
Can we deliver randomized trials of focal therapy in prostate cancer?
10
NATURE REVIEWS | CLINICAL ONCOLOGY ADVANCE ONLINE PUBLICATION | 1 Introduction The management of men with localized prostate cancer is controversial. The current diagnostic pathway—serum prostate-specific antigen (PSA) measurement followed by transrectal ultrasonography (TRUS)-guided prostate biopsies—is limited because the screening test (PSA) lacks specificity and the verification test (biopsy) lacks sensitiv- ity. 1 Accordingly, this diagnostic process cannot accurately discriminate between men with or without clinically significant cancer, which has led to well-recognized errors of overdiagnosis and overtreatment as well as underdiagnosis and ineffective risk stratification of patients. 2,3 Nonetheless, active surveillance—a treatment option relying on repeat PSA measurement and biopsy that is recommended for men with low-risk disease—is associated with poor uptake; only four in 10 men in the UK 4 and one in nine men in the USA are managed with active surveillance. 5 At the same time, the Scandinavian Prostate Cancer Group-4 (SPCG-4) and Prostate Intervention Versus Observation Trial (PIVOT) have confirmed a clinically important survival benefit in treating men with high-risk and possibly intermediate-risk localized prostate cancer. 6,7 Radical surgery (prostatectomy) or radio- therapy have been the mainstay treatment for such men, although both options carry the risk of urinary incontinence, erectile dysfunction and rectal problems. 8 Prostate cancer treatment is unusual com- pared with most other solid tumours in that typically the whole organ is treated, rather than just the malignant lesion. However, tissue-preserving focal therapies (Box 1) have emerged as potential interventions for localized prostate cancer that might reduce the rate of adverse effects associated with whole-gland treatment while maintain- ing acceptable disease control rates. If fea- sible, the ‘collateral damage’ to the external urinary sphincter, bladder neck, neuro- vascular bundles and rectal mucosa could be minimized. 9,10 Early proof-of-concept studies have shown low rates of such adverse effects and encouraging data on early disease control following focal therapy. 11 However, there is a pressing need to design, plan and implement randomized controlled trials (RCTs) comparing focal therapy with standard of care. 12 Why do we need RCTs? In surgical inno- vation, change is often based on case series or large registry datasets. Although inno- vations, including prosthetic hip implants and partial nephrectomy for renal cancer, have been adopted on the basis of such studies, considerable biases as well as residual confounding factors are involved in nonrandomized data. In the literature on focal therapy, one systematic review of focal therapy case series has shown that >2,000 patients have been treated in this way. 11 Despite these numbers, adoption of focal therapy has been slow, perhaps due to a lack of randomized comparative data. A lack of robust comparative data can have important implications, depending on the (as yet unknown) true effects of focal therapy. For example, if focal therapy actually has a clinically meaningful role in treating men with prostate cancer, a lack of robust data means that an effec- tive treatment will not be widely adopted. Conversely, paucity of robust data might instead lead to ‘treatment creep’, with infor- mal dissemination and diffusion of a treat- ment strategy that might, at best, have no clinically meaningful role and, at worst, lead to deleterious effects on rates of metastasis and overall survival and disease-specific survival. Only robust comparative data can allow good strategic decision-making. The Prostate Cancer RCT Consensus Group (Box 2) met in London, UK on 26 April 2012 to discuss the optimal approach to design, develop and deliver a RCT evaluating the role of novel inter- ventions, particularly focal therapy, in men with localized prostate cancer with dis- cussions of the key issues on trial design. OPINION Can we deliver randomized trials of focal therapy in prostate cancer? Hashim U. Ahmed, Viktor Berge, David Bottomley, William Cross, Rakesh Heer, Richard Kaplan, Tom Leslie, Chris Parker, Clare Relton, Richard Stephens, Matthew R. Sydes, Lindsay Turnbull, Jan van der Meulen, Andrew Vickers, Timothy Wilt, Mark Emberton and the Prostate Cancer RCT Consensus Group Abstract | Tissue-preserving focal therapies, such as brachytherapy, cryotherapy, high- intensity focused ultrasound and photodynamic therapy, aim to target individual cancer lesions rather than the whole prostate. These treatments have emerged as potential interventions for localized prostate cancer to reduce treatment-related adverse- effects associated with whole-gland treatments, such as radical prostatectomy and radiotherapy. In this article, the Prostate Cancer RCT Consensus Group propose that a novel cohort-embedded randomized controlled trial (RCT) would provide a means to study men with clinically significant localized disease, which we defined on the basis of PSA level (≤15 ng/ml or ≤20 ng/ml), Gleason grade (Gleason pattern ≤4 + 4 or ≤4 + 3) and stage (≤cT2cN0M0). This RCT should recruit men who stand to benefit from treatment, with the control arm being whole-gland surgery or radiotherapy. Composite outcomes measuring rates of local and systemic salvage therapies at 3–5 years might best constitute the basis of the primary outcome on which to change practice. Ahmed, H. U. et al. Nat. Rev. Clin. Oncol. advance online publication 22 April 2014; doi:10.1038/nrclinonc.2014.44 Competing interests H.U.A. has received research funding from the following companies: Advanced Medical Diagnostics, GlaxoSmithKline and Sonacare. M.E. has received research funding from the following companies: Advanced Medical Diagnostics, GlaxoSmithKline, Steba Biotech and Sonacare. M.E. is a paid consultant for GlaxoSmithKline, Steba Biotech and Sonacare. M.E. is a director on the board of and has share options in Nuada Medical. The other authors declare no competing interests. PERSPECTIVES © 2014 Macmillan Publishers Limited. All rights reserved
-
Upload
independent -
Category
Documents
-
view
7 -
download
0
Transcript of Can we deliver randomized trials of focal therapy in prostate cancer?

NATURE REVIEWS | CLINICAL ONCOLOGY ADVANCE ONLINE PUBLICATION | 1
IntroductionThe management of men with localized prostate cancer is controversial. The current diagnostic pathway—serum prostate- specific antigen (PSA) measurement followed by transrectal ultrasonography (TRUS)-guided prostate biopsies—is limited because the screening test (PSA) lacks specificity and the verification test (biopsy) lacks sensitiv-ity.1 Accordingly, this diagnostic process cannot accurately discriminate between men with or without clinically significant cancer, which has led to well-recognized errors of over diagnosis and overtreatment as well as underdiagnosis and ineffective
risk stratification of patients.2,3 Nonetheless, active surveillance—a treatment option relying on repeat PSA measurement and biopsy that is recommended for men with low-risk disease—is associated with poor uptake; only four in 10 men in the UK4 and one in nine men in the USA are managed with active surveillance.5 At the same time, the Scandinavian Prostate Cancer Group-4 (SPCG-4) and Prostate Intervention Versus Observation Trial (PIVOT) have confirmed a clinically important survival benefit in treating men with high-risk and possibly intermediate-risk localized prostate cancer.6,7 Radical surgery (prostatectomy) or radio-therapy have been the mainstay treatment for such men, although both options carry the risk of urinary incontinence, e rectile d ysfunction and rectal problems.8
Prostate cancer treatment is unusual com-pared with most other solid tumours in that typically the whole organ is treated, rather than just the malignant lesion. However, tissue-preserving focal therapies (Box 1) have emerged as potential interventions for localized prostate cancer that might reduce
the rate of adverse effects associated with whole-gland treatment while maintain-ing acceptable disease control rates. If fea-sible, the ‘collateral damage’ to the external urinary sphincter, bladder neck, neuro-vascular bundles and rectal mucosa could be minimized.9,10 Early proof-of-concept studies have shown low rates of such adverse effects and encouraging data on early disease control following focal therapy.11 However, there is a pressing need to design, plan and implement randomized controlled trials (RCTs) comparing focal therapy with s tandard of care.12
Why do we need RCTs? In surgical inno-vation, change is often based on case series or large registry datasets. Although inno-vations, including prosthetic hip implants and partial nephrectomy for renal cancer, have been adopted on the basis of such studies, considerable biases as well as residual confounding factors are involved in non randomized data. In the literature on focal therapy, one systematic review of focal therapy case series has shown that >2,000 patients have been treated in this way.11 Despite these numbers, adoption of focal therapy has been slow, perhaps due to a lack of randomized comparative data.
A lack of robust comparative data can have important implications, depending on the (as yet unknown) true effects of focal therapy. For example, if focal therapy actually has a clinically meaningful role in treating men with prostate cancer, a lack of robust data means that an effec-tive treatment will not be widely adopted. Conversely, paucity of robust data might instead lead to ‘treatment creep’, with infor-mal dissemination and diffusion of a treat-ment strategy that might, at best, have no clinically meaningful role and, at worst, lead to deleterious effects on rates of metastasis and overall survival and disease-specific survival. Only robust comparative data can allow good strategic decision-making.
The Prostate Cancer RCT Consensus Group (Box 2) met in London, UK on 26 April 2012 to discuss the optimal approach to design, develop and deliver a RCT evaluating the role of novel inter-ventions, particu larly focal therapy, in men with localized prostate cancer with dis-cussions of the key issues on trial design.
OPINION
Can we deliver randomized trials of focal therapy in prostate cancer?Hashim U. Ahmed, Viktor Berge, David Bottomley, William Cross, Rakesh Heer, Richard Kaplan, Tom Leslie, Chris Parker, Clare Relton, Richard Stephens, Matthew R. Sydes, Lindsay Turnbull, Jan van der Meulen, Andrew Vickers, Timothy Wilt, Mark Emberton and the Prostate Cancer RCT Consensus Group
Abstract | Tissue-preserving focal therapies, such as brachytherapy, cryotherapy, high-intensity focused ultrasound and photodynamic therapy, aim to target individual cancer lesions rather than the whole prostate. These treatments have emerged as potential interventions for localized prostate cancer to reduce treatment-related adverse-effects associated with whole-gland treatments, such as radical prostatectomy and radiotherapy. In this article, the Prostate Cancer RCT Consensus Group propose that a novel cohort-embedded randomized controlled trial (RCT) would provide a means to study men with clinically significant localized disease, which we defined on the basis of PSA level (≤15 ng/ml or ≤20 ng/ml), Gleason grade (Gleason pattern ≤4 + 4 or ≤4 + 3) and stage (≤cT2cN0M0). This RCT should recruit men who stand to benefit from treatment, with the control arm being whole-gland surgery or radiotherapy. Composite outcomes measuring rates of local and systemic salvage therapies at 3–5 years might best constitute the basis of the primary outcome on which to change practice.
Ahmed, H. U. et al. Nat. Rev. Clin. Oncol. advance online publication 22 April 2014; doi:10.1038/nrclinonc.2014.44
Competing interestsH.U.A. has received research funding from the following companies: Advanced Medical Diagnostics, GlaxoSmithKline and Sonacare. M.E. has received research funding from the following companies: Advanced Medical Diagnostics, GlaxoSmithKline, Steba Biotech and Sonacare. M.E. is a paid consultant for GlaxoSmithKline, Steba Biotech and Sonacare. M.E. is a director on the board of and has share options in Nuada Medical. The other authors declare no competing interests.
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved

2 | ADVANCE ONLINE PUBLICATION www.nature.com/nrclinonc
The meeting was supported by a research grant provided by the Medical Research Council (UK) and logistical support was provided by the Pelican Cancer Foundation charity. We had no commercial support. In total, 60 partici pants attended from multi disciplinary backgrounds, with five patient representatives, three representa-tives from the major stakeholder charities, three nurses, six oncologists, 29 urolo-gists, three radio logists and 11 represen-tatives of clinical epidemio logy, health economics, statis tics and clinical trials (a c omplete list of participants is provided in Supplementary Table 1 online). The first half of the day involved short present ations (each followed by discussions) on current errors and potential solutions to the local-ized prostate cancer pathway, RCTs that have evaluated different treatment strategies for localized prostate cancer, challenges in delivering large multi centre RCTs, the role of multi parametric MRI (mpMRI) in pros-tate cancer diagnosis and follow-up moni-toring, the current state-of-the-art of focal therapies, novel RCT designs and integrat-ing comparative effectiveness research into electronic healthcare systems.
Participants were then divided into four subgroups that were predetermined to ensure multidisciplinary discussion. All four break-out groups were tasked with considering the same issues and questions
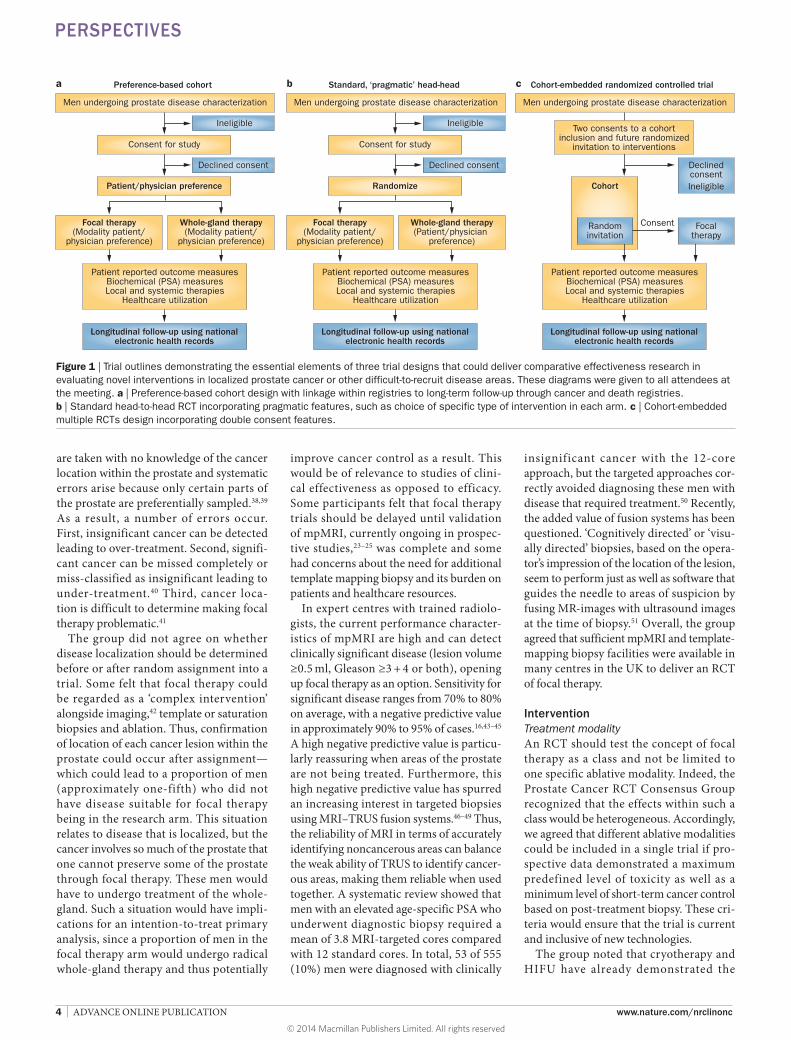
within the context of designing a compara-tive effectiveness trial evaluating the role of focal therapy in localized prostate cancer. Firstly, the groups were asked to consider whether focal therapy merited research and, if so, to consider the following issues using the population, intervention, comparator, outcomes (PICO) structure: the patient population suitable for focal therapy; tests and technologies that should form part of this complex intervention (localization of cancer, targeted therapy to individual lesions and follow-up care); the composition of the suitable comparator arm(s) for the relevant population; and the outcome measures that would provide robust, clinically meaningful data that might change practice if a future RCT was in favour of focal therapy, or reject the focal therapy hypothesis if the results were negative. Secondly, the groups were asked to consider which of the three trial designs (Figure 1) might be suitable. Finally, the subgroups discussed the potential barri-ers to the successful implementation of such a study and possible strategies to overcome them. The whole group met together to dis-cuss individual group feedback in the after-noon session. This Perspective is the result of that meeting. Here, we explore whether randomized trials in prostate cancer surgi-cal innovation are possible and how novel trial designs could take the field beyond the current state of the art.
Rationale for research questionFocal therapy aims to target areas of clini-cally significant prostate cancer in a selective manner, affecting only a minimal margin of normal tissue to minimize adverse effects to the nearby neurovascular bundles, exter-nal urinary sphincter, bladder neck and rectal mucosa. Advances in technological improvements in imaging (namely, multi-parametric (mp)MRI),13–17 biopsy (template mapping or saturation biopsies)18–22 and ablative therapies now enable us to entertain the possibility of treating only the cancerous areas in approximately one-fifth to as many as three- quarters of men with localized pros-tate cancer. Ablative therapies—i ncluding cryosurgery, high-intensity focused ultra-sound (HIFU), brachytherapy, electro-poration, photo thermal, photodynamic and radio frequency—have the potential to deliver focal therapy. However, mpMRI in particular has not yet been conclusively validated in prospective studies to be effec-tive for guiding targeted focal approaches, although these studies are ongoing.23–25
Published nonrandomized cohort studies with small numbers of patients and short follow-up durations with median range of 17–47 months have shown that cryo-therapy,26,27 HIFU28–30 and photo thermal therapy31,32 are associated with low rates of adverse effects across all cancer risk categor-ies, with encouraging early disease control rates showing absence of clinically signifi-cant cancer ranging from 83% to 100% on the basis of biopsy findings.11 Among the group, there was consensus that focal therapy might offer a strategy to reduce harm in those men that stand to benefit from treatment, but cancer control data were required with follow-up of at least 3 years.
Framing the clinical questionPopulationWe reached a consensus that focal therapy should be assessed only in a particular subgroup of patients. To set the lower end of the spectrum, research should focus on men with clinically significant cancer who are likely to benefit from some form of immediate treatment. To set the upper end of the spectrum, the disease should be morphologically amenable to a focal tissue-preserving approach (on the basis of the size and location of individual lesions).
Clinically significant cancerThe potential selection criteria for a patient to qualify for focal therapy were discussed in terms of PSA level, Gleason grade and
Box 1 | Energy-based modalities that can deliver focal therapy for prostate cancer
Cryotherapy ■ Cryoprobes inserted into the prostate via the perineum undergo freezing to temperatures
of -40°C. Two freeze-thaw cycles are required to destroy cells using coagulative necrosis
High-intensity focused ultrasound (HIFU) ■ HIFU uses both thermal (temperatures >56°C) and mechanical effects to destroy tissue. It is
usually delivered using a transrectal probe under ultrasound guidance, but new devices using MRI-guidance and intra-urethral HIFU are being evaluated
Photodynamic therapy ■ Involves the activation of a photosensitizer (via injected intravenous) by a specific wavelength
of light transmitted through laser fibres inserted tranperineally into the prostate to create cell damage and tissue necrosis through the production of reactive oxygen species. This technique is being evaluated within regulatory trials
Laser-based photothermal therapy ■ Laser fibres, inserted transperineally or transrectally, cause coagulative necrosis through
a direct thermal effect, with monitoring of effect using MRI-thermometry
Brachytherapy ■ Low dose-rate brachytherapy involves implantation of small radioactive seeds. High dose-rate
brachytherapy involves inserting a source of high dose-rate radiation into the prostate gland for a few minutes
Irreversible electroporation therapy ■ Uses an electric field to open nano-sized pores in the cell membrane, which when applied
with sufficient amplitude and duration causes permanent damage to the cell membrane
Radiofrequency therapy ■ High frequency alternating current (in the range of 350–500kHz) is used to generate heat
capable of causing coagulative necrosis
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CLINICAL ONCOLOGY ADVANCE ONLINE PUBLICATION | 3
stage of the cancer. PSA level should be as high as is clinically acceptable. In other words, by having a high threshold, more men would be eligible and hence this would improve external validity; however, it should not be so high that the prob-ability of metastases would be increased. Therefore, the proposed thresholds for intervention were PSA levels of either ≤15 ng/ml or ≤20 ng/ml. These two thresh-olds included men with intermediate- risk disease and while the majority of the group accepted ≤20 ng/ml was clinically accept-able some wanted to lower this so that the risk of metastases was lower. Furthermore, no lower limit of PSA should be set, pro-vided the patient fulfilled other criteria for c linically significant cancer.
These criteria included Gleason grade, for which there was general agreement that grade, as with PSA and for the same reasons, be as high as clinically acceptable. Although an overall grade threshold of Gleason pattern ≤4 + 4 was considered by some attendees, most felt that Gleason ≤4 + 3 would be more acceptable as it mini-mized the probability that men would have metastases. Furthermore, some stated that a Gleason 4 + 4 lesion, which is morpho-logically suitable for focal therapy, should be included, but the majority of participants felt that men with such lesions should be excluded because regardless of the volume of such a lesion the probability of metastases was clinically unacceptable.
We agreed that the disease should be localized (that is, ≤cT2cN0M0) on clini-cal examination, but radiological stage ≤T3aN0M0 was also acceptable.33 Multi-focality is a feature of many other solid organ cancers and was, therefore, not considered a contraindication to focal therapy in pros-tate cancer. Treatment should be targeted to areas defined as clinically significant by volume (≥0.5 ml) and grade (Gleason ≥3 + 4),34–37 in accordance with what has been termed ‘index lesion ablation’.10
The diagnostic pathwayPSA testing, Gleason grading and staging should ideally occur as part of the diagnos-tic pathway before random assignment into a focal therapy trial. However, current clini-cal practice relies heavily on TRUS-guided biopsy, which all attendees recognized as insufficient for accurate disease localization for the purpose of delivering focal therapy. These limitations of TRUS-guided biopsy are due to its random and systematic errors. Random errors occur because the biopsies
Box 2 | The Prostate Cancer RCT Consensus Group participants
Acher, Peter Southend Hospitals NHS Trust, Essex, UKAhmed, Hashim Uddin University College London, UCLH NHS Foundation Trust, London, UKAllen, Clare UCLH NHS Foundation Trust, London, UKAlonzi, Roberto Mount Vernon Cancer Centre and University College London, London, UKArya, Manit Queen Mary’s University, St Bart’s Hospital NHS Trust, UCLH NHS Foundation Trust, London, UK Banks, Freddy West Hertfordshire NHS Trust, Hertfordshire, UKBarratt, Dean Centre for Medical Image Computing, University College London, London, UKBerge, Viktor Oslo University Hospital, Oslo, NorwayBott, Simon Frimley Park Hospital NHS Foundation Trust, Surrey, UKBottomley, David Leeds Teaching Hospitals NHS Trust, West Yorkshire, UKBurgess, Meg Prostate Cancer Charity, London, UKCathcart, Paul Barts and The London NHS Trust and UCLH NHS Foundation Trust, London, UKChinegwundoh, Frank Barts and The London NHS Trust, London, UKCoe, Jane UCLH NHS Foundation Trust, London, UKCrane, Sarah Pelican Cancer Foundation, Basingstoke, UKCross, William Leeds Teaching Hospitals NHS Trust, West Yorkshire, UKDickinson, Louise University College London, London, UKDobbs, Christopher Patient/Public Representative 2, London, UKEmberton, Mark University College London, UCLH NHS Foundation Trust, London, UKFawcett, Derek Department of Urology, Royal Berkshire NHS Foundation Trust, Reading, UKHargrave, David Patient/Public Representative 6, London, UK Heer, Rakesh Newcastle University, Newcastle, UKHellawell, Giles Department of Urology, Northwick Park Hospital, London, UKHenderson, Alastair Maidstone and Tunbridge Wells NHS Trust, Kent, UKHindley, Richard Hampshire Hospitals NHS Foundation Trust, Hampshire, UKHrouda, David Imperial College NHS Trust, London, UKKaplan, Rick MRC Clinical Trials Unit, London, UKKhoo, Vincent Institute of Cancer Research and The Royal Marsden Hospital, London, UKKirkham, Alex University College London Hospitals NHS Foundation Trust, London, UKLangley, Stephen Royal Surrey Hospitals NHS Trust, Surrey, UKLarner, Tim Brighton and Sussex University Hospitals NHS Trust, Sussex, UKLeslie, Tom Oxford University and Oxford Radcliffe NHS Trust, Oxford, UKLovatt, David Patient/Public Representative 5, London, UK Malcolm, Emma Prostate Action, London, UKMcCartan, Neil UCLH NHS Foundation Trust, London, UKMcGinn, Brian Patient/Public Representative 3, London, UK Miller, Paul Brighton and Sussex University Hospitals NHS Trust, Sussex, UKMills, Robert Norfolk and Norwich University Hospitals NHS Foundation Trust, Norwich, UKMoore, Caroline University College London, London, UKParker, Chris Institute of Cancer Research and The Royal Marsden Hospital, London, UKPatel, Shraddha University College London, London, UKPersad, Raj Bristol Urology Institute and Bristol Royal Infirmary and Southmead Hospital, Bristol, UKPope, Alvan The Hillingdon Hospitals NHS Trust Foundation Trust, Uxbridge, UKRelton, Clare School of Health and Related Research, University of Sheffield, Sheffield, UKRobertson, Nicola University College London, London, UKRobinson, Angus Brighton and Sussex University Hospitals NHS Trust, Sussex, UKScott, Rebecca University College London, London, UKSidhu, Sabeena Royal Surrey County Hospital, Surrey, UKSimmons, Lucy University College London, London, UKSimms, Matthew Hull and East Yorkshire NHS Trust, Hull, UKStephens, Richard Patient/Public Representative 1, London, UKStone, Helena University College London, London, UKSydes, Matthew MRC Clinical Trials Unit, London, UKTurnbull, Lindsay Centre for Magnetic Resonance Investigations, University of Hull, Hull, UKVan As, Nicholas Institute of Cancer Research and The Royal Marsden Hospital, London, UKvan der Meulen, Jan London School of Hygiene and Tropical Medicine, London, UKVickers, Andrew Memorial Sloan–Kettering Cancer Center, New York, USAWillis, Sarah London School of Hygiene and Tropical Medicine, London, UKWilt, Timothy University of Minnesota, Minneapolis, USAWinkler, Matthias Imperial College Healthcare NHS Trust, London, West Middlesex University Hospital NHS Trust, Isleworth, UKWood, Wendy Southampton University Clinical Trials Unit, Southampton, UK
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved
4 | ADVANCE ONLINE PUBLICATION www.nature.com/nrclinonc
are taken with no knowledge of the cancer location within the prostate and systematic errors arise because only certain parts of the prostate are preferentially sampled.38,39 As a result, a number of errors occur. First, insignificant cancer can be detected leading to over-treatment. Second, signifi-cant cancer can be missed completely or miss-classified as insignificant leading to under-treatment.40 Third, cancer loca-tion is difficult to d etermine making focal therapy problematic.41
The group did not agree on whether disease localization should be determined before or after random assignment into a trial. Some felt that focal therapy could be regarded as a ‘complex intervention’ alongside imaging,42 template or saturation biopsies and ablation. Thus, confirmation of location of each cancer lesion within the prostate could occur after a ssignment—which could lead to a proportion of men (approximately one-fifth) who did not have disease suitable for focal therapy being in the research arm. This situation relates to disease that is localized, but the cancer involves so much of the prostate that one cannot preserve some of the prostate through focal therapy. These men would have to undergo treatment of the whole-gland. Such a situation would have impli-cations for an intention-to-treat primary analysis, since a proportion of men in the focal therapy arm would undergo radical whole-gland therapy and thus potentially
improve cancer control as a result. This would be of relevance to studies of clini-cal effectiveness as opposed to efficacy. Some participants felt that focal therapy trials should be delayed until validation of mpMRI, currently ongoing in prospec-tive studies,23–25 was complete and some had concerns about the need for additional template mapping biopsy and its burden on patients and healthcare resources.
In expert centres with trained radiolo-gists, the current performance character-istics of mpMRI are high and can detect clinically significant disease (lesion volume ≥0.5 ml, Gleason ≥3 + 4 or both), opening up focal therapy as an option. Sensitivity for significant disease ranges from 70% to 80% on average, with a negative predictive value in approximately 90% to 95% of cases.16,43–45 A high negative predictive value is particu-larly reassuring when areas of the prostate are not being treated. Furthermore, this high negative predictive value has spurred an increasing interest in targeted biopsies using MRI–TRUS fusion systems.46–49 Thus, the reliability of MRI in terms of accurately identifying noncancerous areas can balance the weak ability of TRUS to identify cancer-ous areas, making them reliable when used together. A systematic review showed that men with an elevated age-specific PSA who underwent diagnostic biopsy required a mean of 3.8 MRI-targeted cores compared with 12 standard cores. In total, 53 of 555 (10%) men were diagnosed with clinically
insignificant cancer with the 12-core approach, but the targeted approaches cor-rectly avoided diagnosing these men with disease that required treatment.50 Recently, the added value of fusion systems has been questioned. ‘Cognitively directed’ or ‘visu-ally directed’ biopsies, based on the opera-tor’s impression of the location of the lesion, seem to perform just as well as software that guides the needle to areas of suspicion by fusing MR-images with ultrasound images at the time of biopsy.51 Overall, the group agreed that sufficient mpMRI and template-mapping biopsy facilities were available in many centres in the UK to deliver an RCT of focal therapy.
InterventionTreatment modalityAn RCT should test the concept of focal therapy as a class and not be limited to one specific ablative modality. Indeed, the Prostate Cancer RCT Consensus Group recog nized that the effects within such a class would be heterogeneous. Accordingly, we agreed that different ablative modalities could be included in a single trial if pro-spective data demonstrated a maximum predefined level of toxicity as well as a minimum level of short-term cancer control based on post-treatment biopsy. These cri-teria would ensure that the trial is current and inclusive of new technologies.
The group noted that cryotherapy and HIFU have already demonstrated the
a Preference-based cohort b Standard, ‘pragmatic’ head-head c Cohort-embedded randomized controlled trial
Men undergoing prostate disease characterization
Ineligible
Declined consent
Focal therapy(Modality patient/
physician preference)
Whole-gland therapy(Modality patient/
physician preference)
Consent for study
Patient/physician preference
Patient reported outcome measuresBiochemical (PSA) measuresLocal and systemic therapies
Healthcare utilization
Longitudinal follow-up using nationalelectronic health records
Men undergoing prostate disease characterization
Ineligible
Declined consent
Focal therapy(Modality patient/
physician preference)
Whole-gland therapy(Patient/physician
preference)
Consent for study
Randomize
Patient reported outcome measuresBiochemical (PSA) measuresLocal and systemic therapies
Healthcare utilization
Longitudinal follow-up using nationalelectronic health records
Men undergoing prostate disease characterization
DeclinedconsentIneligible
Two consents to a cohortinclusion and future randomized
invitation to interventions
Cohort
Patient reported outcome measuresBiochemical (PSA) measuresLocal and systemic therapies
Healthcare utilization
Longitudinal follow-up using nationalelectronic health records
Randominvitation
Focaltherapy
Consent
Figure 1 | Trial outlines demonstrating the essential elements of three trial designs that could deliver comparative effectiveness research in evaluating novel interventions in localized prostate cancer or other difficult-to-recruit disease areas. These diagrams were given to all attendees at the meeting. a | Preference-based cohort design with linkage within registries to long-term follow-up through cancer and death registries. b | Standard head-to-head RCT incorporating pragmatic features, such as choice of specific type of intervention in each arm. c | Cohort-embedded multiple RCTs design incorporating double consent features.
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY ADVANCE ONLINE PUBLICATION | 5
necessary level of safety and disease con-trol to represent the focal therapy class.11 However, HIFU has approval in the Euro-pean market, but not in the USA; results from regulatory trials of HIFU are cur-rently being reviewed by the FDA, but these data were obtained from trials evaluating whole-gland therapy.52,53 Although the FDA recently convened a panel discussion to determine the levels and type of evidence needed to approve novel therapies for local-ized disease, no clear ruling on trial design could be determined going forward. While there was agreement that focal thera pies conferred fewer treatment-related adverse events, there was disagreement as to what constituted a cancer control benefit in the medium term (3–5 years follow-up).54 This lack of consensus might prevent clinical innovation in this disease as a result since commercial entities have no clear route for commercialisation of new therapies. Over all, we agreed that brachytherapy, image- guided radiotherapy, irreversible electro poration, photothermal therapy, photo dynamic ther-apy and injectables (for example, magnetic nanoparticles, toxins and antiandrogens) do not currently have enough toxicity and effectiveness data to support their inclusion in a trial of focal therapy.
Treatment protocolThe type of focal ablation to be delivered in the trial would be left to local physician preference, administered according to the published data. The choice would be multi-factorial, including physician experience and the modality available. The extent of tissue ablation could also vary, with experi-enced focal therapists delivering lesion-based plans and less-experienced centres delivering hemiablation (treatment of an entire side of the prostate) for predefined periods of training or until a certain number of patients had been treated, perhaps with centralized quality control review. We agreed that retreatment of an area initially treated focally should be permitted because this represented an element of the focal therapy intervention. The choice of abla-tive therapy should be nominated before random assignment and used as a stratifi-cation factor. For example, in a trial of focal therapy versus radical prostatectomy, both cryotherapy and HIFU could be permitted in the experimental arm. Physicians would have to nominate which approach they chose to use and the randomization strategy would ensure that equal numbers of both cryotherapy and HIFU patients were treated
so that comparisons could be made between focal-cryotherapy and focal-HIFU.
ComparatorFocal therapy should be evaluated in men with clinically significant disease; thus, the comparator arm should be an established and widely used whole-gland therapy with long-term safety and efficacy data. That is, surgery or radiotherapy comprise the only appropriate comparators for a trial of focal therapy. The choice of whole-gland therapy should be nominated before random assign-ment and used as a stratification factor. For instance, in a trial comparing focal therapy to radical therapy, one would assume that radical prostatectomy was an effective and conferred similar toxicity rates as radical radiotherapy so they could form the con-trol arm as a ‘class’ of radical therapies. However, in order to ensure that there were similar numbers of men in the control arm undergoing radical radiotherapy as there were undergoing radical prostatectomy, the type of radical therapy would need to be declared before randomization so that the process could be stratified to equalize the two subgroups.
OutcomesWe could not reach a consensus on the most appropriate primary outcome measure for a trial of focal therapy. However, further work on deriving core outcome measures for localized prostate cancer clinical trials would be a worthy endeavour and could be drawn from a number of common themes, such as overall health-related quality of life, harms (such as erectile dysfunction, urinary incontinence, lower urinary tract symptoms and rectal side-effects), and metastases /cancer- specific survival and overall survi val. Such an endeavour is c urrently u nderway in the UK.55
Composite medium-term outcomesWith the long natural history of localized prostate cancer, even when classified as clini-cally significant, determining the rates of mortality and metastasis would require long follow-up periods (≥10 years). The group agreed that these outcomes were impor-tant, but a medium-term outcome measure at 3–5 years was preferred by many, as physi-cians and patients would be r eassured to adopt and accept new therapies shown to be beneficial in a timely manner without the requirement for follow-up of 10–15 years. We agreed that mortality and freedom-from-distant-metastases could be amalgamated
into a composite measure to inform power calculations. Indeed, c omposite medium-term outcomes should be clinically relevant and important to patients. The composite measure might include change in genito-urinary and rectal functional status (for example, continent to incontinent, potent to impotent), need for salvage local therapy and need for systemic (hormonal or chemo-therapeutic) therapy as well as mortality and freedom-from- metastases. Initiatives such as Core Out come Measures in Effective ness Trials (COMET) are attempting to derive core outcomes that experts will agree on, as m easured within clinical trials.56 However, ‘need’ can be perceived subjectively. Thus, the need for commencement of these therapies must be objectively defined and verified and the indications for their use standardized, which would minimize physi-cian bias.57 Finally, with such a composite outcome measure, subsequent, long-term mortality data might then be embedded into a national cohort or a registry. These data could be linked to national hospital and cancer databases—similar to post approval postmarketing phase IV surveillance.58 The benefits of such an approach would be to ensure that long-term disease control out-comes are collected on mortality so that any detrimental effect of focal therapy, which would only become evident with 10–15 years of follow-up, can be detected and focal therapy halted.
Quality of lifeThe group agreed that any new treat-ment strategy would need to address the treatment- related harms of whole-gland radical therapies. Generic measures of qual-ity of life, such as the EuroQol EQ-5D ques-tionnaire, might not be sensitive enough to detect differences between strategies, especial ly in the presence of patient accep-tance bias following treatment. However, quality-adjusted life years and instruments to measure this are also required to deter-mine cost-effectiveness as this is increas-ingly required by funders and regulatory bodies. Disease-specific and symptom- specific patient-reported outcome m easures are preferable. Accordingly, a non- inferiority design might be most appropri-ate because focal therapy is unlikely to be superior to radical therapy in terms of long-term and medium-term efficacy. However, if cancer control for focal therapy was found to be noninferior at 5 years with a more- favourable adverse-effect profile, it would likely be adopted.
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved

6 | ADVANCE ONLINE PUBLICATION www.nature.com/nrclinonc
Trial designOver the past few years, 11 RCTs evaluat-ing novel interventions in localized prostate cancer have closed prematurely because of slow recruitment, despite the fact pre-piloting questionnaires demonstrating that physi cians and patients regarded the speci fic research questions as important in the defined population. In all instances, the failures resulted predominantly from lack of equipoise from individual patients and physi cians (Table 1),59–71 in spite of having taken into account lessons learned from the piloting phases of previous and historically successful RCTs.72 Although certain exemplar RCTs have succeeded with recruitment, the cost to achieve this has been high; for example, the UK Prostate Testing for Cancer and Treatment (ProTECT) study assessing screening
against treatment, cost £35 million.73 More-over, such academic trials have been slow to initiate (2–4 years from funding deci-sion to the start of recruit ment) and report (10–15 years), which can often lead to issues regarding external validation owing to differing population character istics.74,75 Indeed, this lack of timely delivery of RCTs might not be an issue speci fic to prostate cancer research. Recently, there has been much discussion around the increasingly rigid and slow-moving pace of funders and the regu latory framework within which researchers are working. It has been sug-gested that the degree of scrutiny by funders and research governance checks are often burdensome and disproportionate to the risk posed by many trials.76 The group con-sidered a number of trial designs, which are detailed below.
Nonrandomized cohort preferenceA nonrandomized cohort patient- preference study design meets the NIH definition of comparative effectiveness research, namely that “comparative effectiveness research is the conduct and synthesis of research com-paring the benefits and harms of differ-ent interventions and strategies to prevent, diagnose, treat and monitor health condi-tions in ‘real world’ settings”.77 We agreed that a cohort patient-preference study, which would allow a patient and their physician to choose the treatment alloca-tion (focal therapy or radical therapy) to then compare the two groups, stood a high chance of success ful recruitment (Figure 1a). However, we also agreed that this design would not represent the highest level of evi-dence and would be subject to imbalances in the study populations through selection and
Table 1 | Abandoned trials of focal therapy in localized prostate cancer*
Trial (years open) Location (number of centres)
Study design Primary outcome(s) Accrual (actual/expected)
Accrual rate (patients per year)
Reason for closure
CROP (2011–2013)88
UK (>10) Whole-gland cryotherapy vs expectant management with delayed hormones
Metastases 7/540 7 Lack of physician equipoisePatient choice
START (2007–2011)59
USA, Canada and UK (~16)
Active surveillance vs radical prostatectomy or radical radiotherapy
Disease-specific survival 180/2,130 43 Lack of physician equipoisePatient choice
LOPERA (2010–2011)60,61
UK (4) Laparoscopic radical prostatectomy vs robot-assisted radical prostatectomy vs open radical prostatectomy
Feasibility of recruitment 28/75 35 Lack of physician equipoisePatient choice
SABRE (2009–2011)62
UK (5) Low-dose-rate brachytherapy vs radical prostatectomy
Feasibility of recruitment 0/400 NA Lack of physician equipoisePatient choice
SPIRIT (2002–2004)63,64
USA and Canada (31)
Brachytherapy vs radical prostatectomy
Overall survival;Metastasis-free survival and probability of survival without symptoms;Adverse effects
56/1,980 24 Lack of physician equipoisePatient choice
University of Calgary (1997–2003)65,66
Canada (1) Whole-gland cryotherapy vs external-beam radiotherapy
No evidence of disease progression at 36 months (radiological, biochemical, further treatment) (non-inferiority)
244/480 40 Lack of physician equipoisePatient choice
University of Western Ontario (NR)67
Canada (1) Whole-gland cryotherapy vs external-beam radiotherapy
Biopsy;Biochemical disease-free survival;Disease-specific and overall survival
64/150 NR Change in radiotherapy practice
SWOG-8890 (1990–1992)68
USA (NR) Radical prostatectomy vs external-beam radiotherapy
Overall and disease-specific survival
6/1,128 3 Lack of physician equipoisePatient choice
Northwest Uro-Oncology Group (1999–2000)69
UK (2) Radical prostatectomy vs radical radiotherapy
Feasibility 1 (Target NR)
1 Lack of physician equipoisePatient choice
MRC PR06 (1994–1996)70
Europe (NR) Radical prostatectomy vs radical radiotherapy
Overall survival 35/1,800 17 Lack of physician equipoisePatient choice
SPCG-10 (NR)71 Scandinavian countries (NR)
Radical prostatectomy vs radical radiotherapy
Overall survival 0 (Target NR)
NA Abandoned due to poor accrual
*Information obtained from literature reports, trial registries or by contacting investigators directly. Abbreviations: NA, not applicable; NR, not reported; vs, versus.
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | CLINICAL ONCOLOGY ADVANCE ONLINE PUBLICATION | 7
work-up biases resulting from preferences for each arm. Thus, trials of focal therapy employing this design would unlikely lead to widespread acceptance of their findings in either direction.
Standard explanatory RCTA well-designed, standard, prospective RCT of whole-gland therapy versus focal therapy would provide excellent compara-tive evidence. However, the standard head-to-head RCT (Figure 1b) stands a risk of failing to recruit. This failure could result from patients and physicians being unable or unwilling to accept randomized assignment of treatment, for reasons that might include a lack of individual physician equipoise (despite there being genuine uncertainty at the professional ‘community’ level), lack of individual patient equipoise and professional resistance (for example, desire to maintain expertise in a pro cedure or monetary gain in certain health systems). The group were not convinced that pragmatic features—such as allowing physician–patient pairs to choose the method of disease localization, the type of focal therapy in the intervention arm and the type of whole-gland therapy in the research arm (that is, ‘your choice of whole-gland therapy’ versus ‘your choice of focal-therapy’)—were likely to result in greater accrual and acceptance rates, and might be limited in interpretability. The feasibly of a standard RCT could be evaluated in a pilot study to quantify and to assess if these potential problems with recruitment could be accounted for in a full study. However, in light of the difficulties that numerous trials have already demonstrated (Table 1), the consensus within the working party was to consider alternative methods in preference to standard RCTs.
Cohort-embedded RCTOne possible alternative to the standard RCT trial design is the cohort-embedded RCT, which has four key features.78 Firstly, the trial involves the recruitment of a large cohort of patients who have explicitly given consent with the condition of interest. Secondly, these trials regularly measure the relevant outcomes for the whole cohort over a long period of time. For instance, in the example of focal therapy, erectile function and continence would be measured annually for up to 5–10 years using validated patient questionnaires. Next, cohort-embedded RCTs have the capacity for multiple RCTs over time. For instance, in localized pros-tate cancer, the first embedded RCT would
be to evaluate focal therapy compared with radical therapy in men with intermediate-risk to high-risk disease. The second RCT might be to evaluate the role of radical pros-tatectomy in men with locally advanced prostate cancer versus standard of care, which is radiotherapy. A third RCT might involve an evaluation of the clinical utility in using regular MRI scans to monitor disease in active surveillance compared to regular prostate biopsies. Finally, these trials have ‘patient-centred’ informed consent—that is, the process of obtaining patient information and consent aims to replicate what occurs in the real-world healthcare setting (Figure 1c).
For each embedded RCT, the process would begin with identification of all eli-gible patients in the whole cohort. Then, some patients from all eligible patients in the cohort would be randomly selected and invited to have the trial intervention. After the intervention has been given, the trialists would compare the outcomes in the ran-domly selected patients with the outcomes in eligible patients not randomly selected. This approach is currently being evaluated in chronic noncancer diseases for which the interventions are n onsurgical—i ncluding depression,79 obesity,80 back pain, falls in the elderly,81 ulcerative colitis82 and sclero-derma83 as well as radiotherapy and chemo-therapy interventions in breast cancer, colo rectal cancer and metastatic cancers from any site.84
Although the cohort-embedded RCT has its strengths in terms of focal therapy trials, concerns were raised that, although the design is not inherently unethical, it has chal-lenges that are specific to cancer and surgical treatments that would need to be carefully and explicitly addressed.85,86 Firstly, some concerns centred on the impact of patient refusal rates on outcome measures and the statistical methods that could be used to overcome this. In other words, as patients in only one arm of the RCT have the oppor-tunity to reject the allocated treatment there may be imbalances in baseline character istics of disease or comorbidity between the ran-domly selected group and the group eligible but not randomly selected (and thus forming the control arm). Secondly, the potential high degree of heterogeneity in the control group embedded within the cohort might be a concern, although some pointed out that such heterogeneity would reflect standard practice in real life and, therefore, would improve external validity. Thirdly, those attendees who had active clinical research portfolios with phase II (and some phase III)
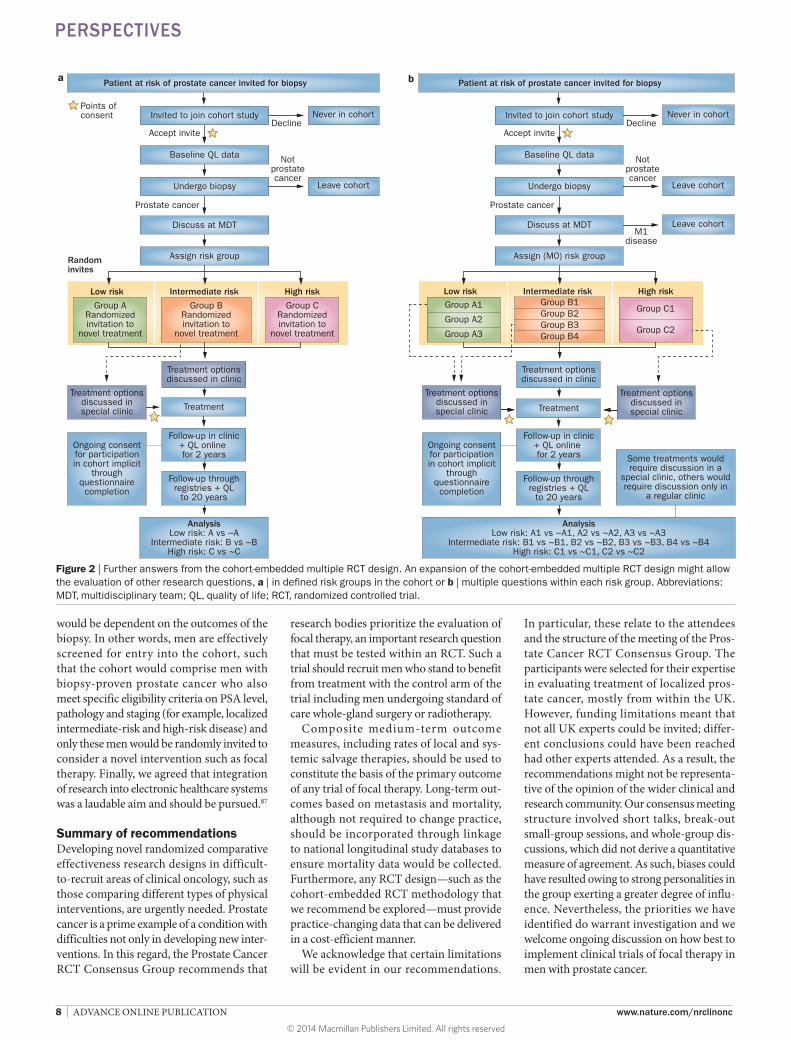
studies recruiting from this population of men had concerns that an over arching cohort RCT could negatively affect their trial accrual. Finally, the exact information that would be given to patients when asked to join the cohort might cause concern, as would the time liness of the random ization. For example, if focal therapy would be the primary (or only) research intervention that a randomly selected proportion of men would be invited to consider, would this have to be declared to all potential participants in the patient information and consent process at the time of inclusion into the cohort? The alternative is that only men randomly selected to undergo focal therapy follow-ing inclusion into the cohort are informed and the control group to which they are being compared are not informed that they were eligible for random selection to focal therapy, but were not selected. The rationale for this approach would be that men in the cohort had given informed consent for such a process. The group concluded that reveal-ing information about the inter vention before random assignment would result in men refusing to participate, disappoint-ment in those who chose to participate but were not selected to receive the intervention or both, which could undermine the study. However, disappoint ment over the selection process might be mitigated by the inclusion of additional randomized trials that would be incorporated into the cohort in a similar manner with random selection to undergo other experimental interventions, including those that are relevant for late-stage disease (locally advanced or recurrent or metastatic, Figure 2).
Ideally, recruitment into the prostate cancer cohort would have to occur before biopsy to mitigate healthcare professional influence on patient choice about random-ization. However, a number of concerns were voiced that such an approach would lead to a very large number of patients, requiring consider able resource to manage, recruited into the cohort, and who were not likely to be eligible for future randomized trials since most would test negative for cancer. Some felt that this problem could be solved by recruit-ing all men under going biopsy to the cohort, and then narrowing the cohort for further follow-up and random ized evaluation to a select subgroup of men (for example, on the basis of their cancer risk category). Such an approach might also enable specific research interventions to be declared to patients upfront because the decision on whether they would be eligible for that intervention
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved
8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrclinonc
would be dependent on the outcomes of the biopsy. In other words, men are effectively screened for entry into the cohort, such that the cohort would comprise men with biopsy-proven prostate cancer who also meet specific eligibility criteria on PSA level, pathology and staging (for example, localized intermediate-risk and high-risk disease) and only these men would be randomly invited to consider a novel intervention such as focal therapy. Finally, we agreed that integration of research into electronic healthcare systems was a laudable aim and should be pursued.87
Summary of recommendationsDeveloping novel randomized comparative effectiveness research designs in difficult-to-recruit areas of clinical oncology, such as those comparing different types of physical interventions, are urgently needed. Prostate cancer is a prime example of a condition with difficulties not only in developing new inter-ventions. In this regard, the Prostate Cancer RCT Consensus Group recommends that
research bodies prioritize the evaluation of focal therapy, an important research question that must be tested within an RCT. Such a trial should recruit men who stand to benefit from treatment with the control arm of the trial including men undergoing standard of care whole-gland surgery or radiotherapy.
Composite medium-term outcome m easures, including rates of local and sys-temic salvage therapies, should be used to constitute the basis of the primary outcome of any trial of focal therapy. Long-term out-comes based on metastasis and mortality, although not required to change practice, should be incorporated through linkage to national longitudinal study databases to ensure mortality data would be collected. Furthermore, any RCT design—such as the cohort-embedded RCT methodology that we recommend be explored—must provide practice-changing data that can be delivered in a cost-efficient manner.
We acknowledge that certain limitations will be evident in our recommendations.
In particular, these relate to the a ttendees and the structure of the meeting of the Pros-tate Cancer RCT Consensus Group. The partici pants were selected for their expertise in evaluating treatment of localized pros-tate cancer, mostly from within the UK. However, funding limitations meant that not all UK experts could be invited; differ-ent conclusions could have been reached had other experts attended. As a result, the recommendations might not be representa-tive of the opinion of the wider clinical and research community. Our consensus meeting structure involved short talks, break-out small-group sessions, and whole-group dis-cussions, which did not derive a quantitative measure of agreement. As such, biases could have resulted owing to strong personalities in the group exerting a greater degree of influ-ence. Nevertheless, the priori ties we have identified do warrant investigation and we welcome ongoing discussion on how best to implement clinical trials of focal therapy in men with prostate cancer.
Leave cohort
Patient at risk of prostate cancer invited for biopsya b
Points ofconsent
Accept invite
Never in cohort
Leave cohort
Notprostatecancer
Decline
Prostate cancer
Discuss at MDT
Randominvites
Baseline QL data
Invited to join cohort study
Undergo biopsy
Assign risk group
Group ARandomizedinvitation to
novel treatment
Group CRandomizedinvitation to
novel treatment
Treatment optionsdiscussed in clinic
Treatment
Follow-up throughregistries + QL
to 20 years
AnalysisLow risk: A vs ~A
Intermediate risk: B vs ~BHigh risk: C vs ~C
Treatment optionsdiscussed inspecial clinic
Ongoing consentfor participationin cohort implicit
throughquestionnairecompletion
Follow-up in clinic+ QL online for 2 years
Patient at risk of prostate cancer invited for biopsy
Accept invite
Never in cohort
Leave cohort
Notprostatecancer
Decline
Prostate cancer
Discuss at MDT
Baseline QL data
Invited to join cohort study
Undergo biopsy
Assign (M0) risk group
Treatment optionsdiscussed in clinic
Treatment
Follow-up throughregistries + QL
to 20 years
AnalysisLow risk: A1 vs ~A1, A2 vs ~A2, A3 vs ~A3
Intermediate risk: B1 vs ~B1, B2 vs ~B2, B3 vs ~B3, B4 vs ~B4High risk: C1 vs ~C1, C2 vs ~C2
Ongoing consentfor participationin cohort implicit
throughquestionnairecompletion
Follow-up in clinic+ QL online for 2 years
M1disease
High riskIntermediate riskLow risk
Group BRandomizedinvitation to
novel treatment
High riskIntermediate riskLow risk
Treatment optionsdiscussed inspecial clinic
Group B1Group B2Group B3Group B4
Group A1
Group A2
Group A3
Treatment optionsdiscussed inspecial clinic
Group C1
Group C2
Some treatments wouldrequire discussion in a
special clinic, others wouldrequire discussion only in
a regular clinic
Figure 2 | Further answers from the cohort-embedded multiple RCT design. An expansion of the cohort-embedded multiple RCT design might allow the evaluation of other research questions, a | in defined risk groups in the cohort or b | multiple questions within each risk group. Abbreviations: MDT, multidisciplinary team; QL, quality of life; RCT, randomized controlled trial.
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | CLINICAL ONCOLOGY ADVANCE ONLINE PUBLICATION | 9
Division of Surgery, University College London, UK (H.U.A., M.E.). Oslo University Hospital, Oslo, Norway (V.B.). St James’s Institute of Oncology, Leeds, UK (D.B., W.C.). Newcastle University and Freeman Hospital, Newcastle, UK (R.H.). MRC Clinical Trials Unit, London, UK (R.K., M.R.S.). University of Oxford, Oxford, UK (T.L.). Royal Marsden Hospital, London, UK (C.P.). University of Sheffield, Sheffield, UK (C.R.). National Cancer Research Institute, London, UK (R.S.). University of Hull, Hull, UK (L.T.). London School of Hygiene and Tropical Medicine, London, UK (J.v.d.M.). Memorial Sloan–Kettering Cancer Center, New York, USA (A.V.). University of Minnesota School of Medicine, Minnesota, USA (T.W.). Correspondence to: H.U.A. [email protected]
1. Wilt, T. J. & Ahmed, H. U. Prostate cancer screening and the management of clinically localized disease. BMJ 346, f325 (2009).
2. Welch, H. G. & Albertsen, P. C. Prostate cancer diagnosis and treatment after the introduction of prostate-specific antigen screening: 1986–2005. J. Natl Cancer Inst. 101, 1325–1329 (2009).
3. Chou, R. et al. Screening for prostate cancer: a review of the evidence for the U. S. preventive services task force. Ann. Intern. Med. 155, 762–771 (2011).
4. McVey, G. P. et al. Initial management of low-risk localized prostate cancer in the UK: analysis of the British Association of Urological Surgeons Cancer Registry. BJU Int. 106, 1161–1164 (2010).
5. Cooperberg, M. R. et al. The changing face of low-risk prostate cancer: trends in clinical presentation and primary management. J. Clin. Oncol. 22, 2141–2149 (2004).
6. Bill-Axelson, A. et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N. Engl. J. Med. 364, 1708–1717 (2011).
7. Wilt, T. J. et al. Radical prostatectomy versus observation for localized prostate cancer. N. Engl. J. Med. 367, 203–213 (2012).
8. Resnick, M. J. et al. Long-term functional outcomes after treatment for localized prostate cancer. N. Engl. J. Med. 368, 436–445 (2013).
9. Ahmed, H. U. et al. Will focal therapy become a standard of care for men with localized prostate cancer? Nat. Clin. Pract. Oncol. 4, 632–642 (2007).
10. Ahmed, H. U. The index lesion and the origin of prostate cancer. N. Engl. J. Med. 361, 1704–1706 (2009).
11. Valerio, M. et al. The role of focal therapy in the management of localised prostate cancer: a systematic review. Eur. Urol. http:// dx.doi.org/10.1016/j.eururo.2013.05.048.
12. Ahmed, H. U. et al. Transatlantic consensus group on active surveillance and focal therapy for prostate cancer. BJU Int. 109, 1636–1647 (2012).
13. Arumainayagam, N. et al. Multiparametric MR imaging for detection of clinically significant prostate cancer: a validation cohort study with transperineal template prostate mapping as the reference standard. Radiology 268, 761–769 (2013).
14. Kasivisvanathan, V. et al. Transperineal magnetic resonance image targeted prostate biopsy versus transperineal template prostate biopsy in the detection of clinically significant prostate cancer. J. Urol. 189, 860–866 (2013).
15. Puech, P. et al. Prostate cancer diagnosis: multiparametric MR-targeted biopsy with cognitive and transrectal US-MR fusion guidance versus systematic biopsy—prospective multicenter study. Radiology 268, 461–469 (2013).
16. Puech, P. et al. Dynamic contrast-enhanced- magnetic resonance imaging evaluation of intraprostatic prostate cancer: correlation with radical prostatectomy specimens. Urology 74, 1094–1099 (2009).
17. Turkbey, B. et al. Correlation of magnetic resonance imaging tumor volume with histopathology. J. Urol. 188, 1157–1163 (2012).
18. Losa, A. et al. Complications and quality of life after template-assisted transperineal prostate biopsy in patients eligible for focal therapy. Urology 81, 1291–1296 (2013).
19. Crawford, E. D. et al. Clinical-pathologic correlation between transperineal mapping biopsies of the prostate and three-dimensional reconstruction of prostatectomy specimens. Prostate 73, 778–787 (2013).
20. Huo, A. S. et al. Accuracy of primary systematic template guided transperineal biopsy of the prostate for locating prostate cancer: a comparison with radical prostatectomy specimens. J. Urol. 187, 2044–2049 (2012).
21. Ahmed, H. U. et al. Characterizing clinically significant prostate cancer using template prostate mapping biopsy. J. Urol. 186, 458–464 (2011).
22. Taira, A. V. et al. Performance of transperineal template-guided mapping biopsy in detecting prostate cancer in the initial and repeat biopsy setting. Prostate Cancer Prostatic Dis. 13, 71–77 (2010).
23. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/show/NCT01492270 (2011).
24. Simmons, L. A. et al. The PICTURE study—Prostate Imaging (multi-parametric MRI and Prostate HistoScanning™) Compared to Transperineal Ultrasound guided biopsy for significant prostate cancer Risk Evaluation. Contemp. Clin. Trials 37, 69–83 (2014).
25. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/show/NCT01138527 (2014).
26. Bahn, D. et al. Focal cryotherapy for clinically unilateral, low-intermediate risk prostate cancer in 73 men with a median follow-up of 3.7 years. Eur. Urol. 62, 55–63 (2012).
27. Ward, J. F. & Jones J. S. Focal cryotherapy for localized prostate cancer: a report from the national Cryo On-Line Database (COLD) Registry. BJU Int. 109, 1648–1654 (2012).
28. Ahmed, H. U. et al. Focal therapy for localised unifocal and multifocal prostate cancer: a prospective development study. Lancet Oncol. 13, 622–632 (2012).
29. Ahmed, H. U. et al. Focal therapy for localized prostate cancer: a phase I/II trial. J. Urol. 185, 1246–1254 (2011).
30. Ahmed, H. U. et al. Focal salvage therapy for localized prostate cancer recurrence after external beam radiotherapy: A pilot study. Cancer 118, 4148–4155 (2012).
31. Lindner, U. et al. Image guided photothermal focal therapy for localized prostate cancer: phase I trial. J. Urol. 182, 1371–1377 (2013).
32. Oto, A. et al. MR Imaging-guided focal laser ablation for prostate cancer: phase I trial. Radiology 267, 932–940 (2013).
33. Preston, M. A., Harisinghani, M. G., Mucci, L., Witiuk, K. & Breau, R. H. Diagnostic tests in urology: magnetic resonance imaging (MRI) for
the staging of prostate cancer. BJU Int. 111, 514–517 (2013).
34. Ahmed, H. U., Arya, M., Freeman, A. & Emberton, M. Do low-grade and low-volume prostate cancers bear the hallmarks of malignancy? Lancet Oncol. 13, e509–e517 (2012).
35. Nevoux, P. et al. Quantitative tissue analyses of prostate cancer foci in an unselected cystoprostatectomy series. BJU Int. 110, 517–523 (2012).
36. Karavitakis, M., Ahmed, H. U., Abel, P. D., Hazell, S. & Winkler, M. H. Tumor focality in prostate cancer: implications for focal therapy. Nat. Rev. Clin. Oncol. 8, 48–55 (2011).
37. Mazzucchelli, R. et al. Pathology of prostate cancer and focal therapy (‘male lumpectomy’). Anticancer Res. 29, 5155–5161 (2009).
38. Ahmed, H. U., Emberton, M., Kepner, G. & Kepner, J. A biomedical engineering approach to mitigate the errors of prostate biopsy. Nat. Rev. Urol. 9, 227–231 (2012).
39. Han, M. et al. Geometric evaluation of systematic transrectal ultrasound guided prostate biopsy. J. Urol. 188, 2404–2409 (2012).
40. Wong, L. M. et al. A negative confirmatory biopsy among men on active surveillance for prostate cancer does not protect them from histologic grade progression. Eur. Urol. http://dx.doi.org/10.1016/j.eururo.2013.04.038.
41. Tsivian, M., Hruza, M., Mouraviev, V., Rassweiler, J. & Polascik, T. J. Prostate biopsy in selecting candidates for hemiablative focal therapy. J. Endourol. 24, 849–853 (2010).
42. MRC. Developing and evaluating complex interventions: new guidance [online], http://www.mrc.ac.uk/complexinterventionsguidance (2008).
43. Arumainayagam, N. et al. Multiparametric MR imaging for detection of clinically significant prostate cancer: a validation cohort study with transperineal template prostate mapping as the reference standard. Radiology 268, 761–769 (2013).
44. Muller, B. G. et al. The role of magnetic resonance imaging in focal therapy for prostate cancer: recommendations from a Consensus Panel. BJU Int. http://dx.doi.org/10.1111/bju.12243.
45. Yerram, N. K. et al. Low suspicion lesions on multiparametric magnetic resonance imaging predict for the absence of high-risk prostate cancer. BJU Int. 110, E783–E788 (2012).
46. Robertson, N. L., Emberton, M. & Moore, C. M. MRI-targeted prostate biopsy: a review of technique and results. Nat. Rev. Urol. 10, 589–597 (2013).
47. Puech, P. et al. Prostate cancer diagnosis: multiparametric MR-targeted biopsy with cognitive and transrectal US-MR fusion guidance versus systematic biopsy—prospective multicenter study. Radiology 268, 461–469 (2013).
48. Sonn, G. A. et al. Targeted biopsy in the detection of prostate cancer using an office based magnetic resonance ultrasound fusion device. J. Urol. 189, 86–91 (2013).
49. Kasivisvanathan, V. et al. Transperineal magnetic resonance image targeted prostate biopsy versus transperineal template prostate biopsy in the detection of clinically significant prostate cancer. J. Urol. 189, 860–866 (2013).
50. Moore, C. M. et al. Image-guided prostate biopsy using magnetic resonance imaging-derived targets: a systematic review. Eur. Urol. 63, 125–140 (2013).
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved
10 | ADVANCE ONLINE PUBLICATION www.nature.com/nrclinonc
51. Wysock, J. S. et al. A prospective, blinded comparison of magnetic resonance (MR) imaging-ultrasound fusion and visual estimation in the performance of MR-targeted prostate biopsy: the PROFUS trial. Eur. Urol. http:// dx.doi.org/10.1016/j.eururo.2013.10.048.
52. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/show/NCT00772317 (2014).
53. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/show/NCT00295802 (2014).
54. Jarow, J. P. et al. Drug and device development for localized prostate cancer: report of a Food and Drug Administration/American Urological Association Public Workshop. Urology http://dx.doi.org/10.1016/j.urology.2013.10.087.
55. Williamson, P. R. et al. Developing core outcome sets for clinical trials: issues to consider. Trials 13, 132 (2012).
56. Williamson, P., Altman, D., Blazeby, J., Clarke, M. & Gargon, E. Driving up the quality and relevance of research through the use of agreed core outcomes. J. Health Serv. Res. Policy 17, 1–2 (2012).
57. Freemantle, N. & Calvert, M. J. Interpreting composite outcomes in trials. BMJ 341, c3529 (2010).
58. Hagberg, K. W., Taylor, A., Hernandez, R. K. & Jick, S. Incidence of bone metastases in breast cancer patients in the United Kingdom: results of a multi-database linkage study using the general practice research database. Cancer Epidemiol. 37, 240–246 (2013).
59. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/ct2/show/NCT00499174 (2013).
60. US National Library of Medicine. ClinicalTrials.gov [online], http://www.controlled-trials.com/ISRCTN59410552 (2011).
61. Mayer, E. et al. Randomised controlled trial (RCT) of Laparoscopic, OPEn and Robot-Assisted prostatectomy as treatment for organ-confined prostate cancer. LopeRA Feasibility Study (CRUK/09/008) [abstract]. NCRI UK Annual Conference, a49 (2011).
62. Eccles, B. K. et al. SABRE 1 (Surgery Against Brachytherapy—a Randomised Evaluation): feasibility randomised controlled trial (RCT) of brachytherapy vs radical prostatectomy in low-intermediate risk clinically localised prostate cancer. BJU Int. 112, 330–337 (2013).
63. Crook, J. M. et al. Comparison of health-related quality of life 5 years after SPIRIT: Surgical Prostatectomy Versus Interstitial Radiation Intervention Trial. J. Clin. Oncol. 29, 362–368 (2011).
64. Wallace, K., Fleshner, N., Jewett, M., Basiuk, J. & Crook, J. Impact of a multi-disciplinary patient
education session on accrual to a difficult clinical trial: the Toronto experience with the surgical prostatectomy versus interstitial radiation intervention trial. J. Clin. Oncol. 24, 4158–4162 (2006).
65. Donnelly, B. J. et al. A randomized trial of external beam radiotherapy versus cryoablation in patients with localized prostate cancer. Cancer 116, 323–330 (2010).
66. Robinson, J. W. et al. A randomized trial of external beam radiotherapy versus cryoablation in patients with localized prostate cancer: quality of life outcomes. Cancer 115, 4695–4704 (2009).
67. Chin, J. L. et al. Randomized trial comparing cryoablation and external beam radiotherapy for T2C-T3B prostate cancer. Prostate Cancer Prostatic Dis. 11, 40–45 (2008).
68. Crawford, E. D. et al. Southwest Oncology Group strategies in prostatic carcinoma. Semin. Surg. Oncol. 11, 60–64 (1995).
69. O’Reilly, P., Martin, L. & Collins, G. Few patients with prostate cancer are willing to be randomised to treatment. BMJ 318, 1556 (1999).
70. PR06 Collaborators. Early closure of a randomized controlled trial of three treatment approaches to early localised prostate cancer: the MRC PR06 trial. BJU Int. 94, 1400–1401 (2004).
71. Scandinavian Prostate Cancer Group–SPCG. http://www.spcginfo.com/ (2014).
72. Donovan, J. et al. Quality improvement report: Improving design and conduct of randomised trials by embedding them in qualitative research: ProtecT (prostate testing for cancer and treatment) study. Commentary: presenting unbiased information to patients can be difficult. BMJ 325, 766–770 (2002).
73. The ProtecT trial—evaluating the effectiveness of treatments for clinically localised prostate cancer. http://www.nets.nihr.ac.uk/projects/hta/962099 (2012).
74. Thompson, I. M. Jr & Tangen, C. M. Prostate cancer—uncertainty and a way forward. N. Engl. J. Med. 367, 270–271 (2012).
75. Wilt, T. J. et al. Systematic review: comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann. Intern. Med. 148, 435–448 (2008).
76. Al-Shahi Salman, R. et al. Increasing value and reducing waste in biomedical research regulation and management. Lancet 383, 176–185 (2014).
77. National Research Council. Initial National Priorities for Comparative Effectiveness Research [online], http://www.iom.edu/~/media/ Files/Report%20Files/2009/ComparativeEffectivenessResearchPriorities/CER%20report%20brief%2008-13-09.ashx (2009).
78. Relton, C., Torgerson, D., O’Cathain, A. & Nicholl, J. Rethinking pragmatic randomised controlled trials: introducing the “cohort multiple randomised controlled trial” design. BMJ 340, c1066 (2010).
79. Collaborative care in screen-positive elders (CASPER) trial. http://www.controlled-trials.com/ ISRCTN02202951 (2012).
80. Relton, C. et al. South Yorkshire Cohort: a ‘cohort trials facility’ study of health and weigh—protocol for the recruitment phase. BMC Public Health 11, 640 (2011).
81. Multifaceted podiatry intervention for fall prevention in patients over 65 years of age. http://www.controlled-trials.com/ISRCTN68240461 (2013).
82. Comparison of infliximab and ciclosporin in steroid resistant ulcerative colitis: a trial. http://www.controlled-trials.com/ISRCTN22663589 (2012).
83. Thombs, B. D. et al. New directions for patient-centred care in scleroderma: the Scleroderma Patient-centred Intervention Network (SPIN). Clin. Exp. Rheumatol. 30 (Suppl. 71), S23–S29 (2012).
84. Verkooijen, H. M., Roes, K. & van Gils, C. H. Cohort multiple randomized controlled trial: a solution for the evaluation of multiple interventions. Ned. Tijdschr. Geneeskd. 157, A5762 (2013).
85. Altman, D. G. et al. Randomised consent designs in cancer clinical trials. Eur. J. Cancer 31A, 1934–1944 (1995).
86. Ergina, P. L. et al. Challenges in evaluating surgical innovation. Lancet 374, 1097–1104 (2009).
87. Vickers, A. J. et al. Feasibility study of a clinically-integrated randomized trial of modifications to radical prostatectomy. Trials 13, 23 (2012).
88. Current Controlled Trials. www.controlled-trials.com [online], http://www.controlled-trials.com/ISRCTN72677390 (2011).
AcknowledgementsThe Medical Research Council (UK) provided support for travel and accommodation costs to all attendees (ref G1002509). Pelican Cancer Foundation charity provided logistical support in organizing the event. No commercial bodies were involved.
Author contributionsH.U.A. wrote the first draft. All named co-authors provided editorial input to revisions and authorized the final draft. All attendees named in Box 2 were sent the draft manuscript and had input into the drafting and editing process. All attendees gave
PERSPECTIVES
© 2014 Macmillan Publishers Limited. All rights reserved




















