
Case management for the mentally ill: a comparative evaluation of client satisfaction
10
Health and Social Care in the Community 5(2), 106-1 15 Case management for the mentally ill: a comparative evaluation of client satisfact ion Deborah Cullen’ BA(Hons), Allyson Waite’ BSc(Hons), Nicolas Oliver’ MA, Jerome Carson’ BA(Hons), MSc, CPsychol and Frank Holloway2 MA, MRCPsych ‘Psychology Department, Institute of Psychiatry and ‘Maudsley Hospital, Denmark Hill, London, UK Correspondence Frank Holloway Maudsley Hospital Denmark Hill London SE5 8AZ UK Abstract This paper reports on client satisfaction with community mental health services. A Client Satisfaction Interview was used as one outcome measure in a randomized controlled study of clinical case management vs. standard community care. The Interview had high internal consistency reliability (Cronbachs alpha = 0.89) with very high inter-rater reliability for overall scores (Y = 0.99) and good inter-rater reliability for individual items (kappa over 0.9 for 18 of 22 items). Case management clients had significantly higher total satisfaction scores than control group clients who received standard community care at 9 months (t = 2.02 P = 0.05) but not at baseline (t = 0.59, P = 0.55) or 18 months (t = 1.76, P = 0.09). In addition to a quantitative measure of satisfaction, clients were asked to provide more qualitative accounts of their experience with services. The findings are discussed in relation to the team’s model of case management and the differences between case management and control services. The limitations of this study are considered in the context of methodological issues surrounding measurement of client satisfaction and the study’s own methodological shortcomings. Keywords: case management, mental illness, satisfaction Accepted for publication 5 March 1996 Introduction Satisfaction with services has been widely acknowl- edged to influence patient behaviours in terms of care seeking, compliance with treatment and maintaining contact with practitioners (Locker & Dunt 1978). However, it is only relatively recently that consumer views have been taken into account in the evaluation of mental health services in Britain. This has occurred in part as a response to Government initiatives that have emphasized the consumer perspective in the evaluation and monitoring of health services (Williams & Wilkinson 1995).However, the process of measuring consumer satisfaction has been fraught with numerous methodological difficulties (Webb 1993, Ruggeri 1994). Studies of patient satisfaction with medical care tend to report high levels of satisfaction. Studies of satisfaction with psychiatric services show similar results (e.g. Raphael 1972, Polowczyk et al. 1993). Where hospital-based care has been compared with community services greater satisfaction with commu- nity services has been found (Bene-Kociemba et al. 1982, Hoult et al. 1983).There is a tendency in evaluat- ing client satisfaction to use global measures of satis- faction, although these often show little differences across settings and client groups (Essex 1981). A more fruitful approach is to examine satisfaction and dissat- isfaction with specific aspects of the service being assessed (Holloway 1993). In addition qualitative data involving the comments of service users can usefully complement quantitative satisfaction data (Wykes & Carroll 1993). Recently case management has been advocated as a solution for the perceived failings of community care for people with long-term mentally illness. The broad 106 0 1997 Blackwell Science Ltd
Transcript of Case management for the mentally ill: a comparative evaluation of client satisfaction

Health and Social Care in the Community 5(2), 106-1 15
Case management for the mentally ill: a comparative evaluation of client sat isfact ion
Deborah Cullen’ BA(Hons), Allyson Waite’ BSc(Hons), Nicolas Oliver’ MA, Jerome Carson’ BA(Hons), MSc, CPsychol and Frank Holloway2 MA, MRCPsych ‘Psychology Department, Institute of Psychiatry and ‘Maudsley Hospital, Denmark Hill, London, UK
Correspondence Frank Holloway Maudsley Hospital Denmark Hill London SE5 8AZ UK
Abstract This paper reports on client satisfaction with community mental health services. A Client Satisfaction Interview was used as one outcome measure in a randomized controlled study of clinical case management vs. standard community care. The Interview had high internal consistency reliability (Cronbachs alpha = 0.89) with very high inter-rater reliability for overall scores (Y = 0.99) and good inter-rater reliability for individual items (kappa over 0.9 for 18 of 22 items). Case management clients had significantly higher total satisfaction scores than control group clients who received standard community care at 9 months ( t = 2.02 P = 0.05) but not at baseline ( t = 0.59, P = 0.55) or 18 months ( t = 1.76, P = 0.09). In addition to a quantitative measure of satisfaction, clients were asked to provide more qualitative accounts of their experience with services. The findings are discussed in relation to the team’s model of case management and the differences between case management and control services. The limitations of this study are considered in the context of methodological issues surrounding measurement of client satisfaction and the study’s own methodological shortcomings.
Keywords: case management, mental illness, satisfaction
Accepted for publication 5 March 1996
Introduction
Satisfaction with services has been widely acknowl- edged to influence patient behaviours in terms of care seeking, compliance with treatment and maintaining contact with practitioners (Locker & Dunt 1978). However, it is only relatively recently that consumer views have been taken into account in the evaluation of mental health services in Britain. This has occurred in part as a response to Government initiatives that have emphasized the consumer perspective in the evaluation and monitoring of health services (Williams & Wilkinson 1995). However, the process of measuring consumer satisfaction has been fraught with numerous methodological difficulties (Webb 1993, Ruggeri 1994).
Studies of patient satisfaction with medical care tend to report high levels of satisfaction. Studies of
satisfaction with psychiatric services show similar results (e.g. Raphael 1972, Polowczyk et al. 1993). Where hospital-based care has been compared with community services greater satisfaction with commu- nity services has been found (Bene-Kociemba et al . 1982, Hoult et al. 1983). There is a tendency in evaluat- ing client satisfaction to use global measures of satis- faction, although these often show little differences across settings and client groups (Essex 1981). A more fruitful approach is to examine satisfaction and dissat- isfaction with specific aspects of the service being assessed (Holloway 1993). In addition qualitative data involving the comments of service users can usefully complement quantitative satisfaction data (Wykes & Carroll 1993).
Recently case management has been advocated as a solution for the perceived failings of community care for people with long-term mentally illness. The broad
106 0 1997 Blackwell Science Ltd

Case management: satisfaction with care
aims of case management are to ’enhance the continu- ity of care and its accessibility, accountability and efficiency’ (Intagliata 1982). Outcome studies of case management, including a satisfaction measure, report a trend towards improved satisfaction with services (Wasylenki et al. 1985, Goering et al. 1988, Wright et al. 1989, Muijen et al. 1992) compared with traditional ser- vices. In addition, case managed clients have been reported to receive more services, to have fewer unmet service needs (Bigelow 1991) and to be more likely to still stay in contact with services 6 months after dis- charge from hospital (Wright et al. 1989).
There have been few controlled studies of case man- agement in Britain (Holloway et al. 1995). This paper reports on the findings of a randomized controlled trial of an intensive case management service vs. stan- dard care for patients with severe mental illness. An integral outcome measure was client satisfaction with services and the results are presented along with qual- itative comments from service users. In the light of existing research, it was hypothesized that case man- agement clients would report greater levels of satisfac- tion with services.
Methods
Participants were clients involved in the evaluation of an intensive clinical case management service com- pared with standard control services in a London inner-city area. All clients in the study were aged between 16 and 65 years and lived in a defined inner urban catchment area. All clients had a diagnosis of functional psychosis and had evidence of previous unsatisfactory engagement with mental health ser- vices, manifested by previous non-compliance with treatment, frequent readmission or poor symptomatic response to conventional management. Admission to the project was by referral from psychiatrists and other members of the multidisciplinary team. After baseline assessment clients were allocated randomly to the case management or control groups. Clients were inter- viewed at baseline (before randomization) and then 9 and 18 months later. The design was of an ’intention to treat’ type and attempts were made to follow up all 70 patients who gave consent to be entered into the study. Randomization was by sealed envelope utilizing ran- dom permuted blocks.
The case management service was delivered by a multidisciplinary team (four psychiatric nurses, one occupational therapist, with sessional input from a clinical psychologist and psychiatrist). The team worked to the model of clinical case management delineated by Kanter (1989). There were four aspects to the team’s functioning: engagement and assessment,
direct ’clinical’ work, ’social care’, and brokerage or advocacy. Interventions included: the assessment of mental state, the provision and monitoring of medica- tion, intervention in crisis, psycho-education and fam- ily therapy and assistance with practical aspects of daily living (including welfare benefits). The team sought to be accessible to clients with an ’open door’ policy at their base, in addition offering a regular socially orientated drop-in service. The case managers advocated on behalf of their clients with other health and social welfare agencies. Project clients’ care plans were reviewed regularly in a multidisciplinary meet- ing. The day-to-day running of the service is described in more detail elsewhere (Holloway ef al. in press).
The control group received the standard services available in the catchment area including input from community psychiatric nurses, social workers and a depot anti-psychotic clinic. Staff working with clients in both the case management and the control group referred to other services as appropriate, subject to the normal local service provision constraints.
This paper presents the findings from the investiga- tion of clients’ satisfaction with the services received during the course of the study. The measure used was developed by the research team but strongly influ- enced by other published measures (e.g. the General Satisfaction Questionnaire, Huxley & Mohamad 1991-2). The questionnaire had 22 satisfaction items each rated on a 4-point scale (0 = dissatisfied to 3 = very satisfied). During the course of the interview clients were also asked what they considered to be the positive and negative aspects of the service and how this could be improved; verbatim comments are used to complement quantitative data.
Results
Client characteristics
Socio-demographic characteristics of all the clients involved in the study are presented in Table 1. Project clients were typically male, in their 30s and had been suffering from a schizophrenic illness for over a decade. The majority were from ethnic minorities (largely Afro-Caribbean).
Reliability of the satisfaction interview
Twenty-one pairs of satisfaction interviews were car- ried out by members of the research team who had had previous training. The correlation between overall sat- isfaction scores (calculated by summing across all items) was high (Y = 0.99). For individual items reliabil- ity was very high (kappa > 0.9 for 18 of 22 items). Cronbach’s alpha for the scale was 0.89.
0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15 107

D. Cullen eta/.
Table 1 Socio-demographic characteristics of control and case management groups at baseline interviews
Case management Control n = 35 n=35
Number % Number %
Sex Male Female
Age group (years) < 20 20-29 30-39 40-49 50-59 60 +
22 63 24 69 13 37 11 31
0 0 1 3 9 26 14 40
17 49 11 31 5 14 6 17 2 5 2 5 2 6 1 3
Hospital diagnosis Schizophrenia and related disorders 29 83 35 100
Bipolar affective disorder 6 17 0 0
Ethnic origin White Non-white
Years since
17 49 15 43 18 51 20 57
onset of illness Mean (standard deviation) 12.7 (8.3) 10.5 (8.9)
Fifty-seven per cent of control and 68% of case man- agement clients agreed to a full satisfaction interview at 9 months and 51 % of control and 60% of case man- agement clients agreed to a full satisfaction interview at an 18-month follow-up
failed to reach significance (MANOVA F= 2.8, P = 0.076). For the two groups combined satisfaction improved significantly over time (MANOVA F = 16.9, P < 0.001).
Individual satisfaction items
Overall satisfaction
The mean total satisfaction scores at baseline, 9-month and 18-month follow-up are shown in Table 2. There was no significant difference between groups at base- line (t = 0.59, P = 0.55) or at 18 months (t = 1.76, P = 0.09), but the difference at 9 months was significant (t = 2.02, P = 0.05). A multivariate analysis of variance of the effect of project status on satisfaction scores at 9 and 18 months with baseline scores as a co-variate
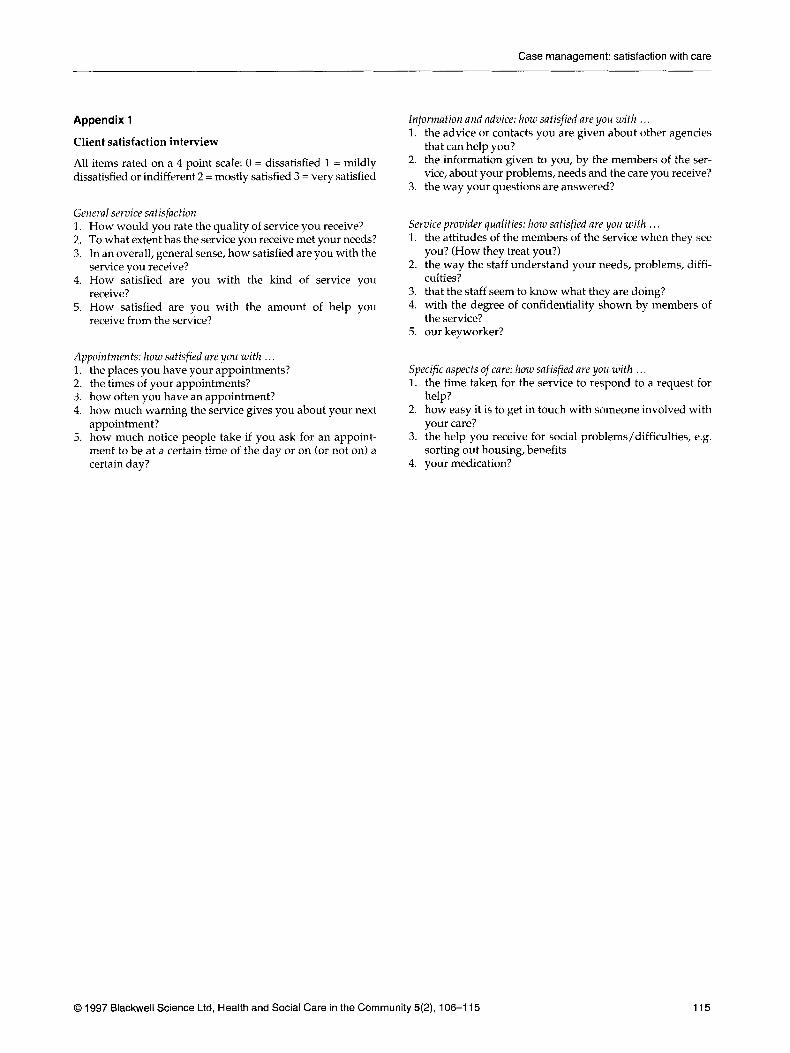
For the purposes of presentation individual items of the satisfaction interview were grouped a priori into five categories: general satisfaction (five items), appointments (five items), service provider qualities (five items), provision of information (three items), and specific aspects of treatment and care (four items). The items comprising these categories are presented in Appendix 1.
Responses on each item were recoded into ’satisfied’ (scores of 3 and 2) and ‘dissatisfied‘ (scores of 1 and 0).
Table 2 Total satisfaction scores for case
months and 18 months Baseline 9 months 18 months management control patients at baseline, 9
Case management n = 2 8 II = 26 n = 22 mean (standard deviation) 39.2 (18.1) 55.4 (9.1) 56.0 (9.7)
Control n = 31 n = 21 n = 1 8 mean (standard deviation) 41.8 (5.4) 49.0 (12.6) 48.3 (17.6) significance test t = 0.59, P = 0.55 t = 2.02, P = 0.05 t = 1.76, P = 0.09
108 0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15

Case management: satisfaction with care
The data were analysed using the chi-square statistic or Fisher’s exact test as appropriate in two-by-two contin- gency tables (control/case management vs. dissatis- fied/satisfied). The frequencies for the contingency tables at baseline, 9 months and 18 months are presented in Tables 3,4,5,6 and 7. There were no sigruficant differ- ences in levels of satisfaction found at baseline between those clients who were later to drop out of the interview process and those who completed it. Given the numbers of significance tests carried out, the results which follow should be considered as mainly suggestive.
General satisfaction
Case management clients were significantly more sat- isfied at 9 months than control patients on three of the five general items (see Table 3). There were no signifi- cant differences between the two groups at baseline and at 18-month follow-up, mainly due to an increase in satisfaction by control patients between nine and 18 months.
Case management clients spoke of being particu- larly satisfied with the range of help that was offered. This covered a broad spectrum of tasks and activities:
Any problem, she’ll sort it out -welfare, letters, medication’ ‘I never encountered help like this before - money, financial difficulties, hobbies, activities, making sure that I’m keeping myself organized - it’s been different.
There were also many comments highlighting the dif- ference between the case management service and pre- vious help clients had received:
Before, people just told me to keep taking the medication, but now people talk to me.
The help now is much better than before - people are con- cerned that my day is structured properly.
My case manager used to come to the flat, make cups of tea and chat with me - it was very helpful. No one from the hos- pital has ever done that before.
Appointments
There were no differences between case manage- ment and control patients in items relating to appointments (see Table 4) at any time point, and generally satisfaction was high. Many clients spoke of the importance of seeing someone regularly. The following comments, the first from a case manage- ment client and the second from a control group client illustrates the importance of regular help and support and the potential consequences of being without it:
When something happens, it might start building over the course of a few weeks. Before, I might start drinking heavily and end up in hospital. Seeing someone every week puts things into perspective.
When I get ill, I get no help at all. I can’t manage myself. I was going insane in my bedroom for four months ... social worker was contacted and didn’t come .... she doesn’t give me enough help.
There was, however, considerable individual variation as to the ideal frequency of visits by workers. Some individuals cited almost daily contact as optimum, whereas others felt they were seen ‘more than enough’ and would have been satisfied with contact once a month. Clients also showed some understanding of the difficulties and demands facing their workers. One client remarked that giving enough help to those who needed it was like ‘feeding the five thousand’, a seem- ingly impossible task. Many clients echoed the feelings of one who commented that:
. . . it would be better if there was more time, more nurses.
Baseline 9 months 18 months
(n = 28) ( n = 31) ( n = 26) (n = 21) ( n = 22) ( n = 18) CM(%) CTR(%) CM(%) CTR(%) CM(%) CTR(%)
Service quality 68 59 100 65 73 65% x2 = 7.9, P = 0.005
Needs met 53 54 88 53 90 71 % x2 = 6.8, P = 0.009
Overall satisfaction 74 68 96 71 100 82% Fisher P = 0.035
Type of service 78 70 96 75 95 76%
Help you get 72 69 88 81 91 67%
Table 3 Percentage of respondents reporting satisfaction at baseline, 9 month and 18 month follow-up for case management (CM) and control (CTR) clients: (overall satisfaction items)
0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15 109

D. Cullen eta/.
Table 4 Percentage of respondents reporting satisfaction at baseline, 9 month
management (CM) and control (CTR) clients: (appointments items)
Baseline 9 months 18 months
( n = 28) (n = 31) (n = 26) (n 21) ( n = 22) (n = 18) CM (%) CTR (%) CM (%) CTR (96) CM (%) CTR (%) and 18 month follow-up for
Place of
Time of
Frequency of
Warning of
Timing of
appointment 83 86 84 95 95 82
appointment 78 90 96 95 91 87
appointment 67 67 89 80 86 89
appointment 80 81 96 95 100 88
appointment 82 68 2 94 75 72
Service provider qualities
Respondents were generally positive about their professional carers (see Table 5). At 18 months the case management clients were significantly more satisfied than controls about the understanding shown by staff of their problems but there were otherwise no significant differences between the two groups.
Many case management clients reported the impor- tance of having someone they liked and trusted around:
They‘re there to talk to, if you want a chat, any worries you can just have a chat and they put your mind at rest.
. . . [my case manager] kept me alive - if I didn’t meet her I think I’d be a lot worse.
. . . [my case manager] is everything rolled into one: counsel- lor, nurse, someone to talk to, a shoulder to cry on - she’s like my ’spiritual sister’.
The more I get to know her, the more I can talk to her and tell her things.
They understand me now, it took a bit of time.
A common complaint in both the control and case
management group was the lack of contact with their psychiatrist, which occurred, on average, once every 4 or 6 weeks. This may have contributed to the difficul- ties communicating with and the alienation from some doctors that some clients reported:
There’s a barrier between me and the doctors; they don’t really want to talk to me but X [case manager] does.
. . . [my case manager] really wants to help me; she’s on my side whereas the doctors are against me.
... [my case manager] doesn’t agree that John the Baptist spoke to me, but she has an open mind. The doctors just think I’m mad.
Clients also reported dissatisfaction with the tempo- rary nature of doctors’ placements, a consequence of the rotation of junior medical staff:
X [the doctor] listens and accepts, but she is only there for six months and then she’s gone. It’s frustrating and annoying.
I see X [my consultant] once in a blue moon; that’s OK as long as the junior doctor listens to me. She [the junior doctor] is nice, I’d like her to be permanent. They should have someone there [at the day hospital] permanently, like a GP, not in tran- sit all the time.
Table 5 Percentage of respondents Baseline 9 months 18 months reporting satisfaction at baseline, 9 month CM (%) CTR (%) CM (%I CTR (%) CM (%) CTR (%) and 18 month follow-up for case (n = 28) ( n = 31) (n = 21) (n = 26) ( n = 22) ( n = 18) management (CM) and control (CTR)
clients (service provider items) Staff attitudes 71 81 96 91 91 89
Staff understanding 61 74 89 81 95 65 Fisher P = 0.02
Staff competence 78 83 100 85 95 78 Staff confidentiality 85 89 91 95 95 93 Keyworker 87 80 100 94 96 100
110 0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15

Case management: satisfaction with care
The provision of information
At baseline patients were notably dissatisfied with the information that they received from staff. Satisfaction with these items improved markedly by the nine month follow-up for both case-managed and control patients (see Table 6). The case management group were significantly more satisfied than controls at 18 months on one of the three items (staff understanding of the client’s problems). Respondents noted the diffi- culties they experienced in communicating with staff, not just their doctors:
It’s like a glass between the staff and me.
The style of the communication was also identified as important:
It’s not all rigid and formal -you can talk about anything.
She gives me answers that I can understand ... we seem to understand each other.
However, the mere provision of information and advice may not be perceived as adequate to meet clients’ needs:
They give me advice but nothing seems to be done.
Specific aspects of treatment and care
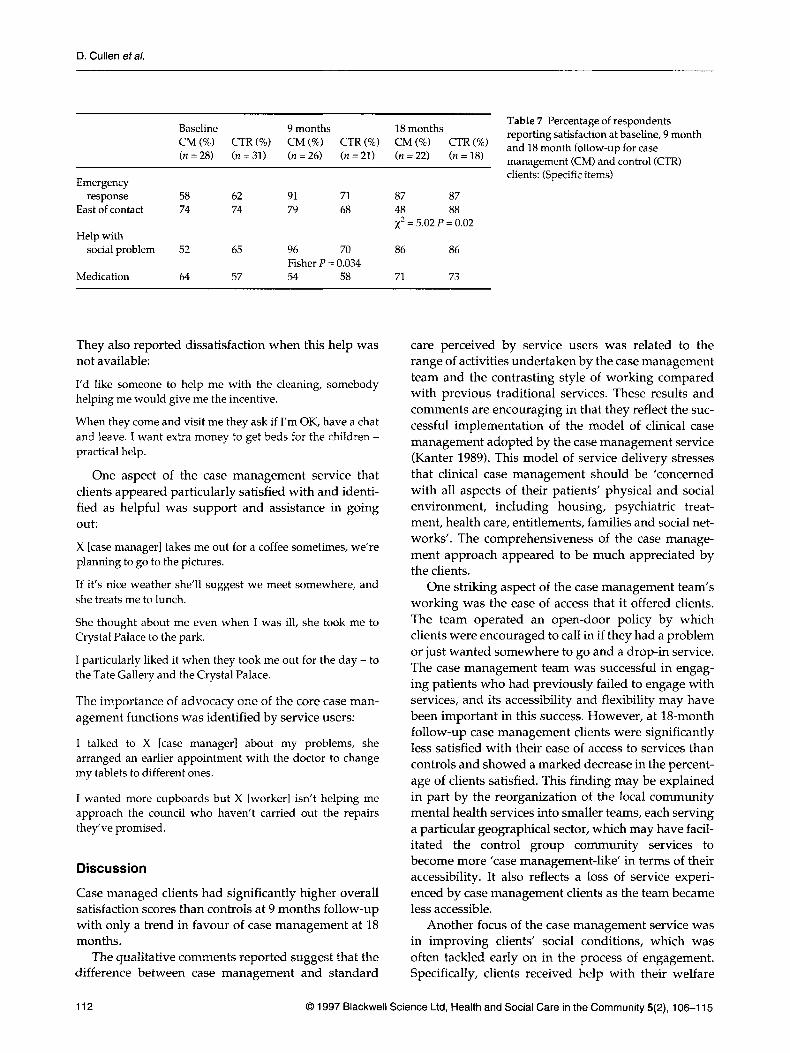
Case managed clients were significantly more satisfied with the help they received with their social problems at 9 months but not at 18 months: this was due to an increase in satisfaction by control patients between 9 and 18 months (see Table 7). There were no differences between the two groups regarding attitudes to medi- cation (an area where it had been predicted that case management would have an impact) and little evi- dence of change over time for this item. Satisfaction with the ease of contact with services became signifi- cantly worse for case managed clients at 18 months.
Although clients in both groups noted an improve- ment in the response of services to requests for help in an emergency over time, they remarked on the diffi-
culty of obtaining help ’out of hours’. Whereas some clients were not actively dissatisfied with this situation others expressed dissatisfaction that their only option would be to contact the local emergency psychiatric clinic and be treated by people unfamiliar with them and their circumstances. Some clients did not turn to services at all at these times:
Outside of 9-5 I rely on my friends.
At weekends I’d turn to my parents.
Within service hours clients held widely differing opinions on ease of access, ranging from ’impossible’ to ’easy on weekdays’. Most mentioned the possibility of telephoning workers in their offices if they needed help, but many talked about the frustrations of engaged lines or having to leave messages on answer- phones. The comments of the case management clients suggested they were gratified by the option of being able to come in and see somebody directly:
If phoning, the lines are engaged; if I come in myself I‘ve been seen straight away.
I usually come in [if I need help]. If X [case manager] isn’t here there’s always someone else.
This direct access diminished during the life of the research project (Holloway et aZ. in press). Clients’ comments indicated that they valued the practical help that was avaiIable from the case management service very highly:
I haven’t any problems with bills now X [case manager] helps me with them if I have any queries, she sorts something out.
I’m mostly satisfied with the treatment; there’s been lots of practical help, they’ve helped me get grants.
I enjoy chatting with X [case manager] and getting help with shopping and cooking.
They give me help with buying things for the flat and help at home like clearing away rubbish.
X [case manager] helped me with personal problems, poll tax, the council . . . without her help I’d have been lost.
Table 6 Percentage of respondents Baseline 9 months 18 months reporting satisfaction at baseline, 9 month CM (%) CTR (%) CM (%) CTR (%) CM (%) CTR (%) and 18 month follow-up for case (n = 28) (n = 31) (n = 21) (?7 = 26) (n = 22) ( n = 18) management (CM) and control (CTR)
clients: (information items) Informa tion
from staff 64 59 84 81 100 76 Fisher P = 0.02
Staff answers
Advice re to questions 62 59 84 95 86 82
other services 46 56 88 71 76 71
0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15 111
D. Cullen eta/.
Table 7 Percentage of respondents reporting satisfaction at baseline, 9 month
management (CM) and control (CTR) clients: (Specific items)
Baseline 9 months 18 months
(n = 28) (n = 31) (n = 26) (n = 21) (n = 22) (n = 18) CM (%) CTR (%) CM (%) CTR (%) CM (%) CTR (%) and 18 month follow-up for
Emergency response 58 62 91 71 87 87
East of contact 74 74 79 68 48 88
Help with x2 = 5.02 P = 0.02
social problem 52 65 96 70 86 86
Medication 64 57 54 58 71 73 Fisher P = 0.034
They also reported dissatisfaction when this help was not available:
I’d like someone to help me with the cleaning, somebody helping me would give me the incentive.
When they come and visit me they ask if I’m OK, have a chat and leave. I want extra money to get beds for the children - practical help.
One aspect of the case management service that clients appeared particularly satisfied with and identi- fied as helpful was support and assistance in going out:
X [case manager] takes me out for a coffee sometimes, we’re planning to go to the pictures.
If it’s nice weather she’ll suggest we meet somewhere, and she treats me to lunch.
She thought about me even when I was ill, she took me to Crystal Palace to the park.
I particularly liked it when they took me out for the day - to the Tate Gallery and the Crystal Palace.
The importance of advocacy one of the core case man- agement functions was identified by service users:
I talked to X [case manager] about my problems, she arranged an earlier appointment with the doctor to change my tablets to different ones.
I wanted more cupboards but X [worker] isn’t helping me approach the council who haven’t carried out the repairs they’ve promised.
Discussion
Case managed clients had significantly higher overall satisfaction scores than controls at 9 months follow-up with only a trend in favour of case management at 18 months.
The qualitative comments reported suggest that the difference between case management and standard
care perceived by service users was related to the range of activities undertaken by the case management team and the contrasting style of working compared with previous traditional services. These results and comments are encouraging in that they reflect the suc- cessful implementation of the model of clinical case management adopted by the case management service (Kanter 1989). This model of service delivery stresses that clinical case management should be ’concerned with all aspects of their patients’ physical and social environment, including housing, psychiatric treat- ment, health care, entitlements, families and social net- works’. The comprehensiveness of the case manage- ment approach appeared to be much appreciated by the clients.
One striking aspect of the case management team’s working was the ease of access that it offered clients. The team operated an open-door policy by which clients were encouraged to call in if they had a problem or just wanted somewhere to go and a drop-in service. The case management team was successful in engag- ing patients who had previously failed to engage with services, and its accessibility and flexibility may have been important in this success. However, at 18-month follow-up case management clients were significantly less satisfied with their ease of access to services than controls and showed a marked decrease in the percent- age of clients satisfied. This finding may be explained in part by the reorganization of the local community mental health services into smaller teams, each serving a particular geographical sector, which may have facil- itated the control group community services to become more ’case management-like’ in terms of their accessibility. It also reflects a loss of service experi- enced by case management clients as the team became less accessible.
Another focus of the case management service was in improving clients’ social conditions, which was often tackled early on in the process of engagement. Specifically, clients received help with their welfare
112 0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15

Case management: satisfaction with care
benefits which often resulted in a significant increase in their income. That this was successful can be inferred from the marked increase observed in case managed respondent’s satisfaction with the help they received for their social problems at 9 months. At 18 months control patients had shown similar increases in satisfaction, possibly reflecting a change in the ori- entation of the reorganized local services towards a more holistic approach to community mental health care. It had been expected that intensive case manage- ment would improve patient understanding of and compliance with medication: case managers spent con- siderable time discussing medication issues with their clients. This activity was not reflected in any noticeable change in clients’ attitudes towards their medication.
Respondents in both groups were consistently posi- tive about the staff who cared for them (except their psy- chiatrists) and the arrangements for appointments with staff. They were initially much less positive about the information and advice received from staff, although this improved over time in both groups. The clinical case management service was a time intensive service with clients being seen at least fortnightly and often more than once a week and at times daily. Choice of appoint- ment or visit location was client determined as was fre- quency. For the control group, visits were much more likely to be fortnightly to monthly with little choice about location. However, these differences in provision were not reflected in differences in rated satisfaction.
As with other studies of satisfaction the present study suffers from methodological limitations com- mon to the literature on satisfaction with care (Ruggieri 1994). Clearly these must be considered when interpreting the data and considered by future researchers of users’ views of psychiatric care.
The measure used in the current study was designed in-house, albeit partly modelled on existing scales, and was not piloted before use in the study. Initial experience with the scale suggests that it is reli- able and produces results that are interpretable. Researchers may wish to utilize an scale with well- established psychometric properties, e.g. the General Satisfaction Questionnaire (Huxley & Mohamad 1991-92) or the Verona Service Satisfaction Scale (Ruggeri & Dall’Agnola 1993), although this might mean a failure to investigate areas of satisfaction spe- cific to a service.
Specific to this study, the sample size was relatively small and therefore there are problems in generalizing to other populations. However, the sample is likely to be representative of ’hard to treat’ patients with psy- chotic illnesses in contact with inner-city services.
Related to small sample size, there was a significant proportion of clients who refused to participate in the
interviews (17% at baseline; 33% at first follow-up and 44% at second follow-up). It is possible that the clients who did complete the interviews were not representa- tive of the whole sample, although there were no sig- nificant differences between refusers and respondents on a range of baseline sociodemographic and clinical measures. In general, unsatisfied clients are more likely to drop out of studies of satisfaction (El-Guebaly ef al. 1983). There were more drop-outs from the con- trol than the case managed condition at 9 and 18 months, which is consistent with the apparent increased satisfaction amongst the case management clients who did respond to the interview.
Assessors were not blind to the treatment condition. This raises the possibility of assessor bias (although the reliability of the interview was high). Attempts to blind assessors to treatment condition would have made it impossible to collect the qualitative data which we sought.
The method of analysis by which responses are dichotomized into satisfied vs. dissatisfied may obscure more subtle group differences. It could be that with a sensitive enough measure, differences in ’amount’ of satisfaction might be investigated rather than gross comparisons of satisfaction/dissatisfaction. In this study an overall satisfaction score was calcu- lated to provide a measure of overall satisfaction: the overall scores differentiated between groups at 9 months but not at 18 months. It is argued that over the study period the control condition took on many of the characteristics of the case management service.
A major problem in this field of research is the lack of an agreed definition of satisfaction - ’the term sat- isfaction is defined differently by individuals as a result of varying backgrounds and experiences’ (Ware 1983). There are additional conceptual prob- lems with the measurement of client satisfaction simi- lar to those encountered in the measurement of sub- jective quality of life (Oliver et al . 1995). The cognitive processes involved in making a judgement of satis- faction are not transparent to the administrator of a satisfaction questionnaire. To compare ratings of sat- isfaction across individuals implies a universality of rating; that ‘mostly satisfied’ means the same for dif- ferent people. Even to compare within individuals longitudinally has its problems. Stimson & Webb (1975) suggest that satisfaction is related to the extent to which services meet clients’ expectations. It is con- ceivable that such expectations change over time but this is not an issue that is addressed by current mea- sures. In the current study case managed respondents initially reacted favourably to the accessibility of the service but became less satisfied as this extreme degree of availability was decreased.
0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15 113

D. Cullen eta/.
Studies report high levels of satisfaction, typically between 70 and 90% (Damkot et al. 1983). This may well be explained by the effects of social desirability in responding and acquiescence. High baseline levels of satisfaction make detection of change difficult due to a ceiling effect, apparent in this study in the very positive responses to questions about staff qualities and arrange- ments about appointments. It is notable however, in the current study that there were a number of individual items where 40% or more of the sample reported dissat- isfaction at baseline: the extent to which respondents felt their needs were met, the help that they received for their social problems, their medication, responses to urgent requests for help, staff responses to questions, and the advice respondents received about other agen- cies. All these areas improved substantially over time except satisfaction with medication.
The collection of qualitative data highlights impor- tant service satisfaction dimensions often overlooked by existing measures. Consistent with this Elbeck & Fecteau (1990) advocate the use a more unstructured, qualitative approach to elicit clients’ feelings regard- ing the services they receive. Keeping in mind the limi- tations outlined above, the current paper presents insights into factors contributing to clients’ satisfaction with community mental health services. It suggests that services that are comprehensive, flexible and accessible will be valued and positively regarded by the clients who receive them.
References Bene-Kociemba A,, Cotton P.G. & Fortgang C. (1982)
Assessing patient satisfaction with state hospital and after- care services. American Journal of Psychiatry 139,660-662.
Bigelow, D.A. & Young D.J. (1991) Effectiveness of a case management program. Community Mental Health Journal
Damkot D.K., Pandiani J.A. & Gordon L.R. (1983) Development, implementation and findings of a continu- ing client satisfaction survey. Community Mental Health Journal 19,265-278.
Elbeck M. & Fecteau G. (1990) Improving the validity of mea- sures of patient satisfaction with psychiatric care and treat- ment. Hospital and Community Psychiatry 41,998-1001.
El-Guebaly N., Towes J., Leckie A. & Harper D. (1983) On evaluating patient satisfaction: Methodological issues. Canadian Journal of Psychiatry 28,24-29.
Essex D. (1981) The development, factor analysis and revi- sion of a client satisfaction form. Community Mental Health Journal 17,226-235.
Goering P.N., Wasylenki D.A., Farkas M., Lancee W.J. & Ballantyne R. (1988) What difference does case manage- ment make? Hospital and Community Psychiatry 39,272-276.
Holloway F. (1993) The User Perspective on Mental Health Services: its Value and Limitations. In Lieper. R. & Field V (Eds) Counting for Something in Mental Health Services. Avebury, Aldershot.
27,115-123.
Holloway F., Oliver N., Collins E. & Carson J. (1995) Case management: a critical review of the outcome literature. European Psychiatry 10,113-128.
Holloway F., Murray M., Squire C. & Carson J. (in press) Intensive case management: putting it into practice. Psychiatric Bulletin.
Hoult J., Reynolds I., Charbonneau-Powis M., weeks P. & Briggs J. (1983) Psychiatric hospital vs. community treat- ment: the results of a randomised trial. Australian and New Zealand Journal of Psychiatry 17,160-7.
Huxley P. & Mohamad H. (1991-2) The development of a general satisfaction questionnaire for use in programme evaluation. Social Work and Social Sciences Review 3,63-74.
Intagliata J. (1982) Improving the quality of community care for the chronically mentally disabled: the role of case man- agement. Schizophrenia Bulletin 8,655-74.
Kanter J. (1989) Clinical case management: definition, princi- ples, components. Hospital and Community Psychiatry 40,
Locker D. & Dunt D. (1978) Theoretical and methodological issues in sociological studies of consumer satisfaction with medical care. Social Science and Medicine 12,283-292.
Muijen M., Marks I., Connolly J. & Audini B. (1992) Home based care for patients with severe mental illness: a ran- domised controlled trial. British Medical Journal304,749-754.
Oliver N., Holloway F. & Carson J. (1995) Deconstructing Quality of Life, Journal @Mental Health 4,1-4.
Polowczyk D., Brutus M., Orvieto A.A., Vidal, J. & Cipriani D. (1993) Comparison of patient and staff surveys of con- sumer satisfaction. Hospital and Community Psychiatry 44,
Raphael W. (1972) Psychiatric Hospitals Viewed by their Patients. King Edward’s Hospital Fund for London, London.
Ruggeri M. (1994) Patients’ and relatives’ satisfaction with psychiatric services: the state of the art and its measure- ment. Social Psychiatry and Psychiatric Epidemiology 29,
Ruggeri M. & Dall’Agnola R. (1993) The development and use of the Verona Expectations for Care Scale (VECS) and the Verona Service Satisfaction Scale (VSSS) for measuring expectations and satisfaction with community-based psy- chiatric services in patients, relatives and professionals. Psychological Medicine 23,511-523.
Stimson G. & Webb B. (1975) On Going To See the Doctor. Routledge & Keagan Paul, London.
Ware J.E., Snyder M.K., Wright W.R. & Davies A.R. (1983) Defining and measuring patient satisfaction with medical care. Evaluation and Programme Planning 6,247-263.
Wasylenki D.A., Goering P.N., Lancee W.J., Ballantyne R. & Farkas M. (1985) Impact of a case manager program on psychiatric aftercare. The Journal of Nervous and Mental Disease 173,303-308.
Webb Y. (1993) Consumer surveys: an overview. In Lieper. R. & Field V. (Eds) Counting for Something in Mental Health Services. Avebury, Aldershot.
Williams 8. & Wilkinson G. (1995) Patient satisfaction in mental health care. British Journal of Psychiatry 166,559-562.
Wright R.G., Heiman J.R., Shupe J. & Olvera G. (1989) Defining and measuring stabilisation of patients during 4 years of intensive community support. American Journal of Psychiatry 146,1293-1298.
Wykes T. & Carroll S. (1993) Patient satisfaction with inten- sive care psychiatric services: can it be assessed? Journal of Mental Health 2,339-347.
361-368.
589-91.
21 2-227.
114 0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15
Case management: satisfaction with care
Appendix 1
Client satisfaction interview
All items rated on a 4 point scale: 0 = dissatisfied 1 = mildly dissatisfied or indifferent 2 = mostly satisfied 3 = very satisfied
General service satisfaction 1. How would you rate the quality of service you receive? 2. To what extent has the service you receive met your needs? 3. In an overall, general sense, how satisfied are you with the
4. How satisfied are you with the kind of service you
5. How satisfied are you with the amount of help you
service you receive?
receive?
receive from the service?
Appointments: how satisfied are you with . . . 1. the places you have your appointments? 2. the times of your appointments? 3. how often you have an appointment? 4. how much warning the service gives you about your next
appointment? 5. how much notice people take if you ask for an appoint-
ment to be at a certain time of the day or on (or not on) a certain day?
Information and advice: how satisfied are you with . . . 1. the advice or contacts you are given about other agencies
that can help you? 2. the information given to you, by the members of the ser-
vice, about your problems, needs and the care you receive? 3. the way your questions are answered?
Service provider qualities: how satisfied are you with . . . 1. the attitudes of the members of the service when they see
2. the way the staff understand your needs, problems, diffi-
3. that the staff seem to know what they are doing? 4. with the degree of confidentiality shown by members of
the service? 5. our keyworker?
you? (How they treat you?)
culties?
Specific aspects of care: how satisfied are you with . . . 1. the time taken for the service to respond to a request for
2. how easy it is to get in touch with someone involved with
3. the help you receive for social problems/difficulties, e.g.
4. your medication?
help?
your care?
sorting out housing, benefits
0 1997 Blackwell Science Ltd, Health and Social Care in the Community 5(2), 106-1 15 115















![APPLYING METHOD TO THE MADNESS [FN1]: THE RIGHT TO COURT APPOINTED GUARDIANS AD LITEM AND COUNSEL FOR THE MENTALLY ILL IN IMMIGRATION PROCEEDINGS](https://static.fdokumen.com/doc/165x107/6317d16ebc8291e22e0e6e67/applying-method-to-the-madness-fn1-the-right-to-court-appointed-guardians-ad.jpg)


