Caesarean Section on Request: A Comparison of Obstetricians??? Attitudes in Eight European Countries
10
Caesarean section on request: a comparison of obstetricians’ attitudes in eight European countries M Habiba, a M Kaminski, b M Da Fre `, c K Marsal, d O Bleker, e J Librero, f H Grandjean, g P Gratia, h S Guaschino, i W Heyl, j D Taylor, a M Cuttini k a Reproductive Sciences Section, Department of Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK b INSERM Unit 149, Epidemiological Research Unit on Perinatal Health and Women’s Health, Villejuif Cedex, France c Unit of Epidemiology, Regional Health Agency of Tuscany, Florence, Italy d Department of Obstetrics and Gynaecology, Lund University Hospital, Lund, Sweden e Department of Obstetrics and Gynecology, Amsterdam Medical Centre, Amsterdam, The Netherlands f Fundacio ´ n Instituto de Investigacio ´ n en Servicios Salud, Valencia, Spain g INSERM Unit 558, Research Unit in Epidemiology and Public Health, Toulouse Cedex, France h Department of Gynecology and Obstetrics, Centre Hospitalier de Luxembourg, Luxembourg i Obstetrics and Gynaecology Unit, Istituto per l’Infanzia ‘‘Burlo Garofolo’’, Trieste, Italy j Klinikum Ludwigsburg, Frauenklinik, Ludwigsburg, Germany k Unit of Epidemiology, Ospedale Pediatrico Bambino Gesu ` , Rome, Italy Correspondence: Dr M Habiba, Reproductive Sciences Section, Department of Cancer Studies and Molecular Medicine, University of Leicester, Robert Kilpatrick Building, Leicester Royal Infirmary, PO Box 65, Leicester LE2 7LX, UK. Email [email protected] Accepted 17 February 2006. Published OnlineEarly 2 May 2006. Objective To explore the attitudes of obstetricians to performe a caesarean section on maternal request in the absence of medical indication. Design Cluster sampling cross-sectional survey. Setting Neonatal Intensive Care Unit (NICU) associated maternity units in eight European countries. Population Obstetricians with at least 6 months clinical experience. Methods NICU-associated maternity units were chosen by census in Luxembourg, Netherlands and Sweden and by geographically stratified random sampling in France, Germany, Italy, Spain and UK. An anonymous, self-administered questionnaire was used for data collection. Main outcome measures Obstetricians’ willingness to perform a caesarean section on maternal request. Results One hundred and five units and 1530 obstetricians participated in the study (response rates of 70 and 77%, respectively). Compliance with a hypothetical woman’s request for elective caesarean section simply because it was ‘her choice’ was lowest in Spain (15%), France (19%) and Netherlands (22%); highest in Germany (75%) and UK (79%) and intermediate in the remaining countries. Using weighted multivariate logistic regression, country of practice (P < 0.001), fear of litigation (P = 0.004) and working in a university-affiliated hospital (P = 0.001) were associated with physicians’ likelihood to agree to patient’s request. The subset of female doctors with children was less likely to agree (OR 0.29, 95% CI 0.20–0.42). Conclusions The differences in obstetricians’ attitudes are not founded on concrete medical evidence. Cultural factors, legal liability and variables linked to the specific perinatal care organisation of the various countries play a role. Greater emphasis should be placed on understanding the motivation, values and fears underlying a woman’s request for elective caesarean delivery. Keywords Caesarean, maternal request, obstetricians’ attitude. Please cite this paper as: Habiba M, Kaminski M, Da Fre ` M, Marsal K, Bleker O, Librero J, Grandjean H, Gratia P, Guaschino S, Heyl W, Taylor D, Cuttini M. Caesarean section on request: a comparison of obstetricians’ attitudes in eight European countries. BJOG 2006; 113:647–656. Introduction Caesarean section performed at patients’ request in the absence of a medical indication is a focus of considerable attention both for clinical and ethical reasons. 1–5 The reported rates range from 2.6% in Flanders 6 to 26.8% in Western Australia. 7 Different sampling frameworks and the inconsist- ent use of the term ‘on demand’ may, at least partially, explain such wide variation. 8,9 Nevertheless, there are indications that maternal request is becoming increasingly relevant in situa- tions where medical justification may not—in itself—be suf- ficient to recommend a caesarean delivery. 10–12 The caesarean section rate is rising in most developed countries, and evi- dence from North Carolina suggests that the rising primary DOI: 10.1111/j.1471-0528.2006.00933.x www.blackwellpublishing.com/bjog Intrapartum care ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology 647
Transcript of Caesarean Section on Request: A Comparison of Obstetricians??? Attitudes in Eight European Countries
Caesarean section on request: a comparisonof obstetricians’ attitudes in eightEuropean countriesM Habiba,a M Kaminski,b M Da Fre,c K Marsal,d O Bleker,e J Librero,f H Grandjean,g
P Gratia,h S Guaschino,i W Heyl,j D Taylor,a M Cuttinik
a Reproductive Sciences Section, Department of Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK b INSERM Unit 149,
Epidemiological Research Unit on Perinatal Health and Women’s Health, Villejuif Cedex, France c Unit of Epidemiology, Regional Health Agency of
Tuscany, Florence, Italy d Department of Obstetrics and Gynaecology, Lund University Hospital, Lund, Sweden e Department of Obstetrics and
Gynecology, Amsterdam Medical Centre, Amsterdam, The Netherlands f Fundacion Instituto de Investigacion en Servicios Salud, Valencia, Spaing INSERM Unit 558, Research Unit in Epidemiology and Public Health, Toulouse Cedex, France h Department of Gynecology and Obstetrics, Centre
Hospitalier de Luxembourg, Luxembourg i Obstetrics and Gynaecology Unit, Istituto per l’Infanzia ‘‘Burlo Garofolo’’, Trieste, Italy j Klinikum
Ludwigsburg, Frauenklinik, Ludwigsburg, Germany k Unit of Epidemiology, Ospedale Pediatrico Bambino Gesu, Rome, Italy
Correspondence: Dr M Habiba, Reproductive Sciences Section, Department of Cancer Studies and Molecular Medicine, University of Leicester,
Robert Kilpatrick Building, Leicester Royal Infirmary, PO Box 65, Leicester LE2 7LX, UK. Email [email protected]
Accepted 17 February 2006. Published OnlineEarly 2 May 2006.
Objective To explore the attitudes of obstetricians to performe a
caesarean section on maternal request in the absence of medical
indication.
Design Cluster sampling cross-sectional survey.
Setting Neonatal Intensive Care Unit (NICU) associated maternity
units in eight European countries.
Population Obstetricians with at least 6 months clinical
experience.
Methods NICU-associated maternity units were chosen by census
in Luxembourg, Netherlands and Sweden and by geographically
stratified random sampling in France, Germany, Italy, Spain and
UK. An anonymous, self-administered questionnaire was used for
data collection.
Main outcome measures Obstetricians’ willingness to perform
a caesarean section on maternal request.
Results One hundred and five units and 1530 obstetricians
participated in the study (response rates of 70 and 77%,
respectively). Compliance with a hypothetical woman’s request for
elective caesarean section simply because it was ‘her choice’ was
lowest in Spain (15%), France (19%) and Netherlands (22%);
highest in Germany (75%) and UK (79%) and intermediate in
the remaining countries. Using weighted multivariate logistic
regression, country of practice (P < 0.001), fear of litigation
(P = 0.004) and working in a university-affiliated hospital
(P = 0.001) were associated with physicians’ likelihood to agree
to patient’s request. The subset of female doctors with children
was less likely to agree (OR 0.29, 95% CI 0.20–0.42).
Conclusions The differences in obstetricians’ attitudes are not
founded on concrete medical evidence. Cultural factors, legal
liability and variables linked to the specific perinatal care
organisation of the various countries play a role. Greater emphasis
should be placed on understanding the motivation, values and
fears underlying a woman’s request for elective caesarean delivery.
Keywords Caesarean, maternal request, obstetricians’ attitude.
Please cite this paper as: Habiba M, Kaminski M, Da Fre M, Marsal K, Bleker O, Librero J, Grandjean H, Gratia P, Guaschino S, Heyl W, Taylor D, Cuttini M.
Caesarean section on request: a comparison of obstetricians’ attitudes in eight European countries. BJOG 2006; 113:647–656.
Introduction
Caesarean section performed at patients’ request in the
absence of a medical indication is a focus of considerable
attention both for clinical and ethical reasons.1–5 The reported
rates range from 2.6% in Flanders6 to 26.8% in Western
Australia.7 Different sampling frameworks and the inconsist-
ent use of the term ‘on demand’ may, at least partially, explain
such wide variation.8,9 Nevertheless, there are indications that
maternal request is becoming increasingly relevant in situa-
tions where medical justification may not—in itself—be suf-
ficient to recommend a caesarean delivery.10–12 The caesarean
section rate is rising in most developed countries, and evi-
dence from North Carolina suggests that the rising primary
DOI: 10.1111/j.1471-0528.2006.00933.x
www.blackwellpublishing.com/bjogIntrapartum care
ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology 647

caesarean section rate is not explained by changes in patients’
characteristics.13 A growing awareness of consumer preferen-
ces is said to play a major role.14 However, physicians’ atti-
tudes can significantly influence or motivate patients’ choice,15,16
a point which acquires prominence in the light of the evidence
that a significant proportion of obstetricians in the USA (46%)
and of female obstetricians in London (31%) would favour
a caesarean section for themselves or for their partners in an
uncomplicated pregnancy.17,18 Yet, this view was shared by
only 16% of Scottish female obstetricians,19 15% of female UK
trainees,20 7% of obstetricians in the Republic of Ireland,21 2% of
Norwegian22 and Flemish6 obstetricians and by only 1.4% of
those in the Netherlands.23
That a proportion of obstetricians would prefer a caesarean
section for themselves or for their partner may reflect their
perception of its overall safety or other advantages compared
with vaginal delivery.24 There is also an evidence of an
increased willingness of obstetricians to accept their patients’
request for a caesarean delivery in the absence of ‘mitigating’
circumstances. When surveyed, 69% of consultant obstet-
ricians in England and Wales indicated that they would per-
form an elective caesarean birth on maternal request due to
fear of litigation and pressure from the patients,25 and
approximately 50% of obstetricians in Israel were willing to
perform a caesarean section on request in support of patient’s
autonomy.26 That this be the case despite the generalised
concerns about the rising caesarean section rates represents
a significant shift from the position held by most obstetricians
two decades ago.27 The exact reasons for this change remain
to be explored.
Data that allow direct comparison between countries and
provide insight about the factors influencing clinical decision
making are scarce. A European multicenter study project
(EUROBS) on ethical issues in pre- and perinatal care offered
the opportunity to describe the attitudes of a large represen-
tative sample of obstetricians in eight European countries
towards a request for caesarean delivery in the absence of
compelling medical reasons and to explore the possible
underlying factors.
Methods
SampleEight European countries took part in the EUROBS project
(Developments of Perinatal Technology and Ethical Decision-
Making during Pregnancy and Birth: the Obstetricians’ Per-
spective): France, Germany, Italy, Luxembourg, Netherlands,
Spain, Sweden and UK. In every country, only maternity units
associated with a third-level Neonatal Intensive Care Unit
(NICU) were sampled. The cluster sampling strategy mir-
rored the one adopted in a previous European study on
ethical issues in neonatal medicine (EURONIC).28,29 In Lux-
embourg, The Netherlands and Sweden, all the existing
NICU-associated maternity units were recruited (census sam-
pling); whereas in France, Germany, Italy, Spain and UK,
random samples stratified by geographical area were selected.
In every recruited unit, all physicians with at least 6 months
experience in obstetrics were invited to participate in the
study.
Data collectionData collection took place in 2001–02. Structured question-
naires were used to record information on unit organisation
and policies and to survey the obstetricians’ practices and
attitudes in six major areas: prenatal ultrasound examination,
late termination of pregnancy, management of severe prema-
turity, situations of conflicting opinions between staff and the
women, legal concerns in obstetric practice and maternal
request for caesarean section. The head or the clinical director
of each unit was contacted inviting the unit to participate and,
in case of agreement, to identify a local study coordinator. The
local study coordinator undertook the distribution of the staff
questionnaires to eligible obstetricians. Completed question-
naires were returned in sealed envelopes to the coordinating
centre in Italy either directly or via the local coordinator.
The staff questionnaire was anonymous and self-administered
to protect confidentiality. Thus, nonresponders were not
identified and no reminders were sent. It was developed in
English and translated into national languages; a back-
translation into English was performed to check the accuracy
of the translation and ensure identical semantic content. A
pilot study was carried out to assess the questionnaires’ read-
ability and suitability to the different national contexts.
This study explores obstetricians’ attitudes to a woman’s
request for caesarean delivery in case of uncomplicated term
pregnancy as an area of potential conflict between staff and
women. Respondents were asked to consider whether or not
they would perform a caesarean section on a 25-year-old
woman, with a singleton uncomplicated pregnancy in cephalic
presentation at 39 weeks of gestation, who requests cae-
sarean section despite the obstetrician’s recommendations
for vaginal delivery and despite her being informed of the
higher morbidity and mortality associated with surgical birth.
Respondents were also asked to consider their response in
case the patient’s preference was based on one of the following
distinct scenarios: a) her personal choice, b) fear of vaginal
delivery, c) previous caesarean section, d) previous traumatic
vaginal delivery, e) previous intrapartum fetal death, f) that
her first child was disabled and g) the patient were a colleague.
Respondents who indicated compliance with maternal
request based on any of these reasons were then asked to
clarify their rationale by selecting one or more of the follow-
ing nonexclusive options: a) out of respect for the woman’s
autonomy, b) to avoid possible problems with noncompli-
ance during delivery and c) to avoid possible legal consequen-
ces in case something goes wrong. Space was allowed to write
Habiba et al.
648 ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology
in additional answers beyond the preset ones. Different sec-
tions of the questionnaire addressed doctors’ demographic
and professional characteristics and their perception of the
effect of litigation on their practice. The latter question aimed
at establishing the number of obstetricians who felt that their
personal medical practice was influenced ‘often’, ‘occasionally’
or ‘not at all’ by fear of litigation.
Statistical analysisQuestionnaire coding and data entry were performed at the
coordinating centre in Italy. Statistical analysis was carried
out with the STATA statistical package (version 8.0).30
Weights, computed as the inverse of the probability for a given
maternity unit to be selected within a certain country and
geographical stratum, were applied to take into account the
different sampling fractions adopted in the participating
countries.28,29,31 Standard errors were adjusted for intracluster
correlation, that is the nonindependence of observations
within the same maternity unit.31
Unless stated otherwise, results are presented as weighted
proportions and 95% CI. Multivariate logistic regression
analysis was used to explore factors associated with an obstet-
rician’s agreement with the request for caesarean delivery
solely because it was the woman’s personal choice. The doctor-
related variables considered as predictive factors included age,
sex, having had children, current religion and religiousness,
length of experience in obstetrics, involvement in private
practice, involvement in research and self-reported feelings
that fear of litigation influences one’s clinical practice. The
unit-related variables included number of deliveries per year,
number of obstetric beds, unit proportion of caesarean deliv-
eries, whether or not the hospital and/or the unit was univer-
sity affiliated and whether or not the unit was a referral centre
for high-risk pregnancies. The final model retained the vari-
ables significantly associated with the outcome of interest at
the 0.05 level. A statistically significant interaction (P = 0.01)
was found between the obstetricians’ gender and having had
children; therefore, the odds ratios for women versus men
were reported separately according to whether or not they
had children.
Results
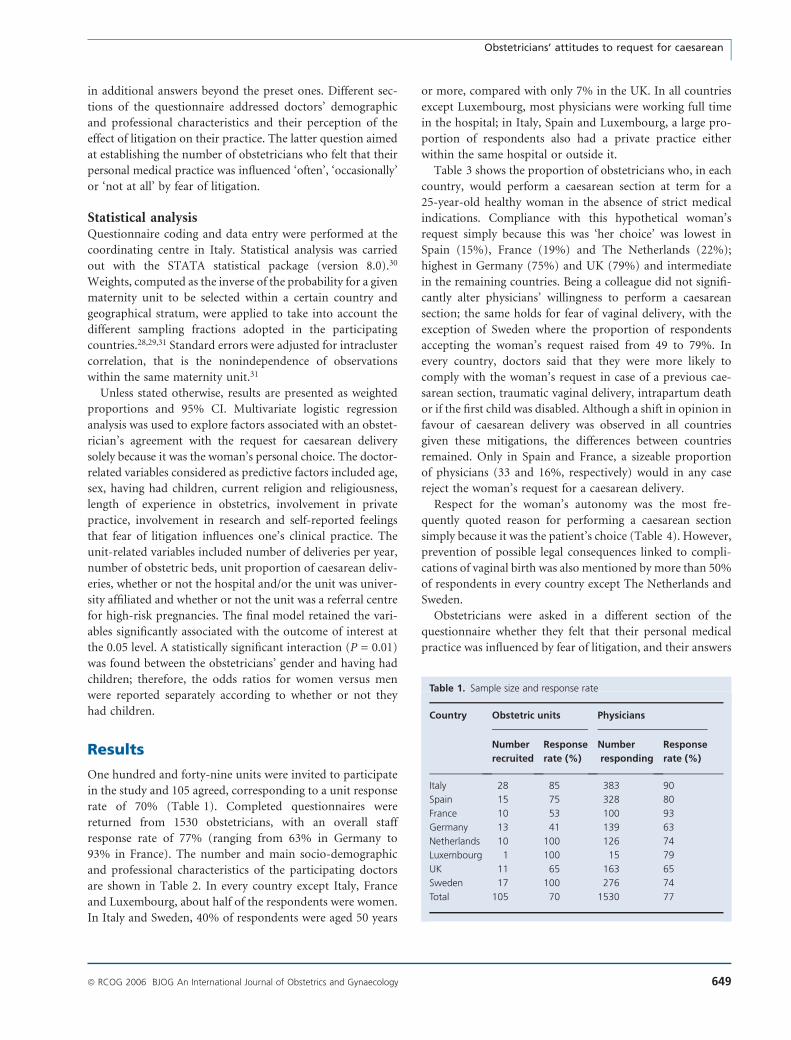
One hundred and forty-nine units were invited to participate
in the study and 105 agreed, corresponding to a unit response
rate of 70% (Table 1). Completed questionnaires were
returned from 1530 obstetricians, with an overall staff
response rate of 77% (ranging from 63% in Germany to
93% in France). The number and main socio-demographic
and professional characteristics of the participating doctors
are shown in Table 2. In every country except Italy, France
and Luxembourg, about half of the respondents were women.
In Italy and Sweden, 40% of respondents were aged 50 years
or more, compared with only 7% in the UK. In all countries
except Luxembourg, most physicians were working full time
in the hospital; in Italy, Spain and Luxembourg, a large pro-
portion of respondents also had a private practice either
within the same hospital or outside it.
Table 3 shows the proportion of obstetricians who, in each
country, would perform a caesarean section at term for a
25-year-old healthy woman in the absence of strict medical
indications. Compliance with this hypothetical woman’s
request simply because this was ‘her choice’ was lowest in
Spain (15%), France (19%) and The Netherlands (22%);
highest in Germany (75%) and UK (79%) and intermediate
in the remaining countries. Being a colleague did not signifi-
cantly alter physicians’ willingness to perform a caesarean
section; the same holds for fear of vaginal delivery, with the
exception of Sweden where the proportion of respondents
accepting the woman’s request raised from 49 to 79%. In
every country, doctors said that they were more likely to
comply with the woman’s request in case of a previous cae-
sarean section, traumatic vaginal delivery, intrapartum death
or if the first child was disabled. Although a shift in opinion in
favour of caesarean delivery was observed in all countries
given these mitigations, the differences between countries
remained. Only in Spain and France, a sizeable proportion
of physicians (33 and 16%, respectively) would in any case
reject the woman’s request for a caesarean delivery.
Respect for the woman’s autonomy was the most fre-
quently quoted reason for performing a caesarean section
simply because it was the patient’s choice (Table 4). However,
prevention of possible legal consequences linked to compli-
cations of vaginal birth was also mentioned by more than 50%
of respondents in every country except The Netherlands and
Sweden.
Obstetricians were asked in a different section of the
questionnaire whether they felt that their personal medical
practice was influenced by fear of litigation, and their answers
Table 1. Sample size and response rate
Country Obstetric units Physicians
Number
recruited
Response
rate (%)
Number
responding
Response
rate (%)
Italy 28 85 383 90
Spain 15 75 328 80
France 10 53 100 93
Germany 13 41 139 63
Netherlands 10 100 126 74
Luxembourg 1 100 15 79
UK 11 65 163 65
Sweden 17 100 276 74
Total 105 70 1530 77
Obstetricians’ attitudes to request for caesarean
ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology 649

are shown in Figure 1. In every country, more than 50% of
respondents answered that ‘occasionally’ this was the case.
Fear of litigation was quoted as ‘often’ influencing decision
making more frequently in Italy and Spain, while the opposite
was true in Sweden and The Netherlands.
Table 5 shows the results of the multivariate logistic analy-
sis exploring the factors associated with obstetricians’ likeli-
hood to comply with the woman’s request for a caesarean
section purely because it was her choice. Differences between
countries remained statistically significant after potential
Table 2. Socio-demographic and professional characteristics of responding obstetricians (unweighted proportions)*
Italy,
n (%)
Spain,
n (%)
France,
n (%)
Germany,
n (%)
Netherlands,
n (%)
Luxembourg,
n (%)
UK,
n (%)
Sweden,
n (%)
Sex
Male 241 (64) 169 (52) 63 (63) 71 (51) 64 (51) 10 (67) 84 (52) 127 (46)
Female 133 (36) 155 (48) 37 (37) 68 (49) 61 (49) 5 (33) 76 (47) 147 (54)
Age (years)
Younger than 30 35 (9) 68 (21) 17 (17) 24 (17) 10 (8) 2 (13) 18 (11) 3 (1)
30–39 67 (18) 103 (32) 46 (46) 73 (53) 65 (52) 5 (33) 85 (53) 60 (22)
40–49 124 (33) 78 (24) 22 (22) 23 (17) 27 (22) 6 (40) 45 (28) 102 (37)
50 and more 149 (40) 75 (23) 15 (15) 19 (14) 23 (18) 2 (13) 12 (7) 109 (40)
Having had children
Yes 264 (70) 195 (60) 71 (71) 58 (42) 80 (64) 9 (60) 102 (64) 249 (91)
No 111 (30) 128 (40) 29 (29) 81 (58) 45 (36) 6 (40) 58 (36) 25 (9)
Length of experience in obstetrics (in years)
Less than 1 0 16 (5) 5 (5) 5 (4) 0 1 (7) 3 (2) 4 (1)
1–5 59 (15) 89 (27) 21 (21) 68 (49) 38 (30) 2 (13) 39 (24) 51 (19)
More than 5 322 (85) 222 (68) 74 (74) 65 (47) 87 (70) 12 (80) 120 (74) 219 (80)
Full-time work in the hospital
Yes 329 (86) 288 (88) 97 (97) 130 (94) 109 (87) 6 (40) 149 (92) 246 (89)
No 52 (14) 40 (12) 3 (3) 8 (6) 17 (13) 9 (60) 13 (8) 29 (11)
Private practice activity
Yes 298 (78) 134 (41) 26 (26) 11 (8) 1 (0.8) 8 (57) 22 (14) 19 (7)
No 84 (22) 193 (59) 74 (74) 128 (92) 125 (99) 6 (43) 139 (86) 256 (93)
*Within countries, discrepancies between totals and number of responding obstetricians as presented in Table 1 are due to missing values.
Table 3. Respondents’ attitudes towards a request for caesarean delivery for an uncomplicated term pregnancy (weighted proportions)*
Italy, %
(95% CI)
Spain, %
(95% CI)
France, %
(95% CI)
Germany, %
(95% CI)
Netherlands, %
(95% CI)
Luxembourg, %
(95% CI)
UK, %
(95% CI)
Sweden, %
(95% CI)
Proportion of physicians who would comply with this woman’s request for a caesarean delivery for each of the following reasons
1. This is her choice 55 (46–64) 15 (9–23) 19 (14–26) 75 (57–87) 22 (17–29) 57 (33–78) 79 (72–85) 49 (42–57)
2. Fear of vaginal delivery 46 (38–54) 10 (6–16) 14 (8–24) 85 (72–92) 30 (24–37) 50 (24–76) 76 (69–82) 79 (71–85)
3. Previous caesarean
section
93 (90–95) 38 (30–48) 49 (38–60) 92 (83–97) 62 (48–75) 86 (76–92) 98 (93–99) 73 (67–77)
4. Previous traumatic
vaginal delivery
78 (70–84) 38 (30–47) 77 (61–88) 97 (89–99) 81 (76–86) 86 (76–92) 99 (96–100) 94 (91–96)
5. Previous intrapartum
death
81 (76–85) 60 (50–70) 67 (54–78) 94 (88–97) 90 (86–93) 93 (88–96) 98 (95–99) 90 (86–93)
6. Her first child is disabled 80 (73–85) 54 (45–63) 55 (43–67) 96 (89–99) 76 (67–83) 86 (76–92) 94 (89–97) 86 (80–90)
7. This patient is a colleague 47 (40–55) 21 (16–28) 26 (18–36) 78 (67–86) 27 (21–34) 57 (33–78) 76 (68–82) 58 (51–64)
Proportion of physicians who would in any case refuse to comply with this woman’s request for a caesarean delivery
2 (0.8–5) 33 (25–43) 16 (9–27) 2 (0.5–10) 6 (3–12) 7 (4–12) 0 6 (3–9)
*A 25-year-old pregnant woman starts labour at 39 completed weeks. The fetus was apparently normally formed, healthy and in cephalic
presentation. Despite being informed that a vaginal delivery is indicated, and of the higher morbidity and mortality associated with caesarean
delivery, the woman insists on a caesarean section.
Habiba et al.
650 ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology

confounders were controlled for. Caesarean section on
demand appeared more likely to be accommodated in the
UK and Germany and less likely in Spain, France and The
Netherlands. Physicians from university-affiliated units were
twice as likely to perform a caesarean section on demand. In
contrast, being a female doctor decreased the probability of
accepting a patient’s request for a caesarean section, but the
effect was statistically significant only among physicians who
had children themselves (OR 0.29, 95% CI 0.20–0.42). A con-
sistent, statistically significant trend emerged between obstet-
ricians’ self-reported feeling that their clinical practice was
influenced, occasionally or often, by fear of litigation and
the willingness to perform a caesarean delivery at the patient’s
request. Factors not associated with the likelihood of agreeing
to a woman’s request for a caesarean section were the doctor’s
age, current religion and religiousness, length of experience in
obstetrics, involvement in private practice or research, the
unit’s annual delivery rate, the number of obstetric beds,
the unit’s caesarean rates and whether the unit was a referral
centre for high-risk pregnancies (data not shown).
Discussion
This study presents the findings of a large representative sam-
ple of obstetricians from NICU-associated maternity units in
eight European countries. The census or the random sam-
pling strategy that was adopted and the overall high physi-
cians’ response rate within the recruited units (77%) support
the validity of our data, although in some countries, a lower
unit recruitment fraction might have impaired the represen-
tativeness of the results at national level.
When confronted with a woman’s request for a caesarean
delivery in the absence of clinical indication, the attitude of
European obstetricians varied within as well as between coun-
tries. Obstetricians from Spain, France and The Netherlands
were the least likely and those from UK and Germany the
Table 4. Reasons for supporting this woman’s choice for a caesarean delivery independently from other medical or nonmedical indications
(weighted proportions)
Italy, %
(95% CI)
Spain, %
(95% CI)
France, %
(95% CI)
Germany, %
(95% CI)
Netherlands, %
(95% CI)
Luxembourg, %
(95% CI)
UK, %
(95% CI)
Sweden, %
(95% CI)
Proportions of physicians indicating the following reasons*
Out of respect for the
woman’s autonomy
93 (87–97) 83 (61–94) 79 (62–90) 95 (80–99) 96 (78–99) 100 97 (92–99) 97 (93–99)
To avoid possible problems
of noncompliance during
delivery
45 (33–58) 40 (30–51) 53 (33–72) 49 (41–58) 37 (22–55) 62 (50–74) 33 (29–37) 52 (39–64)
To avoid possible legal
consequences if
something goes wrong
63 (54–71) 81 (70–89) 89 (50–99) 69 (59–77) 30 (13–53) 87 (69–96) 52 (40–63) 31 (25–37)
*Proportions computed on physicians who would perform a caesarean section simply because it was the woman’s choice. Answers were
not mutually exclusive.
0
10
20
30
40
50
60
70
80
90
100
Italy Spain France Germany Netherlands Luxembourg UK SwedenNo Yes, occasionally Yes, often
Figure 1. Proportion of physicians feeling that their personal medical practice is influenced ’occasionally’ or ’often’ by fear of litigation.
Columns indicate weighted proportion; vertical bars indicate 95% CI.
Obstetricians’ attitudes to request for caesarean
ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology 651
most likely to accept a request for a caesarean section based
exclusively on patient’s choice. International variability was
not explained by differences in physicians’ demographic and
professional characteristics or by characteristics of the units.
Thus, it is likely that cultural factors, as well as elements
related to the national organisation of perinatal care, play
a role. Differences in physicians’ attitudes across countries
have been reported also by other studies. Doctors from
Greece, Spain and Italy appeared less likely and those from
the Netherlands most likely to give complete information in
relation to intensive care interventions.32 Neonatologists were
less likely to involve parents in decisions concerning their
preterm babies in the NICUs of France, Italy and Spain, com-
pared with the northern countries such as Sweden and UK.28
Medical paternalism is said to be a more dominant tradition
in France, while in the Anglo-Saxon cultures, patient’s con-
sent is given more prominence.33 These patterns may partially
explain our findings in Spain and France on the one hand and
the UK on the other hand. In the Netherlands, a very low
national caesarean section rate34 is coupled with a policy of
prenatal care delivered, in case of low-risk pregnancy, by GPs
and midwives rather by obstetricians:23: a pattern consistent
with the lower agreement with caesarean on demand docu-
mented in our study as well as in others.23,35
Obstetricians’ attitudes, however, are also dependent on
the clinical question asked. According to our data, in most
countries, a maternal request for a caesarean delivery
appeared more likely to be accepted when backed up by
a medical or quasi-medical justification, even when question-
able from an evidence-based perspective (e.g. previous cae-
sarean section, traumatic delivery, intrapartum death or
disabled child). Physicians’ acceptance of such reasoning
seemed to be high in every country except Spain. In the Neth-
erlands, the resulting change in attitudes was quite remark-
able, suggesting that a shift from the ‘normal pregnancy’
paradigm moved the woman’s request to a different level of
consideration. In Spain, however, despite the overall high
caesarean section rate,34 none of the mitigating quasi-medical
indications was sufficient to persuade a significant proportion
of doctors to accept a caesarean delivery on request. The
marked contrast between Spain and other countries such as
UK and Germany is unlikely to be explained by differences in
the interpretation of medical evidence; rather, it seems to
emphasise the value attributed to patient’s choice.
Although ‘country’ is an important explanatory variable for
doctors’ attitudes towards maternal choice, responses within
countries were not uniform, pointing to the role of unit policies
or even practitioners as individuals. Physicians’ age as well as
other personal and professional characteristics such as religion,
length of clinical experience, private practice and involvement in
research were not significant explanatory variables. Female gen-
der was only associated with a lower likelihood of accepting the
woman’s request for a caesarean delivery among female doctors
who themselves had children: a finding which might explain the
inconsistencies that emerged in previous studies between the
obstetrician’s gender and the preferences for caesarean delivery
for themselves or for their partners.18,20,21
In this study, personal financial incentives did not seem to
influence doctors’ decision with regards to caesarean section
on demand. Obstetricians from the three countries with the
highest percentage of respondents engaged in private practice
(Italy, Luxembourg and Spain) had an average or low accep-
tance for caesarean section on request, whereas in countries
with the highest acceptance rate for caesarean on demand,
a smaller percentage of obstetricians engaged in private prac-
tice. Also, in multivariate analysis, private practice was not
a significant predictive variable.
In contrast, a physician’s self-reported feeling that ‘fear of
litigation influences his/her clinical practice’ emerged as the
variable more strongly and consistently associated with will-
ingness to perform a caesarean delivery on maternal request,
with odds ratios raising from 1.84 for those reporting ‘occa-
sional’ influence to 3.01 if it was ‘often’. Although respect for
patient’s autonomy was the most widely quoted reason by
physicians’ willing to accept the woman’s request, a relevant
proportion (from about 30% in the Netherlands and Sweden
to more than 80% in Spain, Luxembourg and France) also
mentioned the wish to avoid legal consequences in case of
complications during vaginal birth. Taken together, these
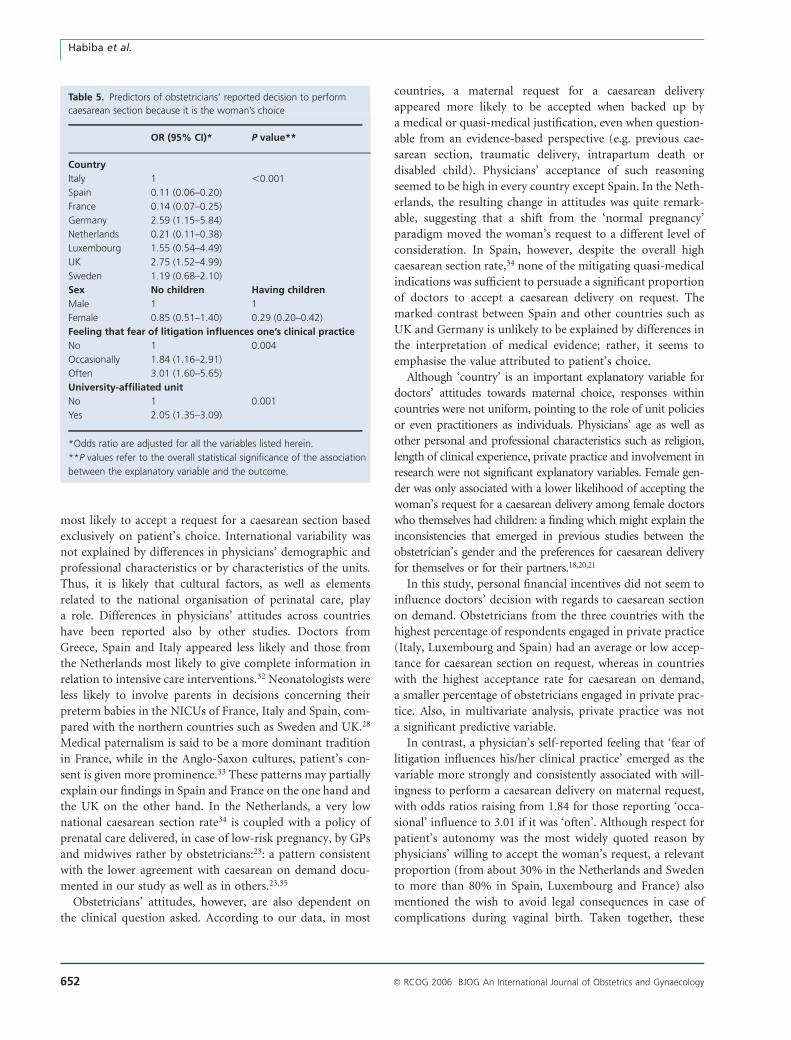
Table 5. Predictors of obstetricians’ reported decision to perform
caesarean section because it is the woman’s choice
OR (95% CI)* P value**
Country
Italy 1 ,0.001
Spain 0.11 (0.06–0.20)
France 0.14 (0.07–0.25)
Germany 2.59 (1.15–5.84)
Netherlands 0.21 (0.11–0.38)
Luxembourg 1.55 (0.54–4.49)
UK 2.75 (1.52–4.99)
Sweden 1.19 (0.68–2.10)
Sex No children Having children
Male 1 1
Female 0.85 (0.51–1.40) 0.29 (0.20–0.42)
Feeling that fear of litigation influences one’s clinical practice
No 1 0.004
Occasionally 1.84 (1.16–2.91)
Often 3.01 (1.60–5.65)
University-affiliated unit
No 1 0.001
Yes 2.05 (1.35–3.09)
*Odds ratio are adjusted for all the variables listed herein.
**P values refer to the overall statistical significance of the association
between the explanatory variable and the outcome.
Habiba et al.
652 ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology

findings indicate that the issue of respect for autonomy may
be compounded by the practice of defensive medicine, which
has been linked to higher caesarean section rates in some
countries,36–38 although supportive evidence remain contro-
versial.36,39,40
Fear of litigation appeared less relevant to physicians’ deci-
sion making in Sweden and The Netherlands, a finding con-
sistent with the low medico-legal burden in these countries.
Yet, there was an important difference between the two coun-
tries with regards to accepting the patient’s ‘choice’ of a cae-
sarean section. Clearly, several factors interact to determine
obstetricians’ attitudes towards caesarean section on demand
in various countries; the relative weight of these factors seems
to be modulated by the specific national or regional character-
istics of medical practice and perinatal care organisation.
A study published in 1986 found that only 2% of US obstet-
ricians would agree to carry out a caesarean section on a pri-
migravid woman at term with no other medical problems and
that a higher risk of litigation swayed 3% towards performing
a caesarean section.27 A later study conducted in 2000
reported that most practitioners in the Portland, Oregon met-
ropolitan area, would not perform a caesarean section based
on patients’ request or in the absence of clear medical indi-
cation.41 In the study by Ghetti et al.,41 only 9% of female
responders and 29.2% of male responders said that they
would consider a caesarean section for fear of urinary incon-
tinence after vaginal delivery. This, however, contrasts with
the higher acceptance of maternal request reported by Kenton
et al.,42 where 67% of recently trained obstetricians and
gynaecologist were willing to perform a primary caesarean
section specifically to prevent pelvic floor disorders. The US
findings that age, years in practice and practice type were not
associated with willingness to perform caesarean section on
request41,42 are in agreement with the findings in our study.
Many publications have mentioned about the risk of fur-
ther increase in caesarean section rate should caesarean sec-
tion on demand become widespread. So far, however, the
relationship between obstetricians’ willingness to perform
a caesarean section based on patient’s request and caesarean
section rates in the respective countries has been inconsistent.
Spain, where our study has shown a low acceptance of mater-
nal request, has the second highest caesarean section rate after
Italy.34 The UK, which has the highest level of acceptance for
maternal request, ranks fourth with regards to its caesarean
section rate.34 On the other hand, The Netherlands features
both a low caesarean section rate and a low acceptance of
maternal request.4 Up to now, the proportion of pregnant
women who actively ask for and are granted an elective cae-
sarean section has probably been quite limited in Europe.16
Should such demand increase, it is hard to believe that we
would not witness a rise of caesarean section rates. In that
situation, issues of costs and resource allocation should also
be considered.43
Traditionally, caesarean delivery has been associated with
a higher maternal mortality and morbidity, both short and
long term, and with neonatal respiratory distress.2,5,44 How-
ever, most of the published literature is based on women who
required a caesarean section because of medical reasons,45 and
it is difficult to disentangle the adverse effects of surgery from
those of its underlying indications. Advances of medical care
have certainly rendered caesarean delivery safer.37 At the same
time, medicalisation of vaginal birth has been linked to
adverse effects such as pelvic floor injury and its sequelae,
which are now quoted as major reasons in favour of caesarean
delivery.46 Reliable data allowing an unbiased comparison of
maternal and fetal benefits and risks, both short and long
term, of planned caesarean versus vaginal delivery are
scarce.5,45,46 Thus, the elements for evidence-based decision
making about the most appropriate way of delivery for the
individual, healthy woman who request an elective caesarean
section are lacking.
In principle, the existence of clinical uncertainty about
alternative treatment strategies makes a good case for allow-
ing the patient’s preferences to prevail.39 However, compli-
ance with patients’ request for caesarean delivery has been
criticised as the easy short cut, which exempts physicians from
dealing with the anxiety associated with childbirth and pro-
viding proper counselling and support.47 Ultimately, the
‘choice’ in favour of caesarean section might be disempower-
ing to women.48 Against this background, it is interesting that
in both our study and that by Ghetti et al.,41 female obstet-
ricians were less likely to agree with the woman’s request,
particularly when they had children themselves.
Apart from financial incentives, obstetricians may see other
advantages in elective caesarean section, such as better control
of the birth process and timing of delivery.15,49 The relation-
ship between the physicians’ attitudes towards caesarean on
demand and the fear of litigation, highlighted in ours as well
as in previous studies,25,35 represents an additional warning.
So far, litigation has largely centred on fetal damage and on
withholding rather than performing medical procedures.47–49
Thus, elective caesarean birth seems less risky than labour
from a liability standpoint.49
One potential criticism of our study is the choice of the
cutoff point for inclusion, which allowed the inclusion of
obstetricians who may not themselves be finally responsible
for making such controversial decisions. However, as the
questions posed addressed values and beliefs, we were inter-
ested in the views of all respondents (of whom only 71 had
between 6 and 12 months of experience in obstetrics). The
choice of 12 months experience as a cutoff point did not alter
the overall results, and furthermore, neither the obstetricians’
age nor the length of experience were significant predictors in
the multivariate analysis.
Despite the appeal of autonomy and ‘consumer’s ethics’,14
women are still highly dependent on the information provided
Obstetricians’ attitudes to request for caesarean
ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology 653

by their physician. Rather than expressing a free, informed
choice for caesarean delivery, they may become trapped
between the obstetricians’ attitudes,15 lack of opportunities
for nonmedicalised vaginal birth16 and media-publicised fash-
ionable trends featuring vaginal delivery as unsafe, archaic,
disfiguring and ultimately socially unacceptable.48 The cur-
rent controversy surrounding this topic suggests the need
for further research to better characterise the cost-benefit bal-
ance and risks of caesarean section in uncomplicated preg-
nancies compared with truly nonmedicalised spontaneous
vaginal birth. Both short- and long-term outcomes should
be considered.
Until better evidence becomes available, individual obstet-
ricians faced with a request for elective caesarean delivery are
charged with the delicate task of fostering their patient’s
autonomy and freedom of choice by exploring the motivation
and fears underlying such request5,45,46 and ultimately act
according to what they believe to better promote the health
and welfare of mother and fetus.50
Acknowledgements
We acknowledge the contribution of Michael Hills as stati-
stical advisor and of the IRTEF Institute in data management.
We are very grateful to our colleagues who answered our
questionnaire.
Conflict of interest
None.
Funding
The results presented in this study are part of the European
Concerted Action project EUROBS on ‘Developments of
perinatal technology and ethical decision-making during
pregnancy and birth: the obstetricians’ perspective’, funded
by the European Commission (Contract no. BMH4-CT98-
3376, Project coordinator: Marina Cuttini, IRCCS Burlo Gar-
ofolo, Trieste). The views expressed are those of the authors
and the sponsor has played no part in study design, execution,
analysis, preparing or reviewing the manuscript. The decision
to submit for publication it that of the authors and the cor-
responding author. Dr M.C acts as custodian for the data.
Other members of the EUROBS studygroup
C Arnaud and M Garel (France); P Benciolini, C Viafora and
R Saracci (Italy), Manuel Marın Gomez (Spain), G Lingman
and T Nilstun (Sweden), I de Beaufort (Netherlands).
List of participating obstetrics units
• France
Hopital Maison Blanche, Reims (R Gabriel, C Quereux); Centre
Hospitalier Universitaire, Amiens (J Gondry, JC Boulanger); Cen-
tre Hospitalier Universitaire Jean Bernard, Poitiers (G Magnin);
Centre Hospitalier, Saint Brieuc (B Cloup, A Renaud-Giono); Cen-
tre Hospitalier Universitaire, Caen (M Dreyfus, M Herlicoviez);
Centre Hospitalier Universitaire, Rouen (L Marpeau); Hopital
Antoine Beclere, Clamart (F Audibert, R Frydman); Hopital Robert
Debre, Paris (P Blot); Hopital Nord, Saint Etienne (MN Varlet, P
Seffert); Hopital Francxois Mitterand, Pau (C Belcikowski, M Che-
valier); Hopital Bretonneau, Tours (J Lansac); Maternite Port-
Royal, Paris (D Cabrol); Hopital Jeanne de Flandre, Lille (F Puech).
• Germany
Marienkrankenhaus, Hamburg (U Blasshof, P Scheidel); Stadt.
Krankenhaus, Luneburg (E Walbrodt, J Gille); Stadt. Kranken-
haus Koln-Holweide, Koln (U Schellenberger, F Wolff); Klinikum
Frauenklinik, Bamberg (J Peisl, R v Hugo); Universitatsklinik,
Gottingen (W Heyl, G Emons); Universitatsklinikum Virchow
Klinikum, Berlin (U Buscher, JW Dudenhausen); Universitatskli-
nikum, Dresden (A Riehn, W Distler); Universitatsklinikum,
Leipzig (B Viehweg, M Hockel); Universitats-Frauenklinik, Mun-
ster (W Klockenbusch, L Kießl); Frauenklinik der Universitat,
Gießen (M Zygmunt, W Kunzel); Frauenklinik der Universitat,
Mainz (P Brockerhoff, PG Knapstein); Frauenklinik der Univer-
sitat, Munchen (F Kainer, G Kindermann); Universitatsklinikum,
Tubingen (B Schauff, D Wallwiener); Stadt. Krankenhaus Mun-
chen-Schwabing, Munchen (EM Grischke); Stadt. Krankenanstal-
ten, Krefeld (W Poleska, J Baltzer).
• Italy
Ospedale Santa Croce, Moncalieri To (ME Renzetti, R Monti);
Ospedale Niguarda Ca’ Granda, Milano (A Ragusa, S Garsia);
Ospedale di Circolo e Fondazione Macchi, Varese (P Clerici, G
Maffioli, D Balestreri, PF Bolis); Azienda Ospedaliera S Anna, Como
(G Bonifacino, F Colombo); Ospedale Bolognini, Seriate Bg (G
Palmerio, LD Moretti); Ospedale Policlinico G B Rossi, Verona
(E Zardini, D Pecorari, V Silvestre, L Fedele); Universita degli
Studi di Padova, Padova (DM Paternoster, A Ambrosiani, F
Lauri, S Mazzer, M Rondinelli, P Grella); Istituto per l’Infanzia
Burlo Garofolo, Trieste (S Guaschino); Policlinico Universitario
di Udine, Udine (F Petraglia); Presidio Ospedaliero di Gorizia,
Gorizia (C Gigli); Policlinico S Orsola-Malpighi, Bologna
(LF Orsini, D De Aloysio); Ospedale Maggiore, Bologna (M
Lenzi, C Melega); Ospedale S Maria Annunziata, Firenze (C
Campatelli, Gaggi); Ospedale Civile Spirito Santo, Pescara (V
Palladoro, R Lotti); Presidio Ospedaliero di Belcolle, Viterbo
(G Palla); Policlinico Umberto I, Roma (M Anceschi, EV Cosmi);
Ospedale SS Annunziata, Napoli (C Picardi, R Arienzo); Azienda
Ospedaliera S Giovanni di Dio e Ruggi d’Aragona, Salerno (C
Lomiento, A Fasolino, De Angelis, R Quirino); Ospedale A Per-
rino, Brindisi (S Burlizzi, ER Poddi); Azienda Ospedaliera Vito
Fazzi, Lecce (F Totaro Aprile, A Perrone, FG Tinelli); Ospedali
Riuniti di Foggia, Foggia (Maruotti, F Pietropaolo, G Arciuolo,
P Lauriola, C Napolitano, CM Troysi); Ospedali Riuniti Bianchi
Melacrino Morelli, Reggio Calabria (N Bitto, PF Tropea);
Habiba et al.
654 ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology

Presidio Ospedale Civico e Benfratelli, Palermo (P Bellipanni, C
Giannola, C Vicari, V Giambanco); Universita degli Studi di
Cagliari, Ospedale San Giovanni di Dio, Cagliari (S Ajossa, GB
Melis).
• Luxembourg
Luxembourg Hospital Centre (P Gratia).
• Spain
Hospital Clınico Universitario de Santiago, Santiago de Campos-
tela (R Ucieda Somoza, M Iglesias Dıaz); Hospital Central de
Asturias, Oviedo (A Escudero Gomis, S Villaverde Fernandez);
Hospital de Basurto, Bilbao (T Martinez-Astorquiza, JM Usandizaga
Pombo); Hospital Ntra. Sra. de Aranzazu, San Sebastian (JJ
Urtiaga Unda, JJ Larraz Soravilla); Hospital Infantil Miguel Servet,
Zaragoza (JJ Tobajas Homs, C Gonzalez Batres); Casa de Mater-
nitat, Barcelona (E Barrau Vernia, V Caradach); Hospital Ntr Sra
de Candelaria, Tenerife (JA Cortell Olcina, F Martin Casanas);
Hospital Universitario Virgen de la Arrixaca, Murcia (JL Delgado
Martın, JJ Parrilla); Hospital Universitario de Canarias, Tenerife
(J Parache); Hospital Son Dureta, Palma de Mallorca (A Marques
Bravo, M Usandizaga Calparsoro); Hospital Clınico S Carlos,
Madrid (MA Herraiz, M Escudero Fernandez); Hospital
Universitario Santa Cristina, Madrid (E Soto Sanchez,
F Izquierdo Gonzalez); Hospital Materno-Infantil de Malaga Car-
los Haya, Malaga (J Carrera Rodriguez, M Abehsera Bensabat);
Hospital San Pedro de Alcantara, Caceres (JI Morinigo Yague, C
Alcon Alcon); Hospital Clınico San Cecilio de Granada, Granada
(A Cano Aguilar, M Dolz Romero); Hospital General Universi-
tario de Alicante, Alicante (JC Martınez Escoriza).
• Sweden
Centrallasarettet, Falun (I Westman, A-C Cachrimanidou); Cen-
tralsjukhuset, Karlstad (J Hareide, G Wadsten); Sundsvalls Sju-
khus, Sundsvall (L Berglund); Centralsjukhuset, Kristianstad (H
Strom, G Helm); Universitetssjukhuset MAS, Malmo (S Montan);
Malarsjukhuset, Eskilstuna (B Moller, M Rom); Karnsjukhuset,
Skovde (J Leyon, G Wallstersson); Centrallasarettet, Vasteras
(LOW Svensson); Lanssjukhuset Ryhov, Jonkoping (R Boij, R
Lenrick); Centrallasarettet, Boras (T Solum); Sahlgrenska Univer-
sitetssjukhuset/Ostra, Goteborg (U-B Wennerholm, M Wennerg-
ren); Akademiska Sjukhuset, Uppsala (U Hansson); Norrlands
Universitetssjukhus, Umea (P-A Holmgren, I Sjoberg); Region-
ssjukhuset i Orebro, Orebro (G Falk, M Lood); Regionssjukhuset i
Linkoping, Linkoping (A Jeppsson, G Berg, S Kjellberg); Univer-
sitetssjukhuset i Lund, Lund (G Lingman, K Marsal); Karolinska
Sjukhuset, Stockholm (O Bakos, V Odlind).
• The Netherlands
Maxima Medical Center, Veldhoven (MY Bongers); Isala Clinics,
Zwolle (J van Eyck); Academic Medical Centre at the University of
Amsterdam, Amsterdam (M Pel, OP Bleker); Free University Med-
ical Centre, Amsterdam (JIP de Vries, HP van Geijn); Academic
Hospital Groningen, Groningen (MP Heringa, JP Holm); Leiden
Academic Medical Centre, Leiden (J van Roosmalen, HHH Kan-
hai); Academic Hospital Maastricht, Maastricht (LLH Peeters, JG
Nijhuis); Academic Medical Centre St Radboud, Nijmegen (PP Van
den Berg, DDM Braat); Academic Medical Centre Utrecht, Utrecht
(HW Bruinse, G Visser); Erasmus Medical Centre, Rotterdam (EAP
Steegers, JW Wladimiroff).
• The UK
Derriford Hospital, Plymouth (I Montague, AD Falconer); Leices-
ter Royal Infirmary, Leicester (A Akkad, C Stewart); King’s Col-
lege Hospital, London (M Marsh); Southmead Hospital, Bristol
(D Bisson); Nottingham City Hospital, Nottingham (H Hamoda,
DT Liu); Birmingham Womens Hospital, Birmingham (MJ Whit-
tle); St James University Hospital, Leeds (G Mason); Rosie Hos-
pital, Cambridge (P Plumpton, C Lees); North Staffordshire
Maternity Hospital, Stoke on Trent (GV Sunanda, G Masson);
Royal Gwent Hospital, Newport (R Gonsalves); University Hos-
pital of Wales, Cardiff (K Sidhu, N Amso). j
References
1 Paterson-Brown S. Should doctors perform an elective caesarean
section on request? Yes, as long as the woman is fully informed.
BMJ 1998;317:462–3.
2 Amu O, Rajendran S, Bolaji II. Should doctors perform an elective
caesarean section on request? Maternal choice alone should not deter-
mine method of delivery. BMJ 1998;317:463–5.
3 Bewley S, Cockburn J. The unethics of ‘request’ caesarean section.
BJOG 2002;109:593–6.
4 Feinmann J. How to limit caesareans on demand—too NICE to push?
(Editorial). Lancet 2002;359:774.
5 Nygaard I, Cruikshank DP. Should all women be offered elective cesarean
delivery? Obstet Gynecol 2003;102:217–19.
6 Jacquemyn Y, Ahankour F, Martens G. Flemish obstetricians’ personal
preference regarding mode of delivery and attitude towards caesarean
section on demand. Eur J Obstet Gynecol Reprod Biol 2003;111:164–6.
7 Quinlivan JA, Petersen RW, Nichols CN. Patient preference the leading
indication for elective caesarean section in public patients—results of
a 2-year prospective audit in a teaching hospital. Aust N Z J Obstet
Gynaecol 1999;39:207–14.
8 Meikle SF, Steiner CA, Zhang J, Lawrence WL. A national estimate of
the elective primary cesarean delivery rate. Obstet Gynecol 2005;
105:751–6.
9 Gamble JA, Health M, Creedy DK. Women’s request for a cesarean
section: a critique of the literature. Birth 2000;4:256–63.
10 Wilkinson C, McIlwaine G, Boulton-Jones C, Cole S. Is a rising caesarean
section rate inevitable? Br J Obstet Gynaecol 1998;105:45–52.
11 Kolas T, Hofoss D, Daltveit AK, Nilsen ST, Henriksen T, Hager R, et al.
Indications for cesarean delivery in Norway. Am J Obstet Gynecol
2003;188:864–70.
12 Singer B. Elective cesarean sections gaining acceptance. CMAJ
2004;170:775.
13 Bailit JL, Love TE, Mercer B. Rising caesarean rates: are patients sicker?
Am J Obstet Gynecol 2004;191:800–3.
14 Anderson GM. Making sense of rising caesarean section rates. BMJ
2004;329:696–7.
15 Hopkins K. Are Brazilian women really choosing to deliver by cesarean?
Soc Sci Med 2000;51:725–40.
16 Gamble JA, Creedy DK. Women’s request for a cesarean section: a
critique of the literature. Birth 2000;27:256–63.
17 Gabbe GS, Holzman GB. Obstetricians’ choice of delivery. Lancet
2001;357:722.
18 Al-Mufti R, McCarthy A, Fisk NM. Survey of obstetricians’ personal
preference and discretionary practice. Eur J Obstet Gynecol Reprod
Biol 1997;73:1–4.
19 MacDonald C, Pinion SB, MacLeod UM. Scottish female obstetricians’
views on elective caesarean section and personal choice for delivery.
J Obstet Gynaecol 2002;22:586–9.
Obstetricians’ attitudes to request for caesarean
ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology 655
20 Wright JB, Wright AL, Simpson NAB, Bryce FC. A survey of trainee
obstetricians’ preferences for childbirth. Eur J Obstet Gynecol Reprod
Biol 2001;97:23–5.
21 Mc Gurgan P, Coulter-Smith S, O’Donovan PJ. A national confidential
survey of obstetrician’s personal preferences regarding mode of delivery.
Eur J Obstet Gynecol Reprod Biol 2001;97:17–19.
22 Backe B, Salvesen KA, Sviggum O. Norwegian obstetrician prefer
vaginal route of delivery. Lancet 2002;359:629.
23 Does van der J, Roosmalen van J. Obstetricians’ choice of delivery. Eur J
Obstet Gynecol Reprod Biol 2001;99:139.
24 Land R, Parry E, Rane A, Wilson D. Personal preferences of obstetricians
towards childbirth. Aust N Z J Obstet Gynaecol 2001;41:249–52.
25 Cotzias CS, Paterson-Brown S, Fisk NM. Obstetricians say yes to mater-
nal request for elective caesarean section: a survey of current opinion.
Eur J Obstet Gynecol Reprod Biol 2001;97:15–16.
26 Gonen R, Tamir A, Degani S. Obstetricians’ opinions regarding patient
choice in cesarean delivery. Obstet Gynecol 2002;99:577–80.
27 Johnson SR, Elkins TE, Strong C, Phelan JP. Obstetric decision-making:
responses to patients who request cesarean delivery. Obstet Gynecol
1986;67:847–50.
28 Cuttini M, Rebagliato M, Bortoli P, Hansen G, de Leeuw R, Lenoir S,
et al. Parental visiting, communication and participation in ethical deci-
sions: a comparison of neonatal unit policies in Europe. Arch Dis Child
Fetal Neonatal Ed 1999;81:F84–91.
29 Cuttini M, Nadai M, Kaminski M, Hansen G, de Leeuw R, Lenoir S, et al.
End-of-life decisions in neonatal intensive care: physicians’ self-reported
practices in seven European countries. Lancet 2000;355:2112–18.
30 StataCorp. 2003. Stata Statistical Software: Release 8.0. College
Station, TX: Stata Corporation.
31 Lemeshow S, Letenneur L, Dartigues JF, Lafont S, Orgogozo JM,
Commenges D. Illustration of analysis taking into account complex
survey considerations: the association between wine consumption and
dementia in the PAQUID study. Am J Epidemiol 1998;148:298–306.
32 Vincent JL. Information in the ICU: are we being honest with our
patients? The results of a European questionnaire. Intensive Care
Med 1998;24:1251–6.
33 Maio G. The cultural specificity of research ethics—or why ethical
debate in France is different. J Med Ethics 2002;28:147–50.
34 World Health Organisation Regional Office for Europe. Caesarean section
per 1000 live births. European health for all database (HFA-DB). Updated
Jan 2006 [www.data.euro.who.int/hfadb]. Accessed 21 March 2006.
35 Kwee A, Cohlen BJ, Kanhai HH, Bruinse HW, Visser GH. Caesarean
section on request: a survey in The Netherlands. Eur J Obstet Gynecol
Reprod Biol 2004;113:186–90.
36 Localio AR, Lawthers AG, Bengtson JM, Hebert LE, Weaver SL, Brennan
TA, et al. Relationship between malpractice claims and cesarean deliv-
ery. JAMA 1993;269:366–73.
37 Vimercati A, Greco P, Kardashi A, Rossi C, Loizzi V, Scioscia M, et al.
Choice of cesarean section and perception of legal pressure. J Perinat
Med 2000;28:111–17.
38 Grant D, McInnes MM. Malpractice experience and the incidence of
cesarean delivery: a physician-level longitudinal analysis. Inquiry
2004;41:170–88.
39 Baldwin LM, Hart LG, Lloyd M, Fordyce M, Rosenblatt RA. Defensive
medicine and obstetrics. JAMA 1995;274:1606–10.
40 Dubay L, Kaestner R, Waidmann T. The impact of malpractice fears on
cesarean section rates. J Health Econ 1999;18:491–522.
41 Ghetti C, Chan BKS, Guise J-M. Physicians’ responses to patient-
requested cesarean delivery. Birth 2004;31:280–4.
42 Kenton K, Brincat C, Mutone M, Brubaker L. Repeat cesarean section
and primary elective cesarean section: recently trained obstetrician-
gynecologist practice patterns and opinions. Am J Obstet Gynecol
2005;192:1872–6.
43 MacKenzie IZ. Should women who elect to have caesarean sections
pay for them? (Letter). BMJ 1999;318:1070.
44 National Collaborating Centre for Women’s and Children’s Health.
Caesarean section. Clinical Guideline 13, National Institute for Clinical
excellence. 2004 [www.nice.org.uk/pdf/CG013NICEguideline.pdf].
Accessed 21 March 2006.
45 Minkoff H, Chervenak FA. Elective primary cesarean delivery. N Engl J
Med 2003;348:946–50.
46 Johanson R, Newburn M, MacFarlane A. Has the medicalisation of
childbirth gone too far? BMJ 2002;324:892–5.
47 Harris LH. Counselling women about choice. Best Pract Res Clin Obstet
Gynaecol 2001;15:93–107.
48 Wagner M. Choosing caesarean section. Lancet 2000;356:
1677–80.
49 McFarlin B. Elective cesarean birth: issues and ethics of an informed
decision. J Midwifery Womens Health 2004;49:421–9.
50 American College of Obstetricians and Gynecologists. Surgery and
patient choice. In: Morales AJ, chair. Ethics in Obstetrics and Gynecol-
ogy, 2nd edn. Washington, DC: ACOG; 2004. p. 21–5.
Habiba et al.
656 ª RCOG 2006 BJOG An International Journal of Obstetrics and Gynaecology