
Childhood facial emotion recognition and psychosis-like symptoms in a nonclinical population at 12...
23
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [University of Bristol Library] On: 9 November 2010 Access details: Access Details: [subscription number 773509252] Publisher Psychology Press Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Cognitive Neuropsychiatry Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713659088 Childhood facial emotion recognition and psychosis-like symptoms in a nonclinical population at 12 years of age: Results from the ALSPAC birth cohort Andrew Thompson ab ; Sarah Sullivan a ; Jon Heron c ; Kate Thomas c ; Stanley Zammit ad ; Jeremy Horwood c ; David Gunnell c ; Chris Hollis e ; Glyn Lewis a ; Dieter Wolke f ; Glynn Harrison a a The Academic Unit of Psychiatry, University of Bristol, Bristol, UK b ORYGEN Research Centre, Department of Psychiatry, University of Melbourne, Melbourne, Australia c Department of Social Medicine, University of Bristol, Bristol, UK d Department of Psychological Medicine, Cardiff University, Cardiff, UK e Division of Psychiatry, University of Nottingham, Nottingham, UK f Department of Psychology, University of Warwick, Warwick, UK First published on: 05 October 2010 To cite this Article Thompson, Andrew , Sullivan, Sarah , Heron, Jon , Thomas, Kate , Zammit, Stanley , Horwood, Jeremy , Gunnell, David , Hollis, Chris , Lewis, Glyn , Wolke, Dieter and Harrison, Glynn(2010) 'Childhood facial emotion recognition and psychosis-like symptoms in a nonclinical population at 12 years of age: Results from the ALSPAC birth cohort', Cognitive Neuropsychiatry,, First published on: 05 October 2010 (iFirst) To link to this Article: DOI: 10.1080/13546805.2010.510040 URL: http://dx.doi.org/10.1080/13546805.2010.510040 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Childhood facial emotion recognition and psychosis-like symptoms in a nonclinical population at 12...

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [University of Bristol Library]On: 9 November 2010Access details: Access Details: [subscription number 773509252]Publisher Psychology PressInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Cognitive NeuropsychiatryPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713659088
Childhood facial emotion recognition and psychosis-like symptoms in anonclinical population at 12 years of age: Results from the ALSPAC birthcohortAndrew Thompsonab; Sarah Sullivana; Jon Heronc; Kate Thomasc; Stanley Zammitad; Jeremy Horwoodc;David Gunnellc; Chris Hollise; Glyn Lewisa; Dieter Wolkef; Glynn Harrisona
a The Academic Unit of Psychiatry, University of Bristol, Bristol, UK b ORYGEN Research Centre,Department of Psychiatry, University of Melbourne, Melbourne, Australia c Department of SocialMedicine, University of Bristol, Bristol, UK d Department of Psychological Medicine, CardiffUniversity, Cardiff, UK e Division of Psychiatry, University of Nottingham, Nottingham, UK f
Department of Psychology, University of Warwick, Warwick, UK
First published on: 05 October 2010
To cite this Article Thompson, Andrew , Sullivan, Sarah , Heron, Jon , Thomas, Kate , Zammit, Stanley , Horwood, Jeremy, Gunnell, David , Hollis, Chris , Lewis, Glyn , Wolke, Dieter and Harrison, Glynn(2010) 'Childhood facial emotionrecognition and psychosis-like symptoms in a nonclinical population at 12 years of age: Results from the ALSPAC birthcohort', Cognitive Neuropsychiatry,, First published on: 05 October 2010 (iFirst)To link to this Article: DOI: 10.1080/13546805.2010.510040URL: http://dx.doi.org/10.1080/13546805.2010.510040
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Childhood facial emotion recognition and psychosis-like
symptoms in a nonclinical population at 12 years of age:
Results from the ALSPAC birth cohort
Andrew Thompson1,2, Sarah Sullivan1, Jon Heron3,Kate Thomas3, Stanley Zammit1,6, Jeremy Horwood3,
David Gunnell3, Chris Hollis4, Glyn Lewis1, Dieter Wolke5,and Glynn Harrison1
1The Academic Unit of Psychiatry, University of Bristol, Bristol, UK,2ORYGEN Research Centre, Department of Psychiatry, University of
Melbourne, Melbourne, Australia, 3Department of Social Medicine, University
of Bristol, Bristol, UK, 4Division of Psychiatry, University of Nottingham,
Nottingham, UK, 5Department of Psychology, University of Warwick,
Warwick, UK, 6Department of Psychological Medicine, Cardiff University,
Cardiff, UK
Introduction. Nonclinical psychotic symptoms (for example, low intensity or low
frequency psychotic symptoms such as ideas of reference or single word auditory
hallucinations) are common in adolescents and may be associated with an increased
risk of developing a psychotic disorder in adulthood. Those at high risk of developing
a psychotic disorder appear to perform poorly on facial emotion recognition tasks
Correspondence should be addressed to Andrew Thompson, Orygen Youth Health and
Research Centre, 35 Poplar Rd, Parkville, VIC 3205, Australia. E-mail: andy.thompson@mh.
org.au
We are extremely grateful to all the families who took part in this study, the midwives for
their help in recruiting them, and the whole ALSPAC team, which includes interviewers,
computer and laboratory technicians, clerical workers, research scientists, volunteers, managers,
receptionists, and nurses. AT designed the study along with GL and SS. KT and JH assisted with
analysis of the data along with AT and provided statistic support. GH was principal investigator
on the grant and provided supervision on all aspect of the study. All other authors were involved
in the design and collection of the primary outcome measure and provided comments and
feedback on the manuscript. All authors report no competing interests. All the authors had full
access to all of the data in the study and take responsibility for the integrity of the data and the
accuracy of the data analysis. The UK Medical Research Council, the Wellcome Trust, and the
University of Bristol provide core support for ALSPAC. The Wellcome Trust funded this
particular research (Grant No. 072043). DG and GL are NIHR Senior Investigators. This
publication is the work of the authors who will serve as guarantors for the contents of this paper.
COGNITIVE NEUROPSYCHIATRY
0000, 00 (00), 1�22
# 2010 Psychology Press, an imprint of the Taylor & Francis Group, an Informa business
http://www.psypress.com/cogneuropsychiatry DOI: 10.1080/13546805.2010.510040
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

but the relationship between facial emotion recognition and nonclinical ‘‘psychosislike symptoms’’ (PLIKS) in children is unclear. We aimed to examine the associationbetween childhood facial emotion recognition and PLIKS in adolescents.Methods. Longitudinal study using a large birth cohort. 6455 subjects completed asemistructured clinical assessment for psychotic symptoms (the PLIKSi) at the meanage of 12.9 (SD� 0.23). Facial emotion recognition (using the DANVA) waspreviously assessed at the age of 8 in the cohort.Results. There was no increase in odds of reporting any PLIKS either in relation tothe total score on the measure of facial emotion recognition or for the individualemotion scores of fear, sadness, anger, and happiness. Similar results were also foundwhen examining more intense and/or more frequently experienced psychoticsymptoms.Conclusions. Deficits in facial emotion recognition in 8-year-olds do not appearto predict later reporting of nonclinical psychotic symptoms in early adolescence.The results do not support the proposal that recognition of emotion is a traitphenomenon in those individuals at increased risk for psychosis. However, furtherresearch is warranted in older children/adolescents when more subtle emotionrecognition deficits can be investigated.
Keywords: Cognition; Cohort studies; Populations at risk; Psychotic disorders;
Social cognition.
INTRODUCTION
Several studies have found that nonclinical psychotic symptoms (‘‘psychosis-
like symptoms’’; PLIKS) are relatively common in both the general
community adult (Bijl, Ravelli, & van Zessen, 1998; Johns et al., 2004;
Kendler, Gallagher, Abelson, & Kessler, 1996; Kessler et al., 1994) and childand adolescent populations (Laurens et al., 2007; Poulton et al., 2000;
Yoshizumi, Murase, Honjo, Kaneko, & Murakami, 2004). The reporting of
PLIKS in these populations has been associated with an increased risk of
later developing a psychotic disorder (Hanssen, Bak, Bijl, Vollebergh, & van
Os, 2005; Poulton et al., 2000); PLIKS are thought to represent the less
severe end of a continuum of psychosis (van Os, Hanssen, Bijl, & Ravelli,
2000). There has therefore been increased interest in examining the
relationship between known or putative risk factors for schizophrenia andPLIKS as evidence of a possible intermediate phenotype (Cannon et al.,
2002; Horwood et al., 2008).
Social cognition, defined as a domain of cognition that involves the
perception, interpretation, and processing of social information (Ostrum,
1984) has received increased attention within schizophrenia research in the
past decade. One of the most widely studied of the proposed social cognitive
skills has been the perception and the recognition of emotions (Edwards,
Jackson, & Pattison, 2002; Penn, Corrigan, Bentall, Racenstein, & Newman,1997). Two main modalities for receiving information regarding emotion
2 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010
perception and recognition are: visual, specifically facial expressions; and
auditory in the form of prosody (the emotional state of speech). Authors
have shown deficits in the recognition of emotions in both these domains
in patients with schizophrenia (Edwards et al., 2002) and those in the
first episode of psychosis (Edwards, Pattison, Jackson, & Wales, 2001;
Kucharska-Pietura, David, Masiak, & Phillips, 2005), with stronger evidencefor facial emotion recognition deficits (Edwards et al., 2002; Kohler, Walker,
Martin, Healey, & Moberg, 2009). Although often a global deficit is seen in
facial emotion recognition in schizophrenia, the most consistent findings
have been for negative emotions especially the recognition of fear and
sadness (Gaebel & Wolwer, 1992) as well as anger (Mandal, Pandey, &
Prasad, 1998).
There is emerging evidence that those in putative ‘‘high-risk’’ groups for
developing psychosis may also have difficulties recognising and discriminat-ing emotions (Phillips & Seidman, 2008). Deficits in facial emotion
recognition have been demonstrated in individuals at genetic high risk (on
the basis of family history) in the majority of studies (Eack et al., 2009; Kee,
Horan, Mintz, & Green, 2004; McCown, Johnson, Austin, & Shefsky, 1988),
in those at clinical high risk (‘‘at risk mental state’’) for psychosis
(Addington, Penn, Woods, Addington, & Perkins, 2008; Schloegelhofer,
Schaefer, Papageorgiou, Werneck-Rohrer, & Amminger, 2006), and in
individuals with schizotypy (Poreh, Whitman, Weber, & Ross, 1994; Shean,Bell, & Cameron, 2007; Williams, Henry, & Green, 2007), although often the
degree of deficit is less pronounced compared to those with schizophrenia.
This has led some authors to suggest that emotion recognition may be a
possible trait marker or endophenotype for schizophrenia (Eack et al., 2009;
Edwards et al., 2001; Phillips & Seidman, 2008) and represent a potential
vulnerability to psychosis (Penn et al., 1997). However, not all studies in
these groups have demonstrated differences between ‘‘at risk’’ individuals
and control subjects (Bolte & Poustka, 2003; Shean et al., 2007; Toomey,Seidman, Lyons, Faraone, & Tsuang, 1999).
Children appear to recognise emotions in faces from an early age (Bruce
et al., 2000; Camras & Allison, 1985; Mondloch, Geldart, Maurer, & Le
Grand, 2003). The ability to recognise different emotional states may occur at
different stages of development especially during adolescence. Although the
basic emotion recognition building blocks appear to be present at primary
school age (Harrigan, 1984; Kirouac, Dore, & Gosselin, 1985), they continue
to develop past this age (Thomas, de Bellis, Graham, & LaBar, 2007;Tremblay, Kirouac, & Dore, 2001). It is not known whether such basic facial
affect recognition skills are related to, or risk factors for, the development of
psychotic symptoms or psychotic disorder. There have been no prospective
studies of early emotion recognition skills and either schizophrenia or PLIKS
as a potential, intermediate phenotype (or ‘‘at risk’’ group) for schizophrenia.
FACIAL EMOTION RECOGNITION AND PLIKS 3
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010
Our study uses a large population-based cohort to investigate the
relationship between performance on a facial emotion recognition task in
childhood and the presence of PLIKS in early adolescence. The specific
research questions were: (1) what is the association between the facial
emotion recognition of a child at the age of 8 and PLIKS at the age of 13
in the ALSPAC cohort?; (2) are specific negative emotions more or lessassociated with risk of PLIKS?; (3) are any associations stronger with stricter
definitions of PLIKS?; and (4) are any associations affected by confounding
factors?
METHODS
Participants
The study examined longitudinal data from the Avon Longitudinal Study of
Parents and Children (ALSPAC) birth cohort (www.alspac.bris.ac.uk). The
cohort consists of children born to residents of the former Avon Health
Authority area in South West England who had an expected date of delivery
between 1 April 1991 and 31 December 1992. The former County of Avon
includes both urban and rural areas and the population is broadlyrepresentative of children in the United Kingdom (Golding, Pembrey, &
Jones, 2001). Parents of the study children have completed regular postal
questionnaires about their child’s health and development since birth, and all
the children have been invited to attended annual assessment clinics since the
age of 7 years. A range of face-to-face interviews and psychological and
physical assessments were carried out at these clinics. The cohort has been
described in detail previously (Golding et al., 2001). The ALSPAC birth
cohort consists of 14,541 pregnancies that resulted in 14,062 live births:13,988 infants were still alive at 1 year. The current study is based on the
6455 children who completed the PLIKS interview as part of the annual
ALSPAC assessment clinic at mean age 12.9 (95% CI, 12.5�13.3 years).
Outcome variable: Psychosis-like symptoms
Psychosis-like symptoms (PLIKS) were measured at the ALSPAC clinic
using the PLIKS semistructured face-to-face interview (Horwood et al.,
2008). The PLIKS interview (PLIKSi) consists of 12 core questions covering
past 6-month occurrence of hallucinations (visual and auditory); delusions(delusions of being spied on, persecution, thoughts being read, reference,
control, grandiose ability, and other unspecified delusions); and experiences
of thought interference (thought broadcasting, insertion, and withdrawal).
For these 12 core items, seven stem questions were derived from DISC-IV
4 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

(Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000) (modified slightly
after piloting), and five stem questions from Section 17 of the Schedules
for Clinical Assessment in Neuropsychiatry (SCAN) version 2.0 (World
Health Organisation, 1994). Definitions of all items followed the glossary
definitions in SCAN, and clinical cross-questioning and probing was used
to establish the presence or absence of symptoms. Interviewers ratedsymptoms as either not present, suspected, or definitely present. Interviewers
(psychology graduates) underwent initial training with experienced SCAN
trainers and attended regular booster training sessions and monthly
workshops with two of the authors (GH and AT). The average kappa value
for interrater reliability was .72 and test�retest reliability was .48 (Horwood
et al., 2008).
Our study examined three primary PLIKSi outcomes reflecting increasing
‘‘severity’’ of psychotic symptoms: (1) presence of any suspected or definitesymptoms (broad PLIKS), (2) a narrower outcome of definite symptoms
only (narrow PLIKS), and (3) an even narrower outcome of any definite
symptoms occurring monthly or more frequently (strict PLIKS).
We also examined associations using a fourth PLIKS outcome: those with
third-person auditory hallucinations and ‘‘first-rank’’ delusions (delusions of
control or delusions of thought broadcast, insertion, or control) (Schneider,
1959). These symptoms were selected because they are frequently thought of
as more characteristic of schizophrenia, in concordance with both DSM-IVand ICD-10 criteria. These two groups of symptoms were combined as a
‘‘bizarre PLIKS’’ outcome. With this outcome we aimed to examine whether
the associations were similar for those with more ‘‘schizophrenia-like’’
symptoms.
Exposure variable: Facial emotion recognition
Previous information on facial expression recognition was available in the
cohort. This was collected using the DANVA (Diagnostic Analysis of Non-
Verbal Accuracy) child faces subtest at the age of 8 (Nowicki & Carton,
1993; Nowicki & Duke, 1994). The faces subtest comprises 24 photos of
child faces, with each face showing one of four emotions: fear, happiness,
sadness, and anger. The faces were colour photos of both male and female
children of primary school age. The photos are presented to the child for 2 s
and then the child has to respond by indicating which emotion is displayedin the photo. The pictures shown are classified as either high or low intensity
(i.e., the emotion displayed was easier to identify or a little harder). The
test was performed as part of the assessment clinic at age 8 and was
computerised to aid completion, with the tester providing only minimal
prompts to the child throughout the testing procedure.
FACIAL EMOTION RECOGNITION AND PLIKS 5
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

The DANVA child faces test gives a total score out of 24 for facial emotion
recognition, a score for emotion misattribution, and individual summary
scores for the four emotions and low and high intensity emotions. The total
DANVA score and the scores for each of these individual summary scores
were used as continuous variables. A binary variable, based on the upper 20th
percentile, was also created and used in the analysis (DANVA total binary)(Nowicki, personal communication). This was chosen as the scores on the
DANVA were somewhat right skewed and this would give a measure of the
more extreme responders on the measure. Similar binary variables using 20th
percentile cutoffs (or as near as possible) were created for the individual
emotions and these were analysed separately. The DANVA has been shown to
have good internal consistency, test�retest reliability, and convergent validity
and construct validity (Nowicki & Carton, 1993; Nowicki & Duke, 1994).
Potential confounders
A number of sociodemographic variables were included as potential
confounders. Previous studies have demonstrated associations between
psychosis-like symptoms and social class, ethnicity, and parental education
(Horwood et al., 2008; Laurens, West, Murray, & Hodgins, 2008). Ques-
tionnaires completed by the parents during the antenatal period providedinformation on child’s ethnic background (nonwhite vs. white), parental social
class based on the higher of the mother or partner’s occupational social class
(using the 1991 Office of Population Census and Statistics classification; Dale
& Marsh, 1993; OPCS, 1991), and maternal education (O-level or more vs. less
than O-level; O-levels were the standard school-leaving qualifications taken
around age 16 years until recently in the United Kingdom).
We thought that additional factors in the child’s development including
IQ and previous childhood psychiatric disorder may also act as potentialconfounders to any relationship as they may affect both facial affect
recognition and PLIKS. This was based on previous research demonstrating
a potential association with these factors and development of psychotic-like
symptoms (Cannon et al., 2002; Horwood et al., 2008; Kim Cohen et al.,
2003). An abbreviated form of the Wechsler Intelligence Scale for Children
(WISC)-III (United Kingdom version) was used to derive an overall
Intelligence Quotient (IQ) of the children at the ALSPAC 8-year clinic
(Wechsler, 1991). DSM-IV psychiatric diagnoses were made at 91 months(7.6 years) using the Developmental and Wellbeing Assessment (DAWBA;
Goodman, Ford, Richards, Gatward, & Meltzer, 2000) based on parent and
teacher reports. The presence of any Axis 1 diagnosis of attention deficit/
hyperactivity disorder, conduct disorder, oppositional defiant disorder,
depression, or anxiety versus no diagnosis was used in the analysis.
6 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010
Statistical analysis
All analyses were carried out using STATA version 9.0 (Stata Corporation,
2005). The sample that attended the PLIKS interview was compared with the
rest of the cohort. Logistic regression was used to calculate odds ratios (ORs)
and 95% confidence intervals (CIs) for PLIKS, with total score on the DANVA
and each of the six subscores as independent variables. The crude associations
(without adjustment for possible confounding variables) between the DANVAscores (independent variables) and broad, narrow, strict, and bizarre PLIKS
(dependent variables) were computed. The analyses were repeated controlling
for potential confounders in multiple logistic regression analyses. This was
done to determine the extent that these variables may have on the observed
associations. The first set of analyses included parents’social class, educational
level, and child’s sex, ethnicity, and age at PLIKS interview. Further
adjustment was made for IQ (WISC score) and presence of one or more
DAWBA diagnoses (psychiatric diagnosis) in a second analysis. Finally, theanalysis was repeated including all the potentially confounding variables.
For continuous dependent variables, linear regression models with mean
differences (MDs) were used.
Because information on the confounding factors was not available for all
participants for each set of confounders, we calculated the association based
on the reduced sample size for which information was available (controlled
for age and gender). In a separate step we then also added the respective
confounding variables.
Ethical approval
Ethical approval for the study was obtained from the ALSPAC Law and
Ethics Committee and the Local Research Ethics Committees. Informed
consent was obtained from the parents of the children after explanation of
the nature of the study.
RESULTS
6455 children completed the PLIKSi during the annual ALPSAC assessment
clinic at mean age 12.9 years. There were 880 children (13.7% of all those
interviewed) who were rated as having ‘‘broad’’ PLIKS, 363 (5.6% of those
interviewed) ‘‘narrow’’ PLIKS, and 164 (2.5% of those interviewed) childrenwith ‘‘strict’’ PLIKS. There were 233 children (3.6%) who were rated as
having suspected or definite ‘‘bizarre’’ PILKS.
6703 children in the total cohort completed the DANVA at the age of 8,
of these children 5267 (78.6%) also had complete data for the PLIKSi at
FACIAL EMOTION RECOGNITION AND PLIKS 7
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010
mean age 12.9. Overall the mean number of errors on the DANVA was 4.61
(range�0�22, SD�2.73). There was no difference in the overall score on
the DANVA faces between those who completed the PLIKSi and those who
did not (4.61 for completers compared to 4.63 for noncompleters).
A summary of potential confounders in relation to total DANVA score is
presented in Table 1 (DANVA and confounders dichotomised only for thepurpose of this table) along with the outcome variables by high/low total
DANVA scores. The high scorers on total DANVA errors were more likely to
be male, white, of a lower social class, have a mother with a lower level of
education, a lower individual IQ, and have at least one previous psychiatric
diagnosis.
Associations between PLIKS outcomes and DANVAemotion recognition scores
Table 2 shows the associations between each of the PLIKS outcomes and the
total and individual subscores of the DANVA. There was no suggestion of
a relationship between total errors on the DANVA and PLIKS at anydefinition of PLIKS. For the individual emotions subscores there was no
suggestion that worse performance on recognition of faces of negative
emotions (fear, sadness, and anger) were more associated with PLIKS. The
majority of the odds ratios were less than one. In fact those who reported
the strictest definition of PLIKS (‘‘strict’’) appeared to perform better on
recognition of fearful faces than those without PLIKS (OR�0.86, 95%
CI�0.75�1.00, p-value�.045). However, such a relationship was not seen
for other PLIKS variables with this emotion. There was also no relationshipbetween performance with regard to the intensity (high/low) of the facial
emotions displayed and reporting of PLIKS of any definition.
Given that some of the scores on the DANVA were right skewed, the
analysis was repeated with DANVA scores dichotomised into a binary
variable on the basis of scores being above or below the 80th percentile.
Again there were no consistent associations between both total DANVA
score and reporting of PLIKS nor individual emotion sub-scores and PLIKS.
Associations adjusting for potential confounders
Table 3 summarises the multivariable logistic regression models investigating
the impact of a series of potential confounding factors on the association ofDANVA individual emotions with ‘‘narrow’’ PLIKS only.
None of the sets of confounders were responsible for any substantial
change in the association between DANVA scores and PLIKS, although
all confounders reduced the odds ratios. The same was true for all of the
8 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

TABLE 1Frequency of potential confounders and primary outcome (PLIKS scores) by total DANVA errors binary score (dichotomised into
below and above the 80th centile) with corresponding odds ratios (ORs), 95% confidence intervals, and p-values
Low total DANVA errors score High total DANVA errors score Low vs. high total DANVA errors score
Binary confounding variables N (%) N (%) OR (95% CI) p-value
Gender
Male 2524 (75.1) 839 (24.9) 1 (reference) B.001
Female 2655 (79.5) 684 (20.5) 0.77 (0.69 to 0.87)
Social class
Low 1838 (75.9) 585 (24.1) 1 (reference) .007
High 2974 (78.8) 800 (21.2) 0.85 (0.75 to 0.95)
Maternal education
Below O level 1031 (73.4) 373 (26.6) 1 (reference) B.001
Above O level 3976 (78.5) 1088 (21.5) 0.76 (0.66 to 0.87)
Ethnicity
White 4722 (77.2) 1397 (22.8) 1 (reference) .03
Nonwhite 204 (83.3) 41 (16.7) 0.68 (0.48 to 0.96)
DAWBA
No diagnosis 4151 (77.8) 1184 (22.2) 1 (reference) .02
One or more diagnoses 281 (72.4) 107 (27.6) 1.33 (1.06 to 1.68)
FA
CIA
LE
MO
TIO
NR
EC
OG
NIT
ION
AN
DP
LIK
S9
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

TABLE 1 (Continued)
Low total DANVA errors score High total DANVA errors score Low vs. high total DANVA errors score
Binary confounding variables N (%) N (%) OR (95% CI) p-value
None 2726 (77.7) 783 (22.3) 1 (reference) .53
At least one 398 (79.0) 106 (21.0) 1.06 (0.88 to 1.30)
Narrow PLIKS
None 2959 (77.8) 845 (22.2) 1 (reference) .66
At least one 165 (79.0) 44 (21.0) 1.07 (0.80 to 1.43)
Strict PLIKS
None 3050 (77.8) 869 (22.2) 1 (reference) .51
At least one 74 (78.7) 20 (21.3) 1.16 (0.74 to 1.81)
Bizarre PLIKS
None 3949 (77.5) 1149 (22.5) 1 (reference) .68
At least one 141 (78.8) 38 (21.2) 1.08 (0.75 to 1.55)
Continuous confounding
variables Mean (SD) Mean (SD) OR (95% CI) p-value
Age in days* 4689 (80.1) 4693 (73.0) 1.00 (1.00 to 1.00) .19
IQ# 105.7 (15.7) 99.4 (17.6) 0.98 (0.97 to 0.98) B.001
N�number; OR�odds ratio; CI�confidence interval; DAWBA�diagnostic assessment of wellbeing; IQ� intelligence quotient; DANVA�diagnostic
analysis of nonverbal accuracy; PLIKS�psychosis-like symptoms. *N�5289. #N�6068.
Outcome variables
10
TH
OM
PS
ON
ET
AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010
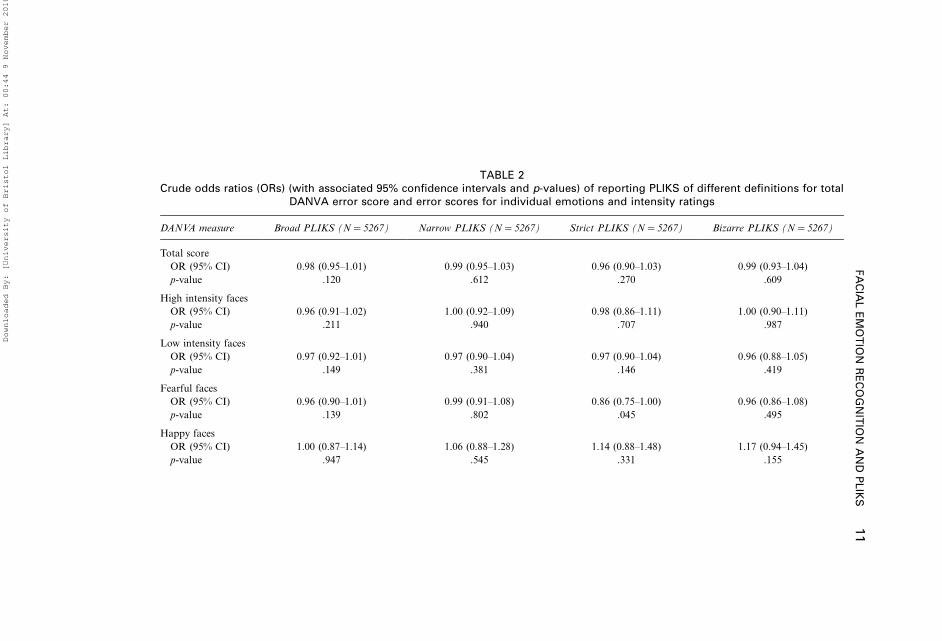
TABLE 2Crude odds ratios (ORs) (with associated 95% confidence intervals and p-values) of reporting PLIKS of different definitions for total
DANVA error score and error scores for individual emotions and intensity ratings
DANVA measure Broad PLIKS (N�5267) Narrow PLIKS (N�5267) Strict PLIKS (N�5267) Bizarre PLIKS (N�5267)
Total score
OR (95% CI) 0.98 (0.95�1.01) 0.99 (0.95�1.03) 0.96 (0.90�1.03) 0.99 (0.93�1.04)
p-value .120 .612 .270 .609
High intensity faces
OR (95% CI) 0.96 (0.91�1.02) 1.00 (0.92�1.09) 0.98 (0.86�1.11) 1.00 (0.90�1.11)
p-value .211 .940 .707 .987
Low intensity faces
OR (95% CI) 0.97 (0.92�1.01) 0.97 (0.90�1.04) 0.97 (0.90�1.04) 0.96 (0.88�1.05)
p-value .149 .381 .146 .419
Fearful faces
OR (95% CI) 0.96 (0.90�1.01) 0.99 (0.91�1.08) 0.86 (0.75�1.00) 0.96 (0.86�1.08)
p-value .139 .802 .045 .495
Happy faces
OR (95% CI) 1.00 (0.87�1.14) 1.06 (0.88�1.28) 1.14 (0.88�1.48) 1.17 (0.94�1.45)
p-value .947 .545 .331 .155
FA
CIA
LE
MO
TIO
NR
EC
OG
NIT
ION
AN
DP
LIK
S11
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

TABLE 2 (Continued)
DANVA measure Broad PLIKS (N�5267) Narrow PLIKS (N�5267) Strict PLIKS (N�5267) Bizarre PLIKS (N�5267)
Sad faces
OR (95% CI) 1.00 (0.92�1.09) 0.96 (0.84�1.10) 0.97 (0.80�1.18) 0.93 (0.78�1.09)
p-value .972 .554 .789 .362
Angry faces
OR (95% CI)
p-value 0.95 (0.89�1.01) 0.97 (0.89�1.06) 0.97 (0.85�1.11) 0.98 (0.88�1.10)
.100 .525 .660 .723
The odds ratios represent the change in odds of reporting PLIKS per unit change in DANVA score. Odds ratios of less than 1 indicate that the odds of
reporting PLIKS are reduced when the number of DANVA errors increase; an odds ratio of greater than 1 indicates that the odds of reporting PLIKS increase
as the number of DANVA errors increase.
12
TH
OM
PS
ON
ET
AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

potential confounders combined. Table 3 shows these associations for the
narrow outcome of PLIKS. This finding was the same for all of the other
definitions of PLIKS investigated (‘‘broad’’, ‘‘strict’’, and ‘‘bizarre’’) (results
not shown but available on request).
DISCUSSION
Poor facial emotion recognition at aged 8 was not associated with an
increased risk of PLIKS in early adolescence. This was the case for overall
performance in facial emotion recognition, different intensity emotions, aswell as both positive and negative emotional states. The relationship
remained similar after adjusting for potential confounders.
This is contrary to our hypotheses and in contrast to most of studies in
individuals deemed to be at high risk for schizophrenia or psychosis (family
history of schizophrenia, individuals with schizotypy, and those with ‘‘at risk
mental states’’) (Phillips & Seidman, 2008). However, not all studies have
consistently shown deficits in these groups and the evidence base is not
substantial. There are a number of possible explanations for this negativefinding that warrant further discussion.
First, it is possible that the assessment of emotion recognition used is not
sensitive enough to detect any subtle differences in emotion recognition.
Although this is possible, the DANVA has good validity and reliability in
this age group as a brief measure (Nowicki & Carton, 1993; Nowicki &
Duke, 1994; Nowicki & Mitchell, 1998). Recent studies using the DANVA
have demonstrated facial affect recognition deficits in schizotypy (Shean
et al., 2007), as well as those with ‘‘at risk’’ for bipolar illness (Brotman et al.,2008), providing some support for the face validity of the DANVA in similar
populations. Deficits in facial affect recognition using the DANVA have also
been found in schizophrenia patients (Hooker & Park, 2002; Pan, Chen,
Chen, & Liu, 2009). Rather than being chosen on the basis of any particular
theory of emotional development or on ‘‘anatomically objective’’ criteria
such as the position of facial features or specific facial muscle tensions (e.g.,
Ekman & Friesen, 1975; Izard, 1971), DANVA test items were selected
primarily on empirical-normative grounds (Nowicki & Duke, 1974). How-ever, it does not test all of the six basic emotions (disgust and surprise are
not included in the DANVA) suggested by Ekman (Ekman, 1994; Ekman,
Freisen, & Ellsworth, 1972) that are often used in emotion recognition
tests in the schizophrenic population (Edwards et al., 2001). Authors have
suggested that disgust and surprise may be less developed in 8-year-old
children (Camras & Allison, 1985) and neither of these emotions have been
implicated as important deficits in those individuals with schizophrenia
(Edwards et al., 2002).
FACIAL EMOTION RECOGNITION AND PLIKS 13
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010
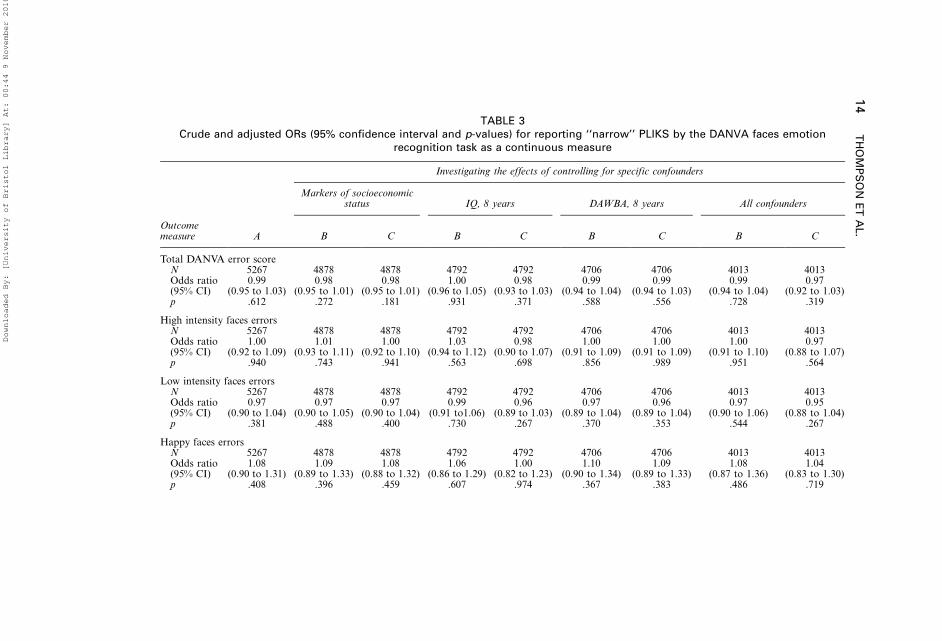
TABLE 3Crude and adjusted ORs (95% confidence interval and p-values) for reporting ‘‘narrow’’ PLIKS by the DANVA faces emotion
recognition task as a continuous measure
Investigating the effects of controlling for specific confounders
Markers of socioeconomicstatus IQ, 8 years DAWBA, 8 years All confounders
Outcomemeasure A B C B C B C B C
Total DANVA error scoreN 5267 4878 4878 4792 4792 4706 4706 4013 4013Odds ratio(95% CI)
0.99(0.95 to 1.03)
0.98(0.95 to 1.01)
0.98(0.95 to 1.01)
1.00(0.96 to 1.05)
0.98(0.93 to 1.03)
0.99(0.94 to 1.04)
0.99(0.94 to 1.03)
0.99(0.94 to 1.04)
0.97(0.92 to 1.03)
p .612 .272 .181 .931 .371 .588 .556 .728 .319
High intensity faces errorsN 5267 4878 4878 4792 4792 4706 4706 4013 4013Odds ratio(95% CI)
1.00(0.92 to 1.09)
1.01(0.93 to 1.11)
1.00(0.92 to 1.10)
1.03(0.94 to 1.12)
0.98(0.90 to 1.07)
1.00(0.91 to 1.09)
1.00(0.91 to 1.09)
1.00(0.91 to 1.10)
0.97(0.88 to 1.07)
p .940 .743 .941 .563 .698 .856 .989 .951 .564
Low intensity faces errorsN 5267 4878 4878 4792 4792 4706 4706 4013 4013Odds ratio(95% CI)
0.97(0.90 to 1.04)
0.97(0.90 to 1.05)
0.97(0.90 to 1.04)
0.99(0.91 to1.06)
0.96(0.89 to 1.03)
0.97(0.89 to 1.04)
0.96(0.89 to 1.04)
0.97(0.90 to 1.06)
0.95(0.88 to 1.04)
p .381 .488 .400 .730 .267 .370 .353 .544 .267
Happy faces errorsN 5267 4878 4878 4792 4792 4706 4706 4013 4013Odds ratio(95% CI)
1.08(0.90 to 1.31)
1.09(0.89 to 1.33)
1.08(0.88 to 1.32)
1.06(0.86 to 1.29)
1.00(0.82 to 1.23)
1.10(0.90 to 1.34)
1.09(0.89 to 1.33)
1.08(0.87 to 1.36)
1.04(0.83 to 1.30)
p .408 .396 .459 .607 .974 .367 .383 .486 .719
14
TH
OM
PS
ON
ET
AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

TABLE 3 (Continued)
Investigating the effects of controlling for specific confounders
Markers of socioeconomicstatus IQ, 8 years DAWBA, 8 years All confounders
Outcomemeasure A B C B C B C B C
Angry faces errorsN 5267 4878 4878 4792 4792 4706 4706 4013 4013Odds ratio(95% CI)
0.98(0.90 to 1.07)
0.98(0.89 to 1.08)
0.98(0.89 to 1.07)
1.00(0.92 to 1.11)
0.99(0.89 to 1.08)
0.97(0.88 to 1.07)
0.96(0.88 to 1.06)
0.98(0.88 to 1.09)
0.97(0.87 to 1.08)
p .669 .667 .626 .849 .767 .497 .469 .692 .535
Fearful faces errorsN 5267 4878 4878 4792 4792 4706 4706 4013 4013Odds ratio(95% CI)
0.99(0.90 to 1.08)
0.99(0.90 to 1.09)
0.98(0.89 to 1.07)
0.99(0.90 to 1.09)
0.95(0.87 to 1.05)
0.98 (0.90 to1.08)
0.98(0.90 to 1.08)
0.97(0.87 to 1.08)
0.94(0.85 to 1.05)
p .766 .834 .635 .820 .309 .732 .725 .587 .256
Sad faces errorsN 5267 4878 4878 4792 4792 4706 4706 4013 4013Odds ratio(95% CI)
0.96(0.85 to 1.10)
0.97(0.85 to 1.12)
0.97(0.84 to 1.11)
1.00(0.87 to 1.14)
0.95(0.83 to 1.10)
0.95(0.83 to 1.10)
0.95(0.82 to 1.09)
0.99(0.85 to 1.16)
0.96(0.82 to 1.12)
p .586 .706 .628 .985 .494 .503 .475 .936 .597
Model A�The model adjusts for age at PLIKS interview and gender. B�The model is based on participants with available data for the potential
confounder of interest (as indicated by the column header), adjusting for age at PLIKS interview and gender. C�The model adjusts for age at PLIKS
interview, gender, and the potential confounder. N�number; OR�odds ratio; CI�confidence interval; PLIKS�psychosis-like symptoms; IQ�intelligence
quotient; DAWBA�developmental and Wellbeing Assessment; DANVA�diagnostic analysis of nonverbal accuracy.
FA
CIA
LE
MO
TIO
NR
EC
OG
NIT
ION
AN
DP
LIK
S15
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

Second, it is possible that the DANVA was prone to ceiling effects in
performance. Older children and adolescents might be able to recognise and
label emotions, but they might not be as sensitive to nuances in facial
expression conveyed in blends of emotions or emotions of lesser intensity.
From our data it does appear that the mean number of errors is relatively
low (4.6 out of a possible 24) so we cannot discount this possibility. Moredifficult tasks such as those of morphing neutral faces to emotional faces
(Norton, McBain, Holt, Ongur, & Chen, 2009) might be considered in future
studies.
Third, and related to the previous suggestion, is the possibility that more
subtle social cognitive skills develop later on in adolescence and that any
deficits in these more subtle processes might be related to PLIKS, but were
not apparent at the age of 8. Research on facial affect recognition in early
childhood has suggested that such skills are fully developed in earlychildhood (Bruce et al., 2000; Camras & Allison, 1985; Mondloch et al.,
2003). However, recently others have suggested that more subtle skills,
especially relating to negative emotions such as anger and fear, may be
developed later, in adolescence (Camras & Allison, 1985; Kolb, Wilson, &
Taylor, 1992; Thomas et al., 2007). This could be a reason why we do not
find an association in this study. The finding of poorer performance on the
DANVA in an 18-year-old college population in another ‘‘at risk’’ group
with schizotypy (Shean et al., 2007) supports this suggestion.Further to this, authors have suggested that emotion recognition skills for
particular emotions may have different developmental trajectories from
adolescence to adulthood (Thomas et al, 2007). Evidence suggests that these
may be more likely to be the negative emotions such as fear and anger, that
are often poorly recognised by patients with psychotic symptoms (Edwards
et al., 2002; Mandal et al., 1998). The neuroanatomical changes and synaptic
pruning in structures believed to be involved in processing social information
are subject to relative change during early and late adolescence (Blakemore,2005). For example, there are substantial age-related changes in the
amygdala volume between 7.5 years and 18 years (Schumann et al., 2004)
and significant growth in the prefrontal cortex including grey matter growth
in the dorsolateral prefrontal cortex during adolescence/early adulthood
(Giedd, 2004). Therefore, early age deficits in social cognition may be of less
importance in the development of psychosis or psychotic symptoms than
those acquired in adolescent/early adulthood, a time of greatest risk for
developing such a disorder. Our results would suggest that ‘‘gross’’ deficits insocial cognition, that may be more apparent at the age of 8, are not
associated with early psychotic symptoms.
Fourth, it could be that the emotion recognition skills in those at risk for
developing schizophrenia are acquired normally in early childhood and
then lost in later adolescence/adulthood. There is currently no evidence to
16 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

support this hypothesis. However, authors have suggested that pronounced
emotional recognition problems may appear at a relatively late stage in the
developmental course of a mental disorder, or may only be associated with
more severe levels of schizophrenia-spectrum symptomatology (Toomey &
Schuldberg, 1995).
Last, it is possible that measures of psychotic like symptoms are not astrong marker for being at risk for psychosis which therefore explains why
we did not find an association. Although initial studies showed a strong
correlation between PLIKS developing a schizophreniform illness (Poulton
et al., 2000), and association between a number of putative risk factors
for schizophrenia and PLIKS (Cannon et al., 2002), recent evidence from
our group has suggested that PLIKS may not represent such a strong
intermediate phenotype for schizophrenia as first suspected, but rather an
additional risk factor that is more closely linked to other expressions ofemotional distress such as depression (Schreier et al., 2009; Thomas et al.,
2009). However, this study examined the 6-month prevalence of these
symptoms, whereas others have looked at the lifetime prevalence of such
symptoms (Kelleher, Harley, Murtagh, & Cannon, 2009; Laurens et al.,
2007). Research in this cohort and other such longitudinal approaches will
allow us to explore these hypotheses further.
Strengths and limitations
There are several strengths to our study. First, ALSPAC is a large
population-based cohort and because of the large sample size (in spite of
attrition from the original sample), we believe we had sufficient power to
detect potentially important associations. Second, the PLIKSi was derived
from widely used assessment tools for psychotic symptoms, and interviewers
were carefully trained and the interrater reliability thoroughly assessed andwas very good (average kappa�.72) (Horwood et al., 2008) and derived
similar rates of symptoms to previously used assessments in this population
(Cannon et al., 2002). Last, as the cohort study has collected information on
a number of factors in both child and the parent, we were able to control for
a number of important potential confounders in the analysis.
With regard to the limitations of the study, it is acknowledged that there
was substantial attrition in the ALSPAC cohort and likely selection biases in
the sample of participants (49.3%) that completed the PLIKS interviewcompared to the total birth cohort and were therefore included as the
primary outcome in this study. These selection biases have been investigated
in previous papers using the PLIKS interview (Horwood et al., 2008).
However, these levels of losses to follow up are similar to those seen in other
large-scale longitudinal studies (Callaway et al., 2007; Plewis, Calderwoof,
FACIAL EMOTION RECOGNITION AND PLIKS 17
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

Hawkes, & Nathan, 2004). In particular, lower social classes and ethnic
minorities were under represented in this sample compared to the whole
cohort but the overall symptom levels obtained show minimal change when
adjusting for these differences. Previous research using the DANVA has
suggested that both lower social classes and certain ethnic minorities may
perform more poorly on facial emotion recognition (Collins & Nowicki,2001; Nowicki & Duke, 1994). As there was no measure of PLIKS taken at
age 8, we cannot rule out the issue of reverse causality. However, this appears
to be less of a problem, as our results show a lack of association.
In conclusion, using data from a large birth cohort, there appears to be no
specific relationship between emotion recognition deficits at the age of 8 and
an increased risk of reporting psychotic symptoms in early adolescence. Our
findings do not lend support to the proposal that facial emotion recognition
is a trait or risk factor for developing a psychotic disorder. Althoughthere was no relationship found in this cohort, other measures of either
emotion recognition (such as prosody) or social cognition were not
investigated. Other related social cognition deficits such as ‘‘theory of
mind’’ and attributional bias in particular have been suggested as other
vulnerability markers for psychotic illnesses. We plan to investigate such
skills in this cohort to further explore the relationship between social
cognitive abilities and the development of both PLIKS and psychotic
illnesses.
Manuscript received 15 December 2009
Revised manuscript received 20 April 2010
First published online month/year
REFERENCES
Addington, J., Penn, D., Woods, S. W., Addington, D., & Perkins, D. O. (2008). Facial affect
recognition in individuals at clinical high risk for psychosis. British Journal of Psychiatry, 192,
67�68.
Bijl, R. V., Ravelli, A., & van Zessen, G. (1998). Prevalence of psychiatric disorder in the
general population: results of The Netherlands Mental Health Survey and Incidence Study
(NEMESIS). Social Psychiatry and Psychiatric Epidemiology, 33, 587�595.
Blakemore, S. (2008). The social brain in adolescence. Nature Reviews Neuroscience, 9, 267�277.
Bolte, S., & Poustka, F. (2003). The recognition of facial affect in autistic and schizophrenic
subjects and their first-degree relatives. Psychological Medicine, 33, 907�915.
Brotman, M. A., Guyer, A. E., Lawson, E. S., Horsey, S. E., Rich, B. A., Dickstein, D. P., et al.
(2008). Facial emotion labeling deficits in children and adolescents at risk for bipolar disorder.
American Journal of Psychiatry, 165, 385�389.
Bruce, V., Campbell, R. N., Doherty-Sneddon, G., Import, A., Langton, S., McAuley, S., et al.
(2000). Testing face processing skills in children. British Journal of Developmental Psychology,
18, 319�333.
18 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

Callaway, L. K., McIntyre, H. D., O’Callaghan, M., Williams, G. M., Najman, J. M., & Lawlor,
D. A. (2007). The association of hypertensive disorders of pregnancy with weight gain over the
subsequent 21 years: Findings from a prospective cohort study. American Journal of
Epidemiology, 166, 421�428.
Camras, L., & Allison, K. (1985). Children’s understanding of emotional facial expressions and
verbal labels. Journal of Nonverbal Behavior, 9, 84�94.
Cannon, M., Caspi, A., Moffitt, T. E., Harrington, H., Taylor, A., Murray, R. M., et al. (2002).
Evidence for early-childhood pan-developmental impairment specific to schizophreniform
disorder: Results from a longitudinal birth cohort. Archives of General Psychiatry, 59, 449�457.
Collins, M., & Nowicki, S., Jr. (2001). African American children’s ability to identify emotion in
facial expressions and tones of voice of European Americans. Journal of Genetic Psychology,
162, 334�346.
Dale, A., & Marsh, C. (1993). The 1991 Census user’s guide. London, UK: Office for National
Statistics.
Eack, S. M. E., Mermon, D., Montrose, D. M., Miewald, J., Gur, R. E., Gur, R. C., et al. (2009).
Social cognition deficits among individuals at familial high risk for schizophrenia.
Schizophrenia Bulletin. Advance online publication.
Edwards, J., Jackson, H. J., & Pattison, P. E. (2002). Emotion recognition via facial expression and
affective prosody in schizophrenia: A methodological review. Clinical Psychology Review, 22,
789�832.
Edwards, J., Pattison, P. E., Jackson, H. J., & Wales, R. J. (2001). Facial affect and affective prosody
recognition in first-episode schizophrenia. Schizophrenia Research, 48, 235�253.
Ekman, P. (1994). Strong evidence for universals in facial expressions: A reply to Russell’s mistaken
critique. Psychological Bulletin, 115, 268�287.
Ekman, P., & Friesen, W. V. (1975). Unmasking the face. Upper Saddle River, NJ: Prentice Hall.
Ekman, P., Freisen, W. V., & Ellsworth, P. (1972). What emotion categories or dimensions can
observers judge from facial behaviour? In P. Ekman (Ed.), Emotion in the human face (pp. 39�55). Cambridge, UK: Cambridge University Press.
Gaebel, W., & Wolwer, W. (1992). Facial expression and emotional face recognition in
schizophrenia and depression. European Archives of Psychiatry and Clinical Neuroscience,
242, 46�52.
Giedd, J. N. (2004). Structural magnetic resonance imaging of the adolescent brain. Annals of the
New York Academy of Sciences, 1021, 77�85.
Golding, J., Pembrey, M., & Jones, R. (2001). ALSPAC*the Avon Longitudinal Study of Parents
and Children. I. Study methodology. Paediatric and Perinatal Epidemiology, 15, 74�87.
Goodman, R., Ford, T., Richards, H., Gatward, R., & Meltzer, H. (2000). The Development and
Well-Being Assessment: Description and initial validation of an integrated assessment of child
and adolescent psychopathology. Journal of Child Psychology and Psychiatry, 41, 645�655.
Hanssen, M., Bak, M., Bijl, R., Vollebergh, W., & van Os, J. (2005). The incidence and outcome of
subclinical psychotic experiences in the general population. British Journal of Clinical
Psychology, 44, 181�191.
Harrigan, J. A. (1984). The effects of task order on children’s identification of facial expressions.
Motivation and Emotion, 8, 157�169.
Hooker, C., & Park, S. (2002). Emotion processing and its relationship to social functioning in
schizophrenia patients. Psychiatry Research, 112, 41�50.
Horwood, J., Salvi, G., Thomas, K., Duffy, L., Gunnell, D., Hollis, C., et al. (2008). IQ and non-
clinical psychotic symptoms in 12-year-olds: Results from the ALSPAC birth cohort. British
Journal of Psychiatry, 193, 185�191.
Izard, C. E. (1971). The face of emotion. New York, NY: Appleton-Century-Crofts.
FACIAL EMOTION RECOGNITION AND PLIKS 19
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

Johns, L. C., Cannon, M., Singleton, N., Murray, R. M., Farrell, M., Brugha, T., et al. (2004).
Prevalence and correlates of self-reported psychotic symptoms in the British population. British
Journal of Psychiatry, 185, 298�305.
Kee, K. S., Horan, W. P., Mintz, J., & Green, M. F. (2004). Do the siblings of schizophrenia
patients demonstrate affect perception deficits? Schizophrenia Research, 67, 87�94.
Kelleher, I., Harley, M., Murtagh, A., & Cannon, M. (2009). Are screening instruments valid for
psychotic-like experiences? A validation study of screening questions for psychotic-like
experiences using in-depth clinical interview. Schizophrenia Bulletin. Advance online publica-
tion.
Kendler, K. S., Gallagher, T. J., Abelson, J. M., & Kessler, R. C. (1996). Lifetime prevalence,
demographic risk factors, and diagnostic validity of nonaffective psychosis as assessed in a US
community sample: The National Comorbidity Survey. Archives of General Psychiatry, 53,
1022�1031.
Kessler, R. C., McGonagle, K. A., Zhao, S., Nelson, C. B., Hughes, M., Eshleman, S., et al. (1994).
Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States:
Results from the National Comorbidity Survey. Archives of General Psychiatry, 51, 8�19.
Kim-Cohen, J., Caspi, A., Moffitt, T. E., Harrington, H., Milne, B. J., & Poulton, R. (2003). Prior
juvenile diagnoses in adults with mental disorder: Developmental follow-back of a prospective-
longitudinal cohort. Archives of General Psychiatry, 60, 709�717.
Kirouac, G., Dore, F. Y., & Gosselin, F. (1985). The recognition of facial expressions of emotions.
In R. E. Tremblay, M. A. Porovost, & F. F. Strayer (Eds.), Ethologie et development de l’enfant
(pp. 131�147). Paris, France: Stock.
Kohler, C. G., Walker, J. B., Martin, E. A., Healey, K. M., & Moberg, P. J. (2009). Facial emotion
perception in schizophrenia: A meta-analytic review. Schizophrenia Bulletin. Advance online
publication.
Kolb, B., Wilson, B., & Taylor, L. (1992). Developmental changes in the recognition and
comprehension of facial expression: Implications for frontal lobe function. Brain and Cognition,
20, 74�84.
Kucharska-Pietura, K., David, A. S., Masiak, M., & Phillips, M. L. (2005). Perception of facial and
vocal affect by people with schizophrenia in early and late stages of illness. British Journal of
Psychiatry, 187, 523�528.
Laurens, K. R., Hodgins, S., Maughan, B., Murray, R. M., Rutter, M. L., & Taylor, E. A. (2007).
Community screening for psychotic-like experiences and other putative antecedents of
schizophrenia in children aged 9�12 years. Schizophrenia Research, 90, 130�146.
Laurens, K. R., West, S. A., Murray, R. M., & Hodgins, S. (2008). Psychotic-like experiences and
other antecedents of schizophrenia in children aged 9�12 years: A comparison of ethnic and
migrant groups in the United Kingdom. Psychological Medicine, 38, 1103�1111.
Mandal, M. K., Pandey, R., & Prasad, A. B. (1998). Facial expressions of emotions and
schizophrenia: A review. Schizophrenia Bulletin, 24, 399�412.
McCown, W., Johnson, J., Austin, S., & Shefsky, M. (1988). Deficits in ability to decode facial
affects in families of schizophrenics. Psychotherapy in Private Practice, 6, 93�101.
Mondloch, C. J., Geldart, S., Maurer, D., & Le Grand, R. (2003). Developmental changes in face
processing skills. Journal of Experimental Child Psychology, 86, 67�84.
Norton, D., McBain, R., Holt, D. J., Ongur, D., & Chen, Y. (2009). Association of impaired facial
affect recognition with basic facial and visual processing deficits in schizophrenia. Biological
Psychiatry, 65, 1094�1098.
Nowicki, S., Jr., & Carton, J. (1993). The measurement of emotional intensity from facial
expressions. Journal of Social Psychology, 133, 749�750.
Nowicki, S., & Duke, M. P. (1974). A preschool and primary internal-external control scale.
Developmental Psychology, 10, 874�881.
20 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

Nowicki, S., & Duke, M. P. (1994). Individual differences in the nonverbal communication of
affect: The Diagnostic Analysis of NonVerbal Accuracy scale. Journal of Nonverbal Behavior,
18, 9�35.
Nowicki, S., & Mitchell, J. (1998). Accuracy in identifying affect in child and adult faces and
voices and social competence in preschool children. Genetic, Social and General Psychology
Monographs, 124, 39.
Office of Population Surveys and Statistics. (1991). Standard occupational classification. London,
UK: Her Majesty’s Stationery Office.
Ostrum, T. M. (1984). The sovereignty of social cognition. In R. F. Wyer & T. K. Skrull (Eds.),
Handbook of social cognition. Mahwah, NJ: Lawrence Erlbaum Associates, Inc.
Pan, Y.-J., Chen, S.-H., Chen, W. J., & Liu, S.-K. (2009). Affect recognition as an independent
social function determinant in schizophrenia. Comprehensive Psychiatry, 50, 443�452.
Penn, D. L., Corrigan, P. W., Bentall, R. P., Racenstein, J. M., & Newman, L. (1997). Social
cognition in schizophrenia. Psychological Bulletin, 121, 114�132.
Phillips, L. K., & Seidman, L. J. (2008). Emotion processing in persons at risk for schizophrenia.
Schizophrenia Bulletin, 34, 888�903.
Plewis, I., Calderwoof, L., Hawkes, D., & Nathan, G. (2004). National Child Development Study
and 1970 British Cohort Study technical report: Changes in the NCDS and BCS70 populations
and samples over time. London, UK: Centre for Longitudinal Studies, Institute of Education.
Poreh, A. M., Whitman, R. D., Weber, M., & Ross, T. (1994). Facial recognition in hypothetically
schizotypic college students: The role of generalized poor performance. Journal of Nervous and
Mental Disease, 182, 503�507.
Poulton, R., Caspi, A., Moffitt, T. E., Cannon, M., Murray, R., & Harrington, H. (2000).
Children’s self-reported psychotic symptoms and adult schizophreniform disorder: A 15-year
longitudinal study. Archives of General Psychiatry, 57, 1053�1058.
Schloegelhofer, M., Schaefer, M., Papageorgiou, K., Werneck-Rohrer, S., & Amminger, G. P.
(2006). Emotion recognition in individuals at ultra high risk for psychosis. Schizophrenia
Research, 86, S94�S95.
Schneider, K. (1959). Clinical psychopathology. New York, NY: Grune & Stratton.
Schreier, A., Wolke, D., Thomas, K., Horwood, J., Hollis, C., Gunnell, D., et al. (2009). Prospective
study of peer victimization in childhood and psychotic symptoms in a nonclinical population at
age 12 years. Archives of General Psychiatry, 66, 527�536.
Schumann, C. M., Hamstra, J., Goodlin-Jones, B. L., Lotspeich, L. J., Kwon, H., Buonocore,
M. H., et al. (2004). The amygdala is enlarged in children but not adolescents with autism; the
hippocampus is enlarged at all ages. Journal of Neuroscience, 24, 6392�6401.
Shaffer, D., Fisher, P., Lucas, C. P., Dulcan, M. K., & Schwab-Stone, M. E. (2000). NIMH
Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): Description,
differences from previous versions, and reliability of some common diagnoses. Journal of the
American Academy of Child and Adolescent Psychiatry, 39, 28�38.
Shean, G., Bell, E., & Cameron, C. D. (2007). Recognition of nonverbal affect and schizotypy.
Journal of Psychology, 141, 281�291.
STATA Corporation. (2005). STATA Statistical Software, Release 9. College Station, TX: Author.
Thomas, K., Harrison, G., Zammit, S., Lewis, G., Horwood, J., Heron, J., et al. (2009). Association
of measures of fetal and childhood growth with non-clinical psychotic symptoms in 12-year-
olds: The ALSPAC cohort. British Journal of Psychiatry, 194, 521�526.
Thomas, L. A., de Bellis, M. D., Graham, R., & LaBar, K. S. (2007). Development of emotional
facial recognition in late childhood and adolescence. Developmental Science, 10, 547�558.
Toomey, R., & Schuldberg, D. (1995). Recognition and judgment of facial stimuli in schizotypal
subjects. Journal of Communication Disorders, 28, 193�203.
FACIAL EMOTION RECOGNITION AND PLIKS 21
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010

Toomey, R., Seidman, L. J., Lyons, M. J., Faraone, S. V., & Tsuang, M. T. (1999). Poor perception
of nonverbal social-emotional cues in relatives of schizophrenic patients. Schizophrenia
Research, 40, 121�130.
Tremblay, C., Kirouac, G., & Dore, F. Y. (2001). The recognition of adults’ and children’s facial
expressions of emotions. Journal of Psychology, 121, 341�350.
Van Os, J., Hanssen, M., Bijl, R. V., & Ravelli, A. (2000). Straus (1969) revisited: A psychosis
continuum in the general population? Schizophrenia Research, 45, 11�20.
Wechsler, D. (1991). Wechsler Intelligence Scale for Children (third edition). New York, NY:
Psychological Corporation.
Williams, B. T., Henry, J. D., & Green, M. J. (2007). Facial affect recognition and schizotypy. Early
Intervention in Psychiatry, 1, 177�182.
World Health Organisation. (1994). Schedules for clinical assessment in neuropsychiatry.
Washington, DC: American Psychiatric Association.
Yoshizumi, T., Murase, S., Honjo, S., Kaneko, H., & Murakami, T. (2004). Hallucinatory
experiences in a community sample of Japanese children. Journal of the American Academy of
Child and Adolescent Psychiatry, 43, 1030�1036.
22 THOMPSON ET AL.
Downloaded By: [University of Bristol Library] At: 00:44 9 November 2010




















