................... 260
Appendix 17: Example ephemeral reflective notes page ......................................................................... 260
Appendix 18: Example of peer debrief meeting minutes ......................................................................... 261
Appendix 19: MIE Approval emails ........................................................................................................... 262
Appendix 20: Adverse event flow chart .................................................................................................... 263
Appendix 21: Client factors in Castonguay and Beutler (2006) ................................................................ 264
Appendix 22: Demographic information sheet......................................................................................... 265
Appendix 23: Definitions of causal relationships in research ................................................................... 266
Appendix 24: Included studies with social factors findings ...................................................................... 266
Appendix 25: Helpful elements density table ........................................................................................... 268
Appendix 26: Unhelpful elements density table....................................................................................... 270

5 of 271
Word count: 52,183
List of tables
Table 1: Participant demographic characteristics ....................................................................................... 83
List of figures
Figure 1: Thinking, behaving, experiencing, reconceptualising cycle ......................................................... 13
Figure 2: Referents, concepts and meanings .............................................................................................. 20
Figure 3: Role of concept analysis ............................................................................................................... 21
Figure 4: Causal influence flow diagram ..................................................................................................... 31
Figure 5: Incorrect causal assumption ........................................................................................................ 32
Figure 6: Simple causal assumption ............................................................................................................ 33
Figure 7: Smoking cessation flow diagram ................................................................................................. 34
Figure 8: Wampold's pie ............................................................................................................................. 46
Figure 9: Concept analysis method steps flow diagram ............................................................................. 80
Figure 10: Example notes of preliminary interview summary .................................................................... 89
Figure 11: Participant data extraction spreadsheet sample ....................................................................... 91
Figure 12: Hand notations for spreadsheet data cleansing ........................................................................ 92
Figure 13: Initial sketching for participant-informed concept hierarchy .................................................... 96
Figure 14: Intermediate sketch of participant informed hierarchy ............................................................ 97
Figure 15: Participant-informed concept framework ................................................................................. 98
Figure 16: Helpful super-factors and stages of change ............................................................................ 100
Figure 17: Unhelpful super-factors and stages of non-change ................................................................. 101
Figure 18: Categories of activity ............................................................................................................... 102
Figure 19: Categories of inactivity ............................................................................................................ 102
Figure 20: Elements of helpful activity categories 7 to 9 .......................................................................... 103
Figure 21: Unhelpful elements connoting non-change categories 7 to 9 ................................................ 104
Figure 22: Study selection flow chart........................................................................................................ 105
Figure 23: Manual interpretation of study data tags ................................................................................ 111
Figure 24: Labelled research data tags ..................................................................................................... 112
Figure 25: Portion of data analysis spreadsheet ....................................................................................... 113
Figure 26: Research-informed concept framework .................................................................................. 115
Figure 27: Reconstructed concept framework ......................................................................................... 119
Figure 28: Example of color-coding on reconstructed concept framework ............................................. 120
Figure 29: Helpful factors in the reconstructed concept framework ....................................................... 128
Figure 30: Unhelpful factors in the concept reconstruction framework .................................................. 148
Figure 31: Therapist relational skill causal influence ................................................................................ 167
Figure 32: Reconstructed helpful client factors causal influence ............................................................. 168
Figure 33: Reconstructed unhelpful client factors causal influence ......................................................... 169

6 of 271
Abstract
Background and objective
Common factors theory proposes that clients make significant contributions to psychosocial change
processes and outcomes in psychological therapy. However, the client factors concept contains such a
wide range of client activities, characteristics and extratherapeutic circumstances that without some form
of structural logic, it is difficult to understand how clients contribute to change processes, or how
counselling psychology theory might be shaped to work with the most potent client factors. Using first-
hand participant experience and published peer-reviewed psychotherapy outcomes research, this study
sets out to identify client factors associated with psychosocial change and non-change, and to organise
them into a conceptual framework.
Method
A deductive qualitative ‘hierarchy of abstraction’ concept analysis method is used to interpret and
organise data from nine participant interviews and 68 research studies. Graphic frameworks derived from
each data source are compared, then combined into a single reconstructed concept framework.
Findings
The resulting conceptual hierarchy model presents client factors associated with change and non-change
over four levels of abstraction. The detail of experience is located at the least abstract elemental and
categorical levels of change-related activity and inactivity; then abstracted to stages of change and non-
change; then further abstracted to two broad client factors. In this provisional model, the first of these
factors is client use of available social support resources, which inspires and reinforces the second factor,
which is reflective and experiential learning. Inadequate social support is implicated in the learning and
experiential stagnation associated with non-change. The adequacy of the reconstructed concept is
assessed against seven criteria; and by comparing its fit with two social learning theories.
Conclusion and implications
In view of the importance of reflective and experiential learning in this conceptual model, social learning
theory is proposed as relevant for informing future developments in counselling psychology theory and
research. In this model, the term ‘social learning factors’ more accurately points to the potentially major
constellation of wider client and extratherapeutic social contributions to therapy outcomes currently
indicated by ‘client factors’ in common factors theory.
Key words: client factors; concept analysis; concept adequacy; psychotherapy process; psychotherapy
outcome; common factors theory.

7 of 271
Declaration No portion of the work referred to in this thesis has been submitted in support of an
application for another degree or qualification of this or any other institute of learning.
Copyright (i) The author of this thesis (including any appendices and/or schedules to this
thesis) owns certain copyright or related rights in it (the “Copyright”) and she
has given the University of Manchester certain rights to use such Copyright,
including for administrative purposes.
(ii) Copies of this thesis, either in full or in extracts and whether in hard or
electronic copy, may be made only in accordance with the Copyright, Designs
and Patents Act 1988 (as amended) and regulations issued under it or, where
appropriate, in accordance with licensing agreements which the University
has from time to time. This page must form part of any such copies made.
(iii) The ownership of certain Copyright, patents, designs, trademarks and other
intellectual property (the “Intellectual Property”) and any reproductions of
copyright works in the thesis, for example, graphs and tables
(“Reproductions”), which may be described in this thesis, may not be owned
by the author and may be owned by third parties. Such Intellectual Property
and Reproductions cannot and must not be made available for use without
the prior written permission of the owner(s) of the relevant Intellectual
Property and/or Reproductions.
(iv) Further information on the conditions under which disclosure, publication and
commercialisation of this thesis, the Copyright and any Intellectual Property
and/or Reproductions described in it may take place is available in the
University IP Policy (see
http://documents.manchester.ac.uk/DocuInfo.aspx?DocID=24420), in any
relevant thesis restriction declarations deposited in the University Library, the
University Library’s regulations (see
http://www.library.manchester.ac.uk/about/regulations/) and in the University’s
policy on Presentation of Theses.

8 of 271
Acknowledgements Thank you to the nine participants who graciously contributed time and experience to
this research.
Thank you to my husband Mark for your unfailing encouragement. Through the happy
times and the difficult times, you are my security. I could not have completed this work
without you by my side. It is a privilege to share this life with you.
Thank you to my sons Ben and James for bringing me home time and again with stories
of intrepid learning journeys, which cannot be completed without our daemons: The
White Mare of the Light, Pantalaimon, Shadowmere, and Aslan to name a few.
Thank you to my colleagues at Oakwood Psychology Services for your tireless, kind
and enthusiastic support. In particular, Joanne Blezard, Julie Keir, Fiona Whelan, Sue
Haywood, Rachel Burgon, Molly Keir, Jane Oldfield, Ros Rheinberg, Dan Owens-
Cooper, Ellie Fretwell, Marie Mellor, Susan Murnane and David Fenton.
Thank you to members of the Chorlton Home Group for praying with me for endurance
to complete this project, which has rightly taken its place behind family and work
priorities.
Thank you to Dr Terry Hanley and Dr Laura Winter for supervising this project with
patience and wisdom.
Thank you to fellow students Didier Danillon and Nicky Toor. Our thesis meetings have
been reassuring and motivating. Special thanks to Lina Efthyvoulou for your solidarity
particularly through the toughest parts of the past four years.
Thank you to the composers and musicians whose performances have been uplifting
companions on this long learning journey. In particular, Brian Eno, David Sylvian,
Robert Fripp, Steve Reich, Bill Laswell, Jim White, Joe Frank, Laraaji, Nils Frahm,
Ólafur Arnalds, Klaus Schulze, Poppy Ackroyd, Sophie Hutchings, Kai Engel, Arvo Pärt,
Max Corbacho, Daniel Segerstad and Johannes Hedberg (Carbon Based Lifeforms),
Hidetoshi Kolzumi and Andre Scheffer (Connect.Ohm), Joe Acheson (Hidden
Orchestra); Markus Sieber (Aukai), Kieran Hebden (Four Tet), Simon Green (Bonobo)

9 of 271
and Skip McDonald (Little Axe). Super-thanks to John Schaefer (newsounds.org) for
pinning back my ears for the past thirty five years with your brotherly erudition. It is a
privilege to share a lifetime with you all.
And within all, thank you to God of love, the beating heart of generous creativity.
Dedication This research is dedicated to the memory of a participant.
The Author I earned my Master’s degree in Counseling Psychology (M.Ed) from Rutgers University,
New Jersey, USA in 1994. I earned another Master’s degree in Counselling Studies
(MA) from University of Manchester, UK in 2010. I have worked in full-time practice in a
range of mental health settings since 1994. Since 2006 I have worked in social sector
counselling service development and leadership. My academic research to date
includes this thesis; and my 2010 Master’s thesis on the cost-effectiveness of a guided
self-help intervention. I have published articles, guidance and textbook chapters in the
area of counselling psychology theory and practice including social entrepreneurship.

10 of 271
Flower in the crannied wall,
I pluck you out of the crannies,
I hold you here, root and all, in my hand,
Little flower – if I could understand
What you are, root and all, and all in all,
I should know what God and man is.
Alfred Tennyson, 1863
CHAPTER 1: INTRODUCTION
1.1 Chapter overview This chapter aims to orient the reader to the study. It is set out over five sections. In the
first I explain the problem this study addresses, which is the disorganised state of the
client factors concept within common factors theory. I justify the need for an evidence-
based conceptual framework that accommodates a wide range of known client factor
dimensions, states and behaviours over various levels of conceptual abstraction; that
accounts for the temporality of change processes; and that includes unhelpful as well as
helpful factors.
In the second section, to reduce possible doubt for the reader about why I chose a
concept analysis methodology for this study, I explain why I treat the term ‘client factors’
as a concept. I then explain why empirical concept analysis is a better fit than more
‘mainstream’ qualitative methodologies including thematic analysis, interpretive
phenomenological analysis and grounded theory. I also explain the tradition and context
for the reconstructive ‘ladder of abstraction’ concept analysis used here.
In the third section I detail the study’s two-fold purpose, which is to reconstruct the client
factors concept and then to consider the utility of the reconstructed concept to
counselling psychology theory. This section also includes the four research questions
that guide me in achieving these aims.
In the fourth section I define and discuss key terms including concepts; psychotherapy;
causal syntax; and outcome.

11 of 271
The chapter concludes in the fifth section with an overview of the study’s chapter layout
and content.
1.2 Study problem Sometimes, when reading textbooks and research articles that are relevant to my work,
I encounter an abstract technical term whose precise meaning, structure or function is
not fully explained. When I am particularly committed to the topic, I am troubled by an
under-defined term. It is likely to be derived from a detailed set of conceptually
interrelated phenomena, but I cannot extrapolate its significance if I don’t understand
what the concept encompasses, how its components hang together, or where its
mechanisms of action lie. For me, ‘client and extratherapeutic factors’ is such a term. I
became interested in it as an important but incoherent concept when, around the turn of
the century, I enthusiastically read The Heart and Soul of Change, Hubble, Duncan and
Miller’s (1999a; updated by Duncan, Miller, Wampold and Hubble in 2010) textbook
about the common factors that enable psychotherapy to achieve its results. Two key
messages in this book deeply influenced my subsequent thinking and work as a
psychotherapist. The first, from Tallman and Bohart (1999) is that the client is more
responsible than the therapist or therapeutic approach for making therapy work. The
second, from Hubble and Duncan and Miller’s (1999b) concluding chapter, is that the
practice of therapy should not be about classifying disease but about facilitating change.
Here they use the term ‘client and extratherapeutic factors’ to encompass client
characteristics that impact outcome; aspects of client activity within and beyond the
therapy relationship; and social and emotional resources that clients may use to
facilitate change. Overall, 18 disparate client and extratherapeutic factors can be
summarised from chapters contributed to this textbook by Asay and Lambert (1999),
Tallman and Bohart (1999) and Hubble, Duncan and Miller (1999b):
1. Duration and severity of client’s problem
2. Pre-treatment change
3. Stage of change
4. Motivation
5. Hopes and expectations
12 of 271
6. Helpful behaviours outside therapy
7. Nature, strength and quality of social support
8. Client’s theory of change
9. Self-expression and self-disclosure
10. Using self-help media
11. Participation and openness
12. Clarity of goals
13. Agency in pursuing goals
14. Active learning
15. Creative conceptualisation and re-conceptualisation
16. Reflexive self-understanding; gaining new perspective and realisations
17. Exposure and extinction
18. Reality testing, mastery and corrective experiences
In the textbook’s second edition (Duncan, Miller, Wampold and Hubble, 2010) Bohart
and Tallman (2010) add a further seven client factors gathered from literature review:
19. Suitability for therapy
20. Cooperation and interactive collaboration
21. Contribution to the therapeutic bond
22. Perception of therapy
23. Resilience and post-traumatic growth
24. Early change
25. Higher level of distress
Bohart and Tallman (2010) describe this known constellation of client and
extratherapeutic factors as a “potpourri of findings from unrelated research areas”
(p.94). A less charitable metaphor than a bowl of dried flowers and cinnamon sticks
could be applied. For me, the primary problem with this list is its disorganised
randomness. It includes behavioural and cognitive functions, active and passive states,
intra-therapeutic and extratherapeutic elements; intimations of different theories such as
‘stage of change;’ various degrees of abstraction from lived experience; temporally
determined aspects such as ‘pre-therapy change’ and ‘early change;’ and difficult-to-

13 of 271
measure categories such as ‘suitability for therapy’ (see for example Laaksonen,
Lindfors, Knekt and Aalberg, 2010 for discussion of a ‘suitability for therapy’ scale that
predicts outcome on the basis of participant personality function). This potpourri does
not tell me how change comes about, nor why some clients find change difficult to
achieve. In other words, it does not, by itself, offer a cohesive theory of ‘the active
client’, despite its appearance in a textbook dedicated to illuminating conceptual
mechanisms of client change. It requires some sort of analytic technique to render
theoretical coherence to its components.
To this end Tallman and Bohart (1999) briefly hypothesise (after Kolb, 1984) that client
change happens in cycles of thinking, behaviour and experience which lead to shifts in
problem and solution conceptualisation, which in turn lead to further thinking. To assist
reader comprehension I have adapted this change model into the graphic shown in
figure 1.
Figure 1: Thinking, behaving, experiencing, reconceptualising cycle

14 of 271
I find this conceptual model of client change inadequate for five reasons. Firstly, it is
over-simplified and does not show where the range of 25 client factors summarised
above might fit in, or how they make a difference. For example, the influence of social
support is missing. Secondly, it cannot distinguish, accommodate or organise the
various levels of abstraction inherent to the listed client factors. For example, ‘active
learning’ is a more abstract term (i.e. a general category of activity) than ‘exposure’ (i.e.
a behavioural technique associated with active learning). Thirdly, it does not suggest
where this cycle sits in wider temporal planes of change. For example, the client factor
‘stage of change’ implies that different tasks, frames of mind, states of awareness, or
activities are present at different times in a change process. Does this cycle happen
early or late in a change process? Or does it represent the entire change process?
Fourthly, the model does not account for why people struggle, or fail, to make desired
changes, which might be even more important for therapists to understand than how
people successfully change. Lastly, Tallman and Bohart state that there is “no specific
evidence” (p.113) to support their use of the thinking-behaving-experiencing cyclical
model in this way. Further work is required to render theoretical coherence to the
concept of client factors and its component parts.
Client factors as a concept
Before I explain why I chose concept analysis to help me construct a client factors
theoretical framework, I first explain why I believe the term is a concept.
In this study concepts are defined as abstract linguistic entities (for example, nouns)
that mediate between collections of interrelated embodied experiences, and the
meaning or interpretation that is made of them in mental representations such as
thoughts and ideas (Rundle, 1995). Concepts lend themselves to analysis and structural
mapping to assist with theorising and knowledge synthesis (Fauconnier and Turner,
1998; Knafl and Deatrick, 2000). As this study will show, it is possible to create a
structurally logical framework to map the meaning of the term ‘client factors’ through a
process of organising findings from quantitative research, thus determining it is a
concept (Laurence and Margolis, 1999).

15 of 271
The structural prototype that best describes the client factors concept is Laurence and
Margolis’ (1999) ‘containment model:’ an abstract concept that is a composite of
multiple other interrelated, less abstract concepts, as is the case with ‘client factors.’
Concepts as legitimate subjects for research enquiry
Much psychotherapy research over the past fifty years has been devoted to
understanding which therapeutic approaches and therapist attributes produce the best
outcomes. But this vast literature, according to Kazdin (2009), offers little explanation
about why psychotherapy works, or how client change comes about. Kazdin suggests
that “fresh approaches are needed in conceptualisation” of key change mechanisms
(p.419). Similarly, Beutler (1991) asserted that while a wide range of client variables are
theoretically important predictive constructs, they lack consensual or consistent
meaning, are poorly defined, and have weak conceptual linkages to psychotherapy
theories. These views indicate that client factors are worthy of improved
conceptualisation.
My starting point with this study is that I believe Bohart and colleagues are right: as
conceptual entities, client and extratherapeutic factors make more difference in therapy
outcomes than therapist or technique factors. By extension I also believe that the client
factors concept must point to a complex theoretical architecture of process mechanisms
in which most if not all of the factors identified above (and potentially others not listed)
must fit in a logically interrelated manner. I require an analytic method that enables me
to redress the five limitations with the thinking-behaving-experiencing-reconceptualising
model shown in figure 1. So, it must permit me to (a) consider the boundaries of the
concept and the associated rules by which member objects are included and excluded
(even if the rules are provisional and experimental); (b) distinguish and accommodate
various levels of conceptual abstraction amongst the member objects; (c) create a
graphic illustration of influential relationships between member objects in a way that
respects and highlights the temporal nature of human psychosocial change processes;
(d) include non-change factors as well as change factors and, if possible, illuminate
relationships between these; and (e) ensure that the framework is evidence-based.

16 of 271
1.3 Why concept analysis Rennie (2012) helpfully distinguishes three types of qualitative research and the
varieties of methods that suit each type. The first type, ‘experiential’ research,
conceptualises reported experience into structures or categories using methods such as
narrative analysis (McLeod and Balamoutsou, 2006), grounded theory (Strauss and
Corbin, 1998) and interpretive phenomenological analysis (Smith, Flowers and Larkin,
2009). The second type, ‘discursive’ research, is applied to the study of language use,
with methods such as conversation analysis (Sacks, 1972) and discourse analysis
(Parker, 1998). The third type, ‘experiential/discursive’ blends these two, and according
to Rennie is characterised by two methods, thematic analysis (Braun and Clarke, 2013)
and case studies (Stiles, 2003) because each has been applied to both the experiential
and discursive types of research.
This study lies in the experiential type, as its purpose is to conceptualise experience
reported by participants and published literature into a theoretically-informed structure.
In this study, if I had wanted simply to qualitatively describe, list or thematically organise
influential client factors that might be located in research literature or participant
experience I might have chosen thematic analysis, interpretive phenomenological
analysis (IPA) or grounded theory. Any of these methods would facilitate an evidence-
based analysis, but I will here explain why each approach is not the right fit for the aims
of this study, which is to create a tentative theoretically informed framework for the client
factors term.
Why not thematic analysis
Thematic analysis is unsuited to this study’s aims for several reasons. Rennie (2012)
notes that it is best suited to discursive and experiential/discursive - and by
extrapolation, not experiential - types of qualitative research. Although Rennie does not
explicitly explain why he makes this assertion, I wonder if it might be because thematic
analysis is not designed to create, develop or improve theory (University of Auckland,
no date). It tends to suit inductive research (Braun and Clarke, 2013) that creates
concepts from various forms of discourse analysis (Rennie, 2012). By contrast, my
theory-engaged study requires a deductive approach that starts with an existing

17 of 271
theoretical concept and critically examines the particulars of qualitative and quantitative
evidence for the theory. Furthermore, thematic analysis lacks strategies for
distinguishing different levels of conceptual abstraction or temporal zones, and thus
forces the researcher to work within a single plane of interpretation (University of
Auckland, no date). In short, while thematic analysis is useful for locating and analysing
themes and patterns in qualitative material, it is not designed to deal with abstract,
theory-bound concepts.
Why not IPA
Considering IPA next, Rennie (2012) suggests it is useful for experiential qualitative
research that creates structured conceptualisations. IPA permits two levels of thematic
abstraction - emergent and superordinate. But these functions cannot adequately
accommodate the multi-layered abstraction inherent in the client factors concept.
Moreover, IPA tends to focus on the individual participant (Larkin, Watts and Clifton,
2006) which is not suited to the aim here. On a personal note I would not choose IPA
because I do not agree with some terminology used by its proponents. For example I do
not believe that themes ‘emerge’ as foregone ontological entities waiting to be
discovered (see for example Smith and Osborn, 2007) but are epistemologically created
by the researcher. Additionally, I do not like the idea of the IPA researcher claiming the
power to give ‘voice’ to participants (see for example Larkin, Watts, and Clifton, 2006)
especially when participant contributions are sometimes heavily interpreted through the
IPA researcher’s frame of reference.
Why not grounded theory
Grounded theory at first seems an appropriate qualitative methodological choice. It
comprises a taxonomical, hierarchical analytical process, which identifies and organises
associated categories and properties of data under conceptual labels. It deals well with
analyses of social processes which can be translated to graphic models (Morrow and
Smith, 1995). It produces a discursive set of theoretical propositions that account for
causes and consequences related to the examined phenomena (Strauss and Corbin,
1990). It has been adapted for use in research which (as I explain further in Chapter 3,
is the case with this study) is rooted in critical realist ontology (e.g. Hoddy, 2018). It

18 of 271
includes criteria for judging analytic adequacy including fit, relevance, workability and
modifiability (Glaser, 1998). However, upon further consideration grounded theory also
proves inappropriate. Where grounded theory starts with raw data from which it seeks to
inductively draw up abstract concepts, in this case I am starting with an abstract
concept and require a methodology that deductively drills down, examines and maps its
structure and generative mechanisms using selectively chosen data. It is not possible
for me to ignore literature or theory in the topic area (as suggested by Glaser and
Strauss, 2000). Indeed, the starting point for the study is my knowledge of, and
reference to, an influential body of existing theory and research on client contributions to
therapy process and outcomes.
Why concept analysis
My research position is illustrated by the Tennyson poem that opens this chapter. The
mystery of the flower growing in the crack in the rock is like the concept of client factors
in the puzzle of what makes therapy work. If I can pull up and examine the root structure
of this concept I might achieve a better understanding of what clients do to bring about
psychosocial change, as a fundamental aspect of human adaptation and survival.
And so I arrive at concept analysis as the favoured qualitative methodology. Although in
Chapter 3 I describe and distinguish between different types of concept analysis and
related methodologies, and explain the ‘reconstructive hierarchy of abstraction’ method
(Sartori, 1984) chosen for this study, I here briefly orient the reader to concept analysis
methodology. For the avoidance of confusion, it is important that I first distinguish
‘concept analysis’ as an empirical research methodology (as used here) from ‘concept
analysis’ as a process of defining and clarifying key terms at the outset of a study (as
used, for example by Aveyard, Payne and Preston, 2016). Empirical concept analysis
research methodologies are traditionally employed in nursing scholarship (e.g. Rodgers
and Knafl, 2000); sociology (e.g. Fredericks and Miller, 1987); political science (e.g.
Collier and Gerring, 2009); cognitive science (e.g. Laurence and Margolis, 1999); and
gender studies (e.g. Goertz and Mazur, 2007). Each of these disciplines tends to prefer
its own philosophical and ontological schools of thought on the nature of concepts and
the purpose of concept analysis. This study employs a form of concept analysis derived

19 of 271
from the political science work of Sartori (1984) and Gerring (1997; 2012).
‘Reconstructive’ concept analysis aims to map relevant data units to a theoretically
informed hierarchically abstract definitional framework, and also aims to assess the
pragmatic adequacy of the result. Reconstructive concept analysis offers a critical
approach to understanding conceptual terms that have become arbitrarily fixed to
empirical findings, which I will argue later, may be the case with the term ‘client factors.’
As I discuss further in Chapter 3, counselling psychology has yet to engage with
concept analysis methods, even though our work is concerned with innumerable
relatively abstract concepts such as ‘emotional distress,’ ‘resilience,’ ‘collaboration,’
‘facilitation’ ‘goals,’ ‘family’ or ‘multiculturalism.’ Such concepts are ‘tools of the trade,’
but the scientist-practitioner’s ability to teach, practice, research and theorise effectively
using these tools depends on a precise, deep and clear understanding of their meaning
and referents, as well as the ability to measure them or assess their impact in people’s
lives. Achieving such clarity, in turn, depends on research methods that enable analysis
of conceptual structure and linkage to theory.
Empirical concept analysis
One starting point for understanding the role of concepts in language is to distinguish
‘referents,’ ‘concepts,’ and ‘meanings’ (Jackson, 1984). Referents are contextual, social
or personal characteristics, dispositions, processes, events and other phenomena that
are most directly visible in lived experience. Concepts are verbal denotations (linguistic
representations or symbols) for these phenomena. They are created though social
convention. Meanings are the individual and collective mental constructions predicated
by concepts. They are developed socially and are vulnerable to misunderstanding or
distortion if not adequately researched, taught or communicated. Figure 2 provides an
illustration of the relationship between referents, concepts and meanings.

20 of 271
Figure 2: Referents, concepts and meanings
In this diagram we can see that concepts are tools that bridge referents and their
meanings. By extension, concept analysis is a methodology that maintains conceptual
tools in an “orderly condition” (Jackson, 1984, p.206) by epistemologically mediating the
relationship that referents have with their meanings, and by enhancing contextual clarity
and definitional specificity, particularly as a preparatory step where a concept is
required to form part of a scientific investigation. Some types of concept analysis also
strive for ontological depth by pointing to possible mechanisms of action or the nature of
a process in order to advance existing theory (Risjord, 2009), which is the case in this
study. Figure 3 provides a basic illustration of the mediating role of concept analysis
research between concepts and theory development.

21 of 271
Figure 3: Role of concept analysis
1.4 Study purpose and questions Bohart has noted that “the role of the client as an active change agent who makes
significant contributions to the change process has been neglected in the
psychotherapy literature” (2004, p.119). He recommends, “There are now many reviews
of specific aspects of client functioning but none give a comprehensive picture of the
client in therapy….It seems more useful to investigate what these characteristics
mean....” (Bohart and Wade, 2013, p.221, 246).
This study takes up Bohart’s research recommendation. It has two aims. The first, as
previously noted, is to sort out the jumbled meaning of the ‘client and extratherapeutic
factors’ concept by creating a provisional theoretical model of how people participate (or
not) in processes of psychosocial change. The second is to consider the utility of the
concept for counselling psychology theory. I explain these aims further. then detail the
four research questions used to address them.

22 of 271
Aim 1: Analysis and reconstruction of the client factors concept
Clients operate in patchily mapped conceptual space in terms of their contribution to
psychotherapeutic process and outcome. One possible reason for this is that client
factors discussed in empirical or theoretical literature can sometimes be chosen or
described from a ‘therapy-centric’ position (Bickman and Salzer, 1996; Bohart, 2004).
Therapy-centrism refers to an assumption that the therapist (or therapeutic
approach/model, or therapeutic relationship), is the primary active agent in
psychotherapeutic work. Authors adopting a therapy-centric perspective tend to
acknowledge client influences on psychotherapeutic outcome only insofar as they
provide a raison d’etre for the therapist (e.g. functional deficits). Therapy-centrism tends
to position the client in a more passive or impaired role compared to that of the
therapist. Therapy-centrism also refers to professional blindness to these assumptions.
The first aim is therefore to bring a coherent structure to the client factors concept while
attempting to avoid compounding therapy-centrism. To achieve this, it is important to
be careful in choosing the epistemological frame and data sources for the analysis
(which I discuss in Chapter 3). But I acknowledge at the outset that as a therapist
myself I cannot eradicate my personal aim to serve therapy by trying to improve my
knowledge certain theoretical directions in psychotherapy literature.
Concept analyses traditionally examine the context, use, variants and/or definitions of
the concept in question, in data samples drawn from relevant disciplinary research (for
example Olsson, Bond, Burns, Wella-Brodrick and Sawyer’s 2003 study on adolescent
resilience; Burrows’ 1997 concept analysis of facilitation; and Ridner’s 2004 analysis of
psychological distress). In this case, because ‘client factors’ is a multidimensional
containment concept, the aim is to create an organising structure that adds definitional
specificity while respecting its contextual dimensionality.
Once the concept has been analysed, clarified and in some cases tentatively re-defined
through literature review, some researchers use case studies to demonstrate how
concept components work (for example Knafl and Deatrick’s 1990 concept analysis of
family styles for managing life with a chronically unwell child; and Brush, Kirk, Gultekin
and Baiardi’s 2011 concept analysis of overcoming). However the addition of case study

23 of 271
material does not use participant experience to define and structure the concept, only to
illustrate it once it has been derived from the literature.
Penrod (2007) observes that concept analyses derived solely from professional
literature can lack pragmatic utility because the results do not necessarily fit with
people’s experiences. I agree with Penrod’s position, in that some psychotherapy
research focuses too narrowly on professional activity to the exclusion of client activity,
and thus misses valuable information about the mechanics of change. I make an
assumption at the outset of this study that research based solely on diagnostic or
psychometric data, or on therapy-centric questions about therapy’s effectiveness, will
yield some useful information about client characteristics and activities that influence
processes of psychotherapeutic change and outcome. But because this body of
research tends not to explore the extratherapeutic resources and activities clients use to
make desired changes while in therapy, it does not provide a well-rounded picture of the
active client.
In this study I follow Penrod’s (2007) proposal to ‘advance’ literature-based concept
analysis by contrasting and combining the categorical framework derived from
published research data with a similarly-structured framework derived from participant
interview data. In my study, the participant framework is ‘dominant’ (in line with Morse
and Penrod, 1999) – in other words it forms the primary analysis against which the
literature conceptualisation is compared and contrasted (this will be explained further in
Chapter 3). During the process of comparison, the conceptual frameworks are held over
each other to determine which components are shared and which are unique to their
data source. To enhance the reliability of the results (Stavros and Westburg, 2009), the
two are then integrated in a form of data triangulation to advance a single concept
(Hupcey and Penrod, 2003; selective mapping of conceptual properties from different
source domains into a blended space is described further in Fauconnier and Turner,
1998). In the present study, this methodological triangulation approach is used, but
consistent with terminology adopted in Sartori’s (1984/2009) hierarchical concept
analysis methodology (explained further in Chapter 3), the process is termed ‘concept
reconstruction,’ This term will be used for the remainder of the study.

24 of 271
Aim 2: Consider the utility of a reconstructed client factors concept in
counselling psychology theory
An organising framework for understanding, structuring and synthesising the operational
contents of the client factors concept could offer a range of opportunities for the
advancement of counselling psychology theory. Counselling theories are intended to
guide the counsellor’s role, attitude, skills and techniques in the therapeutic encounter,
based on organising principles that represent interpretations of client problem
presentations (Drapela, 1990). Counselling psychology is aligned with humanistic and
integrative counselling theories with various problem-oriented principles. Without
wishing to over-simplify the differences between these theoretical approaches, nor to
trivialise their philosophical rigour, nor their helpful contribution to people’s lives, I
suggest that psychodynamic variants are devised around redressing problematic
attachment history; cognitive-behavioural variants around adjusting maladapted reactive
thoughts and actions; person-centred variants around releasing thwarted emotions;
narrative approaches around externalising and re-authoring the problem and so forth.
To my mind the organising principle of a counselling theory devised around a coherent
and comprehensive client factors concept would focus less on interpreting problems
and more on harnessing psychosocial processes and resources associated with
generative change. It might also inform the counsellor how to help counteract factors
associated with therapeutic failure.
Research questions
Four questions guide me in reaching these aims:
1. What do participants describe as salient factors in their efforts to make desired
psychosocial life-changes, and how are these best conceptualised? This data
informs the primary concept framework.
2. How are client factors represented in psychotherapy research? This data informs
the comparator framework.
3. What are the key helpful and unhelpful components of a reconstructed client
factors framework?
4. What is the utility of the reconstructed concept to counselling psychology theory?

25 of 271
The study’s first aim is addressed and answered by the first three study questions, and
in particular the third question which represents the combination of information from the
first two questions. Its second aim is addressed by the fourth question. The answers to
these questions are discussed in Chapter 5.
1.5 Key terms In this section I define and discuss five relevant terminological areas: Concepts;
psychotherapy; causal syntax in psychotherapy; and outcome.
Concepts Here I describe the role of concepts in mental health theory; the relationship between
concepts and theory; and some difficulties inherent in their abstract nature.
Concepts in mental health theory
Concepts facilitate communication within a knowledge community by linking a class of
referents to their meaning by one (or in the case of ‘client factors’, two) words. Concepts
in mental health care include, but are not limited to, practices, aims, traits, actions,
states of being, and social positions related to the roles of caregiver or care recipient. A
concept is best described in a brief statement of necessary and sufficient conditions.
However, the meanings of concepts in mental health care are rarely so definitionally or
ideologically ‘pure.’ Definitionally they overlap with related terms arising in practical use
in specific contexts over time. Ideologically they represent the language of professional
interests and then enter research analysis and theory as facts of life (Pilgrim, 2016,
2017).
Building blocks of knowledge? Or theoretical niches?
Concepts have been described by some authors as building blocks of theory in the
social sciences because of their inherent explanatory powers (e.g. Chinn and Kramer,
1994; Pintrich, Marx and Boyle, 1993). From this viewpoint, concept research extends
theory by bridging the gap between current theoretical understandings, and intellectual
goals in theory development (Rodgers, 2000b). On the other hand Paley (1996)
reverses the concept-theory equation, stating that theory creates concepts to occupy

26 of 271
meaning ‘niches.’ Paley asserts that “the only way to clarify a concept is to explicitly
adopt a theory that determines what its niche will be” (p.577).
In this study I take the ‘either/both’ ground by conceiving theory and concept
development as interdependent activities. Concepts are the ‘offspring’ of theories in that
theorists invent niche concepts to explain aspects of observed or imputed cause and
effect. For example, ‘client factors’ is an offspring of common factors theory (this will be
discussed further in Chapter 2). Once ‘born’ concepts exert formative influence on their
theoretical ‘parents.’ For example, if one theorises that client factors exert considerable
influence on outcome one can examine and adjust common factors theory in light of
new knowledge about client factors.
It is helpful to remember here that the purpose of theory, and associated concept
clarification, is the advancement of practice. Careful and thorough work on evidencing,
justifying and clarifying concepts makes them better tools with which to reflect on and
refine the theories and practices with which they are associated, but they must be
associated with a theory, even if not the originating theory, to make this work
meaningful.
The problematic nature of concepts
As useful as concepts are as communication devices and holders of meaning, I briefly
discuss here two difficulties inherent in their use and development in psychological
science: contextuality: how concepts are defined by power-interests; and obscuration of
connotation: how vagueness shrouds meaning.
Contextuality
Mental health concepts are created and shaped by the knowledge-contexts in which
they are used. The substantive content of scientific conceptual models, and what is
accepted as ‘core knowledge’ are influenced by sociological and historical factors
(Pintrich, Marx and Boyle, 1993). For reasons I shall explore further in Chapter 2,
common factors theory provides relatively little information about the client factors
concept, although it is potentially the most potent of all the common factors. Thin
descriptions of key concepts within a theory leave room for the representation of

27 of 271
incorrect information or the incorporation of “a false belief or two into [the] essence
placeholder for a concept” (Laurence and Margolis, 1999, p.48). As I will argue further in
Chapter 2 the belief, strongly held by some psychotherapy professionals, that the
therapeutic relationship directly ‘accounts for’ client therapeutic change (see for
example Patterson, Uhlin and Anderson, 2008), while unsubstantiated by research
evidence (Ardito and Rabellino, 2011), represents an example of therapy-centric
extrapolation of common factors theory.
Obscured connotation
Although the client factors concept appears to introduce client activity and
characteristics into a causal argument about the efficacy of psychotherapy, it also
linguistically obscures the magnitude and diversity of client influence on the process. As
abstractions, concepts lose the detail of their implications, particularly where there is
little consensus on their meaning even within their contexts of origin (concepts
described by Pilgrim and Bentall as “woolly,” 1999, p.271). The client factors concept is
such a case, where even in psychotherapy literature, the term does not
comprehensively or coherently point to its connotations, including sociological matters.
Shrouded concepts are uninformative and limit the theorising that can be done with
them. On the other hand, overly narrow or rigid conceptual definitions exclude
knowledge development from diverse sources.
Psychotherapy In this study the term psychotherapy encompasses the work of qualified and in-training
professionals including counsellors, psychologists, CBT therapists, occupational
therapists, social workers, psychiatrists and others who may not uniformly call their work
‘psychotherapy,’ in assisting individuals, families, couples or groups with a recognised
method of talk-therapy to improve mental health; to change problematic behaviours,
personality difficulties or relationship patterns; and/or to pursue personal growth: “self-
efficacy, competence, and mastery” (Luborsky, Crits-Christoph, Mintz and Auerbach,
1988, p. 165). Furthermore, psychotherapy is viewed a relationally-based joint activity
that depends considerably, if not primarily, on the quality of client involvement for its
effectiveness (Bohart and Tallman, 1999; Duncan, Miller and Sparks, 2004).

28 of 271
‘Client’ as a problematic term
‘Client’ connotes the passive role of a person being dealt with by social or medical
services. It is derived from the Latin ‘cliens’ which means “a person under the patronage
or protection of another;” and in ancient Rome referred to a “plebeian under the
protection of a patrician” (Oxford English Dictionary, 2017, no page number). The term
also, less obviously, connotes co-dependency: psychotherapists depend on clients to
make a living; and clients depend on psychotherapists to help with their emotional and
behavioural problems.
Use of the term ‘client’ lends patronising power to the person who uses it to describe
someone with whom they have a working relationship. Psychotherapists commonly use
the term ‘my client,’ as if the client is blessed by ‘belonging’ to the therapist.
‘Client’ also connotes participation in marketised care services in which the ‘customer’
has a choice of provider when they pay privately. But people who access publicly-
funded mental health services are rarely given much choice over type of therapy or
provider. In looking to alternative terms, ‘service user’ and ‘patient,’ are more commonly
associated with public sector services, but are even less apt descriptors for people who
partner with psychotherapists to achieve desired changes in life. McLaughlin (2009)
criticises the term ‘service user’ for prescribing a limited identity that points to the
person’s use of disability services and obscures their preferred, able statuses - which
may involve admirably resourceful and engaged ways of living. The term ‘patient’ is
derived from medicine and invites the sort of ‘pathologisation’ and ‘treatment’ of
individuals and groups of people with mental health difficulties from which some (but not
all) counselling psychologists seek to distance their practice (Woolfe, 2016).
There is no commonly used term for people who access psychotherapy relationships
that does not imply - and maintain - a power difference between the participants that
privileges the therapist as the agent most responsible for outcome. The absence of an
egalitarian term for therapy participants points to a “conceptual practice” (Harding, 2004,
p.30) which is complied with by therapists and clients alike. However, with regret, I have
chosen to retain the term ‘client’ in this study because ‘client factors’ is the subject of the
concept analysis. In Chapter 6 I address changing the concept title.

29 of 271
Where an author whose work I describe in some detail refers to ‘patients’ (e.g. Orlinsky,
2009) I retain this terminology in those passages.
Causal syntax in psychotherapy Bohart, Tallman, Byock and Mackrill (2011) argue against the use of experimental and
randomised controlled trials to judge whether, how, or which psychotherapy or client
factors ‘cause’ changes in client presenting problems. They contrast psychotherapy to
cancer treatment. Radiation might ‘cause’ cancer cells to die in a direct and linear
fashion. But psychotherapy is a complex interactive process in which the relationship
between inputs and outcome is “fundamentally probabilistic” (p.105). Bandura (1978)
also dispenses with unidirectional causal models of human behaviour, and instead
describes how people’s personal and cultural characteristics and social roles may
determine the interaction between environmental events, and internal cognitive
processes such as reflective thought, selective attention, planning and foresight, beliefs
and preferences, incentives, self-evaluation and self-efficacy. In Bandura’s ‘reciprocal
determinism’ model (1978), individuals influence environments and vice versa. Certainly
if one thinks about events in one’s daily life they are hardly separable from preceding
events, cognitive states, free will, chance, social context and so on. The idea that
something happens, or changes because of one entity’s sole influence on another does
not match phenomenological experience.
However, we cannot completely rid psychotherapy theory of an ontology of causality,
because without it, there would be no way of understanding how psychotherapy helps,
or indeed, why it should exist. In this study I suggest that the best we can do is point to
aspects of ‘causal influence’ and ‘causal probability’ in psychotherapy process and
outcome. To describe these we need causal syntax.
Gerring (2012) provides a clear explanation of causal syntax in social science which I
briefly summarise in the remainder of this section.
Independent and dependent variables
Dependent variables are the measured outcome of therapy (Kazdin, 2009).
Independent variables are causal inputs and generally take the form of client and

30 of 271
therapist cognitive, relational or creative activity. Making any causal argument, even
about probable influence, requires one to be able to say that a change in X
(independent variable, input or predictor) generates a change in Y (dependent variable,
outcome or response) relative to what Y would be without the change in X, given certain
background conditions and the scope of the empirical phenomena of interest. How X
changes Y may be obvious and straightforward; or it can occur over a pathway of
intermediary mechanisms. So, the distance between X and Y can be anything from
proximate (i.e. few if any intermediary factors) or distal (indirect effects with complex
and multi-staged mechanics). Intermediary generative mechanisms in the process of
change are known as mediators; while intervening variables and pre-existing conditions
that change the relationship between X and Y are known as moderators (moderators
and mediators are explained further in Appendices 6 and 7 respectively; and a summary
of definitions for mediators, moderators and predictors is available in Appendix 23).
Predictors of treatment outcome are conceptually similar to moderators but are
associated broadly with outcome across all treatment conditions. For example, the
client’s problem complexity or chronicity will have a direct bearing on outcome
regardless of the type of therapy provided (Beutler, Clarkin and Bongar, 2000; Beutler,
2016). Predictors are naturally occurring variables that can be measured and
statistically calculated in experimental research. They may include aspects of therapy,
client factors originating in or before therapy, or extratherapeutic factors.
Causal factors, as independent variables (X) be capable of change, and mediators
capable of activation, even if such dynamism is only a potentiality or cannot be directly
manipulated for example in experimental conditions. Gerring includes a range of related
terms for causal influencers, such as variables, conditions and factors (2012, p.202).
Furthermore, the outcome Y must be clearly specified and in some way measurable.
Gerring also asserts that important, or ambiguous background conditions ought to be
explicitly mentioned. Finally he argues that self-maintaining processes are not causal
because in these cases, X and Y are insufficiently distinguished. Figure 4 shows causal
influence in a flow diagram:

31 of 271
Figure 4: Causal influence flow diagram
In this causal syntax diagram, X (causal factors) lead to M (mechanisms of change)
which in turn leads to Y (changes in outcome). B (constant background factors) have an
antecedent and indirect effect on X and therefore an even less determinable effect on Y.
Incorrect causal assumptions
Beckwith, Dickinson and Kendall (2008) provide an illustrative example of how incorrect
causal inferences arise. An individual attends a smoking cessation class and
subsequently quits smoking (outcome Y). A causal inference could be made that the
causal factor (X) was the individual’s adoption of information and advice provided by the
class, as shown in Figure 5.

32 of 271
Figure 5: Incorrect causal assumption
In the Beckwith et.al. (2008) scenario, the causal influence had actually been the
participant’s partner’s insistence that he quit smoking. If the outcome Y (quit smoking)
happened irrespective of the advice provided in smoking cessation classes, or any other
facilitative factor, the causal assumption diagram would be as shown in figure 6.

33 of 271
Figure 6: Simple causal assumption
One can make further causal extrapolations beyond those made by Beckwith et.al.
(2008), if additional facilitative factors leading to the participant quitting smoking are
considered. For example, background factors include a government campaign to place
graphic health warnings on cigarette packaging. Additionally, alongside attending
classes which the participant found helpful, he obtained a nicotine replacement patch
from his GP which reduced his urge to smoke. He had managed to quit smoking a few
years ago and so had self-efficacy for quitting. The causal assumption diagram for this
scenario is shown in figure 7, where (M) mechanisms of change (or non-change) may
be mediators or moderators.
.

34 of 271
Figure 7: Smoking cessation flow diagram
Outcome In this study, outcome is defined as changes to client symptoms, diagnosis, behaviour,
attitude or psychosocial functioning as a result of having undertaken psychotherapy. In
distinguishing process from outcome, Orlinsky, Grawe and Parks (1994) propose that
process includes all in-session impacts, including the immediate effects on the client of
therapist interventions. Describing outcome, Orlinsky (2009) distinguishes between
outcomes and outputs. Outcomes relate to the aim of therapy (for example reduction in
presenting problems). Outputs are further-reaching consequences on clients’ life-
trajectories and social productivity.
Clients may experience a range of meaningful outcomes and outputs, in addition to the
ones they sought psychotherapeutic help to achieve, or different from those measured
by the therapist or researcher. For example Binder, Holgersen and Nielson, (2010) and
Castonguay et.al. (2010) found that clients deemed good outcome for mental health
psychotherapy to include new ways of relating to others, and improved self-confidence.

35 of 271
It is possible that some clients may only experience or become aware of certain
outcomes and outputs months or years after therapy is complete.
In the current study, where participants could discuss the ‘outcome’ of their choice,
some discussed clinical ‘outcomes’, while all described ‘outputs.’ Several also said the
core problem for which they sought therapy was not fully remitted, which is also an
‘outcome.’
Outcome is a particularly nebulous and unreliably formed concept in psychological
research. Here I briefly describe four problems with the outcome concept: Mis-
conceptualisation; reporting bias; unclear definition of improvement; and the non-linear
nature of change.
Mis-conceptualisation
Outcome mis-conceptualisation refers to an incorrect assumption that an observed
effect or change is an outcome of psychotherapy. It can be seen, for example, when an
aspect of therapist or client experience in therapy is described as an outcome but is
actually a process effect that dissipates soon after therapy ends (Nilsson, Svensson,
Sandell and Clinton, 2007). It may be possible to distinguish ‘lasting outcome’ from
process effects by gathering follow-up data some months after participants finish
therapy in outcome research (Hill and Lambert, 2004).
Another form of mis-conceptualisation is the erroneous conflation of client positive
feedback with therapeutic improvement. Studies have found no relationship between
client satisfaction and treatment efficacy (Stiles, Shapiro and Firth-Cozens, 1990;
Lunnen and Ogles, 1998; Pekarik and Guidry, 1999). Lastly, Kenniston, Boltax and
Almond (1971) explain how what is described as an outcome might actually be a
reflection of the quality of client participation in the social structure of therapy.
Reporting bias
Client change might be judged from the perspective of the researcher, the therapist, an
observer, or the client, but it has been found that therapist and client views of ‘success’
in therapy do not necessarily correspond (Cartwright and Roth, 1957). As Mintz (1972)

36 of 271
showed in a study on the determinants of global outcome, judging ‘successful’
improvement is a process particularly vulnerable to therapist bias. Mintz found that
therapists thought clients who started therapy relatively well and made minor changes
were more ‘successful’ than those who started with more troublesome problems and
nonetheless made unexpected gains. This suggests to me that ‘success’ might
sometimes be conflated by therapists with ‘easier therapy.’
Results of psychotherapy effectiveness studies can be negative or null; but such
findings are less likely than positive results to be reported in the research literature
(Lilienfeld, et.al. 2014). Likewise there is a risk in psychotherapy outcome research that
causal significance can be incorrectly attributed to therapy rather than to potentially
greater influences that take place outside the consulting room (Lilienfeld, et.al. 2014).
Unclear definition of improvement
Examples of studies included in this concept analysis that clearly indicate thresholds for
improvement are Dow et.al., (2007), whose marker of ‘improvement’ was ‘35%
reduction in Y-BOS questionnaire’; and Alonso, Muchon, Pifarre, Malaix-Cols and
Torres (2001) who indicated ‘absence of panic attacks over past 2 weeks.’ Other
studies such as Kleindienst et.al. (2011) indicate that a ‘statistically significant’ change
has been achieved. However, 48/68 (70.6%) of studies did not include a specific
threshold for defining improvement either in terms of changes in outcome measures
from start to end of therapy, or changes in problems reported by other means. Without
such markers it is unclear when outcomes are reported as ‘better’ or ‘worse,’ what the
relative value of this change is.
The non-linear nature of change
Hayes, Laurenceau, Feldman, Strauss and Cardaciotto (2007) discuss how outcome
research might accommodate the idiosyncratic nature of psychotherapeutic change.
Using dynamic systems theory (Thelen and Smith, 1996) they explain how human
cognitive and behavioural change processes tend to be triggered by critical fluctuations
or disturbances in a person’s life that are in turn set off by events that arise in highly
interdependent social systems. Such fluctuations might treated as ‘error’ or ‘noise’ in

37 of 271
traditional pre-and post- therapy designs, which, for convenience, conceptualise change
as gradual and linear. But these disturbances give vital clues to the transformative
impact of destabilisation and reorganisation in clients’ lives. Hayes et.al. (2007) suggest
that if we want to understand what mobilises client change we must study ‘transition
points’ rather than relying solely on time course outcome data. I consider these in the
concept reconstruction.
1.6 Study structure This doctoral study is presented over six standard chapters: Introduction; Literature
Review; Methodology; Results; Discussion; Conclusion. Here I briefly explain the writing
style in which this study is presented; and then provide an overview of each chapter.
Style
In terms of structure, all chapters start with an overview but for the sake of parsimony,
do not end with summaries.
In terms of research design, the job of clarifying what ‘client factors’ are, and how they
can be synthesised into a coherent framework requires a deductive, qualitative,
exploratory and graphically rendered methodology that considers the interrelated
functions of different types of client activities and resources within and beyond
psychotherapy processes. This research approach might be thought of as a counselling
psychology equivalent of a map maker surveying and sketching up a broad and
diversely featured landscape.
In terms of language use, I use first person voice in order to take responsibility and
ownership of the views expressed, while also acknowledging that my work rests on
important ideas rooted in my readings of influential authors in and around
psychotherapy research.
In terms of authorial stance, I examine the client factors concept and its uses in
psychotherapy literature in explicitly critical ways. A fundamental supposition (following
Bohart and Wade, 2013) is that client factors are considerably more potently associated
with process and outcome than most psychotherapy research accounts for. Sometimes
where client factors are identified in the literature they may be those that endorse the

38 of 271
therapist’s role as skilled helper (e.g. ‘preference for type of therapist,’ Beutler,
Harwood, Someah and Miller, 2016) and client’s role as functionally impaired (e.g.
‘resistance,’ Beutler, Harwood, Michelson, Song, and Holman, 2011). Incomplete and
biased conceptualisations of client activity in and beyond therapy limit therapists’ (and
clients’) capacity to perceive and criticise taken-for-granted assumptions about ‘what
works’ in therapy (Beck, 2013).
Consistent with this critical approach I do not bracket off my assumptions about the
topics addressed here as some qualitative researchers advise (e.g. Tufford and
Newman, 2010). I have instead attempted to transparently incorporate them into the text
as I go along, because my views infuse my curiosity about client factors with
investigative vigour. To suppress them would be a form of self-denigration, and a denial
of the socially experiential approach to knowledge-development used here (Fivush,
2000; Rennie, 2012). My assumptions are included to help the reader understand the
perspective from which I interpret the material handled here.
Study overview: Chapter 2: Literature review
The literature review develops my argument for the need for an organising conceptual
framework for client factors. It does this by first situating the client factors concept within
common factors theory, and then by scoping the diversity of client factor dimensions in
relevant literature. I highlight the disjointed nature of knowledge about the active client.
I then look at another common factor, therapeutic alliance, which has received more
research attention than client factors. I find it to be poorly conceptualised. I discuss
evidence that it may not directly influence outcome. I round out the chapter by
introducing change process theory but critiquing the conceptualisation of client factors
found in Orlinsky’s (1986/2009) process model.
Chapter 3: Methodology
The methodology chapter opens with an explanation of the critical realist ontology that
informs my handling of causality in this study. This is followed by a reflection on why
and how the study is shaped by a ‘muted group’ epistemology (Ardener, 1975;
Kramarae, 1981). My selection of a deductive qualitative ‘hierarchy of abstraction’
39 of 271
concept analysis method (Sartori, 2009) is justified in spite of its absence from
counselling psychology research, and in light of the unsuitability of proximate qualitative
analytic approaches. I explain the seven stages of concept analysis fashioned here to
manage, organise, analyse and interpret data from interviews with nine people who
recently completed psychotherapy, and data extracted from 68 psychotherapy outcome
studies, to reach a ‘reconstructed’ concept framework. I explain the structure and
colour-coding used to organise this framework over enhanced fishbone diagrams.
In Chapter 3 I also explain steps I took to ensure research rigour and credibility. I then
conclude with consideration of the ethical issues involved in completing this study
including my deliberations on the death of a participant.
Chapter 4: Results
The results chapter examines and explains the contents of the reconstructed concept
hierarchy. It is divided into two sections: helpful and unhelpful client factors. Each
section is subdivided by four temporal stages of change/non-change. In each stage the
component categories and elements are detailed with evidence from participant and
research data. Each section concludes with a summary of key findings.
Chapter 5: Discussion
To commence the discussion I review and answer my four research questions on the
basis of study results. Then, in order to fruitfully challenge the concept reconstruction I
subject it to analytic review using seven criteria for concept adequacy devised by
Gerring (2012). This review comprises the majority of the chapter. Within the review the
most substantive criterion is considered first, i.e. the concept’s utility for counselling
psychology theory. In this part of the discussion I review causal syntax diagrams that
summarise the study’s findings in relation to client contributions to psychotherapeutic
process. I then discuss the remaining six concept adequacy criteria, including domain,
fecundity, differentiation, resonance, consistency and operationalisation. The chapter
then moves on to discuss recommendations. I propose that social learning theory is an
important area of study for counselling psychologists. The discussion concludes with a
non-exhaustive summary of the study’s limitations.

40 of 271
Conclusion
Concluding the study in Chapter 6, I briefly describe three contributions to knowledge: a
provisional client factors process model; a tentative adjustment to change process
theory that requires further testing and validation; and the introduction of concept
analysis as a potentially relevant methodology for counselling psychology theoretical
research. Finally, the results are reviewed in relation to the aims of the study.

41 of 271
CHAPTER 2: LITERATURE REVIEW
2.1 Chapter overview The aim of this literature review is to locate and describe the relevance of client factors
in common factors theory and psychotherapy process theories, and to deepen my
explanation for why I think the client factors concept requires an organising framework.
The chapter unfolds over four sections. The first section provides a brief history of the
development of common factors theory. I contrast Lambert’s (1992) and Wampold’s
(2001; Wampold and Imel, 2015) theories of the relative distribution of various common
factors in psychotherapy outcome variance. I explain why I think the study of client
factors is important to further development of common factors theory. In the second
section I provide a brief history and meanings for the terms ‘client factors’ and
‘extratherapeutic factors,’ and explain why, in this study, the latter is discarded. I
examine some diverse dimensions of the client factors concept and then provide some
examples of under-conceptualisation of client factors in recent studies. In the third
section I review erratic conceptualisations of the related common factor ‘therapeutic
alliance.’ I review some problems with research on the role of therapeutic alliance in
psychotherapy outcomes. I explain why I think therapeutic alliance might be a reflection
of client and therapist relational factors and other client work factors, rather than a
causal factor in its own right. In the fourth and final section I explain the relationship
between client factors and psychotherapeutic change processes. I illustrate further
consequences of under-conceptualisation of client factors via critique of the treatment of
client activity and social factors in Orlinsky’s (1986/2009) transtheoretical process
model. I conclude the chapter with a brief explanation of why Pascual-Leone,
Greenberg and Pascual-Leone’s (2009) ‘task analysis’ method of psychotherapy
process theory development might be better suited to accommodate client factors, and
how this study might form a preliminary stage in such an endeavour.
2.2 Common factors theory Common factors theory proposes that different types of therapy have elements in
common that account for why, according to some research, they produce generally
equivalent results. This phenomenon is coined the ‘dodo bird hypothesis’ based on a

42 of 271
reference to Lewis Carroll’s Alice in Wonderland made by Saul Rosenzweig in a
prescient, and now famous, 1936 paper. In this story, the dodo bird judged that all
competitors in a race had won. Rosenzweig suggested that the equivalent benefits of
different psychotherapies are caused by “unrecognised factors in any therapeutic
situation that may be even more important than those being purposely employed”
(p.412). He posed a question that has inspired many subsequent studies: “what do
therapies have in common that makes them equally successful?” (p.413).
A landmark text in the development of common factors theory is Frank and Frank’s
1993 comparative study of psychotherapy, Persuasion and Healing (following Frank,
1973). Frank and Frank (1993) suggest a wide range of generic patient,
extratherapeutic and therapy factors are responsible for patient healing in various types
of psychotherapy. Patient factors include expecting to improve; remoralisation;
confession; learning, self-reflection; attitude change; and commitment to new values.
Extratherapeutic factors include peer and family influences; and stressful life
circumstances and events. Therapy factors include the patient-doctor relationship;
provision of education and encouragement for patient behaviour modification;
stimulation of patient emotions and self-reflection; and collaborative construction of new
plots for patient life stories that sustain better patient self-image. Frank and Frank
(1993) describe the psychotherapist as not so much an applied behavioural scientist, as
a hermeneutic interpreter of ‘clients as texts’ of their own life stories: a view that
positions the client as the primary author and the therapist as perhaps a temporary
editor. But they also identify psychological healing with the aid of a therapist as just one
of numerous types of ‘ritual’ people might undertake to achieve the same, or similar
aims of healing – activities that express, connect and reinforce one’s belonging in a
wider socio-ideological group. Opportunities for experiential learning that enhance
mastery and self-efficacy are available through such formal and informal social
memberships. Social memberships, it seems to me, in themselves comprise both the
means and the ends of social help-seeking.

43 of 271
Relative contributions of common factors to variability in outcome
Beside Frank and Frank (1993), other researchers have developed conceptual schemes
for understanding the common mechanisms of client change across various schools of
psychotherapy (for example, Goldfried, 1980; Orlinsky and Howard, 1986; Grencavage
and Norcross, 1990; Kolden, 1991; Castonguay, 1993; Garfield, 1995; Asay and
Lambert, 1999; Lambert and Barley, 2002; Castonguay and Beutler, 2006. See
Wampold and Imel, 2015 for a brief history of common factors conceptual model
development). A commonly cited conceptual scheme was devised by Michael Lambert
(1992) (coined ‘Lambert’s pie,’ see for example Cooper, 2008, p.56). Lambert attempted
to quantify the relative contribution of pan-theoretical factors to variability in outcome: in
other words, the determinants of whether therapy works well or not. He proposed that
30% of “improvement in psychotherapy patients as a function of therapeutic factors”
(p.97). These he described as therapist variables including warmth, empathy,
acceptance, which he subsequently relabelled “therapeutic relationship” (Asay and
Lambert, 1999, p.31), although this usage indicates only the therapist’s contribution to
the therapeutic relationship and does not account for the client’s contribution.
Additionally he attributed 15% to techniques of specific therapies; 15% to client
expectancy and 40% to what he described as “extratherapeutic change” (p.97) including
client factors such as ego strength; and contextual factors such as social support.
Lambert’s 1992 ‘percent of variance accounted for’ common factors model is
problematic for a number of reasons. I will touch on four here. First, “no statistical
procedures were used to derive the percentages that appear in [the figure], which
appears somewhat more precise than is perhaps warranted” (Lambert, 1992, p.98).
Compared to subsequent meta-analytic research by Wampold (2001, discussed below)
Lambert’s model considerably over-estimates the variance in outcome attributable to
therapist and techniques. Second, it obscures client agency by inserting client factors
under the label “extratherapeutic change” which includes spontaneous remission and
fortuitous events (Asay and Lambert, 1999). Third, where specific client factors are
mentioned they are only cursorily described, such as capacity for a meaningful
relationship with the therapist, maturity, motivation, quality of social support and
“personality makeup and ego organisation” (Asay and Lambert, 1999, p.32). Finally,

44 of 271
DeRubeis, Gelfand, German, Fournier and Forand (2014) criticise the ‘percent of
variance accounted for’ model because some of the factors, for example, therapist
technical skill, are not necessarily characterised by high variance within and across
studies, although still representing an essential - and potent - ingredient of therapy.
They suggest that this model also does not account for variability amongst clients in the
degree to which the quality of therapy provided to them will effect their outcomes – in
other words, client factors that render them, as DeRubeis et.al. (2014) describe,
‘spontaneous remitter,’ ‘easy,’ ‘pliant,’ ‘challenging’ or ‘intractable’ patients. DeRubeis
et.al. (2014) also note that Lambert’s common factors model does not facilitate
understanding of causal links between therapy factors and outcome, or the potential for
“patients to improve with the passage of time, irrespective of the quality of therapy
provided to them” (p.421). Regardless of these criticisms, Lambert has continued to
describe his 1992 model as offering an “empirical point of view” showing “percent of
improvement in psychotherapy patients as a function of therapeutic factors” (Lambert,
2013, p.200).
In 2001 Wampold re-evaluated common factors outcomes on the basis of rigorous
meta-analysis. Wampold radically re-drew variance attributions, with significantly
diminished variance attributable to therapy factors, which I will now explain in some
detail, as my argument for the potency of client factors in this study rests in part on
Wampold’s influential work.
Wampold’s pie
Wampold (2001, Wampold and Imel, 2015) developed a common factors conceptual
scheme called the ‘contextual model’ which accounts for the benefit of therapy over
three pathways: first, the foundation of a therapeutic relationship; next, through client
expectations of therapy; and finally, through client mobilisation of “treatment actions”
(Wampold and Imel, 2015, p.53).
Wampold’s statistically transparent, stable and robust research on the relative
contribution of therapeutic common factors found, in line with the ‘dodo bird hypothesis’
“small, if not zero” (2001, p.118) differences in outcome between a variety of treatments
in comparison trials. He also proposed that a range of common factors (not just the

45 of 271
therapeutic relationship as in Lambert’s 1992/1999 model) account for a greater
proportion of variance in outcome than specific components of different therapies.
Wampold (2001) says 13% of variability is due to psychotherapy and the remaining 87%
is due to client and extratherapeutic factors. “Variance attributable to clients is great”
(Wampold, 2001, p.204).
Wampold breaks down psychotherapy’s 13% of variance in somewhat complicated
terms. Factors common to most types of therapy account for approximately 70% of the
13% (in other words, approximately 9% of the whole). These include several therapist
factors: competence, congruence, empathy, affirmation (Wampold and Imel, 2015,
p.209, p.258), allegiance/adherence to a “model” (2001, p.205; Wampold and Imel
2015, p.258) and the ability to culturally adapt the model to fit the client (p.209).
Wampold and Imel (2015) also include two client-therapist collaboration factors: goal
consensus and therapeutic alliance; and two client factors: expectations and placebo
effects (p.258).
Factors attributable to specific therapies account for approximately 8% of the 13%
(approximately 1% of the whole) (Wampold, 2001, p.207). The remaining 22% of the
13% (approximately 3% of the whole) Wampold (2001) says is “unexplained variance”
which he attributes to client factors. Client and extratherapeutic factors account for 90%
of variance (87% + 3%).
Figure 8 shows a graphic representation of variance attributions in ‘Wampold’s pie.’

46 of 271
Figure 8: Wampold's pie
While it is useful to see how important client and extratherapeutic factors are to
psychotherapeutic process and outcome, Bandura (1986) commented that “research
aimed at estimating the relative percentage of behavioural variation due to persons or
situations is ill suited for clarifying the transactional nature of human functioning” (p.29).
This suggests that pie charts showing proportional contributions of different variables to
psychotherapy outcome cannot capture the socially interactive determinants of
psychosocial change. Bandura recommends that social research should examine the
interdependency of causal factors; and the conditions in which people both create and
are influenced by their social climates “in an ongoing sequence of events” (p.29). The
client factors reconstruction created in this study achieves this.
Why study client factors
While psychotherapy outcome research continues to focus attention on the relative
effectiveness of competing models of psychotherapy (Wampold and Imel, 2015) “the
increase in knowledge from this vast enterprise has not been commensurate with the
Sources of variability in outcome: Wampold's Pie
Client and extratherapeutic factors 87% Therapeutic common factors 9%
Effects of specific therapies 1% Unexplained variance (client differences) 3%

47 of 271
investment of time, effort and money and the sophistication of the researchers. Different
studies often yield inconsistent findings, and most of the relationships found, even those
reaching the conventional level of statistical significance, have been too weak to
influence practice” (Frank and Frank, 1993, p.18). It follows from this that common
factors research needs a path to influence practice more meaningfully. I have so far
described two important signposts. First, it is clear from Wampold’s research that
variability of outcome due to the ingredients of psychotherapy is relatively slight.
Second, it is clear from Bandura’s criticism of pie charts that, rather than asking which
type of therapy gets better results, it might be more helpful to study key processes in
client extratherapeutic social interaction. I will now add a third signpost: Clarkin and
Levy (2004) assert, in their authoritative scoping review of influential client factors, that
“non-diagnostic client characteristics may be more useful predictors of psychotherapy
outcome than DSM-based diagnoses,” (p.214). They suggest research “focussed on a
constellation of salient [client] variables will be likely to show the greatest impact on
treatment process and outcome” (p.215). They do warn, however, that “one is faced
with an overwhelming number of client variables to consider” (p.214).
So, in calibrating these three signposts to form a direction for this study, it seems
important first to grasp which non-diagnostic client and extratherapeutic factors most
strongly or generally determine psychotherapy outcome. Then it seems important to
represent client contributions as a cohesive framework of social interaction, influence
and transition points. Task complexity and methodological unfamiliarity do not deter my
aim to make progress in this area.
2.3 Client factors In this section I first offer context for the terms ‘client factors’ and ‘extratherapeutic
factors,’ before providing a review of diverse known helpful and unhelpful phenomena
that comprise the term. This section concludes with some observations on the
obscuration of client factors in common factors studies. Further description and
analysis of specific aspects of the client factors concept found in this study comprise
Chapter 4: Results and Chapter 5: Discussion.

48 of 271
Context
The term ‘client factors’ may have entered published psychotherapy research
terminology around the mid-1980s (e.g. Hoffman, 1985), following ground-breaking
meta-analyses of client variables published by Garfield in 1971 and 1978. It contains
and obscures a large constellation of client activities and circumstances that may
influence outcome in psychotherapy. In medicine, psychiatry, occupational and physical
therapies the concept may be termed ‘patient factors,’ or more specifically, ‘patient
health behaviour.’ The concept is similarly used in nursing and midwifery studies (e.g.
Cox, 1982; Forchuk, 1994; Amoakoh-Coleman et.al. 2016); disability studies (e.g.
Scheirs, Blok, Tolhoek, El Aouat, Glimmerveen, 2012) and management consultancy
(e.g. McLachlin, 1999) but does not have much meaning beyond these professional
fields.
The term ‘client factors’ includes, but is not limited to, client demographic background
and socio-cultural identity; quality of social support; expectations and preferences for
therapy; motivation and readiness to change; learning in and outside sessions;
resilience to adverse life events; and severity of impairment (Beutler, 2016; evidence for
each of these areas will be discussed in the review of client factors that follows).
Extratherapeutic factors are more arbitrarily defined. Some authors (e.g. Addis and
Cardemil, 2006) state that client factors and unexplained and error variance are all
‘extratherapeutic.’ Others (e.g. Wampold and Budge, 2012) combine some therapy-
related factors (client motivation and involvement) with some non-therapy related
factors (social support and spontaneous remission) within the term. I argue here and in
more detail later in the study, that the term ‘extratherapeutic factors’ is redundant, as it
forms a part of client-related influence over the process and outcome of therapy.
However, I retain it where referenced authors have used it.
Review of the diversity of client factors
How clients use therapy depends on their beliefs about ‘normal and healthy’
psychosocial functioning. What clients want from therapy depends on how far their
experience deviates from perceived norms, or is causing suffering to themselves or

49 of 271
others (Boorse, 1976). Additionally, how and when clients access therapy is shaped by
availability, culture and context (World Health Organisation, 2013). So, potentially
influential client factors have diverse sources. For clarity I have broadly organised this
section of the literature review into helpful and unhelpful factors. Firstly I review helpful
demographic, social, cognitive and emotional, behavioural, and learning factors,
agency, and resilience with life events. Then I review unhelpful social, cognitive and
emotional and behavioural factors; and severity of impairment.
Demographic factors
In demographic terms, outcome has been found to be influenced in certain
circumstances by client gender and age (Woodhead, Cronkite, Moos and Timko, 2014).
On the other hand, Clarkin and Levy (2004) found no relationship between age and
outcome except for younger clients with substance abuse, who had worse outcomes
than older clients. Other studies have found no difference in outcome for people of
different ethnic groups (Lambert et.al., 2006), marital or employment statuses
(Davidson, et.al. 2004) or socioeconomic backgrounds (Garfield, 1994; Robinson-
Whelen, Hughes, Taylor, Hall, and Rehm, 2007). Garfield (1994) found a small positive
relationship between client educational level and treatment completion but on the other
hand Yu (2011) found a statistically insignificant link between lower client educational
attainment and therapy dropout.
In general, studies of the relationship between a range of demographic factors and
outcome offer inconsistent or contradictory findings (Bohart and Wade, 2013). It might,
then, be extrapolated that demographic factors per se are not necessarily a useful client
factor category.
Social factors
Outcome has been found to be affected by the nature and quality of clients’ social
support. For example, Bankoff’s (1996) quantitative study of engagement with 57
psychodynamic psychotherapy clients found that strong pre-treatment social network
support had a significant positive association with therapeutic bond, client self-
relatedness and therapeutic realisations in the initial phase of therapy.

50 of 271
More recently, Roehrle and Strouse (2008) conducted a meta-analysis of 27 studies on
the effects of social support on psychotherapy outcomes, and found a modest
correlation (r = 0.13) between social support and outcome, which they note is a similar
level of correlation as that found between therapeutic alliance and outcome. They make
a number of assumptions, including that the influences of social support are similar to
therapeutic help in certain aspects such as empathy and attachment, advice, social
coping and social skill development, and encouragement to put change into practice.
They also note negative social etiological factors, where aversive or controlling
interpersonal relationships, or insufficiently helpful social relations may be a reason
people seek help from a therapist. Roehrle and Strouse recommend that further studies
should examine the interaction effect of social support and therapeutic alliance.
Helpful cognitive and emotional factors
In an influential coding review intended to locate therapeutic common factors present in
a sample of 50 research articles, Grencavage and Norcross (1990) identified client
“positive expectancies and hope for improvement” (p.374) as a distinct common factor.
This finding is problematic because it can be argued that ‘hope’ and ‘expectancy’ are
different constructs. The study’s findings are additionally difficult to interpret because
the authors do not include references or specific inclusion/exclusion criteria for the
literature sample they assessed. I therefore focus on expectancy here, as it may have a
wider evidence base than hope (see for example meta-analyses by Kirsch, 1990 and
Constantino, Arnkoff, Glass, Ametrano and Smith, 2011).
The concept of client expectation can be crudely divided in two definitional realms: firstly
the extent to which clients expect to actively work to bring about desired change; and
secondly, how much they expect the therapist’s help will enable change. On the latter
point, Frank and Frank (1993) found that outcome can be influenced by clients’
expectations that they will be helped by the therapist. This finding may be related to how
credible the client found the therapy or therapist as a helping medium (Hardy, et.al.
1990). On the former point, Patterson, Uhlin and Anderson (2008) found that clients
who expected that in their role as client, they would have to work hard and attend

51 of 271
therapy regularly, experienced better alliance. This finding may be related to how well-
socialised the client was to the nature or type of therapy offered, or how much control
they wished to exert on the process (Greenberg, Constantino and Bruce, 2006).
Alternatively it may reflect how well client and therapist mutual role expectations were
matched or suited (Arnkoff, Glass and Shapiro, 2002); or how well client preferences for
type of therapy or therapist behaviour were met (Swift, Callahan and Vollner, 2011).
Other studies, however, have found minimal predictive capacity for expectancy or
treatment credibility (Ladouceur et.al, 2000; Borkovec et.al., 1987, Borkovic et.al. 2002;
referenced in Newman, Crits-Christoph, Gibbons and Erickson, 2006). In summary,
expectation, treatment credibility, or client preference do not consistently relate to
treatment response (Newman, Crits-Christoph, Gibbons and Erickson, 2006).
Looking next at motivation, this too is a multi-faceted concept. Bohart and Wade (2013;
after Donovan and Rosengren, 1999) differentiate motivation to obtain help from
motivation to change. Motivation has elsewhere been described as a set of dimensions
not limited to readiness to change but also including self-efficacy, decision balancing,
goals and values, and reasons not to change (Substance Abuse and Mental Health
Services Administration, 2012). Perhaps not surprisingly, Lombardi, Button and Westra
(2014) assert that motivation to change is difficult to measure. They found that in-
session client language (‘change-talk’) was a better predictor of outcome in cognitive
behavioural therapy for generalised anxiety than formal self-report measures, but that
arguments against change (‘counter-change talk’) more consistently and potently
predicted negative outcome than arguments in favour of change predicted positive
outcome. Furthermore, Vogel, Hansen, Stiles and Götestam (2006) found that high
motivation to change was not significantly related to outcome in cognitive behavioural
treatment for obsessive compulsive disorder. Inconsistent findings may to some extent
be related to wide variability in term definition and operationalisation.
A concept related to readiness to change but more action oriented, is goal-directedness.
People who are more goal-focussed in therapy may experience early change in therapy,
which has in turn been associated with positive outcome (Hansen and Lambert, 2003).

52 of 271
In particular, clients who articulate ‘approach goals’ rather than ‘avoidance goals’ were
found by Elliot and Church (2002) to have better outcomes.
Self-esteem is noted as a client factor by Bohart and Tallman (2010). A study by Rice,
Ashby and Slaney (1998) found that self-esteem mediated the relationship between
maladaptive perfectionism and depression, through a buffering effect. However this was
not a psychotherapy outcome study. Self-esteem is studied more commonly as an
outcome of psychotherapy rather than as a mediator or moderator of outcome (Smith
and Glass, 1977). In short, self-esteem does not have a strong evidence base as a
client factor associated with variability in outcome.
Helpful behavioural factors
The association between quality of client participation in psychotherapy and outcome
has been made by Orlinsky, Grawe and Parks, 1994; Kazdin and Wassel, 1999; and
Littel, Alexander and Reynolds, 2001. Client willingness to talk about and explore
emotions and experiences, along with willingness to try new behaviours are highlighted
by Bohart and Tallman, 2010. A meta-analysis by Mausbach et.al. (2010) found a
significant association between homework completion in CBT and positive outcome,
although their moderator variables were types and sources of homework completion
ratings rather than types of client homework activity. In terms of specific homework
activities, various forms of client self-monitoring have been associated with positive
outcome in studies by Clarke, Rees and Hardy (2004), Stirman et.al. (2018) and Khattra
et.al. (2017). The latter study also found that relaxation skills learned in therapy helped
clients make meaningful changes in coping. Problem-resolution (Paulson, Truscott and
Stuart, 1999) and associated coping strategies (Carver, Scheier and Weintraub, 1989)
may be taught and assisted via therapeutic intervention, but their operation and long-
term adoption relies on client perseverance and resourcefulness.
Learning, agency and resilience to life events
A key element of problem resolution is client learning (Gershefski, Arnkoff, Glass and
Elkin, 1996). Attainment of insight, new realisation or understanding has been found by
numerous researchers to help people adopt a revised view of reality, and of themselves,

53 of 271
which in turn leads to more constructive or congruent lifestyle choices (see for example
Brady, 1967; Elliott, 1985; Frank and Frank, 1993; Garfield, 1994; Hanna and Ritchie,
1995; Timulak, 2007; Bohart, 2007; Higginson and Mansell, 2008). On the other hand, a
study by Llewelyn, Elliott, Shapiro, Hardy and Firth-Cozens (1988; referenced in
Barkham, 2002) compared therapist and client views of helpful events in therapy. The
study found it was therapists who rated the development of insight as the most helpful
element of therapy, whereas clients rated problem evaluation and resolution as most
helpful.
Gibbard (2014) found clients achieved new realisations through writing, reading and
thinking; self-expression, self-reflection and self-acceptance. These findings are echoed
in studies by Elliott (1985), Clarke, Rees and Hardy (2004) and Binder, Holgersen and
Nielsen (2009) whose participants described how reflexively talking about thoughts,
emotions and experiences led to creating new meaning and improved self-
understanding.
A particular form of reflexive insight described by Rennie (1992, 2002, 2010) is client
agency: a sophisticated form of active learning in which clients intentionally participate,
interpret, assess and transform relational interactions in and beyond therapy in order to
achieve their aims and practise new behaviours. An unpublished study by Greaves
[Wade] (2006, noted in Bohart and Wade, 2013) demonstrates how actively clients use
relationship building skills to develop rapport with their therapist, including building a
common language base, honest engagement, expression of vulnerability, hope and
appreciation. Clients also use agency beyond managing their relationship with their
therapist. In a study of client retrospective narratives about therapy experiences, Adler,
Skalina and McAdams (2008) summarise how their participants described “a struggle
with a discrete and personified problem which is …ultimately vanquished by a
reempowered, agentic protagonist….Their therapeutic work continues even though they
have stopped meeting with a therapist” (p.730) [the protagonist being the client
themselves]. It is my interpretation that participants in this study seemed to own their
process of change, and conceptualised it as a larger and longer process in which
therapy had played a smaller and shorter part. However, despite evidence for the

54 of 271
construct of client agency, Coleman and Neimeyer (2015) found, in a review of
psychometric properties of client agency measures, that associated studies showed that
while agency was positively associated with therapeutic alliance, it did not directly affect
therapy outcome. A qualitative study by Mackrill, 2008 examines client reports of
agency and associates these with specific client-reported goal attainment (but not
psychometric outcomes). Mackrill found that therapists sometimes did not notice client-
reported change strategies. It would seem important therefore, where researchers wish
to develop knowledge of client agency and its impact on outcome, that they analyse
direct client reports in relation to specific outcomes, rather than solely depend on
therapist opinion or experience of client agency (for example as described by Williams
and Levitt, 2007).
Resilience is noted as a client factor by Bohart and Tallman (2010) and Beutler (2016)
however, it is not necessarily well-conceptualised in psychotherapy literature (Fougere,
Daffern and Thomas, 2012). It may refer to a personality trait, an outcome, or a process
of adjustment to adversity (Helmreich et.al., 2017). For example, in a study unrelated to
psychotherapy outcome, Ong, Bergeman, Bisconti and Wallace (2006) provide multiple
definitions for resilience including an outcome: achievement of “positive outcomes in the
face of untoward life events” (p.730) and a capability: “to maintain and preserve the
boundaries between positive and negative emotional states” (p.730). Yi, Vitaliano,
Smith, Yi and Weinger (2008) found that resilience capability mediated the relationship
between psychological adjustment and physical health in patients with diabetes through
a buffering effect. However this too was not a psychotherapy outcome study. Resilience
is studied more commonly as an outcome of psychotherapy rather than as a mediator or
moderator of outcome (see for example Helmreich et.al.’s 2017 protocol for a future
Cochrane Review of psychological interventions for resilience enhancement in adults;
and a meta-analysis of resilience training interventions by Joyce, et.al., 2018). As with
self-esteem, resilience does not have a strong evidence base as a client factor that
mediates variability in outcome.

55 of 271
Unhelpful factors
In a literature review seeking to understand client experiences of hindering factors in
therapy, Henkelman and Paulson (2006) note that researchers find it difficult to elicit
information about unhelpful factors from clients. However, there are some hindering
client factors within and beyond psychotherapy that have been acknowledged in
research.
Unhelpful factors are here divided into social, cognitive and emotional, behavioural
factors, and severity of impairment.
Unhelpful social factors
There is possibly clearer evidence of the detrimental impact of unsupportive, neglectful
hostile or stigmatising client social ecology on psychotherapy outcomes than there is for
the beneficial impact of helpful social ecology. In a trial of psychiatric clinic treatment for
generalised anxiety disorders, Yonkers, Dyck, Warshaw, and Keller (2000) found a
diminished likelihood of remission was associated with poor spousal and family
relationships. Probst, Lambert, Loew, Dahlbender and Tritt (2015) found that inpatients
undertaking psychotherapy treatment were more likely to experience extreme negative
deviation from normal outcomes when they experienced poor social support and
adverse life events. Probst et.al. (2015) recommend that, to improve treatment
outcome, therapists should help poorly responding patients to deal with life events and
build social networks.
Social isolation has been identified as a major health risk (Pantell et.al. 2012) that
inhibits regulatory functions necessary for self-reparatory change (Baumeister and
DeWall, 2005). Related to social isolation, Joutsenniemi, Laaksonen, Knekt, Haaramo
and Lindfors (2012) found that lone parents and divorced people were significantly less
likely to benefit from therapy, or else needed long-term therapy. Castonguay and
Beutler (2006) identified associations between financial or occupational difficulties and
worse outcome in therapy. They also identified that clients with dysphoric disorders are
less likely to benefit from therapy when they are from underserved ethnic or racial
groups. Cochran and Cauce (2006) found that drug and alcohol misuse severity may be
exacerbated by client minority sexual or gender identity, and suggest that “coping with

56 of 271
stigmatised sexual identity, dealing with stressors of being a minority group, and
internalising negative feelings towards the self are possible explanations” (p.144).
Unhelpful cognitive and emotional factors
Client hopelessness, passivity, and self-protective resistance to change negatively
impact client efforts to change (Bohart 2010). Carver et.al. (1989) identified emotional or
behavioural disengagement, denial, and substance misuse as unhelpful to outcome
particularly when participants felt they had low control over adverse stressors.
Laaksonen et.al. (2012) found that participant inability to clearly define a problem-focus
contributed to lower levels of symptom change at one-year follow-up. Low goal-
directedness has been linked in older adults with higher levels of stress and lower levels
of engagement with social support (Payne, Robbins and Doughty, 1991). Walker and
Rosen (2004) identified client self-blame or self-criticism as precursors of poor outcome;
and similarly Powers, Milyavskaya and Koestner (2012) found self-criticism to be
negatively associated with goal progress across a variety of domains. Unwanted
thoughts were reported by Llewelyn et.al. (1988) as correlated with negative outcome.
Kim, Zane and Blozis (2012) found that somatic symptoms were negative predictors of
outcome.
Severity of impairment
Outcome may be negatively impacted by client initial symptom severity or functional
impairment. Lorenzo-Luaces, DeRubeis and Webb (2014) found that people with three
or more prior depressive episodes were significantly less likely to benefit from CBT,
regardless of the quality of therapeutic alliance. Castonguay and Beutler (2006) found
evidence that, regardless of diagnosis, clients are less likely to benefit from therapy
when they have higher levels of impairment; have been diagnosed with a personality
disorder; have low internal locus of control; or “negative self-attribution” (p.356). Similar
findings regarding severity of impairment have been described in studies by Keijsers,
Hoogduin and Schaap, 1994; Yonkers, Dyck, Warshaw, and Keller 2000; and in analytic
reviews by Clarkin and Levy, 2004; Keeley, Storch, Merlo and Geffken, 2008; and
Beutler, 2016). However, research findings relating to the impact of severity of

57 of 271
impairment on outcome should be interpreted with caution. Bohart and Wade (2013)
note that “when discussing the relationship between initial levels of disturbance and
outcome it is important to know if outcome means amount of change, or final status
(return to normal levels of functioning)” (p.227). Earliness of change is another
outcome-influencing variable related to severity of impairment. Hansen and Lambert
(2003) found that “a patient’s pretreatment functioning…influenced time to change, with
higher pretreatment distress producing more immediate change than lower pretreatment
distress” (p.7). In summary, severity of impairment is not necessarily a unilaterally
negative client factor. As a client factor associated with outcome, severity can be
mediated by other factors including client motivation to reduce distress; or the curative
effects of client efforts to curb more extreme problem behaviours.
Obscuration of client involvement in therapy
Clients’ views of how and when change occurs, and which changes are important can
differ from psychotherapists’ views (Kazdin, 1999). Similarly, clients’ views of what is
helpful and unhelpful in therapy can differ from therapists’ views (Wark, 1994). When
clients’ views on their role in therapy are considered, their participation can sometimes
be downplayed. For example, a study of helpful therapeutic processes by Watson,
Cooper, McArthur, and McLeod (2012) says the research allows “clients’ contributions
to the change process to come to the fore” (p.77). But in the resulting analytic map,
therapist speaking activity is expanded to 13 discrete categories, while client speaking
activity is reduced to just one, ‘talking’ (p.84).
To conclude this section on known client factors, I suggest that common factors theory
‘short-circuits.’ It shows that the client is the most potent common factor in
psychotherapy outcome, but it does not fully explain how and why that is the case, and
what could be done with this knowledge to improve therapy. Castonguay observed in
1993 that “not all of the common factors identified at a conceptual level have been the
object of thorough empirical investigation….Among the variables that need to be better
understood are the cognitive, emotional and behavioral aspects of client’s [sic]
involvement in therapy” (p.275). Perhaps more research attention has been paid to a
single therapy factor, therapeutic alliance, than to all client factors.

58 of 271
2.4 Therapeutic alliance Common factors theorists have tended to focus on the importance of the therapeutic
relationship, with ensuing debates about how to conceptualise it (Gaston, 1990; Horvath
and Bedi, 2002); measure it (Lambert, 2010; Ardito and Rabellino, 2011) and optimise it
(Wampold, 2008; Rousmaniere, 2016; Castonguay, 2017). This focus may be because
the working relationship is the factor some therapists believe they have the most
responsibility for, or control over.
By way of brief definition, therapeutic relationship is an umbrella term for what some
authors following Greenson (1967) have broken down into three components including
transference, alliance and ‘real relationship.’ Each of these components could be
viewed as inconsistently conceptualised, as I will now explain.
Transference
Transference has been defined as client activation and application of the mental
representation of a significant other to the therapist (Glassman and Andersen, 1999).
However King and O’Brien (2011) suggest that transference is difficult to differentiate
from other aspects of therapeutic relationship and constitutes only “a small part of the
feelings that exist between therapist and client” (p.12).
Alliance
Alliance is contrarily defined across the psychotherapeutic literature. For example Gelso
(2014) says it is the “joining together of the reasonable self or ego of the client and the
therapist’s analysing or therapizing side for the purpose of the work.” Bordin (1979)
suggests it is client-therapist development of a trusting bond, and joint agreement on
goals and tasks of therapy. Some non-directive approaches might not recognise task
assignment as a purpose of therapy. Horvath and Bedi (2002) acknowledge that there
is no universally accepted definition of the alliance concept.
‘Real relationship’
Turning to the third component, the ‘real relationship’ is also nebulously and potentially
controversially defined. Gelso (2014) says it is the combination of client and therapist

59 of 271
‘genuineness’ with their ‘realistic perceptions’ of one another. Genuineness is a
contextually determined construct. On the therapist’s side it is certainly delimited by
judicious self-disclosure required by the professional role; and on the client’s side by
their knowledge that therapy is a temporary working relationship within which they
perform to the therapist’s evaluative gaze (even ‘unconditional positive regard’ has
conditions). ‘Realistic perception’ is impossible to assess or measure as our
intersubjective ideas about others are socially constructed, highly idiosyncratic, and in
constant flux.
Contested research on the role of alliance as a common factor
Major research contributions on alliance (e.g. Horvath, Del Re, Flückiger and Symonds,
2011) are correlation studies, which suggest only an association between alliance and
outcome, not a causal influence. Wampold and Imel (2015) provide a lengthy appraisal
of various other methodological problems with alliance research including halo effects,
rater bias, publication bias, research allegiance, inappropriate timing of measurements,
and differential importance of the alliance within various approaches. While alliance may
be important to most therapists, Bachelor (1995) and Bedi, Davis and Williams (2005)
found that therapists and clients hold divergent understandings of relationship factors,
with some clients paying little regard to collaboration with the therapist.
Studies of therapist and client relative contributions to therapeutic relationship produce
conflicting findings. For example Krupnick et.al. (1996) found that client early-treatment
contributions to the therapeutic alliance were significantly related to therapeutic
outcome, while therapist contributions were not related to outcome. Contradictorily,
Baldwin, Wampold and Imel (2007) found that while therapist variability in therapeutic
alliance affected outcome, client variability in therapeutic alliance made no difference to
outcome, leading Wampold and Imel (2015) to conclude, “there is no relationship
between the patient’s contribution to alliance and outcome….The alliance, with the
possible exception of the bond, is not directly therapeutic. Agreement on the goals and
tasks of therapy are needed to ensure that collaborative work proceeds in therapy”
(pp.190, 194). An inference I make from these findings (which I develop further in
Chapter 5: Discussion), is that the effectiveness of the therapeutic alliance mirrors client

60 of 271
social adjustment, capacity for initiation of relationships, and perseverance in using
relational social learning both within and beyond therapy. Therapeutic alliance is from
this standpoint an indicative client factor rather than a therapy factor. It is my view that
client relational skill generates numerous causal influences on the process and outcome
of therapy, and may go some way to explaining the correlation between alliance and
outcome. This view is supported by discussion of the impact of client ‘social ecology’ on
therapeutic bond by Bankoff (1996), who found that clients who formed a better
therapeutic bond at the beginning of treatment “entered treatment feeling cared for by
each of their significant ties. They are people who discussed entering treatment with
their romantic partner, and who eventually did enter with the support and blessing of
their [parents], their romantic partner and their two best friends. They are people who
also felt pressured by their friends to get help through therapy” (p.58) and ultimately “got
much more out of their therapy” (p.59).
2.5 Change process theory This literature review has so far examined knowledge and conceptualisations of client
factors associated with psychotherapy outcome. The chapter concludes by looking at
how client factors are positioned in change process theory, and in particular, Orlinsky’s
(2009) well-known ‘Generic Model of Psychotherapy.’
Orlinsky’s Generic Model
Orlinsky’s process framework maps the interrelationships of “all the actions, events and
experiences that occur in psychotherapy – and the individual and social contexts in
which psychotherapy occurs” (2009, pp.321-322). Based on meta-analysis of a
substantial number of studies, the first version appeared in Orlinsky and Howard (1986)
and has since been developed in stages over several decades. The purpose of the
review that follows is to explain the model but also to critique its passive conception of
the client and its restricted view of social influences surrounding the therapeutic
process. In this way I further build my argument that client factors require clearer
conceptualisation before they can inform and evolve psychotherapy process theory.

61 of 271
Orlinsky distinguishes between the systems of action that take place in therapy, and
those that take place in the social milieux surrounding therapy, which I explain in turn.
Systems of action within therapy
Orlinsky, Grawe and Parks (1994) describe six aspects of process that appear in all
forms of therapy: contractual implementation (in particular, patient suitability and
therapist skill for therapy); technical operations (in particular, interpretive conversations
about life problems and core personal relationships); interpersonal bond (in particular,
the patient’s perspective on their therapist’s usefulness); intrapersonal self-relatedness
(in particular openness to experience versus defensiveness); clinical in-session impacts
(particularly insight, emotional relief and hope for the future, and negative
‘psychonoxious’ impacts); and sequential flow (the timing of significant events early,
middle or late in therapy).
Systems of action in the social milieux
Orlinsky acknowledges that therapy process is influenced by the patient’s social
conditions and the “adequacy and predictability of support from the economic, political
and social structures that support communal life” (p. 338) prior to entering therapy.
Orlinsky calls these influences “inputs” (p.332). Consequences resulting from the
patient’s engagement in psychotherapy process are “outputs” (p.332). These include
some influence over the quality and character of the patient’s “involvements with family,
friends and intimates and a public life of dealings with teachers, employers, colleagues
and officials in varied organisations” (p.335) but he does not discuss how these
relational involvements might have a reciprocal influence on what happens in therapy.
The powerful therapist and the passive patient
My first critique of Orlinsky’s (2009) process model is that it describes the role of the
patient in explicitly passive and receptive terms. The “compliant and cooperative”
(p.324) patient shows the “ability to perceive and absorb the input stemming from
therapeutic operations and from the quality of the therapeutic bond” (p.327).
Furthermore, Orlinsky’s framework diagram positions the therapist’s contribution to the
therapeutic bond as the most potent ‘active ingredient’ in therapy, while the patient’s

62 of 271
contribution – notwithstanding its essential nature in therapy - is omitted. Nonetheless
Orlinsky obliquely alludes to the power of the client’s contribution, when he proposes
that the ‘dodo bird effect’ in common factors theory is caused by the benefit derived by
“well-disposed, high functioning persons” from “almost any sort of therapeutic
intervention….yet even very skilful and experienced therapists find it difficult to succeed
with patients (e.g. ‘borderlines’ or psychotics) who have difficulty forming a secure
therapeutic bond” (p.330). This interpretation of the ‘dodo bird hypothesis’ illuminates
the flawed logic of privileging the therapist’s contribution to the therapeutic bond if it is
the client’s disposition that more powerfully predicts the outcome of therapy.
Separation of therapy from social context
My second criticism is that Orlinsky distinguishes therapy as a social activity separate
from the rest of the patient’s life, while nonetheless asserting therapy has a primary
impact on the patient’s capacity for engagement with “the ‘never-ending story’ of finding,
fostering or failing in intimate relationships” (p.338). He positions the ‘treatment milieu’
as the therapist’s office rather than the client’s social life. He does not directly consider
the possibility that, for the client, therapy is just another ‘intimate relationship’ which
reflects, more than it changes, their capacity for relational engagement - although he
notes that therapists encounter difficulties forming therapeutic bonds with clients who
have difficulties forming bonds outside therapy.
In summary, Orlinsky’s model in my opinion inadequately accounts for the influence of
client factors on therapy process.
Task analysis: Towards a process model for the active client
Research that seeks to answer ‘how did the client and their social context (in which
therapy plays a part) achieve that outcome?’ might employ task analysis as a method
for mapping and understanding psychotherapy change processes.
Pascual-Leone, Greenberg and Pascual-Leone (2009) describe task analysis as a
three-step research method, involving discovery, validation and dynamic modelling
phases. It starts with a declared set of theoretical assumptions and uses these in the
discovery phase to inform observations from the top down, while using systematically

63 of 271
gathered empirical data to deductively inform the model from the bottom back to theory.
It values the subjective experience of the client and positions client work within internal
(cognitive-affective) and external (social) worlds as the “true causal mechanisms for the
individual expression of internal experience and of outward behaviour” (p.528). Task
analysis places the therapist in the “conceptual background in order to focus on optimal
client processes” (p.532). It aims to illuminate how clients approach specific tasks in
therapy, in order to build more abstract causal models “that hold true for clients in
general.” Empirical concept analysis, as used here, is an essential preliminary step to
provide process context, before task analysis can produce process detail.
I expect that by clarifying the concept of the active client, change processes will also be
observed and clarified. In this case, once the concept analysis is complete, Pascual-
Leone, Greenberg and Pascual-Leone’s (2009) three-phase task analysis approach
informs possible next steps for validation, then dynamic modelling for the development
of measurement tools for further research as potential follow-on projects to this thesis.

64 of 271
CHAPTER 3: METHODOLOGY
3.1 Chapter overview This chapter provides a full explanation of how the concept analysis was carried out,
presented over twelve sections.
The first section explains why a critical realist ontology is useful for exploring the
influence of client factors in research. The second section describes my epistemological
assumption that knowledge creation occurs through social processes. I describe muted
group epistemology and explain why I have chosen it for this study. I counter some
criticism of muted group theory.
In the third section I describe the concept analysis design used here. I first explain
concept analysis as a deductive qualitative method. I then explain the relevance of
concept analysis to counselling psychology and remark on its absence from counselling
psychology literature. I rule out concept mapping, content analysis, framework analysis
and evolutionary concept analysis. I then differentiate replacement from reconstructive
concept analysis and explain why I chose the latter, in particular Sartori’s (1984/2009)
method. The section concludes with an overview of the stages and tasks of concept
reconstruction Sartori recommends.
The fourth, fifth and sixth sections deal with participant data management for creating
the participant-informed concept framework. In particular in the fourth section I explain
participant recruitment, characteristics and data collection. I also cover the semi-
structured interview design, interview style and transcription method. In the fifth section I
explain how I summarised interviews, created a data extraction and analysis
spreadsheet and organised data hierarchically through processes of data cleansing and
data immersion. In the sixth section I explain data interpretation through the creation of
a fishbone framework for organising and representing the data, and the delineation of
four levels of concept abstraction.
The seventh, eighth and ninth sections deal with research data management for
creating the research-informed concept framework. In particular in the seventh section I
explain the study selection process and characteristics of included studies. In the eighth

65 of 271
section I explain how I extracted research data to an extraction spreadsheet. In the
ninth section I explain research data interpretation to its own fishbone framework.
In the tenth section I explain the process of contrasting the participant-informed and
research-informed frameworks, and the removal of elements deemed marginal due to
contradictory evidence. I then explain how the two frameworks were combined into one,
using color-coding to differentiate the elements and categories that were based on (a)
participant-only data; (b) research-only data; and (c) participant and research data.
In the eleventh, penultimate section I explain how I ensured research rigour including
data triangulation, researcher reflexivity, audit trail, participant checks and catalytic
validity.
The chapter concludes in the twelfth section by explaining ethical issues including
approval, consent, confidentiality and risk, as well as a researcher dual role and a
participant death.
3.2 Critical realism and theoretical assumptions The need to balance clarity against flexibility in conceptual research is an ontological
matter: it requires a philosophy of the nature of being and reality. Concepts are abstract,
definitional, theoretical words; but they find their expression and formation in everyday
human activity and conversation which is naturally pragmatic, diverse, local, and
evolving. So, the process of analysing and developing concepts requires the researcher
to take a position on the nature of reality: Do concepts point to fixed, timeless,
decontextualized truths; or are they culturally-rooted linguistic constructions that only
exist insofar as the words and their meanings usefully promote the interests of a
particular power-group?
The former position is compatible with ‘realist’ or ‘essentialist’ philosophies, which hold
that reality exists in a pure or essential form independent of human representations of it.
The latter is more compatible with ‘relativist,’ ‘interpretivist’ or ‘social constructionist’
views which hold that reality is created through shared human activity, values and
languages; or ‘phenomenological’ views, which hold that knowledge is related to human
consciousness and objects of direct experience.

66 of 271
A strength of the ‘realist’ position in concept analysis is that it seeks to precisely define
and locate concepts in order to render them researchable ‘scientific’ entities. A
weakness of the ‘realist’ position in social science more generally is that it can reduce
reality to observable events, and discount theoretical entities with material impact such
as paradigms (Mingers, 2006).
A strength of the ‘relativist’ position is that it respects historically and culturally specific
social processes and language in the creation of knowledge. It allows some scope for
non-dominant representations in the production or sharing of knowledge (Crombie and
Nightingale, 1999). A weakness of the ‘relativist’ position, according to critical realist
philosopher Roy Bhaskar, is that several forms of ‘reality’ cannot be accounted for as
products of discourse. These include materiality (such as atomic structures) and
physical realities (such as gravity), and some moral and political ‘realities’ that ensue
from human activity such as social, financial and military power and oppression; and
more positively, trust and solidarity. A further weakness of the relativist position is that it
cannot fully accommodate a possible intransitive “ontological domain separate from the
activities and cognitions of human beings” (Mingers, 2006, p.20). Consequently relativist
knowledge of reality can be mistaken for reality itself; and thereby ontology confused
with epistemology.
Critical realism
It is of course possible to hold an ontological position in relation to concepts that lies
somewhere between the ‘realist’ and ‘relativist’ realms. Bhaskar’s critical realist
ontological model is useful here. A ‘critical’ ontology is appropriate in this concept
analysis because it attempts to detect and redress beliefs and practices that lead to
psychological therapy research focussing preferentially on therapy factors over client
factors (Usher, 1996). A ‘realist’ ontology is appropriate, because although absolute
knowledge of the real is impossible, it is possible to research social potentialities that
may or may not be galvanised in psychotherapy and the wider material and social
context in which psychotherapy takes place.
Critical realism stands in opposition to empiricism that reduces reality to observable
events, and posits instead that reality exists over three stratified and inter-related levels:

67 of 271
the ‘real,’ the ‘actual’ and the ‘empirical.’ Here I will explain these three realities and how
they apply in critical concept analysis of ‘client factors.’
The Real
Critical realism proposes that reality is the potentiality of causal properties and
mechanisms that shape the world as we experience it. However, this potentiality is
independent of human experience; it is transcendental and extra-linguistic. Its
properties are emergent, and may change their nature. However, we can materially
transact with the mutable nature of reality, and to some extent change its manner of
emergence.
Contextual, relational and individual agency are ‘real’ in that they are intrinsically
implicated in causal processes (Parr, 2015), although these processes may be only
partially – or incorrectly - understood in socially constructed terms. I can assert that
aspects of psychosocial un-wellness, and people’s efforts to address them, point to the
‘real’ in that they make a profound material and social difference in people’s lives,
irrespective of socially constructed debates about diagnostic labels or psycho-medical
mental health theory and treatment.
The Actual
The activation of generative potentialities under certain temporal, local or social
conditions produces changes in states of affairs. It is only in such actual activity of the
world that the unseen mechanisms of the real might be detected. We create and refine
imaginary models (theories) about causal realities on the basis of limited
phenomenological perceptions and language. In the case of client factors research, it is
in the context-bound manifestations of client change-work that we might find clues to
generative properties and mechanisms.
The Empirical
Bhaskar asserts that the move from the ‘actual’ realm of imaginary models to an
adequate account of ‘real’ causality is through empirical testing. “Science is an ongoing

68 of 271
social activity….Its aim is the production of knowledge of the independently existing and
transfactually [structurally generative] active mechanisms of nature” (2008, p.138).
Realism thus becomes critical as it assumes the possibility of an intransitive realm of
reality while also acknowledging the transitive dimension of human knowledge
construction through culture-bound language systems. Concept development and
theory improvement occur synergistically through analytic social research methods. So
in this concept analysis, in order to try to capture the essence of client change
processes and potentialities as they occur in clinical practice and research studies, I am
limited to using the language and existing knowledge of my historical, social and cultural
location, and the obtainable knowledge of others who have either studied or
experienced aspects of the concept. It may also be, as is my intention, that in studying
actual observations of the concept, I change the way the concept is formed in my own
language and perspectives. Additionally, the activity and motivation of my research in
itself may be reflexive evidence of “universals that are themselves implicated in their
own identification” (Scott, 2005, p.637).
Social relationships and first-hand accounts as evidentiary in critical realist
research
Critical realist research is suitable for counselling psychology because it accommodates
social relationships as causal influences. Just as counselling psychology research
prioritises and values individuals’ subjective and intersubjective experiencing (Kasket,
2016), Scott (2005) explains the importance of first-hand accounts in critical realist
social research:
Critical realists prioritise social actors’ descriptions of their experiences,
projects and desires. This does not imply that social actors can always
provide complete and accurate accounts of their activities, plans, projects
and histories. However, critical realists argue that such phenomena are
central to any investigation they may undertake (p.644).

69 of 271
Researcher theoretical assumptions
In terms of research ontology I assume that properties and mechanisms related to client
cognitive, behavioural and relational factors are an actual (in the critical realist sense)
influence in psychotherapy processes. I assume that knowledge of the meaning,
structure and implications of the client factors concept is underdeveloped because (a)
the inherent diversity of its components makes it difficult to draw up what is known into a
single theoretical framework; and (b) there is little professional incentive for
psychotherapists to research clients’ role in making therapy work.
Furthermore, I think it is possible to hold a social constructionist epistemology in my
development of psychological knowledge (elaborated in section 3.3) while also believing
that aspects of the material and mechanical world are not socially constructed. The
material world and its events would exist regardless of whether or not we talked about
them; although language and human relations may be necessary for much of the
material and mechanical world to have been created and activated. So for example, life
and death are real, not socially constructed events - although our knowledge of them is
understood through social means. Importantly, I believe God is real as a force of such
generative magnitude that it (not he or she) remains largely beyond human
comprehension or capability to describe, other than through the term ‘love.’ This
understanding maps onto Bhaskar’s transcendent realm of the real: “this is a beautiful
world. If you go into anything deeply enough, you will find it there. You could describe it
as inner emptiness, but I describe it as bliss…. I call this the ‘cosmic envelope.’ Spirit is
real. At a very deep level we are all spiritual beings” (Bhaskar, 2014, no page number).
Finally, I also believe, like Bhaskar, that “agency is real. We really do make a difference
in the world. Within any social context we as agents must take responsibility for our
action individually and collectively” (Bhaskar, 2014, no page number).
3.3 Muted group epistemology In counselling psychology, a phenomenological perspective leads us to respect human
subjective experience and consciousness as primary sources of knowledge about how
our world works (McLeod, 2003). Bhaskar says, “You start from a human experience.
You start from epistemology. That is where you are” (2014, no page number). While

70 of 271
some qualitative researchers assert that critical realism can function as both ontology
and epistemology (e.g. Fletcher, 2017), in this study I differentiate critical realism as a
relevant ontology of the nature of reality, from my epistemological stance on the nature
of knowledge. I recognise that while the ultimate truth of existence may lie beyond
human comprehension, I also believe human knowledge is constructed from subjective
experience, and in particular, relational activity and language (Gergen, 2015).
Epistemological assumptions
As a practitioner I observe that therapeutic processes and outcomes are shaped by
clients and their social circumstances, far more than by what I do to support their efforts
to make desired psychosocial changes. My thinking about the mechanisms and purpose
of psychotherapy is further influenced by Jordan’s (2010) relational-cultural theory; and
forerunning collaborative theoretical work about women’s development in relationships
from the Wellesley College Stone Center (e.g. Jordan, Kaplan, Miller, Stiver and Surrey,
1991). In particular I rely here on Miller’s idea that “official definitions of reality” (1991,
p.26) do not sufficiently draw upon complex processes of knowledge development that
occur in people’s day-to-day emotional and social connections with each other. While I
acknowledge the practical feminist stance inherent in these epistemological influences,
this study does not explicitly draw on feminist methodology and does not seek to make
a particular contribution to the psychology of women.
While asserting that this study’s epistemology is based on an assumption that
knowledge exists and is created in social interaction, I do not go quite as far as some
postmodern feminists might by saying that “there are no criteria for determining which
version of reality is better” (Fivush, 2000, p.88). If such total relativism were the case
then there would be no point, for example, in qualitative researchers taking steps to
demonstrate the trustworthiness of their work. Advances in knowledge would be
impossible (Parr, 2015).
Lowman (2012) reminds us that the focus of the scientist-practitioner psychologist’s
work should be to ensure that research informs practice in order to improve its
usefulness to clients. I try here to re-present client experience (a) to earn the public trust
placed in psychologists (Donati, 2016); and (b) to respect clients, their activity and
71 of 271
social contexts as integral to the construction of counselling psychology knowledge. I
have tried to create a study that moves beyond therapist experience, and even beyond
established therapy-centric perspectives of how people change in therapy.
This point leads to the relevance in this study of an epistemology derived from muted
group theory (E. Ardener, 1975; Kramarae, 1981). This theory allows client
autobiographic narrative as valid data for knowledge construction (Howard, Maerlender,
Myers and Curtin,1992; Fivush, 2000).
Muted group theory
Muted group theory was developed by anthropologists Edwin Ardener (1975) and
Shirley Ardener (2005) as a theory of communication and language. It highlighted how
socially subordinate groups are not permitted access to participate equally in the
generation of categories of thought, conceptualisation, and ideas about social
structures, and the encoding of these types of knowledge into discourse. The values
and experiences of people in muted groups are thereby kept private, or inadequately
recognised, or mis-represented in dominant communication, including in the design and
presentation of social research. “The astounding deficiency of a method, supposedly
objective, is starkly revealed: the failure to include half the people in the total analysis”
(E. Ardener, 1975, p.4). Another assumption I make, in linking the muted group
epistemology to the critical realist ontology adopted here (after Parr, 2015) is that
despite the socially-constructed nature of knowledge, it is possible for us to distinguish
between more and less successful methods for knowledge development (as Ardener
did in the quote above). Consequently, in seeking to better understand client factors,
this study asks clients directly what they do to make desired changes.
While muted group theory was subsequently adopted and developed as a feminist
theory (Kramerae, 1981), I draw from it in its original form as a theory that befits any
social group that is ‘spoken for’ by those with more social power. Ardener described the
mutually affecting spheres of dominant and muted groups as “simultaneities” (Ardener,
2005, p. 52). Interdependency is acknowledged here because psychotherapists need
clients to lend fundamental credence to their professional identity.

72 of 271
To illustrate how muted group theory epistemologically informs this study, I have
replaced the terms ‘men’ and ‘women’ with ‘psychotherapists’ and ‘clients’ in muted
group’s three main premises as follows (Oregon State University, undated):
1. Therapists cannot validly speak for clients: Psychotherapists and clients
perceive what happens in therapy differently. They have different aims,
perspectives and perception-shaping experiences.
2. Therapists use therapy-centric language: Psychotherapists enact their
language in ways that perpetuate their power, while insufficiently querying, or
being informed by, clients’ experiences about how the work of therapy is
achieved.
3. Client perspectives need translating if the dominant discourse is to adopt
them: Client agency in making desired life-change must be converted into
psychotherapist language and publicised in psychotherapist media in order to be
recognised.
While it may be challenging to practitioners to consider how these premises might apply
in psychotherapy, it been observed that such power imbalances in psychotherapy and
its research are subtle and pervasive (Harrison, 2013; Proctor, 2017).
Criticisms of muted group theory
Here I will address, insofar as they may impact its use in this study, three criticisms
made about muted group theory: it essentialises men and women; it is not empirically
tested; and it is dated (West and Turner, 2003).
Essentialisation
In this research I am not using muted group theory to consider male and female
communication patterns. It is used in a focussed way to address the muting of clients
and the side-lining of other forms of social support in psychotherapy research. I am not
‘essentialising’ that all psychotherapy research is therapy-centric; nor that all clients
behave the same way in therapy. On the contrary, I am seeking to thicken what is
known about the complexities of client influence on psychotherapeutic outcomes.

73 of 271
Empirically untested
An extensive body of literature supports and describes the use of muted group theory
(see Ardener, 2005 for a bibliography).
Dated
If we did not use today ideas that were considered radical in the 1970s we would have
abandoned the work of Carl Rogers and Aaron Beck. The dismissive accusation that
muted group theory is dated possibly betrays a discourse that feminist theories should
not age. “Many in our field have found that muted group theory has helped inform us
about how power functions in our talk and writing, and language….It helps explain
what’s going on in a way that is easily understood, believable and useful (Kramarae,
2005, pp.55, 56).
3.4 Concept analysis design As explained in the introduction on pages 15-19 I have employed a reconstructive
concept analysis method derived from political science (Sartori, 1984; Collier and
Gerring, 2009) to define, map and assess the client factors concept. This work is
intended to represent an initial stage before further research can validly explore or
develop measures for its intrinsic phenomena (Sartori, 1970; Robson, 2002), for
example by using task analysis as described on pages 62-63.
Before explaining concept analysis methodology and design in detail, I first explain the
process by which I found and decided on this method. I initially proposed to create a
client resources survey instrument that therapists might use in routine practice to
understand the role of particular client factors in assisting and hindering client-desired
change. This idea was not supported by my advisors who preferred I attempt a
qualitative thematic analysis of participant interviews around client factors. During this
developmental stage, with further reading into my topic and analytic strategy, it became
clearer to me that the term ‘client factors’ represented an abstract, theoretical shorthand
for a wide range of more specific categories of client experience and activity, and as
such it was a concept (as I have justified on page 14). From here I fixed on the idea that
the vagueness of the concept in itself posed the research problem I should tackle. After

74 of 271
undertaking training in thematic analysis with Virginia Braun, I observed that, despite its
popularity in counselling psychology research, thematic analysis was not the ideal
method for my task. Its principal aim is to identify and analyse patterns in qualitative
data (Braun and Clarke, 2013; 2014), while I needed to create conceptual anatomical
definition. In other words, I sought not simply to put ‘meat on the bones’ of the client
factors concept but to describe its ‘musculoskeletal structure’: a theoretically and
structurally coherent framework linked to existing theory into which to organise my
analysis. I therefore needed an analytic method that respected concepts as multi-
layered abstract linguistic entities, while permitting synthesis of findings from outcome
studies with participant interviews. From here, my ongoing methodological reading
brought me to Gerring’s (2012) appealing and relevant work on social science concept
analysis. Gerring in turn pointed me to Sartori (1984; 2009), whose antipathy for vague
concepts and practical methodology captured my imagination and determined the
direction for the completion and write-up of this study.
Concept analysis as a deductive qualitative method
Hupcey and Penrod (2003) recommend qualitative methods for reconstructive concept
analysis (which I have previously explained, aims to map relevant data units to a
theoretically informed hierarchical definitional framework, then assess the adequacy of
the result). Hupcey and Penrod (2003) combine source material from previous research
with client knowledge. Furthermore, Gilgun (2014) recommends a deductive qualitative
approach when working in theory-guided research with ‘sensitising concepts,’ which, as
with ‘client factors,’ give only a “general sense of reference” and lack “specification of
attributes and consequently [do] not enable the user to move directly to the relevant
content” (Blumer, 1954, p.7). The purpose of deductive analysis is to clarify or revise the
concept’s dimensions, and to show theoretical patterns in a way that “helps the
researcher see what they might not otherwise have noticed” (Gilgun, 2014, p.5). The
process moves from working first with thick descriptions, to interpreting an organising
framework, then assessing the pragmatic utility of the framework against existing
theory.

75 of 271
Concept analysis as a potentially useful method in counselling psychology
Concept analysis straddles academic and clinical knowledge development. Counselling
psychologists could use it to improve the explanatory and predictive nature of theory-
relevant concepts, with the ultimate aim of evolving practice (Forsyth, 1980) as relevant
scientist-practitioner activity (Corrie and Callahan, 2000).
Concept analysis is not used in counselling psychology
A total contents search of The Counseling Psychologist and the Journal of Counseling
Psychology conducted on 11.02.2018 located only one concept analysis study by
Hogan (1975) which describes a Q-sort used to create an empathy scale. A method
more commonly found is concept mapping (e.g. Goodyear, Tracey, Claiborn and
Lichtenberg, 2005) which is used to illustrate knowledge structures underlying concepts
through the use of diagrams of spacial and relational groupings of meanings. In this
regard concept mapping might be useful here as a comparative method. However
concept mapping is ultimately unsuitable for two reasons. First, it is an
expository/descriptive rather than a critical method. Second, it is positioned as a ‘post-
positive’ method that claims to “make use of an objective, impartial researcher and
standardised procedures” (Goodyear et.al., 2005, p. 236). A key premise of this critical
realist study is that no social research can be impartial. “Our theories and methods are
shaped by social forces and informed by interests” (Pilgrim and Bentall, p.262).
Another related method used in counselling psychology research is content analysis.
This may include the identification of conceptual themes relevant to the research topic,
for example in a literature review, but without a specific methodological analysis or
critical appraisal process (e.g. Shin, et.al. 2017; Pilgrim and Bentall, 1999; Olsson,
Bond, Burns, Vella-Brodrick and Sawyer, 2003; Hargons, Mosley and Stevens-Watkins,
2017). Such an approach would be insufficiently rigorous for the purposes of this study
as it is a form of literature review.
Framework analysis (Ritchie and Lewis, 2003) shares a similar method to concept
analysis, but likewise does not appear to be favoured by counselling psychologists. It

76 of 271
starts with a conceptual framework to which data is tagged (an etic process, Morrow
and Smith, 2000), whereas concept analysis (at least as I have used it as a
reconstructive process) starts with organising the data into thematically related groups
which are increasingly differentiated through processes of familiarisation, data
cleansing, and conceptual structuring, before a suitably shaped, theoretically-informed
framework is finalised towards the end (an emic process, Morrow and Smith, 2000).
Framework analysis uses concepts as ‘givens’ against which to locate and organise
appropriate data; while reconstructive concept analysis uses data units as ‘given’
connotations around which to locate and organise appropriate conceptual extensions to
link with existing theory.
Why I did not use a nursing concept analysis method
Nursing concept analysis methods in the tradition of Walker and Avant (2014), Rodgers
(1989) and Chinn and Jacobs (1987) provide clear descriptions of their analytic purpose
and methods. However they were not chosen here for several reasons. Firstly, these
approaches require the creation of ‘model’ or ‘exemplary’ cases. This points to their
realist stance that ‘truth’ is a fixed or universal entity that can be pinned down with
language and specifically located in experience. While this ontology may be suitable for
mathematical and other hard science concepts it is not in my opinion fitting for social
science concepts where meaning is fluidly context-bound (Duncan, Cloutier and Bailey,
2007). A criticism of nursing concept analysis methods, such as Rodgers’ ‘evolutionary’
approach (2000b) that rely solely on literature is that they can replicate professional
bias. They do not actively address language ownership about client experiences
(Wuest, 1994). Beckwith, Dickinson and Kendall (2008) argue that these nursing
concept analysis approaches are uncritical and derivative simplifications of a textbook
(Wilson, 1970) that offers a stepwise strategy for enabling grammar school pupils to
pass Oxbridge university exams. They also propose that these analytic methods lack
processes for evaluation of their findings.
Replacement versus reconstruction
The chapter now moves on to explain in more detail the concept analysis design used
here. In concept analysis an early decision must be made whether the aim is to replace

77 of 271
a defective concept by formulating a new one; or to improve an existing concept through
reconstruction (Sartori, 1984). An example of replacement concept formation can be
found in Pilgrim and Bentall (1999), where concept analysis is described as a “strategy
for replacing biased or misleading concepts with ones that are more useful scientifically
and clinically” (p. 262). However, the purpose here, while still intending to improve the
concept’s scientific utility, is to reconstruct it by clarifying its meaning using multiple
perspectives (Caron and Bowers, 2000). In this way I lend epistemic privilege both to
first-hand participant knowledge and to processed research data on client factors in line
with Hupcey and Penrod (2003).
Sartori’s concept analysis method
Sartori’s concept analysis method (1984; 2009) derives from political science. His
‘ladder of generality’ method used here has been described by Goertz (2006) as a
“classic” (p.69) contribution to the literature on concepts. It fits a critical realist ontology
in that Sartori dismisses any notion that concepts are fixed definitions of essential
phenomena. As objects of language he describes them as “arbitrary conventions”
(2009, p.89). While I argue that language use in an epistemological sense is hardly
arbitrary but results from, and contributes to, complex social structures, the ontology is
appropriate for this study. Sartori devised a process for creating a ‘reconstructed’
information-organising concept hierarchy that values the discriminative use of qualitative
and quantitative data. A hierarchy of abstraction aims to define a concept over several
layers of connotations that are incrementally less ambiguous than their aggregated
‘parent’ terms. Furthermore, Gerring (2012) offers seven criteria with which to evaluate
the adequacy of a reconstructed concept (applied in Chapter 5). The Sartori method is
indicative rather than prescriptive, which is useful here as it offers the researcher some
freedom to adjust the process to the context. I have made alterations and additions in
order to complete this study’s objectives. The following process explains the Sartori
method and how I have modified it:
1. Data collection: To commence, Sartori (1984) calls the researcher to collect a
“representative set of definitions” from “pertinent literature” (p.41). Because
‘representativeness’ has elsewhere been proscribed as too difficult to prove in

78 of 271
qualitative research (Barbour, 2001), I created a purposive literature dataset on
the basis of inclusion/exclusion criteria I devised to locate a diverse range of
client factors in outcome studies. Because ‘client factors’ is a term that
encompasses many other concepts, instead of seeking definitions, I aimed to
locate its component attributes and operations. Additionally Sartori recommends
the researcher strive for “historical depth” (p.41) in the data sample. In this study
this meant reviewing studies back to 1960 although in the included dataset the
oldest article is dated 1983. Study selection is explained in section 3.8 (pp.103-
108). My study is enhanced in line with Hupcey and Penrod (2003)’s advice to
triangulate the concept analysis with participant data, which in this case,
consistent with muted group epistemology, forms the primary structure for the
findings and analysis. The collection of participant data is explained in section 3.5
(pp. 80-87; for an example of a Sartori-inspired concept analysis that follows his
instructions without triangulation, see Knafl and Deatrick, 1990).
2. Data extraction: Sartori then calls the researcher to extract the relevant
characteristics, although he does not explain how this might be done. I achieved
this with the use of spreadsheets which are discussed and illustrated in sections
3.6 (pp. 88-92) and 3.9 (p.109).
3. Data interpretation for concept hierarchy construction: The next step is
creating what Sartori calls a “ladder of abstraction” (p.44) ‘matrix’ diagram that
organises denotative labels for clusters of included phenomena (‘intensions’ or
‘connotations’ of the concept, Sartori, 2009) over levels of abstraction. I replaced
the term ‘matrix’ with ‘framework,’ because ‘matrix’ connotes a total source
context while this study does not aim for comprehensive or conclusive findings.
However I am looking for explanatory mechanisms, associations or tendencies
between client input and therapeutic outcome where possible (Fletcher, 2017;
Sartori, 2009). In terms of framework structure, following the rule that the more
abstract the term, the fewer its connotations, the least abstract terms are
granular context-specific phenomena. These are thematically clustered under
category labels with mid-range abstraction. Further connotative reductions are
made to link mid-range abstractions to the generalised original concept.

79 of 271
Hierarchical conceptualisation strategy yields maximal, mid-range and minimal
definitions of the concept (Gerring, 2012). A further step in the structuring
process is deciding the “conceptual frontiers” (Sartori, 1984, p.43): which
phenomena and denotations are, and are not, part of the concept. In this study,
factors with contradictory or marginal evidence were ruled out (this is explained
further in section 3.11, pp. 115-117). In terms of language use within the concept
framework, the coherence and precision of the “semantic field” (Sartori 1984,
p.51) should be ensured. Jargonistic terms, which Sartori says “add to
obfuscation” (p.54) should be avoided. Neighbouring terms within the hierarchy
should relate well. Synonymies, which Sartori calls “terminological waste” (p.39),
should appear neither laterally nor vertically in the hierarchy. In terms of visually
presenting the findings, in this study I have used an enhanced fishbone graphic
for displaying the interpreted frameworks, and this process is explained in
sections 3.7 (pp. 92-99) and 3.10 (pp.109-115). Encouragingly, Sartori leaves
organising matrices “to the perceptiveness and ingenuity of the analyst” (2009,
p.116).
4. Concept reconstruction: In this study, the meaning of ‘reconstruction’ involves
comparing and combining the participant and research hierarchies into a single
final framework. This process is explained in section 3.11 (pp116-119).
Figure 9 summarises the study design’s parallel process in diagrammatic form over
seven steps. Steps one to three, data collection, extraction and interpretation are
conducted for participant data, then repeated over steps four to six for research data. In
step seven the resulting concept hierarchy frameworks are compared and combined
into one.

80 of 271
Figure 9: Concept analysis method steps flow diagram
Steps one to seven are explained in the following sections 3.5 – 3.11, along with the
labelling of the structural hierarchy at the more abstract levels. The content of the
concept reconstruction is described in detail in Chapter 4.
3.5 Participant recruitment and data collection In explaining how I handled Step 1: Participant data collection (see figure 9, p.80), I
cover the following topics in this section: participant recruitment process; recruitment
objective; participant characteristics; interview design; data collection; power dynamics;
and interview transcription.
Recruitment process
In qualitative research the process of attracting participants is an important contextual
aspect of the study. Participant sites determine to an extent who in included and
therefore the nature of the light shed on the topic (Morrow and Smith, 2000). In this
study I needed to talk to people who had recently finished a course of counselling.
Following Spradley’s (1980) strategies for locating participants, simplicity, permissible
accessibility and unobtrusiveness were key guiding principles. In spring 2016 I obtained

81 of 271
permission to recruit participants from a suburban third sector general counselling
service with a primarily person-centred approach (TS1); and an urban university student
and staff counselling service (US1) with generally short-term CBT and solution-focussed
approaches. An additional suburban site (TS2) is a specialist third sector service I
manage, which predominantly serves clients within an NHS adult community eating
disorder service using integrative, CBT and group-based approaches. This service was
chosen for ease of access and unobtrusiveness. I met with therapy teams from each
service to provide a brief talk about the purpose and method of my research. I asked
them to invite clients who were about to finish counselling to participate. I suggested 4+
sessions of therapy should have been completed, to roughly accommodate advice from
Kadera, Lambert and Andrews (1996) that it takes at least 2 sessions, and for most
clients, 8 or more sessions to achieve significant changes. I also placed recruitment
posters (Appendix 9) in the waiting areas of TS1 and TS2 and the therapy room in US1.
Dataset adequacy and the question of data saturation
I aimed to recruit 12 adults aged 18+ which is the minimum recommended for qualitative
research by Baker and Edwards (2012). However I stopped at nine (a) to manage the
volume of data within project timescale (b) because nine came forward on my first
recruitment exercise; and (c) upon data analysis it was clear that no further interviews
would be needed, because in terms of dataset adequacy I was able to meet the
information requirements of the study with the obtained sample, in that it was large
enough to capture a range of experience but not so large as to be unduly repetitious
(O’Reilly and Parker, 2012).
The question of achieving data saturation with participant interviews as a quality marker
was problematic in this study for two reasons. Firstly, data saturation is described in
grounded theory methodology as a process that assures theoretical categories are fully
accounted for in theory-generating analysis of unstructured participant interviews
(Aldiabat and Le Navenec, 2018). While this may be appropriate for inductive theory-
building research, it is not necessarily a suitable notion in deductive theory-clarifying
research (which is the purpose of this study). The nature and direction of data
collection in deductive research (particularly within a critical realist ontology) means the

82 of 271
researcher cannot capture all possible categories of meaning. This renders the
achievement of saturation “an unrealistic target” (O’Reilly and Parker, 2012, p.194). The
second reason is related to the first. Data saturation is not a recognised aim of
reconstructive concept analysis where instead, data triangulation is recommended (see
p.23 in section 1.4 for Hupcey and Penrod’s 2003 triangulation recommendations).
Fusch and Ness (2015) assert that methodological data triangulation “goes a long way
towards ensuring” data saturation (pp.1411-1412).
In terms of data adequacy, my participant data analysis spreadsheet (figure 11, p.91)
represented what Brod, Tesler and Christiansen (2009) have called a ‘saturation grid,’
albeit modified here for deductive research intended to locate categories rather than
inductively validate categories determined from preceding interviews. The major
categories and elements were listed on the columns and the participants were listed on
the rows. All categories and elements represented in the reported results contained
quotes from at least two participants, in line with Brod, Tesler and Christiansen (2009)
who included data from at least two interviews per category.
Participant characteristics
I hoped for a diverse participant group, but recruitment was non-purposive due to the
exploratory nature of the research design. Because I took no steps to ensure greater
diversity, the actual self-selected group was comprised of white women aged from 18
years into their 30s. With hindsight it was predictable that the services I accessed would
tend to yield participants in this stratum. The composition of this sample was determined
by their having recently accessed counselling and having an interest in the topic of how
clients make therapy work, and/or an interest in participating in research.
A homogenous comparison sample is an advantage in critical realist research where the
investigation probes the mechanism of a generalised concept derived from research to
see if it actually affects clinical outcomes as expected in specific contexts (Miller and
Tsang, 2011). While my research focus is not concerned with specific contexts it could
not evade the contextuality of the settings where I sourced participants.

83 of 271
Participants were predominantly highly educated, childless, working fulltime and in long-
term relationships. Table 1 provides a summary of participant demographics.
Categories were chosen to correspond to those frequently included in the research
literature sample (discussed in section 3.8). I applied culturally appropriate pseudonyms
to avoid the de-humanisation of numerical labels. Although Allen and Wiles (2016)
recommend that participants choose their own pseudonyms at the outset, this issue
only came to my attention at write-up stage.
Table 1: Participant demographic characteristics
Par
tici
pan
t
nu
mb
er
Pse
ud
on
ym
Inte
rvie
w
sch
edu
le
Gen
der
Eth
nic
ity
Age
Edu
cati
on
Emp
loym
ent
Sou
rce
1 Dana A F White
British
31-40 BA Fulltime TS1
2 Ella B F White
British
31-40 BA No TS2
3 Luka B F White non-
European
31-40 Doctorat
e
Fulltime TS2
4 Kyra B F White
British
31-40 Masters Fulltime TS2
5 Lucy A F White
British
26-30 Masters Fulltime TS2
6 Zoey A F White
British
31-40 BA Fulltime US1
7 Thea B F Mixed
White
British and
other
White
European
18-25 A-Levels Part
time
TS2
8 Lily B F White
British
18-25 Masters Fulltime TS2
9 Esme A F White
British
18-25 Masters Fulltime TS2

84 of 271
Interview design
Briefly reviewing the structure of the causal syntax behind the concept analysis, a
change in independent variable X is a mechanism directly or indirectly associated with a
change in outcome Y. In this case X is client factors, which I am seeking to elucidate. Y
is conceptualised here as desired psychosocial life-change, which I am not seeking to
elucidate. A generic outcome is used here for two reasons: (a) participants in this study
had attended psychotherapy for help with a range of different psychosocial issues; (b)
participants could pick the outcome that was meaningful to them, not necessarily the
original reason they sought therapy.
In devising questions for a semi-structured interview to elicit from participants why, from
their point of view, change did and did not happen in therapy, I ruled out some existing
interview schedules. The Client Change Interview (Elliott, 1996) was unsuitable
because it does not explore client perceptions of causality in therapeutic change (e.g.
Klein and Elliott, 2006). I also ruled out the Helpful Aspects of Therapy (HAT, Llewellyn,
1988) and Patients' Perceptions of Corrective Experiences in Individual Therapy
(PPCEIT, Constantino et.al. 2011a) because of their bias in eliciting therapy-validating
information (e.g. Constantino et.al. 2017; Constantino and Angus, 2017). It was
important to the concept reconstruction that participant narratives were not shaped by
therapy-centric questions; and that the starter questions were not leading in terms of
explanatory attributions for change or non-change. After piloting multi-question
interviews with two doctoral student peers, I removed questions relating to whether
participants thought personal demographics had a bearing on the therapy outcome
because (a) they were leading and (b) participant feedback was that they were
irrelevant.
I decided that a semi-structured interview format would provide flexibility for participants
to expand upon topics of relevance to them while being guided by subject-relevance for
the research (Kvale, 2007). This type of interview also permits the researcher freedom
to tailor their responses to the participant (Morrow and Smith, 2000). I chose simply-
framed interview questions that were tightly focussed to the aim of the study (Agee,
2009). These questions assumed that participants and their contexts had exerted

85 of 271
important effects on therapy outcomes, and that participants could identify and describe
what these effects were. The ‘what’ changes and non-changes were not the objects of
enquiry, but needed to be established in order to frame ‘why’ questions aimed to access
participant experience of causal attributions for change and non-change processes
(Swan, 2017).
Schedule A, used with four participants, comprised four open-ended interview
questions:
1. Please describe one positive or desired change that has happened in your life since you
started therapy
2. Why do you think this change happened?
3. Please describe one thing that hasn’t changed in your life as you hoped since you
started therapy
4. Why do you think this change did not happen?
Schedule B, used with five participants, placed the non-change questions (3 and 4) first,
followed by the change questions (1 and 2). This was done to balance the ‘warm-up
effect’ in interviews where participants may provide information more freely in later
stages of the interview (Mellon, 1990).
Data collection
No participant was excluded and none declined to take part once they had read the
information sheet (Appendix 10). Interviews were set up at participant convenience to
occur between one and six months after their last counselling session. This timeframe
was chosen so that there was sufficient interval for participants to reflect on their role in
therapy; while not being so distal that experiential memory might have faded. All
participants were sent the interview questions (Appendix 11) at least a week in advance
so they could think about them before their interview if they wished. All participants gave
consent (Appendix 12) and provided demographic information prior to interviews
commencing (Appendix 22, with results in Table 1, p.83).

86 of 271
Interviews were conducted in summer and autumn of 2016. One interview took place on
Skype and the remainder in-person at TS2 in a confidential consulting room.
Interview lengths were determined by how much the participant had to say on each
question although I more actively wound up two interviews in order to keep to an hour in
line with the participant information sheet which said interviews would be 30-60 minutes.
The shortest interview was 30 minutes (Luka) and the longest was 62 minutes (Esme).
The average interview length was 46.7 minutes.
By way of interview manner my style is warm and relatively informal, although focussed
on the job at hand without engaging in tangential chit-chat or offering information about
myself other than an introduction to my role as student-researcher. Prior to commencing
recording I started interviews with an explanation of the research topic and answered
participant queries in relation to the topic or the information sheet provided. Upon
commencing recording, besides asking the four interview questions my interjections
were restricted to eight types:
Summarising prompts intended to invite participant to discuss a relevant topic
further (for example: So all of these things you are attributing to helping you get
to the point where things are really good now.)
Summarising interpretations seeking correction (Kvale, 2007) (for example, So
there was a sense of escape there…? Dana: Yeah! I think so. Well, not escape,
but, just, new beginnings. Kind of, ‘yes I want to go away from here but I do
actively want to go where I’m going.’)
Questions inviting further discussion of a specific topic (for example: How did you
decide upon each one of those helpful activities?)
Questions seeking deeper meaning or relevance of the topic in the participant’s
life (for example: What does that mean for you making that really big decision,
something that you’d been thinking about for a long time, that you were actually
able to do it?)
Questions seeking clarification of a process (for example, Do you think that’s as
a result of sleeping better, feeling better, having taken the steps that you’ve
taken? Or did that actually contribute to your being able to sleep better?

87 of 271
Open questions testing for further information (for example: Is there anything else
about this process of change that you feel is important to tell me about?)
Directing the conversation to areas of relevance (for example: Well, moving
house was another decision there.)
Brief joining affirmations, emotionally mirroring something the participant said (for
example: Definitely! [Laughing with participant])
Power dynamics
I was aware of mild but not detrimental role power imbalances fluctuating between me
and the participants (Vähäsantanen and Saarinen, 2013). Participants understood from
the information sheet that it was my role to ask questions and theirs to share relevant
personal experience (Kvale, 2007). Implicit in this arrangement was my role to listen,
understand, interpret and learn (although this was not, and probably should have been
spelled out in the information sheet). In terms of researcher power, I devised the
questions, managed the commencement and conclusion of the interviews, the timing
and introduction of the four questions, and I sometimes guided conversations to optimal
relevance for the research topic (Kvale, 2007). In terms of participant power, I was
dependent on their willingness to donate time and to provide analysable information. It
is my observation that the interviews unfolded in a spirit of mutual cooperation, in which
power balanced itself by homeostasis-seeking social grace. I felt it would have been
inappropriate, in terms of my ethical obligation not to burden or exploit participants, to
de-stabilise this power balance, for example by introducing my personal experiences
into the conversations (Karnieli-Miller, Strier and Pessach, 2009).
Interview transcription
I transcribed all interviews verbatim within four weeks of their recording date while they
were still fresh in my memory (Sreenan, Smith and Frost, 2015). Visible body language,
facial expressions and hand gestures were not noted. Audible sighs, laughter and crying
were noted, as were pauses lasting five seconds or longer. Participant anonymity was
protected by the use of codes for diagnoses, services attended and named staff,
geographical places. The names of significant others and types and places of work
were removed. A partial transcript is available in Appendix 13. My decision-making

88 of 271
regarding removing diagnostic terms is presented in Appendix 14, along with how I
handled transcribing local pronunciations, punctuation and speech fillers (Oliver,
Serovich and Mason, 2015).
3.6 Participant data extraction Step 2 (see figure 11, p.91) was carried out over the following stages: Interview
summaries; data extraction spreadsheet; data cleansing; and data immersion. I will now
explain each of these stages.
Interview summaries
While transcribing, I simultaneously kept a notebook of hand-written observations.
These briefly summarised each participant’s answers to the four interview questions. I
also noted some key themes along with initial interpretations which helped me monitor
and limit my “intrusion into the text” (Borland, 1991, p.70). Figure 10 shows my notes on
points Ella makes in her interview, plus observations, for example, that she did not
seem to give herself credit for the changes she’d achieved; and that she said she
sought security. I also jotted down ideas for working up the analysis, for example, that
‘personal factors’ and ‘relational factors’ are interdependent.

89 of 271
Once all interviews were transcribed I typed up summaries which are presented in
Appendix 15. Six participants chose as their desired change the primary reason they
attended therapy, while the remaining three chose other issues. In terms of changes not
achieved, four participants said they had not satisfactorily reached the goal for which
they attended therapy; and four identified other issues that remained unresolved. One
participant said there were no outstanding issues after therapy.
Data extraction spreadsheet
While transcribing I simultaneously built a spreadsheet in which I organised and
categorised all conceptual data related in any way to helpful and unhelpful factors
participants described. Over a lengthy data extraction and analysis process these data
were organised and re-organised into increasing levels of abstraction:
Figure 10: Example notes of preliminary interview summary

90 of 271
(a) Elements are mildly abstract, person-level, labelled groupings of direct activities
and experiences associated with processes of change and non-change.
Elements are built up from, and illustrated by non-abstract participant quotes.
Quotes are the ‘thick descriptions’ with which Gilgun (2014) encourages the
deductive researcher to start the analysis. I used at least one and in many cases,
several quotes from one or more participants to illustrate each element. The
labelling of elements represented the first stage of interpretation. Labels were
revised several times over the course of data extraction to best summarise the
meaning of the element.
(b) Categories are groups of elements that belong best together in classes of action
or inaction, although it was only after some time working with the data that I
discerned that action and inaction were defining pattern characteristics at the
categorical level. Categories are labelled with terms that indicate the particular
‘state of doing’ indicated by their component elements on the helpful factors side;
and the ‘state of being’ indicated by component elements on the unhelpful factors
side. Abstracted away from actual experience, categories form chains of inter-
related factors comprising processes of change on the helpful side, and non-
change on the unhelpful side. The creation of categories represented a further
stage of interpretation.
(c) Super-factors are highly abstract features of the most abstract term ‘client
factors.’ Without a specific definition, super-factors depend on reader epistemic
experience to extrapolate their meaning. These factors were derived from my
interpretation and management of the data, informed non-specifically by
counselling theory, and were imposed on the data at the outset to provide a
preliminary deductive basis for concept categorisation.
Data was used at ‘face value’ as honest explanations of experience. I did not, as other
qualitative researchers might, listen for ‘distortions,’ ‘self-deception,’ or ‘groundless
assertions’ (Elliott, 2010). While my previous knowledge from personal and
professional observations and reading about how people make desired life-changes
informed this interpretive activity, I tried to minimize seeking, interpreting, interposing or
inventing meaning beyond what participants said. In this way I assumed there was no

91 of 271
failure (or veiling) in participant communication of meaning nor in my listening and
understanding. This was done to reduce risk of ‘therapy-centrism’ in my use of
participant data. So my guiding questions as I familiarised myself with the interviews
and developed the data extraction spreadsheet was, ‘What factors enabled this
participant to make desired changes? What factors posed obstacles to change?’
Figure 11 shows how the hierarchy of super-factors, categories and elements were
constructed within descending rows of the spreadsheet, with illustrative participant
quotes within each element’s column.
Figure 11: Participant data extraction spreadsheet sample
Data cleansing
Once notations from all transcripts were added into element columns, I printed out the
labelling rows of the entire spreadsheet (Appendix 16). This was then cut into
manageable sections for close review and data cleansing, which involved collapsing
Super-factors
Categories Elements
Participant quotes

92 of 271
duplicates; re-positioning those that seemed to be under the wrong super-factor;
renaming those that required more accurate labels; and deleting entries which, upon
consideration, were not elements because, for example, they were not precisely
evidenced by participant data.
Figure 12 shows my editorial notations on a section of the spreadsheet print-out.
Figure 12: Hand notations for spreadsheet data cleansing
Data immersion
To further immerse myself in the data I carefully re-read each transcript several times to
locate exact quotes for the conceptual themes and added these to the spreadsheet
(figure 11 on p.91 shows location of quotes). Over 270 quotes were added, although
only 68 were chosen to present in this write-up. All participants gave clear and
descriptive answers to each of the four interview questions. Material from all participants
was well-dispersed across the spreadsheet. There were no participants whose data was
sparsely represented.

93 of 271
3.7 Participant data interpretation Step 3 (see figure 9, p.80) interpretation was carried out over two interrelated tasks:
development of a fishbone framework diagram to illustrate the interrelationship of
helpful and unhelpful client factors over time; and the delineation and expression of four
levels of conceptual abstraction within the framework. While more detailed discussion of
the contents of the framework is presented in Chapter 4, I explain here how I used the
interview data as the basis for the fishbone structure. First I explain the central spine of
the framework, then follow this with explanation of how the ribs were built up.
Fishbone spine: Process of change over time
All participants, in providing detailed accounts of how they made desired life change,
naturally embedded significant events in unfolding time. The ‘time-stamp’ on key
activities and experiences in client narratives permitted me to design the concept
framework using ‘process of change over time’ as the spine. I could then position
change and non-change elements in a general chronological order based on where they
were positioned in participant life-narratives.
Temporal descriptions had various purposes. Most participants provided a timeline to
orient me to the history of their problems as well as their decisions and efforts to
change. For example, Kyra explained that she had recently left a job she had held for
seven years, in which colleagues had accommodated her mental and physical health
problems. She did not want these to carry on in her new job, So I decided at the start of
[the current year] that I probably needed some additional support to try and break the cycle for
good….There’s been probably a lot of things over the past six to twelve months, that have
accumulated in me thinking that I need to, I need to make some real life changes. Zoey
explained how several geographical moves over time were part of her increasing
recognition of the need for help: And then shortly after moving to [English city 2], about six
months, I went to the doctor and asked for some more counselling.
Change processes were described as requiring active work over extended periods of
time during and after psychotherapy. For example, Luka said, I’ve done probably quite a
lot of work since it was a really, really bad relapse in Christmas, so last six months I’ve done

94 of 271
quite a lot. And it just gradually happened. Kyra said, [my therapist] sent me an app to
download, that I’ve used. I’ve been using that for a good few months now [since therapy ended],
to look at, and then you can pull off your sheets of progress to see patterns of how you’ve been
feeling at the same time, and when you’ve had blips. Thea explained, Each time [I’ve had
psychotherapy] I’ve been a bit more able to try and get on board with [therapist suggestions].
Although it did take five-ish years.
Contrasting how slowly positive changes came about for some participants, Lily
described how quickly problems emerged: I just didn’t get…how things could change so
quickly from one month, in January, feeling completely fine and [asymptomatic] on Christmas
Eve, then five months later, [symptomatic of D3] and terrified of anything. Others reported a
chronic pattern of difficulties going back to childhood. For example, Lucy said, I want to
break away from all the rules and restrictions that I’ve imposed on myself for so many
years….I’m confronting years and years and years of behaviours that have become so
engrained. Zoey explained, I went to see…my mum, and I said, ‘I’m not coming round here
anymore.’ There’s been over the years, so many conversations.
Some participants recounted time lost within developmental trajectories due to the
impact of recurrent or debilitating problems. For example, Dana explained how she had
to take time out from her training course and work: I was missing a lot of time off work and I
had major stomach upsets and, that I’ve now recognised was [D2] and [D1]. Ella said, I’d gone
from [less improved to more improved]…. That was last Christmas, not the Christmas just gone,
the Christmas before. Or was it this Christmas? No it was last Christmas. So then I [relapsed]
beginning of the year. Thea explained how she had had to defer starting university a few
years previously, due to mental health problems: I couldn’t do my personal statement so
that’s why I couldn’t apply to Uni the first year.
Another form of reflective time description related to how long participants had recently
enjoyed the fruits of their change efforts. For example Dana said because I’ve been
sleeping well for a good couple of months I can now watch the news and then go to bed. Luka
said, I very rarely, actually, for the last few weeks I think, I’ve not thought that I hate myself.
Some participants remarked how long it had been since they had last functioned as

95 of 271
well. For example, Ella said, I saw people I’ve not seen for twelve months on Saturday night.
We had a big reunion. Thea noted, A few months into the relationship with [girlfriend] I
managed to go for a month without [specific difficulty occurring]. Which was the longest it had
been in six years.
Some participants described reflecting back to the past to see how far their life had
since changed for the better, to motivate themselves to keep going. For example, Ella
said, All I have to do is look back at those times and think, ‘do you really wanna be there? Do
you really want to be the ones that you felt sorry for in [Service A programme]? Do you really
want to feel as low as them, as isolated as them?’ On the other hand, Esme projected into
the future to motivate herself to make changes: So in ten years, do I want to be childless,
friendless, still [unwell], miserable? No.
In summary, participants described taking a series of large and small, complementary
steps over quite lengthy periods of time before they achieved their desired aim; and in
aggregate these steps brought about wider changes in their quality of life and
relationships.
Fishbone ribs
Once the data extraction spreadsheet was complete, using A3 paper I sketched out and
worked up a provisional framework in order to clarify and organise all aspects of the
hierarchy and its component categories and elements. Meaning was created from
participant material at the elemental level. Quotes from at least two different participants
were required to qualify each element. Meaning elements were grouped via a mildly
interpretive process into categories of activity and inactivity. Categories and elements
were reviewed and adjusted in terms of contents and labels until best fit was achieved.
Categories were then further condensed and abstracted to stages of change, which
were then abstracted to super-factors, in a process similar to content analysis (see for
example Erlingsson and Brysiewicz, 2017). Figures 13 and 14 show some of this work
in progress.

96 of 271
Figure 13: Initial sketching for participant-informed concept hierarchy

97 of 271
Figure 14: Intermediate sketch of participant informed hierarchy
Through data extraction a fundamental distinction was made between helpful and
unhelpful factors. Because these largely mirrored each other, a fishbone structure fit for
interpreting and presenting client factors as components of a process that unfolds over
time. The finalised participant-informed client factors hierarchy is shown in figure 15. It
should be noted that this diagram is intended to be viewed in A3/200% size. It is
reproduced here at A4 size to give the reader an indication of the fishbone but it is
acknowledged that detail at the elemental level is lost in this format. Final elements are
explained in detail in Chapter 4.

98 of 271
Figure 15: Participant-informed concept framework

99 of 271
Hierarchy of abstraction
The following description explains how the concept framework was built and labelled.
This is a structural, methodological explanation which is distinguished from the results
presented in Chapter 4, although for illustrative purposes I explain here the labels I used
and why.
The blue-spined participant-informed concept framework shows participant social,
behavioural, cognitive and identity factors organised into holistic chains of change and
non-change occurring over time. The area above the spine of the fishbone shows
helpful factors and the corresponding area below the spine shows unhelpful factors. The
helpful and unhelpful sides are each divided vertically into four levels of conceptual
abstraction from highly abstract super-factors, to moderately abstract stages of
change/non-change, to less abstract categories of activity/inactivity and finally specific
elements which are non-exhaustive connotations of each category. Elements include
illustrative participant quotes and research findings which are the “real world
counterparts” (Sartori 1984, p.22) of conceptual terms.
I will now explain the four levels of abstraction in turn. Each of the concept labels is
shown in bold throughout the remainder of the write-up for highlighting purposes.
Level Four: Super-factors
Super-factors are the most abstract level of intension -or connotation- of the concept, of
which there are two. Super-factor 1, social support is subdivided as (A) a moderator
(inspiration), and (B) a mediator (facilitation and reinforcement) for super-factor 2, which
is reflective learning. These helpful super-factors form a concatenated trajectory that
leads to ongoing inter- and intrapersonal growth cycles across the lifespan.
On the unhelpful side of the framework, super-factor 1: inadequate social support
refers to various types of non-generative relational impairment or injustice in the familial,
community or cultural context. An impoverished social environment contributes to, and
is reinforced by super-factor 2: psychosocial stagnation. Here this term refers to living
in a state of cognitive and social inflexibility that hinders reflective learning and adaptive
growth.
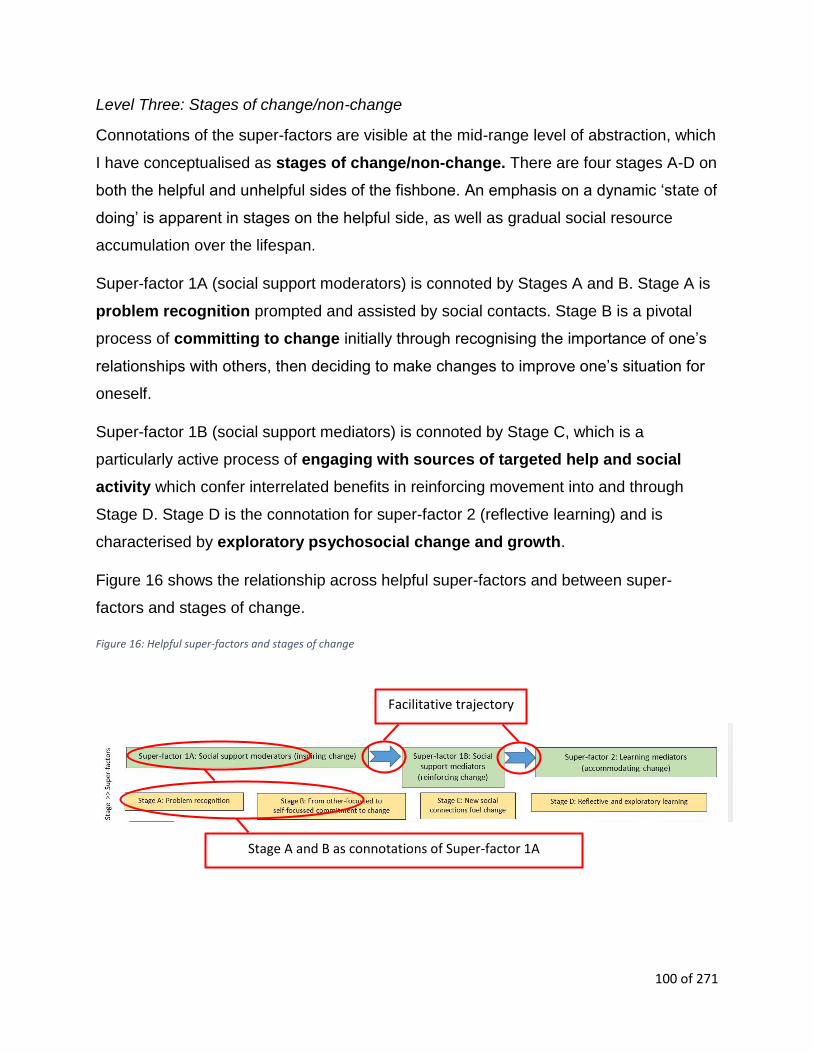
100 of 271
Level Three: Stages of change/non-change
Connotations of the super-factors are visible at the mid-range level of abstraction, which
I have conceptualised as stages of change/non-change. There are four stages A-D on
both the helpful and unhelpful sides of the fishbone. An emphasis on a dynamic ‘state of
doing’ is apparent in stages on the helpful side, as well as gradual social resource
accumulation over the lifespan.
Super-factor 1A (social support moderators) is connoted by Stages A and B. Stage A is
problem recognition prompted and assisted by social contacts. Stage B is a pivotal
process of committing to change initially through recognising the importance of one’s
relationships with others, then deciding to make changes to improve one’s situation for
oneself.
Super-factor 1B (social support mediators) is connoted by Stage C, which is a
particularly active process of engaging with sources of targeted help and social
activity which confer interrelated benefits in reinforcing movement into and through
Stage D. Stage D is the connotation for super-factor 2 (reflective learning) and is
characterised by exploratory psychosocial change and growth.
Figure 16 shows the relationship across helpful super-factors and between super-
factors and stages of change.
Figure 16: Helpful super-factors and stages of change
Facilitative trajectory
Stage A and B as connotations of Super-factor 1A

101 of 271
On the unhelpful side of the framework, a less mobile ‘state of being’ is apparent in
stages of non-change. Unhelpful super-factor 1 (Inadequate social support) is connoted
by Stages A and B. Stage A Non-change is a problem-maintaining social
environment. From this ensues Stage B Non-change which is characterised by no
commitment to change.
Unhelpful super-factor 2 (psychosocial stagnation) is connoted by Stages C and D. In
stage C Non-change, no new generative social connections compounds the effects
of the previous two stages to propel the individual into stage D Non-change, a cycle of
resource depletion, which re-connects with stage A Non-change. Here I define
resource depletion as adverse socio-cultural or emotional circumstances that overtax
one’s health, social support, coping skills, self-efficacy or sense of identity, to the point
that one can no longer reflect, learn, explore or develop one’s potential.
Figure 17 shows the self-maintaining relationship across unhelpful super-factors and
between super-factors and stages of non-change.
Figure 17: Unhelpful super-factors and stages of non-change
Level Two: Categories of activity/inactivity
The connotations of the stages of change are visible in the next less abstract level
which comprises nine categories of activity on the helpful side, and nine obverse
categories of inactivity on the unhelpful side. On the positive side, most categories
are labelled with participles to capture the ‘state of doing’ that characterises participant
work at this level.
Self-maintaining relationship
Stages A and B non-change as connotations of unhelpful super-factor 1

102 of 271
Figure 18 shows categories of activity as connotations of respective stages of change.
Figure 18: Categories of activity
Figure 19 shows categories of inactivity as connotations of respective stages of non-
change.
Figure 19: Categories of inactivity
Level One: Elements
Elements are the densest and least abstract level of the concept hierarchy because
they are built from non-conceptual raw data. However, as interpretations from the data,
they are mild abstractions. They are illustrated by constituent participant quotes and
research references to assist the reader understand their formation. There are 38
helpful and 22 unhelpful elements, 60 in total. Element contents are described in
Chapter 4.
Categories 7 to 9 as connotations of change Stage D
Category 5 as a connotation of change Stage B and C
Categories of inactivity 1 and 2 as connotations of Stage A non-change
Inactivity category 5 as a connotation of stages B and C non-change

103 of 271
Figure 20 shows a narrated screenshot of helpful elements that connote helpful
categories 7, 8 and 9 (which in turn are connotations of change stage D).
Figure 20: Elements of helpful activity categories 7 to 9
Figure 21 shows a narrated screenshot of unhelpful elements that connote unhelpful
categories 7, 8 and 9 (which in turn are connotations of non-change stage D).
Elements connoting their respective helpful categories

104 of 271
Figure 21: Unhelpful elements connoting non-change categories 7 to 9
3.8 Research data collection Step 4 (see figure 9, p.80) research data collection is now presented over two parts:
study selection; and a summary of characteristics of the 68 included studies.
Study selection
Study selection took place over four phases which are shown in the flow chart in figure
22 (adapted from Moher, Liberati, Tetzlaff and Altman, 2009). This chart is included to
assist the reader in following the stages of the literature selection process. Although this
‘PRISMA’ style chart is commonly seen in systematic reviews it is stressed that the
review conducted here was selective in line with concept analysis methodology (Sartori,
1984; Rodgers, 2000b) not systematic. Phases included identification; screening;
application of eligibility criteria; and inclusion. Each phase is next described in further
detail.
Elements connoting their respective non-change categories

105 of 271
Figure 22: Study selection flow chart
Articles located in search of
PsycINFO (n-677), ScienceDirect
(n=410), Mendeley Open Access
(n=2056) & Sage Journals (n=197)
(Total n=3340)
2. S
cree
nin
g 4
. In
clu
ded
3
. Elig
ibili
ty
1.
Iden
tifi
cati
on
Articles located in existing files and
textbook reference lists
(n=299)
Articles screened for relevance
by title (n=3639) Records excluded (n=3564)
Full-text articles assessed for
eligibility against quality control
criteria (n=124)
Full-text articles excluded (n=56)
Measures/ timepoints not specified (n= 10)
Client factor not found, not described or not
a significant predictor (n= 9)
Predictor or moderator not clearly a client
factor (n= 8)
Outcome or predictor judged by therapist
(n=7)
Client factor is an aspect of presenting
problem (n= 6)
Design or analysis does not explain change
mechanisms (n= 5)
Client factor not operationally defined (n= 3)
Involuntary treatment participants (n=2)
Analytic focus on therapist action (n= 2)
Minimum 3 sessions not specified (n= 2)
Therapy not described (n= 1)
Therapy outcome not specified (n= 1)
Studies included in concept
analysis (n=68)
Abstracts screened for relevance
(n= 697)
Articles located in systematic
reviews and meta-analyses
(n=49)

106 of 271
Identification
The search for relevant research about client factors associated with process and
outcome was conducted in January 2018. Three sources were used: databases, select
textbook bibliographies, and my existing collection of articles.
In considering which databases to search, although Penrod and Hupcey (2004) advise
that in concept analysis, multidisciplinary sources should be sampled in order to capture
the concept’s use in different contexts, in this study, due to the discipline-specific nature
of the client factors concept, databases were restricted to those likely to yield articles
about client activity in psychotherapy. These included Sage Journals, Science Direct,
PsycINFO and the Mendeley open access catalogue. The Science Direct search was
limited to 2017-18 for manageability and to yield up-to-date indications of the concept
while providing some balance with the text book searches which yielded older studies.
Search terms were searched for within ‘all fields’ rather than restricted to ‘keywords’
and/or ‘title’ to increase the scope and credibility of the search (Rodgers, 2000b). Terms
included ‘client factors,’ client characteristics,’ ‘extratherapeutic factors,’ ‘client agency’
(altered in PsycINFO to ‘empowerment’), ‘client variables,’ ‘moderators’ ‘mediators,’ and
‘predictors of therapeutic change.’ In PsycINFO these terms were exploded to additional
relevant terms and then associated with exploded terms for ‘counselling.’ Appendix 1
shows screen shots of the searches conducted.
Textbook reference lists were searched including Garfield 1978, 1994; Clarkin and
Levy, 2004; and Bohart and Wade 2013. These were chosen to ensure the inclusion of
studies that preeminent researchers relied on for the concept’s development over time
(a precedent for this type of hand search can be found in Bernd and Strouse, 2008).
Relevant articles from my existing library of research articles (collected in preparatory
work from 2015-2018) were included.
Screening
3340 study titles were reviewed and 2643 were excluded as irrelevant. 697 were
retained for abstract review against primary inclusion criteria (Appendix 2), and a further
608 studies were excluded. 89 studies remained.

107 of 271
Among the 89 remaining studies were 14 meta-analyses/systematic reviews. Because
the final sample could include only primary research, 49 relevant primary studies were
retrieved from the bibliographies of these studies, which were themselves removed
(detail of studies included from removed meta-analyses is shown in Appendix 3). 124
studies remained for full text review.
Eligibility
Under full-text review the 124 remaining studies were subjected to quality control. The
baseline quality threshold was the study’s publication in a peer-reviewed journal. Then,
because I required data relating as exclusively as possible to client or extratherapeutic
factors (rather than therapist, technique or diagnostic factors); and because I was
seeking either statistical inference of mediation, moderation or prediction (rather than
simple correlation); or client asserted association between client factor and outcome,
further exclusion criteria were applied (detailed in Appendix 5. Results of exclusion are
in Figure 22 ‘full text articles excluded’ text box).
Inclusion
After the application of these exclusion criteria, 68 studies remained for full data
extraction and concept analysis. A distinction was made between those where outcome
was analysed from follow-up data gathered at least 1 month after therapy finished
(41.2%, n=28/68), and those where outcome was measured at the end of therapy
(58.8%, n=40/68). Client factors reported from follow-up data might be less likely to be
temporary artefacts of the therapeutic process. However due to the relatively small
number of studies in each subgroup, I decided not to create concept analyses
comparing any differences, but treated the 68 studies as a complete dataset.
Dataset adequacy
Study sample dataset adequacy in concept analysis is indicated by its capacity to
support the study. The appropriateness of the sample is indicated by its capacity to offer
a sketch of how the concept is operationalised (Penrod and Hupcey, 2005). Both
requirements were attained with this sample. Penrod and Hupcey (2005) note ‘modest’
single-researcher concept analysis studies have included 83 and 107 studies, whereas

108 of 271
Rodgers (2000b) notes that an effective concept analysis may include anywhere from
30 to over 4,000 articles in studies that do not triangulate with qualitative interviews.
The data from 68 included studies was triangulated in this study with nine interviews as
discussed in sections 3.5–3.7 above.
Characteristics of 68 included studies
The following characteristics of included studies are summarised here: nationality,
journals, participant demographics, presenting issues and type of therapy, study design
and type of analysis.
Nationality and journals
15 countries were represented in the complete set of 68 studies although more than half
(55.9%, n=38) were from USA. They appeared in a total of 35 journals with the most
appearing in the Journal of Consulting and Clinical Psychology (42.9%, n=15).
Publication dates spanned 1983 – 2018.
Participant demographics
The number of participants in each study ranged from 2 to 1383. Gender was specified
in 86.8% of studies (n=59) from 0% - 100% female, with 92.6% of studies (n=63)
reporting cohorts > 50% female. Participant ethnic background was reported by 42.6%
of studies (n=29), ranging from 19.5% to 100% white/causasian. Participant mean age
was reported in 91% of studies (n=62) and ranged from 20.5 years to 69.2 years.
Participant cohabiting/marital status was specified in 54.4% (n=37) studies, ranging
from 0.8% to 100% cohabiting/married, with 37.8% (n=14) studies reporting more than
half the participants were cohabiting/married. Education levels were specified in 42.6%
(n=29) of studies either as mean years (ranging from 11.3 to 16.8 years) or percentage
who had some university education or more (ranging from 14.8% to 85.3%).
Employment status was specified in 23.2% (n=16) studies, ranging from 33.3% to 100%
of participants in part-time or full-time employment.

109 of 271
Presenting issues and types of therapy
14 specific problem areas were covered as well as cohorts with mixed diagnoses. The
largest problem segment was depression (30.9%, n=21). In terms of types of therapy,
22 studies compared therapies using multiple orientations and the remaining 44 studies
examined single therapies, with variants of cognitive and behavioural therapy
predominating (77.2%, n=32). Therapy modality was stated in 53 (77.9%) of studies,
including individual (58.5%, n=31), multimodal (22.6%, n=12), group (n=9) and couples
(n=1). Treatment setting was mentioned in 48 (70.6%) of studies, the largest segment
being university hospitals and research training clinics (56.3%, n=27). Participant
cohorts in more than half the studies (n=38) were treated on an outpatient basis. 60%
(n=41) of studies mentioned therapists’ professional disciplines including
multidisciplinary teams (26.8%, n=11); qualified and trainee psychologists (24.4%,
n=10), qualified and trainee psychological therapists (19.5%, n-8), and one study each
for CBT therapist, psychiatrist and generic mental health staff.
Study design and analysis
The majority of studies (85.3%, n=58) were quantitative designs, with the remainder
mixed methods (7.35%, n=5) and qualitative designs (7.35%, n=5). The qualitative
studies used grounded theory (n=3), consensual (n=1) and thematic phenomenological
(n=1) analyses. The majority of the remaining studies (76.2%, n=48) used variants of
regression analysis including hierarchical linear, logistic, univariate, multiple, stepwise
and Cox proportional hazards. “Hierarchical linear modelling allows coefficients to vary
contingent on moderating and mediating effects at other levels of analysis and as such
is [a] tool suitable for critical realist interest in testing the effects of intervening
mechanisms on theoretical relations” (Miller and Tsang, 2011, p.151). In terms of types
of causal relationships between client factor and outcomes, the majority (72%, n=49)
were predictive. Associations, including those relying on participant reports, were
identified in 14 (20.6%). The remaining five studies analysed mediators (n=4) and
moderators (n=1) of outcome.

110 of 271
3.9 Research data extraction For step 5 (see figure 9, p.80) I created a colour-coded data extraction spreadsheet in
which I entered and organised relevant data from the 124 studies identified at eligibility
stage. Appendix 4 shows a screenshot of a portion of this spreadsheet and lists all
column headings. Identified client factors were listed according to whether the research
found they were predictors, mediators, moderators or in other ways associated with
outcome, although this distinction ultimately proved to be of limited utility because the
majority (72%, n=49) were prediction studies.
3.10 Research data interpretation Research data interpretation for step 6 (see figure 11) took place over the following
phases: manual interpretation of findings tags; labelling the tags; entering the tags into
the analysis spreadsheet; creating the research-informed concept hierarchy framework;
and comparison of this with the participant-informed framework. I now explain these five
phases.
Manual interpretation of tags
In order to work with the extracted client factor findings from the 68 studies included in
the research sample, I printed these out from the data extraction spreadsheet, cut each
into a tag, and arranged these over the large sketch which had formed the basis for the
participant-informed concept framework (see figures 15, 16 and 17). In this way I
privileged the participant framework as the organising principle for interpretation. Figure
23 shows this work in progress.

111 of 271
Figure 23: Manual interpretation of study data tags
112 of 271
Labelling the tags
Once all 68 research tags were organised into elements, I labelled them with sticky
notes. Elements contained from one to seven studies. Figure 24 shows this job when it
was finished.
Entering the tags onto data analysis spreadsheet
I created a research data analysis spreadsheet labelled identically to the participant
data extraction sheet, and entered the tags and associated references. A screenshot of
a portion of the data analysis spreadsheet is shown in figure 25.
Figure 24: Labelled research data tags

113 of 271
Figure 25: Portion of data analysis spreadsheet

114 of 271
Creating the research-informed concept hierarchy framework
The red-spined research-informed framework, shown in figure 26, is structured over the
same hierarchy of abstraction as the participant-informed framework. It should be noted
that this diagram is intended to be viewed in A3/200% size. It is reproduced here at A4
size to give the reader an indication of the fishbone but it is acknowledged that detail at
the elemental level is lost in this format. Final elements are explained in detail in
Chapter 4.

115 of 271
Figure 26: Research-informed concept framework

116 of 271
Comparison of participant and research frameworks
Here I revisit the advice given by Hupcey and Penrod (2003; noted in Chapter 1), that
the process of reconstruction involves comparing the participant- and research-informed
frameworks to observe differences. The reader can do this by comparing figure 15
(p.98) to figure 26 (p.115).
In the research-informed framework, the super-factors remain the same as the
participant-informed framework on both the helpful and unhelpful sides of the fishbone.
There is generally good concordance between the participant and research-based
frameworks on the other three levels of the hierarchy as well. However, the following
differences appear at abstraction Level Three (stages of change).
Stage A (problem recognition) lacks connotative Category 2Positive: Hitting rock
bottom. Stage B (commitment to change) is less dynamic, as it lacks connotative
Category 3Positive: Precluding relational loss. Impoverishment of connotation in the
early stages of change is because most included studies investigated what happened
in, and in some cases, after therapy, not what prompted clients to access therapy.
The connotations for Stage C (new social connections) and Stage D (exploratory
learning) replicate their counterparts in the participant-informed framework.
On the unhelpful side of the fishbone, Category 4Negative: Unready to change is
missing from stage B Non-change (no commitment to change), because people
uncommitted to change generally do not start or complete therapy, and my research
sample excluded drop-out studies.
3.11 Combining participant and research frameworks The seventh and final stage of the method (see figure 9, p.80) involves removing
marginal denotations that do not fit an operational definition of the concept (Sartori
1984), then combining the frameworks into one.

117 of 271
Removed denotations
I removed four client factors comprised of contradictory evidence, all of which appeared
in the research-informed framework (figure 26). These include education and age;
therapeutic alliance and experiencing emotions.
Education and age
Two demographic factors, education and age appeared in the research-informed
framework (categories 10 and 11 in figure 26 on p.115) but not in the participant-
informed framework. However, the findings in both these categories were contradictory.
For example, more education was associated with positive outcome in one study
(Kyrios, Hordern and Fassnacht, 2015) and negative outcome in another (McCrady,
Hayaki, Epstein and Hirsch, 2002). Likewise younger age was found to predict better
outcome in three studies (McCrady, Hayaki, Epstein and Hirsch, 2002; Fournier, et.al.
2009; and Reddy and Jagannathan, 2017) potentially because of the advantages of
early intervention. On the other hand Hendriks et.al. (2012) and Chambless et.al.
(2017) found that later age of illness onset also predicted better outcomes, potentially
because earlier-onset illness is more likely to become part of a person’s identity. Given
the contradictory and treatment-dependent findings in the education and age
categories, they were cancelled out of the framework.
Therapeutic alliance
In category 5, counselling appears at element 5F in the participant-informed framework
(figure 15 on p.98) and 5B in the research-informed framework (figure 26 on p.115). As
an aspect of counselling, therapeutic alliance was not included in either framework due
to contradictory evidence in the research data and insufficient evidence in the
participant data. Evidence in the research data for the predictive role of client
contributions include studies by Hartmann, et.al. (2010) and Goldman, Greenberg and
Pos (2007) who found therapeutic alliance was of little significance to outcome.
Mallinckrodt (1996) found it was associated with outcome in so far as it promoted
change in client’s social support outside therapy. Findings by Shahar, et.al. (2004),
Hawley et.al., (2006), Liebert, Smith and Agaskar (2011) and Hartzler et.al. (2011)

118 of 271
suggested that participant contribution to the therapeutic alliance replicated participant
relational engagement or difficulties in other areas of life and that these social
influences in turn had a mediating impact on outcome. Castonguay et.al. (1996) and
Zuroff et.al. (2007) reported a simple positive association between working alliance and
outcome.
In terms of participant data on therapeutic alliance, although all participants mentioned
the helpful and unhelpful influence of things therapists said, did and did not do, as well
as their learning from regular counselling contact, only one mentioned their relationship
with their therapist having an impact on the changes they made, which did not meet the
threshold of quotes from two participants for element inclusion.
Element 8PositiveG: Experiencing emotions in the research-informed framework
(figure 26, p.115) was cancelled out due to inconsistent evidence. Goldman, Greenberg
and Pos (2007), and Castonguay, Goldfried, Wiser, Raue, and Hayes (1996) found that
experiencing emotions in therapy predicted positive outcome. Somewhat contradictory
findings were presented by Dingemans, Spinhoven, and van Furth (2007), who found
lower expression of emotion after treatment predicted better outcome at 1-year follow-
up. Participant data lent further support to my decision to remove this category. No
participants credited being emotional in therapy for helping them achieve change. On
the contrary, one said she preferred online therapy because it helped contain
emotionality.
Combining participant-informed and research-informed frameworks into one
The reconstructed framework (green spine) appears in figure 27. It should be noted that
this diagram is intended to be viewed in A3/200% size. It is reproduced here at A4 size
to give the reader an indication of the fishbone but it is acknowledged that detail at the
elemental level is lost in this format. Final elements are explained in detail in Chapter 4.

119 of 271
Figure 27: Reconstructed concept framework

120 of 271
The reconstructed concept framework repeats the structure presented in Section 3.7
(see in particular pp. 99-104) for the participant-informed concept hierarchy. It relies on
colour-coding at the elemental and categorical levels of the concept hierarchy to
differentiate their evidence bases. Green categories and elements are those that
contain both participant and research data. Blue categories and elements are those that
contain only participant data. Pink elements are those that contain only research data.
Figure 28 provides a screenshot from a portion of the (non-finalised) unhelpful side of
the framework to show examples of colour-coding with explanations.
Figure 28: Example of color-coding on reconstructed concept framework
Blue categories and
elements =
participant-only data
Pink elements = research-only data
Green categories and
elements = participant
and research data

121 of 271
3.12 Rigour Rigour in this study is defined as the quality control measures I took to ensure credibility
and trustworthiness. These include providing sufficient raw data to evidence my
interpretations; data triangulation; researcher reflexivity; an audit trail; and participant
checks.
Raw data to back interpretations
In Chapter 4, I present the findings that comprise the categorical and elemental levels of
the helpful and unhelpful factors sides of the reconstructed concept framework. All
elements are explained with data examples: either participant quotes or key research
findings and references, or both in many cases. Faithful inclusion of original material
provides an indication of the interpretive process they have been subjected to (White,
Woodfield and Ritchie, 2003).
Data triangulation
While triangulation in qualitative research has various definitions, in this study it means
the methodological choice to use two data sources for contrast and complementariness
(Jensen, 2008; see also section 1.4 p.78 above).
Researcher reflexivity
In this study I am careful to differentiate researcher reflectivity from reflexivity.
Reflectivity is here defined as the introspective activity of reviewing important episodes
of personal or professional activity in order to make sense of how things happened and
why certain choices were made (Dallos and Stedman, 2009). While my mind has
certainly been preoccupied with this project for much of the past two years, I did not, as
some counselling psychology researchers do, keep a contemporaneous reflective
journal as a qualitative research tool (e.g. Demarco and Willig, 2011) due to uncertainty
of its worth. I did however create hundreds of pages of ephemeral reflective notes in the
writing-up process (example in Appendix 17). Overall, for me as I assume for others,
academic writing involves innumerable reflective decisions about discursive expansion
and editorial contraction.

122 of 271
Reflectivity is a thinking activity that both informs and critically reviews the action of
reflexivity, which I discuss next.
Reflexivity in a critical realist paradigm involves critically attending to what our data,
theories and concepts are claiming about the world, focusing particularly on explanatory
mechanisms in social processes (Archer, et.al. 2016), as I am in this study. It also
involves making conscious choices to either follow existing cultural practices, or else
make efforts to change them (Archer, 2007). In this regard reflexivity is demonstrated in
this study where, for example, I have transparently justified methodological choices to
either align with, or divert from, the work of previous researchers, particularly other
concept analysts. I have also assessed and explained the reflexive influence of my
assumptions and experiences on this study. In its totality this study is a large reflexive
act built on thousands of undocumented reflective actions. Reflexive practice demands
honesty, courage and wisdom in order to make “changes, alterations and adjustments”
(Pope, 1999, p.180) and to divert from taken-for-granted practices, which I have done
by pursuing concept analysis in the first place.
Audit trail
Confirmability, as an aspect of credibility in qualitative research is demonstrated by an
audit trail (Anney, 2014). This type of evidence makes the “building blocks used by
researchers in arriving at their interpretations clearly visible to the reader” (Snape and
Spencer, 2003, p.21). I have taken this instruction literally by providing in the body and
appendices of this study, a number of screenshots and photos of work in progress,
including the literature selection process (Appendices 1-5, 24). Additionally, regular,
formalized debriefing sessions with fellow doctoral students helped me to describe and
justify the developmental stages in completing this study, and deepen my reflexive
analysis of the work (Anney, 2014; See Appendix 18 for anonymised minutes of a peer
meeting).

123 of 271
Participant checks
To promote data dependability as an aspect of study credibility (Anney, 2014), I asked
each participant to review their interview transcript for accuracy. This process is
elsewhere referred to as a “member check” (e.g. Guba and Lincoln, 1982, p.247; Elliott,
Rennie and Fischer, p.218). However, the term ‘member’ did not fit the context of this
study, as participants did not identify as belonging to a common group (Billig, 1999).
I attached their transcript in an email to the participant with thanks for their participation
and a request for transcript review and correction. All participants replied. Three added
comments for clarity which were adopted into the transcripts.
In line with the muted group epistemology I requested participants do a follow-up check
of my use of their quoted material in the results chapter. Five replied, two were happy
with the text and three made minor clarifications that were incorporated.
Catalytic validity
Stiles (1993) suggests that research with catalytic validity will re-orient, focus or
energise the participants. Regarding transcript checks, Kyra said, “It has been really
interesting to reflect back on the interview with you.” Lily said, “That was such an
interesting [read] and to see how things have changed (positively!) over the past few
months.”
Regarding the interpretation checks, Zoey said, “It’s been quite a revelation reading this
to confirm how much progress I have made since I did this interview with you.” Thea
said, “I think reading this was very good for me, I will probably read it again.”
3.13 Ethics This section explains how I complied with relevant British Psychological Society (2014)
and University of Manchester (2014) codes of ethics for the conduct of research with
human subjects. It includes my consideration of ethical issues related to the death of a
participant during the completion of this study.
124 of 271
University approval
This study was approved as medium risk by the University Research Ethics Committee
(UREC) in November 2015 with minor amendments approved in March 2016 (Appendix
19). No adults classified as vulnerable by UREC were recruited.
Informed consent
Prior to interviews, all participants were given an information sheet (Appendix 10) which
presented information about the topic and purpose of the research, what they were
being asked to do, method of data collection, risks of participating, confidentiality and
right to withdraw. Consent was obtained from all participants (Appendix 12).
Confidentiality
Participant information and consent sheets were stored in a secure filing cabinet in my
home. Interviews were audio-recorded to MP3 and stored in my secure dropbox.
Transcription adjustments were made to protect participant anonymity. No person-
identifiable information was used in the write-up of this study.
Risk to participants
Participants were informed there was a small chance of feeling upset when discussing
the interview questions. Most interviews unfolded relatively unemotionally but Kyra cried
when thinking about the potential loss of relationships she faced if she did not address
her problems. Similarly Esme cried as she expressed regret about the impact of her
illness on her life and relationships. Zoey cried when recounting family indifference to
her poor mental state, and also when describing the impact of an adverse event on her
life. I provided empathic responses. These participants self-stabilised and continued
with the interview without further distress.
Risk to participants of becoming upset when reading the transcript came to light after I
sent the first transcript to Dana for review. She was bothered by the number of speech
fillers such as ‘um’ and ‘you know’ appearing in the verbatim script. I explained I would
remove these. With all subsequent transcripts I removed these before sending to
participants in line with the editing notes provided in Appendix 14.

125 of 271
Mitigating researcher dual role
In consideration of my dual role as researcher and manager at TS2 I prepared an action
plan should a TS2 participant express a complaint about their therapy (Appendix 20; in
the event no complaints arose). Although the focus of the research was not clients’
therapy experiences, I also considered the risk with TS2 participants knowing I was the
service manager, that they might avoid saying if they found TS2 therapy or staff
unhelpful in any regard which might skew the results. However I deemed this risk low
because I was not asking about therapy experience. In the event 5/7 TS2 participants
mentioned helpful therapy experiences and 1/7 mentioned a non-adverse experience of
under-engagement with therapy.
Participant death
Thirteen months after her interview, while I was still working on study write-up, I was
informed by a family member that a TS2 participant had suddenly and unexpectedly
died. I had two ethical concerns related to this tragic event. The first was whether I
ought to mention her death in the study. The second related to appropriate use of her
data, because at that time participants had not yet been asked to review how I used
their quotes in the analysis.
I discussed the matter with my research supervisor who did not feel university
involvement was required in this instance. Neither the British Psychological Society
Code of Human Research Ethics (2014) or the Health and Care Professions Council
Standards of Conduct, Performance and Ethics (2016) mention participant death.
Qualitative research around participant death is sparse, and what I found did not speak
to my concerns. For example Burles (2017) discusses the impact of predictable
participant death on the welfare of the psycho-oncology researcher, but she does not
deal with ethical use of data from participants who die before the completion of a study.
I considered the following matters in favour of not mentioning her death in the study:
News that she died did not come to me in my role as researcher, but in my role
as director of the service where she had received care in previous years.

126 of 271
Although I did not know the cause of death it clearly was in no way related to
her participation in this study.
Her death neither invalidated her data nor impacted the findings and analysis.
On the other hand, these facts were over-ridden by my belief that it would be
disrespectful to not mention her death in the study. In critical realist terms, death is real.
In personal and professional terms, it was terribly sad, and especially so for TS2
colleagues and clients who knew her well. Furthermore it was necessary to address in
some way the difficulty that I could not ask her to review the final draft. For this reason I
considered removing her data from the study, but as the analysis was at that point
almost finished, it would have been difficult to un-weave her valuable contributions. A
family member told me in a conversation following her death that it would have been
very important to her that her contribution be included.
On balance, her original consent to participate in my mind over-rode her not being able
to review the write-up. To further protect her anonymity I have deliberately not disclosed
which participant she was.

127 of 271
CHAPTER 4: RESULTS
4.1 Chapter overview The aim of this chapter is to explain in detail the content of the categories and elements
in reconstructed concept framework. The chapter is organised over two sections: helpful
client factors and unhelpful client factors. Each section is subdivided at the hierarchy
level ‘stage of change’ of which there are four in each section. Within each stage I
explain the meaning of the categories that comprise each stage. I then explain the
elements that comprise each category, including whether they are evidenced by
participant-only, research-only or participant and research data. I provide illustrative
examples from participant quotes and research references for the 38 elements that
comprise the helpful factors, and 22 elements that comprise the unhelpful factors. Each
section concludes with a summary of key findings.
The results are presented with coded references to diagnoses to protect participant
confidentiality. In line with the muted group epistemology, the results are presented with
close reference to participant experience across all relevant elements, which makes
their exposition lengthy.
4.2 Helpful client factors In this section I provide detailed descriptions the elements for each category of action
along the helpful factors side of the reconstructed framework, which for reader
convenience is shown in figure 29, with the caveat previously noted that this should be
viewed at A3/200% for clarity).
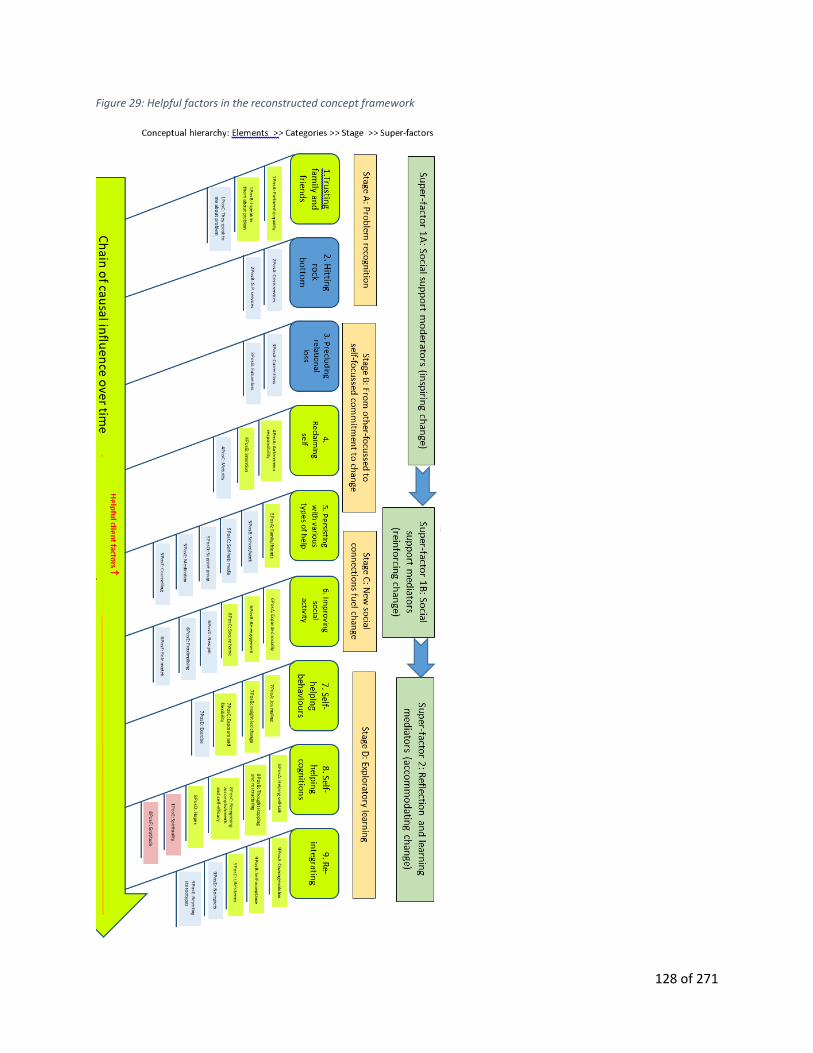
128 of 271
Figure 29: Helpful factors in the reconstructed concept framework
129 of 271
The following section is broken down by stages of change, of which there are four:
Stage A: Problem recognition; Stage B: Self-commitment; Stage C: New social
connections; and Stage D: Exploratory learning.
Stage A: Problem recognition Stage A: Problem recognition is connoted by two categories: Trusting family and
friends; and hitting rock bottom. I explain the meaning of each along with its connotative
elements.
Category 1Positive: Trusting family and friends which means allowing and engaging
in conversations with supportive family and friends around problem recognition. It is
connoted by four elements: partnership quality, speaking to others about the problem;
others speak to me about the problem; and spirituality.
1PositiveA: Partnership quality (participant and research data)
Five participants spoke about the importance of a loving long-term partner or friend in
helping them overcome their problem. Dana said, my partner massively supported me,
forever. Similarly, Zoey credited my best friend who has been an absolute rock to me
throughout everything. The idea of her partner being a ‘rock’ was echoed by Ella: I’m
lucky, my fiancé is an absolute rock. He’s an absolute star.
The association of clients’ marital quality with positive outcomes was supported by client
reports in five studies, including Fournier et.al. (2009); Jarrett, Eaves, Grannemann, and
Rush, A.J. (1991); and Hooley and Teasdale (1989). Studies by Renneberg,
Chambless, Fydich and Goldstein, (2002) and McCrady, et.al. (2002) also made this
finding, the latter at 6 months follow-up.
1PositiveB: Speaking to family/friends (participant-only data)
Opening up to trusted people was identified as an early step in problem recognition by
all nine participants. Luka said, My sister was over and she noticed that I was really ill. And I
did ask her, ‘do you think I’m ill?’ because I don’t think [I had] the realisation that I was actually
really ill. And she said, ‘yeah, I think you are.’ And I did ask her, ‘Do you think I need to do

130 of 271
something about it?’ And when I decided…I really wanted to do something, then I think the
changes slowly started to happen.
1PositiveC: Family/friends raised the problem (participant-only data)
Six participants spoke about the helpful impact of trusted people being prepared to raise
and discuss the problem before they had fully acknowledged it to themselves. Lily said,
The first time [boyfriend] ever met me, he said, ‘that’s not [healthy behaviour].’ And then from
then I felt like, he gets it. He encouraged me then to go to the doctor. Esme said, [My friends]
learned they had to go, ‘You know what? You’re being ridiculous!’ And actually confront me
with it. A lot of the time I just needed a good shake.
Category 2Positive: Hitting rock bottom means experiencing a crisis as a result of
the problem where ensuing contacts with healthcare professionals spur resolve to
address the problem. It is connoted by two elements: accessing crisis services; and GP
services.
2PositiveA: Crisis services (participant-only data)
Four participants identified health or psychiatric crises that propelled them to attend
emergency services for help. These experiences were identified as turning points in
problem recognition. Lucy said, I was actually taken from work into hospital. And I think that
was the wake-up call.
2PositiveB: GP services (participant-only data)
Seven participants explained how conversations with GPs represented turning points
either in problem recognition or in accessing help. Kyra said, So I was referred through to
[service A] by my GP because for quite a long time I’d had probably underlying [D3] and [D2]
issues. Zoey recalled, [My GP] said, ‘just try [counselling] once more and see how you get on.
And if it doesn’t work again, I’ll get you to somebody else.’ And she, the doctor, was amazing.
Stage B: From other-focussed to self-focussed commitment to change The active Stage B: From other-focussed to self-focussed commitment to change
is connoted by three ‘state of doing’ categories of action: Precluding relational loss; self-

131 of 271
reclamation; and persistently accessing help. Each is now explained along with its
connotative elements.
Category 3Positive: Precluding relational loss means wishing to preserve and
protect relationships from damage the problem has caused (or could potentially cause).
It is connoted by two elements: current relationships and future relationships.
3PositiveA: Preserving current relationships (participant-only data)
The risk of one’s unaddressed problems damaging important relationships was
highlighted as a motivating factor by six participants. Dana explained how her partner
warned her: She was like, ‘just stop it. It’s really, making me want to leave.’ I thought, ‘Ohh hoo
– oh okay!’ Ella described her partner and father’s reactions when they visited her in
hospital during a crisis: And that gave me another kick just to say, ‘Look, you’ve got to get
right.’ I can’t see him broken again. Really wrecked me, that. And my dad, his face just coming
in.
3PositiveB: Protecting future relationship opportunity (participant-only data)
In this participant sample, the wish to preclude loss also applied to future relationships.
The importance of not losing the chance of parenthood was mentioned by four
participants as motivating change. Kyra said, I’m at an age where we might think about a
family. And I worry about the impact of all the years of self-abuse on my chances of being able
to have children. And I thought that if we even want to consider that angle, then I need to do
something to change.
Category 4Positive: Self-reclamation is a pivotal transition point of committing
responsibility to salvage oneself from the problem. It is connoted by three elements:
autonomous responsibility; intention; and maturity.
4PositiveA: Autonomous responsibility (participant and research data)
Stage B pivots from making changes for others to making changes for oneself.
Autonomous responsibility requires a degree of self-worth that translates the value of
preserving important relationships into self-mobilisation. Three clients expressed
reaching a point of readiness to change for one’s own sake. Ella, who was initially

132 of 271
motived by a desire not to hurt loved ones, said, I wouldn’t have come out of it until I
decided for myself.
Two studies were represented in this element. In a qualitative study based on client
report at end of treatment and 12-month follow-up, Khattra et.al. (2017) found that a
cognitive shift from other-focussed to self-focussed motivation was associated by
participants with leading to meaningful adjustments in coping. A similar finding was
made by Zuroff et.al. (2007) based on end-of-treatment data.
4PositiveB: Intention (participant and research data)
This element encompasses self-determining motivation and commitment to change,
expectancy that help will be effective, and willingness to do what is necessary to create
a better life. Six participants described aspects of this experience. Luka said, What made
it possible? I think I was just really committed to get better, because I was really in a very bad
place. Lily said, I was desperate, willing to do anything.
Six studies are represented in this element. Hartmann, Orlinsky, Weber, Sandholz and
Zeeck (2010) found that client positive expectancy early in therapy predicted symptom
remission at 3-month follow-up. Similar expectancy findings based on end of therapy
data are presented by Chambless, et.al. (2017) and Safren, Heimberg, and Juster
(1997). Meyer at.al. (2002) found that the benefits of the therapeutic alliance on
outcome were mediated by client expectancy.
Motivation was conceptualised by Keijsers, Hoogduin and Schaap (1994) as willingness
to participate in therapy, and was associated with symptom reduction in therapy. Burns
and Nolen-Hoeksema (1991) found that client willingness to learn new coping strategies
was correlated with being less unwell at the start of therapy and with being more
improved at 12 weeks. This suggests that people who are more prepared to change
may seek help sooner.
4PositiveC: Maturity (participant-only data)
Seven participants asserted that an increasing sense of maturity in the form of their
advancing age assisted their motivation to change. Kyra described it like this: I’ve

133 of 271
decided that I can’t go on in that cycle, I’m in my mid-thirties now, can’t continue to keep going
round the same old vicious circle. And maybe (laughing), with age comes wisdom! Thea
described how coping with mental illness also promoted maturity: I think the [D1] itself has
made me wiser. So the [D1] in a weird way helped me get over it because I would not have got
as mature without it.
Category 5Positive: Persistently accessing help is characterised by resourcefully
tapping different types of social help, over time, with repeated attempts where
approaches may initially fail or fall short. It is connoted by six elements, two of which
contain participant and research data and four, participant-only data.
5PositiveA: Help from family/friends (participant and research data)
Four participants described receiving valuable emotional and practical help from family
and friends after they had commenced a period of active change. For example, Ella
said, My dad’s an angel. He worries as much as I do….He will say, ‘You alright, love? You sound
a bit down.’ I’m like, ‘Dad, you alright?’ ‘Oh,’ he says, ‘I’m having a shit day!’ (laughing). Dana’s
mother lent money to help her move, an important step in improving her situation.
Six studies support the element of help given by family and friends. Steinmetz,
Lewinsohn and Antonuccio (1983) and Toth, et.al. (2013) found that client experience of
family social support was predictive of better outcomes at 6-8 months post-therapy.
Mallinckrodt (1996) made a similar finding without follow-up data. Drilling into specific
types of helpful support, Davidson, Borg, Marin, Topor and Sells (2005) found
participants’ significant others’ focus on their capabilities, interests and successes was
associated with positive outcome, as was their help in making important decisions.
Leibert, Smith, and Agaskar (2011) found that participants with higher subjective social
support had less severe symptoms when starting therapy. The authors suggested this
means that socially supported clients may seek help earlier. Mallinckrodt (1996) found
that the therapeutic alliance mediated participant social support by promoting it, but that
the association between change in alliance and symptoms was not significant. This
suggests that therapy outcome may be related to how much it helps people improve
their social support, rather than directly linked to therapeutic alliance.

134 of 271
5PositiveB: Help from staff at school/work
5PositiveC: Self-help and social media including apps
5PositiveD: Support groups
5PositiveE: Medication
Use of each of these elements was endorsed by several participants, and all
participants used at least one of them. Three participants received supportive help from
staff at school or work. For example, Thea said: The school nurse supported me for the five
years. I could always go to her for a hot chocolate or just sit in her room. Seven participants
used a range of self-help media, for example Zoey wrote blogs and Dana read blogs for
advice; Luka and Kyra used apps; Lucy and Thea used social media; and Zoey, Esme
and Thea used books or other reading material. Five participants used support groups.
Dana, Luka and Thea mentioned psychotropic medication as useful.
No studies are included in these helpful elements, although this does not indicate a lack
of evidence for their role in supporting psychotherapy outcomes. The absence of
studies in these areas is related to my study selection process. Self-help and support
groups were excluded from the research sample, which only included professionally-
facilitated treatments (further study in this area should include self-help activity).
Medication outcomes were not included in data extraction, because in those studies
where it was used (Hendriks, et.al. 2012; Fournier, et.al. 2009) medication was
positioned as a comparison treatment factor rather than a client factor.
5PositiveF: Persistence with counselling (participant-only data)
This element refers to participant persistence with accessing counselling and also
tenacity with forming and appreciating therapeutic relationships, sometimes in spite of
previous experiences of unsatisfactory therapy encounters. All participants discussed
persistence, which I have here divided into four areas to elucidate its dimensions.

135 of 271
Seeking and attending counselling
Participants demonstrated considerable perseverance in seeking and attending
counselling. Ella, Kyra and Thea recounted having attended multiple services over time.
Thea said: Starting with [service D] then going to [service E then service A]. And the same
things have come up. And each time I’ve been a bit more able to try and get on board with
them. Although it did take five-ish years.
Giving counselling another try
Kyra, Lucy and Zoey sought different types of therapy after previous sub-optimal
experiences. Zoey recalled, I said [to my GP] I needed more than a counsellor. Because I
wasn’t coping very well. The counsellors were nice, and they listened, and they tried to show
support, but I needed someone…to give me direction and sort myself out. Then I started seeing a
CBT therapist….I started to make big steps forward. She was really good.
Trying counselling alongside other types of help
Dana credited her mental health improvement to using a range of different types of help
simultaneously: As well as going to see the counsellor, I saw a homeopath, I’ve
changed my diet, started doing yoga every day and I really did make changes. And I
was on the medication as well.
On the other hand using several types of therapy simultaneously left Luka unsure which
had been helpful. When not wholly satisfied with online therapy, she simultaneously
sought and attended face-to-face CBT, and a support group. However, she said, Really
hard for me to tell…what actually worked. I don’t know what specific, why, and what time.
Steinmetz, Lewinsohn and Antonuccio (1983) found participant reports of being in
concurrent therapy predicted negative variance in outcome at 6-month follow-up.
Appreciating therapist contributions
Although the focus of this research is on client contributions to outcome it should be
noted that all participants mentioned helpful or unhelpful contributions of therapy and
therapists either in the therapy just concluded, or in previous therapy. Successful

136 of 271
therapist relational engagement was highlighted particularly where the therapist
matched their approach to the participant’s preferred way of working. For example, Kyra
said, The thing with [therapist], she sussed me out quite quickly. So when we talked about
methodology at the start, of how I can take some practical steps, she delved quite deep about
my professional role and about how I work and how I think. And then approached the next few
sessions in that way.
Stage C: New social connections fuel change Stage C: New social connections fuel change is connoted by two categories, first,
accessing forms of help (category 5Positive above). Category 6: improving social
activity also occurs at this stage and is explained here along with its connotative
elements.
Category 6Positive: Improving social activity has the double meaning of actively
extending, enriching or re-engaging with social life; and self-improving through
broadened social contact. Social reinforcement and social self-efficacy energises
motivation to make further changes. This category synergistically links participant efforts
to access help with specific further self-improvement pursued in the categories that
connote stage D: Exploratory learning. Category 6Positive is connoted by six elements:
expanded sociality; engagement; secure home; new job; proximalising; and role
models.
6PositiveA: Expanded sociality (research and participant data)
This element means the commencement of new (or resumption of old) social activity,
including pro-socially helping others. Six participants described benefits of expanded
sociality, Ella particularly persuasively: The amount of sense of security I’ve had around me
over these last two years [from family, friends, therapy and social life]. Without that whole
structure I don’t think I’d have come this far. I’ve been going out loads at the moment….It’s
probably helping as well. I saw people I’ve not seen for twelve months on Saturday night….So I
felt more of the group.
Three included studies supported this element. Binford et.al. (2005) and Zywiak,
Longabaugh and Wirtz (2002) confirmed that participants who sought more social

137 of 271
contact directly after therapy had better outcomes at 6-month follow-up. Davidson et.al.
(2005) found that clients associated prosocial behaviour with positive outcome.
6PositiveB: Re-engagement (participant and research data)
This element refers to client efforts to improve existing relationships with better
communication skills, along with positive reception of these efforts by others. Four
participants reported this element. For example, Dana said she had become more
patient and respectful with her partner. Similarly Esme reported controlling her partner
less. Both participants said these changes were appreciated by their partners and
contributed to desired change.
Two studies supported this element. Constantino et.al. (2017) found that participants
credited ‘corrective experiences’ for leading to positive outcome. These included
reduced need for control, and improved communications such as disclosure,
assertiveness and accommodation of others’ views. Khattra et.al. (2017) found that
participants who reported becoming more adaptive in interpersonal relationships also
reported better therapy outcomes; but the authors solely credit therapy for this change
without acknowledging that it could only have happened in the context of welcoming
social milieux.
6PositiveC: Secure private home (research and participant data)
Dana and Zoey reported that improving their housing was important to the change
process. This is supported by a study by Davidson et.al. (2005) who found that
participants associated better outcome with having safe, private accommodation.
6PositiveD: New job (or leaving bad job) (participant-data only)
Six participants described how either getting a new job or leaving a bad job was a
helpful step that indicated improvement in their situation and also propelled self-concept
development (which is an element of Category 9Positive: Reintegrating). Dana said,
I’ve found a job that is perfect for me. I’m good at it….I can see very clear steps up the ladder.
Kyra explained how her new job helped her adopt a healthier identity: It’s a positive thing
that I’ve moved jobs. I leave quite a lot of the baggage…I’m trying to draw a line in the sand

138 of 271
with the [D2] that I’ve suffered and how it’s impacted on my health and wellbeing….There are
too many ghosts in the closet from where I’ve been for the last 7-8 years.
Ella explained how leaving a bad job opened space for therapeutic work: I didn’t realise
how exhausting it can be, getting better (laughing). But it is. And I’m so glad I’ve not been at
work through it. She was an absolute cow I was working for. So, what did I do? She offered me
voluntary redundancy because she knew damn well I wasn’t happy. So I took that and I thought
‘I’ll just have some months, me.’
6PositiveE: Proximalising and distalising (participant-data only)
Three participants were attached to this element.
Proximalisation is a vascular surgery term for an arterial attachment and grafting
procedure. Here it is useful for describing how participants moved geographically closer
to well-loved family (‘my blood’) or to places of personal significance (‘my roots’) to
improve or repair their sense of belonging. For example Lily said about moving near her
family, I’m moving down to [English city 1] in a few weeks and…I just feel so much more
positive. And my sister said, ‘it’s so nice to have my sister back because you were just a different
person a few years ago.’ Dana observed, My roots are up here. We were so miserable in
[English city 1]. And we have family up here. So we decided to move. I love it here.
Distalising is the converse action of taking important steps to move away from unhelpful
family or places associated with bad memories. Zoey said, I needed to get out of [English
city 6] because of just too many negative things and I didn’t know how to sort myself out living
in it all. When I moved away…I came into my own.
6PositiveF: Role models (participant-data only)
Four clients described using either positive or negative role models in a helpful way.
Lucy described the importance of having recovered people in her social network who
she could emulate: People who are living…who are where your goal is. Who are living life, and taking
more of an advocate role. Three participants described consciously endeavouring to not be
like people they pitied or disliked. For example, Dana said, I used my step-mum as a kind

139 of 271
of image of everything that I don’t want to be. I’m really horrified (laughing) to think anyone
would think that I was like her.
Stage D: Reflective and exploratory learning Stage D: Reflective and exploratory learning is connoted by three categories that
represent inter-related types of work on oneself: Self-helping behaviours; helpful
thinking; and re-integrating. Each category is now explained along with its connotative
elements.
Category 7Positive: Self-helping behaviours are actions identified by participants as
being directly helpful in obtaining desired change, primarily through experiential
learning. Some, but by no means all can occur in the context of therapy. The
occurrence of these actions depends on preceding conditions of social support in order
to understand what might be helpful and to promote willingness to try them. There is an
inherent interplay between self-helping behaviours and the subsequent category,
8Positive: Helpful thinking.
Category 7Positive is connoted by five elements: Journaling; insight-led change;
exposure; exercise; and pacing.
7PositiveA: Journaling (participant and research data)
Five participants endorsed the value of reflective writing, including self-monitoring,
journaling and blogging, to improving insight. Lily described how self-monitoring helped
her externalise and de-fuse worry. It also helped her respond pro-actively to stress: On
Monday when I got really lonely, I knew the triggers, where they were going to be, which I didn’t
know before. And it meant I felt in control of what I was doing. It was so eye-opening.
Four studies endorsed this element. Participant reports in studies by Clarke, Rees and
Hardy (2004), Constantino, et.al. (2017), and Stirman et.al. (2018) verifed the
therapeutic value of reflective writing. These results are further supported by Khattra
et.al. (2017) in a study using 12-month follow-up data, who found that keeping thought
records was associated by participants with achieving meaningful differences in coping.
7PositiveB: Insight-led behavioural change (participant and research data)

140 of 271
This element comprises a synergistic interplay of self-awareness, new behaviour and
improved self-guidance and was described by eight participants. Thea described it like
this: I sometimes watch candles to self-soothe or listen to music. I was taking care of myself, it
felt sort of like a mum taking care of you. But you’re doing it for yourself, making sure you get to
bed nice and properly. Lily observed, I recognise where things might go wrong during the day,
and I can just think, ‘right, you need to change this.’
Four studies are included in this element. Simons, Lustman, Wetzel and Murphy (1985)
describe ‘learned resourcefulness’ as an insight-led ability to minimise undesirable
behaviours. Their study found that participant pre-therapy learned resourcefulness
accounted for 57% variance in therapy outcome.
Matos et.al. (2009) describe ‘re-conceptualisation’ as a metacognitive ability to observe
and describe personal change processes over time, which was associated in their study
with better outcomes.
‘Mentalization’ is a label for the ability to understand how one’s own and others’ mental
states and behaviour effect each other. It was operationalised as ‘reflective functioning’
in a study by Ekeblad, Falkenstrom and Holmqvist (2016) who found that participant
higher baseline and mid-therapy reflective functioning predicted better outcome.
Hanna and Ritchie (1995) found that insight-led change was the most potent factor
reported by participants in recounting helpful therapeutic experiences.
7PositiveC: Exposure and flexibility (participant and research data)
Exposure means pushing oneself out of ‘comfort zones’ to face and manage fears.
‘Psychological flexibility’ is defined by Gloster at.al. (2014) as the ability to mindfully
accept cognitions and emotions to promote a meaningful life. Flexibility must be
activated to prevent exposure strategies from backfiring.
In this participant group, exposure was demonstrated by five participants who described
both honest self-examination, and courageous behavioural experimentation. Lucy said
about the self-reflecting aspect of therapy, It’s been a very difficult journey (laughing) and
it’s probably been one of the hardest things I’ve had to do in my life. Because I’m confronting

141 of 271
years…of behaviours that have become so engrained. Esme said that through planned
behavioural experimentation she pushed herself to a position where I was uncomfortable
and had to let go of control. Each time I did, it became easier.
Ella described psychological flexibility in this way: I think it’s pushing myself to go [to social
activity] for the first time. Seeing it was fun, it was great. The world didn’t collapse because Ella
left the house (laughing).
Exposure and behavioural activation were well-evidenced for predicting positive
outcome by four studies in the sample, including Mörtberg, Hoffart, Boecking and Clark
(2015); Ryba, Lejuez and Hopko (2014); Mörtl and Wietersheim (2008); and Leung and
Heimberg (1996).
7PositiveD: Exercise (participant-only data)
Three clients mentioned how an adjusted relationship with exercise promoted desired
change. For Thea starting a new sport was not simply a means to fitness but an
accomplishment: It was really good to be able to practise [new sport]. The achievement was
quite, well, instantaneous. I was strong and getting stronger. For Lily, reducing her athletics
was a precursor to improved self-concept: I like [sport E] being a smaller part of my life. I
can go to work and…forget about [sport E] and not over-analyse it.
Category 8Positive: Helpful thinking includes imagining how and what to do
differently; reflecting on the results of therapeutic and non-therapeutic behaviours; and
changing thought climates to realise potential for emotional and relational growth. This
category is connoted by five elements: helpful self-talk; thought stopping and
restructuring; recognising accomplishments and self-efficacy; hopes; and gratitude.
8PositiveA: Helping self-talk (participant and research data)
All nine participants gave detailed descriptions of helpful inner dialogue, such as
debates that spurred their ‘better self’ to make a decision. Some included using an
‘internal therapist,’ as Lucy described: There’s two sides to my thought process. There is the
[D4] voice…and there is me, who actually is very logical….When those [D4] voices start to take
over, it’s having that conversation…you’d have with the therapist, but having it with yourself! In

142 of 271
the sense of, ‘right, now this is what you need to do, actually this is the right decision and this is
the reasons why, regardless of how you may feel.’
Two studies including Hartmann et.al. (2010) and Zeeck and Hartmann (2005) found
that participant recreation of therapeutic dialogue predicted better outcomes.
8PositiveB: Thought-stopping and restructuring (participant and research data) Seven participants described ways they actively averted unhelpful thinking. Ella said,
I’ve been doing diversion. Trying to get my mind off. I’ll take the dog out around the block.
You’ve got to find a way to ride over it. Esme said, I read about trying to recognise when your
thoughts are [D3] thoughts, and then go, ‘well, you can ignore that then.’
Thea said she used cognitive restructuring. Neimeyer and Feixas (1990) define this as
identifying and scaling intensity of upset, then identifying associated negative automatic
thoughts, then developing adaptive alternatives. They found that participant use of this
skill at the end of therapy predicted maintenance of treatment gains six months later.
8PositiveC: Recognising accomplishments and self-efficacy (participant and
research data)
Eight participants expressed admiration for themselves, particularly in relation to
achieving desired change. Ella said: When I noticed…that I was actually being logical, and I
wasn’t feeling as down, I was like, ‘sommat’s good!’ I make steps myself to enjoy life, believe in
myself more.
Self-efficacy, rather than being the retrospective confidence participants described, is a
prospective expectation of being able to achieve specific goals in future. Interestingly no
participants described this expectation. However, four studies noted its predictive power
on outcome including Gomes and Pascual-Leone (2015); Kavanaugh and Wilson,
(1985); Hartzler, Witkiewitz, Villarroel, and Donovan (2011) and Khattra et.al. (2017)
(the latter three based on follow-up data).

143 of 271
8PositiveD: Hope for the future (participant and research data)
Hopes were voiced by seven participants. They are similar to self-efficacy in intention,
but more broadly aspirational. Dana intended to get married and have children. Lucy
intended to return to work. Luka hoped she would fully recover. Esme used a negative
life-forecast to prompt changes: So in ten years, do I want to be childless, friendless, still
[unwell], miserable? No.
Davidson et.al. (2005) in their qualitative study of recovery processes found hope
offered participants the possibility of an improved life.
8PositiveE: Spirituality (research-only data)
No participants mentioned that faith or spirituality played a part in their change process.
However, three studies were included here. Rosmarin et.al. (2013a) found that belief in
God improved client expectancy in therapy. Rosmarin et.al. (2013b) found religious
coping predicted a positive therapy outcome. Similarly a qualitative study by Mohr et.al.
(2011) found that at 3-year post-therapy follow-up, the subjective importance of religion
in coping was a predictive factor for participant global wellbeing.
8PositiveF: Gratitude (research-only data)
Krentzman (2017) found baseline trait gratitude (a life-orientation towards noticing and
appreciating the positive) was a predictor of positive outcome at six months after
treatment but not 12 months. No participants expressed quotable gratitude although
several had appreciative attitudes towards aspects of their life.
9Positive: Reintegrating has a dual meaning. The first is ‘coming into oneself’ in an
evolved form; and the second, negotiating new relationships with one’s social contexts,
including accepting the inevitability of discordance in life. While this category could be
viewed as a plateau of attainment resulting from preceding participant efforts to change,
the findings here suggest that it is actually a dynamic springboard for participants’
anticipated future personal and relational growth. Only one participant did not have data
in this category but perhaps not coincidentally she decided to return to therapy around

144 of 271
the time she was interviewed. This category is connoted by five elements: owning
evolution; self-acceptance; life on life’s terms; minding regret; and rejecting stereotypes.
9PositiveA: Owning evolution (research and participant data)
This element means a sense of ownership of a lifespan evolutionary process of ‘coming
into oneself’ through new or reframed relationships. Seven participants discussed this
element. Kyra was redefining herself using a preferred healthy identity in her new job:
And it’s leaving that [troubled identity] behind, because in my new role I don’t want people to
know that about me. In Lily’s case this process meant negotiating family resistance to
her evolving identity: I can be anyone I want. I said to my mum ‘I can call myself Lily rather
than [nickname]’ and she said, ‘no you’re [nickname], don’t do that!’ (laughing). But I thought,
it’s nice, it’s so refreshing to think I can.
In Constantino et.al. (2017)’s qualitative study of participant ‘corrective experiences,’ the
findings are organised into two parts: (a) participant views of what was corrected; and
(b) of how correction was caused. In the former section under the heading ‘A balanced
outlook’ a participant is quoted, “I finally found that balance where I can be me and I can be
part of society and finding this mindset has made things a lot better” (p.143). I interpret this
quote as more than merely evidence of personal evolution, but a client factor belonging
on the causal side of the analysis, where wider integration has the potential to promote
further growth.
9PositiveB: Self-acceptance (research and participant data)
Four participants provided evidence of the role of improved self-acceptance in coming
to terms with the flawed nature of life experiences. Luka said, I am happy with what I am
now, more or less….Just having my internal self-confidence constant and not being affected
by…something else. Ella invoked the ‘serenity prayer’ when she said, Everything that I am
able to change, I have changed. Things that I am unable to change I have to live with or find a
coping mechanism.
Goldin et.al. (2013) found that participants’ increased self-endorsement mediated
therapy’s effect on outcome. It was also correlated with sustained improvement in

145 of 271
mental health at 1-year follow-up. However the authors did not examine the mechanism
of action of self-endorsement on outcome, which I propose is, in part, its role in facing
life on life’s terms, which forms the next element.
9PositiveC: Life on life’s terms (participant-only data)
This expression from the 12-Step tradition means acceptance that life is never problem-
free and that one will continually encounter challenges that require personal adaptation.
Three clients noted this element, with Lucy expressing it this way: Ownership…is the
foundation of continuing [recovery], outside of the support network, when you…get back into
society and you get back onto your life. Because I don’t know whether all these thoughts or
voices will completely disappear….But it’s about coping with it.
Esme echoed this: You go to counselling, so you’ve obviously got a problem. But [after
therapy] you’ve just got normal-people problems, that I’m going to have to deal with…like I did
before.
9PositiveD: Minding regret (participant-only data)
This element represents an advanced accommodative step in personal evolution that
involves coming to terms with, and seeking restoration from mental illness’ devastating
toll on one’s life. Two participants expressed this point. Ella said: I feel…like I’ve wasted a
big chunk of my life. And I don’t think I’ll ever get rid of that feeling, but I’ve got to just look
forward. I can’t keep saying, ‘Right, you’ve wasted thirteen years.’ Now…is a hell of a better place
than where I was.
Esme said, It’s the idea that you wasted your time and other people’s time, and hurt people
and yourself, and put yourself through stuff that just didn’t need to happen. And then you come
out of it the other end in the same place that you would have been if you’d just been like you
were. Ultimately achieved nothing. I mean I probably have achieved something in a
way….You’ve got to take the good things from it.

146 of 271
9PositiveE: Rejecting unhelpful stereotypes (participant-only data)
This final helpful element, endorsed by two participants, represents being aware of and
consciously disputing taken-for-granted social norms that might contribute to mental un-
wellness. Esme expressed this, with the following observation about body image
consciousness: But I think I’m hyper-sensitive and opinionated on things about women
and…well, not just women and body image - people and body image. And media and shit. And I
think it’s almost sad that you’re in a culture where even once you’re healthy, you’re not happy.
And I do think that’s the culture, it’s not people. Kyra said in rejection of a social expectation
she felt that she should be preoccupied with dieting, I’m hoping I’ve thrown away all the
whole problems I had with disciplined eating etcetera.
I will briefly summarise the key findings from the helpful elements, including a density
table which shows the number of participants and studies that yielded findings for each
helpful element.
I will then move on to describe in detail the unhelpful categories and elements.
Summary of key findings: Helpful client factors 1. Helpful client factors are conceptualised as a chain of causal influences over
time. The chain is characterised by discernible transition points in client
awareness, commitment to self and others, learning activity and relational
engagement.
2. At the most abstract level of the hierarchy, various forms of engagement with
social resources play a predominant role in promoting and supporting participant
reflective and exploratory learning, which is both the product of, and the catalyst
for, psychosocial growth across the lifespan.
3. I applied active, doing-as-being labels at the low-abstraction categorical level
which captured the personal and relational evolutionary nature of participant
change process narratives.
4. Even though the participant group was homogenous (therapy-seeking white
women under the age of 40) and the research sample was heterogeneous, there
was considerable overlap between the two data pools in the combined

147 of 271
(reconstructed) conceptual framework. To briefly summarise the non-matching
areas, there was no participant evidence to support research evidence of
demographic client factors, or the elements of spirituality and gratitude. There
was no research evidence to support participant evidence of speaking with
trusted family/friends to promote problem recognition; experiencing crisis as a
turning point; sensing maturity; using self-help media; making occupational
adjustments; relocating; using role models; addressing regrets; or rejecting social
stereotypes.
5. Contradictory findings were rare, both within and across the participant and
research pools. However, studies of the role of education, age, therapeutic
alliance, and experiencing emotions on outcome yielded contradictory findings.
These factors were therefore cancelled out of the reconstructed framework.
6. Participants were resourceful and persistent in making desired mental health
changes, which for all, took several years, different forms of help, and/or multiple
attempts. In narrating how they achieved their desired changes, all participants
described using wide-ranging social gambits in which attending therapy took a
partial, intermittent, minor and sometimes fallible role.
7. For participants, psychological therapy represented an occasional, partial or
limited form of assistance in these long change trajectories. All participants
described therapeutic work linked with their social contexts. In contrast to this,
only 18/68 (26%) of the included studies found participant social factors predicted
or were otherwise associated with outcome (see Appendix 24 for the list of these
studies).
The helpful elements density table in Appendix 25 shows the number of participants and
studies that yielded findings for each element.
I now explain the elements on the unhelpful side of the reconstructed framework.
4.3 Unhelpful client factors In this section I provide detailed descriptions of the elements for each category of action
along the unhelpful factors side of the framework, which for reader convenience is
shown in its entirely in the screenshot in figure 30 (best viewed at A3/200%) ::

148 of 271
Figure 30: Unhelpful factors in the concept reconstruction framework

149 of 271
The section is broken down by stages of non-change, of which there are four.
Stage A Non-change: Problem-maintaining social environment Stage A Non-change: Problem-maintaining environment is connoted by two
categories: Compromised support and no problem attribution. Each is now explained
along with its connotative elements.
Category 1Negative: Compromised support means the presence of family care and
communication characteristics in which the participant’s mental health problem is
unrecognised or efforts to address it are unfulfilled. It is connoted by two elements:
Difficult family relationships, and family mental health issues.
1NegativeA: Difficult family/friend relationships (research and participant data)
Four participants gave examples of family or friends not being helpful and/or not
understanding their difficulties, which compounded their problems or posed obstacles to
working on them. Zoey explained: Every time I go speak to mum and try to get to the bottom
of why I feel the way I feel, I’m constantly going round in circles, I’m crying all the time, I’m
confused, I’m distressed. And every time I went to see her, I’d come out…more confused…more
distracted and upset.
Thea said, We are not as close as most families….We had two family therapy sessions. They
were very eye-opening but extremely uncomfortable….I didn’t enjoy those and I’d prefer my
parents weren’t there or that I wasn’t there.
The four studies offering research findings in this category fell into two distinct types of
family difficulty that predicted less, or slower, symptom change. The first was hostile or
dysfunctional family climates (Beevers, Wells and Miller, 2007; and Hooley and
Teasdale, 1999). The other was fear of abandonment (Yen, Johnson, Costello and
Simpson, 2009) or separation (Aaronson et.al. 2008) associated with fear of danger to
significant others.
1NegativeB: Family member with mental health issues (participant-only data)
Three participants described how dealing with a family member with mental illness
made it considerably more difficult for them to work on their own problems.

150 of 271
Category 2Negative: Ignored problem means that in spite of experiencing crises as a
result of the problem, the problem is not attributed by the participant as contributory; or
no decision to address the problem is made in spite of crises. It is connoted by only one
element.
2NegativeA: Unrecognised crisis (Research-only data)
A study by Barnett et.al. (2010) found that patients who did not attribute problem
behaviour to a problem-related event for which they were treated in accident and
emergency did not reduce problem behaviour at 12-month follow-up.
Only one participant endorsed this element, which fell below the minimum to be counted
as a participant-endorsed element. However it seems worth mentioning that Kyra
described how her own and others’ habituation to crises precluded change: I’d had a few
being (laughing) carted away in ambulance and things when I’ve lost consciousness. It almost,
to some extent, to some people, defined me, …a group of people that knew the background to
the illness that I had…for quite a long time.
Stage B Non-change: No commitment to change The non-dynamic Stage B: No other- or self-directed commitment to change is
connoted by three corresponding ‘state-of-being’ categories: socially disconnected;
unready to change; and not minded to use help. Each is now explained along with its
connotative elements.
Category 3Negative: Socially disconnected means the experience of social isolation
but may also involve participants taking more or less active steps to cut themselves off
from others. It is connoted by three elements: alienation; guardedness; and social
difficulties.
3NegativeA: Alienation (participant and research data)
This element, mentioned four participants, means feeling one does not belong culturally,
relationally or geographically which compounded or led to problems. Lily described it
like this: Dana recalled, I wasn’t going anywhere in [English city 1]. A lot of my friends had
moved away. My parents had moved away. So expensive. We were absolutely stifled. This type

151 of 271
of alienation can for some people provide an impetus for element 6Positive E:
Proximalising/Distalising. None of the participants spoke about experiencing stigma
as a form of alienation, Ritsher and Phelan (2004) who found that participants who felt
out of place or like “less than a full member of society” (p.260) particularly in mental
illness stigma predicted greater subjective demoralisation and dysphoria at 4-month
follow-up.
3NegativeB: Guardedness (research and participant data)
All participants, when well, experienced no difficulty talking with hindsight about their
problems and feelings. But this category means being reticent about problems when
unwell. It is the counterpoint of 1PositiveB: Speaking with others about the problem.
Six participants described experiencing it in the past, including Lucy who said, I found it
very secretive, the [D4] side of me wanted to protect what was happening, and I think that’s
where you shut everybody out and not realise you’re doing it. And stop your life, basically.
Leweke, Bausch, Leichsenring, Walter, and Stingl (2009) found that alexithymic
difficulty in verbalising feelings mildly predicted poorer outcome.
3NegativeC: Social difficulty (research and participant data)
This category encompasses social withdrawal and social maladjustment. Six
participants described this as an aspect of being unwell. For example, Zoey said, I cut
myself off. I’d go aggressive, didn’t want anyone near me.
Four studies, all conducted with follow-up data, found that social difficulty predicted
worse outcome or treatment failure (Ritsher and Phelan, 2004; Dow et.al. 2007; Nakano
et.al. 2008 and Hartmann et.al. 2010).
Category 4Negative: Unready to change is the sequel to deficits in social connection.
It is likely for some that mental health problems are artefact of these deficits, but
problems remain unperceived, unacknowledged, or are deemed too formidable to
change. It is connoted by two elements: fear and denial.

152 of 271
4NegativeA: Fear (participant-only data)
Three participants explained how fear held them back from making desired changes.
Zoey explained why she did not want to mention a serious problem: Because I thought if I
say it then it becomes real and it needs to be addressed, and it’s out there, then I’m scared of
doing that. Lucy explained fear of change this way: I’ve not come much further [in
wellness]. So I’m preventing myself from doing that, in some ways. So why can’t I do the next
one? It’s breaking through the fear barriers…because it’s the unknown.
4NegativeB: Denial (participant-only data)
Six participants described being in degrees of denial about their problems along the
way. Lily explained how fear and denial can be connected: I don’t think I acknowledged I
had an issue until I actually said it out loud. I think I was almost scared to admit something was
wrong.
Category 5Negative: Unable to use help means not wholeheartedly pursuing social
help; or, where help is accessed, limited commitment or capacity to engage. It is
connoted by just one element.
5NegativeA: Find counselling fruitless (participant and research data)
This element encompasses experiences of therapy that doesn’t ‘work.’ It includes (a)
participant lack of motivation and (b) therapist inability to strike a useful working
alliance. It was mentioned by four participants. It also includes how people may be less
inclined or capable of engaging in therapy when demoralised or immobilised by mental
illness.
Kyra described the effects of being insufficiently motivated in previous therapy: I half-
heartedly went to counselling and things like that but never really felt like I got…what I needed
to out of it….Sometimes because the fit wasn’t right between me and the counsellor. Or possibly
because I wasn’t in the right frame of mind to make positive changes in my life.
Therapist inability to strike a useful working relationship tended to be framed in terms of
relational clumsiness. Zoey recalled, I saw this guy. The first session didn’t go very well. I

153 of 271
was ready to sit down and tell somebody. And he went all around the houses, talking about all
the admin and I was starting to get panicky. And it went really badly, because I…when I was
telling him things, the expression on his face, I think he was in a lot of shock about what was
coming out of my mouth. Similarly Ella recalled, The first counsellor I had said, ‘I don’t know
what your problem is. Just pull yourself together. I had [D3] as a child.’ And I’m like, ‘Are you a
counsellor?’ It wasn’t really the right thing to say. Thea explained about an earlier course of
therapy, I didn’t like my therapist, which was the first bad thing. And so, I didn’t like the work
we did together and I viewed it as something stupid that didn’t make sense, and I was very
cynical of it.
Therapy may also be fruitless if not sensitively tailored to the client capabilities or level
of functioning. A study by Scheel, Seaman, Roach, Mullin and Mahoney (1999) found
that client perception of the difficulty of the therapist’s recommendation predicted non-
implementation.
Stage C Non-change: No new connections Stage C Non-change: No new connections is connoted by two categories, first,
unable to use help (category 5Negative above). Category 6: Oppressed also occurs at
this stage and is explained here along with its connotative elements.
Category 6Negative: Feeling oppressed refers to participant experience of a socially
or culturally oppressive environment that impedes psychosocial growth. It is connoted
by two elements: adverse work, and adverse partnership.
6NegativeA: Adverse work (participant-only data)
Seven participants spoke about being in situations where they felt strained by too much,
or unpleasant occupational or academic work, which caused or worsened their
problems. Dana said about her circumstances at university, leading up to becoming
unwell: Basically, the course was really stressful, and everything around it. It just wasn’t
plausible for a human being to get that amount of work done.

154 of 271
6NegativeB: Adverse partnership (research-only data)
A study of narrative therapy for women in abusive partnerships by Gonçalves, et.al.
(2011) found that failed therapy (indicated by participant ongoing ‘problem narratives’)
was associated, unsurprisingly, with ongoing abuse in their relationships.
Stage D Non-change: Resource-depletion cycle Stage D non-change: resource-depletion cycle is connoted by three categories that are
counterpoints to their positive counterparts: retained behaviours, retained thinking and
unwell identity. These are explained here along with their connotative elements.
Category 7Negative: Retained unhelpful behaviours are identified by participants as
things they do that tend to keep themselves stuck; or that represent areas where further
work is needed. Research refers to hard-to-change unhelpful behaviours or coping
styles. Retained behaviours reinforce retained thinking (the next category). This
category is connoted by two elements: unhelpful reactions, and avoidance.
7NegativeA: Unhelpful reactions (research and participant data)
Participants described different types of unhelpful reactivity when stressed. For example
Zoey described regressive anxiety: I tend to react in a childlike way when something bad
happens. Or I panic. I’m not calm like a grown woman…I’m quite immature. Both Thea and
Lucy experienced complacency, which Thea described like this: What felt challenging in
the…early stages of recovery is now very easy…I’ve got to a point where I’ve become very, very
comfortable. So it’s about challenging, re-challenging yourself. Lily described indecisiveness:
I don’t trust myself with decisions sometimes, because…I over-analyse everything so I don’t
know why I’m making a particular decision. Esme found her tendency for organising and
leading could turn to unhelpful control of herself and others.
Dingemans, Spinhoven and van Furth (2007) noted another kind of unhelpful stress
response which they call ‘palliative reacting:’ turning to food, alcohol, drugs, smoking
(and, oddly, relaxation) for distraction and comfort. Their study found that palliative
reacting was a predictor for treatment failure at 12-month follow-up.

155 of 271
7NegativeB: Avoidance (research and participant data)
Six participants described how being unwell shielded them from facing potentially
growth-inducing social experiences. Kyra put it like this: In a weird sort of way, it’s another
crutch in my life, that I can let myself get absorbed by the feelings that you have with [D2]. And
sometimes that means you don’t have to make the really tough decisions. If I think about my
relationships with good friends...I can use it as a cop-out.
Three studies supported this element. An experientially avoidant coping style was found
to predict worse outcome in studies by Kim, Zane, and Blozis, (2012) and Berking,
Neacsiu, Comtois, and Linehan (2009). Also, in counterpoint to positive expectancy,
Hartmann et.al. (2010) found that where participants expected painful challenge in
therapy, this predicted treatment failure at 3-month follow-up.
Category 8Negative: Retained unhelpful thinking means unchanged and sometimes
engrained ways of seeing oneself, and of interpreting internal and external stimuli, that
perpetuate psychosocial stagnation. It is a later consequence of social disconnection
and can be experienced as ‘living in my own world with my own rules.’ This category
also refers to hard-to-change, unhelpful thinking styles and cognitive events. It is
connoted by five elements: perfectionism; negative self-talk; obsessions; low
metacognition; and dissociation.
8NegativeA: Perfectionism (research and participant data)
Five participants described how variants of perfectionism were implicated in their
problems. For example, Lily said, Before I even had any [D3] issues…I’d obsessively plan all
my clothes I was going to wear. And…I’m so competitive. [But] I told my mum, ‘I feel like a failed
perfectionist’ because I think I am, but I’m not, because sometimes I have a vision and I don’t do
it.
Three studies supported this element, Hawley, Ho, Zuroff and Blatt (2006) found that
perfectionism slowed the rate of participant symptom reduction, while Kyrios, Hordern
and Fassnacht (2015) found that it predicted treatment failure at 3-month follow-up.
Shahar, Blatt, Zuroff, Krupnick and Sotsky (2004) provide one explanation for

156 of 271
perfectionism’s hindering properties. They found that pre-treatment perfectionism
impeded social relations, which in turn predicted persistence of mental ill-health
symptoms after therapy.
8NegativeB: Unhelpful self-talk (research and participant data)
Six participants gave detailed descriptions of different types of low self-worth, self-put-
downs and inner criticism. Thea interpreted symptoms of mental illness like this: At the
time I just thought ‘I’m lazy, and a bad person which is why I don’t do these things.’ …I thought I
was a terrible person. Generalised ‘negative cognition’ was found by Beevers, Wells and
Miller (2007) to predict slower change in symptoms.
Ella recreated therapeutic dialogue in an unhelpful way: I won’t take compliments.
[Therapist] says, ‘You’re doing so well!’ And I’m like, ‘No I’m not, it’s you! Will you stop!’…In my
head I took, ‘That’s because I’m not good enough. I’m not a good person.’ Altimir et.al. (2010)
found that participant recreation of therapeutic dialogue with negative emotions
predicted non-remission at 3-month follow-up. Although shame is a different construct
than self-criticism, it too can induce a sense of worthlessness. Brown, Linehan,
Comtois, Murray and Chapman (2009) found shame was found to predict ongoing
symptom severity during therapy.
8NegativeC: Obsessions (research-only data)
Alonso, Menchon, Pifarre, Mataix-Cols and Torres (2001) found that greater sexual or
religious obsessions predicted poorer outcome at long term (1-5 years) follow-up.
8NegativeD: Low metacognition (research-only data)
Metacognition refers to awareness and ability to distinguish thoughts and other mental
events from the self. A study by Teasdale at.al. (2002) found that lower metacognitive
processing of memories of depressing events occurring in the 5 months preceding
therapy assessment significantly predicted earlier relapse by 11-month follow-up.

157 of 271
8NegativeE: Dissociation (research-only data)
Kleindienst et.al. (2011) found that dissociation predicted poor improvement in general
psychological functioning at one month follow-up. They proposed that dissociative
disturbances in psychotherapeutic learning may account for this.
Only one participant endorsed this element, which fell below the minimum to be counted
as a participant-endorsed element. However it seems worth mentioning that Zoey
described why dissociative experiences delayed her accessing help: I’d been suffering
from flashbacks and I’d not told anybody. I kept it to myself for six-seven years, because I was
terrified as to what it was, what it meant.
Category 9Negative: Unwell identity means, at varying levels of awareness, living
with psychosocial debility and decreasing hope of recovery. It is connoted by three
elements: endorsed stereotypes; problem-enmeshment and long illness. These are now
explained along with their connotative elements.
9NegativeA: Endorsed unhelpful stereotypes (research and participant data)
This element refers to the extent to which participants aligned themselves with unhelpful
cultural mores or beliefs. Five endorsed the social expectation that women should be
dissatisfied with their bodies, although only Esme noted its cultural origins and
pervasive impact.
Ritsher and Phelan (2004) found that when participants endorsed negative 'mental
health patient' self-stigmatising stereotypes for themselves, this predicted greater
subjective demoralisation and dysphoria at 4-month follow-up.
9NegativeB: Problem-enmeshment (participant-only data)
This element refers to the merging of personal and problem identity. Subtle evidence
was present in the use of possessive pronouns by eight participants to describe aspects
of the problem, such as ‘my episodes,’ ‘my relapse,’ ‘my tablets’ ‘my [diagnostic label]’
and so on. Problem identity enmeshment was clearly voiced by Lily, who said, I didn’t
realise how much my [D3]…had become a part of me.

158 of 271
9NegativeC: Long illness (research and participant data)
This element encompasses hopelessness of overcoming mental health problems when
people have suffered repeated, severe or unremitting problems for years. It is a key
factor in the cycle of resource depletion, and six participants described it, including Ella
who said, I don’t think I’ll ever get rid of it basically. My [D2], I’ve had that since I was a kid.
Luka said, I’m quite realistic about the fact that I can go back into relapse at some point. So I
don’t think it’s been cured. I think I just happened to go into remission. Whether because of
counselling or not. Lucy poignantly described the impact of having had problems since
childhood: It’s always been there, from a very young age and I didn’t recognise it, never got any
help or support. And I think that makes it…tricky going into adulthood, and getting treatment
when you’re in adult services rather than as a child. Because actually you’ve founded your whole
life on something you thought was normal. When now, I can see, it’s not.
Studies by Ramnerö and Ost, (2004) and Nakano et.al. (2008) both found that
participants with longer duration of illness had worse outcomes at 12-month follow-up.
Nakano et.al. (2008) suggest that people with long-term mental health problems may
have more impaired social role functioning which in turn reduces the benefit of therapy.
Summary of key findings: Unhelpful client factors
1. Unhelpful client factors are conceptualised as a cycle of gradual deterioration in
psychosocial functioning over time, if unchecked.
2. At the most abstract ‘super-factor’ level of the hierarchy, inadequate social
support leads to psychosocial stagnation, where difficulties on an individual and
social level obstruct reflective and exploratory learning (Hendry and Kloep,
2002).
3. I applied passive adjectival labels at the categorical level to represent participant
narratives about experiencing states of non-change (or insufficient positive
change). The personally overwhelming nature of these circumstances leads, for
some, to the adoption of an ‘unwell identity’ which is both a signal and promoter
of further personal and social resource depletion.

159 of 271
4. Categories of unhelpful client factors form thematic counterpoints to identified
helpful factors.
5. To briefly summarise the non-matching areas on the unhelpful side of the
reconstructed framework, there was no participant evidence to support research
evidence for difficult counselling recommendations not being followed by clients;
or for the unhelpful impact of partner abuse, religious or sexual obsessions or low
metacognition. There was no research evidence to support participant evidence
of fear or denial preventing change or the unhelpful impact of adverse work
conditions.
An unhelpful elements density table is available in Appendix 26, which shows the
number of participants and studies that yielded findings for each element.

160 of 271
CHAPTER 5: DISCUSSION
5.1 Chapter overview The purpose of this discussion is to answer the four research questions and to review
the adequacy of the concept reconstruction. The chapter is organised over twelve
sections.
In the first four sections I answer each of the research questions set out in the
introduction (p.24), recapped here:
1. What do participants describe as salient factors in their efforts to make desired
psychosocial life-changes, and how are these best conceptualised? This data
informed the primary concept framework.
2. How are client factors represented in psychotherapy research? This data
informed the comparator framework.
3. What are the key helpful and unhelpful components of a reconstructed client
factors framework?
4. What is the utility of the reconstructed concept to counselling psychology theory?
The first two questions are answered relatively briefly as a lead-in to lengthier
discussion of the third question which represents the first aim of the study, to
reconstruct the client factors concept.
The answer to the fourth question regarding the utility of the concept to counselling
psychology theory addresses the first of seven criteria for concept adequacy suggested
by Gerring (2012). Each of Gerring’s remaining six criteria is discussed over a further
six sections. These comprise domain (scope); fecundity (richness and depth);
differentiation (sufficiently contrasted from neighbouring concepts); resonance
(familiarity with existing terminology and meanings; avoidance of neologism);
consistency (same meaning in different contexts) and operationalisation (ease of
observation and measurement)
The chapter rounds out with two further sections: recommendations for further study;
and study limitations.

161 of 271
5.2 Study question 1: Factors salient to participants For the participants in this study, client factors that directly facilitated therapeutic change
included capacity for, and persistence with, reflective and exploratory learning; insight-
led behavioural and cognitive change; and personal and social reintegration and
adaptation. These occur within wider social contexts, assisted by attuned professionals
when participants are in the right frame of mind to engage and benefit from problem-
specific therapeutic psychoeducation. It could be argued that these client factors might
be exclusive to the young, educated, female participant sample that volunteered for this
study. But there were clear similarities and considerable overlap between these
participant results and those yielded by 68 international studies with broad participant
demographic strata (discussed on pp.108-109 in section 3.8 above and also in section
5.3 below).
In terms of factors that posed barriers to desired change reported by participants in this
study, psychosocial stagnation and inadequate social support are linked in cycles of
mutual influence that can for some lead to increasing social isolation or withdrawal
which in turn compounds emotional and behavioural suffering, and can for some have
profoundly negative consequences on self-identity.
5.3 Study question 2: Client factors in psychotherapy research The research sample in this study offered a picture of the client factors concept which
mapped well onto the participant concept framework but with smaller subject-territory
boundaries (with exceptions as explained further below). My study exclusion criteria
account for the absence of research on self-help resources, which feature prominently
in the participant framework (as noted in study limitations in section 5.13 below, future
work on conceptualisation of client factors ought to include research on self-help
resources and strategies). A larger research sample might have extended or deepened
the conceptual framework. However a possible explanation for the narrower footprint in
the research-informed framework is that psychotherapy research tends to focus on how
therapy works, and client factors that account for it not working, rather than on how
clients work to make desired changes within broader social systems, over periods of
time that for some, extend before and after they are ‘in therapy.’

162 of 271
Where the research contributed information that was not present in the participant
framework, it was more on the side of unhelpful client factors, particularly in the area of
hard-to-change cognitive features associated with psychological distress, including
obsessionality, perfectionism and low metacognition. Demographic features proved to
be a contested area with contradictory findings within the research sample and no
findings in the participant data sample, and were thus removed. It can be argued
however that people are unlikely to know, or to assert, how demographic characteristics
such as their gender, age, intelligence, education, social class and so forth have a direct
bearing on how they achieve desired psychosocial changes.
5.4 Study question 3: Key components of the reconstructed concept I have organised the discussion of question 3 to first consider what the reconstructed
concept framework tells us about the resources, processes and activities that comprise
the client factors concept. I then propose a revised title for client factors: social learning
factors. I conclude this section with discussion of conceptual boundaries and scope with
reference to Bronfenbrenner’s (2005) bioecological model.
Resources
Resources for therapeutic change with this participant and research sample fall into two
overarching factors which are represented as super-factors on the concept hierarchy.
The primary resource is reliable, long-term, generative social support that inspires and
reinforces adaptive change over the lifespan, and across close interpersonal and wider
cultural fields of social influence. Caring family members, enduring friendships, loving
life-partnerships, meaningful work and leisure activities, and a sense of belonging are
examples here. Educational, recreational, health care and counselling services also
play an important role, as do a range of self-help media. The availability and
accessibility of these resources is a wider social issue. While the determination to
access and make the most of these resources is a personal issue, it depends in part,
according to the information shared by the participants in this study, on the
encouragement of caring others.

163 of 271
The other resource found to be relevant in this study is the capacity for persistent and
resilient reflective learning. This is facilitated by a range of naturally occurring, and self-
and other-fostered activities that stretch self-knowledge and one’s ability to deal with
life’s ‘slings and arrows.’
Insufficiencies in either of these two factors were implicated in this model in the
psychosocial stagnation that characterises the inability to make desired psychosocial
life-change.
Processes
Processes of therapeutic change for all in the participant sample took place over years,
and for most involved passage through overlapping stages and turning points that are
represented at Level 3 of the concept hierarchy. Starting with problem recognition, this
process evolves through commitment, to tapping social resources for assistance and
reinforcement (of which therapy is only one of a range of elements), to reflective and
exploratory learning, which in turn promotes personal and social integration and realised
potential. The helpful process can be summarised in lifespan terms, as ‘coming into
oneself as a social being.’ Processes of non-change can be described, on the basis of
information provided by participants in this study, as a cycle of personal and social
resource depletion. Compromised social or familial support can for some, lead to social
disenfranchisement and mental ill-health, with concomitant difficulties recognising,
obtaining help for, or finding energy to address problems. Ensuing psychosocial
stagnation is a result of unchanged or unhelpful thinking and behaviour that can
become entrenched over time as ‘coming into an unwell identity.’ Mental health stigma
and detrimental cultural expectations can propel personal deterioration within this cycle.
Activities
Activities that participants identified as most helpful in making desired change are
represented at the categorical and elemental levels of the concept hierarchy. Helpful
activities included trusting and using social resources; persistently seeking and trying
different forms of help; engaging in a range of insight-led and insight-promoting
behaviours; consciously being open to changing thought-climates; and consolidating

164 of 271
personal gains and losses into a new outlook on self and life. Conversely, participants
described difficulties engaging in these activities when they were in a resource-depleted
state, particularly if they had been there for years or since childhood. They also
described how this state deteriorates, for example through mistrust of self and others,
fear, and avoidance of challenge.
Retitling ‘client factors’
In the reconstructed concept framework I found social learning processes were centrally
associated with psychosocial change. Fields of learning included family of origin,
partners, friends; self-help materials; and educational, recreational, health and
counselling service resources. This leads me to wonder if the concept title might be
fruitfully changed so that its definition is no longer predicated on the semantic
component ‘client,’ which indicates dependence on the ‘practitioner.’ ‘Social learning
factors’ might more accurately point to the potentially major constellation of wider client
and extratherapeutic social contributions to psychological therapy outcome. Concept
reconstruction has thus brought me to the brink of concept replacement (see pp. 76-77
above for related discussion).
Conceptual boundaries
I discarded the term ‘extratherapeutic factors’ in this concept reconstruction because
client work and outcomes within therapy are ultimately inseparable from engagement
with wider social resources. Bronfenbrenner’s bioecological systems theory (2005) is
useful here in considering conceptual boundaries. He describes human biopsychosocial
development as occurring via ‘proximal processes’ of regular interaction between
individuals and their immediate social environments over extended periods of time. This
is illustrated in the concept reconstruction diagram (figure 27, p.119) particularly in
Category 1Positive: Trusting family and friends; 5Positive: Persisting with help;
6Positive: Improving social activity and 9Positive:Reintegrating. These socially-
oriented categories are tessellated with self-oriented categories 2Positive: Hitting rock
bottom; 3Positive: Precluding relational loss; 7Positive: Self-helping behaviours
and 8Positive: Helpful thinking. I would go further by suggesting that the definition of
‘client factors’ includes interactions taking place across Bronfenbrenner’s (1993) entire

165 of 271
‘bioecological’ system of person, process, context and time. This system is laid out over
four levels. I will illustrate how each fit with the concept reconstruction using just one
spine, 2Positive: Hitting rock bottom as an example, although any spine might
similarly fit the ‘bioecological’ system:
The ‘microsystem’ context involves direct activities and interactions, which can be seen
for example in element 2PosB: GP services which involves conversations between
doctors and patients.
The ‘mesosystem’ involves networked interactions between parts of the microsystem
including direct effects of indirect events such as accidents and health incidents and
consequential interactions with care services that sparked participant awareness that
one had ‘hit rock bottom.’
The ‘exosystem’ involves strengths and weaknesses in social policies and services
surrounding the microsystem, for example the relative availability, quality, relevance and
accessibility of care services.
The ‘macrosystem’ involves enveloping social structures such as shared values, beliefs,
hazards, lifestyles and opportunities within temporal cultural-political shifts. These can
be seen in the life courses available to persons repeatedly experiencing helpful versus
unhelpful factors. The macrosystem is also responsible for creating and expanding the
diagnostic labelling system applied to people experiencing disturbance, loss,
disconnection or inequality (Bronfenbrenner, 1967; Walker and Rosen 2004; Wilkinson
and Pickett, 2010).
5.5 Study question 4: Concept utility for counselling psychology theory As one of Gerring’s (2012) seven criteria for concept adequacy, causal utility refers to
how well the concept serves as a component of a larger causal argument regarding the
relationship between independent and dependent variables (for want of better terms to
describe ‘the changing’ and ‘the changed’). It is important to note that the research
studies upon which the concept reconstruction is based were predominantly predictive
designs. This means that (within the considerable limitations in scope and size of this
study as discussed in section 5.13 below) any causality implied here is not materially

166 of 271
but socially mechanistic in that there may be a potential or emergent causal
interdependence between the variables in the arguments I now discuss.
The causal utility discussion evolves over two parts in order to establish a learning
theory into which the concept reconstruction fits. In the first part I contrast evidence for
the contributions of therapeutic alliance to therapy outcomes, against the tentative
causal argument made in this study’s concept reconstruction, for reflective and
experiential learning mediated by broader sources of social support. In the second part
I examine aspects of two social learning theories that the concept reconstruction maps
onto well: Margaret Archer’s (2007) ‘internal conversations’ model; and Albert Bandura’s
(1986) ‘social cognitive’ theory. My fourth and final research question, about the causal
utility of the concept to counselling psychology is answered here as I explain how they
speak differentially to the causal influences I have interpreted from the findings in this
study.
Causal influence A: Therapeutic alliance
Some psychotherapy research positions the therapeutic relationship, alliance or bond
as a primary healing factor in therapeutic outcomes (e.g. Orlinsky, Graves and Parks,
1994). Further to this positioning, the therapist is credited by some authors for the
relational skill required to maintain a therapeutic relationship, while the client’s role is
side-lined or rendered void. An example is found in this statement by Norcross (2002),
“The [therapeutic] relationship does not exist apart from what the therapist does in terms
of technique, and we cannot imagine any techniques that would not have a relational
impact” (p.8). Recalling from Chapter 2 that in causal syntax, X is the independent
variable input that facilitates change in dependent variable outcome Y, the causal
influence diagram in the case of Norcross’ statement is set out in figure 31:

167 of 271
Figure 31: Therapist relational skill causal influence
However, the concept reconstruction suggests a differently structured causal syntax.
Therapeutic alliance is not present in the concept framework as its role is disputed by
contradictory and null research findings (for further discussion of the contested
relationship between therapist interpersonal skills and therapy outcome see Truax,
1963; Lambert, DeJulio and Stein, 1978; and Wampold and Imel, 2015). Conducting
this study has led me to propose that the potency of the therapeutic alliance is a
reflection of client capacity for forming and using relationships more generally to assist
in ‘learning by doing.’ To illustrate this reasoning with an example, Lorenzo-Luaces, De
Rubeis and Webb (2014) found the predictive relationship between alliance and
outcome was related to a critical client factor, namely, the number of depressive
episodes the client had previously had. For those with more depressive episodes, the
alliance had less predictive value. Perhaps this finding was due to the likelihood that
recurrent depressive episodes might cause a person to be more socially resource-
depleted and therefore over time less able to form and use relationships, including
therapeutic relationships.

168 of 271
This argument does not say that the collaborative bond between client and therapist
(Krupnick et.al. 2014) is unimportant. On the contrary: without it, clients might
understandably quit therapy, or not engage well in joint efforts of goal formulation,
action planning and strategy exploration that forms some therapy models (see for
example Cooper and McLeod’s 2011 pluralistic approach, which, on a side note, does
not use the term ‘alliance’). But the amount of research, practise and theoretical interest
paid to therapist contributions to alliance may be disproportionate to their causal
association with outcome.
Causal influence B: Client relational and learning resources
The causal influence of helpful client factors arising from the reconstructed concept is
set out in figure 32:
Figure 32: Reconstructed helpful client factors causal influence
As discussed on p.117 in section 3.11 above), in this framework background
demographic factors B (e.g. age, gender, level of education, socioeconomic heritage)
appear to have an indirect, contradictory, contested or hard-to-measure effect on causal

169 of 271
factors involved in the achievement of desired psychosocial change (dependent
variable) Y. Causal super-factor M (mediating/moderating variable) is social support
from proximal sources. Adequate social support facilitates and mediates second super-
factor X (independent variable) which is the persistent and committed efforts
participants made, using a range of relational, social and self-help resources, to learn
via exploration and reflection how to make generative relational, behavioural, cognitive
changes, and to self-redefine; which in turn led to outcome Y. This model therefore
suggests why therapy works well for people who are socially well-prepared to help
themselves. Murphy, Cramer and Lillie (1984) found that, in the context of an
understanding therapeutic relationship, helpful advice given by the therapist was clients’
most valued curative factor derived from attending therapy. Centralising client learning
in this way, according to cognitive psychologist Albert Bandura, can “place the therapist
in a less glamorous role, and this may create some reluctance on the part of therapists
to part with the procedures currently in use” (1961, p.156).
Turning now to review the results for unhelpful client factors, the causal influence of
client factors in the resource-depletion cycle is set out in figure 33:
Figure 33: Reconstructed unhelpful client factors causal influence

170 of 271
Persistently inadequate social support, particularly from proximal sources over time
(independent variable X) leads to alienation, psychosocial stagnation, non-change, and
social resource depletion (dependent variable Y) which can for some, if not ameliorated,
turn to a chronic cycle of un-wellness. The model suggests why therapy tends not to
work as well for people who are socially distressed, disadvantaged or resource-depleted
(Brunner, 2017), because they cannot as effectively ‘convert’ social support to create
the critical ‘independent variable’ of experiential and reflective learning. Counselling is
chiefly concerned with supporting client strategies for psychosocial change. However,
altering or improving clients’ wider social learning environment, would, in this model, be
a helpful prerequisite to priming the capacity for change.
Learning theory and counselling psychology
To recap, in theoretical terms, the concept reconstruction positions client reflective and
exploratory learning enabled by, and interdependent with, social support, as the area
where psychological therapy makes its contribution, via active therapist behaviours such
as providing appropriately tailored psychoeducation and encouraging client growth-
inducing relational connections outside therapy. I now turn therefore to discuss the
relevance of learning theory in counselling psychology.
In addressing the position of learning theory in psychotherapy, cognitive psychologist
Edward Shoben said in 1948, “Psychotherapy is essentially a learning process and
should be subject to study as such” (p.112). He decried the lack of attempts at that time
to formulate therapy in terms of learning theory. Subsequently, Albert Bandura said in
1961, “While it is customary to conceptualise psychotherapy as a learning process, few
therapists accept the full implications of this position.”
To check if, half a century later, this might still be the case in contemporary British
counselling psychology, I searched articles published in Counselling Psychology
Review over the past twelve years (2006 – 2018) for clues to social learning theories
that counselling psychologists might use to inform their work. I found articles in the
areas of cognitive behaviour therapy (Boucher, 2006; Davis, McCabe and Winthrop,
2010; Beaumont, Galpin and Jenkins, 2012); pluralistic therapy (Shorrock, 2012);
solution-focussed group work (Proudlock and Wellman, 2011); neuroscience (Rizq,

171 of 271
2007; Goss, 2015); working with older adults (McIntosh and Sykes, 2016), and people
with HIV diagnosis (Harris and Larson, 2008) that mentioned the transformative role of
client psychosocial or relational learning in therapy outcomes. However, none
referenced a learning theory that might underpin or support their observations. One
article by Gianakis and Carey (2008) reviewed four theories of psychotherapeutic
change including Stiles’ (2002) ‘assimilation of problematic experiences’ model;
Prochaska and Norcross’ (2001) ‘stages of change’ model; Powers’ (2005) ‘perceptual
control theory’; and Bohart and Tallman’s (1999) ‘inherent self-healing’ theory. Key
aspects of all these theories echo those that appear in the reconstructed concept,
including problem awareness/clarification, experiential ‘learning by doing,’ and personal
reorganisation through metacognitive awareness. However, Gianakis and Carey point
out that none of these models reveal what enables these processes to occur. In the
reconstructed concept, the enabling factors are interpreted as the interdependencies of
reflective and experiential learning and social support, as previously discussed.
I also conducted an index search of all four Handbooks of Counselling Psychology
(Woolfe and Dryden 1996; Woolfe, Dryden and Strawbridge, 2003; Woolfe,
Strawbridge, Douglas and Dryden (2010); Douglas, Woolfe, Strawbridge, Kasket and
Galbraith, 2016) and found learning theory referenced as follows: John McLeod
describes client experiential learning in therapy as a relational process including
behavioural change, insight and reframing, and emotional catharsis. The concept
reconstruction resonates with these ideas. He and Donati (2016) reference David Kolb’s
(1984/2014) experiential learning cycle. However, Jarvis (2018) has criticised Kolb’s
(2014) model for not emphasising enough the interactive and social aspects of
experiential and reflective learning, which were fundamental aspects of the concept
reconstruction. It will therefore not be further explored here.
Ontologies of the ‘learning self’
Before unpacking relevant learning theories to compare fit with the concept
reconstruction, it is helpful to first set out three ontological bases for the notion of the
‘learning self,’ to understand how learning theory might describe learning process.

172 of 271
Perspectives on the nature of ‘the self’ can be described as falling along a spectrum
from individualism to social diffusion. On the individualistic side is the humanistic idea of
the ‘separate self.’ This philosophy considers the self to be a functional reality. It values
freedom, self-reliance and independence from the influence of culture and relationships.
Aspects of Rogers’ ideas about learning can be seen to fit on this end of the self-
ontological spectrum. Rogers (1983) describes how good teachers create encouraging
conditions in which students become responsible for self-directed learning via personal
creativity, curiosity and independence. On the opposite side is the social constructionist
notion of the ‘dependent self’ who is entirely a product of relationships, society, culture
and contingency. For example Gergen (2009) dispatches notions of the individual
‘coherent self.’ Instead he describes ‘multi-selves:’ human constellations of potentials
for action existing within the relational dimension.
Lying on the middle ground between these two philosophies is the notion of a
‘transactional self’ who has personal concerns, choice and agency that impact the
material and social world in a real way, and whose sense of identity and self-knowledge
are mediated through interactions with the material and social world. Here the ‘self’ and
the material world are mutually formative.
This ontological middle ground is consistent with a critical realist ontology of the self that
acknowledges the neurological basis of the mind and consciousness from which arises
epistemologically created selfhood and personal identity, from which in turn emerges
social agency (O’Mahoney, 2011; although I would say that personal identity does not
precede social agency in order of emergence, but they are interdependent processes).
Next I examine two learning theories that lie in this self-ontology middle ground:
Archer’s ‘reflexive social action’ theory, and Bandura’s ‘social cognitive’ theory.
Archer: reflexive social action
Relational sociologist Margaret Archer (2007) defines reflexivity as internal
conversations in which one is both subject and object (speaker and listener). She
positions inner dialogue as a vital (and empirically overlooked) means by which people
achieve social and occupational mobility. She describes three types of reflexive self-
talk: communicative, autonomous and meta-reflexivity.
173 of 271
Communicative reflexivity is intersubjective in that it involves sharing one’s inner
dialogue with others for affirmation, information, deliberation, or ascertaining others’
needs. Autonomous reflexivity is task-oriented and kept to oneself, because input from
others is not required or desired for self-injunctions or self-directed action. Meta-
reflexivity is value-driven and involves reflecting on one’s reflections, for example
through self-monitoring, self-analysis, daydreaming, or staging imaginary conversations
with others. Meta-reflexivity involves engaging with the possibility that there are at least
“two sides to the story” (2007, p.131).
Participants in my study voiced all three types of self-talk and all gave examples of
helpful internal dialogue that described and assisted their changing outlook, behaviours
and self-understanding (captured in element 8PositiveA: Helpful self-talk). Some also
gave examples of unhelpful self-talk that tended to confirm or reinforce a stagnant or
resource-depleted state (captured in element 8NegativeB: Negative self-talk).
Archer’s theory fits well with the reconstructed client factors concept, in that she
ascribes causal power to self-talk as a method people use for responding to
circumstances and enacting desired life-changes:
[Reflexivity enables] subjects to design and determine their responses to
the structured circumstances in which they find themselves, in the light of
what they personally care about most….Outcomes vary enormously with
agents’ creativity in dreaming up brand new responses, even to situations
that may have occurred many times before. Ultimately the precise
outcome varies with subjects’ personal concerns, degrees of commitment,
and with the costs different agents will pay to see their projects through in
the face of structural hindrances. Equally they vary with subjects’
readiness to avail themselves of enablements (pp. 11-12).
Archer offers a three-stage model of reflexive learning that sits within a larger
ontological philosophy of ‘relational realism’ (2014; Tilly, 2002) which proposes that
social interactions constitute society:

174 of 271
1. Advantageous or disadvantageous social features exist across four orders of reality
(Archer, 2014). These include (a) the natural environment including human
embodiment; (b) evolving technological resources; (c) the social realm including
education, politics, economics, culture and personal relationships; and (d)
transcendental reality, which Archer describes as belief in God and leads to
detachment from over-riding concern with the previous three realms of reality. This
bears similarities both with Rogers’ ego-less universe and Bhaskar’s transcendent-
emergent realm of the real – although Archer (2014) assigns individual formative
moral drive, free will and determinism to this order of reality.
One or more of these orders of reality becomes a generative interactive power in
relation to people’s projects when…
2. …they ask themselves, ‘what do I want?’ and ‘how do I go about getting it?’ Archer
proposes that, following these questions comes three phases of self-determining life-
long internal conversations: (a) discernment of predominant satisfactions and
dissatisfactions with one’s current way of life, and which of the realms of reality it
falls into (which maps onto Stage A: Problem recognition in the concept
reconstruction); (b) deliberation over which concerns, in which realm of reality one
should prioritise and commit to pursuing (which maps onto Stage B: Other-
focussed and self-focussed commitment to change); and (c) dedication to
persevere with a particular area of concern even with the possibility that one’s
actions might fail; while giving up concerns in other areas (which maps onto
Category 5Positive: Persisting with help).
3. Then the chosen course of action is reviewed, adapted, adjusted, abandoned or
enlarged with the aim of becoming “what we care about most in society” (p.21)
(which maps onto Super-factor 2: Reflective learning with the aim of achieving
Category 9Positive: Reintegrating). Where people are unable to conceive or
execute their concerns in any realm, they tend to experience shame, withdrawal and
“loss of relational goods” (2014, no page number) with which to engage in social
interaction. This maps onto Stage D Non-change: resource depletion cycle.
Archer’s theory and my concept reconstruction also overlap where the catalyst for
action is desire for a particular way of being that is different than one’s current state.

175 of 271
The major mapping gap is where the reconstructed client factors concept ascribes some
causal influence to social relations in inspiring and reinforcing psychosocial change,
whereas Archer solely ascribes this agency to individual inner dialogue. Archer’s
theoretical framework positions constructs similar to psychosocial change (social
actualisation and occupational mobility) as the outcome of reflexive learning, but she
describes reflexive learning as if it originates and develops in a mental vacuum,
“relatively autonomous from…structural or cultural properties” (p.15) and originating
from “first-personhood…as distinct from any social ‘concept of the self’” (p.27).
Reflexivity is examined in Archer’s model insofar as it mediates the intra-personal
relationship between deliberation and action in people’s social lives. But in my opinion
(which is heavily influenced by relational-cultural theory e.g. Jordan, 2010), the contents
of reflexive inner dialogue (the what, why and how one talks to oneself) originate in, and
are structured and limited by the socio-cultural foundations of language, relationships,
resources and potentialities in which one’s life is embedded. Furthermore, the power of
relationality can sometimes override autonomous reflexive agency as a primary
determinant of behaviour. These two points are voiced by Archer’s research
participants. Some described self-talk that addressed inherently relational, interactive
problems in their work (and working identities). Others described occupational decision
making based on the influence of trustworthy ‘similar and familiar’ friends; or based on
the emotional pull to maintain contextual and relational continuity, over and above
following one’s own reflexive inclinations. In this way, ‘learning by doing’ was shown to
be a relationally-informed rather than solely reflexivity-informed activity. Nonetheless,
Archer does not view self-talk as dependent on social moderators and mediators.
Bandura: Social cognitive theory
The ‘self’ in Albert Bandura’s social cognitive theory is a stable single entity that can
perform multiple cognitive and behavioural functions, although not simultaneously. He
ascribes five reflective capabilities to human nature, which he sees as being formed
neither solely by inner mental forces nor by external stimuli, but by a mutually
determinative reciprocity between personal behavioural and cognitive factors, and
environmental factors. Interestingly, although Bandura does not describe it this way,

176 of 271
four of the five capabilities depend on forms of inner dialogue (as Archer argues):
symbolizing (translating experience into internal models that serve as guides for future
action); forethought (symbolic representation of future possibilities exerting causal
impact on present action); self-regulation (attempting to bring oneself in line with internal
standards as well as the expectations of others); and self-reflection (knowledge
development and self-alteration through self-analysis). The fifth capability is vicarious
learning through modelling and imitative observation.
All five of these capabilities are clearly found in elements and categories of the concept
reconstruction. For example, symbolising was found in element 7PositiveB: Insight-led
change. Reflexive forethought was seen in 8PositiveD: Hopes for the future as well
as Category 3: Precluding relational loss and Category 4: Reclaiming self. Self-
regulation was seen in Category 8: Self-helping behaviours and Category 9: Self-
helping cognitions. Self-reflection was evident throughout all categories and stages of
the helpful factors side of the concept analysis, particularly in Stage D: Exploratory
learning. Vicarious learning was present particularly in element 6PositiveF: Role
models and more implicitly in some forms of help participants accessed such as
5PositiveD: Support groups and 5PositiveF: Counselling.
Bandura also describes how the individual and their social environment reciprocally
influence each other. Idiosyncratic individual behaviour brings about certain interactive
responses in others. People select and create environments in a way that can
reproduce generative change or stagnation. This is evident on the concept
reconstruction in Unhelpful superfactors 1 and 2: Inadequate social support and
psychosocial stagnation. Group behaviour can empower individuals. But in different
circumstances groups can form detrimental (e.g. coercive) reciprocal systems, or
impacts that are felt to be coercive by member participants.
Bandura also describes the determining influence of “chance encounters” in people’s
life paths, well as the influence of wider historical and political events. On an individual
level he describes how self-evaluative standards (acquired from proximal social
influences) give direction to life by guiding choices. This is seen on the reconstruction in
categories 9Positive: Reintegrating; and 9Negative: Unwell identity.

177 of 271
Bandura also discusses incentive to action as motivated by two-way interpersonal
interaction, and the accommodation of social influence. This is captured in the concept
reconstruction in category 1Positive: Trusting family and friends particularly in the
elements of communication to and from supportive people as an aspect of problem
recognition.
Two areas included in the concept reconstruction that are not explicitly covered by
Bandura’s theory are (a) the recognition of a personal crisis by oneself and/or trusted
others as a catalyst for decisive action in seeking life-change; and (b) the requirement of
trust for generative social relations.
Utility of the concept reconstruction to counselling psychology
The concept reconstruction framework suggests that counselling psychology might
beneficially develop learning theories to help clients make therapy work through
engagement with social resources beyond the consulting room. Bandura’s social
learning theory is explicitly devised to hypothesise mechanisms at work in psychological
therapy. It provides a clear, detailed and deep account of how dependent psychosocial
learning is on pre-existing and concurrent social resources, the importance of enacted
and reflective learning, and, consequently the role of insufficient social support in
obstructing the natural human drive to learn and adapt over time.
A potential lack of utility in the concept reconstruction is that it does not explicitly label
empathy anywhere within the hierarchy. Empathy has been positioned as a change-
producing relational element by a number of researchers (Davis, 1996; Bohart and
Greenberg, 1997; Bohart, 2004; Jordan, 2010; Martinez, 2017). However Bandura
proposes that empathy is not a unitary phenomenon, but comprises three constructs
which are not particularly closely related to one another, as I discuss further here.
Three constructs of empathy
The first construct, social perspective taking, can be seen across category 9Positive:
Reintegrating. The second, imaginative self-involvement, can be seen in reflective
activities including elements 5PositiveF: Counselling and 7PositiveA: Journaling.
The third, emotional responsiveness, is present across a number of categories,

178 of 271
particularly 1Positive: Trusting family and friends; 3Positive: Precluding relational
loss; 6Positive: Improving social activity and 9Positive: Re-integrating. In the
concept reconstruction, empathy is subsumed (and therefore assumed to exist) within
Super-factor 1: Social support.
I now move on to discuss Gerring’s (2012) remaining six criteria for concept adequacy:
domain, fecundity, differentiation, resonance, consistency and operationalisation.
5.6 Domain Gerring recommends that the researcher stipulate the conceptual domain, or ‘language
communities’ the concept relates to, for example, lay or academic audiences; or
‘schools’ and ‘cultures’ within a discipline. Domain also refers to the distance from lay
usage the author has travelled to create scientifically precise terminology.
In this concept reconstruction I have attempted to rely on everyday language rather than
psychotherapeutic terminology in line with the ‘muted group’ epistemology that suggests
the concept should be meaningful to those who experience it (Wuest, 1994). Tight
space on the framework diagrams leaves some labels requiring explanation for example
4PositiveC: Maturity means participant sense of ‘with age comes responsibility and
wisdom’ rather than their numerical age. No participants offered suggestions to change
my conceptual labels after second participant review, but this does not necessarily
indicate that the linguistic domain was entirely relevant for them.
I have also tried to retain non-pathologising and context-informed terminology in line
with the feminist paradigm in counselling psychology (Taylor, 1996). The reconstructed
concept also reflects relational-cultural theory (Jordan 2010) that positions amelioration
of social disconnection as the purpose of therapy rather than the removal of ‘symptoms.’
5.7 Fecundity Descriptive concepts help explain causal influences in human science by interpreting
and illustrating intersections of circumstances, events, intentions and reactions over a
set of cases. Good concepts “reveal the structure within the realities they attempt to
describe” (Gerring, 2012, p. 125). The large size of the conceptual fishbone frameworks
permits the fecund inclusion of detail to the least abstract level. This in turn helps to

179 of 271
clarify the types of elements and categories that belong to the concept; to show
coherent relationships between levels of abstraction and over temporal stages; and to
delimit conceptual borders. Such delimitation help with the next criterion, differentiation.
5.8 Differentiation This criterion refers to how well the concept is differentiated from contiguous or similar
concepts. The concept reconstruction collapsed extratherapeutic factors into client
factors because they were insufficiently distinguished. Then, because the concept
includes a wide range of activities and causal influences beyond therapy, I have
proposed that the title is inaccurate and could be replaced with ‘social learning factors’
(see discussion on p.164 in section 5.4 above). In this way the concept may be clearly
differentiated from contiguous concepts such as therapist or therapy factors.
5.9 Resonance In assessing the linguistic resonance and conceptual familiarity of the reconstructed
client factors concept against existing usage, it is useful to compare and contrast how
client factors are presented in this study against how they are represented in well-
researched ‘treatment matching’ theory.
Treatment matching approaches shape therapy around client factors known to mediate
or moderate therapy processes (which I here differentiate from ‘outcome informed’
approaches that match therapeutic approaches to elicited client preferences for working
style or approach e.g. Duncan, Miller and Sparks, 2004). A number of such approaches
have evolved over the past quarter century, for example culturally adapted treatments
(Benish, Quintana and Wampold, 2011; Smith, Rodríguez and Bernal, 2011); phase-
based therapies based on clients’ ‘stage of change’ (Kanfer and Schefft, 1988;
Prochaska, DiClemente and Norcross, 1992; Prochaska, Norcross and DiClemente,
1994) or stage of ‘assimilation of problematic experiences’ (Stiles, et.al., 1990; Stiles,
2002, 2005). Norcross and colleagues have developed a treatment matching approach
called ‘customized/tailored therapy relationship’ (TTR) (Norcross, 2002; Norcross and
Lambert, 2010, 2011; Norcross and Wampold, 2010; Norcross and Wampold, 2011;
also called ‘treatment adaptation’ and ‘prescriptive matching’ in Norcross and Karpiak,
2012).

180 of 271
Systematic treatment selection (STS)
The treatment matching approach I focus on here is Larry Beutler and colleagues’
‘systematic treatment selection’ (STS) (Beutler and Consoli, 1992; Castonguay and
Beutler, 2006; Beutler et.al., 2016; also called ‘prescriptive therapy’ in Beutler 2016).
STS has been chosen because it conceptualises client factors as impacting outcome in
their own right, where other approaches (e.g. TTR) conceptualise client dimensions only
in so far as they inform therapist contributions which are in turn viewed as the primary
outcome mediators.
Based on decades of direct and meta-analytic research work, STS is a set of technically
eclectic treatment principles (Beutler, 1983, 2016) that are tailored to clients’ non-
diagnostic ‘predisposing trait-like tendencies’ and problem dimensions. The range of
salient client dimensions identified by Beutler and colleagues has been adjusted over
time (for development of STS see Beutler 1983; Beutler, Patterson, Jacob, Shoham,
Yost and Rohrbaugh, 1994; Beutler and Clarkin, 1999; Beutler, Clarkin and Bongar,
2000; Beutler and Harwood, 2000; Groth-Marnat, Roberts and Beutler, 2001;
Castonguay and Beutler, 2006; Beutler, Harwood, Kimpara, Verdirame and Blau, 2011;
Beutler et.al. 2011b; Beutler and Forrester, 2014).
Client factors in STS
Beutler et.al. (2016) mention eight client factors that comprise STS (the first four from
Beutler, Clarkin and Bongar 2000 and the second four from Beutler at.al. 2006). They
explain that these dimensions are not equally well-established in the research literature,
and that they are descriptive and atheoretical. At the end of the list of eight I have added
a further two relevant client factors that appear in Beutler and Clarkin (1999) but for
unknown reasons were subsequently dropped from the model. I describe only the client
factors and not the associated treatment recommendations. I concurrently map these
factors against the labels and the conceptual footprint of the reconstructed framework to
check its resonance with established use in STS.
1.Functional impairment: This dimension includes symptom intensity,
chronicity and comorbidity as well as the presence of family problems and/or

181 of 271
isolation from social, school or occupational activity and/or lack of friendships. In
previous iterations (e.g. Beutler 1983) this dimension was called ‘symptom
complexity’ and highlighted negative social reinforcement for the continuation of
client symptom patterns. In the reconstructed concept this relatively vague
dimension is redrawn as unhelpful super-factors 1 and 2: Inadequate social
support and psychosocial stagnation. It is also associated with non-change
stages A and D: Problem-maintaining environment and resource-depletion.
The main difference is that Beutler et.al. use terminology that locates the problem
within the individual whereas the framework here tends to identify problem
sources as transactions between the individual and their social environment.
2. Coping Style is characterised by internalising or externalising traits (people can
display aspects of both). Internalising traits include self-responsibility; self-blame
and constricted affect. Externalising traits include self-dramatisation, and
experiencing anxiety “only when deprived of a direct, active method of coping
with stress or when blame cannot be transferred” (Beutler and Clarkin, 1999.
p.78). Neither internalising nor externalising traits are located on the
reconstructed concept because they did not appear in this study as contributing
to outcome.
3. A. Resistance is defined in STS as a psychopathological trait based in
unconscious avoidance of threatening personal material. It may involve passive
obstructionism or outright refusal to engage in aspects of therapy (Beutler,
Harwood, Michelson et.al. 2011). It can be seen in the reconstructed framework
in Stage B Non-change: No commitment to change. Beutler et.al. use
terminology that ascribes to clients more detrimental causal force than the
passive description I used.
B. Reactance within normal personality expression is the forcefulness of one’s
efforts to resist threats to one’s freedom from the surrounding environment.
Reactance is not found on the reconstructed concept.

182 of 271
4. Degree of subjective distress may be a feature of reactance or functional
impairment. More distress was experienced by participants when they were
anywhere within the cycle of non-change featured on the unhelpful factors side
of the concept reconstruction.
5. Stage of readiness: Prochaska and Norcross’ (1999) transdiagnostic theory of
change proposes that people use different attitudes, intentions and behaviours to
effect change over time in five stages: pre-contemplation, contemplation,
preparation, action and maintenance. STS refers to stage of readiness theory to
inform therapy (Beutler et.al., 2016). Contemplation, preparation and action
stages are found in the reconstructed concept in Stages A-D: problem
recognition, commitment to change, new social connections and
exploratory learning.
6. Preference for type of therapist: Although this dimension is included in Beutler
et.al’s (2016) list of salient client factors, I have not been able to find any
research by Beutler that discusses the role of client preference for type of
therapist. It appears to have been adopted into STS from Norcross’ (2002;
Norcross and Wampold, 2011) TTR. The suitability of the match between type of
therapist/therapy and client is found on the reconstructed concept framework in
the element 5PositiveF: Counselling and 5NegativeA: Find counselling
fruitless.
7 & 8. The interactive effect of demographic and symptom variables:
Castonguay and Beutler (2006) examine the impact of age, gender, ethnicity,
socioeconomic status and religion in studies on diagnostic categories including
dysphoria, anxiety, substance misuse and personality disorders. The chart for
interactive effects of demographic client factors on symptom variables that I
extracted from Castonguay and Beutler (2006) is in Appendix 21. Socioeconomic
status had the strongest evidence-base as a cross-diagnostic, outcome-
mediating client factor. It is not found on the reconstructed concept, because

183 of 271
neither the participant or research data pools highlighted social class,
employment status or income as having a bearing on outcome.
9. Client expectation as Beutler uses the term refers to considerably more than
expectations about the type of therapy and the therapist (e.g. Arnkoff, Glass and
Shapiro, 2002), the outcome (e.g. Constantino, Arnkoff, Glass, Ametrano and
Smith, 2011) or even of themselves as clients (e.g. Beitel et.al., 2009). In
summary, they are the “accumulation of wisdom gained through observed or
experienced cause and effect relationships. [They] may be situation specific
(states) or general (traits) that bear a relationship to one’s age, gender, social
position and personal background” (p.58). In the concept reconstruction this
dimension is Super-factor 2: Reflective learning. The multiple meanings of the
term ‘expectations’ in psychotherapy lexicon reduces the resonance of Beutler’s
use of the term here.
10. Environmental resources refers to social support systems including work,
school, friends, partners and family. People with well-established social and
familial support systems were found by Beutler and Clarkin (1999) to respond
less pathologically to stressful events, and to have higher self-concepts than their
counterparts who are more socially isolated. In the reconstructed framework this
dimension is Super-Factor 1 A and B: Social support moderators and
mediators.
Summary of resonance
In terms of conceptual resonance, abstraction levels four (super-factors) and three
(stages of change) on the helpful and unhelpful sides of the reconstructed framework
were well-covered by STS dimensions 1 (functional impairment), 3B (resistance), 5
(stage of readiness), 9 (expectations) and 10 (environmental resources). Dimension 6
(preference for type of therapist) matched helpful and unhelpful counselling elements.
Four STS dimensions were not present in the concept reconstruction (2:
internalising/externalising coping style; 3B: reactance; 4: subjective distress; and 7/8

184 of 271
socioeconomic status). The main feature of the concept reconstruction that is missing in
STS is Stage C non-change: No new social connections as a crucial maintaining
aspect of the psychosocial stagnation cycle.
There was little terminological resonance between STS and the reconstructed concept.
Some terms in STS hold specialist definitions whereas the reconstructed framework
generally uses lay terms (with the exception of the term ‘proximalising’), in line with
Gerring’s advice to avoid technical jargon and neologisms. STS terminology tends to
adopt a ‘deficit perspective’ in which client factors are framed as problems upon which
the therapist operates; whereas the reconstructed concept takes a much broader and
more strengths-based view, in line with counselling psychology philosophy (Gelso and
Fretz, 1992). However the primary terminological dissonance is minimal mention of
social support in STS, in comparison to the central stage it takes across the
reconstructed concept. This may be because STS focusses on the therapist’s role in
adapting therapy to best help remediate client dysfunctional stress responses, rather
than helping clients harness healing resources beyond the consulting room, which in
turn may be viewed as falling beyond the therapist’s preferred or perceived domain of
influence. Consequently, the client factors concepts upon which treatment matching
approaches are based are skewed by a focus on aspects of client functioning that are
within direct awareness and influence of the psychotherapist. The mediating effects of
extratherapeutic client factors such as social support and culture tend not to be
represented as directly influencing outcome.
Gerring (2012) provides reassurance to the researcher of specialised concepts that they
can break with established usage, and thus, as shown above, incur a cost to resonance.
Reckoning with this cost requires embedding the concept in concrete, representational
data, in other words, at a low level of abstraction. The hierarchy of abstraction method
is therefore particularly useful for working with a concept that is relevant within a limited
context. I will discuss context further with the following criterion, consistency.
5.10 Consistency “A concept ought to carry the same meaning…in each empirical context in which it is
applied” (Gerring, 2012, p.121). The consistency of the client factors concept is easy to

185 of 271
assure because it only appears in psychotherapeutic literature that relies on common
factors theory.
5.11 Operationalisation “A concept that cannot be measured cannot be tested – at least not very precisely”
(Gerring, 2012, p. 205). The process of linking the more- and less-abstract connotations
in the reconstructed concept to empirical indicants poses numerous challenges. I will
touch on just two here. Firstly, causal events and processes in psychosocial change,
and their manifestations in subjective experience, can be difficult to observe, let alone to
capture, because they are best described in “actor-defined meanings and motivations”
(Gerring, 2012, p.157) via personal, subjective, narrative material that requires careful
interpretation to convert for use in research or practice. Qualitative and mixed methods
research do make this obstacle surmountable. However, a second challenge is that
ideally, the causal factor should be amenable to manipulation by the researcher to
understand its impact on outcome. Social support from family, friends, colleagues and
so on, is not particularly amenable to manipulation. This may go some way to explaining
why social support is rarely considered in psychotherapy outcome research. Likewise,
reflective and exploratory learning as the other major client factor relies on mental
states and conditions that “stem partly from…free will” (Gerring, 2012, p.208). Such
volitional states are not particularly amenable to direct or ethical manipulation.
5.12 Recommendation for further study On the basis of the results of the client factors concept reconstruction I here make a
tentative recommendation for theory development in counselling psychology, in the area
of relational learning networks.
It has been proposed by Goertzen (2010, after Royce, 1987) that psychology produces
too much empirical data and not enough integrative theoretical research. Evolving
theory is a difficult, time-consuming, trial-and-error process that inevitably courts
controversy. The idea that therapy works best for people who are already socially
positioned to help themselves is not new (Orlinsky, 2009). Likewise, the related idea
that clients make therapy work is not new (Bohart and Tallman, 1996), but it has not had
the impact it could have had because, I propose here, descriptions of client

186 of 271
presentations have tended to be limited to features that lend purpose to 20th century
therapy models that position the ‘problem’ within the individual and the ‘cure’ in the
techniques or personal attributes of the psychotherapist. Furthermore, the theory that
therapy is a social learning process is not new (e.g. Bandura, 1961) but counselling
psychology does not seem to actively embrace – or develop – theories that explicitly
embrace client social learning. I further contend that academic circles tend to produce
theory in esoteric, self-referential language that is incomprehensible and irrelevant to
the ‘labouring class’ of practitioners who have a vital need for theory to inform and
develop their work (Beck, 2013).
I therefore suggest that an interesting route for theory development in counselling
psychology is in the area of learning exchange via relational networks. From a
sociological perspective Crossley (2015) considers the focal points of various networks
in which social ties are made. These might include shared values, preferences and
interests; ethnic or cultural backgrounds; or professional, educational and income
brackets and so forth. Furthermore, I propose that simple proximity determines relatively
superficial yet nonetheless influential social exchanges, although deeper affinities may
endure tests of time, social mobility and geographic distance. Social learning results
from active and interdependent participation in, and identification with, networks and
power-alliances within networks. Trust and empathy are essential inputs and outputs in
successful relational interaction histories. Crossley (2011) suggests that personal
reflexive dialogue tends to be characterised by greater or lesser degrees of interactional
trust and empathy, just as social networks are.
Even more theoretically relevant might be the integration of social network analysis with
relational-cultural theory (RCT: Jordan, 2000, 2010). RCT proposes that people grow
through and towards trusting, empathic, ‘authentic’ relationships over the lifespan. A
goal of relational-cultural therapy is the development of relational competence and
capability by promoting flexible relational expectations and reducing the isolation,
disempowerment, shame and marginalising impact of relational disconnections and
relational abuse. Therapy formed from these theories would of necessity be rooted in a
formulation process that, insofar as this is acceptable and makes sense to clients,
187 of 271
attends closely to relationship stories; accounts for actual and potential relational-
cultural resources within social networks; identifies areas of intra-psychic and relational
resource depletion or power inequalities; and sets out a strategy for exploratory and
reflective learning through social resource enrichment. This process would de-
centralise the therapist and even the therapeutic relationship in favour of focus on the
client’s social world. This recommendation that mental health providers develop and
embrace methods for increasing extratherapeutic social support for clients identified as
socially resource-depleted is in line with studies by Turner, 1981; Kelly, 2006;
Radomski, 2014; Budge and Wampold, 2015; Probst, Lambert, Loew, Dahlbender and
Tritt, 2015; and Amati, Banks, Greenfield and Green, 2017.
This chapter concludes with discussion of some of the study’s limitations.
5.13 Study limitations In this section I provide a non-exhaustive overview of the study’s limitations in six areas.
Ontological limitation
Critical realist research in some cases, as here, does not seek to make final judgements
or generalisable truth claims on an issue but simply to make revisions to previous
understandings (Pawson, Greenhalgh, Harvey and Walshe, 2005). Additionally, Scott
(2005) brings our attention to the way all social research inevitably lags behind the
evolving and emergent nature of reality. However, when we create new knowledge, we
can in turn change some small aspect of reality through adjusted human action, but in
such evolution, reality once again makes our revised actions obsolete. Over the two
years it has taken me in this study to make the obvious-sounding recommendation that
therapists can enhance their work by focussing on helping clients enrich experiential
learning through active use of social resources - further work has been done in the area
of relational sociology, for example into art space and social spaces (Crossley, 2015).
Epistemological limitation
Given the assumptions set out in the introduction to this study, it could be argued that
my results confirm what I already believed: that emotional wellness, and recovery from
episodes of mental un-wellness depend on social resources and generative relational

188 of 271
events; and that psychological therapy is only as useful as the client’s social resources
(or social potentialities) outside the consulting room. Gerring (2012) reminds us that in
social science, “descriptive inferences draw from a standard itinerary of tropes” (p.141),
and in the case with this study the trope is the recent ‘relational turn’ in social science
(see for example, Eacott, 2018). But to balance my partiality I have been clear about
my assumptions and views; and I have provided a methodological audit trail so the
reader can see how the contents and boundaries of the concepts have been drawn up.
And although the result does perhaps reflect the ‘relational turn’ in the social sciences,
this does not necessarily reduce the value of its message, that counselling psychology
perhaps needs to engage with learning theory for direction.
Procedural limitation
Concept analysis has been described as “best done as a collaborative endeavour”
(Knafl and Deatrick, 2000, p. 43). This recommendation resonates with my belief that
knowledge construction proceeds through social interaction. While my mental
interaction with the literature and participant data surrounding my topic could, at a
stretch, be considered a social process, this study’s potential scope, richness and reach
is restricted by its being of necessity a single-author project. The generalisability of the
findings are limited by the small scale of the study, its qualitative design, and its
epistemological assumption that knowledge is “situated and perspectival” (Hekman,
1997). The timing of my decision to replace thematic analysis with concept analysis in
the design of this study does not have a material bearing on the generalisability of the
findings.
Data limitations: Literature sample
The research literature sample excluded comparison studies that found different client
factors to be salient predictors of outcome dependent on the type of therapy received.
This was because the analytic strategies in those studies were designed to demonstrate
differential treatment effects on clients rather than client effects on treatment and
outcome. It could therefore be argued that it is impossible to completely separate, or
distinguish, client factors from treatment and therapist factors, especially when outcome
data is collected in or at the end of therapy. I had considered conducting the concept

189 of 271
analysis only with studies based on long-term follow-up data, where time elapsed after
therapy provides some assurance that the client factor measured is not an immediate
‘halo effect’ of the therapeutic encounter. However, after an extensive and time-
consuming literature search, only 28 relevant studies were found with follow-up data,
which was insufficient for a concept analysis. This led to my decision to include the
remaining 40 studies that were based on end-of-therapy data. Future research in this
area might see if any difference is found if solely studies using follow-up data are used.
Studies included in the literature concept analysis were chosen on the basis of the
presence of client factors associated with outcome. Other studies may find that the
same client factors are not associated with outcome, but such studies were not included
or analysed due to their null findings relative to this study.
In this study I did not explore client predictors of premature termination, non-completion
or drop-out from therapy; nor whether there is a difference in salient client factors
between people who do and do not access psychological therapy for help. While drop-
out is certainly an ‘outcome’ of therapy that is mediated by client factors, I made this
decision for two reasons. First, the process of drop-out did not directly address the
research questions (although it might have contributed valuable data to the unhelpful
factors side of the research framework). Second, the participant sample had all
completed the course of therapy about which they spoke in their interview, so it made
sense to match this with the published material.
My literature search excluded self-help resources, which turned out to feature
prominently in the participant framework. Future work on conceptualisation of client
factors ought to include research on self-help resources and strategies.
Data limitations: Participant sample
The white, young, mostly European, female participant sample was relatively socially
homogenous. This raises questions about whether people in other demographic groups
might approach psychosocial change using different activity and social factors; or may
experience different obstacles to change. Further studies might use the same general
client factors concept derived from international research and reconstruct it with data

190 of 271
from groups with other socio-cultural identities (insofar as this is possible given the
middle-class western phenomenon of individual talking therapy as socially approved
help). While the heterogeneity of the research literature sample led to some research-
informed elements (client age, education, therapeutic alliance and experiencing
emotions) being cancelled out of the framework due to contradictory findings, no
contradictions arose between participants in participant-led elements, so none were
cancelled out. It might be possible that a more heterogeneous participant sample could
produce contradictory findings that cancel out some participant-informed elements.
It is possible that the homogeneity of the participant group led to a certain loss of
individuality in their voices in the results chapter. There was considerable harmony
across their narratives in terms of the elements and categories their interviews
endorsed. None were found to report factors that were particularly outstanding from the
rest of the cohort.
A further limit in the participant sample is that they all accessed counselling for help with
debilitating and in some cases potentially life-threatening mental health problems. It
could be argued that the ‘recovery trajectory’ these participants followed required a
different kind of work – and thus results in a differently shaped client factors concept,
than had they, for example, sought counselling for personal development.
Limitation in scope: There are doubtlessly other salient client factors that might belong
on the detailed elemental level of the concept hierarchy that this study, given its limited
data pools, did not pick up. Also, at the most abstract level, the key mediating super-
factor ‘reflective and experiential learning’ may have been differently constructed had
the participant sample been comprised of people with learning or communication
difficulties. This study also does not consider macro-system political, economic, legal or
cultural conditions involved in super-factor social resource enrichment or depletion.
These are however extremely important considerations, particularly for counselling
psychology theory, training and practice development, for example in the area of
culturally informed work (Chung and Bemak, 2012). Lastly, this study does not
specifically consider differential client factors that might be at work in group or couple
therapy (see Perkins, 2010 for consideration of client factors in couple therapy).

191 of 271
As all that lives keep movin' on When all is said and done
The breeze come down and touch our domes The raindrops fall on every home
Cause there ain't nothin' set in stone.
Stereo MCs, Breeze, Deep Down & Dirty, 2001
CHAPTER 6: CONCLUSION The conclusion is set out over two sections. In the first, I propose three contributions to
knowledge offered by the concept reconstruction. In the second review the study’s
results in relation to its aims.
6.1 Contributions to knowledge This study contributes a provisional process model of client factors; a tentative
adjustment to psychotherapeutic change process causal theory; and it introduces
concept analysis as a potentially relevant methodology to advance theoretical research
in counselling psychology. Each of these contributions is framed under a rubric of ‘risky
territory’ as I will now explain further.
A provisional process model of client factors
This study’s main argument is that ‘client factors’ is an under-conceptualised term in
psychotherapeutic literature. It requires a coherent theoretical structure to bring forth its
meaning and ensure its grounding in lived experience. Based on my analysis and
interpretation of participant reports and carefully selected research articles, this study
presents a graphic concept framework and description that depicts a system client
factors associated with process and outcome in psychotherapy. The model enhances
the contextual clarity and definitional specificity of the client factors concept. A practical
risk with this model, however, is its size. Its A3 format is not reproducible in any
publication format (as the reader will observe in figures 15, 26 and 27 above). On the
other hand, while the model is provisional due to its numerous limitations, it is unique in
several ways. I touch on four here:
1. It is derived from open participant interviews, rather than questionnaires that
force participants to confirm existing client factor theories (as in Thomas, 2006);
or that ask about corrective experiences of therapy (as in Constantino and

192 of 271
Angus, 2017). The interview questions used here permitted participants to
introduce and discuss factors that were evident and important to them (rather
than factors that are important to therapists). This widened the client factors
scope to include a diverse range of potent social resources that exert influence
beyond therapy, as well as obstacles to achieving desired change.
2. Participant information is complemented with information from published
research to enhance the pragmatic utility of the concept analysis (Penrod, 2007).
Both types of data are considered valuable but in this study the participant data,
as ‘muted group’ evidence (in line with study epistemology), formed the primary
framework template against which the research evidence was compared.
3. Arranged over a conceptual hierarchy, the model offers ‘close up’ ‘midrange’ and
‘overview’ perspectives that could assist with further theorising about key
mechanisms and stages in client change and non-change processes over time.
In particular, it highlights the vital influence of social support before and during
participants’ active change processes. It also highlights the role of social
resource depletion that makes psychosocial change difficult.
4. The model positions therapy and the therapeutic relationship and learning
resources, while client agency within therapy and wider social contexts as the
primary driver of change.
A tentative adjustment to change process causal theory
A second contribution to knowledge is this model’s spotlight on the causal potentialities
of client reflective and exploratory learning within social contexts. This in turn highlights
that the experience of being supported with trust, solidarity and empathy may help
people to make desired psychosocial changes, particularly where these relational
resources are available outside therapy. Without the presence of these extratherapeutic
resources there is a risk that for some clients, the effects of therapy may last only as
long as therapy does.
Causal theory is risky territory for counselling psychology research (whether
quantitative, qualitative, or mixed methods) because from a critical realist ontological
standpoint, human intelligence may be unable to fully grasp causality, and can at best

193 of 271
only interpret its signs through faulty epistemologies and contestable concepts. So,
through doing this study I have come to understand better how, in the words of
philosopher Alan Watts, “your concepts will be attempts to catch water in a sieve”
(1960, no page number). I may be no closer to knowing at the end of this work the
reality of what client factors are, than I was at the beginning. I have however learned a
tremendous amount about the representation of client factors. My learning is illustrated
by the Stereo MCs lyrics that open this chapter: Nothing is set in stone, including the
little flower with its roots deep in the soil in the rock crack, which this study commenced.
We struggle to explain with words the rain and wind of life and relationships.
Introducing concept analysis as a relevant method for counselling psychology
research
Abstract, complex or contested concepts represent epistemological quagmires: poor
places to build a research project. Concepts that are vague and important require
critical examination and meaningful reconstruction as a foundational step for any
research. I have found concept analysis to be a helpful methodological tool for this job.
I am puzzled why, when it enjoys a reputable position in nursing scholarship and social
science (both disciplinarily adjacent to counselling psychology) concept analysis is not
featured on counselling psychology’s standard menu of favoured qualitative research
methodologies (for example, ethnography; empirical phenomenology; grounded theory;
narrative, discourse and conversation analysis; protocol analysis; and thematic analysis,
Creswell, 1998; Elliott and Timulak, 2005; Braun and Clarke, 2013; Finlay, 2015).
Sartori (2009) asserts that because “thinking is language-wrapped” (p.101) concept
analysis “plays a non-replaceable role in the process of thinking.…At no stage of the
methodological argument does…taxonomical unpacking lose weight and importance”
(p.19). I worry that lacking a repertoire of critical concept analysis approaches on the
‘acceptable’ list of counselling psychology research methods we struggle to evolve
concept-based theories in psychological therapy. This in turn risks counselling
psychologists relying on 20th century individualistic theories and therapies that neither
acknowledge nor tackle unequal access to social resources in the aetiology of
psychosocial distress (Vermes, 2017).

194 of 271
Learning surprises
While the results are provisional and limited, the concept analysis process has proven
to be gratifyingly effective for organising and representing the interrelationship of
potentially powerful helpful and unhelpful client factors across planes of abstraction. I
could never have imagined creating the resulting graphics when I started the study.
However, my most important learning is the eye-opening relevance of Bandura’s social
learning theory to my findings. Shockingly, given how long I have been a therapist and
how many advanced trainings I have undertaken, I do not recall reading or being taught
much, if anything, about Bandura’s theories prior to doing this study. Despite my
previous ignorance of his work, the extensive mapping of Bandura’s theories to my
concept framework may point to the enormous influence and absorption of Bandura’s
theories into the zeitgeist of much counselling theory I have read over the past 25 years.
The comprehensiveness and accuracy of the mapping also, for me, indicate that my
framework is reassuringly ‘on the right track’ and makes me determined to read and rely
on Bandura’s work more extensively in future.
6.2 Closing remarks: Results in relation to aims In closing, I return to the concerns with which I opened the study. Bohart and Tallman
(1996, 1999) asserted that the common factor that makes therapies equally effective, is
the client working in a therapeutic relationship. With this study, however, I conclude that
client work outwith the therapeutic relationship largely accounts for therapeutic
outcome. People need generative, long-term and evolving learning relationships with
people, places and cultures, not therapy per se, to be as well as possible. In closing
their chapter Tallman and Bohart (1999) argue that “truly taking seriously the active,
generative nature of how clients change in therapy would fundamentally re-structure
how we view the process of therapy…Finally, researchers would focus their study on
clients rather than on therapists” (p.119). Here, I have proposed that if we are to
account for the active role of the client, we require theories about the mechanisms and
purpose of therapy that centre on client factors. And if this theory is ultimately to
improve therapy, we must not only conceptualise how the active client achieves change,
but also why clients don’t manage to achieve change. This study has produced one

195 of 271
such conceptualisation of the ‘grand theatre’ of how people do, and don’t make desired
psychosocial life-changes, in which psychotherapy and its practitioners are bit players
amongst a large cast of more important characters. Wampold and Imel (2015) describe
“the therapist as an agent of change and patients as active participants” in therapy
(p.34). On the basis of participant narratives in this study I have played with reversing
this proposition: Clients and their social resources are agents of change, while
therapists may be active participants in limited ways for partial aspects of the process.

196 of 271
REFERENCES References with an asterisk indicate those included in the concept analysis. Those with a double asterisk included client follow-up data.
*Aaronson, C. J., Shear, M. K., Goetz, R.R., Allen, L.B., Barlow, D. H. and White, K.S. (2008). Predictors and time course of response among panic disorder patients treated with cognitive-behavioral therapy. The Journal of Clinical Psychiatry, 69(3), 418-424. DOI: 10.4088/JCP.v69n0312.
Addis, M.E. and Cardemil, E.V. (2006). Does manualization improve therapy outcomes? In J.C. Norcross, L.E. Beutler and R.F. Levant (Eds), Evidence-Based Practices in Mental Health (131-160). Washington DC: American Psychological Association. ISBN: 1-59147-290-3.
Adler, J.A., Skalina, L.M. and McAdams, D.P. (2008). The narrative reconstruction of psychotherapy and psychological health. Psychotherapy Research, 18(6), 719-734. DOI: 10.1080/10503300802326020.
Agee, J. (2009). Developing qualitative research questions: A reflective process. International Journal of Qualitative Studies in Education, 22(4), 431-447. DOI: 10.1080/09518390902736512.
Aldiabat, K.M. and LeNavenec, C-L. (2018). Data saturation: The mysterious step in grounded theory method. The Qualitative Report, 23(1), 245-261. Downloaded from https://nsuworks.nova.edu/cgi/viewcontent.cgi?article=2994&context=tqr on 05.01.2019.
Allen, R.E.S. and Wiles, J.L. (2016). A rose by any other name: Participants choosing research pseudonyms. Qualitiative Research in Psychology, 13(2), 149-165. DOI: 10.1080/14780887.2015.1133746.
**Alonso, P., Menchon, J.M., Pifarre, J., Mataix-Cols, D., Torres, L., Salgado, P. and Vallejo, J. (2001). Long-term follow-up and predictors of clinical outcome in obsessive-compulsive patients treated with serotonin reuptake inhibitors and behavioral therapy. Journal of Clinical Psychiatry, 62(7). DOI: 10.4088/JCP.v62n07a06.
Altimir, C., Capella, C., Nunez, L., Abarzua, M. and Krause, M. (2017). Meeting in difference: Revisiting the therapeutic relationship based on patients’ and therapists’ experiences in several clinical contexts. Journal of Clinical Psychology, 73(11), 1510-1522. DOI: 10.1002/jclp.22525.
**Altimir, C., Krause, M., Parra, G. De, Dagnino, P., Tomicic, A., Valdés, N., Perez, J.C., Echavarri, O. and Vilches, O. (2010). Clients’, therapists’, and observers' agreement on the amount, temporal location, and content of psychotherapeutic change and its relation to outcome. Psychotherapy Research, 20(4), 472-487. DOI: 10.1080/10503301003705871.
Amati, F., Banks, C., Greenfield, G. and Green, J. (2017). Predictors of outcome for patients with common mental health disorders receiving psychological therapies in community settings: A systematic review. Journal of Public Health, 39(4), 1-13.
American Psychological Association Task Force on Psychological Intervention Guidelines (1995). Template for developing guidelines: interventions for mental disorders and psychosocial aspects of physical disorders. Washington, DC: American Psychological Association.
Amoakoh-Coleman, M., Agyepong, I.A., Zuithoff, N.P.A., Kayode, G.A., Grobbee, D.E., Klipstein-Grobusch, K., and Ansah, E.K. (2016). Client factors affect provider adherence to clinical guidelines during first antenatal care. PLoS ONE, 11(6) e0157542. DOI: 10.1371/journal.pone.0157542.
Anney, V.N. (2014). Ensuring the quality of the findings of qualitative research: Looking at trustworthiness criteria. Journal of Emerging Trends in Educational Research and Policy Studies, 5(2), 272-281. ISSN: 2141-6990.
Archer, M. (2007). Making Our Way Through The World: Human Reflexivity and Social Mobility. Cambridge: Cambridge University Press. ISBN: 978-0-521-69693-7.

197 of 271
Archer, M. (2014). We are what we love: Love and identity. Accessed on www.socialontology.org on 11.06.2018.
Archer, M., Decoteau, C., Gorski, P., Little, D., Porpora, D., Rutzou, T., Smith, C., Steinmetz, G. and Vendenberghe, F. (2016). What is Critical Realism? Downloaded from http://www.asatheory.org/current-newsletter-online/what-is-critical-realism on 30.05.2018.
Ardener, E. (1975). Belief and the problem of women. In S. Ardener, S. (Ed.) Perceiving Women. London: Malaby Press, 1-17. ISBN: 0-460-14006-x.
Ardener, S. (1975). Introduction. In S. Ardener, S. (Ed.) Perceiving Women. London: Malaby Press, vii-xxiii. ISBN: 0-460-14006-x.
Ardener, S. (2005). Ardener’s ‘Muted groups’: The genesis of an idea and its praxis. Women and Language, 28(2), 50-54.
Ardito, R.B. and Rabellino, D. (2011). Therapeutic alliance and outcome of treatment: Historical excursus, measurements and prospects for research. Frontiers in Psychotherapy, 2:270, 1-11. DOI: 10.3389/fpsyg.2011.00270.
Arnkoff, D.B., Glass, C.R. and Shapiro, D.A. (2002). Expectations and preferences. In In J.C. Norcross (Ed.), Psychotherapy Relationships That Work: Therapist Contributions and Responsiveness to Patients (335-356). Oxford: Oxford University Press. ISBN: 978-0-19-514346-1.
Asay, T.P. and Lambert, M.J. (1999). The empirical case for the common factors in therapy: Quantitative findings. In M.A. Hubble, B.L. Duncan and S.D. Miller (Eds), The Heart and Soul of Change: What Works in Therapy (23-55). Washington, D.C: American Psychological Association. ISBN: 1-55798-557-X.
Aveyard, H., Payne, S. and Preston, N. (2016). A Post-Graduate’s Guide to Doing a Literature Review in Health and Social Care. Maidenhead: Open University Press. ISBN: 978-0-33-526368-4.
Bachelor, A. (1995). Clients’ perception of the therapeutic alliance: A qualitative analysis. Journal of Counseling Psychology, 42(3), 323-337. DOI: 10.1037/0022-0167.42.3.323.
Baker, S.E. and Edwards, R. (2012). How many qualitative interviews is enough? National Centre for Research Methods. DOI: 10.1177/1525822X05279903.
Baldwin, S.A., Wampold, B.E. and Imel, Z.E. (2007). Untangling the alliance-outcome correlation: Explaining the relative importance of therapist and patient variability in the alliance. Journal of Consulting and Clinical Psychology, 75(6), 842-852. DOI: 10.1037/0022-006X.75.6.842.
Bandura, A. (1961). Psychotherapy as a learning process. Psychological Bulletin, 58(2). 143-159.
Bandura, A. (1978). The self system in reciprocal determinism. American Psychologist, 33(4), 344-358. Downloaded from https://www.uky.edu/~eushe2/Bandura/Bandura1978AP.pdf on 02.08.2018.
Bandura, A. (1986). Social Foundations of Thought and Action. Englewood Cliffs, NJ: Prentice-Hall. ISBN: 0-13-815614-X.
Bankoff, E.A. (1996). Pre-treatment social support and effective psychotherapy process: A panel study. Psychotherapy: Theory, Research, Practice, Training, 33(1), 51-60. ISSN: 00333204.
Barbour, R.S. (2001). Checklists for improving rigour in qualitative research: A case of the tail wagging
the dog? British Medical Journal, 322. DOI: 10.1136/bmj.322.7294.1115.
Barkham, M. (2002). Methods, outcomes and processes in the psychological therapies across four successive research generations. In W. Dryden (Ed.), Dryden’s Handbook of Individual Therapy (4th Ed.). London: Sage, 373-433. ISBN: 978-0761969433.

198 of 271
**Barnett, N.P., Apodaca, T.R., Magill, M., Colby, S.M., Gwaltney, C., Rohsenow, D. J. and Monti, P.M. (2010). Moderators and mediators of two brief interventions for alcohol in the emergency department. Addiction, 105(3), 452-465. DOI: 10.1111/j.1360-0443.2009.02814.x.
Baron, R.M. and Kenny, D.A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173-1182. DOI: 10.1037/0022-3514.51.6.1173.
Beaumont, E., Galpin, A. and Jenkins, P. (2012). Being kinder to myself. Counselling Psychology Review, 27(1), 31-43. ISSN: 0269-6975.
Beck, J. (2013). Powerful knowledge, esoteric knowledge, curriculum knowledge. Cambridge Journal of Education, 43(2), 177-193. DOI: 10.1080/0305764X.2013.767880.
Beckwith, S., Dickinson, A. and Kendall, S. (2008). The “con” of concept analysis: A discussion paper which explores and critiques the ontological focus, reliability and antecedents of concept analysis frameworks. International Journal of Nursing Studies, 45(12), 1831-1841. DOI: 10.1016/j.ijnurstu.2008.06.011.
Bedi, R., Davis, M. and Williams, M. (2005). Critical incidents in the formation of the therapeutic alliance from the client’s perspective. Psychotherapy: Theory, Research, Practice, Training, 42(3), 311-323. DOI: 10.1037/0033-3204.42.3.311.
*Beevers, C.G., Wells, A. T. and Miller, I.W. (2007). Predicting response to depression treatment: The role of negative cognition. Journal of Consulting and Clinical Psychology, 75(3), 422-431. DOI: 10.1037/0022-006X.75.3.422.
Beitel, M., Hutz, A., Sheffield, K., Gunn, C., Cecero, J., and Barry,D. (2009). Do psychologically minded clients expect more from counselling? Counselling and Psychotherapy: Theory, Research and Practice, 82, 369-383. DOI: 10.1348/147608309X436711.
Benish, S.G., Quintana, S. and Wampold, B.E. (2011). Culturally adapted psychotherapy and the legitimacy of myth: A direct-comparison meta-analysis. Journal of Counseling Psychology, 58(3), 279-289. DOI: 10.1037/a0223626.
*Berking, M., Neacsiu, A., Comtois, K.A. and Linehan, M.M. (2009). The impact of experiential avoidance on the reduction of depression in treatment for borderline personality disorder. Behavior Research and Therapy, 47(8), 663-670. DOI: 10.1016/j.brat.2009.04.011.
Bernd, R. and Strouse, J. (2008). Influence of social support on success of therapeutic interventions: A meta-analytic review. Psychotherapy: Theory, Research, Practice and Training, 45(4), 464-476. DOI: 10.1037/a0014333.
Beutler, L.E. (1983). Eclectic Psychotherapy: A Systematic Approach. New York: Pergamon. ISBN: 978-0-08028-842-0.
Beutler, L.E. (1991). Have all won and must all have prizes? Revisiting Luborsky et. al.’s verdict. Journal of Consulting and Clinical Psychology, 59(2), 226-232. ISSN: 0022-006X.
Beutler, L.E. (2016). Selecting the most appropriate treatment for each patient. Accessed at https://www.youtube.com/watch?v=BpmKDqpbLzo on 15.09.2017.
Beutler, L.E., & Clarkin, J.F. (1999). Systematic treatment selection: Toward targeted therapeutic interventions. New York, NY: Routledge. ISBN: 978-0-87630-576-8.
Beutler, L.E., Clarkin, J.F. and Bongar, B. (2000). Guidelines for the systematic treatment of the depressed patient. New York: Oxford University Press. ISBN: 978-0756763800.
Beutler, L.E. and Consoli, A. (1992). Systematic Eclectic Psychotherapy. In J.C. Norcross and M.R. Goldfried (Eds). Handbook of Psychotherapy Integration (264-299). New York: Basic Books

199 of 271
Beutler, L.E. and Forrester, B. (2014). What needs to change: Moving from “research informed” to “empirically effective” practice. Journal of Psychotherapy Integration, 24, 168-177. DOI:10.1037/a0037587.
Beutler, L.E. and Harwood (2000). Prescriptive psychotherapy: A Practical Guide to Systematic Treatment Selection. New York: Oxford University Press. ISBN: 978-0-19513-669-2.
Beutler, L.E., Harwood, M., Kimpara, S., Verdirame, D. and Blau, K. (2011a). Coping Style. Journal of Clinical Psychology, 67(2), 176-183. DOI: 10.1002/jclp.20752.
Beutler, L.E., Harwood, M., Michelson, A., Song, X. and Holman, J. (2011b). Resistance/reactance level. Journal of Clinical Psychology, 67(2), 135-142. DOI: 10.1002/jclp.20753.
Beutler, L. E., Patterson, K. M., Jacob, T., Shoham, V., Yost, E., & Rohrbaugh, M. (1994). Matching treatment to alcoholism subtypes. Psychotherapy: Theory, Research, Practice, Training, 30, 463– 472. DOI:10.1037/0033-3204.30.3.463
Beutler, L., Someah, K., Kimpara, S. and Miller, K. (2016). Selecting the most appropriate treatment for each patient. International Journal of Clinical and Health Psychology, 16, 99-108. DOI: 10.1016/j.ijchp.2015.08.001.
Bhaskar, R. (2008). A Realist Theory of Science. London: Routledge. ISBN: 978-0-203-89263-3.
Bhaskar, R. (2014). Critical realism. Accessed on https://www.youtube.com/watch?v=TO4FaaVy0Is on 24.08.2017.
Bickman, L. and Salzer, M. S. (1996). Dose-response, disciplines, and self-help: Policy implications of Consumer Reports findings. Paper presented as part of a symposium on ‘Consumer Reports Mental Health Survey Results: Practice and Policy Implications’, 104th Annual Convention of the American Psychological Association, Toronto, Canada, August 1996.
Billig, M. (1999). Whose terms? Whose ordinariness? Rhetoric and ideology in conversation analysis. Discourse and Society, 10(4), 543-558. Downloaded from http://www.jstor.org/stable/42888872 on 03.06.2017.
Binder, P.E., Holgersen, H. and Nielsen, G.H. (2009). Why did I change when I went to therapy? A qualitative analysis of former patients’ conceptions of successful psychotherapy. Counselling and Psychotherapy Research, 9(4), 250-256. DOI: 10.1080/14733140902898088.
Binder, P.E., Holgersen, H. and Nielsen, G.H. (2010). What is a ‘good outcome’ in psychotherapy? A qualitative exploration of the former patient’s point of view. Psychotherapy Research, 20(3), 285-294. DOI: 10.1080/10503300903376338.
**Binford, R.B., Mussell, M.P., Crosby, R.D., Peterson, C.B., Crow, S.J, and Mitchell, J.E. (2005). Coping strategies in bulimia nervosa treatment : Impact on outcome in group cognitive – behavioral therapy. Journal of Consulting and Clinical Psychology, 73(6), 1089-1096. DOI: 10.1037/0022-006X.73.6.1089.
Blumer, H. (1954). What is wrong with social theory? American Sociology Review, 18, 3-10.
Bohart, A.C. (2004). How do clients make empathy work? Person-Centred and Experiential Psychotherapies, 3(2), 102-116. DOI: 10.1080/14779757.2004.9688336.
Bohart, A.C. (2007). Insight and the active client. In L.G. Castonguay and C.E. Hill (Eds), Insight in Psychotherapy (257-277). Washington, DC: American Psychological Association. ISBN: 978-1-59147-477-7.
Bohart, A.C. and Greenberg, L.S. (1997). Empathy Reconsidered: New Directions in Psychotherapy. Washington DC: American Psychological Association. ISBN: 978-1557984104.

200 of 271
Bohart, A.C. and Tallman, K.L. (2010). Clients: The neglected common factor. In B. Duncan, S.D. Miller, B.E. Wampold and M.A. Hubble (Eds). The Heart and Soul of Change: Delivering What Works in Therapy (2nd Ed; 83-111). Washington, DC: American Psychological Association. ISBN: 978-1433807091.
Bohart, A.C. and Tallman, K.L. (1996). The active client: Therapy as self-help. Journal of Humanistic Psychology, 36, 7-30. DOI: 10.1177/00221678960363002.
Bohart, A.C. and Tallman, K.L. (1999). How Clients Make Therapy Work: The Process of Active Self-Healing. Washington, DC: American Psychological Association. ISBN: 978-1557985712.
Bohart, A.C., Tallman, K.L., Byock, G. and Mackrill, T. (2011). The “Research Jury” Method: The application of the jury trial model to evaluating the validity of descriptive and causal statements about psychotherapy process and outcome. Pragmatic Case Studies in Psychotherapy, 7(1), 101-144. Accessed from https://ejbe.libraries.rutgers.edu/index.php/pcsp/article/viewFile/1075/2524 on 29.08.2018.
Bohart, A. and Wade, A.G. (2013). The client in psychotherapy. In M.J. Lambert (Ed.) Bergin and Garfield’s Handbook of Psychotherapy and Behaviour Change (6th Edition, 219-257). Hoboken, NJ: Wiley. ISBN 978-1-118-03820-8.
Boorse, C. (1976). What a theory of mental health should be. Journal for the Theory of Social Behavior, 6(1), 61-84. DOI: 10.1111/j.1468-5914.1976.tb00359.x.
Bordin, E.S. (1979). The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy: Theory, Research and Practice, 16, 252-260. DOI: 10.1037/h0085885.
Borkovec, T.D., Mathews, A.M., Chambers, A, Ebrahimi, S, Lytle, R and Nelson, R. (1987). The effects of relaxation training with cognitive or nondirective therapy and the role of relaxation-induced anxiety in the treatment of generalized anxiety. Journal of Consulting and Clinical Psychology, 55, 883-888.
Borkovec, T.D., Newman, M.G., Pincus, A.L. and Lytle, R. (2002). A component analysis of cognitive-behavioral therapy for generalized anxiety disorder and the role of interpersonal problems. Journal of Consulting and Clinical Psychology, 70, 288-298. DOI: 10.1037//0022-006X.70.2.288.
Borland, K. (1991). That’s not what I said: Interpretive conflict in oral narrative research. In S.B. Gluck and D. Patai (Eds), Womens’ Words: The Feminist Practice of Oral History. New York: Routledge, 63-75. ISBN: 978-0415903721.
Boucher, T. (2006). In cognitive therapy, how would the therapist understand and work with difficulties that arise in the therapeutic relationship. Counselling Psychology Review, 21(3), 12-18. ISSN: 0269-6975.
Brady, J.P. (1967). Psychotherapy, learning theory and insight. Archives of General Psychiatry, 16, 304-311.
Braun, V. and Clarke, V. (2013). Successful Qualitative Research. London: Sage. ISBN: 978-1-84787-582-2.
Braun, V. and Clarke, V. (2014). What can “thematic analysis” offer health and wellbeing researchers? International Journal of Qualitative Studies on Health and Wellbeing, 9. DOI: 10.3402/ghw.v9.26152.
British Psychological Society (2014). Code of Human Research Ethics. Downloaded from https://www.bps.org.uk/sites/bps.org.uk/files/Policy%20-%20Files/BPS%20Code%20of%20Human%20Research%20Ethics.pdf on 29.05.2018.
Brod, M., Tesler, L. E., & Christiansen, T. L. (2009). Qualitative research and content validity: Developing best practices based on science and experience. Quality of Life Research, 18(9), 1263-1278. doi:10.1007/s11136-009-9540-9.
Bronfenbrenner, U. (1967). The psychological costs of quality and inequality in education. Child Development, 38, 909-925.

201 of 271
Bronfenbrenner, U. (1993). The ecology of cognitive development: Research findings and fugitive findings. In R. Wonziak and K. Fisher (Eds). Development in Context: Acting and Thinking in Specific Environments (3-44). Hillsdale, NJ: Erlbaum.
Bronfenbrenner, U. (2005). The ecobiological theory on human development. In U. Bronfenbrenner (Ed). Making Human Beings Human: Bioecological Perspectives on Human Development (1-15). London: Sage.
Brown, L.S. (1994). Subversive Dialogues: Theory in Feminist Therapy. New York: Basic Books. ISBN: 978-0-46508-321-3.
*Brown, M.Z., Linehan, M.M., Comtois, K.A., Murray, A. and Chapman, A.L. (2009). Shame as a prospective predictor of self-inflicted injury in borderline personality disorder: A multi-modal analysis. Behaviour Research and Therapy, 47(10), 815-822. DOI: 10.1016/j.brat.2009.06.008.
Brunner, R. (2017). Why do people with mental distress have poor social outcomes? Four lessons from the capabilities approach. Social Science and Medicine, 191, 160-167. DOI: 10.1016/j.socscimed.2017.09.016 0277.
Budge, S.L. and Wampold, B.E. (2015). The relationship: How it works. In O.C.G. Gelo, O. Pritz and B. Rieken (Eds). Psychotherapy Research (213-228). DOI: 10.1007/978-3-7091-1382-1_11.
Burles, M.C. (2017). Negotiating post-research encounters: Reflections on learning from participant deaths following a qualitative study. Mortality, 22(2), 170-180. DOI: 10.1080/13576275.2017.1291605.
*Burns, D.D. and Nolen-Hoeksema, S. (1991). Coping styles, homework compliance, and the effectiveness of cognitive-behavioral therapy. Journal of Consulting and Clinical Psychology, 59(20), 305-311. DOI: 10.1037/0022-006X.59.2.305.
Brush, B.L., Kirk, K., Gultekin, L. and Baiardi, J.M. (2011). Overcoming: A concept analysis. Nursing Forum, 46(3), 160-168. DOI: 10.1111/j.1744-6198.2011.00227.x
Carey, T.A., Carey, M., Stalker, K., Mullan, R.J., Murray, L.K. and Spratt, M.B. (2007). Psychological change from the inside looking out: A qualitative investigation. Counselling and Psychotherapy Research, 7(3), 178-187. DOI: 10.1080/14733140701514613.
Caron, C.D. and Bowers, B.J. (2000). Methods and application of dimensional analysis: A contribution to concept and knowledge development in nursing. In B.L. Rodgers and K.A. Knafl (Eds). Concept Development in Nursing: Foundations, Techniques and Applications (2nd Edition, 285-319). Philadelphia, PA: Saunders/Elsevier. ISBN: 978-0-7216-8243-3.
Cartwright, D.A. and Roth, I. (1957). Success and satisfaction in psychotherapy. Journal of Clinical Psychology, 13(1), 20-26. ISSN: 0021-9762.
Carver, C.S., Scheier, M.F. and Weintraub, J.K. (1989). Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology, 56 (2), 267-283. DOI: 10.1037/0022-3514.56.2.267. Castonguay, L.G. (1993). ‘Common factors’ and ‘non-specific variables’: Clarification of the two concepts and recommendations for research. Journal of Psychotherapy Integration, 3, 267-286. DOI: 10.1037/h0101171. Castonguay, L.G. (2017). How and Why are Some Therapists Better Than Others? Understanding Therapist Effects. Washington, DC: American Psychological Association. ISBN: 978-1-433-82771-6.
Castonguay, L.G. and Beutler, L.E. (2006). Common and unique principles of therapeutic change: what do we know and what do we need to know? In L.G. Castonguay and L.E. Beutler (Eds.), Principles of Therapeutic Change that Work. New York: Oxford University Press, 353-370. ISBN: 978-0-19-515684-3.

202 of 271
Castonguay, L.G., Boswell, J.F., Zack, S.E., Baker, S., Boutselis, M.A., Chiswick, N.R., Damer, D.D., Hemmelstein, N.A., Jackson, J. S., Morford, M., Ragusea, S.A., Roper, J.G., Spayd, C, Weiszer, T., Borkovec, T.D., Grosse Holtforth, M. (2010). Helpful and hindering events in psychotherapy: a practice research network study. Psychotherapy: Theory, Research, Practice and Training, 47, 327-344. DOI: 10.1037/a0021164.
*Castonguay, L.G., Goldfried, M.R., Wiser, S., Raue, P.J., and Hayes, A.M. (1996). Predicting the effect of cognitive therapy for depression: A study of unique and common factors. Journal of Consulting and Clinical Psychology, 64(3), 497-504. DOI: 10.1037/0022-006X.64.3.497.
*Chambless, D. L., Milrod, B., Porter, E., Gallop, R., McCarthy, K. S., Graf, E., Rudden, M., Sharpless, B.A. and Barber, J.P. (2017). Prediction and moderation of improvement in cognitive-behavioral and psychodynamic psychotherapy for panic disorder. Journal of Consulting and Clinical Psychology, 85(8), 803-813, DOI: 10.1037/ccp0000224.
Chinn, P. and Jacobs, M. (1987). Theory and Nursing: A Systematic Approach (2nd Ed). St Louis: C.V. Mosby. ISBN: 978-0-80-160988-6.
Chinn, P.L. and Kramer, M.K. (1994). Theory and Nursing: A Systematic Approach (3rd Ed.). St Louis MO: Mosby Year Book. ASIN: B00IF1YR96
Chung, R.C. and Bemak, F.P. (2012). Social Justice Counseling. London: Sage. ISBN: 978-1-4129-9952-6.
Claes, C., Van Hove, G., Vandevelde, S., van Loon, J., Schalock, R. (2012). The influence of supports strategies, environmental factors and client characteristics on quality of life related personal outcomes. Research in Developmental Disabilities, 33, 96-103. DOI: 10.1016/j.ridd.2011.08.024.
*Clarke, H., Rees, A. and Hardy, G.E. (2004). The big idea: clients' perspectives of change processes in cognitive therapy. Psychology and Psychotherapy: Theory, Research and Practice, 77, 67-89. DOI: 10.1348/147608304322874263.
Clarkin, J.E. and Levy, K.N. (2004). The influence of client variables on Psychotherapy. In M.J. Lambert (Ed.), Bergin and Garfield’s Handbook of Psychotherapy and Behaviour Change (5th Edition, 194-226). New York: Wiley. ISBN: 0-471-37755-4.
Cochran, B.N. and Cauce, A.M. (2006). Characteristics of lesbian, gay, bisexual and transgender individuals entering substance abuse treatment. Journal of Substance Abuse Treatment, 30(2), 135-146. DOI: 10.1016/j.jsat.2005.11.009.
Coleman, R.A. and Neimeyer, R.A. (2015). Assessment of subjective client agency in psychotherapy: A review. Journal of Constructivist Psychology, 28(1), 1-23. DOI> 10.1080/10720537.2014.939791.
Constantino, M.J. and Angus, L. (2017). Clients’ retrospective accounts of corrective experiences in psychotherapy: An international multisite collaboration. Journal of Clinical Psychology, 73(2), 153-167. DOI: 10.1002/jclp.22427.
Constantino, M.J., Angus, L., Friedlander, M.L., Messer, S.B. and Moertl, K. (2011a). Patients’ perceptions of corrective experiences in individual therapy. Unpublished interview protocol.
Constantino, M.J., Arnkoff, D.B., Glass, C.R., Ametrano, R.M. and Smith, J.Z. (2011). Expectations. Journal of Clinical Psychology, 67(2), 184-192. DOI: 10.1002/jclp.20754.
*Constantino, M.J., Morrison, N.R., Coyne, A.E., Goodwin, B.J., Santorelli, G.D. and Angus, L. (2017). Patients' perceptions of corrective experiences in naturalistically delivered psychotherapy. Journal of Clinical Psychology, 73(2), 139-152. DOI: 10.1002/jclp.22428.
Collier, D. and Gerring, J. (2009). Introduction. In D. Collier and J. Gerring (Eds), Concepts and Method in Social Science. London: Routledge (1-10). ISBN: 978-0-415-77578-6.

203 of 271
Cooper, M. (2008). Essential Research Findings in Counselling and Psychotherapy: The Facts are Friendly. London: Sage. ISBN: 978-1847870438.
Cooper, M. and McLeod, J. (2007). A pluralistic framework for counselling and psychotherapy: Implications for research. Counselling and Psychotherapy Research, 7 (3). pp. 135-143. DOI: 10.1080/14733140701566282.
Corrie, S. and Callahan, M.M. (2000). A review of the scientist-practitioner model: Reflections on its potential contributions to counselling psychology within the context of current health care needs. British Journal of Medical Psychology, 73, 413-427. DOI: 10.1348/000711200160507.
Cox, C.L. (1982). An interaction model of client health behaviour: Theoretical prescription for nursing. Advances in Nursing Science. 5(1), 41-56.
Creswell, J.W. (1998). Qualitative Inquiry and Research Design: Choosing Among Five Traditions. London: Sage. ISBN: 0-7619-0144-2.
Crits-Christoph, P. (1997). Limitations of the dodo bird verdict and the role of clinical trials in psychological research: Comment on Wampold et.al. (1997). Psychological Bulletin, 122(3), 216-220. DOI: 10.1037/2F0033-2909.122.3.216.
Crossley, N. (2011). Towards Relational Sociology. Abingdon, Oxford: Routledge. ISBN: 978-0-415-48014-7.
Crossley, N. (2015). Relational sociology and culture: A preliminary framework. International Review of Sociology, 25(1), 65-85. DOI: 10.1080/03906701.2014.997965.
Dallos, R. and Stedmon, J. (2009). Reflective Practice in Psychotherapy and Counselling. Open University Press. ISBN: 978-0335233618.
*Davidson, L., Borg, M., Marin, I., Topor, A. and Sells, D. (2005). Processes of recovery in serious mental Illness: Findings from a multinational study. American Journal of Psychiatric Rehabilitation, 8(3), 177-201. DOI: 10.1080/15487760500339360.
Davidson, J. R. T., Edna, B., Hupperty, J. D., Keefe, F. J., Franklin, M. E., Compton, J. S., Zhao, N., Connor, K.M., Lynch, T.R. and Gadde, K. S. (2004). Fluoxetine, comprehensive cognitive behavioral therapy, and placebo in generalized social phobia. Archives of General Psychiatry, 61, 1005–1013. doi:10.1001/archpsyc.61.10.1005
Davis, M.H. (1996). Empathy: A Social Psychological Approach. New York: Routledge. ISBN: 978-0-8133-3001-3.
Davis-Mccabe, C. and Winthrop, A. (2010). Computerised CBT: University students’ experiences of using an online self-help programme. Counselling Psychology Review, 25(4), 46-55. ISSN: 0269-6975.
De Hoog, N., Bolman, C., Bernt, N., Kers, E., Mudde, A., De Vries, H. and Lechner, L. (2016). Smoking cessation in cardiac patients: the influence of action plans, coping plans and self-efficacy on quitting smoking. Health Education Research, 31(3), 350-362. DOI:10.1093/her/cyv100.
Department of Health (2018). The Common Law Duty of Confidence. Accessed at https://www.health-ni.gov.uk/articles/common-law-duty-confidentiality on 29.05.2018.
DeRubeis, R., Gelfand, L.A., German, R.E., Fournier, J.C. and Forand, N.R. (2014). Understanding processes of change: How some patients reveal more than others – and some groups of therapists less – about what matters in psychotherapy. Psychotherapy Research, 24(3), 419-428. DOI: 10.1080/10503307.2013.838654.
**Dingemans, A.E., Spinhoven, P. and van Furth, E.F. (2007). Predictors and mediators of treatment outcome in patients with binge eating disorder. Behaviour Research and Therapy, 45(11), 2551-2562. DOI: 10.1016/j.brat.2007.06.003.

204 of 271
Donald, I. and Carey, T. (2017). Improving knowledge about the effectiveness of psychotherapy. Psychotherapy and Politics International, e.1424. DOI: 10.1002/ppi1424.
Donati, P. (2016). The ‘relational subject’ according to a critical realist relational sociology. Journal of Critical Realism, 15(4), 352-375. DOI: 10.1080/14767430.2016.1166728.
Donovan, D.B. and Rosengren, D.B. (1999). Motivation for behavior change and treatment among substance abusers. In J.A. Tucker, D.M. Donovan and A.G. Marlett (Eds), Changing Addictive Behavior: Bridging Clinical and Public Service Strategies (127-159). New York: Guilford. ISBN: 978-1572306776.
Douglas, B., Woolfe,R., Strawbridge, S., Kasket E. and Galbraith, V. (Eds.), The Handbook of Counselling Psychology (4th Ed, 169-184). London: Sage. ISBN: 978-1-4462-7632-7.
**Dow, M.G.T., Kenardy, J.A., Johnston, D.W., Newman, M.G., Taylor, C.B. and Thompson, A. (2007). Prognostic indices with brief and standard CBT for panic disorder: II. Moderators of outcome. Psychological Medicine, 37(10), 1503-1509. DOI: 10.1017/S0033291707000682.
Drapela, V.J. (1990). The value of theories for counselling practitioners. International Journal for the Advancement of Counselling, 13, 19-26. DOI: 10.1007%2FBF00154639.
Duncan, B., Miller, S.D., Wampold, B.E. and Hubble, M. (2010). The Heart and Soul of Change: Delivering What Works in Therapy (2nd Ed). Washington, DC: American Psychological Association. ISBN: 978-1433807091.
Duncan, B., Miller, S.D. and Sparks, J.A. (2004). The Heroic Client. San Francisc, CA: Jossey Bass. ISBN: 0-7879-7240-1.
Duncan, C., Cloutier, J.D. and Bailey, P.H. (2007). Concept analysis: The importance of differentiating the ontological focus. Journal of Advanced Nursing, 58(3), 293-300. DOI: 10.1111/j.1365-2648.2007.04277.x.
Eacott, S. (2018). Beyond Leadership: A Relational Approach to Organizational Theory in Education. London: Springer. ISBN: 978-981-10-6568-2.
*Ekeblad, A, Falkenström F. and Holmqvist R. (2016). Reflective functioning as predictor of working alliance and outcome in the treatment of depression. Journal of Consulting and Clinical Psychology, 84(1), 67-78. DOI: 10.1037/ccp0000055.
Elkins, A. (2009). The medical model in psychotherapy: Its limitations and failures. Journal of Humanistic Psychology, 49(1), 66-84. DOI: 10.1177/0022167807307901.
Elliot, A.J. and Church, M.A. (2002). Client-articulated avoidance goals in the therapy context. Journal of Counseling Psychology, 49, 243-254. DOI: 10.1037//0022-0167.49.2.243.
Elliott, R. (1985). Helpful and non-helpful events in brief counselling interviews: An empirical taxonomy. Journal of Counseling Psychology, 32, 307-322. Elliott, R. (1996). Client change interview schedule. Unpublished research instrument. Department of Psychology, Toledo University.
Elliott, R. (2010). Psychotherapy change process research: Realizing the promise. Psychotherapy Research, 20(2), 123-135. DOI: 10.1080/10503300903470743.
Elliott, R., Fischer, C.T. and Rennie, D.L. (1999). Evolving guidelines for publication of qualitative research studies in psychology and related fields. British Journal of Clinical Psychology, 38(3), 215-229. DOI: 10.1348/014466599162782.
Elliott, R. and Timulak, L. (2005). Descriptive and interpretive approaches to qualitative research. In J. Miles and P. Gilbert (Eds.), A Handbook of Research Methods for Clinical and Health Psychology. Cary, N.C: Oxford University Press USA, 147-159. ISBN: 978-0198527565.

205 of 271
Erlingsson, C. and Brysiewicz, P. (2017). A hands-on guide to doing content analysis. African Journal of Emergency Medicine, 7, 93-99. DOI: 10.1016/j.afjem.2017.08.001 2211-419X.
Farley, L. (2017). The replacement of child figure: An allegory for scholars of education, psychology and childhood. Critical Discourses in the Academy Seminar Series, University of Manchester, 08.06.2017.
Fauconnier, G. and Turner, M. (1998). Conceptual integration networks. Downloaded from http://www.cogsci.ucsd.edu/~faucon/BEIJING/CIN.pdf on 29.08.2018.
Feltham, C. (2013). Counselling and Counselling Psychology: A Critical Examination. Ross-on-Wye: PCCS Books. ISBN: 978-1-906254-58-2.
Finlay, L. (2015). Qualitative methods. In A. Vossler and N. Moller (Eds). The Counselling and Psychotherapy Research Handbook. London: Sage. ISBN: 978-1-4462-5527-8.
Fivush, R. (2000). Accuracy, authority and voice: Feminist perspectives on autobiographical memory. In P.H. Miller and E.K. Scholnick (Eds), Towards a Feminist Developmental Psychology (85-105). New York: Routledge. ISBN: 0-415-92177-5.
Fleetwood, S. (2004). The ontology of organisation and management studies. Downloaded from http://eprints.uwe.ac.uk/16278/2/Download.pdf on 15.09.2017.
Fletcher, A.J. (2017). Applying critical realism in qualitative research: Methodology meets method. International Journal of Social Research Methodology, 20(2), 181-194. DOI: 10.1080/13645579.2016.1144401.
Forchuk, C. (1994). The orientation phase of the nurse-client relationship: testing Peplau’s theory. Journal of Advanced Nursing, 20(3), 532-537.
Forsyth, G.L. (1980). Analysis of the concept of empathy: Illustration of one approach. Advances in Nursing Science, 2(2), 33-42. ISSN: 0161-9268.
Fougere, A., Daffern, M. and Thomas, S. (2012). Towards an empirical conceptualisation of resilience in young adult offenders. Journal of Forensic Psychiatry and Psychology, 23(5-6), 706-721. DOI: 10.1080/14789949.2012.719536.
*Fournier, J.C., De Rubeis, R.J., Shelton, R.C., Hollon, S.D., Amsterdam, J.D. and Gallop, R. (2009). Prediction of response to medication and cognitive therapy in the treatment of moderate to severe depression. Journal of Consulting and Clinical Psychology, 77(4), 775-787. DOI: 10.1037/a0015401.
Frank, J.D. (1973). Persuasion and Healing: A Comparative Study (2nd Ed.). Baltimore, MD: Johns Hopkins University Press. ISBN: 978-0801814433.
Frank, J.D. and Frank, J.B. (1993). Persuasion and Healing: A Comparative Study (3rd Ed.). Baltimore, MD: Johns Hopkins University Press, ISBN: 978-0-801-84636-6.
Frazier, P.A., Tix, A.P. and Barron, K.E. (2004). Testing moderator and mediator effects in counseling psychology research. Journal of Counseling Psychology, 51(1), 115-134. DOI: 10.1037/0022-0167.51.1.115.
Fredericks, M. and Miller, S.I. (1987). The use of conceptual analysis for teaching sociology courses. Teaching Sociology,15(4), 392-398. DOI: 10.2307/1317995.
Fusch, P.I. and Ness, L.R. (2015). The Qualitative Report, 20(9), 1408-1416. Downloaded from https://cpb-us-e1.wpmucdn.com/sites.nova.edu/dist/a/4/files/2015/09/fusch1.pdf on 05.09.2019.
Garfield, S.L. (1971). Research on client variables in psychotherapy. In A.E. Bergin and S.L. Garfield (Eds.), Handbook of Psychotherapy and Behaviour Change: An Empirical Analysis. New York: Wiley.

206 of 271
Garfield, S.L. (1978). Research on client variables in psychotherapy. In A.E. Bergin and S.L. Garfield (Eds.), Handbook of Psychotherapy and Behaviour Change (2nd Edition, 191-232). New York: Wiley. ISBN: 978-0-471-06968-3.
Garfield, S.L. (1994). Research on client variables in psychotherapy. In A.E. Bergin and S.L. Garfield (Eds.), Handbook of Psychotherapy and Behaviour Change (3rd Edition, 190-228). New York: Wiley. ISBN: 0-471-54513-9.
Garfield, S.L. (1995). Psychotherapy: An Eclectic-Integrative Approach (2nd Ed.). Hoboken, NJ: Wiley. ISBN: 978-0471595564.
Gaston, L. (1990). The concept of the alliance and its role in psychotherapy: Theoretical and empirical considerations. Psychotherapy: Theory, Research, Practice, Training, 27(2), 143-153. DOI: 10.1037/2F0033-3204.27.2.143.
Gelso, C.J. (2014). A tripartite model of the therapeutic relationship: Theory, research, practice. Psychotherapy Research, 24(2), 117-131. DOI: 10.1080/10503307.2013.845920.
Gelso, C.J. and Fretz, B.R. (1992). Counseling Psychology. Fort Worth, TX: Harcourt-Brace. ISBN: 0-03-027858-9.
Gergen, K.J. (2009). Relational Being: Beyond Self and Community. New York: Oxford Universtiy Press. ISBN: 978-0-19-984626-9.
Gergen, K.J. (2015). Towards a relational humanism. Journal of Humanistic Counselling, 54(2), 149-165. DOI: 10.1002/johc.12009.
Gerring, J. (1997). Ideology: A definitional analysis. Political Research Quarterly, 50(4), 957-994. DOI: 10.2307/448995.
Gerring, J. (1999). What makes a concept good? A criterial framework for understanding concept formation in the social sciences. Polity, 31(3), 357-393. Downloaded from http://blogs.bu.edu/jgerring/files/2013/06/Conceptformation.pdf on 29.09.2017.
Gerring, J. (2012). Social Science Methodology: A Unified Framework (2nd Ed.). Cambridge University Press. ISBN: 978-0-521-13277-0.
Gershefski, J.J., Arnkoff, D.B. Glass, C.R. and Elkin, I. (1996). Clients’ perceptions of treatment for depression: I Helpful aspects. Psychotherapy Research, 6, 233-247. DOI: 10.1080/10503309612331331768. Gianakis, M. and Carey, T.A. (2008). A review of the experience and explanation of psychological change. Counselling Psychology Review, 23(3), 27-38. ISSN: 0269-6975.
Gibbard, I. (2014). Clients’ experiences of change in cognitive behavioural therapy and person-centred therapy. Unpublished thesis. Available from: https://ethos.bl.uk/OrderDetails.do;jsessionid=31AD135B7A46811D92C206685830938C?uin=uk.bl.ethos.632280.
Gilgun, F. (2014). An introduction to deductive qualitative analysis. International Congress on Qualitative Inquiry. Downloaded from https://www.slideshare.net/JaneGilgun/an-introduction-to-deductive-qualitative-analysis on 06.09.2018.
Glaser, B.G. (1998). Doing Grounded Theory: Issues and Discussions. Mill Valley, CA: Sociology Press. ISBN: 978-1884156113.
Glaser, B.G. and Strauss, A.L. (2000). The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago, IL: Aldine. ISBN: 978-0202302607.

207 of 271
Glassman, N.S. and Andersen, S.M. (1999). Transference in social cognition: Persistence and exacerbation of significant-other-based inferences over time. Cognitive Therapy and Research, 23(1), 75-91. DOI: 10.1023%2FA%3A1018762724798.
**Gloster, A.T., Klotsche, J., Gerlach, A.L., Hamm, A., Ströhle, A., Gauggel, S., Kircher, T., Alpers, G.W., Deckert, J. and Wittchen, H. (2014). Timing matters: change depends on the stage of treatment in cognitive behavioral therapy for panic disorder with agoraphobia. Journal of Consulting and Clinical Psychology, 82(1), 141-153. DOI: 10.1037/a0034555.
Goertz, G. (2006). Social Science Concepts: A User’s Guide. Princeton University Press. ISBN: 978-0-691-12411-7.
Goertz, G. and Mazur, A.G. (Eds), (2007). Politics, Gender and Concepts: Theory and Methodology. Cambridge University Press. ISBN: 978-0-521-72342-8.
Goertzen, J.R. (2010). Dialectical pluralism: A theoretical conceptualisation of pluralism in psychology. New Ideas in Psychology, 28, 201-209. DOI: 10.1016/j.newideapsych.2009.09.013.
Goldfried, M.R. (1980). Toward the delineation of therapeutic change principles. American Psychologist, 35, 991-999.
**Goldin, P.R., Jazaieri, H., Ziv, M., Kraemer, H. Heimberg, R.G. and Gross, J.J. (2013). Changes in beliefs about the social competence of self and others following group cognitive-behavioral treatment. Clinical Psychological Science, 1(3), 301-310. DOI: 10.1177/2167702613476867.
*Goldman, R.N., Greenberg, L.S. and Pos, A.E. (2007). Depth of emotional experience and outcome. Psychotherapy Research 15(3), 248-260. DOI: 10.1080/10503300512331385188.
*Gomes, K. and Pascual-Leone, A. (2015). A resource model of change: Client factors that influence problem gambling treatment outcomes. Journal of Gambling Studies, 31(4), 1651-1669. DOI: 10.1007/s10899-014-9493-y.
*Gonçalves, M.M., Ribeiro, A. P., Stiles, W. B., Conde, T., Matos, M., Martins, C., and Santos, A. (2011). The role of mutual in-feeding in maintaining problematic self-narratives: Exploring one path to therapeutic failure. Psychotherapy Research, 21(1), 27–40. DOI: 10.1080/10503307.2010.507789.
Goodyear, R., Tracey, T.J.G., Claiborn, C.D. and Lichtenberg, J. (2005). Ideographic concept mapping in counselling psychology research. Journal of Counseling Psychology, 52(2), 236-242. DOI: 10.1037/0022-0167.52.2.236.
Gopen, G.D. and Swan, J.A. (1990). The science of scientific writing. American Scientist, 78(6), 550-558.
Gordon, R. (2012). Where oh where are the clients? The use of common factors in counselling psychology. Counselling Psychology Review, 27 (4), 8-17.
Goss, D. (2015). Affective neuroscience. Counselling Psychology Review, 30(1), 52-63.
Goss, D. and Parnell, T. (2017). Integrating neuroscience into counselling psychology. Counselling Psychology Review, 32(4), 4-17.
Greaves, A.L. (2006). The active client: A qualitative analysis of thirteen clients’ contributions to the psychotherapy process. Unpublished doctoral dissertation, University of Southern California.
Greenberg, R.P., Constantino, M.J. and Bruce, N. (2006). Are patient expectations still relevant for psychotherapy process and outcome? Clinical Psychology Review, 26, 657-678. DOI: 10.1016/j.cpr.2005.03.002.
Greenson, R.R. (1967). The Technique and Practice of Psychoanalysis (vol. 1). New York: International Universities Press. ASIN: B00M0QWR0I.

208 of 271
Grencavage, L. and Norcross, J. (1990). Where are the commonalities among the therapeutic common factors? Professional Psychology: Research and Practice, (21)5, 372-378. DOI: 10.1037/0735-7028.21.5.372.
Groth-Marnat, G., Roberts, R. and Beutler, L.E. (2001). Client characteristics and psychotherapy: Perspectives, support, interactions and implications for training. Australian Psychologist, 36(2), 115-121. DOI: 10.1080/00050060108259643.
Guba, E.G. and Lincoln, Y.S. (1982). Epistemological and methodological bases of naturalistic enquiry. Educational Communication and Technology Journal, 30(4), 233-252. DOI: 10.1126/science.146.3642.347.
**Hanna, F.J. and Ritchie, M.H. (1995). Seeking the active ingredients of psychotherapeutic change: Within and outside the context of therapy. Professional Psychology: Research and Practice, 26(2), 176-183. DOI: 10.1037/0735-7028.26.2.176.
Hansen, N.B. and Lambert, M. (2003). An evaluation of the dose-response effect in naturalistic treatment settings using survival analysis. Mental Health Services Research, 5. 1-11. DOI: 10.1023/A:102175130.
Harding, S. (2004). A socially relevant philosophy of science? Resources from standpoint theory’s controversiality. Hypatia, 19(1), 25-47. Downloaded from https://muse.jhu.edu/article/53922/pdf on 10.09.2017.
Hardy, G.E., Barkham, M., Shapiro, D.A., Reynolds, S., Rees, A. and Stiles, W.B. (1995). Credibility and outcome of cognitive-behavioral and psychodynamic-interpersonal therapy. British Journal of Clinical Psychology, 34, 555-569. DOI: 10.1111/j.2044-8260.1995.tb01489.x
Hargons, C., Mosley, D.V. and Stevens-Watkins, D. (2017). Studying sex: A content analysis of sex research in counselling psychology. The Counseling Psychologist, 45(4), 528-546. DOI: 10.1177/0011000017713756.
Harris, G.E. and Larson, D. (2008). High-risk behaviours following an HIV diagnosis, Counselling Psychology Review, 23(3), 48-61. ISSN: 0269-6975.
Harrison, K. (2013). Counselling psychology and power: Considering therapy and beyond. Counselling Psychology Review, 28(2), 107-117. ISSN: 0269-6975.
**Hartmann, A., Orlinsky, D., Weber, S., Sandholz, A., Zeeck, A. (2010). Session and intersession experience related to treatment outcome in bulimia nervosa. Psychotherapy Theory, Research, Practice and Training, 47(30), 355-370. DOI: 10.1037/a0021166.
**Hartzler, B., Witkiewitz, K., Villarroel, N. and Donovan, D. (2011). Self-efficacy change as a mediator of associations between therapeutic bond and one-year outcomes in treatments for alcohol dependence. Psychology of Addictive Behavior, 25(2), 269-278. DOI: 10.1037/a0022869.
*Hawley, L.L., Ho, M.R., Zuroff, D.C and Blatt, S.J. (2006). The relationship of perfectionism, depression, and therapeutic alliance during treatment for depression: Latent difference score analysis. Journal of Consulting and Clinical Psychology, 74(5), 930-942. DOI: 10.1037/0022-006X.74.5.930.
Hayes, A.M., Laurenceau, J-P., Feldman, G., Strauss, J.L. and Cardaciotto, L. (2007). Change is not always linear: The study of non-linear and discontinuous patterns of change in psychotherapy. Clinical Psychology Review, 27, 715-723. DOI: 10.1016/j.cpr.2007.01.008.
Health and Care Professions Council (2016). Standards of Conduct, Performance and Ethics. Downloaded from https://www.hcpc-uk.org/assets/documents/10004EDFStandardsofconduct,performanceandethics.pdf on 09.09.2018.
Hekman, S. (1997). Truth and method: Feminist standpoint revisited. Signs, 22(2), 341-365. Stable URL: http://www.jstor.org/stable/3175275.

209 of 271
Helmreich, I., Kunzler, A., Chmitorz, A., König, J., Binder, H., Wessa, M., Lieb, K. (2017). Psychological interventions for resilience enhancement in adults (Protocol). Cochrane Database of Systematic Reviews Issue 2. Art. No.: CD012527. DOI: 10.1002/14651858.CD012527.
*Hendriks, G.J., Keijsers, G. P.J., Kampman, M., Hoogduin, C. A.L. and Voshaar, R. C.O. (2012). Predictors of outcome of pharmacological and psychological treatment of late-life panic disorder with agoraphobia. International Journal of Geriatric Psychiatry, 27(2), 141-150. DOI: 10.1002/gps.2700.
Hendry, L. B. and Kloep, M. (2002). Lifespan Development: Resources, Challenges and Risks. Cengage Learning. ISBN: 978-1861527547.
Henkelman, J. and Paulson, B. (2006). The client as expert: researching hindering experiences in counselling. Counselling Psychology Quarterly, 19(2), 139-150. DOI: 10.1080/09515070600788303. Higginson, S. and Mansell, W. (2008). What is the mechanism of psychological change? A qualitative analysis of six individuals who experienced personal change and recovery. Psychology and Psychotherapy: Theory, Research and Practice, 81, 309-328. DOI: 10.1348/147608308X30125. Hill, C. and Lambert, M. (2004). Methodological issues in studying psychotherapy processes and outcomes. In M.J. Lambert (Ed), Bergin and Garfield's Handbook of Psychotherapy and Behavior Change (5th ed., pp. 84-135). 0-471-37755-4.
Hoddy, E. (2018). Critical realism in empirical research employing techniques from grounded theory methodology. International Journal of Social Research Methodology. DOI: 10.1080/13645579.2018.1503400.
Hoffman, J.J. (1985). Client factors related to premature termination of psychotherapy. Psychotherapy: Theory, Research, Practice, Training 22(1), 83-85. DOI: 10.1037/2Fh0088530.
Hogan, R. (1975). Empathy: A conceptual and psychometric analysis. The Counseling Psychologist. 5(2), 14-18. DOI: 10.1177/001100007500500204.
*Hooley, J.M. and Teasdale, J.D. (1999). Expressed emotion and behavior therapy outcome: A prospective study with OCD and agoraphobic outpatients. Journal of Consulting and Clinical Psychology, 67(5), 658-665.
*Hooley, J.M. and Teasdale, J.D. (1989). Predictors of relapse in unipolar depressives: Expressed emotion, marital distress, and perceived criticism. Journal of Abnormal Psychology, 98(3), 229-235. DOI: 10.1037/0021-843X.98.3.229.
Horvath, A.O. and Bedi, R.P. (2002). The alliance. In J.C. Norcross (Ed.), Psychotherapy Relationships That Work: Therapist Contributions and Responsiveness to Patients (37-70). Oxford: Oxford University Press. ISBN: 978-0-19-514346-1.
Horvath, A.O., Del Re, A.C., Flückiger, C. and Symonds, D. (2011) Alliance in individual psychotherapy. In J.C. Norcross (Ed.), Psychotherapy Relationships That Work: Therapist Contributions and Responsiveness to Patients (2nd Ed., 25-69). Oxford: Oxford University Press. ISBN: 978-0199737208.
Hougaard, E. (1994). The therapeutic alliance – a conceptual analysis. Scandinavian Journal of Psychology, 35(1), 67-85. DOI: 10.1111/j.1467-9450.1994.tb00934.x
Howard, G.S., Maerlender, A.C., Myers, P.R. and Curtin, T.D. (1992). In stories we trust: Studies of the validity of autobiographies. Journal of Counseling Psychology, 39(3), 398-405. DOI: 10.1037/0022-0167.39.3.398.
Hoyle, R.H. and Robinson, J.C. (2004). Mediated and moderated effects in social psychological research: Measurement, design and analysis issues. In C. Sansone, C. Morf and A.T Panter (Eds). The Sage Handbook of Methods in Social Psychology (213-234). Thousand Oaks, CA: Sage. ISBN: 978-0-761925354.

210 of 271
Hubble, M.A., Duncan, B.L. and Miller, S.D. (1999a). The Heart and Soul of Change: What Works in Therapy. Washington, DC: American Psychological Association. ISBN: 1-55798-557-X.
Hubble, M.A., Duncan, B.L. and Miller, S.D. (1999b). Directing attention to what works. In M.A. Hubble, B.L. Duncan and S.D. Miller (Eds), The Heart and Soul of Change: What Works in Therapy (407-448). Washington, DC: American Psychological Association. ISBN: 1-55798-557-X.
Hupcey, J.E. and Penrod, J. (2003). Concept advancement: Enhancing inductive validity. Research and Theory for Nursing Practice, 17, 19-30.
Iacoboni, M. (2008). Mirroring People: The New Science of How We Connect with Others. New York: Farrar, Straus and Giroux. ISBN: 978-0-374-21017-5.
Ivey, A.E. and Zalaquett, C.P. (2011). Neuroscience and counselling: Central issue for social justice leaders. Journal for Social Action in Counselling and Psychology, 3(1), 103-116. Downloaded from http://psysr.org/jsacp/ivey-v3n1-11_103-116.pdf on 02.12.17.
Jackson, R.H. (1984). Ethnicity. In G. Sartori (Ed). Social Science Concepts (206-238). Beverley Hills, CA: Sage. ISBN: 0-8039-2177-2.
*Jarrett, R.B., Eaves, G.G., Grannemann, B.D. and Rush, A.J. (1991). Clinical, cognitive, and demographic predictors of response to cognitive therapy for depression: A preliminary report. Psychiatry Research, 37, 245-260. DOI: 10.1016/0165-1781(91)90061-S.
Jarvis, P. (2018). Learning to be a person in society. In K. Illeris (Ed). Contemporary Theories of Learning (2nd Ed., 15-28). London: Routledge. ISBN: 978-1-138-55049-0.
Jensen, D. (2008). Credibility. In L.M. Gi ven (Ed.) The Sage Encyclopedia of Qualitative Research Methods (138-139). London: Sage. ISBN: 978-1412941631.
Johansson, P. and Høglend, P. (2007). Identifying mechanisms of change in psychotherapy: Mediators of treatment outcome. Clinical Psychology and Psychotherapy, 14(1), 1-9. DOI: 10.1002/cpp.514.
Jordan, J.V. (2000). The role of mutual empathy in relational/cultural therapy. Journal of Clinical Psychology. In Session 56(80), 1005-1016. DOI: 10.1002/1097-4679(200008)56:8<1005::AID-JCLP2>3.0.CO;2-L
Jordan, J.V. (2010). Relational-Cultural Therapy. Washington, DC: American Psychological Association. ISBN: 978-1-4338-0463-2.
Jordan, J.V., Kaplan, A.G., Miller, J.B., Stiver, I.P. and Surrey, J.L. (Eds). Women’s Growth in Connection. New York: Guilford. ISBN: 0-89862-465-7.
Joutsenniemi, K., Laaksonen, M.A., Knekt, P., Haaramo, P. and Lindfors, O. (2012). Prediction of the outcome of short- and long-term psychotherapy based on social-demographic factors. Journal of Affective Disorders, 141, 331-342. DOI: 10.1016/j.jad.2012.03.027. Joyce, S., Shand, F., Tighe, J., Laurent, S.J., Bryant, R.A. and Harvey, S.B. (2018). Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open,
8(6),1-9. DOI: 10.1136/bmjopen-2017-017858. Kadera, S.W., Lambert, M.J. and Andrews, A.A. (1996). How much therapy is really enough? A session-by-session analysis of the psychotherapy dose-effect relationship. Journal of Psychotherapy Practice and Research 5(2), 132-151. Kaldo, V., Ramnerö, J. and Jernelöv, S. (2015). Involving clients in treatment methods: A neglected interaction in the therapeutic relationship. Journal of Consulting and Clinical Psychology, 83(6), 1136-1141. DOI: 10.1037/ccp0000039.

211 of 271
Karnieli-Miller, O., Strier, R. and Pessach, L. (2009). Power relations in qualitative research. Qualitative Health Research, 19(2), 279-289. DOI: 10.1177/1049732308329306.
Kanfer, F.H. and Schefft, B.K. (1998). Guiding the Therapeutic Process of Change. Champaign, IL: Research Press. ISBN: 978-0-87822-285-8.
Kasket, E. (2016). Carrying out research. In B. Douglas, R. Woolfe, S. Strawbridge, E. Kasket and V. Galbraith (Eds.), The Handbook of Counselling Psychology (4th Ed, 228-243). London: Sage. ISBN: 978-1-4462-7632-7.
**Kavanagh, D.J. and Wilson, P.H. (1985). Prediction of outcome for group cognitive therapy for depression. Behavior Research and Therapy. 27(4), 333-343.
Kazdin, A.E. (1999). The meanings and measurement of clinical significance. Journal of Clinical and Consulting Psychology, 67, 322-339. DOI: 10.1037/0022-006x.67.3.332.
Kazdin, A. E. (2009). Understanding how and why psychotherapy leads to change. Psychotherapy Research, 19(4-5), 418-428. DOI: 10.1080/10503300802448899.
Kazdin, A.E. and Nock, M.K. (2003). Delineating mechanisms of change in child and adolescent therapy: Methodological issues and research recommendations. Journal of Child Psychotherapy and Psychiatry, 44(8), 1116-1129. DOI: 10.1111/1469-7610.00195.
Kazdin, A. E. and Wassel, G. (1999). Barriers to treatment participation and psychological change among children referred for conduct disorder. Journal of Clinical Child Psychology, 28, 160-172.
Keeley, M.L. , Storch, E.A., Merlo, L.J. and Geffken, G.R. (2008). Clinical predictors of response to cognitive-behavioral therapy for obsessive-compulsive disorder. Clinical Psychology Review, 28, 118-130. DOI: 10.1016/j.cpr.2007.04.003.
*Keijsers, G.P.J, Hoogduin, C.A.L. and Schaap, C.P .D .R. (1994). Predictors of Treatment Outcome in the Behavioural Treatment of Obsessive-Compulsive Disorder. British Journal of Psychiatry, 165, 781-786. DOI: 10.1192/bjp.165.6.781.
Kelly, J. (2006). Being ecological. An Expedition into Community Psychology. New York, NY: Oxford University Press. ISBN: 978-0-19517-379-6.
Kenniston, K, Boltax, S. and Almond, R (1971). Multiple criteria of treatment outcome. Journal of Psychiatry Research, 8, 107-118. DOI: 10.1016/0022-3956(71)90012-4.
**Khattra, J., Angus, L., Westra, H., Macaulay, C., Moertl, K, and Constantino, M. (2017). Client perceptions of corrective experiences in cognitive behavioral therapy and motivational interviewing for generalized anxiety disorder: An exploratory pilot study. Journal of Psychotherapy Integration, 27(1), 23-34. DOI: 10.1037/int0000053.
*Kim, J.E., Zane, N.W. and Blozis, S.A. (2012). Client predictors of short-term psychotherapy outcomes among Asian and White American outpatients. Journal of Clinical Psychology, 68(12), 1287-1302. DOI: 10.1002/jclp.21905.
Kindt, M., Buck, N., Arntz, A. and Soeter, M. (2007). Perceptual and conceptual processing as predictors of treatment outcome in PTSD. Journal of Behavior Therapy and Experimental Psychiatry, 38(4), 491-506. DOI: 10.1016/j.jbtep.2007.10.002.
King, R. and O’Brien, T. (2011). Transference and countertransference: Opportunities and risks as two technical constructs that migrate beyond their psychoanalytic homeland. Psychotherapy in Australia, 17(4). Downloaded from http://www.psychotherapy.com.au/fileadmin/site_files/pdfs/Transference_and_Countertransference.pdf on 28.07.2018.
Kirsch, I. (1990). Changing Expectations: A Key to Effective Psychotherapy. Belmont, CA: Brroks/Cole. ISBN: 978-0534126483.

212 of 271
Klein, M.J. and Elliott, R. (2006). Client accounts of personal change in process-experiential psychotherapy: A methodologically pluralistic approach. Psychotherapy Research, 16(1), 91-105. DOI: 10.1080/10503300500090993
**Kleindienst, N., Limberger, M.F., Ebner-Priemer, U.W., Keibel-Mauchnik, J., Dyer, A., Berger, M., Schmahl, C. and Bohus, M. (2011). Dissociation predicts poor response to dialectial behavioral therapy in female patients with borderline personality disorder. Journal of Personality Disorders, 25(4), 432-447. DOI: 10.1521/pedi.2011.25.4.432.
Knafl, K.A. and Deatrick, J.A. (1990). Family management style: Concept analysis and development. Journal of Pediatric Nursing, 5(1), 4-14.
Knafl, K.A. and Deatrick, J.A. (2000). Knowledge synthesis and concept development in nursing. In B.L. Rodgers and K.A. Knafl (Eds). Concept Development in Nursing: Foundations, Techniques and Applications (2nd Edition, 39-54). Philadelphia, PA: Saunders/Elsevier. ISBN: 978-0-7216-8243-3.
Kolb, D.A. (1984). Experiential Learning. Englewood Cliffs, NJ: Prentice-Hall.
Kolb, D.A. (2014). Experiential Learning: Experience as the Source of Learning and Development. Pearson Education. ISBN: 978-0-13-389240-6.
Kolden, G.G. (1991). The generic model of psychotherapy: An empirical investigation of patterns of process and outcome relationships. Psychotherapy Research, 1(1), 62-73. DOI: 10.1080/10503309112331334071.
Kraemer, H.C., Wilson, G.T., Fairburn, C.G. and Agras, W.S. (2002). Mediators and moderators of treatment effects in randomised clinical trials. Archives of General Psychiatry, 59(10), 877-883. DOI: 10.1001/archpsyc.59.10.877.
Kramarae, C. (1981). Women and Men Speaking: Frameworks for Analysis. Rowley, MA: Newbury House. ISBN: 978-0-883-77179-2.
Kramarae, C. (2005). Muted group theory and communication: Asking dangerous questions. Women and Language, 28(2), 55-61.
**Krentzman, A.R. (2017). Gratitude, abstinence, and alcohol use disorders: Report of a preliminary finding. Journal of Substance Abuse Treatment, 78, 30-36. DOI: 10.1016/j.jsat.2017.04.013.
Krupnick, J.L., Sofsky, S.M., Simmens, S., Moyer, J., Elkin, I., Watkins, J. and Pilkonis, P.A. (1996). The role of the therapeutic alliance in psychotherapy and pharmacotherapy outcome: Findings in the NIMH Treatment of Depression Collaborative Treatment Programme. Journal of Consulting and Clinical Psychology, 64, 532-539.
Kuyken, W, Watkins, E., Holden, E., White, K., Taylor, R.S., Byford, S., Evans, A., Radford, S., Teasdale, J.D. and Dalgleish, T. (2010). How does mindfulness based cognitive therapy work? Behavior Research and Therapy, 48, 1105-1112. DOI: 10.1016/j.brat.2010.08.003.
Kvale, S. (2007). Doing Interviews (2-10). London: Sage. ISBN: 978-0-76194-977-0.
**Kyrios, M., Hordern, C. and Fassnacht, D.B. (2015). Predictors of response to cognitive behaviour therapy for obsessive-compulsive disorder. International Journal of Clinical and Health Psychology, 15(3), 181-190. DOI: 10.1016/j.ijchp.2015.07.003.
Laaksonen, M.A., Lindfors, O., Knekt, P. and Aalberg, V. (2012). Suitability for Psychotherapy Scale and its reliability, validity and prediction. British Journal of Clinical Psychology, 51, 351-375. DOI: 10.1111/j.2044-8260.2012.02033.x. Ladouceur, R., Dugas, M.J., Freeston, M.H., Leger, E., Gagnon, F. and Thibodeau, N. (2000). Efficacy of a cognitive-behavioral treatment for generalised anxiety disorder: Evaluation in a controlled clinical trial. Journal of Consulting and Clinical Psychology, 68, 957-964. DOI: 10.1037/0022-006X.68.6.957.

213 of 271
Lambert, M.J. (1992). Implications of outcome research for psychotherapy integration. In J.C. Norcross and M.R. Goldfried (Eds.), Handbook of Psychotherapy Integration (94-129). New York: Basic Books. ASIN: B01A64LX0A.
Lambert, M.J. (2010). Preventing Treatment Failure: The Use of Measuring, Monitoring and Feedback in Clinical Practice. Washington, DC: American Psychological Association. ISBN: 978-1433807824.
Lambert, M.J. (2013). The efficacy and effectiveness of psychotherapy. In M.J. Lambert (Ed), Bergin and Garfield’s Handbook of Psychotherapy and Behaviour Change (6th Edition, 169-218). Hoboken, N.J: Wiley. ISBN 978-1-118-03820-8.
Lambert, M.J. and Barley, D.E. (2002). Research summary on the therapeutic relationship and psychotherapy outcome. In J.C. Norcross (Ed.), Psychotherapy Relationships that Work: Therapist Contributions and Responsiveness to Patients (17-32). New York: Oxford University Press. ISBN: 973-0-19-514346-1.
Lambert, M.J., DeJulio, S.S. and Stein, D. (1978). Therapist interpersonal skills: Process, outcome, methodological considerations and recommendations for future research. Psychological Bulletin, 85, 467-489. AN: 00006823-197805000-00002.
Lambert, M.J., Smart, D.W., Campbell, M.P., Hawkins, E.J., Harmon, C. and Slade, K.L. (2006). Psychotherapy outcome as measured by the OQ-45 in African American, Asian/Pacific Islander, Latino/a and Native American clients compared to matched Caucasian clients. Journal of College Student Psychotherapy, 20, 17-29. DOI: 10.1300/J035v20n04_03.
Larkin, M., Watts, S. and Clifton, E. (2006). Giving voice and making sense in interpretive phenomenological analysis. Qualitative Research in Psychology, 3, 102-120. DOI: 10.1191/1478088706qp062oa.
Laurence, S. and Margolis, E. (1999). Concepts and cognitive science. In E. Margolis and S. Laurence (Eds), Concepts: Core Readings. MIT Press, 3-81. ISBN: 978-0262631938.
*Leibert, T. W., Smith, J. B. and Agaskar, V. R. (2011). Relationship between the working alliance and social support on counseling outcome. Journal of Clinical Psychology, 67(7), 709-719. DOI: 10.1002/jclp.20800.
Lemmens, L.H.J.M., Müller, V.N.L.S., Arntz, A. and Huibers, M.J.H. (2016). Mechanisms of change in psychotherapy for depression: An empirical update and evaluation of research aimed at identifying psyshcological mediators. Clinical Psychology Review, 50, 95-107. DOI: 10.1016/j.cpr.2016.09.004.
*Leung, A.W. and Heimberg, R.G.(1996). Homework compliance, perceptions of control and outcome of cognitive-behavioral treatment of social phobia. Behavior Research and Therapy, 34(5), 423-432. DOI: 10.1016/0005-7967(96)00014-9.
*Leweke, F., Bausch, S., Leichsenring, F., Walter, B. and Stingl, M.(2009). Alexithymia as a predictor of outcome of psychodynamically oriented inpatient treatment inpatient treatment, Psychotherapy Research, 19(3), 323-331. DOI: 10.1080/10503300902870554.
Lilienfeld, S., Ritschel, L.A, Lynn, S.J., Cautin, R.L. and Latzman, R.D. (2014). Why ineffective psychotherapies appear to work: A taxonomy of causes of spurious therapeutic effectiveness. Perspectives on Psychological Science, 9(4), pp.355–387. 10.1177/1745691614535216.
Littel, J., Alexander, L. and Reynolds, W. (2001). Client participation: Central and underinvestigated elements of intervention. Social Service Review, 75(1), 1-28. DOI: 10.1086/591880.
Llewelyn, S. (1988). Psychological therapy as viewed by clients and therapists. British Journal of Clinical Psychology, 27(3), 223-238. DOI: 10.1111/j.2044-8260.1988.tb00779.x.

214 of 271
Llewelyn, S.P., Elliott, R., Shapiro, D.A., Hardy, G.E. and Firth-Cozens, J. (1988). Client perceptions of significant events in prescriptive and exploratory periods of individual therapy. British Journal of Clinical Psychology. 27, 105-114. DOI: 10.1111/j.2044-8260.1988.tb00758.x. Lombardi, D.R., Button, M. and Westra, H.A. (2014). Measuring motivation: Change talk and counter-change talk in cognitive behavioral therapy for generalised anxiety. Cognitive Behavioral Therapy, 43(1) [no page numbers]. DOI:10.1080/16506073.2013.846400. Lorenzo-Luaces, L., De Rubeis, R.J. and Webb, C.A. (2014). Client characteristics as moderators of the relationship between the therapeutic alliance and outcome in cognitive therapy for depression. Journal of Consulting and Clinical Psychology, 82(2), 368-373. DOI: 10.1037/a0035994.
Lowman, R.L. (2012). The scientist-practitioner consulting psychologist. Consulting Psychology Journal: Practice and Research. 64(3), 151-156. DOI: 10.1037/a0030365.
Luborsky, L., Crits-Christoph, Mintz, J. and Auerbach, A. (1988). Who Will Benefit from Psychotherapy?
New York: Basic Books. ISBN: 0-465-09189-X.
Luborsky, L., Singer, B. and Luborsky, L. (1975). Comparative studies of psychotherapies: Is it true that ‘Everyone has won and all must have prizes’? Archives of General Psychiatry, 32(8), 995-1008. DOI: 10.1001/archpsyc.1975.01760260059004.
Luborsky, L., Rosenthal, R., Diguer, L., Andrusyna, T.P., Berman, J.S., Levitt, J.T., Seligman, D.A. and Krause, E.D. (2002). The dodo bird verdict is alive and well – mostly. Clinical Psychology: Science and Practice, 9(1), 2-12. DOI: 10.1093/clipsy.9.1.2/pdf.
Lunnen, K. M., & Ogles, B. M. (1998). A multiperspective, multivariable evaluation of reliable change. Journal of Consulting and Clinical Psychology, 66, 400–410. DOI: 10.1037/0022-006X.66.2.400.
Lynch, J. (2017). Reframing inequality: the health inequalities turn as a dangerous frame shift. Journal of
Public Health, 4(1), 653-660. DOI: 10.1093/pubmed/fdw140.
Mackrill, T. (2008). Exploring psychotherapy clients’ independent strategies for change while in therapy. British Journal of Guidance and Counselling, 36(4), 441-453. DOI: 10.1080/03069880802343837.
*Mallinckrodt, B. (1996). Change in working alliance, social support, and psychological symptoms in brief therapy. Journal of Counseling Psychology, 43(4), 448-455. DOI: 10.1037/0022-0167.43.4.448.
Mansell, W. (2011). Core processes of psychopathology and recovery: ‘Does the dodo bird have wings’? Clinical Psychology Review, 31(2), 189-192. DOI: 10.1016/j.cpr.2010.06.009.
Martin, P. (2009). Book review of ‘Reflections on Human Potential: Bridging the Person-centered Approach and Positive Psychology’ by B.E. Levitt. British Journal of Guidance and Counselling, 37(3), 387-402. DOI: 10.1080/03069880903007844.
Martinez, R. (2017). Empathy. London: Cannongate. ISBN: 9781786892379
**Matos, M., Santos, A., Gonçalves, M., Martins, C. (2009). Innovative moments and change in narrative therapy. Psychotherapy Research, 19(1), 68-80. DOI: 10.1080/10503300802430657.
Mausbach, B.T., Moore, R., Roesch, S., Cardenas, V. and Patterson, T.L. (2010). The relationship between homework compliance and therapy outcomes: An updated meta-analysis. Cognitive Therapy
and Research, 34(5), 429-438. DOI: 10.1007/s10608-010-9297-z.
**McCrady, B.S., Hayaki, J., Epstein, E.E. and Hirsch, L.S. (2002). Testing hypothesized predictors of change in conjoint behavioral alcoholism treatment for men. Alcoholism: Clinical and Experimental Research, 26(4), 463-470. DOI: 10.1111/j.1530-0277.2002.tb02562.x.
McIntosh, M. and Sykes, C. (2016). Older adults’ experience of psychological therapy, Counselling Psychology Review, 31(1), 20-30.

215 of 271
McLachlin, R. (1999). Factors for consulting engagement success. Management Decision, 37(5), 354-404.
McLaughlin, H. (2009). What's in a name: ‘Client’, ‘patient’, ‘customer’, ‘consumer’, ‘expert by experience’, ‘service user’—What's next? British Journal of Social Work, 39(6), 1101-1117. DOI: 10.1093/bjsw/bcm155.
McLeod, J. (2003). Qualitative research methods in counselling psychology. In R. Woolfe, W. Dryden and S. Strawbridge (Eds). Handbook of Counselling Psychology (2nd Ed., 74-92). London: Sage.
McLeod, J. and Balamoutsou, S. (2006). A method for qualitative narrative analysis of psychotherapy transcripts. In J. Frommer and D.L. Rennie (Eds), Qualitative Psychotherapy Research: Methods and Methodology (2nd Ed, 128-152). Lengerich, Germany: Pabst Science.
Mellon, C.A. (1990), Naturalistic Inquiry for Library Science: Methods and Applications for Research, Evaluation, and Teaching. New York: Greenwood Press. ISBN: 978-0313256530.
*Meyer, B., Pilkonis, P.A., Krupnick, J.L., Egan, M.K., Simmens, S.J. and Sotsky, S.M. (2002). Treatment expectancies, patient alliance and outcome: Further analyses from the National Institute of Mental Health Treatment of Depression Collaborative Research Program. Journal of Consulting and Clinical Psychology, 70(4), 1051-1055. DOI: 10.1037/0022-006X.70.4.1051.
Miller, J.B. (1991). The development of women’s sense of self. In J.V. Jordan, A.G. Kaplan, J.B. Miller, I.P Stiver and J.L. Surrey (Eds). Women’s Growth in Connection (11-26). New York: Guilford.
Miller, K.D. and Tsang, E.W.K. (2011). Testing management theories: Critical realist philosophy and research methods. Strategic Management Journal, 32(2), 139-158. Downloaded from http://www.jstor.org/stable/41000104 on 27.05.2018.
Mingers, (2006). Realising Systems Thinking: Knowledge and Action in Management Science. Springer. ISBN: 978-0387281889.
Mintz, J. (1972). What is “success” in psychotherapy. Journal of Abnormal Psychology, 81(1), 11-19. DOI: 10.1037/h0033225.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med 6(6): e10000097. DOI:10.1371/journal.pmed10000097.
**Mohr, S., Perroud, N., Gillieron, C., Brandt, P.Y., Rieben, I., Borras, L. and Huguelet, P. (2011). Spirituality and religiousness as predictive factors of outcome in schizophrenia and schizo-affective disorders. Psychiatry Research, 186(2-3), 177-182. DOI: 10.1016/j.psychres.2010.08.012.
Mones, A.G. and Schwartz, R.C. (2007). The functional hypothesis: A family systems contribution towards an understanding of the healing process of the common factors. Journal of Psychotherapy Integration, 17(4), 314-329. DOI: 10.1037/1053-0479.17.4.314.
Morrow, S.L. and Smith, M.L. (1995). Constructions of survival and coping by women who have survived childhood sexual abuse. Journal of Counseling Psychology, 42(1), 24-33. DOI: 10.1037/0022-0167.42.1.24.
Morrow, S.L. and Smith, M.L. (2000). Qualitative research for counseling psychology. In S.D. Brown and R.W. Lent (Eds), Handbook of Counseling Psychology (3rd Ed., 199-230). New York: Wiley and Sons. ISBN: 0-471-25458-4.
Morse, J.M. and Penrod, J. (1999). Linking concepts of enduring, uncertainty, suffering and hope. Journal of Nursing Scholarship, 31, 145-150. DOI: 10.1111/j.1547-5069.1999.tb00455.x.
*Mörtberg, E., Hoffart, A., Boecking, B. and Clark, D.M. (2015). Shifting the focus of one's attention mediates improvement in cognitive therapy for social anxiety disorder. Behavioural and Cognitive Psychotherapy, 43(1), 63-73. DOI: 10.1017/S1352465813000738.

216 of 271
**Mörtl, K. and Wietersheim, J.V. (2008). Client experiences of helpful factors in a day treatment program: A qualitative approach. Psychotherapy Research, 18(3) 281-293. DOI: 10.1080/10503300701797016.
Murphy, P.M., Cramer, D. and Lillie, F.J. (1984). The relationship between curative factors perceived by patients in their psychotherapy and treatment outcome: An exploratory study. British Journal of Medical Psychology, 57, 187-192. 10.1111/j.2044-8341.1984.tb01599.x.
Najavits, L.M. and Strupp, H. (1994). Differences in the effectiveness of psychodynamic therapists: A process-outcome study. Psychotherapy, 31, 114-123. DOI: 10.1037/0033-3204.31.1.1114.
**Nakano, Y., Lee, K., Noda, Y., Ogawa, S., Kinoshita, Y., Funayama, T., Watanabe, N., Chen, J., Noguchi, Y. and Furukawa, T.A. (2008). Cognitive-behavior therapy for Japanese patients with panic disorder: Acute phase and one-year follow-up results. Psychiatry and Clinical Neurosciences, 62(3), 313-321. DOI: 10.1111/j.1440-1819.2008.01799.x.
**Neimeyer, R.A. and Feixas, G. (1990). The Role of Homework and Skill Acquisition in the Outcome of Group Cognitive Therapy for Depression. Behavior Therapy, 21, 281-292. DOI: 10.1016/S0005-7894(05)80331-4.
Newman, M.G., Crits-Christoph, P., Gibbons, M.B.C. and Erickson, T.M. (2006). Participant factors in treating anxiety disorders. In L.G. Castonguay and L.E. Beutler (Eds), Principles of Therapeutic Change that Work. New York: Oxford University Press, 121-153. ISBN: 978-0-19-515684-3.
Nilsson, T., Svenson, M., Sandell, R. and Clinton, D. (2007). Patients’ experiences of change in cognitive-behavioral therapy and psychodynamic therapy: A qualitative comparative study. Psychotherapy Research, 17(5), 553-566. DOI: 10.1080/10503300601139988.
Norcross, M.J. (2002). Empirically supported therapy relationships. In J.C. Norcross (Ed.), Psychotherapy Relationships that Work: Therapist Contributions and Responsiveness to Patients (3-16). New York: Oxford University Press. ISBN: 973-0-19-514346-1.
Norcross, J.C. and Karpiak, C.P. (2012). Teaching clinical psychology: four seminal lessons that all can master. Teaching of Psychology, 39(4), 301-307. DOI: 10.1177/0098628312461486.
Norcross, J.C. and Lambert, M.J. (2010). Evidence-based therapy relationships. In J.C. Norcross (Ed.), Evidence-based Therapy Relationships (1-4). Downloaded from http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.463.7645&rep=rep1&type=pdf on 26.11.2017.
Norcross, J.C. and Lambert, M. (2011). Psychotherapy relationships that work II. Psychotherapy, 48, 4-8. DOI: 10.1037/a0022180.
Norcross, J.C. and Wampold, B.E. (2010). Adapting the relationship to the individual patient. In J.C. Norcross (Ed.), Evidence-based Therapy Relationships (27-31). Downloaded from http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.463.7645&rep=rep1&type=pdf on 26.11.2017.
Oliver, D.G., Serovich, J.M. and Mason, T.L. (2005). Constraints and opportunities with interview transcription: Towards reflection in qualitative research. Social Forces, 84 (2), 1273-1289. DOI: 10.1353/sof.2006.0023.
Olsson, C.A., Bond, L., Burns, J.M., Vella-Brodrick, D.A., and Sawyer, S.M. (2003). Adolescent resilience: A concept analysis. Journal of Adolescence, 26, 1-11. DOI: 10.1016/S0140-1971(02)00118-5.
O’Mahoney, J. (2011). Critical realism and the self. Journal of Critical Realism, 10(1), 122-129. DOI: 10.1558/jcr.v10i1.122.
O’Reilly, M., & Parker, N. (2012). Unsatisfactory saturation: A critical exploration of the notion of saturated sample sizes in qualitative research. Qualitative Research Journal, 1-8. DOI:10.1177/1468794112446106.

217 of 271
Ong, A.D., Bergeman, C.S., Bisconti, T.L. and Wallace, K.A. (2006). Psychological resilience, positive emotions and successful adaptation to stress in later life. Journal of Personality and Social Psychology, 91(4), 730-749. DOI: 10.1037/0022-3514.91.4.730.
Oregon State University (undated). Muted group theory. Downloaded from http://oregonstate.edu/instruct/theory/mutedgrp.htmlon 04.11.2017.
Orlinsky, D.E. (2009). The ‘Generic Model of Psychotherapy’ after 25 years: Evolution of a research-based metatheory. Journal of Psychotherapy Integration, 19(4), 319-339. DOI: 10.1037/a0017973.
Orlinsky, D.E. and Howard, K.I. (1986). Process and outcome in psychotherapy. In A.E. Bergin and S.L. Garfield (Eds.), Handbook of Psychotherapy and Behaviour Change (3rd Edition, 331-381). New York: Wiley. ISBN: 0-471-54513-9.
Orlinsky, D.E., Grawe, K. and Parks, B.K. (1994). Process and outcome in psychotherapy: Noch einmal [once again]. In A.E. Bergin and S.L. Garfield (Eds.), Handbook of Psychotherapy and Behavior Change (4th Ed, 270-376). New York: Wiley. ISBN: 978-0471545132.
Oxford English Dictionary (2017). Accessed at https://en.oxforddictionaries.com/definition/client on 10.09.2017.
Paley, J. (1996). How not to clarify concepts in nursing. Journal of Advanced Nursing, 24, 572-578. DOI: 10.1046/j.1365-2648.1996.22618.x.
Pantell, M., Rehkopf, O., Jutte, D., Syme, S.L., Balmes, J. and Adler, N. (2012). Social isolation: A predictor of mortality comparable to traditional clinical risk factors. American Journal of Public Health, 103 (11), 2056–2062. DOI: 10.2105/AJPH.2013.301261. Parker, I. (Ed.) (1998). Social Constructionism, Discourse and Realism. London: Sage. ASIN: B01JXPARY6
Parker, I. (2007). Critical psychology: What it is and what it is not. Social and Personal Psychology Compass, 1(1), 1-15. DOI: 10.1111/j.1751-9004.2007.00008.x.
Parr, S. (2015). Integrating critical realist and feminist methodologies: Ethical and analytical dilemmas. International Journal of Social Research Methodology, 18(2), 193-207. DOI: 10.1080/13645579.2013.868572.
Patterson, C.L., Uhlin, B. and Anderson, T. (2008). Clients’ pretreatment counselling expectations as predictors of the working alliance. Journal of Counseling Psychology, 55, 528-534. DOI: 10.1037/a0013289.
Paulson, B.L., Truscott, D. and Stuart J. (1999). Clients’ perceptions of helpful experiences in counseling. Journal of Counseling Psychology, 46, 317-324. ISSN: 0022-0167. Pawson, R., Greenhalgh, T., Harvey, G. and Walshe, K. (2005). Realist review: A new method of systematic review designed for complex policy interventions. Journal of Health Services Research and Policy, 10(1), 21-34. DOI: 10.1258/1355819054308530.
Payne, E.C., Robbins, S.B. and Doughty, L. (1991). Goal-directedness and older adult adjustment. Journal of Counseling Psychology, 38 (3), 302-308. DOI: 10.1037/0022-0167.38.3.302. Pekarik, G. and Guidry, L. (1999). Relationship of satisfaction to symptom change, follow-up adjustment and clinical significance in private practice. Professional Psychology: Research and Practice, 27(2), 202-208. DOI: 10.1037//0735-7028.27.2.202.
Penrod, J. (2007). Living with uncertainty: Concept advancement. Journal of Advanced Nursing, 57(6), 658-667. DOI: 10.1111/j.1365-2648.2006.04008.x.

218 of 271
Penrod, J. and Hupcey, J. (2005). Enhancing methodological clarity: Principle-based concept analysis. Journal of Advanced Nursing, 50(4), 403-409, DOI: 10.1111/j.1365-2648.2005.03405.x.
Perkins, S.N. (2010). Influential client factors: Understanding and organising therapists’ perceptions of client factors that influence reported outcome of therapy. Unpublished PhD thesis. Virginia Polytechnic Institute and State University. Downloaded from https://vtechworks.lib.vt.edu/bitstream/handle/10919/27631/sperkins_dissertation_2010.pdf?sequence=1&isAllowed=y on 23.09.2017.
Pilgrim, D. (2017). Key Concepts in Mental Health (4th Ed). London: Sage. ISBN: 978-1-4739-7301-5.
Pilgrim, D. (2016). Diagnosis and formulation in medical contexts. In B. Douglas, R. Woolfe, S. Strawbridge, E. Kasket and V. Galbraith (Eds.), The Handbook of Counselling Psychology (4th Ed, 169-184). London: Sage. ISBN: 978-1-4462-7632-7.
Pilgrim, D. and Bentall, R. (2009). The medicalisation of misery: A critical realist analysis of the concept of depression. Journal of Mental Health, 8(3), 261-274. DOI: 10.1080/09638239917427.
Pintrich, P.R., Marx, R.W., Boyle, R.A. (1993). Beyond cold conceptual change: the role of motivational beliefs and classroom contextual factors in the process of conceptual change. Review of Educational Research, 63(2), 167-199. Downloaded from http://links.jstor.org/sici?sici=0034-6543%28199322%2963%3A2%3C167%3ABCCCTR%3E2.0.CO%3B2-1 on 16.11.2017.
Pope, C.A. (1999). Reflection and refraction: A reflexive look at an evolving model for methods instruction. English Education, 31(3), 177-200.
Porter, N. (2002). Contextual and developmental frameworks in diagnosing children and adolescents. In M. Ballou and L.S. Brown (Eds.), Rethinking Mental Health and Disorder, New York: Guilford, 262-278. ISBN: 978-1-57230-799-5.
Powers, W.T. (2005). Behavior: The Control of Perception. San Diego, CA: Benchmark Publications. ISBN: 987-0-96971-217-1.
Powers, T.A., Milyavskaya, M. and Koestner, R. (2012). Mediating the effects of self-criticism and self-directed perfectionism on goal pursuit. Personality and Individual Differences, 52, 765-770. DOI:
10.1016/j.paid.2011.12.031. Probst, T., Lambert, M.J., Loew, T.H., Dahlbender, R.W. and tritt, K. (2015). Extreme deviations from expected recovery curves and their associations with therapeutic alliance, social support, motivation and life events in psychosomatic in-patient therapy. Psychotherapy Research, 25(6), 714-723. DOI: 10.1080/10503307.2014.981682.
Prochaska, J.O., DiClemente, C.C. and Norcross, J.C. (1992). In search of how people change: Applications to addictive behaviors. American Psychologist, 47, 1102-1114. DOI: 10.1037/0003-066X.47.9.1102.
Prochaska, J.O. and Norcross, J.C. (1999). Systems of Psychotherapy: A Transtheoretical Analysis (4th Ed). Pacific Grove, CA: Brooks/Cole. ISBN: 0-534-35704-0.
Prochaska, J.O., Norcross, J.C. and DiClemente, C.C. (1994). Changing for Good: A Revolutionary Six-Stage Program for Overcoming Bad Habits and Moving Your Life Positively Forward. New York: Harper Collins. ISBN: 0-380-72572-X.
Proctor, G. (2017). The Dynamics of Power in Counselling and Psychotherapy: Ethics, Politics and
Practice (2nd Ed.). Ross-on-Wye: PCCS Books. ISBN: 978-1910919187.
Proudlock, S. and Wellman, N. (2011). Solution-focussed groups - the results look promising. Counselling Psychology Review 26(3), 45-54. ISSN: 0269-6975.

219 of 271
Radomski, M.V. (2014). Assessing context: Persona, social and cultural. In M.V. Radomski and C.A. Trombly Latham (Eds). Occupational Therapy for Physical Dysfunction. Lippincott, Williams and Wilkins. ISBN: 9781451189216.
**Ramnerö, J. and Ost, L. (2004). Prediction of outcome in the behavioural treatment of panic disorder with agoraphobia. Cognitive Behaviour Therapy, 33(4), 176-180. DOI: 10.1080/16506070410031691.
*Reddy, A.S. and Jagannathan, A. (2017). Predictors of coping and perceived expressed emotions in persons with alcohol dependence in India: a pilot study. Asian Journal of Psychiatry, 28, 38-40. DOI: 10.1016/j.ajp.2017.03.011.
*Renneberg, B., Chambless, D.L., Fydich, T. and Goldstein, A.J. (2002). The relationship of affect balance in family interactions to behaviour therapy outcome: A study with agoraphobic outpatients and their relatives. Clinical Psychology and Psychotherapy, 9(2), DOI: 10.1002/cpp.306.
Rennie, D.L. (1992). Qualitative analysis of the client’s experience of psychotherapy: The unfolding of reflexivity. In S.G. Toukmanian and D.L. Rennie (Eds), Psychotherapy Process Research: Paradigmatic and Narrative Approaches (211-233). London: Sage. ISBN: 978-0803943551.
Rennie, D.L. (2002). Experiencing psychotherapy: Grounded theory studies. In D.J. Cain and J. Seeman (Eds), Humanistic Psychotherapies: Handbook of Research and Practice (117-144). Washington, DC: American Psychological Association. ISBN: 978-1557987877.
Rennie, D.L. (2010). Humanistic psychology at York University: Retrospective: Focus on clients’ experiencing in psychotherapy: Emphasis of radical reflexivity. Humanistic Psychologist, 38, 40-56. DOI: 10.1080/08873261003635856.
Rennie, D.L. (2012). Qualitative Research as Methodological Hermeneutics. Psychological Methods, 17(3), 385-398. DOI: 10.1037/a0029250.
Rice, K.G., Ashby, J.S. and Slaney, R.B. (1998). Self-esteem as a mediator between perfectionism and depression: A structural equations analysis. Journal of Counseling Psychology, 45(3), 304-314.
Ridner, S. (2004). Psychological distress: Concept analysis. Journal of Advanced Nursing, 45(5), 536-545. DOI: 10.1046/j.1365-2648.2003.02938.x.
Ritchie, J. and Lewis, J. (2003). Qualitative Research Practice. London: Sage. ISBN: 978-0-7619-7110-8.
**Ritsher, J.B. and Phelan, J.C. (2004). Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Research, 129(3), 257-265. DOI: 10.1016/j.psychres.2004.08.003.
Rizq, R. (2007). Tread carefully: Counselling psychology and neuroscience. Counselling Psychology Review, 22(4), 5-18. ISSN: 0269-6975.
Robinson-Whelen, S., Hughes, R.B., Taylor, H.B., Hall, J.W. and Rehm, L.P. (2007). Depression self-management programme for rural women with physical disabilities. Rehabilitation Psychology, 52, 254–262. doi:10.1037/0090-5550.52.3.254.
Robson, C. (2002). Real World Research. Malden, MA: Blackwell. ISBN: 978-0-631-21304-8.
Rodgers, B.L. (1991). Using concept analysis to enhance clinical practice and research. Dimensions of Critical Care Nursing (10)1, 28-34. ISSN: 0730-4625.
Rodgers, B.L. and Knafl, K.A. (Eds). Concept Development in Nursing: Foundations, Techniques and Applications (2nd Edition, 77-102). Philadelphia, PA: Saunders/Elsevier. ISBN: 978-0-7216-8243-3.
Rodgers, B.L. (2000a). Philosophical foundations of concept development. In B.L. Rodgers and K.A. Knafl (Eds). Concept Development in Nursing: Foundations, Techniques and Applications (2nd Edition, 7-37). Philadelphia, PA: Saunders/Elsevier. ISBN: 978-0-7216-8243-3.

220 of 271
Rodgers, B.L. (2000b). Concept analysis: An evolutionary view. In B.L. Rodgers and K.A. Knafl (Eds). Concept Development in Nursing: Foundations, Techniques and Applications (2nd Edition, 77-102). Philadelphia, PA: Saunders/Elsevier. ISBN: 978-0-7216-8243-3.
Roehrle, B. and Strouse, J. (2008). Influence of social support on success of therapeutic interventions: A meta-analytic review. Psychotherapy: Theory, Research, Practice, Training, 45(4), 464-476. DOI: 10.1037/a0014333.
Rogers, C.R. (1983). Freedom to Learn for the 80’s. Columbus, OH: Charles E. Merrill. ISBN: 978-0-67-509519-8.
Rosenzweig, S. (1936). Some implicit common factors in diverse methods of psychotherapy. American Journal of Orthopsychiatry, 6(3), 412-415. DOI: 10.1111/j.1939-0025.1936.tb05248.x.
*Rosmarin, D.H., Bigda-Peyton, J.S., Kertz, S.J., Smith, N., Rauch, S.L. and Björgvinsson, T. (2013a). A test of faith in God and treatment: The relationship of belief in God to psychiatric treatment outcomes. Journal of Affective Disorders, 146(3), 441-446. DOI: 10.1016/j.jad.2012.08.030.
*Rosmarin, D.H., Bigda-Peyton, J.S., Öngur, D., Pargament, K.I. and Björgvinsson, T. (2013b). Religious coping among psychotic patients: Relevance to suicidality and treatment outcomes. Psychiatry Research, 210(1), 182-187. DOI: 10.1016/j.psychres.2013.03.023.
Rounsaville, B.J. and Carroll, K. (2002). Commentary on ‘Dodo bird revisited’: Why aren’t we dodos yet? Clinical Psychology: Science and Practice, 9(1), 17-20. DOI:10.1093/clipsy.9.1.17.
Rounsaville, B.J., Weissman, M.M. and Prusoff, B.A. (1981). Psychotherapy with depressed outpatients: Patient and process variables as predictors of outcome. British Journal of Psychiatry, 138, 67-74. PMID: 7023593.
Rousmaniere, T. (2016). Deliberate Practice for Psychotherapists: A Guide to Improving Clinical Practice. New York: Routledge. ISBN: 978-1138203204.
Royce, J.R. (1987). A strategy for developing unifying theory in psychology. In A.W. Staats and L.P. Mos (Eds). Annals of Theoretical Psychology, Vol 5, 275-286.
Rundle, B. (1995). Concept. In T. Honerich (Ed.). The Oxford Companion to Philosophy (146). Oxford: Oxford University Press.
*Ryba, M. M., Lejuez, C. W. and Hopko, D. R. (2014). Behavioral activation for depressed breast cancer patients: The impact of therapeutic compliance and quantity of activities completed on symptom reduction. Journal of Consulting and Clinical Psychology, 82(2), 325-333. DOI: 10.1037/a0035363.
Ryle, G. (1971). Collected Papers (Volume 2). London: Hutchinson.
Sacks, H. (1972). An initial investigation of the usability of conversational data for sociology. In D.N. Sudnow (Ed.), Studies in Social Interaction (31-74). New York: Free Press. ISBN: 978-0029323601.
*Safren, S.A., Heimberg, R.G. and Juster, H.R. (1997). Clients' expectancies and their relationship to pretreatment symptomatology and outcome of cognitive-behavioral group treatment for social phobia. Journal of Consulting and Clinical Psychology, 65(4), 694-698.
Sartori, G. (1970). Concept misinformation in comparative politics. American Political Science Review. 64, 1033-1046. DOI: 10.2307/1958356. Sartori, G. (1984). Guidelines for concept analysis. In G. Sartori (Ed). Social Science Concepts: A Systematic Analysis (15-88). London: Sage. ISBN: 0-8039-2177-2.
Sartori, G. (2009). Part 1: Sartori on concepts and method. In D. Collier and J. Gerring (Eds.), Concepts and Method in Social Science: The Tradition of Giovanni Sartori. London: Routledge (11-178). ISBN: 0-415-77578-7.

221 of 271
*Scheel, M.J., Seaman, S., Roach, K., Mullin, T. and Mahoney, K.B. (1999). Client implementation of therapist recommendations predicted by client perception of fit, difficulty of implementation and therapist influence. Journal of Counseling Psychology, 46(3) 308-316. DOI: 10.1037/0022-0167.46.3.308.
Scheirs, J.G.M., Blok, J.B., Tolhoek, M.E.; El Aouat, F., Glimmerveen, J.C. (2012). Client factors as predictors of restraint and seclusion in people with intellectual disabilities. Journal of Intellectual and Developmental Disability, 37(2), 112-120. DOI: 10.3109/13668250.2012.682357.
Shoben, E.J. (1949). Psychotherapy as a problem in learning theory. Psychological Bulletin, 46, 366-392. DOI: 10.1037/h0061680.
Scott, D. (2005). Critical realism and empirical research methods in education. Journal of Philosophy of Education, 39(4), 633-646. DOI: 10.1111/j.1467-9752.2005.00460.x.
*Shahar, G., Blatt, S.J., Zuroff, D.C., Krupnick, J.L. and Sotsky, S.M. (2004). Perfectionism impedes social relations and response to brief treatment for depression. Journal of Social and Clinical Psychology, 23(2), 140-154. DOI: 10.1521/jscp.23.2.140.31017.
Shin, R.Q., Welch, J.C., Kaya, A.E., Yeung, J.G., Obana, C., Sharma, R., Vernay, C.N. and Yee, S. (2017). The intersectionality framework and identity intersections in the Journal of Counseling Psychology and The Counseling Psychologist: A content analysis. Journal of Counseling Psychology, 64(5), 458-474. DOI: 10.1037/cou0000204.
Shorrock, M. (2012). The pragmatic case of Ed. Counselling Psychology Review, 27(2), 23-35. ISSN: 0269-6975.
Siegel, D.J. (2012). Pocket Guide to Interpersonal Neurobiology. New York: Norton. ISBN: 978-0-393-70713-7.
*Simons, A. D., Lustman, P.J., Wetzel, R.D., Murphy, G.E. (1985). Predicting response to cognitive therapy of depression: The role of learned resourcefulness. Cognitive Therapy and Research, 9(1), 79-89. DOI: 10.1007/BF01178752.
Smith, J.A., Flowers, P. and Larkin, M. (2009). Interpretive Phenomenological Analysis: Theory, Method and Research. London: Sage. ISBN: 978-1412908344.
Smith, J.A. and Osborn, M. (2007). Interpretive Phenomenological Analysis. In J.A. Smith (Ed), Qualitative Psychology: A Practical Guide to Research Methods, 53-80. ISBN: 978-141-293084-0.
Smith, M.L., Glass, G.V. and Miller, T.I. (1980). The Benefits of Psychotherapy. Baltimore: Johns Hopkins University Press. ISBN: 0-8018—382-8.
Smith, T. B., Rodríguez, M. D., & Bernal, G. (2011). Culture. In J. C. Norcross (Ed.), Psychotherapy Relationships that Work (2nd ed., 316-335). New York: Oxford University Press. ISBN: 978-0-19973-720-8.
Snape, D. and Spencer, L. (2003). The foundations of qualitative research. In J. Lewis and J. Ritchie (Eds). Qualitative Research Practice: A Guide for Social Science Students and Researchers (1-23). Thousand Oaks, CA: Sage. ISBN: 0761971092.
Spradley, J.P. (1980). Participant Observation. Cengage Learning. ISBN: 978-0030445019.
Sreenan, B., Smith, H. and Frost, C. (2015). Student top tips. In A. Vossler and N. Moller (Eds). The Counselling and Psychotherapy Research Handbook, 245-256. London: Sage. ISBN: 978-1-4462-5527-8.
Stavros, C., & Westberg, K. (2009). Using triangulation and multiple case studies to advance relationship marketing theory. Qualitative Market Research, 12(3), 307-320. doi:10.1108/13522750910963827.
**Steinmetz, J.L., Lewinsohn, P.M. and Antonuccio, D.O. (1983). Prediction of individual outcome in a group intervention for depression. Journal of Consulting and Clinical Psychology, 51(3), 331-337. DOI: 10.1037/0022-006X.51.3.331.

222 of 271
Stiles, W.B. (1993). Quality control in qualitative research. Clinical Psychology Review, 13, 593-618. DOI: 10.1016/0272-7358(93)90048-Q.
Stiles, W.B. (2002). Assimilation of problematic experiences. In J.C. Norcross (Ed.), Psychotherapy Relationships That Work: Therapist Contributions and Responsiveness to Patients (357-365). Oxford: Oxford University Press. ISBN: 978-0-19-514346-1.
Stiles, W.B. (2003). When is a case study scientific research? Psychotherapy Bulletin, 38, 6-11. Downloaded from file:///C:/Users/Admin/Downloads/Stiles2003PsychotherapyBulletin.pdf on 01.01.2019.
Stiles, W.B. (2005). Extending the Assimilation of Problematic Experiences Scale: Commentary on the Special Issue. Counselling Psychology Quarterly, 18, 85-94. DOI: 10.1080/09515070500136868.
Stiles, W.B., Elliott, R., Llewelyn, S., Firth-Cozens, J, Margison, F.R., Shapiro, D.A. and Hardy, G. (1990). Assimilation of problematic experience by clients in psychotherapy. Psychotherapy, 27, 411-420. Downloaded from https://www.researchgate.net/profile/William_Stiles/publication/232578783_Assimilation_of_problematic_experiences_by_clients_in_psychotherapy/links/09e415089403714e77000000/Assimilation-of-problematic-experiences-by-clients-in-psychotherapy.pdf on 02.12.2017.
Stiles, W.B., Shapiro, D.A. and Elliott, R. (1986). Are all psychotherapies equivalent? The American Psychologist, 41(2), 165-180. DOI: 10.1037/0003-066X.41.2.165.
Stiles, W.B., Shapiro, D., Firth-Cozens, J. (1990). Correlations of session evaluations with treatment outcome. British Journal of Clinical Psychology, 29(1), 13-21. DOI: 10.1111/j.2044-8260.1990.tb00844.x.
*Stirman, S.W., Gutner, C.A., Suvak, M. K., Adler, A., Calloway, A. and Resick, P. (2018). Homework Completion, Patient Characteristics, and Symptom Change in Cognitive Processing Therapy for PTSD. Behavior Therapy, In press as of 06/2018. DOI: 10.1016/j.beth.2017.12.001.
Strauss, A. and Corbin, J. (1990). Basics of Qualitative Research: Grounded Theory Procedures and Techniques. London: Sage. ISBN: 978-0803932517.
Strauss, A. and Corbin, J. (1998). Basics of Qualitative Research: Grounded Theory Procedures and
Techniques (2nd Ed). London: Sage. ISBN: 978-0803959408.
Street, E. (2003). Counselling psychology and naturally occurring systems (Families and couples). In R. Woolfe, W. Dryden and S. Strawbridge (Eds). Handbook of Counselling Psychology (2nd Ed., 419-441). London: Sage.
Substance Abuse and Mental Health Services Administration (2012). Enhancing Motivation for Change in Substance Abuse Treatment. Rockville, MD: United States department of health and Human Servoces. Downloaded from https://www.ncbi.nlm.nih.gov/books/NBK64967/pdf/Bookshelf_NBK64967.pdf on 05.01.2019.
Swan, E. (2017). How to use a fishbone diagram. GoLeanSixSigma. Accessed on https://www.youtube.com/watch?v=OPxSbRuv3Cw on 03.06.2017.
Swift, J. K., Callahan, J. L., & Vollmer, B. M. (2011). Preferences. In J. C. Norcross (Ed.), Psychotherapy Relationships that Work (2nd ed., pp. 301---315). New York: Oxford University. ISBN: 978-0-19973-720-8.
Tallman, K. and Bohart, A.C. (1999). The client as a common factor: Clients as self-healers. In M.A. Hubble, B.L. Duncan and S.D. Miller (Eds), The Heart and Soul of Change: What Works in Therapy (91-132). Washington, DC: American Psychological Association. ISBN: 1-55798-557-X.
Taylor, M. (1996). The feminist paradigm. In In R. Woolfe and W. Dryden (Eds). Handbook of Counselling Psychology (201-239). London: Sage.
**Teasdale, J. D., Moore, R.G., Hayhurst, H., Pope, M., Williams, S. and Segal, Z.V. (2002). Metacognitive awareness and prevention of relapse in depression: Empirical evidence. Journal of Consulting and Clinical Psychology, 70(2), 275-287. DOI: 10.1037//0022-006X.70.2.275.

223 of 271
Thelen, E. and Smith, L.B. (1996). A Dynamic Systems Approach to the Development of Cognition and Action. Cambridge, MA: MIT Press. ISBN: 978-0-26-270059-7.
Thomas, M.L. (2006). The contributing factors of change in a therapeutic process. Contemporary Family Therapy, 28, 201-210. DOI 10.1007/s10591-006-9000-4.
Tilly, C. (2002). Stories, Identity and Political Change. Lanham, MD: Rowman and Littlefield. ISBN: 978-1-461-642-602.
Timulak, L. (2007). Identifying core categories of client-identified impact of helpful events in psychotherapy: A qualitative meta-analysis. Psychotherapy Research, 17(3), 305-314. DOI: 1080/10503300600608116.
**Toth, S. L., Rogosch, F. A., Oshri, A., Gravener-Davis, J., Sturm, R. and Morgan-Lopez, A.A. (2013). The efficacy of interpersonal psychotherapy for depression among economically disadvantaged mothers. Development and Psychopathology, 25, 1065-1078. DOI: 10.1017/S0954579413000370.
Truax, C.B. (1963). Effective ingredients in psychotherapy: An approach to unravelling the patient-therapist interaction. Journal of Counseling Psychology, 10, 256-263.
Tufford, L. and Newman, P. (2010). Bracketing in qualitative research. Qualitative Social Work, 11(1), 80-96. DOI: 10.1177/1473325010368316.
Turner, J. (1981). Social support as a contingency in psychological wellbeing. Journal of Health and Social Behaviour, 22, 357-367. Downloaded from http://www.jstor.org/stable/pdf/2136677.pdf on 11.12.2017.
University of Auckland (no date). Questions about thematic analysis. Accessed on https://www.psych.auckland.ac.nz/en/about/our-research/research-groups/thematic-analysis/frequently-asked-questions-8.html on 26.08.2018.
University of Manchester (2014). Manchester Institute of Education Ethical Practice Policy Guidance. Downloaded from http://documents.manchester.ac.uk/display.aspx?DocID=22801 on 29.05.2018.
Usher, R. (1996). A critique of the neglected epistemological assumptions of educational research. In D. Scott and R. Usher (Eds), Understanding Educational Research. London: Routledge. ISBN: 0-415-13131-6.
Vähäsantanen, K., & Saarinen, J. (2013). The power dance in research interview: Manifesting power and powerless. Qualitative Research, 13 (5), 493-510. DOI:10.1177/1468794112451036
Vayrynen, P. (2015). The Lewd, The Rude and The Nasty: A Study of Thick Concepts in Ethics. Oxford: Oxford University Press. ISBN: 978-0-1902-6217-4.
Vermes, C. (2017). The individualism impasse in counselling psychology. Counselling Psychology Review, 32(1), 44-53.
Vogel, P.A., Hansen, B., Stiles, T.C. and Götestam, K.G. (2006). Treatment motivation, treatment expectancy and helping alliance as predictors of outcome in cognitive behavioral treatment of OCD. Journal of Behaviour Therapy, 37, 247-255. DOI: 10.1016/j.jbtep.2005.12.001.
Walker, L.O. and Avant, K.C. (2014). Strategies for Theory Construction in Nursing (5th Ed.). Harlow, Essex: Pearson Education Limited. ISBN: 978-1-2920-2776-0.
Walker, M. and Rosen, W.B. (2004). How Connections Heal. New York: Guilford Press. ISBN: 1-59385-032-8. Wampold, B.E. (2001). The Great Psychotherapy Debate. Mahwah NJ: Earlbaum. ISBN: 0-8058-3202-5.
Wampold, B.E. (2008). Qualities and actions of effective therapists. American Psychological Association. Accessed from http://www.apa.org/education/ce/effective-therapists.pdf on 18.09.2017.

224 of 271
Wampold, B.E. and Budge, S.L. (2012). The 2011 Leona Tyler Award Address: The relationship – and its relationship to the common and specific factors of psychotherapy. The Counseling Psychologist, 40(4), 601-623. DOI: 10.1177/0011000011432709.
Wampold, B.E. and Imel, Z. (2015). The Great Psychotherapy Debate: The Evidence for What Makes Psychotherapy Work (2nd Ed). Hove, East Sussex: Routledge. ISBN: 978-0-8058-5709.
Wark, L. (1994). Therapeutic change in couples’ therapy: Critical change incidents perceived by therapists and clients. Contemporary Family Therapy, 16(1), 39-52. DOI 10.1007/BF02197601.
Watson, V.C., Cooper, M., McArthur, K. and McLeod, J. (2012). Helpful therapeutic processes: Client activities, therapist activities and helpful effects. European Journal of Psychotherapy and Counselling, 14(1), 77-89. DOI: 10.1080/13642537.2012.652395.
West, R. and Turner, L.H. (2003). Muted group theory. Introducing Communication Theory: Analysis and Application. ISBN: 0767430344. Downloaded from http://highered.mheducation.com/sites/0767430344/student_view0/chapter28/index.html on 18.11.2017.
Westra, H.A., DoZois, D.J. and Marcus, M. (2007). Expectancy, homework compliance and initial change in cognitive-behavioural therapy for anxiety. Journal of Consulting and Clinical Psychology, 75(3), 363-373. DOI: 10.1037/0022-006X.75.3.363.
Watts, A. (1960). The World as Emptiness. Accessed from http://project.unicorn.holtof.com/watts/the_world_as_emptiness.htm on 05.09.2018.
White, C., Woodfield, K. and Ritchie, J. (2003). Reporting and presenting qualitative data. In J. Lewis and J. Ritchie (Eds). Qualitative Research Practice: A Guide for Social Science Students and Researchers (287-300). Thousand Oaks, CA: Sage. ISBN: 0761971092.
Williams, D.C. and Levitt, H.M. (2007). Principles for facilitating agency in psychotherapy. Psychotherapy Research, 17(1), 66-82. DOI: 10.1080/10503300500469098.
Wilson, G.T., Fairburn, C.G., Agras, W.S., Walsh, B.T. and Kraemer, H. (2002). Cognitive-behavioral therapy for bulimia nervosa: Time course and mechanisms of change. Journal of Consulting and Clinical Psychology, 70(2), 267-274. DOI:10.1037//0022-006X.70.2.267.
Wilson, J. (1970). Thinking with Concepts. Cambridge: Cambridge University Press. ISBN: 978-0-52109-6010.
Woodhead, E.L., Cronkite, R.C., Moos, R.H. and Timko, C. (2014). Coping strategies predictive of adverse outcomes among community adults. Journal of Clinical Psychology, 70(12), 1183-1195. DOI: 10.1002/jclp.21924.
Woolfe, R. (2016). Mapping the world of helping: The place of counselling psychology. In B. Douglas, R. Woolfe, S. Strawbridge, E. Kasket and V. Galbraith (Eds.), The Handbook of Counselling Psychology (4th Ed, 5-19).
Woolfe R. and Dryden, W. (Eds). Handbook of Counselling Psychology. London: Sage. ISBN: 0-8039-8992-X.
Woolfe, R., Dryden, W. and S. Strawbridge (Eds). (2003) Handbook of Counselling Psychology (2nd Ed). London: Sage. ISBN: 0-7619-7207-2.
Woolfe, R., Strawbridge, S., Douglas, B. and Dryden, W. (Eds), Handbook of Counselling Psychology (3rd Ed), London: Sage. ISBN: 978-1-84787-079-7.
World Health Organisation (2013). Counselling for Maternal-Newborn Health: A Handbook for Building Skills. Geneva: World Health Organisation. Downloaded from https://www.ncbi.nlm.nih.gov/books/NBK304190/pdf/Bookshelf_NBK304190.pdf on 28.10.2017.

225 of 271
Wuest, J. (1994). A feminist approach to concept analysis. Western Journal of Nursing Research, 16(5), 577-586. DOI: 10.1177/019394599401600509.
*Yen, S., Johnson, J., Costello, E. and Simpson, E.B. (2009). A 5-day dialectical behavior therapy partial hospital program for women with borderline personality disorder: Predictors of outcome from a 3-month follow-up study. Journal of Psychiatric Practice, 15(3), 173-182. DOI: 10.1097/01.pra.0000351877.45260.70.
Yi, J.P., Vitaliano, P.P., Smith, R.E., Yi, J.C. and Weinger, K. (2008). The role of resilience on psychological adjustment and physical health in patients with diabetes. British Journal of Health Psychology, 13, 311-325. DOI: 10.1348/135910707X186994.
Yonkers, K.A., Dyck, I.R., Warshaw, M. and Keller, M.B. (2000). Factors predicting the clinical course of generalised anxiety disorder. British Journal of Psychiatry, 176, 544-549. Downloaded from http://bjp.rcpsych.org/content/bjprcpsych/176/6/544.full.pdf on 28.10.2017.
Yu, J.J. (2011). Predicting psychotherapy client dropout from in-treatment client-reported outcome. Texas A&M University Unpublished doctoral thesis. Downloaded from http://oaktrust.library.tamu.edu/bitstream/handle/1969.1/ETD-TAMU-2011-12-10356/YU-DISSERTATION.pdf?sequence=2 on 30.12.2018.
*Zeeck, A. and Hartmann, A. (2005). Relating therapeutic process to outcome: Are there predictors for the short-term course in anorexic patients? European Eating Disorders Review, 13, 245-254. DOI: 10.1002/erv.646.
*Zuroff, D.C., Koestner, R., Moskowitz, D.S., Mcbride, C., Marshall, M. and Bagby, M.R. (2007). Autonomous motivation for therapy: A new common factor in brief treatments for depression. Psychotherapy Research, 17(2), DOI: 10.1080/10503300600919380.
**Zywiak, W.H., Longabaugh, R. and Wirtz, P. (2002). Decomposing the relationships between pretreatment social network characteristics and alcohol treatment outcome. Journal of Studies on Alcohol, 63(1), 114-121. DOI: 10.15288/jsa.2002.63.114.

226 of 271
APPENDICES
Appendix 1: Database search screenshots
Science Direct
PsycInfo
Step one
Step two

227 of 271
Step Three

228 of 271
Sage Journals
Appendix 2: Primary study inclusion criteria (a) quantitative, qualitative, mixed method outcome studies, meta-analyses or
systematic reviews of outcome studies that identify client factors that mediate,
moderate, predict or are otherwise associated with psychotherapeutic outcomes
(no theory papers)
(b) dated 1960 or later
(c) published in English in a peer-reviewed journal, and freely obtainable through the
University of Manchester library or Google Scholar
(d) participants aged 18+
(e) studies of treatment participants or completers (not predictors/mediators of early
termination or drop-out)
(f) face-to-face therapy modalities including group, family, couples and individual
psychological therapy (excluding on-line modalities)
(g) bona fide therapy and psychoeducation (excluding pure self-help)
(h) delivered by trainee or qualified practitioners
(i) inpatient, day patient, outpatient, community, home, educational and
organisational settings
(j) clients in voluntary therapy (excluding people receiving mandatory or
probationary treatment or those legally detained for mental health treatment)

229 of 271
(k) psychological or behavioural presenting problems including addictions
(excluding health promotion therapy such as HIV programmes or pain
management)
(l) client factor is demographic, behavioural, cognitive, emotional or experiential
(excluding neurological, learning, communication or health conditions)
(m) client factor is a clearly defined personal variable (e.g. demographic
characteristics), process variable (i.e. activity or learning initiated within therapy)
or extra-therapeutic variable (e.g. events and circumstances) whose positive or
negative effects (i.e. mediation, moderation, prediction, or other association) on
outcome of the intervention were demonstrated through the use of recognised
statistical methods in quantitative studies; or client quotes in qualitative studies
(n) the interaction between outcome and the associated client variable in
quantitative studies was statistically significant to p < 0.05
(o) the predictor/mediator is a client-originating circumstantial, demographic,
psychological, cognitive, or behavioural variable, not a variable that is dependent
on therapy configuration, for example, client satisfaction with therapy. To further
illustrate this distinction, for example where client marital happiness is a positive
predictor for reduced risk of depression relapse, this is a client-originating factor;
but where client minority status is a positive predictor of outcome only in therapy
groups comprised of more than half minorities, this is a treatment process factor

230 of 271
Appendix 3: 49 studies extracted from 14 reviews/analyses

231 of 271
Appendix 4: Research data extraction spreadsheet All column headings in data extraction spreadsheet
Date of extraction No. of P’s Setting Significance of
interaction b/w
OM and
predictor
variables
Search source % white/cauc Inpt/day pt/
outpt
Negative
predictors
Included/excluded % female Staff profile Positive
predictors
Reason for
exclusion
Mean age Time points for
OMs
Negative
mediators
Authors %
Married/cohab
Type of design Positive
mediators
Year of pub. Education Analysis Negative
moderators
Title % in
employment
Primary OM Positive
moderators
Journal Presenting
issues
Outcome
variable
Associated
w/neg outcome
Issue, pages, DOI Therapy model Threshold of
improvement
Associated
w/pos outcome
Country Therapy
modality
Predictor OM TA not assoc
w/OM
Quant/qual/mixed # sessions/tx
length
Predictor
variable
TA assoc w/OM
Screenshot of a portion of the research data extraction spreadsheet
Green = excluded after full-text review
White = included after full-text review – studies with no follow-up data
Yellow = included after full-text review – studies including follow-up data
Pink = column titles

232 of 271

233 of 271
Appendix 5: Quality control exclusion criteria (1) The predictive client factor was an aspect of the presenting problem, for example
specific symptoms (e.g. avolition as a predictor of outcome in treatment for
schizophrenia), because these conflate the independent and dependent variables in the
causal argument
(2) No therapy was mentioned; less than 3 sessions of therapy were provided; or length of
therapy is not mentioned
(3) The outcome and/or predictor variable or measures were not specified
(4) The outcome or client variable was partially or wholly judged by the treating therapist,
introducing unacceptably high risk of bias
(5) the relationship between client factors and treatment, or client factors and outcome, was
not discussed
(6) where studies by author(s) with same findings were already included
Additionally in quantitative studies further exclusions were made where:
(7) outcome or predictor measures were not named
(8) outcomes were measured using tests with disputed validity (i.e. Rorschach)
(9) treatment comparison studies that found the predictor variable had differential effects
depending on type therapy (indicating the client factor was confounded with a co-
occurring process mediator)
(10) the predictor variable could not be sufficiently distinguished from a process
variable, for example where a predictor was not a baseline measurement; or where a
mediator represented a therapeutic technique (for example, mindfulness skills as a
predictor of outcome in mindfulness-based cognitive therapy)
(11) the design (e.g. cross-sectional) or statistical analysis (e.g. simple correlation)
inadequately explained the relationship between client factor and outcome
(12) time points for outcome measures were not provided
Additionally, in qualitative studies further exclusions were made where:
(13) the analytic focus was on therapist not client action
(14) the analytic focus was on the ‘meaning of change’ rather than participants’
understanding of how they made change happen

234 of 271
Appendix 6: Tests, variants and causal syntax chart for moderators Moderators are qualitative or quantitative variables that influence the direction or
strength of relationship between the independent and dependent variables in
experimental psychological therapy studies (Baron and Kenny, 1986). Conceptually,
moderators help identify for whom and under what circumstances therapies have
different effects (Kraemer, Wilson, Fairburn and Agras, 2002). Moderators tend to be
contextual factors such as client or therapist demographics, state/trait characteristics,
competencies, enduring attitudes, or extratherapeutic events and circumstances.
In causal syntax, moderators exist prior to the commencement of the independent
variables they interactively moderate, in the following order:
[Moderator A: Extratherapeutic, client or therapist state/trait characteristic] pre-exists the
application of [Independent variable X: client and/or therapist therapeutic activity] and
exerts [specific impedance or facilitation quality C in relation to a control or comparison
group] on B’s potential to achieve [Dependent variable Y: outcome of interest]
Using variables from an actual study (Beutler et.al. 2011b) moderation causal syntax is
illustrated here:

235 of 271
Tests for moderation
Baron and Kenny (1986) describe moderator data types as either continuous, for
example age; or categorical, for example gender. It can however be argued that a
variety of psychologically relevant observable human traits are categorised according to
potentially oppressive, oversimplified, biased, irrelevant or value-laden social
constructs. But for statistical purposes, tests for moderation where the independent and
moderator variables are categorical or continuous are conducted using hierarchical
multiple regression. Where both variables are categorical, ANOVA can be used. The
significance of continuous data moderators can be calculated with single degree of
freedom F-tests; and of categorical moderators with multiple degrees of freedom
omnibus F-tests (Frazier, Tix and Barron, 2004). More detailed statistical procedures for
moderator-outcome research can be found in Baron and Kenny (1986); Hoyle and
Robinson (2004); and Frazier, Tix and Barron (2004).
Variants

236 of 271
Frazier, Tix and Barron (2004) describe three moderator interaction patterns: (a)
‘enhancing,’ where treatment (or other independent variable) and moderator effect the
outcome in the same direction, and together lend a stronger-than-additive effect; (b)
‘buffering,’ where the moderator weakens the effect of the independent variable; and (c)
‘antagonistic,’ where treatment (or other independent variable) has the same effect on
outcome but in the opposite direction. Hoyle and Robinson (2004) add a further
interaction, (d) ‘crossover,’ where the independent variable has opposite effects on the
dependent variable at the two extreme ends of the moderator’s expression.
Categorical moderators are variables that have certain effects in certain therapies and
not others. For example a client who likes observing and documenting their daily
activities might gain more insight into how to change certain behaviours by doing self-
monitoring in CBT, than might someone who finds self-monitoring difficult or boring.
Continuous moderators are variables that have the same effects regardless of the type
of therapy. For example a client who has a firm belief that God loves him may be
emotionally protected by this in difficult times regardless of secular theories of change
his therapist might offer him.
The trajectory of moderator effects might be described as ‘linear’ (i.e. increase in effect
is proportional to increase in application of the moderator); ‘quadratic’ (i.e. moderator
effects are compounded either by time or strength of application); or ‘stepped’ (i.e. time
or strength of application yields a smaller then larger effect, or vice versa) (Baron and
Kenny 1986).
Causal syntax charts
The following chart shows illustrative examples of moderator relationships from four
actual studies.
Study
A. Moderator
(pre-existing
circumstance
that impacts
relationship
between B and
D)
B.
Independent
variable (input
element)
C.
Direction or
strength of
moderator
impact
D.
Dependent
variable
(measured
outcome of
interest)

237 of 271
Example 1:
Beutler et.al.
2011b
Therapist
directiveness
[Therapist factor]
Client reactivity
[Client factor]
Facilitates
Client tardiness
for appointments
Example 2:
Lorenzo-Luaces,
DeRubeis and
Webb, 2014
Number of
previous
depressive
episodes
[Client factor]
Therapeutic
alliance
[Process factor]
Reduces
Depressive
symptom change
Example 3:
Burns and
Nolen-
Hoeksema, 1991
Client
willingness to
learn new coping
strategies
[Client factor]
CBT for affective
disorders
[Therapy factor]
Enhances
Degree of
improvement in
mood
Example 4:
Leibert, Smith
and Agaskar
(2011)
Level of social
support
[Extratherapeutic
factor]
Lower initial
symptom level
[Client factor]
Slows
Change in
symptom level
Appendix 7: Tests, variants and causal syntax chart for mediators Mediators are transformational mechanisms which are activated or changed by events
in the therapeutic process in a way that at least partially accounts for the outcome of the
therapy. Some researchers define mediating processes as correlated with treatment
type, and that mediators are of necessity treatment effects (e.g. Wilson, Fairburn,
Agras, Walsh and Kraemer, 2002). However other researchers allow for mediators to
represent client response or activity in relation to treatment effects (e.g. Berking,
Neacsiu, Comtois, and Linehan 2009), such as cognitive (e.g. insight), emotional (e.g.
dissonance) or behavioural factors (e.g. task diligence) (Baron and Kenny, 1986) that
offer explanatory value about why therapy works (Johansson and Høglend, 2007).
Descriptions of mediation should explain the relational role of the mediator between
relevant variables, for example, “early homework compliance mediates the relationship
between expectancy for anxiety change and initial change in CBT” (Westra, Dozois and
Marcus, 2007, p. 363). Descriptions should also indicate that mediation occurred prior to
outcome, thereby ensuring that the mediator was a result of therapeutic activity.

238 of 271
Building on the A-X-C-Y causal sentence developed in Appendix 6 above, mediators
are introduced as follows:
[Moderator A: Extratherapeutic, client or therapist state/trait characteristic] pre-exists the
application of [Independent variable X: client and/or therapist therapeutic activity].
Moderator exerts [specific impedance or facilitation quality C in relation to a control or
comparison group] on X’s potential to promote [Mediator D: client transformational
thoughts, feelings and behaviours] which partially or completely cause [Dependent
variable Y: outcome of interest]
It is important to note that the syntax above is idealised. The impact of moderators and
mediators are not commonly examined in the same study, although they undoubtedly
simultaneously exert influence on each other and on outcome. The syntax diagram
shown here is not based on a specific study:
Lemmens, Muller, Arntz and Huibers (2016) explain various difficulties in demonstrating
causal relationships between change in the mediator and change in outcome. Where
researchers describe a mediator only in relation to its outcome but not the antecedent

239 of 271
variable it mediates, the relationship is predictive rather than mediating. The majority of
quantitative studies included in this concept analysis describe a predictive relationship
between independent and dependent variables. Only 9.5% (n=6) identified mediators of
change and, interestingly, none identified moderators.
Tests for mediation
Tests of mediation are generally carried out via multiple linear (for quantitative
measures) or logistic (for binary measures) regression analyses; multiple regression
over four steps, or structural equation modelling. These methods are explained in detail
in Frazier, Tix and Baron (2004). In order to establish that change in the mediator
precedes change in the outcome it is important that mediator and outcome are
assessed at multiple points in therapy, not just pre-and post (Johansson and Høglend,
2007).
Mediation is suggested if (a) outcome is significantly related to treatment; (b) treatment
is significantly related to changes in the mediating variable; and (c) the relationship
between treatment and outcome decreases or goes to zero when change in the
mediating variable is entered into the equation (Baron and Kenny, 1986; Dingemans,
Spinhoven and van Furth, 2007).
Variants
While moderators and mediators have distinct and separate roles in influencing
outcomes, Frazier, Tix and Barron (2004) describe two ways mediators and moderators
can interact in certain circumstances: moderated mediation, and mediated moderation.
In moderated mediation, a mediated relation between input and outcome varies across
levels of a moderator. Using smoking cessation in this fictional example, the moderator
is client quit-self-efficacy based on the number of previous failed attempts to quit. The
client undertakes a group-based smoking cessation programme (the input). One of the
treatment mediators is social encouragement to quit provided by group members. The
higher the number of previous failed quit attempts, the less beneficial impact social
encouragement has on the client, and the lower the likelihood of permanent abstinence.

240 of 271
In mediated moderation, a mediator variable accounts for the relation between the
moderator and outcome. Reusing the smoking cessation example where the moderator
remains the client’s quit-self-efficacy based on number of previously failed attempts,
another mediator in the group programme is targeted self-efficacy enhancement
techniques, which interacts with the moderator’s influence on smoking abstinence (de
Hoog, Bolman, Bernt, Kers, Mudde et.al., 2016).
Causal syntax charts
The following chart shows illustrative examples of mediator relationships from actual
studies.
A.
Moderator
(pre-
existing
circumstan
ce that
facilitates
or impedes
B’s impact
on D and
thus E)
B.
Independe
nt variable
(input
element)
C.
Direction or
strength of
moderator
impact on
Mediator D
D.
Mediator (client
thoughts,
feelings and
behaviours
arising or
changing as a
result of therapy
that partially or
completely
cause E)
E.
Dependent
variable
(measured
outcome of
interest)
Example 1:
Dingemans,
Spinhoven
and van Furth
(2007)
Cognitive
behaviour
therapy for
binge
eating
[Therapy
factor]
Reduction in
weight concern
Abstinence
from binge
eating
Example 2:
Wilson,
Fairburn,
Agras, Walsh
and Kraemer
(2002)
CBT and
IPT for
bulimia
[Therapy
factor]
Reduction in
dietary restraint
Reduction
in binge
eating and
purging

241 of 271
Example 3:
Moscovich,
Hofmann,
Suvak and In-
Albon (2005)
Passage
of time
[Extrather
apeutic
factor]
Change in social
anxiety
Change in
depression
Example 4:
Teasdale
et.al. (2002)
Cognitive
therapy
and
mindfulnes
s cognitive
therapy
[Therapy
factor]
Change in
accessibility of
alternative
perspectives
Reduction
in risk of
relapse
In Example 4 (Teasdale, et.al. 2002) low meta-cognitive awareness is a moderator of
outcome which is directly addressed by the mediator, but the researchers do not
discuss or analyse its moderating impact on outcome, only the possible mediating
impact of improving this in therapy.
Appendix 8: Tests and causal syntax chart for predictors Tests
Predictors are calculated using multiple regression analyses. Predictors should be
measured at least at the outset and end of therapy.
Causal syntax charts
The following chart shows illustrative examples of types of predictors from actual
studies.
Study Predictor
variable
Type of
therapy
Time
predictor
was
measured
Function
of
correlation
Outcome
Example 1:
Kindt,
Buck,
Arntz and
Conceptual
processing
[client skill
CBT
Imagery
Rescripting
for PTSD
Pre- and
post-
treatment
Positive
Decrease in
PTSD
symptoms
after therapy

242 of 271
Soeter
(2007)
developed
in therapy]
Example 2:
Dingemans
,
Spinhoven
and van
Furth
(2007)
Palliative
reacting
i.e.
eating/drin
king in
response
to stress
[client
factor]
CBT for
binge
eating
disorder
Pre-, mid-
and post-
treatment
Negative
Abstinence
from binge
eating at end
of therapy
Example 3:
McCrady,
Hayaki,
Epstein
and Hirsch
(2002)
Quality of
pre-
treatment
marital
relationship
[extrathera
peutic
factor]
Alcohol-
related
behavioural
couples
therapy for
men
Pre- and
monthly
post-
treatment
for 6
months
Positive
Abstinence
from drinking
alcohol at 6
month follow-
up
Example 4:
Rounsavill
e,
Weissman
and
Prusoff
(1981)
Psychother
apy
techniques
exploratory
, reflective
and
directive
[Therapy
factor]
Psychother
apy for
depression
Pre-therapy
and at 16
weeks after
commence
ment
Zero
Improvement
in depressive
symptoms

243 of 271
Appendix 9: Participant recruitment poster
Study on how people make counselling work
Are you aged 18+?
Will your counselling finish in May, June or July 2016?
After your counselling is finished, are you interested in confidentially sharing with a
researcher your experience of desired changes happening or not happening?
If you answered YES to these questions, you may be eligible to participate in a Counselling
Psychology doctoral research study.
The purpose of this research is to learn directly from counselling clients how and why
they were able (or not able) to make desired changes in life. And to explore personal and
social factors that can be helpful and unhelpful when trying to make desired changes in
life.
Research interviews take approximately 30-60 minutes of your time and will be held at
Oakwood House, Davenport. You will need to spend a further 15-30 minutes reviewing the
researcher’s transcript/analysis of your interview sometime after your interview.
If you are eligible to participate you will be given a participant information form and a list
of questions to think about in advance of your interview. Your informed consent will be
obtained before commencing. Some demographic details will be collected.
Contact: This study is being conducted by Caroline Vermes, MA, M.Ed, MBACP (Accred.)
who is undertaking the Doctorate in Counselling Psychology at University of Manchester.
You can contact her at [email protected]. Alternatively speak to
your therapist who will pass on your details to the researcher.
Ethical approval granted by University of Manchester Institute of Education

244 of 271
Appendix 10: Participant information sheet
Personal and social factors associated by clients
with change and non-change since the commencement of therapy
Participant Information Sheet
You are being invited to take part in a research study as part of a student project on the Doctorate in
Counselling Psychology. Before you decide to participate it is important for you to understand why the
research is being done and what it will involve. Please take time to read the following information carefully
and discuss it with others if you wish. Please ask if there is anything that is not clear or if you would like
more information. Take time to decide whether or not you wish to take part. Thank you for reading this.
Who will conduct the research? Caroline Vermes
Title of the Research: Personal and extratherapeutic factors associated by clients with change and non-
change since the commencement of therapy.
What is the aim of the research? This study is designed to explore and analyse how psychological therapy clients describe their own efforts to make desired changes. It aims to understand how and what personal and social resources clients use to help themselves; and what sorts of obstacles clients describe as getting in the way of making desired change. The study seeks a better understanding of how clients work towards therapeutic outcomes. The results may ultimately seek to extend theory about client agency. This will help educate practitioners so they can adapt therapy to identify, work with and support client self-healing capabilities; and understand and address barriers to well-being.
Why have I been chosen? You responded to an invitation to participate. You may have been selected
on the basis of demographic characteristics requested in the call for participants.
What would I be asked to do if I took part? You will take part in a confidential interview for 30 - 60
minutes with the researcher about recent desired changes you may and may not have made in your life.
About a week in advance of your interview, to help you prepare, you will be sent a short list of questions
to think about. Your thoughts about these questions will be discussed in the interview. Afterwards, within
12 months of your interview, you will also be asked to read and comment on a summary of the
researcher’s analysis of the anonymised information you and others have shared. This is likely to happen
over email so you will be asked to supply an email address that you access regularly. If you do not use
email, another communication method will be agreed with you. Reading and commenting on the research
summary may take 15 – 60 minutes depending on how much time you want to give it.
Are there any risks if I participate? There is a small chance some participants may become upset when
discussing their thoughts about the research questions. This could happen before, during and/or after the
interview. It may be related to thinking about or describing any difficulties encountered when trying to
make desired changes in life. The researcher will check this with you in the interview. You will be given
contact details for support services, along with the researcher and research supervisor’s contact details,
should you need to further discuss your reactions to participating in this research.
What happens to the data collected? The interview will be digitally audio-recorded by the interviewer.
The audio file will be stored on securely encrypted memory stick that can only be accessed by the
researcher. The recording will be transcribed and anonymised. Transcripts will be analysed by the

245 of 271
researcher for salient themes. The audio files will be kept securely in electronic storage for up to 5 years
by the researcher then will be permanently deleted by the researcher.
How is confidentiality maintained? Participant identifying information will be anonymised upon
transcription. This means any personal information you share in your interview that could identify you will
be removed before the data is analysed. Basic demographic information including gender, age range,
ethnicity and education will be attached to the transcript for differential analysis purposes. The information
you share with the researcher is confidential. The researcher cannot disclose to anyone that you
participated in the research. However, if you disclosed in your interview any information that suggested
that a child or adult was at risk of neglect or abuse, the researcher would have an ethical responsibility to
report some details to the appropriate authority. Quotes from your interview may be used in the final write
up to illustrate themes or other important findings. These quotes will not include any personal information
that could identify you.
What happens if I do not want to take part or if I change my mind? It is up to you to decide whether
or not to take part. If you do decide to take part you will be given this information sheet to keep and be
asked to sign a consent form. If you decide to take part you are still free to withdraw up to the date that
data from your interview transcript is entered into analysis software 30th September 2016.
Will I be paid for participating in the research? No
What is the duration of the research? 1 x 30-60 minute interview. Then, within 12 months of your
interview you will be sent one or two follow up emails asking for your comments and views on the work.
This may take 15-30 minutes depending on how much time you want to spend on it.
Where will the research be conducted? By prior arrangement at Oakwood House, 104 Kennerley
Road, Stockport, SK2 6EY
Will the outcomes of the research be published? This research may be submitted for publication. It
may also form background research for further research which may be submitted for publication.
Criminal Records Check (if applicable) DBS clearance has been obtained on behalf of the researcher
by the University of Manchester.
Contact for further information [email protected]
What if something goes wrong? If there are any issues regarding this research that you would prefer
not to discuss with Caroline Vermes, please contact the research supervisor Terry Hanley on 0161 275
8815 or [email protected]. If there are issues with the research you wish to discuss with
the researcher, please contact Caroline Vermes on 0786 333 7965 or

246 of 271
Appendix 11: Interview schedule Form A:
1. Please describe one positive or desired change that has happened in your life since you
started therapy
2. Why do you think this change happened?
3. Please describe one thing that hasn’t changed in your life as you hoped since you
started therapy
4. Why do you think this change did not happen?
Form B:
1. Please describe one thing that hasn’t changed in your life as you hoped since you
started therapy
2. Why do you think this change did not happen?
3. Please describe one positive or desired change that has happened in your life since you
started therapy
4. Why do you think this change happened?

247 of 271
Appendix 12: Participant consent form
CONSENT FORM
If you are happy to participate, please read, tick the boxes and sign the consent form below:
1. I confirm I have read and understand the attached information sheet about the above
study and have had the opportunity to consider the information. I have had the
opportunity to ask questions and have had these answered satisfactorily
2. I understand that my participation in the study is voluntary and that I am free to withdraw
at any time up to the stipulated deadline without giving a reason
3. I consent to my therapist passing my contact details to the researcher
4. I understand that the interviews will be audio-recorded
5. I agree to the researcher creating an anonymised transcript of the audio-recording
6. I agree to the transcript being subject to research analysis
7. I agree to anonymised quotes from my interview appearing in written versions of the
study
8. I agree that any data collected may be published in anonymous form in academic books
or journals
I agree to take part in this project
________________________ _______________ ______________________________
Name of participant Date Signature
________________________ _______________ ______________________________
Name of researcher Date Signature

248 of 271
Appendix 13: Transcript portion [blue highlighted text included in concept analysis]
CV: So to kick off the interview [P4] is there anything in particular that hasn’t changed as you hoped it
might, since you’ve done your therapy?
P4: So yeah, I’ve had a think about this, they’re quite probing questions actually. The main thing…is it
okay to start with a bit of background about me?
CV: It certainly is. And only go as far as you want to with anything that we’re talking about.
P4: Okay. So I was referred through to [service A] by my GP because for quite a long time I’ve had
probably underlying [D3] and [D2] issues. So, I’ve had quite a lot of change over the past few months. So
I decided at the start of the year that I would need...that I probably needed some additional support to
try and break the cycle for good. Because I’ve been through cycles of counselling etcetera before and
possibly not taken it a seriously as I should have done, or given as much into it as I should have done in
the past. So, (sigh) but off the back of that, having come for therapy or counselling to tackle [symptom
of D3] and the associated [D3], the main thing that hasn’t gone as well as I want was the overcoming
[D2].
So I still don’t think that I manage that particularly well. And I think I still have times when I feel quite
overwhelmed with that feeling of anxiousness. And I’m hoping with time, because I, trying to think when
I started with [therapist 4A], it was maybe back in March? And I think…at the time, yeah, it’s probably
got a little bit better. But not to the extent that I would have hoped it would have done. And I’m hoping
now my one-to-one sessions have stopped with [therapist 4A] I’ll go into group sessions for overcoming
[D2] and that will potentially help tackle that a little bit more head on. And also dealing with interacting
with other people that have similar issues might actually be quite useful for me because I’m a bit of a
“heart on my sleeve” type of person. So, I like to talk things through. So I think that…and bounce off
other people, so I do think potentially that will be maybe a more conducive environment to help me get
a better balance over those issues. But I think certainly that would be the one key thing for me, that.
CV: So reduce [D2], overall, that would be something you would hope to have gotten out of therapy, and
feel like you still got a ways to go with that.
P4: yeah, yeah, maybe I put too much of an expectation on what I’d hoped to achieve. And maybe it…I
think part of it is untangling the two issues, although they are very interlinked. I think that, yeah, the

249 of 271
[D2], I’d hoped that that might…because I’d always explain my [D2] on (clicking fingers) causing the [D3].
So, almost like the emotional crutch. So I’d have hoped, and it’s been weird in some sense because, I’ll
come onto why, the thing that has got better, that my [D3] is more under control, but my [D2] is still
quite high.
CV: Yes, yes. So you untangled them.
P4: So that’s a good thing, which I’ll talk a little bit more about later. So I think I’ve been able to separate
the two issues which have been good. But the one that’s benefitted the most over what, the past four-
five months, is the [D3] side of things. The bit that’s still quite bad for me is the [D2].
CV: Do you have any thoughts about why the [D2] is still as bad as it is at this point?
P4: yes. So I think it’s because I’ve had quite a lot of transition recently. I’ve been, I’ve changed roles
recently. I probably put myself under an awful lot of pressure both from an academic and from a
professional point of view. I’ve just moved into quite a senior role. And having left, I was with [previous
workplace], I left [previous workplace] after seven and a half years. So it’s where I grew up, [previous
workplace], from when I graduated. So it’s been quite a big step for me to leave that support network
behind. And moving somewhere that’s completely unknown, and operating at a higher professional
level. I think almost because of those pressures that have been put on, that’s probably kept my [D2] up
here (demonstrating with hand). And maybe had I not gone through that at the time I’ve been going
through therapy, at the moment I may not have had, it may have come down, but I don’t know.
CV: It may have come down but you don’t know. But you’re certainly thinking that the therapy
coinciding with this significant change in your workplace social support, and your workplace
expectations may have something to do with the [D2] being still quite profound?
P4: Yeah. I think so. I think, well, I haven’t learned yet to be able to drop the expectations that I have on
me. And again, that’s compounded by the fact that (clicking fingers) I want to be able to perform well
and create a good impression where I’ve gone. So that’s I think, part of the…it’s all tangled up, but yeah.
And I haven’t learn to re-programme yet. My, almost setting my expectations of myself lower. Not that
necessarily anyone else has that high expectation of me.
CV: Okay, yes. So you see this as coming actually from inside of you, that even though you’ve been
through these external changes, leaving [previous workplace], starting your new job, that there’s
something going on within you that you want to recalibrate.

250 of 271
P4: Yes. And I think I struggle with that, and I don’t know why. I think that I’m a quite practical person
generally. But it’s something that, I don’t know, I’m scared of failing but then I set myself up to fail.
Which is probably (laughing) where the [D2] comes from!
CV: (laughing) But you push yourself to, or your expectations are so high that then there is a chance that
you might not meet them. And then that causes more [D2].
Appendix 14: Transcription considerations I gave considerable thought ‘for and against’ replacing references to formal diagnostic
terms participants used to describe problems they sought counselling help for (such as
‘depression,’ ‘anxiety,’ ‘bulimia’ and so on). There were several reasons I wanted to
replace diagnostic terms with codes. A practical reason was to enhance participant
anonymity. An epistemological reason was that this research is expressly not about
understanding how therapists work with clients with particular diagnoses - a focus that I
believe serves the politics and economics of the psy-professions. I did not want readers,
likely to be psy-professionals, to be tempted to make assumptions about the
participants’ therapeutic journeys, based on particular knowledge and views about
specific diagnoses and their treatment. Ideological reasons to replace diagnostic terms
is that they may obscure the contexts in which my female participants described their
efforts to overcome health and emotional difficulties (Porter 2002); or may pathologise
common female responses to demanding maturational journeys (Chesler, 1972; Brown,
1994). Removing diagnostic terms could assist my intention to contribute to theory
about the complexities of people’s efforts at life improvement “beyond the individualizing
and pathologizing force of psychological categories” (Farley, 2017).
On the other hand, I also had two reasons not to replace participant references to
diagnostic labels. The first was that even with diagnosis terms removed, there was
sufficient description in most interviews of participants’ symptoms and therapeutic goals
that diagnoses might be guessed by a psychologically trained reader. Additionally, all
participants chose to name at least one diagnosis without any prompting from me, and
chose to describe their experience of its impact on their life, so I questioned my use of
authorial power to obscure terms that were clearly important to participants.

251 of 271
I ultimately opted, on the balance of arguments above, to replace diagnostic terms with
coded descriptors. No participant commented on this in their transcript check.
The final transcripts were not wholly verbatim documents. I made three significant
modifications from the spoken to written words of the participants:
A. Locally accented pronunciations were transcribed in standard written English, for
instance the spoken term, “It sounds good that, dunnit?” was transcribed as “It
sounds good that, doesn’t it?” On the other hand, local sentence structure and
word choice were unaltered, for instance, “It were wrote all over her face.”
B. Participant speech fillers were removed, including “um” and “you know.” “Sort of”
and “kind of” were removed where they were qualifiers that did not change the
meaning of the words they preceded; but they were kept where they indicated “a
type of something.” “Like” was removed where it acted as a filler, for example ‘Do
you mean you, like, didn’t stop at the red light?’ However, it was retained where it
was a preposition meaning “for example;” where it was an adjective meaning
“similar;” where it was a verb indicating “finds agreeable;” or where it indicated
the participant’s introduction to retelling someone else’s speech, for example, ‘My
sister was like, ‘Are you coming down the pub with us?’ Response tokens such
as “yes” and “mm-hmm” were also removed from my interjections where they
were simply given as encouragement to participants’ narrative, or indicated that I
was following what they were saying.
C. Punctuation was added. Where a participant spoke in run-on sentences, these
were broken down to briefer segments. For example, the following transcribed
text from Participant 4 was actually spoken as one sentence: ‘I probably put
myself under an awful lot of pressure both from an academic and from a
professional point of view. And I’ve just moved into quite a senior role. And
having left…I was with [previous workplace], I left [previous workplace] after
seven and a half years. So it’s where I grew up, [previous workplace], from when
I graduated. So it’s been quite a big step for me to leave that support network
behind. And moving somewhere that’s completely unknown, and operating at a
higher professional level.’ While adding punctuation I was careful to retain the

252 of 271
meaning and substance of what was said in the conversations, and to be
respectful of participants’ intentions at all times.
Interview texts were tidied or “denaturalised” (Oliver, Serovich and Mason, 2005,
p.1277) in this way for two reasons. First, I was interested in what people said about
their experiences, thoughts, beliefs, feelings and actions, rather than the mechanics of
how they said it. As I planned to include that a substantial number of participant quotes
in my findings and analysis chapters, the addition of punctuation and removal of filler
words improved the readability of the text (Kvale, 2007). Secondly, this editing was
intended to make reading their transcripts more agreeable to participants. My decision
to edit the text this way was reinforced when I sent the first transcribed interview to
Participant 1 as a completely unredacted verbatim document. In her reply, she
expressed disbelief that the transcript accurately replicated her speech patterns:
‘There's one thing that jumps out at me, which is all the ‘um’s’ and ‘kind of’s.’ At first I
thought maybe I just wasn’t aware of how much I said it.’ I did not want to inadvertently
adopt a position of ‘academic power’ over my participants by presenting them with
transcripts that could distract them from checking that I’d accurately transcribed their
narrative; or worse, that could cause them dismay about their conversational speech
patterns. “Our scholarly representations of those performances, if not sensitively
presented, may constitute an attack on our collaborators’ carefully constructed sense of
self” (Borland, 1991, p.71). I explained to P1 I would remove the filler words. After this, I
tidied each text as above before sending completed transcripts to the remaining
participants.
Addition of descriptive statistics and key attributes to transcripts
Date of interview
Length rounded to the closest minute
Total word count
Words per minute (combined speakers)
Number of participant mentions of different types of helping professionals and
services (to assist with analysis of how self-directed versus professional-directed
participants were)

253 of 271
Appendix 15: Interview summaries
1. Dana 6732 words 48 mins (140.25 wpm) 06.06.2016
The change in practical terms:
Sleeping well
What brought this about?
[Attended counselling, used self-help materials]
Sleep inducing medication
Not watching t.v. before bed
Trying not to worry
Confidence arising from landing the perfect job
Yoga
Homeopathy
Got to a really bad place – calling Samaritans
The non-change in practical terms:
Sexual intimacy with partner
Obstacles to change?
[relative]
History of health issues
Negative change in self-image
[relative]
2. Ella 8886 words 50 mins (177.72 wpm) 16.06.2016
The change in practical terms
No more D3 behaviour
Growing the angel, reducing the devil
Stopped dependence on others pushing me. Doing it for myself and others
What brought this about?
[Attended CBT, service A programme, participating in a combination of modalities]

254 of 271
Got to a really bad place – coma
Not letting things bother me
Taking better care of self, thinking more clearly
Changed my goals from unrealistic to healthy
Journaling to understand personal susceptibilities
Change in ‘mindset’ (CBT language)
Pushing myself out of (dis)comfort zone to go out socially
Diversion from upsetting thoughts
Setting self-limits
Becoming part of the group
Being loved and needed
Family party
Awareness of ageing process, time ticking, need to be a grown up
Seeing others not getting better; not wanting to be like others
Creating a different version of me
I have to pick myself up rather than relying on others
Stopping avoiding taking care of myself by over-doing for others. Caring more for others by taking better
physical and emotional care of myself
The non-change in practical terms
Still experiencing symptom of D4
Obstacles to change?
This won’t change, I’m stuck with this (it’s not a treatment shortcoming)
Had [D2] since I was a child
Resignation/acceptance that I might be stuck with this
3. Luka 4113 words 30 mins (137.10 wpm) 14.07.2016
The change in practical terms
In remission from disease
Self-acceptance

255 of 271
What brought this about?
[Attended CBT, analytic and online therapy, support group and used self-help materials]
Decision to just deal with it
Got to a really bad place – emergency GP
Asked sister if I was ill and she said yes
Sought help from a range of sources
It just happened naturally, subconsciously; but also through application of “techniques” e.g. goal
modification to more realistic self-care
Non-change in practical terms
Underlying issues unchanged
Obstacles to change
Sporadic attendance
I was distracted, not focussed in sessions, did not know what to say
No in-person relationship with therapist
4. Kyra 7885 words 48 mins (164.27 wpm) 14.07.2016
The change in practical terms
Separating D2 from D3 as different problems to work on
What has brought this about?
[Telephone and online counselling an advantage as not “fluffy,” helps contain emotion]
Realising I need to make life changes – frustrated with the unwell cycle
Wanting the option to have children
Not wanting to lose relationships with loved ones especially partner
I don’t want to be defined by a problem that has caused multiple emergency hospitalisations (don’t
want to seem vulnerable)
New job, need to be my best
Seeing the problems as a “snappable cycle”
Going to the GP as an entry point
Self-monitoring and reflective learning
Non-change in practical terms

256 of 271
D2 not reduced enough
Obstacles to change
Difficult to change “habits of a lifetime”
Still need to understand and explore causes of D2
Think a group might help better than 1:1
Higher professional expectations in new job
High personal expectations
I’m scared to fail but then set myself up to fail
5. Lucy 7654 words 51 mins (151 wpm) 17.08.2016
The change in practical terms
Getting passion for life back
Getting relationships with friends, family and husband back.
What helped bring this about
Realising I’d become isolated and lonely due to D1
Fear of losing relationships/wanting to preserve relationships
Sharing problems with others; allowing others to help
Seeing I have a choice how to behave, how to look after myself
Physical health deterioration – health crisis
Friends interested in psychology
Self-reflection
Taking ownership of recovery
Reading recovery stories, other people’s experiences in print
Other people’s experiences – known friends
Use of social media support groups
Switching/converting drive for illness to drive for wellness
Using certain character traits as a force for good rather than a force for self-destruct e.g. goal-oriented;
perfectionistic; stubborn
Facing the problem; stopping denial; challenging myself to change old habits and beliefs

257 of 271
Turning point: Friend wanting to talk to me about the problem. Going to the GP
Non-change in practical terms
Not overcome D4
Obstacles
Complacency
Denial
False sense of security due to some improvement
The D4 still is strong in my thoughts and feelings
Fear of the unknown
6. Zoey 6609 words 51 mins (129.59 wpm) 22.08.2016
The change in practical terms
More self-awareness. Understanding why I react certain ways and why I have behaved certain ways in
the past. Understanding how D2 has been present in my life. Seeing D2 as a problem and isolating it
from other issues
What helped bring this about
[Opening up to therapist and trusting them after a difficult start; using CBT techniques]
Confiding in friends.
Reading The Empathy Trap.
Put things in boxes and label them
Online support group
Reflective/autobiographical writing in blog
Non-change in practical terms
How people hurt me and how I react to this in a childlike way – I just put it to one side and keep going.
Obstacles/perpetuators
Friends hurt me. They don’t know how to react to my disclosure about abuse.
Negative reaction to blog
Not being able to trust my friends
Being lonely

258 of 271
7. Thea 5656 words 38 mins (148.84 wpm) 31.08.2016
Change in practical terms
Happier
Going to Uni
Self-worth improved
What helped bring this about
[Got on well with therapy team and TS2 therapist]
Met gf on Tinder
She made me happier
I trusted her so could accept her compliments which improved how I felt about myself
Physical activity club made me feel strong and capable, sense of mastery
Extended social life though physical activity club
I took therapy more seriously – I was ready – I asked to practice known CBT techniques
Non-change in practical terms
Motivation to do routine self-care activities and domestic maintenance (making bed, drawing curtains)
Obstacles/perpetuators
This goal wasn’t the focus of therapy, not what I was referred for, not a pressing health issue
Family did not acknowledge D1 as a problem for me
8. Lily 8037 42 mins (191.35 wpm) 06.09.2016
Change in practical terms
[Improved D3 through CBT techniques and therapist instructions]
Realising relationship with [exercise] isn’t healthy. Realised there are other things in life. Don’t want to
worry about it any more
More confident
Moving to [English city 1]: fresh start, getting away from environment that reminds me of being ill. Hope
of establishing new routine
What helped bring this about
Planning ahead. Weekly lists. Awareness of perfectionism and how it works. Internalised therapist tells
me how to respond

259 of 271
Pie chart of self-evaluation
New job
Non-change in practical terms
Still bothered by D3 and feelings. Hoped they would go away completely.
Obstacles/perpetuators
2 months of therapy isn’t enough to help me change thoughts and feelings. All it can do is help me
change how I can react. I have innate traits i.e. perfectionism and inner competitiveness that I have to
learn to channel the right way. D3 voice – how to disentangle that from an activity I love and that
defines me.
9. Esme 8730 62 mins (140.84 wpm) 07.02.2017
Change in practical terms
Relaxing over-self-control without letting go completely
What helped bring this about
[therapist helped me realise I was too controlling. She didn’t mollycoddle me. She pushed me]
Giving some control over housework to bf and generally being less controlling with him
Pushing myself out of my comfort zone
Getting impatient with myself
Trusting bf’s view of the problem and its effect on our relationship
Reducing self-absorption, improving empathy
Seeing myself through others eyes – adjusting self-perception
Not being able to deny impact of behaviour on health
Aiming to help a friend then realising I should take my own advice
Non-change in practical terms
Nothing. But I regret having gone through this experience. It wasted part of my life and didn’t make
anything any better
Obstacles/perpetuators
Culture makes women discontented with themselves

260 of 271
Appendix 16: Entire interview data spreadsheet
Appendix 17: Example ephemeral reflective notes page

261 of 271
Appendix 18: Example of peer debrief meeting minutes Thesis progress meeting
Online meeting minutes Wed 26/09/17
Chair: [redacted]
Minutes: [redacted]
Attended: Caroline, [redacted], [redacted]
Apologies: [redacted]
Caroline:
- 'Old' intro chapter now split into more usual format intro + short lit. review.
- Meeting with Terry on Tuesday 03/10
- Methodology needs some more work, but not re-opened yet.
- Submission planned in May
Aims: next week 04/10/17
Complete both intro and lit review complete for the meeting with Terry (by Monday)
Restart the methods chapter
[remainder of minutes redacted]
Next meeting
Proposed time Weds 04/10/17, 10:30am

262 of 271
Appendix 19: MIE Approval emails
Ethics Education
To:
Caroline Vermes
Cc:
Terry Hanley
Inbox
Tuesday, November 24, 2015 10:28 AM
Dear Caroline Ref: PGR-7232175 Project Title: Personal and extratherapeutic factors associated by clients with change and non-change since the commencement of therapy. I am pleased to confirm that your ethics application has now been approved by the School Research Integrity Committee (RIC) against a pre-approved UREC template. If anything untoward happens during your research then please ensure you make your supervisor aware who can then raise it with the RIC on your behalf This approval is confirmation only for the Ethical Approval application. Regards Georgia Irving
minor MIE ethics change
Terry Hanley
Actions
To:
Caroline Vermes
Tuesday, March 08, 2016 11:58 AM
For info – your thesis change is approved
Terry
Dr Terry Hanley CPsychol AFBPsS | Senior Lecturer in Counselling Psychology | Ellen Wilkinson Building, A6.15 | University of Manchester |
Oxford Road | M13 9PL | tel: +44 (0)161 275 8815 | email: [email protected] (preferred contact) | skype: terry.s.hanley | new
twitter accounts @DrTerryHanley [personal twitter] @UoMCounsPsych [programme twitter]

263 of 271
Appendix 20: Adverse event flow chart

264 of 271
Appendix 21: Client factors in Castonguay and Beutler (2006) Dysphoria
disorders
Anxiety disorders Substance misuse Personality
disorders
Age Age of adult clients
is inversely related
to the quality of
outcome
Evidence that age
has no prognostic
value
Better outcome
associated with
abstinence-based
social support for
adolescents
Not assessed in
Castonguay and
Beutler (2006)
Gender Young male clients
more likely to drop
out
Mixed evidence
favouring the
conclusion that
gender has no
prognostic value
Mixed and
contradictory
evidence
Insufficient evidence
Ethnicity Insufficient evidence Evidence that
ethnicity has no
prognostic value
(further research
recommended)
Insufficient evidence Not assessed in
Castonguay and
Beutler (2006)
Socioeconomic status Clients from lower
SES more likely to
drop out
Clients from lower
SES more likely to
drop out
Employed clients
have better
outcomes
Clients from lower
SES more likely to
drop out
Religion Insufficient evidence Insufficient
evidence
Not assessed in
Castonguay and
Beutler (2006)
Not assessed in
Castonguay and
Beutler (2006)

265 of 271
Appendix 22: Demographic information sheet Research participant information sheet
Participant number________________________ Counselling at _____________________
Gender (please circle the best option)
Female Male Trans Other Prefer not to say
Age (please circle one)
18-25 26-30 31-40 41-50 51-60 61+ Prefer not to say
Relationship status (circle all that apply)
Single Boyfriend/girlfriend Married (heterosexual) Married/civil partnership (same-sex)
Same-sex long term relationship Heterosexual long-term relationship Divorced
Widowed/Widower Other Prefer not to say
Ethnic group (please circle the best option)
British White Irish White Other White (state)__________________________
British Black (Caribbean) British Black (African) Other Black (state)_________________
Mixed Black Mixed heritage Black and White
Indian (Asian or British Asian) Pakistani (Asian or British Asian) Bangladeshi (Asian or British Asian)
Other Asian Mixed Asian Mixed heritage Asian and White
Other ethnicity (state)_________________________ Prefer not to say
Last level of education completed (circle best option)
Primary school Secondary GCSE A Level/ A Level equivalent
Apprenticeship Vocational training
University Bachelors
University Masters
University Doctorate
Other (state)___________________________
Prefer not to say
Current employment (circle all that apply)
Homemaker Self-employed Full-time employed Part-time employed
Full-time student Part-time student Jobseeker Apprentice Volunteer
Other (state) ______________________________________________
Email address: _________________________________________________________________

266 of 271
Appendix 23: Definitions of causal relationships in research
Definition
Negative predictor The presence of this factor during therapy predicts a poorer
outcome at end of therapy or at follow-up. Statistical analyses
include variants of hierarchical multiple regression
Positive predictor The presence of this factor during therapy predicts a better
outcome at end of therapy or at follow-up.
Negative mediator This factor arises during therapy and mediates between therapy
factors (or other client factors) and a poorer outcome at end of
therapy
Positive mediator This factor arises during therapy and mediates between therapy
factors (or other client factors) and a poorer outcome at end of
therapy
Negative moderator Client characteristic present before the commencement of therapy
that negatively effects outcome
Positive moderator Client characteristic present before the commencement of therapy
that positively effects outcome
Other association with negative
outcome
Non-statistically derived client factors that negatively effect
outcome
Other association with positive
outcome
Non-statistically derived client factors that positively effect
outcome
Appendix 24: Included studies with social factors findings
A. Negative prediction (i.e. adverse social circumstance predicts worse outcome)
*Hartmann, Orlinsky, Weber, Sandholz, Zeeck, (2010)
* Nakano, Lee, Noda, Ogawa, Kinoshita, Funayama, Watanabe, Chen, Noguchi and Furukawa
(2008)
* Dow, Kenardy, Johnston, Newman, Taylor and Thompson (2007)
*Ritsher and Phelan (2004)
Hooley and Teasdale (1999)
Hooley and Teasdale (1989)
B. Positive prediction (i.e. supportive social circumstance predicts better outcome)
*Binford, Mussell, Crosby, Peterson, Crow and Mitchell, J.E. (2005)

267 of 271
* McCrady, Hayaki, Epstein, and Hirsch (2002)
*Zywiak, Longabaugh and Wirtz (2002)
*Steinmetz, Lewinsohn and Antonuccio, D.O. (1983)
* Toth, Rogosch, Oshri, Gravener-Davis, Sturm and Morgan-Lopez (2013)
Mallinckrodt (1996)
Renneberg, Chambless, Fydich and Goldstein (2002)
Jarrett, Eaves, Grannemann and Rush, A.J. (1991)
Fournier, De Rubeis, Shelton, Hollon, Amsterdam and Gallop (2009)
C. Positive association (i.e. supportive social circumstance associated with better outcome)
* Khattra, Angus, Westra, Macaulay, Moertl and Constantino (2017)
Davidson, Borg, Marin, Topor, and Sells (2005)
Constantino, Morrison, Coyne, Goodwin, Santorelli and Angus (2017)
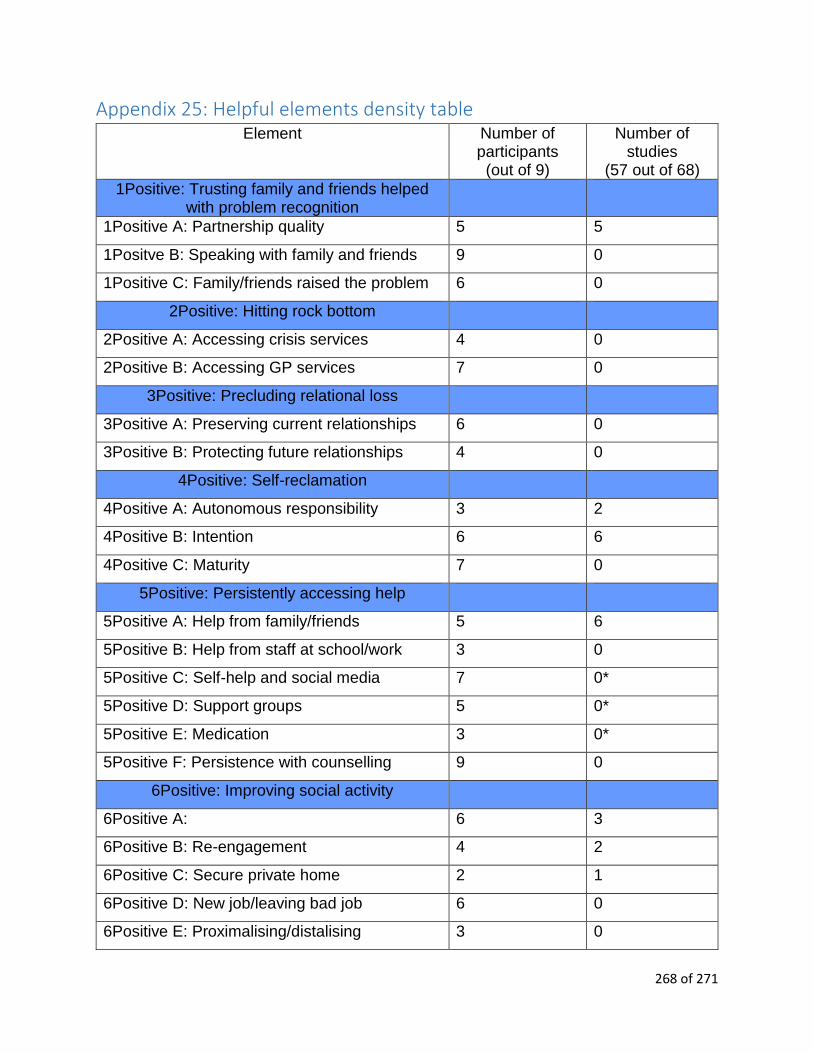
268 of 271
Appendix 25: Helpful elements density table Element Number of
participants (out of 9)
Number of studies
(57 out of 68)
1Positive: Trusting family and friends helped with problem recognition
1Positive A: Partnership quality 5 5
1Positve B: Speaking with family and friends 9 0
1Positive C: Family/friends raised the problem 6 0
2Positive: Hitting rock bottom
2Positive A: Accessing crisis services 4 0
2Positive B: Accessing GP services 7 0
3Positive: Precluding relational loss
3Positive A: Preserving current relationships 6 0
3Positive B: Protecting future relationships 4 0
4Positive: Self-reclamation
4Positive A: Autonomous responsibility 3 2
4Positive B: Intention 6 6
4Positive C: Maturity 7 0
5Positive: Persistently accessing help
5Positive A: Help from family/friends 5 6
5Positive B: Help from staff at school/work 3 0
5Positive C: Self-help and social media 7 0*
5Positive D: Support groups 5 0*
5Positive E: Medication 3 0*
5Positive F: Persistence with counselling 9 0
6Positive: Improving social activity
6Positive A: 6 3
6Positive B: Re-engagement 4 2
6Positive C: Secure private home 2 1
6Positive D: New job/leaving bad job 6 0
6Positive E: Proximalising/distalising 3 0

269 of 271
6Positive F: Role models 4 0
7Positive: Self-helping behaviours
7Positive A: Journalling 5 4
7Positive B: Insight-led behavioural change 8 4
7Positive C: Exposure and flexibility 5 4
7Positive D: Exercise 3 0
8Positive: Helpful thinking
8Positive A: Helping self-talk 8 2
8Positive B: Thought-stopping and restructuring 7 1
8Positive C: Recognising accomplishments and self-efficacy
8 4
8Positive D: Hope for future 7 1
8Positive E: Spirituality 0 3
8Positive F: Gratitude 0 1
9Positive: Reintegrating
9Positive A: Owning evolution 7 1
9Positive B: Self-acceptance 4 7
9Positive C: Life on life’s terms 3 0
9Positive D: Minding regret 2 0
9Positive E: Rejecting unhelpful stereotypes 2 0
*study exclusion criteria precluded possible entries

270 of 271
Appendix 26: Unhelpful elements density table Element Number of
participants Number of
studies (29 out of 68)
1Negative: Compromised support
1Negative A: Difficult family relationships 4 4
1Negative B: Family mental health issues 3 0
2Negative: Ignoring problem
2Negative A: Unrecognised crisis 1* 1
3Negative: Socially disconnected
3Negative A: Alienation 4 2
3Negative B: Guardedness 6 1
3Negative C: Social difficulty 6 4
4Negative: Unready to change
4Negative A: Fear 3 0
4Negative B: Denial 6 0
5Negative: Unable to use help
5Negative A: Find counselling fruitless 4 1
6Negative: Feeling oppressed
6Negative A: Adverse work 7 0
6Negative B: Adverse partnership 0 1
7Negative: Retained unhelpful behaviours
7Negative A: Unhelpful reactions 5 1
7Negative B: Avoidance 6 3
8Negative: Retained unhelpful thinking
8Negative A: Perfectionism 5 3
8Negative B: Unhelpful self-talk 6 2
8Negative C: Obsessions 0 1
8Negative D: Low meta-cognition 0 1
8Negative E: Dissociation 1* 1
9Negative: Unwell identity

271 of 271
9Negative A: Endorsed unhelpful stereotype 5 1
9Negative B: Problem enmeshment 8 0
9negative C: Long illness 6 2
*1 fell beneath threshold of 2 to be considered a participant-informed element
Copyright © 2022 FDOKUMEN