Blood Markets
252
Blood Markets Rures adquireret umbraculi, etiam tremulus matrimonii libere senesceret app November 2008 Kalorama Information A division of MarketResearch.com 38 East 29th Street Sixth Floor New York, New York 10016 212.807.2660 t 800.298.5603 t 212.807.2676 f www.kaloramainformation.com
-
Upload
nwfsc-noaa -
Category
Documents
-
view
0 -
download
0
Transcript of Blood Markets

Blood Markets
Rures adquireret umbraculi, etiam tremulus matrimonii libere senesceret app November 2008
Kalorama InformationA division of MarketResearch.com
38 East 29th Street Sixth FloorNew York, New York 10016
212.807.2660 t800.298.5603 t212.807.2676 f
www.kaloramainformation.com


Copyright © 2008 Kalorama Information Reproduction without prior written permission, in any media now in
existence or hereafter developed, in whole or in any part, is strictly prohibited
BLOOD: THE WORLDWIDE MARKET FOR BLOOD PRODUCTS,
BLOOD TESTING, BLOOD EQUIPMENT, AND SYNTHETIC
BLOOD PRODUCTS Blood Markets has been prepared by Kalorama Information. We serve business/ industrial clients worldwide with a complete line of information services and research publications. Kalorama Information Market Intelligence Reports are specifically designed to aid the action-oriented executive by providing a thorough presentation of essential data and concise analysis.
Editor: Bruce Carlson Author: Allison Sahoo Publication Date: October 2008
641 Avenue of the Americas New York, New York 10011-2002
(800) 298-5699 • Outside the U.S. (212) 807-2657 FAX: (212) 807-2676
http://www.KaloramaInformation.com E-MAIL: [email protected]
KLI1816262
COPYRIGHT © 2008 Kalorama Information a division of MarketResearch.com, Inc.

Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 3 -

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 4 -
T A B L E O F C O N T E N T S
CHAPTER ONE: EXECUTIVE SUMMARY ....................................................................... 1 Blood Collection...................................................................................................................... 3 Blood Typing and Testing for Diseases ................................................................................ 6 Blood Storage And Processing .............................................................................................. 8 Blood Transfusions............................................................................................................... 10 Blood Management And Safety Issues ............................................................................... 12 Synthetic Blood Products..................................................................................................... 12 Blood Products Market........................................................................................................ 14 Table 1-1: Global Blood Products Market, 2007: Blood Testing
And Typing Products Market................................................................................... 16 Table 1-2: Global Projected Blood Banking and Plasmapheresis
Molecular Diagnostics Testing Market Estimate: 2007–2014 ................................ 17 Plasma and Blood Collection Equipment Market............................................................. 18 Table 1-3: Global Market for Blood Collection Equipment: 2007–2014............... 19 Synthetic Blood Products Market....................................................................................... 19 Table 1-4: Recombinant Factor and High Blood Loss Market: 2007-2014........... 20
CHAPTER TWO: OVERVIEW............................................................................................. 21 The Global Blood Industry .................................................................................................. 21
History of the Blood Industry.............................................................................................. 21 Table 2-1: Timeline of Global Blood Industry Development 1922 - 2008 ............. 23 Blood and its Components ................................................................................................... 27
Plasma................................................................................................................................ 29 Figure 2-1: Composition of Blood Plasma................................................................ 30 Immunoglobulin Products ................................................................................................... 30 Blood Transfusions............................................................................................................... 31 Efforts to Create a Virus-Free Blood Supply..................................................................... 35 Table 2-2: Viral Inactivation Methods for Viruses Found in Platelets.................. 38 Table 2-3: Viral Inactivation Methods for Viruses Found in Red Blood Cells..... 39 Synthetic Blood Products..................................................................................................... 39

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 5 -
Hemoglobin Based Oxygen Carriers .............................................................................. 41 Perflurocarbon (PFC) Based Blood Products................................................................ 44 Factor Products for Hemophilia A ................................................................................. 46 Synthetic Platelets............................................................................................................. 46
CHAPTER THREE: BLOOD MANAGEMENT, BLOOD COLLECTION,
PROCESSING AND USE .............................................................................................. 49 Blood Collection.................................................................................................................... 49 Organizations Collecting Blood........................................................................................... 50 Donor Donation Demographics........................................................................................... 54 Donor Recruitment............................................................................................................... 55 Blood Screening and Evaluation ......................................................................................... 56 Methods for Collecting Blood from Donors....................................................................... 57 Figure 3-1:Worldwide Annual Blood Collection by Component (Red Cells,
Platelets, Plasma, Whole Blood) ................................................................................ 59 Cord Blood Collection.......................................................................................................... 62 Plasma Collection ................................................................................................................. 63 Blood Typing and Testing for Diseases .............................................................................. 65
Table 3-1: Basic Blood Types..................................................................................... 67 Table 3-2: Blood Transfusion Compatibility............................................................ 67 Blood Testing ........................................................................................................................ 69 Table 3-3: PCR-Based Screening Tests Licensed by CBER ................................... 74 Table 3-4: Comparison of Direct and Indirect ELISA Tests.................................. 78 Blood Processing................................................................................................................... 83 Figure 3-2: Results of Cohn Fractionation Method................................................. 85 Table 3-5: Plasma Proteins of Therapeutic Interest................................................ 86
Cascade Plasma Fractionation ........................................................................................ 88 Automated Fractionation................................................................................................. 89
Blood Transfusions............................................................................................................... 89 Types of Transfusions .......................................................................................................... 93 Blood Management Issues ................................................................................................. 103 Safety Issues ........................................................................................................................ 105 Table 3-6: Risk of Contamination ........................................................................... 110 Table 3-7: Viral Inactivation by Procedure............................................................ 111
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 6 -
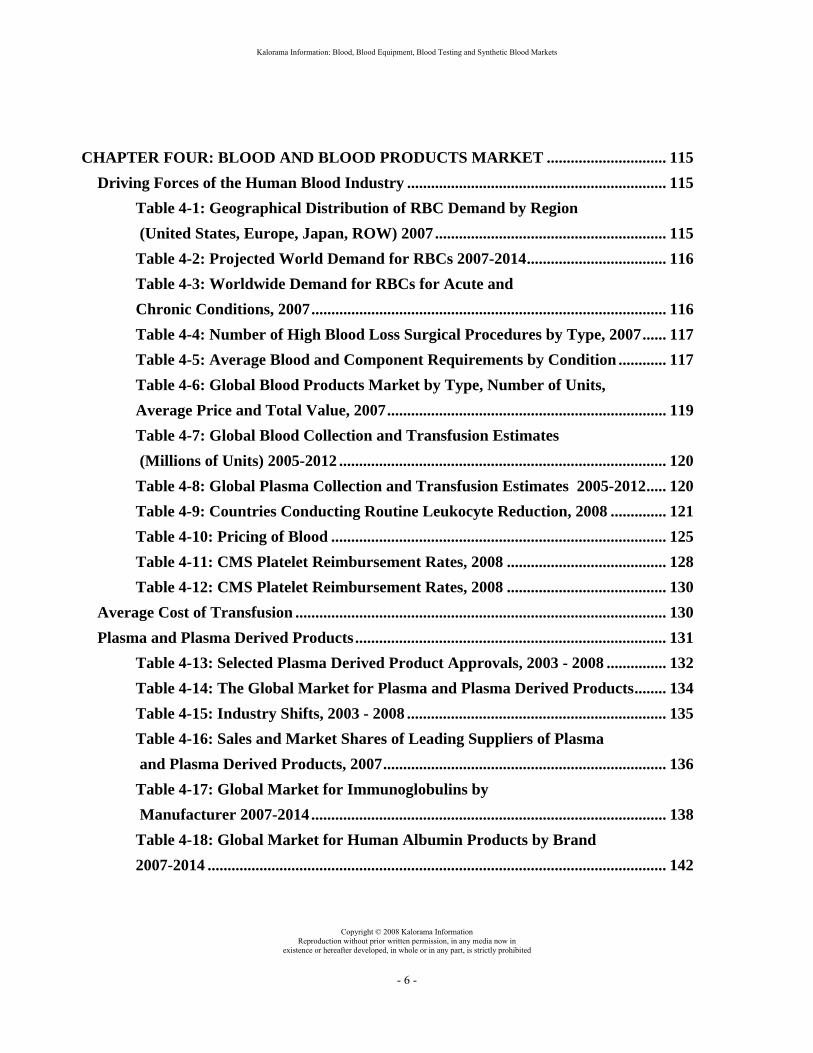
CHAPTER FOUR: BLOOD AND BLOOD PRODUCTS MARKET .............................. 115
Driving Forces of the Human Blood Industry ................................................................. 115 Table 4-1: Geographical Distribution of RBC Demand by Region
(United States, Europe, Japan, ROW) 2007.......................................................... 115 Table 4-2: Projected World Demand for RBCs 2007-2014................................... 116 Table 4-3: Worldwide Demand for RBCs for Acute and
Chronic Conditions, 2007......................................................................................... 116 Table 4-4: Number of High Blood Loss Surgical Procedures by Type, 2007...... 117 Table 4-5: Average Blood and Component Requirements by Condition ............ 117 Table 4-6: Global Blood Products Market by Type, Number of Units,
Average Price and Total Value, 2007...................................................................... 119 Table 4-7: Global Blood Collection and Transfusion Estimates
(Millions of Units) 2005-2012 .................................................................................. 120 Table 4-8: Global Plasma Collection and Transfusion Estimates 2005-2012..... 120
Table 4-9: Countries Conducting Routine Leukocyte Reduction, 2008 .............. 121 Table 4-10: Pricing of Blood .................................................................................... 125 Table 4-11: CMS Platelet Reimbursement Rates, 2008 ........................................ 128 Table 4-12: CMS Platelet Reimbursement Rates, 2008 ........................................ 130 Average Cost of Transfusion ............................................................................................. 130 Plasma and Plasma Derived Products.............................................................................. 131 Table 4-13: Selected Plasma Derived Product Approvals, 2003 - 2008 ............... 132 Table 4-14: The Global Market for Plasma and Plasma Derived Products........ 134 Table 4-15: Industry Shifts, 2003 - 2008 ................................................................. 135 Table 4-16: Sales and Market Shares of Leading Suppliers of Plasma
and Plasma Derived Products, 2007....................................................................... 136 Table 4-17: Global Market for Immunoglobulins by
Manufacturer 2007-2014 ......................................................................................... 138 Table 4-18: Global Market for Human Albumin Products by Brand
2007-2014 ................................................................................................................... 142

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 7 -
Table 4-19: Prevalence of Conditions Requiring Prothrombin Complex Concentrates.............................................................................................. 143
Table 4-20: Leading Factor IX Products, 2008 ...................................................... 143 CHAPTER FIVE: BLOOD TESTING AND TYPING MARKETS................................. 147
Blood Testing Products for Donor Screening .................................................................. 147 Table 5-1: Global Blood Banking and Plasmapheresis Testing by Molecular
Diagnostics: 2007–2014 (HIV, Hep C, Hep B, Hep A, HTLV, West Nile, Others) ..................................................................................................... 150
Table 5-2: U.S. Blood Banking and Plasmapheresis Testing by Molecular Diagnostics: 2007–2014 (HIV, Hep C, Hep B, Hep A, HTLV, West Nile, Others).................................................................................................... 150
Table 5-3: Global Projected Blood Banking and Plasmapheresis Molecular Diagnostics Testing Market Potential: 2007–2014 (HIV, Hep C, Hep B, Hep A, HTLV, West Nile, Others)........................................................................... 151
Table 5-4: Projected Blood Banking and Plasmapheresis Molecular Diagnostics Testing Market Potential in the United States: 2007–2014 (HIV, Hep C, Hep B, Hep A, HTLV, West Nile, Others)...................................... 152
Table 5-5: Selected Commercially Available Molecular (Nucleic Acid) Tests for Blood, Plasma and Organ Donor Screening in the United States, 2001 - 2008... 154
Blood Typing Products....................................................................................................... 156 Plasma and Blood Collection Equipment......................................................................... 158 Table 5-6: Total Global Market for Blood Collection Equipment: 2007–2014... 159 Table 5-7: Global Market for Automated Blood Collection
Equipment: 2007–2014 ............................................................................................ 160 CHAPTER SIX: SYNTHETIC BLOOD PRODUCTS MARKET.................................... 163
Driving Forces of the Synthetic Blood Products Industry.............................................. 163 Recombinant Factor Market ............................................................................................. 166 Table 6-1: Oxygen Carrier Market ......................................................................... 168

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 8 -
Table 6-2: High Blood Loss Market HBOC and PFC Agent Revenues 2007-2012................................................................................................. 168
Synthetic Blood Products in Clinical Development......................................................... 169 Table 6-3: Recombinant Factor Products in Clinical Trials................................. 183 Other Research Initiatives ................................................................................................. 184
CHAPTER SEVEN: TOTAL BLOOD PRODUCTS MARKET ...................................... 187
The Blood Products Industry ............................................................................................ 187 Figure 7-1: Global Blood Products Market by Segment (Blood Collection
Equipment, Molecular Diagnostic Tests, Albumin, Blood Typing, RBCs, Recombinant Factors, Immunoglobulins), 2007 ........................................................ 188
Table 7-1: Global Blood Products Market Forecast by Segment, 2007 – 2014 (Blood Collection Equipment, Molecular Diagnostic Tests, Albumin, Blood Typing, RBCs, Recombinant Factors, Immunoglobulins) ............................. 189
Figure 7-2: Global Blood Products Market Forecast by Segment, 2014 (Blood Collection Equipment, Molecular Diagnostic Tests, Albumin, Blood Typing, RBCs, Recombinant Factors, Immunoglobulins) ............................ 190
CHAPTER EIGHT: COMPANY PROFILES: .................................................................. 191
AABB................................................................................................................................... 191 Abbott Laboratories........................................................................................................... 193 Alliance Pharmaceuticals................................................................................................... 198 America’s Blood Centers ................................................................................................... 200 American Red Cross........................................................................................................... 201 Baxter International........................................................................................................... 203 Biopure Corp. ..................................................................................................................... 205 Bio-Rad Laboratories......................................................................................................... 206 BioTime Inc. ........................................................................................................................ 208 Chiron.................................................................................................................................. 210 CSL Behring........................................................................................................................ 212 Gen-Probe Inc. .................................................................................................................... 214

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 9 -
Fenwal.................................................................................................................................. 218 Grifols Biologicals, Inc. ...................................................................................................... 219 Haemonetics, Inc................................................................................................................. 221 Hemosol Corp. .................................................................................................................... 223 JP Laboratories Inc............................................................................................................ 226 Northfield Laboratories ..................................................................................................... 229 Novo Nordisk A/S ............................................................................................................... 231 Perftoran ............................................................................................................................. 235 Sanguine Corp. ................................................................................................................... 237 Oxygen Biotherapeutics ..................................................................................................... 239 Talecris Biotherapeutics .................................................................................................... 240


Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 1 -
C H A P T E R O N E
Executive Summary
THE GLOBAL BLOOD INDUSTRY
The U.S. long care industry has experienced strong growth from 2002 through
2007 and this is expected to continue through the forecast period. Growth will be fueled
by aging populations in the U.S., Europe and Japan
SCOPE AND METHODOLOGY
Sales estimates for each market segment represent global revenues and are
expressed in current dollars. Estimates are provided for the historic 2002 to 2007period
and forecasts are provided through 2014. Historical information for this report was
gathered from a wide variety of published sources including company reports and filings,
government documents, legal filings, trade journals, newspapers and business press,
analysts’ reports and other sources. Interviews with company representatives were
conducted to capture the perspectives from industry participants’ point of view and assess
trends, and form the basis of the forecasting and competitive analysis.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 2 -
OVERVIEW
The modern blood industry developed primarily in response to World War II and
the unprecedented need for blood in the medical treatment of casualties. Developments in
the large-scale storage and use of blood between the first and second world wars laid the
groundwork for progress that was rapidly made in the late 1940s and beyond.
Blood performs two major functions: it transports materials such as oxygen and carbon dioxide, as well as heat, through the body; it also defends the body against infections and foreign materials. The blood itself is comprised largely of watery plasma, in which are suspended seven types of cells and cell fragments:
• red blood cells (RBCs) or erythrocytes, which transport of oxygen and carbon dioxide;
• five kinds of white blood cells (WBCs), which protect the body from infection.;
• platelets or thrombocytes, representing cell fragments;
• three types of granulocytes;
• neutrophils;
• eosinophils;
• basophils.
Found in the blood, tissue fluids as well as many secretions, immunoglobulins are
glycoproteins (molecules composed of proteins and carbohydrates) that function as
antibodies. Often, the terms antibody and immunoglobulin are used interchangeably.
Immunoglobulin products are polyclonal antibody-rich fractions obtained from pooled fractionated and purified human blood plasma, or from animal plasma. Immunoglobulin products are generally used for passive immunization, as antibody-based immunity can be immediately transferred to a person by injection of immunoglobulin preparations.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 3 -
BLOOD COLLECTION Donated blood is collected by specialized collection centers. After collection,
whole blood is separated into its three main components: red blood cells (RBCs),
platelets, and plasma. Sometimes a fourth component called cryoprecipitate (a fraction of
plasma highly concentrated in some clotting factors such as Factor VIII or antihemophilic
factor, fibrinogen, and von Willebrand factor) is also generated. Several different types of
organizations currently collect blood. While most operate on a not for profit basis, some
pay donors. To date, about 40 countries have developed national blood policies, though
the implementation rate has been slow. In the developed countries, blood donation is
predominantly operated on a voluntary basis, with unpaid donors encouraged to donate
blood for humanitarian reasons. Since there is no uniform set price for blood, the cost
can vary considerably between different regions and collection centers. Cost also varies
with the component, with the most expensive blood component being RBCs.
Around the world, for-profit blood collection is comprised largely of plasma
donation (plasmapheresis). This is because the donation process is much more arduous
and time-consuming than for red blood cells, and the platelet shortage is more severe.
First created in 1991 by the Plasma Protein Therapeutics Association (PPTA), the
National Donor Deferral Registry (NDDR) is a database of permanently deferred plasma
donors. It was established to help ensure the safety of plasma and plasma-derived
products by ensuring that permanently deferred donors would not be inadvertently
allowed back into the donation pool. About 3% of donors are deferred each year.
Blood donor recruitment involves education, information and motivation
techniques to encourage individuals to donate blood. Most blood collection centers
employ recruitment directors who focus exclusively on increasing the numbers of donors.
Different blood collection centers utilize different techniques, particularly across different
countries and cultures. Some provide all donors with inexpensive gifts, many of which
may be donated by local businesses. These include food and refreshments, coupons for
free or discounted products and services, and give-aways such as T-shirts, pens, mugs,
etc. Other centers randomly select a small number of donors to win a larger prize, such as
a television or vacation.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 4 -
To be eligible to donate blood, donors must be at least 17 years of age, weigh at
least 110 lbs. and be in good health. Donors must also meet other medical criteria, such
as having no history of hepatitis or risk of HIV. Many centers refuse to accept donations
from persons who have accepted money in exchange for sex, or men who have had
sexual relations with other men, since 1977. Other conditions for exclusion include living
in or traveling to certain African or Caribbean countries; having been in juvenile
detention, jail or prison within the past 12 months; having had syphilis, gonorrhea or
venereal disease within the past year; or having had sexual contact with any person who
meets that criteria. Potential donors who are ineligible are deferred, on either a
temporary, indefinite or permanent basis.
Blood collection procedures and systems are often referred to as either "manual"
or "automated." In a manual process, whole blood is withdrawn from a donor and
collected in a container that typically includes an amount of anticoagulant. After
collection, the blood is subjected to a separation procedure. This contrasts with automated
collection (ABC), or apheresis, in which the donor is directly connected to a blood
collection device that separates a desired component and returns remaining components
to the donor. A single ABC donation can supply patients with a unit of red blood cells
and enough platelets and plasma for a complete transfusion. While six to eight regular
whole blood donations are required to supply enough platelets for one transfusion, just
one ABC donation from a single donor can provide enough platelets for one to three
transfusions. However, automated blood collection continues to represent less than half
of all blood collection.
The process by which blood plasma is collected, known as plasmapheresis,
largely consists of automated collections. Plasma companies produce a wide range of
medical products, ranging from vaccines to products used in the manufacture of clotting
agents such as Factor VIII. In the procedure, plasma is removed from the body then
mixed with an anticoagulant solution that separates the plasma from the red blood cells.
The plasma is then diverted into a storage contained, while the RBCs are re-infused back
into the body.
Plateletpheresis (also called thrombapheresis or thrombocytapheresis) is a process
in which only the blood clotting cells, or platelets, are extracted from the blood. More

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 5 -
modern automatic plateletpheresis allows the blood donor to give a portion of his
platelets, while retaining the red blood cells and a portion of the plasma.
Leukopheresis is the process of withdrawing leukocytes, one type of white blood
cell, from the blood. Leukopheresis units may be utilized in transfusions; they may also
be processed to obtain stem cells. In a procedure similar to that of plasmapheresis and
plateletpheresis, blood is drawn from one arm by a needle and processed automatically
through a machine that removes white cells.
Like other apheresis techniques, red blood cell apheresis refers to the process of
separating red blood cells from donated blood while unused components are returned to
the body. This allows greater collection of red blood cells (two units compared with one),
which is beneficial since about 60% of all transfusions require RBCs.
Cord blood is human blood from the placenta and umbilical cord that are left over
after birth. Although still a small segment of the overall blood collection industry, cord
blood collection is becoming increasingly popular as a means to access valuable stem
cells. As of mid 2008, several dozen storage companies were in operation, up from about
12 in 2001. However, the donation of cord blood remains extremely low compared with
conventional blood and plasma donation.
Plasma fractionators collect human plasma and separate it into components. In
terms of amount, the major products prepared are human serum albumin and intravenous
immunoglobulin, although a variety of other important products are also prepared. Due to
the significant level of investment required to establish a fractionation facility ($25
million - $50 million in construction costs, which includes engineering, building and
equipment for a plant producing 100,000 to 300,000 liters per year), fractionators tend to
be large, well-capitalized players.
Plasma brokers and distributors represent a diverse and fragmented group. In
addition to some larger pharmaceutical distributors such as AmeriSourceBergen and
Cardinal Health, the market also includes a large number of smaller, privately held
companies that trade plasma between fractionators and users such as hospitals.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 6 -
BLOOD TYPING AND TESTING FOR DISEASES Blood typing and testing represents the cornerstone of ensuring that transfused
blood is safe for the recipient and free of disease.
Blood Typing The differences in human blood are due to the presence or absence of certain
antigens located on the surface of the red blood cells and antibodies in the blood plasma.
Individuals with different blood types have varying combinations of these molecules. Not
all blood groups are compatible with each other, and mixing incompatible blood groups
during transfusions leads to blood clumping or agglutination. These clumped red cells
can crack and cause toxic reactions with potentially fatal consequences when the receiver
of a blood transfusion has antibodies against the donor blood cells. While there are more
than 20 genetically determined blood group systems known today, the AB0 and Rh
systems are the most important ones used for blood transfusions. In the U.S., type O+ is
the most common, accounting for about 38% of the population, while type AB- is the
least common at just 1%. In terms of compatibility, those with type AB+ are the easiest
to match, since they can safety received blood from donors of any type, while those with
type O- may only receive blood from others of type O-.
A variety of different methods are currently used to determine blood type. These
may be either manual or automated. Manual blood typing methods include slide/tile
testing, tube testing and microplate, which differ mainly in terms of the surface on which
the blood is test. For each test, blood type is determined by testing for the presence or
absence of Rh factor and blood group antigens A and B on the surface of red blood cells.
Automated blood typing systems employ similar biochemical mechanisms to classify
blood but replace the human component with artificial intelligence. Several devices are
currently available, which generally utilize microtiter plates to determine ABO and Rh
types, solid phase red cell adherence assays for antibody detection and/or modified solid
phase red cell adherence plates for IgG cross matches.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 7 -
Blood Testing A variety of infectious agents can be present in blood, including viruses (e.g.,
HIV-1, hepatitis B and C, HTLV, West Nile virus), bacteria, protozoans, Chagas disease,
Lyme Disease and prions (e.g., the agent of variant Crueutzfeldt-Jakob disease, which is
the human form of mad cow disease). As of mid 2008, the main residual risk is due to
hepatitis B virus - ranging from 10 in Spain to 1.6 per million donations in France and
Germany – although other conditions such as variant Creutzfeldt-Jakob disease (vCJD)
may pose relatively high risk in certain regions.
Nonetheless, blood safety is relatively high, due to the widespread usage of blood
testing. In the United States, the risk of acquiring an infectious disease from allogenic
blood ranges from 1:60,000 for hepatitis B to 1:500,000 for HIV, with transmission rates
for other viruses, such as hepatitis C and the human T-cell leukemia virus, intermediate
between these.
There is a continuing trend toward the use of molecular diagnostics in the
screening of donated blood, plasma and organs for transplantation. Before 1985, all
donated blood, plasma and organs were tested only for syphilis and hepatitis B surface
antigen (HBsAg). From 1985 through 1989, serologic testing for HIV-1 and HTLV were
added to the requirements. In the following years, tests for alanine-aminotransferase
(AAT) hepatitis B core antibody (antiHBc) and HCV have also been implemented.
Nucleic acid amplification testing (NAT), also known as “molecular diagnostics”,
is a newer technology whose investigation has been encouraged by the FDA since 1994.
In 2001, the FDA licensed the first NAT systems for screening of plasma donors with the
expectation that NAT would permit earlier detection of HIV and HCV infections in
donors. NAT allows detection of very small amounts of genetic material (DNA or RNA),
allowing highly sensitive detection of targets. This has resulted in lower rates of
infectious disease transmission.
Polymerase chain reaction (PCR) amplification is now the most widely used
nucleic acid amplification method. Because PCR can amplify even very tiny amounts of
target DNA within a few hours, the assays can quickly and accurately detect the presence
of slow-growing microorganisms, such as chlamydia, mycoplasmas, mycobacteria,

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 8 -
herpesviruses and enteroviruses and are now routinely used in many diagnostic
laboratories for the diagnosis of tuberculosis and genital C. trachomatis infection.
An immunoassay is a biochemical test that measures the level of a substance in
the plasma by measuring the reaction of an antibody to its antigen. Monoclonal
antibodies, which are antibodies that are identical because they are clones of a single
parent immune cell, are often used in immunoassays since they only usually bind to one
site of a particular molecule. They therefore provide a more specific and accurate test,
which is less easily confused by the presence of other molecules. The presence of both
antigens and antibodies can be measured by immunoassays. In tests designed to detect
infection, the presence of antibodies against the pathogen is measured; for measuring the
levels of hormones such as insulin, the insulin acts as the antigen and is measured
directly.
The Enzyme-Linked Immunosorbent Assay (ELISA for short) is a technique used
to detect the presence of an antibody or antigen in a plasma sample. It utilizes two
antibodies, one of which is specific to the antigen and the other of which is coupled to an
enzyme. This second antibody will cause a chromogenic or fluorogenic substrate to
produce a signal. Several variations of the test are currently in use.
The most serious barrier to the use of molecular diagnostic technologies in blood
screening is cost. Each molecular assay costs as much as 10 times that of the most
expensive immunoassay now used in blood banks. Although blood banks are, for the
most part, not-for-profit organizations, but they must still cover their costs and the use of
molecular assay methods would mean an increase in blood pricing. To deal with the
issue of costs, blood banks and plasmapheresis centers do not test individual donations
but use a pooling method.
BLOOD STORAGE AND PROCESSING Blood can be stored as whole blood (with all of the plasma present) or, much
more commonly, as packed red blood cells in which about 70% of the plasma has been
removed. After this occurs, blood and/or blood components are commonly refrigerated or

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 9 -
frozen to extend their usefulness, with storage times based upon the physiological
qualities of those materials.
Blood processing typically involves the breaking down of blood into its
components (fractions), which are then utilized for a variety of purposes. Several
different methods are used including Cohn fractionation, standard fractionation and more
advanced methods.
The process of fractionation represents the separation of proteins from the blood
plasma and dates to the work of Harvard biochemist Edwin Cohn in 1940. Searching for
a substitute for whole plasma, Cohn determined that different proteins (fractions) in the
blood could be separated from each other by using different temperatures and
biochemical conditions and by the use of solvents like cold ethanol. His method used
these biochemical techniques to separate the blood plasma into five fractions, allowing
the isolation of fibrinogen (Fraction or Factor I), gamma globulin (Fraction II and III),
and albumin (Fraction V). Although the original Cohn fractionation method continues to
be used since it offers high yields of albumin, many improvements have been made to the
original technique, including the use of other solvents such as acetone or salts
(ammonium sulfate) or heat to separate the albumin from other plasma components.
These have arisen due to several shortfalls with the Cohn ethanol technique.
Modern fractionation methods address the limitations of Cohn fractionation while
allowing the separation of a larger number of proteins. In addition to Factors I – V, these
include several hundred proteins of therapeutic value that are found in much lower
concentrations. These methods employ selective precipitation of proteins by precipitation
and/or chromatographic procedures.
Ongoing advances in fractionation methods provide increasing yields of desired
proteins with higher purity. This is important, since human plasma sources represent as
much as 45% of the total cost of operating a plasma fractionation facility and higher
yields lead to greater revenue from the same amount of plasma. Additionally, increasing
purity offers lower levels of risk. Many of these changes are driven by the industry’s
safety consciousness and incorporate the latest procedures for virus reduction and
clearance of prions. To this end, manufacturers continue to introduce new membranes for
virus filtration (nanofiltration), sterilizing grade filters, process chromatography sorbents

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 10 -
and membrane chromatography devices. Other developers are working on novel
fractionation methods, including cascade plasma fractionation.
BLOOD TRANSFUSIONS
Blood transfusion is the process of transferring whole blood or blood-based
products from one person (the donor) into the circulatory system of another (the
recipient). A transfusion may be undertaken in connection with the treatment of various
medical conditions in which the recipient sustains significant blood loss or the
mechanism of producing red blood cells (or another essential blood component) fails,
such as trauma, surgery or shock. Patients who require blood transfusions generally fall
into two categories: those who require transfusions resulting from acute blood loss that
might be associated with surgery; or those requiring chronic transfusions associated with
treatment for chronic anemia, chemotherapy, or bone marrow transplant. More than 50%
of transfusions occur in patients over the age of 65.
In the developed countries, testing of blood is conducted routinely prior to
transfusion to insure that donated blood will be compatible with recipients’ blood. A
variety of tests are used that determine blood type by identifying the presence of
antibodies.
Although early transfusions focused on the transfer of whole blood, this is now
generally reserved only for special cases and more commonly, just the specific
components needed by the recipient are transfused. This provides for more economical
usage of blood supplies, as each unit of blood can be utilized for multiple recipients, and
also reduces the risk of causing hypertension in recipients. Each pint of whole blood
contains one transfusible dose of RBCs, one-half to one transfusible dose of plasma, and
one-fifth to one-eighth of a transfusible dose of platelets.
Because red blood cells are the only cells in the body that transport oxygen, they
are the blood component most frequently used for transfusion. A transfusion of RBCs
increases the amount of oxygen that can be carried to the tissues of the body. RBCs that
have been separated from the liquid plasma (packed RBCs) are given to persons who
have anemia or have lost a significant amount of blood.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 11 -
A key factor in blood clotting, platelets are another component frequently given
by transfusion. Platelets are extracted from donated blood and concentrated for use.
Along with other clotting factors, platelets are typically used to correct a deficiency in
either platelet number (thrombocytopenia) or platelet function (thrombocytopathy or
qualitative platelet disorders).
Transfusion with fresh frozen plasma (FFP), which represents the remaining
plasma after removal of red blood cells and platelets from whole blood, is commonly
indicated for the treatment of microvascular bleeding due to congenital and acquired
coagulopathies. FFP may also be used to reverse the anticoagulation effects of warfarin
prior to surgery or during active bleeding episodes.
Cryoprecipitated antihemophilic factor, or cryoprecipitate, is prepared from fresh
frozen plasma (FFP). It is the white precipitate that forms when FFP is thawed at 1º to
6ºC. Cryoprecipitate is utilized for the treatment of congenital or acquired fibrinogen and
Factor VIII and XIII deficiencies.
Derived from large pools of human donors and administered as intramuscular
immunoglobulin (IMIG) or intravenous immunoglobulin (IGIV), immune serum globulin
contains IgG antibodies against a wide spectrum of normal human proteins and anti-
idiotypic antibodies as well as a broad range of immune antibodies directed against
foreign antigens and pathogens. Immune serum globulin is therefore indicated for a wide
range of conditions.
Factor VIII concentrate is a lyophilized powder purified from plasma to treat
patients with hemophilia A or von Willebrand’s disease, and is an important product
since about 80% of hemophiliacs lack sufficient amounts of Factor VIII in their blood.
Coagulation Factor IX and Factor IX Complex are indicated for the treatment of
Factor IX deficiency (hemophilia B, Christmas disease) and Recombinant Coagulation
Factor IX (rFIX) is used for new patients with hemophilia B and for those with limited
exposure to human-derived Factor IX products.
Recombinant human Factor VIIa, a coagulation factor that is primarily
synthesized in the liver, is FDA approved for treatment of bleeding episodes in patients
with hemophilia A or B, when inhibitors to these factors are present. It is also being

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 12 -
investigated for treatment in episodes of severe life-threatening bleeding, stem cell
transplantation, intra-cerebral hemorrhage and trauma.
Thrombin, also known as activated Factor II, is a serine protease that converts
fibrinogen, a soluble plasma glucoprotein that is synthesized by the liver, into fibrin. It is
topically applied to help control bleeding, particularly from small, sometimes
inaccessible, blood vessels during surgery when conventional surgical techniques are not
feasible.
BLOOD MANAGEMENT AND SAFETY ISSUES The effective management of blood supplies is a critical issue for the blood
industry, which continues to be challenged with a growth in demand that exceeds any
increases in supply. While many blood collection groups have ramped up donor
recruitment campaigns and thereby increased overall donations, demand continues to rise
with aging populations so that in most countries, the available supply of blood for
transfusion does not meet demand. Part of the reason for this reduced availability is
increasing safety measures, designed to reduce incidence of viral transmission through
blood transfusions.
Although the blood supplies in the developed nations are, to a very high degree,
free of disease-causing viruses, the risk of transfusion-related infection is nonetheless
present. Because these supplies contain human blood, achieving 100% virus eradication
is unlikely. However, efforts continue to reduce the risk of virus transmission as much as
possible. These include a variety of initiatives including plasma treatments, platelet
treatments, utilization of red blood cells, improved donor screening, improved viral
screening, increasing repeat donation rates, enhancing viral inactivation processes and the
selective use of blood derivative products.
SYNTHETIC BLOOD PRODUCTS Synthetic blood products are not derived from human blood, but instead represent
oxygen-carrying volume-replacement solutions. Although efforts are underway to
develop artificial cells or to culture red blood cells (RBCs) from stem cells, present

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 13 -
synthetic blood products do not contain cells, antibodies, coagulation factors, or any of
the other myriad components of blood itself. Synthetic blood substitutes have long been
sought for treatment of chronic and acute anemias, and rapid replacement of blood lost
after trauma and are commonly used a variety of applications. One of the primary reasons
for their development is to ease the projected shortage in the blood supply.
Blood volume expanders are large molecular weight solutions, which when
introduced into the body, tend to pull water from the extracellular fluid compartment into
circulation, such as into plasma and intracellular space. They may be used for a variety of
different applications including hrmorrhagic shock, cardiopulmonary bypass, septic
shock, obstetrics, thermal injury, vascular surgery or organ transplantation.
Hemoglobin-based oxygen carriers (HBOCs) are investigational agents designed
to deliver oxygen to tissues and organs as a result of blood loss during surgery, life-
threatening blood loss or other situations in which the body may have diminished oxygen
delivery. They do not have the same properties as whole blood, such as fighting
infections or coagulating blood during wound healing, but rather they are designed solely
to deliver oxygen. In early attempts to use Hb solutions as oxygen carriers, anaphylactoid
side effects were common. These were mainly due to the phospholipid content of residual
RBC stroma that nonspecifically activated the complement cascade. Today, ultrafiltration
and purification techniques result in stroma-free HBOC solutions. Another immunologic
challenge facing the nonhuman HBOC products is the possibility of specific immune
responses to the foreign Hb molecule.
Perflurocarbon (PFC) based blood products are chemically inert, water insoluble,
synthetic aromatic or aliphatic compounds with fluorine substituted for all hydrogen
atoms. The first clinical trials with PFC as an oxygen carrier began in the early 1980s and
since then, improvements in the oxygen capacity and emulsion properties of PFCs have
led to second-generation PFC-based oxygen carriers. Despite product improvements and
ongoing clinical trials, the products appear to cause several unwanted side effects,
therefore, development is proceeding slowly.
Synthetic platelets have been developed for treating thrombocytopenia associated
with the cancer chemotherapy. They mimic platelet activity in that they target the site of
hemorrgage where clot formation is enhanced or initiated. However, treatment with

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 14 -
platelet preparations has several problems including potential infectivity with blood borne
viral contaminants, alloimmunization in 30% to 70% of patients, a short half-life, and
febrile reactions with transfusions.
Other synthetic blood products include factor products for the treatment of
hemophilia, which have been successfully commercialized.
BLOOD PRODUCTS MARKET The market for human blood and blood components continues to expand as a
result of the growing and aging populations, particularly in the developed nations. In
2007, worldwide demand for non-infected blood exceeded 200 million pints. Of this, red
blood cells (RBCs) comprised 85 million units. Through 2014, global demand for RBCs
is expected to reach 133 million units. Much of this need is for the management of acute
blood loss, with approximately 50 million units required in 2007. Aside from RBCs,
other blood products are also often required in such procedures. Organ transplants, for
example, typically require 30 units of platelets, 20 bags of cryoprecipitate and 25 units of
fresh frozen plasma while burn treatment requires 20 units of platelets, on average.
In 2007, the total global value of all human-derived blood products was $16.2
billion, as shown in Table 1-1. Of this, an estimated $9.2 billion was attributable to red
blood cells while $3.3 billion was from immunoglobulins, $759 million to albumin and
$2.8 billion to other human plasma-derived products such as plasma, platelets, clotting
factors, prothrombin complex concentrates, fibrin sealants and alpha-1 proteinase
inhibitor (API).
While some countries such as India and the Philippines set prices for blood and
blood components, in many of the developed nations including the U.S., there is no
uniform, fixed price for blood. Rather, the cost varies from country to country and region
to region, with even nearby centers often charging different prices and fluctuations often
occurring. Established in 1953 by the American Association of Blood Banks, the
Washington, D.C.-based National Blood Exchange (NBE) coordinates the distribution of
more than 300,000 units of blood and blood components throughout the U.S. each year.
In return for a transaction fee of 1% charged to both the shipper and the receiver, the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 15 -
NBE responds to requests for blood from hospitals facing shortfalls in their supply,
locating blood resources and arranging deliveries.
Table 1-1
Global Blood Products Market, 2007
Market value in millions RBCs $9,265 Immunoglobulins 3,300 Albumin 759 Other Plasma Products 2,880 Total $16,204
Source: Kalorama Information
Of red blood cells (RBCs), platelets, plasma and cryoprecipitate, RBCs are
generally the most expensive component of whole blood. The unit price of RBCs,
however, varies with a number of factors including blood type and special preparation
methods but overall, has continued to rise through the years. This trend is expected to
continue through the foreseeable future.
Plasma collection continues to rise, with more than 26 million liters collected in
2007, as compared with about 10 million liters in 1995. In 2007, worldwide sales of
plasma and plasma derived products comprised approximately $7.0 billion. This includes
plasma, albumin, platelets, fibrin sealants, immunoglobulins, alpha-1 proteinase
inhibitors, clotting factors such as Factor VIII and other products. Through 2014,
compound annual growth will accelerate to 8.5% per year from an estimated 7.0% per
year during the 2002 – 2007 period. The U.S. will remain the single largest global
market, accounting for more than half of all plasma product sales.
Global demand for immunoglobulins, or antibodies, is rising by 6% - 8% per year
and remains the driving force behind plasma collection. The total worldwide market for
all immunoglobulin products is estimated at about $3.3 billion in 2007. The bulk of this is
comprised of IVIG, particularly broad spectrum, polyvalent products.
The market for albumin products for all applications, including usage as a blood
volume expander, other therapeutic uses and experimental use, comprised a significant

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 16 -
portion of the overall market for plasma products at more than $0.7 billion in 2007. The
market is mature and has become subject to a high level of generic competition. Low
product differentiation and declining prices are the key reasons for the rapid value decline
in the market. However, prices have begun to stabilize so that through the forecast period,
rising demand will lead to compound annual growth of 2.2%.
BLOOD TESTING AND TYPING PRODUCTS MARKET Because of the need to continually utilize the most advanced technologies that
will provide the lowest level of blood contaminants, particularly in the developed
markets, sales of older immunoassay technology remain relatively flat while sales of
newer nucleic acid tests are growing briskly. Global sales of immunoassays are expected
to rise by about 2% per year from $610 million in 2007 to $700 million in 2014 while
nucleic acid tests will increase by 11.5% from $953 million to about $2,046 million
during this time. Due to their lower cost, immunoassays and/or in-lab developed PCR
tests tend to be utilized more frequently in the developing nations while nucleic acid
testing is used predominantly in the developed countries, although this is slowly
changing.
In 2007, the global market for HIV tests was the largest, at $336 million, followed
by HCV with $269 million, WNV at $257 million and HBV at $254 million, as shown in
Table 1-2.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 17 -
Table 1-2
Global Projected Blood Banking and Plasmapheresis Molecular Diagnostics Testing Market Estimate: 2007–2014
Type of Test Year HIV HCV HBV HAV HTLV WNV Others Total 2007 $336 $269 $254 $235 $0 $257 $214 $1,564 2014 $437 $350 $334 $306 $239 $328 $284 $2,279
Source: Kalorama Information
Due to the significant technological barriers to entry, the market for immunoassay
blood testing products is dominated by a handful of companies. Outside of Asia, the
market for immunoassay blood screening is controlled by two companies—Abbott
Laboratories and Ortho Clinical Diagnostics. Abbott and Ortho hold approximately 75%
of the blood screening business with Bio-Rad/Sanofi/Genetic Systems, Diasorin and
bioMérieux taking the remaining 25%. In Asia, primarily Japan, Thailand, Korea and
Taiwan, the majority of blood banks use Fujirebio's RPHA (Rapid Particle
Hemagglutination) tests run on Olympus Optical's PK instruments for HIV and HTLV
testing. A number of nucleic acid tests are commercially available for use in donor
screening by blood banks and plasmapheresis centers. First to come to market, the Chiron
Procleix HIV-1/HCV assay and system have been used in IND clinical trials at the
American Red Cross, America's Blood Centers, and the Association of Independent
Blood Centers since April 1999. In 2007, Chiron owned more than three quarters of the
U.S. market.
Blood typing reagents and instruments are used by blood transfusion services,
hospital and private blood banks, and hospital laboratories that prepare blood units for
transfusion to patients. More than 80% of blood typing is done in hospitals. In 2007, this
market segment is valued at $510 million and with 2% expected annual growth will
increase to $585 million in 2014. The sector has seen significant growth in the past
several years related to investment in automated and gel-based techniques in the U.S. that
remove the subjectivity of reading blood group tests and also free technologists to
perform other tasks. Despite recent expansion, only three major companies remain active
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 18 -
in the market for blood grouping reagents - Olympus, Ortho Clinical Diagnostics and
Immucor. These three companies hold 90% of the market with local suppliers and in-lab
developed tests used in less regulated emerging countries.
PLASMA AND BLOOD COLLECTION EQUIPMENT MARKET The market for plasma and blood collection equipment is broad, encompassing
both manual and automatic systems for collection, leukocyte reduction, post-collection
component processing and storage as well as IT applications for blood centers. Although
automated collection systems are more expensive than manual systems, they are also
faster, more efficient and offer greater safety to blood donors. Because of this, their usage
is growing relatively briskly.
The market for blood equipment has been expanding at a steady pace over the
past several years, although the plasma collection segment has experienced some recent
flux due to shifts in the number of plasma collection centers. In 2007, the total global
market for all blood center equipment reached $2.1 billion, as shown in Table 1-3, with
automated equipment comprising $500 million of this. By 2014, total sales of blood
collection equipment will reach $2.9 billion, of which automated equipment will account
for $829.4 million.
The market for automated blood and plasma collection equipment is controlled by
Haemonetics, Abbott Laboratories and Baxter International. Competition is based on
performance, as measured by the time and efficiency of component collection and the
quality of the components collected. The top players in the leukocyte reduction segment
tend to be distinct from those in the automated collection equipment market. In 2007, BD
Biosciences remained the market leader with its BD LeucoCOUNT assay, which is used
on an automated or manual flow cytometer. Other developers are also working on novel
automated systems, particularly focusing on optimization of bacteria and virus
inactivation. This is in part a result of the AABB’s guidelines, published in March 2004,
instructing blood centers to test all platelet components for the presence of bacteria.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 19 -
Table 1-3
Global Market for Blood Collection Equipment: 2007–2014
Year
Total Market Revenue in $ Billion
Automated Equipment Revenue in $ Billion
2007 2.1 0.5 2014 2.9 0.8
Source: Kalorama Information
SYNTHETIC BLOOD PRODUCTS MARKET Around the world, demand for blood continues to exceed supply. Because they
are not dependent upon voluntary donations, and therefore can be manufactured in
quantities that will meet demand, synthetic blood products represent an important means
to address shortfalls between supply and demand for human blood.
The market for recombinant factors stands at more than $5.6 billion in 2007 and is
expected to rise to more than $10.1 billion by 2014, as shown in Table 1-4. While in the
past, growth was driven by conversion from plasma-derived therapies, adequate dosing
and compliance, and increasing prophylactic use of recombinant therapies, future gains
will be fueled by continuing improvements in products, including expanded indications
and enhanced delivery systems. Baxter remains the undisputed leader in the recombinant
factor market with its Advate, although competitors such as NovoNordisk and Bayer
continue to expand usage of their products.
The market for emerging hemoglobin-based oxygen carriers (HBOCs) and PFC-
based products is projected to reach nearly $1.1 billion by 2014, as major HBOC and
PFC products reach the market by 2010. Developers with high potential products include
Biopure and Northfield Laboratories.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 20 -
Table 1-4
Recombinant Factor and High Blood Loss Market: 2007-2014
Year
Recombinant Factor Revenues(in millions)
HBOC and PFC Agent Revenues (in millions)
2007 $5,608 $0 2014 10,189 1,150
Source: Kalorama Information
White Blood Cells (Leukocytes)

Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 21 -
C H A P T E R T W O
Overview
THE GLOBAL BLOOD INDUSTRY The global blood industry represents a diverse assortment of companies, groups
and organizations that have evolved over time to provide for the safe collection, testing,
storage and delivery of human blood, synthetic blood and blood products for transfusion.
These blood transfusions are of critical importance to those with both acute and chronic
medical conditions in which blood is depleted or non-functioning: according to U.S.
statistics, 4.5 million Americans would die each year without blood transfusions and the
National Blood Service of England and Wales says that in 2007, more than one million
persons received blood donations.
The following sections provide highlights of the blood industry’s technological
development and a background on the physiological aspects of human and synthetic
blood.
HISTORY OF THE BLOOD INDUSTRY Although the notion of using one person's blood to heal another is less than 100
years old, scientists had experimented with transfusing animal blood as early as the
1600s. Later, the first transfusion experiments utilizing human blood involved stitching a
donor's vein (in early cases the physician's) to a patient's vein.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 22 -
The modern blood industry, however, developed primarily in response to World
War II and the unprecedented need for blood in the medical treatment of casualties. The
world’s deadliest war to date, World War II resulted in more than 72 million military and
civilian casualties. Particularly outside the U.S. and Western Europe, many of these could
have been prevented with greater usage of blood collection, storage and transfusion
technology. However, developments in the large-scale storage and use of blood between
the first and second world wars laid the groundwork for progress that was rapidly made
in the late 1940s and beyond. Table 2-1 shows key events in the development of blood
collection technology.
United States
The United States is among the leaders in the development of the global blood
industry, although the country continues to experience long-standing problems related to
blood supply safety. In 1941, at the request of the Surgeon General of the U.S. Army and
Navy, the American Red Cross organized a civilian blood donor service to collect blood
plasma for the war effort. The first center opened in New York and the Red Cross
collected over 13 million units of blood over the course of World War II. Following the
attack on Pearl Harbor, victims were successfully treated with albumin to increase blood
volume. As scientists learned to separate blood into its components, such as freeze-dried
plasma and clotting factors, battlefield survival improved significantly.
After the war, the Red Cross initiative gave way to a nationwide network of blood
banks that collected blood for civilian hospitals with the first federal license allowing an
establishment to manufacture whole blood in 1946. The American Association of Blood
Banks was officially established the following year.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 23 -
Table 2-1
Timeline of Global Blood Industry Development 1922 - 2008
Year Event 1922 Percy Lane Oliver begins operating a blood donor service out of his London home, recruiting
volunteers who travel to local hospitals to give blood. 1930 Dr. Serge Yudin in Moscow is the first to test the efficacy of transfusing humans with cadaver
blood. He successfully resuscitates a young man who slashed his wrists by injecting him with 420 cc of blood from a cadaver. The Soviets become the first to establish a network of facilities to collect and store blood for use in transfusions at hospitals.
1935 The Mayo Clinic in Rochester, MN, having organized a transfusion service two years earlier, is the first to begin storing citrated blood and using it for transfusions at a U.S. hospital.
1936 Physician Federico Duran-Jorda establishes the Barcelona Blood-Transfusion Service. The service collects blood, tests it, pools it by blood group, preserves and stores it in bottles under refrigeration, and transports it to front line hospitals during the Spanish Civil War.
1939 Baxter introduces the Transfuso-Vac container, the first sterile, vacuum-type blood collection and storage unit. Before this, blood could be stored for only a few hours; the new container allowed storage for up to 21 days, making blood banking practical.
1940 A plasma shortage in Britain during World War II prompts the U.S. to organize the Plasma of Britain campaign, run by Dr. Charles Drew at Presbyterian Hospital in New York. Using techniques to separate and preserve blood plasma, Dr. Drew devises a sterile system to process, test, and store plasma for shipment overseas by the Red Cross. Separately, Harvard biochemist Edwin Cohn invents a method to separate out different proteins (or fractions) from plasma, allowing isolation of fibrinogen (Fraction I), gamma globulin (Fraction II and III), and albumin (Fraction V).
1941 Baxter introduces the Plasma-Vac container, providing the first means of separating plasma from whole blood and storing it for future use.
1948 Dr. Carl W. Walter develops a plastic bag for the collection of blood, revolutionizing blood collection. Prior to this, glass bottles were used to store blood, which were both fragile and susceptible to contamination.
1959 Using X-ray crystallography, Dr. Max Perutz at Cambridge University, England, unravels the structure of hemoglobin, the oxygen-carrying protein in red blood cells.
Late 1960s Drs. Ken Brinkous of UNC Chapel Hill and Ed Shanbrom of Hyland Labs produce a highly concentrated form of Factor VIII by pooling large quantities of plasma that generate vast amounts of cyro. The powder's clotting power is 100 times stronger than raw plasma, easily stored in a portable vial, and injectable.
1979 Baxter introduces the first automated blood-cell separator, the CS-3000 system. 1981 The first cases of GRID (Gay-related Immunodeficiency Disease) are reported. It is later
renamed AIDS (Acquired Immune Deficiency Syndrome) as hemophiliacs and others outside the gay community are affected.
1984 Dr. Robert Gallo of the NIH identifies the virus that causes AIDS. 1985 After dozens of Americans are infected with AIDS from blood transfusions, the first blood-
screening test to detect the presence or absence of HIV antibodies - the ELISA test - is licensed by the U.S. government and is universally adopted by U.S. blood banks and plasma centers.
1987 - 2008 A series of more sensitive tests are developed to screen donated blood for infectious diseases: tests that screen for indirect evidence of hepatitis; the anti-HTLV-I test; the hepatitis C test; the HIV-1 and HIV-2 antibodies test; the HIV p24 antigen test; and Nucleic Acid Amplification Testing (NAT) that directly detects the genetic material of viruses like HCV and HIV.
Source: Educational Broadcasting Corporation.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 24 -
In 1971, the Secretary of Health, Education, and Welfare transferred the
responsibility of regulating the blood banking industry from the Division of Biologics
Standards (DBS) to the U.S. Food and Drug Administration (FDA). The FDA
subsequently established an annual inspection program that monitors donor screening,
blood testing, labeling, storage and handling, record keeping and other practices. Blood
centers must promptly correct any and all problems, and investigators typically verify
resolution of deficiencies through follow-up inspections. As technology develops and
new information about the transmission of infectious diseases becomes available, FDA's
Center for Biologics Evaluation and Research (CBER) issues written guidance to all
blood establishments. This guidance is incorporated into standard operating procedures
for all blood facilities and is also supported by the country’s major blood organizations,
including the American Red Cross, the American Association of Blood Banks, the
Council of Community Blood Centers, and the American Blood Resources Association.
Improvements continue to be made in blood screening techniques, with a
significant reduction in the release of unsuitable blood compared with the late 1980s and
early 1990s. The identification of the HIV virus in the mid 1980s led to the 1996
introduction of the first test kit to screen blood for antigens to HIV-1 (the virus that is
responsible for the vast majority of U.S. AIDS cases). Three years later, Ortho
Pharmaceuticals introduced the first fully automated blood and plasma screening system.
However, these improvements have fallen far short of necessary updates. Since
1993, the American Red Cross (ARC), which currently controls 43% of the U.S. blood
supply, has been under a federal court order to improve its collection and processing
systems. Yet despite $21 million in fines imposed since 2003, the first year in which the
FDA could levy penalties against the organization, the ARC continues to fall short. In
January 2008, FDA commissioner Andrew C. von Eschenbach attended a Red Cross
board meeting and warned that members could face criminal charges for their failure to
meet compliance objectives. Lapses include the distribution of more than 200 potentially
contaminated blood products between December 2006 and April 2008, 134 cases of
suspected post-transfusion hepatitis from January 2000 to June 2002, as well as faulty
internal monitoring processes and a history of falsified records. Critics of the
organization note that while blood revenues, at $2.1 billion in 2007, represent more than

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 25 -
two thirds of the ARC’s business, the organization continues to focus most of its fund-
raising and other activities on its much smaller disaster relief operations.
In parallel with the development of a whole blood industry, a large U.S. plasma
industry has evolved to supply both medical and research facilities. As of mid 2008, the
U.S. supplies about 60% of the world’s plasma and about 40% of the plasma used in
Europe alone. While the U.S., like France, had formerly obtained plasma from its prison
population, this practice was discontinued in the early 1980s after prison plasma was
linked to high rates of contamination from infectious disease. However, the U.S. remains
one of the few countries that allows for payment of plasma donors, permitting donors to
give twice a week. This compensation, which is typically about $40 for twice-a-week
contributions, offsets the unpleasantness of the plasmapheresis procedure, in which the
blood is drained through a drinking straw-sized needle over the course of 45 minutes
while plasma is removed and red cells are cycled back in.
Europe
The European blood industry developed largely in tandem with its U.S.
counterpart, as a means to improve survival of World War II soldiers. Some countries,
however, lagged others.
Nazi Germany, for example, accepted only blood from Aryan donors in an effort
to maintain racial purity of its population. This resulted in significantly lower supplies of
blood, which stalled the development of modern transfusion products. During this time, a
variety of largely unfruitful experiments were conducted including draining blood from
prisoners of war (POWs) and injecting them with horse blood or polymers.
Following the war, products and procedures to improve the safety of blood
products continued to be implemented at a somewhat slower pace in Europe than in the
U.S. In postwar France, giving blood was viewed as a patriotic act and volunteer donors
were rarely questioned about their medical history or sexual or drug practices. This led to
blood banks collecting blood from high-risk groups as late as 1990, well into the HIV
crisis. France and Britain further stalled the approval and distribution of safer, American
heat-treated plasma products when they became available to give their domestic
companies time to catch up with scientific advances. In Germany, officials at Coblenz-
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 26 -
based UB Plasma were brought to trial in 1994 for repeatedly ignoring information given
by blood donors suggesting the donors might be carrying the AIDS virus.
Asia
Although Asia has since closed the gap in blood transfusion technology, the
region significantly lagged Europe and the U.S. following World War II. Like Germany,
Japan sought to preserve its racial purity and was slow to adopt war-time transfusion
techniques. When blood was collected and transfused, techniques were often primitive,
resulting in a high number of transfusion-related casualties.
Following the war, blood collection procedures improved with the reorganization
of the Japanese Red Cross (JRC) under American advisers. This affiliation provided for
much needed technology transfer that modernized Japan’s blood industry. Improvements
continued to be made and by 1966, Japan had become a primary source for the whole
blood used in the Vietnam War. Mobile bleeding teams were dispatched from the 406th
Medical Laboratory in Japan to donor resources in Japan, Korea, Okinawa, and Taiwan to
collect, screen, test and store blood for the rising wartime demand. Screening for
infectious diseases has continued to progress, with improvements made concurrent with
or only shortly after improvements in U.S. and European technology. In 1989, for
example, the Japan Red Cross started screening donated blood for anti-HCV.
However, the contamination issues that have plagued other blood supplies have
also been present in Japan. In the mid 1990s, Japanese patients charged that the
government and drug companies criminally concealed the contamination of blood
products, resulting in the arrest and incarceration of some of the nation's most revered
doctors. In 2004, JRC officials said that blood potentially tainted with HIV, which had
been collected from eight donors at risk of having HIV, had been used in transfusions.
Around the new millennium, the Japanese Ministry of Health launched a national
initiative to become self-sufficient in plasma collection, announcing plans to gradually
reduce the import of plasma fractionated products from other countries while increasing
domestic plasma collections. This is an attempt to meet the country's need for plasma-
derived pharmaceuticals, including albumin, globulin, and Factor VIII products. As of

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 27 -
mid 2008, the Japanese Red Cross collected less than 1 million liters of plasma each year,
but needs to reach 1.5 million liters.
BLOOD AND ITS COMPONENTS
Blood performs two major functions. It transports materials such as oxygen and carbon dioxide, food molecules (glucose, lipids, amino acids), ions (e.g., Na+, Ca2+, HCO3
−), wastes and hormones, as well as heat through the body. Blood also defends the body against infections and foreign materials.
A liquid tissue, the blood is comprised largely of watery plasma. Suspended in the plasma are seven types of cells and cell fragments:
• red blood cells (RBCs) or erythrocytes;
• five kinds of white blood cells (WBCs) or leukocytes including two types of leukocytes without granules in their cytoplasm - lymphocytes and monocytes;
• platelets or thrombocytes;
• three types of granulocytes;
• neutrophils;
• eosinophils;
• basophils.
All of these types of blood cells are produced in the bone marrow—about one
trillion of them each day in an adult human – and arise from stem cells. The stem cells
are very rare, representing only about one in 10,000 bone marrow cells. They are attached
to osteoblasts lining the inner surface of bone cavities and produce, by mitosis, two kinds
of cells: more stem cells and cells that begin to differentiate along the paths leading to the
various kinds of blood cells.
Normally, the human body will replace lost plasma volume, platelets, and red
cells in about 24 hours, 2 days, and 56 days, respectively. Each donation of one pint of
blood burns about 650 calories, according to the Mayo Clinic.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 28 -
Red Blood Cells (Erythrocytes) Red blood cells (RBCs) are responsible for the transport of oxygen and carbon
dioxide. They are the most numerous types of cell in the blood, outnumbering white
blood cells, for example, by about 700:1. Women average about 4.8 million RBCs per
cubic millimeter (mm3) or microliter (µl) of blood. Men average about 5.4 million x 106
per µl. These values can vary significantly depending on such factors as health and
altitude. For example, Peruvians living at high 18,000 foot altitudes have been found to
have as many as 8.3 x 106 RBCs per µl. As RBC precursors mature in the bone marrow,
they manufacture hemoglobin until it accounts for 90% of the dry weight of the cell. As
this occurs, the nucleus is squeezed out of the cell. Nearby macrophages then ingest the
extruded nuclei and break down their DNA.
Thus RBCs are terminally differentiated; that is, they can never divide. They live
about 120 days and then are ingested by phagocytic cells in the liver and spleen. Most of
the iron in their hemoglobin is reclaimed for reuse. The remainder of the heme portion of
the molecule is degraded into bile pigments and excreted by the liver. About 3 million
RBCs die each second. Transfusions of RBCs are typically used to treat trauma, anemia
and surgery patients.
White blood cells (WBCs) are much less numerous than the RBCs. The WBCs
participate in protecting the body from infection, consist of lymphocytes and monocytes
with relatively clear cytoplasm, and three types of granulocytes (neutrofils, eosinofils and
basofils), whose cytoplasm is filled with granules.
There are several kinds of lymphocytes, each with different functions to perform.
The most common types of lymphocytes are B lymphocytes ("B cells"). These are
responsible for generating antibodies. T lymphocytes ("T cells") include several
subtypes:
• inflammatory T cells that recruit macrophages and neutrophils to the site of infection or other tissue damage;
• cytotoxic T lymphocytes (CTLs) that kill virus-infected and tumor cells;
• helper T cells that enhance the production of antibodies by B cells.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 29 -
Both B cells and T cells reside in the lymph nodes, spleen and other tissues where
they encounter antigens; they divide by mitosis and mature into fully functional cells.
Monocytes leave the blood and become macrophages. Macrophages are large,
phagocytic cells that engulf foreign material (antigens) that enter the body.
Neutrophils are the most abundant of the WBCs. These granulocytes squeeze
through the capillary walls into infected tissue where they kill bacteria and then engulf
the remnants by phagocytosis. The number of eosinophils in the blood is normally quite
low (up to 450/µl). However, their numbers increase sharply in certain diseases,
especially infections by parasitic worms. Eosinophils are cytotoxic, releasing the contents
of their granules on the invader. The number of basophils also increases during infection.
Basophils leave the blood and accumulate at the site of infection or other inflammation.
There they discharge the contents of their granules, releasing a variety of mediators such
as histamine, serotonin, prostaglandins and leukotrienes, which increase blood flow and
add to the inflammatory process. The mediators released by basophils also play an
important part in some allergic responses such as hay fever and an anaphylactic response
to insect stings.
Platelets Platelets are cell fragments produced from megakaryocytes. Blood normally
contains 150,000 to 350,000 platelets per microliter (µl). If this value drops much below
50,000/µl, there is a danger of uncontrolled bleeding because of the essential role that
platelets play in blood clotting. When blood vessels are cut or damaged, the loss of blood
from the system must be stopped before shock and possible death occur. This is
accomplished by the solidification of the blood, a process called coagulation or clotting.
A blood clot consists of a mass of platelets enmbedded in a network of insoluble fibrin
molecules. Platelet transfusions are typically used for cancer patients receiving
chemotherapy, particularly to alleviate the effects of bone marrow suppression.
Plasma Plasma is the straw-colored liquid in which blood cells are suspended. As shown
in Figure 2-1, it is comprised mainly of water, and to a considerably lesser extent, of
proteins, salts, lipids and glucose.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 30 -
Plasma transports materials needed by cells and materials that must be removed
from cells, including: various ions; glucose and traces of other sugars; amino acids; other
organic acids; cholesterol and other lipids; hormones; and urea and other wastes.
Transfusions of plasma are mainly used for burn patients while fresh frozen plasma is
used for massive transfusions.
Figure 2-1
Composition of Blood Plasma
Water, ~92.0%
Salts, 0.8%
Glucose, 0.1%
Lipids, 0.6%
Proteins, 6% to 8%
Source: Kalorama Information
IMMUNOGLOBULIN PRODUCTS Found in the blood, tissue fluids as well as many secretions, immunoglobulins are
glycoproteins (molecules composed of proteins and carbohydrates) that function as
antibodies. Often, the terms antibody and immunoglobulin are used interchangeably. In
terms of structure, immunoglobulins are one of the two types of serum proteins, the other
being albumin. Immunoglobulins primarily contain immunoglobulin type G (IgG) as the
active component and are synthesized and secreted by plasma cells that are derived from
the B cells. These B cells are activated upon binding to their specific antigen and
differentiate into plasma cells. In some cases, the interaction of the B cell with a T helper
cell is also necessary.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 31 -
Immunoglobulin products are polyclonal antibody-rich fractions obtained from
pooled fractionated and purified human blood plasma. They may also be derived from
animal plasma, in the case of antivenins and antitoxins. Immunoglobulin products are
generally used for passive immunization, as antibody-based immunity can be
immediately transferred to a person by injection of immunoglobulin preparations.
To assure a consistent and broad spectrum of antibodies in the product and
economies of scale, non-specific or regular immunoglobulin products are usually
produced from pooled plasma from at least 1,000 donors.
However, immunoglobulins derived from selected plasma obtained from persons
with high titers of specific antibodies (from prior antigen exposure) can be used to
produce specialized preparations enriched with these specific antibodies. For example,
immunoglobulin prepared from plasma with high hepatitis B virus surface antigen
(HBsAg) antibodies, which is derived from persons immunized with a hepatitis B virus
vaccine, can be used to prepare immunoglobulin with a high level of HBsAg antibodies,
i.e., Hepatitis B Immunoglobulin.
BLOOD TRANSFUSIONS Over 40 million red cell units are transfused annually in North America, Europe
and Japan, making blood transfusions one of the most frequently utilized therapeutics in
medicine. Some of these units (whole blood) are transfused directly into patients to
replace blood lost by trauma or during surgery. Most are further fractionated into
components, including:
• RBCs, which when refrigerated can be used for up to 42 days;
• platelets, which must be stored at room temperature and thus can be saved for only 5 days;
• plasma, which can be frozen and stored for up to a year.
Patients who require blood transfusions generally fall into two categories: those
who require transfusions resulting from acute blood loss that might be associated with
surgery; or those requiring chronic transfusions associated with treatment for chronic

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 32 -
anemia, chemotherapy, or bone marrow transplant. More than 50% of transfusions occur
in patients over the age of 65.
Although the global demand for blood increased over the last decade, the supply
of blood has declined. The current worldwide supply of blood for transfusions stands at
60 million pints per year, while the worldwide demand for blood has reached 180 million
pints per year. This trend is expected to continue, particularly since the over 65
population in the U.S., Europe and Japan is increasing at a faster pace than the overall
population. In the U.S., for example, the 65+ years segment is expected to double in the
next 30 years. Thus, as the "baby boomer" population in the United States ages and
requires more blood, the prime donor age population will shrink, exacerbating the
shortfall.
Diseases Contracted from Blood Transfusions and Related Identification Testing A variety of infectious agents can be present in blood, including viruses (e.g.,
HIV-1, hepatitis B and C, HTLV, West Nile virus), bacteria, protozoans, Chagas disease,
Lyme Disease and prions (e.g., the agent of variant Crueutzfeldt-Jakob disease or vCJD,
which is the human form of mad cow disease). In the United States, the risk of acquiring
an infectious disease from allogenic blood ranges from 1:60,000 for hepatitis B to
1:500,000 for HIV, with transmission rates for other viruses, such as hepatitis C and the
human T-cell leukemia virus, intermediate between these. Blood supply safety in Europe
is similarly high due to the introduction of viral nucleic acid testing (NAT) in the mid
1990s. As of mid 2008, the main residual risk is due to hepatitis B virus - ranging from
10 in Spain to 1.6 per million donations in France and Germany – although other
conditions may pose relatively high risk in certain regions.
Regulators in the developed nations continue to monitor blood supply safety and
implement methods to improve safety risks. In the U.K., 50 persons who received blood
transfusions were warned they may have been exposed to vCJD and a similar warning
was issued to around 100 blood donors whose blood had been given to recipients who
later developed the brain disease. To reduce the possibility of further transmission, the
donors were asked not to donate blood, tissue, or organs, and to inform doctors of their
position if they require surgery. In Canada, a criminal trial in 2006 charged a physician

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 33 -
with allowing HIV-infected blood-clotting product to be given to hemophilia patients in
the 1980’s and 1990’s. More than 1,000 people became infected with HIV and up to
20,000 others contracted hepatitis C through the transfusion of blood and blood products
during what is considered by some to be Canada’s worst public health disaster.
To minimize such occurrences, the red cell antibody screening and identification
methods that have long been in place in the developed countries continue to be expanded
and improved. Typical safeguards include:
• donor screening: potential donors are informed about risks and must provide information about factors that may affect the safety of their blood;
• donor deferral: potential donors with a history of intravenous drug abuse are routinely deferred; those who have lived in European countries with reported or suspected cases of mad cow disease may also be deferred;
• donor lists: blood collection centers keep lists of deferred donors and ensure that they do not collect blood from anyone on the list;
• blood testing: all donated blood is tested for a series of infectious diseases;
• quarantine: donated blood is quarantined until it is shown to be free of infectious agents;
• problems and deficiencies: blood collection centers must investigate manufacturing problems, correct deficiencies, and notify regulators of deviations.
Because of these precautions, disease transmission through tainted blood in the
developed nations remains relatively rare, while the risks of infectious disease
transmission, particularly HIV and hepatitis, in developing countries are considerably
higher. For example:
• while screening of donated blood for HIV is routine in South America, screening for hepatitis B and hepatitis C is not, despite Pan American Health Organization initiatives to do so;
• the prevalence of HIV in Kenyan blood donor populations in 1994 was 20%, and is believed to be even higher now, with 1 in 50 blood transfusions in Kenya transmitting HIV;
• in 2004, 80% of the population of the Chinese village of Donghu was infected with HIV as a result of an unsanitary blood collection and pooling process. At
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 34 -
three blood-collection stations where villagers routinely sold their blood, it was standard practice to pool blood from dozens of sellers, from which plasma was separated. Red cells from the pool were then divided and transfused back into the sellers without prior screening tests on the RBCs. As a result, just one HIV-infected blood seller could taint the entire pool;
• in December 2005, Russian health authorities reported that hundreds of patients were given HIV-infected blood; the tainted blood in the country’s pooled supply was traced to one 35-year-old female donor;
• in June 2008, the World Bank warned of tainted blood transfusions in Central Asia, saying that over the past two years, hundreds of persons have been infected with HIV/AIDS.
Transfusion-Associated Risks Other safety issues regarding the blood supply relate to severe transfusion
reactions. These are most often the result of clerical errors and are estimated to occur at a
frequency of about 1:12–30,000. These can occur for several reasons. For example, fluid
overload can occur when too much fluid is delivered through transfusions, especially if
the patient has not experienced blood loss before the transfusion. Fluid overload may
require treatment with medications to increase urine output (diuretics) to rid the body of
the excess fluid. Additionally, iron overload may occur if a large amount of whole blood
or packed red blood cells is transfused. When red blood cells die, the iron from the
hemoglobin is released and must be stored by the body. Since iron is only slowly lost by
the body, large increases in the amount of iron may overload the body’s ability to store it
and as a result may need to be treated with medications that bind iron.
Additionally, allogeneic blood has been shown to be immunosuppressive, which
may lead to increased risks for certain hospital-related or other infections after
transfusion. These may be mild, moderate or severe:
• nonhemolytic fever reactions cause fever and chills without destruction (hemolysis) of the red blood cells. This is the most common transfusion reaction and can occur even when the blood has been correctly matched and administered;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 35 -
• hemolytic transfusion reactions destroy the transfused red blood cells when they are attacked by the person's immune system. This most commonly occurs if there is a mismatch with the ABO or Rh blood types and can be life-threatening;
• allergic reactions range from mild itching, hives, and wheezing to severe reactions can such as anaphylactic shock, a life-threatening reaction;
• an immune reaction to platelets in transfused blood results in the destruction of the transfused platelets;
• an immune reaction attacking the person's lungs (transfusion-related acute lung injury), resulting in difficulty breathing and other symptoms.
It is also possible for blood, especially platelets, to become contaminated with
bacteria during or after donation. Transfusion with blood containing bacteria can result in
a systemic bacterial infection, which may be difficult to treat depending upon the nature
of the infection and level of bacterial resistance. Because of the precautions taken in
drawing and handling donated blood, this risk is small. The risk of bacterial infection
from transfusions with platelets is somewhat higher since, unlike many other blood
components, platelets are stored at room temperature. Therefore, any bacteria present will
proliferate and cause an infection when the platelets are used for transfusion.
Despite the increased public awareness of issues relating to the safety of the blood
supply, the overall risk of death after allogeneic transfusion is estimated at 1:500,000–
1,000,000 in the United States. When compared with the annualized 1:50,000 risk of
death in an automobile accident, this represents an extremely high and acceptable level of
safety.
EFFORTS TO CREATE A VIRUS-FREE BLOOD SUPPLY Although much progress has been made in the past 50 years to protect the safety
of the blood supply by identifying and screening out donors that may carry harmful
viruses, varying degrees of risk of viral transmission from transfused blood remain
present throughout the world’s blood supply. A variety of methods are being used to
continue to reduce this risk, including plasma treatments, platelet treatments and
utilization of red blood cells.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 36 -
Plasma Treatment Several different plasma treatment methods are currently utilized to inactivate
viruses in donated blood, including pasteurization, vapor heating, low pH and solvent
detergent. Pasteurization and vapor heating may be used on either lipid-enveloped or
non-enveloped viruses, while low pH and solvent detergent treatment are effective only
on enveloped viruses. The development of methods for inactivation of these latter non-
encapsulated viruses remains challenging, since the outer coats of such viruses generally
include proteins similar to the proteins one wishes to retain.
Pasteurization is one of the oldest pathogen inactivation techniques and involves
heat treatment at 60 degrees C for 10 hours in solution. The process, which is also used to
kill viruses in a number of common foods including milk and orange juice, has been
shown to significantly reduce the risk of transmission of hepatitis B, HIV and herpes
viruses from transfused blood. With pasteurization as the sole method of pathogen
inactivation, no cases of transmission of HBV, HAV, HIV, HCV, or HGV (hepatitis G)
have been documented. However, pasteurization is not effective against prions, the
molecules that carry mad cow disease.
Effective viral inactivation may also be achieved by wet or vapor heating under
pressure as well as exposure of the virus to a low pH environment.
Another currently used method is solvent-detergent treatment, which is effective
against lipid-encapsulated viruses (HBV, HCV, HIV), that are susceptible to membrane
disruption by solvents and detergents. This phenomenon has been confirmed by
numerous research groups and the method is now applied worldwide for treatment of
plasma products. For example, incubating plasma at 30° C for four hours using the
organic solvent tri (N butyl) phosphate (TNBP) and the anionic detergent Triton X-100
inactivates more than ten million infectious units of hepatitis B virus, over one million
infectious units of hepatitis C virus, and more than 100 billion infectious units of HIV.
The solvent/detergent compounds are then chromatographically removed after plasma
treatment is completed and have been shown to cause little functional change in plasma
proteins, such as clotting factors. However, this method is not effective against HAV and
parvovirus, which are not lipid encapsulated.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 37 -
These conventional methods are also applicable to emerging threats. In March
2006, Baxter Healthcare announced results of a study confirming that the potentially
deadly Asian bird flu virus (H5N1), an enveloped virus, was readily inactivated through
pasteurization, vapor heating, low pH exposure and/or usage of solvent detergent.
Platelet Treatments Virus inactivation methods focused on platelets dates to the early 1990s with the
investigation of various photoactive compounds, although there are no currently
approved methods for pathogen inactivation of platelet concentrates in the U.S. As shown
in Table 2-2, compounds under investigation include psoralens and dyes activated by
visible light that act by oxygen-dependent generation of reactive molecular species and
UV-activated, intercalating compounds that form covalent adducts with nucleic acids.
In 2003, Cerus Corp. introduced its Intercept system for virus inactivation in
platelets to Europe. Developed in collaboration with Baxter, European trials of the
psoralen-based compound showed comparable efficacy to control platelet concentrates in
thrombocytopenic patients. In vitro experiments with the compound showed elimination
of bacteria, viruses, and parasites on the order of 5 logs. Similar results were found in the
corresponding American study using single donor platelets. Commercialization of the
system is proceeding slowly but steadily, with Cerus announcing various orders and
collaborations in Germany, Spain, Portugal and other countries in 2007 and 2008. In the
U.S., Intercept is in Phase III testing for usage with plasma and platelets. A Phase III
clinical trial evaluating Intercept’s usage for red blood cells was halted after two study
patients developed antibodies to red blood cells treated with S-303, the compound used in
the system.
CaridianBCT (formerly Gambro BCT) subsidiary Navigant Biotechnologies has
also introduced a platelet treatment device, with its Mirasol Pathogen Reduction
Technology (PRT) demonstrating high recovery and survival of platelets similar to those
reported from the Cerus product. Both products are CE-Marked.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 38 -
Table 2-2
Viral Inactivation Methods for Viruses Found in Platelets
Viruses Method VSV, SIN, HIV Aluminum phthalocyanine tetrasulfonates HSV, VSV, PRV Merocyanine VSV Phenothiazine dyes HIV, CMV, SIV Porphyrin derivatives and sapphyrin HIV, DHBV, BVDV, CMV Psoralens, S-59 HIV, DHBV, VSV Psoralens, 8-MOP VSV, SIN, HIV Psoralens, AMT Polio Pulsed laser–UVB radiation BVDV, HIV, VSV, HepA Riboflavin
Source: BioPharm International; company reports.
Red Blood Cell Treatments Virus inactivation treatments for red blood cells are in a considerably earlier stage
of development than platelet therapies, largely due to antibody reactivity challenges.
Table 2-3 shows methods investigated over the past 15 years.
Psoralens are activated at wavelengths at which hemoglobin absorbs (300nm –
400 nm) and interferes with their activation, so they are not useful for red blood cell
treatment. Light-activated dyes that bind with viruses, such as Methylene blue (MB) and
dimethymethylene blue (DMMB), may be used in virus inactivation, but they can have
negative effects on cells. Inactivation by merocyanine 540 has also been proposed, but
albumin inhibits the molecule’s ability to make enveloped viruses sensitive to
photoinactivation, and its activity spectrum overlaps with that of hemoglobin at 570 nm.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 39 -
Table 2-3
Viral Inactivation Methods for Viruses Found in Red Blood Cells
Viruses Method VSV, SIN, HIV Aluminum phthalocyanine tetrasulfonates VSV, FeLV Benzoporphyrin derivative HIV Hypericin PRV, BVDV, VSV, SV-40, PPV Inactine VSV, SIN, HIV Merocyanine 540 VSV, DHBV, VSV, PRV, SIN, HIV Phenothiazine dyes HIV, DHBV, BVDV S-303 VSV Silicon phthalocyanines VSV Phthalocyanines HIV-1, CMV, SIV Porphyrin derivatives, sapphyrin Source: BioPharm International.
SYNTHETIC BLOOD PRODUCTS Synthetic blood products are not actually blood, but oxygen-carrying volume-
replacement solutions. Although efforts are underway to develop artificial cells or to
culture red blood cells (RBCs) from stem cells, present synthetic blood products do not
contain cells, antibodies, coagulation factors, or any of the other myriad components of
blood itself. Synthetic blood substitutes have long been sought for treatment of chronic
and acute anemias, and rapid replacement of blood lost after trauma and are commonly
used a variety of applications including:
• elective surgery;
• preoperative ANH;
• perioperative volume replacement;
• cardiovascular surgery;
• pump priming;
• volume replacement/stabilization;
• trauma;
• perfusion of ischemic tissue;
• thrombolytic therapy;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 40 -
• PTCA;
• sickle cell crisis;
• stroke;
• peripheral vascular disease;
• oxygenation of solid tumors;
• radiotherapy;
• chemotherapy.
However, synthetic blood products are not appropriate in many clinical settings,
such as anemia caused by chronic renal failure, severe blood loss after trauma, leukemic
anemia, or chemotherapy-induced anemia.
Blood Volume Expanders Blood volume expanders are large molecular weight solutions, which when
introduced into the body, pull water from the extracellular fluid compartment into
circulation, such as into plasma and intracellular space. They may be used for a variety of
different applications including hemorrhagic shock, cardiopulmonary bypass, septic
shock, obstetrics, thermal injury, vascular surgery or organ transplantation. In general,
there are two categories of intravenous products available for blood-volume expansion:
crystalloids and colloids.
A crystalloid is a substance in solution that can pass through a semipermeable
membrane, such as the veins. Crystalloids are usually sugar or salt solutions (e.g.,
dextrose or saline) that contain some combination of electrolytes (e.g., sodium, chloride,
potassium) or trace elements. Two of the most popular are normal saline and lactated
Ringer's solutions. In general, crystalloids are inexpensive, easy to obtain and safe. They
work quickly, and excess fluids can be easily eliminated through diuresis. However, since
they contain small particle size solutes, crystalloids rapidly leak out of the vasculature
into the surrounding tissues and therefore, their effects do not last long. Also, large
volumes are required to achieve the desired effect and this may cause edema in certain
patients.
A colloid is a substance in solution that cannot pass through a semipermeable
membrane. These materials include whole blood, plasma, packed red cells and the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 41 -
different types of prepared colloid solutions, both natural and synthetic. Albumin is a
natural colloid since its solutions contain a protein derived from human plasma. Synthetic
colloid solutions are made from sugar or starch molecules. Due to their large molecular
size, they are capable of mimicking some of the properties of naturally occurring plasma
proteins such as albumin.
Hemoglobin Based Oxygen Carriers Oxygen therapeutics are investigational agents designed to deliver oxygen to
tissues and organs as a result of blood loss during surgery, life-threatening blood loss or
other situations in which the body may have diminished oxygen delivery. They do not
have the same properties as whole blood, such as fighting infections or coagulating blood
during wound healing, but rather are designed solely to deliver oxygen.
The delivery of oxygen within the human body is normally provided by the
hemoglobin in RBCs. However, during acute anemia, a short-term condition where RBCs
are not sufficient and oxygen is not adequately delivered, it is critical that oxygen be
delivered safely and effectively. Because oxygen therapeutics are very small molecules,
at just a fraction of the size of an RBC, they can travel in the plasma outside the red cells
and are in immediate contact with the tissue. As a result of this better penetration, oxygen
may be supplied more efficiently along the capillaries between the red cells. Thus,
researchers are studying whether oxygen therapeutics may further enhance oxygen
delivery since they can freely pass obstructions, such as blood clots, clogged arteries and
fat emboli. This may provide benefits in situations where the ischemic rescue of
compromised tissue is needed (e.g. acute myocardial infarction, stroke), in life
threatening blood loss including trauma, and in chemotherapy-induced anemia. These
agents are also being studied for their use during coronary artery bypass grafting (CABG)
surgery, as well as other general surgery procedures including elective orthopedic,
vascular, transplant and urologic surgery in which the loss of RBCs can result in acute
anemia.
In addition to these important therapeutic applications, oxygen therapeutics also
offer several other benefits including the ability to:
• reduce the need for donated blood from a blood bank;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 42 -
• help avoid or reduce the need for donated (allogeneic) red blood cells when used
with blood conservation techniques;
• reduce the transmission of viruses and other contaminants due to a manufacturing
process that includes heat-treatment and filtration;
• avoid the need to be cross-matched since they are free of cell-surface antigens,
which can cause transfusion reactions.
Potential sources of acellular hemoglobin for the preparation of hemoglobin-
based oxygen carriers (HBOCs) include outdated human red blood cells, bovine
hemoglobin, and recombinant technologies. Substantial progress has been achieved in the
development of oxygen therapeutics. There are several HBOCs in Phase II and III of
clinical development. The primary focus of these trials is to determine the safety and
efficacy of HBOCs to reduce or eliminate patient exposure to donated RBCs. Data from
these studies are expected to support the use of these products as treatments for acute
anemia or as adjuncts to blood conservation techniques used during surgery.
One of the primary reasons for developing oxygen carriers is to ease the projected
shortage in the blood supply, although some approaches for creating HBOCs face similar
supply challenges. It is estimated that 70,000 kg of Hb would be required to replace 20%
of the RBC transfusions in the United States, presenting a considerable challenge to
human HBOC products. Producers of human HBOCs utilize the Hb from expired RBC
products and the projected blood supply shortage might be expected to adversely affect
this approach.
Production of human Hb by recombinant DNA technology is another approach
taken by some producers but it is unclear whether this technology is capable of producing
these massive quantities. One interesting twist on recombinant technology is the
engineering of transgenic pigs that are reported to stably produce up to 50% human Hb.
This source is estimated to require ~100,000 transgenic pigs and is an expensive and
lengthy proposition. In contrast, HBOC manufacturers that base their products on bovine
Hb are unlikely to face a supply problem.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 43 -
Immunologic Properties
In early attempts to use Hb solutions as oxygen carriers, anaphylactoid side effects
were common. These were mainly due to the phospholipid content of residual RBC
stroma that nonspecifically activated the complement cascade. Today, ultra filtration and
purification techniques result in stroma-free HBOC solutions.
Another immunologic challenge facing the nonhuman HBOC products is the
possibility of specific immune responses to the foreign Hb molecule. These concerns
have been lessened by studies demonstrating that Hbs in general are very poor
immunogens and that the intravenous route of administration is a poor way to generate an
immune response. Immune responses to foreign Hb have not been a significant concern in
phase I and II trials, but whether a patient has ever received multiple doses of these
products is unknown. Finally, there are conflicting animal studies that report that soluble
Hbs are immunosupressive and increase the risk of acquiring infections. Several studies
suggest that the Hb molecule suppresses macrophage function, thereby increasing the risk
of peritonitis and other infections.
Vasoactive Properties
A significant challenge facing development of HBOCs is their effect on vascular
tone as manifested by the hypertension observed in early studies of soluble Hb. Animal
studies with current HBOCs continue to demonstrate this vasoconstrictive effect but are
also helping scientists to understand the mechanisms of this effect. Increases in diastolic
and systolic pressures of 10% to 35% peaking 15 minutes to 30 minutes after
administration and returning to baseline by 2 hours have been observed in some animal
studies.
The clinical significance of the vasoconstrictive properties of soluble HBOCs in
humans is currently unknown, although several anecdotal accounts of early clinical trials
report that hypertension was not observed. Furthermore, as phase II trials of several
products are nearing completion and with phase III trials planned, this property likely has
not raised significant safety questions. In addition to polymerization that prevents
extravasation into the endothelium, other methods under investigation to overcome this
property of soluble Hb have focused on genetic engineering. These include modifying

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 44 -
cysteine residues on the Hb molecule that are important for NO binding and transport and
cross-linking the Hb molecule to SOD or catalase.
Performance
The HBOC trials currently in progress include their use in trauma, acute
normovolemic hemodilution (ANH), and cardiopulmonary bypass surgery. Although
information from the phase I and II safety and dose escalation trials with HBOC products
is closely guarded, recent animal data with current HBOC products is promising. For
instance, one study in sheep replaced 95% of blood volume with a bovine Hb HBOC
product, and these animals showed only minor increases in blood pressure, normal cardiac
output, normal venous PO2 and O2 content, and recovery to a hematocrit of 20% by day
10. Similar impressive results have been observed in studies involving other HBOC
products in baboons and rats. Preliminary reports of HBOC products suggest few side
effects and satisfactory outcomes. These suggest that the use of HBOC products in
humans may be possible in the not-too-distant future as one means to minimize allogeneic
blood exposure.
Perflurocarbon (PFC) Based Blood Products PFCs are chemically inert, water insoluble, synthetic aromatic or aliphatic
compounds with fluorine substituted for all hydrogen atoms. Initially developed during
World War II’s atomic bomb-making Manhattan Project as a chemically inert solvent for
handling highly reactive uranium compounds, PFCs are also the basis of several
important commercial products, such as Teflon and Scotchguard. The electron-dense
fluorine atoms result in little intramolecular interaction and low surface tension making
PFC molecules excellent solvents for gases. Indeed, some PFC products can dissolve 100
times more O2 per volume than plasma. Unlike the cooperative binding of O2 by Hb, the
O2 capacity of PFCs is linearly related to PO2 and obeys Henry's law.
The first clinical trials with PFC as an oxygen carrier began in the early 1980s
with Fluosol from the Green Cross Corp. of Japan. However, the insolubility of PFCs in
water necessitates their use as emulsions. One drawback of this product for use as an
oxygen carrier was the high viscosity of the emulsion, which limited the concentration of
Fluosol that could be infused and thus its capacity to carry and deliver O2. Even at a PO2

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 45 -
of 66.6 kPa (500 mmHg), the 20% Fluosol that could be infused contained only 50 mL/L
O2. In an early clinical trial of patients with acute anemia, Fluosol did not provide
sufficient oxygenation to improve outcomes. Nevertheless, Fluosol is the only blood
substitute product currently approved by the FDA for clinical use. Fluosol is approved for
supplemental oxygenation of ischemic tissue in PTCA because of its ability to diffuse
into poorly vascularized tissue.
Developmental Status
Since the mid-1980s, improvements in the oxygen capacity and emulsion
properties of PFCs have led to the investigation of second-generation PFC-based oxygen
carriers. These new products can be infused at PFC concentrations as high as 900 g/L
without encountering viscosity problems, however, few of these have progressed beyond
late advanced stage testing. For example, Alliance Pharmaceuticals terminated
development of its Phase III LiquiVent on disappointing clinical study results. The
eight-carbon aliphatic molecule (perfluorooctyl bromide or perflubron) contains one Br
atom and 17 F atoms, emulsified in egg yolk phospholipids, similar to that used for total
parenteral nutrition. A 900 g/L emulsion of perflubron has an O2 capacity of >160 mL/L
O2 at a PO2 of 66.6 kPa (500 mmHg). Perflubron is stable at 4 °C for up to 4 years,
enhancing its attractiveness as an oxygen carrier.
Commercialization Challenges
Aside from efficacy limitations, PFC-based substances face other challenges to
routine clinical use. These include the linear relation of O2 capacity to PO2, short half-
lives, and a series of reported side-effects in human volunteers.
Probably the most significant limitation for widespread use of PFCs as oxygen
carriers is the linear relation of O2 dissolved to the PO2. At room air PO2 [18 kPa (~135
mmHg)], the O2 content of 900 mL/L Perflubron is <50 mL/L, whereas at a PO2 of 66.6
kPa (500 mmHg) the O2 content is >160 mL/L. The latter content is nearly equal to that
of whole blood at ambient PO2.
The duration of effective use of PFC is also limited by its short half-life. PFCs are
eliminated from the body unmetabolized through the lungs. They are also cleared from
the circulation by RES (reticuloendothelial system) phagocytosis from which they are
ultimately excreted by exhalation. This clearance is rapid, with reported half-lives of up

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 46 -
to 4 hours. The RES clearance also results in slight splenomegaly and hepatomegaly and
possibly some other side effects as discussed below. The short half-life of PFCs will
likely limit their clinical utility to settings where prolonged volume expansion and
restoration of oxygen-carrying capacity is not anticipated. These would include
oxygenation of poorly vascularized tissues and tumors, the priming of cardiopulmonary
bypass pumps, and ANH.
Like the HBOC blood substitutes, PFCs are reported to manifest several side
effects, the clinical significance of which is not currently fully understood. In healthy,
conscious human volunteers a transient "flu-like" syndrome has been described when
Perflubron was administered as a contrast agent. Symptoms included back pain, malaise,
flushing, and a transient fever of several hours. These symptoms are most likely cytokine-
mediated, as the PFC particles are cleared by cells of the RES. One commonly observed
side effect is a transient thrombocytopenia. Thus, current PFC products are unlikely to be
administered to thrombocytopenic patients.
Factor Products for Hemophilia A Hemophilia is an inherited disorder characterized by severe, spontaneous bleeding
that affects an estimated 400,000 people worldwide. Hemophilia A, which comprises
50,000 of these patients worldwide, is caused by a deficiency or defect in coagulation
caused by inadequate amounts of a protein called Factor VIII. Patients with the disease
experience acute, debilitating, and often life-threatening bleeding episodes. Depending on
the severity of the disease, bleeding may occur spontaneously or after minor trauma.
Conventional treatment consists of temporarily increasing the patient's Factor VIII levels
through infusions of plasma-derived or recombinantly-produced Factor VIII. There are
two types of treatments available and in development: recombinant factor therapy and
gene therapy.
Synthetic Platelets Synthetic platelets have been developed for treating thrombocytopenia associated
with the cancer chemotherapy. They mimic platelet activity in that they target the site of
hemorrgage where clot formation is enhanced or initiated. Treatment with platelet
preparations has several problems—potential infectivity with blood borne viral

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 47 -
contaminants, alloimmunization in 30% to 70% of patients, a short half-life, and febrile
reactions with transfusions.


Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 49 -
C H A P T E R T H R E E
The Blood Management System: Blood Collection, Processing
and Use
BLOOD COLLECTION Donated blood is collected by specialized collection centers. In the U.S., these are
FDA-licensed specifically for the collection, processing and storage of blood. Almost
half of the U.S. blood supplies are collected by the American Red Cross, and the other
half is collected by independent collection centers which are loosely banded together by
an organization known as America's Blood Centers (formerly the Council of Community
Blood Centers).
After collection, whole blood is separated into its three main components: red
blood cells (RBCs), platelets, and plasma. Sometimes a fourth component called
cryoprecipitate (a fraction of plasma highly concentrated in some clotting factors such as
Factor VIII or antihemophilic factor, fibrinogen, and von Willebrand factor) is also
generated. Up to four blood components may then be processed and sold.
Hospital blood banks obtain their supplies from regional blood centers, which
may be affiliated either with the Red Cross or independent centers. In each region,
several blood suppliers may compete for hospital business. This can affect pricing, since
blood banks must balance commitment to a single supplier for lowest pricing against the
need to maintain necessary supplies. Hospital blood banks may also supplement their
supply by acquiring blood from out-of-state suppliers as well as by in-house collections.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 50 -
Since there is no uniform set price for blood, the cost can vary considerably
between different regions and collection centers. Cost also varies with the component,
with the most expensive blood component being RBCs. The price of a unit of RBCs
depends upon a number of factors including the blood type (type O, universal-donor
blood is usually the most expensive) and whether the unit has any special attributes
required by the intended recipient. These may include, for example, white-blood-cell
reduction (a technique used to remove contaminating white blood cells), special-antigen
typing (necessary when the intended recipient has become sensitized to certain RBC
antigens as a result of prior RBC transfusion or, occasionally, pregnancy), or other
characteristics.
The allowed frequency of blood donation varies widely by country. Red blood
cells are the limiting step for whole blood donations, as they take the longest to replace of
all blood components at 56 days. In Hong Kong, subsequent blood donations may be
made from 12 to 24 weeks; in Australia, they may be made at 12 weeks; and in the
United States, they may be made in 56 days (eight weeks).
ORGANIZATIONS COLLECTING BLOOD Several different types of organizations currently collect blood. While most
operate on a not for profit basis, some pay donors. To date, about 40 countries have
developed national blood policies, though the implementation rate has been slow.
Not For-Profit Blood Collection
In the developed countries, blood donation is predominantly operated on a
voluntary basis, with unpaid donors encouraged to donate blood for humanitarian
reasons. Many physicians and blood industry experts believe that in addition to
containing supply costs, a not for-profit blood collection system also leads to a safer
blood supply by selectively discouraging donation from persons in high risk groups that
might seek to donate solely to obtain compensation. While donors often receive various
non-monetary benefits from donation including coupons for free or heavily discounted
products and services from local businesses, paid time off from work, etc., these benefits

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 51 -
are largely viewed as having no transferable cash value. With a few exceptions (such as
Zimbabwe), the developing nations are more willing to pay for blood, as supplies are
considerably lower than in developed countries.
The World Health Organization (WHO), for example, says that according to its
Global Database on Blood Safety, only 38% of blood collected is from low- and medium-
income countries where 82% of the world’s population lives, with 60% of the world’s
blood supply used by 18% of its population. Moreover, 95% of blood donations in high-
income countries are voluntary and unpaid, compared to only 25% in low-income
countries. In 1997, the WHO set a goal for all blood donations to come from volunteers,
but as of mid 2008, less than half of the 124 countries surveyed had established this
standard. In a few countries, such as Brazil, it is illegal to receive any compensation,
monetary or otherwise, for the donation of blood or other human tissues.
The amount of blood collected also varies by country, from 200 ml to 550 ml, although
450 ml to 500 ml is typical.
In the U.S., all blood components intended for transfusion to patients is collected
from volunteer donors, such that all of the country’s blood collection industry is currently
operated on a not for-profit basis. In 2008, the American Red Cross (ARC) continues to
collect most donated blood:
• the American Red Cross collects 43%;
• community blood centers collect 49%;
• hospital blood banks collect 8%.
This represents a decline in the ARC’s share from the mid 1990s when it accounted for
more than 55% of blood collections, and may be related to ongoing problems with the
ARC’s screening and collection methods that continue to result in relatively high
contamination rates. About 80% of the ARC’s blood supply is collected through its
mobile units.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 52 -
Red Cross
Comprised of individual organizations in more than 80 countries, the International
Red Cross and Red Crescent Movement is the world’s largest group of humanitarian,
non-governmental organizations. As part of the groups’ extensive health and safety
services, they also organize the collection and delivery of donated human blood to
hospitals. The American Red Cross is the largest single member of the International Red
Cross - in fiscal 2007, the ARC’s blood business generated $2.1 billion in revenues, more
than twice the size of the second largest blood collection organization.
Community Blood Banks
Community blood banks are located across the U.S., Europe and Asia and often
participate in larger networks of regional or national blood collection centers. Founded in
1962, America's Blood Centers is the country’s largest network of not-for-profit,
independent community blood centers with more than 450 blood collection centers
nationwide. Many states and provinces also operate associations of community blood
donation centers.
Although they compete with the American Red Cross for blood collection market
share and turf wars for donors are not uncommon, U.S. community blood banks are
increasingly cooperating with the ARC to improve blood safety practices and increase the
availability of blood supplies throughout the U.S. For example, many ARC chapters work
with community blood banks in areas where the Red Cross does not collect blood to
ensure that local communities have enough blood for patients in need. Many centers also
work cooperatively to improve information technology, education and training and share
knowledge.
Hospitals
Hospitals comprise a very small portion of blood donations and often engage in
collection activities to supplement blood obtained from other suppliers and/or reduce the
costs of obtaining blood. This latter consideration can be important, since blood
collection centers may raise prices for a variety of reasons connected with their own

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 53 -
increasing collection costs and double digit price increases are not uncommon. However,
because hospital collection centers must adhere to the same regulatory requirements
imposed on external blood collection centers, operations must be large enough to offset
these often high costs.
Other Blood Collection Sites
Although local Red Cross and community blood centers are equipped to collect
blood on site, for reasons of convenience, many donations occur off site. About four
fifths of blood donations occur at mobile blood drives sponsored by blood centers. These
are often highly publicized events and may be held at various public facilities such as
schools and colleges, shopping malls, offices, etc. Besides minimizing donors’ time lost
during the process and thereby accommodating donors who may not otherwise have been
able to schedule blood donation, locating blood drives in such public areas also helps to
recruit donors who may otherwise not have been aware of the need for donated blood.
For-Profit Blood Collection
Around the world, for-profit blood collection is comprised largely of plasma
donation (plasmapheresis). This is because the donation process is much more arduous
and time-consuming than for red blood cells, and the platelet shortage is more severe.
The global plasma industry continues to be dominated by a small number of large
U.S. pharmaceutical companies that supply the majority of plasma used in the U.S. and
Europe. More than 400 for-profit plasmapheresis centers in the U.S. collect blood from as
many as 2 million paid donors each year. About 70% of those donate regularly. Because
the body replenishes plasma more quickly than whole blood, plasma donations can be
made twice weekly, to a maximum of 104 times a year. In contrast, whole blood can be
donated only about once every two months.
Rising numbers of donors are migrating from unpaid whole blood donation to
paid plasma donation. A study conducted by Ohio University, for example, found that
10% of college students have sold their blood plasma at least once for payments ranging
from $9 to $20 per donation. In that group, three out of five were former Red Cross
donors who stopped donating blood when they started selling their plasma.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 54 -
National Donor Deferral Registry
First created in 1991 by the Plasma Protein Therapeutics Association (PPTA), the
National Donor Deferral Registry (NDDR) is a database of permanently deferred plasma
donors. It was established to help ensure the safety of plasma and plasma-derived
products by ensuring that permanently deferred donors would not be inadvertently
allowed back into the donation pool. While the original NDDR was a telephone-based
system, an Internet-based system was subsequently introduced to provide real-time data
at lower cost. The NDDR, which has obtained 510k clearance from the FDA, now allows
all U.S.-based plasma collection centers access to the national listing of permanently
deferred plasma donors. About 3% of donors are deferred each year.
DONOR DONATION DEMOGRAPHICS In the developed nations, less than 5% of the population donates blood although a
significantly larger proportion is eligible. In the U.S., for example, just 8 million persons
each year donate about 15 million units (pints) of blood. This represents less than 3% of
the population, although about 37% is eligible. Reflecting research published in a July
2007 issue of Transfusion, this is significantly lower than earlier eligibility estimates of
about 60%, due to new methods of calculating donor population size that include high-
risk behavior, disease exposure, presence of chronic diseases and age.
Despite recent efforts to publicize the need for donated blood to younger persons,
blood donation remains an activity dominated by the aging World War II generation. This
group was the first to donate blood, and tends to view donation as a patriotic duty. Many
have made it an ongoing part of their lives. For example, while 24% of donors are
between the ages of 17 and 24, they tend to give just once. Those age 55 and older,
however, comprise just 17% of donors but give regularly four to six times per year. Many
of these donors are affiliated with veterans groups, Masonic lodges, rotary clubs and
other organizations that perform public service. Although the leading blood collection
agencies continue to target younger adults in advertising and other promotional
campaigns, and certain events, such as the 2001 World Trade Center attack and
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 55 -
Hurricane Katrina in 2005, have temporarily increased interest in blood donation among
this group, older adults continue to comprise the mainstay of blood donors.
DONOR RECRUITMENT Blood donor recruitment involves education, information and motivation
techniques to encourage individuals to donate blood. Most blood collection centers
employ recruitment directors who focus exclusively on increasing the numbers of donors.
Trade associations, such as the Association of Donor Recruitment Professionals, have
emerged to help recruitment professionals share information and best practices.
Different blood collection centers utilize different techniques, particularly across
different countries and cultures. Some provide all donors with inexpensive gifts, many of
which may be donated by local businesses. These include food and refreshments,
coupons for free or discounted products and services, and give-aways such as T-shirts,
pens, mugs, etc. Other centers randomly select a small number of donors to win a larger
prize, such as a television or vacation. Standard ongoing recruitment techniques at all
blood centers, however, involve meeting with various groups of people to disseminate
material on blood donation and its importance; and enlisting the aid of these groups in
recruiting donors from among their constituencies. Specific ongoing efforts include:
• the establishment of June 14 as World Blood Donor Day by the World Health
Assembly; June 14 is the birthday of Karl Landsteiner, the scientist that
developed the ABO blood typing system;
• the U.S. celebration of Blood Collectors Week during each third week of
September;
• designation of January as National Blood Donor month in the U.S., during which
many blood collection centers run highly publicized blood drives, particularly to
reach new donors.
Many individual collection centers also conduct special events to increase
excitement for blood donation. These include barbeques and other parties; contests and
sweepstakes; talks at schools, institutions, community groups and companies; and

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 56 -
programs connecting patients who have received donated blood with blood donors so that
donors, volunteers, blood drive sponsors and others can see the results of their efforts.
BLOOD SCREENING AND EVALUATION To be eligible to donate blood, donors must be at least 17 years of age, weigh at
least 110 lbs. and be in good health. There is no standard upper age limit, but the blood
donation must be deemed to be medically safe to the donor during the screening process.
Donors must also meet other medical criteria, such as having no history of hepatitis or
risk of HIV. Many centers refuse to accept donations from persons who have accepted
money in exchange for sex, or men who have had sexual relations with other men. Other
conditions for exclusion include living in or traveling to certain African or Caribbean
countries; having been in juvenile detention, jail or prison within the past 12 months;
having had syphilis, gonorrhea or venereal disease within the past year; or having had
sexual contact with any person who meets those criteria.
Potential donors who are ineligible are deferred, on either a temporary, indefinite
or permanent basis. Persons placed on temporary deferral, for example, include those
who have recently had dental work, received certain toxoids or vaccines, used certain
medicines, have been diagnosed with alcoholism, potentially been exposed to the SARS
virus and/or received certain blood donations. An indefinite deferral may result from the
birth or residence since 1997 in certain African countries, potential exposure to variant
Crueutzfeldt-Jakob disease (vCJD) and/or evidence of parental drug use. Persons with
certain severe chronic medical illnesses (insulin-dependent diabetes, adrenal disease,
severe renal disease, etc.) and those with certain infectious diseases (hepatitis, HIV) will
be put on permanent deferral. The U.S. Centers for Disease Control and Prevention
(CDC) maintains a list of blood deferrals for common health problems and international
travel, while the U.S. Department of Defense maintains a list of deferrals for drugs,
medications and immunizations.
Actual blood collection takes about 10 minutes, with the entire process, including
screening, preparation and post collection steps, taking about one hour. Typical steps
include:

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 57 -
• registration, during which the donor signs a document indicating that he has provided truthful information about himself, understands the donation process and is making a voluntary donation;
• medical screening, when a medical history is taken and various tests for
infectious disease are administered;
• blood collection;
• documentation of any adverse events;
• post-collection refreshments.
Complications from blood donation are rare, occurring in just 2% of all donors,
according to an American Red Cross study. Most side effects are mild, including bruising
at the injection site; reactions to the sodium citrate used in apheresis collection; and
hypovolemic reactions such as light headedness and, in the worst cases, fainting. An
analysis of all U.S. blood donation reports from October 2004 to September 2006
evaluated 22 events and found no deaths related to donation.
METHODS FOR COLLECTING BLOOD FROM DONORS
Blood collection procedures and systems are often referred to as either "manual"
or "automated." In a manual process, whole blood is drawn from a donor and collected in
a container that typically includes an anticoagulant such as sodium citrate, phosphate,
dextrose and/or adenine. After collection, the blood is subjected to a separation procedure
to isolate various components. This contrasts with automated collection, in which the
donor is directly connected to a blood collection device that separates a desired
component and returns remaining components to the donor. In the automated process, the
initial collection of whole blood and the separation of the whole blood into the desired
components or fractions can be achieved in a single procedure.
Manual Blood Collection
Manual blood collection is a technique that is little changed over the past 50
years. It involves several steps, and therefore does not lend itself to standardization across

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 58 -
different collection centers. This introduces several areas of variability, as outlined by the
American Association of Blood Banks:
• whole blood collection volumes may vary by up to 10% of the collected volume,
resulting in varying red cell contents of the final product;
• separation methodology and/or centrifugation can affect final red cell content;
• the type of filter used can affect the leucodepletion performance and red cell
recovery;
• donor haematocrit may range from 38% to 55%, affecting final product
haematocrit;
• fixed amount of preservation solution, regardless of red cell content, may affect
haematocrit.
Automated Blood Collection
Automated Blood Collection (ABC), or apheresis, is a specialized collection
process that significantly increases the yield of blood components and includes the
collection of platelets. During the two to three hour ABC process, blood flows into a
sterile disposable collection container and is separated into red blood cells, platelets and
plasma. Required blood components are collected and the remaining portion is returned
to the donor. Each ABC donation is customized for the donor based on height, weight,
blood cell counts and blood type.
A single ABC donation can supply patients with a unit of red blood cells and
enough platelets and plasma for a complete transfusion. While six to eight regular whole
blood donations are required to supply enough platelets for one transfusion, just one ABC
donation from a single donor can provide enough platelets for one to three transfusions.
However, automated blood collection continues to represent less than 40% of all
blood collection, as shown in Figure 3-1. Worldwide, about 40 million whole blood
collection procedures are conducted, compared to just 20 million for plasma collection
(most of which is for the production of pharmaceuticals), 3 million for platelet collection
and about 600,000 for retrieval of RBCs. About 800,000 ABC procedures are performed
on patients during surgery. In the U.S., automated collection systems are used to collect

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 59 -
more than 700,000 RBC units each year and about one million "single donor" platelet
units.
Figure 3-1
Worldwide Annual Blood Collection by Component (Red Cells, Platelets, Plasma, Whole Blood)
Automated Red Cells0.6M0.9%
Platelets3M
4.7%
Plasma20M
31.4%
Whole Blood40M
62.9%
Source: Haemonetics
Plasmapheresis
The process by which blood plasma is collected, known as plasmapheresis, was
developed in the 1940s. While early plasma collection consisted of a labor-intensive
manual process, the majority of plasma collections worldwide now consist of automated
collections. Although plasma may be used in a therapeutic setting, since it does not
contain red blood cells so patients can receive a transfusion regardless of their blood type,
the primary use for plasma today is in the manufacture of medical products. Plasma
companies produce a wide range of medical products, ranging from vaccines to products
used in the manufacture of clotting agents such as Factor VIII.
Non-Automated

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 60 -
In the procedure, plasma is removed from the body then mixed with an
anticoagulant solution that separates the plasma from the red blood cells. The plasma is
then diverted into a storage contained, while the RBCs are re-infused back into the body.
This process takes about 45 minutes. During this procedure, a sterile kit is used and the
donor’s blood never leaves the system.
Unlike whole blood donation, however, plasma donation suffers from greater
concerns over quality. Because plasmapheresis centers pay for plasma donations, they
have long attracted donors from the underclass and/or homeless populations. These
groups tend to suffer from malnutrition, drug and/or alcohol addiction and a range of
other health problems. To counter this effect, college students have been targets of paid
donor recruiting strategies since the 1970s. However, research from Ohio University
suggests that these donors also suffer from health issues. Researchers found that paid
college student donors were more than three times as likely as non-donors and four times
as likely as Red Cross unpaid blood donors to drink alcohol five or more days a week.
And while about 12% of non-donors and 25% of Red Cross donors were smokers, more
than 33% of paid donors smoked cigarettes.
Plateletpheresis Plateletpheresis (also called thrombapheresis or thrombocytapheresis) is a process
in which only the blood clotting cells, or platelets, are extracted from the blood. Early
forms of the procedure were accomplished manually from the separation of platelets from
multiple bags of whole blood. In North America, the platelet-rich plasma (PRP)
technique while in Europe, Buffy Coat is more popular. Since each 250 ml or 500 ml bag
of blood contains a relatively small number of platelets, 5 to 10 bags of whole blood are
usually required to accumulate a single unit of platelets sufficient for one patient. Each
unit of platelets separated from donated whole blood is called a "platelet concentrate".
More modern automatic plateletpheresis allows the blood donor to give a portion
of his platelets, while retaining the red blood cells and a portion of the plasma. While the
basic principles of the technique are the same as in the manual procedure, automatic
plateletpheresis uses a computer-controlled machine to process the donor’s blood in a
sterile single-use centrifuge, and return unwanted components to the donor. This allows

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 61 -
repetition of the draw-centrifuge-return cycle to obtain more platelets. Using this
technique, six or more units of platelets are can be harvested in a single sitting, depending
upon the donor’s platelet count.
Most newer apheresis devices can separate a dose of platelets in about 60 to 120
minutes depending on the donor's health. Due to the length of the donation procedure and
the size of the machine, though, most platelet donations are conducted in blood centers
instead of during mobile blood drives.
Emerging devices attempt to address pathogens in harvested platelets. In Europe,
for example, CaridianBCT (formerly Gambro BCT) has launched a pathogen reduction
system for platelets. The Mirasol system applies riboflavin and light to reduce the
pathogen load in blood products, and the company claims that it is the first technology to
show indications of working in all three major blood components (platelets, plasma, and
red blood cells). Studies have demonstrated Mirasol’s effectiveness on a broad range of
viruses, bacteria and parasites.
Leukopheresis Also known as leukoreduction, leukopheresis is the process of removing
potentially harmful white blood cells from the blood. Leukopheresis units may utilized in
transfusions; they may also be processed to obtain stem cells. In a procedure similar to
that of plasmapheresis and plateletpheresis, blood is drawn from one arm by a needle and
processed automatically through a machine that removes white cells. The remainder of
the blood is returned by a needle in the other arm. The procedure is continuous and
requires 3 - 4 hours. The process may also be used to extract granulocytes, white blood
cells whose cytoplasm contains tiny granules. These cells, which are formed in the bone
marrow, are used to treat infections that are unresponsive to antibiotic therapy.
Leukopheresis has been adopted in many countries and about 80% of all red
blood cells collected in the U.S. are now leukoreduced. However, there is some
disagreement on the benefits of the process. An April 2007 meta-analysis covering 3,093
patients who received leukoreduced blood found that the treated blood reduced the
frequency of post-transfusion infection by 50%; a similar study conducted at Strong
Memorial Hospital at University of Rochester found that a change to universal use of
leukoreduced blood reduced post-transfusion infection by 33% - 45%. However, studies

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 62 -
conducted at University of South Alabama Medical Center and University of Washington
found no reduction of mortality or length of hospital stay in patients receiving
leukoreduced blood. Furthermore, leukoreduction removes about 10% of red blood cells
from each processed unit of RBCs.
Red Blood Cell Apheresis Like other apheresis techniques, red blood cell apheresis refers to the process of
separating red blood cells from donated blood while unused components are returned to
the body. This allows greater collection of red blood cells (two units compared with one),
which is beneficial since about 60% of all transfusions require RBCs.
During the procedure, blood is drawn from the arm through sterile tubing into a
centrifuge. The centrifuge spins the blood to separate the components by weight and
density. A port is opened which allows the red cells to be drawn into a collection bag,
while the other components are returned to the donor through another vein. The entire
process takes about 1-2 hours, slightly longer than regular whole blood donation. Since
the body typically requires about 8 weeks to replenish red blood cells from conventional
donation, the recommended interval between RBC apheresis procedures is double that
time, or about 112 days. However, RBC apheresis donors often recover much faster
because they receive fluid replacement during the procedure. Many donors also find it
more comfortable because a smaller needle is used.
CORD BLOOD COLLECTION Cord blood is human blood from the placenta and umbilical cord that are left over
after birth. Although still a small segment of the overall blood collection industry, cord
blood collection is becoming increasingly popular as a means to access valuable stem
cells.
There are 2 main methods of harvesting cord blood from the umbilical vein -
before the placenta is delivered (in utero) or after (ex utero.) With ex utero collection, the
cord blood is collected after the placenta is delivered and the umbilical cord is clamped
off from the newborn. The placenta is placed in a sterile supporting structure with the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 63 -
umbilical cord hanging through the support. The cord blood is drained under the
influence of gravity, yielding between 40-150 ml. A similar technique is employed in the
in utero method, except that the cord blood is collected after the baby has been delivered
but before the delivery of the placenta. In both methods, the cord blood is shipped to a
specialized cord blood bank facility after collection, analyzed for infectious agents and
tissue-typed. It is then processed and depleted of red blood cells before being stored in
liquid nitrogen for later use.
Since the stem cells in cord blood have been successfully used to treat a rising
number of serious medical conditions, and cord blood is more likely to match its donor or
a family member than stem cells collected from the bone marrow of a non-relative, a
rising number of parents are saving the cord blood of their newborns for possible use in
the future. Private blood banking facilities charge about $2,000 to collect cord blood and
$100 per year for storage. As of mid 008, several dozen storage companies were in
operation, up from about 12 in 2001.
However, the donation of cord blood remains extremely low compared with
conventional blood and plasma donation. This is likely to a variety of factors including
limited public awareness of the value and need for cord blood as well as a lack of cord
blood collection programs within hospitals.
PLASMA COLLECTION Blood plasma transfusions benefit trauma patients, transplant recipients, and
patients with clotting disorders, although most often, plasma is sold to pharmaceutical
companies for manufacture into medicines such as IVIG and Factor VIII.
The blood plasma industry continues to undergo significant shifts, following costs
increases of raw material (human plasma) as well as rises in processing costs associated
with the implementation of new safety measures such as inventory hold and plasma pool
testing. Furthermore, demand in the U.S. and Europe (although not Asia) continues to
exceed supply, driven in part by the increase in patients requiring new plasma-derived
therapies. Against this backdrop, competition within the two key groups of players –
fractionators, which collect plasma, and distributors, which sell it – remains strong and

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 64 -
consolidation among leaders has significantly reduced the number of players while
increasing their size and scope.
Plasma Fractionators Plasma fractionators collect human plasma and separate it into components. In
terms of amount, the major products prepared are human serum albumin and intravenous
immunoglobulin, although a variety of other important products are also prepared
including:
• alpha1 protease inhibitor (treatment for emphysema caused by genetic
deficiency);
• Factor VIII concentrate (prophylaxis and treatment of hemophilia A
bleeding episodes and von Willebrand disease);
• anti-inhibitor coagulant complex (treatment of bleeding episodes in
presence of Factor VIII inhibitor);
• anti-thrombin III (prevention of clotting and thromboembolism associated
with liver disease and anti-thrombin III deficiency);
• factor IX Complex (prophylaxis and treatment of hemophilia B bleeding
episodes and other bleeding disorders);
• factor XIII (prophylaxis and treatment of bleeding episodes due to factor
XIII deficiency).
Due to the significant level of investment required to establish a fractionation
facility ($25 million - $50 million in construction costs, which includes engineering,
building and equipment for a plant producing 100,000 to 300,000 liters per year),
fractionators tend to be large, well-capitalized companies.
The leading plasma fractionators are currently operating at or near manufacturing
capacity, processing more than 25 million liters of plasma annually to produce over 500
metric tons of human serum albumin and over 50 tons of immunoglobulins worldwide.
Four plasma fractionators – Talecris Biotherapeutics, CSL Behring, Grifols, and Baxter -
currently account for about 50% of the worldwide plasma derivatives market, as large
capital costs and regulatory tend to restrict the entry of new participants into the market.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 65 -
Talecris is a new company formed in April 2005 to acquire the fractionating business of
Bayer Biological Products, as this latter company divested its plasma business in an effort
to focus on its Rx and OTC drug and diagnostics operations. The market leaders continue
to invest in plant improvements that will boost efficiency and utilize less plasma to
generate similar quantities of vaccines and pharmaceutical products.
Distributors/Brokers Unlike plasma fractionators, which are primarily large, well-funded enterprises,
plasma brokers and distributors represent a diverse and fragmented group. In addition to
some larger pharmaceutical distributors such as AmeriSourceBergen and Cardinal
Health, the market also includes a large number of smaller, privately held companies that
trade plasma between fractionators and users such as hospitals. These include Blood
Diagnostics, Carolina Purchasing Alliance and FloMed, among others.
Because larger players are able to offer greater service options, smaller
distributors often must discount prices to compete. For example, Cardinal Health offers
three-hour or less emergency access to coagulation factors in select areas of the country.
The company also publishes its shipping schedule and product recall news on a
dedicated, plasma services website and offers after-hours telephone assistance.
BLOOD TYPING AND TESTING FOR DISEASES Blood typing and testing represents the cornerstone of ensuring that transfused
blood is safe for the recipient and free of disease. The following sections describe
commonly used methods of blood testing and typing.
Blood Typing The differences in human blood are due to the presence or absence of certain
antigens located on the surface of the red blood cells and antibodies in the blood plasma.
Individuals with different blood types have varying combinations of these molecules. Not
all blood groups are compatible with each other, and mixing incompatible blood groups
during transfusions leads to blood clumping or agglutination. These clumped red cells

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 66 -
can crack and cause toxic reactions with potentially fatal consequences when the receiver
of a blood transfusion has antibodies against the donor blood cells. This occurs because
red blood cells contain hemoglobin which becomes toxic when outside the cell. The
agglutinated red cells can also clog blood vessels and inhibit blood circulation to various
parts of the body.
While there are more than 20 genetically determined blood group systems known
today, the AB0 and Rh systems are the most important ones used for blood transfusions.
According to the AB0 blood typing system there are four different kinds of blood types:
A, B, AB or 0 (null):
• persons with blood type A have A antigens on the surface of the red blood cells
and B antibodies in the blood plasma; in the U.S., about 40% of Caucasians, 27%
of African-Americans, 28% of Asians, and 16% of Native Americans are type A;
• those with blood type B have B antigens on the surface of the red blood cells and
A antibodies in the plasma; in the U.S., about 11% of Caucasians, 20% of
African-Americans, 27% of Asians, and 4% of Native Americans are type B;
• in blood type AB, individuals have both A and B antigens on the surface of the
red blood cells and no A or B antibodies at all in the plasma; in the U.S., about
4% of the white population, 4% of African-Americans, 5% of Asians, and less
than 1% of Native Americans are type AB;
• persons with blood type O have neither A nor B antigens on the red blood cells
but both A and B antibodies in the plasma; in the U.S., about 45% of the white
population, 49% of African-Americans, 40% of Asians, and 79% of Native
Americans are type O.
Many persons also have a Rhesus or Rh factor on the surface of the red blood
cells. This antigen was name after the Rhesus monkey, in which the factor was first
identified.
Those with the Rh antigen are deemed Rh+ while those without it are called Rh-.
A person with Rh- blood does not have Rh antibodies naturally in the plasma (as one can
have A or B antibodies). But a person with Rh- blood can develop Rh antibodies if he

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 67 -
receives blood from a person with Rh+ blood, whose Rh antigens can trigger the
production of Rh antibodies in the plasma, which could lead to subsequent hemolysis.
An individual with Rh+ blood can safely receive blood from a person with Rh- blood.
Using just the A/B and Rh systems, therefore, each person’s blood type can be
classified into one of eight different types, as shown in Table 3-1. In the U.S., type O+ is
the most common, accounting for about 38% of the population, while type AB- is the
least common at just 1%. Distribution varies in other populations.
Table 3-1
Basic Blood Types
Type A Type B Type AB Type O Rh+ A + B + AB + O + Rh- A - B - AB - O -
Source: Medscape
In terms of compatibility, those with type AB+ are the easiest to match, since they
can safety received blood from donors of any type, while those with type O- may only
receive blood from others of type O-, as shown in Table 3-2.
Tabke 3-2
Blood Transfusion Compatibility
Recipient Blood Type Must Be AB+ Any blood type AB- O- A+ B - AB- A+ O- O+ A- A+ A- O- A- B+ O- O+ B - B- B- O- B - O+ O- O+ O- O-
Source: Medscape

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 68 -
Methods of Blood Typing A variety of different methods are currently used to determine blood type. These
may be either manual or automated, as discussed below.
Manual Blood Typing Methods
Manual blood typing methods include slide/tile testing, tube testing and
microplate, which differ mainly in terms of the surface on which the blood is test. For
each test, blood type is determined by testing for the presence or absence of Rh factor and
blood group antigens A and B on the surface of red blood cells. This is accomplished
with the addition of anti-A, anti-B and anti-Rh antibodies. The interaction of antibodies
with antigen produces aggregates that result in agglutination and indicates the presence of
that antigen in the blood.
Automated Blood Typing and Screening Methods
A relatively newer development, automated blood typing systems employ similar
biochemical mechanisms to classify blood but replace the human component with
artificial intelligence. Several devices are currently available, which generally utilize
microtiter plates to determine ABO and Rh types, solid phase red cell adherence assays
for antibody detection and/or modified solid phase red cell adherence plates for IgG cross
matches. Interpretation of the reactions is done by artificial intelligence software.
Automated blood typing has several advantages over manual typing in terms of
cost, efficiency and errors. First, a shortage of health care personnel often requires
transfusion services to utilize cross-trained, less-experienced staff from other areas of the
laboratory. Use of automation may allow the blood bank to conduct tests without need for
costly specialized technical staff. Furthermore, since interpretation of the
immunohematology reaction is done by the instrument without subjective interpretation
by the technologist, human errors are reduced. In a study published in a 2005 issue of
Laboratory Medicine, researchers evaluated 254 specimens tested by Immucor’s
ABS2000 automated blood typing machine and found no discrepancies over manual
testing. The device required 5.63 hours per day less technologist hands-on-time and no

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 69 -
technologist interpretation of reactions. Other studies have similarly demonstrated high
efficiency and accuracy of automated systems.
BLOOD TESTING There is a continuing trend toward the use of molecular diagnostics in the
screening of donated blood, plasma and organs for transplantation. This trend took shape
in the late 1990s with the development of molecular assays for HIV and, later, HCV and
HBV. The development of a screening molecular assay for HAV is now also under way.
For many years, the blood/plasma supply has been successfully screened for
infectious agents using automated immunoassay systems. Before 1985, all donated
blood, plasma and organs were tested only for syphilis and hepatitis B surface antigen
(HBsAg). From 1985 through 1989, serologic testing for HIV-1 and HTLV were added
to the requirements. In the following years, tests for alanine-aminotransferase (AAT)
hepatitis B core antibody (antiHBc) and HCV have also been implemented. Donor
testing for the HIV p24 antigen began in 1996 and a third generation HBsAg test is now
used with the third version of a highly sensitive serologic assay for HCV. For the most
part, these are surrogate assays, that is, they test for some product of the infection rather
than the infecting agent itself.
Moreover, despite continued revision and expansion of the pre-donation screening
interview, infectious donors may fail to respond accurately to questions about
transmissible disease risk factors at the time of blood donation. They may also not be
detected, if infected, using the classic testing methodologies. Thus, while the risks of
transmitted HIV and HCV may be low (one in 1,900,000 units transfused and one in
1,000,000 units transfused for HIV and HCV, respectively), these risks may be further
lowered by molecular testing.
In early 1999, the American Red Cross and 16 member laboratories of the
American Blood Centers began testing donated blood for HIV and HCV using gene
amplification technologies on an IND application protocol. These trials subsequently
proved successful and, in 2001, the first nucleic amplification tests for HIV and HCV
became available for blood bank and plasmapheresis center screening.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 70 -
The implementation of nucleic acid testing for HIV and HCV accomplished
several things. First, it brought American blood banks in compliance with a European
Committee for Proprietary Medical Products (CPMP) requirement that all plasma
derivatives distributed in the European Union after July 1, 1999 be harvested from
plasma that has tested negative for HCV by molecular methods, and subsequently for
HIV and HBV.
Second, the FDA policy established under former Commissioner Kessler had
directed blood products manufacturers and encouraged blood banking establishments to
implement cutting-edge technology to decrease or eliminate the period during which a
patient is infectious but found non-reactive by immunoassay screening methods.
Molecular testing methods have closed this period to approximately 10 days (from 16
days) for HIV and to between 10 and 30 days (from 70 to 80 days) for HCV.
Third, it has served to reassure the American public that everything is being done
to reduce transfusion risks through advanced technology. Since the public sees such
issues in black and white, it is insufficient that the risk of contracting HIV or HCV is
extremely small – the risk must be nonexistent and only efforts to make it so, despite the
cost, are acceptable. This belief persists, despite the fact that a person’s chance of dying
in a car accident is much higher than their risk of their contracting transfusion-related
HIV infection.
The following sections describe these tests in more detail.
Nucleic Acid Amplification Testing (NAT) Nucleic acid amplification testing (NAT), also known as “molecular diagnostics”,
is a newer technology whose investigation has been encouraged by the FDA since 1994.
In 2001, the FDA licensed the first NAT systems for screening of plasma donors with the
expectation that NAT would permit earlier detection of HIV and HCV infections in
donors. The tests were developed by National Genetics Institute (NGI) for screening
plasma used in manufacturing of products such as clotting factors and immune globulins.
NAT allows detection of very small amounts of genetic material (DNA or RNA)
by a process of massive copying (amplification) of a gene fragment, allowing highly
sensitive detection of targets. The use of pooled plasma samples for testing makes use of

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 71 -
the NAT system cost-effective. If a test pool is positive for virus, the individual donation
that is suspected of containing the virus can be identified and not used for manufacturing,
and the donor can be deferred and notified.
Although several strategies for the amplification of nucleic acids have been
developed, including amplification of the nucleic acid target (polymerase chain reaction
or PCR, strand-displacement amplification, self-sustaining sequence replication),
amplification of a nucleic acid probe (ligase chain reaction, Qß replicase) and signal
amplification (branched-probe DNA assay), PCR is now the most widely used
amplification method.
Alternative approaches to NAT identify antibodies to HCV, antibodies to HIV,
and HIV-1 antigens, which are the virus' own proteins. However, there is still a period
during which a donor can be infected, but have negative screening tests. Using NAT for
HCV, this detection window is reduced by 57 days from an average of 82 days to 25
days. For HIV-1, the average window period with antibody tests is 22 days and 16 days
with antigen tests; NAT further reduces this period to 12 days. This has resulted in lower
rates of infectious disease transmission, with one study estimating that NAT has helped
prevent the transmission of approximately five HIV-1 infections and 56 hepatitis C virus
(HCV) infections each year since it began being used in the United States as an
investigational screening test in mid-1999.
NAT technology has also been implemented in blood testing procedures for other
viruses. After 23 documented cases of West Nile virus (WNV) transmission through
blood transfusions in the U.S. during 2002, for example, national blood donor screening
for WNV RNA using mini-pool nucleic acid amplification testing (MP-NAT) was
implemented in July 2003 and in December 2005, Gen-Probe received FDA approval to
market its WNV assay commercially.
CBER Licensed NAT Screening Tests A number of NAT screening tests have been licensed by CBER. Gen-Probe alone,
for example, has received FDA approvals for more than 50 NAT-based products that
detect a wide variety of infectious microorganisms, including those causing sexually
transmitted diseases, tuberculosis, strep throat, pneumonia and fungal infections. The
company also developed the first FDA approved blood screening assay for the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 72 -
simultaneous detection of HIV-1 and HCV. The Procleix HIV-1/HCV Assay, which is
currently marketed by Chiron, was approved by FDA in 2002 and is used to screen more
than 80% of blood samples donated to the American Red Cross, America's Blood
Center's affiliates, the Association of Independent Blood Centers and the U.S. military
screen; it is also approved and used in 15 other countries. NAT tests identifying other
types of blood-borne viruses are under development.
Polymerase Chain Reaction (PCR) Amplification PCR is now the most widely used nucleic acid amplification method. Because
PCR can amplify even very tiny amounts of target DNA within a few hours, the assays
can quickly and accurately detect the presence of slow-growing microorganisms, such as
Chlamydia, mycoplasmas, mycobacteria, herpesviruses and enteroviruses and are now
routinely used in many diagnostic laboratories for the diagnosis of tuberculosis and
genital C. trachomatis infection. PCR assays have also been developed that can detect
antimicrobial resistance and are used to identify the cause of infection by organisms that
cannot be cultivated. The value of viral load measurement by nucleic acid amplification
in the management of patients with HIV infection or hepatitis C has also been established.
During the nucleic acid amplification procedure, DNA is cyclically denatured,
annealed and extended to produce millions of copies of the original target DNA. In the
initial step of the procedure, DNA is extracted from the specimen of interest. Heat of
approximately 95 degrees C is used to denature the extracted double-stranded DNA,
separating it into single strands. Cooling to 55 degrees C then allows primers specifically
designed to flank the target nucleic acid sequence to adhere to the target DNA in
annealing process. Following this, the enzyme Taq polymerase and nucleotides are added
to create new DNA fragments complementary to the target DNA in the extension step.
After approximately 30 cycles, the result is the accumulation of a specific PCR product
with sequences located between the 2 flanking primers.
Reverse transcription PCR is a modification of this method that is used when the
initial template is RNA rather than DNA. In this process, the enzyme reverse

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 73 -
transcriptase first converts the RNA target into a DNA copy (cDNA). This cDNA can
then be amplified by standard PCR methods. Reverse transcription PCR can be used to
amplify the much higher numbers of copies of messenger or ribosomal RNA than the
number of DNA copies present in bacteria or fungi. It may also detect the expression of
certain genes during the course of infection, since the detection of cDNA using reverse
transcription PCR of messenger RNA encoded by a pathogen could indicate an active
infection, in contrast to the detection of DNA from nonviable organisms using standard
PCR.
Other modifications have also been made to the original PCR technique. These
include:
• Nested PCR, which reduces the contaminations in products due to the
amplification of unexpected primer binding sites;
• Inverse PCR, which allows PCR when only one internal sequence is known;
• Asymmetric PCR, which preferentially amplifies one strand of the original DNA
more than the other;
• Linear-After-The-Exponential-PCR (LATE-PCR), a modification on asymmetric
PCR, which maintains reaction efficiency as the limiting primer concentration
decreases mid-reaction;
• Quantitative PCR, which provides an indirect method for quantitatively
measuring starting amounts of DNA, cDNA or RNA by rapidly measuring the
quantity of PCR product;
• Touchdown PCR, which reduces nonspecific primer annealing by more gradually
lowering the annealing temperature between cycles;
• Colony PCR, which allows bacterial clones such as E. coli to be screened for the
correct ligation products.
CBER Licensed PCR Screening Tests In order to be used for blood screening, tests must be approved by the FDA’s
Center for Biologics Evaluation and Research (CBER). Several PCR screening tests have
been licensed by CBER, as shown in Table 3-3, many of which have been approved
relatively recently.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 74 -
Table 3-3
PCR-Based Screening Tests Licensed by CBER
Condition Manufacturer Approval Test Name Indication West Nile Virus (WNV) Roche 8/28/2007
COBAS TaqScreen West Nile Virus Test
Qualitative detection of West Nile Virus (WNV) RNA in plasma specimens from individual human donors, donors of whole blood and blood components, and other living donors. Also intended for use in testing plasma specimens to screen organ donors when specimens are obtained while the donor’s heart is still beating.
Human Immuno-deficiency Virus-1 (HIV-1) Roche 5/11/2007
COBAS AmpliPrep/COBAS TaqMan HIV-1 Test
Quantitation of Human Immunodeficiency Virus Type 1 (HIV-1) nucleic acid. Not intended to be used as a donor screening test.
Human Immuno-deficiency Virus-1 (HIV-1) Abbott 5/11/2007
Abbott RealTime HIV-1 Amplification Kit
Quantitation of Human Immunodeficiency Virus type 1 (HIV- 1) on the automated m2000 System. Not intended to be used as a donor screening test.
Hepatitis C Virus (HCV)
BioLife Plasma Services 2/9/2007
Hepatitis C Virus (HCV) Reverse Transcription (RT) Polymerase Chain Reaction (PCR) assay
Qualitative detection of HCV ribonucleic acid (RNA) in pools of human Source Plasma comprised of equal aliquots of not more than 512 individual plasma samples.
Human Immuno-deficiency Virus-1 (HIV-1)
BioLife Plasma Services 1/31/2007
Human Immunodeficiency Virus, Type 1 (HIV-1) Reverse Transcription (RT) Polymerase Chain Reaction (PCR) assay
Qualitative detection of HIV-1 ribonucleic acid (RNA) in pools of human Source Plasma comprised of equal aliquots of not more than 512 individual plasma samples.
Hepatitis B Virus (HBV) Roche 8/2/2005
COBAS AmpliScreen HBV Test
Testing for HBV DNA in post-mortem cadaveric (non-heart-beating) donors; individual testing
Hepatitis B Virus (HBV) Roche 4/21/2005
COBAS AmpliScreen HBV Test
Qualitative in vitro test for direct detection of HBV DNA in human plasma from donations of whole blood and blood components and source plasma; testing individual plasma samples from other living donors and organ donors (when specimens are obtained while the donor's heart is still beating)
Hepatitis C Virus (HCV) Roche
3/9/2005
COBAS Ampliscreen HCV Test, version 2.0
Testing of individual cadaveric specimens (obtained from non-heart-beating donors)
(continued)

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 75 -
Table 3-3 (continued)
PCR-Based Screening Tests Licensed by CBER
Condition Manufacturer Approval Test Name Indication
Hepatitis C Virus (HCV)
Roche
5/13/2004 COBAS Ampliscreen HCV
Testing for source plasma donors in a mini-pool format of up to 96 donations with single unit resolution testing; testing individual plasma samples from other living donors and organ donors (when specimens are obtained while the donor's heart is still beating)
Hepatitis C Virus (HCV) Roche
12/3/2002
COBAS Ampliscreen HCV Test
Detecting HCV RNA, in conjunction with licensed tests for detecting antibodies to HCV
Hepatitis C Virus (HCV)
National Genetics Institute
9/18/01
UltraQual HCV-
RT-PCR-Assay
Qualitative detection of HCV ribonucleic acid (RNA) in pooled human source plasma comprised of equal aliquots of not more than 512 individual plasma samples
Human Immuno-deficiency Virus-1 (HIV-1) Roche
3/9/2005
COBAS AmpliScreen HIV-1 Test, version 1.5
Testing for HIV-1 in post-mortem
cadaveric (non-heart-beating) donors Human Immuno-deficiency Virus-1 (HIV-1) Roche
12/19/2003
COBAS
AmpliScreen HIV-1 Test, version 1.5
Testing for Source Plasma donors in a mini-pool format of up to 96 donations with single unit resolution testing; testing individual plasma samples from other living donors and organ donors
Human Immuno-deficiency Virus-1 (HIV-1)
National Genetics Institute
9/18/2001
UltraQual HIV-1
RT-PCR (Reverse PCR)
Qualitative detection of human HIV-1on RNA in pooled human source plasma comprised of equal aliquots of not more than 512 individual plasma samples
Source: FDA
Immunoassay An immunoassay is a biochemical test that measures the level of a substance in
blood plasma by measuring the reaction of an antibody to its antigen. (Each protein-based
antibody recognizes and binds to a specific antigen). Monoclonal antibodies, which are
antibodies that are identical because they are clones of a single parent immune cell, are
often used in immunoassays since they only usually bind to one site of a particular
molecule. They therefore provide a more specific and accurate test, which is less easily
confused by the presence of other molecules.
The presence of both antigens and antibodies can be measured by immunoassays.
In tests designed to detect infection, the presence of antibodies against the pathogen is
measured; for measuring the levels of hormones such as insulin, the insulin acts as the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 76 -
antigen and is measured directly. The quantity of antibodies or antigens can be detected
through various methods, with the labeling of either the antigen or antibody being among
the most common. This label may consist of an enzyme (as in an enzyme immunoassay),
a radioisotope such as I-125 or fluorescence. Other methods to measure antibody and/or
antigen levels include agglutination, nephelometry, turbidimetry and Western Blot.
Immunoassays can be competitive or noncompetitive. In a competitive
immunoassay, the antigen in the unknown sample competes with labeled antigen to bind
with antibodies. The amount of labeled antigen bound to the target antibody is then
measured. In this method, the response is inversely proportional to the concentration of
antigen in the unknown. This is because the greater the response, the less antigen in the
unknown was available to compete with the labeled antigen. In noncompetitive
immunoassays (sandwich assays), antigen in the unknown is bound to the antibody site,
then labeled antibody is bound to the antigen. The amount of labeled antibody on the site
is then measured. Unlike the competitive method, the results of the noncompetitive
method are directly proportional to the concentration of the antigen since labeled
antibody will not bind if the antibody is not present in the unknown sample.
Additionally, immunoassays may be either homogeneous or heterogeneous. A
heterogeneous immunoassay requires an extra step to remove unbound antibody or
antigen from the site. Homogeneous assays do not require this step, making them faster
and easier to perform.
Enzyme-Linked Immunosorbent Assay The Enzyme-Linked Immunosorbent Assay (ELISA for short) is a technique used
to detect the presence of an antibody or antigen in a plasma sample. It utilizes two
antibodies, one of which is specific to the antigen and the other of which is coupled to an
enzyme. This second antibody will cause a chromogenic or fluorogenic substrate to
produce a signal. Several variations of the test are currently in use. While some of these
provide improvements over the basic ELISA test, in some cases, ELISA can yield a
relatively high rate of false positives. This is because other microbes can often trigger the
same antibodies as the microbes being evaluated. False positive rates as high as 70%, for
example, have been measured in the usage of ELISA tests in central Africa where the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 77 -
microbes responsible for tuberculosis, malaria and leprosy can interfere with the
measurement of antibodies to HIV.
Basic ELISA
The basic ELISA test may be either direct (in which antigen concentrations are
measured) or indirect (in which serum antibody concentrations are measured). Table 3-4
compares the advantages and disadvantages of each. The direct method consists of:
• applying a sample of known antigen to a surface, typically the well of a microtiter plate, and fixing the antigen to the surface to immobilize it;
• coating the surface with serum samples of unknown antibody concentration. This serum is usually taken from another species to prevent non-specific antibodies in the patient's blood from binding to the antigen;
• washing the plate to remove unbound antibody, leaving only the antibody-antigen complexes remaining attached to the surface;
• adding the second antibodies to the surface, which then bind to any antigen-antibody complexes. These second antibodies are coupled to the substrate-modifying enzyme;
• washing the plate to remove excess unbound antibodies;
• applying a substrate which is converted by the enzyme to emit a chromogenic or fluorescent signal; the enzyme acts as an amplifier, so that even if only few enzyme-linked antibodies remain bound, the enzyme molecules will produce many signal molecules.
• quantifying the result with a spectrophotometer or other optical device.
ELISA may be run in either a qualitative or quantitative format. Qualitative
results provide a simple positive or negative result while in quantitative ELISA, the
optical density of the sample is interpolated into a standard curve which is typically a
serial dilution of the target. The assay can also be modified for the detection of cytokines
or other proteins.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 78 -
Table 3-4
Comparison of Direct and Indirect ELISA Tests
Advantages Disadvantages Direct ELISA
Quick methodology since only one antibody is used.
Immunoreactivity of the primary antibody may be reduced as a result of labeling.
Cross-reactivity of secondary antibody is eliminated.
Labeling of every primary antibody is time-consuming and expensive.
No flexibility in choice of primary antibody label from one experiment to another.
Limited signal amplification. Indirect ELISA A wide variety of labeled secondary
antibodies are available commercially.
Cross-reactivity may occur with the secondary antibody, resulting in nonspecific signal.
Versatile, since many primary antibodies can be made in one species and the same labeled secondary antibody can be used for detection.
An extra incubation step is required in the procedure.
Immunoreactivity of the primary antibody is not affected by labeling.
Sensitivity is increased because each primary antibody contains several epitopes that can be bound by the labeled secondary antibody, allowing for signal amplification.
Different visualization markers can be used with the same primary antibody.
Source: Pierce Biotechnology
Alternate ELISA Methods
An alternate ELISA technique involves competitive binding. In this method, the higher the original antigen concentration, the weaker the final signal. Competitive ELISA consists of:
• incubating unlabeled antibody in the presence of its antigen;
• adding the bound antibody/antigen complexes to an antigen-coated surface;
• washing the plate to remove unbound antibody. The more antigen in the sample, the less antibody will be able to bind to it, creating competition for the antigen;
• adding the secondary antibody, specific to the primary antibody; this second antibody is coupled to the enzyme;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 79 -
• applying a substrate which is converted by the enzyme to emit a chromogenic or fluorescent signal;
• quantifying the result with a spectrophotometer or other optical device.
Sandwich Method
Sandwich ELISA is a common method used to detect the antigen concentration in unknown samples. This technique comprises:
• preparing a surface to which a known quantity of antibody is bound;
• applying the antigen-containing sample;
• washing the plate to remove unbound antigen;
• applying the enzyme-linked antibodies which are also specific to the antigen;
• washing the plate to remove unbound enzyme-linked antibodies;
• applying a chemical which is converted by the enzyme into a signal;
• viewing the result.
The accuracy of this technique depends upon a number of factors including the
number of molecules of the first antibody that are bound to the solid phase, the avidity of
the first and second antibodies for the antigen and the specific activity of the second
antibody.
Reverse Sandwich Method
The reverse sandwich ELISA (or double antigen sandwich) dates to the late 1980s
when researchers were seeking an assay that would allow the identification of low-
concentration antibodies and comparison of results among different species. While in the
sandwich method, an antigen is sandwiched by two antibodies, in the reverse sandwich
method, an antibody is sandwiched by two antigens. Subsequent studies comparing the
technique with conventional indirect ELISA have demonstrated that it offers higher
specificity and sensitivity as well as the ability to comparably titrate antibodies between
species. This latter characteristic allows the hyperimmune serum produced in animals to
be used as the reference antiserum for quality control of this ELISA; it also enables
seroepidemiologic surveys of zoonoses, in which antibody prevalence rates and geometric
mean concentrations are compared between humans and different animal species.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 80 -
Reverse Sandwich Inhibition Method
The reverse sandwich inhibition (or simply inhibition) method is similar to
competitive ELISA, but in this system, the test sample antigen and the enzyme-labeled
antigen are added one after the other. This is useful when the test serum contains both an
antigen and an antibody of interest. Inhibition ELISA may also be used to determine the
identity of a specific antigen or antibody. For example, in studies comparing the assay to
other ELISA tests, inhibition ELISA was found to be superior to sandwich ELISA in the
detection of active filarial infection.
Costs and Other Barriers The most serious barrier to the use of molecular diagnostic technologies in blood
screening remains cost. Each molecular assay costs as much as 10 times that of the most
expensive immunoassay now used in blood banks. Although blood banks are largely not-
for-profit organizations, but they must still cover their costs and the use of molecular
assay methods would mean an increase in blood pricing. Similarly, plasma collection
and processing organizations would also have to raise their prices, putting a further strain
on a healthcare system already suffering under rising costs and ongoing criticism from
both the government and the people.
To deal with the issue of costs, blood banks and plasmapheresis centers do not
test individual donations but use a pooling method. If a pool tests positive for HIV or
HCV, then the individual donations comprising that pool are tested to identify the
infected unit(s). In the beginning, this pooling approach was seen as problematic. First,
since HCV circulates in concentrations of only 10,000 to 100,000 genome equivalents per
milliliter, pooling of one positive sample with many other negative samples was thought
to make detection of the virus more difficult. The initial approach to this issue was the
concentration of the virus in the pool by ultracentrifugation prior to gene amplification.
This was not seen as a guarantee that the virus would concentrate in the centrifuge pellet.
HCV can bind to serum lipids, which float to the top of the serum during
ultracentrifugation and are discarded during decanting and washing.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 81 -
Others have suggested that pools of fifty or fewer samples might not need
concentration. As long as a highly sensitive amplification method is used, these smaller
pools might be adequate for accurate analysis. Additional objections include the:
• inadvertent pooling of endogenous inhibitors of the amplification, leading to false negative results;
• need for personnel trained in the specialized amplification procedures and techniques;
• use of instrumentation that has been foreign to the blood bank;
• length of time necessary to provide data can be up to 48 hours, delaying release of blood resources.
Since testing began in 1999, however, experience with nucleic acid testing in the
blood banks and plasmapheresis centers has been extensive. Each of these issues has
been investigated and evaluated.
At their current stage of development, therefore, molecular methods are probably
not ideal for the blood bank and plasmapheresis center. However, since the European
Union has decided that it will accept only those blood products that have been assayed
for HCV by gene amplification approaches, the blood banks will stretch to accept
molecular testing technology. Resisting its implementation is a hard argument to make
since blood banking and plasmapheresis products centers have publicly signed off on the
concept that their facilities must accept leading edge technology to protect the blood
supply. Therefore, they cannot be seen as going back on this pledge for any reason.
Eventually, though, costs will come down. The size of the blood banking and
plasmapheresis markets is such that it is large enough for instrument manufacturers to
come up with more practical, high throughput instrumentation. The molecular biologists
will also be pressured to develop faster, simpler analytical methods. Now that the blood
banks have accepted HCV and HIV testing by molecular methods, it is only a matter of
time before other pathogens, with the possible exception of syphilis, will fall under the
same umbrella, further justifying dedicated instrumentation. (Syphilis assays are too
cheap and too quick as it is, and the molecular methods are unlikely to make a significant
difference with regard to this test.) This is because it is more economically feasible for

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 82 -
the blood bank to do all of its testing using one set of instrumentation instead of doing it
some of it by immunoassay and some by gene amplification.
Blood Storage Blood can be stored as whole blood (with all of the plasma present) or, much
more commonly, as packed red blood cells from which about 70% of the plasma has been
removed. After this occurs, blood and/or blood components are commonly refrigerated or
frozen to extend their usefulness, with storage times based upon the physiological
qualities of those materials:
• red blood cells may be stored under refrigeration for a maximum of 42 days and
frozen for up to 10 years;
• plasma is frozen at -70o Celsius and then stored at -20o Celsius up to one year;
• cryoprecipitate, which contains clotting factors, is made from fresh-frozen plasma
and may be stored frozen for one year;
• platelets may be kept for five days in an agitator at 22o Celsius, with some newer
technologies providing storage up to seven days.
In selected cases, long term cryopreservation of RBC's may be performed to store
certain RBC's. In the deglycerolization procedure, the RBC's are first incubated in a 40%
glycerol solution which acts as an antifreeze within the cells. The units are then placed in
sterile containers in a deep freezer at less than -60o Celsius. When they are ready to be
used, the cryopreserved units are thawed and washed free of glycerol prior to use as
saline suspended RBC's. The washed units are depleted of plasma and leukocytes and
must be used in 2 - 4 hours to prevent possible bacterial contamination. Because of the
expense of the process, however, it is reserved for rare RBC’s that are not normally
obtainable through conventional collection methods.
As with blood collection, storage is closely regulated to ensure product safety,
with blood storage bags and other materials requiring regulatory approval. Other
equipment used in the process is specially designed to ensure optimum performance.
Blood storage refrigerators, for example, are typically designed with transparent doors so

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 83 -
that labels may be read without opening the door and products will not be affected by
slight resulting temperature differentials.
Freezing systems are also designed to maximize product integrity. Newer systems
enable the freezing of red blood cells for up to 10 years and when needed, thawing those
cells. The technology automates the blood freezing process in a closed system, which
allows for multi-day storage of the thawed red blood cells. Previous technologies
required thawed blood to be used within 24 hours after thawing or be discarded.
Recent studies, however, indicate that storage bags for refrigerated blood may
cause safety risks. Around the world, red blood cells are stored in polyvinyl chloride
(PVC) bags plasticized with di-2-ethylhexyl phthalate (DEHP) or a similar plasticizer. In
a report published in the Indian Journal of Experimental Biology, researchers claim that a
significant amount of DEHP (as much as 0.15 gram per liter of blood) leaches out into
the blood, and can inhibit a key enzyme called Na-K-A TPase in the liver, brain and red
blood cells. Decreases in the levels of this enzyme have been linked with various
neurological disorders, heart disease, stroke and brain tumors.
BLOOD PROCESSING Blood processing typically involves the breaking down of blood into its
components (fractions), which are then utilized for a variety of purposes. The following
sections describe both established and emerging fractionation methods.
Cohn Fractionation
The process of fractionation represents the separation of proteins from the blood
plasma and dates to the work of Harvard biochemist Edwin Cohn in 1940. At that time, a
great need existed for material that could serve the life-saving functions of blood plasma
but would be easier and more practical to store, transport and administer. To this end,
methods were sought to divide blood plasma into its active components and find stable
substitutes for whole plasma. Searching for such a substitute, Cohn determined that
different proteins (fractions) in the blood could be separated from each other using
different temperatures and biochemical conditions as well as solvents like cold ethanol.
His method used these biochemical techniques to separate blood plasma into five

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 84 -
fractions, allowing the isolation of fibrinogen (Fraction or Factor I), gamma globulin
(Fraction II and III), and albumin (Fraction V). Albumin proved to be an excellent
substitute for human plasma, by helping to expand the volume of blood and leading to
speedier recovery. Additionally, Cohn's method was gentle enough so the protein retained
its biological activity. The process also dramatically reduced viral infectivity. Figure 3-2
shows the proportion of components obtained from the Cohn fractionation method.
Although the original Cohn fractionation method continues to be used since it
offers high yields of albumin, many improvements have been made to it, including the
use of other solvents such as acetone, salts (ammonium sulfate) or heat to separate the
albumin from other plasma components. These have arisen due to several shortfalls with
the Cohn ethanol technique.
First, traditional Cohn fractionation can be dangerous and environmentally
unfriendly since ethanol is a highly explosive, controlled substance. It can also be
unsanitary as it requires open tanks and filter presses that increase the risk of
contamination. The use of ethanol may also be too gentle to kill certain kinds of viruses
that require heat inactivation. This is particularly true when the process is used to produce
bovine serum albumin, as the BSA is often contaminated with immunoglobulins, which
cause regulatory problems in pharmaceutical production and can interfere with diagnostic
assays. Additionally, newer methods are able to isolate a wider variety of plasma
proteins.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 85 -
Figure 3-2
Results of Cohn Fractionation Method
Source: Cohn, E.J.: The Separation of Blood into Fractions of Therapeutic Value, Ann, Int. Med. 26: 341-
352, March 1947.
Classical Fractionation Methods Modern fractionation methods address the limitations of Cohn fractionation while
allowing the separation of a larger number of proteins. In addition to Factors I – V, these
include several hundred proteins of therapeutic value that are found in much lower
concentrations, as shown in Table 3-5. These methods employ selective precipitation of
proteins by precipitation and/or chromatographic procedures.
In a precipitation technique, the composition of a buffer is altered to force the
precipitation of a portion of the proteins. This takes advantage of the differential
solubility of proteins under varying conditions as well as the high protein concentration
of plasma which allows aggregates of protein to form over a period of several minutes to

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 86 -
several hours. Precipitated proteins are then separated from other proteins that remain in
solution by low speed centrifugation.
Table 3-5
Plasma Proteins of Therapeutic Interest
Protein
Concentration in Plasma
Indication
Albumin 40 g/L Volume restoration after trauma, shock, burns Alpha1 proteinase inhibitor 1.5 mg/mL Hereditary emphysema Anti-D IgG Varies Rh prophylaxis in pregnancy and childbirth Antithrombin III 100µg/mL Antithrombin III deficiency C1-inhibitor 170µg/mL Hereditary angioedema Factor IX 10 µg/mL Hemophilia B Factor VIII 0.5 µg/L Factor VII deficiency Factor XI 0.3 µg/mL Hemophilia B Factor XIII 30 µg/mL Factor XIII deficiency Fibrinogen 3 g/L Tissue sealant component Fibronectin 300 µg/mL Wound healing Hepatitis B IgG Varies Hepatitis immunity Immunoglobulin G Up to 12.5 g/L Primary and secondary immune deficiency Measles IgG Varies Measles protection and treatment Protein C 4 µg/mL Neonatal thrombosis Rabies IgG Varies Rabies risk Tetanus IgG Varies Tetanus protection and treatment Thrombin 150 µg/mL Tissue sealant component Varicella Zoster IgG Varies Chicken pox protection Von Willebrand factor 10 µg Von Willebrand’s disease
Source: BioPharm International.
Precipitation may be induced by salts, isoelectric change and/or solvents.High salt
concentrations promote precipitation, since with increasing ionic strength, proteins begin
to interact via hydrophobic patches on their surface, as proteins and salt compete for the
residual water. Ammonium sulfate is used as the salt of choice, since it preserves protein
activity and promotes precipitation at lower concentrations than other salts. Isoelectric
precipitation is induced by varying the pH level of the solution. This occurs as the pH
level approaches the isoelectric pH (pI) of a given protein, causing weak electrostatic
attractive forces on the protein to lead to aggregation and precipitation. Solvent
precipitation, as with ethanol (Cohn fractionation) or acetone, occurs by a similar

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 87 -
mechanism as isoelectric precipitation. The addition of a solvent reduces the availability
of water for salvation, with precipitation most likely to occur at the pI of the protein.
Chromatographic techniques include a variety of methods in which proteins are
fractionated by partitioning between a mobile or buffer and an immobile or matrix, phase.
The most widely used technique involves a matrix packed in a column through which the
protein sample is passed. Specific techniques include gel filtration and adsorption
chromatography.
Gel filtration (also called size exclusion or gel permeation chromatography)
separates proteins on the basis of their size and shape. Large proteins do not enter the
pores of the chromatographic matrix, but pass through, while smaller molecules are
retained. Proteins do not bind significantly to the matrix and sorting does not occur as a
result of differential binding but of differential exclusion from pores in the beads. Gel
filtration resins are composed of a variety of materials, including dextran, agarose, and
polyacrylamide and are available in various pore sizes.
In adsorption chromatography, a sorbent is selected that binds proteins with
different affinities. Binding of protein to the matrix is most simply achieved by mixing
them. This type of batch adsorption is especially popular with hydroxyapatite, but can
also be performed with ion exchange resins. One advantage of the adsorptive method is
the ability to use high volumes of sample, eliminating concentration steps. This saves
time and generally leads to higher overall yields in protein preparations. Various forms of
adsorption chromatography techniques include:
• ion exchange chromatography, in which the charged groups on the surface of a
protein bind to an insoluble matrix with opposite charge;
• hydrophobic interaction chromatography, which takes advantage of hydrophobic
patches on the protein surface that interact with non-polar materials under non-
denaturing conditions;
• hydroxyapatite chromatography, which allows fractionations that often are not
attainable with any other method such as separation of isozymes or of antibodies
that only differ in their light chains.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 88 -
Advanced Fractionation Methods Ongoing advances in fractionation methods provide increasing yields of desired
proteins with higher purity. This is important, since human plasma sources represent as
much as 45% of the total cost of operating a plasma fractionation facility and higher
yields lead to greater revenue from the same amount of plasma. Additionally, increasing
purity offers lower levels of risk. Many of these changes are driven by the industry’s
safety consciousness and incorporate the latest procedures for virus reduction and
clearance of prions. Following contamination fears in many of the world’s largest blood
supplies, the fear of infectious agents remains omnipresent, and extends to both known
and unknown pathogens.
To this end, manufacturers continue to introduce new membranes for virus
filtration (nanofiltration), sterilizing grade filters, process chromatography sorbents and
membrane chromatography devices. Other developers are working on novel fractionation
methods, including cascade plasma fractionation.
Cascade Plasma Fractionation Developed over the past few years by ProMetic and its partners and tested by
Hemosol, the Cascade process is a specific sequence of capture steps to optimize the
protein recovery yield from plasma. The process consists of a series of filters through
which human plasma is processed to increase the recovery yield of plasma proteins and
allows for the recovery of additional new proteins. This allows fractionators to use less
plasma for the same output or increase production output with the same level of plasma.
Proteins targeted by the process include Factor VIII/von Willebrand Factor complex,
plasminogen, fibrinogen, alpha 1-antitrypsin, immunoglobulin G and human serum
albumin.
The procedure also has advantages in therapeutic plasmapheresis. Until recently,
the plasma containing the pathogenic protein(s) was discarded after treatment, resulting
in the sacrifice of about 180 g of normal protein to eliminate a few grams of the
pathogenic protein species. A potentially significant side effect of this standard procedure
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 89 -
was a depletion of essential plasma proteins, putting the patient at risk to suffer from
protein depletion or risk the transmission of diseases from infected substitution fluids.
Automated Fractionation In March 2008, U.K.-based RTS Life Science unveiled an automated blood
fractionation system, which provides high throughput processing capable of handling up
to 500 samples per day. Offering significant time and cost savings compared with manual
methods, the approach also removes the risk of human error and provides automated
sample tracking and auditing. The system incorporates technology which measures the
height of each fraction and calculates the volume of each layer following fractionation
via centrifugation.
BLOOD TRANSFUSIONS Blood transfusion is the process of transferring whole blood or blood-based
products from one person (the donor) into the circulatory system of another (the
recipient). A transfusion may be undertaken in connection with the treatment of various
medical conditions in which the recipient sustains significant blood loss or the
mechanism of producing red blood cells (or another essential blood component) fails,
such as trauma, surgery or shock.
While accounts of unsuccessful attempts at blood transfusion date to the 1400s,
only in the 19th century was the reason for transfusion-related deaths linked to the
existence of blood types and resulting incompatibility between donor and recipient. This
problem was addressed by mixing some blood from the donor and the receiver before the
transfusion and allowed a greater number of successes. The development of
anticoagulation and refridgeration methods in the early 1900s permitted the storage of
blood and paved the way for the substantial blood banking industry that exists today.
Testing Before Transfusion In the developed countries, testing of blood is conducted routinely prior to
transfusion to insure that donated blood will be compatible with recipients’ blood. A
variety of tests are used, as described below, that determine blood type by identifying the
presence of antibodies.
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 90 -
Coombs Test The Coombs test (also known as an antiglobulin test or AGT) was developed in
the 1940s by Cambridge immunologists Robin Coombs, Arthur Mourant and Rob Race.
It now refers to two clinical blood tests:
• Direct Coombs test, also direct antiglobulin test or DAT;
• Indirect Coombs test, also indirect antiglobulin test or IAT.
The Direct Coombs test is used to determine if antibodies or complement system
factors have bound to RBC surface antigens in vivo. It is used when immune-mediated
haemolytic anemia (antibody-mediated destruction of RBCs) is suspected. A positive
Coombs test indicates that an immune mechanism is attacking the patients own RBCs.
This could result from an autoimmune or alloimmune response, as well as from a drug
induced immune mediated mechanism.
In the DAT procedure, the patients’RBCs are washed then incubated with
antihuman globulin (also known as Coombs reagent). If immunoglobulin or complement
factors have adhered onto the RBC surface, the Coombs reagent will agglutinate the
RBCs and the test is deemed positive.
The Indirect Coombs test can detect very low concentrations of antibodies. It is
used to screen for a wide range of antibodies in blood transfusion preparation. Prior to
transfusion, the IAT may be used to test a sample of the recipients serum against a
sample of the blood donor’s RBCs, in a technique also sometimes called cross matching.
The IAT is also used to screen pregnant women for IgG antibodies that may pass through
the placenta into the fetal blood to cause hemolytic disease of the newborn.
The IAT is a two step test. In the first stage, washed test RBCs are incubated with
a test serum. If the serum contains antibodies to antigens on the RBC surface, the
antibodies will bind onto the surface of the RBCs. In the second stage, the RBCs are
washed several times with isotonic saline and then incubated with antihuman globulin. If
antibodies have bound to RBC surface antigens in the first stage, RBCs will agglutinate
when incubated with the antihuman globulin (Coombs reagent) and the indirect Coombs
test will be positive.
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 91 -
Manual Cross-Match Techniques Cross-match testing is widely used to prevent incompatibility of transfused blood.
It is typically performed on each unit of blood that may used prior to a transfusion and
offers several benefits by:
• avoiding the sensitization of the recipient to future incompatible transfusions;
• preventing a transfusion reaction in a previously sensitized recipient;
• preventing formation of isoantibodies, which may induce a delayed transfusion reaction and subsequent hemolytic anemia.
However, cross-match techniques do not guarantee the survival of donor cells and
like other manual procedures, are subject to clinical errors. Further, the hemolyzing
antibody may not be detected in a cross-match seeking agglutination.
The procedure, as described above, is a two-step process that involves incubating
washed test RBCs with a test serum, then washing the RBCs with isotonic saline and
incubating them with antihuman globulin. If antibodies have bound to RBC surface
antigens in the first stage, RBCs will agglutinate when incubated with the Coombs
reagent and the test will be positive, indicating incompatiblity of donor and recipient
blood.
To ensure that sufficient blood is available for a particular procedure, more blood
is typically ordered and tested than will be transfused. In some hospitals and for some
procedures, the ratio of ordered blood to transfused blood is as high as five to one. Once
blood is cross-matched for surgery, it is unavailable to other patients for 24 to 48 hours.
However, without cross-matching, RBCs can be stored for over a month.
In some cases, cross-matching prior to transfusion is not possible and universally
compatible O- blood must be used. These include emergencies in which patients need
blood immediately and transfusions for premature infants in which cross-matching and
blood-typing procedures are not possible.
Major Cross-Match In a major cross-match, donor RBCs are reacted with recipient serum or plasma to
detect antibodies that would attack transfused cells. This test is often performed in
addition to blood typing in a previously transfused patient to detect unexpected blood
group antibodies and is considered an important test.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 92 -
In some less common cases, major cross-matches do not always provide
conclusive results. For example, in patients receiving methyldopa, both a direct and an
indirect Coombs test are typically performed. In the absence of hemolytic anemia, usually
only the direct Coombs test is positive and this generally does not interfere with typing or
cross-matching. However, if the indirect Coombs test is also positive, reflecting problems
in the major cross-match, a hematologist or transfusion expert is asked to interpret
results.
Minor Cross-Match In a minor cross-match, recipient RBCs are reacted with donor serum or plasma to
detect antibodies that could destroy transfused cells. The minor cross match is not as
important as the major cross-match because it detects antibodies in the donor serum
which typically undergo significant dilution by the recipient's blood, thus reducing their
effect. If the donor antibody screening is routinely employed, the minor cross-match is
not essential and in emergencies, donor blood with a minor cross-match incompatibility
is often considered to be acceptable.
Antibody Screen
While cross-matches test the reactivity of a recipient’s blood against antigens
present on donor RBCs, antibody screens are used to detect unexpected antibodies to red
cell antigens in the recipient’s blood. If the antibody screen is negative, indicating that no
such antibodies are present, no further testing is performed unless a request is specifically
made for a cross-match on the sample. If the antibody screen is positive, indicating that
an unexpected red cell antibody is detected, or the patient has a history of a clinically
significant red cell antibody, a complete cross-match is then performed.
In the antibody screen, the patient’s serum is combined with known red cells
displaying significant minor red cell antigens (e.g. Kell, Duffy, Rhesus). The sample is
incubated, centrifuged and washed and then anti-human IgG is added to detect any
antigen antibody reaction. The sample is centrifuged again and observed for
agglutination.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 93 -
TYPES OF TRANSFUSIONS Although early transfusions focused on the transfer of whole blood, this is now
generally reserved only for special cases and more commonly, just the specific
components needed by the recipient are transfused. This provides for more economical
usage of blood supplies, as each unit of blood can be utilized for multiple recipients, and
also reduces the risk of causing hypertension in recipients. Each pint of whole blood
contains one transfusible dose of RBCs, one-half to one transfusible dose of plasma, and
one-fifth to one-eighth of a transfusible dose of platelets.
Whole Blood Whole blood is not commonly used in transfusion because a patient's medical
condition can often be treated with a blood component. Furthermore, too much whole
blood can raise a recipient's blood pressure, resulting in adverse effects. From the point of
view of the medical industry, the use of blood components represents a more efficient
way to utilize a limited blood supply, because blood that has been fractionated into
components can be used to treat more than one person. It is also more considerably more
convenient in terms of storage and distribution.
Believing that autologous blood (ie. blood collected earlier from the transfusion
patient) or allogeneic blood transfused within 12 hours of collection might reduce blood
loss and the need for platelets and FFP, some researchers have studied the use of fresh
whole blood as an alternative to using red blood cells, platelets and other components in
cardiac surgery. Although one study published in a 1991 issue of Blood showed less
postoperative blood loss in infants, most concluded that the logistic problems of obtaining
fresh whole blood from a prescreened donor outweighed any advantages. At present,
therefore, whole blood tends to be used when:
• specific components required by the recipient are not available;
• the recipient has lost a lot of blood, such as following an injury or surgical procedure. In this case, whole blood is given to help restore blood volume, which is essential for maintaining healthy blood pressure levels;
• there is reason to believe that the recipient’s body tissues may not be receiving sufficient oxygen;
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 94 -
In addition to these special cases, the donation of whole blood is generally
reserved for treating young children and remote areas where the hospital summons
donors when it needs them.
Packed Red Blood Cells Because red blood cells are the only cells in the body that transport oxygen, they
are the blood component most frequently used for transfusion. A transfusion of RBCs
increases the amount of oxygen that can be carried to the tissues of the body. RBCs that
have been separated from the liquid plasma (packed RBCs) are given to persons who
have anemia or have lost a significant amount of blood.
Platelets A key factor in blood clotting, platelets are another component frequently given
by transfusion. Platelets are extracted from donated blood and concentrated for use.
Along with other clotting factors, platelets are typically used to correct a deficiency in
either platelet number (thrombocytopenia) or platelet function (thrombocytopathy or
qualitative platelet disorders).
One unit of platelets generally increases the platelet count by about 5-10 x 109/L
in the average adult. Surgical and obstetrical patients with microvascular bleeding usually
require platelet transfusion if the platelet count is less than 50 x 109/L but generally do
not require therapy if it is greater than 100 x 109/L.
Leukocytes Leukapheresis, or the collection of white blood cells with the return of other blood
components to the donor, is relatively rare since the transfusion of leukocytes is not a
common practice. Occasionally, leukapheresis may be used in a research setting to obtain
blood cells from virus-infected patients to study various therapies.
More common is the cleansing of donated blood of leukocytes to prevent against
reactions in recipients. Four major types of reactions are associated with leukocyte
transfusion:

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 95 -
• febrile non-hemolytic transfusion reactions (FNHTR);
• alloimmunization and platelet refractoriness;
• transfusion-associated viruses;
• immunosuppression.
FNHTR is defined as a rise in temperature by at least one degree Celsius during
or within 24 hours of the completion of the transfusion. Flu-like symptoms of chills,
shaking and, in some cases, headache and nausea typically result. Fever can sometimes
be severe, reaching 104 degrees Fahrenheit, requiring the use of medication to bring the
temperature down. FNHTR is believed to occur in approximately 3% - 7% of patients
receiving red blood cell transfusions and 20% to 30% of platelet transfusion recipients
who receive blood that has not been leukocyte reduced.
Refractoriness to platelet transfusions that accompanies alloimmunization is one
of the most serious and difficult to manage of all transfusion therapy hazards. It occurs
when the body reacts to transfused leukocytes and creates antibodies against them. This
immune response, called alloimmunization, can cause patients to become refractory
(resistant) to subsequent platelet transfusions so that they do not benefit from the
transfusion. About 50% of patients undergoing multiple blood transfusions experience
this response, and subsequently require platelets matched to their specific blood type.
Patients receiving leukocyte reduced blood products are at a much lower risk for
refractoriness to platelet transfusion than are recipients of blood that is not leukocyte
reduced.
Transfused leukocytes can transmit several blood-borne viruses to patients
through transfusions. Most of these viruses belong to the herpes virus groups and exist
primarily as latent or inactive infections in the leukocytes of persons who carry the
disease but do not have symptoms. However, more serious viruses such as
cytomegalovirus (CMV) can also be transmitted. In certain patients, CMV infection can
cause fever, hepatitis, pneumonia and severe brain damage, and can ultimately lead to
death. In North America, 50% or more of the adult population has been exposed to this
virus, making transfusion-transmitted CMV a high risk. Other leukocyte-associated
viruses include Epstein-Barr (EBV), Human Herpes Virus type 6, and Human T-
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 96 -
lymphotropic virus type I (HTLV-I). These viruses are associated with infectious
mononucleosis, high fever and transient rash and adult leukemia, respectively.
Immunosuppression may also result and can lead to life-threatening events, such
as multiple organ failure, increased risk of infection after surgery and/or diminished
prospect of cure in patients with certain malignancies.
In 1998, the FDA’s Blood Products Advisory Committee unanimously agreed that
the "benefit-to-risk ratio associated with leukoreduction is sufficiently great to justify
requiring universal leukoreduction of all non-leukocyte cellular transfusion blood
components", as of mid 2008, however, the FDA has not issued a rule requiring universal
leukocyte reduction. In 2001, the agency issued guidance encouraging U.S. blood
collection centers to adopt the practice, and many of the largest, such as the American
Red Cross, have so that approximately 80% of the U.S. blood supply is now routinely
leukoreduced. Despite ongoing calls from health experts, however, leukoreduction is not
required by law. Opposition to mandatory leukoreduction generally focuses on cost
concerns. On average, a unit of leukoreduced blood costs about $30 more to produce than
a unit of non-leukoreduced blood, forcing hospitals to increase the amount of money
spent on their blood supply. Leukocyte depletion by either prestorage or poststorage
filtration has also been instituted for all blood components by the United Kingdom,
Canada, France, Spain, Portugal, Ireland and other countries.
Fresh Frozen Plasma (FFP) After removal of red blood cells and platelets from whole blood, the remaining
plasma contains all the blood coagulation factors, fibrinogen and other proteins in a
volume of 170 to 250 mL. The plasma is then frozen within six to eight hours of
phlebotomy to prevent inactivation of temperature-sensitive coagulation factors V and
VIII. At temperatures below -18º C, FFP can be stored for up to one year with minimal
loss of coagulant activity.
Transfusion with FFP is commonly indicated for the treatment of microvascular
bleeding due to congenital and acquired coagulopathies resulting in a prolongation of
either the activated partial thromboplastin time (aPTT) or prothrombin time (PT) greater
than 1.5 times normal, or a coagulation factor assay of less than 25%. FFP may also be

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 97 -
used to reverse the anticoagulation effects of warfarin prior to surgery or during active
bleeding episodes. (While parenteral vitamin K will produce the same effect in six to 12
hours without exposing patients to the risks associated with human blood components,
sufficient time for this treatment may not always be available). When FFP is indicated, it
is typically administered in a dosage that will result in a minimum of 30% of plasma
factor concentration. This usually requires 10 to 15 mL/kg of FFP, although a dose of 5 to
8 mL/kg is often adequate to quickly reverse warfarin anticoagulation. Over the past
decade, the usage of FFP has increased tenfold with almost two million units transfused
annually in the U.S. alone.
Cryoprecipitate Cryoprecipitated antihemophilic factor, or cryoprecipitate, is prepared from fresh
frozen plasma (FFP). It is the white precipitate that forms when FFP is thawed at 1º to
6ºC. This cold-insoluble material is removed following centrifugation and immediately
refrozen at -18ºC, at which temperature it can be stored for up to one year. Each unit of
cryoprecipitate contains 80 to 150 units of Factor VIII, 150 to 250 mg of fibrinogen, von
Willebrand Factor, Factor XIII, and fibronectin in a volume of 5 to 15 mL.
Cryoprecipitate is utilized for the treatment of congenital or acquired fibrinogen
and Factor VIII and XIII deficiencies. It may also be administered prophylactically in
non-bleeding perioperative or peripartum patients with congenital fibrinogen deficiencies
or von Willebrand's disease. Although cryoprecipitate has been the traditional approach
to managing patients with hemophilia A and von Willebrand's disease, select
intermediate purity Factor VIII concentrates are now preferred for von Willebrand's
disease and recombinant or highly purified Factor VIII concentrate is preferred for
hemophilia A because of their greater efficacy and safety, although many hospitals still
routinely stock cryoprecipitate. In fibrinogen replacement therapy, one unit of
cryoprecipitate per 10 kg body weight increases plasma fibrinogen by approximately 50
mg/dL in the absence of massive bleeding. Other indications for cryoprecipitate
transfusion include bleeding from excessive anticoagulation, massive hemorrhage and
disseminated intravascular coagulation.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 98 -
Immune Serum Globulin/IMIG/IGIV Derived from large pools of human donors and administered as intramuscular
immunoglobulin (IMIG) or intravenous immunoglobulin (IGIV), immune serum globulin
contains IgG antibodies against a wide spectrum of normal human proteins and anti-
idiotypic antibodies as well as a broad range of immune antibodies directed against
foreign antigens and pathogens. Immune serum globulin is therefore indicated for a wide
range of conditions including:
• primary immune deficiency (congenital agammaglobulinemia, common variable immunodeficiency, x-linked agammaglobulinemia, Wiskott-Aldrich syndrome);
• secondary immune deficiency (bone marrow transplant, septicemia prophylaxis, acute Graft-vs-Host Disease prophylaxis, chronic lymphocytic leukemia and pediatric HIV);
• Kawasaki syndrome, adisease primarily affecting young children, resulting in inflammation of the blood vessels and other tissues, such as heart muscle;
• idiopathic thrombocytopenic purpura, a disease that results in a decrease in the
number of circulating platelets. Low levels of platelets can result in bleeding
problems;
• various neurological disorders (acute Guillain-Barré syndrome, chronic
inflammatory demyelinating polyradiculoneuropathy, dermatomyositis and
others).
A variety of commercial products are available, which are typically prepared by
cold ethanol fractionation (the Cohn process) and further purified by a variety of steps
such as enzymatic treatment at a low pH, fractionation, filtration and chromatography.
The final products contain more than 95% IgG (not less that 90% in monomeric), less
than 2.5% IgA, and a negligible amount of IgM.
Immunoglobulin is distinct from a vaccine, however, since many vaccines require
repeated injections over several months to work effectively while immunoglobulin,
which contains antibodies that fight a virus, works immediately and seems to stay
effective for several months. Because of this, vaccines are sometimes administered
concurrently with immunoglobulins.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 99 -
FactorVIII Factor VIII concentrate is a lyophilized powder that is purified from plasma to
treat patients with hemophilia A or von Willebrand’s disease. An essential blood clotting
factor, about 80% of hemophiliacs lack sufficient amounts of Factor VIII in their blood.
Factor VIII is therefore also known as anti-hemophilic factor.
One unit of concentrate equals the clotting activity in 1 ml of fresh plasma,
although prepared Factor VIII concentrates differ in their purification levels. Highly
purified Factor VIII is stabilized by adding 98% of pasteurized human albumin. Porcine
Factor VIII concentrate may be used for patients with high titer anti-human Factor VIII
allo or autoantibody inhibitors. Because it is cell free and therefore poses no risk of
antibody-related incompatibility, Factor VIII is administered without regard to patient or
donor ABO or Rh type.
The product is generally stored refrigerated at 2 - 8° C for up to two years from
the date of manufacture, although some concentrates may be kept at room temperature for
longer. Once reconstituted, it should not be refrigerated. Factor VIII concentrate should
be infused within 4 hours of preparation to reduce the risk of bacterial growth. While
vials are usually shipped to a hospital pharmacy, blood service or nursing unit, many
patients receive them directly for home care.
Factor VIII concentrate is indicated for the treatment of bleeding or invasive
procedures in patients with hemophilia A and those with low titer Factor VIII inhibitors.
Prophylactic doses are sometimes used in addition to regular daily doses by some
hemophilic inhibitor patients to try to induce immune tolerance. Dosage depends on the
degree of factor deficiency, the weight of the patient and the presence and level of Factor
VIII inhibitors. The half life of circulating Factor VIII is 8 to 12 hours, therefore
transfusions may need to be repeated every 12 to 24 hours to maintain hemostatic levels.
This is necessary following surgery to prevent delayed bleeding and promote wound
healing in hemophilic patients.
Over the past several years, many improvements have made in Factor VIII
production to increase patient safety. While the transfer of a plasma byproduct into the
blood stream of a hemophilia patient often led to the transmission of HIV, HBV and
HCV, the introduction of recombinant synthesized factor products in the early 1990s

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 100 -
halted the transmission of nearly all forms of disease during replacement therapy.
However, antibody formation to Factor VIII remains a problem, with incidence linked to
many factors including the Factor VIII product itself.
Factor IX and Factor IX Complex Coagulation Factor IX and Factor IX Complex are indicated for the treatment of
Factor IX deficiency (hemophilia B, also known as Christmas disease) and Recombinant
Coagulation Factor IX (rFIX) is used for new patients with hemophilia B and for those
with limited exposure to human-derived Factor IX products. These preparations are
generally derived from three sources:
• human-derived Coagulation Factor IX is highly purified through chromatography or monoclonal antibody affinity columns, but may contain non-therapeutic traces of Factors II, VII, and X;
• Factor IX Complex is a less pure preparation of human plasma that also contains some Factors II, VII, and X, as well as proteins C and S. Some products also contain small amounts of heparin;
• Recombinant Coagulation Factor IX (rFIX) is produced in a Chinese hamster ovary tissue cell-line under serum-free conditions and is extensively purified. It is therefore free of risk of transmission of human disease.
Human-derived Factor IX concentrates and complex are treated with heat,
nanofiltration and/or solvent/detergent to reduce the risk of viral transmission. While
none of the currently available formulations have been known to transmit HIV or HCV,
there is a small risk of non-enveloped virus and/or prion disease transmission.
Factor IX preparations are typically stored as lyophilized powders at 2 - 8°
Celsius. One unit of Factor IX is equivalent to that found in 1 mL of normal human
plasma. Each unit of Factor IX concentrate or complex infused per kilogram of body
weight will cause about a 1% rise in the circulating Factor IX level, while each unit of
rFIX will yeild a 0.8 IU/ml rise. Factor IX concentrates are infused intravenously over
several minutes or administered by continuous infusion. The half-life in the blood ranges
from 18 to 32 hours.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 101 -
Factor VIIa Recombinant human Factor VIIa is a serine protease and vitamin K-dependent
coagulation factor that is primarily synthesized in the liver. Recombinant Factor VIIa is
FDA approved for treatment of bleeding episodes in patients with hemophilia A or B,
when inhibitors to these factors are present. It is also being investigated for treatment of
episodes of severe life-threatening bleeding, stem cell transplantation, intra-cerebral
hemorrhage and trauma.
Factor VIIa promotes hemostasis by enhancing thrombin generation through
direct activation of FX after complexing with Tissue Factor at the site of injury. In
normal individuals, a small amount of thrombin activates FVIII as well as platelets
accumulated at the injury site. The activated platelets then provide negatively charged
surfaces for further thrombin generation. The administration of recombinant Factor VIIa
enhances thrombin generation through direct activation of FX independent of FVIII.
To produce recombinant human factor VIIa, the gene for human FVII is isolated
from chromosome 13 and transfected into a baby hamster kidney cell line that secretes
FVII into the culture medium. The product is purified with murine monoclonal anti-FVII
antibodies and is subjected to treatment with 0.1% Triton X-100 to inactivate enveloped
viruses. Subsequent ion exchange chromatography further purifies the product and causes
auto-activation, producing an activated form of FVII.
C1 Inhibitor C1 inhibitor is a serine protease inhibitor (serpin) protein, whose main function is
the inhibition of the complement system to prevent spontaneous activation. C1-inh also
inhibits proteinases of the fibrinolytic, clotting, and kinin pathways, and is the most
important physiological inhibitor of plasma kallikrein, Factor XIa and Factor XIIa.
Patients with C1 inhibitor deficiency experience recurrent, unpredictable, debilitating,
and potentially life threatening attacks of inflammation affecting the larynx, abdomen,
face, extremities and urogenital tract. Severe cases of C1-inh deficiency, known as
hereditary angioneurotic edema (HAE), are significantly debilitating and life threatening
although these cases are relatively rare, with just 10,000 HAE sufferers in the U.S.
While there is no approved therapy for acute HAE attacks in the U.S., C1
inhibitor has been used in Europe to treat HAE for more than 35 years. In May 2008, Lev

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 102 -
Pharmaceuticals submitted a Biologics License Application (BLA) to the FDA for its
Cinryze C1 inhibitor for the treatment of HAE.
Fibrin/Thrombin Thrombin, also known as activated Factor II, is a serine protease that converts
fibrinogen, a soluble plasma glucoprotein that is synthesized by the liver, into fibrin. A
fibrillar protein, fibrin is polymerised into a mesh that, together with platelets, form a clot
over a wound site to prevent further bleeding. Thrombin also activates Factor XI, Factor
V, and Factor VIII, thereby accelerating the production of more thrombin.
In 1998, the FDA approved the first commercial fibrin sealant. The product,
whose main active ingredient is fibrinogen, is topically applied to help control bleeding,
particularly from small, sometimes inaccessible, blood vessels during surgery when
conventional surgical techniques are not feasible. This encompasses a large and growing
number of indications including cardiopulmonary bypass and colostomy operations as
well as situations when a traumatic injury to the spleen has occurred. In addition to
addressing blood loss, fibrin sealants have also been shown to help control leakage of air
and other body fluids. Fibrin sealant sprays can be used instead of sutures or staples for
fixation of skin grafts, to avoid complications such as pain on staple removal, as well as
suture- or staple-induced ischemia, fistualization, granuloma formation and foreign body
reaction. While initial products were derived from bovine blood, newer fibrin sealants are
prepared from human blood plasma.
Therapeutic Apheresis Therapeutic apheresis applies apheresis or blood exchange technology to the clinical
treatment of various autoimmune diseases and blood disorders by removing selected,
abnormal components or cells and returning all other components. It is used in a wide
variety of therapeutic areas including hematology, oncology, neurology, nephrology and
rheumatology, and can be applied to a range of techniques including:
• cytopheresis (cell reduction);
• leukapheresis;
• low density lipoprotein apheresis;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 103 -
• plasmapheresis;
• plateletpheresis;
• red blood cell exchange;
• stem cell harvesting.
For some conditions, therapeutic apheresis techniques are the only appropriate
therapy. For example, low density lipoprotein apheresis is used for patients suffering
from severe hyperlipidemia and coronary heart disease who do not respond to lipid-
lowering drugs. Circulating bone marrow stem cells are often used in transplantation
procedures. In some cases of leukemia with very high white blood cell counts, removal of
excess leukocytes may help to prevent complications of thrombosis. In some
myeloproliferative disorders, the platelet count can sometimes be very high
(thrombocytosis) and removal of platelets can help to avoid complications of thrombosis
and bleeding. Replacement of the plasma with saline solution can help to reduce
circulating antibodies and immune complexes in circumstances where excess blood
proteins cause circulatory problems. This can occur in a variety of diseases including
Waldenstrom's macroglobulinemia, myasthenia gravis, Guillain-Barré syndrome,
hyperviscosity syndrome, paraproteinemia, cryoglobulinemia and Goodpasture's
syndrome.
BLOOD MANAGEMENT ISSUES The effective management of blood supplies is a critical issue for the blood
industry, which continues to be challenged with a growth in demand that exceeds
increases in supply. While many blood collection groups have ramped up donor
recruitment campaigns and thereby increased overall donations, demand continues to rise
with aging populations so that in most countries, the available supply of blood for
transfusion does not meet demand.
Availability
The availability of blood for transfusion represents the net result of a complicated set of circumstances including:

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 104 -
• volume of blood collection;
• efficiency of blood collection and processing, such that the maximum utility is derived from each unit of collected blood;
• adequacy of storage and distribution systems;
• pricing levels and fluctuations;
• regulatory restrictions.
With the exception of regulatory restrictions, all of these factors are primarily
market driven. Blood collection volume tends to fluctuate with the levels of promotion
and advertising invested by blood banks. It can also be affected by external events, such
as highly publicized disasters and catastrophes. The efficiency of collection and
processing is largely based on the technology utilized to separate components, which in
turn is a function of the research invested by equipment manufacturers. Storage systems
are also technology-based. These factors can significantly impact availability, to both
increase and decrease it. On one hand, expanded collection and more effective equipment
that maximizes yields will increase availability; on the other, these improvements can
also lead to rising costs for collection centers, which can result in substantial price
increases for hospitals.
Regulatory activity tends to decrease availability, as the primary objective of such
oversight is to improve blood supply safety, particularly regarding the transmission of
infectious disease. This often involves restrictions on potential donors, which can limit
collection volume, but can also include requirements to implement costly new safety-
enhancing technologies. In 1997, for example, the FDA initiated a Blood Action Plan to
increase the effectiveness of its scientific and regulatory actions. The plan addressed key
areas of concern such as emergency operations, response to emerging diseases, and
updating of regulations. The FDA’s Blood Products Advisory Committee continues to
meet regularly to discuss issues of interest, recommending the implementation of a
leukocyte reduction process in all donated blood in 1998; voting to restrict blood
donation from persons who might have been exposed to the human variant of mad cow
disease in 2001; and continuing to monitor the threat to the blood supply of West Nile
virus. From time to time, however, regulatory activity can increase availability as with

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 105 -
FDA’s February 2007 draft guidance related to the collection and storage of cord blood.
This document offers cord blood banks a more straightforward path to licensure, allowing
them to cite existing data rather than supply their own clinical data.
SAFETY ISSUES Although the blood supplies in the developed nations are, to a very high degree,
free of disease-causing viruses, the risk of transfusion-related infection is nonetheless
present. Because these supplies contain human blood, achieving 100% virus eradication
is unlikely. However, efforts continue to reduce the risk of virus transmission as much as
possible. These include a variety of initiatives including the reduction of blood typing
errors, improved donor screening, improved viral screening, increasing repeat and/or
voluntary donation rates, enhancing viral and bacterial inactivation processes and
biovigilence.
Reducing Blood Typing Errors Errors related to transfusing the wrong type of blood remain a significant source
of preventable risk. In September 2003, the sixth annual report on Serious Hazards of
Transfusions (SHOT) produced by the U.K. Royal College of Pathologists showed at
least 15 patients died and dozens of others were placed in intensive care because of the
blood mistakes, an increase of 20% from 2002. SHOT also recorded a 7% rise in near
misses, or potentially disastrous mistakes that were spotted in time.
One approach to reducing errors is the use of a barcode patient identification
system involving hand-held computers for blood sample collection for compatibility
testing and the administration of blood. The International Society of Blood Transfusion
has set up a working group on automation and data processing to establish a replacement
for the currently used ABC Codabar that will be used worldwide.
In February 2004, the FDA proposed a finalized rule requiring bar codes on the
labels of drugs and biological products. The rule requires machine-readable information
on container labels of blood and blood components intended for transfusion. The FDA
estimates that the rule will help prevent nearly 500,000 adverse events and transfusion
errors while saving $93 billion in health costs over 20 years.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 106 -
European countries such as France and Slovakia have already passed legislation
that requires that patients be tested at bedside for blood type prior to blood transfusions.
In response to this several companies have launched rapid blood typing devices
including, Micronics' ABO Card and Akers' HealthTEST Blood Transfusion
Match/Screen Test.
Improving Donor Screening Blood collection groups continue to refine their screening techniques to reduce
the risk of accepting contaminated blood. This typically involves identifying high risk
individuals and ensuring that blood is not collected from these persons. To do this,
screening managers refer to detailed lists prepared by the collection group that set forth
factors (medical conditions, travel to certain countries, sexual contact with high risk
persons, etc.) which would preclude a donation. These guidelines also provide deferral
periods, following which blood donations may be accepted from individuals in each
specified group. Collection centers often maintain and share comprehensive databases on
deferred individuals so that such persons may not inadvertently be allowed to donate
blood during a deferral period. In an effort to continuously improve donor screening
techniques, these lists of exclusion conditions are reviewed and updated on an ongoing
basis. The multi-step process includes:
• identification of conditions that may increase the risk of contamination in a
donor’s blood;
• evaluation of the magnitude of this risk in the context of known instances of blood
contamination linked to the condition;
• determination of an appropriate deferral period for the condition;
• formal update of the donor screening guidance;
• periodic review of the condition and validation of its continued inclusion in the
guidance.
Many blood collection groups conduct such reviews several times each year,
which often augment their exclusion conditions. The factors to consider are numerous, as
evidenced by the 287-page reference guide issued by the AABB (formerly known as the
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 107 -
American Association of Blood Banks) in September 2007 titled, Screening Blood
Donors: Science, Reason, and the Donor History Questionnaire.
Improving Viral Screening Like donor selection, viral screening is an effective means to reduce blood supply
risk, particularly in the developed nations. The U.S., Europe and Japan have extremely
high safety requirements regarding viral testing of donated blood and because of this,
these blood supplies have very low rates of contamination. This is not always true in the
developing world, however. In 2000, for example, the World Health Organization
estimated that 1 million new HIV infections around the world resulted from inadequate
blood screening, most of which occurred in the developing countries. This trend persists,
with about 40% of all blood donations in emerging countries remaining unscreened for
HIV, HCV or HBV in 2007 and HIV-contaminated blood accounting for approximately
5% of all HIV infections in Africa.
In an effort to reduce the risk of false negative tests, most major blood collectors
in the developed nations have adopted the usage of more sensitive nucleic acid
amplification (NAT) testing. Although infected donors can still test negative with NAT,
the length of time between initial infection and a positive test result is shorter, resulting in
fewer false negatives.
Furthermore, as with donor screening practices, the developed nations continue to
review viral screening requirements and as new threats become apparent, update
procedures. In June 2005, in response to rising incidence of West Nile virus, the FDA
issued new guidance recommending that blood donors be deferred on the basis of a
reactive investigational screening test for WNV. At their discretion, blood establishments
may reenter such donors after 120 days from the date of their reactive donation.
Increasing Repeat Donation Rates The average donor gives blood just 1.6 times per year. However, repeat donation
can provide an effective means to selectively improve blood supply safety since past
donors have already passed medical screens and are therefore more likely to continue to
meet health requirements than entirely new donors. Additionally, the cost of encouraging
repeat donation is lower than the cost of acquiring new donors, providing added incentive

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 108 -
for collection centers to increase donor retention. Although several small studies have
been undertaken to identify conditions under which blood donors tend to become repeat
donors, this research remains in its infancy and practices to encourage repeat donation
tend to remain focused on ancedotal beliefs that donors with positive, side effect-free
experiences will be more likely to make subsequent donations than those without. To this
end, practices to increase repeat donation have focused on procedural improvements.
Because the initial donor screening step can be time consuming and repetitive,
plasma collectors began using an abbreviated questionnaire in the early 1990s to collect
information from donors who had previously completed a full-length questionnaire. The
shorter version eliminates donor characteristics that do not change (demographics, and
medical/behavioral history information documented from previous donations), making
the initial screening process shorter and easier for both donors and staff. A small number
of whole blood collectors submitted prior-approval license amendments for
implementation of a similar abbreviated questionnaire to the FDA and the first approval
was granted in 1998 for repeat whole blood donors who meet specified criteria, as well as
for RBC and platelet apheresis donors. In late 2003, the American Association for Blood
Banks (AABB) standardized this concept, formally proposing to the FDA an abbreviated
questionnaire for established repeat blood donors, who maintain a pattern of regular
donation as defined in the blood center standard operating procedures. The form was
subsequently approved.
Enhancing Viral Inactivation Processes Despite ongoing efforts to screen out potentially contaminated blood from
donations, some small amounts of virus can still creep into the blood supply, as shown in
Table 3-6. This is due to the narrow but finite window within which a donor may be
infected but the virus would not appear on a test. Viral inactivation technologies,
therefore, continue to be required to address these situations. These processes, including
heat, chemical, and/or ultraviolet radiation, are largely effective but may continue to
leave some small levels of virus in treated blood. As shown in Table 3-7, they may also
not address fully address certain less serious viruses such as parvovirus B19 and
enteroviruses. Development of new technologies, therefore, continues in an effort to

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 109 -
achieve complete viral inactivation in blood supplies. Emerging techniques include
Aphios’s critical-fluid inactivation (CFI) sterilization technology, which uses a fluid like
carbon dioxide that is raised above its critical temperature and pressure; and
CaridianBCT’s (formerly Gambro BCT) pathogen reduction system for platelets,
Mirasol, which applies light and riboflavin to alter the nucleic acids of pathogens,
rendering them inactive.
Component manufacturers also continue to experiment with new purification
techniques. In July 2005, for example, Talecris announced new product labeling for its
Gamunex (Immune Globulin Intravenous [Human], 10% Caprylate/Chromatography
Purified) indicating that the product now incorporates several manufacturing steps to
Remove pathogenic prions, such as those associated with the development of (vCJD).
The Caprylate/Chromatography process for improved product purity and prolonged
biological activity is a result of research with experimental agents and includes several
individual steps within the production process such as cloth filtration and depth filtration.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 110 -
Table 3-6
Risk of Contamination
Virus
Historical Evidence for Transmission from Plasma
Risk of Contamination
Virus for which all blood donors are tested HIV Yes Less than 1/10 million Hepatitis C virus Yes Yes Less than 1/10 million Hepatitis B virus Yes Less than 1/10 million HTLV types I, II Yes Only theoretical risk Other viruses Cytomegalovirus No Only theoretical risk Parvovirus B19 Yes
Only theoretical risk if heat inactivated; otherwise,1/100,000 to 1/1,000,000
West Nile virus No Much lower than 1/600,000, only theoretical risk Parasites Malaria No Only theoretical risk Chagas No Only theoretical risk Babesiosis No Only theoretical risk Prions vCJD Unknown Theoretical risk of less than 1/100,000,000
Source: Paediatrics & Child Health.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 111 -
Table 3-7
Viral Inactivation by Procedure
Procedure Agents Inactivated Agents Not Inactivated Inactivation By Heat
CMV, HAV, HBV, HCV, HIV, WNV, parvovirus B19
Inactivation Using Solvent/Detergent
CMV, HBV, HCV, HIV, WNV HAV, parvovirus B19, enteroviruses
Ultrafiltration using 35 nm and 15 nm filters
Removes even small viruses but also macromolecules (eg, Factor VIII is decreased)
Leukocyte depletion Decreases CMV, HTLV type I, II Non-WBC-associated viruses
Source: Paediatrics & Child Health.
Increasing Voluntary Donation While not an issue in the developed nations, the emerging nations continue to face
challenges resulting from the collection of blood from high risk groups such as prison
populations. To decrease the likelihood of contamination in donated blood, developing
countries are increasingly soliciting voluntary donations though increased advertising and
publicity of blood donation programs. Some progress in this area has been made, with the
WHO reporting that:
• in China, voluntary blood donation went from 45% of donations in 2000 to over
90% in 2007;
• Cuba and Suriname have introduced 100% voluntary donation since they created
their national blood transfusion services
• in Bolivia, the establishment of a national blood program has brought the rate of
voluntary, unpaid donations from 10% in 2002 to over 50% in 2007;
• South Africa has had 100% voluntary, unpaid donation since it established a
national blood service. Because of this even with HIV prevalence of 23.3% in the
adult population, only 0.02% of its regular blood donors have contracted HIV.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 112 -
Preventing Bacterial Infections Most blood bank services feel fairly confident about their ability to screen for
viruses but systems to screen for bacterial infection, which remains one of the major life-
threatening hazards related to blood transfusion, are less advanced. A number of new
bacterial screening, prevention and control guidelines are therefore being adopted.
Platelets, which are used to treat immuncompromised patients with serious
illnesses such as cancer and leukemia, are the blood component most vulnerable to
bacterial contamination since they must be stored at room temperature to retain their
blood clotting functions. At least 16 different species of bacteria have been found to
contaminate donated platelets. The risk of receiving a bacteria-contaminated unit of
platelets may be 50 - 250 times higher than the combined risk of transfusion-related
infections per unit associated with HIV and hepatitis. AABB data indicate that bacterial
contamination of platelets is the number one cause of morbidity and mortality from a
transfusion-transmitted infection and as many as 1 in every 2,000 platelet units transfused
and 1 in every 20,000 red cell units transfused may be contaminated with bacteria. It is
estimated that up to one in 4,000 transfusions leads to a severe septic reaction and as
many as one in 17,000 transfusions can lead to death due to bacterial contamination.
There are a number of strategies underway to decrease bacteria in blood products
including: improving the method of skin preparation at the site of venipuncture, diverting
the first milliliters of blood during collection (a new bag now available), filtering the
leukocytes from the unit and treating blood units to kill or remove pathogens. The AABB
recently published guidelines instructing blood centers to test all platelet components for
the presence of bacteria as of March 2004. At the same time, Haemonetics received FDA
clearance to integrate a new blood sampling system for bacterial detection into its platelet
collection disposables. The Haemonetics system allows simplified testing, unlike other
systems that require manual connection and extraction of a sample, thereby extending
platelet processing time and reducing the usable shelf life of platelets. In September
2007, France-based Hemosystem received FDA approval to market its Scansystem
bacterial screening technology in the U.S.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 113 -
Biovigilence In late 2008, the U.S. will launch the first nationwide data collection program for
the blood industry. The new U.S. Biovigilance Network collect and analyze data to
identify trends and recommend best practices to reduce adverse reactions and incidents
associated with blood transfusion, particularly focusing on a centralized and standardized
reporting process. The Network is a public/private collaboration with shared
responsibilities for program development, operation and management, and funding with
the U.S. Centers for Disease Control and Prevention providing the platform for initial
surveillance through the National Healthcare Safety Network.
The first stage of the pilot phase will be implemented with nine hospitals across
the country. This will allow for fine-tuning of the surveillance system and analysis of
initial data collected. Additional organizations are voluntarily registering to contribute
data, with full participation and system launch expected in 2009. Until the launch of the
new network, the U.S. was the only developed nation that did not have a national system
to track and monitor the safety of blood collection and transfusion. Instead, the U.S.
relied on information from hemovigilance systems in other countries and on tracking by
individual hospitals, transfusing organizations and blood centers. Countries with
surveillance systems tend to have lower morbidity and mortality rates for both patients
and donors.
Other Safety Precautions Blood collection centers may also take other precautions to enhance the safety of
donated blood. These are often implemented on an ad hoc basis, in response to specific
threats. For example, when the mosquito-borne West Nile virus (WNV) emerged in the
U.S. in 1999 as a potential risk factor, blood centers began stockpiling frozen blood
components before the start of mosquito season.


Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 115 -
C H A P T E R F O U R
The Human Blood
and Blood Products Market
DRIVING FORCES OF THE HUMAN BLOOD INDUSTRY The market for human blood and blood components continues to expand as a
result of the growing and aging populations, particularly in the developed nations. In
2007, worldwide demand for non-infected blood exceeded 200 million pints per year. Of
this, red blood cells (RBCs) comprised the most heavily consumed blood product at 85
million units, with Europe accounting for the single largest market, as shown in Table 4-
1. Through 2014, total global demand for RBCs is expected to reach 133 million units, as
shown in Table 4-2.
Table 4-1
Geographical Distribution of RBC Demand by Region (United States, Europe, Japan, ROW)
2007
Region Units of RBCs (in millions)
United States 15 Europe 22 Japan 12 ROW 36 Total 85
Source: Kalorama Information

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 116 -
Table 4-2
Projected World Demand for RBCs 2007-2014
Year Units of RBCs (in millions)
2007 85 2008 89 2009 93 2010 99 2011 106 2012 114 2013 123 2014 133
Source: Kalorama Information
Much of the need for RBCs is for the management of acute blood loss, as shown
in Table 4-3, with approximately 50 million units required in 2007. As shown in Table 4-
4, many of these were required for high blood loss surgical procedures, such as
gastrointestinal, cardiovascular, orthopedic, urologic and thoracic interventions. With
more than 9.0 million procedures in 2007, over 29 million units of RBCs were transfused
for these procedures alone, at a market value of more than $3.2 billion. Usage of blood
during surgery continues to rise, despite efforts to contain demand through the increasing
utilization of perioperative blood salvage techniques and/or minimally invasive surgical
procedures. Transfusions for chronic blood loss, such as that associated with chronic
anemias, chemotherapy, or bone marrow transplant, represented the balance.
Table 4-3
Worldwide Demand for RBCs for Acute and Chronic Conditions, 2007
Blood loss segment Units RBCs (in millions)
Acute Blood loss 50 Chronic Blood loss 35 Total 85
Source: Kalorama Information

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 117 -
Table 4-4
Number of High Blood Loss Surgical Procedures by Type, 2007
Type of Surgery Number of Procedures
Units RBCs per Procedure
Total Units Transfused
Total Market Value (in millions)
Gastrointestinal 2,650,000 3.6 9,540,000 $1,039.86 Cardiovascular 2,440,000 3.8 9,272,000 1,010.65 Orthopedic 1,695,000 2.7 4,576,500 498.84 Urologic 850,000 2.6 2,210,000 240.89 Thoracic 335,000 3.3 1,105,500 120.50 Other 1,083,000 2.5 2,707,500 295.12 Total 9,053,000 3.2 29,411,500 $3,205.85 Source: Kalorama Information
Aside from RBCs, other blood products are also often required in such
procedures, as shown in Table 4-5. Organ transplants, for example, typically require 30
units of platelets, 20 bags of cryoprecipitate and 25 units of fresh frozen plasma while
burn treatment requires 20 units of platelets, on average.
Table 4-5
Average Blood and Component Requirements by Condition
Cause of Blood Need Average Number of Units Required
Automobile Accident 50 units of blood Heart Surgery 6 units of blood 6 units of platelets Organ Transplant 40 units of blood 30 units of platelets 20 bags of cryoprecipitate 25 units of fresh frozen plasma Bone Marrow Transplant 120 units of platelets 20 units of blood Burn 20 units of platelets
Source: Kalorama Information

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 118 -
Variables Influencing the Demand for Blood Transfusions
With an aging population in the developed nations and advances in medical
treatments requiring blood transfusions, the demand for blood continues to increase at
rate of about 6% each year, overall. Nonetheless, other factors can influence the demand
for blood transfusions, including:
• seasonality – demand tends to be higher in summer;
• rising utilization of alternative therapies – non-invasive alternatives to surgery can
reduce demand for blood;
• blood pricing and availability – as blood becomes more difficult or costly to
obtain, some patients defer elective procedures, thereby decreasing demand;
• new technologies – researchers are experimenting with various ways to stimulate
the body to produce more blood, to reduce the need for transfusions.
This latter area is particularly promising although moving slowly. It includes, for
example, administration of synthetic erythropoietin, a hormone that stimulates RBC
production. Critically patients do not produce sufficient levels of erythropoietin to induce
the production of RBCs, however, research published in an article appearing in a 2003
issue of the Journal of the American Medical Association reported that in clinical studies,
patients who were given a man-made erythropoietin required 20% less transfused blood
than those not receiving the hormone. Similarly, in late 2005 the FDA approved
Celgene’s Revlimid for patients with a subgroup of myelodysplastic syndromes (MDS).
MDS are a group of rare diseases where the body does not produce enough healthy,
properly functioning blood cells and patients therefore become transfusion dependent. In
clinical trials, most patients treated with Revlimid no longer required transfusions after
the first three months of treatment and remained transfusion free for up to 44 weeks.
Market Size
In 2007, the total global value of all human-derived blood products was $16.2
billion, as shown in Table 4-6. Of this, an estimated $9.2 billion was attributable to red
blood cells while $3.3 billion was from immunoglobulins, $759 million to albumin and
$2.8 billion to other human plasma-derived products such as plasma, platelets, clotting

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 119 -
factors, prothrombin complex concentrates, fibrin sealants and alpha-1 proteinase
inhibitor (API). Average global costs for each product are somewhat lower than U.S.
prices, which tend to be higher.
Table 4-6
Global Blood Products Market by Type, Number of Units, Average Price and Total Value, 2007
Units in millions Cost/unit
Market value in millions
RBCs 85 109 $9,265 Immunoglobulins 60 55 3,300 Albumin 23 33 759 Other Plasma Products 36 80 2,880 Total 204 79 $16,204
Source: Kalorama Information
Through 2014, the total number of collected units worldwide will reach 104.5 million, as shown in Table 4-7, assuming that collection centers ramp up their efforts to meet rising demand with new donor recruitment initiatives.
As this occurs, the number of transfused units (which includes RBCs, plasma, platelets and other components fractionated from each single collected unit) will rise from an estimated 204.0 million units in 2007 to 250.9 million units in 2014. Each pint of whole blood contains one transfusible dose of RBCs, one-half to one transfusible dose of plasma, and one-fifth to one-eighth of a transfusible dose of platelets, although automated blood collection, which enables the collection of one full dose of platelets and other components from a single donor, is becoming more popular.
The number of units of collected and transfused plasma will also increase during this time, rising from an estimated 26 million liters in 2007 to 32 million liters in 2014, as shown in Table 4-8.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 120 -
Table 4-7
Global Blood Collection and Transfusion Estimates (Millions of Units) 2005-2012
2007 2008 2009 2010 2011 2012 2013 2014 Collected units 85.0 87.6 90.2 92.9 95.7 98.5 101.5 104.5 Transfused units 204.0 210.1 216.4 222.9 229.6 236.5 243.6 250.9
Source: Kalorama Information
Table 4-8
Global Plasma Collection and Transfusion Estimates 2005-2012
2007 2008 2009 2010 2011 2012 2013 2014 Millions of Liters 26.0 26.8 27.6 28.4 29.3 30.1 31.0 32.0
Source: Kalorama Information
CHANGING PATTERNS OF TRANSFUSION PROCEDURES In an effort to both ensure greater safety of transfused blood and conserve
shrinking blood resources, blood collection agencies are increasingly standardizing their
processes. In December 2002, for example, the European Parliament and Council
approved the EU Blood directive that legislated blood donated anywhere in the European
Union will be taken and treated in a uniform fashion. To reduce the risk of
contamination in donated blood, the directive also outlined the necessity of using the
latest technologies for the detection, inactivation and elimination of pathogens in blood
products, such as leukocyte reduction. Thus some technologies that have not yet been
commercialized in the United States are already being used in Europe. Key transfusion-
related trends are described below.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 121 -
Leukocyte Reduction
To address complications associated with the transfusion of leukocytes, many
countries now implement routine leukocyte filtration, as shown in Table 4-9. Canada was
the first country to move to 100% leukocyte reduction, while in the U.S., Rhode Island
was the first state to provide 100% leukocyte reduced blood products for its health care
system. As of mid 2008, however, the U.S. does not have a national requirement
mandating leukocyte reduction.
Table 4-9
Countries Conducting Routine Leukocyte Reduction, 2008
Country Leukocyte Reduction Policy Austria In 1996, the Austrian Red Cross introduced leukocyte reduction, filtering all
donated blood. The ARC subsequently introduced leukocyte reduction by filtration into other Austrian blood banks.
Canada Canadian Blood Services and Hema-Quebec introduced pre-storage leukoreduction for all blood products. In 1998, following a directive issued by the Canadian Government, Canada was one of the first countries in the world to implement filtering of all platelets for transfusion.
France France committed to 100% leukocyte reduction in 1998, both on clinical grounds and as a precautionary tool to ensure the safety of its blood supply.
Ireland Ireland moved to 100% leukocyte reduction of its transfused red cells and plasma in 1998 as a precautionary measure against nvCJD. The decision was based on the findings of experiments involving scrapie (a disease similar to nvCJD that occurs in sheep and goats).
Germany Germany mandated routine filtration of all blood products in 2000, based on clinical studies demonstrating the benefits of removing donor white blood cells from transfusion products.
New Zealand New Zealand moved to 100% filtration of platelets in 2000, followed by 100% filtration of blood bank red blood cells in 2001.
Norway In Norway, 100% leukocyte reduction is required. Portugal Portugal introduced filtration of all donated blood and platelets in 1999 to
reduce the risk of infection with nvCJD. UAE United Arab Emirates, a federation composed of the seven emirates of Abu
Dhabi, Dubai, Sharjah, Ajman, Umm al-Qaiwain, Ras al-Khaimah and Fujairah, moved to 100% filtered collections in 2001.
U.K. The U.K. introduced filtration of all blood components for transfusion, red cells, platelets and plasma in 1999. This was a move to minimize the risk of nvCJD as well as a response to the U.K.'s Spongiform Encephalopathy Advisory Committee (SEAC), which advised the government to leukoreduce blood for transfusion as a precautionary measure.
U.S. In 2001, the FDA issued guidance encouraging U.S. blood collection centers to implement leukocyte reduction procedures but as of mid 2008 has not issued a formal rule requiring it due to conflicting scientific evidence and cost concerns.
Source: Kalorama Information
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 122 -
Several manufacturers active in the blood processing space have introduced lines
of leukocyte reduction filters for red blood cells and platelets including Fenwal Blood
Technologies (formerly Baxter Transfusion Therapies), Pall and others. Pall has a
particularly extensive product portfolio, including the EZ Prime High Efficiency,
LeukoGuard line, Leukotrap line, LPS High Efficiency and the Purecell line.
Impact of Autologous Donations
Autologous donations represent blood collected from, and transfused to, the same
patient. This may occur in expectation of upcoming surgery, when patients collect and
store their own blood for future use. Although it is an option for many surgical patients, it
tends to be more common for those with rare blood types and/or when donated blood
would be crossmatched. The use of autologous blood ensures that the blood type will
always match; reduces the risk of infectious disease transmission; and minimizes the risk
of allergic reactions. However, it is significantly more expensive and arrangements must
be made well in advance. Furthermore, it is possible that donated blood would still have
to be used if more blood is required than has been set aside. The use of autologous blood
is also not recommended for patients who are medically unable to give blood, such as
cardiac patients, small children and infants.
In the U.S., autologous donations account for about 5% of all transfusions overall
and in some surgical centers, they comprise as much as half of transfusions. Such
collections may be performed by hospital staff or a contract extracorporeal service
provider, such as Hospital Clinical Services Group (formed in May 2007 when Specialty
Care Services Group acquired Fresenius Medical Care Extracorporeal Alliance, the
largest and longest continuously operating provider of outsourced perfusion,
autotransfusion, and other blood management services in the U.S.) which serves more
than 300 hospitals across the country.
Types of Autologous Donations
Autologous donations are collected in several different scenarios:
• preoperative donations;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 123 -
• intra-operative blood salvage;
• postoperative blood salvage;
• acute normovolemic hemodilution (ANH).
Preoperative donations are typically collected from healthy patients undergoing
elective surgery whose blood would otherwise need to be cross-matched with donor
blood. Many patients can give blood as frequently as every 3 days, although once a week
is more common. The optimal donation period begins 4 to 6 weeks before surgery in
order for a sufficient number of units to be donated and to enable more complete RBC
regeneration, with the last donation occurring no less than 72 hours before surgery to
allow for restoration of intravascular volume. However, there are several significant
disadvantages to preoperative donation including the risk of patients entering surgery
with anemia and thereby incurring potentially longer hospital stays. Cost is also an issue,
since preoperative blood donation can cost as much as $800 per patient compared with
less than $500 for peri-operative blood salvage.
Intra-operative blood salvage represents the collection and reinfusion of blood lost
during surgery. Once used almost exclusively during cardiac procedures, intra-operative
blood salvage is now commonly used for orthopedic surgeries, some solid organ
transplants and some trauma cases, as shown in Table 4-10, and may be used in some
procedures where postoperative blood salvage is not appropriate, such as major vascular
surgery and certain neurological procedures. The amount of RBCs recovered during
intra-operative blood salvage varies with the surgical procedure but may amount to 50%
or more of that lost. Blood salvaged intra-operatively may be transfused directly after
collection or washed prior to infusion. Although data regarding the safety of unwashed
salvaged blood is limited, this form of autologous blood is usually infused in relatively
small amounts of less than 2 liters without significant adverse effects; washed blood
tends to be utilized more often, as it reduces infusion of free hemoglobin, tissue pro-
coagulants, and debris.
Postoperative blood salvage is most commonly used for cardiac and orthopedic
surgical patients. Blood is typically collected from chest and joint drains, then transfused
without washing.
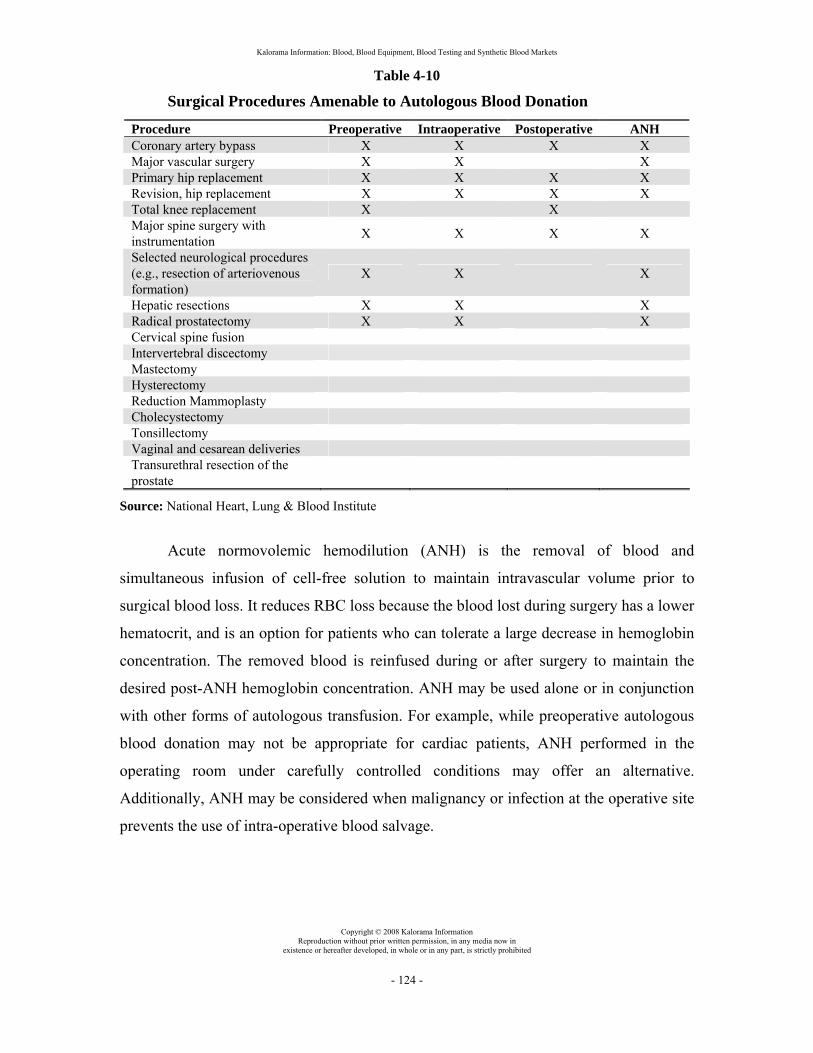
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 124 -
Table 4-10
Surgical Procedures Amenable to Autologous Blood Donation
Procedure Preoperative Intraoperative Postoperative ANH Coronary artery bypass X X X X Major vascular surgery X X X Primary hip replacement X X X X Revision, hip replacement X X X X Total knee replacement X X Major spine surgery with instrumentation X X X X
Selected neurological procedures (e.g., resection of arteriovenous formation)
X X X
Hepatic resections X X X Radical prostatectomy X X X Cervical spine fusion Intervertebral discectomy Mastectomy Hysterectomy Reduction Mammoplasty Cholecystectomy Tonsillectomy Vaginal and cesarean deliveries Transurethral resection of the prostate
Source: National Heart, Lung & Blood Institute
Acute normovolemic hemodilution (ANH) is the removal of blood and
simultaneous infusion of cell-free solution to maintain intravascular volume prior to
surgical blood loss. It reduces RBC loss because the blood lost during surgery has a lower
hematocrit, and is an option for patients who can tolerate a large decrease in hemoglobin
concentration. The removed blood is reinfused during or after surgery to maintain the
desired post-ANH hemoglobin concentration. ANH may be used alone or in conjunction
with other forms of autologous transfusion. For example, while preoperative autologous
blood donation may not be appropriate for cardiac patients, ANH performed in the
operating room under carefully controlled conditions may offer an alternative.
Additionally, ANH may be considered when malignancy or infection at the operative site
prevents the use of intra-operative blood salvage.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 125 -
PRICING OF BLOOD While some countries such as India and the Philippines set prices for blood and
blood components, in many of the developed nations including the U.S., there is no
uniform, fixed price for blood. Rather, the cost varies from country to country and region
to region, with even nearby centers often charging different prices. (In the U.S. the
Centers for Medicare and Medicaid Services or CMS sets government reimbursement
rates but blood collection facilities determine their own pricing and private insurers
determine their own coverage levels. Because of this, hospitals often pay more than CMS
rates for certain products, particularly during periods of shortage). Furthermore, the
various components of blood are priced quite differently, with additional processing
generally adding to the cost. Other factors than can affect pricing include:
• short and long term supply fluctuations;
• competition within a particular area;
• contract issues with hospitals;
• regulatory requirements.
This latter factor can have a significant impact on prices. Although the cost of
blood had remained fairly stable for many years with increases below the rates of
inflation, between 1999 and 2004 blood costs nearly doubled as a result of new Good
Manufacturing Practices (GMPs) and quality processes required by FDA as well as new
safety measures such as donor screening by Nucleic Acid Tests for HCV and HIV, and
later for West Nile virus.
National Blood Exchange
Established in 1953 by the AABB (formerly the American Association of Blood
Banks), the Washington, D.C.-based National Blood Exchange (NBE) coordinates the
distribution of more than 240,000 units of blood and blood components throughout the
U.S. each year. In return for a transaction fee of 1% charged to both the shipper and the
receiver, the NBE responds to requests for blood from hospitals facing shortfalls in their
supply, locating blood resources, arranging deliveries and coordinating payments. This
provides blood centers with the opportunity to move surplus blood to areas in need. The
NBE also:

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 126 -
• tracks national market trends;
• obtains type and component-specific blood information on a daily, weekly and
annual basis;
• provides daily assessments of the blood supply including current prices.
While the NBE provides assistance with surplus issues and blood supply
questions during business hours, it maintains a 24-hour, 7-day per week telephone
network to assist with blood shortage and emergency issues. In January 2006, the NBE
launched the Web-based NBExchange system, allowing participants to manage account
information, broadcast emergency shortages and view shipment details at any time.
RBCs and Leukoreduced RBCs
Of red blood cells (RBCs), platelets, plasma and cryoprecipitate, RBCs are
generally the most expensive component of whole blood. The unit price of RBCs,
however, varies with a number of factors including blood type and special preparation
methods. In general, the universal donor type O is the most expensive because it is in
highest demand. Other factors that can add to the cost include the utilization of leukocyte
reduction techniques and/or special-antigen typing. This latter procedure is necessary
when the intended recipient has become sensitized to certain RBC antigens as a result of
prior RBC transfusion or pregnancy.
Costs for RBCs have risen over the past several years, with CMS reimbursement
rates for a single unit of RBCs increasing from $86.41 in 2004 to $129.66 in 2008. The
cost for leukocyte reduced RBCs has increased at an even faster pace, rising from
$119.26 in 2004 to $185.15 in 2008. While just 20% of RBCs provided to U.S. hospitals
were leukoreduced in 1999, by 2007 this proportion had risen to 80%.
Washed Red Blood Cells
Washing red blood cells with sterile normal saline removes about 99% of plasma
proteins, electrolytes and antibodies. These washed RBCs are used for patients who have
allergic reactions to plasma components of the blood as well as patients with antibodies
to IgA or IgE immunoglobulins or thalassemic patients. Peri-operative autotransfusion of

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 127 -
washed RBCs may also be used to reduce peri-operative transfusion requirements. Until
recently, the procedure was limited to adults because the processing of less than 300 ml
of salvaged blood was considered a contraindication to intra-operative transfusion and the
centrifugation bowls used by such devices were too large compared with the small blood
volume of children. However, newer devices with smaller bowls have extended the
procedure to pediatric use. In 2008, CMS increased reimbursement rates for washed
RBCs to $277.03 per unit from $211.03 the prior year and just $160.69 in 2004.
Deglycerolized Red Blood Cells
Frozen, rejuvenated and deglycerolized RBCs are similar in function to liquid
stored red blood cells. Each unit contains at least 80% of the original RBCs following the
deglycerolization process, with virtually all plasma, platelets and leukocytes removed.
However, the deglycerolization process enables long term storage of RBCs up to 10
years, compared with 42 days for refrigerated RBCs. Such cryopreserved blood can help
to maintain stores of Rh negative blood, provide units for persons with antibodies to
high-incidence antigens or persons difficult to cross-match because of multiple
alloantibodies and to provide plasma-free blood to persons with IgA deficiency.
In 2008, CMS reduced reimbursement rates for deglycerolized RBCs by 3% to
$347.23, based upon the prior year’s hospital claims. However, this nonetheless
represents a significant increase from 2004 rates of $183.44.
Single-Donor Platelets and Random-Donor Platelets
Each year, approximately 4 million doses of platelets are transfused in the U.S.
and Europe. Single-donor platelets are obtained through apheresis, while random-donor
platelets are obtained through the pooling of blood from many donors. Platelets from a
single donor are generally viewed as possessing a higher degree of safety since random-
donor platelets carry about five times the risk of post-transfusion sepsis and fatality that
apheresis platelets do. Additionally, apheresis platelets tend to be used before random-
donor platelets, making them fresher and less likely to develop significant bacteria. (To
maintain their functionality, platelets cannot be refrigerated but must be stored at room
temperature, making them susceptible to bacterial contamination). One study conducted

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 128 -
at Johns Hopkins Medical Institutions showed that over a 12-year period, increasing the
use of single-donor platelets from 51.7% of all platelet transfusions to 99.4% reduced
septic platelet transfusion reactions from three events annually to one.
Since they require costly apheresis equipment to collect, apheresis platelets are
significantly more expensive than random-donor platelets. One apheresis unit from a
blood supplier may be priced at about $500, while a pool of five or six $50 platelet units
costs about $250 - $300. In 2008, CMS reimbursed platelet units at a variety of different
rates, depending upon the type of processing involved, as shown in Table 4-11. However,
many hospitals own their own apheresis equipment, making the costs of single-donor
platelet acquisition comparable to or even lower than what they would pay for random-
donor units from an outside supplier.
Table 4-11
CMS Platelet Reimbursement Rates, 2008
CPT/HCPCS Code Description Price P9019 Individual platelets $69.50 P9031 Leukocyte reduced platelets 107.51 P9032 Irradiated platelets 121.72 P9033 Leukocyte reduced, irradiated platelets 139.94 P9034 Platelet pheresis 441.03 P9035 Platelet pheresis, leukocyte reduced 499.53 P9036 Platelet pheresis, irradiated 417.71 P9037 Platelet pheresis, leukocyte reduced, irradiated 630.08
Source: CMS
Fresh Frozen Plasma and Pooled Frozen Plasma
In the U.S., prices of fresh frozen plasma (FFP) have recently stabilized after a
steep decline. While CMS reimbursed purchases of plasma frozen within 8 hours of
collection at a rate of $63.35 in 2005, this represented a 33.3% decline over 2004
reimbursement rates of $95.00. The reimbursement rate for pooled frozen plasma was
similarly lowered from $124.31 to $78.00 in 2005. The changes were made following an
evaluation of 2003 hospital claims and subsequent removal of the products from CMS’s
low volume blood products list, in line with CMS’s new methodology of calculating

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 129 -
blood product reimbursement rates. This price decline was due in part to ongoing
increases in production volume and was experienced in other countries as well. From
1999 to 2002, for example, South Africa increased its domestic production of FFP from
50,000 liters to 110,000 liters. In 2008, CMS reimbursement rates for fresh frozen plasma
remained relatively steady at $67.03, and prices for pooled frozen plasma were increased
by 28.5% to $73.87 after a steep reduction in 2006.
Cryoprecipitate
Prices of cryoprecipitate have pulled back somewhat after a strong rise in 2005.
During that year, CMS raised reimbursement rates to $48.25 per unit from $29.31 in
2004 with the agency’s new process of determining reimbursement rates for blood
products. The increase reflected rising costs that result from the difficulty of producing
high-quality product in light of the need to optimize Factor VIII yield, minimize protein
content and address cryoprecipitate’s resistance to many viral inactivation techniques. In
subsequent years, however, cryoprecipitate prices were lowered until they finally reached
$41.24 in 2008.
Granulocytes
Granulocytes are white blood cells whose cytoplasm contains tiny granules, and
are named according to the staining characteristics of the granules. They are formed in
the bone marrow and collected by apheresis for transfusion into patients within 24 hours
after collection. Although their efficacy has not been well established, granulocytes may
be used to treat infections that are unresponsive to antibiotic therapy. They are therefore
used in relatively low volumes.
CMS reimbursement rates for granulocytes have fluctuated dramatically over the
past several years, falling from $1,248.66 in 2004 to $750.36 in 2007 then increasing
again in 2008 to $1,387.55. Used relatively infrequently, granulocytes are particularly
vulnerable to hospital claim volume.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 130 -
Gamma-Irradiated Blood
Red blood cells are exposed to gamma radiation to inactivate any lymphocytes
present. The use of irradiated blood and blood products in transfusions is recognized as
the most effective way of preventing transfusion associated graft versus host disease (TA-
GVHD). This occurs when T-lymphocytes from the donor's blood divide at a rapid rate
and target the cells of the recipient, whose immune system is unable to reject them.
Patients with severely weakened immune systems, such as bone marrow transplant
patients, those with congenital immunodeficiencies, transplant recipients, newborn
infants and leukemia patients require irradiated blood when given a transfusion.
Approximately 10 - 15% of all blood in North America is irradiated for this purpose.
A variety of different irradiated blood products are sold, as shown in Table 4-12.
CMS reimbursement rates on most of these products changed little from the prior year,
with some increasing slightly and others decreasing somewhat.
Table 4-12
CMS Platelet Reimbursement Rates, 2008
CPT/HCPCS Code Description Price P9032 Irradiated platelets 121.72 P9033 Leukocyte reduced, irradiated platelets 139.94 P9036 Platelet pheresis, irradiated 417.71 P9037 Platelet pheresis, leukocyte reduced, irradiated 630.08 P9038 Irradiated red blood cells 195.18 P9040 Irradiated, leukocyte reduced RBCs 240.27 P9056 Irradiated, leukocyte reduced blood 147.13 P9057 Irradiated, leukocyte reduced, deg, washed RBCs 373.99 Source: CMS
AVERAGE COST OF TRANSFUSION The cost of transfusion varies widely with a number of factors including:
• country and state where the transfusion is performed;
• material transfused (red blood cells, platelets, plasma, etc.);
• presence of alloimmunization;
• condition for which the transfusion is required;
• whether the patient is an adult or a child.
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 131 -
For example, studies have shown that patients with hematologic tumors tend to
require more red blood cells at a higher average cost than patients with solid tumors who
require blood. Other variations across different conditions and tumor types have also
been identified. While the American Red Cross supplies blood for transfusion at about
$150 - $250 per 400 ml bag, other costs related to processing, distribution and storage
can drive the per-bag cost as high as $1,000. However, the average CMS reimbursement
rate is less than $200 per bag.
On average, the cost of transfusion therapy in the U.S. is estimated at about $6
billion - $8 billion per year. America’s Blood Centers estimates the total number of
transfusions at about 5 million, with a cost per transfused unit of about $500 - $800, and
many transfusions requiring two or more units. This results in a net loss for hospitals and
surgicenters on blood transfusions, which must be made up elsewhere. In other parts of
the world, most blood services are funded by government programs, which are also
feeling the weight of increased blood processing costs.
PLASMA AND PLASMA DERIVED PRODUCTS Plasma and plasma derived products continue to experience expanding usage as
demand continues to rise with aging populations in the U.S., Europe and Japan and
companies introduce new recombinant products. Table 4-13 shows selected new plasma
derived products.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 132 -
Table 4-13
Selected Plasma Derived Product Approvals, 2003 - 2008
Year Product Manufacturer Indication Benefit 2003 Crosseal Fibrin
Sealant Omrix Hemostasis in liver
surgery patients Ease of preparation and use
2003 Zemaira Alpha-1 proteinase inhibitor (API)
Aventis Behring (CSL)
API deficiency and evidence of emphysema
15 min. infusion time compared with 30 min for other products
2003 Advate rFactor VIII plasma/albumin free method
Baxter Hemophilia A No plasma products used in MAb production or as additives; no prior risk
2003 Gamunex IVIG, 10% by Chromatography Process
Bayer Primary immune deficiency and ITP
High efficacy, new safety paradigm
2003 Flebogamma IVIG
Grifols Primary immune deficiency
Liquid, ready to use
2003 (Germany)
Octaplex Prothrombin Complex
Octapharma Prophylaxis, treatment of bleeding in patients with congenital or acquired deficiencies of clotting factors II, VII, IX or X
Two independent virus inactivation steps
2004 Octagam IVIG
Octapharma Primary immune deficiency
Only liquid and double virus inactivated IVIG that can be stored at room temperature
2004 (Spain)
High Purity Factor IX Concentrate
Grifols Treatment and prophylaxis of hemorrhages in patients with hemophilia B
Prepared with two additional purification steps
2005 Gammagard 10% IVIG
Baxter Primary immune deficiency
Ready to use liquid
2005 (Germany)
Wilate Factor VIII
Octapharma Treatment of von Willebrand Disease (VWD) and hemophilia A
First high purity VWF/FVIII-concentrate with two independent virus inactivation steps
2006 Vivaglobin immune globulin
CSL Primary immune deficiency
First and only FDA-approved subcutaneous Ig treatment
2007 Evithrom thrombin
Omrix Biopharmaceuticals
Aid to hemostasis in minor capillaries
First human thrombin approved since 1954
2007 Privigen IVIG
CSL Behring Primary immune deficiency
Only Proline-Stabilized liquid form IVIG
2007 Ceprotin
Baxter Prevention and treatment of venous thrombosis and purpura fulminans
First FDA approved therapy for patients with severe congenital Protein C deficiency
2008 ARTISS human fibrin sealant
Baxter Skin grafts Slow setting, allows for controlled manipulation of skin grafts
Source: BioProcess International; FDA; company filings.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 133 -
Manufacturers also continue to improve products, obtaining expanded labeling
particularly to allow room temperature storage. This increases convenience and
simplifies storage options.
Plasma Market Size
Plasma collection continues to rise, with more than 26 million liters collected in
2007, as compared with about 10 million liters in 1995. In 2007, worldwide sales of
plasma and plasma derived products comprised approximately $7.0 billion, as shown in
Table 4-14. This includes plasma, albumin, platelets, fibrin sealants, immunoglobulins,
alpha-1 proteinase inhibitors, clotting factors such as Factor VIII and other products.
Through 2014, compound annual growth will accelerate to 8.5% per year from an
estimated 7.0% per year during the 2002 – 2007 period. The U.S. will remain the single
largest global market, accounting for more than half of all plasma product sales.
Market Dynamics
The plasma industry continues to experience consolidation and as a result, the
positions of leading players have shifted dramatically. Australia-based CSL, for
example, has become one of the world’s leading fractionators through a series of
acquisitions including its 2000 buyout of ZLB (the Central Laboratory of the Swiss Red
Cross Blood Transfusion Service in Bern, Switzerland) and 2004 purchase of Aventis
Behring. This latter acquisition was unexpected, and followed an announcement that a
previously proposed merger between Aventis Behring and Bayer’s plasma operations
would not occur. Bayer subsequently divested its plasma business to Cerberus and
Ampersand and Fenwal was established in March 2007 with the sale of Baxter’s
Transfusion Therapies business to Texas Pacific Group and Maverick Capital. Table 4-15
shows some significant industry shifts since year 2000.
These shifts have occurred against a backdrop of rising costs related to the
obtaining of raw material (plasma) and implementation of safety measures such as
inventory hold and plasma pool testing, causing major chemical-pharmaceutical
companies to exit the business, as dedicated plasma companies consolidate and
strengthen their positions. For example, plasma processing costs have risen by more than

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 134 -
40% since the late 1990s and nucleic-acid testing alone adds $5 – 15 per liter of plasma.
At the same time, however, product prices have come under pressure as a result of newer
plasma fractionation processes that utilize less plasma to make similar quantities of
pharmaceuticals and vaccines.
Table 4-14
The Global Market for Plasma and Plasma Derived Products 2002 - 2014
Year Revenue in $
Billion Percent Change
2002 $5.0 - 2003 5.3 6.0% 2004 5.7 6.6% 2005 6.1 7.1% 2006 6.5 7.4% 2007 7.0 7.7% 2008 7.6 7.9% 2009 8.2 8.1% 2010 8.8 8.3% 2011 9.6 8.5% 2012 10.4 8.7% 2013 11.4 8.9% 2014 12.4 9.0%
Period
Compound Annual Growth Rate (CAGR)
2002 - 2007 7.0% 2007 - 2014 8.5% 2002 - 2014 7.8%
Source: Kalorama Information.
In 2004 and 2005, fewer plasma collection procedures were performed as a result
of a global oversupply of source plasma. This oversupply persisted through early 2006 in
Japan, although plasma collections in the U.S. and Europe then rebounded. Throughout
the world, health care reimbursement guidelines continue to inhibit demand for plasma-
derived therapeutics, although in some areas, regulatory restrictions are easing.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 135 -
Table 4-15
Industry Shifts, 2003 - 2008
Year Event 2003 Bayer and Aventis terminate plans to merge their plasma products businesses. 2003 Baxter announces plans to close 26 of its 120 plasma collection centers in the
U.S. as well a 700,000-L plant in Michigan. 2003 Probitas Pharma and Baxter each acquire certain Alpha Therapeutic assets
from Mitsubishi Pharma; Baxter sells or closes all of Alpha’s 41 plasma collection centers while Probitas rebrands under the Grifols name.
2003 Octapharma completes acquisition of Mexican fractionator Probifasa SA de CV.
2003 Aventis Bio-Services sells 21 of its 80 plasma collection centers to International Bioresources.
2003 Bayer divests the plasma operations of its Biological Products Division. 2003 CSL acquires Aventis Behring, creating ZLB Behring, in a deal valued at
$295 million. 2004 Baxter further reduces fractionation capacity by around 13%. 2004 ZLB Behring closes 35 collection centers, reducing collection volume by one
million liters and leaving 65 centers in operation, saving $100 million in operating costs.
2004 Cerberus Capital and Ampersand Ventures buy Bayer’s plasma fractionation business for over $590 million. The new company thus created, NPS Biotherapeutics, Inc., will also incorporate Precision Pharma.
2005 The American Red Cross exits the plasma therapeutics business, restructuring its relationship with Baxter from a contract manufacturing agreement to a supply agreement.
2005 Talecris, incorporating a variety of Bayer plasma products, becomes operational.
2006 Cerus acquires the rights to Baxter’s Intercept blood system. 2006 Grifols acquires U.S.-based PlasmaCare, adding 14 plasma collection centers. 2006 Talecris expands into Canada. 2006 Biotest AG and the Sanquin Blood Supply Foundation merge their plasma
product manufacturing activities. 2006 Talecris establishes a European headquarters in Frankfurt to serve more than
15 European countries Talecris acquires 58 plasma collection centers from International
BioResources 2007 Biotest AG acquires Nabi Pharmaceuticals’ biologics division. 2007 Talecris acquires another 3 plasma collection centers from International
BioResources and enters into an agremenet o open an additional 10 centers 2008 Grifols signs an agreement with Stough Development Corp. to open 10 new
U.S. plasma collection centers 2008 Baxter Healthcare Corporation’s Transfusion Therapies business is sold to
Texas Pacific Group and Maverick Capita to form Fenwal.
Source: BioProcess International; company filings.
As a result of these changes, the industry remained closely held in 2007, with a
handful of companies occupying leading positions, as shown in Table 4-16. Baxter took
first place, with approximately $2.1 billion in sales of plasma proteins and antibodies

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 136 -
(immunoglobulins). It was followed by CSL, Octapharma, Talecris and Grifols. A large
number of other suppliers are also active in the market including Biotest Pharmaceuticals
(which acquired Nabi Pharmaceuticals’ biologics group in late 2007), Cangene, DynPort
Vaccine Company, Haemacure Corp, Kamada, Medimmune (which has recently been
acquired by AstraZeneca), Omrix Pharmaceuticals, Vivostat (formerly Vivolution),
Wyeth and others.
Table 4-16
Sales and Market Shares of Leading Suppliers of Plasma and Plasma Derived Products, 2007
Company Sales ($ Million) Market Share Baxter $2,138 30.5% CSL 1,743 24.9% Octapharma 860 12.3% Talecris 825 11.8% Grifols 550 7.9% Others 884 12.6% Total $7,000 100.0%
Source: Kalorama Information
Immunoglobulins
Global demand for immunoglobulins, or antibodies remains the driving force behind plasma collection, with some sources estimating that global demand outstrips current supply several-fold. The group comprises both intravenous (IVIG) and intramuscular (IMIG) products derived from human plasma that are used to address either a variety of conditions (polyvalent immunoglobulins) or certain specific conditions.
Immunoglobulin Market Dynamics
While immunoglobulins have been available for many years and a large
proportion of health care providers view the products as interchangeable, newer products
are being introduced with expanded capabilities and marketers are now trying to change
the perception of immunoglobulins as commodities. In 2003, for example, Bayer
introduced Gamunex IVIG, the first completely new immunoglobulin launched in more

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 137 -
than a decade. Now owned by Talecris after Bayer divested its plasma business,
Gamunex is manufactured using a new process that reportedly offers increased efficacy,
tolerability, safety and convenience. Other manufacturers including Grifols, Octapharma
and CSL have since introduced new products, particularly liquid formats that replace
older lyophilized IVIG. This, along with continued price increases in the U .S. and
Europe, has supported market growth in 2006 and 2007.
According to Talecris, patients are able to identify differences in the performance
of these different products. The company conducted a survey of IGIV patients and found
that:
• 58% of patients have preferences for specific products, which are based primarily
on side effects;
• 34% of patients avoid certain products due to side effects.
Immunoglobulin Market Size
Although IVIG prices had tumbled recently along with overall plasma industry
prices, immunoglobulin prices have since stabilized with many manufacturers, such as
Baxter, reporting sales gains, particularly for new IVIG products. As shown in Table 4-
17, the total worldwide market for all immunoglobulin products is estimated at about
$3.3 billion in 2007. The bulk of this is comprised of IVIG, particularly broad spectrum,
polyvalent products. The following sections describe selected specialty immunoglobulin
products.
Through 2014, the overall market for immunoglobulin is expected to expand by
6.7% per year to reach almost $5.2 billion, although if new uses for the products are
identified, growth could be much higher. For example, while IVIG continues to be used
primarily in antibody replacement therapy for persons with compromised immune
systems, there is also growing evidence that they may be used to address Alzheimer’s
disease. In this regard, Baxter is conducting a phase III clinical trial of its Gammagard as
a treatment for patients with mild to moderate forms of Alzheimer’s. Early stage studies
have shown significant improvement in cognitive function for patients receiving
Gammagard, although these results must now be validated in larger scale trials.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 138 -
Table 4-17
Global Market for Immunoglobulins by Manufacturer 2007-2014
Company 2007 2008 2009 2010 2011 2012 2013 2014 Baxter 985 1,054 1,128 1,207 1,291 1,382 1,478 1,582 CSL 693 748 808 873 943 1,018 1,100 1,188 Talecris 460 497 537 579 626 676 730 788 Others 1,162 1,220 1,281 1,345 1,412 1,483 1,557 1,635 Total 3,300 3,519 3,754 4,004 4,272 4,559 4,865 5,193
Source: Kalorama Information
RSV Immunoglobulin
RSV immunoglobulin is designed to address respiratory syncytial virus, and was
pioneered by Medimmune (which was acquired by global pharmaceutical company
AstraZeneca in mid 2007). Medimmune introduced RespiGam, an intravenous immune
globulin containing neutralizing antibodies against RSV, indicated for the prevention of
RSV disease in children less than 24 month of age with bronchopulmonary dysplasia
(BPD) or a history of premature birth (i.e., born at 35 weeks or less gestation). RespiGam
has since been replaced in the marketplace by Synagis, a humanized monoclonal
antibody approved for the prevention of serious lower respiratory tract disease caused by
RSV in pediatric patients, and is no longer produced. In 2007, total global sales of
Synagis exceeded $1.2 billion.
CMV Immunoglobulin
CMV immunoglobulin protects against cytomegalovirus, a herpesvirus. It is
indicated for the prevention of CMV disease associated with solid organ transplantation.
Leading manufacturers include Medimmune, which offers CytoGam, and CSL. Sales of
the products, however, are low with 2007 sales for CytoGam estimated at under $30
million.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 139 -
Hepatitis B Immunoglobulin
Hepatitis B immunoglobulin (HBIG) is used to selectively address hepatitis B in
individuals who may have been exposed to the virus. Several manufacturers offer the
product including CSL and Cangene, whose HepaGam B was approved by the FDA in
early 2006.
However, research remains inconclusive as to HBIG’s usefulness. Several studies,
for example, have shown that HBIG used in combination with antiviral medications can
prevent recurrence of hepatitis B after liver transplantation. On the other hand, other a
small study conducted at Erasmus Medical Centre in Rotterdam, The Netherlands
concluded in 2002 that passive immunization with immunoglobulin in patients infected
with the hepatitis B virus is only likely to be effective in those on antiviral treatment who
have low pre-treatment levels of the hepatitis B surface antigen.
RhoD Immunoglobulin
RhoD immunoglobulin (RHIG) containing anti-RhoD is used to prevent the
formation of Rh antibodies in an Rh negative individual who has received Rh positive
blood as a result of carrying an Rh positive infant or the transfusion of Rh positive blood.
One leading RHIG product is WinRho SDF [Rho(D) Immune Globulin
Intravenous (Human)], which was developed by Cangene and licensed by Baxter in 2005.
In the first quarter of 2006, Baxter introduced a liquid formulation of the product.
Currently currently sold in more than 40 countries worldwide, WinRho’s sales continue
to rise but in 2007 are estimated at less than $100 million.
Tetanus Immunoglobulin
Tetanus immunoglobulin (TIG) is used to treat individuals who are at risk of
tetanus. This includes persons with serious wounds who have had toxoid injections more
than 10 years earlier, had an incomplete course of injections, or do not know their
immunity status. TIG is available as both an intramuscular agent for prophylaxis of
tetanus prone wounds and in an intravenous preparation for treatment of clinical tetanus.
It is often used concurrently with tetanus vaccine for persons with serious wounds who
are at risk of tetanus. Several manufacturers offer relatively small products including
Baxter, Cangene and CSL.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 140 -
Rabies Immunoglobulin
Rabies is a zoonotic viral disease that infects domestic and wild animals. It is
transmitted to other animals and humans through saliva from infected animals (ie. bites,
scratches, licks on broken skin and mucous membranes). Once symptoms develop, the
disease is fatal to both animals and humans, therefore, rabies immunoglobulin is
administered to any person who may have been in contact with a rabies-infected animal.
In most developing countries where canine rabies is common, human-derived
rabies immunoglobin is very expensive. It is therefore often in short supply or not
available at all; in these areas, highly purified equine rabies immunoglobulin is used as a
cheaper substitute. There are some exceptions, however. In July 2008, Kamada’s
KamRAB was approved in Israel; the injectable drug is manufactured from human
plasma enriched with anti rabies Immune Globulin, and administered after contact with
an animal suspected to be infected with rabies. KamRAB was first launched in 2003 and
is available in Asia and South America.
Varicella Immunoglobulin
Varicella immunoglobulin (VZIG) has been available since 1978 and is used to
address chicken pox in exposed, susceptible individuals at risk for complications. These
may include immunosuppressed individuals, pregnant females, neonates and health
personnel, who are seronegative and have been exposed to varicella.
The market for VZIG is small, however, and the only U.S.-licensed manufacturer
of a product recently discontinued production. Because of the resulting risk of a product
shortage, the FDA approved an expanded access investigational new drug protocol (IND)
for Cangene’s VariZIG in January 2006. The approval allows at-risk patients to receive
VariZIG if they have been exposed to Varicella roster.
Vaccinia Immunoglobulin
Vaccinia immunoglobulin (VIG) is the antibody to the virus used to produce
small pox vaccine; it is therefore used to counteract certain side effects that can arise
from the vaccine, such as infections in persons who have skin conditions such as burns,
impetigo, varicella-zoster, or poison ivy.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 141 -
Because global use of the smallpox vaccine was believed to have virtually
eradicated smallpox by 1980, the market for VIG has been small. However, recent threats
of the utilization of smallpox as a biological weapon have led to the stockpiling of
smallpox vaccine and associated interest in VIG. Several manufacturers offer products
including Cangene, which received FDA approval for its VIG product in 2005.
Albumin
Accounting for 55% - 60% of the volume of human plasma, albumin is one of the
most important blood products due to its usage as a blood volume expander. Blood
volume expanders are primarily albumin-based products that are used to pull water from
the extracellular fluid compartment into circulation. Standard Cohn fractionation
methods, which were developed to separate albumin, continue to be used as these provide
high yields, although newer methods offering even greater yields are also utilized.
Albumin Market Dynamics
A relatively recent global overproduction of plasma and albumin has led to price
instability, with albumin prices declining by as much as 50% over the past several years.
This occurred as a result of broader shifts in the plasma industry, including consolidation
amongst the leading players. By mid 2006, however, supply and demand had become
more closely aligned, leading to greater price support in 2007 and beyond.
Albumin Market Size
The market for albumin products for all applications, including usage as a blood
volume expander, other therapeutic uses and experimental use, comprised a significant
portion of the overall market for plasma products at an estimated $759 million in 2007.
However, the market is mature and has become subject to a high level of generic
competition. This has resulted in product differentiation and flat to declining prices.
Through the forecast period, rising demand is expected to lead to compound annual
growth of 2.2%, resulting in total global albumin product sales of $883 million in 2014,
as shown in Table 4-18.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 142 -
Table 4-18
Global Market for Human Albumin Products by Brand 2007-2014
Brand Company 2007 2008 2009 2010 2011 2012 2013 2014 AlbuRx 5, 25, others
CSL $160 $165 $170 $175 $181 $187 $193 $199
Buminate, Flexbumin
Baxter 143 145 147 150 153 156 159 162
Plasbumin Talecris 124 126 128 130 132 134 136 138 Albutein 5%, 20%, 25%, others
Grifols 81 84 88 92 96 100 104 108
Albumin 5%, 20%, 25%
Octapharma 52 53 55 57 59 61 63 65
Actovegin Nycomed 43 42 41 40 39 38 37 36 Others Various 156 159 162 165 168 171 173 175 Total $759 $774 $791 $809 $828 $847 $865 $883
Source: Kalorama Information
CSL was the market leader in 2007 with several albumin products used primarily
in critical care applications. Baxter followed closely with an estimated $143 million in
revenues for Buminate and Flexbumin. Introduced in early 2006, Flexbumin is the first
preparation of human albumin to be packaged in a flexible container. (Other products are
packaged in glass bottles, which pose risk of breakage and are often cumbersome to store.
This was a result of technical requirements related to manufacturing, including inertness,
sturdiness and a high water vapor and oxygen barrier that no single plastic material had
previously been able to fulfill).
Prothrombin Complex Concentrates
Prothrombin complex concentrates (PCCs), also known as low-purity FIX
products, are used for the prophylaxis, peri-operative substitution and treatment of
bleeding in patients with congenital or acquired deficiencies of clotting factors II, VII, IX
and/or X. With the exception of Factor IX (FIX) deficiencies, these conditions affect a
relatively small number of persons, as shown in Table 4-19.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 143 -
Table 4-19
Prevalence of Conditions Requiring Prothrombin Complex Concentrates
Deficient Factor Prevalence II < 50 cases documented worldwide VII 2.0 cases/million IX 1 case/30,000 X 1.5 cases/million
Source: Octapharma
The use of PCCs has been largely abandoned for the high-purity FIX products
that have lower thrombogenic potential and undergo more rigorous viral inactivation
methods. For example, in August 2003, Octapharma received approval in Germany to
market a new PCC, Octaplex, prepared using two distinct virucidal technologies to
provide a high level of purity. This compares with standard PCCs that typically undergo
just one viral inactivation procedure. Recombinant FIX (BeneFix), which is not derived
from human plasma, offers an advantage over plasma-derived concentrates, but plasma
levels of factor per unit may be lower than for plasma-derived products. Table 4-20
shows leading FIX products available in the U.S.
Table 4-20
Leading Factor IX Products, 2008
Product
Manufacturer
Source Viral Inactivation Procedure
MonoNine CSL Human plasma Sodium thiocyanate AlphaNine Grifols Human plasma Solvent and
detergent Nanotiv, Octanine F
Octapharma Human plasma Nanofiltration
BeneFix Wyeth Recombinant Immunoaffinity chromatography
Source: Cleveland Clinic; company filings

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 144 -
Alpha-1 Proteinase Inhibitors
Alpha-1 proteinase inhibitors (APIs) address antitrypsin deficiency (Alpha-1), a
genetic disorder that can cause liver and lung disease in both children and adults. There
are about 100,000 persons with API deficiency in the U.S. alone, but according to the
Alpha-1 Foundation, at least 90% of these remain undiagnosed and untreated.
A handful of API products are currently available. The most established of these
is Talecris Biotherapeutics’ Prolastin, a product originally developed by Bayer nearly
twenty years ago. For many years, Prolastin remained the preeminent API, despite
ongoing product shortages, until Alpha Therapeutic (whose API business was
subsequently acquired by Baxter) introduced Aralast in 2002 and Aventis Behring (which
was later bought out by CSL) launched Zemaira the following year. Zemaira offers a 15
minute infusion time, compared with 30 minutes for other products. This important
advantage has resulted in strong continued sales growth for Zemaira.
Israel-based Kamada has introduced an API product in Europe and in March
2006, announced the removal of the FDA’s clinical hold status on the drug enabling the
company to begin Phase III testing in anticipation of U.S. approval. Kamada’s API
production capacity currently ranks among the world’s largest, according to the company,
and its intravenous AAT is the only ready-to-use AAT therapy that does not require
reconstitution with water.
Fibrin Sealants
Fibrin sealants are topically applied adhesive gels that help control bleeding,
particularly from small, sometimes inaccessible, blood vessels during surgery when
conventional surgical techniques are not feasible. This includes the major blood-loss
surgeries of the cardiovascular, pulmonary, and liver regions as well as the sealing of
needle holes, pulmonary leaks, oozing wounds, skin grafts, and plastic surgery
procedures. Their commercial use dates to 1998, when the FDA approved the first fibrin
sealant for sale; however, this has been limited due to high costs of initial products and
Factor V antibody risks associated with the use of bovine thrombin for platelet gels. In

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 145 -
2007, the global market for fibrin sealants is estimated at about $180 million, with $100
million of this derived from U.S. sales.
Although a number of companies are investigating commercial fibrin sealants,
only a handful have received FDA approval to market their products in the U.S. Baxter
remains the market leader with its Tisseel, and in mid 2007 signed licensing agreements
with Intercytex and Spinal Restoration to evaluate Tisseel’s use in novel regenerative
medicine therapies. In October 2004, Johnson & Johnson Wound Management acquired
the exclusive marketing and distribution rights for Omrix’s Crosseal human fibrin sealant
in North America from Omrix. Crosseal is the first all-human protein, bovine component-
free fibrin sealant approved for sale in the U.S. In May 2007, the product’s indications
were expanded from livery surgery to vascular surgery and it was re-launched as Evicel.
CSL markets Beriplast in Europe and Japan, but the product is not available in the U.S.
While first generation fibrin sealants are sourced from pools of thousands of
purchased units of plasma, newer products such as ThermoGenesis’ CryoSeal FS System
simultaneously produces fibrin sealant components (fibrinogen-rich cryoprecipitate and
thrombin) from a single unit of a patient’s own blood. This eliminates the antibody risks
associated with earlier products. As of mid 2008, CryoSeal was available in selected
regions outside the U.S.
Clotting Factors and Factor VIIa Human plasma-derived clotting factors, including Factor VIIa and Factor VIII, are
rapidly being replaced by recombinant products which offer higher levels of safety due to
lower levels of potential virus contamination. Usage has also been boosted with increased
government funding in Europe for conversion from plasma-derived Factor VIII to
recombinant Factor VIII. Recombinant factors are discussed in more detail in Chapter 6.
In the developing countries, however, which cannot afford more expensive recombinant
products, sales of human-derived clotting factors continue to rise.


Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 147 -
C H A P T E R F I V E
The Blood Testing and Typing Markets
BLOOD TESTING PRODUCTS FOR DONOR SCREENING Unlike many other medical equipment markets, the unusual characteristic of the
markets for blood bank testing technology is that, particularly in the developed nations,
they immediately embrace new approaches that are declared the standard for blood
safety. This is due to the requirement, both stated and implied, that blood and plasma
collection facilities use the most up-to-date technology to ensure the safety of the blood
supply. These centers are not able to argue, for example, that they would rather use
immunoassay because of its cost advantages or that they already possess instrumentation
for the procedure. Once a technology is declared the new standard, all blood banks and
plasmapheresis centers must adopt it or be left open to major lawsuits should a person
become infected with a disease via their blood or plasma products.
Therefore, in the blood bank and plasmapheresis testing markets, dollar volume
closely parallels sample volume. Moreover, with the introduction of molecular
diagnostics, a strong increase in the cost-per-test is expected with the introduction of each
new method over the next ten years. Part of this cost increase will be due to inflationary
effects, but most of it will result from three conditions in the market for blood
bank/plasmapheresis center testing products.
First, in an effort to get to market quickly, manufacturers will introduce assay
methods that adequately serve their initial purpose but leave room for improvement, such
as tests that run on manual or semi-automatic systems rather than fully automatic tests.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 148 -
This means that subsequent generations of improved test products will be introduced in
short order. Improved performance generally means higher pricing.
Second, the competition for blood/plasma testing will remain limited. For
molecular diagnostics, it is expected to be even more limited than for immunoassay
products—especially where related high-throughput instrumentation becomes involved.
Because of this, there will be virtually no price competition through the foreseeable
future, allowing companies to recoup their development costs earlier through scheduled
price increases.
Third, the market for blood banking and plasmapheresis testing reagents is
inelastic. Blood banks must use the latest technology and reagents. Therefore, with
limited competition, companies have considerable discretion over pricing and can
maintain market share once blood banks and plasmapheresis centers have adopted the
assays and purchased the necessary instrumentation. Blood banks and plasmapheresis
centers also cannot effectively “cherry pick” their reagents from various molecular
diagnostics suppliers, even as new competition appears. Pricing and discounting for
reagents and supplies is generally based on total volume, therefore attempts to spread the
business around could actually leave the blood bank or plasmapheresis center with less
than optimal pricing overall.
Market Size Because of this need to continually utilize the most advanced technologies,
particularly in the developed markets, sales of older immunoassay technology remain
relatively flat while sales of newer nucleic acid tests continue to grow briskly. Global
sales of immunoassays are expected to rise by about 2% per year from $610 million in
2007 to $700 million in 2014 while nucleic acid tests will increase by 11.5% from $953
million to about $2,046 million during this time. Due to their lower cost, immunoassays
and/or in-lab developed PCR tests tend to be utilized more frequently in the developing
nations while nucleic acid testing is used predominantly in the developed countries,
although this is slowly changing.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 149 -
Immunoassays
Immunoassays for HIV, hepatitis B, hepatitis C and syphilis have been the routine
approach to testing blood units for blood borne infectious agents. All blood banks in
Latin America also screen donated units for Chagas disease. Blood banks in some
developing countries additionally screen for Dengue fever and malaria, diseases which
are both common and deadly in many tropical nations.
The range of immunoassays and screened diseases continues to expand, however,
as with the December 2006 FDA approval of Ortho’s test for Chagas’ disease.
Representing the first test licensed in the U.S. for the condition, 241 blood donations
tested position for donor exposure in the first ten months of using the test. As of mid
2008, more than 70% of the U.S. blood donations were being screened for Chagas’.
The 2007 market for blood screening immunoassays performed by blood public,
private and hospital-based transfusion services is estimated at $610 million worldwide.
This market will see a modest growth of 2% per year to $700 million in 2014.
Nucleic Acid Testing
Nucleic acid testing (NAT) has allowed blood banks to detect viral contamination,
including West Nile Virus, HIV and hepatitis C, sooner and prevent them from slipping
into blood transfusions, and has now become an integral part of the concerted effort to
make blood transfusions safer. For example, Gen-Probe estimates that in the course of 30
months, its Procleix WNV assay intercepted approximately 1,500 units of blood invested
with West Nile virus from among the 29 million units tested. This prevented the
transfusion of contaminated blood to as many as 4,500 recipients.
As shown in Table 5-1, once a test is introduced to the blood bank/plasmapheresis
arena, it is rapidly accepted - by necessity. In 2007, more than 8.2 million tests were
utilized around the world, with the U.S. accounting for about 4.1 million of these, as
shown in Table 5-2. HIV was the most widely utilized test, followed by HCV and HBV.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 150 -
Table 5-1
Global Blood Banking and Plasmapheresis Testing by Molecular Diagnostics: 2007–2014 (HIV, Hep C, Hep B, Hep A, HTLV, West
Nile, Others)
Number of Tests (in thousands) Year HIV HCV HBV HAV HTLV WNV Others Total 2007 1,745 1,396 1,396 1,222 0 1,222 1,222 8,202 2008 1,753 1,402 1,402 1,227 1,227 1,227 1,227 9,464 2009 1,763 1,410 1,410 1,234 1,234 1,234 1,234 9,518 2010 1,770 1,416 1,416 1,239 1,239 1,239 1,239 9,558 2011 1,780 1,424 1,424 1,246 1,246 1,246 1,246 9,612 2012 1,790 1,432 1,432 1,253 1,253 1,253 1,253 9,666 2013 1,800 1,440 1,440 1,260 1,260 1,260 1,260 9,720 2014 1,810 1,448 1,448 1,267 1,267 1,267 1,267 9,774
Source: Kalorama Information
Table 5-2
U.S. Blood Banking and Plasmapheresis Testing by Molecular Diagnostics: 2007–2014 (HIV, Hep C, Hep B, Hep A, HTLV, West
Nile, Others)
Number of Tests (in thousands) Year HIV HCV HBV HAV HTLV WNV Others Total 2007 698 698 698 698 0 698 698 4,188 2008 701 701 701 701 701 701 701 4,907 2009 705 705 705 705 705 705 705 4,935 2010 708 708 708 708 708 708 708 4,956 2011 712 712 712 712 712 712 712 4,984 2012 716 716 716 716 716 716 716 5,012 2013 720 720 720 720 720 720 720 5,040 2014 724 724 724 724 724 724 724 5,068
Source: Kalorama Information
In 2007, almost all of the blood drawn in North America, Europe and Japan was
tested for West Nile virus, HIV and HCV by NAT. In Western countries, it costs
approximately $10 to NAT-test each unit of pooled blood. Table 5-3 presents the
projected global blood banking and plasmapheresis molecular diagnostics testing market
potential for the period 2007 to 2014, while Table 5-4 shows similar information for the
U.S. market. In 2007, the global market for HCV tests was the largest, at $336 million,

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 151 -
followed by HCV with $269 million, WNV at $257 million and HBV at $254 million. It
should be noted that blood banks and plasmapheresis centers, in an attempt to reduce the
cost-per-unit of molecular diagnostic testing procedures will continue to test blood on a
pooled basis, pooling samples from 10 to 25 units of collected blood/plasma and testing
these pools instead of individual units. This helps contain costs and is possible because of
the extremely high sensitivity of molecular diagnostics procedures compared with
immunoassay testing. Other blood screening tests include those for SARS, BSE, babiosis
and other tick-borne infections as well as malaria.
Table 5-3
Global Projected Blood Banking and Plasmapheresis Molecular Diagnostics Testing Market Potential: 2007–2014 (HIV, Hep C, Hep
B, Hep A, HTLV, West Nile, Others)
Year HIV HCV HBV HAV HTLV WNV Others Total Tests* 1,745 1,396 1,396 1,222 0 1,222 1,222 8,202 ECPT $193 $193 $182 $193 $0 $210 $175 $191
2007
Market (MM) $336 $269 $254 $235 $0 $257 $214 1,564 Tests* 1,753 1,402 1,402 1,227 1,227 1,227 1,227 9,464 ECPT $200 $200 $189 $200 $147 $217 $182 $191
2008
Market (MM) $350 $280 $265 $245 $180 $266 $223 1,809 Tests* 1,763 1,410 1,410 1,234 1,234 1,234 1,234 9,518 ECPT $207 $207 $196 $207 $154 $224 $189 $198
2009
Market (MM) $364 $291 $276 $255 $190 $276 $233 1,886 Tests* 1,770 1,416 1,416 1,239 1,239 1,239 1,239 9,558 ECPT $214 $214 $203 $214 $161 $231 $196 $205
2010
Market (MM) $378 $302 $287 $265 $199 $286 $243 1,961 Tests* 1,780 1,424 1,424 1,246 1,246 1,246 1,246 9,612 ECPT $221 $221 $210 $221 $168 $238 $203 $212
2011
Market (MM) $392 $314 $299 $275 $209 $297 $253 2,039 Tests* 1,790 1,432 1,432 1,253 1,253 1,253 1,253 9,666 ECPT $228 $228 $217 $228 $175 $245 $210 $219
2012
Market (MM) $407 $326 $311 $285 $219 $307 $263 2,118 Tests* 1,800 1,440 1,440 1,260 1,260 1,260 1,260 9,720 ECPT $235 $235 $224 $235 $182 $252 $217 $226
2013
Market (MM) $422 $338 $323 $295 $229 $318 $273 2,198 Tests* 1,810 1,448 1,448 1,267 1,267 1,267 1,267 9,774 ECPT $242 $242 $231 $242 $189 $259 $224 $233
2014
Market (MM) $437 $350 $334 $306 $239 $328 $284 2,279
*Tests in thousands
ECPT = Estimated Cost per Test in $; market in millions
Source: Kalorama Information

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 152 -
Table 5-4
Projected Blood Banking and Plasmapheresis Molecular Diagnostics Testing Market Potential in the United States: 2007–2014 (HIV, Hep
C, Hep B, Hep A, HTLV, West Nile, Others)
Year HIV HCV HBV HAV HTLV WNV Others Total
Tests* 698 698 698 698 0 698 698 4,188 ECPT $275 $275 $260 $275 $0 $300 $250 273
2007
Market (MM) $192 $192 $181 $192 $0 $209 $175 1,141 Tests* 701 701 701 701 701 701 701 4,907 ECPT $285 $285 $270 $285 $210 $310 $260 272
2008
Market (MM) $200 $200 $189 $200 $147 $217 $182 1,335 Tests* 705 705 705 705 705 705 705 4,935 ECPT $295 $295 $280 $295 $220 $320 $270 282
2009
Market (MM) $208 $208 $197 $208 $155 $226 $190 1,392 Tests* 708 708 708 708 708 708 708 4,956 ECPT $305 $305 $290 $305 $230 $330 $280 292
2010
Market (MM) $216 $216 $205 $216 $163 $234 $198 1,448 Tests* 712 712 712 712 712 712 712 4,984 ECPT $315 $315 $300 $315 $240 $340 $290 302
2011
Market (MM) $224 $224 $214 $224 $171 $242 $206 1,506 Tests* 716 716 716 716 716 716 716 5,012 ECPT $325 $325 $310 $325 $250 $350 $300 312
2012
Market (MM) $233 $233 $222 $233 $179 $251 $215 1,564 Tests* 720 720 720 720 720 720 720 5,040 ECPT $335 $335 $320 $335 $260 $360 $310 322
2013
Market (MM) $241 $241 $230 $241 $187 $259 $223 1,624 Tests* 724 724 724 724 724 724 724 5,068 ECPT $345 $345 $330 $345 $270 $370 $320 332
2014
Market (MM) $250 $250 $239 $250 $195 $268 $232 1,683
*Tests in thousands
ECPT = Estimated Cost per Test in $; market in millions
Source: Kalorama Information
Market Participants
Due to the significant technological barriers to entry, the market for blood testing products is dominated by a handful of companies, as described below. These players tend to be different for immunoassays and nucleic acids tests, and also vary geographically.
Immunoassays
Outside of Asia, the market for blood screening is controlled by two companies—
Abbott Laboratories and Ortho Clinical Diagnostics. Together, Abbott and Ortho hold
approximately 75% of the blood screening business with Bio-Rad/Sanofi/Genetic

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 153 -
Systems, Diasorin and bioMérieux taking the remaining 25%. The bulk of Ortho’s
market share is HCV tests which were produced in a joint venture with Chiron
Diagnostics (who discovered and holds the patent on Hepatitis C, then was acquired by
Novartis in mid 2006). However Chiron has now licensed the rights to its HCV assay to
Abbott, Bio-Rad and Bayer.
The Chiron HCV license along with the 1999 FDA approval of Abbott's Prism, a
fully automated multi-channel analyzer, has given Abbott an edge in this market.
Worldwide, Abbott has been replacing its older Commander blood screening systems
with the newer Prism, although Commander remained available as of mid 2008. In
January 2008, Abbott received approval for the first fully automated HTLV-I/HTLV-II
blood screening test for use on Prism. The test is intended for use by laboratories to
screen individual donations of blood and plasma for antibodies to human T –
lymphotropic virus Type I and/or human T – lymphotropic virus Type II (anti-HLTV-
I/HTLV-II). Prism is currently used in over 30 countries, to screen more than 25% of the
global blood supply.
In March 2008, Ortho received FDA approval for Bitros ECi/ECiQ, an
immunoassay used to detect antibodies to HIV-1 and HIV-2 in less than 50 minutes. It is
the first such test that can be run in full random access with other tests for immediate
result reporting upon test completion. The approval follows the December 2006 approval
of the first U.S. test for Chagas disease, Ortho’s T.cruzi ELISA Test System.
In Asia, primarily Japan, Thailand, Korea and Taiwan, the majority of blood
banks use Fujirebio's RPHA (Rapid Particle Hemagglutination) tests, which run on
Olympus Optical's PK instruments for HIV and HTLV testing.
Nucleic Acid Testing
A number of nucleic acid tests are commercially available for use in donor
screening by blood banks and plasmapheresis centers, as shown in Table 5-5. Because
blood collection centers often utilize equipment that is being studied under an
Investigational New Drug (IND) application, FDA approval dates do not necessarily
represent the time at which equipment becomes available, although widespread usage is
precluded until approval is granted.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 154 -
Table 5-5
Selected Commercially Available Molecular (Nucleic Acid) Tests for Blood, Plasma and Organ Donor Screening in the United States,
2001 - 2008
Tradename Format Sample Use Manufacturer Approval Date
UltraQual HIV-1 RT-PCR Assay
PCR Plasma Donor Screen National Genetics Institute
9/18/2001
UltraQual HCV RT-PCR Assay
PCR Plasma Donor Screen National Genetics Institute
9/18/2001
Procleix HIV-1/HCV
HIV-1/HCV Nucleic Acid Test (TMA)
Plasma Donor Screen Gen-Probe Chiron Corp.
2/8/2002
COBAS AmpliScreen HCV Test
PCR Plasma Donor Screen Roche Molecular Systems
12/3/2002
COBAS Ampliscreen HIV-1 Test
PCR Plasma Donor Screen Roche Molecular Systems, Inc
12/20/2002
Procleix WNV West Nile Virus Nucleic Acid Test (TMA)
Plasma Donor Screen Gen-Probe Chiron Corp
6/18/2003
ADVIA Centaur HAV Total Assay
HAV Nucleic Acid
Plasma Donor Screen Bayer 3/7/2005
Procleix Ultrio HIV-1/HCV Nucleic Acid Test (TMA)
Plasma Donor Screen Gen-Probe Chiron Corp
10/4/2006
Procleix Tigris WNV
Automated West Nile Virus Nucleic Acid Test (TMA)
Plasma Donor Screen Gen-Probe Chiron Corp
3/2/2007
AmpliPrep/ COBAS TaqMan HIV-1 Test
PCR Plasma Donor Screen Roche Molecular Systems, Inc
5/14/2007
COBAS TaqScreen West Nile Virus Test
Automated West Nile Virus Nucleic Acid Test (TMA)
Plasma Donor Screen Roche Molecular Systems, Inc
8/27/2007
PRISM HTLV-I/HTLV-II test
HTLV-I/HTLV-II Nucleic Acid Test (TMA)
Plasma Donor Screen Abbott 1/21/2008
Source: Kalorama Information
For example, the Chiron Procleix HIV-1/HCV assay and system have been used
in IND clinical trials at the American Red Cross, America's Blood Centers, and the
Association of Independent Blood Centers since April 1999. Developed as a joint
venture between Chiron and Gen-Probe, the Procleix system is marketed by Chiron.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 155 -
Once FDA approved in 2002, Chiron had the major U.S. blood banks sign multi-year
contracts for the use of the novel system. Thus in 2008, Chiron owned 80% share in the
United States, by virtue of its early market entry.
In 2005, Chiron announced the opening of a nucleic acid testing lab at the Beijing
Blood Center, China, paving the way for increased NAT testing in Asia. The Chiron
NAT Lab is utilized as a clinical trial site required for product registration in China and
uses Procleix HIV-1/HCV Assays.
Roche Diagnostic's COBAS AmpliScreen System and COBAS AmpliScreen
HCV (Hepatitis C Virus), Version 2.0 and the COBAS AmpliScreen HIV-1 test, Version
1.5 have the majority market share outside the United States, amounting to about 90% of
the market. COBAS AmpliScreen tests are also used in other countries where product
registration is not required. Roche's AmpliNAT multiplex system - the first to test for
HIV-1, Hepatitis B, or Hepatitis C in a single triplex reaction - has been used exclusively
by the Japanese Red Cross since 1999 to screen Japan's entire blood supply. Canada’s
entire blood supply is screened using Roche COBAS AmpliScreen tests, and France
recently chose to screen more than 75% of its donated blood with Roche COBAS
AmpliScreen products. The COBAS AmpliScreen Hepatitis B Test is approved for use
in the EU and is currently in clinical trials in the United States.
One particularly noteworthy new nucleic acid test is Gen-Probe’s Procleix test for
identification of West Nile virus (WNV). WNV is spread by the bite of an infected
mosquito and can infect people, horses, many types of birds, and some other animals. It
was first detected in the United States in 1999, with the first documented cases of WNV
transmission through organ transplantation and transfusion noted in 2002. Since then,
more than 4,000 persons per year become infected. Although about 80% of people
infected with WNV remain without symptoms, and 20% develop mild symptoms, one in
150 to 200 persons infected with WNV develops a more severe form of the disease that
may be fatal. The introduction of the Procleix WNV Assay is a case study in diagnostics
development, with GenProbe and Chiron developing the assay in about half the normal
development time for such a product. This was largely due to unprecedented cooperation
given to the company by the FDA and members of the blood banking community, as a
result of the public health threat posed by WNV. FDA began allowing national

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 156 -
deployment of investigational nucleic acid tests to screen blood for West Nile virus in
early 2003, and Procleix subsequently become available at the end of June.
GenProbe and Chiron subsequently introduced an automated version of the test,
Procleix Tigris. The world’s first fully automated NAT instrument system, the Procleix
Tigris significantly reduces labor costs and contamination in high-volume diagnostic
testing environments and enables large blood collection centers to individually test each
donor’s blood. Many experts believe there will be significant demand for automation if
blood collection centers begin the screening of individual blood donations rather than the
testing of pooled samples, in an effort to further improve the safety of the nation’s blood
supply. Individual unit screening at larger blood centers currently is impractical without
automated instrumentation because of the throughput limitations of current semi-
automated instruments. However, automation will encourage adoption of additional
blood screening tests, such as tests for HBV, West Nile virus, parvo B-19 and HAV.
Since then, other WNV tests have been approved, underscoring the speed at
which the NAT market moves. In August 2007, the FDA approved Roche's TaqScreen
West Nile Virus Test. With an ability to also detect other viruses of the Japanese
encephalitis family, total automation and the option to isolate the generic material of any
infectious agent in a donated blood sample, the test is expected to capture a significant
portion of the WNV testing market.
BLOOD TYPING PRODUCTS Blood typing reagents and instruments are used by blood transfusion services,
hospital and private blood banks, and hospital laboratories that prepare blood units for
transfusion to patients. More than 80% of blood typing is done in hospitals. Each unit is
assessed for its ABO and Rh grouping and the presence of blood antibodies.
Facing efficiency pressures similar to those of other lab disciplines, blood banks
have a rising need for automation, reduced cost through improved assay performance and
improved laboratory clinical good manufacturing (cGMP) compliance. Historically,
blood bank procedures called crossmatch identified the ABO group and D type of blood
donors and recipients, as well as unexpected red blood cell alloantibodies. Crossmatch

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 157 -
was performed by a manual hemagglutination antibody/antigen test and read visually.
These tests are now being replaced by new gel-based techniques that can be automated,
with some 30% to 40% of hospital labs having transferred to gel-based systems. These
systems remove the subjectivity of reading blood group tests and also free technologists
to perform other tasks.
Market Size In 2007, this market segment is valued at $510 million and with 2% expected
annual growth will increase to $585 million in 2014. Geographically, the EU accounts
for some 35% of the market, N. America comprises 38%, Japan holds 13% and the ROW
takes the remaining 14% with most of that supplied by local companies and in-lab
developed tests.
Market Participants Despite recent expansion, only three major companies are active in the market for
blood grouping reagents - Olympus, Ortho Clinical Diagnostics and Immucor. These
three companies hold 90% of the market with local suppliers and in-lab developed tests
used in less regulated emerging countries.
Ortho Clinical Diagnostics remains the market leader. In March 2002, Ortho
acquired Micro Typing Systems of Pompano Beach, FL. MTS manufactured the ID-
Micro Typing System that is now marketed by Ortho while Diamed AG, Switzerland
markets the ID-Micro Typing System in Europe. In 2003, Ortho Clinical Diagnostics
introduced the Ortho ProVue Analyzer, a fully automated blood banking system for use
with MTS' Gel Test. It is estimated that Ortho and Diamed hold about 30% of the world
market for non traditional techniques; Immucor has about 35%.
Immucor has been very aggressive, since blood grouping is its only business.
(This compares with Ortho, for which blood grouping is a very small component and one
which consumes considerable resources for relatively low returns). Immucor developed
the Galileo, a fully automated gel-based instrument that offers a broad assay menu and
features similar to a chemistry analyzer: continuous access, linear rack, and bidirectional
interface, and multitasking for high volume testing. In June 2007, the company
introduced Galileo Echo, an automated walk-away instrument for small to medium sized

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 158 -
testing facilities, of which Immucor estimates there are approximately 6,000 worldwide.
Immucor continues to expand, reporting revenues of $223 million in 2007 compared with
$183 million in 2006 and $144 million in 2005.
Olympus Medical markets the PK line of high throughput systems that run
reagents manufactured by Immucor's subsidiary, Gamma Biologicals. These systems are
generally used by large blood services, however Olympus is beginning to target smaller
blood banks with the TANGO, a fully automated blood bank benchtop analyzer, that
came to market in 2005.
PLASMA AND BLOOD COLLECTION EQUIPMENT The market for plasma and blood collection equipment is broad, encompassing
both manual and automatic systems for collection, leukocyte reduction, post-collection
component processing and storage as well as IT applications for blood centers. Although
automated collection systems are more expensive than manual systems, they are also
faster, more efficient and offer greater safety to blood donors. Because of this, their usage
is growing relatively briskly.
Market Size The market for blood equipment has been expanding at a steady pace over the
past several years, although the plasma collection segment has experienced some recent
flux due to shifts in the number of plasma collection centers. For example, Baxter closed
many of the Alpha Therapuetics plasma collection centers it acquired in 2003, spurring a
multi-million dollar lawsuit from Haemonetics when it repudiated Haemonetics’ plasma
collection equipment contracts. (Haemonetics subsequently prevailed in a lawsuit,
obtaining a $27.8 million award in May 2005). In 2007, the total global market for all
blood center equipment reached $2.1 billion, as shown in Table 5-6. Over the next
several years, average annual growth of 4.6% will result in 2014 sales of an estimated
$2.9 billion.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 159 -
Table 5-6
Total Global Market for Blood Collection Equipment: 2007–2014
Year Revenue in $ Billion Percent Change
2002 1.7 - 2003 1.7 4.2% 2004 1.8 5.3% 2005 1.9 4.2% 2006 2.0 4.5% 2007 2.1 4.6% 2008 2.2 4.7% 2009 2.3 4.8% 2010 2.4 4.9% 2011 2.5 5.0% 2012 2.6 5.1% 2013 2.7 5.2% 2014 2.9 5.3%
Period
Compound Annual Growth Rate (CAGR)
2002 - 2007 4.3% 2007 - 2014 4.6% 2002 - 2014 4.5%
Source: Kalorama Information.
Automated blood collection equipment comprises a significant portion of this
market, at an estimated at $500 million in 2007, as shown in Table 5-7. Historic growth
has been steady, averaging 5.8% per year over the past several years. Through 2014, total
sales are expected to rise by 7.5% per year to reach $829.4 million. Many of these
devices can be used to collect plasma as well as platelets and RBCs.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 160 -
Table 5-7
Global Market for Automated Blood Collection Equipment: 2007–2014
Year Revenue in $ Million Percent Change
2002 377.2 2003 401.3 6.4% 2004 418.0 4.2% 2005 440.0 5.3% 2006 468.6 6.5% 2007 500.0 6.7% 2008 534.5 6.9% 2009 572.4 7.1% 2010 614.2 7.3% 2011 660.3 7.5% 2012 711.1 7.7% 2013 767.3 7.9% 2014 829.4 8.1%
Period
Compound Annual Growth Rate (CAGR)
2002 - 2007 5.8% 2007 - 2014 7.5% 2002 - 2014 6.8%
Source: Kalorama Information.
Market Participants The market for automated blood and plasma collection equipment is controlled by
Haemonetics, Abbott Laboratories and Baxter International. In general, competition is
based on performance, as measured by the time and efficiency of component collection
and the quality of the components collected.
Haemonetics invented the first automated red blood cell collection system, known
as the MCS+ Mobile Collection System, which has reportedly been used in more than
one million blood donations around the world. Prior to this, all plasma was collected
manually. Today the company offers a variety of equipment for the collection and storage

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 161 -
of red cells, plasma and platelets. These include portable devices as well as systems for
surgical blood salvage. With over a half billion dollars in sales in ifs fiscal year ended
March 2008, Haemonetics continues to be known for high quality products, introducing
both new and upgraded devices and accessories at a steady pace:
• In December 2005, Haemonetics received FDA clearance to market its redesigned
cardioPAT surgical blood salvage system. The device was originally cleared in
January, but Haemonetics identified areas for technology improvement during
early customer trials and postponed full market introduction to incorporate
enhancements;
• In April 2006, the company announced the European launch of the Cymbal
system, a portable device for collecting two units of non-leukoreduced red blood
cells from a single blood donor in one donation. Cymbal represents a portable
version of Haemonetics’ double-red cell collection technology, enabling broader
usage of a system that can significantly enhance donation yields;
• In May 2008, the company received FDA clearance for eLynx, a data capture and
temporary storage system that streamlines and consolidates workflow activities in
blood collection centers;
• In June 2008, Haemonetics introduced a plasma collection software for its PCS2
plasma collection system that reduces plasma donation time by 20%.
Baxter is attempting to expand the usage of its Alyx automated double-red cell
collection system. The portable device was launched in 2003, and in 2005, won the
Medical Design Excellence Awards (MDEA) competition. Baxter offers several other
automated blood collection systems including the Amicus and CS-3000 blood separators.
Along with Abbott Laboratories, Pall Corporation, Terumo and others, it also sells a
variety of manual tools for blood collection including needles, plastic blood bags,
solutions and tubing.
CaridianBCT (formerly Gambro BCT) offers several systems for automated blood
collection including Spectra, Trima Accel, Atreus and OrbiSac. The Trima Accel is the
first automated blood collection system to collect a combination of leukoreduced red
blood cells, platelets and plasma. Introduced in 2007, the OrbiSac allows automated
separation of manually collected whole blood, automatically separating the buffy coat

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 162 -
platelets (the layer of white blood cells and platelets remaining between plasma and
RBCs) after whole blood is centrifuged. FDA approved in June 2008, the Atreus is the
first self-contained, automated manufacturing system for whole blood that includes both
automation and informatics capabilities. The system includes a web application that
configures the device, defines workflow, automates data capture, generates managerial
reports and centralizes documentation.
The top players in the leukocyte reduction segment tend to be distinct from those
in the automated collection equipment market. In 2007, BD Biosciences remained the
market leader with its BD LeucoCOUNT assay, which is used on an automated or
manual flow cytometer. In March 2004, BD Biosciences' BD IMAGN system and the
residual WBC assay received FDA clearance for analysis of leucoreduced blood
products, such as platelet and red cell concentrates. The system had a successful history
of usage in Europe and Asia.
In January 2004, Pall Corporation received FDA clearance to market its blood
Sample Diversion Pouch on its Leukotrap blood collection and filtration systems. The
Sample Diversion Pouch is used to divert up to 45 mL of blood for testing during
collection, which can contain the highest levels of bacteria. Research has shown that
bacteria present at the skin site can contaminate the first few milliliters of blood collected
during blood donation. A venipuncture site can contain more than 3,000 bacteria colony-
forming units.
Other developers are also working on novel automated systems, particularly
focusing on optimization of bacteria. This is in part a result of the AABB’s March 2004
guidelines instructing blood centers to test all platelet components for the presence of
bacteria. For example, France-based Hemosystem SA currently markets the CE-Marked
Scansystem bacterial screening technology in Europe and in September 2007, obtained
FDA approval to market Scansystem in the United States. Three years earlier,
Haemonetics reached an agreement with Hemosystem to market Scansystem in Europe,
the Middle East, Africa, and Latin America. As part of the agreement, Haemonetics also
assumed right of first refusal to market the product in major Asian countries. Future
applications for Scansystem including bacterial detection in red cell units are currently
under development.

Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 163 -
C H A P T E R S I X
Synthetic Blood Products Market
DRIVING FORCES OF THE SYNTHETIC BLOOD PRODUCTS INDUSTRY
Around the world, demand for blood continues to exceed supply. According to the
National Blood Data Resources Center (NBDRC), an independent not-for-profit
corporation founded by the American Association of Blood Banks, about 10% of U.S.
hospitals must occasionally cancel or postpone elective surgery because of a lack of red
cell units. Half of those hospitals do this for at least two days. Additionally, one-fourth of
hospitals cannot meet their non-surgical blood requests at least one day, and for those
experiencing such shortages, half are not able to meet it on at least five days.
Because they are not dependent upon voluntary donations, and therefore can be
manufactured in quantities that will meet demand, synthetic blood products represent an
important means to address shortfalls between supply and demand for human blood.
However, while some synthetic products, such as recombinant factors, are well
established, others like oxygen carriers are in a much earlier stage of development.
Variables Influencing the Supply and Demand of Donated Blood While a major reason for the blood shortage is that people are unwilling or unable
to donate blood, there are five main reasons for the shrinking numbers:

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 164 -
• changing demographics;
• increasing need for blood;
• increasing blood donor rejections;
• seasonality and weather;
• decreasing public awareness of the importance of blood donation.
Since blood transfusions became commonplace in the 1950s, blood centers have
depended on the World War II generation for donations. As this generation ages, there
are fewer Baby Boomers living and the generations that follow do not donate as much.
Experts suspect this may be related to differences in lifestyle, the level of altruism, and
the fact that the blood community is not effectively marketing to these younger
generations. Since people older than 65 use 43% of all donated blood, the demand for
blood will increase as the global population ages.
As this occurs, the need for blood will rise. Lengthening lifespans and increasing
complexity of surgeries will also contribute to greater demand for blood. The U.S., for
example, uses about 5% more blood every year.
However, the donor rejection rate is increasing. Beginning with the AIDS
epidemic in the early 1980s, the blood supply has become much safer. But achieving this
has required turning away more and more potential donors. Today, increasingly
sophisticated and sensitive tests, coupled with significantly more questions designed to
eliminate donors who may transmit blood-borne diseases, means there are fewer people
who are able to donate blood. For instance, people who have spent three or more months
in the UK between 1980 and 1996 cannot donate blood in the United States for fear they
could introduce the human version of mad-cow disease, variant Creutzfeldt-Jakob
Disease (vCJD), into the blood supply.
Seasonality also plays a role. Blood donations tend to decline in the summer
months when donors often take vacations and during hard winters when inclement
weather makes travel to donation centers difficult.
There are other reasons for the shortage as well. Blood products are perishable.
Red blood cells have a shelf life of 42 days, and platelets just five days, so blood
donations are required on a daily basis. People’s perceptions about blood donation also

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 165 -
contribute to blood shortages. For example, a recent study evaluating why people do not
donate blood and other organs found that a persistent mistrust of doctors and hospitals as
well as religious misconceptions played a major role. Minorities were particularly likely
to avoid making donations for these reasons. The study, which involved 20-minute phone
interviews with 339 Baltimore, MD residents, found that Caucasian women were far less
willing to donate blood than Caucasian men (36% compared to 86%), while just 41% of
African-American women surveyed said they would donate blood. But the greatest
barrier that prevents people from donating is a lack of convenience and a lack of
knowledge of the importance of donating.
For the purposes of this report, synthetic blood products that would help address
this imbalance between blood demand and blood supply include:
• recombinant factor for hemophilias, such as Factor VIII (TKT);
• hemoglobin-based oxygen carriers (HBOCs);
• perflurocarbon-based oxygen carriers (PFCs);
• synthetic platelets.
Recombinant factors are widely available; research continues into HBOCs, PFCs
and synthetic platelets, with new products expected to be introduced over the next several
years.
However, it should also be noted that there are still many questions about blood
substitute products such as HBOCs and PFCs that must be addressed. For example, will
they be used for initial resuscitation, prior to transfusion with human-derived blood, or as
an adjunctive therapy? Will pharmacies or blood banks control the products? Who will
oversee issues such as initial and total dose, monitoring of utilization, clinical laboratory
measurements, quality control, and transfusion/infusion reactions? The FDA also has
questions about whether blood substitutes that may be approved for certain specific
indications could be used more widely than indicated, potentially compromising patient
safety.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 166 -
RECOMBINANT FACTOR MARKET Hemophilia A affects about 70,000 people in the world’s developed drug markets.
One of the keys to successfully managing this genetically transmitted disease involves
administering treatments with recombinant factors. These include genetically engineered
or cloned clotting factors (Factor VIII or antihemophilic factor) that are not derived from
human or animal plasma as well as a recombinant Factor VIIa (NovoSeven) that is also
produced without human serum proteins. Certain plasma-derived products, such as
immunoglobulins and albumin, are generally not manufactured by recombinant means.
Market Size The market for recombinant factors stands at more than $5.6 billion in 2007 and is
expected to rise by 8.9% per year to more than $10.1 billion by 2012, as shown below in
Table 6-1.
Table 6-1
World Recombinant Factor Market by Brand, 2009-14
Revenues (in millions) Product Company 2007 2008 2009 2010 2011 2012 2013 2014 Recombinate, Advate
Baxter $1,714
$1,920
$2,150
$2,408
$2,697
$3,021
$3,383
$3,789
Kogenate Bayer AG 1,273 1,349 1,430 1,516 1,607 1,704 1,806 1,914 Novoseven NovoNordisk 1,224 1,346 1,481 1,629 1,792 1,971 2,168 2,385 Helixate CSL 357 378 401 425 451 478 506 537 ReFacto Wyeth 330 350 371 393 417 442 468 496 Others Various 710 753 798 846 896 950 1,007 1,068 Total $5,608 $6,096 $6,631 $7,217 $7,860 $8,565 $9,339 $10,189
Source: Kalorama Information
While growth has been driven by conversion from plasma-derived therapies,
adequate dosing and compliance, and increasing prophylactic use of recombinant
therapies, future gains will be fueled by continuing improvements in products, including
expanded indications and enhanced delivery systems. The products are primarily
consumed in the developed Western nations: according to the Plasma Protein
Therapeutics Association (PPTA), the Americas and Europe continue to consume more

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 167 -
than three quarters of plasma-derived Factor VIII. European use continues to rise,
particularly with increased government funding for conversion from plasma-derived
Factor VIII to recombinant Factor VIII.
Market Participants Baxter remains the undisputed leader in the recombinant factor market, although
competitors continue to expand usage of their products. In 2007, global sales of Baxter’s
Advate recombinant Factor VIII for hemophilia A exceeded $1.2 billion and continue to
rise as Advate is introduced into new global markets; during the year, Argentina became
the first country in Latin America to launch the product. Advate was also recently
introduced in Japan and New Zealand with upcoming launches in Venezuela, Taiwan and
Hong Kong. Baxter continues to work on ways to increase Advate’s half life, which
would decrease the number of injections required, and introduce higher potency
formulations, such as the 3000 IU dosage, which was launched in 2007. In January 2008,
Baxter began a program to develop a recombinant form of Factor IX.
Sales of Bayer’s Kogenate exceeded $1.2 billion in 2007 with the June launch of
the 2000 IU vial size. The larger Grab & Go package is designed help to reduce
reconstitution time and provide added convenience for users. The company is also in
Phase II testing of a new patented pegylated liposome technology and in July 2008,
acquired Maxygen’s hemophilia program assets, including a next-generation recombinant
Factor VIIa protein known as MAXY-VII. The lead therapeutic candidate is expected to
enter Phase I clinical testing in the third quarter of 2008.
Sales of NovoNordisk’s NovoSeven also continue to expand strongly. In 2004,
NovoNordisk obtained European approval to market its Novoseven for the control of
bleeding in patients with factor VII deficiency and Glanzmanns thrombasthenia
refractory to platelet transfusions and the company continues to conduct clinical studies
evaluating the product for use in connection with intracerebral hemorrhage (ICH). In
2007, NovoNordisk completed Phase II safety studies for the use of NovoSeven in
cardiac surgery, with preliminary results confirming the product’s safety profile as well
as its biologic haemostatic effect. During the year, NovoNordisk submitted heat-stable
versions of NovoSeven to regulators in the U.S., EU and Japan.
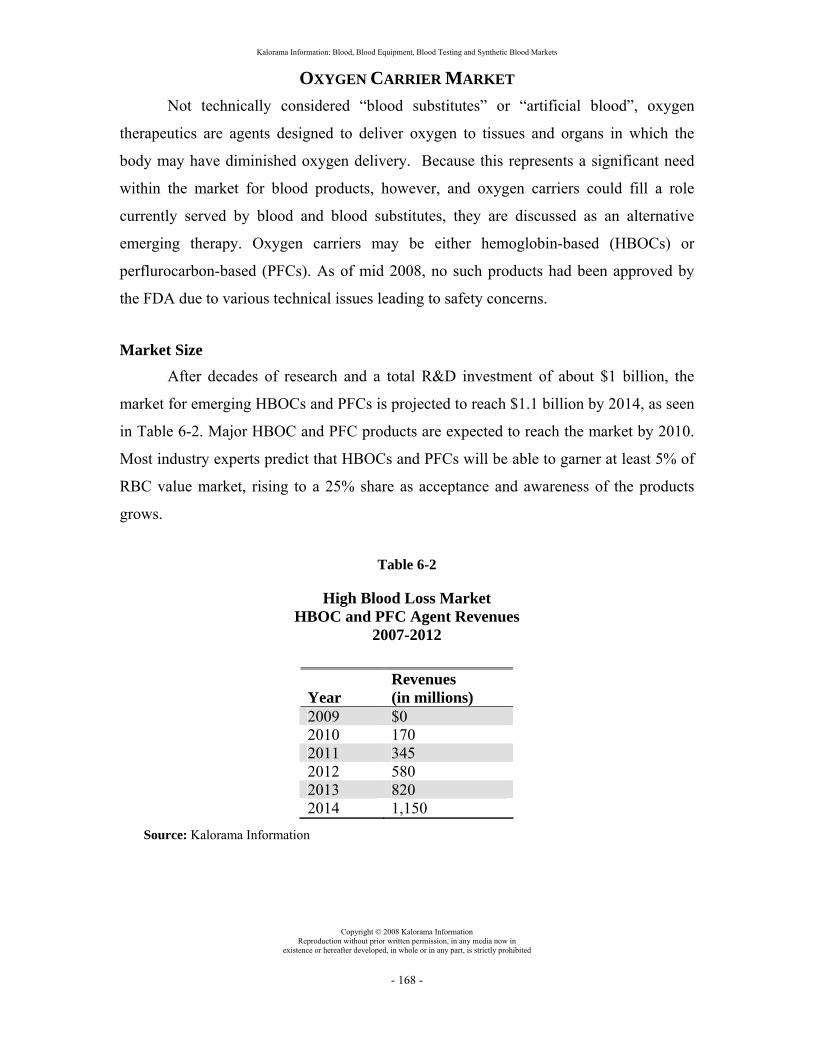
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 168 -
OXYGEN CARRIER MARKET Not technically considered “blood substitutes” or “artificial blood”, oxygen
therapeutics are agents designed to deliver oxygen to tissues and organs in which the
body may have diminished oxygen delivery. Because this represents a significant need
within the market for blood products, however, and oxygen carriers could fill a role
currently served by blood and blood substitutes, they are discussed as an alternative
emerging therapy. Oxygen carriers may be either hemoglobin-based (HBOCs) or
perflurocarbon-based (PFCs). As of mid 2008, no such products had been approved by
the FDA due to various technical issues leading to safety concerns.
Market Size After decades of research and a total R&D investment of about $1 billion, the
market for emerging HBOCs and PFCs is projected to reach $1.1 billion by 2014, as seen
in Table 6-2. Major HBOC and PFC products are expected to reach the market by 2010.
Most industry experts predict that HBOCs and PFCs will be able to garner at least 5% of
RBC value market, rising to a 25% share as acceptance and awareness of the products
grows.
Table 6-2
High Blood Loss Market HBOC and PFC Agent Revenues
2007-2012
Year Revenues (in millions)
2009 $0 2010 170 2011 345 2012 580 2013 820 2014 1,150
Source: Kalorama Information

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 169 -
SYNTHETIC BLOOD PRODUCTS IN CLINICAL DEVELOPMENT Major blood-loss surgical procedures, cardiothoracic surgeries, and trauma are the
primary settings in which Phase I and II safety and dose-escalation trials are currently
being conducted with new Hb- and PFC-based oxygen carriers. Both Hb-based oxygen
carrier (HBOC) molecules and PFC emulsion particles (<0.1 µm in diameter) are
significantly smaller than RBCs, which are about 7 µm in diameter. As such, they are
much better able to diffuse into and deliver O2 to poorly vascularized hypoxic tissues.
The PFC emulsion Fluosol (Green Cross Co.) has FDA approval for use in percutaneous
transluminal coronary angioplasty (PTCA). Other uses that could potentially take
advantage of the ability of oxygen carriers to diffuse into the microcirculation include
delivering oxygen to poorly vascularized radiosensitive tumors and ischemic crises in
sickle cell disease.
Product development, however, continues to be controversial, with a report
appearing in a May 2008 issue of the Journal of the American Medical Association
(JAMA) linking HBOCs to safety issues. The article described a statistical meta-analysis
examining the incidence of myocardial infarction and death as reported in the published
clinical trial data from five different HBOCs. It cited a total of 164 deaths among HBOC-
treated patients and 123 deaths among subjects in the control groups. Overall, the HBOCs
were associated with a 30% increased risk of death. There were a total of 59 heart attacks
among HBOC-treated patients and 16 heart attacks among patients in the control groups.
Across all five studies, there was a 270% increased risk of heart attack among patients
receiving HBOCs.
The following sections profile notable product candidates.
Hemolink (Hemosol)
Drug: Hemoglobin raffimer
Brand Name: Hemolink
Synonyms: Hemoglobin raffimer; Human hemoglobin - Hemosol; Human hemoglobin - Hemosol
Chemical Name: The polyaldehyde ((2R,4S,6R,8R,11S,13R)-1,14-dihydroxy-4- hydroxymethyl-3,5,7,10,12-pentaoxatetradecane-2,4,6,8,11,13- hexacarbaldehyde)

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 170 -
derived from raffinose (beta-D-fructofuranosyl- alpha-D-galactopyranosyl-(1->6)-alpha-D-glucopyranoside) by treatment with sodium periodate is reacted with human hemoglobin A sub(0) at the 2,3-DPG binding pocket. Both intermolecular and intramolecular crosslinking occurs. This product is reduced to generate covalent amine bonds with >95% crosslinked hemoglobin of which about 55% is polymerized.
Therapeutic Class: Blood substitutes and plasma protein fractions
Mechanism of Action: Hemoglobin agonists
Originator Company: Hemosol Corp. (Canada); Hemosol Corp. (United States)
Parent Company: Hemosol Corp.
Highest Phase: Preregistration
Development Status:
• Preregistration, Canada, Hypovolaemia
• Preregistration, United Kingdom, Hypovolaemia
• Suspended II, United States, Anemia
• Suspended II, United States, Hypovolaemia
Ontario-based Hemosol is developing several products hemoglobin-based oxygen
carriers, however, development remains stalled following the company’s November 2005
announcement of insolvency and its filing of Notices of Intention to Make a Proposal to
its creditors under Canada’s Bankruptcy and Insolvency Act.
One of these products is hemoglobin raffimer, a solution of highly purified, o-
raffinose cross-linked human hemoglobin-based oxygen carrier in lactated Ringer's. It
combines both polymerized and non-polymerized hemoglobin components of varying
molecular weights. Hemoglobin raffimer is designed to facilitate delivery of oxygen to
vital organs and tissues in patients undergoing cardiac, orthopedic and other surgery, as
well as in patients undergoing chemotherapy. Other potential indications for hemoglobin
raffimer include hypovolaemia associated with trauma or surgery, oxygen delivery for
cancer patients, ischemic rescue in patients with stroke or myocardial infarction, and
tissue perfusion in angioplasty and organ transplants. However, unlike whole blood, it
can be stored for more than a year at normal refrigeration temperatures of 40C, or for two

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 171 -
or more months at ambient room temperature. Preclinical studies have shown that
hemoglobin raffimer enhances the growth of new red blood cells.
Eight clinical trials of hemoglobin raffimer involving over 500 patients have been
completed. The most advanced trial to be completed is a Phase III trial, which was
conducted in 299 patients undergoing CABG surgery in the UK and Canada. The trial
was completed in 2000. In the primary efficacy endpoint, 17% of hemoglobin raffimer
recipients received a transfusion of donor red blood cells compared with 27% of the
control group; a statistically significant relative reduction of 37%. In addition,
hemoglobin raffimer use was associated with a 20% reduction in the amount of donor red
blood required in patients receiving a transfusion and a longer overall time (14 hours)
required to transfusion, compared with patients in the control group. Results further
indicate that treatment with hemoglobin raffimer meant that the use of donated blood was
avoided to a greater extent in patients receiving hemoglobin raffimer, relative to those
receiving a standard blood volume expander - Hespan.
Based on the results from this Phase III trial Hemosol filed for approval of
hemoglobin raffimer in Canada and the UK. However, in March 2002, Health Canada
advised Hemosol that hemoglobin raffimer would not be approved and that additional
data would be required for a refiled New Drug Submission. In the U.S., clinical trials of
hemoglobin raffimer have been suspended.
Hemopure (Biopure)
Drug: Hemoglobin glutamer-250 (bovine)—Biopure
Brand Name: Hemopure
Synonyms: Bovine hemoglobin - Biopure; Bovine hemoglobin - Biopure; Hemoglobin glutamer-250 (bovine); Hemoglobin glutamer - Biopure; Hemoglobin- bovine - Biopure; HBOC-201; Hemoglobin glutamer - Biopure; Hemoglobin- bovine—Biopure.
Therapeutic Class:
• Blood and Related Products
• Whole Blood and Plasma Fractions
• Irrigating Solutions

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 172 -
Mechanism of Action: Hemoglobin agonists
Originator Company: Biopure Corporation (United States)
Parent Company: Biopure Corporation
Licensee: Braun Melsungen; Tshepo Pharmaceuticals
Highest Phase: Launched
Development Status:
• Launched, South Africa, Surgical Anemia
• Preregistration, United States, Anemia
• Preregistration, UK, Anemia
• Phase II, United States, Coronary Occlusion/Acute Coronary Syndrome
• Phase II, United States, Coronary Artery Disease
• Phase II, United States, Peripheral Vascular Disease
• Phase II, United States, Wounds and Injuries
• Phase II, Europe, Cardiopulmonary Bypass Surgery
• Phase II, Europe, Percutaneous Coronary Intervention (PCI)
Hemopure is Biopure's stable formulation of ultrapurified, polymerised bovine
hemoglobin with an average mass of 250kD for use in transfusions. It is formulated in a
balanced salt solution similar to Ringer's lactate and has a viscosity lower than that of
human whole blood. One unit of Hemopure contains 30g of hemoglobin in 250mL of
solution. On a gram-for-gram basis, Hemopure carries the same amount of oxygen as
hemoglobin in red blood cells. However, as it circulates in plasma rather than red blood
cells, Hemopure can carry oxygen through constricted or partially-blocked blood vessels
to tissues that red blood cells cannot access under such circumstances.
Tshepo Pharmaceuticals had been the licensee for Hemopure in South Africa. In
2003, Biopure gave notice that it was terminating its distribution agreement with Tshepo
and in 2006, the company began marketing Hemopure in South Africa with a new sales
agent. Hemopure is approved in South Africa for the treatment of acute anemia and
avoidance of red blood cell transfusions in adults undergoing surgery.
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 173 -
A single-center, phase II trial has also been approved in South Africa to evaluate
Hemopure among trauma patients in the hospital setting. In July 2004, Biopure initiated a
phase II trial among trauma patients at the Johannesburg General Hospital, South Africa,
commencing with a target of approximately 50 subjects. The randomized, single-blind,
parallel- group, standard therapy-controlled trial is investigating Hemopure's application
in emergency treatment of unstable patients with significant blood loss (hypovolaemia)
caused by blunt or penetrating trauma. In 2007, an independent data safety and
monitoring board (DSMB) reviewed the data from the first 21 patients in this trial and
recommended that the trial continue without modification.
In 2006, Biopure began patient enrollment in a Phase II clinical trial investigating
Hemopure in patients undergoing multi-vessel coronary artery bypass graft (CABG)
surgery. The objective of this trial is to assess the safety and feasibility of Hemopure in
reducing heart damage, as measured by cardiac enzyme elevation, and enhancing tissue
preservation during CABG surgery. Secondary endpoints include measurements of major
adverse cardiac events, kidney function, transfusion requirements, cognitive impairment
and length of hospital stay. As of mid 2008, the trial had enrolled 53 patients with a target
of 60.
Hemopure has also shown potential in other areas with Phase II trials in patients
with sickle cell disease and phase I development as an adjunct to radiotherapy in patients
with cancer.
In 33 patients receiving Hemopure infusions (0.6-2 g/kg) once during and once
after elective surgery, no significant hemodynamic changes were seen, and no increases
in blood pressure were observed. In a phase III study, the administration of Hemopure to
approximately 350 patients resulted in transient, slight to modest increases in blood
pressure compared to the red blood cell group. A mean increase of 14.4 mm/Hg in mean
arterial pressure (MAP) was observed in the Hemopure group, compared to 7.3 mm/ Hg
in the red blood cell group. Similar changes in MAP from pre- treatment to 30 minutes
post-infusion were observed following the first infusion in the Hemopure (17.3 mm/Hg
+- 0.9) and red blood cell groups (1.9 mm/Hg +- 0.8).
In clinical studies, a single Hemopure infusion given to patients with sickle cell
disease produced a reduction in the exercise-induced increase in heart rate compared with

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 174 -
placebo recipients in a single-blind, placebo-controlled study. None of the patients were
in sickle cell crisis and all received a single dose of 0.2, 0.4 or 0.6 g/kg (n = 12) or
placebo (6). The change in total hemoglobin was small but the amount of free
hemoglobin detected in plasma was 0.48 g/dl in recipients of the lowest dose to 0.75 g/dl
in patients receiving the highest dose of Hemopure.
Plasma hemoglobin levels significantly and dose-dependently increased compared
with baseline in 33 patients receiving Hemopure infusions (0.6-2 g/kg) once during and
once after elective surgery. Patients were participating in a single-blind, randomized,
placebo-controlled trial. Hemopure was administered after a blood loss of 500mL or
more.
The administration of Hemopure reduced the requirements for red blood cell
transfusions in patients requiring transfusions after cardiac surgery in a multicenter,
double-blind Phase II trial. Nearly 100 patients were randomized to receive either
Hemopure or allogenic red blood cells for up to 3 transfusions during the first 72 hours
after cardiopulmonary bypass surgery. Subsequent transfusions used red blood cells in
both groups of patients. About 34% (17/50) of Hemopure recipients did not require red
blood cell transfusions after surgery. The hemocrit was similar for both groups of patients
at the time of discharge, suggesting that Hemopure may promote the production of red
blood cells.
In a similar study, Hemopure eliminated the requirement for allogeneic red blood
cell transfusions in a significant number of patients. In a single-blind Phase II study,
patients undergoing elective surgery for abdominal aortic aneurysms (n = 72) were
randomized to receive either Hemopure (n = 48) or allogeneic red blood cells (n = 24) at
the first transfusion decision during or after surgery. The 48 patients received an initial
dose of 2 units of Hemopure and up to 3 more units within 96 hours, if needed. Any
additional infusions in these patients were of allogeneic red blood cells. Red blood cell
transfusions over the 28-day study period were not required in 27% of patients who
received Hemopure. In addition, on the day of surgery and during the 96-hour treatment
period, 39 and 66% respectively of Hemopure-recipients did not require allogeneic blood.
Furthermore, the hematocrit at time of hospital discharge was similar in both Hemopure
and control patients.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 175 -
In a Phase III orthopedics study reported in a June 2008 issue of the Journal of
Trauma, the product eliminated the need for transfusion in the majority of the nearly 700
patients participating. Researchers also concluded that patients less than 80 years of age
with moderate clinical need for additional oxygen carrying capacity could safely avoid
transfusion when treated with up to 10 units of Hemopure.
Biopure intends to shortly initiate a U.S. clinical trial of Hemopure in patients
suffering from Acute Myelogenous Leukemia (AML) who refuse transfusion with blood
components, meeting with the FDA in July 2008 to develop protocols for the
identification of appropriate patients. This application represents an unmet medical need
because of an expected 100% mortality within 6 months in the absence of induction
chemotherapy.
PolyHeme (Northfield Laboratories)
Drug: Human hemoglobin—Northfield Laboratories
Brand Name: PolyHeme
Therapeutic Class:
• Blood substitutes and plasma protein fractions
• Whole Blood and Plasma Fractions.
Mechanism of Action: Hemoglobin agonists
Originator Company: Northfield (United States).
Parent Company: Northfield
Highest Phase: Preregistration
Development Status:
• Preregistration, United States, Hypovolaemia
PolyHeme is a chemically modified hemoglobin solution derived from human
blood. It has been developed by Northfield Laboratories as an alternative to transfused
blood for the treatment of acute blood loss, such as occurs in trauma or surgery. Single
molecules of hemoglobin are toxic to the kidneys and cause vasoconstriction. The
hemoglobin molecules in PolyHeme are polymerized to create small chains of linked

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 176 -
tetramers. This chemically modified human hemoglobin that requires no cross matching
and is therefore compatible with all blood types. It has a shelf life in excess of 12 months.
In early trials, PolyHeme was shown to be as effective as donated blood in the
transfusion of seriously injured, bleeding trauma patients. A randomized study of 44
trauma patients showed that patients who received 6 units of PolyHeme during initial
blood replacement needed only 6.8 additional units of donated blood, whereas those who
received donated blood needed 10.4 units altogether. A survival rate of 75% was reported
in 171 patients receiving PolyHeme who had essentially no remaining red cells in their
circulation.
In March 2003, Northfield announced that it had received clearance from the
FDA to proceed with the pivotal Phase III trial and in December of the year, it received
notification of the first full approval by an institutional review board (IRB) to proceed
with enrollment in the PolyHeme urban ambulance trial. This trial is a controlled study
designed to evaluate the safety and efficacy of PolyHeme in treating severely injured and
bleeding patients when blood is not immediately available. The study aimed to enroll 720
patients spread across 25 - 30 Level I trauma centers across the United States, with a
primary endpoint of survival at 30 days. In October 2004, the Independent Data
Monitoring Committee (IDMC) recommended that the pivotal Phase III trial continue
without modification. This follows the second planned interim analysis of the study.
In late 2006, Northfield Labs released preliminary results of the trial, indicating
disappointing mortality data: 13.2% of patients receiving PolyHeme died versus 9.6%
among the control group. After a subsequent analysis, however, the company released
more detailed findings in May 2007 indicating no significant difference in mortality
between patients who received the standard of care, including early blood transfusion,
and PolyHeme. The company is currently preparing a Biologics License Application, or
BLA, for PolyHeme for submission to the FDA later in 2008.
Oxygent (Alliance Pharmaceutical)
Drug: Perflubron—Oxygent
Synonyms: AF 0144; AF0144; Oxygent

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 177 -
Chemical Name: Octane, 1-bromo-1,1,2,2,3,3,4,4,5,5,6,6,7,7,8,8,8-heptadecafluoro-
Molecular Formula: C8BrF17
CAS® Registry Number: 423-55-2
Therapeutic Class:
• B05A-Fluorocarbon Blood Substitutes
• Other Hematological Agents.
Mechanism of Action: Membrane permeability enhancers.
Originator Company: Alliance Pharmaceutical Corp.
Parent Company: Alliance Pharmaceutical Corp.
Licensee: Il-Yang; PFC Therapeutics
Highest Phase: Phase III
Development Status:
• Phase II, China, Various Applications
Perflubron (Oxygent) is a biologically inert, oxygen-carrying perfluorochemical
liquid, a concentrated stable emulsion of perflubron and lecithin, which was originally
developed by Alliance Therapeutics as an intravascular oxygen carrier during surgery.
Administration of perflubron emulsion in combination with blood conservation and
transfusion techniques (using the patient's own blood) is intended to reduce the need for
donor blood transfusions during elective surgery. Perflubron emulsion is administered
using Alliance's proprietary Augmented Acute Normovolemic Hemodilution (A-ANH)
technique. It is in phase III trials in Europe and the United States.
The current formulation of Alliance's perflubron (AF 0144) is a 60%
weight/volume perflubron-based formulation, emulsified with phospholipid as its
surfactant, with an initial median particle diameter of 0.16-0.18microm and a shelf-life of
up to 2 years. In contrast, red blood cells can only be stored for just 6 weeks.
Baxter Healthcare had licensed exclusive rights to perflubron emulsion in Europe
and North America during May 2000 in a deal valued at $50 million. At Baxter's request,
Alliance and Baxter then formed a joint venture, called PFC Therapeutics. PFC

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 178 -
Therapeutics was set up to conduct further development and to commercialize perflubron
emulsion in Europe and North America.
In August 2002, Alliance Pharmaceuticals sent PFC Therapeutics a notice of
intended termination of its exclusive license to commercialize perflubron emulsion, on
the grounds that PFC Therapeutics had not met all of its obligations under the licensing
agreement. In June of the following year, Alliance acquired the balance of ownership
interest in the joint venture, and will pay Baxter a royalty on the sales of Oxygent
following regulatory approval.
Clinical testing of Oxygent remains ongoing, although some trials have been
scaled back due to a lack of funding. Alliance has estimated its esearch and development
costs to date for its oxygen-therapeutic product candidates, including Oxygent, at
approximately $161 million; it further estimates that the completion of clinical trials for
Oxygent will cost at least an additional $70 million and take several more years.
In January 2007, the French Ethics Committee (IRB) and the French Competent
Authority (regulatory agency) granted approval to start the Phase IIb clinical trial for
Oxygent to prevent postoperative ileus resulting from hypoxia during major surgery trial.
Subsequently, Alliance submitted a clinical trial protocol revision to the French Ethics
Committee and the French Competent Authority, which modified the dosing regimen to a
dose-escalation protocol. Alliance initiated the trial, but in November 2007, discontinued
enrollment in the French study to focus on development of Oxygent in China.
In May 2005, PFC Therapeutics and Beijing Double-Crane Pharmaceutical Co.,
Ltd, the market leader for IV solutions and one of the largest pharmaceutical companies
in China, entered into a development, license and supply agreement to develop Oxygent
for the Chinese market. As of mid 2008, Phase II trials in China were ongoing.
In previous clinical trials, perflubron emulsion was shown to be well tolerated in
patients undergoing surgery and significantly more effective than blood in reversing
transfusion triggers. These multicenter studies involved a total of 256 patients undergoing
orthopedic, gynecologic or urologic elective surgery that usually results in moderate to
high blood loss. Patients were randomized to receive either perflubron emulsion and
100% oxygen, a unit of fresh autologous blood (collected during hemodilution before
surgery), or a volume expander and 100% oxygen when the patient reached a first

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 179 -
transfusion trigger. Perflubron emulsion also delayed the requirement for a subsequent
blood transfusion significantly longer than blood.
Oxycyte (Oxygen Biotherapeutics) Oxycyte is a perfluorocarbon (PFC) based blood substitute that can carry five
times more oxygen than hemoglobin. Oxygen Biotherapeutics (formerly Synthetic Blood
International) is looking at different applications for Oxycyte in surgery patients.
In August 2005, Synthetic Blood submitted an amendment to its Investigational
New Drug (IND) application with the FDA to initiate a Phase II proof-of-concept study
to evaluate the safety and biological effects of Oxycyte in patients with traumatic brain
injury. In this eight-patient, open label, Phase II pilot study, Oxycyte was administered to
patients with severe traumatic brain injury within 24 hours of the injury's occurrence. In
April 2006, the company announced that Oxycyte increased cerebral oxygen tension in
the first three patients treated in the study.
Oxygen Biotherapeutics expects to begin a Phase IIb clinical trial of Oxycyte in
traumatic brain injury in the third quarter of 2008. The multi-center, double-blind,
placebo-controlled study will enroll up to 300 patients; of these, 200 patients will be
allowed for enrollment through a recently approved $1.9 million grant from the United
States Department of Defense. Other studies may include evaluation of Oxycyte in
orthopedic surgery patients who lose modest amounts of blood during surgery;
administration to patients undergoing coronary bypass or heart valve replacement surgery
on a heart-lung machine; as well as surgical patients who lose enough blood during
surgery to require a blood or red cell transfusion.
PHER-O2 (Sanguine)
Sanguine's PHER-O2 is a synthetic red blood cell product with potential
applications in a variety of specialties, including transfusions, CAT scans, cardioplegia
and the treatment of heart attacks, strokes, head and neck tumors, and hemorrhagic shock.
It represents a second generation product to Sanguine’s Fluosol, an FDA-approved

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 180 -
synthetic red blood substitute for medical use in connection with blood supplementation.
Fluosol is not presently marketed, however, due to its need for frozen storage, low (20%)
PFC content and short intra-vascular residency time; however, in the three years of its
highest usage, Fluosol was transfused into approximately 15,000 human patients each
year.
Fluosol represents a combination of the carbohydrate decalin (C10 H18) that
replaces the hydrogen atoms with flourine atoms, resulting in a fluorocarbon.
PHER-O2 has successfully completed animal toxicity and efficacy trials at the
University of Alberta in Canada. Sanguine believes that Fluosol’s acceptance should
enable it to pursue the fast track for PHER-O2 through clinical trials and the FDA
approval process.
Albrec (Mitsubishi Pharma)
Drug: Recombinant human serum albumin - Mitsubishi Pharma
Brand Name: Albrec
Synonyms: GB-1057
Therapeutic Class:
• Blood substitutes and plasma protein fractions
• Protein Solutions
Mechanism of Action: Osmosis stimulants non-diuretic
Originator Company: Mitsubishi Pharma Corp.
Parent Company: Mitsubishi Chemical
Highest Phase: Registered
Development Status: Registered, Japan, Hypovolaemia
• Phase I, U.S., Stabilizing Agent
Welfide Corp. (formerly Yoshitomi) developed a recombinant form of human
serum albumin (GB-1057, also known as Albrec) derived from yeast, for use in blood
volume replacement in hemorrhagic shock and other conditions. In October 2001,
Welfide merged with Mitsubishi-Tokyo Pharmaceuticals to form Mitsubishi Pharma.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 181 -
At the BIO 2004 Annual International Convention (BIO-2004) in June 2004,
Mitsubishi Pharma announced that recombinant human serum albumin had been
approved by Japanese health authorities following regulatory submission, which was
originally lodged in 1997. Construction of a plant to produce recombinant human serum
albumin was completed in Japan in 1999. The plant uses Streamline and Chromaflow
technology developed by the Swedish-based Amersham Pharmacia Biotech.
Clinical evaluation of GB-1057 outside Japan is in a much earlier stage, with
Phase I U.S. trials ongoing.
Hemospan (Sangart) Sangart’s Hemospan combines low hemoglobin concentration with high-oxygen
transport capability. The product uses components harvested from outdated human blood
combined with polyethylene glycol (PEG) to eliminate the toxicity of free hemoglobin. In
laboratory testing, this “pegylation” of the hemoglobin has been shown to help mitigate
against immunologic reactions. In November 2005, the company announced positive
results from a Phase II clinical trial of Hemospan in hip surgery patients. The
investigation included 90 patients aged 50 to 89 undergoing hip arthroplasty procedures
at six hospital sites in Sweden. Patients were randomized to receive either 250 mL or
500 mL of Hemospan or a control solution prior to induction of spinal anesthesia. The
objectives of the trial were to further assess the safety of Hemospan and demonstrate
preliminary efficacy. Hemospan was found to be well tolerated in the study group with
no serious adverse events attributable to the product noted during the trial. Additionally,
the percentage of patients with hypotensive episodes was significantly lower in the
Hemospan groups (46% in the 250 mL group, 42% in the 500 mL group) compared to
87% in the control group. In May 2008, Sangart completed enrollment in a second Phase
II study of Hemospan after an independent data safety monitoring board (DSMB)
recommended the continuation of its Phase III clinical trials under current protocols
Advate (Baxter) Baxter’s Advate (antihemophilic factor (recombinant) plasma/albumin-free
method, rAHF-PFM) was approved in July 2003 in the United States and subsequently in
the EU for the prevention and control of bleeding episodes in subjects with hemophilia A.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 182 -
It is the only hemophilia A therapy made without any plasma protein additives in the cell
culture process, purification and final formulation, thereby eliminating the risk of
infection from viruses and infectious prions. The genetically engineered full-length
clotting factor VIII is similar to the natural clotting factor found in the healthy body.
Phase II and III data demonstrated that Advate is effective in controlling bleeding
episodes and has equivalent pharmacokinetic properties to Recombinate, the full-length
rAHF molecule and a leading recombinant Factor VIII therapy which Baxter introduced
in 1992.
There are several ongoing studies of Advate, including a continuation study in
previously treated patients, a surgery study and a pediatric study, as well as plans to
launch Advate in additional markets. As of late 2007, Advate was available in 36
countries worldwide, including Japan.
Recombinant Factors In January 2008, the U.S. FDA approved ZymoGenetics' Recothrom Thrombin,
topical (recombinant) for sale. Previously referred to as recombinant thrombin
(rThrombin), Recothrom, is the first and only recombinant, plasma-free thrombin
approved for use as a topical hemostat. The product is indicated as an aid to hemostasis
whenever oozing blood and minor bleeding from capillaries and small venules is
accessible and control of bleeding by standard surgical techniques is ineffective or
impractical. A Phase III pivotal clinical trial showed that Recothrom had comparable
efficacy and a significantly lower incidence of antibody formation compared to bovine
thrombin. While the bovine-derived product has been used for more than 30 years, it has
been associated with the development of antibodies that may cross-react with human
blood proteins, leading to serious bleeding complications.
Other recombinant factor products under development are shown in Table 6-3.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 183 -
Table 6-3
Recombinant Factor Products in Clinical Trials
Product Pharmacological Class Company Phase II rFVIIa short-acting analogue Factor VII NovoNordisk OBI-1 Factor VIII Ipsen Phase I rFVIIa long-acting analogue Factor VII NovoNordisk rFXIII Factor XIII NovoNordisk Pre-clinical Factor VIII Gene Therapy Oxford BioMedica
Source: Kalorama Information
Synthocytes Synthocytes are microcapsules to which fibrinogen has been chemically linked.
Although considerably larger than platelets, they mimic platelet activity in that they
target the site of hemorrhage, where presumably clot formation is enhanced or initiated.
Acute thrombocytopenia occurs secondary to cancer chemotherapy (induced by bone
marrow suppression. Synthocytes therefore are a substitute for platelet transfusions.
Early Phase I studies conducted at the University of Nottingham in the U.K. showed
promising results in patients with thrombocytopenia secondary to cancer chemotherapy.
Synthocytes may also have a role in the perioperative arena. Intraoperative
thrombocytopenia may occur during major blood loss, when blood is replaced with blood
products that do not contain platelets. Thrombocytopenia may occur secondary to
cardiopulmonary bypass following the consumption of synthocytes or damage within the
extracorporeal circuit. Many patients take antiplatelet drugs to minimize platelet
stickiness as a prophylaxis against coronary or cerebral ischemic events. While platelet
counts are normal, platelet function in these patients may be severely compromised. This
is termed thrombasthenia. As mentioned previously, ANH-induced thrombocytopenia is
one of the stated endpoints and theoretical disadvantages of this technique. The use of
synthetic platelets, in conjunction with an oxygen-transport blood substitute, might

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 184 -
enhance a practitioner’s ability to sequester larger volumes of whole blood without the
sequelae of thrombocytopenia.
However, development of synthocytes appears to have slowed after their original
developer, Andaris Group, was acquired after completing preliminary Phase IIa studies of
synthrocytes. Other developers working on similar platelet-substitute type products
include U.K.-based Haemostatix.
Gene Therapy
A number of gene therapy projects targeting Factor VIII have been suspended and/or abandoned by various companies. For instance, Targeted Genetics, Wyeth and Cell Genesys have all abandoned their Factor VIII programs, with Wyeth suspending its program in Phase III.
OTHER RESEARCH INITIATIVES
In addition to these initiatives conducted by corporate and/or private-sector researchers, several well established public-sector groups are also investigating novel blood substitutes. Selected initiatives are profiled below.
Jerome H. Holland Laboratory A division of the American Red Cross, the Jerome H. Holland Laboratory was
established in 1987 to expand the ARC’s 25 year old research initiatives. Since then, the
JHL has grown to become one of the world's foremost blood research facilities with work
supplemented by a dozen Red Cross Blood Services regions conducting their own local
research and development. In 2008, the laboratory has more than 250 scientists working
on both basic and applied research programs in biochemistry, coagulation proteins,
experimental pathology, product development, transmissible diseases and virology,
immunology, molecular biology, platelet biology and plasma derivatives. Development
initiatives are conducted both in-house and in collaboration with other groups such as the
U.S. Army, with key areas of research including:

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 185 -
• improving the safety and efficacy of U.S. blood services;
• studying the molecular biology of blood and the immune response;
• developing new biomedical products and technologies.
Immune Disease Institute Founded in 1953, the Immune Disease Institute (formerly known as the Center for
Blood Research) is a non-profit organization affiliated with Harvard Medical School.
However, while its investigators hold appointments in departments of HMS, CBRI
remains independent in its governance, finance, and research direction. Scientists
associated with Harvard have been responsible for a long list of blood research
milestones, beginning with Dr. Edwin Cohn’s historic fractionation of blood plasma in
1941. In 2007, IDI’s budget is estimated at about $50 million, of which funding from the
National Institutes of Health (NIH) comprised approximately three quarters. More than
six dozen peer-reviewed research papers were published during the year, on a broad
variety of blood and disease related topics.
National Blood Foundation Established in 1983, the National Blood Foundation supports research and
education that advances transfusion medicine and blood banking to benefit both patients
and donors. Funds are raised annually from corporations, blood centers, foundations, and
individuals, to provide grants for scientific research and educational initiatives.
Since 1985, the AABB-affiliated NBF has awarded approximately $5 million in
grants to 145 researchers. Transfusion medicine is a key focus area of research, including
immunology, hematology, tissue and transplantation medicine, cellular therapies,
emerging infectious disease, immunohematology, donor health and recruitment and
retention, and implementation of technological devices. Priority is given to new
investigators and innovative projects that may have a practical impact on patients and
blood donors. In 2008, the following projects were funded:
• Hematopoietic Stem Cell Mobilization by Cannabinoids;
• Notch-induced NK Cells for Cell Therapy in Hematologic Maligancy;
• Cytoadherence in Pediatric Malaria (CPM) Study;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 186 -
• Identification of Novel H-Y Antigens using Artificial Neural Network;
• The Role of Platelets in Experimental Transfusion-related Acute Lung Injury;
• Platelet Cold Receptors: Potential for Improving Platelet for Improving Cold Storage;
• Blood Donation considerations in African Americans.

Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 187 -
C H A P T E R S E V E N
Total Blood Products Market
THE BLOOD PRODUCTS INDUSTRY The blood products industry is primarily composed of several key segments that
span the collection and testing processes as well as therapies designed to address blood
deficiencies:
• blood collection equipment;
• blood typing reagents and instruments;
• molecular diagnostic tests;
• red blood cells (RBCs) and other plasma-derived products such as platelets, fibrin sealants, alpha-1 proteinase inhibitors, etc., excepting albumin and immunoglobulins;
• albumin;
• immunoglobulins;
• recombinant factors;
• synthetic blood products including hemoglobin-based oxygen carriers (HBOCs) and perflurocarbon based blood products (PFCs).
Of these, RBCs and Other Plasma Products comprised the single largest segment
with 46.7% of the market, as shown in Figure 7-1. It was followed by recombinant
factors with 21.6% and plasma-derived immunoglobulins with 12.7%. Overall, these and
other products for transfusion comprised about 84% of the market, while blood collection

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 188 -
equipment, molecular diagnostic tests and blood typing reagents and instruments
accounted for just 16%.
Figure 7-1
Global Blood Products Market by Segment (Blood Collection Equipment, Molecular Diagnostic Tests, Albumin, Blood Typing, RBCs, Recombinant Factors,
Immunoglobulins), 2007
Molecular Diagnostic Tests
6.0%
Albumin2.9%
Blood Typing Reagents and Instruments
2.0%
RBCs and Other Plasma Products
46.7%
Blood Collection Equipment
8.1%
Immunoglobulins12.7%
Recombinant Factors21.6%
Source: Kalorama Information
Market Size In 2007, the total global market for blood collection equipment and products
reached $25.9 billion, as shown in Table 7-1. Through 2014, the overall market is
expected to expand by 6.2% per year to reach $39.6 billion, driven by aging populations
in the largest markets of U.S., Europe and Japan, as well as increasing life spans and
nominal price and population growth. The recombinant factor segment will experience
the greatest gains at 8.9% per year, followed by immunoglobulins at 6.7% and molecular
diagnostic tests at 5.5%.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 189 -
Table 7-1
Global Blood Products Market Forecast by Segment, 2007 – 2014 (Blood Collection Equipment, Molecular Diagnostic Tests, Albumin, Blood Typing, RBCs,
Recombinant Factors, Immunoglobulins, HBOCs and PFCs)
Revenues (in $ millions) Product 2007 2008 2009 2010 2011 2012 2013 2014 CAGR RBCs and Other Plasma Products 12,145 12,692 13,263 13,859 14,483 15,135 15,816 16,528 4.5% Recombinant Factors 5,608 6,096 6,631 7,217 7,860 8,565 9,339 10,189 8.9% Immunoglobulins 3,300 3,519 3,754 4,004 4,272 4,559 4,865 5,193 6.7% Blood Collection Equipment 2,100 2,200 2,300 2,400 2,500 2,600 2,735 2,880 4.6% Molecular Diagnostic Tests 1,564 1,809 1,886 1,961 2,039 2,118 2,198 2,279 5.5% Albumin 759 774 791 809 828 847 865 883 2.2% Blood Typing Reagents and Instruments 510 520 531 541 552 563 574 586 2.0% HBOCs and PFCs 0 0 0 170 345 580 820 1,150 n/a Total 25,986 27,610 29,155 30,962 32,879 34,967 37,212 39,687 6.2%
Source: Kalorama Information
As this occurs, recombinant factors will comprise a significantly larger portion of
the overall market, as shown in Figure 7-2, but nonetheless will remain second to RBCs
and Other Plasma Products in terms of size. In 2014, RBCs will account for a lower
41.6% of the market, with recombinant factors having increased to 25.7% and
immunoglobins having also expanded slightly to 13.1%.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 190 -
Figure 7-2
Global Blood Products Market by Segment, 2014 (Blood Collection Equipment, Molecular Diagnostic Tests, Albumin, Blood Typing, RBCs, Recombinant Factors,
Immunoglobulins, HBOCs and PFCs)
Albumin2.2%
Molecular Diagnostic Tests
5.7%
Blood Typing Reagents and Instruments
1.5% HBOCs and PFCs2.9%
Blood Collection Equipment
7.3%
Immunoglobulins13.1%
Recombinant Factors25.7%
RBCs and Other Plasma Products
41.6%
Source: Kalorama Information

Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 191 -
C H A P T E R E I G H T
Company Profiles
AABB 8101 Glenbrook Road Bethesda, MD 20814
Phone: (301) 907-6977 Fax: (301) 907-6895
www.aabb.org
The AABB, formerly known as the American Association of Blood Banks, was set up in 1947 to establish and promote the highest standards of care for patients and donors in blood banking. This voluntary and professional association brings together all individuals and institutions are associated in blood banking, tissue banking, transfusion medicine and tissue transplantation.
The group develops and promotes quality management programs at blood centers, transfusion services and tissue banks to ensure the safest blood and tissues supplies possible. It provides professional educational programs related to transfusion medicine, establishes a good legal and regulatory policy environment, promotes the application of scientific discoveries to the improvement and enhancement of blood transfusion and tissue transplantation practices and maintains symbiotic relationships with other organizations, including state and regional blood banking associations. It also helps to develop acceptance and understanding of AABB member activities and their roles in the health care profession, with the public sectors and other professionals.
Other programs and services offered by AABB include the National Blood Foundation (NBF), the National Blood Data Resource Center (NBDRC) and the National Blood Exchange (NBE). The NBF was established in 1983 to support research and education in the areas of transfusion medicine and blood banking to benefit both patients and donors. Funds here are raised annually from corporations, blood centers, foundations,

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 192 -
and individuals by NBF, providing grants for scientific research in the fields of transfusion medicine and blood banking and support education initiatives that benefit the transfusion medicine community. NBDRC is the premier source of national blood data and it conducts surveys of blood services activities in the United States. It also monitors and forecasts blood supply and demand, and performs commissioned research for the Federal Government and other clients. Its current research activities include collection of monthly blood supply monitoring data from a representative sample of U.S. blood centers and biennial nationwide blood collection and utilization survey. NBE was established as a resource sharing program in 1953, and today continues to support the blood banking and transfusion medicine community. With a nationwide network of blood facilities, NBE is the primary resource-sharing program in the U.S. Each year, NBE coordinates the distribution of more than 300,000 units of blood and blood components.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 193 -
ABBOTT LABORATORIES 100 Abbott Park Road Abbott Park, IL 60064 Phone: (847) 937-3500
Fax: (847) 937-1511 www.abbottdiagnostics.com
Abbott Laboratories is one of only two pharmaceutical companies that have had
major success in the diagnostics industry. The other is Hoffmann-LaRoche. During the
1960s and early 1970s, pharmaceutical companies saw the diagnostics markets as a
lucrative, growing opportunity that were a “natural extension” of their healthcare
products business strategies. As a result, they applied business approaches and strategies
that proved successful in pharmaceuticals to the diagnostics markets, where these same
business approaches and strategies were totally inappropriate. Abbott was not one of
these.
Instead, Abbott acquired several mildly successful, but not particularly exciting,
diagnostics businesses and united them into a separate division of the company. This
consolidation approach lent itself to maximizing the synergy of these newly acquired
businesses and minimizing the associated overhead. In a further effort to increase the
potential of this business strategy and rapidly being new products to market, Abbott
recruited key management from Texas Instruments, a company that, at that time, was
lauded for its ability to bring technology rapidly from concept through research and
development to market. The pharmaceutical division of Abbott was kept separate from
diagnostics and interference from corporate management in the affairs of the diagnostics
operations was minimized, while support was maximized.
Abbott quickly brought clinical chemistry instrumentation (the ABA series) and
reagents to market, and dove into the emerging immunoassay markets, focusing primarily
on new homogeneous immunoassay technologies. Efforts in this latter area successfully
yielded products that provided strong competition for Syva’s EMIT line, which was very
popular at that time. This was followed by pioneering work in fluorescence polarization
immunoassays and the TDx and ADx instruments (both of which had little-known
capabilities for also performing clinical chemistry assays), and later the IMx. Over time,
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 194 -
Abbott has brought to market clinical diagnostics instrumentation, reagent products, and
laboratory data management systems to automate the entire clinical laboratory and its
data/patient management systems.
Abbott has been and continues to be highly successful in blood bank, hospital,
and commercial clinical laboratories. For example, the company launched the first
radioimmunoassays and enzyme immunoassays for hepatitis B antigens. It was one of
the first companies to market an HIV assay and, later, an HCV assay. The outstanding
profits that Abbott experienced from its blood bank testing business helped to make other
diagnostic testing development possible.
During the early-to-mid-1990s, Abbott made a major effort to get into the
molecular diagnostics market. It pushed the development and marketing of its LCx
system and reagents. The LCx is a semi-automated system for amplifying target genes
using the ligase chain reaction (LCR), and then capturing/analyzing the results by MEIA
technology, the same technology as is used in the company’s IMx immunoassay system.
The LCx was originally offered with only two assays—Chlamydia trachomatis and
Mycobacterium tuberculosis, with the latter available only in Europe.
The LCx has not been successful. While the ligase chain reaction is a viable
amplification technology, the semi-automated approach of the LCx is not one that offers
a significant improvement over other approaches. Moreover, the company had several
design problems with disposable products associated with the system. For example, the
sealable tubes used to perform the assays were very difficult to manufacture by injection
molding because of their small size and tight tolerance requirements. For any
amplification technology to work properly, samples must be protected from
contamination. The LCx tubes would not seal properly and were, therefore,
contamination risks.
When the LCx was first introduced at the 1995 national meeting of the American
Association for Clinical Chemistry, it was during a period of time when women’s health
issues were in focus. The LCx was introduced, flying high, with a women’s health theme
and emphasis on its first assay, Chlamydia trachomatis, was evidence of Abbott’s
commitment to these issues. This was to be the first of a long series of LCR-based
assays, including one for Neisseria gonorrhoeae, which were envisioned for the LCx. A

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 195 -
decade after its introduction, the LCx is below the market radar, having been quietly
pulled from the U.S. market.
In 1999, Abbott and Chiron Corporation signed an agreement through which
Chiron licensed to Abbott its hepatitis C virus (HCV) patent rights for nucleic acid
diagnosis. This worldwide, semi-exclusive license, which excludes blood screening
applications, allowed Abbott to research, develop, make and sell HCV nucleic acid probe
products for in vitro diagnostics. This has been translated to the Abbott HCV ASR and
HCV Genotyping ASR kits.
Abbott took another major step in the molecular diagnostics market by acquiring
Vysis in December of 2001. Vysis has been a leader in the field of Fluorescence In Situ
Hybridization (FISH) assays. The company now markets the Vysis AneuVysion assays
for prenatal diagnosis (multicolored probes for the assessment of aneuploidies in fetal
cells), Vysis PathVysion assay for HER-2 assessments in breast cancer, and the Vysis
UroVysion assay for recurrent bladder cancer.
Abbott also markets a molecular diagnostic assay for cystic fibrosis (CFTR) gene
that assesses 33 core mutations for the disease, including the 25 ACMG Panel-1, plus
5/7/9T and Exon 10 Reflex Testing. Cystic fibrosis transmembrane conductance
regulator (CFTR) gene comprises 27 exons and spans ~250 kb on the long arm of
chromosome 7. Since the cloning of the CFTR2 gene, more than 900 mutations have
been identified. Mutations in the CFTR protein affect the ability of epithelial cells to
secrete chloride ions in response to cytosolic cyclic AMP.
The Abbott CFTR assay uses PCR/OLA/SCS technology. This approach
combines target amplification using PCR with oligo ligation assay (OLA) to produce
allele specific fragments which are then analyzed by electrophoretic sequence coded
separation (SCS). OLA exploits the ability of DNA ligases to join adjacent nucleotides
covalently only when they perfectly complement a single-stranded DNA template.
One of Abbott’s leading blood banking products is the Prism, the first fully-
automated blood screening instrument and analyzer to test for Hepatitis B, HIV and
HTLV. Suitable for high volume blood centers and blood banks, the system combines
most tests into a single system, thus reducing the risk of mistakes, tampering and
accidents. Abbott Prism has a built-in quality control system that monitors critical
Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 196 -
functions and verifies proper processing of each sample. Also, the system is a completely
closed one, thus minimizing the chance for operator errors during sample processing. In
October 2005, the company announced the launch of Abbott Prism in the United States
and made it available to all blood banks across the country. In November 2005, Puget
Sound Blood Center became the first blood center in the U.S. to use the Abbott Prism
blood screening system. Outside the United States, the Prism system is used in more than
30 countries, nearly half of which rely on Abbott Prism to screen 100% of their blood
donations.
The Abbott Prism HBcore is the first hepatitis B test approved by the FDA for use
on the Abbott Prism system. Additional hepatitis and retrovirus screening tests, which
includes a test for HIV, are currently under FDA review. Abbott also has other Prism
assays in development and in January 2008, received approval for the first fully
automated HTLV-I/HTLV-II blood screening test for use on Prism. The test is intended
for use by laboratories to screen individual donations of blood and plasma for antibodies
to human T – lymphotropic virus Type I and/or human T – lymphotropic virus Type II
(anti-HLTV-I/HTLV-II). Just six month earlier, Abbott received approval for a Prism
HCV test to screen individual donations of blood and plasma for antibodies to hepatitis C
(HCV).
In October 2005, Abbott and Intermountain Health Care (IHC), the largest
integrated health care system in Utah, entered a nine-year contract for Abbott's
immunoassay diagnostic instruments and tests. This agreement brings several
ARCHITECT i2000 SR immunoassay systems into IHC's network during the course of
the contract period. In addition, Abbott will continue to supply tests for IHC's current
AxSYM , IMx and TDx immunoassay systems. Three years later, Abbott introduced the
next generation ARCHITECT ci4100 Integrated System, an automated diagnostic
analyzer that integrates immunoassay and clinical chemistry testing.
In December 2005, Abbott submitted pre-market approval (PMA) applications
with the U.S. FDA seeking approval of a hepatitis anti-HBs test for use on its
ARCHITECT instrument and a hepatitis HBsAg/Confirmatory test for use on its AxSYM
instrument. In April 2006, the company signed a group purchasing agreement with the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 197 -
Greater New York Hospital Association Services, Inc. This agreement allows Abbott to
provide instruments and related products to the over-250 members of GNYHA Services.
In mid 2008, Abbott introduced Emerald, a new device for performing complete
blood counts (CBCs). The Emerald has the ability to complete CBC results in 60 seconds
and report results in easy-to-read histograms representing white blood cells, red blood
cells and platelets. Following regulatory approval, the system will expand Abbott's
hematology platform with a premium, robust low-volume solution for small to mid-sized
clinical laboratories; intuitive software and onboard reagents enable Emerald to offer
faster and simpler data entry.
Abbott recorded total revenues of $25.9 million in 2007, up from $22.4 million
the prior year.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 198 -
ALLIANCE PHARMACEUTICALS 6175 Lusk Blvd.
San Diego, CA 92121 Phone: (858) 410-5200
Fax:(858) 410-5201 www.allp.com
Alliance Pharmaceuticals is a pharmaceutical research and development company
focusing on the commercialization of Oxygent, an intravascular oxygen carrier that
reduces the need for donor blood during surgeries and for other patients at risk of acute
tissue hypoxia (oxygen deficiency).
Oxygent (perflubron emulsion) will augment oxygen delivery to tissues when a
patient is expected to experience substantial blood loss. It is estimated that approximately
8 million to 10 million patients worldwide annually receive at least one unit of donor
blood during elective surgeries, including, cardiovascular, orthopedic, and general
surgical procedures. An oxygen carrier could be used instead of donor blood for a portion
of these patients.
A single unit of Oxygent is expected to provide the equivalent oxygen delivery of
1 to 2 units of red blood cells. Oxygent is a sterile emulsion that is compatible with all
blood types and is expected to have a shelf life of approximately two years. It is
manufactured using a cost-effective, proprietary process at Alliance’s commercial-scale
facility that has the potential to produce approximately 800,000 units annually. Oxygent
may be used with other blood sparing techniques, including Alliance’s proprietary
Augmented Acute Normovolemic Hemodilution technique. In September 2000, the
company announced that its analysis of the data from a Phase III study in Europe
demonstrated that the product provided a statistically significant reduction in the need for
donor blood in patients undergoing a variety of general surgery procedures.
A few months later, however, Alliance voluntarily suspended enrollment in a
Phase III cardiac surgery study in the U.S. due to an imbalance in certain adverse events,
primarily the incidence of stroke. While the frequency of these adverse events in the
Oxygent treatment group was consistent with published data for patients undergoing

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 199 -
cardiac bypass surgery, the control group frequency was remarkably low, causing a
disparity in the proportion between the treatment and control patients. Alliance met with
the FDA regarding the continuing clinical development of Oxygent and presented a data
analysis that explained reasons for the imbalance.
In January 2007, the French Ethics Committee (IRB) and the French Competent
Authority (regulatory agency) granted approval to start the Phase IIb clinical trial for
Oxygent to prevent postoperative ileus resulting from hypoxia during major surgery trial.
Subsequently, Alliance submitted a clinical trial protocol revision to the French Ethics
Committee and the French Competent Authority, which modified the dosing regimen to a
dose-escalation protocol. Alliance initiated the trial, but in November 2007, discontinued
enrollment in the French study to focus on development of Oxygent in China.
In May 2005, PFC Therapeutics and Beijing Double-Crane Pharmaceutical Co.,
Ltd, the market leader for IV solutions and one of the largest pharmaceutical companies
in China, entered into a development, license and supply agreement to develop Oxygent
for the Chinese market. As of mid 2008, Phase II trials in China were ongoing.
In 2007, the development-stage company had no product revenue, and regulatory
approval for Oxygent is several years away.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 200 -
AMERICA’S BLOOD CENTERS 725 15th Street NW Suite 700
Washington, DC 20005 Phone: (202) 393-5725 Fax: (202) 393-1282
www.americasblood.org
America’s Blood Centers is one of the largest networks of non-profit, community blood centers in North America. The organization was founded in 1962 when seven community-based blood centers came together with the assistance of local hospitals, physicians and civic groups to establish America's Blood Centers. With top of the line medical expertise, good customer service and a community-first blood banking philosophy as its basic principles, America's Blood Centers today operates in 45 U.S. states and Canada.
The U.S. members of ABC are licensed and regulated by the United State’s Food
and Drug Administration while the Canadian members are regulated by Health Canada.
These members participate in the process by serving over 180 million people at over 600
collection sites spread throughout the country. These members also provide blood
products and services to over 4,200 hospitals and health care facilities across North
America.
ABC’s members are also active in research and receive the maximum number of
blood-related NIH research funds. These funds have been utilized in ground-breaking
research activities that have led to successful results in varied cases. For example, the
New York Blood center, a member of ABC, invented the hepatitis B vaccine and solvent-
detergent plasma sterilization. This center also operates the largest cord blood bank in
America. BloodSource, another ABC member, received the first FDA accreditation for
Fresh Frozen Plasma Donor Retested (FFP-DR).
ABC runs a variety of programs including ‘National Donor Day’, which is
celebrated on February 14, and “World Blood Donor Day’ on June 14. Over the past 11
years, Saturn/UAW and the over 300 retail Saturn outlets have partnered to encourage
Americans to pledge to donate five points of life that include, blood, platelets, cord blood,
bone marrow and organs and tissue.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 201 -
AMERICAN RED CROSS 2025 E Street, NW
Washington, DC 20006 Phone: (202) 303-4498
www.redcross.org
The American Red Cross (ARC) is a premier emergency response organization for the U.S. Since its founding in 1881 by Clara Barton, the ARC has been a part of a worldwide movement that offers neutral humanitarian care to the victims of war and to those affected by devastating natural disasters. Over the years, the organization has expanded its services, always with the aim of preventing and relieving suffering. Over four million people each year give blood through the Red Cross, making it the largest supplier of blood and blood products in the United States. Each year the organization spends over $25 million in scientific research activities at its laboratories to improve the safety, purity and efficacy of the blood products it collects and supplies.
The blood donated at ARC is tested at one of eight National Testing Laboratories (NTLs). With a strong organizational network, ARC has the capability to direct blood donations to any part of the country or the world where it is needed most. The Charles Drew training institute also allows the Red Cross to provide training and educational resources to the ARC personnel. A centrally managed blood inventory system has also been put in place to ensure consistent availability of blood and its components throughout all ARC centers and the world.
In 1999, the ARC became the first center to implement a Nucleic Acid Testing (NAT) study, which is unique as it looks for the genetic material of HIV and Hepatitis C rather than the body’s response to the disease. Now these tests have been licensed by the FDA and are able to detect the genetic material of a transfusion-transmitted virus like HIV without needing to wait for the body to form antibodies. This technique thus offers a potential time advantage over current techniques. Other testing procedures include tests for hepatitis, hepatitis B, hepatitis C, syphilis, human T-cell lymphotropic virus (HTLV), HIV/AIDS and West Nile virus.
However, despite ongoing improvements in ARC’s collection and processing procedures, ARC continues to fall short. Since 1993, the ARC has been under a federal court order to improve its systems and since 2003, the first year in which the FDA could levy penalties against the organization, has been fined $21 million. In January 2008, FDA commissioner Andrew C. von Eschenbach attended a Red Cross board meeting and

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 202 -
warned that members could face criminal charges for their failure to meet compliance objectives. Lapses include the distribution of more than 200 potentially contaminated blood products between December 2006 and April 2008, 134 cases of suspected post-transfusion hepatitis from January 2000 to June 2002, as well as faulty internal monitoring processes and a history of falsified records. Critics of the organization note that while blood revenues, at $2.1 billion in 2007, represent more than two thirds of the ARC’s business, the organization continues to focus most of its fund-raising and other activities on its much smaller disaster relief operations.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 203 -
BAXTER INTERNATIONAL One Baxter Parkway
Deerfield, IL 60015-4625 Phone: (847) 948-2000 Fax: (847) 948-3642
www.baxter.com
Baxter International Inc. operates on a global scale through its various
subsidiaries in assisting healthcare professionals and their patients with treatment of
complex medical conditions including hemophilia, immune disorders, kidney disease,
cancer, trauma and other conditions.
The company’s blood and blood related products include automated component
collection systems, blood collection and processing systems and ancillary products. The
automated component collection systems comprise blood collection systems and products
that are used for the automated separation and collection of blood components. Blood
collection and processing systems comprise products and systems like blood pack units
and leukocyte reduction filters. These are used for the collection and preparation of
blood, blood components and for the reduction of leukocytes by filtration from whole
blood, red cells and platelet products. Ancillary products include systems that help to
collect, process, store and transfuse blood and its components.
Baxter continues to both develop new blood products and expand usage of
existing products. In November 2005, Baxter received clearance from the US FDA for
the seven day storage of leukoreduced, apheresis platelets collected on the AMICUS
Separator and stored in Baxter's PL 2410 collection container. This allows for the
transfusion of these platelets when coupled with 100% release testing for bacterial
contamination using the bioMérieux BacT/ALERT Microbial Detection System, and
licensed by blood centers as determined by the FDA. Also in 2005, the company
announced collaborative research agreements with organizations Nektar Therapeutics and
Lipoxen Technologies to develop longer acting therapeutic forms of blood clotting
factors that would reduce the frequency of injections required to treat blood clotting
disorders.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 204 -
Baxter has long been a pioneer in this area. In 1992, the company introduced
Recombinate Antihemophilic Factor (recombinant), the first genetically manufactured
Factor VIII product for the treatment of hemophilia. In 2003, Baxter obtained FDA
approval for Advate, the first Factor VIII made without any added human or animal
plasma proteins and albumin, for the prevention and control of bleeding episodes in
persons with hemophilia A. The company received the European Commission Marketing
Authorization for Advate in 2004 and since then has continued to expand the product’s
global reach. In 2007, worldwide sales of Advate exceeded $1.2 billion, surpassing sales
of Recombinate; during the year, Argentina became the first country in Latin America to
launch the product. Advate was also recently introduced in Japan and New Zealand with
upcoming launches in Venezuela, Taiwan and Hong Kong. Baxter continues to work on
ways to increase Advate’s half life, which would decrease the number of injections
required, and introduce higher potency formulations, such as the 3000 IU dosage, which
was launched in 2007. In January 2008, Baxter began a program to develop a
recombinant form of Factor IX.
In 2007, the company reported revenues of $11.2 billion, up from $10.3 billion
the prior year.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 205 -
BIOPURE CORP. 11 Hurley St.
Cambridge, MA 02141 Phone: (617) 234-6500
Fax: (617) 234-6505 www.biopure.com
Biopure is developing products that deliver oxygen through the body in a manner
similar to human blood. The company has led in the development and manufacture of
oxygen therapeutics, a new class of pharmaceuticals that are intravenously administered.
Biopure's products represent a new Oxygen Bridge treatment approach for managing
patients' oxygen requirements in a broad range of potential medical applications.
Hemopure [hemoglobin glutamer - 250 (bovine)], or HBOC-201, Biopure's first-
in-class product for human use, is approved in South Africa for treating adult surgical
patients who are acutely anemic. It also is used for eliminating, reducing or delaying the
need for allogenic red blood cell transfusion in these patients. In a Phase III orthopedics
study reported in a June 2008 issue of the Journal of Trauma, the product eliminated the
need for transfusion in the majority of the nearly 700 patients participating. Researchers
also concluded that patients less than 80 years of age with moderate clinical need for
additional oxygen carrying capacity could safely avoid transfusion when treated with up
to 10 units of Hemopure.
Biopure intends to shortly initiate a U.S. clinical trial of Hemopure in patients
suffering from Acute Myelogenous Leukemia (AML) who refuse transfusion with blood
components, meeting with the FDA in July 2008 to develop protocols for the
identification of appropriate patients. This application represents an unmet medical need
because of an expected 100% mortality within 6 months in the absence of induction
chemotherapy.
In 2007, publicly traded Biopure reported $2.5 million in sales, up from $1.7
million in 2006. Virtually all of this was derived from the company’s veterinary product,
Oxyglobin [hemoglobin glutamer - 200 (bovine)], or HBOC-301, the only hemoglobin-
based oxygen therapeutic approved by the FDA and the European Commission.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 206 -
BIO-RAD LABORATORIES 1000 Alfred Nobel Drive
Hercules, CA 94547 Phone: (510) 741-1000 Fax: (510) 741-5817
www.bio-rad.com
Bio-Rad Laboratories is actively involved in the manufacture and sales of clinical
diagnostic systems and instruments used in life sciences research, medical screening and
diagnostics. The organization ranks among the top ten clinical diagnostics companies
throughout the world. Its products are supplied to a global range of over 70,000 research
and industry customers that include hospitals, universities, government agencies,
biotechnology firms and pharmaceutical companies. One third of the company is owned
by the Schwartz family.
Bio-Rad’s broad range of products includes various disease tests and
technological applications like image analysis, molecular detection, chromatography, and
gene transfer. This includes precast gels, blotting membranes & reagents, acrylamide,
agarose & gel reagents, premixed buffers, IPG strips, protein assays, protein & DNA
standards, stains & dyes, DNA purification & preparation kits. In addition to blood virus
testing products, the company also provides high quality control systems, toxicology, in
vitro and genetic disorders testing, specialty chemistry, molecular pathology, and
internet-based software. Recognized globally as the "Gold Standard" in diabetes
monitoring, broad-spectrum drug screening, and hospital epidemiology; the group
recently introduced new products for use in the areas of diabetes monitoring, HIV testing,
and proteomics
In January 2006, Bio-Rad Laboratories renewed its collaboration with the Institut
Pasteur of Paris, France for an additional four years and in April of the year, Bio-Rad
signed a three-year agreement with Premier, one of the largest group purchasing
organizations in the United States. This agreement allows Premier a three-year sole-
source contract for Bio-Rad Laboratories' diabetes monitoring instruments and products.
Premier member hospitals and health care systems would enjoy preferred pricing on Bio-
Rad's comprehensive menu of Hemoglobin A1c instruments and diabetes testing

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 207 -
solutions. Bio-Rad's product offering in the Hemoglobin A1c category includes the
VARIANT II, VARIANT II TURBO, D-10 and Micromat II instruments. The company
continues to introduce new products, launching the Syphilis IgG kit and Epstein Barr
virus kits for use on its BioPlex 2200 system in 2007 and the Vasculitis kit for use on
BioPlex 2200 in February 2008.
In 2007, Bio-Rad reported sales of $1.4 billion, up from $1.2 billion in 2006.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 208 -
BIOTIME INC. 935 Pardee St.
Berkeley, CA 94710 Phone: (510) 845-9535 Fax: (510) 845-7914 www.biotimeinc.com
BioTime is developing aqueous-based synthetic solutions that may be used as
plasma expanders, organ preservation solutions, or as solutions to replace blood volume
during low temperature surgery. These products are intended for the treatment of
hypovolemia caused by surgical blood loss, the emergency treatment of blood loss due to
traumatic injury, the replacement of all of a patient's circulating blood during cardiac
surgery and neurosurgery that involve lowering the patient's body temperature to
hypothermic levels, and the preservation of body organs and tissues awaiting transplant
other biomedical applications.
The company’s products include Hextend, which has completed regulatory
review; Pentalyte, which is in Phase II clinical trials; Hetacool, which has not yet entered
clinical testing; and Hetafreeze, which is in the discovery phase.
Hextend (6% Hetastarch in Lactated Electrolyte Injection) is an artificial colloidal
solution, pharmacologically classified as a plasma volume expander. It is intended to
support oncotic pressure as well as provide electrolytes. PentaLyte is a solution that is
almost identical to Hextend. But it contains a lower molecular weight starch
(pentastarch), which is substituted with fewer hydroxyethyl groups. Its lower molecular
weight and degree of substitution results in its removal from the blood more rapidly than
hetastarch.
HetaCool is a modified formulation of Hextend designed for use at low
temperatures. Interruption of blood flow can be maintained only for short periods of time
at normal body temperatures because many critical organs, particularly the brain, are
quickly damaged by any loss of oxygen. As a result, certain surgical procedures are
performed at low temperatures because a lower body temperature helps to minimize the
chance of damage to organs by reducing the patient's metabolic rate. This decreases the

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 209 -
patient's needs during surgery for oxygen and nutrients which normally flow through the
blood. As of mid 2008, BioTime was preparing an IND application to conduct clinical
trials using HetaCool to replace all of a patient's circulating blood volume during
profound hypothermic surgical procedures, such as repair of the aortic arch, during which
heart and brain activity could be arrested for 2 hours or more.
In 2007, publicly traded BioTime reported $1.0 million in sales, down slightly
from the prior year; most of this was derived from sales of Hextend.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 210 -
CHIRON 4560 Horton Street
Emeryville, CA 94608 Phone: (510) 655-8730 Fax: (510) 655-9910
www.chiron.com
Chiron is known primarily as a biopharmaceutical firm rather than a diagnostics
firm. It’s genomic and biotechnology expertise, however, can easily be translated into
molecular diagnostic applications and be used to provide some of the more unique assays
that may become available for diagnostic and pharmacogenetic testing. At this time,
Chiron is spending much of its diagnostics developments efforts in collaborations with its
partners, Gen-Probe and Ortho Diagnostics. In late 2006, Chiron was acquired by
Novartis, but continues to retain much of its individual character as a business enterprise.
Chiron’s relationship with Ortho was established in 1989 and involved the
development of immunodiagnostic blood screening methods and reagents for the
determination of HIV and hepatitis viruses in the blood bank and plasmapheresis settings.
This business area now consists of a full line of immunoassay tests for hepatitis viruses
and retroviruses, and provides supplemental tests and microplate-based instrument
systems to automate test performance and data collection. Chiron conducts certain
research functions and manufactures viral antigens and supplemental hepatitis tests.
Ortho manufactures and sells assays and instrument systems. Chiron and Ortho share
equally in the pretax operating earnings generated by this business. The joint operation
holds the immunodiagnostics rights to Chiron’s hepatitis and retrovirus technology and
receives royalties from the sale of HCV and HIV tests by Abbott, and from the sale of
HCV tests by Bio-Rad Laboratories, Inc. and certain other licensees.
In 1998, Chiron and Gen-Probe formed a strategic alliance focused on introducing
Procleix nucleic acid testing products to improve the safety of the world’s blood supply.
The target market for these products includes blood banks and plasmapheresis centers.
These tests are intended to provide much greater sensitivity than he current
immunodiagnostics tests, allowing direct detection of viruses in much earlier stages of

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 211 -
infection. Under this collaboration, Gen-Probe performs certain product development,
assay, and instrument manufacturing functions, while Chiron and Gen-Probe jointly
participate in new assay and instrument research and development. Chiron sells the
collaboration’s products and Gen-Probe receives a fixed percentage of Chiron’s sales
revenues for this product line.
Chiron’s blood testing business is healthy and growing, largely due to the
introduction of the Procleix system. Once FDA approved in 2002, Chiron had the major
U.S. blood banks sign multi-year contracts for the use of the novel system. In March
2007, the FDA cleared the Procleix Tigris, the first system to fully automate every step of
Nucleic Acid Testing for West Nile Virus detection. Thus in 2008, Chiron owned 80%
share in the United States, by virtue of its early market entry and ongoing introduction of
ancillary products.
In July 2003, Chiron announced that it had granted to Baxter AG, a subsidiary of
Baxter International, a license to use its HIV and hepatitis C virus (HCV) intellectual
property in combination with Baxter’s own technology for screening plasma for use with
plasma fractionation in Europe. These licenses allow Baxter to continue to enhance and
develop its own large-scale plasma-testing technology for screening plasma. The
financial terms and other details of the license were not disclosed. This license represents
the first usage of Chiron’s intellectual property in plasma fractionation. Source plasma is
used in the processing of various therapeutic proteins for the treatment of serious
disorders, such as hemophilia and immune system deficiencies, and to make products
used to help treat and prevent disease like tetanus, rabies, measles, rubella and hepatitis
B.
Following its acquisition by Novartis in 2006, Chiron no longer reports revenues.
However, Novartis includes revenues from Chiron businesses in its new Vaccines and
Diagnostics Division. In 2007, this operating unit, which includes Novartis’s broad
portfolio of vaccine products, reported sales of $1.5 billion, up 25% on a comparable full-
year basis over the prior year’s sales on strong growth in seasonal influenza vaccines as
well as NAT blood testing products.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 212 -
CSL BEHRING 1020 First Ave.
King of Prussia, PA 19406 Phone: (610) 878-4000 Fax: (610) 878-4009 www.cslbehring.com
CSL Behring is a producer of plasma products. The organization is a subsidiary of
CSL Limited, a pharmaceutical company that operates worldwide from its headquarters
in Melbourne, Australia. It has plants located in Bern, Switzerland; Marburg, Germany;
and Kankakee, Illinois, employing more than 7,500 persons in 19 countries. The
organization also operates one of the world’s largest, fully-owned plasma collection
networks. Besides its large network of plasma centers in the U.S., the company also runs
significant plasma procurement programs in Europe and the USA.
CSL’s offerings comprise therapies that include products for the treatment of
hemophilia and other bleeding and coagulation disorders. It also offers immunoglobulins
for the prevention and treatment of immune disorders, treatments that inhibit the
formation of blood clots, wound-healing agents used during major surgical procedures,
and plasma expanders for the treatment of a variety of conditions such as shock, burns
and circulatory disorders. The organization offers coagulation products like Helixate FS,
which is an antihemophilic factor (recombinant) formulated with sucrose. In late 2005,
FDA approved the room temperature storage of the drug. This extended storage labeling
provides greater flexibility for those having the disease. Its Monoclate-P is also an
antihemophilic factor (human) while its Stimate is a nasal spray with the active ingredient
of desmopressin acetate. Mononine is used for treating people with hemophilia B. It
comprises coagulation Factor IX (human) monoclonal antibody purified. Humate-P
(marketed in Europe as Haemate-P) is a factor replacement therapy for the von
Willebrand disease. It comes in the form of an injectable drug that helps to achieve
hemostasis by replacing the most active forms of VWF (high molecular weight VWF
multimers) and Factor VIII that are missing in patients with von Willebrand Disease
(VWD).
In May 2006, CSL Behring signed a major plasma acquisition contract with
Blood Centers of America. As per this five year contract, BCA will provide at least

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 213 -
500,000 liters of plasma annually to the company. This will assist the organization further
in producing immunoglobulin products, plasma-derived clotting factors, Alpha-1
proteinase inhibitor, and critical care and wound-healing therapies.
CSL continues to introduce new products, and in July 2007, received FDA
approval of Privigen, [Immune Globulin Intravenous (Human), 10% Liquid], an
intravenous immunoglobulin (IVIg) for treating patients diagnosed with primary
immunodeficiency. The first praline-stabilized 10% liquid IVIG, Privigen is also
indicated for the treatment of chronic immune thrombocytopenic purpura to rapidly raise
platelet counts to prevent bleeding. Earlier in the year, the company’s Humate-P
(Antihemophilic Factor/von Willebrand Factor Complex [Human]), for the treatment of
hemophilia A and von Willebrand disease (WWD) was approved by the FDA to prevent
excessive bleeding during and after surgery, in patients with severe VWD and mild to
moderate VWD where the use of desmopressin is not adequate. The company has also
recently obtained FDA approval for an additional indication for Rhophylac Rh0(D)
(Immune Globulin Intravenous [Human]), an anti-D Rh immunoglobulin (Ig). This
additional indication is for the treatment of immune thrombocytopenic purpura (ITP), to
raise platelet counts in Rh0(D)-positive, non-splenectomized adult patients with chronic
ITP. The company has also submitted applications in the U.S. and Canada requesting
approval of its C1-esterase inhibitor concentrate for the treatment of hereditary
angioedema.
CSL Behring runs an assurance program, which is designed to help ensure that
patients who rely on its recombinant and plasma-derived therapies can continue to
receive these treatments even if they experience a lapse in their third-party, private health
insurance. This program is available to those who use factor replacement therapies,
intravenous immune globulin therapy and Alpha 1 augmentation therapy.
In 2007, CSL reported total sales of $2.1 billion, of which 33% was derived from
immunology products, 22% was from plasma-derived coagulation, 18% was due to
critical care products, 17% was comprised of recombinant FVIII, and the remainder was
from wound healing and other products.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 214 -
GEN-PROBE INC. 10210 Genetic Center Drive
San Diego, CA 92121 Phone: (858) 418-8000 www.gen-probe.com
Gen-Probe is a global leader in the development, manufacture and marketing of
rapid, accurate and cost-effective nucleic acid probe-based products used for the clinical
diagnosis of human diseases and for screening donated human blood. Founded in 1983,
the company pioneered the scientific and commercial development of nucleic acid testing
(NAT). By using nucleic acid probes that specifically bind to nucleic acid sequences
known to be unique to target organisms, NAT enables detection of microorganisms that
are difficult or time-consuming to detect with traditional laboratory methods.
In December 2001, Chugai Pharmaceutical Co., Ltd., Gen-Probe’s former indirect
parent, announced its intention to spin off the company as a separate, stand alone firm by
distributing all of its shares of Gen-Probe’s common stock to its shareholders. In
September 2002, Chugai Pharmaceutical completed the distribution, and Gen-Probe’s
common stock began trading on the NASDAQ National Market.
To date, Gen-Probe has received United States FDA approvals for more than
50 products that detect a wide variety of infectious microorganisms. In February 2002,
the FDA approved the company’s Biologics License Application, or BLA, for its
biochemical test used to screen donated blood for human immunodeficiency virus-type 1
(HIV-1) and hepatitis C virus (HCV). At the time, the Gen-Probe assay was the only
FDA-approved NAT assay available for screening donated blood. Today, it is used to
screen more than two thirds of the U.S. donated blood supply for HIV-1 and HCV.
The company generates its revenues primarily from the sale of clinical diagnostic
and blood screening assays. Gen-Probe’s clinical diagnostic products are marketed to
laboratories and public health institutions in the United States and Canada through a
direct sales force. Gen-Probe also has agreements with Bayer, bioMérieux and Fujirebio
(through their subsidiary Rebio Gen, Inc.) to market several of its clinical diagnostic
products in various global markets. In addition to product sales, the company also

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 215 -
generates revenues through research collaborations with government organizations and
healthcare companies and through licenses of its patented NAT technologies.
Gen-Probe has achieved a leading position in the NAT industry because of its
technologically advanced and reliable assays and instruments, as well as its strong sales
force and technical support group. The company’s investment in research and
development has enabled it to develop a portfolio of proprietary and patented
technologies that it combines to create NAT products to meet changing customer needs
for rapid, accurate and cost-effective assays. Gen-Probe has also worked with outside
vendors to develop a range of instrument systems for performing its assays. The
company has recently received FDA approval and is currently developing additional
assay for the world’s first fully automated NAT instrument system, the Procleix Tigris.
This instrument significantly reduces labor costs and contamination in high-volume
diagnostic testing environments and enables large blood collection centers to individually
test each donor’s blood.
Gen-Probe has developed one of the broadest arrays of core NAT technologies in
the industry. When used in combination, these technologies have significantly advanced
NAT assays, making them more specific, more sensitive, easier to use and faster than
products based on competing NAT technologies. In the past, the company has leveraged
its core technologies to develop products that have achieved leading positions in new
NAT markets, such as blood screening and tuberculosis testing. The company plans to
continue to use its core NAT technologies as a platform for the development of additional
products addressing emerging segments of the NAT market. These could include:
• Targeting Ribosomal RNA – The company has developed and patented a
technique that detects and identifies organisms by targeting their ribosomal RNA,
or rRNA. Most NAT assays target DNA, which is present in only one or two
copies in each target organism cell. By using a probe that hybridizes to rRNA,
the sensitivity of the test is increased thousands of times because there is much
more rRNA target present than DNA. Targeting of rRNA also reduces the
likelihood of obtaining a false negative result and enables design of diagnostic
products for infectious diseases caused by any bacteria, fungi and parasites;

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 216 -
• Target Capture Technology – Gen-Probe has developed target capture techniques,
which when used in conjunction with its patented amplification methods,
concentrate the target organisms and also remove materials in the sample that
might otherwise interfere with amplification resulting in its current generation of
amplified assays;
• Transcription-Mediated Amplification - Gen-Probe’s patented TMA technology
is designed to overcome the many problems faced with other target amplification
methods such as PCR. The simple test is suitable for automation, minimizes the
possibility of carry-over contamination and false positive test results, and often
can be used with clinical samples with little or no purification. It is also able to
amplify RNA and DNA targets, whereas PCR requires additional reagents and
steps to amplify RNA;
• Chemiluminescent Technologies and Hybridization Protection Assay - Gen-
Probe’s DNA probes use chemiluminescent acridinium esters (AE molecules) that
generate light as a label for detection. The AE technology is much more sensitive
than fluorescence or absorbance techniques used by other companies. Gen-
Probe’s Dual Kinetic Assay (DKA) technology uses two types of AE molecules—
one that “flashes” and another one that “glows.” By using DKA, the company has
created NAT assays that can detect two separate targets simultaneously;
In early 2004, FDA granted marketing clearance for sexually transmitted disease
testing on Gen-Probe’s Tigris System. Tigris has been approved to run Gen-Probe’s
APTIMA Combo 2 Assay, an FDA-approved amplified nucleic acid test for
simultaneously detecting Chlamydia trachomatis and Neisseria gonorrhoeae. Tigris can
process approximately 500 samples in an eight-hour shift and up to 1,000 samples in
about 13 hours. Because one trained operator can run two or three Tigris machines
simultaneously, the productivity of a single technician using Tigris could be as much as
ten times greater than a technician using current semi-automated systems.
Gen-Probe continues to receive regulatory approvals expanding its product line,
with the FDA granting approval in 2007 for the Procleix Ultrio assay, which
simultaneously detects HIV-1, HCV and HBV, on the Tigris system and European

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 217 -
regulators approving the APTIMA HPV Assay for detection of human papillomavirus in
2008.
The company expects that the markets for new applications of NAT technology
will continue to develop in both clinical and non-clinical fields. Among the clinical
fields that are expected to grow, the company sees NAT technology being utilized in the
areas of new analytes, such as the West Nile Virus, cancer diagnosis and
pharmacogenomics. Gen-Probe is also looking to emerging non-clinical markets for
NAT technology, including food, beverage, bioterrorism and environmental testing.
Today, these markets predominately use traditional methods for microbiological testing,
such as culture. There is, however, an increasing demand for NAT technology to provide
more rapid and efficient tests.
In 2007, Gen-Probe reported total sales of $403.0 million, up from $354.7 million
the prior year.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 218 -
FENWAL 3 Corporate Drive
Lake Zurich, IL 60047 Tel. (847) 550-2300 www.fenwalinc.com
Fenwal was established in March 2007 upon the sale of Baxter Healthcare
Corporation’s Transfusion Therapies business to Texas Pacific Group and Maverick
Capital, Ltd.
The company offers a range of automated component collection, whole blood
technology and ancillary equipment to blood collection centers. These include the ALYX
portable, continuous flow pneumatic component collection system; the Autopheresis-C
plasmapheresis instrument; and two whole blood centrifugal separators, the AMICUS
Separator and the CS 3000. Whole blood products include leukoreduction filters and
Blood-Pack sampling devices.
Shortly after its inception, Fenwal entered into an alliance with Data Innovations
to develop a data capture and reporting system for Fenwal’s automated blood component
collection systems. Such a device will allow blood centers to export data from Fenwal’s
automated blood collection devices into a system that will generate standard and
customized reports analyzing critical donor and procedural information.
A privately held company, Fenwal does not report financial results.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 219 -
GRIFOLS BIOLOGICALS, INC. 5555 Valley Boulevard
Los Angeles. California 90032. EUA Tel. (800) 421-0008 Fax. (323) 227-7616
www.grifols.com Grifols Biologicals is a world leader in developing and manufacturing blood
typing instruments.
The company has a rich history dating to the development of plasmapheresis by
Dr. Josep Antoni Grifols in 1951. This led to the establishment of an enterprise for
manufacturing scientific instrumentation for hematology and diagnostics. In 1966, the
company received U.S. grants patent for a centrifuge that automatically washes red blood
cells and performs the Coombs test, and in 1994, it began to market blood bags for blood
and plasma collection and storage. In 1995, the company inaugurated the new production
plant for blood bags and plastic bags for parenteral solutions in Las Torres de Cotillas,
Murcia and subsequently introduced NAT testing to detect hepatitis C (HCV) virus in
plasma fractionation pools, two years before it became compulsory in 1997.
Grifols’ product portfolio is impressive. Its bioscience division offers plasma-
derived clotting factors for the treatment of coagulation disorders, intravenous
immunoglobulin for the treatment of immune deficiency disorders and albumin for
volume expansion or replacement. Its diagnostic division focuses on the research,
development, manufacturing and marketing of diagnostics products for laboratory
analysis, including products for hospital blood banks and transfusion centers. Hemostasis
products include screening reagents, thrombophilia reagents, hemophilia reagents and
instrumentation as well as standard blood bags for the extraction, separation, storage and
transfusion of blood components. The Grifols Leucored System of blood bags includes a
filtration system for closed circuit leukocyte depletion of blood components.
Instrumentation products for blood banks include the Centrifuge JyM, Grifols Hemo-
stock refrigerators with a system controlling stocks of blood by blood groups and Grifols
mixers.
Over the past few years, Grifols has been building out its plasma collection
business. In 2006, Grifols acquired U.S.-based PlasmaCare, adding 14 plasma collection

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 220 -
centers; two years later, Grifols signed an agreement with Stough Development Corp. to
open 10 more U.S. plasma collection centers, then obtained a $10.7 million loan to
finance the purchase of another 4 U.S. centers.
As this occurs, its revenues continue to rise, with 2007 sales increasing 8.4% to
703.3 million euros ($1.0 billion). Sales outside Spain are rising faster than domestic
revenues, and now account for 72.6% of all company revenue.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 221 -
HAEMONETICS, INC. 400 Wood Rd.,
Braintree, MA, 02184, U.S.A. Tel. (800) 225-5242
www.haemonetics.com
Haemonetics has been a global leader in blood processing technologies for over
thirty years. The company is known for its innovative products, top of the line
technologies, and operational excellence. Today the organization employs over 1,800
people in sixteen countries. Its products are marketed in over 50 countries.
The company offers a range of products for the collection of red blood cells,
freezing and thawing of RBCs, collection of platelets and plasma and surgical cell
salvage. The Haemonetics MCS+8150 system collects two units of red cells from each
donor, helping blood collection agencies to double their red cell yield from the same
number of donors. The company offers two proprietary anticoagulant and storage
solutions, including the AS-3 for healthy storage of red cells and the CP2D used for
anticoagulation of donor’s blood. It also offers the TCD total containment device for
blood collection. This is a sterile connection that is compact, secure and easy to use. Red
cell freezing and thawing devices include the ACP 215 automated cell processing system
that enhances the shelf life of thawed blood from 24 hours to 14 days. Platelet collection
devices include the MCS+ automated system.
Haemonetics continues to enhance its product line, introducing new plasma
collection software in mid 2008 that reduces donation time by 20%. FDA-cleared in May,
the PCS2 software can be used with existing Haemonetics PCS2 plasma collection
devices so no device replacement or additional operator training is required. In April
2006, Haemonetics announced the launch of the Cymbal system, its latest blood
collection system. This portable device helps to collect two units of red blood cells from a
single blood donor in one donation. Half the size of Haemonetics' first generation
technology, this device helps to cost effectively collect more blood on community blood
drives.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 222 -
Net revenues for Haemonetics stood at $516.4 million in its fiscal year ending
March 2008, up from $449.6 million in the corresponding the year ago period.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 223 -
HEMOSOL CORP. 2585 Meadowpine Blvd.
Mississauga, Ontario Canada, L5N 8H9
Tel. (905) 286-6200 Fax. (905) 286-6300 www.hemosol.com
Hemosol Corporation is primarily involved in the discovery, development and
manufacture of life sustaining therapeutic products that are based on human blood
proteins. The company has a strong presence in the purification of proteins from a
biological source and offers cGMP manufacturing, development and testing large and
small volume parenterals, biologics and blood products to satisfy U.S., European and
Canadian regulatory requirements. Its processing systems can handle the purification of
up to 100kgs of protein per batch.
Hemosol is attempting to develop an oxygen carrier. The company’s lead product
is Hemolink, a hemoglobin raffimer made by purifying and then modifying outdated
human red blood cells. Units of blood are mixed together, the cells are washed and then
burst open to release the hemoglobin. Two units of expired blood create one unit of
Hemolink. The product has a longer shelf life than red blood cells, and can be stored for
up to a year in refrigeration. Despite this seemingly significant potential, however, the
compound remains in a state of suspended animation.
Based on the results from a favorable Phase III trial Hemosol filed for approval of
hemoglobin raffimer in Canada and the UK. However, in March 2002, Health Canada
advised Hemosol that hemoglobin raffimer would not be approved and that additional
data would be required for a refiled New Drug Submission. In the U.S., clinical trials of
hemoglobin raffimer have been suspended following a review of safety data.
After laying off most of its 130-person staff in 2003, the company filed a Notice
of Insolvency in November 2005, indicating its inability to continue funding ongoing
operations.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 224 -
IMMUCOR 3130 Gateway Drive
P.O. Box 5625 Norcross, GA 30091-5625 Telephone: (800) 829-2553
Fax: (770) 441.3807 www.immucor.com
Immucor is a global in vitro diagnostics company that specializes in pre-
transfusion diagnostics. The company was established in 1982 and develops,
manufactures and sells products that are used by hospital blood banks, clinical
laboratories, and blood donor centers to detect and identify certain properties of human
blood prior to patient transfusion. Immucor is particularly known for automating various
manual processes in blood banking laboratories.
Two acquisitions have been central to Immucor’s growth. In 1998, Immucor
acquired Gamma Biologicals, Inc., a manufacturer of diagnostic equipments whose
products were marketed to over 3,500 hospitals, blood centers and laboratories in over 50
other countries. In 1999, Immucor acquired the BCA blood bank division of Biopool
International, Inc. This group had been acquired by Biopool in 1997 from Organon
Teknica Corp. and offers a wide range of reagents and test kits used in blood grouping,
detection of Rh antigens, cross matching of blood and for the detection of rare antigens in
patient or donor blood. Today, Immucor employs over 600 people worldwide.
Immucor’s Capture system was first cleared to market in 1986. This solid phase
technology performs antibody screening and identification assays, in an easy-to-use,
standardized test with high sensitivity. As of 2008, Immucor reports that on a global
basis, Capture continues to be used more than 30 million times each year. Its blood bank
automation products include the ABS2000, the first FDA-cleared (1998) instrument for
full automation of blood typing and antibody screening assays. Immucor's second
generation blood automation system, the Galileo, was launched in Europe in 2002 and
received FDA clearance to market in the U.S. in April 2004. Galileo is a fully automated
gel-based instrument that offers a broad assay menu and features similar to a chemistry
analyzer: continuous access, linear rack, and bidirectional interface, and multitasking for
high volume testing. In June 2007, the company introduced Galileo Echo, an automated

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 225 -
walk-away instrument for small to medium sized testing facilities, of which Immucor
estimates there are approximately 6,000 worldwide. In addition, Immucor also offers
various blood bank reagents that include reagent red blood cells, blood grouping reagents,
anti human globulin, proficiency kits and specialty products for antibody investigation.
In March 2008, Immucor announced the acquisition of molecular diagnostics
company BioArray Solutions for $117 million. BioArray has developed diagnostic
systems based on its BeadChip system to determine antigens for donors and recipients of
blood transfusions. Immucor will acquire an IP portfolio with roughly 100 issued or
pending patents, as well as a 19% stake in a new company formed to commercialize
BioArray technologies outside of the blood transfusion and transplantation areas. The
deal will allow Immucor to deliver more precise genotyping solutions while maximizing
the value of BeadChip products through an established distribution network.
In 2007, Immucor reported revenue of $261.2 million, up from $223.6 million the
prior year.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 226 -
JP LABORATORIES INC. 120 Wood Avenue
Middlesex, NJ 08846 Phone: (732) 469 6670 Fax: (732) 469 6680
www.jplabs.com
JP Laboratories is a product research and development company. The firm
develops new products and processes and then licenses them to other companies for
manufacturing and marketing fees on royalty basis. Under grants from the National
Heart, Lung and Blood Institute of the National Institutes of Health, the company is
exploring a unique class of compounds that can carry oxygen, in which researchers
synthesize fluorocarbons with water soluble groups.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 227 -
MEDIMMUNE/ASTRAZENECA
One MedImmune Way Gaithersburg, MD 20878 Phone: (301) 398-0000 www.medimmune.com
Founded in 1987, MedImmune is a biotech company that develops, manufactures
and commercializes products for the treatment of infectious diseases, inflammatory
diseases, and cancer. With its headquarters in Maryland, the company also has facilities
in the United Kingdom and the Netherlands, employing over 2,000 people worldwide. In
mid 2007, MedImmune was acquired by global pharmaceutical company AstraZeneca for
$15.2 billion, then combined with AstraZeneca’s own biologics R&D group and
Cambridge Antibody Technology, which it acquired in May 2006, to form the company’s
new Global Biologics Organization (GBO). The GBO, however, is physically centered at
MedImmune’s Maryland offices and retains much of MedImmune’s pre-acquisition
character.
The company’s main product is Synagis (palivizumab), a blood derived product,
and the first monoclonal antibody successfully developed to combat an infectious disease.
Synagis helps to prevent serious lower respiratory tract disease caused by the respiratory
syncytial virus (RSV) in children at high risk for the disease. The drug was approved by
the FDA in 1998 and received approval by the European Medicines Evaluation Agency
soon in 1999. In 2002, it also received approval by the Japanese Ministry of Health,
Labor and Welfare. In 2003, the U.S. label for Synagis was expanded by the FDA for use
in young children with hemodynamically significant congenital heart disease at risk of
RSV disease. Synagis is now approved in more than five dozen countries, including the
United States. More importantly, this drug has been used to vaccine over half a million
babies since 1998. In 2007, worldwide sales of the product reached $1.2 billion.
A considerably smaller product for MedImmune is Cytogam (cytomegalovirus
immune globulin intravenous), a blood derived product that, like Synagis, is also used in
transfusion. It is indicated for prophylaxis against CMV disease associated with the
transplantation of the kidney, lung, liver, pancreas, and heart. In transplants of these

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 228 -
organs from CMV seropositive donors into CMV seronegative recipients, prophylactic
CMV-IGIV needs to be considered in combination with ganciclovir. In 2007, total
worldwide sales of Cytogam are estimated at less than $30 million.
MedImmune’s revenues continue to increase, with 2007 sales estimated at more
than $1.4 billion, as compared with $1.2 billion in 2006.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 229 -
NORTHFIELD LABORATORIES 1560 Sherman Ave.
Evanston, Illinois 60201 Phone: (847) 864-3500
www.northfieldlabs.com
Northfield Laboratories is developing an oxygen-carrying blood substitute for the
treatment of urgent, large volume blood loss in trauma and surgical settings. Northfield’s
product, PolyHeme, is a hemoglobin-based oxygen-carrying blood substitute. PolyHeme
simultaneously restores lost blood volume and hemoglobin levels and is designed for
rapid, massive infusion. PolyHeme is a solution of chemically modified human
hemoglobin which simultaneously restores lost blood volume and hemoglobin levels and
can be rapidly and massively infused.
PolyHeme requires no cross-matching. It is compatible with all blood types and
therefore immediately available for infusion. It has an extended shelf life of more than 12
months. The product has been safely infused in clinical trials in sufficiently massive
quantities to be useful in the treatment of large volume blood loss. In clinical trials to
date, patients who received PolyHeme had improved survival compared to historical
patients who did not receive blood.
In March 2003, Northfield received clearance from the FDA to proceed with a
pivotal Phase III trial and in December of the year, it received notification of the first full
approval by an institutional review board (IRB) to proceed with enrollment in the
PolyHeme urban ambulance trial. This trial is a controlled study designed to evaluate the
safety and efficacy of PolyHeme in treating severely injured and bleeding patients when
blood is not immediately available. The study aimed to enroll 720 patients spread across
25 - 30 Level I trauma centers across the United States, with a primary endpoint of
survival at 30 days. In October 2004, the Independent Data Monitoring Committee
(IDMC) recommended that the pivotal Phase III trial continue without modification,
however, conclusions drawn from study data have been mixed.
In late 2006, Northfield Labs released preliminary results of the trial, indicating
disappointing mortality data: 13.2% of patients receiving PolyHeme died versus 9.6%
among the control group. However, the company released more detailed findings in May

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 230 -
2007 indicating no significant difference in mortality between patients who received the
standard of care, including early blood transfusion, and PolyHeme. Northfield is currently
preparing a Biologics License Application for submission to the FDA later in 2008.
As a development stage company, Northfield Labs reported no revenue in 2007.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 231 -
NOVO NORDISK A/S Novo Allé
2880 Bagsværd Denmark
Phone: 45 4444 8888 Fax: 45 4449 0555
www.novonordisk.com
Novo Nordisk has one of the broadest diabetes product portfolios in the industry,
including advanced products within the area of insulin delivery systems. In addition,
Novo Nordisk has a leading position in areas such as hemostasis management,
growth hormone therapy and hormone replacement therapy.
The company has developed NovoSeven, a recombinant Factor Vlla for the
treatment of bleeds in hemophilia A and B patients with inhibitors. This recombinant
protein is expressed from cloned human FVII genes in baby hamster kidney cells. No
material of human origin is used in the production process or in the final product.
NovoSeven induces hemostasis in pharmacologic doses by converting FX to FXa
on the surface of activated platelets. Following a series of complex steps, FXa will lead to
the development of a blood clot at the site of injury. It is important to know that under
normal circumstances, platelets only become activated at the site of injury—thus
preventing blood clots from forming in areas where they are not wanted. This distinct
mechanism of action explains NovoSeven’s potential for safe and effective hemostasis,
even in the absence of Factors VIII or IX.
In Europe, NovoSeven is indicated for the treatment of spontaneous bleeding
episodes in hemophilia A and B patients with inhibitors and in patients with acquired
hemophilia. It is also indicated for the treatment of bleeding episodes due to surgery in
patients with inhibitors. Those inhibitors are the antibodies that develop in patients with
hemophilia A following a replacement therapy. Inhibitors develop in about 15% to 30%
of hemophilia A patients. Hemophilia affects 1 in 10,000 live male births worldwide.
NovoSeven is approved in the United States as well.
In 2007, NovoNordisk completed Phase II safety studies for the use of
NovoSeven in cardiac surgery, with preliminary results confirming the product’s safety

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 232 -
profile as well as its biologic haemostatic effect. During the year, NovoNordisk also
submitted heat-stable versions of NovoSeven to regulators in the U.S., EU and Japan.
In 2007, Novo Nordisk reported sales of 41.8 billion Danish kroners, or about
$8.6 billion, up from 38.7 billion Danish kroners, or $8.0 billion, in 2006. Of this,
NovoSeven accounted for about $1.2 billion.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 233 -
ORTHO CLINICAL DIAGNOSTICS
1001, U.S. Hwy. 202, Raritan, New Jersey 08869
Phone: (908) 218-1300 Fax: (908) 704-3649 Raritan, New Jersey
www.orthoclinical.com
Ortho-Clinical Diagnostics (OCD) is a subsidiary of Johnson & Johnson, a
leading global provider of diagnostic products and services. It was formed in 1997 from
the merger of two Johnson & Johnson companies: Ortho Diagnostic Systems, a
worldwide leader in diagnostic reagents and instrument systems, and Johnson & Johnson
Clinical Diagnostics (formerly a division of Eastman Kodak Co. that was acquired by
J&J in 1994), a worldwide leader in clinical laboratory systems. Today the organization
has headquarters in New Jersey and research headquarters in Rochester, New York. It
also maintains facilities in Canada, the United Kingdom, France, Germany, Italy, Spain,
Japan, Singapore and Australia.
Products and therapies are classified into two key areas: transfusion medicine and
clinical laboratories. Transfusion medicine includes products offered for blood screening,
blood banking and immunohematology. The blood screening division develops
instrument systems and reagents are developed for screening blood for AIDS and
hepatitis. Blood banking includes products such as the ID-Micro Typing System (ID-
MTS) Gel Test, a flexible automation system which currently has over 2,400 users in
North America. This technology is based on column agglutination and can standardize
the complete menu of testing for a blood bank; it offers ABO & Rh typing, antibody
screening & identification, and antigen typing. Immunohematology products include
instrumentation and reagent systems that enable blood typing. Products for the blood
banking industry include automation and reagent systems for a range of blood bank
applications including pretransfusion testing, transfusion software and information
management systems. The company also offers a range of traditional antisera and reagent
red blood cell products to meet testing needs.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 234 -
In January 2006, the company announced the release of two new MicroTip assays
for sale on the VITROS 5,1 FS Chemistry System. These additional assays would help to
further enhance the testing capabilities of the VITROS 5,1 FS Chemistry System. The
assays are Antistreptolysin O* (ASO), to aid in the diagnosis of post-streptococcal
diseases such as glomerulonephritis, rheumatic fever, bacterial endocarditis and scarlet
fever; and Alpha-1 Antitrypsin (AAT), to aid in the diagnosis of cirrhosis of the liver and
pulmonary emphysema.
Ortho continues to expand its capabilities in the blood testing arena, particularly
through acquisitions of technology developers. In August 2008, Johnson & Johnson
completed the acquisition of Immunicon, the developer of the FDA-approved CellSearch
System. This represents the first diagnostic test to automate the detection and
enumeration of circulating tumor cells (CTCs), cancer cells that detach from solid tumors
and enter the blood stream. Two months earlier, J&J acquired Amic, a privately held
Swedish developer of novel in vitro diagnostic (IVD) technologies for use in Point-of-
Care (POC) and near-patient settings. Amic is currently working to develop a chip-based
micro-fluidic platform that would enable fully quantitative, immunoassay tests.
Johnson & Johnson’s total sales through its more than 200 operating companies,
including Ortho Clinical Diagnostics, reached $61.1 billion in 2007, up from $53.3
billion the prior year.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 235 -
PERFTORAN Russian Academy of Science
142290, Pushchino of the Moscow Region Russia
Phone: +7 (0967) 73-39-82 Fax: +7 (0967) 33-05-46
www.perftoran.ru
Perftoran was formed in 1997 by the Ministry of Public Health and Medical
Institute of Russian Federation. The company’s product, also known as Perftoran, is a
perfluorocarbon-based oxygen carrier (PBOC), consisting of perfluorodecalin,
perfluoromethylcyclohexylpiperidine and proxanol. Perftoran is similar to Fluosol
(Green Cross and Alpha Therapeutic), the first PBOC to be used in the late 1970s, with
the exception that the emulsifier is new and improved. Fluosol was associated with
several problems, including cumbersome preparation procedures, side-effects and modest
oxygen transport characteristics. However, the number of side effects associated with
Perftoran is considerably lower. This is probably related to the emulsifier (less
complement activation). Perftoran has a small particle size, i.e. 0.07 mm. Smaller
particles evade the reticuloendothelial system more easily, which results in longer
intravascular persistence and fewer side effects. In addition, smaller particles traverse the
microcirculation with less resistance.
Perftoran is marketed as "a multipurpose substance able to correct various type of
hypoxia." Several clinical studies have been conducted using Perftoran in patients
undergoing neurosurgery for cranial trauma and kidney transplantation, revealing
improved morbidity and mortality. In one study, 757 wounded and critically ill patients
were treated with Perftoran. The indications included hypovolemia, DIC (disseminated
intravascular coagulation), bronchopulmonary lavage and regional perfusion of
extremities. The results were compared to a control group of 976 patients. Perftoran
performed extremely well as an oxygen transport medium. Hemodynamic function
improved in hypovolemic patients while hepatic function recovery was accelerated. The
need for allogeneic blood decreased, while the incidence of ARDS (acute respiratory
distress syndrome) was less in patients treated with Perftoran. Perftoran was also used

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 236 -
during cardiac surgery as a blood substitute during cardiopulmonary bypass and in
cardioplegic solutions. The results were similarly impressive - decreased hemolysis of
red blood cells, rapid restoration of cardiac activity.
Perftoran must be stored frozen and has a shelf life of two years. It may be
thawed and refrozen five times. As a "new and improved" first-generation PBOC, these
initial results suggest that Perftoran has considerable clinical efficacy in a variety of
settings. It is uncertain whether Perftoran will be available on a worldwide basis.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 237 -
SANGUINE CORP. 101 East Green Street, Suite 11
Pasadena, CA 91105 Phone: (801) 746-3570
Fax: (801) 532-1765 www.sanguine-corp.com
Sanguine is developing PHER-O2, a perfluorocarbon (PFC) emulsion with
oxygen carrying properties that has immediate applications as an intravenous supplement
to red blood cell function. Sanguine is a well-established organization with experts in the
field of synthetic blood chemistry and development. Dr. Thomas C. Drees was involved
in the creation of Fluosol, the only synthetic blood supplement approved to date for
human use by the FDA. The FDA approved Fluosol for angioplasty use only in 1989 but
Fluosol was withdrawn from the market in 1994 because of the difficulty of storing it
frozen and then bringing it to ambient temperature prior to use.
PHER O2 is a second-generation formulation of the perfluorocarbon (PFC)
emulsion and in fact, is the pioneering PFC in the field of synthetic substitutes for blood.
As such, PHER O2 was designed to overcome some of the deficiencies of the original
Fluosol product - the need for frozen storage, low (20%) PFC content and short intra-
vascular residency time. Fluosol was chemically derived and is a combination of the
carbohydrate decalin (C10 H18) that replaces the hydrogen atoms with flourine atoms,
resulting in a fluorocarbon. Although refuted by the FDA as a blood substitute, it remains
the first and only blood substitute approved to date by the FDA for medical use in
connection with blood supplementation. The United States and eight other countries
approved Fluosol for use in cardiac angioplasty to “reduce the amount of allogeneic
blood units transfused.”
PHER-O2 does not need to be typed and cross matched. It has a long shelf life,
and offers no risk of AIDS, Hepatitis, nor mad cow disease. PHER-O2 is designed to
carry more oxygen than blood and to be much smaller than a red blood cell. It should be
useful in transfusions, heart attack, stroke cancer and many other hypoxic and ischemic

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 238 -
diseases, such as burns, shock, eye surgery, transplant organ perfusion and sickle cell
anemia.
PHER-O2 has successfully completed animal toxicity and efficacy trials at the
University of Alberta in Canada. Sanguine believes that Fluosol’s acceptance should
enable it to pursue the fast track for PHER-O2 through clinical trials and the FDA
approval process, although testing is proceeding slowly.
As a development stage company, Sanguine reported no product revenue in 2007.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 239 -
OXYGEN BIOTHERAPEUTICS 3189 Airway Ave., Building C
Costa Mesa, CA 92626 Phone: (714) 427-6363 Fax: (714) 427-6361
www.sybd.com
Oxygen Biotherapeutics (formerly Synthetic Blood International) specializes in
pharmaceuticals and medical devices in the fields of liquid ventilation, oxygen
therapeutics, blood substitutes and implanted glucose sensing.
The company is developing Oxycyte, an oxygen-carrying intravenous emulsion
that can carry five times more oxygen than hemoglobin, making it an effective means of
transporting oxygen to tissues and carbon dioxide to the lungs for disposal. New
applications of oxygen therapeutic agents include stroke, myocardial infarction, and
certain malignant diseases. Oxygen Biotherapeutics expects to begin a Phase IIb clinical
trial of Oxycyte in traumatic brain injury in the third quarter of 2008. The multi-center,
double-blind, placebo-controlled study will enroll up to 300 patients. Other studies may
include evaluation of Oxycyte in orthopedic surgery patients who lose modest amounts of
blood during surgery; administration to patients undergoing coronary bypass or heart
valve replacement surgery on a heart-lung machine; as well as surgical patients who lose
enough blood during surgery to require a blood or red cell transfusion.
As a development stage company, Oxygen Biotherapeutics reported no product
revenue in 2007.

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 240 -
TALECRIS BIOTHERAPEUTICS 4101 Research Commons, 79 T.W. Alexander Drive
Research Triangle Park North Carolina, 27709 Phone: (919) 316-6300
www.talecris.com
Talecris Biotherapeutics is a relatively new organization formed in early 2005
from a group of leading blood industry players. The company was organized by private
investment firms Cerberus Capital management and Ampersand ventures, which acquired
the assets of the global plasma business of Bayer Biological Products. Shortly thereafter,
Talecris added the acquired plasma fractionation and contract manufacturing facilities of
Precision Pharma Services in Melville, N.Y. and the blood derived products of Cutter
Laboratories. Talecris now offers top of the line technologies through state of the art
fractionation and production facility located in Clayton, North Carolina.
The company’s leading products include Gamunex immune globulin (IGIV),
Koate DVI antihemophilic factor, Plasbumin human albumin, hyperimmune globulin
therapies, Prolastin Alpha 1 proteinase inhibitor and hemostasis products.
In January 2006, Talecris along with Jeffrey Modell Foundation, opened the
Jeffrey Modell diagnostic center for Primary Immunodeficiencies at the University of
Miami Leonard M. Miller School of Medicine. This center is one among 24 centers that
focuses on the diagnosis, treatment and care of people with primary immunodeficiencies.
Two months later, Food and Drug Packaging selected the Talecris Plasma fractionation
plant for its ‘Plants of the year’ award. The organization stated that Talecris handled
immunoglobulin products with extreme care, before, during and after packaging.
Talecris continues to expand the depth and breadth of its product line. In August
2007, it introduced latex-free Gamunex, wherein all product going forward will be
packaged without latex in the rubber stoppers used in product packaging. The
modification was made to address ongoing concerns in the medical community related to
latex allergies. A year later, Talecris announced that the European Commission granted
orphan drug designation to the company’s alpha1 proteinase inhibitor [human] for

Kalorama Information: Blood, Blood Equipment, Blood Testing and Synthetic Blood Markets
Copyright © 2008 Kalorama Information
Reproduction without prior written permission, in any media now in existence or hereafter developed, in whole or in any part, is strictly prohibited
- 241 -
inhalation use in the treatment of congenital Alpha-Antitrypsin Deficiency (also known
as AAT Deficiency or Alpha-1). Currently, there are no approved aerosolized treatments
available for augmentation therapy for this condition.
As a privately traded company, Talecris Biotherapeutics does not report financial
results.