
Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain
Upload
zi-mannheimCategory
view
1download
0
ORIGINAL ARTICLE
Pain Ratings and Somatosensory Evoked Responses toRepetitive Intramuscular and Intracutaneous Stimulation in
Fibromyalgia Syndrome
Martin Diers,* Caroline Koeppe,* Pinar Yilmaz,* Kati Thieme,* Jaana Markela-Lerenc,*Marcus Schiltenwolf,† Klaus van Ackern,‡ and Herta Flor*
Summary: To determine the presence of perceptual sensitizationand related brain responses we examined 15 patients with fibromy-algia syndrome and 15 healthy controls comparable in age and sex.Multichannel EEG recordings and pain ratings were obtained duringthe presentation of 800 painful electrical intramuscular and intracu-taneous stimuli to the left m. erector spinae and the left m. extensordigitorum. The stimulus intensity was adjusted to 50% between painthreshold and tolerance. Detection and pain thresholds were signifi-cantly lower in the fibromyalgia syndrome group. Sensitization oc-curred for both groups during intramuscular stimulation. In the EEGdata the fibromyalgia syndrome patients showed higher N80 ampli-tudes compared with the healthy controls. Arm stimulation andintramuscular stimulation yielded higher N80 and N150 amplitudescompared with intracutaneous stimulation or stimulation of the back.These results indicate lower pain thresholds in the fibromyalgia syn-drome patients after electrical stimulation and a higher N80 amplitudeboth indicative of enhanced sensory processing in this group.
Key Words: EEG, Fibromyalgia syndrome, Event-related poten-tials, Electrical stimulation, Needle electrodes, Sensitization.
(J Clin Neurophysiol 2008;25: 000–000)
Fibromyalgia syndrome (FMS) is characterized by chronicwidespread pain and tenderness at specific sites (Wolfe et
al., 1990). The etiology of FMS remains unclear, however,the generalized hyperalgesia, widespread pain, and spontane-ous pain in FMS have been related to central changes. Forexample, Gibson et al. (1994) reported that heat and mechan-
ical pain thresholds were significantly lower in FMS patientscompared with healthy controls (HC). The change in thermalpain sensitivity was noted following the stimulation of thedorsal surface of the hand, rather than over designated “ten-der points.” Based on such results it seems likely that fibro-myalgia patients display a generalized change in pain sensi-tivity. Sorensen et al. (1998) found lowered pain levels byrepeated electrical stimulation at the anterior tibial muscle inpatients with FMS compared with HC. Although thresholdsfor pain evoked by electrical stimulation of the skin were notsignificantly different in the two groups, pain thresholds torepeated intramuscular electrical stimulation were signifi-cantly lower for the fibromyalgia patients. In a study byMontoya et al. (2005) patients with fibromyalgia showedsensitization during blocks of pressure pain stimulation. In astudy by Stevens et al. (2000) patients with FMS perceivedcold pressure pain earlier and judged it earlier as intolerablethan control subjects. Equivalent results were found byPetzke et al. (2003) who noted that expectancy effects play arole in FMS. In the study by Gibson et al. (1994) patients withFMS also displayed a significant increase in the peak-to-peakamplitude of the cerebral potential evoked by painful CO2
laser stimulation in a time window 207 and 370 millisecondspoststimulus. Similar results were found by Lorenz et al.(1996) and Lorenz (1998). Fibromyalgia patients exhibitedsignificantly lower heat pain thresholds than matched controlsand had higher amplitudes of the laser-evoked potentialcomponents N170 and P390. The observation of amplitudeenlargement of the N170 suggests enhanced nociceptive ac-tivation and neuronal synchronization in secondary somato-sensory cortex by radiant heat. The P390 enhancement inFMS patients might indicate greater attention to or cognitiveappraisal of painful stimuli. Lorenz et al. (1996) documentedthat this hyperreactivity was not present in auditory evokedpotentials, suggesting that general hypervigilance is notpresent in FMS patients. Using functional MRI, Gracely et al.(2002) reported that comparable levels of subjectively re-ported painful stimulation resulted in activation patterns thatwere similar in FMS patients and HC, whereas similar ob-jective pressure intensities resulted in greater effects in pa-tients in regions specific for pain processing. This applies toregions involved in the sensory-discriminative component ofpain, such as primary somatosensory cortex and secondary
From the *Department of Clinical and Cognitive Neuroscience, CentralInstitute of Mental Health, University of Heidelberg, Mannheim; †Or-thopedic University Hospital Heidelberg, Schlierbacher Landstr. 200a,Heidelberg; and ‡Department of Anesthesiology and Critical Care Med-icine, Medical Faculty Mannheim at the University of Heidelberg,Theodor-Kutzer-Ufer, Mannheim, Germany.
This work was supported by a grant from the Deutsche Forschungsgemein-schaft (Clinical Research Unit 107 “Neuronal plasticity and learningprocesses in pain chronicity,” FL 156/26).
Address correspondence and reprint requests to Herta Flor, Ph.D., Depart-ment of Clinical and Cognitive Neuroscience, Central Institute of MentalHealth, University of Heidelberg, J 5, D-68159 Mannheim, Germany;e-mail: [email protected].
Copyright © 2008 by the American Clinical Neurophysiology SocietyISSN: 0736-0258/08/2503-0001
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008 1
AQ: 1
AQ: 4
<zjs;Original Article> • <zjss;Original Article> • <zdoi;10.1097/WNP.0b013e31817759c5>

somatosensory cortex as well as to those involved in theaffective-motivational component, such as insular and ante-rior cingulate cortex (ACC). These findings support thehypothesis that FMS is characterized by cortical augmenta-tion of pain processing.
Most research with painful electrical stimulation hasused either transcutaneous (eg, Babiloni et al., 2001; Dow-man, 1994; Dowman and Darcey, 1994) or intracutaneousstimulation (for a review see Bromm, 2001). Fewer studiesused intramuscular painful electrical stimulation as a morespecific model for muscle pain (Niddam et al., 2001, 2002;Shimojo et al., 2000; Svensson et al., 1997). Overall, painfulelectrical intramuscular stimulation evokes activity in aboutthe same brain areas as painful electrical cutaneous stimula-tion. These brain regions include the contralateral primarysomatosensory cortex, the secondary somatosensory cortexbilaterally, and the ACC as well as the posterior cingulatecortex (Bromm, 2004; for a review see Bromm and Lorenz,1998). Shimojo et al. (2000) found similar topographic pat-terns and source generators in response to intramuscular andintracutaneous stimulation. The vertex-measured magnitudeof the P260 component, thought to originate from the ACC(Babiloni et al., 2001; Bromm, 2001; for review see Apkarianet al., 2005) was found to be positively related to stimulusintensity for both modalities. With PET, Svensson et al.(1997) found a substantial overlap of the activation caused bycutaneous and intramuscular painful electrical stimulation,with ACC activity in response to the intramuscular stimula-tion being larger. On the subjective level, Shimojo et al.(2000) reported higher values in detection, pain, and toler-ance thresholds for intramuscular compared with intracuta-neous stimulation, and Chen et al. (2000) reported likewisethat intramuscular compared with intracutaneous stimulationneed higher stimulation intensity to achieve a comparablepain level. Lower somatosensory evoked potential amplitudesat most recording sites and slightly prolonged latencies werereported for muscle compared with skin stimulation when thesame pain level was used (Niddam et al., 2001).
The purpose of the present study was the comparison ofbrain activation patterns in response to painful stimulationand the comparison of intramuscular and intracutaneous stim-ulation in chronic fibromyalgia patients and matched healthycontrol subjects. Three components of the nociceptive re-sponse related to somatosensory event-related potentials wereexamined; N80 thought to originate from primary somato-sensory cortex, N150 thought to originate from secondarysomatosensory cortex, and P260 thought to originate fromACC. We expected lower pain thresholds, enhanced percep-tual sensitization as well as enhanced early and late corticalresponses in the FMS patients compared with the controls. Inaddition, we expected higher responsivity in the FMS patientscompared with the control group in the intramuscular stimu-lation condition related to their muscle pain.
METHOD
ParticipantsFifteen FMS patients and 15 HC participated in the
study. The patients were mainly recruited through a joint
case management unit established by several pain researchcenters in the Mannheim/Heidelberg area. All patients under-went medical examination. The HC were recruited throughnewspaper advertisement. Exclusion criteria for all subjectswere (a) neurologic complications; (b) pregnancy; (c) psy-chosis; (d) cardiac pacemaker; (e) allergy to plaster; (f) drugabuse; (g) centrally acting medication such as opiates. Fibro-myalgia syndrome was diagnosed according to the criteria ofthe American College of Rheumatology (Wolfe et al., 1990).Tender points were determined according to the manual ofOkifuji et al. (1997). The FMS patients’ average age was51.47 years (SD � 8.30, range: 34–62), 87% were women.The HC were on average 49.33-year-old (SD � 10.80, range:30–64), 67% were women. There was no significant differ-ence between the groups with respect to age (t(28) � 0.61,NS) or gender (�2(1) � 0.20, NS). The fibromyalgia patientshad been suffering from their pain for a minimum of 6months (M � 99.42 months, SD � 140.28, range: 8–396).Informed consent was obtained and the study was approvedby the local ethics committee and adhered to the Declarationof Helsinki.
Psychologic AssessmentAll FMS patients completed the German Version of the
West Haven-Yale Multidimensional Pain Inventory (Flor etal., 1990), the Pain Related Self-Statement Scale (Flor et al.,1993), the German version of the Fear-Avoidance BeliefsQuestionnaire (Pfingsten et al., 2000), the Pain ExperienceScale (Geissner, 1995), the German version of the Center forEpidemiological Studies Depression Scale (Hautzinger andBailer, 1993), the General Somatic Complaints Scale (vonZerssen and Koeller, 1976), and the Fibromyalgia ImpactQuestionnaire (Burckhard et al., 1991). Depression and so-matic complaints were also assessed in the HC. The FMSpatients had significantly more somatic complaints comparedwith the HC (t(27) � �8.18, P � 0.001). Likewise, the FMSpatients scored significantly higher on the depression scale(t(28) � �3.97, P � 0.001). Table 1 presents the demo-graphic, psychometric, and clinical data for the FMS patientsand the HC.
Stimulation ProcedureIn each recording block, 800 painful electrical bipolar
pulses with a duration of 0.5 milliseconds were administeredin random order at a frequency of 2.5 Hz by a DigitimerDS7A stimulator to the m. extensor digitorum in the leftlower arm (arm intramuscular, AIM), and the m. erectorspinae at L3 in the left lower back (back intramuscular, BIM).Intracutaneous stimulation was applied at the same sites at thelower arm (AIC) and the lower back (BIC). The short inter-stimulus-interval was chosen to provoke temporal summationeffects (cf. Staud et al., 2003). Both intramuscular and intra-cutaneous stimuli were presented with a pair of disposableneedle electrodes (20 mm long, 3 mm un-insulated tip, 2 mm2
stimulation area, 1 cm separation. Model: 13R27, 28G, Dan-tec, Denmark, cf. Niddam et al., 2001).
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
M. Diers et al. Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008
Copyright © 2008 by the American Clinical Neurophysiology Society2
T1
AQ: 2
Threshold Determination and SubjectiveRatings
Individual perception and pain thresholds as well aspain tolerance were measured by the method of limits, aver-aging over the last two of three ascending and descendingseries. The painful stimulus intensity that was applied was setto 50% between pain threshold and tolerance. After 20 and atthe end of 800 stimuli of the four recording blocks a rating ofstimulus intensity and unpleasantness was obtained on an11-point visual analog scale (0 � no pain; 10 � strongestimaginable pain; 0 � not at all unpleasant; 10 � extremelyunpleasant) to obtain separate self-report measures for thesensory-discriminative and the affective-motivational aspectsof pain. If the intensity was rated as too close to unbearable(values �8), stimulus intensity was lowered to a tolerablelevel before the recording trial. A lowering of the intensitywas necessary in 18% of all trials. Fibromyalgia syndromepatients and HC were not significantly different with respectto lowered stimulus intensities. Typically, intensities rated asbearable were only marginally lower than the calculatedintensities (Table 2). To obtain a measure of perceptualsensitization, we compared the first and the last rating. Thepatients were also asked to rate the severity and unpleasant-ness of their habitual pain before and after each stimulationblock using the same scale. The mean stimulation intensity
was used as covariate for the sensitization and the event-related potential data.
EEG RecordingsSomatosensory event-related potentials (SEPs) were
recorded from 57 electrodes using a standard EEG cap(Electrocap, Dayton, OH) based on the extended international10 to 20 system. The scalp recordings were referenced to thevertex electrode CZ. Electrode impedances were kept below5 k�. Additionally, eye movements were monitored withsupra- and infraorbital electrodes and with electrodes on theexternal canthi. EEG signals were sampled at 2.5 kHz andfiltered online with a 500 Hz analog low pass filter. Somato-sensory event-related potentials were segmented into 400milliseconds epochs (50 milliseconds before and 350 milli-seconds after each stimulus; cf. Babiloni et al., 2001). Epochswith eye movements, drifts and muscle artifacts were manu-ally rejected. After baseline correction and averaging, digitalfiltering (30 Hz low pass and 1.6 Hz high pass) was per-formed. The data were rereferenced to a common averagereference. As the International Federation of Clinical Neuro-
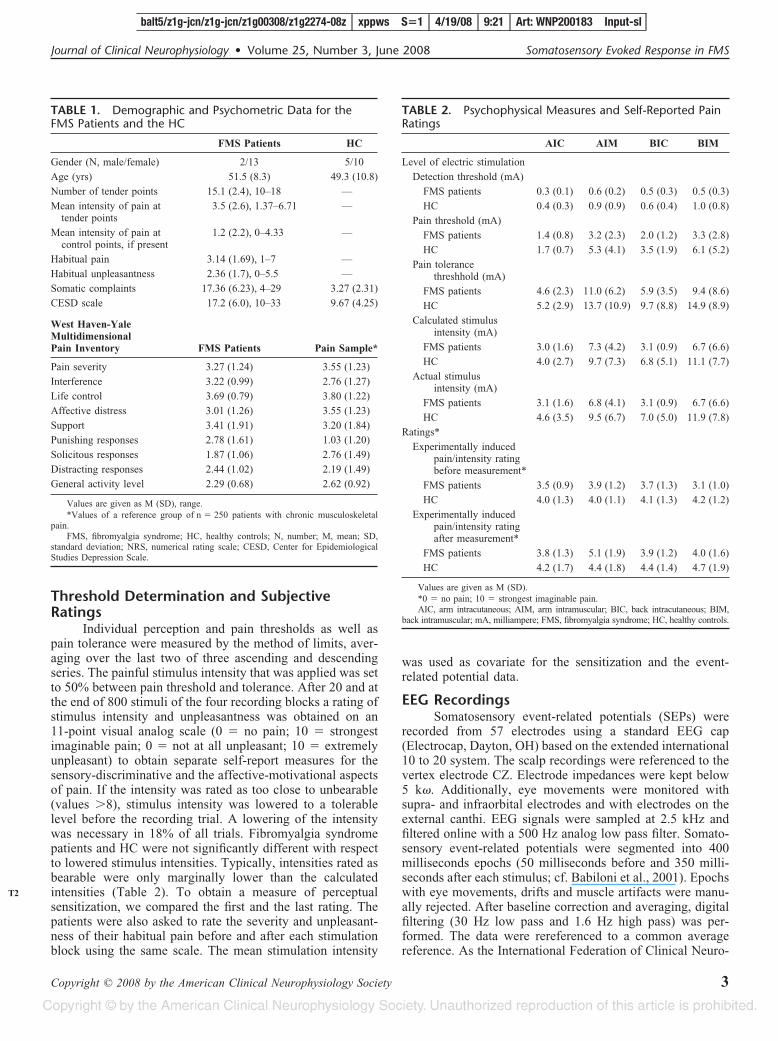
TABLE 1. Demographic and Psychometric Data for theFMS Patients and the HC
FMS Patients HC
Gender (N, male/female) 2/13 5/10
Age (yrs) 51.5 (8.3) 49.3 (10.8)
Number of tender points 15.1 (2.4), 10–18 —
Mean intensity of pain attender points
3.5 (2.6), 1.37–6.71 —
Mean intensity of pain atcontrol points, if present
1.2 (2.2), 0–4.33 —
Habitual pain 3.14 (1.69), 1–7 —
Habitual unpleasantness 2.36 (1.7), 0–5.5 —
Somatic complaints 17.36 (6.23), 4–29 3.27 (2.31)
CESD scale 17.2 (6.0), 10–33 9.67 (4.25)
West Haven-YaleMultidimensionalPain Inventory FMS Patients Pain Sample*
Pain severity 3.27 (1.24) 3.55 (1.23)
Interference 3.22 (0.99) 2.76 (1.27)
Life control 3.69 (0.79) 3.80 (1.22)
Affective distress 3.01 (1.26) 3.55 (1.23)
Support 3.41 (1.91) 3.20 (1.84)
Punishing responses 2.78 (1.61) 1.03 (1.20)
Solicitous responses 1.87 (1.06) 2.76 (1.49)
Distracting responses 2.44 (1.02) 2.19 (1.49)
General activity level 2.29 (0.68) 2.62 (0.92)
Values are given as M (SD), range.*Values of a reference group of n � 250 patients with chronic musculoskeletal
pain.FMS, fibromyalgia syndrome; HC, healthy controls; N, number; M, mean; SD,
standard deviation; NRS, numerical rating scale; CESD, Center for EpidemiologicalStudies Depression Scale.
TABLE 2. Psychophysical Measures and Self-Reported PainRatings
AIC AIM BIC BIM
Level of electric stimulation
Detection threshold (mA)
FMS patients 0.3 (0.1) 0.6 (0.2) 0.5 (0.3) 0.5 (0.3)
HC 0.4 (0.3) 0.9 (0.9) 0.6 (0.4) 1.0 (0.8)
Pain threshold (mA)
FMS patients 1.4 (0.8) 3.2 (2.3) 2.0 (1.2) 3.3 (2.8)
HC 1.7 (0.7) 5.3 (4.1) 3.5 (1.9) 6.1 (5.2)
Pain tolerancethreshhold (mA)
FMS patients 4.6 (2.3) 11.0 (6.2) 5.9 (3.5) 9.4 (8.6)
HC 5.2 (2.9) 13.7 (10.9) 9.7 (8.8) 14.9 (8.9)
Calculated stimulusintensity (mA)
FMS patients 3.0 (1.6) 7.3 (4.2) 3.1 (0.9) 6.7 (6.6)
HC 4.0 (2.7) 9.7 (7.3) 6.8 (5.1) 11.1 (7.7)
Actual stimulusintensity (mA)
FMS patients 3.1 (1.6) 6.8 (4.1) 3.1 (0.9) 6.7 (6.6)
HC 4.6 (3.5) 9.5 (6.7) 7.0 (5.0) 11.9 (7.8)
Ratings*
Experimentally inducedpain/intensity ratingbefore measurement*
FMS patients 3.5 (0.9) 3.9 (1.2) 3.7 (1.3) 3.1 (1.0)
HC 4.0 (1.3) 4.0 (1.1) 4.1 (1.3) 4.2 (1.2)
Experimentally inducedpain/intensity ratingafter measurement*
FMS patients 3.8 (1.3) 5.1 (1.9) 3.9 (1.2) 4.0 (1.6)
HC 4.2 (1.7) 4.4 (1.8) 4.4 (1.4) 4.7 (1.9)
Values are given as M (SD).*0 � no pain; 10 � strongest imaginable pain.AIC, arm intracutaneous; AIM, arm intramuscular; BIC, back intracutaneous; BIM,
back intramuscular; mA, milliampere; FMS, fibromyalgia syndrome; HC, healthy controls.
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008 Somatosensory Evoked Response in FMS
Copyright © 2008 by the American Clinical Neurophysiology Society 3
T2
physiology Guidelines (Nuwer et al., 1994) do not refer tonociceptive response related somatosensory potentials, theEEG data were preprocessed according to the literature (eg,Dowman, 2002; Reinert et al., 2000; Valeriani et al., 2002;Shimojo et al., 2000). Before digital filtering, the stimulusartifact was eliminated from the SEP by a linear interpolationof the datapoints between 4 milliseconds before and 4 milli-seconds after the stimulus.
Data Management and Statistical AnalysisPeak maxima were determined by visual inspection of
the SEP waveforms at the C2 electrode over the somatosen-sory cortex contralateral to the stimulation site for the 40 to90 milliseconds time window (N80), the 90 to 180 millisec-onds time window (N150), and the 240 to 300 millisecondstime window (P260). For the N80, N150, and P260 compo-nents, peak amplitudes at all electrodes were calculated at thelatencies determined at C2 and then used in the calculation ofthe root mean square activities in frontocentral (F3, F1, FZ,F2, F4, C3A, C1A, CZA, C2A, C4A) and central (C5, C3,C1, CZ, C2, C4, C6, C3P, C1P, PZA, C2P, C4P) electrodesubsets. These electrodes were chosen because they werelocated over the generators of the neuroelectrical signal in thesomatosensory and the cingulate cortex. For all dependentmeasures, analyses of covariance with group as between andlocation (back vs. arm) and stimulation method (intramuscu-lar vs. intracutaneous) as within-subject factors were calcu-lated. The mean of all four implicated stimulus intensitieswas used as a covariate. Dependent measures were the psy-chophysical thresholds, the stimulus intensities, the pain andunpleasantness ratings and the root mean square activities inthe electrodes of interest for the N80, N150, and P260
components. Variables were tested for normal distributionusing the Kolmogorov-Smirnov test. The data were correctedfor outliers by winsorisation [up to two values more thanthree box lengths (interquartile distance) from the upper orlower edge of the box were replaced by values three boxlengths from the upper or lower edge of the box; Dixon andTukey, 1968; Tukey and McLaughlin, 1963]. For the SEPdata the mean stimulation intensity of the four conditions wasused as covariate, because baseline values differed signifi-cantly between the groups (see below).
Statistical analyses were performed using SPSS for Win-dows (version 12.0.1; SPSS Inc., 2002). ANOVAs and analysesof covariances with Bonferroni as post hoc-test were calculatedas applicable. We chose a significance level of P � 0.05.
RESULTS
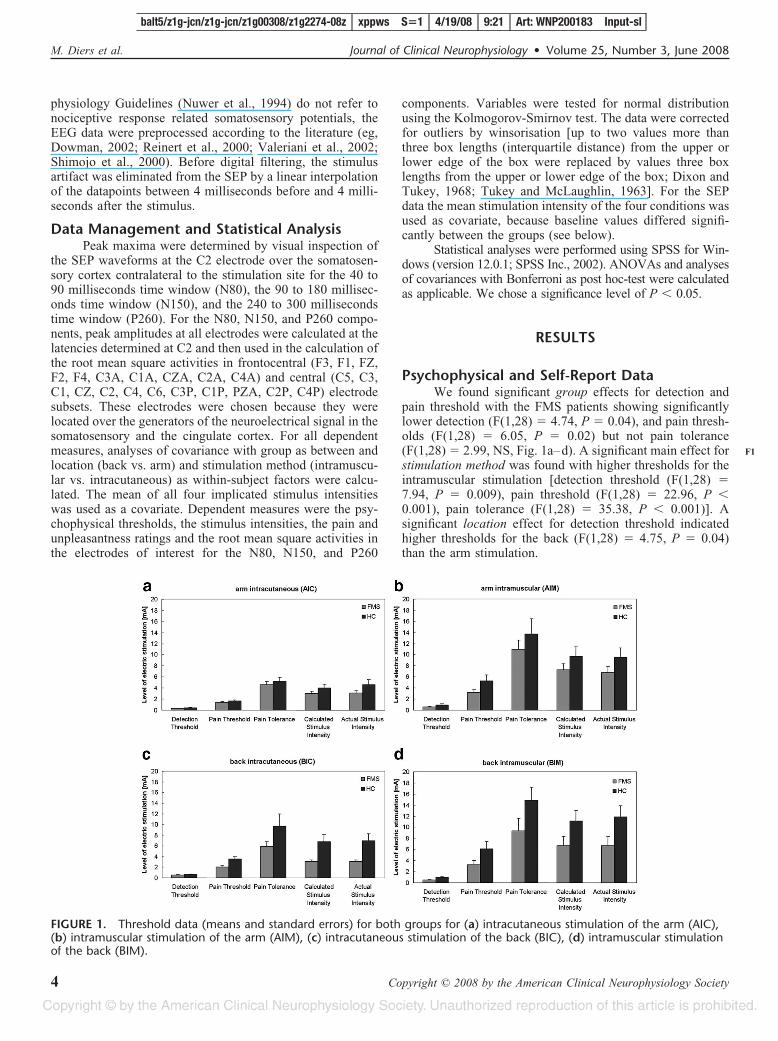
Psychophysical and Self-Report DataWe found significant group effects for detection and
pain threshold with the FMS patients showing significantlylower detection (F(1,28) � 4.74, P � 0.04), and pain thresh-olds (F(1,28) � 6.05, P � 0.02) but not pain tolerance(F(1,28) � 2.99, NS, Fig. 1a–d). A significant main effect forstimulation method was found with higher thresholds for theintramuscular stimulation [detection threshold (F(1,28) �7.94, P � 0.009), pain threshold (F(1,28) � 22.96, P �0.001), pain tolerance (F(1,28) � 35.38, P � 0.001)]. Asignificant location effect for detection threshold indicatedhigher thresholds for the back (F(1,28) � 4.75, P � 0.04)than the arm stimulation.
FIGURE 1. Threshold data (means and standard errors) for both groups for (a) intracutaneous stimulation of the arm (AIC),(b) intramuscular stimulation of the arm (AIM), (c) intracutaneous stimulation of the back (BIC), (d) intramuscular stimulationof the back (BIM).
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
M. Diers et al. Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008
Copyright © 2008 by the American Clinical Neurophysiology Society4
F1
From the threshold data we calculated the stimulationintensity. The patients and controls showed a significantgroup difference in the actual stimulation intensity with FMSpatients displaying significantly lower intensities (F(1,28) �6.46, P � 0.02). A significant effect for stimulation method(F(1,28) � 30.09, P � 0.001) revealed higher thresholds forthe intramuscular than the intracutaneous stimulation.
For self-reported pain intensity in response to the acutestimulation, no significant group effects were observed.Stimulation method was significant with higher pain rat-ings for the intramuscular than the intracutaneous stimulation(F(1,28) � 6.427, P � 0.02). Pain unpleasantness ratingsyielded no significant group effect.
To test whether sensitization had occurred during the800 painful stimulation trials, we compared the perceivedintensity of the stimulation at the beginning (after 20 trials)and at the end of the stimulation (after 800 trials). Both, FMSpatients and HC sensitized during the course of the stimula-tion (see Table 2 for means before and after the 4 stimulationconditions). Both groups perceived the stimuli as more pain-
ful at the end as compared with the beginning of the stimu-lation blocks as indicated by the significant factor “time”(F(1,27) � 5.123, P � 0.03). We found no significant groupor interaction effects although the FMS patients receivedsignificantly lower levels of stimulation.
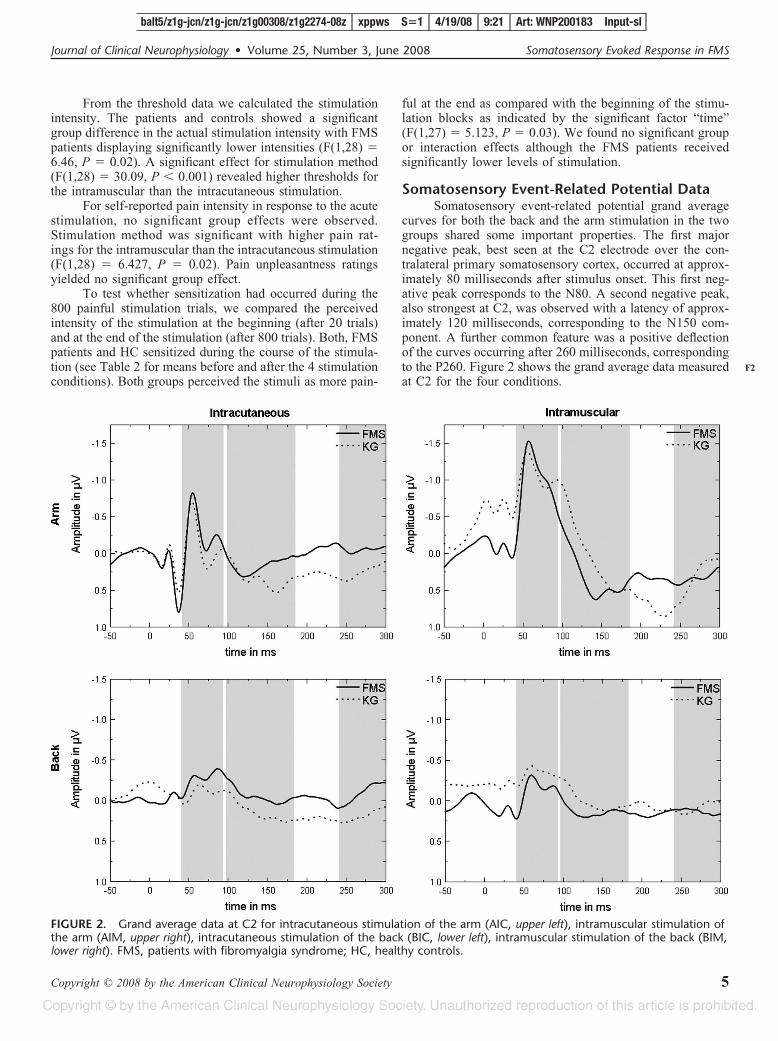
Somatosensory Event-Related Potential DataSomatosensory event-related potential grand average
curves for both the back and the arm stimulation in the twogroups shared some important properties. The first majornegative peak, best seen at the C2 electrode over the con-tralateral primary somatosensory cortex, occurred at approx-imately 80 milliseconds after stimulus onset. This first neg-ative peak corresponds to the N80. A second negative peak,also strongest at C2, was observed with a latency of approx-imately 120 milliseconds, corresponding to the N150 com-ponent. A further common feature was a positive deflectionof the curves occurring after 260 milliseconds, correspondingto the P260. Figure 2 shows the grand average data measuredat C2 for the four conditions.
FIGURE 2. Grand average data at C2 for intracutaneous stimulation of the arm (AIC, upper left), intramuscular stimulation ofthe arm (AIM, upper right), intracutaneous stimulation of the back (BIC, lower left), intramuscular stimulation of the back (BIM,lower right). FMS, patients with fibromyalgia syndrome; HC, healthy controls.
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008 Somatosensory Evoked Response in FMS
Copyright © 2008 by the American Clinical Neurophysiology Society 5
F2

The most prominent difference between the FMS pa-tients and the HC was a higher negativity at approximately 80milliseconds after stimulus onset in the FMS patients’ wave-form. At 80 milliseconds the central cluster yielded a signif-icant “group” effect (F(1,28) � 5.542, P � 0.05) with theFMS patients showing higher activity than the HC. A signif-icant “stimulation method” � “group” effect was found at 80milliseconds at the central cluster (F(1,28) � 4.257, P �0.05) with the FMS showing higher activity than the controlsand higher activity in the intramuscular stimulation condition.No group differences were found for the N150 or the P260component of the somatosensory evoked potential.
The most prominent differences between the locationsarm and back were higher root mean square amplitudes forthe arm at approximately 80 and 150 milliseconds afterstimulation onset and higher root mean square amplitudes forintramuscular stimulation compared with intracutaneousstimulation at approximately 80 and 150 milliseconds afterstimulation onset. Specifically root mean square activityyielded a significant “location” � “covariate” effect at 80milliseconds for the frontal cluster (F(1,28) � 5.25, P �0.05), at 150 milliseconds for the frontal cluster (F(1,28) �15.606, P � 0.001) and for the central cluster (F(1,28) �4.686, P � 0.05) with higher activity at the arm. A significant“stimulation method” � “covariate” effect was found at 80milliseconds for the frontal cluster (F(1,28) � 6.377, P �0.05) and for the central cluster (F(1,28) � 9.834, P � 0.005)and at 150 milliseconds for the frontal cluster (F(1,28) � 4.11,P � 0.05) and the central cluster (F(1,28) � 5.586, P � 0.05)with higher activity at the intramuscular stimulation (Fig. 3).In addition, the “location” � “stimulation method” � “co-variate” effect was significant at 80 milliseconds at the centralcluster (F(1,28) � 4.897, P � 0.05) with higher activity at theintramuscular arm stimulation compared with the intracuta-neous back stimulation as well as higher activity at theintracutaneous arm stimulation compared with intramuscularback stimulation and at 150 milliseconds at the central cluster(F(1,28) � 4.566, P � 0.05) with higher activity at theintramuscular arm stimulation compared with the intracuta-neous back stimulation as well as higher activity in intramus-cular back stimulation compared with the intracutaneous armstimulation.
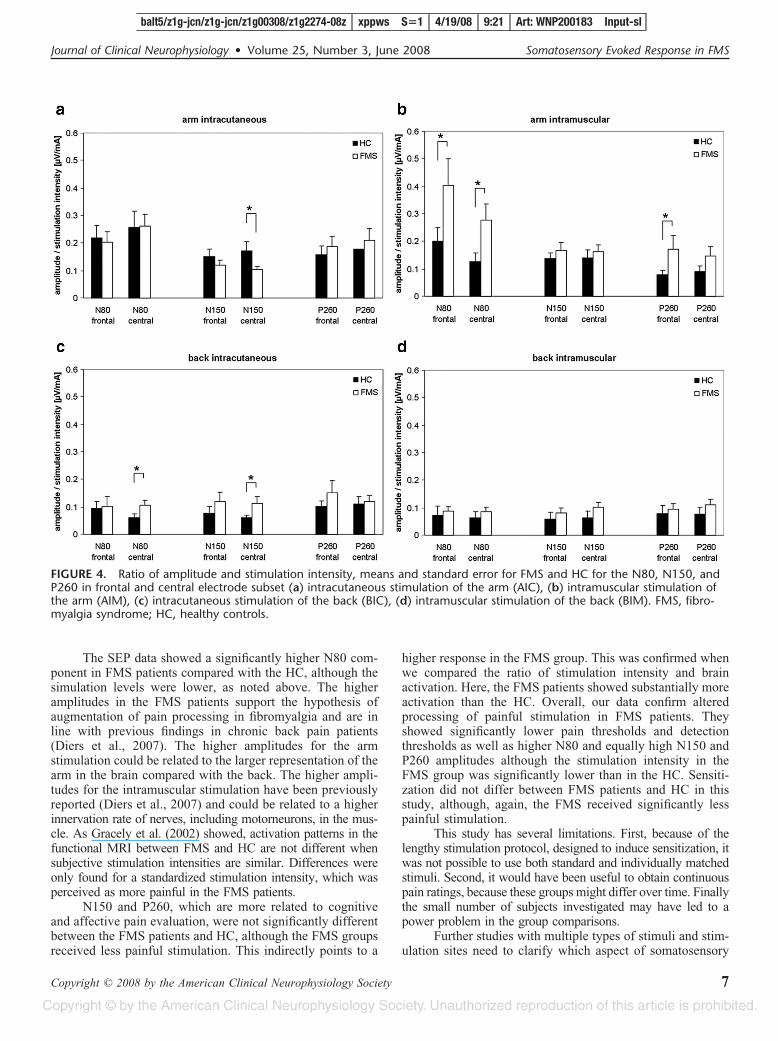
A comparison of the ratio of amplitude and stimulationintensity showed that FMS patients needed lower stimulationintensities for a similar level of brain activation compared
with the HC. The ration was significantly higher in the FMSpatients for intracutaneous stimulation of the arm at 150milliseconds (central cluster: t(28) � �1.746, P � 0.05), forintramuscular stimulation of the arm at 80 milliseconds (fron-tal cluster: t(28) � 1.816, P � 0.05, central cluster: t(28) �2.236, P � 0.05) and at 260 milliseconds (frontal cluster:t(28) � 1.712, P � 0.05), as well as for intracutaneousstimulation of the back at 80 milliseconds (central cluster:t(28) � 1.845, P � 0.05) and at 150 milliseconds (centralcluster: t(28) � 1.878, P � 0.05) (Figs. 4a–d).
DISCUSSIONThe data of this study showed significant sensitization
for AIM and BIM in both groups, chronic fibromyalgiapatients, and HC, although the FMS group received signifi-cantly lower levels of noxious stimulation. This is in contra-diction to a number of previous studies (eg, Petzke et al.,2003; Staud et al., 2003) that reported more perceptualsensitization in the FMS patients compared with HC. Staud etal. (2003) stimulated the flexor digitorum muscle of theforarm mechanically, Petzke et al. (2003) the right thumbnailand left thumb mechanically and the left forearm with heatstimuli. We delivered electrical stimuli, which may not havethe same effect. Because our HC showed sensitization ratherthan habituation, the larger number of painful stimuli and thehigh frequency might have prevented habituation in the HC.Our HC group consisted of more men than our FMS group,although the difference was not significant. To eliminate apossible gender effect we reduced the sample to archive aidentical number of men in both groups (age-matched). How-ever, also a perfectly matched sample showed no significantgroup effect of sensitization. Using the stimulation intensityas a covariate also lead to no significant group difference.However, as noted above FMS patients were stimulated at amuch lower level than the HC. Thus, the equivalence of thesensitization of both groups suggests that the FMS group wasactually more affected by the pain.
Sorensen et al. (1998) found lowered pain levels afterrepeated electrical stimulation at the anterior tibial muscle inpatients with FMS compared with HC. Scudds et al. (1987)and Arroyo and Cohen (1993) found lowered pain thresholdsand pain tolerance to electrical stimuli in patients with fibro-myalgia. This is in accordance with our findings, where weobserved significantly lower thresholds in the FMS group.
FIGURE 3. Means and standard errors of the root mean square activity of the central electrode subset in the four stimulationconditions for the 80 milliseconds (a), the 150 milliseconds (b), and the 260 milliseconds time window (c). FMS, fibromyalgiasyndrome; HC, healthy controls.
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
M. Diers et al. Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008
Copyright © 2008 by the American Clinical Neurophysiology Society6
F3, AQ:3
F4
The SEP data showed a significantly higher N80 com-ponent in FMS patients compared with the HC, although thesimulation levels were lower, as noted above. The higheramplitudes in the FMS patients support the hypothesis ofaugmentation of pain processing in fibromyalgia and are inline with previous findings in chronic back pain patients(Diers et al., 2007). The higher amplitudes for the armstimulation could be related to the larger representation of thearm in the brain compared with the back. The higher ampli-tudes for the intramuscular stimulation have been previouslyreported (Diers et al., 2007) and could be related to a higherinnervation rate of nerves, including motorneurons, in the mus-cle. As Gracely et al. (2002) showed, activation patterns in thefunctional MRI between FMS and HC are not different whensubjective stimulation intensities are similar. Differences wereonly found for a standardized stimulation intensity, which wasperceived as more painful in the FMS patients.
N150 and P260, which are more related to cognitiveand affective pain evaluation, were not significantly differentbetween the FMS patients and HC, although the FMS groupsreceived less painful stimulation. This indirectly points to a
higher response in the FMS group. This was confirmed whenwe compared the ratio of stimulation intensity and brainactivation. Here, the FMS patients showed substantially moreactivation than the HC. Overall, our data confirm alteredprocessing of painful stimulation in FMS patients. Theyshowed significantly lower pain thresholds and detectionthresholds as well as higher N80 and equally high N150 andP260 amplitudes although the stimulation intensity in theFMS group was significantly lower than in the HC. Sensiti-zation did not differ between FMS patients and HC in thisstudy, although, again, the FMS received significantly lesspainful stimulation.
This study has several limitations. First, because of thelengthy stimulation protocol, designed to induce sensitization, itwas not possible to use both standard and individually matchedstimuli. Second, it would have been useful to obtain continuouspain ratings, because these groups might differ over time. Finallythe small number of subjects investigated may have led to apower problem in the group comparisons.
Further studies with multiple types of stimuli and stim-ulation sites need to clarify which aspect of somatosensory
FIGURE 4. Ratio of amplitude and stimulation intensity, means and standard error for FMS and HC for the N80, N150, andP260 in frontal and central electrode subset (a) intracutaneous stimulation of the arm (AIC), (b) intramuscular stimulation ofthe arm (AIM), (c) intracutaneous stimulation of the back (BIC), (d) intramuscular stimulation of the back (BIM). FMS, fibro-myalgia syndrome; HC, healthy controls.
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008 Somatosensory Evoked Response in FMS
Copyright © 2008 by the American Clinical Neurophysiology Society 7
processing is altered in FMS. The data of our study supportintervention techniques aimed at reducing sensitization inFMS (eg, Thieme et al., 2006).
REFERENCESApkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mecha-
nisms of pain perception and regulation in health and disease. Eur JPain 2005;9:463–484.
Arroyo JF, Cohen ML. Abnormal responses to electrocutaneous stimulationin fibromyalgia. J Rheumatol 1993;20:1925–1931.
Babiloni C, Babiloni F, Carducci F, et al. Mapping of early and late humansomatosensory evoked brain potentials to phasic galvanic painful stim-ulation. Hum Brain Mapp 2001;12:168–179.
Bromm B, Lorenz J. Neurophysiological evaluation of pain. Electroencepha-logr Clin Neurophysiol 1998;107:227–253.
Bromm B. Brain images of pain. News Physiol Sci 2001;16:244–249.Bromm B. The involvement of the posterior cingulate gyrus in phasic pain
processing of humans. Neurosci Lett 2004;361:245–249.Burckhard CS, Clark SR, Bennett RM. The fibromyalgia impact question-
naire: development and validation. J Rheumatol 1991;18:728–733.Chen AC, Shimojo M, Svensson P, Arendt-Nielsen L. Brain dynamics of scalp
evoked potentials and current source densities to repetitive (5-pulse train)painful stimulation of skin and muscle: central correlate of temporalsummation. Brain Topogr 2000;13:59–72.
Diers M, Koeppe C, Diesch E, et al. Central processing of acute muscle painin chronic low back pain patients: a EEG mapping study. J ClinNeurophysiol 2007;24:76–83.
Dixon WJ, Tukey JW. Approximate behavior of the distribution of Win-sorized t (Trimming/Winsorization II). Technometrics 1968;10:83–98.
Dowman R. SEP topographies elicited by innocuous and noxious sural nervestimulation. I. Identification of stable periods and individual differences.Electroencephalogr Clin Neurophysiol 1994;92:291–302.
Dowman R, Darcey TM. SEP topographies elicited by innocuous andnoxious sural nerve stimulation. III. Dipole source localization analysis.Electroencephalogr Clin Neurophysiol 1994;92:373–391.
Dowman R. Pain-evoked anterior cingulate activity generating the negativedifference potential may reflect response selection processes. Psycho-physiology 2002;39:369–379.
Flor H, Behle DJ, Birbaumer N. Assessment of pain-related cognitions inchronic pain patients. Behav Res Ther 1993;31:63–73.
Flor H, Rudy TE, Birbaumer N, et al. Zur Anwendbarkeit des WestHaven-Yale Multidimensional Pain Inventory im deutschen Sprach-raum. Der Schmerz 1990;4:82–87.
Geissner E. Die Schmerzempfindungsskala SES - Ein differenziertes undveranderungssensitives Verfahren zur Erfassung chronischer und akuterSchmerzen. Rehabilitation 1995;34:XXXV–XLIV.
Gibson SJ, Littlejohn GO, Gorman MM, et al. Altered heat pain thresholdsand cerebral event-related potentials following painful CO2 laser stim-ulation in subjects with fibromyalgia syndrome. Pain 1994;58:185–193.
Gracely RH, Petzke F, Wolf JM, Clauw DJ. Functional magnetic resonanceimaging evidence of augmented pain processing in fibromyalgia. Ar-thritis Rheum 2002;46:1333–1343.
Hautzinger M, Bailer M. Allgemeine Depressions Skala (ADS) [GeneralDepression scale]. Beltz Test, Weinheim; 1993.
Lorenz J, Grasedyck K, Bromm B. Middle and long latency somatosensoryevoked potentials after painful laser stimulation in patients with fibro-myalgia syndrome. Electroencephalogr Clin Neurophysiol 1996;100:165–168.
Lorenz J. Hyperalgesia or hypervigilance? An evoked potential approach to thestudy of fibromyalgia syndrome. Z Rheumatol 1998;57(suppl 2):19–22.
Montoya P, Sitges C, Garcıa-Herrera M, et al. Abnormal affective modula-tion of somatosensory brain processing among patients with fibromy-algia. Psychosom Med 2005;67:957–963.
Niddam DM, Graven-Nielsen T, Arendt-Nielsen L, Chen AC. Non-painfuland painful surface and intramuscular electrical stimulation at the thenarand hypothenar sites: differential cerebral dynamics of early to latelatency SEPs. Brain Topogr 2001;13:283–292.
Niddam DM, Yeh TC, Wu YT, et al. Event-related functional MRI study oncentral representation of acute muscle pain induced by electrical stim-ulation. Neuroimage 2002;17:1437–1450.
Nuwer MR, Lehmann D, da Silva FL, et al. IFCN guidelines for topographicand frequency analysis of EEGs and EPs. Report of an IFCN committee.The International Federation of Clinical Neurophysiology. Electroen-cephalogr Clin Neurophysiol 1994;91:1–5.
Okifuji A, Turk DC, Sinclair JD, et al. A standardized manual tender pointsurvey. I. Development and determination of a threshold point for theidentification of positive tender points in fibromyalgia syndrome.J Rheumatol 1997;24:377–383.
Petzke F, Clauw DJ, Ambrose K, et al. Increased pain sensitivity infibromyalgia: effects of stimulus type and mode of presentation. Pain2003;105:403–413.
Pfingsten M, Kroner-Herwig B, Leibing E, et al. Validation of the Germanversion of the Fear-Avoidance Beliefs Questionnaire (FABQ). Eur JPain 2000;4:259–266.
Reinert A, Treede R, Bromm B. The pain inhibiting pain effect: an electro-physiological study in humans. Brain Res 2000;862:103–110.
Scudds RA, Rollman GB, Harth M, McCain GA. Pain perception andpersonality measures as discriminators in the classification of fibrositis.J Rheumatol 1987;14:563–569.
Shimojo M, Svensson P, Arendt-Nielsen L, Chen AC. (2000) Dynamic braintopography of somatosensory evoked potentials and equivalent dipolesin response to graded painful skin and muscle stimulation. Brain Topogr2000;13:43–58.
Sorensen J, Graven-Nielsen T, Henriksson KG, et al. Hyperexcitability infibromyalgia. J Rheumatol 1998;25:152–155.
Staud R, Cannon RC, Mauderli AP, et al. Temporal summation of pain frommechanical stimulation of muscle tissue in normal controls and subjectswith fibromyalgia syndrome. Pain 2003;102:87–95.
Stevens A, Batra A, Kotter I, et al. Both pain and EEG response to coldpressor stimulation occurs faster in fibromyalgia patients than in controlsubjects. Psychiatry Res 2000;97:237–247.
Svensson P, Minoshima S, Beydoun A, et al. Cerebral processing of acuteskin and muscle pain in humans. J Neurophysiol 1997;78:450–460.
Thieme K, Flor H, Turk DC. Psychological pain treatment in fibromyalgiasyndrome: efficacy of operant behavioral and cognitive behavioraltreatments. Arthritis Res Ther 2006;8:R121.
Tukey JW, McLaughlin DH. Less vulnerable confidence and significanceprocedures for location based on a single sample: trimming/Winsoriza-tion I. Sankhya Series A 1963;25:331–352.
Valeriani M, Le Pera D, Niddam D, et al. Dipolar modelling of the scalpevoked potentials to painful contact heat stimulation of the human skin.Neurosci Lett 2002;318:44–48.
von Zerssen D, Koeller DM. Beschwerden-Liste [General Somatic Com-plaints Scale]. Hogrefe, Gottingen; 1976.
Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheuma-tology 1990 criteria for the classification of fibromyalgia. report of themulticenter criteria committee. Arthritis Rheum 1990;33:160–172.
balt5/z1g-jcn/z1g-jcn/z1g00308/z1g2274-08z xppws S�1 4/19/08 9:21 Art: WNP200183 Input-sl
M. Diers et al. Journal of Clinical Neurophysiology • Volume 25, Number 3, June 2008
Copyright © 2008 by the American Clinical Neurophysiology Society8
JOBNAME: AUTHOR QUERIES PAGE: 1 SESS: 1 OUTPUT: Sat Apr 19 09:21:34 2008/balt5/z1g�jcn/z1g�jcn/z1g00308/z1g2274�08z
1—The abstract has been set as a single paragraph and the internal heads have been deleted, asstructured abstracts are not allowed per journal style.
2—Please check whether Tables 1 and 2 are OK as typeset.
3—Please provide better quality of figure 3.
4—Kindly provide the department/division details of second affiliation.
AUTHOR QUERIES
AUTHOR PLEASE ANSWER ALL QUERIES 1
Copyright © 2022 FDOKUMEN




















