Chordoma: Brief review of the literature and report of a case with widespread metastases
6
CHORDOMA: BRIEF REVIEW OF THE LITERATURE AND REPORT OF A CASE WITH WIDESPREAD METASTASES C. C. WANG, MD, AND A. EVERETTE JAMES, JR., MU The natural course and management of chordoma are reviewed. A report of an unusual case of widespread metastatic chordoma is reported. Radiation therapy, though primariIy palliative in nature, is of value. HORDOMA IS A MALIGNANT TUMOR ORIGINAT- C ing from the remnants of the embryonic notochord. It was first described by Luschka in Virchow’s laboratory in 1857.7 Because of the microscopic appearance of the tumor- chords of polygonal and vacuolated cells separated by homogeneous m u c h matrix- Virchow was of the opinion that this tumor was of cartilaginous origin and described it as an ecchondrosis. The following year Mul- ler7 found that the microscopic appearance of this tumor was similar to that found in chorda dorsalis. He reasoned that this tumor developed from notochordal remnants and first used the term chordoid tumor or chor- doma. The theory of the notochordal origin of this tumor was generally accepted follow- ing the work of Rippert13 in 1894, who, by puncturing the anterior spinal ligament and rupturing the nucleus pulposus, was able to produce chordoma-like neoplasms in the area of the puncture site. Histopathologically, chordoma appears as a soft fleshy encapsulated tumor divided by fibrous trabeculae and contains chords of nonvacuolated polygonal and (the more char- acteristic) vacuolated mucin-containing cells. Interspersed between this lobar arrangement of cells is a homogeneous mucin matrix. Ex- cellent discussions of the pathological find- ings in chordomas are to be found in the There are 548 cases of cliordoma reported: 240 intracranial, 227 sacrococcygeal and 81 vertebral.11 The largest series from a single 3. 6, l3 From the Departments of Radiology, Harvard Med- ical School, and the Massachusctts General Hospital, Boston, Mass. Address for reprints: Dr. C. C. Wang, Department of Radiology, Massachusetts General Hospital, 30 Fruit Street, Boston, Mass. 021 14. Received for publication October 3, 1967. hospital (59 cases) showed 54.2% occurring in the sacrococcygeal r e g i ~ n . ~ These tumors have been found in all age groups with the peak incidence in the fifth decade. There is a definite male preponderance with a ratio of 3:1.14 Because of the slow growth rate of this tumor, the onset of symptoms is gradual; there is an average duration of symptoms before diagnosis of 20 months.8 The clinical symptoms and signs of a chordoma are often associated with its local extension. The sacrococcygeal chordoma may present externally as a subcutaneous midline soft-tissue mass or intrapelvically it may mimic pelvic tumors with obstruction of the urinary or gastrointestinal tracts. When the tumor involves the base of the skull and clivus, it may resemble a pituitary adenoma. Roentgenographic findings often reveal an expanded lesion with osteoblastic and/or osteolytic process and calcification within the tnmor mass.5~ 17 Chordomas most commonly have a slow growth rate that is locally aggressive in na- ture. Although not rapid, the growth rate is inexorably progressive. Because of the loca- tions of the disease, complete surgical extir- pation is rarely-if at all-possible. The pa- tient often succumbs to the disease by its local extension. Metastatic chordomas are rare but do oc- cur. Gentil and Coley reported that approxi- mately lOyo of the cases have distant metas- tases.8 Because of the rarity of metastatic chordoma a case is reported here. CASE REPORT A 59-year-old Caucasian man first entered Massachusetts General Hospital because of pain and fullness at the base of his spine, which had been present for 2 years. Rectal 162
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Chordoma: Brief review of the literature and report of a case with widespread metastases

CHORDOMA: BRIEF REVIEW OF T H E LITERATURE AND REPORT OF A CASE WITH WIDESPREAD
METASTASES C. C. WANG, MD, AND A. EVERETTE JAMES, JR., MU
The natural course and management of chordoma are reviewed. A report of an unusual case of widespread metastatic chordoma is reported. Radiation therapy, though primariIy palliative in nature, is of value.
HORDOMA IS A MALIGNANT TUMOR ORIGINAT- C ing from the remnants of the embryonic notochord. It was first described by Luschka in Virchow’s laboratory in 1857.7 Because of the microscopic appearance of the tumor- chords of polygonal and vacuolated cells separated by homogeneous m u c h matrix- Virchow was of the opinion that this tumor was of cartilaginous origin and described it as an ecchondrosis. The following year Mul- ler7 found that the microscopic appearance of this tumor was similar to that found in chorda dorsalis. He reasoned that this tumor developed from notochordal remnants and first used the term chordoid tumor or chor- doma. The theory of the notochordal origin of this tumor was generally accepted follow- ing the work of Rippert13 in 1894, who, by puncturing the anterior spinal ligament and rupturing the nucleus pulposus, was able to produce chordoma-like neoplasms in the area of the puncture site.
Histopathologically, chordoma appears as a soft fleshy encapsulated tumor divided by fibrous trabeculae and contains chords of nonvacuolated polygonal and (the more char- acteristic) vacuolated mucin-containing cells. Interspersed between this lobar arrangement of cells is a homogeneous mucin matrix. Ex- cellent discussions of the pathological find- ings in chordomas are to be found in the
There are 548 cases of cliordoma reported: 240 intracranial, 227 sacrococcygeal and 81 vertebral.11 The largest series from a single
3. 6, l3
From the Departments of Radiology, Harvard Med- ical School, and the Massachusctts General Hospital, Boston, Mass.
Address for reprints: Dr. C. C. Wang, Department of Radiology, Massachusetts General Hospital, 30 Fruit Street, Boston, Mass. 021 14.
Received for publication October 3, 1967.
hospital (59 cases) showed 54.2% occurring in the sacrococcygeal r e g i ~ n . ~ These tumors have been found in all age groups with the peak incidence in the fifth decade. There is a definite male preponderance with a ratio of 3:1.14 Because of the slow growth rate of this tumor, the onset of symptoms is gradual; there is an average duration of symptoms before diagnosis of 20 months.8
T h e clinical symptoms and signs of a chordoma are often associated with its local extension. The sacrococcygeal chordoma may present externally as a subcutaneous midline soft-tissue mass or intrapelvically it may mimic pelvic tumors with obstruction of the urinary or gastrointestinal tracts. When the tumor involves the base of the skull and clivus, i t may resemble a pituitary adenoma. Roentgenographic findings often reveal an expanded lesion with osteoblastic and/or osteolytic process and calcification within the tnmor mass.5~ 17
Chordomas most commonly have a slow growth rate that is locally aggressive in na- ture. Although not rapid, the growth rate is inexorably progressive. Because of the loca- tions of the disease, complete surgical extir- pation is rarely-if at all-possible. T h e pa- tient often succumbs to the disease by its local extension.
Metastatic chordomas are rare but do oc- cur. Gentil and Coley reported that approxi- mately lOyo of the cases have distant metas- tases.8 Because of the rarity of metastatic chordoma a case is reported here.
CASE REPORT
A 59-year-old Caucasian man first entered Massachusetts General Hospital because of pain and fullness at the base of his spine, which had been present for 2 years. Rectal
162

No. 1 CHORDOMA: l<EVIEIV AND CASE REPORT * Ll/aiig and Jamej 163
examination revealed a firm mass in the region of the coccyx. Roentgenograms of the spine showed an area of bone destruction in the sacrum (Fig. 1). Because of this finding, a subtotal resection was performed with only partial removal of an encapsulated tumor. Microscopic examination of the removed tis- sue showed a chordoma (Fig. 2).
Approximately 8 months following initial surgery the patient was readmitted for evalu- ation of paresthesia of the perineum. A cystogram showed evidence of neurogenic clys- function of the bladder. He was discharged and returned the following year with bilateral gluteal masses and complaints of buttock pain, consistent with local recurrence. Roent- genograms of the vertebral spine revealed an increase in bone destruction. A series of multiple local partial excisions of recurrent chordoma were performed.
Approximately 16 months after his initial admission the patient was given external radiation therapy to the sacral area for re- current tumor. He received a total of appros- imately 4000 R to the tumor, 2 mev radiation, at the rate of 150 to 200 R per day. Following the course of radiotherapy his condition improved and there was definite decrease in the size of the tumor mass.
Two years following the external radio- therapy the patient returned with multiple recurrent skin nodules in the buttock region which were repeatedly treated with palliative radiotherapy. On each occasion the recurrent
nodules responded quite satisfactorily to a close of 1500 to 2000 R in one week's time.
Approximately 5 % years after first admis- sion he underwent a colostomy and later additional palliative radiotherapy because of multiple abscesses and fistulae in the rectal area with recurrent tumor. A few months later he noted masses in the right axillary and infraclavicular regions and subsequently a large mass in the anterior aspect of the right deltoid. Each lesion was treated with a combination of iadiation therapy and chem- otherapy with satisfactory shrinkage of the tumor. A large mediastinal mass was discov- ered on follow-up chest roentgenograph (Fig. 3). The mediastinal mass was not treated by radiation therapy because of its lack of symptoniatology.
During the next 3 years the patient had severe problems with widespread metastatic disease for which he received multiple courses of palliative radiotherapy. Multiple recurrent abscesses and draining sinuses subsequently developed and required numerous incisions and drainages. After an extended period of debilitation and gradual deterioration the patient died approximately 11 years after the onset of the disease.
Necropsy revealed a chordoma of the sac- rum with extension to the pelvis associated with extensive necrosis. There were wide- spread metastases to the lung, pleura, peri- cardium, myocardium, retroperitoneum, liver, muscle and subcutaneous tissues. The subcu-
k"c. 1 . Roentgenograin of the pelvis shows bone destruction of the s:icruni and coccyx.

CANCER Jz i ly 1968 1'01. 22
FIG. 2. Photomicro- graph of the lesion shows chordoma with typical cells in mucin- oils matrix (x260).
taneous nodules were extremely extensive This case apparently represents an unu- (Fig. -1. 5). sually slow-growing but relentlessly uncontrol-
lable metastasizing chordoma. I t is probably the result of hematogenous dissemination of
It is commonly recogni7ed that most chor- the disease. Whether multiple surgical exci- doinas remain locali7ed. T h e reason for the sions and drainages are responsible for its low incidence of distant metastases from distant spread is indeed a matter of specula- choldoma is not readily evident. tion.
COMMENTS
FIG. 3. A (left), posteroanterior and B (right) lateral roentgenograms of the chest reveal a metastatic tumor in the right upper niediastinurn in the region of the azygos node.
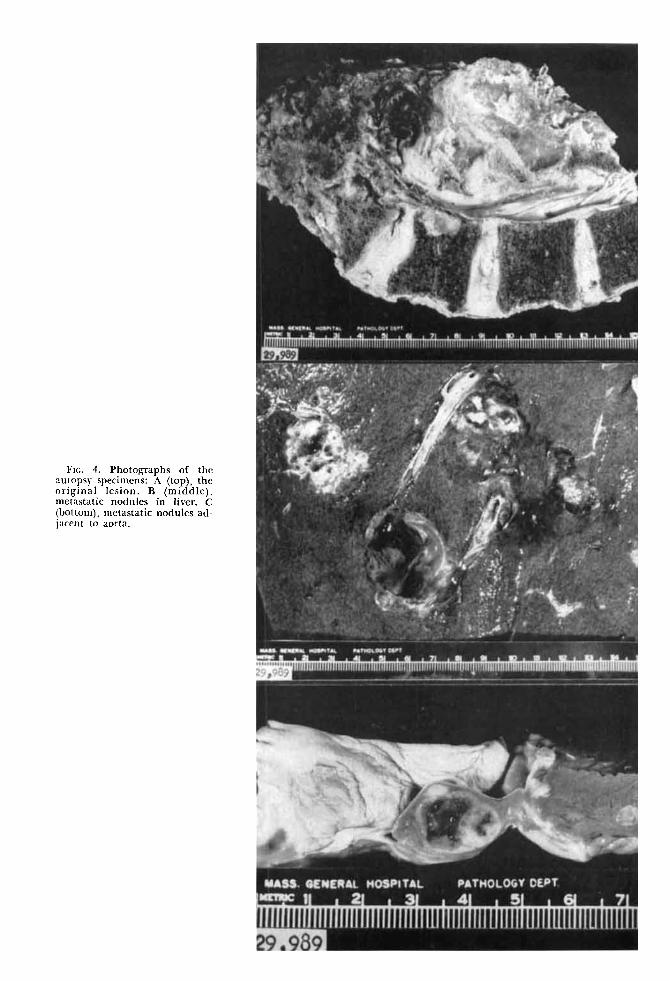
Frc. 4. Photographs of the autopsy specimens: A (top), the original lesion. B (middle), metastatic nodules in liver. C (bottom), metastatic nodules ad- jacent to aorta.
166 CANCER July 1968 Vol. 22
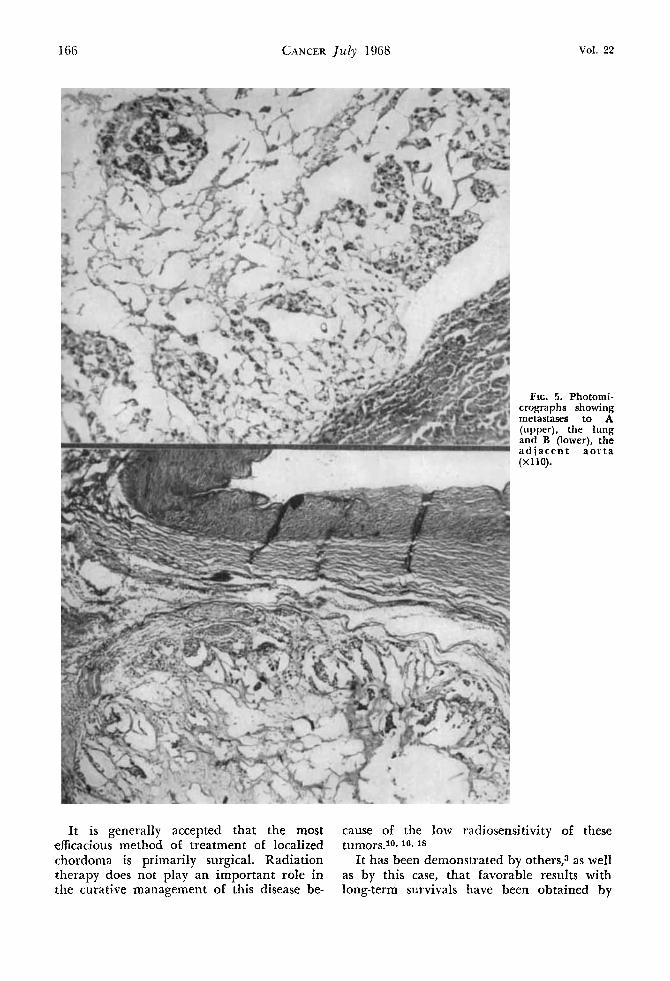
FIG. 5. Photomi- crographs showing metastases to A (upper), the lung and B (lower), the adjacent aor ta (X 110).
It is generally accepted that the most cause of the low radiosensitivity of these efficacious method of treatment of localized tumors.l0.16.1* chordoma is primarily surgical. Radiation It has been demonstrated by others? as well therapy does not play an important role in as by this case, that favorable results with the curative management of this disease be- long-term survivals have been obtained by

No. 1 CHORDOMA: REVIEW AND CASE REPORT * IVang and ]antes 167
the combined use of surgery and aggressive radiation therapy.l.4, 11, 14, 2O In order to achieve a significant growth restraint of resid- ual disease following surgical removal of chordoma, it is believed that a dose of 5000 to 6000 r in 5 to 6 weeks, time is necessary for long-lasting effects. A dose of such magnitude -close to the tolerance level of most of the normal tissues lying adjacent to a chordoma
-should be given with extreme caution, otherwise, permanent complications may en- sue. For the skin and bone sparing effects, the use of supervoltage radiation in the man- agement of these commonly eccentric lesions is advantageous. To palliate symptoms of metastatic chordoma such as pain, massive tumor, and draining sinuses, a dose of 2000 to 3000 r should suffice.
REFERENCES
1. Bouchard, J.: Radiation therapy of tumors and diseases of the nervous system. Philadelphia, Lea and Febiger, 1966.
2. Cappell, D. F.: Chordoma of the vertebral column with three new cases. 1. Path. Bart. 31:797-814, 1928.
3. Dahlin, D. C., and MacCarthy: Chordoma. Cancer
4. Davis, J. C., and Baldwin, N.: Chordoma, JAMA
5. Debcnhani, G. P.: Chordoma in the gluteus maximus muscle. Canad. Med. Ass. J . 93588-561, 1956.
6. Faust, D. B., Gilmore, H. R., Jr.. and Mudgett, C. S.: Chordomata-A review of the literature with report of a sacrococcygeal case. An?i. Intern. Aled. 21:
7. Friedman, I., Harrison, D. F. N., and Biid, E. S.: The fine structures of chordoma with particular refer- ence to the physaliphorous cell. J. Clin. Path. 15:116- 125, 1962.
8. Gentil, F., and Colcy, B. L.: Sacrococcygeal chor- donia. Ann. Surg. 127:432-455, 1948.
9. Gould, S. E., Hincrman, D. L., Batsakis, J. G., and Beamer, P. R.: Diagno5tic pattern-Diseases of bone. A m . J. Clin. Path. 39:178-181, 1963.
10. Hass, G. M.: Chordomas of the cranium and cervical portion of the spine-Review of literature with a rcport of case. Arch. Neural. Psychiat. 32:300, 1934.
5: 1170-1 178, 1952.
33~104-112, 1963.
678-698, 1944.
11. Kamrin, R. P., Potanos, J. N., and Pool, J . L.: An evaluation of the diagnosis and treatment of chordoma. 1. Neurol. Nezcrosurg. Psychiat. 27:157-165, 1964.
12. Littman, L.: Sacro-coccygeal chordoma. Ann. Surg. 137:SO-90, 1953.
13. Mabrey, R. E.: Chordoma--A study of 150 cases. Am. 1. Cancer 25:501-517, 1935.
14. MacCarthy, C., Waugh, J. M., Coventry, M. B., and O’Sullivan, D. C.: Sacrococcygeal chordomas. Surg. Gyizec. Obstet. 113:551-554, 1961.
15. McCune, W. S.: Management of sacrococcygeal tumors, Ann. Surg. 159:911-918, 1964.
16. Montgomery, A. H., and Wolman, I. J.: Sacro- coccygeal chordomas in children. Am. 1. Dis. Child. 46:1269, 1933.
17. Sennett, E. J.: Chordoma, its roentgen diagnostic aspects and its response to roentgen therapy. A m . 1. Roentgen. 69:613-622, 1953.
18. Ridpath, R. F.: Chordoma-Report of two cases.
19. Spjut, H., and Luse, S. A.: Chordoma-An elec- tron-microscopic study, Cancer 17:643-656, 1964.
20. Wood, E. H., and Himedi, Geo. M.: Chordomas- Roentgenologic study of sixteen cases previously unre- ported. Radiology 54:706-716, 1950.
21. Worthy, T. S.: Sacrococcygeal chordoma, two cases with unusual features. Cliiz. Radiol. 16:412-413, 1965.
Ann. Otol. 47:649-658, 1938.