Chest wall resection and reconstruction for locally recurrent breast cancer: From technical aspects...
7
Chest wall resection and reconstruction for locally recurrent breast cancer: From technical aspects to biological assessment Francesco Petrella a, *, Davide Radice b , Alessandro Borri a , Domenico Galetta a , Roberto Gasparri a , Monica Casiraghi a , Adele Tessitore a , Alessandro Pardolesi a , Piergiorgio Solli a , Giulia Veronesi a , Stefania Rizzo c , Stefano Martella d , Mario Rietjens d , Lorenzo Spaggiari a,e a Department of Thoracic Surgery, European Institute of Oncology, Italy b Department of Epidemiology and Biostatistics, European Institute of Oncology, Italy c Department of Radiology, European Institute of Oncology, Italy d Department of Plastic and Reconstructive Surgery, European Institute of Oncology, Italy e University of Milan School of Medicine, Italy article info Article history: Received 14 October 2013 Received in revised form 22 February 2014 Accepted 3 March 2014 Available online xxx Keywords: Breast cancer Chest wall resection Chest wall reconstruction abstract Introduction: Breast cancer is the leading cause of cancer death among women in the industrialized countries. The incidence of local recurrences after mastectomy and breast- conserving therapy varies between 5% and 40% depending on risk factors and primary therapy. Methods: From April 1999 to April 2011, 40 patients underwent chest wall resection and reconstruction for locally recurrent breast carcinoma with chest wall invasion. The main goal of surgery was local disease control to palliate clinical symptoms. Results: Local radical resection was achieved in 26 patients (65%). One, 2 and 5 year overall survival rates were 94.4%, 82.0% and 68.5%; 1, 2 and 5 year disease-free survival rates were 94.4%, 73.6% and 45.5% respectively. Univariate analysis indicated age (p ¼ 0.002) and synchronous distant metastases (p ¼ 0.020) as factors having a negative impact on overall survival; multivariate analysis disclosed age (p ¼ 0.052) and synchronous metastases (p ¼ 0.059) as factors with a slight negative impact on overall survival. Older age was associated with improved overall survival. Univariate analysis indicated synchronous distant metastases (p ¼ 0.029) and the need of post resectional additional treatments (p ¼ 0.022) as factors adversely conditioning disease-free survival or time to progression; multivariate analysis disclosed the need of post resectional additional treatments (p ¼ 0.036) as the only factor adversely conditioning disease-free survival or time to progression. * Corresponding author. Department of Thoracic Surgery, European Institute of Oncology, Via Ripamonti, 435, 20141 Milan, Italy. Tel.: þ39 0257489362; fax: þ39 0294379218. E-mail addresses: [email protected], [email protected] (F. Petrella). Available online at www.sciencedirect.com ScienceDirect The Surgeon, Journal of the Royal Colleges of Surgeons of Edinburgh and Ireland www.thesurgeon.net the surgeon xxx (2014) 1 e7 Please cite this article in press as: Petrella F, et al., Chest wall resection and reconstruction for locally recurrent breast cancer: From technical aspects to biological assessment, The Surgeon (2014), http://dx.doi.org/10.1016/j.surge.2014.03.001 http://dx.doi.org/10.1016/j.surge.2014.03.001 1479-666X/ª 2014 Royal College of Surgeons of Edinburgh (Scottish charity number SC005317) and Royal College of Surgeons in Ireland. Published by Elsevier Ltd. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Chest wall resection and reconstruction for locally recurrent breast cancer: From technical aspects...
ww.sciencedirect.com
t h e s u r g e on x x x ( 2 0 1 4 ) 1e7
Available online at w
ScienceDirectThe Surgeon, Journal of the Royal Colleges
of Surgeons of Edinburgh and Irelandwww.thesurgeon.net
Chest wall resection and reconstruction for locallyrecurrent breast cancer: From technical aspects tobiological assessment
Francesco Petrella a,*, Davide Radice b, Alessandro Borri a,Domenico Galetta a, Roberto Gasparri a, Monica Casiraghi a,Adele Tessitore a, Alessandro Pardolesi a, Piergiorgio Solli a,Giulia Veronesi a, Stefania Rizzo c, Stefano Martella d, Mario Rietjens d,Lorenzo Spaggiari a,e
aDepartment of Thoracic Surgery, European Institute of Oncology, ItalybDepartment of Epidemiology and Biostatistics, European Institute of Oncology, ItalycDepartment of Radiology, European Institute of Oncology, ItalydDepartment of Plastic and Reconstructive Surgery, European Institute of Oncology, ItalyeUniversity of Milan School of Medicine, Italy
a r t i c l e i n f o
Article history:
Received 14 October 2013
Received in revised form
22 February 2014
Accepted 3 March 2014
Available online xxx
Keywords:
Breast cancer
Chest wall resection
Chest wall reconstruction
* Corresponding author. Department of Thora0257489362; fax: þ39 0294379218.
E-mail addresses: francesco.petrella@ieo
Please cite this article in press as: PetrellFrom technical aspects to biological asse
http://dx.doi.org/10.1016/j.surge.2014.03.0011479-666X/ª 2014 Royal College of SurgeonsPublished by Elsevier Ltd. All rights reserved
a b s t r a c t
Introduction: Breast cancer is the leading cause of cancer death among women in the
industrialized countries. The incidence of local recurrences after mastectomy and breast-
conserving therapy varies between 5% and 40% depending on risk factors and primary
therapy.
Methods: From April 1999 to April 2011, 40 patients underwent chest wall resection and
reconstruction for locally recurrent breast carcinoma with chest wall invasion. The main
goal of surgery was local disease control to palliate clinical symptoms.
Results: Local radical resection was achieved in 26 patients (65%). One, 2 and 5 year overall
survival rates were 94.4%, 82.0% and 68.5%; 1, 2 and 5 year disease-free survival rates were
94.4%, 73.6% and 45.5% respectively.
Univariate analysis indicated age (p ¼ 0.002) and synchronous distant metastases
(p ¼ 0.020) as factors having a negative impact on overall survival; multivariate analysis
disclosed age (p ¼ 0.052) and synchronous metastases (p ¼ 0.059) as factors with a slight
negative impact on overall survival. Older age was associated with improved overall
survival.
Univariate analysis indicated synchronous distant metastases (p ¼ 0.029) and the need
of post resectional additional treatments (p ¼ 0.022) as factors adversely conditioning
disease-free survival or time to progression; multivariate analysis disclosed the need of
post resectional additional treatments (p ¼ 0.036) as the only factor adversely conditioning
disease-free survival or time to progression.
cic Surgery, European Institute of Oncology, Via Ripamonti, 435, 20141 Milan, Italy. Tel.: þ39
.it, [email protected] (F. Petrella).
a F, et al., Chest wall resection and reconstruction for locally recurrent breast cancer:ssment, The Surgeon (2014), http://dx.doi.org/10.1016/j.surge.2014.03.001
of Edinburgh (Scottish charity number SC005317) and Royal College of Surgeons in Ireland..

t h e s u r g e on x x x ( 2 0 1 4 ) 1e72
Please cite this article in press as: PetrellaFrom technical aspects to biological asse
Conclusions: Chest wall resection and reconstruction for locally recurrent breast cancer is a
feasible and safe procedure providing adequate local disease control and an excellent
palliation of very disabling symptoms in a selected group of patients.
ª 2014 Royal College of Surgeons of Edinburgh (Scottish charity number SC005317) and
Royal College of Surgeons in Ireland. Published by Elsevier Ltd. All rights reserved.
Introduction
Breast cancer is the leading cause of cancer death among
women in the industrialized countries.1 The incidence of local
recurrences after mastectomy and breast-conserving therapy
varies between 5% and 40% depending on risk factors and
primary therapy.2
The first-line treatments in recurrent breast cancer are
endocrine therapy for patients with estrogen or progesterone
receptor positive cancer, and chemotherapy for patients with
receptor-negative cancers.3e5 However, local therapies such
as radiotherapy or surgery may be required in selected cases
for local disease control and palliation of disabling symptoms
like pain, bleeding, ulceration, malodorous secretion, infec-
tion and fungating lesions.6,7
On the one hand, locoregional recurrence of breast cancer
following breast surgery may be a systemic disease and in
many patients it tends to occur at the same time as distant
metastases, making the indication for surgical resection
questionable.8,9 On the other, although the primary goal of
chest wall resection is to achieve local tumor control, it may
lead to long-termpalliation and even cure for a small subset of
patients with isolated chest wall recurrence of breast cancer
after multimodal treatment failure.10
Early detection of locoregional recurrence and small tumor
size predicted a better prognosis.11e13 Options for local treat-
ment of locoregional recurrence include wide local excision
and/or radiotherapy whether or not in combination with hy-
perthermia14; however, for small lesions, the type of local
treatment did not affect the final outcome.15
Whether complete resection of local recurrence offers a
merely palliative or possibly curative approach or a major
prolongation of survival remains unsettled.16 The aim of this
study was to define the role of chest wall resection for locally
recurrent breast cancer as a salvage treatment for a selected
group of symptomatic patients.
Methods
The present study was conducted in accordance with the
Declaration of Helsinki.17 Written informed consent was ob-
tained from all subjects before any procedure was done. The
investigators explained all the planned procedures verbally to
all subjects who received and signed a subject information
sheet to acquaint themselves with details of the planned
therapeutic schedule. All patients authorized the in-
vestigators to use their data anonymously only for scientific
purposes according to Italian legislation (law no. 675/1996).
F, et al., Chest wall resssment, The Surgeon (2
Data were collected prospectively and entered into our
institutional general thoracic database at the point of care.
The database was reviewed retrospectively.
From April 1999 to April 2011, 40 patients underwent chest
wall resection and reconstruction for locally recurrent breast
carcinoma with chest wall invasion proven by routine pre-
operative chest computed tomography (CT) or by chest wall
magnetic resonance imaging (MRI) in selected cases. Themain
goal of surgical therapy was local disease control to palliate
clinical symptoms like pain, cutaneous ulceration and
discomfort related to chest wall deformity. For this reason a
distant metastasis was not a contraindication. Selection
criteria for surgery weremultimodal treatment failure and life
expectancy of more than 6 months.
The surgical approach involved soft tissue resection with
broad margins and chest wall resection with total or partial
sternectomy and resection of one or more ribs. In case of
major tissue defect following resective surgery reconstruction
was performed using different types of prostheses covered by
a vascularized pedicle muscle flap.
Technical aspects of demolition and reconstructive pro-
cedures were reviewed (sternectomy, ribs resection, soft tis-
sue resection, endothoracic organ resection, type of
prosthesis, type of flap and technical complications) together
with oncologic history including previous type and date of
breast operation, histology and biology of breast and thoracic
surgical specimens (Ki67%, Her2 neu expression, estrogen and
progesterone receptor expression), and the interval between
breast and thoracic surgery.
Patients were defined as triple negative if estrogen, pro-
gesterone and Her2 neu expression were negative; otherwise,
they were defined as non-triple negative.10
Recurrence was defined as the return of cancer after
treatment and after a period of time during which the cancer
could not be detected. Local recurrence was defined as the
reappearance of disease in locoregional lymph nodes or in the
chest wall adjacent to the site of thoracic excision. Distant
recurrence was defined as distant sites of visceral disease,
including malignant pleural effusions or implants.
Progression was defined as cancer growthwithout a period
of time duringwhich the cancer could not be detected. Distant
progression was defined as cancer spreading to distant sites;
locoregional progression was defined as cancer worsening
close to the surgical field.
A complete resection (R0) was defined as pathologic
demonstration of negative tissue margins and an assessment
by the operating surgeon that all detectable disease had been
removed. Microscopically incomplete resection (R1) was
defined as complete macroscopic resection with positive
margins found on final pathologic review. Macroscopically
ection and reconstruction for locally recurrent breast cancer:014), http://dx.doi.org/10.1016/j.surge.2014.03.001
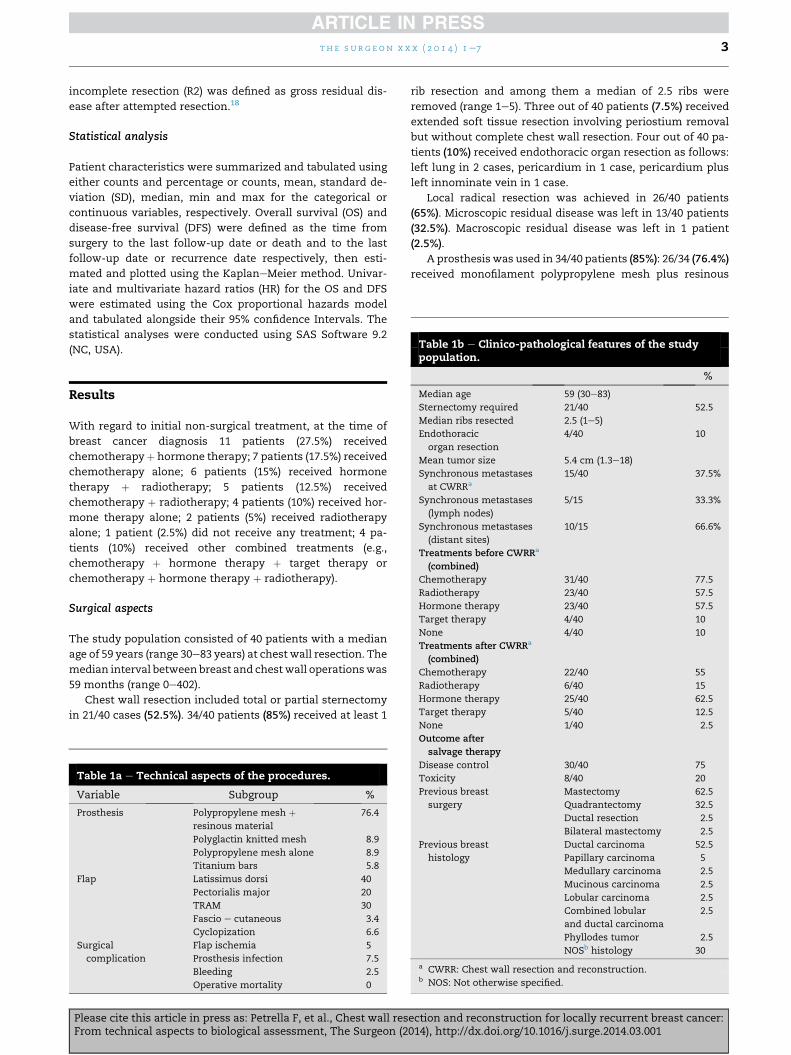
Table 1b e Clinico-pathological features of the studypopulation.
t h e s u r g e on x x x ( 2 0 1 4 ) 1e7 3
incomplete resection (R2) was defined as gross residual dis-
ease after attempted resection.18
Statistical analysis
Patient characteristics were summarized and tabulated using
either counts and percentage or counts, mean, standard de-
viation (SD), median, min and max for the categorical or
continuous variables, respectively. Overall survival (OS) and
disease-free survival (DFS) were defined as the time from
surgery to the last follow-up date or death and to the last
follow-up date or recurrence date respectively, then esti-
mated and plotted using the KaplaneMeier method. Univar-
iate and multivariate hazard ratios (HR) for the OS and DFS
were estimated using the Cox proportional hazards model
and tabulated alongside their 95% confidence Intervals. The
statistical analyses were conducted using SAS Software 9.2
(NC, USA).
%
Median age 59 (30e83)
Sternectomy required 21/40 52.5
Median ribs resected 2.5 (1e5)
Endothoracic
organ resection
4/40 10
Mean tumor size 5.4 cm (1.3e18)
Synchronous metastases
at CWRRa
15/40 37.5%
Synchronous metastases
(lymph nodes)
5/15 33.3%
Synchronous metastases
(distant sites)
10/15 66.6%
Treatments before CWRRa
(combined)
Chemotherapy 31/40 77.5
Radiotherapy 23/40 57.5
Hormone therapy 23/40 57.5
Target therapy 4/40 10
None 4/40 10
Treatments after CWRRa
(combined)
Chemotherapy 22/40 55
Radiotherapy 6/40 15
Hormone therapy 25/40 62.5
Target therapy 5/40 12.5
Results
With regard to initial non-surgical treatment, at the time of
breast cancer diagnosis 11 patients (27.5%) received
chemotherapyþ hormone therapy; 7 patients (17.5%) received
chemotherapy alone; 6 patients (15%) received hormone
therapy þ radiotherapy; 5 patients (12.5%) received
chemotherapy þ radiotherapy; 4 patients (10%) received hor-
mone therapy alone; 2 patients (5%) received radiotherapy
alone; 1 patient (2.5%) did not receive any treatment; 4 pa-
tients (10%) received other combined treatments (e.g.,
chemotherapy þ hormone therapy þ target therapy or
chemotherapy þ hormone therapy þ radiotherapy).
Surgical aspects
The study population consisted of 40 patients with a median
age of 59 years (range 30e83 years) at chest wall resection. The
median interval between breast and chest wall operationswas
59 months (range 0e402).
Chest wall resection included total or partial sternectomy
in 21/40 cases (52.5%). 34/40 patients (85%) received at least 1
Table 1a e Technical aspects of the procedures.
Variable Subgroup %
Prosthesis Polypropylene mesh þresinous material
76.4
Polyglactin knitted mesh 8.9
Polypropylene mesh alone 8.9
Titanium bars 5.8
Flap Latissimus dorsi 40
Pectorialis major 20
TRAM 30
Fascio e cutaneous 3.4
Cyclopization 6.6
Surgical
complication
Flap ischemia 5
Prosthesis infection 7.5
Bleeding 2.5
Operative mortality 0
Please cite this article in press as: Petrella F, et al., Chest wall resFrom technical aspects to biological assessment, The Surgeon (2
rib resection and among them a median of 2.5 ribs were
removed (range 1e5). Three out of 40 patients (7.5%) received
extended soft tissue resection involving periostium removal
but without complete chest wall resection. Four out of 40 pa-
tients (10%) received endothoracic organ resection as follows:
left lung in 2 cases, pericardium in 1 case, pericardium plus
left innominate vein in 1 case.
Local radical resection was achieved in 26/40 patients
(65%). Microscopic residual disease was left in 13/40 patients
(32.5%). Macroscopic residual disease was left in 1 patient
(2.5%).
A prosthesis was used in 34/40 patients (85%): 26/34 (76.4%)
received monofilament polypropylene mesh plus resinous
None 1/40 2.5
Outcome after
salvage therapy
Disease control 30/40 75
Toxicity 8/40 20
Previous breast
surgery
Mastectomy 62.5
Quadrantectomy 32.5
Ductal resection 2.5
Bilateral mastectomy 2.5
Previous breast
histology
Ductal carcinoma 52.5
Papillary carcinoma 5
Medullary carcinoma 2.5
Mucinous carcinoma 2.5
Lobular carcinoma 2.5
Combined lobular
and ductal carcinoma
2.5
Phyllodes tumor 2.5
NOSb histology 30
a CWRR: Chest wall resection and reconstruction.b NOS: Not otherwise specified.
ection and reconstruction for locally recurrent breast cancer:014), http://dx.doi.org/10.1016/j.surge.2014.03.001
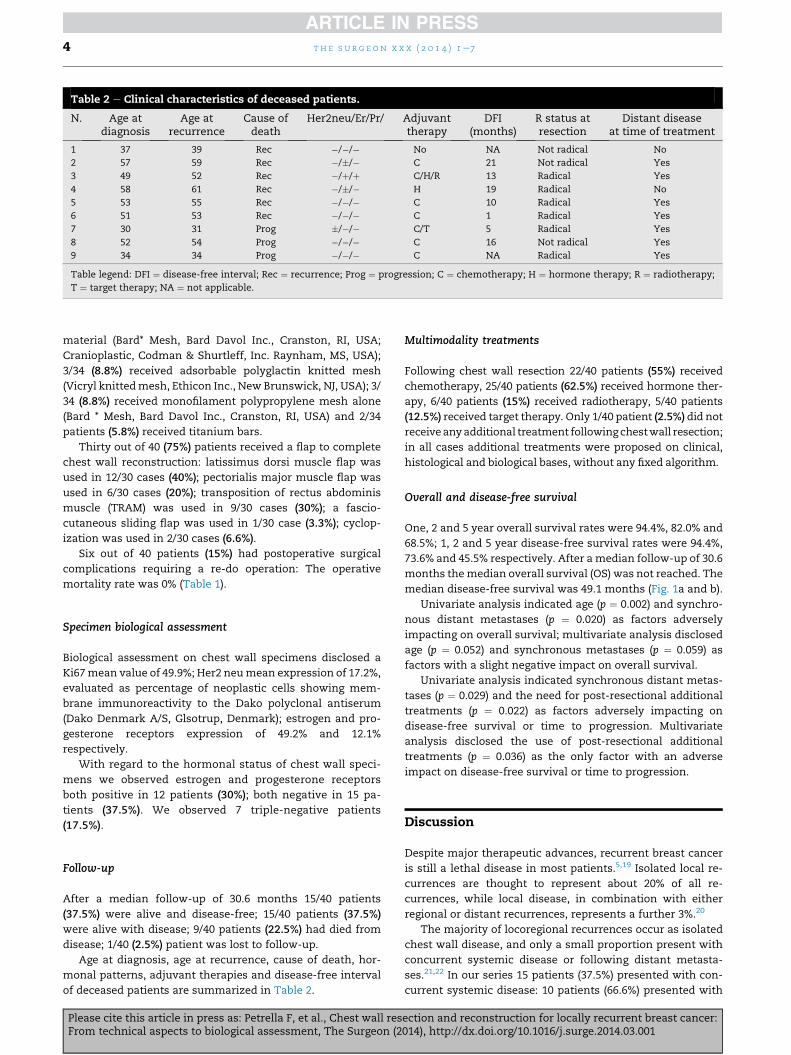
Table 2 e Clinical characteristics of deceased patients.
N. Age atdiagnosis
Age atrecurrence
Cause ofdeath
Her2neu/Er/Pr/ Adjuvanttherapy
DFI(months)
R status atresection
Distant diseaseat time of treatment
1 37 39 Rec �/�/� No NA Not radical No
2 57 59 Rec �/�/� C 21 Not radical Yes
3 49 52 Rec �/þ/þ C/H/R 13 Radical Yes
4 58 61 Rec �/�/� H 19 Radical No
5 53 55 Rec �/�/� C 10 Radical Yes
6 51 53 Rec �/�/� C 1 Radical Yes
7 30 31 Prog �/�/� C/T 5 Radical Yes
8 52 54 Prog �/�/� C 16 Not radical Yes
9 34 34 Prog �/�/� C NA Radical Yes
Table legend: DFI ¼ disease-free interval; Rec ¼ recurrence; Prog ¼ progression; C ¼ chemotherapy; H ¼ hormone therapy; R ¼ radiotherapy;
T ¼ target therapy; NA ¼ not applicable.
t h e s u r g e on x x x ( 2 0 1 4 ) 1e74
material (Bard* Mesh, Bard Davol Inc., Cranston, RI, USA;
Cranioplastic, Codman & Shurtleff, Inc. Raynham, MS, USA);
3/34 (8.8%) received adsorbable polyglactin knitted mesh
(Vicryl knittedmesh, Ethicon Inc., New Brunswick, NJ, USA); 3/
34 (8.8%) received monofilament polypropylene mesh alone
(Bard * Mesh, Bard Davol Inc., Cranston, RI, USA) and 2/34
patients (5.8%) received titanium bars.
Thirty out of 40 (75%) patients received a flap to complete
chest wall reconstruction: latissimus dorsi muscle flap was
used in 12/30 cases (40%); pectorialis major muscle flap was
used in 6/30 cases (20%); transposition of rectus abdominis
muscle (TRAM) was used in 9/30 cases (30%); a fascio-
cutaneous sliding flap was used in 1/30 case (3.3%); cyclop-
ization was used in 2/30 cases (6.6%).
Six out of 40 patients (15%) had postoperative surgical
complications requiring a re-do operation: The operative
mortality rate was 0% (Table 1).
Specimen biological assessment
Biological assessment on chest wall specimens disclosed a
Ki67mean value of 49.9%; Her2 neumean expression of 17.2%,
evaluated as percentage of neoplastic cells showing mem-
brane immunoreactivity to the Dako polyclonal antiserum
(Dako Denmark A/S, Glsotrup, Denmark); estrogen and pro-
gesterone receptors expression of 49.2% and 12.1%
respectively.
With regard to the hormonal status of chest wall speci-
mens we observed estrogen and progesterone receptors
both positive in 12 patients (30%); both negative in 15 pa-
tients (37.5%). We observed 7 triple-negative patients
(17.5%).
Follow-up
After a median follow-up of 30.6 months 15/40 patients
(37.5%) were alive and disease-free; 15/40 patients (37.5%)
were alive with disease; 9/40 patients (22.5%) had died from
disease; 1/40 (2.5%) patient was lost to follow-up.
Age at diagnosis, age at recurrence, cause of death, hor-
monal patterns, adjuvant therapies and disease-free interval
of deceased patients are summarized in Table 2.
Please cite this article in press as: Petrella F, et al., Chest wall resFrom technical aspects to biological assessment, The Surgeon (2
Multimodality treatments
Following chest wall resection 22/40 patients (55%) received
chemotherapy, 25/40 patients (62.5%) received hormone ther-
apy, 6/40 patients (15%) received radiotherapy, 5/40 patients
(12.5%) received target therapy. Only 1/40 patient (2.5%) did not
receiveanyadditional treatment following chestwall resection;
in all cases additional treatments were proposed on clinical,
histological and biological bases, without any fixed algorithm.
Overall and disease-free survival
One, 2 and 5 year overall survival rates were 94.4%, 82.0% and
68.5%; 1, 2 and 5 year disease-free survival rates were 94.4%,
73.6% and 45.5% respectively. After a median follow-up of 30.6
months themedian overall survival (OS) was not reached. The
median disease-free survival was 49.1 months (Fig. 1a and b).
Univariate analysis indicated age (p ¼ 0.002) and synchro-
nous distant metastases (p ¼ 0.020) as factors adversely
impacting on overall survival; multivariate analysis disclosed
age (p ¼ 0.052) and synchronous metastases (p ¼ 0.059) as
factors with a slight negative impact on overall survival.
Univariate analysis indicated synchronous distant metas-
tases (p ¼ 0.029) and the need for post-resectional additional
treatments (p ¼ 0.022) as factors adversely impacting on
disease-free survival or time to progression. Multivariate
analysis disclosed the use of post-resectional additional
treatments (p ¼ 0.036) as the only factor with an adverse
impact on disease-free survival or time to progression.
Discussion
Despite major therapeutic advances, recurrent breast cancer
is still a lethal disease in most patients.5,19 Isolated local re-
currences are thought to represent about 20% of all re-
currences, while local disease, in combination with either
regional or distant recurrences, represents a further 3%.20
The majority of locoregional recurrences occur as isolated
chest wall disease, and only a small proportion present with
concurrent systemic disease or following distant metasta-
ses.21,22 In our series 15 patients (37.5%) presented with con-
current systemic disease: 10 patients (66.6%) presented with
ection and reconstruction for locally recurrent breast cancer:014), http://dx.doi.org/10.1016/j.surge.2014.03.001
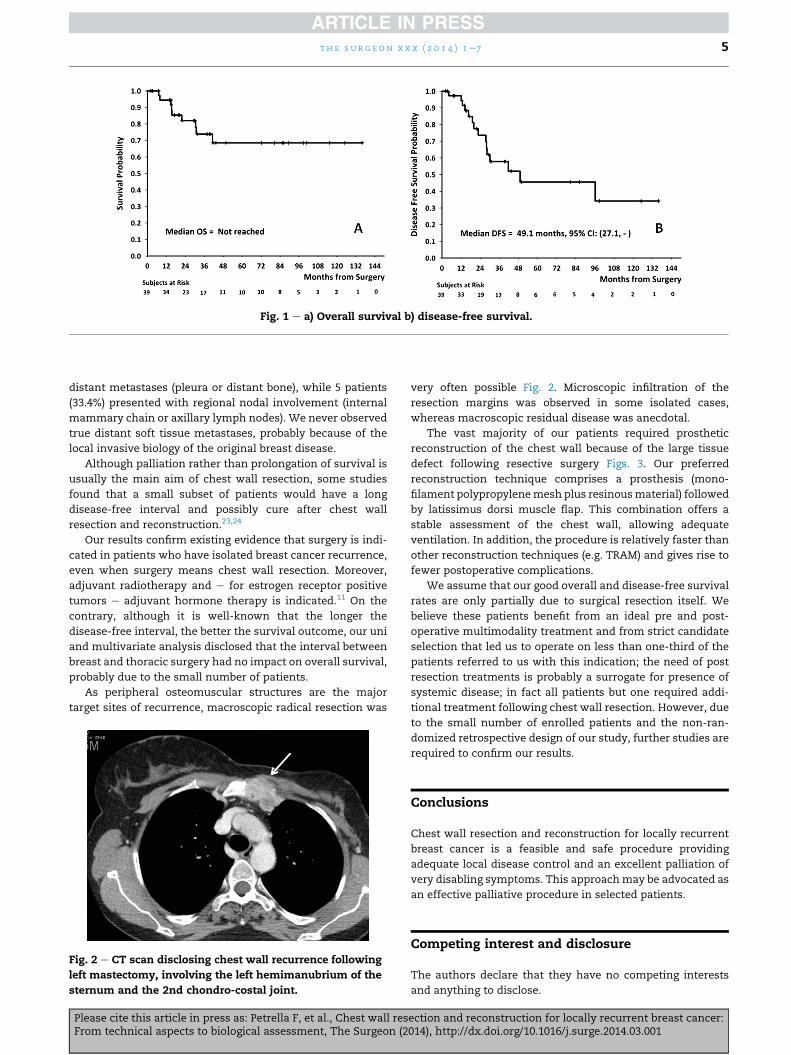
Fig. 1 e a) Overall survival b) disease-free survival.
t h e s u r g e on x x x ( 2 0 1 4 ) 1e7 5
distant metastases (pleura or distant bone), while 5 patients
(33.4%) presented with regional nodal involvement (internal
mammary chain or axillary lymph nodes). We never observed
true distant soft tissue metastases, probably because of the
local invasive biology of the original breast disease.
Although palliation rather than prolongation of survival is
usually the main aim of chest wall resection, some studies
found that a small subset of patients would have a long
disease-free interval and possibly cure after chest wall
resection and reconstruction.23,24
Our results confirm existing evidence that surgery is indi-
cated in patients who have isolated breast cancer recurrence,
even when surgery means chest wall resection. Moreover,
adjuvant radiotherapy and e for estrogen receptor positive
tumors e adjuvant hormone therapy is indicated.11 On the
contrary, although it is well-known that the longer the
disease-free interval, the better the survival outcome, our uni
and multivariate analysis disclosed that the interval between
breast and thoracic surgery had no impact on overall survival,
probably due to the small number of patients.
As peripheral osteomuscular structures are the major
target sites of recurrence, macroscopic radical resection was
Fig. 2 e CT scan disclosing chest wall recurrence following
left mastectomy, involving the left hemimanubrium of the
sternum and the 2nd chondro-costal joint.
Please cite this article in press as: Petrella F, et al., Chest wall resFrom technical aspects to biological assessment, The Surgeon (2
very often possible Fig. 2. Microscopic infiltration of the
resection margins was observed in some isolated cases,
whereas macroscopic residual disease was anecdotal.
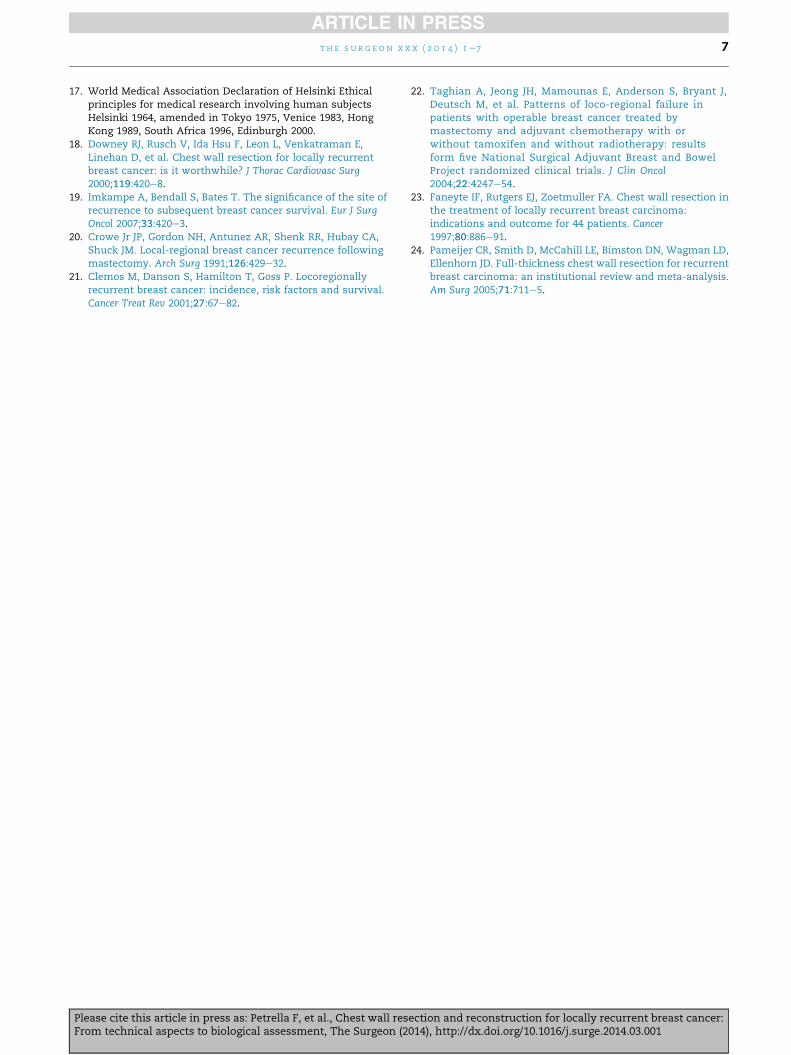
The vast majority of our patients required prosthetic
reconstruction of the chest wall because of the large tissue
defect following resective surgery Figs. 3. Our preferred
reconstruction technique comprises a prosthesis (mono-
filament polypropylenemesh plus resinousmaterial) followed
by latissimus dorsi muscle flap. This combination offers a
stable assessment of the chest wall, allowing adequate
ventilation. In addition, the procedure is relatively faster than
other reconstruction techniques (e.g. TRAM) and gives rise to
fewer postoperative complications.
We assume that our good overall and disease-free survival
rates are only partially due to surgical resection itself. We
believe these patients benefit from an ideal pre and post-
operative multimodality treatment and from strict candidate
selection that led us to operate on less than one-third of the
patients referred to us with this indication; the need of post
resection treatments is probably a surrogate for presence of
systemic disease; in fact all patients but one required addi-
tional treatment following chest wall resection. However, due
to the small number of enrolled patients and the non-ran-
domized retrospective design of our study, further studies are
required to confirm our results.
Conclusions
Chest wall resection and reconstruction for locally recurrent
breast cancer is a feasible and safe procedure providing
adequate local disease control and an excellent palliation of
very disabling symptoms. This approachmay be advocated as
an effective palliative procedure in selected patients.
Competing interest and disclosure
The authors declare that they have no competing interests
and anything to disclose.
ection and reconstruction for locally recurrent breast cancer:014), http://dx.doi.org/10.1016/j.surge.2014.03.001
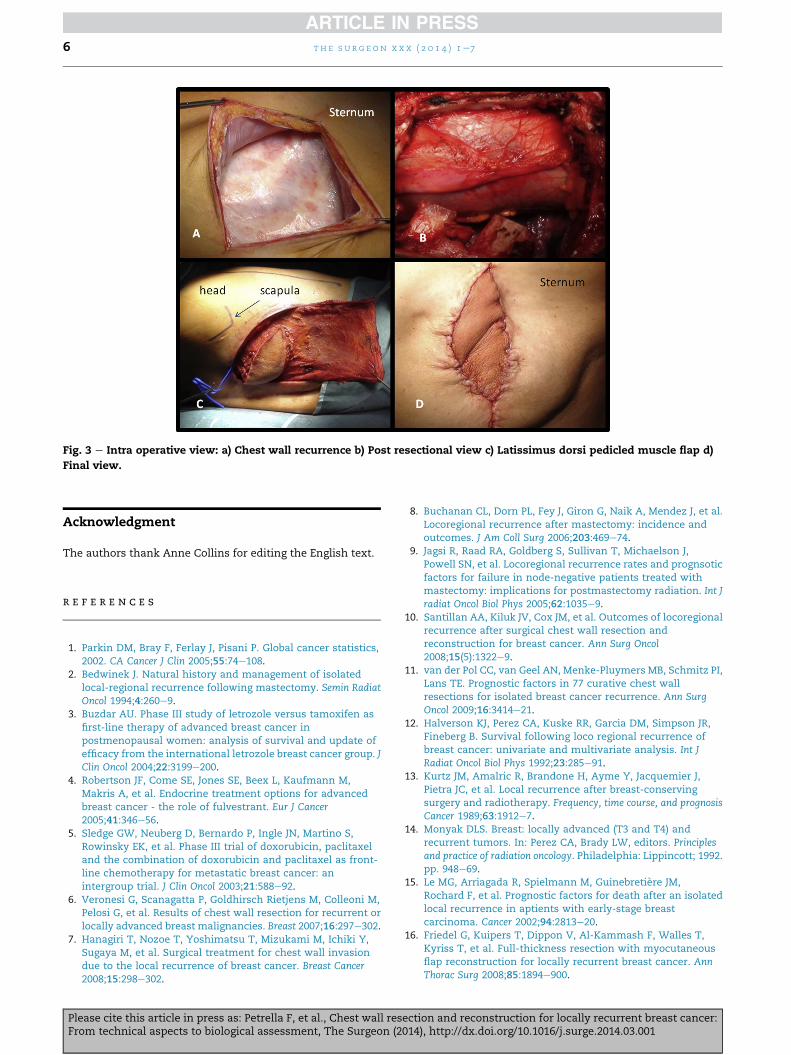
Fig. 3 e Intra operative view: a) Chest wall recurrence b) Post resectional view c) Latissimus dorsi pedicled muscle flap d)
Final view.
t h e s u r g e on x x x ( 2 0 1 4 ) 1e76
Acknowledgment
The authors thank Anne Collins for editing the English text.
r e f e r e n c e s
1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics,2002. CA Cancer J Clin 2005;55:74e108.
2. Bedwinek J. Natural history and management of isolatedlocal-regional recurrence following mastectomy. Semin RadiatOncol 1994;4:260e9.
3. Buzdar AU. Phase III study of letrozole versus tamoxifen asfirst-line therapy of advanced breast cancer inpostmenopausal women: analysis of survival and update ofefficacy from the international letrozole breast cancer group. JClin Oncol 2004;22:3199e200.
4. Robertson JF, Come SE, Jones SE, Beex L, Kaufmann M,Makris A, et al. Endocrine treatment options for advancedbreast cancer - the role of fulvestrant. Eur J Cancer2005;41:346e56.
5. Sledge GW, Neuberg D, Bernardo P, Ingle JN, Martino S,Rowinsky EK, et al. Phase III trial of doxorubicin, paclitaxeland the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: anintergroup trial. J Clin Oncol 2003;21:588e92.
6. Veronesi G, Scanagatta P, Goldhirsch Rietjens M, Colleoni M,Pelosi G, et al. Results of chest wall resection for recurrent orlocally advanced breast malignancies. Breast 2007;16:297e302.
7. Hanagiri T, Nozoe T, Yoshimatsu T, Mizukami M, Ichiki Y,Sugaya M, et al. Surgical treatment for chest wall invasiondue to the local recurrence of breast cancer. Breast Cancer2008;15:298e302.
Please cite this article in press as: Petrella F, et al., Chest wall resFrom technical aspects to biological assessment, The Surgeon (2
8. Buchanan CL, Dorn PL, Fey J, Giron G, Naik A, Mendez J, et al.Locoregional recurrence after mastectomy: incidence andoutcomes. J Am Coll Surg 2006;203:469e74.
9. Jagsi R, Raad RA, Goldberg S, Sullivan T, Michaelson J,Powell SN, et al. Locoregional recurrence rates and prognsoticfactors for failure in node-negative patients treated withmastectomy: implications for postmastectomy radiation. Int Jradiat Oncol Biol Phys 2005;62:1035e9.
10. Santillan AA, Kiluk JV, Cox JM, et al. Outcomes of locoregionalrecurrence after surgical chest wall resection andreconstruction for breast cancer. Ann Surg Oncol2008;15(5):1322e9.
11. van der Pol CC, van Geel AN, Menke-Pluymers MB, Schmitz PI,Lans TE. Prognostic factors in 77 curative chest wallresections for isolated breast cancer recurrence. Ann SurgOncol 2009;16:3414e21.
12. Halverson KJ, Perez CA, Kuske RR, Garcia DM, Simpson JR,Fineberg B. Survival following loco regional recurrence ofbreast cancer: univariate and multivariate analysis. Int JRadiat Oncol Biol Phys 1992;23:285e91.
13. Kurtz JM, Amalric R, Brandone H, Ayme Y, Jacquemier J,Pietra JC, et al. Local recurrence after breast-conservingsurgery and radiotherapy. Frequency, time course, and prognosisCancer 1989;63:1912e7.
14. Monyak DLS. Breast: locally advanced (T3 and T4) andrecurrent tumors. In: Perez CA, Brady LW, editors. Principlesand practice of radiation oncology. Philadelphia: Lippincott; 1992.pp. 948e69.
15. Le MG, Arriagada R, Spielmann M, Guinebretiere JM,Rochard F, et al. Prognostic factors for death after an isolatedlocal recurrence in aptients with early-stage breastcarcinoma. Cancer 2002;94:2813e20.
16. Friedel G, Kuipers T, Dippon V, Al-Kammash F, Walles T,Kyriss T, et al. Full-thickness resection with myocutaneousflap reconstruction for locally recurrent breast cancer. AnnThorac Surg 2008;85:1894e900.
ection and reconstruction for locally recurrent breast cancer:014), http://dx.doi.org/10.1016/j.surge.2014.03.001
t h e s u r g e on x x x ( 2 0 1 4 ) 1e7 7
17. World Medical Association Declaration of Helsinki Ethicalprinciples for medical research involving human subjectsHelsinki 1964, amended in Tokyo 1975, Venice 1983, HongKong 1989, South Africa 1996, Edinburgh 2000.
18. Downey RJ, Rusch V, Ida Hsu F, Leon L, Venkatraman E,Linehan D, et al. Chest wall resection for locally recurrentbreast cancer: is it worthwhile? J Thorac Cardiovasc Surg2000;119:420e8.
19. Imkampe A, Bendall S, Bates T. The significance of the site ofrecurrence to subsequent breast cancer survival. Eur J SurgOncol 2007;33:420e3.
20. Crowe Jr JP, Gordon NH, Antunez AR, Shenk RR, Hubay CA,Shuck JM. Local-regional breast cancer recurrence followingmastectomy. Arch Surg 1991;126:429e32.
21. Clemos M, Danson S, Hamilton T, Goss P. Locoregionallyrecurrent breast cancer: incidence, risk factors and survival.Cancer Treat Rev 2001;27:67e82.
Please cite this article in press as: Petrella F, et al., Chest wall resFrom technical aspects to biological assessment, The Surgeon (2
22. Taghian A, Jeong JH, Mamounas E, Anderson S, Bryant J,Deutsch M, et al. Patterns of loco-regional failure inpatients with operable breast cancer treated bymastectomy and adjuvant chemotherapy with orwithout tamoxifen and without radiotherapy: resultsform five National Surgical Adjuvant Breast and BowelProject randomized clinical trials. J Clin Oncol2004;22:4247e54.
23. Faneyte IF, Rutgers EJ, Zoetmuller FA. Chest wall resection inthe treatment of locally recurrent breast carcinoma:indications and outcome for 44 patients. Cancer1997;80:886e91.
24. Pameijer CR, Smith D, McCahill LE, Bimston DN, Wagman LD,Ellenhorn JD. Full-thickness chest wall resection for recurrentbreast carcinoma: an institutional review and meta-analysis.Am Surg 2005;71:711e5.
ection and reconstruction for locally recurrent breast cancer:014), http://dx.doi.org/10.1016/j.surge.2014.03.001