Beginning of a molecular era in hearing and deafness
11
Clin Genet 1999: 55: 149–159 Printed in Ireland. All rights reser6ed Developmental Biology: Frontiers for Clinical Genetics Section Editor: Roderick R McInnes e-mail: [email protected] Beginning of a molecular era in hearing and deafness Robertson ND, Morton CC. Beginning of a molecular era in hearing and deafness. Clin Genet 1999: 55: 149–159. © Munksgaard, 1999 Nahid G Robertson and Cynthia C Morton Departments of Pathology, Obstetrics, Gynecology and Reproductive Biology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA Corresponding author: Cynthia C. Morton, Department of Pathology, Brigham and Women’s Hospital, 75 Francis Street, Boston, MA 02115, USA. Fax: +1 617 738 6996; e-mail: ccmor- [email protected] Received 23 December 1998, revised and accepted for publication 13 January 1999 Despite detailed studies of physiological processes of the inner ear (1, 2), as well as advances in the understanding of clinical aspects of hearing and deafness (3–5), much remains to be known about the actual genes and molecular mechanisms in- volved in the processes of hearing and balance maintenance. However, significant progress has been made in this area largely in the last two years. The era for identifying genes involved in deafness has begun and is now moving at a rapid pace. What have been some obstacles to overcome in starting the process of identification of genes and molecular mechanisms in hearing? In part, there are problems inherent in the study of single genes in communities of deaf individuals where assorta- tive mating, due to linguistic homogamy and a shared common culture, may confound tradi- tional genetic approaches due to genetic hetero- geneity and environmental factors contributing to the phenotype. Some of the problems in this sys- tem have been circumvented by studying geo- graphically isolated, sometimes consanguineous families. In conjunction with intensive efforts to sequence the human genome, which are continu- ally providing a large number of human chromo- somal markers, isolated deafness disorders have been mapped by linkage analysis to specific inter- vals on human chromosomes, narrowing down regions for the search of a mutated gene. In ad- dition, utilization of mouse models has proven invaluable, by first finding the gene defect in a mutant strain of deaf mice and then identifying the human gene through comparison of regions of homologous synteny between human and mouse chromosomes. Another problem in identifying genes in the inner ear has been the difficulty in accessing the cochlear and vestibular labyrinths, the sensory end organs for hearing and balance, which are embedded in the petrous portion of the temporal bone, the densest bone in the human body. However, the construction of a human fetal cochlear cDNA library (6), as well as cDNA libraries from auditory tissues of other organisms (7, 8) is now providing a repertoire of genes that are expressed in the cochlea, therefore identifying candidate genes for deafness by a tissue- specific approach. To date, over 4000 cochlear expressed sequence tags (ESTs) have been se- quenced from the human fetal cochlear cDNA library and deposited in GenBank databases (9). Analysis of these cochlear cDNAs provides a win- dow into known and novel genes expressed in the cochlea (10). 149
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Beginning of a molecular era in hearing and deafness

Clin Genet 1999: 55: 149–159Printed in Ireland. All rights reser6ed
Developmental Biology: Frontiers for Clinical GeneticsSection Editor: Roderick R McInnese-mail: [email protected]
Beginning of a molecular era in hearing anddeafness
Robertson ND, Morton CC. Beginning of a molecular era in hearingand deafness.Clin Genet 1999: 55: 149–159. © Munksgaard, 1999
Nahid G Robertson andCynthia C MortonDepartments of Pathology, Obstetrics,Gynecology and Reproductive Biology,Brigham and Women’s Hospital, HarvardMedical School, Boston, MA, USA
Corresponding author: Cynthia C. Morton,Department of Pathology, Brigham andWomen’s Hospital, 75 Francis Street,Boston, MA 02115, USA. Fax: +1 617738 6996; e-mail: [email protected]
Received 23 December 1998, revised andaccepted for publication 13 January 1999
Despite detailed studies of physiological processesof the inner ear (1, 2), as well as advances in theunderstanding of clinical aspects of hearing anddeafness (3–5), much remains to be known aboutthe actual genes and molecular mechanisms in-volved in the processes of hearing and balancemaintenance. However, significant progress hasbeen made in this area largely in the last twoyears. The era for identifying genes involved indeafness has begun and is now moving at a rapidpace.
What have been some obstacles to overcome instarting the process of identification of genes andmolecular mechanisms in hearing? In part, thereare problems inherent in the study of single genesin communities of deaf individuals where assorta-tive mating, due to linguistic homogamy and ashared common culture, may confound tradi-tional genetic approaches due to genetic hetero-geneity and environmental factors contributing tothe phenotype. Some of the problems in this sys-tem have been circumvented by studying geo-graphically isolated, sometimes consanguineousfamilies. In conjunction with intensive efforts tosequence the human genome, which are continu-ally providing a large number of human chromo-somal markers, isolated deafness disorders have
been mapped by linkage analysis to specific inter-vals on human chromosomes, narrowing downregions for the search of a mutated gene. In ad-dition, utilization of mouse models has proveninvaluable, by first finding the gene defect in amutant strain of deaf mice and then identifyingthe human gene through comparison of regionsof homologous synteny between human andmouse chromosomes.
Another problem in identifying genes in the innerear has been the difficulty in accessing the cochlearand vestibular labyrinths, the sensory end organsfor hearing and balance, which are embedded in thepetrous portion of the temporal bone, the densestbone in the human body. However, the constructionof a human fetal cochlear cDNA library (6), as wellas cDNA libraries from auditory tissues of otherorganisms (7, 8) is now providing a repertoire ofgenes that are expressed in the cochlea, thereforeidentifying candidate genes for deafness by a tissue-specific approach. To date, over 4000 cochlearexpressed sequence tags (ESTs) have been se-quenced from the human fetal cochlear cDNAlibrary and deposited in GenBank databases (9).Analysis of these cochlear cDNAs provides a win-dow into known and novel genes expressed in thecochlea (10).
149

Robertson and Morton
Heterogeneity in hearing loss: involvement of manygenes
The complexity of gene expression in the cochleais reflected by a great number of genes tran-scribed in this organ. The finding of a large per-centage (13%) of cochlear ESTs not identified todate in any other tissue, as apparent from theanalysis of the human cochlear cDNA library,may indicate the existence of genes that areunique to the cochlea (9). This is not surprisingconsidering the intricate nature of this organ(Figs. 1 and 2), which is comprised of a largevariety of different cell types and maintains aprecise structure and ionic state necessary forproper functioning. In addition, the great degreeof genetic heterogeneity, reflecting many differenttypes of, and loci for, deafness is indicative ofthe involvement of a large number of genes or-chestrating the hearing process (11).
The most common sensory deficit in humans ishearing loss, including perturbations due to bothenvironmental (e.g. acoustic trauma, ototoxicity,viral or bacterial infections) and genetic causes,with varying times of onset ranging from congen-ital deafness to presbycusis (hearing loss relatedto aging). One in a thousand children is esti-
mated to be born deaf, with approximately halfof the cases due to genetic causes. By age 65,one-third of the human population has significanthearing impairment with a higher incidence inmales as compared to females. Approximately75% of genetic cases are estimated to have anautosomal recessive mode of inheritance, 10–15%are autosomal dominant and the remainder areX-linked, mitochondrial, or chromosomal (i.e.,aneuploidies) in origin (12–14).
Hearing loss can be conductive, sensorineural,or mixed in nature. The conductive portions ofthe auditory apparatus, the external and middleear, are air-filled cavities which contain the tym-panic membrane and the three ossicles whichtransmit sound vibrations to the oval window(Fig. 1). The inner ear, consisting of the cochlearand vestibular labyrinths, contains sensorineuralorgans where mechanoelectrical transduction oc-curs to carry neural signals to higher corticalcenters for integration, processing, and feedback.
Clinical categories of hearing loss haveemerged based on conductive versus sensorineuralcauses, as well as other factors such as audiologicprofile, environmental influences, severity, age ofonset, mode of inheritance, and accompanying
Fig. 1. Diagram of a frontal section of the human ear illustrating the outer, middle, and inner sections. The inner ear consists ofthe cochlear and vestibular labyrinths. Modified and reprinted with permission from Netter FH: Atlas of Human Anatomy.Summit. New Jersey: Ciba-Geigy Corporation, 1993.
150

Beginning of a molecular era in hearing and deafness
Fig. 2. Diagrams of a cross section of the cochlear duct (above) and the vestibular sense organs, macula utriculi and cristaampullaris (below). Hair cells are shown in green and overlying membranes in blue. Modified and reprinted with permission fromBarr ML and Kiernan JA: The Human Nervous System: An Anatomical Viewpoint. Philadelphia: JB Lippincott Company, 1993.
symptoms in other organ systems. Genetic hetero-geneity is seen within some clinically identified typesof hearing loss, indicating that accurate diagnosisand classification of types of deafness can occur onlywith elucidation of specific gene involvement andfundamental understanding of molecular mecha-nisms. Clinical and genetic assessments have beenhelpful in creating a framework to begin identifyinggenes and teasing out specific deafness disorders.Two broad categories are syndromic disorders(Table 1), where hearing loss is accompanied byinvolvement of one or several other organ systems,and nonsyndromic disorders (Table 2), where theinner ear appears to be the only affected organ.
Syndromic hearing loss
Hundreds of syndromes that include hearing lossas an associated finding have been described (15);however, only a relatively small number ofcausative genes have been characterized. Thepleiotropic effects of a single mutated gene, asdemonstrated by perturbation of its function inseveral tissues, may reflect a common role of thatgene in the development, structure, and function ofseveral different organ systems.
One category of genes with roles in neural crestdevelopment, with involvement in the auditoryprocess and in pigmentation by melanocyte migra-
151
Robertson and Morton
tion and differentiation, is exemplified by the genesfound to be mutated in the different types ofWaardenburg syndrome, and include the transcrip-tion factors PAX3 (16, 17), MITF (18), SOX10(19), as well as the growth factor endothelin-B(EDN3) (20, 21) and its receptor (EDNRB) (22,23). Defects in EYA1, the human homolog of theDrosophila eyes absent gene, is mutated in bran-chio-oto-renal (BOR) syndrome, suggesting thecommon developmental role of this gene in theinner ear and kidney (24).
Other genes implicated in a common mechanismhave roles in the maintenance of ionic balance. Inthe inner ear, sensory hair cells of the cochlea andvestibule are bathed in potassium-rich endolymph,which upon mechanical stimulation will cause de-polarization of these cells by rapid influx of potas-sium ions. Two genes encoding potassium channelproteins, KVLQT1 (25) and KCNE1 (26, 27), aremutated in Jervell and Lange–Nielsen syndrome,resulting in deafness and cardiac arrhythmias. An-other gene involved in ion transport is PDS, mu-tated in Pendred syndrome, a disorder withcongenital deafness and variable thyroid goiterfindings (28). The encoded protein, pendrin, hashomology to known sulfate transporters, and hasrecently been implicated in transport of the anionschloride and iodide (29).
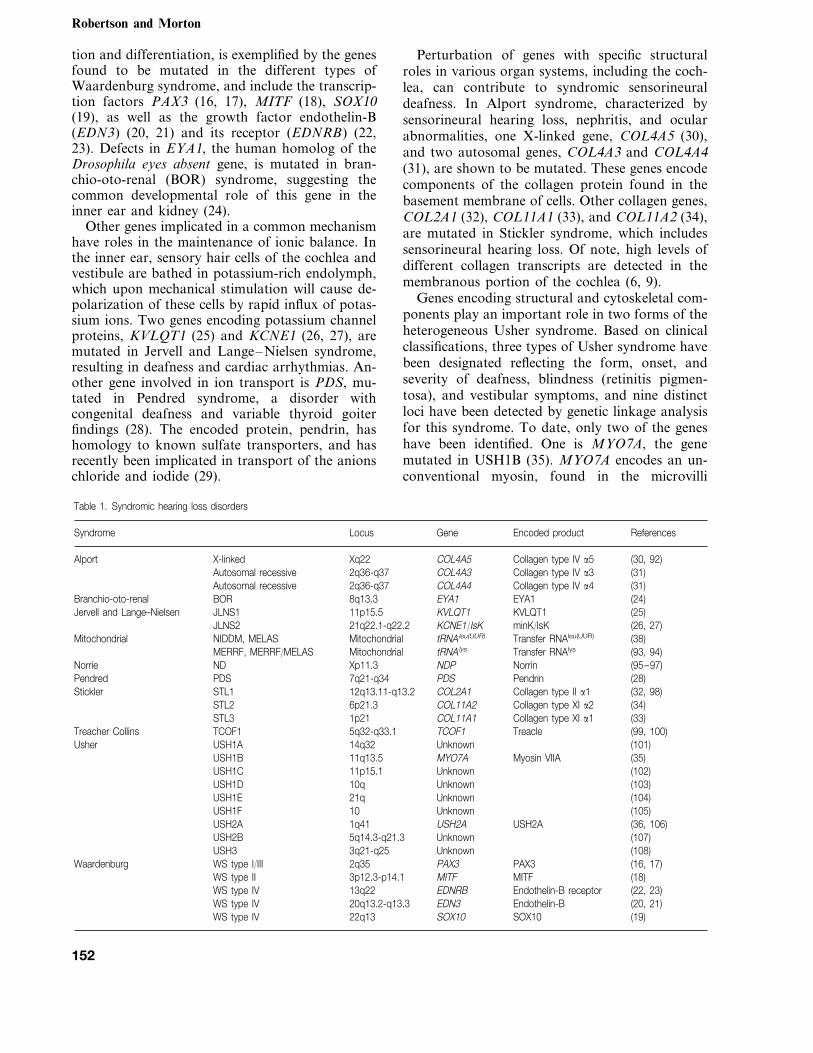
Perturbation of genes with specific structuralroles in various organ systems, including the coch-lea, can contribute to syndromic sensorineuraldeafness. In Alport syndrome, characterized bysensorineural hearing loss, nephritis, and ocularabnormalities, one X-linked gene, COL4A5 (30),and two autosomal genes, COL4A3 and COL4A4(31), are shown to be mutated. These genes encodecomponents of the collagen protein found in thebasement membrane of cells. Other collagen genes,COL2A1 (32), COL11A1 (33), and COL11A2 (34),are mutated in Stickler syndrome, which includessensorineural hearing loss. Of note, high levels ofdifferent collagen transcripts are detected in themembranous portion of the cochlea (6, 9).
Genes encoding structural and cytoskeletal com-ponents play an important role in two forms of theheterogeneous Usher syndrome. Based on clinicalclassifications, three types of Usher syndrome havebeen designated reflecting the form, onset, andseverity of deafness, blindness (retinitis pigmen-tosa), and vestibular symptoms, and nine distinctloci have been detected by genetic linkage analysisfor this syndrome. To date, only two of the geneshave been identified. One is MYO7A, the genemutated in USH1B (35). MYO7A encodes an un-conventional myosin, found in the microvilli
Table 1. Syndromic hearing loss disorders
Syndrome Locus Gene Encoded product References
(30, 92)Collagen type IV a5Alport COL4A5Xq22X-linkedAutosomal recessive 2q36-q37 COL4A3 Collagen type IV a3 (31)
2q36-q37 COL4A4 (31)Autosomal recessive Collagen type IV a48q13.3 EYA1 EYA1BOR (24)Branchio-oto-renal
KVLQT1Jervell and Lange–Nielsen (25)JLNS1 11p15.5 KVLQT1minK/IsK (26, 27)JLNS2 21q22.1-q22.2 KCNE1/IsK
(38)Transfer RNAleu(UUR)tRNAleu(UUR)MitochondrialNIDDM, MELASMitochondrialMitochondrial tRNAlys Transfer RNAlys (93, 94)MERRF, MERRF/MELAS
(95–97)NorrinNDPXp11.3NDNorriePendrinPDS7q21-q34 (28)PDSPendred
12q13.11-q13.2 COL2A1 Collagen type II a1 (32, 98)Stickler STL1STL2 6p21.3 COL11A2 Collagen type XI a2 (34)STL3 1p21 COL11A1 Collagen type XI a1 (33)
(99, 100)TreacleTCOF15q32-q33.1TCOF1Treacher CollinsUsher USH1A 14q32 Unknown (101)
USH1B 11q13.5 MYO7A Myosin VIIA (35)Unknown (102)USH1C 11p15.1
USH1D 10q Unknown (103)USH1E 21q Unknown (104)USH1F 10 Unknown (105)USH2A 1q41 USH2A USH2A (36, 106)USH2B 5q14.3-q21.3 Unknown (107)
(108)Unknown3q21-q25USH3Waardenburg WS type I/III 2q35 PAX3 PAX3 (16, 17)
WS type II 3p12.3-p14.1 MITF MITF (18)Endothelin-B receptorEDNRB13q22WS type IV (22, 23)
WS type IV 20q13.2-q13.3 EDN3 Endothelin-B (20, 21)WS type IV 22q13 SOX10 SOX10 (19)
152

Beginning of a molecular era in hearing and deafness
Table 2. Nonsyndromic hearing loss disorders
Locus Encoded product ReferencesGeneGenetic classification Designation
5q31 DIAPH1 Diaphanous 1 (58, 109)Autosomal dominant DFNA1UnknownDFNA2 1p34 (80)
(75, 110)GJB2 Connexin 2613q12DFNA3(111)DFNA4 19q13 Unknown
DFNA5 DFNA5DFNA5 7p15 (56, 112)Unknown (113)4p16.3DFNA6UnknownDFNA7 1q21-q23 (114)
(59, 115)a-TectorinTECTA11q22-q24DFNA8/A1214q12-q13 COCH COCH (50, 116)DFNA9
(117)Unknown6q22-q23DFNA10(69, 118)Myosin VIIADFNA11 11q12.3-q21 MYO7A
UnknownDFNA13 6p21 (119)Unknown (120)4p16.3DFNA14POU4F3 POU4F3DFNA15 5q31 (62)
(121)Unknown2q24DFNA1622q Unknown (122)DFNA17
(123)Unknown3q22DFNA1810 (pericentromeric) Unknown (124)DFNA19
GJB2 Connexin 26Autosomal recessive DFNB1 (72, 125)13q12MYO7A (67, 68, 126)Myosin VIIA11q13.5DFNB2MYO15 Myosin XVDFNB3 (54, 127)17p11.2
(70, 128)PendrinPDS7q31DFNB414q12 Unknown (129)DFNB5
(130)Unknown3p14-p21DFNB69q13-q21 Unknown (131)DFNB7
UnknownDFNB8 21q22 (132)Unknown (133)2p22-p23DFNB9
21q22.3 Unknown (134)DFNB10UnknownDFNB11 9q11-q21 (135)
(136)Unknown10q21-q22DFNB12UnknownDFNB13 7q34-q36 (137)
DFNB14 reservedUnknown (11)3q21-q25 19p13DFNB15UnknownDFNB16 15q21-q22 (138)
(139)Unknown7q31DFNB1711p14-p15.1 Unknown (140)DFNB18
(141)Unknown18p11DFNB19DFNB20 reserved
DDP DDPX-linked DFN1 (41, 42)Xq22Unknown (142)Xq22DFN2POU3F4 POU3F4DFN3 (43)Xq21.1
(143)UnknownXp21.2DFN4reservedDFN5
(144)UnknownXp22DFN6reservedDFN7
DFN8 reserved
12S rRNA (44)12S rRNAMitochondrialMitochondrialtRNAser(UCN) transfer RNAser(UCN)Mitochondrial (145)
known as stereocilia, which are actin-filled struc-tures present on the apical surface of the sensoryhair cells in the cochlea and vestibular systems.These stereocilia harbor the ‘tip links’, which arethought to be the mechanical springs for physi-cally opening the ion channels, leading to depo-larization of hair cells upon bending of thestereocilia due to the shearing force from theoverlying tectorial membrane upon stimulationby sound. The other known gene for Usher syn-
drome is designated USH2A, encoding a novelprotein with sequence similarities to motifs foundin basal lamina, extracellular matrix, and cell ad-hesion molecules (36).
In addition to nuclear genes, mitochondrialmutations (37) have also been shown to be re-sponsible in several syndromes usually affecting awide range of organs. Interestingly, one syn-drome includes sensorineural hearing loss in asso-ciation with diabetes mellitus type II (38).
153
Robertson and Morton
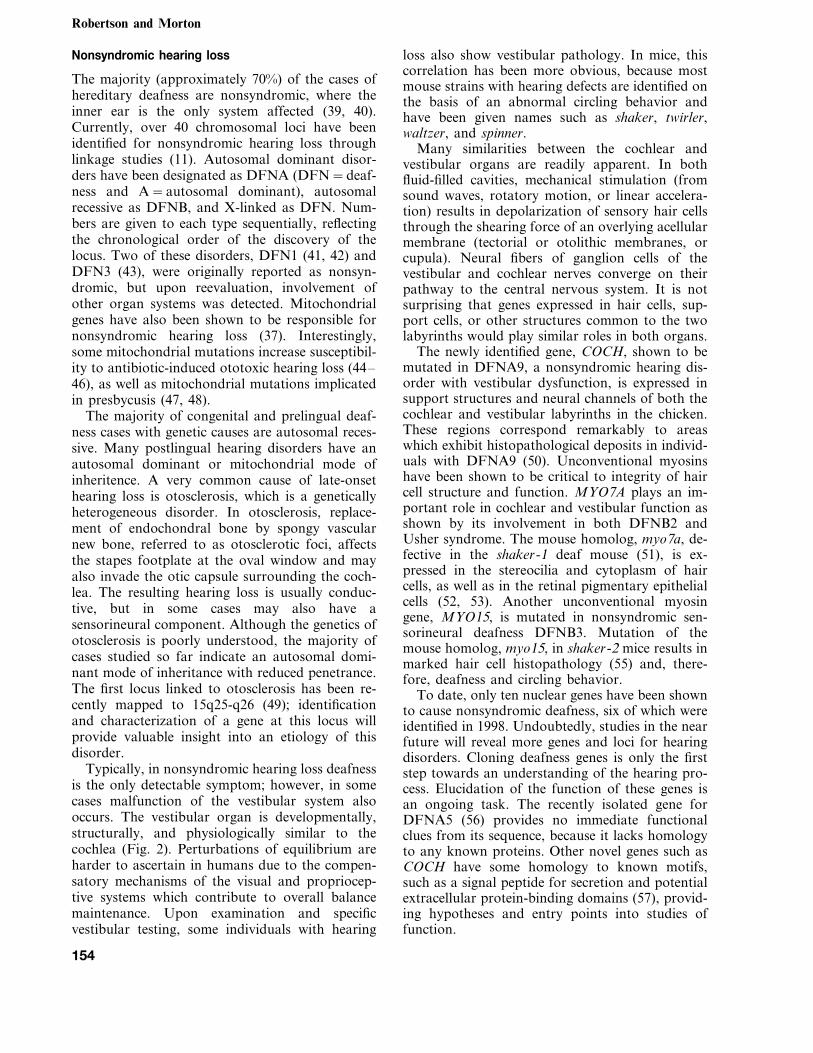
Nonsyndromic hearing loss
The majority (approximately 70%) of the cases ofhereditary deafness are nonsyndromic, where theinner ear is the only system affected (39, 40).Currently, over 40 chromosomal loci have beenidentified for nonsyndromic hearing loss throughlinkage studies (11). Autosomal dominant disor-ders have been designated as DFNA (DFN=deaf-ness and A=autosomal dominant), autosomalrecessive as DFNB, and X-linked as DFN. Num-bers are given to each type sequentially, reflectingthe chronological order of the discovery of thelocus. Two of these disorders, DFN1 (41, 42) andDFN3 (43), were originally reported as nonsyn-dromic, but upon reevaluation, involvement ofother organ systems was detected. Mitochondrialgenes have also been shown to be responsible fornonsyndromic hearing loss (37). Interestingly,some mitochondrial mutations increase susceptibil-ity to antibiotic-induced ototoxic hearing loss (44–46), as well as mitochondrial mutations implicatedin presbycusis (47, 48).
The majority of congenital and prelingual deaf-ness cases with genetic causes are autosomal reces-sive. Many postlingual hearing disorders have anautosomal dominant or mitochondrial mode ofinheritence. A very common cause of late-onsethearing loss is otosclerosis, which is a geneticallyheterogeneous disorder. In otosclerosis, replace-ment of endochondral bone by spongy vascularnew bone, referred to as otosclerotic foci, affectsthe stapes footplate at the oval window and mayalso invade the otic capsule surrounding the coch-lea. The resulting hearing loss is usually conduc-tive, but in some cases may also have asensorineural component. Although the genetics ofotosclerosis is poorly understood, the majority ofcases studied so far indicate an autosomal domi-nant mode of inheritance with reduced penetrance.The first locus linked to otosclerosis has been re-cently mapped to 15q25-q26 (49); identificationand characterization of a gene at this locus willprovide valuable insight into an etiology of thisdisorder.
Typically, in nonsyndromic hearing loss deafnessis the only detectable symptom; however, in somecases malfunction of the vestibular system alsooccurs. The vestibular organ is developmentally,structurally, and physiologically similar to thecochlea (Fig. 2). Perturbations of equilibrium areharder to ascertain in humans due to the compen-satory mechanisms of the visual and propriocep-tive systems which contribute to overall balancemaintenance. Upon examination and specificvestibular testing, some individuals with hearing
loss also show vestibular pathology. In mice, thiscorrelation has been more obvious, because mostmouse strains with hearing defects are identified onthe basis of an abnormal circling behavior andhave been given names such as shaker, twirler,waltzer, and spinner.
Many similarities between the cochlear andvestibular organs are readily apparent. In bothfluid-filled cavities, mechanical stimulation (fromsound waves, rotatory motion, or linear accelera-tion) results in depolarization of sensory hair cellsthrough the shearing force of an overlying acellularmembrane (tectorial or otolithic membranes, orcupula). Neural fibers of ganglion cells of thevestibular and cochlear nerves converge on theirpathway to the central nervous system. It is notsurprising that genes expressed in hair cells, sup-port cells, or other structures common to the twolabyrinths would play similar roles in both organs.
The newly identified gene, COCH, shown to bemutated in DFNA9, a nonsyndromic hearing dis-order with vestibular dysfunction, is expressed insupport structures and neural channels of both thecochlear and vestibular labyrinths in the chicken.These regions correspond remarkably to areaswhich exhibit histopathological deposits in individ-uals with DFNA9 (50). Unconventional myosinshave been shown to be critical to integrity of haircell structure and function. MYO7A plays an im-portant role in cochlear and vestibular function asshown by its involvement in both DFNB2 andUsher syndrome. The mouse homolog, myo7a, de-fective in the shaker-1 deaf mouse (51), is ex-pressed in the stereocilia and cytoplasm of haircells, as well as in the retinal pigmentary epithelialcells (52, 53). Another unconventional myosingene, MYO15, is mutated in nonsyndromic sen-sorineural deafness DFNB3. Mutation of themouse homolog, myo15, in shaker-2 mice results inmarked hair cell histopathology (55) and, there-fore, deafness and circling behavior.
To date, only ten nuclear genes have been shownto cause nonsyndromic deafness, six of which wereidentified in 1998. Undoubtedly, studies in the nearfuture will reveal more genes and loci for hearingdisorders. Cloning deafness genes is only the firststep towards an understanding of the hearing pro-cess. Elucidation of the function of these genes isan ongoing task. The recently isolated gene forDFNA5 (56) provides no immediate functionalclues from its sequence, because it lacks homologyto any known proteins. Other novel genes such asCOCH have some homology to known motifs,such as a signal peptide for secretion and potentialextracellular protein-binding domains (57), provid-ing hypotheses and entry points into studies offunction.
154

Beginning of a molecular era in hearing and deafness
Some functional categories are starting toemerge from characterization of hearing genes. Inaddition to the unconventional myosins, which arenecessary for actin organization in the stereociliaof hair cells, another cytoskeletal gene, DIAPH1,the human homolog of the Drosophila diaphanousgene, shown to be mutated in DFNA1, is thoughtto regulate actin polymerization (58). Anotherstructural protein, alpha-tectorin, encoded by thegene TECTA, is mutated in DFNA8/12 (59). Spe-cific to the inner ear, alpha-tectorin is an extracel-lular protein that is a component of thenoncollagenous matrix of the tectorial membrane(60, 61).
Two members of the POU-domain transcriptionfactor genes, POU3F4 and POU4F3, are involvedin hearing disorders DFN3 (43) and DFNA15 (62),respectively. Genes in this family have a highlyconserved homeodomain and a POU-specific do-main with high-affinity DNA binding (63, 64).Mice which are homozygous null for Pou4f3 showprofound deafness and vestibular dysfunction,reflecting the role of this gene in hair cell differenti-ation (65, 66).
An interesting question arises regarding whysome nonsyndromic deafness genes are exclusivelyor preferentially expressed in the inner ear as ex-pected, while other deafness genes are expressed ina variety of tissues, yet pathology resulting fromthese latter gene defects is manifested in only oneorgan. The alterations of a single gene’s functionmay be compensated for by redundancy of its roleby other genes in tissues other than the inner ear.It is also possible that perturbations of a gene’sfunction are apparent only within the context ofthe tight cellular structure and precise physiologi-cal environment of the cochlea, as well as theunique interactions with other components of thistissue.
A theme that is becoming apparent from thecloning of deafness genes is that mutations in onegene can result in two or three different types ofhearing loss, (i.e., syndromic and nonsyndromic,autosomal dominant and recessive). For example,different defects in MYO7A can result in either thesyndromic USH1B (35), the nonsyndromic autoso-mal recessive DFNB2 (67, 68), or the autosomaldominant DFNA11 (69). Mutations in PDS cancause either Pendred syndrome (28) or the nonsyn-dromic deafness DFNB4 (70).
One gene that has turned out to be a majorcontributor in a large percentage of nonsyndromicdeafness, as well as in sporadic cases, is GJB2. Thisgene encodes connexin 26, a gap junction proteinthought to have an important role in intercellularcommunication by recycling of potassium ions
back to the endolymph following depolarization ofhair cells (71). GJB2 mutations cause the autoso-mal recessive hearing loss, DFNB1, as well as theautosomal dominant disorder DFNA3 (72–75). Insome populations, mutations in GJB2 are esti-mated to be responsible for 50% of severe to pro-found recessive nonsyndromic hearing loss and for20% of childhood genetic deafness (74, 76–78).The carrier rate for GJB2 mutations varies in dif-ferent populations, but is estimated to be as muchas 3–4% in some ethnic groups (73, 74, 78, 79).Another member of the connexin family, GJB3,which maps to the DFNA2 locus (80), was recentlyshown to be mutated in an autosomal dominanthearing impairment (81). Other mutations in GJB3were shown to cause a skin disease, erythrokerato-dermia variabilis (82).
Implications of deafness gene discovery and futuredirections
With the continual discovery of genes mutated inhearing loss, issues regarding genetic testing, diag-nosis, and possible treatments are being raised thatwill need careful evaluation. The elucidation ofspecific gene alterations resulting in hearing lossand balance deficits provides the possibility of pre-cise diagnosis by prenatal or postnatal genetic test-ing. With this opportunity comes a host of ethical,social, and logistical issues for individuals withhearing loss, some of whom are part of a well-es-tablished ‘deaf culture’, as well as for medicalprofessionals who now have these genetic tools athand.
One study of individuals attending a meeting forthe deaf indicates that many of the hearing-im-paired feel their culture may be threatened bygenetic studies (83). Another recent and more com-prehensive study shows a more positive attitude ofone population of deaf and hearing adults towardsgenetic testing (84). Some deaf participants in bothstudies indicate that they would prefer deaf chil-dren. Further consideration of opinions of largergroups of individuals with different types of hear-ing loss is needed. As with any other genetic test,appropriate interpretation and counseling are im-portant, and of course personal decisions ulti-mately rest with the individuals and families forwhom these services are provided. Genetic testingmay offer valuable information regarding decisionsfor educational approaches; choices in modes oflanguage acquisition, including sign or spoken lan-guage; career and lifestyle decisions; and potentialintervention and treatments such as amplificationdevices or cochlear implants.
155
Robertson and Morton
Aside from the immediate implications of ge-netic studies, scientific endeavors in the moleculargenetics of the sensory perception of the inner earare crucial for solving the mysteries of complexbiological processes. Genes that are being iden-tified in the context of specific types of deafness inisolated kindreds are shown to play critical roles inproper cochlear functioning. Therefore, these samegenes and mechanisms are important in a spectrumof hearing impairment, including progressive lossdue to aging or to environmental factors such assound trauma, infections, or pharmacologicalagents. One fascinating area of study has been thatof the regeneration of damaged cochlear andvestibular hair cells. Scientists in this field haverecognized that, unlike mammals, in lower verte-brates such as sharks and birds, hair cells eithercontinue to form throughout life or regenerateafter damage or death by proliferation and differ-entiation of the progenitor supporting cells; effortsare concentrated on making this phenomenon pos-sible in mammals (85–91). Elucidation of the exacttriggers and cues for hair cell regeneration may oneday provide the means to prevent or reverse hear-ing loss and balance deficits in humans.
Detailed molecular studies will undoubtedly leadto a more fundamental and thorough understand-ing of the development, structure, and function ofthe auditory and vestibular systems that serve ascritical gateways to an enriched perception of acomplex set of stimuli in our outside world.
References
1. Hudspeth AJ. How the ear’s works work. Nature 1989:341: 397–404.
2. Teas DC. Auditory physiology: present trends. Ann RevPsychol 1989: 40: 405–429.
3. Nance WE, Sweeney A. Genetic factors in deafness ofearly life. Otol Clin N Amer 1975: 8: 19–48.
4. Bieber FR, Nance WE. Hereditary hearing loss. In: Jack-son LG, Schimke RN, eds. Clinical Genetics – A Source-book for Physicians. New York: John Wiley and Sons,1979: 443–461.
5. Bieber FR: Genetic Studies of Questionnaire Data from aResidential School for the Deaf. Medical College of Vir-ginia, 1981.
6. Robertson NG et al. Isolation of novel and known genesfrom a human fetal cochlear cDNA library using subtrac-tive hybridization and differential screening. Genomics1994: 23: 42–50.
7. Wilcox ER, Fex J. Construction of a cDNA library frommicrodissected guinea pig organ of Corti. Hear Res 1992:62 (1): 124–126.
8. Heller S et al. Molecular markers for cell types of theinner ear and candidate genes for hearing disorders. ProcNatl Acad Sci USA 1998: 95 (19): 11400–11405.
9. Skvorak AB et al.: Human cochlear expressed sequencetags provide insight into cochlear gene expression andidentify candidate genes for deafness, Hum Mol Genet1998 (in press).
10. http: //www.partners.org/pathology11. http: //dnalab-www.uia.ac.be/dnalab/hhh12. Morton NE. Genetic epidemiology of hearing impair-
ment. Ann NY Acad Sci 1991: 630: 16–31.13. Reardon W. Genetic deafness. J Med Genet 1992: 29 (8):
521–526.14. Marazita ML et al. Genetic epidemiological studies of
early-onset deafness in the U.S. school-age population.Am J Med Genet 1993: 46 (5): 486–491.
15. Gorlin RJ, Toriello HV, Cohen MM. Hereditary HearingLoss and Its Syndromes. New York: Oxford UniversityPress, 1995.
16. Tassabehji M et al. Waardenburg’s syndrome patientshave mutations in the human homologue of the Pax-3paired box gene. Nature 1992: 355 (6361): 635–636.
17. Hoth CF et al. Mutations in the paired domain of thehuman PAX3 gene cause Klein–Waardenburg syndrome(WS-III) as well as Waardenburg syndrome type I (WS-I). Am J Hum Genet 1993: 52 (3): 455–462.
18. Tassabehji M, Newton VE, Read AP. Waardenburg syn-drome type 2 caused by mutations in the human microph-thalmia (MITF) gene. Nature Genet 1994: 8 (3): 251–255.
19. Pingault V et al. SOX10 mutations in patients with Waar-denburg–Hirschsprung disease. Nature Genet 1998: 18(2): 171–173.
20. Edery P et al. Mutation of the endothelin-3 gene in theWaardenburg–Hirschsprung disease (Shah–Waarden-burg syndrome). Nature Genet 1996: 12 (4): 442–444.
21. Hofstra RM et al. A homozygous mutation in the en-dothelin-3 gene associated with a combined Waardenburgtype 2 and Hirschsprung phenotype (Shah–Waardenburgsyndrome). Nature Genet 1996: 12 (4): 445–447.
22. Puffenberger EG et al. A missense mutation of the en-dothelin-B receptor gene in multigenic Hirschsprung’sdisease. Cell 1994: 79 (7): 1257–1266.
23. Attie T et al. Mutation of the endothelin-receptor B genein Waardenburg–Hirschsprung disease. Hum Mol Genet1995: 4 (12): 2407–2409.
24. Abdelhak S et al. A human homologue of the Drosophilaeyes absent gene underlies branchio-oto-renal (BOR) syn-drome and identifies a novel gene family. Nature Genet1997: 15 (2): 157–164.
25. Neyroud N et al. A novel mutation in the potassiumchannel gene KVLQT1 causes the Jervell and Lange–Nielsen cardioauditory syndrome. Nature Genet 1997: 15(2): 186–189.
26. Schulze-Bahr E et al. KCNE1 mutations cause Jervelland Lange–Nielsen syndrome. Nature Genet 1997: 17(3): 267–268.
27. Tyson J et al. IsK and KvLQT1: mutation in either of thetwo subunits of the slow component of the delayed rec-tifier potassium channel can cause Jervell and Lange–Nielsen syndrome. Hum Mol Genet 1997: 6 (12):2179–2185.
28. Everett LA et al. Pendred syndrome is caused by muta-tions in a putative sulphate transporter gene (PDS). Na-ture Genet 1997: 17: 411–422.
29. Scott DA et al.: The Pendred syndrome gene productfunctions as an iodine, chloride transporter. The Molecu-lar Biology of Hearing and Deafness, Bethesda, MD,1998: 63.
30. Barker DF et al. Identification of mutations in theCOL4A5 collagen gene in Alport syndrome. Science1990: 248 (4960): 1224–1227.
31. Mochizuki T et al. Identification of mutations in thealpha 3 (IV) and alpha 4 (IV) collagen genes in autosomalrecessive Alport syndrome. Nature Genet 1994: 8 (1):77–81.
156

Beginning of a molecular era in hearing and deafness
32. Williams CJ et al. A-2�G transition at the 3% acceptorsplice site of IVS17 characterizes the COL2A1 gene muta-tion in the original Stickler syndrome kindred. Am J MedGenet 1996: 63 (3): 461–467.
33. Richards AJ et al. A family with Stickler syndrome type2 has a mutation in the COL11A1 gene resulting in thesubstitution of glycine 97 by valine in alpha 1 (XI) colla-gen. Hum Mol Genet 1996: 5 (9): 1339–1343.
34. Vikkula M et al. Autosomal dominant and recessiveosteochondrodysplasias associated with the COL11A2.Cell 1995: 80 (3): 431–437.
35. Weil D et al. Defective myosin VIIA gene responsible forUsher syndrome type 1B. Nature 1995: 374 (6517): 60–61.
36. Eudy JD et al. Mutation of a gene encoding a proteinwith extracellular matrix motifs in Usher syndrome typeIIA. Science 1998: 280 (5370): 1753–1757.
37. Fischel-Ghodsian N. Mitochondrial genetics and hearingloss: the missing link between genotype and phenotype.Proc Soc Exp Biol Med 1998: 218 (1): 1–6.
38. van den Ouweland JMW et al. Mutation in mitochondrialtRNALeU(UuR) gene in a large pedigree with maternallytransmitted type II diabetes mellitus and deafness. NatureGenet 1992: 1: 368–371.
39. http: //www.ncbi.nlm.nih.gov/omim40. Cohen MM, Gorlin RJ. Epidemiology, etiology, and ge-
netic patterns. In: Gorlin RJ, Toriello HV, Cohen MM,eds. Hereditary Hearing Loss and Its Syndromes. NewYork: Oxford University Press, 1995: 9–21.
41. Tranebjaerg L et al. A new X-linked recessive deafnesssyndrome with blindness, dystonia, fractures, and mentaldeficiency is linked to Xq22. J Med Genet 1995: 32 (4):257–263.
42. Jin H et al. A novel X-linked gene, DDP, shows muta-tions in families with deafness (DFN-1), dystonia, mentaldeficiency and blindness. Nature Genet 1996: 14 (2): 177–180.
43. de Kok YJ et al. Association between X-linked mixeddeafness and mutations in the POU domain genePOU3F4. Science 1995: 267 (5198): 685–688.
44. Prezant TR et al. Mitochondrial ribosomal RNA muta-tion associated with both antibiotic-induced and non-syn-dromic deafness. Nature Genet 1993: 4 (3): 289–294.
45. Fischel-Ghodsian N et al. Mitochondrial gene mutation isa significant predisposing factor in aminoglycoside oto-toxicity. Am J Otolaryngol 1997: 18 (3): 173–178.
46. Estivill X et al. Familial progressive sensorineural deaf-ness is mainly due to the mtDNA A1555G mutation andis enhanced by treatment of aminoglycosides. Am J HumGenet 1998: 62 (1): 27–35.
47. Fischel-Ghodsian N et al. Temporal bone analysis ofpatients with presbycusis reveals high frequency of mito-chondrial mutations. Hear Res 1997: 110 (1–2): 147–154.
48. Corral-Debrinski M et al. Mitochondrial DNA deletionsin human brain: regional variability and increase withadvanced age. Nature Genet 1992: 2 (4): 324–329.
49. Tomek MS et al. Localization of a gene for otosclerosisto chromosome 15q25-q26. Hum Mol Genet 1998: 7 (2):285–290.
50. Robertson NG et al. Mutations in a novel cochlear genecause DFNA9, a human nonsyndromic deafness withvestibular dysfunction. Nature Genet 1998: 20 (3): 299–303.
51. Gibson F et al. A type VII myosin encoded by the mousedeafness gene shaker-1. Nature 1995: 374 (6517): 62–64.
52. Hasson T et al. Expression in cochlea and retina ofmyosin VIIa, the gene product defective in Usher syn-
drome type 1B. Proc Natl Acad Sci USA 1995: 92 (21):9815–9819.
53. Hasson T et al. Unconventional myosins in inner-earsensory epithelia. J Cell Biol 1997: 137 (6): 1287–1307.
54. Wang A et al. Association of unconventional myosinMY015 mutations with human nonsyndromic deafnessDFNB3. Science 1998: 280 (5368): 1447–1451.
55. Probst FJ et al. Correction of deafness in shaker-2 miceby an unconventional myosin in a BAC transgene. Sci-ence 1998: 280 (5368): 1441–1447.
56. Van Laer L et al. Nonsyndromic hearing impairment isassociated with a mutation in DFNA5. Nature Genet1998: 20 (2): 194–197.
57. Robertson NG et al. Mapping and characterization of anovel cochlear gene in human and in mouse: a positionalcandidate gene for a deafness disorder, DFNA9. Genom-ics 1997: 46: 345–354.
58. Lynch ED et al. Nonsyndromic deafness DFNA1 associ-ated with mutation of a human homolog of theDrosophila gene diaphanous. Science 1997: 278: 1315–1318.
59. Verhoeven K et al. Mutations in the human a-tectoringene cause autosomal dominant nonsyndromic hearingimpairment. Nature Genet 1998: 19: 60–62.
60. Richardson GP et al. Polypeptide composition of themammalian tectorial membrane. Hear Res 1987: 25 (1):45–60.
61. Legan PK et al. The mouse tectorins. Modular matrixproteins of the inner ear homologous to components ofthe sperm–egg adhesion system. J Biol Chem 1997: 272(13): 8791–8801.
62. Vahava O et al. Mutation in transcription factorPOU4F3 associated with inherited progressive hearingloss in humans. Science 1998: 279: 1950–1954.
63. Ingraham HA et al. The POU-specific domain of Pit-1 isessential for sequence-specific, high affinity DNA bindingand DNA-dependent Pit-1–Pit-1 interactions. Cell 1990:61 (6): 1021–1033.
64. Wegner M, Drolet DW, Rosenfeld MG. POU-domainproteins: structure and function of developmental regula-tors. Curr Opin Cell Biol 1993: 5 (3): 488–498.
65. Erkman L et al. Role of transcription factors Brn-3.1 andBrn-3.2 in auditory and visual system development. Na-ture 1996: 381 (6583): 603–606.
66. Xiang M et al. Essential role of POU-domain factorBrn-3c in auditory and vestibular hair cell development.Proc Natl Acad Sci USA 1997: 94 (17): 9445–9450.
67. Liu X-Z et al. Mutations in the myosin VIIA gene causenonsynaronuc recessive deafness. Nature Genet 1997: 16:188–190.
68. Weil D et al. The autosomal recessive isolated deainess,DFNB2, and the Usher 1B syndrome are allelic defects ofthe myosin VIIA gene. Nature Genet 1997: 16: 191–193.
69. Liu X-Z et al. Autosomal dominant nonsyndromic deaf-ness caused by a mutation in the myosin VIIA gene.Nature Genet 1997: 17: 268–269.
70. Li XC et al. A mutation in PDS causes non-syndromicrecessive deafness. Nature Genet 1998: 18 (3): 215–217.
71. Kikuchi T et al. Gap junctions in the rat cochlea: im-munohistochemical and ultrastructural analysis. AnatEmbryol (Berl) 1995: 191 (2): 101–118.
72. Kelsell DP et al. Connexin 26 mutations in hereditarynon-syndromic sensorineural deafness. Nature 1997: 387:80–83.
73. Scott DA et al. Connexin mutations and hearing loss.Nature 1998: 391 (6662): 32.
157

Robertson and Morton
74. Kelley PM et al. Novel mutations in the connexin 26 gene(GJB2) that cause autosomal recessive (DFNB1) hearingloss. Am J Hum Genet 1998: 62: 792–799.
75. Denoyelle F et al. Connexin 26 gene linked to a dominantdeafness. Nature 1998: 393 (6683): 319–320.
76. Denoyelle F et al. Prelingual deafness: high prevalence ofa 30delG mutation in the connexin 26 gene. Hum MolGenet 1997: 6 (12): 2173–2177.
77. Zelante L et al. Connexin 26 mutations associated withthe most common form of non-syndromic neurosensoryautosomal recessive deafness (DFNB1) in Mediter-raneans. Hum Mol Genet 1997: 6 (9): 1605–1609.
78. Estivill X et al. Connexin-26 mutations in sporadic andinherited sensorineural deafness. Lancet 1998: 351 (9100):394–398.
79. Morell RJ et al. Mutations in the connexin 26 gene(GJB2) among Ashkenazi Jews with nonsyndromic reces-sive deafness. N Engl J Med 1998: 339 (21): 1500–1505.
80. Coucke P et al. Linkage of autosomal dominant hearingloss to the short arm of chromosome 1 in two families. NEngl J Med 1994: 331 (7): 425–431.
81. Xia JH et al. Mutations in the gene encoding gap junctionprotein beta-3 associated with autosomal dominant hear-ing impairment. Nature Genet 1998: 20 (4): 370–373.
82. Richard G et al. Mutations in the human connexin geneGJB3 cause erythrokeratodermia variabilis. Nature Genet1998: 20 (4): 366–369.
83. Middleton A, Hewison J, Mueller RF. Attitudes of deafadults toward genetic testing for hereditary deafness. AmJ Hum Genet 1998: 63 (4): 1175–1180.
84. Middleton A, Hewison J, Mueller RF. Attitudes of deaf,hard of hearing and hearing adults toward genetic testingfor inherited deafness. Am J Hum Genet 1998: 63 (4Supplement): A203.
85. Cotanche DA. Regeneration of hair cell stereociliary bun-dles in the chick cochlea following severe acoustictrauma. Hear Res 1987: 30 (2-3): 181–195.
86. Cruz RM, Lambert PR, Rubel EW. Light microscopicevidence of hair cell regeneration after gentamicin toxicityin chick cochlea. Arch Otolaryngol Head Neck Surg1987: 113 (10): 1058–1062.
87. Corwin JT, Cotanche DA. Regeneration of sensory haircells after acoustic trauma. Science 1988: 240 (4860):1772–1774.
88. Warchol ME et al. Regenerative proliferation in inner earsensory epithelia from adult guinea pigs and humans.Science 1993: 259 (5101): 1619–1622.
89. Corwin JT, Oberholtzer JC. Fish n’ chicks: model recipesfor hair-cell regeneration? Neuron 1997: 19 (5): 951–954.
90. Cotanche DA. Hair cell regeneration in the avian cochlea.Ann Otol Rhinol Laryngol Suppl 1997: 168: 9–15.
91. Kil J, Warchol ME, Corwin JT. Cell death, cell prolifera-tion, and estimates of hair cell life spans in the vestibularorgans of chicks. Hear Res 1997: 114 (1-2): 117–126.
92. Zhou J et al. Deletion of the paired alpha 5(IV) and alpha6(IV) collagen genes in inherited smooth muscle tumors.Science 1993: 261 (5125): 1167–1169.
93. Shoffner JM et al. Myoclonic epilepsy and ragged-redfiber disease (MERRF) is associated with a mitochondrialDNA tRNA(Lys) mutation. Cell 1990: 61 (6): 931–937.
94. Zeviani M et al. A MERRF/MELAS overlap syndromeassociated with a new point mutation in the mitochon-drial DNA tRNA(Lys) gene. Eur J Hum Genet 1993: 1(1): 80–87.
95. Berger W et al. Mutations in the candidate gene forNorrie disease. Hum Mol Genet 1992: 1 (7): 461–465.
96. Berger W et al. Isolation of a candidate gene for Norriedisease by positional cloning. Nature Genet 1992: 2 (1):84.
97. Chen ZY et al. Isolation and characterization of a candi-date gene for Norrie disease. Nature Genet 1992: 1 (3):204–208.
98. Ahmad NN et al. Stop codon in the procollagen II gene(COL2A1) in a family with the Stickler syndrome (arthro-ophthalmopathy). Proc Natl Acad Sci USA 1991: 88:6624–6627.
99. Anonymous: Positional cloning of a gene involved in thepathogenesis of Treacher Collins syndrome. The TreacherCollins Syndrome Collaborative Group. Nature Genet1996: 12 (2): 130–136.
100. Dixon MJ. Treacher Collins syndrome. Hum Mol Genet1996: 5 (Spec No): 1391–1396.
101. Kaplan J et al. A gene for Usher syndrome type I(USH1A) maps to chromosome 14q. Genomics 1992: 14(4): 979–987.
102. Smith RJ et al. Localization of two genes for Ushersyndrome type I to chromosome 11. Genomics 1992: 14(4): 995–1002.
103. Wayne S et al. Localization of the Usher syndrome typeID gene (UshlD) to chromosome 10. Hum Mol Genet1996: 5 (10): 1689–1692.
104. Chaib H et al. A newly identified locus for Usher syn-drome type I, USH1E, maps to chromosome 21q21. HumMol Genet 1997: 6 (1): 27–31.
105. Wayne S et al. Localization of the Usher syndrome typeIF (UshlF) to chromosome 10. Am J Hum Genet 1997:61 (4 Supplement): A300.
106. Kimberling WJ et al. Localization of Usher syndrometype II to chromosome lq. Genomics 1990: 7 (2): 245–249.
107. Pieke Dahl S et al.: Localization of USH2B to 5ql4.3-q21.3. The Molecular Biology of Hearing and Deafness,Bethesda, MD, 1998: 88.
108. Sankila EM et al. Assignment of an Usher syndrome typeIII (USH3) gene to chromosome 3q. Hum Mol Genet1995: 4 (1): 93–98.
109. Leon PE et al. The gene for an inherited form of deafnessmaps to chromosome 5q31. Proc Natl Acad Sci USA1992: 89 (11): 5181–5184.
110. Chaib H et al. A gene responsible for a dominant form ofneurosensory non-syndromic deafness maps to theNSRD1 recessive deafness gene interval. Hum Mol Genet1994: 3 (12): 2219–2222.
111. Chen AH et al. Linkage of a gene for dominant non-syn-dromic deafness to chromosome 19. Hum Mol Genet1995: 4 (6): 1073–1076.
112. Van Camp G et al. Localization of a gene for non-syn-dromic hearing loss (DFNA5) to chromosome 7p15.Hum Mol Genet 1995: 4 (11): 2159–2163.
113. Lesperance MM et al. A gene for autosomal dominantnonsyndromic hereditary hearing impairment maps to4p16.3. Hum Mol Genet 1995: 4 (10): 1967–1972.
114. Fagerheim T et al. Identification of a new locus forautosomal dominant non-syndromic hearing impairment(DFNA7) in a large Norwegian family. Hum Mol Genet1996: 5 (8): 1187–1191.
115. Verhoeven K et al. A gene for autosomal dominantnonsyndromic hearing loss (DFNA12) maps to chromo-some 11q22-113. Am J Hum Genet 1997: 60 (5): 1168–1173.
116. Manolis EN et al. A gene for non-syndromic autosomaldominant progressive postlingual sensorineural hearingloss maps to chromosome 14q12-13. Hum Mol Genet1996: 5: 1047–1050.
158

Beginning of a molecular era in hearing and deafness
117. O’Neill ME et al. A gene for autosomal dominant late-onset progressive non-syndromic hearing loss, DFNA10,maps to chromosome 6. Hum Mol Genet 1996: 5 (6):853–856.
118. Tamagawa Y et al. A gene for a dominant form ofnon-syndromic sensorineural deafness (DFNA11) mapswithin the region containing the DFNB2 recessive deaf-ness gene. Hum Mol Genet 1996: 5 (6): 849–852.
119. Brown MR et al. A novel locus for autosomal dominantnonsyndromic hearing loss, DFNA13, maps to chromo-some 6p. Am J Hum Genet 1997: 61 (4): 924–927.
120. Van Camp G et al. Linkage of a second family to theDFNA6 deafness locus on chromosome 4p16.3, and iden-tification of a deaf patient with a chromosomal inversionthrough this region. Am J Hum Genet 1997: 6 (4 Supple-ment): A298.
121. Fukushima K et al.: Autosomal dominant non-syndromicdeafness locus (DFNA16) maps to chromosome 2q24.The Molecular Biology of Hearing and Deafness,Bethesda, MD, 1998: 103.
122. Lalwani AK, Wilcox ER, Castelein CM: DFNA17, a newlocus for nonsyndromic hearing loss maps to chromo-some 22. The Molecular Biology of Hearing and Deaf-ness, Bethesda, MD, 1998: 104.
123. Boensch D et al. Mapping of a further type of autosomaldominant, nonsyndromic hearing impairment (DFNA18)to chromosome 3q22. Am J Hum Genet 1998: 63 (4Supplement): A282.
124. Green G et al.: Identification of a new locus –DFNA19 – for dominant hearing impairment. The
Molecular Biology of Hearing and Deafness, Bethesda,MD, 1998: 107.
125. Guilford P et al. A non-syndrome form of neurosensory,recessive deafness maps to the pericentromeric region ofchromosome 13q. Nature Genet 1994: 6 (1): 24–28.
126. Guilford P et al. A human gene responsible for neurosen-sory, nonsyndromic recessive deafness is a candidate ho-mologue of the mouse sh-1 gene. Hum Mol Genet 1994:3 (6): 989–993.
127. Friedman TB et al. A gene for congenilal, recessive deaf-ness DFNB3 maps to the pericentromeric region of chro-mosome 17. Nature Genet 1995: 9 (1): 86–91.
128. Baldwin CT et al. Linkage of congenital, recessive deaf-ness (DFNB4) to chromosome 7q31 and evidence forgenetic heterogeneity in the Middle Eastern Druze popu-lation. Hum Mol Genet 1995: 4 (9): 1637–1642.
129. Fukushima K et al. Consanguineous nuclear families usedto identify a new locus for recessive non-syndromic hear-ing loss on 14q. Hum Mol Genet 1995: 4 (9): 1643–1648.
130. Fukushima K et al. An autosomal recessive nonsyn-dromic form of sensorineural hearing loss maps to 3p-DFNB6. Genome Res 1995: 5 (3): 305–308.
131. Jain PK et al. A human recessive neurosensory nonsyn-dromic hearing impairment locus is potential homologueof murine deafness (dn) locus. Hum Mol Genet 1995: 4(12): 2391–2394.
132. Veske A et al. Autosomal recessive non-syndromic deaf-ness locus (DFNB8) maps on chromosome 21q22 in alarge consanguineous kindred from Pakistan. Hum MolGenet 1996: 5 (1): 165–168.
133. Chaib H et al. A gene responsible for a sensorineuralnonsyndromic recessive deafness maps to chromosome2p22-23. Hum Mol Genet 1996: 5 (1): 155–158.
134. Bonne-Tamir B et al. Linkage of congenital recessivedeafness (gene DFNB10) to chromosome 21q22.3. Am JHum Genet 1996: 58 (6): 1254–1259.
135. Scott DA et al. An autosomal recessive nonsyndromic-hearing-loss locus identified by DNA pooling using twoinbred Bedouin kindreds. Am J Hum Genet 1996: 59 (2):385–391.
136. Chaib H et al. Mapping of DFNB12, a gene for anon-syndromal autosomal recessive deafness, to chromo-some 10q21-22. Hum Mol Genet 1996: 5 (7): 1061–1064.
137. Mustapha M et al. A sensorineural progressive autosomalrecessive form of isolated deafness, DFNB13, maps tochromosome 7q34-q36. Eur J Hum Genet 1998: 6 (3):245–250.
138. Campbell DA et al. A new locus for non-syndromal,autosomal recessive, sensorineural hearing loss(DFNB16) maps to human chromosome 15q21-q22. JMed Genet 1997: 34 (12): 1015–1017.
139. Greinwald JH Jr et al. Localization of a novel gene fornonsyndromic hearing loss (DFNB17) to chromosomeregion 7q31. Am J Med Genet 1998: 78 (2): 107–113.
140. Jain PK et al. A gene for recessive nonsyndromic sen-sorineural deafness (DFNB18) maps to the chromosomalregion 11p14-p15.1 containing the Usher syndrome type1C gene. Genomics 1998: 50 (2): 290–292.
141. Green GE et al.: Identification of a novel locus(DFNB19) for nonsyndromic autosomal recessive hearingloss in a consanguineous family. The Molecular Biologyof Hearing and Deafness, Bethesda, MD, 1998: 108.
142. Tyson J et al. Mapping of DFN2 to Xq22. Hum MolGenet 1996: 5 (12): 2055–2060.
143. Lalwani AK et al. A new nonsyndromic X-linked sen-sorineural hearing impairment linked to Xp21.2. Am JHum Genet 1994: 55 (4): 685–694.
144. del Castillo I et al. A novel locus for non-syndromicsensorineural deafness (DFN6) maps to chromosomeXp22. Hum Mol Genet 1996: 5 (9): 1383–1387.
145. Reid FM, Vernham GA, Jacobs HT. A novel mitochon-drial point mutation in a maternal pedigree with sen-sorineural deafness. Hum Mutat 1994: 3 (3): 243–247.
159