Change in Glenohumeral Rotation and Scapular Position After Competitive High School Baseball
12
125 Journal of Sport Rehabilitation, 2010, 19, 125-135 © 2010 Human Kinetics, Inc. Change in Glenohumeral Rotation and Scapular Position After Competitive High School Baseball Stephen J. Thomas, Kathleen A. Swanik, Charles “Buz” Swanik, Kellie C. Huxel, and John D. Kelly IV Context: Pathologies such as anterior instability and impingement are common in baseball and have been linked to decreases in internal rotation (IR) and concurrent increases in external rotation (ER). In addition, alterations to scapular position have been identified in this population, but the chronology of these adaptations is uncertain. Objectives: To determine whether there is a change in range of motion and scapular position after a single baseball season. Design: Prospective cohort. Setting: High school. Participants: 19 high school baseball players (age 16.6 ± 0.8 y, mass 78.6 ± 12.0 kg, height 180.3 ± 6.2 cm). Interventions: Subjects were measured for all depen- dent variables at preseason and postseason. Main Outcome Measures: Participants were measured for glenohumeral (GH) IR and ER with the scapula stabilized. Total GH range of motion was calculated as the sum of IR and ER. Scapular upward rota- tion was measured at 0°, 60°, 90°, and 120° of GH abduction in the scapular plane, and scapular protraction, at 0°, hands on hips, and 90° of GH abduction. Results: Overall, the dominant arm had significantly less GH IR (11.4°, P = .005) and sig- nificantly more ER (4.7°, P = .001) than the nondominant arm. Total motion in the dominant arm was significantly less than in the nondominant arm (6.7°, P = .001). Scapular upward rotation in the dominant arm significantly increased at 0° (2.4°, P = .002) and significantly decreased at 90° (3.2°, P = .001) and 120° (3.2°, P < .001) of abduction from preseason to postseason. Scapular protraction in the nondominant arm significantly decreased at 45° (0.32 cm, P = .017) and 90° (0.33 cm, P = .006) from preseason to postseason. Conclusion: These data suggest that scapular adapta- tions may be acquired over a relatively short period (12 wk) in a competitive baseball season. Competitive high school baseball players also presented with significant GH motion differences between their dominant and nondominant arms. Total motion was also significantly less in the dominant arm than in the nondominant arm. Keywords: scapular dyskinesis, posterior capsule, GIRD, subacromial impinge- ment syndrome Thomas is with the McKay Orthopaedic Research Laboratory, University of Pennsylvania, Philadelphia, PA. K. Swanik is with the Dept of Nursing and Health Science, Neumann University, Aston, PA. C. Swanik is with the Dept of Health, Nutrition and Exercise Sciences, University of Delaware, Newark, DE. Huxel is with Interdisciplinary Health Sciences, A.T. Still University, Mesa, AZ. Kelly is with the Dept of Orthopaedic Surgery, University of Pennsylvania Hospital, Philadelphia, PA. ORIGINAL RESEARCH REPORTS
Transcript of Change in Glenohumeral Rotation and Scapular Position After Competitive High School Baseball

125
Journal of Sport Rehabilitation, 2010, 19, 125-135© 2010 Human Kinetics, Inc.
Change in Glenohumeral Rotation and Scapular Position After
Competitive High School Baseball
Stephen J. Thomas, Kathleen A. Swanik, Charles “Buz” Swanik, Kellie C. Huxel, and John D. Kelly IV
Context: Pathologies such as anterior instability and impingement are common in baseball and have been linked to decreases in internal rotation (IR) and concurrent increases in external rotation (ER). In addition, alterations to scapular position have been identified in this population, but the chronology of these adaptations is uncertain. Objectives: To determine whether there is a change in range of motion and scapular position after a single baseball season. Design: Prospective cohort. Setting: High school. Participants: 19 high school baseball players (age 16.6 ± 0.8 y, mass 78.6 ± 12.0 kg, height 180.3 ± 6.2 cm). Interventions: Subjects were measured for all depen-dent variables at preseason and postseason. Main Outcome Measures: Participants were measured for glenohumeral (GH) IR and ER with the scapula stabilized. Total GH range of motion was calculated as the sum of IR and ER. Scapular upward rota-tion was measured at 0°, 60°, 90°, and 120° of GH abduction in the scapular plane, and scapular protraction, at 0°, hands on hips, and 90° of GH abduction. Results: Overall, the dominant arm had significantly less GH IR (11.4°, P = .005) and sig-nificantly more ER (4.7°, P = .001) than the nondominant arm. Total motion in the dominant arm was significantly less than in the nondominant arm (6.7°, P = .001). Scapular upward rotation in the dominant arm significantly increased at 0° (2.4°, P = .002) and significantly decreased at 90° (3.2°, P = .001) and 120° (3.2°, P < .001) of abduction from preseason to postseason. Scapular protraction in the nondominant arm significantly decreased at 45° (0.32 cm, P = .017) and 90° (0.33 cm, P = .006) from preseason to postseason. Conclusion: These data suggest that scapular adapta-tions may be acquired over a relatively short period (12 wk) in a competitive baseball season. Competitive high school baseball players also presented with significant GH motion differences between their dominant and nondominant arms. Total motion was also significantly less in the dominant arm than in the nondominant arm.
Keywords: scapular dyskinesis, posterior capsule, GIRD, subacromial impinge-ment syndrome
Thomas is with the McKay Orthopaedic Research Laboratory, University of Pennsylvania, Philadelphia, PA. K. Swanik is with the Dept of Nursing and Health Science, Neumann University, Aston, PA. C. Swanik is with the Dept of Health, Nutrition and Exercise Sciences, University of Delaware, Newark, DE. Huxel is with Interdisciplinary Health Sciences, A.T. Still University, Mesa, AZ. Kelly is with the Dept of Orthopaedic Surgery, University of Pennsylvania Hospital, Philadelphia, PA.
ORIGINAL RESEARCH REPORTS

126 Thomas et al
Repetitive stress placed on the shoulder complex during the overhead throw-ing motion is thought to be one of several factors in the development of shoulder injuries in throwers.1–3 Injuries such as anterior instability, rotator-cuff-tendon injury, internal impingement, SLAP lesions (superior labral tear from anterior to posterior), and elbow pain are common in these athletes. Throwers typically present with decreases in internal- and concurrent increases in external-rotation motion in the dominant arm.4–9 More recently, scapular alterations in this population have been described.3,10–12 Although alterations in scapula motion and position appear prevalent in overhead throwers, the chronology and mechanism behind these changes remain somewhat controversial. Some believe that increases in external rotation occur over several years and are associated with repetitive stretching of the anterior capsule.6,7,13–15 Others have suggested that the internal-rotation deficits are a result of an acquired tight posterior capsule.1,8,9,16 Finally, others have identified humeral retro-version as a contributor to both external-rotation gain and internal-rotation loss.17–19
Scapular dyskinesis is defined as an observable alteration in the position of the scapula and the patterns of scapular motion in relation to the thoracic cage.20,21 Alterations identified in baseball players include increased protraction and ante-rior tilting and decreased upward rotation. These changes in motion are thought to be detrimental to normal function of the shoulder complex and over time place increased stress on the static and dynamic restraints of the shoulder.3,10–12,21
The sequential manifestation and potential time frame of these motions and position changes have yet to be characterized. If the mechanical changes manifest rapidly (over the course of a single season), perhaps they can be remedied equally rapidly. Furthermore, prospective studies in overhead athletes are lacking. For these reasons, the purpose of this study was to measure glenohumeral internal and external rotation in conjunction with scapular positioning in baseball players throughout the course of a single scholastic sports season.
MethodsDesign
A pre–post design was used to assess 2 independent variables and 5 dependent vari-ables. The 2 independent variables were the point in time that the evaluation was performed (preseason and postseason) and arm (dominant and nondominant). The dependent variables were dominant and nondominant glenohumeral internal rotation, glenohumeral external rotation, total glenohumeral rotation, and scapular upward rotation and protraction. Total motion was calculated as glenohumeral internal plus external rotation. Scapular upward rotation (rest and 60°, 90°, and 120° of glenohu-meral abduction) and scapular protraction (rest, hands on hips, and 90° glenohumeral abduction) were tested at each of these positions. The rest position is considered to be 0° of glenohumeral abduction, and the hands-on-hips position is considered to be 45° of glenohumeral abduction with the hands resting on the participant’s iliac crests. The measurements were recorded twice, before and after the 12-week season.
Participants
Twelve position players and 7 pitchers, a total of 19 high school baseball players (age 16.6 ± 0.8 y, mass 78.6 ± 12.0 kg, height 180.3 ± 6.2 cm), volunteered to

Glenohumeral Rotation and Scapular Position 127
participate in this study. Pitchers were identified by the coach and were consistently used throughout the season. Exclusion criteria consisted of previous surgery to either shoulder or current shoulder pathology or symptoms. The study was approved by a university institutional review board. Informed constant was obtained from participants or, for those who were under the age of 18, the participants’ parents, and a health-history questionnaire and Health Insurance Portability and Account-ability Act forms were all completed before testing.
Instrumentation
Glenohumeral internal and external rotation were measured using a Saunders digital inclinometer (Saunders Group Inc, Chaska, MN). A priori test–retest reliability of glenohumeral range of motion was assessed by the primary investigator. Twenty healthy shoulders were measured and then remeasured 3 to 5 days later. Intraclass correlation coefficients (ICC2,1) and standard errors of measurement (SEM) for glenohumeral range of motion were calculated to be .989 and 1.03° and .943 and 2.55° for internal and external rotation, respectively.22
Scapular upward rotation was measured using a Saunders digital inclinometer modified to rest evenly on the scapular spine. The digital inclinometer was modified using methods described by Johnson et al.23 A priori test–retest reliability of the scapular upward-rotation measurements was assessed by the primary investigator. Thirty-six healthy shoulders were measured and then remeasured 3 to 5 days later. ICC and SEM values for scapular upward rotation were calculated to be .967 and 0.70°, .946 and 1.55°, .974 and 0.86°, and .965 and 0.89° at rest and 60°, 90°, and 120° of glenohumeral abduction, respectively.22
Scapular protraction was measured using Kibler’s Lateral Scapular Slide Test20 with a Vernier caliper (Mitutoy model number 505-633-50, Measurement Technology, UK) and recorded in centimeters. A priori test–retest reliability of the scapular-protraction measurements was assessed by the primary investiga-tor. Thirty-six healthy shoulders were measured and then remeasured 3 to 5 days later. ICC and SEM values for scapular protraction were calculated to be .935 and 0.328 cm, .970 and 0.186 cm, and .975 and 0.231 cm at rest, hands on hips, and 90° of glenohumeral abduction, respectively.22
Procedures
Passive internal- and external-rotation measurements were taken in the supine posi-tion, with the glenohumeral joint in 90° of abduction perpendicular to the plane of the body. The scapula was then stabilized by the tester’s hand, and the arm was rotated until scapular motion was detected.24 The inclinometer was then placed on the dorsal surface of the forearm, and the hold button was pressed to record the measurement. This was repeated 3 times, and the average of the 3 measurements was taken. All measurements were taken bilaterally by the primary investigator, who was blinded to the arm dominance of the athletes, and the order of testing was alternated.
Scapular upward-rotation measurements were taken with the subject standing with normal relaxed posture. A guide pole was used to help position the subject’s arm at 60°, 90°, and 120° of abduction. When the appropriate amount of abduction was determined a pin was inserted into the guide pole, and that location was then

128 Thomas et al
recorded for consistency in the postseason measurement. The subject was asked to abduct the arm until it was positioned against the pin. This position was maintained until the measurement was recorded. The lateral arm of the inclinometer was then placed over the posterior lateral acromion, and the medial arm was placed over the root of the scapular spine. The hold button was pressed to record the measure-ment. This was repeated twice and the average of the 2 measurements was taken. All measurements were taken bilaterally by the primary investigator, who was blinded to the arm dominance of the athlete, and the order of testing was alternated.
Scapular-protraction measurements were taken with the subject standing with normal relaxed posture. The measurements were taken in 3 different positions (rest, hands on hips, and 90° glenohumeral abduction with maximum internal rotation25). First, the inferior angle of the scapula was palpated and the lateral arm of the calipers was placed at the tip of the inferior angle. The medial arm of the calipers was then positioned at the corresponding spinous process, and the measurement was recorded. This was repeated 3 times, and the average of the 3 measurements was used for analysis.
Statistical Analyses
Data analysis consisted of descriptive statistics. Statistical tests included separate 1-way multivariate analyses of variance (MANOVA) with repeated measures on time for dominant- and nondominant-arm scapular upward rotation and protraction. Separate post hoc analyses of variance (ANOVA) were then performed when statisti-cal significance was found at the MANOVA level. Separate 1-way ANOVAs with repeated measures on time were performed for dominant- and nondominant-arm internal rotation, external rotation, and total glenohumeral motion. Separate 1-way ANOVAs were performed comparing dominant- and nondominant-arm internal rotation, external rotation, and total glenohumeral motion (α ≤ .05). Because of the small sample size no statistical comparisons were made between pitchers and position players. The SPSS for Windows statistical program (Version 13.0, SPSS, Inc., Chicago, IL) was used for data analysis.
ResultsOverall, combining the preseason and postseason measurements, the dominant arm had significantly less internal rotation (P = .05), significantly more external rota-tion (P = .001), and significantly less total motion than the nondominant arm (P = .001; Table 1). No significant main effects for time were observed in glenohumeral rotation or total motion.
Significant main effects for time were found for dominant-arm upward rotation (P < .001) and scapular protraction (P = .009; Table 2 and 3). Follow-up ANOVAs revealed that scapular upward rotation significantly increased from preseason to postseason at 0° abduction (P = .002) and decreased from preseason to postseason at 90° (P = .001) and 120° (P < .001) abduction (Table 2). Scapular protraction signifi-cantly decreased from preseason to postseason at 90° (P = .006) abduction (Table 3).
Significant main effects for time were found for nondominant-arm upward rotation (P = .003) and scapular protraction (P = .028; Table 2 and 3). Follow-up ANOVAs revealed that scapular upward rotation significantly decreased from
Glenohumeral Rotation and Scapular Position 129
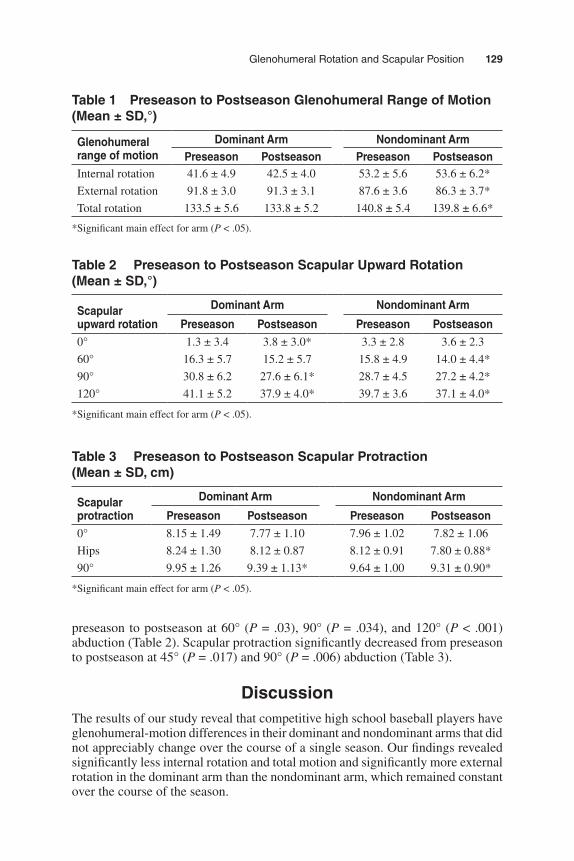
preseason to postseason at 60° (P = .03), 90° (P = .034), and 120° (P < .001) abduction (Table 2). Scapular protraction significantly decreased from preseason to postseason at 45° (P = .017) and 90° (P = .006) abduction (Table 3).
DiscussionThe results of our study reveal that competitive high school baseball players have glenohumeral-motion differences in their dominant and nondominant arms that did not appreciably change over the course of a single season. Our findings revealed significantly less internal rotation and total motion and significantly more external rotation in the dominant arm than the nondominant arm, which remained constant over the course of the season.
Table 1 Preseason to Postseason Glenohumeral Range of Motion (Mean ± SD,°)
Glenohumeral range of motion
Dominant Arm Nondominant ArmPreseason Postseason Preseason Postseason
Internal rotation 41.6 ± 4.9 42.5 ± 4.0 53.2 ± 5.6 53.6 ± 6.2*
External rotation 91.8 ± 3.0 91.3 ± 3.1 87.6 ± 3.6 86.3 ± 3.7*
Total rotation 133.5 ± 5.6 133.8 ± 5.2 140.8 ± 5.4 139.8 ± 6.6*
*Significant main effect for arm (P < .05).
Table 2 Preseason to Postseason Scapular Upward Rotation (Mean ± SD,°)
Scapular upward rotation
Dominant Arm Nondominant Arm
Preseason Postseason Preseason Postseason0° 1.3 ± 3.4 3.8 ± 3.0* 3.3 ± 2.8 3.6 ± 2.3
60° 16.3 ± 5.7 15.2 ± 5.7 15.8 ± 4.9 14.0 ± 4.4*
90° 30.8 ± 6.2 27.6 ± 6.1* 28.7 ± 4.5 27.2 ± 4.2*
120° 41.1 ± 5.2 37.9 ± 4.0* 39.7 ± 3.6 37.1 ± 4.0*
*Significant main effect for arm (P < .05).
Table 3 Preseason to Postseason Scapular Protraction (Mean ± SD, cm)
Scapular protraction
Dominant Arm Nondominant Arm
Preseason Postseason Preseason Postseason0° 8.15 ± 1.49 7.77 ± 1.10 7.96 ± 1.02 7.82 ± 1.06
Hips 8.24 ± 1.30 8.12 ± 0.87 8.12 ± 0.91 7.80 ± 0.88*
90° 9.95 ± 1.26 9.39 ± 1.13* 9.64 ± 1.00 9.31 ± 0.90*
*Significant main effect for arm (P < .05).

130 Thomas et al
Motion differences in overhead athletes are well documented.1,6,8,9,26,27 How-ever, the etiology of these changes remains debatable. The results of our study reveal that passive internal rotation was significantly less in the dominant arm than the nondominant arm. This finding is in agreement with previous research in adolescent, college, and professional overhead athletes.6,8,9,13,14,16,27,28 Burkhart et al1 stated that larger glenohumeral internal-rotation deficits (GIRD) create higher risk of shoulder injury. They postulate that GIRD reflects a tight posteroinferior capsule, which results from a healing response of the posterior rotator-cuff tendon and capsule to chronic distractive forces.1 Any posterior soft-tissue adaptation is thought to alter the arthrokinematics of the humeral head into a posterosuperior direction.29,30 This shift in arthrokinematics is thought to put the shoulder at risk for SLAP lesions, rotator-cuff-tendon tears, and impingement syndrome.1,31 Kibler et al14 found a correlation between loss of internal rotation and years of play in junior elite tennis players. This suggests that the loss of internal rotation may occur as a “dose response” to the duration of exposure to chronic eccentric distractive forces experienced during the deceleration phase of the overhead throw.
Passive external rotation was significantly greater in the dominant arm than the nondominant arm. This finding is in agreement with what several studies examining range of motion in overhead athletes have found.5,6,13,14,32 Many authors suggest that repetitive overhead motions cause anterior capsule stretching, which is demonstrated by increases in external rotation.2,33 However, when examining external rotation throughout a 12-week competitive season we did not observe any significant changes. This suggests that the anterior static restraints do not attenuate over a single season. Osbahr et al18 and Regan et al19 suggest that the external-rotation torque placed on the humeral epiphyseal plate in young overhead athletes will increase humeral retroversion. This causes a shift in the total arc of motion into increased amounts of external rotation.18,19 In the current study, the bilateral difference in external rotation may be a result of, at least in part, increased humeral retroversion, which has been thought of as a positive adaptation because of the gain of external rotation without soft-tissue attenuation.17 A gain of external rotation has also been viewed as a positive adaptation, in addition to several other kinematic variables, because of its correlation with increased ball velocity.34,35 More prospective studies are warranted to examine the contributions of boney- versus soft-tissue remodeling to increased humeral external rotation.
Wilk et al36 developed the total-motion concept, in which they state that if the total motion is equal bilaterally then the change in the arc of motion is a result of humeral retroversion and should not be a concern. However, we found significantly less total motion in the dominant arm than the nondominant arm. This decrease in total motion is best explained by the appreciably greater amount of GIRD than external-rotation gain. We believe these changes most likely occurred because of a contribution of humeral retroversion coupled with soft-tissue adaptations. According to Burkhart et al,1 the soft-tissue adaptation is a tightened and thickened posterior capsule. However, other authors have generalized this adaptation to posterior shoul-der tightness, which may include tightness of the posterior rotator-cuff-tendon, as well as the posterior capsule.8,9
Scapular dyskinesis is commonly linked to glenohumeral-joint pathology in overhead athletes.3,11,15,20,21 A decrease in scapular upward rotation is thought to cause subacromial impingement at higher degrees of glenohumeral abduction.37–39

Glenohumeral Rotation and Scapular Position 131
Recently, several researchers have begun to objectively measure scapular upward rotation in overhead athletes using a digital inclinometer.23,27,28,39 Although inclina-tion measures only 1 aspect of a 3-dimensional issue, it nonetheless depicts side-to-side differences, and therefore dyskinesis, in the involved scapulas. However, to date there have not been any studies that assessed scapular upward rotation throughout a competitive high school baseball season.
The results of our study revealed that dominant-arm scapular upward rotation at 90° and 120° of glenohumeral abduction significantly decreased from preseason to postseason. The 90° and 120° positions, which presented with changes of 3.2° and 3.2°, respectively, may be clinically meaningful and place these healthy athletes at a heightened risk of impingement syndrome. This finding suggests that the repetitive stresses placed on the shoulder throughout the season caused a decrease in neuro-muscular control or balance of the upper trapezius, lower trapezius, and serratus anterior. These muscles are involved in the force couple for scapular upward rota-tion, and alterations in neuromuscular control would affect the kinematics. These results are similar to changes seen in individuals with impingement syndrome.37,38 Studies examining electromyography (EMG) and kinematics of the scapular sta-bilizers in a group with impingement syndrome have demonstrated decreases in the activity of the lower trapezius and serratus anterior along with decreases in scapular upward rotation.37,40 These deficits, which are thought to cause a decrease in the subacromial-space dimensions, may be placing the shoulder at risk for future impingement syndrome or rotator-cuff-tendon irritation during forward flexion and abduction.38,41,42 Burkhart et al1 believe that the first culprit in shoulder injuries in throwers is GIRD. They suggest that GIRD places increased stress on the scapula-stabilizing muscles because of scapula “windup” during follow-through. This may eventually lead to fatigue-related inhibition and stretching of scapular restraints and ultimately a malpositioned, or “SICK” (scapular malposition, inferior medial scapu-lar winging, coracoid tenderness, and scapular dyskinesis), scapula.10 Although this cannot be ascertained in the current study it could be important because it may suggest that if internal-rotation deficits are identified and treated early, it could offset or prevent motion alterations (decreased upward rotation). There was also an increase in dominant-arm scapular upward rotation at 0° of glenohumeral abduction from preseason to postseason. This increase in upward rotation may be the result of a multitude of factors, which include slouching, rounded shoulders, and increased thoracic kyphosis. Previous studies have found that scapular upward rotation in the resting position ranges from –2° to 5° in healthy subjects because of subject posture. 12,28,39,40,43–46 These possible changes in posture may place the resting scapula in altered upward rotation compared with an upright posture.44,45
Scapular upward rotation in the nondominant arm also decreased at 60°, 90°, and 120° of glenohumeral abduction from preseason to postseason. These decreases may suggest that there is a neuromuscular negative cross-transfer effect that occurs over the course of a single baseball season. Cross-transfer effects have been associ-ated with increased neuromuscular strength and endurance in the nondominant arm caused solely by training in the dominant arm.46–48 This study may indicate that cross-transfer can occur with inhibitory effects, as well. More studies are warranted to further investigate this observation.
Scapular protraction is also critical to overall performance in overhead throw-ing. During the deceleration and follow-through phases of the overhead throw, the

132 Thomas et al
scapula must protract around the thoracic wall to help dissipate the large forces placed on the glenohumeral joint.3,15 However, excessive protraction has been linked to increased internal impingement, increased anterior shoulder instability, potentiated supraspinatus impingement, and rotator-cuff-tendon weakness.3 In an attempt to supply an objective measure of scapular protraction, Kibler et al3 developed the Lateral Scapular Slide Test, a reliable clinical method of evaluating scapula-stabilizing strength.
The results of the current study demonstrated that dominant-arm protraction at the 90° abducted position decreased from preseason to postseason. This suggests that the scapula moved into a more retracted position, which is beneficial for overhead athletes, allowing for optimal function. It may be that the increased protraction noted in more mature throwers with symptoms does not manifest until later.3,10,12 In other words, the decreased protraction demonstrated in these less mature athletes may serve as an early protective mechanism. However, the observed change was only 0.57 cm, which may not be clinically significant. Further research is required to determine the magnitude of change required for a clinically meaningful result.
Scapular protraction in the nondominant arm also decreased from preseason to postseason at the hands-on-hips and 90°-abduction positions. These results are similar to those in the dominant arm and may suggest a protective mechanism in these healthy baseball players. Again, the observed changes were only 0.32 cm and 0.33 cm, respectively, which may not be clinically significant.
LimitationsThere are some limitations to this study that should be acknowledged. First, pitch-ers and position players were combined and analyzed together. It has been dem-onstrated in the literature that pitchers subject their shoulders to additional stress because of the high number of repetitions each game. However, in a recent study conducted in our laboratory using the current methodology, pitchers had more GIRD and less total motion than position players. No differences were observed between pitchers and position players for scapular measurements.49 Next, only 2 of the possible 5° of freedom were measured for the scapula. This is a limitation because of the potential injury risk of alterations in the other motions of the scapula. However, to our knowledge scapular upward rotation and protraction are the only valid and reliable measurements that can be observed clinically.3,20,23,43 Currently a 3-dimensional electromagnetic tracking system can be used to measure all 5° of scapular motion. However, this technique does not translate well to the clinic, and there is still some question of its validity and reliability because of skin motion between the sensor and the scapula.50 A reason for the observed changes in both dominant- and nondominant-arm scapular protraction may be an inherent error in the measurement technique. For this measurement the distance from the inferior angle of the scapula to the spinous process is taken. There was a measured decrease in protraction at the 90° position and also a decrease in scapular upward rotation. Because of the decrease from preseason to postseason in scapular upward rota-tion at the 90° position, the inferior angle should be closer to the spinous process solely as a result of a change in upward rotation and not protraction. This would give a measure of scapular protraction that is less than the preseason measurement. Therefore, the amount of protraction may not have changed over the season. This

Glenohumeral Rotation and Scapular Position 133
is a limitation of the measurement, and future methods should be developed to account for this error.
ConclusionCompetitive high school baseball players demonstrate significantly less internal rotation and total motion and significantly more external rotation in the domi-nant arm at the beginning of the season. Over the course of a single season, decreases in scapular upward rotation and protraction manifest themselves in this asymptomatic cohort. We posit that decreased protraction may serve as an early protective mechanism for throwers, whereas decreased upward rotation may be the sentinel maladaptive development regarding the maintenance of shoulder homeostasis. A proper preventive posterior-capsule-stretching program and scapular strengthening may be warranted to help slow the progression of these early scapular adaptations.
References 1. Burkhart SS, Morgan CD, Kibler BW. The disabled throwing shoulder: spectrum of
pathology, part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19:404–420. 2. Jobe FW, Kvitne RS, Giangarra CE. Shoulder pain in the overhand or throwing ath-
lete. the relationship of anterior instability and rotator cuff impingement. Orthop Rev. 1989;18(9):963–975.
3. Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med. 1998;26:325–337.
4. Bigliani LU, Codd TP, Connor PM, Levine WN, Littlefield MA, Hershon SJ. Shoulder motion and laxity in the professional baseball player. Am J Sports Med. 1997;25:609–613.
5. Brown LP, Niehues SL, Harrah A, Yavorsky P, Hirshman PH. Upper extremity range of motion and isokinetic strength of the internal and external shoulder rotators in Major League Baseball players. Am J Sports Med. 1988;16:577–585.
6. Ellenbecker TS, Roetert EP, Bailie DS, Davies GJ, Brown SW. Glenohumeral joint total rotation range of motion in elite tennis players and baseball pitchers. Med Sci Sports Exerc. 2002;34:2052–2056.
7. Meister K, Day T, Horodyski M, Kaminski TW, Wasik MP, Tillman S. Rotational motion changes in the glenohumeral joint of the adolescent/Little League baseball player. Am J Sports Med. 2005;33(5):693–698.
8. Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006;34(3):385–391.
9. Tyler TF, Nicholas SJ, Roy T, Gleim GW. Quantification of posterior capsule tight-ness and motion loss in patients with shoulder impingement. Am J Sports Med. 2000;28:668–673.
10. Burkhart SS, Morgan CD, Kibler BW. The disabled throwing shoulder: spectrum of pathology, part III: the SICK scapula, scapular dyskinesis, the kinetic chain, and reha-bilitation. Arthroscopy. 2003;19:641–661.
11. Laudner KG, Myers JB, Pasquale MR, Bradley JP, Lephart SM. Scapular dysfunc-tion in throwers with pathologic internal impingement. J Orthop Sports Phys Ther. 2006;36(7):485–494.
12. Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Scapular position and orientation in throwing athletes. Am J Sports Med. 2005;33:263–271.

134 Thomas et al
13. Ellenbecker TS, Roetert EP, Piorkowski PA, Schulz DA. Glenohumeral joint internal and external rotation range of motion in elite junior tennis players. J Orthop Sports Phys Ther. 1996;24:336–341.
14. Kibler WB, Chandler TJ, Livingston BP, Roetert EP. Shoulder range of motion in elite tennis players. effect of age and years of tournament play. Am J Sports Med. 1996;24:279–285.
15. Meister K. Injuries to the shoulder in the throwing athlete. part one: biomechanics/pathophysiology/classification of injury. Am J Sports Med. 2000;28:265–275.
16. Spigelman TH, Swanik KA, Hamstra KL, Swanik CB. Glenohumeral range of motion in pre-pubescent swimmers over a twelve-week season. J Athl Train. 2003;38:S-71–S-72.
17. Crockett HC, Gross LB, Wilk KE, et al. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002;30(1):20–26.
18. Osbahr DC, Cannon DL, Speer KP. Retroversion of the humerus in the throwing shoulder of college baseball pitchers. Am J Sports Med. 2002;30:347–353.
19. Reagan KM, Meister K, Horodyski MB, Werner DW, Carruthers C, Wilk KE. Humeral retroversion and its relationship to glenohumeral rotation in the shoulder of college baseball players. Am J Sports Med. 2002;30:354–360.
20. Kibler BW. Role of the scapula in the overhead throwing motion. Contemp Orthop. 1991;22:525–532.
21. Warner JJP, Micheli LJ, Arslenian LE, Kennedy J, Kennedy R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impinge-ment syndrome. a study using Moiré topographic analysis. Clin Orthop Relat Res. 1992;285:191–199.
22. Weir JP. Quantifying test–retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19(1):231–240.
23. Johnson MP, McClure PW, Karduna AR. New method to assess scapular upward rota-tion in subjects with shoulder pathology. J Orthop Sports Phys Ther. 2001;31:81–89.
24. Awan R, Smith J, Boon AJ. Measuring shoulder internal rotation range of motion: a comparison of 3 techniques. Arch Phys Med Rehabil. 2002;83:1229–1234.
25. Thomas SJ, Swanik KA, Swanik C, Huxel KC. Glenohumeral rotation and scapular position change following a single competitive high school female sports season. J Athl Train. 2009;44(3):230–237.
26. Cavallo RJ, Speer KP. Shoulder instability and impingement in throwing athletes. Med Sci Sports Exerc. 1998;30:18–25.
27. Mourtacos SL, Sauers EL, Downar JM. Adolescent baseball players exhibit differences in shoulder mobility between the throwing and non-throwing shoulder and between divisions of play. J Athl Train. 2003;38:S-72.
28. Downar JM, Sauers EL. Clinical measures of shoulder mobility in the professional baseball player. J Athl Train. 2005;40:23–29.
29. Clabbers KM, Kelly JD, IV, Bader D, et al. Effect of posterior capsule tightness on glenohumeral translation in the late-cocking phase of pitching. J Sport Rehabil. 2007;16:41–49.
30. Huffman GR, Tibone JE, McGarry MH, Phipps BM, Lee YS, Lee TQ. Path of gleno-humeral articulation throughout the rotational range of motion in a thrower’s shoulder model. Am J Sports Med. 2006;34(10):1662–1669.
31. Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three sub-types and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998;14(6):553–565.
32. Beach ML, Whitney SL, Dickoff-Hoffman SA. Relationship of shoulder flexibility, strength, and endurance to shoulder pain in competitive swimmers. Journal of Sport and Physical Therapy. 1992;16:262–268.
33. Jobe CW, Pink MM, Jobe FW. Anterior shoulder instability, impingement, and rota-tor cuff tear: theories and concepts. In: Jobe FW, ed. Operative Techniques in Upper Extremity Sports Injuries. St. Louis, MO: Mosby; 1996:164–176.

Glenohumeral Rotation and Scapular Position 135
34. Matsuo T, Escamilla RF, Fleisig GS, Barrentine SW, Andrews JR. Comparison of kinematic and temporal parameters between different pitch velocity groups. J Appl Biomech. 2001;17(1):1–13.
35. Werner SL, Suri M, Guido JA Jr, Meister K, Jones DG. Relationships between ball velocity and throwing mechanics in collegiate baseball pitchers. J Shoulder Elbow Surg. 2008;17(6):905–908.
36. Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med. 2002;30(1):136–151.
37. Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activ-ity in people with symptoms of shoulder impingement. Phys Ther. 2000;80(3):276–291.
38. Lukasiewicz AC, McClure PW, Michener L, Pratt N, Sennett B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;29:574–586.
39. Su KPE, Johnson MP, Gracely EJ, Karduna AR. Scapular rotation in swimmers with and without impingement syndrome: practice effects. Med Sci Sports Exerc. 2004;36:1117–1123.
40. Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther. 1996;24(2):57–65.
41. Hébert LJ, Moffet H, McFadyen BJ, Dionne CE. Scapular behavior in shoulder impinge-ment syndrome. Arch Phys Med Rehabil. 2002;83:60–69.
42. Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech (Bristol, Avon). 2003;18(5):369–379.
43. Borsa PA, Timmons MK, Sauers EL. Scapular-positioning patterns during humeral elevation in unimpaired shoulders. J Athl Train. 2003;38:12–17.
44. Finley MA, Lee RY. Effect of sitting posture on 3-dimensional scapular kinematics measured by skin-mounted electromagnetic tracking sensors. Arch Phys Med Rehabil. 2003;84(4):563–568.
45. Kebaetse M, McClure PW, Pratt NA. Thoracic position effect on shoulder range of motion, strength, and three-dimensional scapular kinematics. Arch Phys Med Rehabil. 1999;80:945–950.
46. Shaver LG. Cross transfer effects of conditioning and deconditioning on muscular strength. Ergonomics. 1975;18(1):9–16.
47. Yasuda Y, Miyamura M. Cross transfer effects of muscular training on blood flow in the ipsilateral and contralateral forearms. Eur J Appl Physiol Occup Physiol. 1983;51(3):321–329.
48. Yuza N, Ishida K, Miyamura M. Cross transfer effects of muscular endurance during training and detraining. J Sports Med Phys Fitness. 2000;40(2):110–117.
49. Thomas SJ, Swanik KA, Swanik C. Internal rotation and total motion differences: a comparison of baseball pitchers and position players. J Athl Train. 2008;43(3):s-21.
50. McClure PW, Michener LA, Sennett B, Karduna AR. Direct 3-dimensional measure-ment of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:269–277.

Copyright of Journal of Sport Rehabilitation is the property of Human Kinetics Publishers, Inc. and its content
may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express
written permission. However, users may print, download, or email articles for individual use.