Middle East Journal of Anesthesiology
157
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Middle East Journal of Anesthesiology


Consultant Editors
Assem Abdel-Razik (Egypt)
Bassam Barzangi (Iraq)
Izdiyad Bedran (Jordan)
Dhafir Al-Khudhairi (Saudi Arabia)
Mohammad Seraj (Saudi Arabia)
Abdul-Hamid Samarkandi (Saudi Arabia)
Mohamad Takrouri (Saudi Arabia)
Bourhan E. Abed (Syria)
Mohamed Salah Ben Ammar (Tunis)
M. Ramez Salem (USA)
Elizabeth A.M. Frost (USA)
Halim Habr (USA)
Editorial Executive Board
Editor-In-Chief: Ghassan Kanazi
Executive Editors Maurice A. Baroody
Editors Chakib Ayoub Marie Aouad Sahar Siddik-Sayyid
Managing Editor Mohamad El-Khatib [email protected]
Founding Editor Bernard Brandstater
Emeritus Editor-In-Chief Anis Baraka
Honorary Editors Nicholas Greene Musa Muallem
Webmaster Rabi Moukalled
Secretary Alice Demirdjian [email protected]
MIDDLE EAST JOURNAL OF ANESTHESIOLOGY
Department of Anesthesiology American University of Beirut Medical Center P.O. Box 11-0236. Beirut 1107-2020, Lebanon
The Middle East Journal of Anesthesiology is a publication of the Department of Anesthesiology of the American University of Beirut, founded in 1966 by Dr. Bernard Brandstater who coined its famous motto:“For some must watch, while some must sleep” (Hamlet-Act. III, Sc. ii).and gave it the symbol of the poppy flower (Papaver somniferum), it being the first cultivated flower in the Middle East which has given unique service to the suffering humanity for thousands of years. The Journal’s cover design depicts The Lebanese Cedar Tree, with’s Lebanon unique geographical location between East and West. Graphic designer Rabi MoukalledThe Journal is published three times a year (February, June and October) The volume consists of a two year indexed six issues. The Journal has also an electronic issue accessed at www.aub.edu.lb/mejaThe Journal is indexed in the Index Medicus and MEDLARS SYSTEM.E-mail: [email protected]: +961 - (0)1-754249
All accepted articles will be subject to a US $ 100.00 (net) fee that should be paid prior to publishing the accepted manuscript
Please send dues via:
WESTERN UNIONTo Mrs. Alice Artin DemirjianSecretary, Middle East Journal of Anesthesiology OR TOCredit Libanaise SALAG: Gefinor.Ras.BeyrouthSwift: CLIBLBBX
Name of BeneficentMiddle East Journal of AnesthesiologyAcc. No. 017.001.190 0005320 00 2
(Please inform Mrs. Demirjian [email protected] - Name and Code of article - Transfer No. and date (WESTERN UNION) - Receipt of transfer to (Credit Libanaise SAL)
Personal checks, credit cards and cash, are not acceptable

“For some must watch, while some must sleep”
(Hamlet-Act. III, Sc. ii)

134

Kingdom of Saudi Arabiah
National Guard Health Affairs
CARDIAC SCIENCE DEPARTMENT
The National Guard Health Affairs is considered a flagship facility in the Middle East, providing primary and tertiary healthcare services to the National Guard forces, their dependents and civilian employees. The National Guard group comprises of four major hospitals and sixty healthcare center, which operate to American JCI standards. As a Center Of Excellence, it performs all major surgeries-including cardiac surgery, liver transplants and conjoined twin separation. We are currently inciting applications for the following post:
We, in turn can offer a generous tax-free salary, generous holidays, annual flights and exceptional benefits.
If you are interested please send your CV indicating which journal advert you are responding to, along with copies of your certificates to the recruitment office of the KAMC for the attention of John Quinn at Email:[email protected], or fax# +966-1-2520056. Your application will be treated in strictest of confidence and all initial enquiries or requests for more information are welcomed. For more information please visit our website at www.ngha.med.sa
Consultant in Cardiac Critical Care and Assistant Consultants in Cardiac Critical Care
Responsibilities include peri-operative care of critically ill cardiac patients.
Our requirements in terms of academics and experience are as follows:
• Consultant Cardiac Critical CareFRCS-Irish / UK, North American or Australian Boards coupled with minimum 3 years post Board experience in Anaesthesia and fellowship in Cardiac Anaesthesia and Critical Care desirable
• Assistant Consultant Cardiac Critical CareFRCS-Irish / UK, North American, Australian Boards/Arab or Saudi Board/MRCP or equivalent coupled with minimum 0-1 year post Board experience in Anaesthesia and fellowship in Cardiac Anaesthesia and Critical Care desirable


767 M.E.J. ANESTH 21 (6), 2012
Middle East Journal of Anesthesiology
Vol. 21, No. 6, October 2012
CONTENTS
EDITORIAL15th WFSA WORLD CONGRESS OF ANAESTHESIOLOGISTS
���������������������������������������������������������������������������������������������������������������������������������Anis Baraka 769REVIEW ARTICLES
PREvENTION AND MANAGEMENT OF COMPLICATIONS OF REGIONAL ORbITAL ANESTHESIA
������������������������������������������������������������������������������������ Nalini Vadivelu, Yili Huang, Alan Kaye, Vijay Kodumudi, Alice Kai , Ron A Adelman 775
AIDS FOR FACILITATION OF DIFFICULT TRACHEAL INTUbATION REvIEW AND RECENT ADvANCES
������������������������������������������������������������������������������������������������������ Musa Muallem, Anis Baraka 785LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIvE ANESTHETIC CONSIDERATIONS
���������������������������������������������������������������� Alan Kaye, Tyler Stout, Ira Padnos, Brian Schwartz, Amir R� Baluch, Charles Fox, Henry Liu 793
CEREbRAL OXIMETRY: A REPLACEMENT FOR PULSE OXIMETRY?
SCIENTIFIC ARTICLESTENS COMPARED TO OPIOIDS IN POSTOPERATIvE ANALGESIC THERAPY AFTER MAJOR SPINAL SURGERY WITH REGARD TO COGNITIvE FUNCTION
���������������������������������������������������������������������Axel Unterrainer, Franz Uebleis, Franziska Groß, Gabriela Werner, Martin Krombholz, Wolfgang Hitzl 815
INTERObSERvER vARIAbILITY FOR NON-INvASIvE PREDICTION OF DIFFICULT INTUbATION IN DIFFERENT YEARS OF ANESTHESIOLOGY RESIDENCY
��������������������������������������������������������������������������������� Nalan Celebi, Ozgur Canbay, Hemra Cil, Zeliha Korkmaz Disli, Ayse Heves Karagoz 823
COMbINED USE OF METOCLOPRAMIDE AND DEXAMETHASONE AS A PROPHYLACTIC ANTIEMETIC IN ELECTIvE CESAREAN SECTION UNDER SPINAL ANESTHESIA
������������������������������������������������������������������������������������������������� Frikha M, Dhouib F, Bouhlel R, Djemel W, Smaoui L, Karoui A 829
ULTRASONOGRAPHIC MODIFICATION OF CORMACK LEHANE CLASSIFICATION FOR PRE-ANESTHETIC AIRWAY ASSESSMENT
������������������������������������������������������������ Deepak Gupta, Arvind Srirajakalidindi, Bryant Ittiara, Leigh Apple, Gokul Toshniwal, Halim Haber 835
vIDEOLARYNGOSCOPIC ENDOTRACHEAL INTUbATION (GLIDESCOPE®) OF MORbIDLY ObESE PATIENTS IN SEMI-ERECT POSITION: A COMPARISON WITH RAPID SEQUENCE INDUCTION IN SUPINE POSITION
����������������������������������������������������������������������������������������������� Deepak Gupta, Konstantin Rusin 843
��������������������������������������������������������������������������������������������������������������������������� Elizabeth Frost 807

768768
NALOXONE vERSUS METOCLOPRAMIDE FOR THE TREATMENT OF ESTAbLISHED POSTOPERATIvE NAUSEA AND vOMITING IN PATIENTS FOLLOWING GENERAL ANESTHESIA WITH FENTANYL SUPPLEMENTATION
������������������������������������������������������������������������������������������������ Aliyyah Dabbous, Fouad Souki, Anis Baraka, Samar Jabbour-Khoury 851
LONG-TERM USE OF INTRATHECAL DROPERIDOL AS AN EXCELLENT ANTIEMETIC IN NONMALIGNANT PAIN – A RETROSPECTIvE STUDY
Mohammad-Hazem I� Ahmad-Sabry, Gholamreza Shareghi 857CASE REPORTS
INHALATIONAL INDUCTION WITH “vASOPARALYTIC” SEvOFLURANE: ARE WE “HYPEROXYGENATING” WHILE ANESTHETIZING DEvELOPING bRAINS? A CASE SERIES DISCUSSION
������������������������������������������������������������������ Deepak Gupta, Jaspreet Sangha, Edward Kaminski 863INCORRECT FIXATION OF ENDOTRACHEAL TUbE: A CAUSE OF NON-INFLATION OF THE CUFF
���������������������������������������������������������������������������������������������������� Kiran Jangra, S�K� Malhotra 869KETAMINE INFUSION AS A TREATMENT FOR MAJOR DEPRESSIvE DISORDER: A NEW ROLE FOR ANESTHESIOLOGISTS?
������������������������������������������������������������������� Joshua Dilley, W� Brooks Gentry, Kimberly Golden 871A CASE OF SEvERE SAM FOLLOWING A DAvID PROCEDURE
���������������������������������������������������������������������������� Menachem M� Weiner, Cesar Rodriguez-Diaz 875RESPIRATORY SUPPORT INCLUDING EMERGENT EXTRACORPOREAL MEMbRANE OXYGENATION AS A bRIDGE TO AIRWAY DILATATION FOLLOWING PERIOPERATIvE bRONCHIAL OCCLUSION
����������������������������������������������������������������������������������������������������� Arlyne Thung, Don Hayes Jr, Thomas Preston, Joseph Tobias 879
GENERAL ANESTHESIA IN A PATIENT WITH CLEIDOCRANIAL DYSPLASIA
����������������������������������������������������������������������������������������������������� Cindy Wang, Steven Neustein 889ACUTE QUADRIPLEGIA SECONDARY TO CERvICAL bODY EROSION AND EPIDURAL AbSCESS
���������������������������������������������������������������������������������������������� Jahan Porhomayon, Nader Nader 891INFERIOR WALL DIvERTICULUM OF LEFT vENTRICLE COEXISTING WITH MENTAL RETARDATION AND ATRIAL SEPTAL DEFECT
������������������������������������������������������������������������������������������������� Henry Liu, Ting Zhou, Jiao Liu, Yiru Tong, Jack Shanewise 895
ENDOTRACHEAL TUbE CUFF LEAK WITH MYSTERIOUS LARYNGOTRACHEAL PATHOLOGY
�������������������������������������������������������������������� J� L� La Fleur, K� Boddu, Amir Baluch, Alan Kaye 899SAFE REMOvAL OF EPIDURAL CATHETER - A DILEMMA IN PATIENTS WHO ARE STARTED ON DUAL ANTI PLATELET THERAPY POSTOPERATIvELY FOR ACUTE CORONARY SYNDROME.
������������������������������������������������������������������� Jyoti Burad, Rajini Kausalya, Mohammed Ismaili, Qutaiba Tawafic, Rohit Date 905
CRICOTHYROID APPROXIMATION USING A SILASTIC SHEATH: A NEW APPROACH
�������������������������������������������������������������������������������������������������������������������� Abdul-latif Hamdan 909

769 M.E.J. ANESTH 21 (6), 2012
EDITORIAL
15TH WFSA WORLD CONGRESS OF ANAESTHESIOLOGISTS
The 15th WFSA World Congress of Anaesthesiologists was held in Buenos Aires- Argentina (25-30 March 2012). (Fig. 1a, 1b)
The President of WFSA-Angela Enright (Canada) (Fig. 2)
The Secretary of WFSA-David Wilkinson (United Kingdom) (Fig. 3)
Chairman of WCA 2012-Alfred Cattaneu (Argentina) (Fig. 4)
The WCA Congress is the most important opportunity we have to meet our anesthesiology colleagues from allover the World, and exchange ideas, share knowledge, and most importantly renew old friendship and develop new ones.
The scientific program has been carefully crafted to include scientific presentations, panels and workshops, as well as the exhibit of the different anesthetic equipments. The sessions were presented in English, but also included Spanish and Portuguese sessions. One of the most important sessions chaired by Angela Enright our President of WFSA was the Harold Griffith Symposium which introduced the these “Making the dream reality” (Fig. 5, Fig. 6).
During the WFSA meeting in Buenos Aires, Dr. David Wilkinson of the UK was elected as the next President of WFSA, and Dr. Yehia Khater of Egypt was elected as the Chairman of the Executive Committee of WFSA. Congratulations!
I was honored by being nominated as a Faculty of the 15th WCA Congress, and as a speaker who delivered four subjects (Fig. 7):
Revisiting Preoxygenation
Pathophysiology of one lung ventilation during thoracotomy and thoracoscopy
Neuromuscular disorders in children – the response of muscle relaxants
Difficult airway management in pediatrics
The Congress started on Saturday 25 March by the Opening Ceremony and welcome reception, and was closed on Friday 30 March by the closing ceremony and the Farewell Barbecue. The Tango dances, the famous dance of Argentina was practiced everywhere, in the streets, in the exhibit area, as well as during the Welcome and the closing ceremonies (Fig. 8a, 8b, 8c).
Good Bye and thank you Argentina. We are looking forward to the 16th World Congress of Anaesthesiologists which will be held in Hong Kong on 28 August - 2 September 2016 (Fig. 9).
Anis Baraka, MD, FRCA (Hon)Emeritus Professor-American University of Beirut
Emeritus Editor-in-Chief-Middle East Journal of Anesthesiology

770 BARAKA A.
Fig� 1a, 1b 15th WFSA World Congress of
Anaesthesiologists -Buenos Aires Argentina 25-30 March 2012
M.E.J. ANESTH 21 (6), 2012
77115TH WFSA WORLD CONGRESS OF ANAESTHESIOLOGISTS
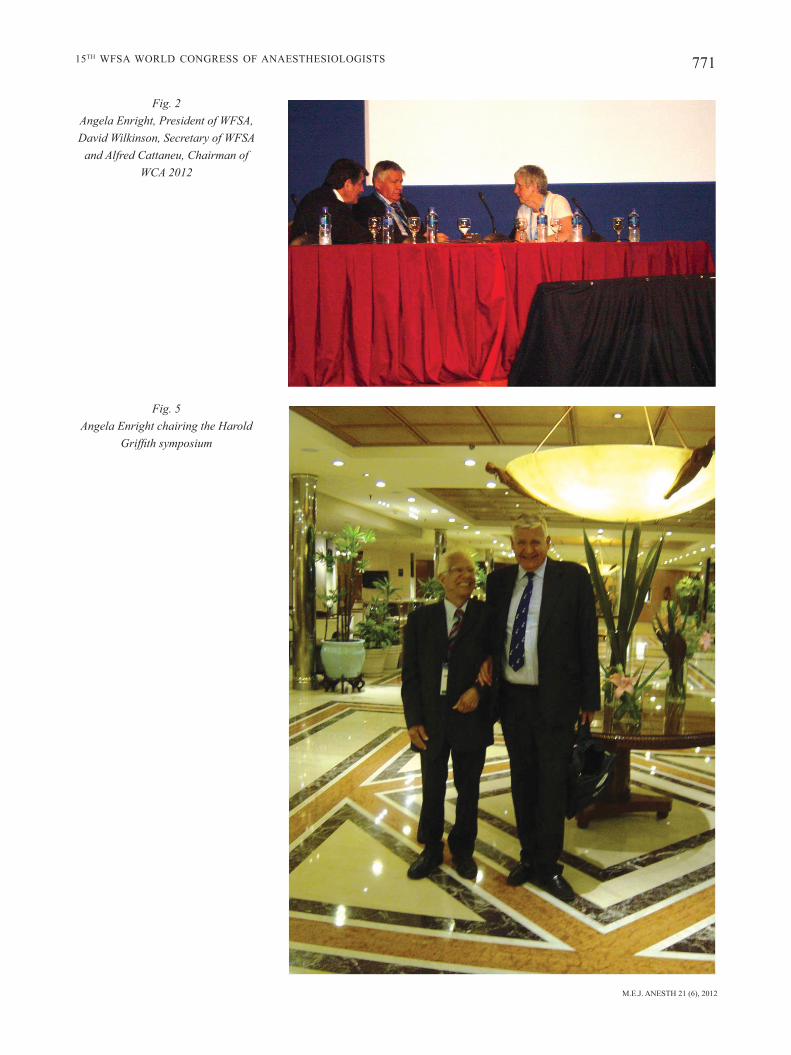
Fig� 5 Angela Enright chairing the Harold
Griffith symposium
Fig� 2 Angela Enright, President of WFSA, David Wilkinson, Secretary of WFSA
and Alfred Cattaneu, Chairman of WCA 2012

772 BARAKA A.
Fig� 4 Alfred Cattaneu and Anis Baraka
Fig� 5Angela Enright chairing the Harold
Griffith symposium
Fig� 6 The theme of the Global Oximetry Project- Making the dream reality

M.E.J. ANESTH 21 (6), 2012
77315TH WFSA WORLD CONGRESS OF ANAESTHESIOLOGISTS
Fig� 7 Dr Anis Baraka Faculty of the WCA
2012 representing Lebanon
Fig� 8 The famous tango Dancing of Argentina
practiced everywhere in the streets, at the scientific exhibit and at the Gala
Dinner
Fig� 9 The ad of the 16th WCA Hong Kong


775 M.E.J. ANESTH 21 (6), 2012
REVIEW ARTICLES
PREVENTION AND MANAGEMENT OF COMPLICATIONS OF REGIONAL ORBITAL ANESTHESIA
NALINI vADIvELU*, YILI HUANG**, ALAN DAvID KAYE***, vIJAY KODUMUDI****, ALICE KAI*****, RON A ADELMAN******
Abstract
The majority of ophthalmic procedures are performed under regional anesthesia, but the proximity of important structures such as the blood vessels, optic nerve and the brainstem lead to increased risks associated with these blocks. The most serious of these complications is brainstem anesthesia. As the number of outpatient freestanding surgical centers increase, the significance of these potential complications is expected to increase from orbital blocks for ocular surgical procedures such as cataract removal and vitrectomy. An understanding of these complications, which may sometimes be life-threatening, are thus vital to the anesthesia practitioner. Procedural improvements include a close evaluation of the precise anatomy of the region, with particular attention to injection sites, depth of injection, position of the globe, and techniques to avoid nerve damage and accidental injection into surrounding structures, including blood vessels, globe and cerebrospinal fluid. This literature review emphasizes the importance of the prevention, recognition and management of these complications, which includes the extremely serious complication of brainstem anesthesia.
Disclosure Statement: The authors have no relationships with pharmaceutical companies or products to disclose, nor do they discuss off-label or investigative products in this manuscript.
Introduction
The majority of ophthalmic surgeries utilize either topical anesthesia or regional anesthesia by the injection of local anesthetic (LA) around or behind the eye, either by ophthalmologists or anesthesiologists. Over the past three decades, anesthesiologists have become increasingly involved in eye blocks that were previously performed by surgeons. The three most common techniques to supply anesthesia include retrobulbar, peribulbar, and topical anesthesia (TA). The proximity of the targeted nerves to vital structures predisposes retrobulbar and peribular techniques in particular to inherent potential complications.
One rare, but life-threatening complication is brainstem anesthesia and is associated primarily with retrobulbar injection. It is estimated to accompany anywhere between 0.01% to 0.79% of
* M.D, Associate Professor, Department of Anesthesiology, Yale University school of Medicine, New Haven Connecticut.** M.D, Resident, Department of Anesthesiology, Yale University school of Medicine, New Haven Connecticut.*** M.D, PhD, Professor and Chairman, Department of Anesthesiology, Professor, Department of Pharmacology, Louisiana
State University Health Science Center, New Orleans, Louisiana.**** Undergraduate, School of Liberal Arts and Sciences, University of Connecticut, Storrs, Connecticut.***** BA, National Institutes of Health Fellow, National Institutes of Health, Neuroplasticity Unit, Bethesda, Maryland.****** M.D, Professor of Ophthalmology and Visual Science, Yale University School of Medicine, New Haven, Connecticut. Corresponding Author: Alan D. Kaye, MD., Ph.D., DABA, DABPM, Director Pain Services, Professor and Chairman,
Department of Anesthesiology, Louisiana State University School of Medicine, 1542 Tulane Ave, Room 656, New Orleans, LA 70112, Tele: (504) 568-2319; Fax: (504) 568-2317. E-mail: [email protected]

776 VADIVELU N. et. al
muscles. The apex of the cone is the site of entry of the optic nerve into the orbit. The four rectus muscles (superior, medial, inferior and lateral) insert near the equator of the globe, which is suspended in the anterior part of the orbit and is the base of the retrobulbar cone. These four rectus muscles stem from the annulus of Zinn, a fibrous ring at the orbital apex that surrounds the optic foramen and the medial aspect of the superior orbital fissure. The muscle cone divides the orbit into the extraconal, conal, and intraconal compartments5. With the exception of the trochlear nerve, the motor supply to the extraocular muscles also passes through this muscular cone. It is, therefore, highly likely that the administration of LA inside the muscular cone should provide intense operative akinesia and anesthesia as well as post-operative analgesia for ocular surgeries6,7. However, this practice is associated with risks. Many other structures are located in this muscular cone including the meningeal sheaths of the optic nerve, the optic nerve and the blood supply to the orbit. Perforation of these structures can lead to injury, risk of toxicity to the nerve and hemorrhage by damage to the blood vessels supplying the orbit8. Additionally, injection of LA can lead to spread from the orbital apex via the submeningeal pathways to the central nervous system9. Intraconal space (inside the cone formed by the rectus muscles) is the location for retrobulbar injection. It is anatomically different than extraconal space, which is the site for peribulbar injection. These techniques will be discussed in greater detail later in the manuscript.
Transmitting Nerves and Vessels from the Orbits
The nerves and vessels that innervate the optic foramen and medial portion of the superior orbital fissure extend through the annulus of Zinn in order to supply structures in the muscle cone. The three cranial nerves that supply the motor innervations to the extraocular muscles are the trochlear nerve (cranial nerve IV), the abducens nerve (cranial nerve VI) and the oculomotor nerve (cranial nerve III). The oculomotor nerve supplies the medial, superior and inferior rectus, the inferior oblique, and the levator palpebrae superioris muscles. The abducens nerve supplies the lateral rectus muscle and the trochlear nerve supplies the superior
regional ophthalmologic blocks and the consequences can be deadly1,2,3. Symptoms range from drowsiness and slurred speech to respiratory depression and hemodynamic instability4. It is important for anesthesia providers to be cognizant of the potential complications of LA injections for orbital anesthesia, to recognize the signs and symptoms particular to possible adverse events, and to be knowledgeable of the preventive measures and the management of these complications.
In this review, we discuss the anatomical considerations, LA pharmacological considerations, regional anesthetic techniques, and potential complications, which include hemorrhage, blindness, cardiopulmonary arrest and brain stem anesthesia.
Anatomic Considerations
Ophthalmic surgery is challenging on many fronts. Immobility and analgesia are paramount to surgical success. Basic knowledge of orbital anatomy is important for effective analgesia, successful surgery, and reduction of potential complications.
Orbit Anatomy
It is important to be intimately familiar with the anatomy of the orbit in order to prevent and treat the complications that can arise from the administration of LAs for eye surgeries. With the exception of the inferior oblique, all of the six extraocular muscles (lateral rectus, medial rectus, superior rectus, inferior rectus, superior oblique, and inferior oblique) form a cone in the bony orbit, through which several sensory and motor innervations make their passage, including the first branch of the trigeminal nerve (ophthalmic nerve) through the ciliary ganglion, which supplies sensory innervation to the globe. Motor innervation is supplied by the oculomotor nerve, trochlear nerve, abducens nerve, and the temporal division of the facial nerve. The branches of the ophthalmic division of the trigeminal nerve along with most of the motor nerves to the orbit travel behind the globe within a space for which LA can be deposited (except for the temporal division of the facial nerve). It should be noted that the cone is anatomically incomplete and that there is no structure which links all of the extrinsic ocular

M.E.J. ANESTH 21 (6), 2012
777PREVENTION AND MANAGEMENT OF COMPLICATIONS OF REGIONAL ORBITAL ANESTHESIA
nerve block to achieve eyelid akinesia.
The anesthetic solution is usually a 2-6 mL mixture of 0.75% bupivacaine (or 0.5% ropivacaine) and 2% lidocaine that is injected with a 25-gauge, 3-cm needle, aiming toward the orbital muscle cone16. Epinephrine is sometimes added to reduce hemorrhage and to extend the duration of action of the LA, while hyaluronidase is sometimes used as another adjunct, which acts by increasing the potency of the bupivacaine (or ropivacaine)17 and expediting its onset18.
ii. Peribulbar anesthesia (PBA)
RBA was the predominant regional eye block for much of the last century19 but has recently given way to the similarly efficacious pericone block, the peribulbar anesthesia block (PBA), which theoretically leads to fewer complications because it does not involve introducing a needle into the muscular cone, which is close to numerous vulnerable structures20. However, it should be noted that RBA is still being practiced all over the world.
PBA was first reported by Davis and Mandel in 198521. With peribulbar block the local anesthetic is deposited within the orbit but not in the muscular cone. Widespread use of the phacoemulsification technique has changed anesthesia requirements in which total akinesia is no longer essential. The block consists of two injections: a superior injection above the medial canthus nasally and an inferior injection given at the junction of the outer two thirds and the inner one third of the inferior rim of the orbit. A common local anesthetic mixture used is 5 cc of 2% lidocaine with 1: 200,000 epinephrine, along with 5 cc of 0.75% bupivacaine (or 0.5% ropivacaine) for the block.
iii. Topical Anesthesia (TA)
LA drops are effective for many uncomplicated ophthalmologic procedures. It is estimated that approximately half of all cataract procedures and 90% of those utilizing phacoemulsification are performed with TA. Limitations include lack of akinesia and short duration of action. Whenever phacoemulsification is not employed, total akinesia is required making TA largely inadequate. Intraoperative comfort is diminished with TA and the use of lidocaine jelly instead of eye drops has been demonstrated to enhance the quality of analgesia. Specific patients, who are on anticoagulants
oblique muscle. The zygomatic nerve, a branch of the maxillary nerve in the floor of the orbit splits into the zygomaticotemporal and zygomaticofacial branches. The anterior and posterior ethmoidal foramina are the exit points for the ethmoidal nerves and vessels as they leave the orbit7.
As previously mentioned, three of the most common techniques for ophthalmogical procedures include retrobulbar block, peribulbar blocks, and TA. Though not suitable for open globe surgery, these blocks are adequate for many different types of surgery. Significant growth in topical anesthesia for certain lens and anterior chamber procedures has become accepted in clinical practice and has evolved in technique over the past two decades.
i. Retrobulbar Block
Since its first description by Knapp in 1884, the retrobulbar block has commonly been utilized for intraocular surgeries10. Anesthetic injection into the muscular cone by the retrobulbar block gives retrobulbar anesthesia (RBA). The purpose of the block is to anesthetize the cornea, the ciliary body, the ciliary ganglion located between the ophthalmic artery and the optic nerve all of which are supplied by the ophthalmic cranial nerves (II, III, & VI).
Atkinson refined the retrobulbar block in 193611 with a technique that involves having the patient look in and up, allowing the inferior oblique muscle and the fascia between the lateral and inferior rectus muscles to be out of the way of the needle tip12. However, CT analysis of cadaveric orbits has revealed that this technique leads to stretching of nerves and the conformation of the optic nerve, ophthalmic artery, and superior orbital vein to be precariously close to the needle tip, increasing the potential risk of accidental puncture and systemic anesthetic toxicity13. The current recommendation to increase safety is to position the eye either into a primary gaze or an infranasal position14.
The current technique of RBA involves advancing the needle into the temporal lower lid, through the orbital septum, and then following the orbit toward the muscle cone and orbital apex. The needle is aspirated after entering the muscle cone space. After determination via aspiration that the needle is not in the vasculature, LA is administered15. In addition, some practitioners will administer a separate facial

778 VADIVELU N. et. al
whereas amide LAs undergo hepatic metabolism.
Lidocaine is an intermediate-duration amide LA with significant potency, fast onset, good tissue penetration, and low cardiac toxicity. The concentration of lidocaine used for regional anesthesia ranges from 1-2%, with orbital techniques typically employing a 2% preparation, and a single injection can provide up to approximately 6 hours of analgesia. As with many regional techniques, lidocaine is often used in combination with a long-acting LA, such as bupivacaine in order to achieve both rapid and enduring analgesia for orbital anesthesia.
Bupivacaine was the first long-acting amide LA created. The concentration of bupivicaine used for regional nerve blockade ranges from 0.25-0.75%, and a single injection can provide up to approximately 16-24 hours of analgesia. It is more hydrophobic than lidocaine and has a slower onset. Bupivicaine is highly protein-bound which allows for a longer duration; however, this also contributes to the potential for cardiotoxicity. Due to its narrow therapeutic index, bupivacaine has been replaced in many locations by ropivacaine.
Levobupivacaine is the levorotatory enantiomer of bupivacaine. Commercial bupivacaine is a racemic mixture of both enantiomers (R and S). Levobupivacaine is approximately equivalent to its racemic bupivicaine with respect to onset, duration and dosing in regional anesthesia. However, cardiac and CNS toxicity of levobupivacaine is approximately 35% less than racemic bupivacaine.
Exparel™ is a bupivacaine liposome injectable suspension (1.3% 266 mg/20 mL or 13.3 mg/mL). DepoFoam, which is a multivesicular lipososme, consists of tiny 10-30 microns in diameter lipid-based particles which contain discrete water-filled chambers of bupivacaine dispersed through a lipid matrix. This novel preparation allows for increased duration of efficacy and pain relief up to 72 hours after injection. This drug preparation recently came to market in 2012 and to date, there are no clinical trials for this agent in orbital anesthesia.
Ropivacaine is a long-acting amide local anesthetic derived from mepivacaine and is a structural analog of bupivacaine. Ropivacaine differs from bupivacaine in that exists as a pure S enantiomer, and it demonstrates significantly reduced cardiac and CNS
including daily aspirin or NSAIDs, would benefit from TA to minimize the risk of bleeding.
Choice of Local Anesthetic
LAs are the key agents used to achieve neural blockade in regional anesthesia, including orbital blocks. The basic structure of LAs consists of an aromatic end and an amine end linked to each other through an ester or and amide chain. These molecules act primarily via targets on neuronal sodium channels thereby blocking the conduction of action potentials along the course of nerves. The susceptibility of a nerve to blockade by LAs depends on characteristics of the individual drug (e.g. potency, pKa, buffering), characteristics of the tissue (e.g. presence of local inflammation and acidosis), and characteristics of individual nerve fibers (e.g. diameter, myelination, activity). LAs tend to block small nerve fibers both earlier and at lower concentrations than large nerve fibers, and blockade resolves in the reverse order. For example, blockade of 0.15μm C-fibers (post-ganglionic autonomic, pressure, dull pain, and temperature) occurs before 1.5μm Aδ fibers (sharp pain), and blockade of 15μm Aα (motor) is the last to occur. In addition to blocking sodium channels on sensory and motor fibers, at high doses or after inadvertent intravascular injection, LAs can block sodium channels in the brain and heart, potentially resulting in morbidity or mortality, including loss of consciousness, seizures, myocardial depression, and even cardiac arrest.
LAs can be broadly divided into two categories: those with an amide linking chain and those with an ester linking chain. Ester LAs can generally be identified as those with only one “i” in their names, and they include cocaine, chloroprocaine, and tetracaine. Amide LAs can generally be identified as those with two “i’s.” Amides are more commonly available and tend to be utilized for orbital regional techniques, and include lidocaine, mepivicaine, bupivicaine, and ropivicaine. Allergy to ester LAs is much more common than amide LAs, due to the metabolism of ester LAs to the common allergen para-aminobenzoicacid (PABA). Amide LAs can generally be safely used in patients with a history of allergy to ester LAs. Ester LAs are primarily metabolized by pseudocholinesterase,

M.E.J. ANESTH 21 (6), 2012
779PREVENTION AND MANAGEMENT OF COMPLICATIONS OF REGIONAL ORBITAL ANESTHESIA
CNS Toxicity
At sufficient doses or after intravascular injection, LAs cause CNS stimulation. Early symptoms can include lightheadedness, metallic taste, tinnitus, and circumoral numbness. This can progress to restlessness, unconsciousness, and tonic clonic seizures. At higher doses, CNS depression occurs which can result in respiratory failure and death.
Cardiovascular Toxicity
LAs can additionally cause cardiovascular toxicity, though this generally occurs at doses higher than those causing CNS symptoms. LAs act on the myocardium, decreasing electrical excitability, conduction rate, and contractile force. On rare occasions LAs have caused cardiovascular collapse and death without preceding CNS symptoms. This may be due to either an action on the pacemaker or the sudden onset of ventricular fibrillation. Ventricular tachycardia and fibrillation are relatively uncommon consequences of local anesthetics but can occur, particularly with bupivacaine. Bupivacaine associated cardiotoxicity is very resistant to resuscitation and defibrillation. In addition to ACLS, treatment should include rapid administration of lipid emulsion.
Therefore, the choice of LA can play a large role in determining the risk of toxicity. Of the commonly used LAs, lidocaine and bupivacaine, it is clear that the latter has the greater toxic potential. Of note is that lidocaine has a relatively short duration compared to bupivacaine and accidental intraocular injections of preservative free lidocaine has not been found to cause permanent neuroretinal damage but has been seen to temporarily paralyze the pupil in mydriasis. Permanent visual damage has been attributed to the retinal injury from the needle penetration and increased intraocular pressure causes by the volume of injected LA22. Bupivacaine, by virtue of its high lipid solubility is highly potent but severe cardiotoxicity can occur with inadvertent intravascular administration23.
Like all LA toxicity, signs of bupivacaine toxicity start with central nervous system (CNS) excitation including dizziness, tremors, and nervousness followed by CNS and cardiovascular depression,
toxicity. Concentrations of ropivicaine ranging from 0.2-1% are used for regional anesthesia, and a single injection can provide up to approximately 16 hours of analgesia.
Mixtures of lidocaine with a long-acting local anesthetic such as bupivacaine or ropivacaine are commonly used for regional anesthesia techniques. This combination does achieve a quicker onset of analgesia; however, the plasma levels of the long-acting LA are lower than when using only long-acting LAs.
Additives to LAs
Vasoconstrictors such as epinephrine, typically administered for orbital regional blocks, or phenylephrine are often added to LAs to improve the duration and quality of neural blockade. Vasoconstriction slows the rate of systemic absorption, which can allow for the administration of higher doses of LAs before encountering toxicity. The addition of epinephrine to LAs can also serve as a marker of intravascular injection. If LA with epinephrine is injected intravascularly, the patient will demonstrate signs of tachycardia, hypertension, or T-wave peaking on EKG. Epinephrine may also improve the quality of neuraxial LA blockade independent of vasoconstriction through α-2 adrenergic activity.
Toxicity of LAs
The primary concern in the administration of LAs is the risk of systemic LA absorption resulting in CNS and cardiac toxicity. This can occur from inadvertent intravascular injection of LA or from systemic absorption of LA. The risk of systemic toxicity depends on the LA agent and the site of administration. For example, even a very small dose of lidocaine can rapidly cause unconsciousness and seizure if inadvertently injected into an artery. Even without intravascular injection, rates of absorption and risk of systemic toxicity vary by location of administration. Toxicity also varies with specific LA agents. The potent, lipophilic, long-acting amide agent bupivicaine presents a much higher risk of cardiotoxicity than any of the other commercially available agents.

780 VADIVELU N. et. al
brainstem anesthesia and promptly provide treatment because, left untreated, the associated cardiovascular and systemic sequalae can be life-threatening. Vigilant perioperative monitoring, with assistance from the anesthesia care team, is essential25. Although the incidence of brainstem anesthesia following RBA is only between 1:500 and 1:350, a wide range of symptoms include aphasia, apnea, bradycardia, tachycardia, cyanosis, impaired hearing, cardiac arrest, confusion, diaphoresis, dilatation of the contralateral pupil drowsiness, dysphagia, facial paralysis, gaze palsy, hypertension, loss of consciousness, nausea and vomiting, seizures and shivering. It is advisable to observe the patient for at least 15 minutes post-injection to detect and to manage these complications promptly26,27.
It is estimated that the incidence of brainstem anesthesia complicating eye block anesthesia is one in 350 to 500 patients. A variety of interventions have been utilized depending on the symptoms including reassurance, use of vasoconstrictors or vasodilators, ventilation and endotracheal intubation28.
Two possible etiologies have been postulated for the development of brainstem anesthesia. First, simian studies have revealed that reversal of blood flow from the ophthalmic artery towards the anterior cerebral artery or internal carotid artery occurs upon accidental arterial anesthetic injection into the ophthalmic artery. LA solution may then reach the brain causing the symptoms of brainstem anesthesia29,30. The second possible etiology postulated is that inadvertent injection of the anesthetic solution into the dura mater sheath of the optic nerve or intrathecally through the optic foramen reaches the cerebrospinal fluid compartment causing the symptoms of brainstem anesthesia31,32.
Since the symptoms of brainstem anesthesia often appear minutes after injection, it is thought that perforation of the meningeal sheath of the optic nerve triggers a diffusion mechanism, which is responsible for the symptoms33. This theory was verified by monitored injection of contrast material into the optic nerve dural sheath in cadavers. The material was seen to diffuse through the ophthalmic artery into the subdural space and chiasm, ultimately reaching the respiratory center34.
Brainstem anesthesia’s hemodynamic and respiratory manifestations are due to blockade of the
including hypotension, respiratory depression, and cardiac arrhythmias and/or arrest24. The toxic potential of LAs makes it essential that LA orbital blocks are administered with extreme perioperative vigilance and complications are dealt with promptly and effectively.
Strict sterile technique including antibiotic skin preparation, sterile gloves, hat, and mask should be used for all regional blocks. Monitoring patients for regional anesthesia is additionally important, as patients may require procedural sedation, and complications such as LA toxicity, nerve injury, vascular puncture and bleeding can occur. Standard monitoring should include pulse oximetry, electrocardiography, and blood pressure monitoring. Some centers use capnography to ensure adequate ventilation, but pulse oximetry and frequent verbal communication with the patient are often adequate.
Resuscitation equipment should also be available, including a self-inflating bag-valve-mask, oxygen source with face-mask, suction, intravenous access, laryngoscope, and endotracheal tubes. Resuscitation medications such as vasopressors and lipid emulsion should also be readily available.
Complications
Complications from regional anesthesia in ophthalmic surgery could be seen immediately after the administration of the LA orbital block or could take up to 40-60 minutes for symptoms to become clear. It is, therefore, recommended to observe the patient for up to an hour after a block. Complications from retrobulbar injection include trauma to adjacent structures, retrobulbar hemorrhage, oculocardiac reflex, misplaced injections, intra-arterial injections, subarachnoid injection, extraocular muscle damage, optic nerve damage, globe perforation, and brainstem anesthesia. Complications from peribulbar anesthesia include trauma to adjacent structures, peribulbar hemorrhage, central retinal artery occlusion, oculocardiac reflex, toxic injury to rectus muscles, and globe perforation.
Brainstem Anesthesia
It is imperative that the healthcare practitioner is cognizant of and able to recognize the symptoms of

M.E.J. ANESTH 21 (6), 2012
781PREVENTION AND MANAGEMENT OF COMPLICATIONS OF REGIONAL ORBITAL ANESTHESIA
Brain stem anesthesia can occur as a complication of a regional block involving any cranial nerve though most commonly it has been discussed in setting of ophthalmologic surgeries. Nique et al described a case of brain stem anesthesia in a patient who presented with dysarthria and hypertension following the administration of V2-V3 blocks in the diagnosis of trigeminal neuralgia. Rapid progression to unconsciousness and apnea followed. Endotracheal intubation with ventilatory support was needed to regain hemodynamic stability41. Endotracheal intubation and Intensive Care Unit admission was needed in other cases involving anesthetic blocks for ocular surgeries such as cataract and trabeculectomies with seizures and signs of brainstem anesthesia to prevent catastrophic outcomes42,43.
3. Examination of the fundus after administration of peribulbar or retrobulbar blocks by indirect opthalmoscope. Globe perforation is a serious complication with the potential for vision loss. It is possible for globe penetration or perforation to go undetected most commonly in cataract removal often until the completion of the procedure. For this reason and in order to decrease the morbidity of the its complication, it is recommended that immediately following the administration of peribubar or retrobulbar blocks, the fundus be checked with an indirect opthalmoscope to ensure that the retinal vessels are patent and that the sclera has not been inadvertently penetrated44. The presence of Hyptony or dark red reflex could indicate the presence of a potential ocular globe penetration45. To avoid the risk of hemorrhage from the choroidal and retinal blood vessels, and the risk of retinal detachement, it is recommended that ocular surgery be cancelled if globe penetration is suspected. Treatments of globe perforation include retinopexy of the perforation site, photocoagulation and retinal repair. If the cataract permits indirect opthalmoscopy of the penetration site, arrangements should be made for retinopexy of the perforated site1.
4. Positioning can play a large role in the prevention of complications. Correct positioning consists of the globe being in the primary or in the slightly downward and outward position, and directing the needle toward the inferior section of the orbital fissure, and not cross the mid-sagittal plane with
cranial nerves by caudal flow, specifically the vagus (X) and the glossopharyngeal (IX) in contrast to the cephalad flow of LA drugs, seen in high lumbar spinal anesthesia, thoracic sympathetic blockade (hypotension, bradycardia) and apnea due to thoracic intercostal paralysis. The parasympathic blockade of the vagus nerve leads to a period of tachycardia and hypertension that is prolonged by abolition of the regulation of the carotid sinus reflex caused by the blockade of the glossopharyngeal nerve. Severe apnea is usually the result, when blunting of diaphragmatic respiration occurs35.
There have been reports of other cranial nerves being affected, including a case of immediate contralateral amaurosis, which may be caused by optic nerve injection, or cortical stroke by ventricular emboli36. Transient bilateral hearing loss following RBA has also been seen37.
Globe Perforation
Inadvertent globe perforations by regional eye blocks has a reported incidence of 0.9 in 10,000 RBA and 1 in 16,000 PBA38. Intraglobal hemorrhage can lead to globe rupture. It must be remembered that a highly myopic eye with an axial length exceeding 26 mm is a contraindication for regional ophthalmologic anesthesia39. There is a twenty-fold increase in incidence of globe perforation in highly myopic individuals leading to an incidence to approximately 1 in 500 in these patients. Vitrectomies have had to be performed because on severe intraocular hemorrhage or retinal detachments. Less severe bleeds may be undetected in up to a third of cases40,41.
Prevention and management of complications
1. Vigilance and prompt treatment are keys to the management of the complications arising from the administration of local anesthetic regional blocks for eye surgeries. Informed consent should be obtained from all patients before the administration of LA regional orbital blocks40.
2. Ventilatory support and intensive care facilities should be immediately available especially in cases where brainstem anesthesia is suspected.

782 VADIVELU N. et. al
entirely eliminates the risks associated with both RBA and PBA. Although not possible in all kinds of ophthalmologic procedures, topical anesthesia may be employed in some ocular procedures57. However, since pain sensations may not be completely eliminated with topical anesthesia the need exists for the use of RBA or PBA58. If RBA or PBA is to be employed, ropivacaine is far less toxic than bupivacaine and substitution should be considered. Bupivacaine mediated pathophysiological processes, including cardiovascular collapse from inadvertent intravascular injection, are, in general, extremely difficult to treat.
Conclusion
As an increasing number of ophthalmologic surgeries are performed in freestanding surgical centers where full anesthesia care may not be available, it is vital for health care providers to be cognizant of the anesthetic concerns and risks and complications with the administration of regional anesthesia for ophthalmologic surgeries. The complications resulting from the administration of LAs are numerous including confusion, diaphoresis, nausea and vomiting, aphasia, apnea, bradycardia, tachycardia, cyanosis, impaired hearing, cardiac arrest, confusion, dilatation of the contralateral pupil, dysphagia, drowsiness, facial paralysis, gaze palsy, hypertension, loss of consciousness, shivering, seizures, and cardiovascular collapse.
Loss of vision and even death can occur if complications are not promptly recognized and treated. The proximity of the eye to vital structures makes the administration of regional anesthesia for ocular surgery particularly risky. Hence, every attempt must be made to prevent the life-threatening and devastating consequences of the complications of LA blocks. Health care providers should be familiar with the types of anesthesia available, the inherent toxicities of the LAs being used, positioning of the eye, the type of needles, site of injection and techniques of injection. Recognition of complications should be quick and with immediate treatment of complications as appropriate. Facilities for advanced surgical procedures, ventilatory support, and intensive care should be immediately available.
the needle. This adjustment has the disadvantage of increasing the risk of incomplete nerve blockage46.
5. Modification of techniques to decrease complications have been developed to improve the effectiveness of the block and to decrease the incidence of accidental punctures. The first such technique, developed by Gills and Lloyd, is to apply a lidocaine post anesthetic injection to reduce site burning, and then to apply pressure for 60 minutes. Another method is to place an additional injection into the subcutaneous space as the first injection is being withdrawn to increase the flow of LAs towards the lateral canthus, thereby increasing the paralysis of the orbicularis oculi muscles47.
6. It is also thought that the use of the appropriate needle type may reduce adverse events. It is recommended that needles used should be less than 35 mm long. The use of blunted needles is also encouraged after making a skin wheal with the local anesthetic at the site of injection. Though blunted needles can cause more injection site pain, they may also be associated with less inadvertent perforations48.
7. The site of injection also plays an important role. Currently PBA is often the preferred alternative to RBA as it is considered theoretically safer than RBA. The needle only advances until it is parallel to the floor or roof of the orbit and does not enter inside the muscle cone. This results in an even distribution of anesthesia between the lower and the upper peribulbar spaces49. It is seen that PBA achieves better lid akinesia though it has a greater chance of having incomplete ocular akinesia due to uncertain local anesthetic flow compared to RBA. Other disadvantages of the PBA also exist. Some studies have shown that the risk of globe perforation remains unaltered50 and PBA has also been linked to an increased risk of neurogenic pulmonary edema51. Different mechanisms exist for the development of acute neurogenic pulmonary edema and subsequent respiratory distress after peribulbar block52,53,54. Acute neurogenic pulmonary edema occurs primarily due to changes in Starling’s forces, acute rise in hydrostatic pressures55 and alteration in the permeability between the alveolar-capillary interfaces56.
8. Lastly, the type of anesthesia plays an important role. It is recommended to consider topical or general anesthesia in high risk cases. This almost

M.E.J. ANESTH 21 (6), 2012
783PREVENTION AND MANAGEMENT OF COMPLICATIONS OF REGIONAL ORBITAL ANESTHESIA
25. MCGOLDRICK K: Complications of regional anesthesia for ophthalmic surgery. Yale J� Biol� Med; 1993, 66(5):443-5.
26. HAMILTON R: Brain-stem anesthesia as a complication of regional anesthesia for ophthalmic surgery. Can� J� Ophthalmol; 1992, 27(7):323-5.
27. DAHLE J, ISERSON K: ED treatment of brainstem anesthesia after retrobulbar block. Am� J� Emerg� Med; 2007, 25(1):105-6.
28. HAMILTON R, GIMbEL H, ET AL: Regional anaesthesia for 12,000 cataract extraction and intraocular lens implantation procedures. Can� J� Anaesth; 1988, 35(6):615-23.
29. ALDRETE J, NARANG R, ET AL: Reverse carotid blood flow--a possible explanation for some reactions to local anesthetics. J� Am� Dent� Assoc; 1977, 94(6):1142-5.
30. ALDRETE J, ROMO-SALAS F, ET AL: Reverse arterial blood flow as a pathway for central nervous system toxic responses following injection of local anesthetics. Anesth� Analg; 1978, 57(4):428-33.
31. DRYSDALE D: Experimental subdural retrobulbar injection of anesthetic. Ann Ophthalmol; 1984, 16(8):716-8.
32. JAvITT J, ADDIEGO R, ET AL: Brain stem anesthesia after retrobulbar block. Ophthalmology; 1987, (6):718-24.
33. CHANG J, GONZALEZ-AbOLA E, ET AL: Brain stem anesthesia following retrobulbar block. Anesthesiology; 1984, 61(6):789-90.
34. DRYSDALE D: Experimental subdural retrobulbar injection of anesthetic. Ann Ophthalmol; 1984, 16(8):716-8.
35. HAMILTON R: Brain stem anesthesia following retrobulbar blockade. Anesthesiology; 1985, 63(6):688-90.
36. BISHARA S, ESTRIN I, ET AL: Immediate contralateral amaurosis after retrobulbar anesthesia. Ann� Ophthalmol; 1990, 22(2):63-5.
37. GEORGE R, HACKETT J: Bilateral hearing loss following a retrobulbar block. Can� J� Anaesth; 2005, 52(10):1054-7.
38. EKE T, THOMPSON J: National Survey of Local Anaesthesia for Ocular Surgery in the United Kingdom. Ophthalmology; 2000, 107(5):817.
39. DUKER J, BELMONT J, ET AL: Inadvertent globe perforation during retrobulbar and peribulbar anesthesia. Patient characteristics, surgical management, and visual outcome. Ophthalmology; 1991, 98(4):519-26.
40. SCHRADER W, SCHARGUS M, ET AL: Risks and sequelae of scleral perforation during peribulbar or retrobulbar anesthesia. J� Cataract Refract; Surg. 2010, 36(6):885-9.
41. NIQUE T, BENNETT C: Inadvertent brainstem anesthesia following extraoral trigeminal V2-V3 blocks. Oral Surg� Oral Med� Oral Pathol; 1981, 51(5):468-70.
42. AGUIRRE J, VITTA-VELIS G, ET AL: Essentials of Regional Anesthesia Ch. 5, Springer, New York 2012.
43. Dahle J, Iserson K: ED treatment of brainstem anesthesia after retrobulbar block. Am� J� Emerg� Med; 2007, 25(1):105-6.
44. FEIbEL R: Ocular penetration by anesthetic injection. Ophthalmology; 1992, 99(3):301.
45. RINKOFF J, DOFT B, ET AL: Management of ocular penetration from injection of local anesthesia preceding cataract surgery. Arch� Ophthalmol; 1991, 109(10):1421-5.
46. GRIZZARD W, PAUTLER SE: Complications from retrobulbar injection. Poster 87, Annual Meeting, American Academy of Ophthalmology, 1984.
47. GILLS J, LOYD T: A technique of retrobulbar block with paralysis of orbicularis oculi. Am� In� Ocular Implant Sot� J; 1983, 9:339-340.
48. PAUTLER S, GRIZZARD W, ET AL: Blindness from retrobulbar injection
References
1. MATbERS W: Letter to the editor. Ann� Ophthalmo1; 1987, 19:91.2. NICOLL J, ACHARYA P, ET AL: Central nervous system complications
after 6000 retrobulbar blocks. Anesth� Analg; 1987, 66:1298-302.3. WITTPPENN J, RAPOZA P, ET AL: Respiratory arrest following
retrobulbar anesthesia. Ophthalmology;. 1986, 93:867-70.4. RODMAN D, NOTARO S, ET AL: Respiratory depression following
retrobulbar bupivacaine: Three case reports and literature review. Ophthal; 1987, Surg. 18:768-771.
5. RHOTON A: The orbit. Neurosurgery; 2002 Oct, 51(4 Suppl):S303-34.6. DAHLE J, ISERSON K: ED treatment of brainstem anesthesia after
retrobulbar block. The American Journal of Emergency Medicine; 2007, 25(1):105-106.
7. AvIv R, CASSELMAN J: Orbital imaging: Part 1. Normal anatomy. Clin Radiol; 2005 Mar, 60(3):279-87.
8. NOUvELLON E, CUvILLON P, ET AL: Regional anesthesia and eye surgery. Anesthesiology; 2010, 113(5):1236-42.
9. HAMILTON R: Brain-stem anesthesia as a complication of regional anesthesia for ophthalmic surgery. Can� J� Ophthalmol; 1992, 27(7):323-5.
10. WONG D: Regional anaesthesia for intraocular surgery. Can� J� Anaesth; 1993, 40(7):635-57.
11. ATKINSON W: Retrobulbar injection of anesthetic within the muscular cone (cone injection). Arch� Ophthalmol; 1936, 16:494-50318.
12. UNSOLD R, STANLEY J, ET AL: The CT-topography of retro-bulbar anesthesia; anatomic-clinical correlation of complications and suggestion of a modified technique. Albrecht von Graefes Arch. Klin� Ophthalmol; 1981, 217:125-136.
13. FEIbEL R: Current concepts in retrobulbar anesthesia. Surv� Ophthalmol; 1985, 30(2):102-10.
14. GRIZZARD W, KIRK N, ET AL: Perforating ocular injuries caused by anesthesia personnel. Ophthalmology; 1991, 98(7):1011-6.
15. SCHRADER W, SCHARGUS M, ET AL: Risks and sequelae of scleral perforation during peribulbar or retrobulbar anesthesia. J� Cataract Refract; 2010, Surg. 36(6):885-9.
16. DONLON J, DOYLE D, ET AL: Anesthesia for eye, ear, nose, and throat surgery, Miller’s Anesthesia, pp. 2527-31, Elsevier Churchill Livingstone, Philadelphia 2005.
17. FEIbEL R: Current concepts in retrobulbar anesthesia. Surv� Ophthalmol; 1985, 30(2):102-10.
18. CHIN G, ALMQUIST H: Bupivacaine and lidocaine retrobulbar anesthesia. A double-blind clinical study. Ophthalmology; 1983, 90(4):369-72.
19. HAMILTON R: Retrobulbar block revisited and revised. J� Cataract Refract� Surg; 1996, 22(9):1147-50.
20. RIPART J, LEFRANT J, et al: Peribulbar versus retrobulbar anesthesia for ophthalmic surgery: an anatomical comparison of extraconal and intraconal injections. Anesthesiology; 2001, 94(1):56-62.
21. DAvIS D, ANDMANDEL M: Efficacy and complication rate of 16, 224 consecutive peribulbar blocks. A prospective multicenter study. J� Cataract Refract; 1994, Surg. 20(3):327-37. Erratum in: J� Cataract Refract; 1994, Surg. 20(6):673.
22. LINCOFF H, ZWEIFACH P, ET AL: Intraocular injection of lidocaine. Ophthalmology; 1985, 92(11):1587-91.
23. DE LA COUSSAYE J, ELEDJAM J, ET AL: Cardiotoxicity of local anesthetics. Cah� Anesthesiol; 1993, 41(6):589-98.
24. ALbRIGHT G: Cardiac arrest following regional anesthesia with etidocaine or bupivacaine. Anesthesiology; 1979, 51(4):285-7.

784 VADIVELU N. et. al
54. GOMEZ R, ANDRADE L, ET AL: Costa JRR. Brainstem anaesthesia after peribulbar anaesthesia. Can� J� Anaesth; 1997, 44:732-734.
55. MALIK B: Mechanisms of neurogenic pulmonary edema. Circ� Res; 1985, 57(1):1-18.
56. COLICE G, MATTHAY M, ET AL: Neurogenic pulmonary edema. Am� Rev� Respir� Dis; 1984, 130(5):941-8.
57. YEPEZ, J, DE YEPEZ, J, ET AL: Topical anesthesia for phacoemulsification, intraocular lens implantation, and posterior vitrectomy. J� Cataract Refract� Surg; 1999, 25:1161-1164.
58. FRIEDMAN D, BASS E, ET AL: Synthesis of the literature on the effectiveness of regional anesthesia for cataract surgery. Ophthalmology; 2001, 108(3):519-29.
into the optic nerve. Ophthalmic Surg; 1986, 17(6):334-7.49. DAvIS D, MANDEL M: Posterior peribulbar anesthesia: an alternative
to retrobulbar anesthesia. J� Cataract Refract� Surg; 1986, 12:182-4.50. BLOOMbERG L: Anterior periocular anesthesia: five years experience.
J� Cataract Refract� Surg; 1991, 17:508-511.51. SCHRADER W, SCHARGUS M, ET AL: Risks and sequelae of scleral
perforation during peribulbar or retrobulbar anesthesia. J� Cataract Refract; 2010, Surg. 36(6):885-9.
52. ASHAYE A, UbAH J, ET AL: Respiratory arrest after retrobulbar anaesthesia. West Afr� J� Med� 2002, 21:343-344.
53. BORET H, PETIT D, ET AL: Brainstem anesthesia after peribulbar anesthesia. Ann� Fr� Anesth� Reanim; 2002, 21:725-727.

785 M.E.J. ANESTH 21 (6), 2012
AIDS FOR FACILITATION OF DIFFICULT TRACHEAL INTUBATION REVIEW AND RECENT ADVANCES
MUSA MUALLEM*, ANIS bARAKA**
Abstract
Management of difficult tracheal intubation has been facilitated by different techniques which include the use of stylets, introducers, intubating laryngeal mask airway, as well as by the development of special laryngoscope blades and fiberoptic laryngoscopes.
The most recent advances for facilitation of difficult tracheal intubation is the introduction of the video-assisted laryngoscopes
The management of difficult tracheal intubation by video-assisted laryngoscopy can be further facilitated by using suspension laryngoscopy which frees the hands of the anesthesiologist to handle the insertion of the endotracheal tube with the aid of an endotracheal tube introducer, and a curved pipe stylet, under an umbrella of pharyngeal oxygen insufflation
Background
With the introduction of muscle relaxants by Harold Griffith in the forties, failure to ventilate and/or intubate became a major concern and a nightmare to anesthesiologists because of the serious morbidity and mortality that may follow. The usual scenario of a difficult airway resulting in morbidity or even death is difficult mask ventilation, and repeated trials at laryngoscopy by one or more individuals, resulting in pharyngeal trauma and edema. Ventilation becomes more and more difficult, complicated with hypoxemia, brain damage, and cardiac arrest1,2.
Causes of difficult airway
The causes of difficult airway and difficult tracheal intubation can be due to the:
1. Anesthesiologist being inadequately trained,
2. Short of equipment, or
3. due to the patient’s anatomic condition.
The following patient’s conditions have been found to contribute to difficult airway and difficult tracheal intubation
* MD, DA. Emeritus Professor.** MD, FRCA (Hon.) Emeritus Professor. Corresponding Author: Musa Muallem MD, Anesthesiology Department, American University of Beirut Medical Center,
Beirut, Lebanon. E-mail: [email protected]
786 MUALLEM M. et. al
= 1. History of difficult airway= 2. Obesity = 3. Pregnancy= 4. Short neck = 5. Receding Jaw= 6. Short thyromental distance less than 4 cm3
= 7. Tumors, polyps, of larynx and pharynx= 8. Trauma or burn to face and neck= 9. Cervical Spine Injury= 10. Carious front teeth, or expensive dental
appliances = 11. Short atlanto-occipital distance and angle= 12. Restricted neck movement= 13. Class III&IV Mallampatti on pharyngeal
examination4
= 14. Grade III, IV Cormack airway during laryngoscopy5
Evaluation and prediction of difficult airway
A difficult airway can usually be predicted during the preoperative anesthesia visit by history and physical examination of the patient considering the above mentioned contributing factors,
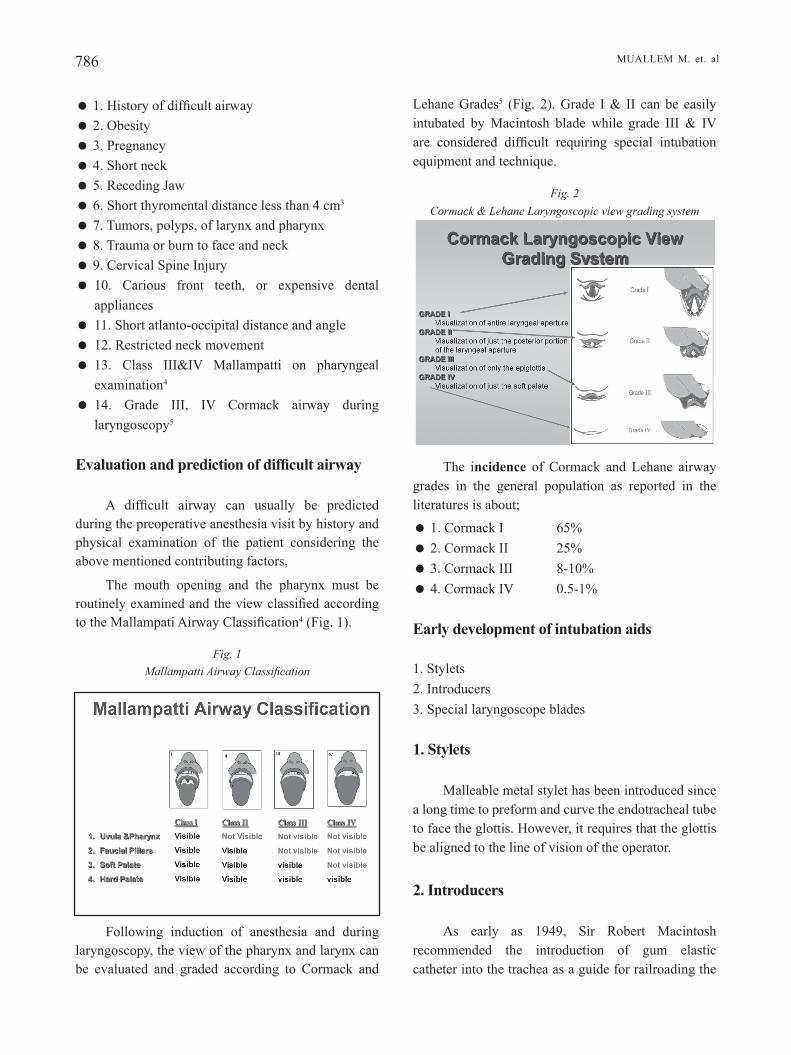
The mouth opening and the pharynx must be routinely examined and the view classified according to the Mallampati Airway Classification4 (Fig. 1).
Fig� 1 Mallampatti Airway Classification
Following induction of anesthesia and during laryngoscopy, the view of the pharynx and larynx can be evaluated and graded according to Cormack and
Lehane Grades5 (Fig. 2). Grade I & II can be easily intubated by Macintosh blade while grade III & IV are considered difficult requiring special intubation equipment and technique.
Fig� 2 Cormack & Lehane Laryngoscopic view grading system
The incidence of Cormack and Lehane airway grades in the general population as reported in the literatures is about;
= 1. Cormack I 65%= 2. Cormack II 25%= 3. Cormack III 8-10%= 4. Cormack IV 0.5-1%
Early development of intubation aids
1. Stylets2. Introducers3. Special laryngoscope blades
1. Stylets
Malleable metal stylet has been introduced since a long time to preform and curve the endotracheal tube to face the glottis. However, it requires that the glottis be aligned to the line of vision of the operator.
2. Introducers
As early as 1949, Sir Robert Macintosh recommended the introduction of gum elastic catheter into the trachea as a guide for railroading the

M.E.J. ANESTH 21 (6), 2012
787AIDS FOR FACILITATION OF DIFFICULT TRACHEAL INTUBATION REVIEW AND RECENT ADVANCES
endotracheal tube over it6. Not until the 1980, with the introduction into the market of the multiple-use Eichmann Gum Elastic Bougie and later several other single-use introducers with a curved tip, that the use of introducers and the technique of railroading the endo-tracheal tube over it became popular as an aid for difficult intubation7,8,9.
The disadvantage of the Eichmann Gum Elastic Bougie and many other similar introducers was that they all have a hard rigid tip that could injure the tracheal wall and produce pneumothorax or mediastinal emphysema10.
This prompted the author of this review to develop a home-made prototype introducer with a soft curved rounded tip and semi rigid body that could be safely introduced into the trachea11. Based on this prototype, the VBM Medizintechnik GmbH Company manufactured and put on the market in 2004 a new introducer, the Muallem endotracheal tube introducer (METTI) with the above mentioned characteristics12 (Fig. 3).
Fig� 3 METTI Introduce
3. Special laryngoscope blades
Several laryngoscope blades for improving the glottic view have been developed. The McCoy blade is worth mentioning. However, all these blades require the operator to see directly the epiglottis and glottis.
Still we had about 8% of the cases when we cannot see directly the glottis, and an instrument that allows us to see around the corner is required.
Development of the fiberscope
1. Rigid Fiberscopes (the Bullard),
These scopes will allow visualization of the glottis around a curve through an eyepiece that can be fitted with a camera and screen
The Bullard scope is one example that gives a good view of the glottis. It is recommended in tight jaw opening where other thicker blades could not be introduced. Intubation with this scope may be difficult in spite of the good view. This scope had to be modified by the authors by adding a side channel and using an introducer as a guide to successful intubation13,14,15 (Fig. 4).
Fig� 4 Bullard scope as modified with the side channel
and the METTI
Introducer
2. Semi rigid fiberscope -The Bonfil
The Bonfils acts as a stylet with vision at its tip. It has been recommended as the first line of management of a difficult airway. It has similar drawbacks as the flexible fiberscope as will be mentioned below.
3. Flexible fiberscope
The flexible fiberscope for the past decade has been considered as the gold standard of difficult airway management. It serves like an introducer with vision at its tip. It can be curved to follow the mouth and pharyngeal and laryngeal curves into the trachea. When it is introduced into the trachea, the endotracheal tube is railroaded over it. However, the railroading is blind and the tube can be stuck along its way at the arytenoids or the vocal cords. Other drawbacks are, a narrow field of vision, and its tip can fog frequently or get covered by secretions or blood. Training in its use has a long learning curve, and it is quite expensive to purchase and maintain.
788 MUALLEM M. et. al
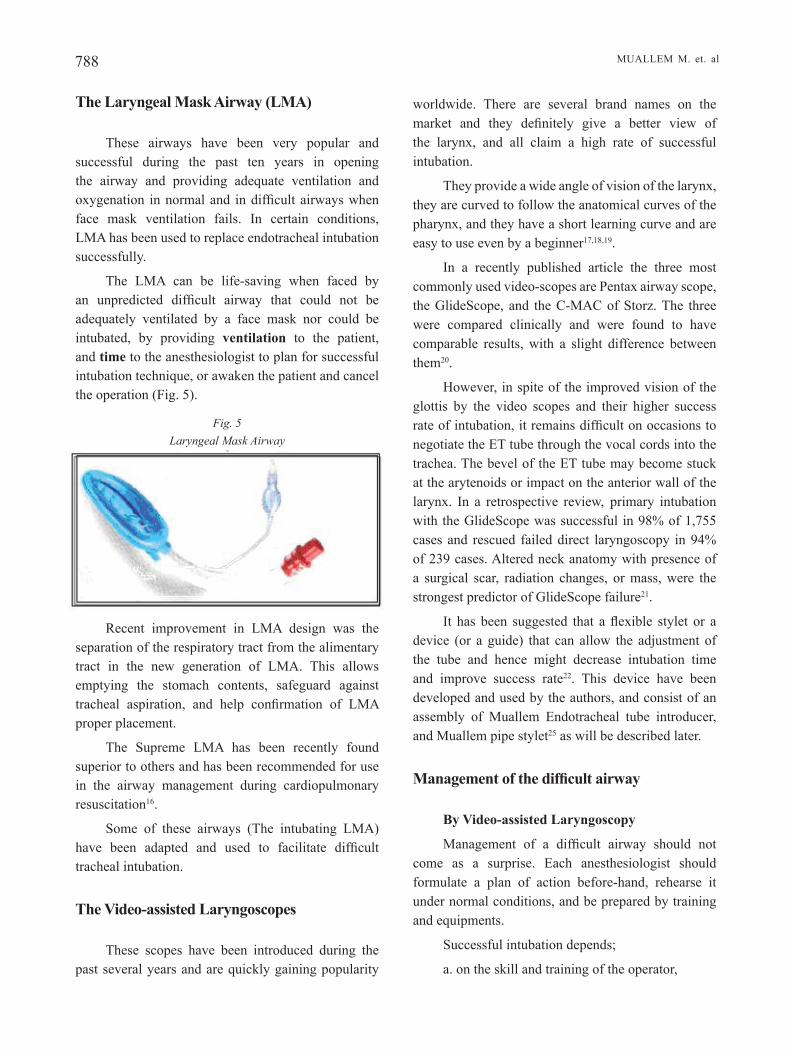
The Laryngeal Mask Airway (LMA)
These airways have been very popular and successful during the past ten years in opening the airway and providing adequate ventilation and oxygenation in normal and in difficult airways when face mask ventilation fails. In certain conditions, LMA has been used to replace endotracheal intubation successfully.
The LMA can be life-saving when faced by an unpredicted difficult airway that could not be adequately ventilated by a face mask nor could be intubated, by providing ventilation to the patient, and time to the anesthesiologist to plan for successful intubation technique, or awaken the patient and cancel the operation (Fig. 5).
Fig� 5 Laryngeal Mask Airway
Recent improvement in LMA design was the separation of the respiratory tract from the alimentary tract in the new generation of LMA. This allows emptying the stomach contents, safeguard against tracheal aspiration, and help confirmation of LMA proper placement.
The Supreme LMA has been recently found superior to others and has been recommended for use in the airway management during cardiopulmonary resuscitation16.
Some of these airways (The intubating LMA) have been adapted and used to facilitate difficult tracheal intubation.
The Video-assisted Laryngoscopes
These scopes have been introduced during the past several years and are quickly gaining popularity
worldwide. There are several brand names on the market and they definitely give a better view of the larynx, and all claim a high rate of successful intubation.
They provide a wide angle of vision of the larynx, they are curved to follow the anatomical curves of the pharynx, and they have a short learning curve and are easy to use even by a beginner17,18,19.
In a recently published article the three most commonly used video-scopes are Pentax airway scope, the GlideScope, and the C-MAC of Storz. The three were compared clinically and were found to have comparable results, with a slight difference between them20.
However, in spite of the improved vision of the glottis by the video scopes and their higher success rate of intubation, it remains difficult on occasions to negotiate the ET tube through the vocal cords into the trachea. The bevel of the ET tube may become stuck at the arytenoids or impact on the anterior wall of the larynx. In a retrospective review, primary intubation with the GlideScope was successful in 98% of 1,755 cases and rescued failed direct laryngoscopy in 94% of 239 cases. Altered neck anatomy with presence of a surgical scar, radiation changes, or mass, were the strongest predictor of GlideScope failure21.
It has been suggested that a flexible stylet or a device (or a guide) that can allow the adjustment of the tube and hence might decrease intubation time and improve success rate22. This device have been developed and used by the authors, and consist of an assembly of Muallem Endotracheal tube introducer, and Muallem pipe stylet25 as will be described later.
Management of the difficult airway
By Video-assisted Laryngoscopy
Management of a difficult airway should not come as a surprise. Each anesthesiologist should formulate a plan of action before-hand, rehearse it under normal conditions, and be prepared by training and equipments.
Successful intubation depends;
a. on the skill and training of the operator,

M.E.J. ANESTH 21 (6), 2012
789AIDS FOR FACILITATION OF DIFFICULT TRACHEAL INTUBATION REVIEW AND RECENT ADVANCES
b. on the equipment and intubation aids available
c. on the patient’s airway and type of the anatomical difficulty present.
Faced with difficult tracheal intubation, we should avoid repeated trials, and aim for maintaining adequate ventilation and oxygenation, keeping the patient alive until a proper plan of action is developed.
During the past fifteen years different guidelines and algorithms have been developed and recommended by the ASA and other societies for the difficult airway management. These guidelines have been very useful and have reduced the incidence of complications since their introduction23,24.
Following the introduction of the video-assisted laryngoscopes many of the steps of the guidelines could be omitted, and if the proper equipment is available, we can go directly to the most recently recommended technique.
In spite of the advance in vedeoscope, we still find some airways difficult to intubate. Providing a good view of the glottis with the video-scope does not always correlate with successful tracheal intubation.
Muallem and Baraka have added to the video-scope the use of an assembly of an introducer (METTI-VBM) and a curved pipe stylet Muallem pipe stylet (MPS-VBM) to facilitate tracheal intubation using the GlideScope. After visualization of the glottis, the ET tube introducer (METTI) is inserted into the trachea by the help of the pipe stylet (MPS), and the ET tube is railroaded over the introducer into the trachea, Their technique could be used for oral or nasal difficult tracheal intubation25,26 (Fig. 6).
Fig� 6 An assembly of ET Tube, M Pipe stylet,
and METTI Introducer
The assembly of (METTI) introducer and (MPS) pipe stylet (or J tube) makes one device where each component can be maneuvered independently. The
pipe stylet or J tube is used to curve the introducer and the ET tube, and METTI to guide the tube into the trachea (Fig. 7). The tip of the introducer can be rotated for 360 degree circle by rotating the body of the introducer inside the pipe stylet.
Fig� 7 An assembly of Muallem pipe stylet (J tube) and introducer
METTI
The GlideScope have been used in combination with the flexible fiberscope instead of the assembly described above, where the fiberscope was used as a flexible introducer (an expensive alternative) over which the endotracheal tube was railroaded successfully into the trachea.
Intubation of the difficult airway should always be done under an umbrella of pharyngeal oxygen insufflation. These patients desaturate quickly after induction of anesthesia and the production of apnea. Baraka and al. have shown in obese patients that pharyngeal oxygen insufflation can maintain apneic oxygenation and prolong apneic time, and safe intubation time27. Intubation becomes unhurried atraumatic and safe procedure.
Pharyngeal oxygen insufflation following mask preoxygenation can be simply produced by naso- pharyngeal oxygen catheter or by the curved disposable dental evacuator hooked to the angle of the mouth and used as an oral oxygen insufflator (Fig. 8).
Fig 8 Nasal oxygen catheter and oral oxygen insufflator
During the railroading of the endotracheal tube over the introducer (METTI), the tube may get stuck
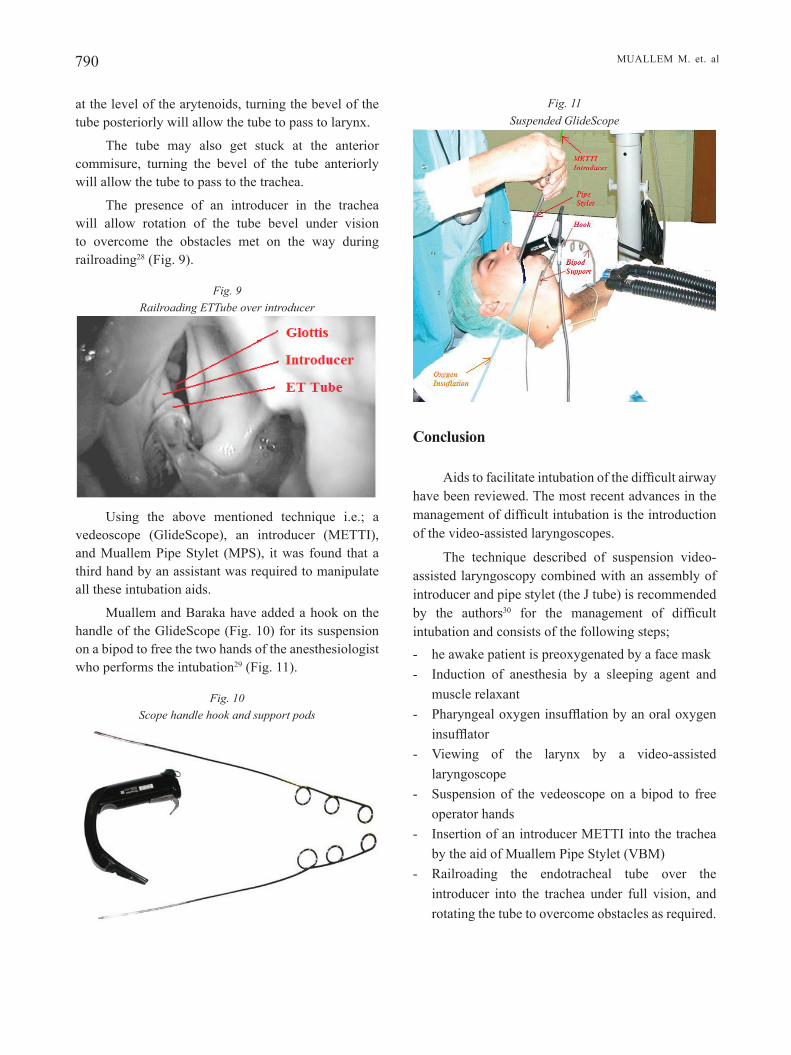
790 MUALLEM M. et. al
at the level of the arytenoids, turning the bevel of the tube posteriorly will allow the tube to pass to larynx.
The tube may also get stuck at the anterior commisure, turning the bevel of the tube anteriorly will allow the tube to pass to the trachea.
The presence of an introducer in the trachea will allow rotation of the tube bevel under vision to overcome the obstacles met on the way during railroading28 (Fig. 9).
Fig� 9 Railroading ETTube over introducer
Using the above mentioned technique i.e.; a vedeoscope (GlideScope), an introducer (METTI), and Muallem Pipe Stylet (MPS), it was found that a third hand by an assistant was required to manipulate all these intubation aids.
Muallem and Baraka have added a hook on the handle of the GlideScope (Fig. 10) for its suspension on a bipod to free the two hands of the anesthesiologist who performs the intubation29 (Fig. 11).
Fig� 10 Scope handle hook and support pods
Fig� 11 Suspended GlideScope
Conclusion
Aids to facilitate intubation of the difficult airway have been reviewed. The most recent advances in the management of difficult intubation is the introduction of the video-assisted laryngoscopes.
The technique described of suspension video-assisted laryngoscopy combined with an assembly of introducer and pipe stylet (the J tube) is recommended by the authors30 for the management of difficult intubation and consists of the following steps;- he awake patient is preoxygenated by a face mask- Induction of anesthesia by a sleeping agent and
muscle relaxant- Pharyngeal oxygen insufflation by an oral oxygen
insufflator- Viewing of the larynx by a video-assisted
laryngoscope- Suspension of the vedeoscope on a bipod to free
operator hands- Insertion of an introducer METTI into the trachea
by the aid of Muallem Pipe Stylet (VBM)- Railroading the endotracheal tube over the
introducer into the trachea under full vision, and rotating the tube to overcome obstacles as required.

M.E.J. ANESTH 21 (6), 2012
791AIDS FOR FACILITATION OF DIFFICULT TRACHEAL INTUBATION REVIEW AND RECENT ADVANCES
References
1. GENE N, PETERSON, MD., PHD, ET AL: Management of the Difficult Airway. A Closed Claims Analysis. Anesthesiology; 2005, 103:33-9.
2. DOMINIC BELL: Avoiding adverse outcomes when faced with ‘difficulty with ventilation. Anesthesia; 2003, 58, pp. 945-950.
3. AYOUb C, BARAKA A, EL-KHATIb M, MUALLEM M, KAWKAbANI N, SOUEIDE A: A new Cut-off point of thyromental distance for prediction of difficult airway. Middle East Journal of Anesthesiology; 2000, vol. 15, (6):619-633.
4. MALLAMPATI SR, GATT SP, GUGINO LD, DESAI SP, WARAKSA B, FREIbERGER D, LIU PL: A clinical sign to predict difficult tracheal intubation: A prospective study. Can Anesth Soc Journal; 1985, 32:429-34.
5. CORMACK RS, LEHANE J: Difficult tracheal intubation in obstetric. Anaesthesia; 1984, 39:1105-1115.
6. SIR RObERT MACINTOSH: An Aid for oral Intubation. British Medical Journal; 1949, 1:28.
7. NOLAN JP, WILSON ME: An evaluation of the gum elastic bougie. Anaesthesia; 1992, vol. 47, pp. 878-88.
8. HAMES KC, ET AL: Use of the boujie in simulated difficult intubation. I. Comparison of single-use bougie with the fiberscope. Anaesthesia; 2003, 58, pp. 845-851.
9. MARFIN AG, ET AL: Use of the boujie in simulated difficult intubation. II. Comparison of the single-use boujie with multiple use bougie. Anaesthesia; 2003, 58, pp. 852-855.
10. BARAKA AS: Tension Pneumothorax complicating jet ventilation via a Cook Airway exchange catheter. Anesthesiology; 1999, 91:557-558.
11. MUALLEM M: Endotracheal tube introducer, An aid for the difficult airway. Middle East Journal of Anesthesiology; 2000, vol. 15 (6):687-692.
12. MUSA K. MUALLEM, MIREILLE S. AZAR, FREDERIC J. GERGES, VIvIANE NASR, ANIS BARAKA: Muallem Endo-Tracheal Tube Introducer (METTI)-An Aid for the Difficult Airway-.Middle East Journal of Anesthesiology; 2005, 18:(2)385-390.
13. BARAKA A, MUALLEM M, SIbAI A, LOUIS F: Bullard laryngoscopy for tracheal intubation of patients with cervical spine pathology. Can� J� Anesth; 1992, 39(5)513-522.
14. BARAKA A, MUALLEM M: Bullard laryngoscopy for tracheal intubation n a neonate with Pierre-Robin syndrome. Paediatric Anaesthesia; 1994, 4:111-113.
15. BARAKA A, MUALLEM M, SIbAI A: Facilitation of difficult tracheal intubation by the Fiberoptic Bullard Laryngoscope. Middle East Journal of Anesthesiology; 1991, 11(1)73-77.
16. HANAKO KOHAMA, ET AL: Comparison of supreme and soft seal
LMA for management during cardiopulmonary resuscitation in novice: a manikin study; Journal of Anesthesia, Japanese society of Anesthesiologists Dec. 2010.
17. COOPER RM: Early experience with a new video laryngoscope. Can J Anesth; 2005, 52:191-198.
18. DOYLE DJ. ZURA, RAMACHANDRAN M: Video-laryngoscopy in the management of the difficult airway, Can J Anesth; 2004, 51:95.
19. PANDIAN A, RAvAL M, BAILEY CR: A nonairway management use of the Video Laryngoscope (GlideScope). EJA; 2008, 25:511.
20. TEOH WHL, et al: Comparison of three video-laryngoscopes: Pentax Airway Scope, C-MAC™, GlideScope® vs. the Macintosh laryngoscope for tracheal intubation. Anaesthesia; Nov. 2010; volume 65, Issue 11, pp. 1126-1132.
21. MICHAEL F. AZIZ, MD, ET AL: Routine Clinical Practice Effectiveness of the GlideScope in Difficult Airway Management. Anesthesiology; January 2011, vol. 114, no 1, pp. 34-41.
22. RAI MR, DERING A, VERGHESE C: The GlideScope system: A clinical assessment of performance. Anaesthesia; 2005, 60:60-64.
23. American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway. An updated report. Anesthesiology; 2003, 98-5, pp. 1269-1277.
24. HENDERSON, et al: Difficult Airway Society guidelines For management of the unanticipated difficult intubation. Anaesthesia; 2004, 59, pp. 675-692.
25. MUALLEM M, BARAKA A: Tracheal intubation using the GlideScope with a combined curved pipe stylet and endotracheal tube introducer. Can� J� Anesth; 2007, 54(1)77-78.
26. MUALLEM M, BARAKA A: The use of the GlideScope to facilitate naso-tracheal intubation in patients with a difficult airway. European Journal of Anesthesiology; 2009, vol. 26, no. 2.
27. BARAKA A, et al: Supplementation of pre-oxygenation in morbidly obese patients using nasopharyngeal oxygen insufflation. Anesthesia; 2007, 62:769-773.
28. BARAKA A, ET AL: Posterior-beveled vs. lateral- beveled tracheal tube for fiberoptic intubation. Can� J� Anesth; Oct. 2002, 49(8)889-890.
29. MUALLEM M, BARAKA A: Suspension laryngoscopy using the GlideScope. Middle East Journal of Anesthesiology; 2009, 20(1)127-128.
30. MUALLEM MUSA, BARAKA ANIS: A novel technique for oral and nasal tracheal intubation using the video assisted laryngoscope (the GlideScope) in patients with difficult and normal airway. Middle East Journal of Anesthesiology; 2010, 20(5), pp. 763-764.


793 M.E.J. ANESTH 21 (6), 2012
LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIVE ANESTHETIC CONSIDERATIONS
ALAN D. KAYE*, TYLER b. STOUT**, IRA W. PADNOS***, bRIAN G. SCHWARTZ****, AMIR R. bALUCH*****,
CHARLES J. FOX******, HENRY LIU*******
Abstract
Congenital heart disease (CHD) affects roughly 8/1000 live births. Improvements in medical and surgical management in recent decades have resulted in significantly more children with left-to-right cardiac shunts surviving into adulthood. Surgical care of these patients for their original cardiac defect(s) or other non-cardiac medical conditions requires thorough understanding of cardiopulmonary changes and mastery of treatment options. Commonly encountered CHD with left-to-right shunt include atrial septal defect (ASD), ventricular septal defect (VSD), endocardial cushion defect (ECD) and patent ductus arteriosus (PDA). The key pathological change is increased pulmonary vascular resistance (PVR) and pressure secondary to increased blood flow from the left-to-right shunt. Increasing PVR and pulmonary arterial hypertension (PAH) will lead to reversed direction of blood flow through the cardiac defect (Eisenmenger Syndrome) and heart failure. Cardiac defects with left-to-right shunt generally require surgical or trans-catheter repair at an early age. We review the current concepts and general principles of perioperative anesthetic management of CHD, including neuraxial anesthesia. Current techniques and unique pharmacodynamic and pharmacokinetic effects of some commonly used anesthetic agents in patients with left-to-right shunt are also reviewed.
Introduction
Congenital heart disease (CHD) affects about 8/1000 live birth1,2. Both genetic and environmental factors play important roles in the pathogenesis of CHD. However, those identifiable environmental risk factors can only be identified in 10% of clinical patients2. The number of infants born with CHD has increased significantly over the past fifty years, largely due to advancement in medical imaging technology which allows for the detection of a greater number of cardiac abnormalities2,3. With the advancement in medical and surgical management of those patients
* M.D, PhD, Professor and Chairman, Department of Anesthesiology, Louisiana State University Health Sciences Center, New Orleans, LA.
** M.D, Resident, Department of Anesthesiology, University of Alabama, Birmingham, AL.*** M.D, Director of Cardiac Anesthesia, Department of Anesthesiology, Louisiana State University Health Science Center,
New Orleans, LA.**** M.D, Department of Cardiology, Baylor Healthcare Systems, Dallas, TX.***** M.D, Attending Staff, Metropolitan Anesthesia Consultants, Dallas, TX.****** M.D, Vice Chairman, Department of Anesthesiology, Tulane University Medical Center, New Orleans, LA.******* M.D, Director of Cardiac Anesthesia, Department of Anesthesiology, Tulane University Medical Center, New Orleans,
LA. Corresponding Author: Alan D. Kaye, MD, Ph.D., DABA, DABPM, Professor and Chairman. Department of
Anesthesiology, Louisiana State University School of Medicine 1542 Tulane Ave, Room 656, New Orleans, LA 70112, Tel: (504) 568-2319; Fax: (504) 568-2317. E-mail: [email protected]

794 KAYE A. D. et. al
with CHD, many of them now survive into adulthood. Currently, it is estimated that there are nearly one-million adult CHD patients in the USA alone, which outnumbers children with CHD4. These patients will need surgical interventions in their adult life either for their original cardiac abnormalities or other non-cardiac co-existing medical conditions. A thorough understanding of the anatomy, pathophysiology, clinical presentation, preoperative evaluation, and management of those patients with left-to-right (systemic to pulmonary) cardiac shunt is essential for the optimal anesthetic management for cardiac and non-cardiac surgical procedures.
CHD can be cyanotic and noncyanotic. CHD can be atrial, ventricular, septal, or vascular if categorized according to the site of the abnormality. CHD has been divided into 5 major categories according to the pathophysiology of the congenital cardiac lesions5 (Table 1).
Table 1 Pathophysiological classification of CHD5
CHD w CHD with increased pulmonary blood flow (septal defects without pulmonary obstruction and left-to-right shunt)
CHD w CHD with decreased pulmonary flow (septal defects with pulmonary obstruction and right-to-left shunt)
CHD C CHD with obstruction to blood progression and no septal defects (no shunt)
CHD S CHD so severe as to be incompatible with postnatal blood circulation
CHD si CHD silent until adult age
This review will focus on left-to-right cardiac shunts and the anesthetic considerations for patients with these malformations undergoing cardiac or noncardiac surgical procedures. The commonly-encountered congenital cardiac defects with left-to-right shunt include ventricular septal defect (VSD), atrial septal defect (ASD), endocardial cushion defect (ECD), and patent ductus arteriosus (PDA). Though these cardiac defects are not always isolated entities, often times they are associated with other congenital abnormalities. For the convenience of discussion, single lesions rather than various syndromes with multiple defects will be discussed.
Pathophysiological changes induced by left-to-right cardiac shunt
In the presence of a cardiac septal defect, blood flows through the defect secondary to a pressure gradient existing at the different sides, usually from the left side (higher pressure) to the right side of the heart. The direction and the quantity of the blood flow through the defect are dependent upon the pressure gradient. A Left-to-right shunt sends some oxygenated blood back through the pulmonary circulation instead of entering the systemic circulation. Therefore, the patient does not develop cyanosis, at least at earlier stages, which may potentially delay the patient from seeking medical intervention and establishing the correct diagnosis. Some patients will develop cyanosis later in life due to reversed direction of the blood flow through the cardiac defect secondary to pulmonary hypertension. The persistently increased pulmonary blood flow due to left-to-right shunt may result in the following pathophysiological changes:
1. Increase in pulmonary vascular resistance (PVR) and development of pulmonary arterial hypertension (PAH): The increased blood flow and potentially higher pressure due to the left-to-right shunt leads to damage of small pulmonary arteries and arterioles with intimal and medial smooth muscle cell proliferations, arteriolitis and necrosis of the arterial wall, aneurysmal dilatation, and glomoid-like plexiform lesions5. These changes consequently result in obstructive vascular lesions (or pulmonary vascular disease) due to the arterial wall thickening and lumen narrowing, as shown in Figure-1, which increase vascular resistance5. When PVR increases to a certain extent, the quantity of shunted blood will decrease due to lowered pressure gradient across the cardiac defect. With increase of PVR, the shunting volume of blood will decrease and the ratio of pulmonary circulation/systemic circulation (Qp/Qs) will decrease. With increases in pulmonary blood pressure, the direction of blood flow through the defect may be reversed from "left-to-right" to "right-to-left" if right-sided pressure surpasses that of the left side. This converts the noncyanotic congenital cardiac defect into a cyanotic disease (as Eisenmenger Syndrome). To prevent the pathogenesis of the permanent/irreversible pulmonary vascular changes and eventual pulmonary hypertension

M.E.J. ANESTH 21 (6), 2012
795LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIVE ANESTHETIC CONSIDERATIONS
and Eisenmenger Syndrome, it is highly recommended that these cardiac defects be repaired within 1-2 years of life either surgically or non-surgically5.
With an ever-increasing PVR, PAH will ensue. PAH is a serious complication of CHD which will ultimately lead to heart failure. Without early surgical intervention, about one-third of pediatric CHD patients will develop significant PAH. Data from the Netherlands indicates that more than 4% of adult CHD patients have PAH5. The incidence is higher in those with septal defects and left-to-right shunt. Pulmonary hypertension seems to occur more likely in patients with VSD. Eisenmenger’s syndrome, characterized by reversed pulmonary-to-systemic (right-to-left) shunt, represents the most advanced form of PAH in patients with CHD and affects as many as 50% of those with PAH and left-to-right shunts. It is associated with the poorest outcome among CHD patients with PAH5. Morbidity increases as older patients are at increased risk of arrhythmia, heart failure, valve regurgitation and PAH. Data demonstrates that the probability of PAH increases with age in patients with cardiac defects6. The increase in pulmonary pressure is due to increased volume load to the right heart and physical narrowing of pulmonary vascular lumen. It can also be caused by the increased pulmonary vascular tonicity and impaired
relaxation induced by the left-to-right shunt-associated endothelial dysfunction and its associated biochemical changes. The support for this theory is the study of MacLean with experimental pulmonary hypertension associated with left-to-right shunt. This study revealed that intracellular cAMP was reduced due to increased degradation of cAMP by phosphodiesterase7. In humans with pulmonary vascular disease associated with left-to-right shunt, PGI2-synthase has been shown to be reduced, which may lead to decreased synthesis of PGI2, an arachidonic acid metabolite, which relaxes arterial vessels8. However, Loukanov et al reported plasma cAMP levels in patients with left-to-right shunt do not correlate with hemodynamic findings. This observation should be taken into account when assessing potential changes in plasma cAMP in patients treated with vasoactive substances known to interfere with the synthesis of cAMP9.
Genetic factors appear to predispose certain patient to develop pulmonary hypertension. A recent study correlated the Glu298Asp polymorphism of the endothelial nitric oxide synthase gene and pulmonary hypertension in children with congenital cardiac diseases10. They looked at a total of 80 children with congenital cardiac diseases at a median age of 3.8 years, ranging 0.136.2- years. The Glu298Asp
Fig� 1 CHD with increased pulmonary blood flow
(A) Pulmonary vascular disease in a patient with complete AV septal defect. Postmortem injection of contrast material in the pulmonary arteries showing the typical “winter tree” appearance of the distal arterial circulation.(B) Histology of the lung of the same patient showing subocclusion of the lumen of a small artery due to concentric intimal fibrosis5. (Copyright of Elsevier Inc, permission received)

796 KAYE A. D. et. al
polymorphism was identified using PCR and restriction fragment length polymorphism. The study found that although gene frequency for Glu298Glu, Glu298Asp, and Asp298Asp was not different in the control group compared to these patients, the endothelial nitric oxide synthase polymorphism was related to acute post-operative elevation of pulmonary artery pressure (genotypic frequency 53.3% versus 25%; Armitage trend test: p50.038). In addition, the allelic frequency of the Glu298Asp was related to post-operative pulmonary hypertension (Fischer’s exact test: p50.048). The authors believe that patients with left-to-right shunt are more likely to develop acute elevation of pulmonary artery pressure after cardiopulmonary bypass when presenting with the Glu298Asp polymorphism of the gene endothelial nitric oxide synthase10. This could be used as a genetic marker for the predisposition for the development of pulmonary hypertension after intra-cardiac repair10. Yap et al found that PAH is a high risk predictor of postoperative complications for patient with CHD and PAH to have cardiac and non-cardiac surgical procedures11.
2. Cardiomegaly and cardiac remodeling: Persistent left-to-right shunting of blood can lead to the enlargement of the right atrium and/or right ventricle depending upon the location of the CHD and the severity of the volume and/or pressure overload. Dilated cardiomegaly has been reported in patients with ASD12. Chronic blood overload in the cardiac chambers potentially initiate a cardiac remodeling process. Sugimoto et al studied serum level of procollagen type III N-terminal amino peptide (PIIIP) and the severity of CHD. The increased serum PIIIP levels in proportion to the severity of ventricular load or cyanosis suggest enhanced myocardial synthesis of collagen type III in patients with CHD. Suppression of the PIIIP level by an angiotensin converting enzyme (ACE) inhibitor suggests the involvement of the renin-angiotensin-aldosterone system in myocardial fibrosis. This remodeling mechanism seems to be similar to other pathological condition-related cardiac hypertrophy and remodeling, in which the renin-angiotensin-aldosterone system (RAA) is contributing. There is plenty of evidence that ACE inhibitors and direct RAA inhibitors are effective in affecting cardiac remodeling process13,14. Additional future understanding of the cellular mechanism of this
remodeling process will likely provide the basis for the development of newer diagnostic and therapeutic strategies in patients with CHD.
3. Dysrhythmias: Atrial, ventricular and other types of dysrhythmias can occur in patients with left-to-right cardiac shunt. These rhythm disturbances likely are due either to the intrinsic nature of the anomaly or to morphological changes secondary to blood overloading the right-side of the heart, or surgical palliation. Tachyarrhythmias, either supraventricular or ventricular, and bradyarrhythmias, either sinus node dysfunction or atrioventricular block, may occur frequently. Technological advances in intervention and surgical approaches have led to prophylactic and therapeutic reduction in arrhythmias15. Nagao et al� studied the relationship of duration of ASD and the occurrence of atrial fibrillation, and found that the incidence of atrial fibrillation in patients with CHD is highly related to the aging/duration of ASD16.
4. Myocardial ischemia: Left-to-right shunt related hemodynamic overload in patients with CHD may induce myocardial ischemia. Sugimoto et al� studied the changes of troponin I and Brain Natriuretic Peptide (BAP) and its N-terminal prohormone fragment (NT-proBNP) in 412 children with CHD (30 ASD, 32 VSD) and 350 normal children (control group) over a five year period. Troponin I is currently believed to be the most sensitive marker of myocardial injury. The study found that serum troponin I levels in healthy children with CHD are increased17 and troponin I levels in pediatric patients with ASD and VSD are significantly higher than in those of healthy children. More interestingly, patients with VSD and significantly elevated levels of troponin I were associated with pulmonary hypertension17.
Anatomical changes of left-to-right cardiac shunt
ASD: Based on the portion of the atrial septum that has failed to develop normally, ASDs are anatomically classified into four types: ostium secundum (85%), ostium primium (10%), sinus venosus (5%), and coronary sinus defects (rare)18. Spontaneous closure occurs by 18 months in almost all patients born with ASDs <3 mm diameter and in 80% of those with

M.E.J. ANESTH 21 (6), 2012
797LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIVE ANESTHETIC CONSIDERATIONS
defects 3-8mm19,20. Defects with diameters >8 mm rarely close spontaneously and may require surgery later in life20.
VSD: Ventricular septum is composed of a smaller membranous part and a larger muscular portion. The membranous part of the septum is separated into the pars atrioventricularis and the pars interventricularis by the tricuspid valve. True membranous VSD lesion is completely bordered by fibrous tissue. If the lesion penetrates into any portion of the muscular septum, the defect is named a perimembranous, paramembranous, or infracristal defect21. The muscular portion is composed of three sections: inlet, trabecular, and infundibular. Inlet VSDs are located in the inlet portion of the muscular septum which is inferioposterior in relation to the membranous section of the septum. There are no muscular fibers that separate this type of defect from the atrioventricular valve. The muscular portion that makes up the majority of the septum is termed the trabecular subunit. Lesions within this section that are encompassed by muscular tissue are termed muscular lesions. Finally, the infundibular subunit is the portion of the septum that divides the outflow tracts of both ventricles21. Depending on the size of the lesion, small VSDs are usually clinically insignificant, whereas the larger ones usually cause more hemodynamic instability and can lead to other pathologies, such as CHF and PAH22. Generally, only a portion of the patients with VSD become clinically symptomatic. Moderate to large defects become hemodynamically significant left-to-right shunts in the first 2-6 weeks of life23. The size and morphology of a VSD are important determinants of spontaneous closure and to the need for surgical intervention. Early age at presentation, in contrast, is not predictive of the need for surgical intervention. In early childhood, there appears to be very little risk of endocarditis or aortic valvular prolapse.
ECD: Endocardial cushion defects (also referred to as atrioventricular canal defects) are the result of irregular development of the fetal heart. The endocardial cushions are the portions of the fetal heart that form the adult atrioventricular valves. They also develop into the contiguous portions of the atrial and ventricular septums24. When the endocardial cushions fail to fuse and develop properly, the result can be
either a single defect in the atrial septum known as an atrial primum defect or a defect that involves any of the structures that the endocardial cushions develop into. When all of the structures that the endocardial cushions develop into are abnormal, it is known as a complete atrioventricular canal defect25. ECDs are not among the most common forms of congenital heart defects in the general population. On the contrary, those with Down’s syndrome have a much higher chance of being affected. This is particularly true for the complete form of endocardial cushion defect-those with abnormal atrioventricular valves and septums25. It is thought that approximately 33 % of patients with the complete form also suffer from Down syndrome21. Although a single defect in the atrial septum may not pose a huge problem for a patient, a complete atrioventricular canal defect can cause major dilemmas. The issues arise from left-to-right shunts that form at the points of both the atrial and ventricular septal defects25. As mentioned earlier, this allows blood to flow from the systemic circulation into the pulmonary circulation. Because of the significance of the shunt, early onset CHF is common. Surgical repair is generally recommended when CHF is present. Surgery is usually suggested prior to one year of age26.
PDA: Patent ductus arteriosis is not an intracardiac left-to-right shunt; but, it causes similar pathophysiological alterations as other left-to-right cardiac abnormalities. PDA is not considered an abnormality until it persists beyond 2 to 3 days post-natal27. With some functional similarities, PDA is like a mild form of ASD. PDA usually does not have a detrimental effect on the developing child. However, it is generally recommended that these be surgically corrected at an early age to prevent future complications, such as pulmonary hypertension and CHF2. Interestingly, there are some associated congenital heart abnormalities that require a patent PDA in order for survival. In such cases as tricuspid or aortic atresia, it may be necessary to give PGE1 in order to maintain the patency of the ductus2.
Clinical Presentation
The clinical manifestations of left-to-right cardiac shunt depends on the age of the child, site and

798 KAYE A. D. et. al
size of the anomaly. Failure to thrive is a very common presentation in children with CHD and influences the metabolic response to injury and outcome after corrective cardiac surgery. Energy imbalance is a major contributing factor. The age and time of corrective surgery affects the potential for nutritional recovery. Although the immediate postoperative period is characterized by a hypermetabolic state, low total and resting energy expenditure are reported within 24 hours of surgery. After 5 days, resting energy expenditure returns to preoperative levels. Significant improvements in weight and growth occur within months after corrective surgery. However, limited postoperative recovery in nutritional status and growth occurs in infants with a low birth weight, intellectual deficit, or residual malformation. Further studies are needed to elucidate the timing of corrective cardiac surgery to maximize nutritional outcomes and to identify those infants who may benefit from aggressive preoperative nutrition support28. Avitzur et al� studied the Resting Energy Expenditure (REE) in 29 children younger than 3 years of age with CHD (14 cyanotic and 15 noncyanotic CHD) before and after open heart surgery. The study found that REE was similar in the cyanotic and the noncyanotic children before and after surgery. These parameters, REE, VCO2, and VO2, were similar in children with cyanotic versus noncyanotic CHD, similar before and after surgery. The Schofield equation is more accurate than the WHO equation in predicting energy needs of children with CHD, but measurement of REE is preferred over calculation of REE29.
ASD: Small ASDs are usually asymptomatic in early life and the defects may close spontaneously19. Larger defects will cause symptoms such as shortness of breath, fatigue, and lethargy. Later in life, some patients may present with atrial dysrhythmias and even Eisenmenger's syndrome. Severe defect may present with symptoms of CHF as early as the first year of life.
VSD: Moderate to large VSDs can cause delayed growth and development, decreased exercise tolerance, pulmonary infections, and congestive heart failure during infancy. On physical examination, a systolic thrill at the left lower sternal border, increased P2 intensity, regurgitant holosystolic or early systolic murmur, or an apical diastolic rumble may be heard.
ECD: ECD usually presents in the immediate neonatal period with cyanosis due to large intracardiac communications and relatively high pulmonary vascular resistance. Undernourishment with failure to thrive, repeated respiratory infections, tachycardia, tachypnea, and CHF present early in infancy. Physical examination usually reveals a systolic thrill, holosystolic regurgitant murmur, and a mid-diastolic rumble at the left sternal border.
PDA: Large PDAs may cause atelectasis, lower respiratory tract infections, CHF, tachycardia, exertional dyspnea, tachypnea, and poor weight gain. When pulmonary vascular obstructive disease ensues (Eisenmenger's syndrome), cyanosis in the lower half of the body and left arm develops. On physical examination, a continuous “machinery” murmur, a systolic thrill at the left upper sternal border and bounding peripheral pulses with wide pulse pressure can be appreciated.
Diagnosis
With current medical technologies, it is generally not too difficult to make a diagnosis for most CHDs. Physical examination, auscultation with stethoscope, EKG, chest radiograph (CXR), and echocardiography offer reasonably accurate diagnosis. There are occasions in which other strategies are needed for the establishment of diagnosis or assessment of cardiac functions or hemodynamic status. Additionally, transesophageal echocardiography may be required in older children and adults when transthoracic 2-D echocardiography cannot adequately visualize all cardiac structures. Cardiac catheterization can be a useful technique not only in establishing the correct diagnosis, but also in assessing cardiac functions. It can be especially important for preoperative evaluation for certain surgical procedures. Angiographic CT imaging has been used in the cardiac catheterization laboratory for the diagnosis of congenital heart disease.
Clinically, a patient with a small PDA defect is usually asymptomatic. If the PDA shunt is large, an apical diastolic rumble may be heard. A PDA patient usually has left ventricular hypertrophy, left atrial hypertrophy, right ventricular hypertrophy, and cardiomegaly on x-ray. 2-D echocardiography is

M.E.J. ANESTH 21 (6), 2012
799LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIVE ANESTHETIC CONSIDERATIONS
diagnostic and dimensions of the left atrium and left ventricle provide important assessment of the size of the left-to-right shunt across the PDA30.
An ECD patient has an accentuated S1, a narrowly split S2, and an accentuated P2 present. ECD patients usually have superior axis deviation of the QRS complex, which lies between 0 and-150 degrees. The symptoms of patients with VSD are dependent upon the size of the shunt; Cardiomegaly involving the left atrium, left ventricle, and right ventricle may be seen on chest X-ray with increased pulmonary vascular markings. 2-D echocardiography with Doppler can identify the size and exact location of the defect31.
Predictors of clinical outcome
1. Pulmonary hypertension and Eisenmenger Syndrome: Without early surgical repair, about one third of patients with CHD will develop PAH6. Eisenmenger's syndrome, characterized by reversed pulmonary-to-systemic (right-to-left) shunt, represents the most advanced form of PAH-CHD and affects as many as 50% of those with PAH and left-to-right shunts. It is associated with the poorest outcome among patients with PAH-CHD6. In patients with suspected pulmonary vascular disease anticipating a two-ventricle repair, although preoperative testing via cardiac catheterization with vasodilators is reasonable, the preoperative parameters and the precise values of these parameters that best correlate with early and late outcome remain unclear32.
2. Vasodilator responders have a better outcome: Krasuski et al studied 215 patients with PAH. The vasoreactivity of patients was assessed during inhalation of 40 parts per million nitric oxide (iNO) and vasodilator responders were defined as those participants who achieved a mean pulmonary artery pressure (PAP) of ≤40 mm Hg and a drop in mean PAP ≥ the median for the cohort (13%). There were 51 deaths (25.9%) over a mean follow-up period of 2.3 years. It was found that vasodilator responders had significantly improved survival regardless of whether or not they had idiopathic or nonidiopathic PAH or whether or not they had Dana Point class 1 or non-Dana Point class 1 PAH. In multivariate modeling, advanced age, elevated right atrial pressure,
elevated serum creatinine, and worsened functional class significantly predicted shorter survival, whereas vasodilator response predicted improved survival. It was concluded that vasodilator responsiveness to iNO is an important method of risk stratifying PAH patients, with results that apply regardless of clinical etiology33.
3. Older age: As discussed previously, older patients with CHD have higher morbidity and mortality rate if they undergo a surgical procedure. They are at increased risk of arrhythmia, valve regurgitation, PAH and heart failure. Data showed that probability of PAH increases with age in patients with cardiac defects6.
4. Gender: Shapiro et al� investigated the gender differences in patients with CHD and pulmonary hypertension. 2318 female and 651 male patients were studied and a greater number of females had PAH associated with connective tissue disease (P <0.001). Further, more males had portopulmonary hypertension (P <0.001); more females had congenital heart disease-associated PAH (P = 0.017), thyroid disease (P <0.001), and depression reported (P ≤0.001). At diagnosis, males had higher mean pulmonary arterial pressure (53 ± 14 vs. 51 ± 14.3 mm Hg; P = 0.013) and mean right atrial pressure (10 ± 6 vs 9 ± 6 mm Hg; P = 0.031). Females had better survival estimates for 2 years from enrollment and for 5 years from diagnosis34. However, Klitzer et al� showed the opposite results in mortality with the female gender associated with an 18% higher in-hospital and 30-day post-discharge mortality as compared with male gender. There was no difference in length of hospital stay between males and females35. Therefore, the precise effect of gender on the short-term and long-term survival of patients with CHD will require additional investigation.
Treatment
ASD: Management of an ASD is by either surgical or trans-catheter correction of the defect. Usually, small ASDs require no treatment, whereas larger ones are corrected surgically at an early age. And correction of an ASD should not occur prior to 2 years of age owing to the chance of natural closure of the defect19, Defects that close on their own are generally located within the ostium secundum portion of the atrial septum26. The degree of shunt should

800 KAYE A. D. et. al
be determined prior to correcting an ASD. This can be determined by cardiac catheterization or pulsed Doppler echocardiography which will both show the pulmonary-to-systemic blood flow ratio (Qp/Qs)36. A ratio greater that 2:1 is indicative of a significant left-to-right shunt37. Surgical correction of ASDs has been demonstrated to be slightly more effective than trans-catheter methods; however, the latter are less invasive and therefore have shorter hospital stays and fewer complications38. Defects that require surgical repair are usually located within the ostium primum or sinus venosus portion of the atrial septum26. Following successful repair, children usually have no significant future problems. There are no special considerations for these patients if they were to undergo future non-cardiac surgery26.
VSD: Medical management is the first choice for infants with a moderate to large VSD who develop CHF and growth failure. If improvement is not noted, a trans-catheter or surgical closure should be performed before 6 months of age39,40. Surgical mortality is 2%-5% after the age of 6 months and is higher for those <2 months old, infants with associated defects, or those with multiple VSDs. The surgical approach is preferably through the right atrium as opposed to a ventriculotomy because of an increased risk of right bundle branch block with the ventriculotomy approach39.
ECD: One distinguishing feature is the superior axis deviation of the QRS complex that generally lies between 0 and-150 degrees. Most patients with ECD are refractory to medical treatment and need surgical repair. Mortality rate is 5%. Mitral valve replacement may be necessary, which increases the risk of complete heart block after surgery41,42. Repair is usually performed around 3-8 months old. Early repair is extremely important in Down’s syndrome infants with complete ECD due to the increased risk of developing early pulmonary vascular obstructive disease, PAH and even Eisenmenger Syndrome.
PDA: PDA is usually ligated not long after birth and these patients generally do not develop significant complications. However, there are some adult patients with PDA. All PDAs identifiable by physical examination should be closed41,42. In premature infants, this can usually be done with indomethacin.
The dosage of indomethacin is generally 0.2mg/kg given intravenously in 2 doses that are separated by approximately 12 hours43. In term infants and children, closure must be through a catheter or through surgery. Catheter closure has varying degrees of success with hemolysis, residual leaks, left pulmonary artery stenosis, peripheral coil embolization, and femoral vessel occlusion presenting as potential complications. Surgical closure is performed between 6 months to 2 years old or with first diagnosis in an older patient. Infants with CHF, pulmonary hypertension, or recurrent pneumonia usually require emergent surgery. The procedure is classically performed through a left posterolateral thoracotomy without cardiopulmonary bypass. Newer techniques include video-assisted thoracoscopy. The mortality of surgery is usually less than 1%41,44.
Considerations in anesthetic management
Pre-operative anesthetic evaluation
1. Assessment of hemodynamic status: In addition to basic preoperative tests including ECG, chest x-ray, hemoglobin and hematocrit, and type and cross-match of blood, hemodynamic assessment is an important component of preoperative evaluation. There are other critical clinical, radiological, and echocardiographic correlates of changes in the pulmonary vasculature that assist the clinician in decision-making regarding operability. Early in the course of the disease (left-to-right shunt), when the shunt is operable, there is often clear evidence of increased pulmonary blood flow. With the increase in PVR to generate right atrial pressure higher than left atrial pressure, patients develop clinical cyanosis from shunt reversal (Eisenmenger syndrome). Notwithstanding the uncertainties surrounding the predictive value of preoperative hemodynamics on postoperative outcomes, accurate hemodynamic assessment is of particular importance in determining the operability, at intermediate levels of elevation in PVR where clinical signs can be subtle. Decision-making regarding operability can be critical in some patients as closure of the defect can potentially cause

M.E.J. ANESTH 21 (6), 2012
801LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIVE ANESTHETIC CONSIDERATIONS
progression of pulmonary hypertension and adversely affect the natural history of a disease that would otherwise allow survival into the third or fourth decade of life44. Hemodynamic assessment is especially pivotal for those less invasive repair strategies such as trans-catheter closure. Hemodynamic assessment assists in appropriate device selection in trans-catheter closure. The fenestrated ASD device, which has been used in patients with pulmonary hypertension and in the closure of ASDs in the elderly with decreased left ventricular compliance, can be considered in selected patients with elevated PVR. In similar fashion, the ASD or VSD device has been used in patients with PDA patients with pulmonary hypertension. However, using an Amplatzer PDA plug possesses the risk of embolization to the aorta because of absence of a retention disc on the pulmonary arterial end45.
2. Cardiac function: Cardiac functional status not only determines the operability of patients with CHD, but also helps intraoperative anesthetic management. CHF does not necessarily preclude surgical repair of patients with CHD. Some of these patients with CHF may need surgery to improve the symptoms, as in the case of patients with ECD who present with CHF26. Some patients with significantly decompensated cardiac dysfunction may not be ideal candidates for surgical intervention, as in the case of moderate to large VSD patients who develop CHF and growth failure, requiring medical treatment for optimization before surgery39,40.
3. Existence of complications: Preoperative existence and severity of pulmonary complications are a key element of a preoperative workup. Pneumonia secondary to pulmonary congestion due to cardiac dysfunction may require optimization before elective surgical repair.
4. Co-existing medical issues: other co-existing medical illnesses either related to CHD or not, may determine the candidacy of a patient for surgery.
Intraoperative management
1. General Considerations:
Throughout the perioperative period, the goals of anesthetic management for left-to-right shunts are to
decrease the shunt flow and maintain cardiovascular and respiratory stability to provide adequate tissue perfusion and oxygenation. The strategies potentially affecting the shunt flow are discussed below:
(1). Effects of Ketamine versus propofol in children with cardiac shunting: the principal hemodynamic effect of propofol is a decrease in systemic vascular resistance (SVR). Thus, in patients with intracardiac shunting, this decrease in SVR results in an increase in right-to-left shunting and a decrease in the ratio of pulmonary to systemic blood flow, which may lead to arterial desaturation46. This effect is especially detrimental in patients with congenital right-to-left shunt, where a patient may develop a reversed direction of shunting (Eisenmenger Syndrome) from left-to-right shunt46. Williams et al� studied the hemodynamic effects of propofol in children with CHD and found that after intravenous administration of propofol, systemic MAP and SVR decreased significantly and systemic blood flow increased significantly in all patient groups. However, heart rate, pulmonary MAP, and PVR were unchanged. The Qp/Qs ratio increased. In patients with cardiac shunt, propofol resulted in decreased left-to-right flow and increased right-to-left flow; the pulmonary to systemic flow ratio significantly decreased47. Ketamine did not produce the changes induced by propofol. The authors suggested that during pediatric cardiac catheterization, both anesthesiologists and cardiologists need to know that anesthetic agents can significantly alter the hemodynamic status in children with complex congenital heart defects and affect the results of hemodynamic calculations that are important for decision-making and treatment of these patients46. In this regard, loss of an airway for a patient with CHD can cause quicker decompensation due to limited reserve and potential morbidity and mortality. Securing intravenous access is prudent, whenever possible, prior to anesthetic induction as CHD patients have, in general, limited and reduced cardiopulmonary physiology.
(2). Inhaled iloprost (prostaglandin): Zhang et al� looked into the effects of inhaled iloprost on mean PAP and PVR in 50 adult patients with CHD and significantly PAH. This study found that PAP decreased in 39 out of 50 patients and PVR reduced

802 KAYE A. D. et. al
in 43 out of 50 patients. Intravenous adenosine also decreased PAP but not PVR48, indicating that inhaled iloprost can have selective pulmonary vasodepressor effects and potentially be beneficial for patients with PAH48. Other prostaglandin analogs have also been found to be beneficial to patients with PAH49. Recently, Ruan et al� converted gene-transfected cells into a stable cell line and planted them into mice, in which the cells constantly expressed the hybrid enzyme and were capable of producing large-amounts of PGI2. The PGI2-producing cell line not only exhibited an approximate 50-fold increase in PGI2 biosynthesis, but demonstrated superior anti-platelet aggregation in vitro and increased reperfusion in a mouse ischemic hindlimb model in vivo. They concluded that gene-transfected cells provide an experimental intervention for PGI2-diminished heart diseases, such as PAH50.
(3). ACE inhibitors: The renin-angiotensin II-aldosterone axis is a critical regulator of blood pressure and fluid homeostasis. Local renin-angiotensin II systems have been discovered and novel actions of angiotensin peptides have emerged: AngII can act as an immunomodulator and profibrotic molecule. The enzyme responsible for its synthesis, Angiotensin-converting-enzyme (ACE), is present in high concentrations in lung tissue. A literature review revealed AngII and functional polymorphisms of the ACE gene increase ACE activity with increased susceptibility for asthma, chronic obstructive pulmonary disease (COPD), and for PAH. Drugs that inhibit the synthesis of AngII (ACE inhibitors) or that antagonize its actions on its receptors (AT1 receptor antagonists) have been shown to provide beneficial effects51. enalaprilat and captopril were also found to benefit patients with VSD and heart failure in children. All patients showed clinical improvement in weight gain, respiration and echocardiographic findings52.
(4). Avoiding airway obstruction, hypoventilation, and hypoxemia: These pathological states are known factors which result in increased pulmonary arterial pressure45. For those patients with Eisenmenger Syndrome, further increase in pulmonary blood pressure will worsen symptoms. However, in patients with PAH and existing left-to-right shunting, further increases in pulmonary pressure will potentially decrease left-to-right shunting volume through the
defect, theoretically benefiting the patient but may lead to right heart failure45.
2. Special considerations:
(1). Neuraxial anesthesia decreases SVR, which may decrease left-to-right shunt. However, if a parturient is hypovolemic, decreased CVP due to epidural or spinal administration may increase left-to-right shunt. Other changes may offset this potential benefit. The net result of shunting volume through the cardiac defect is difficult to generalize during epidural or spinal administration in obstetric patients, and is dependent upon volume status and the severity of pulmonary hypertension. Niijima et al� reported that intraoperatively, neuraxial anesthesia decreased the ratio of Qp/Qs53.
(2). Parturient with CHD: Parturient with unrepaired left-to-right shunt pose challenges for surgical and anesthesia teams. As more women with CHD survive into reproductive age and become pregnant, Anesthesia providers need to mitigate the negative impact of the escalated hemodynamic demands of labor and delivery. Continuous epidural analgesia attenuates increased sympathetic activation associated with labor and delivery. Avoidance of hypoxemia in patients with PAH and appropriate fluid management can be pivotal in the management of these patients. Appropriate blood volume assists in providing adequate intravascular volume and to minimize the vasodilation with drop in blood pressure or cardiac failure from overload. This may be a daunting task because of increased hemodynamic demand due to labor and delivery. CVP may be needed to help manage the parturient with uncorrected left-to-right shunt, especially in those with cardiac failure54. Parturient mortality is ~0.1-1% in low risk patients, 1-5% in patients with moderate risk, and mortality increases to 5-30% with high risk heart disease. Even in the first 20 weeks of gestation, the parturient may experience significant cardiac problems due to increased cardiac output (CO) (40% above normal levels by 20 weeks) and blood volume by 50%55. These changes place great strain on an already overworked heart. Specifically, decrease in SVR may facilitate right-to-left shunt. Maternal and fetal oxygen requirements increase dramatically in a parturient while functional respiratory capacity reduces in pregnancy, causing

M.E.J. ANESTH 21 (6), 2012
803LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIVE ANESTHETIC CONSIDERATIONS
potential maternal and fetal hypoxemia55. Parturient with unrepaired left-to-right shunt may theoretically have decreased left-to-right shunting volume related to reduction in SVR, however, this theoretical benefit may be offset by other maternal changes during pregnancy such as increased CO and blood volume, decreased FRC, and increased metabolism. Under-resuscitation of intravascular volume will be hazardous because it may increase left-to-right shunt. Left-to-right shunt volume may increase with lowered CVP from vena cava compression induced reduction in venous return.
Effects of oxytocin on hemodynamic parameters during the peripartal period in patients with CHD and left-to-right shunt: The cardiovascular side effects of standard doses of oxytocin are well-described with decreased MAP by 30% and SVR by 50%; decreasing shunting flow in left-to-right shunt. However, oxytocin also increases cardiac output by 50% and heart rate and stroke volume by 20-30%, which may be problematic for the parturient. This creates a dilemma in terms of withholding oxytocin after delivery55.
(3). Patients with PDA are more vulnerable to coronary ischemia due to ongoing pulmonary runoff during the diastolic phase of the cardiac cycle and potential for low diastolic blood pressure. Fluri et al� reported a case of fatal myocardial ischemia in a patient with PDA56. Therefore, patients with PDA should be monitored closely for hemodynamic changes and for EKG changes indicating myocardial ischemia.
(4). Trans-Catheter repair of cardiac defects: Significant hemodynamic instability exists during trans-catheter cardiac defect repair. The anesthetic records and catheterization data of 70 consecutive trans-catheter VSD closures between February 1989 and September 1992 were reviewed by Laussen et al�, and risk factors associated with hemodynamic instability evaluated. In 28 of 70 procedures (40%), hypotension (>20% decrease in systolic blood pressure from baseline) occurred; 12 patients responded to intravascular fluid administration alone, while 16 patients required additional acute resuscitation. Significant dysrhythmias occurred during 20 (28.5%) anesthetics associated with hypotension and requiring treatment or catheter withdrawal. American Society of Anesthesia (ASA) physical status, precatheterization indication for device placement, and patient size
were not predictive of hemodynamic instability during the procedure57. Blood transfusions were necessary in 38 (54.4%) cases and were size-related, with patients weighing less than 10 kg requiring a significantly larger transfusion volume (25.1 +/-12.4 mL/kg). After 35 procedures (50%) patients were admitted directly to Intensive Care Unit due to hemodynamic instability or procedure duration; 24 (68%) required mechanical ventilation. No deaths occurred; there was no late morbidity due to catheterization-related events. Intravenous sedation was used for the initial catheterizations, maintained with a combination of midazolam, ketamine, and morphine. Subsequently, general intravenous or inhaled anesthesia was predominantly used during transesophageal echocardiography and internal jugular vein cannulation. Hemodynamic instability, therefore, is common during device closure of VSDs, and is likely to be an inescapable feature of these procedures in many patients because of the technique necessary for device placement57. The utilization of transesophageal echocardiography (TEE) is a routine tool for guidance of trans-catheter closure of secundum-type ASD and has demonstrated excellent results57.
(5). Intracardiac echocardiography (ICE) has currently been studied to determine its efficacy compared to other monitoring modalities such as TEE for guiding trans-catheter device closure of ASD, patent foramen ovale (PFO), and VSD. Rigatelli et al� studied 258 patients over a period of 5 years to look into the efficacy of ICE as a guiding tool for transcatheter repair of cardiac defects. ICE helped decision-making in cancelling 18 patients for transcatheter closure due to unsuitable rims, atrial myxoma not diagnosed by preoperative transesophageal echocardiography or inaccurate transesophageal echocardiography measurement of defects more than 40 mm. The remaining 240 patients underwent transcatheter closure: transesophageal echocardiography-planned device type and size were modified in 108 patients (45%). Rates of procedural success, predischarge occlusion and complication were 100%, 94.2% and 5%, respectively. On mean follow-up of 65±15.3 months, the follow-up occlusion rate was 96.5%. There were no cases of aortic/atrial erosion, device thrombosis or atrioventricular valve interferences. This study indicated that intracardiac echocardiography-guided interatrial

804 KAYE A. D. et. al
shunt transcatheter closure is safe and effective and appears to have excellent long-term results, potentially minimizing the complications resulting from incorrect device selection and sizing58. Bartel et al. also found that Intracardiac echocardiography is superior to conventional monitoring for guiding device closure of interatrial communications59.
(6). Opioid use in CHD surgery: There is a commonly held belief that short-acting opioids possess more beneficial hemodynamic profiles and may help patient recovery. However, Akpek et al� did not find any difference regarding the effects of remifentanil and fentanyl on hemodynamics and respiration intraoperatively or 24 hours postoperatively in pediatric patients aged from 3 months to 6 years old with CHD60.
Postoperative management
1. Postoperative monitoring: Postoperatively patients with left-to-right shunt or other CHD should be continuously monitoring hemodynamically, until major vital signs, metabolic status, and vital organ functions return to normal levels.
2. Postoperative Pain Control: Adequate postoperative analgesia enhances deep breathing and minimizes respiratory complications after thoracotomy. In recent years, the use of regional techniques in cardiothoracic anesthesia have gained significant popularity and improved cardiac surgery outcomes. Ultrasound guided epidural placement is one such example of a technique that reduces postoperative pain and discomfort. Continuous infusion epidurals have led to shorter ICU stays, decreased occurrence of
postoperative emesis, earlier oral feedings, and overall shorter hospital stays61. Opioid agent use in patients with left-to-right shunt can have potential benefits because it lowers systemic MAP, and SVR. The drop in MAP and SVR may decrease left-to-right shunt and decrease the ratio of Qp/Qs.
Summary
More and more children with left-to-right CHD now survive into adulthood. These patients with CHD typically will need surgical care for their original cardiac defect(s) or other non-cardiac medical conditions. Commonly encountered CHD with left-to-right shunt include ASD, VSD, ECD and PDA. The key pathological change is the increased pulmonary vascular resistance due to arterial wall thickening, increased tonicity and impaired relaxation secondary to increased blood flow from the left-to-right shunt. Increasing PVR will lead to PAH and the reversed direction of flow through the cardiac defect (Eisenmenger Syndrome). The main causes of death are heart failure and dysrhythmia. To prevent permanent PAH and Eisenmenger Syndrome, cardiac defects with left-to-right shunt generally require surgical repair at an early age. However, some patients may survive into adult life even without repair. Surgical care for those patients with un-repaired left-to-right shunt poses many challenges for the anesthesiologist due to alterations in cardiopulmonary physiology. For this reason, it is imperative that the anesthesiologist maintain a thorough understanding of pathophyiological changes and possess up-to-date strategies of managing these patients.

M.E.J. ANESTH 21 (6), 2012
805LEFT-TO-RIGHT CARDIAC SHUNT: PERIOPERATIVE ANESTHETIC CONSIDERATIONS
References
1. http://www.chdinfo.com/chdaware/chdoverview.htm2. COTRAN RS, KUMAR V, COLLINS T: Robbins Pathologic Basis of
Disease, edition 7, chapter 12. Philadelphia: WB Saunders 2004, 564.
3. PILLUTLA P, SHETTY KD, FOSTER E: Mortality associated with adult congenital heart disease: Trends in the US population from 1979 to 2005. Am Heart J; 2009, 158:874-9.
4. PAREKH DR: A review of heart failure in adults with congenital heart disease. Methodist Debakey Cardiovasc J; 2011 Apr-Jun, 7(2):26-32.
5. THIENE G, FRESCURA C: Anatomical and pathophysiological classification of congenital heart disease. Cardiovascular Pathology; 2010, 19:259-274.
6. MULDER BJ: Changing demographics of pulmonary arterial hypertension in congenital heart disease. Eur Respir Rev; 2010 Dec 1, 19(118):308-13.
7. MACLEAN MR, JOHNSTON ED, MCCULLOCH KM, ET AL: Phosphodiesterase isoforms in the pulmonary arterial circulation of the rat: changes in pulmonary hypertension. J Pharmacol Exp Ther; 1997, 283:619-24.
8. TUDER RM, COOL CD, GERACE MW, ET AL: Prostacyclin synthase expression is decreased in lungs from patients with severe pulmonary hypertension. Am J Respir Crit Care Med; 1999, 159:1925-32.
9. LOUKANOv T, TAKAHASHI H, TONCHEv P, GROSS J, BETTENDORF M, GORENFLO M: Plasma Cyclic 3=,5=-Adenosine Monophosphate in Patients With Elevated Pulmonary Pressure Due to Left-to-Right Shunt. Canadian Journal of Cardiology; 2011, 27:523.e25–523.e29.
10. LOUKANOv T, HOSS K, TONCHEv P, KLIMPEL H, ARNOLD R, SEbENING C, KARCK M, GORENFLO M: Endothelial nitric oxide synthase gene polymorphism (Glu298Asp) and acute pulmonary hypertension post cardiopulmonary bypass in children with congenital cardiac diseases. Cardiol Young; 2011 Apr, 21(2):161-9.
11. YAP SC, HARRIS L, CHAUHAN VS, OECHSLIN EN, SILvERSIDES CK: Identifying high risk in adults with congenital heart disease and atrial arrhythmias. Am J Cardiol; 2011 Sep 1, 108(5):723-8.
12. ENNEZAT PV, JUTHIER F, MARéCHAUX S, MOUQUET F, BAUCHART JJ, AUFFRAY JL, MONTAIGNE D, ASSEMAN P, VINCENTELLI A: Atrial septal defect associated with dilated cardiomyopathy in the setting of acute cardiac failure: importance of comprehensive bedside echocardiography in ICU. Eur J Echocardiogr; 2010 May, 11(4):E11.
13. GAJARSA JJ, KLONER RA: Left ventricular remodeling in the post-infarction heart: a review of cellular, molecular mechanisms, and therapeutic modalities. Heart Fail Rev; 2011 Jan, 16(1):13-21.
14. WESTCOTT KV, HUANG BS, LEENEN FH: Brain renin-angiotensin-aldosterone system and ventricular remodeling after myocardial infarct: a review. Can J Physiol Pharmacol; 2009 Dec, 87(12):979-88.
15. LAM W, FRIEDMAN RA: Electrophysiology issues in adult congenital heart disease. Methodist Debakey Cardiovasc J; 2011 Apr-Jun, 7(2):13-7.
16. NAGAO K, TSUCHIHASHI K, TANAKA S, IIMURA O: Studies on atrial arrhythmias in atrial septal defect. The influences of aging on atrial fibrillation. Nihon Ronen Igakkai Zasshi; 1995 Jan, 32(1):27-32.
17. SUGIMOTO M, MANAbE H, NAKAU K, FURUYA A, OKUSHIMA K, FUJIYASU H, KAKUYA F, GOH K, FUJIEDA K, KAJINO H: The role of N-terminal pro-B-type natriuretic peptide in the diagnosis of congestive heart
failure in children. -Correlation with the heart failure score and comparison with B-type natriuretic peptide. Circ J; 2010 May, 74(5):998-1005.
18. JACObS JP, QUINTESSENZA JA, BURKE RP, MAvROUDIS C: Congenital Heart Surgery Nomeclature and Database Project: atrial septal defect. Ann Thorac Surg; 2000, 69:S18-S24.
19. RADZIK D, DAvIGNON A, vAN DOESbURG N, FOURNIER A, MARCHAND T, DUCHARME G: Predictive factors for spontaneous closure of atrial septal defects diagnosed in the first 3 months of life. J Am Coll Cardiol; 1993 Sep, 22(3):851-3.
20. MAHONEY LT, TRUESDELL SC, KRZMARZICK TR, LAUER RM: Atrial septal defects that present in infancy. Am J Dis Child; 1986 Nov, 140(11):1115-8.
21. MINETTE MS, SAHN DJ: Ventricular septal defects. Circulation; 2006, Nov 14, 114(20):2190-7.
22. KAPLAN, JA: “Anesthesia for Patients with Congenital Heart Disease”. Ed. David L. Reich and Steven N. Konstadt. Cardiac Anesthesia. Fourth ed. Philadelphia: W.B. Saunders, 1999, 789.
23. WERNOvSKY G, GRUbER PJ: Common congential heart disease: presentation, management, and outcomes. In: Ballard RA, ed. Avery’s Diseases of the Newborn. 8th ed. Philadelphia, PA: WB Saunders, 2004.
24. SILvERMAN NH, ZUbERbUHLER JR, ANDERSON RH: Atrioventricular septal defects: crosssectional echocardiographic and morphologic comparisons. Int J Cardiol; 1986, 13:309-31.
25. BOPE ET, RAKEL RE, kELLERMAN R: “Cardiovascular Disease: Congenital Heart Disease”. Bope: Conn’s Current Therapy. First ed. Philladelphia, PA: Saunders Elsevier, 2009.
26. LITMAN RS: Pediatric Anesthesia: The Requisites in Anesthesiology, ed 1, chapter 3, Philidelphia, PA, 2004 Mosby, 19-33.
27. SCHNEIDER DJ, MOORE JW: “Congenital Heart Disease for the Adult Cardiologist: Patent Ductus Arteriosus”. Circulation: Journal of the American Heart Association; 2006, 114:1873-882.
28. NYDEGGER A, BINES JE: Energy metabolism in infants with congenital heart disease. Nutrition; 2006 Jul-Aug, 22(7-8):697-704.
29. AvITZUR Y, SINGER P, DAGAN O, KOZER E, AbRAMOvITCH D, DINARI G, SHAMIR R: Resting energy expenditure in children with cyanotic and noncyanotic congenital heart disease before and after open heart surgery. JPEN; 2003 Jan-Feb, 27(1):47-51.
30. REIN AJ, OMOKHODION SI, NIR A: Significance of a cardiac murmur as the sole clinical sign in the newborn. Clin Pediatr; 2000, 39:511-20.
31. ROSENFELD HM, vAN DER VELDE ME, SANDERS SP, ET AL: Echocardiographic predictors of candidacy for successful transcatheter atrial septal defect closure. Cathet Cardiovasc Diagn; 1995, 34:29-34.
32. GIGLIA TM, HUMPL T: Preoperative pulmonary hemodynamics and assessment of operability: is there a pulmonary vascular resistance that precludes cardiac operation? Pediatr Crit Care Med; 2010 Mar;11(2 Suppl):S57-69.
33. KRASUSKI RA, DEvENDRA GP, HART SA, WANG A, HARRISON JK, BASHORE TM: Response to inhaled nitric oxide predicts survival in patients with pulmonary hypertension. J Card Fail; 2011 Apr, 17(4):265-71.
34. SHAPIRO S, TRAIGER GL, TURNER M, MCGOON MD, WASON P, BARST RJ: Gender Differences in the Diagnosis, Treatment, and Outcome of Patients With Pulmonary Arterial Hypertension Enrolled in

806 KAYE A. D. et. al
the Registry to Evaluate Early and Long-Term PAH Disease Management (REVEAL). Chest; 2011, in press.
35. KLITZNER TS, LEE M, RODRIGUEZ S, CHANG RK: Sex-related disparity in surgical mortality among pediatric patients. Congenit Heart Dis; 2006 May, 1(3):77-88.
36. DITTMANN, H, JACKSCH, R, VOELKER, W, ET AL: Accuracy of Doppler echocardiography in quantification of left to right shunts in adult patients with atrial septal defect. J Am Coll Cardiol; 1988, 11:338.
37. VICK, GW III: Defects of the atrial septum including atrioventricular septal defects. In: Science and Practice of Pediatric Cardiology, 2nd ed. Garson, A Jr, Bricker, JT, Fisher, DJ, Neish, SR (EDs), Williams & Wilkins, Baltimore 1998, 1141.
38. DU ZD, HIJAZI, ZM, KLEINMAN, CS, ET AL: Comparison between transcatheter and surgical closure of secundum atrial septal defect in children and adults: results of a multicenter nonrandomized trial. J Am Coll Cardiol; 2002, 39:1836.
39. WAIGHT DJ, BACHA EA, KAHANA M, CAO QL, HEITSCHMIDT M, HIJAZI ZM: Catheter therapy of Swiss cheese ventricular septal defects using the Amplatzer muscular VSD occluder. Catheter Cardiovasc Interv; 2002 Mar, 55(3):355-61.
40. TURNER SW, HORNUNG T, HUNTER S: Closure of ventricular septal defects: a study of factors influencing spontaneous and surgical closure. Cardiol Young; 2002, 12:357-63.
41. OHYE RG, BOvE EL: Advances in congenital heart surgery. Curr Opin Pediatr; 2001, 13:473-81.
42. KAMbAM J: Endocardial cushion defects. In: Kambam J, Fish FA, Merrill WH, eds. Cardiac Anesthesia for Infants and Children. St. Louis, MO: CV Mosby, 1994, 203-210.
43. ARCHER N: “Patent Ductus Arteriosus in the Newborn”. Archives of Disease in Childhood; 1993, 69:529-32.
44. RANGEL A, PéREZ-REDONDO H, FARELL J, BASAvE MN, ZAMORA C: Division or occlusion of patent ductus arteriosus? Angiology; 2003 Nov-Dec, 54(6):695-700.
45. VISWANATHAN S, KUMAR RK: Assessment of operability of congenital cardiac shunts with increased pulmonary vascular resistance. Catheter Cardiovasc Interv; 2008 Apr 1, 71(5):665-70.
46. OKLü E, BULUTCU FS, YALçIN Y, OZbEK U, CAKALI E, BAYINDIR O: Which anesthetic agent alters the hemodynamic status during pediatric catheterization? Comparison of propofol versus ketamine. J Cardiothorac Vasc Anesth; 2003 Dec,17(6):686-90.
47. WILLIAMS GD, JONES TK, HANSON KA, MORRAY JP: The hemodynamic effects of propofol in children with congenital heart disease. Anesth Analg; 1999 Dec, 89(6):1411-6.
48. ZHANG DZ, ZHU XY, MENG J, XUE HM, SHENG XT, HAN XM, CUI CS, WANG QG, ZHANG P: Acute hemodynamic responses to adenosine and iloprost in patients with congenital heart defects and severe pulmonary arterial hypertension. Int J Cardiol; 2011 Mar 17, 147(3):433-7.
49. PAPIERNIAK ES, LOWENTHAL DT, MUbARAK K: Pulmonary Arterial Hypertension: Classification and Therapy With a Focus on Prostaglandin Analogs. Am J Ther; 2011 Jun 3.
50. RUAN KH, MOHITE A, SO SP, RUAN CH: Establishing novel prostacyclin-synthesizing cells with therapeutic potential against heart diseases. Int J Cardiol; 2011, in press.
51. KAPARIANOS A, ARGYROPOULOU E: Local Renin-Angiotensin II Systems, Angiotensin-Converting Enzyme and its Homologue ACE2: Their Potential Role in the Pathogenesis of Chronic Obstructive Pulmonary Diseases, Pulmonary Hypertension and Acute Respiratory Distress Syndrome. Curr Med Chem; 2011, 18(23):3506-15.
52. MOMMA K: ACE inhibitors in pediatric patients with heart failure. Pediatric Drugs; 2006, 8(1):55-69.
53. NIIJIMA K, SETO A, UEHARA H, TAKENAKA I, KADOYA T: Anesthetic management for an adult patient with secundum atrial septal defect associated with a large left-to-right shunt. Masui; 2000 Jun, 49(6):646-8.
54. GOLDSMITH RJ, HENDERSON JL, REYNOLDS JD, PENNING DH. Management of a parturient with an uncorrected atrioventricular canal defect. Int J Obstet Anesth; 1998 Jul, 7(3):181-4.
55. DOb DP, YENTIS SM: Practical management of the parturient with congenital heart disease. Int J Obstet Anesth; 2006 Apr, 15(2):137-44.
56. FLURI S, PAvLOvIC M, WAGNER BP: Patent arterial duct, bottle-meal, and fatal myocardial ischaemia. Cardiol Young; 2010 Feb, 20(1):108-10.
57. LAUSSEN PC, HANSEN DD, PERRY SB, FOX ML, JAvORSKI JJ, BURROWS FA, LOCK JE, HICKEY PR: Transcatheter closure of ventricular septal defects: hemodynamic instability and anesthetic management. Anesth Analg; 1995 Jun, 80(6):1076-82.
58. RIGATELLI G, DELL'AvvOCATA F, CARDAIOLI P, GIORDAN M, BRAGGION G, AGGIO S, RONCON L, CHEN-SCARAbELLI C, SCARAbELLI TM, FAGGIAN G: Five-year follow-up of transcatheter intracardiac echocardiography-assisted closure of interatrial shunts. Cardiovasc Revasc Med; 2011, in press.
59. BARTEL T, KONORZA T, ARJUMAND J: Intracardiac echocardiography is superior to conventional monitoring for guiding device closure of interatrial communications. Circulation; 2003, 107(6):795-7.
60. AKPEK EA, ERKARA C, DONMEZ A, MERCAN S, ESEN A, ASLAMACI S, ARSLAN G: Remifentanil use in children undergoing congenital heart surgery for left-to-right shunt lesions. J� Cardiothoracic and Vascular Anesthesia; 2005, 19(1):60-66.
61. LIN YC, SENTIvANY-COLLINS SK, PETERSON KL, ET AL: Outcomes after single injection caudal epidural versus continuous infusion epidural via caudal approach for postoperative analgesia in infants and children undergoing patent ductus arteriosus ligation. Paediatr Anaesth; 1999, 9(2):139-43.

807 M.E.J. ANESTH 21 (6), 2012
CEREBRAL OXIMETRY: A REPLACEMENT FOR PULSE OXIMETRY?
ELIZAbETH A.M. FROST*
Abstract
Cerebral oximetry has been around for some 3 decades but has had a somewhat checkered history regarding application and reliability. More recently several monitors have been approved in the United States and elsewhere and the technique is emerging as a useful tool for assessing not only adequate cerebral oxygenation but also tissue oxygenation and perfusion in other organs.
Conflict of Interest
The author has no financial relationships with any of the products discussed and has not received any funding for production of this paper.
Introduction
Cerebral oximetry has been studied for over thirty years1 and has been commercially available to clinicians for over two decades2. But, while pulse oximetry has been a standard of care for decades, only recently has cerebral oximetry been not only extensively studied but also adapted to investigate changes in oxygen delivery to the brain and how the monitor may be used as a “first alert” of impending organ dysfunction in other parts of the body3. It is a noninvasive technology using near-infrared spectroscopy (NIRS) to monitor regional cerebral tissue oxygen saturation (rSO2). NIRS has been widely used for assessing cerebral tissue oxygenation in a variety of populations including the fields of neonatology, anesthesiology, neurology, and cardiac surgery.
Mechanism of action
Cerebral oximetry estimates regional tissue oxygenation by transcutaneous measurement of the cerebral cortex, an area of the brain that is most susceptible to changes in oxygen supply and demand and has limited oxygen reserve. Measurement is based on the ability of light to penetrate the skull and determine hemoglobin oxygenation according to the amount of light absorbed by hemoglobin (near-infrared spectroscopy, NIRS)4 (Fig. 1) Unlike pulse oximetry, NIRS cerebral oximetry uses 2 photo-detectors with each light source, which allows selective sampling of tissue beyond a specified depth beneath the skin. Near-field photo-detection can then be subtracted from far-field photo-detection to provide selective tissue oxygenation measurement. Adhesive pads are applied over the frontal lobes that both emit and capture reflected near-infrared light passing through the cranial bone to and from the underlying cerebral tissue.
* Corresponding Author: Elizabeth A. M. Frost MD, Department of Anesthesiology, Mount Sinai Medical Center, New York, NY.

808 FROST E.A.M.
blood flow in any monitored tissue.Normal cerebral rSO2 values are published for
each manufacturer’s device (e.g., the Somanetics INVOS 5100 normal value for an adult cardiac surgical patient is 67 ± 9%). Bilateral room air baseline rSO2 values should be established prior to the induction of general anesthesia or measurement by secure adherence of the pads to the skin. Values must be interpreted in the context of available clinical information as many factors alter measurements including cardiac output, blood pressure, hypo/hypercapnia, arterial pH, inspired oxygen concentration, temperature, local blood flow, hemoglobin concentration, hemorrhage, embolism, pre-existing disease (e.g., cerebral infarction) and position changes among others. With so many variables there is as yet no gold standard test to unequivocally validate that cerebral oximetry reflects regional oxygenation of frontal lobe cerebral tissue. Also, given that the technology of the several devices differs, individual validation is required. It may be reasonable to suggest that invasive and direct measurement of regional tissue oxygen pressure (tiPO2) might be equivalent to rSO2 but these are not the same parameters although some correlations may exist.
The adequacy of global oxygen delivery depends also on central venous saturation. Traditional techniques required the placement of invasive central venous access devices. A recent study of 40 patients compared two non-invasive technologies for the estimation of regional venous saturation (reflectance plethysmography and NIRS), using venous blood gas analysis as the gold standard.5In the first group a reflectance pulse oximeter probe was placed on the skin overlying the internal jugular vein. In the second group, a cerebral oximeter patch was placed on the skin overlying the internal jugular vein and overlying the ipsilateral cerebral hemisphere. Oxygen saturation estimates from both groups were compared with measured saturation from venous blood. Correlation was statistically significant for near infrared spectroscopy, but not for transcutaneous regional oximetry. Placement of cerebral oximetry patches directly over the internal jugular vein (as opposed to on the forehead) appeared to approximate internal jugular venous saturation better, suggesting this modality may offer additional clinically useful information regarding global cerebral oxygen supply and demand matching.
Fig 1 Near-infrared light passes readily through skin and skull and is absorbed by biological molecules in the brain� A spectroscopic window exists in the wavelength range of 660-940nm. (figure
courtesy of G Fischer MD)
Tissue sampling by cerebral oximetry is mainly from venous (70-75%) rather then arterial (25%) blood and is independent of pulsatile flow (Fig. 2). Monitoring is non invasive and can provide an early warning of decreased oxygen delivery. Many cardiothoracic and vascular anesthesiologists have adopted the technique to provide continuous intraoperative insight into brain perfusion and oxygenation dynamics.
Fig� 2 Cerebral oxygenation values are between arterial and venous
levels� (Figure courtesy o f G Fischer MD)
Presently four commercially available cerebral oximeters have been approved by the United States Food and Drug Administration (FDA) for adult use: Somanetics INVOS, CASMED Fore-Sight, OrNim Cerox, and Nonin Equanox. The Somanetics’ INVOS device has also been shown to improve outcome in patients >2.5 kg who were at risk for reduced or absent

M.E.J. ANESTH 21 (6), 2012
809CEREBRAL OXIMETRY: A REPLACEMENT FOR PULSE OXIMETRY
critical lower threshold for a total of 10 minutes for the entire surgical procedure then the left sided AUC value would be 150 min •%. Five and six fields record rSO2 values that are present at skin closure. The final variable asks if the use of rSO2 monitoring during the procedure was a first indicator, or “first alert” of an intraoperative event that could lead to a potential adverse outcome. These newly captured rSO2-related data fields will provide further insight into the clinical utility of rSO2 monitoring.
The Duke Clinical Research Institute (DCRI) examined the STS Adult Cardiac Surgery Database cerebral oximetry parameters collected from January 2008 through December 2009 specifically enquiring if item 7 were a “first alert”. This analysis established that in 23% (8,406 of 36,548) of procedures, the use of cerebral oximetry provided the first indication of impending potential clinical problem3. The statistical analysis is ongoing.
Several large clinical trials of cerebral oximetry have been conducted. In a retrospective study of 2,279 cardiac surgical patients, Goldman et al assessed two groups of patients9. Only group 1 employed rSO2 monitoring. Significant reduction of stroke (0.97% rSO2 group vs. 2.5% control; p <0.044), postoperative mechanical ventilation time (6.8% rSO2 group vs. 10.6% control; p <0.0014) and the length of postoperative hospital stay (p <0.046) were established in the monitored group. The most notable differences in these outcomes were found among the New York Heart Association Class I patients, indicating that monitoring benefits not only the sickest patients. Prospective, randomized controlled trials examining the effects of employing rSO2 monitoring in cardiac surgical patients also have been conducted. Murkin et al examined the results in patients in whom
These findings have also been confirmed by Marimon et al in a study of 20 pediatric patients undergoing cardiac surgery.6Cerebral oximetry and somatic renal oxygen saturation correlated significantly with continuous oxygen saturation from a central venous catheter.
Applications
Beyond providing continuous insight into regional oxygenation of the brain, cerebral oximetry may allow clinicians to use the brain as an index organ that points to the adequacy of tissue perfusion and oxygenation of other vital organs, a concept supported by multiple clinical outcome studies3, 7, 8. Data from the Society of Thoracic Surgeons (STS) National Database strongly suggest that the intraoperative use of cerebral oximetry in cardiac surgical patients frequently (23%) served as a “first alert” indicator of an intraoperative dynamic that could lead to a potentially adverse clinical outcome in both adult and pediatric patients. This Society (STS) collects the world’s largest database for cardiothoracic cases with more than 500 participating centers contributing procedural data for over 3.77 million cardiothoracic surgical procedures (www.sts.org). Seven cerebral oximetry-related data fields are presently being collected. (Fig. 3) One and two collect right and left pre-anesthesia induction baseline rSO2 values. Three and four relate to both left and right cumulative saturation values below the threshold (baseline-25%). The cumulative values are captured as the area under the curve (AUC) and include both the time spent below the lower threshold as well as the magnitude of these excursions; thus, the units of AUC are minute •%. For example, if a patient had a unilateral (left-sided) oxygen desaturation of 15% below the
Fig 3 The Society of Thoracic Surgeons (STS) National Database Fields related to cerebral oximetry
Cerebral Oximetry: Data Collection from the Society of Thoracic SurgeonsPre-Induction Baseline Regional Oxygen Saturation: Left: __________ (%) Right ____________ (%)Cumulative Saturation Below Threshold: Left: __________ (minute-%) Right __________ (minute-%)Skin Closure Regional Oxygen Saturation: Left: __________ (%) Right __________ (%)Cerebral Oximeter Provided the First Indication: Yes /No

810 FROST E.A.M.
oximetry and capnography was shown in 100 children between the ages of 9 months to 18 years. Various agents were used including ketamine, fentanyl, dexmedetomidine and propofol. Changes in rSO2 occurred in 2.1% of patients and were associated with changes in SPO2 23% only of the time and changes in ETCO2 29% of the time. Very few hypoxic events resulted in changes in rSO2 but most of the changes in rSO2 were not accompanied with any changes in cardiorespiratory parameters. However, most of the children were otherwise healthy and deemed suitable for off site sedation. It would appear that rSO2 is a more sensitive measure of cerebral oxygenation than pulse oximetry but isolated decreases in rSO2 in children may not correlate well with short or long-term neurologic complications. Clearly more studies are indicated.
Other studies in children have compared tissue oximetry in somatic sites to that of the cerebral cortex. Mittnacht summarized recent developments and available data on the use of NIRS in children at risk for low perfusion, postulating that during states of low cardiac output, cerebral blood flow and thus cerebral NIRS may be better preserved than in somatic tissue sites14. Sites other than the frontal cerebral cortex (e.g. abdomen, flank, and muscle) have been investigated for a possible correlation with invasive measures of systemic perfusion and oxygenation. The abdominal site seems preferable to the flank site NIRS (kidney region) application. Thus, to increase the sensitivity, specificity, and positive predictive value of tissue oximetry to detect systemic hypoperfusion, multisite NIRS such as a combination of cerebral and somatic site NIRS has been suggested. NIRS has also been used to assess systemic perfusion in patients undergoing first-stage palliation for hypoplastic left heart syndrome. Multi site measuring is in the early stages and certainly more investigation is indicated as NIRS has been shown predictive in the detection of low-flow states (low cardiac output).
In the field of trauma, cerebral oximetry may also have found a place. Taussky et al compared NIRS cerebral oximetry with CT perfusion in 8 brain injured patients and found that mean cerebral blood flow measured by CT perfusion was 61ml/100gm/min for the left side and 60ml/100g/min on the right
saturations fell below 75% of preoperative levels and were treated and compared the outcome to patients who were not treated.7 Patients in the control group had longer intensive care unit stays (p = 0.029) than in the active treatment group. Morbidity and mortality were significantly lower in the treatment group than that observed in the control group (p = 0.048). More recently, Baraka has also commented on the efficacy of cerebral oximetry monitoring during cardiopulmonary bypass10.
Pedrini et al indicated the potential reliability of cerebral oximetry monitoring during carotid endarterectomy under general anesthesia, using a cutoff of -25% or a cutoff of -20% for prolonged hypoperfusion in a study of 473 patients with a mean age of 7311. Three patients presented with transient ischemic deficits at awakening but there were no cases of death or stroke. Shunting was required in 41 patients; in 30 the decision was made based on initial rSO2 and in 11 after decrease of rSO2 intraoperatively. Using the area under the curve analysis, for a >25% reduction from baseline, sensitivity was 100% and specificity was 91%.
Other studies in general surgery and geriatric patients have found similar improvement when rSO2 falling below 75% of baseline was aggressively treated8. Control patients experiencing intraoperative cerebral desaturation had significantly longer PACU stays and lower postoperative day seven mean Mini-Mental Status Exam score (p = 0.02) compared with patients who were treated for desaturation. Another study by Tang et al of 76 patients undergoing thoracic surgery with single lung ventilation showed that early cognitive dysfunction related positively to intraoperative decline of rSO212. In fact more than 600 peer-reviewed retrospective studies, prospective observational studies and case reports attest to the clinical value of rSO2 monitoring in critical care operative situations3.
Outside of the Operating Room
Although rSO2 monitoring has been used mainly in the operating room, Padmanabhan et al reported a procedural emergency room study in 200913. Poor correlation between NIRS cerebral oximetry, pulse

M.E.J. ANESTH 21 (6), 2012
811CEREBRAL OXIMETRY: A REPLACEMENT FOR PULSE OXIMETRY
a registry in 2012 to gather information about this critical complication. Murphy et al collected data on 124 patients undergoing elective shoulder arthroscopy in the beach chair (61 subjects) or lateral decubitus (63 subjects)19.Anesthetic management was standardized in all patients. Baseline heart rate, mean arterial blood pressure, arterial oxygen saturation, and rSO2 were measured before patient positioning and then every 3 minutes for the duration of the surgical procedure. rSO2 values below a critical threshold (> or = 20% decrease from baseline or absolute value < or = 55% for >15 seconds) were defined as a cerebral desaturation event (CDE) and treated using a predetermined protocol. Anesthetic management was similar in the beach chair and lateral decubitus positions. Intraoperative hemodynamic variables did not differ between groups. rSO2 values were lower in the beach chair group throughout the intraoperative period (P <0.0001). The incidence of CDEs was higher in the beach chair group (80.3% vs. 0% in the lateral decubitus position group), as was the median number of CDEs per subject (4, range 0-38 vs. 0, range 0-0 lateral position group, all P <0.0001). Among all study patients without interscalene blocks, a higher incidence of nausea (50.0% vs. 6.7%, P = 0.0001) and vomiting (27.3% vs. 3.3%, P = 0.011) was observed in subjects with intraoperative CDEs compared with subjects without CDEs. This study alone would suggest that cerebral oximetry monitoring be included for all patients to be operated in a beach chair position, especially if some level of hypotension is added.
Possible conditions for errors in interpretation
It should, however, be noted that rSO2 may not provide early warning of a low hematocrit immediately after initiation of hypothermic coronary artery bypass in cardiac surgery as demonstrated by Sung et al in a study of 151 surgical patients20. Also, interdevice technologic differences may impose potential variation in the ability to accurately acquire brain oxygenation signals. In twelve healthy volunteers each of three NIRS devices were randomly applied to the forehead21. Then, a circumferential pneumatic head cuff was positioned such that when inflated, hypoxia-ischemia would be produced in the extracranial
side15. Mean NIRS values were 75 on the right and 74 on the left. Linear regression analysis demonstrated a statistically significant probability value (p = 0.0001) comparing NIRS frontal oximetry and CT perfusion-obtained CBF values. Other investigators have used cerebral oximetry as an additional monitor in trauma patients at the scene and during transport in 33 road ambulances and 32 helicopters16. For outdoor monitoring, adequacy of signal was around 50% which improved to 100% during road transport and 86% during helicopter transport. The authors felt that not only was cerebral oximetry possible but it added valuable information.
The feasibility of evaluating the role of cerebral oximetry in predicting return of spontaneous circulation after cardiac arrest was examined by Nasir et al17. Patients with return of spontaneous circulation after in-hospital arrest had significantly higher overall mean rSO2; patients with return of circulation had an rSO2 above 30% for >50% of the time of resuscitation. Non-survivors had rSO2 <30% for >50% of the time. Also, survivors had a significantly higher change in rSO2 from baseline as compared to non-survivors (310% vs. 150%).
In yet another study outside of the operating room, Rifai et al monitored 30 patients in cardiac failure18. All patients had New York Heart Association (NYHA) functional class I to III. All patients were on cardiac failure medical therapy. rSO2 measurements were recorded from the left and right forehead simultaneously. The mean rSO2 value was 67.4% (range, 47.6%-76.3%), while the mean peripheral tissue saturation SPO2 was 97% (range, 92%-100%). The mean difference between cerebral and peripheral tissue oxygenation (SpO2-rSO2) was 29.2% (range, 19.2%-51.4%). There was also a significant positive correlation between rSO2 and mean arterial blood pressure (0.55, P <.01). Statistically significant lower rSO2 values were observed in patients with diabetes (P = <026) and in patients with dyslipidemia. Thus rSO2 may be an important biomarker to measure in patients in cardiac failure and may be a useful indicator of target organ perfusion.
Concerned about the incidence of cerebral injury following shoulder surgery in the beach chair position, the American Society of Anesthesiologists established

812 FROST E.A.M.
continuously monitor cerebral tissue oxygenation and has the potential to improve clinical outcomes in gastric, orthopedic, pediatric, urologic and essentially any general surgical patient population both in and out of hospital. The brain may act as an index organ of how well all of the vital organs are perfused and oxygenated.
Finally it might be noted that on at least two occasions to the author’s knowledge, cerebral oximetry has featured in medical malpractice cases. In the first one, the anesthesiologist informed the surgeon (and also documented his remarks) that the rSO2 had decreased on several occasions after cross clamping of the carotid but had rebounded with fluid administration. The surgeon declined to insert a shunt. The patient suffered mild hemiparesis postoperatively. In a second case, the rSO2 declined 40% for about 30 minutes during carotid endarterectomy and no action was documented. The patient suffered a stroke. In one case the anesthesiologist was helped and in the other he was not although in both situations, it was argued that rSO2 is not the standard of care… but that may soon change.
scalp tissue beneath the NIRS cerebral oximeters. Comparisons among the three devices indicated that the induction of extracranial hypoxia-ischemia resulted in a significant reduction in regional cerebral oxygen saturation measurements in all three NIRS devices studied. Thus extracranial contamination appears to significantly affect NIRS measurements of cerebral oxygen saturation. However, while the authors suggest that the clinical implications of these apparent inaccuracies require further study, they note that the oxygen saturation measurements provided by cerebral oximetry do not solely reflect that of the brain alone.
Concluding Comments
These and other studies in a wide range of patient populations and ages indicate that cerebral oximetry has the potential to provide a measurable clinical benefit not only in cardiovascular and thoracic procedures. An aging population with decreasing organ functional reserve is an increasing part of anesthesia practice. This, to date underutilized, monitor can provide anesthesiologists with a noninvasive tool to

M.E.J. ANESTH 21 (6), 2012
813CEREBRAL OXIMETRY: A REPLACEMENT FOR PULSE OXIMETRY
Surgery? Stroke Res Treat 2012: 2012: 156975 Epub 2011 Nov 912. TANG L, KAZAN R, TADDEI R, ET AL: reduced cerebral oxygen
saturation during thoracic surgery predicts early postoperative cognitive dysfunction. Br J Anaesth; 2012, 108(4):623-9.
13. PADMANAHAN P, BERKENbOSCH JW, LORENZ D, ET AL: Evaluation of cerebral oxygenation during procedural sedation in children using near infrared spectroscopy. Ann Emerg Med; 2009, 54(2):205-13.
14. MITTNACHT AJ: Near infrared spectroscopy in children at high risk of low perfusion. Curr Opin Anaesthesiol; 2010 Jun, 23(3):342-7.
15. TAUSSKY P, O'NEAL B, DAUGHERTY WP, ET AL: Validation of frontal near-infrared spectroscopy as noninvasive bedside monitoring for regional cerebral blood flow in brain-injured patients. Neurosurg Focus; 2012 Feb, 32(2):E2.
16. WEATHERALL A, SKOWNO J, LANSDOWN A, ET AL: Feasibility of cerebral near-infrared spectroscopy monitoring in the pre-hospital environment. Acta Anaesthesiol Scand; 2012, 56(2):172-7.
17. NASIR A, SHAH C, PATEL R, ET AL: A feasibility study evaluating the role of cerebral oximetry in predicting return of spontaneous circulation in cardiac arrest Resuscitation, 2012 Feb 6th.
18. RIFAI L, WINTERS J, FRIEDMAN E, SILvER MA: Initial description of cerebral oximetry measurement in heart failure patients Congest Heart Fail. 2012 Mar; 18(2):85-90. doi: 10.1111/j.1751-7133.2011.00284.x. Epub; 2012 Feb 16.
19. MURPHY GS, SZOKOL JW, MARYMONT JH, GREENbERG SB, AvRAM MJ, VENDER JS, VAUGHN J, NISMAN M: Cerebral oxygen desaturation events assessed by near-infrared spectroscopy during shoulder arthroscopy in the beach chair and lateral decubitus positions. Anesth Analg; 2010 Aug, 111(2):496-505.
20. SUNG TY, KANG WS, HAN SJ, KIM JS, CHEE HK, SHIN JK, KIM SH: Does near-infrared spectroscopy provide an early warning of low haematocrit following the initiation of hypothermic cardiopulmonary bypass in cardiac surgery. J Int Med Res; 2011, 39(4):1497-503.
21. DAvIE SN, GROCOTT HP: Impact of extracranial contamination on regional cerebral oxygen saturation: a comparison of three cerebral oximetry technologies. Anesthesiology; 2012 Apr; 116(4):834-40.
References
1. JObSIS FF: Non-invasive monitor of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science ;1977 ,198:1264-7.
2. MCCORMICK PW, STEWART M, GOETTING MG, ET AL: Regional cerebrovascular oxygen saturation measured by optical spectroscopy in humans. Stroke; 1991, 22:596-602.
3. AvERY EG: Cerebral Oximetry: A “First Alert” Indicator Of Adverse Outcomes http://www.surgicalproductsmag.com/scripts/ShowPR~PUBCODE~0S0~ACCT~0000100~ISSUE~1010~RELTYPE~FEA~PRODCODE~0000~PRODLETT~HC.asp accessed Feb 14th 2012
4. FERARI M, MOTTOLA L, QUARESIMA V, ET AL: Principles, techniques and limitations of near-infrared spectroscopy. Can J Appl Physiol; 2004, 29:463-87.
5. COLQUHOUN DA, TUCKER-SCHWARTZ JM, DURIEUX ME, THIELE RH: Non-invasive estimation of jugular venous saturation: a comparison between near infrared spectroscopy and transcutaneous venous oximetry Stroke Res Treat. 2012; 2012:156975. Epub; 2011 Nov 9.
6. MARIMON GA, DOCKERY WK, SHERIDAN MJ, ET AL: near-infrared spectroscopy cerebral and somatic (renal) oxygen saturation correlation to continuous venous oxygen saturation via intravenous oximetry catheter. J Crit care; 2012; 27(3): 314e 12-8.
7. MURKIN JM, ADAMS SJ, NOvICK RJ, ET AL: Monitoring brain oxygen saturation during coronary bypass surgery: a randomized, prospective study. Anesth Analg; 2007, 104:51-8.
8. CASATI A, FANELLI G, PIETROPAOLI P, ET AL: 2005 Continuous monitoring of cerebral oxygen saturation in elderly patients undergoing major abdominal surgery minimizes brain exposure to potential hypoxia. Anesth Analg; 2005, 101:740-7.
9. GOLDMAN S, SUTTER F, FERDINAND F, ET AL: Optimizing intraoperative cerebral oxygen delivery using noninvasive cerebral oximetry decreases the incidence of stroke for cardiac surgery patients. Heart Surg Forum; 2004, 7(5):1062-7.
10. BARAKA A: Cerebral oximetry during cardiopulmonary bypass. Middle East J Anesthesiol; 2011, 21(1):7-7.
11. PEDRINI L, MAGNONI F, SENSI L, ET AL: Is Near-Infrared Spectroscopy a Reliable Method to Evaluate Clamping Ischemia during Carotid


815 M.E.J. ANESTH 21 (6), 2012
SCIENTIFIC ARTICLES
TENS COMPARED TO OPIOIDS IN POSTOPERATIVE ANALGESIC THERAPY AFTER MAJOR SPINAL
SURGERY WITH REGARD TO COGNITIVE FUNCTION
AXEL F. UNTERRAINER*, FRANZ XAvER UEbLEIS**, FRANZISKA ANDREA GROs***, GAbRIELA GERTRAUD WERNER****
MARTIN AUGUST KROMbHOLZ***** WOLFGANG HITZL******
Abstract
Background: Long term use of opioids causes cognitive decline. Transcutaneous nerve stimulation (TENS) applied preincisionally and postoperatively reduces postoperative opioid requirement and provides sufficient analgesia after major spinal surgery. Aim of this study was to find out the impact of TENS compared to opioids, prescribed for postoperative analgesia on early postoperative cognitive function.
Methods: This study was prospective and randomised-controlled. Patients and observers were blinded to the study design.
Forty-one patients of both sexes planned for lumbar interbody fusion were admitted and divided randomly into 2 groups. 35 Patients finished the study. Group A received TENS preincisionally and postoperatively, group B received piritramide intravenously (IV) by patient-controlled analgesia pump. The adjuvant analgesic therapy diclofenac 75 mg IV and the rescue medication paracetamol 1g IV was the same for all patients. Pain intensity was assessed by visual analogue scale (VAS). A battery of objective, standardized psychological tests was administered in the same order the day before surgery and 24 to 30 hours postoperatively.
Results: The two groups were compared by pairs. Pre- and postoperative attention and memory differed significantly in both groups (p <0,05). The postoperative fatigue was lower in group A (p <0,05). Neither age, sex, body mass index, duration of operation, the need of rescue medication nor the incidents of hypotensive phases showed any significant association with postoperative cognitive decline.
* MD, D.E.A.A, department of Neuroanesthesiology Paracelsus Medical University Salzburg; study design, conduct of study; data collection, manuscript preparation
** PhD, department of Clinical Psychology; data collection.*** MSc, department of Clinical Psychology, data collection; manuscript preparation.**** MSc, department of Clinical Psychology; data collection.***** MD, department of Neurosurgery; data collection.****** PhD, department of Biostatistics; data analysis; manuscript preparation. Corresponding author: Axel Friedrich Unterrainer. Department of Neuroanesthesiology, Paracelsus Medical University
Salzburg, Ignaz-Harrer-Strasse 79, A 5020 Salzburg. Tel: 0043 662 4483 56410, Fax: 0043 662 4483 3204. E-mail: [email protected]

816 UNTERRAINER A.F. et. al
blinded study was designed to test the hypothesis that the patient controlled intravenous administration of PCA pump filled with piritramide (PCA-IV) impacts the cognitive function differently compared to TENS for postoperative analgesia within 24 hours.
Patients were divided randomly in 2 groups by rolling the die. According to a former study on TENS patients of the two groups were treated in the following manner6. Group A received TENS therapy for 30 minutes prior to skin incision, for 24 hours after the end of operation and PCA pump filled with saline; group B-sham TENS therapy for 30 minutes prior to skin incision, for 24 hours after the end of operation and PCA pump filled with piritramide. Due to necessity of postoperative analgesic treatment a control group without either TENS or PCA-IV was not created. In both groups TENS or sham TENS was started immediately after skin closure still under anesthesia.
In both groups 4 cutaneous self-adhesive electrode pads, sized 16 cm² (tens/ems, Promed GmbH, D-82490, Farchant, Germany) were attached on either side in a distance of 4 cm to the planned skin incision at dermatomal levels.
The TENS electrodes were connected to the TENS device (tens 1000 s, D-82490, Farchant, Germany). Stimulation was set in a synchronized mode. With a bidirectional electrical current wave a pulse width of 0.25 ms without bursts. The frequency was regulated on 100 Hz. Depending on the individual tolerance patients of group A received an intensity of 10 to 20 mA. The intensity of the electrical stimulation was set on 0mA for group B. Patients in group B were told that they cannot feel the electrical stimulation. The flashing “in use” light on TENS device was shown to them with intent to prove its correct mode of operation. The treatment by TENS or sham TENS lasted for 24 to 30 hours postoperative, shortly interrupted by changing the bandage on the postoperative day.
In both groups propofol was used for induction and sevoflurane for maintenance of anesthesia; analgesia was provided by fentanyl during the intra operative period. Rocuronium was used to facilitate intubation and for intra operative muscle relaxation. A forced air patient warming system was used to keep body temperature over 36°C during the whole operation.
Conclusions: Augmentation of fatigue in early postoperative phase was less in patients treated with TENS than with opioids for analgesic therapy after major spinal surgery. Further investigations on the duration of opioid therapy when cognitive functions decline are necessary.
Key words: transcutaneous electrical nerve stimulation; major spinal surgery, postoperative neurobehavioral manifestation, opioid, fatigue.
Introduction
The impact of anesthetics and oxygen desaturation on postoperative cognitive dysfunction was investigated recently1-3.
The advantage concerning postoperative cognitive function of epidural analgesia versus patient-controlled opioid based analgesia after abdominal operation has been shown4. Long term treatment with opioids causes cognitive dysfunction5. Transcutaneous electrical nerve stimulation (TENS) was proved efficient and opioid sparing in postoperative analgesia after major spinal surgery6.
The intention of this study was to clarify a possible difference in early postoperative cognitive function between patients treated for postoperative analgesia with TENS and patients treated with piritramide given by a patient controlled analgesia (PCA)-pump after major spinal surgery. A visual analogue scale (VAS) score of pain of 3 or less was considered to be sufficient.
Material and Methods
Ethical approval of this study (Ethical Committee N° 1236) was provided by the appropriate Ethical Committee on 28 July 2010.
Forty-one opioid naïve patients of both sexes American Society of Anesthesiologists Grade I to III planned for elective posterior interbody fusion of 2 or 3 lumbar vertebrae were included into the study on the preoperative day. Written informed consent was obtained from all patients
No participant had been treated by TENS before. A prospective randomized patient and observer

M.E.J. ANESTH 21 (6), 2012
817TENS COMPARED TO OPIOIDS IN POSTOPERATIVE ANALGESIC THERAPY AFTER MAJOR SPINAL SURGERY WITH REGARD TO COGNITIVE FUNCTION
and explained before the patients were dismissed on ordinary ward. The bolus dose in group B was piritramide 2mg, the lockout time was 20 minutes, and the maximum dose within 4 hours was piritramide 15mg. Concerning the injected volumes the PCA pump was adjusted equally in group A.
Paracetamol 1g IV was administered as an additional rescue medication if either TENS or PCA therapy failed to achieve a VAS of 3 or less.
A battery of psychological tests was administered to the patients on the day before operation and was repeated 24 hours to 30 hours after surgery. The order of administration of the tests was the same in both sessions.
The Mini Mental State Examination (MMSE) is a short neuropsychological test for the assessment of cognitive deficit7. The MMSE is divided into two sections: The first requires vocal responses only and covers orientation, memory and attention. The second tests ability to name, follow verbal and written commands, write a sentence spontaneously and copy a complex figure. The test is not timed, requires 5-10 minutes and has several parallel forms. The maximum total score is 30.
The Short Cognitive Performance Test (SCT) is
Depending on the cause either fluids or phenylephrine were administered to improve hypotension.
Blood haemoglobin levels were kept over 8g dl-1 by autotransfusion of salvaged erythrocytes. Patients of both groups received piritramide 0.08mg kg-1 intravenously (IV) and diclofenac 75 mg IV 20 minutes before the expected end of skin closure. All patients received diclofenac 75 mg IV 12 hours after operation.
Patients’ level of pain (from 0 no pain to 10 worst pain imaginable) was assessed by a standard 10 cm visual analogue scale (VAS) (DoloMeter, Mundipharma Ges.m.b.H., A-1072 Wien, Austria) during analgesic therapy.
The pain score was evaluated when the patients were awake and able to obey simple commands before leaving the recovery room, before psychological testing, and if necessary before administration of rescue medication. With intention to achieve a VAS of 3 or less single injections of piritramide were administered by the medical staff until the discharge from the recovery room.
The PCA pump, in group A filled with saline and in group B filled with piritramide, was connected
Table 1 Range, Mean and SD of Age, BMI, Sex distribution and OP duration by groups
Treatment Groups P
All Patients (n = 35) A (n = 17) B (n = 18) (Student t-test)Age Range 41-75 41-74 43-75
Mean (± SD) 60.49 (± 9.96) 56.65 (± 11.07) 64.33 (± 8.86) 0.031
Age > 65 y 15/35 4/17 (24%) 11/18 (61%) P = 0.041
BMI Range 20.42-35.02 21.25-31.99 20.42-35.02
Mean (± SD) 27.30 (± 3.45) 26.46 (± 3.17) 28.13 (± 3.73) NS (0.16)
Sex Male N = 18 (51.4%) N = 8 N = 10
P = 1.0 Female N = 17 (48.6%) N = 9 N = 8
Length of operation (min) Range 88-237 90-237 88-228
Mean (± SD) 161.86 (± 37.84) 160.82 (± 39.07) 162.89 (36.61) NS (0.87)
BMI: Body-Mass-Index

818 UNTERRAINER A.F. et. al
(A-E). The maximum total score is 24.
The Profile of Mood States (POMS) is a self-report instrument to assess current mood states with 35 adjectives9-11.
The 4 POMS subscales are measuring: “depressive state” (maximum score 98), “fatigue” (maximum score 49), “vigour” (maximum score 49)
a brief neuropsychological test battery that consists of nine subtests to measure neuropsychological functions as memory, attention and related cognitive functions, taking into account the speed of information processing8. The SCT has been used in the assessment of treatment responses in numerous clinical trials for treatment of dementia in our institution. It requires 10-15 minutes to administer and has five parallel forms
Table 2 Rescue medication and hypotensive phases by groups
All Patients (n = 35) Treatment Groups P
N % A (n = 17) B (n = 18) Rescue medication 0 gramme 23 65.7 12 11
P = 0.58 1 gramme 11 31.4 5 6 2 gramme 1 2.8 0 1Hypotensive phases no 30 85.7 15 15
P = 1.0Blood pressure systolic between 71 and 80 mmHg yes 5 14.3 2 3 Exact Pearson Chi-Square based on Monte Carlo method.
Table 3 MMSE, SCT & POMS for all patients and different groups
All Patients (n=35) Treatment Groups
A (n=17) B (n=18) A vs. B
pre post pre post P pre post P P
MMSEMean (± SD) 28.29 (±2.07) 28.49 (±1.82) 29 (±1.41) 28.65 (±1.97) NS (0.42) 27.61 (±2.38) 28.33 (±1.71) NS
(0.09)NS (0.14)
SCTMean (± SD) 2.71 (±2.86) 4.71 (±3.63) 2.59 (±2.94) 5.06 (±3.90) 0.0003 2.83 (±2.85) 4.39 (±3.43) 0.014 NS (0.84)
POMS_dMean (± SD) 31.37
(±16.16)30.86
(±19.11)32.12
(±18.16)27.82
(±15.29)NS
(0.251)30.67
(±14.58)33.72
(±22.20)NS (0.4) NS (0.69)
POMS_fMean (± SD) 21.69 (±7.18) 25.2 (±8.60) 21.12 (±5.87) 23.35 (±8.12) NS (0.25) 22.22 (±8.36) 26.94 (±8.91) 0.016 NS (0.32)
POMS_vMean (± SD) 25.57 (±6.80) 23.17 (±6.61) 25.06 (±6.79) 22.88 (±6.05) NS (0.26) 26.06 (±6.97) 23.44 (±7.27) NS
(0.17)NS (0.69)
POMS_aMean (± SD) 13.91 (±8.55) 13.46 (±9.00) 14.47
(±10.09)13.29 (±9.45) NS (0.53) 13.39 (±7.04) 13.61 (±8.84) NS (0.9) NS (0.89)
MMSE: Mini Mental State Examination, SCT: Short Cognitive Performance Test, POMS: Profile of Mood States (d: depressive state, f: fatigue, v: vigour, a: anger).

M.E.J. ANESTH 21 (6), 2012
819TENS COMPARED TO OPIOIDS IN POSTOPERATIVE ANALGESIC THERAPY AFTER MAJOR SPINAL SURGERY WITH REGARD TO COGNITIVE FUNCTION
Fig� 1 SCT score for group A vs� B, before and after the operation�
Higher scores mean lower cognitive function
Fig� 2 Scores for the POMS scale “fatigue” group A vs� B, before and
after the operation� Higher scores mean higher fatigue
Concerning the fatigue of the patients evaluated with POMS it was found a significant augmentation within group B (sham TENS plus piritramide, PB = 0.016), but not in group A (TENS, PA = 0.25). Consequently patients treated with TENS showed an equal fatigue before and after the operation.
Discussion
Because participants could not be encouraged to be tested for longer than 20 minutes, the simple, just for screening reasons used SCT was performed. Intending to deepen findings concerning attention, memory, and especially cognitive processing speed, more specific tests for verbal memory, visual memory, and attention should be done12. Connect-the-number-test would gain
and “anger” (maximum score 49). The POMS requires about 5 minutes.
Repeated measures analysis of variance (ANOVA) with one fixed factor (group A vs group B) were applied to analyze data. For post-hoc comparisons, paired and unpaired Student t-tests were used. Exact Pearson Chi square tests were used to analyze distributions of sex, rescue medication and hypotensive phases. Whiskerplots with 95% confidence intervals were used to illustrate data. A p-value less than 0.05 indicates a statistically significant result. All computations were done with STATISTICA 6.1 (StatSoft, Inc. (2004). STATISTICA (data analysis software system), version 6).
Results
Thirty-five patients finished the study. Five patients were cancelled for surgical reasons after the preoperative testing. One patient dropped out because another than the planned operation was performed.
Concerning age (P = 0.03) and age over 65 years (P = 0.041) the groups differed significantly (Table 1). Regarding height (P = 0.37), weight (P = 0.47), sex (P = 1.0), body mass index (BMI) (P = 0.16), length of operation (P = 0.87)(Table 1) and necessity of rescue medication no significant difference was found between the groups (Table 2).
No significant difference was found between the two groups with respect to the frequency of hypotensive phases (P = 1.0) (Table 3).
MMSE was analyzed with a repeated measure ANOVA to compare the means with the fixed factor “group”. No significant differences between the two groups were found (P = 0.14).
Furthermore, no effect was found concerning the mood states within the groups A and B, before and after the operation for the scales “depressive state” (PA
= 0.25, PB = 0.40) “vigour” (PA = 0.26, PB = 0.17) and “anger” (PA = 0.53, PB = 0.90) of the POMS.
The pair wise comparisons (Student t-tests) showed statistically significant differences in the Short Cognitive Performance Test within both groups (PA = 0.0003, PB = 0.014) (Fig. 1). Score augments in both groups, which means the cognitive function of the patients declined postoperatively.

820 UNTERRAINER A.F. et. al
equal in both groups. We assume that both analgesic methods are of the same value in treating postoperative cognitive deficits caused by pain.
This study proves that postoperative cognitive ability declines within 24 hours to 30 hours postoperatively in both groups independently from analgesic treatment. On the one hand this might be caused by an overhang of sevoflurane, on the other hand by post operative sleep disturbances, inflammatory stress response and environmental factors19-21.
Orientation concerning time and place, retentiveness, ability of memorization, speech, the understanding of speech, reading, writing, drawing, and calculating were not influenced differently by postoperative analgesic treatment.
Further studies will be necessary to find out the duration of opioid therapy when cognitive functions decline.
This study shows that the augmentation of postoperative fatigue was less in analgesic treatment by TENS than by opioids. Free of doubt this contributes to patients’ comfort.
more findings on cognitive processing speed13.
Because it is not possible to design a true ‘‘control’’ for the electrical tapping sensation, patients were told that the perception of the electric pulse depends on one´s individual threshold of sensibility14. Although a double-blind study design would have been preferable, the study was not biased by interviewers. They were blinded in regard to randomization.
In order to increase patients’ comfort and to reduce oxygen consumption by avoiding shivering after anesthesia participants were warmed throughout the whole operation15. This probably contributed to the postoperative decline in cognitive function within both groups16.
Our findings concerning the necessity of rescue medication interfere with Unterrainer’s and Dawood’s studies which showed a non opioid analgesic sparing effect of TENS6,17.
Particularly with regard on Hudetz’s findings cognitive function was not influenced by metabolic syndrome18. BMI did not differ significantly within the groups.
The investigated cognitive functions were

M.E.J. ANESTH 21 (6), 2012
821TENS COMPARED TO OPIOIDS IN POSTOPERATIVE ANALGESIC THERAPY AFTER MAJOR SPINAL SURGERY WITH REGARD TO COGNITIVE FUNCTION
12. HäRTUNG C, MARKOWITSCH HJ, NEUFELD H, CALAbRESE P, DEISINGER K, KESSLER J: German version of Wechsler Memory Scale. manuscript. University Bern 2000.
13. OSWALD WD, ROTH E: German version of the Connect the Number Test. manuscript University Göttingen 1987.
14. HAMZA MA, WHITE PF, AHMED HE, GHONAME EA: Effect of the frequency of transcutaneous electrical nerve stimulation on the postoperative opioid analgesic requirement and recovery profile. Anesthesiology; 1999 Nov, 91(5):1232-8.
15. RALLEY FE, WYNANDS JE, RAMSAY JG, CARLI F, MACSULLIvAN R: The effects of shivering on oxygen consumption and carbon dioxide production in patients rewarming from hypothermic cardiopulmonary bypass. Can J Anaesth; 1988 Jul, 35(4):332-7.
16. SALAZAR F, DOñATE M, BOGET T, BOGDANOvICH A, BASORA M, TORRES F, ET AL: Intraoperative warming and post-operative cognitive dysfunction after total knee replacement. Acta Anaesthesiol Scand; 2011 Feb, 55(2):216-22.
17. DAWOOD MY, RAMOS J: Transcutaneous electrical nerve stimulation (TENS) for the treatment of primary dysmenorrhea: a randomized crossover comparison with placebo TENS and ibuprofen. Obstet Gynecol; 1990 Apr, 75(4):656-60.
18. HUDETZ JA, PATTERSON KM, AMOLE O, RILEY AV, PAGEL PS: Postoperative cognitive dysfunction after non cardiac surgery: effects of metabolic syndrome. J Anesth; 2011 Jun, 25(3):337-44.
19. RöRTGEN D, KLOOS J, FRIES M, GROTTKE O, REX S, ROSSAINT R, ET AL: Comparison of early cognitive function and recovery after desflurane or sevoflurane anaesthesia in the elderly: a double-blinded randomized controlled trial. Br J Anaesth; 2010 Feb, 104(2):167-74.
20. TERRANDO N, MONACO C, MA D, FOXWELL BM, FELDMANN M, MAZE M: Tumor necrosis factor-alpha triggers a cytokine cascade yielding postoperative cognitive decline. Proc Natl Acad Sci U S A; 2010 Nov 23, 107(47):20518-22.
21. KRENK L, RASMUSSEN LS, KEHLET H: New insights into the pathophysiology of postoperative cognitive dysfunction. Acta Anaesthesiol Scand; 2010 Sep, 54(8):951-6.
References
1. SCHOEN J, HUSEMANN L, TIEMEYER C, LUELOH A, SEDEMUND-ADIb B, BERGER KU, ET AL: Cognitive function after sevoflurane-vs propofol-based anaesthesia for on-pump cardiac surgery: a randomized controlled trial. Br J Anaesth; 2011 Jun, 106(6):840-50.
2. ROYSE CF, ANDREWS DT, NEWMAN SN, STYGALL J, WILLIAMS Z, PANG J, ET AL: The influence of propofol or desflurane on postoperative cognitive dysfunction in patients undergoing coronary artery bypass surgery. Anaesthesia. 2011 Jun, 66(6):455-464.
3. SUEHIRO K, OKUTAI R: Duration of cerebral desaturation time during single-lung ventilation correlates with mini mental state examination score. J Anesth; 2011 Jun, 25(3):345-9.
4. BEILIN B, HOOFIEN D, PORAN R, GRAL I, GRINEvIC G, BUTIN B, ET AL: Comparison of two patient-controlled analgesia techniques on neuropsychologogical function in the postoperative period. Journal of Clinical and Experimental Psychology; 2008, 30(6):674-682.
5. KURITA GP, LUNDORFF L, PIMENTA CA, SJøGREN P: The cognitive effect of opioids in cancer: a systemic review. Support Care Cancer; 2009, 17(1):11-21.
6. UNTERRAINER AF, FRIEDRICH C, KRENN MH, PIOTROWSKI WP, GOLASZEWSKI SM, HITZL W: Postoperative and Preincisional Electrical Nerve Stimulation TENS reduce postoperative opioid requirement after major spinal surgery. J Neurosurg Anesthesiol; 2010 Jan, 22(1):1-5.
7. FOLSTEIN MF, FOLSTEIN SE, MCHUGH PR: Mini-Mental State: A practical method for grading the state of patients for the clinician. Journal of Psychiatric Research; 1975, 12:189-198.
8. LEHFELD H, ERZIGKEIT H: SCT. Short Cognitive Performance Test. Int Psychogeriatr; 1997, 9 Suppl1: 115-21.
9. MCNAIR DM, LORR M, DOPPLEMAN LF: Eits manual for the profile of mood states. San Diego: Educationals and Industrial Testing Service, 1971.
10. BIEHL B, LANDAUER A: The Profile of Mood States POMS. manuscript. University Mannheim, 1975.
11. DANGEL S: German version of Profile of Mood States of McNair D, Lorr M, Doppleman L. manuscript University Mannheim, 1979.


823 M.E.J. ANESTH 21 (6), 2012
INTEROBSERVER VARIABILITY FOR NON-INVASIVE PREDICTION OF DIFFICULT INTUBATION
IN DIFFERENT YEARS OF ANESTHESIOLOGY RESIDENCY*
NALAN CELEbI, OZGUR CANbAY, HEMRA CIL, ZELIHA KORKMAZ DISLI, AYSE HEvES KARAGOZ
Abstract
Background. The incidence of a difficult laryngoscopy/intubation, which could lead to failed intubation is in the range of 1.5%-13%. Failed intubation may lead to hypoxia, brain damage or death. Preoperative evaluation of the airway can be accomplished by non-invasive bedside clinical tests during physical examination. We studied interobserver variability for non-invasive prediction of difficult intubation in different anesthesiology residency years.
Methods. Three hundred eighty four adult patients undergoing elective surgery with general anesthesia and endotracheal intubation were enrolled this study. The investigators were divided in to two groups: three of them were in 4th (Group 1) and the other three were in 1st (Group 2) year of their anesthesiology residency. The variables evaluated were age, weight, height, submental-cervical angle, measurements of mandibular space, deviation of trachea, jaw-hyomental distance, swelling or scar tissue at neck, limited mouth opening, small mouth cavity, macroglossia, cleft lip-palate, long teeth and modified Mallampati score.
Results. The incidence of difficult intubation is %4.9. Group 1 is more successful than Group 2 in predicting difficult intubation.
Conclusions. Regarding Mallampati score, measurements of mandibular space, jaw-hyomental distance, mouth opening and mouth cavity; interobserver variability is detected in predicting difficult intubation among different years of anesthesiology residency. In means of submental-cervical angle, tracheal deviation, swelling or scar tissue at neck and macroglossia, similar results which are statistically significant, are obtained.
* Faculty of Medicine, Department of Anaesthesiology, Hacettepe University, 06100 Sihhiye/Ankara, Turkey. Corresponding Author: Hemra Cil, MD, Hacettepe University, Department of Anesthesiology and Reanimation, Tel:
+90-312-3051265. E-mail: [email protected]
This work was supported by the Department of Anesthesiology and Reanimation, Hacettepe Hospital, Ankara, Turkey.None of the authors has any conflict of interest.

824 CELEBI N. et. al
Introduction
Predicting difficult airway is one of the most important responsibilities of an anesthesiologist and the incidence of a difficult laryngoscopy/intubation, which could lead to failed intubation range between 1.5% to 13%1-5. Failed intubation can cause hypoxia, brain damage or death6. Problems in the airway management can be predicted based on previous anesthesia records, the medical history of the patient and a physical examination1. Difficult mask ventilation can be a sign of difficult intubation7.
American Society of Anesthesiology Closed Claims study provided that large percentage of claims is about respiratory adverse events. Difficult intubation is one of the most common reasons leading to injury8. Death or brain damage occurred in 85% of cases6-9. This respiratory adverse events ratio decreased in 19931999- (%35) compared with 1985199210-. Some preoperative test and examination methods are expected to predict difficult intubation with high sensitivity-specificity and positive predictive value. But there are some disadvantages like inter-observer difference and deficiency of common consensus11.
Preoperative evaluation of the airway can be accomplished by some measurements of the non-invasive bedside clinical test during physical examination. The aim of this study is to investigate whether an interobserver variability exists in different years of anesthesiology residency concerning certain measurements of non-invasive prediction of difficult intubation.
Methods
A written informed consent was received from 384 adult patients (i.e. older than 18 years old) who will undergo elective surgery with general anesthesia and endotracheal intubation between 2-6 November 2010. The patients have no airway pathology. The study protocol was approved by Ethics Committee of Hacettepe University on 23 July 2010 (Protocol number: HEK 10/47 642) (Chairperson of the ethics committee: Prof.Dr.Rustu Onur).
Preoperative evaluation of the patients was performed by investigators using a standard sheet.
The variables evaluated were age, height, weight, and measurements of submental-cervical angle, mandibular space, jaw-hyomental distance, mouth opening and cavity. In addition existence of deviation of trachea, swelling or scar tissue at neck, macroglossia, cleft lip-palate and long teeth were recorded. Modified Mallampati score were obtained from each patient; and class III and IV were predicted as candidates for difficult intubation.
Measurement of mandibular space is the straight distance from the angle of mandibula to the symphysis-menti12. Reference point hyomental distance is body of the hyoid bone and symphysis of mandibula13. Interincisor gap is measured between the maxillary and mandibular incisors in the midline with the mouth fully opened and with the head neutral position3,5,14. Interincisor gap is graded by distance measured: grade1 = <3.5 cm, grade2 = 3.5-5 cm, grade3 = >5 cm.
Although the prognostic value is poor, Mallampati score is one of most commonly used bedside tests for predicting difficult intubation. It is determined by inspecting the oral cavity of the patient. Recommended test way is the patient in sitting position, the head in extension position, the tongue protruded outside the mouth without phonation, with maximal mouth opening15. Score evaluate the visibility of the base of uvula, faucial pillars (the arches anterior and posterior to the tonsils). Also head and neck mobility is important for the score but not included2. In 1985 Mallampati et.al reported three class score based on oropharyngeal anatomical structure16. Then in 1987 Samsoon ve Young reported Modified Mallampati score17. The modified Mallampati test was better at predicting tracheal intubation than original1,5,16,18. Sensitivity was 0.55 and the overall specificity was 0.8418. Class III and IV Mallampati have a high positive predictive accuracy for identifying difficult intubation18.
Modified Mallampati classification (is based on visibility of oropharyngeal anatomical structure)17:
Class I: Soft palate, fauces, uvula, pillars;
Class II: soft palate, fauces, portion of uvula;
Class III: soft palate, base of uvula;
Class IV: hard palate only.

M.E.J. ANESTH 21 (6), 2012
825INTEROBSERVER VARIABILITY FOR NON-INVASIVE PREDICTION OF DIFFICULT INTUBATION IN DIFFERENT YEARS OF ANESTHESIOLOGY RESIDENCY
The investigators participated in this study were divided in to two groups: three of them were in 4th (Group 1); the other three were in 1st (Group 2) year of their anesthesiology residency. Preoperative visit of each patient was performed both physicians from each group, at different time points.
The patients did not receive any premedication. Anesthesia was induced by combination of propofol, fentanyl and rocuronium. Then orotracheal intubation was performed by the same anesthesiologist who was at the 4th year of their residency. Endotracheal tube size, necessity of guide usage during intubation, difficulty in mask ventilation-intubation was evaluated by using standardized anesthesia sheets prospectively. Intubation in more than three attempts or total duration of 10 min was defined as difficult intubation19.
Before the study we made a pretest for 20 patients to calculate kappa and power. Then by using PASS 2008 program we provided minimum 250 sample size was enough for the study. The statistical analysis was performed by using SPSS 18.0. Mallampati scores of patients attributed by Group 1 and Group2 were compered by using weighted kappa. Due to different prevalence, other test results were compared with PABAK kappa (prevalence-adjusted, bias-adjusted κ)20. Predicting difficult intubation is compared by using ROC curvey.
Results
Three hundred eighty four patients (n = 384) were included in the study. Demographic data of the patients is shown in table 1.
Table 1 Demogrphic data of the Patients� Data are given as mean ±
Variable
Age (year) 51.12 ± 15.96
Weight (kg) 73.67 ± 15.33
Height (m) 1.64 ± 0.085
Body Mass index (kg/m2) 27.47 ± 5.84
Weighted kappa was 0.942 (p: 0.00) for Group
1, which indicates a very good agreement among the residents in Group 1. Weighted kappa was 0.922 (p: 0.00) for Group 2, which also indicates a very good agreement among the residents in Groups 2.
Mallampati scores of patients evaluated by Group 1 (4th year residents) and Group 2 (1st year residents) are compared at the table 2. Weighted kappa between two groups is 0.2328 which points out low correlation between the groups. Standard error is 0.0397 and p <0.001.
Table 2 Comparison of Mallampati scores according to groups
Group 1 Mallampati score
Total
1 2 3 4
Gro
up 2
Mal
lam
pati
scor
e 1 278 14 8 1 3012 43 11 5 2 61
3 9 5 0 2 16
4 3 2 1 0 6
Total 333 32 14 5 384
Intubation was difficult in 19 patients (4.9% of all patients) and 10 of who were obese. Prevalence of difficult intubation in obese patients is 9.5%. Guide usage was necessary in 21 patients and 12 of them is difficult intubation.
ROC curve was used to compare determination of difficult intubation. Area under the Group 1’s ROC curve was 0.806 (± 0.066) and the Group 2 curve was 0.758 ± (0.065). Although Group 1 is more successful than Group 2 both groups can be considered successful in predicting difficult intubation, as long as both groups predicted 13 of 19 difficult intubation patients.
Statistically significant similar results were obtained in both groups in means of determining submental-cervical angle, tracheal deviation, swelling or scar tissue at neck and macroglossia (p <0.05). Results of measurements mandibular space, jaw-hyomental distance, mouth opening, mouth cavity size were also similar in both groups statistically not significant (p >0.05). Agreement on existence cleft lip-palate and long teeth were 100%.

826 CELEBI N. et. al
Discussion
Predicting difficult airway is one of the most important priorities of an anesthesiologist. Curtain non-invasive bedsides tests are used in order to predict difficult intubation. Interobserver difference is one of disadvantages of these tests. In this study, it is detected that results of Mallampati score has low correlation between two different groups of residents. There is interobserver variability due to different anesthesiology residency years in Mallampati score and similarly in predicting difficult intubation. In spite of this, similar results were obtained in both groups in means of determining submental-cervical angle, tracheal deviation, swelling or scar tissue at neck and macroglossia.
There are various studies in large populations using different bed-side predictive tests for difficult intubation2,4,21. Interobserver Mallampati score variability was similar to previous demonstrated between two anesthetist11,22 and between nurse and anesthetist14. Karkouti et al. studied interobserver reliability of ten tests for predicting difficult tracheal intubation with one rater for each group. Similarly Hilditch et.all studied interobserver reliability with one rater for each group.
Interobserver variability depends on factors like poor communication between anesthesiologist and patient, poor instruction and unknown technique. Already Mallampati test has complicated and modified maneuvers. Already in our study interobserver Mallampati score variability was obtained like in other studies. Unlike previous studies, interobserver agreement between was very good in both groups. But despite of having same education program at the beginning of anesthesiology residency, agreement between two groups was fair. This might be related to the different level of experiences of the groups. The other studies do not mention about the rater’s experience. On the other hand both groups predicted difficult airway successfully. This may suggest that,
factors other than Mallampati score, also influences the decision of the raters on predicting difficult intubation. Another interesting point in our study is that, the total number of patients with scores of Mallampati III and IV (indicating difficult intubation) was similar between two groups (19 to 22).
In our study the incidence of difficult intubation was 4.9 %, which was comparable to the literature. However Bilgin et. al found 8% incidence of difficult intubation in their study with Turkish population5.
All anesthetists studied lessons about predicting difficult intubation and non-invasive bedside tests at the beginning of their residency. However in our study, we showed that experience of anesthetist effects tests results.
The study of Karkouti et. al suggested more than two raters for excluding variability due to rater factors11. Because of this, in our study we accepted three anesthetists for each group. At the same time larger sample size was compared to previous studies investigating interobserver variability for prediction of difficult intubation.
One negative aspect of our study was the lack of laryngeal view grade of laryngoscopy.
In our study, unlike previous studies, we accepted more than one rater for each group and our study revealed very good agreement among raters of the same group, although the agreement between groups with different experience groups was fair. Despite that, both groups predicted difficult intubation successfully. This indicates that other factors than Mallampati score, also play an important role when assessing and predicting difficult airway.
Acknowledgements
The authors wish to thank Jale Karakaya University of Hacettepe for her help with statistical analysis.

M.E.J. ANESTH 21 (6), 2012
827INTEROBSERVER VARIABILITY FOR NON-INVASIVE PREDICTION OF DIFFICULT INTUBATION IN DIFFERENT YEARS OF ANESTHESIOLOGY RESIDENCY
References
1. RANDELL T: Prediction of difficult intubation. Acta Anaesthesiol Scand; 1996, 40:1016-23.
2. SHIGA T, WAJIMA Z, INOUE T, SAKAMOTO A: Predicting difficult intubation in apparently normal patients: a meta-analysis of bedside screening test performance. Anesthesiology; 2005, 103(2):429-37.
3. KHAN ZH, MOHAMMADI M, RASOULI MR, FARROKHNIA F, KHAN RH: The diagnostic value of the upper lip bite test combined with sternomental distance, thyromental distance, and interincisor distance for prediction of easy laryngoscopy and intubation: a prospective study. Anesth Analg; 2009, 109(3):822-4.
4. YILDIZ TS, KORKMAZ F, SOLAK M, TOKER K, ERCIYES N, BAYRAK F, GANIDAGLI S, TEKIN M, KIZILKAYA M, KARSLI B, TURAN A, OZCAN U: Prediction of difficult tracheal intubation in Turkish patients: a multi-center methodological study. Eur J Anaesthesiol; 2007, 24(12):1034-40.
5. BILGIN H, OZYURT G: Screening tests for predicting difficult intubation. A clinical assessment in Turkish patients. Anaesth Intensive Care; 1998, 26(4):382-6.
6. CAPLAN RA, POSNER KL, WARD RJ, CHENEY FW: Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology; 1990, 72(5):828-33.
7. vAN KLEI WA, GD, RUTTEN CL, HENNIS PJ, KNAPE JT, KALKMAN CJ, MOONS KG: Role of history and physical examination in preoperative evaluation. Eur J Anaesthesiol; 2003, 20(8):612-8.
8. CHENEY, FW: The American Society of Anesthesiologists Closed Claims Project: what have we learned, how has it affected practice, and how will it affect practice in the future?. Anesthesiology; 1999, 91(2):552-6.
9. NAGUIb M, SCAMMAN FL, O'SULLIvAN C, AKER J, ROSS AF, KOSMACH S, ENSOR JE: Predictive performance of three multivariate difficult tracheal intubation models: a double-blind, case-controlled study. Anesth Analg; 2006, 102(3):818-24.
10. PETERSON, GN, DOMINO KB, CAPLAN RA, POSNER KL, LEE LA, CHENEY FW: Management of the difficult airway: a closed claims analysis. Anesthesiology; 2005, 103(1):33-9.
11. KARKOUTI K, ROSE DK, FERRIS LE, WIGGLESWORTH DF, MEISAMI-FARD T, LEE H: Inter-observer reliability of ten tests used for predicting
difficult tracheal intubation. Can J Anaesth; 1996, 43(6): 554-9.12. MERAH NA, WONG DT, FOULKES-CRAbbE DJ, KUSHIMO OT, BODE
CO: Modified Mallampati test, thyromental distance and inter-incisor gap are the best predictors of difficult laryngoscopy in West Africans. Can J Anaesth; 2005, 52(3):291-6.
13. TURKAN S, ATES Y, CUHRUK H, TEKDEMIR I: Should we reevaluate the variables for predicting the difficult airway in anesthesiology? Anesth Analg; 2002, 94(5):1340-4.
14. HILDITCH WG, KOPKA A, CRAWFORD JM, ASbURY AJ: Interobserver reliability between a nurse and anaesthetist of tests used for predicting difficult tracheal intubation. Anaesthesia; 2004, 59(9):881-4.
15. LEWIS M., KERAMATI S, BENUMOF JL, bERRY CC: What is the best way to determine oropharyngeal classification and mandibular space length to predict difficult laryngoscopy? Anesthesiology; 1994, 81(1):69-75.
16. MALLAMPATI SR, GATT SP, GUGINO LD, DESAI SP, WARAKSA B, FREIbERGER D, LIU PL: A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J; 1985, 32(4):429-34.
17. SAMSOON GL, YOUNG JR: Difficult tracheal intubation: a retrospective study. Anaesthesia; 1987, 42(5):487-90.
18. LEE A, FAN LTY, GIN T, KARMAKAR MK, NGAN KEE WD: A Systematic Review (Meta-Analysis) of the Accuracy of the Mallampati Tests to Predict the Difficult Airway. Anesthesia & Analgesia; 2006, 102(6):1867-78.
19. JANSSENS M, HARTSTEIN G: Management of difficult intubation. Eur J Anaesthesiol; 2001, 18(1):3-12.
20. NAM JM: Comparison of validity of assessment methods using indices of adjusted agreement. Stat Med; 2007, 26(3):620-32.
21. LUNDSTROM LH, MOLLER AM, ROSENSTOCK C, ASTRUP G, GATKE MR, WETTERSLEv J: A documented previous difficult tracheal intubation as a prognostic test for a subsequent difficult tracheal intubation in adults. Anaesthesia; 2009, 64(10):1081-8.
22. MERINO GARCIA M, MARCOS VIDAL JM, GARCIA PELAZ R, DIEZ BURON F, ESPANA FUENTE L, BERMEJO GONZALEZ JC: Evaluation of a protocol for predicting difficult airway in routine practice: interobserver agreement. Rev Esp Anestesiol Reanim; 2010, 57(8):473-8.


829 M.E.J. ANESTH 21 (6), 2012
COMBINED USE OF METOCLOPRAMIDEAND DEXAMETHASONE AS A PROPHYLACTIC ANTIEMETIC
IN ELECTIVE CESAREAN SECTION UNDER SPINAL ANESTHESIA*
Frikha MohaMed, dhouib Firas, bouhlel riadh, djeMel Walid, sMaoui lasaad, karoui abdelhaMid
Abstract
Background: Nausea and vomiting during regional anesthesia for cesarean section still remain a major problem. We compared the efficacy of dexamethasone plus metoclopramide with dexamethasone alone for preventing nausea and vomiting during and after spinal anesthesia for cesarean section in parturients.
Methods: The study was performed in 72 full term parturient women of ASA I & II (American Society of Anesthesiology Grade I & II), aged between 19 and 37 years with uncomplicated pregnancies. The group I (n = 36) received 8 mg of dexamethasone intravenously immediately when the surgery started, while group II (n = 36) received 8 mg of dexamethasone plus 10 mg of metoclopramide. The type and number of episodes of nausea and emesis were recorded, as well as any other adverse effects.
Results: During the intraoperative period, a complete response (no emesis, no rescue) was noticed in 83% of patients in Group I and in 86% of patients in Group II. The incidence of nausea during both intra and postoperative periods was not different between the two groups. Metoclopramide was associated with impaired taste and smell and hot flushes.
Conclusions: 10 mg of metoclopramide did not improve the incidence of emetic symptoms in patients undergoing cesarean section when combined with 8 mg of dexamethasone.
Introduction
Cesarean delivery under regional anesthesia has become increasingly popular over the past decade as a result of increased patient acceptability, improved fetal condition at birth and greater maternal safety1,2.
Nausea and vomiting during regional anesthesia for cesarean section still remain a significant problem not only for the patient, but also for the surgeon and the anesthesiologist as well. The etiology of intraoperative nausea and vomiting is complex; it may be attributed to surgical stimulation, hypotension, vagal stimulation and uterotonic drugs. Patient demographic data and anesthetic technique also can play a role3.
* Department of Anesthesiology and Surgical Intensive Care. Habib Bourguiba Hospital. Sfax. Tunisia.Corresponding author: Dhouib Firas, Department of Anaesthesiology and Surgical Intensive Care, Habib Bourguiba Hospital, Sfax, Tunisia. Address: Menzel Chaker Road Km 0.5, El Ferdawss Street, 3029 Sfax Tunisia, Tel: 00216 22761151. E-mail: [email protected]

830 FRIKHA M. et. al
drug solutions in all groups were prepared by one anesthesiologist and they looked identical. Another anesthesiologist, who was blinded to the study, gave the drugs.
All parturients received 1000 ml of lactated Ringer’s solution IV over 30 min before spinal injection. All patients received oxygen via a face mask at a flow rate of three liters per minutes starting from the induction of spinal anesthesia. Patients were positioned in the left lateral decubitus or sitting position and a 25 gauge spinal needle was introduced through mid-line approach at the L3-L4 inter-space. Patients received a subarachnoid injection including 2 ml of 5% isobaric bupivacaine with 10 µg fentanyl. Surgery started when a sensory block up to T5 dermatome was obtained. Hypotension was defined as a reduction of more than 20% from baseline pressure or if systolic blood pressure was less than 90 mmHg and managed with intravenous lactated Ringer’s solution and ephedrine bolus in 3 mg increments.
Each patient was observed by an anesthesiologist blinded to which antiemetic the patients had received and asked for the intra-operative and postoperative occurrence of nausea and vomiting.
The number of episodes of emesis and type were recorded. Nausea was defined as a subjectively unpleasant sensation associated with awareness of the urge to vomit; Vomiting was defined as the forceful expulsion of gastric contents from the mouth5.
Repeated vomiting within 1 to 2 minutes period was recorded as single emesis. The data were taken as follows:
- No vomiting: complete control
- 1 to 2 vomiting episodes: Nearly complete control
- 3 to 5 vomiting episodes: Partial control
- >5 vomiting episodes: Failure
- No nausea: 0
- Mild nausea: 1
- Moderate nausea: 2
- Severe nausea: 3
The details of any other adverse effects were noted throughout the study after general questioning
A number of treatments has been introduced in order to reduce post operative nausea and vomiting (PONV), such as 5-HT3 antagonists (ondansetron and granisetron), dopamine receptor antagonists, and antihistamine drugs. However, each of these treatments is associated with critical limiting factors, namely cost with 5-HT3 antagonists, extrapyramidal symptoms with dopamine receptor antagonists, excessive sedation and tachycardia with antihistamine drugs4.
Almost all previous researches on PONV prevention were using single prophylactic antiemetic drug. We hypothesized that a metoclopramide-dexamethasone combination is more effective than dexamethasone alone in reducing the incidence of emetic symptoms. To test this hypothesis, we compared the efficacy of dexamethasone plus metoclopramide with dexamethasone alone for preventing nausea and vomiting during and after spinal anesthesia for cesarean section in parturients.
Parturients and Methods
After local ethics committee approval and informed consent from the participants, the study was performed in 72 full term parturient women of ASA I & II (American Society of Anesthesiology Grade I & II), aged between 19 and 37 years with uncomplicated pregnancies, who were scheduled for elective cesarean delivery under spinal anesthesia. Exclusion criteria were contraindications for metoclopramide, use of antiemetic or antidepressive drugs, patient classified as American Society of Anesthesiologists grade III or IV, presence of extrapyramidal motoric disease such as malignant hyperthermia, hepatic insufficiency, pheochromocytoma, mechanical ileus or epilepsy, intended or probable postoperative administration of propofol, stomach tube, and current participation in another clinical trial.
The study period was between August 2010 and April 2011. Parturients were randomly assigned to the following study groups using a sealed envelope technique: Group I (n = 36) received 8 mg of dexamethasone intravenously immediately when the surgery started, while group II (n = 36) received 8 mg of dexamethasone plus 10 mg of metoclopramide intravenously at the beginning of the surgery. The
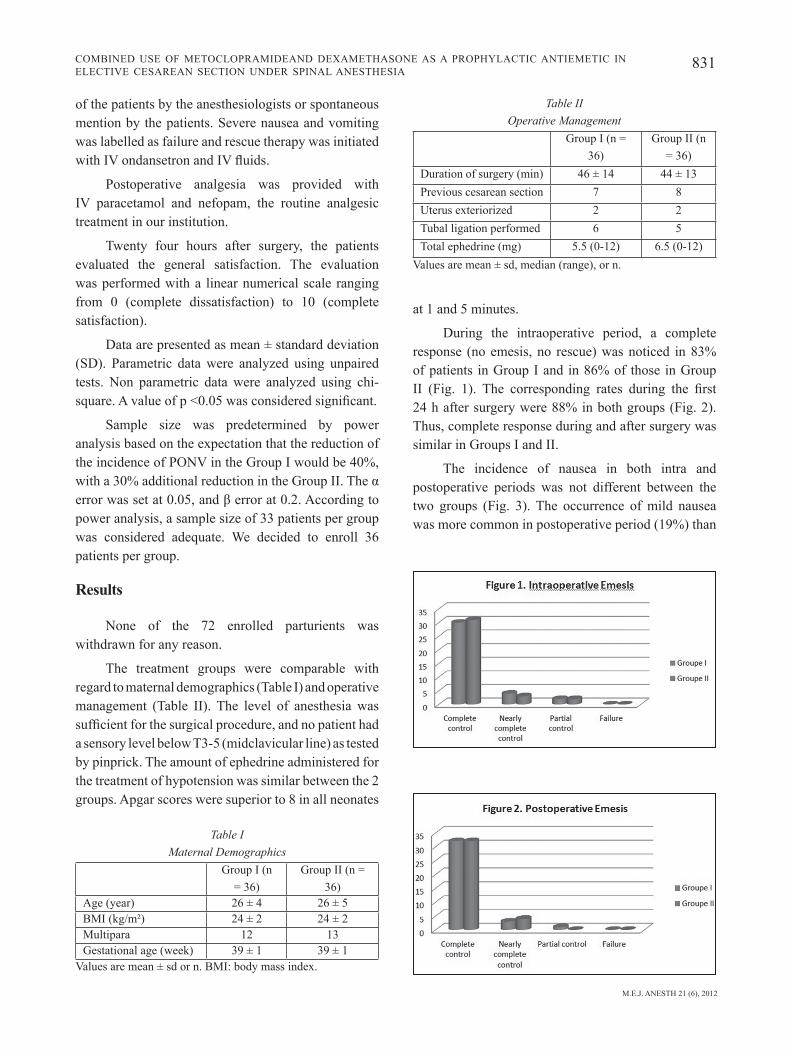
M.E.J. ANESTH 21 (6), 2012
831COMBINED USE OF METOCLOPRAMIDEAND DEXAMETHASONE AS A PROPHYLACTIC ANTIEMETIC IN ELECTIVE CESAREAN SECTION UNDER SPINAL ANESTHESIA
at 1 and 5 minutes.
During the intraoperative period, a complete response (no emesis, no rescue) was noticed in 83% of patients in Group I and in 86% of those in Group II (Fig. 1). The corresponding rates during the first 24 h after surgery were 88% in both groups (Fig. 2). Thus, complete response during and after surgery was similar in Groups I and II.
The incidence of nausea in both intra and postoperative periods was not different between the two groups (Fig. 3). The occurrence of mild nausea was more common in postoperative period (19%) than
of the patients by the anesthesiologists or spontaneous mention by the patients. Severe nausea and vomiting was labelled as failure and rescue therapy was initiated with IV ondansetron and IV fluids.
Postoperative analgesia was provided with IV paracetamol and nefopam, the routine analgesic treatment in our institution.
Twenty four hours after surgery, the patients evaluated the general satisfaction. The evaluation was performed with a linear numerical scale ranging from 0 (complete dissatisfaction) to 10 (complete satisfaction).
Data are presented as mean ± standard deviation (SD). Parametric data were analyzed using unpaired tests. Non parametric data were analyzed using chi-square. A value of p <0.05 was considered significant.
Sample size was predetermined by power analysis based on the expectation that the reduction of the incidence of PONV in the Group I would be 40%, with a 30% additional reduction in the Group II. The α error was set at 0.05, and β error at 0.2. According to power analysis, a sample size of 33 patients per group was considered adequate. We decided to enroll 36 patients per group.
Results
None of the 72 enrolled parturients was withdrawn for any reason.
The treatment groups were comparable with regard to maternal demographics (Table I) and operative management (Table II). The level of anesthesia was sufficient for the surgical procedure, and no patient had a sensory level below T3-5 (midclavicular line) as tested by pinprick. The amount of ephedrine administered for the treatment of hypotension was similar between the 2 groups. Apgar scores were superior to 8 in all neonates
Table I Maternal Demographics
Group I (n = 36)
Group II (n = 36)
Age (year) 26 ± 4 26 ± 5BMI (kg/m²) 24 ± 2 24 ± 2Multipara 12 13Gestational age (week) 39 ± 1 39 ± 1
Values are mean ± sd or n. BMI: body mass index.
Table II Operative Management
Group I (n = 36)
Group II (n = 36)
Duration of surgery (min) 46 ± 14 44 ± 13Previous cesarean section 7 8Uterus exteriorized 2 2Tubal ligation performed 6 5Total ephedrine (mg) 5.5 (0-12) 6.5 (0-12)
Values are mean ± sd, median (range), or n.
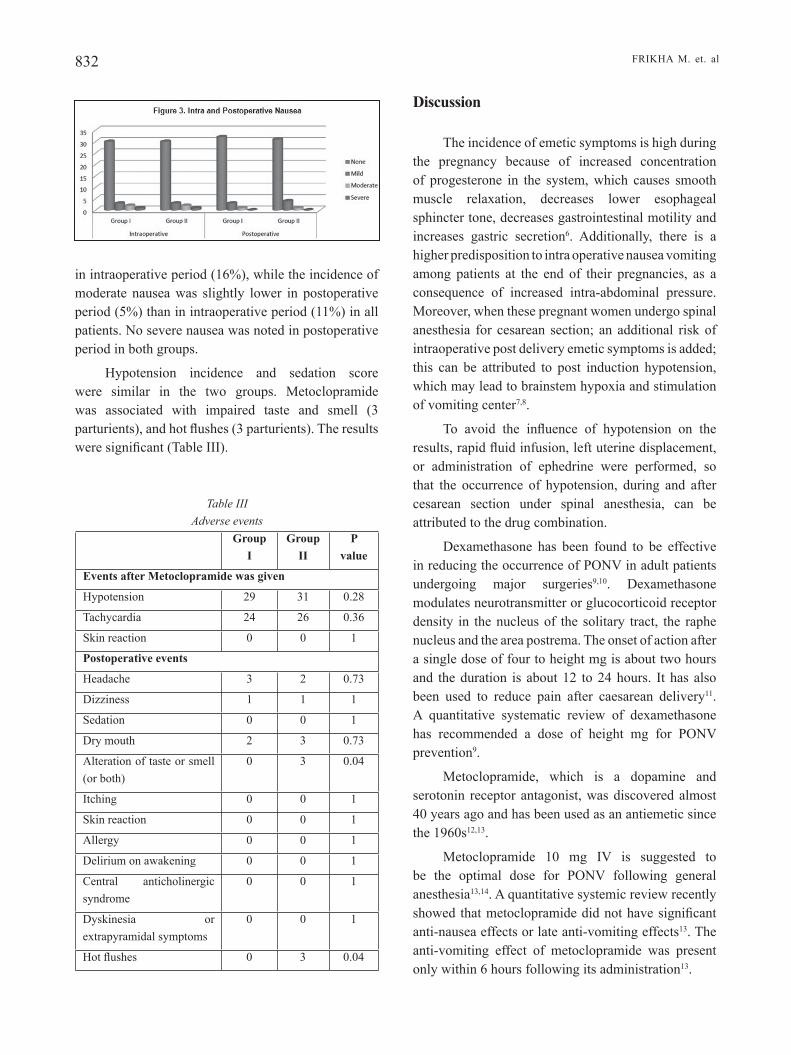
832 FRIKHA M. et. al
Discussion
The incidence of emetic symptoms is high during the pregnancy because of increased concentration of progesterone in the system, which causes smooth muscle relaxation, decreases lower esophageal sphincter tone, decreases gastrointestinal motility and increases gastric secretion6. Additionally, there is a higher predisposition to intra operative nausea vomiting among patients at the end of their pregnancies, as a consequence of increased intra-abdominal pressure. Moreover, when these pregnant women undergo spinal anesthesia for cesarean section; an additional risk of intraoperative post delivery emetic symptoms is added; this can be attributed to post induction hypotension, which may lead to brainstem hypoxia and stimulation of vomiting center7,8.
To avoid the influence of hypotension on the results, rapid fluid infusion, left uterine displacement, or administration of ephedrine were performed, so that the occurrence of hypotension, during and after cesarean section under spinal anesthesia, can be attributed to the drug combination.
Dexamethasone has been found to be effective in reducing the occurrence of PONV in adult patients undergoing major surgeries9,10. Dexamethasone modulates neurotransmitter or glucocorticoid receptor density in the nucleus of the solitary tract, the raphe nucleus and the area postrema. The onset of action after a single dose of four to height mg is about two hours and the duration is about 12 to 24 hours. It has also been used to reduce pain after caesarean delivery11. A quantitative systematic review of dexamethasone has recommended a dose of height mg for PONV prevention9.
Metoclopramide, which is a dopamine and serotonin receptor antagonist, was discovered almost 40 years ago and has been used as an antiemetic since the 1960s12,13.
Metoclopramide 10 mg IV is suggested to be the optimal dose for PONV following general anesthesia13,14. A quantitative systemic review recently showed that metoclopramide did not have significant anti-nausea effects or late anti-vomiting effects13. The anti-vomiting effect of metoclopramide was present only within 6 hours following its administration13.
in intraoperative period (16%), while the incidence of moderate nausea was slightly lower in postoperative period (5%) than in intraoperative period (11%) in all patients. No severe nausea was noted in postoperative period in both groups.
Hypotension incidence and sedation score were similar in the two groups. Metoclopramide was associated with impaired taste and smell (3 parturients), and hot flushes (3 parturients). The results were significant (Table III).
Table III Adverse events
Group I
Group II
P value
Events after Metoclopramide was given
Hypotension 29 31 0.28
Tachycardia 24 26 0.36
Skin reaction 0 0 1
Postoperative events
Headache 3 2 0.73
Dizziness 1 1 1
Sedation 0 0 1
Dry mouth 2 3 0.73
Alteration of taste or smell (or both)
0 3 0.04
Itching 0 0 1
Skin reaction 0 0 1
Allergy 0 0 1
Delirium on awakening 0 0 1
Central anticholinergic syndrome
0 0 1
Dyskinesia or extrapyramidal symptoms
0 0 1
Hot flushes 0 3 0.04

M.E.J. ANESTH 21 (6), 2012
833COMBINED USE OF METOCLOPRAMIDEAND DEXAMETHASONE AS A PROPHYLACTIC ANTIEMETIC IN ELECTIVE CESAREAN SECTION UNDER SPINAL ANESTHESIA
delivery performed under regional anesthesia.
Patients receiving metoclopramide showed a significant increased incidence of impaired taste and smell, and hot flushes, but otherwise, no extrapyramidal symptoms or other unpleasant side effects were experienced. These events may cause a discomfort for parturients.
Our study has some limitations that might have influenced the findings. First, our sample size was small. The second deficiency in this study design is the failure to include a third group receiving metoclopramide alone.
Conclusion
Combined use of dexamethasone and metoclopramide as a prophylactic antiemetic did not show any significant results compared to the use of dexamethasone alone. In addition to that, the increase of the incidence of hot flushes and impaired taste and smell suggest reconsidering the utility of metoclopramide as a prophylactic antiemetic. A bigger sample or a third group receiving metoclopramide alone could lead to break new grounds.
None of the currently available antiemetics is entirely effective, perhaps because most of them act through the blockade of one type of receptor15. Therefore, it is possible that a combination of antiemetics with different sites of activity would be more effective than one drug alone.
The use of 5-HT3 antagonists in prevention of PONV is more common nowadays. We were able to use ondansetron only as a rescue therapy due to lack of the product and its high cost.
We chose to evaluate the use of a metoclopramide-dexamethasone combination in comparison with dexamethasone alone for reducing nausea and vomiting in patients during and after spinal anesthesia for cesarean section.
Our results showed that 10 mg of metoclopramide did not improve the incidence of emetic symptoms in patients undergoing cesarean section when combined with height mg of dexamethasone. These results are in agreement with a multicenter study which recommended a combination of 8 mg of dexamethasone and highly dose of metoclopramide (25 or 50 mg)16. Unfortunately, this multicenter study did not evaluate the efficacy of combinating these two antiemetic therapies for reducing emetic episodes during cesarean

834 FRIKHA M. et. al
10. Fujii Y, Tanaka H, Toyooka H: The effects of Dexamethasone on antiemetics in female patients undergoing gynecologic surgery. Anesth Analg; 1997, 85:913-7.
11. Wu JI, Lo Y, Chia YY, Liu K, Fong WP, Yang LC, et al: Prevention of postoperative nausea and vomiting after intrathecal morphine for cesarean section: a randomized comparison of Dexamethasone, droperidol, and a combination. International Journal of Obstetric Anesthesia; 2007, 16:122-127.
12. Polati E, Verlato G, Finco G, et al: Ondansetron versus Metoclopramide in the treatment of postoperative nausea and vomiting. Anesth Analg; 1997, 85:395-9.22.
13. Henzi I, Walder B, TraMe`r MR: Metoclopramide in the prevention of postoperative nausea and vomiting: a quantitative systematic review of randomized, placebo-controlled studies. Br J Anaesth; 1999, 83:761-71.
14. Fujii Y, Tanaka H, Toyooka H: Prevention of nausea and vomiting in female patients undergoing breast surgery: a comparison with granisetron, properidol, Metoclopramide and placebo. Acta Anaesthesiol Scand; 1998, 42:220-4.
15. RoWbothaM DJ: Current management of postoperative nausea and vomiting. Br J Anaesth; 1992, 69:46S-59S.
16. Jan Wallenborn, Götz Gelbrich, DetleF Bulst, Katrin Behrends, Hasso Wallenborn, Andrea Rohrbach, et al: In BMJ British Medical Journal (2006).
References
1. Ong BY, Cohen MM, Palahniuk RJ: Anesthesia for cesarean delivery - effect on neonates. Anesth Analg; 1989, 68:270-5.
2. Reynolds F: Epidural analgesia in obstetrics. Pros and cons for mother and baby. BMJ; 1989; 299, 751-2.
3. Balki M, Kasodekar S, DhuMne S, Carvalho JA: Prophylactic granisetron does not prevent postdelivery nausea and vomiting during elective cesarean delivery under spinal anesthesia. Anesth Analg; 2007, 104:679-83.
4. Gan TJ: Postoperative nausea and vomiting-can it be eliminated? JAMA; 2002, 287:1233-6.11.
5. Watcha MF, White PF: Postoperative nausea and vomiting: its etiology, treatment, and prevention. Anesthesiology; 1992, 77:162-84.
6. Tarhan O, Canbay N, Celebi S, Uzun A, Sahin F, Coskun U: Subhypnotic doses of midazolam prevent nausea and vomiting during spinal anesthesia for cesarean section. Minerva Anesthesiol; 2007, 73:629-33.
7. Datta S, Alper MH, OstheiMer GW, Weiss JB: Methods of ephedrine administration and nausea and hypotention during spinal anesthesia for cesarean section. Anesthesiology; 1982, 56:68-70.
8. Patra CK, Badola RP, Bhargava KP: A study of factors concerned in spinal anesthesia. Br J Anaesth; 1972, 44:1208-11.
9. Henz I, Walder B, TraMe´r M: Dexamethasone for the prevention of postoperative nausea and vomiting: a quantitative systemic review. Anesth Analg; 2000, 90:186-94.

835 M.E.J. ANESTH 21 (6), 2012
ULTRASONOGRAPHIC MODIFICATION OF CORMACK LEHANE CLASSIFICATION FOR PRE-ANESTHETIC
AIRWAY ASSESSMENT*
DEEPAK GUPTA, ARvIND SRIRAJAKALIDINDI, bRYANT ITTIARA, LEIGH APPLE, GOKUL TOSHNIWAL, HALIM HAbER
Abstract
Background: The major drawback of Cormack Lehane classification for airway assessment is its dependence on invasive direct laryngoscopy and hence it is inapplicable for pre-anesthetic assessment of airway in patients with no prior history of tracheal intubation.
Study Objectives: The purpose of the study was to compare and correlate the ultrasound view of the airway and the Cormack Lehane classification of the direct laryngoscopy.
Methods/Study Procedures: The present study was conducted on patients scheduled for elective surgery and requiring general anesthesia with direct laryngoscopy and endotracheal intubation. In the pre-operative holding area, the following measurements were obtained with the oblique-transverse ultrasound view of the airway: (a) the distance from the epiglottis to the midpoint of the distance between the vocal folds, (b) the depth of the pre-epiglottic space, and (c) the total time taken by the operator to achieve the final ultrasonic image. The data was then compared with the Cormack Lehane classification during direct laryngoscopy in the operating room. Subsequently based on the correlation data, the ultrasonographic modification of Cormack-Lehane Classification was developed.
Results: It was observed that there was a correlation of the distance between the epiglottis and the vocal cords (E-VC) with the Cormack Lehane Grading; correlation was strong negative with regression coefficient of -0.966 (95% CI -1.431 to -0.501; p = 0.0001). Subsequently, the correlation of the pre-epiglottis space (Pre-E) with the Cormack Lehane Grading was strong in positive direction with regression coefficient of 0.595 (95% CI 0.261 to 0.929; p = 0.0008). Finally the ratio of Pre-E and E-VC distances with the Cormack Lehane Grading had the strongest positive correlation with regression coefficient of 0.495 (95% CI 0.319 to 0.671; p <0.0001). Based on these statistical calculations and after rearranging the data, we found that prediction of Cormack Lehane (CL) grades can be adequately (67%-68% sensitivity) made by the ratio of Pre-E and E-VC distances (Pre-E/E-VC) {0<[Pre-E/E-VC]<1 ≈ CL grade 1; 1<[Pre-E/E-VC]<2 ≈ CL grade 2; and 2<[Pre-E/E-VC]<3 ≈ CL grade 3}. The average time taken to complete the ultrasound examination of airway in the preoperative area was 31.7 ± 12.4 seconds.
Conclusion: The non-invasive ultrasonographic modification of invasive Cormack Lehane classification for pre-anesthetic airway assessment can supplement the presently available non-invasive modalities of pre-anesthetic airway assessment including the Mallampati Classification.
* Department of Anesthesiology, Wayne State University/Detroit Medical Center, Detroit, MI 48201, United States. Corresponding Author: Halim Haber, M.D., Clinical Associate Professor, Anesthesiology, Wayne State University, Box
No 162, 3990 John R, Detroit, Michigan 48201, United States, Tel: 1-313-745-7233, Fax: 1-313-993-3889. E-mail: [email protected]

836 GUPTA D. et. al
Introduction
The Cormack Lehane classification is frequently used to describe the best view of the larynx seen during laryngoscopy. Although it is perhaps one of the most widely used classifications, one major drawback is that it cannot be applied for predicting difficulty in tracheal intubation in patients undergoing intubation for the first time. Direct laryngoscopy is simply too invasive of a technique to be used to assess and classify an airway in an awake patient.
Ultrasound imaging is a safe, simple, painless, and non-invasive modality through which soft tissues can be visualized and identified. However, there is limited information regarding the feasibility and potential opportunities to use ultrasound imaging for examining the upper airway1-4. Previous studies have utilized an external on-skin cricoid-level transverse scanning technique4-5, and an internal intraoral sublingual technique1-2 to visualize the trachea and the esophagus, and reported difficulties associated with each technique. The major problem with the external technique is the difficulty in maintaining good probe-skin contact over an uneven and curved surface.
The purpose of this study was to compare and correlate the ultrasound view of the airway and the Cormack Lehane classification of the direct laryngoscopy.
Methods
After institutional review board approval for the study protocol, 72 patients were enrolled in the study after obtaining the written informed consent. Only ASA class I-III patients aged 18-80 years and undergoing elective surgery requiring general anesthesia with direct laryngoscopy (Macintosh blade) and endotracheal intubation were included in the study. The patients with mouth opening too small to pass Macintosh blade 4, edentulous patients, and the patients with head and neck anatomical pathologies that might have unpredictable effect on the ultrasound assessment of the airway were excluded from the study. The patients who were not able to extend their neck >30 degrees were also excluded.
In the pre-operative holding area, the Mallampati
Classification of the pre-anesthetic airway assessment was documented as follows:
Class 1: Full visibility of tonsils, uvula and soft palate
Class 2: Visibility of hard and soft palate, upper portion of tonsils and uvula
Class 3: Soft and hard palate and base of the uvula are visible
Class 4: Only Hard Palate visible
Subsequently, the ultrasound view of the airway of all study patients was assessed by the same anesthesia resident with a high frequency linear probe (A SonoSite® MicroMaxx® ultrasound system (SonoSite INC, Bothell, WA) HFL38/13-6 MHz transducer). The patients were asked to lie down supine with active maximal head tilt-chin lift. The probe was then placed in the submandibular area in the midline. Without changing the position of the probe, the linear array of the ultrasound probe was rotated in the transverse planes from cephalad to caudal or plane “A” (a coronal plane to see the mouth opening) to plane “G” (an oblique transverse plane that bisects the epiglottis and posterior most part of vocal folds with arytenoids in one 2-dimensional view) (Fig. 1). The further rotation of the ultrasound array was ceased at the first simultaneous visualization (in the same ultrasonic frame) of the epiglottis and posterior most part of vocal folds with arytenoids (Fig. 2). The following study measurements were obtained with
Fig� 1 Ultrasonic Planes (Planes A-G) for the Ultrasound Assessment
of the Airway

M.E.J. ANESTH 21 (6), 2012
837ULTRASONOGRAPHIC MODIFICATION OF CORMACK LEHANE CLASSIFICATION FOR PRE-ANESTHETIC AIRWAY ASSESSMENT
the oblique-transverse ultrasound view of the airway (Plane “G”): (a) the distance from the epiglottis to the midpoint of the distance between the vocal folds, and (b) the depth of the pre-epiglottic space (Fig. 2). The total time taken by the operator to achieve the final ultrasonic image (Plane “G”) was also recorded.
The patients were then taken to the operating room and the standard general anesthesia procedure was performed as per the discretion of the attending anesthesiologist and in accordance with good clinical practice, and per standard of care. During the intra-operative direct laryngoscopy the anesthesia providers were asked to fill out the Cormack and Lehane grading for the vocal cord view during direct laryngoscopy as per following:
Grade 1, visualization of the entire laryngeal aperture
Grade 2, visualization of parts of the laryngeal aperture or the arytenoids
Grade 3, visualization of only the epiglottis
Grade 4, visualization of only the soft palate
The Bland Altman plot with limits of agreement was drawn for the correlation of the standard of care Pre-operative Mallampati Classification with Intraoperative Cormack Lehane Grading. Subsequently, the
regression coefficients for correlating the ultrasound parameters with Cormack Lehane grading were determined and P <0.05 was considered significant. Similar to the plots described by Carvalho et al6, the logistic plots of the cumulative probability were drawn to assess the ED 50 and ED 95 for the prediction of the Cormack Lehane Grades I, II and III. Subsequently, the Receiver Operating Characteristic graphs were drawn to determine the cut-point (a whole number value of ultrasound parameter or the derivative ratio) for the most appropriate prediction of the Cormack Lehane Grades.
Results
Out of the 72 patients enrolled in the study, first 23 enrolled patients were excluded from the final analysis as the ultrasound measurements and related technical data collection was incompletely recorded due to the initial stages of investigators’ proficiency in assessing the ultrasound imaging parameters and collection of data as the utility of the ultrasound imaging for airway assessment was very new to the research investigators. Based on the improved proficiency in appreciation of the ultrasound parameters and the collection of the complete study data in the remaining 49 patients, it was observed that there was a correlation of the distance between the epiglottis and the vocal cords (E-VC) with the Cormack Lehane Grading; correlation was strong negative with regression coefficient of -0.966 (95% CI -1.431 to -0.501; p = 0.0001). Subsequently, the correlation of the pre-epiglottis space (Pre-E) with the Cormack Lehane Grading was strong in positive direction with regression coefficient of 0.595 (95% CI 0.261 to 0.929; p = 0.0008). Finally the ratio of Pre-E and E-VC distances with the Cormack Lehane Grading had the strongest positive correlation with regression coefficient of 0.495 (95% CI 0.319 to 0.671; p <0.0001). Though logistic data interpretation and analysis of our study patients (Fig. 3) suggested that ED 50 (Pre-E/E-VC values below which 50% probability for the corresponding Cormack Lehane Grade) were 0.55, 1.49 and 2.41 for Cormack Lehane Grade 1, II and III respectively and ED 95 (Pre-E/E-VC values below which 95% probability for the corresponding Cormack Lehane Grade) were 1.17, 3.33 and 4.86
Fig� 2 Ultrasonic View in the Plane G for Ultrasonographic
Modification of Cormack Lehane Grading

838 GUPTA D. et. al
for Cormack Lehane Grade 1, II and III respectively, after rearranging the data (Fig. 4-5) for simplification, we found that prediction of Cormack Lehane (CL) grades can be adequately (67%-68% sensitivity) made by the ratio of Pre-E and E-VC distances(Pre-E/E-VC) {0<[Pre-E/E-VC]<1 ≈ CL grade 1; 1<[Pre-E/E-VC]<2 ≈ CL grade 2; and 2<[Pre-E/E-VC]<3 ≈ CL grade 3} (Fig. 6). The Bland-Altman scatter plot for pre-operative Mallampati Classification and intra-operative Cormack Lehane Grading (Fig. 7) showed large and wide limits of agreement (-1.66 to + 1.70) but these differences between the two grading systems
were statistically insignificant. The average time taken to complete the ultrasound examination of airway was 31.7 ± 12.4 seconds.
Discussion
The presently available non-invasive modality of airway assessment primarily include (but not limited to) Mallampati Classification, thyromental distance assessment, and atlanto-occipital (neck) extension; and in the pre-operative holding areas, the anesthesiologists usually come to a conclusion of a predicted difficult
Fig� 3 Crude Data Analysis of the Study Patient Population
Fig� 4 Probability and Cumulative Probability Graphs of the Cormack Lehane Classification in correlation with Ultrasound Assessment of the Airway

M.E.J. ANESTH 21 (6), 2012
839ULTRASONOGRAPHIC MODIFICATION OF CORMACK LEHANE CLASSIFICATION FOR PRE-ANESTHETIC AIRWAY ASSESSMENT
Fig� 5 Incidence Graph of the Cormack Lehane Classification and its correlation
with Ultrasound Assessment of the Airway
Fig� 6 Receiver Operating Characteristic Graphs for the Development
of the Ultrasonographic Modification of Cormack Lehane Grading

840 GUPTA D. et. al
approximately 30 seconds to reach a conclusion as regards to the ultrasonographic modification grade of Cormack Lehane Classification. This fast and quick airway assessment can be a good supplementary tool in the busy anesthesiologists’ armamentarium wherein the anesthesia care teams can rest assured that before transferring the patients to the operating room they have insightful visuals of the patients’ airways that was obtained non-invasively and without much delays in the daily routines of anesthesia caregiving.
We devised the oblique G plane (Fig. 1) to document the ultrasonographic modification grade of Cormack Lehane Classification that was quick to achieve and easy to calculate the ratio of the distances (Pre-E/E-VC). Even though the sensitivity was only 67%-68% (possibly due to the small number of patients), the rapidity of this ultrasound application in the airway assessment may pave a way for future pre-anesthetic airway assessment wherein the intra-operative Cormack Lehane Classification can be routinely predicted based on the ratio of the pre-epiglottic space depth and the epiglottis-to-vocal-cords distance. We devised this ratio for the classification because it is our understanding that the larger pre-epiglottic space as well as smaller E-VC distance will have correlation with increasing difficulty in the airway instrumentation (laryngoscopy and intubation) in terms of the Cormack Lehane Classification grading. Moreover if the pre-epiglottic space is very large in a patient but the ratio is small because of larger E-VC distance in the patient, the predicted airway in the patient will be easy and intraoperative Cormack Lehane grade in the patient will be low; the only concern for airway management in the patient will be that the laryngoscopy to achieve the low grade of Cormack Lehane classification will be tedious secondary to larger force required to lift the large epiglottis as reflected by the deep pre-epiglottis space.
We acknowledge the limitations of our classification. The number of the patients was small. We did not have any Cormack Lehane grade IV patients in our study. Based on the assessment of the Receiver Operating Characteristic curves (Fig. 6) for each Cormack Lehane Grades, it will be more prudent to say that as the Cormack Lehane Classification is a continuum of the four grades (only three grades were
or easy airway based on their combined assessment of the above mentioned predictors with other external observations like mouth opening and head and neck pathologies (LEMON Score)7-9. However, it is not always feasible to do a complete airway examination in urgent/emergent clinical scenarios in agitated, non-cooperative or unconscious patients. Moreover, as observed in our analysis, the intra-operative laryngoscopy grade (Cormack Lehane Classification) may not always correlate adequately well with the pre-operative predictors of airway assessment. Hence there is always a need of non-invasive but more accurate airway assessment of the airway in the pre-operative holding area as researchers have documented questionable feasibility of the invasive transnasal flexible fiberoptic airway assessment in the pre-operative area10-11. Additionally, the time constraints of operating room complexes may limit the possibility of testing for any new modalities of airway assessment in the pre-operative holding areas unless the innovative applications for assessing the airway is not time consuming for both the patients and the anesthesia care providers.
The present study demonstrates that Cormack Lehane Classification can be appropriately assessed by the ultrasound examination of the neck that takes
Fig� 7 Bland Altman Plot for Correlation of Preoperative Mallampati Classification and Intraoperative Cormack Lehane Grading

M.E.J. ANESTH 21 (6), 2012
841ULTRASONOGRAPHIC MODIFICATION OF CORMACK LEHANE CLASSIFICATION FOR PRE-ANESTHETIC AIRWAY ASSESSMENT
Conclusion
The ultrasonographic modification of Cormack-Lehane Classification was developed with 67%-68% sensitivity as per the ratio of the distances [Pre-E/E-VC]:
0< [Pre-E/E-VC] <1 ≈ CL grade 1
1< [Pre-E/E-VC] <2 ≈ CL grade 2
2< [Pre-E/E-VC] <3 ≈ CL grade 3
The non-invasive ultrasonographic modification of invasive Cormack Lehane classification for airway assessment can supplement the presently available non-invasive modalities of pre-anesthetic airway assessment including the Mallampati Classification.
observed and studied in our study patient population), the extremes of the Cormack Lehane grade (grade I and III) will be better assessed and predicted by the ratio of the distances (Pre-E/E-VC) than the Cormack Lehane grade II. Even though we did not have any Cormack Lehane grade IV patients, it may be easily theorized by our results and analysis that in Cormack Lehane grade IV patients, the pre-epiglottic space will be very large with very high probability of the large epiglottis obscuring the ultrasonographic visualization of the non-phonating vocal cords in the ultrasonic plane “G”, and the calculation of the ratio of the distances (Pre-E/E-VC) may be impossible in the indirectly predicted (prediction by exclusion) Cormack Lehane grade IV patients. For a better neck skin surface contact, the concave curve high frequency transducer has yet not been developed and this may delay the routine use of ultrasound in the airway assessment as standard of care.

842 GUPTA D. et. al
7. SOYUNCU S, EKEN C, CETE Y, BEKTAS F, AKCIMEN M: Determination of difficult intubation in the ED. Am J Emerg Med; 2009, 27:905-10.
8. REED MJ, DUNN MJ, MCKEOWN DW: Can an airway assessment score predict difficulty at intubation in the emergency department? Emerg Med J; 2005, 22:99-102.
9. REED MJ, RENNIE LM, DUNN MJ, GRAY AJ, ROBERTSON CE, MCKEOWN DW: Is the 'LEMON' method an easily applied emergency airway assessment tool? Eur J Emerg Med; 2004, 11:154-7.
10. ROSENBLATT W, IANUS AI, SUKHUPRAGARN W, FICKENSCHER A, SASAKI C: Preoperative endoscopic airway examination (PEAE) provides superior airway information and may reduce the use of unnecessary awake intubation. Anesth Analg; 2011, 112:602-7.
11. AKçA O, LENHARDT R, HEINE MF: Can transnasal flexible fiberoptic laryngoscopy contribute to airway management decisions? Anesth Analg; 2011, 112:519-20.
References
1. TSUI BC, HUI CM: Sublingual airway ultrasound imaging. Can J Anaesth; 2008, 55:790-1.
2. TSUI BC, HUI CM: Challenges in sublingual airway ultrasound interpretation. Can J Anaesth; 2009, 56:393-4.
3. SINGH M, CHIN KJ, CHAN VW, WONG DT, PRASAD GA, YU E: Use of sonography for airway assessment: an observational study. J Ultrasound Med; 2010, 29:79-85.
4. LAKHAL K, DELPLACE X, COTTIER JP, TRANQUART F, SAUVAGNAC X, MERCIER C, FUSCIARDI J, LAFFON M: The feasibility of ultrasound to assess subglottic diameter. Anesth Analg; 2007, 104:611-4.
5. ADHIKARI S, ZEGER W, SCHMIER C, CRUM T, CRAVEN A, FRROKAJ I, PANG H, SHOSTROM V: Pilot study to determine the utility of point-of-care ultrasound in the assessment of difficult laryngoscopy. Acad Emerg Med; 2011, 18:754-8.
6. CARVALHO B, DURBIN M, DROVER DR, COHEN SE, GINOSAR Y, RILEY ET: The ED50 and ED95 of intrathecal isobaric bupivacaine with opioids for cesarean delivery. Anesthesiology; 2005, 103:606-12.

843 M.E.J. ANESTH 21 (6), 2012
VIDEOLARYNGOSCOPIC ENDOTRACHEAL INTUBATION (GLIDESCOPE®) OF MORBIDLY OBESE PATIENTS
IN SEMI-ERECT POSITION: A COMPARISON WITH RAPID SEQUENCE
INDUCTION IN SUPINE POSITION*
DEEPAK GUPTA, KONSTANTIN RUSIN
Abstract
Background: In regards to peri-anesthetic morbidity considerations, morbidly obese patients often have full stomach for extended periods secondary to delayed gastric emptying. Additionally, they may have difficulty lying supine because of multiple reasons.
Study Objectives: The purpose of the study was to compare endotracheal intubation of morbidly obese patients placed in semi-erect position with the rapid sequence induction in the supine position using GlideScope® video laryngoscopy.
Methods: A prospective randomized study was conducted in ASA I-III patients aged 18-65 years who were scheduled for bariatric surgery. Group A (Study Group): General anesthesia was induced in the semi-erect position, and endotracheal intubation was performed by the investigator positioned in front of the patient. The GlideScope® blade was held in the right hand of the investigator during intubation and endotracheal tube with rigid stylet was inserted using the left hand. Group B (Control Group): General anesthesia was induced and patient’s trachea intubated in the standard supine position.
Results: 39 patients underwent endotracheal intubation in semi-erect position (Study Group) and 37 patients underwent endotracheal intubation in supine position (Control Group). No differences were observed in the intubation parameters or patient safety. Intubation times required to secure patients’ airways were not significantly insignificant (p = 0.42) between the two groups; desaturation episodes occurred 50% less frequently (though insignificant p = 0.42) in the semi-erect group.
Conclusion: This is the first prospective study demonstrating endotracheal intubation with GlideScope® in the semi-erect position as comparable to standard supine position intubation. Moreover, gravity-directed and aligned biomechanics in the semi-erect position may be ergonomically more efficient for intubating morbidly obese patients.
* Department of Anesthesiology, Wayne State University/Detroit Medical Center, Detroit, MI 48201, United States. Corresponding Author: Konstantin Rusin, M.D., Ph.D. Associate Medical Director, Anesthesiology, Wayne State
University, Box No 162, 3990 John R, Detroit, Michigan 48201, United States, Tel: 1-313-745-7233, Fax: 1-313-993-3889. E-mail: [email protected]

844 GUPTA D. et. al
using standard general anesthetic techniques.
The laryngoscopy and intubation procedure was performed as follows:
• Group A (Study Group): The patient was seated on the operating room table adjusted to the semi-erect angle in which the patient felt most comfortable. After standard ASA monitors application, patient was pre-oxygenated in the semi-erect position. General anesthesia was induced in the semi-erect position, and endotracheal intubation was performed by the investigator positioned in front of the patient. The GlideScope® blade was held in the right hand of the investigator during intubation and endotracheal tube with rigid stylet was inserted using the left hand.
• Group B (Control Group): The patient was pre-oxygenated and general anesthesia was induced in the standard supine position. Subsequently, patient’s trachea was intubated with GlideScope® in the standard supine position.
The following observations were recorded pre-operatively: body mass index (BMI), past medical history of gastro-esophageal reflux disease, obstructive sleep apnea and continuous positive airway pressure (CPAP) use, and pre-existing intolerances to lay supine with corresponding causes for these intolerances. Intra-operatively, following parameters were recorded: the total time for video laryngoscopy and intubation, incidence of failure to intubate in the first attempt, incidence of desaturation episodes (pulse oximetry readings decreasing below 90%), incidence of the need for bag-mask ventilation interrupting laryngoscopy and intubation, and incidence of gross visible regurgitation of gastric contents into the oropharynx during video-laryngoscopy.
For statistical analysis, an ANOVA single factor test was applied to compare the means and variance of the continuous data. A Fisher exact probability test (two tailed) was utilized to compare all categorical data. Normality/distribution of data was evaluated by histogram and probability plots. For non-parametric data Mann Whitney tests was used. A p-value of <0.05 was considered significant.
Introduction
The rising incidence of morbid obesity necessitates that anesthesia care providers search for safer and optimal techniques to secure these patients’ airways. In regards to peri-anesthetic morbidity considerations, morbidly obese patients often have full stomach for extended periods secondary to delayed gastric emptying. Additionally, they may have difficulty lying supine because of multiple reasons. Therefore, to perform surgery in this patient population, anesthetic induction and intubation in a semi-erect position may be required. Postural change from supine to sitting position significantly reduces collapsibility of pharyngeal airway in anesthetized and paralyzed patients with obstructive sleep apnea1. However, intubation in the semi-erect position may be difficult, if not impossible, with a conventional direct laryngoscope. In such difficult cases, flexible fiberoptic bronchoscope intubation has been the standard technique, with the practitioner positioned at the patient’s right side facing the patient. Recently cases studies have reported awake intubation performed with video laryngoscopy by Airtraq (Prodol, Vizcaya, Spain)2 and Pentax-AWS airway Scope systems (AWS; Hoya, Tokyo, Japan)3 in patients placed in the semi-erect position. Thus far there have been no prospective human studies with GlideScope® (Verathon Inc., Bothell, WA, United States) aided endotracheal intubation in obese semi-erect patients.
The purpose of the study was to assess the feasibility in regards to patient safety considerations and ease for operator’s use in general anesthesia induction and endotracheal intubation of morbidly obese patients placed in semi-erect position and to compare this technique with the rapid sequence induction in the supine position using GlideScope® video laryngoscopy.
Methods
After institutional review board approval for the study protocol and written informed consent, a prospective randomized study was conducted in 85 ASA I-III patients aged 18-65 years who were scheduled for bariatric surgery under general anesthesia

M.E.J. ANESTH 21 (6), 2012
845VIDEOLARYNGOSCOPIC ENDOTRACHEAL INTUBATION (GLIDESCOPE®) OF MORBIDLY OBESE PATIENTS IN SEMI-ERECT POSITION: A COMPARISON WITH RAPID SEQUENCE INDUCTION IN SUPINE POSITION
(Table 1). There were also no significant differences in regards to preoperative characteristics except a higher BMI in supine controls (51.6 ± 10.5 kg/m2 control group; 46.8 ± 8.9 kg/m2 study group), which was statistically significant (P = 0.04).
Discussion
In this first prospective study to compare anesthesia induction and endotracheal intubation with GlideScope® in semi-erect position versus supine position, no differences were observed in the intubation parameters or patient safety. Intubation times required to secure patients’ airways were not significantly between the two groups; desaturation episodes occurred 50% less frequently (though insignificant p = 0.42) in the semi-erect group.
Results
A total of 85 patients were recruited for inclusion in the study protocol. However, after written informed consent and completed recruitment, nine patients were excluded from the study because tracheal intubation was performed with Mac-Miller laryngoscopes instead of GlideScope® due to unforeseen unavailability of the GlideScope®. Among the remaining 76 eligible patients, 39 patients underwent endotracheal intubation in semi-erect position (Study Group) and 37 patients underwent endotracheal intubation in supine position (Control Group). In comparing the two groups the intubation times (control group 51.8 ± 17.8s; study group 54.6 ± 13.2 s) were not significantly different (P = 0.42). In comparing the two groups there were no significant differences in the intubation parameters
Table 1 Pre-Operative Demographics and Intra-Operative Intubation Characteristics
Characteristic Semi-Erect Intubation Group (n = 39)
Supine Intubation Group(n = 37)
P value(*significant if <0.05)
Body Mass Index (kg/m2) 46.8 ± 8.9 51.6 ± 10.5 0.04*Pre-Existing Co-Morbidities Diagnosed Gastro-esophageal Reflux Disease (n) 38% (15/39) 54% (20/37) 0.25Diagnosed Obstructive Sleep Apnea (n) 36% (14/39) 41% (15/37) 0.81CPAP Treatment for Sleep Apnea at Home (n) 28% (11/39) 35% (13/37) 0.62Symptomatic Intolerance to Supine Position (n) 77% (30/39) 76% (28/37) >0.99Underlying Reason for Intolerance to Supine Position Dyspnea 53% (16/30) 50% (14/28) >0.99Heartburn 23% (7/30) 32% (9/28) 0.56Gastropharyngeal Reflux 13% (4/30) 21% (6/28) 0.50Backache 60% (18/30) 79% (22/28) 0.16Others 23% (7/30) 7% (2/28) 0.15Multiple 47% (14/30) 50% (14/28) >0.99Tolerance to Supine Position Despite Symptoms 11% (1/9) (Despite
Dyspnea and Heartburn)56% (5/9) (Despite
Heartburn or Pharyngeal Reflux)
0.13
Intubation Parameters Intraoperative Time Taken to Intubate (s) 54.6 ± 13.2 51.8 ± 17.8 0.42Intraoperative Failure to Intubate in First Attempt (n)
8% (3/39) 5% (2/37) >0.99
Intraoperative Desaturation Episodes (n) 5% (2/39) 11% (4/37) 0.42Intraoperative Bag-Mask Ventilation before Second Intubation Attempt (n)
3% (1/39) 0% (0/37) >0.99
Visible Gross Regurgitation during Intubation (n) 5% (2/39) 3% (1/37) >0.99

846 GUPTA D. et. al
case reports observed that different models of video-laryngoscopes (Airtraq2 and Pentax-AWS airway Scope systems3) might have been equivalently useful to accomplish sleep endotracheal intubation in semi-erect position (this can be a domain for future endeavors by the airway researchers).
One of the major alternative positions for endotracheal intubation in morbidly obese patients is the ‘Ramped’ position4-7. The ‘ramped’ position is achieved by arranging blankets, pillows, solution bags or the Rapid Airway Management Positioner (RAMP, Airpal Inc., Center Valley, PA)6 beneath the patient’s shoulders and head before anesthesia induction. Some RAMP devices are placed beneath the patient’s shoulders after anesthetic induction7 and then inflated to elevate patient’s shoulders and upper thorax. Disadvantage with ‘ramped’ position is the need for patient re-positioning after endotracheal intubation to remove blankets, pillows, or RAMPs beneath the patient. This maneuvering can risk injury to patients as well as operating room personnel. Semi-erect positioning of patient nullifies the need for ‘ramped’ positioners and video laryngoscopy nullifies the need for the operator to be at patient’s head end for intubation. This technique is similar to flexible fiberoptic bronchoscope guided awake intubation performed in semi-erect position.
To demonstrate anatomical maneuverability advantages, the positions used in our study have been described as schematic diagrams with manikins in Figs. 1 and 2 for control group (supine position intubation) and study group (semi-erect position intubation) respectively. Positioning shown in Fig. 3 (a schematic diagram of the conventional method for semi-erect position intubation with operator’s position at the patient’s head-end) was not used in our study, and is only shown as a comparative method for endotracheal intubation. From an operator’s perspective, potentially favorable biomechanics (Table 2) for performing intubation in the semi-erect position (Fig. 2) are evident with (a) maintained neutral cervical spine position for operator (b) patient’s mouth and video display aligned in one line of sight for operator (c) forces required for laryngoscopy primarily directed towards gravity and (d) minimal force requirement for lower jaw depression to achieve an optimal video-laryngoscopic view. The favorable biomechanics for patients in the studied semi-
Induction and intubation in morbidly obese patients can be challenging. While performing endotracheal intubation in morbidly obese patients, the anesthesia care providers may encounter; (a) large redundant oropharyngeal tissues compressing on the lax glottic opening (b) low functional residual capacity that markedly reduces allowable apneic time (c) large breasts (male or female) and (d) less cervical spine mobility with potentially increased risk of dental or oropharyngeal injuries during laryngoscopy. Pre-anesthetic sleep patterns may predict patients’ physiological responses at the time of induction of anesthesia before the cellular and molecular effects of inhalational anesthesia, mechanics of positive pressure ventilation and technicalities of the operative procedures charter patients’ pathophysiology into domains unpredictable from their pre-anesthetic sleep patterns. It is reasonable to hypothesize that the cardiorespiratory variables of morbidly obese patients are more favorable when they are lying in their comfortable sleeping positions. Majority of these patients have intolerance to supine position and are either using ergonomically incorrect multitude of pillows or biomechanically correct reclining beds. These intolerances arise from a variety of reasons that are similar to as observed in our study (Table 1) and may caution the anesthesia care provider to anticipate difficult airway secondary to failure to ventilate/intubate, gross pulmonary aspirations, rapid desaturation episodes, and severely labile hemodynamics.
The next step for designing the present study was to utilize an ergonomically correct method that would be less strenuous on the patients’ airways that are being intubated as well as on the operators performing the intubation. Presently, unless an extraordinarily difficult airway is predicted, most practitioners prefer sleep induction and endotracheal intubation as compared to an awake state endotracheal intubation. Therefore, to compare the endotracheal intubation with GlideScope® in morbidly obese patients in two different positions, sleep induction protocol was chosen for the present study. The additional reasons for sleep induction as the choice was that the videolaryngoscopy method used in this study (GlideScope®) requires rigid stylet (GlideRite®), which may not be safe to manipulate within the un-relaxed airways of awake patients. Other
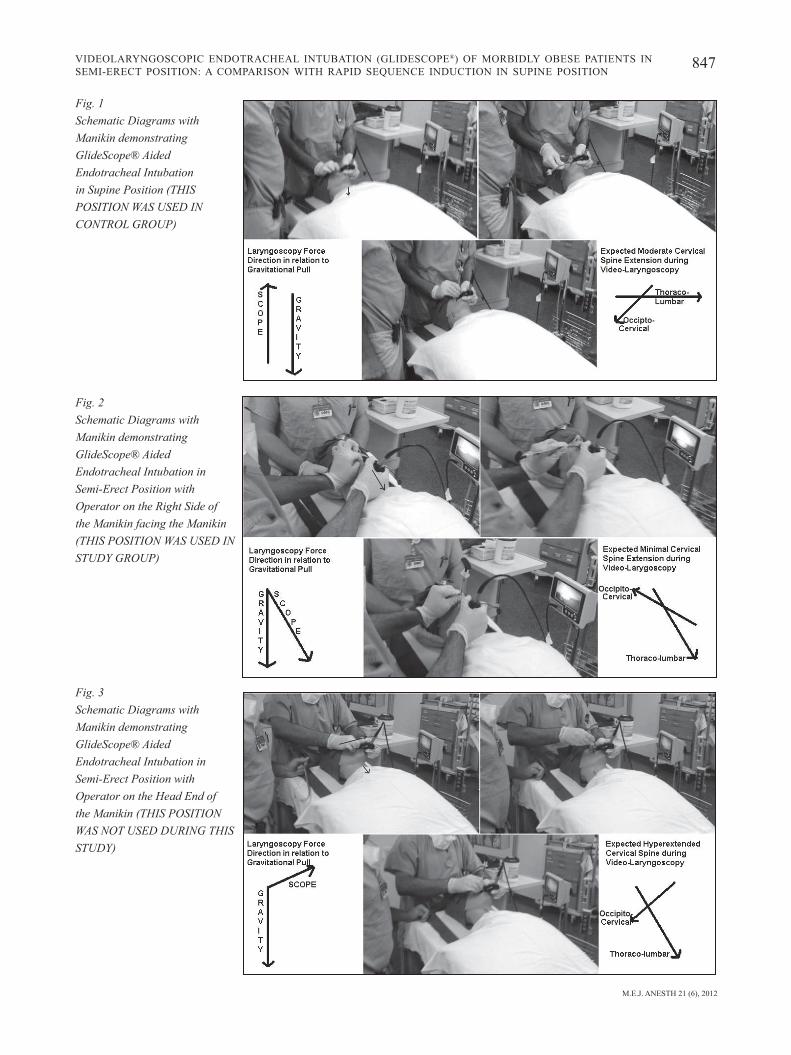
M.E.J. ANESTH 21 (6), 2012
847VIDEOLARYNGOSCOPIC ENDOTRACHEAL INTUBATION (GLIDESCOPE®) OF MORBIDLY OBESE PATIENTS IN SEMI-ERECT POSITION: A COMPARISON WITH RAPID SEQUENCE INDUCTION IN SUPINE POSITION
Fig� 1 Schematic Diagrams with Manikin demonstrating GlideScope® Aided Endotracheal Intubation in Supine Position (THIS POSITION WAS USED IN CONTROL GROUP)
Fig� 2 Schematic Diagrams with Manikin demonstrating GlideScope® Aided Endotracheal Intubation in Semi-Erect Position with Operator on the Right Side of the Manikin facing the Manikin (THIS POSITION WAS USED IN STUDY GROUP)
Fig� 3 Schematic Diagrams with Manikin demonstrating GlideScope® Aided Endotracheal Intubation in Semi-Erect Position with Operator on the Head End of the Manikin (THIS POSITION WAS NOT USED DURING THIS STUDY)

848 GUPTA D. et. al
erect position (Fig. 2) are evident with (a) operators’ hands staying away from their eyes and (b) avoidance of laryngoscopic forces on the patients’ maxillary teeth and upper lips. However while intubating from the patient’s right side, caution is required to avoid un-warranted forceful lower jaw depression that may cause injuries to mandibular teeth, lower lips and tongue. Even though GlideScope® is known to cause moderate cervical spine extension in classical supine position8, the semi-erect position (Fig. 2) may achieve video-laryngoscopic
view for intubation with minimal neck extension.
The limitations of the semi-erect position (Fig. 2) are (a) operator’s side position while intubation (instead of head-end position) (b) exchange of hands for using GlideScope® blade and holding the endotracheal tube (c) difficult ergonomics while performing the jaw-pull maneuver for face-mask seal and bag-mask ventilation from the right side of the patient (sometimes may require the assistance of secondary operators at the head end). Secondary anesthesia operators will have
Table 2 Biomechanical Comparisons between the Various Positions for GlideScope® Aided Endotracheal Intubatio�
Characteristic Supine Position as in Control Group
See Fig� 1
Semi-Erect Position as in Study Group
See Fig� 2
Alternative Semi-Erect Position (NOT USED in this
study)See Fig� 3
Patient Position Laying Flat on Surgical Table Table Back End Up to Patient Comfort Level
Table Back End Up to Patient Comfort Level
Primary Operator Position Head End of Patient Right Side of Patient Head End of Patient
Face-Mask Seal Using Jaw Thrust Away from Operator180º to Gravity
Using Jaw Pull Towards Operator90º to Gravity
Using Jaw Thrust Away from Operator120º-150º to Gravity
GlideScope® Blade In Left Hand In Right Hand In Left Hand
Endotracheal Tube In Right Hand In Left Hand In Right Hand
Video Display on Left Side of Patient
Operator’s Eyes, Patient’s Opened Mouth and Video Display: NOT ALIGNED in one line of sight
Operator’s Eyes, Patient’s Opened Mouth and Video Display: all ALIGNED in one line of sight
Operator’s Eyes, Patient’s Opened Mouth and Video Display: NOT ALIGNED in one line of sight
Neutral Cervical Spine Motion of Operator
Not Maintained as NOT ALIGNED line of sight
Maintained as ALIGNED line of sight
Not Maintained as NOT ALIGNED line of sight
Upper Extremity Movements of Operator
Left Arm Flexion;
Pronation of Supinated Right Arm
Right Arm Abductionand External Rotation;
Supination of Pronated Left Arm
Left Forearm Extension with Left Arm Flexion;Pronation of Supinated Right Arm
Direction for Laryngocopy Movement
180º to Gravity(Against Gravity)
30-60º to Gravity(Towards Gravity)
120-150º to Gravity(Away from Gravity)
Primary Force for Laryngoscopy Strong Force for Lower Jaw Lifting
Minimal Force for Lower Jaw Depression
Moderate Force for Lower Jaw Thrusting and then Lifting
Oral Injury Cautions For Maxillary TeethFor Upper Lip
For Mandibular TeethFor Lower Lip
For Both TeethFor Both Lips
Patient’s Cervical Spine Motion Moderate Extension Minimal ExtensionPrimarily Neutral
Hyperextension Likely
Secondary Operator Right Side of PatientFor Cricoid Pressure;Second Pairs of Hand
Head End of Patient For Stabilizing Head;Second Pairs of Hand
Right Side of PatientFor Cricoid Pressure;Second Pairs of Hand

M.E.J. ANESTH 21 (6), 2012
849VIDEOLARYNGOSCOPIC ENDOTRACHEAL INTUBATION (GLIDESCOPE®) OF MORBIDLY OBESE PATIENTS IN SEMI-ERECT POSITION: A COMPARISON WITH RAPID SEQUENCE INDUCTION IN SUPINE POSITION
BMI in semi-erect position (P = 0.04) may have a role to play in equivalent results between the two groups; however both study group patients as well as controls were morbidly obese with mean BMI above 45 kg/m2. Additionally, though 50% decrease in the oxygen desaturation episodes among the semi-erect group patients may require validation in larger adequately powered studies, the prevention of oxygen desaturation elicited in our study may still be clinically significant.
Conclusion
This is the first prospective study demonstrating endotracheal intubation with GlideScope® in the semi-erect position. There were no statistical differences in any intubating parameters in the semi-erect position as compared to the standard supine intubation. Moreover, gravity-directed and aligned biomechanics in the semi-erect position may be ergonomically more efficient for intubating morbidly obese patients.
Acknowledgement
The authors are thankful to Dr George Mckelvey, Research Associate, Department of Anesthesiology, Wayne State University for completing the statistics and copyediting the final manuscript.
to perform additional tasks including (a) stabilization of relaxed patient’s head (b) assisting with jaw-thrust maneuver if jaw-pull maneuver fails, and (c) bag-mask ventilation in case of unanticipated difficult airway or prolonged anesthesia induction period. This may appear to increase the anesthesia personnel requirements in the operating rooms. However, this is not a major concern as there is always a certified registered nurse anesthetist or a resident anesthesiologist as the primary operator at the time of anesthesia induction under the direct supervision of attending anesthesiologist as the secondary operator in most of the hospitals in the United States. A potential future study will be to quantify whether this more optimal ergonomic intubation positioning leads to its generalized acceptance for semi-erect position endotracheal intubation.
There were some limitations to the present study. Based on the intubation times as the primary outcome, the power of the study was 0.29. To adequately power this study (1-β = 0.8), the total patients required would have been approximately 800. However, even this large number of patients will only give a statistical advantage to the classical supine position intubation (51.8 sec) as compared to studied semi-erect position intubation (54.6 sec). This 3-second gain may be statistically significant but in our opinion will not be clinically significant. Despite randomization of the patients’ allocation between the two groups, lower

850 GUPTA D. et. al
OCHROCH EA: Obstructive sleep apnea is not a risk factor for difficult intubation in morbidly obese patients. Anesth Analg; 2009, 109:1182-6.
6. CATTANO D, MELNIKOv v, KHALIL Y, SRIDHAR S, HAGbERG CA: An evaluation of the rapid airway management positioner in obese patients undergoing gastric bypass or laparoscopic gastric banding surgery. Obes Surg; 2010, 20:1436-41.
7. bRZEZINSKI M, LEE A, HOLAK EJ, PAGEL PS: A simple method for obtaining a "ramped" laryngoscopy position after anesthetic induction. J Cardiothorac Vasc Anesth; 2010, 24:537-9.
8. TURKSTRA TP, CRAEN RA, PELZ DM, GELb AW: Cervical spine motion: a fluoroscopic comparison during intubation with lighted stylet, GlideScope®, and Macintosh laryngoscope. Anesth Analg; 2005, 101:910-5.
References
1. TAGAITO Y, ISONO S, TANAKA A, ISHIKAWA T, NISHINO T: Sitting posture decreases collapsibility of the passive pharynx in anesthetized paralyzed patients with obstructive sleep apnea. Anesthesiology; 2010, 113:812-8.
2. UAKRITDATHIKARN T, ASAMPINAWAT T, WANASUWANNAKUL T, YOOSAMRAN b: Awake intubation with Airtraq laryngoscope in a morbidly obese patient. J Med Assoc Thai; 2008, 91:564-7.
3. SUZUKI A, TERAO M, AIZAWA K, SASAKAWA T, HENDERSON JJ, IWASAKI H: Pentax-AWS airway Scope as an alternative for awake flexible fiberoptic intubation of a morbidly obese patient in the semi-sitting position. J Anesth; 2009, 23:162-3.
4. COLLINS JS, LEMMENS HJ, bRODSKY Jb, bROCK-UTNE JG, LEvITAN RM: Laryngoscopy and morbid obesity: a comparison of the "sniff" and "ramped" positions. Obes Surg; 2004, 14:1171-5.
5. NELIGAN PJ, PORTER S, MAX b, MALHOTRA G, GREENbLATT EP,

851 M.E.J. ANESTH 21 (6), 2012
NALOXONE VERSUS METOCLOPRAMIDE FOR THE TREATMENT OF ESTABLISHED POSTOPERATIVE NAUSEA AND VOMITING
IN PATIENTS FOLLOWING GENERAL ANESTHESIA WITH FENTANYL SUPPLEMENTATION
- PILOT STUDY -
DAbbOUS A*, SOUKI M**, bARAKA A*, JAbbOUR-KHOURY S*
Introduction
Postoperative nausea and vomiting (PONV) remains a common adverse event associated with surgery and anesthesia. Despite significant advances in the area of PONV and the introduction of new antiemetic agents, the overall incidence of PONV is currently estimated to be around 20 to 30%1.
PONV can cause prolonged post anesthesia care unit (PACU) stay and unanticipated admissions following ambulatory surgery, therefore increasing medical costs1. Nausea and vomiting are also among the most unpleasant experiences associated with surgery and one of the most common reasons for poor patient satisfaction rating in the postoperative period2. Because PONV is multi-factorial and several neurotransmitters are involved in the emetic response, effective management remains challenging.
Intraoperative opioids are considered one of the anesthesia related factors for PONV3-5. In a review of 27,626 patients admitted to the PACU, administration of opioids during surgery increased the risk of PONV four folds6. Roberts et al7 also confirmed that incidence of nausea and vomiting both increased in a dose dependent manner by the amount of opiate administered postoperatively. Prophylactic administration of an antiemetic had no influence on the risk of PONV in the PACU related to opioids6.
Low dose naloxone infusion (0.25mcg-1mcg/kg/hr) has been shown to decrease epidural and patient controlled analgesia (PCA) opioid related side effects (nausea, vomiting and pruritis) without affecting pain scores8-12, and hence naloxone administration may also decrease the incidence of PONV following general anesthesia including fentanyl supplementation. Metoclopramide has been used for the treatment of PONV in the PACU13-14, and for breakthrough PONV after prophylaxis15.
The purpose of this study is to compare the antiemetic effectiveness of bolus intravenous naloxone 0.5mcg/Kg versus metoclopramide 10mg for the treatment of PONV in the PACU, in patients undergoing general anesthesia including fentanyl supplementation.
* Department of Anesthesiology, P.O. Box 11-0236, Beirut, Lebanon. Fax: 961 1 745249. E-mail: [email protected]* Department of Anesthesiology, American University of Beirut-Medical center, Beirut, Lebanon.** Fouad Souki, Assistant professor, clinical anesthesia, University of Miami, Fl. Corresponding Author: Alia Dabbous, MD, American University of Beirut.

852 DABBOUS A. et. al
Methods
After obtaining Institutional review board approval and informed consent for this randomized controlled prospective study; ASA I and II patients aged 18-70 years, scheduled for elective surgery under general anesthesia including fentanyl supplementation were recruited. Exclusion criteria included patient’s refusal, renal or liver diseases, pregnant or lactating mothers and patients who were on antiemetic drugs preoperatively. Using standardized monitoring techniques of EKG, pulse oximetry, and blood pressure, induction of general anesthesia was done using propofol 2mg/Kg, lidocaine 1.5 mg/Kg and fentanyl 2mcg/Kg. Muscle relaxation was achieved with rocuronium 0.6mg/Kg. For maintenance of anesthesia, nitrous oxide/ oxygen mixture with sevoflurane was used. Additional doses of fentanyl and muscle relaxants were administered as needed. At the end of the surgical procedure reversal of the neuromuscular blockade was achieved with neostigmine 0.05mg/Kg and glycopyrrolate 0.01mg/Kg. The total dose of fentanyl used, as well as, the duration of the operation were recorded. Upon arrival to the PACU, assessment of nausea was done according to a four points verbal descriptive scale (VDS)16 (0 = no nausea, 1 = mild, 2 = moderate, 3 = severe). The assessment was done by one PACU nurse involved in the study. Vomiting was recorded as either present of absent.
Treatment for PONV was given if nausea was moderate to severe and lasted for 10 minutes, more than one episode of vomiting occurred, or at any time the patient requested treatment. A total of 44 patients experienced PONV in the PACU and warranted treatment. Patients were randomly selected to receive either metoclopramide 10mg or naloxone 0.5mcg/kg, both drugs diluted to 10ml.
The person administering the medications was unaware of the treatment drugs. Assessment of the patients was done at 2, 5, 10 minutes following the study medication. Response was documented as complete(i.e no nausea and vomiting and no antiemetics given) or partial (i.e improvement in the nausea score). After 10minutes, if the patient continued to complain of nausea or vomiting, or had a partial response to either naloxone or metoclopramide and requested treatment,
ondansetron 4mg intravenously was given.
Assessment of pain was also recorded according to the 10 point verbal analogue scale (zero being = no pain, and 10 being = the worst pain ever). As regards to safety, we reported all possible drug-related side effects and observed vital signs before and 10 minutes after treatment.
Continuous variables were analyzed using Student t-test, and quantitative variables were analyzed using Fisher’s Exact Test. All tests performed were two-sided with significance level set at P <0.05.
Results
Twenty two patients were treated with Naloxone and 22 with Metoclopramide. Both groups were comparable in terms of age, sex, operative duration, total intraoperative fentanyl used, and number of PONV risk factors (Table 1).
Table 1 Demographic and Clinical characteristics of Patient
Population (N = 44)
Naloxone (N = 22)
Metoclopramide (N = 22)
Age (years) 46 ± 14 46 ± 17
M:F 7:15 7:15
Weight (Kg) 78 ± 19 78 ± 22
Operative duration (hours) 2.5 ± 1.6 2.2 ± 1
Total fentanyl (μg) 236 ± 137 322 ± 194
Risk Factor Score (median) 1.5 1
Total response (ie the total number of patients who responded partially or completely) to naloxone was comparable to the effect of metoclopramide at five minutes14 patients (64%) versus 16 patients (73%) respectively. Also, at 10 minutes14 patients (64%) naloxone versus 18 patients (82%) metoclopramide (P = 0.255) as shown (Table 2). However, the number of patients who were free of nausea and vomiting (complete response) in the naloxone group at 5 minutes (27%, n = 6) was statistically higher than in the metoclopramide group (5%, n = 1), (P = 0.046). Complete response at 10 minutes was 7 patients (32%)

M.E.J. ANESTH 21 (6), 2012
853NALOXONE VERSUS METOCLOPRAMIDE FOR THE TREATMENT OF ESTABLISHED POSTOPERATIVE NAUSEA AND VOMITING IN PATIENTS FOLLOWING GENERAL ANESTHESIA WITH FENTANYL SUPPLEMENTATION
in the naloxone group versus 3patients (14%) in the metoclopramide group. The antiemetic effect was not related to the total amount of fentanyl used, operative time, age, weight, or initial pain score (Tables 3, 4). Pain did not increase after treatment with naloxone, and the mean pain score was 4.1/10 at 2, 5 and 10 minutes. In the metoclopramide group, mean pain score did not change significantly (Table 5).
Table 2 Response at 2,5 and 10 minutes
Naloxone Group
Metoclopramide Group
Partial Response 7 (32%) 9 (41%)
2 Minutes Complete Response 4 (18%) 1 (5%)
Total Response 11 (50%) 10 (45%)
Partial Response 8 (36%) 15 (68%)
5 Minutes Complete Response 6 (27%)* 1 (5%)*
Total Response 14 (64%) 16 (73%)
Partial Response 7 (32%) 15 (68%)
10 Minutes Complete Response
7 (32%) 3 (14%)
Total Response 14 (64%) 18 (82%)
* The difference is statically significantComplete response: no nausea and vomiting and no antiemetics given.Partial response: improvement in the nausea score.Total response: partial and complete response
Table 3 Clinical characteristics of patients who responded to naloxone
compared to those who did not respondDid not respond (N = 8)
Responded (N = 14)
56 ± 12 41 ± 14 Age
65 ± 15 80 ± 20 Weight
171 ± 70 176 ± 74 Total amount of fentanyl
2.5 ± 1.6 2.1 ± 1.1 Operative Duration
4.3 ± 1.1 4.0 ± 1.5 Pain score
Table 4 Clinical characteristics of patients who responded to
metoclopramide compared to those who did not respondDid not respond
(N = 8)Responded (N = 14)
51 ± 20 45 ± 17 Age67 ± 12 81 ± 23 Weight
275 ± 210 332 ± 196 Total amount of fentanyl1.9 ± 0.9 2.3 ± 1.1 Operative duration2.8 ± 3.5 3.4 ± 2.3 Pain score
Table 5 Pain score
Initial 2 Minutes 5 Minutes 10 Minutes
Naloxone 4.1 ± 1.4 4.1 ± 1.4 4.1 ± 1.4 4.1 ± 1.3
Metoclopramide 3.3 ± 2.4 3.2 ± 2.3 3.2 ± 2.3 3.0 ± 2.2
With regards to the vital signs, no variations of blood pressure or heart rate, compared to pretreatment values, were recorded in any group during the study period, with no reported side effects. Also, 4 patients in the naloxone group, as well as, 4 patients in the metoclopramide group received rescue antiemetic therapy by ondansetron 4mg intravenously. Patients who received ondansetron were nausea free and did not request further treatment.
Discussion
Despite the increasing use of prediction models and guidelines for PONV prophylaxis, PONV remains a “10-20% problem” in the postoperative period. There is evidence that patients at a considerable high risk of developing PONV can benefit from prophylactic antiemetic treatment. However, applying the same approach for patients at a low or moderate risk is not unequivocally supported and fails to improve patient satisfaction compared to symptomatic treatment in the PACU17.
The rescue treatment of PONV has not been well studied, because of the difficulty in performing therapeutic trials, as compared to preventive studies. Only about 10%-20% of patients can be expected to experience PONV in the first 2 hours in the PACU. Drugs given prophylactically cannot be used to treat

854 DABBOUS A. et. al
PONV in the PACU which means that a different class of drugs has to be used1,5.
Postoperative nausea and vomiting seem to have many causes, and it is perhaps naive to think that an anti-emetic, working at one specific receptor, should be universally effective18. Nausea and vomiting can be mediated via peripheral and/or central nervous pathways. Within the peripheral nervous system, vagal afferents are of importance. While the chemoreceptor trigger zone, an important center for the control of emesis, is located outside the blood-brain barrier, other centers which modulate emesis are located within the brain, e.g. the nucleus tractus solitaries (NTS). Ligands of the mu-opiate receptor (MOR) are known to influence many functions that involve vagal afferent input to the nucleus tractus solitarius (NTS), including cardiopulmonary responses, gastrointestinal activity, and cortical arousal. MOR ligands modulate either the presynaptic release from or the postsynaptic responses to largely separate populations of vagal afferents in the intermediate NTS19. Hence the direct effect of opioids and opioid antagonists which can cross the blood-brain barrier.
Low dose naloxone infusion, has been shown to decrease epidural and PCA opioid related side effects (nausea, vomiting and pruritis) without increasing pain score8-12. However, the efficacy of naloxone as a treatment for PONV following general anesthesia with fentanyl supplementation has not been reported. Efficacy data of several antiemetics, particularly metoclopramide has been previously published. Metoclopramide was found to be significantly better than propofol for the treatment of PONV in the PACU13, and was comparable to ondansetron20.
Anesthesiologists have used metoclopramide for the treatment of PONV in the PACU13,14,20. 11% of anesthesiologists in the USA use metoclopramide for the treatment of PONV when no prophylaxis is given14, or for breakthrough PONV despite prophylaxis15.
Our study is the first to show, in patients receiving general anesthesia including fentanyl, that naloxone in a dose of 0.5 µg/Kg can be used to treat PONV in the PACU without increasing pain scores. Naloxone is found to be comparable to metoclopramide. However at 5 minutes, complete response was significantly better with naloxone than with metoclopramide. It is known
that the initial distribution half-life phase of naloxone is 4 minutes. Whereas, its half life in serum following distribution is 64 minutes. Based on animal studies, the rapid onset of the narcotic antagonist action of naloxone can be related to its rapid entry into the brain, whereas its potency stems in part from its high lipid solubility which allows a high brain concentration to be achieved23.
Defining the success of the treatment as partial or complete is only arbitrary. What matters most is the patient’s request of further treatment for PONV. Only 4 patients in each group needed rescue ondansetron treatment, the clinical effectiveness of naloxone and metoclopramide would be comparable and is >80% in this small group of patients. This constitutes higher numbers than would be expected by placebo. It has been reported that the chance of recurrence of PONV after a first episode, treated with placebo, is 65% during the early period of 0-2 hours22. Polati et al reported a 66.7% early effectiveness of metoclopramide in PONV treatment compared to 35% in the placebo group21.
Why would a small-dose naloxone infusion prevent opioid-induced side effects and, in some studies, even paradoxically enhance analgesia? Opioid receptors are linked to G proteins23,24. Opioids have traditionally been thought to produce their analgesic effects via agonist binding to Gi/o receptor-coupled complexes23. Crain and Shen25,26 have proposed that opioids also bind at remarkably small doses to Gs-coupled receptors. Opioid binding to Gs protein-coupled receptors may be responsible for the hyperalgesia occasionally reported with opioid administration and with some opioid-induced side effects, such as pruritus and nausea and vomiting. Crain and Shen also hypothesized that small doses of opioid antagonists may decrease opioid-induced side effects and improve pain control by inhibiting only the excitatory G protein receptor complexes and leaving the inhibitory complexed receptors available for pain control25,26. Thus, this theory would predict that, in patients receiving opioids for pain, a small-dose infusion of an opioid antagonist would prevent side effects and produce a paradoxical enhancement of analgesia. Indeed, Gan et al.11 observed these results in adult patients being treated with Intravenous morphine and naloxone. Similarly, Maxwell et al. saw a dramatic

M.E.J. ANESTH 21 (6), 2012
855NALOXONE VERSUS METOCLOPRAMIDE FOR THE TREATMENT OF ESTABLISHED POSTOPERATIVE NAUSEA AND VOMITING IN PATIENTS FOLLOWING GENERAL ANESTHESIA WITH FENTANYL SUPPLEMENTATION
diminution of opioid-induced side effects with small-dose naloxone therapy in children and adolescents27.
Conclusion
Single low dose naloxone (0.5mcg/kg) was found to be effective in relieving PONV in the PACU, in patients receiving general anesthesia including fentanyl supplementation, without increasing pain scores. The
total response was comparable to metoclopramide.However, the complete response at 5 minutes was even better with naloxone.
Acknowledgment
We thank Mrs Nawal Menassa Gergi RN for patient assessment and drug administration in the PACU.

856 DABBOUS A. et. al
References
1. HAbIb A, GAN T: Evidence-based management of postoperative nausea and vomiting: a review. Can J Anesth; 2004, 51:326-341.
2. MYLES P, WILLIAMS D, HENDRATA M, ET AL: Patient satisfaction after anesthesia and surgery: results of a prospective survey of 10 811 patients. Br J anaesth; 2000, 84:6-10.
3. TRAMER M: A rational approach to the control of postoperative nausea and vomiting: evidence from systematic reviews. Part II. Recommendations for prevention and treatment, and reach agenda. Acta Anaesthesiol Scand; 2001, 45:14-19.
4. GAN T: Postoperative nausea and vomiting-can it be eliminated? JAMA; 2002, 287:1233-6.
5. GAN T, MEYER T, APFEL C, ET AL: Consensus guidelines managing postoperative nausea and vomiting. Anesth Analg; 2003, 97:62-71.
6. JUNGER A, HARTMANN B, BENSON M, ET AL: The use of an anesthesia information management system for prediction of antiemetic rescue treatment at the postanesthesia care unit. Anesth Analg; 2001, 92:1203-9.
7. RObERTS G, BECKER T, CARLSEN H, ET AL. Postoperative nausea and vomiting is strongly influenced by postoperative opioid use in a dose dependant manner. Anesth Analg; 2005, 101:1343-8.
8. RAWAL N, SCHOTT U, DAHLSTROM B, ET AL: Influence of naloxone infusion on analgesia and respiratory depression following epidural. Anesthesiology; 1986, 64:194-201.
9. CEPEDA M, ALvAREZ H, MORALES O, CARR D: Addition of ultralow dose naloxone to postoperative morphine PCA: unchanged analgesia and opioid requirement but decreased incidence of opioid side effects. Pain; 2004, 107:41-6.
10. KIM M, NAM S, CHO M, SHIN Y: Epidural naloxone reduces postoperative nausea and vomiting in patients receiving epidural sufentanil for postoperative analgesia. Br J anaesth; 2007, (2)99:270-5.
11. GAN T, GINSbERG B, GLASS P, ET AL: Opioid sparing effects of a low-dose infusion of naloxone in patient-administered morphine sulfate. Anesthesiology; 1997, 87:1075-81.
12. SPOSITO JA, HAbIb AS: Low-dose naloxone infusion for the treatment of intractable nausea and vomiting after intrathecal morphine in a parturient. Int J Ostet Anesth; 2010 Jan, 19(1):119-21.
13. LACROIX G, LESSARD M, TRéPANIER C: Treatment of postoperative nausea and vomiting: comparison of propofol, droperidol and metoclopramide. Can J Anaesth; 1996, 43:115-20.
14. MACARIO A, CLAYbON L, PERGOLIZZI J: Anesthesiologists' practice
patterns for treatment of postoperative nausea and vomiting in the ambulatory Post Anesthesia Care Unit. BMC Anesthesiol; 2006, 6:6.
15. WHITE P, WATCHA M:. Postoperative nausea and vomiting: prophylaxis versus treatment. Anesth Analg; 1999, 89:1337-9.
16. BOOGAERTS J, VANACKER E, SEIDEL L, ET AL: Assessment of postoperative nausea using a visual analogue score. Acta Anaesthesiol Scand; 2000, 44:470-4.
17. SCUDERI P, JAMES R, HARRIS L, MIMS G: Antiemetic prophylaxis does not improve outcomes after outpatient surgery when compared to symptomatic treatment. Anesthesiology; 1999, 90:360-37.
18. TRAMER M, MOORE A, REYNOLDS D, ET AL: A quantitative systemic review of ondansetron in treatment of established postoperative nausea and vomiting. BMJ; 1997, 314:1088-90.
19. AICHER SA, GOLDbERG A, SHARMA S, ET AL: Mu opioid receptors are present in vagal afferents and their dendritic targets in the medial nucleus tractus solitaries. J Comp Neurol; 2000, 422(2):181-90.
20. POLATI E, VERLATO G, FINCO G, ET AL: Ondansetron versus metoclopramide in the treatment of postoperative nausea and vomiting. Anesth Analg; 1997, 85:359-9.
21. EbERHART L, FRANK S, LANGE H, ET AL: Systemic review on the recurrence of postoperative nausea and vomiting after a first episode in the recovery room-implications for the treatment of PONV and related clinical trials. BMC Anesthesiology; 2006, 6:14.
22. BERKOWITZ BA: The relationship of pharmacokinetics to pharmacological activity: morphine, methadone and naloxone. Clin Pharmacokinet; 1976, 1(3):219-30.
23. SNYDER SH, PASTERNAK GW: Historical review: opioid receptors. Trends Pharmacol Sci; 2003, 24:198-205.
24. STANDIFER KM, PASTERNAK GW: G proteins and opioid receptor mediated signalling. Cell Signal; 1997, 9:237-48.
25. CRAIN SM, SHEN KF: Antagonists of excitatory opioid receptor functions enhance morphine’s analgesic potency and attenuate opioid tolerance/dependence liability. Pain; 2000, 84:121-31.
26. CRAIN SM, SHEN KF: Modulation of opioid analgesia, tolerance and dependence by Gs-coupled, GM1 ganglioside-regulated opioid receptor functions. Trends Pharmacol Sci; 1998,19:358-65.
27. MAXWELL L, KAUFMANN S, BITZER S, ET AL: The effects of a small-dose naloxone infusion on opioid-induced side effects and analgesia in children and adolescents treated with intravenous patient controlled analgesia: A double-blind, prospective, randomized, controlled study. Anesth Analg; 2005, 100:953-8.

857 M.E.J. ANESTH 21 (6), 2012
LONG-TERM USE OF INTRATHECAL DROPERIDOL AS AN EXCELLENT ANTIEMETIC IN NONMALIGNANT
PAIN-A RETROSPECTIVE STUDY
MOHAMMAD-HAZEM I. AHMAD-SAbRY*, GHOLAMREZA SHAREGHI**
Abstract
Over the past five years our pain practice encountered eight patients (5 female, 3 male) with chronic non-malignant pain syndromes, in whom any meaningful pain reduction via opioid analgesics (either by oral or systemic and/or intraspinal route) had resulted in profound nausea and/or vomiting despite generous use of available and/or affordable anti-emetics. After obtaining proper consents, small, incremental doses of intrathecal droperidol were added to these patients having implanted intrathecal narcotic drug delivery system. Significant reduction of nausea and vomiting without any side effects from droperidol was obtained while adequate pain reduction is achieved.
Procedure
All patients had implanted programmable Medtronic Synchromed pumps with intrathecal access catheters. The intrathecal catheter tip placement varied depending on the pain pathology of the patient. Six of eight patients were started and remained on morphine sulfate intrathecally for their opioids. Two patients with contraindications to morphine had fentanyl and hydramorphone as their intrathecal opioid respectively. The intrathecal dose of droperidol was started low (22.7 ± 18.6 micrograms/day). All patients were on simple continuous pump dosing during the study.
Results
All patients achieved statistically significant antiemesis (77 ± 10% P< 0.001) as well as statistically significant pain relief (84 ± 7% P < 0.005) early on (within two pump refills). As the intrathecal dose/day of droperidol was increased to 124.7 ± 114.8 micrograms/day as well as their intrathecal pain medication use, the degree of significance of antiemesis improved to 86 ± 9% (P < .001) which was a statistically significant improvement of P ≤ 0.05 level from the starting dose of droperidol in each patient.
For the six patients on morphine the antiemesis improved to 88 ± 10% (P≤ .003), also statistically significantly different at P ≤ 0.05 level from the starting antiemesis level. During this period the intrathecal morphine dose was doubled from 4.76 ± 2.43 mg/day to 9.5 ± 6.5 mg/day (P ≤ .001).
* Lecturer of Anesthesiology, Alexandria Faculty of Medicine, Alexandria University, Alexandria, Egypt.** Gholamreza Shareghi, Ph.D, M.D. Attending anesthesiologist, Advanced Pain Therapeutics of Knoxvile, Knoxville, TN,
USA. Correspinding Author: Mohammad-Hazem I. Ahmad-Sabry. Alexandria Faculty of Medicine, Alexandria University,
Alexandria, Egypt. E-mail: [email protected]

858 AHMAD-SABRY M. H. I. et. al
nausea to many opioids, regardless of dose, type or duration of therapy, thus preventing adequate opioid dosing for adequate pain relief. In this group of unfortunate people sometimes even the strongest available and affordable antiemetics offered via (oral, subcutaneous, transdermal, transmucosal, intramuscular, and intravenous) routes do not counter the nausea and/or vomiting enough so adequate pain relief can be obtained on a chronic basis.
Control of nausea and vomiting is via two centers in the brain1-7. The involved centers are the emesis center and the chemoreceptor trigger zone (CTZ). Baroreceptors, vagus, peripheral pain receptors (via histamine neural involvement), vestibular area (via acetylcholine involvement), cerebral cortex and CTZ all send provocative signals to the emesis center. Dopamine, emetic drugs, 5HT3, opioid analgesics, cisplatin, and nitrogen mustard all provoke CTZ. The CTZ/ area postrema is located at the floor of the fourth ventricle. The CTZ has at least five different receptor types that may be provoked (dopamine D2, histamine, 5HT3, muscarinic and substance P).
We took advantage of the presence of opioid receptors in the spinal cord and brain for pain reduction, as well as the presence of dopaminergic D2 receptors in CTZ and used a dopamine D2 antagonist (droperidol) in small quantities intrathecally to see if effective antiemesis as well as pain relief could be simultaneously achieved on a chronic basis.
Materials And Methods
- Over the past five years we took eight patients who fit the above category: four patients with Complex Regional Pain Syndrome (CRPS), three patients with lower back syndrome (two failed back syndrome, one multilevel degenerative joint disease), one patient with short bowel syndrome/abdominal pain.
- We obtained proper and appropriate informed consents regarding use of droperidol in the pain clinic institution. We followed all the guidelines dictated in Declaration of Helsinki (http://www.wma.net/e/policy/pdf/17c.pdf) for the use of preservative-free compounded antiemetic droperidol in the intrathecal space. Then we obtained consent as a new and not yet FDA-approved drug for this purpose from each patient.
Patients had no adverse effects from the use of droperidol at these doses (no sedation, changes in mental status, no signs or symptoms of arachnoiditis, no new sensory or motor disturbance, or any other indications of nerve toxicity detected.). Serial neurological studies involving MRI and CT, with contrast, EMG every 6-12 month showed no intrathecal catheter tip irritation sequelae in our patients either.
Conclusions
We find droperidol in microgram doses of 5-300/day intrathecally a safe antiemetic to use along with opioid analgesics. We did not use droperidol intrathecally alone as its use systemically without an opioid companion base is fraught with concern in anesthesia literature (“calm looking on the outside-agitated on the inside”). We would suggest a minimal starting dose of 20-30 micrograms/day of droperidol, adjust most probably upwards by 25-50% on subsequent pump refills until the desired effect is established. The scientific literature is rich with references to the brainstem chemoreceptor trigger zone, the floor of the fourth ventricle, and other nausea center locations (area postrema, the circumventricular organ, etc.). We would like to suggest that droperidol’s direct actions on these centers are involved with antiemesis at these small doses.
Keywords
1. Intrathecal Opioids 2. Intrathecal Droperidol 3. Long Term Profound Antiemesis 4. Non-Malignant and Malignant pain
Introduction
Since discovery of opioid sensitive receptors in the spinal cord intraspinal opioids have become of great value in both the understanding and management of many acute and chronic pain conditions.
Opioid analgesics are administered by many routes (oral, subcutaneous, transmucosal, transdermal, intramuscular, intravenous, epidural and subarachnoid). Some patients will have refractory

M.E.J. ANESTH 21 (6), 2012
859LONG-TERM USE OF INTRATHECAL DROPERIDOL AS AN EXCELLENT ANTIEMETIC IN NONMALIGNANT PAIN-A RETROSPECTIVE STUDY
Results
The intrathecal dose of droperidol was always started low (22.7 ± 18.6 micrograms/day).
Depending on the patient’s antiemetic response to this dose, and the pain relief response to increasing doses of the opioid used intrathecally, we increased our daily dose of droperidol by 15-50 micrograms/day on subsequent pump refills, if it was needed.
The use of non-intrathecal antiemetics significantly decreased (86 ± 9% P< 0.01) in all patients. One patient with CRPS, prior to visiting our pain clinic, had a pump and intrathecal catheter placed with trial of morphine and fentanyl, and then the pump and catheter removed. She had been unable to take any type of opioids (severe emesis) despite trial of high doses of all available antiemetics and/or passage of time to get used to the opioids. After the addition of intrathecal droperidol this patient was able to gradually tolerate intrathecal fentanyl as well as oral oxycontin up to 40 mg p.o. QID within three months of the start of intrathecal droperidol.
One of our CRPS patients’ pump was removed
- For six of the above patients we used morphine sulfate as the intrathecal opioid. For one patient we used hydromorphone and another patient had fentanyl. The tip of the intrathecal catheter placement was in the lumbar spine for one patient, lower thoracic spine for two patients, midthoracic spine for one, and very high thoracic spine for three CRPS patients. The pertinent data of patients are tabulated in Table 1.
Intrathecal narcotics and droperidol were all preservative-free, made specifically under strict aseptic conditions in “clean rooms”. They were placed in 20 cc luerlock capped, marked syringes and airmailed via Federal Express overnight to our clinic. The drugs in the syringes were then used within two weeks of their arrival. For all the patients in this study the interval between subsequent pump refills was less than ninety days. We have not done any in-vitro or in-vivo (the removed portion of pump solution before fresh drug is injected during pump refill) of the stability of the opioid/droperidol combination. There was no incidence of precipitation out of solution (removed portion of pump solution) during any pump refill. There was no clinical evidence of loss of antiemesis during the study.
Table 1
Patient # Year of birth
Disease state for which pump was implemented
Site of intrathecal catheter tip
Year of implantation
Currently (2006) using the system
Intrathecal narcotic used
I 1955 CRPS-left upper extremity*
CRPS-right lower extremityT1-T2 2002 Yes Fentanyl
II 1957 CRPS-right upper extremity*
CRPS-right lower extremityT1-T2 2002 Yes Morphine sulfate
III 1949 CRPS-right upper extremityCRPS-right lower extremity*
T5-T6 2002 No-removed in 2004 due to insurance problems
Morphine sulfate
IV 1949 CRPS-right upper extremity *CRPS-right lower extremity
T1-T2 2003 Yes Morphine sulfate
V 1928 Short bowel syndrome, abdominal pain with chronic nausea
T10-T11 2002 No-deceased in 2004 secondary to pneumonia
Morphine sulfate
VI 1942 Severe multilevel degenerative lumbar disc disease
T12-L1 2003 Yes Morphine sulfate
VII 1958 Failed back surgery syndrome T12-L1 1998 ⊗ 2003 ¾ Yes Morphine sulfate
VIII 1957 Failed back surgery syndrome L3-L4 2001 Yes Dilaudid *- site of worst symptoms⊗ - implanted by another pain physician¾ - year droperidol was added

860 AHMAD-SABRY M. H. I. et. al
Discussion
The proximity of most of the brainstem nausea/vomiting centers to the walls of the fourth ventricle, and the ease by which a partly lipophilic drug like droperidol gets to the active site of action of nausea centers is a promising new avenue for treatment of intractable nausea/vomiting. To optimize antiemesis we hoped for the lowest effective dose, with the least number of negative side effects, no toxicity and as close to the nausea centers as possible.
The chemoreceptor trigger zone (CTZ) has been known, so far, to have at least five kinds of receptors that may activate nausea. It would be very interesting to see what the antagonist of each receptor system, if placed appropriately intrathecally, either singular or in combination would do in management of intractable nausea/vomiting.
Intrathecal droperidol, an effective antiemetic, was recently reported by Dr. Stearns in the literature18. Their patient population had malignant disease. In the retrospective portion of their study, in 41 patients, intractable nausea was caused by opioid intolerance in 46%, abdominal tumors in 49%, and chemotherapy or radiation in 5%. Intrathecal droperidol either reduced or resolved nausea in over 95% of their patients. The droperidol dose in their study ranged from 25 to 455 micrograms per day. Both the percentage of the patients in that study who had significant nausea reduction and the dose range of intrathecal droperidol that allowed antiemesis is in general agreement with our study.
There has been a reported rat study involving intrathecal droperidol administration, with or without morphine to evaluate antinociception19. In this study droperidol had no effect on antinociception intrathecally. Droperidol exerted no histopathological effects on the rat spinal cord.
Epidural drug delivery is a potent weapon in the anesthesiologist and pain specialist’ armamentarium. It is well known that most drugs injected epidurally must cross the dura to achieve proximity to the site(s) of action. We did not use epidural droperidol, but a quick look through the literature shows its use as conceivable and appropriate in both an acute and chronic setting.
Epidural droperidol has been reported as a potent
eighteen months after implantation secondary to insurance problems. An elderly patient with short bowel syndrome/abdominal pain who, prior to our pump placement, was living only on hyperalimentation for two-and-one-half years was able to take some oral food after the pump placement (morphine/droperidol). The patient was able to enjoy eating and partially absorb food. The patient died two years afterwards secondary to COPD complications.
Conclusion
We find droperidol a rather safe drug at the above doses intrathecally. Droperidol was given a “black box warning” by the Food and Drug Administration in 2001. If it is given as an intravenous bolus, at a dose of 0.1 mg/kg, there is an increased chance of ventricular arrhythmia of Torsades de Pointes type, and even at a much lower dose (from 0.675 to 1.25 mg) droperidol intravenously will prolong QT. The Medwatch Report that spurred the FDA was by Habib and Gan13. The represented cases in that study were not so clear cut. There have been a number of other editorials from respected sources agreeing to safety and efficiency of droperidol in intravenous doses from 0.625 to 1.25 mg to prevent nausea and vomiting14,15,16.
Recent studies comparing droperidol and ondansetron17,18,19,20 revealed that QT does increase by a small but significant percentage within 2-3 minutes after giving from 0.625 to 1.25 mg droperidol in men and women, and to about the same extent in the same 2-3 minutes after giving 4 mg of intravenous ondansetron both of the “mild” prolongation of QT moved towards normal within ninety minutes.
In our study the dose of droperidol given over 24 hours is below a single dose given IV as above.
All of our patients on the combination of intrathecal droperidol/opioid reduced use of almost all forms of (oral/rectal) antiemetics (86% ± 9% P < 0.001 reduction in use). If the ratio of droperidol to opioid in the pump was to be drastically adjusted (to manage increasing pain level in a patient) we offered short term oral Antiemetics until the new steady state was established. Over time we increased the dose of droperidol along with the opioid in those situations, as to be more proactive to the patient’s needs.

M.E.J. ANESTH 21 (6), 2012
861LONG-TERM USE OF INTRATHECAL DROPERIDOL AS AN EXCELLENT ANTIEMETIC IN NONMALIGNANT PAIN-A RETROSPECTIVE STUDY
suggest a useful role for central neuroaxis use of droperidol in the perioperative setting. The reduction of cisplatin-induced emesis by epidural droperidol, as well as the reduction in intractable nausea in a significant number of patients undergoing chemotherapy and/or radiation18 also suggests a useful role for central neuroaxis use of droperidol in oncology.
We recently took our own advice: in August 2006 a 45-year-old male with metastatic rectal adenocarcinoma to the pelvis, large bowel and retroperitoneal area was referred for pain management. He was on 2000-2500 mg/day MS Contin and 1500 mg/day MS-IR. He had significant pain in his abdomen, pelvis and lower back, pain upon micturition, and neuropathic lower pelvis pain. He also had severe nausea, anorexia and mild confusion from the oral.
Opioids and had failed transdermal opioids. An implanted intrathecal access catheter (tip at T9 level) and totally implanted programmable pump was installed. We started him on simple continuous dose of 30 mg/day of morphine sulfate and 300 mcg/day of droperidol. Within two weeks he had no more nausea/anorexia or pain. He remains that way three months later and has gained ten pounds.
antinausea, antiemetic and excellent anti-pruritic when given along with epidural fentanyl. Single bolus of epidural droperidol (2.5 mg) significantly reduced epidural fentanyl’s induced pruritus. Continuous infusion of epidural droperidol (2.5 mg/day for 2 days) also significantly reduced fentanyl’s pruritus as well as postoperative nausea and vomiting22*. Epidural droperidol bolus of 2.5 mg also decreased the incidence of nausea, emesis and pruritus associated with epidural sufentanil23*. Continuous epidural droperidol (2.5 mg/day) inhibited nausea, vomiting and pruritus during epidural morphine analgesia24. Epidural droperidol, in a group of women undergoing cesarean section delivery, induced a dose-related reduction in the incidence of pruritus (2.0 mg of morphine + 1.25 mg or 2.5 mg or 5.0 mg of droperidol as a single epidural bolus)21*. The mechanism(s) by which pruritus inhibition occurs is not yet clear.
Epidural droperidol, as 50 mcg/kg body weight, given as a bolus and repeated every six hours x three, has been reported for short term use to suppress cisplatin-induced emesis with good success20.
The above representative epidural droperidol studies in battling postoperative nausea and vomiting

862 AHMAD-SABRY M. H. I. et. al
Warning on the Preoperative Use of Droperidol: A Review of Cases� Anesth Analg; 2003, 965:1377-1379.
14. MILLER DP: Arrhythmogenic Potential of Antiemetics: Perspective on Risk-Benefit� Can J Anaesh; 2003, 50:215-220.
15. DERSHWITZ M, DROPERIDOL: Should the Black Box be Light Gray? J Clin Anesth; 2002, 14:298-603.
16. WHITE PF, DROPERIDOL: A Cost-Effective Antiemetic for Over Thirty Years, Anesth Analg; 2002, 95:789-790.
17. SAMUEL HASSENbUSCH, MD, PHD, KIM bURCHIEL MD, FACS, RObERT J. COFFEX, MD, MICHAEL J. COUSINS, MbbS, TIM DEER, MD, MARC b. HAHN, DO, STURARD DU PEN, MD, KENNETH FOLLETT, MD, PHD, ELLIOT KRAMES, MD, JAMES N. ROGERS, MD, OREN SAGHER, MD, PETER S. STAATS, MD, MARK WALLACE, MD, AND KENNETH DEAN WILLIS, MD: Management of Intrathecal Catheter-Tip Inflammatory Masses: A Consensus Statement, Pain Medicine; 2002, 3:313-323.
18. STEARNS LJ: Intrathecal Droperidol Found to Relieve Intractable Nausea. Clinical Anesth; 2006, (32).
19. GRIP G, SvENSSON bA, GORDTH JR T, POST C, HARTvIG P: Histopathology and Evaluation of Potentiation of Morphine-induced Antinociception by Intrathecal Droperidol in the Rat. Acta Anaesthesia Scand; 1992, (36):145-152.
20. IWAMA H, ARAI M: Epidural Administration of Droperidol Suppresses Cisplatin-induced Emesis: Preliminary Findings. Surgery Today, publisher Springer Japan; 1998, (28):231-234.
21. HORTA ML, RAMOS L, GONCALvEZ R: The Inhibition of Epidural Morphine-induced Pruritus by Epidural Droperidol. Anesthesia and Analgesia; 2000, (90):638-641.
22. LEE IH, LEE IO: Antipruritic and Antiemetic Effect of Epidural Droperidol: Comparative Study between Single and Continuous Epidural Injection. Eur� J� Anesthesiol; 2006, (23):213-218.
23. WILDER-SMITH CH, WILDER-SMITH OH, FARSCHTSCHIAN F, NAJI P: Epidural Droperidol Reduces the Side Effects and Duration of Analgesia of Epidural Sufentanyl. Anesthesia and Analgesia; 1994, (79):98-104.
24. NAKATA K, MAMMOTO T, KITA T, TANIGUCHI H, KANbARA N, AKAMATSU T, SAKAI T, KISHI Y: Continuous Epidural, Not Intravenous Droperidol Inhibits Pruritus, Nausea and Vomiting During Epidural Morphine Analgesia. Journal of Clinical Anesthesia; 2002, 121-125.
References
1. vANDER KOOY D, KODA LY: Organization of the Projections of a Circumventricular Organ: The Area Postrema in the Rat. The Journal of Comparative Neurology; 2004, 219(3):328-338.
2. PEDIGO NW JR, bRIZZEA KR: Muscarinic Cholinergic Receptors in Area Postrema and Brainstem Areas Regulating Emesis� Brain Research Bulletin; 1985, 14:169-177.
3. HARDING RK, HUGANINOLTZ, HEARNEY M, KUCHARCZKY J: Discrete Lesions of the Area Postrema Abolish Radiation-induced Emesis in the Dog. Neurosci Lett; 1985, 1:95-100.
4. bAKER PC, bERNAT JL: The Neuro Anatomy of Vomiting in Man: Association of Projectile Vomiting with Solitary Metastasis in the Lateral Tegmentum of the Pons and the Middle Cerebellar Peduncle� J Neurol Neurosurg Psychiatry; 1985, (48):1165-1168.
5. ISNETSOv vv: The Central Neurophysiological and Neurochemical Mechanisms of Vomiting (a Review of the Literature)� {Article in Russian}. Aviakosm Ekolog Med; 1992, 26:10-18.
6. CARPENTER DO: Neural Mechanisms of Emesis. Can� J� Physiolo Pharmacol; 1990, (68):230-236.
7. MILLER AD, NONAKA S, JAKUS J: Brain Areas Essential or Nonessential for Emesis. Brain Res; 1994, (647):255-264.
8. HYDE TM, GIbbS M, PEROUTKA SJ: Distribution of Muscarinic Cholinergic Receptors in the Dorsal Vagal Complex and Other Selected Nuclei in the Human Medulla. Brain Res; 1988, (447):287-292.
9. bODIS S, ALEXANDER E III, KOOY H, LOEFTER JS: The Prevention of Radiosurgery Induced Nausea and Vomiting by Ondansetron: Evidence of a Direct Effect on the Central Nervous System Chemoreceptor Trigger Zone� Surg Neurol; 1994, (42):249-252.
10. FAbLING JM, GRAN TJ, EL-MOALEM HE, WARNER DS, bOREL CO: A Randomized, Double-Blinded Comparison of Ondansetron, Droperidol and Placebo for Prevention of Post-Operative Nausea and Vomiting After Supratentorial Craniotomy� Anesth Analg; 2000, (91):358-361.
11. HYDE TM, KNAbLE Mb, MURRAY AM: Distribution of Dopamine D1-D4 Receptor Subtype in Human Dorsal Vagal Complex. Synapse, 1996, (24):224-232.
12. STAHL SM: The Ups and Downs of Novel Antiemetic Drugs, Part 1: Substance P, 5-HT, and the Neuropharmacology of Vomiting. J� Clin Psychiatry; 2003, 64:498-499.
13. HAbIb AND GAN TJ: Food and Drug Administration Black Box

863 M.E.J. ANESTH 21 (6), 2012
CASE REPORTS
INHALATIONAL INDUCTION WITH “VASOPARALYTIC” SEVOFLURANE: ARE WE “HYPEROXYGENATING” WHILE ANESTHETIZING DEVELOPING BRAINS?
A CASE SERIES DISCUSSION*
DEEPAK GUPTA, JASPREET SANGHA, EDWARD KAMINSKI
Abstract
Background: The concerns for hyperoxia-related brain tissue injury are well known to the medical community. The cerebro-vasodilatory properties of sevoflurane may create relative cerebral tissue “hyperoxia” during inhalational induction as compared to a propofol-based intravenous induction of anesthesia.
Study Objectives: The objective for this case series discussion was to identify any differences in cerebral tissue oxygenation secondary to induction of anesthesia with sevoflurane versus propofol.
Methods/Study Procedures: After institutional review board approval, the computer data of tissue cerebral oximetry of pediatric patients (1-18 years age group) undergoing non-cardiac surgeries was comparatively analyzed for changes over time between the groups of children who received sevoflurane induction versus propofol induction of anesthesia. “Hyperoxia” (“hyperoxygenation”) was defined as significant percent changes from the baseline values as recorded in tissue cerebral oximetry.
Results: In this case series, seven patients underwent inhalational (INH) induction with high concentrations (8%) sevoflurane with nitrous oxide in 33% oxygen and four patients underwent intravenous (IV) induction with 2 mg/kg propofol and nitrous oxide in 33% oxygen. As compared to propofol, significant cerebral tissue “hyperoxia” occurred with sevoflurane induction (p = 0.003). This did not resolve over time.
Conclusion: As compared to intravenous induction with propofol, inhalational induction with “vasoparalytic” sevoflurane “hyperoxygenates” developing brains. This observation requires validation in larger trials to conclude appropriate effect on our practice of pediatric anesthesia and pediatric patient safety under anesthesia.
* Department of Anesthesiology, Childrens Hospital of Michigan, Wayne State University/Detroit Medical Center, Detroit, MI 48201, United States.
Corresponding Author: Edward Kaminski, M.D., Staff Pediatric Anesthesiologist, 3901, Beaubien St, Suite 3B-17, Detroit, Michigan 48201, United States, Tel: 1-313-745-5535; Fax: 1-313-745-5448. E-mail: [email protected]

864 GUPTA D. et. al
Abstract entitled, “Inhalational Induction with Vasoparalytic Sevoflurane: Are we Hyperoxygenating while Anesthetizing Developing Brains?” was presented as Digital Poster plus Oral Presentation at the SPA/AAP Pediatric Anesthesiology 2012 meeting in Tampa, Florida, on Saturday, February 25 and was selected as the third prize winner of the American Academy of Pediatrics John J. Downes Resident Research Award.
Financial Disclosures NONE; Conflicts of Interest NONE
Introduction
The concerns for hyperoxia-related brain tissue injury are well known to the medical community1-3 and may contribute to neuroapoptosis in developing brains of children undergoing anesthesia. The concerns include but are not limited to widespread apoptotic neurodegeneration, induction of pro-inflammatory cytokines and inhibition of growth factor signaling cascades2.
Sevoflurane, a potent cerebro-vasodilator, is the agent of choice for inhalational induction of anesthesia. The cerebro-vasodilatory properties of sevoflurane may create relative cerebral tissue “hyperoxia” during inhalational induction as compared to a propofol-based intravenous induction of anesthesia. The hyperoxia created for even a few minutes maybe detrimental3.
The objective for this case series discussion was to identify any differences in cerebral tissue oxygenation secondary to induction of anesthesia with sevoflurane versus propofol.
Methods
After institutional review board approval, the computer data of tissue cerebral oximetry of pediatric patients (1-18 years age group) undergoing non-cardiac surgeries was analyzed. We analyzed the data for patients in whom INVOS®™ Cerebral/Somatic Oximeter (®Somanetics Corporation, Troy, Michigan, United States; ™Covidien, Mansfield, Massachusetts, United States) was used during May-June 2011 at Childrens Hospital of Michigan, Detroit Medical
Center, Detroit, Michigan, United States. Oximetry data was compared between the groups of children who received sevoflurane induction versus propofol induction of anesthesia. The changes from the baseline in the tissue cerebral oximetry were statistically compared at different points of recorded times starting from the baseline time point immediately before the induction of anesthesia to about one hour after the initiation of induction. Though computer data of tissue cerebral oximetry extended beyond one hour time-period, these extended data points were only used for graphical extrapolation because of insufficient comparative data after the one hour timeperiod.
For the purposes of this case series discussion, “hyperoxia” (“hyperoxygenation”) was defined as significant percent changes from the baseline values as recorded in tissue cerebral oximetry. Absolute tissue cerebral oximetry values were also recorded.
Results
Cerebral tissue oximetry data was available for eleven pediatric patients. Seven patients underwent inhalational (INH) induction with high concentrations (8%) sevoflurane with nitrous oxide in 33% oxygen. Four patients underwent intravenous (IV) induction with 2 mg/kg propofol and snitrous oxide in 33% oxygen. All patients were maintained on 1.5% isoflurane with medical air in 33% oxygen. Per our analysis, as compared to propofol, significantly marked cerebral tissue “hyperoxia” occurred with sevoflurane induction (p = 0.003). This did not resolve over time (Fig. 1). As anesthesia period progressed beyond the one-hour time-period, children who had received propofol induction showed cerebral tissue “hyperoxia” secondary to vasodilatory characteristics of isoflurane maintenance. However, the levels of “hyperoxia” never reached the levels as observed in patients who had undergone sevoflurane induction (Fig. 1). Conversely, the statistical significance was not appreciated in the absolute values (p = 0.687) of the tissue cerebral oximetry between the two groups of patients (Fig. 2); this may have been secondary to very small number of patients, short duration of total anesthesia time studied, and higher baseline absolute oximetry values in patients who underwent propofol induction.

M.E.J. ANESTH 21 (6), 2012
865INHALATIONAL INDUCTION WITH “VASOPARALYTIC” SEVOFLURANE: ARE WE “HYPEROXYGENATING” WHILE ANESTHETIZING DEVELOPING BRAINS? A CASE SERIES DISCUSSION
Fig� 1 Mean Percent Changes in Cerebral Tissue Oximetry over Time
Fig� 2 Absolute Values of Cerebral Tissue Oximetry over Time
Discussion
The safety of anesthesia for children has gained limelight because animal studies have reported neuroapoptotic properties of most anesthetic agents. The only differences elicited in those studies are the possible differences in the severity of the neuroapoptosis induced by the different anesthetic agents4-7. Additionally, the concerns for hyperoxia-related brain tissue injury are not new to the medical community1,8-10. The only paradigm shift is that hyperoxia-related tissue injury (most common to lungs and brain) may be a continuum of spectrum. Hyperoxia-related lung injury occurs more often at normobaric conditions and hyperoxia-related cerebral injury occurs more often at hyperbaric conditions10.
However, this continuum cannot rule out the possibility of the hyperoxia-related cerebral injury at normobaric conditions. The ideal anesthetic technique and choice of agents used differ in pediatric anesthesia. The inhalational induction of anesthesia is often standard of care in the pediatric anesthesia work environments where avoidance of needle sticks often precludes intravenous induction of anesthesia. Sevoflurane (the agent of choice for inhalational induction) decreases cerebral metabolic rate despite being a cerebral vasodilator. Conversely, propofol (the agent of choice for intravenous induction) decreases cerebral blood flow as well as the cerebral metabolic rate. Therefore, sevoflurane creates a potential physiological dilemma for the cerebral tissues due to increased ratio of oxygen supply to oxygen demand as compared to propofol. As cerebral tissue oximetry may provide an estimate of tissue oxygen tension11 or saturation, the dilemmatic physiological phenomenon of luxury oxygenation was reflected in our case series as the significantly different changes in the cerebral tissue oximetry incurred by sevoflurane induction (Fig. 1). Additionally, nitrous oxide (used during induction of anesthesia for ‘second gas’ effect12 on sevoflurane-induction and for reducing propofol injection pain) induces transient diffusion hyperoxia secondary to ‘concentrating effect’ or ‘second gas’ effect on oxygen13-14 that was reflected as the initial V-shaped peaks in the graphical presentation of changes in cerebral tissue oximetry (Fig. 1).
There are few study limitations for this case series. Firstly, it is difficult to interpret these observations in regards to quantifying potential neuroapoptotic or hyperoxia cerebral injury because this case series had a very small number of patients with short duration of observation period without any short-term or long-term follow up to quantifiably assess the abovementioned obscure injuries. Secondly, higher baseline absolute values of cerebral tissue oximetry were observed in the intravenous induction group (Fig. 2) because these patients had pre-existing intravenous access and were well rehydrated with maintenance infusions; and they received intravenous induction of anesthesia only because of their pre-existing intravenous access as inpatients. In contrast to these inpatients, the fasting outpatients had received inhalational induction of anesthesia per universal practice protocols based on prevailing patient/provider choices. Reciprocally, the

866 GUPTA D. et. al
difference in the baseline absolute values of cerebral tissue oximetry may be suggestive that fasting patients are exposed to starvation induced hypovolemia15 and its deleterious effects on cerebral tissue environments and it may be uncertain how these hyperosmolar and susceptible environments respond to sudden luxury oxygenation with sevoflurane induction. Finally, as the cerebral tissue oximetry has been primarily quantified to indirectly and non-invasively assess the degree of cerebral ischemia/cerebral hypoxia, the higher values of cerebral tissue oximetry have not been quantified to appropriately reflect the degree of cerebral “hyperoxia” that may be cumulative reflection of increased oxygen delivery (cerebral vasodilation), and/or decreased oxygen extraction (increased anesthetic depth) and/or increased oxygen content (cerebral hypoxemia). Based on these limitations, the future projects should assess (a) whether the results of this small case series can be validated in larger retrospective and prospective trials (b) whether sevoflurane induction would have increased the oximetry levels if patients were well hydrated before induction of anesthesia, (c) whether the higher doses of sevoflurane (8%) required to
rapidly achieve induction of anesthesia is the major contributing factor for the changes observed in our case series.
Conclusion
As compared to intravenous induction with propofol, inhalational induction with “vasoparalytic” sevoflurane “hyperoxygenates” developing brains. This observation requires validation in larger trials to conclude appropriate effect on our practice of pediatric anesthesia and pediatric patient safety under anesthesia.
Acknowledgement
The authors are deeply grateful to Dr Harold Michael Marsh, Vice-Chair, Department of Anesthesiology, Wayne State University and Dr Maria Markakis Zestos, Chief of Anesthesiology, Childrens Hospital of Michigan for their input and guidance for this manuscript.

M.E.J. ANESTH 21 (6), 2012
867INHALATIONAL INDUCTION WITH “VASOPARALYTIC” SEVOFLURANE: ARE WE “HYPEROXYGENATING” WHILE ANESTHETIZING DEVELOPING BRAINS? A CASE SERIES DISCUSSION
neonates and young children. Anesth Analg; 2007, 104:509-20.8. AHOTUPA M, MäNTYLä E, PELTOLA V, PUNTALA A, TOIvONEN H: Pro-
oxidant effects of normobaric hyperoxia in rat tissues. Acta Physiol Scand; 1992, 145:151-7.
9. MASAMOTO K, TANISHITA K: Oxygen transport in brain tissue. J Biomech Eng; 2009, 131:074002.
10. ALLEN BW, DEMCHENKO IT, PIANTADOSI CA: Two faces of nitric oxide: implications for cellular mechanisms of oxygen toxicity. J Appl Physiol; 2009, 106:662-7.
11. TASKER RC: Brain tissue oxygen tension is more indicative of oxygen diffusion than oxygen delivery and metabolism in patients with traumatic brain injury. Crit Care Med; 2009, 37:378-9.
12. KORMAN B, MAPLESON WW: Concentration and second gas effects: can the accepted explanation be improved? Br J Anaesth; 1997, 78:618-25.
13. MARKELLO R, MACEDA L, GOPLERUD, D: Diffusion Hyperoxia, A “Concentrating” Effect. Anesth Analg; 1974, 53:233-8.
14. RACKOW H, SALANITRE E: The pulmonary absorption-excretion volume effect. Anesth Analg. 1976, 55:51-6.
15. WRIGHT JW, REYNOLDS TJ, KENNY JT: Plasma hyperosmolality at the onset of drinking during starvation induced hypovolemia. Physiol Behav; 1976, 17:651-7.
References
1. DICKENS F: The toxic effects of oxygen on brain metabolism and on tissue enzymes; tissue enzymes. Biochem J; 1946, 40:171-87.
2. SIFRINGER M, BRAIT D, WEICHELT U, ZIMMERMAN G, ENDESFELDER S, BREHMER F, VON HAEFEN C, FRIEDMAN A, SOREQ H, BENDIX I, GERSTNER B, FELDERHOFF-MUESER U: Erythropoietin attenuates hyperoxia-induced oxidative stress in the developing rat brain. Brain Behav Immun; 2010, 24:792-9.
3. SOLA A, SALDEñO YP, FAvARETO V: Clinical practices in neonatal oxygenation: where have we failed? What can we do? J Perinatol; 2008, 28 Suppl1: S28-34.
4. ISTAPHANOUS GK, HOWARD J, NAN X, HUGHES EA, MCCANN JC, MCAULIFFE JJ, DANZER SC, LOEPKE AW: Comparison of the neuroapoptotic properties of equipotent anesthetic concentrations of desflurane, isoflurane, or sevoflurane in neonatal mice. Anesthesiology; 2011, 114:578-87.
5. LIANG G, WARD C, PENG J, ZHAO Y, HUANG B, WEI H: Isoflurane causes greater neurodegeneration than an equivalent exposure of sevoflurane in the developing brain of neonatal mice. Anesthesiology; 2010, 112:1325-34.
6. CATTANO D, YOUNG C, STRAIKO MM, OLNEY JW: Subanesthetic doses of propofol induce neuroapoptosis in the infant mouse brain. Anesth Analg; 2008, 106:1712-4.
7. MELLON RD, SIMONE AF, RAPPAPORT BA: Use of anesthetic agents in


869 M.E.J. ANESTH 21 (6), 2012
INCORRECT FIXATION OF ENDOTRACHEAL TUBE: A CAUSE OF NON-INFLATION OF THE CUFF*
KIRAN JANGRA, S.K. MALHOTRA
Introduction
Adequate control of endotracheal tube (ETT) cuff volume and pressure is essential during mechanical ventilation under general anesthesia or for ventilatory support in the Critical Care Unit. Over-inflation can lead to tracheal wall injury while under-inflation can result into a leak that can lead to difficulties in ventilating and oxygenating patients as well as an increase in the risk of aspiration. There are few case reports in the literature describing the causes of endotracheal tube cuff leak or inability to inflate or deflate the endotracheal tube cuff. We report the case of endotracheal tube cuff that could not be inflated/deflated due to the kinking/ obstruction of the inflation tube secondary to the fixation of the endotracheal tube.
Case Report
A 45-year-old male patient was admitted to Emergency Department with polytrauma following road traffic accident. After initial resuscitation and subsequent amputation of both lower limbs, patient was shifted to Intensive Care Unit for further ventilatory support. The 8 mm cuffed endotracheal tube (Portex blue-line, Smiths Medical, USA) was fixed at 21 cm with adhesive tape (Durapore, 3M, US).The initial fixation of ETT was done in operating room and as per our protocol, refixation of the ETT was done in ICU. However, no subsequent manipulation of the ETT was undertaken, thereafter. Four hours later, an audible leak from ETT was noticed. An attempt was made to inflate the cuff but there was a resistance. The cuff leak persisted, though pilot balloon was getting inflated normally. At this point, it was decided to change the ETT. After removal of the ETT, we examined the inflation tube underneath the adhesive tape. It was found that the tape was tightly applied over folded inflation tube at its junction with ETT, leading to its kinking and inability to inflate the ETT cuff (Fig. 1). After straightening the inflation tube, both the pilot balloon as well as the endotracheal tube cuff could be easily inflated and deflated.
Discussion
Endotracheal tube cuff leak is commonly observed in Anesthesia and Intensive Care set up. It may result in inadequate ventilation and potential risk of pulmonary aspiration. Leak in endotracheal cuff or inability to inflate the cuff may be due to problem in Inflation system i.e. inflation tube, valve or pilot balloon. Laurent et al1 reported a similar problem but that was due to kinking of inflation tube in nasotracheal tube, as a result of its anatomical route. In another case report, inflation tube got cut after fixation causing leaky ETT cuff 2.
* Department of Anesthesia and Intensive Care, PGIMER, Chandigarh, INDIA. Corresponding Author: Kiran Jangra, Tel: 0091-9914844330, Fax: 0091-172-2744401. E-mail: drkiransharma0117@
gmail.com

870 JANGRA K. et. al
Conclusion
We recommend that whenever adhesive tape is applied for tube fixation; ensure that the inflation tube underneath is not acutely folded at its point of insertion into ETT, so that its kinking and subsequent failure to inflate the ETT cuff is prevented.
In our case, the ETT cuff leak occurred due to acute folding of inflation tube at its junction with ETT leading to inability to inflate the ETT cuff. The cuff leak was not detected before shifting the patient to ICU as the refixation of ETT in ICU was inappropriate. The pilot balloon was inflating but the intraballoon pressure was not being transmitted to the ETT cuff.
Fig� 1 Kinking of inflation tube following its folding
on itself� (indicated by arrow)
References
1. LAURENT CS, LEE D, BENUMOF J: Kinking of the Pilot Tube Prevents Inflation of the Cuff. Anesth� Analg; 2003, 96(2):632-633.
2. GUPTA B, FAROOQUE K, JAIN D, KAPOOR R: Improper tube fixation causing a leaky cuff. J� Emerg� Trauma Shock; 2010, 3:182-184.

871 M.E.J. ANESTH 21 (6), 2012
KETAMINE INFUSION AS A TREATMENT FOR MAJOR DEPRESSIVE DISORDER:
A NEW ROLE FOR ANESTHESIOLOGISTS?
JOSHUA D. DILLEY*, W. bROOKS GENTRY**,KIMbERLY J. GOLDEN***
A 2003 study indicates that the lifetime prevalence of major depressive disorder (MDD) is 16.2% and that in a 12 month period 13.1 to 14.2 million US adults will suffer from MDD1. MDD can be a devastating illness, affecting every aspect of a person’s life. An emerging therapy involving ketamine administration for the treatment of MDD has shown promise in treating those who have not been responsive to conventional pharmacological therapy, as well as those unresponsive to ECT therapy2-6. We report the first administration of this therapy by anesthesiologists. Written informed consent was obtained from the patient granting permission for publication of this article.
Case Report
A 42 yo, 80 kg woman presented from home with MDD, diagnosed at age 17, and a recent suicide attempt. She had been treated with conventional biogenic amine antidepressant medications, her symptoms remained unresponsive however. Her depression was complicated by inhalant abuse and unemployment. Her past medical history included irritable bowel syndrome and low back pain. Her past surgical history was insignificant. She was not interested in receiving ECT.
After a thorough history and physical exam, including labwork (CBC, BMP, and urinalysis) and EKG, she was received in the PACU for ketamine infusion therapy. Standard ASA monitors were placed and oxygen was given via a simple oxygen mask. A 22 gauge IV was placed in her left hand. Ketamine (50 mg) was diluted in a 50 mL bag of normal saline and 40 mL were delivered via an infusion pump. The infusion was delivered as per recommendations from our psychiatry department and current literature, with a dose of 0.5 mg/kg delivered over ten minutes7. She was subsequently monitored and remained under anesthesia care for 40 minutes in total.
During the infusion, typical signs of ketamine administration including nystagmus, confusion, and hallucinations, as well as increased blood pressure and heart rate were exhibited. She maintained spontaneous respirations and was communicative throughout therapy. She did experience some agitation that was treated successfully with two, 1 mg doses of IV midazolam.
* Resident.** Professor.*** Assistant Professor. Corresponding Author: Joshua D. Dilley, 4301 W. Markham Street, slot #515, Tel: 501-454-1018. E-mail: joshuaddilley@
gmail.com Department of Anesthesiology, University of Arkansas for Medical Sciences. Dr. Gentry is Chief Medical Officer of InterveXion Therapeutics, LLC, an AR Bioventures Company. His work in the
company is unrelated to this case report.

872 DILLEY J. D. et. al
After therapy she remained under the care of the psychiatric department and was discharged three days later. Her mood and symptoms improved beginning with the ketamine infusion and lasted throughout her admission. Initially, she had rated her guilt on a visual analog scale at a 9/10. Upon discharge, she rated it at 4.5/10. She also reported to psychiatry staff that before she had received the ketamine therapy, she was planning on committing suicide upon discharge. She stated that after receiving the therapy, she no longer had this desire and felt positive about her future. She returned to psychiatric clinic for follow-up two weeks later. At this time, she reported that she felt “wonderful” for ten days but relapsed into depression thereafter.
Upon interview 6 months after the treatment, she reported that her depression was less than what it had been for years for a period of 2-3 months. She also reported that before the treatment she took 3-4 ibuprofen daily for her low back pain. Since the treatment, her back pain has completely resolved.
Discussion
A lot of questions remain unanswered regarding the unexpected effectiveness of this therapy. Based on current literature and supported by our case, NMDA antagonism as a treatment for refractory depression appears promising3,7-8. With conventional biogenic-amine-based antidepressants (SSRI’s/MAOI’s), a period of several weeks is typically needed in order for these medications to take effect. Ketamine has been shown to exert its antidepressant effects within 2 hours
of infusion; a clear advantage3. Although, it is unclear at this point how long the effects of a single ketamine infusion may last, a recent case study reported sustained positive results for 3 months with a trial of 6 infusions over 2 weeks8. This, unfortunately, is also a case report from a single patient. Larger studies report more modest results with peak effect occurring at 2 days and lasting around one week3,7.
Ketamine has also been studied extensively as an adjuvant to opioid use in pain control. It has been suggested that the antidepressant properties contribute to pain relief. The magnitude of this effect, has not been thoroughly described. Depression is 3-4 times more common in patients with chronic back pain than reported in the general population9-11. Given the evidence of ketamine’s antidepressant effects and high prevalence of depression amongst those with chronic pain, it is likely that its antidepressant effects are playing a role in decreased opioid requirements in chronic pain patients, as pain can often be a symptom of depression.
Conventional biogenic-amine-based antidepressants have also been shown to produce functional and quantitative changes of AMPA receptors, indicating the receptor’s involvement in depression12-13. Work is continuing in this area. With the recent interest in ketamine as an antidepressant and the ability of anesthesiologists to safely and effectively administer this medication, it is likely that anesthesia providers will be more commonly involved in delivering this therapy.

M.E.J. ANESTH 21 (6), 2012
873KETAMINE INFUSION AS A TREATMENT FOR MAJOR DEPRESSIVE DISORDER: A NEW ROLE FOR ANESTHESIOLOGISTS?
References
1. KESSLER RC, BERGLUND P, DEMLER O, JIN R, KORETZ D, MERIKANGAS KR, RUSH AJ, WALTERS EE, WANG PS: The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication. JAMA; 2003, 289(23):3095-105.
2. BERMAN RM, CAPPIELLO A, ANAND A, OREN DA, HENINGER GR, CHARNEY DS, KRYSTAL JH: Antidepressant effects of ketamine in depressed patients. Biol Psychiatry; 2000, 47(4):351-4.
3. ZARATE CA JR, SINGH JB, CARLSON PJ, BRUTSCHE NE, AMELI R, LUCKENbAUGH DA, CHARNEY DS, MANJI HK: A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry; 2006, 63(8):856-64.
4. MATHEW SJ, MURROUGH JW, AAN HET ROT M, COLLINS KA, REICH DL, CHARNEY DS: Riluzole for relapse prevention following intravenous ketamine in treatment-resistant depression: a pilot randomized, placebo-controlled continuation trial. Int J Neuropsychopharmacol; 2010, 13(1):71-82.
5. IbRAHIM L, DIAZGRANADOS N, LUCKENbAUGH DA, MACHADO-VIEIRA R, BAUMANN J, MALLINGER AG, ZARATE CA JR: Rapid decrease in depressive symptoms with an N-methyl-d-aspartate antagonist in ECT-resistant major depression. Prog Neuropsychopharmacol Biol Psychiatry; 2011, 35(4):1155-9.
6. LI N, LIU RJ, DWYER JM, BANASR M, LEE B, SON H, LI XY, AGHAJANIAN G, DUMAN RS: Glutamate N-methyl-D-aspartate Receptor Antagonists Rapidly Reverse Behavioral and Synaptic Deficits Caused by Chronic Stress Exposure. Biol Psychiatry; 2011, 69(8):754-61.
7. DIAZGRANADOS N, IbRAHIM L, BRUTSCHE N, NEWbERG A, KRONSTEIN P,
KHALIFE S, KAMMERER W, QUEZADO Z, LUCKENbAUGH D, SaLvADORE G, MACHADO-VIEIRA R, MANJI H, ZARATE CA JR: A Randomized Add-on Trial of an N-methyl-D-aspartate Antagonist in Treatment-Resistant Bipolar Depression. Arch Gen Psychiatry; 2010, 67(8):793-802.
8. MURROUGH JW, PEREZ AM, MATHEW SJ, CHARNEY DS: A case of sustained remission following an acute course of ketamine in treatment-resistant depression. J Clin Psychiatry; 2011, 72(3):414-5.
9. LOFTUS RW, YEAGER MP, CLARK JA, BROWN JR, AbDU WA, SENGUPTA DK, BEACH ML: Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology; 2010, 113(3):639-46.
10. SULLIvAN MJ, REESOR K, MIKAIL S, FISHER R: The treatment of depression in chronic low back pain: review and recommendations. Pain; 1992, 50(1):5-13.
11. CURRIE SR, WANG J: Chronic back pain and major depression in the general Canadian population. Pain; 2004, 107(1-2):54-60.
12. MARTINEZ-TURRILLAS R, DEL RIO J, FRECHILLA D: Neuronal proteins involved in synaptic targeting of AMPA receptors in rat hippocampus by antidepressant drugs. Biochem Biophys Res Commun; 2007, 353:750-755.
13. SvENNINGSSON P, TZAvARA ET, LIU F, FIENbERG AA, NOMIKOS GG, GREENGARD P: DARPP-32 mediates serotonergic neurotransmission in the forebrain. Proc Natl Acad Sci� U� S� A; 2002, 99:3188-3193.


875 M.E.J. ANESTH 21 (6), 2012
A CASE OF SEVERE SAM FOLLOWING A DAVID PROCEDURE
MENACHEM M. WEINER*, CESAR A. RODRIGUEZ-DIAZ*
Abstract
We report a case of hemodynamically significant systolic anterior motion of the mitral valve following a David procedure. Although systolic anterior motion of the mitral valve has been reported following mitral valve repair or replacement and aortic valve replacement, it has not been previously described following isolated ascending aortic surgery.
Introduction
Systolic Anterior Motion (SAM) of the mitral valve leaflets and chordae with associated turbulent flow through the left ventricular outflow tract (LVOT) as well as mitral regurgitation (MR) has been described following cardiac surgery particularly mitral valve repair or replacement1 and aortic valve replacement2,3. It has not been previously described following isolated ascending aortic surgery. We present a patient who developed SAM with left ventricular outflow obstruction and mitral regurgitation following the David procedure4.
Case Report
A 47-year-old gentleman with history of hypertension and a recent episode of chest pain and shortness of breath was found to have an ascending aortic aneurysm. Preoperative transthoracic echocardiography revealed a 5.7 ascending aorta and aortic root aneurysm. The aortic valve was trileaflet with moderate aortic valve insufficiency. No SAM and only trivial MR was seen (fig. 1). No significant subaortic gradient was measured. A valve sparing root replacement with coronary artery reimplantation as well as replacement of the ascending aorta with a graft (David procedure) was performed. Following separation from cardiopulmonary bypass, transesophageal echocardiography revealed normal biventricular function without the aid of ionotropic support. However, turbulent flow was seen in the LVOT with a gradient of 64 mm Hg demonstrated by continuous flow Doppler with coexistent severe mitral regurgitation. SAM of the anterior mitral leaflet and part of the subvalvular apparatus was seen (fig. 2). This was associated with increasing pulmonary arterial pressures and profound systemic arterial hypotension (62/33 mm Hg). The patient was treated by decreasing the paced heart rate to 70 beats per minute, increasing the mean arterial pressure and volume expansion. A mean arterial pressure of greater than 80 mm Hg was required to prevent SAM with resolution of the LVOT obstruction and the MR.
* M.D, Assistant Professor of Anesthesiology, Department of Anesthesiology, Mount Sinai School of Medicine, New York, NY.
Corresponding Author: Menachem M. Weiner MD,Department of Anesthesiology, The Mount Sinai Medical Center, One Gustave L. Levy Place, Box 1010, New York, NY, 10029-6574, Tel: 212 241-7467, Fax: 212 876-3906. E-mail: [email protected]

876 WEINER M. M. et. al
We believe that this is the first report of SAM occurring after a David procedure. While the valve is not replaced in a David procedure, it is reimplanted inside a tube graft9. This reimplantaion may change the relationship between the aortic and mitral valves. Veronisi and colleagues10 have described a phenomenon of mitral-aortic coupling which demonstrated that both valves have synchronous and reciprocal dynamic behavior. Further work showed that this relationship was altered by the placement of an annuloplasty ring on the mitral valve11. Perhaps performing a David procedure similarly alters this relationship and in so doing can lead to the development of SAM.
The cardiac anesthesiologist and the echocardio-grapher need to be able to anticipate SAM as its presence after cardiac surgery has been correlated with increased mortality12. The treatment of SAM is to increase both preload and afterload, thereby increasing left ventricular size, and preventing obstruction. This can be accomplished with the use of beta-blockers which both decrease heart rate increasing preload and decrease the force of left ventricular ejection, alpha-1 vasoconstrictors which increase afterload and volume expansion.2 The use of positive ionotropes, diuretics, or vasodilators needs to be avoided as much as possible.
Discussion
SAM of the mitral leaflets and chordae as seen in the midesophageal views on transesophageal echocardiography causing LVOT obstruction and MR is often found in patients with hypertrophic cardiomyopathy5. Other echocardiographic features of SAM include turbulent flow through the LVOT seen with color flow Doppler and high outflow velocity seen with continuous wave doppler which is usually described as late peaking. The mechanism by which this occurs has been described as a high velocity flow caused by the narrowed LVOT creating a Venturi effect on the mitral valve leaflets, causing the leaflets to move anteriorly thereby further narrowing the LVOT and causing obstruction6. It has also been described to occur after cardiac surgical procedures including mitral valve repair1 and aortic valve replacement particularly for aortic stenosis2,3. A number of predictors of SAM after mitral valve surgery have been elucidated. These include an anterior leaflet length greater than 1.8 cm and less than 2.5 cm distance between the coaptation point and the septum7. The presence of SAM following AVR has been attributed to the increase in blood velocity through the LVOT once the obstruction due to the stenotic valve has been relieved and end systolic pressures fall8.
Fig� 1 Transesophageal echocardiography� Midesophageal
aortic valve long axis view demonstrating an unobstructed left ventricular outflow tract.
LA-left atrium, LVOT-left ventricular outflow tract, Ao-Ascending aorta
Fig� 2 Transesophageal echocardiography� Midesophageal aortic
valve long axis view demonstrating an obstructed left ventricular outflow tract due to systolic anterior motion of
the mitral valve. LA-left atrium, LVOT-left ventricular outflow tract, Ao-Ascending aorta

M.E.J. ANESTH 21 (6), 2012
877A CASE OF SEVERE SAM FOLLOWING A DAVID PROCEDURE
References
1. CRESCENZI G, LANDONI G, ZANGRILLO A, GUARRACINO F, ROSICA C, LA CANNA G, ALFIERI O: Management and decision-making strategy for systolic anterior motion after mitral valve repair. J Thorac Cardiovasc Surg; 2009, 137:320.
2. KERUT EK, HANAWALT C, DEARSTINE M, FRANK R, EvERSON C: Mitral Systolic Anterior Motion (SAM) with Dynamic Left Ventricular Outflow Obstruction Following Aortic Valve replacement. Echocardiography; 2007, 24:658.
3. XU J, WEN J, SHU L, LIU C, ZHANG J, ZHAO W: Mechanism and Correlated factors of SAM Phenomenom after Aortic Valve replacement. Journal of Huazhong University of Science and Technology; 2007, 27:72.
4. DAvID TE, FEINDEL CM: An aortic valve-sparing operation for patients with aortic incompetence and aneurysm of the ascending aorta. J Thorac Cardiovasc Surg; 1992, 4:617.
5. SHERRID MV, CHAUDRY FA, SWISTEL DG: Obstructive hypertrophic cardiomyopathy: Echocardiography, pathophysiology, and the continuing evolution of surgery for obstruction. Ann Thorac Surg; 2003, 75:620.
6. NAKATANI S, MARWICK TH, LEvER HM, THOMAS JD: Resting echocardiographic features of latent left ventricular outflow tract obstruction in hypertrophic cardiomyopathy. Am J Cardiol; 1996, 78:662.
7. MASLOW AD, REGAN MM, HAERING JM, JOHNSON RG, LEvINE RA: Echocardiographic predictors of left ventricular outflow tract obstruction and systolic anterior motion of the mitral valve after mitral valve reconstruction for myxomatous valve disease. J Am Col Cardiol; 1999, 34:2096.
8. ROUTLEDGE T, NASHEF SAM: Severe mitral systolic anterior motion complicating aortic valve replacement. Interactive Cardiovasc Thorac Surg; 2005, 4:486.
9. FEINDEL CM, DAvID TE: Aortic valve sparing operations: Basic concepts. International Journal of Cardiology; 2004, 97:61.
10. VERONISI F, CORSI C, SUGENG L, MOR-AvI V, CAIANI EC, WEINERT L, LAMbERTI C, LANG RM: A study of functional anatomy of aortic mitral valve coupling using 3D matrix transesophageal echocardiography. Circ Cardiovasc Imaging; 2009, 2:24.
11. VERONESI F, CAIANI EG, SUGENG L, FUSINI L, TAMbORINI G, ALAMANNI F, PEPI M, LANG RM: Effect of mitral valve repair on mitral-aortic coupling: A real-time three-dimensional transesophageal echocardiography study. J Am Soc Echocardiogr; 2012, 25:524.
12. AURIGEMMA G, BATISTA S, ORSINELLI D, SWEENEY A, PAPE L, CEUNOUD H: Abnormal left ventricular intracavity flow acceleration in patients undergoing aortic valve replacement for aortic stenosis: A marker for high postoperative morbidity and mortality. Circulation; 1992, 86:926.


879 M.E.J. ANESTH 21 (6), 2012
RESPIRATORY SUPPORT INCLUDING EMERGENT EXTRACORPOREAL MEMBRANE OXYGENATION
AS A BRIDGE TO AIRWAY DILATATION FOLLOWING PERIOPERATIVE BRONCHIAL OCCLUSION
ARLYNE K. THUNG*, DON HAYES, JR**,
THOMAS J. PRESTON***, JOSEPH D. TObIAS*
Abstract
During the perioperative period, various factors may lead to intraoperative and postoperative respiratory failure including upper airway obstruction, bronchospasm, acid aspiration, laryngospasm, and pulmonary hypertension. Regardless of the etiology, prompt recognition with treatment of the inciting event is required to ensure a successful recovery. We report the intraoperative development of respiratory insufficiency and failure in a 17-year-old girl who was status post lung transplant undergoing bronchoscopy. During bronchoscopy, complete left main stem obstruction occurred due to a fibrinous mass near the bronchial anastomosis site. Various modalities were used to support the patient intraoperatively and then postoperatively including low tidal volume/high PEEP ventilation, inhaled nitric oxide (iNO), and high frequency oscillatory ventilation (HFOV). In the CTICU, emergent bedside venovenous extracorporeal membrane oxygenation (ECMO) was used as a bridge to the recovery of respiratory function which was achieved with removal of the occluding fibrinous airway tissue followed by balloon dilatation and stenting of the left main stem bronchus. The potential perioperative causes of respiratory failure are reviewed and support techniques including conventional ventilator strategies, iNO, HFOV and ECMO discussed.
Introduction
Despite continued advancements and improvements in monitoring, pharmacologic agents, and the skill of anesthesia providers, anesthesia entails the potential risk of morbidity and even mortality1,2. In the majority of cases, perioperative cardiovascular arrest and death are the result of either cardiac or respiratory failure. The term respiratory failure is generally used to describe inadequate pulmonary gas exchange resulting in hypoxemia and hypercarbia. During the perioperative period, various factors may be responsible for intraoperative and postoperative respiratory failure including upper airway obstruction, laryngospasm, bronchospasm, acid aspiration and pulmonary arterial hypertension. Regardless of the etiology, prompt recognition and
* MD, Department of Anesthesiology & Pediatrics, Nationwide Children’s Hospital and The Ohio State University, Columbus, Ohio.
** CCP, Department of Pediatrics, Division of Pulmonary Medicine, Nationwide Children’s Hospital and The Ohio State University, Columbus, Ohio.
*** MD, Perfusion Services, The Heart Center & Nationwide Children’s Hospital, Columbus, Ohio. Corresponding Author: Arlyne Thung, MD, Department of Anesthesiology & Pain Medicine, Nationwide Children's
Hospital, 700 Children's Drive, Columbus, Ohio 43205, Tel: (614) 722-4200, Fax: (614) 722-4203. E-mail: [email protected]

880 THUNG A. K. et. al
treatment of the inciting event are required to ensure a successful recovery. However, despite aggressive therapy, progressive respiratory dysfunction may require increased support to provide adequate oxygenation and ventilation. Various strategies may be employed to provide support while the inciting event is treated and recovery ensues. We report the use of emergent bedside venovenous extracorporeal membrane oxygenation (ECMO) in a patient who developed perioperative respiratory failure due to acute occlusion of the left main bronchus following flexible fiberoptic bronchoscopy and biopsy. Prior to the initiation of ECMO, other modalities of support to treat the patient’s life-threatening hypoxemia in both the operating room and the cardiothoracic intensive care unit (CTICU) included low tidal volume/high positive end expiratory pressure (PEEP) ventilation, inhaled nitric oxide (iNO) and high frequency oscillatory ventilation (HFOV). ECMO effectively reversed the hypoxemia and provided the bridge to recovery of respiratory function, which was achieved with removal of the occluding fibrinous airway tissue followed by balloon dilatation and stenting of the left bronchus. The potential perioperative causes of respiratory failure are reviewed and support techniques, including conventional ventilator strategies, iNO, HFOV and ECMO are discussed.
Case Report
Institutional Review Board approval for single case reports is not required at Nationwide Children’s Hospital (Columbus, Ohio). A 17-year-old adolescent with a history of cystic fibrosis (CF), who was status post lung transplantation 6 months prior to the current admission presented to the operating room for direct laryngoscopy with bronchoscopy and sinus debridement. The patient had been hospitalized for the past 2 weeks and had tolerated flexible fiberoptic bronchoscopy with biopsy without complications, which was performed due to concerns of allograft rejection. The procedure was performed with intravenous sedation using propofol. During the course of her admission, she was also treated for cytomegalovirus (CMV) viremia and pneumonitis. Due to progressive respiratory distress
as evidenced by the development of biphasic stridor (inspiratory greater than the expiratory component) and concerns for worsening graft function due to the CMV pneumonitis, the decision was made for a repeat bronchoscopy. The planned procedure was biopsy and an airway evaluation by the otorhinolaryngology service to investigate the etiology for the new onset stridor. Upon arrival to the operating room, the patient was in no acute respiratory distress with no active audible stridor. Preoperative vital signs included blood pressure 117/78 mmHg, heart rate 109 beats per minute, respiratory rate 24 breaths per minute and oxygen saturation of 100% on room air. The patient was held nil per os for 6 hours. Routine American Society of Anesthesiologists’ monitors were placed. Anesthesia was induced with propofol (50 mg) and the incremental inhalation of increasing concentrations of sevoflurane in 100% oxygen. Spontaneous ventilation was maintained during anesthetic induction. Once an adequate depth of anesthesia was achieved, direct laryngoscopy was performed and the vocal cords were sprayed with 5 mL of 2% lidocaine. Direct laryngoscopy and bronchoscopy revealed no signs of tracheal narrowing and a normal airway. A 6.0 mm endotracheal tube was placed by otorhinolaryngology and the pulmonology service proceeded with the flexible fiberoptic bronchoscopy and biopsy. During bronchoscopy, a fibrinous mass in the left main stem bronchus was noted (Fig. 1). Approximately one hour after the start of the bronchoscopy and biopsy, the patient acutely became increasingly more difficult to ventilate with the oxygen saturation decreasing from 100% to 92-94%. Using a metered dose inhaler, albuterol was administered through the endotracheal tube for presumptive bronchospasm. Although there was no change in the depth of placement of the endotracheal tube positioning, auscultation revealed decreased breath sounds on the left side. Repeat bronchoscopy was performed to investigate the changes. Although the endotracheal tube was correctly positioned in the mid-trachea, there was edema of the left bronchial mucosa and complete occlusion of the left bronchus along the suture lines of the graft. An additional 8 mg of dexamethasone was administered (total for the case of 12 mg) and neuromuscular blockade achieved with the administration of rocuronium (20 mg) in an attempt to facilitate ventilation. Despite hand-ventilation with

M.E.J. ANESTH 21 (6), 2012
881RESPIRATORY SUPPORT INCLUDING EMERGENT EXTRACORPOREAL MEMBRANE OXYGENATION AS A BRIDGE TO AIRWAY DILATATION FOLLOWING PERIOPERATIVE BRONCHIAL OCCLUSION
100%, the oxygen saturation continued to decrease to 72-74%. A radial arterial cannula was placed. Ventilatory settings included FiO2 1.0, respiratory rate 24 breaths per minute, peak inflating pressure 42 cmH2O which was necessary to generate a tidal volume 5-6 mL/kg, and PEEP 16 cmH2O. Intraoperative chest radiograph showed complete opacification of the left lung, proper positioning of the ETT and no evidence of pneumothorax (Fig. 2). Arterial blood gas analysis revealed pH 7.211, PaCO2 54 mmHg, and PaO2 55 mmHg. Nitric oxide was started at 20 ppm, and the ETT was advanced into the right main stem bronchus. The remainder of the procedure was aborted and the patient was transported to the pediatric cardiothoracic intensive care unit (CTICU). During transportation, the oxygen saturation varied from 85-89% utilizing a FiO2 of 1.0. Shortly after arrival to the CTICU, there was an abrupt decrease of the oxygen saturation to 40-50%. Repeat laryngoscopy was performed and the endotracheal tube was changed to a 7.0 and placed into the right bronchus using fiberoptic guidance. Inhaled NO was increased to 40 ppm; however, the oxygen saturation remained at 50-60%. Given the ongoing hypoxemia, HFOV was initiated with settings of mean airway pressure (MAP 24) cmH2O, amplitude 50, and Hz 3 without therapeutic effect. Thirty minutes later, a 20 French Avalon Elite™ catheter (Avalon Laboratories LLC, Rancho Dominguez, CA) was placed by the cardiothoracic surgery service into the patient's right internal jugular vein for venovenous ECMO (VV-ECMO). Following the initiation of VV-ECMO, flexible fiberoptic bronchoscopy was performed by the pulmonology service and demonstrated edema and near 100% occlusion of the left main stem bronchus with tissue and airway debris. Vigorous lavage was performed and small lumens were created into both subsegments of the left bronchus using pediatric size biopsy forceps followed by the instillation of 10 mg of dexamethasone. The next morning, the interventional pulmonology service performed bedside flexible fiberoptic bronchoscopy with balloon dilatation of the left bronchus and debridement of the fibrinous tissue while the patient was still on VV-ECMO. Following this procedure, there was gradual expansion of the left lung over the next 8-12 hours (Fig. 3). The patient was decannulated from ECMO and transitioned from HFOV to conventional ventilation on the 2nd
postoperative day and her trachea was extubated on the 3rd postoperative day. She was supported with non-invasive ventilation for 48 hours and subsequently weaned to room air. There was no change in her baseline neurological status. The remainder of her postoperative course was unremarkable and she has returned to her baseline status.
Fig� 1 Intraoperative photograph taken during bronchoscopy showing edema of the left bronchial mucosa and total
occlusion of the left bronchus just above the suture site for the graft
Fig� 2 Intraoperative chest radiograph showing complete
opacification of the left lung, proper positioning of the endotracheal tube, and no evidence of pneumothorax

882 THUNG A. K. et. al
Fig� 3 Repeat chest radiograph following interventional
bronchoscopy and balloon dilatation of the left bronchus� The single lumen catheter for venous-venous extracorporeal
oxygenation can be seen in the right internal jugular vein
Discussion
The care of the patient with postoperative respiratory failure begins with the identification of its etiology. In general, there are 5 primary causes of hypoxemia including 1) a low inspired concentration of oxygen, 2) hypoventilation, 3) ventilation-perfusion inequalities, 4) shunt, and 5) diffusion abnormalities. Although a low inspired oxygen concentration is frequently not considered in the differential diagnosis of hypoxemia, it must be considered in the operating room setting and its possibility ruled out by ensuring that the inspiratory oxygen concentration is 100%. In our patient, prompt evaluation with auscultation of the chest during manual ventilation with 100% revealed an inequality of breath sounds that prompted investigation via bronchoscopy. Although movement of the ETT is the most likely scenario resulting in inequality of breath sounds, we noted that the placement of the ETT (depth of insertion) had not changed. Rather, the acute onset of edema and plugging with debris of the left main stem bronchus resulted in total obstruction and significant ventilation-perfusion mismatch resulting in hypoxemic respiratory failure.
In the setting of hypoxemia, an evaluation of the severity of the lung disease may be based on the difference between the PaO2 and the partial pressure of
oxygen in the alveoli. This is commonly referred to the A-a (alveolar-arterial) oxygen gradient. In our patient, the severity of the respiratory failure was demonstrated by an A-a gradient of approximately 600 with a PaO2 of 55 mmHg and an FiO2 of 1.0. Another measure of severity of lung injury that is used is if PaO2:FiO2 ratio. When the ratio is less than 300 mmHg, acute lung injury (ALI) is considered to be present while adult respiratory distress syndrome (ARDS) is present when the ratio is less than 200 mmHg. In our patient, the PaO2:FiO2 ratio was 55.
During conventional positive pressure ventilation, oxygenation is regulated by the FiO2 and the mean airway pressure (MAP). MAP is determined by the PIP, PEEP and the inspiratory time3. Increasing the MAP by manipulation of any of these variables recruits alveoli, improves ventilation-perfusion matching and decreases intrapulmonary shunting. In addition to reducing ventilation-perfusion inequalities and increasing functional residual capacity (FRC), increasing MAP may also result in a significant improvement in respiratory compliance thereby allowing for more effective spontaneous ventilation and decreasing the PIP required to provide adequate tidal ventilation. This may limit the potential for barotrauma during mechanical ventilation4,5. Intraoperatively, a relatively simple maneuver to increase MAP is to lengthen the inspiratory time, a technique that is frequently accomplished by setting an inspiratory to expiratory ratio of 1:1. A longer inspiratory time such that the ratio exceeds 1:1 is not recommended as expiratory time is compromised which may result in insufficient time to exhale with the development of auto-PEEP and an increased risk of barotrauma.
Mechanical ventilation also provides the minute ventilation for CO2 removal, calculated as the respiratory rate (RR) times the tidal volume. PaCO2 is directly related to the body’s production of CO2 during the catabolism of fats and carbohydrates and is inversely related to alveolar ventilation. In most clinical circumstances, the control of PaCO2 is via alterations in the minute ventilation; however, some control of the body’s endogenous CO2 production is possible through the use of fats versus carbohydrates for nutrition or by control of body temperature. Prevention of hyperthermia and even induction of mild

M.E.J. ANESTH 21 (6), 2012
883RESPIRATORY SUPPORT INCLUDING EMERGENT EXTRACORPOREAL MEMBRANE OXYGENATION AS A BRIDGE TO AIRWAY DILATATION FOLLOWING PERIOPERATIVE BRONCHIAL OCCLUSION
hypothermia (35oC) can be used clinically to control hypercarbia as well as hypoxemia and limit mechanical ventilatory requirements.
In patients with severe lung disease, ventilation to normocarbia is not necessary and may in fact be harmful. Current practice in the ICU during the care of patients with ALI and ARDS includes permissive hypercarbia or allowing the PaCO2 to increase, provided that the pH is above 7.25. This strategy has been shown to improve outcome in patients with adult respiratory distress syndrome (ARDS)6. When dealing with a critically ill patient in the operating room, although new models of anesthesia machines provide newer modalities of ventilatory support, older versions may be incapable of supporting the critically ill patient. In such cases, the early switch to a standard ICU ventilator is suggested. These ICU ventilators not only provide higher working pressures with the delivery of effective PIP and PEEP, but also allow for newer modalities of ventilation which may be helpful in patients with ALI such as pressure-regulated, volume controlled ventilation (PRVC).
Low tidaL voLume ventiLation: The 2000 ARDS Network publication in the New England Journal of Medicine is viewed as a milestone in the practice of critical care medicine. In a prospective randomized trial of adults with ARDS, ventilation was provided with a tidal volume of either 6 mL/kg or 12 mL/kg7. Survival was greater in the low tidal volume group (31% versus 39.8%). In addition, ventilator-free days and number of days without non-pulmonary organ system failure were significantly increased in the low tidal volume treated group. Despite the compelling results set forth from the adult trials, lingering controversy remains whether the lung protective strategy of low tidal volume should be universally applied to all patients with ARDS/ALI and specifically the pediatric population. Detractors to the universal approach have instead advocated an approach more tailored to the individual patient, based on the underlying pulmonary process8,9. In the operating room, during the short term support of patients, such strategies cannot be universally advocated, especially when dangerously low oxygen saturations are present. In such scenarios, the short term consequences of the increased PIP relate primarily to its effects on preload and cardiovascular performance as well as the risk of
barotrauma resulting in pneumothorax.
Extrapolation of low tidal volume ventilation to pediatric patients has been challenging given the scarcity of date to support its use in this younger patient population and the controversy that exists even among the adult patient population. Critics of a universal application of low tidal volume to pediatric patients have cited specific concerns. Neonates and infants may not be as susceptible to the barotrauma seen with high tidal volume ventilation as demonstrated by animal models10,11. Additionally, low tidal volumes may inadequately ventilate infants and neonates who at baseline have higher respiratory compliance versus their adult counterparts making them more prone to atelectasis.
Despite the arguments against low tidal volume ventilation in younger patients, some studies have suggested undeniable benefits in patients with ARDS/ALI. In a retrospective study examining pediatric patients ranging in age from 1 week to 17 years with ALI who were mechanically ventilated from 1988-1992 versus patients from 2000-2004, Albuali et al12 reported that the group cared for during the 1988-1992 time frame were ventilated with significantly higher mean tidal volumes (10.2 ± 1.7 versus 8.1 ± 1.4 ml/kg), lower levels of PEEP (6.1 ± 2.7 versus 7.1 ± 2.4 cm H2O) and higher PIP (31.5 ± 7.3 versus 27.8 ± 4.2 cmH2O). Most importantly, those cared for during the 2000-2004 period had a lower mortality (21% versus 34%) and greater number of ventilator free days. In our patient, we chose low tidal volume/high PEEP ventilation as an appropriate ventilatory strategy because of her age, the history of a pre-existing CMV pneumonitis, and the requirements of a high PEEP to main adequate oxygenation. As such, the tidal volume was decreased to limit the PIP during use of a high PEEP technique. Although the decision to use low tidal volume ventilation may be more straightforward in older pediatric patients whose pulmonary mechanics are similar to their adult counterparts, the decision still remains unclear in younger patients. It has been suggested that until this clinical dilemma is resolved by more definitive randomized controlled trials examining the use of low tidal volume ventilation in younger pediatric patients, application of adult data to pediatric patients still remains a valid endeavor13,14.

884 THUNG A. K. et. al
nitric oxide: First described in 1987 as endothelial-derived growth factor15, iNO was introduced into clinical practice during the early part of the 1990’s16. Currently, the only FDA-approved indication for iNO is the treatment of hypoxic respiratory failure for term or near-term infants due to conditions such as primary pulmonary arterial hypertension, diaphragmatic hernia, aspiration, sepsis, or infectious pulmonary processes. The pulmonary vasodilatory effects of iNO are mediated through activation of guanylate cyclase with increased production of intracellular cyclic guanine monophosphate (cGMP) leading to decreased intracellular calcium concentration, smooth muscle relaxation and decreased pulmonary vascular resistance. Alterations in the pulmonary vascular tone result in the optimization of ventilation-perfusion matching with improvement of oxygenation via preferential dilatation of vessels in the better ventilated alveoli17,18. Rapid inactivation of iNO occurs through hemoglobin binding and formation of methemoglobin thereby limiting its systemic effects. Methemoglobin is metabolized to hemoglobin by methemoglobin reductase within the erythrocytes. The incidence of methemoglobinemia is low with inhaled NO concentration ≤40 ppm19-21.
The use of iNO in both adult and pediatric patients for acute hypoxemic respiratory failure has been reported in multiple studies. In neonates >34 weeks gestation who had hypoxic respiratory failure, the Neonatal Research Network reported that iNO reduced the use of ECMO but had no effect on mortality22. Van Meurs et al reported similar findings in a cohort of premature infants with severe respiratory failure23. More recently, meta-analyses looking at the use of iNO in both pediatric and adult patients with ALI concluded that iNO could not be recommended in patients with acute hypoxemic respiratory failure. Despite the transient improvement in oxygenation that occurred for the first 24 hours, no reduction in mortality was noted24,25.
Although the use of iNO as a definitive treatment for ALI is controversial, its use as a temporizing measure to improve oxygenation is promising in specific clinical scenarios. Dietrich and Tobias reported the successful intraoperative administration of iNO in a pediatric patient who developed hypoxemia
following institution of one lung ventilation during thoracoscopic lung resection26. In our patient, iNO was administered to optimize oxygenation and facilitate an uneventful transport to the CTICU. Inhaled NO at a concentration of 20 ppm was administered to the manual resuscitation bag for use during transport. Following the patient’s acute decompensation with profound hypoxemia after arrival to the CTICU, iNO proved ineffective even when increased to 40 ppm. When iNO is administered intraoperatively using the anesthesia machine ventilator, specific modifications in the intraoperative ventilator technique are needed to prevent rebreathing and disruption of the normal function of the delivery system27.
HigH frequency osciLLatory ventiLation: High frequency oscillatory ventilation (HFOV) is a subtype of high frequency ventilation, which uses a piston to generate small tidal volumes with very high rates. It was been introduced into ICU care to provide ventilation and oxygenation in patients with respiratory failure while limiting the risk of barotrauma. Barotrauma is limited by avoiding high PIP’s. High frequency ventilator techniques rely on respiratory rates greater than 120 breaths per minute (2 Hz) with tidal volumes less than dead space. Gas exchange is thought to occur via convection rather than bulk flow28. HFOV uses a piston-driven, diaphragm oscillator to provide a constant mean or distending airway pressure. Lung volumes are maintained above FRC thereby providing a constant distending pressure for alveoli while avoiding PIP’s. Superimposed around the MAP are the oscillations provided by the inward and outward movement of the diaphragm. The movement of the diaphragm provides not only active inspiration, but also active expiration thereby decreasing gas trapping and inadvertent PEEP29. Unlike conventional mechanical ventilation, HFOV is unique in that oxygenation and ventilation are separated. Oxygenation is determined by the independent adjustments of MAP and FiO2. Ventilation is manipulated by adjustments of the amplitude (delta P), frequency (Hz), and inspiratory time. In general, when caring for patients with ALI, the MAP is set at 2-4 cmH2O above the MAP on conventional ventilation and adjusted up as needed to allow for a decrease of the FiO2 to the desired level. The efficacy of the MAP and its effect on alveolar recruitment is assessed by a chest

M.E.J. ANESTH 21 (6), 2012
885RESPIRATORY SUPPORT INCLUDING EMERGENT EXTRACORPOREAL MEMBRANE OXYGENATION AS A BRIDGE TO AIRWAY DILATATION FOLLOWING PERIOPERATIVE BRONCHIAL OCCLUSION
radiograph with the goal of achieving lung expansion of 8-9 ribs. Ventilation is controlled primarily by adjusting the amplitude (delta P) using the power setting on the ventilator. The power knob is adjusted to control the amplitude that is changed in increments of 2-4 cmH2O to provide for adequate chest movement and CO2 removal. HFOV has been utilized in full range of ICU patients including adults, children, infants, and neonates. Despite its theoretical advantages over conventional mechanical ventilation, there are limited and conflicting evidence-based data to demonstrate its impact on morbidity and mortality30-32.
In our patient, HFOV was selected over conventional mechanical ventilation after the hypoxemia failed to improve with ensuring correct placement of the ETT, iNO at 40 ppm, and manual bag ventilation. Given the severity of her lung disease and total left lung obstruction, HFOV did not result in a clinically significant improvement in oxygenation. Following the initiation of ECMO, HFOV was continued to provide a constant distending pressure and optimal recruitment of the left lung. This proved efficacious once the obstructing etiology was removed and treated. Following treatment, the patient tolerated the transition to conventional ventilation without difficulty.
extracorporeaL membrane oxygenation: ECMO was first described in 1972 as a salvage treatment for an adult patient who developed acute respiratory failure following blunt trauma32. Since the earliest days of its clinical use, ECMO’s role in the treatment of patients with acute respiratory failure has fluctuated. The initial success of ECMO in the adult population was attenuated seven years later following a randomized controlled prospective study evaluating prolonged ECMO therapy for acute respiratory failure34. With a 90% mortality rate in both groups, ECMO was soon dismissed as an ineffective treatment for adult patients with acute respiratory failure. However, as the use ECMO waned in the adult population, its use in the neonatal population took over with reports of success in various causes of respiratory failure in the neonate including sepsis, meconium aspiration, congenital diaphragmatic hernia and congenital heart disease. Following success in the neonatal population and with improvements in the technology and techniques used
for ECMO, it has become a popular means of rescue for patients of all ages with potentially reversible respiratory or cardiac failure that is unresponsive to conventional therapy. The publication of the CESAR (Conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure) trial in 2009 solidified ECMO’s role in the treatment of adult patients with reversible respiratory failure35. In evaluating the 180 patients who were randomized to either ECMO or conventional management, 6-month survival without disability was greater in ECMO patients (63% versus 47%) than those patients treated with conventional management. ECMO’s role as an invaluable means of support for patients with reversible respiratory failure was further bolstered by the 2009-2010 Influenza A/H1N1 global pandemic in which patients with H1N1-related ARDS treated with ECMO demonstrated a significantly lower mortality rate than those patients who were not referred for ECMO (23.7% versus 52.5%, p <0.05)36.
Although the majority of ECMO was originally performed using the venoarterial (VA) route, there has been significant progress made in the development of technology to allow for support of oxygenation and ventilation using the VV route in patients with normal cardiovascular function. VA-ECMO requires both an arterial and venous cannula and at times involves ligation of the carotid artery. Currently, this approach is typically reserved for patients requiring cardiovascular support. In VA-ECMO, a cannula is placed in the jugular vein to drain blood from the right atrium. A pump propels the blood through an oxygenator and then into the arterial cannula which returns the blood via direct cannulation of the aorta, carotid, axillary or femoral artery. Given its more invasive nature, there is an increased risk of significant morbidity with VA-ECMO. These issues have led to the increased use of VV-ECMO by most centers when treating isolated respiratory failure. In VV-ECMO, blood is drained from the right atrium and reenters the central venous circulation while preserving normal pulmonary blood flow and without the need for placement of a cannula into an artery. Although initially performed using two cannula (one placed into the internal jugular and the other into the femoral vein), VV-ECMO can now be performed using a single catheter placed into the internal jugular vein37. As used in our patient, a

886 THUNG A. K. et. al
significant innovation that has enhanced the capability of extracorporeal support was the development of a bicaval dual lumen catheter (Avalon Laboratories, Rancho Dominguez, CA) that allows respiratory support through a single catheter for application of ECMO38. This specially designed catheter drains venous blood from the superior and inferior vena cava and then returns oxygenated blood from the ECMO circuit to the right atrium ideally directed at the inlet of the tricuspid valve. This designs limits venous admixture and improves oxygenation during VV-ECMO. Additional modalities of extracorporeal respiratory support are being developed with may offer additional benefits over conventional VV or VA-ECMO techniques. The reader is referred to reference 39 for full descriptions of these modalities39.
As was noted in our patient, in addition to its role as a therapeutic modality for patients with ARDS and ALI, ECMO can be used as a bridge to definitive treatment in patients with acute upper and lower airway obstruction. Wilms et al reported the use VA-ECMO in a 39-year-old man who experienced total obstruction of a distal tracheal stent by a tumor mass40. The occluding tracheal mass was removed with the use of forceps, suctioning and lavage while on ECMO. The authors reviewed 12 other reports in patients ranging from the neonatal period to 73 years of age with obstructing lesions of the upper and lower airway, which were managed with either VV or VA-ECMO before definitive treatment41-52. No mortality was reported in any of these cases.
In summary, we present the use of various modalities of respiratory support in an adolescent who was status post lung transplant and developed intraoperative respiratory failure. In addition to identifying the etiology of the respiratory failure, keys in the successful management of such patients includes the ability to move rapidly along a treatment algorithm to treat hypoxemic respiratory failure (Table 1). Key in the management of such patients includes consideration for the use of manipulations of ventilator
techniques to augment MAP and oxygenation including low tidal volume/high PEEP techniques, permissive hypercarbia, use of an ICU ventilator in the OR, the addition iNO, as well as none conventional modes of ventilation such as HFOV. When these techniques fail, extracorporeal support may be life-saving especially for acute upper and lower airway obstruction.
Table 1 Algorithm for treatment of perioperative respiratory
failure1. Identify etiology (hand ventilate with 100% oxygen).2. Treat etiology if feasible.3. Correct or treat simple problems (auscultation for breath sounds, obtain chest radiograph
a. Malpositioned endotracheal tubeb. Secretions and mucus plugging (suction
endotracheal tube)c. Bronchospasm
4. Adjust ventilator to increase mean airway pressure (use ICU ventilator as needed)
a. Lengthen inspiratory timeb. Increase PEEPc. Increase PIP (tidal volume)
5. Whenever feasible, use low tidal volume strategy with plateau pressure of less than 32 cmH2O. Permissive hypercarbia (pH ≥7.2) and permissive hypoxemia (oxygen saturations 80%).6. Maintain normothermia and treat hyperthermia aggressively to limit oxygen consumption and CO2 production.7. Limit the use of anesthetic agents that impair hypoxic pulmonary vasoconstriction.8. Consider use of an ICU ventilator in the operating room with switch to total intravenous anesthesia. Alternative modes of ventilation including pressure-regulated volume controlled (PRVC) may be helpful. 9. Consider prone positioning if technically feasible.10. Add inhaled nitric oxide starting at 20 ppm.11. Consider switching to non-conventional mode of ventilation (high frequency).12. Extracorporeal life support technology.

M.E.J. ANESTH 21 (6), 2012
887RESPIRATORY SUPPORT INCLUDING EMERGENT EXTRACORPOREAL MEMBRANE OXYGENATION AS A BRIDGE TO AIRWAY DILATATION FOLLOWING PERIOPERATIVE BRONCHIAL OCCLUSION
References
1. RAMAMOORTHY C, HAbERKERN CM, BHANANKER SM, DOMINO KB, POSNER KL, CAMPOS JS, MORRAY JP: Anesthesia-related cardiac arrest in children with heart disease: data from the Pediatric Perioperative Cardiac Arrest (POCA) registry. Anesth Analg; 2010, 110:1376-1382.
2. BHANANKER SM, RAMAMOORTHY C, GEIDUSCHEK JM, POSNER KL, DOMINO KB, HAbERKERN CM, CAMPOS JS, MORRAY JP: Anesthesia-related cardiac arrest in children: update from the Pediatric Perioperative Cardiac Arrest Registry. Anesth Analg; 2007, 105:344-350.
3. BOROS SJ, MATALON SV, EWALD R, LENARD AS, HUNT CE: The effect of independent variations in inspiratory-expiratory ratio and end-expiratory pressure during mechanical ventilation in hyaline membrane disease: the significance of mean airway pressure. J Pediatr; 1977, 91:794-798.
4. WEISMAN IM, RINALDO JE, ROGERS RM, SANDERS MH: Intermittent mandatory ventilation. Am Rev Respir Dis; 1983, 127:641-647.
5. TObIAS JD: Conventional mechanical ventilation. Saudi J Anaesth; 2010, 4:86-98.
6. HICKLING KG, WALSH J, HENDERSON S, JACKSON R: Low mortality rate in adult respiratory distress syndrome using low-volume, pressure-limited ventilation with permissive hypercapnia. Crit Care Med; 1994, 22:1568-1578.
7. The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med; 2000, 342:1301-1308.
8. DEANS KJ, MINNECCI P: Mechanical ventilation in ARDS: One size does not fit all. Crit Care Med; 2005, 33:1141-1142.
9. GATTIONI L: “Counterpoint: is low tidal volume mechanical ventilation preferred for all patients on ventilation? No”. Chest; 2011, 140:9-15.
10. COPLAND IB, MARTINEZ F, KAvANAGH BP, ET AL: High tidal volume ventilation causes different inflammatory responses in newborn versus adult lung. Am J Respir Crit Care Med; 2004, 169:739-748.
11. HAUbER HP, KARP D, GOLDMANN T, ET AL: Effect of low tidal volume ventilation on lung function and inflammation in mice. BMC Pulmonary Medicine; 2010, 10:21.
12. ALbUALI WH, SINGH RN, FRASER DD, ET AL: Have changes in ventilation practice improved outcome in children with acute lung injury? Pediatr Crit Care Med; 2007, 8:324-330.
13. CHEITFETZ IM: Management of acute lung injury: sharing data between adults and children. Respiratory Care; 2011, 56:1258-1272.
14. HANSON JH, FLORI H: Application of the acute respiratory distress syndrome network low-tidal volume strategy to pediatric acute lung injury. Respir Care Clin; 2006, 12:349-357.
15. PALMER RM, FERRIGE AG, MONCADA S: Nitric oxide release accounts for the biological activity of endothelium-derived-relaxing factor. Nature; 1987, 327:524-526.
16. ROSSAINT R, FALKE KJ, LOPEZ F, ET AL: Inhaled nitric oxide for adult respiratory distress syndrome. N Engl J Med; 1993, 328:399-405.
17. MILLER CC, MILLER JW: Pulmonary vascular smooth muscle regulation: the role of inhaled nitric oxide gas. Respir Care; 1992, 37:1175-85.
18. HADDAD E, LOWSON SM, JOHNS RA, ET AL: Use of inhaled nitric oxide perioperatively and in intensive care patients. Anesthesiology; 2000,
92:1821-1825.19. TAYLOR M, CHRISTIAN K, PATEL N, ET AL: Methemoglobinemia:
Toxicity of inhaled nitric oxide therapy. Pediatr Crit Care Med; 2001, 2:99-101.
20. HEAL CA, SPENCER SA: Methaemoglobinaemia with high-dose nitric oxide administration. Acta Paediatr; 1995, 84:1318-1319.
21. NAKAJIMA W, ISHIDA A, ARAI H, ET AL: Methaemoglobinaemia after inhalation of nitric oxide in infant with pulmonary hypertension. Lancet; 1997, 350:1002-1003.
22. The Neonatal Inhaled Nitric Oxide Study Group. Inhaled nitric oxide in full-term and nearly full-terms infants with hypoxic respiratory failure. N Engl J Med; 1997, 336:597-604.
23. VAN MEURS KP, WRIGHT LL, EHRENKRANZ R, ET AL: Inhaled nitric oxide for premature infants with severe respiratory failure. N Engl J Med; 2005, 353:13-22.
24. ADHIKARI NK, BURNS KE, FRIEDRICH JO, ET AL: Effect of nitric oxide on oxygenation and mortality in acute lung injury: systematic review and meta-analysis. BMJ; 2007, 334:779-786.
25. AFSHARI A, BROK J, MOLLER AM, ET AL: Inhaled nitric oxide for acute respiratory distress syndrome and acute lung injury in adults and children: A systematic review with meta-Analysis and trial sequential analysis. Anesth Analg; 2011, 112:1411-1421.
26. DIETRICH CC, TObIAS JD: Intraoperative administration of nitric oxide. J Intensive Care Med; 2003, 18:146-149.
27. TObIAS JD, GRUEbER RE: Nitric oxide administration using an anesthesia machine ventilator. Am J Anesthesiol; 2000, 27:137-139.
28. BANCALARI A, GERHARDT T, BANCALARI E, ET AL: Gas trapping with high-frequency ventilation: jet versus oscillatory ventilation. J Pediatr; 1987, 110:617-622.
29. MAMMEL MC, OPHOvEN JP, LEWALLEN PK, ET AL: High-frequency ventilation and tracheal injuries. Pediatrics; 1986, 77:608-613.
30. DOCTOR A, ARNOLD JH: Mechanical support of acute lung injury: Options for strategic ventilation. New Horizons; 1999, 7:359-373.
31. ARNOLD JH, HANSON JH, TORO-FIGUERO LO, GUTIERREZ J, BERENS RJ, ANGLIN DL: Prospective, randomized comparison of high-frequency oscillatory ventilation and conventional mechanical ventilation in pediatric respiratory failure. Crit Care Med; 1994, 22:1530-1539.
32. ARNOLD JH, TRUOG RD, THOMPSON JE, FACKLER JC: High-frequency oscillatory ventilation in pediatric respiratory failure. Crit Care Med; 1993, 21:272-278.
33. HILL JD, ObRIEN TG, MURRAY JJ: Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock lung syndrome). New Engl J Med; 1972, 286:629-634.
34. ZAPOL WM, SNIDER MT, HILL JD, ET AL: Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA; 1979, 242:2193-2196.
35. PEEK GJ, MUGFORD M, TIRUvOIPATI R, ET AL. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised control. Lancet; 2009, 374:1351-1363.
36. NOAH MA, PEEK GJ, FINNEY SJ, ET AL: Referral to an Extracorporeal Membrane Oxygenation Center and Mortality Among Patients With Severe 2009 Influenza A (H1N1). JAMA; 2011, 306:1659-1668.
37. HAYES D JR, KUKREJA J, TObIAS JD, bALLARD HO, HOOPES CW: Ambulatory venovenous extracorporeal respiratory support as a bridge for cystic fibrosis patients to emergent lung transplantation. J

888 THUNG A. K. et. al
Cystic Fibrosis; 2012, 11:40-45.38. BERMUDEZ CA, ROCHA Rv, SAPPINGTON PL, TOYODA Y, MURRAY
HN, bOUJOUKOS AJ: Initial experience with single cannulation for venovenous extracorporeal oxygenation in adults. Ann Thorac Surg; 2010, 90:991-995.
39. HAYES D JR, TObIAS JD, KUKREJA J, KIRKbY S, PRESTON TJ: A review of extracorporeal life support for acute respiratory distress syndrome. Heart Lung (in press).
40. WILMS DC, MENDEZ R, NORMAN v, ET AL: Emergency bedside extracorporeal membrane oxygenation for rescue of acute tracheal obstruction. Resp Care; 2012, 57:646-649.
41. HIGASHI K, TAKESHITA J, TERASAKI H, ET AL: A case of acute airway obstruction with sharp sawdust particles, successfully treated with extracorporeal lung assist. Crit Care Med; 1990, 18:239-240.
42. MORNEAULT L, JOHNSTON A, PERREAULT T: Management of acute airway obstruction using extracorporeal membrane oxygenation. ASAIO J; 1996, 42:321-323.
43. ISSACSON G. Acute airway obstruction in the hospitalized infant: four hard lessons in the distal trachea. Ann Otol Rhinol Laryngol; 1996, 105:532-535.
44. ROSA P JR, JOHNSON EA, bARCIA PJ: The impossible airway: a plan. Chest; 1996, 109:1649-1650.
45. SHIRAISHI T, KAWAHARA K, SHIRAKUSA T, ET AL: Primary tracheal fibrosarcoma in a child: a case of tracheal resection under ECMO
support. Thorac Cardiovasc Surg; 1997, 45:252-254.46. STEWART AS, SMYTHE WR, AUKbURG S, ET AL: Severe acute extrinsic
airway compression by mediastinal tumor successfully managed with extracorporeal membrane oxygenation. ASAIO J; 1998, 44:219-221.
47. BELMONT MK, WAX MK, DESOUZA FN: The difficult airway: cardiopulmonary bypass - the ultimate solution. Head Neck; 1998, 20:266-269.
48. BROWN KL, SHEFLER A, COHEN G, ET AL: Near-fatal grape aspiration with complicating acute lung injury successfully treated with extracorporeal membrane oxygenation. Pediatr Crit Care Med; 2003, 4:243-245.
49. CHAO vT, LIM DW, TAO M, ET AL: Tracheobronchial obstruction as a result of a mediastinal mass. Asian Cardiovasc Thorac Ann; 2006, 14:e17-18.
50. IGNACIO RC JR, FALCONE RA JR, bROWN RL: A case report of severe tracheal obstruction requiring extracorporeal membrane oxygenation. J Pediatr Surg; 2006, 41:E1-E4.
51. COLLAR RM, TAYLOR JC, HOGIKYAN ND, ET AL: Awake extracorporeal membrane oxygenation for management of critical distal tracheal obstruction. Otolaryngol Head Neck Surg; 2010, 142:618-620.
52. HOLLIDAY T, JACKSON A: Emergency use of extracorporeal membrane oxygenation for a foreign body obstructing the airway. Crit Care Resusc; 2010, 12:273-275.

889 M.E.J. ANESTH 21 (6), 2012
GENERAL ANESTHESIA IN A PATIENT WITH CLEIDOCRANIAL DYSPLASIA
CINDY JESSICA WANG*, STEvEN MARK NEUSTEIN**
Introduction
Cleidocranial dysplasia (CD) is a rare disorder that involves developmental abnormalities of bony structures. CD is characterized as an autosomal dominant skeletal dysplasia with a variety of clinical manifestations; most commonly supernumerary teeth, brachycephalic skull, short stature, and hypoplastic or aplastic clavicles. In a systematic review of a study population comparing CD individuals with non-affected relatives as controls, scoliosis and upper respiratory complications (including recurrent sinus infections, collapsing nasal passages, sleep apnea, and wheezing) were noted to be significantly increased in CD individuals in comparison with controls1. Other possible manifestations of CD that involve upper airway structures include maxillary hypoplasia, high vaulted palate, and palatal clefting2. The variety of CD associated structural abnormalities can potentially pose challenges to anesthetic management; however, there is limited literature describing anesthetic implications of CD patients undergoing surgery. Potential difficulties for airway management and neuraxial placement are described in the anesthetic management of a patient with CD who underwent a variety of obstetrical procedures3. We present our approach to airway assessment and anesthetic management of a patient with CD undergoing a general surgical procedure.
Case Description
A 24 year-old male with CD presented to our operating room for repair of pelvic prolapse. He had complaints of worsening urinary and fecal incontinence over the past several years and was scheduled for repair of both rectal and bladder prolapses (low anterior resection with rectopexy and urethral sling). It was unknown if his pelvic prolapse was related to cleidocranial dysplasia. Past medical history was significant for prior surgeries at an outside hospital related to developmental abnormalities from cleidocranial dysplasia. He had three prior back surgeries related to scoliosis (mainly in the thoracic region) and jaw surgery 3 years prior. Family history was significant for a mother with CD.
During pre-operative evaluation on the day of surgery, our patient was noted to have a limited mouth opening (Mallampati Class III), brachycephaly, frontal bossing, and short stature (the patient’s height and weight were 165 cm and 57 kg respectively). He had full flexion, extension, and range of motion of his neck. Since his prior surgeries were at an outside
Department of Anesthesiology, Mount Sinai School of Medicine, New York, N.Y.* MD, Resident.** MD, Professor. Corresponding Author: Steven Neustein, Department of Anesthesiology, Mount Sinai School of Medicine, New York,
NY, Tel: 201-241-7467. E-mail: [email protected]

890 WANG C. J. & NEUSTEIN S. M.
dysplasia undergoing various obstetric procedures. Int J Obstet Anesth; 2010 Jan, 19(1):106-8.
4. AZIZ MF, HEALY D, KHETERPAL S, FU RF, DILLMAN D, BRAMbRINK AM: Routine clinical practice effectiveness of the Glidescope in difficult airway management: an analysis of 2,004 Glidescope intubations, complications, and failures from two institutions. Anesthesiology; 2011, 114:34-41.
hospital, no history was available on the ease of prior intubations. Upon assessment of the airway, it was felt that airway management could potentially be challenging and a video laryngoscope was made available in the operating room. Upon entering the operating room, ASA monitors were placed and our patient was pre-medicated with midazolam. After pre-oxygenation and intravenous induction with propofol and fentanyl, mask ventilation was uncomplicated and a neuromuscular blocking agent was given. We decided to first assess our patient’s airway with direct laryngoscopy. With a Macintosh 3 blade and external laryngeal manipulation, a limited Cormack-Lehane Grade 2 view was obtained. The video laryngoscope (GlideScope, Verathon, Bothell, WA) was then used to facilitate the endotracheal intubation. The GlideScope provided full visualization of the vocal cords allowing for atraumatic intubation with a 7.0 standard cuffed endotracheal tube with the assistance of the GlideScope rigid stylet. Our patient was maintained on inhaled anesthetic and the case proceeded uneventfully with successful extubation at the end of the case. He recovered fully with no anesthetic complications.
Discussion
There is very little information available regarding anesthetic care for patients with CD presenting for surgery. In particular, patients with CD have a variety of structural abnormalities that can potentially interfere with the patency of their airway requiring careful assessment by the anesthesiologist involved in their care. Anatomic abnormalities of the skull and facial structures (including dentition) may impede with mask ventilation and endotracheal intubation while spinal abnormalities may pose challenges to neuraxial techniques. In addition to performing a standard history and physical, there should be preparation to deal with a potentially difficult airway. Additional equipment such as a video laryngoscope or fiberoptic scope should be readily available. In a recent analysis of intubations at two academic medical centers, the GlideScope video laryngoscope assisted in successful intubation in 94% of cases after a failed direct laryngoscopy attempt4. Our patient did have a difficult intubation that was successfully managed with the use of the GlideScope. Our case report demonstrates how patients with CD may have skeletal abnormalities that require careful assessment of the airway and preparation with appropriate equipment to manage a potentially difficult airway.
References
1. COOPER SC, FLAITZ CM, JOHNSTON DA, LEE B, HECHT JT: A natural history of cleidocranial dysplasia. American Journal of Medical Genetics; 2001, 104:1-6.
2. NEbGEN D, WOOD RS, SHAPIRO RD: Management of a mandibular fracture in a patient with cleidocranial dysplasia: report of a case and review of the literature. J� Oral Maxillofac Surg; 1991, 49:405-409.
3. IOSCOvICH A, BARTH D, SAMUELOFF A, GRISARU-GRANOvSKY S, HALPERN S: Anesthetic management of a patient with cleidocranial

891 M.E.J. ANESTH 21 (6), 2012
ACUTE QUADRIPLEGIA AFTER INTERSCALENE BLOCK SECONDARY TO CERVICAL BODY EROSION
AND EPIDURAL ABSCESS
JAHAN PORHOMAYON*, NADER D. NADER**
Abstract
Although the incidence of neurological complications after shoulder surgery with regional anesthesia remains low but serious negative outcomes have been reported in the literature. Here we report a case of acute quadriplegia secondary to cervical epidural abscess and possible neck manipulation.
Keywords
Brachial Plexus, Interscalene, Nerve Block, Postoperative Complications, Spinal Cord, Cervical Vertebrae, Anesthesia, Conduction, Shoulder Surgery
Authors do not have any financial and personal relationships with other people or organizations that could inappropriately influence (bias) their work. Examples of potential conflicts of interest include employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, and grants or other funding.
Introduction
The interscalene approach to the brachial sheath effectively provides analgesia for surgery on the shoulder or upper arm by providing blockade of the lower cervical plexus and the cephalic portion of the brachial plexus1. Neurological complications attributed to the administration of interscalene anesthesia have been reported2-5, including the permanent loss of cervical spinal cord function6. This report describes a case in which our patient developed acute postoperative quadriplegia following the intraoperative administration of combined interscalene and general anesthesia that was initially attributed to an inadvertent subdural injection of local anesthetic. Rapid and appropriate multidisciplinary intervention resulted in the complete return of neurological function for this patient although the occurrence was subsequently demonstrated to have arisen from a preexisting medical condition.
* MD, FCCP, FABHP, Associate Professor of Anesthesiology and Critical Care Medicine, VA Western New York Health Care System, State University of New York at Buffalo, Buffalo, NY 14215.
** M.D., Ph.D., FCCP, Professor of Anesthesiology, Surgery, Pathology and Anatomical Sciences, VA Western New York Health Care System, State University of New York at Buffalo, Buffalo, NY 14215.
Corresponding Author: Jahan Porhomayon, Department of Anesthesiology & Critical Care Medicine, VA Western New York Healthcare System, State University of New York at Buffalo, 3495 Bailey Avenue, Buffalo, NY 14215, Tel: 716 862-8707, Fax: 716 862-8707. Email: [email protected]

892 PORHOMAYON J. et. al
Case Report
A 59 year-old, male presented for drainage of a left shoulder abscess and biopsy of the head of the right humerus. His past medical history was significant for hypertension and type II diabetes melitus. Preoperative sedation was provided with midazolam 1 mg intravenously (IV). Even though patient consented to regional anesthesia but also he firmly requested to have general anesthesia for the procedure. A right interscalene block and inhalational general anesthesia (GA) via laryngeal mask airway (LMA) was planned. The induction of GA was accomplished with propofol 100 mg to facilitate LMA insertion and maintained with spontaneous respirations of Sevoflurane 0.7 vol% and 60% nitrous oxide. No muscle relaxants or narcotics were administered. The interscalene block was performed under sterile technique by inserting an insulated 22 gauge 1¼ inch Stimuplex (B. Braun Medical, Bethlehem, PA) needle connected to a peripheral nerve stimulator into the right interscalene groove in a caudad direction. Contraction of the right biceps muscle was present at a depth of 1.6 cm with stimulation at 0.4 mA. Levobupivacaine (Chirocaine) 0.25% 20 ml was injected in incremental doses after negative aspirations for blood and cerebrospinal fluid. Surgical exposure was optimized by placing a thyroid pillow between the patient’s shoulders providing cervical extension and the head was rotated to the contra lateral operative side during the two stages of the surgery. The patient’s vital signs remained stable throughout the 90-minute intraoperative period and no adverse events were noted.
After arrival in the recovery room, the patient’s heart rate dropped to 47 beats per minute and his blood pressure decreased to 73/40 mmHg. Hemodynamic stabilization was accomplished by administering 500 ml 0.9 normal saline and ephedrine 10 mg IV. Respiratory parameters were unremarkable, respiratory rate of 22 per minute, pulse oximetery reading was 100% on 2 liters/nasal cannula, arterial blood gas was within normal limit, however the patient complained of mild dyspnea. Physical examination revealed hypophonia and quadriplegia. Sensation was present only above T4. In light of respiratory stability and the lack of an ensuing mitigation of sensation or the return of strength,
it was suspected that an inadvertent subdural injection of the local anesthetic had occurred. Dexamethasone 10 mg IV was administered to attenuate possible spinal cord inflammation. A neurology consult and CT of the cervical spine were obtained.
Six hours after termination of surgery, the patient then began showing mild improvement, with the return of bilateral lower extremity proprioception, contraction of the left biceps, and the recovery of phonation. The computed tomography of cervical spine excluded spinal hematoma but demonstrated intrathecal and subcutaneous air around the cervical spinal cord. Fourteen hours following surgery, there was no further recovery. Magnetic resonance imaging of the cervical spine revealed a severe case of osteomyelitis with complete destruction of the vertebral bodies and spinal cord compression due to an epidural abscess at the level of C5-C6 (Fig. 1). Retrospective reviews of the preoperative bone scan (Fig. 2) and cervical X-ray films revealed this lesion was a preexisting inflammatory process. Emergent neurosurgical intervention to relieve the spinal cord compression consisting of C4-5, C5-6, and C6-7 discectomy; C5-6 vertebrectomy; C4-C7 anterior fusion with fibular strut and plate, and C4-T1 posterior fusion with mass fixation and allograft was performed. Antibiotic therapy with Vancomycin and Ceftazadime was instituted. The patient regained full sensory and motor function over the next 10 days.
Fig� 1 Cervical spine magnetic resonance imaging performed post- interscalene block showing vertebral body erosion at C5-6 (indicated by the small solid arrows) and the presence of a
large epidural abscess (large hollow arrow)

M.E.J. ANESTH 21 (6), 2012
893ACUTE QUADRIPLEGIA AFTER INTERSCALENE BLOCK SECONDARY TO CERVICAL BODY EROSION AND EPIDURAL ABSCESS
Fig� 2 Preoperative bone scans demonstrating cervical and bilateral
shoulders inflammatory processes
Discussion
Timing of interscalene block after general anesthesia remains a controversial topic in anesthesiology mostly because it may contribute to delay in diagnosis of neurological complications. However, Bogdanov et al was able to demonstrate no permanent or long-term neurological complications related to interscalene block after induction of general anesthesia in 548 consecutive cases of arthroscopic shoulder surgery patients7. Based on finding from his study and request by our patient to have general anesthesia for the procedure, we proceeded with combined general and regional techniques. Interscalene block would also provide post operative pain relief.
This case highlights some of the major neurologic complications of interscalene block including acute postoperative quadriplegia that was thought to be related to inadvertent injection of LA into subdural space. Neurologic complications after interscalene block have been well described in the literature including reported cases of postoperative quadriplegia
or quadreparesis secondary to diverse etiologies2, 8-9.
Norris10 and his group suggested anatomical explanations of injected anesthetics into dural cuff and Reina et al.11-12 suggested spread of local anesthetic from epidural fat storage site to epidural and subdural space. Alternative etiologies described include the presence of space-occupying lesions13, trauma14, inadvertent injection of local anesthetics into the substance of the cervical spinal cord6, epidural, subdural4, or subarachnoid space3, continuous infusion of cisatracurium and steroids, intraoperative hypotension resulting in cord ischemia and injection of LA into vertebral artery. Acute quadriplegia may also arise from odontoid process dislocation or fracture15-16, and rarely secondary to cobalamin deficiency or bilateral medullary pyramid infarctions17.
The initial diagnosis of subdural blockade was based on clinical presentation of a slow onset neural blockade, extensive involvement of dermatomes outside of the brachial plexus distribution, the absence of apnea, relative lack of sympathetic block, and the delayed resolution of symptoms4. Total spinal anesthesia and cord ischemia was ruled out since he was hemodynamic ally compensated and was breathing spontaneously during his entire operative and post operative course. Intraneuronal injection was unlikely since patient usually complain of severe pain both intra-operatively and in post operative phase of recovery.
In conclusion, it is important to note that quadriplegia in this case was not related to the interscalene block, but we must mention that interscalene block may have contributed to the complexity of diagnosing neurologic injury in this case. Such diagnostic uncertainty may contribute to a delay in the definitive treatment of spinal cord compression where early diagnosis and surgical intervention are crucial. Therefore, we recommend a comprehensive diagnostic strategy when there are atypical neurologic findings following interscalene block.

894 PORHOMAYON J. et. al
References
1. bROWN DL: Brachial plexus anesthesia: an analysis of options. Yale J Biol Med;� Sep-Oct 1993, 66(5):415-431.
2. bORGEAT A, EKATODRAMIS G, KALbERER F, bENZ C: Acute and nonacute complications associated with interscalene block and shoulder surgery: a prospective study. Anesthesiology; Oct 2001, 95(4):875-880.
3. IOCOLANO CF: Total spinal anesthesia after an interscalene block. J Perianesth Nurs; Jun 1997, 12(3):163-168; quiz 169-170.
4. TETZLAFF JE, YOON HJ, DILGER J, bREMS J: Subdural anesthesia as a complication of an interscalene brachial plexus block. Case report. Reg Anesth; Sep-Oct 1994, 19(5):357-359.
5. TETZLAFF JE, YOON HJ, bREMS J: Interscalene brachial plexus block for shoulder surgery. Reg Anesth; Sep-Oct 1994, 19(5):339-343.
6. bENUMOF JL: Permanent loss of cervical spinal cord function associated with interscalene block performed under general anesthesia. Anesthesiology; Dec 2000, 93(6):1541-1544.
7. bOGDANOv A, LOvELAND R: Is there a place for interscalene block performed after induction of general anaesthesia? Eur J Anaesthesiol; Feb 2005, 22(2):107-110.
8. bORGEAT A, EKATODRAMIS G: Nerve injury associated with regional anesthesia. Curr Top Med Chem; Aug 2001, 1(3):199-203.
9. EKATODRAMIS G, bORGEAT A: Convulsions after the administration of high dose ropivacaine following an interscalenic block. Can J Anaesth; Jun 2001, 48(6):613-614.
10. NORRIS D, KLAHSEN A, MILNE b: Delayed bilateral spinal anaesthesia
following interscalene brachial plexus block. Can J Anaesth; Mar 1996, 43(3):303-305.
11. REINA MA, PULIDO P, CASTEDO J, vILLANUEvA MC, LOPEZ A, SOLA RG: [Characteristics and distribution of normal human epidural fat]. Rev Esp Anestesiol Reanim; Jun-Jul 2006, 53(6):363-372.
12. REINA MA, vILLANUEvA MC, MACHES F, CARRERA A, LOPEZ A, DE ANDRES JA: The ultrastructure of the human spinal nerve root cuff in the lumbar spine. Anesth Analg; Jan 2008, 106(1):339-344, table of contents.
13. SCHNEIDER M, SAbO D, GERNER HJ, bERND L: Destructive osteoblastoma of the cervical spine with complete neurologic recovery. Spinal Cord; May 2002, 40(5):248-252.
14. ANDERSON DK, DEMEDIUK P, SAUNDERS RD, DUGAN LL, MEANS ED, HORROCKS LA: Spinal cord injury and protection. Ann Emerg Med; Aug 1985, 14(8):816-821.
15. FAIRHOLM D, LEE ST, LUI TN: Fractured odontoid: the management of delayed neurological symptoms. Neurosurgery; Jan 1996, 38(1):38-43.
16. vACCARO AR, URbAN WC, AIKEN RD: Delayed cortical blindness and recurrent quadriplegia after cervical trauma. J Spinal Disord; Dec 1998, 11(6):535-539.
17. MARX A, GLASS JD, SUTTER RW: Differential diagnosis of acute flaccid paralysis and its role in poliomyelitis surveillance. Epidemiol Rev; 2000, 22(2):298-316.

895 M.E.J. ANESTH 21 (6), 2012
INFERIOR WALL DIVERTICULUM OF LEFT VENTRICLE COEXISTING WITH MENTAL RETARDATION
AND ATRIAL SEPTAL DEFECT
HENRY LIU*, TING ZHOU*, JIAO LIU, MD*, YIRU TONG*, JACK S. SHANEWISE**
Abstract
We report a case of congenital inferior wall left ventricular diverticulum (LVD), atrial septal defect and mental retardation detected by intraoperative transesophageal echocardiography. The combination of three features strongly suggests that genetic factors play important role in the pathogenesis of the disorder. Most LVDs are asymptomatic. Echocardiographers and cardiac anesthesiologists should be aware of this anomaly, and include it in the differential diagnosis of abnormally shaped ventricular wall and seek other congenital abnormalities if LVD is detected.
Key words: Cardiovascular, Left ventricular diverticulum, Atrial septal defect, Mental retardation
Ventricular diverticula are rare congenital cardiac malformations1,2,3, especially in the adult population, even though there are significantly more reports in the literatures from the last two decades mainly due to improved technology in establishing the diagnosis. The majorities of these diverticula arise from the apex of the left ventricle and are usually diagnosed in early childhood4. Seventy percent of patients with left ventricular diverticulum (LVD) have associated midline thoracoabdominal defects5. LVD coexisting with atrial septal defect (ASD) has been reported6,7. However LVD coexisting with mental retardation plus ASD has never been reported. Here we report a case that LVD is located in the inferior wall of the left ventricle in association with mental retardation and ASD in an adult patient. The combination of LVD, ASD and mental retardation implies genetic factor(s) contribute to the pathogenesis of this condition.
Case Report
A fifty-one year old white female presented with shortness of breath and poor exercise tolerance. She is 61 inches tall and weighs 65 kilograms. She has history of mental retardation. No chest wall or abdominal wall defects were found. Evaluation by transthoracic echocardiography (TTE) revealed an atrial septal defect (ASD) with left-to-right shunt. The patient was referred for ASD repair. Preoperatively chest X-ray revealed mild cardiac enlargement with prominence of both left and right pulmonary arteries and clear lung fields. The electrocardiogram showed normal sinus rhythm and heart rate of 90/minute with occasional premature ventricular beats. After
* Department of Anesthesiology, Tulane University Hospitals & Clinics, New Orleans, LA 70112, Tel: (504)8134983, Fax: (504)9881743. E-mail: [email protected]
* M.D, Department of Anesthesiology, Tulane University Hospitals & Clinics, New Orleans, LA 70112.** M.D, Department of Anesthesiology, Columbia University Presbyterian Medical Center Columbia/Cornell Health
System, New York, NY 10032. Corresponding Author: Henry Liu, M.D, Division of Cardiothoracic & Vascular Anesthesia.

896 LIU H. et. al
induction and endotracheal intubation, intraoperative transesophageal echocardiography (TEE) confirmed the presence of a large ostium secundum ASD. A LVD located at the base of the inferior wall, measuring approximately 1.5 cm by 2 cm was also found. The diverticulum was seen to get smaller during systole and larger during diastole, indicating that LCD has synchronized contraction with the left ventricle (Fig. 1). The patient had a successful closure of the ASD and postoperative recovery was uneventful. She was discharged three days after surgery.
Discussion
Ventricular diverticula are rarely seen in the adult population. The actual prevalence is unknown. There were only 10 cases in more than 13000 congenital heart disease operations at the Texas Heart Institute over a 20-year period7. The majority of ventricular diverticula are congenital, but a small percentage of ventricular diverticula can be caused by other pathological conditions, such as ischemic heart disease8. There are two types of ventricular diverticula: muscular and fibrous diverticulum. Muscular diverticulum is characterized by having all three layers of cardiac tissue including endocardium, myocardium and pericardium in the wall. Fibrous diverticulum arises in the subvalvular areas and histologically has predominantly fibrous tissue in the wall. Although the location of the ventricular diverticulum in the majority of patients is in the apex of left ventricle4, ventricular diverticula can
also occur in other locations, as in our case. The etiology and mechanism of LVD are unknown. LVD appears to be a developmental abnormality characterized by a local embryological development failure of the ventricular muscle3,9. The coexistence of LVD in our patient with mental retardation and ASD implies that genetic factor(s) contribute to the pathogenesis. There has been one report of familial occurrence of LVD involving siblings10.
Ventricular diverticula can be isolated or coexist with other clinical conditions. Seventy percent of patients are found to be associated with congenital midline thoracoabdominal defects5. Ventricular diverticula has also be reported with other cardiac anomalies, such as ventricular septal defect, ASD, dextrocardia, Tetralogy of Fallot, endocardial cushion defect, persistent truncus arteriosus, tricuspid atresia, anomalous pulmonary or systemic venous return and hypertrophic cardiomyopathy11.
The morbidity and mortality associated with LVD varies. Most ventricular diverticula are asymptomatic for many years, but some may have complications including acute rupture and cardiac tamponade12, peripheral embolism, chest pain syndrome, dysrhythmia13 and endocarditis11. LVD may present a dilemma. The current asymptomatic status must be weighed against the potential fatal risk of ventricular rupture. Some advocates surgery and there are reports of successful surgical resection of diverticula in order to prevent acute rupture and cardiac tamponade14.
Fig� 1 Mid-esophageal two chamber transesophageal echocardiographic view of the left ventricular diverticulum (arrow) during diastole (left) and systole (right)� The diverticulum has synchronized contraction with the left ventricle� The mitral valve is indicated by arrowheads� (LA = left atrium, LV = left ventricle)

M.E.J. ANESTH 21 (6), 2012
897INFERIOR WALL DIVERTICULUM OF LEFT VENTRICLE COEXISTING WITH MENTAL RETARDATION AND ATRIAL SEPTAL DEFECT
LVD can be diagnosed by various imaging modalities. Most diverticula are detected by echocardiography, left ventricular angiography, magnetic resonance imaging, or computed tomography15. It is possible to establish a fetal diagnosis16. With echocardiography ventricular diverticulum generally appears as an echo-free space with a narrowed neck communicating with left ventricle and should be visible in multiple views to exclude the possibility of imaging artifacts. Ventricular diverticula should be differentiated from ventricular aneurysms and ventricular pseudoaneurysms. Generally, a
ventricular aneurysm has a broad-based connection with left ventricle and has paradoxical movement with each cardiac cycle, while a ventricular diverticulum has synchronized contraction with ventricle. Ventricular pseudoaneurysm is a chronic contained rupture of the left ventricle, its wall consisting only of pericardium and thrombus3. Echocardiographers and cardiac anesthesiologists should be aware of this anomaly, and include it in the differential diagnosis of abnormally shaped ventricular wall and seek other congenital abnormalities if LVD is detected.

898 LIU H. et. al
caused by ischemic heart disease. Am� Heart J; 1997, 133(4):481-483.
9. CIANCIULLI TF, DEL CARMEN GONZALEZ COLASO P, ET AL: Left ventricular diverticulum, a rare cechocradiographic finding: two adult patients and review of the literature. Cardiology J; 2009, 16(1):76-81.
10. SHIZUKUDA Y, MURAKAMI H, IWAKURA M, ET AL: Siblings with left ventricular diverticulum and hypertrophic cardiomyopathy. J� cardiology (Japan); 1988, 18:867-974.
11. WALTON-SHORLEY M, SMITH SM, TALLEY JD: Left ventricular diverticulum: case report and review of the literature. Catheterization and Cardiovascular Diagnosis; 1992, 26(1):31-33.
12. GOWITT GT, ZAKI SA: Rupture of a cardiac diverticulum resulting in sudden death. Am� J� Forensic med Pathology; 1988, 9:155-58.
13. SHEN EN, FUKUYAMA O, HERRE JM, ET AL: Ventricular tachycardia with congenital ventricular diverticulum. Chest; 1991, 100:283-285.
14. SUILEN C, BEAT F, RUTISHAUSER W: Congenital intrathoracic left ventricular diverticulum in an adult. Chest; 1990, 98:750-751.
15. GObAL F, SACHDEvA R, URETSKY BF: Computed tomography and angiography of left ventricular diverticulum. J Am Coll Cardiol; 2011 Aug 23, 58(9):e17.
16. BRACHLOW A, SAbLE C, SMITH S, SLACK M, MARTIN G: Fetal diagnosis and postnatal follow-up of an asymptomatic congenital left ventricular diverticulum. Pediatr Cardiol; 2002, 23:658-660.
References
1. HAEGELI LM, ERCIN E, WOLbER T, Brunckhorst C, TANNER FC, JENNI R, LüSCHER TF, DURU F: Arrhythmic manifestations in patients with congenital left ventricular aneurysms and diverticula. Am J Cardiol; 2011 Dec 15, 108(12):1826-30.
2. CHEN HW, CHEN ML, YANG B, JU WZ, ZHANG FX, HOU XF, CHEN C, SHAN QJ, ZOU JG, XU DJ, CAO KJ: Clinical characteristics of congenital ventricular aneurysm and diverticula in inland China. Zhonghua Xin Xue Guan Bing Za Zhi. 2011 Sep, 39(9):865-8.
3. OHLOW MA: Congenital left ventricular aneurysms and viverticula: definition, pathophysiology, clinical relevance and treatment. Cardiology; 2006, 106(2):63-72.
4. YAMASHITA H, MOMOMURA S, MOCHIZUKI T, SUZUKI J, TAKENAKA K, SERIZAWA T: Congenital left ventricular diverticulum with septal defect, mitral and tricuspid regurgitation, and coronary disease. Am Heart J; 1993, 126:461-463.
5. CANTRELL JR, HALLER JA, RAvITCH MM: A syndrome of congenital defects involving the abdominal wall, sternum, diaphragm, pericardium, and heart. Surg� Gynecol� Obstet; 1958, 107:602-614.
6. VICTOR S, RAvINDRAN P, MARAGATHAM, ET AL: Congenital diverticulum of muscular interventricular septum in association of atrial septal defect. Indian Heart J; 1984, 36(6):401-2.
7. OKEREKE OUJ, COOLEY DA, FRAZIER OH: Congenital diverticulum of the left ventricule. J� Thoracic & Cardiovascular Surgery; 1986, 91:208-14.
8. BASHOUR TT, ET AL: Left ventricular narrow-neck large diverticulum

899 M.E.J. ANESTH 21 (6), 2012
ENDOTRACHEAL TUBE CUFF LEAK WITH MYSTERIOUS LARYNGOTRACHEAL PATHOLOGY
J. LANCE LAFLEUR*, KRISHNA bODDU**, AMIR R. bALUCH***, ALAN D. KAYE****
Abstract
A 63 year-old obese man with gastroesophageal reflux disease, hiatal hernia, and no known history of airway pathology was to undergo a total knee arthroplasty. After intubation, however, repeated cuff leaks, decreasing tidal volumes, and desaturations prompted five additional endotracheal tube placements. Findings on radiography, computed tomography, and fiberoptic laryngoscopy and tracheoscopy were equivocal. Factors contributing to this challenge of persistent and repeated cuff leaks in the absence of known airway pathology could include various laryngotracheal abnormalities.
Keywords include endotracheal tube cuff, tracheal stenosis, and tracheomalacia
Case Description
A 63 year-old man suffered from chronic left knee osteoarthritis secondary to remote trauma. After unsuccessful medical management and multiple knee surgeries, a total knee arthroplasty was planned. His medical history included gastroesophageal reflux disease (GERD), hiatal hernia, dyslipidemia, and benign prostatic hypertrophy. His surgical history included multiple left knee surgeries, right knee arthroscopy, lumbar diskectomy, and lipoma excision. He denied any previous anesthetic complications, intensive care unit admissions, or prolonged periods of endotracheal intubation or mechanical ventilation. His daily medications included fenofibrate, atorvastatin, tamsulosin, esomeprazole, and aspirin. His exercise tolerance was severely limited by knee pain, and he was unable to walk 1 block.
Upon physical examination his weight was 125 kg (276 lb), height 193 cm (6 ft 4 in), and body mass index (BMI) was 33.6 (obese). Airway evaluation revealed a Mallampati Class II, beard, adequate grade I cervical mobility, normal Wilson’s (upper lip bite test) position A, intact dentition, and moderate micrognathia. His airway distances were within normal limits: inter-incisors 5 cm, thyromental 12 cm, sternomental 22 cm, neck circumference 36 cm1,2,3,4. His renal and liver function tests, complete blood count, coagulation studies, electrocardiogram, chest radiograph, and adenosine nuclear cardiac study were all within normal limits.
* MD, MBA, Attending Physician, , The Spine Diagnostic & Pain Treatment Center, Baton Rouge, Louisiana.** MBBS, MD, DNB, FANZCA, Consultant Anaesthetist, Director of Regional Anaesthesia, Royal Perth Hospital, Perth,
Australia*** MD, Attending Physician, Metropolitan Anesthesia Consultants, Dallas, Texas.**** MD, PhD, Professor and Chairman, Department of Anesthesiology, Louisiana State University Health Science Center,
New Orleans, Louisiana. Corresponding Author: K. Boddu, MBBS, MD, DNB, FANZCA Department of Anaesthesia & Pain Medicine, 197
Wellington Street, Royal Perth Hospital, Perth, WA 6000, Australia, Tel: +61416030020. E mail: [email protected]

900 LA FLEUR J. L. et. al
a lateral cervical spine radiograph were then ordered (Table 2), and otolaryngology (ENT) was consulted for rigid bronchoscopic evaluation to rule out tracheal stenosis, mass, or rupture. The patient was given additional muscle relaxant, and rigid laryngoscopy and tracheoscopy (Video 1-3) were then performed by ENT with intermittent ventilation using a 6.0 ETT. The patient was then extubated successfully in the operating room and taken to the post-anesthesia care unit. The
On the day of surgery, the patient was premedicated with midazolam 2 mg, and monitored with standard ASA monitors, including noninvasive blood pressure, temperature, end-tidal carbon dioxide (ETCO2), electrocardiogram, and pulse oximeter in the operating room. The blood pressure was 159/94, the heart rate was 62 beats per minute (BPM), and the oxygen saturation (SpO2) was 100%. The patient was preoxygenated with 100% oxygen at 10 liters per min (L/min) for three minutes. A rapid sequence induction was planned for frequent GERD symptoms and a history of hiatal hernia, which were controlled on esomeprazole. General anesthesia was induced with lidocaine 50 mg, fentanyl 150 mcg, propofol 200 mg, and succinylcholine 100 mg. After one failed intubation attempt by a medical student, the patient was tracheally intubated using a Macintosh 4 laryngoscope. A grade 2a view was achieved with cricoid pressure.
The 8.0 endotracheal tube (ETT) cuff was inserted, inflated, ETCO2 was detected, and breath sounds were bilateral and equal upon auscultation. The ETT was secured at 24 cm at the lip, no leak was present at 30 cm H2O, and the SpO2 was 100%. Then, cisatracurium 10 mg was administered, end-tidal sevoflurane was increased to 2%, and the fraction of inspired oxygen (FiO2) was decreased to 50% at 2 L/min. Vital signs, capnogram, ETCO2, tidal volumes, and peak inspiratory pressures were normal for ten minutes. Subsequently, tidal volumes decreased from 700 cc to 400-500 cc, the SpO2 decreased to the low 90s, and an ETT cuff leak was apparent at less than 20 cm H20 after an additional 10-20 cc of injected air.
Five subsequent ETT placements were performed (Table 1). After each successful ETT placement, the cuffs were inflated, breath sounds were bilateral, and no leak was present at 30 cm H2O. A period of normal vital signs, capnogram, ETCO2, tidal volumes, and peak inspiratory pressures followed. Afterwards, tidal volumes decreased from 700 cc to 400-500 cc, the SpO2 decreased to the low 90s, and an ETT cuff leak was apparent at less than 20 cm H20 after 10-20 cc of injected air. All cuffs were confirmed as functional prior to intubation. Except for the final ETT, each tube was unable to be advanced past 24 cm. The final successful ETT was secured at 26 cm.
An intraoperative chest radiograph (Fig. 1) and
Fig� 1Red arrow, tracheal stenosis; Green arrow, post-stenotic
tracheal dilation
Fig� 2Red arrow, tracheal stenosis; Green arrow, post-stenotic
tracheal dilation

M.E.J. ANESTH 21 (6), 2012
901ENDOTRACHEAL TUBE CUFF LEAK WITH MYSTERIOUS LARYNGOTRACHEAL PATHOLOGY
permitted passage distal to the stenosis preventing supraglottic herniation. Our serial ETT dilations may provide a reason for both our eventual sustained ability to ventilate the patient with a sufficient seal, and for the absence of stenosis on endoscopy. In part, our attempts to secure the airway of this patient may have been curative of the patient’s stenosis.
Over time, ulcerative tracheal lesions, which can be formed from a period of hypoperfusion as a result of an overinflated ETT cuff, may be replaced by membranes or webs5. This may represent another explanation in this case. The membrane or web would have not allowed for advancement of the ETT past 24 cm. The successful, sustained placement of the 6.0 ETT at 26 cm was possible only after perforation of the membrane or web. Subsequent tracheoscopy may have failed to visualize the membrane or web as it would have been obliterated by serial intubations or by the removal of the final ETT by ENT with the cuff fully inflated.
Ideally, the ETT should be advanced 2 cm after the cuff completely passes through the cords, or when the external tube markings are 22 to 24 cm at the lower incisors. This places the tip of the tube 2 to 4 cm above the carina in the midtrachea. After ETT placement, the cuff should be inflated to 22 – 32 cm H20 (generally should not exceed 25 cm H20) until adequacy of ventilation is demonstrated. In the absence of a cuff pressure gauge, moderate tension should be felt in the pilot balloon5.
The majority of stenosis occurs at the cuff site, although it can also happen at the ETT tip site5.
patient was admitted to the surgical intermediate unit, and his hospital course was uncomplicated. He denied dyspnea or hoarseness, and auscultation revealed clear lungs without stridor or wheezing. Computed tomography (CT) of the chest (Fig. 2) was ordered to further characterize chest radiograph findings.
A total of six ETT were used in this case including two 8.0, two 7.0, and two 6.0 tubes. The cuff viability of one 7.0 ETT was unable to be assessed as its pilot balloon inflating tube was torn. One 6.0 ETT was not recovered postoperatively. Testing of the remaining four cuffs by saline injection showed that both 8.0 and one 6.0 cuffs were intact, and one 7.0 cuff was ruptured. Thus, out of the six cuffs, there were three intact cuffs, one ruptured cuff, and two cuffs which were unable to be assessed.
Discussion
The present case describes a patient with repeated cuff leaks from multiple ETTs with an uncertain explanation. One possible reason for the repeated cuff leaks is tracheal stenosis which appears on chest radiograph and chest CT. The first five ETT were unable to be advanced past 24 cm, which may have been a region of subglottic stenosis. After the cuffs were inflated, there was gradual supraglottic herniation with a resulting loss of tidal volume, desaturation, and cuff leak. Further inflation then led to cephalad migration of the cuff and ETT which impeded ventilation and oxygenation. The successful, sustained placement of a 6.0 ETT at 26 cm occurred as the smaller diameter
Table 1: Endotracheal Tube Placements
ETT (mm ID)
Intubation Technique
Depth (cm)
Sustained function (min) Comments
8.0 DL, Mac 4 24 10 Leak after OGT attempted x 3; cuff not visible on DL
8.0 Cook 24 5 Advancement past 24 cm unsuccessful
7.0 Cook 24 4 Flexible FOB view through ETT showed carina
7.0 Cook 24 2 Case cancelled after development of cuff leak
6.0 DL, Mil 3 24 2 Performed by ENT
6.0 Cook 26 >120 Flexible FOB view through ETT showed carina
DL, direct laryngoscopy; Mac 4, Macintosh 4 laryngoscope; OGT, orogastric tube; Cook, Cook airway exchange catheter; FOB, flexible bronchoscope; ETT, endotracheal tube; Mil 3, Miller 3 laryngoscope; ENT, otolaryngologist.

902 LA FLEUR J. L. et. al
Excessive mucosal pressure is the principal cause of post-intubation ETT cuff site induced tracheal stenosis6. When the cuff pressure is greater than 30 mm Hg, it can exceed capillary perfusion pressure7. This can lead to mucosal edema and ischemia, which can ultimately progress to inflammation, desquamation, ulceration, and necrosis of the trachea5,6,7. In hypotensive patients, capillary perfusion pressure is more easily overcome, and ulceration occurs at even lower cuff pressures8,9. Resulting circumferential lesions heal by fibrosis and contraction, which can eventually lead to tracheal stenosis. Using a cuff with high volume, low pressure, and a larger contact area minimizes mucosal pressure and decreases the incidence of post-intubation tracheal stenosis10. However, the benefits of using such high volume, low pressure cuffs can be negated by cuff overinflation.
Symptoms of tracheal stenosis include dyspnea, stridor, and wheezing6. Upper airway obstruction classically presents with monophonic wheezing, whereas lower, small airway obstruction (asthma, COPD) is classically polyphonic wheezing. Post-intubation tracheal stenosis commonly misdiagnosed as asthma or COPD in up to 44% of patients. Symptoms may not manifest at rest until the trachea lumen has decreased to 30% of its original size which may take up to 3 months. A diagnosis of tracheal stenosis should be considered in patients with progressive dyspnea and wheezing which is unresponsive to bronchodilators, or in patients with a recent or prolonged period of endotracheal intubation. Confirmation can be obtained with radiography, computed tomography, or
endoscopy. Treatment options include steroids and surgery for symptomatic lesions. Rigid bronchoscopy and tracheal dilation with possible stent placement is the definitive treatment for mild to moderate lesions, or can be used as a temporizing measure for more severe lesions. Tracheal reconstruction is considered for severe lesions when the lumen diameter is 4 to 5 mm6,11.
Another possible explanation for the persistent cuff leak is tracheomalacia and dilation, as the increased tracheal compliance and diameter did not allow for an effective cuff seal. Also, luminal narrowing from concomitant tracheal collapse may have obstructed ETT advancement past 24 cm. During the chest radiograph with positive pressure ventilation and the chest CT with spontaneous ventilation, there was evidence of tracheomalacia and dilation. Conversely, during endoscopy when the patient was paralyzed and apneic, there was no airway pressure gradient and thus no visible tracheal collapse. The staff radiologists suggested live fluoroscopy and rigid or flexible FOB without paralysis to identify possible dynamic tracheal compression during spontaneous ventilation. Lastly, the rigid bronchoscope may have masked any tracheal collapse by altering the mechanical integrity of the trachea. The endoscopy did, however, provide evidence of tracheal dilation.
Tracheomalacia is abnormal tracheal flaccidity resulting in dynamic airway collapse when extraluminal pressure is greater than intraluminal pressure, such as during expiration or coughing5. Tracheal cartilage erosion from previous ischemic
Table 2: Imaging Results
Imaging Results
Lateral Cervical Spine Nondiagnostic
Chest X-Ray Report 1) Mass extending out of the superior mediastinum or in the lungs in the right upper lobe cannot be excluded.Report 2) Possible proximal tracheal stenosis, possible distal tracheal dilation, and possible right upper lobe mass.
Rigid Laryngoscopy and Tracheoscopy
Normal from the supraglottis to the main bronchi except for an enlarged trachea in the steep slope of the trachea.
Chest Computed Tomography Report 1) No mediastinal mass. Small hiatal hernia. (No mention of airway.) Report 2) Vocal cord thickening, possible edema or hematoma, cannot rule out laryngeal mass, no intrathoracic mass. Possible proximal tracheal stenosis, possible distal tracheal dilation, possible tracheomalacia, possible tracheal membrane or web.

M.E.J. ANESTH 21 (6), 2012
903ENDOTRACHEAL TUBE CUFF LEAK WITH MYSTERIOUS LARYNGOTRACHEAL PATHOLOGY
with no known history of airway pathology that required five additional endotracheal tube placements. Factors contributing to this challenge of persistent and repeated cuff leaks in the absence of known airway pathology could include various laryngotracheal abnormalities. Clinical anesthesiologists must appreciate the differential diagnosis and potential treatment plan when confronted with such a challenging problem.
Acknowledgments
The authors would like to express their gratitude for Dr. Evan Pivalizza who provided editorial assistance with the manuscript.
insult can lead to tracheomalacia5. The cartilage softens and the posterior membranous wall widens with possible anterior ballooning into the lumen. The average female tracheal diameter is approximately 2 cm, while the average male tracheal diameter is 2.4 cm12. Whenever increasing cuff volumes are necessary to sustain a seal, tracheomalacia and tracheal dilation should be considered9. Symptoms include dyspnea, cough, wheezing, dysphagia, and recurrent respiratory infections. Difficulty weaning from mechanical ventilation or repeated failed extubations may also indicate functional tracheal collapse. Short term treatment may include non-invasive positive pressure ventilation such as CPAP or BIPAP5.
In summary, the present case describes a patient

904 LA FLEUR J. L. et. al
2000, 321:1000-2.7. KNOWLSON GTG, BASSETT HFM: The pressures exerted on the
trachea by tracheal inflatable cuffs. Br J Anaesth; 1970, 42:834-837.8. O’DONNELL JM: Orotracheal tube intracuff pressure initially and
during anesthesia including nitrous oxide. CRNA; 1995, 6:79-85.9. HARRIS R, JOSEPH A: Acute tracheal rupture related to endotracheal
intubation: Case Report. J Emerg Med; 2000, 18:35-39.10. MATHIAS DB, WEDLEY JR: The effects of cuffed tracheal tubes on the
tracheal wall. Br J Anaesth; 1974, 46:849-852.11. MCENERY JT: Surgical management of tracheal stenosis. Ann Surg;
1974, 179:819-824.12. ROLLINS J, TOCINO I: Early radiographic signs of tracheal rupture.
AJR; 1987, 148:695-8.
References
1. WILSON ME, SPIEGELHALTER D, RObERTSON JA, LESSER P: Predicting difficult intubation. Br J Anaesth; 1988, 61:211-216.
2. PATIL VU, STEHLING LC, ZAUDER HL: Fiberoptic Endoscopy in Anesthesia. Chicago, USA: Year Book Medical Publishers, 1983.
3. SAvvA D: Prediction of difficult tracheal intubation. Br J Anaesth; 1994, 73:149-153.
4. HIRESMATH AS, HILLMAN DR, JAMES AL, NOFFSINGER WJ, PLATT PR, SINGER SL: Relationship between difficult tracheal intubation and obstructive sleep apnoea. Br J Anaesth; 1998, 80:606-611.
5. HAGbERG C: Benumof’s Airway Management: Principles and Practice. 2nd ed. Philadelphia: Mosby Elsevier, 2007: 82, 388-389, 817-818, 1191-1192.
6. SPITTLE N, MCCLUSKEY A: Tracheal stenosis after intubation. BMJ;

905 M.E.J. ANESTH 21 (6), 2012
SAFE REMOVAL OF EPIDURAL CATHETER-A DILEMMA, IN PATIENTS WHO ARE STARTED ON DUAL
ANTI PLATELET THERAPY POSTOPERATIVELY FOR ACUTE CORONARY SYNDROME
- A Case Report -
JYOTI bURAD*, RAJINI KAUSALYA**, MOHAMMED ISMAILI***, QUTAIbA TAWAFIC****, ROHIT DATE****
Abstract
Epidural catheter insertion or removal in patients receiving antiplatelet therapy for acute coronary syndrome poses a high risk for epidural hematoma. Though practice guidelines suggest stopping clopidogrel for at least 7 days before such intervention. Withholding anti-platelet drugs for such a long duration represents a great risk to these patients.
We present a case of a 53 year old male patient who underwent an exploratory laparotomy. He had an epidural catheter inserted for analgesia. He developed acute myocardial infarction on the first postoperative day, which was treated with dual antiplatelet therapy and percutaneous coronary angioplasty. The removal of epidural catheter in this patient required a clinical decision, balancing the risk of epidural hematoma with continuation of antiplatelet therapy against the risk of coronary re-thrombosis with discontinuation of the medication.
We followed a strategy that combined a short duration of discontinuation of therapy, assessment of platelet functions by laboratory test, transfusion of platelets and removal of catheter, followed by restart of anticoagulation, which proved safe for the patient.
Key words: Antiplatelets, epidural catheter, platelet function assay, neuro-axial complications.
We declare that we have no funding support, no conflict of interest, no commercial or non-commercial affiliations or consultancies with regard to this case.
* Department of Anesthesia and ICU, Sultan Qaboos University Hospital, Muscat, Oman.* M.D, E.D.I.C, Senior Registrar.** M.D, Senior Consultant.*** M.D, F.R.C.P.C, Consultant.**** M.D, Registrar. Corresponding Author: Jyoti Burad, M.D, (Anesthesia), E.D.I.C, Senior Registrar, Department of Anesthesia and ICU,
Sultan Qaboos University Hospital, Muscat. P.O. Box: 239, PC 115, Madinat Qaboos, Muscat, Oman, Tel: 00968 99578636. E-mail: [email protected]

906 BURAD J. et. al
Case Report
A 53 year old male patient was admitted to our hospital with small bowel ischemia with past medical history of stable ischemic heart disease and no active episodes in the last six months. The surgeon decided for emergency laparotomy. Epidural catheter was inserted at T8-T9 level using aseptic technique and an infusion of bupivacaine and fentanyl was started. Subsequently, general anesthesia was induced. Intraoperative analgesia was achieved effectively with epidural infusion. Intraarterial blood pressure and central venous pressure were monitored. Patient was hemodynamically and metabolically stable throughout. He was transfused with two units of packed red blood cells to compensate for surgical blood loss. At the end of the surgery, the patient was stable and he was extubated on operating table. Patient was shifted to Intensive Care Unit (ICU) for overnight observation. Baseline investigations 2 hours postoperative, revealed an acute anterior-inferior ST elevation myocardial infarct on ECG (electrocardiogram) and the first Troponin-I value reported was 11 (normal <.04 µg/l). The patient was comfortable, completely pain-free on epidural infusion. Surprisingly, he was hemodynamically stable with normal central venous pressure and urine output. The cardiologist decided for immediate Percutaneous Coronary Intervention (PCI). He was given antiplatelet drugs (loading dose of clopidogrel 600mg and aspirin 300mg). Angioplasty and balloon dilatation of the involved coronaries were performed. The patient tolerated the procedure well. He was started on therapeutic dose of low molecular weight heparin (LMWH; Enoxaparin 60mg) twice daily.
A decision to remove the epidural catheter by the end of the first post operative week was made to prevent infection of the neuraxial compartment.
A multidisciplinary meeting with cardiologist, general surgeon, hematologist and intensivist was held and it was decided that the antiplatelet drugs can temporarily be withheld for the purpose of removing the epidural catheter. On fourth postoperative day clopidogrel and aspirin were put on-hold. As per the advice of the hematologist and availability of the test, platelet function was assessed twenty four hours later
by Platelet function analyzer (PFA 100); Closure time was found to be 197 seconds (normal range of 96-197 seconds).
Despite of the normal closure time, it was decided to transfuse platelets to the patient after 48 hours of stopping aspirin and clopidogrel. Enoxaparin was discontinued on day 4. Twelve hours after enoxaparin cessation, infusion of un-fractionated heparin was started. Activated partial thromboplastin time (APTT) was maintained at 2 to 2.5 times of the normal.
The heparin infusion was stopped after 12 hours. Coagulation profile was checked and was reported to be normal. Platelets were transfused and epidural catheter was removed after 2 hours. The antiplatelet drugs and LMWH were restarted 2 hours later. Patient was observed in the ICU for another two days, for development of neurologic or cardiac complications. He developed neither and was discharged to the ward.
Discussion
The incidence of ischemic heart disease is rising. So is the use of antiplatelet drugs in managing such cases. The safety of regional anesthesia in patients who are already on antiplatelet drugs is controversial. Our patient had an epidural catheter in place before the antiplatelets were given for acute myocardial infarction in the postoperative period.
Combined therapy with clopidogrel and aspirin increases the bleeding time through a synergistic antiplatelet action1. Guidelines recommend that clopidogrel be stopped at least 7 days prior to epidural catheter insertion or removal. However, if the patient has had an acute myocardial infarction, dual anti-platelet therapy is imperative for PCI procedures. The risk of coronary re-thrombosis and further deterioration in myocardial status is likely to be considerable if clopidogrel is stopped in patients with recent acute coronary syndrome2.
We, therefore, stopped the antiplatelets, but continued the low molecular weight heparin in therapeutic dose. After 24 hours, platelet function assay (PFA 100) was done which reflected that the platelet aggregation was not completely inhibited by antiplatelets. Percentage platelet aggregation after

M.E.J. ANESTH 21 (6), 2012
907SAFE REMOVAL OF EPIDURAL CATHETER-A DILEMMA, IN PATIENTS WHO ARE STARTED ON DUAL ANTI PLATELET THERAPY POSTOPERATIVELY FOR ACUTE CORONARY SYNDROME
clopidogrel has been shown to be inversely correlated with CYP3A4 activity3. A recent study of platelet function using optical light aggregometry found that only 50% of platelets had a definitive response to clopidogrel4. A similar resistance to aspirin has been described, with a failure of aspirin to reduce platelet production of thromboxane A2 by irreversible acetylation of cycloxygenase-1(COX-1) and thus failing to prevent platelet activation and aggregation5.
The bleeding time is the most accurate test to assess platelet function and the effect of anti-platelet drugs, However, it is impractical, subjective and does not correlate well with the degree of bleeding.
Similarly, PFA and other tests have their limitations. Because of the unreliability of platelet function tests4,6-8, it was decided to transfuse the platelets prior to removal of the epidural catheter. Infusion of unfractionated heparin was started after discontinuation of LMWH as an “off-label bridging therapy” to reduce the risk of coronary re-thrombosis during the time of subtherapeutic antithrombotic effect. As per ASRA 2010 guidelines, the heparin was stopped 2 hours before catheter removal and coagulation status was assessed immediately before removing the catheter.
As widely known, platelet transfusion carries risks of infection, transfusion reactions and clerical errors. Cost, scarcity and risk of coronary re-thrombosis due to platelet transfusion was weighed against the risk of epidural hematoma due to manipulation of catheter with deranged platelet functions. The acknowledgement of ASRA 2010 guidelines that additive effects of multiple hemostasis altering medications may affect the hemostasis more than expected, led us to consider administration of platelets9. The effect of transfused platelets was normal for two hours, long enough to prevent formation of hematoma. This could lead to coronary rethrombosis hence therapy with antiplatelets and LMWH was resumed after two hours.
Conclusion
In conclusion, we managed to safely remove an epidural catheter in a patient with acute coronary syndrome on dual antiplatelets. This case represents a clinical scenario that is not uncommon. It may present in one way or another in anesthesia practice. There are no clear-cut guidelines for such scenarios. By putting forward this case, we propose a possible strategy to be considered when dealing with such patients.

908 BURAD J. et. al
during surgery in patients receiving anticoagulant and/or antiplatelet therapy: pharmacokinetic and pharmacodynamic considerations. Clin Pharmacokinet; 2004, 43:963-81.
7. CRAFT RM, CHAvEZ JJ, SNIDER CC, MUENCHEN RA, CARROLL RC: Comparison of modified Thrombelastograph and plateletworks whole blood assays to optical platelet aggregation for monitoring reversal of clopidogrel inhibition in elective surgery patients. J Lab Clin Med; 2005, 145:309-15.
8. HOCHHOLZER W, TRENK D, FRUNDI D, NEUMANN FJ: Whole blood aggregometry for evaluation of antiplatelet effects of clopidogrel. Thromb Res; 2007, 119:285-91.
9. HORLOCKER TT, WEDEL DJ, ROWLINGSON JC, ENNEKING FK, KOPP SL, bENZON HT, bROWN DL, HEIT JA, MULROY MF, ROSENQUIST RW, TRYbA M, YUAN CS: Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med; 2010 Jan-Feb, 35(1):64-101.
References
1. PAYNE DA, HAYES PD, JONES CI, bELHAM P, NAYLOR AR, GOODALL AH: Combined therapy with Clopidogrel and aspirin significantly increases the bleeding time through a synergistic antiplatelet action� J Vasc Surg; 2002, 35:1204-9�
2. HOWARD-ALPE GM, DE bONO J, HUDSMITH L, ORR WP, FOEX P, SEAR JW: Coronary artery stents and non-cardiac surgery. Br� J� Anaesth; 2007, 98:560-74.
3. LAU WC, GURbEL PA, WATKINS Pb, ET AL: Contribution of hepatic cytochrome P450 3A4 metabolic activity to the phenomenon of clopidogrel resistance. Circulation; 2004, 109:166-71.
4. AGARWAL S, COAKELY M, REDDY K,RIDDELL A, MALLETT S: Quantifying the effect of antiplatelet therapy: a comparison of the platelet function analyzer (PFA-100) and modified thromboelastography (mTEG) with light transmission platelet aggregometry. Anesthesiology; 2006, 105:676-83.
5. HANKEY GJ, EIKELbOOM JW: Aspirin resistance. Lancet; 2006, 367:606-17.
6. HARDER S, KLINKHARDT U, ALvAREZ JM: Avoidance of bleeding

909 M.E.J. ANESTH 21 (6), 2012
CRICOTHYROID APPROXIMATION USING A SILASTIC SHEATH: A NEW APPROACH
AbDUL-LATIF HAMDAN*
Abstract
Transsexualism is a gender identity disorder in which affected individuals believe themselves to be born into the wrong sex. Hormonal therapy and many surgical interventions were adopted in order to change their appearances. Cricothyroid approximation is the most acceptable surgical intervention to raise the vocal pitch in male to female transsexuals. Long term follow up of this surgery revealed some failure partially due to cutting of the sutures through the cricoid and thyroid cartilages. In this report we would like to describe the first case of cricothyroid approximation using a silastic sheath interposed between the cartilages and the mattress suture to circumvent such a complication.
Introduction
Transsexualism is a gender identity disorder in which affected individuals believe themselves to be born into the wrong sex. The prevalence is increasing and is estimated at 1 in 37,000 with the majority being male to female transsexuals1. It is thought to be a complex and permanent transposition, the causes of which are not known. The presence of a large nucleus suprachiasmaticus in the hypothalamus is recently being investigated as an organic etiological factor in transsexuality2,3. Hormonal therapy and many surgical interventions were adopted in order to change their appearances. The use of female hormones leads to larger breasts and a smoother skin. Surgical procedures include genital conversion in addition to mandibular angle contouring and breast augmentation. It is well known that the larynx is a hormonal target and hormonal receptors have been described in the vocal folds. The use of male hormones results in an irreversible deepening of the female voice, however, in male to female transsexuals, the voice and the laryngeal framework are not affected by estrogen treatment4. Consequently there is persistence of the masculine voice and the prominence of Adam’s apple in these patients. Speech therapy to achieve a perceived feminine voice often results in a functional increase in pitch that is not always controllable by the patient. This is more pronounced in situations when primal unconditioned sounds prevail. This has lead to the emergence of new functional laryngeal procedures such as thyroplasty type IV or cricothyroid approximation, which was initially described by Ishhiki et al in an attempt to bring the thyroid and cricoid cartilages together5-8. The rationale behind such surgery is to increase the tension in the vocal folds without damaging the rima glottides. Despite the popularity of this procedure, there is growing evidence of long term failure to maintain the elevated pitch in these patients. In a study by Matai et al on 45 patients who had cricothyroid approximation, 79% thought their voice improved, 55% attributed the improvement to surgery and 21% to speech therapy9. The decrease in the efficacy of this surgery is not very well understood. Ishhiki et al has reported a possible
** Corresponding Author: Abdul-latif Hamdan, MD, EMBA, MPH, FACS, Department of Otolaryngology-Head & Neck Surgery, American University of Beirut Medical Center, Beirut, Lebanon. Email: [email protected]

910 HAMDAN AL/
needle was then curved upward in the reverse direction from the silastic sheath, cricoid cartilage, tunneled upward through the cricothyroid membrane to exit from the thyroid cartilage and the overlying silastic sheath. Same procedure was done on the opposite side and the threads were tied in order to approximate the cricoid to the thyroid cartilage (Fig. 2). This was done while the patient is phonating in order to better tune her voice.
Fig� 1 A transverse skin incision showing the cricoid, thyroid and
cricothyroid muscle
Fig� 2 Two 5 × 10 mm silastic sheaths positioned on the left thyroid lamina and cricoid cartilage with a mattress suture running
across
Discussion
The history of surgical management of the transsexual voice has evolved over the last two decades. The aim of the surgery is to increase the fundamental frequency or mean frequency of the voice while maintaining a feminine color to it. As we know the major determinants of vocal pitch are
natural decrease in tension within the vocal folds with time10. In some cases, the failure has been attributed to the mattress sutures cutting through the cricoid and thyroid cartilages prior to the maturation of the scar in this region. This has been counteracted by using miniplates made of titanium or Lactosorb to avoid such complications 11. In this report we would like to describe the first case of cricothyroid approximation using a silastic sheath interposed between the cartilages and the mattress suture.
Case Presentation
A 29 year old male to female transsexual presented to us with discontent of her male voice. Speech therapy did not provide a satisfactory outcome. Patient had genital conversion surgery, breast augmentation and has been on estrogen therapy. Medical history and system inquiry were negative. Patient was a heavy smoker and had no history of voice abuse or overuse. Laryngeal video-endostroboscopy was normal. Patient was informed about the surgical procedure and was admitted for cricothyroid approximation. Post-operatively there was a noticeable improvement in her voice and the patient was referred to a speech therapist for vocal training. One year follow up revealed further improvement in her vocal pitch.
Surgical Procedure
Under local anesthesia and with the patient fully awake, the neck was scrubbed and draped in the usual manner. A 5 cm transverse incision was made through the skin and subcutaneous tissues at the level of the cricothyroid membrane after infiltrating the skin with Xylocaine 1/100,000 epinephrine. Skin flaps were raised superiorly and inferiorly and strap muscles were reflected laterally. The cricothyroid muscles were identified (Fig. 1). Two 5 × 10 mm silastic sheaths were cut and positioned on both thyroid laminate and another two were placed on the cricoid cartilage. Non absorbable 3-0 Nylon mattress sutures were placed initially through the silastic sheath, then through the thyroid cartilage and were tunneled inferiorly and submucosally across the cricothyroid membrane into the cricoid cartilage and through the silastic sheath. The

M.E.J. ANESTH 21 (6), 2012
911CRICOTHYROID APPROXIMATION USING A SILASTIC SHEATH: A NEW APPROACH
surgeries is to decrease the mass per unit length of the vocal folds resulting in a subsequent increase in vocal pitch15.
In a nutshell, cricothyroidopexy seems to be the most acceptable surgical intervention for raising the pitch in male to female transsexuals, with the effect being more pronounced on the modal frequency rather than the mean frequency 16. One technical problem commonly encountered during the surgery is cutting of the sutures within the thyroid or cricoid cartilages. Various authors have described the usage of miniplate to prevent such complications. In this report, we are describing the usage of a silastic sheath that can be interposed between the cartilage and the sutures in order to circumvent breaking of the sutures or cutting through the cartilages. It is a simple and cheap material that is available in most hospital and can be cut and tailored according to the individual’s needs. In the above described case, after a one year of follow up, the patient maintained his post-operative pitch. We believe that using a silastic sheath is an innovative method that can be used in cricothyroid approximation. A future study on a large number of cases is needed to document the efficacy of this new approach.
tension, mass and length. The tension within the vocal folds can be increased by contraction of either bellies of the cricothyroid muscle. The pars recta is believed to tenses the vocal fold by the mechanism of rotation, thereby narrowing the visor angle between the thyroid and cricoid cartilages. On the other hand, pars obliqua is believed to tenses the vocal fold by the mechanism of translation12. The virtual increase in the tension within the vocal folds observed with the natural contraction of the cricothyroid muscle has led various authors to simulate the action of this later. Cricothyroid approximation is a perfect example for such a simulation. The increase in tension is thought to be far more important than the increase in length with this procedure. In a study by Neumann et al, the increase in tension resulted in an increase in the vocal pitch by five halftones on the average, in 94% of the cases13. To further increase the efficacy of cricothyroid approximation, this procedure has been coupled with sublaxation of the thyroid cartilage over the cricoid14. Attempts to incise the vocal cords longitudinally or to ablate part of the thyroarytenoid muscle have been described in conjunction with cricothyroidopexy or as separate procedures. The rational behind these

912 HAMDAN AL/
References
1. LANDEN M, WALINDER J, LUNDSTROM B: Prevalence, incidence and sex ration of transexualism. Acta Psych Scand; 1996, 93:221-223.
2. In: EICHER W, ED: Transsexualismus: moglichkeiten und grenzen der geschlechtsumwandlung. Stuttgart: Fischer; 1992, 17-20.
3. GOOREN LJ, TRANSSEKSUALITEIT I: Omschrijving, etiologie, hulpverlening. Ned Tijdschr Genesskd; 1992, 136:1893-1895.
4. EDGERTON MT: The surgical treatment of male transsexuals. Clin Plastic Surg; 1974, 1:285-323.
5. ISSHIKI N, MORITA H, ODAMURA H, HIRAMOTO M: Thyroplasty as a new phonosurgical technique. Acta Otolaryngol; 1974, 78:451-457.
6. ISSHIKI N, TAIRA T, TANAbE M: Surgical alteration of the vocal pitch. J Otolaryngol; 1983, 12(5):335-340.
7. TANAbE M, HAJI T, HONJO I, ISSHIKI N: Surgical treatment for androphonia. An Experimental study. Folia Phoniat; 1985, 37:15-21.
8. ISSHIKI N: Vocal mechanics as the basis of phonosurgery. Laryngoscope; 1998, 108:1761-1766.
9. MATAI V, CHEESMAN A, CLARKE PM: Cricothyroid approximation and thyroid chondroplasty: A patient survey. Otolaryngol Head Neck Surg; 2003, 128(6):841-847.
10. ISSHIKI N: Mechanical and dynamic aspects of voice production as
related to voice therapy and phonosurgery. Otolaryngol Head Neck Surg; 2000, 122(6):782-793.
11. NEUMANN K, WELZEL C, BERGHAUS A: Resorbable material for osteosynthesis or titanium for the cricothyroidopexy? Laryngorhinootologie; 2003, 82(6):428-435.
12. HONG KH, YE M, KIM YM, KEvORKIAN KF, KREIMAN J, BERKE GS: Functional differences between the two bellies of the cricothyroid muscle. Otolaryngol Head Neck Surg; 1998, 118(5):714-722.
13. NEUMANN K, WELZEL C, BERGHAUS A: Operative voices pitch raising in male-to-female transsexuals. A survey of our technique and results. HNO; 2003, 51(1):30-37.
14. KANAGALINGAM J, GEORGALAS C, WOOD G, AHLUWALIA S, SANDHU G, CHEESMAN AD: Cricothyroid approximation and subluxation in 21 male-to-female transsexuals. The Laryngoscope; 2005, 115:611-618.
15. ISSHIKI N, TAIRA T, TANAbE M: Surgical alteration of the vocal pitch. J Otolaryngol; 1983, 12(5):335-340.
16. BROWN M, PERRY A, CHEESMAN AD, PRING T: Pitch change in male to female transsexuals: has phonosurgery a role to play? Int J Lang Comm Dis; 2000, 35:129-136.

M.E.J. ANESTH 21 (6), 2012
Clinical or laboratory investigations:The following structured format is required:
1. Cover Letter 7. Discussion
2. Title page 8. Acknowledgements
3. Abstract 9. References
4. Introduction 10. Tables
5. Methods 11. Figures
6. Results
1. Cover LetterManuscripts must be accompanied by a cover letter, signed by all authors and stating that:
- All authors have contributed intellectually to the manuscript and the manuscript has been read and approved by all the authors.
- The manuscript has not been published, simultaneously submitted or accepted for publication elsewhere.
2. Title PageStarts at page 1 and includes:
- A concise and informative title (preferably less than 15 words). Authors should include all information in the title that will make electronic retrieval of the article both sensitive and specific.
- Authors listing: first name, middle initial and last name with a superscript denoting the academic degrees as footprints.
- The name of the department(s) and institutions(s) to which the work should be attributed.
- The name, address, telephone, fax numbers and e-mail address of the corresponding author.
- Disclose sources of financial support (grants, equipment, drug etc…).
- Conflict of interest: disclosure of any financial relationships between authors and commercial interests with a vested interest in the outcome of the study.
- A running head, around 40 characters.- Word count of the text only (excluding abstract,
acknowledgements, figure legends and references).
3. AbstractAbstract should follow the title page. It should be
structured with background, methods, results and conclusion.
The Middle East of Anesthesiology publishes original work in the fields of anesthesiology, intensive care, pain, and emergency medicine. This includes clinical or laboratory investigations, review articles, case reports and letters to the Editor.
Submission of manuscripts:The Middle East Journal of Anesthesiology accepts
electronic submission of manuscripts as an e-mail attachment only.
Manuscripts must be submitted via email attachment to:
Editor-In-Chief,
Department of Anesthesiology,
American University of Beirut Medical Center
Beirut, Lebanon
E-mail: [email protected]
Human SubjectsManuscripts describing investigations performed in
humans must state that the study was approved by the appropriate Institutional Review Board and written informed consent was obtained from all patients or parents of minors.
Language:Articles are published in English.
Manuscript PreparationManuscript format required:
Double-spaced lines
Wide margins (1.5 inches or 3.8 cm)
Page numbers start on title page
Word count should reflect text only (excluding abstract, references, figures and tables).
Editorial 1500
Abstract 250 (General articles)100 (Case Reports)
Review article 4000
Original article 3000
Case Reports 800
Letter to Editor 500
GUIDELINES FOR AUTHORS

8. AcknowledgementsThey should be brief. Individuals named must be given
the opportunity to read the paper and approve their inclusion in the acknowledgments.
9. References- References should be indicated by Arabic numerals in
the text in the form of superscript and listed at the end of the paper in the order of their appearance. Please be accurate, giving the names of all authors and initials, the exact title, the correct abbreviation of the journal, year of publication, volume number and page numbers.
- The titles of journals should be abbreviated according to the style used in the list of Journals Indexed for MEDLINE.
Example: (1) from a journal (2) from a book.1. SHAWW: AND ROOT B: Brachial plexus anesthesia
Comparatives study of agents and techniques. Am. J. Surg.; 1951, 81:407.
2. ROBINSON JS: Modern Trends in Anaesthesia, Evans and Gray Ch. 8, Butterworth Pub. Co., London 1967.
10. TablesTables capture information concisely and display it
efficiently: They also provide information at any desired level of details and precision. Including data in tables rather than text frequently makes it possible to reduce the length of the text.
- Type or print each table with double spacing on a separate sheet of paper.
- Number tables consecutively in the order of their first citation in the text.
- Supply a brief title for each.- Place explanatory matter in footnotes, not in the
heading.- Explain all nonstandard abbreviations in footnotes.- Identify statistical measures of variations, such as
standard deviation and standard error of the mean.
11. Figures- Figures should be submitted in JPEG or TIFF format
with a minimum of 150 DPI in resolution.- Colored data if requested by author is chargeable.- If a figure has been published previously, acknowledge
the original source and submit written permission from the copyrights holder to produce the figure.
Abbreviations and symbols:- Use only standard abbreviations.- Avoid abbreviations in the title of the manuscript.- The spelled-out abbreviations followed by the
abbreviation in parenthesis should be used in first mention.
It should state, the specific purpose of the research or hypotheses tested by the study, basic procedures, main findings and principal conclusions.
Provide separate word count for the abstract.
4. IntroductionProvide the nature of the problem and its significance.
State the specific purpose or research objectives or hypothesis tested. Provide only directly pertinent references and do not include data or conclusions from the work being reported.
5. MethodsA. Selection and description of participants:
- Describe selection of participants (including controls) clearly, including eligibility and exclusion criteria.
B. Technical information:- Identify the methods, apparatus (give the
manufacturer’s name and address in parentheses), and procedure in sufficient detail to allow others to reproduce the results. Give references to established methods. Provide references and brief descriptions for methods that have been published. Identify precisely all drugs and chemicals used, including generic names(s), dose(s) ands routes(s) of administration.
C. Statistics-describe statistical methods with enough detail to enable a knowledgeable reader with access to the original date to verify the reported results. Define statistical terms, abbreviations and most symbols. Specify the computer software used. Provide a power analysis for the study.
6. ResultsPresent your results in logical sequence in the text, tables
and illustrations, giving the main or most important findings first. Do not repeat all the data in the tables or illustrations in the text: emphasize or summarize only the most important observations. Extra or supplementary materials and technical details can be placed in an appendix.
7. DiscussionEmphasize the new and important findings of the study
and the conclusions that may be drawn.
Do not repeat in details data or other information given in the Introduction or the Results sections. For experimental studies, it is useful to begin the discussion by summarizing briefly the main findings, then explore possible mechanisms or explanations for these findings, compare and contrast the results with other relevant studies. State the limitations of the study, and explore the implications of the findings for future research and for clinical practice. Link the conclusions with the goals of the study, but avoid unjustified statements and conclusions not adequately supported by the data.


Printed by Arab Scientific PublishersAin Al-Tineh, Beirut, LebanonTelefax: + 961 (1) 785107 / 8Email: [email protected]