Child Fatality Review in Colorado
80
Child Fatality Review in Colorado: A History 1989–2006 by Donna Andrea Rosenberg, M.D.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Child Fatality Review in Colorado

Child Fatality Review in Colorado:
A History 1989–2006by Donna Andrea Rosenberg, M.D.

ACKNOWLEDGEMENTS
The assistance of the Colorado Department of Human Services,in particular Ms. Shirley Mondragón, for facilitating the use ofCAPTA/Children’s Justice Act grant funds in the preparation ofthis monograph, is gratefully acknowledged, as is the guidanceand technical support of Shannon Breitzman, RochelleManchego, and Mary Chase of the Colorado Department ofPublic Health and Environment.
This report is published by the Colorado Department of HumanServices and the Colorado Department of Public Health andEnvironment with funds from the CAPTA/Children’s Justice Actgrant from the National Center for Child Abuse and NeglectAdministrations for Children, Youth and Families, U.S.Department of Health and Human Services.
Cover: Child with Flowersby Theodore Clement Steele,1918, oil on canvas, private collection
i
Child Fatality Review in Colorado:
A History 1989–2006by Donna Andrea Rosenberg, M.D.
Prepared by:
Colorado Department of Public Health and Environment.
2008
Additional copies may be obtained from:
Colorado Department of Public Health and EnvironmentPrevention Services Division
Injury, Suicide and Violence Prevention Unit4300 Cherry Creek Drive South
Denver, CO 80246-1530(303) 692-2573
or on the web at:
http://www.cdphe.state.co.us/pp/cfrc

U N I ON
CONSTITUTION
AN
D
Bill Ritter, Jr., GovernorJames B. Martin, Executive Director
Dedicated to protecting and improving the health and environment of the people of Colorado
4300 Cherry Creek Dr. S. Laboratory Services DivisionDenver, Colorado 80246-1530 8100 Lowry Blvd.Phone: (303) 692-2000 Denver, Colorado 80220-6928TDD Line (303) 691-7700 (303) 692-3090Located in Glendale, Colorado
http://www.cdphe.state.co.us
ii
Historically, the deaths of children have been far less understood than those of adults. In 1989,the Colorado Child Fatality Review Committee was formed in an effort to better understand whychildren were dying in our state, and with a view to preventing as many of those deaths aspossible. Colorado has been a national leader in this endeavor.
Over the years, dozens of people have contributed their time and passion to this effort. Weacknowledge with gratitude their work, persistence, and professionalism.
This monograph documents the history of Colorado’s Child Fatality Review Team, from itsbeginning in 1989, a time when surveys of children’s deaths nationwide were nascent andprimitive, to today, when Colorado stands as an exemplary standard in a nation that has muchexpanded and refined its focus on death in childhood, but that still has a long way to go.
Donna Rosenberg, M.D. Co-chair, Colorado State Child Fatality Prevention Review Team—2005–2008

iii
PREFACE
A fter 17 years in operation, the Colorado ChildFatality Review Committee had the resourcesavailable to write a brief history of our
activities over that time. Having been a member ofthe Committee since its inception, I thought thatwriting this history would be easy. I was wrong.Though some memories have faded or blurred, andsome administrative files have decomposed withage, there was still a vast amount of material, pro-cedural and statistical, to condense into readableshape that informs, without being too graphic or too dull.
The process involved first combing through themany, many boxes of administrative files that grewduring these years, whose contents document theefforts of the people who gave birth to, and thenguided, the child fatality review process in Colorado.Most of them are now elsewhere, doing other things,retired, even, unfathomably, having migrated to otherstates. All were diligent, but all were also idiosyn-cratic organizers, each with a filing system that was,to say the least, unique. Some documents had dates.Others did not, especially various incarnations of ourdata collection instrument, all of this being a sourceof both frustration and future caution to your tem-porary historian.
An early decision was taken to maximize the infor-mation about our process and to not make this adata-dense monograph. Our aggregate data hasbeen published in previous monographs, and wehope to continue to publish our ongoing data. Abroad-brush approach to statistics was deemedbest.
I am grateful to all those who spoke to me abouttheir recollections and experiences.
I write this preface as I conclude the writing of themonograph, and I see that what is absent from thesepages is a sense of what it has felt like to be a
member of the child death review team, closelyscrutinizing the details of every child’s death in ourstate, month in and month out, year in and year out.One is sometimes asked the question, “You get usedto it after a while, don’t you?” One small story:
We had been a team for many years, with very littlechange in our composition. We knew one another’sexpertise, experience, verbal habits, even hand-writing, quite intimately. We had, by then, reviewedmany thousands of cases of child death together,been over much rocky and sad human terraintogether.
The case was that of a 3-year old boy. He had beendropped off in an emergency room in the dead ofwinter. The cause of death was hypothermia. He hadbeen left outside naked, to punish him for some perceived wrong. Police investigation had found photographs in the glove compartment of the familytruck, showing that the boy had repeatedly beensuspended outside the window of the speedingvehicle, the adults taking pictures of his terrorizedface. At autopsy, he was covered in bruises, fromrepeated beatings. His penis was mottled and someof the tissue had died before he did, from its havingbeen clamped. The marks appeared to have beencaused by a large alligator clip.
I looked up from the paperwork to see one of my colleagues with tears streaming down her face. Shewas a long-time member of our team, a veteransocial worker and social services administrator. Iwordlessly passed her my clean handkerchief. Shewordlessly accepted it. A week later, I received bypost my washed and ironed handkerchief. There wasno note. None was necessary.
So, in response to the question, “You do get used toit, don’t you?” The answer is, No. Never. I suspectthe same is true of my colleagues, past and present,in this necessary and sorrowful business of childdeath review.
—Donna Andrea Rosenberg, M.D.

iv

1
Table of Contents
Background and Accomplishments of Child Fatality Review in Colorado: Highlights . . . . . . . . . . . . . . 2
The Beginning: Two Ladies Were Talking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Colorado Child Fatality Review in the Context of the USA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Confidentiality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Data Collection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Data Collection Instruments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13–23
Natural Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13SIDS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Accidental Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Drowning. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Motor Vehicle Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Suicide Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Homicide Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Firearm Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Undetermined Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Preventability of Childhood Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Problems and Solutions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Local Teams . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Goals of Colorado Child Fatality Review: Past to Present . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Goals of Colorado Child Fatality Review: Future. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Appendix A: Data Collection Instruments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36–63Data Collection Instrument 1989 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Data Collection Instrument 1990 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38Data Collection Instrument 1991–92 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Data Collection Instrument 1994 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Data Collection Instrument 2006. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46Child Fatality Prevention System Clinical Review Process Documents 2006 . . . . . . . . . . . . . . . . . . . . . 62
Appendix B: Activities of the Child Fatality Review Team: Publications, Conferences, Teaching . . . 64–70Publications—Annotated List . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Conferences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67Teaching . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
Appendix C: Membership—Past and Present . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71–72Colorado Child Fatality Review Committee, 1989–2006 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71Colorado Child Fatality Prevention System Review Team Current Membership . . . . . . . . . . . . . . . . . . . 72

2 Child Fatality Review in Colorado: A History 1989–2006
Background andAccomplishments of ChildFatality Review in Colorado:Highlights
AChild Fatality Review Committee has been incontinuous operation in Colorado since 1989,when a memorandum of agreement was
signed between the Colorado Department of Healthand the Colorado Department of Social Services (asthey were formerly named).
At its inception, the Committee was exceptional inthe United States—and the world—because itundertook an ongoing and comprehensive reviewof every single child death in the entire state.
The Committee’s process and methods have subse-quently been widely emulated throughout thecountry.
The Committee reviews approximately 750 childdeaths annually. At this time of this writing, the totalnumber of pediatric deaths reviewed is approxi-mately 12,500.
The Committee, under the auspices of the ColoradoDepartment of Public Health and Environment, hasbeen legislatively mandated since 2005.
Funding for the Committee covers administrativecosts only and comes from a federal grant. Therewas no fiscal note that accompanied the legislativemandate. The Committee operates largely becauseof the volunteer efforts of many professionalsthroughout the state of Colorado.
Accomplishments of the Colorado Child FatalityReview Committee involve system changes, inter-agency cooperation, public education, improvedcriminal investigation, product safety, protection ofsurviving siblings or family members, legislation,traffic safety, better understanding of specific causesof death, professional education and research.
The Child Fatality Review Committee and itsmembers have been integral to these changes andaccomplishments in Colorado:
• Graduated Driver’s License and child passengersafety legislation.
• Coroners can now access social services recordson children.
• Death certificates now have instructions for com-pletion on the back.
• Local child death review teams exist in severalColorado counties / judicial districts.
• Improved communications between coroners’offices and other agencies involved in childfatality.
• Linkage of prevention efforts among agenciesand systems.
• Support for Shaken Baby Syndrome preventionactivities.
• Clarification of public information on variousissues including Shaken Baby Syndrome, SuddenInfant Death Syndrome (SIDS), Baby Doe regu-lations.
• Interaction with media outlets both to clarifypublic misinformation and to promote preventionstrategies.
• Re-opening of criminal investigations.
• Press releases regularly issued by the HealthDepartment, relating to prevention of childhoodinjuries.
• Funding for distribution of car seats.
• Training on proper installation of car seatsthroughout state.
• Institution by local teams of safety measures atdangerous intersections following child fatalities.
• Intervention by social services for safety ofsiblings of deceased children.
• Multidisciplinary training on child death investi-gation, over several years, throughout state.
Child Fatality Review in Colorado: A History 1989–2006 3
• Many presentations of child fatality data atacademic meetings by members.
• Publications in peer-review medical journals ofchild fatality data.
• “How To” manual for development of local childfatality review teams published and distributedthroughout state.
The Beginning: Two Ladies Were Talking
Sometime in 1988, Ms. Pat West and Ms. JaneBeveridge had a troubling conversation. It was about dead children in Colorado. Ms.
Beveridge, from her vantage point at the ColoradoDepartment of Social Services, knew of 48 childrenwho had been fatally abused or neglected during theprevious several years. But the number of childrenwho died of abuse or neglect, according to Ms. Westat the Colorado Department of Health, was far fewer.The immediate question was, “Why is there such a large discrepancy between what our agenciesbelieve to be the truth of child maltreatmentdeaths?” A larger question was “Why are childrendying in Colorado?”
And the central question, the one that is the mostimportant reason for looking closely at deaths inchildhood is, “What can we do about it?”
Any answer is a work in progress because deathtrends change over time, some causes of deathbeing reasonably preventable, others not. This reporttells the story of child death review in Colorado: howit came to be, how it has evolved, the milestones, the successes, the troubles, the questions we haveanswered and the questions to which we hope toone day have an answer.
The reader should understand that looking atchildren’s deaths was a novel, even revolutionary,idea. Our two ladies talking started it all in Colorado.
They created a model for child death review that has now been emulated in countless other places. Itwas not hitherto an endeavor in the world of publichealth. It had no money to fund it at the start, andvery little thereafter. It has depended upon the vigorand commitment of dozens of people over the years(16 dozen, to be precise), some supported by theirown agencies to participate, others simply volun-teering their expertise, for a total of many ofthousands of hours, in the interest of Colorado’schildren, today and for the future.
The conversation between the two ladies wasfounded on years of individual experience. Ms.Beveridge had come to the Department of SocialServices in 1985, after twelve years in the field ofchild protection. She began to collect data on childabuse and neglect deaths around the state, becauseshe perceived a need to reform the investigation andreporting of childhood deaths by departments ofsocial services. Ms. West brought her unique per-spective from her public health vantage point, inparticular from her 1988 state-wide survey of allcounty nursing offices and public health nurses. The purpose of the survey had been to secure apurchase on the role and activities of the nursingdepartments with respect to child abuse and neglect.In 1988 Ms. West and her colleagues at theDepartment of Health wrote an internal paperColorado’s Public Health Issues in Child Physical andSexual Abuse and Neglect, the intent of which was
Pat West (left) and Jane Beveridge, Co-founders, Colorado ChildFatality Review Committee. Ms. West moved to Philadelphia in1991 and continued her work in child fatality review there. Ms.Beveridge remained with the Colorado Child Fatality team andwas co-chair for 15 years, until her retirement in 2005

4 Child Fatality Review in Colorado: A History 1989–2006
“to create the basis for, and an outline of, a statepublic health plan for child abuse.” The paperaddressed needs in “surveillance, policy andprogram development, and translation of scientificknowledge into action at the state and communitylevel.” Viewing child abuse and neglect as a publichealth matter, rather than one strictly within thepurview of social services departments, was anunusual and innovative perspective. The paperbegins, “The Colorado Department of Health is reexamining its role relative to child physical andsexual abuse and neglect.”
The survey work and the resulting paper were, in a sense, precursors to the eventual focus on childfatality review.
After considerable research, the two ladies decided it was time to broaden the conversation. In January1989, a multiagency / multidisciplinary group of 40professionals was invited to gather together andfigure out what to do next about childhood deaths inour state. This group was the Ad Hoc Child FatalityTask Force. It included people from medicine, law,public health, coroners’ offices and social services.The opinion was decisive: “The time has come todetermine why children die and to evaluate whetherthose deaths were preventable.” In the words of Dr.Harry Wilson, pediatric pathologist who, for the nextseveral years until his 1993 move to Texas, com-mitted massive time and effort, we needed to createan “inventory of childhood deaths.” Only if weunderstood the “what” and the “why” would wehave a chance at understanding the “how” of prevention. The Ad Hoc Task Force gave the rec-ommendation that a permanent child deathreview process must be started in Colorado. “Thepreliminary discussions confirmed that therewere widespread problems in identifying thecauses of children’s deaths.”
The bureaucracy of creating a wholly newpublic health survey, especially one thatdepended in part upon the participation ofexperts outside of public health, could havebeen monumental. There were a number of cumbersome options: seek a statutoryamendment within the ColoradoDepartment of Health, seek a bill (and afiscal note) through the state legislature,and perhaps others. The ladies chose the most practical and immediate route:look within the existing mandates of the
Colorado Department of Health and those of theColorado Department of Social Services and see ifthe already-established charges of those agencieswould include child death review. The AttorneyGeneral’s office was asked to address the question.The answer was, Yes: The Department of Health hasthe statutory authority to investigate and determinethe epidemiology of conditions that contribute to
1988 internal paper of the Colorado Department of Health,discussing child abuse and neglect as a public health matter.

Child Fatality Review in Colorado: A History 1989–2006 5
death, and to use Vital Records forresearch conducted in the publicinterest. The Colorado Department ofSocial Services, under the ChildProtection Act, has the responsibilityto protect the well-being of childrenand their families.
And so, a formal InteragencyAgreement was signed in September1989, by the executive directors ofthe two state agencies.
In a later document, the ladiesmodestly comment that, “…bureau-cratic hurdles can be overcomequickly if the multiagency support for such a Committee to exist ispresent.” They do not note howmuch effort, time and skillful campaigning had gone into theirsingle-minded goal for a child deathreview team.
So the documents and, at least theo-retically, the structure were in place.But no one really knew quite how toproceed. The public health memberswere especially helpful, becausethey were the ones with expertise in doing other death surveys. Thesingle most important decision wasthis: We will look at all child deathsin the state; not just the apparenthomicides; not just the apparentaccidents, and so on. The originalproblem identified by the two ladieswas that childrens’ deaths had beenmislabeled. The only way to develop
Interagency Agreement betweenColorado Department of Health and
Colorado Department of Social Services,establishing the Colorado Child Fatality
Review Committee, September 1989.

6 Child Fatality Review in Colorado: A History 1989–2006
an accurate inventory of child death was to look atevery single death and understand it sufficiently inorder to correctly label it and record its details insome consistent way. Then, we would be able toknow what the true numbers were for homicides,accidents and other manners of death.
Death is an event, a moment in time. But everydeath is also a narrative, a story, with antecedentevents, a collection of circumstances and the people
around it. As importantly, therefore, we would have a richer understanding of the series of events thatresulted in death.
From the files, 1989: Without computerrecords or any existing analyses, DebFrench searched and hand-tabulatedthe Colorado Health Department’srecords in an attempt to see how accu-rately child deaths were being reported.

Child Fatality Review in Colorado: A History 1989–2006 7
Colorado Child Fatality Review in the Context of the USA
In 1989, in other parts of the United States, a small number of child death review teams were forming. Colorado’s Child Fatality Review
Committee was exceptional for its decision to do an ongoing and comprehensive review of allchildhood deaths in the entire state.
At the time that the Colorado Child Fatality ReviewCommittee (CFRC) was formed, the landscapeacross the United States for the survey and analysisof child deaths was irregular and, in many areas,entirely barren. For example, it was virtuallyimpossible to estimate the incidence of fatal childabuse. The National Committee for Prevention ofChild Abuse annually surveyed all states, but did notuse a rigorous case definition and excluded casesnot known to either Social Services or other childabuse agencies. Its incidence rate regularly differedfrom that of the Centers for Disease Control, whichused the Uniform Crime Reports from the FederalBureau of Investigation.
The first interagency child death review team wasformed in Los Angeles County in 1978. It incor-porated professionals from criminal justice andhuman services. Dr. Michael Durfee, a psychiatrist inLos Angeles, and Deanne Tilton Durfee have shep-herded the process of child death review towardgreater accountability and visibility both in LosAngeles County and around the United States. By1992, child death review teams had been estab-lished at the state and/or local level in 21 states,covering 100 million Americans or 40% of thenation’s population. Missouri became the first stateto establish a complete functioning network of stateand local teams in all jurisdictions. Also, in 1992, the U.S. Department of Health and Human Servicesheld a national hearing on fatal child abuse in LosAngeles and began an interagency task force toaddress implementation of the process nationally.The U.S. Public Health Service articulated an
objective for the year 2000, including a recommen-dation that state child death review teams beestablished in 45 states. By 2001, according to asurvey done at Brown Medical School, 49 states(including the District of Columbia) had child fatalityreview of some sort, with 40 states having eitherstate or both state and local level child fatality reviewof some scope, though not necessarily as compre-hensive as Colorado’s; another 9 had child fatalityreview at the local level only. Of the 49 states, 32(65%) had child death review legislation in place, but Colorado was not amongst them.
In 2005, the legislation for child death review in Colorado was passed and the Child FatalityPrevention Act was incorporated into the ColoradoRevised Statutes. The purpose of the legislation wasto establish a statewide, multidisciplinary, multi-agency system to prevent child fatalities, and theexisting team that had been functioning since 1989was re-named the Colorado State Child FatalityPrevention Review Team, and was re-organized. The Team remains housed, and under the auspices of the Colorado Department of Public Health andEnvironment, in the Injury, Suicide and ViolencePrevention Section of the Prevention ServicesDivision. There was no fiscal note attached to thelegislation; therefore the process was mandated, but without a budget with which to operate.
Funding
I t would be the rare children’s services effort thatcould boast of having enough funding to fulfill itsgoals. The Child Fatality Review Committee is in
the majority of those that cannot so claim. From1989 until 1995, the committee had a limitedamount of federal funds that were available from the Colorado Department of Human Services (CDHS)and the Colorado Department of Public Health andEnvironment’s (CDPHE) Preventive Health BlockGrant.

8 Child Fatality Review in Colorado: A History 1989–2006
From July 1995 onwards, the funds to support theadministrative costs of the committee have comethrough the CDPHE’s Maternal Child Health BlockGrant. The figures available for July 1995 throughJune 2002 vary annually from $16,728 to $48,073.In addition, the committee was awarded a separateproject grant directly by the Maternal and ChildHealth Bureau for the three-year period 1998–2001.Funding, even at this minimal level, was sometimesuncertain.
From the files: Operating on a shoestring. A 1991apologetic note from the CFRC’s staff assistant to acoroner’s office thanking them for their continuedsupport by sending autopsy records to us. “We havereceived a bill for some reports. When the Committeewas formed, there was no vehicle built in to pay forreports. We are working on setting up a system to do this now and I hope to be able to satisfy your billshortly.” The file copy of the note is inexplicably butpoignantly against a background of a page of detailon several Colorado childrens’ deaths.

Child Fatality Review in Colorado: A History 1989–2006 9
Apart from administrative costs, themajority of the work undertaken by the Child FatalityReview Committee remains unsupported by directfunds. Some of the members of the Committee arepermitted by their own agencies to participate as afunction of their agency duties. Others contributetheir time pro bono.
Confidentiality
Because identified information about each child is reviewed and needs to be protected,every member of the Child Fatality Review
Committee (CFRC) is required to sign a confiden-tiality agreement. Further, no identifying material may be taken from a meeting by persons other thanthose whose agency provided the data, only non-identifying data is maintained in the CFRC database,and data is reported in aggregate form only.
From the files: 2002 newspaperarticles reported on threatened
funding to Colorado’s ChildFatality Review Committee.

10 Child Fatality Review in Colorado: A History 1989–2006
Every member ofColorado’s Child FatalityReview Committee must
sign a confidentialityagreement.
Remarkably few difficulties have arisen with respectto the CFRC’s ability to obtain confidential records,even after the Health Insurance Portability andAccountability Act (HIPAA) federal regulations of1996 (with implementation beginning 2003 andonwards) put highly formalized procedures andpaperwork in place to protect confidential patient
information. This has largely been due to theexcellent and ongoing communication between theadministrative coordinator of the CFRC (a positionwhich historically has had very little turnover) and theagency that holds the records (ex. coroner’s office)because all due authority for the CFRC to have therecords is properly presented and current.

Child Fatality Review in Colorado: A History 1989–2006 11
Data Collection
Everything follows from data collection: dataanalysis, identification of death trends, identifi-cation of preventable types of deaths, and,
most importantly, design of primary preventionstrategies. Since the inception of the Child FatalityReview Committee, data collection has been thesingle greatest challenge. At the time that theCommittee was formed, there was no existing datacollection instrument and one had to be devised. Itwas primitive but functional, and versions of it were
adapted as the years went by. One of the problemswith data analysis over the 17 year time period thatthis history covers is that somewhat different datawas collected on cases, depending upon the yearand the particular incarnation of the data collectioninstrument. In general, however, more detail, notless, was collected as time proceeded.
The starting point for child death review was the col-lection of all death certificates for children under 17years (later, under 18 years) from Vital Records, adivision of the Colorado Department of Health.
For those children who diedat a year of age or less, thebirth certificate was also col-lected. Then, for each of thechildren’s deaths, additionalrecords were sought: socialservices records, autopsyreports and law enforcementrecords. It became clearearly on that having pre-mortem medical records wasnecessary in a considerablenumber of cases every year,in order to better understanda child’s death. For example,if a child’s cause of death isnoted as “seizure” on thedeath certificate, one neededto know if the child had apremortem history ofseizures, that is, if this was aknown underlying condition,or if the seizures were newand unexpected. Now andthen, as another example,the cause of death will havebeen noted as “cardiopul-monary arrest,” with nounderlying cause provided.This is inadequate—car-diopulmonary arrest is not a
Colorado Death Certificate

12 Child Fatality Review in Colorado: A History 1989–2006
cause of death in children, it is death—and moreinformation was needed. The existing rules and regulations of the health department did not at theoutset specifically allow the CFRC to obtain ante-mortem medical records. Therefore, in 1993,application was made to the health department foran amendment, testimony was formally taken at apublic hearing on the matter, and the amendmentwas passed. Thereafter, the team was able to gatherantemortem medical records for due cause. Thishelped immeasurably in many cases to clarify thesometimes inadequate information on the death certificate.
The attention to detail with which the DeathCertificate had been completed was uneven at thebeginning of CFRC and has improved steadily overthe years. In Colorado’s Coroner system, the personcertifying a death is an elected coroner, who is oftennot a medical doctor, though may have training in amedical field. For the most part, a forensic or generalpathologist will determine the cause of death byautopsy, and the coroner will determine the mannerof death based on investigative information. Thedeath certificate may then be completed and signedby the coroner, a coroner’s representative, and/or afuneral home staff person. There are inconsistenciesin how deaths were/are certified in a coronersystem, but with representation from the coronercommunity/association, improvements have beenmade through education and communication.
Data Collection Instruments
The collection of data means that one needs a form (instrument) for each child fatality onwhich to record the same types of data that
one is collecting on all other child fatality cases. The data collection instrument for the Child FatalityReview Committee has undergone many incar-nations and much change since the committeebegan in 1989. Most changes to the data collectioninstrument have resulted from the perception that
having certain more specific data would help betterunderstand aggregate data in terms of preventability.Occasionally, items were deleted from the data col-lection instrument because, however valuable thedata may have been theoretically, it was simply notavailable in the overwhelming majority of cases. Thehigh percentage of missing data might improperlyskew the statistics or lead one to form wrong con-clusions based upon an inadequate sample.
Until the early 2000s, the Colorado Child FatalityReview Committee independently designed its datacollection instrument and the various incarnations of it.
In 2002, the Michigan Public Health Institute wasawarded funding from the Maternal and Child HealthBureau to create and serve as the National Centerfor Child Death Review (NCCDR). Part of the NationalCenter’s charge was to develop a uniform data col-lection instrument for childhood deaths to be usednationally. During 2003–2004, Colorado was one of 18 states working with the National Center todevelop a set of standardized elements and datadefinitions, toward the goal of a finalized uniformdata collection instrument. The committee’s adminis-trative coordinator, Rochelle Manchego, has workedclosely with the NCCDR to revise the data collectioninstrument. This standardized Child Death ReviewCase Reporting System was piloted in 14 states andis now available for national use. The system is web-based, allowing teams to enter case data, accessand download their data and standardized reports viathe internet, and complete data analysis and developreports. With data use agreements between states,we will be able to compare data with other statesand with national compilations of statistics.
Space does not permit a comprehensive inclusion in this History of all the data collection instrumentsthat have been used by the Colorado Child FatalityReview Committee, but a sampling of them showsthe development of the instrument from a very basicone to a highly complex one. These may be found inAppendix A.

Child Fatality Review in Colorado: A History 1989–2006 13
Data
Between 1989–2004, 11,835 children died inColorado. During this 16-year time period, thedeath rate dropped very significantly, from
1989 when the rate was 94.1/100,000 to 2004,when the rate was 65.8/100,000.
Natural DeathsBetween 1989–2004, 8,351 children died naturaldeaths. Over the sixteen years, there was a very significant decrease in the rate of childhood naturaldeaths. The rate fell from 71.5/100,000 in 1989 to 45.7/100,000 in 2004.
Most of the decrease in the naturaldeath rate is accounted for by adecrease in the infant natural mor-tality rate of neonates and infants.Because this decrease occurred inthe context of an overall decrease inthe natural manner of death for allage groups, it signifies a real drop inthe neonatal and infant death rates,not just a prolongation of morbiditythat resulted in death at a later age.
Sudden Infant Death Syndrome(SIDS)
Sudden infant death syndrome is theunexpected death of an infantyounger than one year of age thatremains unexplained after a completeand negative death scene investi-gation, autopsy, and review of theclinical history. The cause of SIDS isunknown, and there may be several.Despite this, SIDS itself is considereda cause of death and can be writtenon a death certificate. When thecause of death is recorded as SIDSon a death certificate, the manner ofdeath is recorded as natural.
Though the definition of SIDS has, throughout theUnited States, remained the same for many years, itis difficult to know how reliable many of the nationalSIDS statistics are, because the working use of thedefinition may be significantly looser than the formaldefinition. For example, in some regions, SIDS maybe noted on the death certificate as the cause ofdeath, when there has not been an adequate sceneinvestigation, or an adequate review of the clinicalhistory, or the autopsy showed abnormalities thatwere not taken into account when finalizing thecause of death.
0
10
20
30
40
50
60
70
80
90
100
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Crude Death Rates: Colorado Occurrences, Ages 0–17, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Source: Health Statistics Section, Colorado Department of Public Health and Environment.
0
10
20
30
40
50
60
70
80
90
100
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Crude Natural Death Rates: Colorado Occurrences, Ages 0–17, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Source: Health Statistics Section, Colorado Department of Public Health and Environment.

14 Child Fatality Review in Colorado: A History 1989–2006
Since Colorado’s Child Fatality Review Committeelooks at every child death in the state with consistentdiagnostic criteria for SIDS that conform to theformal definition, our statistics are some of the mostreliable.
Over a nine-year period, 1990–1998, the rate ofSIDS in Colorado decreased from 2.2 deaths/1,000live births to 0.8 deaths/1,000 live births. This is asignificant decrease. How does one account for therate drop? It is possible that the Back-to-Sleepcampaign initiated in 1992 by the AmericanAcademy of Pediatrics (Pediatrics, 1992; 89:1120-26) has resulted in sufficient response by parents toput babies to sleep on their backs. This appears tobe the trend in Colorado and nationwide. Data fromthe PRAMS (Pregnancy Risk Assessment MonitoringSystem) project in Colorado, which surveyed parentson the sleeping position of infants, showed that thepercentage of babies put to sleep prone (on theirstomachs) decreased from 9.4 percent in 1997 to7.7 percent in 1999. Other explanations, such as arate shift on the basis of definitional change with, forexample, commensurate increases in the rates ofinfant homicide, undetermined or natural manners ofdeath, are not borne out by the statistics. Between1989 and 2004, the rates of infant homicide havenot changed significantly, varying in the rangebetween 1.9/100,000 to 3.8/100,000. The rates of natural manner of death from 1989 to 2004 have decreased steadily from 71.5/100,000 to45.7/100,000. The rates of undetermined manner ofdeath have not changed significantly, varying from0.9/100,000 to 2.5/100,000. Overall, the infantmortality rate has dropped significantly in Coloradobetween 1989–2004, largely due to the drop innatural deaths, with a small portion of those beingdue to the decrease in SIDS deaths.
Since 1998, the rate for SIDS has fluctuatedsomewhat but has neither overall increased norfallen.
The SIDS rate for male infants is almost twice that offemale infants (2.0/1,000 live births compared to
1.1/1,000 live births). Also, the SIDS rate is morethan 2.5 times higher for black infants than for eitherwhite or Hispanics in Colorado. The SIDS rate forblack infants dropped dramatically between 1993and 1995, although even at its lowest, it is still morethan twice the rate for that of white non-Hispanicand Hispanic infants.
The seasonal distribution of SIDS shows that, whileSIDS deaths occur every month of the year, thelargest number of deaths occurs between Decemberand March.
While the reported national peak incidence of SIDS isbetween 2–4 months of age, Colorado’s SIDS agedistribution shows a peak incidence of 1–4 monthsof age. Approximately 95 percent of SIDS deaths inColorado occur before the age of 6 months, which iscongruent with national figures.
But the matter of SIDS is a problematic one. The1989 National Institute of Child Health andDevelopment definition on page 13, is probablyflawed, because the way the definition wasdetermined was probably flawed. Certain deceasedchildren were classified as having died of SIDS.There was probably variability in the quality of sceneinvestigation, forensic autopsy and review of clinicalhistory within this pool of deceased children. Thus,the pool of children whose deaths were ascribed toSIDS was probably made up of children whosedeaths were related to a number of causes. In otherwords, the pool of deaths may have been called SIDSdeaths, but the pool was contaminated. It was datafrom this pool of deceased children that werestudied to discern not only “risk factors” for SIDS, but also to arrive at a definition of SIDS itself.
This is the problem, by analogy: let us say that onecollects all the information on a group of animals,each of which is called a pig. One then studies theinformation to determine what is encompassed andexcluded by pigdom. Unbeknownst to one, mixedinto the data is information on some ducks andgeese, wrongly thought to have been pigs. Here’s theconclusion: pigs fly.

Child Fatality Review in Colorado: A History 1989–2006 15
Now, let us say theoretically that an 11-month-oldchild died unexpectedly, and an investigation of hisdeath yielded no clear diagnosis. His cause of deathwas signed out as SIDS, but in fact he died ofhypothermia. Data about his life and death wereentered into a data pool, along with data from otherdeceased infants. Within the data pool is informationfrom two other theoretical 11-month old infants. Onedied of undetected poisoning, the other of unde-tected inflicted asphyxiation. In both cases, thecause of death was erroneously listed as SIDS. Thepooled data were studied to determine, amongstother things, the age range for SIDS. In conse-quence, it was concluded that SIDS occurs in infantsup to 1 year of age.
There are said to be risk factors for SIDS. Thisbasically means that there are conditions or circum-stances that are more highly associated with SIDS.For example, the following are generally held to berisk factors for SIDS:
The list of risk factors for SIDS has changed over the years. At one time, twin babies (i.e. multiple-gestation infants) were said to be at increased risk of SIDS. This is because when twins would die eitherat the same time or both as infants, and the deathswould be signed out as SIDS, the conclusion was
drawn that twins were at increased risk of SIDS. Infact, twins are not at increased risk of SIDS. Whenno other causes of death are immediately apparent,such as lethal heart malformations, the deaths ofinfant twins are far more likely to be related to environmental causes (ex. carbon monoxide,hypothermia), neglect (dehydration & acute star-vation), genetic causes (inborn errors of metabolism,other genetic anomalies), or some kind of assault(asphyxiation, poisoning).
Also, SIDS has been said to be familial, that is, ababy would be at increased risk if a prior siblingwere dead of SIDS. While it is true that more thanone infant in certain families die, and the cause isdesignated as SIDS, this is almost always becauseSIDS is a wrong diagnosis in multiple infant deaths in the same family. Some of the more likely causesappear above.
The term “risk factor” as applied to SIDS issomething of a misnomer. “Risk factor” usuallymeans that it is the factor itself that causallyincreases the risk of acquiring the condition. Forexample, smoking is a risk factor for lung cancer.However, when the term “risk factor” is used withrespect to SIDS, it really means that the factor is more highly associated with SIDS than with
Maternal Factors Infant Factors Other Factors
• Cigarette smoking
• Absent or delayed prenatal care
• Teen mother
• Older mother
• Unmarried mother
• Poorer mother
• Short time between pregnancies
• Drug abuse
• ? Heavy caffeine use
• Low blood pressure in last trimester of pregnancy
• Anemia
• Preterm birth
• Low birth weight
• ? Prone (on belly) sleep position (accepted by some, notothers)
• Paternal smoking
• Related to waged income in family

16 Child Fatality Review in Colorado: A History 1989–2006
non-SIDS deaths or with non-deaths. The risk factorsfor SIDS themselves are not known to causallyincrease the risk of dying of SIDS.
Indeed, what are called “risk factors” are more likelyto be proxy measures for other, as yet undiscovered,causal agents. A “proxy measure” is the storefrontdisplay; the real goods are in the back room. Forexample, let us say that one is more likely to developlung cancer if one lives in the hypothetical town ofSleepyville, but living in Sleepyville is not a risk factorfor lung cancer. Reason: it is not the living inSleepyville that increases one’s risk of lung cancer; itis that, there being little else to do in Sleepyville, oneis more likely to smoke. Living in Sleepyville is theproxy measure for the real risk factor: smoking. Inthe same way, a mother having no money in thebank, in and of itself, doesn’t cause her baby to diein his sleep.
It is not simply the term “risk factor” that is prob-lematic. Underlying the semantic problem is a logicproblem. For example, pediatricians now routinelyadvise new parents to lay a baby on his back. Theydo this because the American Academy of Pediatrics(AAP) has interpreted the studies to indicate that thereduction in prone sleeping (on belly) in babiesreduces the incidence of SIDS. Presumably, thismeans that there are babies out there who would be dead except that they were put to sleep on theirbacks. Presumably, this in turn means that a baby’srisk of dying of SIDS is reduced if he sleeps on hisback.
On the other hand, from a public health point of view,SIDS is considered a non-preventable cause ofdeath. Hence the question: how can one say thatSIDS is non-preventable and, at the same time, saythat back sleeping has prevented some infants’deaths?
There is considerable contention about the use-fulness of the term “SIDS”. At one end are those who contend that the term “SIDS” serves a usefuland humanitarian purpose: it helps identify aresearchable problem and group of patients; itrelieves distraught, innocent parents of unwarrantedsuspicion; it gives parents a reason—howevermeager—for the child’s death, and affords themaccess to a community of fellow sufferers in SIDSsupport groups.
In the middle are those who contend that, becausethe data pool was contaminated by an unknownnumber of children who had died of causes otherthan SIDS, and manners other than natural, the “riskfactors” for SIDS and the definition of SIDS itself arevery possibly flawed. Some would say they areflawed to the point of meaninglessness.
At the other end, some maintain that the term “SIDS”should be abandoned altogether, because it meansonly one thing: the cause and manner of death areunknown. As such, writing SIDS as the cause ofdeath on a death certificate is simply substituting theappearance of knowledge for knowledge itself, andthe death certificate should say that both cause andmanner of death are unknown.
In Colorado, the approach remains the traditionalone, using the classic definition of SIDS, using it as acause of death on the death certificate, with thosedeaths being signed out as natural.

Child Fatality Review in Colorado: A History 1989–2006 17
Accidental Deaths Between 1989–2004, 2,254 childrendied accidentally. Over the sixteenyears, the rate of accidental death fellfrom 16.3/100,000 in 1989 to12.7/100,000 in 2004, accountingfor the second largest contribution tothe overall decrease in total childdeaths.
All the accidental death rate decreasewas accounted for by children 14years of age and younger, especiallyfor children under age 9. For children15–17 years of age, the accidental death rateslightlyincreasedoverall.
Between 1989and 2004, theaccidental deathrate for childrenaged 1–4decreased from20.4/100,000(possibly anunusually highfigure for thatyear) to11.6/100,000.During the sameyears, the rate decreased from 9.1/100,000 to5.8/100,000 for children aged 5–9. The accidentaldeath rate for children aged 10–14 fell from10.9/100,000 in 1989 to 5.9/100,000 in 2004, butit is as yet unclear if this really represents a true ratedecrease, because the low figure for 2004 may bean anomaly.
Two types of accidental death, drowning deaths andmotor vehicle deaths, were particularly studied bythe CFRC and are summarized below.
Drowning
Over a five-year period, 80 children died of acci-dental drowning, on average 16 children per year.Most (74 percent) were boys. While there was nosignificant rate difference between race/ethnicity,there is a large rate difference amongst age groups.The rate for 1-year old children is more than twicethat of all other age groups (4.3/100,000) except 15 year olds (2.7/100,000). Children 4 years of ageand under constituted 39 percent of all drowningfatalities.
0
2
4
6
8
10
12
14
16
18
20
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Crude Accident Death Rates: Colorado Occurrences, Ages 0–17, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Source: Health Statistics Section, Colorado Department of Public Health and Environment.
0
5
10
15
20
25
30
35
40
45
15–17 Years
10–14 Years
5–9 Years
0–4 Years
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Age-specific Accident Death Rates: Colorado Occurrences, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Rates based on small numbers may fluctuate and should be viewed with caution.
Source: Health Statistics Section, Colorado Department of Public Health and Environment.
18 Child Fatality Review in Colorado: A History 1989–2006
Most children (60 percent) died in open bodies ofwater—lakes, ponds, reservoirs, rivers, creeks andirrigation ditches. Irrigation ditches were the greatestthreat to children ages 2–12; none of the childrenwho drowned in irrigation ditches were under directadult supervision at the time. Lakes and rivers andponds were the greatest threat to teenagers ages13–17. None of the children who died in theseincidents was wearing any, or adequate, life jackets(if they were wearing them, the life jackets were lostbecause they were improperly fastened or too large.)
Bathtub drownings accounted for 14 percent of alldrowning fatalities. These children were either unsu-pervised infants and toddlers, or children andadolescents with a medical history of seizures.
Most drowning fatalities to children in Coloradooccur in rural areas, because most occur in outdoorbodies of water, and most occurred betweenJune–August annually.
Prevention strategies recommended by the ChildFatality Review Committee include:
• Rivers and streams have undercurrents that areextremely dangerous and are not always visible.These are not safe places for children to play.
• Always wear a Coast Guard-approved life jacketwhen on a boat, jet ski, or near open bodies ofwater. “Water wings” or other air-filled swimmingaids are not safe substitutes for life jackets.
• Children and adolescents with a history ofseizures should be monitored during bathing.
• Around a pool, install four-sided fencing thatcompletely surrounds the pool, at least 5 feethigh, equipped with self-closing, self-latching,and locking gates.
• Never leave a child unsupervised in or aroundwater.
Motor Vehicle Deaths
Motor vehicle-related deaths were the leading causeof death for children 1–17 years. They include motorvehicle, bicycle and pedestrian collisions, as well asa few rare cases, for example of a child struck by amotor vehicle while riding a go-cart, or a child leftalone in a car who then engaged the gears.
Only 17 percent of children who died while anoccupant of a motor vehicle were seat-belted in.
Rural rates of fatal motor vehicle crashes are higherthan those for metropolitan areas.
Young drivers: 58 percent of crashes in whichchildren died involved drivers less than 21 years ofage, of which the majority was 16–17 years of age.
Law enforcement determined that at least 27percent of crashes involving young drivers involveddriver inexperience, whereas the Child FatalityReview Committee considered 75 percent to involvedriver inexperience. “The multidisciplinary nature ofthe child fatality review process, along with its focuson prevention, probably accounts for the committee’ssignificantly stronger emphasis on this issue.”
Excessive speed was a factor in 62 percent of thecrashes in which at least one driver was under 21years of age. In 15 percent, blood alcohol waselevated (BAC >0.05), and drugs were found in 14percent.
The Child Fatality Review Committee concluded thatcrashes are not “accidents” in the conventionalsense of the word, because that implies that nothingcould have been done. They are, rather, “predictableand preventable events.”
The Child Fatality Review Committee made publicthe following recommendations, based upon its statistics and analysis:
• Begin safe pedestrian, bicycle, and drivingmessages early…elementary, middle school, andhigh school.
Child Fatality Review in Colorado: A History 1989–2006 19
• Pedestrians should be taught to cross at des-ignated intersections or crosswalks after alwayslooking in both directions.
• Education on rural driving safety, includingcaution at intersections, reduced speed on gravelroads, and stop sign compliance.
• All occupants in vehicle should be appropriatelyrestrained with a car seat or a seat belt,according to size and age.
• Graduated licensing allows young drivers to gainthe experience they need to become safe drivers.
• Encourage mandatory driver’seducation, including a safe drivingcomponent, in high school.
• Increase awareness of adverseweather driving safety—lowerspeeds and extra room betweenvehicles.
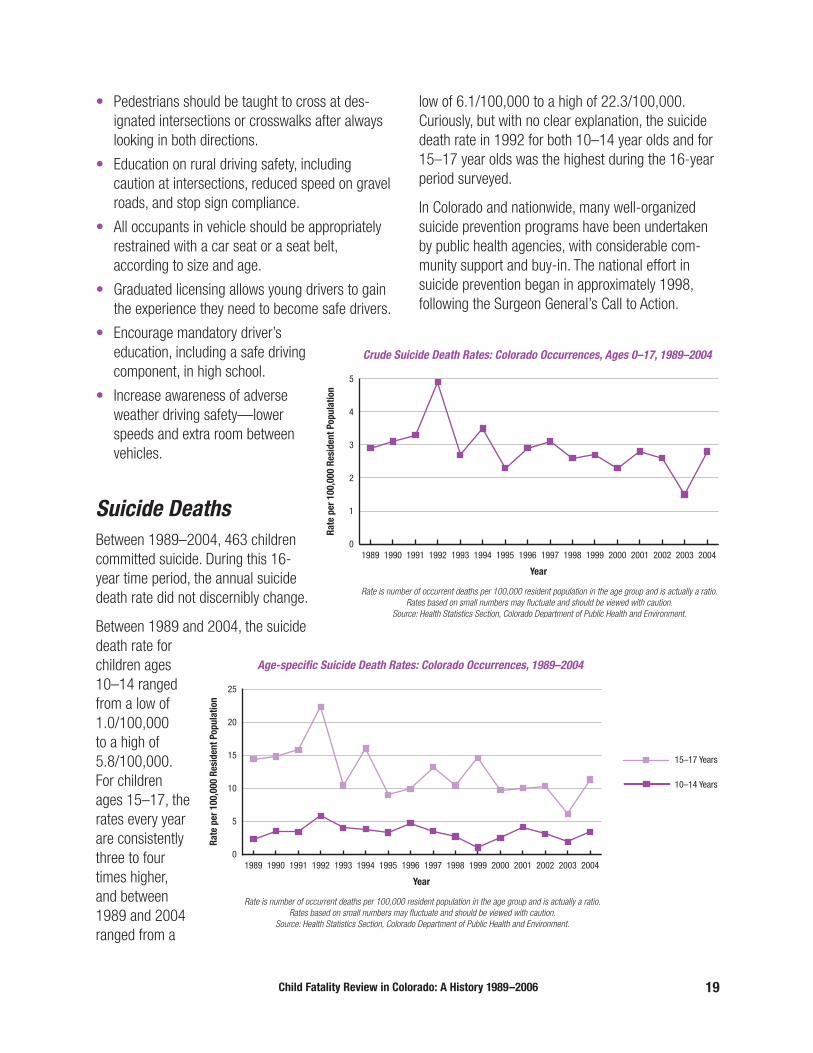
Suicide DeathsBetween 1989–2004, 463 childrencommitted suicide. During this 16-year time period, the annual suicidedeath rate did not discernibly change.
Between 1989 and 2004, the suicidedeath rate forchildren ages10–14 rangedfrom a low of1.0/100,000 to a high of5.8/100,000.For childrenages 15–17, therates every yearare consistentlythree to fourtimes higher,and between1989 and 2004ranged from a
low of 6.1/100,000 to a high of 22.3/100,000.Curiously, but with no clear explanation, the suicidedeath rate in 1992 for both 10–14 year olds and for15–17 year olds was the highest during the 16-yearperiod surveyed.
In Colorado and nationwide, many well-organizedsuicide prevention programs have been undertakenby public health agencies, with considerable com-munity support and buy-in. The national effort insuicide prevention began in approximately 1998, following the Surgeon General’s Call to Action.
0
1
2
3
4
5
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Crude Suicide Death Rates: Colorado Occurrences, Ages 0–17, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Rates based on small numbers may fluctuate and should be viewed with caution.
Source: Health Statistics Section, Colorado Department of Public Health and Environment.
0
5
10
15
20
25
15–17 Years
10–14 Years
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Age-specific Suicide Death Rates: Colorado Occurrences, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Rates based on small numbers may fluctuate and should be viewed with caution.
Source: Health Statistics Section, Colorado Department of Public Health and Environment.
20 Child Fatality Review in Colorado: A History 1989–2006
In Colorado, efforts began in 2000. Nationally, theyouth suicide rates have been falling, althoughColorado’s rates are not yet showing any consistentreduction. Perhaps this is because many of theknown risk factors for suicide in adolescents—stressful life events, hopelessness, poor impulsecontrol, alcohol or other substance abuse, genderidentity conflicts, disturbed interpersonal rela-tionships—are sufficiently common in theadolescent population as a whole that no risk factoritself nor any particular combination of them is suffi-ciently discriminative. The Rocky Mountain region
has one of the higher suicide rates in the country (all ages). Firearms and hanging/strangulation/suffo-cation are the most common methods of suicide.Access to firearms and its relationship to suicide arediscussed below in the section on firearms.
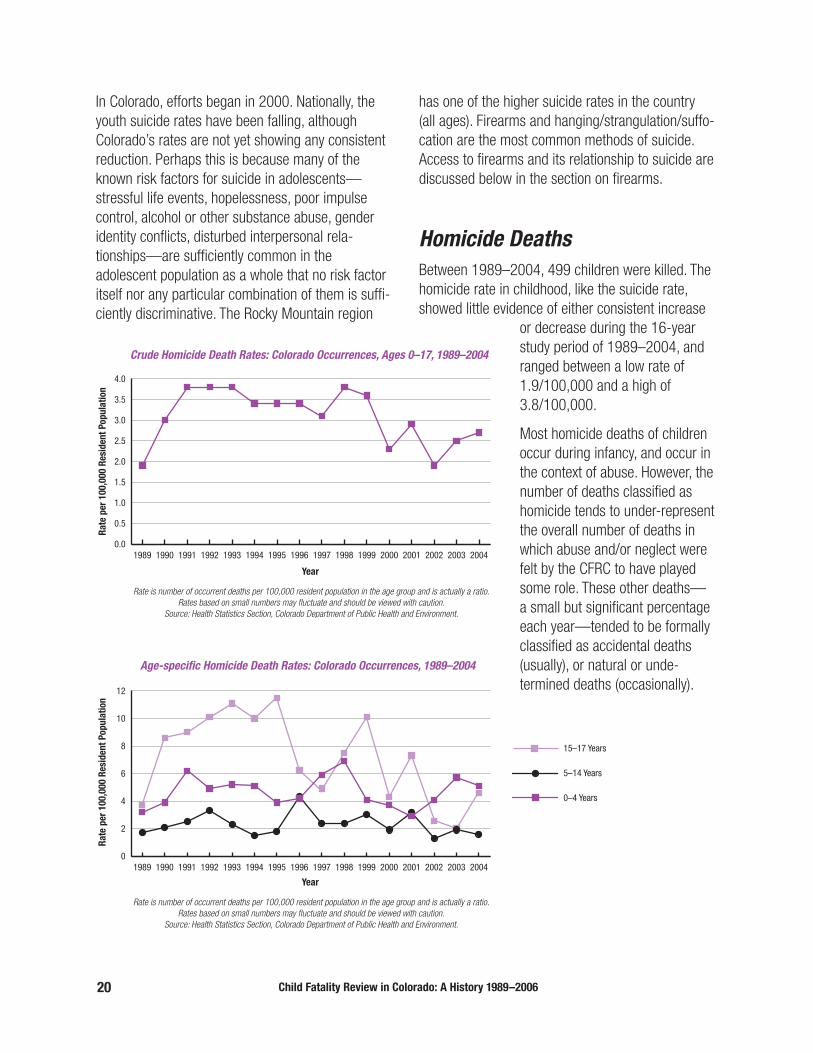
Homicide Deaths Between 1989–2004, 499 children were killed. Thehomicide rate in childhood, like the suicide rate,showed little evidence of either consistent increase
or decrease during the 16-yearstudy period of 1989–2004, andranged between a low rate of1.9/100,000 and a high of3.8/100,000.
Most homicide deaths of childrenoccur during infancy, and occur inthe context of abuse. However, thenumber of deaths classified ashomicide tends to under-representthe overall number of deaths inwhich abuse and/or neglect werefelt by the CFRC to have playedsome role. These other deaths—a small but significant percentageeach year—tended to be formallyclassified as accidental deaths(usually), or natural or unde-termined deaths (occasionally).
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Crude Homicide Death Rates: Colorado Occurrences, Ages 0–17, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Rates based on small numbers may fluctuate and should be viewed with caution.
Source: Health Statistics Section, Colorado Department of Public Health and Environment.
0
2
4
6
8
10
12
15–17 Years
5–14 Years
0–4 Years
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Age-specific Homicide Death Rates: Colorado Occurrences, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Rates based on small numbers may fluctuate and should be viewed with caution.
Source: Health Statistics Section, Colorado Department of Public Health and Environment.

Child Fatality Review in Colorado: A History 1989–2006 21
This is a complex matter, because manner of deathis a unifactorial designation, whereas the complexcircumstances that lead up to death may be bothmultifactorial and difficult to penetrate. As waswritten in one of the CFRC’s reports (June 1998),“Most of the maltreatment deaths fall into the cate-gories of physical abuse, supervisional neglect, ormedical neglect. There are cases, however, that arenot so simple to classify. A case in which a child’smother’s boyfriend physically abuses the child clearlyfalls into the abuse category, but should it be codedas neglect as well if the mother was aware of pastabuse but failed to protect the child? Many motorvehicle-related deaths have associated factors whichcould fall into the category of neglect—failure torestrain the child properly or a parent driving whileintoxicated. Is there a point at which this could beconsidered abusive?”
In about a quarter to a third of all maltreatmentdeaths, there had been a prior child protectioncontact with the victim, a sibling or the perpetrator.Because social services is the agency to which suspected abuse or neglect are mandated to bereported by various types of professionals, it istherefore assumed that social services will be posi-tioned to prevent fatal child abuse. The evidencefrom the Child Fatality Review Committee overalldoes not support this assumption because, whenone looks carefully at the types of problems that hadprecipitated the contact with social services, theywere generally mild to moderate problems, the sortsof problems that social services daily encounters incountless other families. In other words, the natureof the pre-existing family problem could not forewarnsocial services as to the child’s risk, because theproblem was sufficiently pervasive in the generalpopulation and could not serve to discriminatebetween the thousands of families who would not goon to fatally harm their child, and the one that would.
Firearm Deaths
Over a five-year period, there were 193 child deathsfrom firearms, approximately 39 per year, and 18percent of all injury-related childhood deaths.Although the manner of death is recorded on each of the death certificates (of the 193, 46 percent were suicides; 40 percent homicides; 10 percentaccidents; 4 percent undetermined), the manner ofdeath is not always clear. For example, a gun-shotwound that is clearly self-inflicted in a teenager with a high blood alcohol could be determined to besuicide, accident, or undetermined, depending uponthe perspective of the particular coroner completingthe death certificate.
Overall, the great majority of firearm deaths aremales ages 10–17 (80 percent) and Blacks are disproportionately represented (11/100,000compared to a rate of 5.5/100,000 in Hispanics and3.1/100,000 in Whites). However, in the subset ofsuicide firearm deaths, blacks are least represented(11 percent) with Hispanic (26 percent) and whitechildren (63 percent) more likely to kill themselveswith a firearm.
Almost all firearm deaths of children occurred tochildren of the most highly populated counties,though not necessarily the largest urban areas. Byfar the most common weapon used was a handgun,in at least two thirds of all the child deaths.
More than half of all children (52 percent) died at hisor her own home and another 18 percent died at thehome of a relative, friend or acquaintance, meaningthat of all children killed by firearms, 70 percent diedin a home, paradoxically the place that should besafest for children.
Children as young as three years are strong enoughto pull the trigger on many of the handguns availablein the USA. The Child Fatality Review Committeedetermined that access to firearms must be con-trolled by adults, by locking guns and storing lockedammunition separately, with no access to keys by

22 Child Fatality Review in Colorado: A History 1989–2006
From the files: A 1999 Denver Post article highlights necessity for parents to find out if their children are visiting homes withfirearms. Dr. Larry Matthews, of the Colorado Child Fatality Review Committee, is interviewed about the Committee’s findings.
Child Fatality Review in Colorado: A History 1989–2006 23
children. But since 86 percent of all the firearmdeaths were intentional (suicide or homicide),children who may be at risk should have no potentialaccess to firearms, meaning that firearms should beremoved from the home. People living in ahousehold with guns have a five times greater risk ofsuicide than those without a gun in the home.
Gun ownership is both legal and dangerous. Accessis the issue.
Prevention strategies recommended by the ChildFatality Review Committee include:
• Teach children never to touch a gun and to tell anadult if they find a gun.
• Use gun locks and load indicators on all firearms.
• If you own a gun, take lessons on how to properlyhandle a firearm. Make sure children also takelessons if they will be using afirearm.
• Remove firearms from homeswith troubled adolescents.
• Ask relatives, friends andneighbors if they own afirearm and how it’s stored.Don’t allow a child to play ina home where guns areimproperly stored.
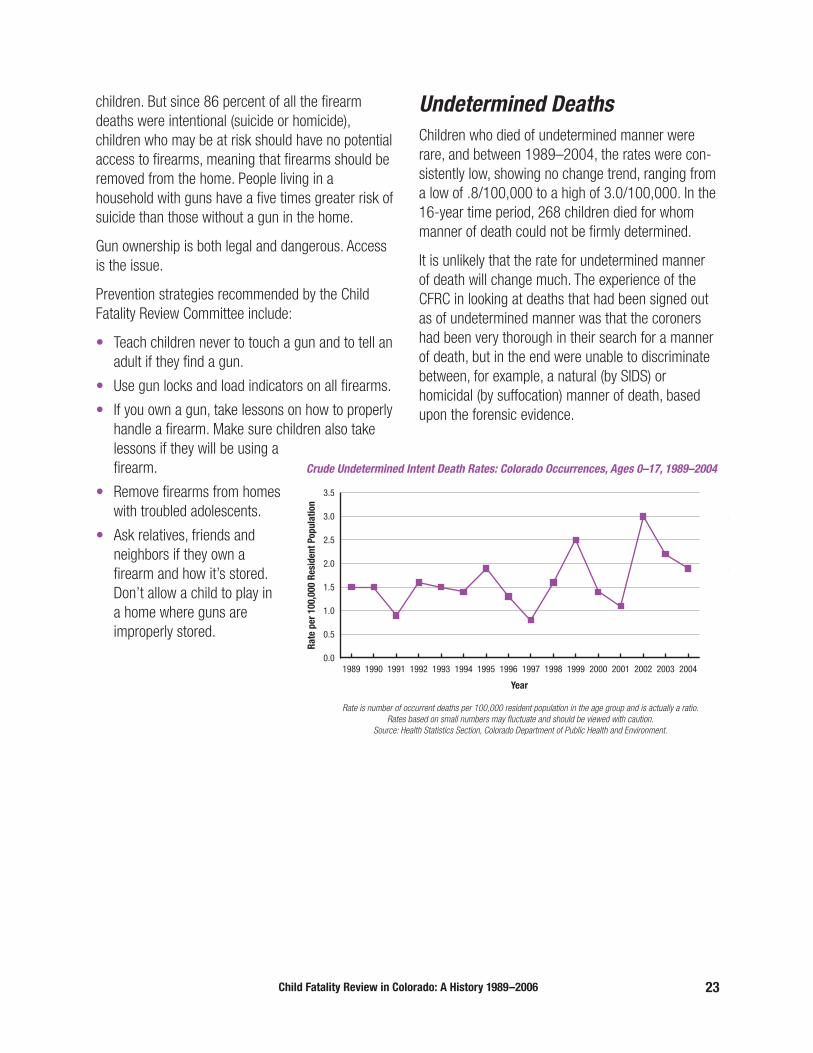
Undetermined Deaths Children who died of undetermined manner wererare, and between 1989–2004, the rates were con-sistently low, showing no change trend, ranging froma low of .8/100,000 to a high of 3.0/100,000. In the16-year time period, 268 children died for whommanner of death could not be firmly determined.
It is unlikely that the rate for undetermined mannerof death will change much. The experience of theCFRC in looking at deaths that had been signed outas of undetermined manner was that the coronershad been very thorough in their search for a mannerof death, but in the end were unable to discriminatebetween, for example, a natural (by SIDS) orhomicidal (by suffocation) manner of death, basedupon the forensic evidence.
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
2004200320022001200019991998199719961995199419931992199119901989
Rate
per
100
,000
Res
iden
t Pop
ulat
ion
Year
Crude Undetermined Intent Death Rates: Colorado Occurrences, Ages 0–17, 1989–2004
Rate is number of occurrent deaths per 100,000 resident population in the age group and is actually a ratio.Rates based on small numbers may fluctuate and should be viewed with caution.
Source: Health Statistics Section, Colorado Department of Public Health and Environment.

24 Child Fatality Review in Colorado: A History 1989–2006
Preventability of ChildhoodDeaths
Preventability is a robust concept in the world ofpublic health, and Colorado’s Department ofPublic Health and Environment successfully
directs much of its efforts to the prevention of mor-bidity and mortality.
For the purposes of the Child Fatality ReviewCommittee, a preventable death was defined as onein which, with retrospective analysis, a reasonableintervention (for example, medical, educational,social, legal or psychological) might have preventedthe death. ‘Reasonable’ was defined by taking intoconsideration the conditions, circumstances orresources available.
The definition is loose, and leaves quite a bit of roomfor subjective determination. It was not alwayspossible to determine whether or not a death waspreventable, either because of inadequate infor-mation collected at the time of death, insufficientinformation made available to the committee, or noclear consensus among committee members thatthe death was preventable.
The Child Fatality Review Committee estimated that one in four childhood deaths was preventable.During a five-year span, 1990–1994, almost allhomicides (95 percent) were thought to have beenpreventable, similarly almost all accidents (94percent), more than half of the undeterminedmanner of death cases (58 percent), all of thesuicides (100 percent) but very few of the naturaldeath cases (4 percent). As is clear from this data,the overwhelming majority of deaths that aredetermined to have been preventable fall into thelarger category of injury, which includes suicide,homicide, and accident.
Unlike public health interventions that can bedirected at natural manners of death, for example,infectious diseases that are blood-borne or causedby insect-to-human transmission, interventions that
can be put in place to prevent homicide, suicide andaccident are significantly more problematic, becausethey may largely depend upon changing humanbehavior or impulse, notoriously difficult to do, especially quickly. However, this by no meanssuggests that intervention into human behavior isimpossible—witness the vast changes that havebeen made in smoking behavior (and thereforesecond-hand smoke exposure) through variousmeans, mostly legislation that is informed by datafrom, and lobbying by, public health bureaus.
In relation to homicide, data show that almost allthese deaths are of infants, with a few toddlers andpre-school children. Because of deeply valued andnecessary rights of privacy in this country, theseyears from 0–5 tend to be the “invisible years,” i.e.,years when there is no public oversight of children.Most of the children who were murdered had nothad direct referral or intervention by social servicesbefore they died. It is problematic to try to balancehomicide prevention efforts in this age range, effortswhich would at least require legislated oversight ofall children in this cohort, with rights of privacy thatare a cornerstone of our legal system and a foun-dation of our culture. When children enter school,there is a public system that regularly sees childrenand is legally charged to monitor them for abuse,neglect, and absence. Homicide rates in the school-age child are low, probably the result of acombination of the child being more physicallyrobust and less attackable, being at school for manyhours each day, i.e., having decreased exposure topotential harm, and being monitored at school sothat signs of abuse or neglect can be perceivedearly, reported to social services, and early sec-ondary prevention strategies hopefully put into place.
Whether the majority of homicidal child fatalities aretruly preventable, given the age at which most occurand the fact that no public agency is likely to havehad access to the child, is still questionable.Anecdotally, however, it appears that few if anychildren are killed with more than two adults in the

Child Fatality Review in Colorado: A History 1989–2006 25
home. This “light of day” phenomenon may helpguide resources so that more young children havebetter access to pre-school care by a group ofadults.
Public health experience with accidents, anothertype of preventable death in childhood, is more successful, and data from the Child Fatality ReviewCommittee have helped inform some public healthmeasures that have resulted in legislativechanges. For example, rates of teen motorvehicle deaths did not diminish even with driver’straining. Therefore, in 1999, Colorado introducedthe Graduated Drivers Licensing Law, and madeit stricter in 2005. The law is designed to givenovice drivers more experience behind the wheeland limit high-risk situations while they are stillmastering the task of driving. The law aimed toreduce the number of vehicle-related deathsamongst teens by gradually introducing them todriving. According to the law, a teenager mustgo through stages before he or she can obtain afull driver’s license. At age 15, a teen mayobtain a driver’s permit if heor she presents proof ofenrollment in a driver’s edu-cation course approved bythe Department of Motor
Vehicles. Teens are subject to various restrictions,including driving only when accompanied by alicensed driver 21 years of age or older while accu-mulating at least 50 hours of behind the wheelinstruction, 10 hours of which must be done atnighttime. Drinking and driving is prohibited, as arecell phone use and traffic violations. After a year of alearner’s permit, and passing a provisional driver’s
From the files: Articles in the Denver Post focus on
graduated driving for teens.

26 Child Fatality Review in Colorado: A History 1989–2006
license test, a teen still has restrictions for 12 moremonths, including:
• No driving between midnight and 5 a.m.,
• No passengers under 21, unless a licensed driverover 21 is present for the first six months,
• Only one passenger under 21 for twelve months,
• Not more than one passenger in the car fordrivers under 17,
• Recommended seatbelts.
These laws were based upon public health data thatanalyzed driver age, passenger composition, time ofday of crashes and other factors, meaning thatrather than try to change behavior, public healthefforts were directed at legal change, i.e., limitingthe opportunity for the dangerous behavior. Thegraduated driver’s license law has shown goodresults in other states, such as Florida, where it isactively enforced.
Suicide, along with homicide and accident, is thethird corner of the injury triangle. Much research andpublic health resources, in Colorado and nationwide,have been directed at suicide prevention. Mostchildhood suicides are teenagers, and close scrutinyof the case material by the Child Fatality ReviewCommittee indicates that most teens who die bysuicide have not previously attempted it and that, in this population, there is a mix of circumstances,some of the teens having experienced very difficulthome and social situations while others had noknown pre-existing risk factors for suicide. (However,it must be noted that access to comprehensive andreliable data about pre-existing risk factors is oftendifficult and therefore makes our conclusions lessrobust.) In the same way that decreasing the oppor-tunity for dangerous behavior in teen drivers hasbeen deployed through legislated driving controls,the single intervention most likely to succeed indiminishing suicide amongst adolescents is fore-closing access to firearms. As noted elsewhere,people living in a household where a gun is kepthave a five times greater risk of suicide than people
living in a household without a gun. At the presenttime, there is little likelihood that any legislativeaction in our state will restrict gun access toteenagers.
This means that adults in the home must be effec-tively educated to make sure that firearms areunavailable or absolutely inaccessible.
We continue to grapple with the issue of preventa-bility, not just in analyzing data and positioning publichealth or legislative strategies to diminish childhooddeaths, but with the definition of “preventability”itself. While it is true that, in theory, most homicides,suicides and accidents are preventable, human life is not so tidy and human beings not so willing toabsorb and act on prevention strategies, howeversensible, that are taught to them. Understanding thatone should act in a certain way is not equivalent toacting in that way. “Preventable,” in the best of allpossible worlds, is not the same as “penetrable” inthis one. It makes most sense to put resources intothose types of childhood deaths that are both pre-ventable and penetrable, i.e., for which there is aclear point where prevention measures are likely tobe effective. This has been done with some forms of accidents, for example preventing swimming pooldrownings by the erection of functioning securityfences around the pools. Seat belt laws for infants,combined with the wide availability of infant carseats through public health programs, have had asignificant impact on the rate of accidental infantvehicular deaths. Teaching still matters but, as notedby Lynn Trefren, a public health nurse with longservice to the Child Fatality Review Committee, “Thebiggest issue we face in our clinics is prioritizing theinformation that we give to families. We know thatthey cannot take in all the information we have tooffer. Looking at major causes of preventable deathscan give us some guidance in choosing the teachingthat might offer the most protection to that child.Another major challenge within our system is thelack of resources our families deal with. No parentcan give total focus to potential injuries when lack offood or shelter is a real, daily issue for them.”

Child Fatality Review in Colorado: A History 1989–2006 27
From the files: A 2000 Rocky Mountain News article on the disputes over gun control in Colorado. The controversy continues.

28 Child Fatality Review in Colorado: A History 1989–2006
Problems and Solutions
In many ways, the Colorado Child Fatality ReviewCommittee/Team is remarkable for having had sofew of the problems experienced by other large
teams, despite the fact that many of our memberspreviously had, at most, a nodding acquaintance withone another, hailed from vastly different disciplines,and jointly undertook a novel endeavor together.Turnover has been very low; participation has beenvery high. Consensus over classification of certainaspects of death (was there neglect? was this a preventable death?) has not been uniform, but theprocess has allowed for discussion and dis-agreement. Administration of the team has beenhandled not only ably, but also with tact andoutreach that has helped the team form good rela-tionships with the coroners’ offices and lawenforcement, and therefore helped greatly with theaccumulation of data. Turnover for this position hasalso been low, with only four sequential adminis-trators of the team in 17 years—Sally Van Manen,Carol Carney, Mary Chase (who has gone on tobecome the Director of the Vital Statistics Unit at the CDPHE) and Rochelle Manchego. We have beenfortunate that the program director of Injury, Suicide,and Violence Prevention Programs at the CDPHE hasconsistently taken an interest in and supported thechild fatality review process. The current director,Shannon Breitzman, continues in that tradition. Therehas also been excellent support from the statisticalexperts at the CDPHE. The state Department ofHuman Services (formerly the Department of SocialServices) has, from the beginning, been pivotallyinvolved with, and supportive of, the Committee. It is unlikely that the team could have formed or con-tinued functioning without them. Active participationby top-level people and the provision of socialservices data have been consistent.
So, what were the problems?
One of the earliest was getting information fromvarious agencies, even though the paperwork was inplace to have it released. Understandably, there wasa sense that “the state was coming in” to criticize
the handling of various cases at the local level. Overtime, and time was an important element here, andwith professionalism and grace, the relationshipswere established with these various agencies by theteam administrator, sometimes with the intervention(a phone call, later on emails) from a member of theteam acquainted with the agency. Mr. Tom Faure, Dr. Tom Henry, and Dr. Amy Martin are specificallymentioned for their sustained efforts in reaching outto their coroner colleagues across the state toenhance the committee’s ability to collect andanalyze data. Jill-Ellyn Straus, prosecutor with theAdams County District Attorney’s Office, was over theyears a tireless ambassador for the Child FatalityReview Committee and immeasurably enhanced ourwork with law enforcement. It is also a measure ofthe competence of the committee’s administratorsthat these issues were rarely brought to the attentionof the team members.
Inevitably, various legal questions arose during theprocess of review. Some of them were: What do wedo if we think a doctor in the community is deliveringsubstandard care? What do we do if we suspect abreach of the Baby Doe laws (protecting the rights of newborns with congenital disabilities)? What if oneof the prosecutors at the team meeting decides tosubpoena one of the doctors also at that meeting,based upon an opinion expressed in a confidentialenvironment, relating to materials protected by confi-dentiality? How do we both adjust to and complywith the new HIPAA regulations? What do we do if we are worried that confidentiality has beenbreached in a case (my recollection is that this was a concern only once in 17 years, and there was nofinal proof of breach)? Most of these, and other, legalmatters were turned over for a response from theteam’s legal counsel, the state’s Attorney General.
One hiatus in the Committee’s work occurredbetween August 2002 and January 2003, when the Committee requested guidance from its legalcounsel, the state Attorney General’s Office, on clari-fication of confidentiality rules that applied to theactivities of the review process, rule clarification onpublic meetings, and guidance on storage of doc-

uments. While waiting for the legal opinion, activitiesof the Committee were suspended. The AttorneyGeneral’s Office undertook major research on thesequestions, and operation thereafter resumed.
Two problems that have beset the team and have notbeen solved are: How do we publish our data on aregular basis, given the tremendous amount of timethat the analysis and writing take and with the verylimited (or no) resources available to do so? How dowe move from collecting data and developing aninventory of child death to creating and evaluatingprimary prevention projects?
Local Teams
However detailed the information about achild’s death that is reviewed by the stateChild Fatality Review Committee, it is likely
that a local group, in the county or judicial districtwhere the child resided, will have
better information
and be able to more usefully benefit from that infor-mation. Bringing agencies together at a communitylevel offers the greatest potential for strengtheningintervention and prevention efforts for children andfamilies.
The Child Fatality Review Committee functions at the state level, meaning that it can best see—andpotentially solve—systemic problems, identify policyissues and arrange for statewide data collection.Early on, the state committee realized that it wantedto help maximize an effort to form and sustain localchild death review teams in Colorado. In October1993, the committee published the monograph,“How to” Manual for Local Child Fatality Review. InJanuary 2001, the revised version, titled How toStart a Local Child Fatality Review Team: Guidelinesfor Local Child Fatality Review in Colorado was pub-lished and is available at no cost on the web athttp://www.cdphe.state.co.us/pp/cfrc.
The goals of local team review include improvementof a community’s response to at-risk families; identification and prevention of social and family
circumstances that con-
tribute to child fatalities;promotion of cooperation and communicationamongst agencies; and sharing of information aboutadvances in the fields of investigation, intervention,prevention and prosecution of child death.
Several counties in Colorado have formed local childfatality review teams, valiantly operating on little or
From the files: The convening of a local child fatality review team was newsworthy.
Child Fatality Review in Colorado: A History 1989–2006 29

30 Child Fatality Review in Colorado: A History 1989–2006
no budget. For example, the El Paso CountyDepartment of Social Services contracted with theColorado Department of Social Services, so that the State department agreed, for the period of sixmonths and the sum of not more than $6,050.88, to give total material, technical, on-site and dataanalysis support to the nascent El Paso County childfatality review team.
As of 1999, there were 5 functioning local countyteams in the state: Boulder (established 1997),Denver (established 1996), El Paso (established1996) , La Plata (established 1994, capturingArchuleta and San Juan counties), Mesa (established1995, with cases from an additional 7 surroundingcounties), and Pueblo (established 1994).
A 1998 survey of those teams by our state ChildFatality Review Committee yielded some interestingfindings: most of the counties reported that theywere reviewing cases quickly, within days or weeksof a child’s death. They were clearly more nimbleoutfits compared to our state child death reviewteam, which had to requisition records and wait forthem. They also reported that local prevention, inter-vention and investigation activities could take placemore easily as a result of the review process. Forexample, Denver Child Fatality Review Team reportedthat they had a policy change at social servicesrelated to response time to child death, a new open-door policy with top Denver Department of SocialServices administration, and the ability to get intoplace safety features and signage at a particularlocation after a pedestrian had been struck there bya car. El Paso county reported that they had held agun safety forum with three community meetings as a direct result of child fatality review. They wereattempting to work with the police department todevelop a better surveillance form on firearm-relateddeaths or injuries, including the make and model ofthe weapon, the owner, and where the firearm camefrom. La Plata county reported that the reviewprocess added impetus to prevention activities; forexample, a drapery cord choking emphasized theimportance of the Bright Beginnings Home Safety Kit,and there had been coordination of activities with
groups such as Scared Stiff and Drive Smart. Mesacounty reported that there had been some pre-vention activities coordinated with schools, andPueblo county also reported that they had institutedsafety features and signage after a pedestrian wasstruck by a car. Only Denver county reported thatthere was any funding for their child fatality reviewprocess, with annual funds of about $15,000coming from a portion of the salary of one employeeat the Child Advocacy Center. All the other countychild fatality review teams depended upon the pro-fessionals who volunteered their time.
By 2000, Adams and Arapahoe counties had beenadded to the list of counties that conducted regularchild fatality review.
On 17 July, 2001, the Colorado Child Fatality ReviewCommittee sponsored a Local Team Teleconference.Many team members representing Arapahoe, Denverand El Paso counties child fatality review teams par-ticipated. The main team membership problemshighlighted were that representation from the schooldistrict was important but uneven, as was represen-tation by law enforcement. Data collection tools wereinconsistent amongst counties and there was a realquestion as to what to do with the data, once col-lected. The local teams had various ideas as to howto make use of the data, especially in designingprimary prevention strategies and developing a goodrelationship with the media. Insofar as the teamswere operating on either no budget or very littleindeed, there were no plans made to move forwardwith any specific programs.
As of this writing, the local teams that are inoperation include: Adams, Denver, El Paso, Mesa,and Pueblo counties, but funding has been sparse orabsent, and the teams continue to function largelybecause of the professional volunteers. It is possiblethat these local teams will regularly use the same(complex but thorough) data collection instrumentthat is being used at the state level, but the burdenof the data collection instrument may make it toocumbersome, with diminishing returns.
Child Fatality Review in Colorado: A History 1989–2006 31
Goals of Colorado Child FatalityReview: Past to Present
In the first publication of the Child Fatality ReviewCommittee (Annual Report and ConferenceProceedings, April 1991—See Appendix B), the
goals of the CFRC were published. Let us look atthese goals of over a decade and a half ago and seeif they have been achieved and how, or not achievedand why.
Goal #1: “To describe trends and patterns ofchild deaths in Colorado”.
This goal has been the most successful. Inspectionof the Colorado Child Fatality Review Process showsthat once cases are sorted on the basis of manner ofdeath, the individual case material is then carefullyreviewed by expert groups and/or subcommittees.
Goal #2: “To identify and investigate theprevalence of a number of risks and potentialrisk factors in the population of deceasedchildren.”
This goal has been achieved in part, largely in con-nection with four particular categories of death:motor vehicle deaths, drowning deaths, firearmsdeaths and SIDS deaths. These finding are exploredin the four Briefs, published by the CFRC between1999–2001 and have been briefly summarizedabove (See Appendix B).
Goal #3: “To evaluate the service and systemresponses to children and families who are considered to be at high risk and to offer recommendations for improvement in thoseresponses.”
In fact, this goal has 3 parts: 1) identify high riskfamilies; 2) evaluate service and system response tothose families; 3) recommend improvements inthose responses.
This goal was predicated on the assumption that itwas possible to prospectively identify “families who
are considered to be at high risk” and that theservice and system inadequacies could prevent anumber of deaths. The term “high risk” refers to therisk of child abuse/neglect deaths.
As can be seen, the goal of recommendingservice/system responses depended upon the abilityto identify those families in which a homicidal childabuse/neglect death is most likely. This has notproven possible. Identification depends upon one or several features being present in the “high risk”group and absent in the low risk group.
There are two elements of identification. The first isthat the family has to be known to social services.The second is that the family has to have certainfeatures present that are indicative of “high risk”,i.e., features that do not occur in other families. Both these elements, according to our data, areproblematic.
Consistently, approximately 70 percent of childrenwho die in the context of child abuse/neglect areunknown to social services prior to the death.Therefore, there was never an opportunity to deploypreventive intervention, much less to recommendimprovement in that intervention. Of the approxi-mately 30% of children previously known to socialservices, almost all the families had been reported or investigated for “minor” child abuse or neglect,meaning that they did not differ in any identifiableway from the many thousands of other families alsoreported for “minor” abuse who did not go on to kill a child.
It is common for social services to receive reports of,or investigate, minor abuse or neglect and thereforethis sort of report does not constitute a flag or riskfactor for later homicide, that is, it does not help dis-criminate between the many children reported andinvestigated for minor abuse/neglect who surviveand the few who are reported/investigated who arelater killed. This means that social services is not in a position to prevent child abuse, or neglect,fatalities in the first instance, but may be veryeffective at preventing severe injury or death of

32 Child Fatality Review in Colorado: A History 1989–2006
siblings. It is unlikely that directing resources todepartments of social services for the prevention of a first child abuse death in a family will result in asignificant decrement of the infant fatality rate. Thisgoes against the expectations of the public and the
wishes of the professionals, because we wish thatpouring more money and related resources into theproblem will diminish it. It may not. The point of pen-etration—and therefore prevention—comes onlyafter the first death in a family. This is a tragedy but
Flow chartshowing
Procedurefor CaseAnalysis,
Child FatalityReview
Committee,mid-late
1990s.
Child Fatality Review in Colorado: A History 1989–2006 33
not one that is likely to change without vast changesin the social structure that would involve some sortof prevention (home visitor services for all newmothers, for an extended time; community daycaresor nurseries as in France; the Nurse FamilyPartnership [NFP] Program in the United States andelsewhere—www.nursefamilypartnership.org). Inother words, there does not appear to be a usefulrisk assessment tool for social services to identifythose families more likely to fatally abuse a firstchild. Preventing child abuse or neglect deathsremains the problem it has always been, but havingthese sorts of “negative results” means thatresources are not hopefully, but improperly, directedto measures that are unlikely to result in significantrate changes, and that we must look for otheravenues in the prevention of deaths of childrenunder five years of age.
In 1988, a peer review Social Services Child FatalityReview Team was established that, over the nextthree years, 1989–1991, looked closely at all childhomicide fatalities in our state, publishing theirreport of this review in the June 1993 Annual Reportof the Colorado Child Fatality Review Committee (see Appendix B). Case-specific reports were issued,outlining significant events in the case, strengths,concerns and recommendations for policy, procedureor training. The peer review model was new to thefield of child protection and staff struggled with thelevel of responsibility they feel when a child dies dueto abuse or neglect. Emphasis in the peer reviewchanged over time, increasingly addressing systemicissues such as training needs and policy and pro-cedural concerns. A state consultant was also hiredto provide assistance to those staff who were experi-encing complicated grief as a result of a child’sdeath. There were several policy and practice impli-cations that were identified over the course of thestudy, significantly:
• Neglect is at least as lethal as abuse. Moretraining is needed on standards of care and inter-vention in neglect. Supervision neglect of childrenunder the age of six must be given high priority.
• Domestic abuse is common in many of the childmaltreatment deaths, but the relationshipsbetween child protection workers and domesticviolence staff are marked by misunderstandingand lack of knowledge on both sides.
• In chronically maltreating families, detailed caseplans are critical, in order to measure progress orlack of progress. Progress must be measured byuseful behavioral change by the parents, notsimply by compliance with the treatmentprogram.
• Black and Hispanic children are overrepresentedamongst child maltreatment deaths. The childwelfare system must evaluate which factors areplacing these children at higher risk.
• Any adult in the home of an abused or neglectedchild must be involved in the treatment plan, notonly the female head of household. This includeslive-in companions.
• Since there were a number of child maltreatmentdeaths where there had been prior involvementby social services with a sibling, it is important forcaseworkers to evaluate the safety concerns forall children in the family.
• Vulnerable stages of a case include changes ofcaseworkers or jurisdictions. Increased super-vision is indicated.
• Social services are chronically understaffed todeal with the problem of child maltreatment inour state. Additional caseworkers are needed.
In summary, the goal of evaluating, and recom-mending improvement in the system responding to“high risk children” was a goal worth undertaking,but most children who die in the context of abuseare unknown to the system and therefore notaccessible for intervention. Other preemptivesystems must be implemented.

34 Child Fatality Review in Colorado: A History 1989–2006
Goal #4: “To characterize high risk groups interms that are compatible with the developmentof public policy.”
This goal is an expansion of the previous one, andmeans that those children who die of any manner—natural or one of the injury manners (suicide,accident, homicide beyond the infant/toddler age—should have the characteristics of their deaths, andin particular the group characteristics sufficientlyunderstood as to develop useful public policy.
Certainly, the collection of data by the Child FatalityReview Committee has enriched our understandingof these types of deaths, well beyond what was pre-viously culled only from death certificate information.This is due to the fact that our data sources havebeen far broader, and have included informationfrom social services, law enforcement, trans-portation, schools, pre-mortem medical records andsometimes highly detailed information from othersources, such as the Federal Aviation Administration(on air carrier deaths in private aircrafts). Weperceive, for example, that a fair number of pediatricaircraft deaths occur when a licensed but relativelyinexperienced family member is piloting a privateaircraft and there is aircraft malfunction or difficultweather that might have been manageable bysomeone with more regular piloting experience.Tragically, these also tend to be those situationswhere several members of a family are on board,and die together.
So, the characterization of these high risk groupshas been achieved by the rich data collection. Butthe second part of this goal—translating that char-acterization into public policy—overall has not. Thereisn’t even wide agreement on how to define ‘publicpolicy.’ It can mean: whatever governments chooseto do or not to do; the actions of government and theintentions that determine those actions; politicaldecisions for implementing programs to achievesocietal goals; the outcome of the struggle in gov-ernment over who gets what.
What is clear from all these definitions is that theforce of government is at the center of public policyand that government is both influential and influ-enceable. What is implicit is that public policy almostalways carries a fiscal note, to implement, monitorand evaluate it.
The Child Fatality Review Committee has not, histor-ically, been very influential in developing publicpolicy. A large reason is that good, solid data over aconsiderable period of time is necessary in order tohave credibility for proposals, and most of our effortshave thus far been directed toward data collectionand analysis. A second reason is that, unfunded orunderfunded as the team is, relying as it largely doesupon professional volunteers, there has been littletime left to undertake the heavy lifting involved inwriting, meeting, lobbying and generally beinginvolved in the legislative process. Finally, some ofthe most important issues, such as significantlystricter gun control, are unpopular in our stateamongst both legislators and the populace.
In summary, the characterizations of the high riskgroups are available as a result of a rich data setcollected over many years, but the Child FatalityReview Team has not been as centrally involved inthe development of public policy as the originalmembers had hoped.
Goal #5: “To improve the sources of data col-lection by developing protocols for autopsies,death investigations, and complete recording of cause of death on the death certificate.”
Aggregate data is valuable only when it is accurateand complete, and depends entirely upon the indi-vidual sources of data also being accurate andcomplete. At the beginning of the child death reviewprocess, 39 percent of children’s deaths weredeemed to have been inadequately investigated, and 15 percent of SIDS cases were believed to havebeen inadequately investigated.

Child Fatality Review in Colorado: A History 1989–2006 35
Over the years, Tom Faure, Chief MedicalInvestigator with the Boulder County Coroner’s Officeand active in the state coroner’s association, wasinstrumental in helping the Child Fatality ReviewCommittee forge a relationship with coroners aroundthe state. Recognizing that we had come a long waybut still had a way to go, in 1998, Dr. Tom Henry, ofthe Denver County Coroner’s/Medical Examiner’sOffice, wrote, “The extent of the coroner’s investi-gation is sometimes a concern. There are sixty-threecounties in Colorado, and each must operate withina budget. Some counties may have a full timesalaried pathologist to perform as many autopsies asare required, while other counties pay for autopsieson a per-case basis. The budget for a rural countymay dictate that the coroner be very selective aboutthe expenditures for any autopsy, especially thoseinvolving extensive toxicologic analysis, radiologicexams, etc. When an investigation requires a con-sultant, such as an engineer, toxicologist,anthropologist, or odontologist, costs can quicklyrise. The economic issues will continue to be aconcern for all counties. Ultimately, the adequacy ofthe investigation depends upon the dedication andperseverance of the coroner and support receivedfrom the community.”
As part of that “community support”, the ColoradoChild Fatality Review Committee, between late 1997 and 2001, with the support of a federal grant,sponsored a core team to travel to various parts of Colorado and deliver intensive training on childdeath investigation (see Appendix B for more detail).Professional audiences turned out in large numbersfor these training seminars, which were, by allaccounts, extremely well received.
In summary, we have seen a great improvement inthe quality of data we are able to collect on childfatalities from coroners’ offices, and in the quality ofdeath investigation overall, especially in unexpecteddeath of infants.
Goals of Colorado Child FatalityReview: Future
Following the legislative mandate of 2005 andwith the reorganization in 2005–2006 of theChild Fatality Review Committee, now known
as the Colorado State Child Fatality PreventionReview Team, a new era begins. We have welcomednew team members who bring fresh ideas and vigor.Some old goals, articulated at the start of thisprocess in 1989, are yet to be realized. Mostimportant of these is the conversion of data toaction, meaning the development of primary pre-vention strategies to decrease the death toll ofchildren in our state. Data collection and analysisremain at the heart of the process, but must have auseful outcome. We have 17 years of data that needclose analysis and publication, and will need thefunds to support that. We are currently storing caserecords that are necessary for deeper analysis andeventual publication of aggregate data, but are indanger of being destroyed unless we can find them a permanent home. We also look forward toexpanding the membership of our team to includeexcellent professionals who do not live in the Denvermetro area and who have a great deal to contributeto the process. Improved long-distance interactionaltechnology for meetings is on the horizon. We lookforward to collectively developing a list of practicablegoals. These will only be accomplished throughteamwork.

36 Child Fatality Review in Colorado: A History 1989–2006
Appendix A: Data Collection Instruments Data Collection Instrument 1989
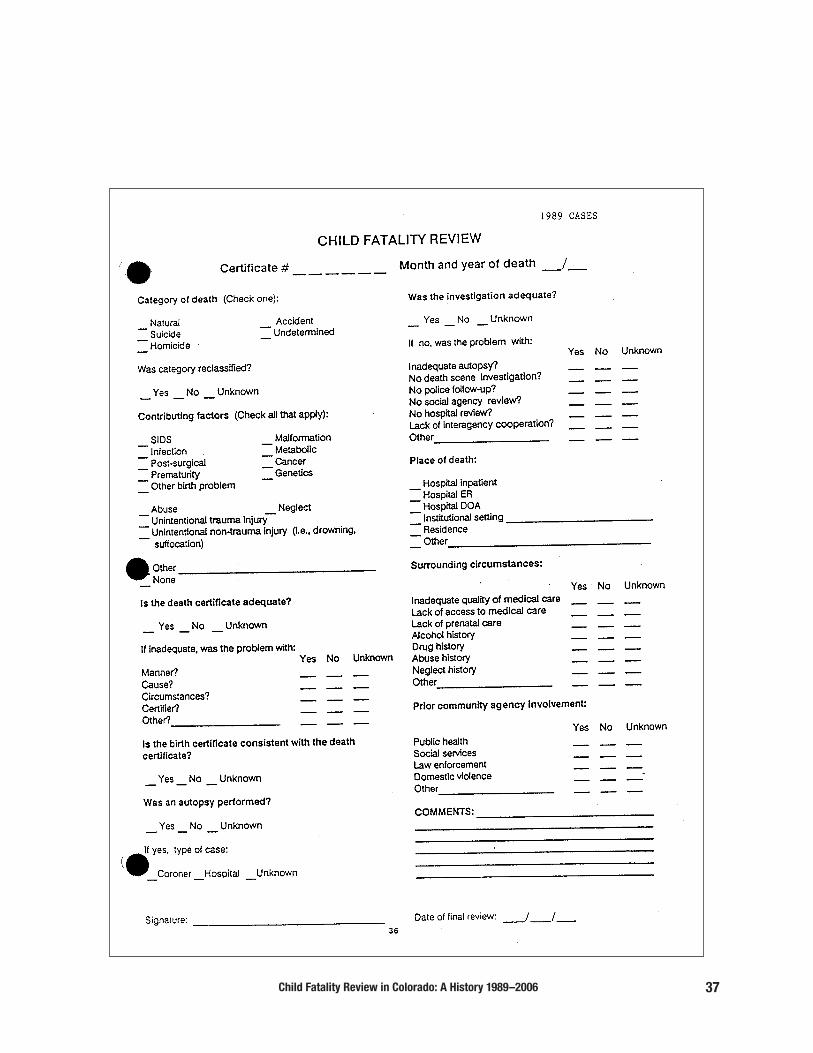
Child Fatality Review in Colorado: A History 1989–2006 37

38 Child Fatality Review in Colorado: A History 1989–2006
Data Collection Instrument 1990

Child Fatality Review in Colorado: A History 1989–2006 39
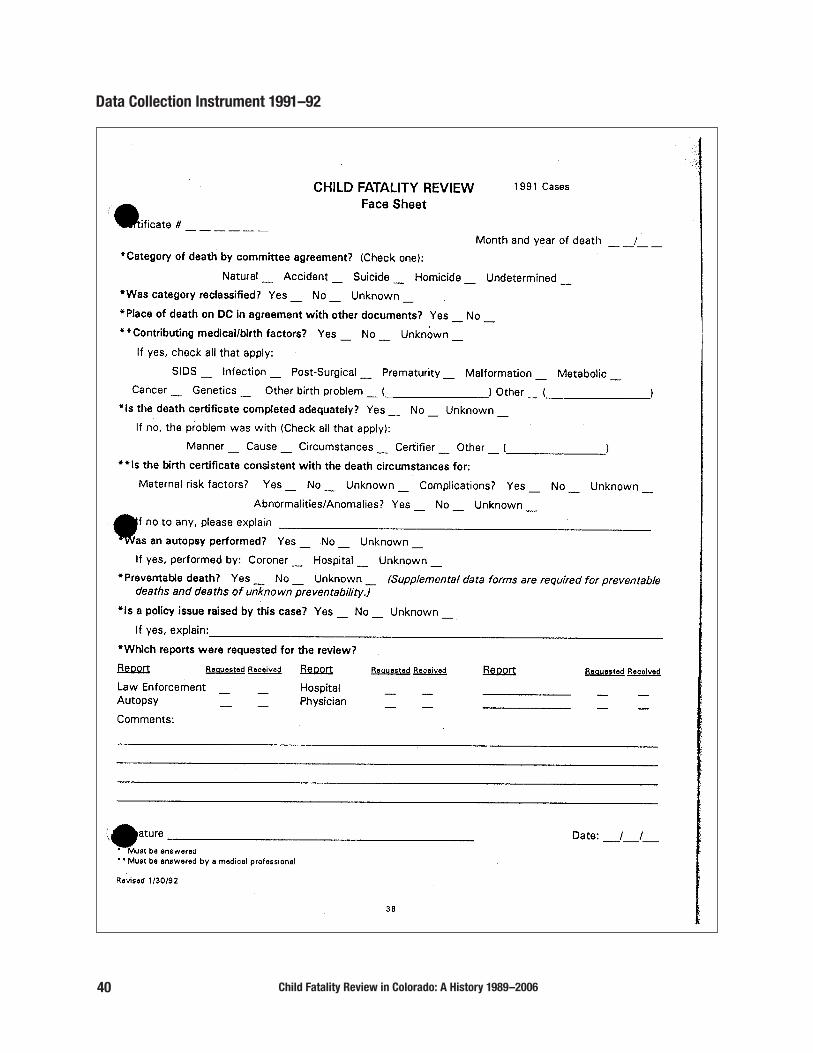
40 Child Fatality Review in Colorado: A History 1989–2006
Data Collection Instrument 1991–92

Child Fatality Review in Colorado: A History 1989–2006 41

42 Child Fatality Review in Colorado: A History 1989–2006
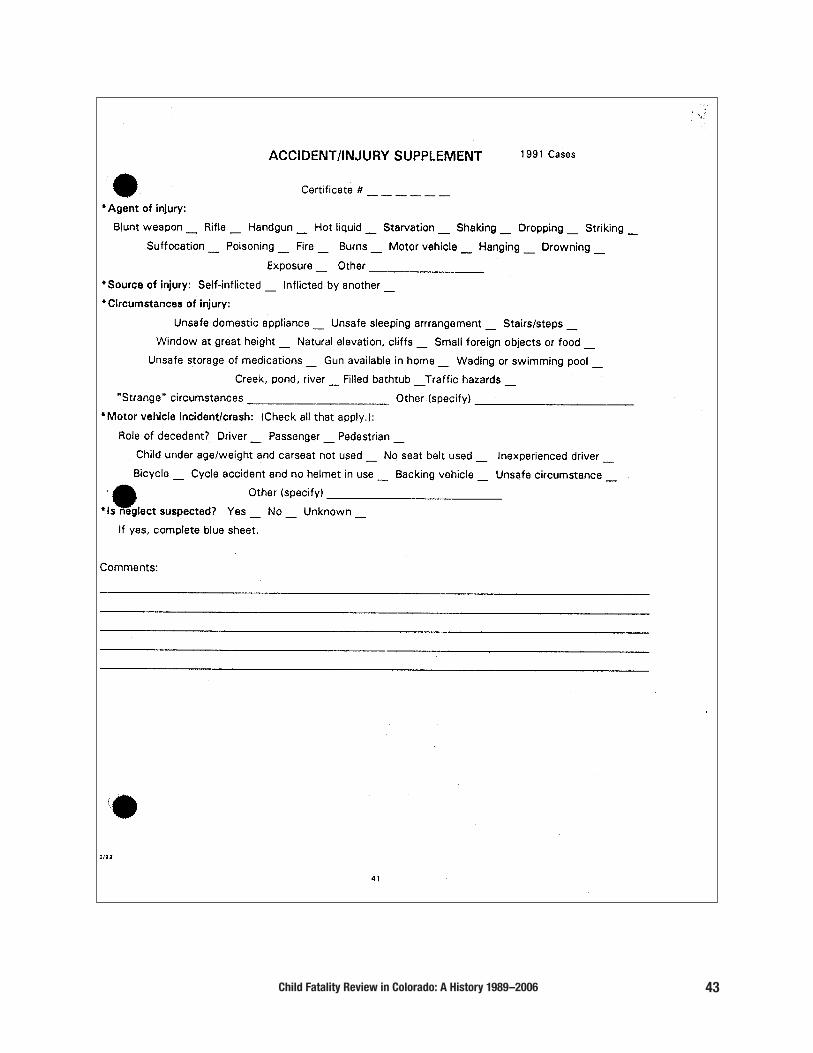
Child Fatality Review in Colorado: A History 1989–2006 43

44 Child Fatality Review in Colorado: A History 1989–2006
Data Collection Instrument 1994
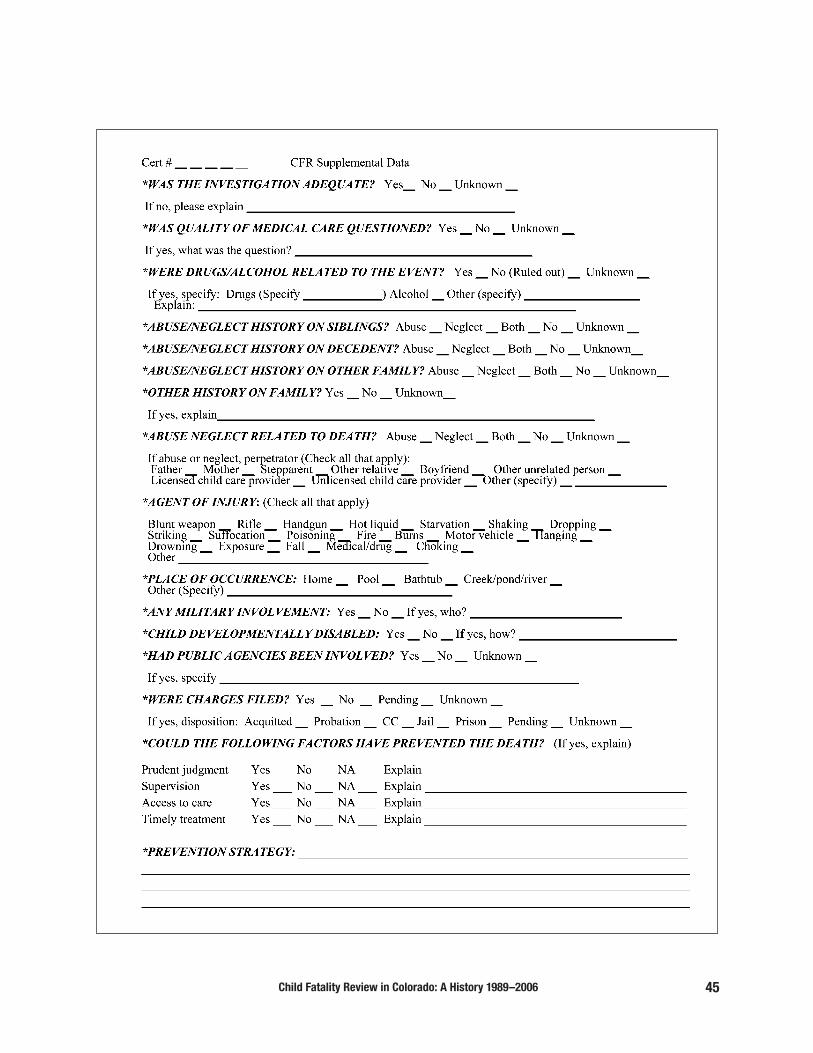
Child Fatality Review in Colorado: A History 1989–2006 45

46 Child Fatality Review in Colorado: A History 1989–2006
Data Collection Instrument 2006

Child Fatality Review in Colorado: A History 1989–2006 47

48 Child Fatality Review in Colorado: A History 1989–2006
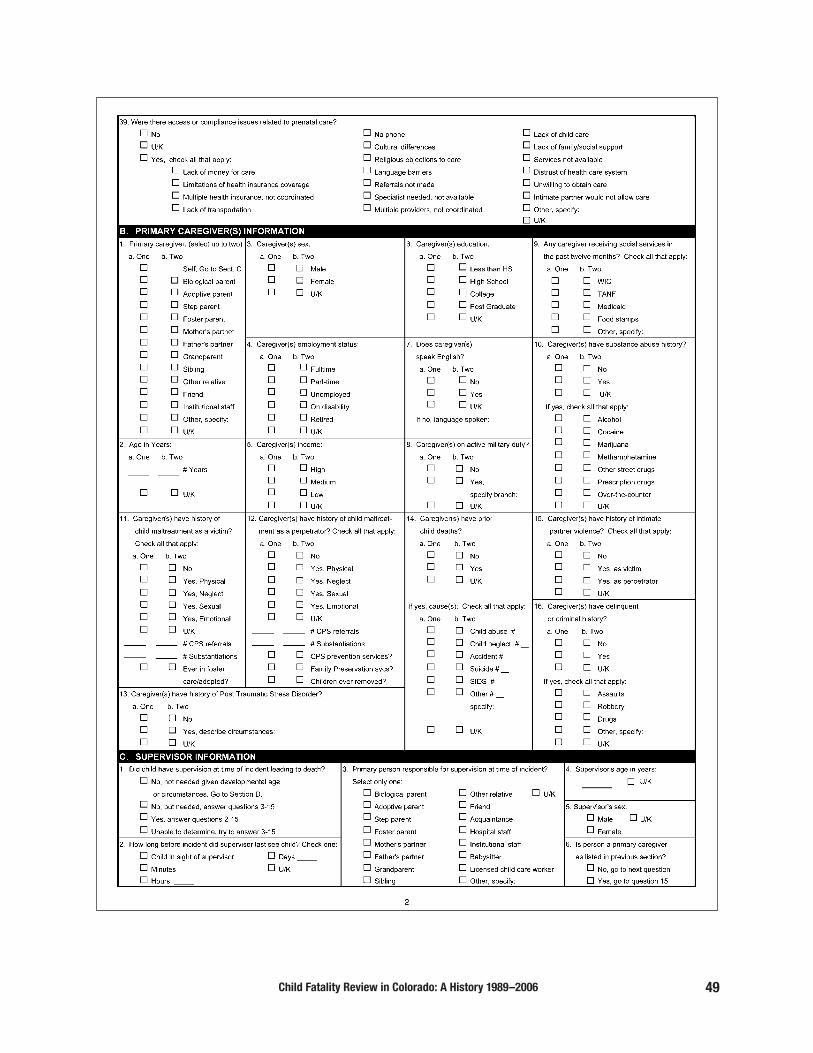
Child Fatality Review in Colorado: A History 1989–2006 49

50 Child Fatality Review in Colorado: A History 1989–2006

Child Fatality Review in Colorado: A History 1989–2006 51
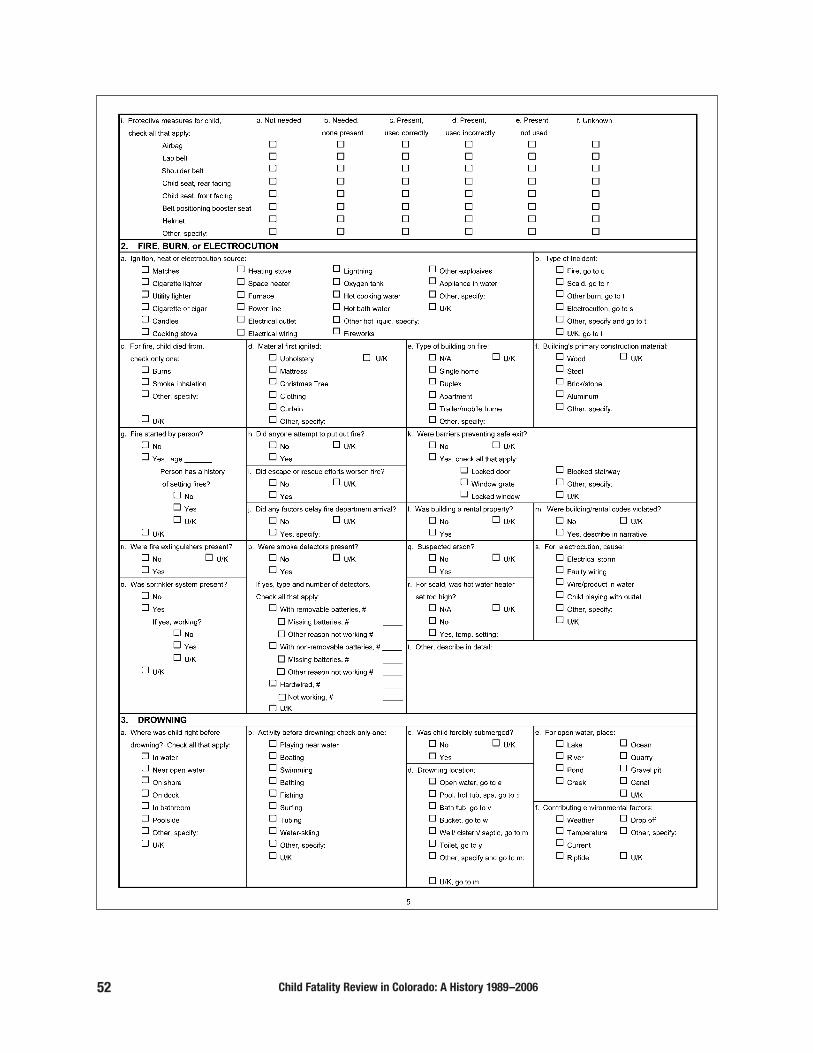
52 Child Fatality Review in Colorado: A History 1989–2006

Child Fatality Review in Colorado: A History 1989–2006 53

54 Child Fatality Review in Colorado: A History 1989–2006

Child Fatality Review in Colorado: A History 1989–2006 55
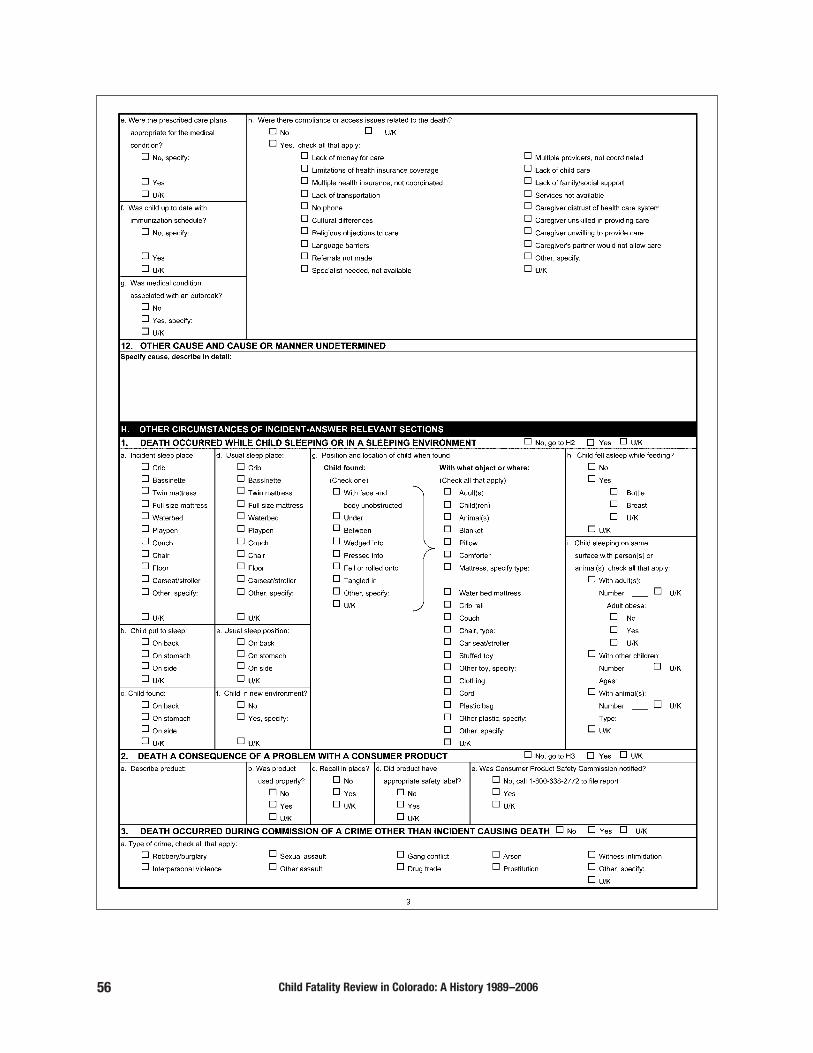
56 Child Fatality Review in Colorado: A History 1989–2006

Child Fatality Review in Colorado: A History 1989–2006 57

58 Child Fatality Review in Colorado: A History 1989–2006
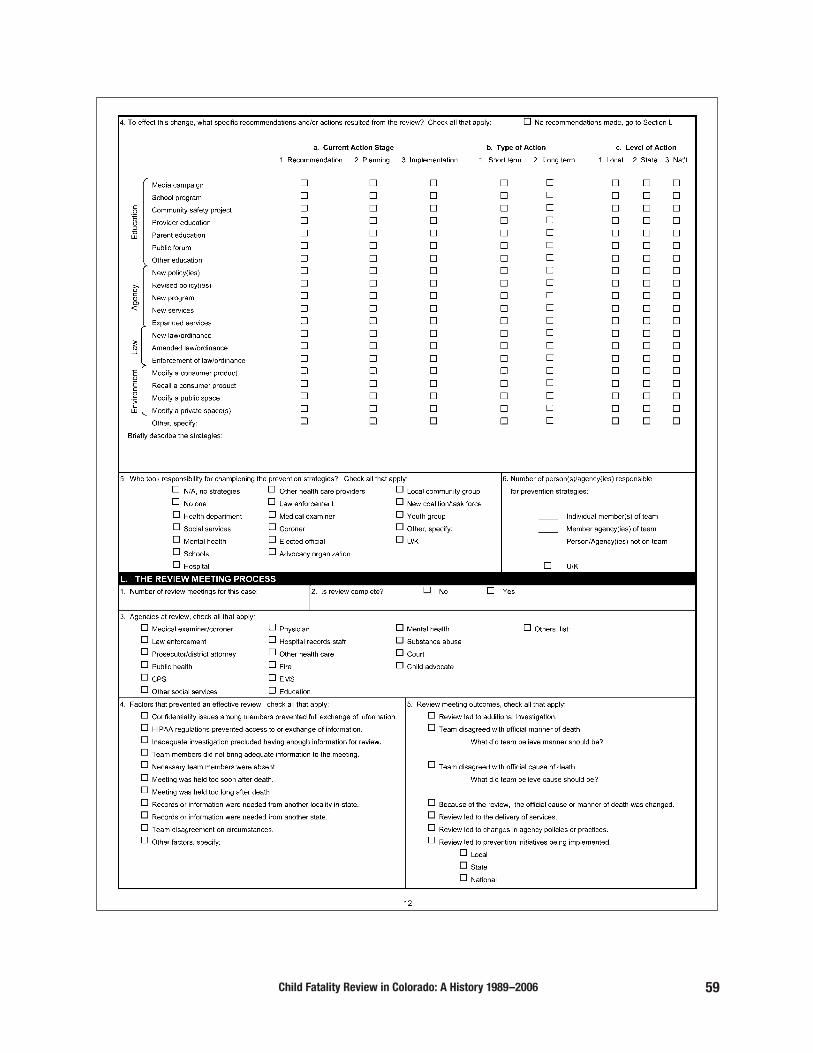
Child Fatality Review in Colorado: A History 1989–2006 59

60 Child Fatality Review in Colorado: A History 1989–2006
Child Fatality Review in Colorado: A History 1989–2006 61

62 Child Fatality Review in Colorado: A History 1989–2006
Child Fatality Prevention System Clinical Review Process Documents 2006

Child Fatality Review in Colorado: A History 1989–2006 63

64 Child Fatality Review in Colorado: A History 1989–2006
Appendix B: Activities of the Child FatalityReview Team—Publications,Conferences, Teaching
Publications—Annotated List
April 1991
Colorado Child Fatality Review CommitteeAnnual Report and Conference Proceedings
Published by the Colorado Department of Health andthe Colorado Department of Social Services
Includes: Development of the Review Process;Committee Findings; Conference Proceedings(October 26, 1990, Denver, Colorado, Designing aBetter Response: Child Death in the 90s).
Appendices: Interagency Agreement; ConfidentialityStatement; Data Collection Sheet; Guidelines forLocal Interagency Case Collaboration; Guidelines for Interagency Notification and Investigation of Child Homicide and Deaths of QuestionableCause/Manner; Departments of Social ServicesGuidelines for Child Death Investigations; LawEnforcement Guidelines for Child DeathInvestigations; Child Deaths by County; DeathCertificate; Glossary.
March 1993
Child Fatality—Colorado: 1989–1990
Published by the Colorado Department of Health andthe Colorado Department of Social Services
Includes: Overview of Child Fatality ReviewProgram; Sources and Limitations of Data; Summaryof Findings; Demographic Characteristics ofDecedents; Infant Deaths; Manner of Death;Underlying Cause of Death; Injury Deaths;Preventable Deaths; Procedures Related to Death;Review of Manner of Death.
Appendices: Data Collection Forms; Membership ofChild Fatality Review Committee.
June 1993
1993 Annual Report—Colorado Child FatalityReview Committee
Published by the Colorado Department of Health andthe Colorado Department of Social Services
Includes: Preventable Deaths; Overview of ChildFatality Review Program; Summary of 1991 ChildDeath Data; Significant Findings in SpecialPopulations; Fatality Review Uncovers PolicyQuestions; Conference Issues andRecommendations – 1993 Child Fatality ReviewConference.
Appendices: Data Collection Forms; CurrentMembership of Child Fatality Review Committee;Death Certificate; Interagency Agreement;Confidentiality Forms; Law Enforcement Guidelines;1993 Child Fatality Review Conference Speakers,Participants, and Organizers.
October 1993
“How to” Manual for Local Child Fatality Review
Published by the Colorado Department of Health andthe Colorado Department of Social Services
Includes: Background on Child Fatality ReviewTeams; Colorado Child Fatality Review Process;Getting Started: Team Formation at the Local Level;Data Collection/Reporting.
Appendices: Childhood Death by County ofResidence: Colorado 1989-1991; ConfidentialityStatement; Sample Death Certificate; Definition ofPreventable Death; Data Collection/Reporting Forms;List of Colorado Child Fatality Team Members.

Child Fatality Review in Colorado: A History 1989–2006 65
October 1996 (available at www.pubmed.gov)
Mortality From Intentional and UnintentionalInjury Among Infants of Young Mothers inColorado, 1986–1992.
Authors: Carol D. Siegel, Patricia Graves, KateMaloney, Jill Norris, Ned Calonge, Dennis Lezotte.
Published in: Archives of Pediatric and AdolescentMedicine, October 1996. Volume 150, pages1,077–1,083.
The objective of this study was to investigate theassociation between maternal age and other riskfactors and infant injury deaths in the state ofColorado from 1986 to 1992. Conclusions: Maternalage and marital status significantly affect the rate ofboth unintentional and intentional infant injury mor-tality. The results suggest that child abuse preventionstrategies should be targeted to teenaged mothers,and that strategies designed to prevent unintentionalinjuries should focus particularly on parents or care-takers of infants born to unmarried mothers in theirearly 20s as well as to married teenagers.
This publication was based, in part, on data collectedby the Child Fatality Review Committee
June 1998 (available at http://www.cdphe.state.co. us/pp/cfrc)
Child Fatalities in Colorado, 1990–1994, ColoradoChild Fatality Review Committee
Published by the Colorado Department of PublicHealth and Environment and the ColoradoDepartment of Human Services
Includes: Overview; Child Fatalities: ColoradoOccurrences 1990–1994; Special Topics (Infants;Sudden Infant Death Syndrome; Unintentional Injury;Motor Vehicles; Suicide; 17-year olds; Firearms;Maltreatment); Perspectives Gained.
Appendices: Law Enforcement Guidelines for ChildDeath Investigations; Sample Death Certificate; DataCollection Forms; Interagency Agreement; CurrentMembership.
April 1999 (available at http://www.cdphe.state.co. us/pp/cfrc)
BRIEF—Motor Vehicle-related Child Fatalities:Colorado 1995–1997, Colorado Child FatalityReview Committee
Published by the Colorado Department of PublicHealth and Environment
Includes: Demographics; Circumstances; YoungDrivers; Prevention Strategies; Conclusions.
December 1999 (available at http://www.cdphe.state.co. us/pp/cfrc)
BRIEF—Firearm Child Fatalities: Colorado1993–1997
Published by the Colorado Department of PublicHealth and Environment
Includes: Demographics; Circumstances;Prevention; Conclusions.
January 2000 (available at www.pubmed.gov)
Impact of infants born at the threshold of via-bility on the neonatal mortality rate in Colorado
Authors: Jacinto Hernandez, DM Hall, EdwardGoldson, Mary Chase, Carol Garrett
Published in: Journal of Perinatology, Jan.–Feb.2000. Volume 20 (1), pages 21–26.
The purpose of the study was to determine the con-tribution of infants born at the threshold of viability(<750 grams) on neonatal mortality in Colorado.

66 Child Fatality Review in Colorado: A History 1989–2006
Conclusions: Future attempts to reduce the Coloradoneonatal mortality rate would best focus on the 500-to 750 gram weight group through the re-regional-ization of high-risk perinatal care.
This publication was based, in part, on data collectedby the Child Fatality Review Committee
March 2000 (available at www.pubmed.gov)
Adolescent suicide and household access tofirearms in Colorado: results of a case-controlstudy
Authors: S. Shah, RE Hoffman, L Wake, WM Marine
Published in: Journal of Adolescent Health, March2000. Volume 26 (3), pages 157–163.
The purpose of the study was to determine whether,compared with age- and sex-matched controls whodid not commit suicide, adolescents who committedsuicide by firearms were more likely to have hadhousehold access to firearms. Conclusions: Towtypes of public health interventions to prevent ado-lescent firearm suicides are likely to be successful:limiting household access to firearms, and identifyingadolescents at high risk of firearm suicide.
This publication was based, in part, on data collectedby the Child Fatality Review Committee
June 2000(available at http://www.cdphe.state.co. us/pp/cfrc)
BRIEF—Accidental Drowning Fatalities: ColoradoChildren 1993–1997
Published by the Colorado Department of PublicHealth and Environment
Includes: Demographics; Location of Drownings;Month of Drowning; Prevention; Conclusions.
January 2001(available at http://www.cdphe.state.co. us/pp/cfrc)
How to Start a Local Child Fatality Review Team:Guidelines for Local Child Fatality Review inColorado
Published by the Injury Prevention Program of theColorado Department of Public Health andEnvironment and Child Welfare Services of theColorado Department of Human Services
IIncludes: Introduction; Background; Local Review;Frequently Asked Questions; Getting Started; CaseIdentification and Selection; Local Review TeamMembership; Team Member Roles; Confidentiality;Data Collection.
July 2001(available at http://www.cdphe.state.co. us/pp/cfrc)
BRIEF—Sudden Infant Death Syndrome AmongColorado Infants 1990–1998
Published by the Colorado Department of PublicHealth and Environment
Includes: Background; Demographics; Risk Factors;Risk Reduction.
August 2001(available at http://www.cdphe.state.co. us/pp/cfrc)
Denver Child Fatality Review Committee—Report 1997–2000
Authors: Sally Holloway, Sheila Marquez, Dr. LoraMelnicoe, Dr. Andrew Sirotnak
Published with direct support from: ColoradoDepartment of Public Health and Environment,Denver Children's Advocacy Center, Denver DistrictAttorney’s Office 2nd Judicial District, Denver PoliceDepartment.

Child Fatality Review in Colorado: A History 1989–2006 67
This publication was not produced by the ColoradoChild Fatality Review Committee but, becauseseveral key members are common to both teams, itis available at its website and therefore listed here.
August 2002(available at www.pubmed.gov or http://www.pedi-atrics.org/cgi/content/full/110/2/e18)
Underascertainment of Child MaltreatmentFatalities by Death Certificates, 1990–1998
Authors: Tessa Crume, Carolyn DiGuiseppi, TimByers, Andrew Sirotnak, Carol Garrett
Published in: Pediatrics, August 2002. Volume 110(2), 6 pages (electronic publication)
The purpose of the study was to address theconcern that systems of child protection, lawenforcement, criminal justice, and medicine do not adequately assess the circumstances sur-rounding child fatality as a result of maltreatment.Conclusions: Only half of the children who died as a result of maltreatment had death certificates thatwere coded consistently with maltreatment. Thedegree of underascertainment is of concern becausemost national estimates of child maltreatmentfatality in the United States are derived from codingon death certificates. In addition, the patterns rec-ognized in this study raise concern about systematicunderascertainment that may affect children ofspecific socioeconomic groups.
This publication was based on data collected by theChild Fatality Review Committee
Conferences
October 26, 1990
Designing a Better Response: Child Death in the1990s; Denver, Colorado
This conference was the first large multidisciplinaryconference to occur in Colorado. It took place at TheChildren’s Hospital, approximately one year after theformation of the Child Fatality Review Committee,and there were more applicants for the conferencethan there was space for them. The attendee list isremarkable for the very large number of people insenior positions from the many different agenciesthat should be participating in child death investi-gation, and for the broad representation from aroundthe state. Altogether, there were 139 participants,many from the Denver metro area, but also includingrepresentatives from: Steamboat Springs, ColoradoSprings, Rifle, Akron, Montrose, Canon City, Delta,Pueblo, Fort Collins, Boulder, Telluride, Cortez,Fairplay, Greeley, Grand Junction, Fort Carson, MonteVista, Alamosa, Fountain, Castle Rock, Salida,Loveland, Georgetown and La Junta.
The focus of the conference was the investigation ofchild deaths, emphasizing adequate evaluation ofcause and manner, with a view to the developmentof prevention strategies.
“…A measure of any society is marked by howwe respect our childhood and how we treat ourchildren… You’ve come with a charge, to ask thequestion, How can we do things differently?”
—Dr. Tom Vernon, Executive Director, Colorado Department of Health
“We have high expectations of all of you. You arehere to do some work with us and for us…”
—Pat West, Co-chair, Child Fatality Review Committee

68 Child Fatality Review in Colorado: A History 1989–2006
“…When you study children’s deaths, you have tohave a hope…How do we get the pieces of thepuzzle put together differently than they havebeen, so that at the end of an investigation, thosepeople who are key to it can sit back and say, Wehave as much as we’re going to get and we knowsomething about what went on here.”
—Jane Beveridge, Co-chair, Child Fatality Review Committee
“…We probably need at least three categories[apart from founded and unfounded, for abuse],and that is the one in between that says, We don’t know. ..The very nature of looking at theseproblems gives us even more questions toask…Our goal for the next decade ought to be tonarrow that down so that the “We don’t know”group is as small as it could possibly be, [though] I don’t think we’ll ever eliminate it...You can’treview child fatality cases without developing anever-increasing and an ever-broadening sense ofhumility about what we don’t know and aboutwhat we are still yet unable to do.”
—Dr. Richard Krugman, Director, C. Henry Kempe National Center for the Prevention
and Treatment of Child Abuse and Neglect; Acting Dean, School of Medicine,
University of Colorado Health Sciences Center
There were six discipline-specific working groupsformed from conference attendants, who spent theafternoon together. Each of the working groups wasasked to address the following questions, and thenreport back to the conference at large:
What would it look like if the system was workingwell? When and how do you start from the point ofinitial referral to complete investigation? What is yourobligation? How do you know when you have fulfilledyour obligation? How do you design a betterresponse within your agency?
The following recommendations came from the conference’s working subgroups, addressing inter-agency collaboration of child death.
• Develop uniform guidelines for the separateagencies responding to children’s death.
• Establish formal interagency county agreementsfor coordinated efforts in investigating children’sdeaths.
• Encourage local interagency review of children’sdeaths.
• Collect data at a state level to give policy makersand professionals a clearer picture as to pre-ventable deaths and necessary resources.
One footnote: Those who study child fatality arealso human, and need respite. Mel Apodaca, ChiefInvestigator at the Denver County Coroner’s Officeand part-time comedian, gave a lunchtime comedyshow. Regrettably, his performance was notrecorded.
March 11–12, 1993
Taking Responsibility, Denver, Colorado
The second conference sponsored by the ChildFatality Review Committee was supported by theColorado Department of Transportation and tookplace at the Holiday Inn on I-70 East. There wereover twenty speakers, including national experts Dr. Michael Durfee of the Los Angeles Child FatalityReview Team, and Professor Susan Baker, of theJohns Hopkins University Injury Prevention ResearchCenter. Many of the other speakers were membersof the Colorado Child Fatality Review Committee.
The conference was attended by a multidisciplinaryaudience, including people from medicine, nursing,social services, coroner’s offices, law enforcement,government, public health, education, counseling,and the legal profession.

Child Fatality Review in Colorado: A History 1989–2006 69
The conference was designed so that participants, at the conclusion, would be able to identify trendsand patterns of child death; would have a betterunderstanding of the many systems involved in childdeath investigation, intervention, and prevention;would be acquainted with current preventionmodels; would have information to support devel-opment and operation of an interagency child fatalityreview committee in their community.
October 4, 1996
When a Child Dies: Developing an EffectiveCommunity Response, Planning a Local ChildFatality Review Team, Denver, Colorado
Sarah Kaplan, of the American Bar Association’sCenter on Children and the Law, was the featuredspeaker at this conference. The conferenceattendees were the members of the Child FatalityReview Committee.
July 17, 2001
Local Team Teleconference, Statewide
The Colorado Child Fatality Review Team sponsoreda teleconference for local teams around the state.The purpose was to bring the local teams together(conversationally though not physically) for jointcommunication about their child fatality reviewprocesses. There were 14 participants from threelocal teams (Arapahoe, Denver, and El Pasocounties) and the state CFRC. The teams discussedteam membership and frequency of meetings,problems in recruiting members, the difficulty ofhaving consistent law enforcement representationdue to the nature of the job, difficulty in knowingwhat to do with information, the conflicts inherent inchild death review because the different agenciesinvolved have different individual purposes, the datacollection process (or lack thereof), and communityprevention efforts that have resulted from fatalityreview.
Teaching
Between 1997 and 2001, a core multidisciplinaryteam from the CFRC traveled around Colorado givingan intensive 2-day seminar on Infant and Child Injuryand Death Investigation. The course was designedfor a multidisciplinary audience, including lawenforcement investigators, attorneys, coroners andcoroners’ investigators, and social services, publichealth and emergency medical services personnel.
The seminars were approved by the ColoradoAssociation of Chiefs of Police and by the CountySheriffs of Colorado.
The CFRC core team was funded by a federal grantand the 2-day seminar cost $10 for participants, andincluded lunch and snacks!
Potential audience members were asked: Are youconfident that your agency would respond effectivelyand appropriately in the event of a sudden unex-plained child death? Are protocols in place in yourcommunity for the investigation of sudden unex-plained child deaths? Do you know the criteria fordesignating and unexplained child death as SuddenInfant Death Syndrome? How can all involvedagencies work together to most effectively and sensitively respond to a sudden unexplained childdeath?
The seminar focused on deaths related to abuseand/or neglect and sudden unexplained deaths. Thegoal was to teach a standard investigative approachtoward all child deaths to a variety of personnel fromdifferent disciplines, with the attendees able tounderstand all aspects of child death investigationsand the benefits of working together toward deter-mining cause of death.
Seminars took place in Highlands Ranch (1997), La Junta (1997), Delta (1997), Steamboat Springs(1997), Fort Collins (1997), Aurora (1998), Aurora(1999), Boulder (1999), Durango (2000), Pueblo(2000), Greeley (2001) and Eagle (2001).
70 Child Fatality Review in Colorado: A History 1989–2006
Over 650 professional participants enrolled for thisseminar throughout Colorado. The seminars alsoattracted some participants from Nebraska, NewMexico, Utah and Wyoming.
Seminars were held at a rather remarkable variety of venues, some in technologically-sophisticatedfacilities such as the National Institute of Standardsand Technology in Boulder, others in down-homeenvironments, such as the Nachos Restaurant inPueblo.
Participating counties included: Adams, Alamosa,Arapahoe, Archuleta, Boulder, Denver, Delta,Douglas, Eagle, El Paso, Fremont, Garfield, Huerfano,Jefferson, Lake, La Plata, Larimer, Las Animas,Loveland, Mesa, Moffat, Montezuma, Montrose,Otero, Prowers, Pueblo, Rio Blanco, Routt, SanMiguel, Summit, Teller, Washington, and Weld.
Hosting agencies included: Sungate Children’sAdvocacy Center, Blue Sky Bridge/Boulder CountyChild and Family Resource Center, Four CornersChild Advocacy Center, La Plata County Sheriff’sOffice, Durango Police Department, Pueblo ChildAdvocacy Center, Pueblo Police Department, PuebloCounty Department of Human Services, GreeleyChild Advocacy Center, Larimer County ChildAdvocacy Center—Fort Collins, Weld CountyDepartment of Human Services, Resource Center ofEagle County, 5th Judicial District Attorney’s Office,Eagle County Sheriff’s Office, and the Eagle CountyDepartment of Health and Human Services.
Members of the traveling team included: Jill-EllynStraus, Tom Henry, Tom Faure, Andy Sirotnak, SheilaMarquez, Susan Ludwig, Fred Walsh, Gerri Burggraff,Holly Nicholson-Kluth, Rochelle Manchego, DianeWaters, and Corey Johnson.
Child Fatality Review in Colorado: A History 1989–2006 71
Karen AbrahamsonRobin AdairBarbara AlexanderRichard AmendScott AnthonyRick ArcherDede ArnholzKathy AtkinsBarbara BaileyBill BaneLori BanksMarilyn BartonChuck BayardR. BeattySusan BeauchampBarbara BellMike BellBonnie BenedettiJane BeveridgeBriana BiancaLynn BindelJane BinghamRose BirchfieldRoberta BoitanoLouise BorisBrock BowersShannon BreitzmanDon BrossDave BroudyGerri BurggraffBrenda BurnettElna CainHendrika CantwellRobin CareyCarol Carney
Joe CarneyVicky CassabaumJennifer CharlesMary ChaseMark ChavezDarci CherryTim ClarkKaren ConnorJane CotlerTessa CrumeRobin DanniDavid DensonMary Pat DeWaldJamie DillonMichael DobersonBetty DonovanMary DregerSue DunnThor EellsMarty EgglehoffChris EhaltTom FaureGreg FerrillReginald FingerGail Finley-RareyLinda FordDeborah FrenchChip FryEd FryerCarol GarrettLori GerzinaRoger GollubDennis GoodwinJudy GrangeMaile Gray
Candace GroszCraig HamiltonTriena HarperSandra HarrisTom HenryJacinto HernandezSusan HiattJeff HimesKirby HodgkinRichard HoffmanRoger HoffnerBarbara HoweJim HughesRick HuntRachel HutsonRonald HymanKathie JacksonJoyce JenningsCarole JennyChristine JorgensenJohn JorgensenAlison KempeJames KramerRichard KrugmanRobert KurtzmanBill LetsonMark LovellSusan LudwigJoan MacEachenPhyllis MaddenRochelle ManchegoAlison MangoldCarol MannCraig MansanaresSheila MarquezAmy MartinAnn MatthewsLarry MatthewsDaniel McCaskyRobert McCurdyJohn McDowellJanet McNallyJohn McPheeMike Merrill
Jan MickishDave MillerDolores MitchellTom MiyoshiShirley MondragonGlen MooreClare MootzJanet MotzGeorge MummaPatsy MundellAmy MurphyJohn MuthHal NeesHolly Nicholson-KluthKim NolenP.A. NorrisMim OrleansEd OrsiniKevin PalettaNancy PetersonKimberly PoyerKevin RainesKaren RamstromTheresa RapstineElinora ReynoldsGreyson RobinsonJohn RomaniecDonna RosenbergDorothy RupertWilliam RushAnita Saranga CoenLinda SatkowiakEric SchmidtAlyson ShupeAllen SimmonsAndrew SirotnakCarla Slatt-BurnsRay SlaughterMark SlavskySteve SmeeMelody SmithVicki SmithKelly Stainback-Tracy
Appendix C: Membership—Past and Present Colorado Child Fatality Review Committee,1989–2006
Following is a list of professionals who served onthe Colorado Child Fatality Review Committee,either in entirety or in part, from 1989–2006.

72 Child Fatality Review in Colorado: A History 1989–2006
Lorann StallonesEllen SteinKaren SteinhauserLes StevesonJill-Ellyn StrausMarie SwigertAnne TaylorCourtney ThomasSharon ThorsonHenry TollLynn TrefrenKaren TrierweilerLee UlshofferMichael ValdezSally VanManenBill Vertrees
Tom WaddillJames WaheJeff WallerFred WalshJames WayheMichelle Weiss-SamarasDavid WellsPat WestMark WhiteCurt WilliamsHarry WilsonJeff WithrowGreg WolgamottSteve WygantSusan Yates
Every effort was made to be inclusive, but thecomplete records of membership going back over17 years were not discovered in their entirety.Sincere apologies are tendered to any who wereinadvertently omitted. It is also remotely possiblethat a few people will be mildly surprised to seetheir names on the above list, even though they didnot actually participate. Some available recordsseemed to lump together those who weremembers, those who agreed to become members(but never did), and those who were simply on themailing list. Apologies also, then, for any unwar-ranted implication of association.
Already mentioned are the four coordinators of ourCommittee. We further wish to acknowledge thoseadministrators of the Child Fatality ReviewCommittee from the Colorado Department of SocialServices and the Colorado Department of PublicHealth and Environment who, over the years, keptthis process going because of their tremendouscommitment, and their ability to keep it functioningby cobbling together the funding and volunteers:
Jane Beveridge Joe CarneyPat West Susan LudwigDeb French Ron HymanCarol Garrett Shannon Breitzman
Colorado State Child Fatality PreventionReview Team (est. CRS 25-20.5-4), Current Membership 2005–2008
Voting members appointed by the Governor onSeptember 1, 2005:
Robin Adair Larry MatthewsMary Pat DeWald Rebecca ParkerMargaret Ferguson Theresa RapstineWilliam Frangis Donna RosenbergAtrelle Jones Christine SchoberKelly Lear-Kaul Charles UrbachBrad Lenderink Laurel VandermeulenDavid Long Kathryn WellsAmy Martin
Ex-Officio members appointed by state agencies:
Karen Abrahamson Holly HedegaardBarbara Bailey Ron HymanLori Banks Bill LetsonScott Bates Susan LudwigShannon Breitzman Rochelle ManchegoBrenda Burnett Shirley MondragonBetty Donovan David Wells
Ex-Officio members selected by appointed Team:
Lori Burkey Sheila MarquezVicky Cassabaum Bonnie McNultyBob Flory Tracey SchlaferDiana Goldberg Andrew SirotnakMaile Gray Linda WeinermanLeah Lamb Peter Werlin

This monograph was written by Donna Rosenberg, M.D.; a long-time member of the Colorado Child Fatality Review Committeeand current chairperson of the Colorado State Child FatalityPrevention Review Team. Dr. Rosenberg has been a respectedexpert in child abuse and neglect in Colorado for many yearsand was asked to write this report/monograph because of herhistory, passion, and dedication to the safety and wellbeing ofchildren. She has been a member of the Child Fatality ReviewTeam for 19 years.
Colorado Department of Public Health and EnvironmentPrevention Services Division
Injury, Suicide and Violence Prevention Unit4300 Cherry Creek Drive South
Denver, CO 80246-1530(303) 692-2573
http://www.cdphe.state.co.us/pp/cfrc