Brazilian Journal of - ANESTHESIOLOGY - Amazon S3
120
Brazilian Journal of Anesthesiology Vol. 71 N. 3 | May-Jun 2021 Brazilian Journal of ANESTHESIOLOGY Revista Brasileira de Anestesiologia Obstetric anesthesia Vol. 71, N. 3 | May-Jun 2021 | ISSN 0104-0014
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Brazilian Journal of - ANESTHESIOLOGY - Amazon S3
Contact us
[email protected] www.bjan-sba.org +55 21 979 770 024
Brazilian Journal ofA n e s t h e s i o l o g y
BJAN Brazilian Journal of Anesthesiology
Vol. 71 N. 3 | M
ay-Jun
2021
Brazilian Journal ofANESTHESIOLOGYR e v i s t a B r a s i l e i r a d e A n e s t e s i o l o g i a
Obstetric anesthesia
Vol. 71, N. 3 | May-Jun 2021 | ISSN 0104-0014

M.S.: 1.0497.1449
Broad range of packaging content sizesAppropriate for every kind of procedure
Short-acting sedation withrapid and safe patient recovery
Packaging content sizes appropriate for all anesthesia steps, from induction to maintenance
Reference: 1. Drug package insert.
For further information, scan the QR Code.
The Revista Brasileira de Anestesiologia/Brazilian Journal of Anesthesiology (BJAN) is the official journal of Sociedade Brasileira de Anestesiologia (SBA). The BJAN only accepts original articles for publication that can be submitted in English or Portuguese, and are published in English. Before submitting a manuscript, authors must read carefully the Instructions to Authors. It can be found at: <https://bjan-sba.org/instructions>Manuscripts must be submitted electronically via the Journal’s online submission system <http://www.editorialmanager.com/bjan>.
The BJAN publishes original work in all areas of anesthesia, surgical critical care, perioperative medicine and pain medicine, including basic, translational and clinical research, as well as education and technological innovation. In addition, the Journal publishes review articles, relevant case reports, pictorial essays or contextualized images, special articles, correspondence, and letters to the editor. Special articles such as guidelines and historical manuscripts are published upon invitation only, and authors should seek subject approval by the Editorial Office before submission.
The BJAN accepts only original articles that are not under consideration by any other journal and that have not been published before, except as academic theses or abstracts presented at conferences or meetings. A cloud-based intuitive platform is used to compare submitted manuscripts to previous publications, and submissions must not contain any instances of plagiarism. Authors must obtain and send the Editorial Office all required permissions for any overlapping material and properly identify them in the manuscript to avoid plagiarism.
All articles submitted for publication are assessed by two or more members of the Editorial Board or external peer reviewers, assigned at the discretion of the Editor- in-chief or the Associate editors.Published articles are a property of Sociedade Brasileira de Anestesiologia, and their total ou partial reproduction can be made with previous authorization. The BJAN assumes no responsibility for the opinions expressed in the signed works.
Edited by | Editada por Sociedade Brasileira de Anestesiologia (SBA)Rua Prof. Alfredo Gomes, 36, Rio de Janeiro/RJ, Brazil – CEP 22251-080Telefone: +55 21 3528-1050E-mail: [email protected]
Published by | Publicada porElsevier Editora Ltda.Telefone RJ: +55 21 3970-9300Telefone SP: +55 11 5105-8555www.elsevier.comISSN: 0104-0014 © 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. All rights reserved.
Editor-in-Chief Maria José Carvalho Carmona – Faculdade de Medicina da Universidade de São Paulo, SP, Brazil
Co-Editor André Prato Schmidt – Hospital das Clínicas da Universidade Federal do Rio Grande do Sul, RS, Brazil
Associate Editors Ana Maria Menezes Caetano – Universidade Federal de Pernambuco, Recife, PE, BrazilCláudia Marquez Simões – Hospital Sírio Libanês, São Paulo, SP, BrazilFlorentino F. Mendes – Universidade Federal de Ciências da Saúde de Porto Alegre, RS, BrazilGabriel Magalhães Nunes Guimarães – Universidade de Brasília, DF, BrazilGuilherme A.M. Barros – Faculdade de Medicina de Botucatu da Universidade Estadual Paulista, SP, BrazilLeonardo Henrique Cunha Ferraro – Universidade Federal de São Paulo, SP, BrazilLiana Maria Torres de Araújo Azi – Universidade Federal da Bahia, Salvador, BA, BrazilLuciana Paula Cadore Stefani – Universidade Federal do Rio Grande do Sul, RS, BrazilLuis Vicente Garcia – Faculdade de Medicina da Universidade de São Paulo, Ribeirão Preto, SP, BrazilLuiz Marcelo Sá Malbouisson – Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, SP, BrazilMarcello Fonseca Salgado-Filho – Universidade Federal Fluminense, Rio de Janeiro, RJ, BrazilNorma Sueli Pinheiro Módolo – Faculdade de Medicina de Botucatu da Universidade Estadual Paulista, São Paulo, SP, BrazilPaulo do Nascimento Junior – Faculdade de Medicina de Botucatu da Universidade Estadual Paulista, São Paulo, SP, BrazilRodrigo Leal Alves – Hospital São Rafael, Salvador, BA, BrazilVanessa Henriques Carvalho – Universidade Estadual de Campinas, SP, BrazilVinicius Caldeira Quintão – Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, SP, Brazil
Editorial Committee Adrian Alvarez – Hospital Italiano de Buenos Aires, BA, ArgentinaAdrian Gelb – University of California, San Francisco, CA, USAAlexandra Rezende Assad – Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, BrazilAngela Maria de Sousa – Hospital das Clínicas da Faculdade de MedicinaAntônio Carlos Aguiar Brandão – Universidade do Vale do Sapucaí, Pouso Alegre, MG, BrazilAugusto Key Takaschima – Serviços Integrados de Anestesiologia, Florianópolis, SC, BrazilBernd W. Böttiger – University Hospital of Cologne, Klinikum Köln, GermanyBobbie Jean Sweitzer – Northwestern Medicine, Chicago, USACarlos Galhardo Júnior – Instituto de Cardiologia, MS/RJ, BrazilCarlos Manuel Correia Rodrigues de Almeida – Hospital CUF Viseu, Viseu, PortugalCarolina Baeta Neves D. Ferreira – Hospital Moriah, São Paulo, SP, BrazilCátia Sousa Govêia – Universidade de Brasília, DF, BrazilCélio Gomes de Amorim – Universidade Federal de Uberlândia, MG, BrazilClarita Bandeira Margarido – Sunnybrook Health Sciences Care, Toronto, Ontário, CanadaClaudia Regina Fernandes – Universidade Federal do Ceará, CE, BrazilClyde Matava – The Hospital for Sick Children, Toronto, Ontário, CanadaDavid Ferez – Universidade Federal de São Paulo, SP, BrazilDeborah Culley – Harvard University, Boston, USADomingos Cicarelli – Hospital das Clínicas da Faculdade de Medicina da USP, SP, BrazilDurval Campos Kraychette – Universidade Federal da Bahia, BA, BrazilEdmundo Pereira de Souza Neto – Centre Hospitalier de Montauban, Tarn-et-Garonne, FranceEduardo Giroud Joaquim – Universidade Federal de São Paulo, SP, BrazilEliane Cristina de Souza Soares – Universidade Federal de Minas Gerais, MG, BrazilEmery Brown – Massachusetts Institute of Technology, Cambridge, Massachusetts USAEric Benedet Lineburger – Hospital São José, Criciúma, SC, BrazilErick Freitas Curi – Hospital Santa Rita, Vitória, ES, BrazilFabiana A. Penachi Bosco Ferreira – Universidade Federal de Goiás, GO, BrazilFábio Papa – University of Toronto, Toronto, Ontario, CanadaFátima Carneiro Fernandes – Universidade Federal do Rio de Janeiro, RJ, BrazilFederico Bilotta – Sapienza Università Di Roma, Rome, ItalyFelipe Chiodini – Faculdade de Medicina da Universidade de São Paulo, SP, BrazilFernando Abelha – Hospital de São João, Porto, PortugalFrederic Michard – MiCo, Consulting and Research, Denens, SwitzerlandGastão Duval Neto – Universidade Federal de Pelotas, RS, BrazilGiovanni Landoni – Vita-Salute San Raffaele University, Milan, ItalyGildásio de Oliveira Júnior – Alpert Medical School - Brown University, Providence, USA Giovanni Landoni – Vita-Salute San Raffaele University, Milano, ItalyHazem Adel Ashmawi – Universidade de São Paulo, SP, BrazilIsmar Lima Cavalcanti – Hospital Geral de Nova Iguaçu, RJ, BrazilJean Jacques Rouby – Pierreand Marie Curie University, Paris, FranceJean Louis Teboul – Paris-Sud University, Paris, France
Jean Louis Vincent – Université Libre De Bruxelles, Brussels, BelgiumJoão Batista Santos Garcia – Universidade Federal do Maranhão, São Luís, MA, BrazilJoão Manoel da Silva Júnior – Hospital do Servidor Público, SP, BrazilJoão Paulo Jordão Pontes – Universidade Federal de Uberlândia, MG, BrazilJudymara Lauzi Gozzani – Universidade Federal de São Paulo, SP, BrazilKurt Ruetzler – Cleveland Clinic, Cleveland, OH, USALaszlo Vutskits – Geneva University Hospitals, Geneve, GE, SwitzerlandLeandro Gobbo Braz – Faculdade de Medicina de Botucatu da Universidade Estadual Paulista, São Paulo, SP, BrazilLuciano Gattinoni – University of Göttingen, Göttingen, GermanyLeopoldo Muniz da Silva – Faculdade de Medicina de Botucatu da Universidade Estadual Paulista, SP, BrazilLigia Andrade da S. Telles Mathias – Irmandade da Santa Casa de Misericórdia de São Paulo, SP, BrazilLuiz Antônio Diego – Universidade Federal Fluminense, Rio de Janeiro, RJ, BrazilLuiz Fernando dos Reis Falcão – Universidade Federal de São Paulo, SP, BrazilLuiz Marciano Cangiani – Hospital da Fundação Centro Médico Campinas, Campinas, SP, Brazil Marcelo Gama de Abreu – University Hospital Carl Gustav Carus, Dresden, SN, GermanyMarcelo Luis Abramides Torres – Faculdade de Medicina da Universidade de São Paulo, SP, BrazilMárcio Matsumoto – Hospital Sírio Libanês, São Paulo, SP, BrazilMarcos Antônio Costa de Albuquerque – Universidade Federal de Sergipe, SE, BrazilMarcos Francisco Vidal Melo – Harvard University, Boston, MA, USAMaria Ângela Tardelli – Universidade Federal de São Paulo, SP, BrazilMariana Fontes Lima Neville – Universidade Federal de São Paulo, SP, BrazilMário José da Conceição – Fundação Universidade Regional de Blumenau, SC, BrazilMassimiliano Sorbello – AOU Policlinico Vittorio Emanuele, Catania, ItalyMatheus Fachini Vane – Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, SP, BrazilMônica Maria Siaulys – Hospital e Maternidade Santa Joana, São Paulo, SP, BrazilNádia Maria da Conceição Duarte – Universidade Federal de Pernambuco, Recife, PE, BrazilNeuber Martins Fonseca – Faculdade de Medicina da Universidade Federal de Uberlândia, MG, BrazilNicola Disma – Istituto Giannina Gaslini, Génova, ItalyOscar César Pires – Universidade de Taubaté, SP, BrazilPaolo Pelosi – Universita Degli Studi Di Genova, Genoa, LI, ItalyPaulo Alípio – Universidade Federal Fluminense, RJ, BrazilPedro Amorim – Centro Hospitalar e Universitário do Porto, PortugalPedro Francisco Brandão – Universidade Federal do Espírito Santo, ES, BrazilPedro Paulo Tanaka – Stanford University School of Medicine, California, USAPhilip Peng – University of Toronto, Toronto, Ontario, CanadaPriscilla Ferreira Neto – Instituto da Criança HCFMUSP, SP, BrazilRaffael Pereira Cezar Zamper – London Health Science Center, London, UKRajinder K. Mirakhur – Royal Hospital, Belfast, Northern Ireland, United KingdomRicardo Antônio Guimarães Barbosa – Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, SP, BrazilRicardo Vieira Carlos – Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, SP, BrazilRodrigo Lima – Queens University, Toronto, Ontário, Canadá Rogean Rodrigues Nunes – Hospital São Lucas, Fortaleza, CE, BrazilRonald Miller – University of California, San Francisco, CA, USASara Lúcia Ferreira Cavalcante – Hospital Geral do Inamps de Fortaleza, CE, BrazilThaís Cançado – Serviço de Anestesologia de Campo Grande, MS, BrazilWaynice Paula-Garcia – Universidade de São Paulo, BrazilWolnei Caumo – Universidade do Rio Grande do Sul, Porto Alegre, RS, Brazil
Previous Editors-in-Chief Oscar Vasconcellos Ribeiro (1951-1957) Zairo Eira Garcia Vieira (1958-1964) Bento Mário Villamil Gonçalves (1965-1979) Masami Katayama (1980-1988) Antônio Leite Oliva Filho (1989-1994) Luiz Marciano Cangiani (1995-2003) Judymara Lauzi Gozzani (2004-2009) Mario José da Conceição (2010-2015) Maria Ângela Tardelli (2016-2018)
Editorial Office Managing Editor – Mel RibeiroCommunications and Marketing Coordinator – Felipe Eduardo Ramos BarbosaEditorial Assistant – Pedro SaldanhaLibrarian – Teresa LibórioTranslator – Emily Catapano

The Brazilian Journal of Anesthesiology is indexed by Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS) since 1989, Excerpta Médica Database (EMBASE) since 1994, Scientific Electronic Library Online (SciELO – Brasil) since 2002, MEDLINE since 2008,
Scopus since 2010 and Web of Science (SCIE - Science Citation Index Expanded) since 2011.
ISSN 0104-0014 • Volume 71 • Number 3 • May-June, 2021
ii Brazilian Journal of Anesthesiology Vol. 71, N. 3, May–Jun, 2021
Editorial
205 Challenges in obstetric anesthesiaAna Maria M. Caetano, André P. Schmidt
Infographic
207 Epidural analgesia in the obese obstetric patientAna Maria M. Caetano, André P. Schmidt
Clinical Research
208 Association of postpartum depression and epidural analgesia in women during labor: an observational studyIpek Saadet Edipoglu, Duygu Demiroz Aslan
214 Epidural analgesia in the obese obstetric patient: a retrospective and comparative study with non-obese patients at a tertiary hospitalClaudia Cuesta González-Tascón, Elena Gredilla Díaz, Itsaso Losantos García
221 Effect of anesthetic technique on the quality of anesthesia recovery for abdominal histerectomy: a cross-observational studyDaniel de Carli, José Fernando Amaral Meletti, Rodrigo Pauperio Soares de Camargo, Larissa Schneider Gratacós, Victor Cristiano Ramos Gomes, Nicole Dutra Marques
228 Pain catastrophizing in daughters of women with fi bromyalgia: a case-control studyRégis Junior Muniz, Mariane Schäffer Castro, Jairo Alberto Dussán-Sarria, Wolnei Caumo, Andressa de Souza
233 Effect of ondansetron on spinal anesthesia-induced hypotension in non-obstetric surgeries: a randomised, double-blind and placebo-controlled trialFabrício Tavares Mendonça, Luis Carlos Crepaldi Junior, Rafaela Carvalho Gersanti, Kamila Christine de Araújo
241 Effect of anesthesia induction on cerebral tissue oxygen saturation in hypertensive patients: an observational studyYasi Taşkaldıran, Özlem Şen, Tuğba Aşkın, Süheyla Ünver
247 Effect of preoperative oral liquid carbohydrate intake on blood glucose, fasting-thirst, and fatigue levels: a randomized controlled studyGökçen Aydın Akbuğa, Mürüvvet Başer
254 General anesthesia for emergency cesarean delivery: simulation-based evaluation of residentsJúlio Alberto Rodrigues Maldonado Teixeira, Cláudia Alves, Conceição Martins, Joana Carvalhas, Margarida Pereira
Brazilian Journal of Anesthesiology iiiVol. 71, N. 3, May–Jun, 2021
259 Intubating conditions and hemodynamic changes during awake fi beroptic intubation using fentanyl with ketamine versus dexmedetomidine for anticipated diffi cult airway: a randomized clinical trialAnil Kumar Verma, Shipra Verma, Amiya Kumar Barik, Vinay Kanaujia, Sangeeta Arya
265 Referral to immediate postoperative care in an intensive care unit from the perspective of anesthesiologists, surgeons, and intensive care physicians: a cross-sectional questionnaireJoão Manoel Silva Jr, Henrique Tadashi Katayama, Felipe Manuel Vasconcellos Lopes, Diogo Oliveira Toledo, Cristina Prata Amendola, Fernanda dos Santos Oliveira, Leusi Magda Romano Andraus, Maria José C. Carmona, Suzana Margareth Lobo, Luiz Marcelo Sá Malbouisson
Experimental Trials
271 Dose-related effects of dexmedetomidine on sepsis-initiated lung injury in ratsGülsüm Karabulut, Nurdan Bedirli, Nalan Akyürek, Emin Ümit Bağrıaçık
Case Reports
278 Thromboelastography as a point-of-care guide for spinal anesthesia in an eclamptic patient: a case reportVendhan Ramanujam, Usama Iqbal, Mary Im
281 Perioperative anesthesia management of a pregnant patient with central airway obstruction: a case reportKeevan Singh, Shenelle Balliram, Rachael Ramkissun
285 Ultrasound-guided quadratus lumborum block for surgical treatment of endometriosis: case reportIdelberto do Val Ribeiro-Junior, Luiz Gustavo Oliveira Brito, Maíra Rossmann-Machado, Rose Luce Gomes do Amaral, Angélica F.A. Braga, Vanessa Henriques Carvalho
288 Evaluation of the density spectral array in the Wada test: report of six casesSusana Pacreu, Esther Vilà, Luis Moltó, Rodrigo Rocamora, Juan Luis Fernández-Candil
292 Pulmonary embolism confounded with COVID-19 suspicion in a catatonic patient presenting to anesthesia for ECT: a case reportB. Naveen Naik, Nidhi Singh, Ashish S. Aditya, Aakriti Gupta, Nidhi Prabhakar, Sandeep Grover
295 Hyperbaric oxygen therapy in the treatment of pneumocephalus associated with epidural block: case reportJoão Castedo, António Pedro Ferreira, Óscar Camacho
299 Combined spinal-epidural anesthesia for abdominoplasty and liposuction in Limb-Girdle Muscular Dystrophy: case reportPlinio da Cunha Leal, Wildney Leite Lima, Eduardo José Silva Gomes de Oliveira, Caio Márcio Barros de Oliveira, Lyvia Maria Rodrigues de Sousa Gomes, Elizabeth Teixeira Noguera Servin, Ed Carlos Rey Moura
Letters to the Editor
302 Donning N95 respirator masks during COVID-19 pandemic: look before you leap!Anju Gupta, Ajisha Aravindan, Kapil Dev Soni
303 Occupational team safety in ECT practice and COVID-19Rujitika Mungmunpuntipantip, Viroj Wiwanitkit
304 Validation of the Surgical Outcome Risk Tool (SORT) in patients with pancreatic cancer undergoing surgeryDimitrios E. Magouliotis, Athina Samara, Maria P. Fergadi, Dimitrios Symeonidis, Dimitris Zacharoulis
305 Airway management in obese patientsManuel Ángel Gómez-Ríos, David Gómez-Ríos, Zeping Xu, Antonio M. Esquinas
306 Medicinal cannabis: new challenges for the anesthesiologistIgor P. Saffi er, Claudia C.A. Palmeira
307 Regional analgesia technique for postoperative analgesia in total knee arthroplasty: have we hit the bull’s eye yet?Kartik Sonawane, Hrudini Dixit, J. Balavenkatasubramanian
309 Challenges of prototyping, developing, and using video laryngoscopes produced by inhouse manufacturing on 3D printersVictor Sampaio de Almeida, Vinicius Sampaio de Almeida, Guilherme Oliveira Campos
311 Reorganization of obstetric anesthesia services during the nationwide COVID-19 lockdown – experience from an Indian tertiary hospitalAnjuman Chander, Vighnesh Ashok, Vanita Suri
313 Perspectives on Pecs I block in breast surgeriesRaghuraman M. Sethuraman
iv Brazilian Journal of Anesthesiology Vol. 71, N. 3, May–Jun, 2021

E
C
SvqGsy
(uGJrp(o
tahqRehva
g(woaiiiqo
adn
h©B
Brazilian Journal of Anesthesiology 2021;71(3):205---206
DITORIAL
hallenges in obstetric anesthesia
itht
(tTrapo
cngqicuugsusag
pewdTal
ince the dawn of humanity, childbirth has taken place in aery painful way, being accepted as such even with biblicaluotes. One of them, possibly the best-known, appears inenesis, chapter 03, verse 16: ‘‘To the woman, He [God]aid: ‘I will surely multiply your pain in childbearing; in painou shall bring forth children’’’.
In October 1846, dentist William Thomas Green Morton1819---1868) successfully demonstrated the first anesthesiasing ether to remove a neck tumor at the Massachusettseneral Hospital in Boston. After this event, the obstetricianames Young Simpson (1811---1870) has used ether and chlo-oform as anesthesia for deliveries in Scotland, and similarlyroceeded John Snow (1813---1858) and Walter Channing1786---1876), respectively in England and the United Statesf America.
At that time, there was great religious and medical resis-ance to this innovation. However, in 1853, Queen Victoriasked John Snow to administer chloroform for the birth ofer eighth child. After this event, the technique becameuite popular, being known in England as ‘‘Anesthesia a laeine’’.1---5 These modalities of labor analgesia were consid-red the standard care for a long time until other techniquesave emerged, including the use of nitrous oxide,6 intra-enous opioids,7 ketamine,8,9 and, eventually, neuroaxialnesthesia for vaginal delivery.
In Brazil, the right to methods of pain relief during labor isuaranteed by law to all women in the Unified Health SystemSUS).10 Nevertheless, for many years, general anesthesiaas the technique of choice for both elective and emergencybstetric procedures. In the last 30 years, there has beenn overall increasing trend towards neuroaxial anesthesianstead of general anesthesia for obstetric women. Neuroax-al anesthesia has become the state-of-the-art essentiallyn all obstetric centers, reflecting the improvement in theuality of care for pregnant women, with many advantagesver the techniques previously used.11
Consensus has not always existed in scientific communitybout neuroaxial labor analgesia. Many controversies andoubts were raised regarding the effects of neuroaxial tech-iques for labor analgesia, especially regarding the potential
ewdt
ttps://doi.org/10.1016/j.bjane.2021.04.025 2021 Published by Elsevier Editora Ltda. on behalf of Sociedade BrasilY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
ncrease in labor duration and the increase in instrumen-al delivery rates. Fortunately, most of these controversiesave been solved by solid scientific evidence, and neuroaxialechniques are currently widely used and accepted.12,13
In this issue of the Brazilian Journal of AnesthesiologyBJAN), three interesting studies may significantly con-ribute to the good practice of obstetric anesthesia.14---16
hose manuscripts have addressed exciting topics in obstet-ic anesthesia, including education strategies for futurenesthesiologists,14 the association of labor pain with post-artum depression,15 and the influence of obesity onbstetric anesthesia outcomes.16
General anaesthesia is mostly performed for emergencyesarean sections and due to a lack of time to administereuraxial anaesthesia.17 However, for most anaesthesiolo-ists, the clinical experience with general anaesthesia isuite low in the obstetric population. Notably, simulations a well-known modern teaching tool, which can greatlyontribute to the training in anesthesiology, especially innusual clinical circumstances. Hence, Teixeira et al.14 eval-ated the ability of anesthesiology residents to performeneral anesthesia for emergency cesarean section in a safeimulation environment. Although the performance eval-ation was satisfactory, authors have recommended thetandardization of simulation techniques in the obstetricrea in order to further improve the development of futureenerations of anesthesiologists.
Furthermore, Edipoglu et al.15 have demonstrated thatatients who underwent epidural analgesia for vaginal deliv-ry, when compared to those in which delivery occurredithout neuroaxial analgesia, displayed lower pain scoresuring labor and lower incidence of postpartum depression.his study has demonstrated the importance of a flawlessnesthetic care for women in labor in order to improveong-term postpartum outcomes.
Finally, González-Tascón et al.16 have retrospectively
valuated approximately one thousand obese obstetricomen who received neuraxial analgesia for labor andelivery, focusing on outcomes related to the neuroaxialechniques and their success rate. Remarkably, the authorseira de Anestesiologia. This is an open access article under the CC.

TORI
oftoprtlo
latitsilo
C
T
R
1
1
1
1
1
1
1
1
1
1
Brazil
∗
EDI
bserved a greater number of puncture attempts to per-orm neuroaxial anesthesia and a surprising increase inhe cesarean section rate in obese as compared with non-bese patients.16 Obesity is currently a major public healthroblem worldwide, overwhelmingly affecting the obstet-ic population. Therefore, more research is warranted inhis field, providing strong scientific evidence and guide-ines to optimize multidisciplinary perinatal care in high-riskbstetric patients.18,19
Obstetric anesthesia is still a hot topic in the anesthesiaiterature. Despite many recent advances in the field, thessistance of obstetric patients is still frequently challengingo the anesthesiologists everywhere. The studies publishedn this issue of BJAN aimed to present new insights intohe obstetric anesthesia scenario. In summary, they havehown that advances in training techniques and understand-ng the potential benefits of anesthetic techniques and theirimitations is essential to improve clinical outcomes in thebstetric setting.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Caton D. Obstetric anesthesia: the first ten years. Anesthesiol-ogy. 1971;33:102---9.
2. Edwards ML, Jackson AD. The historical development of obstet-ric anesthesia and its contributions to perinatology. Am JPerinatol. 2017;34:211---6.
3. Gibson ME. An Early History of Anesthesia in Labor. J ObstetGynecol Neonatal Nurs. 2017;46:619---27.
4. Melzack R, Taenzer P, Feldman P, Kinch RA. Labour is stillpainful after prepared childbirth training. Can Med Assoc J.1981;125:357---63.
5. Whitfield A. A short history of obstetric anaesthesia. Res Medica.1992;III:28---30.
6. Carstoniu J, Levytam S, Norman P, Daley D, Katz J, SandlerAN. Nitrous oxide in early labor. Safety and analgesic efficacy
assessed by a double-blind, placebo-controlled study. Anesthe-siology. 1994;80:30---5.7. McIntosh DG, Rayburn WF. Patient-controlled analgesia inobstetrics and gynecology. Obstet Gynecol. 1991;78:1129---35.
20
AL
8. Akamatsu TJ, Bonica JJ. Ketamine for obstetric delivery. Anes-thesiology. 1977;46:78.
9. Akamatsu TJ, Bonica JJ, Rehmet R, Eng M, Ueland K. Expe-riences with the use of ketamine for parturition. I. Primaryanesthetic for vaginal delivery. Anesth Analg. 1974;53:284---7.
0. Ministério da Saúde. Diretrizes nacionais de assistência ao partonormal: relatório de recomendação; 2017.
1. Rosa T, Ribeiro I. History of the evolution of anesthesiafor obstetrics in a European Hospital. Eur J Anaesthesiol.2014;31:188.
2. Cambic CR, Wong CA. Labour analgesia and obstetric outcomes.Br J Anaesth. 2010;105 Suppl 1:i50---60.
3. Jones L, Othman M, Dowswell T, et al. Pain management forwomen in labour: an overview of systematic reviews. CochraneDatabase Syst Rev. 2012:CD009234.
4. Teixeira J, Carvalhas J, Pereira M, et al. General anesthesia foremergent cesarean delivery: simulation-based resident assess-ment. Braz J Anesthesiol. 2021;71:254---8.
5. Edipoglu IS, Aslan DD. Association of postpartum depressionand epidural analgesia in women during labor: an observationalstudy. Braz J Anesthesiol. 2021;71:208---13.
6. González-Tascón CC, Díaz EG, Losantos I. Epidural analgesia inthe obese obstetric patient: a retrospective and comparativestudy with non-obese patients at a tertiary hospital. Braz JAnesthesiol. 2021;71:214---20.
7. Devroe S, Van de Velde M, Rex S. General anesthesia for cae-sarean section. Curr Opin Anaesthesiol. 2015;28:240---6.
8. Denison FC, Aedla NR, Keag O, et al. Care of women withobesity in pregnancy: green-top guideline No. 72. BJOG.2019;126:e62---106.
9. Mace HS, Paech MJ, McDonnell NJ. Obesity and obstetric anaes-thesia. Anaesth Intensive Care. 2011;39:559---70.
Ana Maria M. Caetano a,∗, André P. Schmidtb
a Universidade Federal de Pernambuco (UFPE),Departamento de Cirurgia, Disciplina de Anestesiologia,
Recife, PE, Brazilb Universidade Federal do Rio Grande do Sul (UFRGS),
Hospital de Clínicas de Porto Alegre (HCPA), Serviço deAnestesia e Medicina Perioperatória, Porto Alegre, RS,
Corresponding author.E-mail: [email protected] (A.M. Caetano).
6

I
E
A
a
b
M
A
h
c
h©B
Brazilian Journal of Anesthesiology 2021;71(3):207
NFOGRAPHIC
pidural analgesia in the obese obstetric patient�
na Maria M. Caetano a,∗, André P. Schmidtb
Universidade Federal de Pernambuco (UFPE), Departamento de Cirurgia, Disciplina de Anestesiologia, Recife, PE, BrazilUniversidade Federal do Rio Grande do Sul (UFRGS), Hospital de Clínicas de Porto Alegre (HCPA), Serviço de Anestesia eedicina Perioperatória, Porto Alegre, RS, Brazil
vailable online 27 April 2021
DOI of original article:ttps://doi.org/10.1016/j.bjane.2021.02.054� Article reference. González-Tascón CC, Díaz EG, Losantos I. Epiduromparative study with non-obese patients at a tertiary hospital. Braz J∗ Corresponding author.
E-mails: [email protected], [email protected] (A.M. Ca
ttps://doi.org/10.1016/j.bjane.2021.04.026 2021 Published by Elsevier Editora Ltda. on behalf of Sociedade BrasilY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
al analgesia in the obese obstetric patient: a retrospective and Anesthesiol. 2021;71:214---20.
etano).
eira de Anestesiologia. This is an open access article under the CC.
C
Aas
I
a
Ib
RA
h©B
Brazilian Journal of Anesthesiology 2021;71(3):208---213
LINICAL RESEARCH
ssociation of postpartum depression and epiduralnalgesia in women during labor: an observationaltudy
pek Saadet Edipoglu a,∗, Duygu Demiroz Aslanb
Marmara University, Faculty of Medicine, Division of Pain Medicine, Department of Physical Medicine and Rehabilitation,stanbul, TurkeyIstanbul Training and Research Hospital, Department of Anesthesiology, Istanbul, Turkey
eceived 28 April 2019; accepted 9 December 2020vailable online 19 February 2021
KEYWORDSPostpartumdepression;Edinburgh postnataldepression scale;Epidural analgesia;Visual AnalogueScale;Vaginal birth
AbstractBackground and objectives: Postpartum depression affects women, manifesting with depressedmood, insomnia, psychomotor retardation, and suicidal thoughts. Our study examined if thereis an association between epidural analgesia use and postpartum depression.Methods: Patients were divided into two groups. One group received epidural analgesia duringlabor while the second group did not. The Edinburgh postnatal depression scale (EPDS) wasadministered to patients prior to birth and 6 weeks postpartum. Pain severity was assessed bythe Visual Analogue Scale (VAS) during labor and at 24 hours postpartum.Results: Of the 92 patients analyzed, 47.8% (n = 44) received epidural analgesia. We detectedsignificantly higher VAS score during labor (p = 0.007) and 24 hours postpartum (p = 0.0001)in the group without epidural analgesia. At 6 weeks postpartum, a significant difference wasobserved between the EPDS scores of both groups (p = 0.0001). Regression analysis revealedhigher depression scores in patients experiencing higher levels of pain during labor (OR = 0.572,p = 0.039). Epidural analgesia strongly correlated with lower scores of depression (OR = 0.29,p = 0.0001).Conclusion: The group that received epidural analgesia had lower pain scores. A high correlationbetween epidural analgesia and lower depression levels was found. Pregnant women givingbirth via the vaginal route and having high pain scores could reduce postnatal depression scoresusing epidural labor analgesia. Pregnant women should opt for epidural analgesia during laborto lessen postpartum depression levels.
© 2021 Published by Elsevier EdThis is an open access article ulicenses/by-nc-nd/4.0/).∗ Corresponding author.E-mail: [email protected] (I.S. Edipoglu).
ttps://doi.org/10.1016/j.bjane.2021.02.021 2021 Published by Elsevier Editora Ltda. on behalf of Sociedade BrasilY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
itora Ltda. on behalf of Sociedade Brasileira de Anestesiologia.nder the CC BY-NC-ND license (http://creativecommons.org/
eira de Anestesiologia. This is an open access article under the CC.

esio
I
CfrbnadsaiiiPotp
tndtsrHtdd
hssSt
M
OmIDIsOpwoswoiuiPss
cet
ewi(aegoapo3taeafdw(ipt(Eotettfdstwdtt(sts
S
SsmTpdldatti
Brazilian Journal of Anesth
ntroduction
urrently, increasing the rates of vaginal deliveries is theocus of attention because giving birth by the vaginaloute is one of the most important factors associated withoth maternal and infant health.1,2 Unfortunately, vagi-al delivery is not completely free of complications, suchs its association with postpartum depression.3 Postpartumepression, manifested as a depressed mood, insomnia oromnolence, marked weight loss, psychomotor retardation,
lowered self-esteem and self-worth, and suicidal thoughtss a disorder of pregnant women after giving birth.3,4 Thencidence of postpartum depression may be as high as 1n every 10 postpartum women in developed countries.5
ostpartum depression may lead to behavioral and devel-pmental problems both in the mother and the infant, andhose problems may extend into childhood and adolescenceeriods.6
Among women who deliver vaginally, a number prefero receive epidural analgesia for delivery while some doot. Epidural analgesia is commonly used to alleviate painuring labor and is well tolerated by both the mother andhe infant. Several studies and meta-analyses have demon-trated that epidural analgesia is an effective method toeduce the severity of pain during normal vaginal delivery.7
owever, there are only a few studies in the literature inves-igating the effect of epidural labor analgesia on postpartumepression which reported a decreased risk of postpartumepression with epidural labor analgesia.4
In this study, our primary hypothesis was that women whoad epidural labor analgesia would have lower depressioneverity scores 6 weeks postpartum. Our secondary hypothe-is was that those patients would have lower Visual Analoguecale (VAS) scores during labor and 24 hours postpartum ifhey received epidural analgesia.
ethods
ur study is a prospective observational study over a 6-onth period. The institutional ethics committee of the
stanbul Education and Research Hospital’s Anesthesiologyepartment approved this study. It is registered via the
SRCTN registry with study ID ISRCTN84174861 (recruitmenttart date of March 25, 2018 and recruitment end date ofctober 25, 2018). Women aged 18-45 years, who werelanning to give birth electively via a normal vaginal routeith or without epidural analgesia, with American Societyf Anesthesiologists (ASA) physical status I-III, and who con-ented to participate were included in the study. Patientsere excluded if they had a history of schizophrenia, bipolarr obsessive-compulsive disorders in the prepartum period,f they had any hematological disorders that contraindicatedse of regional anesthesia, and if they had skin infectionsn the lumbar area or inadequate fetal vitality concepts.atients were also excluded if the route of delivery waswitched to a cesarean section or have prepartum depres-ion (Edinburgh Postnatal Depression Scale ≥ 10).
Upon admission to our hospital, when patients met theriteria of inclusion, informed consent was obtained fromach patient in the waiting room and they were allocatedo one of the two groups. Initially we used ‘‘patient prefer-
Pfat
20
logy 2021;71(3):208---213
nce’’ for the decision of the technique. But for patientsho have contraindications for regional anesthesia, we
nformed and inclined the patient for the indicated approachinfection in the intervention site, bleeding, pathologies,nd intracranial disorders were our contraindications forpidural analgesia). One group consisted of women whoave birth without receiving epidural analgesia and the sec-nd group consisted of women who gave birth with epiduralnalgesia. The second group received an epidural catheter,laced in the intervertebral space between either L3---L4r L4---L5, when cervical dilatation of the patient reached---5 cm, while the other group received no intervention forheir labor. Patients in the epidural analgesia group received
bolus dose of bupivacaine 0.125% + 100 �g fentanyl via thepidural catheter. This was followed by patient-controllednalgesia (PCA) containing 0.125% bupivacaine + 2 �g.mL-1
entanyl with 6 ml.h-1 continuous infusion and 6 ml PCAemand dose with 10-minute lockouts. Prior to birth and 6eeks postpartum, an Edinburgh Postnatal Depression Scale
EPDS) was administered to both patient groups. The EPDSs a commonly used 10-item scale validated for our studyopulation. A score ≥ 10 was the cut-off score for postpar-um depression. If a patient responded positively to item 10the thought of harming myself has occurred to me) of thePDS, they were evaluated for overt depression regardlessf the patient’s total score and were reported to our hospi-al’s psychiatric department. EPDS were applied by the samexperienced anesthesiologist. Both groups received postpar-um analgesia. One group received epidural PCA containinghe previously started dose (0.125% bupivacaine + 2 �g.mL-1
entanyl with 6 ml.h-1 continuous infusion and 6 ml PCAemand dose with 10-minute lockouts) until discharge. Theecond group received intravenous (IV) tramadol 1 mg.kg-1
wice a day and 15 mg.kg-1 paracetamol three times a day asell as rescue tramadol doses of 1 mg.kg-1 if necessary, untilischarge. The patient’s severity of the pain was assessed byhe VAS during the birth and 24 hours postpartum. In the VAS,he lowest score is 0 (no pain at all) and the highest is 10worst pain imaginable). The aim was to keep patient VAScores below 4. We recorded demographic parameters, ges-ational age, number of pregnancies, VAS scores, and EPDScores.
tatistical analysis
PSS 21.0 software was used for the statistical analysis. Thetudy data were summarized with the descriptive statisticalethods (mean, standard deviation, frequency, and ratio).he Mann---Whitney U test was used for inter-group com-arisons of quantitative data not conforming to a normalistribution. The correlation between the use of epiduralabor analgesia, VAS score, and occurrence of postpartumepression was assessed with multivariate logistic regressionnalysis. The Hosmer---Lemeshow test was used for the logis-ic regression model. Qualitative data was compared withhe Student’s t test. Results were evaluated in a confidencenterval of 95% and at a significance level of p < 0.05. The
ower and Sample Size program (PS version 3.1.2) was usedor patient number analysis. If the change in the EPDS wasssumed to be at least 20%,4 the lowest number of patientso be included in the study should be 88 to meet an � = 0.059

I.S. Edipoglu and D.D. Aslan
F artuw
aht
R
OfAatl
4TTdT
ga
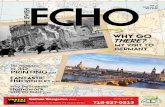
igure 1 Flow Diagram. A comparison of the severity of postpithout epidural analgesia.
nd a power = 0.80. It was assumed that there would be aigh number of drop-outs in the study, therefore we plannedo include 127 patients at baseline.
esults
f the 198 patients analyzed for eligibility, 166 wereound eligible according to the exclusion/ inclusion criteria.
mong these 166 eligible patients, 129 patients gave consentnd participated in the study. After excluding patients losto follow-up and change of delivery, 92 patients were ana-yzed in the final evaluation (Fig. 1). Of these 92 patients,a
rs
21
m depression in women who gave normal vaginal birth with or
7.8% (n = 44) preferred delivery with epidural analgesia.he remaining patients did not receive epidural analgesia.he mean age of the patients was 29.81 ± 7.19 years. Theemographic data of the study patients are presented inable 1.
No statistically significant differences in patient demo-raphics were detected between the epidural labornalgesia group and the group who did not receive epidural
nalgesia (p > 0.05). These data are presented in Table 2.In the group of women who gave birth without epidu-al analgesia, we detected significant differences in the VAScores both during labor (p = 0.0001) and 24 hours after deliv-
0

Brazilian Journal of Anesthesiology 2021;71(3):208---213
Table 1 Patient Demographic Data.
Epidural analgesia group 47.8% (n = 44)Age (years) 29.81 ± 7.19Body Mass Index (BMI) 28.24 ± 4.39Gestation (weeks) 38.47 ± 0.79Number of pregnancies 1.88 ± 1.16VAS score during labor 5.58 ± 2.52VAS 24 hours postpartum 4.17 ± 2.18Prepartum EPDS scores 8.32 ± 4.66EPDS score 6 weeks postpartum 6.08 ± 4.58ASA score
II 60 (64.5%)III 32 (34.4%)
VAS, Visual analogue scale; EPDS, Edinburgh Postnatal Depres-sion Scale; ASA, American Society of Anesthesiologists physicalstatus.
Table 2 Comparison of the demographic data between thetwo groups.
Epiduralanalgesia(n = 44)
No epiduralanalgesia(n = 48)
p-value
Age (years) 28.88 ± 6.81 30.64 ± 7.49 0.243Body Mass Index (BMI) 28.07 ± 4.12 28.4 ±4.65 0.723Gestational age (weeks)38.43 ± 0.72 38.52 ± 0.85 0.593Number of pregnancies 1.28 ± 0.48 2.31 ± 1.33 0.076ASA score
II 29 (65.9%) 31 (64.5%) 0.894III 15 (34.1%) 17 (35.5%)
ASA, American Society of Anesthesiologists physical status.
ebpipsbde
s
Table 4 Multiple regression analysis of EPDS scores.
Odds Ratio (OR) p-value
VAS score 24 hours postpartum 0.288 0.117VAS score at labor 0.572 0.039*Epidural analgesia 0.290 0.0001*
VAS, Visual analogue scale; EPDS, Edinburgh Postnatal Depres-sion Scale.An EPDS score ≥ 10 equals depression.
ldonwd
D
Iebdibchairwsbd
pltr
ciation between epidural analgesia and decreased severity
Mann---Whitney U test and Student’s t test were used.p < 0.05 was determined statistically significant.
ry (p = 0.007). Overall, we report that the women givingirth with epidural analgesia experienced significantly lowerain levels (Table 3). There was not a significant differencen the EPDS scores between the groups in the prepartumeriod (p = 0.191); however, we detected a high degree ofignificant difference in the EPDS scores 6 weeks postpartumetween the two groups (p = 0.0001). Therefore, postnatalepression score was lower among women who received
pidural analgesia (Table 3).Multiple regression analysis (Table 4) revealed that EPDScores correlated with receiving epidural analgesia during
otl
Table 3 Comparison of VAS and EPDS scores between groups.
Epiduralanalgesia(n = 44)
VAS score during labor 3.28 ± 0.95
VAS score 24 hours postpartum 2.71 ± 0.82
Prepartum EPDS score 7.63 ± 4.72
EPDS score 6 weeks postpartum 3.89 ± 3.43
VAS, Visual analogue scale; EPDS, Edinburgh Postnatal Depression ScaMann---Whitney U test and Student’s t test were used.
a p < 0.05 was determined statistically significant.
21
The Hosmer---Lemeshow test was used for the logistic regressionmodel.
abor and with VAS scores during delivery. Higher scores ofepression were found in patients experiencing higher levelsf pain during labor (OR = 0.572, p = 0.039). This finding wasot detected 24 hours postpartum in VAS scores. In addition,omen who received epidural analgesia had lower scores ofepressions (OR = 0.29, p = 0.0001) (Table 4).
iscussion
n this study, we investigated the relationship betweenpidural analgesia and depression score in women who gaveirth vaginally. The EPDS, which is widely used and vali-ated, was selected to assess the probability of depressionn the women included in the study.8,9 This scale has alsoeen validated for the pregnant patient population in ourountry.10 We observed that pain severity was significantlyigher in the women who did not prefer to receive epiduralnalgesia during labor, with significantly higher VAS scoresn both the prepartum and postpartum periods. Logisticegression analysis identified that the VAS score at laboras correlated with the development of postnatal depres-
ion (OR = 0.572, p = 0.039). We report a very high correlationetween the use of epidural analgesia and lower postpartumepression levels (OR = 0.29, p = 0.0001).
In a recent study, Lim et al. reviewed a total of 201atients retrospectively and reported that alleviation ofabor pain with epidural analgesia resulted in a reduction inhe severity of depression symptoms.6 We reported similaresults in this observational and prospective study.
Again, similar to our results, Ding et al. reported an asso-
f depression in a study including 200 individuals.4 We addi-ionally evaluated patient depression levels both beforeabor and in the postpartum period. In our study, there was
No epiduralanalgesia(n = 48)
p-value
7.21 ± 1.93 0.0001a
5.30 ± 2.26 0.007a
8.91 ± 4.58 0.1918.08 ± 4.61 0.0001a
le; ASA: American Society of Anesthesiologists physical status.
1

and
nptarbsdaObd
ibwebasttiectecma
wpeargVobs
adAresaarcoc
nwlmfce
ttAtcet
C
IapgsdtIg
T
Or
C
T
R
I.S. Edipoglu
o difference in depression levels between the two groupsrior to labor, however, there was a significant difference inhe EPDS scores 6 weeks postpartum (p = 0.0001). Regressionnalysis demonstrated the correlation between the epidu-al analgesia and depression effectively. A study performedy Badou et al. with 43 patients was the first to demon-trate an association between the severity of labor pain andepression.11 Contrary, some studies were unable to detect
relationship between depression and labor pain severity.ur study is in line with that published by Badou et al. Weelieve the discrepancy in outcomes are due to insufficientata regarding pain scores.4
There are a wide range of studies in the literaturenvestigating the outcomes of postpartum depression onoth mother and infant. One study investigated patientsho underwent a cesarean section and those who deliv-red vaginally, and they suggested a significant relationshipetween severe pain and postpartum depression.12 Theylso reported that postpartum depression may be respon-ible for 17% of late-phase maternal deaths.12 In addition tohose studies, a number of studies in the literature reporthat postpartum depression adversely affected nursing thenfant.13,14 In their study including 2,729 patients, Verbeekt al. reported that postpartum depression affected thehildhood period unfavorably. Furthermore, they added thathose effects may be so extensive that they negatively influ-nce the adolescent period.15 These findings lead to theonclusion that postpartum depression is a major cause oforbidity in women and attempts to lower its incidence rate
re needed.In our current study, we report that the VAS score 6
eeks postpartum was correlated with development ofostnatal depression. Several studies, available in the lit-rature, report similar results to those of our study in whichdministration of epidural analgesia resulted in a significanteduction in VAS scores.16---18 We believe that epidural anal-esia is the main determinant for pain reduction and lowerAS scores. We also assume that this reduction in pain wasne of the most important factors creating the correlationetween epidural analgesia and lower postpartum depres-ion rates.
On the other hand, other studies report that epiduralnalgesia in pregnant women cause unfavorable or contra-icting results. In a meta-analysis including 9,658 patients,nim et al. reported results different from those summa-ized above.7 They found that women who received anpidural mode of administration experienced more hypoten-ion compared to women that did not.7,19---21 Other studieslso reported that epidural modes of administration caused
delay in the second phase of labor.7,22,23 Although epidu-al analgesia allows for better pain control, the authorsould not demonstrate significant differences in the levelsf maternal satisfaction, reporting that there were someontradicting findings.7
The limitations of our study are the low number of preg-ant women included. Increasing the number of patientsould maybe enhance the value of our findings. Another
imitation is that VAS scores are a subjective means of assess-
ent for pain. However, a more effective scoring systemor pain assessment is not available. Therefore, the VAS isommonly used in the literature. One of the best ways ofvaluating postoperative pain is the opioid consumption of
21
D.D. Aslan
he patient but we could not use this approach because ofhe different methods of analgesia for postpartum period.lso, there are other confounding factors that may influencehe chance of postpartum depression like patients’ socioe-onomic class and postpartum BMI at the time of the secondvaluation but we did not investigate these variables andhis is another limitation for our study.
onclusion
n conclusion, our study found an association between favor-ble VAS scores and lower depression severity 6 weeksostpartum in women who received epidural analgesia andave birth vaginally. In addition, we report that increasedcores of pain at labor were correlated with postpartumepression score and there was a very high correlation withhe use of epidural analgesia and lower depression levels.n light of these results, we suggest that pregnant womeniving birth via the vaginal route should use analgesia.
rial registry
ur study was registered February 15, 2016 via the ISRCTNegistry with study ID ISRCTN84174861.
onflict of interest
he authors declare no conflicts of interest.
eferences
1. World Health Organization. Monitoring Emergency ObstetricCare: A Handbook. Geneva, Switzerland: WHO Press; 2009.WHO.
2. Bayrampour H, Salmon C, Vinturache A, et al. Effect of depres-sive and anxiety symptoms during pregnancy on risk of obstetricinterventions. J. Obstet Gynaecol Res. 2015;41:1040---8.
3. American Psychiatric Association. Diagnostic and StatisticalManual of Mental Disorders. 4th edition; text revision Washing-ton, DC: American Psychiatric Press; 2000.
4. Ding T, Wang DX, Qu Y, et al. Epidural Labor Analgesia IsAssociated with a Decreased Risk of Postpartum Depression: AProspective Cohort Study. Anesth Analg. 2014;119:383---92.
5. Orbach-Zinger S, Landau R, Harousch AB, et al. The RelationshipBetween Women’s Intention to Request a Labor Epidural Anal-gesia, Actually Delivering With Labor Epidural Analgesia, andPostpartum Depression at 6 Weeks: A Prospective ObservationalStudy. Anesth Analg. 2018;126:1590---7.
6. Lim G, Farrell LM, Facco FL, et al. Labor Analgesia as a Predic-tor for Reduced Postpartum Depression Scores: A RetrospectiveObservational Study. Anesth Analg. 2018;126:1598---605.
7. Anim-Somuah M, Smyth RM, Jones L. Epidural versus non-epidural or no analgesia in labor. Cochrane Database Syst Rev.2011;7:CD000331.
8. Zanardo V, Giliberti L, Volpe F, et al. Cohort study of thedepression, anxiety, and anhedonia components of the Edin-burgh Postnatal Depression Scale after delivery. Int J GynaecolObstet. 2017;137:277---81.
9. Matthey S, Souter K, Mortimer K, et al. Routine antenatal mater-nal screening for current mental health: evaluation of a changein the use of the Edinburgh Depression Scale in clinical practice.Arch Womens Ment Health. 2016;19:367---72.
2
esio
1
1
1
1
1
1
1
1
1
1
2
2
2
Brazilian Journal of Anesth
0. Aksu S, Varol FG, Hotun Sahin N. Long-term postpartum healthproblems in Turkish women: prevalence and associations withself-rated health. Contemporary Nurse. 2017;53:167---81.
1. Boudou M, Teissèdre F, Walburg V, et al. Association betweenthe intensity of childbirth pain and the intensity of postpartumblues. Encephale. 2007;33:805---10.
2. Eisenach JC, Pan PH, Smiley R, et al. Severity of acute pain afterchildbirth, but not type of delivery, predicts persistent pain andpostpartum depression. Pain. 2008;140:87---9.
3. Dias CC, Figueiredo B. Breastfeeding and depression: a system-atic review of the literature. Affect Disord. 2015;171:142---54.
4. Figueiredo B, Canário C, Field T. Breast feeding is nega-tively affected by prenatal depression and reduces postpartumdepression. Psychol.Med. 2014;43:1---10.
5. Verbeek T, Bockting CL, van Pampus MG, et al. Postpartumdepression predicts offspring mental health problems in ado-lescence independently of parental lifetime psychopathology. JAffect Disord. 2012;136:948---54.
6. Pugliese PL, Cinnella G, Raimondo P, et al. Implementation ofepidural analgesia for labor: is the standard of effective anal-gesia reachable in all women? An audit of two years. Eur RevMed Pharmacol Sci. 2013;17:1262---8.
2
21
logy 2021;71(3):208---213
7. Sikdar I, Singh S, Setlur R, et al. A prospective review of thelabor analgesia programme in a teaching hospital. Med J ArmedForces India. 2013;69:361---5.
8. Sweed N, Sabry N, Azab T, et al. Regional versus IV analgesicsin labor. Minerva Med. 2011;102:353---61.
9. El-Kerdawy H, Farouk A. Labor analgesia in preeclampsia:remifentanil patient controlled intravenous analgesia versusepidural analgesia. Middle East Journal of Anesthesiology.2010;20:539---45.
0. Head B, Owen J, Vincent R, et al. A randomized trial ofintrapartum analgesia in women with severe preeclampsia.Obstetrics & Gynecology. 2002;99:452---7.
1. Gambling DR, Sharma SK, Ramin SM, et al. A randomizedstudy of combined spinal epidural analgesia versus intravenousmeperidine during labor: impact on cesarean delivery rate.Anesthesiology. 1998;89:1336---44.
2. Lian Q, Ye X. The effects of neuraxial analgesia of combinationof ropivacaine and fentanyl on uterine contraction. Anesthesi-
ology. 2008;109:A1332.3. Long J, Yue Y. Patient controlled intravenous analgesiawith tramadol for pain relief. Chinese Medical Journal.2003;116:1752---5.
3

C
Erp
C
a
b
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):214---220
LINICAL RESEARCH
pidural analgesia in the obese obstetric patient: aetrospective and comparative study with non-obeseatients at a tertiary hospital
laudia Cuesta González-Tascón a,∗, Elena Gredilla Díaz a, Itsaso Losantos Garcíab
Servicio de Anestesiología y Reanimación, Hospital universitario La Paz, Madrid, SpainDepartamento de Bioestadística, Hospital universitario La Paz, Madrid, Spain
eceived 18 February 2020; accepted 27 February 2021vailable online 9 April 2021
KEYWORDSObesity;Neuraxial anesthesia;Labor analgesia;Cesarean section
AbstractBackground and objectives: Obesity is becoming a frequent condition among obstetric patients.A high body mass index (BMI) has been closely related to a higher difficulty to perform theneuraxial technique and to the failure of epidural analgesia. Our study is aimed at analyzingobese obstetric patients who received neuraxial analgesia for labor at a tertiary hospital andassessing aspects related to the technique and its success.Methods: Retrospective observational descriptive study during one year. Women with a BMIhigher than 30 were identified, and variables related to the difficulty and complications ofperforming the technique, and to analgesia failure rate were assessed.Results and conclusions: Out of 3653 patients, 27.4% had their BMI ≥ 30 kg.m-2. Neuraxialtechniques are difficult to be performed in obese obstetric patients, as showed by the numberof puncture attempts (≥ 3 in 9.1% obese versus 5.3% in non-obese being p < 0.001), but theincidence of complications, as hematic puncture (6.6%) and accidental dural puncture (0.7%)seems to be similar in both obese and non-obese patients. The incidence of cesarean section inobese patients was 23.4% (p < 0.001). Thus, an early performance of epidural analgesia turnsout to be essential to control labor pain and to avoid a general anesthesia in such high-riskpatients.
© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).∗ Corresponding author.E-mail: [email protected] (C.C. González-Tascón).
ttps://doi.org/10.1016/j.bjane.2021.02.054 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
itora Ltda. This is an open access article under the CC BY-NC-ND
esio
B
OcentO3no3tIowladt
nittprb3fpmtptrttwa
otsadc
ota
M
Bnmrhwb
ninappgca
wocwdow
mdtctwottp
a
awmtdctinftllN
R
D
Ta7g
Brazilian Journal of Anesth
ackground
besity has become an increasi ng concern worldwide andontinues to rise in developed countries, both among gen-ral and obstetric population. Body mass index (BMI) isowadays considered a reliable and well-known indica-or used worldwide in overweight and obesity diagnosis.verweight and obesity are defined as a BMI ≥ 25 and ≥0 kg.m-2, respectively. According to the World Health Orga-ization (WHO), obesity is classified in three categories:besity grade I (BMI range, 30---34.9 kg.m-2), grade II (range,5---39.9 kg.m-2), and grade III (> 40 kg.m-2). According tohe last data published by the Spanish National Statisticsnstitute in 2017, 44.3% of men and 30% of women wereverweight, and obesity rate was 18.2% in men and 16.7% inomen.1 BMI has in fact increased up to 0.4% during the
ast 30 years worldwide.2 Overweight and obese patientsre associated with greater comorbidity, such as coronaryiseases, hypertension, obstructive sleep apnea, or gas-rointestinal reflux.2
Obesity during pregnancy is also implicated in the mater-al and perinatal outcome. On one hand, obesity is anmportant risk factor of hypertensive disorders and gesta-ional diabetes during pregnancy.3,4 Hypertension can evolveo preeclampsia, which considerably increases maternal anderinatal morbimortality, and causes intrauterine growthetardation of the fetus. Moreover, a BMI ≥ 25 kg.m-2 haseen associated to a greater risk of miscarriage (58% versus7% in non-obese pregnant women) and congenital mal-ormations, mainly spina bifida, neural tube defects, cleftalate and congenital heart diseases.5 A delayed diagnoseay be due to the greater difficulty of using ultrasound in
hese patients. On the other hand, the placenta of obeseregnant women weighs around 60---80 grams more at theime of birth, and it is just placenta weight that has a greaterelation to the weight of the newborn.5 Therefore, it seemshat fetal macrosomia index, defined as a weight at theime of birth over 4000---4500 grams, is greater among obeseomen, which justifies a higher odd of cesarean sectionmong these patients.5---7
The greater rates of instrumental or cesarean delivery inbese pregnant women turns neuraxial anesthesia into theechnique of choice. The key is to avoid general anesthe-ia in patients, whose pregnant condition plus their obesityltogether, increase complications dramatically, such as aifficult airway or failed resuscitation after hemodynamicollapse.4
Therefore, we will discuss the impact of obesity in thebstetric and anesthetic management, as well as focus onhe importance of a suitable neuraxial technique on time sos so guarantee the safety of this kind of patient.
aterial and methods
ased on the increasing prevalence of obesity among preg-ant women and the close relationship between obesity andaternal and perinatal outcomes, we have carried out a
etrospective observational descriptive study at a tertiaryospital among pregnant women (obese and non-obese),ho received neuraxial analgesia for labor at our centeretween January and December 2017.
1ir(
21
logy 2021;71(3):214---220
The main purpose was to analyze the features of all preg-ant women over 18 years old, as well as different variablesn relation to the difficulty of performing the neuraxial tech-ique, and the maternal and neonatal outcomes, so as to beble to establish a comparison with the non-obese obstetricopulation for the same period. For such reason, we pro-osed the hypotheses that a high BMI was associated withreater maternal and neonatal comorbidity, a higher diffi-ulty to perform the neuraxial technique and failure rate,s well as a higher cesarean section rate.
Out of the whole sample, women with a BMI ≥ 30 kg.m-2
ere identified, while variables related to the difficultyf performing the technique, to analgesia failure rate andomplications were evaluated. Maternal body mass indexas calculated based on the recorded height and weight atelivery. Thus, patients were classified into two groups: non-bese pregnant women (BMI < 30 kg.m-2) and obese pregnantomen (BMI ≥ 30 kg.m-2).
Demographic data related to maternal age, to BMI andaternal pathologies, were collected as well as obstetricata (i.e. gestational age, parity, single or twin pregnancy,ype of labor (spontaneous or instrumental delivery, andesarean section), and neonatal data. Information on theechnique performed (epidural or combined spinal-epidural)as collected as well. On the bases of the complicationsf the technique, we defined the success or failure of ourechnique as the number of puncture attempts, as well ashe incidence of hematic puncture (HP) and accidental duraluncture (ADP).
Finally, we identified those cases that required generalnesthesia due to a failed neuraxial technique.
Qualitative data description was made in the form ofbsolute frequencies and percentages. Quantitative dataere presented through an average ± typical deviation,inimum and maximum when they were continuous and
hrough the percentile and the interquartile range whenealing with ordinary variables. Qualitative variable asso-iation was analyzed by the chi-square test or Fisher’s exactest. Mann-Whitney U test was used for comparing qual-tative and quantitative data, for independent data, ason-parametric evidence, and the Student’s t-student testor independent data as parametric evidence. All statisticests were considered bilateral and those including p-valuesower than 0.05 were considered significant. Data were ana-yzed by the statistics software SAS 9.3 (SAS Institute, Cary,C, USA).
esults
emographic data
he study covered a total number of 3653 patients with anverage age of 32.82 ± 5.8 years and an average weight of4.51 ± 12.16 kg (average BMI 27.51 ± 5.75 kg.m-2). Averageestational age was 38.83 ± 2.49 weeks.
Out of the total number of patients observed (n = 3653),
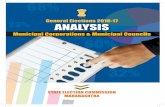
001 patients (27,4%) had a BMI ≥ 30 kg.m-2 (Fig. 1). Accord-ng to the BMI, 747 patients (74.62%) had obesity grade I (BMIange, 30---34.99), 189 patients (18.88%) had obesity grade IIBMI range, 35---39.99), 63 patients (6.3%) had obesity grade5

C.C. González-Tascón, E.G. Díaz and I.L. García
74.62%
18.88%
6.30%0.20%
G R A D E 1 G R A D E 2 G R A D E 3 G R A D E 4
DISTRIBUT ION OF OBESI TY GRADE INPREGNANT PATIENTS
Figure 1 Distribution of obesity grade among obese pregnant women.
Table 1 Hypertensive disorders in obese and non-obesepregnant women (p = 0,799).
Hypertensive disorders in pregnancy PATIENT COLLECTION
NON-OBESES 2,3% (n = 60)OBESES 2,1% (n = 20)
Obesity grade I 2,1% (n = 15)Obesity grade II 1,6% (n = 3)Obesity grade III 3,3% (n = 2)
Ih
O
GIipw(ot
HItnhsI(
N
IbbpucOot
Table 2 Difficulty of neuraxial technique regarding punc-ture attempts (p < 0,001).*
PUNCTURE ATTEMPTS % OBESE % NON-OBESES
1---2 90,8% (n = 883) 94,8% (n = 2373)3---4 8,3% (n = 81) * 5,2% (n = 129) *> 4 0,8% (n = 8) * 0,1% (n = 2) *
qp
icoawua(oortonosip(pptl
gaasg
Obesity grade IV 0%
II or extreme (BMI range, 40---49.99), and 2 patients (0.2%)ad obesity grade IV or morbid (BMI 50 or greater).
bstetric pathology
estational Diabetes (GD)n our study, gestational diabetes rate was slightly highern obese women (5.2% versus 5% in non-obese), being
= 0.757. Out of the total number of obese pregnant womenith GD (n = 51), 39 patients presented obesity grade I
76.5%), 9 patients obesity grade II (17.6%) and 3 patientsbesity grade III (5.9%). We did not find any patient amonghe population studied with obesity grade IV who had GD.
ypertensive disorders in pregnancyn spite of the fact that the incidence of gestational hyper-ension has turned out to be greater in non-obese (2.3%,
= 60) versus obese (2.1%; n = 20), being p = 0.799, it must beighlighted that there was a greater presence of hyperten-ive disorders in those pregnant women with obesity gradeII (3.3%) versus the other obese patients, with p = 0.882Table 1).
euroaxial technique and complications
t was performed 3237 epidural techniques and 416 com-ined spinal-epidural (CSE). The technique was required toe repeated in 52 patients out of the total number of obeseregnant women (5.19%) due to the lack of analgesia 45 min-tes after the placement of the catheter, and this time, a
ombined spinal-epidural (CSE) technique was performed.ne or two puncture attempts were needed in 94.8% of non-bese compared to 90.7% of obese. According to our data,he need of three or more attempts was clearly more fre-E
A(
21
* These results are statistically significant (p < 0,001).
uent among obese, 9.1% against 5.3% of non-obese, being < 0.001 (Table 2).
If all possible complications related to the neurax-al technique are taken into account, the odds of theseomplications altogether were 72.7% (n = 2021) in the groupf non-obese and 27.3% (n = 758) in the obese one. Whennalyzing each of the complications separately, HP incidenceas 6,6% in both groups, being n = 50 among the obese pop-lation against n = 133 in non-obese, with p = 0,659, as wells the odds of ADP, which was 0,7% (n = 5) in obese and 0,7%n = 15) in non-obese with p = 0.659. However, the numberf patients who had headache after delivery was higher (8bese and 37 non-obese women) than the number of ADPecorded in both groups. This can be explained because ofhe fact that post-dural puncture headache (PDPH) is onef the most common postpartum complications followingeuraxial block, but dural puncture is not the only causef postpartum headache. Other possible causes can be ten-ion headache, migraine or cortical vein thrombosis, whosencidence is increased during pregnancy and in the puer-erium. A blood patch was performed in only two patients25%) out of the total obese pregnant women with post-artum headache (n = 8), against 22 out of 37 non-obeseregnant women with postpartum headache (Table 3). Inhis case, p-value could not be calculated because of theack of data.
Despite the fact that the number of HP and ADP alto-ether was greater among non-obese population, whennalyzing these complications among the obese population,nd depending on the BMI of the patient, we faced in ourtudy a greater incidence in those patients with obesityrade III (16.36%, n = 9), being p = 0.022.
xpulsive phase of labor
mong our studied population, labor was induced in 63.1%n = 632) of obese versus 26.2% (n = 694) of non-obese. On
6

Brazilian Journal of Anesthesio
Table 3 Incidence of postpartum headache and accidentaldural puncture (ADP) and the need of blood patch in obeseand non-obese parturients.
OBESE(IMC > 30)
NON-OBESE(IMC < 30)
Accidental duralpuncture (ADP)
5/1001 15/2652
Postpartum headache 8/1001 37/2652
OBESE(IMC > 30)
NON-OBESE(IMC < 30)
ooO(F2=cb
aawe
naoap
D
Boat
imioocsittotaah
apvp
ganat
totstcua
padh
BLOOD PATCH 2 (25%) 22 (59,45%)NO BLOOD PATCH 6 (75%) 15 (40,54%)
ne hand, delivery was spontaneous in 79% (n = 2096) of non-bese, against 67,6% (n = 677) of obese, where p < 0,001.n the other hand, instrumental delivery was recorded in 9%
n = 90) of obese, contrary to 9.2% (n = 246) of non-obese.inally, cesarean section rate in obese pregnant women was3,4% (n = 234), whereas among non-obese was 11.7% (n
310), being p < 0,001. In our study, the main reason foresarean section was failure of induction or disproportionetween the fetus and the uterus (Table 4).
In our population, seven of the patients who underwent cesarean section required sedation besides the epiduralnesthesia due to the lack of pain control. In addition, fiveomen needed general anesthesia because of an incompletepidural block.
On the bases of our database, the average weight of aewborn child was 3187.26 ± 455.53 grams in non-obesend 3326.67 ± 485.12 grams in obese, being the incidencef fetal macrosomia higher in this latter group (5.6%, n = 51)gainst 2.6% (n = 64) in non-obese pregnant women, where
< 0.001.
iscussion
ased on our study results, the prevalence of overweight andbesity in obstetric patients is markedly high in our centre,s it has recently become a reference center nationwide forhe obstetric follow-up of obese pregnant women. Accord-
bls
Table 4 Delivery in obese and non-obese parturients (p < 0,001).
OBESE (IM
SPONTANEOUS DELIVERY 677 (67INSTRUMENTAL DELIVERY 90 (9
Spatula 29 (2Forceps 47 (4
Ventouse 14 (1
OBESE
CESAREAN SECTION 234
- FI or disproportion (NICE III) 19- NRFS (NICE I) 44
NON CESAREAN SECTION 767
* FI (Failed Induction); NRFS (Non-reassuring Fetal Status).
21
logy 2021;71(3):214---220
ng to test results, obese pregnant women show greateredical comorbidity, which had been widely studied and
dentified in previous studies. Our findings suggest that thedds of gestational diabetes are slightly higher in the groupf obese pregnant women, although statistical significanceould not be reached. However, the incidence of hyperten-ive disorders was 25% (n = 20) in obese against 75% (n = 60)n non-obese. Therefore, although it has not been possibleo find a close relation between obese women and hyper-ensive conditions, it is quite interesting the higher ratef hypertension in obesity grade III. We should be awarehat obesity is only one of the multiple risk factors associ-ted with hypertensive disorders during pregnancy, such asdvanced gestational age or medical conditions (e.g. chronicypertension, diabetes mellitus or chronic renal disease).
In our center, the epidural technique is the first option inny case, but when pregnant women show a breakthroughain related to strong uterine dynamics or advanced cer-ical dilatation, then the CSE technique will be preferablyerformed.
Recent studies show that a high BMI is correlated to4,5,7,8:reater complication to perform the technique, determineds a higher number of puncture attempts and more timeeeded to find the epidural space; greater failure of epiduralnalgesia; and greater delay in detecting the failure of theechnique.
Despite the fact that a high BMI means a risk factor forhe failure of the technique, in our daily practice, we do notbserve such a high failure rate in obese pregnant women ashe one described in the literature. In our hospital, analge-ia for delivery is performed by residents from second up toheir last year of training. However, neuraxial techniques inomplicated patients (e.g. obese patients or scoliosis) aresually carried out by residents in their last year or thettending anesthesiologist.
In most cases, locating the epidural space in obeseregnant women becomes complicated due to the loss ofnatomical references and because the epidural skin-spaceistance (ESD) may be bigger than usual.4,8 Previous studiesave already recorded the directly proportional association
etween BMI and ESD, although this distance is not normallyonger than 8 cm in most patients.9,10 Our study did not mea-ure ESD, but has collected a greater number of puncture*.
C >30) NON-OBESE (IMC < 30)
,6%) * 2096 (79%) *%) * 246 (9,2%) *,9%) 91 (3,4%),7%) 101 (3,8%),4%) 54 (2%)
(IMC >30) NON-OBESE (IMC < 30)
(23,4%) * 310 (11,7%) *0 (19%) 234 (8,8%)
(4,4%) 76 (2,9%)(76,6%) * 2342 (88,2%) *
7

E.G
ad
rtpicTplmtn(trturTnasrtUotntioiotenftldnttnttgsrypitp
r1aha
tcitewAPtetiltsn
tiltsehSnrfwai
iastIess
smwcibraS
peienoc
C.C. González-Tascón,
ttempts in obese pregnant women, which confirms a higherifficulty in locating epidural spaces in this type of patient.
Air or saline solution can be used to identify the loss ofesistance when finding the epidural space. It is importanto highlight that ligaments are softer in obese and pregnantatients due to the influence of progesterone. Based on this,t seems that the feeling of losing resistance using air is moreonfusing and so the likelihood of false positives increases.herefore, we can state that the greater the BMI of theatient, the more difficult the puncture becomes, and so theoss of resistance technique with saline solution is recom-ended for these patients.11 However, we should be aware
hat epidural space localization using loss of resistance tech-ique with saline can hinder the identification of an ADPinadvertent dural puncture). When air is used to identifyhe epidural space, any cerebrospinal leak can be easilyecognized, unlike when saline is used. Hence, the idealechnique for identification of the epidural space remainsnclear. Moreover, accurate identification of the anatomicaleferences in the obese patient can be widely complicated.he risk of a general anesthesia in such patients is so high,ot only because of the pregnancy but also the obesity, thatn adequate epidural analgesia must be achieved. Ultra-ound (US) techniques are proposed to improve the successate during epidural catheter insertion, as well as to reducehe complications related to the accidental dural puncture.S imaging of the spine is thought to reduce the likelihoodf a failed and traumatic catheterization. Several studiesried to investigate the ease of catheter insertion, the timeeeded for the procedure and the rate of success, comparedo the traditional palpation technique. Some of these stud-es compared the US examination of the spine in lean andbese patients12 and others analyzed the US guidance onlyn obese patients scheduled for elective cesarean section13
r otherwise only in patients with BMI < 35 kg.m-2.14 Givenhe results of these studies, US imaging helps locate thepidural space in the obese parturient, and so reduces theumber of puncture attempts and the time needed to per-orm the technique. Nonetheless, the use of US appears noto be that helpful in lean parturients, in which anatomicalandmarks are clearly palpable. Thus, there is some evi-ence that US guidance may improve the success of theeuraxial block in the obese parturient, as well as reducehe rate of procedure-related adverse events. Furthermore,he impact of US on patient satisfaction regarding the tech-ique and analgesia has been highly positive.15 However,he learning curve can be complicated and so US-guidedechniques are recommended only when the anesthesiolo-ist is used to perform and interpret US images. In fact, thetudies mentioned above have been carried out by expe-ienced anesthesiologists trained in US scanning. In recentears, the use of ultrasonography has become increasinglyopular in anesthesiology. Hence, it should be consideredn obstetric anesthesia because of its potential benefits inhe obese parturient, avoiding a general anesthesia in theseatients.
According to the literature, ADP incidence in the obstet-ic population is up to 4% in obese pregnant women versus
% in non-obese ones.16---18 In our study, complications suchs ADP or HP seem to be similar in both groups, although weave not been able to demonstrate that such associationsre statistically significant. When all complications relatedccan
21
. Díaz and I.L. García
o the neuraxial technique are considered, the rate of theseomplications in the obese patient is not higher compar-ng to non-obese in our study. As previously mentioned, theechnique in the obese parturient has been performed byxperienced anesthesiologists, so the probability of successas higher in such patients. Around 50-80% of patients withDP develop PDPH.19---22 Our study has not found a higherDPH incidence among obese population, which matcheshe results obtained in previous studies. In fact, the Peraltat al. study16 demonstrated that a BMI ≥ 35 kg.m-2 was a pro-ective factor against the development of PDPH. The reasons related to a higher pressure in the epidural space, whichimits the leak of cerebral spinal fluid (CSF) just throughhe dural rent. Nonetheless, once PDPH has developed, itseverity and treatment (analgesia and/or blood patch) doot seem to be related to the BMI of the patient.
As there is not still a standard definition of failure ofhe epidural technique, it appears to be difficult to reportts real incidence. A widely acceptable definition is theack of analgesia during the first 45 minutes after placinghe catheter in the epidural space.8 Kula et al., in theirtudy,4 mentioned the assessment of the number of nec-ssary attempts to place a catheter as the way to estimateow difficult the technique was and the likelihood of failure.aravanakumar et al. found in their study that 74% of preg-ant women needed more than one attempt, and up to 14%equired three or more attempts, being the total failure rateor this technique 42% in this kind of patient.23 In our study,e have been able to assess the success of the techniqueccording to the number of puncture attempts and we diddentify a correlation with data obtained in the literature.
Finally, we noted a higher rate of cesarean deliveryn obese pregnant women. The literature states a greaternesthetic risk among obese women who undergo cesareanection under general anesthesia, as it is expected due tohe physiological and anatomical changes during pregnancy.n this sense, Brick et al. do mention a higher cesarean deliv-ry rate among obese multiparous pregnant women, whileuch relation between BMI and the likelihood of cesareanection is not found in obese nulliparous pregnant women.24
Eventually, we observed in our population significanttatistics when referring to a greater incidence of fetalacrosomia in obese pregnant women, which is in lineith the latest breakthroughs in the literature. Thisan be related to a greater concentration of leptin andnterleukin-6 (IL6) in the umbilical cord of babies deliveredy obese mothers, which seems to be in relation to a higheresistance to insulin and long-term metabolic disordersmong these newborn children, according to Catalano andhankar studies.5
To sum up, neuraxial techniques are preferred for obesearturient, in who the placement of a well-functioningpidural catheter is one of the safest methods of provid-ng labor analgesia. It must be taken into account that laborpidural analgesia can be converted to surgical anesthesia ifeeded for cesarean delivery and, given the increased riskf fetal macrosomia, a well-functioning epidural catheteran be helpful in the management of a shoulder dysto-
ia. Therefore, regular assessment of the labor epiduralatheter is paramount to ensure that the block can be reli-bly extended to provide adequate surgical anesthesia ifeeded.23,25,268

esio
l
-
-
C
Oracsitlbcw
oddraoaEteprfl
ntist
C
T
E
Cmn
R
1
1
1
1
1
1
1
1
1
Brazilian Journal of Anesth
Our results should be interpreted in the context of study’simitations:
As it is a retrospective study, information has not beencollected systematically, and the lack of data makes it dif-ficult to find statistically relevant relations in some cases,in spite of being in line with what is described in theliterature.
Due to the retrospective nature of this study, maternalBMI was calculated based on the recorded weight andheight in the third trimester of pregnancy. As we didnot have previous data, the accurate weight before preg-nancy could not be recorded. This makes us consider obese(BMI ≥ 30 kg.m-2) those pregnant women who may be notbefore pregnancy.
onclusion
ur study is aimed at analyzing obese obstetric patients whoeceived neuraxial analgesia for labor at a tertiary hospitalnd assessing aspects related to the technique and its suc-ess. Given the number of puncture attempts, our findingsuggest evidence of greater difficulty in performing neurax-al anesthesia in obese pregnant women. However, it seemshat complications related to neuraxial blockade are simi-ar in both groups although statistical significance could note reached. Lastly, it must be noted the higher incidence ofesarean section and macrosomia among the obese pregnantomen.
Due to the increasing incidence of obesity in general andbstetric population, the anesthesiologist must be ready toeal with any potential complications that may develop atelivery. These parturients remain challenging for obstet-ic and anesthesia providers. Thus, the experience of thenesthesiologist with this kind of patients becomes a piv-tal point to achieve a satisfactory neuraxial analgesia andn adequate management of the obese pregnant woman.arly epidural anesthesia in these patients is the best optiono guarantee an appropriate analgesia and avoid a gen-ral anesthesia. Given their pregnancy and obesity, theseatients are therefore considered to be at high anestheticisk. It is thus crucial to closely watch over these patientsrom the moment of inserting the epidural catheter untilabor.
Summing up, given the high prevalence of obese preg-ant women in the last years, a multidisciplinary approacho this profile of patient turns out to be necessary, includ-ng anesthesiologists and obstetricians, in order to reduceuch complications and warrant an adequate analgesia inhe obese pregnant women.
onflicts of interest
he authors declare no conflict of interests.
thical approval
EIm approval (Comité de Etica de la Investigación conedicamentos del Hospital Universitario La Paz). Project
umber: PI-3730
1
21
logy 2021;71(3):214---220
eferences
1. Instituto Nacional de Estadística (INE). Índice de masa corporalsegún grupos de edad (% población de 18 y más años), recuper-ado de: http://www.ine.es.
2. Riveros-Perez E, McClendon J, Xiong J, et al. Anesthetic andobstetric outcomes in pregnant women undergoing cesareandelivery according to body mass index: Retrospective analysisof a single-center experience. Ann Med Surg. 2018;36:129---34.
3. Sullivan EA, Dickinson JE, Vaughan GA, et al. and on behalfof the Australasian Maternity Outcomes Surveillance System(AMOSS) --- Maternal super-obesity and perinatal postcomes inAustralia: a national population-based cohort study. Sullivanet al. BMC Pregnancy Childbirth. 2015;15:322.
4. Kula AO, Riess ML, Ellinas EH. Increasing body mass index pre-dicts increasing difficulty, failure rate, and time to discovery offailure of epidural anesthesia in laboring patients. J Clin Anesth.2017;37:154---8.
5. Catalano PM, Shankar K. Obesity and pregnancy: mechanisms ofshort term and long term adverse consequences for mother andchild. BMJ. 2017;360:j1.
6. Crane JMG, Murphy P, Burrage L, et al. Maternal and perinataloutcomes of extreme obesity in pregnancy. J Obstet GynaecolCan. 2013;35:606---11.
7. Tonidandel A, Booth J, D’Angelo R, et al. Anesthetic andObstetric outcomes in morbidly obese parturients: a 20-yearfollow-up retrospective cohort study. Int J Obstet Anesth.2014;23:357---64.
8. Guasch E, Iannuccelli F, Brogly N, et al. Failed epidural for labor:what now? Minerva Anestesiol. 2017;83:1207---13.
9. Guasch E, Ortega R, Gilsanz F. Analgesia epidural para parto enla gestante obesa. Rev Soc Esp Dolor. 2006;13:468---74.
0. Eley VA, Chin A, Sekar R, et al. Increasing body mass indexand abdominal subcutaneous fat thickness are associated withincreased skin-to-epidural space distance in pregnant women.Int J Obstet Anesth. 2019;38:59---65.
1. Espinoza-Hernández CY, Estrada-Utrera MS, Islas-Ruíz FG, et al.Técnica de Nesi para identificación del espacio epidural vs téc-nica de Pitkin en cirugía obstétrica. Anest Méx. 2016;28:11---8.
2. Sahin T, Balaban O, Sahin L, et al. A randomized con-trolled trial of preinsertion ultrasound guiadance for spinalanesthesia in pregnancy: Outcomes among obese and leanparturients: Ultrasound for spinal anesthesia in pregnancy. JAnesth. 2014;28:413---9.
3. Li M, Ni X, Xu Z, et al. Ultrasound-assisted technology versus theconventional landmark location method in spinal anesthesia forcesarean delivery in obese parturients: A randomized controlledtrial. Anesth Anal. 2019;129:155---61.
4. Tawfik MM, Atallah MM, Elkharboutly WS, et al. Does preproce-dural ultrasound increase the first-pass success rate of epiduralcatheterization before cesarean delivery? A randomized con-trolled trial. Anesth Analg. 2017;124:851---6.
5. Gredilla E, Pérez Ferrer A, Canser E, et al. Factores asociados ala satisfacción materna con analgesia epidural para control deldolor del trabajo de parto. Med Prevén. 2008;14:22---7.
6. Peralta F, Higgins N, Lange E, et al. The relationship of bodymass index with the incidence of postdural puncture headachein parturients. Anesth Analg. 2015;121:451---6.
7. Miu M, Paech MJ, Nathan E. The relationship between body massindex and post-dural puncture headache in obstetric patients.Int J Obstet Anesth. 2014;23:371---5.
8. An X, Zhao Y, Zhang Y, et al. Risk assessment of morbidly obeseparturient in cesarean section delivery. A prospective cohort,
single-center study. Medicine. 2017;96:42.9. López Correa T, Garzón Sánchez JC, Sánchez Montero FJ, et al.Cefalea postpunción dural en obstetricia. Rev Esp AnestesiolReanim. 2011;58:563---73.
9
E.G
2
2
2
2
2
2thesia: current insights. Local Reg Anesth. 2019;12:111---24.
C.C. González-Tascón,
0. Anne MacGregor E. Headache in pregnancy. Neurol Clinics.2012;30:835---66.
1. Franz AM, Jia SY, Bahnson HT, et al. The effect of second-stagepushing and body mass index on postdural puncture headache.J Clin Anesth. 2017;37:77---81.
2. Song J, Zhang T, Choy A, et al. Impact of obesity on postduralpuncture headache. Int J Obstet Anesth. 2017;30:5---9.
3. Saravanakumar K, Rao SG, Cooper GM. Obesity and obstetricanaesthesia. Anaesthesia. 2006;61:36---48.
2
22
. Díaz and I.L. García
4. Brick A, Layte R, McKeating A, et al. Does maternal obesityexplain trends in caesarean section rates? Evidence from a largeIrish maternity hospital. Ir J Med Sci. 2020;189:571---9.
5. Taylor CR, Dominguez JE, Habib AS. Obesity and Obstetric Anes-
6. McCall SJ, Li Z, Kurinczuk JJ, et al. Maternal and perinataloutcomes in pregnant women with BMI & 50: An internationalcollaborative study. PLoS ONE. 2019;14:e0211278.
0
C
Eac
DRV
a
b
c
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):221---227
LINICAL RESEARCH
ffect of anesthetic technique on the quality ofnesthesia recovery for abdominal histerectomy: aross-observational study
aniel de Carli a,b,∗, José Fernando Amaral Meletti a,b,odrigo Pauperio Soares de Camargoa,c, Larissa Schneider Gratacósa,ictor Cristiano Ramos Gomesa, Nicole Dutra Marquesa
Faculdade de Medicina de Jundiaí, Jundiaí, SP, BrazilCET-Sociedade Brasileira de Anestesiologia, Disciplina de Anestesiologia da Faculdade de Medicina de Jundiaí, Jundiaí, SP, BrazilUniversidade Estadual de Campinas, Obstetrícia e Ginecologia, Campinas, SP, Brazil
eceived 27 August 2019; accepted 12 January 2021vailable online 27 April 2021
KEYWORDSPostoperative period;Patient satisfaction;Quality of HealthCare;Anesthesia;Anesthesia recoveryperiod
AbstractIntroduction: Spinal anesthesia combined with sedation and general anesthesia combined withepidural are two techniques often used for patients undergoing abdominal hysterectomy. Thereis no consensus that one of these techniques is superior regarding the perception of patientstowards the quality of postoperative recovery. This observational cross-sectional study aimed toassess the quality of postoperative recovery in women undergoing open abdominal hysterectomyby comparing both anesthetic techniques.Method: We recruited 162 women aged between 30 and 74 years to be submitted to abdom-inal hysterectomy. The anesthetic technique used followed the preference of the attendinganesthesiologist without interference of the investigators. After applying the exclusion crite-ria, 80 patients underwent spinal anesthesia combined with sedation (Group 1) and 62 womenunderwent epidural anesthesia combined with general anesthesia (Group 2). The quality ofpostoperative recovery was evaluated using the questionnaire Quality of Recovery-40 (QoR-40)completed 24 hours after the end of the surgery.Results: Eighty patients in Group 1 answered the QoR-40 questionnaire with an average ratingof 179.4 points, median of 186.5, standard deviation of 17.4 and a confidence interval of 3.8.The 60 patients in Group 2 answered the QoR-40 with an average of 174.9 points, median of178 points, standard deviation of 16 points and a confidence interval of 4.0 (p = 0.024).Conclusion: Women who received spinal anesthesia combined with sedation considered qualityof postoperative recovery better.
© 2021 Sociedade Brasileira dis an open access article undlicenses/by-nc-nd/4.0/).∗ Corresponding author.E-mail: [email protected] (D. Carli).
ttps://doi.org/10.1016/j.bjane.2021.01.013 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
e Anestesiologia. Published by Elsevier Editora Ltda. Thiser the CC BY-NC-ND license (http://creativecommons.org/
itora Ltda. This is an open access article under the CC BY-NC-ND

ti, R
I
Hfpafs
odtaoostr
saPotmqhir
hrit
tiacaa
M
Taeos(i5stal2
oRo
sstIttfdeo
7th
pdptsa
tttpawc
pfbt(
ffecmwnprclrw
iaoohda
D. Carli, J.F. Melet
ntroduction
ysterectomy consists of surgical removal of the uterus and,ollowing C-section, it is the second most common surgeryerformed in female patients. This surgery is associated with
high emotional burden related to fertility, sexuality, andemininity, and can elicit strong physical, psychological, andocial changes.1
Although surgical procedures focus on the improvementf health and feeling of well-being, they can also engen-er enough discomfort and emotional fragility to lead tohe perception of decreased quality of life, even in thebsence of specific complications.2 Frequently, a poor post-perative recovery period can lead to prolonged lengthf stay, increasing hospital costs and diminishing patientatisfaction.3,4 Thus, the multidisciplinary team should seekechniques that offer patients fast recovery and expeditiouseturn to daily activities.5
Most studies assessing the quality of postanesthetic andurgical recovery, most of the time analyze elements suchs recovery time, cardiorespiratory complications, pain,ostoperative Nausea and Vomiting (PONV), length of stayr other complications.6 When they are considered alone,hese aspects do not necessarily mirror the recovery ofost patients undergoing anesthesia and surgery. Therefore,uality-of-life assessment from the patient’s point of viewas become an important factor to be considered in studiesnvestigating the anesthesia and surgery effect on patientecovery and satisfaction.
Two anesthesia approaches commonly used for abdominalysterectomy are general anesthesia combined with epidu-al and spinal anesthesia combined with sedation. No studiesn the literature used adequate tools to compare these twoechniques regarding the quality of postoperative recovery.
The present study aimed to evaluate the perception ofhe quality of postoperative recovery in women undergo-ng hysterectomy by comparing two techniques: generalnesthesia combined with epidural and spinal anesthesiaombined with sedation. Our hypothesis was that spinalnesthesia offers better quality of recovery 24 hours afternesthesia.
ethod
his cross-sectional observational study was conductedccording to the international standards for human researchthics established by the Declaration of Helsinki, and Res-lution 466/12 from the Ministry of Health of Brazil. Thetudy was approved by the regional ethics committee033125/2016) and by the national system for register-ng research involving humans (Plataforma Brasil: CAAE5339616.5.0000.5412). All patients included in the studyigned an informed consent form. Data were collected inwo hospitals located at an inland city of São Paulo State,ssisted by the same anesthesiology team. The data col-ecting period occurred between September 2016 and March018.
The sample size calculation was based on the primaryutcome, that is, the total score obtained in the Quality ofecovery-40 (QoR-40) questionnaire applied 24 hours post-peratively to women undergoing hysterectomy, from a pilot
wate
22
.P. Camargo et al.
ample of 90 patients included in the total sample of thistudy, comparing spinal anesthesia combined with sedationo general anesthesia combined with epidural anesthesia.n this sample, there was a difference of 8 points betweenhe mean scores for spinal anesthesia combined with seda-ion (186, standard deviation ± 13), and the mean scoresor general anesthesia combined with epidural (178, stan-ard deviation ± 12). Based on these data, the sample sizestimated was 55 individuals per Group, to obtain a powerf 90% and a type I error of 5%.
The study included patients, aged between 30 and4 years, physical status ASA (American Society of Anes-hesiologists) I or II to be submitted to open abdominalysterectomy proposed by the gynecology surgeon.
Exclusion criteria were refusal to participate in the study;resence of impaired cognitive function; use of psychoactiverugs; fear of intraoperative anesthetic technique failure;resence of a complication that would lead to anestheticechnique conversion, the need for re-operation or admis-ion to the intensive care unit; and patients opting tobandon research.
We recruited 162 patients to participate in the study, andhe anesthetic technique was decided by the attending anes-hesiologist, in agreement with the patient and the surgicaleam, without the influence of the investigators, but com-lying with the techniques and doses recommended in thenesthetic protocol of the team of anesthesiologists thatorked at the two institutions in which the research wasonducted.
In Group 1 with 80 patients, the anesthetic techniqueerformed was sedation with intravenous midazolam and/orentanyl combined with spinal anesthesia using 0.5% hyper-aric bupivacaine and morphine. At the end of the surgery,he patients were sent to the PostAnesthesia Care UnitPACU).
In Group 2 with 62 women, the anesthetic technique per-ormed was sedation with intravenous midazolam and/orentanyl and single-shot epidural anesthesia using 50%nantiomeric excess levobupivacaine hydrochloride in con-entrations ranging from 0.25---0.5% with epinephrine andorphine. Then, the patients received general anesthesiaith intravenous injection of fentanyl, propofol and rocuro-ium. Tracheal intubation and mechanical ventilation wereerformed, and anesthesia was maintained using sevoflu-ane. Atropine and neostigmine were administered upononclusion of the surgery. After confirmation of neuromuscu-ar function recovery (monitoring of the train of four > 0.9),eturn of spontaneous breathing and awakening, the tracheaas extubated, and the patient sent to PACU.
Both anesthetic techniques were completed with thenstitution’s standard prescription of intravenous analgesiand antiemetic drugs that started one hour before the endf surgery, comprising intravenous administration of 100 mgf ketoprofen every 12 hours and 1 g of dipyrone every 6ours for pain control, and 10 mg dexamethasone (singleose) combined with 8 mg ondansetron every 8 hours asntiemetics.
Upon PACU admission, and every 20 minutes, patients
ere assessed for pain and PONV using an 11-point numericalnalog scale (where zero means no symptoms and ten meanshe highest intensity of symptoms possible). When pain scorexceeded 3 points, the patient received 2 mg of morphine2

esio
appo1d
mcctochia
4ficsefbqphaasQhcaips
ptpbt
aaor
S
Aaounitcp
R
Assccotaue
degwdG
tdtTc
4ptictoa
ito1
tr
D
Ttpsccwdoot
Brazilian Journal of Anesth
t 20-minute intervals, until the pain score was less than 4oints. When the PONV assessment exceeded 3 points, theatient received 10 mL of medication consisting of 3 mg.mL-1
f dimenhydrinate, 5 mg.mL-1 of pyridoxine hydrochloride,00 mg.mL-1 of glucose and 100 mg.mL-1 fructose in a singleose.
After reaching a score equal to or greater than nine in theodified Aldrete and Kroulik assessment, patients were dis-
harged from the PACU and were sent to the floor where theyontinued receiving the analgesic and antiemetic medica-ions initiated in the operating room. When they complainedf pain, they received 100 mg of tramadol as rescue medi-ation for pain, with a minimum interval of 8 hours. If theyad PONV, they would be medicated with 10 mL of the med-cation comprised of dimenhydrinate, pyridoxine, glucose,nd fructose every 12 hours.
The quality of recovery was assessed using the QoR-0 questionnaire. It consists of 40 questions divided intove dimensions: emotional state; physical comfort; psy-hological support; physical independence; and pain. Itscore varies between 40 (worst evaluation) and 200 (bestvaluation) and each question is scored according to therequency in which it occurs in an interval that variesetween 1 to 5 points, according to the Likert scale. Theuestionnaire has two parts. In Part A, questions indicateositive aspects, and the highest score is attributed to theighest occurrence. In Part B, questions indicate negativespects and the higher the occurrence, the lower the scorettributed.7,8 Validity, reliability, user-friendliness, respon-iveness and cross-cultural adaptation to Portuguese of theoR-40 were established in previous studies, revealing aigh reliability coefficient.4,9,10 Several clinical trials suc-essfully used QoR-40 to assess the quality of post-surgicalnd postanesthesia recovery.11---13 The score of 142 pointss a cut-off point and higher values indicate good qualityostanesthetic satisfaction.11 The questionnaire used in thistudy is found in Annex 1.
Twenty-four hours after the end of the surgery, theatients were asked to complete the questionnaire by inves-igators who had no knowledge of the anesthetic procedureerformed. The investigator remained close to the patient’sed, without interfering in the answers, only paying atten-ion to clarify any possible doubt.
In addition to the QoR-40 total score, other data werelso collected: 1) age, duration of surgery; and 2) evalu-tion of pain and PONV occurrence in the initial 24 hoursf the postoperative period, through the specific questionsegarding these issues in the dimensions of QoR-40.
tatistical analysis
fter data acquisition, quantitative data were entered inton Excel® database, then transferred and analyzed by meansf SPSS® software version 24. The Mann-Whitney test wassed for comparing groups regarding the ordinal data andon-Gaussian continuous data (presented as median and
nterval), whose results did not show normal distribution byhe Komolgorov-Smirmov test. Student’s t-test was used toompare the parametric quantitative data. We accepted aower of 90% and a type 1 error of 5%.drft
22
logy 2021;71(3):221---227
esults
total of 162 patients were recruited to participate in thetudy and 20 were excluded. The reasons for exclusion were:even patients refused to participate, eight patients did notomplete the questionnaire correctly, two patients requiredonversion of the chosen anesthetic technique due to intra-perative pain, two patients were submitted to anestheticechniques different from the two techniques evaluated,nd one patient required admission to the intensive carenit due to surgical complications. Thus, 142 patients werevaluated (Fig. 1).
Table 1 shows the mean age of the patients and the meanuration of the surgery, regarding the anesthetic techniquesvaluated. There was no difference observed between theroups regarding the mean age of participants, but thereas a difference between the groups regarding the meanuration of the surgery, with a longer mean duration forroup 2.
Table 2 shows the scores attributed by the patients tohe quality of postoperative recovery, using the Qor-40, itsimensions, and the sum of the three questions related tohe presence of PONV in the initial 24 hours postoperatively.hese three questions were then inserted into the physicalomfort dimension.
Table 2 shows that in Group 1 patients had a QoR-0 total score higher than those in Group 2 (p = 0.024),redominantly in the dimensions of physical comfort, emo-ional states, and psychological support. In the physicalndependence and pain dimensions, there was no statisti-al difference between the groups. We can also observehat Group 1 had a higher score related to the presencef PONV in the first 24 hours, which reveals greater comfortnd better quality regarding this item (p < 0.001).
Table 3 compares the two anesthetic techniques accord-ng to the QoR-40 cut-off score, which divides patients intowo categories: good quality of recovery (scores greater thanr equal to 142) and poor quality of recovery (scores below42).
In Table 3, there was no statistical difference betweenhe Groups regarding the classification of the quality ofecovery of patients.
iscussion
his cross-sectional observational study examined 142 ques-ionnaires that assessed the perception of the quality ofostoperative recovery 24 hours postoperatively in womenubmitted to open abdominal hysterectomy, comparing twoommonly used anesthetic managements: spinal anesthesiaombined with sedation (Group 1), and epidural combinedith general anesthesia (Group 2). The study revealed noifference between the groups regarding the mean agef the patients assessed. Concerning surgery duration, webserved that Group 2 had a longer surgical time comparedo Group 1 (p < 0.001). This is because the investigators
id not interfere with the anesthetic technique when usingandomization, leaving the anesthesiologist free to decideor the anesthesia technique whose duration is more con-rollable (Group 2) in patients expected to undergo longer3

D. Carli, J.F. Meletti, R.P. Camargo et al.
Figure 1 Flowchart describing allocation of patients.
Table 1 Comparison between groups according to age and duration of surgery.
Type of anesthesia n Mean Standard deviation (±) pa
Age Spinal + Sedation 80 44.98 6.129 0.501Epidural + General Anesthesia 62 46.23 6.959Total 142 45.64 6.521
Duration of thesurgery
Spinal + Sedation 80 99.44 22.385 <0.001Epidural + General Anesthesia 62 142.38 39.047
Total 142 119.14 37.732
a Student t test.
224
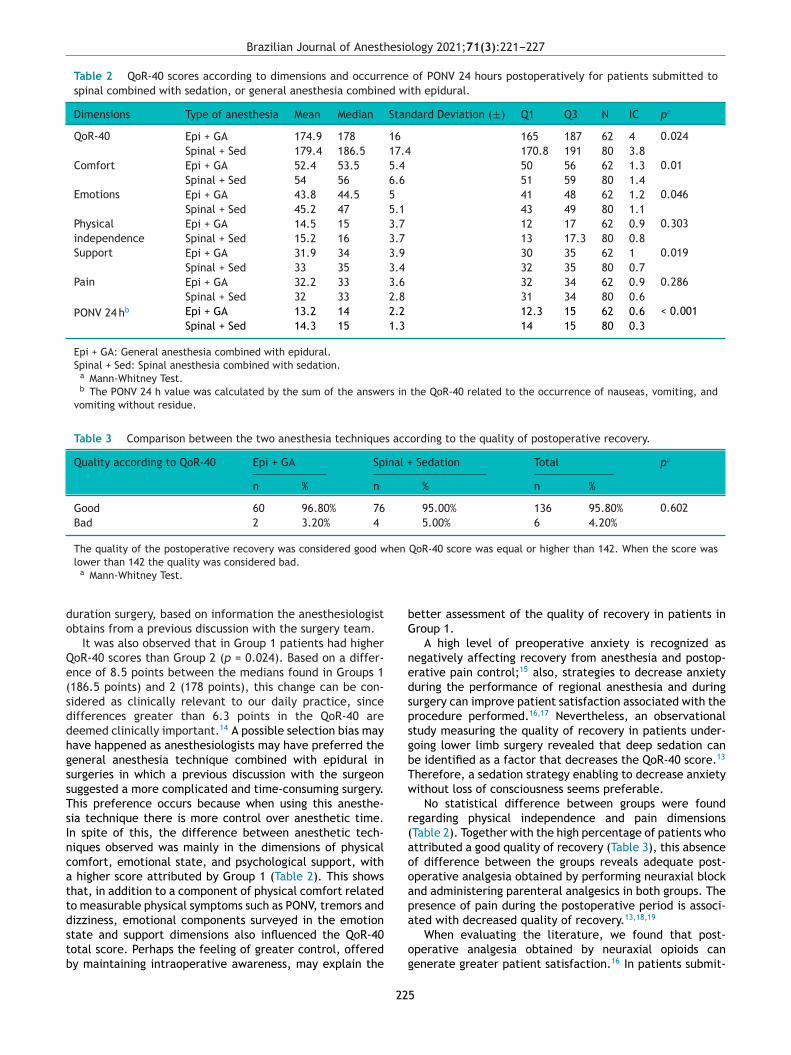
Brazilian Journal of Anesthesiology 2021;71(3):221---227
Table 2 QoR-40 scores according to dimensions and occurrence of PONV 24 hours postoperatively for patients submitted tospinal combined with sedation, or general anesthesia combined with epidural.
Dimensions Type of anesthesia Mean Median Standard Deviation (±) Q1 Q3 N IC pa
QoR-40 Epi + GA 174.9 178 16 165 187 62 4 0.024Spinal + Sed 179.4 186.5 17.4 170.8 191 80 3.8
Comfort Epi + GA 52.4 53.5 5.4 50 56 62 1.3 0.01Spinal + Sed 54 56 6.6 51 59 80 1.4
Emotions Epi + GA 43.8 44.5 5 41 48 62 1.2 0.046Spinal + Sed 45.2 47 5.1 43 49 80 1.1
Physicalindependence
Epi + GA 14.5 15 3.7 12 17 62 0.9 0.303Spinal + Sed 15.2 16 3.7 13 17.3 80 0.8
Support Epi + GA 31.9 34 3.9 30 35 62 1 0.019Spinal + Sed 33 35 3.4 32 35 80 0.7
Pain Epi + GA 32.2 33 3.6 32 34 62 0.9 0.286Spinal + Sed 32 33 2.8 31 34 80 0.6
PONV 24 hb Epi + GA 13.2 14 2.2 12.3 15 62 0.6 < 0.001Spinal + Sed 14.3 15 1.3 14 15 80 0.3
Epi + GA: General anesthesia combined with epidural.Spinal + Sed: Spinal anesthesia combined with sedation.
a Mann-Whitney Test.b The PONV 24 h value was calculated by the sum of the answers in the QoR-40 related to the occurrence of nauseas, vomiting, and
vomiting without residue.
Table 3 Comparison between the two anesthesia techniques according to the quality of postoperative recovery.
Quality according to QoR-40 Epi + GA Spinal + Sedation Total pa
n % n % n %
Good 60 96.80% 76 95.00% 136 95.80% 0.602Bad 2 3.20% 4 5.00% 6 4.20%
The quality of the postoperative recovery was considered good when QoR-40 score was equal or higher than 142. When the score was
do
Qe(sddhgssTsIncattdstb
bG
nedspsgbTw
r(aooap
lower than 142 the quality was considered bad.a Mann-Whitney Test.
uration surgery, based on information the anesthesiologistbtains from a previous discussion with the surgery team.
It was also observed that in Group 1 patients had higheroR-40 scores than Group 2 (p = 0.024). Based on a differ-nce of 8.5 points between the medians found in Groups 1186.5 points) and 2 (178 points), this change can be con-idered as clinically relevant to our daily practice, sinceifferences greater than 6.3 points in the QoR-40 areeemed clinically important.14 A possible selection bias mayave happened as anesthesiologists may have preferred theeneral anesthesia technique combined with epidural inurgeries in which a previous discussion with the surgeonuggested a more complicated and time-consuming surgery.his preference occurs because when using this anesthe-ia technique there is more control over anesthetic time.n spite of this, the difference between anesthetic tech-iques observed was mainly in the dimensions of physicalomfort, emotional state, and psychological support, with
higher score attributed by Group 1 (Table 2). This showshat, in addition to a component of physical comfort relatedo measurable physical symptoms such as PONV, tremors and
izziness, emotional components surveyed in the emotiontate and support dimensions also influenced the QoR-40otal score. Perhaps the feeling of greater control, offeredy maintaining intraoperative awareness, may explain thea
og
22
etter assessment of the quality of recovery in patients inroup 1.
A high level of preoperative anxiety is recognized asegatively affecting recovery from anesthesia and postop-rative pain control;15 also, strategies to decrease anxietyuring the performance of regional anesthesia and duringurgery can improve patient satisfaction associated with therocedure performed.16,17 Nevertheless, an observationaltudy measuring the quality of recovery in patients under-oing lower limb surgery revealed that deep sedation cane identified as a factor that decreases the QoR-40 score.13
herefore, a sedation strategy enabling to decrease anxietyithout loss of consciousness seems preferable.
No statistical difference between groups were foundegarding physical independence and pain dimensionsTable 2). Together with the high percentage of patients whottributed a good quality of recovery (Table 3), this absencef difference between the groups reveals adequate post-perative analgesia obtained by performing neuraxial blocknd administering parenteral analgesics in both groups. Theresence of pain during the postoperative period is associ-
ted with decreased quality of recovery.13,18,19When evaluating the literature, we found that post-perative analgesia obtained by neuraxial opioids canenerate greater patient satisfaction.16 In patients submit-
5

ti, R
tqsctAbstAebbb
Qwtg
poisFa2cdab
ifqyltdd
seil
C
We2sr
A
Dlm
w
c
s
l
p
F
TA(
C
T
A
Sf1
R
1
D. Carli, J.F. Melet
ed to hysterectomy, neuroaxis anesthesia provides betteruality of recovery, when compared to general anesthe-ia without associated blockade. In addition, a decreasedonsumption of parenteral opioids due to neuraxial anes-hesia was also related to better quality of recovery.20
nother meta-analysis described the importance of the com-ination of neuraxial blockade with general anesthesia,howing decrease of mortality and incidence of respira-ory, cardiovascular and gastrointestinal complications.21
nother prospective cohort study, with patients under gen-ral anesthesia submitted to orthopedic surgeries performedelow the knees --- associated or not with peripheral nervelockades --- observed that the patients who received thelockades were more satisfied and with less intensity pain.22
It can also be observed that Group 1 scored higher in theoR-40 questions related to PONV in the initial 24 hours,hich indicates greater comfort and better quality regarding
hese three questions (p < 0.001), and mirroring a bettereneral perception of the quality of recovery.13,18,19
From the data depicted in Table 3, we observed that mostatients (95.8%) attributed a QoR-40 total score greater thanr equal to 142 points, a score associated with good qual-ty recovery. Only six patients (4.2%) reported a QoR-40 totalcore below 142. There were no differences between groups.rom this finding, it can be concluded that the two evalu-ted anesthetic techniques allowed good quality recovery4 hours postoperatively. This is ascribed to the multidis-iplinary team’s concern with the main factors that canetermine worse quality of recovery (pain and PONV), thatre prevented with anesthetic techniques combined withlocks23 and parenteral drugs.7,24
The major limitations found in this study were thendividuality and subjectivity of the issue, which causes dif-erent interpretations regarding questions present in theuestionnaire selected for the study. Questions like: ‘‘Doou feel support from family or friends?’’ and ‘‘Do you feelonely?’’ are examples of questions in which the interpreta-ion of the influence of the anesthetic technique becomesifficult. Undeniably, new tools and new studies must beesigned so that the matter can be better understood.
Nevertheless, the QoR-40 proved to be valuable as atarting tool for the quantification of the quality of postop-rative recovery, enabling to compare anesthetic techniquesn a perspective that is still less approached in the scientificiterature: through the patient’s eyes.
onclusion
e concluded that the perception of the quality of postop-rative recovery in patients who underwent hysterectomy4 hours after surgery was higher in patients who underwentpinal anesthesia combined with sedation compared to thoseeceiving general anesthesia combined with epidural.
uthors’ contributions
aniel de Carli: Study design and planning, collecting, ana-
yzing and interpretating of data, wrote and reviewed theanuscript.José Fernando Amaral Meletti: Study design and planning,rote and reviewed the manuscript.
1
22
.P. Camargo et al.
Larissa Schneider Gratacós: Obtained informed consents;ollected intraoperative data and questionnaires.
Victor Cristiano Ramos Gomes: Obtained informed con-ents; collected intraoperative data and questionnaires.
Nicole Dutra Marques: Obtained informed consents; col-ected intraoperative data and questionnaires.
Rodrigo Pauperio Soares de Camargo: Study design andlanning.
unding
he study received a grant from Coordenação deperfeiçoamento de Pessoal de Nível Superior --- BrazilCAPES) --- Grant Code 001.
onflicts of interest
he authors declare no conflicts of interest.
ppendix A. Supplementary data
upplementary material related to this article can beound, in the online version, at doi:https://doi.org/10.016/j.bjane.2021.01.013.
eferences
1. Melo MCB, Barros ÉND. Histerectomia e simbolismo do útero:possíveis repercussões na sexualidade feminina. Rev SBPH.2009;12:80---99.
2. Lee WK, Kim MS, Kang SW, Kim MS, Lee JR. Type of anaesthesiaand patient quality of recovery: a randomized trial compar-ing propofol-remifentanil total i.v. anaesthesia with desfluraneanaesthesia. Br J Anaesth. 2015;114:663---8.
3. Poitras S, Beaule P, Dervin GF. Validity of a short-term qualityof life questionnaire in patients undergoing joint replacement:the Quality of Recovery-40. J Arthroplasty. 2012;27:1604---8.
4. Kluivers KB, Riphagen I, Vierhout ME, Brölmann HA, de Vet HC.Systematic review on recovery specific quality-of-life instru-ments. Surgery. 2008;143:206---15.
5. Murphy GS, Szokol J, Greenberg SB, et al. Preoperative dex-amethasone enhances quality of recovery after laparoscopiccholecystectomy: effect on in-hospital and postdischarge recov-ery. Anesthesiology. 2011;114:882---90.
6. Estivalet FF, Bagatini A, Gomes CR. Remifentanil associated topropofol or sevoflurane for videolaparoscopic cholecystectomy:a comparative study. Rev Bras Anestesiol. 2002;52:385---93.
7. Myles PS, Weitkamp B, Jones K, Melick J, Hensen S. Validityand reliability of a postoperative quality of recovery score: theQoR-40. Br J Anaesth. 2000;84:11---5.
8. Myles PS, Hunt JO, Nightingale CE, et al. Development and psy-chometric testing of a quality of recovery score after generalanesthesia and surgery in adults. Anesth Analg. 1999;88:83---90.
9. Gornall BF, Myles PS, Smith CL, et al. Measurement of qualityof recovery using the QoR-40: a quantitative systematic review.Br J Anaesth. 2013;111:161---9.
0. Eduardo AHA, Santos CB, Carvalho AMP, Carvalho EC. Validationof the Brazilian version of the Quality of Recovery - 40 Item
questionnaire. Acta Paul Enferm. 2016;29:253---9.1. Pereira LG, Costa M, Sousa G, Abelha F. Quality of recovery afteranaesthesia measured with QoR-40: a prospective observationalstudy. Braz J Anesthesiol. 2016;66:369---75.
6
esio
1
1
1
1
1
1
1
1
2
2
2
2
Brazilian Journal of Anesth
2. Mihara T, Ishii T, Ka K, Goto T. Effects of steroids on quality ofrecovery and adverse events after general anesthesia: meta-analysis and trial sequential analysis of randomized clinicaltrials. PLoS One. 2016;11:e0162961.
3. Moro ET, Silva MA, Couri MG, Issa DD, Barbieri JM. Qualityof recovery from anesthesia in patients undergoing ortho-pedic surgery of the lower limbs. Rev Bras Anestesiol.2016;66:642---50.
4. Myles PS, Myles DB, Galagher W, Chew C, MacDonald N, DennisA. Minimal clinically important difference for three quality ofrecovery scales. Anesthesiology. 2016;125:39---45.
5. Ali A, Altun D, Oguz BH, Ilhan M, Demircan F, Koltka K. Theeffect of preoperative anxiety on postoperative analgesia andanesthesia recovery in patients undergoing laparascopic chole-cystectomy. J Anesth. 2014;28:222---7.
6. Wu CL, Rowlingson AJ, Partin AW, et al. Correlation of postoper-ative pain to quality of recovery in the immediate postoperativeperiod. Reg Anesth Pain Med. 2005;30:516---22.
7. Kubulus C, Schmitt K, Albert N, et al. Awake, sedated or anaes-thetised for regional anaesthesia block placements?: a retro-spective registry analysis of acute complications and patientsatisfaction in adults. Eur J Anaesthesiol. 2016;33:715---24.
8. Royse CF, Chung F, Newman S, Stygall J, Wilkinson DJ. Predic-tors of patient satisfaction with anaesthesia and surgery care: acohort study using the Postoperative Quality of Recovery Scale.Eur J Anaesthesiol. 2013;30:106---10.
2
22
logy 2021;71(3):221---227
9. Myles PS, Williams DL, Hendrata M, Anderson H, Weeks AM.Patient satisfaction after anaesthesia and surgery: resultsof a prospective survey of 10,811 patients. Br J Anaesth.2000;84:6---10.
0. Castro-Alves LJS, De Azevedo VLF, Braga TFDF, Goncalves AC,et al. The effect of neuraxial versus general anesthesia tech-niques on postoperative quality of recovery and analgesiaafter abdominal hysterectomy: a prospective, randomized, con-trolled trial. Anesth Analg. 2011;113:1480---6.
1. Pöpping D, Elia N, Van Aken H, et al. Impact of epidural analge-sia on mortality and morbidity after surgery: systematic reviewand meta-analysis of randomized controlled trials. Annals Surg.2014;259:1056---67.
2. Elkassabany N, Cai LF, Mehta S, et al. Does regional anes-thesia improve the quality of postoperative pain managementand the quality of recovery in patients undergoing operativerepair of tibia and ankle fractures? J Orthopaedic Trauma.2015;29:404---9.
3. Abdallah FW, Morgan PJ, Cil T, et al. Ultrasound-guided mul-tilevel paravertebral blocks and total intravenous anesthesiaimprove the quality of recovery after ambulatory breast tumorresection. Anesthesiology. 2014;120:703---13.
4. Schraag S, Pradelli L, Alsaleh Ajo, et al. Propofol vs. inhalationalagents to maintain general anaesthesia in ambulatory and in-patient surgery: a systematic review and meta-analysis. BMCAnesthesiol. 2018;18:162.
7

C
Pfi
RW
a
b
c
ed
N
RA
B
h©l
Brazilian Journal of Anesthesiology 2021;71(3):228---232
LINICAL RESEARCH
ain catastrophizing in daughters of women withbromyalgia: a case-control study�
égis Junior Muniza, Mariane Schäffer Castroa, Jairo Alberto Dussán-Sarriab,d,olnei Caumob,c,d, Andressa de Souza a,d,∗
Universidade La Salle, Programa de Pós-Graduação em Saúde e Desenvolvimento Humano, Canoas, RS, BrazilUniversidade Federal do Rio Grande do Sul (UFRGS), Programa de Pós-Graduação em Ciências Médicas, Porto Alegre, RS, BrazilUniversidade Federal do Rio Grande do Sul (UFRGS), Hospital de Clínicas de Porto Alegre (HCPA), Serviço de Tratamento de Dor
Medicina Paliativa, Porto Alegre, RS, BrazilUniversidade Federal do Rio Grande do Sul (UFRGS), Hospital de Clínicas de Porto Alegre (HCPA), Laboratório de Dor eeuromodulação, Porto Alegre, RS, Brazil
eceived 16 July 2019; accepted 18 October 2020vailable online 6 February 2021
KEYWORDSFibromyalgia;Catastrophizing;Anxiety;Depression
Abstract Fibromyalgia is a syndrome characterized by chronic pain related to the muscu-loskeletal system. Patients feel incapable and show catastrophic thoughts (exaggeration of thesensations) related to painful events. This study aimed to compare catastrophic thoughts of painbetween daughters of women with fibromyalgia and daughters of women without fibromyal-gia, no daughter having the syndrome. It was a case-control study in which 76 women wereincluded: 38 daughters of women diagnosed with fibromyalgia (case group), and 38 daughtersof women without fibromyalgia (control group). The Brazilian versions of the Profile of ChronicPain: Screen, the Pittsburgh Sleep Quality Index, the Pain Catastrophizing Scale, ResilienceScale, Beck Depression Inventory-II, and the State-Trait Anxiety Inventory were used. Datawere tabulated and analyzed using SPSS 20.0. Continuous variables were compared betweenthe groups using the Mann-Whitney U test or Student’s t-test for independent samples. A sig-nificant difference was considered at p < 0.05. Regarding catastrophism, the case group hadhigher total catastrophism compared to the control group (p = 0.025). Daughters of patientswith fibromyalgia showed higher rumination and magnification levels related to pain (p = 0.028and p = 0.007, respectively) but did not show hopelessness. This study concludes that daugh-ters of women with fibromyalgia are more likely to have symptoms of fibromyalgia due to theirvisualization of the syndrome. This indicates that emotional aspects may induce changes, andadditional research on an individual basis is necessary.
© 2021 Sociedade Brasileira deopen access article under theby-nc-nd/4.0/).
� Study conducted at the Pain and Neuromodulation Laboratory at Hosrazil.∗ Corresponding author.
E-mail: [email protected] (A. Souza).
ttps://doi.org/10.1016/j.bjane.2020.10.012 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Anestesiologia. Published by Elsevier Editora Ltda. This is anCC BY-NC-ND license (http://creativecommons.org/licenses/
pital de Clínicas de Porto Alegre (HCPA---UFRGS), Porto Alegre, RS,
itora Ltda. This is an open access article under the CC BY-NC-ND

esio
I
GpsaPc
Icnatgpoafwgoa
‘aipslftapgi
ewstw
M
TSTCicNdH
P
Ttw
WPrfiwgwp
I
Tooipanoaaa
I
PPbnPtSoiade
ema
S
Tb0aata1wp
S
Brazilian Journal of Anesth
ntroduction
eneralized pain is a sign of nervous system sensitization inatients with chronic pain.1 Pain intensity varies from per-on to person, depending on the cause and psychologicallterations.2 The International Association for the Study ofain (IASP) defined chronic pain as pain persisting over threeonsecutive months.3
Fibromyalgia presents with hyperalgesia and allodynia.4
t is characterized by abnormal pain processing, which isaused by neurobiological alterations that deregulate theociceptive mechanism controlling biophysical responsesssociated with pain.5 The American College of Rheuma-ology (ACR) defined fibromyalgia as the manifestation ofeneralized pain for at least three consecutive months, withain on palpating at least 11 of the 18 trigger points.6 Drugr non-drug therapy5 can manage chronic pain. Chronic painffects sleep quality, resulting in fatigue and decreased per-ormance of the activities of daily living.7,8 Patients whoere exposed to physical, emotional, environmental, orenetic presents increased pain perception in cases of notnly fibromyalgia but also autoimmune diseases, infections,nd inflammations.9
Catastrophizing is a cognitive process defined as‘exaggerated negative thinking brought to bear during anctual or anticipated painful experience’’.10,11 Catastrophiz-ng related to pain can change pain perception. The fearrovoked by catastrophizing influence the perception oftimuli and pain intensity.12,13 Studies suggest that higherevels of catastrophizing thoughts are associated with higherunctional incapabilities.14 Emotions may influence the painhreshold through psychiatric or somatoform disorders inddition to catastrophizing.15 Several studies revealed theresence of pain catastrophizing in patients with fibromyal-ia. A domain of catastrophizing is magnification, which mayncrease the patient’s attention to painful symptoms.16,17
Therefore, the aim of this study was to compare the lev-ls of pain catastrophizing between daughters of womenith fibromyalgia and daughters of healthy women. The
tudy hypothesis was that catastrophizing is higher in daugh-ers of women with fibromyalgia than in daughters of healthyomen.
ethods
his article has addressed the checklist of items in theTROBE Statement for case-control observational studies.he study protocol was approved by the Ethics and Researchommittee of Hospital de Clínicas de Porto Alegre/RS (reg-
stration no 140635). The use of protocols followed theonditions established in the resolution no 466/12 of theational Health Council. This case-control study was con-ucted at the Pain and Neuromodulation Laboratory ofospital de Clínicas de Porto Alegre (HCPA).
opulation and study design
his is a case-control observational study in which daugh-ers of women with fibromyalgia and daughters of womenithout fibromyalgia aged above 18 years were included.
Ccw
22
logy 2021;71(3):228---232
omen with fibromyalgia treated at the Pain Treatment andalliative Medicine Ambulatory of HCPA were contacted toecruit their daughters, while daughters of women withoutbromyalgia were recruited using the snowball technique, inhich each recruited daughter of a woman with fibromyal-ia indicates another person who is the daughter of a womanithout fibromyalgia. Written informed consent for partici-ation in the study was obtained from all participants.
nclusion and exclusion criteria
he inclusion criteria were age over 18 years, no diagnosisf fibromyalgia, and a mother with (case group) or with-ut (control group) fibromyalgia. Participants received thenformed consent form, understood the study objective androtocol, and signed the form. The exclusion criteria were
diagnosis of fibromyalgia or of a serious psychiatric or cog-itive disorder that could interfere with the understandingf scales used in the study, such as a neurologic disorder,
systemic disease-causing decompensation, or an associ-ted inflammatory disease, including lupus and rheumatoidrthritis.
nstruments and evaluations
articipants were evaluated in a single appointment at theain Treatment and Palliative Medicine Ambulatory of HCPAy the research team using: Sociodemographic Question-aire for epidemiologic analysis; the Brazilian version of therofile of Chronic Pain: Screen (B-PCP:S)18 for characteris-ics of chronic pain; the Brazilian version of the Pittsburghleep Quality Index19 for sleep quality; the Brazilian versionf the Pain Catastrophizing Scale (B-PCS)20 for catastrophiz-ng; the Resilience Scale (RS)21 for the capacity to deal withdversities; the Beck Depression Inventory-II (BDI-II)22 forepression; State-Trait Anxiety Inventory (STAI)23 for anxi-ty.
Volunteers were asked to remember a nociceptive painfulxperience for B-PCP:S and B-PCS. Data regarding otheredical conditions and previous diagnosis of depression or
nxiety were not collected.
ample size calculation
he sample size was calculated based on a study performedy Montoya et al. in 2005.24 The estimated effect size was.68 (Cohen’s d). With the independent samples t-test for
difference between mean values up to 0.68, a two-tailedlpha error of 0.05, power of 80%, and same sample size, aotal of 70 women were required: 35 for the control groupnd 35 for the case group. Considering that approximately0% of participants could not complete all tests, 76 patientsere recruited to compensate for possible losses. The sam-le size was calculated using the G*Power program.
tatistical analysis
ontinuous and categorical variables were resumed withonventional descriptive statistics. Normality was verifiedith the Shapiro-Wilk test. Continuous variables were com-
9

R.J. Muniz, M.S. Castro, J.A. Dussán-Sarria et al.
Table 1 Epidemiological and clinical characteristics.
Variable Control (n = 38) Case (n = 38) p-valuea
Median (25th---75th) Median (25th---75th)
Age 27.50 (19.0---34.0) 30.00 (23.75---35.0) 0.160Body mass index 23.00 (20.99--- 24.85) 24.1 (22.26---27.97) 0.132Formal Education (years of study) 14.00 (13.00---16.00) 13.00 (12.00---16.00) 0.139
Values are described as median and interquartile ranges (interquartile 25---75) (n = 76).a Mann Whitney test.
Table 2 Catastrophizing, resilience, depression, and anxiety behavior profile of the sample.
Variable Control (n = 38) Case (n = 38) p-value Effect sizeMedian (25th---75th) Median (25th---75th)
Total B-PCS 12.50 (2.00---24.50) 21.50 (11.00---31.75) 0.025a,b 0.50B-PCS --- Hopelessness 5.00 (2.00---10.00) 7.00 (3.75---12.0) 0.135b ---B-PCS --- Magnification 3.00 (0.00---5.25) 5.00 (2.00---7.25) 0.028a,b 0.48B-PCS --- Rumination 6.00 (0.00---9.25) 9.00 (5.00---11.00) 0.007a,b 0.68Resilience Scale 136.50 (132.00---145.25) 134.50 (126.75---140.25) 0.137b ---BDI-II 6.00 (3.75---9.00) 10.00 (5.00---15.25) 0.005a,b 0.78STAI --- State 29.00 (27.75---32.25) 28.00 (25.00---31.00) 0.011a,c 0.60STAI --- Trait 24.00 (22.00---27.00) 24.00 (22.75---27.25) 0.628b ---
Values described as median and interquartile ranges (interquartile 25---75) (n = 76).a Significant difference from control group.
powDT
R
Tig(aptfc
lapRnppgtmtasa
ttcts
P(t(ti(p
D
Ificmhecrih
b Mann Whitney test.c t-test for independent samples.
ared between the groups using the Mann-Whitney U testr Student’s t-test for independent samples. The differenceas considered significant if p < 0.05 (error tax of type I).ata were analyzed using SPSS 20.0 (SPSS, Chicago, IL, USA).here were no missing data to be addressed.
esults
his study presents the results of the analyses of 76 women,ncluding 38 daughters of women with fibromyalgia (caseroup) and 38 daughters of women without fibromyalgiacontrol group). Age, years of study and BMI were considereds non-parametric variables (Shapiro Wilk Test; p = 0.002,
< 0.001 and p < 0.001, respectively). Both groups hadhe same baseline profile (Table 1), with no significant dif-erences between the groups (p > 0.05) in the presentedharacteristics.
Pain catastrophizing thought scale and its domains (hope-essness, magnification, and rumination) were considereds non-parametric variables (Shapiro Wilk Test; p = 0.009,
= 0.005, p < 0.001 and p = 0.003, respectively).esilience Scale, BDI and STAI-Trait were also consideredon-parametric (Shapiro Wilk Test; p = 0.012, p < 0.001 and
= 0.025, respectively). Only STAI-State was considered as aarametric variable (Shapiro Wilk Test; p = 0.149). The caseroup has a higher total pain catastrophizing level comparedo the control group (Table 2); p = 0.025. In its domains,agnification and rumination were significantly higher in
he case group compared to the control group (p = 0.028nd p = 0.007, respectively). However, hopelessness was notignificantly different between the groups (p = 0.135). Inddition, the RS score did not significantly differ between
ioes
23
he two groups (p = 0.137). The BDI-II score was significan-ly higher (p = 0.005) in the case group compared to theontrol group. The STAI-trait score did not differ significan-ly between the groups (p = 0.628), while STAI-state had aignificant difference between groups (p = 0.011).
B-PCP:S was used to characterize pain in both groups.ain frequency was considered a parametric variableShapiro Wilk Test; p = 0.311), while interference in activi-ies and emotions were considered non-parametric variablesShapiro Wilk Test; p = 0.001 and p < 0.001, respectively) Theotal B-PCP:S scores of its domains were significantly highern daughters of women with fibromyalgia: pain frequencyp < 0.001), pain interference in activities (p < 0.001), andain interference in emotions (p < 0.001) (Table 3).
iscussion
n both groups, participants had no medical diagnosis ofbromyalgia, but pain catastrophizing levels were signifi-antly different between them in terms of rumination andagnification of thoughts related to pain. This allow to
ypothesize that patients who have contact with their moth-rs’ condition may be more susceptible to higher levels ofatastrophizing. However, this study has not investigated theelationship between mothers and daughters, and thereforet cannot conclude that their relationship is the cause ofigher results.
Environmental and psychosocial factors can trigger phys-
ological alterations and directly affect the mental healthf women with fibromyalgia.25 Fitzcharles et al. (2014)26valuated 120 individuals with fibromyalgia and verifiedignificant differences in catastrophizing, evidencing that
0

Brazilian Journal of Anesthesiology 2021;71(3):228---232
Table 3 Pain characteristics profile according to each group.
Variable Control (n = 38) Case (n = 38) p-valuea Effect sizeMean ± SD Mean ± SD
B-PCP:S 22.18 ± 15.75 40.05 ± 17.46 < 0.001 0.71Pain frequency 12.05 ± 7.50 18.52 ± 6.32 < 0.001 0.93Pain interference in activities 5.36 ± 4.98 12.60 ± 9.32 < 0.001 0.97Pain interference in emotions 4.76 ± 4.64 8.92 ± 4.78 < 0.001 0.88
an ±rol gr
eeclwhscm
aficrtra
waattfiifeaetm
baiaiea
atfiladdd
poatosSvhtt
fievqufiham
C
T
R
Profile of Chronic Pain scale (B-PCP:S), values are described as mea t-tests for independent samples, significant difference in cont
nvironmental factors, such as familial or work atmosphere,xposure to stressors, physical or emotional, and psychoso-ial factors resulting from socioeconomic and educationalevels can influence mental health. In the present study,e concluded that daughters of women with fibromyalgiaave higher levels of catastrophizing. According to previoustudy, environmental factors, such as seeing their mothers’ondition affect psychosocial characteristics, may influenceental health.RS score showed no significant difference, which is
ttributable to the fact that women of neither group suf-ered from fibromyalgia. As for the possibility that resiliences associated with fibromyalgia, therefore this study’s parti-ipants did not present resilience, McAllister et al. (2015)27
eported few negative effects with fewer symptoms. Emo-ional aspects related to daily activities and interpersonalelationships can influence emotional well-being and medi-te this relation to pain.28
Responses from case group showed that preoccupationith the possibility of developing fibromyalgia can provokelterations in the emotional state, causing depressive andnxious thoughts and feelings, since daughters witnessedhe emotional and physical discomfort provoked by pain inheir mothers. This generates a negative notion regardingbromyalgia, possibly leading to a psychosomatic effect in
ts homeostasis.28 Regarding environmental and psychosocialactors that could cause higher levels of stress,25 Fitzcharlest al. (2014)28 found a significant correlation betweennxiety and depression. According to previous study, thenvironmental factor, such as seeing their mothers’ condi-ion affecting psychosocial characteristics, influence in theirental health, such as pain catastrophizing.25
In contrast to depression, trait-anxiety did not differetween the groups. Fibromyalgia seems to be related ton anguish that could develop from painful symptoms: painntensity, daytime drowsiness, fatigue, cognitive disturbs,nxiety, and depression.29,30 It has been evidenced that anx-ety is a symptom of fibromyalgia. Since patients who werevaluated did not have fibromyalgia, they also did not havenxiety.
Daughters of women with fibromyalgia showed emotionalnd behavior alterations, which warrants medical atten-ion because some characteristics shown by women withbromyalgia are seen in their daughters, although in smaller
evels. Possibilities of pain catastrophizing, depression, and
nxiety may be associated with mothers’ condition and theaughters’ somatization, or could have a genetic trace, andaughters of mothers with fibromyalgia in the study couldevelop symptoms of fibromyalgia.23
standard deviation (n = 76).oup.
The present study had the strength of not having anyatient loss or missing data. The limitations include the lackf investigating other medical conditions since it could be
possible confounder for the results of the study. Besideshat, the snowball technique is one of the main limitationsf this study, since it has a high risk of bias, in which thisampling method could affect outputs of questionnaires.ampling method used in this study for the case group (con-enience sampling), in which patients were called from aospital ambulatory, is a method that has no way to know ifhe sample is representative of all population, meaning thathis reduces external validity from this study.
Therefore, even for the daughters of women withbromyalgia who do not have a diagnosis, studies shouldvaluate catastrophizing, anxiety, and depression as a pre-entive measure with appropriate guidelines for a betteruality of life. Further studies should be conducted to eval-ate possible genetic factors in daughters of women withbromyalgia and to compare daughters with mothers whoave the same syndrome. Studies should be performed tonalyze the time to event (fibromyalgia) and possible treat-ents to avoid the development of the syndrome.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Barbero M, Fernández-de-las-Peñas C, Palacios-Ceña M, et al.Pain extent is associated with pain intensity but not withwidespread pressure or thermal pain sensitivity in women withfibromyalgia syndrome. Clin Rheumatol. 2017;36:1427---32.
2. Bushnell MC, Čeko M, Low LA. Cognitive and emotional controlof pain and its disruption in chronic pain. Nat Rev Neurosci.2013;14:502---11.
3. Steingrímsdóttir ÓA, Landmark T, Macfarlane GJ, et al. Definingchronic pain in epidemiological studies: A systematic review andmeta-analysis. Pain. 2017;158:2092---107.
4. Choy EHS. The role of sleep-in pain and fibromyalgia. Nat RevRheumatol. 2015;11:513---20.
5. Boomershine C. Fibromyalgia: The Prototypical Central Sensi-tivity Syndrome. Curr Rheumatol Rev. 2015;11:131---45.
6. Arnold LM, Fan J, Russell IJ, et al. The fibromyalgia fam-ily study: A genome-wide linkage scan study. Arthritis Rheum.2013;65:1122---8.
7. Góes SM, Stefanello JMF, Homann D, et al. Torque and muscleactivation impairment along with insulin resistance are asso-ciated with falls in women with fibromyalgia. J Strength CondRes. 2016;30:3155---64.
1
, J.A
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2014;7:313---26.30. Nugraha B, Karst M, Engeli S, et al. Brain-derived neurotrophic
R.J. Muniz, M.S. Castro
8. Soriano-Maldonado A, Amris K, Ortega FB, et al. Associationof different levels of depressive symptoms with symptomatol-ogy, overall disease severity, and quality of life in women withfibromyalgia. Qual Life Res. 2015;24:2951---7.
9. Efrati S, Golan H, Bechor Y, et al. Hyperbaric oxygen therapycan diminish fibromyalgia syndrome - Prospective clinical trial.PLoS One. 2015;10:e0127012.
0. Block PR, Thorn BE, Kapoor S, et al. Pain catastrophizing, ratherthan vital signs, associated with pain intensity in patients pre-senting to the emergency department for pain. Pain Manag Nurs.2017;18:102---9.
1. Reiter S, Eli I, Mahameed M, et al. Pain Catastrophizing andpain persistence in temporomandibular disorder patients. J OralFacial Pain Headache. 2018;32:309---20.
2. Henderson LA, Akhter R, Youssef AM, et al. The effects ofcatastrophizing on central motor activity. Eur J Pain (UnitedKingdom). 2016;20:639---51.
3. Dunn LK, Durieux ME, Fernández LG, et al. Influence ofcatastrophizing, anxiety, and depression on in-hospital opioidconsumption, pain, and quality of recovery after adult spinesurgery. J Neurosurg Spine. 2018;28:119---26.
4. Craner JR, Sperry JA, Koball AM, et al. Unique contributions ofacceptance and catastrophizing on chronic pain adaptation. IntJ Behav Med. 2017;24:542---51.
5. Lee JE, Kim SH, Shin SK, et al. Attentional Engagementfor Pain-Related Information among Individuals with ChronicPain: The Role of Pain Catastrophizing. Pain Res Manag.2018;2018:6038406.
6. Loggia ML, Berna C, Kim J, et al. The Lateral Prefrontal Cor-tex Mediates the Hyperalgesic Effects of Negative Cognitions inChronic Pain Patients. J Pain. 2015;16:692---9.
7. Burns JW, Gerhart JI, Post KM, et al. The Communal CopingModel of Pain Catastrophizing in Daily Life: A Within-CouplesDaily Diary Study. J Pain. 2015;16:1163---75.
8. Caumo W, Ruehlman LS, Karoly P, et al. Cross-Cultural Adapta-tion and Validation of the Profile of Chronic Pain: Screen for a
Brazilian Population. Pain Med (United States). 2013;14:52---61.9. Bertolazi AN, Fagondes SC, Hoff LS, et al. Validation of theBrazilian Portuguese version of the Pittsburgh Sleep QualityIndex. Sleep Med. 2011;12:70---5.
23
. Dussán-Sarria et al.
0. Sehn F, Chachamovich E, Vidor LP, et al. Cross-Cultural Adap-tation and Validation of the Brazilian Portuguese Version ofthe Pain Catastrophizing Scale. Pain Med (United States).2012;13:1425---35.
1. Wagnild GM, Young HM. Development and psychometric evalu-ation of the Resilience Scale. J Nurs Meas. 1993;1:165---78.
2. Warmenhoven F, Van Rijswijk E, Engels Y, et al. The BeckDepression Inventory (BDI-II) and a single screening questionas screening tools for depressive disorder in Dutch advancedcancer patients. Support Care Cancer. 2012;20:319---24.
3. Kaipper MB, Chachamovich E, Hidalgo MPL, et al. Evalua-tion of the structure of Brazilian State-Trait Anxiety Inventoryusing a Rasch psychometric approach. J Psychosom Res.2010;68:223---33.
4. Montoya P, Pauli P, Batra A, et al. Altered processing of pain-related information in patients with fibromyalgia. Eur J Pain.2005;9:293---303.
5. Andreoli L, Tincani A. Undifferentiated connective tissue dis-ease, fibromyalgia, and the environmental factors. CurrentOpinion in Rheumatology. 2017;29:355---60.
6. Fitzcharles MA, Rampakakis E, Ste-Marie PA, et al. The associ-ation of socioeconomic status and symptom severity in personswith fibromyalgia. J Rheumatol. 2014;41:1398---404.
7. McAllister SJ, Vincent A, Hassett AL, et al. Psychologicalresilience, affective mechanisms, and symptom burden in atertiary-care sample of patients with fibromyalgia. Stress Heal.2015;31:299---305.
8. Sturgeon JA, Zautra AJ, Arewasikporn A. A multilevel structuralequation modeling analysis of vulnerabilities and resilienceresources influencing affective adaptation to chronic pain. Pain.2014;155:292---8.
9. Gerdle B, Ghafouri B, Ernberg M, et al. Chronic musculoskele-tal pain: Review of mechanisms and biochemical biomarkersas assessed by the microdialysis technique. J Pain Res.
factor, and exercise in fibromyalgia syndrome patients: A minireview. Rheumatol Int. 2012;32:2593---9.
2

C
Ehd
FK
H
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):233---240
LINICAL RESEARCH
ffect of ondansetron on spinal anesthesia-inducedypotension in non-obstetric surgeries: a randomised,ouble-blind and placebo-controlled trial
abrício Tavares Mendonça ∗, Luis Carlos Crepaldi Junior, Rafaela Carvalho Gersanti,amila Christine de Araújo
ospital de Base do Distrito Federal, Departamento de Anestesiologia, Brasília, DF, Brazil
eceived 17 June 2020; accepted 12 December 2020vailable online 22 March 2021
KEYWORDSElderly;Hypotension;Ondansetron;Spinal anesthesia
AbstractBackground and objectives: Spinal anesthesia is an effective technique for many surgical pro-cedures, but it is often associated with an increased risk of potentially deleterious hemodynamicdisturbances. The benefits of prophylactic ondansetron for preventing spinal anesthesia-induced hypotension are still uncertain. Therefore, this study aimed to compare the effectof ondansetron and placebo before spinal block on the incidence of hypotension in patientshaving non-obstetric surgeries.Methods: Randomized, double-blind, parallel-group, superiority trial with a 1:1 allocationratio. A total of 144 patients scheduled for non-obstetric surgeries with an indication for spinalanesthesia were randomized. Patients received intravenous ondansetron (8 mg) or placebobefore standard spinal anesthesia. The primary outcome was the rate of hypotension in thefirst 30 minutes after spinal anesthesia.Results: Hypotension occurred in 20 of 72 patients (27.8%) in the ondansetron group and in 36of 72 patients (50%) in the placebo group (Odds Ratio---OR = 0.38; 95% Confidence Interval---CI0.19 to 0.77; p = 0.007). Fewer patients in the ondansetron group required ephedrine comparedto the placebo group (13.9% vs. 27.8%; OR = 0.42; 95% CI 0.18 to 0.98; p = 0.04). Exploratoryanalyses revealed that ondansetron may be more effective than placebo in patients aged 60years or older (OR = 0.12; 95% CI 0.03 to 0.48; p = 0.03). No difference in heart rate variationswas observed.Conclusion: Our findings suggest that ondansetron can be a viable and effective strategy toreduce both the incidence of spinal anesthesia-induced hypotension and vasopressors usage innon-obstetric surgeries.
© 2021 Sociedade Brasileira deopen access article under the Cnc-nd/4.0/).∗ Corresponding author.E-mail: [email protected] (F.T. Mendonça).
ttps://doi.org/10.1016/j.bjane.2020.12.028 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Anestesiologia. Published by Elsevier Editora Ltda. This is anC BY-NC-ND license (http://creativecommons.org/licenses/by-
itora Ltda. This is an open access article under the CC BY-NC-ND

ldi Ju
I
BfacTib
io8ltaspirrdimtse
oarBssdpta
wbds
M
T
TsadfadiDb(tT
iTT
P
WeSbSEaupadppo
I
Iisb0aaoesbaSptds
O
Tht9ptamubht
F.T. Mendonça, L.C. Crepa
ntroduction
esides being the most common anesthesia techniqueor cesarean section, spinal anesthesia has become thenesthetic approach of choice for many general surgical pro-edures on the lower limbs, perineum and lower abdomen.1
his technique is of easy execution, providing not only fastntraoperative anesthesia with a lower respiratory impact,ut also better pain control, favoring a rapid recovery.1,2
Despite its many advantages, spinal anesthesia hasmportant side effects including hypotension, which isbserved in approximately 40% of non-obstetric patients and0% of the obstetric patients.3,4 Arterial hypotension canead to a reduction in blood flow and cardiac output, resul-ing in a state of systemic hypoperfusion. Following spinalnesthesia, hypotension results mainly from a decrease inystemic vascular resistance secondary to a blockage of sym-athetic fibers and an increase in vagal tone. This reductionn venous return can trigger the Von Bezold-Jarisch (BJ)eflex, mediated by serotonin receptors (subtype 5-HT3),esulting in increased efferent vagal signaling and bradycar-ia, ultimately exacerbating hypotension.3,5---7 Importantly,f associated with bradycardia and without proper treat-ent, hypotension can progress to cardiac arrest.8 Thus,
herapeutic strategies that can reduce the risk of hypoten-ion after spinal anesthesia may prevent more critical sideffects related to this technique.9
Ondansetron is a drug employed as prophylaxis for Post-perative Nausea and Vomiting (PONV), whose antiemeticctivity involves the selective inhibition of the 5-HT3
eceptors.10 As a result, ondansetron can suppress theJ reflex, and it has been postulated as a therapeutictrategy to prevent hypotension in patients undergoingpinal anesthesia.6,11 In this respect, several studies haveemonstrated the effectiveness of ondansetron on obstetricatients.6,11---13 However, only a few trials have investigatedhe prophylactic use of ondansetron to prevent hypotensionfter spinal anesthesia in non-obstetric patients.7,14
The aim of the present study was, therefore, to assesshether the intravenous administration of ondansetronefore spinal anesthesia is more effective to reduce the inci-ence of hypotension in patients undergoing non-obstetricurgical procedures compared to placebo.
ethods
rial design and trial setting
his was a prospective, randomized, parallel-group,uperiority placebo-controlled, fase IV trial with a 1:1llocation ratio carried out at the Hospital de Baseo Distrito Federal, Brasília, Distrito Federal, Brazil,rom March 2019 to December 2019. The study waspproved by the local Research Ethics Committee (Comitêe Ética em Pesquisa do Instituto de Gestão Estratég-ca de Saúde do Distrito Federal---CEP/IGESDF, Brasília,F, Brazil) on February 26, 2019, with record num-
er 3.172.436, and registered in the Plataforma Brazilhttp://aplicacao.saude.gov.br/plataformabrasil) underhe number CAAE 03627118.3.0000.8153, and at Clinicalrials (NCT03973411). All patients gave formal writtendweo
23
nior, R.C. Gersanti et al.
nformed consent, and all information were deidentified.his trial followed the Consolidated Standards of Reportingrials (CONSORT) reporting guideline.
articipants
e included patients that were scheduled for urgent orlective surgical procedures requiring spinal anesthesia.urgeries from all medical specialties were allowed. Eligi-le patients were 18 years of age or older with Americanociety of Anesthesiologists (ASA) physical status I, II, or III.xclusion criteria were patients with any contraindication or
history of hypersensitivity to the drugs used in the study,se of clonidine during the spinal anesthesia, patients usingrophylactic or therapeutic anticoagulation treatments. Welso excluded patients with atrioventricular block in anyegree, diagnosed with cardiac arrhythmias, heart failureatients, kidney disease, liver diseases, any type of sus-ected systemic or localized infection at the puncture site,r any contraindication to the neuroaxial anesthesia.
nterventions
n the operating room, all patients received standard mon-toring, which included electrocardiography, pulse oxygenaturation, noninvasive blood pressure monitoring, andody temperature. After venous access, patients received.05 mg.kg−1 midazolam Intravenous (IV). Crystalloids weredministered at a volume of 10 mL.kg−1 before to spinalnesthesia. Deidentified syringes (20 mL) containing eitherndansetron (8 mg) or placebo (distilled water) was deliv-red to the theatre and administered 5 minutes beforepinal anesthesia, which was then performed with hyper-aric bupivacaine (15 mg or more), and adjuvants opioidst the discretion of the anesthesiologist, except clonidine.pinal anesthesia was performed in a sitting position andatients were placed in a supine position immediately afterhe injection. Patients remained in a supine position for theuration of the study (30 minutes). After this period, theurgery was started.
utcomes
he primary outcome was the proportion of patients withypotension during surgery. Hypotension was defined as sys-olic blood pressure (SBP) below 80% of control or below0 mmHg. Secondary outcomes included the proportion ofatients with bradycardia, vasopressors usage, and varia-ions in blood pressure and Heart Rate (HR). Baseline SBPnd HR values were recorded, as well as after anxiolysis, 5inutes, 10 minutes, 15 minutes, 20 minutes, and 30 min-
tes after spinal anesthesia. We calculated the differenceetween the highest and lowest systolic blood pressure andeart rate (reported as change in SBP and HR) and identifiedhe lowest value noted during the study time. Bradycar-
ia was defined as an HR of below 50 beats/min. Patientsere also given atropine 0.5 mg in case of bradycardia andphedrine 5 mg in case of hypotension. All patients receivedxygen (100%) through a face mask after spinal anesthesia.4

esio
S
BtMwc1ttdciptep
R
WridtEoir
B
Tpgtv
S
NticvwaeFiwapcsays(i
tdmRS
S
Bsa
R
Focictbas
P
Tog
S
Fcvpsatsc
S
Fapooi0o
Brazilian Journal of Anesth
ample size
ased on data from a pilot study, we assumed that 45% ofhe patients would have hypotension after spinal anesthesia.oreover, we hypothesized that treatment with ondansetronould result in a 30% risk difference in the rate hypotensionompared to placebo (15% vs. 45%). Thus, a sample size of00 patients (50 per group) was initially planned to give therial 90% power an alpha level of 5% (two-sided). However,he sample size was recalculated with the availability of trialata, and we updated sample size parameters for a moreonservative treatment difference (17.5% vs. 45%). Allow-ng for a potential 20% dropout rate, we calculated that 70atients per group (a total of 140) would be required to givehe trial 90% power to detect this updated treatment differ-nce. Sample size calculations were performed with the weblatform (https://clincalc.com/stats/samplesize.aspx).
andomization sequence, allocation concealment
e used a computer-generated, centrally concealed 1:1andomization sequence. An independent investigator notnvolved in patient surgery or follow-up generated the ran-om sequence list and randomly allocated patients intowo groups via the Sequentially Numbered Opaque Sealednvelopes (SNOSE) technique. Syringes containing eitherndansetron or placebo were prepared centrally by the samenvestigator, precoded, and sent sequentially to the surgicaloom right before its administration.
linding
his is a double-blind study at the level of patients, careroviders, and outcome assessors. Anesthesiologists, sur-eons, and operating personnel did not know which studyreatment was used. Syringes were identical in terms ofolume, color, viscosity, and odor.
tatistical methods
ormality assumptions were assessed with the Shapiro-Wilkest. Between-group differences at baseline were exam-ned with Chi-Square or Fisher’s Exact tests for binary andategorical outcomes. Continuous variables were comparedia unpaired Student’s t-tests. A logistic-regression modelas fitted with binary dependent variables and stratifiedccording to age. We used linear mixed-effects models toxamine the effect of ondansetron vs. placebo over time.ixed effects were time and treatment group. Time wasncluded in the models as a categorical variable. Modelsere constructed with interactions terms between timend treatment group and had a random intercept for eachatient. Holm-Šídák correction was applied for multipleomparisons. In a non-prespecified analysis, we fitted theame models with interaction terms for time, treatment,nd age, defined as a binary variable (≥ 60 years vs. < 60
ears).15 A two-tailed p < 0.05 was considered statisticallyignificant. Analyses were based on the Intention-To-TreatITT) principle, in which all randomized patients werencluded in the analyses as randomized and contributedggtw
23
logy 2021;71(3):233---240
o the analyses. Results are summarized as mean (Stan-ard Deviation---SD), mean (95% Confidence Interval---95% CI),ean difference (95% CI), counts (percentage), or Oddsatio (OR) with 95% CI. All analyses were performed withtata 16.0 (CollegeStation, TX, USA).
ubgroup analyses
ased on clinical grounds, we performed a non-prespecifiedubgroup analysis comparing elderly patients (60 years ofge or older) to non-elderly patients (< 60 years of age).
esults
rom July 2019 through December 2019, we screened a totalf 188 patients for eligibility. Of these, 144 met all inclusionriteria and were randomized (72 per group). Four patientsn the placebo group received a dose of hyperbaric bupiva-aine below the recommended by the study protocol, buthey were included in the ITT analysis (Figure 1). Overall,oth groups were comparable with respect to demographicnd baseline clinical characteristics (Table 1). No deaths orerious complications occurred.
rimary outcomes
he risk of hypotension was 27.8% (20 of 72 patients) in thendansetron group and 50% (36 of 72 patients) in the placeboroup (OR = 0.38; 95% CI 0.19 to 0.77; p = 0.007) (Table 2).
econdary outcomes
ewer patients in the ondansetron group required ephedrineompared to the placebo group (13.9% [10 of 72 patients]s. 27.8% [20 of 72 patients]; OR = 0.42; 95% CI 0.18 to 0.98;
= 0.04) (Table 2). Other prespecified secondary outcomes,uch as blood pressure levels at 5, 10, 15, 20, and 30 minutesfter anxiolysis, did not differ substantially between thewo groups (Table 2). No secondary outcomes remainedtatistically significant after a Holm-Šídák multiple testingorrection.
ubgroup analyses
or the primary outcome, elderly patients demonstrated greater benefit with ondansetron compared to youngeratients (p = 0.03 for interaction) (Figure 2). Hypotensionccurred in 5 out of 18 elderly patients (27.8%) in thendansetron group and in 19 out of 25 elderly patientsn the placebo group (76%) (OR = 0.12; 95% CI 0.03 to.48; p = 0.003). In the non-elderly subgroup, hypotensionccurred in 15 out of 54 patients (27.8%) in the ondansetron
roup and in 17 out of 47 patients (36.2%) in the placeboroup (OR = 0.68; 95% CI 0.29 to 1.58; p = 0.37) (Supplemen-ary Tables S1 and S2). This age-related interaction effectas not observed in any secondary outcome.5

F.T. Mendonça, L.C. Crepaldi Junior, R.C. Gersanti et al.
Foll ow-Up
AnalysisInclu ded i n analys is (n=72)� ITT analys is (n=72)
All oca tion
Inclu ded i n analys is (n=72)� ITT analys is (n=72 )
Lost to follow-up ( n=0)
Discontinued i nterventi on (n=0)
Lost to follow-up (n=0)
Discontinued i nterventi on (n=4) pati ents receive d s maller anaest hetic do ses
Enrollment
Allocated to placebo (n=72)�Rec eive d pla cebo (n=72 )� Did not receive placebo (n=0)
Allocated to ondan setron (n=72)�Rec eive d ondan setron (n=72 )� Did not receive ondan setron (n=0)
Rando mize d (n=14 4)
Excluded (n=44)� Not meeting inclusion criteria (n=42)� Declin ed to particip ate (n=2)� Othe r rea sons (n=0)
Ass essed for eligibil ity (n=18 8)
Figure 1 Study flow chart (CONSORT standard).
Figure 2 Efficacy of ondansetron vs. placebo to prevent spinal anesthesia-induced hypotension in patients undergoing non-obstetric surgeries. Results were stratified by age (elderly [≥ 60 years] vs. non-elderly [< 60 years]). Squares represent Odds Ratio(OR) estimates computed via logistic regression models (ITT analyses). Horizontal lines depict 95% Confidence Intervals (95% CI).The center of the diamond summarizes the overall effect, and its width represents the overall 95% CI. P for interaction is the resultf udeds el, n
D
IucohpgcmcoFttp2a
ac
chtnittmbrwta
rom a likelihood-ratio test, indicating that the model that inclignificantly better compared to the simpler model (nested mod
iscussion
n this randomized, double-blind trial involving patientsndergoing urgent or elective surgeries of different medi-al specialties, the prophylactic intravenous administrationf ondansetron resulted in a significantly lower rate ofypotension induced by spinal anesthesia when compared tolacebo. Consequently, fewer patients in the ondansetronroup required ephedrine during the surgical procedureompared to the placebo group. Although this result wasarginally significant at the statistical level, at the clini-
al level we believe that the observed difference betweenndansetron and placebo can be of major clinical relevance.or instance, as a measure of projected impact, based onhe observed control event rate of 28%, we calculated that
he use of ondansetron would result in a reduction of 139atients requiring ephedrine per 1,000 surgeries (95% CI: 5 to13). Interestingly, we also noticed that older patients hadhigher risk of hypotension and that ondansetron may have
vtB
23
an age × treatment interaction term fitted the observed datao interaction).
more pronounced anti-hypotensive effect in the elderlyompared to younger patients.
Although spinal anesthesia is considered a safe pro-edure, it may be associated with complications such asypotension and bradycardia. Previous studies indicate thathe rate of hypotension and bradycardia after the subarach-oid block is substantial, ranging from 10% to 80%.1,2,4 Its believed that the hypotension during spinal anesthesia isriggered by the Bezold-Jarisch (BJ) reflex, a cardiorespira-ory reflex evoked by the stimulation of serotonin-sensitiveechanoreceptors and chemoreceptors (5-HT3 receptors),ut also by 5-HT1B/1D, 5-HT7 and 5-HT2A/2B receptors. Theeceptors are in the ventricular walls, the afferent path-ay is nonmyelinated vagal C-fibers to the medulla, and
he efferent pathway includes an increased vagal activitys well as an inhibition of sympathetic outflow producing
asodilation, bradycardia, and hypotension. These recep-ors can be activated not only by hypervolemia (i.e., ‘‘true’’J reflex) but also by hypovolemia, such as that caused by6

Brazilian Journal of Anesthesio
Table 1 Baseline demographic and clinical characteristicsof the study participants.
Placebo(n = 72)
Ondansetron(n = 72)
Age, mean (SD), y 51.0 (17.3) 47.4 (16.5)Height, mean (SD), cm 166.7 (8.8) 169.7 (9.5)Weight, mean (SD), kg 72.9 (17.8) 72.7 (13.5)Males, n (%) 41 (56.9) 49 (68.1)ASA, n (%)I 14 (19.4) 21 (29.2)II 46 (63.4) 40 (55.6)III 12 (16.7) 11 (15.3)Hypertension, n (%) 25 (34.7) 23 (31.9)ACE inhibitors or ARBs usage,
n (%)23 (31.9) 18 (25.0)
Type-2 diabetes, n (%) 13 (18.1) 11 (15.3)Obesity, n (%) 8 (11.1) 10 (13.9)Elderly, n (%) 25 (34.7) 18 (25.0)Medical speciality, n (%)General surgery 4 (5.6) 2 (2.8)Oncological surgery 3 (4.2) 2 (2.8)Vascular surgery 13 (18.1) 7 (9.7)Urology 13 (18.1) 20 (27.8)Proctology 6 (8.3) 4 (5.6)Gynecology 2 (2.8) 3 (4.2)Orthopedics 31 (43.1) 34 (47.2)Bupivacaine, mean (SD), mg 15.4 (2.7) 16.0 (2.6)Morphine usage, n (%) 61 (84.7) 61 (84.7)Morphine dose, mean (SD),
mcg94.4 (24.4) 92.3 (16.1)
Analgesia level, n (%)T4 5 (6.9) 2 (2.8)T6 21 (29.2) 19 (26.4)T8 20 (27.8) 18 (25)T10 24 (33.3) 23 (31.9)T12 2 (2.8) 10 (13.9)
setaipbBsdilcdopatia
FseaTpTca
ttst(oaahpaaTeataawiusdsyrveva
ebirbiittjpma
tsa
ASA, American Society of Anesthesiologists physical status; SD,Standard Deviation. ACE, Angiotensin-Converting Enzyme; ARBs,Angiotensin Receptor Blockers.
pinal anesthesia due to its vasoconstriction-inhibiting prop-rties. Another mechanism exists during spinal anesthesia,he reverse Bainbridge reflex.16 During high and low spinalnesthesia, BP, HR and right atrial pressure are all decreasedn the same proportion, and the intensity of bradycardia isroportional to the drop in BP. Concerning this reverse Bain-ridge reflex, the pathway shares the same vagal way thanJ, but this reverse BR facilitates vagal outflow and inhibitsympathetic outflow to the sinoatrial node causing bradycar-ia. If 5-HT3 are associated with cardioreceptors involvedn the BR response to inhibit sympathetic neurons at theevel of the brainstem, other systems are potentially asso-iated with the physiology of hypotension/low heart rateuring spinal anesthesia. The Medial Septum/vertical limbf the Diagonal Band complex (MSDB) influences the hip-ocampus through projections from cholinergic, GABAergic,
nd glutamatergic neurons, and is implicated in the con-rol of BP. 5-HT3 receptors at the MSDB produce a tonicnhibitory action of the sympathetic pathway that is medi-ted via the local release of angiotensin in the MS/vDB.17mwse
23
logy 2021;71(3):233---240
rom a physiological point of view, during spinal anesthe-ia, the cardioinhibitory afferents fibers act as a protectiveffect to counteract the redistributive hypovolemic statend do not represent, strictly speaking, a pure BJ reflex.hese effects can occur at any point during anesthesia mayrogress to cardiac arrest without proper treatment.5,8,18
hus, the identification of therapeutic strategies that effi-iently prevent these reflexes in patients undergoing spinalnesthesia can be highly valuable for anesthesiologists.
Herein, we showed that the prophylactic administra-ion of ondansetron is an attractive alternative to decreasehe incidence of hypotension induced by spinal anesthe-ia in non-obstetric patients. Most notably, we show thathis effect was significantly evident in elderly patients≥ 60 years). Consistent with previous reports showing thatndansetron prevents complications related to spinal block-de in geriatric patients,7,19,20 we also observed that thedministration of ondansetron prior to anesthesia preventsypotension without affecting the heart rate of theseatients. In older patients, inflammation, oxidative stress,nd endothelial dysfunction can lead to an increased inrterial stiffness and a decreased vascular distensibility.he consequences are higher SBP and pulse pressure lev-ls, augmented left ventricular contraction and afterload,s well as a reduction in coronary perfusion and left ven-ricular early diastolic filling.21 We observed that patientsged over 60 years displayed higher baseline SBP levels and
greater mean change than younger. Aging is also associatedith a decreased response to beta-adrenergic drugs and an
ncrease in the parasympathetic state which, in turn, atten-ates cardiopulmonary reflex and baroreflex.22 A previoustudy on low-dose spinal anesthesia study detected a higherrop in cardiac index, left ventricular stroke volume andystemic vascular resistance in older patients compared toounger.20 Another plausible explanation for these resultselies on the fact that approximately 80% of the bloodolume is stored in veins and that age-related vessel stiff-ning may dampen the ability to cushion changes in bloodolume, such as that caused by vasodilation during spinalnesthesia.23
Moreover, we cannot fully exclude that the preventiveffect observed predominantly in the elderly group might beecause these patients are more susceptible to hypotensionnduced by the BJ reflex. In line with this hypothesis, it isecognized that geriatric patients usually display decreasedlood flow from the superior and inferior vena cava thats gradually intensified with advancing age.24 The decreasen blood flow related to vascular stiffness associated withhe vasodilation provoked by neuraxial block could explainhe important reduction in preload in geriatric patients andustify why the BJ reflex is more active in this group ofatients. Thus, it is conceivable that ondansetron would beore effective in preventing hypotension induced by spinal
nesthesia in elderly patients by blocking this reflex.Previous studies involving obstetric patients observed
hat patients that received 4 mg of ondansetron before toubarachnoid block had a lower incidence of hypotensionnd consumption of vasopressors, suggesting the involve-
ent of the inhibition of the BJ reflex.13,25,26 While our trialas conducted with a non-obstetric population, it is still pos-ible to draw a parallel between pregnant women and thelderly since both have an important physiological reduction
7
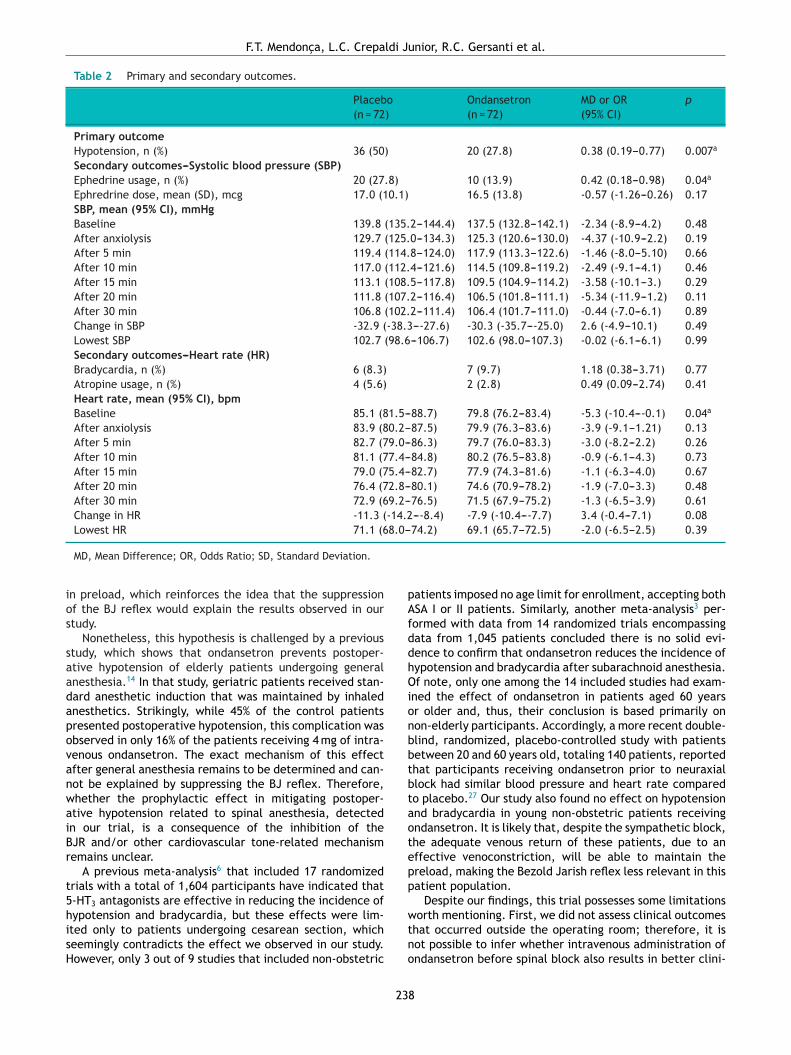
F.T. Mendonça, L.C. Crepaldi Junior, R.C. Gersanti et al.
Table 2 Primary and secondary outcomes.
Placebo(n = 72)
Ondansetron(n = 72)
MD or OR(95% CI)
p
Primary outcomeHypotension, n (%) 36 (50) 20 (27.8) 0.38 (0.19---0.77) 0.007a
Secondary outcomes---Systolic blood pressure (SBP)Ephedrine usage, n (%) 20 (27.8) 10 (13.9) 0.42 (0.18---0.98) 0.04a
Ephredrine dose, mean (SD), mcg 17.0 (10.1) 16.5 (13.8) -0.57 (-1.26---0.26) 0.17SBP, mean (95% CI), mmHgBaseline 139.8 (135.2---144.4) 137.5 (132.8---142.1) -2.34 (-8.9---4.2) 0.48After anxiolysis 129.7 (125.0---134.3) 125.3 (120.6---130.0) -4.37 (-10.9---2.2) 0.19After 5 min 119.4 (114.8---124.0) 117.9 (113.3---122.6) -1.46 (-8.0---5.10) 0.66After 10 min 117.0 (112.4---121.6) 114.5 (109.8---119.2) -2.49 (-9.1---4.1) 0.46After 15 min 113.1 (108.5---117.8) 109.5 (104.9---114.2) -3.58 (-10.1---3.) 0.29After 20 min 111.8 (107.2---116.4) 106.5 (101.8---111.1) -5.34 (-11.9---1.2) 0.11After 30 min 106.8 (102.2---111.4) 106.4 (101.7---111.0) -0.44 (-7.0---6.1) 0.89Change in SBP -32.9 (-38.3----27.6) -30.3 (-35.7----25.0) 2.6 (-4.9---10.1) 0.49Lowest SBP 102.7 (98.6---106.7) 102.6 (98.0---107.3) -0.02 (-6.1---6.1) 0.99Secondary outcomes---Heart rate (HR)Bradycardia, n (%) 6 (8.3) 7 (9.7) 1.18 (0.38---3.71) 0.77Atropine usage, n (%) 4 (5.6) 2 (2.8) 0.49 (0.09---2.74) 0.41Heart rate, mean (95% CI), bpmBaseline 85.1 (81.5---88.7) 79.8 (76.2---83.4) -5.3 (-10.4----0.1) 0.04a
After anxiolysis 83.9 (80.2---87.5) 79.9 (76.3---83.6) -3.9 (-9.1---1.21) 0.13After 5 min 82.7 (79.0---86.3) 79.7 (76.0---83.3) -3.0 (-8.2---2.2) 0.26After 10 min 81.1 (77.4---84.8) 80.2 (76.5---83.8) -0.9 (-6.1---4.3) 0.73After 15 min 79.0 (75.4---82.7) 77.9 (74.3---81.6) -1.1 (-6.3---4.0) 0.67After 20 min 76.4 (72.8---80.1) 74.6 (70.9---78.2) -1.9 (-7.0---3.3) 0.48After 30 min 72.9 (69.2---76.5) 71.5 (67.9---75.2) -1.3 (-6.5---3.9) 0.61Change in HR -11.3 (-14.2----8.4) -7.9 (-10.4----7.7) 3.4 (-0.4---7.1) 0.08Lowest HR 71.1 (68.0---74.2) 69.1 (65.7---72.5) -2.0 (-6.5---2.5) 0.39
ios
saadapovanwaiBr
t5hisH
pAfddhOionbbtbtaotepp
MD, Mean Difference; OR, Odds Ratio; SD, Standard Deviation.
n preload, which reinforces the idea that the suppressionf the BJ reflex would explain the results observed in ourtudy.
Nonetheless, this hypothesis is challenged by a previoustudy, which shows that ondansetron prevents postoper-tive hypotension of elderly patients undergoing generalnesthesia.14 In that study, geriatric patients received stan-ard anesthetic induction that was maintained by inhalednesthetics. Strikingly, while 45% of the control patientsresented postoperative hypotension, this complication wasbserved in only 16% of the patients receiving 4 mg of intra-enous ondansetron. The exact mechanism of this effectfter general anesthesia remains to be determined and can-ot be explained by suppressing the BJ reflex. Therefore,hether the prophylactic effect in mitigating postoper-tive hypotension related to spinal anesthesia, detectedn our trial, is a consequence of the inhibition of theJR and/or other cardiovascular tone-related mechanismemains unclear.
A previous meta-analysis6 that included 17 randomizedrials with a total of 1,604 participants have indicated that-HT3 antagonists are effective in reducing the incidence of
ypotension and bradycardia, but these effects were lim-ted only to patients undergoing cesarean section, whicheemingly contradicts the effect we observed in our study.owever, only 3 out of 9 studies that included non-obstetricwtno
23
atients imposed no age limit for enrollment, accepting bothSA I or II patients. Similarly, another meta-analysis3 per-ormed with data from 14 randomized trials encompassingata from 1,045 patients concluded there is no solid evi-ence to confirm that ondansetron reduces the incidence ofypotension and bradycardia after subarachnoid anesthesia.f note, only one among the 14 included studies had exam-
ned the effect of ondansetron in patients aged 60 yearsr older and, thus, their conclusion is based primarily onon-elderly participants. Accordingly, a more recent double-lind, randomized, placebo-controlled study with patientsetween 20 and 60 years old, totaling 140 patients, reportedhat participants receiving ondansetron prior to neuraxiallock had similar blood pressure and heart rate comparedo placebo.27 Our study also found no effect on hypotensionnd bradycardia in young non-obstetric patients receivingndansetron. It is likely that, despite the sympathetic block,he adequate venous return of these patients, due to anffective venoconstriction, will be able to maintain thereload, making the Bezold Jarish reflex less relevant in thisatient population.
Despite our findings, this trial possesses some limitations
orth mentioning. First, we did not assess clinical outcomeshat occurred outside the operating room; therefore, it isot possible to infer whether intravenous administration ofndansetron before spinal block also results in better clini-
8

esio
catebosoprrHasis
C
IohtOogsle
C
T
A
WAes
B
A
Sbj
R
1
1
1
1
1
1
1
1
1
1
2
2
2
Brazilian Journal of Anesth
al outcomes after surgery. Second, Postoperative Nauseand Vomiting (PONV) is a patient-relevant endpoint, buthese outcomes were not considered in this trial because theffectiveness of ondansetron in the prophylaxis of PONV haseen established previously.28---30 Third, the generalizabilityf our results for the elderly population may be limited,ince older patients accounted for approximately one-thirdf our patients only. Fourth, the sample size for the non-respecified subgroup analyses (elderly vs. non-elderly) iselatively small. This reduced sample size for each subgroupestricts the conclusions that can be drawn from our trial.ence, our findings suggesting a treatment-by-age inter-ction should be regarded as exploratory only, and largertudies are needed to elucidate the role of ondansetronn the prevention of spinal anesthesia-induced hypotensionpecifically in older populations.
onclusion
n conclusion, the prophylactic administration ofndansetron resulted in significantly lower rates ofypotension induced by spinal anesthesia when comparedo placebo, especially in patients aged 60 years or older.ur results indicate not only that the prophylactic use ofndansetron can reduce the usage of ephedrine duringeneral non-obstetric surgical procedures that requirepinal anesthesia, but also that ondansetron may help toimit the side effects related to spinal block particularly inlderly patients.
onflicts of interest
he authors declare no conflicts of interest.
cknowledgements
e would like to thank all colleagues in the Department ofnesthesiology of the Hospital de Base do Distrito Federal,specially Dr. Nadja Glória Correa Graça, for supporting thetudy.
Preliminary data for this study were presented at therazilian Anesthesiology Congress (CBA) in November 2019.
ppendix A. Supplementary data
upplementary data associated with this article cane found, in the online version, at doi:10.1016/.bjane.2020.12.028.
eferences
1. Carpenter RL, Caplan RA, Brown DL, et al. Incidence and riskfactors for side effects of spinal anesthesia. Anesthesiology.1992;76:906---16.
2. Liu SS, McDonald SB. Current issues in spinal anesthesia. Anes-thesiology. 2001;94:888---906.
3. Terkawi AS, Mavridis D, Flood P, et al. Does ondansetronmodify sympathectomy due to subarachnoid anesthesia?:meta-analysis, meta-regression, and trial sequential analysis.Anesthesiology. 2016;124:846---69.
2
2
23
logy 2021;71(3):233---240
4. Pereira IDF, Grando MM, Vianna PTG, et al. Retrospective analy-sis of risk factors and predictors of intraoperative complicationsin neuraxial blocks at Faculdade de Medicina de Botucatu-UNESP. Rev Bras Anestesiol. 2011;61:574---81.
5. Campagna JA, Carter C. Clinical relevance of the Bezold-Jarischreflex. Anesthesiology. 2003;98:1250---60.
6. Heesen M, Klimek M, Hoeks SE, et al. Prevention of spinalanesthesia-induced hypotension during cesarean delivery by5-hydroxytryptamine-3 receptor antagonists: a systematicreview and meta-analysis and meta-regression. Anesth Analg.2016;123:977---88.
7. Owczuk R, Wenski W, Twardowski P, et al. Ondansetron attenu-ates the decrease in blood pressure due to spinal anesthesia inthe elderly: a double blind, placebo-controlled study. MinervaAnestesiol. 2015;81:598---607.
8. Kashihara K. Roles of arterial baroreceptor reflex during bezold-jarisch reflex. Curr Cardiol Rev. 2009;5:263---7.
9. Walsh M, Devereaux PJ, Garg AX, et al. Relationship betweenintraoperative mean arterial pressure and clinical outcomesafter noncardiac surgery: toward an empirical definition ofhypotension. Anesthesiology. 2013;119:507---15.
0. Tyers MB, Freeman AJ. Mechanism of the anti-emetic activityof 5-HT3 receptor antagonists. Oncology. 1992;49:263---8.
1. Owczuk R, Wenski W, Polak-Krzeminska A, et al. Ondansetrongiven intravenously attenuates arterial blood pressure drop dueto spinal anesthesia: a double-blind, placebo-controlled study.Reg Anesth Pain Med. 2008;33:332---9.
2. Wang M, Zhuo L, Wang Q, et al. Efficacy of prophylactic intra-venous ondansetron on the prevention of hypotension duringcesarean delivery: a dose-dependent study. Int J Clin Exp Med.2014;7:5210---6.
3. Trabelsi W, Romdhani C, Elaskri H, et al. Effect of ondansetronon the occurrence of hypotension and on neonatal parame-ters during spinal anesthesia for elective caesarean section: aprospective, randomized, controlled, double-blind study. Anes-thesiol Res Pract. 2015;2015:158061.
4. Golparvar M, Saghaei M, Saadati MA, Farsaei S. Effect ofondansetron on prevention of post-induction hypotension inelderly patients undergoing general anesthesia: A randomized,double-blind placebo-controlled clinical trial. Saudi J Anaesth.2015;9:365---9.
5. Carmona MJC, Simões CM. Paciente 4.0---O desafio do cuidadoaos pacientes muito idosos. Rev Bras Anestesiol. 2020;70:1---2.
6. Crystal GJ, Salem MR. The Bainbridge and the ‘‘Reverse’’ Bain-bridge Reflexes: History. Physiology, and Clinical Relevance.Anesth Analg. 2012;114:520---32.
7. Urzedo-Rodrigues LS, Ferreira HS, Almeida DO, et al. Blockadeof 5-HT3 receptors at septal area increase blood pressure inunanaesthetized rats. Auton Neurosci. 2011;159:51---61.
8. Kinsella SM, Tuckey JP. Perioperative bradycardia and asystole:relationship to vasovagal syncope and the Bezold-Jarisch reflex.Br J Anaesth. 2001;86:859---68.
9. Raghu K, Kumar S, Rajaram G, et al. Effect of ondansetron inthe prevention of spinal anesthesia-induced hypotension. J SciSoc. 2018;45:125.
0. Lairez O, Ferré F, Portet N, et al. Cardiovascular effects oflow-dose spinal anaesthesia as a function of age: An obser-vational study using echocardiography. Anaesth Crit Care PainMed. 2015;34:271---6.
1. Wu J, Xia S, Kalionis B, Wan W, Sun T. The Role of OxidativeStress and Inflammation in Cardiovascular Aging. Biomed ResInt. 2014:2014.
2. Monahan KD. Effect of aging on baroreflex function in humans.Am J Physiol Regul Integr Comp Physiol. 2007;293:R3---12.
3. Alvis BD, Hughes CG. Physiology considerations in geriatricpatients. Anesthesiol Clin. 2015;33:447---56.
4. Wehrum T, Lodemann T, Hagenlocher P, et al. Age-relatedchanges of right atrial morphology and inflow pattern assessed
9
ldi Ju
2
2
2
2
2
3
postoperative nausea and vomiting in obese adult patientsundergoing laparoscopic sleeve gastrectomy during closed-looppropofol-remifentanil anaesthesia: A randomised double-blind
F.T. Mendonça, L.C. Crepa
using 4D flow cardiovascular magnetic resonance: results ofa population-based study. J Cardiovasc Magnetic Res. 2018;20:38.
5. Rashad MM, Farmawy MS. Effects of intravenous ondansetronand granisetron on hemodynamic changes and motor and sen-sory blockade induced by spinal anesthesia in parturientsundergoing cesarean section. Egypt J Anaesth. 2013;29:369---74.
6. Marciniak A, Owczuk R, Wujtewicz M, et al. The influence ofintravenous ondansetron on maternal blood haemodynamicsafter spinal anaesthesia for caesarean section: a double-blind,placebo-controlled study. Ginekol Pol. 2015;86:461---7.
7. Tatikonda CM, Rajappa GC, Rath P, et al. Effect of intra-venous ondansetron on spinal anesthesia-induced hypotensionand bradycardia: a randomized controlled double-blinded study.Anesth Essays Res. 2019;13:340---6.
24
nior, R.C. Gersanti et al.
8. Figueredo ED, Canosa LG. Ondansetron in the prophylaxisof postoperative vomiting: a meta-analysis. J Clin Anesth.1998;10:211---21.
9. Cox F. Systematic Review of Ondansetron for the Prevention andTreatment of Postoperative Nausea and Vomiting in Adults. BritJ Theat Nurs. 1999;9:556---66.
0. Bataille A, Letourneulx J-F, Charmeau A, et al. Impact of aprophylactic combination of dexamethasone-ondansetron on
placebo-controlled study. Eur J Anaesthesiol. 2016;33:898---905.
0

C
Eoa
Y
AR
RA
A
h©l
Brazilian Journal of Anesthesiology 2021;71(3):241---246
LINICAL RESEARCH
ffect of anesthesia induction on cerebral tissuexygen saturation in hypertensive patients:n observational study�
asin Taşkaldıran ∗, Özlem Şen, Tuğba Aşkın, Süheyla Ünver
nesthesiology and Reanimation, Health Sciences University Dr. Abdurrahman Yurtaslan Oncology Health Application andesearch Center, Ankara, Turkey
eceived 7 January 2019; accepted 25 October 2020vailable online 6 February 2021
KEYWORDSAnesthesia induction;Cerebral tissueoxygen saturation;Hypertension
AbstractObjective: In hypertensive patients, the autoregulation curve shifts rightward, making thesepatients more sensitive than normotensive individuals to hypotension. Hypotension followingthe induction of anesthesia has been studied in normotensive patients to determine its effectson brain tissue oxygenation, but not enough studies have examined the effect of hypotensionon brain oxygenation in hypertensive patients. The current study aimed to use near-infraredspectroscopy to evaluate brain tissue oxygen saturation after the induction of anesthesia inhypertensive patients, who may have impaired brain tissue oxygen saturation.Methods: The study included a total of 200 patients aged > 18 years old with ASA I---III. Measure-ments were taken while the patient was breathing room air, after the induction of anesthesia,when the lash reflex had disappeared following the induction of anesthesia, after intubation,and in the 5th, 10th, and 15th minutes of surgery. The patients were divided into nonhyperten-sive and hypertensive groups.Results: There was a significant difference in age between the groups (p = 0.000). No corre-lation was found between cerebral tissue oxygen saturation and age (r = 0.015, p = 0.596).Anesthesia induction was observed to decrease mean arterial blood pressure in both groups(p = 0.000). Given these changes, there was no significant difference in brain tissue oxygensaturation between the nonhypertensive and hypertensive groups (p > 0.05).Conclusion: There was no difference between hypertensive and normotensive groups in termsof the change rates in cSO2 values. However, there was a difference between the groups interms of cSO2 values.
© 2021 Sociedade Brasileira deopen access article under the Cnc-nd/4.0/).� Study conducted at the ‘‘Anesthesiology and Reanimation, Health
pplication and Research Center’’.∗ Corresponding author.
E-mail: [email protected] (Y. Taşkaldıran).
ttps://doi.org/10.1016/j.bjane.2021.02.010 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Anestesiologia. Published by Elsevier Editora Ltda. This is an
C BY-NC-ND license (http://creativecommons.org/licenses/by-Sciences University Dr. Abdurrahman Yurtaslan Oncology Health
itora Ltda. This is an open access article under the CC BY-NC-ND

. Şen
I
DaahbchwCmsattikhTsho
M
Twaptttrbcctip
PPzricsCwnwbitmtTamO
waMOaw-iaiwd
shtlci
tCtbwwffblsp0
R
Atr0w((ot4dttsmtaaMi
Y. Taşkaldıran, Ö
ntroduction
uring anesthesia induction, hypotension occurs and mayffect the blood supply to the organs.1 The cerebralutoregulation mechanism protects the blood supply fromypotension. When an individual’s mean blood pressure isetween 60 and 150 mmHg, cerebral blood flow remainsonstant.2 However, when this autoregulation changes,ypotension may lead to a decrease in cerebral blood flow,hich may then cause a decrease in cerebral oxygenation.3
erebral oxygenation can be measured using a noninvasiveethod, the Near-Infrared Spectroscopy (NIRS). In hyperten-
ive patients, there is a change in cerebral autoregulation,nd this alteration causes the cerebral autoregulation curveo shift rightward.4 Hypotension due to anesthesia induc-ion has been studied in normotensive patients in terms ofts effects on brain tissue oxygenation, but to the best of ournowledge, not enough studies have examined the effect ofypotension on brain oxygenation in hypertensive patients.he current study aimed to use NIRS to evaluate brain tis-ue oxygen saturation after the induction of anesthesia inypertensive patients, who may have impaired brain tissuexygen saturation.
ethods
wo hundred patients who were aged over 18 years old,ith American Society of Anesthesiologists (ASA) status I---III,nd scheduled to undergo elective general anesthesia, wererospectively enrolled in the study after ethics commit-ee approval (local ethics committee number: 2017---12/6,rial registry no ACTRN12618000506291) was obtained, andhe patients signed informed consent forms. Patients whoepresented emergency cases, were pregnant, had unsta-le hemodynamics, had cerebrovascular disease, underwentranial surgery, had known carotid disease or previousarotid surgery, were allergic to the drugs of interest inhe current study, or did not want to participate were notncluded in the study. In addition, patients who had a bloodressure > 180/90 mmHg were also excluded.
Oral intake was stopped 8 hours before the operation.atients were given fluids at 100 mL.h−1 until the operation.rior to the operation, 0.01 mg.kg−1 intravenous (IV) mida-olam premedication was administered. In the operatingoom, standard monitoring of the patients was performed,ncluding electrocardiography, noninvasive blood pressure,apnography, and pulse oximetry. In addition, two NIRS sen-ors were placed on the frontal region of the patients.erebral tissue oxygen saturation (cSO2) measurementsere obtained using an INVOSTM 5100C (Medtronic, Min-esota, USA) cerebral/somatic oximeter. Preoxygenationas induced by asking the patient to take three deepreaths of 100% O2 (total flow: 6 L.min−1) prior to thenduction of anesthesia. The induction of general anes-hesia was performed using 2 mg.kg−1 propofol, 0.7---0.9g.kg-1rocuronium, 1 mg.kg-1 lidocaine and 1 �g.kg−1 fen-
anyl and was followed by endotracheal tube placement.
here were no pharmacological interventions betweennesthesia induction and tracheal intubation. Anestheticanagement was ensured using 1 MAC of sevoflurane, 50%2 and N2O. Volume-controlled ventilation was establishedm1so
24
, T. Aşkın et al.
ith a tidal volume: 6 mL.kg−1, PEEP: 5 mmHg, I/E: 1/2,nd FiO2: 40% at a frequency of 12 minutes. All patients’ean Arterial Pressure (MAP), Heart Rate (HR), Peripheralxygen Saturation (SpO2), End-Tidal Carbon Dioxide (ETCO2)nd bilateral cSO2 were measured. The measurement timesere as follows: T1 --- First measurement in room air; T2
-- After the induction of anesthesia; T3 --- After orotrachealntubation; T4 --- 5 minutes after induction; T5 --- 10 minutesfter induction; and T6 --- 15 minutes after induction. Dur-ng anesthesia induction and measurements, noxious stimuliere not applied to the patients, and only the cleaning andisinfection procedures were performed.
The patients were divided into two groups. The Hyperten-ive Group (HT) included patients who were diagnosed withypertension before surgery and received anti-hypertensiveherapy. Hypertension was diagnosed by doctors who fol-owed up the patients; in addition, the diagnosis washecked by health reports. The nonhypertensive groupncluded patients not diagnosed with hypertension.
All data were analyzed using the Statistical Package forhe Social Sciences (SPSS), version 24.0 (SPSS Company,hicago, IL, USA). The Kolmogorov-Smirnov test was usedo determine normality of data distribution. Differencesetween mean values for normally distributed variablesere compared by using the Student’s t-test. For dataithout normal distribution, Mann Whitney U test was per-
ormed. Chi-Squared test and Fisher’s Exact test were usedor categorical data where appropriate. The relationshipsetween the variables were evaluated with Pearson corre-ation tests. A p-value < 0.05 was considered statisticallyignificant. It was estimated that including 200 patients (100atients in each group) would provide a power of 94% (� =.05, d = 0,5).
esults
total of 200 patients were evaluated. In terms of age,he patients in the hypertensive group were older. No cor-elation was found between age and cSO2 (cSO2, Right: r =.015, p = 0.596; cSO2, Left: r = 0.022, p = 0.448). Thereere no differences between the groups in terms of sex
Table 1). The mean length of time to a diagnosis was 8.0± 5.8) years. For hypertensive patients, the mean lengthf time the patients had taken anti-hypertensive drugs prioro surgery was 5.6 (± 2.3) hours. In the hypertension group,2% of the patients used a single medication, and 58% usedouble medication (Table 2). After the induction of anes-hesia, the mean arterial blood pressure decreased, but ithen increased after intubation (p = 0.000). After anesthe-ia induction, the SpO2 levels of the patients increased toore than 98%. End-Tidal CO2 levels did not differ between
he groups (p > 0.05) (Figure 1). The differences in MAPnd cSO2 measurements at T2 and T1 were evaluated forll patients. A weak correlation was detected between theAP and cSO2 levels (r = 0.287, p = 0.000) (Figure 2). After
nduction of anesthesia, MAP decreased from 113.1 (±14.5)
mHg to 85.3 (±18.1) mmHg in hypertensive group and from09.6 (±15.3) mmHg to 87.5 (±17.6) mmHg in nonhyperten-ive group. The decreased rate of MAP in both groups wasver 20%.
2
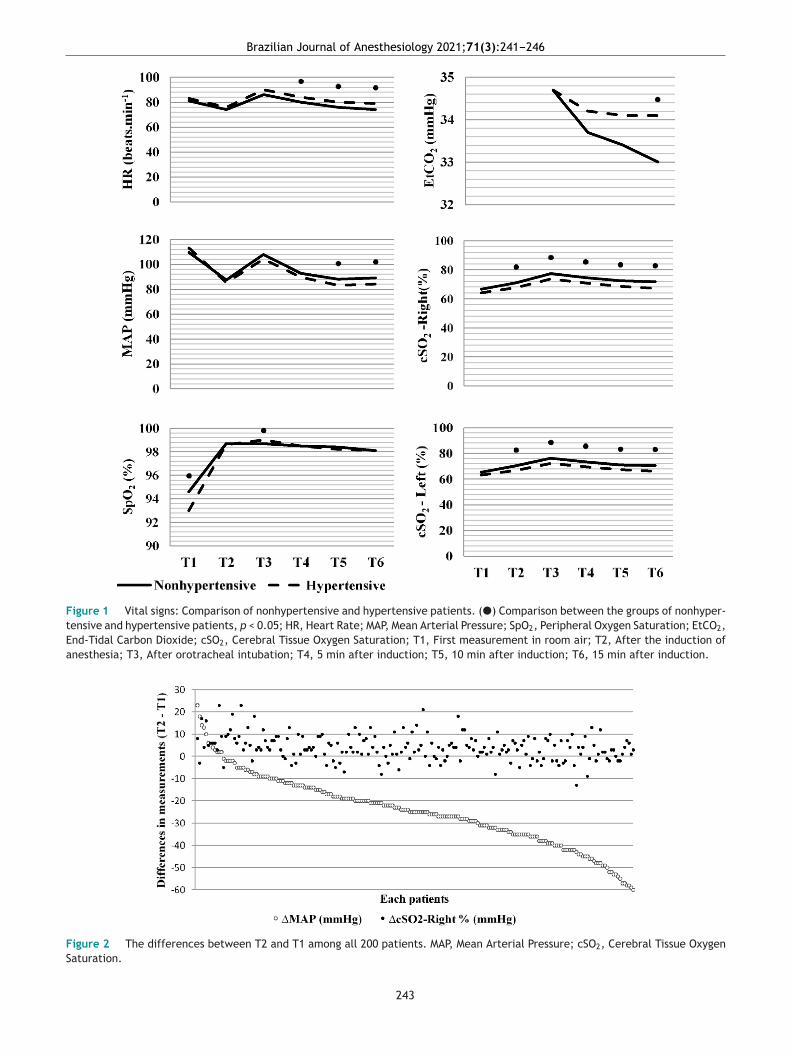
Brazilian Journal of Anesthesiology 2021;71(3):241---246
Figure 1 Vital signs: Comparison of nonhypertensive and hypertensive patients. (�) Comparison between the groups of nonhyper-tensive and hypertensive patients, p < 0.05; HR, Heart Rate; MAP, Mean Arterial Pressure; SpO2, Peripheral Oxygen Saturation; EtCO2,End-Tidal Carbon Dioxide; cSO2, Cerebral Tissue Oxygen Saturation; T1, First measurement in room air; T2, After the induction ofanesthesia; T3, After orotracheal intubation; T4, 5 min after induction; T5, 10 min after induction; T6, 15 min after induction.
Figure 2 The differences between T2 and T1 among all 200 patients. MAP, Mean Arterial Pressure; cSO2, Cerebral Tissue OxygenSaturation.
243
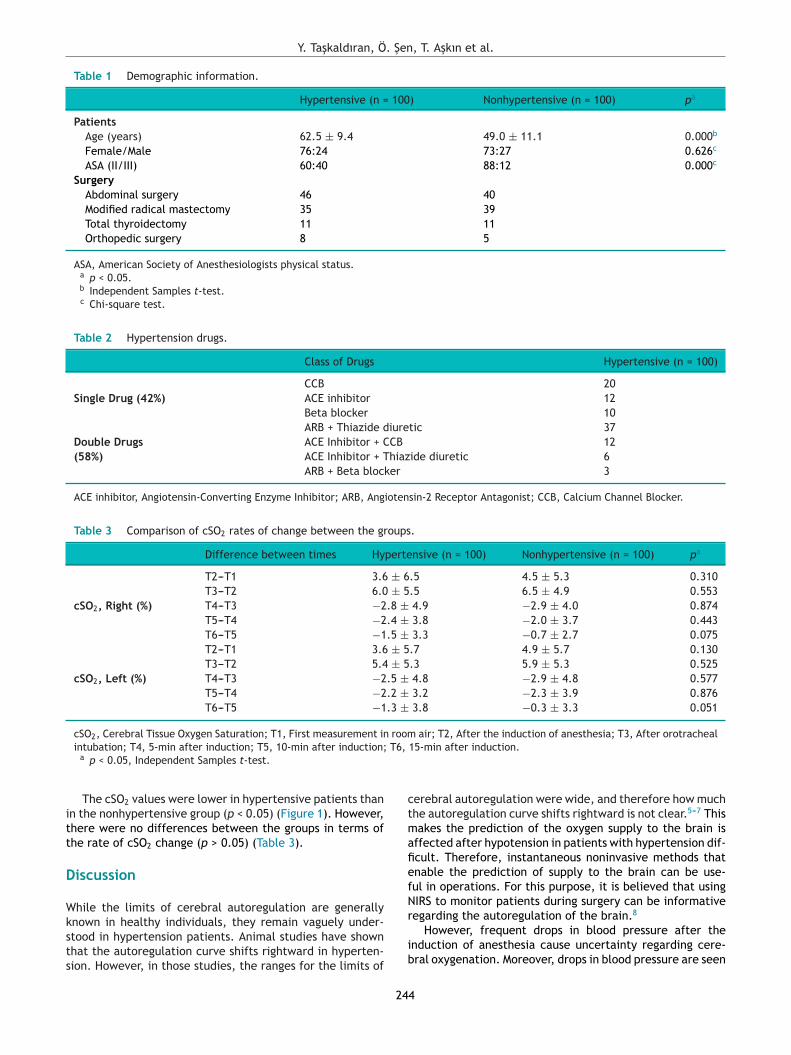
Y. Taşkaldıran, Ö. Şen, T. Aşkın et al.
Table 1 Demographic information.
Hypertensive (n = 100) Nonhypertensive (n = 100) pa
PatientsAge (years) 62.5 ± 9.4 49.0 ± 11.1 0.000b
Female/Male 76:24 73:27 0.626c
ASA (II/III) 60:40 88:12 0.000c
SurgeryAbdominal surgery 46 40Modified radical mastectomy 35 39Total thyroidectomy 11 11Orthopedic surgery 8 5
ASA, American Society of Anesthesiologists physical status.a p < 0.05.b Independent Samples t-test.c Chi-square test.
Table 2 Hypertension drugs.
Class of Drugs Hypertensive (n = 100)
Single Drug (42%)CCB 20ACE inhibitor 12Beta blocker 10
Double Drugs(58%)
ARB + Thiazide diuretic 37ACE Inhibitor + CCB 12ACE Inhibitor + Thiazide diuretic 6ARB + Beta blocker 3
ACE inhibitor, Angiotensin-Converting Enzyme Inhibitor; ARB, Angiotensin-2 Receptor Antagonist; CCB, Calcium Channel Blocker.
Table 3 Comparison of cSO2 rates of change between the groups.
Difference between times Hypertensive (n = 100) Nonhypertensive (n = 100) pa
cSO2, Right (%)
T2---T1 3.6 ± 6.5 4.5 ± 5.3 0.310T3---T2 6.0 ± 5.5 6.5 ± 4.9 0.553T4---T3 −2.8 ± 4.9 −2.9 ± 4.0 0.874T5---T4 −2.4 ± 3.8 −2.0 ± 3.7 0.443T6---T5 −1.5 ± 3.3 −0.7 ± 2.7 0.075
cSO2, Left (%)
T2---T1 3.6 ± 5.7 4.9 ± 5.7 0.130T3---T2 5.4 ± 5.3 5.9 ± 5.3 0.525T4---T3 −2.5 ± 4.8 −2.9 ± 4.8 0.577T5---T4 −2.2 ± 3.2 −2.3 ± 3.9 0.876T6---T5 −1.3 ± 3.8 −0.3 ± 3.3 0.051
cSO2, Cerebral Tissue Oxygen Saturation; T1, First measurement in room air; T2, After the induction of anesthesia; T3, After orotracheal T6,
itt
D
Wksts
ctmafiefN
intubation; T4, 5-min after induction; T5, 10-min after induction;a p < 0.05, Independent Samples t-test.
The cSO2 values were lower in hypertensive patients thann the nonhypertensive group (p < 0.05) (Figure 1). However,here were no differences between the groups in terms ofhe rate of cSO2 change (p > 0.05) (Table 3).
iscussion
hile the limits of cerebral autoregulation are generally
nown in healthy individuals, they remain vaguely under-tood in hypertension patients. Animal studies have shownhat the autoregulation curve shifts rightward in hyperten-ion. However, in those studies, the ranges for the limits ofr
ib
24
15-min after induction.
erebral autoregulation were wide, and therefore how muchhe autoregulation curve shifts rightward is not clear.5---7 Thisakes the prediction of the oxygen supply to the brain is
ffected after hypotension in patients with hypertension dif-cult. Therefore, instantaneous noninvasive methods thatnable the prediction of supply to the brain can be use-ul in operations. For this purpose, it is believed that usingIRS to monitor patients during surgery can be informative
8
egarding the autoregulation of the brain.However, frequent drops in blood pressure after thenduction of anesthesia cause uncertainty regarding cere-ral oxygenation. Moreover, drops in blood pressure are seen
4

esio
msowBik
Ttaocmirs
titwo
ittibnnbiatbddttdbnsai
iririlgcggeWbjw
fthtt
aiabweEmMh
Wabaioiwd
oeotbnup
S
Ihaucdi
T
A
C
T
R
Brazilian Journal of Anesth
ore frequently in hypertensive patients than in normoten-ive patients.9 In normotensive patients, when cerebralxygenation was assessed upon a drop in blood pressure, itas found that cerebral oxygenation was maintained.10,11
ut the effect of hypotension on oxygenation after thenduction of anesthesia in hypertensive patients is notnown.
Propofol causes a decrease in cerebral blood flow.12
his may affect brain oxygenation when combined withhe hypotension that occurs following the induction ofnesthesia.3 However, propofol may preserve cerebralxygenation due to the depression of cerebral electroen-ephalographic activity13 and a decrease in the cerebraletabolic rate.14 In addition, propofol is also effective
n maintaining cerebral autoregulation15 or masking theelationship between hypotension and cerebral oxygenaturation.10
The body’s oxygen reserve also affects cerebral oxygena-ion. With preoxygenation, the SpO2 levels of patients can bencreased to more than 97%.16 Because we used preoxygena-ion to increase our patient’s SpO2 levels from 93% to 98%,e might have contributed to the maintenance of cerebralxygenation by increasing the oxygen reserve.
One of the factors that affects cerebral autoregulations hypertension treatment, but there are differences amonghe efficacies of the drugs used in this treatment. For ins-ance, it was found that angiotensin-converting enzymenhibitors and beta-blockers have only little effect on cere-ral blood flow and cerebral autoregulation.17---19 There isot enough consensus regarding the effects of calcium chan-el antagonists on cerebral autoregulation and cerebrallood flow. Studies on baboons revealed that there was anncrease in cerebral blood flow and no change in cerebralutoregulation,20 while studies performed in rats showedhat cerebral blood flow did not change and that the cere-ral autoregulation curve shifted leftward.21 Due to theifferences and uncertainties among the efficacy of therugs used in hypertension treatment, we did not grouphe patients according to the anti-hypertensive medicationhey were using. Nevertheless, it is known that despite theifferences among these drugs, with treatment, the cere-ral autoregulation curve of these patients verges on that oformotensives.22,23 We believe that the rates of cerebral tis-ue oxygenation changes were similar between hypertensivend normotensive patients as a result of this improvementn autoregulation.
Normal cSO2 levels can be between 55% and 80%, whichs a wide range. Thus, it would be useful to monitor theate of change in measured cSO2 levels instead of check-ng whether the measured cSO2 levels are within the normalange. In this regard, medical intervention is recommendedf basal cSO2 levels drop by 20% or 25% or if the measuredevels are below 50%.24---26 In our study, we found that bothroups exhibited parallel cSO2 changes, and their rates ofhange in cSO2 levels were similar (Figure 1). Moreover, theraphs showed that there is a difference between the tworoups in terms of cSO2 levels; however, while this differ-nce was not clinically significant, it was numerically clear.
e believe that this is due to the difference in cerebrallood flow caused by hypertension. In a study on this sub-ect, follow-up was performed in hypertensive patients whoere treated for 9 years. These follow-ups showed that pre-24
logy 2021;71(3):241---246
rontal blood flow was lower in hypertensive patients underreatment than in normotensive patients. It appears thatypertension treatment is useful for cerebral autoregula-ion but unable to prevent blood flow to different areas ofhe brain.27
While blood pressure is one of the important factorsffecting cerebral blood flow, it is not the single determin-ng factor for cerebral blood flow in patients whose cerebralutoregulation is maintained. In our study, the correlationetween the rate of MAP change and the rate of cSO2 changeas weak. As shown in Figure 2, the changes in cSO2 lev-ls were not affected by the amount of decrease in MAP.nd-organ injury might occur when MAP decreases below 80mHg for more than 10 minutes.28 In our study, the meanAP did not decrease below 80 mmHg by induction. This mayave led to a weak relationship between MAP and cSO2.
Another factor that affects brain metabolism is age.hile aging affects brain metabolism, its effect on cerebral
utoregulation is uncertain. Cerebral autoregulation haseen shown to be similar between individuals between 50nd 75 years old and younger individuals. There is not enoughnformation on the cerebral autoregulation of individualsver 75 years old.29 In our study, the cSO2 changes observedn the older hypertensive group and the normotensive groupere found to be similar. Moreover, a weak correlation wasetected between age and cSO2 levels.
Limitations of this study include the observational naturef this study and the recruitment of patients undergoinglective surgery alone, which prevented an investigationf the effect of nonregulated hypertension. Another limita-ion was the noninvasiveness of the method used to monitorlood pressure. Since the mean MAP value in our study didot decrease below 80 mmHg, this was a limitation to eval-ate to brain tissue oxygen saturation levels at lower bloodressure.
ummary
n conclusion, the results of the study demonstrated thatypotensive response to anesthesia induction did not makeny difference in terms of the change rates in cSO2 val-es in patients receiving antihypertensive therapy whenomparing to normotensive patients. However, there was aifference between hypertensive and normotensive groupsn terms of cSO2 values.
rial registry number
CTRN12618000506291
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Stephan H, Sonntag H, Schenk H, et al. Effects of propofol oncardiovascular dynamics, myocardial blood flow and myocar-dial metabolism in patients with coronary artery disease. Br JAnaesth. 1986;58:969---75.
5
. Şen
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
29. Van Beek AH, Claassen JA, Rikkert MGO, et al. Cerebral autoreg-ulation: an overview of current concepts and methodology
Y. Taşkaldıran, Ö
2. Lassen NA. Cerebral blood flow and oxygen consumption in man.Physiol Rev. 1959;39:183---238.
3. Jaeger M, Soehle M, Schuhmann M, et al. Correlation of contin-uously monitored regional cerebral blood flow and brain tissueoxygen. Acta Neurochir. 2005;147:51---6.
4. Strandgaard S, Olesen J, Skinhøj E, et al. Autoregulation ofbrain circulation in severe arterial hypertension. Br Med J.1973;1:507---10.
5. Strandgaard S, MacKenzie ET, Sengupta D, et al. Upper limit ofautoregulation of cerebral blood flow in the baboon. Circ Res.1974;34:435---40.
6. Strandgaard S, Jones JV, MacKenzie ET, et al. Upper limit ofcerebral blood flow autoregulation in experimental renovascu-lar hypertension in the baboon. Circ Res. 1975;37:164---7.
7. Jones JV, Fitch W, Mackenzie ET, et al. Lower limit of cerebralblood flow autoregulation in experimental renovascular hyper-tension in the baboon. Circ Res. 1976;39:555---7.
8. Moerman A, De Hert S. Recent advances in cerebral oxime-try. Assessment of cerebral autoregulation with near-infraredspectroscopy: myth or reality? F1000Res. 2017;6:1---9.
9. Prys-Roberts C, Meloche R, Foex P, et al. Studies of anaesthe-sia in relation to hypertension I: cardiovascular responses oftreated and untreated patients. Br J Anaesth. 1971;43:122---37.
0. Meng L, Gelb A, McDonagh D. Changes in cerebral tissue oxy-gen saturation during anaesthetic - induced hypotension: aninterpretation based on neurovascular coupling and cerebralautoregulation. Anaesthesia. 2013;68:736---41.
1. Nissen P, Van Lieshout JJ, Nielsen HB, et al. Frontallobe oxygenation is maintained during hypotension followingpropofol-fentanyl anesthesia. AANA J. 2009;77:271---6.
2. Ludbrook GL, Visco E, Lam AM, Ludbrook GL, Visco E, LamAM. Propofol Relation between brain concentrations, elec-troencephalogram, middle cerebral artery blood flow velocity,and cerebral oxygen extraction during ınduction of anesthesia.Anesthesiology. 2002;97:1363---70.
3. Kochs E, Hoffman WE, Werner C, et al. The effects of propofolon brain electrical activity, neurologic outcome, and neuronaldamage following incomplete ischemia in rats. Anesthesiology.1992;76:245---52.
4. Alkire MT, Haier RJ, Barker SJ, et al. Cerebral metabolism duringpropofol anesthesia in humans studied with positron emissiontomography. Anesthesiology. 1995;82:393---403.
5. Ederberg S, Westerlind A, Houltz E, et al. The effects of propofol
on cerebral blood flow velocity and cerebral oxygen extractionduring cardiopulmonary bypass. Anesth Analg. 1998;86:1201---6.6. Nimmagadda U, Chiravuri SD, Salem MR, et al. Preoxygena-tion with tidal volume and deep breathing techniques: the
24
, T. Aşkın et al.
impact of duration of breathing and fresh gas flow. Anesth Analg.2001;92:1337---41.
7. Waldemar G, Schmidt JF, Andersen AR, et al. Angiotensinconverting enzyme inhibition and cerebral blood flow autoreg-ulation in normotensive and hypertensive man. J Hypertens.1989;7:229---35.
8. Britton KE, Granowska M, Nimmon CC, et al. Cerebral bloodflow in hypertensive patients with cerebrovascular disease:technique for measurement and effect of captopril. Nucl MedCommun. 1985;6:251---61.
9. Globus M, Keren A, Eldad M, et al. The effect of chronic propra-nolol therapy on regional cerebral blood flow in hypertensivepatients. Stroke. 1983;14:964---7.
0. McCalden T, Nath R. Cerebrovascular autoregulation is resistantto calcium channel blockade with nimodipine. Cell Mol Life Sci.1989;45:305---6.
1. Cai H, Yao H, Ibayashi S, et al. Amlodipine, a Ca2+ chan-nel antagonist, modifies cerebral blood flow autoregulation inhypertensive rats. Eur J Pharmacol. 1996;313:103---6.
2. Strandgaard S. Autoregulation of cerebral blood flow inhypertensive patients. The modifying influence of prolongedantihypertensive treatment on the tolerance to acute, drug-induced hypotension. Circ Res. 1976;53:720---7.
3. Tryambake D, He J, Firbank MJ, et al. Intensive blood pressurelowering increases cerebral blood flow in older subjects withhypertension. Hypertension. 2013;61:1309---15.
4. Murkin JM, Adams SJ, Novick RJ, et al. Monitoring brain oxy-gen saturation during coronary bypass surgery: a randomized,prospective study. Anesth Analg. 2007;104:51---8.
5. Slater JP, Guarino T, Stack J, et al. Cerebral oxygen desaturationpredicts cognitive decline and longer hospital stay after cardiacsurgery. Ann Thor Surg. 2009;87:36---45.
6. Edmonds HL. Detection and treatment of cerebral hypoxia keyto avoiding intraoperative brain injuries. J Clin Monit Comput.2000;16:69---74.
7. Beason-Held LL, Moghekar A, Zonderman AB, et al. Longitudinalchanges in cerebral blood flow in the older hypertensive brain.Stroke. 2007;38:1766---73.
8. Wesselink EM, Kappen TH, Torn HM, et al. Intraoperativehypotension and the risk of postoperative adverse outcomes:a systematic review. Br J Anaesth. 2018;121:706---21.
with special focus on the elderly. J Cereb Blood Flow Metab.2008;28:1071---85.
6

C
Eor
G
a
b
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):247---253
LINICAL RESEARCH
ffect of preoperative oral liquid carbohydrate intaken blood glucose, fasting-thirst, and fatigue levels: aandomized controlled study
ökçen Aydın Akbuğa a,∗, Mürüvvet Başerb
Bozok University, Faculty of Health Sciences/Surgery Nursing, Yozgat, TurkeyErciyes University, Faculty of Health Sciences/Women’s Health and Childbirth Nursing, Kayseri, Turkey
eceived 19 August 2019; accepted 25 February 2021vailable online 15 April 2021
KEYWORDSFasting;Thirst;Fatigue;Blood glucose
AbstractBackground: This study aimed to analyze the effects of preoperative oral intake of liquid carbo-hydrate on postoperative blood glucose, fasting-thirst, and fatigue levels in patients undergoingarthroscopic surgery.Methods: This randomized controlled clinical trial enrolled 82 patients, who were scheduledto undergo arthroscopic surgery, and divided them into two groups: (1) those who consumed acarbohydrate-rich drink, and (2) those not consuming anything after midnight. Pre- and postop-erative fasting-thirst (visual analog scale) and blood glucose levels were measured. Likewise,the Brief Fatigue Inventory was applied to patients 24 hours after surgery.Results: The mean blood glucose levels in the first postoperative hour were 90.90 ± 13.56mg.dL-1 and 107.00 ± 15.84 mg.dL-1 in the intervention group and control group, respectively(p < 0.001). The postoperative mean thirst scores were 4.70 ± 1.59 and 6.36 ± 2.07 in the inter-vention group and control group, respectively (p < 0.001). Their corresponding postoperativemean fasting scores were 5.54 ± 1.76 and 5.86 ± 1.79 (p > 0.05) and the mean fatigue levelsin the 24th postoperative hour were 4.80 ± 2.13 and 5.48 ± 1.46, respectively (p > 0.05).Conclusions: Oral intake of liquid carbohydrate before spinal anesthesia was found to havepositive effects on patients’ postoperative blood glucose and thirst levels.
© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).∗ Corresponding author.E-mails: [email protected] (G.A. Akbuğa), mbaser@erciyes
ttps://doi.org/10.1016/j.bjane.2021.02.053 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
.edu.tr (M. Başer).
itora Ltda. This is an open access article under the CC BY-NC-ND

a an
I
ScawtapCeocm
uasrfarsem
pAfudc
ggrobtaft
cl
M
T
Toif2risn
t
aosurrpssdnswrSHfnwaragi
S
Asdiwtigrd5ew
gttoa
i
D
AcBd
G.A. Akbuğ
ntroduction
urgical procedures performed for therapeutic reasons canause physiological and psychological stress in the organismnd can result in catabolism.1,2 This is closely associatedith factors that influence the management of symp-
oms, such as the duration of preoperative fasting, typend length of anesthesia, surgical techniques, hemorrhage,ostoperative pain, nausea-vomiting, ileus, and fatigue.2,3
atabolism also causes patients to experience fatigue, low-rs their resistance, prolongs their recovery and lengthf hospital stay, and increases their risk for postoperativeomplications; thus, it can result in an increased risk forortality and morbidity.3,4
New evidence-based protocols have been developed. These of traditional approaches for perioperative treatmentnd care of individuals has been avoided to lower theirtress response and to accelerate their recovery. Enhancedecovery after surgery (ERAS) is a cycle-based protocolor perioperative strategies that requires multidisciplinarypproaches.5---7 The protocol aims to enable individuals toeturn to their basic performance and functions within thehortest time possible. ERAS also suppresses catabolism andnhances their quality of life because it prevents develop-ent of postoperative complications.6,7
Two of the protocol’s predictors include shortenedreoperative fasting duration and carbohydrate loading.ccordingly, individuals are told that they can consume solidoods up to 6 hours prior to surgery, clear liquid-based foodp to 2 hours prior to surgery, 800 mL carbohydrate-richrink at any time until midnight before surgery, and 400 mLarbohydrate-rich drink 2---3 hours before surgery.5---7
Many studies have reported that a diet of clear liquidiven 2 hours before surgery does not increase patients’astric fluid volumes or gastric acidity and it poses noisk of aspiration.8,9 Some other studies have revealed thatral intake of liquid carbohydrate suppresses catabolismy lowering the stress response induced both by surgicalrauma and fasting, decreases insulin resistance, minimizeslterations in postoperative glucose levels, and reducesasting-thirst feelings, nausea and vomiting, defecationime, length of hospital stay, and fatigue.4,8---12
This study aimed to investigate whether preoperativearbohydrate improves fasting-thirst, fatigue, and glucoseevels compared with standard therapy.
ethods
rial design
his randomized controlled trial was conducted at therthopedic clinic of a research and application hospitaln Turkey. The ethics committee approval was obtainedrom the Clinical Trials Ethics Committee (07/10/2016-016/523). Institutional permission was obtained from theelated research and application hospital. Participants werenformed about the purpose of the study, and they had all
igned the informed consent form. Blinding or masking wasot performed in the study.If scheduled for surgeries performed under spinal anes-hesia at the orthopedic clinic, patients should not eat
PTri
24
d M. Başer
nything after midnight; moreover, they start to eat basedn regimen I (pulpless, grain-free clear liquid diet) at theecond postoperative hour. Arthroscopy lasts for 45---90 min-tes. Then, patients are sent home after undergoing theecommended blood tests and physical examinations andeturn to the clinic on the morning of surgery. In this study,atients were told to come to the clinic 2 hours beforeurgery. The first patients who underwent arthroscopicurgery between 08:00 and 10:00 a.m. by the same orthope-ic surgeon were included in the sample. The patients wereot administered any intravenous fluid after surgery. As atandard, a 10---15 mL.kg-1 of balanced solution (Isolen-S)as given to the patients in the intraoperative period. They
eceived 1000---1500 mL of intravenous fluid on average.pinal anesthesia took place using 15 mg of 0.5% bupivacaineCl (Marcaine) through the intervertebral space (L3---4). As
ar as is known, bupivacaine, used for spinal anesthesia, haso effect on glucose metabolism. Those included in the studyere ≥ 18 years old, indicated for arthroscopic surgery,nd could communicate enough to be able to answer theesearch questions. Individuals diagnosed with any psychi-tric disorder, endocrine disorder, renal and hepatic failure,astroesophageal reflux, sour cherry allergy, and body massndex of > 25 kg.m-2 were excluded from the study.
ample size calculation and patient randomization
power analysis was carried out to determine the sampleize of the study. For this purpose, the arithmetic meanifference (3.3) between the blood glucose levels of thentervention and control groups mentioned by Yagci et al.8
as used. After the arithmetic mean and standard devia-ion were used to calculate the sample size (95% confidencenterval, 95% power), 30 patients should be included in eachroup. When the desired number of the calculated data waseached, the power analysis was repeated over the studyata. The margin of error in the post-hoc power analysis was%. According to the blood glucose level in the first postop-rative hour, the effect size of 1.095 and power of the studyas calculated as 99%.
Therefore, 70 patients were randomly divided into tworoups using a computerized table of random numbers. Afterhe random numbers were placed in opaque envelopes,he envelopes were numbered sequentially, and they werepened just before the start of the procedure. Patients weressigned to the intervention and control groups.
The study was conducted on a total of 61 patients includ-ng 31 in the intervention group and 30 in the control group.
ata collection tool
patient information form, physiological measurementhart, visual analog scale (VAS) for fasting-thirst levels, andrief Fatigue Inventory (BFI) were all used to collect theata.
atient information formhis form was prepared by the researcher upon literatureeview.4,8,12 It includes 10 questions about the character-stics of the patients such as age, sex, marital status,
8

Brazilian Journal of Anesthesiology 2021;71(3):247---253
Inter vention Group• Obtaining verbal and written consents • Filling out the Patient Information
Form • Measurement of blood glucose value
and fasting-thirst levels • Giving 400 mL sour cherry juice 2
hours before the operation• Measurement of the blood glucose
value and fasting-thirst levels justbefore the operation (2 hou rs afterdrinking the juice)
• Me asurement of the blood gluc oseval ue and fastin g-thi rst lev els 1 hourafte r the o peration
• Dete rmination of fatigue level 24hours afte r t he op eration
Control Group • Obtaining verbal and written consents• Filling out the Patient Information
Form • Measurement of blood glucose value
and fasting-thirst levels • Measurement of the blood glucose
val ue and fasti ng-thir st level ju stbefore the op eration
• Measurement of the blood glucosevalue and fasting-thirst levels 1 hourafte r the o peration
• Dete rmination of fat igue lev el 24 hou rs
after the operation
The measurements and applications for the intervention and control group
ation
ea
BTaCifo4tia
I
Fi
AB-oot(
AThr
S
PbWwfscd
tomgcw
R
T3(t>fiig0
Figure 1 The measurements and applic
ducational level, occupation, income level, presence ofny chronic disease, and surgery duration.
FIhis inventory was developed by Mendoza et al.13 anddapted by Cinar et al.14 for the Turkish population.ronbach’s alpha internal consistency coefficient of the
nventory is 0.98. BFI has nine items and evaluates theatigue severity (now, always, worst) (1, 2, 3) and the effectf fatigue on the activities of daily living (4a, 4b, 4c, 4d, 4e,f). Each item is rated between 0 and 10 points. The higherhe score, the more severe the fatigue is, and the more doest affect daily living activities.15 In this study, Cronbach’slpha internal consistency coefficient of BFI was 0.74.
ntervention
igure 1 shows the measurements and applications for thentervention and control groups.
pplications in the intervention groupased on the literature review and opinions of three experts
-- a dietitian, an anesthesiologist, and a biochemist ---400 mLf grain-free sour cherry juice from a fixed brand (with valuef 200 kcal and deemed suitable for a clear diet) was given tohe patients in the intervention group 2 hours before surgeryFig. 1).4
pplications in the control grouphose in the control group did not drink the liquid carbo-ydrate (i.e., sour cherry juice). Rather, they only receivedoutine treatment and hospital care services (Fig. 1).
ss
2
24
s for the intervention and control group.
tatistical analysis
atients’ descriptive characteristics are presented in num-er and percentage distributions in tables. The Shapiro---Wilk
test was used to determine whether the numerical dataere normally distributed. Parametric tests were applied
or analysis of normally distributed data. The independentamples t-test was used to identify whether the blood glu-ose, fasting-thirst, and fatigue levels of both groups areifferent from one another.
Repeated measures analysis of variance was employedo determine the difference between the mean scoresf the repeated measures in both groups. The Bonferroniultiple comparison test was applied to identify which
roup caused the difference between intervention andontrol groups. The significance level in all comparisonsas 0.05.
esults
he study was completed on a total of 61 patients, including1 in the intervention group and 30 in the control groupFig. 2). Table 1 shows the demographic characteristics ofhe patients. Both groups had comparable characteristics (p
0.05, Table 2), and the mean blood glucose levels in therst postoperative hour were 90.90 ± 13.56 mg.dL-1 in the
ntervention group and 107.00 ± 15.84 mg.dL-1 in the controlroup, and their difference was statistically significant (p <.001).
The fasting mean scores of both groups 2 hours before
urgery, immediately before surgery, and 1 hour afterurgery were similar to one another (p > 0.05, Table 3).The mean thirst score just before surgery was 4.90 ±.11 in the intervention group and 6.20 ± 1.98 in the control
9
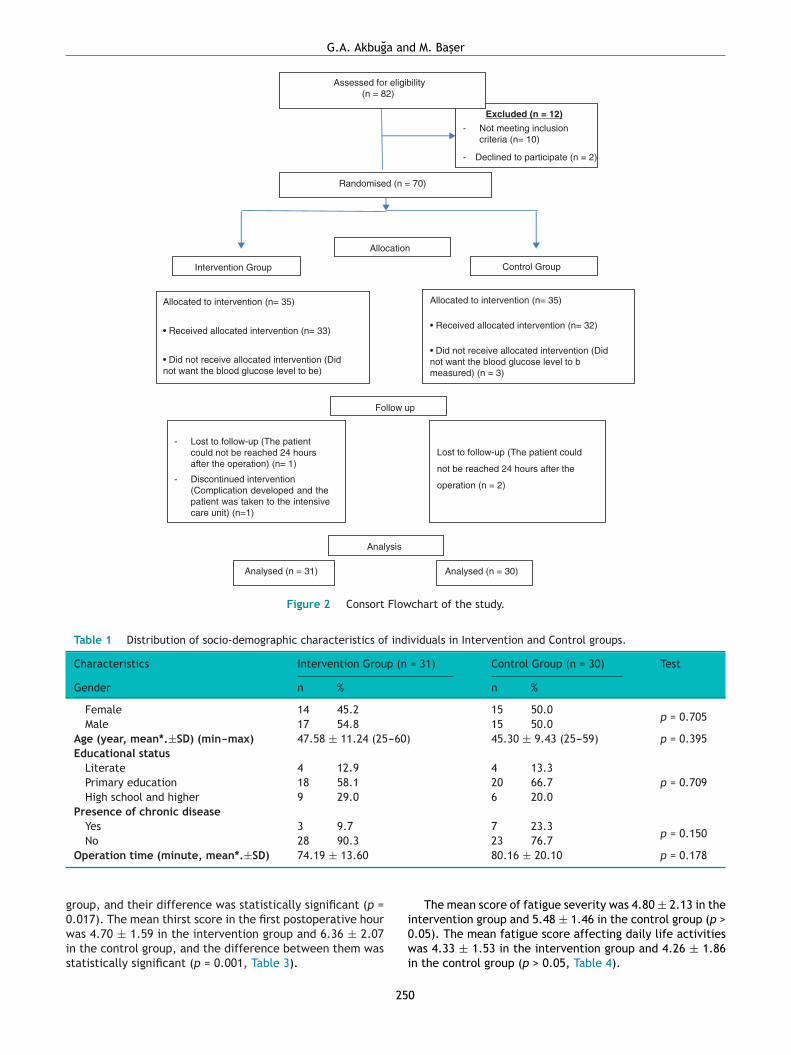
G.A. Akbuğa and M. Başer
Excluded (n = 12)
- Not meeting incl usioncriteria (n= 10)
- Declined to participate (n = 2)
Assessed for eli gibility(n = 82)
Randomised (n = 70)
Allo cat ed to in terventio n (n= 35)
• Received allo cat ed int ervention (n= 33)
• Did not receive alloc ated inte rvention (Didnot want the blood glucose level to be)
Allo cat ed to in terventio n (n= 35)
• Received allocated intervention (n= 32)
• Did not receive alloc ated inte rvention (Didnot want the blood gluc ose l evel to bmeasured ) (n = 3)
- Lost to follow-up (The patientcould not be reached 24 hoursafte r the operation ) (n= 1)
- Discontinued intervention(Complication developed and th epatient was taken to the intensivecare unit) (n=1)
Analysed (n = 3 1)
Lost to follow-up (The patient could
not be reach ed 24 hou rs afte r the
operation (n = 2)
Analysed (n = 3 0)
Allo cation
Follow up
Analysis
Intervention Group Control Group
Figure 2 Consort Flowchart of the study.
Table 1 Distribution of socio-demographic characteristics of individuals in Intervention and Control groups.
Characteristics Intervention Group (n = 31) Control Group (n = 30) Test
Gender n % n %
Female 14 45.2 15 50.0p = 0.705
Male 17 54.8 15 50.0Age (year, mean*.±SD) (min---max) 47.58 ± 11.24 (25---60) 45.30 ± 9.43 (25---59) p = 0.395Educational status
Literate 4 12.9 4 13.3p = 0.709Primary education 18 58.1 20 66.7
High school and higher 9 29.0 6 20.0Presence of chronic disease
Yes 3 9.7 7 23.3p = 0.150
No 28 90.3 23 76.7
g0wis
Operation time (minute, mean*.±SD) 74.19 ± 13.60
roup, and their difference was statistically significant (p =
.017). The mean thirst score in the first postoperative houras 4.70 ± 1.59 in the intervention group and 6.36 ± 2.07n the control group, and the difference between them wastatistically significant (p = 0.001, Table 3).
i0wi
25
80.16 ± 20.10 p = 0.178
The mean score of fatigue severity was 4.80 ± 2.13 in the
ntervention group and 5.48 ± 1.46 in the control group (p >.05). The mean fatigue score affecting daily life activitiesas 4.33 ± 1.53 in the intervention group and 4.26 ± 1.86n the control group (p > 0.05, Table 4).
0
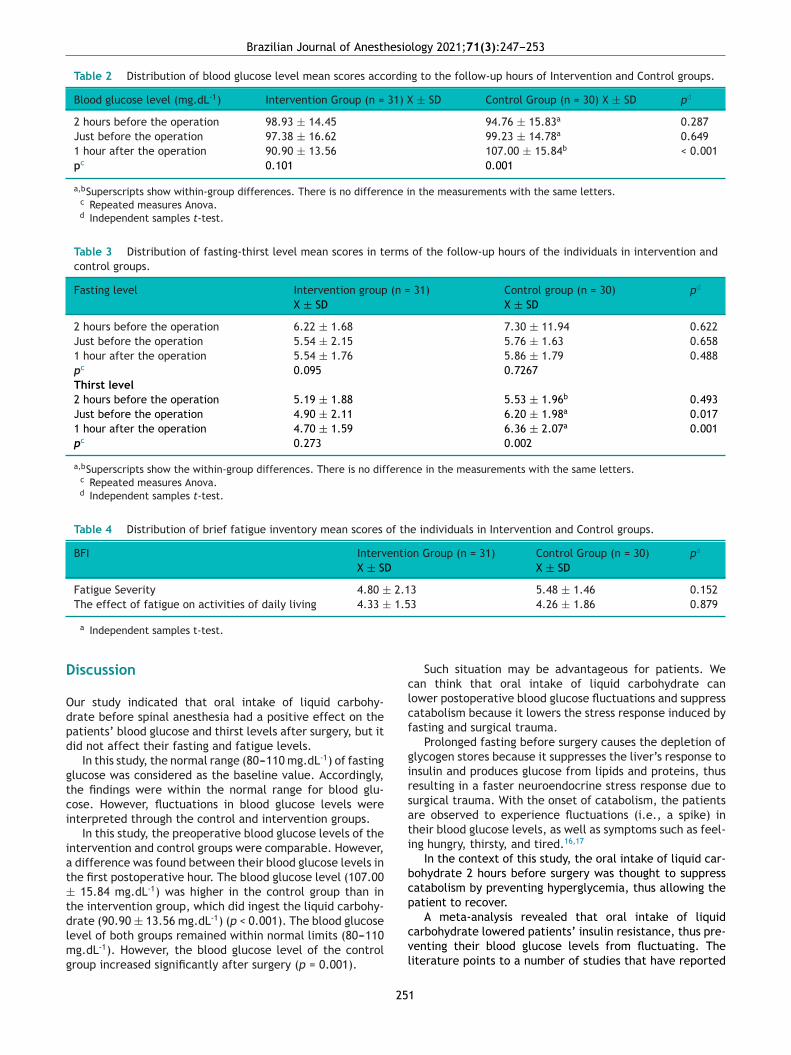
Brazilian Journal of Anesthesiology 2021;71(3):247---253
Table 2 Distribution of blood glucose level mean scores according to the follow-up hours of Intervention and Control groups.
Blood glucose level (mg.dL-1) Intervention Group (n = 31) X ± SD Control Group (n = 30) X ± SD pd
2 hours before the operation 98.93 ± 14.45 94.76 ± 15.83a 0.287Just before the operation 97.38 ± 16.62 99.23 ± 14.78a 0.6491 hour after the operation 90.90 ± 13.56 107.00 ± 15.84b < 0.001pc 0.101 0.001
a,bSuperscripts show within-group differences. There is no difference in the measurements with the same letters.c Repeated measures Anova.d Independent samples t-test.
Table 3 Distribution of fasting-thirst level mean scores in terms of the follow-up hours of the individuals in intervention andcontrol groups.
Fasting level Intervention group (n = 31) Control group (n = 30) pd
X ± SD X ± SD
2 hours before the operation 6.22 ± 1.68 7.30 ± 11.94 0.622Just before the operation 5.54 ± 2.15 5.76 ± 1.63 0.6581 hour after the operation 5.54 ± 1.76 5.86 ± 1.79 0.488pc 0.095 0.7267Thirst level2 hours before the operation 5.19 ± 1.88 5.53 ± 1.96b 0.493Just before the operation 4.90 ± 2.11 6.20 ± 1.98a 0.0171 hour after the operation 4.70 ± 1.59 6.36 ± 2.07a 0.001pc 0.273 0.002
a,bSuperscripts show the within-group differences. There is no difference in the measurements with the same letters.c Repeated measures Anova.d Independent samples t-test.
Table 4 Distribution of brief fatigue inventory mean scores of the individuals in Intervention and Control groups.
BFI Intervention Group (n = 31) Control Group (n = 30) pa
X ± SD X ± SD
Fatigue Severity 4.80 ± 2.13 5.48 ± 1.46 0.152The effect of fatigue on activities of daily living 4.33 ± 1.53 4.26 ± 1.86 0.879
D
Odpd
gtci
iat±tdlmg
clcf
girsati
bcp
a Independent samples t-test.
iscussion
ur study indicated that oral intake of liquid carbohy-rate before spinal anesthesia had a positive effect on theatients’ blood glucose and thirst levels after surgery, but itid not affect their fasting and fatigue levels.
In this study, the normal range (80---110 mg.dL-1) of fastinglucose was considered as the baseline value. Accordingly,he findings were within the normal range for blood glu-ose. However, fluctuations in blood glucose levels werenterpreted through the control and intervention groups.
In this study, the preoperative blood glucose levels of thentervention and control groups were comparable. However,
difference was found between their blood glucose levels inhe first postoperative hour. The blood glucose level (107.00
15.84 mg.dL-1) was higher in the control group than inhe intervention group, which did ingest the liquid carbohy-
rate (90.90 ± 13.56 mg.dL-1) (p < 0.001). The blood glucoseevel of both groups remained within normal limits (80---110g.dL-1). However, the blood glucose level of the controlroup increased significantly after surgery (p = 0.001).
cvl
25
Such situation may be advantageous for patients. Wean think that oral intake of liquid carbohydrate canower postoperative blood glucose fluctuations and suppressatabolism because it lowers the stress response induced byasting and surgical trauma.
Prolonged fasting before surgery causes the depletion oflycogen stores because it suppresses the liver’s response tonsulin and produces glucose from lipids and proteins, thusesulting in a faster neuroendocrine stress response due tourgical trauma. With the onset of catabolism, the patientsre observed to experience fluctuations (i.e., a spike) inheir blood glucose levels, as well as symptoms such as feel-ng hungry, thirsty, and tired.16,17
In the context of this study, the oral intake of liquid car-ohydrate 2 hours before surgery was thought to suppressatabolism by preventing hyperglycemia, thus allowing theatient to recover.
A meta-analysis revealed that oral intake of liquidarbohydrate lowered patients’ insulin resistance, thus pre-enting their blood glucose levels from fluctuating. Theiterature points to a number of studies that have reported
1

a an
sf2g
ta
iboh
tfCs0Iteiad
fmidcuepbEiom
wtwwi
eihgrfgatt
h(s
ct
sRsho
haanspfotdfiste
puamo
C
Owwbn
C
T
R
Univ Faculty Health Sci Nurs E-J. 2014;2.7. Bozkırlı OB, Gündoğdu HR, Ersoy EP, et al. ERAS protokolü
G.A. Akbuğ
imilar findings.4,8,9,18,19 In their study, Svanfeldt et al.20
ound that giving patients 400 mL of liquid carbohydrate hours before surgery prevented stress-induced hyper-lycemia.
Ozdemir et al.8 reported that the blood glucose levels ofhe control and placebo groups returned to normal 24 hoursfter surgery and then gradually increased.
However, some other studies have indicated that oralntake of liquid carbohydrate has no significant effect onlood glucose levels.3,13 The type and length of surgery, typef anesthesia used, and type of liquid carbohydrate mightave influenced these findings.
Gunawardhana21 investigated preoperative fasting prac-ices and revealed that 51.5% of patients who had not eatenor 13 hours did not feel hungry. Similarly, in their study,renshaw and Winslow22 asked patients who fasted beforeurgery to score their fasting level on a scale between
and 10 and found that their mean fasting level was 5.n this study, the oral intake of liquid carbohydrate washought not to have created any difference in fasting lev-ls between the intervention and control groups becauset is liquid and therefore stays in the stomach only for
short time period and does not lead patients to feeliscomfort.
Another problem caused by preoperative fasting is theeeling of thirst. A long-term interruption in nourish-ent can decrease gastrointestinal and salivary secretions,
ncrease thirst and mouth dryness and even lead to dehy-ration. Hausel et al.23 found that patients who underwentolorectal surgery consumed either a carbohydrate-rich liq-id or water to reduce the feeling of thirst. George15
xamined preoperative fasting practices and found thatatients consuming oral drinking liquid carbohydrate 2 hoursefore surgery felt significantly less thirsty based on theRAS protocol. Gebremenhn and Nagaratnam24 also exam-ned patients who fasted before surgery and found that 49%f the patients experienced severe thirst as the most com-on symptom.Likewise, this study revealed that that intervention group
as less thirsty 2 hours after surgery (4.90 ± 2.11) thanhe control group (6.20 ± 1.98) (p = 0.001). Similar findingsere obtained 1 hour after surgery as well: the control groupas thirstier 1 hour after surgery (6.36 ± .2.07) than the
ntervention group (4.70 ± 1.59) (p = 0.017).One of the postoperative symptoms is fatigue. Unnec-
ssary preoperative fasting intensifies fatigue because itncreases cell destruction products; leads to catabolism,ydrogen, and lactic acid accumulation; and stimulateslucose production from lactates and amino acids, thusesulting in protein degradation. Additionally, postoperativeatigue can occur because of tissue damage caused by sur-ical intervention, immobility, and stress. Fatigue adverselyffects patients’ physical and mental well-being, prolongsheir recovery and length of hospital stay, and increasesheir stress response to surgical trauma.25,26
In this study the intervention group had less fatigue 24ours after surgery (4.80 ± 2.13) than the control group5.48 ± 1.46); this difference, however, was not statisticallyignificant (p > 0.05).
Ozdemir et al.8 discovered that patients who drank liquid
arbohydrate had less fatigue 12 hours after surgery thanhose who did not.25
d M. Başer
Kaya and Sentura26 found that fatigue began beforeurgery and increased mostly immediately after surgery.ubin et al.27 revealed that patients who underwent a majorurgery (abdominal, gynecology, or cardiovascular surgery)ad higher fatigue levels than those who underwent anrthopedic surgery.
In this study, patients’ fatigue levels were assessed 24ours after surgery and were found not affected by fastinglone. Other subjective factors such as anxiety, insomnia,nd pain were found to play a role, albeit such factors wereot identified in any of the participants. Given that arthro-copic surgery can be categorized as a minor operation,atients are likely to feel more energetic and vigorous. Theatigue levels did not differ between the groups becausef these reasons. Further studies involving cases with long-erm follow-up are needed to determine the effects ofrinking liquid carbohydrate on fatigue. In light of thesendings, further studies are needed on cases with longurgery duration as well as in cases undergoing anesthesiaechniques other than spinal anesthesia to determine theffect of drinking liquid carbohydrate on fatigue and fasting.
As limitations of the study, findings were obtained fromatients without history of genetic or chronic diseases, whonderwent arthroscopic surgery, and were directed to spinalnesthesia. Moreover, their body mass indexes were noteasured. This study’s findings cannot be generalized to
ther patients undergoing surgery under spinal anesthesia.
onclusion
ral intake of liquid carbohydrate before spinal anesthesiaas found to have a positive effect on patients who under-ent arthroscopic surgery, in terms of their postoperativelood glucose and thirst levels. However, it appeared to haveo effect on their fasting feel and fatigue levels.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Aksoy G, Kanan N, Akyolcu N. Surgery Nursing 1. Nobel Book-store; 2012. p. 11---26.
2. Erdil F, Özhan NÖ. Surgery Nursing. Ankara, IV. Printing, AydoğduOfset; 2001. p. 101---13.
3. Çeliksular C, Saraçoğlu A, Yentür E. The Influence of oral car-bohydrate solution intake on stress response before total hipreplacement surgery during epidural and general anaesthesia.Turk J Anaesthesiol Reanim. 2016;44:117---23.
4. Awad S, Varadhan KK, Ljungqvist O, et al. A meta-analysis ofrandomised controlled trials on preoperative oral carbohydratetreatment in elective surgery. Clin Nutr. 2013;32:34---44.
5. Hübner M, Addor V, Slieker J, et al. The impact of an enhancedrecovery pathway on nursing workload: A retrospective cohortstudy. Int J Surg. 2015;24:45---50.
6. Demirhan İ, Pınar G. Enhanced recovery after surgery and nurs-ing practicesenhanced recovery and nursing. Yıldırım Beyazıt
kolorektal cerrahi sonuçlarımızı etkiledi mi? Turkish J Surg.2012;28:149---52.
2
esio
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
Brazilian Journal of Anesth
8. Yağci G, Can Fatih M, Özturk E, et al. Effects of preoperativecarbohydrate loading on glucose metabolism and gastric con-tents in patients undergoing moderate surgery: A randomized,controlled trial. Nutrition. 2008;24:212---6.
9. American Society of Anesthesiologists. ‘‘Committee practiceguidelines for preoperative fasting and the use of pharma-cologic agents to reduce the risk of pulmonary aspiration:Application to healthy patients undergoing elective proceduresreport by the American Society of Anesthesiologists Committeeon Standards and Practice Parameters’’. Anesthesiology. 2011;114:495.
0. Zareba K, Czygier M, Kamocki Z, et al. Parenteral Nutri-tion and preop preparation in prevention of post-operativeinsulin resistance in gastrointestinal carcinoma. Adv Med Sci.2013;58:150---5.
1. Soop M, Nygren J, Myrenfors P. Preoperative oral carbohydratetreatment attenuates immediate postoperative insulin resis-tance. Am J Physiol Endocrinol Metab. 2001;280:576---83.
2. Özdemir F, Eti Z, Dinçer P, et al. The Effect of preopera-tive oral carbohydrate loading on stress response in patientsundergoing major or minor surgery. Türkiye Clinics J Med Sci.2011;31:1392---400.
3. Mendoza TR, Wang SX, Cleeand SC, et al. The rapid assess-ment of fatigue severity ın cancer patients: use of brief fatigueinventory. Cancer. 1999;85:1186---96.
4. Çınar S, Sezerli M, Sarsmaz N, et al. Hemodiyaliz akut yorgunluksendromuna neden olabilir mi? J Nurs Forum. 2000;3:28---33.
5. Kobe JA. Assessing Preoperative Fasting Practice Among AdultPatients At Kenyatta National Hospital, Surgical Department,
Thesis (MNutr (Human Nutrition). University of Stellenbosch;2015, 101.6. Yıldız H. New approaches during preoperative poverty process.AÜTD. 2006;38:1---5.
2
25
logy 2021;71(3):247---253
7. Azhar RA, Bochner B, Catto J, et al. Enhanced recoveryafter urological surgery: a contemporary systematic reviewof outcomes, key elements, and research needs. Eur Urol.2016;70:176---87.
8. Crenshaw JT. Preoperative Fasting: Will the Evidence Ever BePut into Practice? Am J Nurs. 2011;111:38---43.
9. Korkmaz Ö. Operasyon Öncesi Oral sıvı karbonhidrat SolüsyonuAlımının Stres Yanıta Etkisi, Specialization thesis. Department ofAnesthesiology, Istanbul University Cerrahpaşa Medical Faculty;2004, 58.
0. Svanfeldt M, Thorell A, Hausel J, et al. Effect ofp̈reoperativeöral carbohydrate treatment on insulin action----arandomised cross-over unblinded study in healthy subjects.Clin Nutr. 2005;24:815---21.
1. Gunawardhana A. Knowledge, attitudes and practice of preop-erative fasting guidelines in the National Hospital of Sri Lanka.Sri Lankan J Anaesthesiol. 2012;20:92---5.
2. Crenshaw JT, Winslow EH. Preoperative fasting: old habits diehard. Am J Nurs. 2002;102:36---44.
3. Hausel J, Nygren J, Lagerkranser M, et al. A carbohydrate-rich drink reduces preoperative discomfort in elective surgerypatients. Anesth Analg. 2001;93:1344---50.
4. Gebremedhn EG, Nagaratnam VB. Audit on preoperative fast-ing of elective surgical patients in an african academic medicalcenter. World J Surg. 2014;38:2200---4.
5. Yurtsever S. The fatigue in chronic illnesses and nursing care.Cumhuriyet Univ J Nurs School. 2000;4:16---20.
6. Kaya S, Şenturan L. The investigation of fatigue of the patientsundergoing coronary artery by-pass graft surgery. JAREN.
2016;2:59---67.7. Rubin GJ, Hardy R, Hotopf M. A systematic review and meta-analysis of the incidence and severity of postoperative fatigue.J Psychosom Res. 2004;57:317---26.
3

C
Gs
JC
C
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):254---258
LINICAL RESEARCH
eneral anesthesia for emergency cesarean delivery:imulation-based evaluation of residents
úlio Alberto Rodrigues Maldonado Teixeira ∗, Cláudia Alves,onceição Martins, Joana Carvalhas, Margarida Pereira
entro Hospitalar e Universitário de Coimbra, Serviço de Anestesiologia, Coimbra, Portugal
eceived 15 January 2020; accepted 12 February 2021vailable online 30 April 2021
KEYWORDSGeneral anesthesia;Emergency cesarean;Simulation;Resident evaluation
AbstractIntroduction: Decreased rates of General Anesthesia (GA) for Cesarean Section (C-section) cre-ate a learning problem for anesthesia trainees. In this context, training the management ofGA for C-section using simulation techniques allows a safe environment for exposure, learning,performance improvement, and capability retention.Objective: Analyze anesthesia residents’ performance regarding a simulated clinical case ofGA for emergency C-section and identify specific deficits in skill acquisition.Methods: Between 2015 and 2018, we evaluated the performance of 25 anesthesiology residentschallenged by a simulated clinical case of GA for emergency C-section after the conclusion ofthe obstetric anesthesia rotation. Each resident performed the clinical case once followed bythe assessment of their performance. Final scores were given according to the completion rateof 14-tasks, going from 0% to 100%. Two study groups were considered according to residencyyear for subsequent comparison of results (Group 1, second and third residency years and Group2, fourth and fifth residency years).Results and discussion: Mean score was 64.29% ± 13.62. Comparatively, Group 1 obtained ahigher score than Group 2 (70.63% ± 14.02 vs. 60.27% ± 11.94), although with no statisti-cally significant difference (p = 0.063). The tasks most frequently accomplished were opioidadministration (100%), rapid sequence technique (100%), pre-oxygenation (92%), gastric contentaspiration prophylaxis (84%), and previous clinical history (84%). Conversely, the tasks less fre-quently accomplished were confirming presence of pediatrician (64%), oxytocin administration(56%), PONV prophylaxis (56%), and preoperative airway assessment (48%).Conclusion: The performance of the residents observed in this study was comparable to resultspreviously published. The final score did not depend on the residency year.
© 2021 Sociedade Brasileira deopen access article under theby-nc-nd/4.0/).
∗ Corresponding author.E-mail: [email protected] (J.A. Teixeira).
ttps://doi.org/10.1016/j.bjane.2021.02.059 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Anestesiologia. Published by Elsevier Editora Ltda. This is anCC BY-NC-ND license (http://creativecommons.org/licenses/
itora Ltda. This is an open access article under the CC BY-NC-ND

esio
I
CfyfSCtteosa
rtaiaaat
lrcgc
fptcc
eBdma
apiC
aaotwp
M
Bodc
yy
aficoettpatat
SmSciatoastoa
sscd
eddatni(pwaGmat
bdrct
Brazilian Journal of Anesth
ntroduction
-Section delivery (CS) is one of the most frequently per-ormed surgeries worldwide. There has been, in recentears, an increase in the cesarean rate and the trendor continuous growth in the future has been observed.1
imultaneously, a change in the anesthetic management for-section has been observed favoring regional anesthesiaechniques, with a significant decrease in General Anes-hesia (GA) use, which has been used preponderantly formergency CS.2,3 Given the low frequency and complexityf obstetric emergencies and minimal exposure of anesthe-iology residents to the GA technique for CS, major learningnd performance deficits may occur in this specific area.3,4
Within this scenario, simulation training is particularlyelevant as a learning tool,3---5 and represents an alternativeo provide clinical exposure to this scenario, without posing
risk to patient safety.6,7 Simulation training enables activenvolvement of participants and contributes to fast forwardcquisition of competences, improve long-term retention,nd preclude loss of competences already acquired.7,8 Itlso allows multidisciplinary training aimed at optimizinghe efficiency of team work.8
There is evidence that critical event training using simu-ation improves performance of residents to deliver certainequired tasks when faced with these critical events inlinical practice.4,6,8 The simulation scenario of GA for emer-ency CS has been often used to improve individual technicalapacities and non-technical capacities.8
Although there are several performance assessment toolsor simulation not yet validated,3,8 they are used to assessractice of anesthesiology residents, because they enablehe identification of gaps in training and detect failure inritical competences, frequently not revealed by the classi-al assessment tools.9
The Centro Hospitalar e Universitário de Coimbra (CHUC)ncompasses two maternities, Daniel de Matos (MDM) andissaya Barreto (MBB), and performs, on average, 4,500eliveries a year, with a CS rate of approximately 27%. Theean GA rate for CS is 13%. Each resident performs, on
verage, 5 GA for CS during the rotation.At this hospital center, for four years, one of the evalu-
tion components of the obstetric anesthesia rotation waserformed with a practical exam, solving two simulated clin-cal cases. All exams included a case of GA for emergencyS.
The primary objective of the present paper was tonalyze the performance of anesthesiology residents on
clinical case of GA for emergency CS. The secondarybjectives were the identification of specific deficiencieso acquire competences, and the possible relationshipith the residency year (earlier or later) of the trainingrogram.
ethods
ased on an assessment table, we conducted a retrospectivebservational study to analyze the performance of 25 resi-ents of anesthesiology on solving a simulation of a clinicalase of general anesthesia for emergency C-section.
csc
25
logy 2021;71(3):254---258
In Portugal, the anesthesiology training program lasts 5ears. Obstetric anesthesia training occurs after the secondear of the program and lasts 3 to 4 months.
It was a convenience sample based on the rotation ofnesthesiology residents at CHUC between the second andfth years of residency, and who, between 2015 and 2018oncluded training in obstetric anesthesia. At the beginningf the training period, residents were informed about thevaluation method, and that the practice exam would beaken after concluding training. The clinical case was simul-aneous for different year residents. Due to logistics androfessional factors the participants, senior residents, had
longer gap between conclusion of obstetric rotation andhe evaluation. Residents were familiar with the simulatornd environment but were not aware of the clinical caseshey would be involved with.
Simulated clinical cases were conducted at the Centro deimulação Biomédica de Coimbra, recreating the environ-ent of a surgical block, and using high-fidelity simulator
imMan (Laerdal, Wappingers Falls, NY, USA). The clinicalase and respective assessment table were prepared by fournstructors, anesthesiologists with experience in obstetricsnd working regularly with clinical simulation. The design ofhe clinical case was based on simulation strategies previ-usly published, adapted to the objectives of the proposedssessment.3,4,9,10 The team of four instructors held all theimulation exams during the study period, alternating func-ion of anesthesia nurse/actress, simulator operator andbserver. Each resident took one individual exam and wasssessed only once.
For each case, one of the instructors made a summary,upplying information on the clinical case, by reading acript to the resident who would be the anesthesiologist inharge. During the progression of the scenario, additionaletails were provided only upon resident request.
The obstetric case focused on the management of anmergency C-section due to acute fetal distress (car-iotocographic registration with multiple and prolongedeaccelerations with slow recovery and meconium in themniotic fluid). The pregnant patient did not present cri-eria for difficult airway or co-morbidities. Patient refusedeuraxial anesthesia. She was connected to a device reg-stering the standard American Society of AnesthesiologistsASA) monitoring parameters. The anesthesia nurse (actress)resented the scenario and informed that the obstetric teamas present, prepared, and requesting to start the C-sections soon as possible. The scenario continued as if it were aA for C-section in real-life, including pre-anesthesia assess-ent, choice of drugs, choice and preparation of intubation
nd ventilation material, integration into the dynamics ofhe team involved, and management of the clinical case.
Each case lasted approximately 10 to 15 minutes followedy debriefing with each resident that lasted 20 minutes, con-ucted by two instructors (operator and observer), based onegistrations of the four instructors on the assessment table,omprising also the non-technical capacities revealed duringhe scenario.
The assessment table included 14 tasks. Each item was
lassified as ‘‘completed’’ and ‘‘not completed’’. The finalcore was calculated according to the percentage of tasksompleted. At that time, due to the educational and training5
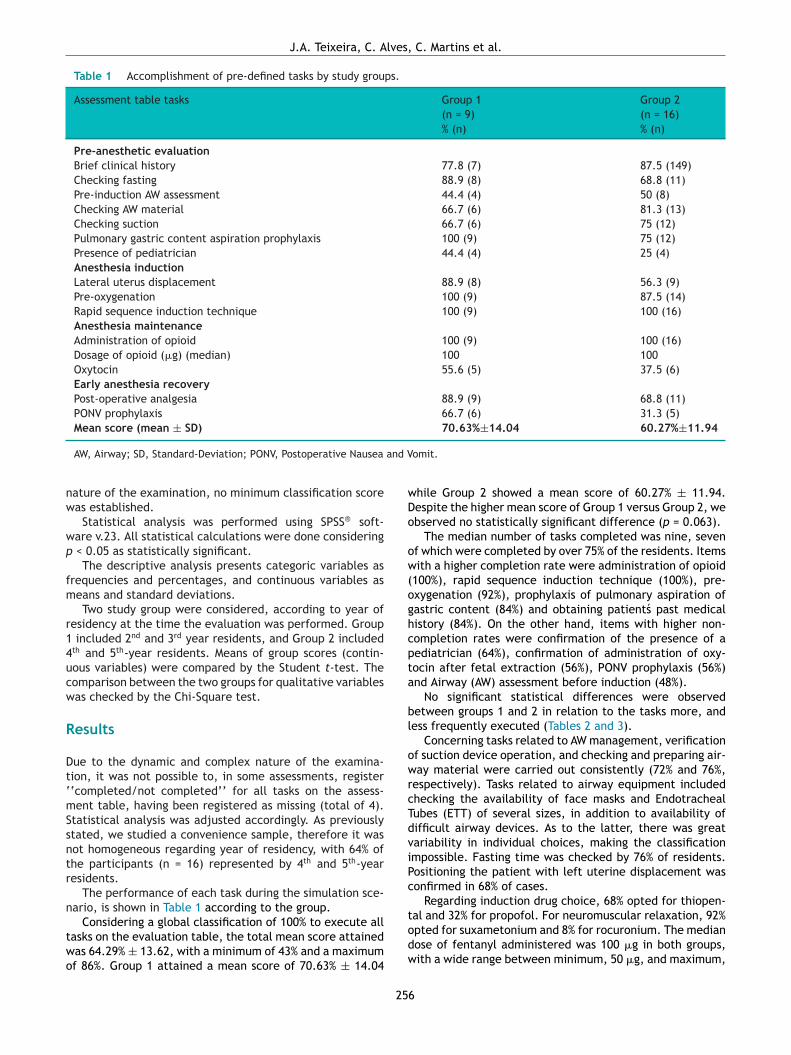
J.A. Teixeira, C. Alves, C. Martins et al.
Table 1 Accomplishment of pre-defined tasks by study groups.
Assessment table tasks Group 1 Group 2(n = 9) (n = 16)% (n) % (n)
Pre-anesthetic evaluationBrief clinical history 77.8 (7) 87.5 (149)Checking fasting 88.9 (8) 68.8 (11)Pre-induction AW assessment 44.4 (4) 50 (8)Checking AW material 66.7 (6) 81.3 (13)Checking suction 66.7 (6) 75 (12)Pulmonary gastric content aspiration prophylaxis 100 (9) 75 (12)Presence of pediatrician 44.4 (4) 25 (4)Anesthesia inductionLateral uterus displacement 88.9 (8) 56.3 (9)Pre-oxygenation 100 (9) 87.5 (14)Rapid sequence induction technique 100 (9) 100 (16)Anesthesia maintenanceAdministration of opioid 100 (9) 100 (16)Dosage of opioid (�g) (median) 100 100Oxytocin 55.6 (5) 37.5 (6)Early anesthesia recoveryPost-operative analgesia 88.9 (9) 68.8 (11)PONV prophylaxis 66.7 (6) 31.3 (5)Mean score (mean ± SD) 70.63%±14.04 60.27%±11.94
and V
nw
wp
fm
r14ucw
R
Dt‘mSsntr
n
two
wDo
ow(oghcpta
bl
owrcTdviPc
AW, Airway; SD, Standard-Deviation; PONV, Postoperative Nausea
ature of the examination, no minimum classification scoreas established.
Statistical analysis was performed using SPSS® soft-are v.23. All statistical calculations were done considering
< 0.05 as statistically significant.The descriptive analysis presents categoric variables as
requencies and percentages, and continuous variables aseans and standard deviations.Two study group were considered, according to year of
esidency at the time the evaluation was performed. Group included 2nd and 3rd year residents, and Group 2 includedth and 5th-year residents. Means of group scores (contin-ous variables) were compared by the Student t-test. Theomparison between the two groups for qualitative variablesas checked by the Chi-Square test.
esults
ue to the dynamic and complex nature of the examina-ion, it was not possible to, in some assessments, register‘completed/not completed’’ for all tasks on the assess-ent table, having been registered as missing (total of 4).
tatistical analysis was adjusted accordingly. As previouslytated, we studied a convenience sample, therefore it wasot homogeneous regarding year of residency, with 64% ofhe participants (n = 16) represented by 4th and 5th-yearesidents.
The performance of each task during the simulation sce-ario, is shown in Table 1 according to the group.
Considering a global classification of 100% to execute allasks on the evaluation table, the total mean score attainedas 64.29% ± 13.62, with a minimum of 43% and a maximumf 86%. Group 1 attained a mean score of 70.63% ± 14.04
todw
25
omit.
hile Group 2 showed a mean score of 60.27% ± 11.94.espite the higher mean score of Group 1 versus Group 2, webserved no statistically significant difference (p = 0.063).
The median number of tasks completed was nine, sevenf which were completed by over 75% of the residents. Itemsith a higher completion rate were administration of opioid
100%), rapid sequence induction technique (100%), pre-xygenation (92%), prophylaxis of pulmonary aspiration ofastric content (84%) and obtaining patient́s past medicalistory (84%). On the other hand, items with higher non-ompletion rates were confirmation of the presence of aediatrician (64%), confirmation of administration of oxy-ocin after fetal extraction (56%), PONV prophylaxis (56%)nd Airway (AW) assessment before induction (48%).
No significant statistical differences were observedetween groups 1 and 2 in relation to the tasks more, andess frequently executed (Tables 2 and 3).
Concerning tasks related to AW management, verificationf suction device operation, and checking and preparing air-ay material were carried out consistently (72% and 76%,
espectively). Tasks related to airway equipment includedhecking the availability of face masks and Endotrachealubes (ETT) of several sizes, in addition to availability ofifficult airway devices. As to the latter, there was greatariability in individual choices, making the classificationmpossible. Fasting time was checked by 76% of residents.ositioning the patient with left uterine displacement wasonfirmed in 68% of cases.
Regarding induction drug choice, 68% opted for thiopen-
al and 32% for propofol. For neuromuscular relaxation, 92%pted for suxametonium and 8% for rocuronium. The medianose of fentanyl administered was 100 �g in both groups,ith a wide range between minimum, 50 �g, and maximum,6
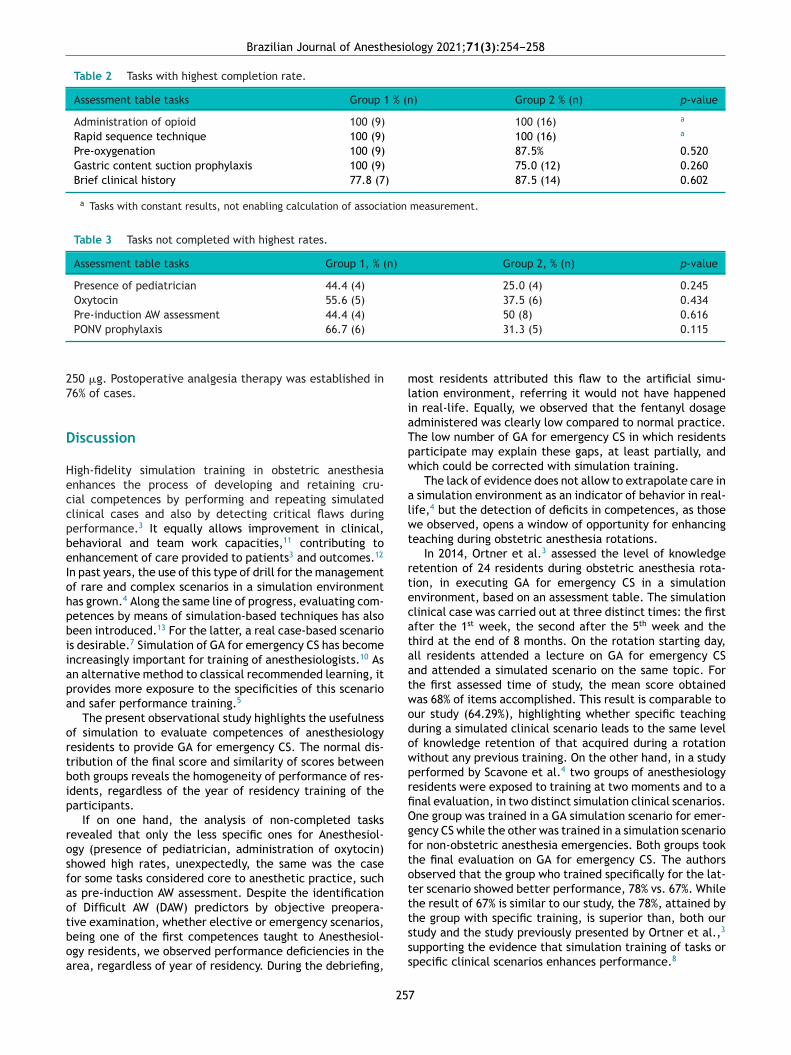
Brazilian Journal of Anesthesiology 2021;71(3):254---258
Table 2 Tasks with highest completion rate.
Assessment table tasks Group 1 % (n) Group 2 % (n) p-value
Administration of opioid 100 (9) 100 (16) a
Rapid sequence technique 100 (9) 100 (16) a
Pre-oxygenation 100 (9) 87.5% 0.520Gastric content suction prophylaxis 100 (9) 75.0 (12) 0.260Brief clinical history 77.8 (7) 87.5 (14) 0.602
a Tasks with constant results, not enabling calculation of association measurement.
Table 3 Tasks not completed with highest rates.
Assessment table tasks Group 1, % (n) Group 2, % (n) p-value
Presence of pediatrician 44.4 (4) 25.0 (4) 0.245Oxytocin 55.6 (5) 37.5 (6) 0.434Pre-induction AW assessment 44.4 (4) 50 (8) 0.616
27
D
HeccpbeIohpbiiapa
ortbip
rosfaotboa
mliaTpw
alwt
rtecataatwodowprfiOgftott
PONV prophylaxis 66.7 (6)
50 �g. Postoperative analgesia therapy was established in6% of cases.
iscussion
igh-fidelity simulation training in obstetric anesthesianhances the process of developing and retaining cru-ial competences by performing and repeating simulatedlinical cases and also by detecting critical flaws duringerformance.3 It equally allows improvement in clinical,ehavioral and team work capacities,11 contributing tonhancement of care provided to patients3 and outcomes.12
n past years, the use of this type of drill for the managementf rare and complex scenarios in a simulation environmentas grown.4 Along the same line of progress, evaluating com-etences by means of simulation-based techniques has alsoeen introduced.13 For the latter, a real case-based scenarios desirable.7 Simulation of GA for emergency CS has becomencreasingly important for training of anesthesiologists.10 Asn alternative method to classical recommended learning, itrovides more exposure to the specificities of this scenariond safer performance training.5
The present observational study highlights the usefulnessf simulation to evaluate competences of anesthesiologyesidents to provide GA for emergency CS. The normal dis-ribution of the final score and similarity of scores betweenoth groups reveals the homogeneity of performance of res-dents, regardless of the year of residency training of thearticipants.
If on one hand, the analysis of non-completed tasksevealed that only the less specific ones for Anesthesiol-gy (presence of pediatrician, administration of oxytocin)howed high rates, unexpectedly, the same was the caseor some tasks considered core to anesthetic practice, suchs pre-induction AW assessment. Despite the identificationf Difficult AW (DAW) predictors by objective preopera-
ive examination, whether elective or emergency scenarios,eing one of the first competences taught to Anesthesiol-gy residents, we observed performance deficiencies in therea, regardless of year of residency. During the debriefing,tsss
25
31.3 (5) 0.115
ost residents attributed this flaw to the artificial simu-ation environment, referring it would not have happenedn real-life. Equally, we observed that the fentanyl dosagedministered was clearly low compared to normal practice.he low number of GA for emergency CS in which residentsarticipate may explain these gaps, at least partially, andhich could be corrected with simulation training.
The lack of evidence does not allow to extrapolate care in simulation environment as an indicator of behavior in real-ife,4 but the detection of deficits in competences, as thosee observed, opens a window of opportunity for enhancing
eaching during obstetric anesthesia rotations.In 2014, Ortner et al.3 assessed the level of knowledge
etention of 24 residents during obstetric anesthesia rota-ion, in executing GA for emergency CS in a simulationnvironment, based on an assessment table. The simulationlinical case was carried out at three distinct times: the firstfter the 1st week, the second after the 5th week and thehird at the end of 8 months. On the rotation starting day,ll residents attended a lecture on GA for emergency CSnd attended a simulated scenario on the same topic. Forhe first assessed time of study, the mean score obtainedas 68% of items accomplished. This result is comparable tour study (64.29%), highlighting whether specific teachinguring a simulated clinical scenario leads to the same levelf knowledge retention of that acquired during a rotationithout any previous training. On the other hand, in a studyerformed by Scavone et al.4 two groups of anesthesiologyesidents were exposed to training at two moments and to anal evaluation, in two distinct simulation clinical scenarios.ne group was trained in a GA simulation scenario for emer-ency CS while the other was trained in a simulation scenarioor non-obstetric anesthesia emergencies. Both groups tookhe final evaluation on GA for emergency CS. The authorsbserved that the group who trained specifically for the lat-er scenario showed better performance, 78% vs. 67%. Whilehe result of 67% is similar to our study, the 78%, attained by
he group with specific training, is superior than, both ourtudy and the study previously presented by Ortner et al.,3upporting the evidence that simulation training of tasks orpecific clinical scenarios enhances performance.8
7

lves,
G2sdtmotar
rtdgih
ttsgi
eteppi
C
Ogpm
tna
wgatoc
F
Ts
C
T
R
1
1
12. Park CS. Simulation and quality improvement in anesthesiology.
J.A. Teixeira, C. A
Even though the best results attained by residents ofroup 1 (2nd and 3rd years) in comparison to those of Group
(4th and 5th years) did not show statistical significance,uch findings deserve some consideration. Although confi-entiality was recommended to all participants regardinghe clinical scenario evaluated, it is likely that some infor-ation sharing occurred. Moreover, the fact that residents
f Group 1 were evaluated right after the end of the rota-ion, unlike residents of Group 2, who were evaluated after
longer time frame, may also explain the difference inesults.
Our study has some limitations. The small sample sizeeduced the power of statistical analysis. The retrospec-ive design of the study decreased accuracy of registrations,one by direct observation, without using video imaging,enerating missing data in the final sample. The impossibil-ty of assuring no information sharing among residents mayave been a bias factor.
Among the strong aspects of the study, stands out the facthat it is the first performed in Portugal based on an innova-ive evaluation tool: holding a clinical case in a high-fidelityimulation environment and conducting it by anesthesiolo-ists with major experience in obstetrics and regular activityn the clinical simulation field.
This study highlights the potential of simulation as anvaluation tool in this scenario, but also shows the needo develop a standardized, practical, and straightforwardvaluation model that reflects objective acquisition of com-etences by residents during obstetric anesthesia rotation,articularly dealing with rare and complex clinical scenar-os.
onclusion
verall performance of residents in a GA scenario for emer-ency CS was satisfactory and comparable to other resultsreviously published. The year of residency was not a deter-ining factor for the final score.Transposition of management in a simulated environment
o clinical practice, although pointed out as likely, shouldot be taken for granted, and should deserve more amplend detailed investigation.
The definition of the training methods and acquaintanceith less frequent clinical scenarios is essential for futureenerations of health professionals. Therefore, designing
nd improving education plans to improve anesthesiologyeaching should be a priority, and the results of this andther similar studies may be the starting point for this pro-ess.1
25
C. Martins et al.
unding
he authors performed the study without receiving financialupport.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Boerma T, Ronsmans C, Melesse DY, et al. Global epidemiol-ogy of use of and disparities in caesarean sections. Lancet.2018;392:1341---8.
2. Bucklin BA, Hawkins JL, Anderson JR, Ullrich FA. Obstetric anes-thesia workforce survey: twenty-year update. Anesthesiology.2005;103:645---53.
3. Ortner CM, Richebé P, Bollag LA, Ross BK, Landau R. Repeatedsimulation-based training for performing general anesthesia foremergency cesarean delivery: long-term retention and recur-ring mistakes. Int J Obstet Anesth. 2014;23:341---7.
4. Scavone BM, Toledo P, Higgins N, Wojciechowski K, McCarthy RJ.A randomized controlled trial of the impact of simulation-basedtraining on resident performance during a simulated obstetricanesthesia emergency. Simul Healthc. 2010;5:320---4.
5. Lipman S, Carvalho B, Brock-Utne J. The demise of generalanesthesia in obstetrics revisited: prescription for a cure. IntJ Obstet Anesth. 2005;14:2---4.
6. Tofil NM, Dollar J, Zinkan L, et al. Performance of anesthe-sia residents during a simulated prone ventricular fibrillationarrest in an anesthetized pediatric patient. Paediatr Anaesth.2014;24:940---4.
7. Murray DJ. Current trends in simulation training in anesthesia:a review. Minerva Anestesiol. 2011;77:528---33.
8. Schornack LA, Baysinger CL, Pian-Smith MCM. Recent advancesof simulation in obstetric anesthesia. Curr Opin Anaesthesiol.2017;30:723---9.
9. Blum RH, Muret-Wagstaff SL, Boulet JR, et al. Simulation-based assessment to reliably identify key resident performanceattributes. Anesthesiology. 2018;128:821---31.
0. Scavone BM, Sproviero MT, McCarthy RJ, et al. Developmentof an objective scoring system for measurement of residentperformance on the human patient simulator. Anesthesiology.2006;105:260---6.
1. Lorello GR, Cook DA, Johnson RL, Brydges R. Simulation-basedtraining in anaesthesiology: a systematic review and meta-analysis. Br J Anaesth. 2014;112:231---45.
Anesthesiol Clin. 2011;29:13---28.3. Wong AK. Full scale computer simulators in anesthesia training
and evaluation. Can J Anaesth. 2004;51:455---64.
8

C
Idkd
AS
a
b
c
d
e
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):259---264
LINICAL RESEARCH
ntubating conditions and hemodynamic changesuring awake fiberoptic intubation using fentanyl withetamine versus dexmedetomidine for anticipatedifficult airway: a randomized clinical trial�
nil Kumar Vermaa, Shipra Verma b,∗, Amiya Kumar Barikc, Vinay Kanaujia d,angeeta Aryae
G.S.V.M. Medical College, Department of Anaesthesiology and Critical Care, Kanpur, IndiaS.M.M.H. Medical College, Department of Anaesthesiology and Critical Care, Saharanpur, IndiaAIIMS, Department of Anaesthesiology and Critical Care, Bhopal, IndiaS.M.M.H. Medical College, Department of Physical Medicine & Rehabilitation, Saharanpur, IndiaGovernment Medical College, Department of Obstetrics and Gynaecology, Banda, India
eceived 10 June 2019; accepted 23 January 2021vailable online 17 March 2021
KEYWORDSAirway management;Fiberoptic intubation;Fentanyl;Ketamine;Dexmedetomidine
AbstractBackground and objectives: Awake fiberoptic intubation (AFOI) is usually performed in patientswith an anticipated difficult airway. Various sedation regimens are used during AFOI, however,most of them cause respiratory depression. The present study aims to compare the effectivenessof fentanyl with ketamine versus dexmedetomidine in search of a better sedation regimenwhich would achieve desirable intubating conditions and hemodynamic stability without causingrespiratory depression.Methods: This is a single centered randomized, double-blind clinical trial. Patients of bothsexes between age 18---55 years and ASA (American Society of Anesthesiologists) physical statusI---II with an anticipated difficult airway were randomly divided into two groups of thirty each.Group FK patients received intravenous fentanyl and ketamine, and group DX patients receiveddexmedetomidine, until Ramsay sedation scale ≥ 2. Heart rate (HR), mean blood pressure(MBP), oxygen saturation (SpO2), respiratory rate (RR), endoscopy time, intubation time, firstend-tidal carbon dioxide (ETCO2) after intubation, endoscopist satisfaction score, and patientdiscomfort score were recorded during the study period. The level of recall was assessed onthe next postoperative day.
Results: Endoscopist satisfaction score was better in group DX patients (p < 0.05). There wasa smaller variation in HR and MBP from baseline with dexmedetomidine compared to fentanylwith ketamine. First ETCO2 after intubation was higher in group FK patients (p < 0.05). Nosignificant difference was found in patient discomfort score, intubation time, RR, SpO2 andlevel of recall of the event.� Study conducted at G.S.V.M. Medical College, Department of Anaesthesiology and Critical Care, Kanpur, India.∗ Corresponding author.
E-mail: [email protected] (S. Verma).
ttps://doi.org/10.1016/j.bjane.2021.01.005 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).

A.K. Verma, S. Verma, A.K. Barik et al.
Conclusions: The use of dexmedetomidine in AFOI provides better intubating conditions andhemodynamic stability compared to fentanyl with ketamine.© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
I
Mai(mcwTacipsA
ialdmaDw
tdTctr
M
A(paftbcBceacrfd
9prineAI3ewlhos
gIaSdbs
l2pa
cpcItuXecoAlwti0a
ntroduction
anagement of difficult airway is a routine affair for thenesthesiologists. A meticulous approach is paramount forts successful management. Awake fiberoptic intubationAFOI) is considered the gold standard technique for theanagement of an anticipated difficult airway.1 An ideal
ondition for AFOI requires a calm, cooperative patientith blunted airway reflex to facilitate easy intubation.herefore, it is necessary to provide adequate anxiolysis,nalgesia, and topical anesthesia for the airway withoutausing respiratory depression. Previously, various drug reg-mens either alone or in combinations has been tried for thisurpose. However, most of them cause respiratory depres-ion leading to airway obstruction, which is undesirable forFOI.
Fentanyl with ketamine could offer hemodynamic stabil-ty with little respiratory side effects.2 Besides, ketaminettenuates the fentanyl-induced reduction in minute venti-ation and suppresses fentanyl-induced cough.2,3 Whereas,exmedetomidine has gained popularity as a preferrededication for conscious sedation.4 It also has anxiolytic,
mnestic, analgesic, as well as antisialogogue properties.5
exmedetomidine has a respiratory sparing effect evenhen administered in large doses.6,7
Thus, we hypothesized that better intubating condi-ions and hemodynamic stability will be achieved withexmedetomidine as compared to fentanyl with ketamine.his study was carried out with the primary objective toompare the AFOI conditions and with the secondary objec-ive to compare the hemodynamic parameters and level ofecall between the two groups.
ethods
fter approval from the Institutional Ethical CommitteeEC/29/09/16/05), this randomized, double-blind study waslanned, and written informed consent was obtained fromll the patients. The study was carried out at our instituteor over one year. Block randomization was performed usinghe opaque sealed envelope technique to get an equal num-er of patients in each group. All the patients included gaveonsent for the present study, and there was no dropout.oth patients and the anesthesiologist assigned for dataollection were kept blinded throughout the study. Differ-nt anesthesiologists were assigned for performing sedationnd AFOI. For blinding, patients of both the groups were
onnected to intravenous (IV) infusion, group FK patientseceived 0.9% normal saline after receiving study drugs (IVentanyl with ketamine), and group DX patients receivedexmedetomidine infusion as per the recommended dose.pcae
26
Based on the previous literature,8 taking a power of0% and � error of 0.05 for this study, the minimum sam-le size was calculated to be twelve per group with a 20%eduction in endoscopy time. So finally, 30 patients werencluded in each group to meet the minimum number oformal distribution. After randomization, 60 patients ofither sex between 18---55 years of age, belonging to themerican Society of Anesthesiologists (ASA) physical status
---II with an anticipated difficult airway (Mallampati grade and 4 with mouth opening less than 5 cm) planned forlective surgery enrolled for the study. Exclusion criteriaere patient’s refusal to consent, a nasal mass, coagu-
ation disorder, allergy to study medication, uncontrolledypertension, pregnancy, ischemic heart disease, hepaticr renal disorders, and history of recent nasopharyngealurgery.
Enrolled patients were randomly allocated into tworoups with 30 patients each. Group FK: patients receivedV fentanyl 2 �g.kg-1 and IV ketamine 0.25 mg.kg-1 with andditional equivalent dose to achieve a Ramsay Sedationcale (RSS) score of ≥ 2.9 Group DX: patients received IVexmedetomidine 1 �g.kg-1 over 10 minutes bolus followedy an infusion of 0.2 to 0.7 �g.kg-1.hour-1 to achieve an RSScore of ≥ 2.9
Ramsay Sedation Scale (RSS) was used to assess the awakeevels: 1) patient anxious and agitated, or restless, or both,) patient cooperative, orientated, and tranquil, 3) theatient responds to commands only, 4) a brisk response, 5)
sluggish response, and 6) no response.9
Patients were shifted to the operation room (OR) afteronfirming nil per oral status. Standard ASA monitors likeulse oximetry, noninvasive blood pressure (NIBP), electro-ardiogram (ECG), and temperature probe were attached.V access secured with 18G cannula and ringer lactate solu-ion infused. Preoperatively nasal patency test carried outsing cotton and nostril with better patency was preferred.ylometazoline 0.1 % (as a nasal decongestant) two drops inach nostril instilled 15 minutes before the start of the pro-edure. The patients received topical anesthesia with 5 mLf 4% lignocaine as nebulization for about 10---15 minutes.ll the patients were premedicated with IV glycopyrro-
ate 0.2 mg 10 minutes before the planned procedure andith ondansetron 4 mg. Study drugs were administered to
he patients as per group allocation. All the patients werentubated awake using a fiberoptic bronchoscope (IPX7 S/N5148). The same anesthesiologist performed the AFOI forll the patients. After the successful passage of the appro-riate-sized endotracheal tube (ETT) through the vocal
ord, the tube position was confirmed with capnographynd bilateral symmetrical air entry on auscultation. Gen-ral anesthesia was induced using IV propofol 2 mg.kg-10
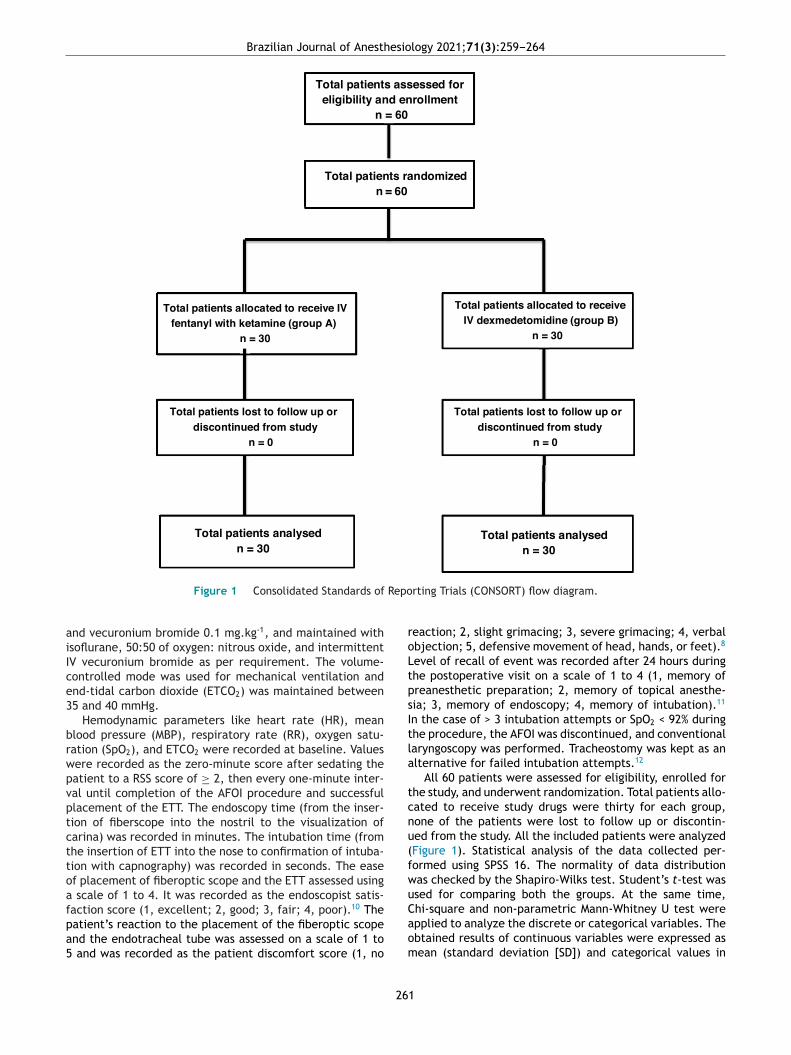
Brazilian Journal of Anesthesiology 2021;71(3):259---264
Total patients ass ess ed for eli gibili ty and enroll ment
n = 60
Total patients randomizedn = 60
Total patients allocated to rece ive IVfentanyl with ketamine (group A)
n = 30
Total patients allocated to re ceive IV dexmedetomidine (group B)
n = 30
Total patients lost to follow up or discontinued from study
n = 0
Total patients lost to follow up or discontinued from study
n = 0
Total patients analysed n = 30
Total patients analysed n = 30
Repo
aiIce3
brwpvptcttoafpa5
roLtpsItla
tcnu(fwuC
Figure 1 Consolidated Standards of
nd vecuronium bromide 0.1 mg.kg-1, and maintained withsoflurane, 50:50 of oxygen: nitrous oxide, and intermittentV vecuronium bromide as per requirement. The volume-ontrolled mode was used for mechanical ventilation andnd-tidal carbon dioxide (ETCO2) was maintained between5 and 40 mmHg.
Hemodynamic parameters like heart rate (HR), meanlood pressure (MBP), respiratory rate (RR), oxygen satu-ation (SpO2), and ETCO2 were recorded at baseline. Valuesere recorded as the zero-minute score after sedating theatient to a RSS score of ≥ 2, then every one-minute inter-al until completion of the AFOI procedure and successfullacement of the ETT. The endoscopy time (from the inser-ion of fiberscope into the nostril to the visualization ofarina) was recorded in minutes. The intubation time (fromhe insertion of ETT into the nose to confirmation of intuba-ion with capnography) was recorded in seconds. The easef placement of fiberoptic scope and the ETT assessed using
scale of 1 to 4. It was recorded as the endoscopist satis-action score (1, excellent; 2, good; 3, fair; 4, poor).10 The
atient’s reaction to the placement of the fiberoptic scopend the endotracheal tube was assessed on a scale of 1 toand was recorded as the patient discomfort score (1, no
aom
26
rting Trials (CONSORT) flow diagram.
eaction; 2, slight grimacing; 3, severe grimacing; 4, verbalbjection; 5, defensive movement of head, hands, or feet).8
evel of recall of event was recorded after 24 hours duringhe postoperative visit on a scale of 1 to 4 (1, memory ofreanesthetic preparation; 2, memory of topical anesthe-ia; 3, memory of endoscopy; 4, memory of intubation).11
n the case of > 3 intubation attempts or SpO2 < 92% duringhe procedure, the AFOI was discontinued, and conventionalaryngoscopy was performed. Tracheostomy was kept as anlternative for failed intubation attempts.12
All 60 patients were assessed for eligibility, enrolled forhe study, and underwent randomization. Total patients allo-ated to receive study drugs were thirty for each group,one of the patients were lost to follow up or discontin-ed from the study. All the included patients were analyzedFigure 1). Statistical analysis of the data collected per-ormed using SPSS 16. The normality of data distributionas checked by the Shapiro-Wilks test. Student’s t-test wassed for comparing both the groups. At the same time,hi-square and non-parametric Mann-Whitney U test were
pplied to analyze the discrete or categorical variables. Thebtained results of continuous variables were expressed asean (standard deviation [SD]) and categorical values in1

A.K. Verma, S. Verma, A.K. Barik et al.
Table 1 Demographic characteristics and ASA physical status.
Parameters Group FK (n = 30) Group DX (n = 30) p-value
Age (years) 31.2 (13.7) 28.6 (15.9) 0.511Gender (male/female) 13/17 8/22 0.176Weight (kg) 57.1 (6.3) 59.9 (6.4) 0.074ASA class (I/II) 18/12 24/6 0.091
n, number; ASA, American Society of Anesthesiologists.Data expressed as mean (standard deviation) or as a number.Using Unpaired t-test for age and weight, Chi-Square test for gender and ASA class.
Table 2 Awake fiberoptic intubation parameters among groups.
AFOI Parameters Group FK (n = 30) Group DX (n = 30) p-value
Endoscopy time (minutes) 3.5 (1.1) 2.7 (0.8) 0.001a
Intubation time (seconds) 39.2 (10.5) 38.0 (11.2) 0.538First end tidal CO2 after intubation 41.2 (4.3) 39.3 (2.7) 0.015a
n, number; AFOI, awake fiberoptic intubation.Data are expressed as the mean (standard deviation).Using Unpaired t-test.Endoscopy time (from the insertion of fiberscope into the nostril to the visualization of carina).
nose
peapc0
R
TcAati(svg3gsawwFhpawo(
bk
diw(
recwndt
D
TkcarAhcDwtetwid
Intubation time (from the insertion of endotracheal tube into thea Significant (p < 0.05).
ercentage (%). The values obtained were dichotomized forndoscopist satisfaction score as good satisfaction score (1nd 2) and poor satisfaction score (3 and 4), similarly foratient discomfort score as some discomfort (1 and 2), andonsiderable discomfort (3, 4, and 5). A p-value of less than.05 was considered to be significant.
esults
he demographic variables and ASA physical status wereomparable (p > 0.05) between the two groups (Table 1).ll the patients underwent successful AFOI in a singlettempt. There was a significant difference in endoscopyime between the two groups (p < 0.05), which was moren group FK (3.45 ± 1.02 minutes) compared to group DX2.70 ± 0.80 minutes) (Table 2). The intubation time wasimilar between both the groups (p > 0.05). The first ETCO2
alue after tracheal intubation was significantly higher inroup FK compared to group DX (41.20 ± 4.25 mmHg vs.9.26 ± 2.72 mmHg) (Table 2). Endoscopists experienced aood satisfaction score for 22 versus 28 patients and pooratisfaction scores for 8 versus 2 patients among groups FKnd DX, respectively. So, the endoscopist satisfaction scoreas significantly better in group DX. Patient discomfort scoreas comparable between both groups. Among the groupK patients, 24 experienced slight or no discomfort, and 6ad considerable or severe discomfort, similarly among theatients of group DX, 29 experienced slight or no discomfort,nd one had significant or severe discomfort (Table 3). Thereas no difference in recall or awareness among the patientsf both the groups during the AFOI procedure (p > 0.05)
Table 3).There was a smaller variation in HR and MBP fromaseline with dexmedetomidine compared to fentanyl withetamine combination. Statistically, significant intergroup
TM
s
26
to confirmation of intubation with capnography).
ifferences were observed in HR and MBP from the start-ng of the AFOI procedure and 5 minutes thereafter, whichas significantly higher in group FK compared to group DX
p < 0.05) (Table 4).Patients of both groups maintained arterial oxygen satu-
ation within the satisfactory level (97% to 99%) during thentire procedure of AFOI, and changes were found statisti-ally insignificant (Table 4). Changes in RR of both groupsere comparable throughout the procedure. There wereo hemodynamic complications like bradycardia, tachycar-ia, hypotension, hypertension, arrhythmia, desaturationhroughout the procedure in both the groups.
iscussion
his study compared the effectiveness of fentanyl withetamine versus dexmedetomidine in achieving a favorableondition for AFOI. The role of fentanyl as an effectivenalgesic and anxiolytic drug is well known, but it causesespiratory depression, which is not desirable for AFOI.dding a low dose of ketamine to fentanyl enhances theemodynamic stability. However, fentanyl with ketamineauses a simultaneous increase in oxygen consumption.11
exmedetomidine is a selective �2 agonist, causes sedationithout loss of consciousness or respiratory depression. In
his study, ETCO2 value was recorded for confirmation ofndotracheal intubation as well as to assess the respira-ory depressant effect of the study drugs.13 The first ETCO2
as significantly higher in group FK compared to group DX,ndicating that fentanyl associated with ketamine may pro-uce more respiratory depression than dexmedetomidine.
his study result is in agreement with the trial conducted byidth et al.2The endoscopic procedures are commonly used for bothcreening as well as therapeutic purposes. For a successful
2
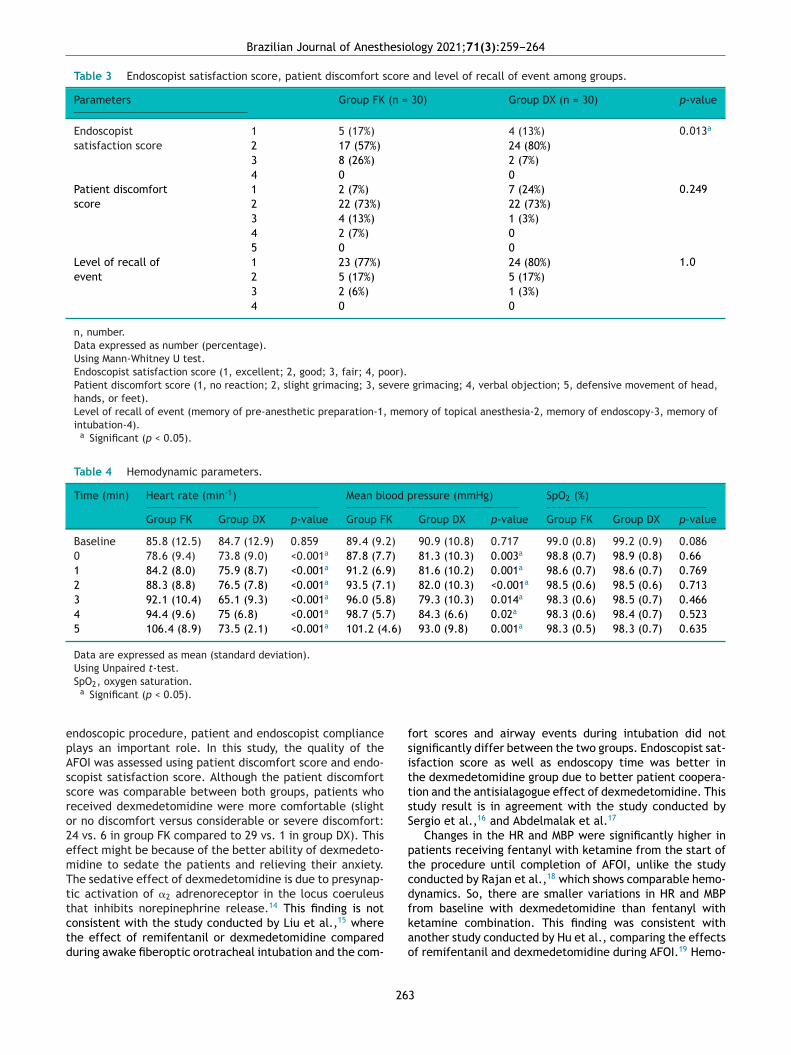
Brazilian Journal of Anesthesiology 2021;71(3):259---264
Table 3 Endoscopist satisfaction score, patient discomfort score and level of recall of event among groups.
Parameters Group FK (n = 30) Group DX (n = 30) p-value
Endoscopistsatisfaction score
1 5 (17%) 4 (13%) 0.013a
2 17 (57%) 24 (80%)3 8 (26%) 2 (7%)4 0 0
Patient discomfortscore
1 2 (7%) 7 (24%) 0.2492 22 (73%) 22 (73%)3 4 (13%) 1 (3%)4 2 (7%) 05 0 0
Level of recall ofevent
1 23 (77%) 24 (80%) 1.02 5 (17%) 5 (17%)3 2 (6%) 1 (3%)4 0 0
n, number.Data expressed as number (percentage).Using Mann-Whitney U test.Endoscopist satisfaction score (1, excellent; 2, good; 3, fair; 4, poor).Patient discomfort score (1, no reaction; 2, slight grimacing; 3, severe grimacing; 4, verbal objection; 5, defensive movement of head,hands, or feet).Level of recall of event (memory of pre-anesthetic preparation-1, memory of topical anesthesia-2, memory of endoscopy-3, memory ofintubation-4).
a Significant (p < 0.05).
Table 4 Hemodynamic parameters.
Time (min) Heart rate (min-1) Mean blood pressure (mmHg) SpO2 (%)
Group FK Group DX p-value Group FK Group DX p-value Group FK Group DX p-value
Baseline 85.8 (12.5) 84.7 (12.9) 0.859 89.4 (9.2) 90.9 (10.8) 0.717 99.0 (0.8) 99.2 (0.9) 0.0860 78.6 (9.4) 73.8 (9.0) <0.001a 87.8 (7.7) 81.3 (10.3) 0.003a 98.8 (0.7) 98.9 (0.8) 0.661 84.2 (8.0) 75.9 (8.7) <0.001a 91.2 (6.9) 81.6 (10.2) 0.001a 98.6 (0.7) 98.6 (0.7) 0.7692 88.3 (8.8) 76.5 (7.8) <0.001a 93.5 (7.1) 82.0 (10.3) <0.001a 98.5 (0.6) 98.5 (0.6) 0.7133 92.1 (10.4) 65.1 (9.3) <0.001a 96.0 (5.8) 79.3 (10.3) 0.014a 98.3 (0.6) 98.5 (0.7) 0.4664 94.4 (9.6) 75 (6.8) <0.001a 98.7 (5.7) 84.3 (6.6) 0.02a 98.3 (0.6) 98.4 (0.7) 0.5235 106.4 (8.9) 73.5 (2.1) <0.001a 101.2 (4.6) 93.0 (9.8) 0.001a 98.3 (0.5) 98.3 (0.7) 0.635
Data are expressed as mean (standard deviation).Using Unpaired t-test.
epAssro2emTttctd
fsittsS
ptcdf
SpO2, oxygen saturation.a Significant (p < 0.05).
ndoscopic procedure, patient and endoscopist compliancelays an important role. In this study, the quality of theFOI was assessed using patient discomfort score and endo-copist satisfaction score. Although the patient discomfortcore was comparable between both groups, patients whoeceived dexmedetomidine were more comfortable (slightr no discomfort versus considerable or severe discomfort:4 vs. 6 in group FK compared to 29 vs. 1 in group DX). Thisffect might be because of the better ability of dexmedeto-idine to sedate the patients and relieving their anxiety.he sedative effect of dexmedetomidine is due to presynap-ic activation of �2 adrenoreceptor in the locus coeruleushat inhibits norepinephrine release.14 This finding is not
onsistent with the study conducted by Liu et al.,15 wherehe effect of remifentanil or dexmedetomidine compareduring awake fiberoptic orotracheal intubation and the com-kao
26
ort scores and airway events during intubation did notignificantly differ between the two groups. Endoscopist sat-sfaction score as well as endoscopy time was better inhe dexmedetomidine group due to better patient coopera-ion and the antisialagogue effect of dexmedetomidine. Thistudy result is in agreement with the study conducted byergio et al.,16 and Abdelmalak et al.17
Changes in the HR and MBP were significantly higher inatients receiving fentanyl with ketamine from the start ofhe procedure until completion of AFOI, unlike the studyonducted by Rajan et al.,18 which shows comparable hemo-ynamics. So, there are smaller variations in HR and MBProm baseline with dexmedetomidine than fentanyl with
etamine combination. This finding was consistent withnother study conducted by Hu et al., comparing the effectsf remifentanil and dexmedetomidine during AFOI.19 Hemo-3

rma,
daT
cbtli
bmhfa
C
T
R
1
1
1
1
1
1
1
1
1
1
20. Patel CR, Engineer SR, Shah BJ, et al. Effect of intravenousinfusion of Dexmedetomidine on perioperative hemodynamicchanges and post-operative recovery. Indian J Anaesth.2012;56:542---6.
A.K. Verma, S. Ve
ynamic stability with the use of dexmedetomidine waslso favoured by another study conducted by Patel et al.20
hroughout the procedure, RR and SpO2 were comparable.However, this study has certain limitations, like single
enter trial, small sample size, problems in maintaininglinding, and variation in tolerance to fiberoptic intuba-ion among patients. In future, multicentric trials involvingarger sample size could be carried out to validate the find-ngs of this study.
In summary, our study has demonstrated that, althoughoth strategies seem to be safe and effective, dexmedeto-idine provides better intubating conditions with smaller
emodynamic variation compared to fentanyl with ketamineor awake fiberoptic intubation in patients with a difficultirway.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Popat M. Practical Fiberoptic Intubation. 1st edition Oxford:Butterworth-Heinemann Publishers; 2001. p. 75---95.
2. Mildh L, Taittonen M, Leino K, et al. The effect of low-dose Ketamine on Fentanyl-induced respiratory depression. Adouble blinded randomized controlled trial. J Clin Anesth.1998;53:965---70.
3. Yeh CC, Wu CT, Huh BK, et al. Premedication with intravenouslow-dose ketamine suppresses fentanyl-induced cough. J ClinAnesth. 2007;19:53---6.
4. Bergese SD, Khabiri B, Roberts WD, et al. Dexmedetomidinefor conscious sedation in difficult awake fibre optic intubationcases. J Clin Anesth. 2007;19:141---6.
5. Bergese SD, Patrick Bender S, McSweeney TD, et al. A compara-tive study of Dexmedetomidine with Midazolam and Midazolamalone for sedation during elective awake fibre optic intubation.J Clin Anesth. 2010;22:35---40.
6. Kamibayashi T, Maze M. Clinical uses of alpha2-adrenergic ago-nists. Anesthesiol. 2000;93:1345---9.
7. Ebert TJ, Hall JE, Barney JA, et al. The effects of increasingplasma concentrations of Dexmedetomidine in humans. Anes-thesiol. 2000;93:382---94.
8. Dhasmana Sc. Nasotracheal fiberoptic intubation: Patient com-fort, intubating conditions and hemodynamic stability duringconscious sedation with different doses of Dexmedetomidine. JMaxillofac Oral Surg. 2014;13:53---8.
26
A.K. Barik et al.
9. Ramsay MA, Savege TM, Simpson BR, et al. Controlled sedationwith alphaxalone-alphadolone. Br Med J. 1974;2:656---9.
0. Masoud S, El-Tohamy S, Amin A. Dexmedetomidine versus mida-zolam/propofol or midazolam/Fentanyl for conscious sedationduring awake fiberoptic intubation. Ain-Shams J Anaesthesiol.2013;6, 30---30.
1. Sinha SK, Joshiraj B, Chaudhary L, et al. A comparison ofDexmedetomidine plus Ketamine combination with Dexmedeto-midine alone for awake fiberoptic nasotracheal intubation: Arandomized controlled study. J Anaesthesiol Clin Pharmacol.2014;30:514---9.
2. Ovassapian A, Tuncbilek M, Weitzel EK, et al. Airway manage-ment in adult patients with deep neck infections: a case seriesand review of the literature. Anesth Analg. 2005;100:585---9.
3. Apfelbaum JL, Hagberg CA, Caplan RA, et al. Practice guidelinesfor management of the difficult airway: an updated report bythe American Society of Anesthesiologists Task Force on Manage-ment of the Difficult Airway. Anesthesiology. 2013;118:251---70.
4. Hall JE, Uhrich TD, Barney JA, et al. Sedative, amnestic, andanalgesic properties of small --- dose dexmedetomidine infu-sions. Anesth Analg. 2000;90:699---705.
5. Liu HH, Zhou T, Wei JQ, et al. Comparison between remifen-tanil and Dexmedetomidine for sedation during modified awakefiberoptic intubation. Exp Ther Med. 2015;9:1259---64.
6. Bergese SD, Dzwonczyk R. A comparative study of Dexmedeto-midine with midazolam and midazolam alone for sedationduring elective awake fibre optic intubation. J Clin Anesth.2010;22:35---40.
7. Abdelmalak B, Makary L, Hoban J, et al. Dexmedetomidine assole sedative for awake intubation in management of the criticalairway. J Clin Anesth. 2007;19:370---3.
8. Rajan S, Talukdar R, Tosh P, et al. Hemodynamic Responses andSafety of Sedation Following Premedication with Dexmedeto-midine and Fentanyl during Fiberoptic-assisted Intubation inPatients with Predicted Difficult Airway. Anesth Essays Res.2018;12:11---5.
9. Hu R, Liu JX, Jiang H. Dexmedetomidine versus remifentanilsedation during awake fibre optic nasotracheal intubation:A double --- blinded randomized controlled trial. J Anesth.2013;27:211---7.
4

C
Riap
JFCLS
a
b
Bc
d
e
B
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):265---270
LINICAL RESEARCH
eferral to immediate postoperative care in anntensive care unit from the perspective ofnesthesiologists, surgeons, and intensive carehysicians: a cross-sectional questionnaire
oão Manoel Silva Jr a,b,c,d,∗, Henrique Tadashi Katayamab,elipe Manuel Vasconcellos Lopesa, Diogo Oliveira Toledob,c,ristina Prata Amendolad, Fernanda dos Santos Oliveiraa,eusi Magda Romano Andrausa, Maria José C. Carmonab,uzana Margareth Loboe, Luiz Marcelo Sá Malbouissonb
Hospital Servidor Público Estadual de São Paulo, Departamento de Anestesiologia, São Paulo, SP, BrazilUniversidade de São Paulo (USP), Faculdade de Medicina (FM), Hospital das Clínicas, Divisão de Anestesiologia, São Paulo, SP,razilHospital Israelita Albert Einstein, Departamento de Pacientes Graves, São Paulo, SP, BrazilHospital de Câncer de Barretos, Departamento de Anestesiologia e Terapia Intesiva, Barretos, SP, BrazilFaculdade de Medicina de São José do Rio Preto (FAMERP), Hospital de Base de São José do Rio Preto, São José do Rio Preto, SP,razil
eceived 3 June 2019; accepted 13 March 2021vailable online 27 April 2021
KEYWORDSSurgical procedures;Post-operative care;Patient selectioncriteria;Intensive care;Anesthesiologists;Surgeons
AbstractIntroduction and objective: Due to the high cost and insufficient offer, the request for IntensiveCare (ICU) beds for postoperative recovery needs adequate criteria. Therefore, we studied thecharacteristics of patients referred to postoperative care at an ICU from the perspective ofanesthesiologists, surgeons, and intensive care physicians.Methods: A questionnaire on referrals to postoperative intensive care was applied to physiciansat congresses in Brazil. Anesthesiologists, surgeons, and intensive care physicians who agreedto fill out the questionnaire were included. The questionnaire consisted of hypothetical clinicalscenarios and cases for participants to choose which would be the priority for referral to the
ICU.Results: 360 physicians participated in the study, with median time of 10 (5---18) years aftergraduation. Of the interviewees, 36.4% were anesthesiologists, 30.0% surgeons, and 33.6% inten-sive care physicians. We found that anesthesiologists were more conservative, and surgeons less∗ Corresponding author.E-mail: [email protected] (J.M. Silva Jr).
ttps://doi.org/10.1016/j.bjane.2021.03.025 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).

J.M. Silva Jr, H.T. Katayama, F.M. Lopes et al.
conservative in ICU referrals. As to patients with risk of bleeding, 75.0% of the surgeons wouldrefer them to the ICU, in contrast with 52.1% of the intensive care physicians, and 43.5% of theanesthesiologists (p < 0.001). As to elderly persons with limited reserve, 62.0% of the surgeonswould refer them to the ICU, in contrast with 47.1% of the intensive care physicians, and 22.1%of the anesthesiologists (p < 0.001). As to patients with risk of respiratory complications, 64.5%of the surgeons would recommend the ICU, versus 43.0% of the intensive care physicians, and32.1% of the anesthesiologists (p < 0.001). Intensive care physicians classified priorities betterin indicating ICU, and the main risk indicator was the ASA physical status in all specialties(p < 0.001). There was no agreement among the specialties and surgeries on prioritizing post-operative intensive care.Conclusion: Anesthesiologists, surgeons, and intensive care physicians presented different per-spectives on postoperative referral to the ICU.© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
I
Tchpstctppdpd
tietaat
sabm
arsttt
M
ACtr
mA
caphtttticigaso
mmooip
ottasferFaeoM
ntroduction
he criteria for referring postoperative patients to intensiveare are unclear and, for this reason, physicians commonlyave different opinions.1,2 Based on ethical and scientificrinciples, front-line physicians making such critical deci-ions should be able to go through this process according tohe best evidence.3 To make this decision, they take intoonsideration, in addition to diagnosis and clinical status ofhe patient, bed availability and the actual benefit for theatient of the proposed therapy and prognosis.4 In general,atients who are in the terminal phases of their diseases andying patients without a chance of recovery are not appro-riate for admission to an ICU, except as potential organonors.5
Deciding about the need for intensive care are amonghe responsibilities of physicians of different specialties:nternal medicine, anesthesiologists, and surgeons. How-ver, there are interpersonal discrepancies with regard tohe interpretation of clinical cases, severity, effectiveness,nd potential resolution with intensive care.6---8 This discrep-ncy makes different professionals have different visions ofhe criteria for referral to intensive care.
In this manner, in assessing referral to intensive care forurgical patients, it is appropriate to define which criteriare considered the most important, in addition to the possi-ility of finding discrepancies in interferences on the correctanagement of these patients in the postoperative period.The objective of the present study was to assess, through
questionnaire answered by physicians, how postoperativeeferrals of surgical patients to the ICU would be from thetandpoint of anesthesia, surgery, and intensive care prac-itioners. To do that, different standpoints were comparedo find trends in referrals to the ICU, according to the par-icipants’ profiles.
ethods
fter approval by the ethics committee of Hospital deâncer de Barretos, a questionnaire (Annex 1: Supplemen-ary Materials) on physicians’ decision about postoperativeeferral of surgical patients to an ICU was applied at major
atn
26
edical congresses in Brazil (World Intensive Care Congress,CERTO, São Paulo State’s Congress of Anesthesiology).
Surgeons, anesthesiologists, and intensive care physi-ians who agreed to fill out the questionnaire handed outt medical congresses and who did it adequately and com-letely were included in the study. However, non-medicalealthcare practitioners and physicians who graduated lesshan 2 years before were excluded. Participation was volun-ary and consent for participation was implied by filling outhe questionnaire. The survey was anonymous, although par-icipants had the choice of leaving comments or requestingnformation at a station inside the congresses. The medi-al specialties were compared as to their decisions. Thentention was to apply the questionnaire at medical con-resses that were not specialized on a single surgical area,nd for this reason, it included a broad range of surgeries,o that we could obtain better performance in the answersf participants.
The questionnaire consisted of six main segments withultiple choice and direct questions, and the first two wereeant to identify the participants and characteristics of the
rganizations where they work, taking into account the typef hospital (private, public, university), and their capabil-ties (total number of beds, ICU beds, monthly surgeries,atients sent to the ICU).
The third segment of the questionnaire had the intentionf presenting situations of surgical patients for participantso decide if they would, hypothetically, refer the patient tohe intensive care unit or not. Seven cases were reported,ll referring to postoperative intensive care for several rea-ons (potential blood loss, limited reserve, acute respiratoryailure, major surgery, sepsis, and hemodynamic instability),xcept for one of the cases, which did not meet crite-ia for recommendations of postoperative intensive care.or each of those hypothetical situations, participants weresked if they would recommend admission to an ICU forach patient’s postoperative care. There was no mentionf priorities or shortage of beds (Annex 1: Supplementaryaterials).
In the following segment, surgical cases were presented,
nd participants classified each situation according to aable of priorities: 1) Critically ill and unstable patient whoeeds intensive care that cannot be provided outside an6

esio
Inrifi
ci
ptcaa
am
S
AccnpebI
apwvt
(mnvw
(s
R
TbatoftN13a4(w
wiatf
cIttotmw(
dwtepgewerP-mppt
pic
tf
to
seolb(
D
Iit
Brazilian Journal of Anesth
CU; 2) Patient who needs intensive monitoring and mayeed immediate intervention; 3) Critically ill patient witheduced likelihood of survival; and 4) Patients generallynappropriate for admission in an ICU. This priority classi-cation has already been reported before.1,4
All scenarios reported in the questionnaire are based onriteria that define high surgical risk patients, as describedn the literature.9
The fifth segment presented the profile of a patient withhysical status II according to the American Society of Anes-hesiologists (ASA), with eight types of surgery which he/sheould have, and participants were asked to classify surgeriesccording to the priority for referral to postoperative ICUdmission.
Last, participants were asked to choose the criteria usedt their hospital to identify surgical risk (ASA, SAPS3, Shoe-aker, POSSUM, or other).
tatistical analysis
ccording to clinical experience and using the minimallinically significant difference among the groups for thealculation, a sample of at least 400 participants would beecessary to produce a 30% chance (answer differentiationercentage between specialties) of an alternative hypoth-sis and a 2% chance (answer differentiation percentageetween specialties) of a null hypothesis, accepting a type
error of 0.05 (unilateral) and 0.95 power.Data were analyzed and results are expressed as aver-
ge ± standard deviation, median (interquartile interval), orercentage. For the statistical analysis, continuous variablesere evaluated by ANOVA and Kruskal Wallis. Categoricalariables were evaluated by the contingency Chi-Squareest.
Agreement analysis was done by applying Kappa statisticsK), which considered: K = 1 when there is perfect agree-ent; K = 0 when agreement is no better than chance;
egative K when agreement is worse than chance. The p-alues presented were two-tail tests and those below 0.05ere considered statistically significant.
The Statistical Package for the Social Sciences softwareSPSS-IBM Corp., Armonk, NY, USA) 25.0 was used for thetatistical analyses.
esults
he survey was made available at three congresses attendedy more than 5,000 physicians from all over Brazil; 420greed to answer the questionnaire and 360 physicians ofhe specialties of surgery, intensive care and anesthesiol-gy filled out the survey appropriately, of which 77.6% wererom the Southeast region, 11% from the Northeast, 6% fromhe South, 3.3% from the Center-West, and 2.1% from theorth. The median time after graduation of physicians was0 (5---18) years. Of those, 36.4% were anesthesiologists,0.0% surgeons, and 33.6% intensive care physicians. Of
ll participants, 40.0% worked mainly in public hospitals,1.4% in private hospitals, and 18.6% in university hospitalsdefined as a hospital that has a link to a medical school,ithout specification on funding) (Table 1).ttpt
26
logy 2021;71(3):265---270
Of the surgeons, 92.6% were from the Southeast region,hile no surgeon from the Midwest or North regions partic-
pated in the survey. Among intensive care physicians andnesthesiologists, in contrast, there was a predominance ofhe Southeast region, but proportions were better balancedor the other regions (Table 1).
On the profile of hospitals, similar percentages of spe-ialists said they worked in public and private hospitals.nterestingly, 28.3% of the anesthesiologists declared thatheir main workload was in university hospitals, whereashat was the case of only 11.1% of the surgeons, and 14.9%f intensive care physicians. In spite of these differences,he answers on the number of ICU beds, type of ICU, esti-ated number of surgical patients referred to the ICU, andork logistics were similar and compatible among all groups
Table 1).As to the questionnaire on referral to the ICU, seven
escriptions of fictitious patients and their surgical plansere provided. In this part, 75% of the surgeons would refer
o the ICU patients whose surgeries would bring an inher-nt risk of intense hemorrhage, in contrast with a smallerroportion of intensive care physicians and anesthesiolo-ists. Surgeons were also more likely to recommend ICU forlderly patients with limited physiological reserve, patientsith risk of respiratory complications, and for major surg-ries. Sepsis patients undergoing urgent surgeries would beeferred to the ICU by most of the intensive care physicians.atients without clear referral criteria for ICU admission
-- controlled comorbidities, surgeries in between minor orajor --- would also be referred by most of the intensive carehysicians. Finally, surgeons would be less likely to referatients with hemodynamic instability and acute anemia tohe ICU (Table 2).
In the second part, six examples of clinical cases wererovided, and participants were asked to rank them by prior-ty. Intensive care physicians, followed by anesthesiologistslassified cases more adequately than surgeons (Table 2).
The main surgical risk indicator was ASA physical sta-us for all specialties, followed by SAPS 3, which is morerequently used by intensive care physicians (Table 2).
On the priority classification for referral to the ICU byype of surgery, the three specialties did not agree on anyf the cases (Fig. 1).
The agreement indicated by Kappa was poor, with inten-ive care physicians more likely to recommend ICU forsophagectomy and pelvic exenteration, while anesthesi-logists for colectomies and, lastly, surgeons were moreikely to recommend post-operative ICU for intestinal biliaryypass, total gastrectomy, and perforated acute abdomenFig. 1).
iscussion
n the comparison among surgeons, anesthesiologists andntensive care physicians with similar demographic charac-eristics, this study found that surgeons were less strict in
he process of screening patients for postoperative ICU, andhe opposite happened with anesthesiologists. Moreover, theerception of priority to indicate post-operative ICU seemedo be more adequate among intensive care physicians; and7

J.M. Silva Jr, H.T. Katayama, F.M. Lopes et al.
Table 1 Characteristics of participants and workplace.
Variables All Surgeons Intensive Care physicians Anesthesiologists p-value(n = 360) (n = 108) (n = 121) (n = 131)
Time since graduation (years) 10 (5.0---18.0) 11 (7.0---20.0) 10 (6.0---18.0) 10 (4.0---24.5) 0.74Characteristics of workplaceRegion of BrazilSoutheast 78.6% 92.6% 74.4% 71.0% 0.75South 5.8% 2.8% 7.4% 6.9% 0.18Northeast 10.6% 4.6% 10.7% 15.3% 0.01central 3.8% 0.0% 5.0% 3.8% 0.76North 1.9% 0.0% 2.5% 3.1% 0.70Type of hospitalPublic 40.0% 49.1% 35.5% 36.6% 0.59Private 41.4% 39.8% 49.6% 35.1% 0.19University 18.6% 11.1% 14.9% 28.3% < 0.001Type of ICU 0.09Mixed 85.3% 81.5% 90.9% 83.2%Surgical 14.7% 18.5% 9.1% 16.8%Hospital beds 200 (120---00) 150 (105---300) 150 (100---300) 200 (140---500) 0.001ICU beds 20 (17.5---40) 20 (20---30) 20 (13---40) 20 (15---40) 0.60Hospital operation logisticsSurgeries performed in the
past month400 (150---700) 400 (50.0---600.0) 200 (80.0---500.0) 500 (375---1000) < 0.001
Surgical patients sent to theICU in the past month
40 (20---80) 37.5 (10---80) 36 (20---80) 50 (25---80) 0.13
ICU operation logisticsNurse to patient ratio 0.31< 1/10 37.0% 28.0% 43.5% 36.4%1/10 25.3% 28.0% 23.5% 25.3%> 1/10 37.7% 44.0% 33.0% 38.4%Physician to patient ratio 0.09< 1/10 28.6% 20.7% 35.9% 26.7%1/10 37.8% 40.2% 38.5% 35.2%> 1/10 33.6% 39.0% 25.6% 38.1%
ta
cmaoeftiaolas
mwil
s
ccaeu
ppmBuirabwsc
ICU, Intensive Care Unit.
he three specialties did not agree on the type of surgerynd referral to the ICU for the post-operative period.
The criteria used in the selection of ICU beds may belassical if we consider patients with higher morbidity andortality,10 however, we saw conflicting answers among
nesthesiologists, surgeons and intensive care physiciansn the referrals and prioritization of surgical patients, forxample, 43% of the surgeons recommended ICU admissionor patients who did not present a clear need, and in con-rast, only 50% would do the same for cases of hemodynamicnstability --- against 82.6% of the intensive care physiciansnd 80.9% of the anesthesiologists. Nevertheless, only 22.1%f the anesthesiologists considered elderly patients withimited physiological reserve eligible for post-operative ICU,gainst 47.1% of the intensive care physicians and 75% of theurgeons.
The appropriate use of intensive care resources is funda-ental, given the scarcity of ICU beds in Brazil and in theorld,11,12 in addition to the fact that these centers special-
zed in providing care to critical patients require very highevels of investment.13,14
Because of that, some priority criteria for ICU admis-ion have been designed,4,15 but they are less applied in
aast
26
linical practice, especially for surgical patients. For medi-al patients, independent factors for ICU admission are oldge, high prognostic scores and the presence of chronic dis-ases (especially cardiovascular).16 However, there are stillncertainties for surgical patients.
The rate of refusal of ICU beds is lower for surgicalatients, but this fact does not lead to more requests forost-operative intensive care by surgical teams.17,18 A largeulticenter study, conducted in many ICUs in all regions ofrazil, found that only 3.5% (95% IC 3.3---3.8) of the patientsndergoing major surgeries were sent to post-operativentensive care; however, the rate of surgical complicationsemains high.19 Therefore, it seems evident that there is
lack of clear definitions on which surgical patients mayenefit from intensive care. In our study, when surgeriesere classified as to their priorities for ICU referral, inten-
ive care physicians, followed by anesthesiologists classifiedases more strictly than surgeons.
The lack of consensus among the members of the surgical
nd perioperative care teams may lead to judgement errorsnd harm to patients.20 Based on these assumptions, in thistudy, we found very poor agreement among physicians onhe referral to intensive care after certain major surgeries,8

Brazilian Journal of Anesthesiology 2021;71(3):265---270
Table 2 Comparison between the three specialties on post-operative referrals to the ICU and surgical risk indicators.
Variables All Surgeon Intensive Care physician Anesthesiologist p-value(n = 360) (n = 108) (n = 121) (n = 131)
Causes that would determine referral to the ICU according to specialty1- Risk of bleeding 55.8% 75.0% 52.1% 43.5% < 0.0012- Elderly with limited reserve 42.5% 62.0% 47.1% 22.1% < 0.0013- Risk of respiratory complication 45.4% 64.5% 43.0% 32.1% < 0.0014- Major surgery 63.8% 74.8% 74.4% 45.0% < 0.0015- Sepsis 72.1% 69.2% 81.8% 65.6% 0.0126- Without recommendation for ICU 21.4% 16.8% 43.0% 5.3% < 0.0017- Hemodynamic instability 72.3% 50.0% 82.6% 80.9% < 0.001Number of correct answers according to priority classificationP1 66.1% 48.1% 76.9% 71.0% < 0.001P2 66.7% 48.1% 76.9% 72.5% < 0.001P2 60.0% 51.9% 72.7% 55.0% 0.002P2 66.4% 51.9% 80.2% 65.5% < 0.001P3 55.0% 63.9% 68.6% 35.1% < 0.001P4 52.2% 49.5% 62.0% 45.3% 0.025Surgical risk criteria used for referral to the ICUSAPS 3 10.2% 1.9% 21.7% 6.3% < 0.001ASA physical status 82.2% 97.2% 67.5% 83.5% 0.14POSSUM 0.8% 0.0% 0.8% 1.6% 0.56Shoemaker 0.8% 0.9% 0.0% 1.6% 0.56Other 3.7% 0.0% 6.7% 3.9% 0.40None 2.3% 0.0% 3.3% 3.1% 1.00
ICU, Intensive Care Unit; P, Priority scale.
F to prn
tIss
s
igure 1 Agreement between specialties and type of surgery
eed of postoperative intensive care).
hat is, none of the specialties was unanimous in considering
CU admission for the proposed surgeries. Interestingly, inpite of not being very sensitive in determining the worseurgical outcomes,2,21 the main risk indicator chosen by allc
d
26
ioritize ICU admission. (The higher the priority, the greater the
pecialties was ASA physical status, maybe because of the
onvenience of the score.The heterogeneity of the answers obtained in this studyenotes a vast difference in the way specialists of the area
9

ayam
ta(soratp
gfwonqmssttltmia
C
Ahctcsr
C
T
A
TPor
A
Sib
R
1
1
1
1
1
1
1
1
1
1
2
Crit Care Med. 2003;31:45---51.21. Silva Junior JM, Malbouisson LM, Nuevo HL, et al. Applicability
J.M. Silva Jr, H.T. Kat
hink, something that should be tackled with educationalctions and implementation of organizational protocolssystematization of processes), also bearing in mind the pos-ibility of complications in case of emergencies that areutside this scope. This study sought to diagnose the cur-ent situation to serve as the basis for the design of moreppropriate policies for a consensus among physicians onhe identification of the patients who should be referred toost-operative intensive care.
However, the study has limitations including the geo-raphical distribution of surgeons, who were predominantlyrom the southeast region. In order to avoid bias, thereas no type of communication with participants to clarifyr explain what was asked in each part of the question-aire, which may have left doubts. They could also haveuestions about the clinical cases used, whether they wereajor or minor surgeries, but as everyone answered the
ame cases, the comparison remained valid. Moreover, thecenarios described did not include some surgical special-ies, like vascular, neurosurgery, thoracic, and others. Lastly,he comparison among other groups, like private versus pub-ic, or among the regions of Brazil, was not done becausehey were outside the scope of the study; in addition,ore detailed questions were not asked, because they could
ncrease time to answer the questionnaire and thus reducedherence to the survey.
onclusion
nesthesiologists, surgeons, and intensive care physiciansave different perspectives when it comes to referring surgi-al patients to post-operative intensive care. This should beaken into account in professional improvement actions tolarify the benefits and limitations of post-operative inten-ive care, aiming to improve the use of a finite and high-costesources.
onflicts of interest
he authors declare no conflicts of interest.
cknowledgements
he authors thank the organizers of Project ACERTO, Sãoaulo’s Congress of Anesthesiology, and the World Congressf Intensive Care jointly with AMIBnet for the support to theesearch.
ppendix A. Supplementary data
upplementary material related to this article can be found,n the online version, at doi:https://doi.org/10.1016/j.jane.2021.03.025.
eferences
1. Blanch L, Abillama FF, Amin P, et al. Triage decisions for ICUadmission: report from the Task Force of the World Federationof Societies of Intensive and Critical Care Medicine. J Crit Care.2016;36:301---5.
27
a, F.M. Lopes et al.
2. Silva JM Jr, Rocha HM, Katayama HT, et al. SAPS 3 score as apredictive factor for postoperative referral to intensive careunit. Ann Intensive Care. 2016;6:42.
3. Nates JL, Nunnally M, Kleinpell R, et al. ICU admission, dis-charge, and triage guidelines: a framework to enhance clinicaloperations, development of institutional policies, and furtherresearch. Crit Care Med. 2016;44:1553---602.
4. Caldeira VM, Silva Junior JM, Oliveira AM, et al. Criteria forpatient admission to an intensive care unit and related mortalityrates. Rev Assoc Med Bras (1992). 2010;56:528---34.
5. Smith G, Nielsen M. ABC of intensive care. Criteria for admis-sion. BMJ. 1999;318:1544---7.
6. Forward E, Konecny P, Burston J, et al. Predictive validity of theqSOFA criteria for sepsis in non-ICU inpatients. Intensive CareMed. 2017;43:945---6.
7. Orsini J, Blaak C, Shamian B, et al. Assessing the util-ity of ICU admission for octogenarians. Aging Clin Exp Res.2016;28:745---51.
8. Solligard E, Damas JK. SOFA criteria predict infection-relatedin-hospital mortality in ICU patients better than SIRS criteriaand the qSOFA score. Evid Based Med. 2017;22:211.
9. Silva ED, Perrino AC, Teruya A, et al. Brazilian consensus onperioperative hemodynamic therapy goal guided in patientsundergoing noncardiac surgery: fluid management strategy -produced by the São Paulo State Society of Anesthesiology(Sociedade de Anestesiologia do Estado de São Paulo - SAESP).Rev Bras Anestesiol. 2016;66:557---71.
0. Rocco JR, Soares M, Gago Mde F. Referred medical patientsnot admitted to the Intensive Care Unit: prevalence, clin-ical characteristics and prognosis. Rev Bras Ter Intensiva.2006;18:114---20.
1. Franklin C, Rackow EC, Mamdani B, et al. Triage considera-tions in medical intensive care. Arch Intern Med. 1990;150:1455---9.
2. Simchen E, Sprung CL, Galai N, et al. Survival of criticallyill patients hospitalized in and out of intensive care unitsunder paucity of intensive care unit beds. Crit Care Med.2004;32:1654---61.
3. Vasilevskis EE, Chandrasekhar R, Holtze CH, et al. The cost ofICU delirium and coma in the intensive care unit patient. MedCare. 2018;56:890---7.
4. Yamauchi LY. Cost analysis in the ICU from the standpoint ofphysical therapy. J Bras Pneumol. 2018;44:175.
5. Guidelines for intensive care unit admission, discharge, andtriage. Task force of the American College of Critical CareMedicine, Society of Critical Care Medicine. Crit Care Med.1999;27:633---8.
6. Sinuff T, Kahnamoui K, Cook DJ, et al. Rationing critical carebeds: a systematic review. Crit Care Med. 2004;32:1588---97.
7. Consensus statement on the triage of critically ill patients.Society of Critical Care Medicine Ethics Committee. JAMA.1994;271:1200---3.
8. Marshall MF, Schwenzer KJ, Orsina M, et al. Influence of politicalpower, medical provincialism, and economic incentives on therationing of surgical intensive care unit beds. Crit Care Med.1992;20:387---94.
9. Silva Junior JM, Chaves RCF, Correa TD, et al. Epidemiology andoutcome of high-surgical-risk patients admitted to an intensivecare unit in Brazil. Rev Bras Ter Intensiva. 2020;32:17---27.
0. Higgins TL, McGee WT, Steingrub JS, et al. Early indicators ofprolonged intensive care unit stay: impact of illness severity,physician staffing, and pre-intensive care unit length of stay.
of the simplified acute physiology score (SAPS 3) in Brazilianhospitals. Rev Bras Anestesiol. 2010;60:20---31.
0

E
Ds
G
a
b
c
RA
h©l
Brazilian Journal of Anesthesiology 2021;71(3):271---277
XPERIMENTAL TRIALS
ose-related effects of dexmedetomidine onepsis-initiated lung injury in rats
ülsüm Karabulut a,∗, Nurdan Bedirli a, Nalan Akyürekb, Emin Ümit Bağrıaçıkc
Gazi University, Faculty of Medicine, Department of Anesthesiology and Reanimation, Ankara, TurkeyGazi University, Faculty of Medicine, Department of Pathology, Ankara, TurkeyGazi University, Faculty of Medicine, Department of Immunology, Ankara, Turkey
eceived 28 May 2019; accepted 27 February 2021vailable online 15 April 2021
KEYWORDSSepsis;Lung injury;Dexmedetomidine
AbstractBackground: Sepsis is one of the leading causes of death in intensive care units. Dexmedeto-midine is a sedative agent with anti-inflammatory properties. This study is designed todifferentiate the impact of two different doses of dexmedetomidine on lung injury inducedby sepsis.Methods: Adult male Wistar rats were randomly divided into four groups: sham (n = 6), control(n = 12), 5DEX (n = 12), and 10DEX (n = 12). Cecal ligation puncture (CLP) was applied for sepsisinitiation. The 5DEX group received 5 �g.kg-1.h-1 and the 10DEX group received 10 �g.kg-1.h-1
dexmedetomidine intravenous infusions for a 1-hour period. Six hours after CLP, tumor necrosisfactor-� (TNF-�), interleukin-1� (IL-1�), and intercellular adhesion molecule-1 (ICAM-1) levelswere analyzed in blood samples. Twenty-four hours after CLP, lung samples from the remainingrats were collected for the measurement of myeloperoxidase (MPO) activity, histological exam-ination, and TdT- (terminal deoxynucleotidyl transferase) mediated fluorescent-dUTP labelingstaining for apoptosis detection.Results: Serum cytokine release, MPO activity, and apoptosis in the lung were significantlyincreased in the CLP group compared with the sham and dexmedetomidine groups (p < 0.05).TNF-�, ICAM-1, and MPO were significantly lower in the 10DEX group compared with both 5DEXand control groups, while IL-1�, total injury score, and apoptotic cell count had significantlylower values in both 10DEX and 5DEX groups compared with the control group (p < 0.05).Conclusion: Dexmedetomidine administration played a protective role against CLP-induced lunginjury. High-dose dexmedetomidine was needed for suppressing the leukocyte-mediated lunginjury and apoptosis of lung tissue.
© 2021 Sociedade Brasileira deopen access article under the Cnc-nd/4.0/).∗ Corresponding author.E-mail: [email protected] (G. Karabulut).
ttps://doi.org/10.1016/j.bjane.2021.02.051 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Anestesiologia. Published by Elsevier Editora Ltda. This is anC BY-NC-ND license (http://creativecommons.org/licenses/by-
itora Ltda. This is an open access article under the CC BY-NC-ND

dirli
I
Stindlsscmmnaer
ltTmetodai
tavarstHsrc
tlwdneti
M
E
TamadC
Ad
HiEAitwsctAixarvbotgataimta
tasirmtsawatIiiwcdl
C
Svxd
G. Karabulut, N. Be
ntroduction
epsis is a life-threatening clinical syndrome that disruptshe host response to infectious pathogens.1 Sepsis syndromes related to major clinical problems, including hemody-amic instability, coagulation problems, and multiple organysfunctions. The most vulnerable organ to sepsis is theung; acute lung injury (ALI) and acute respiratory distressyndrome (ARDS) are the leading causes of mortality inepsis.2 ALI/ARDS is a multifactorial clinical condition asso-iated with multiple organ failure contributing to increasedortality and morbidity.3 The excessive release of inflam-atory cytokines, the upregulation of adhesion molecules,
eutrophil accumulation, the loss of vascular integrity, andpoptosis of alveolar epithelial and pulmonary vascularndothelial cells are major pathological changes in sepsis-elated lung injury.4---6
Intercellular adhesion molecule 1 (ICAM-1) is found ineukocyte and endothelial cell membranes, and regulateshe interaction between leukocytes and the endothelium.4
herefore, ICAM-1 plays an important role in leukocyte-ediated organ injury and has been even shown to be an
arly marker of lung injury diagnosis.7,8 Neutrophil infiltra-ion into the lung plays an important role in the initiationf ALI by releasing neutrophil proteases, causing alveolaramage.9 Apoptosis of lung epithelial cells may promotelveolar destruction and lung fibrosis, contributing to thenitiation and progression of ALI.10,11
The selective �2 agonist dexmedetomidine has seda-ive, anxiolytic, and analgesic properties and is commonlydministered to patients in intensive care units to pro-ide sedation.12 In addition, potential anti-inflammatorynd antiapoptotic effects of dexmedetomidine have beeneported.13 Moreover, clinical reports of patients withevere sepsis have shown that dexmedetomidine improveshe survival rate via its anti-inflammatory effects.14
owever, the protective impact of dexmedetomidine onepsis-related lung injury and the effective dose thateduces inflammation and alveolar apoptosis are notlear.
The primary objective of this study was to differentiatehe effects of two different doses of dexmedetomidine onung injury induced by sepsis, and the secondary objectiveas to demonstrate whether the effects of dexmedetomi-ine on lung injury are related to systemic ICAM-1 release,eutrophil accumulation, and/or the apoptosis of alveolarpithelial cells. Based on previous findings, we hypothesizedhat dexmedetomidine medication could attenuate sepsisnduced lung injury.
aterials and methods
thics statement
he experimental procedures and the care of animals werepproved by the Instructional Animal Care and Use Com-
ittee of Gazi University (Approval No. GÜET-16.002). Allnimals were maintained in accordance with the recommen-ations of the National Institutes of Health Guidelines for theare and Use of Laboratory Animals.
3cta
27
, N. Akyürek et al.
nimal groups, randomization, and experimentalesign
ealthy adult male pathogen-free Wistar rats (n = 42) weigh-ng 250---300 g (GÜDAM --- Laboratory Animals Raising andxperimental Research Center) were included in this study.ll animals were housed at 21 ◦C to 23 ◦C, 30% to 40% humid-
ty, and on a 12-hour light-dark cycle with ad libitum accesso rat chow and water. The block randomization schemeas generated by a computer-generated random assignment
equence prepared in advance. An independent statisti-ian who was not directly participant in the conduct of therial generated the randomization sequence with computer.nesthesia was induced and maintained by intramuscular
njection of 50 mg.kg-1 ketamine hydrochloride, 5 mg.kg-1
ylazine, and intravenous 2 �g.kg-1.h-1 fentanyl infusion inll rats. Anesthesia depth was determined by the toe pinchesponse method. Hydration and drug infusions were pro-ided through a tail vein catheter. Hydration was maintainedy infusion of isotonic sodium chloride solution at a ratef 0.5 mL.h-1. During the experiment, rats were allowedo breathe spontaneously while monitoring peripheral oxy-en saturation. Rats were randomly divided into four groupsccording to a computer-generated list: sham (n = 6), con-rol (n = 12), 5DEX (n = 12), and 10DEX (n = 12) groups. Therere several murine sepsis models used in experimental stud-es. We decided to use the cecal ligation and puncture (CLP)odel since it is polymicrobial and creates conditions similar
o sepsis and septic shock seen in humans, such as perforatedppendicitis, diverticulitis or colon perforation.15
Cecal ligation puncture was applied to rats in the con-rol, 5DEX, and 10DEX groups, while in the sham group thebdominal cavity was exposed without CLP by a midline inci-ion. After CLP surgery and the sham procedure, the ratsn the 5DEX group received 5 �g.kg-1.h-1 dexmedetomidine;ats in the 10DEX group received 10 �g.kg-1.h-1 dexmedeto-idine intravenous infusions for a 1-hour period; rats in
he sham and control groups received equal volumes ofaline. Six hours after CLP, 3 rats from the sham groupnd 6 rats each from the control, 5DEX, and 10DEX groupsere anesthetized with ketamine/xylazine combination,nd blood samples were withdrawn for the measurements ofumor necrosis factor-� (TNF-�), interleukin-1� (IL-1�), andCAM-1 analysis. Twenty-four hours after CLP, the remain-ng rats from every group were euthanized via intravenousnjection of 200 mg.kg-1 pentobarbital, and lung samplesere collected for the analysis of myeloperoxidase (MPO)oncentration, histological examination, and TdT- (terminaleoxynucleotidyl transferase) mediated fluorescent-dUTPabeling (TUNEL) staining for apoptosis detection.
ecal ligation and puncture procedure
epsis was initiated by cecal ligation and puncture as pre-iously described.16 Briefly, intraperitoneal ketamine andylazine were used to maintain anesthesia, and aseptic con-itions were provided. Laparotomy was performed via a
-cm midline incision to explore, ligate, and perforate theecum. The cecum was ligated with 3-0 silk and perforatedwice with an 18G needle, gently squeezed, and a smallmount of feces was extruded. Then, the cecum was reposi-2
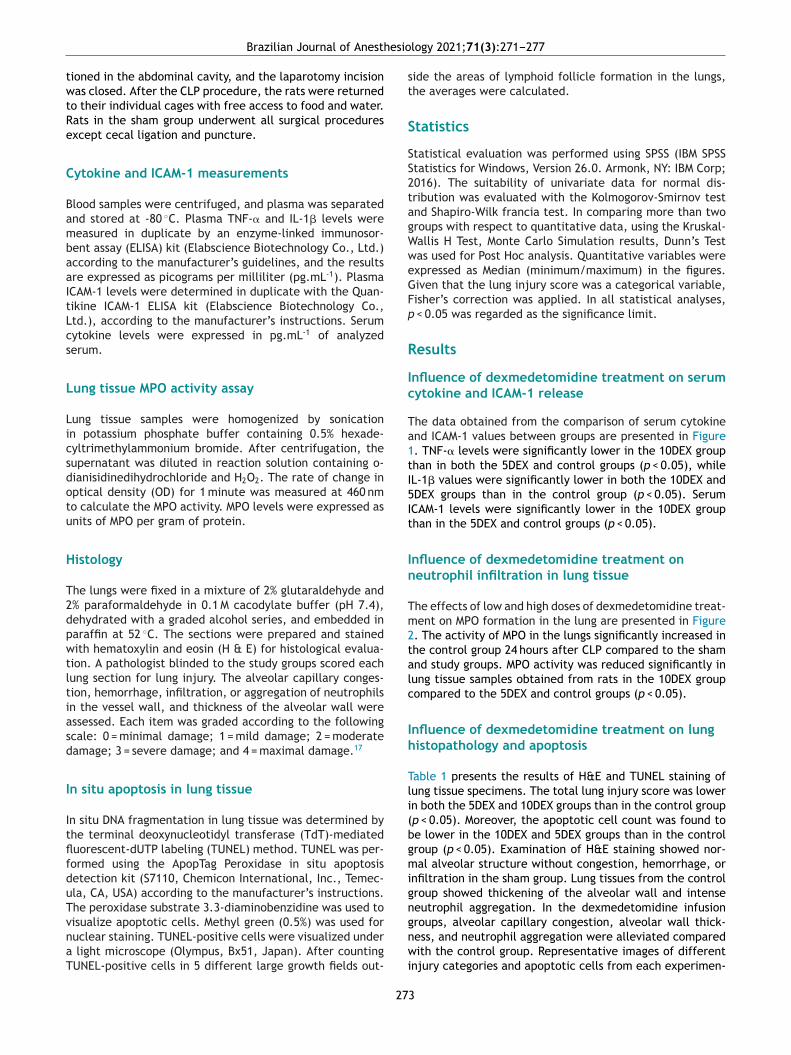
esio
twtRe
C
BambaaItLcs
L
Licsdotu
H
T2dpwtltiasd
I
ItflfduTvnaT
st
S
SS2tagWweGFp
R
Ic
Ta1tI5It
In
Tm2talc
Ih
Tli(bgmign
Brazilian Journal of Anesth
ioned in the abdominal cavity, and the laparotomy incisionas closed. After the CLP procedure, the rats were returned
o their individual cages with free access to food and water.ats in the sham group underwent all surgical proceduresxcept cecal ligation and puncture.
ytokine and ICAM-1 measurements
lood samples were centrifuged, and plasma was separatednd stored at -80 ◦C. Plasma TNF-� and IL-1� levels wereeasured in duplicate by an enzyme-linked immunosor-ent assay (ELISA) kit (Elabscience Biotechnology Co., Ltd.)ccording to the manufacturer’s guidelines, and the resultsre expressed as picograms per milliliter (pg.mL-1). PlasmaCAM-1 levels were determined in duplicate with the Quan-ikine ICAM-1 ELISA kit (Elabscience Biotechnology Co.,td.), according to the manufacturer’s instructions. Serumytokine levels were expressed in pg.mL-1 of analyzederum.
ung tissue MPO activity assay
ung tissue samples were homogenized by sonicationn potassium phosphate buffer containing 0.5% hexade-yltrimethylammonium bromide. After centrifugation, theupernatant was diluted in reaction solution containing o-ianisidinedihydrochloride and H2O2. The rate of change inptical density (OD) for 1 minute was measured at 460 nmo calculate the MPO activity. MPO levels were expressed asnits of MPO per gram of protein.
istology
he lungs were fixed in a mixture of 2% glutaraldehyde and% paraformaldehyde in 0.1 M cacodylate buffer (pH 7.4),ehydrated with a graded alcohol series, and embedded inaraffin at 52 ◦C. The sections were prepared and stainedith hematoxylin and eosin (H & E) for histological evalua-
ion. A pathologist blinded to the study groups scored eachung section for lung injury. The alveolar capillary conges-ion, hemorrhage, infiltration, or aggregation of neutrophilsn the vessel wall, and thickness of the alveolar wall weressessed. Each item was graded according to the followingcale: 0 = minimal damage; 1 = mild damage; 2 = moderateamage; 3 = severe damage; and 4 = maximal damage.17
n situ apoptosis in lung tissue
n situ DNA fragmentation in lung tissue was determined byhe terminal deoxynucleotidyl transferase (TdT)-mediateduorescent-dUTP labeling (TUNEL) method. TUNEL was per-ormed using the ApopTag Peroxidase in situ apoptosisetection kit (S7110, Chemicon International, Inc., Temec-la, CA, USA) according to the manufacturer’s instructions.he peroxidase substrate 3.3-diaminobenzidine was used to
isualize apoptotic cells. Methyl green (0.5%) was used foruclear staining. TUNEL-positive cells were visualized underlight microscope (Olympus, Bx51, Japan). After countingUNEL-positive cells in 5 different large growth fields out-
gnwi
27
logy 2021;71(3):271---277
ide the areas of lymphoid follicle formation in the lungs,he averages were calculated.
tatistics
tatistical evaluation was performed using SPSS (IBM SPSStatistics for Windows, Version 26.0. Armonk, NY: IBM Corp;016). The suitability of univariate data for normal dis-ribution was evaluated with the Kolmogorov-Smirnov testnd Shapiro-Wilk francia test. In comparing more than tworoups with respect to quantitative data, using the Kruskal-allis H Test, Monte Carlo Simulation results, Dunn’s Testas used for Post Hoc analysis. Quantitative variables werexpressed as Median (minimum/maximum) in the figures.iven that the lung injury score was a categorical variable,isher’s correction was applied. In all statistical analyses,
< 0.05 was regarded as the significance limit.
esults
nfluence of dexmedetomidine treatment on serumytokine and ICAM-1 release
he data obtained from the comparison of serum cytokinend ICAM-1 values between groups are presented in Figure. TNF-� levels were significantly lower in the 10DEX grouphan in both the 5DEX and control groups (p < 0.05), whileL-1� values were significantly lower in both the 10DEX andDEX groups than in the control group (p < 0.05). SerumCAM-1 levels were significantly lower in the 10DEX grouphan in the 5DEX and control groups (p < 0.05).
nfluence of dexmedetomidine treatment oneutrophil infiltration in lung tissue
he effects of low and high doses of dexmedetomidine treat-ent on MPO formation in the lung are presented in Figure
. The activity of MPO in the lungs significantly increased inhe control group 24 hours after CLP compared to the shamnd study groups. MPO activity was reduced significantly inung tissue samples obtained from rats in the 10DEX groupompared to the 5DEX and control groups (p < 0.05).
nfluence of dexmedetomidine treatment on lungistopathology and apoptosis
able 1 presents the results of H&E and TUNEL staining ofung tissue specimens. The total lung injury score was lowern both the 5DEX and 10DEX groups than in the control groupp < 0.05). Moreover, the apoptotic cell count was found toe lower in the 10DEX and 5DEX groups than in the controlroup (p < 0.05). Examination of H&E staining showed nor-al alveolar structure without congestion, hemorrhage, or
nfiltration in the sham group. Lung tissues from the controlroup showed thickening of the alveolar wall and intenseeutrophil aggregation. In the dexmedetomidine infusion
roups, alveolar capillary congestion, alveolar wall thick-ess, and neutrophil aggregation were alleviated comparedith the control group. Representative images of differentnjury categories and apoptotic cells from each experimen-
3
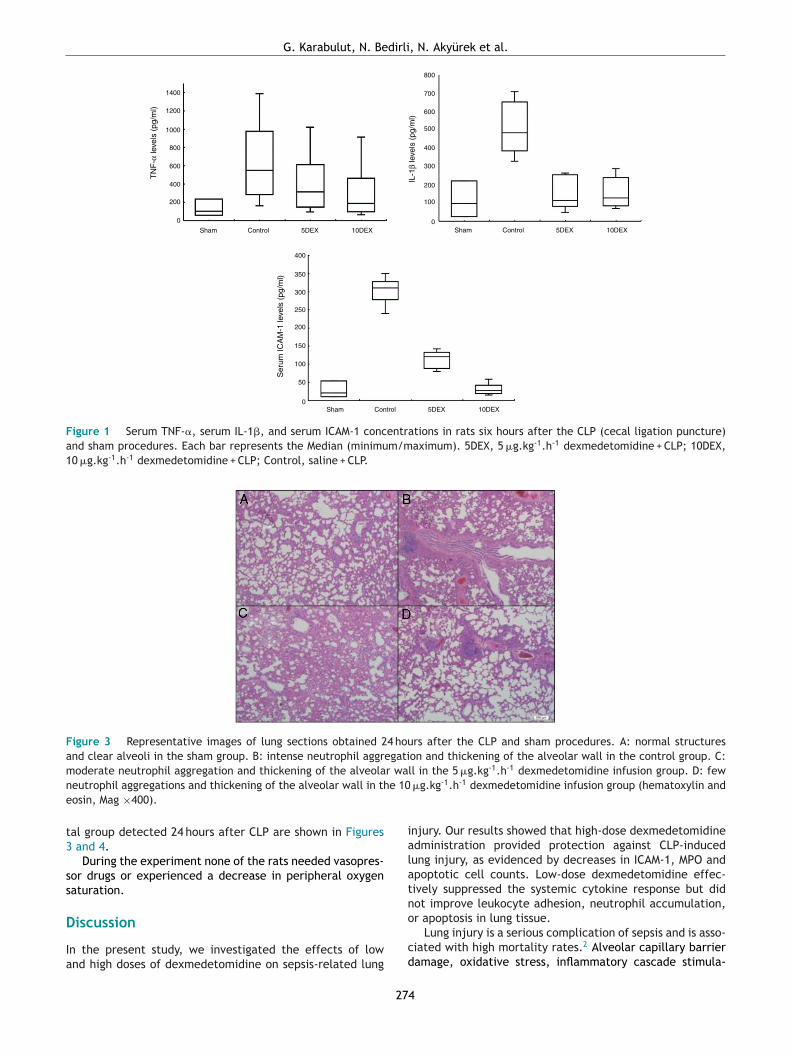
G. Karabulut, N. Bedirli, N. Akyürek et al.
1400
800
700
600
500
400
300
200
100
0
1200
1000
800
400
200
0
400
350
300
250
200
150
100
50
0
Sham Control 5DEX 10DEX
Sham Control 5DEX 10DEX
Sham Control 5DEX 10DEX
600
TN
F-α
leve
ls (
pg/m
l)
Ser
um IC
AM
-1 le
vels
(pg
/ml)
IL-1
β le
vels
(pg
/ml)
Figure 1 Serum TNF-�, serum IL-1�, and serum ICAM-1 concentrations in rats six hours after the CLP (cecal ligation puncture)and sham procedures. Each bar represents the Median (minimum/maximum). 5DEX, 5 �g.kg-1.h-1 dexmedetomidine + CLP; 10DEX,10 �g.kg-1.h-1 dexmedetomidine + CLP; Control, saline + CLP.
Figure 3 Representative images of lung sections obtained 24 hours after the CLP and sham procedures. A: normal structuresand clear alveoli in the sham group. B: intense neutrophil aggregation and thickening of the alveolar wall in the control group. C:m r wa -1 -1
n e 10e
t3
ss
D
Ia
ialatn
oderate neutrophil aggregation and thickening of the alveolaeutrophil aggregations and thickening of the alveolar wall in thosin, Mag ×400).
al group detected 24 hours after CLP are shown in Figures and 4.
During the experiment none of the rats needed vasopres-or drugs or experienced a decrease in peripheral oxygenaturation.
iscussion
n the present study, we investigated the effects of lownd high doses of dexmedetomidine on sepsis-related lung
o
cd
27
ll in the 5 �g.kg .h dexmedetomidine infusion group. D: few �g.kg-1.h-1 dexmedetomidine infusion group (hematoxylin and
njury. Our results showed that high-dose dexmedetomidinedministration provided protection against CLP-inducedung injury, as evidenced by decreases in ICAM-1, MPO andpoptotic cell counts. Low-dose dexmedetomidine effec-ively suppressed the systemic cytokine response but didot improve leukocyte adhesion, neutrophil accumulation,
r apoptosis in lung tissue.Lung injury is a serious complication of sepsis and is asso-iated with high mortality rates.2 Alveolar capillary barrieramage, oxidative stress, inflammatory cascade stimula-
4

Brazilian Journal of Anesthesio
Sham Control 5DEX 10DEX
4,5
4
Tis
sue
mye
lope
roxi
dase
leve
ls (
U/g
tiss
ue)
3,5
3
2,5
2
1,5
1
0,5
0
Figure 2 Lung tissue MPO levels of the rats 24 hours afterthe CLP and sham procedures. Each bar represents theMedian (minimum/maximum). 5DEX, 5 �g.kg-1.h-1 dexmedeto-midine + CLP; 10DEX, 10 �g.kg-1.h-1 dexmedetomidine + CLP;Control, saline + CLP.
Table 1 Injury scores and apoptotic changes in lung tis-sues of the rats twenty-four hours after CLP (cecal ligationpuncture) and sham procedures.
Groups Apoptosis(mean ± SD)
Lung InjuryScores(mean ± SD)
Sham (n = 3) 0.03 ± 0.001ˇ 1.33 ± 0.002ˇ
Control (n = 6) 6.40 ± 0.55 9.60 ± 0.895DEX (n = 6) 4.17 ± 3.06˛ 4.33 ± 1.21˛
10DEX (n = 6) 2.13 ± 1.97˛ 3.67 ± 1.63˛
Values are expressed as mean ± standard deviation; 5DEX,5 �g.kg-1.h-1 dexmedetomidine + CLP; 10DEX, 10 �g.kg-1.h-1
dexmedetomidine + CLP; Control, saline + CLP; ˛ p < 0.05 com-
tmea
tcDrswdeaiiwc
ei
eeirem2atwwHdsdrwt
smsp
tIIilcmiMatpdnammwt2dsewe
triesobf
pared with the control group; ˇ p < 0.05 compared with thecontrol, 5DEX, 10DEX groups.
ion, increased cytokine response, upregulation of adhesionolecules, neutrophil infiltration, and apoptosis of alveolar
pithelium and endothelial cells are pathological processesssociated with lung injury.3,18,19
Patients with sepsis generally require sedation to main-ain effective mechanical ventilation, to ensure patientompliance with this therapy, and to reduce anxiety.exmedetomidine is a potent, highly selective �2-adrenergiceceptor agonist, and it is preferred for sedation in inten-ive care units due to its analgesic and sedative effectsithout respiratory depression. Dexmedetomidine has beenemonstrated to have anti-inflammatory and antiapoptoticffects apart from sedative, anxiolytic, analgesic sparing,nd sympatholytic effects.20 Liu Z et al.21 showed thatntraperitoneal administration of dexmedetomidine inhib-ted the inflammatory response in the lung tissue of miceith sepsis, and this effect was partially mediated by theholinergic anti-inflammatory pathway.
Although the anti-inflammatory and immunomodulatoryffects of dexmedetomidine have been shown in many stud-es, the effective dose range that provided these reported
pit
27
logy 2021;71(3):271---277
ffects was not defined clearly. Ma Y et al.22 studied theffects of low, medium, and high doses of dexmedetomidinenfusion on immunomodulation and mortality; their resultsevealed that dexmedetomidine had immunomodulatoryffects that were initiated within 5 hours, and dexmedeto-idine infusion improved mortality rates dose-dependently
4 hours after CLP. Their results showed that both mediumnd high doses of dexmedetomidine infusion suppressed sys-emic cytokine release and decreased the mortality rate,hile immune regulation was maintained more effectivelyith medium doses of dexmedetomidine, as evidenced byLA-DR levels. However, they did not study the effects ofexmedetomidine on specific organ functions. In the presenttudy, we evaluated the effects of two different doses ofexmedetomidine on lung injury in CLP-induced sepsis inats. Our results showed that high-dose dexmedetomidineas needed for the effective control of systemic inflamma-
ion and neutrophil accumulation in lung tissue.Enhanced levels of serum cytokines and ICAM-1 have been
hown to be associated with endothelial damage in experi-ental studies. Moreover, clinical data has shown that sepsis
urvivors have decreased cytokine and ICAM-1 levels com-ared to nonsurvivors.23
Jing W et al.24 showed that the release of inflamma-ory cascade mediators, such as TNF-�, IL-6, IL-1�, andCAM-1, plays an essential role in lung parenchyma injury.L-1� is an important modulator in the acute phase ofnflammation and is known to participate in alveolar epithe-ial repair.25 TNF-� activates human bronchial epithelialells and facilitates the generation of other inflammatoryediators.26 Moreover, these proinflammatory cytokines are
nvolved in the recruitment of neutrophils and promotion ofPO activity.27 ICAM-1 stimulates the inflammatory cascadend contributes to the migration, accumulation and activa-ion of neutrophils to lung tissue, resulting in ALI.4 In theresent study, 6 hours after CLP, high-dose dexmedetomi-ine decreased the activity of TNF-� and ICAM-1. Pulmonaryeutrophil accumulation is a major marker of inflammationnd tissue damage, and is related to ALI initiation.28 Pul-onary MPO activity has been reported to be a reliablearker of pulmonary neutrophil infiltration.29 Consequently,e determined the MPO activity in the lung tissue of sep-
ic rats treated with different doses of dexmedetomidine4 hours after sepsis initiation. Our results showed thatexmedetomidine provided dose-related protection againstepsis-induced neutrophil accumulation in lung tissue, asvidenced by decreased MPO levels. But in this experiment,e did not investigate the underlining mechanism of thisffect and this needs further studies.
Initiation of the systemic inflammatory cascade and neu-rophil accumulation in lung tissue may promote apoptosis,esulting in lung dysfunction and increased mortality dur-ng sepsis. Alveolar apoptosis has been shown to disruptpithelial barrier function, initiating ALI.30 In the presenttudy, apoptotic cells were detected to identify the effectsf dexmedetomidine on lung injury. Our results showed thatoth low- and high-dose dexmedetomidine were effectiveor controlling sepsis-related lung apoptosis.
There are some limitations to our study. First, the sam-
le size was relatively small. Second, conducting continuousnvasive monitoring and comparing hemodynamic parame-ers might have strengthened the study since the diagnosis5
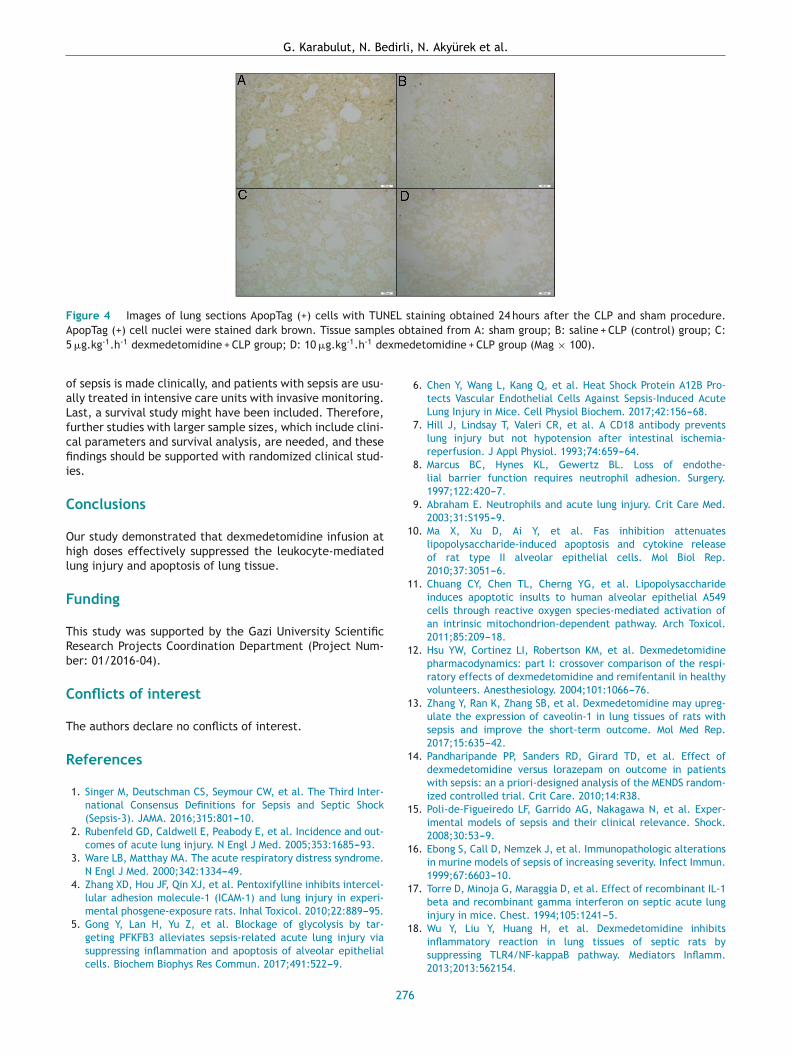
G. Karabulut, N. Bedirli, N. Akyürek et al.
Figure 4 Images of lung sections ApopTag (+) cells with TUNEL staining obtained 24 hours after the CLP and sham procedure.A s ob5 xme
oaLfcfii
C
Ohl
F
TRb
C
T
R
1
1
1
1
1
1
1
1
popTag (+) cell nuclei were stained dark brown. Tissue sample �g.kg-1.h-1 dexmedetomidine + CLP group; D: 10 �g.kg-1.h-1 de
f sepsis is made clinically, and patients with sepsis are usu-lly treated in intensive care units with invasive monitoring.ast, a survival study might have been included. Therefore,urther studies with larger sample sizes, which include clini-al parameters and survival analysis, are needed, and thesendings should be supported with randomized clinical stud-
es.
onclusions
ur study demonstrated that dexmedetomidine infusion atigh doses effectively suppressed the leukocyte-mediatedung injury and apoptosis of lung tissue.
unding
his study was supported by the Gazi University Scientificesearch Projects Coordination Department (Project Num-er: 01/2016-04).
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Singer M, Deutschman CS, Seymour CW, et al. The Third Inter-national Consensus Definitions for Sepsis and Septic Shock(Sepsis-3). JAMA. 2016;315:801---10.
2. Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and out-comes of acute lung injury. N Engl J Med. 2005;353:1685---93.
3. Ware LB, Matthay MA. The acute respiratory distress syndrome.N Engl J Med. 2000;342:1334---49.
4. Zhang XD, Hou JF, Qin XJ, et al. Pentoxifylline inhibits intercel-lular adhesion molecule-1 (ICAM-1) and lung injury in experi-mental phosgene-exposure rats. Inhal Toxicol. 2010;22:889---95.
5. Gong Y, Lan H, Yu Z, et al. Blockage of glycolysis by tar-geting PFKFB3 alleviates sepsis-related acute lung injury viasuppressing inflammation and apoptosis of alveolar epithelialcells. Biochem Biophys Res Commun. 2017;491:522---9.
1
27
tained from A: sham group; B: saline + CLP (control) group; C:detomidine + CLP group (Mag × 100).
6. Chen Y, Wang L, Kang Q, et al. Heat Shock Protein A12B Pro-tects Vascular Endothelial Cells Against Sepsis-Induced AcuteLung Injury in Mice. Cell Physiol Biochem. 2017;42:156---68.
7. Hill J, Lindsay T, Valeri CR, et al. A CD18 antibody preventslung injury but not hypotension after intestinal ischemia-reperfusion. J Appl Physiol. 1993;74:659---64.
8. Marcus BC, Hynes KL, Gewertz BL. Loss of endothe-lial barrier function requires neutrophil adhesion. Surgery.1997;122:420---7.
9. Abraham E. Neutrophils and acute lung injury. Crit Care Med.2003;31:S195---9.
0. Ma X, Xu D, Ai Y, et al. Fas inhibition attenuateslipopolysaccharide-induced apoptosis and cytokine releaseof rat type II alveolar epithelial cells. Mol Biol Rep.2010;37:3051---6.
1. Chuang CY, Chen TL, Cherng YG, et al. Lipopolysaccharideinduces apoptotic insults to human alveolar epithelial A549cells through reactive oxygen species-mediated activation ofan intrinsic mitochondrion-dependent pathway. Arch Toxicol.2011;85:209---18.
2. Hsu YW, Cortinez LI, Robertson KM, et al. Dexmedetomidinepharmacodynamics: part I: crossover comparison of the respi-ratory effects of dexmedetomidine and remifentanil in healthyvolunteers. Anesthesiology. 2004;101:1066---76.
3. Zhang Y, Ran K, Zhang SB, et al. Dexmedetomidine may upreg-ulate the expression of caveolin-1 in lung tissues of rats withsepsis and improve the short-term outcome. Mol Med Rep.2017;15:635---42.
4. Pandharipande PP, Sanders RD, Girard TD, et al. Effect ofdexmedetomidine versus lorazepam on outcome in patientswith sepsis: an a priori-designed analysis of the MENDS random-ized controlled trial. Crit Care. 2010;14:R38.
5. Poli-de-Figueiredo LF, Garrido AG, Nakagawa N, et al. Exper-imental models of sepsis and their clinical relevance. Shock.2008;30:53---9.
6. Ebong S, Call D, Nemzek J, et al. Immunopathologic alterationsin murine models of sepsis of increasing severity. Infect Immun.1999;67:6603---10.
7. Torre D, Minoja G, Maraggia D, et al. Effect of recombinant IL-1beta and recombinant gamma interferon on septic acute lunginjury in mice. Chest. 1994;105:1241---5.
8. Wu Y, Liu Y, Huang H, et al. Dexmedetomidine inhibitsinflammatory reaction in lung tissues of septic rats bysuppressing TLR4/NF-kappaB pathway. Mediators Inflamm.2013;2013:562154.
6

esio
1
2
2
2
2
2
2
2
2
2
2
diaphragmatic hernia. J Pediatr Surg. 2001;36:334---7.
Brazilian Journal of Anesth
9. Ma C, Zhu L, Wang J, et al. Anti-inflammatory effectsof water extract of Taraxacum mongolicum hand.-Mazz onlipopolysaccharide-induced inflammation in acute lung injuryby suppressing PI3K/Akt/mTOR signaling pathway. J Ethnophar-macol. 2015;168:349---55.
0. Wang X, Zhao B, Li X. Dexmedetomidine attenuates isoflurane-induced cognitive impairment through antioxidant, anti-inflammatory and anti-apoptosis in aging rat. Int J Clin Exp Med.2015;8:17281---8.
1. Liu Z, Wang Y, Wang Y, et al. Dexmedetomidine atten-uates inflammatory reaction in the lung tissues of septicmice by activating cholinergic anti-inflammatory pathway. IntImmunopharmacol. 2016;35:210---6.
2. Ma Y, Yu XY, Wang Y. Dose-related effects of dexmedetomidineon immunomodulation and mortality to septic shock in rats.World J Emerg Med. 2018;9:56---63.
3. Hein OV, Misterek K, Tessmann JP, et al. Time course of endothe-
lial damage in septic shock: prediction of outcome. Crit Care.2005;9:R323.4. Jing W, Chunhua M, Shumin W. Effects of acteoside onlipopolysaccharide-induced inflammation in acute lung injury
3
27
logy 2021;71(3):271---277
via regulation of NF-kappaB pathway in vivo and in vitro. ToxicolAppl Pharmacol. 2015;285:128---35.
5. Chen T, Mou Y, Tan J, et al. The protective effect of CDDO-Me on lipopolysaccharide-induced acute lung injury in mice. IntImmunopharmacol. 2015;25:55---64.
6. Chen T, Wang R, Jiang W, et al. Protective Effect of AstragalosideIV Against Paraquat-Induced Lung Injury in Mice by SuppressingRho Signaling. Inflammation. 2016;39:483---92.
7. Huang X, Liu Y, Lu Y, et al. Anti-inflammatory effects of eugenolon lipopolysaccharide-induced inflammatory reaction in acutelung injury via regulating inflammation and redox status. IntImmunopharmacol. 2015;26:265---71.
8. Zhou X, Dai Q, Huang X. Neutrophils in acute lung injury. FrontBiosci. 2012;17:2278---83.
9. McCabe AJ, Dowhy M, Holm BA, et al. Myeloperoxidase activ-ity as a lung injury marker in the lamb model of congenital
0. Bardales RH, Xie SS, Schaefer RF, et al. Apoptosis is a majorpathway responsible for the resolution of type II pneumocytesin acute lung injury. Am J Pathol. 1996;149:845---52.
7
C
Ts
V
a
Mb
c
d
RA
I
Radtio
h©l
Brazilian Journal of Anesthesiology 2021;71(3):278---280
ASE REPORTS
hromboelastography as a point-of-care guide forpinal anesthesia in an eclamptic patient: a case report
endhan Ramanujam a,b,∗, Usama Iqbala,c, Mary Ima,d
Drexel University College of Medicine/ Hahnemann University Hospital, Department of Anesthesiology and Perioperativeedicine, Philadelphia, USALPG /Rhode Island Hospital, Department of Anesthesiology, Providence, USANYU Langone Health, Department of Anesthesiology, New York, USAStanford University, School of Medicine, Department of Anesthesiology, Perioperative and Pain Medicine, Stanford, USA
eceived 27 January 2020; accepted 18 October 2020vailable online 3 February 2021
KEYWORDSThrombocytopenia;Cesarean section;Thromboelastography;Neuraxial anesthesia;Preeclampsia;
Abstract Neuraxial anesthesia is a standard of care during parturition. Since bleeding diathesisis a contraindication to neuraxial techniques, data about its safe administration in a thrombo-cytopenic milieu is limited and evolving. Thrombocytopenia associated with preeclampsia oreclampsia and hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndromeleads to significant maternal and neonatal morbidity. We present a case of uneventful spinalanesthesia for urgent cesarean section in an eclamptic patient with a precipitous drop in plateletcount from 124,000 to 97,000 per cubic millimeter under thromboelastography (TEG) guidance.
Eclampsia© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).a1
lt
ntroduction
egional neuraxial techniques are the gold standard fornalgesia and anesthesia during labor as well as cesareanelivery. Bleeding diathesis is an absolute contraindication
o neuraxial anesthesia because of the risk of develop-ng hematoma, which can lead to sensorimotor deficits. Inbstetric patients, the overall risk of developing hematoma∗ Corresponding author.E-mail: [email protected] (V. Ramanujam).
dnTlH(p
ttps://doi.org/10.1016/j.bjane.2020.10.011 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
fter epidural and spinal techniques is estimated to be about:200,000.1
Pregnancy is a state characterized by profound hemato-ogical changes, such as physiological anemia, neutrophilia,hrombocytopenia, increased procoagulant factors, andiminished fibrinolysis. Following anemia, thrombocytope-ia is the second-most common abnormality in pregnancy.hrombocytopenia is either isolated (gestational or immuno-
ogical) or associated with systemic disorders, such asemolysis, Elevated Liver Enzymes, and Low Platelet count
HELLP) syndrome or acute fatty liver of pregnancy. Sincelatelets are an important component of the normal
itora Ltda. This is an open access article under the CC BY-NC-ND

esio
hww
dabw
C
Af2twbHadampaI1r2rrrt(pswoaenTntwwdbm1rmmeadpsdaHt
mracdtbi(aidaspc
baaabugwasfold7ipstmth
D
Tttmfipim
fblpia
Brazilian Journal of Anesth
emostasis coagulation process, there is always a concernhen offering neuraxial anesthesia to a pregnant womanith a low platelet count.
This report describes the case of an obstetric patient whoeveloped eclampsia and low platelet count and underwentn urgent cesarean delivery, under spinal anesthesia, guidedy Thromboelastography (TEG). The patient has providedritten permission to publish this case report.
ase report
t 25-weeks of pregnancy, a 20-year-old African Americanemale (weight 75 kg, height 1.75 meters, body mass index4.5 kg.m-2) presented to the emergency room in a postic-al state following a generalized tonic-clonic seizure thatas reportedly preceded by a new-onset headache. Herlood pressures ranged from 170---140 and 120---90 mmHg.er prenatal care and medical history were unremarkablend negative for any known hypertensive or seizure disor-ers. The initial lab values were abnormal and revealed
platelet count of 124,000 per cubic millimeter (nor-al range: 150,000---450,000 per cubic millimeter), alkalinehosphatase 207 IU.L-1 (normal range: 30---120 IU.L-1),lanine aminotransferase 60 IU.L-1 (normal range: 10---40U.L-1), aspartate aminotransferase 50 IU.L-1 (normal range:0---40 IU.L-1), lactate dehydrogenase 353 IU.L-1 (normalange: 80---255 IU.L-1), uric acid 7.4 mg.dL-1 (normal range:.6---6 mg.dL-1), Prothrombin Time (PT) 9.9 seconds (normalange: 11---13.5 seconds), fibrinogen 463 mg.dL-1 (normalange: 175---400 mg.dL-1), and 3+ urine protein (normalange: negative or trace). The other measured coagula-ion parameters were the International Normalized RatioINR) of 0.9 (normal range: 0.8---1.1) and Partial Thrombo-lastin Time (PTT) of 29.2 seconds (normal range: 25---35econds). If a grand mal seizure occurs in a pregnant womanith a preeclamptic background, such as the new onsetf persistently elevated blood pressures ≥ 140/90 mmHgfter 20 weeks of gestation with accompanying proteinuria,clampsia is considered the predominant differential diag-osis; therefore, a magnesium sulfate infusion was started.he obstetrician decided to manage the patient for theext 24---48 hours with frequent neurological checks, bloodests, and continuous fetal monitoring (to optimize fetalell-being while the fetus was premature). The patientas immediately admitted, and a decision was made toelay any head imaging until clinical stabilization hadeen achieved. Following admission and while receivingagnesium, her blood pressures varied from 160---140 and
00---80 mmHg. Hourly clinical examinations revealed a neu-ologically improving patient who was increasingly becomingore awake, alert, responsive, and oriented with intactotor strength and sensations. There were no more seizure
pisodes, and the patient denied any other symptoms, suchs headache or visual disturbances. She also received aose of betamethasone for fetal lung maturity. Although theatient continued to remain clinically stable with a reas-uring fetal status under monitoring, her platelet counts
ecreased from 124,000 to 97,000 per cubic millimeter over3-hour period. This raised the possibility that she hadELLP syndrome. The repeat coagulation profile, similar tohe initial set, revealed low PT, elevated fibrinogen, and nor-
corp
27
logy 2021;71(3):278---280
al INR and PTT. Given the possibility that she could developecurrent seizures, disseminated intravascular coagulation,nd stroke, the risk of maintaining her pregnancy was per-eived to be greater than that of delivery. Therefore, it wasecided to deliver the fetus under an urgent cesarean sec-ion. By this time, a TEG had been performed to study thelood coagulation efficiency and assess the platelet functionn clot formation. The test yielded normal results: ReactionR) time 5.8 minutes, Kinetics (K) time 1.8 minutes, alphangle 66.2 degrees, and Lysis index 30 (LY30) 0%, includ-ng a Maximal Amplitude (MA) of 66.2 mm. The MA is airect function of the maximum dynamic properties of fibrinnd platelet bonding via glycoprotein IIb/IIIa, which repre-ents the ultimate strength of a fibrin clot and correlates tolatelet function. Hence it was decided to proceed with theesarean section under spinal anesthesia.
Spinal anesthesia was performed using 14.25 mg of hyper-aric 0.75% bupivacaine and 0.02 mg of intrathecal morphinet the level of the lumbar 3---4 intervertebral space using
20G needle introducer and a 24G spinal needle underseptic precautions. An adequate thoracic 4-sensory levellock was achieved, and the cesarean section proceededneventfully. The delivered neonate’s appearance, pulse,rimace, activity, and respiration scores were 7/7/7, and heas sent to the neonatal intensive care unit for observationnd further management. The patient was hemodynamicallytable throughout the delivery, with blood pressures rangingrom 140---130 mmHg to 90---60 mmHg while she remainedn magnesium infusion; she received no other cardiovascu-ar supportive medications. There was no excessive bleedinguring the surgery and the blood loss was estimated to be00 mL. The patient recovered in the recovery unit with nossues and blood pressures in the 140/90 mmHg limits. Theost-spinal anesthesia evaluation was unremarkable for anyymptoms or signs of neuraxial hematoma. Over the nextwo postoperative days, frequent neurological checks wereade, and her platelet counts and liver function tests began
o improve. On postoperative day five, she was dischargedome without any complications.
iscussion
hrombocytopenia is a known contraindication for neuraxialechniques. Half of preeclamptic patients have thrombocy-openia and its pathogenesis remains unknown. The possibleechanisms include vascular endothelial damage, increasedbrin deposition within the vascular bed, and impairedrostacyclin production. Preeclampsia management primar-ly focuses on stabilizing the mother until fetal maturity isore favorable for delivery.As previously reported, the risk of developing hematoma
ollowing neuraxial anesthesia in a parturient with throm-ocytopenia is exceptionally low when platelet counts areess than 100,000 per cubic millimeter but more than 70,000er cubic millimeter2,3; however, when thrombocytopenias accompanied by coagulopathy during pregnancy, therere no formal recommendations from either the Ameri-
an Society of Anesthesiologists or the American Collegef Obstetrics and Gynecology.4,5 Gestational and immune-elated thrombocytopenias have stable platelet counts withreserved functions, but platelet counts fall drastically9

V. Ramanujam, U. Iqbal and M. Im
Table 1 Discrete coagulation cascade values.
Normal Description
R 5---10 min Measures time to initial fibrin formationK 1---3 min Time to clot formationAlpha angle 53---72 degrees Rate of clot formationMA 50---70 mm Maximal amplitude
unpmbfaapetpoc
epPTtoip
mtacrtu
slitsr
roatdaTrwrcul
C
T
R
1
2
3
4
LY30 0---3%
nder preeclampsia- and eclampsia-related thrombocytope-ias, and platelet functions are impaired. Below 100,000er cubic millimeter, a significant hypo-coagulopathic stateight coexist with thrombocytopenia. In such scenarios, itecomes imperative to assess platelet functions during clotormation, rather than just using counts, to determine thedequacy of coagulation for safely administering neuraxialnesthesia. More specific platelet function tests cannot com-rehensively assess coagulation; can be time-consuming,xpensive, and inflexible. But TEG, a dynamic visco-kineticesting allows the assessment of clotting capacity in vivo androvides information regarding the dynamics of clot devel-pment, stabilization, and dissolution. Discrete coagulationascade values provided by TEG are shown in Table 1.
TEG analyzes whole-blood coagulation, including theffects of red blood cells and platelets, compared to testserformed on platelet-poor plasma, such as PT, Activatedartial Thromboplastin Time (aPTT), or fibrinogen levels.hus, clinically, TEG is complete and more descriptive thanhe other tests. PT and aPTT tests performed in centralr core laboratories can result in significant time delaysn getting results, in contrast to TEG, which is done as aoint-of-care hemostasis monitoring test.
As seen in this eclamptic patient, TEG revealed a nor-al R time, which correlates with normal INR and PTT and
herefore normal clotting factor levels. The patient’s K timend alpha angle were normal. However, with the plateletount below 100,000 per cubic millimeter, a normal MAesult suggested adequate platelet function in clot forma-ion, enabling the urgent cesarean section to be performednder spinal anesthesia without any complications.
There are no formal recommendations as to when is itafe to administer neuraxial anesthesia in a parturient withow platelet count, especially during scenarios with coex-
sting coagulopathies, such as preeclampsia or eclampsia;his case suggests that TEG, together with other coagulationtudies, could serve as a point-of-care guide for safe neu-axial anesthesia administration. When there is a concern5
28
Percentage decrease in amplitude at 30 minutes post-MA
egarding aspiration and airway challenges in the motherr whether the side effects of anesthetic medications willffect the baby, regional anesthesia is always preferredo general anesthesia. Urgent scenarios, such as the oneescribed here, should be considered when there are nobsolute contraindications and when time permits. Thus,EG could make it possible for many women to receive neu-axial intervention during labor and delivery, including thoseho would otherwise not be eligible for it. With further
eporting and data analysis from large cohorts of thrombo-ytopenic pregnant women undergoing neuraxial blockadender TEG guidance, the clinical use of TEG can be stream-ined for this specific population.
onflicts of interest
he authors declare no conflicts of interest.
eferences
. Goodier CG, Lu JT, Hebbar L, et al. Neuraxial Anesthesia inParturients with Thrombocytopenia: A multisite retrospectivecohort study. Anesth Analg. 2015;121:988---91.
. American College of Obstetricians and Gynecologists. Thrombo-cytopenia in pregnancy: practice bulletin no 166. Obstet Gynecol.2016;128:e43---53.
. Lee LO, Bateman BT, Kheterpal S, et al. Multicenter perioperativeoutcomes group investigators. Risk of epidural hematoma afterneuraxial techniques in thrombocytopenic parturients: a reportfrom the multicenter perioperative outcomes group. Anesthesi-ology. 2017;126:1053---63.
. American Society of Anesthesiologists task force on obstet-ric anesthesia. Practice guidelines for obstetric anesthesia: anupdated report by the American Society of Anesthesiologists taskforce on obstetric anesthesia. Anesthesiology. 2007;106:843---63.
. Goetzl LM, ACOG committee on practice bulletins-obstetrics.ACOG practice bulletin. Clinical management guidelines forobstetrician-gynecologists Number 36, July 2002. Obstetric anal-gesia and anesthesia. Obstet Gynecol. 2002;100:177---91.
0

C
Pp
K
a
Tb
RA
I
Cgsoii
h©l
Brazilian Journal of Anesthesiology 2021;71(3):281---284
ASE REPORTS
erioperative anesthesia management of a pregnantatient with central airway obstruction: a case report
eevan Singh a,b,∗, Shenelle Ballirama,b, Rachael Ramkissunb
University of the West Indies, Department of Clinical Surgical Sciences, Anaesthesia and Intensive Care Unit, St Augustine,rinidadSan Fernando General Hospital, Anaesthesia & Intensive Care Unit, San Fernando, Trinidad
eceived 9 March 2020; accepted 25 October 2020vailable online 8 February 2021
KEYWORDSTrachealcompression;Pregnancy;Mediastinal mass
Abstract Mediastinal masses in pregnancy, although rare, can present with life threateningcentral airway obstruction if general anesthesia is required. In patients with central airwayobstruction who are classified as being high risk for anesthesia, specific cardiothoracic inter-ventions are usually required when there is no alternative to general anesthesia. We describethe case of a young female who presented in her second trimester with severe tracheal compres-sion and worsening dyspnea secondary to a mediastinal mass. Intravenous dexamethasonewas started, following which her symptoms improved and a drastic reduction in her trachealcompression was observed. The patient subsequently underwent successful vaginal deliveryunder epidural anesthesia. We discuss the complexities in perioperative decision making forthis rare presentation and potential therapeutic options.
© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. Thisis an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).ouepr
ntroduction
entral Airway Obstruction (CAO) in a patient needingeneral anesthesia is harrowing prospect for many anesthe-iologists. Catastrophic and sometimes irreversible airway
bstruction is well documented and is still being reportedn the medical literature.1,2 Fundamental in these patientss the early identification and quantification of the level∗ Corresponding author.E-mail: [email protected] (K. Singh).
ptebcwr
ttps://doi.org/10.1016/j.bjane.2021.02.012 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
f airway obstruction with the development of an individ-alized management plan.2,3 Although general anesthesia,ven if safely performed, is best avoided in many of theseatients who may be classified as high-risk, it may still beequired in the obstetric patient. In non-emergent cases,harmacotherapy (chemotherapy, steroids) can help reducehe degree of obstruction and its use can be facilitated byarly planning.4 Monotherapy with steroids is seldom used
5
ut can be beneficial in certain tumor types. The discussedase illustrates the perioperative management of a patientith central airway obstruction who showed an excellentesponse to perioperative steroid use and emphasizes the
itora Ltda. This is an open access article under the CC BY-NC-ND

K. Singh, S. Balliram and R. Ramkissun
Figure 1 (a) Proximal tracheal compression caused by the mass at the level of the thoracic inlet. Maximal diameter from (b) was0
icea
C
A5sa
watoiwpfbv
swn
shsCftdt
OowsOapo
attmab
hat2i
odaAitnd
edsbeduwbtefil
p�awb
.4 mm.
mportance of an individualized management plan. This spe-ific role for steroids and the potential magnitude of itsffect has been seldom reported in the literature for centralirway obstruction.
ase report
23-year-old female who was previously well presented at-months (20/40) Period Of Gestation (POG) with a rightided neck mass. She noted this to be increasing in size andssociated with worsening dyspnea.
On review by the ENT department, a CT scan of the neckas requested which showed a large (17 × 11 × 10 cm)nterosuperior mediastinal mass. Marked tracheal deviationo the right and significant tracheal compression at the levelf the thoracic inlet was seen (Figure 1). The transverse cal-ber of the compressed trachea was measured to be 4 mmith approximately 70% tracheal compression. The com-ressed proximal segment was 4 cm long and located 6 cmrom the carina. The great vessels were encased and splayedy the mass with compression of the right internal jugularein. No pleural or pericardial effusions were seen.
A biopsy done under local anesthesia showed featuresuggestive of lymphoma but was inconclusive. The patientas then counselled on the possible diagnosis and potentialeed for chemotherapy.
She was subsequently referred to the Obstetric Anesthe-ia High Risk service (OAHRS) at her local tertiary obstetricospital. On review, she was noted to have significant supinehortness of breath with no clinical signs of Superior Venaaval Obstruction. She was assessed as being a high riskor airway complications and an inability to ventilate inhe event that general anesthesia was needed for operativeelivery. Additionally, no thoracic surgeon was available inhe event of airway collapse by the mediastinal mass.
Several multidisciplinary meetings were held by theAHRS that included the ENT, Hematology, Radiology, Oncol-gy, Obstetrics, and Intensive care departments. A referralas made to the local cardiothoracic center, however, they
uggested delivery at her present hospital as they lacked an
bstetric service. Given her worsening shortness of breathnd lack of cardiothoracic intervention at her present hos-ital the multidisciplinary team decided to trial a coursef high dose steroid to facilitate reduction in tumor sizehffi
28
nd airway compression until delivery of the baby. Oncehe baby was delivered the patient could then be referredo a cardiothoracic center for definitive treatment of theass. Dexamethasone 12 mg intravenous (IV) twice daily for
period of 5 days was commenced followed subsequentlyy prednisolone 30 mg orally.
Initiation of steroids was followed by rapid resolution ofer symptoms and a CT scan performed shortly after initi-tion of dexamethasone showed a reduction in the size ofhe mass and significantly less tracheal compression (Figure). The patient was discharged home and followed weeklyn the antenatal clinic.
At 32/40 POG the prednisolone was tapered to 30 mgrally every other day. Due to the potential risk of furthereterioration and the urgent need to commence treatmentn elective induction was planned at 34/40 weeks POG.nother CT (Figure 2) scan performed shortly before her
nduction showed a still present mass effect, but a patentrachea. Echocardiogram showed normal ejection fraction,o mass compression of any of the chambers and no pericar-ial effusion.
In the event of a potential need for an operative deliv-ry and to optimize the chances of a successful vaginalelivery, a lumbar epidural was inserted at the L4---L5 inter-pace, with the epidural having the potential to facilitateoth labor analgesia and a cesarean section if required. Thepidural would also prevent fatigue and excessive straininguring delivery. As a secondary option in the case of fail-re of epidural anesthesia, general anesthesia was plannedith an inhalation induction, spontaneous ventilation, andypass of the area of compression with the endotrachealube under endoscopic guidance if necessary. The laborpidural was inserted in the operating theatre with the dif-cult airway equipment on standby instead of in the normal
abor suite.The labor epidural was successfully used during the
atient’s labor with a 0.125% bupivacaine solution and 2g.mL-1 of fentanyl given via continuous infusion. Adequatenalgesia was achieved with a T8 level block and the patientas comfortable throughout her delivery eventually givingirth to a healthy newborn.
Postoperatively, the patient was closely monitored in theigh dependency unit for 48 hours and then discharged for
urther definitive oncological care. Subsequent testing con-rmed the mass to be a thymoma.2
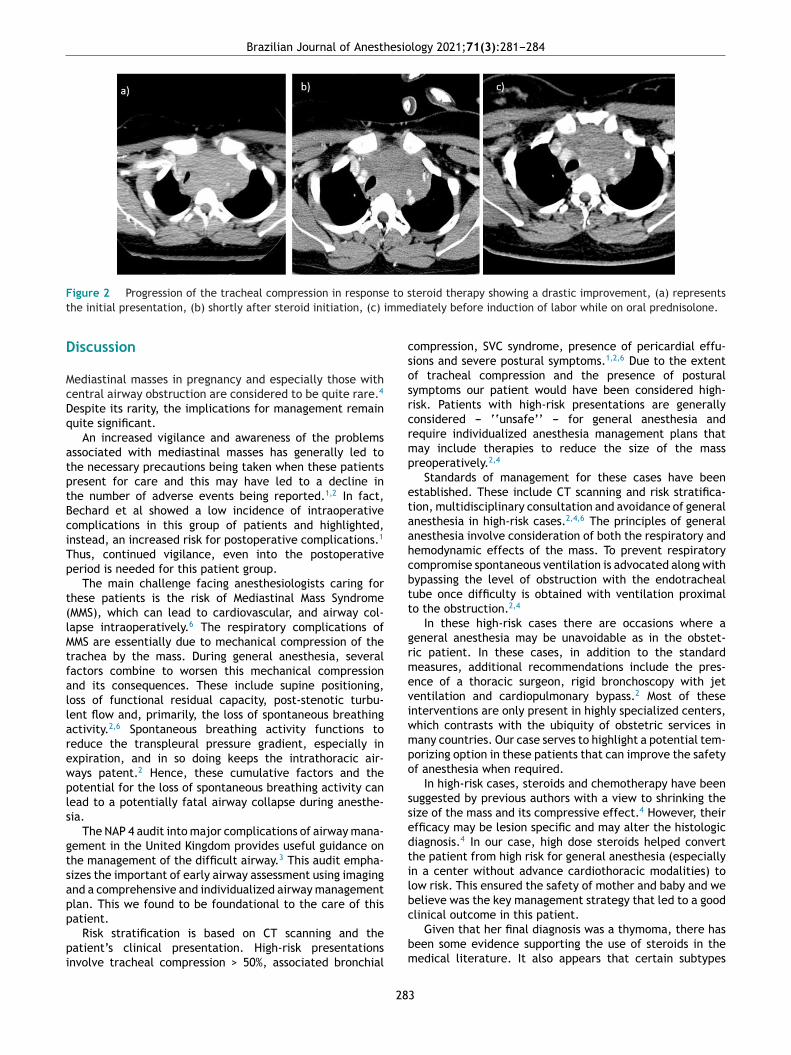
Brazilian Journal of Anesthesiology 2021;71(3):281---284
F to st mme
D
McDq
atptBciTp
t(lMtfallarewpls
gtsapp
pi
csosrcrmp
etaahcbtt
grmeviwmpo
ssedtilb
igure 2 Progression of the tracheal compression in responsehe initial presentation, (b) shortly after steroid initiation, (c) i
iscussion
ediastinal masses in pregnancy and especially those withentral airway obstruction are considered to be quite rare.4
espite its rarity, the implications for management remainuite significant.
An increased vigilance and awareness of the problemsssociated with mediastinal masses has generally led tohe necessary precautions being taken when these patientsresent for care and this may have led to a decline inhe number of adverse events being reported.1,2 In fact,echard et al showed a low incidence of intraoperativeomplications in this group of patients and highlighted,nstead, an increased risk for postoperative complications.1
hus, continued vigilance, even into the postoperativeeriod is needed for this patient group.
The main challenge facing anesthesiologists caring forhese patients is the risk of Mediastinal Mass SyndromeMMS), which can lead to cardiovascular, and airway col-apse intraoperatively.6 The respiratory complications ofMS are essentially due to mechanical compression of the
rachea by the mass. During general anesthesia, severalactors combine to worsen this mechanical compressionnd its consequences. These include supine positioning,oss of functional residual capacity, post-stenotic turbu-ent flow and, primarily, the loss of spontaneous breathingctivity.2,6 Spontaneous breathing activity functions toeduce the transpleural pressure gradient, especially inxpiration, and in so doing keeps the intrathoracic air-ays patent.2 Hence, these cumulative factors and theotential for the loss of spontaneous breathing activity canead to a potentially fatal airway collapse during anesthe-ia.
The NAP 4 audit into major complications of airway mana-ement in the United Kingdom provides useful guidance onhe management of the difficult airway.3 This audit empha-izes the important of early airway assessment using imagingnd a comprehensive and individualized airway managementlan. This we found to be foundational to the care of this
atient.Risk stratification is based on CT scanning and theatient’s clinical presentation. High-risk presentationsnvolve tracheal compression > 50%, associated bronchial
c
bm
28
teroid therapy showing a drastic improvement, (a) representsdiately before induction of labor while on oral prednisolone.
ompression, SVC syndrome, presence of pericardial effu-ions and severe postural symptoms.1,2,6 Due to the extentf tracheal compression and the presence of posturalymptoms our patient would have been considered high-isk. Patients with high-risk presentations are generallyonsidered --- ‘‘unsafe’’ --- for general anesthesia andequire individualized anesthesia management plans thatay include therapies to reduce the size of the massreoperatively.2,4
Standards of management for these cases have beenstablished. These include CT scanning and risk stratifica-ion, multidisciplinary consultation and avoidance of generalnesthesia in high-risk cases.2,4,6 The principles of generalnesthesia involve consideration of both the respiratory andemodynamic effects of the mass. To prevent respiratoryompromise spontaneous ventilation is advocated along withypassing the level of obstruction with the endotrachealube once difficulty is obtained with ventilation proximalo the obstruction.2,4
In these high-risk cases there are occasions where aeneral anesthesia may be unavoidable as in the obstet-ic patient. In these cases, in addition to the standardeasures, additional recommendations include the pres-
nce of a thoracic surgeon, rigid bronchoscopy with jetentilation and cardiopulmonary bypass.2 Most of thesenterventions are only present in highly specialized centers,hich contrasts with the ubiquity of obstetric services inany countries. Our case serves to highlight a potential tem-orizing option in these patients that can improve the safetyf anesthesia when required.
In high-risk cases, steroids and chemotherapy have beenuggested by previous authors with a view to shrinking theize of the mass and its compressive effect.4 However, theirfficacy may be lesion specific and may alter the histologiciagnosis.4 In our case, high dose steroids helped converthe patient from high risk for general anesthesia (especiallyn a center without advance cardiothoracic modalities) toow risk. This ensured the safety of mother and baby and weelieve was the key management strategy that led to a good
linical outcome in this patient.Given that her final diagnosis was a thymoma, there haseen some evidence supporting the use of steroids in theedical literature. It also appears that certain subtypes
3

am a
(w
nwisctifi
C
Astatca
C
T
R
1
2
3
4
5
nism of action. Cancer. 2006;106:1901---7.6. Erdös G, Tzanova I. Perioperative anaesthetic management
of mediastinal mass in adults. Eur J Anaesthesiol EJA.2009;26:627---32.
K. Singh, S. Ballir
type B1) may have significant response to steroid therapy,hich was the case with our patient.5
Although chemotherapy has been safely started in preg-ancy for lymphomas, evidence for its use is limited and itas not started in our patient despite initial testing suggest-
ng a lymphoma. While it may have been a viable option forhrinking the mass our oncologist and hematologist were notonvinced of the adequacy of the biopsy and after consulta-ion with the patient and the multidisciplinary team thoughtt best to expedite delivery and repeat the biopsy. Given thenal diagnosis of thymoma, this was likely the best decision.
onclusion
lthough rare, mediastinal masses in pregnancy can pose aignificant challenge during anesthesia and can be poten-ially fatal. Early detection of such cases can allowppropriate therapy to reduce airway obstruction preopera-ively. In settings without advanced cardiothoracic facilities,onsideration of the use of steroids, in select cases, canllow for a greater margin of safety if anesthesia is required.
onflicts of interest
he authors declare no conflicts of interest.
28
nd R. Ramkissun
eferences
. Béchard P, Létourneau L, Lacasse Y, Côté D, Bussières JS.Perioperative cardiorespiratory complications in adults withmediastinal mass: incidence and risk factors. Anesthesiology.2004;100:826---34, discussion 5A.
. Blank RS, de Souza DG. Anesthetic management of patients withan anterior mediastinal mass: continuing professional develop-ment. Can J Anaesth. 2011;58, 853-9, 860-7.
. NAP4: Major Complications of Airway Management in theUnited Kingdom --- The National Institute of Academic Anaes-thesia [Internet]. [cited 2020 Oct 12]. Available from:https://www.nationalauditprojects.org.uk/NAP4 home.
. Gothard JWW. Anesthetic Considerations for Patients with Ante-rior Mediastinal Masses. Anesthesiol Clin. 2008;26:305---14.
. Kobayashi Y, Fujii Y, Yano M, et al. Preoperative steroid pulsetherapy for invasive thymoma: clinical experience and mecha-
4
C
Us
IMV
a
b
c
RA
I
Qgii
h©B
Brazilian Journal of Anesthesiology 2021;71(3):285---287
ASE REPORTS
ltrasound-guided quadratus lumborum block forurgical treatment of endometriosis: case report
delberto do Val Ribeiro-Juniora, Luiz Gustavo Oliveira Britob,aíra Rossmann-Machadob, Rose Luce Gomes do Amarala, Angélica F.A. Bragac,anessa Henriques Carvalho c,∗
Centro de Atenção Integral à Saúde da Mulher (CAISM), Hospital da Mulher Prof. Dr. J. A. Pinotti, Campinas, SP, BrazilUniversidade de Campinas, Faculdade de Ciências Médicas, Departamento de Obstetrícia e Ginecologia, Campinas, SP, BrazilUniversidade Estadual de Campinas, Faculdade de Ciências Médicas, Departamento de Anestesiologia, Campinas, SP, Brazil
eceived 19 April 2020; accepted 18 October 2020vailable online 6 February 2021
KEYWORDSEndometriosis;VAS;Gynecology;Quadratus lumborumblock
Abstract Quadratus lumborum block (QLB) is a technique that is not widely applied for gyne-cological surgery. Endometriosis affects 10% of the female population and chronic pelvic painis one of the most prevalent symptoms. Laparoscopic surgery for removal of endometriosismay present a long intra-operative duration and this technique might improve postoperativepain control. We described a case report of a patient submitted to general anesthesia asso-ciated to bilateral QLB for pelvic endometriosis. QLB was an adjuvant anesthetic techniquefor endometriosis, providing somatic and visceral analgesia. However, prospective studies areneeded to identify the standard dosage and total duration of analgesia.
© 2021 Published by Elsevier Editora Ltda. on behalf of Sociedade Brasileira de Anestesiologia.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).firQ
ntroduction
uadratus lumborum block (QLB) is an analgesic technique
uided by ultrasonography that introduces a local anestheticnto an interfacial plane that comprises the QL muscle aim-ng to block the thoracolumbar nerves.1 Blanco was the∗ Corresponding author.E-mail: [email protected] (V.H. Carvalho).
opadSpm
ttps://doi.org/10.1016/j.bjane.2021.02.014 2021 Published by Elsevier Editora Ltda. on behalf of Sociedade BrasilY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
rst one to describe it in 20072 and some published caseeports and randomized controlled studies have shown thatLB is effective to provide pain relief after several typesf abdominal surgeries.3 Endometriosis is defined as theresence of endometrial tissue outside the uterine cavitynd one of its common symptoms are chronic pelvic pain,ysmenorrhea, deep dyspareunia, dysuria and dyschezia.4
urgical treatment of endometriosis is mostly indicated forain relief or infertility that is refractory to clinical treat-ent, or advanced clinical spectrum of this disease, such as
eira de Anestesiologia. This is an open access article under the CC.

o, M
dftmpdphmagmrmiaf
C
AocsdthpaapdsltQtse4taSaiitutmnaaQarpcQt2
otwc01hwHhlt4
D
TverpatapciocQubhrfsfctBpseigstthlimbt
a0
I.V. Ribeiro-Junior, L.G. Brit
eep infiltrating endometriosis. Reducing the endometrioticoci is the main goal of surgery.4 There is scant litera-ure regarding the use of QLB in female pelvic surgery,ost of good available data being concentrated in obstetricrocedures. Within gynecological procedures, there is a ran-omized study comparing QLB versus transverse abdominallane (TAP) block in women that underwent total abdominalysterectomy,5 a case report on the postoperative manage-ent of refractory pain after uterine artery embolization,
nd another randomized study assessing quality of life afterynecological laparoscopic surgery with QLB. The use ofyofascial regional block techniques guided by ultrasonog-
aphy, especially for pelvic surgeries such as endometriosis,ay be beneficial as adjuvant strategy for pain control dur-
ng intra and postoperative period. To this moment, therere no reports about the use of QLB for gynecological surgeryor treating endometriosis.
ase report
39-year-old woman, ASA (American Society of Anesthesi-logists) physical status II due to anxiety disorder with nourrent treatment, 70 kg, 1.67 m, nulliparous, with diagno-is of primary infertility and deep infiltrating endometriosisiagnosed by pelvic ultrasound was submitted to surgicalreatment of endometriosis. Preoperative pelvic imagingas found kissing ovaries, endometriotic foci on the upperortion of rectum, left uterosacral ligament, left round lig-ment, left vesicouterine space, and endometriotic lesionst anterior uterine serosae with myometrial infiltration. Sheresented chronic pelvic pain, intense menstrual flow, cycliceep dyspareunia, with no dyschezia or dysuria. A laparo-copic surgery was planned; however, due to the extent ofesions within the abdominal cavity, a conversion to laparo-omy was performed. After informed consent to undergoLB during general anesthesia, patient was admitted inhe operating room with previous venoclysis. Patient wasubmitted to noninvasive monitoring (cardioscopy, periph-ral oxygen saturation, temperature, capnography, NIP),
mg intravenous (IV) midazolam. General anesthesia induc-ion was done with remifentanil, propofol, and rocuronium,nd total IV maintenance with remifentanil and propofol.ubsequently, alcoholic chlorhexidine was applied in thebdominal region bilaterally to posterior axillary line andpsilateral to the region where QLB was performed. Annfragluteal cushion was customized and gave support tohe procedure area (Figure 1A). A curve transducer wassed to obtain the images, and from the median to pos-erior axillary lines, it was identified the abdominal rectususcle, as well as the three muscles of the lateral abdomi-
al wall (external oblique, internal oblique, and transversusbdominus). A more hyperechoic structure with posteriorcoustic shadow was seen (Shamrock signal) where theL and psoas muscles were visualized. Probe was kept in
transverse plane, L4 level between middle and poste-ior axillary line, and a Tuohy 18G needle was introducedostero-anteriorly. After negative aspiration, 35 ml bupiva-
aine 0.25% plus 1:200,000 adrenaline was injected betweenL and psoas muscles (Figure 1B). The duration of the anes-hetic procedure was 340 minutes. In summary, it was used,981 mg of propofol, 3,788 mcg of remifentanil and 50 mgifipt
28
. Rossmann-Machado et al.
f rocuronium. Intraoperatively, 10 mg dexamethasone, 1 granexamic acid, 100 mg ketoprofen, and 8 mg ondansetronere administered. Estimated blood loss was 600 ml andrystalloids were administered, as well as IV metaraminol.5 mg. She remained in the postanesthesia care unit for65 minutes and after 150 minutes post extubation she hader first complaint of pain at the incision area. VAS scoreas 1 (range: 0-10) after 2, 6, 12, and 24 hours after surgery.ospital length stay was of 60 hours and she was dischargedome with normal vital signals, VAS between 0 and 1, ambu-ating. Intravenous sodium dipyrone 1 g 6/6 h and 40 mgenoxicam 12/12 h was applied to this patient within 24 and8 hours.
iscussion
his case report has shown that the QLB use as an adju-ant for pain control after surgical treatment of advancedndometriotic lesions was effective and has meaningfullyeduced the VAS score during immediate postoperativeeriod. Differently from laparoscopic procedures, this wasn open surgery, and if we consider the extensive diseasehat was confirmed intraoperatively, there was a high prob-bility of presenting high VAS scores in the postoperativeeriod, as well as for using intravenous opioids towards painontrol.3 This patient presented minimum VAS score dur-ng the first 24 hours after surgery, and she did not use anypioids at any time. Yousef5 has performed a randomizedontrolled study comparing postoperative pain control usingLB versus transverse abdominus plane block for womenndergoing total abdominal hysterectomy. QLB presentedetter intra and postoperative analgesic control (lower VAS,igher postoperative analgesic duration, and less patientsequesting analgesics), as well as lower administration ofentanyl and morphine. There is a discussion about a pos-ible visceral analgesic effect caused by QLB, differentrom other peripheral blocks where sympathetic innervationould receive the anesthetic by dissection and dispersionhrough pre and paravertebral ganglia.1 Anatomically, aslanco described,2 quadratus lumborum block (QLB) is aosterior abdominal block that allows local anesthetic topread posteriorly to the quadratus lumborum muscle andxpand beyond the middle layer of the thoracolumbar fascian a triangular space called the lumbar interfacial trian-le. This interfacial plane is in close relation with multipleympathetic nerves and connects with the thoracic paraver-ebral space. We believe the local anesthetic effect on thehoracolumbar fascia is the main component for the QLB,owever, further understanding of its anatomic and histo-ogic role is needed, as the true mechanism of the QLB blocks still unknown. The spread into the paravertebral spaceay also have an effect. It seems that a more posteriorlockade approach is more effective than the conventionalransversus abdominus plane (TAP).
Large-volume injections of local anesthetic, typically long-acting amide such as ropivacaine or bupivacaine.125---0.375% (15---30 mL per side, 0.2---0.4 mL.kg−1) injected
nto any of these fascial planes affect the adjacent nervebers, such as the lateral cutaneous branches of the iliohy-ogastric, ilioinguinal, and subcostal nerves, with potentialo track into the paravertebral space. This posterior spread6
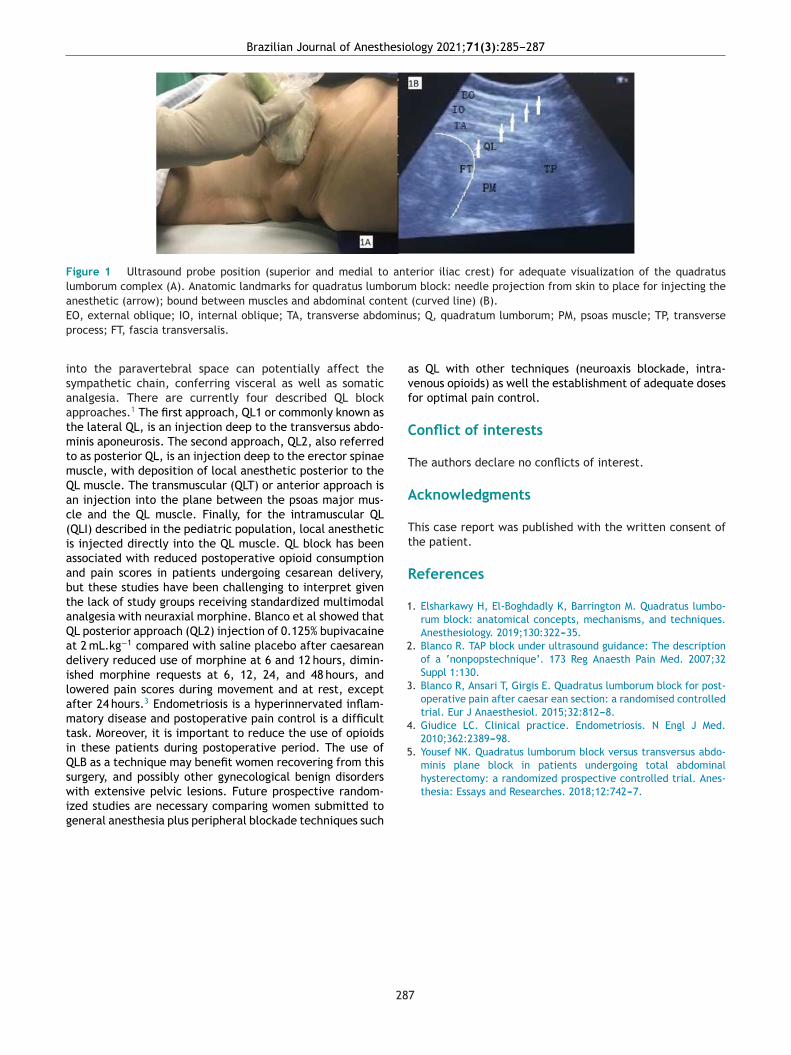
Brazilian Journal of Anesthesiology 2021;71(3):285---287
Figure 1 Ultrasound probe position (superior and medial to anterior iliac crest) for adequate visualization of the quadratuslumborum complex (A). Anatomic landmarks for quadratus lumborum block: needle projection from skin to place for injecting theanesthetic (arrow); bound between muscles and abdominal content (curved line) (B).E minup
isaatmtmQac(iaabtaQadilamtiQswig
avf
C
T
A
Tt
R
1
2
3
4
5. Yousef NK. Quadratus lumborum block versus transversus abdo-minis plane block in patients undergoing total abdominal
O, external oblique; IO, internal oblique; TA, transverse abdorocess; FT, fascia transversalis.
nto the paravertebral space can potentially affect theympathetic chain, conferring visceral as well as somaticnalgesia. There are currently four described QL blockpproaches.1 The first approach, QL1 or commonly known ashe lateral QL, is an injection deep to the transversus abdo-inis aponeurosis. The second approach, QL2, also referred
o as posterior QL, is an injection deep to the erector spinaeuscle, with deposition of local anesthetic posterior to theL muscle. The transmuscular (QLT) or anterior approach isn injection into the plane between the psoas major mus-le and the QL muscle. Finally, for the intramuscular QLQLI) described in the pediatric population, local anesthetics injected directly into the QL muscle. QL block has beenssociated with reduced postoperative opioid consumptionnd pain scores in patients undergoing cesarean delivery,ut these studies have been challenging to interpret givenhe lack of study groups receiving standardized multimodalnalgesia with neuraxial morphine. Blanco et al showed thatL posterior approach (QL2) injection of 0.125% bupivacainet 2 mL.kg−1 compared with saline placebo after caesareanelivery reduced use of morphine at 6 and 12 hours, dimin-shed morphine requests at 6, 12, 24, and 48 hours, andowered pain scores during movement and at rest, exceptfter 24 hours.3 Endometriosis is a hyperinnervated inflam-atory disease and postoperative pain control is a difficult
ask. Moreover, it is important to reduce the use of opioidsn these patients during postoperative period. The use ofLB as a technique may benefit women recovering from this
urgery, and possibly other gynecological benign disordersith extensive pelvic lesions. Future prospective random-zed studies are necessary comparing women submitted toeneral anesthesia plus peripheral blockade techniques such
28
s; Q, quadratum lumborum; PM, psoas muscle; TP, transverse
s QL with other techniques (neuroaxis blockade, intra-enous opioids) as well the establishment of adequate dosesor optimal pain control.
onflict of interests
he authors declare no conflicts of interest.
cknowledgments
his case report was published with the written consent ofhe patient.
eferences
. Elsharkawy H, El-Boghdadly K, Barrington M. Quadratus lumbo-rum block: anatomical concepts, mechanisms, and techniques.Anesthesiology. 2019;130:322---35.
. Blanco R. TAP block under ultrasound guidance: The descriptionof a ‘nonpopstechnique’. 173 Reg Anaesth Pain Med. 2007;32Suppl 1:130.
. Blanco R, Ansari T, Girgis E. Quadratus lumborum block for post-operative pain after caesar ean section: a randomised controlledtrial. Eur J Anaesthesiol. 2015;32:812---8.
. Giudice LC. Clinical practice. Endometriosis. N Engl J Med.2010;362:2389---98.
hysterectomy: a randomized prospective controlled trial. Anes-thesia: Essays and Researches. 2018;12:742---7.
7

C
Et
SJ
a
b
RA
I
Aocsttc
h©l
Brazilian Journal of Anesthesiology 2021;71(3):288---291
ASE REPORTS
valuation of the density spectral array in the Wadaest: report of six cases
usana Pacreu a,∗, Esther Vilàa, Luis Moltóa, Rodrigo Rocamorab,uan Luis Fernández-Candil a
Hospital del Mar, Department of Anestesiología y Reanimación, Barcelona, SpainHospital del Mar, Department of Neurología, Barcelona, Spain
eceived 28 March 2019; accepted 27 February 2021vailable online 8 April 2021
KEYWORDSWada test;Epilepsy;Amobarbital;Alpha waves;Density spectralarray;
Abstract Wada test is an invasive procedure used in the preoperative evaluation for epilepsysurgery to determine language lateralization, postoperative risk of amnesia syndrome, and toassess the risk of memory deficits. It involves injection of amobarbital into internal carotidartery of the affected hemisphere followed by the healthy hemisphere to shut down brainfunction. We performed an observational study evaluating the density spectral array (DSA) ofthe bilateral bispectral index VISTATM Monitoring System (BVMS) in 6 patients with drug-resistantepilepsy undergoing Wada test. DSA revealed the presence of bifrontal alpha waves in absenceof loss of consciousness in all patients.
Loss of consciousness© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).EftBtd
ntroduction
s anesthesiologists we are interested in knowing the effectn processed EEG when an anesthetic is administered inerebral arteries. As an epilepsy reference center we havetudied this effect in the Wada test, a procedure employed
o evaluate language lateralization and memory lateraliza-ion in patients affected by temporal epilepsy, and who areandidates for temporal lobe resection.1 Our center the∗ Corresponding author.E-mail: [email protected] (S. Pacreu).
uabotT
ttps://doi.org/10.1016/j.bjane.2021.02.050 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
pilepsy Group of the Neurological Department uses theunctional magnetic resonance imaging (fMRI), a noninvasiveechnique, to study the language and memory lateralization.ut when the results are inconclusive, the Wada test remainshe most direct method to assess the risk of verbal memoryecline after surgical treatment.
The Wada test consists of an injection of amobarbital (anltrashort acting barbiturate) through the internal carotidrtery (ICA) to reach zones perfused by the middle cere-
ral artery (MCA) and the anterior cerebral one (ACA). Onef the hemispheres is thus either totally or partially anes-hetized in order to evaluate the function of the other.1he expected effect is to produce transient aphasia and
itora Ltda. This is an open access article under the CC BY-NC-ND

esio
cs
fstmtoaptsmpoaiIae
SchptFafabaleqAarhaa
hpt
M
Adfs(Atapapm
wrcrat
t1tbcitbrtcatomaottrpt
R
ThcTttdtpoapilttt
pw
D
Brazilian Journal of Anesth
ontralateral hemiplegia once the drug is injected into thepeech-dominant hemisphere.
A cerebral angiogram is always performed by trans-emoral catheterization of the ICA in order to visualize thehape of intracranial vascularization and the crossflow tohe contralateral hemisphere. This stage is crucial becauseajor vascular fluctuations could influence the results of
he test. In this sense, the medial temporal region and partf the hippocampus are irrigated by the anterior choroidalrtery (ACdA) that usually originates from the ICA, and theosterior two thirds of the hippocampus depend on the pos-erior cerebral artery (PCA), a branch of the vertebrobasilarystem. Patients with PCA thromboembolic disease haveemory deficits frequently, although the contribution of thisosterior part to the memory function is unclear.2 A variationf PCA, named Fetal PCA, originating in the ICA is observed inpproximately 25% of patients making hippocampus functionn this part of the hemisphere totally dependent on the ICA.n this situation, the administration of the barbiturate couldffect all the hippocampus in this hemisphere, and memoryvaluation would totally depend on the other hemisphere.2
The bilateral bispectral index (BIS) VISTATM Monitoringystem (BVMS) includes a bifrontal sensor with four EEGhannels to continuously monitor the frontal lobes of bothemispheres. This monitor shows the distribution of EEGower in relation to frequency across time with a color spec-rogram named density spectral array (DSA). DSA appliesourier’s Transformation converting the EEG signal frommplitudes fluctuating in the time domain to power in therequency domain. Changes in power of the frequency bandss delta (1 to 4 Hz), theta (4---10 Hz), alpha (8---12 Hz), andeta (> 12 Hz) can be used to quantify the brain effect ofnesthetic agents. DSA also shows very low-frequency oscil-ations (approximately 1 Hz). In addition, the 95% spectraldge frequency (SEF 95) can be observed. SEF 95 is the fre-uency below which 95% of the total spectral power lies.nother variable is asymmetry (ASYM), which is processednd indicates the EEG power present in either the left oright hemispheres with respect to total EEG power (bothemispheres).3 When relative values are greater than 50% inmplitude and/or frequency, they are considered significantnd correlate with neuropathological findings.
The aim of this study was to observe DSA evolution in bothemispheres after the administration of amobarbital in sixatients with pharmacoresistant epilepsy and candidates foremporal lobe resection.
aterial and methods
prospective, observational study of the DSA in 6 can-idates for temporal lobe resection of the epileptogenicocus in whom the Wada test had been performed. Thetudy was approved by the Institutional Ethics Committee2020/9448). Three women and three men were included:merican Society of Anesthesiologists (ASA) physical sta-us II/III (3/3), age 35 ± 8.9 years, weight 6.23 ± 21.75 kg,nd height 168.54 ± 10.87 cm. To carry out this test the
atients signed the corresponding informed consent. Annesthetist was present to monitor cardiovascular and res-iratory parameters and deal with any complications thatay have arisen.Tbtt
28
logy 2021;71(3):288---291
Epileptic male and female individuals aged over 18 yearsho were eligible for surgery were included. Exclusion crite-
ia were: hemodynamic instability (arterial hypotension) oromplete auricular-ventricular blockage; moderate/severeenal insufficiency (creatinine clearance < 60 mL.min-1);llergy/hypersensitivity to the active substance; or some ofhe excipients of amobarbital.
The 6 patients attended the neuroangiography area withheir electrode helmets in place following the International0---20 System and EEG measuring commenced together withhe bilateral BVMS. The BVMS DSA shows a spectral rangeetween 0.5 and 30 Hz, but for the purposes of this studyhanges of drug effect above 12 Hz were not evaluated. Dur-ng the procedure systolic/diastolic arterial blood pressure,he electrocardiogram, and percentage oxygen saturationy pulse oximetry were monitored in all patients. A neuro-adiologist introduced a catheter from the femoral arteryowards the ICA in the affected hemisphere. Once theatheter was in place the patient was asked to raise bothrms, amobarbital was then administered until the arm con-ralateral to the injected hemisphere fell. A mean dosagef 125 mg of amobarbital was given. The language test com-enced immediately, including naming objects in a picture,
nd memory exploration through remembering phrases andbjects previously shown. Thirty minutes after finishing theest (the time required between the two injections forhe hypnotic effect to disappear), the same procedure wasepeated in the healthy hemisphere. The Wada test in the 6atients lasted approximately 90 minutes, after completionhey were moved to a hospital ward.
esults
wo of the 6 patients had an extensive connatal lesion in theemisphere where the epileptogenic focus was located. Theerebral angiogram detected fetal PCA in 2 of the 6 patients.he remaining 4 presented a pharmacoresistant focus. Inhese 4 patients the administration of amobarbital, first inhe diseased hemisphere and later in the healthy one, pro-uced the respective contralateral brachial hemiplegia. Athis moment, in patients 1, 2, 3, and 4 the BVMS showed theresence of alpha activity in consonance with low frequencyscillations in both hemispheres but none of them hadmobarbital perfusion in the contralateral hemisphere. Inatient 5 theta and alpha activity were observed (8 Hz), andn patient 6, who presented extensive brain damage in theeft hemisphere, delta activity predominated (Fig. 1). Onlyhe patient 5 showed amobarbital cross-perfusion becausehe left anterior cerebral artery irrigates part of the righterritory.
During the procedure there were no cardiologic or res-iratory complications and the Wada test was performedithout incidents.
iscussion
he DSA provided by the BVMS allowed us to observe theaseline state of the brain and to evaluate the responses tohe anesthetic procedures. The administration of amobarbi-al not only affected the injected hemisphere (ipsilateral)
9
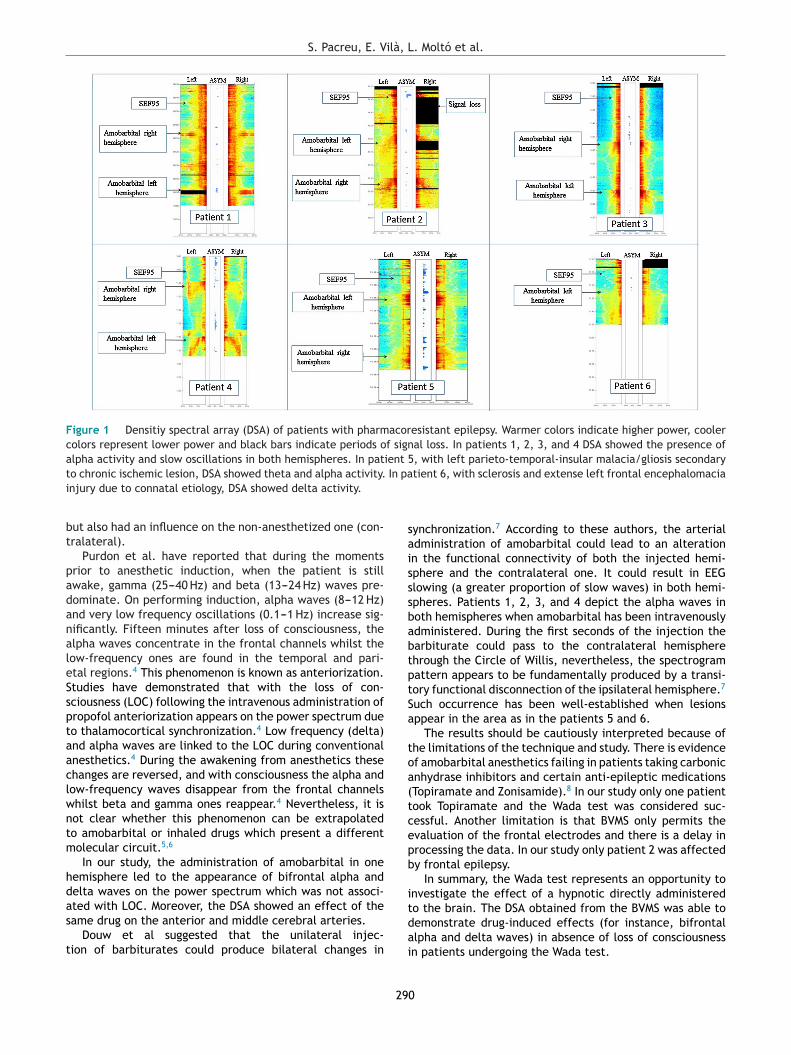
S. Pacreu, E. Vilà, L. Moltó et al.
Figure 1 Densitiy spectral array (DSA) of patients with pharmacoresistant epilepsy. Warmer colors indicate higher power, coolercolors represent lower power and black bars indicate periods of signal loss. In patients 1, 2, 3, and 4 DSA showed the presence ofalpha activity and slow oscillations in both hemispheres. In patient 5, with left parieto-temporal-insular malacia/gliosis secondaryt In pai
bt
padanaleSsptaaclwntm
hdas
t
saisssbabtptSa
toa(tcepb
i
o chronic ischemic lesion, DSA showed theta and alpha activity.njury due to connatal etiology, DSA showed delta activity.
ut also had an influence on the non-anesthetized one (con-ralateral).
Purdon et al. have reported that during the momentsrior to anesthetic induction, when the patient is stillwake, gamma (25---40 Hz) and beta (13---24 Hz) waves pre-ominate. On performing induction, alpha waves (8---12 Hz)nd very low frequency oscillations (0.1---1 Hz) increase sig-ificantly. Fifteen minutes after loss of consciousness, thelpha waves concentrate in the frontal channels whilst theow-frequency ones are found in the temporal and pari-tal regions.4 This phenomenon is known as anteriorization.tudies have demonstrated that with the loss of con-ciousness (LOC) following the intravenous administration ofropofol anteriorization appears on the power spectrum dueo thalamocortical synchronization.4 Low frequency (delta)nd alpha waves are linked to the LOC during conventionalnesthetics.4 During the awakening from anesthetics thesehanges are reversed, and with consciousness the alpha andow-frequency waves disappear from the frontal channelshilst beta and gamma ones reappear.4 Nevertheless, it isot clear whether this phenomenon can be extrapolatedo amobarbital or inhaled drugs which present a differentolecular circuit.5,6
In our study, the administration of amobarbital in oneemisphere led to the appearance of bifrontal alpha andelta waves on the power spectrum which was not associ-
ted with LOC. Moreover, the DSA showed an effect of theame drug on the anterior and middle cerebral arteries.Douw et al suggested that the unilateral injec-ion of barbiturates could produce bilateral changes in
tdai
29
tient 6, with sclerosis and extense left frontal encephalomacia
ynchronization.7 According to these authors, the arterialdministration of amobarbital could lead to an alterationn the functional connectivity of both the injected hemi-phere and the contralateral one. It could result in EEGlowing (a greater proportion of slow waves) in both hemi-pheres. Patients 1, 2, 3, and 4 depict the alpha waves inoth hemispheres when amobarbital has been intravenouslydministered. During the first seconds of the injection thearbiturate could pass to the contralateral hemispherehrough the Circle of Willis, nevertheless, the spectrogramattern appears to be fundamentally produced by a transi-ory functional disconnection of the ipsilateral hemisphere.7
uch occurrence has been well-established when lesionsppear in the area as in the patients 5 and 6.
The results should be cautiously interpreted because ofhe limitations of the technique and study. There is evidencef amobarbital anesthetics failing in patients taking carbonicnhydrase inhibitors and certain anti-epileptic medicationsTopiramate and Zonisamide).8 In our study only one patientook Topiramate and the Wada test was considered suc-essful. Another limitation is that BVMS only permits thevaluation of the frontal electrodes and there is a delay inrocessing the data. In our study only patient 2 was affectedy frontal epilepsy.
In summary, the Wada test represents an opportunity tonvestigate the effect of a hypnotic directly administeredo the brain. The DSA obtained from the BVMS was able toemonstrate drug-induced effects (for instance, bifrontal
lpha and delta waves) in absence of loss of consciousnessn patients undergoing the Wada test.0

esio
C
T
R
1
2
3
4
5
6
7
8. Bookheimer S, Schrader LM, Raush R, et al. Reduced anes-
Brazilian Journal of Anesth
onflicts of interest
he authors declare no conflicts of interest.
eferences
. Abou-Khalil B. An update on determination of language domi-nance in screening for epilepsy surgery: the Wada test and newernon-invasive alternatives. Epilepsia. 2007;48:442---55.
. Zijlmans M, Huibers CJ, Huiskamp GJ, et al. The contribution ofposterior circulation to memory function during the intracarotid
amobarbital procedure. J Neurol. 2012;259:1632---8.. Purdon PL, Sampson A, Pavone KJ, et al. Clinical Elec-troencephalography for anesthesiologists. Anesthesiology.2015;123:1---24.
29
logy 2021;71(3):288---291
. Purdon P, Pierce E, Mukamel E, et al. Electroencephalogram sig-natures of loss and recovery of consciousness from propofol. ProcNatl Acad Sci U S A. 2013;110:E1142---51.
. Löscher W, Rogawski MA. How theories evolved concerning themechanism of action of barbiturates. Epilepsia. 2012;53:12---25.
. Blain-Moraes S, Tarnal V, Vanini G, et al. Neurophysiological cor-relates of sevoflurane-induced unconsciousness. Anesthesiology.2015;122:307---16.
. Douw L, Baayen JC, Klein M, et al. Functional connectivity inthe brain before and during intra-arterial amobarbital injection(Wada test). Neuroimage. 2009;46:584---8.
thetization during the intracarotid amobarbital (Wada) testin patients taking carbonic anhydrase-inhibiting medications.Epilepsia. 2005;46:236---43.
1

C
Psa
BN
a
Cb
Ic
RA
I
Cc
h©l
Brazilian Journal of Anesthesiology 2021;71(3):292---294
ASE REPORTS
ulmonary embolism confounded with COVID-19uspicion in a catatonic patient presenting tonesthesia for ECT: a case report
. Naveen Naik a, Nidhi Singh a, Ashish S. Aditya a, Aakriti Gupta a,∗,idhi Prabhakar b, Sandeep Grover c
Postgraduate Institute of Medical Education and Research (PGIMER), Department of Anaesthesia and Intensive Care,handigarh, IndiaPostgraduate Institute of Medical Education and Research (PGIMER), Department of Radiodiagnosis and Imaging, Chandigarh,
ndiaPostgraduate Institute of Medical Education and Research (PGIMER), Department of Psychiatry, Chandigarh, India
eceived 10 October 2020; accepted 6 February 2021vailable online 22 March 2021
KEYWORDSPulmonary embolism;Deep veinthrombosis;Catatonia;COVID-19
Abstract Catatonic patients may develop deep vein thrombosis (DVT) and pulmonary embolism(PE) due to prolonged periods of immobility. These life-threatening conditions demand promptrecognition and management. We describe the case of a patient with catatonia who presented toanesthesia for electroconvulsive therapy (ECT) at the outset of the current coronavirus disease2019 pandemic. She complained of breathing difficulty and was suspected to have COVID-19infection. On further evaluation, she was found to have DVT and PE and required oxygen therapyand intensive care management. The diagnostic delay in our patient would have probably notoccurred, had it not been for the existing pandemic situation.
© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).D
ntroductionatatonia is a complex condition characterized by signifi-ant psychomotor disturbances including motor immobility.
∗ Corresponding author.E-mail: [email protected] (A. Gupta).
t(epaut
ttps://doi.org/10.1016/j.bjane.2021.02.031 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
ue to immobility, these patients are at risk of several life-hreatening complications such as deep venous thrombosisDVT), pulmonary embolism (PE), aspiration pneumonia, andven death.1---4 Patients with catatonia may occasionally
resent to the anesthesiologist for electroconvulsive ther-py (ECT) sessions. These patients may have pre-existingndiagnosed DVT or may already be on anticoagulation forhe same reason. More importantly, during the coronavirusitora Ltda. This is an open access article under the CC BY-NC-ND

esio
(mnpcicco
C
AtapC(rratpRttuEttatia
mawobmd3iuPsnpptrati(imoytpc
D
Fspl
Brazilian Journal of Anesth
COVID-19) pandemic, the symptoms of DVT and PE may beistaken for COVID-19 infection, which may delay the diag-
osis and increase the risk of morbidity and mortality in suchatients. We describe a case in which PE in a patient withatatonia was confused with COVID-19 infection. This reportntends to make the clinicians dealing with such patientsognizant of this kind of diagnostic fallacy. Written informedonsent was obtained from the patient for the publicationf this case report.
ase description
61-year-old female, diagnosed with catatonia secondaryo severe depression, on pharmacological treatment, wasdmitted for further management. On admission, she com-lained of difficulty in breathing. She was evaluated as aOVID-19 suspect by the Severe Acute Respiratory InfectionsSARI) team of the hospital. Her vitals were as follows: pulseate of 89 bpm, blood pressure of 130/80 mmHg, respiratoryate of 16 breaths/minute, oxygen saturation of 98% on roomir and temperature of 36.5 ◦C. Chest auscultation revealedhe presence of normal vesicular breath sounds. Her com-lete blood count and chest X-ray were within normal limits.everse Transcriptase Polymerase Chain Reaction (RT-PCR)est for COVID-19 infection was found to be negative. Afterhe initial workup, she underwent an uneventful ECT sessionnder general anesthesia. However, two days after the firstCT session, she developed fever (38 ◦C) and desaturation upo 90% on room air. An electrocardiogram (ECG) showed sinusachycardia with a heart rate of 150 bpm. Chest auscultation
nd chest X-ray revealed no abnormality. The differen-ial diagnoses considered included lower respiratory tractnfection, myocardial infarction, congestive heart failure,nd venous thromboembolism. Antipyretics and tablet aug-Vmd
igure 1 Computed Tomography (CT) pulmonary angiography stections showing linear hypodense filling defects suggestive of throulmonary artery and in segmental branch of left pulmonary arterower lobe. (d) Axial CT sections of upper abdomen show contrast re
29
logy 2021;71(3):292---294
enting was started. However, the fever spikes, tachypnea,nd tachycardia persisted. A sepsis workup was negativeith sterile blood and urine culture reports. The valuesf serum myoglobin, CK-MB (creatine kinase myocardialand) and BNP (B-type Natriuretic peptide) were within nor-al limits, hence the possibility of a cardiac event waseemed highly unlikely. The d-dimer value came out to be,900 ng.mL−1 (normal value: < 250 ng.mL−1). This exceed-ngly high value raised a suspicion of DVT. A compressionltrasound, echocardiography, and Computed Tomographyulmonary Angiography (CTPA) was planned. The compres-ion ultrasound revealed the right popliteal vein to beon-compressible suggestive of thrombosis. Echocardiogra-hy revealed normal heart function. CTPA scan revealed theresence of pulmonary thromboembolism with thrombi inhe right pulmonary artery and segmental branches of bothight and left pulmonary arteries. There were areas of lungtelectasis in the right lower lobe. Upper abdomen sec-ions showed contrast reflux in inferior vena cava, whichs an indirect sign of increased right ventricular pressureFigure 1). The patient was transferred to the respiratoryntensive care unit (RICU) of the hospital. Oxygen supple-entation by ventimask and subcutaneous therapeutic dose
f low molecular weight heparin was initiated. No thrombol-sis was required. The patient was discharged home afterhe resolution of thromboembolism and improvement of hersychiatric condition with further ECT sessions and pharma-otherapy.
iscussion
enous thrombosis is caused by the presence of one orore contributing factors of the Virchow’s triad: endothelialamage, venous stasis, and hypercoagulability.5 Catatonic
udy showed pulmonary thromboembolism. (a, b, c) Axial CTmbi in right pulmonary artery extending to right descending
y (arrows). Areas of lung atelectasis were also noted in rightflux in inferior vena cava (arrow).
3

gh, A
plDtTEtthaPw
rCDsnd
foiaqapsdsnpaEpcttdP
lmpcCstft
C
Ta
rchtmamno1sdtc
C
T
R
tion. 2003;107:122---30.10. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for
mortality of adult inpatients with COVID-19 in Wuhan, China: aretrospective cohort study. Lancet. 2020;395:1054---62.
B.N. Naik, N. Sin
atients are susceptible to venous stasis because of pro-onged inactivity and dehydration, thus being at high risk forVT and PE.3 ECT has been established as the most effectivereatment for catatonia accompanied by motor inhibition.6
here are specific concerns for ECT in such patients. Firstly,CT might increase the risk of PE in such patients due tohe possible mobilization of thrombi.2 Secondly, there is aheoretical risk of major bleeding episodes like cerebralemorrhage during ECT among patients already receivingnticoagulant therapy for diagnosed DVT and PE.7 Thirdly,E may mimic clinical features of COVID-19 infection, asas the case in our patient.
The world is facing a rapidly expanding pandemic of lowerespiratory tract infection by a novel coronavirus SARS-oV-2 (severe respiratory syndrome coronavirus 2) sinceecember 2019. COVID-19 infection manifests with a widepectrum of symptoms including fever, fatigue, cough, short-ess of breath, pneumonia, septic shock, and multiorganysfunction.8
Owing to the considerable overlap between the mani-estations of the two conditions, an anesthesiologist mustbtain a meticulous history and conduct a detailed exam-nation of these patients prior to the procedure. Motorctivity should be encouraged in these patients and ade-uacy of hydration must be assessed. We can considerpplication of elastic compression stockings or intermittentneumatic compression devices in high-risk patients. Onehould specifically look for signs of DVT, like swelling, ten-erness, pitting edema, and prominent superficial veins, andigns of PE, such as breathlessness, tachycardia, tachyp-ea, raised jugular venous pressure, and chest pain. Inatients with diagnosed DVT, cardiac function and presencend location of DVT must be evaluated before start of anCT session. There is higher risk of development of PE inatients with proximal DVT (DVT in veins above the knee)ompared to patients with distal DVT (DVT in veins belowhee knee).9 Also, anticoagulants must be adjusted prior tohe procedure. These patients should be monitored in a highependency unit (HDU) after the procedure owing to risk ofE and bleeding episodes.
This patient population presents unprecedented chal-enges during the COVID-19 pandemic. The risks and benefitsust be carefully weighed by the anesthesiologist and thesychiatrist before arriving at a decision to proceed with ECTourse. They are at higher risk for both ECT-associated andOVID-19-related morbidity and mortality.10 Each patienthould be tested for COVID-19 infection close to the time ofheir procedure. It is also prudent to involve the patient’samily and obtain a written and well-informed consent forhe procedure.
onclusion
he COVID-19 pandemic has created an atmosphere of fearnd uncertainty among health care professionals due to their
29
.S. Aditya et al.
isk of infecting themselves as well as their families andolleagues. Since our patient presented to our tertiary careospital at the beginning of the pandemic, we invested ourime and resources towards ruling out COVID-19 infection,eanwhile missing the obvious diagnosis of DVT and PE in
catatonic patient. Many medical centers across the worlday have to wait for 24 hours or longer to get a definitive
egative COVID-19 report. It is easy to miss many diagnosesf significant importance in the crucial situation of COVID-9 pandemic. We may err on the side of caution, but at theame time we must not lose sight of the basic and commoniagnoses first. We must have a high index of suspicion forhe presence of DVT and PE in catatonic patients, so theyan be managed and treated in an expeditious manner.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Marik PE. Aspiration pneumonitis and aspiration pneumonia. NEngl J Med. 2001;344:665---71.
2. Carroll BT. Complications of catatonia. J Clin Psychiatry.1996;57:95.
3. Morioka H, Nagatoma I, Yamada K, et al. Deep venous thrombo-sis of the leg due to psychiatric stupor. Psychiatry Clin Neurosci.1997;51:323---6.
4. Barbuto J. Preventing sudden death during a catatonic episode.Hosp Commun Psychiatry. 1983;34:72---3.
5. Bagot CN, Arya R. Virchow and his triad: a question of attribu-tion. Br J Haematol. 2008;143:180---90.
6. American Psychiatric Association Committee on Electrocon-vulsive Therapy. The practice of electroconvulsive therapy:recommendations for treatment, training, and privileging. 2nded. Washington (DC): American Psychiatric Association; 2001.10.1176/appi.ajp.159.2.331.
7. Utter GH, Dhillon TS, Salcedo ES, et al. Therapeutic Antico-agulation for Isolated Calf Deep Vein Thrombosis. JAMA Surg.2016;151:e161770.
8. Hassan S, Sheikh FN, Jamal S, et al. Coronavirus (COVID-19): AReview of Clinical Features. Diagnosis, and Treatment. Cureus.2020;12:e7355.
9. Kearon C. Natural history of venous thromboembolism. Circula-
4
C
Hpr
J
a
b
RA
I
Pin
h©l
Brazilian Journal of Anesthesiology 2021;71(3):295---298
ASE REPORTS
yperbaric oxygen therapy in the treatment ofneumocephalus associated with epidural block: caseeport
oão Castedo a,∗, António Pedro Ferreira a,b, Óscar Camacho a,b
Unidade Local de Saúde de Matosinhos (ULSM), Departamento de Anestesia, Matosinhos, PortugalUnidade Local de Saúde de Matosinhos (ULSM), Hyperbaric Medicine Unit, Matosinhos, Portugal
eceived 3 January 2020; accepted 6 February 2021vailable online 3 May 2021
KEYWORDSEpidural analgesia;Pneumocephalus;Hyperbaric oxygentherapy;Clinical case
AbstractIntroduction: Pneumocephalus is a rare neuraxial blockade complication, which can be associ-ated with severe neurologic changes.Clinical case: A 51-year-old patient was submitted to left total knee arthroplasty. Postop-eratively, a pneumocephalus associated with decreased consciousness was diagnosed as acomplication of the epidural analgesia. The treatment used was Hyperbaric Oxygen Therapy(HBOT) due to the severity of symptoms. Just after one session of HBOT, there was nearly fullpneumocephalus resorption and significant clinical recovery.Conclusion: This case report enables anesthesiologists to recognize HBOT as a therapeuticoption to be considered when treating severe cases of pneumocephalus.
© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. Thisis an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).nt
ntroduction
neumocephalus is defined as the presence of air in the
ntracranial space, which can occur in any of the centralervous system compartments.1 It is a rare complication of∗ Corresponding author.E-mail: [email protected] (J. Castedo).
too(ta
ttps://doi.org/10.1016/j.bjane.2021.02.058 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Ed
icense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
euraxial blockades that happens when air migrates fromhe site of the spinal puncture to the intracranial space.2---4
The usual treatment for this condition is O2 inhalationhrough a high-output mask, speeding up the reabsorptionf nitrogen into the bloodstream and decreasing the volumef the intracranial gas bubble.1 Hyperbaric Oxygen Therapy
HBOT) is an alternative option to conservative or surgicalreatment due to its fast onset effect of reducing air volumend accelerating gas reabsorption.1itora Ltda. This is an open access article under the CC BY-NC-ND

rreir
lracc
C
AhglsotardeDaoUctop
wAoioTCpoawt
praTma
iina
hmhstet
lrt
vtmahTaT
owrppUmrsh
cwpb
D
Efgaai
tflctt
fti(
aAtoaTn
J. Castedo, A.P. Fe
According to our literature search, there is only one pub-ished case in which HBOT was applied to a pneumocephaluselated to neuraxial anesthesia technique.4 Here we report
patient that presented neurologic changes hours after aombined spinal epidural anesthesia secondary to pneumo-ephalus, successfully managed with HBOT.
linical case
51-year-old woman with past medical history ofypertension, obesity, peripheral venous insufficiency andonarthrosis was submitted to total arthroplasty of theeft knee. The procedure was performed under combinedpinal epidural anesthesia. After intravenous administrationf 100 �g fentanyl as premedication, at 4:30 PM spinal anes-hesia was performed using 9 mg of hyperbaric bupivacainessociated with 5 �g sufentanil and, subsequently, an epidu-al catheter was inserted. The regional anesthesia techniqueetails are unknown, particularly if the identification of thepidural space was performed with saline solution or air.uring surgery, midazolam 3 mg and lidocaine 100 mg weredministered intravenously at the end of surgery. The intra-perative period was uneventful. In the PostAnesthetic Carenit (PACU), 4 mg morphine was administered via epiduralatheter, the first injection being at 7 PM. Upon returningo the ward, drowsiness and slightly slurred speech werebserved, assessed as being compatible with the immediateostoperative period.
At approximately 6:30 AM the medical emergency teamas called due to altered consciousness (torpor state).t the initial assessment, the patient presented airwaybstruction reversed by basic maneuvers, bradypnea requir-ng supplemental O2 (SpO2 92% at 31% FiO2), no signsf respiratory distress, and was hemodynamically stable.he initial neurologic examination was 4 on the Glasgowoma Scale (E2V1M1), associated with poorly reactive mioticupils, outward deviation of left eye, and right eye centeredn the midline. After obtaining the result for blood glucosenalysis of 182 mg.dL-1, 0.4 mg naloxone was administeredith partial improvement of consciousness to 12 points on
he Glasgow Coma Scale (E4V4M4).Neurology evaluation was requested, which reported
ersistent left central facial paresis, with no other neu-ologic deficits. Due to the persistent neurologic findings,fter the administration of naloxone, a brain Computerizedomography (CT) scan was requested, which revealed pneu-ocephalus at the suprasellar cistern, prepontine cistern
nd right Sylvian fissure (Fig. 1).In view of these findings, we proposed the neuraxial
njection of opioid and air as the combined etiology explain-ng the depressed level of consciousness and the focaleurologic deficit (facial paresis) that resulted from thenesthesia/analgesia management.
In view of the clinical severity, urgent treatment withyperbaric oxygen therapy was proposed. Given the requiredanagement of the depressed level of consciousness,
ypoventilation and the need for naloxone infusion, patient
edation and tracheal intubation were performed prior toransferring to the Hyperbaric Medicine Unit (UMH). Thepidural catheter was removed before the patient enteredhe hyperbaric chamber.da
a
29
a and Ó. Camacho
The UMH has a trained team and equipment to deal withevel III medical care (critical patient) in a category 1 multi-oom chamber that is continuously monitored by a staff ofhe attending team (doctor or nurse).
The patient was maintained on invasive mechanicalentilation under sedation and analgesia with propofol, fen-anyl, and muscle relaxation with rocuronium, continuouslyonitored with ECG, invasive blood pressure, urine output,
nd respiratory gases analysis. The protocol consisted of ayperbaric oxygen therapy session according to the US Navyreatment Table 6, maximum pressure of 2.8 ATA (absolutetmospheres) and total run time of 4 hours and 45 minutes.he therapy session was uneventful.
Then, the patient was sent back to the institutionf origin, admitted to the Intensive Care Unit (ICU),here immediate tracheal extubation was performed. The
eassessment brain CT scan showed signs of nearly completeneumocephalus resorption, with only a small air-bubbleresent in the right paramedian side of the Sella turcica.pon neurologic examination, the patient maintained ainor left nasolabial groove erasure, without any other neu-
ologic deficit. Pain control was achieved with multimodalystemic analgesia combined with tramadol 100 mg every 8ours.
The patient was kept in the ICU for two days showing goodlinical progress, except for a respiratory infection treatedith antibiotic therapy, not requiring O2 supplement. Theatient remained in the orthopedic ward for 7 days untileing discharged home.
iscussion
pidural anesthesia/analgesia is a technique widely per-ormed in anesthetic practice, especially for labor anal-esia. However, intracranial hypotension, toxicity by localnesthetics, total spinal anesthesia, unintentional vascularnd dural puncture, low back pain, subdural blockade, andatrogenic pneumocephalus are possible complications.2
The intracranial space behaves as a closed system dueo its rigid structure comprising brain tissue, cerebrospinaluid, and vascular system. Any disruption to this pressurizedlosed system that creates an opening point, has the poten-ial to promote the development of pneumocephalus due tohe entry of air.2
During epidural anesthesia, a path is created that canacilitate the air penetrating into any cranial spaces or intohe cortex tissue itself. This air penetration is classified asntra-axial (cortex, ventricles, vasculature) and extra-axialepidural, subdural, subarachnoid).2
Pneumocephalus is believed to be caused by two mech-nisms: the ball valve and the inverted bottle effect.2
ccording to the ball valve mechanism, air penetrates dueo increased external pressure because of a dura defect thatvercomes intracranial pressure. Once inside the skull, their has no exit due to obstruction by the cranial structures.he inverted bottle mechanism states that when there is aegative intracranial pressure due to a cranial dura-mater
efect or cerebrospinal fluid leak, there are air entries byspiration to balance the pressure differential.2The clinical presentation of pneumocephalus is variablend depends both on intracranial distribution and volume
6

Brazilian Journal of Anesthesiology 2021;71(3):295---298
F rows
oacirscH
ctsdt
etodfsm
oowbttdtip
gctae
ssoc
oetpIadLpcp
ietic
pfrtc
otr
igure 1 CT brain scan performed before HBOT treatment. Ar
f air.2 Most of the cases of patients with pneumocephalusre asymptomatic, however headache is the most commonomplaint. Other symptoms may include nausea, vomit-ng, seizures, syncope, agitation, delirium, changes in deepeflexes and in the level of consciousness.2 This clinicalpectrum overlaps the symptoms of a much more frequentomplication of neuraxial blockades: Postdural Punctureeadache (PDPH).
This case describes a recognized, albeit infrequent,omplication of neuraxial techniques that results from unin-entional administration of drugs and air into the intrathecalpace, with potentially severe and persistent neurologicamage, and which may have variable and late manifesta-ions that delay its early diagnosis.
Of the cases described in the literature in which thepidural technique led to an unintentional dura mater punc-ure and consequent air injection, only one used the lossf resistance technique with saline solution.3 All otherescribed cases, according to our literature search, resultedrom the loss of resistance technique using air.2,4 In thisituation, clinical symptoms are typically immediate andediated by the fast migration of the air.2---4
However, this present case is distinguished by its latenset, which raises some questions related to what causedpioid and air entry into the intrathecal space, and whichas not elucidated by the anesthesia record. Most proba-ly, morphine administered at the PACU was injected intohe intrathecal space and together with an air bubble (dueo an error in the administration technique) promoted theisplacement of a pre-existing air bubble from the spinal tohe intracranial space, driven by the positive pressure of thenjection and the possible slightly head up positioning of theatient on the PACU bed.
This case report highlights the relevance of strin-ent adherence to the techniques for handling epidural
atheters, and administering drugs via this route, in addi-ion to identifying the epidural space using saline solution,s preventive strategies for pneumocephalus of iatrogenictiology.C
T
29
--- pneumocephalus at suprasellar space and prepontine cistern.
Nitrogen makes up 79% of atmospheric air and is a poorlyoluble gas. For this reason, when present in tissues, it per-ists for extended periods, favoring the compressive effectf the air bubble over the nervous system structures, withonsequent injury.
Hyperbaric oxygen therapy consists of the administrationf pure O2 in a high-pressure environment. The therapeuticffect of HBOT derives from the significant increase in par-ial oxygen pressure in all body tissues, according to thehysiological diffusion gradient, i.e., the oxygen cascade.n the case of pneumocephalus, hyperbaric oxygen ther-py works by two mechanisms: high pressure immediatelyecreases the volume of air pocket, according to Boyle’saw (the volume of a gas is inversely proportional to theressure)4; in addition, inhalation of 100% oxygen signifi-antly accelerates nitrogen elimination, consequently, airocket reabsortion.1
HBOT is not an ordinary therapeutic option for treat-ng pneumocephalus. However, the severity of the conditionncouraged us to use this technique, due to its greater effec-iveness in treating the cause, already extensively revealedn cases of gas embolism and decompression illness that areaused by deleterious effects of gas pockets over tissues.5
After just one session, HBOT enabled nearly the com-lete resorption of the intracranial gas pocket and theast and clinically significant neurologic recovery. Theseesults match those described by Shih et al.,4 revealinghe effectiveness of this treatment in this rare anestheticomplication.
This case report allows raising awareness of anesthesi-logists to consider HBOT as a therapeutic option for thereatment of a severe case of pneumocephalus after epidu-al anesthesia.
onflicts of interest
he authors declare no conflicts of interest.
7
rreir
A
Tt
R
1
2
3
4
J. Castedo, A.P. Fe
cknowledgement
he authors are grateful to Dr. Felipe Chehuan for the adap-ation of the manuscript to Brazilian Portuguese.
eferences
. Paiva W, Andrade A, Figueiredo E, Amorim R, Prudente, JacobsenM. Effects of hyperbaric oxygenation therapy on symptomaticpneumocephalus. Ther Clin Risk Manag. 2014;10:769.
5
29
a and Ó. Camacho
. Chacko J, Levis K, Hahn B. Pneumocephalus after Epidural Injec-tion. J Emerg Med. 2018;54, e45---7.
. Jones JM, Gouveia JP, Rodrigues NM. Pneumocephalus andseizures following combined spinal-epidural for labor. J ClinAnesth. 2018;44:123---4.
. Shih C-C, Tsai S-H, Liao W-I, Wang J-C, Hsu C-W. Successful treat-ment of epidural anesthesia-induced severe pneumocephalus
by hyperbaric oxygen therapy. Am J Emerg Med. 2015;33,1116.e1---1116.e3.. Moon RE. Hyperbaric oxygen treatment for decompression sick-ness. Undersea Hyperb Med. 2014;41:151---7.
8

C
CaM
PCE
U
RA
B
Lg
h©B
Brazilian Journal of Anesthesiology 2021;71(3):299---301
ASE REPORTS
ombined spinal-epidural anesthesia forbdominoplasty and liposuction in Limb-Girdleuscular Dystrophy: case report�
linio da Cunha Leal, Wildney Leite Lima, Eduardo José Silva Gomes de Oliveira,aio Márcio Barros de Oliveira, Lyvia Maria Rodrigues de Sousa Gomes,lizabeth Teixeira Noguera Servin, Ed Carlos Rey Moura ∗
niversidade Federal do Maranhão (UFMA), São Luís, MA, Brazil
eceived 3 February 2020; accepted 27 February 2021vailable online 3 April 2021
KEYWORDSCase reports;Limb-Girdle MuscularDystrophy;Anesthesia;Abdominoplasty;Perioperative care
Abstract We report the anesthetic management with combined spinal-epidural in a patientwith limb-girdle muscular dystrophy type 2A, submitted to abdominoplasty and liposuction.The patient had onset of symptoms at 8 years old, diagnosed by muscular biopsy, presentingmuscle weakness in the scapular and pelvic girdles, with reduced mobility. We performed mon-itorization with noninvasive blood pressure, oximeter, thermometer, and electrocardiogram. Inthe postoperative period, she showed no clinical signs of rhabdomyolysis, myotonia, or adverseeffects, maintaining hemodynamic stability. The anesthesia technique allowed spontaneousventilation, monitoring of clinical parameters close to physiological conditions and used smallerdoses of medication, reducing related risks.
© 2021 Published by Elsevier Editora Ltda. on behalf of Sociedade Brasileira deAnestesiologia. This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).p
ackgroundimb-Girdle Muscular Dystrophy (LGMD) is a group of rareenetic syndromes involving muscular dystrophies, which
� Study conducted at Hospital São Domingos, São Luís, MA, Brasil.∗ Corresponding author.
E-mail: [email protected] (E.C. Moura).
dCrc2
tlo
ttps://doi.org/10.1016/j.bjane.2021.02.046 2021 Published by Elsevier Editora Ltda. on behalf of Sociedade BrasilY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
referably affect the muscles of the scapular and hip gir-le, leading to progressive weakness and loss of function.1
lassified as autosomal dominant, with 8 types (1A---1H), orecessive with 26 types (2A---2Z), have a prevalence of 1.68ases per 100,000 inhabitants, the most common being typeA, representing 15% to 40% of all cases.1
The symptoms can start at any age, and get worse overime.1 It often occurs with high serum creatine kinase (CK)evels, but normal levels may be present.1,2 The progressionf the disease varies widely among individuals, who may
eira de Anestesiologia. This is an open access article under the CC.

P.C. Leal, W.L. Lima, E.J. Oliveira et al.
Table 1 Clinical progression.
1992 2008 2015 2016 September/2019 October/05/2019 October/06/2019
Onset ofsymptoms ofmuscleweakness inupper andlower limbs
Progressive lossof musclestrength, withneed ofwheelchair formovement
Muscle biopsywith results forLGMD type 2A
Hysterectomy,withoutcomplications,performed withneuraxialanesthesia
Preoperativeevaluation andanalysis ofexamsrequested
Abdominoplastyand liposuctionwith CSEanesthesia,with local anes-thetic + opioid
Postoperativewithmaintenance ofmonitoring, withdischarge fromhospital afterconfirmation ofhemodynamicstability and nosigns ofrhabdomyolysis
ural.
hfad
rdpdcd
wdouie
g(2lrct
C
WLtamtchcpwsa(t
u0oa
(coswwttiwptpdbaop
finp4
wpeprut
wtd
LGMD, limb-girdle muscular dystrophy; CSE, combined spinal-epid
ave severe impairment of mobility, cardiac and respiratoryunction leading to decreased life expectancy,1,2 due to thisnd the variation in the age range of onset of symptoms, theiagnosis can be difficult and may require genetic testing.2
The benefit of diagnosis arises when these patientsequire surgical interventions, usually orthopedic proce-ures, since the anesthetic management in these individualsresents some particularities due to the higher risk of car-iac complications from malign arrhythmias, respiratoryomplications, malignant hyperthermia (HM), and rhab-omyolysis caused by drugs used in anesthesia.2,3
Few cases of operations performed in patients with LGMDere reported or included in reviews,2,3 and there is no stan-ardization of the anesthetic technique in these patients,nly general recommendations, being necessary to individ-alize the perioperative care according to the degree ofnvolvement to reduce risks and adverse pharmacologicalffects related to neuromuscular diseases.
Thus, this study aims to report, following the CAREuidelines,4 the management with combined spinal-epiduralCSE) anesthesia in a patient diagnosed with LGMD typeA. The patient was submitted to abdominoplasty andiposuction, presented important limb impairment andeduced mobility, requiring adequate monitoring to avoidomplications and also ensure the patient’s comfort duringhis period.
ase report
e present a 35-year-old female patient, diagnosed withGMD type 2A, who underwent abdominoplasty and liposuc-ion in October 2019. The patient had onset of symptomst 8 years of age, with diagnosis at 30 years of age byuscle biopsy with the presence of two pathogenic muta-
ions in heterozygosis in exons 4 and 22, respectively in thealpain gene, characteristic of type 2A. Reported familiaristory of LGMD with diagnosis by muscle biopsy and surgi-al history of hysterectomy with no complications. In thereoperative evaluation, she presented flaccid tetraparesisith proximal muscle strength grade 2 and distal muscle
trength grade 4, not being able to walk alone and requiring wheelchair for movement. The preoperative examinationselectrocardiogram, echocardiogram, pulmonary functionest, and laboratory tests) were normal, except for the val-
93co
30
es of CK and serum creatinine of 315 U.L-1 and value <.17 mg.dL-1 respectively, which were following the patternf LGMD type 2A. The proposed procedure was explainednd the patient consented (Table 1).
It was decided to perform a combined spinal-epiduralCSE) neuraxial anesthesia, spinal anesthesia with bupiva-aine 20 mg and morphine 0.03 mg, epidural (placementf a catheter for additional doses of anesthetic if neces-ary) and fentanyl (intravenous --- IV) 100 mcg in associationith midazolam 5 mg for sedation. The patient’s vital signsere monitored (noninvasive blood pressure, pulse oxime-
ry, electrocardiogram, and axillary thermometer) accordingo ASA standards and with recommendations for monitoringn patients with myopathies3 and spontaneous ventilationith a face mask was maintained during surgery. The tem-erature at the start of the procedure was 36.5 ◦C, and ahermal blanket was used to control the temperature; theatient presented a temperature between 36 ◦C and 36.5 ◦Curing the procedure. The mean blood pressure (MBP) wasetween 78 and 97 mmHg, heart rate (HR) was between 80nd 98 bpm, respiratory rate (RR) of 18 breaths/min andxygen saturation (SatO2) between 98 and 99% during therocedure.
The surgery lasted 240 minutes, without technical dif-culties. Additional doses of local anesthetic were notecessary during the surgery. At the end of the procedure,arecoxib 40 mg, metamizole (dipyrone) 2 mg, ondansetron
mg, and dexamethasone 4 mg were administered.In the postoperative period, hemodynamic stability
as maintained without episodes of myotonia or adverseharmacological effects. The effect of the anesthesianded without complications. The patient remained in theostanesthesia recovery unit for 2 hours, requiring epidu-al administration of fentanyl 20 �g and ropivacaine 2.5 mgsing patient-controlled analgesia (PCA) dispositive to con-rol postoperative pain.
The patient was monitored in the postoperative periodith noninvasive blood pressure, pulse oximetry, thermome-
er. She presented conditions for discharge on the followingay, with MBP between 73 and 93 mmHg, HR between 80 and
0 bpm, RR 18 to 19 breaths/min, SatO2 98%, temperature of6 to 36.7 ◦C, without clinical signs of rhabdomyolysis, withardiorespiratory stability, adequate pain control and with-ut the necessity of additional doses of epidural anesthetic.0

esio
D
IepfaTscciaitpcawepo
tapHvdfm
sawr5idibsondTatfa
trtfsgpit
tcpctmdnott
peesrt
nacftt
E
TC
I
Tc
C
T
R
1
2
3
4
Glob Adv Health Med. 2013;2:38---43.5. Gehling M, Tryba M. Risks and side-effects of intrathecal
morphine combined with spinal anaesthesia: a meta-analysis.Anaesthesia. 2009;64:643---51.
Brazilian Journal of Anesth
iscussion
n a review of the literature, few reports of elective surg-ries were found, the majority of the operations beingerformed under total intravenous anesthesia (TIVA), andew cases with neuraxial anesthesia supplemented withn intrathecal opioid, already included in other studies.2,3
wo operations were performed under neuraxial anesthe-ia, included in the review by Cao et al.,2 one laparoscopicholecystectomy with spinal anesthesia technique and oneesarean section with the CSE technique, which included anntrathecal opioid. They performed neuraxial anesthesia tovoid respiratory complications and the need for intubation,nvasive ventilation, and neuromuscular blockade, reducinghe risks inherent to patients with myopathies, mainly theotential difficulty of weaning from ventilation.2 In theseases, when neuraxial anesthesia was performed, a localnesthetic (bupivacaine) and intrathecal opioid (fentanyl)ere also used, and adequate monitoring in the periop-rative period was maintained3 and in only one case aatient-controlled analgesia device was used in the post-perative period.2
Intrathecal morphine when added to a spinal anes-hesia technique, even in low doses, promotes importantnalgesia, which can extend beyond the first 24 hours ofostoperative, reducing the total consumption of opioids.owever, it is associated with an increased risk of nausea,omiting, itching, urinary retention, and, when in higheroses, with a higher risk of respiratory depression. There-ore, it is recommended prophylaxis for these effects andonitoring to detect complications early.5
In this case, we chose to perform CSE neuraxial anesthe-ia with an intrathecal solution containing local anestheticnd opioid in a low dose and treatment of postoperative painith patient-controlled analgesia by an epidural catheter ---
opivacaine (0.5 mg.mL-1) and fentanyl (4 �g.mL-1), bolus mL, following the recommendations for local anesthesian patients with neuromuscular diseases whenever possible,espite the possibility of acute toxicity of local anesthet-cs. CSE anesthesia is indicated in patients with myopathiesecause it presents a lower risk of complications and allowspontaneous ventilation. Its advantages include a rapidnset of sensorial and motor blockade, reduction of theeed for extra intrathecal doses, allows better control of theuration of anesthesia and holds a desired sensory level.2,3
he option of associating morphine and local anestheticimed to promote an adequate pain control in the periopera-ive period, as well as reducing the consumption of opioids,ollowing the recommendations of prophylaxis for relateddverse effects.
The established anesthetic management contributed tohe patient’s comfort in relation to the pain control andeturn of functions, reducing doses by the combination ofechniques and avoiding drugs that can be potential triggersor cardiorespiratory complications, HM and rhabdomyoly-is. The study had as a limitation the non-performance ofasometry and specific laboratory tests in the postoperativeeriod and because there were no clinical signs that justified
t, besides the fact that the chosen anesthetic technique andhe smaller surgical procedure represented reduced risks.30
logy 2021;71(3):299---301
Considering the possibility of an unpredictable responseo opioids, neuromuscular blockers and their antagonists,ardiorespiratory complications, myotonia, and adverseharmacological effects can be avoided with the use of lowoncentrations of these anesthetics.2,3 It is recommendedo use neuromuscular blockers only when there is neuro-uscular monitoring and to avoid the use of succinylcholineue to the high risk of rhabdomyolysis and HM.2,3 It is worthoting that there is no direct contraindication of the usef inhalational agents due to the possible risk of HM, ashere are no reports of cases of LGMD type 2A presentinghis complication.
Despite the complexity of anesthetic management inatients with MDL, a surgical approach with careful preop-rative planning is possible. A comprehensive preoperativevaluation, including a multidisciplinary team, minimizesurgical risks. Also, adequate perioperative monitoring isequired to detect early cardiopulmonary complications ofhe adverse effects of anesthetics.
The reported case demonstrates a technique of CSEeuraxial anesthesia in a patient with LGMD submitted tobdominoplasty and liposuction without complications. Theombination of local anesthetic and opioids in low dosesacilitated postoperative pain control in combination withhe PCA device, in addition to reducing the total doses ofhe drugs used.
thical approval statement
his case report was approved by the Research and Ethicsommittee of Hospital São Domingos (Number 3.709.613).
nformed consent statement
he patient has provided written consent to present thease.1---5
onflicts of interest
he authors declare no conflicts of interest.
eferences
. Taghizadeh E, Rezaee M, Barreto GE, et al. Prevalence, patho-logical mechanisms, and genetic basis of limb-girdle musculardystrophies: A review. J Cell Physiol. 2019;234:7874---84.
. Cao XQ, Joypaul K, Cao F, et al. Anesthetic management of apatient with limb-girdle muscular dystrophy 2B:CARE-compliantcase report and literature review. BMC Anesthesiol. 2019;19:155.
. Schieren M, Defosse J, Böhmer A, et al. Anaesthetic managementof patients with myopathies. Eur J Anaesthesiol. 2017;34:641---9.
. Gagnier JJ, Kienle G, Altman DG, et al. The CARE Guidelines:Consensus-based Clinical Case Reporting Guideline Development.
1

L
Ddl
D
tHcpt
ttcr
ienndb
rbtdwOCfifv
Brazilian Journal of Anesthesiology 2021;71(3):302---314
ETTER TO THE EDITOR
onning N95 respirator masksuring COVID-19 pandemic:
worn to ensure adequate seal. However, a regular Fit Testis time-consuming, and all sizes may not be available. So,the test may not be practical for every HCW in a pandemic
sfnipsdDmemplfbmuotddtmffmwitself in the middle and stapled (with the staple pin bending
ook before you leap!
ear Editor,The novel Coronavirus Disease (COVID-19) is a respira-
ory disease transmitted by contact, droplets, and fomites.ealthcare Workers (HCWs) taking care of suspected oronfirmed COVID-19 patients need to adhere to strict self-rotection precautions, including N95 masks, to protecthemselves against the virus-containing aerosols.1
A N95 respirator is a respiratory protective mask designedo achieve a very tight facial fit and an efficient filtra-ion of airborne particles. Evidently, its improper use couldompromise its protective effect and may even increase theisk of infection.2,3
Many N95 masks being distributed for use of HCWs comen a single non-adjustable configuration and may not prop-rly fit people of different gender or built. We recentlyoticed that the N95 masks supplied at our institution didot fit well to thin and short people, especially females,uring donning process. A large part of it was left hangingelow the chin (Fig. 1A).
The designation ‘‘N95’’ indicates the respirator is notesistant to oil or solvents (N) and that it is intended tolock at least 95% of exceedingly small (> 0.3 �m in size)est particles. HCWs are at high risk of getting COVID-19ue to repeated exposure from infected patients in theorkplace and may transmit the infection to others. Theccupational Safety and Health Administration (OSHA) (29FR 1910.134) requires an annual ‘‘Fit Test’’ to verify the
t of any respirator that forms a tight seal on the wearer’sace before it is used. After the fit test is made in an indi-idual, a ‘‘User Seal Check’’ should be done every time it isFigure 1 A, N95 mask with leak; B, N95 mask
taa
ituation. Also, during such outbreaks, PPE are searchedrom multiple sources on urgent basis. Hence, end users mayot get time to be familiarized with these, and chances ofmproper usage increase. User Seal check (either positiveressure or negative pressure) is an easily performed mea-ure which should be a mandatory step for N95 respiratoronning process prior to entering the patient care area.4
uring a positive pressure seal check (useful for non-valvedasks and not applicable for valved masks), the person
xhales gently while obstructing the paths for air to exit theask. A successful check is when the facemask is slightlyressurized before the increased pressure causes outwardeakage. During a negative pressure user seal test (usefulor both valved and non-valved masks), the N95 user inhalesriskly while hindering the paths for air to enter the face-ask. A successful check is when the mask collapses slightly
nder the negative pressure thus created. National Institutef Occupational Safety and Health (NIOSH) data indicateshat performing a user seal check leads to higher qualityonning.5 Nonetheless, the OSHA warns that seal checksoes not have the sensitivity and specificity to replace fitests.
We started doing negative pressure seal tests (for valvedasks), and both positive and negative pressure seal tests
or non-valved masks. Unsurprisingly, most of valved masksailed the test for thin built HCWs. Duckbilled non-valvedasks fared best in terms of seal for majority. To curtail theastage, we folded the margin of the mask fitting the chin on
stapled; C, adequate seal after stapling.
owards outside to avoid hurting the person) (Fig. 1B). A neg-tive pressure seal test performed subsequently confirmed
good seal (Fig. 1C). For minor irregularities in fitment,

abhptow
Noot
rccrthr
C
T
R
1
OE
D
‘CbrcmwoteaWi
tsfitCpf
Brazilian Journal of Anesthesiology 2021;71(3):302---314
pplying adhesive tapes all around or wearing the lower tieand more cephalad could rectify the ill fit. Many N95 masksave adjustable tie-band sizes and need to be tightened aser patient’s fitment requirement. While applying any suchapes to the mask, care should be taken to fold one edgef the tape so that it can be easily removed during doffingithout creating additional risk to the HCWs.
No previous study has identified the impact of ill-fitted95 respirators on the transmission of COVID-19. Awarenessf the importance of maintaining an adequate mask seal isf pivotal importance to prevent transmission of infectiono the HCWs during the present COVID-19 outbreak.
We, therefore, would advise caution in the use of theseespirators by ensuring proper seal before entering patient-are areas. The use of positive and/or negative pressure sealheck should be universally adopted by all wearing theseespirators. We also would like to urge the manufacturerso deliberate into mask designs universally acceptable to allealthcare workers irrespective of the race, facial configu-ation, and gender.
onflicts of interest
he authors declare no conflicts of interest.
eferences
. Bessesen MT, Savor-Price C, Simberkoff M, Reich NG, Pavia AT,Radonovich LJ. N95 respirators or surgical masks to protecthealthcare workers against respiratory infections: are we thereyet? Am F J Respir Crit Care Med. 2013;187:904---5.
2. Institute of Medicine. Preparing for an Influenza Pandemic:Personal Protective Equipment for Healthcare Workers. Washing-ton, DC: The National Academies Press. 2008. Available from:10.17226/11980; (accessed: November 25, 2020).
3. National Health Service. Are face masks useful for prevent-ing coronavirus? 2020. Available from: https://www.nhs.uk/conditions/coronavirus-covid-19/commonquestions/; (accessed:December 9, 2020).
4. National Institute for Occupational Safety and Health, DHHS(NIOSH) U.S. How to properly put on and take off a disposablerespirator. Department of Health and Human Services, Centersfor Disease Control and Prevention, Publication No. 2010-133,2010. Available from: https://www.cdc.gov/niosh/docs/2010-133/pdfs/2010-133.pdf; (accessed: December 15, 2020).
5. Viscusi DJ, Bergman MS, Zhuang Z, Shaffer RE. Evaluation of thebenefit of the user seal check on N95 filtering facepiece respira-tor fit. J Occup Environ Hyg. 2012;9:408---16.
Anju Gupta a,∗, Ajisha Aravindana, Kapil Dev Sonib
a Pain Medicine and Intensive Care, Department ofAnaesthesiology, AIIMS, New Delhi, Indiab Department of Critical & Intensive Care, JPN ApexTrauma centre, AIIMS, New Delhi, India
∗ Corresponding author.E-mail: [email protected] (A. Gupta).
Received 22 December 2020; accepted 21 February 2021
https://doi.org/10.1016/j.bjane.2021.02.0340104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.Published by Elsevier Editora Ltda. This is an open access articleunder the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
ccupational team safety inCT practice and COVID-19
ear Editor,We would like to share ideas on the publication
‘Occupational team safety in ECT practice during theOVID-19 pandemic’’. Araujo and Quites noted that ‘‘Weelieve this is a safe and effective way to reduce theisk of contamination from COVID-19 during the ECT pro-edure’’.1 We agree that anesthesiologists should try toitigate COVID-19 spread during ECT procedures. However,e would like to extend the suggestions. Safety must beffered to all patients, not only to the one attending tohe procedure, and there should be no left risk to the oth-rs after the procedure. Complex safety tools used during
procedure must be either easily processed or single-use.aste management is an important topic to be discussed. It
s necessary to prepare for waste disposal and destruction.Finally, the health center administrator should try best
o promote safety of workers.2 During the COVID-19, theafety of both patients and healthcare workers should comerst. It is necessary to plan for both preventive and correc-
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Araujo RF, Quites LO. Occupational team safety in ECT prac-tice during the COVID-19 pandemic. Rev Bras Anestesiol.2020;70:687---8.
2. Saithong C. COVID-19 outbreak, primary health care center andvision of local administrator of primary health care center. CaseStudy Case Rep. 2020;10:17---8.
Rujitika Mungmunpuntipantip a,∗, Viroj Wiwanitkit b
a Private Academic Consultant, Bangkok, Thailandb Dr D. Y. Patil University, Pune, India
∗ Corresponding author.E-mail: [email protected] (R. Mungmunpuntipantip).
Received 24 December 2020; accepted 6 February 2021
https://doi.org/10.1016/j.bjane.2021.02.033
ive actions for any unexpected COVID-19-related incident.OVID-19 outbreak period is a very tough time, and goodolicies from a good administrator can encourage and rein-orce the healthcare workers.
0Pul
30
104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.ublished by Elsevier Editora Ltda. This is an open access articlender the CC BY-NC-ND license (http://creativecommons.org/icenses/by-nc-nd/4.0/).
3
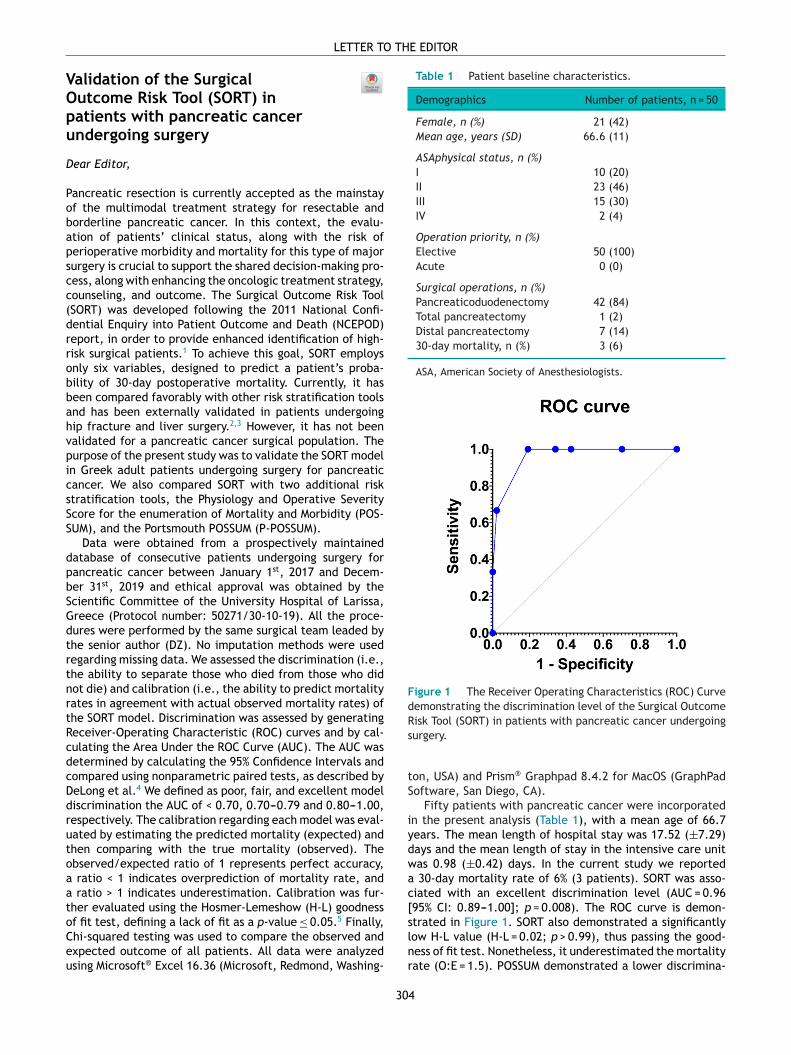
VOpu
D
Pobapscc(drrobbahvpicsSS
dpbSGdtrtnrtRcdcDdrutoaatoCeu
LETTER TO THE EDITOR
alidation of the Surgicalutcome Risk Tool (SORT) inatients with pancreatic cancerndergoing surgery
ear Editor,
ancreatic resection is currently accepted as the mainstayf the multimodal treatment strategy for resectable andorderline pancreatic cancer. In this context, the evalu-tion of patients’ clinical status, along with the risk oferioperative morbidity and mortality for this type of majorurgery is crucial to support the shared decision-making pro-ess, along with enhancing the oncologic treatment strategy,ounseling, and outcome. The Surgical Outcome Risk Tool
Table 1 Patient baseline characteristics.
Demographics Number of patients, n = 50
Female, n (%) 21 (42)Mean age, years (SD) 66.6 (11)
ASAphysical status, n (%)I 10 (20)II 23 (46)III 15 (30)IV 2 (4)
Operation priority, n (%)Elective 50 (100)Acute 0 (0)
Surgical operations, n (%)
FdRisk Tool (SORT) in patients with pancreatic cancer undergoing
SORT) was developed following the 2011 National Confi-ential Enquiry into Patient Outcome and Death (NCEPOD)eport, in order to provide enhanced identification of high-isk surgical patients.1 To achieve this goal, SORT employsnly six variables, designed to predict a patient’s proba-ility of 30-day postoperative mortality. Currently, it haseen compared favorably with other risk stratification toolsnd has been externally validated in patients undergoingip fracture and liver surgery.2,3 However, it has not beenalidated for a pancreatic cancer surgical population. Theurpose of the present study was to validate the SORT modeln Greek adult patients undergoing surgery for pancreaticancer. We also compared SORT with two additional risktratification tools, the Physiology and Operative Severitycore for the enumeration of Mortality and Morbidity (POS-UM), and the Portsmouth POSSUM (P-POSSUM).
Data were obtained from a prospectively maintainedatabase of consecutive patients undergoing surgery forancreatic cancer between January 1st, 2017 and Decem-er 31st, 2019 and ethical approval was obtained by thecientific Committee of the University Hospital of Larissa,reece (Protocol number: 50271/30-10-19). All the proce-ures were performed by the same surgical team leaded byhe senior author (DZ). No imputation methods were usedegarding missing data. We assessed the discrimination (i.e.,he ability to separate those who died from those who didot die) and calibration (i.e., the ability to predict mortalityates in agreement with actual observed mortality rates) ofhe SORT model. Discrimination was assessed by generating
eceiver-Operating Characteristic (ROC) curves and by cal-ulating the Area Under the ROC Curve (AUC). The AUC wasetermined by calculating the 95% Confidence Intervals andompared using nonparametric paired tests, as described byeLong et al.4 We defined as poor, fair, and excellent modeliscrimination the AUC of < 0.70, 0.70---0.79 and 0.80---1.00,espectively. The calibration regarding each model was eval-ated by estimating the predicted mortality (expected) andhen comparing with the true mortality (observed). Thebserved/expected ratio of 1 represents perfect accuracy,ratio < 1 indicates overprediction of mortality rate, and ratio > 1 indicates underestimation. Calibration was fur-her evaluated using the Hosmer-Lemeshow (H-L) goodnessf fit test, defining a lack of fit as a p-value ≤ 0.05.5 Finally,hi-squared testing was used to compare the observed andxpected outcome of all patients. All data were analyzedsing Microsoft® Excel 16.36 (Microsoft, Redmond, Washing-
s
tS
iydwac[slnr
30
Pancreaticoduodenectomy 42 (84)Total pancreatectomy 1 (2)Distal pancreatectomy 7 (14)30-day mortality, n (%) 3 (6)
ASA, American Society of Anesthesiologists.
igure 1 The Receiver Operating Characteristics (ROC) Curveemonstrating the discrimination level of the Surgical Outcome
urgery.
on, USA) and Prism® Graphpad 8.4.2 for MacOS (GraphPadoftware, San Diego, CA).
Fifty patients with pancreatic cancer were incorporatedn the present analysis (Table 1), with a mean age of 66.7ears. The mean length of hospital stay was 17.52 (±7.29)ays and the mean length of stay in the intensive care unitas 0.98 (±0.42) days. In the current study we reported
30-day mortality rate of 6% (3 patients). SORT was asso-iated with an excellent discrimination level (AUC = 0.9695% CI: 0.89---1.00]; p = 0.008). The ROC curve is demon-trated in Figure 1. SORT also demonstrated a significantlyow H-L value (H-L = 0.02; p > 0.99), thus passing the good-ess of fit test. Nonetheless, it underestimated the mortalityate (O:E = 1.5). POSSUM demonstrated a lower discrimina-
4

Brazilian Journal of Anesthesiology 2021;71(3):302---314
tion level (AUC = 0.89 [95% CI: 0.70---1.00]; p = 0.026) anda higher H-L value (H-L = 1.77; p = 0.99). It also underesti-mated mortality (O:E = 1.5). P-POSSUM was also associatedwith an excellent discrimination level (AUC = 0.95 [95% CI:0.87---1.00]; p = 0.010), but lower than SORT, while under-estimating the mortality rate at a higher level comparedwith SORT (O:E = 3). In addition, P-POSSUM was associatedwith a higher H-L value (H-L = 1.58; p = 0.99) in comparisonto SORT.
There are certain limitations to the present study. In fact,the design of the study was retrospective, and the studypopulation was small. Nonetheless, this is the first evidenceregarding the validity of SORT in patients with pancreaticcancer undergoing surgery. In addition, we demonstratedthat SORT is associated with excellent discrimination and anappropriate level of calibration in predicting postoperativemortality. Furthermore, our outcomes suggest the superior-ity of SORT compared with POSSUM and P-POSSUM. Futurestudies should further assess SORT in a greater study popula-tion of patients with pancreatic cancer undergoing surgery,with a greater follow-up, along with comparing it with otherrisk assessment tools.
Ethical approval
Ethical approval was obtained by the Scientific Committeeof the University Hospital of Larissa (Protocol no 50271/30-10-19).
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Protopapa KL, Simpson JC, Smith NC, et al. Development, andvalidation of the Surgical Outcome Risk Tool (SORT). Br J Surg.2014;101:1774---83.
2. Metz CE, Herman BA, Roe CA. Statistical comparison of two ROC-curve estimates obtained from partially paired datasets. Med DecMaking. 1998;18:110---21.
3. Wong GTC, Ang WC, Wong TCL, et al. Surgical Outcome Risk Tool(SORT) validation in hepatectomy. Anaesthesia. 2017;72:1287---9.
4. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areasunder two or more correlated receiver operating character-istic curves: a nonparametric approach. Biometrics. 1988;44:837---45.
5. Hosmer DW, Hosmer T, Le Cessie S, et al. A comparison ofgoodness-of-fit tests for the logistic regression model. Stat Med.1997;16:965---80.
Dimitrios E. Magouliotis a,b, Athina Samarab,Maria P. Fergadib, Dimitrios Symeonidisb,Dimitris Zacharoulis b,∗
a UCL, Faculty of Medical Sciences, Division of Surgery andInterventional Science, London, UKb University of Thessaly, Department of Surgery, Biopolis,Larissa, Greece
∗ Corresponding author.E-mail: [email protected] (D. Zacharoulis).
Received 15 May 2020; accepted 31 October 2020
https://doi.org/10.1016/j.bjane.2020.10.0180104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.Published by Elsevier Editora Ltda. This is an open access articleunder the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Airway management in obesepatients
Dear Editor,
We read with interest the article of Turna et al. 1 on theirrandomized trial of performance of the Airtraq videolaryn-goscope versus the intubating laryngeal mask airway (ILMA)in obese patients. There are several aspects to the study webelieve necessary to consider.
Airway management in obese patients is a challengingissue associated with a high incidence of complications. Theaccumulation of adipose tissue causes several changes inairway anatomy and respiratory function. Thus, obesity isassociated with, among others, decreased pharyngeal area,obstructive sleep apnea, restrictions in neck flexion, narrowjaw opening, enlarged tongue, reduction in functional resid-ual capacity and alveolar oxygen reserve, and increase inO2 consumption. Therefore, obese patients are at increasedrisk of difficult mask ventilation, difficult tracheal intuba-tion, and hypoxemia during the process of securing theairway, even after short periods of apnea. The core recom-mendations of the recent guidelines focus on limiting the
duration and number of attempts at tracheal intubation inorder to achieve early atraumatic intubation, the philoso-phy on which the vortex approach is based. Accordingly,an undue number of attempts to test a device is not jus-tified. Thereby, it was published in 2016 a useful consensuson airway research ethics that every researcher should takeinto account. 2 It recommends limiting to a maximum of twofailed attempts before following the usual progression in theairway management algorithm and restricting the inclusionof patients to ASA I and II to minimize harm.
Likewise, direct laryngoscopy could not be the mostsuitable rescue method after the unsuccessful use of a vide-olaryngoscopy or an ILMA given that its probability of successcan be lower in this situation. Perhaps, it would have beenmore appropriate to use the other device under study asa backup plan. In addition, any blind technique should beavoided due to the significant failure rate, the frequent needfor repeated attempts, and the potential for airway trauma,which can result in deterioration of ventilation. 3 There-fore, fiberoptic intubation through the ILMA is the methodrecommended.
On the other hand, testing a laryngeal video mask as theTotaltrack VLM (Medcomflow S.A., Barcelona, Spain) instead
305

LETTER TO THE EDITOR
of the ILMA versus the Airtraq would allow a more adjustedcomparison. In fact, it is a device similar to Airtraq since ithas a guide channel and a fiberoptic system with LCD screenthat provides a view of the larynx and tracheal tube as itpasses through the vocal cords. 4 It also combines a supra-glottic airway device with the described structure allowingto perform intubation after securing the airway and estab-lishing optimal ventilation limiting the period of apnea. 5
This is especially advantageous in obese patients since theyhave reduced physiological reserves. 5 Similar clinical tri-als are necessary to determine the most reliable and safeairway method for this population.
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Turna CK, Arslan ZI, Okyay K, et al. Comparison of channelledvideolaryngoscope and intubating laryngeal mask airway for tra-cheal intubation in obese patients: a randomised clinical trial:intubation with Airtraq or Fastrach in obese patients. Rev BrasAnestesiol. 2020;70:118---24.
2. Ward PA, Irwin MG. Man vs. manikin revisited --- the ethical bound-aries of simulating difficult airways in patients. Anaesthesia.2016;71:1399---403.
3. Gómez-Ríos MA, Bonome C. The totaltrack VLM: a novelvideo-assisted intubating laryngeal mask. Minerva Anestesiol.2018;84:126---7.
4. Gómez-Ríos MA, Freire-Vila E, Casans-Frances R, et al. The Total-track(TM) video laryngeal mask: an evaluation in 300 patients.Anaesthesia. 2019;74:751---7.
5. Gómez-Ríos MA, Casans-Frances R, Freire-Vila E, et al. Aprospective evaluation of the Totaltrack video laryngeal maskin paralyzed, anesthetized obese patients. J Clin Anesth.2020;61:109688.
Manuel Ángel Gómez-Ríosa,∗, David Gómez-Ríosb,Zeping Xuc, Antonio M. Esquinasd
a Complejo Hospitalario Universitario de A Coruña,Department of Anaesthesiology and PerioperativeMedicine, A Coruña, Spainb Medical University of Pleven, Pleven, Bulgariac Jiangsu Cancer Hospital, Department of Anesthesiology,Nanjing, China
d Hospital General Universitario Morales Meseguer,Intensive Care Unit and Non Invasive Ventilatory Unit,Murcia, Spain
∗ Corresponding author.E-mail: [email protected] (M.Á. Gómez-Ríos).
Received 3 May 2020; accepted 8 December 2020
https://doi.org/10.1016/j.bjane.2020.12.0170104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.Published by Elsevier Editora Ltda. This is an open access articleunder the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Medicinal cannabis: newchallenges for theanesthesiologist
Dear Editor,
Recent years have witnessed a growing debate on usingmedicinal Cannabis for the treatment of several medicalconditions, given its wide-range therapeutic effects andsome research having shown favorable results for its use,such as for difficult control epilepsy disorders, patients withnausea and vomiting resulting from chemotherapy, somepsychiatric disorders as anxiety, and for controlling cancerand non-cancer pain.1---3
Medicinal Cannabis refers to the medicinal use of theplant and its components for medical purposes using someof the active components with pharmacological propertiesand has been used for millennia. The major componentsused are �9-Tetrahydrocannabinol (THC), the major compo-nent presenting psychoactive action on the Central NervousSystem (CNS), and Cannabidiol (CBD), cannabinoid acids,cannabinol, cannabigerol and cannabivarins, componentswith pharmacological properties on the CNS, but with-out psychoactive action. The concentration and quality ofTHC and CBD depend on the plant lineage and type ofcultivation.2---4
In this scenario, it is of interest to anesthesiologists toaccess a wider range of options to control pain, given theseprofessionals are also responsible for analgesia, especiallythose trained in pain and working in the specialty. Whentaking into account relevant issues in pain control, espe-cially side effects due to the chronic use of opioids, andin the pursuit of parsimonious use, medicinal cannabis canbe helpful in this scenario, given it presents less severeside effects such as opioid related respiratory depression,as the use of cannabinoids does not pose a risk of thecomplication.1,5
The major effects of cannabinoids are through theiraction on Cannabinoid receptors (CB), which can be type1 (CB1), located in the central nervous system, mainly inthe frontal cortex, basal ganglia and cerebellum, in additionto spinal cord, adipocytes, gastrointestinal tract, thyroid,adrenal glands, gonads and immune cells; or type 2 Canabi-noid receptors (CB2), expressed mainly in immune cells, CNSglial cells and peripheral tissue.2,4
THC is a partial agonist of type I (CBD I) and type II (CBDII) cannabinoid receptors, which acts on multiple conditionsand symptoms, such as pain, nausea, spasticity, appetitestimulation, and is also responsible for the psychotropiceffects of the plant. Cannabidiol (CBD), in turn, has no psy-choactive effects, has low direct affinity to these receptors,and works as a negative allosteric modulator of CB1, whichattenuates the side effects of THC, in addition to exerting
306
Manuel Ángel Gómez-Ríos a,*, David Gómez-Ríosb,
1. Turna CK,Arslan ZI, OkyayK, et al.Comparison of channelled videolaryngoscope and intubating laryngeal mask airway for tra-cheal intubation in obese patients: a randomised clinical trial: intubation with Airtraq or Fastrach in obese patients. Rev Bras Anestesiol. 2020;70:118−24.
2. Ward PA, Irwin MG. Manvs. manikin revisited − the ethical bound-aries of simulating difficult airways in patients. Anaesthesia. 2016;71:1399−403.
3. Gómez-Ríos MA, Bonome C. Thetotaltrack VLM: a novel video-assisted intubating laryngeal mask. Minerva Anestesiol. 2018;84:126−7.
4. Gómez-Ríos MA, Freire-Vila E, Casans-Frances R, et al. The Total-track(TM) video laryngeal mask: an evaluation in 300 patients. Anaesthesia. 2019;74:751−7.
5. Gómez-Ríos MA,Casans-Frances R, Freire-Vila E, et al. A prospective evaluation of the Totaltrack video laryngeal mask in paralyzed, anesthetized obese patients. J Clin Anesth. 2020;61:109688.
https://doi.org/10.1016/j.bjane.2020.12.017

ia
cctilTtpcc
Busaccttmio
inwiikgta
Rftw
D
TmIapteospb
ei
Brazilian Journal of Anesthesiology 2021;71(3):302---314
ts action on serotoninergic receptors, producing analgesic,nti-inflammatory, anxiolytic and antipsychotic effects.2,5
In 2015, a systematic review with a metanalysis con-luded that there is moderate evidence to the use ofannabinoids to treat chronic pain and spasticity, and thathere is low evidence for the treatment of chemotherapynduced nausea and vomiting, for weight gain in patientsiving with immunodeficiency syndrome, sleep disorders andourette Syndrome, although the authors concluded thathere is very little quality work available.3 Neuropathicain is the most studied pain disorder in clinical trials withannabinoids, with evidence showing mild to moderate effi-acy to attain a 30% reduction in pain intensity.1,3---5
Despite the evidence of the benefits described above, inrazil cannabinoid use in medical practice is still incipient,nlike some countries such as Israel, Australia, Canada, andome parts of the United States, where using the substance islready part of the medical armamentarium to control can-er and non-cancer pain. The use of CBD has been authorizedurrently in Brazil, and is prescribed mainly for difficult con-rol epilepsy, as is the reduced concentration of THC, givenhe substance is responsible for the psychotropic effects ofedicinal cannabis and therefore still has legal barriers to
ts authorization in higher doses, which already is the casef the countries mentioned above.1,4,5
Based on the exposed, and as cannabinoid use has showntself as a new therapeutic option for pain control, we can-ot neglect the importance of anesthesiologists who workith pain to be updated on the use of the substance and have
t in the range of options to offer their patients, if they deemt favorable. It is also indispensable that, as more in-depthnowledge on the topic arises, our colleague anesthesiolo-ists be inspired to develop new studies in the country, givenhe literature available is still scarce and limited, enabling
wide horizon in this field.
Conflicts of interest
The authors declare no conflicts of interest.
References
1. MacCallum CA, Russo EB. Practical considerations in medi-cal cannabis administration and dosing. Eur J Intern Med.2018;49:12---9.
2. Bruni N, Della Pepa C, Oliaro-Bosso S, Pessione E, Gastaldi D,Dosio F. Cannabinoid delivery systems for pain and inflammationtreatment. Molecules. 2018;23:2478.
3. Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids formedical use: a systematic review and meta-analysis. Jama.2015;313:2456---73.
4. Campbell G, Stockings E, Nielsen S. Understanding the evi-dence for medical cannabis and cannabis-based medicines forthe treatment of chronic non-cancer pain. Eur Arch PsychiatryClin Neurosci. 2019;269:135---44.
5. Urits I, Borchart M, Hasegawa M, Kochanski J, Orhurhu V,Viswanath O. An update of current cannabis-based pharmaceuti-cals in pain medicine. Pain and Therapy. 2019;8:41---51.
Igor P. Saffiera, Claudia C.A. Palmeira a,∗
a Universidade de São Paulo, Hospital das Clínicas,Faculdade de Medicina, São Paulo, SP, Brazil
∗ Corresponding author.E-mail: [email protected] (C.C. Palmeira).
Received 11 September 2020; accepted 27 February 2021
https://doi.org/10.1016/j.bjane.2021.02.0560104-0014/ © 2021 Published by Elsevier Editora Ltda. on behalf ofSociedade Brasileira de Anestesiologia. This is an open accessarticle under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
egional analgesia techniqueor postoperative analgesia inotal knee arthroplasty: havee hit the bull’s eye yet?
ear Editor,
otal knee replacement (TKR) is one of the most com-only performed elective lower limb orthopedic surgeries.
t is associated with moderate postoperative pain in 30%nd severe pain in 60% of the patients.1 Inadequate andoorly treated postoperative pain affects the rehabilita-ion process by decreasing the range of motion, delayingarly ambulation, prolonging the length of hospital stay andverall patient satisfaction. It may also be associated witheveral complications like myocardial ischemia, decreasedulmonary function, increased risk of infection, thromboem-olism, and chronic pain development.
pain originates mainly from intra-articular elements dueto damaged cartilage stimulating free nerve endings andnociceptors (Figure 1C). The primary pain generating com-ponents following TKR surgery include skin/subcutaneoustissue over the incision area, medial retinaculum, periostealrim of the cut bones, remnant of the anterior joint capsule,cut nerves along the surgical dissection area, microfracturesand inflammation.2 Structures like the anterior capsule,synovium, meniscus, cruciate, intra-articular ligaments,periosteum of the knee joint, and prepatellar fat pads areremoved during the surgery and hence do not contribute topain generation (Figure 1C-D). The posterior capsule of theknee joint remains untouched, and the intra-articular com-ponents contributing to the posterior knee pain are removedduring surgery. Thus, postoperative knee pain is mainly con-tributed by anterior knee components as compared to theposterior elements.
The anterior knee is innervated by branches from thefemoral nerve (FN) and anterior division of obturator nerve
To provide optimal postoperative analgesia, the knowl-dge of the pain generating components and their neuralnnervations is essential (Figure 1A-B). The preoperative
(Tv
30
ON) through the subsartorial plexus and peripatellar plexus.he posterior knee and intra-articular structures are inner-ated from the branches of the sciatic nerve and posterior
7

FcwF
dcbmastpdsiV
s(mia
LETTER TO THE EDITOR
igure 1 Knee Joint Preop and Postop Pain Generation and Innervations. A, schematic diagram of the knee joint and intra-articularomponents; B, innervation of the knee joint; C, preoperative pain generation with innervations; D, postoperative pain generationith innervations.N, femoral nerve, ON, obturator nerve, FNEs, free nerve endings.
ivision of ON through the popliteal plexus. The adductoranal block (ACB) is given in the true adductor canal (AC)eyond the apex of the femoral triangle. The AC is boundededially by the vasoadductor membrane (VAM), which is
bsent in the femoral triangle. Extrapolating from the dyetudies, a local anesthetic (LA) injection into the AC belowhe VAM enters the adductor hiatus and finally reaches theopliteal region. Thus, ACB targets the saphenous nerveirectly and popliteal plexus indirectly.3 However, the sub-artorial plexus and nerve to vastus medialis, which providemportant innervation to the anterior knee, lie above theAM and outside the AC, do not get involved ACB.
The infiltration between the popliteal artery and the cap-ule of the knee joint (iPACK) and local infiltration analgesiaLIA) was also described as an additional tool in the multi-
covering anterior and posterior innervations of the kneejoint, depending upon the correct placement of LA. TheiPACK directly and ACB indirectly blocks the popliteal plexus,which covers the intra-articular and posterior elementseffectively but leaves the anterior knee pain undertreated.This could be one reason for not achieving optimal pain reliefor reducing perioperative opioid consumption in literature.
Enhanced recovery after surgery (ERAS) has providedevidence-based perioperative care protocol to improve thequality of patient care and minimize complications, therebyimproving outcomes of various surgeries, including TKR.Since RA options like distal femoral triangle block, ACB,selective tibial nerve block, LIA, and iPaCK are consideredmotor-sparing blocks,4 they have been recommended overfemoral and sciatic nerve blocks. The femoral and sciatic
odal management of pain in patients undergoing TKR. ThePACK targets the popliteal plexus, whereas the LIA involves
pericapsular, periarticular, and subcutaneous infiltration
nat
30
erve blocks are not suitable for ERAS protocols as they aressociated with quadriceps and hamstring weakness, respec-ively, leading to the risk of falls.5
8

esiology 2021;71(3):302---314
atptpbBacospcwtotpc
bspfbc
C
T
References
1. Krishna Prasad GV. Postoperative analgesia techniques aftertotal knee arthroplasty: A narrative review. Saudi J Anaesth.2020;14:85---90.
2. Franco CD, Buvanendran A, Petersohn JD, et al. Innervation of theanterior capsule of the human knee: implications for radiofre-quency ablation. Reg Anesth Pain Med. 2015;40:363---8.
3. Vora MU, Nicholas TA, Kassel CA, et al. Adductor canal blockfor knee surgical procedures: review article. J Clin Anesth.2016;35:295---303.
4. Sogbein OA, Sondekoppam RV, Bryant D, et al. Ultrasound-Guidedmotor-sparing knee blocks for postoperative analgesia followingtotal knee arthroplasty: a randomized blinded study. J Bone JointSurg Am. 2017;99:1274---81.
5. Soffin EM, YaDeau JT. Enhanced recovery after surgery for primaryhip and knee arthroplasty: a review of the evidence. Br J Anaesth.2016;117:iii62---72.
Kartik Sonawane ∗, Hrudini Dixit ,J. Balavenkatasubramanian
Department of Anesthesiology, Ganga Medical Centre &Hospitals Pvt. Ltd., Coimbatore, India
∗ Corresponding author.E-mail: [email protected] (K. Sonawane).
Received 13 October 2020; accepted 24 December 2020
https://doi.org/10.1016/j.bjane.2020.12.0240104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.Published by Elsevier Editora Ltda. This is an open access articleunder the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Cdlip
D
TlpmMgaAoabap
bfe
width of layers, number of perimeters, among others. It isworth underscoring that each one of these parameters hasa direct impact on the quality, weight, manufacturing time,and consequently on the final cost of the object.
Polylactic Acid (PLA) is a thermoplastic polyester whoseend features are that of being biocompatible and biodegrad-able, it hydrolyzes in vivo and transforms into lactic acid,ideal for clinical use. Thus, use of PLA has already beena(
ueotamtu
mi
Brazilian Journal of Anesth
Multimodal systemic analgesia using different routeslso plays an essential role in controlling the inflamma-ory process, dealing with the neuropathic component ofain, and thus reducing its severity. The factors otherhan anesthesia and surgical techniques that influenceostoperative pain include the patient’s age, sex, comor-idities, pain threshold, and severity of preoperative pain.1
esides, the patients’ postoperative activity level, the usend duration of tourniquet exsanguinations, preoperativeonsumption of opioids, opioid-induced hyperalgesia, opi-id dependence/resistance/tolerance can also affect theeverity of postoperative pain. A thorough assessment ofostoperative pain is necessary to determine the actualause of pain and prompt management. In our experience,e found that the patient develops tourniquet pain over
he anterior/posterior aspect of the thigh due to regressionf spinal level at 4---6 hours. Many times, patients confusehis with anterior/posterior knee pain. Hence, a thoroughostoperative pain assessment is required to determine theause of pain and rectify mistakes.
To conclude, the ideal RA technique for TKR shoulde procedure-specific, motor-sparing, opioid-sparing, andhould adequately cover both anterior and posterior com-onents of knee pain. Although we have arrows in theorm of different RA techniques, we are yet to hit theull’s eye to provide optimal analgesia and minimize theomplications.
onflicts of interest
he authors declare no conflicts of interest.
hallenges of prototyping,eveloping, and using video
aryngoscopes produced bynhouse manufacturing on 3Drinters
ear Editor,
he limiting factor for routine and widespread use of videoaryngoscopes are their cost and availability. The priceaid by Brazilian public organizations changed a lot in pastonths and figures up to 65,000 reais (R$) can be found.1
oreover, their availability has declined in the currentlobal scenario. Therefore, pursuing low cost and widelyvailable alternatives has become even more important.
Macintosh style acute angle video laryngoscope maden a 3D printer was developed based on a project avail-ble on the airangel.com website. The device is capable ofeing reproduced in large scale with efficacy, low cost, andvailability on a free collaborative platform for the wholeopulation.
During the 3D printing process, some parameters shoulde set up for the model developed to have expected physicaleatures, among which, the main ones are: type of material,xtrusion temperature, model filling, size of printing nozzle,
ad4fi
30
pproved by the National Sanitary Surveillance AgencyANVISA --- Agência Nacional de Vigilância Sanitária).2
In order to seek enhanced cost-benefit for the man-facturing process of the device, the method of finitelements was used. The method consists of discretizationf a continuous medium into small elements, maintaininghe same properties of the original medium. The elementsre described by differential equations and solved by mathe-atical models, so that desired cost results be attained. For
his analysis, tension and fatigue simulations of the materialsing Computer Aided Engineering (CAE)3 were used.
By looking at image A of Figure 1, we can see thatajor tensions lie on the object surface, so parameters that
nfluence size of external walls directly influence stiffnessnd resistance of the device. Thus, for manufacturing the
evice, it is advisable to use at least 4 perimeters, that is,external lines per layer, as shown in image B of the samegure. Moreover, it is recommended to fill out at least 10%
9
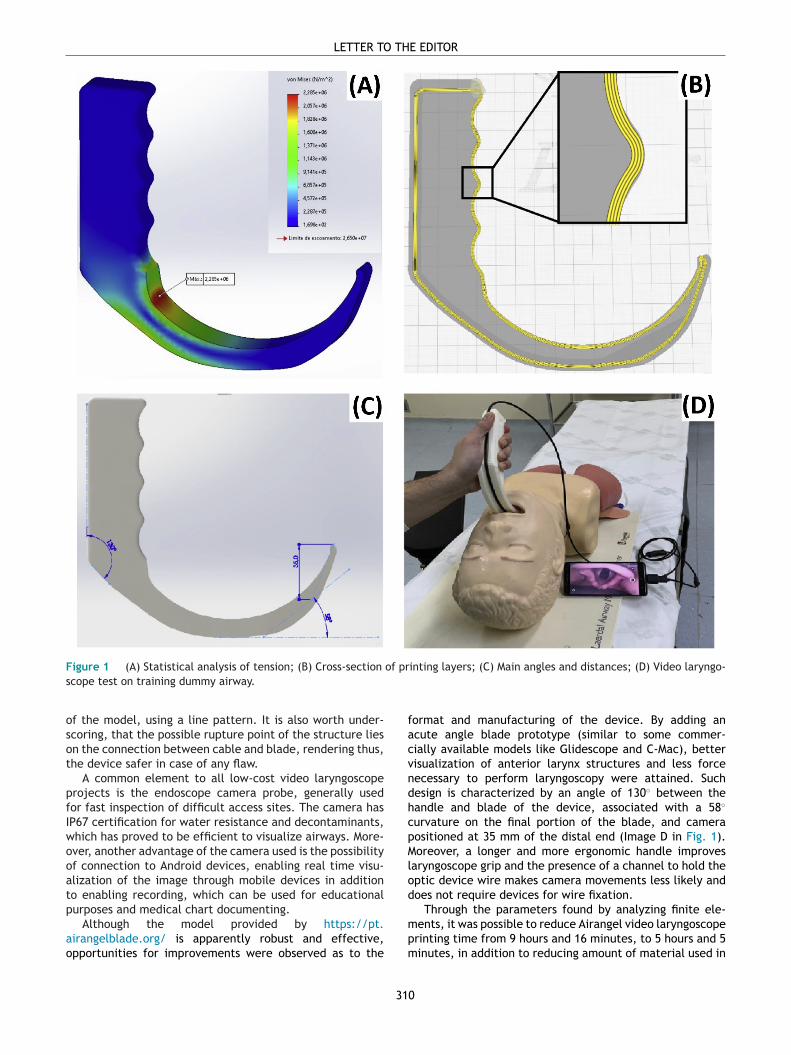
Fs
osot
pfIwooatp
ao
LETTER TO THE EDITOR
igure 1 (A) Statistical analysis of tension; (B) Cross-section of printing layers; (C) Main angles and distances; (D) Video laryngo-cope test on training dummy airway.
f the model, using a line pattern. It is also worth under-coring, that the possible rupture point of the structure liesn the connection between cable and blade, rendering thus,he device safer in case of any flaw.
A common element to all low-cost video laryngoscoperojects is the endoscope camera probe, generally usedor fast inspection of difficult access sites. The camera hasP67 certification for water resistance and decontaminants,hich has proved to be efficient to visualize airways. More-ver, another advantage of the camera used is the possibilityf connection to Android devices, enabling real time visu-lization of the image through mobile devices in additiono enabling recording, which can be used for educationalurposes and medical chart documenting.
format and manufacturing of the device. By adding anacute angle blade prototype (similar to some commer-cially available models like Glidescope and C-Mac), bettervisualization of anterior larynx structures and less forcenecessary to perform laryngoscopy were attained. Suchdesign is characterized by an angle of 130◦ between thehandle and blade of the device, associated with a 58◦
curvature on the final portion of the blade, and camerapositioned at 35 mm of the distal end (Image D in Fig. 1).Moreover, a longer and more ergonomic handle improveslaryngoscope grip and the presence of a channel to hold theoptic device wire makes camera movements less likely anddoes not require devices for wire fixation.
Through the parameters found by analyzing finite ele-
Although the model provided by https://pt.irangelblade.org/ is apparently robust and effective,pportunities for improvements were observed as to the
mpm
31
ents, it was possible to reduce Airangel video laryngoscoperinting time from 9 hours and 16 minutes, to 5 hours and 5inutes, in addition to reducing amount of material used in
0

esiology 2021;71(3):302---314
5Imol
dhaqfsne
vadvtibm
idptdriuetanaafittaitup
The Instagram profile @medical3d.com.br and the web-site www.medical3d.com.br were developed to make thefile with the 3D model of the video laryngoscope and stepby step manufacturing available. As it is an open andcollaborative platform, we believe in the implementationof improvements through the collaboration of the medi-cal community and information acquired as of testing onhumans.
Conflicts of interest
The authors declare no have conflicts of interest.
References
1. DOU 30/04/2020 - Pg. 92 - Seção 3. Diário Oficial da União,https://www.jusbrasil.com.br/diarios/295198992/dou-secao-3-30-04-2020-pg-92 [acesso em 19 de junho de 2020].
2. Medeiros CBS de. Avaliação de peças de Poli (ácidolático) (PLA) impressas para aplicações biomédicas,https://repositorio.ufrn.br/jspui/handle/123456789/26675[acessado em 08 de junho de 2020].
3. Lotti RS, Machado AW, Mazzieiro ÊT, Landre Júnior J. Aplicabili-dade científica do método dos elementos finitos. Rev Dental PressOrtodontia Ortopedia Facial. 2006;11:35---43.
4. Bishop MJ, Harrington RM, Tencer AF. Force applied during tra-cheal intubation. Anesth Analg. 1992;74:411---4.
5. Agência Nacional de Vigilância Sanitária. Resolução da dire-toria colegiada - RDC n185, de 22 de Outubro de 2001,http://www.anvisa.gov.br/legis [acessado em 09 de outubro de2020].
Victor Sampaio de Almeida ∗,Vinicius Sampaio de Almeida ,Guilherme Oliveira Campos
Hospital São Rafael, Salvador, BA, Brazil
∗ Corresponding author.E-mails: [email protected],[email protected] (V.S. Almeida).
Received 28 July 2020; accepted 23 January 2021
https://doi.org/10.1016/j.bjane.2021.01.0120104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.Published by Elsevier Editora Ltda. This is an open access articleu(
Ran-t
D
Tb
WiGt2lt
Brazilian Journal of Anesth
1%, despite the 18% larger volume of the model proposed.t is worth underscoring that despite using less material, theodel proposed still complies with the safety coefficient
f four times the strongest force reported (51.4 N) duringaryngoscopy.4
A wide range of tests were performed on dummies toevelop the most efficient proportions of the blade parts,andle angle and camera positioning. Although of limitedpplicability, studies on dummies have shown excellentuality of visualization of the glottic cleft and success-ul intubation in 100% of cases, including difficult airwayimulation scenarios as with limited mouth opening, promi-ent incisive teeth, and impossibility of performing cervicalxtension.
The low production cost is the major highlight of theideo laryngoscope model. Manufacturing the blade by using
non-industrial 3D printer with PLA bought at specializedealers has an estimated cost of R$ 20. The USB connectionideoscope available in the market has its value linked tohe diameter of the camera, and the price of 7 mm devicess roughly R$ 45. Totaling a cost of R$ 65, this is a negligi-le amount, when compared to classic video laryngoscopeodels available in the market.A low-cost video laryngoscope can save lives, especially
n developing countries or locations where the cost of theevice is unaffordable. In the scenario of the COVID-19andemic, the benefit can be much expanded. However,here is a concern as to the technical aspects for inhouseevelopment and production of these devices, especiallyegarding safety such as ruptures, generation of foreign bod-es in airways and injury to mucosa. In this way, beforesing it in medical practice, studies to prove safety andffectiveness of use in humans are warranted, in additiono registration at regulating agencies of medical products,ccording to Anvisa RDC no 185/2001. However, there areo norms on self-manufactured medical equipment ands to the legal and ethical implication of use. Given weim to improve the model presented, we still have notled for registration at Anvisa. It is worth pointing outhat the estimated cost for patent and registration athis government agency is usually high and can prevent
non-profit project. Another potential hindering factors the requirement for Best Manufacturing Practices Cer-ificate to register medical devices at Anvisa, which isnfavorable to inhouse manufacturing on non-industrial 3Drinters.5
eorganization of obstetricnesthesia services during theationwide COVID-19 lockdown
-- experience from an Indianertiary hospital
ear Editor,
he world is currently facing an unprecedented crisis causedy the severe acute respiratory syndrome coronavirus-2. The
t
ta
31
nder the CC BY-NC-ND licensehttp://creativecommons.org/licenses/by-nc-nd/4.0/).
orld Health Organization declared the novel coronavirusnfection (COVID-19) a pandemic on March 11, 2020. Theovernment of India declared a national-wide lockdown on
he 22nd March, 2020 that lasted for 2 months till 22nd May020. As a tertiary care hospital, we faced significant chal-enges during this 2-month lockdown period which we wisho share with regard to the reorganization of obstetric anes-hesia services in our hospital.
The clinical characteristics of COVID-19 infection in par-urients is consistent with those reported in non-pregnantdults.1 However, many of the symptoms like fatigue, myal-
1

gatcptTwip
tirtasibdha
amuoaOoOthdst
iSbtprtplmseitwpcabnr
lTt
LETTER TO THE EDITOR
ia, tachycardia, and fever may be seen in laboring womens well, making screening difficult in parturients. Due tohese considerations and the fact that COVID-19 infectionsan be asymptomatic,2 we decided to mandatorily test allregnant patients admitted in the delivery suite with real-ime reverse transcriptase --- polymerase chain reaction test.he test has a turnaround time of 6-8 hours, as a result ofhich there were a significant number of patients requir-
ng urgent/emergency cesarean section who did not have areoperative negative test report.
To circumvent this problem, the logistics of operatingwo operating theaters (OT) was discussed, following whicht was decided that parturients with a negative COVID-19eport would be operated in the existing obstetric operatingheater (OOT). Patients who did not have a test report avail-ble (treated as suspects) would be operated in a COVID-19uspect OT in a different part of the hospital. COVID-19 pos-tive parturients were transferred to a separate COVID-19lock for their management. Specific areas for donning andoffing were identified for the COVID-19 suspect OT and allealthcare personnel (HCP) were familiarized with the oper-ting theater floor plan and standard operating procedures.
Arranging adequate manpower to run both operating the-ters was another problem we faced, particularly whenore and more HCP were being deployed in high dependency
nits and intensive care units treating COVID-19 patients inur hospital. From the existing pool of anesthesia residentsnd consultants, 2 separate teams were formed --- one for theOT and one for the COVID-19 suspect OT --- each comprisingf an anesthesia senior resident and a junior resident. TheOT had 2 teams working 12-h shifts which was the usual ros-er schedule in the department. The COVID-19 suspect OTad a single team which was 24-h on-call for a work week of 7ays. Following a consultant-led anesthesia care approach,eparate anesthesia consultants were designated to lead theeams working in the OOT and the COVID-19 suspect OT.
The COVID-19 crisis has resulted in an unprecedentedncrease in the demand for personal protective equipment.tudies have shown that a significant number of HCP haveeen infected, with a disproportionately large number ofhem classified as severe or critical,3 Strategies to minimizeotential COVID-19 exposure of anesthesiologists have beenecommended to limit the consumption of personal pro-ective equipment, including use of video consultations forreanesthesia evaluation and the use of electronic devicesike iPads for remote monitoring and consenting.4 Theseeasures, while suitable in developed countries, are expen-
ive and impractical in low-middle income countries, whereven maintaining effective social distancing in the wardss a challenge. As a uniform policy, all HCP working inhe OOT were instructed to wear N-95 mask with goggleshile those working in the COVID-19 suspect OT used fullersonal protective equipment (bodysuit with hood, shoe-overs, goggles, faceshield, and double-layered gloves inddition to the surgical gown). In order to conserve the num-er of personal protective equipment used, we limited theumber of HCP in the COVID-19 suspect OT to the minimumequired to safely run the theater.
Table 1 Distribution of obstetric surgeries performed inCOVID suspect and obstetric operating theatre during the2-month lockdown period.
COVID-19 suspectoperating theatre
Neuraxialblock
Generalanesthesia
Cesarean deliveryElective --- ---Emergency 22 6
Laparotomy --- 2
Obstetric operating theatre
Cesarean deliveryElective 19 2Emergency 132 37
Laparotomy --- 11Suction and evacuation --- 2Cervical encirclage 1 ---Examination under anesthesia 1 3
for this could be a combination of redistribution of elec-tive cesarean sections and a reduction in referrals fromneighboring states due to the strict COVID-19 mandatednational lockdown in India, that affected interstate trans-port. Of the 218 cesarean deliveries performed, 190 and28 were performed in the OOT and COVID-19 suspect OTrespectively. One hundred seventy three cesarean deliver-ies were performed under neuraxial block, while 45 wereemergency cesarean deliveries performed under generalanesthesia with endotracheal intubation. Following surgery,the patients operated in the OOT were transferred to thestandard postanesthesia care unit and subsequently to thepost-delivery ward, while those operated in the COVID-19 suspect OT completed their postanesthesia recovery inthe theatre whilst awaiting the confirmatory COVID-19 testresults. None of our parturients in the 2-month period oper-ated in the COVID-19 suspect OT turned out positive in theimmediate postoperative period. They were all transferredto the post-delivery ward and had an uneventful postopera-tive course. The newborns were nursed in a separate nurseryand tested at 24 hours after birth. If the test was negative,the babies were reunited with the mothers in the postnatalwards. None of our HCP working in the COVID-19 suspect OTduring the 2-month period developed features of COVID-19infection that required further evaluation and testing.
We now have the rapid point-of-care Xpert Xpress SARS-CoV-2 test that can be processed on the GeneXpert platformin our hospital. With a processing time of 45 minutes, wehave now increased our testing capacity to provide resultsfaster. This has significantly reduced the number of par-turients without a conclusive negative test report requiringurgent/emergency caesarean section, thereby reducing theutilization of personal protective equipment. With the testbeing expensive, geneXpert is currently being used only insituations where patients require immediate or time-boundsurgical interventions, which most of our obstetric patients
The distribution of cases performed during the 2-monthockdown period in our hospital is described in Table 1.he total number of cesarean sections performed is lowerhan the case load that we usually handle. The reason
q
vd
31
ualify for.The undisrupted provision of obstetric anesthesia ser-
ices during the COVID-19 pandemic is challenging, even foreveloped countries.5 Working in a high-volume center in a
2

esiology 2021;71(3):302---314
llhc
F
TC
C
T
R
1
2
3
a summary of a report of 72314 cases from the Chinese Centerfor Disease Control and Prevention. JAMA. 2020;323:1239---42.
4. Melissa B, Kyra B, Emily D, et al. Obstetric anaesthesia duringthe COVID-19 pandemic. Anesth Analg. 2020;131:7---15.
5. Morau E, Bouvet L, Keita H, et al. Anaesthesia and intensive carein obstetrics during the COVID-19 pandemic. Anaesth Crit CarePain Med. 2020;39:345---9.
Anjuman Chandera, Vighnesh Ashok a,∗, Vanita Suri b
a Post Graduate Institute of Medical Education andResearch (PGIMER), Department of Anaesthesia andIntensive Care, Chandigarh, Indiab Post Graduate Institute of Medical Education andResearch (PGIMER), Department of Obstetrics andGynaecology, Chandigarh, India
∗ Corresponding author.E-mail: [email protected] (V. Ashok).
Received 26 October 2020; accepted 13 March 2021
https://doi.org/10.1016/j.bjane.2021.03.0050104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.Published by Elsevier Editora Ltda. This is an open access articleunder the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Pb
D
Ibwtaot
wwtIsIIpmpaabiaoIte
We have to provide a Pecs II block (Pecs I plus pectoralisminor-serratus anterior injection), or Pecs I block plus aserratus anterior plane block (SAPB) for extensive breastsurgeries involving the lateral aspect of the breast, axillarydissection. Here again, I believe that the pectoral compo-nent of Pecs II (i.e. Pecs I) would at least contribute 30% ofthe pain relief.
The authors have stated that this study was the firstone to analyze the role of Pecs I block in breast augmenta-tion procedures.1 However, another study by Ekinci M et al.indeed got published in February 2019 itself which also eval-uated the efficacy of Pecs I block in the same procedure.3
Ekinci M et al. have compared 20 mL versus 30 mL of bupiva-caine 0.25% with placebo and observed that both 20 mL and30 mL groups have significantly reduced the fentanyl con-sumption when compared to the placebo group in contrast totdficf
osStsb
Brazilian Journal of Anesth
ow-middle income country further poses significantly chal-enges. The importance of clear communication betweenealthcare policy officials, administrators and clinicians isrucial and cannot be over-emphasized.
unding
he data collection was approved by the Institute Ethicsommittee (Ref number: NK/6331/Study/308).
onflicts of interest
he authors declare no conflicts of interest.
eferences
. Qiao J. What are the risks of COVID-19 infection in pregnantwomen? Lancet. 2020;395:760---2.
. Rothe C, Schunk M, Sothmann P, et al. Transmission of 2019-NCoVinfection from an asymptomatic contact in Germany. N Engl JMed. 2020;382:970---1.
. Wu Z, McGoogan JM. Characteristics of and important lessonsfrom the coronavirus disease 2019 (COVID-19) outbreak in China:
erspectives on Pecs I block inreast surgeries
ear Editor,
read the article about the clinical investigation of Pecs Ilock in breast augmentation surgeries, published recently,ith profound interest.1 I greatly appreciate the authors for
he wonderful clinical investigation of Pecs I block in breastugmentation procedures. I wish to present my perspectivesn that article which I believe would make more clarity onhis topic.
The authors of this study have observed that Pecs I blockas not superior to placebo in postoperative pain reliefhen the patients themselves participated as their own con-
rol, too. They have also concluded that the role of Pecs block should be ‘‘reconsidered’’ in breast augmentationurgery as well as in breast cancer procedures.1 However,
strongly believe that Pecs I (pectoral component of PecsI) block has definitely some role to play in postoperativeain relief in breast surgeries, particularly in breast aug-entation procedures. This is because of the fact that theectoral nerves do play a role at least in the ‘‘Myofascial’’spect of the pain, although they do not innervate the skinnd subcutaneous tissues of the breast.2 Furthermore, Pecs Ilock alone would not be sufficient in breast cancer surgeriesnvolving the lateral aspect of the breast with or withoutxillary dissection as it would cover mainly the medial aspectf the breast only. Hence, it is misleading to state that Pecs
block needs ‘‘reconsideration’’ in breast cancer surgeriesoo as the surgeries would vary between patients in bothxtent of the incision as well as in depth (multidimensional).
tti
31
he current study. Also, there was no statistically significantifference between 20 mL and 30 mL groups with regard toentanyl consumption.3 Nevertheless, the main differences that Ekinci M et al.3 have not used the same subjects asontrol too as used in this study which I agree as ‘‘unique’’eature of this study.
To conclude, we have the option to choose the vari-us interfascial plane blocks available in the last decadeuch as Pecs blocks, erector spinae plane block (ESPB),APB, etc. It should be based on the two important fac-ors, namely the type and extent of the surgical incision,ensory coverage of the blocks. Hence, we should considerreast surgeries as ‘‘multidimensional entity’’ and choosehe available interfascial plane blocks accordingly, rather
han having an impulse to approach it in only two ways,.e., to block or not to block?43

C
T
R
1
2
3
LETTER TO THE EDITOR
onflicts of interest
he author declares no conflicts of interest.
eferences
. Desroches J, Roy M, Belliveau M, et al. PECS I block for post-operative analgesia in patients undergoing breast augmentationsurgery: a randomized double-blind placebo-controlled study.Rev Bras Anestesiol. 2020;70:333---42.
. Woodworth GE, Ivie RMJ, Nelson SM, et al. Perioperative breastanalgesia: a qualitative review of anatomy and regional tech-niques. Reg Anesth Pain Med. 2017;42:609---31.
. Ekinci M, Ciftci B, Celik EC, et al. The Efficacy of DifferentVolumes on Ultrasound-Guided Type-I Pectoral Nerve Block forPostoperative Analgesia After Subpectoral Breast Augmentation:A Prospective, Randomized, Controlled Study. Aesthetic PlastSurg. 2019;43:297---304.
4. Maniker RB, Johnson RL, Tran De Q. Interfacial Plane Blocksfor Breast Surgery: Which Surgery to Block, and Which Block toChoose? Anesth Analgesia. 2020;130:1556---8.
Raghuraman M. Sethuraman
Sree Balaji Medical College & Hospital, Bharat Institute ofHigher Education & Research, Department ofAnesthesiology, Chennai, IndiaE-mail: [email protected]
Received 24 January 2021; accepted 13 March 2021
https://doi.org/10.1016/j.bjane.2021.03.0040104-0014/ © 2021 Sociedade Brasileira de Anestesiologia.Published by Elsevier Editora Ltda. This is an open access articleunder the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
31
4
Contact us
[email protected] www.bjan-sba.org +55 21 979 770 024
Brazilian Journal ofA n e s t h e s i o l o g y
BJAN Brazilian Journal of Anesthesiology
Vol. 71 N. 3 | M
ay-Jun
2021
Brazilian Journal ofANESTHESIOLOGYR e v i s t a B r a s i l e i r a d e A n e s t e s i o l o g i a
Obstetric anesthesia
Vol. 71, N. 3 | May-Jun 2021 | ISSN 0104-0014