Assessing knowledge, attitudes, and practices of mothers ...
96
College of Nursing National Taipei University of Nursing and Health Sciences Master Thesis Assessing knowledge, attitudes, and practices of mothers regarding childhood immunization in Papua New Guinea Jessica Prabon Advisor: Cheng-Hui Chou, PhD. June 2020
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Assessing knowledge, attitudes, and practices of mothers ...
College of Nursing
National Taipei University of Nursing and Health Sciences
Master Thesis
Assessing knowledge, attitudes, and practices of mothers regarding
childhood immunization in Papua New Guinea
Jessica Prabon
Advisor: Cheng-Hui Chou, PhD.
June 2020
Acknowledgements
Student life at National Taipei University of Nursing and Health Sciences (NTUNHS)
has come to its very end and I give all the praise and glory to my God who has always been
my pillar during this time. I am and will be forever be grateful to God for this amazing
experience.
I would like to express my sincere gratitude to my advisor, Professor Cheng- Hui
Chou for her dedicated supervision, tireless effort, patience, commitment and time. Without
her supervision I would not be able to complete my thesis. Moreover, a special thanks to
Professor Chieh-Yu Liu and Professor Fang-Yi Lin for their valuable input into this work. In
addition, a special thanks to Stephanie Pfeiffer who really gave her time to edit this work.
A heartfelt gratitude to the faculty and staff of NTUNHS, for all their efforts, made it
possible to attain my degree. Also special thanks to Taiwan Ministry of Education, through
NTUNHS school scholarship, that made it possible for my dream to become a reality, attain
my master’s degree. Also a special thanks to my course mates who supported me in words
and deeds.
Special thanks also to Sandaun Provincial Hospital Management for giving me
permission to conduct research, the staff of Outpatient and Family Health Service who
assisted me in collecting my data, and the participants of the study.
Finally special thanks to my husband, daughter and all my family for their continuous
love and support throughout my study. Their heartwarming support motivated and inspired
me to see this study to its completion.
Abstract
Background: Immunization is the most effective public health measure against infectious
diseases like influenza, measles, polio and rubella. However, in recent years, Papua New
Guinea has had frequent outbreaks of vaccine-preventable diseases, such as measles and
polio. Knowledge Attitudes and Practice studies are tools for investigating factors that
influence mothers’ decisions about getting their children immunized.
Purpose: The purpose of this study was to explore the relationships amongmothers’
knowledge, attitudes and practices relating to childhood immunization, in order to identify
factors that could be targeted by interventions aimed at increasing immunization coverage in
Papua New Guinea.
Methods: This cross-sectional correlation study was conducted with 114 mothers who had
children under age five from July to September 2019. This study used a demographic
questionnaire and the Knowledge, Attitude and Practice questionnaire on immunization.
Results were analyzed using ANOVA, t-test, Pearson’s correlation and hierarchical multiple
linear regression.
Results: Age, number of children, education, and urban or rural residence were significant
factors influencing immunization practice. Overall, results showed that the mothers had fairly
good knowledge and favorable attitudes about vaccination, but poor practice. However, in the
hierarchical multiple linear regressions, only knowledge was found to predict practice.
Conclusion: This study found that mothers’ knowledge about vaccines is one factor that
hinders them from getting their children fully vaccinated. Despite the efforts of health
workers to increase coverage by educating mothers, knowledge remains uneven and not all
children are brought in for vaccination. The findings suggest that, on the one hand, current
efforts to educate mothers about vaccines have not yet been completely successful, and on the
other, that health education alone may not be sufficient.

Keywords: Immunization, Knowledge, Attitudes, Practices, Mothers of children under five
Acronym
BCG: Bacillus Calmette Guerin
DTP: Diphtheria Tetanus Pertussis
CDC: Center of Disease Control
EPI: Expanded Program of Immunization
GAVI: Global Alliance for Vaccines and Immunization
HepB: Hepatitis B
IPV: Inactivated Polio Vaccine
KAP: Knowledge, Attitudes and Practices
NHP: National Health Plan
PCV: Pneumococcal Conjugate Vaccine
PHA: Provincial Health Authority
PNG: Papua New Guinea
SPH: Sandaun Provincial Hospital
UNDP: United Nations Development Program
UNICEF: United Nations Children’s Fund
UN: United Nations
VDP: Vaccine Preventable Disease
WHO: World Health Organization
WSP: West Sepik Province
i
Table of contents List of Tables ............................................................................................................................ iii
List of Figures ........................................................................................................................... iv
Chapter I Introduction ............................................................................................................ 1
Section I: Background .......................................................................................................... 1
Section II: Problem statement ............................................................................................... 5
Section III: Study purpose ................................................................................................... 6
Section IV: Research questions ........................................................................................... 6
Section V: Significance of the study .................................................................................... 6
Section I: Introduction of Papua New Guinea ................................................................... 8
Section II: Health System in PNG ....................................................................................... 9
Section III: Under five mortality....................................................................................... 11
Section IV: Expanded Program of Immunization ........................................................... 12
Section V: Relevant studies................................................................................................ 18
2.Knowledge, attitudes and practices of mothers regarding immunization ................. 22
Section VI: Definition of variables .................................................................................... 26
Chapter III: Methodology .....................................................................................................27
Section I: Conceptual Framework .................................................................................... 27
Section II: Research Design ............................................................................................... 28
Section III: Study area and setting ................................................................................... 28
Section IV: Sample size ...................................................................................................... 28
Section V: Sample Selection .............................................................................................. 28
Section VI: Instruments ..................................................................................................... 29
ii
Section VII: Research ethics and statements .......................................................................31
Section VIII: Data collection procedure ........................................................................... 31
Section IX: Data Analysis .................................................................................................. 31
Chapter IV Results and Discussion ......................................................................................34
Section I Results .................................................................................................................. 34
Section II Discussion........................................................................................................... 45
CHAPTER V Conclusion ......................................................................................................57
Section I Implications for future research ....................................................................... 57
1. Health Policy ................................................................................................................ 57
2. Public Health Education ............................................................................................... 58
3. Nursing Practice............................................................................................................ 58
Section II Recommendations of the study ........................................................................ 58
Section III Limitations of the study .................................................................................. 60
Section IV Conclusion ........................................................................................................ 61
Reference ............................................................................................................................. 61
Appendix I: Consent Form ....................................................................................................73
Appendix II: Instrument .................................................................................................... 74
Appendix IV: Permission Request for Instrument.......................................................... 83
Appendix V: Data Collection Plan .................................................................................... 84
Appendix VI: Approval letter from Sandaun Provincial Hospital ...................................85
Appendix VII: Approval letter and number from MRAC PNG .......................................86
iii
List of Tables
Table 1.1 PNG National Immunization Schedule……………………………………………06
Table 2.1 PNG Immunization Coverage in 2014…………………………………………….14
Table 2.2 Immunization Coverage of Momase Region in 2014 …………………………….15
Table 3.1 Statistical Test for Study………………………………………………………......31
Table 4.1 Socio demographic characteristics of mothers………………………………...36-38
Table 4.2 Immunization knowledge score of mother………………………………………..40
Table 4.3 Immunization attitude scores of mothers………………………………………….41
Table 4.4 Immunization practice scores of mothers…………………………………………41
Table 4.5 Mean scores of mothers KAP regarding immunization…………………………...42
Table 4.6 Linear regression analysis of knowledge and demographic characteristics………43
Table 4.7 Linear regression analysis of attitude and demographic characteristics…………..44
Table 4.8 Linear regression analysis of practice and demographic characteristics………….45
Table 4.9 Correlation between knowledge and attitude and the immunization practice…….46
Table 5 Hierarchical multiple regression analysis summary predicting practice……………47

iv
List of Figures
Figure 1 Map of Papua New Guinea…………………………………………………...….....11
Figure 2 Research Framework ………………………………………………………………26
1
Chapter I Introduction
Section I: Background
Immunization is the most effective public health measure against infectious diseases
like influenza, measles, polio, and rubella. Immunization saves the lives of an estimated 2.5
million children every year (Lakew, Bekele, & Biadgilign, 2015). However, due to under-
vaccination, 1.7 million children under the age of five still die from vaccine-preventable
diseases each year, according the WHO (WHO, 2011). Outbreaks of vaccine-preventable
diseases like polio can lead to complications such as acute flaccid paralysis. This complication
has substantial consequences for the social and economic activities of the families
affected(Quilici, Smith, & Signorelli, 2015). For example, when a child has acute flaccid
paralysis, he or she will not go to school and will be a burden on the family. Furthermore,
developing countries such as Papua New Guinea (PNG) are more affected by outbreaks of
VPDs than developed countries, because their health systems lack resources.
Papua New Guinea, which occupies the eastern side of the island of New Guinea, is
located south of the equator and north of Australia and shares a land border with
Indonesia(AusAid, 2015).The country has a tropical climate, characterized by a rainy season
(October to May) and a dry season (June to September). Overall, PNG experiences a high
yearly average of rainfall and average humidity levels are around 70~90%. It also has beautiful
tropical forests, savannah grass plains, big rivers and deltas, swamps, numerous islands,
lagoons, and atolls to the east and north east of the country. Its weather affects the timing and
intensity of disease outbreaks and climate conditions impact the geographical and seasonal
distributions of infectious disease. Additionally, geography and weather can make it difficult
for health workers to provide vaccinations to people in rural areas.
2
Infectious disease is a main factor responsible for the majority of deaths among children
under five around the world. The overall estimated population of Papua New Guinea in 2015
was 7,619,300 (WHO, 2018a). Approximately 40% of PNG’s population consists of children
and adolescents under the age of 15 (AusAid, 2015; National Department of Health, 2010).
Infectious disease is one of the primary causes of death among children under the age of five
in particular (PNG, 2010).
In June 2012 PNG saw the first outbreak of Chikungunya, a fast-spreading infectious
disease, with 1,590 reported cases (Horwood et al., 2013). In late 2013 and 2014, a measles
outbreak spread across the country and into the Solomon Islands and Vanuatu. More than 365
deaths were reported by the end 2014, with a case fatality rate of 0.46% (International
Federation of Red Cross and Red Crescent Societies, 2018). Just three years later, a measles
outbreak occurred again with 57 reported cases, eight of them confirmed by laboratory testing
and two deaths (International Federation of Red Cross and Red Crescent Societies, 2018). The
problem is widespread. A survey of child mortality done in 2015 by searching the WHO,
Centers for Disease Control & Prevention (CDC), the United Nations Children’s Fund
(UNICEF) and the United Nations (UN) websites revealed that each day, 16,000 children die
before reaching their fifth birthday (Khodaee, Khademi, & Saeidi, 2015).
More than 50 countries worldwide have under five mortality of greater than
25 per 1000 live births. Papua New Guinea has an under-five mortality rate of 54.3 per 1000
live births (WHO, 2018a). Although under-five mortality in PNG dropped from 73 per 1000
live births in 2000 to 57.3 per 1000 live births in 2017, it nonetheless missed its 2015 target of
56 per 1000 live births (PNG Govt., 2015). Innovative interventions will be needed to reach
the UN’s Sustainable Development Goals target of less than 25 per 1000 live births by 2030
(Hug et al, 2018). Consequently, the PNG government is prioritizing improving child survival,
3
rolling out immunization programs to address the problem of under-vaccination, with the help
of international agencies such as United Nation agencies and major foundations (PNG, 2010).
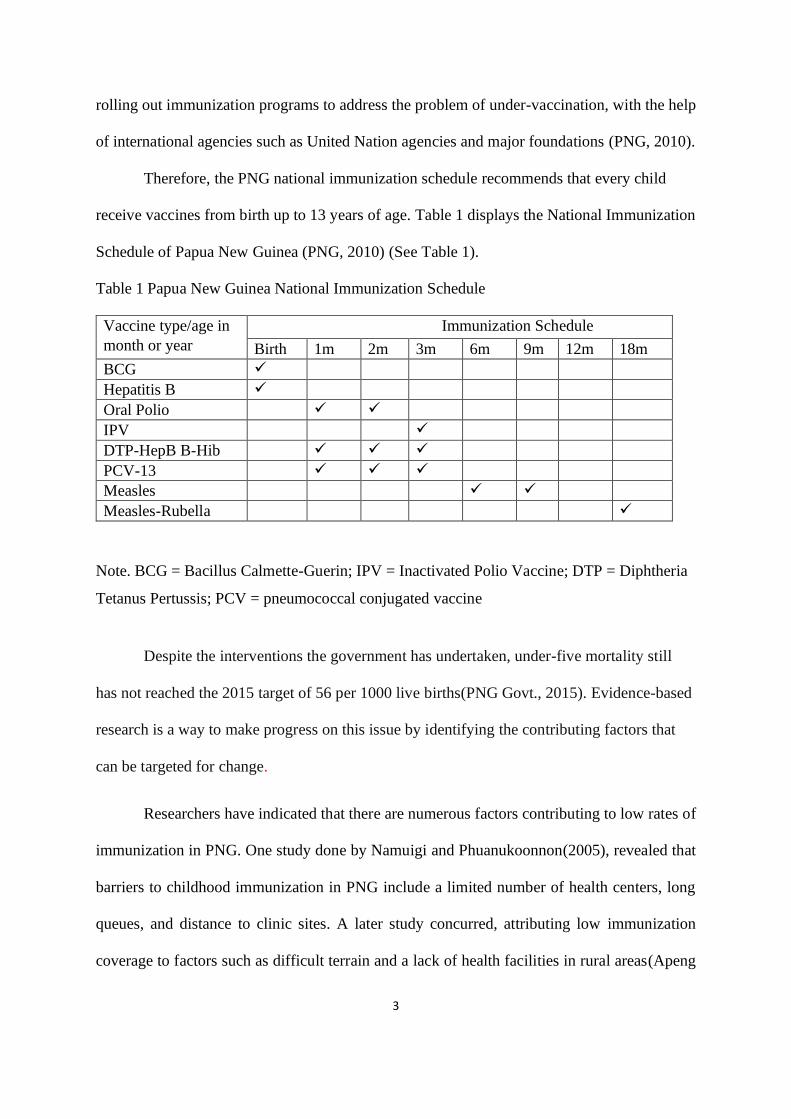
Therefore, the PNG national immunization schedule recommends that every child
receive vaccines from birth up to 13 years of age. Table 1 displays the National Immunization
Schedule of Papua New Guinea (PNG, 2010) (See Table 1).
Table 1 Papua New Guinea National Immunization Schedule
Vaccine type/age in
month or year
Immunization Schedule
Birth 1m 2m 3m 6m 9m 12m 18m
BCG ✓
Hepatitis B ✓
Oral Polio ✓ ✓
IPV ✓
DTP-HepB B-Hib ✓ ✓ ✓
PCV-13 ✓ ✓ ✓
Measles ✓ ✓
Measles-Rubella ✓
Note. BCG = Bacillus Calmette-Guerin; IPV = Inactivated Polio Vaccine; DTP = Diphtheria
Tetanus Pertussis; PCV = pneumococcal conjugated vaccine
Despite the interventions the government has undertaken, under-five mortality still
has not reached the 2015 target of 56 per 1000 live births(PNG Govt., 2015). Evidence-based
research is a way to make progress on this issue by identifying the contributing factors that
can be targeted for change.
Researchers have indicated that there are numerous factors contributing to low rates of
immunization in PNG. One study done by Namuigi and Phuanukoonnon(2005), revealed that
barriers to childhood immunization in PNG include a limited number of health centers, long
queues, and distance to clinic sites. A later study concurred, attributing low immunization
coverage to factors such as difficult terrain and a lack of health facilities in rural areas(Apeng
4
et al., 2010). Yet another study revealed that children were not immunized due to distance to
clinics and travel expenses (Toikilik et al., 2010). Issues with health services transport and
travel challenges are thus well-documented. This study will focus on parental factors in under
vaccination among children under age five in PNG.
Factors such as mothers’ knowledge are vital for improving immunization coverage.
One problem is partial or incomplete knowledge. For example, a study by Karel (1994), found
that village mothers knew the importance of vaccination but did not know the importance of
completing the multiple vaccinations. Also, knowledge about vaccinations is unevenly
distributed across urban and rural areas. One study demonstrated that 60 percent of urban
mothers in PNG knew the importance of immunization and that it prevents illness, leading to
a 70 percent immunization rate in that area (Namuigi & Phuanukoonnon, 2005). (Toikilik et
al., 2010) found five years later that 29 percent of rural mothers remained unaware of the need
for vaccination. Prior studies have emphasized parental knowledge and attitudes about vaccines
in either urban or rural settings, but have not explored how these relate to actual practices. This
study will focus on knowledge, attitudes, and practices related to vaccination among mothers
of children under the age of five living in rural areas.
Mothers in rural and urban areas should have at least some basic idea about
immunization that will motivate them to bring their children in for vaccination. A study has
revealed that the uptake of immunization is determined by parents’ theoretical or practical
understanding of childhood immunization (Alamri, Horaib, & Alanazi, 2018). Another study
done in Pakistan reported that educating mothers about vaccines and VPD was highly effective
and improving mothers’ information increases the immunization coverage rate (Agboatwalla
& Akram, 1997). These studies advise that higher immunization coverage can be achieved by
educating mothers on immunization.
5
It is essential for health workers to understand mothers’ perceptions about
immunization because her judgment strongly influences whether or not her child will be
immunized. Health workers need to provide health education adapted to rural mothers’ current
level of understanding, in particular (Alamri et al., 2018; Alshammari et al., 2018; Alshehri et
al., 2018; Namuigi & Phuanukoonnon, 2005). Nonetheless, no studies have been done on
mothers’ knowledge, attitudes, and practices relating to childhood immunization in PNG.
Therefore, the aim of this study is to fill the gap by identifying the relationships between
mothers’ knowledge, attitudes, and practices regarding childhood immunization in Papua New
Guinea.
Section II: Problem statement
Low immunization coverage is still a problem in Papua New Guinea (Bauri et al., 2019;
United Nations Children's Fund, 2017; WHO, 2015, 2018b; Yarong& Aipit, 2014).Within the
last eight years, there was an outbreak of measles with a case fatality rate of 0.46% and 367
deaths (International Federation of Red Cross and Red Crescent Societies, 2018). In addition,
a polio outbreak in 2018 resulted in 26 confirmed cases of polio, of which 19 were children
under five years of age (Bauri et al., 2019). In PNG, this issue mostly occurred in rural areas
as well urban settlements who are migrants from rural areas seeking economic opportunity by
which, rural mothers are less educated and children have poor uptake of immunization(Bauri
et al., 2019). Contemporary researchers have been urging health workers to provide health
education tailored to mothers’ understanding (Alamri et al., 2018;Alruwaili et al.,
2018;Habib,Alsubhi, &Saadawi,2018; Namuigi & Phuanukoonnon, 2005). Taking into
account factors such as mothers’ knowledge, attitudes, and practices towards immunization
may help with designing more effective public health campaigns aimed at increasing
immunization rates.
6
Section III: Study purpose
The purpose of this study is to explore the relationships among mothers’ knowledge,
attitudes and practices relating to childhood immunization, and to identify the factors that
influence them in Papua New Guinea.
Section IV: Research questions
The questions of this study are:
1. What are the demographic characteristics of mothers with children under age five in Papua
New Guinea?
2. What are the knowledge, attitudes, and practices of mothers regarding childhood
immunization in Papua New Guinea?
3. What are the relationship between mothers’ knowledge, attitude and practices and the
demographic factors of immunization?
4. Which factors are most influential for determining the actual practice of immunization,
when considering demographic characteristics and mothers’ knowledge and attitudes
regarding childhood immunization in Papua New Guinea?
Section V: Significance of the study
The importance of this study is to explore the depth and breadth of mothers’ knowledge,
attitude and practice on childhood immunization in Papua New Guinea. This is for an effective
result of mothers’ knowledge, attitude and practices impacts in the uptake of childhood
immunization.
The findings can be utilized as a strategy to alleviate factors contributing to under
immunization in Papua New Guinea. Health workers should use the findings to improve the
outcome of immunization. Furthermore, this study will add a great deal to literature and public
health and the Ministry of Health in Papua New Guinea, particularly Provincial Health

7
Authorities to draw up health education programs specific to meet mothers’ understanding. In
addition, it will contribute to innumerable articles regarding the mothers’ knowledge, attitude
and practices on childhood immunization in hospital, country and the Western Pacific region.
8
Chapter II Literature Review
This chapter will give a brief introduction of Papua New Guinea and its healthcare
system. And in detail, the knowledge, attitude and practices among mothers’ of under 5
children in Papua New Guinea towards childhood immunization, mothers’ related factors,
socio economic demographic with related studies in line with the study.
Section I: Introduction of Papua New Guinea
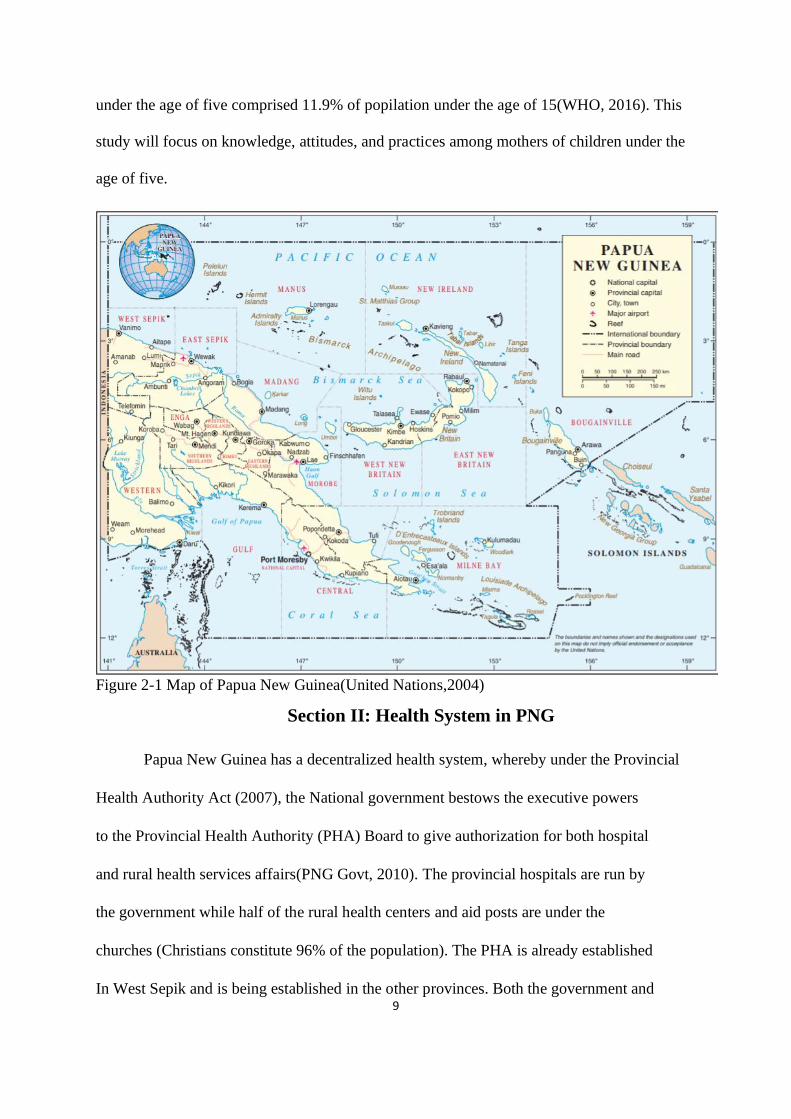
Papua New Guinea has 22 provinces and it’s capital city is Port Moresby. For
administrative purposes, PNG is divided into four regions: the southern region is
comprised of six provinces; the highlands region consists of seven provinces; the islands
region consists of five provinces and the Momase region is comprised of four provinces.
It is a culturally diverse society with ethnic groups organized as clans speaking more
than 800 native languages. The three most common languages are Tok Pisin, Hiri Motu
and English(PNG NDoH, 2010). English is used as a second or third language in addition
to local indigenous languages and is commonly used in government, business, and in
non-governmental organizations(Aquastat Survey, 2011; AusAid, 2015). This study will
be conducted in the Momase region in West Sepik province. The most common language
there is Tok Pisin. The questionnaires used in this study will be translated from English
into Tok Pisin.
In 2015, the country’s population was estimated at 7,619,300, with similar
proportion of women and men. The population growth rate has been estimated at
3.1%. It has a relatively young population with 2.6% of the population over age 65 and
40% of the population under 15 years old(WHO, 2016).Furthermore, about 89% of the
population live in the rural area and has an average literacy rate of 63.4%, by which men and
women have a literacy rate of 65.06% and 61.77% respectively(WHO, 2018a). Children
9
under the age of five comprised 11.9% of popilation under the age of 15(WHO, 2016). This
study will focus on knowledge, attitudes, and practices among mothers of children under the
age of five.
Figure 2-1 Map of Papua New Guinea(United Nations,2004)
Section II: Health System in PNG
Papua New Guinea has a decentralized health system, whereby under the Provincial
Health Authority Act (2007), the National government bestows the executive powers
to the Provincial Health Authority (PHA) Board to give authorization for both hospital
and rural health services affairs(PNG Govt, 2010). The provincial hospitals are run by
the government while half of the rural health centers and aid posts are under the
churches (Christians constitute 96% of the population). The PHA is already established
In West Sepik and is being established in the other provinces. Both the government and
10
non -governmental agencies are collaborating to execute the National Health Plan,
2011~2020. It is a blueprint for the PNG health system and integrates government
policies with international health initiatives such as the UN Millennium Development
Goals. The National Health Plan, 2011-2020 outlines eight major public healthgoals.This study
contributes to two of them: improving child survival and improving preparednessfor disease
outbreaks(PNG Govt, 2010).
Supplementary to the NHP 2011~2020, new National Health Service Standards
recategorized Papua New Guinea’s health services delivery structure into seven levels, as
listed:Level 1 consists ofaid posts, Level 2 is community health posts, Level 3 is the rural
and urban health centers, Level 4 consists of district hospitals, Level 5 indicates provincial
hospitals, Level 6 refers to regional hospitals, and Level 7 is the referral hospital(WHO, 2018a).
Because of limited length of the study period and difficult transportation into rural areas, this
study will be carried out in Level 3 rural and urban health centers and a Level 5 provincial
hospital,Sandaun Provincial Hospital.
The leading causes of morbidity are communicable diseases including pneumonia,
malaria, tuberculosis, diarrheal diseases, meningitis and increasingly, HIV/AIDS. These
account for 50% of mortality (WHO & NDoH, 2012). Specifically, pneumonia accounted for
30% of child mortality, neonatal conditions for 17%, malaria accounted for 15%, diarrheal
diseases for 12%, and malaria for 7% in 2013. In recent years, regular outbreaks of VPDs have
been occurring in PNG. Polio made a comeback in 2018 (International Federation of Red Cross
and Red Crescent Societies, 2018).
At 13,000 per year, PNG has the highest proportion of child deaths in the entire Pacific
region (Duke, Kado, Auto, Amini, & Gilbert, 2015). The WHO and UNICEF launched the
Regional Child Survival Strategy in 2006 (Jayawardena, Subhi, & Duke, 2012), PNG is one
11
of the six countries(Cambodia, China, Laos,Papua New Guinea, Philippines, and Vietnam)
with the highest mortality burden in the Western Pacific region(Jayawardena et al., 2012). In
response, the PNG government introduced the child health policy in 2009 to address the
problem of high child mortality and the policy has been carried over into the 2011-2020
National Health Plan (Jayawardena et al., 2012).. The child health policy has strengthened
immunization programs in PNG.
Most healthcare spending in PNG does not come from patients themselves, but relies on
government funding (Asian Development Bank, 2012). The government reduced health
spending from over 9 percent of GDP in 2010 to 6.8 percent in 2014(World Bank Group, 2017).
International resources also play a vital role in health financing in PNG(World Bank Group,
2017). The health expenditures on health have increased from PGK 137 million per capita in
2011 to an estimated PGK 257 million per capita in 2015(WHO, 2016). The main recipients
of this increased spending were the National Department of Health and urban hospitals. Rural
health services and public programs did not benefit from the allocated budget increase from
PGK 12 million in 2005 to PGK 64 million in 2012(WHO, 2016).
Section III: Under five mortality
The under- five mortality of children in Papua New Guinea has improved in
recent years, as evidenced by the decline in mortality rates of children under five from 100
per 1,000 live births in 1990 to 57.3 per 1,000 live births in 2017 (WHO & NDoH, 2012),
which is still high compared to the other Western Pacific countries(Duke et al., 2015). The
PNG government is addressing child health problems through improved immunization,
periodic supplementary immunization activities, and the joint UNICEF/WHO child survival
strategy, with the focus on an approach that integrates management of childhood illnesses
(PNG Govt, 2010).
12
Section IV: Expanded Program of Immunization
The World Health Organization (WHO) initiated the Expanded Program of
Immunization in 1974 with the intention to vaccinate children around the world (Greenwood,
2014). The program was created with the purpose of expanding immunization services beyond
smallpox to the following six preventable diseases: diphtheria, measles, pertussis, poliomyelitis,
tetanus and tuberculosis (Matapano et al., 2008). Vaccines create immunity by stimulating the
body’s immune system to make its own antibodies, protecting the individual against infection
(Anderson, 2015).Vaccines can be given routinely and alsoin response to outbreaks. Routine
immunization refers to the nationally scheduled administration of vaccines at specific ages.
Parents should take children to clinicswhen they reach the appropriate age for a vaccine. The
WHO recommends that immunization be carried out on specific days of the week to reduce
vaccine wastage, since the vaccines are supplied in multi dose vials to reduce cost. The goal of
routine immunization is to deliver scheduled doses of vaccines in a timely, safe, and effective
way to all children, ultimately inducing immunity against the targeted diseases.
Though efforts at immunization have yielded highly beneficial results and most
developed countries have over 90% coverage, the situation is quite different in developing
countries, especially in Africa and Asia. Like many other countries in the Pacific, Papua New
Guinea is making efforts to strengthen its health system so as to achieve adequate routine
immunization to reduce the burden of VDPs. However, in Papua New Guinea, immunization
coverage is still low.
The low level of immunization coverage in Papua New Guinea may be attributed to factors
such as lack of political will, lack of motivation among the general public and health workers,
poor level of education and awareness, and poor infrastructure().Other factors related to low
immunization coverage could be high illiteracy rates, high fertility rates, and also 89% of the
13
population is living in rural areas with challenging terrain (PNG Govt,2010).
Immunization is a process where an individual is protected from infectious diseases,
by the administration of vaccines, by which it stimulates the body’s immune system to make
its own antibodies to fight against infections(Anderson, 2015). The vaccines defined below
are included in the immunization schedule of PNG.
Bacillus Calmette-Guerin (BCG) is a vaccine used in the prevention of tuberculosis.
It is used in countries with high prevalence of TB in order to prevent childhood tuberculosis,
meningitis, and military tuberculosis (Centers of Disease Control, 2011). BCG vaccine
should be given at birth and the recommended dose is 0.05 ml intra-dermally into the left
upper arm (PNG Pediatric Society, 2016). BCG vaccine is contraindicated to infants of HIV-
positive mothers for whom full assessment of their HIV status has not been completed
(Nuttall & Eley, 2011).Children with HIV are at risk of disseminated BCG disease, meaning
confirmed presence of the bacteria at one or more sites, usually including the vaccine site and
lymph nodes. It has a death rate of over 70% infants infected with HIV.
Hepatitis B vaccine is used to prevent hepatitis B infections which cause liver
disease,which often leads to liver cancer and cirrhosis(Centers for Disease Control and
Prevention, 2018). It should be given at birth and every month for the following three months
as part of the five-in-one vaccine, Pentavalent. The recommended dosage is 0.5ml
intramuscularly into the right thigh(PNG Pediatric Society, 2016). However, it should not be
administered when a child has fever exceeding 38degree Celsius.
Pentavalent vaccines provide protection against five diseases: diphtheria, tetanus,
pertussis (DTP), hepatitis B and Hemophilus influenza type b(UNICEF, 2015).Hepatitis B
vaccine had previously been added to the DTP (diphtheria, tetanus, pertussis) combination
vaccine (DTP-HepB), which has now been replaced by the pentavalent version that includes
influenza. The pentavalent vaccine is administered in a three-dose schedule. The chosen route
14
is intramuscularly into the right thigh. It also should not be given if a child has a fever
exceeding 38 degree Celsius.
Polio vaccine protects children from infection with the polio virus. It is mainly spread
by person-to-person contact and also through the consumption of food or drink products that
are contaminated with fecal matter of an infected person(CDC, 2015c). Most people who get
polio have no symptoms and recover, but others develop paralysis. It can lead to permanent
disability and even death. Some countries have done away with the oral polio vaccine and are
only using injected inactivated polio vaccine, which covers all three types of the polio virus.
PNG is still using the oral polio vaccine and introduced the inactivated polio vaccine in 2015.
Inactivated polio vaccine was not introduced to replace the oral polio vaccine(Expanded
Immunization Programme, 2014). The oral polio vaccine is administered sublingually at one,
two, and three months of age, while the IPV is given intramuscularly into the right thigh at
three months of age together with the oral polio vaccine(PNG Pediatric Society, 2016).
The pneumococcal conjugate vaccine protects against 13 types of pneumococcal
bacteria(CDC, 2015b). It is routinely given at one month of age, then again one month after
the first dose, and again one month after the second dose. The recommended dose is 0.5ml
intramuscularly into the left thigh(PNG Pediatric Society, 2016). It is contraindicated for
children with fever above 38degrees Celsius.
The measles and measles-rubella vaccine are used in the prevention of measles and
rubella(CDC, 2015a) They are viral diseases that have serious consequences. Measles causes
symptoms that can include fever, cough, runny nose, and red watery eyes, commonly
followed by a rash that covers the whole body. While the rubella virus causes fever, sore
throat, rash, headaches and eye irritation. It can lead to ear infections, diarrhea and
pneumonia. It is contagious and can easily spread from person to person. The recommended
15
dose is 0.5ml and it is administered subcutaneously into the right upper arm and is given at
6months, 9months and 18months of age (PNG Pediatric Society, 2016).
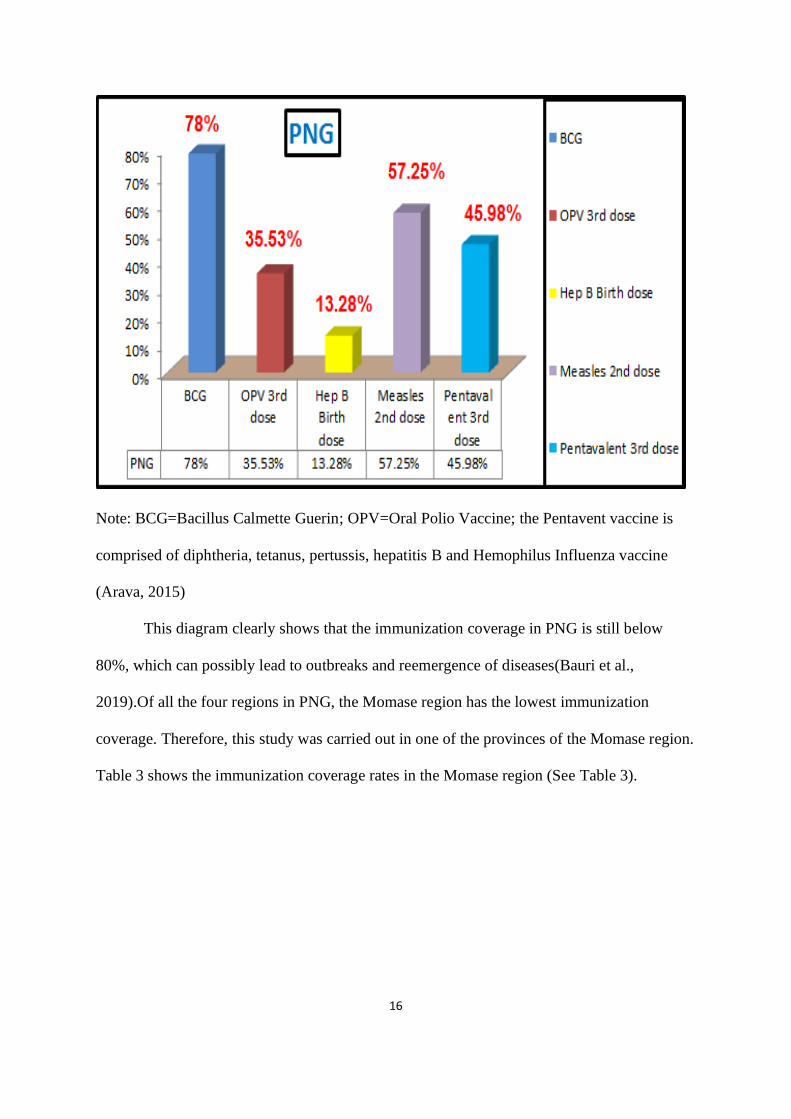
Table 2.1 PNG Immunization coverage of children under the age of five in 2014
16
Note: BCG=Bacillus Calmette Guerin; OPV=Oral Polio Vaccine; the Pentavent vaccine is
comprised of diphtheria, tetanus, pertussis, hepatitis B and Hemophilus Influenza vaccine
(Arava, 2015)
This diagram clearly shows that the immunization coverage in PNG is still below
80%, which can possibly lead to outbreaks and reemergence of diseases(Bauri et al.,
2019).Of all the four regions in PNG, the Momase region has the lowest immunization
coverage. Therefore, this study was carried out in one of the provinces of the Momase region.
Table 3 shows the immunization coverage rates in the Momase region (See Table 3).
17
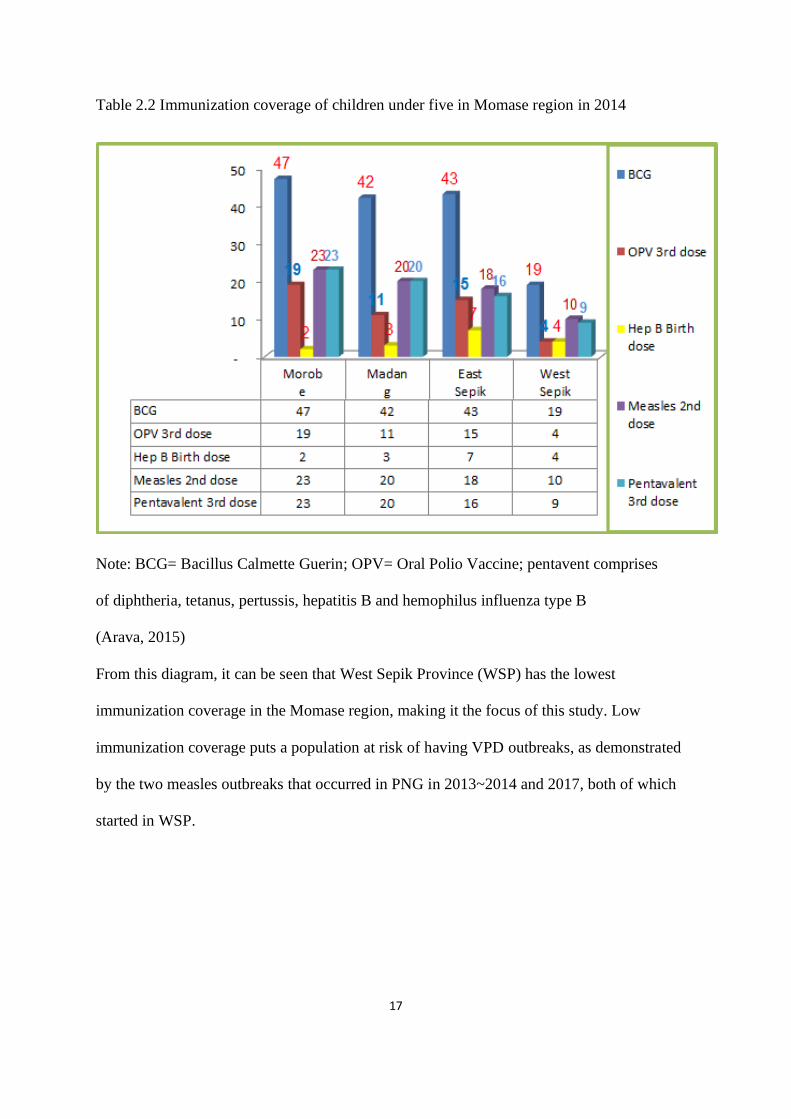
Table 2.2 Immunization coverage of children under five in Momase region in 2014
Note: BCG= Bacillus Calmette Guerin; OPV= Oral Polio Vaccine; pentavent comprises
of diphtheria, tetanus, pertussis, hepatitis B and hemophilus influenza type B
(Arava, 2015)
From this diagram, it can be seen that West Sepik Province (WSP) has the lowest
immunization coverage in the Momase region, making it the focus of this study. Low
immunization coverage puts a population at risk of having VPD outbreaks, as demonstrated
by the two measles outbreaks that occurred in PNG in 2013~2014 and 2017, both of which
started in WSP.
18
Section V: Relevant studies
1.Socioeconomic demographic factors of mothers
The socio-demographic characteristics used in this study include age, number of
children, education level and income, source of information, marital status, transport,
decision-making power, and place of residence.
1.1. Age
Age affects many things, such as a person’s perspective and conduct, their level of
maturity, range of life experience, and their ability to make decisions; thus, mothers’ age can
influence their knowledge, attitudes, and practices regarding vaccination. A study in Yemen
revealed that parents ages 30 years or younger had significantly lower knowledge scores
compared to older parents (Bamatraf& Jawass, 2018).Similarly, a study in the United Arab
Emirates demonstrated that older mothers are less likely to have good knowledge about
childhood immunization(Bersen et al., 2011).However, a study in India showed that there was
no statistical difference in mothers’ knowledge according to age(Dharmalingam, Raghupathy,
Sowmiya, Amudharaj, & Jehangir, 2017). This could mean that, in some contexts, age does
not have much impact on mothers’ knowledge about vaccination.
1.2. Number of children
In general, having more children means more experience and results in better
practices regarding childhood immunization. For example, a study in Saudi Arabia revealed
that having more children resulted in having significantly better KAP scores (Alshehri et al.,
2018). A different study in Saudi Arabia likewise found that having more children was
associated with better KAP scores (Habib et al., 2018).It can be concluded that mothers
having more children have a lot of experience, resulting in positive practices regarding
childhood vaccination.
19
1.3. Education level
Parental education in general and about vaccines in particular has been found in
numerous studies to be related with higher immunization rates, suggesting that parents’
education level plays a significant role in this regard. In a study done in India, the use of health
care services as well as full immunization of children was associated with maternal education
level (Kusuma, Kumari, Pandav, & Gupta, 2010). In a study in Pakistan, immunization of
children was associated with maternal education about vaccination(Mitchell et al.,
2009).Moreover, a study in Guinea Bissau revealed that women and men who have had access
to higher education tend to have better general health knowledge (King.R, Mann.V, &
Boone.P.D, 2010), demonstrating the influence education has on health behaviors including
childhood immunization.
1.4. Income
Income refers to money received on a regular basis for work that can be used to provide
for the child’s basic needs, such as paying for transportation to bring the child to the clinic.
Studies tracking the association between income and immunization have yielded mixed results
in different regions and countries. For example, a study in Uganda revealed that income was
not associated with full vaccination status (Vonasek et al., 2006). In contrast, a study done in
Iraq showed that family’s economic status was positively associated with the uptake of
immunization (Quaitaba et al, 2015). The results of these studies differ, in part, because they
were done in countries with different health systems and different levels of economic
development, which may influence the results.
1.5. Source of information
Sources of information about vaccination include health workers and other people,
media such as pamphlets or TV programs, and clinics and hospitals. A study done in Papua
New Guinea found that participants’ health information came mostly from health workers
20
(Toikilik et al, 2010). Similarly, a study in Egypt revealed that health workers were the main
source of information related to vaccination (Ramadan et al., 2016). These findings
demonstrate that parents often get their knowledge about immunization from health workers.
1.6. Marital Status
For the purposes of this study, marital status is defined as married, single, divorced or
widowed. Marital status can have an impact on mothers’ KAP regarding immunization. One
study done in Nigeria found that married women had significantly higher knowledge of
immunization than separated, single, or divorced women (Chris-Otubor, et al, 2015). Another
study from Nigeria revealed no significant difference regarding the practice of immunization
among mothers of different marital statuses (Kanma-Okafor, et al, 2019). This could suggest
that marital status can have a different influence on immunization knowledge or practice in
according to population group or setting. Differences between countries and ethnic groups
may be due to other factors, including education and culture.
1.7. Transport
Transport is a factor that can prevent caregivers from bringing their children for
vaccination. A study in Nigeria showed that distance to primary health care facilities was
significantly associated with immunization status of the children(Adenike, Adejumoke,
Olufunmi, & Ridwan, 2017).This may be related to socioeconomic factors and cost of
transportation for each immunization, especially where healthcare facilities are not in close
proximity(Adenike et al., 2017). Likewise, a study in Papua New Guinea revealed that distance
and travel expenses are associated with the uptake of immunization (Toikilik et al, 2010). These
findings demonstrate that transportation plays a vital role in the uptake of immunization.
1.8. Women’s role in decision making
21
Several studies have investigated the role of women in health care decisions
(Gakidou.E, Cowling.K, Lozano.R, & Murray.C.J.L, 2010). In many families in Uganda, for
instance, even though mothers are the primary care takers of children, fathers usually make
decisions about participation in government programs and their objections are often one of the
barriers to their children’s vaccination(Nuwuha, Mulindwa, Kabwongyera, & Barenzi, 2000).
Education has been revealed to be one of the main societal factors that impact the role of
women in decisions about childhood vaccination. Many studies have found that maternal
education is the key element in parental adherence to vaccination programs, even though the
education of both parents was found to be essential to health behavior, (Kusuma et al., 2010;
Mitchell et al., 2009; Sullivan, Tegegn, Tessema, Galea, & Hadley, 2009). In this regard, a
study done in sub Saharan Africa revealed that increased health care access in Ethiopia was
related to the high literacy rate among women(Sullivan et al., 2009). In efforts to reduce child
mortality and morbidity, studies have recommended educating mothers about the importance
of family planning, breastfeeding, and immunization programs (Girma.B & Berhane.Y, 2011).
1.9. Place of residence
The 2011 Millennium Development Goal Report describes a higher rate of mortality among
children from rural households. It is thus important to explore whether there are differences in
routine childhood immunization rates between urban and rural communities in low income
countries. A study done in Papua New Guinea demonstrated a significantly higher rate of three-
dose DTP immunization at six months of age in urban compared to rural communities(Toikilik
et al., 2010). Similarly, a study done in Kilifi district in Kenya revealed that children from the
Kilifi Township received pentavalent vaccine doses earlier than children from rural
areas(Moisi, Kabuka, Mitingi, Levine, & Scott, 2010). Likewise, Fernandez, Awofes and
Rammohan(2011) in Indonesia found significantly higher rates of first dose measles
vaccination in urban areas compared to rural areas .That study went on further to state that the
22
differences in immunization coverage between urban and rural children have been linked to
parental education, wealth and the presence of a skilled birth attendant. Furthermore,
misconceptions or lack of knowledge, issues with health services, challenges relating to travel
and transport, and family-related logistic issues have been more frequently reported by
residents of rural areas compared to urban residents(Toikilik et al., 2010). However, a study
that gathered data from multiple African countries revealed that urban communities are not
homogenous with respect to immunization coverage(Cutts, 1991). Specifically, poor urban
residents may represent a large proportion of the population in low income countries. They
may also have a high proportion of migrants or people belonging to different ethnic
groups(Cutts, 1991). Thus, these people may not enjoy the advantages of urban communities
regarding education, proximity to health services, and ease of communication.
2. Knowledge, attitudes and practices of mothers regarding immunization
According to theory of planned behavior, behavior is dependent on a person’s intention
to perform an activity, while intention is determined by an individual’s perspective(The World
Bank, 2010). Therefore, it is important to give information to help shape positive attitudes
towards vaccination and to spread ideas that support the practice of vaccination. A study in
Saudi Arabia demonstrated that parental knowledge and attitudes have a great impact on their
children’s immunization uptake(Alyami et al., 2018). Another study from Saudi Arabia
revealed that the knowledge, attitudes and practices (KAP) of mothers regarding vaccination
is essential for promoting child health as well as the prevention of VPDs(Alshehri et al., 2018).
Supporting a focus on mothers, a study conducted in India revealed that mothers—both urban
and rural—were the main decision makers about children’s vaccination(Mahalingam et al.,
2014). From this, it can be deduced that mothers play a central role in their children’s
immunization status; therefore their KAP regarding immunization should be known.
2.1. Knowledge of childhood immunization
23
It is essential for health workers to develop mothers’ comprehension and positive
perceptions of childhood immunization. Mothers of children under five should be aware of
vaccination services and benefits(Alruwaili et al., 2018).A study done in Uganda revealed that
93.5% of mothers knew that vaccines prevent diseases(Vonasek et al., 2016). A study in Turkey
revealed that parental knowledge is influenced by socio demographic factors(Kara et al., 2018).
Therefore, when communicating with mothers about the importance of vaccination, health
workers should take their socio-demographic factors into consideration.
Lack of knowledge resulted in non-compliance with the immunization schedule. One
study done in Iraq found that insufficient information on vaccination led to children’s poor
immunization status(Qutaiba et al., 2014). This can be solved by health providers describing
the advantages and disadvantages of vaccination and addressing parents’ misconceptions
(Esposito, Principi, Cornaglia, & Group, 2014). Proper communication between health workers
and mothers to offer vaccination information is of vital importance to the uptake of vaccination.
2.2. Attitudes about childhood immunization
Perspectives on and interpretations of health messages have an impact on the outcome
of the child’s vaccination status. A study carried out by analyzing gray literature (e.g., literature
produced by academic, government, or private sources that is not controlled by commercial
publishers)found that having a positive opinion about vaccines is very important(Favin,
Steinglass, Fields, Banerjee, & Sawhney, 2012). Other research done in Papua New Guinea
has revealed that negative outlooks towards vaccination is often due to the side effects of
vaccines(Namuigi & Phuanukoonnon, 2005).It is normal for parents to have both positive and
negative views about vaccination. Information geared towards the parents’ level of
understanding is needed to persuade parents with less intention to vaccinate.
2.3. Practice of childhood immunization
24
It is important for mothers to put into action what they have learned from health workers
based on their opinions and understanding. One study done in Egypt revealed that caregivers’
practice of immunization was good(Ramadan et al., 2016). “Good” referred to adhering to
vaccination schedules and the approaches mothers took to dealing with side effects(Bersen et
al., 2011).In sum, the extent to which mothers translate knowledge from health workers into
practice can assist health care providers to evaluate the effectiveness of their interventions.
3.Relationship between mothers’ knowledge and attitudes about immunization
Researchers have revealed an association between mothers’ knowledge and attitudes
towards childhood immunization. A study carried out in Nigeria by Olujide and colleagues
demonstrated a significant relationship between attitudes and knowledge regarding
vaccination(Olujide, Adekeye, Fred, Olufunke, & Bosede, 2015). Similarly, a study in Uganda
found that mothers’ knowledge and attitudes towards childhood immunization were associated
with practical knowledge about when and how often to go for immunizations, as well as the
site of vaccination(Vonasek et al., 2016). Having a positive perspective and basic knowledge
of immunization is important for mothers to bring their children in for vaccinations.
Studies have also shown that there is a relationship between mothers’ knowledge and
their practices regarding their children’s vaccination. One study in Nigeria has shown that
mothers have good knowledge of immunization. In summary, there is a clear association
between mothers’ knowledge and practices regarding immunization.
Furthermore, many studies have demonstrated an association between mothers’
attitudes and practices regarding immunization. For example, a study in India found that
parents who have a positive attitude about immunization tend to also have good practice with
regards to immunization, compared to parents with a negative attitude(Yadav et al.,
2015).Another study done in Nigeria revealed that mothers with higher level of education have
good knowledge and better attitude regarding immunization(Adefolalu et al,2019).These

25
studies showed that mothers who have high level of knowledge tend to have a positive attitude
towards the practice of immunization.
26
Section VI: Definition of variables
The conceptual and operational definitions of variables in this research are outlined as
follows:
1.Knowledge of immunization
1.1Conceptual definition: For the purposes of this study, knowledge refers to the collection of
information about immunization acquired through education or experience.
1.2. Operational definition: In this study, knowledge will be measured using the KAP
questionnaire regarding immunization created by Sebastian and colleagues(Sebastian,
Parthasarathi, & Ravi, 2017).
2.Attitudesabout immunization
2.1. Conceptual definition: For the purposes of this study, attitude is an individual’s
perspective about immunization, whether positive or negative.
2.2. Operational definition: In this study, attitude will be measured using the KAP
questionnaire regarding immunization(Sebastian et al., 2017).
3.Practice of immunization
3.1. Conceptual definition: For this study, practice refers to the actual application of
immunization information.
3.2. Operational definition: In this study, mothers’ practice will be measured using theKAP
questionnaire regarding immunization (Sebastian et al., 2017).
27
Chapter III: Methodology
The following chapter will discuss the conceptual framework, research design, study
area, population and sample size, and the inclusion and the exclusion criteria. It will also
describe the study setting and sampling selection technique. Lastly, the chapter will also
introduce the instrument, including translation, validity, and reliability. Furthermore, it will
present the procedures for data collection and analysis and plans for obtaining ethical
permission for the study
Section I: Conceptual Framework
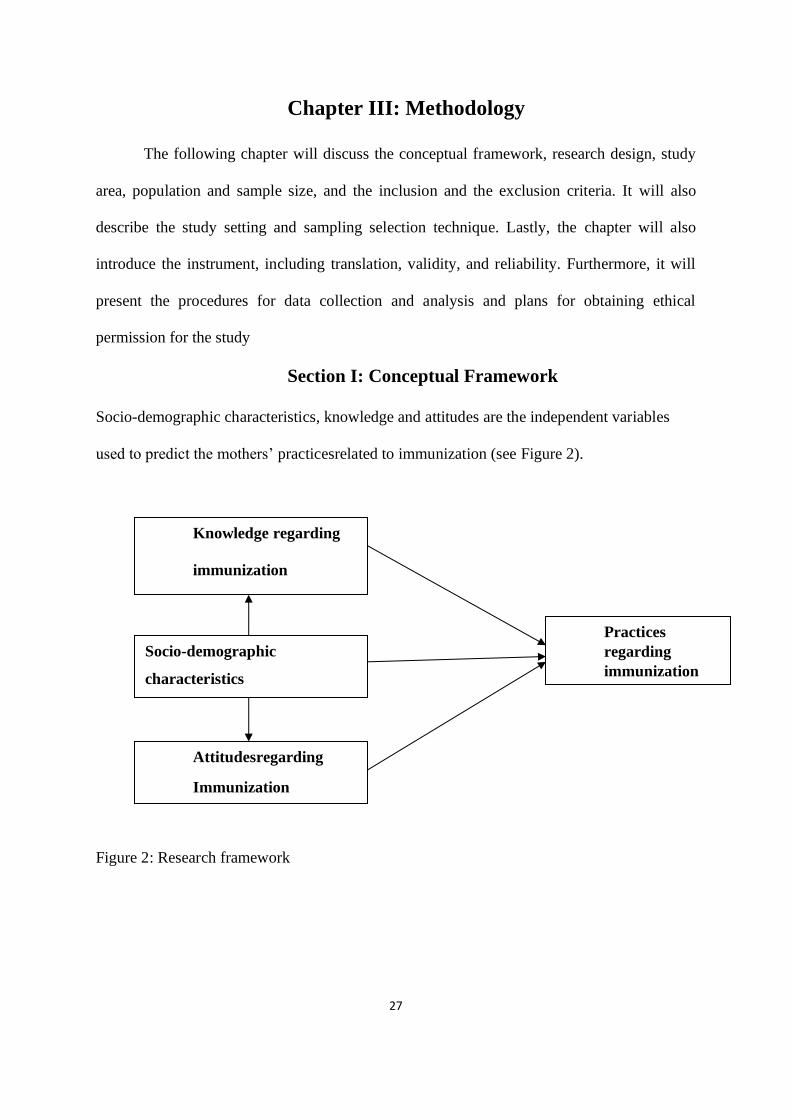
Socio-demographic characteristics, knowledge and attitudes are the independent variables
used to predict the mothers’ practicesrelated to immunization (see Figure 2).
Figure 2: Research framework
Attitudesregarding
Immunization
Knowledge regarding
immunization
Practices
regarding
immunization
Socio-demographic
characteristics
28
Section II: Research Design
This study uses a quantitative cross-sectional correlation design. The aim is to
explore the relationships between the variables, including socio-demographic characteristics,
knowledge, attitudes, and practices regarding childhood immunization in Papua New Guinea.
Section III: Study area and setting
The study was conducted in West Sepik province, also known as Sandaun, which
contains four districts, namely Aitape-Lumi, Nuku, Telefomin and Vanimo Green District.
Data will be collected at Sandaun Provincial Hospital in Vanimo Green District, West Sepik,
which is the referral and teaching hospital in that province. The data was collected in the out-
patient unit, and the well-baby clinic of the hospital. The reason for choosing this hospital was
because the outpatient department operates 24hours a day, well baby clinic every Fridays for
vaccination, and half of the patients are from the rural area.
Section IV: Sample size
We estimated the necessary sample size based on multiple linear regression, assuming
R² deviated from zero, using a medium effect size (f²) of 0.15. The significance level(α) was
set at 0.05(two tailed) and the statistical power was set at 0.8.A sample size of 114 women
was recruited for this study.
Section V: Sample Selection
The inclusion and exclusion criteria of this study are as follows:
1.Inclusion Criteria
1.1 Mothers of children under age 5
1.2 Mothers who read and write Tok pisin
1.3 Mothers age 18 and above
29
2.Exclusion Criteria
Mothers of children with chronic diseases, such as heart problems, or premature babies
Section VI: Instruments
The study used KAP questionnaires regarding immunization created by Sebastian et
al, (2017) and it was modified. Permission was given by the author to use the tool (See
Appendix II).
1. Description
This Knowledge, Attitude, and Practice Questionnaires is a reliable and valid tool to
measure parents’ knowledge, attitudes and practices regarding immunization. The instrument
was initially developed in English in 2017 and it has been translated into a local vernacular
language(Kannada) of India(Sebastian et al., 2017). The scale is considered easy and practical
to use.
The survey instrument was an interview directed questionnaire that explored mothers’
knowledge, attitudes and practices and is comprised of four parts. Part A relates to participants’
socio demographic background and includes age, number of children, education level, marital
status, source of information, income, transport, women’s role in decision making, and place
of residence. Part B examined mothers’ general knowledge regarding vaccination using a 10-
item questionnaire. Part C explored mothers’ vaccination attitudes using a seven-item
questionnaire, and part D assessed practices towards childhood immunization using a five-item
questionnaire.
2.Validity and reliability
Sebastian initially tested the psychometric properties of the twenty-two item scale
among parents in India whose babies were between two to five years old (Sebastian et al., 2017).
The results showed that the instrument was reliable and valid. The authors developed the
30
primary version of the questionnaire in English after an extensive literature search to maintain
consistency with English language published literature. The overall scale content validity score
(S-CVI) and the item-content validity index (I-CVI) were 0.96 and 0.96, respectively
(Sebastian et al., 2017). An I-CVI score of 0.78 or higher indicates excellent content validity,
as does an S-CVI score of 0.8 or higher (Gray, Grove & Sutherland, 2017), demonstrating that
this scale is valid to use. The Cronbach’s alpha was 0.89 (Sebastian et al., 2017). According to
Gray and colleagues, a reliability coefficient should be above 0.7, indicating that this
questionnaire is reliable to use (Gray, Grove & Sutherland, 2017).
3.Scoring
The KAP questionnaire scoring was done by allotting zero and one point for each
incorrect and correct answer, respectively. The maximum score is 22(knowledge
domain:10points, attitude domain: 7 points and practice domain: 5 points). A person who
answers questions correctly and obtains higher scores has a higher level of knowledge, and
better attitudes and practices regarding immunization(Sebastian et al., 2017).
4.Translation
This study used the KAP questionnaire tool to measure mothers’ knowledge, attitudes
and practices in the Tok Pisin language of Papua New Guinea. Content Validity of the
translated questionnaire was established by expert validation. Four experts in the field of
pediatrics in Papua New Guinea who have knowledge about immunization and are fluent
speakers of both Tok Pisin and English validated the content of the translated version. The
questionnaires were translated from English into Tok Pisin and reverse translation was done
by two pediatric nurses who speak both languages fluently. They rated the content relevance,
clarity and simplicity of each item using a four-point Likert scale from 1 (irrelevant, not clear,
and not simple) to 4 (very relevant, very clear, and very simple). The content validity index
(CVI) was calculated to obtain the validity score. The CVIs of the study instrument were 0.94
31
for knowledge about immunization, 0.95 for attitudes towards immunization, and 0.96 for
immunization practice. The average content scale validity score was 0.94.
A pilot study was conducted to determine the reliability of the translated questionnaire.
The purpose of the pilot study is to examine the questionnaire administration technique and the
adequacy of the question items. The result of the pilot study was analyzed to determine the
reliability of the translated scale using SPSS version 20, and was found to be 0.7.
Section VII: Research ethics and statements
This study was approved by the Medical Research Advisory Committee (MRAC) of
Papua New Guinea (MRAC No.19.15) and also approved by the research committee of
Sandaun Provincial Hospital. After providing information about the purpose of the study,
guaranteeing anonymity and credibility, clarifying voluntary participation, and indicating the
benefits of the study. Written consent was obtained from the participants who agreed to take
part in the study. (See Appendix I)
Section VIII: Data collection procedure
Data collection took place after the participants have given their consent. Participants
were mothers of children under the age of five. Interviews were carried out with the revised
questionnaires during the morning shifts. When the participants had completed the
questionnaire, the researcher reviewed it thoroughly to ensure it was complete. (See Appendix
I)
Section IX: Data Analysis
The data was analyzed using the Statistical Packaged for Social Sciences (SPSS)
Version 20. The SPSS showed the results in the form of tables and descriptive statistics. The
demographic variables were analyzed in terms of means, standard deviation, frequency, and
percentages. The researcher calculated the means and standard deviation for knowledge,
32
attitude and practice scores. The variables predicting the practice of immunization was
analyzed using hierarchical multiple linear regression. The table below illustrates each variable
alongside statistical procedures used for data analysis
Table3.1 Statistical test for study
Research question Variables Statistics
1. What are the demographic
characteristics of mothers with
children under age five in
Papua New Guinea?
1.Continuous variables:
-Age
-Number of children
2.Categorical:
-Marital status
-Education
-Transport
-Income
-Source of information
- Women’s decision-
making role
-Place of residence
Descriptive statistics:
1. mean, standard deviation,
and range
2. frequency &percentage
33
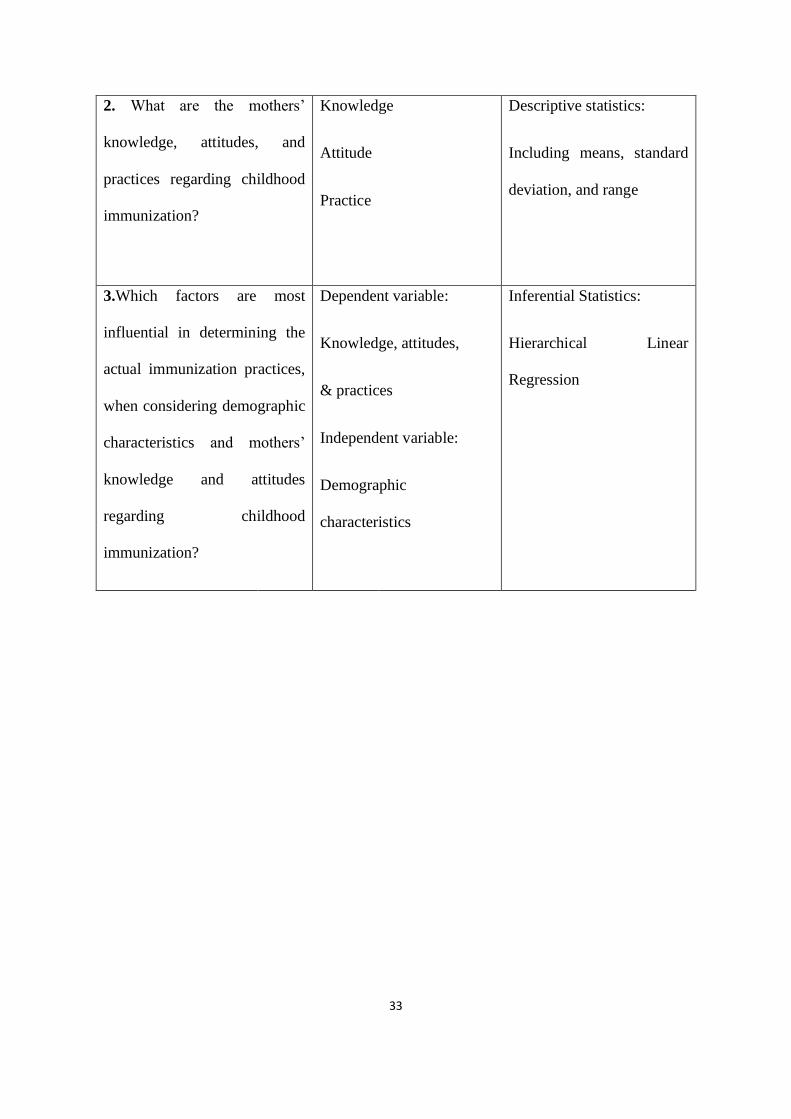
2. What are the mothers’
knowledge, attitudes, and
practices regarding childhood
immunization?
Knowledge
Attitude
Practice
Descriptive statistics:
Including means, standard
deviation, and range
3.Which factors are most
influential in determining the
actual immunization practices,
when considering demographic
characteristics and mothers’
knowledge and attitudes
regarding childhood
immunization?
Dependent variable:
Knowledge, attitudes,
& practices
Independent variable:
Demographic
characteristics
Inferential Statistics:
Hierarchical Linear
Regression
34
Chapter IV Results and Discussion
This section will discuss the results of this study, taking into account the mothers’
knowledge, attitudes and practices regarding immunization. It will also go into detail to
compare the findings of this study with previous studies.
Section I Results
This study explored the knowledge, attitudes, and practices of mothers regarding
childhood immunization in West Sepik, Papua New Guinea. The researcher included 114
mothers from the general outpatient and well-baby clinic of Sandaun Provincial Hospital. The
study took place from the 1st of July to the 4th of September 2019. All questionnaires were
checked to be sure they were properly filled in. To analyze the results, the study used
descriptive statistics, Pearson’s correlation, independent sample t test, ANOVA, post hoc
comparison and hierarchical linear regression.
Research question 1: What are the demographic characteristics of mothers with children
under five in Papua New Guinea?
The demographic characteristics of the mothers were analyzed with a descriptive analysis.
Participants’ average age was 26.24(SD=5.50) years old. The oldest participant was 45 and the
youngest was 18 years old. The mean of the number of children was 2.55(SD=1.83), ranging
from 1 to 10. In regards to education level, half (50%, n=57) had completed less than high
school, nearly one-third (29.8%, n=34) had at least high school or more, and20.2% (n=23) were
illiterate. As regards to the mothers’ income, 93.9% (n=107) earned more than or equal to K200
and only 6.1% (n=7) earned less than or equal to K200. About 93% (n=106) of the mothers
received immunization knowledge from professional sources and only 7.1% (n=8) from
unprofessional sources.
35
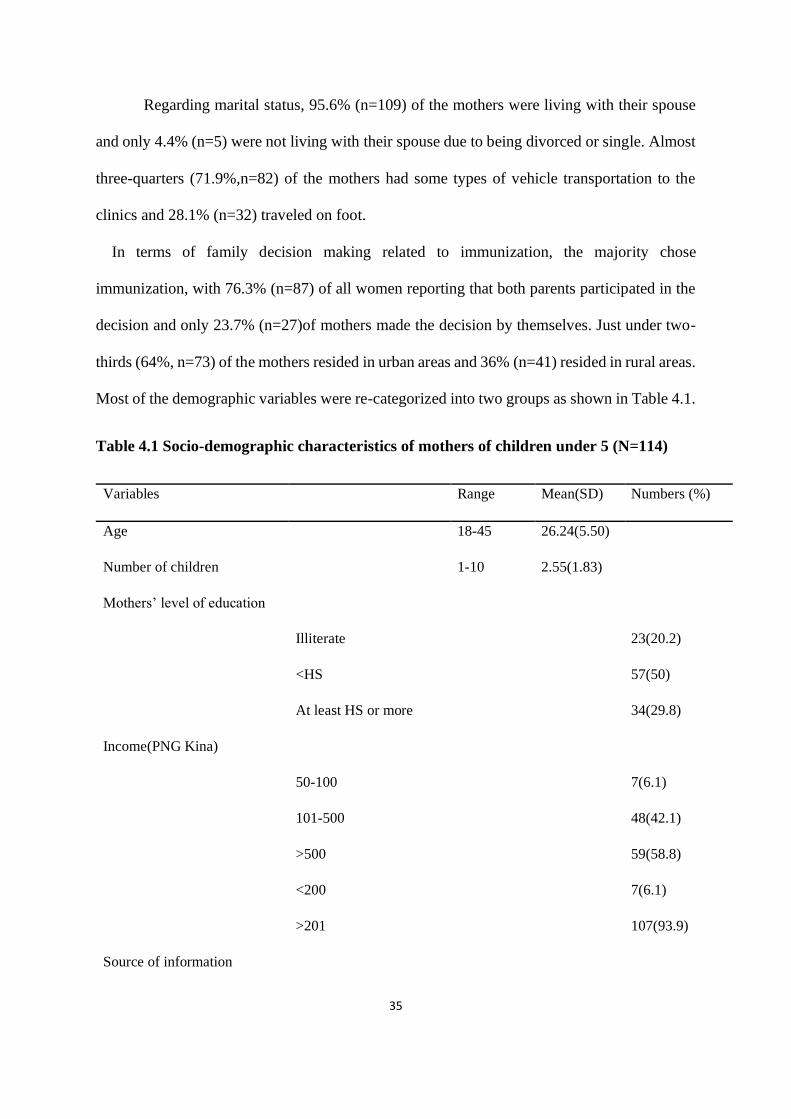
Regarding marital status, 95.6% (n=109) of the mothers were living with their spouse
and only 4.4% (n=5) were not living with their spouse due to being divorced or single. Almost
three-quarters (71.9%,n=82) of the mothers had some types of vehicle transportation to the
clinics and 28.1% (n=32) traveled on foot.
In terms of family decision making related to immunization, the majority chose
immunization, with 76.3% (n=87) of all women reporting that both parents participated in the
decision and only 23.7% (n=27)of mothers made the decision by themselves. Just under two-
thirds (64%, n=73) of the mothers resided in urban areas and 36% (n=41) resided in rural areas.
Most of the demographic variables were re-categorized into two groups as shown in Table 4.1.
Table 4.1 Socio-demographic characteristics of mothers of children under 5 (N=114)
Variables Range Mean(SD) Numbers (%)
Age 18-45 26.24(5.50)
Number of children 1-10 2.55(1.83)
Mothers’ level of education
Illiterate 23(20.2)
<HS 57(50)
At least HS or more 34(29.8)
Income(PNG Kina)
50-100 7(6.1)
101-500 48(42.1)
>500 59(58.8)
<200 7(6.1)
>201 107(93.9)
Source of information
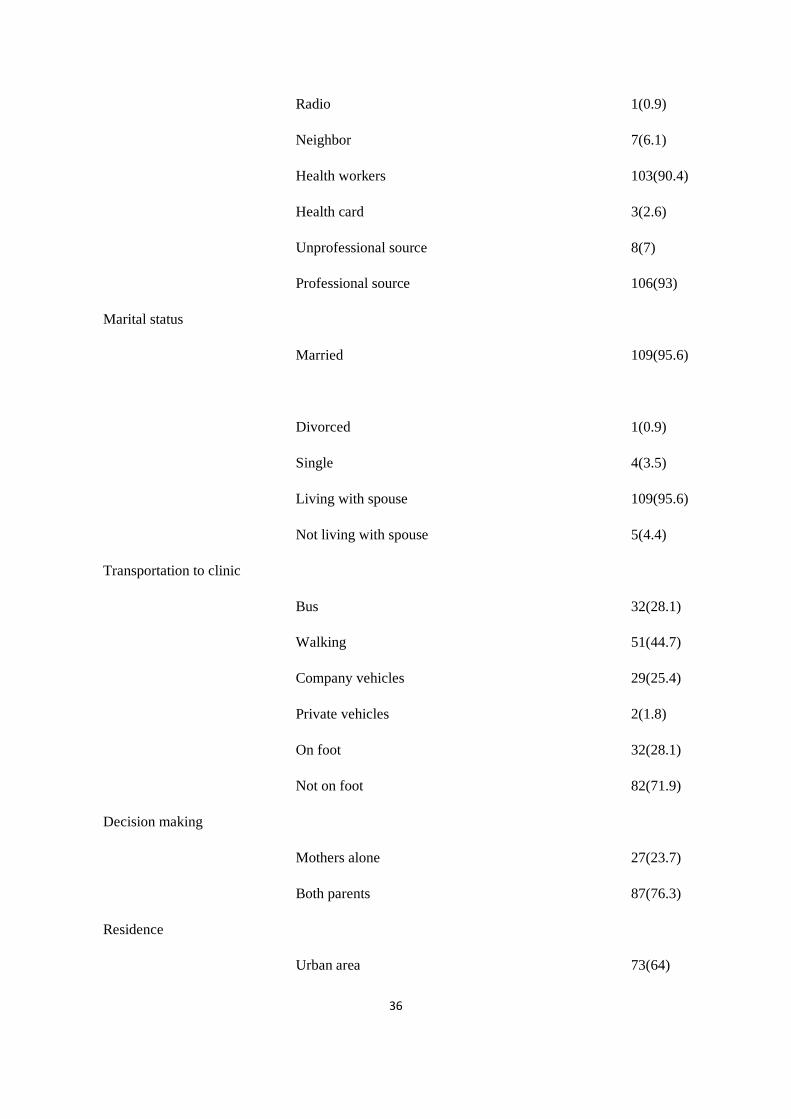
36
Radio 1(0.9)
Neighbor 7(6.1)
Health workers 103(90.4)
Health card 3(2.6)
Unprofessional source 8(7)
Professional source 106(93)
Marital status
Married 109(95.6)
Divorced 1(0.9)
Single 4(3.5)
Living with spouse 109(95.6)
Not living with spouse 5(4.4)
Transportation to clinic
Bus 32(28.1)
Walking 51(44.7)
Company vehicles 29(25.4)
Private vehicles 2(1.8)
On foot 32(28.1)
Not on foot 82(71.9)
Decision making
Mothers alone 27(23.7)
Both parents 87(76.3)
Residence
Urban area 73(64)
37
Rural area 41(36)
SD=standard deviation; HS=high school
Research Question 2: What are the KAP of mothers regarding childhood immunization
in Papua New Guinea?
Mothers’ knowledge, attitudes, and practices regarding childhood immunization were
analyzed by descriptive analysis. Means and standard deviations on knowledge, attitude, and
practice scores were calculated for better assessment. Mothers’ knowledge scores ranged from
5 to 11 with a mean of 9.73(SD=1.42). In general, mothers had good knowledge about
childhood immunization. According to the study findings, 100% (n=114) knew that it was
important to vaccinate their children and that vaccines are safe to use. The high knowledge
scores about immunization among mothers in Papua New Guinea could be due to health
workers giving effective health education on the topic. A total of 99.1% (n=113) knew that it
is important to receive vaccinations during pregnancy. This is so because it protects the mothers
and their children from diseases like tetanus. However, only 80.2% (n=92) of the mothers knew
that the tetanus vaccine is given during pregnancy. Of the participants, 74.6% (n=85) knew that
vaccination enhances immunity and helps the human body fight against diseases. Only 49.1
(n=56) of the mothers knew that fever, swelling and pain at the injection site and rashes are
side effects of vaccination. These findings suggest that health workers education about vaccines
lacks specificity (See table 4.2).
The attitude scores ranged from 5 to7, with a mean of 6.80(SD=0.43), with most
mothers accepting childhood immunization. All (n=114) of the participants knew that
vaccination is important and safe. Also 100% (n=114) of the mothers stated that their culture
has no influence over how they perceive vaccination. A majority of 99.1% (n=113) of the
participants favored vaccination and believed it should be given according to schedule. Nearly
as many, (96.5%,n=110) stated that vaccines should be started in the first week of life. While
38
84.2% (n=96) of the participants said that they would recommend that other mothers bring in
their children for vaccination (See table 4.3).
The vaccination practice scores ranged from 0 to 5, with a mean of 3.17(SD=1.40), with
87.7% (n=100) of the mothers reporting that they would follow the obligatory vaccination
schedule. Seventy-eight (68.4%) of the participants stated that they would get all their children
vaccinated and said they would manage the swelling of the injection site by cold compression.
But 31.6% (n=36) of the mothers stated that they would not get their children vaccinated. This
could be because of the transport issues for those living in the rural areas present obstacles to
getting children vaccinated, although the study did not detect a significant link between
transportation and vaccination. In addition, the cost of transport could present a financial
burden that prevents mothers from bringing their children in for vaccination. About 45.6%
(n=52) of the mothers reported that they would report the minor side effects to the nurse or
health care workers. Just under half (44.7%,n=51) of the mothers stated that they would use
analgesics for swelling and pain after vaccination. This relatively low level of practice to get
children immunized could be due to lack of awareness or lack of understanding among mothers
who are illiterate or who did not complete high school. (See table 4.4)
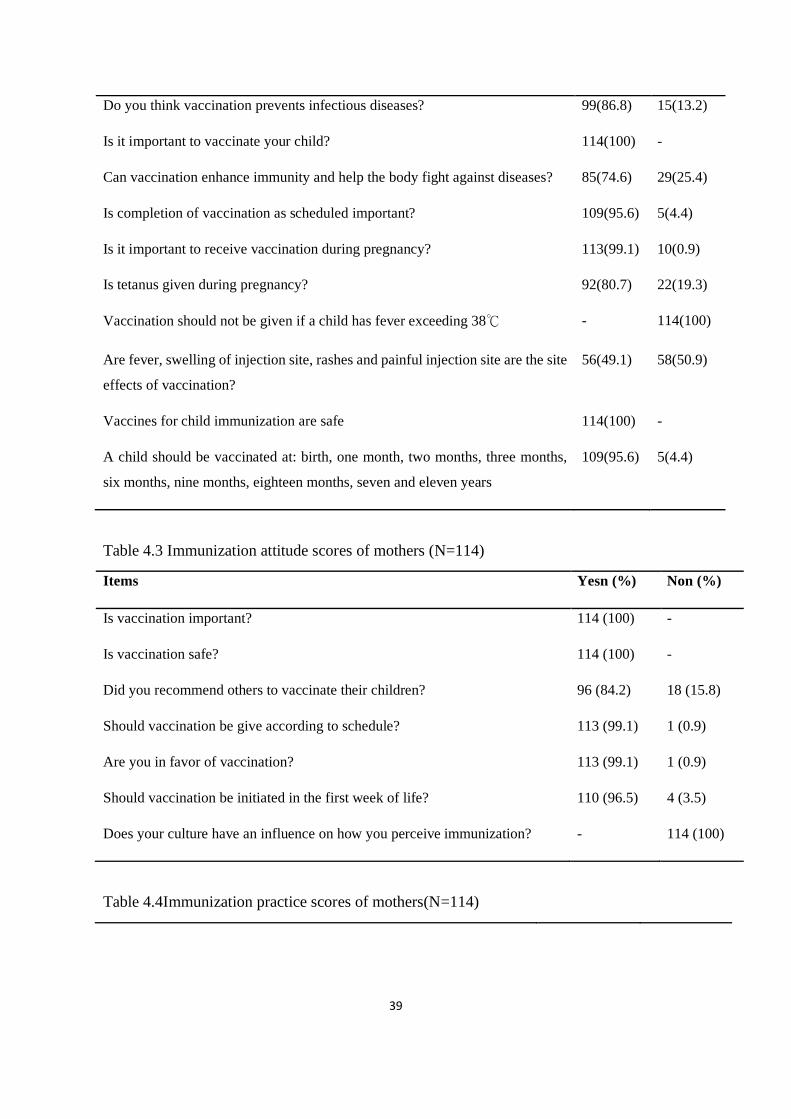
Table 4.2Immunization knowledge scores of mothers(N=114)
Items Yes n (%) No n (%)
39
Do you think vaccination prevents infectious diseases? 99(86.8) 15(13.2)
Is it important to vaccinate your child? 114(100) -
Can vaccination enhance immunity and help the body fight against diseases? 85(74.6) 29(25.4)
Is completion of vaccination as scheduled important? 109(95.6) 5(4.4)
Is it important to receive vaccination during pregnancy? 113(99.1) 10(0.9)
Is tetanus given during pregnancy? 92(80.7) 22(19.3)
Vaccination should not be given if a child has fever exceeding 38℃ - 114(100)
Are fever, swelling of injection site, rashes and painful injection site are the site
effects of vaccination?
56(49.1) 58(50.9)
Vaccines for child immunization are safe 114(100) -
A child should be vaccinated at: birth, one month, two months, three months,
six months, nine months, eighteen months, seven and eleven years
109(95.6) 5(4.4)
Table 4.3 Immunization attitude scores of mothers (N=114)
Items Yesn (%) Non (%)
Is vaccination important? 114 (100) -
Is vaccination safe? 114 (100) -
Did you recommend others to vaccinate their children? 96 (84.2) 18 (15.8)
Should vaccination be give according to schedule? 113 (99.1) 1 (0.9)
Are you in favor of vaccination? 113 (99.1) 1 (0.9)
Should vaccination be initiated in the first week of life? 110 (96.5) 4 (3.5)
Does your culture have an influence on how you perceive immunization? - 114 (100)
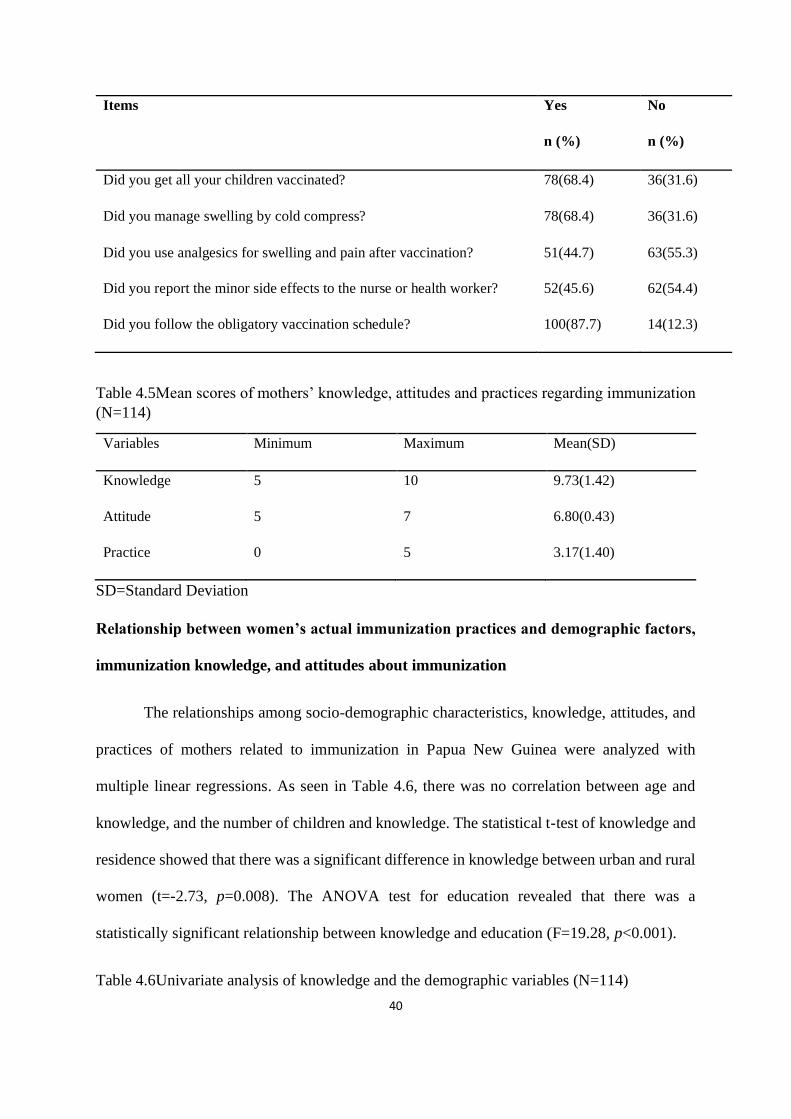
Table 4.4Immunization practice scores of mothers(N=114)
40
Items Yes
n (%)
No
n (%)
Did you get all your children vaccinated? 78(68.4) 36(31.6)
Did you manage swelling by cold compress? 78(68.4) 36(31.6)
Did you use analgesics for swelling and pain after vaccination? 51(44.7) 63(55.3)
Did you report the minor side effects to the nurse or health worker? 52(45.6) 62(54.4)
Did you follow the obligatory vaccination schedule? 100(87.7) 14(12.3)
Table 4.5Mean scores of mothers’ knowledge, attitudes and practices regarding immunization
(N=114)
Variables Minimum Maximum Mean(SD)
Knowledge 5 10 9.73(1.42)
Attitude 5 7 6.80(0.43)
Practice 0 5 3.17(1.40)
SD=Standard Deviation
Relationship between women’s actual immunization practices and demographic factors,
immunization knowledge, and attitudes about immunization
The relationships among socio-demographic characteristics, knowledge, attitudes, and
practices of mothers related to immunization in Papua New Guinea were analyzed with
multiple linear regressions. As seen in Table 4.6, there was no correlation between age and
knowledge, and the number of children and knowledge. The statistical t-test of knowledge and
residence showed that there was a significant difference in knowledge between urban and rural
women (t=-2.73, p=0.008). The ANOVA test for education revealed that there was a
statistically significant relationship between knowledge and education (F=19.28, p<0.001).
Table 4.6Univariate analysis of knowledge and the demographic variables (N=114)
41
Variables N Mean(SD) F/r/t value p value Pos hoc test
Age 26.24(5.50) -.14 .138
Number of children
2.55(1.83) -.14 .132
Residence
Rural 41 9.22(1.61) -2.73 .008**
Urban 73 10.01(1.23)
Education
❶ Illiterate 23 8.43(1.73) 19.28 .001** ❷>❶
❷<HS 57 9.79(1.29) ❸>❷
❸ At least HS or more 34 10.50(0.56) ❸>❶
Note: **p<.001, *p<.005 HS: high school
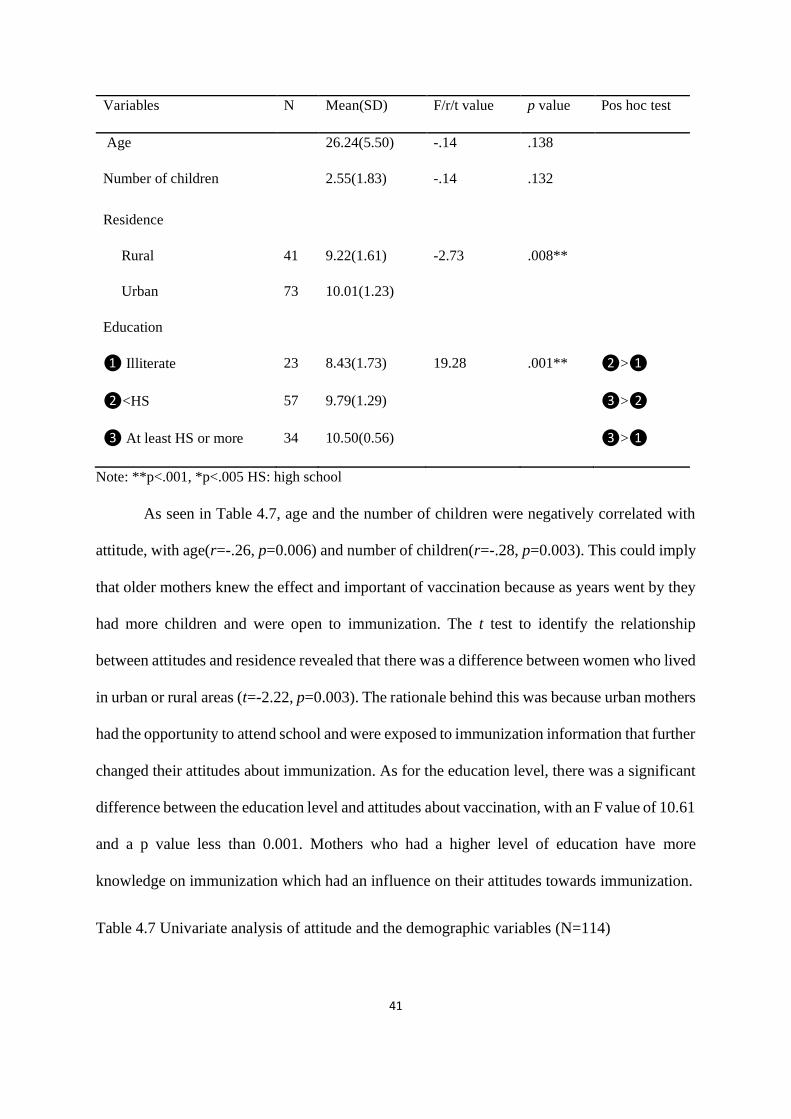
As seen in Table 4.7, age and the number of children were negatively correlated with
attitude, with age(r=-.26, p=0.006) and number of children(r=-.28, p=0.003). This could imply
that older mothers knew the effect and important of vaccination because as years went by they
had more children and were open to immunization. The t test to identify the relationship
between attitudes and residence revealed that there was a difference between women who lived
in urban or rural areas (t=-2.22, p=0.003). The rationale behind this was because urban mothers
had the opportunity to attend school and were exposed to immunization information that further
changed their attitudes about immunization. As for the education level, there was a significant
difference between the education level and attitudes about vaccination, with an F value of 10.61
and a p value less than 0.001. Mothers who had a higher level of education have more
knowledge on immunization which had an influence on their attitudes towards immunization.
Table 4.7 Univariate analysis of attitude and the demographic variables (N=114)
42
Variables n Mean(SD) F/r/t value p value Pos hoc test
Age 26.24(5.50) -.26 .006*
Number of children 2.55(1.83) -.28 .003*
Residence
Rural 41 6.66(0.53) -2.22 .030*
Urban 73 6.86(0.35)
Education
❶ Illiterate 23 6.48(0.51) 10.61 .001** ❷>❶
❷<HS 57 6.81(0.44)
❸ At least HS or more 34 6.97(0.17) ❸>❶
Note:**p<.001, *p<.005 HS: high school
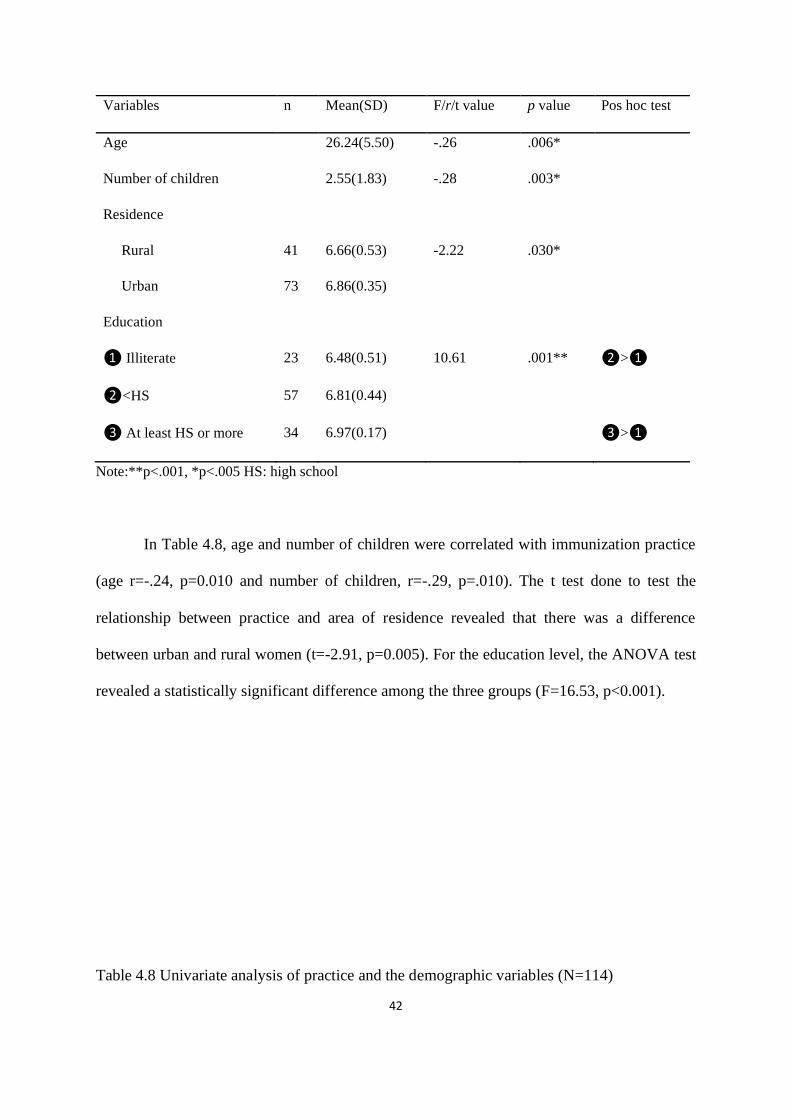
In Table 4.8, age and number of children were correlated with immunization practice
(age r=-.24, p=0.010 and number of children, r=-.29, p=.010). The t test done to test the
relationship between practice and area of residence revealed that there was a difference
between urban and rural women (t=-2.91, p=0.005). For the education level, the ANOVA test
revealed a statistically significant difference among the three groups (F=16.53, p<0.001).
Table 4.8 Univariate analysis of practice and the demographic variables (N=114)
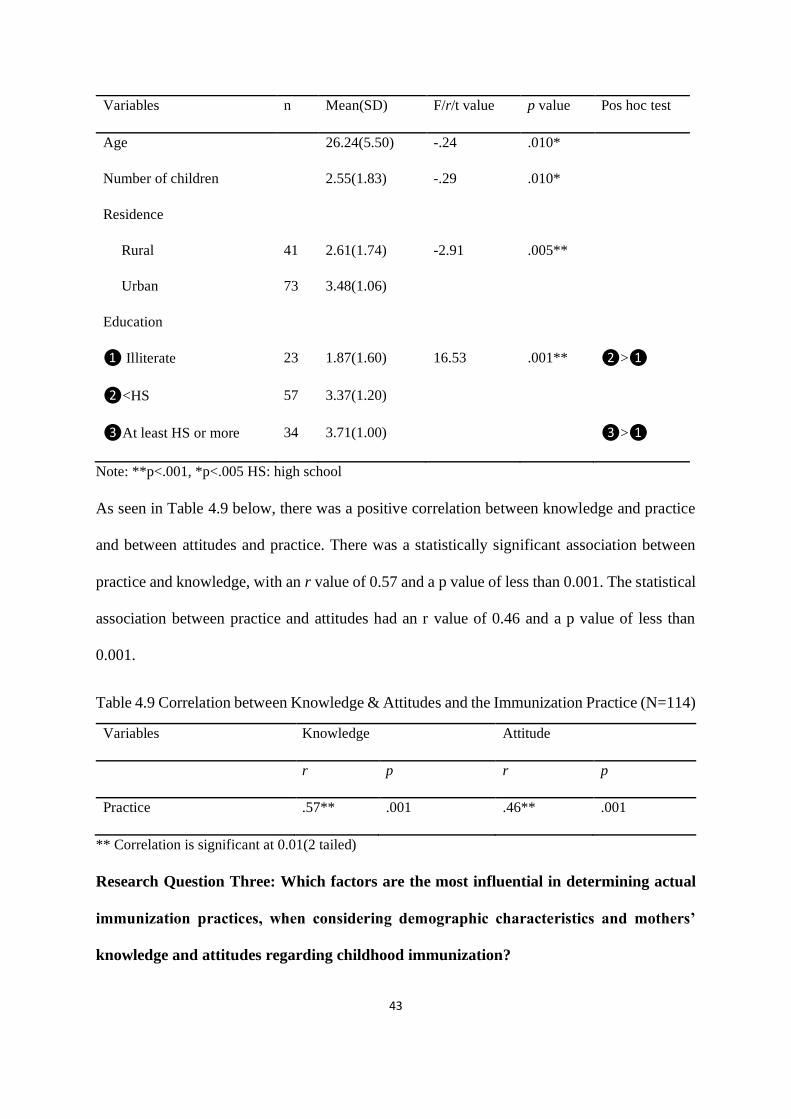
43
Variables n Mean(SD) F/r/t value p value Pos hoc test
Age 26.24(5.50) -.24 .010*
Number of children 2.55(1.83) -.29 .010*
Residence
Rural 41 2.61(1.74) -2.91 .005**
Urban 73 3.48(1.06)
Education
❶ Illiterate 23 1.87(1.60) 16.53 .001** ❷>❶
❷<HS 57 3.37(1.20)
❸At least HS or more 34 3.71(1.00) ❸>❶
Note: **p<.001, *p<.005 HS: high school
As seen in Table 4.9 below, there was a positive correlation between knowledge and practice
and between attitudes and practice. There was a statistically significant association between
practice and knowledge, with an r value of 0.57 and a p value of less than 0.001. The statistical
association between practice and attitudes had an r value of 0.46 and a p value of less than
0.001.
Table 4.9 Correlation between Knowledge & Attitudes and the Immunization Practice (N=114)
Variables Knowledge Attitude
r p r p
Practice .57** .001 .46** .001
** Correlation is significant at 0.01(2 tailed)
Research Question Three: Which factors are the most influential in determining actual
immunization practices, when considering demographic characteristics and mothers’
knowledge and attitudes regarding childhood immunization?
44
A hierarchical multiple regression was carried out to find predictors of immunization
practice among mothers in Papua New Guinea (the assumptions of linearity, normally
distributed errors, and uncorrelated errors were checked and met). In this study, the dependent
variable (DV) is practice related to immunization and the independent variables (IVs) are socio
demographic factors, knowledge and attitudes related to immunization.
Hierarchical multiple regression tests were used to identify the best predictor of
immunization practice among mothers in Papua New Guinea. When age, number of children,
education, and residence were entered, mothers’ education significantly predicted practice with
a beta value of 0.37 and an F value of 13.96. As indicated by R², 25% of the variance in practice
could be predicted by knowing the mothers’ age, number of children, education, and residence.
When knowledge was added, it improved the predictive power, with the R2 changing to 0.39.
Knowledge was found to predict immunization practice with a beta value of 0.45 and an F
value of 13.96. In Model 3, attitude was added; it improved the predictive value, raising the R²
value to 0.41. About 41% of the variance in practice could be predicted by knowing the
mothers’ age, number of children, education, residence, knowledge and attitude. However, the
hierarchical linear regression revealed that knowledge was the best predictor of practice, with
an F value of 12.54 and a beta value of 0.39 (See table 5).
Table 5 Hierarchical Multiple Regression Analysis Summary Predicting Practice (N=114)
B SEB β T F R² ΔR²
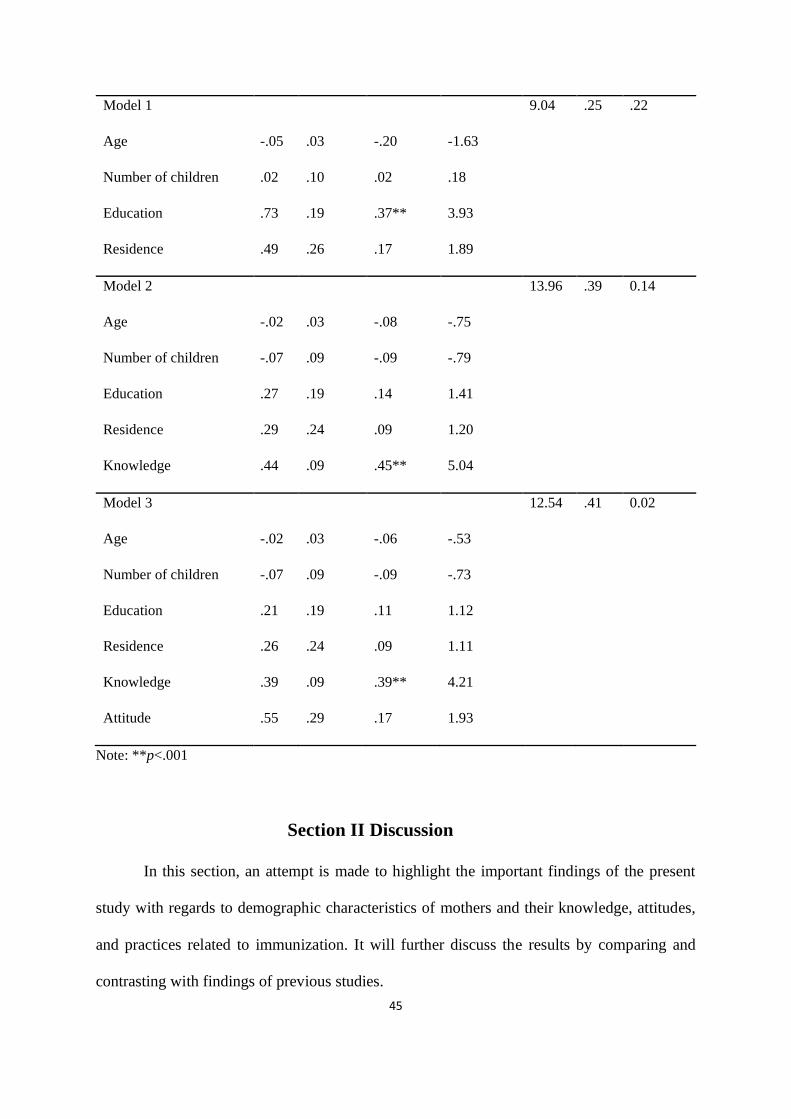
45
Model 1 9.04 .25 .22
Age -.05 .03 -.20 -1.63
Number of children .02 .10 .02 .18
Education .73 .19 .37** 3.93
Residence .49 .26 .17 1.89
Model 2 13.96 .39 0.14
Age -.02 .03 -.08 -.75
Number of children -.07 .09 -.09 -.79
Education .27 .19 .14 1.41
Residence .29 .24 .09 1.20
Knowledge .44 .09 .45** 5.04
Model 3 12.54 .41 0.02
Age -.02 .03 -.06 -.53
Number of children -.07 .09 -.09 -.73
Education .21 .19 .11 1.12
Residence .26 .24 .09 1.11
Knowledge .39 .09 .39** 4.21
Attitude .55 .29 .17 1.93
Note: **p<.001
Section II Discussion
In this section, an attempt is made to highlight the important findings of the present
study with regards to demographic characteristics of mothers and their knowledge, attitudes,
and practices related to immunization. It will further discuss the results by comparing and
contrasting with findings of previous studies.
46
1. Description of the socio demographic characteristics of the study sample
In this study, the average age of mothers with children under age 5 was
26.24(SD=5.504), ranging from 18 to 45. The mean of the number of children under five per
mother was 2.55(SD=1.83), ranging from 1 to 10, indicating that about 76.3% of women had
between 1 and 3 children under age 5. On average, the older a woman gets, the more children
she has. It is common for mothers in rural areas of Papua New Guinea(PNG) to have a
minimum of six children and for urban women to have three children. Health workers offer
contraceptives to mothers, but the women tend to refuse based on cultural beliefs, saying they
will use traditional family planning, consisting of herbs and rituals. However, traditional
planning methods mostly do not turn out as they expected and they come back to the health
clinic with another pregnancy. A survey carried out in 8 provinces(Milne Bay, Gulf, Chimbu,
Southern Highlands, Madang, East Sepik, East New Britain and North Solomons) in PNG
which comprises of the 4 regions, namely Southern, Highlands, Islands and the Momase
regions found that 81% of men from the rural areas and 76% of males from the urban areas
were afraid that the contraceptives might be detrimental to their wives’ health and their future
children (Agyei, 1984).That study went further, stating that another reason was men’s
disapproval for family planning. In addition, they believed benefits of having more children
were financial support in old age and having a happy family. This study was carried in the
Momase region of PNG which shares similar cultural practices to the survey done in 1984 by
Agyei, a Melanesian society, with male having more influence in decision making than women.
.
In this study education level was related to knowledge about immunization. Half of the
participants (50%) of the mothers had primary education. The findings were similar to those of
Adefolalu and colleagues in Nigeria who found that 57.7% of the mothers had primary to
47
secondary education (Adefolalu et al, 2019).A study done in India likewise found that the use
of health care services as well as full immunization of children is associated with the mother’s
level of education (Kusuma, Kumari, Pandav, & Gupta, 2010). Many studies show that
maternal education was one of the factors that contribute to a child’s health. This study was
done in a developing country as well as the other study. Furthermore, both countries that these
studies took place in had a adult literacy rate of about 60%. The high literacy level among
women in this study may partly explain the relatively high knowledge of vaccination. Mothers
who are educated often use the internet and gather as much information they can about
vaccination. In addition, when unsure, they enquire by asking health care professionals during
hospital visits. Many studies have documented that mothers’ education levels influence the
practice of immunization.
In this study, 93.9% of mothers had a family income level of ≥201 Papua New Guinea
Kina and only 6.1% had family incomes ≤200. In PNG, immunization is provided free by the
government. For those mothers living far from health clinics, they only need to pay for their
transport to get to the clinic sites. This study revealed that, 53.3% of the participants travelled
into town by private vehicles or public transportation. However, transportation is a problem in
rural areas due to the difficult terrain, poor conditions and cost. This is supported by a survey
done in PNG by Gibson & Rozelle (2015) which found that health and education services in
rural areas are not easily accessible due to poor road access. This survey was done by collecting
information from the 4 regions in PNG which included Momase region where this study was
conducted. Both of these studies had some participants who lived in rural areas.
Regarding the source of information, 93% of the mothers got their information from
professional sources, specifically health care professionals. This is similar to results of a study
by Hamid and colleagues in a rural area of North Kashmir, India where of the participants
48
(88%) reported that health professionals were their source of information regarding
immunization(Hamid et al,2012).These results could be similar due to the fact that both studies
had participants residing in the rural areas and also both females from these areas have a literacy
of about 60%. This reflects the effective work of the health workers to promote and motivate
mothers about childhood vaccination. Mothers in this study were informed by health
professionals through health education to raise awareness. Only 1% of the mothers got their
information about immunization from radio. This could mean that the radio station in that
province is not being utilized to spread immunization information, as in other provinces. Since
internet data is expensive in PNG and internet coverage in the rural areas is poor, immunization
information should be disseminated via radio as well.
In terms of decision making, 76.3% of the decisions relating to immunization of
children were made by both parents and 23.7% by mothers alone. In this study, more than 95%
of the mothers were living with their spouses. This pattern was similar to a study by Adefolafu
and colleagues in Nigeria where about 95.6% of the mothers were married (Adefolalu et al,
2019).These similarities could be because of the patriarchal society. This could mean that
husband’s involvement has a positive impact on a child’s immunization status. PNG is a
culturally diverse nation, mostly made of patrilineal societies and a handful of matrilineal
societies, but in both, men have dominance over women in terms of decision making (Sai,
2007). In the rural and urban areas of PNG, men commonly hold onto traditional cultural
practices, where tribal discipline and power is given to men who have authority over their clan
and family members. Men make most of the decisions in the family and control most of the
resources, and women are expected to conform to various societal rules and norms, often
having their basic rights denied. This is supported by a United Nations report showing that
PNG has a Gender Inequity Index (GII) value of 0.86(United Nations, 2014). The GII measures
49
three dimensions; reproductive health, empowerment, and economic activity. Women are not
empowered in terms of decision making. In addition, in 2018, PNG had a GII value of 0.74
which ranked it as 161 in terms of gender inequality out of 162 countries, meaning that gender
inequality is exceptionally high(United Nations Development Report, 2019). However, a
minority of men, often those with more education or living in urban areas, are doing away with
these cultural practices.
As for place of residence, in this study, roughly two-thirds most of the women were
living in urban areas (64%), with 36% in rural areas. Residence in urban areas could mean that
they had more opportunity to attend school, which could explain the association between urban
residence and better immunization practices.
2. Mothers’ Knowledge, Attitude and Practices related to immunization
Participants’ knowledge scores ranged from 5 to 11 with a mean of 9.73(1.42), attitude
scores ranged from 5 to 7, with a mean of 6.78(SD=0.43) and, the practice score ranged from
0 to 5, with a mean of 3.17(SD=1.40).About 86.9% of the mothers in this study were aware
that vaccination prevents infectious diseases. This is similar to results of studies conducted in
Egypt, Northern Saudi Arabia and Riyadh, Saudi Arabia, where 93.3%, 85.6% and 82.6%
respectively knew that vaccination prevents infectious diseases(Ramadan et al.,2016; Alruwaili
et al.,2018; Al-zahrani,2013). This could be because immunization is an important public
health intervention effective in preventing infectious diseases to children, public knowledge on
the topic has been boosted and sustained. In addition,74.6% of the mothers knew that
vaccination enhance immunity and so help the body fight against infectious diseases. This
result is similar to findings of study in Riyadh where 89.2% of the parents knew that
vaccination enhance immunity (Al-zahrani, 2013). Another study in India revealed that all
50
(100%) the mothers knew that vaccination boost the immune system(Mereena& Sujatha,
2014). This could be because of the continuous health education by health workers which
enable mothers to grasp the concept of the importance of vaccination.
All (100%) of the mothers knew that it is important to vaccinate their children but what
they knew differed. This result is similar to results of studies conducted in Ikorodu Local
Government Area Nigeria, Democratic Republic of Congo and Kosofe LGA where 100%,
99.8% and 98% of the participants respectively knew about vaccination and the important role
it played in the lives of children under five(Adefolalu et al.,2019; Matapano et
al.,2008;Awodele et al.,2010) These similarities in results could be due to the social structure,
meaning that studies have participants living in tribes who have more knowledge about
immunization educate their fellow tribes’ women, thus increasing their knowledge about
immunization. Furthermore childhood immunization is an important and effective intervention
in the prevention of VDPs.
Knowledge Q4, Attitude Q4 and Practice Q5 are similar and are discussed together here.
In KQ4 95.6% of the mothers knew that completion of child’s vaccination as scheduled is
important. This is contradicting to a study by Angadi and colleagues in India where 97% of the
mothers did not know about the vaccination schedule (Angadi et al., 2013). This difference
observed could be due to the fact that have 20.2% of illiterate mothers while Angadi study
consisted of 38.96% illiterate fathers and 50.32% of illiterate mothers. In Q5 of Attitude
Section, 99.1% of the mothers knew that vaccination should be given according to schedule.
This is similar to results of a study by Ramadan and colleagues in India, where 97.2% of the
mothers knew that children should be vaccinated according to schedule(Ramadan et al.,2016).
While Q5 of Practice section, 87.7% of the mothers followed the obligatory vaccination
schedule and 12.3% did not. This could be due to 20.2% of illiterate mothers in this study.
51
Researchers revealed that maternal education or literacy seemed to be the strongest and the
most important predictor for immunization outcomes(Basu& Stephenson,2005; De &
Bhattacharya, 2002).Education played an important role in this regard.
In Knowledge Q5 and Q6, 99.1% of the mothers knew that it is important to receive
vaccination during pregnancy and 80.7% knew that tetanus vaccine is given during pregnancy.
This is given to protect the mother form tetanus and the baby from neonatal tetanus after the
baby is born. About 90.8% of mothers were aware that tetanus vaccine is important for the
health of the mother and infant (Ramadan et al.,2016).
All(100%) of the mothers knew that vaccines should not be administered if a child has fever
exceeding 38 degree Celsius. A study by Roodpeyma and colleagues in Iran revealed that
45.6% of the mothers knew that fever is a contraindication for vaccines (Roodpeyma et
al.,2007). On this note, there is no contraindication for giving measles/rubella vaccine(Pediatric
Society of Papua New Guinea,2016). This could mean most of the mothers were not aware of
the contraindication of specific vaccines. In supportive, in KQ8, 49.1% of the mothers were
aware that fever, swelling of injection site, rashes are the minor side effects of vaccination and
50.9% did not know that. In PQ2, 68.4% of the participants applied cold compress to swollen
injection site and 31.6% did not. Moreover, in PQ3 44.7% of the mothers used analgesics for
pain and swelling after vaccination and 55.3% did not. Furthermore, in PQ4 45.6% of the
participants reported the minor side effects to the health workers and 54.4% did not. This could
mean that health education given is too general and only emphasized on the benefits and less
emphasis on the minor side effects and contraindications.
In KQ9 AND AQ2, all(100%) of the mothers knew that vaccines for children are safe.
This result is similar to a study by Yousif and colleagues in Saudi Arabia, where 72% of the
mothers knew this (Yousif et al., 2013). This means that participants understood generally
52
knew the benefits of vaccines on their children’s’ health. About 96.5% of the participants knew
that a child should be started at the first week of life(AQ6) and 95.6% of the participants reveled
that a child be vaccinated at birth, one month, two months, three months, six months, nine
months and eighteen months.
The results of this study showed that most of the mothers had a positive attitude towards
immunization. In AQ1, all (100%) of the mothers knew that vaccination is important. This is
congruent to results of studies by Ramadan(98.6%) and Kalyani &Belsiyal(84%) where
mothers knew the importance of vaccination (Ramadan et al.,2016; Kalyani &Balsiyal,2018).
About 84% of the mothers recommend other parents to bring in their children for vaccination.
By extension, almost all the mothers stated that they will follow the recommended vaccination
schedule. This finding was similar to a study in Yemen ( Bamatraf & Jawass, 2010).PNG,
Nigeria and Yemen all offer free immunizations and appear to have had successful campaigns
promoting the idea (Awodele et al.,2010; Bamatraf&Jawass,2010;PNG Pediatric
Society,2016). Furthermore almost all the mothers were in favor of vaccination and all the
mothers revealed that culture did not have an influence on how they perceive immunization.
Though the mothers in this study demonstrated good knowledge and positive attitudes
towards childhood vaccination, their practice towards vaccination appeared to contradict that.
About 36% of the mothers reported that they did not get all their children vaccinated. This
could be because the mothers live in rural areas where accessibility to clinics and going into
town may be a problem due to transportation and financial issues. This is supported by a survey
done in PNG by Gibson &Rozelle(2015) which found that health and education services in
rural areas are not easily accessible due to poor road access.
Relationship between mothers’ Knowledge, Attitude and Practices and demographic
factors
53
The results revealed that age and the number of children did not correlate with
knowledge about immunization. Contrary to this finding, a study done by Mereena and Sujatha
in India reported that age and the number of children correlated with women’s knowledge of
immunization (Mereena& Sujatha, 2014). This could be due to the differences in the number
of sample size and also the study design. The Indian study had more participants (about 300),
compared to the 114 in this study, providing more detailed information that might reveal
differences not apparent in this study, a descriptive research design and used a different KAP
instrument. However, there was a significant difference in knowledge about immunization
according to urban or rural place of residence (t=-2.73, p=.008), with women in urban areas
showing more knowledge about immunization. This finding was similar to results of a study
done by Mugada and colleagues in India, where mothers living in the urban areas also had
greater knowledge of immunization compared to those in rural area s(Mugada et al., 2017).
This may reflect the fact that urban mothers have better access to hospitals and internet and so
are in a better position to get all the information needed. In terms of education, there was a
statistically significant difference in mothers’ knowledge by education level
(F=19.28,p<0.001). This finding was similar to that of a study by Awodele and colleagues in
Nigeria(Awodele et al., 2010).As illustrated in Table 3.1, mothers who were illiterate had less
knowledge than those who had some education but without graduating from high school, and
those with less than high school education did not know as much about immunization as high
school graduates. Mothers who had higher levels of education had more knowledge about
immunization than the mothers with less education.
The results illustrated that there is a negative correlation between age and attitude about
immunization (r=-.26, p=.006) and also between the number of children and attitude about
immunization(r=-.28, p=.003).These findings are similar to results of Mereena and Sujatha’s
54
study in India, which also found a significant difference in attitude related to age and the
number of children. Most of the mothers in that study were between age26 and 30(Mereena&
Sujatha, 2014). This could imply that younger mothers have better attitudesabout
immunization, as the mean age of participants in this study was 26.24.These similarities could
also be due to the fact that the studies were carried out on participants residing in urban and
rural settings and also from low income families. Mereena and Sujatha’s study also found that
attitude about immunization differed according to the number of children, with women who
had more children having a more positive attitude about immunization. This might be explained
by the facts that mothers who have had more than one child have received more information
about immunization over the years, leading to more positive attitudes regarding immunization.
This study also found a statistically significant difference in attitudes towards
immunization by place of residence (r=-2.22, p=.030). Mothers in urban areas have a more
positive attitude towards immunization than mothers in rural areas. As already shown, mothers
in urban areas also have more education and more knowledge about immunization. So their
attitudes about immunization reflect their knowledge, and knowledge can change both
behaviors as well as attitudes. Moreover, there was a significant difference in attitude about
immunization according to level of education (F=10.61, p<0.001). This finding is similar to
results of a study by Adekeye and colleagues in Nigeria (Adekeye et al., 2015),which revealed
that mothers who were illiterate had less positive attitudes towards immunization than mothers
who had primary school education and high school graduates. This shows that having some
form of education is important because it increases one’s level of understanding and changes
attitudes.
The study findings revealed a negative correlation between age and immunization
practice(r=-.24, p=.010) and between the number of children and immunization practice (r=-
55
.294, p=.010). Older mothers had more children than younger women, but were less likely to
immunize all their children than younger mothers. Younger mothers had fewer children but
were more likely to have them all immunized. This is contradictory to a study done by
Adefolalu and colleagues in Nigeria, where older mothers were more mature and brought all
their younger children in for vaccination (Adefolalu et al., 2019). In support of this, a study by
Mohamudand colleagues in Ethiopia found that the rate of complete vaccination of children
increases with the age of their mothers (Mohamud et al., 2014).This could be because the mean
age of those mothers in Ethiopia was 30.96. The results in Ethiopia and Nigeria showing that
mothers with more children were more likely to vaccinate them all could be related to the fact
that mothers received information over the years when having more than one child, leading to
a change in their attitudes and practices regarding immunization.
This study also found that there was a statistically significant difference in practice of
immunization by place of residence (r=-2.91, p=.005). Mothers in the urban areas had better
practice of immunization than mothers in the rural area. Their better immunization practice
reflected their greater knowledge and more positive attitude.
This resultsof this study also showed that there was a significant difference in
immunization practice according to the level of education (F=16.53, p<0.001). This finding is
similar to results of a study by Konwea and colleagues in Nigeria, which likewise found a
significant relationship between education level and immunization, practice (Konwea et al.,
2018). The analysis in this studyrevealed that mothers who were illiterate had less knowledge
than those who had some education without graduating from high school, and those with less
than high school education did not know as much about immunization as high school graduates.
This shows that having some form of education is important because it increases one’s level of
understanding and changes attitudes.
56
Out of the nine demographic factors, only four were found to be significant and have
been discussed above. Factors such as income, source of information about immunization,
marital status, transportation to the clinic, and decision making were not significantly
associated with immunization practice.
The Pearson’s correlation test showed a positive association between knowledge and
practice(r=.57, p<0.001), revealing that mothers who had more knowledge about immunization
were more likely to have their children immunized. This finding was similar to that of a study
by Matapano and colleagues in the Democratic Republic of Congo(Matapano et al.,2018).
Mothers who have higher levels of education tend to have more knowledge, resulting in better
practice of immunization. In addition, there was a positive association between attitude and
practice(r=.46,p<0.001), with better attitude about immunization being associated with greater
likelihood of immunization. Mothers who have some knowledge about immunization have
better attitudes and thus have better practice.
Variables predicting the practice of immunization
This study showed that knowledge (β=0.392) is an important predictor of immunization
practice among mothers in Papua New Guinea. This conclusion, that mothers’ knowledge
about immunization predicts immunization practice, is consistent with findings of the study
done in the Democratic Republic of Congo and the results of a literature review by Favin and
colleagues in Switzerland (Favin et al., 2012; Matapano et al., 2014). Furthermore, knowledge
was identified as an important factor in a study on parents’ decision-making regarding
immunization done in Germany (Zingg & Siergrist, 2012).
57
CHAPTER V Conclusion
This section presents the implications, recommendations, limitations and the conclusions of
the study.
Section I Implications for future research
Knowledge plays a positive and essential role in immunization practice. The
implications of these findings will be discussed as they relate to health policy, public health
education, and nursing practice.
1. Health Policy
Policy makers can use these findings to strengthen and amend health policies of Papua
New Guinea in order to increase childhood immunization coverage. PNG already has good
policies regarding health promotion but they are not being adhered to. Immunization is free
and mandatory in PNG but the vaccination coverage rate remains below eighty percent. The
vaccination rate could be improved if the government puts policies in place such through
58
legislation requiring vaccination for school entry. This has been practiced in many countries
around the world and is found to be effective.
2. Public Health Education
Since knowledge predicted immunization practice, PNG health care workers, especially
the nurses, should take initiative in organizing immunization awareness programs at different
levels of the health care system all the way down to the aid post level. Furthermore, hospitals
and clinics should have visible pamphlets and poster information regarding childhood
immunization available in waiting areas or to be given during health visits. Moreover, health
professionals should go on the radio and talk about the importance of childhood immunization.
And lastly but not least, simple language should be used for ease of comprehension when
targeting the mothers living in both urban settlements and rural areas.
3. Nursing Practice
Nurses should educate mothers at every opportunity about immunization. Nurse
supervisors should draw up schedules regarding health education, including awareness about
immunization as well as other topics, so that nurses do it regularly and routinely. Nurses should
use simple language that mothers can understand when disseminating the information. In
addition, nurse managers should create an incentive structure to reward nurses for providing
health education in the outpatient area or on the wards, and new nurses should be given
encouragement to gain the confidence for doing this. Furthermore illiterate mothers can be
educated with the help of a community leader as a translator because 20.2% of mothers in this
study were illiterate.
Section II Recommendations of the study
Future research could collect data from health cards to match actual immunization
practice with women’s knowledge and attitudes about immunization, which would provide
59
more specific information about the gap between knowledge of immunization and
immunization practice identified in this study. It would also eliminate the possibility of
response bias.
In addition, the findings of this study will serve as a reference for future research
regarding childhood immunization in Papua New Guinea. This study revealed that knowledge
is the best predictor of immunization practice, although the results suggest that a substantial
percentage of children were still not receiving vaccinations. The women scored higher on
knowledge about immunization than on practice. Therefore, a future study should try to
understand the reason for this gap. A qualitative study could provide more insight into the
mothers’ knowledge and attitudes regarding immunization and should be combined with
results of other studies to reduce barriers identified to immunization at clinics to get a fuller
picture of immunization practice in PNG.
The instrument used to measure knowledge, attitudes and practices in this study was
developed by Sebastian and colleagues (2017), however, publication is pending so the results
of the original study are not yet available for comparison. A widely used instrument for another
quantitative study would facilitate comparison. A larger and more representative sample size
would be useful, which would require finding participants in numerous hospitals and clinics in
different parts of the country.
Health education on the benefits of each vaccine should be intensified at health centers
and community gatherings in-order to improve mothers’ knowledge about childhood
immunization. Programs such as female education, adult education and health education should
be strongly encouraged and maintained.
60
Section III Limitations of the study
This study had some limitations in terms of design, sampling and the instrument used.
This was a quantitative cross sectional study with a questionnaire that had all closed questions.
The researcher did not collect information on the actual rate of vaccination to assess the
relationship between intentions and actual practice.Even if the questionnaire asked precise
information about how many children the mother had vaccinated or not vaccinated, it is only
possible to know about her knowledge and attitude about immunization in the present, so it is
not clear what value that information would have. Another limitation of this study was the use
of convenience sampling. Because the mothers were recruited from only one hospital, Sandaun
Provincial Hospital, the study participants consisted of a small portion of Papua New Guinean
mothers. This means the results cannot be generalized to all mothers who have children under
five in PNG. The questionnaire used had all closed questions to avoid the possibility of
misinterpretation of language and to make it easy for both the interviewer and the mothers.
However, closed questions limit the amount of detailed information that could be obtained from
the mothers, as compared to a qualitative study. This questionnaire and was initially in English
then translated in Tok Pisin for the mothers. Although the original intention was to give
participantsa self-administered written quesitonnaire, many women seemed to have difficulty
understanding the questionnaire, so the researcher then conducted an in-person
interview.Therefore, the technique of gathering information was not uniform and may have
introduced some bias, such as social desirability and interview bias. The women knew the
researcher was a health worker, and that health workers expect them to have their children
vaccinated, so in order to please the interviewer they might have been more likely to say they
were getting vaccinations.Furthermore, due to the limited time of data collection; this study
61
was cross sectional in design, so it cannot reflect change in knowledge, attitudes, or practice
over time.
Section IV Conclusion
This study found that mothers’ knowledge about vaccines is one factor that hinders
them from getting their children fully vaccinated. Despite the efforts of health workers to
increase coverage by educating mothers, knowledge remains uneven and not all children are
brought in for vaccination. The findings suggest that, on the one hand, current efforts to educate
mothers about vaccines have not yet been completely successful, and on the other, that health
education alone may not be sufficient. Therefore health education given should be specific on
each vaccine, its benefits and the disadvantages.
Reference
Abdi Nur Mohamud, Amsalu Feleke, WalelegnWorku, ManayKifle and Hardeep Rai
Sharma Immunization coverage of 12–23 months old children and associated factors
in Jigjiga District, Somali National Regional State, Ethiopia. BMC Public Health 2014
14:865.
Adams, A., Boualam, L., Diorditsa, S., Gregory, C., Jee, Y., Mendoza-Aldana, J., & Roesel, S.
(2014). Maintaining polio-free certification in the World Health Organization Western
Pacific Region for over a decade. Journal of Infectious Disease,210 Suppl 1, S259-267.
doi: 10.1093/infdis/jiu164
62
Adefolalu, O.A., Kanma-Okafor, O.J., & Balogun, M.R.,(2019), Maternal knowledge, attitude
and compliance regarding immunization of under five in Primary Health Care centers
in Ikorodu Local Government Area, Laos State, Journal of Clinical Sciences, 16(1)
Adekeye, O.A., Chenube, O.O., Ahmadu, F., & Adekeye, B.T. (2015). Knowledge, Attitude
and Barriers towards Children Immunization among Women in Selected Rural Primary
Health Centres. Ife Psychologia, 23(1), 89–97. Retrieved from
https://core.ac.uk/download/pdf/95550409.pdf
Adenike, O. B., Adejumoke, J., Olufunmi, O., & Ridwan, O. (2017). Maternal characteristics
and immunization status of children in North Central of Nigeria. Pan African Medical
Journal, 26, 159. doi: 10.11604/pamj.2017.26.159.11530
Agboatwalla, & Akram. (1997). Impact of health education on mothers' knowledge of
preventive health practices. Tropica Doctor, 27.
Agyei, W.K.A,1984, Fertility and Family Planning in Papua New Guinea. Journal of
.biosocial .Sciences.16,323
Alamri, E. S., Horaib, Y. F., & Alanazi, W. R. (2018). Knowledge and Attitudes of Parents on
Childhood Immunization in Riyadh, Saudi Arabia. The Egyptian Journal of Hospital
Medicine, 70(2), 251-256. doi: 10.12816/0043085
Alruwaili, A. A. S., El-fetoh, N. M. A., Alruwaili, T. A. S., Alanazi, W. A. S., Alhazmi, H. H.
R., Alanazi, N. A. B., . . . Alrwaili, A. H. (2018). Knowledge, Attitude and Practice of
the Parents Regarding Child Vaccinations in Arar, Northern Saudi Arabia. Egyptian
Journal of Hospital Medicine, 72(9), 5178-5182.
Alshammari, T. M., Alsubaie, Y. S. R., Someili, S. A., Alajmi, N. M., Alanazi Khalid Khalaf,
M., Abdrab Alamir, M. A. M., . . . Alhazmi, A. B. A. (2018). Assessment of Knowledge,
63
Attitude and Practice of Parents about Immunization in Hail City, 2018. Egyptian
Journal of Hospital Medicine, 73(3), 6377-6381.
Alshehri, E. A. H., Alamari, M. A. A., Ahmed, R. H., Abdullh Al-Qahtani, A. H., Abdullah
Alshafa, F. A., & Ali Alsrori, Z. M. (2018). Assessment of Knowledge, Attitude and
Practice of Parents towards Vaccination among Children under 12 Years in Riyadh,
KSA, 2018. Egyptian Journal of Hospital Medicine, 72(1), 3688-3691. doi:
10.12816/0047730
Alyami, A. R., Alhashan, G. M., Nasser, I. A., Alyami, S. R., Al Mardhamah, N. H., Alyami,
M. H., . . . Alanazi, A. M. (2018). Knowledge, Beliefs and Practices of Parents towards
Childhood Vaccination in Najran City, Saudi Arabia. Egyptian Journal of Hospital
Medicine, 70(1), 1-7. doi: 10.12816/0042954
Anderson, V. L. (2015). Promoting Childhood Immunizations. The Journal for Nurse
Practitioners, 11(1), 1-10. doi: 10.1016/j.nurpra.2014.10.016
Angadi MM, Jose AP, Udgiri R, et al. A study of knowledge, attitude and practices on
immunization of children in urban slums of Bijapur city, Karnataka, India. Journal of
Clinical and Diagnostic Research 2013;7:2803–6.
Apeng et al. (2010). The 'Reach Every Village' strategy for community-based health
improvement interventions in the Momase Region of Papua New Guinea. PNG Medical
Journal, 53.
Aquastat Survey. (2011). Papua New Guinea Geography, Climate and Population.
Arawa ,J.(2005), Notes for a lecture on Expanded Immunization Program in Papua New
Guinea, Archives of the National Department of Health, Port Moresby
Asian Development Bank. (2012). The Impact of Out-of-Pocket Expenditures on Families and
Barriers to Use of Maternal and Child Health Services in Papua New Guinea.
AusAid. (2015). Australia's Bilateral Aid Program in Papua New Guinea.
64
Awodele O, Oreagba IA, Akinyede A, Awodele DF, Dolapo DC,(2010)The knowledge and
attitude towards childhood immunization among mothers attending antenatal clinic in
Lagos University Teaching Hospital Nigeria. Tanzania Journal of Health Research.
2010;12(3):172-177.
Bamatraf, F. F., & Jawass, M. A. (2018). Knowledge and Attitude towards Childhood
Immunization among Parents in Al-Mukalla, Yemen. World Family Medicine
Journal/Middle East Journal of Family Medicine, 16(2), 24-31. doi:
10.5742/mewfm.2018.93239
Basu, A. M., & Stephenson, R. (2005). Low levels of maternal education and the
proximate determinants of childhood
mortality:A l itt le learning is not a dangerous thing.
Social Science & Medicine, 60 (9), 2011–2023
Bauri, M., Wilkinson, A. L., Ropa, B., Feldon, K., Snider, C. J., Anand, A., . . . Yoshihiro, T.
(2019). Circulating Vaccine-Derived Poliovirus Type 1 and Outbreak Response --
Papua New Guinea, 2018. MMWR: Morbidity & Mortality Weekly Report, 68(5), 119-
120.
Bersen, R. M., Al-Zahmi, F. R., Al-Ali, N. A., Hamoudi, R. O., Ali, N. A., Schneider, J., . . .
Grivna, M. (2011). Knowledge, Attitude and Practices towards Immunizations among
Mothers in a Traditional City in the United Arab Emirates. Journal of Medical Sciences.
CDC. (2015a). MMR(Measles, Mumps, and Rubella).
CDC. (2015b). Pneumoccocal Conjugate Vaccine(PCV13).
CDC. (2015c). Polio Vaccine. Center for Disease Control and Prevention. (2018). Vaccine
Information Statement-Hepatitis B vaccine,.
Center of Disease Control. (2011). TB Elimination-BCG vaccine
65
Chris-Otubor, G. O., Dangiwa, D. A., Ior, L. D., & Anukam, N. C., (2015), Assessment of
Knowledge, Attitudes and Practices of Mothers in Jos North Regarding Immunization,
IOSR Journal of Pharmacy,5(6), 34-45
Comprehensive Multi-Year Plan(cMYP),(2010), National Immunization Programme 2011-
2015.
Cutts, F. T. (1991). Strategies to improve immunization services in urban Africa. Bulletin of
the World Health Organization.
Dabas, P., Agarwal, C.M., Kumar, R. et al(2005). Knowledge of general public and health
professionals about tetanus immunization. Indian Journal of Pediatrics 72, 1035–1037
(2005).
De, P., & Bhattacharya, B. N. (2002). Determinants of childimmunizat ion in f
our less-developed states of North India.Journal of Child Health Care, 6
(1), 34–50.3.
Dharmalingam, A., Raghupathy, N. S., Sowmiya, M., Amudharaj, D., & Jehangir, H. M.
(2017). Immunization knowledge, attitude and practice among mothers of children
from 0 to 5 years. International Journal of Contemporary Pediatrics, 4(3), 783. doi:
10.18203/2349-3291.ijcp20171488
Esposito, S., Principi, N., Cornaglia, G., & Group, E. V. S. (2014). Barriers to the vaccination
of children and adolescents and possible solutions. Clinical Microbiological Infections
Journal, 20 Suppl 5, 25-31. doi: 10.1111/1469-0691.12447
Expanded Immunization Programme. (2014). Polio and the Introduction of IPV.
Favin, M., Steinglass, R., Fields, R., Banerjee, K., & Sawhney, M. (2012). Why children are
not vaccinated: a review of the grey literature. International Health Journal, 4(4), 229-
238. doi: 10.1016/j.inhe.2012.07.004
66
Fernandez, R. C., Awofes, N., & Rammohan, A. (2011,). Determinants of apparent rural-urban
differentials in measles vaccination uptake in Indonesia,. The International Electronic
Jouranal of Rural and Remote Health Research, Education, Practice and Policy
Gakidou.E, Cowling.K, Lozano.R, & Murray.C.J.L. (2010). Increased educational attainment
and its effect on child mortality in 175 countries between 1970 and 2009: a systematic
analysis. The Lancet, 376.
Girma.B, & Berhane.Y. (2011). Children who were vaccinated, breast fed and from low parity
mothers live longer: A community based case- control in Jimma, Ethiopia. BMC Public
Health.
Gray, J. R., Grove, S. K., & Sutherland, S. (2017). Burns' and Grove's, The Practice of Nursing
Research: Appraisal, Synthesis, and Generation of Evidence, Missouri, Elsevier Inc.
Greenwood, B. (2014). The contribution of vaccination to global health: past, present and
future. Philosophical Transactions of the Royal Society London B Bioogical Sciences,
369(1645), 20130433. doi: 10.1098/rstb.2013.0433
Habib, R. F., Alsubhi, R. A., & Saadawi, D. W. (2018). Assessment of Knowledge, Attitude
and Practice of Parents towards Immunization of Children in Saudi Arabia, 2018. The
Egyptian Journal of Hospital Medicine, 71(2), 2585-2589. doi: 10.12816/0045660
Hamid S, Andrabi SAH, Fazli A and Jabeen R. Immunization of children in a rural area of
North Kashmir India: a KAP study. Online Journal of Health Allied Sciences.2012;
11(1):10.
Horwood, P. F., Reimer, L. J., Dagina, R., Susapu, M., Bande, G., Katusele, M., . . . Pavlin, B.
I. (2013). Outbreak of chikungunya virus infection, Vanimo, Papua New Guinea.
Emerging Infectious Diseases Journal, 19(9), 1535-1538. doi:
10.3201/eid1909.130130
67
Hug et al. (2018). Level & Trends in Child Mortality
International Federation of Red Cross and Red Crescent Societies. (2018). Emergency Plan of
Action Final Report Papua New Guinea: Measles.
Jayawardena, N., Subhi, R., & Duke, T. (2012). The Western Pacific Regional Child Survival
Strategy: progress and challenges in implementation. Journal of Paediatrcs and Child
Health, 48(3), 210-219. doi: 10.1111/j.1440-1754.2010.01926.x
John Gibson & Scott Rozelle,(2015), Poverty and Access to Roads in Papua New Guinea
Kara, S. S., Polat, M., Yayla, B. C., Demirdag, T. B., Tapisiz, A., Tezer, H., & Camurdan, A.
D. (2018). Parental vaccine knowledge and behaviours: a survey of Turkish families.
Eastern Mediterrenean Health Journal, 24(5), 451-458. doi: 10.26719/2018.24.5.451
Khodaee, H. G., Khademi, G. a., & Saeidi, M. (2015). Under-five Mortality in the World(1900-
2015). International Journal of Pediatrics, 3, 1093-1095.
King.R, Mann.V, & Boone.P.D. (2010). Knowledge and reported practices of men and women
on maternal and child health in rural Guinea Bissau:a cross sectional survey. BMC
Public Health.
Konwea EP, David FA, Ogunsile SE (2018) Determinants of compliance with child
immunization among mother of children under five years of age in Ekiti state, Nigeria.
Journal of Health Research 32(3):229–236
Kusuma, Y. S., Kumari, R., Pandav, C. S., & Gupta, S. K. (2010). Migration and immunization:
determinants of childhood immunization uptake among socioeconomically
disadvantaged migrants in Delhi, India. Tropical Medicine and International Health
Journal, 15(11), 1326-1332. doi: 10.1111/j.1365-3156.2010.02628.x
68
Lakew, Y., Bekele, A., & Biadgilign, S. (2015). Factors influencing full immunization
coverage among 12-23 months of age children in Ethiopia: evidence from the national
demographic and health survey in 2011. BMC Public Health, 15, 728. doi:
10.1186/s12889-015-2078-6
Mahalingam, S., Soori, A., Ram, P., Achappa, B., Chowta, M., & Madi, D. (2014). Knowledge,
attitude and perceptions of mothers with children under five years of age about
vaccination in Mangalore, India. Asian Journal of Medical Sciences, 5(4), 52-57.
Mapatano MA, Kayembe K, Piripiri L, Nyandwe K (2014) Immunisation-related knowledge
, attitudes and practices of mothers in Kinshasa, Democratic Republic of the Congo.
South African Family Practice 60: 60-61.
Mereena, Sujatha R (2014) A study on knowledge and attitude regarding vaccines among
mothers of under five children attending pediatric OPD in a selected hospital at
Mangalore. IOSR Journal of Nursing Health Sciences, 5: 39-46. 15.
Merriam-Webster's Collegiate Dictionary (11th edn), Springfield.
Mitchell, S., Andersson, N., Ansari, N. M., Omer, K., Soberanis, J. L., & Cockcroft, A. (2009).
Equity and vaccine uptake: a cross-sectional study of measles vaccination in Lasbela
District, Pakistan. BMC International Health Human Rights, 9 Suppl 1, S7. doi:
10.1186/1472-698X-9-S1-S7
Moisi, J. C., Kabuka, J., Mitingi, D., Levine, O. S., & Scott, J. A. (2010). Spatial and socio-
demographic predictors of time-to-immunization in a rural area in Kenya: Is equity
attainable? Vaccine Journal, 28(35), 5725-5730. doi: 10.1016/j.vaccine.2010.06.011
Mugada V, Chandrabhotla S, Kaja DS, Machara SGK. Knowledge towards childhood
immunization among mothers & reasons for incomplete immunization. Journal
of Applied Pharmaceutical Science. 2017;7(10):157-61
69
Namuigi , & Phuanukoonnon. (2005). Barriers to measles immunization: the beliefs and
attitudes of caregivers in Goroka, Eastern Highlands Province, Papua New Guinea.
PNG Medical Journal.
National Department of Health, P. (2010). Papua New Guinea
Nuttall, J. J., & Eley, B. S. (2011). BCG Vaccination in HIV-Infected Children. Tuberculosis
Research and Treatment, 2011, 712736. doi: 10.1155/2011/712736
Nuwuha, R., Mulindwa, G., Kabwongyera, E., & Barenzi, J. (2000). Causes of low attendance
at National Immunization Days for polio eradication in Bushenyi District,Uganda,.
Tropical Medicine and International Health Journal, 5, 364-369. Olujide, A., Adekeye,
Fred, A., Olufunke, O. C., & Bosede, T. A. (2015). Knowledge, Attitude and Barriers
towards Children Immunization among Women in Selected Rural Primary Health
Centres,Nigeria,An International Journal of Psychology in Africa
PNG & WHO. (2016). PAPUA NEW GUINEA-WHO
WHO.(2017).Country Cooperation Strategy 2016-2020
PNG, Govt. (2010). National Health Plan 2011-2020,Volume One Policies and Strategies
PNG Govt. (2015). Summary Report for Papua New Guinea: Millenium Development Goals
2015.
PNG Pediatric Society. (2016). Standard Treatment for Common Illneses of Children in Papua
New Guinea: A manual for nurses, community health workers, health extension
officers, and doctors.
Qutaiba, B. A.-l. O., Bahari, M. B., Al-Qazaz, H. K., Salih, M. R., Jamshed, S. Q., & Elkalmi,
R. M. (2014). Are parents' knowledge and practice regarding immunization related to
pediatrics' immunization compliance? a mixed method study. BMC Pediatr, 14, 20. doi:
10.1186/1471-2431-14-20
70
Rahman M, Islam MA, Mahalanabis D,1995, Mother's knowledge about vaccine preventable
diseases and immunization coverage in a population with high rate of illiteracy. Journal
of Tropical Pediatrics 1995, 41:376-8
Ramadan, H. A., Soliman, S. M., & Abd El-kader, R. G. (2016). Knowledge, Attitude and
Practice of Mothers toward Children's Obligatory Vaccination. IOSR Journal of
Nursing and Health Science, 05(04), 22-28. doi: 10.9790/1959-0504022228
Roodpeyma S, et al.(2007): Mothers and vaccination: Knowledge, attitudes, and practice in
Iran. Jornal of Pediatrics and Infectious Diseases, 2(1):29–34.
Sai, A. (2007). Tamot: Masculinities in Transition in Papua New Guinea. PhD thesis,
Victoria University, Melbourne.
Šeškutė M, Tamulevičienė E, Levinienė G.(2018) Knowledge and attitudes of postpartum
mothers towards immunization of their children in a Lithuanian tertiary teaching
hospital. Journal of Lithuanian Medical Association
(Medicina).2018;54:2.DOI:10.3390/medicina5401000
Shen, A. K., Clay, R., & Mendez, A. P. (2014). Global Immunization through the Lens of
Development. Public Health Reports, 129(Supplement 3)
Sullivan, M.-C., Tegegn, A., Tessema, F., Galea, S., & Hadley, C. (2009). Minding the
Immunization Gap: Family Characteristics Associated with Completion Rates in Rural
Ethiopia (Vol. 35). Journal of Commuity Helath
The World Bank. (2010). Theories of Behavior Change.
Thorrington, D. (2016). The social and economic impact of community-based transmission of
vaccine-preventable influenzae and measles. London School of Hygiene & Tropical
Medicine. doi: 10.17037/PUBS.03234043
71
Thwaites CL, Beeching NJ, Newton CR. Maternal and neonatal tetanus. Lancet. 2014. doi:
http://dx.doi.org/10.1016/S0140-6736(14)60236-1 PMID: 25149223
Toikilik, S., Tuges, G., Lagani, J., Wafiware, E., Posanai, E., Coghlan, B., . . . Clements, C. J.
(2010). Are hard-to-reach populations being reached with immunization services?
Findings from the 2005 Papua New Guinea national immunization coverage survey.
Vaccine, 28(29), 4673-4679. doi: 10.1016/j.vaccine.2010.04.063
UNDP,2019, Overview Human Development Report, Beyong income, beyong averages,
beyond today: Inequalities in human development in the 21st century, New York, USA.
UNDP(2014),“Sustaining Human Progress: Reducing Vulnerabilities and Building
Resilience” New York, USA.
UNICEF. (2013). UNICEF Annual Report 2013-Papua New Guinea
UNICEF. (2015). Pentavalent vaccine(DTwP-HepB-Hib): Market & Supply Update.
United Nations Children's Fund. (2017). UNICEF PNG Country Programme Strategy Notes-
Health.
Vasantha kalyani C and Xavier Belsiyal C.2016, Knowledge, Attitude And Practice of
Mothers of Under Five Children Regarding Immunization In A Selected Community,
Rishikesh, Uttarakhand, International Journal of Recent Science Research. 7(5), pp.
11301-11305.
Verulava T, Jaiani M, Lordkipanidze A, Jorbenadze R, Dangadze B.(2019), Mothers’
Knowledge and attitudes towards child immunization in Georgia, The Open
Public Health Journal. 2019;12:232-7.DOI:10.2174/1874944501912010232
72
Vonasek, B. J., Bajunirwe, F., Jacobson, L. E., Twesigye, L., Dahm, J., Grant, M. J., . . .
Conway, J. H. (2016). Do Maternal Knowledge and Attitudes towards Childhood
Immunizations in Rural Uganda Correlate with Complete Childhood Vaccination?
PLoS One, 11(2), 1-16. doi: 10.1371/journal.pone.0150131
WHO. (2011). Children: reducing mortality.
WHO. (2015). Regional Framework for Implementation of the Global Vaccine Action Plan in
the Western Pacific.
WHO. (2018a). Papua New Guinea Country Cooperation Strategy at a glance
WHO. (2018b). UHC and SDG Country Profile 2018 Papua New Guinea.
WHO & NDoH. (2012). Health Service Delivery Profile: Papua New Guinea.
Yadav, R., Vaswani, N. D., Khanna, A., Tripathi, P., Singh, A., & Kumar, B. (2015).
Knowledge, attitude and practice of parents regarding immunization at a tertiary care
hospital of Rohtak city. Indian Journal of Health & Wellbeing, 6(3), 341-343.
Yarong T, & Aipit J. (2014). Estmated Immunization Coverage in Children attending Modilon
General Hospital, Madang District, Madang Province, Pediatric Society of Papua New
Guinea
Zingg, A., and Siegrist, M. (2012). Measuring people’s knowledge about vaccination:
developing a one-dimensional scale. Vaccine 30, 3771–3777. doi:
10.1016/j.vaccine.2012.03.01
73
Appendix I: Consent Form
Study Title: Assessing knowledge, attitudes and practices of mothers regarding
immunization in West Sepik Province, Papua New Guinea.
Dear Participant,
You are kindly invited to participate in this study. The aim of this study is to assess
knowledge, attitudes and practices of mothers regarding immunization. Participation is free
and you may withdraw any time during the study. There is no risk to you and you will not be
paid, however, your sincere participation is vital in understanding and educating you as an
important part ofyour child’s health. Your privacy will be protected, so your name will not be
reveal to anyone. Your informatiom will be kept confidential and will not be disclosed to a
third party, but anonymous results may be provided to health care instititutions for the
purpose of improving health education and service care.
Thank you for your time and participation.
I have been informed and understand that by signing this consent form, I give permission to
the reseacher to use my personal information related to the study. I voluntary consent to take
part by answering the questionnaire based on my best knowledge and experience.
Name: ……………………………Signature:………………
(or Finger print)
Date:……………………
Researcher’s Name:………………………………………. Signature: ……………
ID code: …………………………………………………………
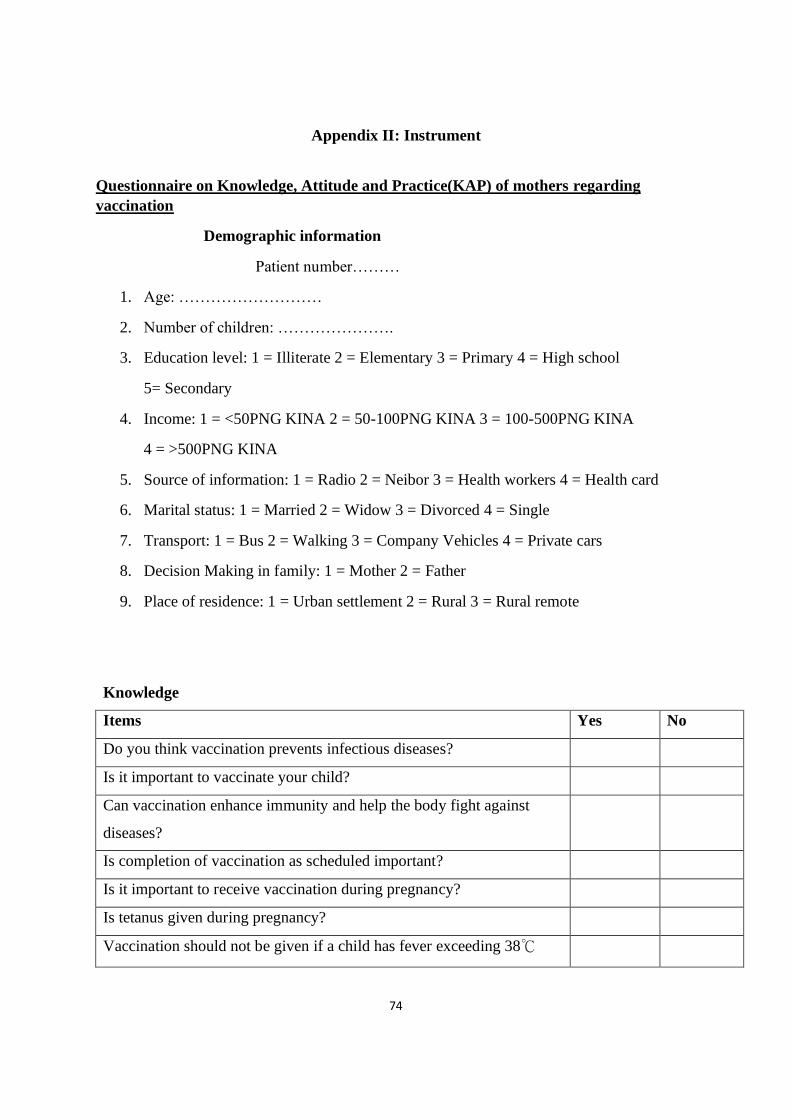
74
Appendix II: Instrument
Questionnaire on Knowledge, Attitude and Practice(KAP) of mothers regarding
vaccination
Demographic information
Patient number………
1. Age: ………………………
2. Number of children: ………………….
3. Education level: 1 = Illiterate 2 = Elementary 3 = Primary 4 = High school
5= Secondary
4. Income: 1 = <50PNG KINA 2 = 50-100PNG KINA 3 = 100-500PNG KINA
4 = >500PNG KINA
5. Source of information: 1 = Radio 2 = Neibor 3 = Health workers 4 = Health card
6. Marital status: 1 = Married 2 = Widow 3 = Divorced 4 = Single
7. Transport: 1 = Bus 2 = Walking 3 = Company Vehicles 4 = Private cars
8. Decision Making in family: 1 = Mother 2 = Father
9. Place of residence: 1 = Urban settlement 2 = Rural 3 = Rural remote
Knowledge
Items Yes No
Do you think vaccination prevents infectious diseases?
Is it important to vaccinate your child?
Can vaccination enhance immunity and help the body fight against
diseases?
Is completion of vaccination as scheduled important?
Is it important to receive vaccination during pregnancy?
Is tetanus given during pregnancy?
Vaccination should not be given if a child has fever exceeding 38℃
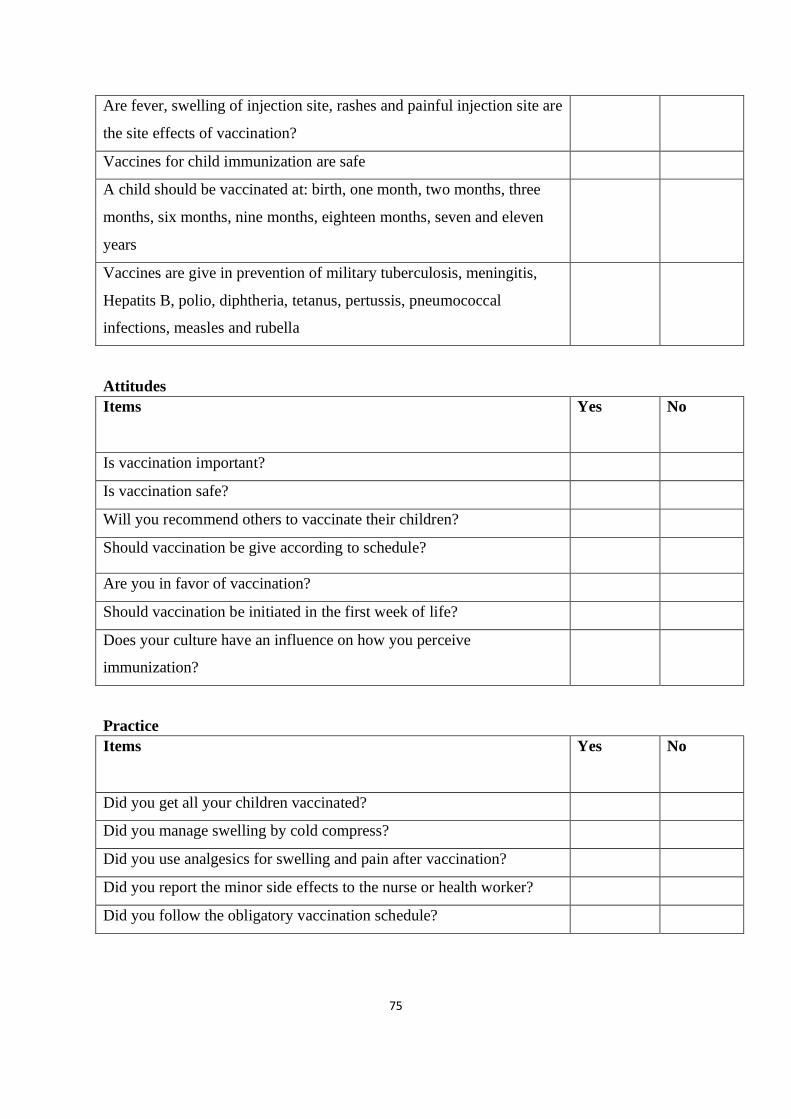
75
Are fever, swelling of injection site, rashes and painful injection site are
the site effects of vaccination?
Vaccines for child immunization are safe
A child should be vaccinated at: birth, one month, two months, three
months, six months, nine months, eighteen months, seven and eleven
years
Vaccines are give in prevention of military tuberculosis, meningitis,
Hepatits B, polio, diphtheria, tetanus, pertussis, pneumococcal
infections, measles and rubella
Attitudes
Items Yes No
Is vaccination important?
Is vaccination safe?
Will you recommend others to vaccinate their children?
Should vaccination be give according to schedule?
Are you in favor of vaccination?
Should vaccination be initiated in the first week of life?
Does your culture have an influence on how you perceive
immunization?
Practice
Items Yes No
Did you get all your children vaccinated?
Did you manage swelling by cold compress?
Did you use analgesics for swelling and pain after vaccination?
Did you report the minor side effects to the nurse or health worker?
Did you follow the obligatory vaccination schedule?
76
Tok Pisin version
Tok OraitPepa
StadiTaitel: Skelim save, pasinnapraktisbilongol mama long tambusutinsait lo West
SipikProvins, Papua Niugini (PNG).
DiaOl Mama,
Yu welkam long stap insait long dispela wok painimaut. As tingting
em lo painim save, pasinnapraktisbilongol mama lo tambusut. Askim i kam sapos yu ken
halivim long givim tingting bilong yu lo ol askim wei bai mi askim yu. Displa olaskim bai
long sait bilong save, pasinnapraktisbilongtambusut. Tingting wei bai yu i givim ba nonap gat
moni bilong em tasol ba i halivim long givimskultoktokinapim save
napasinbilongbringimbebi longkisimtambusut. Ba yui nonap bungim hevi lo taim bilong ol
dispela askim long wanem halivim bilong yu long givim stretpela tingting bilong yu bai i stap
namel long meri weii givim askimpepa na yu weiyu givim tingting. Yu ken lusimdispelastadi
ani taimsaposyulaik. Olgetatingtingyugivim bai halvim long saitbilonglainim and kisim save
lo hausiknaskul.
Sapos yu wabel long givim tingting bilong yu, bikpela tok tenkiu i kam longyu.
Bai mi putim han mak bilong mi long dispela pepa bilongsoimolsem mi wanbel long toktok
wei mi kisim
Nem: ………………………………………Han mak:……………………………
Dei:……………………………………………
Nem bilong merii askim: ……………………… Han mak: ………………………………
ID Namba: ………………………………………
Askim lo tokpisin
Nambabilongsikman………
1.Krimas: ………………………
1. Nambabilongpikinini: ………………….
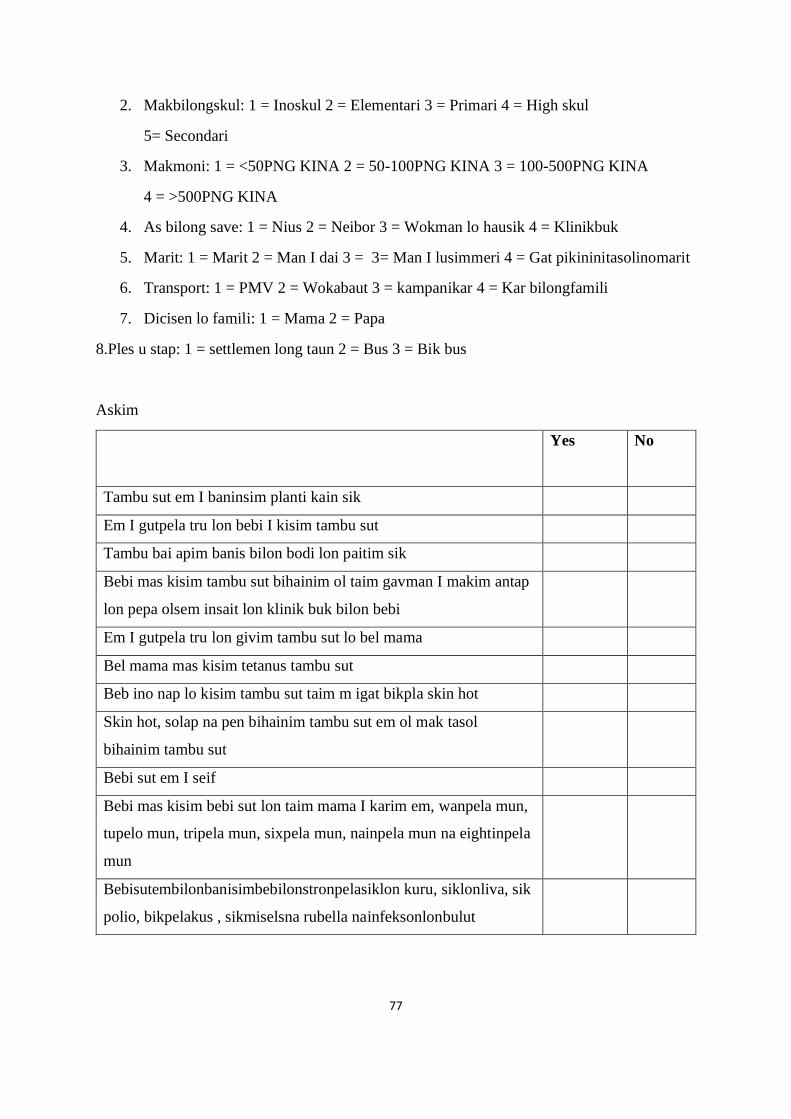
77
2. Makbilongskul: 1 = Inoskul 2 = Elementari 3 = Primari 4 = High skul
5= Secondari
3. Makmoni: 1 = <50PNG KINA 2 = 50-100PNG KINA 3 = 100-500PNG KINA
4 = >500PNG KINA
4. As bilong save: 1 = Nius 2 = Neibor 3 = Wokman lo hausik 4 = Klinikbuk
5. Marit: 1 = Marit 2 = Man I dai 3 = 3= Man I lusimmeri 4 = Gat pikininitasolinomarit
6. Transport: 1 = PMV 2 = Wokabaut 3 = kampanikar 4 = Kar bilongfamili
7. Dicisen lo famili: 1 = Mama 2 = Papa
8.Ples u stap: 1 = settlemen long taun 2 = Bus 3 = Bik bus
Askim
Yes No
Tambu sut em I baninsim planti kain sik
Em I gutpela tru lon bebi I kisim tambu sut
Tambu bai apim banis bilon bodi lon paitim sik
Bebi mas kisim tambu sut bihainim ol taim gavman I makim antap
lon pepa olsem insait lon klinik buk bilon bebi
Em I gutpela tru lon givim tambu sut lo bel mama
Bel mama mas kisim tetanus tambu sut
Beb ino nap lo kisim tambu sut taim m igat bikpla skin hot
Skin hot, solap na pen bihainim tambu sut em ol mak tasol
bihainim tambu sut
Bebi sut em I seif
Bebi mas kisim bebi sut lon taim mama I karim em, wanpela mun,
tupelo mun, tripela mun, sixpela mun, nainpela mun na eightinpela
mun
Bebisutembilonbanisimbebilonstronpelasiklon kuru, siklonliva, sik
polio, bikpelakus , sikmiselsna rubella nainfeksonlonbulut
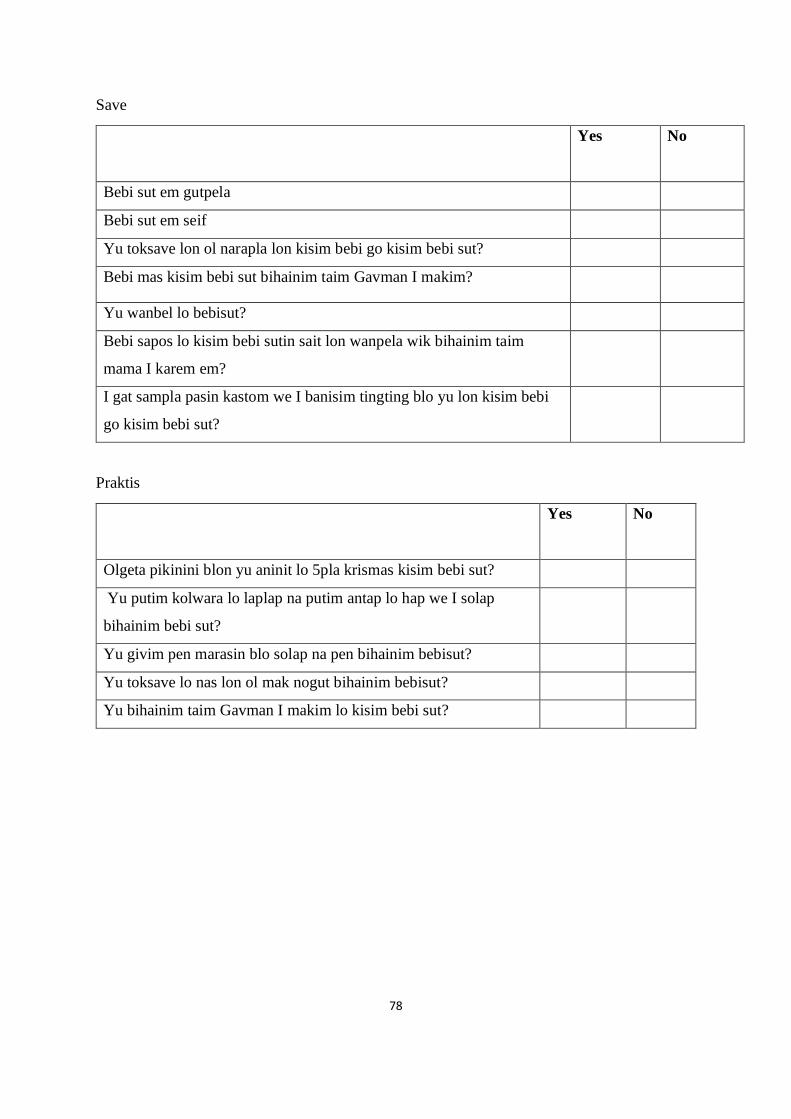
78
Save
Yes No
Bebi sut em gutpela
Bebi sut em seif
Yu toksave lon ol narapla lon kisim bebi go kisim bebi sut?
Bebi mas kisim bebi sut bihainim taim Gavman I makim?
Yu wanbel lo bebisut?
Bebi sapos lo kisim bebi sutin sait lon wanpela wik bihainim taim
mama I karem em?
I gat sampla pasin kastom we I banisim tingting blo yu lon kisim bebi
go kisim bebi sut?
Praktis
Yes No
Olgeta pikinini blon yu aninit lo 5pla krismas kisim bebi sut?
Yu putim kolwara lo laplap na putim antap lo hap we I solap
bihainim bebi sut?
Yu givim pen marasin blo solap na pen bihainim bebisut?
Yu toksave lo nas lon ol mak nogut bihainim bebisut?
Yu bihainim taim Gavman I makim lo kisim bebi sut?
79
Appendix III: Content Validity
Content Validity Index
1. Relevance
1=not relevant
2=relevant but need some revision
3=relevant but need minor revision
4=very relevant
2. Clarity
1=not clear
2=clear but need some revision
3=clear but need minor revision
4=very clear
3. Simplicity
1=not simple
2=simple but need some revision
3=simple but need minor revision
4=very simple
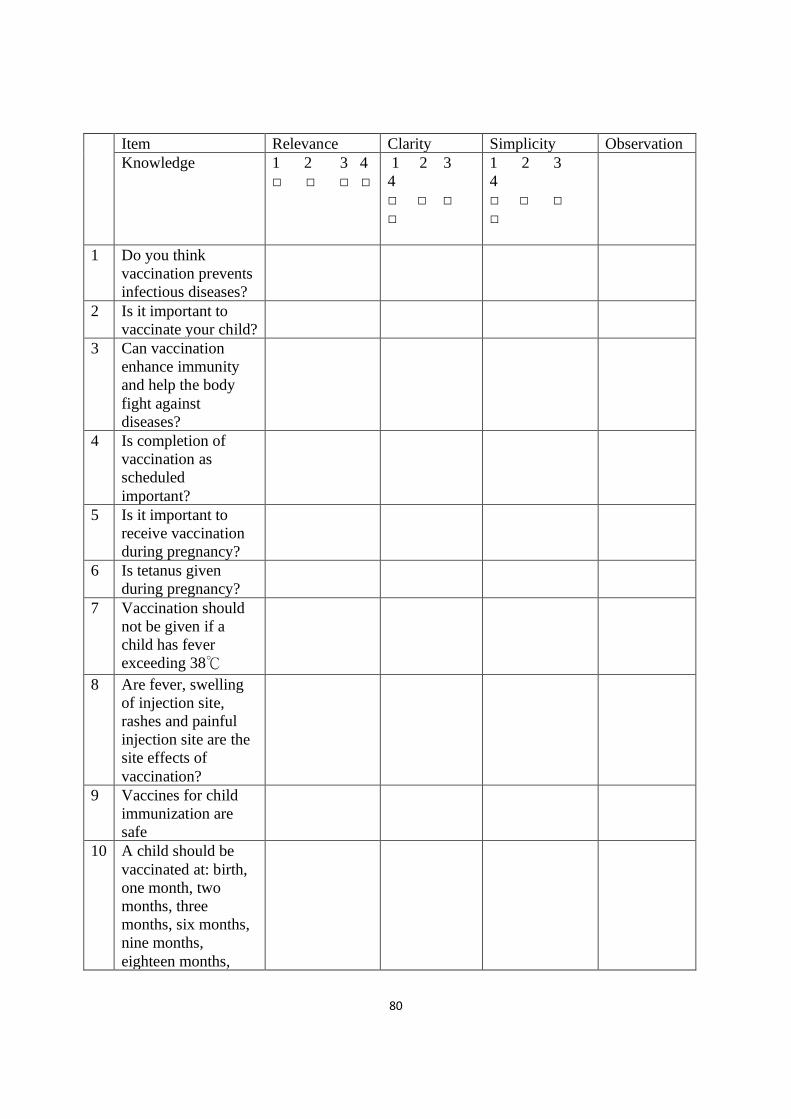
80
Item Relevance Clarity Simplicity Observation
Knowledge 1 2 3 4
□ □ □ □
1 2 3
4
□ □ □
□
1 2 3
4
□ □ □
□
1 Do you think
vaccination prevents
infectious diseases?
2 Is it important to
vaccinate your child?
3 Can vaccination
enhance immunity
and help the body
fight against
diseases?
4 Is completion of
vaccination as
scheduled
important?
5 Is it important to
receive vaccination
during pregnancy?
6 Is tetanus given
during pregnancy?
7 Vaccination should
not be given if a
child has fever
exceeding 38℃
8 Are fever, swelling
of injection site,
rashes and painful
injection site are the
site effects of
vaccination?
9 Vaccines for child
immunization are
safe
10 A child should be
vaccinated at: birth,
one month, two
months, three
months, six months,
nine months,
eighteen months,
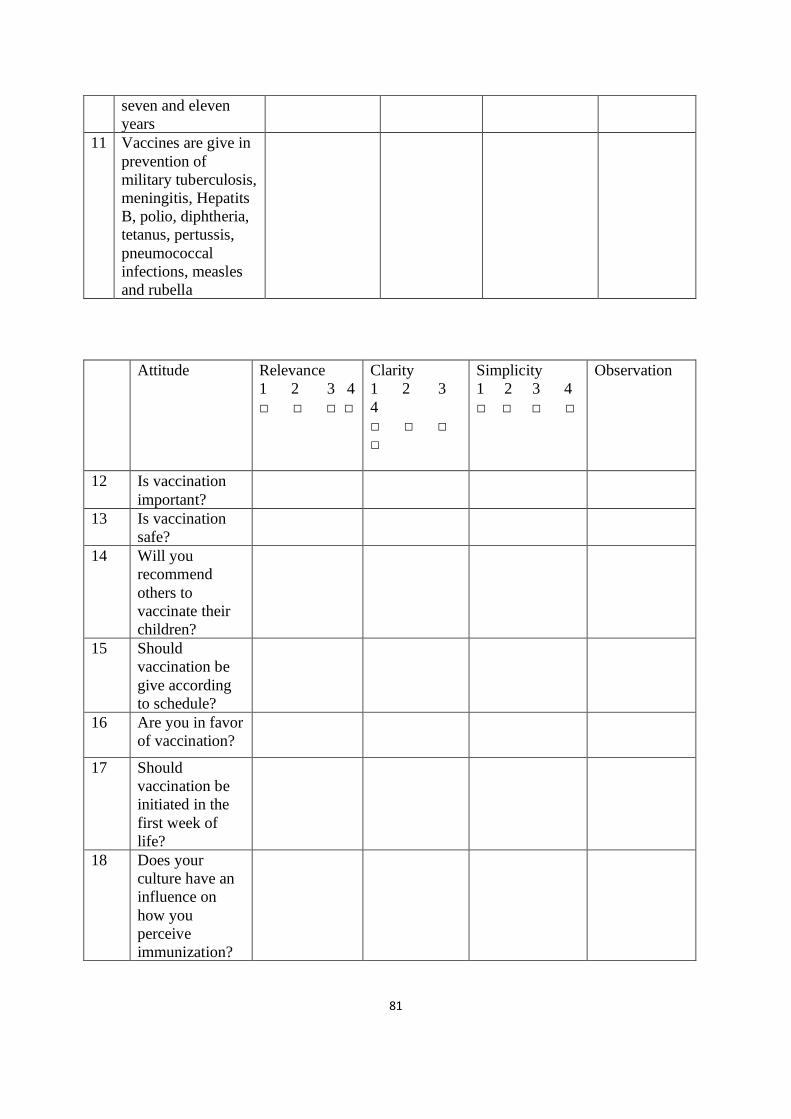
81
seven and eleven
years
11 Vaccines are give in
prevention of
military tuberculosis,
meningitis, Hepatits
B, polio, diphtheria,
tetanus, pertussis,
pneumococcal
infections, measles
and rubella
Attitude Relevance
1 2 3 4
□ □ □ □
Clarity
1 2 3
4
□ □ □
□
Simplicity
1 2 3 4
□ □ □ □
Observation
12 Is vaccination
important?
13 Is vaccination
safe?
14 Will you
recommend
others to
vaccinate their
children?
15 Should
vaccination be
give according
to schedule?
16 Are you in favor
of vaccination?
17 Should
vaccination be
initiated in the
first week of
life?
18 Does your
culture have an
influence on
how you
perceive
immunization?
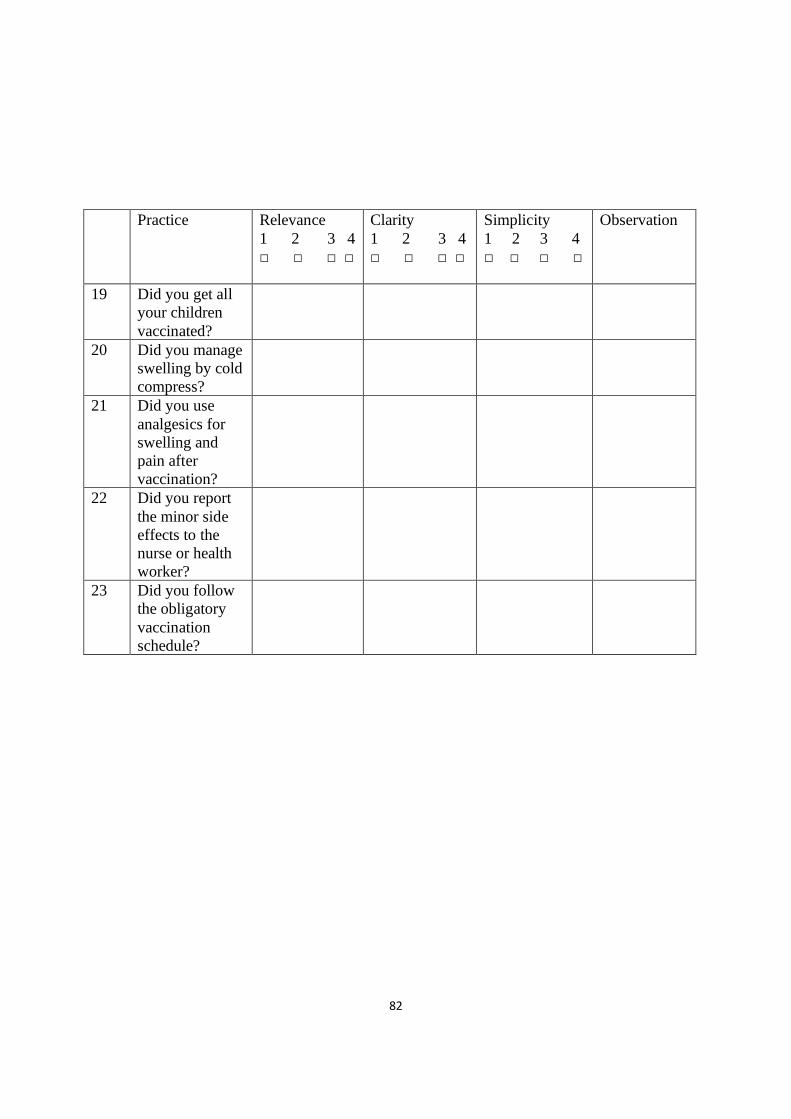
82
Practice Relevance
1 2 3 4
□ □ □ □
Clarity
1 2 3 4
□ □ □ □
Simplicity
1 2 3 4
□ □ □ □
Observation
19 Did you get all
your children
vaccinated?
20 Did you manage
swelling by cold
compress?
21 Did you use
analgesics for
swelling and
pain after
vaccination?
22 Did you report
the minor side
effects to the
nurse or health
worker?
23 Did you follow
the obligatory
vaccination
schedule?
83
Appendix IV: Permission Request for Instrument
Permission to use questionnaire
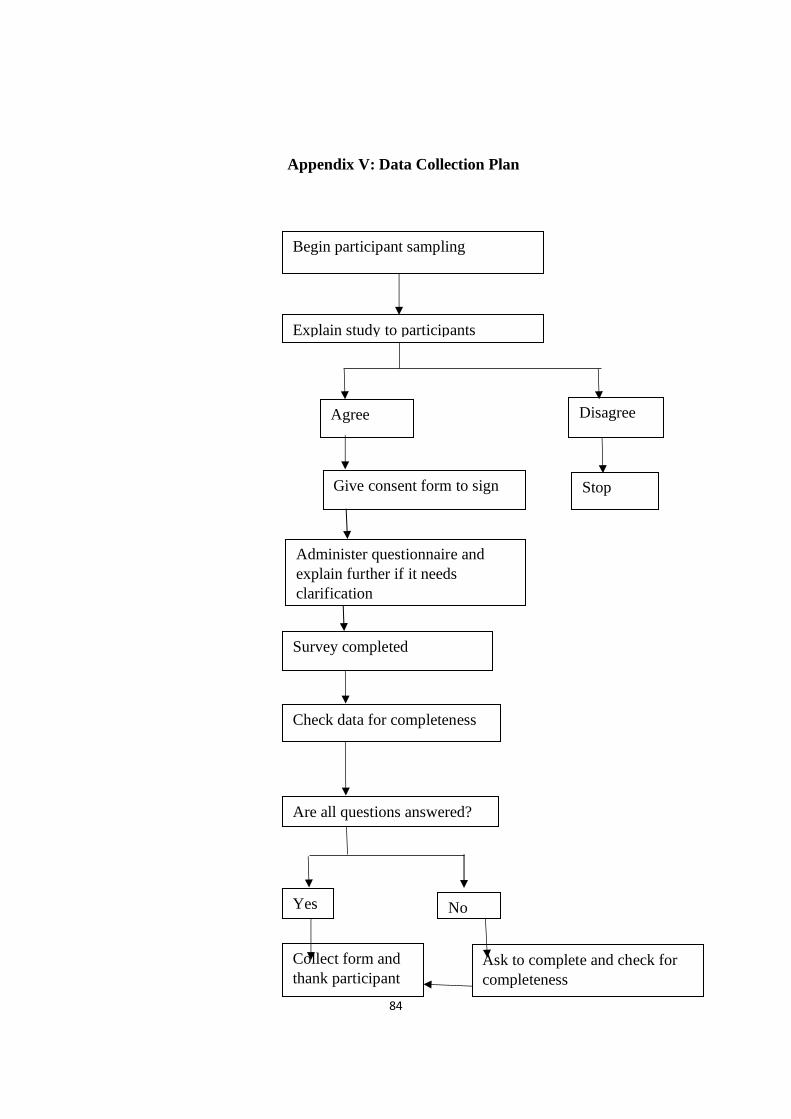
84
Appendix V: Data Collection Plan
Begin participant sampling
Explain study to participants
Agree Disagree
Give consent form to sign
Survey completed
Check data for completeness
Are all questions answered?
Yes No
Collect form and
thank participant
Ask to complete and check for
completeness
Stop
Administer questionnaire and
explain further if it needs
clarification
85
Appendix VI: Approval letter from Sandaun Provincial Hospital
86
Appendix VII: Approval letter and number from MRAC PNG