ATP-supplies in the cold-preserved liver: A long-neglected factor of organ viability
10
SPECIAL ARTICLE ATP-Supplies in the Cold-Preserved liver: A Long-Neglected Factor of Organ Viability Katarina Vajdovi, Rolf Graf, and Pierre-Alain Clavien he goal of liver preservation during transplant surgery is to maintain cellular viability, to allow T early resumption of normal cellular metabolism on reperfusion, and thus to avoid the potential morbidity and mortality associated with poor graft function. The major tool used for liver preservation today is cold organ storage, which reduces metabolic activity by lowering the temperature to between 1 to 4°C.' T o accomplish organ protection during prolonged cold ischemia different cold-storage solutions were de- signed. Belzer's and Southard's University of Wisconsin (UW) solution has been successfullyused worldwide since the first clinical use in 1987. This complex solution sup- ports good graft function even after extended cold preser- vation.2 The preservation principles of the UW solution are based on the prevention of liver-specific cellular fea- tures occurring during cold ischemia. Intracellular edema is prevented by adding nonmetabolizable impermeants such as lactobionate and raffinose. The colloid, hydroxy- ethyl starch, suppresses expansion of extracellular space. The solution contains no glucose to avoid intracellular acidosis and it contains the hydrogen ion buffer KH2P04. Glutathione and allopurinol are added to prevent injury by oxygen radicals. Allopurinol, a xanthine oxidase inhib- itor, can also salvage adenosine triphosphate (ATP) pre- cursors. The purine nucleotide pool for ATP synthesis is further supported by adding adenosine.' Another solution, Bretschneider's histidine-trypto- phan-ketoglutarate (HTK), was designed for cardiac pres- ervation and it was formulated to retard acidosis Abbreviations: L'VZ University of Wisconsin; ATP, adenosine triphospate; HTK; histidine-typtophan-ketoglutarate; SEC, sinusoidal endothelial cells; ADP, adenosine diphophate; AMP, adenosine monophosphate; T m, total adenine nu- cleotidzs; AST, aspartateaminotransferase; PFK-I, phospboficto-I-kinase; NMR, nuclear magnetic resonance; W, S-adenosylmethionine; Pm, pentoxi&line. From the Laboratory of Hepatobiliary and Transplantation Surgery, Depart- ment of Surgey, UniversityHospital Zurich, Zurich, Switzerland Received May 10, 2002; accepted August 17, 2002. Supported by agrantfiom the National Institutes ofHealth (DK54048-OIAI to P.-A.C) and the Swiss National Science Foundation (SNF3200-06l4ll to P.- A. C). K I/. is supported by a grantfiom EMDO foundation, Switzerland. AaYress reprint requests to: Pierre-Akzin Ckzvien, M.D., Ph.D., F.A.C.S., De- partment of Surgery, UniversigHospital Zurich, Raemistmse 100, 8091 Zurich, Switzerland. E-mail: [email protected],ch; fm: (41) I 255 44 49. Copyright 0 2002 by the American Association for the Study of Liver Diseases. doi:l 0.1053/jhep.2002.37189 0270-9I39/02/3606-0032$35.00/0 (histidine), to prevent membrane injury (tryptophan), and to provide a substrate for energy metabolism (keto- glutarate). This solution was also tested by several groups in liver transplantation.3 They showed success in liver preservation comparable with UW solution.3 Although the preservation potential of liver cold stor- age solutions has significantly improved, graft dysfunc- tion after transplantation still occurs at a rate of 5% to 2O%.* A considerable part of primary graft dysfunction is attributable to inadequate cold storage, including an im- perfect storage solution. Graft dysfunction results in in- creased mortality and morbidity rates.5 Subsequent retransplantations further enhance the demands on the short list of donor organs. Thus, new strategies to increase organ protection during cold preservation are still ur- gently needed. Cold ischemia-reperfusion injury of liver is a complex of various events that virtually affect all types of hepatic cells. Generally, characteristic features of ischemic cell in- jury are triggered by ATP depletion,GJ impairment of mitochondria1 respiratory function,8,9 and acidosis from glycolysis.10 Liver parenchymal cells are highly metaboli- cally active and represent the majority (approximately SO%) of liver volume. * This could lead to the assumption that after cold ischemia liver function deteriorates mainly through affected hepatocytes. Hepatocytes, however, are known to be only minimally affected by cold storage. l2 Cold preservation of the liver followed by reperfusion results in loss of viability of sinusoidal endothelial cells (SEC) characterized morphologically by denudation and detachment of the endotheli~m.'~>'3 Disruption of the endothelial wall leads to leukocyte and platelet adhesion, which induces microcirculatory disturbances.'*-'G Our group has shown that apoptosis plays a pivotal role in cold-ischemia-induced SEC injury."-20 Kupffer cells, the resident hepatic macrophages, are activated after reperfusion of stored livers. This is evi- denced by structural changes, release of lysosomal en- zymes and cytokines, formation of oxygen-free radicals, and increased phagocytosis.21,22 Experiments with the isolated perfused rat liver revealed that Kupffer cells par- ticipated in leukocyte- and platelet-induced apoptosis of SEC during cold ischemia and reperfusion.20 The aim of our review is to highlight the deleterious effects of ATP depletion during the ischemic phases of 1543
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of ATP-supplies in the cold-preserved liver: A long-neglected factor of organ viability

SPECIAL ARTICLE
ATP-Supplies in the Cold-Preserved liver: A Long-Neglected Factor of Organ Viability
Katarina Vajdovi, Rolf Graf, and Pierre-Alain Clavien
he goal of liver preservation during transplant surgery is to maintain cellular viability, to allow T early resumption of normal cellular metabolism
on reperfusion, and thus to avoid the potential morbidity and mortality associated with poor graft function. The major tool used for liver preservation today is cold organ storage, which reduces metabolic activity by lowering the temperature to between 1 to 4°C.'
To accomplish organ protection during prolonged cold ischemia different cold-storage solutions were de- signed. Belzer's and Southard's University of Wisconsin (UW) solution has been successfully used worldwide since the first clinical use in 1987. This complex solution sup- ports good graft function even after extended cold preser- vation.2 The preservation principles of the U W solution are based on the prevention of liver-specific cellular fea- tures occurring during cold ischemia. Intracellular edema is prevented by adding nonmetabolizable impermeants such as lactobionate and raffinose. The colloid, hydroxy- ethyl starch, suppresses expansion of extracellular space. The solution contains no glucose to avoid intracellular acidosis and it contains the hydrogen ion buffer KH2P04. Glutathione and allopurinol are added to prevent injury by oxygen radicals. Allopurinol, a xanthine oxidase inhib- itor, can also salvage adenosine triphosphate (ATP) pre- cursors. The purine nucleotide pool for ATP synthesis is further supported by adding adenosine.'
Another solution, Bretschneider's histidine-trypto- phan-ketoglutarate (HTK), was designed for cardiac pres- ervation and it was formulated to retard acidosis
Abbreviations: L'VZ University of Wisconsin; ATP, adenosine triphospate; HTK; histidine-typtophan-ketoglutarate; SEC, sinusoidal endothelial cells; ADP, adenosine diphophate; AMP, adenosine monophosphate; T m , total adenine nu- cleotidzs; AST, aspartate aminotransferase; PFK-I, phospboficto-I-kinase; NMR, nuclear magnetic resonance; W, S-adenosylmethionine; Pm, pentoxi&line.
From the Laboratory of Hepatobiliary and Transplantation Surgery, Depart- ment of Surgey, University Hospital Zurich, Zurich, Switzerland
Received May 10, 2002; accepted August 17, 2002. Supported by agrantfiom the National Institutes ofHealth (DK54048-OIAI to
P.-A.C) and the Swiss National Science Foundation (SNF3200-06l4ll to P.- A. C). K I/. is supported by a grantfiom EMDO foundation, Switzerland.
AaYress reprint requests to: Pierre-Akzin Ckzvien, M.D., Ph.D., F.A.C.S., De- partment of Surgery, Universig Hospital Zurich, Raemistmse 100, 8091 Zurich, Switzerland. E-mail: [email protected],ch; fm: (41) I 255 44 49.
Copyright 0 2002 by the American Association for the Study of Liver Diseases.
doi:l 0.1053/jhep.2002.37189 0270-9I39/02/3606-0032$35.00/0
(histidine), to prevent membrane injury (tryptophan), and to provide a substrate for energy metabolism (keto- glutarate). This solution was also tested by several groups in liver transplantation.3 They showed success in liver preservation comparable with UW solution.3
Although the preservation potential of liver cold stor- age solutions has significantly improved, graft dysfunc- tion after transplantation still occurs at a rate of 5% to 2O%.* A considerable part of primary graft dysfunction is attributable to inadequate cold storage, including an im- perfect storage solution. Graft dysfunction results in in- creased mortality and morbidity rates.5 Subsequent retransplantations further enhance the demands on the short list of donor organs. Thus, new strategies to increase organ protection during cold preservation are still ur- gently needed.
Cold ischemia-reperfusion injury of liver is a complex of various events that virtually affect all types of hepatic cells. Generally, characteristic features of ischemic cell in- jury are triggered by ATP depletion,GJ impairment of mitochondria1 respiratory function,8,9 and acidosis from glycolysis.10 Liver parenchymal cells are highly metaboli- cally active and represent the majority (approximately SO%) of liver volume. * This could lead to the assumption that after cold ischemia liver function deteriorates mainly through affected hepatocytes. Hepatocytes, however, are known to be only minimally affected by cold storage. l2
Cold preservation of the liver followed by reperfusion results in loss of viability of sinusoidal endothelial cells (SEC) characterized morphologically by denudation and detachment of the endotheli~m.'~>'3 Disruption of the endothelial wall leads to leukocyte and platelet adhesion, which induces microcirculatory disturbances.'*-'G Our group has shown that apoptosis plays a pivotal role in cold-ischemia-induced SEC injury."-20
Kupffer cells, the resident hepatic macrophages, are activated after reperfusion of stored livers. This is evi- denced by structural changes, release of lysosomal en- zymes and cytokines, formation of oxygen-free radicals, and increased phagocytosis.21,22 Experiments with the isolated perfused rat liver revealed that Kupffer cells par- ticipated in leukocyte- and platelet-induced apoptosis of SEC during cold ischemia and reperfusion.20
The aim of our review is to highlight the deleterious effects of ATP depletion during the ischemic phases of
1543

1544 VAJDOVA, GRAF, AND CLAVIEN HEPATOLOGY, December 2002
liver transplantation and the role of ATP resynthesis in graft recovery after liver transplantation.
Effect of Cold Ischemia on liver Energy Stores
The liver, a well-differentiated tissue, requires large amounts of oxygen to support its various specialized func- tions. These functions are maintained primarily by energy derived from aerobic metabolism. As cells become anoxic, oxidative phosphorylation ceases and ATP stores are de- pleted, which stops almost all energy-dependent pro- cesses. There is inhibition of RNA and protein synthesis, which affects the equilibrium in the protein composition. One event typical for ischemia involves changes in ion transport with loss of intracellular K+ and increased in- tracellular Na', due to inhibition of Na+/K'-ATPase function.23 Under normal conditions, Na+/K+-ATPase uses high amounts of ATP. During ischemia, when ATP stores are dramatically decreased,G,7 the transport mecha- nism of this pump is inhibited resulting in a significant loss of membrane potential.23 The intracellular accumu- lation of Na' induces cell ~welling.~3 Ischemia also in- duces a redistribution of intracellular Ca2+ ions, which participates in the activation of degradative enzymes and cell membrane disr~ption.~*,~5 Glycolysis is initially accel- erated, and large quantities of lactate are synthesized ac- companied by acidosis. lo
Hypothermia, cooling from 37 to O'C, decreases the metabolic rate in homoiothermic animals theoretically 12 to 13 times using van't Hoff s rule.' Although the meta- bolic rate is decreased during cold storage, energy demand is still higher than the production capacity under anaero- bic conditions by glycolysis. Glycolysis is extremely inef- ficient with respect to ATP production per molecule of glucose during anaerobic conditions, when only approx- imately 6% of the ATP can be generated compared with aerobic metabolism.25
During ischemia, ATP degrades into adenosine diphosphate (ADP), adenosine monophosphate (AMP), and adenosine and further to adenine, inosine, and hypo- xanthine. H ypoxanthine accumulation activates xanthine oxidase, which catalyses the conversion to xanthine.26 This reaction is accompanied by free radical production, which may cause cell injury. The byproducts of AMP metabolism can be easily lost in the process of transplan- tation during organ wash-out following cold Their loss thus limits the availability of AMP for ATP formation during reperfusion. AMP can be reformed in human tissues by de nouo synthesis but is limited by a slow conversion of glucose-6-phosphate to ri bose-5-phosphate and to phosphoribosylpyrophosphate. Alternatively, there is a salvage pathway, which is limited by the avail-
ability of substrates: adenosine, adenine, inosine, and hy- poxanthine.28 Thus, it seems that the level of ATP restoration would also depend on the remaining pool of total adenine nucleotides (TAN = ATP + ADP + AMP) and salvageable precursors for AMP synthesis after cold storage.
The depletion of energy stores during ischemic steps of liver transplantation was shown by using different mod- els. In porcine liver, ATP levels decreased from 9.12 to 0.96 pmol/g dry weight after 12 hours of cold storage in UW s0lution.~9 In rat liver experiments, a drop in con- centration of ATP from 9.5 to 0.5 pmol/g protein and 6.77 to 1.19 pmol/g dry weight was observed after an 8- or 1 8-hour preservation in UW solution, respectively.30,3' In isolated hepatocytes, the cellular ATP content was also shown to be decreased by 50% and 70% after 24 or 48 hours of cold storage, respectively, when preserved in U W and by 75% and 90% when stored in Hanks HEPES- buffered s0lution.3~ The decrease of intracellular ATP correlated with lower viability of cells and enlargement of cell blebs.32
In clinical studies, a correlation between energy stores before reperfusion and primary liver graft function was suggested.33~3~ In addition to cold storage ischemia, the transplanted liver may be exposed to hypotension isch- emia during the donor operation and rewarming ischemia usually occurs during the implantation phase. Thus, the extent of the injury reflects a combination of ischemic insults. This combination of ischemic insults is not often simulated in experimental models.
In human transplantation, Kamiike et al.33 have shown that the level ofATP during cold ischemia did not corre- late with graft function. When all adenine nucleotides (TAN) were taken into consideration, their level at the end of preservation reflected the viability of the graft. An additional analysis of ATP levels in the same organs after reperfusion revealed that they correlated with graft func- tion. This might suggest that the remaining pool of TAN after preservation affects ATP restoration and transplan- tation outcome. In addition, ATP recovery was shown to be inversely related to duration of warm ischemia in this study.
In the study of Lanir et al.,34 a direct correlation be- tween high ATP content and good posttransplant out- come was shown, as defined by aspartate aminotransferase (AST) levels and prothrombin time normalization. How- ever, a group of successfully transplanted patients also included 5 with a low energy charge and low ATP levels. These patients experienced severe postoperative compli- cations. It seems, therefore, that low ATP content and energy charge indicate the severity of ischemic damage but do not necessarily indicate a liver failure. Thus, ac-

HEPATOLOGY, Vol. 36, No. 6 , 2002 VAJDOVA, GRAF, AND CLAVIEN 1545
cording to Kamiike et a1.,33 the viability of liver graft may be better characterized by its ability to resynthetize ATP during reperfusion than by ATP levels after cold storage.
To restore ATP levels after cold ischemic preservation, one should aim at (1) preservation of mitochondrial func- tion, (2) raising levels of precursors for ATP resynthesis, and (3) appropriate reoxygenation during reperfusion.
Mitochondria1 Injury During Cold Storage The injury of mitochondria caused by hypothermic
ischemia could be partially responsible for the inability of hepatic cells to regain complete function after transplan- tation. In the study of Ohkohchi et a1.35 several parame- ters of mitochodrial function, e.g., respiration control ratio, ATPase activity, and ATP content in mitochondria, started to decrease after 12 hours of cold preservation of rat livers in UW solution. O n the other hand, Kim et al.8 have shown that the maximal rate of respiration was not greatly affected by cold ischemia suggesting relatively in- tact electron transport in mitochondria during preserva- tion. However, prolonged cold storage induced a loss of mitochondrial respiration efficiency, which may lead to a diminished capability of mitochondrial ATP synthesis during reperfusion.
The integrity of the mitochondrial membrane is a basic requirement for oxidative phosphorylation to be success- fully carried out. The mitochondrial permeability transi- tion represents a rapid increase of mitochondrial membrane permeability mediated by opening of protein pores.36 This permeability transition can occur during liver ischemia and reperfusion by increased intracellular oxygen free radicals and Ca2+ content.36 After cold stor- age for 24 hours in Krebs-Henseleit medium, followed by isolated organ reperfusion, a mild permeability transition was shown to be induced probably by transition from hypothermia to normothermia.9
These results suggest that mitochondrial membrane integrity is not significantly impaired during cold isch- emia. The slight functional changes may have only a mi- nor effect on impaired organ energy repletion. Thus, since the mitochondrial function is fairly intact after cold stor- age, reduced ATP synthesis during reperfusion is proba- bly caused by other cellular mechanisms.
How to Protect the Transplanted Liver From ATP Loss
Ever since liver transplantation became the major ther- apy for patients with end-stage liver disease there is a continued interest in improving the outcome of this pro- cedure. Numerous studies have been performed to avoid the problems with ATP decrease during the transplanta-
tion process. There are two main strategies employed to solve this problem: (1) prevent or slow down the ATP decrease during cold storage and (2) facilitate ATP recov- ery during reperfusion.
The Prevention of A TP Decrease During CoM Storage Donor Pretreatment. The first step in the transplan-
tation process involves the assessment of donor organ quality. At this point the donor can be manipulated to maximize the potential outcome. A direct relationship between donor nutritional status and liver tissue TAN levels was shown in different animal models.29*30,37 In addition the nutritional status appeared to influence liver graft fun~tion.~9,3~~37 Conversely, some investigators have proposed that malnutrition may contribute to a better function and increase survival after liver transplanta- tion.38,39 Sun et have shown in a rat model that donor fasting for 4 days significantly inhibited liver injury and reduced apoptosis of sinusoidal endothelial cells that oc- curs after liver transplantation.
Glycolysis is the only pathway for ATP production during anoxia. Therefore, modifying the nutritional state was thought to significantly influence the production of ATP and energy state during anoxia. It has been shown that the most important glycolytic enzyme is phospho- fructo-l-kinase (PFK-l), its activity being mainly regu- lated by the celIular concentration of fructose 2,6- bisphosphate.41 Morimoto et al.37 have shown that PFK- 1 is a key enzyme in glycolysis during cold storage of rat livers in UW solution. In this study, donor animals injected with insulin and glucose maintained higher ATP levels and energy charge at least over 12 hours of preser- vation. In comparison to organs from nontreated or fasted donors, an increase of bile production and a decreased liver injury, assessed by cytosolic enzyme release and his- tology, were significant. Through activation of PFK-1, insulin pretreatment enhanced glycolysis in fed donor liv- ers during cold ischemia and improved the energy status and liver function after transplantation. The nutritional deprivation by fasting for 24 hours prior to cold storage was shown to be less effective for maintaining energy stores and recovery of liver function after transplantation.
Accordingly, the results of Morgan et al.42 from an isolated perfused rat liver model have shown that liver bile production and cytosolic enzyme release of cold stored liver are significantly improved when the livers have been nutritionally repleted before harvesting. Subsequently, the same laboratory has provided evidence using a porcine liver ischemic model showing that it is possible to rapidly replenish the glycogen stores of the liver by intraportal infusion of insulin and hexoses.29 Phosphorylated ade- nine nucleotide levels were better maintained over 24

HEPATOLOGY, December 2002 1546 VAJDOVA, CRAF, AND CLAVIEN
hours of cold storage but dropped to the level of the non- infused group after ischemic rewarming. Similar results were provided by the same group in a clinical study, where peak postoperative AST levels showed better function of livers transplanted from glucose-infused donors than from nontreated donors.43
In the study of Morgan et al.,42 SEC morphology changes and cell death were prevented in livers from fed and glucose-injected donors after preservation either in UW or Marshall’s isotonic citrate solution. O n the other hand, Rauen et al. showed that isolated SEC were dying more frequently in UW than in Krebs-Henseleit solu- t i ~ n . ~ ~ ATP levels were higher in those cells that were stored in UW solution. When hypoxia was simulated by KCN or other inhibitors of oxidative phosphorylation, the viability of cells preserved in UW solution was mark- edly increased, while glucose diminished the protective effect of cyanide. These data suggested that SEC injury induced by preservation in UW solution is energy depen- dent. However, additional results of this studf4 revealed that the energy-dependent injury of SEC occurs only at a confluent growth state. Thus, it seems that the final an- swer to energy-dependent injury of cold-stored SEC needs to be answered in whole liver models.
The contradiction of these data with studies showing a protective effect of starvation on liver function after trans- plantation is difficult to explain. It may be possible that prolonged deprivation of food for 4 days, as used in stud- ies by Sumimoto et al. and Sun et al.,39v40 induces defen- sive mechanisms protecting cells against a subsequent injurious challenge. It is hypothesized that long-term fast- ing alters cellular metabolism and different cytoprotective substances are induced. For instance, heat shock protein GRP78 (glucose-regulated protein 78) has been shown to be “overexpressed” after 7 days of fasting. This long fast- ing period increased tolerance to ischemia-reperfusion in- jury in the rat liver transplantation mode1.45
Recent data from our group indicated that a 2-day fasting regimen in the mouse causes a dramatic decrease in ATP concentration in liver tissue with a switch from an apoptotic form of cell death to necrosis along with a poorer tolerance to warm ischemia (unpublished data). Recently, it has been shown in cell culture studies that ATP is required for apoptosis and it can act as a switch in the decision between apoptosis and necrosis.46.47 Leist et al.47 showed in depletion/repletion experiments that re- pletion of the ATP pool by supplying glucose prevented necrosis and restored the ability of the cells to undergo apoptosis. Ischemia-reperfusion-mediated cell death is commonly accompanied by inflammation. Thus, ATP protective strategies in cold preservation may help to di- minish ongoing inflammation during graft reperfusion by
shifting SEC death to the noninflammatory apoptosis. However, further studies evaluating this phenomenon in whole organ cold storage and reperfusion models are still missing.
New Techniques for CoZd Preservation. In compar- ison to simple cold storage, other methods were tested to explore whether they can better maintain tissue energy stores over the preservation period. The technique of hy- pothermic pulsative perfusion using an oxygenated ATP- MgCI2- enriched hyperosmolar colloid solution was shown to be superior to simple cold storage in prevention of dog liver preservation-reperfusion injury.48 The oxy- genated perfusion for 24 hours has improved tissue nu- cleotide levels, decreased liver swelling, and allowed higher bile production during reperfusion. Furthermore, the use of direct ATP supply by an ATP-MgC12 solution showed better results with respect to liver energy stores and functional protection than the hypothermic perfu- sion with UW solution.
In porcine liver transplantation, normothermic extra- corporeal liver perfusion with diluted pig blood for a short preservation time was not shown to be more effective than cold st0rage.~9 However, further results of this study sug- gested that the continued perfusion during cold storage is superior to nonperfused storage organs from non- heart- beating donors to overcome deleterious effects of warm ischemia on energy stores and functional recovery of the liver. The ability to significantly increase adenine nucleo- tide levels during 1 O-hour cold preservation was achieved by either oscillating or continuous organ perhsion with modified UW solution in a rat liver model.5O Oscillating perfusion was shown to be more potent in maintaining energy stores, because oscillating flow did not increase oxidative stress and improved tissue microcirculation. The technique for perfusion storage can be further im- proved by enrichment o f the perfusion-preservation solu- tion with oxygen-carrying agents such as hemoglobin- polyoxyethylene ~onjugate.5~ The effective oxygen supply maintains high tissue ATP levels under low perfusion rates and thus allows gentle manipulation of the liver. A very important advantage of using perfusion techniques for liver cold preservation is the possibility to assess graft function and viability before implantation.
Another alternative for liver preservation has been ex- tensively described by Minor et a1.52,53 They presented a model of organ oxygenation (vascular persuflation),52~53 in which an organ was immersed in hypothermic U W solution. Retrograde gaseous oxygen was infused into the hepatic veins. Oxygen supply during 48-hour cold storage not only prevented the catabolism of high energy sub- strates, but enabled a net synthesis of ATP during preser- vation, reaching tissue concentrations of 17.26 ? 4.81

HEPATOLOGY, Vol. 36, No. 6, 2002 VAJDOVA, GRAF, AND CLAVIEN 1547
pm0l/g,52 which is higher than norma1.28.29 Although during the following ischemic rewarming the energy stores decreased dramatically, they were still far higher than in the group of livers simply stored in UW solution. Due to the prevention of ATP decrease, functional recov- ery of the livers was facilitated, as assessed by higher bile production, decrease of calcium uptake, and vascular re- sistance using the isolated perfused rat liver mode1.52 In the rat liver transplantation model, the extent of lipid peroxidation was not increased by persufflation. In addi- tion, degradation of cytosolic proteins and cytosolic en- zyme release were significantly reduced.53
Modzjications of CoM Storage Solution. The devel- opment of preservation solutions has also focused on the prevention ofATP decline during cold storage. In nuclear magnetic resonance (NMR) studies, Delmas-Beauvieux et a1.I0,5* showed that at the end of the 24-hour cold ischemic period, no ATP was detectable in any of the preserved livers, whatever the type of preservation solu- tion. The nearly complete disappearance of the ATP sig- nal as determined by 3IP NMR spectra, was observed after 8 hours of ischemia for livers preserved in UW, HTK, and histidine-buffered lactobionate s o l ~ t i o n s . ~ ~ ~ 5 ~ In Krebs or Euro-Collins solution5* ATP was depleted in less than 3 hours in stored livers. This suggested that ATP depletion depends on the nature of the cold storage medium.
The widely used UW solution contains allopurinol (1 mmollL), a xanthine oxidase inhibitor, which exerts its effect by salvage of precursors for nucleotide resynthesis and reduction of free radicals.55 In animals, it was shown that the combined pretreatment of donors with allopuri- no1 (50 mg/kg) and, also using it in an organ flush solu- tion (1 mmol/L), improved the hepatic tissue TAN content, probably due to salvage of precur~ors.5~ Further, adenosine ( 5 mmol/L) was added to UW solution as a substrate for the regeneration of adenine nucleotides.' However, simplified variants of UW solution in which adenosine was omitted57 were shown to have similar or even higher protective potential during cold liver storage in animal models.
On the other hand, animal experiments with histidine- buffered lactobionate solution showed that both histidine (100 mmol/L) and lactobionate (50 mmol/L) together caused a more effective ATP and intracellular pH (pHin) reestablishment in liver during reperfusion than UW so- lution.10 The reestablishment of high pHi, values seems to be a necessary factor contributing to ATP synthesis. Delmas-Beauvieux speculated that the increased ATP synthesis was induced by the cellular uptake of histidine. This may lead to glutamate synthesis via the urocanate pathway and consequently stimulate the tricarboxylic acid cycle and ATP synthesis.'O
To reduce the activity of energy consuming processes during liver cold storage, effects of membrane Ca2+ chan- nel antagonists were tested.25 The investigators supposed that a reduction in the passive leakage of calcium ions across membranes would diminish the requirement for active ATP-driven pumps and prevent ATP decrease dur- ing cold ischemia. However, donor pretreatment and modified UW solution fortified with various calcium channel antagonists has not revealed any dramatic effect on liver nucleotide levels. Stabilization of tissue energy stores by verapamil and chlorpromazine over the initial period of storage conferred only minimal protecti0n.~5 The results suggest that partial reduction of energy con- suming processes is not sufficient to prevent liver ATP loss during prolonged cold ischemia.
S-adenosylmethionine (SAM), which is an endoge- nous methyl donor group, as well as a precursor of ATP and glutathion, has been tested by Dunne et al.58 in a rat model of cold ischemia, rewarming, and reperfusion in- jury of liver. SAM was included in a UW preservation solution and added at reperfusion. It limited hemody- namic and metabolic features of the liver damage when administered also to the donor. Furthermore, in another isolated perfused rat liver study of Lee and Lee,59 an en- richment of UW and Ringer's lactate solutions with SAM resulted in significantly higher ATP and AMP levels dur- ing reperfusion in ischemic livers.
In conclusion, we can see that only oscillating perfu- sion5'J and oxygen per~ufflation5~ methods were shown to prevent ATP loss over prolonged liver cold preservation. These techniques of aerobic storage improvement even allowed ATP loading. Comparing these two approaches, the oxygen persufflation appears superior to oscillation perfusion and requires only little additional equipment for clinical use. Both of these promising preservation tools should be taken into consideration for improving liver transplantation technology.
ATP Recovery Following Ischemia Hepatocytes and other eukaryotic cells do not have
storage capacities for nucleotides. Hence, when tissue ad- enine nucleotide levels are depleted during cold storage and/or rewarming ischemia, they need to be resynthesized during reperfusion for full graft recovery. Successful ATP replenishment during liver reperfusion depends on avail- ability of salvageable precursors, oxygen delivery, and mi- tochondrial function.
As already mentioned, the facilitated tissue energy re- covery during liver reperfusion after cold storage can be achieved by nutritional repletion of the donor37 or by donor allopurinol ~retreatment.5~ Further improvement can be gained by using preservation solution, which is

1548 VAJDOVA, GKAF, AND CLAVIEN HEPATOLOGY, December 2002
enriched either with allopurinol,1,56 histidine, lactobion- ate,*O or SAM.s8 However, the salvageable precursors for ATP resynthesis can be rescued only partially following organ flush before implantation. Consequently, initial ATP recovery during liver reperfusion is limited and it should be supported externally.
In the animal experimental models of Palombo et a1.,60 ATP resynthesis after 18-hour cold storage was shown to be markedly improved by exogenous adenosine and ade- nine support. Adenine did not appear to be as effective as adenosine probably because of the kinetic properties of adenosine kinase and phosphoribosylpyrophosphate syn- thetase. The precursor ribose together with adenine for ATP synthesis does not have to be supplemented because in the liver, ribose can be formed, probably via the glyco- lytic pathway.28 Highly active transport and incorpora- tion of adenosine resulted in an increased intracellular ATP pool in isolated hepatocytes.61 A similar observation was made in a whole liver animal model.62 The direct phosphorylation of adenosine to AMP represents the most bioenergetically and kinetically efficient pathway for nucleotide repleti0n.~3 Thus, Palombo et al. proposed that enteral preparations containing at least 3 mmole adenosine (or adenine) should be given postoperatively to liver transplant recipients to replete adenine nucleo- tides.60 Parented administration of adenosine was not suggested to be effective for hepatic ATP repletion be- cause adenosine is rapidly removed from the blood by erythrocytes and vascular endothelium before it reaches the liver.b0
In a study with an isolated perfused rat liver model, Vajdova et al. have shown that prolonged cold ischemia causing a depletion of adenine nucleotides had an effect on hepatocyte function after rewarming ischemia: in- creasing the length of cold storage induced a higher extent of hepatocyte i n j ~ r y . 3 ~ Thus, a direct role of adenine nu- cleotides in maintaining the functional integrity of hepa- tocytes during ischemia was assumed. When ATP recovery was facilitated by short 30-minute oxygenated unsanguinarious perfusion before rewarming ischemia, the liver function did not differ from nonstored livers. These results combined with those of Palombo et al.60 suggest that the effectiveness of this short reperfusion on ATP resynthesis was enhanced by addition of either aden- osine or adenine and ribose to the perfusion solution. In comparison to adenine, the precursor adenosine had su- perior potential to facilitate adenine nucleotide recovery to even higher levels than those found in control nonisch- emic liver. These results suggest that ATP loss may be corrected before implantation rewarming by such a treat- ment, which can help the liver to overcome the warm ischemic insult even after extended preservation time.
Such a perfusion method can also ensure delivery of ade- nine nucleotide precursors directly to the liver cells.
Furthermore, oxygen supply has to be taken into ac- count for establishment of conditions that promote effi- cient ATP recovery during repetfusion. Factors affecting oxygen delivery include cardiac output, hemoglobin con- tent and saturation, and tissue perfusion capacity. Tissue perfusion in turn is affected by flow resistance arising from vasoconstriction, cell edema, endothelial damage, and microcapillary obstruction by cellular debris. In case of a significantly reduced hemoglobin level of the recipi- ent due to perioperative blood loss, either erythrocyte or whole blood is transfused. If there is suspicion of throm- bosis in liver vasculature during reperfusion, heparin is provided to the recipient to improve circulation. In cases requiring vasodilatory therapy after liver transplantation, the recipient can be treated with either cat echo la mine^,^^ epoprosten01,~5 or nitrogly~erine.~5 This leads to im- proved oxygen delivery without impairment of splanch- nic oxygenation.6*,65 Minor and Isselhard66 treated rats with papaverine during preischemia and reperfusion. The livers were then exposed to warm and cold ischemia. They exhibited significantly reduced hepatic vascular resistance and increased hepatic tissue ATP content at the end of reperfusion. As a hemorrheologically active agent, pen- toxifylline (PTX) has been introduced for the treatment of regional microcirculatory defects. PTX, a phosphodi- esterase inhibitor, acts primarily by increasing erythrocyte deformability, by reducing blood viscosity, and by de- creasing the potential for platelet aggregation and throm- bus formation.67 PTX has also been shown to suppress tumor necrosis factor a production in several models in- cluding a rat liver transplantation model and a mouse model ofwarm ischemia-reperfusion when it was used for donor or graft pretreatment.68~69 Its wide range of protec- tive effects against liver ischemic injury should promote its use as a clinical agent for prevention of cold ischemia reperfusion injury and for accompanying microcircula- tion disturbances.
Microcirculation failure in liver transplantation occurs following SEC injury induced by cold ischemia and reper- fusion.'2-'6 Thus, we assume that an intact endothelial wall is a prerequisite for normal physiologic rate of blood flow. It seems that any treatment preventing SEC injury, detachment, or apoptosis could be helpful for a successful ATP recovery. SEC damage, the main feature of cold ischemic injury in liver transplantation, has been exten- sively studied during the last two decades. The data of Upadhya et al.7O suggest that matrix metalloproteinases, which are responsible for detachment of SEC seen during cold preservation, can be blocked and hence prevent en- dothelium denudation. Including inhibitors of apoptosis

HEPATOLOGY, Vol. 36, No. 6, 2002 VAJDOVA, GRAF, AND CLAVIEN 1549
STANDARD PROCEDURE
such as caspase inhibitors's or calpain inhibitors19 to the preservation solution or overexpressing antiapoptotic proteins such as B ~ 1 - 2 ~ ~ prevents SEC apoptosis induced by cold ischemia and reperfusion of the liver. Further- more, flushing the hepatic graft prior to reperfusion with a solution containing glycine, e.g., Carolina rinse solu- tion, prevented a lethal reperfusion injury to SEC.72 In addition to SEC damage prevention, microcirculation disturbances during reperfusion can be ameliorated by blockade of leukocyte and platelet accumulation in liver sinusoids.2OJ3J4
TARGETS FOR IMPROVEMENT
Prevention of Hepatic Mitochondria1 Injury Induced by Cold Storage and Reperfusion
As mentioned previously, the injury of hepatic mito- chondria is not dramatic during liver cold storage and reperfusion.8.35 Yet it may aggravate the injury in combi- nation with other damaging cellular processes. Thus, the recovery of full mitochondrial function, including effec- tive oxidative phosphorylation, immediately after reper- fusion should be attempted, which can be achieved by
various treatments. When rat livers were flushed with Ringer's lactate containing bovine serum albumin after 48-hour preservation, mitochondrial function was im- proved, probably because of the ability of albumin to bind fatty acids, which are known to accumulate during isch- emia and to uncouple mitochondrial respiration.* Cyclo- sporin A, a highly specific inhibitor of mitochondrial permeability transiti0n,3~ induced a high level of liver ATP after the transition from hypothermia to normother- mia due to better recovery of oxidation and phosphoryla- tion rates in mitochondria.9 Thus, cyclosporin A added to the organ rinse solution facilitates tissue recovery of ade- nine nucleotides. Finally, the protective effect of glycine should be mentioned again: its application prevented cold ischemic injury of isolated hepatocytes together with a dramatic improvement of ATP recovery during reperfu- sion. Furthermore, cytotoxicity of mitochondrial uncou- plers was reversed when glycine was present in medium.75 It is anticipated that protection mediated by glycine is related to its ability to stabilize the cell membrane. Since effects of glycine appear to predominate during the
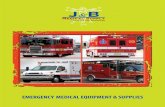
hcxoscs+insulin injcccion; allopuriinol injcclion; PTX injoction
pretreatment
oxygen pnsumation. pulJalivdoscillalive pcrfision, using ATP- MgCII. hiaidinc- ,-, casppssc or calpain
so Preservation lactobionslc. SAM or techniques
inhibitors cnnchcd mcdie
1 Short reperfusion
rinsing with solution stores Organrinse
rcpcrhsion using adcnosinc enriched mcdia
f
solution cnrichcd by glycinc. S A M . cvclosrmrino A or . . BSA
cntml adcnosinc, PTX mnjcction. vascdilatators. prevention oflcukocytc @P Recipient end platelet adhcston treatment
Fig. 1. Improving measures of standard liver transplantation to pro- tect sufficient tissue energy stores. ATP, adenosine triphospate; BSA, bovine serum albumin; PTX, pentoxi- fylline; SAM, S-adenosylmethionine; TAN, total adenine nucleotides.
(&) +;)

1550 VAJDOVA, GRAF, AND CLAVIEN HEPATOLOGY, December 2002
rewarming period, it further argues for providing it in the rinse solution or during infusion of the transplant recipient.
Conclusion ATP loss during prolonged cold storage is one of the
critical events of cold ischemia-reperfusion injury, which occurs in the liver transplantation procedure. The results reviewed above propose various strategies to improve graft energy stores (Fig. 1). The appropriate energy stores for full graft recovery can be either maintained during cold storage or effectively repleted before or during organ reperfusion. The treatments that are necessary to be per- formed when cold storage time is prolonged are (1) to provide oxygen supply during cold preservation, (2) to recharge ATP stores by short prereperfusion before the implantation stage, or (3) to support the recipient with ATP precursors together with improvement of blood flow.
Acknowledgment: The authors thank Dr. B. Stieger from the Department of Clinical Pharmacology and Tox- icology, University Hospital Zurich, for critically reading the manuscript and for helpful suggestions.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Belzer FO, Southard JH. Principles of solid-organ preservation by cold storage. Transplantation 1988;45:673-676. Belzer FO, D’Alessandro AM, Hoffmann RM, Knechtle SJ, Reed A, Pirsch JD, Kalayoglu M, et al. The use o f W solution in clinical transplantation. A 4-yeat experience. Ann Surg 1992;215:579-583. Erhard J, Lange R, Scherer R, Kox WJ, Bretschneider HJ, Gebhard MM, Eigler FW. Comparison of histidine-tryptophan-ketoglucarate (HTK) so- lution versus University of Wisconsin (Uw) solution for organ preserva- tion in human liver transplantation. A prospective, randomized study. Transpl Int 1994;7:177-181. Strasberg SM, Howard TK, Molmenti EP, Hertl M. Selecting the donor liver: risk factors for poor function after orthotopic liver transplantation. HEPATOLOGY 1994;20:829-838. Mor E, Klintmalm GB, Gonwa TA, Solomon H , Holman MJ, Gibbs JF, Watemberg I, et al. The use of marginal donors for liver transplantation. A retrospective study of365 liver donors. Transplantation 1992;53:383-386. Lanir A, Clouse ME, Lee RG. Liver preservation for transplant. Evaluation of hepatic energy metabolism by 31P NMR. Transplantation 1987;43:
Lee RG, Lanir A, Clouse ME. Liver adenine nucleotide metabolism during ischemia and reperfusion of mice livers studied by phosphorous-3 1 nuclear magnetic resonance. Invest Radiol 1987;22:479-483. Kim SK, Belzer FO, Southard JH. Loss of mitochondria1 respiratory func- tion and its suppression during cold ischemic preservation of rat livers with University of Wisconsin solution. HEPATOLOGY 1992; 16:742-748. Leducq N, Delmas Beauvieux MC, Bourdel Marchasson 1, Dufour S, Gallis JL, Canioni P, Diolez P. Mitochondria1 permeability transition dur- ing hypothermic to normotherniic reperfusion in rat liver demonstrated by the protective effect of cyclosporin A. Biochem J 1998;336:501-506. Delmas Beauvieux MC, Gallis JL, Clerc M, Canioni P. 31P NMR studies of rat liver cold preservation with histidine-buffered lactobionate solution. Cryobiology 1993;30:55 1-561
786-790.
11.
12.
13.
14.
15.
16.
17
18
19
20
21
22
23
24
25.
26.
27.
28
29.
30.
31.
Sasse D. Liver structure and inervation. In: Thurman RG, Kauffman FC, Jungerman K, eds. Regulation of Hepatic Metabolism. New York: Ple- num, 1986;3-35. Marzi I, Zhong 2, Lemasters JJ, Thurman RG. Evidence that graft survival is not related to parenchymal cell viability in rat liver transplantation. The importance of nonparenchymal cells. Transplantation 1989;48:463-468. Holloway CM, Harvey PR, Strasberg SM. Viability of sinusoidal lining cells in cold-preserued rat liver allografts. Transplantation 1990;49:225- 229. Marzi I, Knee J, Buhren V, Menger M, Trentz 0. Reduction by superoxide dismutase of leukocyte-endothelial adherence after liver transplantation. Surgery 1992;111:90-97. Takei Y, Marzi I, Gao WS, Gores GJ, Lemasters JJ, Thurman RG. Leu- kocyte adhesion and cell death following orthotopic liver transplantation in the rat. Transplantation 1991;51:959-965. Cywes R, Packham MA, Tietze L, Sanabria JR, Harvey PR, Phillips MJ, Strasberg SM. Role of platelets in hepatic allograft preservation injury in the rat. HEPATOLOGY 1993; 18:635-647. Gao W, Bentley RC, Madden JF, Clavien PA. Apoptosis of sinusoidal endothelial cells ir a critical mechanism of Preservation injury in rat liver transplantation. HEPATOLOGY 1998;27:1652-1660. Natori S, Selzner M, Valentino KL, Fritz LC, Srinivasan A, Clavien PA, Gores GJ. Apopcosis of sinusoidal endothelial cells occurs during liver preservation injuiy by a caspase-dependent mechanism. Transplantation 1999;68:89-96. Sindram D, Kohli V, Madden JF, Clavien PA. Calpain inhibition prevents sinusoidal endothelial cell apoptosis in the cold ischemic rat liver. Trans- plantation 1999;68: 136-140. Sindrain D, Porte RJ, Hoffman MR, Bentley RC, Clavien PA. Synergism between platelets and leukocytes in inducing endothelial cell apoptosis in the cold ischemic rat liver: a KupfFer cell-mediated injury. FASEB J 2001; 15: 1230-1 232. Caldwell Kenkel JC, Currin RT, Tanaka Y, Thurman KG, Lemasters JJ. Kupffer cell activation and endothelial cell damage after storage of rat livers: effects of reperfusion. HEPATOLOGY 1991; 1333-95. Arii S, Monden ti, Adachi Y, Zhang W, Higashitsuji H, Furutani M, Mise M, et al. Pathogenic role ofKupffer cell activation in the reperfusion injury of cold-preserved liver. Transplantation 1994;58:1072- 1077. Macknight AD, LeafA. Regulation of cellular volume. l’hysiol Rev 1977;
Haddad P, Cabrillac JC, Piche D, Musallam L, Huet PM. Changes in intracellular calcium induced by acute hypothermia in parenchymal, en- dothelial, and Kupffer cells of the rat liver. Cryobiology 1999;39:69-79. Churchill TA, Green CJ, Fuller BJ. The importance (of calcium-related effects on energetics at hypothermia: effects of membrane-channel antag- onists on energy metabolism of rat liver. Cryobiology 1995;32:477-486. Yokoyama Y, Bcckman JS, Beckman Tti, Wheat JK, Cash TG, Freeman BA, Parks DA. Circulating xanthine oxidase: potential mediator of isch- emic injury. Am J Physiol 1990;258:G564-G570. Schmidt HC, Gooding CA, James TL. In vivo 31P-MR spectroscopy of the liver in the infant rabbit to study the effect ofhypoxia on the phospho- rus metabolites and intracellular pH. Invest Radiol 1986;21: 156-161. Lee RG, Clouse ME, Lanir A. Liver adenosine triphosphate and pH in fasted and well-fed mice after infusion of adenine nucleotide precursors. Liver 1988;8:337-343. Cywes R, Greig PD, Morgan GR, Sanabria JR, Clavien PA, Harvey PR, Strasberg SM. Rapid donor liver nutritional enhancement in a large animal model. HEPATOLOGY 1992;16:1271-1279. Palombo JD, Pomposelli JJ, Hirschberg Y, Blackburn GL, Bistrian BR. Glycolytic support of adenine nucleotides in rat liver flush-preserved with UW or Collins’ 11. Importance of donor nutritional status. Transplanta- tion 1989;48:901-905. Vajdova K, Smrekova R, Mislanova C, Kukan M, Lutterova M. Cold- preservation-induced sensitivity of rat hepatocyte function to rewarming injury and its prevention by short-term reperfusion. HEPATOLOGY 2000; 32:289-296.
57:510-573.

HEPATOLOGY, Vol. 36, No. 6, 2002 VAJDOVA, GRAF, AND CLAVIEN 1551
32. Sorrentino D, Van Ness K, Ribeiro I, Miller CM. Functional and mor- phological features of isolated hepatocytes preserved in University of Wis- consin solution. HEPATOLOGY 1991 ; 14:33 1-339.
52. Minor T, Isselhard W. Synthesis of high energy phosphates during cold ischemic rat liver preservation with gaseous oxygen insufflation. Trans- plantation 1996;61:20-22.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46
47
Kamiike W , Burdelski M, SteinhoffG, Ringe B, Lauchart W , Pichlmayr R. Adenine nucleotide metabolism and its relation to organ viability in hu- man liver transplantation. Transplantation 1988;45: 138-143. Lanir A, Jenkins RL, Caldwell C, Lee RG, Khettry U, Clouse ME. Hepatic transplantation survival: correlation with adenine nucleotide level in donor liver. HEPATOLOGY 1988;8:471-475. Ohkohchi N, Endoh T, Oikawa K, Seya K, Satomi S. Fragility of the electron transport chain and superoxide generation in mitochondria of the liver graft after cold ischemia. Transplantation 1999;67:1173-1177. Lemasters JJ, Nieminen AL, Qian T , Trost LC, Elmore SP, NishimuraY, Crowe RA, et al. The mitochondrial permeability transition in cell death: a common mechanism in necrosis, apoptosis and autophagy. Biochim Biophys Acta 1998;1366:177-196. Morimoto Y, Kamiike W, Nishida T , Hatanaka N, Shimizu S, Huang TP, Hamada E, et al. Improvement of rat liver graft function by insulin admin- istration to donor. Gastroenterology 1996;111:1071-1080. Sankary H, Foster P, Brown E, Bhattachyaryya A, Williams J. Relevance of the nutritional status of donors in viability of transplanted hepatic allo- grafts. Transplantation 199254: 170- 172. Sumimoro R, Southard JH, Belzer FO. Livers from fasted rats acquire resistance to warm and cold ischemia injury. Transplantation 1993;55:
Sun X, Kimura T, Kobayashi T , Noriki S, Imamura Y, Fukuda M, Yamaguchi A. Viability of liver grafts from fasted donor rats: relationship to sinusoidal endothelial cell apoptosis. J Hepatobiliary Pancreat Surg
Hue L, Rider MH. Role of fructose 2,6-bisphosphate in the control of glycolysis in mammalian tissues. Biochem J 1987;245:313-324. Morgan GR, Sanabria JR, Clavien PA, Phillips MJ, Edwards C, Harvey PR, Strasberg SM. Correlation of donor nutritional status with sinusoidal lining cell Viability and liver function in the rat. Transplantation 1991 ;5 1: 1176-1 183. Cywes R, Greig PD, Sanabria JR, Clavien PA, Levy GA, Harvey PR, Strasberg SM. Effect of intraportal glucose infusion on hepatic glycogen content and degradation, and outcome of liver transplantation. Ann Surg
Rauen U, Noll T, Piper HM, Lauchart W, Becker HD, De Groot H. Endothelial cell toxicity of preservation solutions: comparison of endothe- lial cells of different origin and dependence on growth state. Cryobiology 1994;31:144-153. Nishihara M, Sumimoto R, FukudaY, Southard JH, Asahara T, Kawaishi H, Dohi K. TNF-alpha and heat-shock protein gene expression in isch- emic-injured liver from fasted and non-fasted rats. Role ofdonor fasting in the prevention of reperfusion injury following liver transplantation. Transpl Int 1998;ll Suppl 1:S417-S420. Lelli JL, Jr., Becks LL, Dabrowska MI, Hinshaw DB. ATP converts necro- sis to apoptosis in oxidant-injured endothelial cells. Free Radic Biol Med
Leist M, Single B, Castoldi AF, Kuhnle S, Nicotera P. Intracellular aden- osine triphosphate (ATP) concentration: a switch in the decision between apoptosis and necrosis. J Exp Med 1997;185:1481-1486.
728-732.
2001;8:268-273.
1992;216:235-246.
1998;25:694-702.
48. Toledo Pereyra LH, Bergren CT. Liver preservation techniques for trans- plantation. Artif Organs 1987;11:214-223.
49. Schon MR, Kollmar 0, Wolf S, Schrem H , Matthes M, Akkoc N, Schnoy NC, et al. Liver transplantation after organ preservation with normother- mic extracorporeal perfusion. Ann Surg 2001;233:114-123.
50. Dutkowski P, Odermatt B, Heinrich T, Schonfeld S, Watzka M, Winkel- bach V, Krysiak M, et al. Hypothermic oscillating liver perfusion stimu- lates ATP synthesis prior to transplantation. J Surg Res 1998;80:365-372.
51. Tanaka J, Takino H, Malchesky PS, Walsh RM. Does oxygen supply improve graft viability in liver preservation? Biomater Artif Cells Immobi- lization Biotechnol 199220:545-548.
53. Minor T , Klauke H, Nagelschmidt M, Isselhard W. Reduction of prote- olysis by venous-systemic oxygen persufflation during rat liver preservation and improved functional outcome after transplantation. Transplantation
54. Delmas Beauvieux MC, Gallis JL, Rousse N, Clerc M, Canioni P. Phos- phorus-3 1 nuclear magnetic resonance of isolated rat liver during hypo- thermic ischemia and subsequent normothermic perfusion. J Hepatol 1992; 15: 192-20 1.
55. Minor T, Isselhard W, Yamamoto Y, Obara M, Saad S. The effects of allopurinol and SOD on lipid peroxidation and energy metabolism in the liver after ischemia in an aerobidanaerobic persumation. Surg Today
56. Kusumoto K, Morimoro T, Minor T , Uchino J, Isselhard W. Allopurinol effects in rat liver transplantation on recovery of energy metabolism and free radical-induced damage. Eur Surg Res 1995;27:285-291.
57. Sumimoto R, Jamieson NV, Wake K, Kamada N. 24-hour rat liver pres- ervation using UW solution and some simplified variants. Transplantation 1989;48:1-5.
58. Dunne JB, Davenport M, Williams R, Tredger JM. Evidence that S- adenosylmethionine and N-acetylcysteine reduce injury from sequential cold and warm ischemia in the isolated perfused rat liver. Transplantation 1994;57: 1161 -1 168.
59. Lee YB, Lee SM. Effect of S-adenosylmethionine on hepatic injury from sequential cold and warm ischemia. Arch Pharm Res 2000;23:495-500.
60. Palombo JD, Bowers JL, Clouse ME, McCullough A, Forse RA, Bistrian BR. Hepatic utilization of exogenous nucleotide precursors for restoration ofATP after cold ischemia in rats. Am J Clin Nutr 1993;57:420-427.
61. Lund P, Cornell NW, Krebs HA. Effect of adenosine on the adenine nucleotide content and metabolism of hepatocytes. Biochem J 1975;152: 593-599.
62. Rapaport E, Zamecnik PC. Incorporation of adenosine into ATP: forma- tion ofcompartmentalized ATP. Proc Natl Acad Sci U S A 1976;73:3122- 3125.
63. Fox IH, Kelley WN. Human phosphoribosylpyrophosphate synthetase. Kinetic mechanism and end product inhibition. J Biol Chem 1972;247: 2126-2131.
64. Kaisers U, Pappert D, Langrehr JM, Undi H, Neuhaus P, Rossaint R. Dopamine, dopexamine and dobutamine in liver transplant recipients: a comparison of their effects on hemodynamics, oxygen transport and he- patic venous oxygen saturation. Transpl Int 1996;9:214-220.
65. Kaisers U, Neumann U, Kuhlen R, Sprenger M, Neuhaus P, Rossaint R. Nitroglycerin versus epoprostenol: effects on hemodynamics, oxygen de- livery, and hepatic venous oxygenation after liver transplantation. Liver Transpl Surg 1996;2:455-460.
66. Minor T, Isselhard W. Role of the hepatovasculature in free radical medi- ated reperfusion damage of the liver. Eur Surg Res 1993;25:287-293.
67. Ward A, Clissold SP. Pentoxifylline. A review of its pharmacodynamic and pharmacokinetic properties, and its therapeutic efficacy. Drugs 1987;34:
68. Kozaki K, Egawa H, Bermudez L, Keefe EB, So SK, Esquivel CO. Effects of pentoxifylline pretreatment on Kupffer cells in rat liver transplantation. HEPATOLOGY 1995;21: 1079- 1082.
69. Nishizawa H, Egawa H, Inomata Y, Uemoto S, Asonuma K, Kiuchi T, Yamaoka Y, et al. Efficiency of pentoxifylline in donor pretreatment in rat liver transplantation. J Surg Res 1997;72: 170-176.
70. Upadhya AG, Harvey RP, Howard TK, Lowell JA, Shenoy S, Strasberg SM. Evidence of a role for matrix metalloproteinases in cold preservation injury of the liver in humans and in the rat. HEPATOLOGY 1997;26:922- 928.
71. Bilbao G, Contreras JL, Gomez Navarro J, Eckhoff DE, Mikheeva G, Krasnykh V, Hynes T, et al. Genetic modification of liver grafts with an adenoviral vector encoding the Bcl-2 gene improves organ preservation. Transplantation 1999;67:775-783.
1997;63:365-368.
1993;23:728-732.
50-97.

1552 VAJDOVA, GRAF, AND CLAVIEN HEPATOLOGY, December 2002
72. Arora AS, Nichols JC, DeBernardi M, Steers JL, Krom RA, Gores GJ. Glycine rinse protects against liver injury during transplantation, Trans- plant Proc 1999;31:'505-506.
73. Nishimura Y, Takei Y, Kawano S, Goro M, Nagano K, Tsuji S, Nagai H, et al. The F(ab')2 fragment of an anti-ICAM-1 monoclonal antibody attenuates liver injury after orthotopic liver transplantation. Transplanta- tion 1996;61:99-104.
74. Cywes R, Harvey PR, Packham MA, Cameron R, Strasberg SM. The influence ofprostaglandin E l on platelet adherence and injury in preserved rat liver allografts. Liver Transpl Surg 1996;2:23-36.
75. Marsh DC, Vreugdenhil PK, Mack VE, Belzer FO, Sourhard JH. Glycine protects hepatocyres from injury caused by anoxia, cold itchemia and mi- tochondrial inhibitors, bur not injury caused by calcium ionophores or oxidative stress. HEPATOLOGY 1993; 17:9 1-98.