
Centerline Aug Sept2012
40
VAR VAR VA A IAN IAN ME ME ME M M DIC DIC DIC AL AL L SYS SYS YS YS YS YS YS S Y S YS S S S S S T T T TE TE TE TE TE TE TE TE EM TEM EM E TEM TEM TEM EM T TE EM EM E TE TE E TEM EM E E M EM E EM EM M M TEM M T T TE M T M T T EM EM M TE M T EM T EM EM M EM T M M M M S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S S VAR VAR R AN AN AN AN ME M DIC DI DI AL AL L SY Y S S S SY S T T T E T E TE EM EM EM M E M M E E M S S S S S S S S S S S S S S S S S S S S S S S S S S S S S | | | | | | | | | | | | | | | | | | | | | | N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N EWS EWS EW EWS EWS EWS EWS EWS W EWS W EWS WS EWS EW EWS S S S S EWS EWS S EWS EWS EWS EWS W W EWS EWS E WS W WS E EW E EWS EWS E E W E EWS W W EWS EWS E EWS EW E EWS EWS EWS EWS EWS E EWS W E E W W E WS EW W W W EWS WS W EWS W E FO FO FO FO FO O O O O O O O FO FO O FO FO O O FO FO FO FO FO FO F FO FO FO F FO FO F FO FO FO F O O FO FO F FO O O F F F F F FO F F F F R T R T R T R R R R R R R R HE CLI NIC AL ONC NC O OL LO LO O O G GY GY GY Y G Y Y Y Y Y Y C C C COM OM C C C C O OM CO CO O M MU MU MUN MUN N IT I ITY TY Y T Y | | | A A A UG UG UG UGU U ST– T ST– ST SEP SEP SE S TEM M TEM BER BER BER BER 20 20 20 20 12 12 12 N N N N N N N N N N N N N N EWS S EWS EWS EWS EWS EWS EWS EWS W W W WS EWS W W WS S W S W EWS S S O O O O O O O O O O R T R R HE CLI NIC AL ONC O OLO O O O O G G Y Y COM COM CO MU M M UN IT I T TY Y Y Y I | A A A A UG G U ST– SEP S TEM E ER R ER 20 20 0 12 12 Designing an SABR Program Lahey Clinic Builds In Collaboration, Communication, and QA Radiosurgery Stereotactic Approaches to Treating Early-Stage Lung Cancer Meaningful Use New Mexico Cancer Center Gets Head Start with ARIA System Virtualization Latest Varian Software Moves into the Cloud
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Centerline Aug Sept2012

VARVARVAA IANIAN MEMEMEMM DICDICDICALALL SYSSYSYSYSYSYSYSSYSYSSSSSSSTTTTETETETETETETETEEMTEMEMETEMTEMTEMEMTTEEMEMETETEETEMEMEEMEMEEMEMMMTEMMTTTEMT MTTEMEMMTEMTEMTTEMEMMEMT MMMMT MMSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSVARVARR ANANANAN MEM DICDIDI ALALL SYYSSSSYS TTTTETETEEMEMEMMTEMMMEEMSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSSS ||||||||||||||||||||||||||||| NNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNNEWSEWSEWEWSEWSEWSEWSEWSWEWSWEWSWSEWSEWEWSSSSSEWSEWSSEWSEWSEWSEWSWWEWSEWSEWSWWSEEWEEWSEWSEEWWEEWSWWEWSEWSEEWSEWEEWSEWSEWSEWSEWSEEWSWEEWWEWSEWWWWEWSWSWEWSWEEW FOFOFOFOFOOOOOOOOFOFOOFOFOOOFOFOFOFOFOFOFFOFOFOFFOFOFFOFOFOFOOFOFOFFOOOFFFFFFOFFFFFOR TR TR TR R RRRRRRRR HE CL INICAL ONCNCOOLLOLOOOGGYGYGYYGYYYYYY CCCCOMOMCCCCOOMCOCOO MMUMUMUNMUNNITIITYTYYTY ||| AAAUGUGUGUGUUST–TST–ST SEPSEPSES TEMMTEMBERBERBERBERB 20202020121212NNNNNNNNNNNNNNEWSSEWSEWSEWSEWSEWSSEWSEWSWWWWSEWSWWWSSWEWSWEWSSEWS OOOOOOOOOOR TRR HE CLINICAL ONCOOLOOOOOGGYY COMCOMCO MUMMUNITITTYYYYI | AAAAUGGUST–SEPSS TEM EERRER 202001212
Designing an SABR Program Lahey Clinic Builds In Collaboration, Communication, and QA
RadiosurgeryStereotactic Approaches to Treating Early-Stage Lung Cancer
Meaningful UseNew Mexico Cancer Center Gets Head Start with ARIA System
VirtualizationLatest Varian Software Moves into the Cloud

Centerline magazine is published by
Varian Medical Systems, varian.com.
Centerline welcomes letters to the
editor, contributions for point-of-view
commentaries, and suggestions for ar-
ticles. Reprinting of Centerline articles
may take place with permission from
the editor. Address comments, contri-
butions, inquiries about reprints and
permissions, subscription requests,
and address changes to:
Varian Medical Systems
3100 Hansen Way, M/S MGM
Palo Alto, CA 94304-1038
Attn: Meryl Ginsberg
+1 650.424.6444
On the cover
At the Lahey Clinic’s Sophia Gordon
Cancer Center, Andrea McKee, MD,
is passionate about finding and treat-
ing lung cancer.
© 2012 Varian Medical Systems, Inc. All rights reserved. Varian, Varian Medical Systems, the Varian Medical Systems logo, ARIA, Beacon, Calypso, Clinac, GPS for the Body, On-Board Imager, RapidArc, Smart Segmentation, and Trilogy are registered trademarks and Eclipse, Pivotal, PortalVision, PremierAssurance, ProBeam, TrueBeam, and Tx are trademarks of Varian Medical Systems, Inc. Access 360 and kVue are trademarks of Qfix Systems. EQUICARE CS is a trademark of Cogent Health Solutions. The names of other companies and products mentioned herein are used for identification purposes only and may be trademarks or registered trademarks of their re-spective owners.
CONTENTS AUGUST–SEPTEMBER 2012
FEATURES
Radiosurgery for NSCLC 10A number of clinicians have begun to take a look at the viability of SBRT/ SABR for treating high-risk, operable early-stage NSCLC.
Designing an SABR Program 15At the Lahey Clinic’s Sophia Gordon Cancer Center, a successful SABR program builds in collaboration, communication, and QA.
Rescue Lung, Rescue Life 20Free lung cancer screening programs can save lives with early detection. The Lahey Clinic shares its model.
Prone Breast Treatments 22Recent research suggests that prone positioning may lead to better outcomes for some breast cancer patients. Varian technology can help.
Software Virtualization 25Varian’s ARIA® and Eclipse™ systems move into the cloud—and become accessible from wherever users happen to be.
Meaningful Use 28Establishing “meaningful use” may be easier than you think—especially if you follow the example of New Mexico Cancer Center.
Real-Time Tracking 31Calypso® tumor tracking technology has now been incorporated into Varian’s Pivotal™ Treatment Solution for Prostate Care.
TrueBeam Deployments 34Cancer centers around the world are deploying the TrueBeam™ system for image-guided radiotherapy and radiosurgery.
DEPARTMENTS
Point of View 1At Varian, our job is to innovate, to simplify, and to provide support so that you can focus energy—literally and figuratively—on saving lives, says Kolleen Kennedy, president of Varian’s Oncology Systems business.
News 3
Varian and Siemens Healthcare announce global collaboration
Varian publishes first corporate sustainability report
Campaign educates consumers about RT
Eclipse software features new segmentation and contouring tool
High dose delivery and prone breast treatment capabilities added to Varian linacs
EQUICARE CS™ cancer survivorship software recognized
Surface Beacon® transponder receives FDA clearance
Varian introduces new service and support packages
Treatment planning workshops come to South America
Scripps hits major milestones with proton therapy project
Centers in Puerto Rico and Venezuela launch RapidArc® programs
Contest sends Brazilian medical physicist to Miami for training
Varian establishes training center and help desk in Tokyo
CENTERLINE | AUGUST–SEPTEMBER 2012 | 1
Imagine: a world without fear of cancer. At Varian, that’s the vision that galvanizes us, and we believe it’s at the heart of your vision, too. Every day, millions of people
summon the strength to confront cancer. Cancer treatment professionals the world over do what they can to help patients battle this challenging disease. At Varian, our job is to innovate, to simplify, and to provide support so that you can focus energy—literally and figuratively—on saving lives. Our goal is to unite with you in the common purpose of fighting cancer.
In my nearly 15 years at Varian, I have had the opportunity to be at the helm of our Product Management, Marketing, Engineering, and Customer Support Services organizations. My experiences in these roles, and my interactions with customers across the globe, have helped to shape my current leadership priorities. It all starts with putting patient care first.
As president of Varian’s Oncology Systems business, key values that I emphasize as guiding principles include in-tegrity, collaboration, quality, accountability, innovation, and making sure we are taking a global view by understand-ing the needs of the markets in which we operate, and not assuming that a one-size-fits-all solution will make clinical or economic sense in all settings.
In the spirit of these values, we’re focusing our attention in these areas:
Customer intimacy. We are working to develop our cross-functional ability to deliver a complete and consis-tently attentive end-to-end customer experience. This means speaking with one voice and providing accessible, responsive touch points for customers to interact with our teams, from the product development engineers to the service people, from the sales organization to the education program managers.
A World Without Fear of CancerBy Kolleen Kennedy, president of Varian’s Oncology Systems business
POINT OF VIEW

2 | CENTERLINE | AUGUST–SEPTEMBER 2012
Quality and safety. We recognize that radiotherapy has become a technologically sophisticated process that requires all stakeholders—manufacturers, regulators, and the clinical community—to play an important role. We’re focused on doing our part to build safety elements into our products and training programs. Continuing in the direction we took with ARIA® version 11, we are designing tools that can be configured to support and automate important aspects of your quality program.
Innovation. Building on our long history of developing new tools that make it possible for clinicians to improve the quality of cancer treatment, we’re working to make those tools simpler and easier to use, as well as more efficient. Areas of emphasis are: technologies that simplify SRS and SBRT planning and delivery, specific disease-site solutions, and systems that are customizable to meet different clinical needs and objectives.
Education. Varian’s Global Education and Training team headquarters is in Las Vegas, Nevada, where the company operates the largest corporate radiotherapy training center in the world. Varian has also built a network of education centers, with sites in India, China, Japan, and Europe, to respond to the need for training locally and in multiple languages around the world. In 2012 we announced plans to build a center in Brazil. We have greatly expanded our sponsorship of continuing education programs, online webinars, and peer-to-peer training programs that connect experienced clinicians with those adopting new technology.
Research. Varian spent more than US$170 million on research and development in 2011. Each year we routinely commit significant revenues to support research initiatives, with more than 100 active research projects spanning five continents. Links with partners in academia and industry strengthen our position at the leading edge of science and technology by providing access to thought leaders, novel R&D tools, and data on emerging trends.
This is the “how” of our mission—what we’re doing to join with you to realize the vision of a world without fear of cancer. We want to help you save another 100,000 lives each year. I know that some of the goals articulated here are ambitious and require significant efforts on our part to deliver. I’d love to hear from you as to how we are doing and invite you to get in touch at this e-mail address: ca@varian .com. It’s a pleasure and a privilege to support you. We’re united in purpose to help you fight cancer. n
Kolleen Kennedy, MS, was recently ap-pointed president of Varian’s Oncology Systems business. (Kennedy’s predecessor, Dow Wilson, stepped into the role of chief operating officer.) Kennedy assumed her new position after nearly 15 years at Varian in a variety of management roles. Most
recently, she served as vice president of Varian’s worldwide Customer Support Services (CSS) organization. Under her leader-ship, Varian’s CSS organization was rated the #1 service provider among linear accelerator manufacturers every year by IMV, Ltd., an independent healthcare market research firm that analyzes service trends.
At Varian, our job is to innovate, to simplify, and to provide support so that you can focus energy—literally and figuratively—on saving lives. Our goal is to unite with you in the common purpose of fighting cancer.

CENTERLINE | AUGUST–SEPTEMBER 2012 | 3
Varian and Siemens Healthcare announce global collaboration
Earlier this year, Varian and Siemens Health-care announced a global strategic partner-ship to provide advanced diagnostic and therapeutic solutions and services for treat-ing cancer with image-guided radiotherapy and radiosurgery. The collaboration covers the mutual marketing and representation of products for imaging and treatment in the global radiation oncology business. It also includes the development of software inter-faces between Siemens treatment systems and Varian’s ARIA® oncology information system. The partners will also investigate opportunities for joint development of new products for image-guided radiotherapy and radiosurgery.
Under the agreement, Varian will represent Siemens diagnostic imaging products such as CT, PET/CT, and MRI to radiation oncol-ogy clinics around the world, beginning immediately in most international markets and expanding to North America later this year.
Siemens Healthcare will similarly repre-sent Varian equipment and software for radiotherapy and radiosurgery within its offerings to its healthcare customers. This will enable the two companies to offer com-prehensive solutions to support the entire clinical workflow from imaging to treat-ment. Siemens will continue to service and support its global installed base of approxi-mately 2,000 medical linear accelerators. The agreement will give Siemens custom-ers more choices for therapy equipment, including smooth transition and interface to Varian equipment, as aging accelerators are due for replacement.
Varian and Siemens will also develop in-terfaces that will connect Varian’s ARIA software with Siemens accelerators and imaging systems to give clinics more options for improving workflow and streamlining operations. The collaboration enables Varian and Siemens to codevelop and offer cancer treatment centers new imaging and treatment solutions utiliz-ing the strengths and technology of both companies. n
Varian publishes first corporate sustainability report
Varian has published its first comprehen-sive corporate social responsibility (CSR) report, detailing the company’s policies and achievements in extending care, protect-ing resources, and helping to save lives. The Varian Sustainability Report has been produced as part of the company’s wider investment to continually improve sustain-ability performance and transparency.
“We have a responsibility to achieve our business goals in a socially and environ-mentally responsible manner,” says Tim Guertin, Varian chief executive officer. “While our company continues to develop better therapeutic capabilities for fighting cancer and other diseases as well as better components for X-ray imaging, we strive to do so in ways which extend access to advanced care, improve clinical outcomes, optimize safety, and make a positive impact on the communities where we operate.”
Campaign educates consumers about RTVarian has launched a direct-to-consumer print campaign promoting the TrueBeam™ system, along with an online educational campaign on radiosurgery.
The print ads are designed to educate consumers about radiotherapy and radio-surgery as options for cancer treatment, and to raise awareness of TrueBeam as a powerful treatment technology. The U.S. campaign began in April and will run through November 2012, with ads featured in the Sunday New York Times magazine.
“All ads have a toll-free number that patients can call to request more information and obtain the names of treatment centers near them,” says Lee Wills, Varian’s director of marketing communications. “We believe that patients will also contact their physicians to ask more questions.”
In addition to the print ads, Varian is running a national online campaign that combines banner ads, pay-per-click ads, organic searches, social media, and rich content to educate consumers and referring physicians about radiosurgery. Patients will be guided to a patient portal for more information and to find out how to contact a treatment center near them.
“We encourage sites with Varian technology to leverage our investment in this campaign by promoting their expertise,” says Wills. “We have a variety of programs available to assist in marketing cancer treatment centers equipped by Varian.” For more information, contact [email protected]. n
CENTERLINE NEWS

4 | CENTERLINE | AUGUST–SEPTEMBER 2012
In 2010, Varian commenced a company-wide undertaking to examine sustainability performance and identify challenges and opportunities to be addressed over time. This effort involved the close participation of senior leaders from all divisions, key geographies, and core functions.
The report, based on internationally rec-ognized global reporting initiative (GRI) parameters, reiterates the company’s stated mission to help save an additional 100,000 lives each year, while outlining the governance structure that determines Varian’s sustainability activities and setting goals for future achievements. The report’s content is divided into four key areas: en-vironmental, health access and outcomes, safety and responsibility, and colleagues and communities.
The sustainability report is available for customers, investors, and the general public at varian.com/sustainability. Varian plans to update the report in mid-2012. n
Eclipse software features new segmentation and contouring tool
Varian has received FDA 510(k) clearance for a new radiotherapy treatment planning tool designed to work with the company’s market-leading Eclipse™ treatment plan-ning software to reduce the amount of time needed for contouring images in the radiotherapy treatment planning process.
With Smart Segmentation® Knowledge-Based Contouring, Varian has combined two techniques:
Smart Segmentation, which analyzes anatomical images, drawing on informa-tion about human anatomy to identify and outline organs and other structures.
Knowledge-Based Contouring, which allows the clinician to start the planning process by drawing on a library of expertly precontoured images that have important
High dose delivery and prone breast treatment capabilities added to Varian linacsClinac® and Trilogy® medical linear accelerators have been updated to deliver higher dose rates—up to 2,400 monitor units per minute—a capabil-ity that was previously available only on the TrueBeam™ machine.
Updated control software, which re-ceived 510(k) clearance from the U.S. Food and Drug Administration (FDA) late last year, adds a High-Intensity Mode to the Clinac and Trilogy ma-chines, doubling their former highest output.
“Our High-Intensity Mode enables treatments that are up to 50 percent faster compared to standard treat-ment modes,” says Corey Zankowski, vice president of product manage-ment for Varian’s Oncology Systems business. “High-Intensity Mode is a response to trends toward the use
of hypofractionation and radio-surgery for many types of cancer, which means that higher doses are delivered in just one or a few treat-ment sessions for quick ablation of a tumor. There has been encouraging research supporting this approach for the treatment of cancers of the brain, spine, and lung, as well as for prostate cancer. With High-Intensity Mode, our Clinac and Trilogy machines can deliver these high-dose treatments within a clinically feasible timeframe.”
Varian has also received FDA clear-ance for the Pivotal™ Care Solution for Prone Breast Treatment, an in-novation that allows patients to be treated in the prone position. The new linac control software now makes it possible to use the Clinac or Trilogy machine for prone breast treatments—an approach that allows the breast to move away from the chest wall, often reducing the volume of lung and heart tissue exposed to radiation (see article on page 22).
“The Pivotal Solution makes it pos-sible to treat the breast below the couch top, enabling physicians to choose this approach if it is best for a particular patient,” says Agam Sharda, Varian’s manager of treat-ment solutions marketing. “Varian is committed to providing clinicians with tools that make it possible to offer cancer patients advanced treat-ments that have the best likelihood of a positive outcome.” n
C E N T E R L I N E N E W S

CENTERLINE | AUGUST–SEPTEMBER 2012 | 5
anatomical structures already outlined. The clinician then uses a deformable registra-tion process for matching the precontoured images with those of the patient to create the desired contours.
“It’s similar to building a house from scratch or remodeling. Remodeling is generally faster because you have something to work from,” says Jefferson Amacker, director of clinical solutions at Varian. “Both of these tools give clinicians a head start, so the contouring task can be more easily and quickly completed.”
“Inconsistencies in contouring targets and critical structures can undermine the precision of modern conformal radiation therapy,” says Vincenzo Valentini, MD, professor of radiation oncology at the Università Cattolica del Sacro Cuore in Rome, Italy.
“Inter- and even intraobserver variability remain high,” explains Valentini. “Target delineation remains the only procedure that is largely manual, making it a time-consuming step in radiotherapy planning. The introduction of autosegmentation software is attractive for its potential in terms of time savings, and also for facilitat-ing standardization. It could have a role in training junior staff and residents as they develop their delineation skills. It could also support standardization of the process between centers, to facilitate multicenter research projects as well as networked radiation oncology services.”
Smart Segmentation Knowledge-Based Contouring can be used in conjunction with the Eclipse treatment planning system to create plans for external beam or brachy-therapy treatments. Varian’s proprietary and patented Knowledge-Based Contour-ing tool contains an anatomy atlas that covers many of the areas of the body commonly treated with radiotherapy when cancer has been detected, including the breast, prostate, lung, brain, head and neck, rectum, and gynecological organs. n
EQUICARE CS cancer survivorship case manage-ment software recognized
EQUICARE CS™, the cancer survivorship case management software program jointly offered by Varian and Equicare Health, has been included in the Best Practices Re-pository compiled by the American College of Surgeons Commission on Cancer. The repository is a list of resources designed
to help cancer treatment centers in the United States adopt rigorous standards for high-quality, patient-centered care, in order to qualify to become CoC-accredited cancer programs.
“Cancer survivors benefit most when they have access to coordinated post-treatment care,” says Chris Hanna, IT product spe-cialist at Varian. “Therefore, the CoC has mandated that all organizations seeking
Surface Beacon transponder receives FDA 510(k) clearance
Varian has received 510(k) clearance from the FDA for a new transponder to be used with the Calypso® system as a real-time tracking device for monitoring motion during radiotherapy treatments anywhere on the body. The Surface Beacon® transponder is placed tempo-rarily on the skin for real-time tracking of respiratory and other patient motion during radiotherapy, expanding the number of cancer sites for which the Calypso technology can be used.
“The new surface transponder can be placed on a patient’s chest wall to monitor respiratory motion during radiotherapy,” says Edward Vertatsch-itsch, PhD, general manager of Varian’s
real-time tracking technology organiza-tion. “It is designed to improve target-ing in some of the most prevalent types of cancer, including breast cancer.”
For example, chest wall monitoring during treatment of the left breast can be correlated with the position of the heart. By monitoring this position in real time, clinicians can design treatments that eliminate or significantly reduce dose to the heart.
Varian acquired Calypso in October 2011 to extend the company’s range of real-time tracking tools for enhancing the precision of radiotherapy treatments. n

6 | CENTERLINE | AUGUST–SEPTEMBER 2012
their accreditation will have to create a formal plan for delivering survivorship care by 2014, and they will have to implement that plan by 2015. EQUICARE CS can help them comply with these requirements.”
The EQUICARE CS case management system was specifically designed to help clinics provide cancer survivors with a personalized plan for follow-up care. It is a web-based, patient-centric tool that is intended to help cancer survivors, their caregivers, and their healthcare providers achieve better clinical compliance, which can result in improved patient outcomes following treatment for cancer.
“The EQUICARE CS system guides clini-cians in generating a care plan based on best practices and established guidelines,” says Hanna. “It offers patients round-the-clock access to their care plans through a personalized portal on the Internet. We are very gratified that the American College of Surgeons has recognized the value of this system.” n
Varian introduces new service and support packages
Late last year, Varian introduced a new PremierAssurance™ program offering flex-ible access to a broad spectrum of services from Varian’s world-class customer support organization, through customized, com-prehensive service plans for technology maintenance and upgrades, help desk support, training and education, consult-ing services, and site-specific clinic design solutions. The flexible service packages are designed to help radiotherapy departments maximize technology uptime, predict and control costs, plan for upgrades, and stay abreast of new technology developments.
“In designing the new PremierAssurance program, we focused on how to help cus-tomers get the most out of their invest-ments in Varian technology,” says Kevin O’Reilly, senior director of services market-ing. “The new packages are flexible in order to meet the needs of diverse customers, from large centers with internal service departments to small clinics that depend on Varian for every aspect of service. Pre-mierAssurance is all about choices, and enabling customers to pick the specific levels of service they want and need.”
With PremierAssurance, customers can choose support packages at distinct service levels covering four broad areas: installa-tion, service, help desk, and training and education.
“Varian has been building an extensive portfolio of service capabilities over many years. We have over 2,000 highly skilled professionals, including service engineers, project managers, installation engineers, trainers, and clinical help desk and support
staff located worldwide for fast response to customers’ needs,” O’Reilly says. “Our training teams partner with customers to meet their immediate and long-term goals in maximizing their use of Varian products through carefully structured classroom, onsite, and electronic learning programs. Now, with PremierAssurance, we’re offering these services in more flexible, customiz-able packages.” n
Treatment planning workshops come to South America
Early last year, Varian sponsored a series of Eclipse™ workshops as part of a training course that was organized by the European Society for Therapeutic Radiology and On-cology (ESTRO) at the Centro de Control de Cancer campus in Bogotá, Colombia. A total of 50 physics students attended the workshops, which covered head and neck treatment planning and physics. Worksta-tions were set up for students to obtain hands-on experience.
Then, in the spring of 2012, Varian part-nered with clinicians from McGill University in Montreal, Canada, to offer a two-day contouring workshop for clinicians in Brazil. Focusing mainly on IMRT and radiosurgical approaches to treating tumors of the pelvis and the head and neck, the workshop was the first of what will be an ongoing program of biannual workshops designed to offer clinicians in Brazil an opportunity to obtain advanced treatment planning skills without having to travel abroad.
“Varian’s mission is to help save 100,000 more lives each year, and one way we seek to do that is to support clinical oncology communities in developing areas of the world working to expand their clinical capabilities,” says Tracey Fisher, senior manager of marketing operations and international marketing at Varian. “We all know that technology by itself does not help cancer patients. It’s only in the hands of trained, adept professionals that tech-nology makes a difference. Consequently, we’re committed to training opportunities for radiation oncology professionals around the world.” n
C E N T E R L I N E N E W S

CENTERLINE | AUGUST–SEPTEMBER 2012 | 7
The Scripps Proton Therapy Center being developed in San Diego reached several major milestones since October 2011, when the cyclotron arrived and was installed. At six by nine feet in size, the cyclotron, or proton-generating technology, weighs about 90 tons—about the same as a fully loaded 737 jetliner.
According to Brendan Lyden, manager of the cyclo-tron installation and commissioning group for Varian’s Particle Therapy business, it took two months and two days for the cyclotron to reach Scripps from Varian’s manufacturing facility in Germany. The cyclotron was shipped from the German port of Bremerhaven, and traveled across the Atlantic through the Panama Canal to Port Hueneme in Southern California.
Once the cyclotron arrived at Scripps, an external rigging company used two cranes to lift it and place it into the building. “It took about six hours to rig in the bottom piece and three hours for the top piece, which included the alignment of both pieces,” Lyden says.
Since then, Varian has installed ProBeam™ technology at the Scripps site—including the many components that make up the beam line, which transports protons from their point of origin in the cyclotron to gantries in the treatment rooms. The protons are transported along the beam line by a series of electromagnets attached to structural girders. Once these elements were installed, the on-site team switched to com-missioning the machine. On April 18, a proton beam was accelerated to the clinical energy of 250 MeV (60 percent of the speed of light) and fed into the beam transport system.
The installation covered five treatment rooms, includ-ing three rotational gantries and two fixed-beam delivery systems. Scheduled to begin treating pa-tients in 2013, the Scripps center is being developed through a collaboration between Scripps Health, Scripps Clinic Medical Group, Advanced Particle Therapy (APT), and Varian. The APT website features images and videos showing the project’s progress (advancedparticletherapy.com).
Varian has now signed contracts for provisioning additional proton therapy projects at the King Fahd Medical Center in Riyadh, Saudi Arabia; the St. Pe-tersburg Center of Nuclear Medicine of the Interna-tional Institute of Biological Systems in Russia; and two additional APT projects, the Maryland Proton Treatment Center at the University of Maryland, and the Georgia Proton Treatment Center of Emory Healthcare, in Atlanta, Georgia. n
Scripps hits major milestones with proton therapy project

8 | CENTERLINE | AUGUST–SEPTEMBER 2012
Contest sends Brazilian medical physicist to Miami for training
In June of this year, Marcelo Abib Valentim, a medical physicist from Brazil, attended a one-week training program at Innovative Cancer Center in Miami, Florida, courtesy of Varian Medical Systems. Valentim won the educational trip by taking first prize as a contestant in a game show that Varian conducted at the company’s exhibit last
year during the 13th Annual Congress of the Brazilian Society of Radiotherapy in Rio de Janeiro.
“The game show was quite a produc-tion,” says Milton Munhoz, national sales manager for Varian in Brazil. “People signed up in advance, and they were assigned to compete at particular times in the booth. Almost 100 people competed in 20 rounds of questions about the field of radiotherapy, with just a handful advancing to semifinals
and then finals, which were held on day three of the meeting.”
When he won first prize, Valentim was shocked. “I thought I had a remote chance of winning one of the iPads that were given away to the second and third winners,” he says. “I never imagined I would win the travel. When I saw I made it into the finals, I could barely stand on my feet! The feeling was indescribable.”
C E N T E R L I N E N E W S
In late 2011, the Insituto de Radioterapia Del Este (IRE), a new cancer treatment center in Puerto Rico, installed a Trilogy® system for image-guided radiotherapy and became one of the first Caribbean cancer centers to offer RapidArc® treat-ments. Around the same time, GURVE Radiation Oncology Group (Radioterapia Oncológica GURVE) in Caracas became the first treatment center in Venezuela to offer RapidArc radiotherapy.
“We’re very pleased to offer technologically advanced treat-ments to patients in Puerto Rico,” says Carlos Remedios, MD, president of IRE. “Within two months of installation, we were delivering 25 patient treatments per day on the new Trilogy system, including RapidArc treatments.”
The majority of patients treated at IRE are prostate cancer patients. Plans are to use the new Trilogy machine at IRE for a full spectrum of treatments, including cancer of the prostate, breast, brain, lung, reproductive organs, bladder, and esophagus. “We will add new indications as we gain experience with the technology,” Remedios says.
GURVE, which operates three cancer treatment centers in Venezuela, has treated more than 100 patients to date with RapidArc.
The addition of RapidArc technology at Radioterapia On-cológica GURVE was the culmination of a series of upgrades to a Varian Clinac® 2100C linear accelerator that was installed in 1999. “We have progressed all the way up the learning curve with this linear accelerator,” says Andrés Vera Gimón, MD, director of Radioterapia Oncológica GURVE. “First it was upgraded with a 120-leaf MLC, then a PortalVision™ device.
We also progressed with Varian software, from CadPlan to Eclipse™.”
More recently, the center was upgraded for IMRT, and two years ago, installed an On-Board Imager® device for IGRT, followed by cone-beam CT imaging and RapidArc.
According to Vera, the addition of RapidArc made it possible to increase the number of patients treated during a normal working day from 40 to 46. In addition to lung cancer, clini-cians at the treatment center have now used RapidArc in the treatment of prostate, brain, gynecological, and other types of cancer.
“It’s a true testament to the upgradability of these ma-chines,” Vera says. “Whenever Varian introduces new tech-nology, we install it at one of our centers and learn how to use it. We make sure that it is helpful for our patients, and then order it for the other facilities.”
Radioterapia Oncológica GURVE has now ordered Varian treatment machines with RapidArc for its other two centers in Valencia and Caracas. “We are also working with partners to install a RapidArc-enabled machine at the Hospital Nacional in Panama City, Panama,” Vera says. n
Centers in Puerto Rico and Venezuela
launch RapidArc programs
The lobby at Radioterapia Oncológica GURVE.

CENTERLINE | AUGUST–SEPTEMBER 2012 | 9
Varian has established the company’s first education center in Tokyo, Japan, for serving oncologists, medical physi-cists, and technologists who work with Varian’s cancer treatment systems. In addition, the company has established a help desk to provide phone support for Varian’s customers in Japan.
These services are housed in a new facility that is conveniently located in central Tokyo. The training center features a computer-equipped class-room with 20 workstations and state-of-the-art audio-visual equipment, as well as two customer lounges.
According to the Japanese Society for Therapeutic Radiology and Oncol-ogy (JASTRO), the number of cancer patients who received radiotherapy treatments in Japan doubled over the last decade, rising from roughly 100,000 per year in the late 1990s to more than 250,000 per year today. JASTRO further predicts that the number of Japanese people needing access to radiotherapy services will rise to 360,000 by 2015.
“Varian’s new education center rep-resents our commitment to helping address an expanding need for train-ing in this area,” says Makoto Yamada, sales manager for Varian in Japan. “The new help desk will provide them with phone and e-mail support, when-ever questions come up as they use Varian technology to treat patients.”
Varian’s new offices are located at 5-1 Kabutocho Nihonhashi, Chuo-ku, Tokyo. The first class scheduled in the new training center took place in February 2012, and focused on Var-ian’s Eclipse™ treatment planning software. Additional courses have covered Eclipse operations and the ARIA® oncology information system for managing cancer treatments.
“In the future, we will work with our clinical partners in Japan to develop courses on quality assurance proce-dures, safety, and the newest clinical modalities,” says Jon Hollon, Varian’s director of worldwide training and education. “Radiotherapy use is on the rise in Japan, and our goal is to provide world-class education and customer support on a local basis. The new training center in Tokyo will help us customize our services to the specific needs of Japanese clinicians, and enable them to obtain training without leaving the country.”
The Tokyo project is the sixth such education and training center estab-lished by Varian globally, following similar initiatives in Las Vegas (USA), Beijing (China), Zug (Switzerland), Buc (France), and Mumbai (India). n
Valentim works at the Centro Brasileiro de Oncologia e Mastologia (CEBROM) in Goiânia, in central Brazil, where radio-therapy is now moving from block-based to multileaf beam shaping.
According to Valentim, the training in Miami focused on new technologies, including RapidArc® and cone-beam CT imaging, which are both used routinely at the In-novative Cancer Center. “The multileaf technology opens up a whole new world of possibilities, such as field-in-field forward planning, dynamic IMRT, dynamic arc therapy,” he says. “I hope to expand on my knowledge about these techniques to further improve the treatment quality we offer our patients. In the near future, I’d like to contribute to the implementation of RapidArc radiotherapy, as the natural evolution of the treatment techniques we are using.”
The game show was such a hit last year, Robson Ferrigno, MD, president of the Brazilian Society of Radiotherapy, asked Varian to produce a variation for this year’s meeting. This year, Varian created a scientif-ic contest for radiation oncology residents. The contest has become part of the official program of the Brazilian Congress, with participation from the American Society of Radiation Oncology (ASTRO). n
Varian establishes training center and clinical help desk in Tokyo

10 | CENTERLINE | AUGUST–SEPTEMBER 2012

CENTERLINE | AUGUST–SEPTEMBER 2012 | 11
Lung cancer continues to be the leading cause of cancer-related deaths worldwide.1
Despite recent improvements in survival for many other types of cancer, five-year
survival rates for lung cancer have remained rela-tively poor, mainly because by the time a diagnosis is made, lung cancer is often well advanced and treatment options are limited.2 In 2010, there were estimated to be 1,608,055 new cases of lung cancer worldwide and 1,376,579 deaths, representing 18.2 percent of all cancer deaths.3
In the last decade, stereotactic body radiation therapy (SBRT), which is now also being referred to as stereotactic ablative radiation therapy (SABR), has been used to treat patients who were mostly medically inoperable. From 2008 to 2010, there were more than 40 published clinical papers on SBRT for the treatment of early-stage lung cancer, plus approximately 30 review papers.4, 5
After reviewing the results of medically inoperable patient studies, a number of clinicians have begun to take a look at the viability of SABR/SBRT for treating high-risk, operable early-stage non–small cell lung cancer (NSCLC).
According to Robert D. Timmerman, MD, of the University of Texas Southwestern Medical Center, SABR began to emerge around 1995, facilitated by technological innovation in the areas of immobilization, motion control, 3D dosimetry, and image guidance.
“In the mid-1990s, a new treatment called extracranial stereotactic radioablation was first described in the litera-ture,” explains Timmerman. “The main feature of this ap-proach was to spread out the entrance dose by using many weak beams, moving the patient so that the target corre-sponded to the convergence point of the weak beams, fol-lowing the conduct pioneered for intracranial stereotactic radiosurgery. The use of this approach for extracranial treatments was facilitated by development of immobilization techniques, motion control, and beam-shaping technologies that allowed rapid dose fall-off outside the target, 3D do-simetry, and image guidance. Most importantly, this approach
involves the use of ablative doses—greater than 8–10 Gy per day—over just a few treatment sessions.”
“Historically, early-stage lung cancer was treated by surgical resection, and there is about 30 years’ worth of data regarding outcomes with that approach,” says John Kresl, MD, PhD, medical director of Radiation Oncologists of Central Arizona (ROCA) at Banner Good Samaritan Medical Center in Phoenix, Arizona. “However, between 15 and 45 percent of patients with early-stage lung cancer are not candidates for surgery, and conventional external beam radiotherapy has not been especially effective with this population. We’re in the process today of establishing whether SABR, which delivers high ablative doses more quickly, can play a role.”
Early SABR trials
In the late 1990s, SABR began to be investigated systemati-cally. The first prospective trials in the United States involved medically inoperable patients with NSCLC. The intent was to show local control, which had been poor—in the 15-to-45-percent range—using conventional radiotherapy.6
An early phase 1 trial in 37 patients examined the effects of SABR and dose escalation in the treatment of NSCLC in inoperable, elderly patients, with encouraging results.7
A larger phase 2 single-center trial in 70 patients followed. This trial found that patients whose tumors were in central regions of the lung experienced greater toxicity than did those whose tumors were more peripheral.8
Radiosurgical Approaches to Treating Early-Stage Inoperable and High-Risk
Operable NSCLC
“Between 15 and 45 percent of patients with early-stage lung cancer are not candidates for surgery... We’re in the
process today of establishing whether SABR, which delivers high ablative doses
more quickly, can play a role.”John Kresl, MD, PhD,
Radiation Oncologists of Central Arizona

12 | CENTERLINE | AUGUST–SEPTEMBER 2012
Another phase 2 trial was conducted across multiple treatment centers in North America (Radiation Therapy Oncology Group [RTOG] 0236), encompassing medically inoperable lung cancer patients whose tumors were less than five centimeters, but excluding tumors in the central areas of the lung. The trial enrolled 59 patients, most with T1 tumors.9
“While this was a phase 2 study involving a relatively small patient sample, these results… certainly dictate that further study of SBRT is warranted,” says Timmerman. “We are optimistic that the technique holds promise for these patients.”
Meanwhile, parallel research efforts have been going on in other parts of the world. For example, researchers at VU University Medical Center (VUMC) in Amsterdam, the Netherlands, recently published their analysis of outcomes after delivering SABR to 177 patients with potentially oper-able stage I NSCLC.10
“Approximately two-thirds of patients with early-stage non–small cell lung cancer in the Netherlands currently undergo surgical resection,” says radiation oncologist Suresh Senan, MD, PhD, a coauthor on the study. “As an increasing number of fit patients have elected to undergo SABR in recent years, we were able to retrospectively study outcomes for these potentially operable patients. These findings cer-tainly support ongoing randomized clinical trials comparing surgery and SABR in cases of operable stage I non–small cell lung cancer.”
Just such a study is currently under way and accruing patients. In July of this year, Varian became a supporter of ACOSOG Z4099/RTOG 1021, a phase 3 trial that seeks to compare sublobar resection with SABR in the treatment of high-risk patients with operable early-stage NSCLC. (For more information, see the sidebar on page 14.)
Clinical applications of SABR
Technology developments are making it possible to use Varian linear accelerators to deliver SABR/SBRT treatments quickly, in a typical radiotherapy time slot.11 Using RapidArc® delivery and High-Intensity Mode, which is now available on the TrueBeam™, Trilogy®, and Clinac® iX linear accelera-tors, clinicians around the world are gaining experience with stereotactic ablation of inoperable and high-risk oper-able lung tumors.
The clinical team at VUMC has treated more than 550 lung cancer patients with RapidArc SABR, delivering the treatments on Trilogy, Novalis Tx™ and—most recently—TrueBeam devices.
“RapidArc considerably speeded up the delivery of SABR,” says medical physicist Wilko Verbakel, PhD. “A fraction of 18 Gy can presently be delivered in less than three minutes on the TrueBeam machine.”
At Humanitas Clinic in Milan, Italy, more than 220 lung cancer patients have been treated using RapidArc in High-Intensity Mode on the TrueBeam system since its installation in July 2010. Of these, about 180 had metastatic lung lesions from different primary tumors and the rest had inoperable non–small cell lung cancer.
“Thanks to the High-Intensity Mode, we can explore higher ablative fractionation for small lesions such as oper-able early-stage NSCLC,” says Marta Scorsetti, MD, director of the hospital’s radiotherapy and radiosurgery department. “The beam-on time with unflattened beams is usually shorter compared with flattened beams in our SBRT cases. Beam-on time averaged close to one and a half minutes for the High-Intensity Mode treatments, compared with close to six minutes for the treatments without it.” 12
“While this was a phase 2 study involving a relatively small patient
sample, these results… certainly dictate that further study of SBRT is warranted.
We are optimistic that the technique holds promise for these patients.”
Robert D. Timmerman, MD University of Texas Southwestern Medical Center
Example of tumor response over time in a medically inoperable patient treated at the high end of ablative treatment (12 Gy x 3) in a dose escalation trial at Indiana University.7
Images courtesy of Robert D. Timmerman, MD, University of Texas Southwestern Medcal Center, Dallas, Texas.

CENTERLINE | AUGUST–SEPTEMBER 2012 | 13
A 4D CT is performed on all such patients at Humanitas, and clinicians use different kinds of fractionation schemes according to tumor size and anatomical position. For pe-ripheral lesions up to 2 cm in diameter, they deliver 60 Gy in three fractions, while larger targets (up to 5 cm) receive 48 Gy in four fractions. For lesions that are closer to the chest wall or for central lesions, they deliver 60 Gy in eight fractions, following a “risk-adapted” protocol for treating central tumors that was developed at VU University in Amsterdam.13, 14
In his clinical work, John Kresl of Banner Good Samaritan Medical Center has gained considerable experience treating lung cancer with SBRT, using CyberKnife, Novalis Tx, and now the TrueBeam system.
“Our preferred option is SBRT for the medically inoper-able, based on the data that has accrued over the last decade,” Kresl says. “Also, there is a category of patients who are medically operable but refuse surgery, and we’re treating them with SBRT.”
Kresl anticipates that the success of SBRT for treating some cases of NSCLC may soon be extrapolated to other disease sites. “Data is accruing on the use of SBRT to treat
primary and metastatic liver lesions,” he says. “Because the technology now allows these treatments to be delivered accurately, precisely, and efficiently, it is becoming a rapidly growing discipline within the field of radiation oncology.”
Intrafraction motion review (IMR)
At the University of Alabama at Birmingham (UAB) Health System, SBRT is an option for patients with inoperable, early-stage NSCLC. The treatments are delivered most often in three fractions for small peripheral tumors. According to John Fiveash, MD, associate professor in UAB’s department of radiation oncology, the alternatives are palliative che-motherapy, which many patients don’t want or can’t tolerate, or six to eight weeks of fractionated radiation, which may not work as well.
In late 2011, clinicians at UAB became the first in the United States to utilize intrafraction motion review (IMR), or “triggered imaging,” while delivering a Gated RapidArc radiosurgery treatment for inoperable early-stage lung cancer. IMR, a unique capability of Varian’s TrueBeam system, allows clinicians to continually monitor tumor loca-tion during radiosurgery and provides visual verification that the tumor is being properly targeted.
During a gated treatment, the gating system turns the treatment beam on and off in synchrony with the patient’s breathing to increase treatment precision. With IMR, the gating system also triggers the imager to generate a kV image of the targeted tumor at a specific point in the patient’s respiratory cycle. If the tumor is not where it should be, clinicians can intervene to enhance treatment accuracy.
Dose distribution in color wash on target in the lung (48 Gy prescribed to isodose 95 percent, in red).
Images courtesy of Humanitas Clinic.
“Thanks to the High-Intensity Mode, we can explore higher ablative
fractionation for small lesions such as operable early-stage NSCLC.”
Marta Scorsetti, MD, Humanitas Clinic

14 | CENTERLINE | AUGUST–SEPTEMBER 2012
Lung SABR studies currently under way include:
RTOG 0813 is a phase 2–3 trial for patients with centrally located tumors that uses a five-fraction regimen. Principal investigator: Andrea Bezjak, MD, of Princess Margaret Hos-pital, Ontario, Canada. Target accrual: 94 patients.
RTOG 0915 is a randomized phase 2 trial that is compar-ing two less aggressive dosing regimens (12 Gy x 4 frac-tions versus 34 Gy x 1 fraction) in patients with inoperable peripheral tumors. Coprincipal investigators: Gregory M. Videtic, MD, Cleveland Clinic Foundation; Anurag K. Singh, MD, Roswell Park Cancer Institute; and Joe Y. Chang, MD, PhD, MD Anderson Cancer Center. Closed to accrual at 94 patients.
RTOG 0618 is a small phase 2 study that is investigating SABR in operable patients. This study is looking at a dose regimen of 18 Gy x 3 fractions. Thirty-three high-risk patients have been accrued, and results are expected in mid-2012. Principal investigator: Robert D. Timmerman, MD.
ACOSOG Z4099/RTOG 1021, a randomized phase 3 study, is now under way, enrolling high-risk patients with operable lung cancer and seeking to compare sublobar resection with SABR in this population. The goal is to look at overall survival at three years to see if there is less than a 10 percent difference in survival between the two therapies. If there is, then some patients facing high-risk surgery may have a viable noninvasive option, and clinicians will be able to better inform patients of the risks and benefits of either procedure.
In July of this year, Varian became a supporter of this clinical study, which is being conducted by the Alliance, a National Cancer Institute (NCI)–sponsored cooperative research group formed in March 2011 from the merger of the American College of Surgeons Oncology Group (ACOSOG), Cancer and Leukemia Group B (CALGB), and North Central Cancer Treatment Group (NCCTG). ACOSOG Z4099/RTOG 1021 represents a collaboration between the Alliance and the Radiation Therapy Oncology Group (RTOG). NCI is the sponsor of this prospective randomized trial, and Varian will be providing financial support. The study plans to accrue 420 patients over a five-year period.
“The IMR tool offers us a way of verifying that our gating strategy remains valid throughout an entire treatment,” says Chris Dobelbower, MD, PhD, a radiation oncologist at UAB. “It also gives us the ability to hold the beam should the target wander from isocenter if the patient’s breathing pattern changes.”
To enable the IMR process, thoracic surgeon Douglas J. Minnich, MD, assistant professor at UAB, placed fiducial markers into the lung tumor using electromagnetic naviga-tional bronchoscopy. The markers show up readily in the kV images generated during treatment.
“IMR makes it possible to complete lung cancer treatments with a high level of precision and confidence that you’re treating the area you want to treat,” says Minnich. n
References
1. Youlden D, et al. The international epidemiology of lung cancer. J Thorac Oncol. 2008;3(8):819–831.
2. Ibid.
3. World Health Organization, International Agency for Research on Cancer. GLOBOCAN 2008 website. http://globocan.iarc.fr. Accessed October 6, 2011.
4. Timmerman R, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA. 2010;303(11):1070–1076.
5. Dosoretz DE, et al. Radiation therapy in the management of medically inoperable carcinoma of the lung: results and implications for future treatment strategies. Int J Radiat Oncol Biol Phys. 1992;24:3–9.
6. Ibid.
7. Timmerman R, et al. Extracranial stereotactic radioablation: results of a phase 1 study in medically inoperable stage I non–small cell lung cancer. Chest. 2003;124(5):1946–1955.
8. Timmerman R, et al. Excessive toxicity when treating central tumors in a phase 2 study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J Clin Oncol. 2006:4833–4839.
9. Timmerman, 2010.
10. Lagerwaard FJ, et al. Outcomes of stereotactic ablative radiotherapy in patients with potentially operable stage I non–small cell lung cancer. Int J Radiat Oncol Biol Phys. 2012;83(1):348–353.
11. Prendergast B, et al. Improved clinical efficiency in CNS stereotactic radiosurgery using a flattening filter free linear accelerator. J Radiosurg SBRT. 2011;1(2):117–124.
12. Scorsetti M, et al. Feasibility and early clinical assessment of flattening filter free (FFF) based stereotactic body radiotherapy (SBRT) treatments. Radiat Oncol. 2011;6:113.
13. Bongers EM, et al. Incidence and risk factors for chest wall toxicity after risk-adapted stereotactic radiotherapy for early-stage lung cancer. J Thorac Oncol. 2011;6(12):2052–2057.
14. Lagerwaard FJ, et al. Outcomes of risk-adapted fractionated stereotactic radiotherapy for stage I non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2008;70(3):685–692.
“The IMR tool offers us a way of verifying that our gating strategy
remains valid throughout an entire treatment. It also gives us the ability to hold the beam should the target
wander from isocenter if the patient’s breathing pattern changes.”
Chris Dobelbower, MD, PhD, UAB Health System
Current Lung SABR Studies

CENTERLINE | AUGUST–SEPTEMBER 2012 | 15
Developing a Successful SABR Program
Andrea McKee, MD, chair of the Department of Radiation Oncology at the Lahey Clinic’s Sophia Gordon Cancer Center. Andrea McKee, MD, is passionate about finding
and treating lung cancer. She is also an ardent supporter of the multidisciplinary approach to cancer treatment.
Chair of the Department of Radiation Oncology at the Sophia Gordon Cancer Center of the Lahey Clinic in Burlington, Massachusetts, McKee arrived at the center about 18 months ago, after launching two radiosurgery programs at sites in New Hampshire. Lahey had been outfitted for stereotactic ablative ra-diotherapy (SABR), sometimes referred to as stereotactic body radiotherapy (SBRT), sometime earlier and began delivering such

16 | CENTERLINE | AUGUST–SEPTEMBER 2012
treatments in 2008. McKee was brought on board to expand and improve the SABR program by implementing and for-malizing specific quality measures and other best practices. Along the way, she has become a champion of low-dose CT lung screening for people at high risk for the development of lung cancer, and has established a program for free lung cancer screening at Lahey Clinic (see article on page 20).
Multidisciplinary collaboration
According to McKee, one of the most critical elements of a lung cancer SABR program is multidisciplinary collaboration. She ensures that this happens at several points in the process.
“When we’re first considering how best to treat a lung cancer patient, we discuss the case at a multidisciplinary thoracic oncology team meeting that includes a thoracic surgeon, pulmonologists—including interventional pulmo-nologists—chest and interventional radiologists, thoracic medical oncologists, pathologists, and radiation oncologists,” she says. “Candidates for SABR are patients with stage I or selected stage II non–small cell lung cancer (NSCLC), who are either medically inoperable or who refuse surgery.”
In addition, the team evaluates patients with metastatic lung lesions and patients with recurrent lung cancer, who are sometimes deemed appropriate candidates for SABR. Finally, SABR is sometimes used to treat patients who have peripheral lung tumors along with mediastinal lymph node involvement. “For this highly selected last group, we can administer a combination of radiotherapy and chemotherapy for the mediastinal disease, followed by SABR and/or surgery to remove a primary tumor in the peripheral area of the lung,” McKee explains.
Once a patient is deemed eligible to receive SABR for lung cancer, another important multidisciplinary collaboration occurs within the radiotherapy department in the form of a prospective treatment planning conference. In addition to the radiation oncologists, this conference involves the par-ticipation of radiologists, medical physicists, dosimetrists, radiation therapists, clinical trial personnel, social workers, and nurses.
“In this conference we discuss our patients from a radio-therapy standpoint,” McKee says. “We decide together what films we will use for treatment planning, whether PET, CT, MRI, or a combination of these should be fused for treatment planning purposes. It is important for us to have the radiolo-gists with us to review the films. They are trained to interpret films and help us to see the target in ways that are useful.”
The team also uses the conference to discuss any position-ing or social concerns that might come up for a particular patient during treatment.
“Sometimes, for example, it can be hard to determine whether or not to use radiotherapy a second time when you are dealing with a patient who has received prior radio-therapy,” McKee says. “You want a larger group to take a look and talk about the different radiotherapy options for
“It can be argued that perhaps every case should be reviewed in this
way prior to treatment.”
Andrea McKee, MD, Lahey Clinic
A 3D rendering for a bilateral lung SRS treat-ment, showing dose-limiting structures, tumor volumes (PTVs), and dose clouds.

CENTERLINE | AUGUST–SEPTEMBER 2012 | 17
treatment. This is an important quality measure. It provides extra peer review for these more complicated cases. We hold a similar treatment planning conference as part of our single-fraction brain and spine stereotactic radiosurgery program.”
The value of peer review
Another positive outcome of these meetings is that, when a treatment is subsequently planned and delivered, the entire team knows the whole picture and feels more engaged. “ASTRO is developing a white paper that talks about the importance of peer review, and it can be argued that perhaps every case should be reviewed in this way prior to treatment,” McKee suggests.
The Lahey radiotherapy team also reviews follow-up scans together, to evaluate results after a patient has completed treatment. “This is very interesting because the use of SABR in the treatment of lung cancer is still fairly new,” McKee says. “We’re all still learning about what post-treatment images look like after an ablative dose. They’re different than you might expect, so it’s useful for the whole team, including the radiologists, who can initially find these images somewhat confounding.”
According to McKee, managing these multidisciplinary conferences at the Lahey Clinic is a full-time job that requires the services of a talented coordinator. “We have a specialty procedure coordinator, Fatima Laurenza, who helps to run the conferences,” she says. “She is also a scheduling guru who schedules the more complicated treatments. We keep two SABR treatment slots open per day, one in the morning and one in the afternoon. We can always accommodate more if we need to. There are a lot of people involved when you operate according to this model, and a lot of steps in the
workflow to consider. So you need one person who really understands the program to act as a coordinator and manage the patient’s schedule from initial consultation to the post-treatment conference.”
Established dose constraints and protocols
Lung SABR treatment plans must all comply with a list of dose constraints for important critical structures. “If for some reason every constraint is not being met, the doctor must explain why a deviation is being accepted, and a second doctor signs off on the plan,” McKee explained. “Our plans are based on a variety of different algorithms. Some involve multiple fixed fields; we sometimes use arcs. We keep the number of couch angles to a minimum and they are generally less than 15 degrees.”
The SABR lung treatments follow protocols that have been widely described in the medical literature. For small lesions that are not close to the chest wall or central structures, patients receive three fractions of 18 Gy each, delivered every other day. If there is reason to complete a treatment more quickly, 48–50 Gy can be administered over four consecutive days in fractions of 12–12.5 Gy each. “We determine as a group what is most appropriate for a given patient,” McKee says. “With centrally located tumors, and with tumors close to the chest wall, we follow the literature and back off on daily dose to avoid toxicities such as rib fractures, hemoptysis, or obstructive atelectasis.”
SABR treatments at the Lahey Clinic are delivered using a Varian linear accelerator along with patient positioning and alignment technologies from Brainlab. Daily treatment
A team approach At the Lahey Clinic’s Sophia Gordon Cancer Center, essential elements of the SABR program include multidisciplinary collaboration, rigorous quality assurance, and clear team communication throughout the treatment process.

18 | CENTERLINE | AUGUST–SEPTEMBER 2012
setup is accomplished using cone-beam CT imaging. While most of the treatments are not gated, the team produces a treatment plan based on 4D imaging. “We map tumor motion at the time of simulation and we treat that volume,” McKee says.
During treatment, the patient’s position is checked and verified after every three fields are delivered. “Patients are generally in the room for about 40 minutes,” McKee says. “The treatment itself is a fraction of that time.”
Rigorous quality assurance
The SABR program at the Lahey Clinic incorporates a series of rigorous quality assurance steps that span all phases of treatment. In addition to the specialty program coordinator, the multidisciplinary team meetings, and the checks on the patient’s position, this program includes QA steps that are specific to simulation, as well as a dosimetry checklist to verify prescription, dose constraints, documentation, image guidance, and isocenter verification. The physics team conducts patient-specific QA, including isodose plan review prior to treatment, review of physician and simulation documentation and orders, direct supervision of the first treatment fraction, and weekly and final chart reviews. Equipment QA is based on the American Association of Physicists in Medicine (AAPM) TG-142 frequency with stereotactic tolerances, and isocenter checks of all imaging systems on each day of SRS or SABR treatments.
Treatment QA includes daily output and imaging QA as well as daily Winston-Lutz QA (approved by physics). Checklists must be utilized and initialed by two therapists,
who also review the consent, simulation notes, IGRT guide-lines, beam parameters, and other documentation.
There is a “time-out” with physics on day 1 of treatment. Also on day 1, physics personnel conduct a beam-by-beam verification, including gantry, collimator, couch, and MU settings. Images are approved by the physician prior to treatment. Reimaging takes place in accordance with IGRT guidelines prescribed by the physician at the time of treat-ment planning. For subsequent fractions, the QA program includes patient verification, image approval by the physi-cian, reimaging per IGRT guidelines, beam-by-beam verifica-tion by two therapists, and treatment documentation. The physician writes procedure notes for all fractions.
“We have three chart checks throughout the treatment, as well as verification of the isocenter in three separate venues,” says McKee. Ours is an extensive quality program, with clearly articulated procedures, and a requirement for a “time-out” on the machine for patient identification. We have many ways of checking multiple times that we’re taking the correct actions.”
McKee feels that the cornerstone of the Lahey Clinic quality program is the stereotactic conference.
“That’s where all of the communication happens between the members of a dedicated team all speaking the same language and providing peer review for one other,” she says. “It’s much more rewarding for a therapist, for example, to have intimate knowledge of the treatment plan he or she is delivering. That way, they’re part of the clinical team as highly trained specialists, and not just technicians. We have observed that this not only increases engagement, but also job satisfaction for our clinical team members.”
The stereotactic conference is “where all of the communication happens
between the members of a dedicated team all speaking the same language
and providing peer review for one other.”
Andrea McKee, MD, Lahey Clinic Varian and Brainlab technologies are used to deliver SABR treatments at the Lahey Clinic.

CENTERLINE | AUGUST–SEPTEMBER 2012 | 19
A commitment to early screening
The early-stage NSCLC patients who are nevertheless medi-cally inoperable have a better prognosis after SABR than people who present at stages III or IV, when the disease has spread, McKee observes. “In SABR conference,” she says, “we would review the follow-up outcomes of the medically inoperable group of patients, many of whom came to us by way of ‘screening,’ if you will, because their thoracic oncology team had been following them with yearly CT scans after their first stage I lung cancer was successfully treated surgi-cally, often by lobectomy.”
McKee further explains: “Once diagnosed with their second primary lung cancer years later, these patients would then be referred to us for SABR since they no longer had the pulmonary reserve for surgical management. In radiation oncology, where we have witnessed the dismal prognosis of patients with stage III and IV lung cancer, we were pleas-antly surprised to be part of the excellent results achieved for the medically inoperable patients with stage I and II disease.”
These types of outcomes were also instrumental in creat-ing, among members of the Lahey Clinic team, an abiding commitment to lung cancer screening. “We saw that, if we can catch lung cancer early, then even for patients who are
unable to undergo surgery, SABR is a potentially curative treatment,” says McKee. “Based on prospective data, we can achieve 90 to 95 percent local control rates using this noninvasive approach that is completed on an outpatient basis.” 1, 2
McKee feels that lung cancer screening will result in a paradigm shift in how early-stage screen-detected lung cancer is treated. “As with other malignancies, when we get good at halting the disease, our focus must shift to the survivor’s long-term quality of life,” she says. “If 92 percent of your screened stage I population is surviving 10 years, a main priority becomes alveolar-sparing surgical and SABR techniques in order to best position the patient for their next diagnosis of early-stage screen-detected lung cancer. It’s a dramatically different way of thinking about lung cancer and one that will likely occupy the field of thoracic oncology for the next decade and beyond.” n
References
1. Timmerman R, et al. Stereotactic Body Radiation Therapy for Inoperable Early Stage Lung Cancer. JAMA; 2010;303(11):1070–1076.
2. Lagerwaard FJ, et al. Outcomes of stereotactic ablative radiotherapy in patients with potentially operable stage I non–small cell lung cancer. Int J Radiat Oncol Biol Phys. 2012;83(1):348–353.
Left to right | Stephanie Jalbert, nurse manager, Andrea McKee, MD, and Angela Tambini, chief
therapist, at the Lahey Clinic.
“We have a specialty procedure coordinator who helps to run the conferences. That person is also a
scheduling guru who schedules the more complicated treatments.”
Andrea McKee, MD, Lahey Clinic

20 | CENTERLINE | AUGUST–SEPTEMBER 2012
At the Sophia Gordon Cancer Center of the Lahey Clinic in Burlington, Massa-chusetts, a program for free lung cancer
screening has been established to provide equal access to all people meeting the National Com-prehensive Cancer Network (NCCN) high-risk criteria. Dubbed the “Rescue Lung, Rescue Life” program, it is part of a campaign to increase awareness of the power of low-dose CT screening in the early diagnosis of lung cancer.
According to Andrea McKee, MD, head of the Lahey Clinic’s radiation oncology department, low-dose CT screen-ing can save lives in the fight against lung cancer. “The treatment of lung cancer is stage dependent,” she pointed out in a Varian-sponsored webinar she recently led on the topic of lung cancer screening programs. “The treatment for stage III or IV is usually palliative, but if cancer is caught at stage I or II, it can be treated successfully—more than 90 percent of the time in the case of a screened T1a lesion.1 In the absence of screening, early-stage lung cancer is generally discovered incidentally when the patient is being tested for other reasons, such as a preoperative chest X-ray prior to a hip replacement.”
McKee prefers to detect lung cancer at a more curable stage by intentionally looking for it, when the chances of affecting survival are greatest, rather than finding it by accident when the five-year overall survival probability is small, or waiting for symptoms, by which time the prognosis is usually dismal.
The Rescue Lung, Rescue Life Program

CENTERLINE | AUGUST–SEPTEMBER 2012 | 21
Early detection saves lives
The National Lung Screening Trial (NLST) recently confirmed that screening individuals at high risk for lung cancer with an annual low-dose CT (LDCT) of the chest saves lives. “One life was saved for every 320 high-risk persons screened with LDCT over two years (three screens), resulting in a 20 percent lung cancer–specific mortality benefit versus annual chest radiography,” McKee says, citing a large, NCI-sponsored randomized controlled trial that included more than 53,000 participants who were randomly assigned to one of two groups receiving either chest X-rays or helical CT scans. The groups were followed for at least five years beyond the final screening. The researchers found 20 percent fewer lung cancer deaths among those who were screened with low-dose helical CT compared with those who were screened with chest X-rays. In addition, deaths from all causes (in-cluding lung cancer) were 7 percent lower in those who received the low-dose helical CT scans.2
“As a result, the National Comprehensive Cancer Network (NCCN) recommends that high-risk individuals undergo annual LDCT screening,” McKee says. “The NCCN defined two groups at high risk, including people between the ages of 50 and 74 who have a 20 pack per year smoking history and one other risk factor.” The additional risk factors that the NCCN identified are: any prior lung, lymphoma or smoking-related cancer, a family history of lung cancer among first-degree relatives, chronic lung diseases like emphysema or pulmonary fibrosis, and exposure to specific carcinogens like arsenic, asbestos, cadmium, chromium, diesel fumes, nickel, radon, or silica.
An evidence-based screening program
The Rescue Lung, Rescue Life program at the Lahey Clinic was developed over many months by a multidisciplinary steering com-mittee comprising clinical and administra-tive champions. “We wanted a program that was evidence based,” McKee says. “We
developed a comprehensive business plan based on the NLST experience, to allow ad-
ministrative executives to be comfortable with the use of our CT scanners in this capacity. We enlisted
our legal and compliance departments to give guidance with respect to regulatory issues; we developed a compre-hensive CME and education plan that we continue to develop. We addressed the major issues of informed consent, how and to what degree we would involve people’s primary care physicians, patient education, concerns about enticement or hidden costs to the patient—particularly those who are uninsured—and workload issues.”
McKee recently presented many details of the program in a Varian-sponsored webinar, available online on the MyVarian site (myvarian.com). In addition, the Lahey Clinic is looking to share its lung screening materials with interested parties, who can request a free electronic information package by sending a request to [email protected].
“We developed these materials to minimize, as much as possible, the pain associated with the operational endeavor of starting a responsible, high-volume lung screening program,” McKee says. “More generally, our goals are to save lives through the early detection of lung cancer with responsible CT lung screening, to encourage reimbursement for CT lung screening, to break down barriers and prejudice faced by many who are at risk for lung cancer, to encourage other centers to offer low-cost or free responsible CT lung screening to their patients, and to raise public awareness of the power of CT lung screening to save lives.” n
References
1. The International Early Lung Cancer Action Program Investigators. Survival of patients with stage I lung cancer detected on CT screening. N Engl J Med. 2006;355(17):1763–1771. http://www.nejm.org/doi/full/10.1056/NEJMoa060476. Accessed June 25, 2012.
2. National Lung Screening Trial Research Team. The national lung screening trial: overview and study design. Radiology. 2011;258(1):243–253. http://radiology.rsna.org/content/258/1/243.full. Accessed June 25, 2012.
“The treatment for stage III or IV is usually palliative, but if cancer is caught at stage I or II, it can be treated success-fully—more than 90 percent of the time
in the case of a screened T1a lesion.”
Andrea McKee, MD, Lahey Clinic

22 | CENTERLINE | AUGUST–SEPTEMBER 2012
Turning breast cancer treatment
upside down
Prone positioning may lead to
better outcomes for some patients
Radiation after surgery has been proven to increase survival for breast cancer patients,1 but it has also been shown to increase the
risk of developing heart disease and second-ary lung cancer, sometimes many years after treatment.2 Recent research suggests that placing some breast cancer patients in a prone position (facing down) rather than supine for radiotherapy may lead to better outcomes by limiting the dose reaching the lungs and the heart.
According to Silvia Formenti, MD, radiation oncologist at New York University School of Medicine, using the prone position for some women can enable a significant reduction in the volume of lung and heart tissue exposed. Several trials have investigated treating patients in the prone posi-tion to provide better heart and lung sparing.3, 4, 5, 6

CENTERLINE | AUGUST–SEPTEMBER 2012 | 23
Late last year, Formenti and other clinical researchers from NYU published an article ex-plaining why the prone breast treatment technique is now more feasible than it has been in the past:
With the advent of CT planning, the prone technique has become both feasible and reproducible… The prone setup has been accepted as the best localizing position for both MRI and stereotactic biopsy, but its adoption has been delayed in radiotherapy. New technological advances including intensity-modulated radiation therapy and image-guided radiation therapy have made possible the exploration of accelerated fractionation schemes with a concomitant boost to the tumor bed in the prone position, along with better imaging and verification of reproduc-ibility of patient setup.7
Coral A. Quiet, MD, a partner at Arizona Breast Cancer Specialists in Phoenix, screens all new early-stage breast cancer patients to help determine whether prone or supine treatment is their best option. Screening consists of CT simulation and a patient comfort survey.
Quiet sees considerable advantages to prone positioning for some patients. “The breast creates unique challenges for the targeted delivery of external beam radiation,” she explains. “The prone position can improve setup reproduc-ibility, negate respiratory motion, and pull the breast away from the chest wall. As a result, for some patients, the prone position can be used for postsurgical radiation therapy to
reduce irradiation of cardiac and lung tissue.”
“Treating in the breast can be difficult, whether the patient is in the prone or supine posi-tion,” says Agam Sharda,
manager of treatment solutions marketing at Varian. “Either way, it is our goal to enable a streamlined and reproducible process for treatments in the breast. Our Pivotal™ Treatment Solution for Prone Breast Care, and the recently announced Surface Beacon® transponder for use with Calypso®, are examples of these types of enabling technologies.” n
References
1. Formenti S, et al. Prone accelerated partial breast irradiation after breast conserving surgery: preliminary clinical results and dose-volume histogram analysis. Int J Radiat Oncol Biol Phys. 2004;60:493–504.
2. Buijsen J, et al. Prone breast irradiation for pendulous breasts. Radiother Oncol. 2007;82(3):337–340.
3. Morrow NV, et al. Intra- and interfractional variations for prone breast irradiation: an indication for image-guided radiotherapy. Int J Radiat Oncol Biol Phys. 2007;69(3):910–917.
4. Varga Z, et al. Individual positioning: a comparative study of adjuvant breast radiotherapy in the prone versus supine position. Int J Radiat Oncol Biol Phys. 2009;75(1):94–100.
5. Formenti S, et al. Phase 1–2 trial of prone accelerated intensity modulated radiation therapy to the breast to optimally spare normal tissue. J Clin Oncol. 2007;25(16):2236–2242.
6. Formenti S, et al. Results of NYU 05-181: a prospective trial to determine optimal position (prone versus supine) for breast radiotherapy. Int J Radiat Oncol Biol Phys. 2009;75(3)(suppl):S203–204.
7. Huppert N, et al. The role of a prone setup in breast radiation therapy. Front Oncol. 2011;1. DOI: 10.3389/fonc.2011.00031.
Images courtesy of NYU.
Using the prone position for some women can enable a significant
reduction in the volume of lung and heart tissue exposed.
Silvia Formenti, MD, NYU School of Medicine
Images from prone breast treatment plans. Top: a small-breasted patient (A-cup). Bottom: a large-breasted patient (C-cup).

24 | CENTERLINE | AUGUST–SEPTEMBER 2012
To facilitate breast cancer treatments in the prone position, Varian has developed a new Pivotal™ Treatment Solution for Prone Breast Care, which includes the kVue™ Access 360™ couchtop insert from Qfix, offering 360-degree access to the targeted area of the breast. The board aligns with the couchtop without any obstruction beneath the breast, allowing for full access. In addition, the breast cut-out in the board facilitates access to the sternum and offers therapists the ability to treat the patient using noncoplanar and oblique angles.
The kVue Access 360 is designed for treatments of either the left or right breast, including whole breast, partial breast, and accelerated partial breast treatments. The technology also allows for superclavicular access for treatment of the superclavicular nodes, and is currently the only prone breast solution available that can accommodate this type of treatment.
The Pivotal Treatment Solution for Prone Breast Care requires software upgrades. The package will include a comprehensive marketing kit with materials for explaining prone breast care to patients.
The kVue Access 360 includes many design features that address setup and treatment challenges, addressing provider needs and enhancing patient comfort.
Patient positioning benefits
360-degree access allows for maximum visibility during patient setup, which allows for full utilization of lasers and field lights.
Multiple indexing options are available, and knee positioning guides provide confirmation of patient alignment.
All patient positioning features work together to ensure that the patient is in the same position for each treatment.
Patient comfort benefits
The following features combine to promote patient comfort, leading to a sustainable treatment position:
Patients can more easily get on and off the couchtop because the couch insert has a low profile.
A foam pad contributes to patient comfort while maintaining accuracy.
The inverted wing design adds to patient comfort.
A dual hand grip relieves stress on the patient’s wrists.
Patients with limited arm mobility can use the ipsilateral hand grip.
The patient’s head can be positioned face down or to the side, using one of two headrest options.
Patients can breathe freely, due to the prone headrest design. Lateral light slots promote an open feeling.
Imaging benefits
Less scatter allows for high-quality, low-dose images.
Images are clearer because chest wall motion is reduced in the prone position.
The couch insert is designed specifically to minimize CT image artifacts.
Convenience features
The ergonomically designed insert snaps quickly in and out of position for ease of use by therapists.
A convenient kVue storage cart is included.
Pivotal Treatment Solution for Prone Breast Care and kVue Access 360 couchtop

CENTERLINE | AUGUST–SEPTEMBER 2012 | 25
With version 11, Varian software applications and servers can be virtualized. HIPAA-compliant ARIA® applications can be published via Citrix XenApp servers and served to a variety of remote devices. Users can access their ARIA oncology information system as well as their Eclipse™ treatment planning system from any Windows workstation in the department, from their Macs at home, from laptops on the road, or from tablets at the patient bedside.
Virtualization: Varian software evolves
By Nancy Heifferon

26 | CENTERLINE | AUGUST–SEPTEMBER 2012
It used to be that people had to go wherever the computers were physically located in order to use them. Now, thanks to virtualization
and the Internet, users are being freed from this spatial constraint to operate applications wherever they happen to be.
“The magic occurs at our fingertips, on the keyboard and in the display,” says Chuck Martin, senior manager of en-terprise IT architecture at Varian. “Users don’t care where the hardware with the blinking lights actually resides as long as the data are quickly and easily accessible. That’s virtualization.”
Hospitals and cancer treatment centers are beginning to realize advantages from virtualization, including greater flexibility, higher productivity, and lower costs, as illustrated by the profiles below.
Modernizing an infrastructure
In 2010, Capital Region Medical Center (CRMC) in Jefferson City, Missouri, faced a tough challenge when contemplating a Varian software upgrade. The organization had just built a new comprehensive cancer center to serve both medical and radiation oncology patients. However, the servers they had been using from the previous facility were outdated and out of warranty. It was going to take a large capital expenditure to bring the equipment up to Varian’s recom-mended hardware specifications. The CRMC IT department wanted to modernize its infrastructure and reduce capital expenses by virtualizing the Varian server hardware onto their new VMware vSphere platform and also extending Citrix XenApp capabilities to avoid replacing aging workstations.
Working with Varian, CRMC was able to virtualize its server hardware as well as most of its ARIA and Eclipse applications. This made it possible for the clinical staff to access the applications from every workstation in the depart-ment, regardless of age or specifications. By using virtual-ization, CRMC reduced its total cost of ownership and de-creased the amount of downtime needed during subsequent upgrades. There were other benefits that would not have
been achievable using the previous “traditional” or “non-virtual” system architecture: easy scalability, high avail-ability, and comprehensive monitoring capabilities.
“Virtualization, server or application, offers a lot more reliability, scalability, and ease of management over the more traditional configurations,” observes Jason Cecil, PMP, vice president for information at CRMC. “It simply made much more business sense to invest in a configuration that would ensure business continuity while also preparing us for future needs.”
Serving multiple locations
At CRMC, the IT infrastructure connects the wider organiza-tion via local area networks (LANs). For other organizations, the challenge is to serve geographically separate sites from equipment housed centrally within a secure data center, using only the Internet to connect them. “In cases like this, one or more cancer clinics might be miles away from each other and from the data center,” says Martin. “This is an ideal situation for ‘cloud’ computing.”
The Arizona Breast Cancer Specialists (ABCS) is a radia-tion oncology practice with offices in three communities—Scottsdale, Phoenix, and Gilbert, Arizona. Instead of incur-ring the acquisition and operating costs of identical hardware, software, and databases in three locations, ABCS wanted to simplify, consolidate, and centralize. “The doctors don’t want to be bothered with IT, they want to treat cancer,” says Ed Purkiss, president of Iron Medical Systems, the company that ABCS turned to for IT help.
The answer for ABCS was to go to the cloud and get their computing over the Internet from virtual servers, instead of from hardware on their own premises. The electronic medical record (ARIA) and treatment planning software (Eclipse) use virtual servers that are configured on large physical servers housed in an enterprise data center in Phoenix. The virtual servers can move automatically and without disruption from one physical server to another when glitches happen or when more capacity or higher performance is needed.
“Users don’t care where the hardware with the blinking lights actually resides as long as the data
are quickly and easily accessible. That’s virtualization.”
Chuck Martin, Varian senior manager

CENTERLINE | AUGUST–SEPTEMBER 2012 | 27
Instead of owning and housing servers that have to be maintained, upgraded, and regularly replaced, each ABCS center has only a rack of switches and a VPN appliance in its IT closet. Using inexpensive thin clients or their own devices (Mac laptops, iPads, etc.), the ABCS staff connect to their private cloud and launch their applications.
Iron Medical Systems put ABCS on the cloud. “We use a term called follow-me computing,” explains Purkiss. “When people move around, their network personality follows them, because it’s in the cloud. Whether they’re at home working, stepping into this or that office, or sitting in a café, when they log into the cloud, their experience is the same.”
Ubiquitous access
Virtualization offers a number of advantages, says Purkiss. One is ubiquitous access. With the entire ARIA infrastructure moved to the cloud, everyone can access the Varian suite of applications from anywhere on many types of devices, via many types of connections (DSL, LAN, WiFi, 3G, etc.), eliminating some of the logistical challenges common in busy oncology centers.
Another advantage may be the security that commercial data centers provide. “In the cloud, the databases are housed at commercial server colocation facilities behind armed guards, where retinal scans are used to control access along with other expensive security systems that a hospital or clinic would likely not be able to afford,” says Purkiss.
Cost savings and return on investment (ROI) are powerful incentives to go virtual, as well. Clinics using server and application virtualization methods don’t have to buy ex-pensive servers that take up space, use a lot of power, and require extensive IT resources to manage and service. “Virtualization can contribute to operational consistency, which can have an impact on quality and a clinic’s bottom line,” says Purkiss.
Considerable progress is being made toward cloud com-puting, and ARIA version 11 takes a stride forward in vir-tualization. However, radiation oncology departments and cancer centers are well advised to proceed with caution. “These are not yet simple solutions,” says Purkiss. “We caution people contemplating a cloud solution to know their own comfort level and seek out expert consultation to configure virtual systems.” n
Nancy Heifferon is a freelance healthcare writer.
What is application virtualization, really? Varian ac-complishes this using Citrix XenApp, an on-demand ap-plication delivery solution that centralizes application management in the data center to reduce cost up to 50 percent and deliver instant and secure access to Windows applications to users anywhere. Whether online or offline, virtual application delivery is optimized for each user device, network, and location to ensure a high-definition experience. Read more at the Citrix website at citrix.com/xenapp, or watch a video about how XenApp works at citrix.com/tv/#videos/632.
Speaking the virtual language
“We use a term called follow-me computing.
When people move around, their network personality followsthem, because it’s in the cloud.”
Ed Purkiss, president of Iron Medical Systems

28 | CENTERLINE | AUGUST–SEPTEMBER 2012
“Meaningful use” of an electronic medical record may be easier to prove than you think. Especially if you follow the example of New Mexico Cancer Center.
The phrase “meaningful use” has been on the mind of every healthcare provider in the United States since 2009, when Congress passed the Health Information Technology for Economic and Clinical Health (HITECH) Act to spur the adoption of electronic health records as part of the American Recovery and Reinvestment Act (ARRA). Like all medical providers, oncologists and cancer treatment centers can earn incentives from the U.S. government of up to $44,000 per physician by demonstrating meaningful use of a certified electronic medical record. For physician-owned New Mexico Cancer Center (NMCC) that means an infusion of nearly half a million dollars in revenue over five years, and they aren’t about to leave that money on the table.
For NMCC, qualifying under the stage 1 criteria for mean-ingful use, set by the Centers for Medicare & Medicaid Services (CMS), means more than additional income. It’s a matter of leadership in quality care.
NMCC is a full-service oncology practice that treats ap-proximately one-third of cancer patients in New Mexico from a main clinic in Albuquerque and four others in smaller communities. All the centers are networked and share the ARIA® oncology information system as their electronic
medical record. This allows the practice to standardize care and the 11 physicians to see patients at any location. Cofounder and CEO Barbara McAneny, MD, drives NMCC to be a frontrunner in the adoption of technology for the advancement of patient care, says Agnes Gonzales, RT. Gonzales, who now works in the IT department as a clinical systems implementation and training specialist, is NMCC’s go-to expert on the CMS criteria for meaningful use.
In addition to a culture of technology leadership, Gonzales credits several factors enabling NMCC to qualify early for the maximum financial incentives. She shared the NMCC experience and some lessons learned at the ARIA Medical Oncology User Group meeting in May.
Making Sense of“Meaningful Use”
Agnes Gonzales, RT(R)(T), is NMCC’s go-to expert on the CMS criteria for meaningful use.
By Nancy Heifferon

CENTERLINE | AUGUST–SEPTEMBER 2012 | 29
A head start with ARIA
“We were fortunate at NMCC because we had already con-verted to a paperless environment. We were no longer using charts. Much of the data and documentation required by the CMS objectives were already in our ARIA EMR in some form,” says Gonzales.
“Most of the providers of medical oncology that Varian works with are already collecting data and documenting treatment reasonably well in ARIA because they’re providing holistic care for the patient,” says Ken Hotz, PhD, Varian senior product manager for oncology information systems. “However, the CMS meaningful use criteria require some new capabilities.”
To receive funding under the HITECH Act, practices must first have an EMR that is capable of meeting the CMS objec-tives. Varian has received ARRA/HITECH certification for ARIA medical oncology and radiation oncology software, including e-prescribing. With certification, ARIA clears that first hurdle. Certification means that ARIA is capable of meeting the 25 objectives of stage 1 (15 core and 10 menu objectives), but simply owning a certified system isn’t suf-ficient to merit the incentive payments. Eligible professionals must also show that they are using the capabilities of the system to a meaningful degree.
Varian has added features to ARIA making that easier to accomplish, says Hotz. A dashboard that is updated daily shows at a glance how individual providers—and also, the practice as a whole—are doing at reaching the percentages
required to meet the threshold for meaningful use. For example, a mandatory objective requires that providers record the race and ethnicity of patients in addition to gender, date of birth, and language. In the past, NMCC didn’t record patient race or ethnicity. Now, to comply with meaningful use requirements, they must show that this information is recorded as structured data for more than 50 percent of their patients. The ARIA dashboard displays daily the current total number of eligible patients in the system, the number of patients for whom the data have been recorded appropriately, and the percentage of compliance achieved.
In addition, the dashboard generates reports showing the data that are missing for each patient. The missing-data reports help the provider backfill the EMR with information that they may already have on the patient but which hasn’t been appropriately recorded.
Identify a “meaningful use” expert
NMCC started with ARIA—a certified EMR. The next step was to understand the meaningful use guidelines and the attestation process. “It’s important to have one person who is the central point of contact for all questions that come up,” says Gonzales, who became the center’s expert. As an ARIA superuser and trainer for NMCC staff on Varian soft-ware, with both clinical and IT experience, Gonzales is a natural for the role. Plus she is committed to the challenge. “I’m the expert by default because I was the most ambitious
“We were fortunate at NMCC because we had already converted to a paperless environment. We were no longer using charts. Much of the data and documen-tation required by the CMS objectives were already in our ARIA EMR in some form.” Agnes Gonzales, New Mexico Cancer Center

30 | CENTERLINE | AUGUST–SEPTEMBER 2012
person in the room as far as wanting to learn all about meaningful use,” she says. “I was excited to learn about it.”
Involve IT
Gonzales stresses the importance of involving the IT team from the outset. After all, one of the mandatory requirements is to protect the health information created or maintained by the certified EMR. In many cases, it takes IT expertise to perform the proper security assessment and manage secure user access.
Other objectives involve the electronic exchange of clinical data, making the IT perspective essential to success. The requirement for exchanging Continuity of Care Documents (CCDs) is an example. “Medical oncology practices are generally good about exchanging information with referring doctors, but normally they would do that by sending a printed document by mail or fax,” observes Hotz. The mean-ingful use guidelines require that a CCD be sent as an .xml file of structured data that can be incorporated into another EMR system. “You can’t simply e-mail the information right out of the system,” notes Gonzales. “You have to set it up in the background through an Exchange server. For that you need IT help.”
Providers must also meet one of the public health require-ments—either reporting syndromic surveillance data elec-tronically to a public health agency or sending information electronically to an immunization registry. “Testing the interfaces can be technically daunting, so if you have an IT department like we do, they will take care of that,” says Gonzales.
Map the ripples of change
While many clinics are already collecting and documenting most of the information required by the meaningful use guidelines, there are bound to be procedural changes that have to be made across the organization—from registration to discharge. “Once we had analyzed the core objectives and decided which optional requirements to meet during stage 1, our next task was to figure out which parts of the organization were touched by them,” says Gonzales. “We
had to understand all our processes and identify what needed to change. We did some fact-finding to identify the measures we were already meeting, and then we focused on the measures we weren’t meeting in order to put new or revised processes in place.” Changing the registration process to include capturing data on race was just one example.
Have a physician champion
Attesting for meaningful use requires changes in behavior at every level. Physicians, too, have to be willing to change how they do things. “You may be performing a required task in ARIA, but you have to do it in a specific way so that it can be tracked,” says Hotz. For example, adds Gonzales, “Physicians must be willing to enter diagnoses into the system using structured data in the form of ICD-9 codes.” For this reason, a physician champion is critical to success. NMCC had the best possible champion—the CEO, Barbara McAneny. “She got everyone to embrace the process and the changes,” says Gonzales.
A happy ending is just the beginning
NMCC physicians were well prepared for attesting to mean-ingful use of the ARIA EMR. The required reports were created for them from the ARIA system. Funding for 2011 has been received for eight attesting physicians, and now they are waiting for stage 2 guidelines to be finalized.
Stage 2 will increase the burden on providers. “Practices that haven’t already begun the journey may want to start by doing as much as they can in ARIA now,” advises Hotz. “As the sites are comfortable with the basic documentation, additional capabilities specific to the HITECH Act can be introduced, minimizing the impact to the practice.” ARIA medical oncology customers tend to be fairly sophisticated and deep users of the EMR, he adds, so their transition into meaningful use will likely be easier. They are already used to doing many tasks in the way required for meaningful use attestation.
Gonzales, who worked as a radiation therapist and ap-plications specialist in northern California for several years prior to joining NMCC as chief therapist, subsequently joined the IT department to help implement and adopt ARIA for both medical and radiation oncology. She points out that recording data for meaningful use documentation is con-ceptually quite similar to the practice of “record and verify” that has been in place for some time in the radiation oncology setting. “If you understand the record and verify systems for radiation therapy, you’ll be surprised,” she says. “‘Meaningful use’ will seem familiar.” n
Nancy Heifferon is a freelance healthcare writer.
“We had to understand all our processes and identify what needed to change. We did some fact-finding to identify the measures we were already meeting, and then we focused on the measures we weren’t meeting in order to put new or revised processes in place.” Agnes Gonzales, New Mexico Cancer Center

CENTERLINE | AUGUST–SEPTEMBER 2012 | 31
Last fall, Varian acquired Calypso® Medical Technologies, Inc., the Seattle-based de-veloper and supplier of GPS for the Body®
technology and other specialized tools for real-time tumor tracking and motion management during radiosurgery and radiotherapy. Accord-ing to Varian CEO Tim Guertin, the acquisition enables Varian to offer cancer treatment centers real-time, nonionizing tumor tracking tools for enhancing the precision of their treatments. “These products are a perfect complement for Varian’s motion management technology, includ-ing our TrueBeam™ platform, respiratory gating and dynamic imaging tools for highly focused radiosurgery,” he says.
The Calypso technology has now been incorporated into Varian’s Pivotal™ Treatment Solution for Prostate Care, one of several new Pivotal Treatment Solutions designed to offer disease-specific technologies.
Pivotal Prostate Care accomplishes real-time tracking through the use of electromagnetic Beacon® transponders, which are implanted and then continuously tracked with the 4D localization and tracking system so that beams can be precisely delivered. Cleared by the FDA for use in the prostate and postoperative prostatic bed, Pivotal Prostate Care enables detection of even the slightest tumor movement in real time, allowing the therapist to pause during treatment and readjust the patient if necessary.
Real-time tracking meets real-time treatment delivery
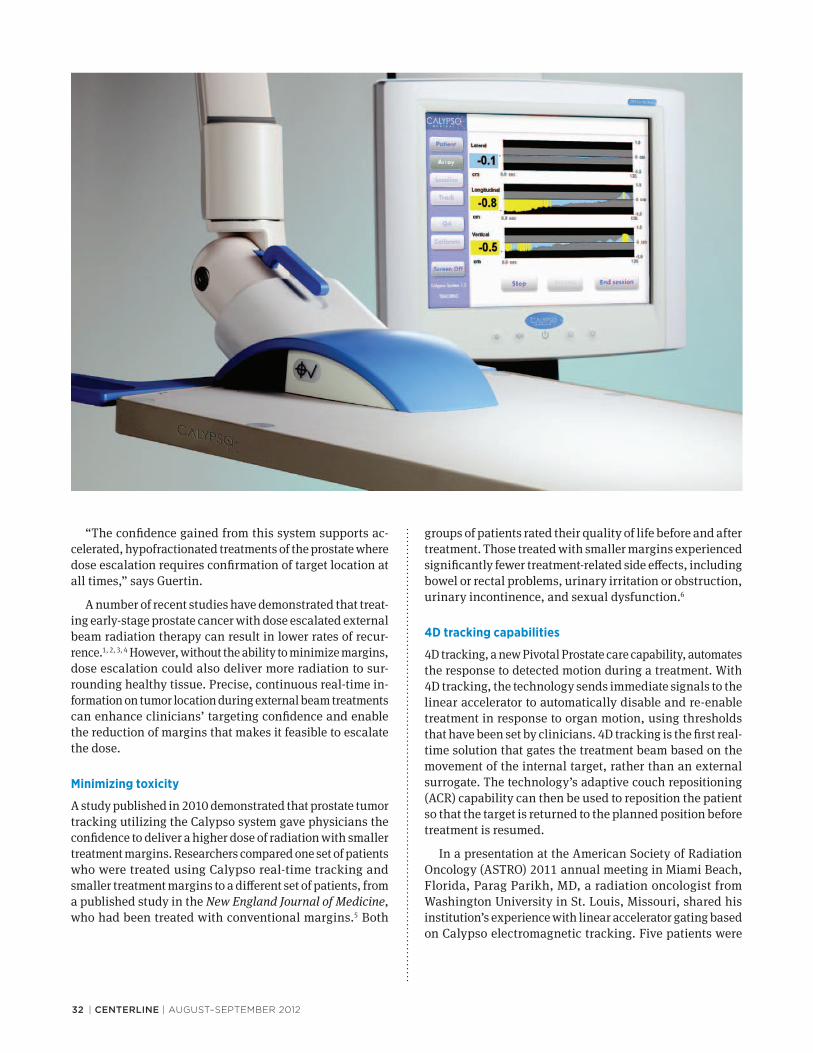
32 | CENTERLINE | AUGUST–SEPTEMBER 2012
“The confidence gained from this system supports ac-celerated, hypofractionated treatments of the prostate where dose escalation requires confirmation of target location at all times,” says Guertin.
A number of recent studies have demonstrated that treat-ing early-stage prostate cancer with dose escalated external beam radiation therapy can result in lower rates of recur-rence.1, 2, 3, 4 However, without the ability to minimize margins, dose escalation could also deliver more radiation to sur-rounding healthy tissue. Precise, continuous real-time in-formation on tumor location during external beam treatments can enhance clinicians’ targeting confidence and enable the reduction of margins that makes it feasible to escalate the dose.
Minimizing toxicity
A study published in 2010 demonstrated that prostate tumor tracking utilizing the Calypso system gave physicians the confidence to deliver a higher dose of radiation with smaller treatment margins. Researchers compared one set of patients who were treated using Calypso real-time tracking and smaller treatment margins to a different set of patients, from a published study in the New England Journal of Medicine, who had been treated with conventional margins.5 Both
groups of patients rated their quality of life before and after treatment. Those treated with smaller margins experienced significantly fewer treatment-related side effects, including bowel or rectal problems, urinary irritation or obstruction, urinary incontinence, and sexual dysfunction.6
4D tracking capabilities
4D tracking, a new Pivotal Prostate care capability, automates the response to detected motion during a treatment. With 4D tracking, the technology sends immediate signals to the linear accelerator to automatically disable and re-enable treatment in response to organ motion, using thresholds that have been set by clinicians. 4D tracking is the first real-time solution that gates the treatment beam based on the movement of the internal target, rather than an external surrogate. The technology’s adaptive couch repositioning (ACR) capability can then be used to reposition the patient so that the target is returned to the planned position before treatment is resumed.
In a presentation at the American Society of Radiation Oncology (ASTRO) 2011 annual meeting in Miami Beach, Florida, Parag Parikh, MD, a radiation oncologist from Washington University in St. Louis, Missouri, shared his institution’s experience with linear accelerator gating based on Calypso electromagnetic tracking. Five patients were

centerline | AUGUST–SEPTEMBER 2012 | 33
implanted with Beacon transponders and received an IMRT treatment on a Trilogy® machine. Gating limits were set at plus or minus 2 mm in each direction. Patients were imaged and the transponder coordinates were recorded relative to the treatment isocenter. These data were entered into the system as a reference for treatment localization and tracking.
At the time of treatment, the electromagnetic array was used to continuously measure the position of the transpon-ders. Patients were localized by comparing detected tran-sponder positions to planned positions. Radiation delivery was automatically held whenever the internal target moved outside the preset patient-specific threshold that had been established by the clinical team. When the target returned within the motion threshold, radiation delivery was auto-matically resumed.
This automated approach was contrasted to a manual process without 4D tracking, with therapists intervening to stop the beam. If the tumor drifted out of position, Parikh’s team utilized a manual option to remotely move the patient back to isocenter. “This gate-and-shift system configuration closes the loop between target tracking and therapy delivery by automatically pausing when the target moves outside the tracking limits,” says Parikh. “It enables us to respond efficiently by repositioning the patient from outside the room.”
Enhanced RapidArc delivery
Pivotal Prostate Care also has the potential to enhance the quality of RapidArc® treatments, which are increasingly being used to expedite delivery of high-dose-rate stereotactic body radiotherapy. “During a rapid, high-dose-rate treatment such as a hypofractionated protocol for prostate cancer, the impact of a geometric miss may be amplified whenever the target volume moves outside the isocenter,” says Chris Toth, vice president of marketing for Varian’s Oncology Systems business. “We believe that Pivotal Prostate Care can play a role in helping to ensure that dose is delivered accurately to the intended target during these treatments.” n
References
1. Zietman AL, DeSilvio ML, Slater JD, et al. Comparison of conventional-dose vs. high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate. JAMA. 2005;294: 1233–1239.
2. Kuban DA, Tucker SL, Dong L, et al. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70:67–74.
3. Peeters ST, Heemsbergan WD, Koper PC, et al. Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase 3 trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol. 2006;24:1990–1996.
4. Dearnaley DP, Sydes MR, Graham JD, et al. Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: first results from the MRC RT01 randomized controlled trial. Lancet Oncol. 2007;8:475–487.
5. Sanda MG, Dunn RL, Michalski J, et al. Quality of life and satisfaction with outcome among prostate-cancer survivors. N Engl J Med. 2008;358:1250–1261.
6. Sandler H, et al. Reduction in patient-reported acute morbidity in prostate cancer patients treated with 81-Gy intensity-modulated radiotherapy using reduced planning target volume margins and electromagnetic tracking: assessing the impact of margin reduction study. Urology. 2010;75(5):1004–1008.
“This gate-and-shift system configuration closes the loop between target tracking and therapy delivery by automatically
pausing when the target moves outside the tracking limits. It enables us to
respond efficiently by repositioning the patient from outside the room.”
Parag Parikh, MD, Washington University

34 | CENTERLINE | AUGUST–SEPTEMBER 2012

CENTERLINE | AUGUST–SEPTEMBER 2012 | 35
Since the introduction in 2010 of the TrueBeam™ system for image-guided radiotherapy and radiosurgery,
hundreds of machines have been ordered by treatment centers around the world. TrueBeam technology has now been deployed at the Cancer Research Center of Languedoc-Roussillon at the Centre Val d’Aurelle in Montpellier, France; the Hong Kong Sanatorium & Hospital; the Welling-ton Hospital in New Zealand; the Chulabhorn Hospital in Thailand; and two treatment centers in India: HCG Ahmedabad and BGS Global Hos-pitals in Bangalore.
First patient treated in France
Toward the end of 2011, a 19-year-old man with a cerebral glioblastoma became the first person in France to be treated using the TrueBeam radiotherapy treatment system. It was one of three TrueBeam devices acquired by the Cancer Research Center of Languedoc-Roussillon at the Centre Val d’Aurelle.
“We believe TrueBeam’s dose delivery speed and its unique ability to image the patient during the treatment will bring considerable benefits for our patients,” says Jean-Bernard Dubois, MD, head of radiotherapy. “With TrueBeam we are able to track the tumor during the treat-ment and adapt the treatment delivery in real time, which helps to better target the tumor and limit damage to sur-rounding healthy organs.”
TrueBeam system adopted in Hong Kong
In Hong Kong, clinicians at the Hong Kong Sanatorium & Hospital used their new system for the treatment of a
metastatic bone lesion as well as to deliver image-guided and intensity-modulated radiotherapy treatments for head and neck cancer.
“The TrueBeam system improves on earlier generations of technology,” says Wing-Hong Kwan, MD, director of the department of radiotherapy, who was particularly excited about the ability to synchronize treatment with a patient’s respiratory motion and to generate real-time images during treatment. “These capabilities enable us to verify and confirm that we are accurately targeting the tumor throughout a course of treatment,” he says. “They provide us with an added measure of accuracy.”
300+ treatments delivered in New Zealand
By the end of 2011, staff at one of New Zealand’s leading hospitals had delivered more than 300 radiotherapy treat-ments using their newly installed TrueBeam device in the first month of its implementation.
Their first TrueBeam patient was an 18-year-old man with Hodgkin’s disease. “He commented on the increased speed with which the treatment was delivered and was enthusiastic to be our first patient treated on TrueBeam,” says Jennifer de Ridder, radiation therapist team leader at Wellington Hospital. “Many of our patients have commented on the streamlined workflow and greater speed, which is a significant factor for those patients who are immobilized during treatment.”
TrueBeam Deployments Continue Around the World
“We believe TrueBeam’s dose delivery speed and its unique ability to image the patient during the treatment will bring considerable benefits for our patients.”Jean-Bernard Dubois, MD Cancer Research Center of Languedoc-Roussillon
“Many of our patients have commented on the streamlined workflow and greater speed, which is a significant factor for those patients who are immobilized during treatment.”Jennifer de Ridder, Wellington Hospital

36 | CENTERLINE | AUGUST–SEPTEMBER 2012
To manage treatment waiting times in New Zealand, the government recently introduced a target that all patients should commence radio-therapy within four weeks of a decision to treat. “We usually meet this target but need to be efficient to continue meeting it in future,” says Carole Johnson, Wellington’s clinical leader of radiation oncology. “So more advanced treatment techniques must be incorporated without making treatment slots longer and without impacting our ability to meet this waiting time target. TrueBeam helps us to achieve this.”
“As well as improving workflow at the hospital, TrueBeam will enable us to introduce stereotactic body radiotherapy treatments for selected patients in 2012,” says Lynne Greig, chief medical physicist. “It clearly positions us for the future and integrates well into our existing suite of equipment.”
Liver cancer treated in Thailand
Clinicians at the Chulabhorn Hospital in Thailand have now used their newly installed TrueBeam system to deliver RapidArc® radiotherapy in the treatment of liver cancer.
“We determined that the lesion could not be excised surgically or treated with radiofrequency ablation because it was too close to critical structures,” says Kanyanee Laebua, MD, head of radiation oncology at the hospital. “The TrueBeam system was ideal for this treatment. We were able to use the TrueBeam system’s High-Intensity Mode, which delivers high doses very quickly. Once the patient was set up on the treatment couch, the actual active treatment time was less than two minutes for each treatment session. The image-guidance tools on the TrueBeam system are easier and faster for our clinicians to operate, compared with earlier genera-tions of technology.”
Two Indian centers deploy TrueBeam
In India, two treatment centers deployed TrueBeam systems within days of each other. At HCG (Health Care Global) Ahmedabad, the first TrueBeam treatments were for a patient who received accelerated partial breast irradiation, allowing her treatment course to be completed in a week instead of the more conventional five. And at BGS Global Cancer Institute in Bangalore, clinicians used a TrueBeam STx machine for treating a 57-year-old female patient with a brain metastasis, who received whole brain radiotherapy followed by stereo-tactic radiosurgical boosts to the lesion.
“The whole procedure, the imaging and treatment, was completed within five minutes,” says Nirmala Srikantia, MD, senior consultant and chief of radiation oncology services at BGS. “TrueBeam STx gives our oncologists the flexibility to deliver multiple high-precision treatments such as this while minimizing the time required and, potentially, the inconvenience to the patient.”
Initial TrueBeam STx treatments at BGS Global Hospitals focused on brain, head and neck, gastrointestinal, and gynecologic cancers using intensity-modulated radiotherapy (IMRT). Early this year, the team began offering stereotactic radiosurgery treatments. “Since the hospital was established, our specialists have routinely treated various types of cancers using medical oncology and surgery, but the TrueBeam STx means we can now offer advanced radiosurgery treatments in addition,” says K. Ravindranath, CMD, chairman and managing director of Global Hospitals Group.
Vivek Bansal, MD, radiation oncologist at HCG Ahmedabad, points to the shorter treatment times, high-quality imaging, and greater throughput as the most significant benefits afforded by the TrueBeam system. “We plan to use TrueBeam to carry out a number of treatments which, as with this first patient, will reduce the length of treatment time as well as enabling overall treatment courses to be carried out in a week rather than several weeks,” he says. “It provides a possibility to address difficult-to-treat cancers such as lung cancer and liver cancer with radiotherapy.”
“We intend to use our TrueBeam devices to treat all forms of cancer, especially those that involve tumor motion, and it enables us to use more complex techniques for the benefit of our patients,” says David Azria, MD, PhD, head of radio-biology and translational research at the Centre Val d’Aurelle in Montpellier, France. “We see TrueBeam as the future development platform in linear accelerators and we wish to be up-to-date for the next 10 years.” n
“We determined that the lesion could not be excised surgically or treated with radiofrequency ablation because it was too close to critical structures. The TrueBeam system was ideal for this treatment.”Kanyanee Laebua, MD, Chulabhorn Hospital
“TrueBeam STx gives our oncolo-gists the flexibility to deliver multiple
high-precision treatments while minimiz-ing the time required.” Nirmala Srikantia, MD, BGS Global Cancer Institute

At Varian, we believe that one of the most powerful tools to battle cancer
is collaboration. Let us partner with you as we deploy our newest oncology
innovations in products, software and services. Together, we can draw on our
collective energy to fight cancer and build a better future.
To learn more, visit varian.com/oncology
© 2012 Varian Medical Systems, Inc. and Varian Medical Systems are registered trademarks of Varian Medical Systems, Inc.
CANCER DIVIDES.SO WE UNITE.

Presort StandardUS Postage
Paid San Jose, CA.
Permit No. 2196
3100 Hansen Way
Palo Alto, CA 94304-1038
make cancerthe victim.
How do you fight cancer? You outsmart it. With radiation treatment so advanced it can locate tumors with pinpoint precision and speed. Make cancer the victim.
TrueBeam from Varian. Visit varian.com/truebeam to find out more.
© 2012 Varian Medical Systems, Inc. All rights reserved. Varian and Varian Medical Systems are registered trademarks and TrueBeam is a trademark of Varian Medical Systems, Inc.
Varian Centerline 5.5x8.5 Ad v1.indd 1 7/18/12 2:11 PM

![arXiv:2208.01009v1 [cs.CL] 1 Aug 2022](https://static.fdokumen.com/doc/165x107/6335a6068502b620dc08ed02/arxiv220801009v1-cscl-1-aug-2022.jpg)


![arXiv:2003.10608v6 [cs.CV] 18 Aug 2020](https://static.fdokumen.com/doc/165x107/632690595c2c3bbfa803c078/arxiv200310608v6-cscv-18-aug-2020.jpg)
![arXiv:1908.11675v1 [cs.CV] 30 Aug 2019](https://static.fdokumen.com/doc/165x107/63275bd25c2c3bbfa8042353/arxiv190811675v1-cscv-30-aug-2019.jpg)

![arXiv:1905.07373v2 [cs.CV] 14 Aug 2019](https://static.fdokumen.com/doc/165x107/631fe7522dde36dbcb013318/arxiv190507373v2-cscv-14-aug-2019.jpg)
![arXiv:1908.05413v2 [math.MG] 2 Aug 2021](https://static.fdokumen.com/doc/165x107/631900411e5d335f8d0af8cb/arxiv190805413v2-mathmg-2-aug-2021.jpg)

![arXiv:2108.07031v1 [cs.PL] 16 Aug 2021](https://static.fdokumen.com/doc/165x107/63154f22c72bc2f2dd04a8d7/arxiv210807031v1-cspl-16-aug-2021.jpg)
![arXiv:1603.05474v4 [cs.CV] 2 Aug 2017](https://static.fdokumen.com/doc/165x107/6325f327e491bcb36c0a8d1b/arxiv160305474v4-cscv-2-aug-2017.jpg)



![arXiv:1704.08381v3 [cs.CL] 18 Aug 2017](https://static.fdokumen.com/doc/165x107/631f5ffd85e2495e151058f9/arxiv170408381v3-cscl-18-aug-2017.jpg)
![arXiv:1108.4223v1 [math.LO] 22 Aug 2011](https://static.fdokumen.com/doc/165x107/631dfc271aedb9cd850f8bc1/arxiv11084223v1-mathlo-22-aug-2011.jpg)
![arXiv:2008.07486v1 [stat.AP] 17 Aug 2020](https://static.fdokumen.com/doc/165x107/631ce10276d2a4450503bd91/arxiv200807486v1-statap-17-aug-2020.jpg)

