Are social-psychological smoking prevention programs effective? The Waterloo study
23
Journal of Behavioral Medicine, Vol. 8, No. 1, 1985 Are Social-Psychological Smoking Prevention Programs Effective? The Waterloo Study Brian R. Flay, t Katherine B. Ryan, 2 J. Allan Best, 2 K. Stephen Brown, 2 Mary W. Kersell, 2 Josie R. d'Avernas, 2 and Mark P. Zanna 3 Accepted for publication: March 20, 1984 Recent evaluations of smoking prevention programs have suggested con- siderable promise for curricula emphasizing resistance of social influences. The present study extends these evaluations by addressing key methodological limitations in previous work. Twenty-two matched schools were randomized to experimental and control conditions. Grade 6 students received a 6-week core curriculum, plus additional sessions through Grades 7 and 8. Questionnaires, and saliva samples to validate self-reported smok- ing behavior, were collected at five times over the 2-year study period. Cross-sectional and longitudinal analyses examined program impact for five levels of initial smoking experience, ranging from "never smoker" through regular, weekly smoker. Significant program effects were documented, most clearly for those having some experience with smoking before the program began and for those with smoking peer and family models. This study provides the methodologically most rigorous test to date of social influence programs for smoking prevention and documents for the first time significant effects for those at high risk for smoking. KEY WORDS: adolescent smoking; smoking prevention; social inoculation; social influences; health promotion. The research reported here was supported by Ontario Ministry of Health Grant CHS-R26 to J. A. Best and B. R. Flay. While writing this paper, B. R. Flay was partially supported by NIDA Grant RI8-DA-03046 to C. A. Johnson, B. R. Flay, and W. B. Hansen. We would like to thank Shelagh Towson for extensive helpful suggestions on early drafts and Debbie Salzman for help with data analysis. Ipresent address: Health Behavior Research Institute, University of Southern California, 1985 Zonal Avenue, Los Angeles, California 90033. 2Health Studies Department, University of Waterloo, Waterloo, Ontario, Canada, N2L 3G1. 3Psychology Department, University of Waterloo, Waterloo, Ontario, Canada, N2L 3G1. 37 0 6 77 5/85/0300 0037S04.50/0 c 1985 Plenum Publishing Corporation
Transcript of Are social-psychological smoking prevention programs effective? The Waterloo study
Journal o f Behavioral Medicine, Vol. 8, No. 1, 1985
Are Social-Psychological Smoking Prevention Programs Effective? The Waterloo Study
Brian R. Flay, t Katherine B. Ryan, 2 J. Al lan Best, 2 K. Stephen Brown, 2 Mary W. Kersell, 2 Josie R. d'Avernas, 2 and Mark P. Zanna 3
Accepted for publication: March 20, 1984
Recent evaluations o f smoking prevention programs have suggested con- siderable promise for curricula emphasizing resistance o f social influences. The present study extends these evaluations by addressing key methodological limitations in previous work. Twenty-two matched schools were randomized to experimental and control conditions. Grade 6 students received a 6-week core curriculum, plus additional sessions through Grades 7 and 8. Questionnaires, and saliva samples to validate self-reported smok- ing behavior, were collected at five times over the 2-year study period. Cross-sectional and longitudinal analyses examined program impact for five levels o f initial smoking experience, ranging from "never smoker" through regular, weekly smoker. Significant program effects were documented, most clearly for those having some experience with smoking before the program began and for those with smoking peer and family models. This study provides the methodologically most rigorous test to date of social influence programs for smoking prevention and documents for the first time significant effects for those at high risk for smoking.
KEY WORDS: adolescent smoking; smoking prevention; social inoculation; social influences; health promotion.
The research reported here was supported by Ontario Ministry of Health Grant CHS-R26 to J. A. Best and B. R. Flay. While writing this paper, B. R. Flay was partially supported by NIDA Grant RI8-DA-03046 to C. A. Johnson, B. R. Flay, and W. B. Hansen. We would like to thank Shelagh Towson for extensive helpful suggestions on early drafts and Debbie Salzman for help with data analysis.
Ipresent address: Health Behavior Research Institute, University of Southern California, 1985 Zonal Avenue, Los Angeles, California 90033.
2Health Studies Department, University of Waterloo, Waterloo, Ontario, Canada, N2L 3G1. 3Psychology Department, University of Waterloo, Waterloo, Ontario, Canada, N2L 3G1.
37
0 6 77 5/85/0300 0037S04.50/0 c 1985 Plenum Publishing Corporation
38 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
INTRODUCTION
Psychological theory and data suggest that successful smoking preven- tion programs should incorporate principles from a wide range of theoretical positions (Flay et al., 1983a). These might include persuasive communications (McGuire, 1968), social inoculation (McGuire, 1964), social learning (Bandura, 1977; Rotter, 1966), attribution (Jones et al., 1972), commitment (Kiesler, 1971), and decision-making (Janis and Mann, 1977) theories. Since the seminal work of Evans et al. (1978), a number of other studies have provided tests of broader psychological approaches to smoking prevention that incorporate principles from such theories. These studies have taken place in Houston (Evans et al., 1981), at Stanford and Harvard (McAlister et al. , 1979, 1980; Perry et al., 1980a, b; Telch et al., 1982), in Minnesota (Arkin et al., 1981; Hurd et al., 1980; Luepker et al., 1983; Murray, et al., 1980), in New York (Botvin and Eng, 1980, 1981, 1982; Botvin et al., 1980), and in Southern California (Flay et al., 1982, 1983b; Johnson et al., 1984). By teaching students how to refuse successfully an offer of a cigarette and to criticize and counterargue advertisements, these research programs have been successful in preventing further increases in cigarette smoking by up to 50O7o for up to 3 years so far. While these studies have differed in many ways, and there has been a gradual refinement of curriculum content, the approaches used are sufficiently similar that they may be considered as variations o f a general social-psychological approach to smoking prevention. See Flay (1985) and Botvin and Wills (1985) for detailed reviews.
Methodological Problems with Past Studies
Fisher (1980) concluded that "It now seems well-established that these interventions work, at least to an appreciable if not totally satisfactory ex- tent" (p. 678). Before accepting the consistency of these results as evidence for the efficacy of social psychological smoking prevention programs,
however, it is necessary to provide a systematic critique of the methodo- logical strengths and weaknesses of the studies on which they are based.
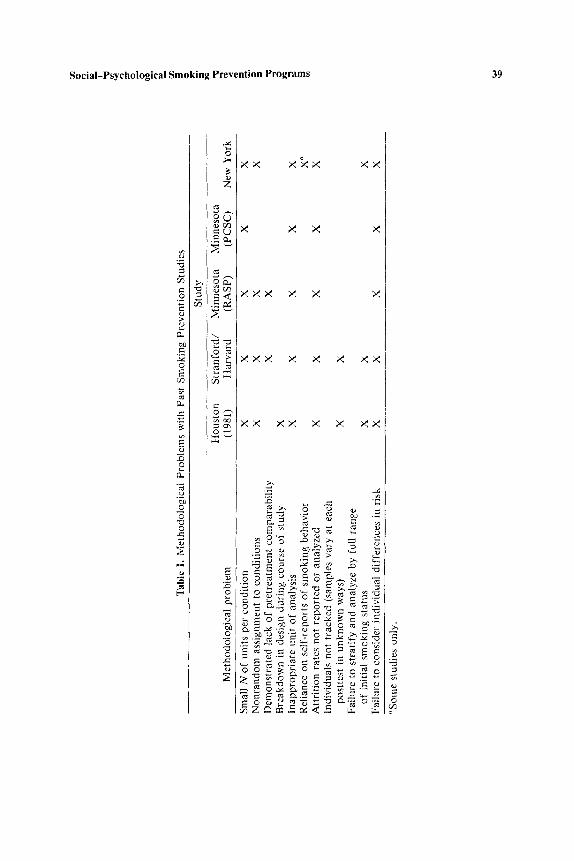
The evaluation of preventive health behavior programs is a complex task (Flay and Best, 1982; Flay and Cook, 1981) and none of the studies reviewed has been without methodological flaws. Table I summarizes the methodological problems with past research on social psychological smok- ing prevention programs. The most common rffethodological concern has to do with the small number of units, usually whole schools, assigned to each condition of an experimental design. In most of the studies reported, only one school was assigned per experimental condition. Thus, condition was confounded with school so that observed posttest differences could be due
Tab
le I
. M
etho
dolo
gica
l P
robl
ems
wit
h P
ast
Sm
okin
g P
reve
ntio
n S
tudi
es
e
Met
hodo
logi
cal
prob
lem
Stu
dy
Ho
ust
on
S
tran
ford
/ M
inn
eso
ta
Min
nes
ota
(1
981)
H
arv
ard
(R
AS
P)
(PC
SC
)
Sm
all
N o
f un
its
per
cond
itio
n
New
Yor
k
X
X
X
X
X
No
nra
nd
om
ass
ignm
ent
to c
ondi
tion
s D
emon
stra
ted
lack
of
pret
reat
men
t co
mpa
rabi
lity
B
reak
dow
n in
des
ign
duri
ng c
ours
e of
stu
dy
Inap
prop
riat
e un
it o
f an
alys
is
Rel
ianc
e on
sel
f-re
port
s of
sm
ok
ing
beh
avio
r A
ttri
tion
rat
es n
ot r
epor
ted
or a
naly
zed
Indi
vidu
als
not
trac
ked
(sam
ples
var
y at
eac
h po
stte
st i
n u
nk
no
wn
way
s)
Fai
lure
to
stra
tify
and
ana
lyze
by
full
ran
ge
of i
niti
al s
mok
ing
stat
us
Fai
lure
to
cons
ider
ind
ivid
ual
diff
eren
ces
in r
isk
X
X
X
X
X
X
X
X
X
X
X
X
X c,
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
O p~
~S
ome
stud
ies
only
.
40 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
to characteristics of the school environment rather than to the treatment program. This confound is clearest when there are documented pretest dif- ferences in smoking rates. For example, in one study the most successful ex- per imental condition was a school which had a lower pretest smoking rate than did schools in other conditions (Hurd et al., 1980). In another study the one school assigned to receive the program was acknowledged to be a "problem" school in terms of smoking among students (McAlister et al., 1980). Before we can be confident that observed effects are due to tested programs, multiple schools or classrooms must be assigned randomly (possibly after matching) to experimental conditions.
Related methodological problems concern sample size and, therefore, statistical power. Most of the studies reviewed had a very small number of children in each condition. Having only zero to three children f rom any one grade level start smoking in a t reatment group while five or six do so in a control group cannot lead to any confidence that the finding is robust. The low expected, and actual, rates of smoking onset during the course of any one study at the elementary or junior high-school level means that large sample sizes are imperative.
Another issue concerns the appropriate unit of analysis. When schools are assigned randomly to conditions, and when the program is delivered to intact classes, the school is the most appropriate unit of statistical analysis for some purposes and the classroom is appropriate for others. It is not en- tirely appropriate to use the individual as the unit of statistical analysis, except for those questions that concern (a) the effects of different levels of attention to or participation in a curriculum on program effectiveness (Bur- stein, 1980a, b) or (b) the effect of the program on individuals with a dif- ferential risk to become smokers (e.g., those with smoking vs nonsmoking parents or friends).
In one sense, the effectiveness of smoking prevention programming is estimated most appropriately f rom program effects on adolescents known to be at high risk of becoming cigarette smokers. The strongest predictors of smoking by adolescents are family and peer smoking [see Flay et al., (1983a) for a review]. Thus, it needs to be shown that smoking prevention programs are effective at preventing adolescents with smoking parents, siblings, and /o r friends f rom becoming smokers themselves. None of the reported studies has done this. Instead, estimates of program effectiveness have been based either on all subjects or on all subjects who had never smoked prior to pretest. Such practices could be leading to under- or overestimates of pro- gram effectiveness if subjects at high risk are being affected, respectively, more or less than subjects at low risk.
Some studies have used questionable methods to control or define samples for statistical analysis. In order to ensure student anonymity, some
Social-Psychological Smoking Prevention Programs 41
studies had no means of identifying students from one test time to another and thus could not exercise control over the history of makeup of their sample at any one time (e.g., Evans et al., 1981; McAlister et al., 1980). Two groups of researchers eliminated pretest smokers from their analyses, thereby completely ignoring possible program effects on from a quarter (Botvin and Eng, 1982) to a half (Evans et al., 1978) of their sample. It would be useful to know the program effects, if any, on students who were smoking or who had already tried it and quit by the pretest. However, it is difficult to compare findings among studies that have considered different levels of smoking, because the categories of smokers (e.g., experimental, regular) used by those researchers have not been the same.
The possible problem of attrition has been addressed hardly at all in reports of smoking prevention research. Attrition figures are rarely reported, even though attribution seems to be of the order of 10% per year (personal communications) and may be as high as 35% (Hansen et al., 1985). This information is particularly important when it may be treatment related. There is some evidence that smokers do less well in school, have lower self-images, and are more likely to be absent on testing occasions than nonsmokers. In addition, demand characteristics of the study might make smokers in program conditions more likely to be absent on testing occasions than smokers in control conditions. The effects of selective attrition on estimates of program effects need to be examined.
Although we have been critical, the reviewed studies were methodologically rigorous in at least three ways. They all included a pretest and a posttest, and all major studies with grade 7 classrooms have had a follow-up test ranging in time from 1 year (Botvin and Eng, 1982) to 3 years (Evans et al., 1981; Luepker et al., 1983; Telch et al., 1982). They also in- cluded control groups, allowing for a comparison of groups receiving the program with groups not receiving it. Finally, all but one study attempted to (a) validate self-reports of smoking behavior by collecting physiological indicators and /or (b) reduce biases of self-reported data by the use of a variation of the bogus pipeline technique (Evans et al., 1977; Jones and Sigall, 1971; Luepker et al., 1981; Williams et al., 1979).
Taken together, the series of studies reviewed have made dramatic ad- vances in the area of smoking prevention research and provide some sup- port for the hypothesis that social-psychological prevention programs help adolescents resist social influences to become cigarette smokers. However, before further investments are made in either programs or large-scale studies designed to test components (Fisher, 1980), it would be well to deter- mine first whether or not the general approach of these smoking prevention programs can be proven to be effective when subjected to a more rigorous test than any one of the previous studies provided. The Waterloo Smoking
42 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
Prevention Project (WSPP) was designed to do just that. It attempts to overcome the methodoloical problems discussed and, therefore, provides a methodologically more rigorous test of the efficacy of the social-psycho- logical approach to smoking prevention.
METHODS
The Program 4
The program consisted of three major components delivered in six 1-hr weekly sessions during grade 6. The first component focused on pro- viding information. The activities were designed to start the development of future attitude and behavior changes and the acquisition of social skills. The information was elicited from the children rather than provided for them. This approach has three major advantages. First, it forces children to search through their belief systems. This is important in that many children believe categorically that smoking is bad but have little supportive knowledge. Elicitation of beliefs, therefore, helps them to discover that they have little information upon which to base their beliefs, and this, in turn, encourages them to begin to search their environment for more informa- tion. Searching for information then was encouraged explicitly and rein- forced throughout the remainder of the program. Second, information elicited from the children themselves is likely to be salient and phrased in such a way that it can be understood by other children. Finally, information gathered collectively from a classroom usually provides a comprehensive coverage of the beliefs of the immediate peer group. Information discussed was also repeated via multiple modes such as video tapes, poster making, and class discussion, to increase the probability of attention, compre- hension, and retention.
The second, and probably most important, component of the pro- gram focused on social influences to smoke (family, peer, media) and the development of skills to resist such pressures. Again, ideas were elicited from the children and repetition achieved by the use of multiple modalities. Specific social coping skills, such as saying "No thank you, I don't smoke," were taught, role played, and practiced.
The third component of the program was concerned with decision making and commitment. Children were asked to integrate individually the information learned in all previous sessions and to consider the social conse-
4A more detailed description of the program is available from the third author.
Social-Psychological Smoking Prevention Programs 43
quences of smoking in their own social environment. Each child then made a decision. Finally, in the public commitment procedure, their decision of whether or not to smoke, along with their main reason for it, was announced to their classmates.
The core curriculum was delivered during the first 3 months of grade 6. Two "maintenance" sessions were given later in grade 6, with the major purpose of maintaining contact with the children. No new information was presented, but a solid review of the three major social influences to smoke was included.
Finally, three "booster" sessions were provided, two in grade 7 and one in grade 8. The booster sessions served to maintain contact with the students and to update the content of the original grade 6 program so that it remained relevant and salient to the maturing students. This is important because the students are exposed to increasing peer pressure at this age. The grade 7 sessions required small groups of students to develop their own smoking prevention program and prescnt a portion of it to their classmates. The grade 8 session had students discuss and present social benefits and consequences of smoking and pressures and influences to smoke; each student again went through a decision-making process.
Design and Sampling
The evaluation of the WSPP was designed to overcome as many of the methodological problems discussed above as possible. A relatively large number of schools were assigned from matched (on socioeconomic status, size, and urban/rura l location) groups to treatment and control conditions. Schools were obtained from two school boards in Southwestern Ontario, the Waterloo County Roman Catholic Separate School Board and the Oxford County Public School Board of Education. In each board, the pro- ject was described to principals who were then asked by a superintendent to volunteer their school for participation. Criteria for participation included the following:
(a) students could be followed easily from grade 6 to the end of grade 8;
(b) schools were willing to be randomly assigned to experimental or control conditions;
(c) all grade 6 students in a selected school who receivcd parental con- sent were to participate in the study; and
(d) schools made a commitment to participate in all intervention and evaluation procedures for the duration of the study.
Seventeen schools in Waterloo and 15 in Oxford that met all of these criteria were volunteered for participation. Six matched pairs were formed
44 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
in Waterloo and five in Oxford. On average, unmatched schools were not different in size, geographic location, or SES from those that were matched and subsequently included in the study. Assignment to treatment or control conditions from the matched groups was random except in three cases in Oxford County, where an administrator thought that principals might not cooperate as fully if their schools were assigned to the control condition. These schools were not significantly different from others in the study.
Most schools in both boards are small, with an average of only one grade 6 class per school. Most Waterloo County schools were located in one of three, closely located cities (combined population, 250,000). Two schools (one pair) were located in nearby small towns. Oxford County schools were predominantly rural and located outside the tobacco-growing areas of the county.
Schools were assigned to either a full testing-full treatment group (program condition) or a full testing-no treatment group (control condi- tion). In the fall of the 1979-1980 school year, grade 6 students in the pro- gram schools received the WSPP curriculum. Grade 6 students in the con- trol schools received only the smoking education that was normally available through the health education curricula of their schools.
Students in both conditions were pretested the week before the core program began (TI) and were posttested immediately following the program (T2), at the end of grade 6 (T3), and at the beginning and end of grade 7 (T4 and TS). Long-term follow-up assessment continues (Best et al., 1985).
Measures
At each testing session students completed a questionnaire and sub- mitted a sample of their saliva to be analyzed for saliva thiocyanate. A videotape, showing how cigarette smoking can be objectively verified through an analysis of saliva, was shown immediately before samples were collected in the earlier (grade 6) sessions. In later sessions, to avoid boredom caused by repeated exposure to the videotape, the modified "bogus pipeline" strategy included giving feedback on smoking rates, an oral question-and-answer session, or a slide presentation.
After giving their samples, students completed questionnaires tapping demographic information, self-reports of smoking behavior, and reports of the smoking habits of parents, siblings, friends, and teachers. [Mediating variables, such as knowledge, attitudes, intentions, and personality variables were also measured--prel iminary results are reported by Flay el al., (1983a).] There were no significant differences between program and
Soc i a l -Psycho log i ca l Smoking Prevention P r o g r a m s 45
control groups at pretest with respect to reported smoking behavior, gender, and reported prevalence of parental, peer, and sibling smoking. 5
Students were classified as being in one of the five following behavioral caegories:
Never smoked: never smoked "even one puff of one cigarette." Tried once: has smoked but "not again since the first time." Quitter: has smoked more than once, but has "quit smoking for good." Experimenter: currently smokes but "usually not every week." Regular smoker: currently smokes "usually every week."
At pretest 42070 of the sample had never smoked, 33% had tried only one cigarette, 12070 were quitters, 9070 were experimenting with cigarette smok- ing, and only 3% were regular smokers.
RESULTS
Participation and Attrition
Ninety-four percent of the children in the total sample received active parental consent to participate, providing a study sample of 697 children in the 22 study schools, 654 of whom were pretested. There was a high level of reported satisfaction with the program, although such findings could be ex- plained by positive demand characteristics. At the end of the core cur- riculum, 84% of the students reported liking it, 72% thought it was the right length, 81% thought it was just the right level of difficulty, 96% felt that they had learned something from it, and 74% found it interesting. The regular classroom teachers who observed the program as it was delivered by specially trained health education specialists felt that all program com- ponents were effective.
Average attrition due to children changing classes or schools was only 4.3% per year. Absenteeism averaged 5.2% per test time. Most of the results to be reported are based on a "reduced" sample of 498 (76.1%) students who were present at pretest and all subsequent tests. However,
5As we repor ted prev ious ly (Flay et al., 1983a) there was a s ta t i s t ica l ly s igni f icant pretest differ- ence in age (mean for p r o g r a m g roup = t0 .91, mean for cont ro l g roup = 11.11 ; t = 3.29, P < 0.001). This could lead to overes t imates of p rog ram effect iveness because older s tudents typical ly are beg inn ing to s m o k e at h igher rates than younger s tudents . To test for this possibi l i ty , we ran all analyses repor ted here on samples tha t inc luded on ly those s tudents wi thin two and wi th in one s t anda rd dev ia t ion of the mean age. In bo lh cases, the pa t te rn of results and the level of s igni f icance of all tests were the same as those repor ted here when not con t ro l l ing for age.
46 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
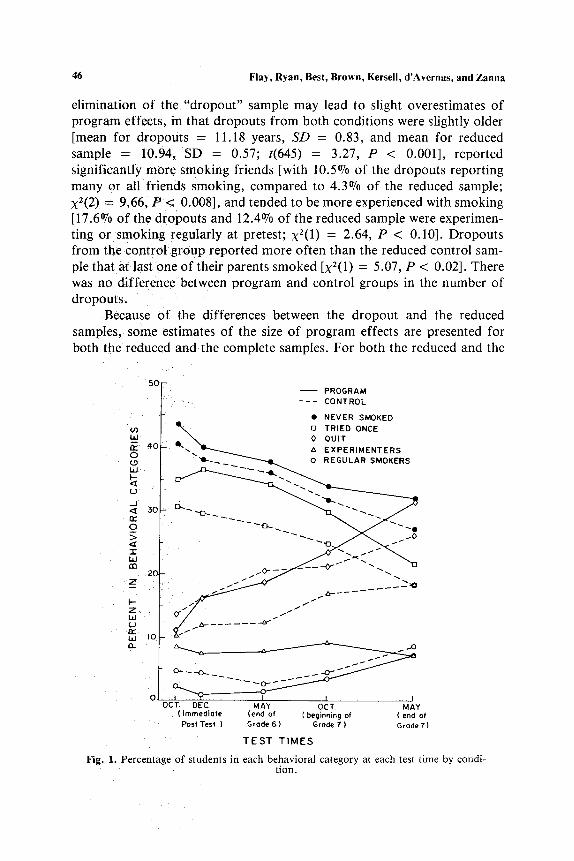
elimination of the "dropout" sample may lead to slight overestimates o f program effects, in that dropouts from both conditions were slightly older [mean for dropouts = 11.18 years, SD = 0.83, and mean for reduced sample = 10.94, SD = 0.57; t(645) = 3.27, P < 0.001], reported significantly m o r e smoking friends [with 10.5% of the dropouts reporting many or all friends smoking, compared to 4.3~ o f the reduced sample; x2(2) = 9.66, P < 0.008], and tended to be more experienced with smoking [17.6~ o f the dropouts and 12.4~ o f the reduced sample were experimen- ting or smoking regularly at pretest; X2(1) = 2.64, P < 0.10]. Dropouts from the control group reported more often than the reduced control sam- ple that at l a s tone o f their parents smoked [x2(1) -- 5.07, P < 0.02]. There was no difference between program and control groups in the number of dropouts.
Because o f the differences between the dropout and the reduced samples, some estimates o f the size o f program effects are presented for both the reduced and the complete samples. For both the reduced and the
50 PROGRAM
- - - CONTROL
�9 NEVER SMOKED r ~ D TRIED ONCE bJ ~ , . 0 0 U I T
t ' . . " o - ~ . ~ ' ~ A EXPERIMENTERS 4( rr"
(.9 ~ o REGULAR SMOKERS ILl ~ ~ ~- .1~
LI
0
I U.I en
20
(.3 I"Y Llul I0
0 I ~ ~-- I I I OCT. DEC. MAY OCT. MAY
( immediote (end of { beginning of ( end of Post Test ) Grode 6) Grode 7 ) Grade7)
T E S T T I M E S
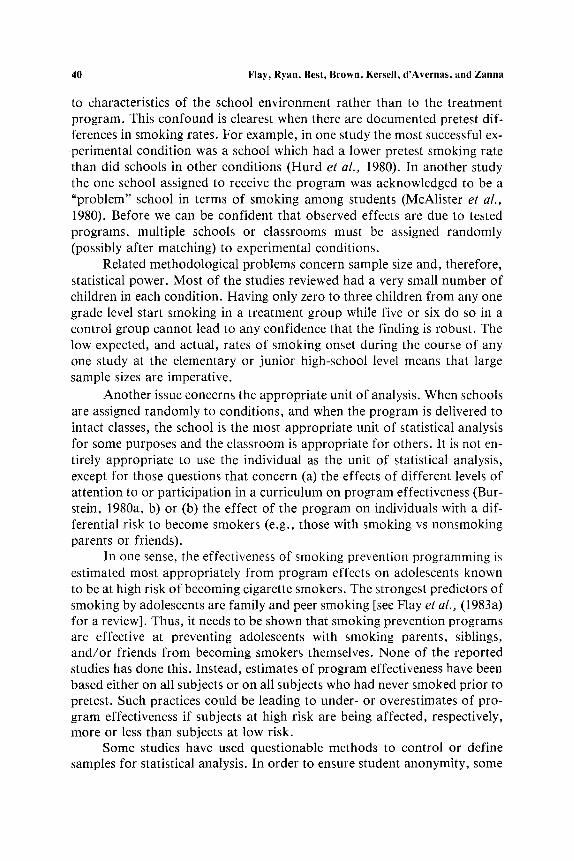
F i g . 1 . Percentage of students in each behavioral category at each test time by condi- tion.
Social-Psychological Smoking Prevention Programs 47
2O
Z - - 18 I--- Z L,J ~E IG rr bJ n 14 x LLI
I,-- 12 Z ELI U I 0 rr LIJ n
8
6
] RECEIVED PROGRAM
] NO PROGRAM
T I T2 T 3 f ~f
GRADE 6
iiiii :!:~:!:i i::iiii!:: !ili:)j :%::::: ::::::::
D T 4
v GRADE
T E S T T I M E S
ill!!;"
iiiiii:~ iiii.:?. ,,..,.-~ ,,,,.,.
T5 /
7
+ 8 , 4 %
3 -i .4Olo
_/
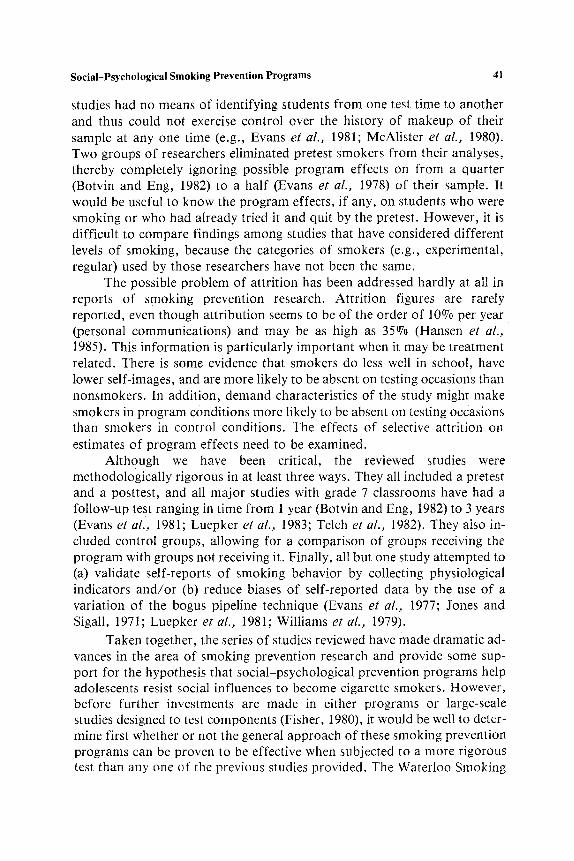
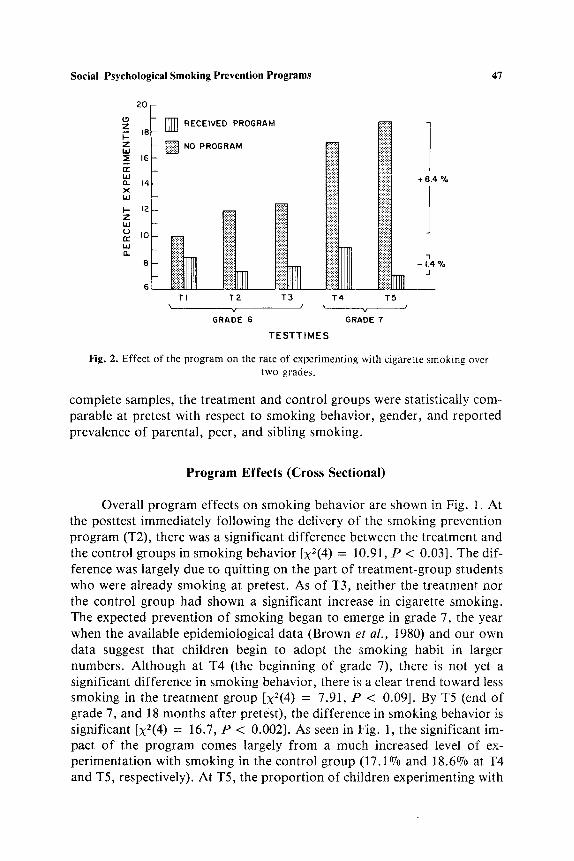
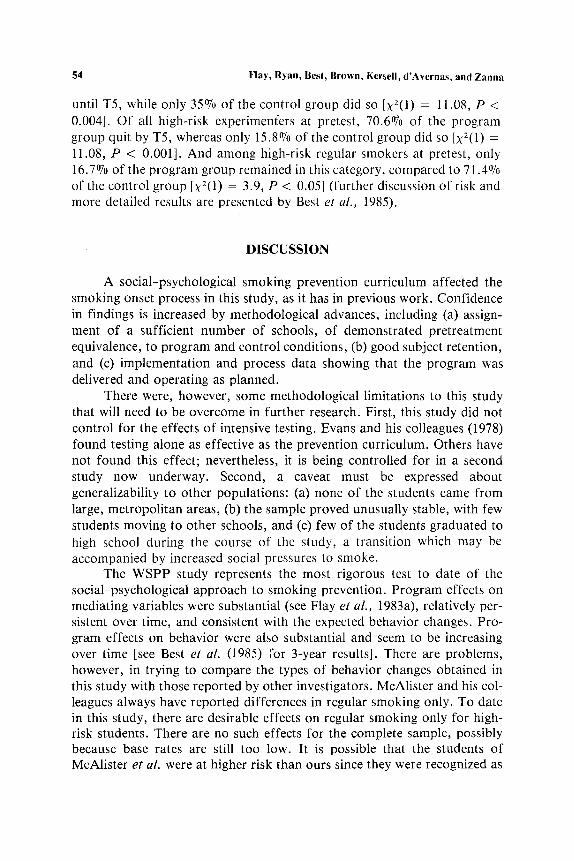
F i g . 2. E f f e c t o f t h e p r o g r a m o n the r a t e o f e x p e r i m e n t i n g w i t h c i g a r e t t e s m o k i n g o v e r
t w o g r a d e s .
complete samples, Lhe treatment and control groups were statistically com- parable at pretest with respect to smoking behavior, gender, and reported prevalence of parental, peer, and sibling smoking.
Program Effects (Cross Sectional)
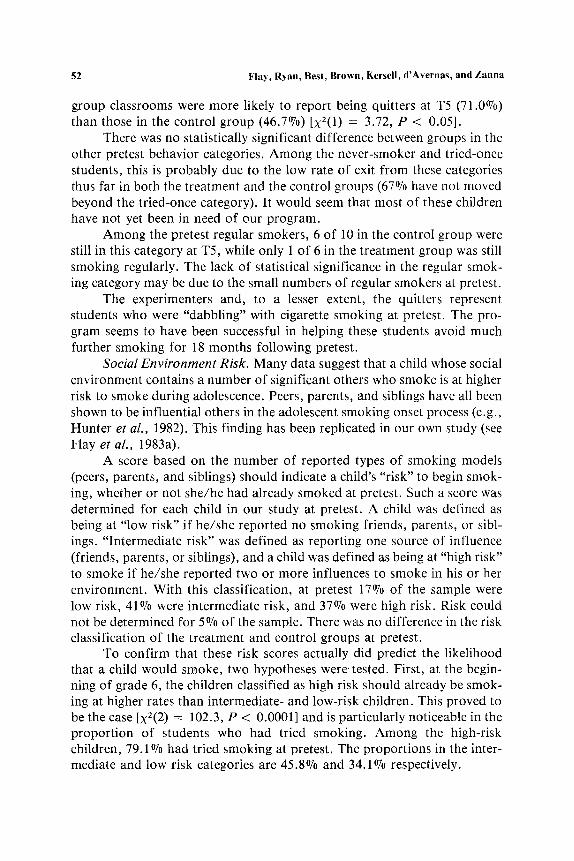
Overall program effects on smoking behavior are shown in Fig. 1. At the posttest immediately following the delivery of the smoking prevention program (T2), there was a significant difference between the treatment and the control groups in smoking behavior [X2(4) = 10.91, P < 0.03]. The dif- ference was largely due to quitting on the part of treatment-group students who were already smoking at pretest. As of T3, neither the treatment nor the control group had shown a significant increase in cigarette smoking. The expected prevention of smoking began to emerge in grade 7, the year when the available epidemiological data (Brown et al., 1980) and our own data suggest that children begin to adopt the smoking habit in larger numbers. Although at T4 (the beginning of grade 7), there is not yet a significant difference in smoking behavior, there is a clear trend toward less smoking in the treatment group [X2(4) = 7.91, P < 0.09]. By T5 (end of grade 7, and 18 months after pretest), the difference in smoking behavior is significant [X2(4) = 16.7, P < 0.002]. As seen in Fig. 1, the significant im- pact of the program comes largely from a much increased level of ex- perimentation with smoking in the control group (17.1% and 18.6% at T4 and T5, respectively). At T5, the proport ion of children experimenting with
48 Flay, Ryan, Besl, Brown, Kersell, d'Avernas, and Zanna
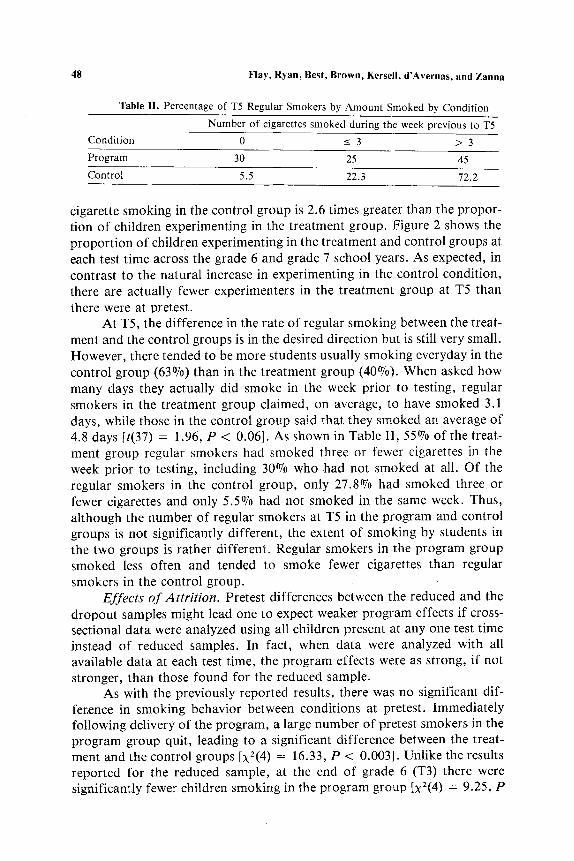
Table lI. Percentage of T5 Regular Smokers by Amount Smoked by Condition
Number of cigarettes smoked during the week previous to T5 Condition 0 _< 3 > 3
Program 30 25 45
Control 5.5 22.3 72.2
cigarette smoking in the control group is 2.6 times greater than the propor- tion of children experimenting in the treatment group. Figure 2 shows the proport ion of children experimenting in the treatment and control groups at each test time across the grade 6 and grade 7 school years. As expected, in contrast to the natural increase in experimenting in the control condition, there are actually fewer experimenters in the treatment group at T5 than there were at pretest.
At T5, the difference in the rate of regular smoking between the treat- ment and the control groups is in the desired direction but is still very small. However, there tended to be more students usually smoking everyday in the control group (63%) than in the treatment group (40%). When asked how many days they actually did smoke in the week prior to testing, regular smokers in the treatment group claimed, on average, to have smoked 3.1 days, while those in the control group said that they smoked an average of 4.8 days [t(37) = 1.96, P < 0.06]. As shown in Table II, 55% of the treat- ment group regular smokers had smoked three or fewer cigarettes in the week prior to testing, including 30% who had not smoked at all. Of the regular smokers in the control group, only 27.8% had smoked three or fewer cigarettes and only 5.5% had not smoked in the same week. Thus, although the number of regular smokers at T5 in the program and control groups is not significantly different, the extent of smoking by students in the two groups is rather different. Regular smokers in the program group smoked less often and tended to smoke fewer cigarettes than regular smokers in the control group.
Effects of Attrition. Pretest differences between the reduced and the dropout samples might lead one to expect weaker program effects if cross- sectional data were analyzed using all children present at any one test time instead of reduced samples. In fact, when data were analyzed with all available data at each test time, the program effects were as strong, if not stronger, than those found for the reduced sample.
As with the previously reported results, there was no significant dif- fer.ence in smoking behavior between conditions at pretest. Immediately following delivery of the program, a large number of pretest smokers in the program group quit, leading to a significant difference between the treat- ment and the control groups [X2(4) = 16.33, P < 0.003]. Unlike the results reported for the reduced sample, at the end of grade 6 (T3) there were significantly fewer children smoking in the program group [X2(4) = 9.25, P
Social-Psychological Smoking Prevention Programs 49
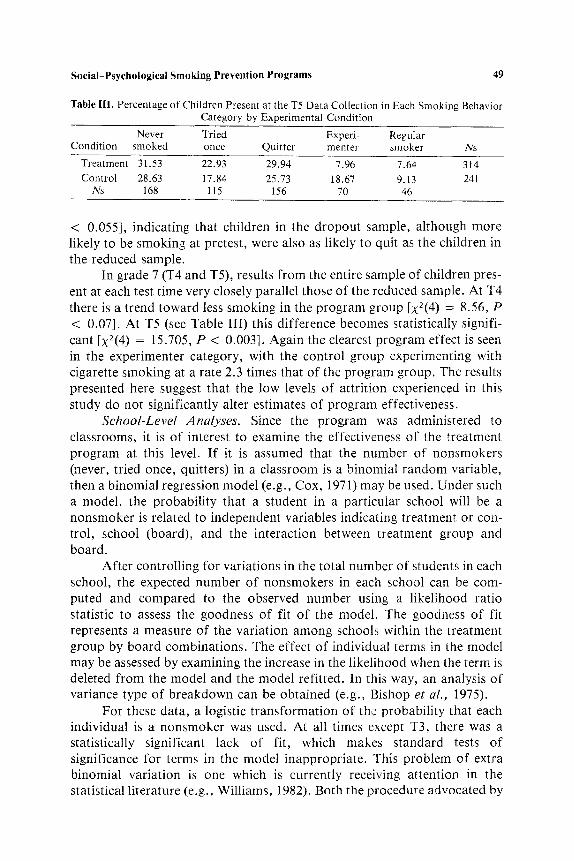
Table III. Percentage of Children Present at the T5 Data Collection in Each Smoking Behavior Category by Experimental Condition
Never Tried Experi- Regular Condition smoked once Quitter menter smoker Ns
Treatment 31.53 22.93 29.94 7.96 7.64 314
Control 28.63 17.84 25.73 18.67 9.13 241 Ns 168 115 156 70 46
< 0.055], indicating that children in the dropout sample, although more likely to be smoking at pretest, were also as likely to quit as the children in the reduced sample.
In grade 7 (T4 and T5), results f rom the entire sample of children pres- ent at each test time very closely parallel those of the reduced sample. At T4 there is a trend toward less smoking in the program group [X2(4) = 8.56, P < 0.07]. At T5 (see Table III) this difference becomes statistically signifi- cant [X2(4) = 15.705, P < 0.003]. Again the clearest program effect is seen in the experimenter category, with the control group experimenting with cigarette smoking at a rate 2.3 times that of the program group. The results presented here suggest that the low levels of attrition experienced in this study do not significantly alter estimates of program effectiveness.
School-Level Analyses. Since the program was administered to classrooms, it is of interest to examine the effectiveness of the treatment program at this level. I f it is assumed that the number of nonsmokers (never, tried once, quitters) in a classroom is a binomial random variable, then a binomial regression model (e.g., Cox, 1971) may be used. Under such a model, the probabil i ty that a student in a particular school will be a nonsmoker is related to independent variables indicating treatment or con- trol, school (board), and the interaction between treatment group and board.
After controlling for variations in the total number of students in each school, the expected number of nonsmokers in each school can be com- puted and compared to the observed number using a likelihood ratio statistic to assess the goodness of fit of the model. The goodness of fit represents a measure of the variation among schools within the treatment group by board combinations. The effect of individual terms in the model may be assessed by examining the increase in the likelihood when the term is deleted f rom the model and the model refitted. In this way, an analysis of variance type of breakdown can be obtained (e.g., Bishop et al., 1975).
For these data, a logistic t ransformat ion of the probabili ty that each individual is a nonsmoker was used. At all times except T3, there was a statistically significant lack of fit, which makes standard tests of significance for terms in the model inappropriate. This problem of extra binomial variation is one which is currently receiving attention in the statistical literature (e.g., Williams, 1982). Both the procedure advocated by
50 Flay, Ryan, Best, Brown, Kersell, d 'Avernas, and Zanna
Williams and that suggested by Finney (1971), in which the lack of fit statistic divided by its degrees of freedom provides the denominator for an approximate F ratio to test hypotheses about main effects and interactions, yield similar results here.
The results indicate that while there is no difference between the treat- ment and the control groups at T l , differences at T2 (P ~- 0.10), T3 (P < 0.10), and T4 (P ~ 0.10) approach statistical significance. At T5, the treat- ment effect is statistically significant (P -- 0.02). Thus even when the classroom (school) is used as the unit of analysis, the program is shown to have produced significant effects. Nevertheless, there is also a great deal of interschool va r iab i l i ty -an in-depth examination of this will be the focus of a future paper.
Longitudinal Analyses of Program Impact
The analyses reported so far may be characterized as successive cross- sectional, and they provide no indication of patterns of change. Longitudinal analyses, which "track" individuals across successive test times, allow for the isolation of patterns of change and, therefore, allow an assessment of how the program works, and for whom.
Two longitudinal strategies were followed in order to assess the pro- gram impact on smoking behavior. Both were an attempt to (a) characterize those children who were likely to be smoking if not for the program and (b) examine the specific impact of the treatment program on these "high-risk" groups.
Pretes t Behavior. Current longitudinal research on adolescent and preadolescent smoking indicates that one of the best predictors of later smoking is earlier experience with it (Pederson et al., 1981). A good indi- cator of "risk," therefore, should be a child's smoking behavior at pretest.
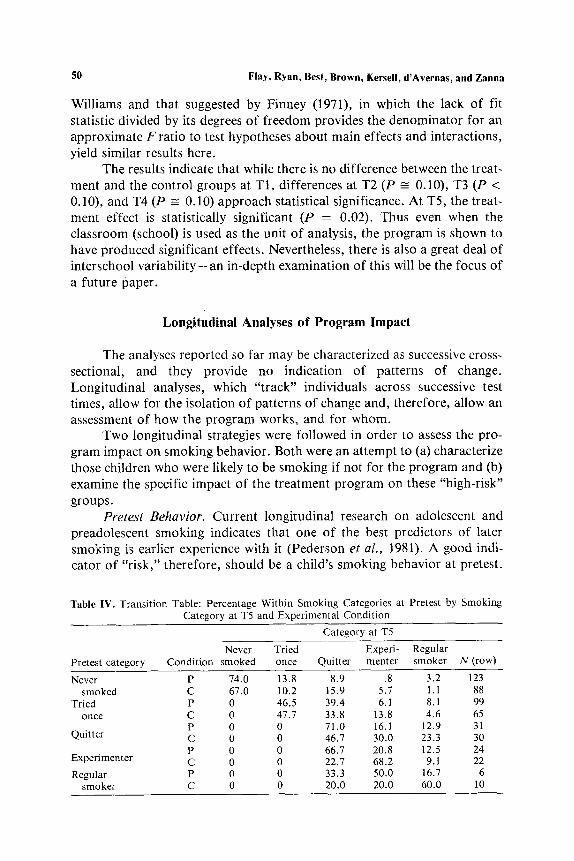
Table IV. Transi t ion Table: Percentage Within Smoking Categories at Pretest by Smoking Category at T5 and Experimental Condit ion
Category at T5
Never Tried Experi- Regular Pretest category Condit ion smoked once Quitter menter smoker N (row)
Never P 74.0 13.8 8.9 .8 3.2 123 smoked C 67.0 10.2 15.9 5.7 1.1 88
Tried P 0 46.5 39.4 6.1 8.1 99 once C 0 47.7 33.8 13.8 4.6 65
P 0 0 71.0 16.1 12.9 31 Quitter C 0 0 46.7 30.0 23.3 30
P 0 0 66.7 20.8 12.5 24 Experimenter C 0 0 22.7 68.2 9.t 22 Regular P 0 0 33.3 50.0 16.7 6
smoker C 0 0 20.0 20.0 60.0 10
Social-Psychological Smoking Prevention Programs 51
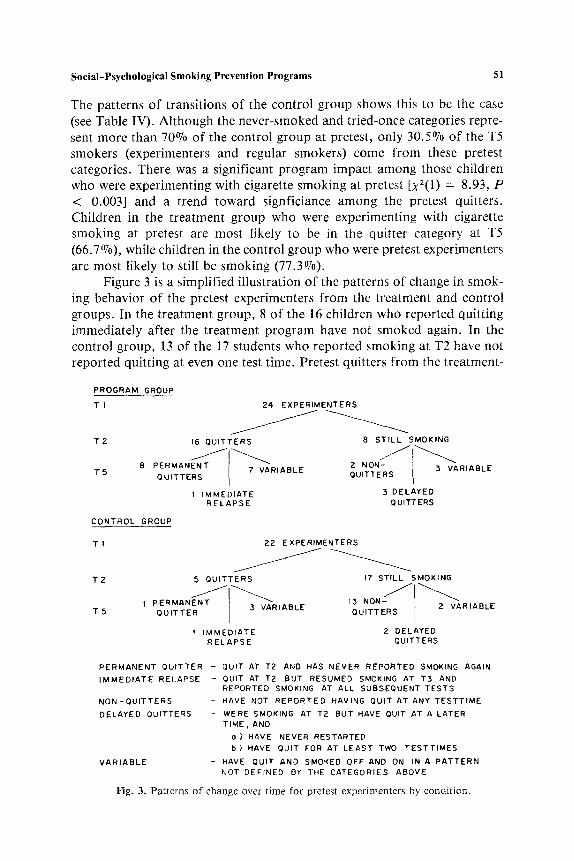
The patterns of transitions of the control group shows this to be the case (see Table IV). Although the never-smoked and tried-once categories repre- sent more than 70% of the control group at pretest, only 30.5% of the T5 smokers (experimenters and regular smokers) come from these pretest categories. There was a significant program impact among those children who were experimenting with cigarette smoking at pretest [xZ(l) = 8.93, P < 0.003] and a trend toward signficiance among the pretest quitters. Children in the treatment group who were experimenting with cigarette smoking at pretest are most likely to be in the ,quitter category at T5 (66.7%), while children in the control group who were pretest experimenters are most likely to still be smoking (77.3%).
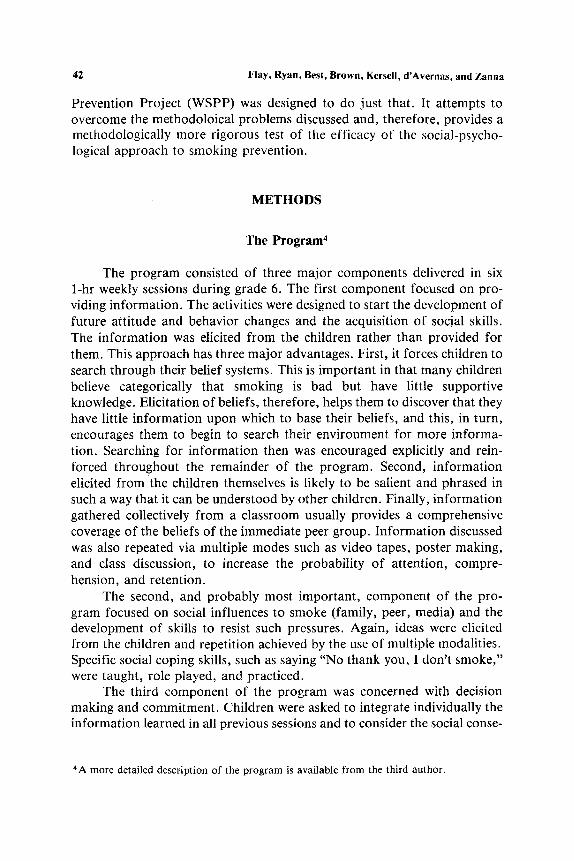
Figure 3 is a simplified illustration of the patterns of change in smok- ing behavior of the pretest experimenters f rom the treatment and control groups. In the treatment group, 8 of the 16 children who reported quitting immediately after the treatment program have not smoked again, In the control group, 13 of the 17 students who reported smoking at T2 have not reported quitting at even one test time. Pretest quitters f rom the treatment-
PROGRAM GROUP
T I
T 2
T 5
16 QUITTERS
8 PERMANENT 7 VARIABLE QUITTERS
I IMMEDIATE RELAPSE
CONTROL GROUP
TI
T 2
TS
24 EXPERIMENTERS
B STILL SMO , G
NON QUITTE;S I VARIABLE 3 DELAYED
QUITTERS
22 EXPERIMENTERS
5 QUITTERS
1 PERMANENT QUITTER 3 VARIABLE
1 iMMEDIATE RELAPSE
17 STILL SMOKING
NJI 13 NO - AR QUITTERS 2 V IABLE
2 DELAYED QUITTERS
PERMANENT QUITTER - QUIT AT T2 AND HAS NEVER REPORTED SMOKING AGAIN
IMMEDIATE RELAPSE - QUIT AT T2 BUT RESUMED SMOKING AT T3 AND REPORTED SMOKING AT ALL SUBSEQUENT TESTS
NON-QUITTERS - HAVE NOT REPORTED HAVING QUIT AT ANY TESTTIME
DELAYED QUITTERS - WERE SMOKING AT T2 BUT HAVE QUIT AT A LATER TIME, AND
o} HAVE NEVER RESTARTED b) HAVE QUIT FOR AT LEAST TWO TESTTIMES
VARIABLE - HAVE QUIT AND SMOKED OFF AND ON IN A PATTERN NOT DEFINED BY THE CATEGORIES ABOVE
Fig. 3. Patterns of change over time for pretest experimenters by condition.
52 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
group classrooms were more likely to report being quitters at T5 (71.0%) than those in the control group (46.7~ Ix2(1) = 3.72, P < 0.05].
There was no statistically significant difference between groups in the other pretest behavior categories. Among the never-smoker and tried-once students, this is probably due to the low rate of exit f rom these categories thus far in both the treatment and the control groups (67% have not moved beyond the tried-once category). It would seem that most of these children have not yet been in need of our program.
Among the pretest regular smokers, 6 of 10 in the control group were still in this category at T5, while only 1 of 6 in the treatment group was still smoking regularly. The lack of statistical significance in the regular smok- ing category may be due to the small numbers of regular smokers at pretest.
The experimenters and, to a lesser extent, the quitters represent students who were "dabbling" with cigarette smoking at pretest. The pro- gram seems to have been successful in helping these students avoid much further smoking for 18 months following pretest.
Social E n v i r o n m e n t Risk . Many data suggest that a child whose social environment contains a number of significant others who smoke is at higher risk to smoke during adolescence. Peers, parents, and siblings have all been shown to be influential others in the adolescent smoking onset process (e.g., Hunter et al., 1982). This finding has been replicated in our own study (see Flay et al., 1983a).
A score based on the number of reported types of smoking models (peers, parents, and siblings) should indicate a child's "risk" to begin smok- ing, whether or not she/he had already smoked at pretest. Such a score was determined for each child in our study at pretest. A child was defined as being at "low risk" if he/she reported no smoking friends, parents, or sibl- ings. "Intermediate risk" was defined as reporting one source of influence (friends, parents, or siblings), and a child was defined as being at "high risk" to smoke if he/she reported two or more influences to smoke in his or her environment. With this classification, at pretest 17% of the sample were low risk, 41% were intermediate risk, and 37% were high risk. Risk could not be determined for 5~ of the sample. There was no difference in the risk classification of the treatment and control groups at pretest.
To confirm that these risk scores actually did predict the likelihood that a child would smoke, two hypotheses were tested. First, at the begin- ning of grade 6, the children classified as high risk should already be smok- ing at higher rates than intermediate- and low-risk children. This proved to be the case [;~z(2) = 102.3, P < 0.0001] and is particularly noticeable in the proport ion of students who had tried smoking. Among the high-risk children, 79.1% had tried smoking at pretest. The proport ions in the inter- mediate and low risk categories are 45.8% and 34.1% respectively.
Social-Psychological Smoking Prevention Programs 53
The second hypothes i s was tha t pre tes t n o n s m o k e r s in the h igh-r i sk ca tegory should be more l ikely to begin smok ing by T5 than in t e rmed ia te - a n d / o r low-r isk n o n s m o k e r s . At T5, 45.5% of the h igh-r i sk pre tes t n o n s m o k e r s had smoked more than once, while only 29 .3% of the inter- med ia te - r i sk and 25 .3% of the low-r isk ch i ld ren had done so [x2(2) = 10.4, P < 0.005].
The t r ea tmen t p r o g r a m did not have a s igni f icant effect on the low- and in t e rmed ia te - r i sk chi ldren. In the low-r isk ca tegory this seems due to the low rate o f smoking in bo th expe r imen ta l cond i t ions . However , at T5 a m o n g the in t e rmed ia te - r i sk chi ldren, there was a be tween-cond i t ion dif- ference in smoking behav io r which a p p r o a c h e d s tat is t ical s ignif icance [X2(4) = 8.73, P < 0.07] with the p r o g r a m g roup having fewer exper imenters (4.8 vs 13.2%) and more qui t ters (27.8 vs 18.4%) t han the con t ro l g roup .
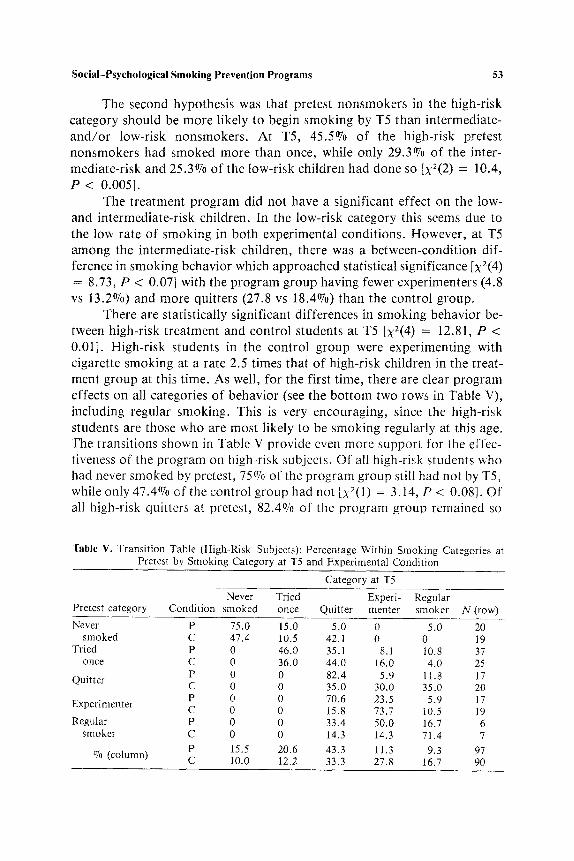
There are s ta t i s t ica l ly s igni f icant d i f ferences in smoking behav io r be- tween high-r isk t r ea tmen t and con t ro l s tudents at T5 [X2(4) = 12.81, P < 0.01]. High- r i sk s tudents in the con t ro l g roup were exper iment ing with c igaret te smoking at a ra te 2.5 t imes tha t o f h igh-r i sk chi ldren in the t rea t - ment g roup at this t ime. As well, for the first t ime, there are clear p r o g r a m effects on all ca tegor ies o f behav io r (see the b o t t o m two rows in Table V), inc luding regula r smoking . This is very encourag ing , since the h igh-r isk s tudents are those who are mos t l ikely to be smok ing regular ly at this age. The t rans i t ions shown in Table V p rov ide even more suppo r t for the effec- t iveness o f the p r o g r a m on high-r isk subjects . O f all h igh-r isk s tudents who had never smoked by pretest , 75% of the p r o g r a m group still had not by TS, while only 47 .4% of the con t ro l g roup had not [•2(1) = 3.14, P < 0.08]. Of all h igh-r isk qui t ters at pretest , 82 .4% of the p r o g r a m g roup remained so
Table V. Transition Table (High-Risk Subjects): Percentage Within Smoking Categories at Pretest by Smoking Category at T5 and Experimental Condition
Category at T5
Never Tried Experi- Regular Pretest category Condition smoked once Quitter menter smoker N (row)
Never P 75.0 15.0 5.0 0 5.0 20 smoked C 47.4 10.5 42.1 0 0 19
Tried P 0 46.0 35.1 8.1 10.8 37 once C 0 36.0 44.0 16.0 4.0 25
P 0 0 82.4 5.9 11.8 17 Quitter C 0 0 35.0 30.0 35.0 20
P 0 0 70.6 23.5 5.9 17 Experimenter C 0 0 15.8 73.7 10.5 19 Regular P 0 0 33.4 50.0 16.7 6
smoker C 0 0 14.3 14.3 71.4 7 P 15.5 20.6 43.3 11.3 9.3 97
07o (column) C 10.0 12.2 33.3 27.8 16.7 90
54 Flay, Ryan, Best, Brown, Kersell, d'Avernas, an{; Zanna
until T5, while only 35% of the control group did so [X2(1) = 11.08, P < 0.004]. Of all high-risk experimenters at pretest, 70.6% of the program group quit by T5, whereas only 15.8% of the control group did so [X2(1) =
11.08, P < 0.001]. And among high-risk regular smokers at pretest, only 16.7% of the program group remained in this category, compared to 71.4% of the control group [x2(1) = 3.9, P < 0.05] (further discussion of risk and more detailed results are presented by Best et al., 1985).
DISCUSSION
A social-psychological smoking prevention curriculum affected the smoking onset process in this study, as it has in previous work. Confidence in findings is increased by methodological advances, including (a) assign- ment of a sufficient number of schools, of demonstrated pretreatment equivalence, to program and control conditions, (b) good subject retention, and (c) implementation and process data showing that the program was delivered and operating as planned.
There were, however, some methodological limitations to this study that will need to be overcome in further research. First, this study did not control for the effects of intensive testing. Evans and his colleagues (1978) found testing alone as effective as the prevention curriculum. Others have not found this effect; nevertheless, it is being controlled for in a second study now underway. Second, a caveat must be expressed about generalizability to other populations: (a) none of the students came from large, metropolitan areas, (b) the sample proved unusually stable, with few students moving to other schools, and (c) few of the students graduated to high school during the course of the study, a transition which may be accompanied by increased social pressures to smoke.
The WSPP study represents the most rigorous test to date of the social-psychological approach to smoking prevention. Program effects on mediating variables were substantial (see Flay et al., 1983a), relatively per- sistent over time, and consistent with the expected behavior changes. Pro- gram effects on behavior were also substantial and seem to be increasing over time [see Best et al. (1985) for 3-year results]. There are problems, however, in trying to compare the types of behavior changes obtained in this study with those reported by other investigators. McAlister and his col- leagues always have reported differences in regular smoking only. To date in this study, there are desirable effects on regular smoking only for high- risk students. There are no such effects for the complete sample, possibly because base rates are still too low. It is possible that the students of McAlister et al. were at higher risk than ours since they were recognized as
Social-Psychological Smoking Prevention Programs 55
being at a problem school. The Minnesota group reported program effects on both regular and experimental smoking, although their monitoring-only (i.e., with saliva collection) control school showed as low an increase in ex- perimental smoking as their program school. They also demonstrated a marked increase in quitting in their program schools at immediate posttest, although this effect was maintained in only one school. As in this study, the Minnesota group was not able to show significant effects on the level of never smokers. Botvin and his colleagues have consistently reported only the number of students becoming smokers from among those students who were never smokers at pretest. This study finds no such effects, though this could be because the number of pretest never smokers shifting categories by T5 is low, and those who do move often try smoking just once.
Two important conclusions can be drawn from the preceding paragraph. First, investigators need to be encouraged to report results on the same dependent variables so that comparisons between studies can be made more easily. Second, results from all levels of smoking behavior need to be reported. Reporting only one level, such as regular smoking, can be misleading. For example, the program tested here would have looked un- questionably effective if we had reported only experimental smoking or only all current smoking (experimental plus regular combined). Similarly, the Minnesota results would have looked more convincing if only regular smoking had been reported. Results for other levels of smoking were not reported in the studies by McAlister et al. or Botvin et al. Without such in- formation, it is difficult to make comparisons across studies.
Our design allowed us to examine important individual differences as they interact with program impact. Experience with smoking before the study was used to stratify students. The program had its greatest effects with those experimenting at pretest. A significant number quit smoking dur- ing the core program, and about half of these remained quitters throughout the follow-up period. This point reflects the value of tracking individuals over time. Cross-sectional analyses suggest a relatively constant proportion across time of quitters in the experimental group. However, only half are the same individuals who quit during the core program. The 50% cessation rate compares favorably to the success in other programs designed to pro- duce cessation (Leventhal and Clearly, 1980; Perry et al., 1980b)and pro- vides evidence of an unexpected positive side effect of good smoking prevention curricula.
This program had somewhat limited effects on regular smokers, in part attributable to small numbers and a consequent inability to demonstrate statistical significance. The importance of an adequate sample size thus is underscored. The cross-sectional analyses also failed to show a significant impact on regular smoking, although others have demonstrated
56 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
this effect at the end of grade 7 (e.g., Botvin and Eng, 1980; McAlister et al., 1979). As noted, the sample for this study was not drawn from metropoli tan areas, and it is possible that students were at a somewhat earlier stage in the onset process than those in other studies. The final data point from this paper still comes quite early in the smoking onset process, and effects on regular smoking may emerge at later follow-up.
The program's impact on pretest experimenters and quitters shows that previous experience with smoking does not preclude prevention of future smoking. Some have argued that prevention programs may have to anticipate initial experimenting, but to the contrary, our program seems to have been well timed and effective when delivered in grade 6.
It remains to be seen what should be done for pretest never smokers. Smoking prevalence in the age range we studied still is far lower than recent surveys indicate for older youth, suggesting that many of these never smokers may begin later. A repetition at a later grade of this type of cur- riculum migh t have proven effective, but alternatively a different kind of program may be required.
The second individual difference we examined was social risk, that is, the variety of smoking models to which children are exposed. The ability of the program to have its greatest impact on the children at greatest social risk is gratifying, since in a sense it is they who need a program most. The fact that the effectiveness of a "social influences" curriculum is a function of social influences in the environment provides convergent validity for the theoretical basis of the program. This pattern of results also suggests ways in which programs of this kind might be extended and refined in the future. It might p rove useful to add components designed to affect directly the various models. For example, a complimentary program to assist parents in quitting might be envisioned (c.f., Flay et al., 1982, 1983b). Our ability to identify individuals at greater risk creates the possibility of additional, sup- plementary programming for them. Alternatively, social influence pro- grams might target schools at high risk with respect to prevalence of student
and parent smoking. The finding that the program influenced current experiments to quit
smoking, and remain quit, is of particular importance. Students at high risk are likely to start smoking at an early age. A program that can lead to successful cessation by early smokers, as well as successful prevention of later starters, seems to provide double value for the effort.
Further long-term results are needed before we can be completely con- fident of the long-term effects of this program. There are still a significant number of high-risk subjects in the control group who have not yet started to smoke. It remains to be seen whether the larger number of high-risk sub- jects remaining in the treatment group can continue to resist pressures to become smokers.
Social-Psychological Smoking Prevention Programs 57
REFERENCES
Arkin, R. M., Roemhild, H. F., Johnson, C. A., Luepker, R. V., and Murray, D. M. (1981). The Minnesota smoking prevention program: A seventh grade health curriculum sup- plement. J. School Health, 51(19): 611-616.
Bandura, A. (1977). Social Learning Theory, Prentice Hall, Englewood Cliffs, N.J. Best, J. A., Flay, B. R., Towson, S. M. J., Ryan, K. B., Perry, C. L., Brown, K. S., Kersell,
M. W., and d'Avernas, J. R. (1985). Smoking prevention and the concept of risk. J. Appl. Soc. Psychol. (in press).
Bishop, Y. M. M., Fienberg, S. E., and Holland, P. W. (1975). Discrete Multivariate Analysis: Theory and Practice, MIT Press, Cambridge, Mass.
Botvin, G., and Eng, A. (1980). A comprehensive school-based smoking prevention program. J. School Health 11: 209-213.
Botvin, G., and Eng, A. (1981). Life skill training and smoking prevention: A one year follow- up. Presented at American Public Health Association meeting, Los Angeles, November.
Botvin, G., and Eng, A. (1982). The efficacy of a multicomponent approach to the prevention of cigarette smoking. Prevent. Med. 11: 199-211.
Botvin, G., Eng, A., and Williams, C. L. (1980). Preventing the onset of cigarette smoking through life skills training. Prevent. Med. 9: 135-143.
Botvin, G., and Wills, T. A. (1985). Personal and social skills training: Cognitive-behavioral approaches to substance abuse prevention. In Bell, C., and Battjes, R. (eds.), Preven- tion research: Deterring drug abuse among children and adolescents. NIDA Research Monograph, Washington, D.C. (in press).
Brown, K. S., Cherry, W. H., and Forbes, W. F. (1980). The smoking habits of Canadian school children. Proceedings o f Conference on Student Smoking, Calgary, Alberta, October, 1978, Canadian Council on Smoking and Health.
Burstein, L. (1980a). The role of levels of analysis in the specification of education effects. In Dreeben, R., and Thomas, J. A. (eds.), The Analysis o f Educational Productivity, Ballinger, Cambridge, Mass.
Burstein, L. (1980b). The analysis of multilevel data in educational research and evaluation. Rev. Res. Educ. 8: 158-233.
Cox, D. R. (1970). The Analysis o f Binary Data, Chapman & Hall, London. Evans, R. I. (1976). Smoking in children: Developing a social psychological strategy of deter-
rence. J. Prevent. Med. 5: 122-127. Evans, R. I., Hansen, W. B., and Mittlemark, M. B. (1977). Increasing the validity of self-
reports of behavior in a smoking in children investigation. J. Appl. Psychol. 62: 521-523.
Evans, R. I., Rozelle, R. M., Mittlemark, M. B., Hansen, W. B., Bane, A. I., and Havis, J. (1978). Deterring the onset of smoking in children: Knowledge of immediate physio- logical effects and coping with peer pressure, media pressure and parent modelling. J. Appl. Soc. Psychol. 8: 126-135.
Evans, R. I., Rozelle, R. M., Maxwell, S. E., Raines, B. E., Dill, C. A., Guthrie, T. J., Henderson, A. H., and Hill, P. C. (1981). Social modelling films to deter smoking in adolescents: Results of a three year field investigation. J. Appl. Psychol. 66(4): 399-414.
Finney, D. J. (1971). Probit Analysis, 3rd ed., Cambridge University Press, London. Fisher, E. B. (1980). Progress in reducing smoking behavior. Am. J. Publ. Health 70: 678-679. Flay, B. R. (1985) What do we know about the social influences approach to smoking pre-
vention? Review and recommendations. In Bell, C., and Battjes, R. (eds.), Prevention research: Deterring drug abuse among children and adolescents, N IDA Research Mono- graph, Washington, D.C. (in press).
Flay, B. R., and Best, J. A. (1982). Overcoming design problems in the evaluation of health behavior change programs. Eval. health Prof. 5: 43-69.
Flay, B. R., and Cook, T. D. (1981). The evaluation of media-based prevention campaigns. In Rice, R. R., and Paisley, W. (eds.), Public Communication Campaigns, Sage, Beverly Hills, Calif.
58 Flay, Ryan, Best, Brown, Kersell, d'Avernas, and Zanna
Flay, B. R., d'Avernas, J. R., Best, J. A., Kersell, M. W., and Ryan, K. B. (1983a). Cigarette smoking: Why young people do it and ways of preventing it. In McGrath, P. J., and Firestone, P. (eds.), Pediatrib and Adolescent Behavioral Medicine, Springer, New York.
Flay, B. R., Hansen, W. B., Johnson, C. A., and Sobel, J. L. (1983b). Involvement of children in motivating parents to quit smoking with a television program. Presented at meetings of American Psychological Association, Anaheim, Calif.
Flay, B. R., Johnson, C. A., Hansen, W. B., Grossman, L. M., Sobel, J. L., and Collins, L. M. (1983c). Evaluation of a school-based, family-oriented, television-enhanced smoking prevention and cessation programs: The importance of impIementation evalua- tion. Presented at Joint Meetings of the Evaluation Network and the Evaluation Research Society, Chicago, October.
Flay, B. R., Johnson, C. A., Hansen,W. B., lJlene, A., Grossman, L. M., Alvarez, L., Sobol, D. F., Hochstein, G., and Sobel, J. L. (1982). Evaluation of a mass media enhanced smoking prevention and cessation program. In Baggaley, J. P., and Janega, P. (eds.), Experimental Research in Televised Instruction, Vol. 5, Concordia University, Mon- treal.
Hansen, W. B., Collins, L. M., Malotte, C. K., Johnson, C. A., and Fielding, J. E. (1985). Attrition in prevention research. J. Behav. Med. (in press).
Hunter, S. MacD., Baugh, J. G., Weber, L. S., Sklov, M. C., and Berenson, G. S. (1982). Social learning effects in trial and adoption of cigarette smoking in children: The Bogalusa Heart Study. Prevent. Med. 11: 29-42.
Hurd, P. D., Johnson, C. A., Pechacek, T., Jacobs, D. R., and Luepker, R. V. (1980). Prevention of cigarette smoking in seventh grade students. J. Behav. Med. 3: 15-28.
Janis, I. L., and Mann, L. (1977). Decision-Making: A Psychological Analysis of Conflict, Choice and Commitment, The Free Press, New York.
Johnson, C. A., Hansen, W. B., Collins, L. M., and Graham, J. W. (1984). Final Report. The High School Anit-Smoking Project. Final report to National Institute on Drug Abuse, University of Southern California, Los Angeles.
Jones, E. E., and Sigall, H. (1971). The bogus pipeline: A new paradigm for measuring affect and attitude. Psychol. Bull. 76: 349-364.
Jones, E. E., Kanouse, D. E., Kelley, H. H., Nisbett, R. E., Valins, S., and Weiner, B. (1972). Attribution: Perceiving the Causes of Behavior, General Learning Press, Morristown, N.J.
Kiesler, C. A. (1971). The Psychology of Commitment, Academic Press, New York. Leventhal, H., and Cleary, P. D., (1980). The smoking problem: A review of the research and
theory in behavioral risk modification. Psychol. Bull. 88: 370-405. Luepker, R. V., Pechacek, T. I., Murray, D. M., Johnson, C. A., Hurd, P., and Jacobs, D. R.
(1981). Saliva tbiocyanate: A chemical indicator of smoking in adolescents. Am. J. Publ. Health 71: 1320-1324.
Luepker, R. V., Johnson, C. A., Murray, D. M., and Pechacek, T. F. (1983). Prevention of cigarette smoking: Three year follow-up of an education program for youth. J. Behav. Med. 6: 53-62.
McAlister, A., Perry, C., and Maccoby, N. (1979). Adolescent smoking: Onset and preven- tion. Pediatrics 63: 650-658.
McAlister, A., Perry C., Killen, J., Slinkard, L., and Maccoby, N. (1980). Pilot study of smoking, alcohol, and drug abuse prevention. Am. J. Publ. Health 70: 719-721.
McGuire, W. J. (1964). Inducing resistance to persuasion. In Berkowitz, L. (ed.), Advances in Experimental Social Psychology (Vol. l), Academic Press, New York.
McGuire, W. J. (1968). The nature of attitudes and attitude change. In Lindzay, G., Aronson, E. (eds.). Handbook of Social Psychology, Vol. 3, 2rid ed., Addison-Wesley, Reading, Mass.
Murray, D. M., Johnson, C. A., Luepker, R. V., Pechacek, T. F., and Jacobs, D. R. (1980). Issues in smoking prevention research. Presented at American Psychological Associa- tion, Montreal, September.
Pederson, L. L., Baskerville, J. C., and Lefcoe, N. M. (1981). Multivariate prediction of cigarette smoking among children in grades six, seven, and eight. J. Drug Educ. 11: 191 - 203.
Social-Psychological Smoking Prevention Programs 59
Perry, C. L., Killen, J., and Slinkard, L. A. (1980a). Peer teaching and smoking prevention among junior high students. Adolescence 15: 277-281.
Perry, C. L., Killen, J., Telch, M. J., Slinkard, L. A., and Danaher, B. S. (1980b). Modifying smoking behavior of teenagers: A school-based intervention. Am. J. Publ. Health, 70: 722-725.
Rotter, J. B. (1966). Generalized expectancies for internal versus external control of reinforce- ment. Psychol. Monogr. 80(1): Whole No. 609.
Telch, M. J., Killen, J. D., McAlister, A. L., Perry, C. L., and Maccoby, N. (1982). Long- term follow-up of a pilot project on smoking prevention with adolescents. J. Behav. Med. 5: 1-8.
Williams, C. L., Eng, A., Botvin, G. C., Hill, P., and Wynder, E. L. (1979). Validation of student's self-reported cigarette smoking status with plasma cotinine levels. Am. J. Publ. Health 69: 1272-1276.
Williams, D. A. (1982). Extra-binominal variationin logistic linear models. Appl. Star. 31: 144-148.