Can young children make active choices? Outcomes of a feasibility trial in seven‐year‐old...
14
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [The University of Notre Dame Australia] On: 1 December 2010 Access details: Access Details: [subscription number 918196760] Publisher Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Early Child Development and Care Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713640830 Can young children make active choices? Outcomes of a feasibility trial in seven-year-old children Beth Hands a ; Dawne Larkin b ; Elizabeth Rose c ; Helen Parker c ; Anne Smith d a Institute for Health and Rehabilitation Research, University of Notre Dame Australia, Fremantle, Australia b School of Sport Science, Exercise and Health, University of Western Australia, Crawley, Australia c School of Health Sciences, University of Notre Dame Australia, Fremantle, Australia d School of Physiotherapy, Curtin University of Technology, Bentley, Australia First published on: 16 June 2010 To cite this Article Hands, Beth , Larkin, Dawne , Rose, Elizabeth , Parker, Helen and Smith, Anne(2010) 'Can young children make active choices? Outcomes of a feasibility trial in seven-year-old children', Early Child Development and Care,, First published on: 16 June 2010 (iFirst) To link to this Article: DOI: 10.1080/03004431003717623 URL: http://dx.doi.org/10.1080/03004431003717623 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Can young children make active choices? Outcomes of a feasibility trial in seven‐year‐old...

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [The University of Notre Dame Australia]On: 1 December 2010Access details: Access Details: [subscription number 918196760]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Early Child Development and CarePublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713640830
Can young children make active choices? Outcomes of a feasibility trial inseven-year-old childrenBeth Handsa; Dawne Larkinb; Elizabeth Rosec; Helen Parkerc; Anne Smithd
a Institute for Health and Rehabilitation Research, University of Notre Dame Australia, Fremantle,Australia b School of Sport Science, Exercise and Health, University of Western Australia, Crawley,Australia c School of Health Sciences, University of Notre Dame Australia, Fremantle, Australia d
School of Physiotherapy, Curtin University of Technology, Bentley, Australia
First published on: 16 June 2010
To cite this Article Hands, Beth , Larkin, Dawne , Rose, Elizabeth , Parker, Helen and Smith, Anne(2010) 'Can youngchildren make active choices? Outcomes of a feasibility trial in seven-year-old children', Early Child Development andCare,, First published on: 16 June 2010 (iFirst)To link to this Article: DOI: 10.1080/03004431003717623URL: http://dx.doi.org/10.1080/03004431003717623
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.
Early Child Development and Care2010, 1–13, iFirst Article
ISSN 0300-4430 print/ISSN 1476-8275 online© 2010 Taylor & FrancisDOI: 10.1080/03004431003717623http://www.informaworld.com
Can young children make active choices? Outcomes of a feasibility trial in seven-year-old children
Beth Handsa*, Dawne Larkinb, Elizabeth Rosec, Helen Parkerc and Anne Smithd
aInstitute for Health and Rehabilitation Research, University of Notre Dame Australia, Fremantle, Australia; bSchool of Sport Science, Exercise and Health, University of Western Australia, Crawley, Australia; cSchool of Health Sciences, University of Notre Dame Australia, Fremantle, Australia; dSchool of Physiotherapy, Curtin University of Technology, Bentley, AustraliaTaylor and FrancisGECD_A_472284.sgm(Received 12 January 2010; final version received 20 February 2010)10.1080/03004431003717623Early Childhood Development and Care0300-4430 (print)/1476-8275 (online)Original Article2010Taylor & [email protected]
This project evaluated the feasibility of a child-centred 24-week physical activityintervention. The Play5 strategy encourages children to choose to play vigorouslyfive times a day for about as long as school recess. The seven-year-old childrenwere randomised to control (n = 176) or intervention groups (n = 132). Data werecollected at baseline and post-intervention. Programme evaluation included parentquestionnaire, teacher records and a seven-day pedometer record with a sub-sample of children. The programme was successful in increasing vigorous activity(p = 0.04), but did not impact on moderate or sedentary activities. Young childrenwere able to choose to be active without parent or teacher direction.
Keywords: children; physical activity; intervention; Play5; MVPA; play
Introduction
Play is important for the optimal development of young children’s physical, psycho-logical and social health and an important opportunity for children to be physicallyactive. As with many behaviours, evidence is mounting that physical activity patternsare established at an early age (Malina, 1996; Pate, Baranowski, Dowda, & Trost,1996). Therefore, the early childhood years are critical for developing healthy lifestylebehavioural patterns, as sufficient physical activity is important for both short- andlong-term health outcomes (Saakslahti et al., 2004).
Primary school-aged Australian children are recommended to participate daily inat least 60 minutes of moderate-to-vigorous physical activity and no more than twohours of recreational screen use (Department of Health and Ageing, 2004). Theseguidelines can be interpreted in a number of ways (Department of Health and Ageing,2007); therefore, the evidence is mixed as to the number of children meeting theseguidelines (Department of Health and Ageing, 2007; Tucker, 2008). Similar to therecommendations developed in other countries (Biddle, Cavill, & Sallis, 1997; Corbin& Pangrazi, 2004), the Australian guidelines are couched in adult, time-constrainedlanguage. Conceptually, 60 minutes has little meaning to young children; therefore,the responsibility for the child’s physical activity level implicitly lies with the parent,caregivers or teacher. Young children are, therefore, dependent on adults to providethem with sufficient opportunities to be active. The revised US guidelines (Corbin &
*Corresponding author. Email: [email protected]
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

2 B. Hands et al.
Pangrazi, 2004) noted the need to encourage children to self-monitor their own phys-ical activity by identifying personal activity patterns and setting target goals.However, the key strategies to do this revolved around counting the number ofminutes per day being active.
To date, most interventions or health promotions involving young children targettheir adult caregivers such as parents or teachers (van Sluijs, McMinn, & Griffin,2007). There is much evidence on the benefits to be derived from active play for bothchildren and their caregivers (for a review, see Baumann, Bellew, Vita, Brown, &Owen, 2002). However, when a child’s activities are completely controlled by anadult, children do not have the opportunity to develop the capacity to choose, select,compare, decide or problem-solve. Yet, the early childhood phase is an important timeto develop self-management skills involving decision-making, goal setting andplanning through play with their peers and siblings (Gallahue & Donnelly, 2003).
We argue that young children have the capacity and motivation to self-manage andregulate their own behaviour (Gallahue & Donnelly, 2003). According to motivationaltheorists (Harter, 1999; Weiss & Williams, 2004), perceptions of competence arecentral to an individual’s intrinsic motivation to engage in mastery and seek outchallenges in a specific domain. Individuals who are more self-determined in theirmotivation are more likely to continue to participate; this is true for children as wellas adults (Motl, 2007). Furthermore, there is a general agreement that movement expe-riences are central to the development of a child’s perception of self. Thus, a child’sperceptions of ability in play, games and sport, and opportunities for success-orientedexperiences are likely to profoundly influence both the level of enjoyment and themotivation to engage in physical activity.
The role of parents and teachers, therefore, is to provide support for children toassist them in making active rather than inactive choices during their recreational time(Elliot, 1994). This support could involve encouraging the child to go outside, walkingwith them to the park, taking them to the beach, buying a ball or skipping rope ordriving them to dance classes.
The purpose of this paper is to report a pilot randomised controlled trial that wasdesigned to test the feasibility and acceptability of an innovative strategy, known asPlay5, to increase the physical activity level of seven-year-old children. Whenengaged in active play, young children typically move in short 10- to 15-minute burstsof activity such as running, jumping or climbing followed by periods of rest (Sallo &Silla, 1997). Mounting evidence supports the notion that activity can be accumulatedin small bouts over one day, without compromising expected health benefits (Corbin& Pangrazi, 2004). The Play5 strategy is based on encouraging children to take owner-ship and make choices about being active rather than inactive in a supportive environ-ment. If a child engages in moderate-to-vigorous activity for about as long as a schoolrecess (10–15 minutes) five times a day, then they will achieve the daily recommendedlevel of physical activity of 60 minutes. Play5 activities, classified as moderate tovigorous, should be fun and make a child huff and puff. They could include walkingto school, playing at recess, playing at lunchtime, walking home from school, skippingrope with a friend, riding a bicycle or playing on the climbing frame in the park. The‘five a day’ concept is easier for young children to understand and follow than ‘60minutes a day’, as it is easy to count the fingers on one hand, and is more compatiblewith their natural intermittent activity patterns. As physical activity and sedentarypatterns may be established in children at a young age (Pate et al., 1996), theimportance of early interventions, such as this project, is heightened.
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

Early Child Development and Care 3
Methods
A group-randomised controlled trial design was used to investigate the feasibility andacceptability of the Play5 strategy over a six-month period. The test battery wascompleted before and immediately after the 24-week intervention with both the inter-vention and control groups. Institutional ethics approval was given for the project.
Participants
Participants were recruited through Year 2 classes in 27 primary schools located in thePerth metropolitan area for the study. The schools were matched according to SESranking and attendance numbers, and each pair of schools was randomly allocated toeither the control or experimental group. Overall, 681 children and their parents(control = 332, experimental = 349) were invited by letter to participate using a passiveconsent protocol. Of these, 599 (87.9%) agreed (control = 288, experimental = 311) toparticipate. At baseline, all parents were asked to complete a questionnaire regardingtheir child’s physical activity level, and responses were received from 308 (45.2%)parents (control = 176, experimental = 132). Of this group, five parents did notcomplete a posttest questionnaire resulting in a posttest sample size of 305 (44.8%).There were 132 in the experimental group (males = 73, females = 59) and 171 in thecontrol group (males = 91, females = 80). This response rate is similar to other school-based studies (Esbenson, Melde, Taylor, & Peterson, 2008). Participant numbers fromeach school ranged from six to 33 with an average of 11. Thirteen schools (seven inexperimental arm) were ranked as high SES rank, five (two in experimental arm) asmedium and nine (four in experimental arm) as low. Baseline demographics charac-teristics for the control and experimental groups are shown in Table 1.
Table 1. Sample characteristics of cohort at baseline.
Intervention (n = 132) Control (n = 171) Total (N = 303)
Age (months) 87.0 87.1 87.0Gender
Male 73 91 164Female 59 80 139
School SESLow (n = 9) 29 43 72Medium (n = 5) 14 26 40High (n = 13) 89 102 191
Language spoken at homeEnglish 129 158 287Other 3 11 14Not reported 2 2
Maternal educationYear 10 or below 27 35 62TEE 20 21 41TAFE Certificate/Diploma 31 47 78University degree 52 66 118Not reported 2 2 4
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010
4 B. Hands et al.
Measures
Parent questionnaire
Physical activity patterns for all participants were determined by parent questionnaire.Parent report for young children is a valid measure of physical activity as young childrenare unable to self-report reliably (Harro, 1997). The questionnaire was based on theAmherst Health and Activity Study Student Survey (Sallis, Taylor, Dowda,Freedson, & Pate, 2002) and asks about the child’s physical activities and sedentarypastimes at home and at school for the previous seven days. The parents reported froman extensive list of active and sedentary pastimes, whether an activity had been under-taken by the child, and if so, the number of occasions and for how many minutes oneach occasion. In addition, demographic information was collected. The questionnairewas completed by parents of both control and intervention groups at pretest and posttest.At posttest, the intervention parents also reported on the number of occasions they hadreminded their child to Play5 and whether they had observed any differences in theirchild’s motivation to be active or their actual physical activity level.
Pedometer study
A sub-sample of 10 children, five boys and five girls, from each class were randomlyselected to wear a Yamax Digiwalker SW200 pedometer on the right hip for sevendays. Objective monitoring of physical activity using pedometers has convergent andconstruct validity (Tudor-Locke, Williams, Reis, & Pluto, 2004), and the model usedfor the study has established reliability (Bassett et al., 1996). Daily step counts, thetime the pedometer was off and the reason why, were recorded in a simple diary. Amean daily step count was derived for those participants recording step counts for aminimum of four days, including at least one weekend day.
Intervention development
Focus groups
Three focus groups were conducted with seven-year-old children located in localprimary schools to identify age-appropriate language to describe physical activity andtime. As a result, Play5 activity was defined as one that made you ‘huff and puff’ andlasted ‘about as long as recess’ or ‘play time’.
Support resources
To evaluate the Play5 concept and provide teachers and parents with ideas to supportthe children, several resources were developed. Teachers received a resource foldercontaining two classroom posters, a set of activity cards for the children to use duringrecess or lunch, classroom-based activities to integrate the Play5 message into eachlearning area, ideas on making play equipment and play equipment such as chalk andelastics. Parents were provided with an information booklet. The final resource hasnow been published (Hands, Parker, Rose, Larkin, & Geneff, 2007).
Even though the parent questionnaires provided the data used to evaluate changesin child physical activity, the key intervention strategy involved the children docu-menting their own physical activity every day. The engagement of young children inthe research process is important, and many effective ways have been identified
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

Early Child Development and Care 5
(Einarsdottir, Dockett, & Perry, 2009; Schiller & Einarsdottir, 2009). In this study, thechildren received a new diary every four weeks in which to record their daily Play5activities. Each diary contained 28 pages, one for each day, each with an attractivedrawing in which up to five activities could be recorded each day. The design of thedrawing changed each week. Every four weeks, the children received a new diary andreturned their completed booklet to the school to be collected by the research team.The data from the diaries are the focus of another paper in preparation. In addition,each child received a fridge poster illustrating the 24-week period and a packet of starsto mark off each week after it was completed.
Intervention
The Play5 strategy was introduced to each class in a 90-minute session by threetrained researchers using classroom-based activities and a practical fun outdoorsession. As part of the presentation, the children brainstormed ideas on Play5 activi-ties that would be classified as moderate to vigorous by adults, were fun, and madethem ‘huff and puff’. The activities could include walking to school, playing at recess,playing at lunchtime, walking home from school, skipping rope with a friend, ridinga bicycle or playing on the climbing frame in the park.
Parents were invited to attend an information session about the project and waysto support the children to be active. An average of 10 parents per class (38%) attended.Over the 24-week intervention period, the children completed the Play5 diary eachevening at home. Midway through the intervention, the research team visited eachschool to provide the teachers and students with some more ideas to Play5.
In order to document the input from significant adults, the teachers were providedwith a simple daily checklist to record if they used a Play5 resource or reminded thechildren to Play5. The parents were also asked to report at the end of the 24-weekperiod how often they reminded their child to Play5.
Data analysis
The child’s physical activities reported in the parent questionnaire were coded assedentary, moderate or vigorous based on metabolic rates (METs). Mean minutes perday for each intensity level were derived. Unreasonably high values were replacedwith values based on the 90th percentile (Sallis et al., 2002). Vigorous activities werethose activities eliciting at least 6 METs, and moderate activities were those elicitingbetween 3 and 5.9 METs. The activities were also coded for active play if they wereinformal activities (not organised sport) and elicited at least 3 METs. Sedentary activ-ities included small screen time (watching television, playing video games), talking onthe phone and reading. Minutes per day engaged in screen time alone were alsoderived.
Statistical analysis was performed using Intercooled Stata 9.2 for Windows(Statacorp, College Station, TX). Activity variables were log-transformed (after addi-tion of constant = 10 due to presence of 0 values) and linear regression was used toestimate intervention effect on post-intervention activity measures adjusting forgender, pre-intervention activity level and school socioeconomic index. Although theintra-school correlation for each physical activity measure was negligible to low(range: .01–.15), robust standard errors were used to account for any misspecificationof correlation structure by assuming independence of observations within schools.
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010
6 B. Hands et al.
Residual analysis was performed to assure adequate model fit and absence of influen-tial outlying observations. A two-way repeated measures ANOVA was used tocompare results over time and group for the smaller pedometer study.
Results
Physical activity
Parent questionnaire
Experimental and control students were comparable on all pre-intervention activitylevels except for vigorous physical activity (VPA), with the control group reportingmore vigorous activity than the experimental group (median 30.6 vs. 24.3 minutes perday, p = 0.04).
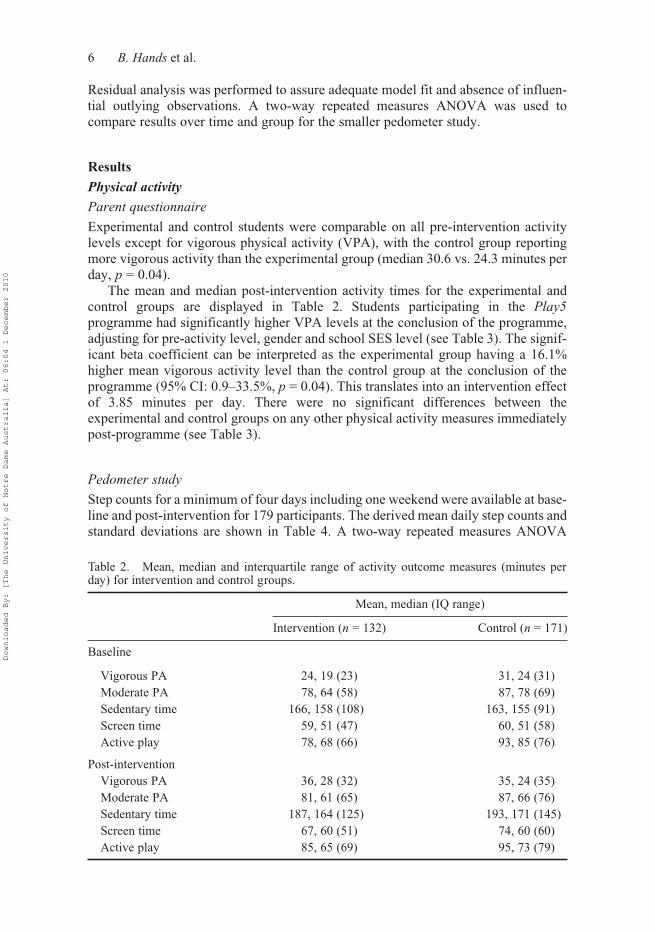
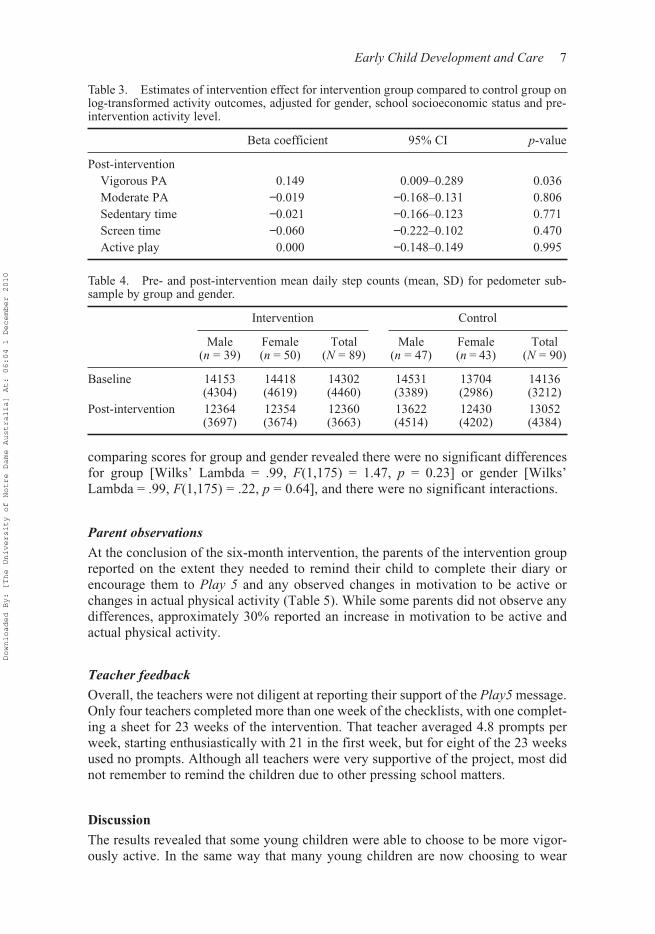
The mean and median post-intervention activity times for the experimental andcontrol groups are displayed in Table 2. Students participating in the Play5programme had significantly higher VPA levels at the conclusion of the programme,adjusting for pre-activity level, gender and school SES level (see Table 3). The signif-icant beta coefficient can be interpreted as the experimental group having a 16.1%higher mean vigorous activity level than the control group at the conclusion of theprogramme (95% CI: 0.9–33.5%, p = 0.04). This translates into an intervention effectof 3.85 minutes per day. There were no significant differences between theexperimental and control groups on any other physical activity measures immediatelypost-programme (see Table 3).
Pedometer study
Step counts for a minimum of four days including one weekend were available at base-line and post-intervention for 179 participants. The derived mean daily step counts andstandard deviations are shown in Table 4. A two-way repeated measures ANOVA
Table 2. Mean, median and interquartile range of activity outcome measures (minutes perday) for intervention and control groups.
Mean, median (IQ range)
Intervention (n = 132) Control (n = 171)
Baseline
Vigorous PA 24, 19 (23) 31, 24 (31)Moderate PA 78, 64 (58) 87, 78 (69)Sedentary time 166, 158 (108) 163, 155 (91)Screen time 59, 51 (47) 60, 51 (58)Active play 78, 68 (66) 93, 85 (76)
Post-interventionVigorous PA 36, 28 (32) 35, 24 (35)Moderate PA 81, 61 (65) 87, 66 (76)Sedentary time 187, 164 (125) 193, 171 (145)Screen time 67, 60 (51) 74, 60 (60)Active play 85, 65 (69) 95, 73 (79)
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010
Early Child Development and Care 7
comparing scores for group and gender revealed there were no significant differencesfor group [Wilks’ Lambda = .99, F(1,175) = 1.47, p = 0.23] or gender [Wilks’Lambda = .99, F(1,175) = .22, p = 0.64], and there were no significant interactions.
Parent observations
At the conclusion of the six-month intervention, the parents of the intervention groupreported on the extent they needed to remind their child to complete their diary orencourage them to Play 5 and any observed changes in motivation to be active orchanges in actual physical activity (Table 5). While some parents did not observe anydifferences, approximately 30% reported an increase in motivation to be active andactual physical activity.
Teacher feedback
Overall, the teachers were not diligent at reporting their support of the Play5 message.Only four teachers completed more than one week of the checklists, with one complet-ing a sheet for 23 weeks of the intervention. That teacher averaged 4.8 prompts perweek, starting enthusiastically with 21 in the first week, but for eight of the 23 weeksused no prompts. Although all teachers were very supportive of the project, most didnot remember to remind the children due to other pressing school matters.
Discussion
The results revealed that some young children were able to choose to be more vigor-ously active. In the same way that many young children are now choosing to wear
Table 3. Estimates of intervention effect for intervention group compared to control group onlog-transformed activity outcomes, adjusted for gender, school socioeconomic status and pre-intervention activity level.
Beta coefficient 95% CI p-value
Post-interventionVigorous PA 0.149 0.009–0.289 0.036Moderate PA −0.019 −0.168–0.131 0.806Sedentary time −0.021 −0.166–0.123 0.771Screen time −0.060 −0.222–0.102 0.470Active play 0.000 −0.148–0.149 0.995
Table 4. Pre- and post-intervention mean daily step counts (mean, SD) for pedometer sub-sample by group and gender.
Intervention Control
Male(n = 39)
Female(n = 50)
Total(N = 89)
Male(n = 47)
Female(n = 43)
Total(N = 90)
Baseline 14153(4304)
14418(4619)
14302(4460)
14531(3389)
13704(2986)
14136(3212)
Post-intervention 12364(3697)
12354(3674)
12360(3663)
13622(4514)
12430(4202)
13052(4384)
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

8 B. Hands et al.
their hats outside, they can also choose to be more physically active. Although manyother physical activity interventions have focused on young children, despite an exten-sive literature search the authors did not identify any other studies that used a similarapproach. The results indicate that such an intervention is feasible and also acceptableto this age group. In a systematic review of controlled trials, van Sluijs et al. (2007)found no strong evidence that school-based, environmental or even multi-componentinterventions were effective with this age group; however, the latter type were effec-tive among adolescents. This present study involved both schools and families byasking them to support, rather than direct, young children being active. The interven-tion effect was encouraging, given that other studies involving children reportedsignificant results ranging from an increase in physical activity of 2.6 minutes duringa physical education class to upwards of 83 minutes per week of moderate-to-vigorousactivity (van Sluijs et al., 2007).
These results would be no surprise to many early childhood professionals. Childdevelopment theorists such as Bruner and Piaget, as well as workers in the field ofchild growth and physical activity, espouse the many developmental benefits ofchild-directed play (Gallahue & Donnelly, 2003). However, this approach seems tobe missing in many physical activity interventions with this age group. A growing
Table 5. Parent responses (N = 134): child involvement and observations for interventiongroup at post-intervention.
N %
Reminded child to complete diaryNone or once 19 14.2Sometimes 31 23.1Almost daily 27 20.1Daily 22 16.4Don’t know or didn’t respond 35 26.1
Encouraged child to Play5None or once 26 19.4Sometimes 34 25.4Almost daily 24 17.9Daily 10 7.5Don’t know or didn’t respond 40 25.4
Change in motivation to be activeMuch less 0 0Less 2 1.5None 70 52.2More 56 41.8Didn’t respond 6 4.5
Change in physical activity levelMuch less 0 0.0Less 2 1.5None 73 54.5More 51 38.1Didn’t respond 8 5.9
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

Early Child Development and Care 9
group of academics and early childhood professionals have raised concerns about thetrend for parents to enrol their young children into adult-supervised structured activi-ties almost every day after school and on weekends. Many young children now haveless down time outside school time to freely plan and participate in their own activi-ties by themselves or with their friends. In 2006, Australian parents reported that37.4% of males and 34.1% of females aged between five and eight years participatedin three hours or more organised sport or dancing in the previous two weeks. Themean hours of participation rose from 4.4 and 3.8 in 2000 to 4.8 and 5.1 in 2006 forthe males and females, respectively (Australian Bureau of Statistics [ABS], 2006).The availability and frequency of a parent to transport a child to activities or sportsexplained a significant, but small amount of variance in physical activity levels ofboys (8%) and girls (1.5%) in Years 4 and 5 (Sallis, Alcaraz, McKenzie, & Hovell,1999). Parents are being exposed to cleverly marketed messages about the need fortheir young children to participate in a wide variety of activities to develop skills at anearly age in order to excel in later life and not be disadvantaged in comparison to theirpeers. Many school- and family-based physical activity interventions are reliant on animportant role for parents and other significant adults. This usually translates intoadult-directed structured activities rather than child-initiated play.
The effectiveness of the Play5 strategy was most likely dependent on the child’srelationship with the important adults in their life, and the willingness of those adultsto encourage and support the growing independence of their child. Although the initialcontact and recruitment was made through the school, the intervention was essentiallyhome based. The teachers did not become actively engaged in the project but wereencouraged to create opportunities for the children to choose to be active. We foundthat few teachers made time to remind the children or to revisit the Play5 concept.This was evidenced by the few who recorded their use of the support materials.Reviews of previous studies show that school-based interventions are not as effectiveas family-based interventions at promoting physical activity in children (Timperio,Salmon, & Ball, 2004; van Sluijs et al., 2007). Given increasing academic require-ments, many schools are limited in the physical activity opportunities they canprovide, so children are likely to participate in more activity outside school hours. Astudy involving New Zealand children in Years 1–6 found the most active childrentook more steps per day outside school hours (Cox, Schofield, Greasley, & Kolt,2006). The present study confirms the need for more family- and community-basedinterventions with this age group.
We also need to better understand young children’s perceptions of activity as theymay be more intrinsically motivated to be active than many perceive. Older childrenreported that choice and self-initiated behaviour change (Ferrar-Caja & Weiss, 2000),along with enjoyment and fun (Burrows, Eves, & Cooper, 1999), increased intrinsicmotivation to participate in physical activity. Almost one-third of the interventiongroup parents observed an increase in motivation to be active as well as a real increasein activity in their child. Anecdotal reports by parents to the research team furtherenriched the results. For example, one child asked their mother to go for a walk afterschool. When the mother replied it was raining, the child replied ‘let’s put on our rain-coats and go anyway’. So they did, and had a lovely time being active together. Theparent realised, with dismay, that she had been discouraging the child’s choice to beactive. It was encouraging that 28% were able to accurately recall the message and afurther 18% still had the general idea of the message even six months after the comple-tion of the intervention.
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

10 B. Hands et al.
No significant differences were identified between experimental and controlgroups for the moderate physical activities, sedentary behaviours and screen time. Onereason moderate physical activity did not increase in the intervention group may havebeen the emphasis on activities that made the children ‘huff and puff’. Sedentarybehaviours or screen time did not significantly reduce among the children in the inter-vention group; however, given the emphasis was on increasing activity not reducinginactivity, the results were encouraging. The second data collection occurred duringwinter when children spend more time indoors and are generally less active(Rowlands & Hughes, 2006). The median time for sedentary activities reported by thecontrol group increased to a greater extent (155–171 minutes) relative to the experi-mental group (158–164 minutes) from baseline to post-intervention. The reduced levelof activity in winter was also observable for the mean daily step counts recorded bythe participants in the pedometer study (Table 4). Both groups reduced their meandaily step counts between baseline (summer) and posttest (winter).
It was surprising there were no gender differences in the physical activity levelsreported by either group or in the pedometer study. In numerous other studies, malesare consistently identified as being more physically active than females from an earlyage (Hinkley, Crawford, Salmon, Okely, & Hesketh, 2008; Sallis, Prochaska, &Taylor, 2000). One explanation could be that the Play5 concept held greater appeal forfemales. Young boys tend to engage in play that is competitive, sport based, andinvolves speed and aggression, whereas girls tend to be more cooperative and taketurns in activities (Ignico, 1989; Kohl & Hobbs, 1998). The Play5 support resourcesand daily diaries were focused on fun and engagement and may have stimulated thegirls to engage in vigorous activities to an equal extent as the boys. Further researchis required to better understand these results.
Limitations and strengths
There were a number of limitations of this study. The length of the intervention was along time for the children to maintain motivation and involvement in the project;however, in order to effect change in deeply entrenched patterns of behaviour, inter-ventions need to be undertaken for a significant duration. Parents and teachers alsofound the intervention time challenging and this may have affected the reporting ofresults as their support for the project was essential. The number of completed ques-tionnaires available for analysis at the completion of the intervention phase was lowerthan hoped; however, they were sufficient to detect change in VPA but not in otheractivity levels and sedentary behaviour. Further, physical activity was based on parentalreport which, although validated with young children, is less accurate than objectivemeasures. van Sluijs et al. (2007) noted that significant positive results were more likelyto be reported if observation or objective physical measures were used. Although a sub-sample of children wore pedometers, no significant results were found. This may beindicative of the sample size and also a limitation of the measure. Finally, the samplewas not representative as it comprised a higher proportion of participants from the highSES group and, given the overall response rate of 44.8% may have some selection bias.However, we do not claim that this strategy will be effective with all children, but willappeal to some. The study also has a number of strengths. We used a novel approachto enhancing physical activity in young children that, to our knowledge, has not beenpreviously evaluated. The message had a strong appeal to the age group and was easyfor them to understand. The 24-week intervention was a significant length of time in
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

Early Child Development and Care 11
comparison to other interventions with children which range from five weeks to sixyears (van Sluijs et al., 2007) and therefore replication may not be feasible. Of the 33controlled trials reported by van Sluijs et al. (2007) involving children, the majoritywere of 12- to 16-week duration.
In evaluating the project, we gathered information from the children (drawings,diaries, questionnaires), their parents (questionnaires) and the teachers (question-naires, record sheets). This rich assortment of data has provided us with insights andideas for future interventions. The Play5 intervention holds much promise as a strat-egy to increase physical activity in young children. In the future, we will evaluate thepublished resources in school settings and test the applicability of the message withother groups such as families and younger children. Future development of the Play5message could also include messages that target sedentary behaviours.
Conclusion
While the importance of the family and school in creating a supportive environmentremains, these results provide support for the argument that young children should beprovided with the opportunity for self-determination by being encouraged to makechoices about being physically active to enhance a healthy future.
AcknowledgementThe authors would like to thank the Telstra Foundation for funding this project.
Notes on contributorsBeth Hands, PhD, is the director of the Institute for Health and Rehabilitation Research at theUniversity of Notre Dame, Australia. Most of her publications relate to children’s physicalactivity, fitness and motor competence, in particular for children with developmental coordina-tion disorder (DCD). She has written a teacher resource for teaching fundamental movementskills and was the project director for a large state-wide survey of physical activity andnutrition in school children aged between seven and 16 years. She conceived the concept ofPlay5 and has explored variations of the concept with families and young children.
Dawne Larkin, EdD, is a senior lecturer in the School of Sport Science, Exercise and Health atthe University of Western Australia. Dawne has published extensively in the area of motorcontrol and motor development with a particular focus on children with DCD. For 20 years,she was the director of the internationally renowned Unigym program for children with move-ment difficulties aged between five and 11 years.
Elizabeth Rose, PhD, is an adjunct senior lecturer in the School of Health Sciences at theUniversity of Notre Dame, Australia. Her area of expertise relates to self-perceptions in thephysical domain among children and adolescents. She has published extensively in this area.
Helen Parker, PhD, is the dean of the School of Health Sciences at the University of NotreDame, Australia. Her field of expertise is motor control and development, with a particularfocus on timing and rhythm.
Anne Smith, PhD, is a bio statistician with the School of Physiotherapy at the Curtin Universityof Technology. Her specialty is analysis of data in longitudinal studies.
ReferencesAustralian Bureau of Statistics (ABS). (2006). Children’s participation in cultural and leisure
activities, Australia (Report 4901.0). Canberra: Australian Bureau of Statistics.
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010
12 B. Hands et al.
Bassett, D.R.J., Ainsworth, B.E., Leggett, S.R., Mathien, C.A., Main, J.A., Hunter, D.C., et al.(1996). Accuracy of five electronic pedometers for measuring distance walked. Medicineand Science in Sports and Exercise, 28(8), 1071–1077.
Baumann, A., Bellew, B., Vita, P., Brown, W., & Owen, N. (2002). Getting Australia active:Towards best practice for the promotion of physical activity. Canberra: CommonwealthDepartment of Health and Ageing.
Biddle, S., Cavill, N., & Sallis, J.F. (1997). Policy framework for young people and health-enhancing physical activity. In S. Biddle, J.F. Sallis, & N. Cavill (Eds.), Young and active(pp. 3–16). London: Health Education Authority.
Burrows, C., Eves, F., & Cooper, D. (1999). Children’s perceptions of exercise – Are childrenmini-adults? Health Education, 99(2), 61–69.
Corbin, C.B., & Pangrazi, R.P. (2004). Physical activity for children: A statement of guide-lines (2nd ed.). Reston, VA: National Association for Sport and Physical Education.
Cox, M., Schofield, G., Greasley, N., & Kolt, G.S. (2006). Pedometer steps in primary school-aged children: A comparison of school-based and out-of-school activity. Journal ofScience and Medicine in Sport, 9, 91–97.
Department of Health and Ageing. (2004). Active kids are healthy kids: Australia’s physicalactivity recommendations for 5–12 year olds. Canberra: Commonwealth of Australia.
Department of Health and Ageing. (2007). Australian national children’s nutrition andphysical activity survey – Main findings. Canberra: Department of Health and Ageing.
Einarsdottir, J., Dockett, S., & Perry, B. (2009). Making meaning: Children’s perspectivesexpressed through drawings. Early Child Development and Care, 179(2), 217–232.
Elliot, A. (1994). Scaffolding learning. Every Child, 1(2), 8–9.Esbenson, F.-A., Melde, C., Taylor, T.J., & Peterson, D. (2008). Active parental consent in
school based research. Evaluation Review, 32(4), 335–362.Ferrar-Caja, E., & Weiss, M.R. (2000). Predictors of intrinsic motivation among adolescent
students in physical education. Research Quarterly for Exercise and Sport, 71, 267–279.Gallahue, D.L., & Donnelly, F.C. (2003). Developmental physical education for all children
(4th ed.). Champagne, IL: Human Kinetics.Hands, B., Parker, H., Rose, E., Larkin, D., & Geneff, R. (2007). Play5 teacher manual: Get
active, at home and at school. Hindmarsh: ACHPER Australia.Harro, M. (1997). Validation of a questionnaire to assess physical activity of children ages
4–8 years. Research Quarterly for Exercise and Sport, 68(4), 259–268.Harter, S. (1999). The construction of the self: A developmental perspective. New York:
Guilford Press.Hinkley, T., Crawford, D., Salmon, J., Okely, A., & Hesketh, K. (2008). Preschool and physi-
cal activity: A review of correlates. American Journal of Preventive Medicine, 34(5),435–441.
Ignico, A.A. (1989). Development and verification of a gender-role stereotyping index forphysical activities. Perceptual and Motor Skills, 68, 1067–1075.
Kohl, H.W., & Hobbs, K.E. (1998). Development of physical activity behaviours amongchildren and adolescents. Pediatrics, 101(3), 549–554.
Malina, R.M. (1996). Tracking of physical activity and physical fitness across the lifespan.Research Quarterly for Exercise and Sport, 67(3), S48–S57.
Motl, R.W. (2007). Chapter 2: Theoretical models for understanding physical activitybehvaiour among children and adolescents – Social cognitive theory and self-determina-tion theory. Journal of Teaching in Physical Education, 26, 350–357.
Pate, R.R., Baranowski, T., Dowda, M., & Trost, S.G. (1996). Tracking of physical activity inyoung children. Medicine and Science in Sports and Exercise, 28(1), 92–96.
Rowlands, A.V., & Hughes, D.R. (2006). Variability of physical activity patterns by type ofday and season in 8–10-year-old boys. Research Quarterly for Exercise and Sport, 77(3),391–395.
Saakslahti, A., Numminen, P., Varstala, V., Helenius, H., Tammi, A., Viikari, J., et al. (2004).Physical activity as a preventive measure for coronary heart disease risk factors in earlychildhood. Scandinavian Journal of Medicine and Science in Sports, 14(3), 143–149.
Sallis, J.F., Alcaraz, J.E., McKenzie, T.L., & Hovell, M.F. (1999). Predictors of change inchildren’s physical activity over 20 months: Variations by gender and level of adiposity.American Journal of Preventive Medicine, 16(3), 222–229.
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010

Early Child Development and Care 13
Sallis, J.F., Prochaska, J.J., & Taylor, W.C. (2000). A review of correlates of physical activityof children and adolescents. Medicine and Science in Sports and Exercise, 32(5), 963–975.
Sallis, J.F., Taylor, W.C., Dowda, M., Freedson, P.S., & Pate, R.R. (2002). Correlates ofvigorous physical activity for children in grades 1 through 12: Comparing parent-reportedand objectively measured physical activity. Pediatric Exercise Science, 14, 30–44.
Sallo, M., & Silla, R. (1997). Physical activity with moderate to vigorous intensity inpreschool and first-grade school children. Pediatric Exercise Science, 9, 44–54.
Schiller, W., & Einarsdottir, J. (2009). Special issue: Listening to young children’s voices inresearch – Changing perspectives/changing relationships. Early Child Development andCare, 179(2), 125–130.
Timperio, A., Salmon, J., & Ball, K. (2004). Evidence-based strategies to promote physicalactivity among children, adolescents and young adults. Journal of Science and Medicinein Sport, 7, 20–29.
Tucker, P. (2008). The physical activity levels of preschool-aged children: A systematicreview. Early Childhood Research Quarterly, 23(4), 547–558.
Tudor-Locke, C., Williams, J.E., Reis, J.P., & Pluto, D. (2004). Utility of pedometers forassessing physical activity: Construct validity. Sports Medicine, 34(5), 281–291.
van Sluijs, E., McMinn, A.M., & Griffin, S.J. (2007). Effectiveness of interventions topromote physical activity in children and adolescents: Systematic review of controlledtrials. British Medical Journal, 335(7622), 703–707.
Weiss, M.R., & Williams, L. (2004). The why of youth sport involvement: A developmentalperspective on motivational processes. In M.R. Weiss (Ed.), Developmental sport andexercise psychology: A lifespan perspective (pp. 223–268). Morgantown, WV: FitnessInformation Technology.
Downloaded By: [The University of Notre Dame Australia] At: 06:04 1 December 2010