
Chapter 1.Orientaion on Conceptual Framework
115
Chapter 1.Orientaion on Conceptual Framework 1.1 Concept of Fieldwork 1.2 Objectives/Goals of Fieldwork 1.3 Historical Background of Fieldwork 1.4 Importance of Fieldwork 1.5 Inter-relationship between Social Work Education and Field Work 1.6 Concept of Clinical Social Work 1.7 Scope of Clinical Social Work 1.8 Standards for Clinical Social Work in Social Work Practice 1
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Chapter 1.Orientaion on Conceptual Framework

Chapter 1.Orientaion on Conceptual Framework
1.1 Concept of Fieldwork
1.2 Objectives/Goals of Fieldwork
1.3 Historical Background of Fieldwork
1.4 Importance of Fieldwork
1.5 Inter-relationship between Social Work Education and Field Work
1.6 Concept of Clinical Social Work
1.7 Scope of Clinical Social Work
1.8 Standards for Clinical Social Work in Social Work Practice
1

Introduction
Social work is a helping profession which fundamental aim is to
help the individuals, groups and community to cope with their
problems through enabling them so that they can solve their
problems. The students of Social Work discipline have to acquire
theoretical knowledge and apply this knowledge in practical
field. Field work gives the opportunities
to the students of Social Work to apply the acquired knowledge in
practical field. In any professional training in Social Work it
is essential to study society and the individual. The department
of Social Welfare is providing the necessary knowledge through
the basic studies courses. Knowledge along is not enough. Social
workers need to have skill to apply this knowledge effectively in
life situation for achievement social improvement. Class room
discussion, plans and theories can not solve the problem. The
social welfare department recognized this and considered
practical work with individual groups and communities.
Concept of Fieldwork
In arena of social work education the term 'fieldwork' is often
used interchangeably with such terms as practicum, field
2

instruction, field education, field practicum and internship
(Horejsi and Garthwait 2002:1). Whatever the term is fieldwork
denotes the practical aspect, one of the two facets, of social
work education. Simply fieldwork is a way of getting social work
students used to with the diverse fields of social work
intervention.
Fieldwork is portrayed in several other ways. In 1952 Council on
Social Work Education observed fieldwork as a method of
instruction in a setting where all the ingredients of the social
work curriculum converge and through their fusion provide an
opportunity of integrating the knowledge, skills, and attitudes
contained in the several content areas of the curriculum
(Boehm,1952:27)
In International Encyclopedia of Social Science vol.5 (1968:418)
has defined- "Field work is the study of people and of their
culture in their nature habitat. Field work came to mean learning
as for as possible way to speak, see and act as a member of its
culture and the same time, as a trained social scientist from a
different culture".
R.R. Sing(19S5:54)in "Field Work in Social Work Education" has defined, "Field
work is an educationally sponsored attachment of social work
students to an institution , agency or a section of community, in
which they are helped to extend their knowledge and understanding
and experience the impact of human need."
3

In Field Work Manual, M, A Momen (1970:1) has said. Field Work
Programme in Social Work education is to provide the student with
actual experience in applying in Social work method and enables
him/her to become familiar with real social work practice .That
is to relate academic theory to create relating as found in the
agency setting.
Field Work provides the students opportunity to realize how
social problems are influencing the individuals, group, family,
organization, and community. Moreover Field Work enables a
student to understand the roles and functions of social policy,
law, and social service related organization, network and
community resources. In total, practical training gives a chance
to a student to observe the role of a social worker in total
problem solving process.
Figure: Process of Social Work practice 4

(Allen Pincus and Anne Minaham, 1973 p- 86)
About this statement it is said that, the objective of the
fieldwork programme in social work education is to provide the
student with actual experience in applying social work methods
and enable him or her to become familiar with real work of
practice. That is to relate academic theory to concrete reality
as found in the agency setting. It also aims to allow the student
to test himself/herself to develop sense of professional
discipline to gain self-confidence and to feel him or herself a
social worker with beginning competence.
From the above discussion Certain Numbers of characteristics of
Field work can be mentioned below.
1. Field work is an educationally sponsored attachment of
social work. Student to an institution, agency or a section
of community
2. Field work helps the students to extend their knowledge and
understanding and experience the Impact as human need.
3. Field work helps the student to realize the theory, methods
and principle of social work in practice.
4. Field work helps the students to became familiar with real
social work practice.
5

5. Field work enable students to apply and integrate previous
learning and current learning.
In the perspective of above discussion, we can say that Field
work is the science of practice in where students can relate
academic theory with social work practice and they can solve
the problems of silent through the application of social work
methods.
Objectives/Goals of Fieldwork:
The fieldwork instruction and classroom teaching are identical
where both are emphasizing "knowledge', 'being' and 'doing'
aspects. Fieldwork helps the students to apply the theory and
principles of social work in actual practice. Students confronted
with real life situations are likely to become more aware of
their own feelings and of his 'professional self or Rifat Rashid
mentioned in his book (1960:70)- "Learn to use himself
creatively, learn to use a body of knowledge and principles
6
creatively through the medium of supervision in a social agency
within a professional pattern",
M.A Momen said in fieldwork Manual (1970:2):
1) The student should learn to apply social work methods in the
solution of given individual group or community problems.
They should be exposed to agency practice in which there is
a planned, a systematic, objective approach to problem
solving. The student should learn to start with a factual
material as the basis for professional intervention and
through appropriate study and diagnosis to move forward
step by step to the implementation of a plan of action.
2) The student should develop facility in the use of
organizational structure particularly the committee. He/she
should learn the technology of the committee process
(professional staffing functions) as well as an
understanding of the human dynamic of task oriented groups
(group development, interaction roles, motivations of
individuals, reference group behavior etc.) within a
structure and gain insight regarding his/her special place
in the network of relationships.
3) The student should achieve self-awareness and disciplined
use of self as a helper and an agent of change in a variety
of individual and group situations. He/she should come to
identify with the profession of social work and its values
and ethics.
7

4) The student needs to learn the organizational framework of
service. He/she must understand agency structure arid
policy and how to facilitate such policy through his/her
practice. He/she should become familiar with the differing
institutional styles tempos of agencies associated with
various field of practice.
5) The student should become familiar with administrative
procedures and processes. He/she should learn how an office
is run, what kind of routines need to be established, how
to facilitate administrative arrangements relevant to the
discharge of the responsibilities of his/her own
assignment. He/she should be aware of how administrative
decisions are made, conveyed and implemented.
6) The student should acquire knowledge regarding community
structure and process. He/she should know the kinds of
formal and informal groups, voluntary and governmental
agencies individuals, institutions and forces that
constitute a community. He/she should be able to analyze
the interplay of forces which bear on a given social
problem. He/she should have the ability to utilize
community resources in support of social welfare goals.
7) The student should acquire significant substantive knowledge
in the specific field of practice characterized by the
agency in which he/she is placed. This means he/she should
be conversant with one or a cluster of social problems
associated with his/her agency or assignment. He/she should
8
become acquainted with the causes of the problem and with
social welfare programmes, agencies, structures, laws and
policies related to its solution.
8) The student should acquire competence in recording and
reporting (process-records, minutes, monthly reports,
administrative correspondence etc.). He/she should know
what to record and how to record. He/she should be
acquainted with the employment of records for the purposes
of planning, evaluating and supervising.
9) The students should acquire and be given an opportunity to
try out a variety of social work methods, skills and
techniques.
Some specific objectives of Field Work Education:
To create a opportunity for the social work student to
justify his acquired knowledge with the field
To help the social work student adjusting with different
work settings
To learn office management, office systems, behavior with
the staffs, dealing with the clients of different agencies
9

To understand the gap between theoretical knowledge and
practical situation
To cope with different working situation in different
agencies
To acquire practical experiences, knowledge, and
understanding the principles, programs, procedures, and
activities of different agencies.
To help students learn how to think critically, analytically
and evaluative, all of which are basic to the teaching of
the problem-solving process.
To help students develop fellings and attitudes appropriate
to the helping process.
To help students develop fellings the and capacity to
establish and maintain professional relationships.
The development of skill in helping, involving the
disciplined use of knowledge in thinking about, analyzing
and understanding professional problems and in the helping
process.
Development of the student’s capacity of cooperative
relationships with his fellow workers and with other
agencies in the community
10

Historical Background of Fieldwork:
The social work activities started as religious practice. In the
feelings of religion people provided protection for the helpless,
windows, orphans and the sick. On the march of time this social
work becomes organized institutionalized and professional. In the
perspective of professionalism, it is needed education, knowledge
and skill for proper practice in social welfare, working field.
For developing knowledge and skill, fieldwork has begun. So, it
is said that the history of fieldwork is related with history of
evolution of social work activities. The history of fieldwork is
discussed below:
In the history of fieldwork practice, at first he who is
mentioriable is Edward Oenison. In 1867 as a volunteer of the
society for the Relief of Distress in London, he became convince
that the mere distribution of alms was futile. He abandoned his
comfortable life and moved to Stepney, a poor quarter in Hast
London to live with the poor in this slum district. There Denison
taught Bible classes, history and economics. The inhabitants of
Stepney found his reluctant to give them the customary meat and
coal tickets unless he was certain they were in dire need. But he
was generous with his time in listening to their problems and
offered his counsel when he felt they were oppressed.The idea of
living among the people who needed help was most effectively
demonstrated by Samuel Augustus Barnett, born in Bristol in 1844.
Barnett had studied theology at Oxford and in 1873 accepted the
11

post of Vicar of St. Judo's Church in white chapel in East
London, one of the poorest parishes in the diocese. Barnett was
encouraged by his fiancee, Henrietta Rowland, who had worked
under Octavia hill. After their marriage Henrietta became her
husband's co-worker. In white chapel, the Barnetts found a great
proportion of the 8,000 parishioner's unemployed or sick, living
in filthy, overcrowded tenements. The Barnetts went to Oxford and
Cambridge and discussed with university students the conditions
they had encountered in St. Jude's. They invited the students to
come to live with them in white chapel to study the life of the
underprivileged, to help in their education and to render
personal aid. Among those who accepted Vicar Barnett's invitation
was Arnold Toynbee, an enthusiastic and gifted young Oxford
graduate.
He was outstanding among his colleagues because of his devotion
and the warm, personal contact he established with the families
of the parish. Unfortunately he was of poor health, contracted
tuberculosis, and died in 1883. In his memory, a number of his
friends built, in 1884, a university settlement in the white
chapel district and called it "Toynbee Hall", the first
settlement house in the world.Toynbee Hall had three main
objectives: education and cultural development of the poor;
information for the students and other residents of the
settlement regarding the condition of the poor and the urgent
need for social reforms; and a general awakening of popular
interest in social and health problems and in social legislation.
12

The basic purpose of the settlement was to bring educated men and
women into contact with the poor for their mutual benefit, so
that by common work and studies they could exercise a cultural
influence beyond the teaching of special subjects. The attitude
of a superior "Lady Bountiful" which still prevailed in charity
societies, was replaced by co-operation and learning on the part
of both instructors and workers at Toynbee Hall.
Later then in 1893, Ann L. Bowes presented a proposal to
international congress of charities conference and philanthropy
in USA for arranging a training education program for social
workers. In 1887, Mary Elen Richmond planed to establish a
training school for applied philanthropy for the purpose of
fieldwork training in social work education. In 1898, a training
course is made run for six weeks. The name of this course was
summer training course.In the early of twenty centuries, the
different courses on social work education and fieldwork training
are established in various universities and colleges in
USA.Social work practice in institutional settings developed
primarily in the Massachusetts General Hospital in 1905. Under
(he guidance of Richard C. Cabot, physician to outpatients Ida
Claim on established the first medical social work department in
a hospital in the United States. Once again there was a precedent
for this service in London. However, social workers in the United
States refused to identify with nursing, because of nurses'
subordinate status, and attempted to develop a professional
identity based on the model of the physician: Medical social
13

workers became interested in professional education as a means of
moving beyond the "warm-heart" position into an understanding of
the psychic or social conditions at the base of patient distress.
Furthermore, with professional education it would be possible to
move into a colleague relationship with the physician. By 1912, a
one-year course in medical social work was established in the
Boston School of Social work. (Morales, shefor, 1986:46-47)
In Pakistan Period
The first short term in service social work training course held
in 1952 at Karachi jointly sponsored by the government of
Pakistan and The United Nations Technical Assistants
Administration, was under the direction and supervision of United
Nations consultants an their Pakistani colleagues. Three days
were given to classroom work and two days to supervised field
demonstration. The curriculum of this course was divided into
three major phases:
o Orientation
o Social work technique
o Fieldwork
Fieldwork consisted of supervised observation and practical work
in seven fields:
Labor welfare
Medical social work
Youth work
14

Rural welfare
Delinquency
Industrial management
Child and family welfare
The next course was held in Dhaka in September, 1953. The
duration of the course was three months. The curriculum of this
course was divided into four major phases:
Orientation course
Techniques course
Fieldwork
Review and examination
Fieldwork as a learning process, involving two days of a Five day
week, was planned to provide observation and practical
demonstration in the field of community organization, rural
welfare, child and family welfare and medical welfare. Fieldwork
was taken as an integral part of the curriculum where
opportunities were provided to lest class room knowledge in
practical situation (Rashid 1960:28-29).The Dhaka training
program was evaluated by the international team. They were
convinced that the field work in particular demonstrated that
modern social work techniques could be applied effectively in
encouraging self help in individuals and in groups. [Ibid, P.
p:28-29] .
15

On the basis of three month training courses conducted in Dhaka
from September 1953, the recommendations of the international
team, Dhaka College and Research Centre was introduced in Dhaka
in 1958. Later on, it is named as Institute of Social Welfare and
Research in 1973. College of social work was established in
Kajshahi in 1964, This college included as a department at Arts
Faculty in Rajshahi University in 1964. Now different
universities and Colleges are teaching professional social work
course under the department of social work in Bangladesh. The
curriculum of these departments has developed including fieldwork
program.
16
Importance of Fieldwork:
Field work has immense importance to the students of social work.
Social work is primarily the professional activity of helping
individuals, groups and communities enhance or restore 'their
capacity for social functioning and creating societal conditions
favorable to that goal (NASW, 1995), and it is fieldwork chat,
for the first time, provides an opportunity for students to
interact professionally with individuals, groups and
organizations (Nelson, 1993). It is believed that in professional
social work education, knowledge alone is not enough and the
development of skills in practice is necessary. On the other
hand, classroom instruction, group discussion, and reading alone
cannot produce professional skills because 'to know' does not
result automatically in the ability 'to do' (Rashid, 1960:3).
"Fieldwork component of the social work curriculum then provides
a structured learning environment to the students for the
development of professional social work skills.
Fieldwork provides students with genuine experience in applying
social work methods and enables them to become familiar with the
real world of practice, i.e. to relate academic theory to
concrete reality as found in the agency setting. It allows the
students to test himself/herself and helps to develop a sense of
professional-self among them. Fieldwork also generates
professional discipline and self-confidence among students and
17

helps them to feel himself/herself a social worker with beginning
competence (ISWR, 1996:1). Moreover, it helps them to identify,
clarify and assess their own needs as social work students as
well as the needs of different types of persons coming to the
agencies as clients. In addition, students become able to
understand the organizational and community context of social
work practice through fieldwork (Corliss and Corliss, 1998:54).
In "Field Work Manual', M.A. Momen (1970:12) has mentioned the following
importance of field work practices:
Students should learn to apply social work methods in the
solution of given individual ground or community problems.
The student should develop facility in the use of
organizational structure; particularly the committee. He/
she should come to know how to foster and use relationships
within structure and gain insight regarding his/ her special
place in the net-work of relationship,
The student should achieve self-awareness and disciplined
use of self as a helper and group situations.
The students need to learn the organizational framework of
services. He/ she must understand agency structure and
18

policy and how to facilitate such policy through his/ he
practice.
The student should become familiar with administrative
procedures and processes,
The student should acquire knowledge regarding community
structure and procures,
The student should acquire significant substantive knowledge
in the specific field of practice characterized by the
agency in which he/ she in placed.
The student should acquire competence in recording and
reporting (process records minutes, monthly reports,
administrative correspondence, etc.).
The student should acquire and be given an opportunity to
try out a variety of social work methods, skills and
techniques,
Field work helps the students to realize the theory, methods
and principles of social work in practice which facilitates
them to develop professional self.
The students acquire and are given an opportunity to try out
a variety of social work methods, skill and techniques. This
may include among others preparing news release public
speaking, arranging and conducting conference, engaging fact
finding and statistical work on specific problem, conducting
finding, personal interviews, preparing budget work schedule
etc.
19

Some other importance of fieldwork
Developing social work skill with emphasis on
individualizing the problem-solving process.
Developing understanding of board policy issues and the
legislative process and administrative process.
To give opportunity for students to learn to work with other
professional and voluntary workers.
To help the student to develop a deeper awareness of himself
and his part in the problem-solving process.
The students learn how to apply social work knowledge and
methods in the solution of given individual, group or
community problems. The students come to know how to
accomplish study, diagnosis and treatment process of
client's problems.
The students can understand how to work under an
administrative and organizational structure and they can
learn how an office is governed and what kinds of routine
needs to be established,
The fieldwork practices in social work education should enable
students, using acquired knowledge of social work methods,
concepts and principles, to work with individuals, groups and
communities, and should further encourage developmental teaching,
leading student from their present status to the desired outcome.
Inter-relationship between Social Work Education and Field Work
20

Mutual relationship between social work education and practice:
Modern social work education has two dimensions: theoretical and
practical. A social worker gains knowledge about society, social
problems, property, social structure, social values, human
behavior, social work process when practical training enable them
to use this knowledge acquired knowledge in this field for real
life purposes. Thus practical training is required for social
worker to solve social problems of human beings/society for
modern social work. Taking notice of this requirement higher
education has been provided with practical training course in its
syllabus about social work, through which students can apply
theoretical knowledge for solution of problems. Social and
Economic Council of United Nations has recognized social work as
a profession in 1951 and formulated the following decisions.
Social Work is a profession based on trained male and female and
who are obtained theoretical and practical knowledge in social
work degree from established and recognized educational
institutions is mandatory to fulfill by them.
Social Work is a practical education, which is learned through
theoretical study of society and social work. This is because
‘public good’ can be affected only by applying theoretical
knowledge in real life in a scientific way. And practical
training helps apprentices to be full-hedged social workers by
making arrangements of applying theoretical knowledge in
practical life. And these together make social work education and
practical training inter-dependent upon each other. Therefore we
21

may say social work education and field work are interrelated
concept just like two branches of a tree.
Figure: Interrelationship between social
work & Field work
From the above discussion, we can say that field work is a
process by which students gather practical experience from the
related field. In social work subject, field work very much
important because of its professional attitude. We know every
profession is composed with academic learning as well as
practical experience.
Clinical social work is a healthcare profession based on theoriesand methods of prevention and treatment in providing mental-health/healthcare services, with special focus on behavioral andbio-psychosocial problems and disorders. Clinical social work’sunique attributes include use of the person-in-environment
22
Social WorkTheoretical PerspectivePractice Perspective

perspective, respect for the primacy of client rights, and strongtherapeutic alliance between client and practitioner. With200,000 practitioners serving millions of client consumers,clinical social workers constitute the largest group of mental-health/healthcare providers in the nation.
Clinical Social Work
Clinical social work is the professional application of social worktheory and methods to the diagnosis, treatment, and prevention ofpsychosocial dysfunction, disability, or impairment, includingemotional, mental, and behavioral disorders (Barker,2003).Clinical social work is broadly based and addresses theneeds of individuals, families, couples, and groups affected bylife changes and challenges, including mental disorders and otherbehavioral disturbances. Clinical social workers seek to provideessential services in the environments, communities, and socialsystems that affect the lives of the people they serve.
Clinical social work has a primary focus on the mental,emotional, and behavioral well-being of individuals, couples,families, and groups. It centers on a holistic approach topsychotherapy and the client’s relationship to his or herenvironment. Clinical social work views the client’s relationshipwith his or her environment as essential to treatment planning.Clinical social work practice also focuses on collaborativeproblem solving, helping clients increase connections with othersand their environment and advocating for the social environmentto be more responsive to the client’s need. Clinicalpractitioners are trained to do this work through use of aprofessional relationship, purposeful conversation, plannedactivity, and resource mobilization. Guiding principles ofclinical practice include worth and dignity of all people, use ofa strengths perspective, confidentiality, and client self-determination in decision making.
The knowledge base of clinical social work includes theories ofbiological, psychological, and social development; diversity andcultural competency; interpersonal relationships; family and
23

group dynamics; mental disorders; addictions; impacts of illness,trauma, or injury; and the effects of the physical, social, andcultural environment. This knowledge is inculcated in social workgraduate school and is fused with direct-practice skills that aredeveloped by the practitioner during a period of at least twoyears of post-graduate experience under clinical supervision.This period should suffice to prepare the clinical social workerfor autonomous practice and state-licensure as a clinical socialwork professional. In the years that follow, clinical socialworkers may pursue an advanced-generalist practice or may decideto specialize in one or more areas. Clinical social workers areoften the first to diagnose and treat people with mentaldisorders and various emotional and behavioral disturbances.Clinical social workers are essential to a variety of client-centered settings, including community mental health centers,hospitals, substance use treatment and recovery programs,schools, primary health care centers, child welfare agencies,aging services, employee assistance programs, and privatepractice settings.
Scope of Clinical Social Work
Clinical social work students are trained to practice within acontext of social policy and macro systems and to consider howthese policies and systems impact clients and worker practices.Clinical social workers are employed in a variety of settingsincluding early childhood intervention programs, hospitals,community health settings, schools, housing developments, nursinghomes, mental health clinics, and child welfare.
Clinical social work is notable for the versatility of itspractitioners and the variety of their roles, including that ofteam member and team leader in a multi-disciplinary setting.Client consumers—individuals, couples, families, and groups—benefit from a variety of direct services, including assessment,diagnosis, treatment planning, intervention/treatment, evaluationof outcomes, and case management. Clinical social work settings
24

and services include, but are not limited to, the following (inalphabetical order):
•child & family services • private practice offices• clinics • public & private schools
• court & forensic venues • public sector health/mentalhealth
• elder care facilities • rehabilitation facilities
• home health care • religious/spiritualorganizations
• hospice • residential treatment• hospitals • rural healthcare• not-for-profit agenciesand organizations agencies
• social services
• palliative andrehabilitative care
• uniformed services andVeterans Affairs
The scope of clinical social work extends across many practicesettings and populations. It is anticipated that these standardswill reinforce and support current clinical practice in allsettings, while affirming the value of clinical social workservices as a discrete practice area.
The flexible and skillful application of knowledge, theories, andmethods in a bio-psychosocial approach is a hallmark of clinicalsocial work. Interventions—the direct person-to-person(s) process—are conducted with people of all ages and range in nature frompreventive, crisis, and psycho-educational services tocollaborative client advocacy and brief and long-term counselingor psychotherapy. Typically, clinical social workers superviseand consult with professional colleagues and may engage inindirect practice (e.g. administration, research, teaching, andwriting). It is a standard of practice for clinical socialworkers to engage in career-long continuing clinical educationand to adhere to a professional code of ethics.
25

Standards for Clinical Social Work in Social WorkPractice
The NASW Board of Directors (2005) adopted following standards
Standard 1. Ethics and Values
Clinical social workers shall adhere to the values and ethics of the social work profession, utilizing the NASW Codes of Ethics as a guide to ethical decision making.
Standard 2. Specialized Practice Skills and Intervention
Clinical social workers shall demonstrate specialized knowledge and skills for effective clinical intervention with individuals, families, and groups.
Standard 3. Referrals
Clinical social workers shall be knowledgeable about community services and make appropriate referrals, as needed.
Standard 4. Accessibility to Clients
Clinical social workers shall be accessible to clients during nonemergency and emergency situations.
Standard 5. Privacy and Confidentiality
Clinical social workers shall maintain adequate safeguards for the private nature of the treatment relationship.
Standard 6. Supervision and Consultation
26

Clinical social workers shall maintain access to professional supervision and/or consultation.
Standard 7. Professional Environment and Procedures
Clinical social workers shall maintain professional offices and procedures.
Standard 8. DocumentationDocumentation of services provided to or on behalf of the client shall be recorded in the client’s file or record of services.
Standard 9. Independent Practice
Clinical social workers shall have the right to establish an independent practice.
Standard 10. Cultural Competence
Clinical social workers shall demonstrate culturally competentservice delivery in accordance with the NASW Standards for CulturalCompetence in Social Work Practice.
Standard 11. Professional Development
Clinical social workers shall assume personal responsibility fortheir continued professional development in accordance with theNASW Standards for Continuing Professional Education and state requirements.
Standard 12. Technology
Clinical social workers shall have access to computer technologyand the Internet, as the need to communicate via e-mail and toseek information on the Web for purposes of education,networking, and resources is essential for efficient andproductive clinical practice.
27

Chapter 2.Concise Delineation on DMC
2.1 History of DMC
2.2 Entrance Examination
2.3 Principals
2.4 Role in National History
2.5 Facilities and Achievements
28

2.6 Clubs and Association
2.7 Alumni Trust
Dhaka Medical College Hospital (DMC)
29

Dhaka Medical College and Hospital (DMCH) is a medical college located in Dhaka, Bangladesh. It is situated inthe Bakshibazar area of Dhaka, the capital city of Bangladesh. The college is close to the University of Dhaka and the Bangladesh University of Engineering and Technology.
History
At the beginning, the college did not have a building of its own.The present building was there before the Partition of Bengal of 1905. The building was first used, in 1904, as the secretariat (headquarters) of the newly formed provinces of East Bengal and Assam. During this period bureaucrats, not doctors, used to roam its busy corridors.In 1921, when the University of Dhaka began its journey, the building was handed over to the University administration. At that time a part of this huge building was used as the University's Medical Center, another part as the students' dormitory and the rest as the administrative wing of the Arts faculty.In 1939, the Dhaka University Council requested that the British Government establishes a medical college in Dhaka. The proposal was postponed due to the Second World War,During World War II it became an American Armed Forces hospital. The Americans left at the end of the war, but the hospital remained.Dhaka Medical College was established in 1946 and the college began admitting students. Academic class started on July 10 whichis celebrated as "DMC DAY". The 1st year was named K-5, 2nd year K-4, 3rd year K-3, 4th year K-2, and 5th year K-1. All the students except K-5 had transferred from the Calcutta Medical College. The main reason behind this was the partition of 1947.
30

At first there were no female students but now about half of the students are females.Over time, the original 100 bed hospital has grown to become Bangladesh's largest hospital. After adding 500 beds on October 3, 2013, DMCH is now a 2300 bed hospital. The new beds were addedin a new building known as DMCH-2. The Medinine (Medical Center) is gradually being shifted to the new building, DMCH-2, which will open with a bone marrow transplantation facility very soon.Major W J Virgin, the head of the committee formed to establish the Dhaka Medical College, was the first principal. At the beginning there were only four departments – Medical,Surgery, Gynecology and Otolaryngology (ENT). Since thecollege did not have'at first, a Anatomy nor a Physiology department the students attended those classes at Mitford Medical School(now the Sir Salimullah Medical College). After a month, Professor of Anatomy Pashupati Basuand and Professor of Physiology Hiralal Saha joined the staff and the classes began in ward number 22 of the hospital.There was no lecture hall or dissection gallery at this time. These needs were met after the foundation of the college buildingin 1955. The institute did not have any student housing. Male students were allowed to reside in the Dhaka University's studenthalls, but girls had to live at home. The college and hospital premises were expanded with temporary sheds, some of which were built for outdoor services of the hospital and some for student housing. New buildings for housing, college and hospital were constructed in phases: a dormitory for girls in 1952, a dormitoryfor male students in 1954–55, a new complex of academic buildingsin 1955, and a dormitory for internee doctors in 1974–75. A new academic and hospital building, Dhaka Medical College Hospital-2 (DMCH-2), was inaugurated by Prime Minister Shiekh Hasina on October 3, 2013.
Entrance examination
Every year, after passing the Higher School Certificate, nearly 65,000 (sixty five thousand) applicants from all over the country
31

sit for the medical college entrance examination. The top 200 students get the opportunity to study at the Dhaka Medical College. Each class of the Dhaka Medical College are named with the prefix K and a number, such as class K-71 (the latest class at the Dhaka Medical College.)
Principals
Serial Name Period
1. Dr. Major W JVirjin
01.07.46 –14.08.47
2. Dr. Colonel E GMontgomery
15.08.47 –19.07.48
3. Professor T Ahmed 19.07.48 –01.01.52
4. Dr. Colonel A KAfridi
01.01.50 –20.03.53
5. Professor NowabAli
21.03.53 –10.04.54
6. Professor A K M AWahed
11.04.54 –20.01.55
7. Professor Nowab 21.01.55 –
32

Serial Name Period
Ali 01.02.57
38. Professor QuaziDeen Mohammad 27.01.08 –
Role in national historyThe Dhaka Medical College has been involved in all the national movements of Bangladesh. Dhaka Medical College dormitory (known as Barrack) was at the heart of thelanguage movement from 1948 to1952. Barrack was formerly situated at Central Shaheed Minar current location.There were about 20 tin shed barracks where the medical students resided. Being close to the Parliament of East Pakistan (presently Jagannath Hall of Dhaka University). For strategic reasons the medical dormitory was chosen as the center of the student movement.In the early hours of February 21, 1952, all the students of Dhaka Medical College gathered in front of the medical college dormitory. In the afternoon the group headed for the parliament which was in session. No procession was allowed due to Section 144. The students decided to break Section 144 at 4:00 PM at the historical "Aam-tola" (which was situated beside the present day Emergency gate).The police fired at the procession, resulting in the deaths of Salam, Barkat, Rafique, Jabbar and Shafiur.After sundown on February 21st, at the site of the deaths, the students of Dhaka Medical College decided to build a monument. They worked continuously on the 22nd and 23rd of February and
33

finished the construction, using bricks, gravel and cement reserved for the hospital.The students of DMC played a vital role in the student and mainstream politics of the 60's as well. When the military government of Ayub Khan started torturing opposing political leaders, the central student leaders took refuge in the Bakshibazar student dormitory. Most of the meetings deciding the upcoming line of action were held on the college campus. During the movement protesting the martial law and the Hamidur Rahman Education Commission, DMC and its dormitories were the only safe refuge for the student leaders. Many students of this institutionactively participated.On January 20, 1969, police charged and fired into a procession of students near the present emergency gate. Student leader Asaduzzaman was severely injured. He was admitted to the hospitalbut died in ward number 8 before any treatment was possible. The students of the medical college led a procession with the blood stained shirt of Shaheed Asad. Shortly after the students of Dhaka University raised the flag of independent Bangladesh in the"Bot tala" of DU. On March 2, 1971, the doctors of DMCH raised itat the peak of present Doctors' Cafeteria. Dhaka Medical College had also made its mark in the mass uprising of the 90's. The doctors actively participated in the movement protesting the anti-health policy of the government of that time under the banner of BMA.[1]
Liberation War, 1971Students, nurse, staff and doctors who had passed from DMC playeda major role in the war of independence. Many of them were engaged in the battlefield, while others risked their lives to treat the injured freedom fighters in the hospital. Almost all the doctors working at DMCH helped the injured freedom fighters by admitting them under false names. Dr. Fazle Rabbi. Moazzem Hossain, Selim ahmed, Ali Hafiz Selim, Abu Yusuf Mia, Iqbal Ahmedfaruq, Muzibul Haque, Mostafa Jalal Mahiuddin, Mozaffar, amzad Hossain, Wali, Osman, Golam Kabir, Zillur Rahim, Dalu,
34

Nurujjuman, Shahadat and many more students took part in the war as liberation fighters. Many of them fought in the Dhaka city.
Facilities and achievmentsIn order for students to post graduate, they must undergo intensive preparation. If desired, one can justify themselves online. To justify your post graduation admission preparation Click here. Sample questions and model tests are provided, which can aid in this process.Dhaka Medical College has two museums. The National Forensic DNA Profiling laboratory is first of its kind in Bangladesh. The laboratory assists in investigations concerning murder, rape, paternity, maternity, immigration, distribution of wealth among successors, deformed dead bodies and other cases needing identification.Shahjahan Hafiz, a student in the fifties was a leading Rabindra song artist in the East Pakistan Radio. The notable alumni of DMCincludes current Foreign Minister Dr Dipu Moni, current Health Minister Professor Dr Ruhul Huq, Health Advisor to the Prime Minister Dr. Syed Modasser Ali, former President of Bangladesh Dr. A.Q.M. Badruddoza and many other distinguished personalities.DMC became champions and runners up in the Debate Competition organised by Bangladesh television more than once and came in third at 'Gyan Jiggasa' (a national general knowledge competitionof Bangladesh Television) in 1985 and Champions in 1987. Dr. Rifat Haider of Batch K59 became champion in 2008 at the Bangladesh chapter of World Quizzing Championship and Dr. Ahmad Fayezi Tamal of Batch K64 became champion four times (2009,2011,2012,2013) in the same competition. Sheikh Mahmood Hasan of Batch K64 and Rajat Das Gupta of Batch K66 became runnerup in that competition in 2010 and 2011 respectively. Dhaka Medical College quiz team became champion in IFIC Bank DQS-SSMC Carnival Captive 2013 competing among 68 teams in 2013. Dhaka Medical College has many voluntary organizations such as the Computer Club of Dhaka Medical College, Debating Club of DMC, Rotaract Club, Medicine Club and so on.
35

Dhaka Medical College Debating Club (DMCDC) is a pioneer in Medical college Debating History. After being established in 2009, DMCDC has hosted two national debate festivals with huge success. Present Debate team of Dhaka Medical College became champion in the TIB-DMCDC National Anti-Corruption Day Debate Competition 2012. They are also runner-up team of SK-F NDFBD DMCDC National Inter-Medical College Debate Competition 2011. TheDebate team also owns the title of runner-up in '1st Bangladesh Television Environmental Debate Competition-2012 ' & the title ofChampion in '2nd Bangladesh Television Environmental Debate Competition'. In Recent Time, Dhaka Medical College Debate Team is the only medical based debate team who reached the final of inter-university debate championship in 2013 JUDS Inter University Debate Championship. By winning 3rd SKF-NDFBD-CMCDC National Inter Medical College Debate Championship In 2014,Dhaka Medical College Debate Team is the present Defending Champion Of Inter Medical College Debate. Present team Consists of team member Ranok Mehedi (K-69),Zahid Hasan (K69),Raisul Arafat (K-71).Dhaka Medical College Football team won Tarubala shield in 1947
which was organised by district sports association. Captain Mirza
Mazharul Islam beat renowned Clubs like Wari on his way to
winning the title. Athletics Secretary of first DMCSU (1949–50)
was Mazharul Islam Damal who expressed his sporting ability by
creating a bang as the opening batsman of Pakistan 'A' cricket
team. Dhaka Medical College Cricket team achieved the pride of
becoming Dhaka division champion in 1962–63 season.
Clubs and associations
36

Medicine Club, DMC Unit Sandhani, DMC branch Computer Club of DMC Ex-Cadets' Association of DMC Debating Club Rotaract club
Alumni trust
Dhaka Medical College Alumni Trust was formed in 1989. Former principal &
professor Wali Ullah was the founder-president.
37

Chapter 3. Introduction to Field Specialization
3.1 Concept of Mental Health
3.2 Concept of Mental Disorder
3.3. Classification and Symptoms of Mental Disorder
38

Concept of Mental Health
Mental health refers to our cognitive, and/or emotional
wellbeing- it is all about how we think, feel and behave. It can
also mean an absence of a mental disorder.
According to WHO ( world Health organization) Mental health
is “a state of well –being in which the individual realizes
his or her own abilities, can cope with the normal stresses
of life can work productively and fruitfully and is able to
make a contribution to his or her community .”
According to the social work Dictionary (1995;231) Mental is
the related state of emotional well –being, freedom from in
capacitating conflicts and the consistent ability to make
and canny out national decisions and cope with environmental
stresses and internal pressure.
At last it can be said that mental health includes a person’s
ability to enjoy life to attain balance between life activities
and efforts to achieve psychological resilience.
The mental health act:
In 1959 mental health act was seen a new era of psychiatric
treatment & care. But less than 10 percent of the psychiatric
39

hospital population is detained, under a section of mental health
act. 1959 Act led to two government publications. The first, a
consultation paper followed in 1978 by a government white paper
entitled review of the mental health act with five main
principles. The Royal assent was given to the Mental Health
(Amendment ) bill in October 1982& the consolidating bill was
passed in the spring of 1983.
Concept of Mental Disorder:
A mental disorder or mental illnesses is a psychological or
behavioral pattern that occurs in an individual and is thought to
cause distress disability.
According to WHO (World Health Organization)
Mental disorders comprise a broad range of problems, with
different symptoms.
However they are generally characterized by some combination of
abnormal thoughts, emotions, behavior and relationship with
others.
According to the Social Work Dictionary
“Mental disorder is impaired psychosocial or cognitive
Functioning due to disturbance in only are or more of the
following process biological, chemical, genetic psychological or
social .
40

Classification & Symptoms of Mental Disorder:
The classification of mental disorders also know as psychiatric
ontology, is a key aspect of psychiatry. Different personalities
and organizations have classified mental disorders in different
ways.
Colemen, divided mental disorders into two general categories in
Abnormal Psychology. These are:
a. Psychotic Disorder.
b. Neurotic Disorders
Psychotic Disorders: Psychotic disorders are divided into two
general categories.
a. Functional psychoses
b. Organic psychoses.
Functional psychoses: Functional psychoses are in turn divided
into four main groups:
I. Schizophrenic disorders (like; Simple reaction, Hebephrenic
reaction, catatonic reaction, paranoid reaction, Childhood
schizophrenia)
II. Paranoid disorders (like; paranoia, Paranoid state).
III. Affective disorders.(Manic- depressive reaction, psychotic
depressive reaction)
IV. Involution Psychotic disorders.
41

Neurotic Disorders: Neurotic Disorders are classified such way
A. Anxiety reaction
B. Aesthetic reaction
C. Hypochondraiacal reaction
D. Conversion reaction.(The most common forms are):
Anesthesia- loss of sensitivity
Hyperesthesia – partial loss of sensations
Paresthesia- exceptional sensations.
E. Dissociative reaction. Such as-
Amnesia,fugue,somnambulism and multiple
personalitly(ideas blocks off)
F . Poblic reaction.(it is a persistent of various fears such
as).
Acrophobia-high places.
Agoraphobia-open places.
Anglophobia-pain.
Astra phobia-storms, thunder and lighting
Clustrophobia- closed places
Hematophobia-blood
Mysophobia- contamination or germs.
Menophobia-being alone.
42
Nyctophobia-. darkness
Ocholophbia - crowds
Pathophobia-diseadse
Pyrophobia-fire.
Syphophobia –syphhilis
Zoophobia-animals or particular animals.
g. Obsessive-compulsive reaction.
h. Neurotic Depressive reaction.
Major Mental Disorders (Psychoses): Major mental disorders are
commonly called psychoses. It is a severe abnormal state of mind
where there is usually disturbance of thinking, felling, mood and
behavior. They are classified into two groups:
a.Organic psychoses
b.Functional psychosis
Organic psychosis: In organic psychoses there are demonstrable
abnormalities in the brain. They may be
1.Acute (Delirium)
2.Chronic(Dementia
)
Delirium: Delirium is the psychoses the commonest organic
disorder seen in the clinical practice. Major symptoms of it-
43
Imparied consciousness
Behavior: Restlessness,
irritability,noisiness,reduced speech.
Motor symptoms: Asterixis, multi-
focal,myoclomous
Thinking: Slow and muddled thinking.
Mood:Anxiety, depression, agitation.
Memory:Disturbance of memory.
Insight:Impaired.
Dementia: Dementia is a chronic organic mental disorder. Major
symptoms of it-
Behavior: Often muddled, distractible,
inappropriate and restless.
Thinking:Thinking slows and becomes impoverished
in content.
Judgment: Judgment is impaired and false idea.
Mood: anxiety, depression and irritability may
be present.
Insight: Insight is lacking into the degree and
nature of the disorders
Functional Psychoses: These are psychoses where there are usually
no demonstrable abnormalities in the brain or in the other
orfgans of the body. Major types of functional psychoses include:
i. Schizophrenia.
44

ii. Mood disorders.
Schizophrenia: Schizophrenia is a major mental disorder. It was
first described by Belgian Psychiatrist Benedict Morel in 1852,
who called it demence precoce. It is a brain disorder and
adversely affect thinking, feeling. Behaviour, social and
occupational functioning. Schizophrenia is grouped into two basic
concepts.
a. Acute Schizophrenia
b. Chronic Schizophrenia
Symptoms of acute schizophrenia:
Lack if insight
Auditory hallucinations
Ideas of reference and suspiciousness.
Flatness of affect and delusional mood.
Thoughts spoken aloud.
Symptoms of acute schizophrenia:
Social withdrawal and slowness.
Lack of drive and initiatives.
Lack of conversation and thought disorders.
Under activity and odd behaviors.
Threats or violence.
45

What Is Schizophrenia?
Schizophrenia is a chronic, severe, and disabling brain disorder
that has affected people throughout history.People with the
disorder may hear voices other people don't hear. They may
believe other people are reading their minds, controlling their
thoughts, or plotting to harm them. This can terrify people with
the illness and make them withdrawn or extremely agitated.People
with schizophrenia may not make sense when they talk. They may
sit for hours without moving or talking. Sometimes people with
schizophrenia seem perfectly fine until they talk about what they
are really thinking. Families and society are affected by
schizophrenia too. Many people with schizophrenia have
What are schizophrenia symptoms and signs?
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM),
symptoms of schizophrenia include the following:
Positive, more overtly psychotic symptoms
Beliefs that have no basis in reality (delusions)
Hearing, seeing, feeling, smelling, or tasting things that
have no basis in reality (hallucinations)
Disorganized speech
Disorganized behaviors
Catatonic behaviors
Negative, potentially less overtly psychotic symptoms
46

Inhibition of facial expressions
Lack of speech
Lack of motivation
Signs & Symptoms
The symptoms of schizophrenia fall into three broad categories:
positive symptoms, negative symptoms, and cognitive symptoms.
Positive symptoms
Positive symptoms are psychotic behaviors not seen in healthy
people. People with positive symptoms often "lose touch" with
reality. These symptoms can come and go. Sometimes they are
severe and at other times hardly noticeable, depending on whether
the individual is receiving treatment. They include the
following:
Hallucinations are things a person sees, hears, smells, or feels
that no one else can see, hear, smell, or feel. "Voices" are the
most common type of hallucination in schizophrenia. Many people
with the disorder hear voices. The voices may talk to the person
about his or her behavior, order the person to do things, or warn
the person of danger. Sometimes the voices talk to each other.
People with schizophrenia may hear voices for a long time before
family and friends notice the problem.
Other types of hallucinations include seeing people or objects
that are not there, smelling odors that no one else detects, and
47

feeling things like invisible fingers touching their bodies when
no one is near.
Delusions are false beliefs that are not part of the person's
culture and do not change. The person believes delusions even
after other people prove that the beliefs are not true or
logical. People with schizophrenia can have delusions that seem
bizarre, such as believing that neighbors can control their
behavior with magnetic waves. They may also believe that people
on television are directing special messages to them, or that
radio stations are broadcasting their thoughts aloud to others.
Sometimes they believe they are someone else, such as a famous
historical figure. They may have paranoid delusions and believe
that others are trying to harm them, such as by cheating,
harassing, poisoning, spying on, or plotting against them or the
people they care about. These beliefs are called "delusions of
persecution."
Thought disorders are unusual or dysfunctional ways of thinking.
One form of thought disorder is called "disorganized thinking."
This is when a person has trouble organizing his or her thoughts
or connecting them logically. They may talk in a garbled way that
is hard to understand. Another form is called "thought blocking."
This is when a person stops speaking abruptly in the middle of a
thought. When asked why he or she stopped talking, the person may
say that it felt as if the thought had been taken out of his or
48
her head. Finally, a person with a thought disorder might make up
meaningless words, or "neologisms."
Movement disorders may appear as agitated body movements. A
person with a movement disorder may repeat certain motions over
and over. In the other extreme, a person may become catatonic.
Catatonia is a state in which a person does not move and does not
respond to others. Catatonia is rare today, but it was more
common when treatment for schizophrenia was not available.
Negative symptoms
Negative symptoms are associated with disruptions to normal
emotions and behaviors. These symptoms are harder to recognize as
part of the disorder and can be mistaken for depression or other
conditions. These symptoms include the following:
"Flat affect" (a person's face does not move or he or she
talks in a dull or monotonous voice)
Lack of pleasure in everyday life
Lack of ability to begin and sustain planned activities
Speaking little, even when forced to interact.
People with negative symptoms need help with everyday tasks. They
often neglect basic personal hygiene. This may make them seem
lazy or unwilling to help themselves, but the problems are
symptoms caused by the schizophrenia.
49

Cognitive symptoms
Cognitive symptoms are subtle. Like negative symptoms, cognitive
symptoms may be difficult to recognize as part of the disorder.
Often, they are detected only when other tests are performed.
Cognitive symptoms include the following:
Poor "executive functioning" (the ability to understand
information and use it to make decisions)
Trouble focusing or paying attention
Problems with "working memory" (the ability to use
information immediately after learning it).Cognitive
symptoms often make it hard to lead a normal life and earn a
living. They can cause great emotional distress.
How is schizophrenia diagnosed?
As is true with virtually any mental-health diagnosis, there is
no one test that definitively indicates that someone has
schizophrenia. Therefore, health-care practitioners diagnose this
disorder by gathering comprehensive medical, family, and mental-
health information. Patients tend to benefit when the
professional takes into account their client's entire life and
background. This includes but is not limited to the person's
gender, sexual orientation, cultural, religious and ethnic
background, and socioeconomic status. The symptom sufferer might
50

be asked to fill out a self-test that the professional will
review if the person being evaluated is able to complete it. The
practitioner will also either perform a physical examination or
request that the individual's primary-care doctor perform one.
The medical examination will usually include lab tests to
evaluate the person's general health and to explore whether or
not the individual has a medical condition that might produce
psychological symptoms.
In asking questions about mental-health symptoms, mental-health
professionals are often exploring if the individual suffers from
hallucinations or delusions, depression and/or manic symptoms,
anxiety, substance abuse, as well as some personality disorders
(for example, schizotypal personality disorder) and developmental
disorders (for example, autism spectrum disorders). Since some of
the symptoms of schizophrenia can also occur in other mental
illnesses, the mental-health screening is to determine if the
individual suffers from schizoaffective disorder or other
psychotic disorder, depressive disorder, bipolar disorder,
anxiety disorder, or a substance-abuse or personality disorder.
Any disorder that is associated with bizarre behavior, mood, or
thinking, like borderline personality disorder or another
psychotic disorder, as well as dissociative identity disorder
(DID), also known as multiple personality disorder (MPD) may be
particularly challenging to distinguish from schizophrenia. In
order to assess the person's current emotional state, health-care
providers perform a mental-status examination as well.
51

In addition to providing treatment that is appropriate to the
diagnosis, determining the presence of mental illnesses that may
co-occur (be comorbid) with schizophrenia is important in
improving the life of individuals with schizophrenia. For
example, people with schizophrenia are at increased risk of
having a substance-abuse, depressive, or anxiety disorder and of
committing suicide.
Treatments
Because the causes of schizophrenia are still unknown, treatments
focus on eliminating the symptoms of the disease. Treatments
include antipsychotic medications and various psychosocial
treatments.
Antipsychotic medications
Antipsychotic medications have been available since the mid-
1950's. The older types are called conventional or "typical"
antipsychotics. Some of the more commonly used typical
medications include:
Chlorpromazine (Thorazine)
Haloperidol (Haldol)
Perphenazine (Etrafon, Trilafon)
Fluphenazine (Prolixin).
52

In the 1990's, new antipsychotic medications were developed.
These new medications are called second generation, or "atypical"
antipsychotics.
One of these medications, clozapine (Clozaril) is an effective
medication that treats psychotic symptoms, hallucinations, and
breaks with reality. But clozapine can sometimes cause a serious
problem called agranulocytosis, which is a loss of the white
blood cells that help a person fight infection. People who take
clozapine must get their white blood cell counts checked every
week or two. This problem and the cost of blood tests make
treatment with clozapine difficult for many people. But clozapine
is potentially helpful for people who do not respond to other
antipsychotic medications.
Other atypical antipsychotics were also developed. None cause
agranulocytosis. Examples include:
Risperidone (Risperdal)
Olanzapine (Zyprexa)
Quetiapine (Seroquel)
Ziprasidone (Geodon)
Aripiprazole (Abilify)
Paliperidone (Invega).
Psychosocial treatments
53

Psychosocial treatments can help people with schizophrenia who
are already stabilized on antipsychotic medication. Psychosocial
treatments help these patients deal with the everyday challenges
of the illness, such as difficulty with communication, self-care,
work, and forming and keeping relationships. Learning and using
coping mechanisms to address these problems allow people with
schizophrenia to socialize and attend school and work. Patients
who receive regular psychosocial treatment also are more likely
to keep taking their medication, and they are less likely to have
relapses or be hospitalized. A therapist can help patients better
understand and adjust to living with schizophrenia. The therapist
can provide education about the disorder, common symptoms or
problems patients may experience, and the importance of staying
on medications. For more information on psychosocial treatments,
see the psychotherapies section on the NIMH website.
Illness management skills. People with schizophrenia can take an
active role in managing their own illness. Once patients learn
basic facts about schizophrenia and its treatment, they can make
informed decisions about their care. If they know how to watch
for the early warning signs of relapse and make a plan to
respond, patients can learn to prevent relapses. Patients can
also use coping skills to deal with persistent symptoms.
Integrated treatment for co-occurring substance abuse. Substance
abuse is the most common co-occurring disorder in people with
schizophrenia. But ordinary substance abuse treatment programs
54

usually do not address this population's special needs. When
schizophrenia treatment programs and drug treatment programs are
used together, patients get better results.
Rehabilitation. Rehabilitation emphasizes social and vocational
training to help people with schizophrenia function better in
their communities. Because schizophrenia usually develops in
people during the critical career-forming years of life (ages 18
to 35), and because the disease makes normal thinking and
functioning difficult, most patients do not receive training in
the skills needed for a job.
Rehabilitation programs can include job counseling and training,
money management counseling, help in learning to use public
transportation, and opportunities to practice communication
skills. Rehabilitation programs work well when they include both
job training and specific therapy designed to improve cognitive
or thinking skills. Programs like this help patients hold jobs,
remember important details, and improve their functioning.
Family education. People with schizophrenia are often discharged
from the hospital into the care of their families. So it is
important that family members know as much as possible about the
disease. With the help of a therapist, family members can learn
coping strategies and problem-solving skills. In this way the
family can help make sure their loved one sticks with treatment
and stays on his or her medication. Families should learn where
to find outpatient and family services.55

Cognitive behavioral therapy. Cognitive behavioral therapy (CBT)
is a type of psychotherapy that focuses on thinking and behavior.
CBT helps patients with symptoms that do not go away even when
they take medication. The therapist teaches people with
schizophrenia how to test the reality of their thoughts and
perceptions, how to "not listen" to their voices, and how to
manage their symptoms overall. CBT can help reduce the severity
of symptoms and reduce the risk of relapse.
Self-help groups. Self-help groups for people with schizophrenia
and their families are becoming more common. Professional
therapists usually are not involved, but group members support
and comfort each other. People in self-help groups know that
others are facing the same problems, which can help everyone feel
less isolated. The networking that takes place in self-help
groups can also prompt families to work together to advocate for
research and more hospital and community treatment programs.
Also, groups may be able to draw public attention to the
discrimination many people with mental illnesses face.
Mood disorders: Mood is defined as a pervasive emotional tone
that profoundly influence ones outlook and perception of self,
others and the environment in general. The major classification
of mood disorders is:
a. Major depressive disorders.
56

b.Bipolar mood disorders.
Major depressive disorders: psychological symptoms of these
desease:
Feelings of unhappiness
Reduced energy, concentration and decreased activity
Helplesssness, hopelessness, forgetfulness.
Hallucination and pessimistic thoughts about past,
present and future
Ideas of self harm( suicide attempt)
Delusions of references, guilt.
Biological symptoms are:
Sleep disturbance
Loss of libido, variation of mood
Loss of appetite and weight.
Bipolar mood disorder: Bipolar mood disorders can be devided
into two types
a. Bipolar 1 disorders
b.Bipolar 2 disorder
57
Bipolar 1 disorders: patient who experience both manic episode
and major depressive episode.
Bipolar 2 disorders: patient has had at least one depressive
episode and no manic episode.
The major symptoms of bipolr mood disorders:
Manic phase
Elated mood, flight of ideas over activity,
pressure of speech.
Irritability, sleep disturbance.
Excessive expenditure and energy, increased
libido.
Out burst of anger.
Hallucination with mood.
Minor mental disorders( Neuroses):we can categorize neurotic
in the following groups….
Anxiety disorder:
58

Anxiety Disorder is an umbrella term that covers several
different forms of a type of common psychiatric disorder
characterized by excessive rumination , worrying, uneasiness,
apprehension and fear about future uncertainities either based
on real or imagined events, which may affect both physical and
psychological health. There are numerous psychiatric and medical
syndromes which may mimic the symptoms of an anxiety disorder
such as hyper thyroidism which may be misdiagnosed as generalized
anxiety disorder.
According to DSM IV, “Anxiety disorders are diagnosed when
subjectively experienced feelings of anxiety are clearly
present.”
Anxiety involves a more general or diffuse emotional reaction
beyond simple fear that is out of proportion to treats from the
environment. Anxiety is a neurotic disorder. The emotions present
in anxiety disorders range from simple nervousness to bouts of
terror (Barker 2003)
Classification of Anxiety Disorder:
Anxiety disorder is divided into generalized anxiety disorder,
phobic disorder, and panic disorder, each has its own
characteristics and symptoms and they require different treatment
( Gelder at al. 2005).
There are mostly common 6 types of Anxiety disorder. These are:
1. General Anxiety Disorder (GAD)
59

2. Acute Stress disorder (ASD)
3. Post-traumatic stress disorder (PTSD)
4. Phobic Anxiety disorder
5. Panic Disorder
6. Obsessive Compulsive Disorder (OCD)
Epidemiology:Globally as of 2010 approximately 273 million (4.5%
of the population) had an anxiety disorder. It is more common in
females (5.2%) than males (2.8%) . According to WHO, the number
of mentally ill people in Bangladesh is about 8.4 million ie, 7%
of the population of 120 million. The following Table shows the
estimated population of Bangladesh who suffers from different
types of mental illness
Table estimated population suffering from mental or related
illness
Problem/illnessPopulation (age
group)Percentage
No. of cases
(million)
Major depression General 3 3.6
Anxiety disorder --- 5 6.0
Obsessions --- 0.5 0.6
Schizophrenia/
psychosis--- 1 1.2
60

Learning
disability--- 2.5 3.0
Chronic illness
(eg, asthma,
diabetes, pain)
--- 10 12.0
Head injury/head
trauma--- .25 0.3
Hypertension/
sleepnessnessAdults 14 8.4
Addictions (inc
smoking)Adults 10 6.0
Dementia (inc
memory impairment)Over 65 years 5 1.2
Source Powell, G. The future of clinical psychology in
Bangladesh, 1995
Definition of different types of Anxiety Disorder:
1.Generalize Anxiety Disorder:
Generalized anxiety disorder is characterized by chronic feelings
of excessive worry and anxiety without a specific cause that
61

person finds difficulty to control and that lead to significant
distress or impairment in occupational or social functioning.
Individuals with generalized anxiety disorder often feel on edge,
tense, and jittery. Someone with generalized anxiety disorder may
worry about minor things, daily events, or the future.GAD variety
of everyday problems for at least 6 months. When their anxiety
level is mild, they can function socially and hold down a job.
Although the years of highest risk are between childhood and
middle age. Women are more affected than men.
Symptoms of Generalized Anxiety Disorder
Feelings of unreality
Hot and cold flushes
Nausea
Shortness of breath
Breathing difficulties
Heart palpitations
Chest pains
Fear of dying, losing control
Sweating
Tingling sensations
Dizziness
Irritability and agitation
Trembling, weakness
Feelings of choking
Feeling of 'going crazy'
62

Difficulties sleeping
2.Acute Stress disorder:
Acute stress disorder is an anxiety disorder which result from a
traumatic experience. Person experienced, witnessed on was
confronted with an event that involve actual treated death or
serious injury self or others. Occurs within minimum 2 days and
maximum 4 weeks after exposure to a traumatic stress.
A person with Acute Stress Disorder may experience difficulty
concentrating, feel detached from their bodies, experience the
world as unreal or dreamlike, or have increasing difficulty
recalling specific details of the traumatic event (dissociative
amnesia).
Symptoms of Acute Stress disorder (ASD):
Derealization
Re-experience ( recurrent image, thought dreams, illusion,
flashback episode)
Avoidance (thought, feeling, conversation, places)
Heighten arousal
Detachment or being in a daze
3.Post Traumatic stress Disorder:
Posttraumatic stress disorder (PTSD) develops after a terrifying
ordeal that involved physical harm or the threat of physical
63

harm.The person who develops PTSD may have been the one who was
harmed,the harm may have happened to aloved one,or the person may
have witnessed a harmful event that happened to loved ones or
strangers. PTSD was first brought to public attention in relation
to war veterans,but it can result from a variety of traumatic
incidents,such as mugging,rape,torture,being kidnapped or held
captive, child abuse,caraccidents,train wrecks,plane
crashes,bombings,or natural disasters such as floods or
earthquakes.
Acute: If duration of symptoms is less than 3 moths
Chronic: If duration of symptoms is more than 3 months
Delayed onset: If onset of symptoms is at least 6 months after
the stressor
Women are more affected than men. Rape and childhood sexual abuse
is the most likely trigger of PTSD.
PTSD affects about 7.7 million American adults,1 but it can occur
at any age,including childhood.7 Women are more likely to develop
PTSD than men,8 and there is some evidence that susceptibility to
the disorder may run in families.9 PTSD is often accompanied by
depression,substance abuse,or one or more of the other anxiety
disorders.
Symptoms of Post Traumatic stress Disorder
Repetitive, distressing thoughts about the event
64

Nightmares and flashbacks
Persistent symptoms of increased anxiety, irritability,
anger, difficulty concentrating
Avoidance or activities or external situation associated
with the trauma
Emotional numbness and detachment
4.Phobic Anxiety disorder:
A persistent, abnormal, and irrational fear of a specific thing.
It is an irrational, intense fear of an object or situation that
poses little or no actual danger. At first glance, a phobia may
seem similar to a normal fear, but it's is the degree to which a
person is affected that determines whether that fear has become a
phobia.
There are three (3) types of Phobia like:
1. Specific / simple phobia: A specific phobia is an intense,
irrational fear of something that actually poses little or
no threat. Some of the more common specific phobias are
heights, escalators, tunnels, highway driving, closed-in
places, water, flying, dogs, spiders and injuries involving
blood. Women are more affected than men.
2. Social phobia: When people become overwhelmingly anxious and
excessively self-conscious in everyday situations that time
is called social phobia. This fear may become so severe that
it interferes with work, school, and other ordinary
65

activities, and can make it hard to make and keep friends.
People with social phobia feel as though all eyes are
focused on them. In extreme cases this intense uneasiness
can progress into a full blown panic attack. In the case of
social phobia that is particularly problematic and in sever
cases can lead to complete social isolation. It is equal
common among men and women.
3. Agoraphobia: The most complex and incapacitating form of
phobic disorder is agoraphobia, which literally means “fear of
the market place (or places of assembly)” and is usually
described as fear of public spaces. Agoraphobia is somewhat
different from the other phobias because it is not so much a fear
of being close to one specific object or situation (animal,
public speaking) as it is of being separated from signals
associated with safety.
Symptoms of Phobic Anxiety disorder:
1. Specific phobia
Is out of proportion to the apparent stimulus
Cannot be explained or reasoned away
Leads to avoidance of the object or situation
2. Social phobia
Symptoms of sympathetic over activity
(tremor,palpitation,sweating)
5.Panic Disorder
66

A panic is a sudden, overwhelming experience of terror or fright
accompanied by a pounding heart, sweatiness, weakness, faintness
and dizziness. It can occur at any time, even during sleep. It
peaks within 10 minutes, but some symptoms may last much longer.
It is common women as men. It often begins in late adolescence or
early childhood. Women are more affected than men. Occurs with
major depression in very high rates.
Three types of panic disorder, these are:
1. Panic disorder with agoraphobia
2. panic disorder without agoraphobia
agoraphobia without history of panic disorder
Symptoms of Panic Disorder
Palpitation, pounding heart or accelerated heart rate
Sweating
Trembling or shaking
Sensation of shortness of breath or smothering
Feeling of choking
Chest pain or discomfort
Nausea or abdominal distress
Feeling dizzy, unsteady, light-headed or faint
Derealization or depersonalization
Fear of losing control or going crazy
67

Fear of dying
Paraestheiae (numbness or tingling sensation)
Chills or hot flushes
DSM IV Panic Disorder Criteria
A) Both (1) and (2)
(1) recurrent unexpected Panic Attacks
(2) at least one of the attacks has been followed by 1 month (or
more) of one (or more) of the following:
(a) persistent concern about having
additional attacks
(b) worry about the implications of the
attack or its consequences (e.g., losing control, having a heart
attack, "going crazy")
(c) a significant change in behavior
related to the attacks
B) The Panic Attacks are not due to the direct physiological
effects of a substance (e.g., a drug of abuse, a medication) or a
general medical condition (e.g., hyperthyroidism).
C) The Panic Attacks are not better accounted for by another
mental disorder, such as Social Phobia (e.g., occurring on
exposure to feared social situations), Specific Phobia (e.g., on
68

exposure to a specific phobic situation), Obsessive-Compulsive
Disorder (e.g., on exposure to dirt in someone with an obsession
about contamination), Posttraumatic Stress Disorder (e.g., in
response to stimuli associated with a severe stressor), or
Separation Anxiety Disorder (e.g., in response to being away from
home or close relatives).
6.Obsessive Compulsive Disorder (OCD):
It is a type of anxiety disorder primarily characterized by
repetitive obsessions and compulsions (urges to perform specific
acts or ritual).
Obsessions : Persistent thoughts, ideas, impulses or images that
are intrusive and inappropriate and that cause marked anxiety or
distress. Individuals with obsessions usually attempt to ignore
or suppress such thoughts or impulses or to counteract them by
other thoughts or actions (compulsions).
Compulsions : Repetitive behaviours (such as hand washing, ordering
or checking) or mental acts (such as praying, counting or
repeating words) that occur in response to an obsession or in a
ritualistic way.
For example, if the people are obsession with germs or dirt, they
may develop a compulsion to wash their hands over and over again.
Being afraid of social embarrassment may prompt people with OCD
to comb their hair compulsively in front of mirror. Sometimes
69

they get ‘caught’ in the mirror and can’t move away from it.
Performing such rituals is not pleasurable.
Healthy people also have rituals, such as checking to see if the
stove is off several times before leaving the house. The
difference is that people with daily life and they find the
repetition distressing, interferes with daily life and they find
the repetition distressing. Women are more affected than men. One
third of young adults had their first symptoms in childhood.
Symptoms of Obsessive Compulsive Disorder (OCD):
Recurrent and persistent thought, impulse or image
Repetitive behavior (hand washing, ordering, checking) or
mental acts (praying, counting, repeating word silently)
Treatment and Management:
Psychological management:
Different psychological techniques given below:
Psychotherapy:
Cognitive behavioral therapy:
Exposure therapy:
Relaxation:
70

Acceptance and Commitment Therapy (ACT)
Dialectical Behavioral Therapy (DBT)
Interpersonal Therapy (IPT)
Eye Movement Desensitization and Reprocessing (EMDR)
Acceptance and commitment therapy
Intolerance of uncertainty therapy
Motivational interviewing
Psycho education
Chapter 4.Dealing with Cases
4.1 Case-1
4.2 Case-2
4.3 Case-3
71

Case- 1
Demographic information
Name: Shabnur
Age: 14 years
Sex: Female
Address: Uzirpur Thana, Barisal
72

Siblings: 4
Position: 3rd
Marital status: Married
Occupation: Nill
Religion: Islam
Economic status: Lower class
Source of referral
The patient was referred to the DMC with the help of his familymember.
Chief complain
Raped
Pregnant
Anxiety
Grandiose idea- She feels that she is nothing but a victim.
History of present illness
According to the patients, Her parents were separated when shewas 10 years. Since she lived with aunt’s family. From thebeginning her uncle always disturbed her. When her aunt waspregnant she(aunt) admitted to the hospital. That time uncle took
73

her to a registry office and threatened her to marry him. Aftercompleting marriage, uncle took her to a rent house and they stayhere for 3 months. At a time she felt that she was pregnant. Atthe same time her family searching her every where and finallyfound her. Then they admit her to the hospital and her uncle wasran away.
Family history
Client’s family members are living in village.
Parents: His father is a laborer and mother is a house wife. Therelationship between family members is disappointing.
Siblings: He has two younger brothers. Both of them are students.
Personal history
Mother’s pregnancy and birth: There was no serious illness andbirth was normal and no complication held after birth.
Early development: Her childhood wasn’t normal and there wasseparation or emotional problem during childhood.
Schooling and higher education: She wasn’t a good student fromher childhood. Her education was finished when she read in class3.
Adolescence and adulthood: Her adolescence and childhood wasnormal and no mentionable crisis had been found.
Sexual history: During interview she mentioned above information.
Occupation: Nothing.
Social circumstances: She didn’t found lives in her familyenvironment. Relationship with family members are not well.
74

History of drug abuse: No.
Forensic history: Pregnant.
Diagnosis
Mental Stress
Management
Psychological management
Counseling
Social management
Counsel the family members to be patience on client
Counsel the family members about medication
Inform the family members about client’s situation
Help client for new beginning of life.
Reduce Prejudice
Treatment techniques
Treatment strategy Purpose
Evidence seeking Reduce Prejudice
Providing information Based on clients needs, suchas medication, disease,readmission.
Pros and cones techniques Aggression
Ventilation Emotional release,
75

identifying hidden cause
Relaxation Physical relaxation
Advice and guidance Medication regularly, consultwith doctor
REBT Build-up confidence
Breathing exercise Remove restlessness
Out comes
The client has given 5 sessions
Problems 2nd session 5th session
Aggression Reducing Reduced
Prejudice Present Reduced
Sleep disturbance Removed Removed
Concentrationproblem
Improving Improving
Delusion Present Decreased
Anxiety Present Decreased
Prognosis
Good prognostic criteria
Client is motivated
She removed tabbies from his hand by himself
Bad prognostic criteria
76

Paranoid personality pattern
Depression
Lack of Seriousness
Comments
Client’s situation is improving slowly and gradually. Clientneeds to take medication for regularly for long time and alsoneeds CBT, counseling and follow-up.
Case- 2
Demographic information
Name: X
Age: 25 years
Sex: Male
Address: Badda, Dhaka
Siblings: 4
Position: 1st
Marital status: Unmarried
Occupation: student-BBA
Religion: Islam
77

Economic status: Middle class
Source of referral
The patient was referred to the DMC with the help of his familymember.
Chief complain
Irrelevant speech, talkativeness
Decreased sleep- sleepless last 10 days
Aggressive behavior
Unwilling to food intake last 4-5 days
Fearfulness
Grandiose idea- he feels that he has some extra capacity fromothers
History of present illness
According to the patients brother he was relatively alright about3 years back. Then he develops irrelevant speech andsleeplessness. He felt hot flash in whole body. He also had theproblem of auditory hallucination .And then he felt frustrationand wanted to take suicide. After that he was admitted in aprivate hospital for 15 days. He was relatively alright for last2 ½ years. Now for last 10 days he develops the previous symptomswith grandiose idea.
Family history 78

Client’s family members are living in village.
Parents: His father is a teacher and mother is a house wife. Therelationship between family members is good.
Siblings: he has two younger brothers. Both of them are students.
There was no history of psychiatric illness in his familymembers.
There was no history of MR in his family members.
There was no history of drug abuse in his family members.
There was no history of Epilepsy in his family members.
Personal history
Mother’s pregnancy and birth: There was no serious illness andbirth was normal and no complication held after birth.
Early development: His childhood was normal and there was noseparation or emotional problem during childhood.
Schooling and higher education: He was an average student formhis childhood. He passed SSC and HSC without any break of study.But he could not continue his study after 6th semester of BBA dueto mental illness.
Adolescence and adulthood: His adolescence and childhood wasnormal and no mentionable crisis had been found.
Sexual history: During interview he mentioned that he has severalextramarital sexual relationships.
Occupation: student, break-up due to psychiatric problem andoccasional involvement in business.
79
Social circumstances: He lives in his family environment.Relationship with family members and neighbors are well.
History of drug abuse: He has been taking cigarette from last 5years. He took energy drink, cannabis and alcohols occasionally.
Forensic history: No forensic history was found.
History of past illness
Past medical illness: Nothing contributory
Past psychiatric illness: First time when he was becomeproblematic was in 2010 and he was under medication of apsychiatrist. He also had to admit in private clinic for 15 daysdue to auditory hallucination and illation.
Pre morbid personality
Relationship: Relationship with his own family members is good.But he has some conflict with his maternal uncle and his family.He thought they will kill him. Very much emotional attached withhis paternal aunt.
Leisure activities: He enjoyed spend time with his friends andloves to play cricket.
Prevailing mood: His prevailing mood was inconsistent.
Character: Paranoid personality.
Attitudes and standards: He was not loyal to his cultural normsand religious values but respects those norms.
Mental State Examination {MSE}
Appearance and behavior:
a. General appearance: A young boy wearing pant, T-shirt and ashirt over the T-shirt. His hair was not combed. He waswearing 3 tabbies in his right hand.
80

b. Rapport: Eye to eye contact was present, sustained and itwas fixed stare. Rapport was established properly.
c. Posture and movement: Restless d. Social behavior: Proper social behavior was absent.
Affect: Grandiosity
Mood: Emotional liability
Speech
a. Quantity: Increase in rate b. Quality: Volume was normal c. Content: Delusion d. Oddity of speech: Repeat same words and sentence. Thought: Hallucination, he feels that he got some supernaturalpower
a. Stream: Pressure of speech b. Content: Delusion c. Form: flight of idea d. Possession: Thought control
Perception: Auditory hallucination has been found
Cognition
a. Consciousness: Impaired b. Orientation: About time place and person is intact c. Attention: Not fully attentive d. Concentration: Poor concentration e. Memory: Immediate: Impaired – due to medication
Recent: Impaired – due to medication
Remote: Intact
Intelligence: Average
81

Abstract thinking: Impaired
Judgment: Impaired
Insight: Lost
Diagnosis
Schizophrenia – According to DSM-IV ant Psychiatrist
Assessment
Clinical interview
Case history
Observation
Assessed problem:
Aggression
Prejudice
Sleep disturbance
Concentration problem
Delusion
Lability
Formulation
Predisposing factors
82

Paranoid personality pattern
Conflict with relatives
Loss of money
Aggressive from childhood
Prejudice
Precipitating factors
Not continue medicine
Conflict with relative
Death of grand mother
Extra marital sexual intercourse
Maintaining factors
Cognitive elements:
Conflict with relatives
Break-up with girlfriend
My girlfriend did black magic on me
My uncle and his family members want to kill me
Affective elements:
Feeling insecure about life
Feeling betrayed by girlfriend
Paranoid personality pattern
83

Management
Pharmacological management
Inj- Halopid
Tab- Cyclid
Tab- V-plen
Tab- Leptic
Tab- Lpoez
Tab- Renidin
Psychological management
Short term goal:
Reduce aggression
Create motivation
Reduce prejudice
Create concentration
Long term goal:
Increase Self-confidence
Make the client stable for long term situation
Social management
Counsel the family members to be patience on client
Counsel the family members about medication
Inform the family members about client’s situation
84
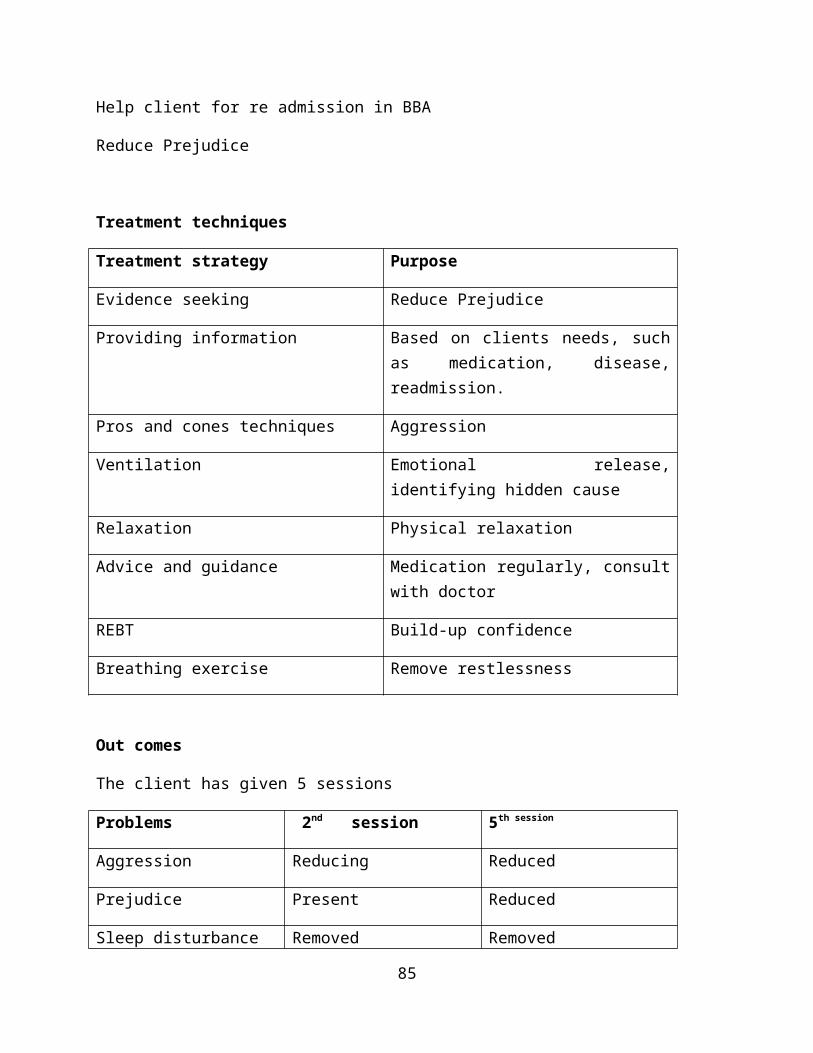
Help client for re admission in BBA
Reduce Prejudice
Treatment techniques
Treatment strategy Purpose
Evidence seeking Reduce Prejudice
Providing information Based on clients needs, suchas medication, disease,readmission.
Pros and cones techniques Aggression
Ventilation Emotional release,identifying hidden cause
Relaxation Physical relaxation
Advice and guidance Medication regularly, consultwith doctor
REBT Build-up confidence
Breathing exercise Remove restlessness
Out comes
The client has given 5 sessions
Problems 2nd session 5th session
Aggression Reducing Reduced
Prejudice Present Reduced
Sleep disturbance Removed Removed
85

Concentrationproblem
Improving Improving
Delusion Present Decreased
Lability Present Decreased
Prognosis
Good prognostic criteria
Client is motivated
He has an educated and understanding family
He removed tabbies from his hand by himself
Bad prognostic criteria
Paranoid personality pattern
Aggression
Comments
Client’s situation is improving slowly and gradually. Clientneeds to take medication for regularly for long time and alsoneeds CBT, counseling and follow-up.
Follow-up
First follow-up after discharge
His condition was improving.
No aggression was seen after discharge {according to his brother}
Restlessness seen in his posture.
86

Readmitted in BBA.
Case No-3
Information of the client:
Name : Labony
Age: 22
Father’s Name: Md. Rejaul Karim
Mother’s Name: Juli
Religion: Muslim
Profession: House wife (before illness)
Sex: Female
Marital Status: Married
Educational Qualification: Illiterate
Present Address: Dhamrai,Savar.
Permanent Address: Dhamrai,Savar.
Information relating to Hospital:
Status of the cabin: Non Paying
Date of Admittance into Hospital: 20-06-14
Date of release: 28-08-14
Date of undertaking case: 08-08-14
Name of Disease:
Duration of Disease: 3 months
87

Family Structure
Sir Name of familymembers
Age EducationalStatus
Occupation Relation
1. Salam 50 Illiterate Driver Husband
2. Md. Rejaul Karim 75 Illiterate Dependent Father
3. Juli 68 Illiterate Housewife Mother
4. Labony 37 Class 3 Housewife Self
5. Akash 03 Illiterate son
12. Mukta 22 Illiterate Housewife Sister-in-law
Source of referral
The client was referred to the Dhaka Medical College Hospital bylocal doctor.
Chief complain
Sleep disturbance
Raped
Anxiety
Not able to cope with her husband
History of Present Illness
According to the patient attendant, she was completely alright 4
months back. Her husband is a CNG driver and she is a housewife.
Some bad boys of local area are disturbing her continuously. Her
husband talked with them but they didn’t stop teasing. One day
88

her husband wasn’t home, when she goes to the outside for
searching him some boys raped her that night. She was found
outside by her husband at next morning. And he discover her as
raped, then he admitted her to the hospital. From then she felt
uncomfortable with her husband.
Rationale of undertaking as case
Being an apprentice psychiatric social worker and as the part of
my academic duty, I decided to take the patient as my case. From
very much professional point of view, I thought I could apply
social work knowledge, skills and values to cure and rehabilitate
Mrs. Labony.
Technique of Data collection:
I collected data through the observation of relevant files,
reports of patient and interview, observation, listening, asking,
and establishing rapport, communication etc basis on the values
and principles of social work profession. The main agents were
Parents, Psycho social worker, doctor (supervisor) & information
desk.
Family history:
Client’s family members are living in village.
There was no history of psychiatric illness in her family.
89

There was no history of MR in her family.
There was no history of drug abuse in her family.
There was no history of Epilepsy in her family.
Personal history
Mother’s pregnancy and birth: During her mother’s pregnancy there was no
serious illness and her birth was normal and no complication held
after birth.
Early development: Her developmental milestones were normal.
According to client’s mother, her childhood was normal and there
was no separation, emotional problem during childhood.
Adolescence and adulthood: Her adolescence was normal and no crisis
has been found.
Sexual history: She was married 4 years back.
Occupation: Housewife
Forensic history: All adult member and she was raped by 3 people.
History of past illness
Past medical illness:
Nothing contributory
Past psychiatric illness:
Nothing contributory
Pre morbid personality
90

Relationship: Relationship with her own family and friends was good.
Still her family is trying their level best to give her support.
Leisure activities: She was productive and hard worker. And she had no
intention to waste time in non productive tasks.
Prevailing mood: Her prevailing mood was depressed.
Character: Hard worker and highly ambitious.
Attitudes and standards: Socially accepted and well mannered.
Mental State Examination (MSE)
Speech: Pressure of Speech (Quantity: Too much speech)
Thought: distractibility
Stream: Pressure of speech Content: Obsession Form: Flight of idea Possession: No possession of thought has been found.
Delusion: Grandiose
Insight: Lest
Rapport: Eye to eye contact was not exactly present and notsustained and rapport was not established properly.
Posture and movement: Abnormal
Social behavior: Normal and culturally appropriate social behaviorwas present.
Perception: No hallucination has been found in any modalities.
Cognition:
91

Consciousness: Not intact Orientation: about time, place and person is not intact. Attention: patient is not attentive. Concentration: Slow concentration. Memory:
Immediate: Slow Recent: intact Remote: intact. Intelligence: Average (based on clinical observation) Abstract thinking: Intact. Judgment: out of order. Insight: Least.
Diagnosis
MAJOR DEPRESSIVE DISORDER (M). (According to Psychiatrist).
Management
Pharmacological management
Tab. Olanap
10mg-----------------------
1+0+1
.Tab. Thyrox 50
mg-----------------------3+0+0
.Tab.Pantonix
20mg-----------------------
1+0+1
.Tab. Cyclid 5 mg
-------------------------1+0+1
.Tab.
Epitra(0.5mg)-----------------
-------0+0+1
Psychological management
Short term goal-
92

Increase activity level
Reduce aggressiveness
Reduce depression
Create motivation &aspiration
Long term goal-
Increase self-confidence
Make the client stablefor long term situation
93

Social Management
Therapist, psycho-social worker and psychiatrist highlightedfollowing issues as the part of social management:
To inform the family members and peer groups about client’ssituation
To counsel the family members to be patience on client
To inform her husband to take care of her and don’t intendto find her guilt’s.
To counsel the peer groups to behave properly with theclient
To give her chance to realize social context.
Prognosis
Good prognostic criteria:
Her family is highly positive & supportive She has value oriented and acceptance the reality DMC team work professionally and cordially.
Bad prognostic criteria:
Feeling uncomfortable with her husband.
Fear
Comment
Client’s situation is improving slowly and gradually. Clientneeds to take medicine regularly for long time and also needscognitive behavior therapy, family therapy, counseling etc. Aftercure from illness, she needs a sound environment to rehabilitatein the society.
94

Chapter 5. Responsibilities and Performance
5.1 Assigned Duties and Responsibilities
5.2 Assigned Task During Fieldwork that I have
Accomplished
5.3 Methods, skills and techniques that I have Applied
5.4 Problems that I Faced During Fieldwork Practice
95
Assigned Duties and Responsibilities
I have to bear some assign duties and responsibilities from this
centre as a social worker. This assignment related with this
agency programs and services are following.
Regular attendance in agency during 60 working days.
To be acknowledge with agency employees, nature, objectives
and services
To know an administrative and organizational structure of
the agency.
To practice social work knowledge.
To achieve knowledge about background and evolution of
Agency
To find out the problems/limitation of this centre
Application of social work method in case preparing
Psycho social study, Diagnosis and treatment plan.
96

Maintaining register paper for process recording in every
working day
To stay at the agency during the prescribed time
Sitting with Institute supervisor every weekly.
Preparing a field work report on the basis of the work what
I have done during field work and submitting it in the field
time to agency supervisor and institute supervisor.
Assigned Task During Fieldwork that I have Accomplished
After being selected as an apprentice social worker at the agencynamed, Dhaka Medical College Hospital(DMC) some respective taskswere fixed up for me and for my other field mates through awritten work plan by the negotiation of the department supervisorand the agency supervisor. They are as fallows:
97

1. Preliminary orientation about the agency
Orientation stage with the agency
Acquaintance with organizational structure
Be familiar with working procedure
Principles of the agency
Objectives of the agency
Introducing with the different welfare projects patronized by theagency
2. I have completed assignments that are bestowed by institutesupervisor.
3. I have studied on different types of diseases through thereading of different kind of books, journals, research papersetc.
4. I have prepared a certain number of cases with the applying ofsocial work method.
5. I attended every sitting class in prescribed time and datewish my Institute supervisor.
6. 1 have tried to diagnosis psycho-social problems of theclients who are taken as long term case study on the behalf ofmine and 1 have followed up and 1 have consulted for removinghis/her psycho-social problem.
7. I have prepared a field practicum paper on selected topics.
98
Methods, skills and techniques that I have Applied
During fieldwork I have applied some techniques of case work aswell as social work for collecting data, diagnosis and treatment.
Case study
This is a kind of qualitative analysis. I used this method tocollect in depth data about the clients and to explore theirprevailing situation of their daily life.
Interviewing
Through face-to-face interview, I collected data, facts andinformation concerning their problem for diagnosis and treatment.
Observation
Following this technique, I observed and took notes on theirphysical expression such excitability, cheerfulness, gloomy andfrustration as well as sulky situation through participation.
Listening
To know the problems of the clients deeply, I did let them speakfirst. Then I talked. I followed the technique due to facilitatethe clients to be free in speaking and express their grievancesto me frankly.
Questioning
In order to obtain specifically necessary information and to leadthe clients' conversation from pointless to fruitful channels, Isometimes questioned them.
99

Case recording
Through this technique, I recorded the discussions anddeliberations of an interview as meaningful as possible.
Treatment
In treating the clients, I used two methods namely SupportiveTreatment Method and Modifying Treatment Method. I have helpedthem through reassurance, logical discussion and advice, guidanceas well as emotional support.
Acceptance
To work with the clients is very important for me as well as the
clients. I tried to accept the clients assuring them my capacity
so that they could accept me as a social worker.
Rapport building
I was careful to buildup successful rapport with the clients.
Through the effective interaction, body language I tried to make
them understand that I could help them.
Diagnosis
Based on the information I have found through interview, I got a
clear concept about the client’s problem. And it was helpful to
find out the actual problem of the client had. In diagnosis I
have used dynamic and etiological diagnosis techniques.
Psycho-social treatment
100

I have used psycho-social treatment techniques to enable the
clients to cope with their problems. Sometimes I have used own
prudence to solve their problems.
Follow up
After solving the problem I ask cordially in following up the
clients. As a social worker I could not let them to turn into the
previous situation again.
Communication skill
For the effective and sustainable solution of the client’s
problem I have communicated with the clients, doctors, nurse and
to help the clients with financial assistance and medicine etc. I
tried to communicate with the social service officer.
Sympathy and empathy
As my clients were the drug addicted person, I used to show them
my highest sympathy and empathy to them and I tried my best to
make them understand that I also feel their problem as they feel.
Process recording
In my field work practice I have used a quite different and
modern format of process recording provided by my institute
supervisor. I tried to abide by his all of the reactions. Besides
the advocacy methods skill and techniques I have used, other
techniques and methods. When I have done official duties in the
agency prepared research report etc. To prepare the research I
101

have used sampling technique and two different questionnaires.
Problems that I Faced During Fieldwork Practice
I have faced manifold problems during my fieldwork at DhakaMedical College Hospital(DMC). They are as follows:
1. Client’s ignorance, superstition, doubtfulness, religiousfanatic etc. are obstacle for build up rapport. On the otherhand, for these reason they express boredom and disagree toprovide real cause about their problems. So it is difficult todiagnosis their problems.
2. There is information gap that are given by clients. So it isdifficult to move forward for solving problems.
3. Poor clients' expectation was to obtain financial assistanceor to get job for their children.
4. But there was no opportunity to fulfill this expectation inDMC. So I could not help them with money and I also could notrehabilitate them by providing job.
5. I have to do case study in office time, so client would havebusy in her family activities. For this reason they could notspend time for providing information.
6. Clients did not know enough about mental illness. So I advisedthem to follow doctor's and therapist consultation and to besincere to their children.
7. It was difficult to find out client's house.
102

Chapter 6. Experience Sharing
6.1 My Experience During Field Practice
6.2 Barrier Regarding Field Practice
103

My Experiences during Field PracticeThere are many experiences I have faced during my field work
practice. Most of the experiences are related to the development
of my life for becoming a professional social worker. These
experiences are briefly discussed below.
I have gathered practical knowledge with respect to the
diagnosis and psychosocial treatment on different types of
mental illness like MSE, Rapport building, Counseling,
Relaxation etc.
The nature of being disciplined with formal dress was very
crucial for me and be present at the agency at regular time
was very important to develop my professional career.
Rapport building and maintain suitable relation with my
clients are also a positive experiences from my field work
practice.
Dealing with different kinds of problems and person are very
effective experiences during my field work practice.
As a student of social work, observing the client and their
family members through home visit was new experiences for
me.
104

I have learnt how to conduct case study and make the report
for case management.
I gathered counseling experience from my field work
practice.
I have learnt the application of case work from social work
perspective.
I tried to apply the principles, skills and techniques of
social work for the development of the psychiatry department
of DMC.
Barriers regarding Field Work PracticeSome barriers I had to face while dealing with the children at
the day care centre that are given following.
1. First few days the agency authority was not cordial and
cooperative enough to work with them effectively; but when
our agency supervisor introduced us with them formally, they
accepted us and helped us to work with them effectively.
105

2. The agency has extreme lack of treatment instruments which
is a great hinder for smooth service delivery.
3. I noticed that there exists a massive disparity in supplying
of opportunities between the paying and non-paying patients.
All the patients are staying in the same floor. When they
see that they are deprived in getting food, medicine and
other benefits; they do not want to cooperate in treatment.
4. There is no specific budget for the novice social worker. So
for the lack of finance social worker cannot work with the
patients. They only conduct psycho-social counseling.
5. There is no separate room and library for the novice social
workers.
6. Lack of coordination and cooperation between the hospital
authority and social service department is also mentionable.
7. Lab, pathology and other equipment are not modern.
8. It has no emergency unit and own blood bank.
9. Indoor and outdoor recreational program is very limited.
10. Lack of essential manpower etc.
106

Chapter 7. Recommendations and Conclusion
7.1 Recommendations
7.2 Conclusion
107

Recommendations
Success depends on proper application of rules and regulations
and other relevant strategies with combination of transparency,
accountability and punctuality. As the social service department
of Dhaka Medical College is now suffering some mighty problems so
some proposal are given to solve this problem and to provide
people friendly service effectively in future to build up a
mostly drug addiction free Bangladesh. Those ares-
The doctors, nurses, & authority of DMC should be more cordialand cooperative
The duration of staying in the hospital for the patients
should be increased.
The institute should take rehabilitation program strongly
The number of the seats should be increased for the patients
To increase the standard of food for the patients of non-
paying ward.
The standard of food of paying ward should also be increased
as they pay a handsome amount of money.
108

To manage an interview room and counseling room for the
apprentice social worker.
To increase co-ordination and integration between the
functions of hospital and social service department.
To take some new programs by social service department; such
as- motivation and rewarding, group counseling, family
counseling, medical allowance etc.
Awareness program on drug abusers should also be increased.
To increase to budget of social service department.
Outsourcing and in sourcing attempt should follow to increase
the budget of this department.
To ensure active involvement of the apprentice social worker
with the entire treatment process so that they could
contribute more for the effective treatment patients.
To take some income generating programs for the released
patients so that they could earn some money which will save
them from economic hardship?
The institute should open a separate unit relating tosubstance dependence mental disorder
To increase indoor games and recreational facilities for the
patients under treatment.
Released patients are very much irregular in weekly follow up
though it is an integral part of complete recovery. So the
agency should set up a communication system with the released
patients so that they come to take follow p service.
Group therapy program should be increased to ensure the
attendance of the patients in therapeutic activities. 109
Bureaucratic formalities should also reduce to get quick
treatment and admission.
Apprentice social worker should give full consent to work with
the patients in their ward which is now is strictly
restricted.
The agency should increase its budget for home visit and after
care treatment.
The number of bed, doctors, therapists, social workers ought
to be increased
To conduct some research and investigative works to find out
more effective way for the treatment of the drug abusers.
Free dispensable medicine program should increase.
110

ConclusionField work is the application of theoretical knowledge in the
practical field. It helps students to be familiar with different
types of practical experience regarding theoretical aspects. At
the end of the report I can say that field work brings a fruitful
result for the theoretical knowledge of social work. By field
practicum a novice social worker may know how to apply the
academic knowledge in various sectors of society. In our society
are fulfilled by different kind of problematic person who have
absolutely failed to solve their problems. In this point a social
worker can deal with this crisis to solve appropriately by their
achieving practical knowledge which is to gain from field
practicum. The impact of field work plays a vital role in
expanding and enriching the theoretical knowledge to overcome my
assigned duties. It can be said that obviously students may
adjust in any sectors in their future life by overcoming all
obstacles that I realize from my experience in field work. I
should say that in some cases I have achieved success and in some
cases I have failed to achieve it due to my lacking. I apologize
for my unintentional mistake. At last recapitulating above all
performance I warmly wish for prosperous and happy life of the
respondents with whom I worked.
111

References
Morales, Armando and Shefor, Bradford W (1986), Social Work:A Profession of Many Faces, Allayn and Bacon, Inc,Massachusetts.
Pincus, Allen and Minahan, Anne (1973), Social Work Practice, F.E. Peacock Publishers, Inc. New York.
Friendlander, Walter, A. & Apte. Robert, Z. (1982).Introduction to Social Welfare, New Delhi, Prentice-Hall of IndiaPrivate Limited.
Institute of Social Welfare and Research. (1996). Field WorkManual, (Abridged), Dhaka University, ISWR.
112

American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders, Text Revision: DSM-IV-TR (Washington, DC, American Psychiatric Publishing).
American Psychiatric Association (APA), (2007) Practice guidelines for the treatment of patients with major depressive disorder, (accessed: 22 December, 2011).
Barker, R. L. (1995) The social work dictionary (NASW Press,Washington DC). 5. Barlow, D. H. (2005) Abnormal psychology:an integrative approach (USA, Thomson Wadsworth).
Beck, A.T., Rush, J., Shaw, B. F. et al. (1987) Cognitive therapy of depression (New York, Guilford Press).
Bradley, W. G. Daroff, R. B. Fenichel, G. M. et al., (2008)Neurology in clinical practice (Philadelphia, Butterworth-Heinemann Elsevier).
Coleman, J. C. (1987) Abnormal psychology and modern life (Chicago, Scott Forman and Company).
Connolly, S. D. & Bernstein, G. A. (2007) Work Group on Quality Issues: Practice parameter for the assessment and treatment of children and adolescents with anxiety disorders, J Am Acad Child Adolesc Psychiatry, 46, 267-283.
DeGruy F. V. (2007) The somatic patient, in: R. E. Rakel, (ed) Textbook of family medicine (Philadelphia, Saunders Elsevier).
Fava, M & Cassano, P. (2008) Mood disorders: Major depressive disorder and dysthymic disorder, in: T. A. Stern,
113

J. F. Rosenbaum, M. Fava, J. Biederman & S. L. Rauch (eds) Massachusetts general hospital comprehensive clinical psychiatry (Philadelphia, Mosby Elsevier).
Feinstein, R. E., & Connelly, J. V. (2007) Personality disorders, in: R. E., Rakel (ed) Textbook of family medicine, (Philadelphia, Saunders Elsevier).
Firoz, A. H. M. (2007) Manual on metal health for primary health care physician (Dhaka, National Institute of Mental Health).
Freudenreich, O., Weiss, A. P., & Goff, D. C. (2008) Psychosis and schizophrenia, in: T. A. Stern, J. F. Rosenbaum, M. Fava, J. Biederman & S. L. Rauch (eds) Massachusetts general hospital comprehensive clinical psychiatry (Philadelphia, Mosby Elsevier).
Friedlander, W. A. (1991) Introduction to social welfare (New Delhi, Prentice-Hall). Goldman L. & Ausiello, D. (2007) Delirium and other mental status problems in the older patient (Philadelphia, SaundersElsevier).
Goodwin, F. K., Jamison, K. R. (2007) Manic-depressive illness: bipolar disorders and recurrent depression (New York, Oxford University Press).
Koran, L. M., Hanna, G. L., Hollander, E. et al. (2007) Practice guideline for the treatment of patients with obsessive-compulsive disorder, Am J Psychiatry, 164, 5-53.
Skidmore, R. A. & Thackeray, M. G. (1964) Introduction to social work (New York, Meredith Publishing Company).
114

http://www.btinternet.com/~david.veale/bddinfo.html (accessed: 10 September, 2012).www.bsmmu.org. (accessed: 10 September, 2012).
s
115




















