Attitudes of Youth Towards Alcohol in Muslim Majority Countries
251
1 Attitudes of Youth Towards Alcohol in Muslim Majority Countries: Insights from Iraq Mustafa Al Ansari A thesis submitted in fulfilment of the requirements of the degree of Doctor of Philosophy The University of Sydney School of Public Health Faculty of Medicine and Health University of Sydney 2021
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Attitudes of Youth Towards Alcohol in Muslim Majority Countries

1
Attitudes of Youth Towards Alcohol in
Muslim Majority Countries: Insights from Iraq
Mustafa Al Ansari
A thesis submitted in fulfilment of the requirements of the degree of
Doctor of Philosophy
The University of Sydney School of Public Health
Faculty of Medicine and Health
University of Sydney
2021

2
Table of Contents
Authorship attribution statement ..................................................................................................................... 6
Statement of originality ..................................................................................................................................... 8
Dedication ......................................................................................................................................................... 9
Acknowledgements ......................................................................................................................................... 10
Transliteration ................................................................................................................................................. 12
Abbreviations .................................................................................................................................................. 13
Glossary ........................................................................................................................................................... 14
List of figures ................................................................................................................................................... 15
List of tables ..................................................................................................................................................... 16
Outcomes arising from this thesis ................................................................................................................... 17
Published manuscripts ................................................................................................................................ 17
Submitted manuscripts ............................................................................................................................... 17
Conference presentations/papers............................................................................................................... 17
Awards ......................................................................................................................................................... 18
Abstract ........................................................................................................................................................... 19
Chapter 1: Introduction ................................................................................................................................... 20
Alcohol in the global context ....................................................................................................................... 20
Alcohol use in Muslim Majority Countries (MMCs) .................................................................................... 21
Alcohol in Iraq .............................................................................................................................................. 23
Iraq at a time of change ............................................................................................................................... 24
Gaps in the research literature .................................................................................................................... 26
Research questions ...................................................................................................................................... 27
Potential outcomes and significance ........................................................................................................... 27
Overview of the thesis ................................................................................................................................. 28
References ................................................................................................................................................... 31
Chapter 2 – Methodology ................................................................................................................................ 34
Socio-historical review: sources of evidence............................................................................................... 34
Scoping review ............................................................................................................................................. 35
Mixed-method approach ............................................................................................................................. 36
Sample selection and setting ................................................................................................................... 37
Possible obstacles, risks and limitations to alcohol research in Iraq....................................................... 38
Mitigations and solutions to risks and obstacles ..................................................................................... 39
Field work and data collection ................................................................................................................ 40
Quantitative component ............................................................................................................................. 40
Survey tools and items ............................................................................................................................ 42
Qualitative component ................................................................................................................................ 44

3
The author as researcher (reflexive statement) .......................................................................................... 47
Ethics approval ............................................................................................................................................ 49
References ................................................................................................................................................... 50
Chapter 3: Alcohol: From Mesopotamia to Modern Iraq ................................................................................ 51
Abstract ....................................................................................................................................................... 52
Introduction ................................................................................................................................................. 52
Methods ...................................................................................................................................................... 53
Findings ........................................................................................................................................................ 54
Alcohol and Iraq in pre-Islamic history .................................................................................................... 55
Alcohol and Islam .................................................................................................................................... 57
Brief history of alcohol during the Islamic era (seventh-20th centuries) in Iraq ...................................... 58
Alcohol and modern Iraq ......................................................................................................................... 59
Data on the prevalence of alcohol use in Iraq ......................................................................................... 63
The next generation: alcohol and Iraqi youth ......................................................................................... 64
Discussion .................................................................................................................................................... 65
Conclusion ................................................................................................................................................... 68
Acknowledgement ....................................................................................................................................... 68
References ................................................................................................................................................... 68
Chapter 4: Alcohol among young people in Iraq: A systematic scoping review ............................................. 75
Abstract ....................................................................................................................................................... 76
Summary ...................................................................................................................................................... 77
Introduction ................................................................................................................................................. 78
Methods ...................................................................................................................................................... 79
Identifying the relevant studies ............................................................................................................... 80
Study selection ........................................................................................................................................ 80
Charting the data ..................................................................................................................................... 81
Patient and public involvement statement ............................................................................................. 81
Results ......................................................................................................................................................... 81
Study descriptions ................................................................................................................................... 83
Prevalence and patterns of alcohol use .................................................................................................. 85
Patterns/locations ................................................................................................................................... 88
Attitudes, behaviours, and motives ........................................................................................................ 88
Discussion .................................................................................................................................................... 93
Limitations ............................................................................................................................................... 95
Conclusion ............................................................................................................................................... 96
References: .................................................................................................................................................. 97
Chapter 5: Alcohol and university students in Iraq: attitudes, availability, and use ..................................... 100

4
Abstract ..................................................................................................................................................... 101
Introduction ............................................................................................................................................... 102
Alcohol consumption among university students in Iraq ...................................................................... 104
Methods .................................................................................................................................................... 105
Ethics approval ...................................................................................................................................... 106
Quantitative survey ............................................................................................................................... 106
Sampling and Recruitment .................................................................................................................... 107
Data Analysis ......................................................................................................................................... 108
Results ....................................................................................................................................................... 109
Sample ................................................................................................................................................... 109
Demographics ........................................................................................................................................ 110
Alcohol consumption ............................................................................................................................. 112
Consumption of other substances ........................................................................................................ 113
Attitudes towards alcohol, alcohol policy and alcohol/drug users ....................................................... 114
Media and war exposure and post-traumatic stress disorder .............................................................. 116
Reliability of the included instruments ................................................................................................. 117
Discussion .................................................................................................................................................. 117
Limitations ............................................................................................................................................. 123
Conclusion ............................................................................................................................................. 125
References ................................................................................................................................................. 126
Chapter 6: Alcohol use in Iraq: Perceptions of students at three Iraqi universities ..................................... 129
Abstract ..................................................................................................................................................... 130
Summary .................................................................................................................................................... 131
Introduction ............................................................................................................................................... 132
Methods .................................................................................................................................................... 134
Settings .................................................................................................................................................. 135
Recruitment ........................................................................................................................................... 135
Qualitative interviews ........................................................................................................................... 136
Translation and transcription ................................................................................................................ 137
Analysis .................................................................................................................................................. 137
Patient and public involvement statement ........................................................................................... 138
Ethics ..................................................................................................................................................... 138
Results ....................................................................................................................................................... 138
Perceived prevalence of drinking .......................................................................................................... 139
Why people drink: “It’s natural for there to be various views” ............................................................ 140
Individual motives ................................................................................................................................. 141
Interpersonal motives ........................................................................................................................... 142

5
Community-related motives .................................................................................................................. 144
Society-related motives and influences ................................................................................................ 145
Globalisation and greater/external society related motives: ............................................................... 147
Perceptions of those who drink – “Not even Christian girls like drinkers” ........................................... 149
Consequences of drinking ..................................................................................................................... 151
View of policies towards alcohol ........................................................................................................... 152
Discussion .................................................................................................................................................. 152
Preventing alcohol misuse in Iraq ......................................................................................................... 154
Limitations ............................................................................................................................................. 158
Reflexivity .............................................................................................................................................. 158
Conclusion ............................................................................................................................................. 159
References ................................................................................................................................................. 160
Chapter 7 - Discussion ................................................................................................................................... 163
Diversity and alcohol in Iraq ...................................................................................................................... 164
Alcohol availability, affordability, and taxation ......................................................................................... 167
Conflict, social unrest, terrorism, and trauma .......................................................................................... 169
Globalisation, media, and social media ..................................................................................................... 170
Alcohol – males and females ..................................................................................................................... 171
Overestimation or underreporting of student drinking? .......................................................................... 172
Risky and harmful behaviour among drinkers ........................................................................................... 173
Importance of tailoring measures and priorities to the Iraqi context ....................................................... 174
Prevention approaches.............................................................................................................................. 175
Screening in a MMC context ..................................................................................................................... 177
Treatment and harm-reduction ................................................................................................................ 178
Sin, stigma, and punishment ..................................................................................................................... 179
Limitations ................................................................................................................................................. 180
Future directions ....................................................................................................................................... 181
Conclusion ................................................................................................................................................. 183
References ................................................................................................................................................. 184
Appendices .................................................................................................................................................... 193
Appendix 1: Ethics approval ...................................................................................................................... 193
Appendix 2: PRISMA statement ................................................................................................................ 194
Appendix 3: Search strategies ................................................................................................................... 196
Appendix 4: English survey ........................................................................................................................ 200
Appendix 5: Arabic survey ......................................................................................................................... 225
Appendix 6: Interview guide (English/Arabic) ........................................................................................... 251

6
Authorship attribution statement
I conducted the research that is contained in this research under the supervision of Professor Kate
Conigrave and Professor Angela Dawson. I conceived and designed the study, with support of my
supervisors and local Iraqi collaborator. I also recruited and liaised with in-country collaborators, and
recruitment sites. With the support of my supervisors and with advice as needed from the in-country
collaborators, I was responsible for:
• The literature reviews
• The design of the survey tool and interview framework
• Field work and ethics application
• Data collection and interviews
• Translation and transcription of interviews
• Quantitative and qualitative data analysis
• Drafting and submitting papers for publication
The results chapters of this thesis are either published or submitted for publication.
Chapter 3 contains an article published as:
Al Ansari M, Dawson A and Conigrave K (2019) Alcohol: from Mesopotamia to Modern Iraq,
Journal of Ethnicity in Substance Abuse, DOI: 10.1080/15332640.2019.1657541.
I designed the study, searched for and analysed the data, and wrote the drafts of the MS with the
support of my supervisors.
Chapter 4 contains a manuscript submitted for publication as:
Al Ansari M, Dawson A and Conigrave K (2020) Alcohol among Young People in Iraq: A
Systematic Scoping Review (submitted for publication)
I designed the study, searched for and analysed the data, and wrote the drafts of the MS with the
support of my supervisors.
Chapter 5 contains a manuscript submitted for publication as:
Al Ansari M, Dawson A, AbdulZahra M, Room R, and Conigrave K (2020) Alcohol and University
Students in Iraq: Attitudes, Availability and Use (Submitted for publication)
I designed the study, collected and analysed the data, and wrote the drafts of the MS with the support
of my supervisors. Professor AbdulZahra assisted with carrying out the study as the in-country
collaborator. Professor Robin Room assisted with devising the appropriate survey tool for the setting.
Chapter 6 contains a manuscript submitted for publication as:

7
Al Ansari M, Dawson A, AbdulZahra M, and Conigrave K (2020) Alcohol Use in Iraq: Perceptions
of Students at Three Iraqi Universities (Submitted for publication)
I designed the study, collected and analysed the data, and wrote the drafts of the MS with the
support of my supervisors and as the in-country collaborator.

8
Statement of originality
This is to certify that to the best of my knowledge; the content of this thesis is my own work. This
thesis has not been submitted for any degree or other purposes.
I certify that the intellectual content of this thesis is the product of my own work and that all the
assistance received in preparing this thesis and sources have been acknowledged.
Signature
Name Mustafa Al Ansari

9
Dedication
The first word I ever said was “Pa” when I first opened my eyes to my father. It was the first time he
had seen me after months– not knowing if I had died in the raging bombings and crossfire on Iraqi
streets. He had not even asked my mother about me, in fear of turning the happiness of their reunion
to grief at my loss.
From the moment I learnt my first words to this moment, my parents have always stood by us through
thick and thin. They dodged bullets and rode the waves (literally) for us, so that we do not experience
the oppression and difficulties they endured.
For that, and for all their sacrifices, support, and love - I dedicate this body of work.

10
Acknowledgements
Thanks be to God (Alhamdolilah). Although there are many that can be thanked during good times -
there is a principle that only God can be thanked at any time – good or bad. As I always remember
God during times of difficulty, I would like to begin with thanking God first during times of success!
I would like to thank my supervisor, Professor Kate Conigrave, who throughout my candidature has
gone above and beyond what anyone can expect from a supervisor, teacher, and mentor. If it were
not for her support and encouragement- even in the most difficult of circumstances - I would not be
clicking the submit button today. I thank her for being an inspiration and for being a role-model to
look up to and follow.
I would also like to thank my auxiliary supervisor, Professor Angela Dawson, who has on numerous
occasions combatted the heat and rain to join our meetings. She has provided irreplaceable guidance
on the research and writing processes.
If it were not for our in-country collaborator, Professor Mohammad AbdulZahra, the whole project
could not have come to fruition. I thank him for dedicating time from his busy schedule as the Dean
of Medicine to support, guide and implement this study. I would also like to thank Dr Jawad Al-
Diwan and Dr Wisam al-Lami who helped facilitate our study and shared their expertise of carrying
out public health research in Iraq.
I would also like to thank the universities, faculties and departments who eased and facilitated our
data collection in Iraq. Similarly, we would like to thank all students and staff who helped us with
recruiting participants for the study, namely students Mohammad Lazim, Sadiq Al-Radhi, Shams al-
Niaimi and Hussain al-Shadidi.
Furthermore, a special thank you is directed to Professor Robin Room who dedicated some of his
busy schedule to advise on and review the quantitative components of our study. I would also like to
thank Dr Michael Livingston for assisting us in devising and reviewing the survey.

11
There were also other great inspirations I met during my time working on this project. I had the
honour of being mentored by Associate Professor Kylie Lee who dedicated her time to guide me
through the research process including training me in systems of organisation. I would like to
acknowledge Dr James Conigrave who shared his expertise and guidance about statistical analysis
and rigour. I still dream of one day being literate in the processes of “R” which always occupy his
screens.
I would also like to thank my mentor and inspiration, Dr Fouad Nagm, for days and nights he
dedicated to assist me with navigating life as a research student. My friends who stood by my side
and endured my absences, tiresome conversations, and repeated complaints – thank you for your
patience and support.
To my loving parents, my appreciation for you is beyond what thoughts can comprehend or words
can express! I owe all my success to my loving family – in Australia and abroad. Firstly, for those in
Iraq who hosted me and assisted me with the day-to-day activities of feeling home and safe while
carrying out my field work. Mostly, I would like to thank my wonderful siblings – from the oldest
Muzaffar, who continuously lifted burden off my shoulders, to my brother, Basim, who shared his
love of study and research and to my beautiful sister Farah who was the first of us to complete a PhD
– I say thank you for supporting me in my pursuit of this dream. Most of all, I would like to thank my
sister and fellow alcohol researcher, Dr Basma Al-Ansari, who introduced me to this amazing project
and team. If it were not for her encouragement, I would still be searching for a PhD topic today!
Finally, I would like to thank my beautiful wife, Sandra, who has stood by my side and peacefully
tolerated my neglect and many sleepless nights in pursuit of completing this thesis.

12
Transliteration
Transliteration from Arabic or Persian languages in this thesis uses the International Journal of
Middle Eastern Studies (IJMES) system (IJMES, 2020).

13
Abbreviations
AUDIT Alcohol Use Disorders Identification Test
AUDIT-C Alcohol Use Disorders Identification Test – Consumption
CIDI Composite International Diagnostic Interview
DALYs Disability Adjusted Life Years
DSM IV Diagnostic and Statistical Manual of Mental Disorders (Version 4)
DSM V Diagnostic and Statistical Manual of Mental Disorders (Version 5)
EMR Eastern Mediterranean Region
ICD International Classification of Diseases
IMF International Monetary Fund
IMHS Iraqi Mental Health Survey
MMC Muslim Majority Country
PC-PTSD Primary Care - Post-Traumatic Stress Disorder test
SDS Severity of Dependence Scale
SSAI Survey of Substance Abuse in Iraq
UN United Nations
UNDESA United Nations Department of Economic and Social Affairs
UNHCR United Nations High Commissioner for Refugees
UNICEF United Nations Children’s Fund
WHO World Health Organization

14
Glossary
ʿaraq Locally made spirit drink with 40%+ alcohol concentration
Ḥayaʾ Modesty/shyness
Manbūẓ Ostracised/outcast
Tafsīr Qur’anic exegesis
Fiqh Islamic jurisprudence
Sunnah The Prophetic tradition (and the tradition of the Imams for Shia Muslims)
Ḥadīth Sayings of the Prophet Mohammad (and the Imams for Shia Muslims)
Khamr Wine (may be inclusive of other intoxicants)
Khamriyyāt Arabic wine poetry (a genre prevalent in pre-Islamic and the medieval eras)

15
List of figures
Figure 1 Overview of thesis structure ............................................................................................................................... 28 Figure 2 Locations of the major historical capitals within Iraq's modern borders. ........................................................... 55 Figure 3 Timeline of alcohol in Iraq's history. .................................................................................................................. 56 Figure 4 Stages of alcohol prohibition in Islam. ............................................................................................................... 57 Figure 5 PRISMA flow chart for literature search ............................................................................................................ 82 Figure 6 Provinces where student/youth specific alcohol data are reported in peer-reviewed original articles ................ 84 Figure 7 Number of participants completing the different survey sections .................................................................... 110 Figure 8 Substance use by participants (respondents re alcohol n=468, re other substances n=450) ............................. 114 Figure 9 Participants’ views on the right response to regular substance use by a friend ................................................ 115 Figure 10 Socio-ecological framework for alcohol use in Iraq complemented by aspects of the motivational model as
presented in Kuntsche et al, 2005 ................................................................................................................................... 135

16
List of tables
Table 1 Laws regarding application for a license to sell alcohol ...................................................................................... 62 Table 2 Laws regarding the operation of licensed stores .................................................................................................. 63 Table 3 Inclusion and exclusion criteria for study selection ............................................................................................. 80 Table 4: Findings of systematic scoping review (studies are ordered by year of data collection) .................................... 90 Table 5 Findings of the included studies .......................................................................................................................... 91 Table 6 Prevalence of lifetime and past-year alcohol consumption by selected demographic data ............................... 111 Table 7 Independent predictors of consumption (using logistic regression) ................................................................... 112 Table 8 Gender and faculty of participants (n = 40) ....................................................................................................... 139

17
Outcomes arising from this thesis
Published manuscripts
Al Ansari M, Dawson A and Conigrave K (2019) Alcohol: from Mesopotamia to Modern Iraq,
Journal of Ethnicity in Substance Abuse, DOI: 10.1080/15332640.2019.1657541.
Submitted manuscripts
Al Ansari M, Dawson A and Conigrave K (2021) Alcohol among Young People in Iraq: A
Systematic Scoping Review (submitted)
Al Ansari M, Dawson A, AbdulZahra M, Room R, and Conigrave K (2021) Alcohol and University
Students in Iraq: Attitudes, Availability and Use (Submitted)
Al Ansari M, Dawson A, AbdulZahra M, and Conigrave K (2021) Alcohol Use in Iraq: Perceptions
of Students at Three Iraqi Universities (Submitted)
Conference presentations/papers
Al Ansari, M.; Dawson, A.; AbdulZahra, M. and Conigrave, K. (2019) University Student
Perceptions of Alcohol Use in Iraq: Insights for Public Health Policy, Presented at the 13th
Annual International Addiction Science Congress (ASC2019), Tehran on 21st of August
2019.
Al Ansari, M.; Dawson, A.; AbdulZahra, M. and Conigrave, K. (2018) Alcohol and University
Students in Iraq: Prevalence and Perception, Presented at the 12th Annual International
Addiction Science Congress (ASC2018), Tehran on 6th of September 2018.
Al Ansari, M.; Dawson, A.; AbdulZahra, M. and Conigrave, K. (2018) Attitudes Towards Alcohol
and its Use Among University Students in Iraq: Policy Implications, Presented at the
Emerging Health Policy Research Conference, University of Sydney on 26th of July 2018.
Al Ansari, M.; Dawson, A.; AbdulZahra, M. and Conigrave, K. (2018) Alcohol and University
Students in Iraq: Perceptions, Availability and Use, Presented at the Kettil Bruun Society
(KBS) Meeting, Chiang Mai on 31st of May 2018.
Al Ansari, M.; Dawson, A.; AbdulZahra, M. and Conigrave, K. (2017) Alcohol and other Drug Use
among Iraq’s University Students: A Possible New Frontier, Presented at the 19th
International Society of Addiction Medicine (ISAM) Conference, Abu Dhabi on 18th of
October 2017.
Al Ansari, M.; Dawson, A.; AbdulZahra, M. and Conigrave, K. (2017) Consumption and Attitudes
towards Alcohol among Iraqi University Students: Impacts on Policy, Presented at the
Global Alcohol Policy Conference (GAPC), Melbourne on 6th of October 2017.

18
Al Ansari, M.; Dawson, A. and Conigrave, K. (2017) Alcohol Consumption among University
Students in Iraq: Preliminary Findings, Presented at the Sydney School of Public Health
Research Conference, University of Sydney on 18th of July 2017.
Al Ansari, M.; Dawson, A. and Conigrave, K. (2017) Student Drinking in Iraq: A Changing Context,
Presented at the World Congress of Public Health, Melbourne on 5th of April 2017.
Al Ansari, M., Dawson, A. and Conigrave, K. (2016) Alcohol: From Mesopotamia to Modern Iraq,
Presented at the Australasian Professional Society on Alcohol and Other Drugs (APSAD)
Conference, Sydney on 31st of October 2016.
Al Ansari, M., Dawson, A. and Conigrave, K. (2016) Alcohol in Iraq’s History and its Potential
Influence on Health Policy, Presented at the Menzies Emerging Health Policy Research
Conference, University of Sydney on 13th of July 2016.
Awards
Bronze Award for Distinguished Research in Addiction Medicine 2019
Esmaeil Zamanian Addiction Medicine Award (EZAMA)
Best Presentation Award 2018
International Addiction Science Congress
Research Training Program Stipend Scholarship 2017-2018
Commonwealth of Australia
Edith Mary Rose (Travelling) Scholarship 2017
The University of Sydney
Australian Postgraduate Award (APA) Scholarship 2015-2016
Commonwealth of Australia

19
Abstract
Background: Anecdotal evidence indicates that alcohol is a growing public health concern in Iraq.
Internal and external factors such as war and resulting trauma, and global alcohol marketing are
possible influences on attitudes towards alcohol among young people in Iraq. However, like many
other Muslim Majority countries, there is scarce data about alcohol in the country.
Method: This research involved four components. The first is an overview of the historical socio-
cultural background of alcohol in Iraq. Then a systematic scoping review identified available data in
local and international peer-reviewed journals about alcohol and young people. This informed mixed-
method research, which included an online survey and semi-structured interviews of university
students. The survey included AUDIT-C and PC-PTSD screening tools, and items on attitudes
towards alcohol and motivations for use.
Results: There have been diverse cultural, historical, and religious influences on attitudes towards
alcohol in Iraq. Data on alcohol and young people is scarce in this context and mostly in non-alcohol-
specific studies. The quantitative survey found a low prevalence of drinking (5.3%; 1.6% females,
10% males). However, two fifths (40%) of male drinking was risky (AUDIT-C score of 4+). Two
fifths of the sample had been exposed to direct conflict and one third tested positive on the PC-PTSD.
Alcohol was said to be easily accessible by both survey and interview participants. Student
interviewees shared a variety of perceived motives for drinking. They also reported on stories of
alcohol harms among drinkers.
Discussion: Although prevalence of drinking is low, alcohol misuse among drinkers is high. Better
health, legal and financial infrastructure in Iraq and ongoing research are needed to help design and
implement tailored, evidence-based approaches. These should aim to maintain or reduce low
prevalence of drinking while ensuring help is available for those with risky drinking.

20
Chapter 1: Introduction
Alcohol in the global context
Alcohol is a major contributor to poor health and social problems worldwide. Globally, alcohol is the
leading risk factor for disease burden in those aged 15-49 years, responsible for almost 10% of deaths
(GBD 2016 Alcohol Collaborators, 2018). Developed countries account for the highest alcohol
consumption levels per capita whilst consumption in Muslim majority countries (MMCs) and Muslim
communities is significantly lower (Alcohol Public Policy Group, 2010; WHO, 2018a). In the
majority of MMCs 80-100% of adults report consuming no alcohol over the past 12 months,
contributing significantly to the global abstinence prevalence of 67.5% (GBD 2016 Alcohol
Collaborators, 2018). However, commercial production and marketing of alcohol is expanding in
countries with low levels of alcohol consumption (Alcohol Public Policy Group, 2010). This is
alarming due to the potential increase in public health problems associated with more widespread use
of alcohol (GBD 2016 Alcohol Collaborators, 2018).
Alcohol is a risky behaviour among young people and can be associated with other risky behaviours.
Globally, alcohol-related burden of disease is highest among young people, with the largest
proportion of disability-adjusted life years (DALYs) lost in those aged 15 to 49 years (GBD 2016
Alcohol Collaborators, 2018). The main contributors to this health burden were traffic accidents and
alcohol use disorders (AUDs). Interpersonal violence is also a major risk associated with drinking,
especially among young people, and may involve violence against strangers or acquaintances as well
as sexual violence resulting in injury or death (WHO, 2006a, 2006c, 2015b). Alcohol use and misuse
has been identified as a concern among university student populations in several countries (Carter et
al., 2010; Linden-Carmichael et al., 2018; Peltzer et al., 2016), including in the Arab world (E. Karam
et al., 2007).

21
Alcohol use in Muslim Majority Countries (MMCs)
Although per capita consumption is stable in developed nations, it is on the increase in several low-
and middle-income countries, especially in the Central African and East Asian regions (Alcohol
Public Policy Group, 2010; WHO, 2010b). Alcohol and drug use is also identified as associated with
health burdens with the highest annual increase in the Eastern Mediterranean region (EMR) (Mokdad
et al., 2016). The latest WHO data on 5-year changes in drinking is from the 2006-2010 period.
Although most MMCs do not have conclusive data in regards to change in alcohol consumption
between 2006 and 2010, an increase in estimates for per capita consumption has been observed for
countries such as Turkey, United Arab Emirates, Qatar, Lebanon and Azerbaijan (WHO, 2010b). On
the other hand, Morocco, Tunisia, Syria, Jordan, and Oman appeared to have a stable per capita
consumption over those 5 years. The only MMCs with a decrease in consumption per capita were
Bahrain, Senegal, and Guinea-Bissau (WHO, 2010b). Although Muslim Middle Eastern countries
were the lowest consumers of alcohol, the last WHO pattern of drinking score in 2006 listed their
pattern of drinking as the second riskiest after the former Soviet countries of Eastern Europe (WHO,
2006a). Similarly, in 2016, among drinkers, the highest alcohol per capita consumption was in the
EMR (WHO, 2018a). The impact of such a drinking pattern may be experienced on an individual
level (e.g. health complications, risk of impulsive behaviour), interpersonal level (e.g. risk of
interpersonal violence), and societal level (e.g. burden on health system) (WHO, 2006c). As of 2016,
there are no national alcohol monitoring systems in any EMR country except for Iran (only for health
consequences) (WHO, 2018a).
MMCs in the EMR, including Iraq and Syria, are amongst the 66% of member states of the World
Health Organization (WHO) which do not have a formal written national alcohol policy (WHO,
2014a). Alcohol policy approaches in MMCs, however, vary. While some MMCs such as Turkey
adopt a western style regulatory policy, other countries, such as Iran, only allow alcohol for non-
Muslims (Al-Ansari et al., 2015). Only five MMCs adopt a total prohibition policy, namely,
Afghanistan, Libya, Saudi Arabia, Somalia and Sudan (Al-Ansari et al., 2015). While some MMCs,

22
such as Oman and Turkey, have a high Alcohol Control Policy Index (ACPI), countries with recent
or ongoing conflict such as Iraq and Syria have one of the lowest ACPI scores indicating their lack
of cohesive alcohol policies (Madureira-Lima et al., 2018).
Religious prohibition and the prominent culture of abstinence may contribute to a perception that
alcohol is not an issue, and to the limited availability of research on alcohol in MMCs. Alcohol is
thus the least studied psychoactive substance in Arab countries (Sweileh et al., 2014). Calls have been
made to increase alcohol research in settings outside of European and Anglophone countries,
particularly in MMCs (Al Ghaferi et al., 2013; Kuntsche et al., 2017; Savic et al., 2016). The growing
investment of the global alcohol industry in developing countries (Alcohol Public Policy Group,
2010) also suggests a need for further research, especially amongst vulnerable sectors such as youth
and student populations. A 2009 review looking at substance use in the Arabian Gulf region identified
that most studies on alcohol have been conducted in male clinical samples (AlMarri & Oei, 2009).
Similarly, a review of alcohol consumption in the Arab region in 2016 reports that less than half the
countries in the region have studies on student consumption (L. Ghandour et al., 2016). Iraq had no
studies focusing on young people or students. Of the four identified studies, three were in clinical
settings and one on a sample of journalists and other professionals.
Despite the limited volume of research, existing studies in the EMR show that youth are a vulnerable
sector of society and are exposed to alcohol. Abstinent older people in Lebanon and among Arabs in
Israel have disclosed that they used to drink in their younger years (Baron-Epel et al., 2015; Yazbek
et al., 2014). A study conducted at two Lebanese universities indicated alcohol use and misuse among
the student population; however, most of the sample was of the Christian faith (L. A. Ghandour et al.,
2009). In Egypt, a single-university study was conducted to research the practice and awareness of
Egyptian students about health risk behaviours (Refaat, 2004). It sampled a total of 687 students (of
which 59% were female) and found a high awareness of the behavioural risks of alcohol amongst
students. Just under a sixth (14.4%) of the sample had tried alcohol in their lifetime with a moderate
correlation (r=0.457) between alcohol and risky sexual behaviour. The study found that no awareness

23
of alcohol was provided by family and that friends and the media were the main source of information
about alcohol and drugs (Refaat, 2004).
Undertaking research on a young population in a MMC within the current evolving social, political,
and cultural situation will contribute to enhanced understanding of the attitudes of youth towards
alcohol and possible changing behaviours in MMCs. Iraq is a prime example of such a country that
can serve to provide further insight into public health strategies that may be required in Iraq and other
comparable MMCs.
Alcohol in Iraq
This section aims to provide a short introduction to highlight the context of this research. A detailed
review of the historical socio-cultural setting and a systematic scoping review of available data on
youth and student drinking in Iraq will be presented in Chapters 3 and 4.
Reported alcohol and drug use prevalence data for Iraq in global reports are typically estimates. For
example, the data in the WHO ATLAS on Substance Use are based on expert estimates rather than
on survey data (WHO, 2010a). However, there are two national household surveys in Iraq, from 2006
and 2014, which collected information about alcohol consumption. Lifetime prevalence of alcohol
consumption among males seems to have increased from 6.8% to 16.7% over those years (US
Department of State et al., 2015; WHO, 2009). In an unpublished 2009 study with no details about
the sample, the lifetime prevalence of alcohol use in Baghdad was found to be 17.8% and increasing
(Al-Hemiary et al., 2014). Together, these figures indicate a likely increase in alcohol consumption.
However, it is unknown whether these increases represent actual drinking behaviours in Iraq or
differences in survey methods. There has been a negligible prevalence of reported alcohol use among
female participants in all Iraqi surveys.
There was a very low prevalence of alcohol abuse (0.1%) in the total sample in the 2006 Iraqi Mental
Health Survey (WHO, 2009). However, among Iraqi drinkers, the rate of alcohol use disorders was
one of the highest from a multinational WHO study: The World Mental Health Survey (Degenhardt

24
et al., 2019; Glantz et al., 2020). The 2014 Survey of Substance Abuse in Iraq (SSAI) indicates that
on average, current drinkers consume more than 6 drinks per day on 10.5 days a month. The SSAI
reports that more than two thirds of drinkers meet the criteria for dependence on the Severity of
Dependence Scale (SDS) (US Department of State et al., 2015). Similarly, a study at youth centres in
Baghdad found over a sixth of the sample met the DSM-IV criteria for alcohol abuse, with an onset
age between 18 and 25 years (Al-Hemiary et al., 2015b).
Alcohol use is a hidden phenomenon in Iraq. This may be due to religious prohibition and social
stigma surrounding drinking. Alcohol users often do not disclose their drinking to family, friends or
anyone outside of their drinking circles in fear of losing face. The lack of clarity surrounding its
prevalence and misuse may pose a challenge in the planning and delivery of effective measures and
interventions by the already struggling Iraqi health system (Al-Hemiary et al., 2014). Iraq’s health
system provides 6.1 physicians for every 10,000 populace, a rate that is half of the regional average
(WHO, 2014b).
Iraq at a time of change
Iraq is an upper-middle income developing country (UN, 2020) with a total population of over 38
million in 2017 (UNDESA, 2017). It is estimated that Iraq’s population is increasing by more than a
million people per annum, with most of the population (60%) under the age of 24. By the year 2030,
it is estimated that Iraq will have at least an additional 15 million people (UNDESA, 2017).
Iraq’s growing population has been subjected to multiple wars resulting in major political, economic,
social and cultural change (Marr, 2018). Any study of mental health in Iraq must be presented against
this backdrop. The Iraq-Iran war lasted eight years between 1980 and 1988. Three years later, the
invasion of Kuwait in 1991 started the First Gulf War. This led to continued sanctions against
Saddam’s regime in Iraq until 2003, which saw the beginning of the second Gulf war. More recently,
Iraq fought a war against Islamic State (IS) after that group established itself in northern Iraq. Iraq

25
continues to be subjected to terrorism and international military presence. Iraqi youth and their parents
have been directly exposed to at least one of these occurrences.
Despite research about the impact of the Gulf Wars on veterans returning to Coalition countries,
public health research has not focused on the Iraqi population. Alcohol misuse was greater amongst
United States and United Kingdom combatants post-deployment than pre-deployment (Browne et al.,
2008; Wilk et al., 2010). There was a correlation between alcohol misuse and combat activity,
amongst other factors. Although the sample of this study is different from both a cultural and
occupational perspective to the Iraqi population, a possible relationship between experience of
conflict and alcohol misuse exists (Lo et al., 2017). Such an association has also been shown in other
MMCs such as Lebanon (Yaacoub et al., 2019). The association of conflict and alcohol misuse is not
surprising, given that alcohol use disorders frequently are triggered by or exacerbate other mental
health disorders including post-traumatic stress disorder (PTSD) (Debell et al 2014 and Shivani et al
2002).
In addition to war and conflict, Iraqis have been exposed to a multitude of local and international
social and mass media since the 2003 Gulf War (Abedalla et al., 2014). Many young people in the
Arab world are shown to regularly consume English-language media (Melki, 2010). English language
exposure is likely to increase among youth given that English as a second language is now taught
from the first year of elementary school instead of at the fifth or third grade as in the pre-2008 and
pre-2013 Iraqi curricula respectively (AlTufaili, 2016). Many of Iraq’s university courses are also
taught completely in English. Exposures to alcohol in the Iraqi setting include direct marketing, and
indirect exposure to alcohol through film, social-media posts, and via other mediums. Such exposures
have been associated with early uptake of alcohol by non-drinking adolescents and with increased
drinking among drinkers (Anderson et al., 2009).
Although WHO indicates that there is no single written alcohol policy in Iraq, there are discrete
alcohol-related policies or regulations imposed by sub-sections of tourism, council or trade laws.

26
Despite Iraq’s changing dynamics most of these regulations date from the pre-2003 conflict. These
approaches have not considered the lived experiences of Iraq’s large and growing young population.
University students in other countries have been shown to be particularly vulnerable to alcohol use
and drink more heavily than their non-student peers (Carter et al., 2010; E. Karam et al., 2007; Linden-
Carmichael et al., 2018; Peltzer et al., 2016). Drinking for social purposes is the main motive for
alcohol use in non-MMCs (Mackinnon et al., 2017). In Iraq, university students are likely to have a
higher exposure to alcohol than their peers in the general community due to their added English
language skills. Universities in Iraq offer social spheres where young people form close bonds and
interact freely with each other. They are also typically the only places where the opposite sexes
interact. Students may be less likely to adopt traditional culture because of higher likelihood of living
away from parents or travelling to locations with less alcohol restrictions. This is particularly
important as, culturally, young Iraqis typically live with and/or are dependent on their parents until
marriage. In addition, students are likely to also drink for coping purposes as in addition to their lived
experiences of social and political instability, they are also under pressure from study load and
social/familial expectations.
Gaps in the research literature
The scarcity of research about alcohol in MMCs, particularly in the Arab region (Sweileh et al., 2014),
as well as the limited research on alcohol in post-conflict civilian populations (Wallace et al., 2013)
demonstrate a need for research in this area. Limited published alcohol-specific studies in Iraq could
be identified, particularly those with a student or youth focus. There is also limited information on
alcohol’s place in Iraqi society and culture, or on attitudes towards alcohol in Iraq. Additionally,
alcohol has not been the subject of any previous reviews or qualitative studies in Iraq. Given these
constraints in the literature, there is a limited understanding of how Iraq’s changing dynamics may
impact attitudes towards alcohol or prevalence of consumption among young people in Iraq.

27
Research questions
To address some of the identified gaps, this thesis set out to examine alcohol among young university
students in Iraq. The definition of “youth” for this study is consistent with the international definition,
as those aged between 17 and 24 (UNDESA, 2013). In particular, this research examines:
1. What is the context of alcohol research in Iraq and what is already known about youth or
student drinking within this context?
2. What are the prevalence and patterns of use/misuse among young Iraqi university students?
3. What are the attitudes towards alcohol and drinkers among young university students in Iraq?
Why do students have these attitudes? (with particular focus on assessing war and
globalisation as influencing factors)
4. How are these attitudes likely to impact the future of alcohol in Iraq, particularly with regards
to prevention and harm reduction?
Potential outcomes and significance
By describing the socio-cultural context of alcohol in Iraq and providing the scope of literature on
young student drinking in Iraq, this thesis will inform a baseline for future alcohol research in Iraq.
The thesis provides the first voice for young Iraqis in alcohol research. This may encourage other
researchers to involve young Iraqis and their perspectives in future health research.
This thesis can inform the potential need for the development of a national alcohol policy in Iraq. It
may contribute to identifying areas where further research or health promotion initiatives are needed,
with a hope to prevent alcohol becoming a greater public health concern in Iraq.
Examination of attitudes towards alcohol use within the selected sample will increase understanding
of the potential factors contributing to changes in drinking behaviour among young people in MMCs.
As Iraq is a post-conflict country with recent exposure to globalisation, this research is likely to
inform alcohol research in post-conflict civil populations, especially in other war-affected MMCs.

28
Understanding the influence of globalisation and war may help inform public health efforts to prevent
alcohol-related harm in developing MMCs with similar contexts to Iraq.
Overview of the thesis
This report has been written as a thesis including publication. Chapter 3 includes an article which has
been published in the journal of Ethnicity and Substance Abuse (Al Ansari et al., 2019). Chapters 4,
5 and 6 include manuscripts submitted for publication in peer-reviewed journals and currently under
Figure 1 Overview of thesis structure

29
review. While this thesis is written to form a cohesive whole, each chapter can also be read
independent of the other chapters. Figure 1 sets out the structure of the thesis.
Chapter 1 introduced the research topic and focused on the research gaps and questions. This chapter
was brief as the detailed background and literature review is presented in Chapters 3 and 4.
Chapter 2 sets out the methodology of this thesis. As detailed methods of chapters 3 to 6 are included
within them, this methodology chapter will only focus on the overall thesis methods and approaches.
This chapter describes the challenges, risks and mitigations involved in conducting research on such
a sensitive topic in Iraq.
Chapter 3 (Alcohol: From Mesopotamia to Modern Iraq) provides a background to understanding
alcohol in the context of Iraq’s diverse ethnicities, religions, and cultures. It briefly summarises
alcohol’s history in Iraq before describing the potential challenges, sensitivities, and socio-cultural
influences in this context.
Chapter 4 is a systematic scoping review of research on student or young people and alcohol in peer-
reviewed original literature. This review includes any study, regardless of alcohol-focus, that had
information on alcohol among young people or students in Iraq. This sets out the need for the mixed-
method study presented in chapters 5 and 6.
Chapter 5 presents the quantitative component of the mixed-method study. This chapter details the
methods and results of the online questionnaire. It describes the prevalence of alcohol use/misuse
using the short Alcohol Use Disorders Identification Test (AUDIT-C). It also presents the overall
reported attitudes of young Iraqi university students towards motives for consumption/abstinence,
alcohol exposure and policy.
Chapter 6 describes the qualitative research carried out as part of this mixed-method study. It presents
the findings from the thematic template analysis of the 40 semi-structured student interviews carried
out at three Iraqi universities. This chapter aims to deepen the understanding of students’ experiences
and perspectives on drinking, and of alcohol harms and influencing factors.

30
As each chapter includes a focused discussion, chapter 7 will consolidate and discuss the findings of
all chapters considering local, MMC and international literature. It will highlight the limitations and
implications of this research before presenting the overall conclusions.

31
References
Abedalla, R. W., et al. (2014). Accessing Information Technology-Social Media in Iraq. International
Journal of Scientific and Research Publications, 4(9).
Al-Ansari, B., et al. (2015). Extent of Alcohol Prohibition in Civil Policy in Muslim Majority
Countries: the Impact of Globalization. Addiction, 111(10), 1703-1713.
doi:10.1111/add.13159
Al-Hemiary, N., et al. (2015). Alcohol and Drug Abuse in Post-Conflict Iraq. Journal of the Faculty
of Medicine, Baghdad, 57(4), 290-294.
Al-Hemiary, N. J., et al. (2014). Drug and Alcohol Use in Iraq: Findings of the Inaugural Iraqi
Community Epidemiological Workgroup. Substance Use & Misuse, 49(13), 1759-1763.
doi:doi:10.3109/10826084.2014.913633
Al Ansari, M., et al. (2019). Alcohol: from Mesopotamia to Modern Iraq. Journal of Ethnicity in
Substance Abuse, 1-23. doi:10.1080/15332640.2019.1657541
Al Ghaferi, H., et al. (2013). Substance Misuse in Arabic Countries: the Need for Published Research.
International Journal of Prevention and Treatment of Substance Use Disorders, 1(1), 7-11.
Alcohol Public Policy Group. (2010). Alcohol: No Ordinary Commodity – a summary of the second
edition. Addiction, 105(5), 769-779. doi:10.1111/j.1360-0443.2010.02945.x
AlMarri, T. S. K., et al. (2009). Alcohol and substance use in the Arabian Gulf region: A review.
International Journal of Psychology, 44(3), 222-233. doi:10.1080/00207590801888752
Anderson, P., et al. (2009). Impact of alcohol Advertising and Media Exposure on Adolescent
Alcohol Use: A Systematic Review of Longitudinal Studies. Alcohol and Alcoholism, 44(3),
229-243. doi:10.1093/alcalc/agn115
Baron-Epel, O., et al. (2015). Alcohol Consumption Among Arabs in Israel: A Qualitative Study.
Substance Use & Misuse, 50(2), 268-273. doi:doi:10.3109/10826084.2014.962051
Browne, T., et al. (2008). How do Experiences in Iraq Affect Alcohol Use Among Male UK Armed
Forces Personnel? Occupational and Environmental Medicine, 65(9), 628-633.
doi:10.1136/oem.2007.036830
Degenhardt, L., et al. (2019). Concordance between the diagnostic guidelines for alcohol and
cannabis use disorders in the draft ICD-11 and other classification systems: analysis of data
from the WHO's World Mental Health Surveys. Addiction, 114(3), 534-552.
doi:10.1111/add.14482
GBD 2016 Alcohol Collaborators. (2018). Alcohol use and burden for 195 countries and territories,
1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet,
392(10152), 1015-1035. doi:10.1016/S0140-6736(18)31310-2
Ghandour, L., et al. (2016). Alcohol consumption in the Arab region: What do we know, why does it
matter, and what are the policy implications for youth harm reduction? International Journal
of Drug Policy, 28, 10-33. doi:http://dx.doi.org/10.1016/j.drugpo.2015.09.013
Ghandour, L. A., et al. (2009). Lifetime alcohol use, abuse and dependence among university students
in Lebanon: exploring the role of religiosity in different religious faiths. Addiction, 104(6),
940-948. doi:doi:10.1111/j.1360-0443.2009.02575.x
Glantz, M. D., et al. (2020). The epidemiology of alcohol use disorders cross-nationally: Findings
from the World Mental Health Surveys. Addictive Behaviors, 102, 106128.
doi:https://doi.org/10.1016/j.addbeh.2019.106128

32
Karam, E., et al. (2007). Alcohol use among college students: an international perspective. Curr Opin
Psychiatry, 20(3), 213-221. doi:10.1097/YCO.0b013e3280fa836c
Kuntsche, E., et al. (2017). Alcohol and other substance use in a cross-cultural perspective. Drug and
Alcohol Review, 36(6), 717-720. doi:doi:10.1111/dar.12625
Lo, J., et al. (2017). A Systematic Review on Harmful Alcohol Use Among Civilian Populations
Affected by Armed Conflict in Low- and Middle-Income Countries. Substance Use & Misuse,
52(11), 1494-1510. doi:10.1080/10826084.2017.1289411
Madureira-Lima, J., et al. (2018). Alcohol control policies and alcohol consumption: an international
comparison of 167 countries. Journal of Epidemiology and Community Health, 72(1), 54-60.
doi:10.1136/jech-2017-209350
Marr, P. (2018). The modern history of Iraq (Fourth edition. ed.). Boca Raton, FL: Routledge, an
imprint of Taylor and Francis.
Melki, J. (2010). Media habits of MENA youth: A three-country survey. Beirut.
Mokdad, A. H., et al. (2016). Health in times of uncertainty in the eastern Mediterranean region,
1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet
Global Health, 4(10), e704-e713. doi:10.1016/S2214-109X(16)30168-1
Refaat, A. (2004). Practice and awareness of health risk behaviour among Egyptian university
students. Eastern Mediterranean Health Journal, 10(1-2), 72-81. Retrieved from
http://apps.who.int/iris/bitstream/10665/119382/1/emhj_2004_10_1_2_72_81.pdf?ua=1
Savic, M., et al. (2016). Defining “drinking culture”: A critical review of its meaning and connotation
in social research on alcohol problems. Drugs: Education, Prevention and Policy, 23(4), 270-
282. doi:10.3109/09687637.2016.1153602
Sweileh, W. M., et al. (2014). Substance use disorders in Arab countries: research activity and
bibliometric analysis. Substance Abuse Treatment, Prevention and Policy, 9, 33.
doi:http://dx.doi.org/10.1186/1747-597X-9-33
UN. (2020). World Economic Situation and Prospects 2020 (9789210046169).
https://www.un.org/development/desa/dpad/publication/world-economic-situation-and-
prospects-2020/
UNDESA. (2017). World Population Prospects: The 2017 Revision, Key Findings and Advance
Tables.
US Department of State, et al. (2015). Survey of Substance Abuse in Iraq. Bethesda, MD.
Wallace, K., et al. (2013). An Exploration of the Alcohol Policy Environment in Post-Conflict
Countries. Alcohol and Alcoholism, 49(3), 356-362. doi:10.1093/alcalc/agt142
WHO. (2006a). Interpersonal Violence and Alcohol.
http://www.who.int/violence_injury_prevention/violence/world_report/factsheets/pb_violen
cealcohol.pdf?ua=1
WHO. (2006b). Youth Violence and Alcohol.
http://www.who.int/violence_injury_prevention/violence/world_report/factsheets/fs_youth.p
df?ua=1
WHO. (2009). Iraq Mental Health Survey 2006/7. http://www.webcitation.org/6mk3pGCJV
WHO. (2010a). ATLAS of Substance Use Disorders. Country Profile: Iraq .
http://www.who.int/substance_abuse/publications/atlas_report/profiles/iraq.pdf
WHO. (2010b). Estimate of 5-year Change in Recorded Alcohol Per Capita (15+) Consumption,
2006-2010. Retrieved from

33
http://gamapserver.who.int/gho/interactive_charts/gisah/consumption_change/atlas.html.
Retrieved 11/05/2015
http://gamapserver.who.int/gho/interactive_charts/gisah/consumption_change/atlas.html
WHO. (2014a). Global Status Report on Alcohol and Health. Geneva.
http://www.webcitation.org/6mk3vWQQm
WHO. (2014b). Iraq: Health Profile.
Wilk, J. E., et al. (2010). Relationship of Combat Experiences to Alcohol Misuse Among U.S.
Soldiers Returning from the Iraq War. Drug and Alcohol Dependence, 108(1–2), 115-121.
doi:10.1016/j.drugalcdep.2009.12.003
Yaacoub, H., et al. (2019). Association of War and Other Factors with Substance Use in a Lebanese
Male Sample. Journal of Drug Issues, 49(1), 106-117. doi:10.1177/0022042618807765
Yazbek, J.-C., et al. (2014). Prevalence and Correlates of Alcohol Abuse and Dependence in
Lebanon: Results from the Lebanese Epidemiologic Survey on Alcohol (LESA). Journal of
Addictive Diseases, 33(3), 221-233. doi:10.1080/10550887.2014.950026

34
Chapter 2 – Methodology
Chapter 1 introduced the focus of this research and the key research questions before presenting an
overview of the thesis components. By investigating the attitudes of young university students in Iraq,
this research aims to better understand the place of alcohol and the factors which influence young
people’s attitudes to alcohol in Iraqi society. As each of next four chapters is written in a form suitable
for publication, the methodological framework is presented within each section. This chapter provides
additional information of the methodological approaches for the research. It also describes the
challenges, risks, and mitigations for carrying out sensitive research of this nature in Iraq. A broad
chronology of correspondence, field trips, engagements and collaborations will also be set out with
the aim of helping future researchers navigate health research in Iraq. Finally, a brief ‘author as
researcher’ statement will be shared to introduce the role of the author in the conduct of this research.
Socio-historical review: sources of evidence
The socio-historical review relied on Arabic, English and Persian primary and secondary literature to
describe the social, cultural, religious, and historical position of alcohol in Iraq. This review was
important to place this research in context by informing the place of alcohol among the overall
population and among ethnically, culturally, and religiously diverse communities.
Below, the three main sections of this chapter and their sources are described:
The first section of this paper looked at alcohol in pre-Islamic Iraq and Arabia. Historical books and
articles as well as linguistic works regarding alcohol were consulted. These were either searched
online or at the University of Sydney library.
The second section provided an overview of alcohol’s place in Islamic jurisprudence and history. The
main sources consulted were Quran Exegesis’ (interpretation of the Quran) and Hadith literature (the
traditions, sayings, and life of the Prophet Muhammad). These were complemented with Islamic
jurisprudential and scholarly works regarding the Islamic views and laws around alcohol as well as
historical works regarding the place of alcohol in Islamic societies. Finally, works of poetry were

35
utilised for sections on khamriyyat (wine poetry). There were also consultations made with an Islamic
religious scholar to help with identification and interpretation of religious resources.
The third section, Alcohol in Modern Iraq, was divided into two parts. One looked at alcohol from a
social and legal perspective while the other provided an overview of health literature relating to
alcohol in Iraq. For this section, sociological books, peer-reviewed alcohol and mental health
literature, news media and WHO, government and non-government reports were consulted.
Scoping review
This systematic scoping review aimed to identify what is known about attitudes towards alcohol and
prevalence of drinking in Iraq. Supplementary research questions assessed screening and diagnostic
tools, influencing factors and preventative strategies for this setting.
A previous review from the region could not identify any student drinking data from Iraq (L.
Ghandour et al., 2016). The authors however limited their search to indexed papers which had a key
focus on alcohol. The aim of this chapter was to identify all data published in peer-reviewed literature
about youth or student drinking in Iraq, including in papers where alcohol was a subsidiary focus.
Indeed, most of the available data were not in alcohol-specific articles. A meta-analysis could not be
employed as studies used varying methods, including a range of screening and diagnostic tools.
Several did not provide sufficient detail on methods to fully describe these. As we were not assessing
an intervention, and our aim was to map out evidence in an emerging research area, a systematic
scoping review was the best suited approach (Arksey et al., 2005; Peters et al., 2015).
As assessing prevalence of alcohol use and misuse is a primary aim, rather than assessing an
intervention, this review utilised the CoCoPop (condition, context, population) approach instead of
the traditional PICO (population, intervention, condition, outcome) (Munn et al., 2018). We also
followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)
statement (Moher et al., 2009).
In addition to the systematic search that was undertaken in five international databases (MEDLINE
(OVID), Embase (OVID), PsycINFO (OVID), Scopus, Web of Science), we identified an online

36
database of local Iraqi journals (IASJ: Iraqi Academic Scientific Journals). We searched this database
to ensure our scope included literature published in local peer-reviewed journals which are not
indexed in international databases. The full strategy is attached as an appendix (Appendix 3). We also
conducted a hand search to identify other articles that meet the inclusion criteria.
We employed broad inclusion criteria to identify any youth or student drinking data in Iraqi general
or student population settings.
Mixed-method approach
To gain an understanding of attitudes to and use of alcohol among university students in Iraq, an
analysis of prevalence of alcohol use and attitudes towards alcohol must be conducted. A mixed
method approach was chosen so that the qualitative and quantitative components adequately
complement each other, and to explain and contextualise the findings (Bryman, 2006; Schoonenboom
et al., 2017). This provides a more complete picture of attitudes towards alcohol and alcohol
consumption in Iraq. While a quantitative approach may provide some information about students’
alcohol use and attitudes, it may not adequately address the events, feelings and experiences that
contribute to students’ behavior or attitudes. On the other hand, a qualitative approach may provide
a lens into their real-life experiences but would stop short of providing a quantifiable estimate of the
magnitude of the issue, behaviour or attitude.
Other possible methods included an observation or ethnographic approach – but due to the sensitivity
of alcohol as a topic in Iraq, both these methods would not be practical. Alcohol is a hidden
commodity within the Muslim majority population, and it is used cautiously – a researcher is not
likely to encounter alcohol use with either of these methods unless they specifically approach certain
locations or population groups. Such an approach is only practical if the research aims to target
drinking populations.
A mixed-method approach (Schoonenboom et al., 2017) was utilised to present a quantifiable figure
of the attitudes, behaviours and influences of alcohol. This is complemented with an in-depth
explanation of the experiences and thoughts of participants about the interaction of the individual and

37
their environment in Iraq. Although change in behaviours and attitudes is not the primary purpose of
this thesis, the use of both qualitative and quantitative research methods provided an opportunity to
compare quantitative data with previous surveys and to enquire from students about alcohol and
previous generations (Question 1 of Appendix 6). Together this helps to better understand the extent
to which changes in the Iraqi context may have impacted on alcohol use or misuse.
This thesis employed an equal-status interactive mixed-method research, where both components are
of equal value and weight (Schoonenboom et al., 2017). The quantitative and qualitative research was
conducted concurrently in a convergent parallel design (Schoonenboom et al., 2017). This meant that
although the research design and plan considered both components, each study was independent in
its data collection and write up. The point of combining the two components was in the overall
interpretation presented in the discussion (Chapter 7).
Sample selection and setting
A university student sample was chosen for this study for a number of reasons. Firstly, we anticipated
that out of all general population groups, university students would be the most open to speak about
this topic and share their thoughts. Secondly, we hypothesised that university students have a greater
exposure to technology, globalisation, and media due to higher levels of English literacy. Thirdly,
Universities are secured locations and students are freer to communicate their thoughts and opinion,
especially regarding sensitive topics. In addition, this setting offers a more acceptable location for
students to communicate with others, especially those of the opposite sex.
Participants were required to be currently enrolled Iraqi university students to access the survey,
however there was no way of verifying this without compromising anonymity. We only analysed data
for students under the age of 24 to be consistent with the internationally accepted definition of youth
(UNDESA, 2013). In the qualitative study, however, it was not appropriate to ask for the participants’
age – especially if they were female. All our interviewees were undergraduate students and the oldest
was a female in her sixth year of medicine. Based on their degree progress, it was assumed that they
all fell within this age limit.

38
Possible obstacles, risks and limitations to alcohol research in Iraq
Some obstacles apply to any research conducted in Iraq, but others are specific to our research topic.
This section will introduce the potential obstacles and risks and then outline the mitigations which
were applied.
The first obstacle was the unpredictable security situation in Iraq. When we set out on this program
of research, Islamic State of Iraq and Syria (ISIS) was in control of the second largest Iraqi city,
Mosul, and controlled almost a third of Iraq’s territory. It was not clear that field work in Iraq would
be possible. However, as the fighting in the ISIS territories intensified, the threat of terrorism in cities
not controlled by ISIS reduced.
The second obstacle was navigating around the sensitivity of the topic in Iraq, where alcohol is largely
forbidden. This involved introducing the topic to stakeholders, participants, and approvers, as well as
people who were not directly involved in this research, such as family, friends and others who assisted
in facilitating transport and accommodation.
Thirdly, confidentiality and anonymity of participants was crucial. Alcohol is a taboo in Iraq and a
drinker may face social isolation, be disowned by his/her family and community, and may face other
lifetime consequences. Given the rise of ISIS and other extremist groups in recent years, admitting to
alcohol consumption could also have security consequences for the participant. For example, alcohol
shops are known to be attacked or burnt and drinkers to be physically punished. Sometimes even
associating with drinkers may have negative consequences for an individual. These concerns may
drive participants to not disclose their drinking habits, or whether they know drinkers or their attitude
towards alcohol and alcohol users. Similarly, because of changing cultures in Iraq, young participants
with more conservative/traditional views of alcohol may also feel uncomfortable to share their
opinions if they assume the interviewer has more liberal views. This may be because they would be
perceived to be backward thinking or overly traditional.

39
Mitigations and solutions to risks and obstacles
We tailored our research design and data collection approaches to consider and mitigate these
potential obstacles. We consulted on and investigated several possible approaches we could utilise to
best collect quantitative and qualitative data in this setting.
When we first set out on this research project, we contacted the Australian Embassy in Baghdad
outlining our research proposal and asking for any guidance or support that is available. The Embassy
explained that they did not foresee a significant safety risk for us to conduct our research if we do not
travel to ISIS controlled regions in Iraq. They provided the contact details of several private security
companies that can provide personal security in Iraq.
The field work was conducted by the author, an Iraqi Australian of the Muslim faith. Although he has
never lived in Iraq, he speaks Arabic fluently and is well versed with the culture and religion. In
consultation with local academics and from experience, the presence of the first author in Iraq was
not deemed more dangerous, eye-catching or risky than for the locals. The risk mitigations were to
never speak English or travel alone outside the University and to always be accompanied by a local
Iraqi relative or friend. Inter-city travel was limited to that with a university-designated driver in a
university-owned vehicle. This helped us to pass through the express lane at busy security checkpoints
on the highway or at the entry of every province and city. The university-designated driver/guard
stayed with the author throughout his travels outside of his main collaborator’s home city – except in
his travel to Kurdistan, which is considered safe, with only one public terrorist attack there since the
2003 conflict.
The author has been to Iraq several times before and although the attacks are at times random, he was
aware that avoiding certain gatherings and areas would largely reduce the risk – especially if one
reduced the time in major cities with higher risk of attacks.
As Iraq is a country with an advisory level of “Do Not Travel” by the Department of Foreign Affairs
and Trade, the insurance provided through the University of Sydney covered any normal occurrences
but did not cover any war or terrorist-related activity. The author carried a portable phone charger

40
along with two mobile phones, one connected to a local Iraqi service and the other to an Australian
roaming service. He checked-in with his supervisor back in Australia every 48 hours. There were
procedures in place for the supervisor to follow if there was a missed check-in.
Field work and data collection
In 2016 the author travelled to Iraq to form collaborations, secure approvals to conduct this study at
Iraqi universities and seek in-country ethics approval.
During this trip, the author visited four universities, three in the Arab middle and south of Iraq and
one in the Kurdistan region of Iraq. His main in-country collaborator, who is the dean of a medical
faculty in Iraq assisted him in contacting all appropriate parties at these universities and seek in-
person meetings were the potential for the conduct of this study can be discussed. The collaborators
will not be identified to protect the confidentiality of the universities were data was collected. These
meetings included a meeting with the president of a university, a dean of a medical faculty and the
head of the department of public health of the third university.
After visiting these universities in person and submitting the proposal, written approvals from two
universities (not included in appendix so as to not identify the universities) and a verbal approval
from a third university was received. The fourth university, in Kurdistan, did not respond to in-person,
phone or email invitations to participate in this study. The leadership of a second university in
Kurdistan was then contacted by email with the help of the in-country collaborator – similarly there
was no response. In total three recruitment sites were secured for our study.
In 2017, the author returned to Iraq to conduct the data collection for this study. By now, Iraqi ethics
approval had been granted, the survey and framework of the interview had been developed and were
ready for in-country checking.
Quantitative component
The quantitative component of this study focused on assessing the prevalence of alcohol use and
misuse within the student sample. It also aimed to quantify the attitudes of this young population
towards different personal and policy approaches to alcohol. A mixture of convenience and snowball

41
sampling was utilised to recruit participants for this research. More details regarding sampling are
contained in Chapter 5.
Several methods were initially assessed for recruitment and administration of the quantitative study.
The first was to conduct a pen-and-paper survey that is administered at the University in specifically-
hired rooms that are divided by partitions, forming a voting-booth like setting. Students were to be
invited to come in and fill the survey in the provided booths and to submit their survey by placing it
in a ‘ballot’ box upon exiting the room. There were several concerns with this method. Firstly,
Universities in Iraq are divided by campuses and each faculty has its own building, even when on the
same campus. This would mean we would either need to inconvenience students to walk to another
campus/faculty or have a research workforce that is able to relocate the survey room to different
faculties and universities. In addition, each survey may take 20 minutes or more and it would be
difficult for students to be away from their studies or to wait for a booth to be available. The logistics
of this was daunting and given the limits of funding, time, and difficulty of securing spaces through
negotiations with buildings across University campuses, this method was deemed impractical for the
purposes of this research.
We also considered conducting an in-lecture survey using software such as Socrative. This was to be
conducted with permission from lecturers around the University campuses. Again, although this may
have given us a larger (and possibly more representative) sample, it was not practical for a few
reasons. Firstly, electricity supply in Iraq is not consistent. There are emergency generators, but these
are not turned on in the faculties except in emergencies and only provide enough power to turn on
lights and several other key devices. Secondly, given that this would be at the beginning or end of a
scheduled university lecture, there will be very limited time to provide instructions, ask the questions
and receive the answers. Such an approach is only practical for short polls and not for formal research
surveys. The time to explain to students how to login and fill in the answers may already fill any time
we are allocated for the entire survey, especially as not all students are tech-savvy. Thirdly,

42
confidentiality cannot be guaranteed as students sit next to each other in lecture theatres and it is
likely they will be able to see each other’s screen and answers.
Both above methods also required navigating the intra- and inter-faculty bureaucracy to seek
approvals and allocations. They also both required the assistance of research assistants to help the
researcher in setting-up, assisting and packing-up.
When the above two possibilities were not found to be practical, we assessed the use of an online
survey tool. SurveyGizmo (now Alchemer) was chosen as the software allows for surveys to be
translated and to appear in various languages. It also includes an optional setting (that we turned on)
that blocks the collection of any IP or device data from the participant – ensuring anonymity and
hence extra safety for the participant. The participants were also able to fill in the survey at any time
and place that is convenient for them, and anytime during the data collection window. SurveyGizmo
also allowed for the data to be directly downloaded in SPSS – the software we used to conduct our
analysis, removing any need for data entry.
Survey tools and items
To survey this Iraqi population group, we generated a self-report survey that addresses our research
questions and provides adequate opportunity for participants to share their viewpoints. To this end,
we formulated a survey based on several validated tools and past alcohol studies within similar or
general populations in other countries. Our survey design mainly focused on two sources. The
Alcohol, Drugs and Student Lifestyle study (Bullock, 2004) is a large Swedish study based on the
2003 National Young Adult’s Drug Use telephone survey in Sweden. This tool was used to inform
the attitude-related component of our survey. The survey assessed the attitudes of young people
towards substances, substance users and to alcohol and drug policy. As alcohol is a culturally
stigmatised substance in Iraq, it is likely to be perceived similarly to the way illicit drugs are perceived
in a European country like Sweden. For this reason, the drug availability, attitudes, and policy
component of this student-targeted Swedish survey were considered to provide appropriate questions
about alcohol in the Iraqi context. In addition, use of published questions allows potential comparison

43
between findings on alcohol in Iraq with findings on alcohol and illicit drugs in western contexts such
as Sweden.
Most questions were changed to suit the local context – for example, items such as “One can’t have
many friends in this university if one doesn’t drink alcohol” were removed or replaced by the
opposing view “One can’t have many friends in this university if one drinks alcohol”. Another
example is that in the following items about illicit drugs, the word “drug” was replaced with “alcohol”
(responses use a Likert scale): “If a teenager tries drugs it is a sign of a much more serious problem”
and “Trying drugs is a normal part of growing up when you are a student at university.” These simple
changes were made based on the author’s own cultural understanding and were checked with local
collaborators
The 2013 Australian National Drug Strategy Household Survey (Australian Institute of Health and
Welfare, 2013) is the largest national household study on alcohol and drugs in Australia. This
validated survey was used to inform the demographic and substance use components of the survey.
In addition, three validated tools were also included: the Alcohol Use Disorders Identification Test
(AUDIT) (T. F. Babor et al., 2001), the Primary Care Post-Traumatic Stress Disorder screening test
(PC-PTSD) (Prins et al., 2003) and the MacArthur Scale of Subjective Social Status (Goodman et al.,
2001).
At first, we decided to include the full ten item AUDIT test to identify alcohol use and misuse within
this sample. Rather than using the full ten item AUDIT, we used the shorter, three item version,
AUDIT-Consumption (AUDIT-C) (Bush et al., 1998). This was done for brevity purposes and
because items of guilt (item 7) and others’ worry about one’s drinking (item 10) have been shown to
be possibly misinterpreted in the Iraqi context (Al Mousawi, 2015). These items were shown to
contribute to false-positive results because Muslim drinkers in abstinent or conservative areas may
feel guilt even with after consuming even a small amount of alcohol. Consumption of any amount
would also trigger friends and family to talk to the drinker about their alcohol consumption.

44
The PC-PTSD (Prins et al., 2003) was used to identify students with potential PTSD symptoms and
triggers. This tool was used because of its brevity and it has been validated in several cultural settings
(4 items).
The MacArthur Scale of Subjective Social Status (Goodman et al., 2001) was used to self-report the
social, economic, and educational level of participants within Iraqi society. We chose to use this
method instead of income report as the social classes that exist within Iraqi society are not always
based on wealth. It is likely one can find an Iraqi considered from a higher social class that is not
considered wealthy relative to the general population and vice versa. Self-reporting also provides a
lens into how students perceived their position within Iraqi society and how this impacted their
reported behaviours and attitudes.
The demographic questions included university, faculty, age, sex, religion, marital and living status.
In our question about religion, we were careful not to ask about sect within Islam (Shia or Sunni) as
the results may contribute to tension in the already sectarian situation in the country. This also did
not impact our findings as all Islamic sects share alcohol prohibition.
The English survey (appendix 4) was first drafted and shared with the in-country collaborator. After
finalising comments and reviews, the survey was translated to Arabic and circulated again (appendix
5). The survey was then piloted by two medical graduates and a student representative who assessed
the content, translation, its cultural appropriateness, and the length of the survey. The survey took
around 20 minutes to complete and although they thought that it was slightly long, they advised that
the survey kept the participant engaged and that it was realistic to complete. Minor changes to
phrasing were made as a result of the piloting. A random selection of translated survey and interview
questions were back-translated by another colleague to assess translation accuracy. No translation
discrepancy was reported.
Qualitative component
Collecting richer qualitative data about the experiences and perceptions of students required a face-
to-face approach. We assessed that conducting the interviews via online video or phone services may

45
have been more challenging and sensitive for the student. This is because the participant could not
see the interviewer or his reactions and may have had concerns about undeclared recording or
interception of the interview.
In the semi-structured interviews, no questions were asked regarding the person’s own alcohol
consumption or attitude towards alcohol. Rapport building prior to the interview increased the
comfort of the student in speaking to the interviewer. In all questions, we asked about stories or things
that the interviewee may know about the prevalence of alcohol in Iraq and of the attitudes of others
towards alcohol. We also asked about their perspectives about what influences alcohol use behaviours
in Iraq. This was done so that the questions did not make the participant feel ‘accused’, scared or
uncomfortable during the interview. We used the assumption that by asking about other people’s
experiences and views, we can have an insight to the participant’s own attitudes and thoughts.
Once the draft interview guide was finalised, the structure was shared with local medical staff (two
medical researchers and a medical graduate) and cultural/religious expert (religious scholar) for
comment. The interview was also practised with two medical graduates and a student representative
to assess its appropriateness for the local setting. No amendments were suggested to the structure of
the interview.
Iraq is a country that culturally practices sex segregation. For this reason, for maximum comfort, the
gender of the interviewer and the interviewee ought to be the same. Ideally, a female research assistant
would have been hired and trained in each study site as it is not always acceptable or possible for
females to travel alone or with strangers in the local culture. Even in the case that we did find a female
research assistant who was able to travel – all the travel costs and accommodation would need to be
covered to each study site. These approaches were not practical considering the unfunded nature of
this study and the limited time the researcher had at each study site in Iraq (due to the security situation
and difficulty to secure trusted transport).
Female participants may not feel comfortable to be interviewed by a man, especially regarding a
sensitive topic such as alcohol. In addition, females may not want to be observed talking privately

46
with a male and they may feel uncomfortable talking to males whom they do not know or are not
related to. Also, in Iraq, it is not appropriate for members of the opposite sex to be in an enclosed
space if they are not related by blood or marriage.
As there was not a female interviewer available, steps were undertaken to maximise comfort and
cultural sensitivity when recruiting female participants. Most participants, regardless of gender, were
recruited using an “arms-length” approach – that is that recruiters other than the researcher
approached the students for participation (Nathan et al., 2019). Females were approached, where
available, by another female who was a volunteer research assistant (at University A and B) or by
other senior male students or staff members known to the students (at University A and C). This was
to ensure that female participants did not feel uncomfortable. It was explained to the potential
interviewee that we prefer to conduct a one-on-one interview at a distance from other students due to
the sensitivity of the topic – but that if they preferred, we may either sit closer to other students or the
female participant may be accompanied by one of her peers. If the interview was to be conducted in
a room, we always ensured the door remained open.
We also tried our best to conduct our interviews in casual or outdoor university spaces – however,
this was not always possible when the faculty provided us with interview rooms or offices (including
the dean or associate dean’s office). The offer of an office was out of respect from the faculty for my
research and me as an international researcher. It was also to ensure that interviews are conducted in
a quiet room without disruption.
Rapport building is essential to ensure that participants share their knowledge and experience honestly
and comfortably with the interviewer (Nathan et al., 2019). Before the interviews, the interviewer
ensured that he introduced himself and the overall topic. The interviewer then casually conversed
with the student about their day and study. The conversation on the research topic usually flowed
naturally. Recording started when the student was comfortable. It was more challenging to build
rapport with female students as they were reluctant to engage in casual conversation or to maintain
eye contact. The interviewer ensured to follow general rapport building techniques such as

47
maintaining an open and approachable body language, eye contact and using visual and verbal cues
throughout the interview. The questions were also first generic before being focused and more
sensitive (Nathan et al., 2019).
All the interviews were translated to English and transcribed in a one-step method (Arabic Audio to
English Text) by the author. Initial interviews were translated verbatim, including anything said by
the interviewer. However, due to the time-consuming nature of this exercise and the lack of funding
for this research, only participants’ answers were translated in most of the interviews. Several (3-5)
transcripts were checked by bilingual colleagues to assess validity. No obvious discrepancy was
identified in the transcripts that were checked. Thematic template analysis method was used to code
and analyse the data (King, 1998). Template analysis encourages the initial use of a priori themes
informed by previous literature and expected to be relevant to the analysis (King, 1998). This template
of themes and codes is then progressively modified as the analysis occurs. The final template serves
as the basis for the overall analysis and interpretation of the data and write up (King, 1998). The
method is explained in more detail in Chapter 6.
The author as researcher (reflexive statement)
The researcher undertaking any study has a conscious and unconscious impact on the entire research
process (Dodgson, 2019). A reflexive statement reflects on the researcher’s involvement and how it
shaped the research outcomes. This process helps identify the actual or potential impact of the
researcher’s personal, contextual, and circumstantial aspects on the research design, data collection,
analysis, and write-up. This in turn assists readers to understand and interpret the research in light of
some of the researcher’s possible influence on the study (Dodgson, 2019).
To give this section some context, I will briefly provide an overview of my own life and experience
in Iraq. Although born in Iraq, I have only ever lived there for the first five months of my life, which
started amid war in 1991. For the next decade, my family and I were refugees, travelling through
several countries in pursuit of a safe place we can call home before arriving to Australia. I mention
this is to bring context to myself as a researcher in this setting – although I am an ‘insider’ (because

48
I speak the language fluently, am aware of the culture, religion, etc.), I am also an outsider, as a
foreign traveler or researcher going to Iraq. This mix of familiarity and distance provided me a
particular lens into the Iraqi situation.
My previous travels to Iraq (since 2008) have been brief and I have stayed the entire period with my
family with limited interactions with outside circles. I was keen to change that from my first trip – I
wanted to know more about Iraq than just my immediate family circle and this drove me to try to
learn more about local peoples, the changing and evolving cultures and attitudes in Iraq as well as the
ever growing tension between ‘tradition’ and ‘modernity’ – and because of this I started observing
more things, asking more questions and having more conversations. This research for me was founded
on these curiosities. Alcohol was the ideal topic to investigate, as opinions about it are so divided –
in a way Iraqis “either love it or hate it”. Furthermore, the uniqueness of Iraq’s situation regarding
vulnerabilities to alcohol and drug use is unmatched – making the research important on a global
scale.
Iraq is unique – it is a MMC with historically considerable populations of non-Muslims and
competing views regarding many social issues, perspectives and behaviours. By observation, alcohol
is one of these examples of competing viewpoints. As described in Chapter 1, Iraq has gone through
continuous war, sanctions, terrorism, and political unrest for at least the past forty years. Iraq’s young
population is also growing at an exponential rate with over 60% under the age of 24. Since 2003, Iraq
changed dramatically – from an enclosed authoritarian socialist state to a liberal capitalist democracy.
This meant that the media and all exposure to the outside world and internationalisation changed from
being non-existent to being inside every household. When one drives past some of the poorest areas
in Iraq, there is little there except large satellite dishes, some bigger than the roof of the sheds they
supply. At the same time, unemployment is rife, social and health facilities are limited, education is
at a low point, poverty and displacement have increased over the past few years and mental health is
almost not mentioned. At the same time, alcohol is a taboo and there is no mention, education, or
awareness about it except in limited health and religious programs and circles. My experience of Iraq

49
has shaped the research questions, helped inform the development and implementation of the
methods, and the interpretation of the data.
Ethics approval
Ethics approval was sought and granted by the Medical Ethics Committee at the College of Medicine
in the University of Kufa, Iraq (MECCM-0028 – appendix 1).

50
References
Al Mousawi, A. (2015). "Alcohol use disorder identification test use in Muslim countries."
International Journal of Prevention and Treatment of Substance Use Disorders 1(3-4): 79-
92.
Arksey, H. and L. O'Malley (2005). "Scoping studies: towards a methodological framework."
International Journal of Social Research Methodology 8(1): 19-32.
Australian Institute of Health and Welfare (2013). National Drug Strategy Household Survey.
Canberra, Australian Institute of Health and Welfare (AIHW),.
Babor, T. F., J. C. Higgins-Biddle, J. B. Saunders and M. G. Monteiro (2001). AUDIT: The Alcohol
Use Disorders Identification Test: Guidelines for Use in Primary Care. Geneva, World
Health Organization.
Bullock, S. (2004). Alcohol, Drugs and student lifestyle: a study of the attitudes, beliefs and use of
Alcohol and Drugs among Swedish University students, Centrum för socialvetenskaplig
alkohol-och drogforskning (SoRAD).
Bush, K., D. R. Kivlahan, M. B. McDonell, S. D. Fihn and K. A. Bradley (1998). "The AUDIT
alcohol consumption questions (AUDIT-C): an effective brief screening test for problem
drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders
Identification Test." Arch Intern Med 158(16): 1789-1795.
Ghandour, L., A. Chalak, A. El-Aily, N. Yassin, R. Nakkash, M. Tauk, N. El Salibi, M. Heffron and
R. Afifi (2016). "Alcohol consumption in the Arab region: What do we know, why does it
matter, and what are the policy implications for youth harm reduction?" International Journal
of Drug Policy 28: 10-33.
Goodman, E., N. E. Adler, I. Kawachi, A. L. Frazier, B. Huang and G. A. Colditz (2001).
"Adolescents' perceptions of social status: development and evaluation of a new indicator."
Pediatrics 108(2): E31.
King, N. (1998). Template analysis. Qualitative Methods and Analysis in Organizational Research:
A Practical Guide. G. Symon and C. Cassell. London, Sage: 118-134.
Moher, D., A. Liberati, J. Tetzlaff, D. G. Altman and P. G. The (2009). "Preferred Reporting Items
for Systematic Reviews and Meta-Analyses: The PRISMA Statement." PLOS Medicine
6(7): e1000097.
Munn, Z., C. Stern, E. Aromataris, C. Lockwood and Z. Jordan (2018). "What kind of systematic
review should I conduct? A proposed typology and guidance for systematic reviewers in the
medical and health sciences." BMC medical research methodology 18(1): 5-5.
Peters, M. D. J., C. M. Godfrey, H. Khalil, P. McInerney, D. Parker and C. B. Soares (2015).
"Guidance for conducting systematic scoping reviews." JBI Evidence Implementation 13(3).
Prins, A., P. Ouimette, R. Kimerling, R. P. Cameron, D. S. Hugelshofer, J. Shaw-Hegwer, A.
Thrailkill, F. D. Gusman and J. I. Sheikh (2003). "The primary care PTSD screen (PC-
PTSD): development and operating characteristics." Primary Care Psychiatry 9(1): 9-14.
Schoonenboom, J. and R. B. Johnson (2017). "How to Construct a Mixed Methods Research Design."
Kolner Zeitschrift fur Soziologie und Sozialpsychologie 69(Suppl 2): 107-131.
UNDESA (2013). Definition of Youth.

51
Chapter 3: Alcohol: From Mesopotamia to Modern Iraq
Chapters 1 and 2 introduced the overall objectives and methods of this thesis. Those chapters pointed
out the scarcity of alcohol research in Iraq. No literature review provides a background to the context
of alcohol in that country. This chapter aims to fill this gap by providing a socio-historic context to
the place of alcohol in Iraqi cultures. We set out with an overview of the diverse groups of ethnicities,
religions and cultures present within the borders of modern Iraq. Many minority groups in Iraq
identify with pre-Islamic indigenous ethno-religious identities that have been in Iraq for millennia.
This chapter also notes the position of Islam, the majority religion in Iraq, on alcohol and describes
how alcohol’s place in Iraqi society shifted in the post-Islamic era and during the past century. By
acknowledging these histories, a clearer insight on alcohol’s place in Iraq’s current diverse society
can be established. This chapter explains the challenges that Iraqi society has faced in the recent
decades and how these experiences may impact the attitudes and choices of young Iraqis today. By
providing an overview of existing alcohol research and policies in Iraq, this chapter also aims to set
out the challenges and sensitivities of alcohol research, policy, and treatment in the country.
The following article has been published in the Journal of Ethnicity in Substance Abuse:
Al Ansari M, Dawson A and Conigrave K (2019) Alcohol: from Mesopotamia to modern Iraq. Journal
of Ethnicity in Substance Abuse, 1-23 DOI: 10.1080/15332640.2019.1657541

REVIEW
Alcohol: from Mesopotamia to Modern Iraq
Mustafa Al Ansaria , Angela Dawsonb , and Kate Conigravea,c
aThe University of Sydney School of Public Health, Faculty of Medicine and Health, University ofSydney, Sydney, Australia; bFaculty of Health, University of Technology, Sydney, Australia; cDrugHealth Services, Royal Prince Alfred Hospital, Sydney, Australia
ABSTRACTAn understanding of alcohol’s place in Iraq’s history and soci-ety can help inform alcohol policy responses in that countryand other Muslim majority countries. This article describes thehistory of alcohol in Iraq from ancient to modern times, withreflection on the challenges facing Iraqi youth today. A searchwas undertaken to identify peer-reviewed and gray literaturethat describes alcohol-related practices, norms, and valuesacross the millennia in Iraq. A historical overview is providedof alcohol’s use and context, with more detail on recent times.Alcohol was an important commodity in Iraq until the rise ofIslam in the seventh century CE. Despite the subsequentIslamic restrictions on alcohol, alcohol remained present inIraq’s society and cultures. Recent studies provide varyingdescriptions of the prevalence of alcohol consumption, andthere are challenges in researching this sensitive topic. Externalforces shaping alcohol use in Iraq include direct and indirectalcohol promotion, globalized media, and conflict and violencewith its associated stress and trauma. Alcohol research andpolicy development in Iraq must consider the country’s uniquecultural, religious, historical, and political context. Iraq’s youthmay be subject to pressures to increase consumption, andthus policies must be informed by an understanding of thecomplex set of current perspectives and pressures.
KEYWORDSAlcohol; Iraq; Muslimmajority countries; Islam;history; youth
Introduction
The fertile lands of Mesopotamia, between the Tigris and Euphrates rivers,are the probable hosts of the first permanent human settlements fromaround 10,000 BCE (Potts, 2012). The desire to brew beer has been citedas a possible trigger for the establishment of grain farming and suchsettlements (Hanson, 2013; Hornsey, 2003). Today, alcohol is linked to 3.3million deaths or 5.9% of deaths worldwide (World Health Organization,2014). Most alcohol consumption occurs in high-income countries. Inresponse, these countries are increasingly regulating alcohol use by restrict-ing availability, limiting marketing, and increasing taxation (Babor, 2010).
CONTACT Mustafa Al Ansari [email protected] Drug Health Services, Lvl 6, King George VBuilding, Royal Prince Alfred Hospital C39, University of Sydney, 2006, NSW, Australia.Color versions of one or more of the figures in the article can be found online at www.tandfonline.com/wesa.� 2019 Taylor & Francis Group, LLC
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSEhttps://doi.org/10.1080/15332640.2019.1657541
52

To maintain income and productivity, the global alcohol industry is nowgrowing its investments in low- and middle-income countries (AlcoholPublic Policy Group, 2010). This is where the largest increase in alcoholuse exposure has occurred (Gakidou et al., 2017). The highest proportionalincrease in drinking is in countries with low baseline levels of alcoholconsumption (Alcohol Public Policy Group, 2010). Young people areparticularly vulnerable to both alcohol marketing and alcohol-related harm(World Health Organization (WHO), 2014) and are most at risk fromdrinking. Alcohol is the leading risk factor globally for burden of diseasein people aged 15–49 years (Gakidou et al., 2017). Accordingly, low- andmiddle-income countries with young populations and high rates ofabstinence may be especially susceptible to emerging alcohol marketing andalcohol-related harm (WHO, 2014). While Muslim majority countries(MMCs) may be protected by strong religious and cultural taboos in relationto alcohol, their population is unlikely to be totally immune. Indeed, MMCshave seen some recent increases in alcohol consumption (WHO, 2011).Iraq is an upper-middle-income country with an estimated population
of over 38 million, of which three out of five are younger than 24 yearsof age (United Nations Department of Economic and Social Affairs[UNDESA], 2017). While only 3.4% of Iraqi adults report current alcoholconsumption (U.S. Department of State, Bureau of International Narcotics& Law Enforcement Affairs, Iraqi Society of Addiction Medicine,University of California LA, & Center for Human Services, 2015), there aremany pressures on young Iraqis that may increase alcohol misuse. Theseinclude exposure to global media, alcohol promotion, and violent conflictwith its associated political and economic instability, stress, and trauma.Insights into the social, cultural, and historical context of alcohol use in Iraq
can help inform an appropriate policy response. In Iraq, the majority populationof Muslim Arabs and the minority religious and ethnic groups continue to iden-tify with religions and cultures dating back centuries or millennia. An examinationof these traditions can contribute to improved understanding of contemporaryIraqi attitudes and practices related to alcohol. This article provides a chrono-logical overview of the history of alcohol in Iraq and of available data on currentattitudes and consumption, including among young people. Finally, it considersthe challenges faced by researchers and policy makers in Iraq and other MMCsin close geographical proximity that share similar cultures and sensitivities.
Methods
A search of databases and websites was undertaken to identify peer-reviewed and gray literature that describes alcohol-related practices, norms,and values across the millennia in Iraq. This search was not exhaustive,
2 M. AL ANSARI ET AL.
53

particularly for periods up to the 20th century, but was undertaken to revealthe range and nature of available material. This research used primary andsecondary sources in English, Arabic, and Persian (Farsi) languages.For the pre-Islamic era, reference books and articles about the origins of
human alcohol consumption were consulted to gather information aboutalcohol in Iraq’s early history. These were identified through GoogleScholar, library database searches, and searching through hard-copy booksin relevant sections of the university library.Arabic primary sources such as Qur’an exegesis (tafsir) and jurispruden-
tial (fiqh) books were consulted to identify the development of the Islamicjurisprudential position on alcohol. Some of these findings have also previ-ously been published in the English literature (Al-Ansari, Thow, Day, &Conigrave, 2016; Enes, n.d.; Feins, 1997; Michalak & Trocki, 2006). Wherethere were commonalities in findings between peer-reviewed papers andthe primary Arabic literature, the English sources were cited as they aremore accessible to non-Arabic readers. A similar approach was undertakenfor the brief overview of alcohol use during the Islamic era. An extensivesearch of Arabic and English publications on the social position of alcoholin Iraq during the 20th century was also conducted online and in theUniversity of Sydney Library.Peer-reviewed literature relating to the place of alcohol in Iraq’s society and
culture and prevalence of its use were identified using the search terms“alcohol” and “Iraq” on Scopus. The search identified almost 400 studies, butmost were on alcohol use among U.S. servicemen returning from Iraq. Afterexcluding the search terms “military or veterans or duty or soldiers or armed”and excluding irrelevant articles (e.g., relating to laboratory studies of ethanol),there were only three articles specifically about alcohol. In addition, eightarticles on other topics included information about alcohol (three about otherdrugs [benzhexol and corticosteroids], three on mental health [e.g., schizophre-nia], one on driving behaviors, and one on health management). Other data-bases revealed even fewer results. These international academic sources werecomplemented with articles from local unindexed academic journals (someaccessed through Research Gate) or gray literature and from conference pre-sentations. Iraq’s alcohol policies were identified using primary legal sources(in Arabic) from legal databases (e.g., the Iraqi Local Governance LawLibrary). Information about implementation of these policies was mostly gath-ered from gray literature such as online media reports (in Arabic and English).
Findings
Iraq has been home to and influenced by many ethnicities, cultures, religions,and civilizations. This is in part due to Iraq’s location at the crossroadsbetween Central Asia, West Asia, Arabia, Africa, and Europe (Figure 1).
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 3
54

The country’s evolving attitude toward alcohol (summarized in Figure 2)provides a lens to better understand the modern Iraqi society.
Alcohol and Iraq in pre-Islamic history
Beer played a central role in ancient Mesopotamia; it provided the necessarycalories to carry out daily work and was clear of the fecal matter that oftenpolluted freshwater sources (Wolf, Bray, & Popkin, 2008). Accordingly, beeris said to have replaced water as the most consumed beverage (Corfield,2015), and it acted as a form of currency (Corfield, 2015; Sinclair & Sinclair,2010). Beer was socially consumed from a large vat using straws (Hornsey,2003; Sinclair & Sinclair, 2010). The straws were sometimes made from goldand silver and measured approximately 1 cm in diameter and 93 cm in length(Sinclair & Sinclair, 2010). The first brewing recipe spread from southernIraq as a hymn to the Sumerian Goddess of brewing, Ninkasi (Corfield,2015; Hornsey, 2003).
Figure 1. Locations of the major historical capitals within Iraq’s modern borders.
4 M. AL ANSARI ET AL.
55

Wine making similarly originated near the borders of Iraq in modern-day Iran in the fifth millennium BCE (Wolf et al., 2008). In southernMesopotamia, Babylonians worshiped wine deities and used both beer andwine for ceremonial purposes (Hanson, 2013). This region is where the firstevidence of alcohol policy can be found, in the 18th century BCEBabylonian code of Hammurabi. The engraved stone tablet set out legisla-tion on tavern trade and restricted priestesses from opening, operating, orconsuming publicly in taverns (Hammurabi, 1904). Jews in southern Iraqwere also known to have written rules around wine as early as the fifthcentury BCE (Feins, 1997). They continued to produce and consume alco-hol into the Islamic era (Feins, 1997).In northern Iraq, wine was seen as a luxury for the Assyrians, given as a
reward to the men and women who were under the service of the king(Joffe, 1998). This region was also home to the first Christian state, theOshoene Kingdom (Rassam, 2005). Wine was seen as a gift from God, aninherently good substance, but its excessive consumption was frownedupon (Hanson, 2013).In neighboring Arabia, consumption of alcoholic beverages was com-
monplace and had cultural and religious importance until the rise of Islam(Feins, 1997; Maraqten, 1993). Indeed, the significance of alcohol is demon-strated by the hundreds of words that exist for alcoholic beverages in clas-sical Arabic (Maraqten, 1993). The word alcohol is thought to be derivedfrom the Arabic al-kohl, a black powder used in cosmetics for the eye(Matthee, 2014; Michalak & Trocki, 2006; Wiedemann & Allan, 2012).Kohl described any substance that cannot be pulverized any further(Wiedemann & Allan, 2012).In Arabic, alcoholic beverages are also referred to as khamr (literally:
grape wine). The word khamr is the root of takhmeer (fermentation). Theroot kh-m-r is also the root of Arabic terms, including covering, clouding,hatred, or enslaving (Enes, n.d.; Ibn Manẓ�ur, 2003). For this reason, theterm khamr is widely believed to be inclusive of all intoxicants and not justgrape wine (Enes, n.d.; Feins, 1997; Ibn Manẓ�ur, 2003).
Figure 2. Timeline of alcohol in Iraq’s history.
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 5
56

Alcohol and Islam
Islam began in western Arabia in the early seventh century, at a time whenalcohol consumption was widespread (Gately, 2008; Maraqten, 1993). Theadvance of Islam, with its teaching of abstinence from alcohol, reducedalcohol production in the region (Wolf et al., 2008). Islam remains the reli-gion of most of Iraq’s population (Pew Forum on Religion & Public Life,2009). Shia Muslims constitute 65%–70% of the Iraqi population, while29%–34% of the population are Sunni (Pew Forum on Religion & PublicLife, 2009). There is a consensus on the prohibition of alcohol in bothschools of thought. However, Abu Hanifa al-Nu’man, one of the main fourSunni jurisprudential authorities, argued that absolute khamr prohibitiononly applies to grape wine (Abb�u Zah�u, 2012; Feins, 1997). Substancesfrom other sources are prohibited if consumed in amounts that causeintoxication (Abb�u Zah�u, 2012; Feins, 1997).
Alcohol in the Qur’an
The Qur’an and the Sunnah form the main basis of Islamic law. TheQur’an is believed to be the word of God, revealed to Prophet Muhammadduring his life.According to some interpretations, the Qur’anic prohibition of alcohol was
gradually revealed via three stages (Figure 3). This was to create an environ-ment that can accommodate the introduction of absolute prohibition(Al-Ansari et al., 2016; Baasher, 1981; Feins, 1997; Michalak & Trocki, 2006).Chronologically, the first verse warned that the harm from intoxicants
outweighs their benefits:
They ask you [Prophet] about intoxicants and gambling: say, “there is great sin in both,and some benefit for people: the sin is greater than the benefit.”(Abdel Haleem, 2005)
Some scholars have interpreted the “benefits” of khamr in the aboveverse to be the temporary pleasure intoxicants provide (Al-Ṭ ab�at:ab�a)ī ,1997). This is consistent with other verses of the Qur’an that speak ofharmless and pure goblets [of wine] in heaven as a reward for good-doers(Qur’an 37:45) (Abdel Haleem, 2005).
Figure 3. Stages of alcohol prohibition in Islam.
6 M. AL ANSARI ET AL.
57

Despite the warnings about the harms of alcohol in this verse, someMuslims continued to drink and even prayed in a state of intoxication(Michalak & Trocki, 2006). Accordingly, the second verse was revealed:
You who believe, do not come anywhere near prayer if you are intoxicated, not untilyou know what you are saying. (Abdel Haleem, 2005)
As Muslims needed to pray five times a day, the verse greatly limited thepossibility of consuming alcohol, but it was not explicitly forbidden untilthe final verse was revealed:
You who believe: intoxicants and gambling, idolatrous practices, and [divining] arrows arerepugnant acts of Satan’s doing—shun them so that you may prosper. With intoxicantsand gambling, Satan seeks only to incite enmity and hatred among you, and to stop youremembering God and prayer. Will you not give them up? (Abdel Haleem, 2005)
While some scholars argue these verses represent three steps toward theprohibition of alcohol, others say khamr was prohibited from the first verseand the latter verses only elaborate on the prohibition (Al-Ṭ ab�at: ab�a)ī ,1997). Although the Qur’anic prohibition may have been initially gradual,this did not mean that alcohol prohibition was implemented gradually innew areas Islam spread to, such as Iraq.
Alcohol in the Sunnah
The Sunnah is the life, sayings, and teachings of the Prophet Muhammad(relayed via hadith, which were initially verbal accounts). In Shia thought,the life and teachings of the 12 Imams are also considered an accurateinterpretation of Islam (Lindsay, 2005).Statements attributed to the Prophet indicate that khamr is anything that
befogs the mind and that whatever intoxicates in large amounts is prohib-ited in small amounts (Feins, 1997; Michalak & Trocki, 2006). It is alsonarrated that God will reward abstainers, regardless of their intention, forprotecting themselves. This is because consumption of khamr is considereda gateway to every evil (Al-Qummī Al-S: ad�uq, 1984; Enes, n.d.).Hadith literature indicates that in addition to consumption, this prohibition
encompassed any association, production, sale, purchase, transport, profit, orservice of alcohol or any other intoxicant (Al-Ansari et al., 2016; Enes, n.d.;Michalak & Trocki, 2006).
Brief history of alcohol during the Islamic era (seventh–20th centuries)in Iraq
Although the Qur’an and Sunnah prohibit alcohol consumption, there isevidence that some Muslims continued to drink well into the Islamic era(Feins, 1997; Matthee, 2014). There are even examples of Muslim rulers
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 7
58

consuming alcohol from the first century after hijra (Islamic calendar, circaseventh century CE) onward (Feins, 1997). Some Umayyad (661–750 CE inSyria) and Abbasid (750–1258 CE in Iraq) Caliphs were well known fortheir excessive drinking (Abb�u Zah�u, 2012; Feins, 1997; Matthee, 2014).This continued even beyond these empires, when Ibn Battuta, the famous14th-century traveler and chronicler, spoke of a king who was whippedin his own palace as a punishment for his drinking (Ibn Bat: t: �ut: a, 1987).Public consumption was also present, and taverns could be found across
the Muslim world, although their reputation was negative (Matthee, 2014).It is also evident that non-Muslims remained free to produce, trade, andconsume alcohol (Feins, 1997; Matthee, 2014). Strict religious prohibitionand punishment only took place periodically and temporarily, dependingon the ruler (Feins, 1997; Matthee, 2014).Another indicator that drinking did occur in some circles during this era
is the rise of the pre-Islamic genre of wine poetry (khamriyyat) (Kennedy,1997, 2012). Unlike mystic poetry, khamriyyat speak of the love of wineand of intoxication. This style of poetry was mastered by Abu Nawas:
If I count my years I find no excuse for grayness to descend upon my head, Theysay, “You have become old and gray,” yet my hand is not so old that it cannot holda cup to my lips! (Kennedy, 1997)
Abu Nawas is still celebrated in Iraq, and a street named after him, fittingly,has become the center of Baghdad’s nightlife and drinking (Raad, 2017).Alcohol was also used in Islamic medicine, including in antidotes (Ibn
Abi Us: aybi(a, 1996). Ibn Sina (Avicenna) dedicated a portion of his Canon
of Medicine to “rules concerning the use of water and wines.” He explainedsome benefits from wine before prescribing alcohol mixed with mossas a sedative. He also prescribed cures for alcohol overdose while advisingagainst youth intoxication:
To give wine to youths is like adding fire to a fire already prepared with matchwood.Young adults should take it in moderation. But elderly persons may take as muchas they can tolerate. (Avicenna, 1973).
Although public Muslim consumption of alcohol was banned, there is evidencethat alcohol continued to be consumed throughout the Muslims lands, includingby the Ottomans, Safavids, Mughals, and Qajar, until the 20th century (Matthee,2014; Matthee, 2005). The last caliphate was abolished on March 3, 1924.
Alcohol and modern Iraq
Brief history of modern IraqBetween the 1500s and early 1900s, Iraq comprised three provinces of theformer Ottoman Empire: Baghdad, Basra, and Mosul (Fontana, 2010;
8 M. AL ANSARI ET AL.
59

Zubaida, 2002). Despite strong resistance, the British occupied Iraq afterthe First World War. The newly created mandate of Iraq, typically labeled“artificial,” included borders with no historic, cultural, or geographic sig-nificance (Fontana, 2010). This Iraqi monarchy became independent fromthe British in 1932 (Zubaida, 2002). In 1958, following an uprising, thecountry became a socialist republic, and soon afterward the Baathist partyoverthrew the government to rule Iraq for the next few decades.Despite this political volatility, Iraq remained one of the most developed
nations in the region, with an annual per capita income of US$3,510 in1989, and 97% of the urban population had access to health care (Ali &Shah, 2000). However, in August 1990, prior to the First Gulf War, inter-national sanctions reduced Iraq’s oil production by 85% and resulted in thedecline of the per capita income to US$450 by 1996 (Ali & Shah, 2000).These sanctions contributed to the death and disability of many Iraqis,especially children (Ali & Shah, 2000; Rowat, 2000). Mortality rates soaredby more than 100% in the space of a few years (Ali & Shah, 2000; Rowat,2000; The United Nations Children’s Fund, 1999). Since 1980 (except for1989), Iraq has been exposed to either war, sanctions, or terrorism.
Alcohol in Iraq in the 20th century CEThere is only limited published work describing alcohol use in Iraq between1932 and the present. From accounts, we know that alcohol production andconsumption was present in the 1940s and 1950s, especially among Iraq’snon-Muslim population (Zubaida, 2014). Zubaida (2014) also speaks of aJewish cooperative of households making their own alcohol for special occa-sions. Alcohol consumption among non-Muslims and in the middle andupper sectors of society was typically in private households or “casinos” andassociated with enjoyment, sociability, and music (Zubaida, 2014).There was, however, another side to drinking in the common pubs (may-
khanas) that were available around Baghdad. These establishments, whereintoxication and fights were not uncommon, were frequented by poorer classes(Zubaida, 2014). In the 1960s, al-Wardi in his Study of the Nature of IraqiSociety mentioned this heavy presence of alcohol in urban environments. Herelayed that men in urban settings drink to prove their masculinity and it isusual to see a drinker trying to engage in physical fights, even if he has notconsumed enough to be particularly intoxicated (Al-Wardī, 1965). This helpsexplain why araq (distilled spirit) was colloquially known as the “lion’s milk”(h: alīb al-Sab
() (Zubaida, 2014). It is postulated that heavy social responsibil-
ities and lack of opportunities for self-expression may have contributed toheavy drinking among Iraqi men (Al-Wardī, 1965; Khayyat, 1990).In 1990, when alcohol was consumed in Iraq at a rate of 0.8 L of pure
alcohol per capita (WHO, 1999), Sana Khayyat (1990) interviewed Iraqi
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 9
60

women (n¼ 50) across the ethnic, religious, and professional spectra. Thewomen reported their husbands typically drank excessively outside thehome and often returned with financial difficulties and an increased chanceof family conflict and domestic violence. Most of the women describedtheir father, husband, or both as “alcoholics” and expressed that men usealcohol to express their adoption of modern attitudes as opposed totraditional customs (Khayyat, 1990).Iraq’s alcohol industry produced both beer and araq and lasted until the
fall of Saddam in 2003 (Jansen, 2006). The Gulf War, international sanctions,and his permissive attitude toward alcohol and nightlife had made Saddamunpopular in religious spheres (Lewis, 1994; Rohde, 2010). As a response, in1994, Saddam introduced the al-H: amla al-�Im�anīyya (faith campaign), whichbanned public alcohol consumption (H: usayn, 1994). Alcohol played sucha role in establishments on Abu Nawas Street (Baghdad’s main entertain-ment quarter) that the space was deemed “dead” following the ban (Raad,2014). The faith campaign was disputed, including by Saddam’s son Uday(Lewis, 1994), who later oversaw Iraq’s largest brewery until the Second GulfWar in 2003 (Jansen, 2006).
Alcohol in contemporary Iraq (21st century)Iraqi legislation allowed the sale and consumption of alcohol within regula-tions until late 2016. Laws enacted in 2001 (Tables 1 and 2) allowed prem-ises with an annual alcohol license to operate. These premises could not besituated in Iraq’s sacred cities or near a mosque, religious establishment,hospital, or school (Makkī, 2001). Such premises were required to be closedduring special religious occasions, including Ramadhan. Individuals had tobe over 21 years of age to work for an alcohol store, and the law permittedalcohol to be sold to anyone over the age of 18 (Makkī, 2001).Most alcohol sales in Baghdad were reported to be conducted by
Christians and Yezidi minorities in Iraq, although some customers wereMuslim (Alive in Baghdad, 2009). Alcohol businesses ceased sales duringthe Islamic holy months of Ramadhan and Muharram (Alive in Baghdad,2009). According to alcohol shop owners, all types of alcoholic beverageswere readily available in their Baghdad stores but were difficult to transportto other provinces for private sale due to the increased presence of policeand security checkpoints (Alive in Baghdad, 2009).These 2001 national regulations remain the most detailed recent laws
regarding alcohol in Iraq. After the 2003 war, alcohol sales declined due toviolent attacks on bottle shops and nightclubs by a mix of government forces,militia, and terrorists (Russia Today, 2014). However, reports from coalitionforces in Iraq suggest that “moonshine,” home-distilled spirit with highalcohol content, was available in Iraq during this time (Von Zielbauer, 2008).
10 M. AL ANSARI ET AL.
61

Following the introduction of the new Iraqi constitution in 2005, someprovincial governments passed their own laws regarding alcohol. A fewprovinces across Iraq, including the port city of Basra, prohibited alcoholproduction, sale, consumption, and import (Agence France-Presse [AFP],2010). Alcohol prohibition in Basra caused anger among the province’snon-Muslim population, who argued that this would drive people to pro-cure their alcohol from illicit sources (AFP, 2009). A number of Christiansalso accused authorities of using the fight against alcohol to drive them outof the country (Leland, 2011).In 2016, the Iraqi parliament introduced a ban on alcohol import,
production, and sale in all Iraqi provinces other than the Kurdistan autono-mous region (Article 14, Municipal Revenue Laws, passed 22 October, 2016)(Al-H: uk�uma al-
(ir�aqiyya [Iraqi Government], 2016). Some analysts have
argued that this ban was initiated by some members of Iraq’s parliament whohad a conflict of interest. They believe that these members used their politicalpower to establish a monopoly on the black-market trade of alcohol in Iraq(Salloum, 2016). Others argue that alcohol has become a political commodity.It is used to differentiate those in support of a secular, pluralist governmentfrom those working on the Islamization of the state (Salloum, 2016).
Table 1. Laws Regarding Application for a License to Sell Alcohol.Applicant One applicant (license cannot be under two or more names)
Iraqi citizenNon-MuslimFemale or male (males must have completed military service)Over the age of 21Not have an existing license for another store for the same purpose
Zoning and location Not be located in the holy cities (Najaf, Karbal�a(, S�amur�a(, K�adhumiyya, andA)dhamiyya)Not be located on freeways, highways, or any other roads connectingtowns or citiesTo be at a minimum distance of (from the boundaries, in all directions):500 meters from Holy Shrines200 meters from Mosques or Islamic centers100 meters from schools or hospitalsIn the correct zoning within the Baghdad council or other municipal councilsApproval from local People’s CouncilThe relevant department will assess whether the location meets all termsand conditions
Size and facilities Wholesale stores:Minimum size of 150 m2, must include rooms for management, budgeting,and to accommodate other staff. Storage facilities or shelters must be includedwith access available for large vehicles. Sanitary facilities must be included.Retail stores:Minimum size of 20 m2.
Other required documents Ownership or lease documents of the potential storeValid business name approved by the Department of TradePermission from the local representative (Mukhtar)License to import alcoholic beverages or primary ingredients for themaking of alcoholic beveragesContract with an alcoholic beverage import or production company
License renewal and conditions The license is annual and must be renewed annually in person before April 1.The Department of Tourism has the authority to limit the number oflicenses given within a district.
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 11
62

Despite this law’s publicity in local and international media, on theground, the alcohol ban was not implemented, and alcohol is still availablein Iraq—mostly in areas famous for their nightlife in Baghdad and Erbil.
Data on the prevalence of alcohol use in IraqAlcohol is an understudied issue in the Muslim world, including in Iraq, whereover half of the alcohol consumed is believed to be unrecorded (WHO, 2014).There have been attempts to fill in this gap by national household studies,such as the Iraqi Mental Health Survey (IMHS) (WHO, 2009) or Survey ofSubstance Abuse in Iraq (SSAI) (U.S. Department of State et al., 2015).However, the results have been limited due to cultural sensitivities in reportingalcohol use in interviews (Al-Hemiery et al., 2017; WHO, 2009). In the avail-able literature, underreporting of alcohol consumption is also indicated by aclear discrepancy between prevalence of self-reported drinking and the preva-lence of knowing someone who has used alcohol (Al-Hemiery et al., 2017).Despite these limitations, anecdotal evidence from the 1980s (Maghazaji
& Zaidan, 1982) and from present-day Iraq (Al-Diwan, Al-Hemiary, &Hashim, 2015) suggests that alcohol consumption in Iraq is increasing.
Table 2. Laws Regarding the Operation of Licensed Stores.Marketing Alcoholic beverages are not to be displayed in a provocative manner
inside or outside the store.All marketing for alcoholic beverages in any media (visual, readable,or audio) is banned.
Age limits Alcohol cannot be sold to those less than 18 years of age.Employees are all to be over the age of 21.
Closing dates All alcohol shops are to shut for the following occasions:Holy month of RamadhanIslamic New Year (1st of Muharram�)Day of Ashura (10th of Muharram)Birth of the holy Prophet MuhammadNight of ascent and descent��All other religious occasions
Operating hours Wholesale stores:Saturday to Thursday 9 a.m. to 6 p.m.Retail stores:Saturday to Thursday from 10 a.m. to 10 p.m. and Friday, 3 p.m. to10 p.m.
Safety measures It is not permitted to amend the type or the label on any alcoholcontainer.Wholesale stores must meet the relevant regulations for the storageof alcoholic beverages (depending on type).Wholesale stores are not permitted to sell individual containers.Retail stores are not permitted to sell wholesale or any alcohol that isnot sealed into individual containers.
Representation or transfer of license If the licensee is away for international travel, he or she must applyprior to travel for a representative to take all responsibility for thestore during the entire period of the licensee’s absence.A licensee may surrender or transfer the license with the permissionof the Department of Tourism to a family member or a shareholderin the company, given that they meet the requirements to holda license.
�Muharram is the first month of the Islamic lunar calendar.��Commemorates the Ascent of the Prophet Muhammad to heaven.
12 M. AL ANSARI ET AL.
63

Reported lifetime alcohol use by male Iraqis has risen from 6.8% to 16.7%in the nine years between the 2006 IMHS and 2016 SSAI. Past 12-monthconsumption has also increased from 2.9% to 6.7% in the same studies.However, it is unclear whether this increase is real or a result of differentsampling and data collection methods. Reported lifetime alcohol use byfemale Iraqis is negligible at 0.6% in both studies, with past 12-month useat 0.4% and 0.1%, respectively.In terms of alcohol abuse, the 2006 IMHS indicated that only 0.1%
of participants met the criteria for DSM-IV alcohol abuse (WHO, 2009). Bycontrast, the 2015 SSAI found that over 70% of current drinkers scoredwithin the dependence range on the Severity of Substance Dependence Scale(SDS) (U.S. Department of State et al., 2015). In other smaller samples,Al-Hemiary and colleagues (2015) interviewed 2,678 people in youth centersacross Baghdad and found 17% of the male sample met DSM-IV criteria foralcohol abuse using the Composite International Diagnostic Interview secondedition (CIDI-2). In this study, alcohol abuse was most common amongthose who were illiterate (73.7%) (Al-Hemiary, Hashim, Al-Diwan, & AbdulRazzaq, 2015). Data from Ibn Rushd Alcohol and Substance Center in 2004revealed that alcohol use disorders accounted for 41% (n¼ 74) of admissionsamong unemployed male patients between the ages of 21 and 30 years(Aqrawi & Hussain, 2010). Similarly, over a third of a sample of medicalresidents and general practitioners (GPs) reported alcohol as the most abusedsubstance in Iraq (Al-Hasnawi, 2006).
The next generation: Alcohol and Iraqi youthIraqi youth are increasingly exposed to alcohol via international media andculture while facing a challenging political, social, and economic situation athome. In 2014, young Iraqis from Anbar province indicated that some youthboast about their drinking and see drug and alcohol use as a way to escapefrom despair, limited rights, and restricted freedoms (United NationsDevelopment Program [UNDP], Ministry of Planning, & Baytul Hikma,2014). They also see intoxication as a way to imitate celebrities. The inter-viewees focused on ease of access and lack of governmental control as factorsin drinking (UNDP et al., 2014).During the ISIS (“Islamic State” of Iraq and Syria) crisis, Iraqi youth
lived under the constant threat of war and violence. Many young Iraqisjoined the ranks of the military to fight against ISIS. Universities alsointroduced voluntary training courses to prepare students to defendagainst potential ISIS advances (Al-J�ami
(a al-Mustans: iriya [University of
al-Mustansiriya], 2015; Al-Rim�ah: ī , 2015; I(l�am al-ta
(līm al-
(�alī [Higher
Education Media Office], 2015; J�ami(at al-K�ufa [University of Kufa], 2015).
Despite the subsequent decline of ISIS in Iraq, almost nine million Iraqis
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 13
64

still require humanitarian assistance. These include two million internallydisplaced persons (IDPs) (United Nations Office for the Coordinationof Humanitarian Affairs (UNOCHA)), 2018) and four million children(The United Nations Children’s Fund [UNICEF], 2018).Mental health issues are a concern among young Iraqis, with a study
revealing that nearly half (47%) of a sample of 600 primary school childrenin Baghdad had been exposed to a major traumatic event in the past twoyears and 14% of the sample had symptoms of posttraumatic stress disorder(PTSD) (Razokhi, Taha, Taib, Sadik, & Gasseer, 2006). In Mosul, before theISIS occupation, 30% of a secondary school student sample suffered PTSDwith the majority (92%) not receiving any treatment (Razokhi et al., 2006).Previous research has drawn an association between conflict exposure andalcohol abuse among veterans (Browne et al., 2008; Kelsall et al., 2015; Wilket al., 2010) and civilian (Weaver & Roberts, 2010) populations in other set-tings. However, there has been no research about alcohol and war on anyIraqi sample and very limited research on alcohol and internally displacedpopulations (Ezard et al., 2011; Roberts & Ezard, 2015).
Discussion
Alcohol’s place in Iraq’s history is as volatile as the political, security, andeconomic tides that continue to affect the country. The relationship betweenIraq and alcohol is a geopolitical one because alcohol as a commodity in Iraqis more than just another beverage or substance that might have negativehealth effects. Due to the long history of alcohol in Iraq and the expandingexternal cultural, economic, and political influences, alcohol is a commoditythat is often seen to demarcate the “traditional” and the “modern,” the“basic” and the “sophisticated,” the “religious” and the “secular.”The conversation about alcohol throughout Iraq’s history has typically
centered on culture and religion more than on health and medicine. Many ofIraq’s minorities are indigenous to the country and have had a culture ofdrinking that has lasted for millennia, even under Muslim rule. Some Muslims,including royalty, consumed alcohol despite the abstinence of the majority(Matthee, 2014; Nahas, 1982). For centuries, Iraq and neighboring countrieshave seen more stigma toward alcohol than toward other drugs. This is due tothe lack of certainty about the prohibition of other intoxicating substance suchas cannabis (hashish) among rulers, scholars, and lay persons (Nahas, 1982;Rosenthal, 2015). Similarly, use of other drugs and treatment seeking forproblems with those drugs are less stigmatized than for alcohol in Iraq(Al-Hasnawi, Aqrawi, Sadik, & Humphreys, 2009; Brandt, 2005; White, 2011).Historically, there have been several policy interventions in the Islamic
era. For example, Al-Mansur Qalawun, the 13th century Mamluk ruler of
14 M. AL ANSARI ET AL.
65

Egypt and Syria, allowed alcohol and cannabis production and trade butimposed excise taxes on the sale of both substances (Nahas, 1982). In othertimes, consumers of alcohol were punished (Ibn Bat: t: �ut: a, 1987) and thetrade outlawed (Nahas, 1982). This is similar to what occurred on a massscale post-2003 when reportedly 95% of alcohol stores closed due to threatsdespite all being owned and operated by non-Muslim minorities (Taneja,2007). This has driven non-Muslim minorities in Iraq to argue that alcoholtrade and use is their “right” (AFP, 2009). This tension about the right toconsume or trade alcohol among non-Muslims is juxtaposed with the reli-gious and cultural conviction of Iraq’s majority Muslim population thattypically abstains from alcohol and frowns upon any alcohol consumption.These contrasting viewpoints set unique challenges for policy makers andresearchers. It also makes it difficult to discuss alcohol without being per-ceived as advocating either “prohibition” or “normalization” of alcohol use.Due to the Islamic prohibition and social stigma around alcohol, reported
prevalence of alcohol use in Iraq is currently low compared to countrieswhere alcohol consumption is culturally accepted. However, the rate ofalcohol abuse and dependence among those who do drink is a concern.More than 70% of current drinkers in the Iraqi nationwide household sur-vey reported symptoms of dependence (2.4% of the total population, withSDS 3þ) (U.S. Department of State et al., 2015). This prevalence of depend-ence among drinkers is strikingly high. By comparison, in Australia, 1.7%of current drinkers (1.4% of the total population) were dependent (usingWMH-CIDI v3.0, DSM-IV criteria) (Teesson et al., 2010). However, SDSincludes items about “worry about drinking” and the respondent’s desire tostop drinking. Some positive responses could be the result of cultural/reli-gious prohibition of alcohol use. Nonetheless, any increase in consumptioncould be associated with an increased demand on treatment services.Currently, there are very limited facilities for alcohol and drug treatment
in Iraq. Al-Rashad Hospital and Ibn Rushd Hospital were reportedly theonly psychiatric hospitals in Baghdad, with only the latter hosting a special-ized alcohol and drug dependence unit (Al-Hasnawi, 2005). There is alsoreportedly a 40-bed center for alcohol and drug treatment currently beingestablished in Basra (Salaheddin, 2018). The shortage of specialists andtreatment facilities in Iraq means that often only those who can affordmedical care in other countries are able to seek treatment (Salaheddin,2018). Although no published information is available on alcohol-specifictreatment, literature on mental health access in Iraq indicates the barriersof stigma and shortage of services and staff (Bolton, 2013; Sadik, Bradley,Al-Hasoon, & Jenkins, 2010). There have been efforts to incorporate mentalhealth in primary health care (Sadik, Abdulrahman, Bradley, & Jenkins,2011) and to train general practitioners in mental health (Al Hilfi, Lafta, &
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 15
66

Burnham, 2013). However, most Iraqis do not feel comfortable speakingabout mental health with primary care health providers or even with familyand friends (Sadik et al., 2010). Anecdotally, primary health care in Iraqhas limited confidentiality guarantees, especially within the public healthsystem, and it is usual for multiple patients to see a practitioner in thesame consultation room at the same time. Although steps such as alcoholor drug treatment integration into primary health care may increase treat-ment access, there is a long way to go until the Iraqi health system cancope with such pressure. This includes having adequate resources to allowconfidentiality and availability of non-local health professionals, so localsare more at ease to share their alcohol-related concerns without fear of los-ing face or being outcast by their community. Religious bodies and scholarsmay also help with easing the path to treatment, even in areas with alcoholprohibition. An example of this is the issuance of a fatwa (ruling) in neigh-boring Iran that decriminalized treatment access (Al-Ansari, Thow,Mirzaie, Day, & Conigrave, 2019). Alternative avenues for treatment mayalso in the future be provided by religious or cultural organizations whomay integrate their own teachings with evidence-based approaches such asbrief interventions or Alcoholics Anonymous’s 12-step program. However,success will rely on guaranteed confidentiality and reduced stigma aroundalcohol treatment access.Available studies, albeit limited, indicate a possible increase in alcohol con-
sumption since the 2003 war in Iraq. Reasons for this are multifaceted but mayinclude war and media exposure. Although an association between exposure totrauma by civilian populations and increased alcohol misuse has been found,studies in this field are scarce (Weaver & Roberts, 2010). However, a systematicreview of longitudinal studies concluded that exposure to alcohol in the mediaincreases the likelihood of adolescents’ onset and/or increase of alcohol con-sumption (Anderson, de Bruijn, Angus, Gordon, & Hastings, 2009).Lebanon, an MMC with some similarities to Iraq, has also experienced
increased alcohol use in the past few decades. Like Iraq, Lebanon has sev-eral other religious and ethnic minorities, although Lebanon’s non-Muslimpopulation is proportionally larger. There was marked increase in alcoholconsumption in the postwar period between 1991 and 1999, especiallyamong females (40.7% to 67.7%) (Karam, Maalouf, & Ghandour, 2004).Similarly, in Egypt, where half of the population is younger than 20, alco-hol consumption has increased in large community samples from 2.2% in2005/2006 (Emad Hamdi et al., 2013) to 5.9% in a study conducted overthe years 2007 to 2014 (E Hamdi, Sabry, Sedrak, Khowailed, & Loza, 2016).In neighboring Iran, an increase in youth drinking is also indicated (S: ir�amī ,Qurb�anī, & Mīn�unī, 2013). In the MMC context, younger people are at higherrisk to initiate or increase their alcohol consumption as they have increased
16 M. AL ANSARI ET AL.
67

exposure to direct and indirect alcohol marketing across traditional and socialmedia platforms (Anderson et al., 2009; Ghandour et al., 2016).
Conclusion
Despite the limited prevalence of alcohol consumption, the Iraqi environmentis potentially conducive for increased drinking, especially among its youthpopulation. Young people in Iraq are exposed to many stressors as well as toglobal alcohol marketing. Iraqi governments, organizations, and families arelikely to be preoccupied with basic survival needs such as safety, security, andaccess to electricity. Currently, due to the lack of developed mental health oralcohol-related policy or strategies in Iraq, the only protective factors are reli-gious prohibition and the cultural stigma that has developed over the centuries.A well-developed alcohol policy that provides adequate strategies, regulations,and treatment facilities to prevent and treat alcohol misuse is needed. Any suchpolicy development needs to make use of the modern evidence base as well as asensitive approach, founded on an in-depth understanding of Iraq’s long anddiverse religious, social, and cultural traditions. This is also needed to shift thedebate from purely a cultural or moral lens to include a focus on health, med-ical, and social needs; this multi-lensed approach may find consensus from thediverse ethnic, religious, and cultural groups of Iraq.
Acknowledgement
We acknowledge Ayatollah Mohammad Hussein Al-Ansari for his help in identifying andexplaining some of the Islamic literature used in this paper.
ORCID
Mustafa Al Ansari http://orcid.org/0000-0003-4989-8686Angela Dawson http://orcid.org/0000-0003-0926-2202
References
Abb�u Zah�u, F. (2012). Maj�alis al-Lah�u Fī Qus: �ur al-Khulaf �a)Fī al-
(as: r al-
)abb�asī al-Awwal
(132-232 AH/750-847 CE). (Masters), J�ami(at al-Naj�ah: al-Wat: aniyya, Nablus.
Abdel Haleem, M. A. S. (2005). The Qur’an: A New Translation by M. A. S. Abdel Haleem.Oxford: Oxford University Press.
Agence France-Presse. (2009, January 13). Masī h: iy�u al-Bas: ra yah: taj�un(ala man
(
al-mashr�ubat al-Kuh�uliya fī Rama :dan [Christians in Basra Protest Ban on AlcoholicBeverages in Ramadan]. Retrieved from http://www.webcitation.org/6fqjnykTZ
Agence France-Presse. (2010, January 13). Th�alith muh: �afaẓa(ir�aqiya yaf�uz bih�a al-M�alikī
tuqarir h: aẓ r bay(al-Khum�ur [Third Iraqi Province Maliki Won that Decides to Ban
Alcohol Sales]. Retrieved from http://www.webcitation.org/6fqjsnZOM
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 17
68

Al-Ansari, B., Thow, A.-M., Day, C. A., & Conigrave, K. M. (2016). Extent of alcoholprohibition in civil policy in muslim majority countries: The impact of globalization.Addiction, 111(10), 1703–1713. doi:10.1111/add.13159
Al-Ansari, B., Thow, A.-M., Mirzaie, M., Day, C. A., & Conigrave, K. M. (2019). Alcoholpolicy in Iran: Policy content analysis. International Journal of Drug Policy, doi: 10.1016/j.drugpo.2019.07.032
Al-Diwan, J., Al-Hemiary, N., & Hashim, M. (2015). Alcohol and drug abuse in post-con-flict Iraq. European Psychiatry, 30(Suppl. 1), 1394. doi:10.1016/S0924-9338(15)31080-4
Al-Hasnawi, S. (2005). Substance use disorders in Iraq. Addiction, 100(10), 1567. doi:10.1111/j.1360-0443.2005.01305.x
Al-Hasnawi, S. (2006). Attitude of residents and general practitioners toward substanceabuse in Iraq. Medical Journal of Babylon, 3(1–2), 107–112.
Al-Hasnawi, S., Al-Hemiary, N., & Lafta, M. (2007). Public attitudes toward substanceabuse. Karbala Medical Journal, 1(2), 162–166.
Al-Hasnawi, S. M., Aqrawi, R., Sadik, S., & Humphreys, K. (2009). Datapoints: Iraqi psy-chiatrists’ perceptions of substance use disorders among patients. Psychiatric Services,60(6), 728–728. doi:10.1176/ps.2009.60.6.728
Al-Hemiary, N., Hashim, M., Al-Diwan, J., & Abdul Razzaq, E. (2015). Alcohol and drugabuse in post-conflict Iraq. Journal of the Faculty of Medicine, Baghdad, 57(4), 290–294.
Al-Hemiery, N., Dabbagh, R., Hashim, M. T., Al-Hasnawi, S., Abutiheen, A., Abdulghani,E. A., … Rawson, R. A. (2017). Self-reported substance use in Iraq: Findings from theIraqi National Household Survey of Alcohol and Drug Use, 2014. Addiction, 112(8),1470–1479. doi:10.1111/add.13800
Al-H: uk�uma al-(ir�aqiyya [Iraqi Government]. (2016). Q�an�un W�arid�at al-Baladiyy�at
[Municipal Revenue Law]. Baghdad, Iraq: Majlis al-Nuw�ab al-(ir�aqi [Iraqi Parliament].
Al-J�ami(a al-Mustans: iriya [University of al-Mustansiriya] (2015, 20/12/2015). al-Tadrī b
al-s: ayfī lilt: alaba lighar :d da(m al-quw�at al-amniya wa al-H: ashd al-Sha
(bī [Summer
Training for Students for the Purpose to Support the Military Forces and the PopularMobilisation Movement]. Retrieved from http://www.webcitation.org/6fqynpc33
Al-Qummī Al-S: ad�uq, M. (1984). Man l�a Yah: :diruh al-Faqīh [For one that is not in thepresence of a Jurist] (Vol. 4). Qom: Jam�a
(at al-Mudarrisīn fī al-H: awza al-
(ilmiyya.
Al-Rim�ah: ī, H: . M. (2015). 20/12/2015). J�ami(at Baghd�ad Takhtatim Mashr�u
(Tadrīb al-Ṭalaba
wa al-As�atidha(ala H: aml al-Sil�ah: [Baghdad University Concludes its Weapons Training
Project for Students and Staff]. Retrieved from http://www.webcitation.org/6fqyzjG9CAl-Ṭab�at: ab�a
)ī , M. H: . (1997). al-Mīz�an fī Tafsīr al-Qur
)�an [The Balance in the Exegesis of
the Qur’an]. Bayr�ut: M�u)assasat al-�A
(lamī Lilmat:b�u
(�at.
Al-Wardī ,(. (1965). Dir�asah Fī Ṭabī ᶜat al-Mujtamaᶜ al-ᶜ ir�aqī [A Study on the Nature of
Iraqi Society]. Baghd�ad: D�ar al-War�aq.Al Hilfi, T. K., Lafta, R., & Burnham, G. (2013). Health services in Iraq. The Lancet,
381(9870), 939–948. doi:10.1016/S0140-6736(13)60320-7Alcohol Public Policy Group. (2010). Alcohol: No ordinary commodity – a summary of the
second edition. Addiction, 105(5), 769–779. doi:10.1111/j.1360-0443.2010.02945.xAli, M. M., & Shah, I. H. (2000). Sanctions and Childhood Mortality in Iraq. The Lancet,
355(9218), 1851–1857. doi:10.1016/S0140-6736(00)02289-3Alive in Baghdad. (2009, 07/12/2015). Liquor shops open for business. [Video Documentary]
Retrieved from http://www.webcitation.org/6marCVbOHAnderson, P., de Bruijn, A., Angus, K., Gordon, R., & Hastings, G. (2009). Impact of alcohol
Advertising and Media Exposure on Adolescent Alcohol Use: A Systematic Review ofLongitudinal Studies. Alcohol and Alcoholism, 44(3), 229–243. doi:10.1093/alcalc/agn115
18 M. AL ANSARI ET AL.
69

Aqrawi, R., & Hussain, A. (2010). A Study of Addicted Inpatients at Ibn-Rushd PsychiatricTeaching Hospital in Baghdad Category. Paper Presented at the National Instituteon Drug Abuse Program.
Avicenna, (1973). A treatise on the canon of medicine of Avicenna (O. C. Gruner, Trans.).New York: AMS Press.
Baasher, T. (1981). The use of drugs in the Islamic world. Addiction, 76(3), 233–243. doi:10.1111/j.1360-0443.1981.tb00230.x
Babor, T. (2010). Alcohol: No ordinary commodity: Research and public policy. Oxford:Oxford University Press.
Bolton, P. (2013). Mental health in Iraq: Issues and challenges. The Lancet, 381(9870),879–881. doi:10.1016/S0140-6736(13)60637-6
Brandt, M. L. (2005, August 24). 5 questions: Humphreys on substance abuse in Iraq.Stanford News. Retrieved from http://news.stanford.edu/news/2005/august24/med-hum-phreys-082405.html
Browne, T., Iversen, A., Hull, L., Workman, L., Barker, C., Horn, O., … Fear, N. T. (2008).How do experiences in Iraq affect alcohol use among male UK armed forces personnel?Occupational and Environmental Medicine, 65(9), 628–633. doi:10.1136/oem.2007.036830
Corfield, J. (2015). Iraq The SAGE encyclopedia of alcohol: social, cultural, and historicalperspectives (pp. 729–731). Thousand Oaks, CA: SAGE Publications, Inc.
Enes, K. (n.d.). Intoxicants. In J. D. McAuliffe (Ed.), Encyclopaedia of the Qur)�an (pp. 2:
555b). Washington DC: Brill.Ezard, N., Oppenheimer, E., Burton, A., Schilperoord, M., Macdonald, D., Adelekan, M., …
van Ommeren, M. (2011). Six rapid assessments of alcohol and other substance use in popu-lations displaced by conflict. Conflict and Health, 5(1), 1–15. doi:10.1186/1752-1505-5-1
Feins, D. S. (1997). Wine and Islam: The Dichotomy Between Theory and Practice in EarlyIslamic History (Doctor of Philosophy). The University of Edinburgh, Edinburgh.Retrieved from http://www.webcitation.org/74pKigXkr
Fontana, G. (2010). Creating nations, establishing states: Ethno-religious heterogeneity andthe British creation of Iraq in 1919–23. Middle Eastern Studies, 46(1), 1–16. doi:10.1080/00263200902760535
Gakidou, E., Afshin, A., Abajobir, A. A., Abate, K. H., Abbafati, C., Abbas, K. M., …
Murray, C. J. L. (2017). Global, regional, and national comparative risk assessment of 84behavioural, environmental and occupational, and metabolic risks or clusters of risks,1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. TheLancet, 390(10100), 1345–1422. doi:10.1016/S0140-6736(17)32366-8
Gately, I. (2008). Drink: A cultural history of alcohol. New York: Penguin PublishingGroup.
Ghandour, L., Chalak, A., El-Aily, A., Yassin, N., Nakkash, R., Tauk, M., … Afifi, R.(2016). Alcohol consumption in the Arab region: What do we know, why does it matter,and what are the policy implications for youth harm reduction? International Journal ofDrug Policy, 28, 10–33. doi: 10.1016/j.drugpo.2015.09.013
Hamdi, E., Gawad, T., Khoweiled, A., Sidrak, A. E., Amer, D., Mamdouh, R., … Loza, N.(2013). Lifetime prevalence of alcohol and substance use in Egypt: A community survey.Substance Abuse, 34(2), 97–104. doi:10.1080/08897077.2012.677752
Hamdi, E., Sabry, N., Sedrak, A., Khowailed, A., & Loza, N. (2016). Sociodemographicindicators for substance use and abuse in Egypt. Journal of Addiction & Prevention, 4(1), 8.
Hammurabi. (1904). The code of Hammurabi King of Babylon about 2250 B.C. (R. F.Harper, Trans.). Chicago: Chicago University Press.
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 19
70

Hanson, D. J. (2013). Historical evolution of alcohol consumption in society. In P. Boyle,P. Boffetta, A. B. Lowenfels, H. Burns, O. Brawley, W. Zatonski, & J. Rehm (Eds.),Alcohol: Science, policy and public health. Oxford: Oxford University Press.
Hornsey, I. S. (2003). A history of beer and brewing. Cambridge: Royal Society of Chemistry.H: usayn, S. (1994). Ighl�aq K�afat Mah: alat Bay
(al-Mashr�ub�at al-Kuh: �uliyya wa al-Mal�ahī
[Closure of all Shops and Clubs Selling Alcoholic Drinks], pp. 48. Majlis Qiy�adat al-Thawra [Revolutionary Command Council].
Ibn Abi Us: aybi(a, A. (1996).
(uy�un al-Anb�a
)fī Ṭabaq�at al-At: ib�a
)[Key News on the Classes
of Physicians] (al-Najj�ar Ed.). al-Q�ahira: D�ar al-Ma(�arif.
Ibn Bat: t: �ut: a, M. (1987). Rih: lat Ibn Bat: t: �ut:a: Tuh: fat al-Nuẓ�ar fī Ghar�a)ib al-�Ams: �ar wa
(aj�a
)ib
al-�Asf�ar [Ibn Battuta’s Journey: A Gift to Those Who Contemplate the Wonders of Cities andthe Marvels of Travelling] (M. al-
(iry�an & M. al-Qas: s: as: Eds.). Bayr�ut: D�ar Ih: y�a
)al-(ul�um.
Ibn Manẓ �ur, M. (Ed.). (2003). Lis�an al-(arab [Language of the Arabs] [‘Tongue of the
Arabs’] (Vols. 5). Bayr�ut: D�ar S: �adir.I(l�am al-ta
(līm al-
(�alī [Higher Education Media Office] (2015, December 12). al-Shahrist�anī
y�uwajih al-J�ami(�at bitadrīb Ṭalabatuh�a wa muntasibīh�a
(ala al-Sil�ah: lim�uw�ajahat D�a
(ish
[al-Shahristani Instructs Universities to Train their Students and Staff on Weapons toConfront Daesh (ISIS)]. Retrieved from http://www.webcitation.org/6fqyKLNrZ
J�ami(at al-K�ufa [University of Kufa] (2015, December 12). I
(l�an h: awl tadrīb al-duf
(a al-
th�aniya min mutat: awi(ī al-H: ashd al-sha
(bī [Announcement Regarding the Training of
the Second Batch of Volunteers for the Popular Mobilisation Movement]. Retrievedfrom http://www.webcitation.org/6fqyc3qpS
Jansen, M. (2006, May 3). Beer-making traditions suffer as sectarianism brews in Iraq. TheIrish Times, Retrieved from http://www.webcitation.org/6c7VbTFIV
Joffe, A. H. (1998). Alcohol and social complexity in ancient Western Asia. CurrentAnthropology, 39(3), 297–322. doi:10.1086/204736
Karam, E. G., Maalouf, W. E., & Ghandour, L. A. (2004). Alcohol use among universitystudents in Lebanon: Prevalence, trends and covariates: The IDRAC UniversitySubstance Use Monitoring Study (1991 and 1999). Drug and Alcohol Dependence, 76(3),273–286. doi: 10.1016/j.drugalcdep.2004.06.003
Kelsall, H. L., Wijesinghe, M. S. D., Creamer, M. C., McKenzie, D. P., Forbes, A. B., Page,M. J., & Sim, M. R. (2015). Alcohol use and substance use disorders in Gulf War,Afghanistan, and Iraq War veterans compared with nondeployed military personnel.Epidemiologic Reviews, 37(1), 38. doi:10.1093/epirev/mxu014
Kennedy, P. F. (1997). The wine song in classical Arabic poetry: Ab�u Nuw�as and the literarytradition. Oxford: Oxford University Press.
Kennedy, P. F. (2012). Abu Nuwas: A Genius of Poetry. Oxford, UK: OneworldPublications.
Khayyat, S. (1990). Honour and Shame: Women in Modern Iraq. London, UK: Saqi Books.Leland, J. (2011, January15). Baghdad raids on alcohol sellers stir fears. The New York
Times. Retrieved from http://www.webcitation.org/6c7X3HLOhLewis, P. (1994, August 12). Iraq bans public use of alcohol. The New York Times.
Retrieved from http://www.webcitation.org/6mamjH9hiLindsay, J. E. (2005). Daily life in the medieval Islamic world. Westport: Greenwood Press.Maghazaji, H. I., & Zaidan, Z. A. (1982). Alcoholism in Iraq. British Journal of Psychiatry,
140(3), 325–326. doi:10.1192/bjp.140.3.325cMakkī ,
(abd al-Karīm. (2001). Ta
(līm�at Ij�azat bay
(al-Mashr�ubat al-Kuh�uliya [Instructions
for Licence to Sell Alcoholic Beverages], (pp. 187-189). Baghdad, Iraq: al-Waqa)i(
al-(ir�aqiya.
20 M. AL ANSARI ET AL.
71

Maraqten, M. (1993). Wine drinking and wine prohibition in Arabia before Islam.Proceedings of the Seminar for Arabian Studies, 23, 95–115.
Matthee, R. (2014). Alcohol in the Islamic Middle East: Ambivalence and ambiguity. Past& Present, 222(Suppl 9), 100–125. doi:10.1093/pastj/gtt031
Matthee, R. P. (2005). The pursuit of pleasure: Drugs and stimulants in Iranian history,1500–1900. Princeton, USA: Princeton University Press.
Michalak, L., & Trocki, K. (2006). Alcohol and Islam: An Overview. Contemporary drugproblems, 33(4), 523–562. doi:10.1177/009145090603300401
Nahas, G. G. (1982). Hashish in Islam 9th to 18th century. Bulletin of the New YorkAcademy of Medicine, 58(9), 814.
Pew Forum on Religion & Public Life (2009). Mapping the Global Muslim Population: AReport on the Size and Distribution of the World’s Muslim Population. WashingtonD.C. Retrieved from http://www.webcitation.org/6xVuV6xdt
Potts, D. T. (2012). A companion to the archaeology of the Ancient Near East (Vol. 1).Chichester, UK: Wiley-Blackwell.
Raad, Y. (2014). Consolidating socio-spatial practices in a militarized public space: Thecase of Abu Nuwas street in Baghdad (Masters). American University of Beirut, Beirut.
Raad, Y. (2017). Diverse socio-spatial practices in a militarized public space: The case ofAbu Nuwas Street in Baghdad. International Journal of Contemporary Iraqi Studies,11(3), 133–159. doi:10.1386/ijcis.11.3.133_1
Rassam, S. (2005). Christianity in Iraq: Its origins and development to the present day.Herefordshire: Gracewing.
Razokhi, A. H., Taha, I. K., Taib, N. I., Sadik, S., & Gasseer, N. A. (2006). Mental health ofIraqi children. The Lancet, 368(9538), 838–839. doi:10.1016/S0140-6736(06)69320-3
Roberts, B., & Ezard, N. (2015). Why are we not doing more for alcohol use disorderamong conflict-affected populations? Addiction, 110(6), 889–890. doi:10.1111/add.12869
Rohde, A. (2010). State-society relations in Ba’thist Iraq: Facing dictatorship: New York, USA:Taylor & Francis.
Rosenthal, F. (2015). The herb: Hashish versus Medieval Muslim Society. In Gutas (Ed.),Man versus Society in Medieval Islam, (pp. 131–198). Leiden: Brill.
Rowat, C. (2000). UN agency reports on the humanitarian situation in Iraq. Cambridge.Retrieved from http://www.webcitation.org/6mautP37w
Russia Today. (2014, September 21). Forced Sobriety: ISIS Harms Baghdad with AlcoholPrice Surge RT. Retrieved from http://www.webcitation.org/6c7WGWu7l
Sadik, S., Abdulrahman, S., Bradley, M., & Jenkins, R. (2011). Integrating mental healthinto primary health care in Iraq. Mental Health in Family Medicine, 8(1), 39–49.
Sadik, S., Bradley, M., Al-Hasoon, S., & Jenkins, R. (2010). Public perception of mentalhealth in Iraq. International Journal of Mental Health Systems, 4(1), 26–26. doi:10.1186/1752-4458-4-26
Salaheddin, S. (2018). Drug use, sales soar in Iraq’s Basra amid nationwide spike. TheAssociated Press. Retrieved from http://www.webcitation.org/6xVubkOaU
Salloum, S. (2016). 02/11/2016). What’s really behind Iraq’s new alcohol ban? Al-Monitor.Retrieved from http://www.webcitation.org/6manwvahQ
Sinclair, T. R., & Sinclair, C. J. (2010). Bread, Beer and the Seeds of Change: Agriculture’sImprint on World History: CAB International.
S: ir�amī , H: ., Qurb�anī , M., & Mī n�unī , M. (2013). Barrisi Chah�ar dah Tah: qī q�at Shuy�u(
Shin�asī I(tiy�ad dar �Ir�an [Review of 14 Prevalence Studies of Addiction in Iran].
Quarterly Journal of Research on Addiction, 7(26), 29–52.
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 21
72

Taneja, P. (2007). Assimilation, Exodus, Eradication: Iraq’s minority communities since 2003.Retrieved from http://minorityrights.org/wp-content/uploads/old-site-downloads/download-280-Assimilation-Exodus-Eradication-Iraqs-minority-communities-since-2003.pdf
Teesson, M., Hall, W., Slade, T., Mills, K., Grove, R., Mewton, L., … Haber, P. (2010).Prevalence and correlates of DSM-IV alcohol abuse and dependence in Australia:Findings of the 2007 National Survey of Mental Health and Wellbeing. Addiction,105(12), 2085–2094. doi:10.1111/j.1360-0443.2010.03096.x
The United Nations Children’s Fund (UNICEF). (1999). Child and Maternal MortalitySurvey 1999: Preliminary Report. Retrieved from https://fas.org/news/iraq/1999/08/990812-unicef.htm
The United Nations Children’s Fund (UNICEF). (2018). Iraq Humanitarian SituationReport September 2018. Retrieved from https://reliefweb.int/sites/reliefweb.int/files/resources/UNICEF%20Iraq%20Humanitarian%20Situation%20Report%20-%20September%202018.pdf
United Nations Department of Economic and Social Affairs (UNDESA). (2017). WorldPopulation Prospects: The 2017 Revision, Key Findings and Advance Tables. Retrievedfrom https://reliefweb.int/sites/reliefweb.int/files/resources/WPP2017_KeyFindings.pdf
United Nations Development Program (UNDP), Ministry of Planning, & Baytul Hikma(2014). Iraqi Youth Challenges and Opportunities. Baghdad. Retrieved from
United Nations Office for the Coordination of Humanitarian Affairs (UNOCHA). (2018).Humanitarian Bulletin Iraq October 2018. Retrieved from
U.S. Department of State, Bureau of International Narcotics and Law Enforcement Affairs,Iraqi Society of Addiction Medicine, University of California LA, & Center for HumanServices (2015). Survey of Substance Abuse in Iraq. Bethesda, MD.
Von Zielbauer, P. (2008). 13/03/2007). For U.S. troops at war, liquor is spur to crime. TheNew York Times. Retrieved from http://www.webcitation.org/6fqjHvGdt
Weaver, H., & Roberts, B. (2010). Drinking and displacement: A systematic review of theinfluence of forced displacement on harmful alcohol use. Substance Use & Misuse,45(13), 2340–2355. doi:10.3109/10826081003793920
White, W. L. (2011). Circles of recovery: An interview with Keith Humphreys, PhD.Counselor 12(6), 48–52.
Wiedemann, E., & Allan, J. (2012). al-KUHL. In P. Bearman, T. Bianquis, C. E. Bosworth,E. v. Donzel, & W. P. Heinrichs (Eds.), Encyclopaedia of Islam, Second Edition (pp.V356a): Leiden, Brill.
Wilk, J. E., Bliese, P. D., Kim, P. Y., Thomas, J. L., McGurk, D., & Hoge, C. W. (2010).Relationship of combat experiences to alcohol misuse among U.S. soldiers returningfrom the Iraq war. Drug and Alcohol Dependence, 108(1–2), 115–121. doi:10.1016/j.dru-galcdep.2009.12.003
Wolf, A., Bray, G. A., & Popkin, B. M. (2008). A short history of beverages and how ourbody treats them. Obesity Reviews, 9(2), 151–164. doi:10.1111/j.1467-789X.2007.00389.x
World Health Organization (WHO). (1999). Global Status Report on Alcohol 1999.Retrieved from http://www.webcitation.org/6mk3iClCG
World Health Organization (WHO). (2009). Iraq Mental Health Survey 2006/7. Retrievedfrom http://www.webcitation.org/6mk3pGCJV
World Health Organization (WHO). (2011). Meeting report: First meeting of the GlobalNetwork of WHO national counterparts for implementation of the Global strategy toreduce the harmful use of alcohol. Retrieved from Geneva: http://www.webcitation.org/74pKrAMJr
22 M. AL ANSARI ET AL.
73

World Health Organization (WHO). (2014). Global Status Report on Alcohol and Health.Retrieved from Geneva: http://www.webcitation.org/6mk3vWQQm
Zubaida, S. (2002). The fragments imagine the nation: The case of Iraq. InternationalJournal of Middle East Studies, 34(2), 205–215.
Zubaida, S. (2014). Drink, meals and social boundaries. In J. A. Klein & A. Murcott (Eds.),Food consumption in global perspective: Essays in the anthropology of food in honour ofJack Goody (pp. 209–223). London: Palgrave Macmillan UK.
JOURNAL OF ETHNICITY IN SUBSTANCE ABUSE 23
74

75
Chapter 4: Alcohol among young people in Iraq: A systematic scoping review
Chapter 3 established the context of alcohol research in Iraq. It set out historical, social, cultural, and
religious factors that may influence the attitudes towards alcohol among young people today. As
established within that chapter, very little is known about the prevalence of alcohol use or the attitudes
of young people towards alcohol in Iraq.
The current chapter will describe the scope and nature of available data about Iraqi youth drinking in
peer-reviewed journals. A systematic scoping review was utilised to provide a complete picture of
what is already known regarding alcohol use among young people in Iraq. Non-alcohol specific
studies were included because of the scarcity of alcohol-specific research, as identified in Chapters 1
and 3. We also included a wider age range than our mixed-method study because we identified that
most national and general studies categorised their participants in bands between 14 to 34 years. This
chapter sets out to identify the gaps in knowledge about prevalence of alcohol use and attitudes
towards alcohol among young people in Iraq.
The following manuscript has been submitted for publication.

76
Abstract
Introduction
Young people in Iraq are exposed to conflict and trauma, and also to uncensored international TV
and media, with its references to alcohol. However previous regional reviews indicate that alcohol is
the least studied substance in Arab countries and no data on young people in Iraq were identified.
Accordingly, we re-examined the scope of available literature on alcohol and Iraqi young people,
including in studies where alcohol was not the primary focus.
Methods
Five major international databases (MEDLINE (OVID), Embase (OVID), PsycINFO (OVID),
Scopus, Web of Science) and one local Iraqi database (Iraqi Academic Scientific Journals (IASJ))
were systematically searched for published articles up to 16th of September 2019. Original articles
that included any alcohol data on general Iraqi young or student samples were included.
Results
Thirteen articles met the inclusion criteria from a total of 3374 results. All studies were cross-sectional
and quantitative. Most alcohol data were incidental rather than the focus of the studies. All but two
studies used face-to-face or pen-and-paper surveys. Each study reported on alcohol differently – with
most not using validated tools. A wide range of drinking prevalence was reported (2.2%-23.7%).
Studies reported a relatively high rate (12.2-56%) of alcohol misuse among those that drink. Alcohol
was associated with risky behaviour in the two studies that reported on this measure.
Conclusion
Results suggest a low prevalence of drinking compared to non-MMCs, however relatively high
prevalence of risk amongst drinkers. More research is needed using study methods and validated
screening or diagnostic tools tailored for the local Iraqi context.

77
Summary
What is already known?
- Alcohol is the least studied substance in the Arab world
- Iraqi young people are exposed to trauma, conflict and change, and are exposed to the tension
between their home cultures and religions and global culture on social and other media (Al Ansari et
al., 2019).
- Studies on alcohol in Iraq can be hard to find and no review is available of such studies
What are the new findings?
- Thirteen studies presented data on alcohol, though for most alcohol was not their primary focus
- Studies reported a wide range of drinking prevalence: 2.2% to 23.7%.
- Among those who do drink, a high prevalence of risky drinking and risk behaviour was reported, at
times more than samples in non-MMCs
What do the new findings imply?
- Due to variations in study approaches and reporting, no clear picture of the prevalence of drinking
or attitudes towards alcohol among young Iraqis can be drawn
- The reported relatively high rates of risky behaviour and alcohol misuse among drinkers suggest a
need for further research, including on prevention.
- Validated and tailored research methods, tools, and early interventions are needed, because of the
sensitivity of alcohol as a topic in Iraq, as in many other Muslim majority countries.

78
Introduction
Globally, alcohol is the leading risk factor for people aged between 15 and 49 (GBD 2016 Alcohol
Collaborators, 2018). Harmful alcohol use has been associated with conflict exposure (Lo et al.,
2017; Roberts et al., 2015) and other mental health conditions such as PTSD (Debell et al., 2014).
Iraq is a nation that has been exposed to international and civil war for the past four decades. Most of
Iraq’s population is under the age of 24 (UNDESA, 2017), and exposed to civil war, directly or
through family or community involvement (see: Al Ansari et al., 2019). In addition, Iraqi young
people are influenced by conflicting principles and cultures – that of their home cultures and religions
and that which they are exposed to with no censorship on television, social and mass media (Al Ansari
et al., 2019). Although each of these challenges may be present in other MMCs, the combination of
these factors in Iraq is unique – especially given the diversity inherent in its deep cultural tradition
(Al Ansari et al., 2019).
Little is known about alcohol use in Muslim Majority Countries (MMCs), especially within the
Eastern Mediterranean region. In Arab countries, research about alcohol was less than research about
other substances including illicit and abused prescription drugs (Sweileh et al., 2014). Previous
reviews have looked at alcohol policy approaches in MMCs (Al-Ansari et al., 2015) as well as
prevalence of drinking in the Eastern Mediterranean (L. Ghandour et al., 2016) and Arab gulf region
(AlMarri & Oei, 2009). In Iraq specifically, a previous review has looked at alcohol’s place in Iraq’s
history, cultures, and societies (Al Ansari et al., 2019). However, none of these reviews outline the
scope of existing academic literature around alcohol use, misuse, and policy in Iraq – including in
relation to young people. For example, L. Ghandour et al. (2016) found no study matching their
inclusion criteria that describes alcohol use among young people or students in Iraq. This may be for
several reasons – firstly, data about alcohol may be found in studies that focus on other research areas
such as smoking, risky behaviours, and other mental health conditions. These articles may employ a
general sample, not specified by age or student status. And finally, other studies may be published in
local journals which may not always be identified in general academic searches.

79
To remedy these gaps, we conducted a systematic scoping review to identify all articles about alcohol
use, misuse or attitudes among young people or students in Iraq. Our objective was to identify what
is known about attitudes towards alcohol and prevalence of drinking among young people in Iraq. To
meet this objective, this review will consider:
1. What studies on the prevalence of alcohol consumption or attitudes of young people towards
alcohol have been undertaken in Iraq?
2. What definitions, questionnaires, tests, diagnostic processes, and outcomes did the studies
employ?
3. When and if available, how were influencing factors (such as war, globalisation, etc) assessed
in relation to alcohol use?
4. What, and if available, when, preventative strategies have been implemented and evaluated
that address the issues related to alcohol in this population?
Methods
This systematic scoping review (Arksey et al., 2005) intends to describe the available literature about
alcohol in young populations in Iraq. This will include any literature regarding alcohol – including
quantitative and qualitative studies that explore alcohol awareness or attitudes to alcohol, and
prevalence of use, misuse, and dependence. By selecting a wide scope, we aim to capture as much as
possible of the scarce literature about this topic.
Because one of the study’s main objectives is to assess the prevalence of alcohol use and misuse –
this review utilised the approach: condition, context, population (CoCoPop) instead of the traditional
approach: population, intervention, condition, outcome (PICO) (Munn et al., 2018).
Condition: Prevalence of drinking/Attitude towards alcohol
Context: Iraq
Population: Young/Student populations in Iraq

80
Identifying the relevant studies
In keeping with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)
statement (Moher et al., 2009), a systematic search of six major health and multi-discipline databases
was undertaken (see appendix 2 for PRISMA checklist). Five major international databases and one
local Iraqi database were searched for published articles up to 13th of September 2019. These
databases were MEDLINE (OVID), Embase (OVID), PsycINFO (OVID), Scopus, Web of Science,
and Iraqi Academic Scientific Journals (IASJ). No earliest year of publication was included in this
search. The search terms were Iraq AND alcohol* OR substance *use OR drinking. A detailed search
strategy is included in the appendix (Appendix 3). The breadth of this search was purposely selected
to identify any literature that included alcohol data.
Further hand-searched articles, identified via consultation with academics and the reference lists of
the included articles, were also screened for eligibility.
Only English literature was searched. This is because English is the main language of medical
research and education in Iraq. Arabic and Kurdish sources either do not exist, are limited or not
accessible.
Study selection
Original peer-reviewed journal articles conducted in Iraq with an Iraqi general or student sample
containing alcohol-specific data provided by age or student status were included (table 1).
Table 3 Inclusion and exclusion criteria for study selection
Criterion Inclusion Exclusion
Context Iraq Studies conducted outside Iraq
Population Iraqis Non-Iraqi sample. Example:
➢ refugee camps
➢ soldiers/journalists from other countries
Sample selection General and student samples (non-specialised
samples only) e.g. household studies, university
samples and primary health settings
Specialised sample (except students). Example:
➢ only drinkers
➢ only cancer patients
➢ emergency (ED) patients (more likely to
misuse alcohol than general population)

81
Alcohol data Must contain alcohol-specific data Not containing alcohol-specific data. Example:
➢ papers about addiction or substance use that
do not provide alcohol-specific data
Age or occupation Alcohol data is reported for young people aged
14-34 or for those who are students.
Alcohol data is not reported separately for young
people or students.
Study type Peer reviewed original journal articles. Not original journal article in a peer reviewed
journal. Example:
➢ grey literature (such as books, reports, etc.)
➢ conference proceedings and abstracts
➢ reviews, editorials, and commentaries
Charting the data
The aims, methods, and results of each included article were described in a spreadsheet. This
included: the main focus, data collection year, sample identifiers (size, type, sampling method),
setting (university, school, clinic, etc.), method of data-collection (online, pen-and-paper, etc), tools
and any criterion (AUDIT, etc.), lifetime or past-year prevalence and any other relevant quantitative
or qualitative results (if any).
Patient and public involvement statement
There was no patient or public involvement in this research.
Results
The search resulted in 3374 articles, of which 1668 were duplicates. None of the papers found in IASJ
were indexed in the other databases. After a title and abstract screen, 64 articles remained and were
included in the full-text screen. Eight of these studies met the inclusion criteria. Five hand-searched
articles also met the criteria (Figure 1), resulting in a total of 13 included studies.

82
Figure 5 PRISMA flow chart for literature search

83
Study descriptions
Research topics
Descriptions of the studies are reported in Table 2. Of the included studies, only four were alcohol
specific (Al-Ameri et al., 2016; Al-Qazzaz et al., 2017; Al Mousawi, 2015; S. Ali et al., 2009); two
were about substance use (Al-Hemiary et al., 2015a; Rahim, 2010) and two about health risk
behaviours (Baker et al., 2016; Saeed, 2016); one each was primarily focused on mental health
disorders (Alhasnawi et al., 2009), smoking (Al Mousawi, 2014), novel psychoactive drugs (Al-Imam
et al., 2017), risky driving (Shabila et al., 2015), and sleep disorders (Abdulah et al., 2018). No
literature was found that related to preventative strategies in relation to alcohol.
Study years
Although no earliest year limits were placed in the search, all the papers were published between
2009 and 2018 with data collected from 2005 to 2017.
Study settings and data collection
Only one study recruited a sample from more than one province (Alhasnawi et al., 2009). Four studies
recruited from Baghdad (Al-Ameri et al., 2016; Al-Hemiary et al., 2015a; Al-Imam et al., 2017; Al-
Qazzaz et al., 2017) and Erbil (S. Ali et al., 2009; Baker et al., 2016; Rahim, 2010; Shabila et al.,
2015). Two recruited students from Karbala (Al Mousawi, 2014, 2015). Kirkuk (Saeed, 2016) and
Dohuk (Abdulah et al., 2018) were the recruitment sites of one study. Figure 2 identifies provinces
where recruitment occurred on the Iraqi map.
All studies were cross-sectional and quantitative. Nine studies were self-administered surveys
(Abdulah et al., 2018; Al-Ameri et al., 2016; Al-Imam et al., 2017; Al Mousawi, 2014, 2015; S. Ali
et al., 2009; Baker et al., 2016; Saeed, 2016; Shabila et al., 2015) - eight of these were paper-and-pen
and one online (Al-Imam et al., 2017). Three studies used face-to-face interviews (Al-Hemiary et al.,
2015a; Alhasnawi et al., 2009; Rahim, 2010) and one used autopsy blood samples (Al-Qazzaz et al.,
2017). Eight studies were conducted in school or college (Abdulah et al., 2018; Al-Ameri et al., 2016;
Al Mousawi, 2014, 2015; S. Ali et al., 2009; Baker et al., 2016; Saeed, 2016; Shabila et al., 2015),

84
two at home (Alhasnawi et al., 2009; Rahim, 2010), one each at a youth centre (Al-Hemiary et al.,
2015a), online (Al-Imam et al., 2017) and at a forensics laboratory (Al-Qazzaz et al., 2017).
Three of the four alcohol-specific studies were self-administered pen-and-paper surveys conducted
in school/college and the fourth was a post-mortem blood alcohol concentration (BAC) study.
Figure 6 Provinces where student/youth specific alcohol data are reported in peer-reviewed original articles

85
Alcohol screening and diagnostic processes
Only four of the eleven studies reporting alcohol prevalence or patterns data reported using validated
alcohol screening or diagnostic tools. Two used the Composite International Diagnostic Interview
(Al-Hemiary et al., 2015a; Alhasnawi et al., 2009; Kessler et al., 2004), one used the Alcohol Use
Disorders Identification Test (AUDIT) (Al Mousawi, 2015; T. F. Babor et al., 2001), and one the
Mini International Neuropsychiatric Interview (MINI) (Rahim, 2010; Sheehan et al., 1998). One
study utilised blood alcohol concentration at autopsy (Al-Qazzaz et al., 2017). The other studies did
not report how alcohol questions were asked.
Samples
Ten of the studies reported randomised recruitment with varying levels of detail. Ten studies included
a student sample: four were general university samples (Al-Ameri et al., 2016; Al Mousawi, 2014,
2015; S. Ali et al., 2009), three were medical students (Abdulah et al., 2018; Al-Imam et al., 2017;
Shabila et al., 2015), two secondary school (Baker et al., 2016; Saeed, 2016) and one did not specify
(Rahim, 2010). Although S. Ali et al. (2009) defined their sample as medical college students, it
included students studying medicine, dentistry, pharmacy and nursing. Similarly, Al-Ameri et al.
(2016) defined medical students as those studying medicine, dentistry or pharmacy. Of the other three
studies, one was a general household sample (Alhasnawi et al., 2009), one a youth centre sample (Al-
Hemiary et al., 2015a) and the third a sample of general autopsies (Al-Qazzaz et al., 2017).
Two samples were male only (Baker et al., 2016; Saeed, 2016), two had a majority male sample (Al-
Hemiary et al., 2015a; S. Ali et al., 2009) and six a majority female sample (Abdulah et al., 2018; Al-
Ameri et al., 2016; Al-Imam et al., 2017; Al Mousawi, 2014, 2015; Shabila et al., 2015). The other
three studies did not provide gender breakdown for young or student subsamples.
Prevalence and patterns of alcohol use
Lifetime drinking
Alcohol-related results of each study are reported in Table 3. There was a wide variation in reported
prevalence of drinking between studies. Two studies reported prevalence of lifetime alcohol use at

86
7.6% and 9.7% (Al-Ameri et al., 2016; Saeed, 2016). Al-Ameri et al. (2016) provides a breakdown
by gender, showing the vast majority of those that drink are males (19.7% vs 0.8%). On multivariable
analysis, lifetime alcohol users more likely lived away from family (prevalence ratio [PR] 2.7; 95%
CI 1.8-4.1); p<0.001 vs. those who lived with family) and were non-medical students (PR 2.6; 95%
CI 1.4-4.7; p 0.002 vs. medical students (medicine, dentistry or pharmacy)) (Al-Ameri et al., 2016).
Baker et al. (2016) and Al-Imam et al. (2017) also provide alcohol use prevalence (6.6% and 0.9%
respectively) without specifying if the figure is for current or lifetime drinking. Although Baker and
Al-Doski’s total sample is 500 students, they only provide the drinking prevalence for the 296
students who reported any risk behaviours. Age of onset of drinking for a student or age-specific
sample was only reported by one secondary school study: 12 years old (unspecified if mode, median
or mean) (Saeed, 2016).
Current drinking
Similarly, the prevalence of current drinking varied widely, from 2.2% (Al Mousawi, 2015) to 23.7%
(S. Ali et al., 2009). Each study reporting current drinking recruited individuals from a different
setting and used different methods for data collection. The two Kurdistan studies, conducted in Erbil
and Dohuk, had the highest prevalence at 23.7% and 11.9%, respectively (Abdulah et al., 2018; S.
Ali et al., 2009). In contrast, the study in Karbala, a conservative Arab city in central Iraq, reported
2.2% (Al Mousawi, 2015). Al-Qazzaz et al. (2017) reported the post-mortem blood alcohol levels in
14-34-year-old Iraqis who were sent for autopsy in Baghdad. A twelfth (8.5%) of the sample had a
blood alcohol concentration of more than 40mg/100mL (0.04 g/dL).
In their study about sleep , Abdulah et al. (2018) report that evening drinking was a predictor of
emotional disturbance (p=0.034) and restless legs syndrome during the night (p=0.003).
Alcohol misuse including abuse and dependence
Five studies reported data on alcohol misuse, with four using validated screening or diagnostic tools.
Al Mousawi (2015) reports that the majority (56%) of drinking students who completed AUDIT

87
scored above eight (0.8% of entire sample)1. A third (36%) of drinkers who completed AUDIT were
hazardous drinkers (8-15), a tenth (10.7%) risky drinkers (16-19) and a tenth (9.3%) were high-risk
or dependent (20+). Al Mousawi (2015) comments that items 7 (guilt) and 10 (others concerned about
your drinking) of the AUDIT may be may be interpreted differently in the Iraqi context. This is
because guilt is common as a reaction to breaking a religious or cultural taboo. Similarly, any drinking
in this context will typically make other people worried about the drinker’s behaviour even if it does
not necessarily represent high-risk or dependence.
Al-Ameri et al. (2016) reported that 1.2% (12.2% of drinkers) of the Baghdad student sample were
heavy/high risk drinkers (consumed 3+ standard drinks [10g ethanol] per day/7+ per week for women;
4+ per day/14+ per week for men). Similarly, A fifth (19.8%) of the student drinkers in Karbala
consumed more than 4 drinks per drinking day (Al Mousawi, 2015). Almost half (46%) of the fifty
students who answered AUDIT question 3 in Karbala reported consuming 6+ drinks on a weekly or
daily basis (Al Mousawi, 2015).
Despite the occurrence of episodic heavy drinking among drinkers, reported prevalence of alcohol
use disorders is low. A national household study from 2006, the Iraqi Mental Health Survey (IMHS),
showed only 0.7% of those aged 18-34 met DSM-IV lifetime criteria for alcohol abuse and 0.3% met
criteria for dependence (Alhasnawi et al., 2009). Similarly, in Baghdad, Al-Imam et al. (2017)
reported that 0.4% (50% of drinkers) had alcohol use disorder (criteria not provided). In contrast, in
Erbil, six students (6.2% of students) met the DSM-IV criteria for past-12-month alcohol abuse and
two (2.5%) for dependence (Rahim, 2010). In a youth centre sample in Baghdad, 20.1% of 18-35-
year-olds met DSM-IV criteria for lifetime alcohol abuse (no female reported drinking) (Al-Hemiary
et al., 2015a). Although the article does not provide specific details about the nature of the youth
centre attendees, this higher figure suggests that this was most likely a high-risk group, and not
representative of the general population.
1 An AUDIT score above 8 indicates risky drinking. This could range from hazardous use through to high-risk or likely dependence (Babor, 2001).

88
Reliability and validity analysis of alcohol screening/survey tools
Al Mousawi (2015) is the only study that conducted an internal reliability test of its alcohol screening
tool in an Iraqi sample. The AUDIT had a Cronbach’s α of 0.66. However, when the guilt question
was removed, the reliability increased to α = 0.73.
The Shabila et al. (2015) survey showed good internal consistency (α = 0.78 to 0.82) for a broad range
of risky driving behaviours. Abdulah et al. (2018) reported the internal consistency of SLEEP-50 (a
survey in relation to sleep consisting of 50 items, that only includes one alcohol question) in previous
non-Iraqi international studies. Other studies did not measure internal consistency of their survey
tools.
Patterns/locations
Frequency of drinking
Drinkers in Iraq mostly reported consuming alcohol infrequently. Student drinkers mostly reported
drinking ‘occasionally’ in Erbil (81.5%) (S. Ali et al., 2009) and Baghdad (64%) (Al-Ameri et al.,
2016). Neither study defined what is meant by ‘occasional’ drinking. Al Mousawi (2015) reports that
40.8% of drinking students in Karbala had alcohol once monthly or less often. A minority (5.8%) of
students in Kirkuk reported regular drinking (frequency undefined) (Saeed, 2016).
Drinking locations
The only study to report on drinking locations was from Erbil. Students most frequently consumed
alcohol in bars or restaurant (44.5%) followed by outdoor settings (25.9%). Only 7.6% of current
drinkers drank at home (S. Ali et al., 2009).
Attitudes, behaviours, and motives
Attitudes
Only one, smoking-focused study reported on attitudes to alcohol. Two percent of the students had
positive attitudes to alcohol (compared with 2% to illicit drugs and 10% to smoking). Smokers had
more positive attitudes to drinking (p<0.001) (Al Mousawi, 2014). An overall negative attitude

89
towards alcohol is also seen with half of student drinkers in Karbala reporting guilt about their
drinking (54.4%) or that people expressed concern about their drinking (49.1%) (Al Mousawi, 2015).
Motives
Only one study reported on the motive for drinking. Most students (51.9%) reported they drink for
pleasure while 44.4% drink to get relief from stress (S. Ali et al., 2009).
Behaviours
Alcohol-related risk behaviours were reported by two studies. The first reported that most students
perceived either driving after ‘mild to moderate’ drinking (80.1%) or drunk driving (72.5%) to be the
riskiest driving behaviours. Despite this, some students reported driving after drinking (after a ‘mild
to moderate intake of alcohol’ 4.5%; or whilst drunk, 6.4%). Further, almost a tenth reported finding
driving under the influence of alcohol enjoyable (Shabila et al., 2015). In Kirkuk, Saeed (2016)
reports 6.5% of the student sample had ridden more than once in a car driven by someone who has
consumed alcohol. About one third (30.6%) of the secondary school students have also driven a
vehicle while drinking alcohol.
This latter statement however is internally inconsistent with the reported 7.6% lifetime use of alcohol
in the same study. The abstract of this study also contains a statement that more than half (52.5%) of
the students were in a vehicle driven by a drinking person. However, these results are not included in
the paper itself. Saeed (2016) also reported that alcohol is associated with carrying a weapon (n=15,
p 0.014) and physical fighting (n=20, p<0.001).

90
Table 4: Findings of systematic scoping review (studies are ordered by year of data collection)
Sample Data collection
Article Focus Data
year Location Random Size Description
Mean age;
Age range
Male
%
Tool;
Criteria Setting Method
Reported
findings
Al Mousawi
(2014)
Smoking 2005 Karbala ✓ 2298 Students
(university)
21.2 ± 2.7
-
48 Unspecified Lecture
rooms
Self-administered survey Prevalence
Attitudes
Alhasnawi et al.
(2009)
Mental health
disorders
2006-
07
All Iraq ✓ - General
household
-
18-34
- CIDI 3.0
DSM-IV
Home Face-to-face interview Prevalence
S. Ali et al.
(2009)
Alcohol use 2007 Erbil X 342 Students
(university)
21.3
17-29
64 Tool unspecified
Moderate/binge#
Classroom Self-administered survey Prevalence
Patterns
Motives
Rahim (2010) Substance use 2008 Erbil ✓ 81 Students
(unspecified)
-
- MINI 5
DSM-IV
Home Face-to-face interview Prevalence
Al-Hemiary et
al. (2015a)
Substance use 2009 Baghdad ✓ 1684 Youth centre
attendees
-
18-35
79.2 CIDI-2
DSM-IV
Youth centre Face-to-face interview Prevalence
Al Mousawi
(2015)
Alcohol use 2010 Karbala ✓ 5446 Students
(university)
-
17+
45.8 AUDIT
Score of 8+
Lecture
rooms
Self-administered survey Prevalence
Patterns
Attitudes
Baker et al.
(2016)
Health risk
behaviours
2012-
13
Erbil ✓ 500 Students
(secondary)
-
100 Unspecified Classroom Self-administered survey Prevalence
Shabila et al.
(2015)
Risky driving 2014 Erbil ✓ 211 Students
(medical)
21.37 ± 1.8
17-26
48.3 N/A In-college Self-administered survey Behaviour
Al-Ameri et al.
(2016)
Alcohol use 2015 Baghdad ✓ 1435 Students
(university)
19.8 ± 1.6
18-24
47 Tool not specified
Moderate/heavy*
Lecture
rooms
Self-administered survey Prevalence
Al-Qazzaz et al.
(2017)
Alcohol
concentration
2015 Baghdad - 473 General
autopsies
-
14-34
- Blood alcohol
>40mg/100ml
Forensics lab Blood alcohol
concentration
Prevalence
Saeed (2016) Health risk
behaviours
2016 Kirkuk ✓ 278 Students
(secondary)
-
16-18
100 Unspecified Classroom Self-administered survey Prevalence
Behaviour
Abdulah et al.
(2018)
Sleep disorders 2017 Duhok ✓ 317 Students
(medical)
20.4 ± 1.9
17-28
43.3 SLEEP-50
(evening use)
In-college Self-administered survey Prevalence
Al-Imam et al.
(2017)
Novel
psychoactive
drugs
2017 Baghdad - 458 Students
(medical)
19.7 ± 1.4
17-24
34.3 Unspecified Online Self-administered survey Prevalence
# Occasional/moderate/binge use not defined.
* Moderate drinking = one standard drink (10g alcohol) for women, two standard drinks for men; heavy/high-risk drinking = 3+ drinks per day/7+ drinks per week for women, 4+
drinks per day/14+ drinks per week for men.

91
Table 5 Findings of the included studies
Article Relevant findings
Prevalence and patterns Attitudes, behaviours, and motives
Al Mousawi (2014) ➢ Alcohol abstinence was inversely associated with smoking (OR = 0.05, p<0.001).
(prevalence of drinking not reported)
➢ 2% had a positive attitude to alcohol (vs. 10% to smoking and
2% to illicit drugs)
➢ Smokers had more positive attitudes to drinking (p<0.001)
Alhasnawi et al. (2009) ➢ 0.7% of those aged 18-34 met criteria for alcohol abuse
➢ 0.3% met criteria for dependence
N/A
S. Ali et al. (2009) ➢ 23.7% (males: 34.7%; females: 4.1%) consumed alcohol in the past 6 months
➢ Of the drinkers, 81.5% drank occasionally and 18.5% drank moderately or binged
(frequency undefined)
➢ Most frequent drinking in bars or restaurant (44.5%) and outdoor settings (25.9%).
Only 7.6% of users drank at home
Data contradiction: Abstract says moderate to binge drinking only among males while
data tables show two of the five females that drink consume alcohol at moderate to
binge levels.
➢ 51.9% reported they drink to get pleasure and 44.4% for relief
from stress
Rahim (2010) ➢ Five students (6.2%) met criteria for abuse and two (2.5%) for dependence
➢ Alcohol dependence more common among unemployed/non-governmental
employees than students/government employees (p <0.001)
N/A
Al-Hemiary et al.
(2015a)
➢ 339 participants aged 18-35 (20.1%) met criteria for lifetime alcohol abuse
➢ No female reported alcohol/drug abuse
N/A
Al Mousawi (2015) ➢ 2.2% (n=116; 4.1% males; 0.4% females) were current drinkers
➢ Of the 75 drinkers who completed AUDIT, 56% scored 8+ (scores of: 8-15, 36%;
16-19, 10.7%; 20+, 9.3%)
➢ Alcohol use associated with smoking (OR =7.16), male gender (OR=10.52), and
taking evening classes (OR for daytime students=0.51), trauma (data not provided)
➢ Most drinkers had 1-2 standard drinks per day (61.2%); 6% had 10+
➢ Many drank once monthly (40.8%); 20.4% drank on >4 times per week
➢ 46% of the 50 drinkers who answered, reported 6+ drinks weekly or daily
➢ More than half reported guilt (54.4%) about their drinking
➢ Almost half said people were concerned about their drinking
(49.1%)
Author reports possible cultural bias in these items of AUDIT.
Baker et al. (2016) ➢ 20 (6.6% of those that reported risk behaviours) reported alcohol use (unspecified if
current or lifetime).
N/A
Shabila et al. (2015) N/A ➢ 4.5% of students reported driving after ‘mild to moderate’
drinking (4.5%) and 6.4% reported drunk driving
➢ These behaviours were considered the riskiest by 80.1% and
72.5% of students, respectively
➢ A tenth of students (10.7%) thought that driving after a mild to
moderate intake of alcohol was enjoyable. While 8.7% found

92
Article Relevant findings
Prevalence and patterns Attitudes, behaviours, and motives
drunk driving as an enjoyable activity. These were the least
common reported enjoyable behaviours.
Al-Ameri et al. (2016) ➢ 9.7% (n= 139; 19.7% males, 0.8% females) reported lifetime alcohol use
➢ Of drinkers, 17 (12.2%) drank heavy, 23.7% moderate and 64% occasional*
➢ Alcohol use higher among those who are male (19.7% vs 0.8%; p<0.001), non-
medical students^ (10.7% vs 5.1%; p=0.006), older (11.7% for 20-24 vs 7.8% for
18-20; p=0.013), rural (23.3% vs 8.3%; p<0.001), living away from family/relatives
(25.1% vs 6.8%;p<0.001)
➢ Multivariable: only living away from family (PR 2.7 (95% CI 1.8-4.1); p<0.001)
and non-medical faculty (PR 2.6 (95% CI 1.4-4.7); p 0.002) remained significant
N/A
Al-Qazzaz et al. (2017) ➢ 8.5% (n = 40) of autopsies in those aged 14-34 had a blood alcohol >40mg/100mL N/A
Saeed (2016) ➢ Lifetime use: 7.6%
➢ Association between drinking, and age/grade (p<0.001), carrying a weapon (n=15,
p 0.014), physical fight (n=20, p<0.001)
➢ Age of onset was 12 years
Results appear internally contradictory (maybe due to limitations in
English expression)
➢ One third (30.6%) drove a vehicle while drinking alcohol
➢ 52.5% of the students were in a vehicle driven by alcohol
drinking person (in abstract only)
➢ 6.5% rode in a car for 2-4 times with a driver who had
consumed alcohol
Abdulah et al. (2018) ➢ 11.9% (n= 37) reported consuming alcohol in the evening
➢ Evening drinking was predictor of emotional disturbance (p=0.034) and restless
legs syndrome during night (p=0.003)
N/A
Al-Imam et al. (2017) ➢ Four students (0.9%) reported drinking (undisclosed if lifetime or current), two
(0.4%) had alcohol use disorder (criteria unspecified)
➢ Alcohol consumption increased as students progressed in medical college
N/A
* Moderate drinking = one standard drink (10g alcohol) for women, two standard drinks for men; heavy/high-risk drinking = 3+ drinks per day/7+ drinks per week for women, 4+ drinks
per day/14+ drinks per week for men.
^ Medical students in Al-Ameri et al are students studying medicine, dentistry, and pharmacy.

93
Discussion
This systematic scoping review is the first review on prevalence, patterns, and attitudes of alcohol
use in Iraq and to our knowledge, is the first review of student or youth drinking in any MMC. The
search methods employed identified alcohol-related data on young Iraqis in local and international
peer-reviewed academic literature. Thirteen articles were included. Most had a non-alcohol focus and
reported alcohol data incidentally.
A wide range of prevalence was reported for lifetime and current alcohol use and misuse. Less than
half the studies employed validated tools to assess alcohol use. Most articles did not document how
they asked about alcohol. Similarly, most authors either do not report whether they asked about
lifetime or current drinking, or how they determined that participants had “alcohol use disorders” or
were “heavy/binge” users and what pattern of drinking each of these terms represents. This makes
these results harder to interpret. Accordingly, no clear pattern of drinking can be discerned in these
Iraqi young and student samples. However, generally, a higher prevalence of alcohol use was reported
by samples from Kurdistan (North Iraq). This is consistent with data from Iraq’s 2015 household
survey that found alcohol consumption is highest in the Northern governorates and lowest in the
South (US Department of State et al., 2015).
All included studies reporting prevalence of consumption by sex, showed a significantly higher
prevalence of alcohol use or misuse by male participants – with two studies indicating no female use.
The prevalence of female consumption is also low in other Iraqi general population studies with self-
report data including the national household surveys (Al-Hemiery et al., 2017; WHO, 2009). In
contrast, the one study employing the objective measure of post-mortem blood alcohol concentration
shows a higher percent of females overall with BAC of over 40mg/100mL (12.2% vs 8.4% males
with BAC above 40mg/100mL) (Al-Qazzaz et al., 2017). In this sample, there were 1136 males and
only 139 females, and 91.4% of the females had died from a traumatic event (vs 78.4% of males).
One explanation for this discrepancy could be that Iraqis, by observation, are more protective of their
female relatives – and some may be less likely to consent for their female relatives to undergo post-

94
mortem examination except where it is legally required. It is possible that the study has an over-
representation of females who have either been victims of abuse and trauma or who are no longer
connected to their families. Nonetheless, it reveals that female consumption of alcohol exists in Iraq
and is associated with harms including death. In the study, there was a significant relation between
traumatic death and higher consumption (p = 0.007) (Al-Qazzaz et al., 2017).
Studies assessing drinking in this context to date have mostly used in-home or in-class self-reported
pen-and-paper surveys or face-to-face interviews. The sensitivity of alcohol use in MMCs makes it
particularly difficult for young people or females to disclose behaviours or attitudes that go against
societal norms. Previous studies have indicated under-reporting of alcohol consumption in MMCs
and particularly in Iraq (Al-Hemiery et al., 2017).
Although prevalence of alcohol use is low in Iraq compared to some other MMCs such as Lebanon
(E. G. Karam et al., 2004) and non-MMCs such as Australia (AIHW, 2020), the prevalence of alcohol
misuse is high among those who drink. This is clear in all studies that report on both alcohol use and
misuse. Most strikingly, the IMHS (Alhasnawi et al., 2009) showed only 0.7% of those aged 18-34
had an AUD and 0.3% had dependence. However, among drinkers of all ages, 45.7% met criteria for
ICD-11 alcohol use disorders, with 32.1% harmful use and 13.7% dependence (compared to 33.3%,
26.6% and 6.8% respectively in Australia) (Degenhardt et al., 2019). In keeping with these findings,
the 2015 Survey of Substance Abuse in Iraq (SSAI) showed that 71% of current drinkers met criteria
for dependence on the Severity of Dependence Scale (SDS) (US Department of State et al., 2015).
Interestingly, Iraq had the highest prevalence of AUDs among drinkers from all ten countries included
in WHO’s World Mental Health Surveys (Degenhardt et al., 2019). These high prevalence of
dependence among drinkers are worrying. However, Al Mousawi (2015) highlighted the potential for
screening or diagnostic tools to be culturally biased. For example, items 7 (guilt) and 10 (worry of
others about your drinking) of AUDIT may be more highly endorsed by Muslim respondents. This is
most likely because of religious, social, and cultural prohibition. Drinkers may feel guilty and trigger
the worry of family and friends even if they consume alcohol in only small amounts. Similarly, the

95
SDS includes items such as “How much did you worry about your use of the drug?” which may also
provide false positive results for dependence. This illustrates the importance of tailoring tools and
interventions for MMCs.
S. Ali et al. (2009) reported that students used alcohol for pleasure (51.9%) or to relieve stress (44.4%)
and Al Mousawi (2014) reported 2% of students view alcohol positively (with no further details).
Other than these two studies, there is no data on influencing factors, attitudes towards alcohol or
preventative strategies. Given Iraq’s history of exposure to globalisation and war, an understanding
of factors influencing drinking is key to understand and predict trends among young Iraqis.
No study reported on harm-reduction or treatment initiatives and measures in Iraq. Iraq has no clear
written or implemented alcohol policy, strategy or harm reduction initiatives (Al-Ansari et al., 2015;
Al Ansari et al., 2019). This is despite at least three studies from diverse cities showing young people
dying or placing themselves and others at risk while under the influence of alcohol (Al-Qazzaz et al.,
2017; Saeed, 2016; Shabila et al., 2015). This is another area of need.
All studies other than the national IMHS (Alhasnawi et al., 2009) report no funding. This is because
medical and health research only began after 2003 and there are no current major government grant
cycles. Most funded research such as the IMHS or SSAI are either directly managed and funded by
the Ministry of Health or externally funded by international organisations (Al-Hemiery et al., 2017;
Alhasnawi et al., 2009). However, because Iraq is now a high-middle income country, it is no longer
eligible for most international government and non-governmental organisational funding initiatives.
In addition, recent wars in Iraq have had a major impact on the national burden of disease. These
factors impede Iraq’s ability to further progress in health research especially in areas such as alcohol.
Limitations
This study was limited to only include studies in English. Although, to our knowledge, there are no
alcohol-specific data published in the Arabic language because English is the main language of
medical and scientific research in Iraq. A meta-analysis of the data could not be conducted because

96
each study reported on alcohol differently (most using their own measures). We were limited in our
ability to compare figures for specific demographics because the studies did not describe their sample
adequately. Because this is a scoping review, limited assessment was made on the quality of the
included studies. Despite this, clear weakness of the methods and reporting of some studies were
noted in this review. This study was limited to original journal articles published in peer-reviewed
academic journals – this meant that age-specific data for the SSAI was not included as these had been
published in a report, but not in refereed journals. Although the Al-Qazzaz et al. (2017) paper fits
within our scope and was included, the sample differed from the other included studies as it was based
on blood samples of autopsies.
Conclusion
Alcohol research is limited in all MMCs, including Iraq. This review shows that most alcohol data is
incidental rather than the focus of the studies. No clear picture of the prevalence of drinking or
attitudes towards alcohol among young Iraqis can be drawn. However, the results indicate that Iraq
is not immune to health concerns resulting from alcohol use. The high rates of heavy use and AUD
among those who consume alcohol as well as the alcohol-related risk behaviour among students are
cause for concern. More research is needed, particularly to understand the concerns, needs and
experiences of young people and their relationship with alcohol, and ways to effectively prevent or
intervene for AUDs. To achieve this effectively, study methods, screening or diagnostic tools,
preventive and therapeutic interventions should be tailored for the local Iraqi context.

97
References:
Abdulah, D. M., & Piro, R. S. (2018). Sleep disorders as primary and secondary factors in relation
with daily functioning in medical students [Article]. Annals of Saudi medicine, 38(1), 57-64.
https://doi.org/10.5144/0256-4947.2018.57
AIHW. (2020). Alcohol, tobacco & other drugs in Australia.
https://www.aihw.gov.au/reports/alcohol/alcohol-tobacco-other-drugs-australia
Al-Ameri, R. J. K., Abd Al-Badri, H. J., & Lafta, R. K. (2016). Prevalence of Alcohol Consumption
among University Students in Baghdad: A Cross-section survey from Iraq [Article].
Epidemiology Biostatistics and Public Health, 13(4), 8, Article e11942 .
https://doi.org/10.2427/11942
Al-Ansari, B., Thow, A.-M., Day, C. A., & Conigrave, K. M. (2015). Extent of Alcohol Prohibition
in Civil Policy in Muslim Majority Countries: the Impact of Globalization. Addiction,
111(10), 1703-1713. https://doi.org/10.1111/add.13159
Al-Hemiary, N. J., Hashim, M. T., Al-Diwan, J. K., & Abdul Razzaq, E. (2015). Alcohol and drug
abuse in post-conflict Iraq Journal of the Faculty of Medicine 57(4), 291-295.
Al-Hemiery, N., Dabbagh, R., Hashim, M. T., Al-Hasnawi, S., Abutiheen, A., Abdulghani, E. A., Al-
Diwan, J. K., Kak, N., Al Mossawi, H., Maxwell, J. C., Brecht, M.-L., Antonini, V., Hasson,
A., & Rawson, R. A. (2017). Self-reported substance use in Iraq: findings from the Iraqi
National Household Survey of Alcohol and Drug Use, 2014. Addiction, 112(8), 1470-1479.
https://doi.org/10.1111/add.13800
Al-Imam, A., Al-Mukhtar, F., Shafiq, A., & Irfan, M. (2017). Knowledge and (Ab)Use in Connection
with Novel Psychoactive Substances: A Cross-Sectional Analysis of Iraqi Medical Students.
Global Journal of Health Science, 9(11), 61.
Al-Qazzaz, M. A., Al-Saffar, A. J., Al-Rubai, H. K., & Al-Qazzaz, E. M. (2017, December 15).
Evaluation of alcohol concentrations in samples referred to the forensic Laboratory in
Baghdad [journal article]. Egyptian Journal of Forensic Sciences, 7(1), 27.
https://doi.org/10.1186/s41935-017-0023-9
Al Ansari, M., Dawson, A., & Conigrave, K. (2019). Alcohol: from Mesopotamia to Modern Iraq.
Journal of Ethnicity in Substance Abuse, 1-23.
https://doi.org/10.1080/15332640.2019.1657541
Al Mousawi, A. (2014). The prevalence of smoking among karbala/iraq university students in iraq in
2005. Tobacco Use Insights, 7, 9-14. https://doi.org/https://dx.doi.org/10.4137/TUI.S12238
Al Mousawi, A. (2015). Alcohol use disorder identification test use in Muslim countries.
International Journal of Prevention and Treatment of Substance Use Disorders, 1(3-4), 79-
92.
Alhasnawi, S., Sadik, S., Rasheed, M., Baban, A., Al-Alak, M. M., Othman, A. Y., Othman, Y.,
Ismet, N., Shawani, O., Murthy, S., AlJadiry, M., Chatterji, S., Al-Gasseer, N., Streel, E.,
Naidoo, N., Ali, M. M., Gruber, M. J., Petukhova, M., Sampson, N. A., & Kessler, R. C.
(2009). The prevalence and correlates of DSM-IV disorders in the Iraq Mental Health Survey
(IMHS) [Review]. World Psychiatry, 8(2), 97-109.
https://www.scopus.com/inward/record.uri?eid=2-s2.0-
67651171639&partnerID=40&md5=b2d0428a7f85b21d2394a4495cc69e6e
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2694515/pdf/wpa020097.pdf

98
Ali, S. K., & Sabir, J. M. (2009). Prevalence of Alcohol Use among Medical College Students in
Hawler Medical University. Zanko Journal of Medical Sciences, 13(1), 17-23. http://zjms-
hmu.org/files/articles/260311041225.pdf
AlMarri, T. S. K., & Oei, T. P. S. (2009, 2009/06/01). Alcohol and substance use in the Arabian Gulf
region: A review. International Journal of Psychology, 44(3), 222-233.
https://doi.org/10.1080/00207590801888752
Arksey, H., & O'Malley, L. (2005, 2005/02/01). Scoping studies: towards a methodological
framework. International Journal of Social Research Methodology, 8(1), 19-32.
https://doi.org/10.1080/1364557032000119616
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., & Monteiro, M. G. (2001). AUDIT: The Alcohol
Use Disorders Identification Test: Guidelines for Use in Primary Care. World Health
Organization.
Baker, J. M. A., & Al-Doski, N. A. S. (2016). Health risk behaviors among male students in secondary
schools in Erbil city. Zanco Journal of Medical Sciences, 20(1), 1199-1205.
Debell, F., Fear, N. T., Head, M., Batt-Rawden, S., Greenberg, N., Wessely, S., & Goodwin, L. (2014,
September 01). A systematic review of the comorbidity between PTSD and alcohol misuse
[journal article]. Social Psychiatry and Psychiatric Epidemiology, 49(9), 1401-1425.
https://doi.org/10.1007/s00127-014-0855-7
Degenhardt, L., Bharat, C., Bruno, R., Glantz, M. D., Sampson, N. A., Lago, L., Aguilar-Gaxiola, S.,
Alonso, J., Andrade, L. H., Bunting, B., Caldas-de-Almeida, J. M., Cia, A. H., Gureje, O.,
Karam, E. G., Khalaf, M., McGrath, J. J., Moskalewicz, J., Lee, S., Mneimneh, Z., Navarro-
Mateu, F., Sasu, C. C., Scott, K., Torres, Y., Poznyak, V., Chatterji, S., Kessler, R. C., &
Collaborators, o. b. o. t. W. W. M. H. S. (2019). Concordance between the diagnostic
guidelines for alcohol and cannabis use disorders in the draft ICD-11 and other classification
systems: analysis of data from the WHO's World Mental Health Surveys. Addiction, 114(3),
534-552. https://doi.org/10.1111/add.14482
GBD 2016 Alcohol Collaborators. (2018). Alcohol use and burden for 195 countries and territories,
1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The
Lancet, 392(10152), 1015-1035. https://doi.org/10.1016/S0140-6736(18)31310-2
Ghandour, L., Chalak, A., El-Aily, A., Yassin, N., Nakkash, R., Tauk, M., El Salibi, N., Heffron, M.,
& Afifi, R. (2016, 2//). Alcohol consumption in the Arab region: What do we know, why does
it matter, and what are the policy implications for youth harm reduction? International
Journal of Drug Policy, 28, 10-33.
https://doi.org/http://dx.doi.org/10.1016/j.drugpo.2015.09.013
Karam, E. G., Maalouf, W. E., & Ghandour, L. A. (2004, 2004/12/07/). Alcohol use among university
students in Lebanon: prevalence, trends and covariates: The IDRAC University Substance
Use Monitoring Study (1991 and 1999). Drug and Alcohol Dependence, 76(3), 273-286.
https://doi.org/https://doi.org/10.1016/j.drugalcdep.2004.06.003
Kessler, R. C., & Üstün, T. B. (2004). The world mental health (WMH) survey initiative version of
the world health organization (WHO) composite international diagnostic interview (CIDI).
International Journal of Methods in Psychiatric Research, 13(2), 93-121.
Lo, J., Patel, P., Shultz, J. M., Ezard, N., & Roberts, B. (2017, 2017/09/19). A Systematic Review on
Harmful Alcohol Use Among Civilian Populations Affected by Armed Conflict in Low- and
Middle-Income Countries. Substance Use & Misuse, 52(11), 1494-1510.
https://doi.org/10.1080/10826084.2017.1289411

99
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The, P. G. (2009). Preferred Reporting Items
for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Medicine, 6(7),
e1000097. https://doi.org/10.1371/journal.pmed.1000097
Munn, Z., Stern, C., Aromataris, E., Lockwood, C., & Jordan, Z. (2018). What kind of systematic
review should I conduct? A proposed typology and guidance for systematic reviewers in the
medical and health sciences. BMC medical research methodology, 18(1), 5-5.
https://doi.org/10.1186/s12874-017-0468-4
Rahim, T. A. (2010, May). Rate of alcohol and substance use disorders among the journalists in Erbil
City [Empirical Study; Interview; Quantitative Study]. Arab Journal of Psychiatry, 21(1), 50-
60.
https://ezproxy.library.usyd.edu.au/login?url=http://ovidsp.ovid.com/ovidweb.cgi?T=JS&C
SC=Y&NEWS=N&PAGE=fulltext&D=psyc7&AN=2010-13479-004
Roberts, B., & Ezard, N. (2015). Why are we not doing more for alcohol use disorder among conflict-
affected populations? Addiction, 110(6), 889-890. https://doi.org/10.1111/add.12869
Saeed, H. M. (2016). Assessment of the health risk behavior in young adulthood: A school-based
health study in Kirkuk City / Iraq. The Medical Journal of Tikrit University 21(2), 172-181.
Shabila, N. P., Ismail, K. H., Saleh, A. M., & Al-Hadithi, T. S. (2015). Risky driving behaviours
among medical students in Erbil, Iraq [Article]. Sultan Qaboos University Medical Journal,
15(3), e390-e397. https://doi.org/10.18295/squmj.2015.15.03.014
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T.,
Baker, R., & Dunbar, G. C. (1998). The Mini-International Neuropsychiatric Interview
(MINI): the development and validation of a structured diagnostic psychiatric interview for
DSM-IV and ICD-10. The Journal of clinical psychiatry.
Sweileh, W. M., Zyoud, S. e. H., Al-Jabi, S. W., & Sawalha, A. F. (2014). Substance use disorders
in Arab countries: research activity and bibliometric analysis. Substance Abuse Treatment,
Prevention and Policy, 9, 33. https://doi.org/http://dx.doi.org/10.1186/1747-597X-9-33
UNDESA. (2017). World Population Prospects: The 2017 Revision, Key Findings and Advance
Tables.
US Department of State, Bureau of International Narcotics and Law Enforcement Affairs, Iraqi
Society of Addiction Medicine, University of California LA, & Center for Human Services.
(2015). Survey of Substance Abuse in Iraq.
WHO. (2009). Iraq Mental Health Survey 2006/7. http://www.webcitation.org/6mk3pGCJV

100
Chapter 5: Alcohol and university students in Iraq: attitudes, availability, and use
Chapter 3 established the historical and socio-cultural context for this research. Chapter 4 presented
a systematic scoping review outlining the scarcity of available research on youth and student drinking
in Iraq. These reviews allowed the contextual positioning of our research within existing alcohol
literature. The gap in research was even wider when we set out on conducting this mixed-method
study in 2015.
This chapter will present the quantitative component of our mixed-method study on attitudes towards
alcohol and the prevalence of alcohol use among young university students in Iraq. As identified in
Chapter 2, we first intended to conduct this study using a “voting booth” style of set up, with
confidential paper-and-pen surveys, before arriving at the current methodology - conducting this
research via an anonymous online questionnaire.
As the design of this project included consultations with local collaborators in Iraq, we were able to
tailor some items such as the socio-economic scale to the local context, and to include local names
for certain psychoactive substances. In addition, internationally validated screening tools and items
on potential influencers of alcohol consumption were included. The full 10-item AUDIT test was
initially utilised. However, because of observed high attrition rate among the early participants, only
the first three consumption questions (AUDIT-C) were later used. That was considered an acceptable
abbreviation, given both the research on the validity of AUDIT-C compared to the full AUDIT, and
concerns about the validity of items 7 and 10 from the full AUDIT on guilt and other’s concern about
drinking in the MMC context.
This quantitative component of the thesis presents the prevalence and patterns of student drinking.
Students’ attitudes towards alcohol, perceptions about alcohol policies as well as media and trauma
exposure are also presented in this chapter.
The following manuscript has been submitted for publication.

101
Abstract
Introduction
Like other Muslim Majority Countries (MMCs), there is little data on alcohol use in Iraq. This study
examines attitudes towards alcohol and its use among Iraqi university students. It considers the likely
impact of the context of conflict and globalisation.
Methods
An online quantitative questionnaire was distributed to students at diverse universities in Iraq. The
survey included questions on alcohol use (AUDIT-C) and availability, drug use, attitudes towards
alcohol policy and a screen for post-traumatic stress disorder (PC-PTSD). Descriptive analysis was
conducted, followed by multivariable logistic regression to determine independent predictors of
drinking.
Results
Of the 468 students who provided alcohol-related data, a minority reported having ever consumed
alcohol (5.3%; 1.6% females, 10% males). Only 21 participants consumed alcohol in the last 12
months, of whom six had an AUDIT-C score of 4+ (all males). Most students indicated that access
to alcohol was “easy”. Of the 220 respondents who completed the PC-PTSD screen, 29.2% (n=63)
had positive scores. Two in five (n=90, 41.7%) reported direct exposure to violent conflict.
Independent predictors of lifetime consumption were being a non-Muslim, male and living away from
family.
Conclusion
While prevalence of drinking is low, 6/15 male current alcohol users in this convenience sample
report drinking at risky levels. There are several challenges conducting research on this sensitive topic
in a MMC. Further research could strive to obtain representative samples, and to ascertain appropriate
prevention and early intervention approaches for the socio-cultural context of Iraq.
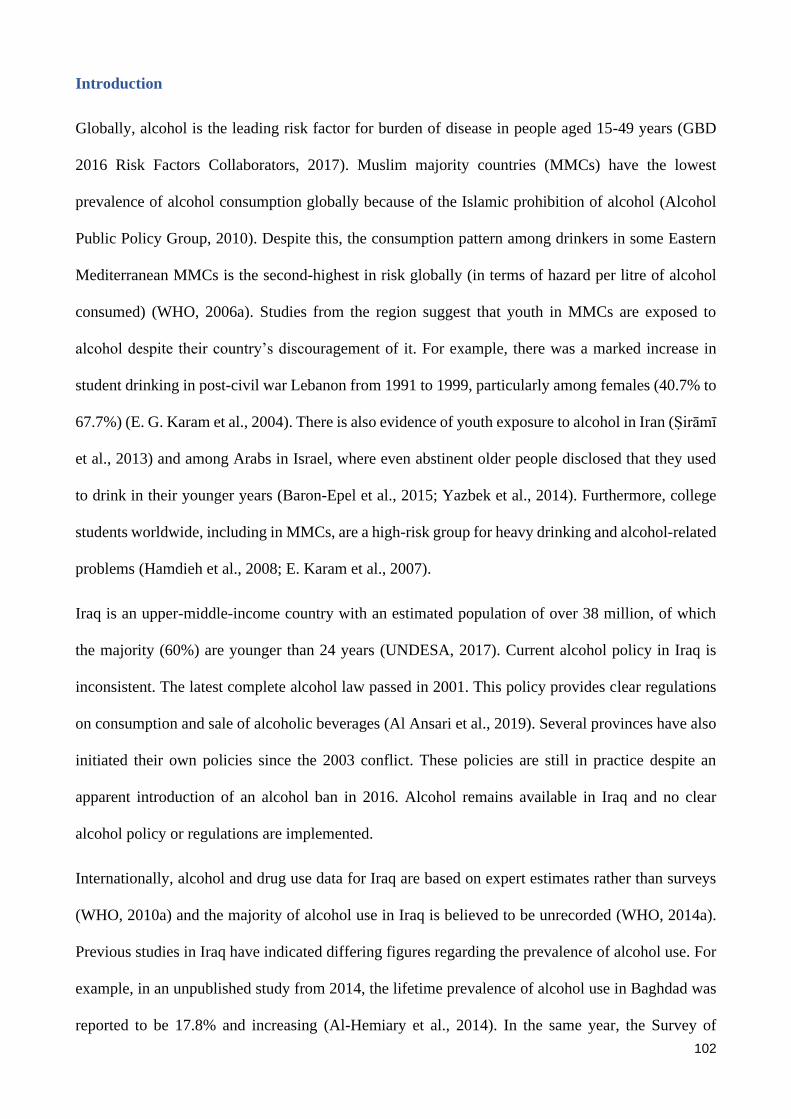
102
Introduction
Globally, alcohol is the leading risk factor for burden of disease in people aged 15-49 years (GBD
2016 Risk Factors Collaborators, 2017). Muslim majority countries (MMCs) have the lowest
prevalence of alcohol consumption globally because of the Islamic prohibition of alcohol (Alcohol
Public Policy Group, 2010). Despite this, the consumption pattern among drinkers in some Eastern
Mediterranean MMCs is the second-highest in risk globally (in terms of hazard per litre of alcohol
consumed) (WHO, 2006a). Studies from the region suggest that youth in MMCs are exposed to
alcohol despite their country’s discouragement of it. For example, there was a marked increase in
student drinking in post-civil war Lebanon from 1991 to 1999, particularly among females (40.7% to
67.7%) (E. G. Karam et al., 2004). There is also evidence of youth exposure to alcohol in Iran (Ṣirāmī
et al., 2013) and among Arabs in Israel, where even abstinent older people disclosed that they used
to drink in their younger years (Baron-Epel et al., 2015; Yazbek et al., 2014). Furthermore, college
students worldwide, including in MMCs, are a high-risk group for heavy drinking and alcohol-related
problems (Hamdieh et al., 2008; E. Karam et al., 2007).
Iraq is an upper-middle-income country with an estimated population of over 38 million, of which
the majority (60%) are younger than 24 years (UNDESA, 2017). Current alcohol policy in Iraq is
inconsistent. The latest complete alcohol law passed in 2001. This policy provides clear regulations
on consumption and sale of alcoholic beverages (Al Ansari et al., 2019). Several provinces have also
initiated their own policies since the 2003 conflict. These policies are still in practice despite an
apparent introduction of an alcohol ban in 2016. Alcohol remains available in Iraq and no clear
alcohol policy or regulations are implemented.
Internationally, alcohol and drug use data for Iraq are based on expert estimates rather than surveys
(WHO, 2010a) and the majority of alcohol use in Iraq is believed to be unrecorded (WHO, 2014a).
Previous studies in Iraq have indicated differing figures regarding the prevalence of alcohol use. For
example, in an unpublished study from 2014, the lifetime prevalence of alcohol use in Baghdad was
reported to be 17.8% and increasing (Al-Hemiary et al., 2014). In the same year, the Survey of

103
Substance Abuse in Iraq (SSAI) suggests that half that number (8.6%; 16.7% male; 0.6% female)
were lifetime consumers (US Department of State et al., 2015). Even this is a marked increase on an
earlier national household study, the 2006 Iraqi Mental Health Survey (IMHS), which found only
3.7% (6.8% of males) consumed alcohol in their lifetime. However, both national household studies
report negligible alcohol use prevalence among females (0.6% in both studies) (US Department of
State et al., 2015; WHO, 2009).
Despite the relatively low prevalence of alcohol use in the general population, risky drinking patterns
are common among drinkers. For example, the SSAI indicates that, on average, current drinkers
consume more than six drinks per day on 10.5 days a month. Two thirds (70%) of current drinkers in
the general population scored within the dependence range on the Severity of Substance Dependence
Scale (SDS) (US Department of State et al., 2015). Interestingly, the Iraqi Mental Health Survey
(IMHS), part of the larger World Mental Health (WMH) Survey, from just ten years prior reported
Iraq as having the lowest overall prevalence of dependence (0.2%) but one of the highest prevalence
of dependence among drinkers (5.4%) (using the Composite International Diagnostic Interview 3rd
edition, CIDI-3) (Glantz et al., 2020; WHO, 2009). Although both national surveys show a high risk
of dependence among drinkers, the difference (70% vs 5.4%) maybe in part due to the tools used and
their validity in the MMC context. SDS is a five-item screen, specific for dependence while CIDI-3
is an in-depth diagnostic interview assessing all sorts of AUDs including dependence. We could not
identify any study that specifically validated either tool in the Iraqi context. However, we identified
that two items of the SDS that may be interpreted differently by participants in MMC contexts and
result in ‘false positive’ scores. These are items 3 and 4 which ask if the drinker is worried about their
drinking and wishes they could stop. We anticipate that most drinkers in MMCs, especially those
adhering to Islam, would often or always worry about their drinking and wish they could stop. This
is because the expected norm in this context is abstinence. In addition to these two surveys, a
specialised sample from youth centres in Baghdad also found that 17% of over 2000 attendees met
criteria for alcohol abuse (using CIDI-2) with an average onset age of 21.7 years (Al-Diwan et al.,

104
2015; Al-Hemiary et al., 2015b). This study however did not report on prevalence of alcohol
consumption among this specialised group.
Alcohol consumption among university students in Iraq
Worldwide, university students drinking is a major health concern, including in some MMCs such as
Lebanon and Egypt (E. Karam et al., 2007; E. G. Karam et al., 2004). However, a systematic review
of alcohol literature in the Arab world identified a scarcity of literature about youth and student
drinking in Iraq (L. Ghandour et al., 2016).
The 2014 household study (SSAI) included 230 students (not specified if university students) reported
that fewer than one in 30 students had ever consumed alcohol (3.0%) and less than one in 50 were
current drinkers (1.7%) (US Department of State et al., 2015). An earlier 2010 study in Karbala
indicated a similarly low prevalence of current drinking among 5446 students (2.2%; male 4.1%;
female 0.4%) (Al Mousawi, 2015).
By contrast, in the large metropolis of Baghdad, results differ across studies. The lifetime
consumption of alcohol was over four times higher than the national or Karbala prevalence, among
three Baghdadi universities (9.7%; 19.7% male; 0.8% female) (Al-Ameri et al., 2016). However, data
collected at around the same time from medical students at Baghdad University indicated a far lower
prevalence at 0.4% (the authors did not specify if this is lifetime or current drinking) (Al-Imam et al.,
2017).
In an earlier (2007) survey in Erbil, a city in Iraqi Kurdistan, the prevalence of drinking (in the past
six months) was even higher - double the prevalence reported at the three Baghdadi universities
(23.7% among 342 students; 34.7% male; 4.1% female) (S. Ali et al., 2009). The tool used to collect
the consumption data is not described. In keeping with this prevalence, a study about student risky
behaviour seven years later at the same university indicated that over a tenth (10.9%) of a sample of
211 students reported having driven a vehicle under the influence of alcohol (Shabila et al., 2015).

105
It is not clear why the prevalence of consumption has varied so greatly in previous studies among
student populations in Iraq. Potential reasons for variability include the method of survey
administration and degree of privacy. Surveys often use interviews or paper surveys in a controlled
setting (e.g. classroom or in-home), where it can be challenging to guarantee confidentiality. Only
one study (about novel psychoactive substances, but including self-report alcohol questions), used an
online questionnaire (Al-Imam et al., 2017). The fact that samples are derived from single universities
or single cities also makes it hard to generalise the findings.
Identifying alcohol use, attitudes, and perceived motives for drinking among students allows for an
assessment of the vulnerability of young Iraqis to take up drinking or to misuse alcohol. We were
only able to identify two studies in local journals that assessed attitudes towards ‘addiction’ in a
general sample and in a sample of medical residents/professionals (Al-Hasnawi, 2006; Al-Hasnawi
et al., 2007). To our knowledge, there is currently no literature about attitudes to alcohol consumption
and alcohol policy in Iraq among Iraqi university students.
To address the challenges of social desirability bias, and collect data on alcohol more sensitively and
accurately, we used online data-collection, designed to maximise anonymity and confidentiality. We
recruited students from multiple universities around Iraq to increase generalisability. We also
collected data on perceived motives for drinking, attitudes on drinking, drinkers, and various alcohol
policies, and a possible connection between war or media exposure and alcohol use. Assessing these
attitudes are important in understanding current behaviour, and potential trends. It is hoped that this
study will help inform policy and preventative measures in Iraq and other MMCs.
Methods
An online cross-sectional survey of Iraqi university students was conducted as the quantitative
component of a larger mixed-method study on attitudes of University students in Iraq towards alcohol.

106
Ethics approval
Ethics approval was granted by the Medical Ethics Committee at the College of Medicine in the
University of Kufa, Iraq (MECCM-0028) (Appendix 1).
Quantitative survey
The survey (Appendix 4 and 5) included 42 questions that were derived from household and college
surveys from other countries, mainly Australia and Sweden (Australian Institute of Health and
Welfare, 2013; Bullock, 2004). The Swedish instrument was designed to assess attitudes towards
drugs in medical student. We considered that alcohol in Iraq shares a similar place to illicit drugs in
the Swedish context, making this instrument relevant. The Australian National Drug Strategy
Household Survey (NDSHS) was used for demographic questions and to assess drinking behaviour,
including drinking location and companions. These instruments were edited to suit the local context
in consultation with local collaborators and international experts. A draft Arabic translation of the
complete survey was produced and then finalised in consultation with local recently graduated
medical doctors in a focus group. The survey was piloted in English and Arabic by members of this
focus group and took 15-20 minutes to complete. The Arabic survey was also shared with religious
and cultural elders for comment. Based on these comments, some minor changes to the Arabic
translation of the survey were made in for cultural sensitivity.
Following a consent question, demographic items enquired into the student’s family and university
background, including internal displacement status, and living situation. Participants were asked if
they had ever consumed alcohol and were screened using the AUDIT-C tool (Bush et al., 1998). This
three-item tool, comprised of the first three items of the AUDIT questionnaire (T. F. Babor et al.,
2001), asks about frequency, amount of usual drinking, and frequency of drinking six or more drinks
(Bradley et al., 1998; T. M. Kelly et al., 2009).
Past or current drinkers were then asked about their drinking location, source of alcohol, and who
they consumed it with. Non-drinkers were asked about any desire to consume alcohol in the future.

107
These alcohol questions were followed by questions regarding use of other substances. Common
substances used in Iraq were identified using literature and in consultation with local collaborators.
Additional items in the survey inquired into attitudes towards alcohol and other drug consumption
and policies. Participants were then asked about exposure to alcohol in the media, and about exposure
to war and violent conflict, before being screened for post-traumatic stress disorder (PTSD) using the
four-item primary care PTSD (PC-PTSD) screening tool. This tool was chosen due to its brevity
(Prins et al., 2003) and suitability for a general population.
To maximise anonymity and confidentiality, and to minimise social desirability bias, the
questionnaire was delivered as an anonymous online survey using the SurveyGizmo platform. No
identifying information or trackable IP addresses were collected. The survey could also be completed
privately at any time of the day and in any location. SurveyGizmo encrypted all data at the disk level.
The data may only be accessed through a password protected site by the author. The data was then
stored on University of Sydney servers after download.
Sampling and Recruitment
A mixture of convenience and snowball sampling was used to recruit participants. These approaches
were chosen as viable approaches to online recruitment for such a sensitive topic. Furthermore, there
were limited central databases of student emails within universities in Iraq, and so random online
sampling would have been difficult. The survey was open for online participation from 5th of March
to 1st of May 2017, although active recruitment only took place from the 8th to the 31st March 2017.
Senior academic representatives of three Iraqi universities gave permission for their students to be
recruited. Initial recruitment took place online by posting the survey link on the e-learning platform
of one of the universities, with lecturers encouraging their students to take part in the survey.
However, it was mentioned by students and staff that other faculties and universities often did not
actively use their e-Learning platforms and that student communication online occurred via student-
only social-media groups. Accordingly, further recruitment was carried out by posting the survey link

108
to these social media groups. As this study was conducted concurrently with the qualitative
component of the larger mixed-method project, interview participants were also asked to distribute
the survey link to their student networks. Initial recruitment was commenced within the Medical
Faculty at each university (via academics, students, and other consultants), and then expanded to other
faculties via students and staff contacts. Names of the universities will not be reported because of the
sensitivity of alcohol in an MMC setting.
The only inclusion criteria for the survey were to be a consenting current student of an Iraqi university
and aged under 24 years. Students could choose to complete the survey in Arabic or English. No
incentives or reimbursement for participation was provided, however, those participating in
interviews received a certificate of participation (if they shared their email address).
Data Analysis
Data were downloaded from SurveyGizmo, then analysed using SPSS Statistics 25. The data was
cleaned and participants who either reported themselves to be not current students at an Iraqi
university, to be above the age of 24 or who had not provided any information regarding their alcohol
consumption were excluded.
Several variables were recoded for the purposes of bivariate analysis. Age was recoded to younger
(17-20 years) and older (21-24 years). A dichotomous variable was created to indicate whether the
student lived with any of parent, partner or relative. Similarly, a variable captured if the student lived
either alone, with friends or in the dorm. All religions or ethnicities other than Islam or Arab were
combined into ‘non-Muslim’ and ‘non-Arab’ respectively. Universities apart from Universities A, B,
C and D were combined to ‘other’ because of small numbers at participants at those institutions.
Similarly, faculties apart from than Medicine, Pharmacy and Engineering were combined to ‘other’.
Drinkers were classified as at risk if the sum of the AUDIT-C items was three or more for females
and four or more for males (Dawson et al. 2012). Those that answered yes to three or more questions
on the PC-PTSD tool were scored positive for this screen (Prins et al., 2003).

109
Chi square tests were used to compare consumption patterns between different demographic groups
(e.g. by age, gender, religion and living location). Fisher’s exact test was used if expected cell values
were less than four. Significance was tested based on p value of less than 0.05.
Predictors that were significant in the bivariate analysis were considered for inclusion in a
multivariable logistic regression analysis to determine their independent predictive effect. The
outcome variables in the two analyses are lifetime and current (past-year) drinking.
Results
Sample
A total of 652 participants accessed the survey link. Five hundred and twenty-five participants were
eligible (students between the age of 17-24 years) and consented and started the survey. Of those, 468
(89%) answered at least one consumption question and were included in further analysis. The alcohol
and drug consumption, availability and use section was completed in full by 448 participants.
However, only 192 students (36.6% of eligible participants) completed the entire survey (Figure 1).
Each table and figure only include the individuals who answered that specific question or section.
There was no association between ever drinking and failure to complete the full questionnaire.
Students responded in either Arabic (n=388) or English (n=80).

110
Figure 7 Number of participants completing the different survey sections
Demographics
Students were aged between 17 and 24 (mean = 20.52 years, standard deviation [sd]= 1.43). Over
half of the sample was female (n=258; 55.1%).
The participating students were from over ten Iraqi universities but most attended four large public
universities from four different provinces in Iraq. Students were from a broad range of regions across
Iraq. However, despite repeated attempts at recruitment, no university from the Kurdistan region
participated. The majority (n=368; 78.6%) of participants were students in faculties of medicine,
followed by 9.6% (n=45) from faculties of pharmacy. Of the 468 students who provided alcohol data,
450 (96.2%) were undergraduate students, eight were postgraduate and ten did not specify.
Islam was the predominant religion (n=448, 95.7%) reported. The majority (76.9%; n=360) of
respondents reported living with relatives, while 23.1% (n=108) lived alone, in dormitories, or with
friends. Most (78%; n = 355) students reported their socio-economic level between steps 4 and 7 on
a ten-step socio-economic ladder. Internally displaced people accounted for 15.8% of the sample
(n=74).
EligibleProvided anyalcohol data
Completedalcohol/drug use
section
Completedattitudes section
Completed war& media section
Respondents (n) 525 468 448 220 192
Percent (%) 100% 89% 85% 42% 37%
0
150
300
450
600

111
Table 6 Prevalence of lifetime and past-year alcohol consumption by selected demographic data
Lifetime abstinence Lifetime use Past-year use Total
n % n % p-value n % p-value^ Total n %
Age
17-20 233 97.5 6 2.5 0.005* 4 1.7 0.003* 239 51.1
21-24 210 91.7 19 8.3 17 7.4 229 48.9
468 100
Gender
Male 189 90.0 21 10 <0.001* 17 8.1 0.001* 210 44.9
Female 254 98.4 4 1.6 4 1.6 258 55.1
468 100
University
University A 211 96.8 7 3.2 4 1.8 218 46.6
University B 42 100 0 0 0 0 42 9
University C 50 87.7 7 12.3 0.028* 6 10.5 0.011* 57 12.2
University D 90 92.8 7 7.2 7 7.2 97 20.7
Other 50 92.6 4 7.4 4 7.4 54 11.5
468 100
Faculty
Medicine 346 94.0 22 6.0
0.361
18 4.9
0.422
368 78.6
Pharmacy 44 97.8 1 2.2 1 2.2 45 9.6
Engineering 23 92.0 2 8.0 2 8.0 25 5.3
Other 30 100 0 0 0 0 30 6.4
468 100
Step on socio-
economic ladder
1-3 32 97.0 1 3.0
0.638
0 0
0.242
33 7.3
4-7 336 94.6 19 5.4 16 4.5 355 78.0
8-10 62 92.5 5 7.5 5 7.5 67 14.7
Missing 13 2.8
468 100
Religion
Muslim 438 97.8 10 2.2 <0.001*
8 1.8 <0.001*
448 95.7
Non-Muslim 5 25 15 75 13 65 20 4.3
468 100
Ethnicity
Arab 415 95.6 19 4.4 0.001*
15 3.5 <0.001*
434 92.7
Non-Arab 28 82.4 6 17.6 6 17.6 34 7.3
468 100
Relationship status
Single 393 95.2 20 4.8
0.002*
16 3.9
<0.001*
413 89.6
Unmarried Couple 19 79.2 5 20.8 5 20.8 24 5.2
Married or engaged 24 100 0 0 0 0 24 5.2
Missing 7 1.5
468 100
Internally
displaced?
Yes 68 91.9 6 8.1 0.249
6 8.1 0.101
74 15.8
No 375 95.2 19 4.8 15 3.8 394 84.2
468 100
Living location
With parent, partner
or relative 347 96.4 13 3.6
0.002*
10 2.8
0.001*
360 76.9
Alone, dorms or
with friends 96 88.9 12 11.1 11 10.2 108 23.1
468 100
* p-value less than 0.05
^ the p-statistics for past-year use are in comparison to past-year abstinence (not shown)

112
Alcohol consumption
Just over one in twenty (5.3%) students had ever consumed alcohol (n=25); the majority of those
were male (n=21) and non-Muslim (n=15). Consumption in the last 12 months was only slightly less
common (4.5%; n=21 of students). However, three of these 21 students with recent consumption later
indicated that they “never” consumed alcohol when asked, “How often do you have a drink containing
alcohol” on AUDIT-1. Of the non-drinkers, 88% (n=373) reported not having any desire to try alcohol
in the future.
Six of the 15 males who had consumed alcohol in the past year scored above four in the AUDIT-C
(40%). None of the four women scored above three. On average, the onset of drinking was at the age
of 17.83 (sd = 3.96). Males, older students (21-24 years), non-Muslims, non-Arab respondents, and
those in a relationship outside of marriage or living away from parents were more likely to have
consumed alcohol (lifetime and past-year; Table 1).
Four of the five dichotomous variables that were significant in the bi-variate analysis were included
in the multi-variate analysis (except non-Arab as closely correlated to non-Muslim). The
multivariable logistic regression model confirmed that being a non-Muslim was the most significant
independent predictor (p<0.001) for lifetime and past-year drinking. Living away from relatives was
also an independent predictor for lifetime and past-year consumption (Table 2). However, being older
was only a significant independent predictor for past-year consumption while being male was only
significant for lifetime consumption.
Table 7 Independent predictors of consumption (using logistic regression)
7a Independent predictors of lifetime consumption
B S.E. Wald df Sig.
Odds
ratio
Older (21-24 years)
(vs. 17-20 years) 1.206 0.673 3.214 1 0.073 3.34
Male
(vs. female) 1.986 0.774 6.586 1 0.010 7.29

113
Live alone, with friends or university dorm
(vs. live with parents, partner, or relatives) 1.415 0.603 5.504 1 0.019 4.12
non-Muslim
(vs. Muslim) 5.310 0.784 45.838 1 < 0.001 202.43
Constant -6.488 0.964 45.271 1 < 0.001 0.002
7b Independent predictors of past-year consumption
B S.E. Wald df Sig. Exp(B)
Older (21-24 years)
(vs. 17-20 years) 1.607 0.748 4.613 1 0.032 4.986
Male
(vs. female) 1.349 0.728 3.431 1 0.064 3.852
Live alone, with friends or university dorm
(vs. live with parents, partner, or relatives) 1.675 0.654 6.565 1 0.010 5.339
non-Muslim
(vs. Muslim) 4.945 0.746 43.929 1 < 0.001 140.513
Constant -6.670 1.002 44.282 1 < 0.001 0.001
A majority of students (54.9%) thought that it was easy or very easy for students to get alcohol if they
wanted it, while only 15.3% reported it being very difficult or impossible; this perception was not
significantly associated with lifetime or past-year consumption. Over half of the 20 respondents to
the source of alcohol question (n=13; 65%) reported that they get their alcohol from bottle shops.
Over half (n=11) of the 21 past-year alcohol consumers reported that they drink with their university
colleagues. A quarter of all participants (n=106/450) reported that they know of friends and/or family
who use alcohol. However, of those, only 28 (6.2% of 450) reported that they know a university friend
who consumes alcohol. Despite this, participants (n=459) on average estimated that over a fifth
(mean=21.1%; SD 17.3) of university students in Iraq drink alcohol. Lifetime and past-year drinkers
estimated a higher prevalence of student drinking than did non-drinkers (p<0.001).
Consumption of other substances
A total of 34 out of 450 respondents (7.3%: 6.5% male, 8.4% female) reported taking prescription
drugs for non-medical reasons. Only seven (1.6%) reported lifetime illicit drug use. One in five

114
participants (n=100; 22.2%) reported tobacco use, with males more than three times as likely as
females to use it (36.8% and 10.4% respectively) (Figure 8)
Figure 8 Substance use by participants (respondents re alcohol n=468, re other substances n=450)
Attitudes towards alcohol, alcohol policy and alcohol/drug users
When asked about motives for drinking or abstinence on a four point Likert-scale (never, rare,
sometimes and often), all students agreed that motives for drinking were sometimes/often perceived
to be either a desire to try forbidden things (87.5%), experiences of trauma (85.7%), fun (82.7%) or
peer pressure (81.2%). On the other hand, lack of religiosity was perceived as a motivating factor by
92.2% of non-drinkers compared to only two thirds (66.7%) of lifetime drinkers (p=0.006).
Participants also perceived that sometimes/often students abstained for religious (93.7%), family
(90.2%) and socio-cultural (89.7%) reasons. In comparison, less than half (44.4%) of lifetime drinkers
and two thirds (69.2%) of non-drinkers perceived that abstinence was sometimes or often for health
reasons (p=0.029). When students (n=257) were asked if alcohol is a moral issue, 67.7% agreed,
while only 43% agreed that it is a medical issue.
Alcohol use Illicit drug usePrescription drug use
(non-medical purposes)Tobacco use
Male 10 2 6.5 36.8
Female 1.6 1.2 8.4 10.4
Total 5.4 1.6 7.6 22.2
0
5
10
15
20
25
30
35
40
Life
tim
e u
se (
%)

115
Of the participants (n=256) who responded to the question asking whether they agree with certain
alcohol policy options, nearly two thirds (n=166; 65.1%) thought that alcohol should be prohibited
entirely. However, 104 (40.8%) agreed with a policy that would allow alcohol production, trade, and
consumption for non-Muslims in Iraq. A sixth of students (n=42; 16.5%) agreed with a policy that
alcohol production, sale and consumption should be permitted for everyone.
Figure 9 Participants’ views on the right response to regular substance use by a friend
9a: If a friend was having alcohol/drugs daily, what would you do? (n=220)
NothingTell them
not toForce them
not toTell them
to get helpReport to
policeCut contact
Tell theirfamily orfriends
Alcohol 6 29 8 22 4 19 10
Drugs 3 24 17 16 7 14 17
0
5
10
15
20
25
30
35
Pe
rce
nta
ge o
f re
spo
nd
en
ts

116
9b: What should happen to someone caught with small amount of alcohol/drugs? (n=231)
Figure 9a shows that students reported that their most likely action if they encountered a friend using
either alcohol or drugs daily would be to advise them to stop (29.1% and 24.1% respectively). More
severe responses (force them not to; tell police, family, or friends) were more likely to be endorsed
for drug use than for alcohol. A similar trend was observed when participants were asked what should
happen if someone was caught with small amounts of alcohol or drugs (Figure 9b).
Media and war exposure and post-traumatic stress disorder
Of the 202 students that were asked if they had been exposed to direct alcohol marketing, more than
half had been exposed on the internet (n=112;55.4%), two fifths on social media (n=84;41.6%) and
satellite TV (n=72;35.6%). A third of the sample indicated they have never had any exposure to
alcohol advertisement (n=74;36.6%). There was a significant association between drinking status and
perception of mass (p=0.035) and social media (p=0.009) as factors contributing to drinking. Two
thirds of non-drinkers perceived that mass or social media influences drinking (n=214,66.7% and
n=212,67.3% respectively), only two-fifth (n=6,40%) and one-third (n=5,33.3%) of lifetime drinkers
respectively agreed.
No actionAdvice, warning
or educationTreatment Fine
Prison orpunishment
Alcohol 10 45 12 22 10
Drugs 1 28 23 19 26
0
5
10
15
20
25
30
35
40
45
50
Pe
rce
nta
ge o
f re
spo
nd
en
ts

117
Of the 220 individuals who answered the questions on exposure to violent conflict and on PTSD
symptoms, two in five (n=90; 41.7%) reported direct experience of war or violent military conflict.
Almost a third (n=63; 29.2%) of the respondents were positive on the PC-PTSD screening test. No
significant association was found between PC-PTSD results and lifetime consumption. No past-year
drinker (n=9) scored positive on the PC-PTSD test.
Reliability of the included instruments
The internal consistency of the 3-item AUDIT-C in this sample was Cronbach’s α 0.70. The PC-
PTSD screen had a Cronbach’s α of 0.73.
Discussion
To our knowledge, this is the first comprehensive study to examine the behaviours and attitudes of
young Iraqi university students towards alcohol and alcohol policy. By doing so, this study addresses
an important gap in the field of alcohol research. This research was conducted with greater anonymity
than past alcohol studies in Iraq and included participants from more universities. This is also the
most current data from university students across several regions in Iraq that provides insight into
student exposure to alcohol, consumption patterns and perceived availability. Our study also provides
insights to improve data collection about sensitive topics such as alcohol in Iraq. Assessing alcohol
use behaviours and attitudes together may help inform efforts to reduce risk factors for drinking in
this context.
Almost one in twenty students in our sample had consumed alcohol (lifetime: 5.4%; past-year: 4.6%).
This is almost double the lifetime use reported by the 2014 national survey’s (SSAI) adult student
sub-sample (3%) and thirteen times the prevalence (0.4%) among medical students surveyed at
Baghdad University in 2016 (Al-Imam et al., 2017). In contrast, students in our sample were only
half as likely to report lifetime consumption of alcohol as respondents in a three-university study in
Baghdad (Al-Ameri et al., 2016). However, in this same study, a similar prevalence of drinking to
our study was reported by medical students (6.0% vs 5.3%) (Al-Ameri et al., 2016).

118
The different consumption rates identified in our research compared to those in other studies may be
explained by contextual factors and the data collection methods. For example, Karbala is a
conservative religious city while Erbil, the capital of Kurdistan, has a higher non-Muslim population,
and is more modernised than the Arab majority regions of Iraq. Correspondingly, Mousawi (2015)
reported the prevalence of past-year drinking in Karbala to be 2.2%, which is half the rate of
consumption identified in our study. In contrast, in Erbil, Ali and Sabir (2009) found that almost half
(44%) of medical students living at colleges in Hawler Medical University had used alcohol in the
past-six months. This is four times the past-year consumption of medical students living away from
family in our sample (10.4%) that did not include students from this location.
In contrast to our study that used an online questionnaire tool, nearly all previous studies collecting
alcohol data in Iraq have used pen-and-paper or face-to-face data collection methods. These
approaches have been found to affect the accuracy of self-reported drinking in non-MMCs cultures
with sensitivities to alcohol (Islam et al., 2012). Pen-and-paper or face-to-face data collection
methods have also been identified as limitations in the two Iraqi national household studies (US
Department of State et al., 2015; WHO, 2009).
On average, students estimated the prevalence of drinking among their fellow students at four times
the actual self-reported prevalence (21.1% vs 5.4%). A quarter of participants reported knowing a
friend or family member that drinks (23.6%). Similar high reports of knowing someone who drinks
have been reported previously in Iraq (US Department of State et al., 2015). Lifetime and current
drinkers estimated a higher prevalence of peer drinking than did non-drinkers. This may indicate that
students under-reported their personal consumption. Alternatively, it may indicate an overestimation
of student drinking norms by drinking participants. The overestimation of drinking norms has been
shown to influence consumption in non-MMCs. Interventions to correct individual misconceptions
of drinking prevalence have been shown to be effective in reducing problem drinking among students
(Lewis et al., 2006; Ridout et al., 2014). These interventions normally require identifying the at-risk
drinkers in the first place – an unlikely possibility in Iraq where alcohol is a sensitive topic. In

119
addition, due to the nature of the sensitivities, it is difficult to establish actual drinking norms.
Students are also unlikely to trust figures presented because they may have themselves underreported
their drinking or know someone who has.
Two fifths (40%) of male drinkers in our sample met the criteria for risky drinking (AUDIT-C score
of 4+). In a 2010 study at Karbala University using the full 10-item AUDIT more than half of drinking
students (56%) reported consuming alcohol at risky levels (AUDIT score of 8+) (Al Mousawi, 2015).
We purposely did not use the full AUDIT because the authors noted possible inflated scores resulting
from items 7 and 10 of the AUDIT (guilt and others’ concern about drinking). Despite that, the
internal consistency of AUDIT-C in our sample was comparable to that of the full AUDIT in Al
Mousawi (2015) study (Cronbach’s α 0.70 vs 0.66). However, the Cronbach’s α score of 0.70 is more
acceptable for a short 3-item instrument (Tavakol et al., 2011). This score inflation is consistent with
the common anti-alcohol sentiment in MMCs. Further research is needed to identify culturally
relevant ways to ask items relating to consequences of drinking – with consideration that guilt and
social concern may be elevated in this setting.
The high prevalence of risky drinking patterns in Iraq is confirmed by two other studies: one in a
national household study and the other in a specialised sample. Almost one in six males that attended
youth centres in Baghdad met DSM-IV criteria for alcohol abuse using the Composite International
Diagnostic Interview (CIDI-2) (Al-Hemiary et al., 2015b). The SSAI reports that 71% of current
drinkers met the criteria for dependence on the Severity of Substance Dependence Scale (SDS) (US
Department of State et al., 2015). This may reflect the over-reporting of guilt/shame in item 3 of the
SDS. WHO estimates show alcohol use patterns among drinkers in EMRO are second in risk to
former soviet Eastern Europe (WHO, 2006b).
Our study is consistent with previous studies in reporting no risky drinking or alcohol misuse among
females. However, sex was associated with lifetime drinking but was no longer significant for past-
year consumption in our multi-variate analysis. A strong association of alcohol use with male sex was
identified in the national household survey (US Department of State et al., 2015) and other studies

120
(Al-Ameri et al., 2016; Al Mousawi, 2015). However, female student in our study reported a higher
consumption of alcohol (and other drugs). For example, compared to the SSAI, females in our sample
provided higher reports of lifetime drinking (1.6% vs 0.6%) and current alcohol use (1.6% vs 0.11%).
They also reported a higher prevalence of lifetime illicit drug use (1.2% vs 0%) and licit drug misuse
(8.4% vs 0.7%) (US Department of State et al., 2015). This could be attributed to sampling differences
or the greater anonymity of our data collection methods.
The gendered role that alcohol plays in Iraq and other MMCs may reflect socio-cultural norms. Haya’
(modesty or shyness) is a universal encouraged trait in Muslim societies particularly for females (M.
Ali, 2014). Drinking is considered an immodest act in Islam and local cultures. Observing haya’ may
also reduce risk factors associated with alcohol consumption. For example, Iraqi females seldom live
or travel alone or with friends – most would stay with relatives even if they study away from home.
Our data indicate that living alone, with friends or at university dormitory was significantly associated
with being male (p = 0.01; data not shown) and in turn, significantly associated with drinking. The
association of drinking and living away from home was also observed in students in Baghdad (Al-
Ameri et al., 2016) and in non-MMCs such as Sweden (Bullock, 2004). This indicates that there may
be an opportunity to focus prevention interventions on males who live in dormitories or with friends.
Interactions between the two sexes are also limited in Iraqi society, especially in conservative areas.
In conservative settings, the university may be the only environment where females closely interact
with their male peers. By observation, in some areas of Iraq, there can be a disparity between the
student’s behaviour at the university and their life in the family home. It is possible that these different
lifestyles, the stress of studies and the stigma around alcohol and illicit drug use may contribute to
prescription drug use for non-medical reasons as observed in our female sample.
As indicated, two thirds (67.6%) of students agreed with the statement that alcohol is a moral issue
(vs 43% that agreed it was a medical issue). Similar observations have been made about attitudes
towards “addiction” in Iraq (Al-Hasnawi, 2006; Al-Hasnawi et al., 2007). Students from our sample
reported most abstain for religious, socio-cultural, and family purposes. They perceived that students

121
in general mostly drink due to lack of religiosity, trauma, for fun or because they find forbidden
actions tempting. Student reactions to those who drink alcohol seem to also be driven by religious
teachings or a sense of social and familial responsibility. For example, a fifth of the sample indicated
they would cut off contact if a friend were using alcohol daily and more than half indicated they
would either tell them to stop, or to get help. Muslims are taught to be a “mirror” for each other and
to encourage good behaviour and discourage anti-social behaviour (amr bil ma’roof wal nahyi ‘an
al-munkar) in their community. If their advice fails, individuals are instructed to avoid the perpetrator
so that he/she may turn back once they realise their ‘bad’ actions have resulted in their isolation
(Dastghaib Shirazi, 1998). This moral worldview may also cause Muslims to underreport their own
drinking. Muslims that drink still consider themselves sinners and Islam discourages confession or
disclosing one’s sin to anyone (M. Ali, 2014). University or social-based interventions may need to
be tailored for settings where alcohol is viewed from a moral (rather than medical) viewpoint. These
may differ from approaches in non-MMCs (Stockings et al., 2016).
Considering that current mental health and substance treatment infrastructure is limited; contextual
measures should be in place to prevent alcohol misuse in Iraq. This may help prevent an increase in
the prevalence of drinking and associated risk behaviours as observed in other post-conflict MMC
settings. For example, Risk behaviours such as drink driving, carrying weapon and physical fights
associated with drinking are high in post-conflict Kirkuk and Erbil (Saeed, 2016; Shabila et al., 2015).
Figures from Lebanon also show an increase in alcohol abuse (DSM-III & DSM-IV) by Muslim
university students within eight years after the end of the civil war (increasing from 3.8% to 6.1%,
from 1991 to 1999) (E. G. Karam et al., 2004).
To prevent alcohol misuse and associated risky behaviours, a consistent and strong alcohol policy is
needed in Iraq. Participants in our study reported a diversity of opinions on policy approaches
Currently, Iraq has a mix of these policies on a federal, provincial and local level (Al Ansari et al.,
2019). For example, currently active federal alcohol laws do not differentiate between faith groups
except that alcohol sellers must be non-Muslim. Consumers, however, can be of any faith, including

122
Muslim. The alcohol ban introduced in 2016 (but not enforced) also applied to all Iraqis, regardless
of faith. In some provinces (e.g. Basra) and local areas (e.g. Khadimiyya in Baghdad), alcohol sales
and drinking are totally prohibited for everyone at a provincial and local level. Consistent with
previous evidence (Stockings et al., 2016), our findings did not suggest that local prohibition impacts
upon reported drinking prevalence or access to alcohol (compared to sites with no alcohol
prohibition). Further details of this analysis have been withheld to avoid identifying participating
universities. These policies may be compromised by weak law enforcement including a lack of
policing at provincial borders.
In addition to strong border control, taxation is known to be the single most impactful preventative
intervention in non-MMCs (T. Babor, 2010; Stockings et al., 2016). Iraq, however, does not have a
digitised tax system and has limited ability to implement import or sales tax on specific commodities
such as alcohol (International Monetary Fund, 2017). Monitoring, controlling, and taxing alcohol will
prove difficult in the current volatile political and economic situation.
Students suggested that advice, warning, or education would be their preferred method of responding
to someone who is caught with alcohol on their person. Given the mixed perceived motives for the
uptake of drinking, this advice could be provided by parents, religious and cultural leaders, or medical
professionals. Such advice could constitute brief interventions or evidence-based approaches to
encourage those already using alcohol in an ‘at-risk’ way to re-think their drinking. The introduction
of brief interventions in primary health settings may help to address harmful drinking. There is
currently an initiative in Iraq to integrate mental health care into primary health care to ease the
associated stigma of seeking such care in specialised facilities (Sadik et al., 2011). This is key given
that trauma is the second highest perceived motive of drinking and that two fifths reported direct
experience of war or violent military conflict. However, mental health is stigmatised in Iraq (Bolton,
2013). In addition, most young people are less likely to visit a medical practitioner to discuss alcohol
use (Humphreys, 2011). The Iraqi health system is struggling to integrate mental health care into

123
primary health care (Sadik et al., 2011). Additionally patient confidentiality is limited as primary
health care practitioners rarely consult in private in Iraqi health settings (Al Ansari et al., 2019).
Information alone has been shown to be ineffective in curbing alcohol use and misuse, however,
programs such as the positive youth development programs (PYDP) or family skill-based
interventions have shown some promising results in curbing alcohol and other drug use (Stockings et
al., 2016). These types of programs equip young people or their parents with psychosocial skills
focusing on resilience, communication, and development without necessarily addressing alcohol
exclusively.
Given that religious, sociocultural and family reasons are the main motives for abstinence and that
drinking is associated with being non-Muslim and living away from family, in the absence of these
protective factors, young people may be vulnerable to alcohol use and misuse. Globalisation has led
to increasing exposure to alcohol advertisements on the internet, social media, and satellite TV. Iraq’s
alcohol policy should therefore be cognisant of this changing contemporary landscape to safeguard
the growing Iraqi youth population into the future. This policy should take into consideration Iraq’s
diverse populace, cultures, and religions as well as evidence-based approaches, locally sourced or
adapted from other MMC and non-MMC experiences.
Limitations
The study sample could not be randomly selected due to the lack of student email databases within
universities. Most collaboration and recruitment occurred within the medical faculties. During visits
to other colleges, we were informed by staff that the use of internet for educational purposes was
relatively new except in faculties such as Medicine, Engineering and Pharmacy. This may have
contributed to limited access from students of other faculties. Because of lack of external funding for
this research, active recruitment at each site only lasted a few days while we were interviewing for
the qualitative component of this study. Funding for further active recruitment could have increased

124
the sample size. Student status and age was self-reported and could not be verified as this was an
anonymous online survey.
Despite our efforts, our sample did not include a University from Kurdistan – a region of Iraq where
previous studies show a higher prevalence of drinking than other provinces. Although no significant
difference was found in drinking based on faculty, our sample had an over-representation of Medicine
and Pharmacy students. Students in Engineering had a higher prevalence of drinking than other
faculties. However, this finding was not significant due to the small number of participants from the
Faculty of Engineering. Student drinking is likely underestimated in our sample and further attention
needs to be paid in future studies to other faculties.
While 448 people (86% of eligible participants) completed the substance use section, less than half
(43.4%) completed the entire survey. We assume that this was because of the survey length (~15-20
minutes) as no association was observed between drinking patterns and the dropout rate. The largest
drop-out rate was found in validation questions that explore similarly concepts in questions with
deliberately reversed phrasing (e.g. motives for drinking). Accordingly, future studies should be
shorter and avoid any perception of repetition. An alternative explanation is that the topic of the
survey (alcohol and drugs) caused offence. There were also some internal contradictions in some
sensitive questions. For example, some people said they have had alcohol in the past 12 months and
then then answered “never” to the first question of the AUDIT (about frequency of drinking in the
last year). This could be because people who do not see themselves as “usual” drinkers answer
“never”. As the PC-PTSD screen and the exposure to war question were placed towards the end of
the survey, less than half of drinkers answered this question – so no conclusions can be drawn about
alcohol use and war exposure.
Young Iraqis who are not university students were not the focus of this study. Drinking prevalence,
patterns and motives may differ among this group. We did not include local laws and prohibition as
an independent variable. However, we analysed by site (some sites had prohibition and others did
not). The impact of policy on alcohol use and attitudes is an area worthy of future investigation.

125
Conclusion
The prevalence of self-reported drinking in Iraq is consistently lower than countries in the developed
world or non-MMCs. However, this study and others have indicated that drinking occurs at risky
levels among many drinkers in this setting. A decline in abstention may lead to an increase in alcohol-
related harm. Iraq’s healthcare system is ill equipped to cope with such an increase and to implement
evidence-based preventive approaches. This reflects an ongoing need to accurately and regularly
measure alcohol use using appropriate tested and tailored tools.
Innovative, low cost evidence-based approaches are required to prevent alcohol-related harms,
including skills-based youth and parental development programs. These initiatives should be tailored
to and evaluated in the local settings. In addition, a clear and implementable alcohol policy that
considers Iraq’s majority youth population and their experiences is needed.

126
References
Al-Ameri, R. J. K., H. J. Abd Al-Badri, and R. K. Lafta. 2016. 'Prevalence of Alcohol Consumption
among University Students in Baghdad: A Cross-section survey from Iraq', Epidemiology
Biostatistics and Public Health, 13: 8.
Al-Ameri, Rawa Jaafar Kadhim, Husham J Abd Al-Badri, and Riyadh K Lafta. 2016. 'Prevalence of
Alcohol Consumption among University Students in Baghdad: A Crosssection survey from
Iraq', Epidemiology Biostatistics and Public Health, 13: e11942-1-8.
Al-Diwan, J., N. Al-Hemiary, and M. Hashim. 2015. "Alcohol and Drug Abuse in Post-conflict Iraq."
In European Psychiatry, 1394.
Al-Hasnawi, Salih. 2006. 'Attitude of Residents and General Practitioners Toward Substance Abuse
in Iraq', Medical Journal of Babylon, 3: 107-12.
Al-Hasnawi, Salih, Nesif Al-Hemiary, and Muhammad Lafta. 2007. 'Public Attitudes toward
Substance Abuse', Karbala Medical Journal, 1: 162-66.
Al-Hemiary, N., M. Hashim, J. Al-Diwan, and E. Abdul Razzaq. 2015. 'Alcohol and Drug Abuse in
Post-Conflict Iraq', Journal of the Faculty of Medicine, Baghdad, 57: 290-94.
Al-Hemiary, Nesif J., Jawad K. Al-Diwan, Albert L. Hasson, and Richard A. Rawson. 2014. 'Drug
and Alcohol Use in Iraq: Findings of the Inaugural Iraqi Community Epidemiological
Workgroup', Substance Use & Misuse, 49: 1759-63.
Al-Imam, Ahmed, Farah Al-Mukhtar, Aisha Shafiq, and Manolia Irfan. 2017. 'Knowledge and (Ab)
Use in Connection with Novel Psychoactive Substances: A Cross-Sectional Analysis of Iraqi
Medical Students', Global Journal of Health Science, 9: 61.
Al Ansari, Mustafa, Angela Dawson, and Kate Conigrave. 2019. 'Alcohol: from Mesopotamia to
Modern Iraq', Journal of Ethnicity in Substance Abuse: 1-23.
Al Mousawi, Ali 2015. 'Alcohol use disorder identification test use in Muslim countries',
International Journal of Prevention and Treatment of Substance Use Disorders, 1: 79-92.
Alcohol Public Policy Group. 2010. 'Alcohol: No Ordinary Commodity – a summary of the second
edition', Addiction, 105: 769-79.
Ali, Mansur. 2014. 'Perspectives on Drug Addiction in Islamic History and Theology', Religions, 5:
912-28.
Ali, Sirwan Kamil , and Jwan Mohammed Sabir. 2009. 'Prevalence of Alcohol Use among Medical
College Students in Hawler Medical University', Zanko Journal of Medical Sciences, 13: 17-
23.
Australian Institute of Health and Welfare. 2013. "National Drug Strategy Household Survey." In.
Canberra: Australian Institute of Health and Welfare (AIHW),.
Babor, Thomas. 2010. Alcohol: No Ordinary Commodity: Research and Public Policy (Oxford
University Press: Oxford).
Babor, Thomas F. , John C. Higgins-Biddle, John B. Saunders, and Maristela G. Monteiro. 2001.
AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care
(World Health Organization: Geneva).
Baron-Epel, Orna, Shiran Bord, Wafa Elias, Chen Zarecki, Yoram Shiftan, and Anat Gesser-
Edelsburg. 2015. 'Alcohol Consumption Among Arabs in Israel: A Qualitative Study',
Substance Use & Misuse, 50: 268-73.
Bolton, Paul. 2013. 'Mental health in Iraq: issues and challenges', The Lancet, 381: 879-81.

127
Bradley, Katharine A., Mary B. McDonell, Kristen Bush, Daniel R. Kivlahan, Paula Diehr, and
Stephan D. Fihn. 1998. 'The AUDIT Alcohol Consumption Questions: Reliability, Validity,
and Responsiveness to Change in Older Male Primary Care Patients', Alcoholism: Clinical
and Experimental Research, 22: 1842-49.
Bullock, Sandra. 2004. Alcohol, Drugs and student lifestyle: a study of the attitudes, beliefs and use
of Alcohol and Drugs among Swedish University students (Centrum för socialvetenskaplig
alkohol-och drogforskning (SoRAD)).
Bush, K., D. R. Kivlahan, M. B. McDonell, S. D. Fihn, and K. A. Bradley. 1998. 'The AUDIT alcohol
consumption questions (AUDIT-C): an effective brief screening test for problem drinking.
Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders
Identification Test', Arch Intern Med, 158: 1789-95.
Dastghaib Shirazi, Sayed Abdul Husain 1998. Greater Sins (Islamic Study Circle: Mumbai).
GBD 2016 Risk Factors Collaborators. 2017. 'Global, regional, and national comparative risk
assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters
of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016', The
Lancet, 390: 1345-422.
Ghandour, Lilian, Ali Chalak, Aida El-Aily, Nasser Yassin, Rima Nakkash, Mitra Tauk, Noura El
Salibi, Meghan Heffron, and Rima Afifi. 2016. 'Alcohol consumption in the Arab region:
What do we know, why does it matter, and what are the policy implications for youth harm
reduction?', International Journal of Drug Policy, 28: 10-33.
Hamdieh, M, N Motalebi, H Asheri, and A Boroujerdi. 2008. 'Prevalence of Alcohol and Drug Abuse
in Young People, 15-35 Year Old, Living in Tehran, Iran', Pejouhesh, 32: 315-19.
Humphreys, Keith. 2011. "Circles of Recovery: An Interview with Keith Humphreys, PhD." In
Counselor, edited by William White, 48-52.
International Monetary Fund. 2017. "Iraq: Selected Issues." In. Washington D.C.: International
Monetary Fund.
Islam, M. Mofizul, Libby Topp, Katherine M. Conigrave, Ingrid van Beek, Lisa Maher, Ann White,
Craig Rodgers, and Carolyn A. Day. 2012. 'The reliability of sensitive information provided
by injecting drug users in a clinical setting: Clinician-administered versus audio computer-
assisted self-interviewing (ACASI)', AIDS Care, 24: 1496-503.
Karam, E., K. Kypri, and M. Salamoun. 2007. 'Alcohol use among college students: an international
perspective', Curr Opin Psychiatry, 20: 213-21.
Karam, Elie G., Wadih E. Maalouf, and Lilian A. Ghandour. 2004. 'Alcohol use among university
students in Lebanon: prevalence, trends and covariates: The IDRAC University Substance
Use Monitoring Study (1991 and 1999)', Drug and Alcohol Dependence, 76: 273-86.
Kelly, Thomas M., John E. Donovan, Tammy Chung, Oscar G. Bukstein, and Jack R. Cornelius.
2009. 'Brief screens for detecting alcohol use disorder among 18-20 year old young adults in
emergency departments: Comparing AUDIT-C, CRAFFT, RAPS4-QF, FAST, RUFT-Cut,
and DSM-IV 2-Item Scale', Addictive Behaviors, 34: 668-74.
Lewis, Melissa A, and Clayton Neighbors. 2006. 'Social norms approaches using descriptive drinking
norms education: A review of the research on personalized normative feedback', Journal of
American College Health, 54: 213-18.
Prins, A., P. Ouimette, R. Kimerling, R. P. Cameron, D. S. Hugelshofer, J. Shaw-Hegwer, A.
Thrailkill, F. D. Gusman, and J. I. Sheikh. 2003. 'The primary care PTSD screen (PC-PTSD):
development and operating characteristics', PRIMARY CARE PSYCHIATRY, 9: 9-14.

128
Ridout, Brad, and Andrew Campbell. 2014. 'Using Facebook to deliver a social norm intervention to
reduce problem drinking at university', Drug and Alcohol Review, 33: 667-73.
Sadik, Sabah, Saad Abdulrahman, Marie Bradley, and Rachel Jenkins. 2011. 'Integrating mental
health into primary health care in Iraq', Mental health in family medicine, 8: 39-49.
Saeed, Hayman M. 2016. 'Assessment of the Health Risk Behavior in Young Adulthood: A school-
based Health Study in Kirkuk City / Iraq', Tikrit Medical Journal, 21: 172-81.
Shabila, Nazar P., Kamaran H. Ismail, Abubakir M. Saleh, and Tariq S. Al-Hadithi. 2015. 'Risky
Driving Behaviours among Medical Students in Erbil, Iraq', Sultan Qaboos University
Medical Journal, 15: e390-e97.
Ṣirāmī, Ḥamīd, Majīd Qurbānī, and Maḥmūd Mīnūnī. 2013. 'Barrisi Chahār dah Taḥqīqāt Shuyūʿ
Shināsī Iʿtiyād dar Īrān [Review of 14 Prevalence Studies of Addiction in Iran]', Quarterly
Journal of Research on Addiction, 7: 29-52.
Stockings, Emily, Wayne D Hall, Michael Lynskey, Katherine I Morley, Nicola Reavley, John
Strang, George Patton, and Louisa Degenhardt. 2016. 'Prevention, early intervention, harm
reduction, and treatment of substance use in young people', The Lancet Psychiatry, 3: 280-96.
UNDESA. 2017. "World Population Prospects: The 2017 Revision, Key Findings and Advance
Tables." In.
US Department of State, Bureau of International Narcotics and Law Enforcement Affairs, Iraqi
Society of Addiction Medicine, University of California LA, and Center for Human Services.
2015. "Survey of Substance Abuse in Iraq." In. Bethesda, MD.
WHO. 2006a. "Interpersonal Violence and Alcohol." In.
———. 2006b. "Public health problems of alcohol consumption in the Region." In.: WHO Regional
Office for the Eastern Mediterranean.
———. 2009. "Iraq Mental Health Survey 2006/7." In.
———. 2010. "ATLAS of Substance Use Disorders. Country Profile: Iraq." In.
———. 2014. "Global Status Report on Alcohol and Health." In. Geneva.
Yazbek, Jean-Claude, Ramzi Haddad, Rami Bou Khalil, Sani Hlais, Grace Abi Rizk, Jihane
Rohayem, and Sami Richa. 2014. 'Prevalence and Correlates of Alcohol Abuse and
Dependence in Lebanon: Results from the Lebanese Epidemiologic Survey on Alcohol
(LESA)', Journal of Addictive Diseases, 33: 221-33.

129
Chapter 6: Alcohol use in Iraq: Perceptions of students at three Iraqi universities
Chapter 5 presented quantitatively the perceptions of young university students in Iraq about the
motives for and influencers of drinking in Iraq, and the prevalence of drinking. Prevalence of self-
reported drinking was low among students, however two fifths of young male drinkers consumed at
risky levels (AUDIT-C score of 4+). Drinkers and non-drinkers alike reported that coping and
socialising were perceived as key motives for drinking. The diversity of views among students is
noted in the quantitative sample. For example, while two-thirds of participants want a policy of total
alcohol prohibition, two fifths prefer allowing alcohol to non-Muslims only, and a sixth want alcohol
production, sale, and consumption to be universally permitted.
This qualitative chapter complements these findings with depth by drawing on personal experiences
of young Iraqis at three Iraqi universities across Iraq. The semi-structured interviews focused on five
guiding questions – these questions aim to chronologically ask about alcohol in Iraq – from the past,
to the present and future. The interview guides were decided in consultation with local experts. As
presented in Chapter 2, due to the sensitive nature of alcohol, no interviewee was asked about their
own drinking behaviour. Students were instead asked about the behaviours and perspectives of other
students.
By describing the experiences and perspectives of young Iraqis, we intend to investigate what lies
behind the behaviours, attitudes, and perspectives of young Iraqis towards alcohol. This will ensure
that perspectives are understood contextually. Preventative measures and alcohol policies can then be
informed by combining quantitative findings from Chapter 5 with in-depth analysis present in this
chapter.
The following manuscript has been submitted for publication.

130
Abstract
Introduction
The people of Iraq have experienced conflict since 1980 and increased exposure to alcohol use in the
media since the lifting of censorship in 2003. While the majority (60%) of Iraq’s population is under
the age of 24, there is a lack of research examining the views of young Iraqis concerning alcohol use
and related contextual factors that could provide insight into drinking behaviour and primary
prevention. We undertook research to explore how the individual, interpersonal and social contexts
of university students influence their experiences and perceptions of alcohol use.
Methods
We undertook a qualitative study underpinned by a socio-ecological framework and the alcohol use
motivational model. Forty students, from eleven disciplines at three universities across Iraq were
interviewed (45% female). Interviews were conducted in English (n = 3) or Arabic (n = 37). Template
analysis was used to examine the data.
Results
Perceptions of the prevalence of alcohol use varied among participants. Perceived motives for
drinking included using alcohol to cope with difficulties associated with grief, loss, poverty, and
unemployment, as well as peer pressure, thrill seeking and social approval. Abstinence was associated
with knowledge of the adverse effects of alcohol and a strong commitment to faith. Students reported
alcohol use as a clandestine activity. Students suggested education, open communication, and
employment opportunities as preventative strategies.
Conclusion
This is the first study to explore young Iraqi views and experiences of alcohol use in the current
context of conflict, political instability, and globalisation. Young Iraqis are a vulnerable population
who may be at risk of alcohol-related harm. Iraq should consider multidimensional preventive
approaches that include evidence-based and culturally appropriate interventions that reflect young
peoples’ real-life experiences and challenges.

131
Summary
What is already known?
- Most Iraqis are under the age of 24 and have experienced conflict, terrorism, social, economic, and
political unrest for all their lives.
- Iraqis have experienced friction between traditional and globalised culture since the second Gulf
War in 2003.
- There have been calls for qualitative alcohol studies in low- and middle-income countries, especially
in the Arab world.
What are the new findings?
- Iraqi university students perceived that drinkers in Iraq always drink excessively; some shared
stories of alcohol-related harm experienced by family or friends.
- Students associated drinking with bad parenting and peer pressure, and abstinence with religiosity
or awareness of alcohol’s harms.
- Alcohol use is hidden - though students perceived that alcohol use is increasing, many (especially
females) denied ever seeing a drinker.
What do the new findings imply?
- Iraq should establish and implement a clear alcohol policy based on a melding of evidence-based
and traditional approaches.
- Research is needed on how best to support young Iraqis and reduce harms from alcohol use or
mental health disorders
-Options that could be examined include tailored parenting and personal development programs to
help prevent alcohol use or misuse.

132
Introduction
Alcohol is linked to 5.3% of deaths globally (WHO, 2018a) and is the leading risk factor for burden
of disease in people aged 15-49 years (GBD 2016 Risk Factors Collaborators, 2017). However, half
of the world’s population is abstinent (in the past 12-months: 57%, lifetime: 44.5%). Muslim majority
countries (MMCs) have the lowest per capita consumption and the largest prevalence of past-year
abstinence that can largely be attributed to the Islamic prohibition of alcohol (WHO, 2018a). However
increased globalisation and local changes in some MMCs may influence drinking.
Iraq is an upper-middle income MMC in the Eastern Mediterranean Region. The country has an
estimated population of 38 million, with the majority (60%) under the age of 24 (UNDESA, 2017).
WHO estimates that 93.8% of Iraq’s population are lifetime abstainers and almost half of those who
have ever consumed alcohol, abstained in the past year (WHO, 2018a). The legal situation regarding
alcohol varies across the country. Although a ban on alcohol consumption and sale was imposed in
2016, this law was not implemented, and Iraq nationally recognises the 2001 laws regarding alcohol
licensing and consumption (Al-Ḥukūma al-ʿirāqiyya [Iraqi Government], 2016; Al Ansari et al.,
2019). These civil laws allow for alcohol to be sold to adults by non-Muslims at a certain distance
from religious and public places (Al Ansari et al., 2019). Despite this, some provincial governments
have introduced local bans on the sale and consumption of alcohol (Al Ansari et al., 2019).
Despite the reported low use of alcohol, the unstable political and economic context in Iraq may place
certain populations, such as young people at risk of substance use disorders. Iraq has been exposed
to war and terrorism, as well as civil unrest since 1980. There are no studies that have examined the
impact of conflict on the exposure to alcohol use and misuse in the Iraqi civilian population. However,
the 2009 Iraqi Mental Health Survey (IMHS) identified that increased exposure to traumatic events
was significantly associated with all mental disorders including substance misuse (WHO, 2009). In
addition, an association between exposure to conflict and mental health conditions including
substance and alcohol use disorders has been noted among coalition military personnel returning from
the Iraq War (Levy et al., 2013). This association has also been noted in studies of conflict-affected

133
civilian populations, including displaced populations in MMCs (Ezard, 2012; Greene et al., 2018; E.
G. Karam et al., 2008; Lo et al., 2017).
Young Iraqis have access to all forms of media, including platforms that market alcohol directly or
indirectly through content that depicts the common use of alcohol such as in film (Al Ansari et al.,
2019). Studies from several countries in the region have found that university students mainly
consume English language media (Melki, 2010). Iraqi university students, who have a higher levels
of English language competence than their non-student peers may be more exposed to alcohol use
and marketing in media. There is strong evidence, mainly from non-MMCs, that alcohol promotion
is linked to the initiation of drinking among young abstainers and increased consumption among
drinkers. Such promotion includes exposure to indirect alcohol marketing present in movies
(Anderson et al., 2009).
While there are some, albeit limited, quantitative studies regarding alcohol consumption in Iraq, there
is no peer-reviewed qualitative research that provides insight into the experiences, perceptions and
views of Iraqi people concerning alcohol use. This lack of data has led to speculation regarding the
factors that influence young people’s alcohol consumption and abstinence. Internationally, experts
have called for research to explore the micro and macro characteristics of drinking in diverse cultures
outside European and Anglophone countries (Kuntsche et al., 2017; Savic et al., 2016). A need for
qualitative research to explore patterns of consumption and the factors influencing substance use
within this cultural context has also been identified (Al Ghaferi et al., 2013).
The current study addresses aspects of this knowledge gap by exploring the attitudes and views of
young Iraqi university students towards alcohol and their related experiences. We sought to
understand why young people drink alcohol, how prevalent they perceive alcohol use to be and what
perceptions they have concerning drinkers and alcohol-related harms. Finally, we aimed to
understand students’ perspectives about the role of health policy in reducing alcohol-related health
risks.

134
Methods
There is a dearth of qualitative mental health research in Iraq, especially in the field of substance use.
Current alcohol policies are based on political and religious inclinations, and rarely account for the
real experiences and circumstances of young Iraqis. Therefore, we applied a constructive descriptive
approach to explore the factors that underpin current attitudes towards alcohol and how these may
influence young people’s decisions to consume or abstain from alcohol. A constructivist approach
allowed for assessing attitudes as constructed by the participants interactions with their environment.
We adopted a social ecological model (Bronfenbrenner, 1977) to explore the relationship between
the individual student’s experiences, perceptions and views of alcohol use and that of the environment
that hosts the individual, family, community, society and beyond. We complemented this framework
with work by Kuntsche and colleagues that examines positive and negative internal and external
factors influencing alcohol use (Kuntsche et al., 2005). Our model combines aspects of this model
with the socio-ecological framework to assess current factors with socio-cultural and environmental
dynamics. We adapted this model to the Iraqi context – assessing macro and micro antecedents to
perceived attitudes and behaviours around alcohol use. In this way, the possible chain of influencing
factors from the global to the individual level can be constructed. Previous literature in other contexts
have shown that a larger number of students in non-MMC countries drink for social and enhancement
motives (Kuntsche et al., 2005; Mackinnon et al., 2017; Wicki et al., 2017). We hypothesise that
while this may also be the case in Iraq, a large proportion of drinkers would be perceived to drink for
reasons of coping and conformity.

135
Figure 10 Socio-ecological framework for alcohol use in Iraq complemented by aspects of the motivational model as
presented in Kuntsche et al, 2005
Settings
To ensure a diversity of insights, four universities in different regions in Iraq were invited to
participate in this study. Three universities were situated in Arabic speaking regions of Iraq and one
in the autonomous region of Kurdistan. The University that was approached in Kurdistan did not
respond to requests via phone, email and in-person and therefore was not included in the study. The
universities who agreed to participate were in diverse Arabic speaking urban settings including a
conservative religious city (University A), a large metropolitan city (University B) and a port city
(University C). The sites selected for this study have varied policies regarding alcohol (regulatory
policy: University B; prohibition: University A and C).
Recruitment
The head of department or Dean in the faculty of medicine was first approached. The Dean then
assigned a staff member or student representative to assist us with recruitment at their faculty as well
as to help with recruitment in other faculties. The interviewer, assisting staff member or student

136
approached students in faculty buildings or university common areas to invite participants. The first
author, a male Iraqi Australian PhD candidate who has been trained in qualitative research methods,
conducted the interviews in Arabic or English according to the participant’s preference.
Due to the sensitive nature of alcohol in Iraq, we attempted to increase participant comfort by
conducting the interviews in a casual relaxed environment, where no one could over-hear the
interview. However, as the interviewer was a male, it was not possible for cultural reasons to
interview a female in a closed area (such as a staff office) unless the door was kept open. Even when
interviews took place in common spaces, some females requested the presence of a colleague or staff
member. All interviews were conducted on campus except for one interview which was conducted
after hours at a nearby café upon the request of the participant. The interview settings included the
empty offices of staff (e.g. office of the Dean, head of school and ICT), University cafes and common
outdoor spaces at the University. All interviews were audio recorded – when there was background
noise the recording device (iPhone) was held up to the participant’s mouth to ensure all words were
captured. Some field notes were taken following the interview to record non-verbal interactions or
reflections of the interviewer. The interviewees and interviewer had not met before except for those
students who had assisted the researcher with recruitment. The researcher engaged in general
conversations with each participant at the beginning of every interview to build rapport and put the
participant at ease.
Qualitative interviews
Qualitative interviewing was used to obtain descriptions of the lived experiences of the interviewees
and how these impacted their attitudes (Brinkmann, 2013). The semi-structure provided flexibility
and scope for the participant to answer freely and to direct the interview while still ensuring the
interview remained on topic and some uniformity in questioning was maintained between participants
(Nathan et al., 2019). The semi-structured interviews were guided by five questions (Appendix 6).
Due to the sensitivity of the topic, no questions were asked about the participant’s own alcohol
consumption or related behaviour. Instead, we enquired about University students as a collective

137
group.
Following verbal consent, the participants were first asked to narrate any story they had heard from
their relatives or friends about alcohol use and attitudes in previous generations (1970’s to 1990’s).
Students were then asked to comment on the influence of sanctions, war and terrorism on attitudes
towards alcohol among students. They were then asked about how common they thought alcohol use
was in Iraqi. After this, participants were invited to comment on the "openness" of Iraq towards the
outside world, including media, economy, culture, etc. and whether it had effects on students’
attitudes towards alcohol. Lastly, participants were asked about tolerance towards minorities and
diverse views about alcohol in Iraq. This was followed by a question about the ideal alcohol policy
that they would adopt in Iraq if they were a decision maker.
Translation and transcription
The transcripts were de-identified, and a pseudonym was assigned for each interview. All
transcription and translation were carried out by the first author, who is fluent in Arabic and English,
in a single step method (Arabic audio to English text). The first 12 recorded audio files were fully
translated and transcribed verbatim. Due to the time-consuming nature of this exercise, only
interviewee responses were transcribed for the remaining interviews (and not the interviewer’s
questions and comments). Some notes and comments/codes were inserted at the translation stage to
assist with analysis.
Analysis
The data was qualitatively analysed using King’s template analysis method (King, 1998). This
method was used as the coding was derived from a priori themes informed by the conceptual
framework (figure 1). Those were complemented and revised by new data-driven themes.
A preliminary template of codes was created a priori using the field exposure and the first eight
transcripts by the first author. These transcripts were circulated to the other authors (AD and KC) for
independent scrutiny. The authors jointly discussed and refined the template over several meetings.

138
A revised template was then used to first analyse data from University A and C by the first author.
These findings were presented and discussed with the authors (AD and KC). The template was further
revised. The further revised template was then used by the first author to analyse data from University
B. The findings were again discussed with the other authors (AD and KC). An audit trail was
maintained of the analysis process.
A reflexivity statement is included in the discussion. Reflexivity places this research in context by
identifying possible influence of the researcher on the study (Dodgson, 2019). This is especially
important in such sensitive research where participants may feel discomfort speaking about the topic.
NVivo 12 software was used for coding and analysis of transcripts.
Patient and public involvement statement
No patients participated in this study. Local collaborators, young medical graduates and student
representatives were consulted in the design, piloting and implementation of this study. We intend to
share published findings from this with local universities and student organisations in Iraq. This
process will also be done in consultation with local collaborators, graduates and students.
Ethics
Ethics approval was granted by the Medical Ethics Committee at the College of Medicine in the
University of Kufa, Iraq (MECCM-0028).
Results
Forty interviews between eight minutes and an hour were conducted. The gender and faculty mix of
the participants are shown in Table 1.

139
Table 8 Gender and faculty of participants (n = 40)
Uni. A (n) Uni. B (n) Uni. C (n) Total (n)
Gender
Male 10 3 9 22
Female 6 4 8 18
Faculty
Medicine 4 2 6 12
Science* 7 2 4 13
Humanities# 2 0 1 3
Engineering^ 3 1 2 6
Social Sciences+ 0 2 4 6
Total (n) 16 7 17 40 *Science includes faculties of science, nursing, geography. #Humanities include faculties of languages and visual arts.
^Engineering includes faculties of engineering and planning. +Social Sciences include faculties of law, education, political science, and media.
The results are presented according to five key themes: perceptions of the prevalence of alcohol use,
perceived motives for abstinence or drinking, attitudes towards those who drink, perceived harms
associated with alcohol use and views of alcohol policy in Iraq. Although participants were
specifically asked questions about student drinking, most students chose to answer with reference to
the alcohol consumption among all young Iraqis. All students spoke about the alcohol use with
reference to men and only one student mentioned drug use (not alcohol use) by females.
Perceived prevalence of drinking
Compared with the pre-war Iraq, students (n=14) reported that the prevalence of alcohol consumption
has increased in Iraq. However, other students (n=7) reported drinking had reduced, and others didn’t
report on prevalence but mentioned that patterns of drinking have become worse. Female students
and those in University A described an increase in prevalence of alcohol use more often than those in
other universities.
Students from all three sites agreed that alcohol use is a clandestine activity.
For example, here in our province, it’s not that alcohol is not present – it’s present, but it’s
hidden. In other provinces it’s present, it’s normal, people go, hang out and drink.
- Said, male, University A

140
However, students in University B reported that alcohol consumption has become more visible in
society:
Now, someone goes out and says publicly that this is me and I am doing this, and I am
drinking. It’s different, very different to before… I feel it’s much more public. Before, in all
honesty, there was none of this, now it’s public.
- Undisclosed, female, University B
Although some students (mainly males) described why they think alcohol use has increased, others
(mainly females) stated they felt that use has increased although they had never witnessed anyone
drinking.
Why people drink: “It’s natural for there to be various views”
Participants reported diverse reasons for alcohol abstinence or consumption. Hisham, a young
medical student from University A, summarised various underlying beliefs – interestingly, motives
for drinking or abstinence were associated students’ world view rather than motives presented in
Figure 10 (such as social or coping, etc.):
It’s natural for there to be various views.
Firstly, those that outright reject it from a religious view.
…Secondly, those that see themselves free from religion, but refuse it for a personal belief.
…mostly, those that are known for alcohol are those that lean towards the secular view, mainly
present in Baghdad.
…I know some people that are secular… [or] Islam is not their faith – but they don’t drink
because they don’t find it suitable, it decreases a person’s aura or they don’t see it as a good
act that has health effects, etc. – so they leave it.
…But religion ensures that most people stay away from it – if they were religious.
- Hisham, Male, University A

141
The following results will be presented according to antecedents to individual perceptions of alcohol
use, as presented in Figure 10. They will start from motives affected by the micro level (individual
motives) to those associated with social, national or global influences.
Individual motives
Students reported perceived personal motives for drinking, one of which was curiosity to know what
the possible effect might be. Participants thought that drinkers belonging to different socio-economic
levels had different motives for drinking. For example, curiosity, and fun/adventure seeking
(enhancement) were particularly associated with young students who could afford to travel to other
countries.
Even when they travel, they’re thinking ‘I am only going to enter this place to have a bit of
fun and while I am at it, might as well drink a bit’ – without a clear reason.
- Hasan, male, University C
Inquisitiveness about alcohol was also connected to a pre-conceived image of alcohol linked to
appearing more sophisticated and cooler or reaching a side of one’s personality that he/she would not
otherwise know.
I am a very curious person, and I tried it…as a joke we say, there are people that think ‘it adds
genius to you!’ Because, what is it? …Alcohol of course gives a strong relaxation to the body.
Through this relaxation, someone can reach their brain – how can I explain it? – how do I
explain it?
- Bilal, male, University C
Although trying alcohol out of curiosity and adventure was condoned, participants were fearful that
drinking for enhancement purposes may lead to ongoing alcohol consumption. One participant,
Batoul (female, University A), described some students as having a “love of adventure, they want to
try everything that is strange…When they try it out once, twice or thrice, they’ll fall for it.” Another

142
female student (Faiza, University C) stated that “they give it, alcohol, to the student without money,
so that the student can get addicted to it”.
Several students argued that young Iraqis’ decisions to drink were the result of their “weak”
personalities. Participants in all three settings explained that young Iraqis were naïve and drank to
conform with others. They suggested that providing health information and education and improving
critical thinking and informed decision making would help enable young people to make better
decisions.
Before we can solve the problem of alcohol… we should focus on the weak and disjointed
personality of a young person here, so that…when they are told that alcohol is harmful to your
health or wrong religiously, then they can simply research it themselves, be convinced or ask
what’s your evidence? Not just accept what you say with a very simple mind of saying – “oh
this is a good guy and he told me [“alcohol is bad”], so it must be correct” – What we need to
do is to know ourselves. This is the main problem you will find among anyone that is addicted
to alcohol or drugs, or all these things [that their earlier abstinence relied on other people’s
opinions].
- Sandra, female, University A
Interpersonal motives
Students also mentioned that social relations with family and friends influenced a person’s alcohol-
related behaviour. Students described “bad” friends and peer pressure as a source of alcohol use.
These encouraged of a mixture of social, enhancement and conformity motives for drinking. For
example, Bilal (male, University C) said “What would my friends think if I rejected their invite?
They’d say, ‘I am not a man.’ I fear that.” Others indicated that young people would drink so that
they can boast about it to their peers.
I have witnessed a lot of cases where people drink and then boast about their drinking saying “I drank
in this place and this funny thing happened to me” – whether to friends, acquaintances or others.

143
- Ibrahim, male, University C
Students also described the important role of families in the choices that young people make about
alcohol use. Careless and strict parenting were both criticised by participants. Students preferred that
parents and teachers educate and raise awareness of the harms of alcohol so that young people develop
long-term “immunity” and are therefore protected from such harms. Current parenting practices, they
argued, were either careless or authoritarian with high expectations that placed pressure on young
people and did not necessarily impact long term behaviour or harm prevention. For example, one
participant shared a story of a friend who had an alcohol problem that was linked to being raised in a
very strict family and a lack of commitment to religion.
There was a student with us, in first year – unfortunately he is now dead…he went to study in
Russia. His religiosity wasn’t very strong, so…he was consuming alcohol… Maybe his
family, they were very strict …As you know, increased pressure eventually causes an
explosion. When he went abroad, naturally, as he was strangled [by strict parenting] at home,
he wanted to open to the world and see what it has to offer.
- Reda, male, University A
It was also indicated that young people found it difficult to talk to their parents about alcohol use. For
example, a female student (University A) shared that students could not communicate with their
parents about alcohol or other socially and religiously sensitive areas because they either did not want
to disappoint their parents or were afraid to lose their parents’ financial support – alluding to the fact
that they may be ‘kicked out’ if exposed. Other students argued that cultural differences affected the
ability of parents to address their child’s drinking. For example, the mother would hide the son’s
drinking in fear of punishment by the father if he found out – or to not reach out for help from others
in fear of long-term social consequences for the child.

144
He was led to this…[by] bad parenting, so for example, his mother might have seen some
things that are worrying about him but didn’t inform his father, so that was the wrong choice,
and so there was no discipline.
- Manal, female, University C
Three students described stories of personal friends who had experienced the death of parents and
family members (some due to conflict), and who had used alcohol for coping purposes. Drinking
within families was also reported by three students who disclosed that their father or close male
relative was a drinker. Two of these participants suggested that they themselves had consumed
alcohol in the past. A father’s regular drinking was also reported to influence the son’s alcohol-related
behaviour. An indication that social motives also exist in Iraq.
[Some] families are strict and religious… he [the young drinker] fears them. So even if it’s
inconvenient, he only drinks when he sleeps over at his friends’ place... If [the son] drinks, he
drinks very little…to a limit where he can go back home, and his family will not find out. But
the person who has a father who drinks, he drinks as much as he wants and gets drunk.
- Ali, male, University B
Community-related motives
The local availability of alcohol was reported to influence the uptake of drinking. Participants from
University B and C reported that alcohol was easily available and some alleged that illegal alcohol
trade was protected by security forces. Some participants said that alcohol (and other drugs) sale
locations were commonly known. A student from University C, where alcohol is banned, offered to
take the interviewer there in person.
Unemployment and lack of alternative recreational activities were also mentioned as possible reasons
for increased alcohol consumption. The lack of activities to fulfil a young person’s social and
enhancement needs encourages alcohol to fill the space.

145
As soon as its sunset, go past the bars where they sell alcohol, you’ll see masses of people
there – it’s very busy (like this – hand gesture showing it’s crowded). Why? ... There is no
alternative. Where should a young person go? With his friends, go out, either to the cafés or
to drink.
- Ali, male, University B
Although many students stated that graduating students seldom find employment, some denied this
was linked to increased alcohol consumption because they believed that education made them more
resistant to alcohol use. However, participants shared their concern about alcohol use among
unemployed young people with limited education for coping or social purposes.
It is not likely that a university student would uptake alcohol after graduating from university.
It’s impossible, because he has…intellectual immunity, he says, ‘I have learnt and struggled
and everything – why now would I destroy myself?’ But as for other young people out there,
there are a lot that went this way [towards alcohol] – even the smallest upset in life, for
example, a lover leaves him, or his father hits him or kicks him out of home, he will go
[towards alcohol]. There is no lack of bad friends [too].
- Mahmoud, male, University C
Society-related motives and influences
Several students (n=12) reported that the unstable political situation and corruption in Iraq led some
to use alcohol as a coping mechanism. One student felt that although religion was currently the
strongest deterrent of alcohol use, this was changing due to perceived corruption and hypocrisy.
They consider that terrorism… [and] limiting of freedoms is because of religion. Most of the
corrupt thieving politicians have a religious side and they scaled up using this side…The
student just wants to escape to anything, as long as it’s not Islam... Anything that is rejected
by Islam, they automatically start wavering towards…In their thinking, Islam has rejected
this, so it must be good.

146
- Hisham, male, University A
Other students stated that they believed that political parties and their militias have a financial interest
in the alcohol and entertainment industries. They gave examples of venues that were attacked by
Islamist militias before later being protected by the same militia after the payment of bribes and
loyalties.
Students spoke of Iraq’s post-war situation and how this had influenced young people’s decisions and
beliefs around alcohol. While participants said that they had limited direct exposure to war, their
words were heavy with allusions to the post-war situation.
They give up on life, or some, their father left them and separated, or as I said, some have
poverty, and others face social pressures. They are not in the same situation as young people
in other countries, especially Europe. That’s why we see they head towards [alcohol].
- Zaman, female, University C
Students in all three settings described alcohol use as a coping mechanism and some participants
described personally knowing people who seek alcohol use for this purpose.
[I know] this person, before the fall of Saddam, he was from a higher socio-economic class.
After the fall, in 2004, there was killing by identity. They took his house and properties and
killed his wife…He started drinking daily under the bridge [homeless] to lessen his suffering.
- Adam, male, University A
Three students from University B and C denied that the Iraqi post-war situation resulted in some
Iraqis to uptake drinking. They argued that the situation might seem traumatic from an outsider’s
perspective – but young Iraqis are familiar to this reality and have become resilient to the situation.
Interestingly, these students shared that their father or male relative used to drink.
People that haven’t lived in Iraq, when they look at us, they see that we live black and dark
lives…Yes, for as long as we know, there’s been war after war, problem after problem. But

147
we are living fine, we are living. When I wake up in the morning, I am exactly like you... As
young people…we see the situation of Iraq as normal. When we come to drink, we don’t drink
because of the [negative] Iraqi situation, because…it is our reality. It is us.
- Sam, male, University B
Globalisation and greater/external society related motives:
Globalisation or “openness” as referred to in Iraq was seen by students considering either “positive”
or “negative” outcomes. All students acknowledged the benefits of media and social media –
especially for facilitating interactions with other cultures and the outside world. In terms of its impact
on alcohol consumption, there were diverse views but summarised in the statement below:
Maybe, it [openness] will increase [consumption]. Because people will see others seek
[alcohol], it will impact them…It could also increase awareness…It really depends on the
person, what side he leans and what his thoughts are.
- Huda, female, University A
Students feared that young people only absorbed “negative” influences such as alcohol use. They
shared that young Iraqis were increasingly “mimicking” what they see on media – where they
believed alcohol is presented in a positive manner.
We say that we like to see the outside world and we will progress through these things. We
will mimic them, and we will become the same as them. But no, this is not true, everything is
different here, we have religion, culture, traditions and for sure these are different from the
outside world.
- Ahlam, female, University B
Religious and social awareness about abstention was also reported to have increased since the 2003
war because of increased freedom of the press that allowed religious channels and media to broadcast
messages to young Iraqis.

148
In Iraq after the fall of the former regime in 2003, it opened to the outside world. This openness
wasn’t just cultural and technological – it was also religious openness. There were religious
lectures that addressed such issues. Permissible drinking now became something very rare
because people heard that [alcohol] is forbidden, and it’s a red line that no one should cross.
So even those who drink alcohol, started drinking secretly or at least started drinking in a way
that emphasises that it’s not permissible.
- Ibrahim, male, University C
Some students (n = 5) inferred that overseas travel was connected to alcohol consumption, with one
describing a friend who returned with an alcohol problem and another narrating a personal story of
colleagues who consumed alcohol for enhancement while travelling with him.
When I travelled, I had friends that would say “Why shouldn’t I try [alcohol], it’s once in a
lifetime. It won’t impact anything, so let me try and see”. Here in Iraq, obviously he can’t do
it, because he is afraid that his family see him, or someone else sees him. So where can he
drink? When he goes out of the country. I have seen over there, it’s easy, there’s nothing
restricting them. They don’t have a reason except wanting to try.
- Adam, male, University A
In contrast, other students did not believe that overseas travel would influence young Muslim Iraqis
to try alcohol.
If they got a chance to travel outside and they saw a bar or something… I don’t think they
will [drink]… [although] it is easy to go there and buy alcohol. Because it’s kind of a stigma
and people think that it’s very hard to drink in public and you should be conservative about
it… and… most of us, as Muslims we are very convinced and… we don’t take these actions
easily.
- Mahdi, male, University A

149
Perceptions of those who drink – “Not even Christian girls like drinkers”
As described earlier, students mentioned coping as a key motive for drinking. Students were
sympathetic towards individuals who drank because they had suffered the loss of loved ones during
the conflict. Others suggested that choices around alcohol use in Iraq weren’t made consciously and
most drinkers (and abstainers) were “imitators” who followed other people. They blamed drinking
on the “weak” personality of young Iraqis who consumed alcohol for conformity and did not make
their own decisions.
In addition to being weak, students viewed drinkers as lacking religious conviction, education and/or
wealth. Although students described alcoholics in a negative tone (“uneducated”, “poor”, etc.), they
typically blamed the social, political and economic environment rather than the individuals
themselves. One student, who shared that he and his relatives drink, praised young people that can
stay away from alcohol, despite peer pressure.
Some students considered any drinker to be an “alcoholic”, while others only used this label for those
who drank excessively, or were addicted to alcohol. Two students reported that if a male student tries
alcohol for curiosity, this would be tolerated. However, according to these students, alcohol is rarely
consumed in amounts that don’t cause intoxication.
In eastern societies…they don’t have a culture of drinking. Drinking of alcohol is a culture.
In the west, there are people that drink for a reason, there are people that stay awake all night
drinking, for a particular reason, but they drink little. But us, here, you won’t be called a
drinker of alcohol unless you’re intoxicated.
- Sam, male, University B
Students suggested that Iraq’s political instability was the primary reason for alcohol use in Iraq.
Students in University B and C stated that before the conflicts and sanctions, drinkers were more
tolerated. However, the political instability and the introduction of religious militias has led to tension
between Iraqis – especially towards minorities. For example, one student indicated that they were not

150
permitted to interact socially with non-Muslims whose religion allowed alcohol use: “our families
don’t allow us to mix with people from other religions…Because they have more alcohol
consumption. So, their assumption is that this will negatively impact us.” (Manal, female, University
C)
Excluding drinkers from social interactions was a consistent theme. Students reported that drinkers
were people that one would not want to associate with.
It’s impossible for a girl to say, “oh it’s okay, I will have a relationship with a drinker” and
same with boys, they’ll say, I will stay away from him and leave.
- Zahra, female, University B
Student differentiated between the attitudes of university students towards drinkers and the attitudes
of young people in the wider society.
“[At] the university… they couldn’t…[have] a drinker of alcohol and put a tick on him. No,
there’s a big X on him. But if you walk outside the university…then yes, a drinker is seen as
normal and even accepted.
- Mahmoud, male, University C
Although many students relayed a negative view towards drinkers, some students mentioned that
drinkers are increasingly perceived in a positive lens which may encourage drinking for social or
enhancement purpose. Firstly, by traditional people who associate alcohol with masculinity and call
it “the milk of lions” and secondly, by students who want to break free from current social and
religious values and beliefs.
The person that drinks is considered a lion [strong, courageous] ... instead of people detesting
him, he became liked… bad things like fornication, drinking and all these things - they [young
people] grouped these and called them “galaat”. [“galaat” are] essentially negative [traits] that
are now used to praise someone.

151
- Yacoub, Male, University A
Despite these differing views, students emphasised the need for young people to be more tolerant
towards people that hold different views regarding alcohol.
We need people that don’t interfere in other people’s business…People must respect our
opinion, respect the differences among us, we aren’t all from the same religion, nor all have
a single opinion…someone must respect diversity. That’s the most important.”
- Naeema, female, University C
Consequences of drinking
Individual and intrapersonal alcohol-related harms were frequently mentioned. One person shared
that his friend died from liver cirrhosis. Losing consciousness, or one’s memory or intellectual
abilities were also mentioned.
At least one student in each of the settings reported that a friend or relative was either a perpetrator
or victim of alcohol-related harms. Two female students from University A spoke about familiar
cases of alcohol-related domestic violence. They both shared the limited ability of females to respond
to any such violence due to a fear of losing their children or their children being left without a father.
“One of my relatives…it gets to the point of hitting her…all I know is he was addicted
to alcohol and he brings his friends home and one thing leads to another – and certainly
this involved girls and such things – she had no solution, she had children, so she
couldn’t do anything.”
- Zaman, female, University A
One girl in University C also shared that she has heard that females were the main target of alcohol-
related violence, even in the streets. Two male students in University C shared specific stories of
how drinking harmed their friends. One of them, Mahmoud, became tearful and expressed his guilt
as he spoke of a friend who died in a fatal car crash: “I was his only friend that didn’t drink, so had

152
I given up some of my time that night, he’d still be here.”
Students in University B did not share specific stories but said that alcohol-related street violence
and car crashes were a daily occurrence in their setting – one narrated this directly from a friend who
works as a police officer.
View of policies towards alcohol
Students were confused and unaware of Iraq’s policy towards alcohol, especially since the 2016 ban.
Students’ opinions of what an ideal alcohol policy in Iraq looks like differed greatly. Some students
(n=7) believed that if social harms are controlled, people should be free to drink by choice. They
suggested regulations, like those in Europe, such as taxes and restricted alcohol hours and venues.
However, many students (n=12) stated that the implementation of immediate prohibition or a phased
approach to this was the most appropriate policy for the Iraqi context.
Students that argued for prohibition did so either for religious reasons or because they believed
prohibition protects health and ensures positive social outcomes. Some participants described
alcohol use as a “right”, stating that people should make their own choices while others thought that
regulation would be more successful in curbing actual alcohol use than a total prohibition policy
because “that which is forbidden is attractive” (al-mamnüʿ marghüb).
Almost all students suggested preventative and health promotional efforts by the state – some
directly blaming the State for the spread of drinking and the lack of awareness about alcohol-related
harm. Students suggested introducing health-related educational programs, improving employment
opportunities, and sport and recreational activities.
Discussion
This is the first qualitative study to explore alcohol consumption in Iraq. This study investigates the
views of students in depth using interviews to shed light on the personal experiences of young Iraqis,
including how exposure to war and to western culture through globalisation may have influenced
perceptions of alcohol use. Drinking in Iraq is a clandestine activity and alcohol remains a sensitive

153
topic (AlMarri & Oei, 2009; L. Ghandour et al., 2016). Students had several views concerning the
prevalence of alcohol use and the possible drinking motives of young Iraqis. A spectrum of opinions
on future policies in Iraq were shared – ranging from complete prohibition to a free-for-all approach.
This diversity of attitudes is understandable in an evolving political, social and economic context and
in light of the Islamic prohibition, local customs, religion and civil laws.
Despite the ban on alcohol marketing in Iraq, young Iraqis are exposed to alcohol advertisement and
normalisation of drinking in international and social media platforms via posts from friends,
celebrities and organisations. Such exposure to alcohol, though indirect via movies and shows, has
been shown to increase young people’s likelihood of alcohol initiation in non-MMCs (Anderson et
al., 2009).
Students in our study indicated that there is a visible increase in the availability and affordability of
alcohol, even in provinces with alcohol prohibition and those affected by the war. The affordability
of alcohol can be confirmed in the media. For example, the cost of a 500mL can of imported beer in
post-ISIS Mosul is 2000 Dinars (~ $1.5 USD) and a 1L bottle of whisky (Alc. 43%) costs 12000
Dinars (~$10 USD) (AP, 2017), which is about the cost of a restaurant meal ($10-20 USD).
Students reported a diverse range of “internal” (coping/enhancement) and “external”
(social/conformity) motives for alcohol consumption. Participants perceived that alcohol use was
linked to coping with exposure to war, grief, poverty, loss of loved ones, unemployment and rejection
of culture and religion. Motives for drinking are important in this context as they are connected with
initiation of drinking and with drinking outcomes (Kuntsche et al., 2005).
While social motives were shared by students, they were normally associated with drinking by
previous generations, drinking in small friend groups or drinking outside of Iraq. Enhancement
motives were associated with traditional and modern perspectives about alcohol. Traditionally, the
feeling of invincibility or being a “lion” was a key factor and currently, the perceptions of
sophistication and modernity. Some perceived that the underlying motive encouraging drinking for

154
social and enhancement purposes was conformity with the positive image of alcohol in global media
and its association with sophistication and modernity.
Alcohol use for coping purposes has been associated with heavier drinking and more adverse personal
and social outcomes for drinkers in our sample and internationally (Kuntsche et al., 2005; Wicki et
al., 2017). Most Iraqis have been exposed to conflict due to the 2003 war, ongoing terrorism and the
war against ISIS. At least 6.7 million Iraqis are currently displaced or in need of urgent assistance
(UNOCHA, 2019). Non-Iraqi displaced people and post-conflict populations have shown an
increased likelihood to use and misuse substances (Greene et al., 2018). Post-traumatic stress disorder
and exposure to trauma, both prevalent among young Iraqis, have also been associated with increased
alcohol misuse (Debell et al., 2014). Iraqi refugees elsewhere have shared that alcohol they have used
alcohol to cope with past experiences of trauma (Dupont et al., 2005).
Iraq is currently experiencing an economic crisis that coupled with the trauma experience could put
young people at risk of harmful drinking (de Goeij et al., 2015). Nationally, one fifth of Iraqis (22%)
and almost half of Iraqis from former ISIS controlled regions (44%) are experiencing poverty
(Bandiera et al., 2019). Over a third (36%) of Iraqi youth are currently unemployed with at least 2.5
million jobs urgently needed (Bandiera et al., 2019). There is evidence, albeit in non-MMCs, that
alcohol use and misuse is associated with poverty (Allen et al., 2018) and long-term unemployment
(Henkel, 2011).
Although a normal outcome of years of conflict and political instability, the underlying social,
economic, and political atmospheres that drive young people to seek alcohol as a coping strategy need
addressing in the long term.
Preventing alcohol misuse in Iraq
By observation, public efforts to address alcohol in Iraq are generally expressed during religious
sermons or during consultations with health professionals. To our knowledge, there is a paucity of
research on alcohol policy in Iraq. Since the 2016 alcohol ban, there has been no clear or centralised

155
alcohol policy in Iraq (Al Ansari et al., 2019). Existing alcohol policy in the country is focused on
the application for and operation of licensed commercial outlets (Al Ansari et al., 2019). These
policies ban the marketing of alcohol, limit the operation hours of premises and regulate the labelling
and bottling of products (Al Ansari et al., 2019).
Illegal sales and smuggling of alcohol make the implementation of a tax on alcohol complicated in
Iraq. While there is strong evidence of the effect of taxation on the reduction of alcohol use (Stockings
et al., 2016), Iraq lacks the infrastructure to implement sale taxes or levies on retail products, including
alcohol. The current taxation model works on a yearly schedule with no firm legal or financial
structure. In 2016 the Government planned to charge a 300% levy on the importation and sale of
alcohol, but this was not implemented. Even if import taxes are imposed, the Iraqi cash-based
economy is not monitored adequately and smuggling is known to be widespread (Bureau for
International Narcotics and Law Enforcement Affairs, 2013).
Universal alcohol prevention efforts typically aim to either reduce overall use, problematic use or
injury/harm (Stockings et al., 2016). Given that prevalence of alcohol use is reportedly low in Iraq
(US Department of State et al., 2015; WHO, 2009), the appropriateness of a universal alcohol
prevention strategy has been questioned in this context (Dabbagh, 2017). However, the vulnerability
of young people in Iraq to alcohol misuse indicates that a long term culturally sensitive strategy that
maintains low levels of consumption while introducing harm reduction and treatment strategies may
be required.
While prohibition with severe consequences for drinking was preferred by some students, they felt
that banning alcohol will increase the desire for consumption among young Iraqis. Although national
or local prohibition may decrease use, evidence on drug prohibition in non-MMCs have found such
bans result in limited or no reduction of problematic use and harm and may result in adverse health
and social effects including increased criminal activity in illegal drug markets (Stockings et al., 2016).
Students suggested alcohol use should be regulated and that a non-prohibition approaches would lead
to increased ‘informed’ abstinence.

156
Iraqis view addiction as a moral rather than a medical issue (Al-Hasnawi et al., 2007; Dabbagh, 2017).
While there is a need to raise awareness of the health aspects of this issue, it is important that
approaches to alcohol-related health promotion take into account this moral worldview (Stockings et
al., 2016). Currently, the biggest deterrent of alcohol use in Iraq is the Islamic prohibition, which
limits alcohol use across all MMCs worldwide (WHO, 2018a). For example, lifetime abstinence rate
is 89.1% in Turkey (WHO, 2018a), despite being a secular nation with alcohol permissibility since
1924 (Evered et al., 2016). Despite the effectiveness of prohibition in other MMCs (WHO, 2018a),
students in our study reported an increasing anti-Islamic sentiment among educated young Iraqis who
blame Islam or the conservative and possibly fundamental Islamist governments for political and
social issues. This negative sentiment is reportedly a reaction to the political, social and economic
governance by Islamist parties leading Iraq since the 2003 conflict. For these reasons, despite keeping
country-wide alcohol use prevalence low, religious intervention may not always be an effective form
of drinking deterrence for the whole population.
Students in our study described the social stigma attached to alcohol use. While this may serve as a
deterrent it may also limit access to treatment and re-integration into society for those affected by
alcohol use disorders. Furthermore, students reported that families often hide an individual’s drinking
in fear of life-long stigma. In some Iraqi settings, alcohol is stigmatised more than other illicit
substances (Humphreys, 2011).
Community-based interventions may be useful in preventing alcohol misuse in the Iraqi setting where
over half of Iraq’s population is under the age of 19 (Bandiera et al., 2019). However, overt
conversations about alcohol might not be possible and substance-specific education programs have
typically been shown to be ineffective (Stockings et al., 2016). Alternatively, conversations about
alcohol could be incorporated into youth development approaches and health promotion efforts. There
are some promising results from generic prevention programs that focus on psychosocial and life
skills in reducing alcohol use, rather than on alcohol-related harm (Stockings et al., 2016).

157
Positive youth development programs (PYDP) are an example of such programs that consist of
training to strengthen young people in general character building and resilience– some also equip
them with some health-related knowledge. Although limited studies found them effective in alcohol-
and drug-related prevention, PYDP has been found effective in strengthening vulnerable populations
and in altering knowledge, attitudes and risky behaviour among young people, including in MMC
settings (Catalano et al., 2019). Accordingly, the use of PYDP in Iraq may strengthen the “weak”
personalities, self-esteem and decision-making processes of young Iraqis that may in turn impact their
attitudes and behaviours around alcohol.
Similar programs to PYDP exist in building parenting skills and parent-child communication. These
programs have had promising results in diverse settings in high, middle and low income countries
(Bo et al., 2018; Giusto et al., 2018; Stockings et al., 2016). In addition to preventing anti-social
behaviour, these interventions delay the child’s onset and frequency of alcohol use (Stockings et al.,
2016). Parenting interventions may be important in Iraq, because the age of transition to financial and
social independence occurs later than other countries, with young people typically living at home
until they are married in their mid-20s.
To reduce drinking for social and enhancement motives, students concern with lack of opportunities
for entertainment and social interactions with other young people should be addressed. Alternative
ways of addressing these social and enhancement needs should be studied and incorporated in future
planning.
A holistic approach to preventing alcohol-related harm that supports young Iraqis to build resilience
in challenging difficult times may be necessary in Iraq. It is important that approaches to addressing
alcohol consider the diverse needs of young people and are sensitive to the socio-cultural context and
Iraq’s already stretched health system.

158
Limitations
Lack of funding and the security situation in Iraq meant that recruitment for the interviews had to
take place over a maximum of two days in each site. This limit in time and resources meant that
participants from Iraqi minorities or internally displaced peoples could not be targeted for
recruitment. It also meant that participants were spontaneously recruited, and the interviews took
place wherever convenient, either in staff rooms or public spaces around campus. Care was taken that
there were no people overhearing, but the lack of privacy may have hindered some participants from
speaking freely. The interviews were all conducted by one male interviewer and thus most female
recruitment was limited to those approached by university staff or interviewed in formal staff
environments. The lack of a female interviewer was reflected in the ten rejections received from
female participants compared to only two from men.
Lack of funding also meant that transcription and translation needed to be done in a one-step process
by the first author. This could have impacted the accuracy of the transcripts and subsequent analysis.
Snippets of a few interviews were back translated to Arabic for verification by someone other than
the first author as a random checking process.
Young Iraqis who are not university students were not the focus of this study. Drinking prevalence,
patterns and motives may differ among this group.
Reflexivity
The first author who conducted, translated and transcribed the interviews is a non-drinking Australian
Iraqi male of the Muslim faith. Although this was not made explicit, interviewees would surmise this
from his name. Being a young insider served positively in that people seemed to identify with the age
and thoughts of the interviewer. However, this could have been perceived negatively as interviewees
might have felt judged or restricted. An example of this is a participant who took a smoking break as
soon as he found out (by accident) that the interviewer was related to one of the University staff.
Being an outsider was positive in that students felt more at ease to share their own opinions but may

159
have potentially influenced them to project a more modern approach. It was the author’s impression
that some interviewees (and some other associates in Iraq) concluded that the author was either
attempting to promote or prohibit alcohol use. This polarisation of views on alcohol policy is
commonly observed in Iraq. At several points in the interviews, the interviewer formed the impression
that students wanted to display what they thought the interviewer wants to hear.
In several interviews, once the participants’ personal view of alcohol became clear – this may have
impacted the interviewer’s understanding of the remainder of the interview. For example, if a student
appeared to be a devout Muslim the interviewer may have unintentionally understood what he said
differently to the same words from a person that appears more liberal.
Conclusion
Alcohol's role in Iraq's youth is multi-dimensional. To some, it represents the difficulties, conflict and
loss young Iraqis have endured and to others, it represents progression towards modern Iraq.
Predominantly, there is a negative perception towards alcohol consumption. Even those with a
positive attitude to alcohol shared that heavy drinking and intoxication are common among drinkers
in Iraq and stressed a need for preventative measures. Others expressed a desire for a staged long-
term plan that gradually leads to an abstinent community.
The challenges that alcohol may present in the upcoming years are unpredictable, especially
considering Iraq’s political, social and economic transition. Currently, prevention is centred on
religious prohibition and social stigma. Increasingly, these preventive methods are becoming less
relevant to some young Iraqis who reportedly choose to initiate or increase their drinking while in
absence of social restraints. To future-proof the prevention of alcohol-related harms, Iraq’s economic
and health infrastructure must be strengthened. This includes providing increased opportunities to
young people, enforcing pricing and taxation policies and initiating youth and parenting development
programs. These programs should consider young people’s lived experiences and attitudes as well as
religion, culture, health (physical and mental), economics and recreation.

160
References
Al-Hasnawi, S., et al. (2007). Public Attitudes toward Substance Abuse. Karbala Medical Journal,
1(2), 162-166. Retrieved from http://www.iasj.net/iasj?func=fulltext&aId=75862
Qānūn Wāridāt al-Baladiyyāt [Municipal Revenue Law], (2016).
Al Ansari, M., et al. (2019). Alcohol: from Mesopotamia to Modern Iraq. Journal of Ethnicity in
Substance Abuse, 1-23. doi:10.1080/15332640.2019.1657541
Al Ghaferi, H., et al. (2013). Substance Misuse in Arabic Countries: the Need for Published Research.
International Journal of Prevention and Treatment of Substance Use Disorders, 1(1), 7-11.
Allen, L. N., et al. (2018). Socioeconomic status and alcohol use in low- and lower-middle income
countries: A systematic review. Alcohol, 70, 23-31.
doi:https://doi.org/10.1016/j.alcohol.2017.12.002
AlMarri, T. S. K., et al. (2009). Alcohol and substance use in the Arabian Gulf region: A review.
International Journal of Psychology, 44(3), 222-233. doi:10.1080/00207590801888752
Anderson, P., et al. (2009). Impact of alcohol Advertising and Media Exposure on Adolescent
Alcohol Use: A Systematic Review of Longitudinal Studies. Alcohol and Alcoholism, 44(3),
229-243. doi:10.1093/alcalc/agn115
AP (Producer). (2017, 22/03/2019). Alcohol shops reopen in Mosul. Retrieved from
https://www.youtube.com/watch?v=9NHtzBr081M
Bandiera, L., et al. (2019). Jobs in Iraq: a primer on job creation in the short-term. In: World Bank.
Bo, A., et al. (2018). Parent-based interventions on adolescent alcohol use outcomes: A systematic
review and meta-analysis. Drug and Alcohol Dependence, 191, 98-109.
doi:https://doi.org/10.1016/j.drugalcdep.2018.05.031
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American
Psychologist, 32(7), 513-531. doi:10.1037/0003-066X.32.7.513
Bureau for International Narcotics and Law Enforcement Affairs. (2013). Money Laundering and
Financial Crimes Country Database.
Catalano, R. F., et al. (2019). Positive Youth Development Programs in Low- and Middle-Income
Countries: A Conceptual Framework and Systematic Review of Efficacy. Journal of
Adolescent Health, 65(1), 15-31. doi:https://doi.org/10.1016/j.jadohealth.2019.01.024
Dabbagh, R. (2017). Current Trends of Substance Use in Iraq: Examining Data from the 2014 Iraqi
National Household Survey of Alcohol and Drug Use. (Doctor of Public Health). UCLA, Los
Angeles. Retrieved from https://escholarship.org/uc/item/2ss660kn
de Goeij, M. C. M., et al. (2015). How economic crises affect alcohol consumption and alcohol-
related health problems: A realist systematic review. Social Science & Medicine, 131, 131-
146. doi:https://doi.org/10.1016/j.socscimed.2015.02.025
Debell, F., et al. (2014). A systematic review of the comorbidity between PTSD and alcohol misuse.
Social Psychiatry and Psychiatric Epidemiology, 49(9), 1401-1425. doi:10.1007/s00127-014-
0855-7
Dupont, H. J. B. H. M., et al. (2005). Killing time: drug and alcohol problems among asylum seekers
in the Netherlands. International Journal of Drug Policy, 16(1), 27-36.
doi:https://doi.org/10.1016/j.drugpo.2004.06.002

161
Evered, E. Ö., et al. (2016). A geopolitics of drinking: Debating the place of alcohol in early
republican Turkey. Political Geography, 50, 48-60.
doi:https://doi.org/10.1016/j.polgeo.2015.06.006
Ezard, N. (2012). Substance use among populations displaced by conflict: a literature review.
Disasters, 36(3), 533-557. doi:10.1111/j.1467-7717.2011.01261.x
Gakidou, E., et al. (2017). Global, regional, and national comparative risk assessment of 84
behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-
2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet,
390(10100), 1345-1422. doi:10.1016/S0140-6736(17)32366-8
Ghandour, L., et al. (2016). Alcohol consumption in the Arab region: What do we know, why does it
matter, and what are the policy implications for youth harm reduction? International Journal
of Drug Policy, 28, 10-33. doi:http://dx.doi.org/10.1016/j.drugpo.2015.09.013
Giusto, A., et al. (2018). A systematic review of interventions targeting men's alcohol use and family
relationships in low- and middle-income countries. Global Mental Health, 5, e10.
doi:10.1017/gmh.2017.32
Greene, M. C., et al. (2018). Alcohol and Drug Misuse Interventions in Conflict-Affected
Populations. In N. Morina & A. Nickerson (Eds.), Mental Health of Refugee and Conflict-
Affected Populations: Theory, Research and Clinical Practice (pp. 221-241). Cham: Springer.
Henkel, D. (2011). Unemployment and Substance Use: A Review of the Literature (1990-2010).
Current Drug Abuse Reviews, 4(1), 4-27. Retrieved from
https://www.ingentaconnect.com/content/ben/cdar/2011/00000004/00000001/art00002
Humphreys, K. (2011) Circles of Recovery: An Interview with Keith Humphreys, PhD/Interviewer:
W. White. Counselor (Vol 12(6)).
Karam, E. G., et al. (2008). Lifetime Prevalence of Mental Disorders in Lebanon: First Onset,
Treatment, and Exposure to War. PLoS Medicine, 5(4), e61.
doi:10.1371/journal.pmed.0050061
King, N. (1998). Template analysis. In G. Symon & C. Cassell (Eds.), Qualitative Methods and
Analysis in Organizational Research: A Practical Guide (pp. 118-134). London: Sage.
Kuntsche, E., et al. (2005). Why do young people drink? A review of drinking motives. Clinical
Psychology Review, 25(7), 841-861. doi:https://doi.org/10.1016/j.cpr.2005.06.002
Kuntsche, E., et al. (2017). Alcohol and other substance use in a cross-cultural perspective. Drug and
Alcohol Review, 36(6), 717-720. doi:doi:10.1111/dar.12625
Levy, B. S., et al. (2013). Adverse health consequences of the Iraq War. The Lancet, 381(9870), 949-
958. doi:http://dx.doi.org/10.1016/S0140-6736(13)60254-8
Lo, J., et al. (2017). A Systematic Review on Harmful Alcohol Use Among Civilian Populations
Affected by Armed Conflict in Low- and Middle-Income Countries. Substance Use & Misuse,
52(11), 1494-1510. doi:10.1080/10826084.2017.1289411
Melki, J. (2010). Media habits of MENA youth: A three-country survey. Beirut.
Savic, M., et al. (2016). Defining “drinking culture”: A critical review of its meaning and connotation
in social research on alcohol problems. Drugs: Education, Prevention and Policy, 23(4), 270-
282. doi:10.3109/09687637.2016.1153602
Stockings, E., et al. (2016). Prevention, early intervention, harm reduction, and treatment of substance
use in young people. The Lancet Psychiatry, 3(3), 280-296.
UNDESA. (2017). World Population Prospects: The 2017 Revision, Key Findings and Advance
Tables.

162
UNOCHA. (2019). Iraq: Humanitarian Bulletin, November 2019.
US Department of State, et al. (2015). Survey of Substance Abuse in Iraq. Bethesda, MD.
WHO. (2009). Iraq Mental Health Survey 2006/7. http://www.webcitation.org/6mk3pGCJV
WHO. (2018). Global status report on alcohol and health. Geneva.

163
Chapter 7 - Discussion
This thesis presented an account of the place of alcohol throughout Iraq’s socio-cultural history. It
then focused on the attitudes to, and experience of alcohol among young people today, amidst Iraq’s
political, social, and economic unrest. In keeping with previous studies, prevalence of alcohol
consumption was relatively low in this Iraqi university student sample, but risky drinking was high
among those who did drink. Corresponding to international and local research, being a non-Muslim
male, and living away from family or relatives was associated with increased odds of consuming
alcohol, even in this conservative country. Overall, our online survey presented a slightly higher
prevalence of drinking among females than previous face-to-face and pen-and-paper surveys in Iraq.
Even in conservative areas, participants said that it was easy to access alcohol. Students in interviews
shared many perceived motives for alcohol consumption among drinkers – chief among those was
drinking for coping, socialising, and entertainment purposes. Young Iraqis either directly or indirectly
connected experiences of unrest resulting from conflict and terrorism with alcohol use or misuse.
Most students perceived alcohol negatively and suggested a mix of regulatory, restrictive, or
prohibitive policies towards alcohol.
This thesis presents the first analysis of factors influencing prevalence of alcohol use and attitudes
towards alcohol among young Iraqis. Chapter 2 set out the special methodological challenges facing
research on the sensitive topic of alcohol among Iraqi youth, and the ways these challenges were
addressed in this setting. Chapter 3 provided the first review on the social, cultural, and historical
context of alcohol in Iraq – an essential precursor to assessing the current perspectives of diverse
young Iraqis. This was followed by the first systematic scoping review on alcohol in Iraq. Chapter 4
described the limited quantity and varying quality of past research on alcohol among young Iraqis.
Together, these two chapters set the base for the mixed-method study. Chapters 5 and 6 presented the
first qualitative and mixed-method data on alcohol prevalence and attitudes towards alcohol among
university students in Iraq.

164
This discussion will synthesise the findings from the two reviews (Chapters 3 and 4) and the mixed-
method studies (Chapters 5 and 6) to enable a clearer understanding of alcohol’s place among young
university students in Iraq. Having both the quantitative and qualitative data enables a holistic
analysis, including key individual and societal vulnerability factors (WHO, 2014a). We will also
contextualise this research within the broader alcohol literature.
Diversity and alcohol in Iraq
Despite the impression sometimes conveyed by the media that MMCs are home to homogenous
societies, our research indicated the existence of a diversity of views on alcohol consumption, how it
is perceived, what leads to alcohol’s misuse and how this should be addressed. Each of our four
studies revealed different dimensions contributing to this heterogeneity. The socio-historical study
showed that many factors have influenced how alcohol is viewed including the presence of diverse
religious, cultural, and family traditions over history.
The scoping review provide further evidence of this diversity by showing that distinct settings in Iraq
have different prevalence of drinking. The quantitative survey showed that views towards drinking
and alcohol policy also differ among students. Even estimation of the prevalence of student drinking
varied widely among participants. The interviews shed further light on this diversity. Most students
view alcohol in a negative light – reasons for this including religious, health and social. However,
those who viewed alcohol in a less negative light also mentioned that alcohol is typically misused in
Iraq because of a lack of culture around drinking. They also expressed the importance for freedom,
self-expression, and self-determination.
As described in Chapter 3, during colonisation by the British after World War I, Iraq’s current borders
were drawn without cultural, religious, or ethnic considerations. This resulted in modern Iraq housing
a multi-faceted population, formed over the millennia at the cross-roads of the East and West. Despite
the Islamic prohibition of alcohol, parts of the Iraqi population have an imbedded historical or cultural
connection with alcohol – sometimes dating to the pre-Islamic era (Al Ansari et al., 2019). Evidently,
the majority Muslim population’s connection to alcohol is also not new. Chapter 3 presents tales of

165
excessive drinking noted throughout most of the post-Islamic era, including by Muslims. Iraq’s
alcohol production and trade, however, has been almost solely in the control of minority religions
over the course of Iraq’s history. Laws typically banned Muslims from participating in alcohol trade
while there was no prohibition for communities of other faiths (Al Ansari et al., 2019; Zubaida, 2014).
Iraq’s main non-Muslim communities are ethno-religious groups that are connected to Iraq ethnically,
culturally, and historically. However, in recent decades, the number of non-Muslim Iraqis declined
rapidly. This displacement started with the persecution of the Jewish population following the
creation of Israel in 1948 (Bashkin, 2012) as well as the displacement of Christian, Mandeans and
Yezidis during the former Baathist government, following the 2003 war (Hanish, 2009) and with the
rise of Daesh (Office of International Religion Freedom, 2019). Iraq’s Christian population, for
example, is estimated to have declined from over a million to only 250,000 in just the past two decades
(Office of International Religion Freedom, 2019). Although non-Muslims account only 3% of Iraq’s
population, over half of the Iraqi-born population of Australia identify with a denomination of
Christianity (ABS, 2016) - a testimony to the grand scale of their displacement in recent years.
Our findings add to the growing literature on alcohol in MMCs showing that prevalence of alcohol
use may be impacted by two key factors: primarily, the proportion of the Muslim population and
secondly, the secularity of government and society. For example, Lebanon is known to have the
highest alcohol use prevalence in the region – mainly due to its large non-Muslim population (44%)
and relatively secular society (Rosentiel et al., 2006). Turkey, although secular, remains relatively
protected from alcohol use because of its overwhelmingly Muslim majority – with more than 87% of
its population lifetime abstainers (Gündüz et al., 2019). Drinking however is reportedly increasing
among young people even in this setting (Gündüz et al., 2019). Our multivariable analysis in Chapter
5 confirmed that being a non-Muslim is a significant predictor of drinking in our Iraqi university
student sample after controlling for other influences such as age and living away from relatives.
As presented in Chapter 6, interview participants also associated drinking behaviour with non-
Muslims – but they differed on whether non-Muslims should be allowed alcohol in Iraq. One

166
participant stated that her parents advised her against having non-Muslim friends, citing “bad
influence” due to alcohol consumption as a primary concern. In extreme cases, such fears escalate to
sectarian conflict centred around alcohol. There have been reports of threats and even actual attacks
on bottle shops and their owners (BBC, 2013). Such sentiments however were not shared by students
in either of our samples. Increasingly, alcohol bans and limitations are seen to infringe on minority
rights in Iraq (UNHCR, 2018). Two fifths (40.8%) of survey participants suggested a policy that
accommodates non-Muslim consumption of alcohol.
Although most traditional drinking in Iraq occurs within ethno-religious minorities, some Muslims
also traditionally consumed alcohol (Zubaida, 2014). Participants in our interviews confirmed that
consumption traditions exist within Muslim families. Consumption by past generations is also in line
with descriptions of drinking araq in Iraq from the mid-20th century (al-Wardī, 1965; Zubaida, 2014).
All students that volunteered information on their drinking in the interviews shared that their father
or other male relatives were drinkers. This is in line with our survey findings on non-drinkers, that
following religion, family was the second most prominent protective factor. Interestingly, all the
interviewees who shared that their older relatives consumed alcohol – stated they were ex-drinkers
who have since ‘repented’. Sharing this detail could be associated with the participant’s desire to be
socially accepted by the interviewer or may be indicative of the resurgence of religious influence in
Iraq following the 2003 conflict (Marr, 2018).
It is likely that as Iraq’s overall population rapidly increases due to high birth rates (UNDESA, 2017),
and religious minorities decrease due to displacement (Office of International Religion Freedom,
2019), the demographics of alcohol use may change in Iraq. Similarly, as the impact of secular
thought and society increases in Iraq, alcohol consumption may increase. However, as Islam remains
the majority religion, it ensures an ongoing protective factor for most of the population – as in the
case of Turkey. Nonetheless, ideally, preventative measures in Iraq should target Muslim and non-
Muslim populations alike.

167
Alcohol availability, affordability, and taxation
Historical accounts relay that the 10th century Abbasid Caliph al-Qāhir ordered taverns shut, alcohol
confiscated and drinkers prosecuted, yet, al-Qāhir himself was never seen sober (Al-Kirmalī, 1919).
In Iraq today, similar contradictions were perceived by students. Even in conservative areas where
alcohol is prohibited, most respondents to the student survey shared that alcohol was easily accessible.
At least one student from a province with an alcohol ban offered to take me to observe places where
alcohol and drugs are sold – apparently under the watch of security forces. Interview participants saw
the mismatch they observed between official policy and the state conduct as hypocrisy. Students
shared that while alcohol is publicly opposed by Islamist political entities and militias, these same
groups were defending other nightclubs, alcohol sellers and bars. When I enquired why they believe
this occurs, their answer was “corruption” and “bribery” – arguing that these same entities supported
the alcohol ban in 2016. It is difficult to decipher between truth and speculation in such accounts.
Such sentiments were also shared in the media following the 2016 ban (Salloum, 2016). However, a
general distrust of the government, political entities and policy makers was sensed from almost all
interviewed students.
One of the arguments made by Islamist groups for alcohol’s ban in Iraq was that all proceeds (or
taxes) resulting from the importation, production, or sale of alcohol were “unclean”. Therefore, they
argued, it is unconstitutional for the government to collect or use such funds (UNHCR, 2018). Iraq’s
constitution guarantees equal rights for minorities, it also sets out that laws cannot be opposed to
Islam – the majority religion. The jurisprudential ruling regarding the permissibility of alcohol
proceeds is however irrelevant as Iraq is a secular state and not a theocracy. While Muslims are the
majority, laws in Iraq are not based on Islamic jurisprudence or theology (The Republic of Iraq, 2005)
– and if they were, alcohol would be prohibited in the first place with no need for financial
justifications. These arguments are also historically questionable considering that non-Muslims in
Iraq and elsewhere in MMCs, such as Iran, have been and are able to produce, sell and consume
alcohol (Al-Ansari et al., 2019; Zubaida, 2014). There is evidence of tax on wine from the 10th

168
century CE (Kennedy, 2015). More recently, there have been customs duties and taxes on alcohol
importation in modern Iraq as early as 1935 (Amīn Rayḥānī, 2015). The government had planned to
increase the levy on alcohol importation to 300% in 2016, a step that was later backtracked
(International Monetary Fund, 2017).
In 1935, there were at least 35 non-Muslim alcohol sellers and 15 importers in Baghdad, most situated
on one street – Shāriʿ al-Rashīd (Ḥarb, 2018). Despite the lower prevalence of non-Muslims, in 2011,
the Russian news outlet, RT reported that there were around 100 licensed alcohol sellers in Baghdad
(RT Arabic, 2011). Today, the landscape seems similar – interviewed students seemed to identify
certain streets with alcohol retailers, nightclubs and other establishments that sell alcohol. By
observation, the presence of alcohol is clear in areas such as Ainkawa, a majority Christian area, in
Erbil. Even fruit shops and outdoor stands display visible alcohol branding. The laws described in
Chapter 3 ban any alcohol marketing and restrict hours of operation and location of alcohol shops to
non-residential areas away from public facilities such as hospitals or schools (Al Ansari et al., 2019).
In theory, Iraq is enacting the enforcement of WHO’s “best buys” of restricted physical availability
of alcohol. However, in practice, licensed stores are reportedly opening in residential areas throughout
central Baghdad, with their hours of operation exceeding those permitted (Ultrasawt Editorial Team,
2019).
Excise taxes on alcohol is another of the WHO “best buys” and a leading preventative measure
(Stockings et al., 2016; WHO, 2018a). Apart from potential moral objections to collecting tax on
alcohol, there is no infrastructure for excise and sales taxes in Iraq (Al-Awwad et al., 2017;
International Monetary Fund, 2017). Reportedly, a full-sized bottle of locally made spirits with over
40% alcohol content is sold for around $8 USD. This is compared to around $40 USD for imported
spirits of the same type (NAS news, 2018). Interview participants in our study also indicate that
alcohol smuggling into provinces with alcohol bans is common. At the time of writing, there were no
publicly accessible data on alcohol smuggling, however, some public figures and news articles have
reported smuggling attempts through domestic and international borders (Ultrasawt Editorial Team,

169
2019). Similarly, The Bureau for International Narcotics and Law Enforcement Affairs (2013) reports
that smuggling is endemic in Iraq, especially of petroleum products and cigarettes.
Market prices of other substances such as tobacco are also low. A packet of cigarettes, by personal
observation, costs as little as half a dollar (USD) and can be bought with no restrictions at any
convenience store. Very often, by observation and anecdotally, young children walk into grocery
shops to buy packets of cigarettes for their parents. Anecdotally, alcohol seems to be similarly
purchased by children. Although there is no data on underage purchase or consumption of alcohol,
one study of secondary school students in Iraq shows the age of onset of drinking as 12 (Saeed, 2016).
In Lebanon, teenage school students reported that they easily purchase alcohol with no questions
asked (Yassin et al., 2018). Similarly, while travelling through Erbil Airport, I enquired if age
restrictions are enforced for alcohol sales – the cashier was unsure. When I asked if they would sell
alcohol to a minor? They answered that they personally would not, however, they were not sure of
any legal enforcement or consequences. A trending video reported on the BBC shows a three-year-
old drinking from a bottle of spirits in a public celebration on 2019 New Year’s Eve in Iraq (BBC
News Arabic, 2019). It is unknown if these videos are real or represent what is more widely happening
in Iraq – but they may impact how Iraqis view alcohol and its potential effect on children.
Conflict, social unrest, terrorism, and trauma
Two fifths (41.7%) of our survey sample reported direct experience of war or violent military conflict
and almost a third (29.2%) scored positive on the PC-PTSD screen. Although no association was
found between PTSD and drinking in our sample, most (85.7%) students attributed drinking motive
to coping with experiences of trauma. Similarly, in the interviews several students shared stories of
friends or people they know who used alcohol to this end. Iraqi refugees in Europe have similarly
shared that drinking occurs for coping purposes (Dupont et al., 2005). Drinking for coping purposes
has also been associated with heavier drinking and worse outcomes in previous international literature
(Wicki et al., 2017). As described in Chapters 1 and 3, Iraqis have experienced continuous war,
sanctions, and terrorism since 1980 (Al Ansari et al., 2019). The biggest decline in living standards

170
was following the two Gulf Wars in 1990 and 2003 (Al Ansari et al., 2019; Marr, 2018). Young Iraqis
born after this period have not seen an Iraq without economic, political, and social turmoil. Even basic
needs such as electricity and running water are limited in Iraq (Marr, 2018). The full impact of this
exposure to conflict and difficulty of living is yet to be established.
Despite these circumstances, some of our interview participants did not feel that war and terrorism
will lead to drinking. They argued that Iraq’s intense circumstances have led to Iraqis becoming more
resilient because terror has become a daily reality for young Iraqis. They perceived that only people
from outside [of Iraq] think that conflict and terrorism are ‘strange to us’ and that ‘we need alcohol
to cope’. By observation, Iraqis reminded of certain health measures or experiencing illnesses,
including COVID-19, commonly make similar statements: “If we survived the bombs that fell on our
houses and the bullets that flew through our walls – do you think we won’t survive a little microbe?”.
Another result of years of conflict in Iraq is the political unrest. Political entities in Iraq are often
accused of contributing to the economic and social unrest. Most of these parties follow Islamist
ideologies. A recurring theme in our interviews was that a large contributor to alcohol use was the
frustration of young people with the perceived hypocrisy and control of Islamist parties. Participants
shared that young people in Iraq are growing increasingly intolerant towards this control and many
are leaving Islam altogether. The apparent contempt of political entities, according to participants,
triggers a reaction among some young people that all things Islamic are wrong and limiting.
Globalisation, media, and social media
In our survey sample, a large portion of students reported seeing alcohol marketing on mainstream
and social media. Although social and mass media were perceived as influencing factors for drinking
by non-drinkers, most drinkers in our survey did not make this association. Students also reported
that drinking was associated with the image of “sophistication”, associating uptake of drinking with
“blind following” of other cultures. They also shared examples of their friends’ consumption while

171
studying or travelling in other countries. Interviewees emphasised that young people should be wise
in their use of the internet and social media.
The survey results also indicate that although students were exposed to pro-alcohol messaging, anti-
alcohol messaging was also prevalent in the Iraqi media (data not shown). Interview participants also
shared that media was a source of religious and health awareness which protected against alcohol use.
As discussed in Chapters 5 and 6, there is increasing evidence in non-MMCs that exposure to alcohol
marketing, including in movies and TV shows, is associated with the earlier uptake of alcohol by non-
drinking adolescents and more drinking by those who already drink (Anderson et al., 2009). Most
young people in Middle Eastern Muslim countries consume English language media (Melki, 2010).
Students also reported that young people normally “imitated” the “negative” behaviours such as
drinking from other cultures. The influence of this exposure is shown in previous media interview
with alcohol sellers in Iraq. An alcohol seller reported that Iraqis often dislike Arabic branding and
labels on their alcoholic beverages and prefer foreign brands and marketing (NAS news, 2018). This
has encouraged local alcohol producers to also use foreign branding such as “Mr Chavez” for their
whisky to appeal to consumers (NAS news, 2018). despite its marketing restrictions on alcohol, Iraq
lacks measures to protect young people from alcohol content on the internet and or via satellite
services. Promotion of alcohol in digital media and especially on the internet remains a global concern
and public health interventions to restrict this promotion have been supported by consistent evidence
(Lobstein et al., 2017).
Alcohol – males and females
In line with these findings and previous studies presented in Chapter 4, our survey (Chapter 5) showed
that males drink significantly more than their female counterparts. Similarly, in chapter 6, all
interviewees consistently used male pronouns when they referred to or described a drinker. All the
stories shared in the interviews were those of male drinkers. Only one female reported knowing a
drinker personally, the other females who reported knowing drinkers connected this to either their

172
occupation or relaying stories they have heard from male relatives. These included stories of female
victims of violence resulting from male alcohol use.
Although still negligible, a higher prevalence of females in our survey reported lifetime or past 12
months alcohol consumption than in other Iraqi studies. As discussed in Chapter 5, in Iraqi culture
there is an additional hayāʾ (modesty) attached to females that is harder to regain if lost. Due to the
sensitivity of alcohol consumption, it is possible that females felt more comfortable to share their
drinking in a self-reported online survey than in past face-to-face interviews or paper-and-pen
surveys.
As indicated in Chapter 3, culturally, alcohol has been associated with masculinity in Iraq (al-Wardī,
1965; Al Ansari et al., 2019). These findings are in line with research from other non-MMCs which
links alcohol with masculinity (de Visser et al., 2007; Wells et al., 2014). Global trend also indicate
alcohol use and misuse is more prevalent amongst males and that many low and middle income
countries have vast differences in prevalence of male and female consumption (GBD 2016 Alcohol
Collaborators, 2018).
Overestimation or underreporting of student drinking?
In MMCs, alcohol is an extremely sensitive topic. This often results in underreporting of drinking by
study participants as with previous studies in Iraq (Al-Hemiery et al., 2017). Previous literature,
however, indicates that students often overestimate their peer consumption which impacts their own
attitudes and behaviours around alcohol (Kypri et al., 2003). Because this study relies on student self-
reported and estimated data – the findings must be viewed in light of this possible underreporting or
overestimation.
Only one in every 20 participants (5.3%) reported lifetime consumption of alcohol. In contrast, one
in four knew a family member or friend who drinks. On average, students estimated that over a fifth
(21.1%) of students drink alcohol. Similarly, interviewees, some of whom reported never having seen
a drinker, shared that drinking is widespread and increasing. The over-estimation of the consumption

173
of others could be due to a perception, shared in the interviews, that young people are increasingly
adapting to globalised western culture and neglecting religious and traditional values. Among
drinkers, the over-estimation could be because drinkers associate more with other drinkers. Also, as
discussed in Chapter 5, students’ perception of the drinking of others influences their own alcohol
consumption in non-MMCs (Kypri et al., 2003). For this reason, norm-resetting interventions have
been proposed but found to have a small long-term effect in university students in non-MMCs
(Foxcroft et al., 2015). The effect of such interventions in Iraq is unknown, especially as most people
are abstainers. Students are also aware of the sensitivities of reporting alcohol use and may not trust
drinking prevalence figures from self-reported studies.
Risky and harmful behaviour among drinkers
Our study reported a range of alcohol-related harms present among young Iraqis today. These
included domestic and other interpersonal violence as well as impact of drinking on health, driving
and other behaviours. These risks and harms may have severe consequences in a country with limited
security, health, and legal infrastructure.
Domestic violence was one of the main alcohol-related harms reported in the interviews. Other studies
in Iraq also associate domestic violence with excessive alcohol use (Abd Azeez et al., 2016; Abdul
Jabbar, 2007; Khayyat, 1990). Interviewees mentioned that women do not often report domestic
violence related to alcohol so that their children do not become outcasts. We could not identify
services that provide help for domestic violence while mitigating risks to the woman or her children.
Students also shared that alcohol-related violence and socially unacceptable behaviour is common in
the city. One female indicated that women are the main victims of alcohol-related street violence and
harassment. Reports of street violence are consistent with evidence from the early 1960s (al-Wardī,
1965; Zubaida, 2014) and with more recent studies described in Chapter 4, associating drinking with
carrying a weapon and physical fights (Saeed, 2016). The association of alcohol with violent

174
behaviour has been demonstrated in many settings internationally (Graham et al., 2011; WHO,
2006a).
Drink driving has also been previously reported as a risk behaviour in North Iraq (Saeed, 2016;
Shabila et al., 2015). Interview participants reported on this phenomenon, with one sharing a personal
account of attending a car accident site following his friend’s death. Although the 2015 Global
Alcohol Report indicates that the national maximum legal blood alcohol concentration (BAC) for
driving in Iraq is 0.08% (WHO, 2015a), it is not clear that these limits are enforced. WHO (2018b)
has scored the enforcement of drink-driving measures in Iraq at 2/10. For comparison, enforcement
in neighbouring Iran is 7/10 and Australia 8/10. However, there are security checkpoints throughout
the Iraqi capital and between cities, so it is likely that a driver who is visibly drunk may be easily
detected in these checkpoints. We could not identify any generalised use of random breath testing or
any active campaigns against drink driving.
Importance of tailoring measures and priorities to the Iraqi context
Iraq is a MMC with high prevalence of lifetime and past-12 months abstinence. Global evidence
increasingly suggests that the only safe level of consumption is zero (GBD 2016 Alcohol
Collaborators, 2018). Internationally, prevention measures should focus on lowering overall
population-level consumption (GBD 2016 Alcohol Collaborators, 2018). For this reason, public
health measures in Iraq should have three priorities: 1. reduce uptake of alcohol use among non-
drinkers, 2. reduce alcohol consumption among those who drink and 3. reduce alcohol-related harm
among risky drinkers.
Tailoring of interventions and their priorities to the cultural context is important. The perception that
a program is “foreign” may limit the program’s reach. For example, announcing “recommended”
drinking guidelines in a MMC will not be seen positively (Al-Ansari et al., 2020). Such a measure
would be interpreted as intending to encourage alcohol consumption. This is because the predominant
social, religious, and cultural guideline is zero consumption. A more contextually sensitive model is

175
that of neighbouring Iran, where despite the legal limit of zero, recommended guidelines are provided
as part of medical treatment for harm reduction (Al-Ansari et al., 2020). In Iraq, a similar approach
may be implemented where general preventative programs campaign for abstinence, but targeted
harm reduction programs advocate for safer limits in clinical settings.
Alcohol sensitivity in Iraq and other MMCs should be also considered contextually. The topic of
alcohol in MMCs is not necessarily comparable to alcohol in non-MMCs, especially in western
countries where alcohol drinking is culturally accepted and prevalent. A more relevant assessment
would be to compare alcohol sensitivity in MMCs to that of illicit substances such as heroin in non-
MMCs. If one is to contextualise alcohol in this way, the perspectives, stigma, and sensitivity around
alcohol in MMCs become easier to understand. In this light, one can also better empathise with the
opposition of many Iraqis to relaxing alcohol restrictions in Iraq, including on its importation,
production, sale, and consumption. Consequently, programs to prevent uptake or harms from illicit
drug use in non-MMCs may provide relevant learnings for this setting.
An example of a tailored measure is the socio-ecological model (Figure 10) used in the qualitative
analysis. This framework helps contextualise motives for alcohol use in the Iraqi context by
considering the global, national, social, inter-personal and individual circumstances of young Iraqis.
The use of such models throws further light on perceptions and helps inform further tailored
approaches for research, prevention, and intervention.
Prevention approaches
Although interviewees suggested a range of preventative measures including educational, sports and
recreational programs, they perceived parenting as the key factor influencing drinking behaviour in
Iraq. Drinkers known to the interview participants were either away from their family, influenced by
family members who drink, or had lost their loved ones during war or conflict. The survey also
showed that living away from relatives was associated with higher prevalence of alcohol use. As
discussed in Chapter 6, in non-MMCs there is mixed evidence for effectiveness of parental education

176
programs to reduce alcohol misuse in young people (Stockings et al., 2016). For parental education
programs to be successful in Iraq they should consider local traditions, incorporate some religious
material, and be tailored to the local context. Programs could emphasise the religious importance of
parental responsibility and include religious and cultural references with every intervention.
Increasing connectedness is an evidence-based approach to prevent alcohol misuse (Bond et al.,
2007). The program could emphasise the importance of connectedness which is also a key principle
in Iraq’s collective culture (Hofstede, 2020).
In addition to parental interventions, students in the interviews and the survey perceived that
education was a key tool in alcohol prevention. Past literature in non-MMCs indicates that education
about alcohol harms alone has limited influence on alcohol behaviours (Lee et al., 2016). However,
as discussed in Chapter 6, literature from non-MMCs and some MMCs indicate programs that include
social skills training, such as positive youth development programs, may be of some benefit.
Interview participants perceived that young Iraqis who drink have “weak personalities” and are
“imitators”, a reference to imitating other cultures and other young people instead of creating their
own identity. Personal development programs could potentially promote the capacity of young Iraqi
people to make informed decisions and create their own identity. Affective skill-based interventions
have been shown to deter drug use in non-MMCs by improving decision-making skills, self-esteem
and peer-pressure avoidance (Faggiano et al., 2008). The same three factors mentioned by our
interviewees that when inadequate lead to “weakened” personalities and alcohol use.
Preventative programs targeted to young people should contain a mix of traditional and modern
approaches. Tailored faith-based or secular approaches can be evaluated in the Iraqi context – this is
so that religious and non-religious problem drinkers alike can have access to treatment facilities. By
observation and through the interviews, some groups of young Iraqis may not follow guidelines unless
they are religiously mandated. On the other hand, other Iraqis may not follow guidelines if they are
perceived as religiously motivated. For this reason, alcohol should be framed in a way that considers
a mixture of moral, health, and social perspectives.

177
Such a “multi-angled” approach may be best to cater for all youth regardless of their attitudes to
religiosity, secularism, traditionality or liberalism. For example, resilience and importance of keeping
good company could include the use of traditional material and proverbs: “Tell me who your friends
are, and I’ll tell you who you are” and “Where did you learn good manners? From the one that lacks
them.” These proverbs emphasise the importance of good company, but also to learn from “bad
company” for self-development. Such tailored programs may be easier to introduce and promote in
Iraq because they will be culturally relevant while not directly addressing sensitive matters such as
alcohol.
Secular and religious aspects may complement each other. While religious programs may focus on
moral and spiritual harms, secular measures may concentrate on the health and social harms of
drinking. Combined, the measures may be relevant to a larger portion of Iraqis. The importance of
including a health angle, even in conservative settings, is to equip young Iraqis even when they are
away from their conservative home environments. Student interviewees emphasised that many young
people do not drink only because it is socially unaccepted. They shared stories of young Iraqis from
conservative areas who consume alcohol excessively when living or travelling away from their
family.
Screening in a MMC context
An investment in culturally safe prevention, early intervention and treatment facilities would be of
benefit in Iraq. However, to assess the need and function of such programs, research is needed to
identify appropriate and tailored screening and diagnostic tools in MMC contexts.. For example, as
presented in Chapter 2 and 4, the Alcohol Use Disorders Identification Test (AUDIT) and the SDS
(Severity of Dependence Scale) include items that may have a different meaning in a MMC. These
items include guilt about using a substance (item 7) or worry of others about one’s use (item 10). An
AUDIT validity study among UAE prisoners identified that AUDIT was valid as a two-factor model
among Arab Muslims, even though items 7 and 10 had a lower standardised factor loading (0.69)
than most other items (Almarri, Oei, et al., 2009).

178
In our survey, we utilised the AUDIT-C screening tool that focuses only on alcohol consumption
items. This removed the potential for the total score to be inflated because of guilt or concern over
drinking. Despite this, there was discrepancy in the way some students answered questions on alcohol.
Some students stated they “consumed alcohol in the past 12 months” in an earlier question then
answered “never” to the first item on AUDIT-C (frequency of drinking). The students may have
interpreted the first item on AUDIT-C as relating to ongoing or regular drinking. They may have only
had alcohol on one occasion in the past year and see their consumption closer to “never” than other
available options. The internal consistency of the 3-item AUDIT-C in our sample was Cronbach’s α
of 0.70. Although this is below the reliability of the AUDIT-C in an American sample (Barry et al.,
2015), it is higher than the Cronbach’s α reported by Al Mousawi (2015) for the full 10-item AUDIT.
Discrepancies on meaning may also impact qualitative results, legal proceedings, and clinical
interviews from the region. For example, in the interviews, students described drinkers as
“alcoholics”, “addicts” or “intoxicated people”. Upon deeper enquiry, students shared that drinkers
in Iraq normally drink excessively and are referred to by these labels.
Such results indicate that without further research and validation of screening and diagnostic tools,
much data generated from the region may not be accurate enough to inform interventions and policy.
Treatment and harm-reduction
Treatment programs in Iraq could utilise evidence-based approaches such as Alcohol Anonymous’
12-step programs (J. F. Kelly et al., 2020) or alcohol relapse prevention pharmacotherapies. Such
programs can be tailored to the local MMC context, as observed in Iran (Al-Ansari et al., 2020).
However, there are currently limited or no alcohol treatment facilities available in Iraq, especially
outside Baghdad (Al Ansari et al., 2019). In Basra, the first rehabilitation facility with 40 beds,
targeted at drug users, was built in 2018 (Ruptly, 2018). Even in MMCs with alcohol treatment
services, sensitivity of alcohol makes providing accessible treatment difficult (Al-Ansari et al., 2020).

179
Religious establishments may encourage treatment seeking. A fatwa in Iran, for example, ensures no
punishment is given to an individual if they seek treatment to stop their consumption – a step that
may likely expand access to alcohol and substance treatment in the country (Al-Ansari et al., 2020).
Religious groups may also support participants through post-treatment social reintegration programs
aimed at re-establishing the ex-drinker’s connection to their family and community. This is likely to
be important given the role of connectedness as a protective factor against youth drinking (Bond et
al., 2007).
Sin, stigma, and punishment
As previously discussed, alcohol in Iraq is mainly viewed from a moral rather than a health
perspective. Chapter 3, for example, presented that alcohol in the Islamic tradition is viewed as the
gateway to other sins and immoralities. This is because in Islamic ethics, the mind is an important
moral compass - and so when intoxicated or addicted, one risks falling into actions that one would
otherwise avoid (Dastghaib Shirazi, 1998; Rizvi; Yaseen et al., 2017). Similarly, from a health-
centred viewpoint, alcohol is increasingly being identified as a gateway drug, leading to the
consumption of other substances (Barry et al., 2016; Kirby et al., 2012).
As presented in Chapter 3, public consumption and intoxication of alcohol has been illegal in Iraq
since 1994. However, anecdotally, alcohol seems to be more socially than legally regulated.
Interviewees did not share any accounts of punitive deterrence taking place in Iraq and only a minority
of survey respondents favoured the approach of physical punishment for drinkers.
Students from both the survey and the interviews reported avoidance as a likely reaction to a drinker.
Student interviewees reported that a drinker becomes “manbūẓ” (outcast) at university. Some Islamic
teachings, presented in Chapters 3 and 5, encourage abstinence through ostracizing of drinkers until
the drinker repents (Dastghaib Shirazi, 1998). Although religious prevention may be effective in this
setting, heightened stigma is a double-edged sword. While isolation may theoretically encourage
turning away from alcohol for reintegration into their social and family community, it may also push

180
the individual into a “rabbit hole”. Once the drinker becomes increasingly isolated from their family
and friends, with their social reputation permanently stained, they may become more attached to their
drinking and form new and more accepting social circles.
This avoidance strategy was especially reported by female interviewees, with several students
emphasising that a female would never speak or be with a person that drinks. One participant added
that avoidance of drinkers by females was not exclusive to Muslim girls.
In Basra, where alcohol is prohibited, drug use is on the rise and prison cells are reportedly crammed
with substance users (Rubin, 2019). More than 1000 people are reportedly arrested each year for
substance use or trade (Rubin, 2019). Although news reports speak of illicit drug and
methamphetamine users, anecdotally, alcohol users may also be prosecuted. Criminalisation of
substance use in non-MMCs has been shown to be largely ineffective in curbing substance misuse
(Hall, 2018). Although there are some Islamic traditions that speak of physical punishments for public
drinking or intoxication as a social deterrent, these traditions forbid personal insults directed at the
drinker (Yaseen et al., 2017) and are seldom carried out (Al Ansari et al., 2019)
Limitations
Limitations for each component of this thesis have been discussed in chapters 3-6. In this section we
discuss limitations which are relevant to this research as a whole. As mentioned in the introduction
to Chapter 4, most studies included in the scoping review were published after we set out on this
research. Although care is given to reference peer-reviewed literature where available, the scarcity of
data meant that media reports, observational and anecdotal data were also consulted in the socio-
historical review (Chapter 3) and in this discussion (Chapter 7).
The sample for the quantitative online survey was not able to be randomly selected and so may not
be representative. Most students were from the medical faculty because that is where recruitment was
targeted. Also, because anecdotally, medical students are more versed in using the internet for non-
social media purposes. The survey length was around 20 minutes. There was a high attrition rate from

181
about the half-way point of the survey. As this is the first paper attempting to record data online
anonymously, there was no past academic literature to use as a guide for optimal length. The piloting
and consultation of the survey did not alert us to this potential issue. Because of the need for
anonymity, we could not follow-up with students with incomplete responses. Future surveys may
consider shortening the time of the survey to a maximum of 10 minutes.
In the interviews, because of sensitivities, we intentionally did not record detailed demographic
information of participants. This meant that we were unable to identify which sector of Iraqi society
participants belonged to. There were 10 rejections from female participants compared to only two
from males. Female participants were more likely to accept if recruited by university staff as opposed
to the interviewee or students assigned by the faculty to assist him. Social conventions prevented the
male interviewee from talking with all participating females in a setting where others could not
overhear the interview. Despite these limitations, almost half (45%) of the interviewees were females.
To ensure greater confidentiality in the interviews, future research should employ both a male and
female interviewer in the Iraqi setting.
As identified in chapter 6, as a researcher I am both an insider and outsider to the young MMC
population being studied. This may have helped me more accurately interpret implied meanings.
However, it may also have made the participants afraid of judgement and so they may have held back
from sharing their thoughts. I did introduce myself as a researcher from Australia and so, interviewees
may have felt more comfortable expressing their opinions. On the other hand, they may have tried to
ensure a correct image of Iraq is represented to the outside world. Despite my Muslim name, being
Australian-Iraqi meant that it was unknown if I was conservative or liberal towards alcohol. In either
case, my personal demographics and characteristics may have impacted their evaluation of what to
share.
Future directions
There is insufficient data to assess change of consumption prevalence since the pre-2003 Second Gulf
War era. However, the local context and the motives for drinking have certainly shifted. The post-

182
2003 era provided opportunities for both traditional conservatism and globalism to become
mainstream. With the absence of a powerful central government, the debate about alcohol, like
debates about other sensitive topics, may not lay to rest. However, if there were an increase in
prevalence of alcohol use or misuse, the added disease burden would pose a challenge for Iraq’s
limited health system. Because the prevalence of abstinence is high in Iraq, the most evidence-based
and practical approach would be to strive to maintain this low prevalence of consumption which
reduces the prospects of increased alcohol burden in Iraq. A mix of religious and secular preventative
measures, such as contextually tailored skill-based personal development programs, may be utilised
to this end. Improvements in infrastructure to support the implementation of WHO’s “best buys” such
as excise sale taxes, restriction of physical availability of alcohol and restrictions on alcohol exposure
in all types of media is important in the current socio-cultural environment.
Regardless of the policy approach to alcohol, clear regulatory guidelines need to be in place to ensure
that minorities and others who choose to drink have a lower risk of harm to themselves and others.
This may include enforcement of policies on drink driving, alcohol licensing, underage sales, and
hours of operation. Students shared, quantitatively and qualitatively, the society’s negative and
unforgiving view towards drinkers. Because of this, a re-integration program would also be key to
help people out of their alcohol-related problems and to connect back to their family and community.
This may require a re-calculated approach and advice by religious authorities to ensure that stigma
does not drive young drinkers into further social and health problems.
Iraqis are still living in an evolving period of conflict, unrest, and lack of essential needs. This
situation may impact their focus on mental and psychological wellbeing. The full extent of the impact
of war and its resulting psycho-social effects will likely not be realised until Iraq approaches some
sort of normality.
Because of increasing number of young Iraqis and the evolving nature of Iraqi society today, there is
a need for ongoing research. Such research should employ culturally sensitive methods that ensure
the confidentiality and anonymity of responders. Given the lack of existing infrastructure and the

183
priorities of local health agencies, the implementation of evidence-based prevention, early
intervention and treatment programs would be challenging. There is a need for research to inform
these processes, and international support from WHO and other agencies to help the overstretched
Iraqi health authorities implement those findings.
Conclusion
Alcohol has been present in Iraq for all recorded history. Over the years various views of alcohol
have been dominant in Iraq and, as seen in this study, attitudes continue to evolve. In today’s Iraq,
Islamic prohibition and its resulting social and cultural stigma have ensured that prevalence of alcohol
consumption remains low. However, given the social, political, and economic unrest in Iraq, these
protective factors may not translate to a continuity of the current pattern of clear majority abstinence.
These factors also do not ensure harm reduction for drinkers in Iraq, who reportedly often drink for
coping purposes and experience alcohol use disorders, including dependence at a higher rate than
many in other countries.
The absence of a clear alcohol policy and strategy in Iraq is worrying. However, it also provides an
opportunity for Iraq to draft new, clear, and consistent policies. These policies should consider Iraq’s
traditional culture, minority groups, as well as secular evidence-based and religious approaches that
relate to the lived experiences of its youthful population. The strategies would ideally maintain
abstinence, prevent alcohol misuse, and provide harm reduction and treatment opportunities for
harmful or dependent drinkers.
Breaking down barriers to targeted and open research among at-risk populations, such as this study,
will ensure more knowledge generation about lived experiences of Iraqis. This will assist in tailoring
preventative, therapeutic and harm reduction measures to the subgroups where they are most needed.

184
References
Abd Azeez, J., et al. (2016). The Extent Exposed of Rural Woman to Domestic Violence in Some
Villages in Diyala Governorate Al-Fatih journal, 12(67), 175-187.
Abdul Jabbar, M. A. (2007). The Prevalence of Violence among a Group of Married Women
Attending Two Teaching Hospitals in Baghdad. The New Iraqi Journal of Medicine, 3(1), 8-
13.
Abdulah, D. M., et al. (2018). Sleep Disorders as Primary and Secondary Factors in Relation with
Daily Functioning in Medical Students. Annals of Saudi Medicine, 38(1), 57-64.
doi:10.5144/0256-4947.2018.57
Abedalla, R. W., et al. (2014). Accessing Information Technology-Social Media in Iraq. International
Journal of Scientific and Research Publications, 4(9).
ABS. (2016). 2016 Census Quickstats Country of Birth: Iraq. Canberra.
https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/4
204_036
AIHW. (2020). Alcohol, Tobacco & Other Drugs in Australia. Canberra.
https://www.aihw.gov.au/reports/alcohol/alcohol-tobacco-other-drugs-australia
Al-Ameri, R., et al. (2016). Prevalence of Alcohol Consumption among University Students in
Baghdad: A Cross-Section Survey from Iraq. Epidemiology Biostatistics and Public Health,
13(4), 8. doi:10.2427/11942
Al-Ansari, B., et al. (2020). Alcohol Treatment Systems in Muslim Majority Countries: Case Study
of Alcohol Treatment Policy in Iran. The International journal of drug policy, 80.
doi:10.1016/j.drugpo.2020.102753
Al-Ansari, B., et al. (2015). Extent of Alcohol Prohibition in Civil Policy in Muslim Majority
Countries: The Impact of Globalization. Addiction, 111(10), 1703-1713.
doi:10.1111/add.13159
Al-Ansari, B., et al. (2019). Alcohol Policy in Iran: Policy Content Analysis. International Journal
of Drug Policy. doi:https://doi.org/10.1016/j.drugpo.2019.07.032
Al-Awwad, A. M. A. W., et al. (2017). Dawr Ḍarībat Al-Mabyaʿāt Fi Tamwīl Al-Muwāzana Al-ʿama
Lil-Dawla [the Role of Sales Tax in Funding State Budget]. [ دور ضريبة المبيعات في تمويل الموازنة
.The Iraqi Journal of Managerial Sciences, 13(54), 81-103 .[العامة للدولة
Al-Diwan, J., et al. (2015). Alcohol and Drug Abuse in Post-Conflict Iraq. Paper presented at the
European Psychiatry. http://www.sciencedirect.com/science/article/pii/S0924933815310804
Al-Hasnawi, S. (2006). Attitude of Residents and General Practitioners toward Substance Abuse in
Iraq. Medical Journal of Babylon, 3(1-2), 107-112.
Al-Hasnawi, S., et al. (2007). Public Attitudes toward Substance Abuse. Karbala Medical Journal,
1(2), 162-166.
Al-Hemiary, N., et al. (2014). Drug and Alcohol Use in Iraq: Findings of the Inaugural Iraqi
Community Epidemiological Workgroup. Substance Use and Misuse, 49(13), 1759-1763.
doi:10.3109/10826084.2014.913633
Al-Hemiary, N., et al. (2015a). Alcohol and Drug Abuse in Post-Conflict Iraq Journal of the Faculty
of Medicine 57(4), 291-295.
Al-Hemiary, N., et al. (2015b). Alcohol and Drug Abuse in Post-Conflict Iraq. Journal of the Faculty
of Medicine, Baghdad, 57(4), 290-294.
Al-Hemiery, N., et al. (2017). Self-Reported Substance Use in Iraq: Findings from the Iraqi National
Household Survey of Alcohol and Drug Use, 2014. Addiction, 112(8), 1470-1479.
doi:10.1111/add.13800
Qānūn Wāridāt Al-Baladiyyāt [Municipal Revenue Law], (2016).
Al-Imam, A., et al. (2017). Knowledge and (Ab)Use in Connection with Novel Psychoactive
Substances: A Cross-Sectional Analysis of Iraqi Medical Students. Global Journal of Health
Science, 9(11), 61.
Al-Kirmalī, A. M. (1919). Khilaṣat Tārīkh Al-ʿirāq: Hindawi.

185
Al-Qazzaz, M. A., et al. (2017). Evaluation of Alcohol Concentrations in Samples Referred to the
Forensic Laboratory in Baghdad. Egyptian Journal of Forensic Sciences, 7(1), 27.
doi:10.1186/s41935-017-0023-9
al-Wardī, ʿ . (1965). Dirāsah Fī Ṭabīᶜat Al-Mujtamaᶜ Al-ᶜirāqī [a Study on the Nature of Iraqi Society].
Baghdād: Dār al-Warāq.
Al Ansari, M., et al. (2019). Alcohol: From Mesopotamia to Modern Iraq. Journal of Ethnicity in
Substance Abuse, 1-23. doi:10.1080/15332640.2019.1657541
Al Ghaferi, H., et al. (2013). Substance Misuse in Arabic Countries: The Need for Published
Research. International Journal of Prevention and Treatment of Substance Use Disorders,
1(1), 7-11.
Al Mousawi, A. (2014). The Prevalence of Smoking among Karbala/Iraq University Students in Iraq
in 2005. Tobacco Use Insights, 7, 9-14. doi:https://dx.doi.org/10.4137/TUI.S12238
Al Mousawi, A. (2015). Alcohol Use Disorder Identification Test Use in Muslim Countries.
International Journal of Prevention and Treatment of Substance Use Disorders, 1(3-4), 79-
92.
Alcohol Public Policy Group. (2010). Alcohol: No Ordinary Commodity – a Summary of the Second
Edition. Addiction, 105(5), 769-779. doi:10.1111/j.1360-0443.2010.02945.x
Alhasnawi, S., et al. (2009). The Prevalence and Correlates of Dsm-Iv Disorders in the Iraq Mental
Health Survey (Imhs). World Psychiatry, 8(2), 97-109.
Ali, M. (2014). Perspectives on Drug Addiction in Islamic History and Theology. Religions, 5(3),
912-928.
Ali, S., et al. (2009). Prevalence of Alcohol Use among Medical College Students in Hawler Medical
University. Zanko Journal of Medical Sciences, 13(1), 17-23.
Allen, L. N., et al. (2018). Socioeconomic Status and Alcohol Use in Low- and Lower-Middle Income
Countries: A Systematic Review. Alcohol, 70, 23-31.
doi:https://doi.org/10.1016/j.alcohol.2017.12.002
AlMarri, T. S. K., et al. (2009). Alcohol and Substance Use in the Arabian Gulf Region: A Review.
International Journal of Psychology, 44(3), 222-233. doi:10.1080/00207590801888752
Almarri, T. S. K., et al. (2009). Validation of the Alcohol Use Identification Test in a Prison Sample
Living in the Arabian Gulf Region. Substance Use & Misuse, 44(14), 2001-2013.
doi:10.3109/10826080902848533
Amīn Rayḥānī. (2015). Qalb Al-ʿirāq Raḥalāt Wa Tārīkh. Cairo: Hindawi.
Anderson, P., et al. (2009). Impact of Alcohol Advertising and Media Exposure on Adolescent
Alcohol Use: A Systematic Review of Longitudinal Studies. Alcohol and Alcoholism, 44(3),
229-243. doi:10.1093/alcalc/agn115
AP (Producer). (2017, 22/03/2019). Alcohol Shops Reopen in Mosul. Retrieved from
https://www.youtube.com/watch?v=9NHtzBr081M
Arksey, H., et al. (2005). Scoping Studies: Towards a Methodological Framework. International
Journal of Social Research Methodology, 8(1), 19-32. doi:10.1080/1364557032000119616
Australian Institute of Health and Welfare. (2013). National Drug Strategy Household Survey.
Canberra.
Babor, T. (2010). Alcohol: No Ordinary Commodity: Research and Public Policy. Oxford: Oxford
University Press.
Babor, T. F., et al. (2001). Audit: The Alcohol Use Disorders Identification Test: Guidelines for Use
in Primary Care. Geneva: World Health Organization.
Baker, J. M. A., et al. (2016). Health Risk Behaviors among Male Students in Secondary Schools in
Erbil City. Zanco Journal of Medical Sciences, 20(1), 1199-1205.
Bandiera, L., et al. (2019). Jobs in Iraq: A Primer on Job Creation in the Short-Term. In: World Bank.
Baron-Epel, O., et al. (2015). Alcohol Consumption among Arabs in Israel: A Qualitative Study.
Substance Use & Misuse, 50(2), 268-273. doi:doi:10.3109/10826084.2014.962051
Barry, A. E., et al. (2015). Evaluating the Psychometric Properties of the Audit-C among College
Students. Journal of Substance Use, 20(1), 1-5. doi:10.3109/14659891.2013.856479

186
Barry, A. E., et al. (2016). Prioritizing Alcohol Prevention: Establishing Alcohol as the Gateway Drug
and Linking Age of First Drink with Illicit Drug Use. Journal of School Health, 86(1), 31-38.
doi:10.1111/josh.12351
Bashkin, O. (2012). New Babylonians : A History of Jews in Modern Iraq. Palo Alto, UNITED
STATES: Stanford University Press.
BBC. (2013, 15/05/2013). Baghdad Alcohol Shops Caught in Deadly Attacks. BBC. Retrieved from
http://www.webcitation.org/6c7XeWApj
BBC News Arabic (Producer). (2019). Fīdīū Iḥtisāʾ Ṭifl ʿiraqi Al-Kuḥūl Yuthīr Ḍajja [Video of Iraqi
Child Drinking Alcohol Causes a Stir]. Retrieved from
https://www.youtube.com/watch?v=Ed26gXLs33E
Bo, A., et al. (2018). Parent-Based Interventions on Adolescent Alcohol Use Outcomes: A Systematic
Review and Meta-Analysis. Drug and Alcohol Dependence, 191, 98-109.
doi:https://doi.org/10.1016/j.drugalcdep.2018.05.031
Bolton, P. (2013). Mental Health in Iraq: Issues and Challenges. The Lancet, 381(9870), 879-881.
doi:http://dx.doi.org/10.1016/S0140-6736(13)60637-6
Bond, L., et al. (2007). Social and School Connectedness in Early Secondary School as Predictors of
Late Teenage Substance Use, Mental Health, and Academic Outcomes. Journal of Adolescent
Health, 40(4), 357.e359-357.e318. doi:https://doi.org/10.1016/j.jadohealth.2006.10.013
Bradley, K. A., et al. (1998). The Audit Alcohol Consumption Questions: Reliability, Validity, and
Responsiveness to Change in Older Male Primary Care Patients. Alcoholism: Clinical and
Experimental Research, 22(8), 1842-1849. doi:doi:10.1111/j.1530-0277.1998.tb03991.x
Brinkmann, S. (2013). Qualitative Interviewing. Cary, UNITED STATES: Oxford University Press,
Incorporated.
Bronfenbrenner, U. (1977). Toward an Experimental Ecology of Human Development. American
Psychologist, 32(7), 513-531. doi:10.1037/0003-066X.32.7.513
Browne, T., et al. (2008). How Do Experiences in Iraq Affect Alcohol Use among Male Uk Armed
Forces Personnel? Occupational and Environmental Medicine, 65(9), 628-633.
doi:10.1136/oem.2007.036830
Bryman, A. (2006). Integrating Quantitative and Qualitative Research: How Is It Done? Qualitative
research, 6(1), 97-113.
Bullock, S. (2004). Alcohol, Drugs and Student Lifestyle: A Study of the Attitudes, Beliefs and Use of
Alcohol and Drugs among Swedish University Students: Centrum för socialvetenskaplig
alkohol-och drogforskning (SoRAD).
Bureau for International Narcotics and Law Enforcement Affairs. (2013). Money Laundering and
Financial Crimes Country Database.
Bush, K., et al. (1998). The Audit Alcohol Consumption Questions (Audit-C): An Effective Brief
Screening Test for Problem Drinking. Ambulatory Care Quality Improvement Project
(Acquip). Alcohol Use Disorders Identification Test. Arch Intern Med, 158(16), 1789-1795.
Carter, A. C., et al. (2010, 2010/09//). The College and Noncollege Experience: A Review of the
Factors That Influence Drinking Behavior in Young Adulthood. Journal of Studies on Alcohol
and Drugs, 71(5), 742+. Retrieved from
https://link.gale.com/apps/doc/A237204853/AONE?u=usyd&sid=AONE&xid=69dc40a2
Catalano, R. F., et al. (2019). Positive Youth Development Programs in Low- and Middle-Income
Countries: A Conceptual Framework and Systematic Review of Efficacy. Journal of
Adolescent Health, 65(1), 15-31. doi:https://doi.org/10.1016/j.jadohealth.2019.01.024
Dabbagh, R. (2017). Current Trends of Substance Use in Iraq: Examining Data from the 2014 Iraqi
National Household Survey of Alcohol and Drug Use. (Doctor of Public Health). UCLA, Los
Angeles. Retrieved from https://escholarship.org/uc/item/2ss660kn
Dastghaib Shirazi, S. A. H. (1998). Greater Sins (S. A. H. S. H. Rizvi, Trans. Vol. 1). Mumbai:
Islamic Study Circle.

187
de Goeij, M. C. M., et al. (2015). How Economic Crises Affect Alcohol Consumption and Alcohol-
Related Health Problems: A Realist Systematic Review. Social Science & Medicine, 131, 131-
146. doi:https://doi.org/10.1016/j.socscimed.2015.02.025
de Visser, R. O., et al. (2007). Alcohol Consumption and Masculine Identity among Young Men.
Psychology & Health, 22(5), 595-614. doi:10.1080/14768320600941772
Debell, F., et al. (2014). A Systematic Review of the Comorbidity between Ptsd and Alcohol Misuse.
Social Psychiatry and Psychiatric Epidemiology, 49(9), 1401-1425. doi:10.1007/s00127-014-
0855-7
Degenhardt, L., et al. (2019). Concordance between the Diagnostic Guidelines for Alcohol and
Cannabis Use Disorders in the Draft Icd-11 and Other Classification Systems: Analysis of
Data from the Who's World Mental Health Surveys. Addiction, 114(3), 534-552.
doi:10.1111/add.14482
Dodgson, J. E. (2019). Reflexivity in Qualitative Research. Journal of Human Lactation, 35(2), 220-
222. doi:10.1177/0890334419830990
Dupont, H. J. B. H. M., et al. (2005). Killing Time: Drug and Alcohol Problems among Asylum
Seekers in the Netherlands. International Journal of Drug Policy, 16(1), 27-36.
doi:https://doi.org/10.1016/j.drugpo.2004.06.002
Evered, E. Ö., et al. (2016). A Geopolitics of Drinking: Debating the Place of Alcohol in Early
Republican Turkey. Political Geography, 50, 48-60.
doi:https://doi.org/10.1016/j.polgeo.2015.06.006
Ezard, N. (2012). Substance Use among Populations Displaced by Conflict: A Literature Review.
Disasters, 36(3), 533-557. doi:10.1111/j.1467-7717.2011.01261.x
Faggiano, F., et al. (2008). School-Based Prevention for Illicit Drugs Use: A Systematic Review.
Preventive Medicine, 46(5), 385-396. doi:https://doi.org/10.1016/j.ypmed.2007.11.012
Foxcroft, D. R., et al. (2015). Social Norms Information for Alcohol Misuse in University and College
Students. Cochrane Database of Systematic Reviews(12).
doi:10.1002/14651858.CD006748.pub4
GBD 2016 Alcohol Collaborators. (2018). Alcohol Use and Burden for 195 Countries and Territories,
1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. The Lancet,
392(10152), 1015-1035. doi:10.1016/S0140-6736(18)31310-2
GBD 2016 Risk Factors Collaborators. (2017). Global, Regional, and National Comparative Risk
Assessment of 84 Behavioural, Environmental and Occupational, and Metabolic Risks or
Clusters of Risks, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study
2016. The Lancet, 390(10100), 1345-1422. doi:10.1016/S0140-6736(17)32366-8
Ghandour, L., et al. (2016). Alcohol Consumption in the Arab Region: What Do We Know, Why
Does It Matter, and What Are the Policy Implications for Youth Harm Reduction?
International Journal of Drug Policy, 28, 10-33.
doi:http://dx.doi.org/10.1016/j.drugpo.2015.09.013
Ghandour, L. A., et al. (2009). Lifetime Alcohol Use, Abuse and Dependence among University
Students in Lebanon: Exploring the Role of Religiosity in Different Religious Faiths.
Addiction, 104(6), 940-948. doi:doi:10.1111/j.1360-0443.2009.02575.x
Giusto, A., et al. (2018). A Systematic Review of Interventions Targeting Men's Alcohol Use and
Family Relationships in Low- and Middle-Income Countries. Global Mental Health, 5, e10.
doi:10.1017/gmh.2017.32
Glantz, M. D., et al. (2020). The Epidemiology of Alcohol Use Disorders Cross-Nationally: Findings
from the World Mental Health Surveys. Addictive Behaviors, 102, 106128.
doi:https://doi.org/10.1016/j.addbeh.2019.106128
Goodman, E., et al. (2001). Adolescents' Perceptions of Social Status: Development and Evaluation
of a New Indicator. Pediatrics, 108(2), E31. doi:10.1542/peds.108.2.e31
Graham, K., et al. (2011). The Relationship between Alcohol and Violence: Population, Contextual
and Individual Research Approaches. Drug and Alcohol Review, 30(5), 453-457.
doi:10.1111/j.1465-3362.2011.00340.x

188
Greene, M. C., et al. (2018). Alcohol and Drug Misuse Interventions in Conflict-Affected
Populations. In N. Morina & A. Nickerson (Eds.), Mental Health of Refugee and Conflict-
Affected Populations: Theory, Research and Clinical Practice (pp. 221-241). Cham: Springer.
Gündüz, A., et al. (2019). Social Norms Regarding Alcohol Use and Associated Factors among
University Students in Turkey. Archives of Clinical Psychiatry (São Paulo), 46, 44-49.
Hall, W. (2018). The Future of the International Drug Control System and National Drug
Prohibitions. Addiction, 113(7), 1210-1223. doi:10.1111/add.13941
Hamdieh, M., et al. (2008). Prevalence of Alcohol and Drug Abuse in Young People, 15-35 Year
Old, Living in Tehran, Iran. Pejouhesh, 32(4), 315-319.
Hanish, S. (2009). Christians, Yazidis, and Mandaeans in Iraq: A Survival Issue. Digest of Middle
East Studies, 18(1), 1-16. doi:10.1111/j.1949-3606.2009.tb00104.x
Ḥarb, Ṭ. (2018, 21/04/2018). Al-Baghdādiyyūn Yufaḍilūn Al-ʿaraq Al-ʿirāqī ʿan Al-Mashrūbāt Al-
Rūḥiyya Al-Ūkhrā Fī Al-Niṣf Al-Āwal Min Al-Qirn Al-ʿishrīn. Kitabat. Retrieved from
https://archive.ph/WFXx5
Henkel, D. (2011). Unemployment and Substance Use: A Review of the Literature (1990-2010).
Current Drug Abuse Reviews, 4(1), 4-27.
Hofstede, G. (2020). Country Comparison: Iraq. https://www.hofstede-insights.com/country-
comparison/iraq/
Humphreys, K. (2011) Circles of Recovery: An Interview with Keith Humphreys, Phd/Interviewer:
W. White. Counselor (Vol 12(6)).
IJMES. (2020). Ijmes Translation and Transliteration Guide In: International Journal of Middle East
Studies.
International Monetary Fund. (2017). Iraq: Selected Issues (IMF Country Report No. 17/252).
Washington D.C.
Islam, M. M., et al. (2012). The Reliability of Sensitive Information Provided by Injecting Drug Users
in a Clinical Setting: Clinician-Administered Versus Audio Computer-Assisted Self-
Interviewing (Acasi). AIDS Care, 24(12), 1496-1503. doi:10.1080/09540121.2012.663886
Karam, E., et al. (2007). Alcohol Use among College Students: An International Perspective. Curr
Opin Psychiatry, 20(3), 213-221. doi:10.1097/YCO.0b013e3280fa836c
Karam, E. G., et al. (2004). Alcohol Use among University Students in Lebanon: Prevalence, Trends
and Covariates: The Idrac University Substance Use Monitoring Study (1991 and 1999). Drug
and Alcohol Dependence, 76(3), 273-286.
doi:https://doi.org/10.1016/j.drugalcdep.2004.06.003
Karam, E. G., et al. (2008). Lifetime Prevalence of Mental Disorders in Lebanon: First Onset,
Treatment, and Exposure to War. PLoS Medicine, 5(4), e61.
doi:10.1371/journal.pmed.0050061
Kelly, J. F., et al. (2020). Alcoholics Anonymous and Other 12‐Step Programs for Alcohol Use
Disorder. Cochrane Database of Systematic Reviews(3).
doi:10.1002/14651858.CD012880.pub2
Kelly, T. M., et al. (2009). Brief Screens for Detecting Alcohol Use Disorder among 18-20 year Old
Young Adults in Emergency Departments: Comparing Audit-C, Crafft, Raps4-Qf, Fast, Ruft-
Cut, and Dsm-Iv 2-Item Scale. Addictive Behaviors, 34(8), 668-674.
doi:https://doi.org/10.1016/j.addbeh.2009.03.038
Kennedy, H. (2015). The Prophet and the Age of the Caliphates: The Islamic near East from the Sixth
to the Eleventh Century: Taylor & Francis.
Kessler, R. C., et al. (2004). The World Mental Health (Wmh) Survey Initiative Version of the World
Health Organization (Who) Composite International Diagnostic Interview (Cidi).
International Journal of Methods in Psychiatric Research, 13(2), 93-121.
Khayyat, S. (1990). Honour and Shame: Women in Modern Iraq: Saqi Books.
King, N. (1998). Template Analysis. In G. Symon & C. Cassell (Eds.), Qualitative Methods and
Analysis in Organizational Research: A Practical Guide (pp. 118-134). London: Sage.

189
Kirby, T., et al. (2012). Alcohol as a Gateway Drug: A Study of Us 12th Graders. Journal of School
Health, 82(8), 371-379. doi:10.1111/j.1746-1561.2012.00712.x
Kuntsche, E., et al. (2005). Why Do Young People Drink? A Review of Drinking Motives. Clinical
Psychology Review, 25(7), 841-861. doi:https://doi.org/10.1016/j.cpr.2005.06.002
Kuntsche, E., et al. (2017). Alcohol and Other Substance Use in a Cross-Cultural Perspective. Drug
and Alcohol Review, 36(6), 717-720. doi:doi:10.1111/dar.12625
Kypri, K., et al. (2003). Perceived Social Norms and Their Relation to University Student Drinking.
Journal of Studies on Alcohol, 64(6), 829. doi:10.15288/jsa.2003.64.829
Lee, N. K., et al. (2016). What Works in School-Based Alcohol Education: A Systematic Review.
Health Education Journal, 75(7), 780-798. doi:10.1177/0017896915612227
Levy, B. S., et al. (2013). Adverse Health Consequences of the Iraq War. The Lancet, 381(9870),
949-958. doi:http://dx.doi.org/10.1016/S0140-6736(13)60254-8
Lewis, M. A., et al. (2006). Social Norms Approaches Using Descriptive Drinking Norms Education:
A Review of the Research on Personalized Normative Feedback. Journal of American College
Health, 54(4), 213-218.
Linden-Carmichael, A. N., et al. (2018). Drinking Patterns of College- and Non-College-Attending
Young Adults: Is High-Intensity Drinking Only a College Phenomenon? Substance Use &
Misuse, 53(13), 2157-2164. doi:10.1080/10826084.2018.1461224
Lo, J., et al. (2017). A Systematic Review on Harmful Alcohol Use among Civilian Populations
Affected by Armed Conflict in Low- and Middle-Income Countries. Substance Use & Misuse,
52(11), 1494-1510. doi:10.1080/10826084.2017.1289411
Lobstein, T., et al. (2017). The Commercial Use of Digital Media to Market Alcohol Products: A
Narrative Review. Addiction, 112(S1), 21-27. doi:10.1111/add.13493
Mackinnon, S. P., et al. (2017). Cross-Cultural Comparisons of Drinking Motives in 10 Countries:
Data from the Drinc Project. Drug and Alcohol Review, 36(6), 721-730.
doi:doi:10.1111/dar.12464
Madureira-Lima, J., et al. (2018). Alcohol Control Policies and Alcohol Consumption: An
International Comparison of 167 Countries. Journal of Epidemiology and Community Health,
72(1), 54-60. doi:10.1136/jech-2017-209350
Marr, P. (2018). The Modern History of Iraq (Fourth edition. ed.). Boca Raton, FL: Routledge, an
imprint of Taylor and Francis.
Melki, J. (2010). Media Habits of Mena Youth: A Three-Country Survey. Beirut.
Moher, D., et al. (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The
Prisma Statement. PLoS Medicine, 6(7), e1000097. doi:10.1371/journal.pmed.1000097
Mokdad, A. H., et al. (2016). Health in Times of Uncertainty in the Eastern Mediterranean Region,
1990-2013: A Systematic Analysis for the Global Burden of Disease Study 2013. The Lancet
Global Health, 4(10), e704-e713. doi:10.1016/S2214-109X(16)30168-1
Munn, Z., et al. (2018). What Kind of Systematic Review Should I Conduct? A Proposed Typology
and Guidance for Systematic Reviewers in the Medical and Health Sciences. BMC medical
research methodology, 18(1), 5-5. doi:10.1186/s12874-017-0468-4
NAS news (Producer). (2018). Al-ʿiraq Yuʿīd Intāj Al-Mashrūbāt Al-Kuhūlīyya Al-Waṭanīyya [Iraq
Returns to Producing National Alcoholic Beverages]. Retrieved from
https://www.youtube.com/watch?v=oZciX0GB_1I
Nathan, S., et al. (2019). Qualitative Interviewing. In P. Liamputtong (Ed.), Handbook of Research
Methods in Health Social Sciences (pp. 391-410). Singapore: Springer Singapore.
Office of International Religion Freedom. (2019). 2019 Report on International Religious Freedom:
Iraq.
Peltzer, K., et al. (2016). Heavy Drinking and Social and Health Factors in University Students from
24 Low, Middle Income and Emerging Economy Countries. Community Mental Health
Journal, 52(2), 239-244. doi:10.1007/s10597-015-9925-x
Peters, M. D. J., et al. (2015). Guidance for Conducting Systematic Scoping Reviews. JBI Evidence
Implementation, 13(3).

190
Prins, A., et al. (2003). The Primary Care Ptsd Screen (Pc-Ptsd): Development and Operating
Characteristics. PRIMARY CARE PSYCHIATRY, 9(1), 9-14.
Rahim, T. A. (2010). Rate of Alcohol and Substance Use Disorders among the Journalists in Erbil
City. Arab journal of psychiatry, 21(1), 50-60.
Refaat, A. (2004). Practice and Awareness of Health Risk Behaviour among Egyptian University
Students. Eastern Mediterranean Health Journal, 10(1-2), 72-81.
Ridout, B., et al. (2014). Using Facebook to Deliver a Social Norm Intervention to Reduce Problem
Drinking at University. Drug and Alcohol Review, 33(6), 667-673. doi:10.1111/dar.12141
Rizvi, S. e. A. Alcohol. Tehran: World Organization for Islamic Services.
Roberts, B., et al. (2015). Why Are We Not Doing More for Alcohol Use Disorder among Conflict-
Affected Populations? Addiction, 110(6), 889-890. doi:10.1111/add.12869
Rosentiel, T., et al. (2006). Lebanon’s Muslims: Relatively Secular and Pro-Christian.
https://www.pewresearch.org/2006/07/26/lebanons-muslims-relatively-secular-and-
prochristian/
RT Arabic (Producer). (2011). Al-ʿirāq.. Tijārat Al-Kuḥūl Taḥmil Al-Mawt Libāʾiʿīhā [Iraq.. Alcohol
Trade Carries Death for It’s Sellers]. Retrieved from
https://www.youtube.com/watch?v=4L3y-OYJiFY
Rubin, A. J. (2019, Sept. 14, 2019). Iraq Faces a New Adversary: Crystal Meth. The New York Times.
Retrieved from https://www.nytimes.com/2019/09/14/world/middleeast/iraq-drug-addiction-
meth.html
Ruptly (Producer). (2018). Iraq: Basra Opens Its First Rehabilitation Centre for Drug Addicts.
Retrieved from https://www.youtube.com/watch?v=BOJo0ByC3cw
Sadik, S., et al. (2011). Integrating Mental Health into Primary Health Care in Iraq. Mental health in
family medicine, 8(1), 39-49.
Saeed, H. M. (2016). Assessment of the Health Risk Behavior in Young Adulthood: A School-Based
Health Study in Kirkuk City / Iraq. The Medical Journal of Tikrit University 21(2), 172-181.
Salloum, S. (2016, 02/11/2016). What's Really Behind Iraq's New Alcohol Ban? Al-Monitor.
Retrieved from http://www.webcitation.org/6manwvahQ
Savic, M., et al. (2016). Defining “Drinking Culture”: A Critical Review of Its Meaning and
Connotation in Social Research on Alcohol Problems. Drugs: Education, Prevention and
Policy, 23(4), 270-282. doi:10.3109/09687637.2016.1153602
Schoonenboom, J., et al. (2017). How to Construct A mixed Methods Research Design. Kolner
Zeitschrift fur Soziologie und Sozialpsychologie, 69(Suppl 2), 107-131. doi:10.1007/s11577-
017-0454-1
Shabila, N. P., et al. (2015). Risky Driving Behaviours among Medical Students in Erbil, Iraq. Sultan
Qaboos University Medical Journal, 15(3), e390-e397. doi:10.18295/squmj.2015.15.03.014
Sheehan, D. V., et al. (1998). The Mini-International Neuropsychiatric Interview (Mini): The
Development and Validation of a Structured Diagnostic Psychiatric Interview for Dsm-Iv and
Icd-10. The Journal of clinical psychiatry.
Ṣirāmī, Ḥ., et al. (2013). Barrisi Chahār Dah Taḥqīqāt Shuyūʿ Shināsī Iʿtiyād Dar Īrān [Review of 14
Prevalence Studies of Addiction in Iran]. Quarterly Journal of Research on Addiction, 7(26),
29-52.
Stockings, E., et al. (2016). Prevention, Early Intervention, Harm Reduction, and Treatment of
Substance Use in Young People. The Lancet Psychiatry, 3(3), 280-296.
Sweileh, W. M., et al. (2014). Substance Use Disorders in Arab Countries: Research Activity and
Bibliometric Analysis. Substance Abuse Treatment, Prevention and Policy, 9, 33.
doi:http://dx.doi.org/10.1186/1747-597X-9-33
Tavakol, M., et al. (2011). Making Sense of Cronbach's Alpha. International Journal of Medical
Education, 2, 53-55.
The Republic of Iraq. (2005). Constitution of the Republic of Iraq [English]. The Republic of Iraq
Retrieved from http://www.webcitation.org/6marXWHp7

191
Ultrasawt Editorial Team. (2019, 20/01/2019). Ṭarīq Al-Kuhūl Ilā Al-ʿiraq.. Tijāra Taḥkimuhā
Mīlīshīāt Dīnīya Wa Aḥzāb Sīyāsīa [the Path to Iraq: A Trade Owned by Religious Militias
and Political Parties]. Ultrasawt. Retrieved from https://archive.is/YujYd
UN. (2020). World Economic Situation and Prospects 2020 (9789210046169).
https://www.un.org/development/desa/dpad/publication/world-economic-situation-and-
prospects-2020/
UNDESA. (2013). Definition of Youth. http://www.un.org/esa/socdev/documents/youth/fact-
sheets/youth-definition.pdf
UNDESA. (2017). World Population Prospects: The 2017 Revision, Key Findings and Advance
Tables.
UNHCR. (2018). Situation of Christians in Baghdad.
UNOCHA. (2019). Iraq: Humanitarian Bulletin, November 2019.
US Department of State, et al. (2015). Survey of Substance Abuse in Iraq. Bethesda, MD.
Wallace, K., et al. (2013). An Exploration of the Alcohol Policy Environment in Post-Conflict
Countries. Alcohol and Alcoholism, 49(3), 356-362. doi:10.1093/alcalc/agt142
Wells, S., et al. (2014). Linking Masculinity to Negative Drinking Consequences: The Mediating
Roles of Heavy Episodic Drinking and Alcohol Expectancies. Journal of Studies on Alcohol
and Drugs, 75(3), 510-519. doi:10.15288/jsad.2014.75.510
WHO. (2006a). Interpersonal Violence and Alcohol. Geneva.
http://www.who.int/violence_injury_prevention/violence/world_report/factsheets/pb_violen
cealcohol.pdf?ua=1
WHO. (2006b). Public Health Problems of Alcohol Consumption in the Region. In: WHO Regional
Office for the Eastern Mediterranean.
WHO. (2006c). Youth Violence and Alcohol.
http://www.who.int/violence_injury_prevention/violence/world_report/factsheets/fs_youth.p
df?ua=1
WHO. (2009). Iraq Mental Health Survey 2006/7. Baghdad: World Health Organization.
WHO. (2010a). Atlas of Substance Use Disorders. Country Profile: Iraq.
http://www.who.int/substance_abuse/publications/atlas_report/profiles/iraq.pdf
WHO. (2010b). Estimate of 5-Year Change in Recorded Alcohol Per Capita (15+) Consumption,
2006-2010. Retrieved 11/05/2015
http://gamapserver.who.int/gho/interactive_charts/gisah/consumption_change/atlas.html
WHO. (2014a). Global Status Report on Alcohol and Health. Geneva.
http://www.webcitation.org/6mk3vWQQm
WHO. (2014b). Iraq: Health Profile.
WHO. (2015a). Global Alcohol Report: Iraq.
http://www.who.int/substance_abuse/publications/global_alcohol_report/profiles/irq.pdf?ua
=1
WHO. (2015b). Preventing Youth Violence: An Overview of the Evidence: World Health
Organization.
WHO. (2018a). Global Status Report on Alcohol and Health. Geneva.
WHO. (2018b). Global Status Report on Road Safety 2018. Geneva.
Wicki, M., et al. (2017). Different Drinking Motives, Different Adverse Consequences? Evidence
among Adolescents from 10 European Countries. Drug and Alcohol Review, 36(6), 731-741.
doi:doi:10.1111/dar.12572
Wilk, J. E., et al. (2010). Relationship of Combat Experiences to Alcohol Misuse among U.S. Soldiers
Returning from the Iraq War. Drug and Alcohol Dependence, 108(1–2), 115-121.
doi:10.1016/j.drugalcdep.2009.12.003
Yaacoub, H., et al. (2019). Association of War and Other Factors with Substance Use in a Lebanese
Male Sample. Journal of Drug Issues, 49(1), 106-117. doi:10.1177/0022042618807765
Yaseen, I. H. M., et al. (2017). Addiction Treatment in the Sunnah. Malaysian Journal Of Islamic
Studies (MJIS), 1(1), 14-24.

192
Yassin, N., et al. (2018). “There Is Zero Regulation on the Selling of Alcohol”: The Voice of the
Youth on the Context and Determinants of Alcohol Drinking in Lebanon. Qualitative Health
Research, 28(5), 733-744. doi:10.1177/1049732317750563
Yazbek, J.-C., et al. (2014). Prevalence and Correlates of Alcohol Abuse and Dependence in
Lebanon: Results from the Lebanese Epidemiologic Survey on Alcohol (Lesa). Journal of
Addictive Diseases, 33(3), 221-233. doi:10.1080/10550887.2014.950026
Zubaida, S. (2014). Drink, Meals and Social Boundaries. In J. A. Klein & A. Murcott (Eds.), Food
Consumption in Global Perspective: Essays in the Anthropology of Food in Honour of Jack
Goody (pp. 209-223). London: Palgrave Macmillan UK.

193
Appendices
Appendix 1: Ethics approval

PRISMA 2009 Checklist
Section/topic # Checklist item Reported on page #
TITLE Title 1 Identify the report as a systematic review, meta-analysis, or both. 72 ABSTRACT Structured summary 2 Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria,
participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number.
73
INTRODUCTION Rationale 3 Describe the rationale for the review in the context of what is already known. 75 Objectives 4 Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons,
outcomes, and study design (PICOS). 76
METHODS Protocol and registration 5 Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide
registration information including registration number. N/A
Eligibility criteria 6 Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale.
76-77
Information sources 7 Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched.
77
Search 8 Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated.
77
Study selection 9 State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis).
77-78 (table 3)
Data collection process 10 Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators.
78
Data items 11 List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made.
78
Risk of bias in individual studies
12 Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis.
N/A
Summary measures 13 State the principal summary measures (e.g., risk ratio, difference in means). N/A Synthesis of results 14 Describe the methods of handling data and combining results of studies, if done, including measures of consistency
(e.g., I2) for each meta-analysis. 78
194Appendix 2:

PRISMA 2009 Checklist
Page 1 of 2
Section/topic # Checklist item Reported on page #
Risk of bias across studies 15 Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies).
N/A
Additional analyses 16 Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified.
N/A
RESULTS Study selection 17 Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at
each stage, ideally with a flow diagram. 79 (figure 5)
Study characteristics 18 For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations.
87 (table 4)
Risk of bias within studies 19 Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). N/A Results of individual studies 20 For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each
intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. 88-89 (table 5)
Synthesis of results 21 Present results of each meta-analysis done, including confidence intervals and measures of consistency. N/A Risk of bias across studies 22 Present results of any assessment of risk of bias across studies (see Item 15). N/A Additional analysis 23 Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). N/A DISCUSSION Summary of evidence 24 Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to
key groups (e.g., healthcare providers, users, and policy makers). 90-92
Limitations 25 Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias).
92
Conclusions 26 Provide a general interpretation of the results in the context of other evidence, and implications for future research. 93
FUNDING Funding 27 Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the
systematic review. N/A
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097
For more information, visit: www.prisma-statement.org.
Page 2 of 2
195

196
Appendix 3: Search strategies
Scopus, Web of Science, and Iraqi Academic Scientific Journals (IASJ)
<until 13th of September 2019>
Search terms/strategy:
1. Iraq
2. alcohol* OR substance *use OR drinking
3. 1 and 2

197
Embase
Database: Embase Classic <1947 to 1973>, Embase <1974 to 2019 September 13>
Search Strategy:
--------------------------------------------------------------------------------
1 alcohol liver disease/ or alcohol.mp. or alcohol test kit/ or drug alcohol interaction/ or alcohol
abuse/ or breath alcohol analyzer/ or alcohol abstinence/ or fetal alcohol syndrome/ or alcohol/ or
alcohol withdrawal seizure/ or fatty alcohol/ or alcohol intoxication/ or alcohol rehabilitation/ or
alcohol rapid test/ or alcohol withdrawal syndrome/ or alcohol liver cirrhosis/ or "Alcohol Use
Disorders Identification Test"/ or alcohol consumption/ (565661)
2 alcoholism.mp. or experimental alcoholism/ or alcohol/ or alcoholism/ (351538)
3 substance abuse/ (52528)
4 drinking.mp. or drinking behavior/ or college drinking/ or drinking/ or binge drinking/ or
underage drinking/ (183381)
5 iraq.mp. or Iraq/ (11433)
6 substance misuse.mp. or addiction/ (50595)
7 1 or 2 or 3 or 4 or 6 (789676)
8 5 and 7 (646)
***************************

198
MEDLINE
Database: Ovid MEDLINE(R) ALL <1946 to September 13, 2019>
Search Strategy:
--------------------------------------------------------------------------------
1 Iraq War, 2003-2011/ or Iraq/ or iraq.mp. (9679)
2 Alcohols/ or alcohol.mp. (299510)
3 alcoholism.mp. or Alcoholism/ or Alcohol-Related Disorders/ or Alcohol Drinking/ (137116)
4 Underage Drinking/ or Alcohol Drinking in College/ or Alcohol Drinking/ or Drinking/ or
drinking.mp. or Binge Drinking/ or Drinking Behavior/ (162100)
5 Substance Withdrawal Syndrome/ or Substance Abuse Detection/ or Substance-Related
Disorders/ (116889)
6 substance misuse.mp. (2347)
7 2 or 3 or 4 or 5 or 6 (504931)
8 1 and 7 (470)
***************************

199
PsycINFO
Database: PsycINFO <1806 to September Week 2 2019>
Search Strategy:
--------------------------------------------------------------------------------
1 exp "Alcohol Use Disorder"/ or exp Alcohol Drinking Patterns/ or exp Alcohol Withdrawal/ or
exp Fetal Alcohol Syndrome/ or exp Alcohol Drinking Attitudes/ or exp Blood Alcohol
Concentration/ or exp Alcohol Intoxication/ or exp Alcohol Abuse/ or Alcohol*.mp. or exp Alcohol
Treatment/ (140955)
2 alcoholism.mp. or exp Alcoholism/ (51384)
3 exp Underage Drinking/ or exp Alcohol Drinking Patterns/ or exp Drinking Behavior/ or exp
Alcohol Drinking Attitudes/ or exp Binge Drinking/ or drinking.mp. or exp Social Drinking/
(56616)
4 exp "Substance Use Treatment"/ or exp "Substance Abuse and Addiction Measures"/ or exp
"Substance Use Disorder"/ or exp "Substance Related and Addictive Disorders"/ (139153)
5 substance misuse.mp. (2960)
6 iraq.mp. (4054)
7 1 or 2 or 3 or 4 or 5 (221985)
8 6 and 7 (393)
***************************

You’re invited to participate in this public health survey about the attitudes of Iraqi university students towards alcohol.
The survey is part of a doctoral research project at the University of Sydney, Australia and is completely anonymous and will not record anyinformation that can link back to you, so please answer honestly.
Your participation is voluntary and you can stop at any time.
Are you willing to participate in this study? *
Are you a university student? *
Yes
No
Yes
No
200200
Appendix 4: English survey

What university do you attend? *
University of Baghdad
University of Basra
University of Kufa
University of Babylon
Salahudin University
Hawler Medical University
University of Mustansiriya
University of Misan
University of Thi Qar
University of Wasit
Nahrain University
University of Technology, Iraq
University of Mosul (alternate campus)
University of Diyala
University of Qadisiya
University of Anbar
Other - please specify
201201

Please select your faculty *
What degree are you currently enrolled in? *
Agriculture
Arts
Business
Engineering
Law
Medicine
Nursing
Pharmacy
Science
Other - please specify
*
Bachelors degree
Graduate diploma
Masters degree
PhD - Doctorate degree
Other - please specify
*
202202

How old are you? *
What is your gender? *
What is your relationship status? *
Male
Female
Single
Cohabited (unmarried couple)
Engaged
Married
Divorced
Widowed
Other - please specify
*
203203

What is your religious affiliation? *
What ethnicity do you identify as? (choose all that apply) *
Muslim
Christian
Jew
Mandaean
Yezidi
Agnostic
Athiest
No religious affiliation
Other - please specify
Arab
Kurd
Assyrian
Chaldean
Turkmen
Armenian
Persian
Other - please specify
204204

Imagine that this ladder represents social, economic and educational levels in Iraqi society.
Choose which step you’d place yourself relative to other people in Iraq. *
Step 1Step 2Step 3Step 4Step 5Step 6Step 7Step 8Step 9Step 10
205205

Are you a refugee or internally displaced person? *
Were you a student before becoming a refugee or an internally displaced person?
Are you living away from your home town during semester (study periods)? *
Where do you normally live during semester (study periods)? *
Yes
No
Yes
No
Yes
No
Live alone
At home with parents
At home with partner
Share accommodations with friends and others
University Dorms
Refugee camp/accommodation
Other - please specify
*
206206

Have you ever tried alcohol? *
Have you ever had a full serve of alcohol? (e.g. a glass of wine, a whole nip of spirits, a glass of beer, etc.) *
About what age were you when you had your first full serve of alcohol? *
Have you had an alcoholic drink of any kind in the last 12 months? *
About what age were you when you last had an alcoholic drink? *
AUDIT 1 *
NeverMonthly or
less2-4 times a
month2-3 times a
week4 or more times a
week
How often do you have a drink containingalcohol?
Yes
No
Yes
No
Yes
No
207207

AUDIT 2 *
1 or2 3 or 4 5 or 6 7 or 9 10 or more
How many drinks containing alcohol do you have on a typical day when you aredrinking?
AUDIT 3 *
Never Less than monthly Monthly Weekly Daily or almost daily
How often do you have six or more drinks on one occasion?
AUDIT 4-8
NeverLess thanmonthly Monthly Weekly
Dailyor
almostdaily
How often during the last year have you found that you were not able to stopdrinking once you had started?
How often during the last year have you failed to do what was normally expected ofyou because of drinking?
How often during the last year have you needed a first drink in the morning to getyourself going after a heavy drinking session?
How often during the last year have you had a feeling of guilt or remorse afterdrinking?
How often during the last year have you been unable to remember what happenedthe night before because of your drinking?
208208

AUDIT 9-10
NoYes, but not in the
last yearYes, during the
last year
Have you or someone else been injured because of your drinking?
Has a relative, friend, doctor, or other health care worker been concerned about yourdrinking or suggested you cut down?
Have you consumed alcohol in: *
Yes No
The city you study in
Elsewhere in Iraq
Another country
Where do you drink alcohol? (choose all that apply)
In my own home
At a friend’s house
At a social gathering or party
Hotels/clubs/bars
In public (e.g. parks, roadside)
At university
In a car or other vehicle
Out of town in orchards, farms or farm houses
Other - please specify
*209209

Where do you get your alcohol from? (choose all that apply)
Friend or acquaintance
Brother or sister
Parent
Spouse or partner
Other relative
Steal it
Purchased it myself from a store
Purchase it illegally (black market seller/dealer)
Get stranger to get it (e.g. online)
Produce/make it myself
Other - please specify
*
210210

Who do you drink alcohol with? (choose all that apply)
Which type of alcoholic beverage do you drink? (choose all that apply)
Alone
Parents
Brother or sister
University friends/colleagues
Friends from outside of university
Strangers
Other - please specify
*
Homemade spirits (e.g. araq)
Homemade beer
Homemade wine
Branded wine
Branded beer (e.g. Heineken, Farida, Corona)
Branded spirits (e.g. vodka, brandy, Chivas Regal whisky)
Other - please specify
*
211211

Have you used any of the following substances (for non-medical reasons)? (choose all that apply)
Tobacco
Marijuana/cannabis/hashish
Meth/amphetamines
Cocaine
Ecstasy
Heroin
Benzodiazepines (e.g. Valium, Clonazepam)
Benzhexol (e.g. Artane)
Anti-depressants/anti-psychotics
Pain-killers/Analgesics/Opioids (e.g. Morphine, Codeine)
Inhalants (e.g. paint thinners, glue)
Steroids
None
Other - please specify
*
212212

Do any of your family and/or friends use alcohol? (choose all that apply)
Do any of your family and/or friends use other drugs? (choose all that apply)
What percentage of university students in Iraq do you think use alcohol? *
Parents
Brothers or sisters
Other relatives
University friends
Other friends
None
Parents
Brothers or sisters
Other relatives
University friends
Other friends
None
0% 100%50%
213213

Do you have a desire to try alcohol?
How difficult do you think it would be to get alcohol if a student wanted it? *
Yes
No
I don't know
Very easy
Easy
Difficult
Very difficult
Impossible
214214

Which of these reasons explain why students choose to NOT USE alcohol? *
Often Sometimes Rarely Never
Health reasons (alcohol isn’t good for their health)
One can become addicted to alcohol
They just don’t want to use alcohol
Influence of mass media (e.g. television, satellite channels)
Influence of social media (e.g. fb, instagram, twitter)
They don’t like how alcohol would influence their behaviour
Alcohol is illegal
Religious reasons (alcohol is forbidden/haram)
They are scared of getting caught
Family reasons (family members think that they shouldn’t drink alcohol)
Societal/cultural reasons (broader society frowns upon drinkers)
Friends (friends don't drink alcohol or think badly of drinkers)
It is not available for them to purchase or drink
Alcohol doesn’t taste good
Enter another option
215215

Which of these reasons explain why students choose to USE alcohol? *
Often Sometimes Rarely Never
Alcohol is available and easily accessible
Influence of social media (e.g. fb, instagram, twitter)
Influence of mass media (e.g. television, satellite channels)
Lack of religiosity
As a way to escape trauma, responsibility or stress
Socialising
Friends drink alcohol (peer pressure)
To rebel against traditional values or show that they are 'modern'
Practising their rights as a minority
Family tradition
‘Forbidden things are always tempting’
For fun and entertainment
Boredom
Relaxation
Enter another option
216216

What do you think of the following statements? *
Stronglyagree Agree Disagree
Stronglydisagree
Drinking alcohol is normal for a young student at University
Alcohol is a bigger problem for Iraq than drugs
People who drink alcohol experiment more with drugs than those who do notdrink
Alcohol is not a problem in Iraq
If a young person tries alcohol it is a sign of a much more serious problem
If alcohol becomes available, there’d be an increase in its use
More treatment facilities are needed in Iraq for people with alcohol problems
Alcohol consumption is a moral issue
Alcohol consumption is a medical issue
Alcohol is a common problem in Iraq
What do you think of the following policy options in relation to Iraq? *
Stronglyagree Agree Disagree
Stronglydisagree
Prohibit alcohol entirely including import and consumption
Allow alcohol for production, sale and consumption by non-Muslims
Alcohol trade and import should be banned, but consumption shouldn’t becriminalised
Alcohol should be permitted to decrease black market trade
Severe punishments for people found in possession of alcohol
Permit alcohol production, sale and consumption for everyone
Enter another option
217217

What do you think should happen to a person found to possess a small quantity of alcohol for personal use? *
No action
A warning only
Advice or brief discussion
Referral to seek counselling or treatment
Education about safety and possible harms
A small fine
A large fine
Short detention
Prison sentence
Physical punishment (e.g. lashes)
Other - please specify
*
218218

What do you think should happen to a person found to possess a small quantity of other drugs for personal use? *
No action
A warning only
Advice or brief discussion
Referral to seek counselling or treatment
Education about safety and possible harms
A small fine
A large fine
Short detention
Prison sentence
Physical punishment (e.g. lashes)
Other - please specify
*
219219

What would you do if you found out that someone you know is: *
Askto
joinin
Try topersuade
them not to
Forcethemnot to
Try topersuade
them to gethelp
Reportthem to the
police
Tell theirfamily and
friends
Cut contactwith them
completely
Shamethem
publicly Nothing
About to tryalcohol for the firsttime
Using alcoholdaily
Selling/supplyingalcohol to others
About to try otherdrugs for the firsttime
Using other drugsdaily
Selling/supplyingdrugs to others
Have you had any direct experience of war or violent military conflict? (been in direct contact or close proximity from terrorist attacks and/oractive military action) *
Yes
No
220220

Have you undertaken military training in preparation for combat?
In your life, have you ever had any experience that was so frightening, horrible, or upsetting that, in the past month, you: *
Yes No
Have had nightmares about it or thought about it when you did not want to?
Tried hard not to think about it or went out of your way to avoid situations that reminded you of it?
Were constantly on guard, watchful, or easily startled?
Felt numb or detached from others, activities, or your surroundings?
Yes, mandatory military service
Yes, at a training program at University
Yes, elsewhere with a militia or brigade
Yes, other - please specify
*
No.
221221

Have you seen an alcohol advertising on any of the following media? *
Satellite television
Newspapers or magazines
Hotels/clubs/bars
Billboards or posters
Internet
Social media
Promotional material
Other - please specify
222222

Have been exposed to alcohol images or mentions in these forms of media? If so, how was alcohol portrayed? *
Noexposure
Fashionableor 'cool'
Stylish,sophisticatedor high class
Fun orrelaxing
Bondingfriendships
Addictingor
controlling
Associatedwith deathor disease
Associatedwith crime
Associatedwith
immorality('evil')
Movies
TV Shows
Novels
Social media (fb,Instagram,twitter)
Reality TV
Advertisements
Religious/culturalchannels
Enter another option
223223

How did you find out about this survey?
University eLearning (e.g. Moodle)
University only social media group
Student society or organisation (e.g. IFMSA-Iraq)
Social media (e.g. facebook, twitter)
Family or friends
During university lecture or tutorial
University Staff or Student
Other - please specify
224224

(. رومخلا ) لوحكلا نع نييقارعلا ةعماجلا ةبلط فقوم لوح ةيحص ةيئاصقتسا ةساردب كراشتل كل ةوعد هذه
.قدص لكب بجا اءاجرف كيلا ، ريشت تامولعم يا لجست نلو ةلوهجم كتيوه نوكتس .ايلارتسا يندس , ةعماج يف هاروتكد ثحب عورشم نم ءزج ةساردلا هذه
.تقو يا فقوتلا عيطتستو ةيعوطت كتكراشم
؟ ةساردلا هذه يف ةكراشملاب بغرت له *
؟ يعماج بلاط تنا له *
معن
ال
معن
ال
225
Appendix 5: Arabic survey

؟ سردت ةعماج يأ يف *
دادغب ةعماج
ةرصبلا ةعماج
ةفوكلا ةعماج
لباب ةعماج
نيدلا حالص ةعماج
ةيبطلا رلواه ةعماج
ةيرصنتسملا ةعماج
ناسيم ةعماج
راق يذ ةعماج
طساو ةعماج
نيرهنلا ةعماج
ةيجولونكتلا ةعماجلا
( ليدبلا عقوملا ) لصوملا ةعماج
ىلايد ةعماج
ةيسداق ةعماج
رابنالا ةعماج
؟ ىرخا ةعماج يأ
226

؟ ةيلاتلا تارايخلا نم كتيلك رتخا اءاجر *
؟ سردت ةلحرم يأ يف *
ةعارزلا
بادآلا
داصتقالاو ةرادالا
ةسدنهلا
نوناقلا
بطلا
ضيرمتلا
ةلديصلا
مولعلا
؟ ىرخا ةيلك يأ *
سويرولاكبلا ةلحرم
يلاعلا مولبدلا ةلحرم
ريتسجاملا ةلحرم
هاروتكدلا ةلحرم
؟ ىرخا ةلحرم يأ *
227

؟ كرمع مك *
؟ كسنج وه ام *
؟ ةيعامتجالا كتلاح يه ام *
ركذ
ىثنا
بزعأ
( لبكم ) جاوزلا لبق ةقالع
بوطخم
جوزتم
قلطم
لمرأ
؟ ىرخا ةلاح يأ *
228

؟ كتنايد يه ام *
ملسم
ينارصن
يدوهي
يئباص
يديزيأ
( يردااللا ) ةيتسونغا
دحلم
ينيد ال
؟ رخآ نيد يأ
229

( قبطني ام لك رتخا ( ؟ يقرعلا كلصا وه ام *
يبرع
يدرك
يروشآ
ينادلك
ينامكرت
ينمرأ
يسراف
؟ رخآ لصا يأ
230

يقارعلا عمتجملا يف ةيملعلاو ةيلاملا ةيعامتجالا , تايوتسملا لثمي ملسلا اذه نا روصت
* قارعلا يف نيرخالا سانلل اتبسن ميركلا كصخش عضت ةجرد يا يف رتخا
Step 1Step 2Step 3Step 4Step 5Step 6Step 7Step 8Step 9
Step 10
231

؟ حزان وا ءيجال تنا له *
؟ حزان وا ءيجال نوكت نا لبق بلاط تنك له
؟ يساردلا لصفلا لالخ كتدلب جراخ شيعت تنا له *
؟ يساردلا لصفلا لالخ اتداع شيعت نيأ *
معن
ال
معن
ال
معن
ال
يدرفمب شيعأ
يدلاو عم تيبلاب
يتكيرش عم تيبلاب
نيرخآ وا ءاقدصا عم ةماقالا ناكم كراشأ
يعماجلا نكسلا
نيئجاللا نكس وا ميخم
؟ رخآ نكسم يأ *
232

؟) رومخلا ) لوحكلا لوانت تبرج نا كل قبس له *
( ةريبلا نم ةبلع وا ةيحورلا تابورشملا نم ةفشر ذيبنلا , نم بوك الثم : ( ؟) رومخلا ) لوحكلا نم لماك اساك تلوانت نا كل قبس له *
؟ ةرم لوال رومخلا ) ) لوحكلا نم الماك اساك تلوانت امدنع كرمع ناك مك *
؟ ةيضاملا رهش لا 12 يف يلوحك بورشم يا تلوانت له *
؟ ةرم رخال يلوحك ابورشم تلوانت امدنع كرمع ناك مك *
معن
ال
معن
ال
معن
ال
233

* AUDIT 1
برشا ال ادبا
ايرهشلقاو
يف تارم ىلا 4 2رهشلا
يف تارم ثالث ىلا نيترم عوبسالا
يف رثكا وا تارم 4عوبسالا
يوتحت يتلا تابورشملل كلوانت لدعم وه ام ؟ لوحكلا ىلع
* AUDIT 2
وا 2 وا 14 وا 36 وا 59 رثكا7,8 وا 10
؟ هيف برشت يذلا مويلا يف ةداع لوانتت ةيلوحكلا تابورشملا نم بوك مك
* AUDIT 3
ادبا كلذ لعفا رهشلاال يف ةرم نم ايمويايعوبساايرهشلقا ابيرقت وا ايموي
؟ ةدحاو ةبسانم يف رثكا وا باوكا ةتيل كلوانت لدعم وه ام
AUDIT 3-8
لصحي مل ادبا يل كلذ
ةرم نم لقا رهشلا ايعوبساايرهشيف
ايمويواابيرقتايموي
؟ فقوتلا عيطتست كناف ال برشلاب ادبت ىتم كنا تدجو مك يضاملا ماعلا لالخ عقوتم وه امب مايقلا نم نكمتت مل برشلا ببسبو كنا تدجو مك يضاملا ماعلا لالخ
؟ كنمعارشلا نم نكمتت يكل حابصلا يف بورشم ىلا جاتحت تنك مك يضاملا ماعلا لالخ
؟ برشلا نم اهيف ترثكا ةسلج دعب كراهب ؟ برشلا دعب مدنلا وا بنذلاب ترعش كنا لصح مك يضاملا ماعلا لالخ
كنال ةقباسلا ةليللا يف لصح ام ركذت نم نكمتت مل كنا لصح مك يضاملا ماعلا لالخ ؟ برشت تنك
234

AUDIT 9-10
الكيف سيل نكل معن و
ةيضاملا ةنسلا لالخ معن ةيضاملا ةنسلا
؟ بورشملل كلوانت ببسب ةباصال رخا صخش وا تنا تضرعت نا لصح له كيدل برشلا ةداع هاجت اقلق يحص فظوم وا بيبط يا وا ءاقدصالا وا ءابرقالا دحا ىدبا نا قبس له
؟ برشلا نم ليلقتلا مهدحا كيلع حرتقا له وا
يف رومخلا ) ) لوحكلا تلوانت له *
المعن
اهيف نكست يتلا ةنيدملا قارعلا يف رخا ناكم
ىرخا ةلود
235

( قبطني ام لك رتخا ( ؟) رومخلا ) لوحكلا لوانتت نيا
يتيب يف
يقيدص تيب يف
ةلفح وا يعامنجا عمجت يف
تاناحلاو يهالملاوا قدانفلا يف
( كرابلا وا عراشلا الثم ) ماع ناكم يف
ةعماجلا يف
ىرخا ةبكرم وا ةرايسلا يف
تاحارتسالا وا عرازملا نيتاسبلا , يف ةنيدملا نم خراخ
؟ رخآ ناكم يا *
236

( قبطني ام لك رتخا ( ؟) رومخلا ) يلوحكلا بارشلا ىلع لصحت نيا نم
فراعملا وا ءاقدصالا نم
يتخا وا يخا نم
يما وا يبا نم
يكيرش وا يجوز نم
نيرخالا يبراقا نم
هقرسا
قاوسالا نم هيرتشا
( ءادوسلا قاوسالا ) ةينوناق ريغ ةقيرطب هيرتشا
( تينرتنالا ربع الثم ) بيرغ صخش نم
هعنصا انا
؟ رخا صخش يا *
237

( قبطني ام لك رتخا ( ؟) رومخلا ) يلوحكلا بارشلا لوانتت نم عم
( قبطني ام لك رتخا ( ؟ اهلوانتت يتلا رومخلا ) ) ةيلوحكلا تابورشملا عاونارنخا
يدرفمب
يما وا يبا عم
يتخا وا يخا عم
ةعماجلا نم يئاقدصا عم
ةعماجلا جراخ نم يئاقدصا عم
ءابرغلا عم
؟ رخآ صخش يا *
تيبلا يف ةعونصملا ةيحورلا ) ) ةرطقملا تابورشملا
تيبلا يف ةعونصم ةريب
تيبلا يف عونصم ذيبن
تاكرش لبق نم ردصملا ذيبنلا
( نيكينياه وا انوروم ةديرف , الثم ) تاكرش لبق نم ةردصملا ةريب
( زافيشت يكسو , اكرف , الثم ) تاكرش نم ةردصملا ةيحورلا ) ) ةرطقملا تابورشملا
؟ رخآ عون يا *
238

( قبطني ام لك رتخا ( ؟) ةيجالع وا ةيبط ريغ بابسال ) ةيتالا داوملا نم يا تلوانت له
( راجيسلا ) غبتلا
( سبيناكاناورام ) شيشحلا
"( نمتلا " لاتسيركلا ) نيماتيفمثيملا
نيياكوكلا
(MDMA بحلا ) يساتسكا
نيوريهلا
( مابيزانولك مويلاف , ) نيبازايدوزنيب
( نياترا ) لوسكيزنيب
ةيبصعلا تاداضمو بائتكالا تاداضم ءاود
( نيفروملا نييادوكلا , ) ملالا تانكسم ةينويفألا , داوملا ةيودا
( قساللا وا غبصلا ) تاقشنتسملا
( زديوريتس ) تاطشنملا
( تاطشنم / تاردخم ) ىرخا داوم يا مدختسا ال
؟ ىرخا داوم يا *
239

( قبطني ام لك رتخا ( ؟) رومخلا ) لوحكلا نولوانتي كئاقدصاوا كتلئاع نم يا له
( قبطني ام لك رتخا ( ؟ ) تاطشنم / تاردخم ) ىرخالا داوملا نولوانتي كئاقدصاوا كتلئاع نم يا له
* قارعلا ؟ يف رومخلا ) ) لوحكلا نولوانتي يذلا نييعماجلا ةبلطلا ةبسن ام
يما وا يبا
يتخا وا يخا
يتلئاع نم نيرخا
ةعماجلا نم يئاقدصا
نيرخالا يئاقدصا
يئاقدصا وا يتلئاع نم دحا ال
يما وا يبا
يتخا وا يخا
يتلئاع نم نيرخا
ةعماجلا نم يئاقدصا
نيرخالا يئاقدصا
يئاقدصا وا يتلئاع نم دحا ال
0% 100%50%
240

؟) رومخلا ) لوحكلا لوانت برجت نا ةبغر كل له
* كلذ ؟ دارا اذا بلاطلا لبق نم رومخلا ) ) يلوحكلا بورشملا ىلع لوصحلا ةبوعص ىدم ام
معن
ال
يردا ال
ادج لهس
لهس
بعص
ادج بعص
ليحتسم
241

* رومخلا ) ) لوحكلا برش مدع ىلع بالطلا زفحت يتلا ةيلاتلا بابسالا نع كيأر وه ام
ادبأاردانانايحأابلاغ
( مهتحص رضي رمخلا ) ) لوحكلا ) ةيحص بابسا ( رمخلا ) لوحكلا ىلع داتعي نا نكمم صخشلا
( رمخلا ) لوحكلا مادختسا نوديري مه ال ( تايئاضفلا نويزفلتلا ، الثم ) ماعلا مالعالا ريثأت
( رتيوت مارغتسنا ، كوبسيف ، الثم ) يعامتجالا لصاوتلا عقاوم ريثأت مهتافرصت ىلع رمخلا ) ) لوحكلا ريثأت نوبحي مه ال
اينوناق عونمم رمخلا ) ) لوحكلا( اعرش مرحم رمخلا ) ) لوحكلا ) ةينيد بابسا ( رمخلا ) لوحكلل مهبرش فشكي نا نوشخي
(( رمخلا ) لوحكلا نوبرشي الا مهل يغبني نا نودقتعي ةلئاعلا ءاضعا ) ةيلئاع بابسا (( رمخلا ) لوحكلا يبراش هركي ماعلا عمتجملا ) ةيفاقثو ةيعامتجا بابسا
(( رمخلا ) لوحكلا يبراش وحن ءوسب نوركفي مهؤاقدصا ) ءاقدصالاهويرشي وا هورتشيل مهل ديلا لوانتمب سيل رمخلا ) ) لوحكلا
ديج سيل رمخلا ) ) لوحكلا معط
Enter another option
242

* رومخلا ) ) لوحكلا برش ىلع بالطلا زفحت يتلا ةيلاتلا بابسالا نع كيأر وه ام
ادبأاردانانايحأابلاغ
ةلوهسب هيلا لوصولا نكممو لوادتم رمخلا ( رتيوت مارغتسنا ، كوبسيف ، الثم ) يعامتجالا لصاوتلا عقاوم ريثأت
( تايئاضفلا نويزفلتلا ، الثم ) ماعلا مالعالا ريثأت نيدلا ةلق
قلقلا وا ةيلوؤسملا وا ىذألا لثم عقاولا نم بورهلل ةقيرط ةيعامتجالا ةرشاعملل
( نارقالا طغض ) نوبرشي مهئاقدصا نال " نويرصع " مهنا راهظاو ةيديلقتلا ميقلا ىلع ةروثلل
تايلقاك مهقوقح ةسراممل يلئاع ديلقت
ةيرغم امئاد ةعونمملا ءايشالا هيفرتلاو ةعتملل
للملا نم ةحارلل
Enter another option
243

* ؟ ةيلاتلا تارابعلاب كيأر ام
ةوقب ةوقبضراعمقفاومقفاوم ضراعم
يعماجلا باشلا بلاطلل يعيبط رمخلا برش قارعلا يف تاردخملا نم ربكا ةلكشم رمخلا
هيبراش مدع نم رثكا ىرخالا تاردخملا نوبرجي رمخلا يبراش قارعلا هجاوت ةلكشم سيل رمخلا
ربكا ةلكشم هدنع باشلا نا ةمالعرمخلل باشلا ةبرجت همادختسا رثك رمخلا لوادت اذا
رمخلا عم لكاشملا يوذل رثكا ةجلاعم قفارمل جاتحي قارعلا يقالخا رمأ رمخلا برش عوضوم
يبط رمأ رمخلا برش عوضوم قارعلاب ةعئاش ةلكشم رمخلا
* قارعلل ؟ ةبسنلاب ةيلاتلا تاسايسلاب كيأر ام
ةوقب ةوقبضراعمقفاومقفاوم ضراعم
همادختسا وا هداريتسا ىتح اتاتب رمخلا عنم نيملسملا ريغل همادختساو هعيبو رمخلا ةعانصب حامسلا
لوحكلا كالهتسا ميرجت يغبني نكلو ال عنمت نا بجي هداريتساو رمخلاب ةرجاتملا ءادوسلا قوسلا يف تالماعتلا ليلقتل لوحكلل حامسلا يغبني لوحكلا ةزايح عم اودجو نيذلا صاخشألل ةمراص تابوقع عيمجلل هعيبو هكالهتساو رمخلا ) ) لوحكلا جاتناب حامسلا
Enter another option
244

* يصخشلا ؟ لامعتسالل لوحكلا نم اليلق هدنع دجو يذلا صخشلل لعفي نا بجي اذام كيأرب
ءيش يأ هل لعفي ال
طقف رذحي نا بجي
اليلق شقاني وا حصني
مزاللا جالعلا وأ هروشملا بلطل لاحي
هلمتحملا رارضا همالسلا و لوح هتيعوت
هريغص همارغب مرغي
هريبك همارغب مرغي
ةريغص ةدمل زجحي
نجسلاب مكحي
( طوصلاب برضي دلجي - الثم ) ايدسج بقاعي رزعي -
؟ رخآ ءيش يأ *
245

* ؟ يصخشلا لامعتسالل تاطشنملا ) / تاردخملا ) ىرخالا داوملا نم اليلق هدنع دجو يذلا صخشلل لعفي نا بجي اذام كيأرب
ءيش يأ هل لعفي ال
طقف رذحي نا بجي
اليلق شقاني وا حصني
مزاللا جالعلا وأ هروشملا بلطل لاحي
لوحكلل هلمتحملا رارضا همالسلا و لوح هتيعوت
هريغص همارغب مرغي
هريبك همارغب مرغي
ةريغص ةدمل زجحي
نجسلاب مكحي
( طوصلاب برضي دلجي - الثم ) ايدسج بقاعي رزعي -
رخآ ءيش يأ *
246

* هفرعت : صخش ناب كل نيبت اذا لعفتس اذام
بلطتمهنمقاحتلالأ
مهب
نأ لواحت نأب مهحصنت
اولعفي ال
مهربجتنأب ال
اولعفي
نأ لواحت نأب مهحصنت
ةدعاسم اوبلطي
غلبتمهنعةطرشلا
ربختمهلئاوع و
مهئقدصأ
يأ عطقت لاصتامهعم
مهريعتانلع
اللعفتيأئيش
لوأل لوحكلا برجي نأ كشو ىلع ةرم
ايموي لوحكلا برشي نيرخآلل رمخلا يطعي عيبي /
داوملا برجي نأ كشو ىلع ( تاطشنملا / تاردخملا ) ىرخألا
ىلوألا ةرملل ىرخألا داوملا برشي
ايموي تاطشنملا ) / تاردخملا )
ىرخألا داوملا يطعي عيبي /نيرخآلل تاطشنملا ) / تاردخملا )
ةيركسعلا تايلمعلا نم وأ يباهرا موجه نم بيرق وأ رشابم لاصتا يف تنك له ( ؟ فينعلا يركسعلا عارصلا وأ برحلا عم ةرشابم ةبرجت يأ كيدل ناك له * ةلاعفلا )
معن
ال
247

؟ لاتقلل دادعتسالل يركسع بيردت يأ تذختا له
* نأ : يضاملا رهشلا يف كتلعج ثيحب ةجعزم ، وأ ةبيهر ةفيخم ، ةبرجت يأب كتايح يف تررم له
المعن
؟ اهركذت نأ ديرت كنا ال نيح يف اهب ركفت تنك اهلوح و سيباوك كيدل تناك ؟ اهب كركذت يتلا فقاوملا بنجتت يك فولؤملا كقيرط نع تجرخ وأ اهركذت نأب ال ةوقب تلواح
؟ ةلوهسب شهدنت قرأ و كيدل رمتسم ، لكشب رذح ىلع تنك ؟ كطيحم نع وأ ةطشنألا ، نع نيرخآلا ، نع لزعمب وأ ردخلاب رعشت تنك
ةيمازلالا ةيركسعلا ةمدخلا يف معن ،
ةعماجلاب يبيردت جمانرب يف معن ،
رخآ ءاول يأ وأ تايشيلملا عم معن ،
(: هعون نييعت ءاجرلا ) رخآ ناكم يف نكلو معن ، *
طق ايركسع بردتا مل ال
248

* ةيلاتلا ؟ ةيمالعالا لئاسولا نم يا يف لوحكلا نع ةياعد يأ تدهاش له
* احورطم ؟ ناك ةروص يأبف كلذك ، وه اذإ هيلاتلا ؟ مالعالا لئاسولا نم يأ يف لوحكلل ركذ وأ ةروصل تضرعت له
ملضرعتأ
طق
قباطمةضوملل
وأ ةثيدحلا عئار
يقار قينأ ،ةجرد وذ وأ ةيلاع
، يلسموأ عتمم
حيرم
ىلإ يدؤي طبارتتاقادصلا
نامدإلا و ببسي ىلع رطيسي
لاعفألا
ةقالع هل وأ توملاب
ضرملا
هلةقالعمئارجلاب
ةقالع هل ، روجفلاب
داسفلارشلاو
مالفألاةينويزفلتلا جمارب
صصقلاو تاياورلا ةيعامتجإلا مالعإلا لئاسو
، مارقتسنإلا كوب ، سيف )( ديرغت
ةيعقاولا نويزفلتلا جمارب تاياعدلاو تانالعإلا
ةيفاقثلا ةينيدلا / تاونقلا
Enter another option
تايئاضفلا
تالجملا وأ دئارجلا
تاناحلا وأ يداونلا قدانفلا ،
تانالعإلا قصلم وأ تاحول
تنرتنإلا
يعامتجإلا لصاوتلا عقاوم
ةيجيورت ةيئاعد تاودأ
( اهنييعت ءاجرلا ) ىرخأ ءايشأ
249

؟ ةيئاصقتسالا ةساردلا هذه ىلا تلصوت قيرط يأ نع
(Moodle الثم ) يعماجلا ينورتكلإلا ملعتلا
طقف ةعماجلاب ةصتخملا ةيعامتجإلا لصاوتلا لئاسو
ةبلطلل ةمظنم وأ ةيعمج
( رتيوت وأ كوب ، سيف ) ةيعامتجإلا لصاوتلا لئاسو
ءاقدصألاوا ةلئاعلا
ةعماجلا يف ةيميلعت ةرود وأ ةرضاحمل كروضح دنع
ةعماجلا يفظوم وأ ةبلط لالخ نم
( اهنييعت ءاجرلا ىرخأ ( ةقيرط نع
250

251
Appendix 6: Interview guide (English/Arabic)
Introduction
As you know Iraq is a nation in a state of change. The country has experienced some difficult times.
I would like to talk with you about the role of alcohol and possibly other drugs in Iraq and your
experiences and views.
من المصاعب. انا اود ان اتكلم معك حول دور الكحول والمخدرات رالكثيلة التغيير. العراق واجه في مرحكما تعلم ان العراق هو دولة
نظرك. ووجهاتاالخرى في العراق خالل تجاربك
Question 1
Have attitudes changed towards alcohol in society over the generations? Can you give some examples
of this i.e. in relation to your friends and family? What has changed and why do you think this is?
ممكن ان تعطيني بعض االمثلة. ما تغير ولماذا حدثت هذه هل تغيرت وجهات النظر نحو الكحول في العراق عبر االجيال؟ هل
التغيرات.
Question 2
Iraq has suffered from sanctions, wars, terrorism and political instability. Do you have any stories to
share where alcohol or other drugs have played a role in the lives of today’s university students who
have lived most of their lives under these conditions? (start with alcohol, then ask about other drugs
if no story)
، ارهاب وعدم استقرار الوضع السياسي. هل لديك اي قصة تحب ان تقولها حروب دولية،كما تعلم ان العراق عانى من عقوبات
؟ الظروف وحتى جميع حياتهم تحت هذه أكثر اعاشوحول كيف الكحول او المخدرات االخرى لعبت دور في حياة طلبة الجامعة الذي
Question 3
Since 2003, Iraq has been at increased exposure to the international world. How do you think Iraqi
students have been influenced by this exposure and how are they conflicted with traditional values –
with specific mention about attitudes towards alcohol.
انفتح 2003منذ العراق ال, االنفتاح ىأكثر هذا ان تعتقد وهل كيف؟ الدولي. العراق أثرالمجتمع في الجامعات – على طالب
ظرهم للكحول؟ نوخصوصا نسبتا الى وجهة
Question 4
One interesting point about Iraq that is overlooked is the diversity that exists within this country –
religious, ethnic, social, and cultural. Do the different groups in Iraq think about and use alcohol
differently? Can you give me some examples?
مكن ان فهل تعتقد ان هذا االمر يؤدي الى افكار مختلفة نحو الكحول في العراق. هل م –يتميز العراق بتعدد الثقافات واالجناس
تعطيني اي امثلة؟
Question 5
Imagine an Iraq where there was the best public health policy related to alcohol; What would it look
like?
ما هي السياسة التي سيتبعها تجاه الكحول؟ وكيف ستكون؟ مثالية،تخيل لو ان العراق دولة
Question 6
Would you like to add anything else?
هل تحب ان تضيف شيئا اخر؟