
Enhancing Mobile Learning Using Speech Recognition Technologies: A Case Study
Upload
khangminh22Category
view
0download
0
Applying Speech Recognition and Language Processing Methods to Transcribe and
Structure Physicians’ Audio Notes to a Standardized Clinical Report Format
by
Syed M. Faizan
Submitted in partial fulfilment of the requirements
for the degree of Master of Computer Science
at
Dalhousie University
Halifax, Nova Scotia
February 2020
© Copyright by Syed M. Faizan, 2020

ii
To my parents, my wife, my son and my sister.
Thank you all for your love and support.

iii
TABLE OF CONTENTS
List of Tables ................................................................................................................... viii
List of Figures ......................................................................................................................x
Abstract .............................................................................................................................. xi
List of Abbreviations Used ............................................................................................... xii
Acknowledgments............................................................................................................ xiii
Chapter 1. Introduction ....................................................................................................1
1.1 Solution Approach................................................................................................ 1
1.2 Research Objectives ............................................................................................. 2
1.2.1 First Objective ................................................................................................2
1.2.2 Second Objective ...........................................................................................3
1.3 Research Scope .................................................................................................... 3
1.4 Thesis Contribution .............................................................................................. 3
1.5 Thesis Organization.............................................................................................. 4
Chapter 2. Background and Related Work ......................................................................5
2.1 Health Record ....................................................................................................... 5
2.1.1 Electronic Health Record (EHR) ...................................................................5
2.2 Clinical Report ..................................................................................................... 5
2.2.1 SOAP .............................................................................................................6
2.3 Clinical Documentation........................................................................................ 9
2.3.1 Challenges ......................................................................................................9
2.3.2 Modes ...........................................................................................................10
2.3.3 Workflows....................................................................................................11
2.3.4 Problems ......................................................................................................12
2.3.5 Summary ......................................................................................................13
2.4 Speech Recognition ............................................................................................ 14
2.4.1 Acoustic Model ............................................................................................15
2.4.2 Language Model ..........................................................................................17
2.4.3 Evaluation Metric.........................................................................................19

iv
2.5 Speech Recognition in Clinical Documentation ................................................ 20
2.5.1 Review Objective .........................................................................................20
2.5.2 Literature Exploration ..................................................................................21
2.5.3 Analysis........................................................................................................21
2.5.4 Findings........................................................................................................22
2.6 Handling Noise in Speech Recognition ............................................................. 25
2.6.1 Feature-space Techniques ............................................................................26
2.6.2 Model-space Techniques .............................................................................27
2.6.3 Summary ......................................................................................................28
2.7 Domain-Specific Speech Recognition ............................................................... 29
2.7.1 Out-of-Domain Model Adaptation ..............................................................29
2.7.2 Domain Relevant Data Generation ..............................................................30
2.7.3 Summary ......................................................................................................31
2.8 Speech Recognition Systems ............................................................................. 32
2.8.1 Deep Speech.................................................................................................32
2.8.2 ESPnet ..........................................................................................................34
2.8.3 Wav2Letter++ ..............................................................................................35
2.8.4 CMUSphinx .................................................................................................36
2.8.5 Kaldi .............................................................................................................36
2.8.6 Julius ............................................................................................................36
2.8.7 Google Speech-to-Text ................................................................................36
2.8.8 Summary ......................................................................................................37
2.9 SOAP Classification ........................................................................................... 38
2.10 Conclusion .......................................................................................................... 39
Chapter 3. Research Methodology ................................................................................40
3.1 Introduction ........................................................................................................ 40
3.2 Layer 1: Transcription of Physicians’ Audio Notes ........................................... 40
3.2.1 Selection of Methods ...................................................................................40
3.2.2 Preliminary Analysis ....................................................................................42
3.2.3 Development of Solution .............................................................................43

v
3.2.4 Evaluation of solution ..................................................................................43
3.3 Layer 2: Autonomous Generation of Clinical Report ........................................ 44
3.3.1 Data Labeling ...............................................................................................44
3.3.2 Selection of Method .....................................................................................44
3.3.3 Development of Solution .............................................................................44
3.3.4 Evaluation of Solution .................................................................................44
3.4 Dataset ................................................................................................................ 44
3.4.1 Data Collection ............................................................................................45
3.4.2 Dataset Preparation ......................................................................................45
3.5 Research Environment ....................................................................................... 46
3.6 Conclusion .......................................................................................................... 47
Chapter 4. Speech Recognition – Methods ...................................................................48
4.1 Introduction ........................................................................................................ 48
4.2 Domain Adaptation ............................................................................................ 48
4.3 Preliminary Analysis .......................................................................................... 49
4.4 Acoustic Modeling ............................................................................................. 51
4.4.1 Audio Pre-Processing...................................................................................51
4.4.2 Fine-tuning ...................................................................................................53
4.5 Language Modeling............................................................................................ 56
4.5.1 Dataset Augmentation with Domain Relevant Data ....................................56
4.5.2 Developing Domain-Specific Language Models .........................................61
4.5.3 Enhancing Pre-Trained Language Model ....................................................63
4.5.4 Summary ......................................................................................................65
4.6 Discussion .......................................................................................................... 66
4.7 Conclusion .......................................................................................................... 66
Chapter 5. Speech Recognition – Evaluations...............................................................67
5.1 Introduction ........................................................................................................ 67
5.2 Setup ................................................................................................................... 67
5.2.1 Evaluation Phases ........................................................................................67
5.2.2 Cross-Validation ..........................................................................................68

vi
5.2.3 Interpretation of Results ...............................................................................68
5.3 Evaluating Acoustic Modeling ........................................................................... 69
5.3.1 Analysis........................................................................................................70
5.4 Evaluating Language Modeling Methods .......................................................... 71
5.4.1 Analysis........................................................................................................72
5.5 Combined Evaluation ......................................................................................... 80
5.5.1 Analysis........................................................................................................80
5.6 Working Examples ............................................................................................. 82
5.6.1 Best Case ......................................................................................................82
5.6.2 Worst Case ...................................................................................................84
5.6.3 Random Cases ..............................................................................................86
5.7 Final Validation .................................................................................................. 91
5.8 Discussion .......................................................................................................... 92
5.9 Conclusion .......................................................................................................... 93
Chapter 6. Classification of Transcription into SOAP Categories ................................94
6.1 Introduction ........................................................................................................ 94
6.2 Methods .............................................................................................................. 94
6.2.1 Assigning SOAP categories to Dataset ........................................................94
6.2.2 Exemplar-based Concept Detection .............................................................98
6.2.3 Exemplar-based Sentence Classification ...................................................100
6.2.4 Summary ....................................................................................................104
6.3 Evaluation......................................................................................................... 105
6.3.1 Experimental Setup ....................................................................................105
6.3.2 Results ........................................................................................................107
6.4 Discussion ........................................................................................................ 124
6.5 Conclusion ........................................................................................................ 125
Chapter 7. Discussion ..................................................................................................126
7.1 Introduction ...................................................................................................... 126
7.2 Observations ..................................................................................................... 126
7.3 3-Layer Solution Framework ........................................................................... 127

vii
7.4 Limitations ....................................................................................................... 128
7.5 Future Work ..................................................................................................... 129
7.6 Conclusion ........................................................................................................ 130
References ........................................................................................................................131
Appendix A. AP Scores for SOAP Classification .......................................................146

viii
LIST OF TABLES
Table 2.1 Documentation Guidelines of SOAP categories adapted from [13] ................... 7
Table 3.1 Summary of Research Environment ................................................................. 46
Table 4.1 Preliminary Results: WER and CER of Cloud and Offline SR ........................ 49
Table 4.2 Examples mistakes by DeepSpeech during preliminary experiments. ............. 49
Table 4.3 Hyperparameters used for acoustic model fine-tuning ..................................... 53
Table 5.1 Training and testing error rates for Acoustic Model training ........................... 70
Table 5.2 Absolute and relative change in error rates after acoustic modeling ................ 70
Table 5.3 List of scenarios for Language Model evaluations ........................................... 71
Table 5.4 Training error rates from each evaluation scenario .......................................... 73
Table 5.5 Cross-validated error rates from each evaluation scenario ............................... 73
Table 5.6 Absolute and relative change in error rates compared to baseline ................... 74
Table 5.7 Variables to analyze each experimented method .............................................. 75
Table 5.8 Comparing error rates between original and augmented corpus ...................... 77
Table 5.9 Comparing error rates between new and enhanced pooled model ................... 78
Table 5.10 Comparing error rates between new and enhanced interpolated model ......... 78
Table 5.11 Error rates after testing with combined models. ............................................. 80
Table 5.12 Performance comparison of DeepSpeech (before and after) with Google ..... 81
Table 5.13 Errors in the best transcribed note .................................................................. 83
Table 5.14 Errors in the worst transcribed note ................................................................ 84
Table 5.15 Errors in the first examined note transcription ............................................... 86
Table 5.16 Errors in the second examined note transcription ........................................... 89
Table 5.17 Error rates on the validation dataset ............................................................... 91
Table 6.1 Patterns observed in subjective category sentences .......................................... 95
Table 6.2 Patterns observed in objective category sentences ........................................... 96
Table 6.3 Patterns observed in assessment category sentences ........................................ 96
Table 6.4 Patterns observed in plan category sentences ................................................... 97
Table 6.5 Cases based on Stop Word, Similarity Function and Exemplar type ............. 105
Table 6.6 Conversion of categorical variables to numeric ............................................. 107

ix
Table 6.7 Confidence scores of sentences from the baseline condition ......................... 109
Table 6.8 Highest and Lowest AP scores for SOAP categories ..................................... 110
Table 6.9 Summary of regression analysis results .......................................................... 110
Table 6.10 Best performing values for maximum n-gram length for each case ............. 112
Table 6.11 Summary of optimal conditions for each SOAP category ............................ 117
Table 6.12 Confidence scores of sentences from case 1 using 8-gram limit .................. 118
Table 6.13 Confidence scores of sentences from case 3 using 11-gram limit ................ 119
Table 6.14 Confidence scores of sentences from case 1 using 1-gram limit .................. 121
Table 6.15 Confidence scores of sentences from case 7 using 6-gram limit .................. 123

x
LIST OF FIGURES
Figure 1.1 Solution approach for clinical documentation ................................................... 2
Figure 2.1 Structure of any SR system in its simplest form ............................................. 15
Figure 2.2 Query Tree for Literature search ..................................................................... 21
Figure 2.3 Structure of Deep Speech Model [77] ............................................................. 33
Figure 2.4 Processing stages in ESPnet recipe [75] .......................................................... 35
Figure 3.1 Steps in Research Methodology spanning over two layers ............................. 40
Figure 4.1 Steps of Pattern Extraction .............................................................................. 58
Figure 4.2 Steps of Knowledge Extraction ....................................................................... 59
Figure 4.3 Steps to Generate Augmented Corpus ............................................................. 61
Figure 5.1 Flow of experiments ........................................................................................ 67
Figure 5.2 Error loss in Acoustic Model training ............................................................. 69
Figure 5.3 Result summary of regression analysis using WER ........................................ 76
Figure 5.4 Result summary of regression analysis using CER ......................................... 76
Figure 6.1 Exemplar based algorithms proposed by Juckett [102] ................................... 98
Figure 6.2 Outline of word-class array [102].................................................................... 99
Figure 6.3 Pseudocode for Exemplar-based Sentence Classification Algorithm ........... 103
Figure 6.4 Precision-Recall curve of the baseline condition .......................................... 108
Figure 6.5 All AP scores over n-gram max length ......................................................... 111
Figure 6.6 Box plots of scores after removing stop words ............................................. 114
Figure 6.7 Comparing performance based on similarity function (Cosine vs Jaccard) .. 115
Figure 6.8 Comparing performance based on exemplar type (sentence vs n-gram) ...... 116
Figure 6.9 Precision-Recall Curve of best performing condition for Subjective ........... 117
Figure 6.10 Precision-Recall Curve of best performing condition for Objective ........... 120
Figure 6.11 Precision-Recall Curve of best performing condition for Assessment ....... 122
Figure 6.12 Precision-Recall Curve of best performing condition for Plan ................... 122
Figure 7.1 Design for 3-Layer Solution Framework ...................................................... 127

xi
ABSTRACT
Clinical documentation is an audio recording of the clinical encounter by the specialist
which is subsequently manually transcribed to be added to the patient’s medical record.
The current clinical documentation process is tedious, error-prone and time-consuming,
more so for specialists working in the emergency department given the rapid turnaround
of high-acuity patients. In this thesis, we investigate methods to automate the clinical
documentation processes for a pediatric emergency department, leading to the generation
of a SOAP report of the clinical encounter. Our approach involves (a) speech recognition
to transcribe the audio recording of the clinical encounter to a textual clinical encounter
report; and (b) identifying and classifying the sentences within the textual report in terms
of the standard SOAP format for clinical reports. For speech recognition, we worked with
the DeepSpeech application and used recurrent neural network and n-gram based methods,
augmented with medical terminologies and heuristics, to develop domain-specific acoustic
and language models. Our approach resulted in a reduction of 49.02% of critical errors as
compared to the baseline acoustic and language models provided by DeepSpeech. For
generating a SOAP report from the clinical text, we extended an exemplar-based concept
detection algorithm to learn a sentence classifier to identify and annotate the clinical
sentences in terms of subjective, objective, assessment and plan. Our SOAP classifier
achieves a precision of 0.957 (subjective), 0.919 (objective), 0.626 (assessment) and 0.82
(plan).

xii
LIST OF ABBREVIATIONS USED
EHR Electronic Health Record
EMR Electronic Medical Record
SR Speech Recognition
ANN Artificial Neural Network
DNN Deep Neural Network
RNN Recurrent Neural Network
CNN Convolutional Neural Network
WER Word Error Rate
CER Critical Error Rate
SOAP Subjective Objective Assessment Plan (Acronym)
NLP Natural Language Processing
CD Clinical Documentation
LM Language Model
AM Acoustic Model
MeSH Medical Subject Headings (Acronym)

xiii
ACKNOWLEDGMENTS
I am deeply thankful and blessed to have Dr. Syed Sibte Raza Abidi as my supervisor on
my journey of this research. I am grateful for his guidance, support, and advice that has
helped me a lot throughout the course of my degree. None of this would have been possible
without him. I also acknowledge the support of all members of the NICHE research group
for their suggestions and constructive feedback that has facilitated this work. I like to thank
Ali Daowd for his assistance on healthcare-related specific questions, William Van
Woensel and Patrice Roy for their expert technical opinions and Brett Tylor for providing
a dataset for this work. I also like to thank Asil Naqvi for keeping himself with me as moral
support in all the blues.

1
Chapter 1. INTRODUCTION
Clinical reports are vital in providing quality healthcare. These reports facilitate physicians
to recall previous episodes of care given to patients [1]. Moreover, these reports ensure
quality healthcare by providing a medium to perform regular audits of the care delivery
process [2]. Clinical documentation is a process in which physicians note down encounter
synopsis and generate clinical reports. It is a challenging (Section 2.3.1) and tedious
process, which can sometimes take twice as much time as it takes for patient interaction
[3], [4]. Clinical documentation is done in three modes (Section 2.3.2): hand-written, type-
written, and dictations; while adhering to two work-flows (Section 2.3.3): front-end and
back-end [6]. Hand-written reports are mostly illegible and unsatisfactory [5]. Type-written
and dictations are currently the most common mode of documentation among physicians.
In general, the process of clinical documentation poses five major problems (Section 2.3.4)
that are caused by either any or all combinations of modes and work-flows. These problems
provide motivation for this thesis to work on methods to automate the process of clinical
documentation.
1.1 Solution Approach
This thesis focuses on using the physician’s dictated audio notes to autonomously generate
structured clinical reports. Dictations are given in audio; therefore, Speech Recognition
(SR) is used to transcribe audio notes. Transcriptions are then analyzed for SOAP
categories, which can be organized to form a standardized clinical report.
After a detailed review of the use of speech recognition in clinical documentation (Section
2.5), this thesis made two recognitions. Firstly, there is a need for more accurate SR
systems. Secondly, physicians prefer to dictate in freestyle; hence there is a need to research
in the direction of autonomous preparation of reports from transcribed notes. This thesis
considers the documentation process from an end-to-end perspective, where physicians can
get the ability to dictate in freestyle. Dictated audio notes should firstly transcribe into text
using a noise-robust domain-specific SR system. Subsequently, transcribed notes should

2
organize to form a structured clinical report using autonomous language processing
techniques. Henceforth, our approach aims to form two separate research objectives, whilst
keeping the focus of this thesis on the individual methods within each objective. Figure 1.1
illustrates the solution design for this thesis.
Figure 1.1 Solution approach for clinical documentation
1.2 Research Objectives
This thesis aims to work as a multi-layer solution pipeline, where each layer possesses its
own set of problems that needs active rounds of research. Two main research problems are
identified that are requisite towards setting a conclusion. These problems act as the
objectives of this thesis, which are defined in the subsections below.
1.2.1 First Objective
The first objective of this thesis is “to accurately recognize speech content from physicians’
dictated audio notes”. To facilitate the better achievement of this objective, this research
forms a set of three research questions.
1. What are the challenges and shortcomings of SR technology in clinical environments?
2. What are the current advancements and in SR that can address those challenges?
3. What are the steps required to develop robust SR systems in clinical environments?

3
The first research question is responded to in Section 2.5, which presents a detailed review
of the use of SR in clinical documentation, its challenges, shortcomings, and reasons for
those shortcomings. For the second question, Section 2.6 and 2.7 presents the current
advancements in SR technology that addresses the challenges of noise-robustness and
domain-robustness. Finally, this thesis responds to the third question by presenting our
methods in Chapter 4, which are evaluated in Chapter 5.
1.2.2 Second Objective
The second objective of this thesis is “to organize transcribed physicians’ dictated audio
notes into meaningful categories of the clinical report structure”. To achieve this objective,
we investigate algorithms to classify the transcribed text into SOAP categories.
1.3 Research Scope
The main scope of this thesis is limited to research problems within the individual layers
of our approached solution pipeline. The feasibility and end-to-end performance of our
solution pipeline are not examined in this work.
Clinical reports are of various types since documentation is done in almost every healthcare
activity. The scope of this thesis is also limited to the pediatric emergency department that
usually generates reports in SOAP (Subjective, Objective, Assessment, and Plan) format;
therefore, this thesis follows the SOAP structure.
In the area of speech recognition, this work considers the single-channel audio input. For
SR systems, the scope of this thesis is limited to open-sourced systems in the offline
domain.
1.4 Thesis Contribution
This thesis spans over two domains of computer science; thus, it contributes to both
domains. This thesis reports five contributions that are listed below.

4
1. This work approaches the process of clinical documentation from an end-to-end
perspective. To the best of our knowledge, this perspective has never approached
before. This thesis seeks freestyle dictations as input and proceeds to generate a
formatted clinical report as output. The operating scope of this solution currently
experiments only within emergency departments following SOAP structure.
Nevertheless, this solution has the potential to expand in other clinical departments and
domains as well.
2. In this work, we demonstrate the use of Project DeepSpeech [7] in the paradigm of the
healthcare domain.
3. We apply methods to adapt out-of-domain pre-trained DeepSpeech models and train
healthcare domain-specific models without requiring a large healthcare dataset.
4. We propose a method to augment the healthcare domain-specific dataset by generating
simulated domain-relevant data using principles of synonym replacement method.
5. Lastly, this thesis contributes by extending an exemplar-based concept detection
algorithm to develop a sentence classifier to classify SOAP categories.
1.5 Thesis Organization
This thesis consists of 7 chapters. Chapter 2 provides background details about the
individual concepts that are frequently referred to in this thesis. Chapter 3 presents the
methodology of this research and all the tools that are used for this research. Chapters 4, 5,
and 6 demonstrate the work that is done for each layer of our solution model. Lastly,
Chapter 7 constructs a thorough discussion upon the observations, limitations and future
work while providing a conclusion to the thesis.

5
Chapter 2. BACKGROUND AND RELATED WORK
2.1 Health Record
A patient’s health record entails chronologically sequenced assortment of a variety of
clinical documents, such as clinical reports, lab reports and x-rays, that are generated over
time by healthcare professionals providing care services to that patient. These records
present medical history and events of care given within the healthcare providers’
institution. The term health record is often used conversely with the medical record or
medical chart.
2.1.1 Electronic Health Record (EHR)
Electronic Health Record (EHR) are software systems that manage patients’ health records
electronically. Like health records and medical records, EHR also often gets interchanged
with Electronic Medical Record (EMR). However, there exists a subtle difference between
both terms. EMR has limited working jurisdiction and can only operate in one provider’s
institutional domain, while EHR’s are designed to serve across multiple institutions i.e.,
available to multiple providers as well as researchers and policymakers [8], [9].
2.2 Clinical Report
A clinical report is a type of clinical document that appends into a patient’s health record.
Clinical reports include details of a patient's clinical status and assessments, recorded by
healthcare providers during the hospitalization visit or in outpatient care [10]. Clinical
reports facilitate communication between healthcare providers [11]. These reports can be
of various types, such as progress reports, visit reports and discharge summaries [12].
Clinical reports can be unstructured, semi-structured, or systematically structured [13].
Unstructured and semi-structured reports include information in free texts, which blends
relevant and vital information with insignificant details and make retrieval of required
information difficult, oftentimes along with adversely increased cognitive load [14].
However, structured reports follow some systematic guidelines to structure the

6
information; thus, important information comes under observation quickly without putting
much effort. In this thesis, we work with systematic reports that follow a defined structure.
2.2.1 SOAP
SOAP is a universally accepted method that provides systematic guidelines to write
structured clinical reports [13], [15]. SOAP is the acronym for Subjective, Objective,
Assessment, and Plan which represents the categories within its structure. SOAP was first
theorized over 50 years ago [16] to advise medical students in writing effective reports
[17], which later accepted widely among healthcare professionals [16]. Table 2.1 mentions
a summary of SOAP guidelines as listed by Sando [13]. There are various benefits that
SOAP formatted reports offer above unstructured or semi-structured reports.
1. SOAP reports follow a defined structure. It lowers mental efforts to extract the required
information efficiently and quickly [14].
2. SOAP reports are clear, concise, accurate, and allows efficient communications
between healthcare providers. Due to this, providers explicitly use these reports to give
recommendations to each other [10], [17].
3. SOAP encourages providers to write complete reports by reminding them about
specific tasks. This way, SOAP ensures complete reports and enhances the quality of
healthcare delivery [16].
4. SOAP reports systematically record encounters of healthcare professionals and
patients. Hence, it can also serve as an evaluation tool for accountability, billing, and
legal documentation [1], [2], [18].
5. When care delivery requires multiple healthcare providers, effectively written SOAP
reports can fasten the delivery process by eliminating the need for redundant history
taking episodes for each provider [18].

7
Table 2.1 Documentation Guidelines of SOAP categories adapted from [13]
Category Documentation Guidelines (Semantic concepts for each category)
Subjective
• Demographics
• Patient concerns and complaints
• Current health problems
• Current medications
• Current allergies
• Past medical history
• Family history
• Social history
Objective
• Drugs administered
• Physical signs and symptoms
• Vital signs
• Medication lists
• Laboratory data
Assessment
• Active problem list with an assessment of each problem
• Actual and potential problems that warrant surveillance
• Therapeutic appropriateness including route and method of
administration
• Goals of therapy for each problem.
• Degree of control for each disease stated
Plan
• Adjustments made to drug dosage, frequency, form or route of
administration
• Patient education and counseling provided
• Oral and written consultations to other health care providers
• Follow-up Plan
• Monitoring parameters

8
On the one hand, SOAP is appraised for its easy to use guidelines. On the other hand, some
studies highlight some limitations as well. Lin [19] questions if swapping the structure of
SOAP to APSO increases any efficiency. Moreover, many studies propose extended
versions of SOAP. However, all those studies, perhaps only add more guidelines above the
basic ones. In this thesis, we focus on the categories of SOAP but not their sequence;
therefore, our produced reports can be sequenced in any order to satisfy any structural
variation of SOAP. Each SOAP category is further explained in later subsections.
• SUBJECTIVE
The subjective category suggests documenting everything that is coming from the
patient’s perspective and experiences [16]. It distinguishes between what a patient is
thinking about the situation from what healthcare providers believe.
• OBJECTIVE
In the Objective category, providers are guided to include all the observations,
examination findings, and diagnostic tests; specifically, those findings that the provider
can objectively confirm. Providing objective measures in a separate category allows
readers to immediately focus on the relevant and clinically verifiable information
without ever needing to know more about the subjective details [18].
• ASSESSMENT
In the Assessment category, providers explicitly mention the diagnosis along with the
rationale that leads to the diagnosis. It might also include all those tradeoffs that were
considered while reaching to the said diagnosis [16].
• PLAN
The plan category is there to document any treatment plans or directions that the
provider might have for the patient or any other provider. This section is also used to
write down secondary treatment plans that will get into consideration if the primary
plan does not show appropriate results [16].

9
2.3 Clinical Documentation
Clinical Documentation (CD) is the process where healthcare providers generate clinical
reports after every patient encounter. These encounters can be of any purpose and of any
length. Even the minor patient-physician interactions must be noted accurately and timely
with the same level of responsibility that is usually taken to prepare reports of surgeries
and other lifesaving treatments. Clinical documentation is a fundamental skill [13] and is
the core responsibility of healthcare providers to generate clinical reports that are accurate
and complete. The process of clinical documentation has multiple aspects of details that
are defined in later subsections.
2.3.1 Challenges
The goal of the clinical documentation process is to generate high-quality and practical
clinical reports to ensure efficient and effective healthcare delivery; however, achieving
this goal is a challenging task. Primarily, the process of clinical documentation poses 5
main challenges.
• ACCURACY
The first challenge of clinical documentation is to produce accurate clinical reports. It
means that all the contents within a report must reflect the truth, and nothing that is in
the report is wrong.
• COMPLETENESS
Completeness is the second challenge, which refers that reports must cover all the
aspects of the patient-provider encounter, and no detail goes unnoticed.
• TURNAROUND TIME
Turnaround time is the time that providers take to perform documentation related tasks
after finishing one encounter and before starting another encounter. The third challenge
of this process is to keep turnaround times as low as possible.

10
• PROVIDER THROUGHPUT
Throughput reflects the efficiency level of a provider. Documentation related tasks can
sometimes take more time and effort than the encounter itself and can overburden the
providers, which can lower the quality of healthcare delivery. Therefore, the fourth
challenge of the clinical documentation process is to keep provider throughput as high
as possible.
• COST
The fifth challenge is to reduce the overall cost. There are two types of costs that are
linked with this challenge; setup cost and report generation cost. Setup cost can be
defined as the cost it takes to set up any tools that assist with the process, while
generation cost can be defined as the cost it takes to generate each report.
2.3.2 Modes
Clinical documentation is usually done in three modes: hand-written, type-written, or
voice-dictated. Institutions adopt one of these ways, whereas many of them use multiple
modes to create redundancy in the documentation. This section will define each mode in
detail.
• HAND-WRITTEN
Classically, clinical reports are produced by hand on a piece of paper. It is the simplest
of all modes, and it consists of a plethora of problems around it. Reports prepared by
hand are illegible to read and are often never consulted again by providers. Moreover,
producing reports in this way takes much time. Handwritten reports are also prone to
damage as they exist in physical format, and making a copy is also a hassle.
• TYPE-WRITTEN
Adaption of EHR changes the way clinicians did documentation tasks. EHR’s require
the digital entry of information within reports. Healthcare providers use the keyboard
and mouse to type-write the reports directly into the software systems of EHR. It
reduces the clutter of illegible paper-based reports and makes comprehension easier.

11
However, healthcare providers are now forced to learn using these new systems.
Without learning, there is still low or no impact on documentation times. A study has
shown that even with EHR, healthcare providers still spend 38.5% of their time in
creating documentation [4].
• VOICE-DICTATED
Voice dictations are not new for healthcare providers. In many institutions’ providers
are facilitated with dedicated transcriptionists who oversee all the documentation
related tasks. Healthcare providers brief transcriptionists about the clinical encounter
by giving them dictations, who then complete the reports. This practice shifts the
burden of documentation away from providers, who are busy with other crucial tasks.
In institutions where no transcriptionist is available, the practice of dictation still
benefits providers. They record dictations after encounters and manage their time on
more important things when needed. At the end of all encounters or later, when they
get time, they then complete the documentation tasks by using pre-recorded dictations.
A number of newer EHR systems are also now providing voice-enabled options to enter
information within reports. These EHR systems use speech recognition technology and
allow providers to use their voice to enter information within individual sections of
clinical reports. An increasing number of institutions are now implementing voice-
enabled EHR systems to facilitate providers; nevertheless, provider adaption of this
documentation mode is still a concerning question.
2.3.3 Workflows
Documentation is usually done in two workflows: front-end and back-end. Both workflows
start when the provider is finished dealing with patients in an encounter and ends when a
report is generated and submitted. Details about both workflows are defined below.

12
• FRONT-END
In the front-end workflow, the provider is responsible for the proper generation and
submission of clinical reports right after the encounter, and before starting any other
encounter.
• BACK-END
In the back-end workflow, the provider has the liberty to delay the report generation
process to the time of their choosing before a deadline that is set by the institution or
any other regulatory body. In this work-flow, the provider can perform encounters back
to back to finish patient queues and can then generate all the clinical reports at once.
2.3.4 Problems
To meet all five challenges of clinical documentation is a challenge in itself.
Documentation modes and workflows usually focus on a subset of these challenges.
Institutions often practice those modes and workflows that are closer to their requirements.
In essence, there is nothing at this moment that can offer to meet all five challenges at the
same time. Therefore, the current practices of the documentation process fail to meet some
challenges and express various problems. There are five major problems. Some of these
problems are caused by specific workflow or mode, while others are due to the overall
process. The problems are defined below.
• LOW QUALITY OF CLINICAL REPORTS
A major problem in the clinical documentation process is the low quality of clinical
reports, which is primarily caused within those institutions that overlook accuracy and
completeness in favor of low turnaround times, high throughput, and low costs.
• HIGH TIME CONSUMPTION
Writing a clinical report takes time. In the case of dictated notes, physicians get the
ability to postpone the development of reports to increase throughput, while also
increasing report turnaround times. With current workflows and modes, this poses a
major problem.

13
• LOSS OF MINOR CLINICAL ENCOUNTERS
Due to the tedious nature of the process, minor encounters are usually ignored, which
in turn poses a high risk of lower quality in healthcare delivery.
• HIGH COST
Many institutions employ dedicated transcriptionists and implement advanced EHR
systems to facilitate providers with the burden of the documentation process. Both
options are costly and require extensive funds.
• LACK OF OPPORTUNITY TO DEVELOP DATASETS FOR RESEARCH
This problem mainly arises due to illegible hand-written reports on paper forms, as
patient records become cluttered, and managing them is a hassle [14]. This problem is
also present in type-written reports to some extent. Physicians get this habit to copy
and paste, and incompleteness is rather common in these reports [20].
2.3.5 Summary
Clinical documentation is the backbone of quality healthcare; however, it often takes more
time than treating patients. There are five main challenges of clinical documentation:
accuracy, completeness, turnaround time, provider throughput, and cost. Each institution
sets policies that focus on a subset of these challenges and practice a workflow and
documentation mode that comply with their policies. There are two commonly practiced
workflows: front-end and back-end; and three documentation modes: hand-written, type-
written and voice-dictated. Currently, no combination of documentation mode and
workflow offers to meet all challenges; therefore, the documentation practices raise a
number of problems. The five major problems of the clinical documentation process are 1)
low quality of reports, 2) high time consumption, 3) loss of minor clinical encounters, 4)
high cost, and 5) lack of opportunity to develop datasets for research.

14
2.4 Speech Recognition
This section provides a background on the fundamental concepts of Speech Recognition
(SR). Speech recognition refers to any machine-based method that functions over speech
input and processes it into text. SR research is generally categorized into three areas:
isolated word recognition, continuous speech recognition, and speech understanding [21].
Isolated word recognition methods are applied to those speech inputs in which speaker
utter individual words, separately. However, continuous speech recognition methods are
used when speech is continuous and in a natural manner. Speech Understanding, whereas,
is used when we are more interested in understanding the sense of speech instead of specific
words. In this thesis, we explore methods from continuous speech recognition, as we work
with natural and continuous speech.
Speech is recorded in the form of audio signals. These signals are defined as the long arrays
of timed sound intensity values. These values represent the acoustic features of the speech
in the form of phonemes that are the basic sound units within a language. Phonemes, when
combined, form the basis for words and other lexicons within the speech. For efficient
recognition, SR requires a prior understanding of such acoustic behaviors, along with the
knowledge of grammatical and other rules that exists within the language. This information
is provided to SR methods using acoustic and language models that are trained on the
speech data from a language. These models are the core components within any SR system.
Firstly, acoustic features from input audio are matched with the given acoustic model to
identify language units (phonemes) which then produce an estimated sequence of words
using the rules from the language model. The robustness of these models is vital in the
performance of Recognition. Figure 2.1 illustrates the structure of any SR system in its
simplest form.

15
Figure 2.1 Structure of any SR system in its simplest form
When a speech input is given, the objective of SR is to obtain the optimal word sequence
for the given speech (𝑿), which is a form of well-known maximum a posteriori (MAP)
problem [22].
Equation 1
�̂� = arg 𝑚𝑎𝑥𝑾 𝑃Λ,Γ(𝑾|𝑿)
In Equation 1, optimal word sequence �̂� is a word sequence 𝑾 that maximizes the
likelihood for the given speech signal 𝑿 by the use of an acoustic model 𝚲 and language
model 𝚪. Both models are the components inside the construction of SR systems that are
further explained in subsequent sections.
2.4.1 Acoustic Model
The acoustic model forms the basis of any SR system [23]. The purpose of the acoustic
model is to provide estimations that a particular phoneme is uttered in a given audio
sequence. Acoustic models are either a statistical or machine learning model that maps the

16
relationship between audio signals and linguistic units. These models are trained upon
hours of speech data to generalize linguistic relationships effectively.
Audio signals are digitally recorded sound waves, which are made up of sequential
samples. The sample rate of an audio file denotes the number of samples recorded in one
second. The resolution of a sample refers to the amount of memory (bits) that is used to
record each sample. For example, a 10-second audio file of sample rate 16000 Hz and
resolution of 16 bits means that it contains a total of 160,000 samples that are recorded in
16 bits each, which translates into a raw size of 312 kilobytes (160,000 x 16 bits) of
memory. Audio signals are long arrays; therefore, these signals are segmented into equal
intervals, called frames, for processing and model construction. Frames are small but
overlapping windows within audio files. Frame size remains fixed throughout the SR
system. As an example, for a 16000 Hz audio signal, if we choose a frame of length 256
samples, then the first frame covers from 0th sample to 255th sample, and then the second
frame starts from 128th sample and so on.
SR systems extract various types of features from frames. The commonly used features are
power spectrum, Mel-frequency cepstral coefficients, and delta features. In continuous
speech recognition systems, features within the frames of training audio files base the
construction of acoustic models. To perform recognition, a query audio file is extracted for
frames, and its features match the acoustic model to get the estimated sequence of linguistic
units.
SR systems from their inception are using statistical acoustic models. These systems use
the Gaussian Mixture Models (GMM) and Hidden Markov Models (HMMs) to recognize
the sequences of phonemes. GMMs detects the phonemes within each frame, and HMMs
estimates the likelihood of having detected phonemes given the prior detected sequence.
Statistical acoustic models then use estimation maximization algorithms to get the optimal
phoneme sequence out of audio signals.

17
The current advancements in machine learning have enabled researchers to develop end-
to-end acoustic models that eliminate the need to use domain expertise as it is required to
train the statistical models. End-to-end models take benefit of powerful machine learning
techniques, such as Artificial Neural Networks (ANN) and Deep Neural Networks (DNN),
to develop acoustic models. These models work on the same inputs, i.e., acoustic features
of audio signals; however, a number of current approaches produce direct word sequences,
as opposed to traditional models that produce phonemes. In such cases, characters are used
as the output sequences.
Since the ultimate goal of SR is to get the optimal word sequence, SR systems take the
output of the acoustic model, either statistical model outputting phoneme sequence or
machine learning model outputting character sequence, and pass it through decoders to
achieve the optimal word sequence. In the decoding part, output sequences are searched in
lexicon dictionaries for matching words. In this step, most SR systems also exploit
language models to refine the output of acoustic models. The details about language models
are in the next subsection.
2.4.2 Language Model
The language model maps the relationship between the words from a given language. In
speech recognition, it provides the contextual information of words by assigning a
probability distribution over the trained word sequences [24]. It is usually trained on large
samples of text from a language. Language models facilitate SR systems to detect
connections between the words in a sentence with the help of a pronunciation dictionary
[23]. Language models also introduce domain-specific vocabulary to the SR paradigm. It
refines the output of SR systems. However, it is not always required for the recognition
task. When language models are used in SR systems, their calculated likelihood
probabilities are merged with the decoded word sequence probabilities from acoustic
models, and then the combined probabilities are used to get the optimal word sequence.
The most common method to construct language models is n-gram language modeling,
where n is the order of language model. An nth order language model calculates the counts

18
for having 1-grams, 2-grams … n-grams from a training corpus. These n-grams occurrence
counts are used to calculate the likelihood of having a word W based on the given sequence
of n-1 preceding words [23].
Equation 2
𝑃(𝑊) = 𝑃(𝑊𝑛|𝑊1, 𝑊2, 𝑊3 … 𝑊𝑛−1) =𝐶(𝑊1, 𝑊2, 𝑊3 … 𝑊𝑛)
𝐶(𝑊1, 𝑊2 … 𝑊𝑛−1)
In Equation 2, 𝑃(𝑊𝑛|𝑊1, 𝑊2, 𝑊3 … 𝑊𝑛−1) denotes the probability of having a word 𝑊𝑛
when given a sequence 𝑊1, 𝑊2, 𝑊3 … 𝑊𝑛−1. 𝐶(𝑊1, 𝑊2, 𝑊3 … 𝑊𝑛) shows the count of
having n-gram within the corpus. 𝐶(𝑊1, 𝑊2, 𝑊3 … 𝑊𝑛−1) shows the count of having (n-1)-
gram.
When dealing with probabilities, n-gram based language models are prone to problems
such as zero probability problem and out of vocabulary problem. The zero probability
problem is due to the unavailability of an n-gram within the training corpus. For these
unseen situations, language modeling techniques offer solutions such as smoothing and
discounting. In smoothing techniques, n-gram counts are manipulated to give weights to
unseen events. Add-one smoothing and add-k smoothing are some examples of smoothing
techniques. In discounting techniques, if an n-gram is unseen, then the counts from (n-1)-
gram are considered with some discounts. This strategy is also known as backing off.
The out of vocabulary problem arises when a language model does not have a word in its
vocabulary. That means not even 1-gram is available for that word. Therefore, solutions to
zero probability problems do not work here. A common strategy to tackle the out of
vocabulary problem is to use pseudowords such as unknown <UNK>, start <S> and stop
</S>. The pseudoword <UNK> is appended with all seen n-1 grams to form a new n-gram,
whereas, the pseudowords <S> and </S> are appended in the start and end of each sentence.
They are then treated as normal words while calculating probabilities and training n-gram
language models.

19
2.4.3 Evaluation Metric
SR systems are evaluated by investigating differences between their output text and ground
truth text. If the SR system works according to expectation, then output text match the
ground truth. However, if there are differences, it highlights the system’s shortcomings and
provides an evaluation of the system. The most commonly adopted evaluation metric for
SR is the Word Error Rate (WER) [25].
• WORD ERROR RATE
Word Error Rate (WER) is an evaluation metric that highlights the ratio of mistakes.
WER returns a value between 0 and 1, where 0 means that the SR system was not able
to recognize a single word correctly, and 1 means that everything was recognized
perfectly. Mistakes are counted in the form of insertions, deletions, and substitutions.
When comparing output text with ground truth, if a word is missing, then it is inserted,
and insertions count is incremented. If a word is in the output sequence and ground
truth does not expect to have it, then it is deleted, and deletions count is incremented.
If for a word found in output sequence ground truth expects a different word, then it is
substituted, and substitutions count is incremented. After finishing comparisons, WER
counts all mistakes and divides them by word count of ground truth to get the error rate.
WER is commonly expressed as a percentage [25], which can be done by multiplying
WER by 100.
𝑊𝐸𝑅 =𝐼 + 𝐷 + 𝑆
𝑊
∴ 𝐼 = # 𝑜𝑓 𝐼𝑛𝑠𝑒𝑟𝑡𝑖𝑜𝑛𝑠
∴ 𝐷 = # 𝑜𝑓 𝐷𝑒𝑙𝑒𝑡𝑖𝑜𝑛𝑠
∴ 𝑆 = # 𝑜𝑓 𝑆𝑢𝑏𝑠𝑡𝑖𝑡𝑢𝑡𝑖𝑜𝑛𝑠
∴ 𝑊 = # 𝑜𝑓 𝑤𝑜𝑟𝑑𝑠 𝑖𝑛 𝐺𝑟𝑜𝑢𝑛𝑑 𝑇𝑟𝑢𝑡ℎ

20
2.5 Speech Recognition in Clinical Documentation
To overcome the challenges of clinical documentation, researchers are looking towards SR
technology since the time of its inception [22]. In theory, the idea of using speech to create
clinical documentation is quite promising. However, multi-factored evaluations show that
it is not as simple to adapt. Changing modes of report generation workflows can open a
plethora of issues that may come with the new mode of input. The introduction of EHR
reformed the process of clinical documentation when it offered typing as the form of input;
however, this input method added up to the already existing issues [26]. With EHR,
providers spend roughly double their time in creating documents as compared to care
delivery [4]. Many healthcare providers are not very good at operating computer systems,
so they still prefer the classical methods of documentation. Since EHR offers much more
than the change of input mode, and it is not possible to use handwriting as the method to
input notes within EHR, many studies have tried to use SR technology as an alternative to
enter notes within EHR. When compared to traditional dictation and transcription methods,
speech assisted EHR significantly reduces turnaround times and costs [27]. Consequently,
as SR technology is improving, the increasing number of institutions are adopting SR
enabled systems to generate clinical reports [27]. However, speech assisted EHR puts the
responsibility of the management of note input and report creation upon healthcare
providers, which limits the provider adoption of this technology. Therefore, in this section,
we investigate the various aspect of SR adoption in documentation workflows and analyze
the limitations and shortcomings of SR in the clinical documentation process.
2.5.1 Review Objective
The purpose of this review is to investigate prior efforts of using SR to overcome the
challenges and problems of documentation. Therefore, we form three main objectives.
1) To explore previous attempts on using speech as a tool for clinical documentation.
2) To scrutinize the methodology and evaluations of explored attempts.
3) To identify all the factors that limit the intended outcomes of explored attempts.

21
2.5.2 Literature Exploration
This thesis deals with a problem in the medical domain; therefore, we primarily used
PubMed [28] as the source to look for literature. We identified a set of keywords that were
combined using ‘AND’ and ‘OR’ operators to retrieve the best matching articles. Figure
2.2 shows the query tree that was used to search PubMed to retrieve the relevant studies.
Figure 2.2 Query Tree for Literature search
2.5.3 Analysis
Healthcare providers use dictations in traditional documentation workflows. However,
they are now required to use an EHR for report generation. Speech-enabled EHRs
contribute more to the challenges of the documentation process. Therefore, in this analysis,
we iterate and analyze the impact of SR on the challenges of the clinical documentation
process.
• ACCURACY AND COMPLETENESS
Accuracy and completeness reflect the overall quality of the report; therefore, studies
usually address these two challenges together. When providers type-write their reports
on EHR, they usually make 0.4 mistakes for every 100 words (0.4% error rate) in back-
end workflow [29]. Zhou conducted a study to test SR on the same workflow, where
he noted an increment of errors by 7.8% [29]. However, he added that reports managed
to achieve the same level of quality after a final review from the provider.
Studies by Hodgson and Goss address the use of SR in front-end workflow. They show
similar results to Zhou, where the report quality significantly declined [27], [30].

22
Although, in a study where experiments were conducted in an ideal environment, with
no real-life constraints and stress, 81% of providers reported improvement in the
overall quality of reports with the use of SR enabled tools [26].
• TURNAROUND TIME AND PROVIDER THROUGHPUT
Providers spend most of their time to generate reports [29]; this means, an efficient
documentation process can reduce turnaround times and boost provider throughput.
Studies report that most of the providers are convinced that SR improves efficiency and
is easy to use [26], [27]. In back-end workflows, SR has shown to reduce turnaround
times and increase productivity [29]. However, when SR is used in front-end
workflows, no significant time difference was reported [30].
• COST
In the clinical documentation process, the cost is the aspect that is the least studied in
the academic domain. One reason could be that costs are primarily a concern of
departments that are not connected with academics. In any case, the cost is a profound
variable in the adoption of any solution, and also plays a vital role in the adoption of
SR in the clinical documentation process. These days, more and more institutions are
tilting towards the adoption of SR enabled solutions since they are thought to reduce
costs [27]. A provider adoption survey done in 2018 has also concluded that SR enabled
systems can reduce monthly transcription costs by 81% [26]. Since we were not able
to find any study that reports any adverse findings in terms of the cost of using SR
enabled systems, there is no reason to disbelieve the above-stated opinions.
2.5.4 Findings
The approach to use SR for documentation is not new. Studies from 1981 [31] and 1987
[32] experimented with SR when this technology was developing as a new concept, where
they found SR to be worsening the problem. SR technology improved a lot since then. This
trend is reflected in the studies done throughout the decade of 1990 [33]–[39]. This trend
remains in the decade of the 2000s [40]–[43]. A study done in 2010 [44] reported that about
two-thirds of their participants feel that SR can improve report quality and can reduce

23
documentation times as well. Another study that was done in 2012 [45] supports the claim
that SR now has the ability to reduce documentation times. Almost all of the recent studies
[27], [46]–[49] affirms that SR has the tendency to overcome problems of documentation.
However, with all the optimism, SR enabled solutions still lack adaption among healthcare
providers [26], [50]. Studies document four main reasons behind the low adoption of SR
enabled solutions.
• HIGH EXPECTATIONS FROM SR ENABLED SYSTEMS.
SR systems are viewed as they can dramatically reduce mistakes and documentation
times. However, current SR technology still struggles to maintain high accuracy due to
real-world issues, such as noise and domain-specific vocabularies. Therefore, noise-
robustness and domain-robustness are real challenges of SR that limit the confidence
of healthcare providers in SR at this point.
• RESPONSIBILITY FOR CORRECTIONS.
SR systems make mistakes, and physicians are responsible for correcting those
mistakes. Due to this, sometimes they spend even more time in corrections. When any
machine-based system makes a mistake, humans are expected to correct for those
mistakes; however, in this scenario, the overall confidence in SR technology can be
increased by making robust systems that do not make mistakes in the first place. The
same challenges apply here as well that are mentioned in the above-stated point.
• CHANGE IN DICTATION STYLE.
SR is merely a tool for note entry in many reporting systems. Physicians are responsible
for controlling the structure of reports where they have to manually select the report
section for which they wish to add the notes. As an example, for the SOAP structured
reports, physicians have to select one of the SOAP categories to enter its content at one
time. This practice breaks their dictation pace as they have to tailor their dictation style
according to the structure of the report. Due to this hassle, physicians prefer recording
conventional dictations where they get the ability to record in freestyle at the time of
encounter. This hassle also calls for autonomous features that are specialized for

24
documentation tasks, and can intelligently separate the content for different sections of
a clinical report from a freestyle recorded dictation.
• PHYSICIANS’ TRAINING
Physicians require training to use SR enabled systems efficiently [51]. A 2010 study
[44] reported positive response when participants got adequate training, whereas, when
they were not satisfied with the training, they reviewed SR enabled systems negatively.
Such training includes teaching physicians to enable SR features within the system and
other reporting features that are linked to SR.

25
2.6 Handling Noise in Speech Recognition
SR is an area of interest with more than three decades of active research [22]. In ideal
environments where noise and distortions do not interfere with speech signals, the latest
developments have enabled SR systems to perform increasingly closer to human speech
recognition performance [52]–[54].
Noise is referred to as any phonetic element in the audio signal that is other than the speech
signal [55]. In real-life environments that are filled with a huge concentration of noise, SR
systems lack that robustness to compete with humans [56]–[58]. This degradation is mainly
due to the difference in the acoustic features from input audio to the ones in the trained
model [59]. Noise from surroundings changes the acoustic features of speech with
unwanted additives from noise. Traditionally, SR-enabled devices used to create an ideal
environment using close-talking microphones and other acoustic adjustments. However,
with the rise in large-scale hand-held mobile devices, it is not further possible to provide
SR with ideal speech inputs. It is inevitable for SR to work in challenging acoustic
environments and noise robustness is now a key challenge for SR to maintain its
performance levels [60].
Noise robustness is a trending problem in the SR domain. Colossal amounts of methods
and techniques have been proposed to provide noise-robust solutions for SR. A number of
systematic reviews of noise-robust speech recognition [22], [23], [61] have presented the
current advancements in systematic manners. In this review, we explain and analyze
techniques about the development of noise-robust systems for domain-specific
environments. We are particularly interested in indoor environments where there are
reverberant distortions and speech overlaps; nevertheless, this review is not limited to such
environments. However, we only review those techniques that deal with single-channel
audio signals.
Noise-robustness techniques can be divided into two main groups: feature-space and
model-space [22]. Feature-space techniques consider the preprocessing of audio signals to
extract clean speech before passing it to SR components. Model-space techniques, on the

26
other hand, deal with the internal construction of noise-robust components. The subsequent
sections explain both groups further and provide an analysis of techniques within each
group.
2.6.1 Feature-space Techniques
SR works well with clean speech. A straightforward and classic solution is to process the
incoming audio to extract clean speech before passing it to the SR system. Feature-space
techniques apply this classic solution by using signal processing techniques to enhance the
acoustic features of speech. These techniques do not change the acoustic model or any
component within SR systems.
Enhancing acoustic features from noisy audio is a difficult problem in single-channel as
compared to multi-channel audio spectrum [62], where techniques, such as acoustic beam-
forming, are performing close to human transcription performance [63]. However, we do
not see such accuracies while using single-channel audio.
Spectral Subtraction [64] and Weiner filtering [65] are classical techniques to filter noise
from the audio signals. These methods do not depend upon training [22]; instead, they use
statistical tools that estimate the noisy speech spectrum and remove any intensity
distribution over that estimated spectrum. These techniques are acceptable when noise is
stationary throughout the span, such as noise from wind, fan, or anything that emits a
continuous stream of sound. However, their performance degrades with the interaction of
varying or convolutional noises such as reverberation and overlapped speeches.
Without prior knowledge of noise or speech patterns, statistical models sometimes over
filter the speech signals, consequently clipping and losing acoustic details [66]. There are
various learning-based techniques to tackle the problems of reverberation and speech
overlap such as Weighted Prediction Error (WPE) using Short-Time Fourier Transform
(STFT) domain [67], de-noising auto-encoder [68] and a statistical-neural hybrid Cepstra
Minimum Mean Squared Error–Deep Neural Network (CMMSE–DNN) based learning
model [69]. However, these techniques shift away from the area of speech recognition

27
while belonging more to the area of signal processing, which is not the working domain of
this thesis.
2.6.2 Model-space Techniques
Model-space techniques aim to develop noise-robust SR components, particularly acoustic
models. These techniques are linked directly with the objective function of acoustic
modeling to absorb the effects of noise and distortion [22]. These techniques have generally
shown to achieve higher accuracies in comparison to feature-space techniques. However,
in comparison, they use significantly more computational resources.
Noise adaptive training [70] and noise aware training [61] are the candidates of the model-
space techniques. In noise adaptive training, acoustic features infused with the noise are
relayed directly into the acoustic models, whereas in noise aware training, an estimated
noise model is generated to calculate corruption in the training noise [61] which then acts
as the mask to filter noise from testing audio. Noise Adaptive techniques are reporting
high-performance gains [71]–[73]. Acoustic models trained using ANN-based noise
adaptive framework were introduced to the same levels of noise that are expected in the
execution life of SR systems, where they have shown performance boosts as high as 20%
[74]. Seltzer [61] shows the use of DNN for noise aware training with a relative
performance boost of 7.5%. Noise based acoustic training works well on the single-
channeled audios and incorporates most of the effects of additive noise. However, models
trained using these techniques are not generalizable [68] to use on environments with
different noise signatures then of where the models were trained.
The development of current end-to-end SR systems has defined a new state-of-the-art [75]–
[78]. These systems are built on the underlined principles of model-space techniques with
the goal to tackle the problem of the noise of real environments. These systems train their
acoustic models in a data-driven way without relying on any expert domain knowledge
[79] such as noise estimates and phonetic dictionaries. Their end-to-end nature allows them
to directly train their model based on paired data, where training audio and its

28
corresponding text is paired. However, to achieve higher accuracies, they require vast
amounts of training data.
2.6.3 Summary
The problem of noise-robustness in SR is addressed using two types of approaches. The
first approach presents techniques that seek treatment to noisy audio before feeding it to
SR systems. These techniques span over unsupervised as well as supervised learning.
However, they shift the problem to the signal processing domain, where the good signal is
enhanced, and undesired signals are suppressed. Variations of such problems are de-
noising and noise removal. The second approach seeks the construction of robust SR
components, particularly the acoustic model. It shows that noise adaptive training is
currently the top-performing technique on which various end-to-end SR systems are
constructed. The review has also mentioned that end-to-end systems are setting the current
state-of-the-art in the technology of SR.

29
2.7 Domain-Specific Speech Recognition
In speech recognition, domain entails the combination of the acoustic domain as well as
the language domain. The acoustic domain includes speakers, audio channels, and
environmental noise. The current state of the art end-to-end SR systems have covered many
grounds of robustness over acoustic domains, though domain robustness is still a
challenging problem [80]. The problem primarily remains due to the domain-specific
language which includes specific words and their relations. Handling the rules of language
is the integral responsibility of the language model within SR systems. However, this
problem broadens when there is a shortage of domain-specific data and language modeling
techniques struggle in training robust language models. Therefore, in this review, we
analyze two major techniques that deal with the development of domain-specific language
models when domain-relevant data are scarce.
2.7.1 Out-of-Domain Model Adaptation
Model adaptation refers to the use of language models that are trained on one language
domain to a different target domain where there is little or no training data available.
Various scenarios are linked to model adaptation that we review one by one. A typical
scenario is that when the available language model is from the general-purpose domain
that seeks adaptation in a specific target domain. In such cases, a direct adaptation of the
out-of-domain language model can give domain agnostic behaviors; therefore, it is better
in such cases to perform some fine-tuning operations. Another scenario is when the source
language model is coming from a domain-specific environment that is different from the
domain of the target environment. Lyer [81] experimented with multiple out-of-domain
models that were combined to form a single model that improved performance on a general
task. You [80] show a 10.4% relative improvement in performance by using an all-rounder
approach where multiple domain-specific models were used to train a single language
model to apply on a general-purpose target.
Adapted models are combined with domain-specific models by either pooling or
interpolation [82]. The pooling technique deals with the creation of one dataset from

30
multiple sources, and then use that dataset to create one combined model [83], whereas, in
interpolation, multiple datasets train multiple language models which are then combined
using interpolation weights.
2.7.2 Domain Relevant Data Generation
Language models work well when there is sufficient domain-specific training data
available. Domain relevant data generation techniques seek various strategies to produce
such domain-specific training data when there is a scarcity problem. There are three main
types of strategies for data generation: conversion, extraction, and augmentation.
Data conversion strategies seek such data sources that exhibit domain-relevant data in
different format or language, then apply techniques to convert such data into the desired
format or language. As an example of data conversion, Horia [84] proposes a technique
that exploits the use of machine translation to convert domain-relevant data that exhibits in
a different language into the language of the target domain.
Data extraction strategies are similar to conversion as it explores domain-relevant data on
other platforms, and instead of conversion, it focuses on the extraction of such data from
the source platform to the target platform. Abhinav [85] has shown relative progress of 6%
by the use of a data extraction technique to extract domain-relevant data from the web and
train language models from extracted data.
Data augmentation strategies offer a different way to generate domain-relevant data. It
focuses on the augmentation of available information within existing data to generate new
data points. Enhancing language models by augmenting domain-specific vocabulary and
synonyms have shown a decrement of absolute recognition error by 5.41% in noisy
environments of tennis championship while having all variety of noises like emotional
outbursts, game noise, crowd noise [86]. Another study shows considerable progress by
using models that were created by web extracted and augmented data using pooling [83].

31
2.7.3 Summary
Domain robustness is a challenge in speech recognition, which is due to the combination
of acoustic and language domains. Approaches of noise-robustness, particularly from end-
to-end SR systems, considerably address the challenges from the acoustic domain.
However, language models still need to be taken care of for robustness. We review two
main techniques that deal with the robustness of language models. The first technique seeks
adaptation of models from different domains to perform tasks on the target domain. These
techniques complement the adaptation process with domain-specific fine-tuning and model
enhancements to achieve higher performance. The second technique focuses on the
generation of domain-relevant data for language models. This technique exploits various
strategies such as data conversion, extraction, and augmentation to artificially generate
domain-relevant data that can then be used to generate domain-specific language models.

32
2.8 Speech Recognition Systems
This section provides an overview of multiple SR systems and toolkits. In this review, we
have a special focus on the state-of-the-art end-to-end open-source offline systems. In SR,
the term “end-to-end” refers to those systems that recognize text from the given speech
without the use of any phonetic representation, which used to be the core of traditional SR
systems [79]. Traditional speech recognition systems used to depend on significant human
expertise for the development of such representations. End-to-end speech recognition is a
recent development that was achieved due to the advancements in Deep Neural Network
(DNN). It was first presented in 2014 [87], in which it reports state-of-the-art accuracy on
the Wall Street Journal corpus. Later, a number of researchers expanded the end-to-end
concept and reported significant performance improvements.
The following SR systems and toolkits are reviewed.
1. Deep Speech
2. ESPnet
3. Wav2Letter++
4. CMUSphinx
5. Kaldi
6. Julius
7. Google Speech-to-Text
2.8.1 Deep Speech
Deep speech is a DNN based end-to-end acoustic modeling technique that uses the
Recurrent Neural Network (RNN) to construct a robust SR system. It is built with the focus
on noise-robustness, by enabling RNN to consume thousands of hours of unaligned,
transcribed audio to train its models. It performs character-level recognition. It was
presented in 2014, where it claimed better performance than other commercial SR systems
on both, clean and noisy datasets [77]. It outperformed previously established SR systems
by achieving 16% WER on the Switchboard corpus [88]. Later in 2015, deep speech
presented a state-of-the-art performance in two vastly different languages: English and

33
Mandarin; and showed that it can be adapted to perform recognition tasks on any other
language [76].
Deep speech models are composed of 6 layers (input + 5 layers) (Figure 2.3), where the
second last layer is a bi-directional recurrent layer [89]. The output layer in deep speech
predicts the character probabilities for the input audio sequence. The structure of deep
speech is straightforward and uncomplicated as compared to other RNN based models [87].
Therefore, deep speech depends upon extensive training data to achieve high-performance
standards. However, due to simplicity in structure, the RNN model is prone to overfitting;
thus, deep speech applies dropout rate in between 5-10% to its layers along with using
techniques to synthesize training data with artificial noise.
Figure 2.3 Structure of Deep Speech Model [77]
One advantage of deep speech is that it provides techniques to accelerate the training
process by using parallelism to enable execution over GPUs. The first technique it provides
takes the approach to train a model on many input examples in parallel. Secondly, it
provides some techniques to parallelize the overall model training process. Since recurrent

34
layers have a sequential nature, it is challenging to parallelize them; therefore, deep speech
approaches to optimize the execution of all other layers.
In November 2017, Mozilla research lab developed project DeepSpeech that implemented
the techniques defined above and released the first stable version of an SR system in the
open-source domain. Under the hood, DeepSpeech uses TensorFlow [90] neural network
toolkit. Training deep speech acoustic model is a compute expensive operation, as it
requires a vast amount of data to efficiently learn the domain characteristics; however, it
has the ability to run inferences in real-time by using a decent sized GPU due to the native
GPU support that TensorFlow provides. To refine its output, DeepSpeech uses an n-gram
based language model. The language model generation is not directly handled by
DeepSpeech; rather, it is dependent upon the implementations by KenLM [91] language
modeling toolkit.
2.8.2 ESPnet
ESPnet is a recent addition to the end-to-end SR systems, presented in 2018 [75]. It is based
on a hybrid DNN/HMM approach. It makes use of two vastly different approaches,
Connectionist Temporal Classification (CTC) and attention mechanism, in the hybrid
manner to train its acoustic models. Although it is a newer edition, it presented comparable
performance as compared to the state-of-the-art systems [75].
ESPnet is based on an attention-based encoder-decoder network to perform recognition
tasks. Attention-based networks do not require explicit acoustic and language models.
However, ESPnet presents a mechanism to develop a hybrid network by fusing the scores
from an attention decoder network with CTC decoder. Moreover, it also provides a
mechanism to make use of explicit language models. The final proposed recipe of ESPnet
works in 6 (1+5) stages (Figure 2.4). Stage 0 prepares the audio data using data preparation
scripts from Kaldi toolkit [92], Stage 1 again uses Kaldi to extract features from training
data. Stage 2 perform data preparation again, although this time preparation is for training
encoders and explicit language models. Stage 3 trains explicit language models. Stage 4
trains SR encoders. Finally, stage 5 performs recognition.

35
Figure 2.4 Processing stages in ESPnet recipe [75]
The first stable version of ESPnet was released in March 2019. It was built on PyTorch
[93], which is a neural network toolkit mainly for research purposes. Therefore, it can have
some issues in the case of scaling applications. Like deep speech, it is also dependent upon
huge datasets for efficient operation.
2.8.3 Wav2Letter++
Wav2Letter++ is the most recently presented end-to-end SR toolkit that is presented in
early 2019 [94]. It is developed entirely on C++ by the Facebook research lab to boost
performance and speed. It reports the lowest error rates on the same datasets on which deep
speech and ESPnet report their performance numbers. The first stable version of
Wav2Letter++ was released in early 2019. As it is based on the end-to-end concept, it also
depends upon massive training data to train efficient acoustic models. However, until the
start of October 2019, it was not offering any pre-trained models with the system.
Wav2Letter++ provides a platform to test various DNN based SR recipes. Recipes in
Wav2Letter++ consists of DNN architectures for acoustic modeling and decoding
information for language models. Currently, the official repository of Wav2Letter++
provides recipes that use Convolution Neural Network (CNN-DNN) based architectures

36
[95], [96]. When using architecture from deep speech, Wav2Letter++ reported 5% WER
on LibriSpeech clean dataset [94].
2.8.4 CMUSphinx
CMUSphinx is not an end-to-end system, as it is built upon traditional pipelines of speech
recognition. It was developed by Carnegie Mellon University (CMU) and was presented in
2004 [97]. We reviewed this system since it has the most recent version of the traditional
HMM-based acoustic model, along with a considerable community presence. Even recent
studies consider to compare it with leading commercial cloud-based SR [98]. However,
with the recent advancements of the end-to-end SR concept, the popularity of CMUSphinx
is now fading away.
2.8.5 Kaldi
Kaldi is a speech recognition toolkit, rather than a standalone system, that was presented
in early 2011 with the purpose of research [92]. The main focus of Kaldi is towards acoustic
model research. However, a number of recent end-to-end systems have borrowed various
components from this toolkit [52], [75]. Kaldi toolkit is built upon traditional HMM/GMM
based SR pipelines.
2.8.6 Julius
Julius was presented in 2009 as a large-vocabulary continuous speech recognition
(LVCSR) system for both research and industrial applications [99]. It was also a traditional
system using HMM-based acoustic models. Its main features were the ability to perform
real-time processes with low memory usage. However, it was last updated in 2014 and has
never updated since.
2.8.7 Google Speech-to-Text
Google speech-to-text [100] is a cloud-based speech recognition service that is currently
leading in real life general-purpose speech recognition [98]. It offers services in 120
languages and supports real-time recognition. The cloud service is based on powerful deep
neural network models and it offers recognition via easy to use API.

37
2.8.8 Summary
This review has covered six open-sourced and one cloud-based SR systems. Within open-
sourced systems, three are built upon end-to-end concept whereas the remaining three are
built upon traditional SR pipelines. This review analyzes these systems upon three factors:
performance, ease of use and scalability. We have shown that performance and scalability
wise, all end-to-end systems are cutting edge. However, training and using them in domain-
specific environments are challenging tasks due to their need for substantial training data.
In terms of noise-robustness, end-to-end systems are the best ones along with the reviewed
cloud-based system. Due to the dependability of traditional systems on accurate training
sets, they usually do not catch up end-to-end systems in real-world environments. When
comparing end-to-end systems with each other, DeepSpeech seems to be the most practical
one to use at this point.

38
2.9 SOAP Classification
Classification is the procedure of assigning one or more classes to some entity. Sentence
classification is the type of classification that falls under the umbrella of NLP and works
on text sentences. It is commonly applied in both medical and non-medical domains. It
stems from the document classification, categorization, or segmentation that works on the
scope of documents. Some examples of classification in NLP are classifying newspaper
articles based on topics and identifying an email as spam. An example of sentence
classification is the sentiment analysis of tweets.
This thesis uses sentence classification to assign SOAP categories to the transcription of
provider dictations. In a clinical report, subjective and objective sections bare most of the
content, whereas the assessment and plan sections are filled with marginally a smaller
number of sentences. This trend has shown in the dataset of this thesis which is also
affirmed by the dataset class proportion reported by Mowery [101]. This trend creates an
imbalanced dataset which may lead to a biased analysis of the performance. Another point
to note while dealing with SOAP format is that each category has a semantic definition,
and a SOAP formatted report expects its content to adhere to those definitions. In this
regard, it is a good idea for a classifier to pick those semantic patterns from the training.
Word sequence of a sentence plays a vital role in highlighting those patterns. It means that
keeping word sequence intact can positively impact the classification performance.
SOAP classification is attempted before by Mowery [101] in which SVM was used and
showed positive gains; however, Mowery did not address the imbalanced nature of SOAP
datasets and also did not exploit the sentence sequences in its solution. We were not able
to find any other study on SOAP classification to compare the results of this study.
Mowery, in its work, also mentioned about this unavailability. However, we reviewed other
studies on similar problems in the medical domain. We adapted an exemplar-based concept
detection algorithm that is defined by Juckett [102] in an effort to extract concepts from
clinical text. This algorithm explicitly takes care of the word sequences and aims to work
efficiently on imbalanced datasets.

39
2.10 Conclusion
In this chapter, we define the clinical documentation process, along with its challenges,
modes, and workflows. We discuss the structure of SR systems along with some recent
developments that are happening in the SR research domain. A literature review presents
the use of SR in the healthcare domain with respect to the challenges of the documentation
process. We also present a review of 6 top-of-the-line speech recognition systems. In the
end, we review techniques to classify sentences into SOAP categories, where we present
an exemplar-based concept detector algorithm with the idea to implement it into a SOAP
classifier.

40
Chapter 3. RESEARCH METHODOLOGY
3.1 Introduction
This chapter describes the methodology undertaken to address the research objectives of
this thesis. The process of research started after performing a systematic review of the
problem, which led us to define a solution approach that spans over two separate layers
and separate domains. The rationale for this multi-layered multi-domain approach is
provided in the introductory chapter (Section 1.1). This chapter now highlights all the steps
that are taken to form a conclusion within each layer. Figure 3.1 highlights the overall
methodology of this thesis.
Figure 3.1 Steps in Research Methodology spanning over two layers
3.2 Layer 1: Transcription of Physicians’ Audio Notes
The focus of this layer is to achieve higher recognition accuracy in the noise rich
environments. It aims to apply the solutions to transcribe physicians’ dictation audio files.
This layer achieves its objective in four steps.
3.2.1 Selection of Methods
Noise-robustness and domain-robustness are two key challenges towards achieving the
first objective of this layer. Both challenges were reviewed in detail (Section 2.6 and 2.7)
to explore the top-of-the-line techniques. After a detailed review (Section 2.8), one Speech
Recognition (SR) system was selected based on the ability to implement our explored

41
techniques. The selection of the SR system and robustness techniques goes hand in hand
to ensure the compatibility between the selections.
• SPEECH RECOGNITION (SR) SYSTEM
We have selected project DeepSpeech [7] in our work. DeepSpeech is an open-source
speech recognition engine that is developed by Mozilla. Project DeepSpeech uses
acoustic models that are trained on the machine learning techniques of deep speech
[77] and language models that are trained using KenLM [91] language modeling
toolkit. When the DeepSpeech engine works with a deep speech acoustic model and a
KenLM language model, the whole combination becomes a complete speech
recognition system.
Name Short Name Description
Project
DeepSpeech
DeepSpeech Speech Recognition Engine requires an acoustic
and a language model to perform recognition
tasks.
Deep Speech
Acoustic Model
Deep speech
model
OR
Acoustic
Model
An acoustic model that is developed using Deep
Neural Network (DNN) based machine learning
techniques.
KenLM Language
Model
KenLM Model
OR
Language
model
A language model that is trained using the
KenLM toolkit.
Deep speech [77] also provides pre-trained acoustic and language models that have
learned from massive datasets. It also provides utilities to train custom models. We
selected the release 0.5.1 for our experiments, which is the latest stable release at this
point in time.

42
• PRE-TRAINED MODELS
Pre-trained acoustic and language models provided by DeepSpeech are trained over
3,000 hours of transcribed audio from Fisher [103], LibriSpeech [104] and Switchboard
[88] datasets. All datasets are in American English. Details of each dataset are given
below.
Corpus
Name Fisher [103]
LibriSpeech
[104] Switchboard [88]
Corpus Size 2,000 hours 1,000 hours 250 hours
Nature of
Data
telephone
conversations audiobooks conversations
Source of
Data 16,000 conversations audiobooks
2,500 conversations by 500
speakers
The pre-trained deep speech model was trained using the following hyperparameters.
Parameter Layer
width
Dropout
rate
Learning
rate
Language model
weight (CTC
Decoder)
Word insertion
weight (CTC
Decoder)
Value 2048 15% 0.00001 0.75 1.85
The language model was trained till 5-grams. The total size of the pre-trained language
model is over 4 gigabytes.
3.2.2 Preliminary Analysis
Cloud-based SR systems generally perform better [105] as compared to offline systems,
but they do not offer customization options as open-sourced offline SR systems offer.
Moreover, in data-sensitive domains, such as the healthcare domain, offline solutions are
preferred due to privacy and such concerns. Therefore, in this work, we will be exploring
robustness techniques to apply them to an open-sourced offline SR system to maximize
accuracy gain. However, we are interested in comparing the performance of the selected
SR system with the top-of-the-line cloud SR system in both settings; before and after

43
applying our solution. In this step, we experimented with DeepSpeech and Google Speech
[100] using our full dataset.
3.2.3 Development of Solution
This step developed a solution to overcome the challenges of this layer. The solution is
motivated by the insights gathered from the preliminary analysis and is based on the
reviewed robustness techniques. It proposes methods to maximize accuracy gains using
both, acoustic and language models.
3.2.4 Evaluation of solution
SR systems are generally evaluated using Word Error Rate (WER) [25], which gives equal
weight to all mistakes. However, in the domain-specific environment, some mistakes can
have more impact than others. For example, in the healthcare domain, a mistaken drug
name or diagnosis is a critical hazard, in comparison to most of the grammatical mistakes.
Therefore, we developed a custom domain-specific evaluation metric, Critical Error Rate
(CER), to evaluate such errors. We evaluated our models on both of these evaluation
metrics (WER and CER).
• CRITICAL ERROR RATE (CER)
Critical mistakes are defined as those mistakes that involve medical concepts. CER
counts critical mistakes and takes its ratio out of all critical concepts within the ground
truth. First, it counts all the critical mistakes, and then it divides the count by the number
of all medical concepts in the ground truth. CER uses Metamap [106] to query the word
to find if it is a critical mistake.
𝐶𝐸𝑅 =𝐶
𝑊
∴ 𝐶 = # 𝑜𝑓 𝐶𝑟𝑖𝑡𝑖𝑐𝑎𝑙 𝑀𝑖𝑠𝑡𝑎𝑘𝑒𝑠
∴ 𝑤 = # 𝑜𝑓 𝐶𝑟𝑖𝑡𝑖𝑐𝑎𝑙 𝐶𝑜𝑛𝑐𝑒𝑝𝑡𝑠 𝑖𝑛 𝐺𝑟𝑜𝑢𝑛𝑑 𝑇𝑟𝑢𝑡ℎ

44
3.3 Layer 2: Autonomous Generation of Clinical Report
A SOAP formatted clinical report contains sections representing all four SOAP categories;
therefore, the focus of this layer is to develop a classifier to categorize sentences from the
transcription of physicians’ notes into one of the SOAP categories. We achieved the
objectives for this layer in four steps.
3.3.1 Data Labeling
In the first step, we labeled the dataset for the classification task.
3.3.2 Selection of Method
In this step, an exemplar-based algorithm was selected, which is proposed by Juckett [102]
for concept detection within clinical texts.
3.3.3 Development of Solution
The selected algorithm detects concepts at the word level, whereas we aim to work at the
sentence level. Thus, in this step, we extended the selected algorithm to give a single
confidence score for each class for the given sentence. We also identified four key areas to
investigate and develop the solution.
3.3.4 Evaluation of Solution
In this step, we evaluated our solution based on the four independent variables that were
formed from the identified areas. For the evaluations, we used Average Precision (AP) as
the primary measure of performance. We did not evaluate the area under the ROC curves
due to the class imbalance in the dataset.
3.4 Dataset
To achieve the objectives of this research, the IWK health center in Halifax, Nova Scotia,
Canada, provided a set of 105 physicians dictated notes, which were then processed into a
structured dataset.

45
3.4.1 Data Collection
Audio clips of clinical dictations were provided by the Pediatric Emergency Department
of IWK health center. 20 out of 105 dictation audio clips contained a complete dictated
note, whereas the rest of the dictations were chunks of incomplete notes. Only 16 dictations
were coupled with gold standard text. In total, all dictations accumulate to 2 hours, 28
minutes, and 14 seconds of audio data. Out of all dictations, 100 were recorded by one
person in different areas of the hospital, whereas, remaining five dictations were recorded
by different persons.
3.4.2 Dataset Preparation
The dataset was prepared in two steps. In the first step, gold standards were generated and
validated. For all those dictation clips where no gold standard was provided, manual
transcription process was completed by three fellow researchers of our lab, one of these
fellows holds a medical degree that helped us in maintaining the exact vocabulary. Every
researcher transcribed all dictation clips; afterward, all three variations were analyzed to
generate gold standards. After generating the missing gold standards, all 105 dictations
were manually validated.
In the second step, the dataset was structured. All dictation and transcription files were
renamed into a sequence of numbers, where a prefix was given to each file. Prefix A was
given to all audio clips, and corresponding text files. A dictation and its respective gold
standard couple were given the same filename; nevertheless, they had separate extensions
(.wav for audio clips, .txt for text files), e.g., (A001.wav, A001.txt).
After setting up all the files for the dataset, we segmented our dataset into two parts. The
first part included 100 dictations that were recorded by one person. We called this an
original dataset and used it for experiments and analysis. The remaining five dictations
form a validation dataset that we used explicitly to validate the final results of our
experiments. We did not use the validation dataset at the time of defining, experimenting
and refining our methods.

46
3.5 Research Environment
This research is performed on two computer systems that were used in parallel. Table 3.1
provides a summary of both systems that were used. System 1 was primarily used for
review, documentation, and light scripting work where the windows operating system is
required. For all the compute-intensive tasks such as model training and fine-tuning,
System 2 was used that was equipped with a well-functioning GPU.
Table 3.1 Summary of Research Environment
System 1 System 2
Processor Intel Core i7 Intel Core i7
RAM 16GB 20GB
GPU - NVIDIA GeForce GTX 960 (2GB VRAM)
Storage HDD SSD
Operating System Windows 10 Pro Ubuntu 18.04 LTS
Metamap [106] was used to extract medical concepts from texts. In this thesis, vocabulary
was limited to MeSH (Medical extended Subject Headings) [107]. Metamap server was
initialized on system 2, which was readily available over the network. We were more
comfortable working with the JAVA implementation of Metamap client; hence all the
scripts that required interaction with Metamap were written in JAVA.
We used Python to experiment with DeepSpeech. We used system 2 for experiments since
DeepSpeech uses TensorFlow [90] libraries to run Deep Learning algorithms that facilitate
execution over NVIDIA based GPU.
Cloud-based SR systems were tested on the JAVA platform. Exemplar based algorithm in
NLP was also implemented in JAVA where results were stored in files which were later
analyzed by python scripts using the scikit-learn library to calculate and plot the precision-
recall graphs.

47
3.6 Conclusion
In this chapter, we present the steps we took in each layer of our solution to address both
of our objectives. We highlight the methods that are selected in each layer, along with the
reasons for such selections. We also mention details about the dataset and working
environment that we used throughout our research.

48
Chapter 4. SPEECH RECOGNITION – METHODS
4.1 Introduction
This chapter presents our methods to explore robust and domain-specific Speech
Recognition (SR) for scenarios when there is a shortage of domain-relevant data. In this
chapter, methods pertaining to both components: acoustic model and language model; are
explored to achieve maximum recognition accuracy. Acoustic models are primarily
focused on achieving noise-robustness, as they are directly responsible for dealing with the
noise within the feature space. Language models, on the other hand, contribute more to
domain-robustness, as they learn from domain-specific language (vocabulary and speech
patterns).
4.2 Domain Adaptation
Domain adaptation is a sub-discipline of machine learning which “deals with scenarios in
which a model trained on a source distribution is used in the context of a different (but
related) target distribution” [108], [109]. In many realistic and low-resourced target
domains, where the collection of data is costly and sometimes impossible, training domain-
specific models become a challenge. In such scenarios, domain adaptation serves as a
highly practical option [110] to bootstrap the model development process [84].
Transfer learning and fine-tuning are two main methods of domain adaptation. In both
methods, models that are already trained on one problem domain are used as the starting
point to use in another problem domain. However, the difference lies in the way these
models are adapted. If the adapted model is shown some training data from a different
target domain to learn the domain specifics, this method is referred to as fine-tuning.
However, if some or all layers of the adapted model are taken to develop a new model, this
method is transfer learning.

49
4.3 Preliminary Analysis
In this section, we address some fundamental questions that require answers to drive this
research. DeepSpeech is a recognition engine that depends on acoustic and language
models to perform recognition tasks; however, we have not trained any domain-specific
models yet. Therefore, our first logical question is, ‘what will be the performance of
DeepSpeech on our dataset by simple domain adaptation of pre-trained (general purpose)
models?’; secondly, ‘what type of mistakes do pre-trained models do on a domain-specific
dataset?’; and thirdly, ‘how does this performance compare with top-of-the-line
commercial cloud-based SR systems like Google SR?’
Table 4.1 Preliminary Results: WER and CER of Cloud and Offline SR
CER WER
DeepSpeech 49.38% 46.63%
Google 20.18% 21.69%
To answer these questions, all 100 audio clips from our original dataset were transcribed
using both SR systems/services (DeepSpeech and Google). Table 4.1 presents the error
rates for both systems. In general, we observed that DeepSpeech, with its pre-trained
models, made a mistake for almost every two words.
In comparison with the cloud-based SR (Google), DeepSpeech made relatively 114.98%
more general mistakes (WER) and 144.69% more critical mistakes (CER). In isolation,
DeepSpeech made more critical mistakes than general mistakes, whereas Google was
better in recognizing domain critical vocabulary. These differences highlight the domain
agnostic behavior of pre-trained models of DeepSpeech.
Table 4.2 Examples mistakes by DeepSpeech during preliminary experiments.
Ground Truth DeepSpeech Google
with the t max of with a tax of with a t maxx of
ibuprofen age profane ibuprofen
tracheal palpation trail at a patient I killed a palpation

50
The reason for a large number of critical mistakes by DeepSpeech is that its models are not
trained on the vocabulary that is deemed critical in our domain. We present some examples
of critical mistakes done by both systems/services in Table 4.2. From the example, one can
observe that DeepSpeech returned hypotheses that are most common in generally spoken
language. For example, ‘t max’ was inferred as ‘tax’, and ‘tracheal’ was conceived as
‘trail’. This behavior is precisely the same that is within the dataset on which the pre-trained
language model is trained, i.e., mostly conversational and general speeches. Thus, we
should investigate techniques to incorporate more domain-specific vocabulary within the
language model.
Google was also not able to conceive many, if not most, of the critical concepts either;
however, we observed that such mistakes were less then DeepSpeech. Most of the time,
when DeepSpeech made a critical mistake, the audio happens to be valid. For example, in
the case of ‘tracheal palpation’, Google recognized ‘palpation’ correctly, while giving a
completely out of context hypothesis for ‘tracheal’, but DeepSpeech did not recognize any
part of that phrase, which is worse. We verified this specific instance manually and found
that the distortion in this audio clip is below the average level of noise within our dataset.
Therefore, for better inferences, there is also a need to explore methods to develop accurate
acoustic models.

51
4.4 Acoustic Modeling
In preliminary experiments, the pre-trained acoustic model was not aware of the acoustic
environment of the target domain. Therefore, we explored methods to train domain-
relevant acoustic models. In this regard, we outlined two research questions. 1) what will
be the impact on performance if the pre-trained acoustic model incorporates the acoustic
environment of our target domain? and 2) how will DeepSpeech perform with a new
acoustic model that is trained solely on our dataset?
Our first question sought domain adaptation of the pre-trained model along with an
enhancement method to incorporate the target domain. There are two methods to do it in a
machine learning paradigm: transfer learning and fine-tuning. Both of these methods adapt
an existing model that is learned in a separate domain. These methods require less training
data from the target domain. In our case, the pre-trained acoustic model has already learned
from general conversations. Moreover, we do not require any change in the input or output
classes. Therefore, we considered using the fine-tuning method to incorporate our target
environment within the pre-trained model.
The second question requires the development of a new acoustic model using supervised
learning. DeepSpeech is an end-to-end system that relies on large datasets to generalize;
therefore, with our dataset of about two and a half hours of audio, we were not able to train
the model to the point of convergence. Even after training a new model for 500 epochs, we
did not observe any reduction in the error rates, whereas, in comparison, the pre-trained
model is only trained for 75 epochs. Hence, we did not pursue this question further.
4.4.1 Audio Pre-Processing
Audio clips in our dataset have an average length of 1:30 mins, whereas the pre-trained
model was trained on the audio files that are of sentence length (4-5 seconds). The length
of audio has a direct correlation on the memory consumption while training deep speech
acoustic models. Therefore, we needed to split the audio clips in shorter chunks to keep the
memory allocation under the affordability of our hardware.

52
A series of considerations were acknowledged before splitting. Firstly, attention was given
towards the completion of words in each split. Any cut in between the utterance of a word
can make it impossible to recognize that splitting word. Secondly, splits were made in a
way to keep the average length around 5 seconds mark.
To effectively break audio clips following all considerations, a silence finding process was
used. The idea is that if a cut is made on silence, that is long enough, then the probability
of breaking a word will greatly diminish. Audio clips were analyzed to find silences upon
various threshold values. There are two thresholds that a silence finder process requires:
max intensity level and duration of silence. Both are defined below.
1) Maximum Intensity Level: This requires a value for maximum sound intensity level
below which everything is considered silence.
2) Duration of silence: This requires a value that denotes time in milliseconds of
continuous silence to mark it as a valid silence period. Whenever sound intensity
drops below the above-defined level a true silence does not need to occur. It is quite
possible that while pronouncing a word, the sound intensity drops below the above-
defined intensity level for a moment; hence this threshold gives an option to select a
duration of silence period, such that only silences of periods more than specific
duration will be marked as true silence.
For each audio clip, the silence finding process was executed with varying threshold levels.
After each execution, all splits were checked for word completion and the average split
length. If any of the considerations failed, thresholds were readjusted, and the process was
re-executed. The whole process was performed manually for each audio clip to ensure that
speech content preserves even after the splits.
Once all the audio clips were broken into smaller splits, they were then stored in a folder
by appending a number from a sequence to their filenames. For Example, the first split of
‘A001.wav’ was given filename ‘A001-01.wav’. All splits were then copied into a folder
that was named ‘A001’. After storing all the splits, their corresponding gold standard

53
transcriptions were also modified in such a way that they contain the same number of lines
as there are splits, where the nth line has the text for the nth split.
4.4.2 Fine-tuning
Project DeepSpeech provides checkpoints for its pre-trained deep speech model.
Checkpoints capture the exact value of all weights and parameters within a model and are
stored in a directory. The checkpointing directory within the project DeepSpeech contains
the latest values for which the deep speech model was exported. Therefore, we used the
provided checkpoints to perform fine-tuning.
Table 4.3 Hyperparameters used for acoustic model fine-tuning
Hyperparameter Value
audio_sample_rate 16000
train_files Path/to/train.csv
alphabet_config_path Path/to/alphabet.txt
export_dir Path/to/export-directory
checkpoint_dir Path/to/checkpointing-directory
train_batch_size 5
n_hidden 2048
epochs 1
dropout_rate 0.15
learning_rate 0.0001
lm_alpha 0.75
lm_beta 1.85
The fine-tuning process is the same as model training in DeepSpeech. While training, if a
checkpointing directory is defined and the directory contains valid checkpoints, then
DeepSpeech starts fine-tuning the existing model; otherwise, it creates a new model. In our
scenario, we downloaded the checkpointing directory and started the training process from
that directory. Table 4.3 provides a list of hyperparameters that we used. Details about
these hyperparameters are as follows.

54
1. Training files.
The parameter train_files expects a path to a comma-separated file (CSV) that contains
three columns: wav_filename, wav_filesize, and transcript. The column wav_filename
record paths of the audio files that we want to use for training the model, wav_filesize
note the sizes of each audio file in bytes, and transcript have the ground truth of each
audio file that other columns enlist. Each row in the CSV represents one audio clip
within the dataset.
2. Alphabet file
The parameter alphabet_config_path expects a path to a text file that contains a list of
all distinct characters that are within the ground truth.
3. Export directory
The parameter export_dir is used to specify the directory in which we wish to export
the trained model. If this parameter is not supplied, then the trained model parameters
will be stored in the checkpointing directory only, without exporting the model for
inference use.
4. Batch size
The parameter train_batch_size is used to set the batch size of training. The pre-trained
deep speech model was trained on a batch size of 24 clips when there were 12 gigabytes
of memory available to the developers of the pre-trained model. With one-sixth of that
memory available to us and while using audio clips of similar lengths (after splits), we
were facing memory exhaustion errors. Therefore, we explored the batch size
iteratively by reducing it on each step. We were able to successfully complete the
training process by using the batch size of 5 audio clips.
5. Epochs
For our evaluations, we were interested in analyzing the error rates after each epoch of
fine-tuning. Therefore, we executed the training one epoch at a time and exported the

55
trained model after each epoch. After each export, the training was resumed from the
same checkpointing directory.
6. Other hyperparameters
Project DeepSpeech reports the hyperparameters that were used to train the pre-trained
model. All other hyperparameters were kept unchanged in this fine-tuning process.
After finishing the fine-tuning process, all generated models are evaluated, whose details
are provided in the next chapter.

56
4.5 Language Modeling
Language is a combination of words (vocabulary) and speech patterns (grammar). Specific
domains may have specialized languages; therefore, domain-specific language model plays
an important role in the domain-robustness of any SR system. Ideally, language models
require training on vast volumes of domain-relevant data [111]. However, in realistic
situations, problems arise when there is little or no domain-specific data available [82]. We
also observed such problems in our preliminary analysis, when we used the pre-trained
model which is an out-of-domain model for our problem domain. Therefore, we explored
various methods to develop robust language models that are specific to our target domain.
The main concern is the insufficiency of domain-relevant training data. In the review, we
highlight two main techniques to develop domain-specific language models when there are
data scarcity problems. The first technique seeks domain adaptation of the out-of-domain
language model while enhancing the adapted model using domain-relevant data and using
various model combination methods. The second technique, on the other hand, focuses on
the generation of domain-relevant data. Therefore, in this work, we experimented with
methods from both techniques. We are also interested to see the recognition performance
without applying any of these techniques. Hence, we also developed standalone language
models using only our original dataset. In summary, we worked on three key tasks to
investigate the impact of language modeling techniques.
1) Dataset Augmentation with Domain-Relevant Data.
2) Developing Domain-Specific Language Models
3) Enhancing Pre-Trained Language Model
4.5.1 Dataset Augmentation with Domain Relevant Data
Our dataset includes clinical notes representing narrated cases of patients’ diagnosis and
treatment, along with rationales and reasons coming from the healthcare provider’s
perspective. These notes contain domain-specific concepts, for example, diseases,
diagnoses, and observations. However, with the limited number of notes having 1966
sentences in total, it is not possible to cover all the concepts within the domain. Therefore,

57
to develop domain-specific and robust language models, it is required to augment our
dataset with most of the domain-relevant information.
We reviewed three techniques for data augmentation: extraction, conversion, and
generation. Extraction and conversion techniques consider that domain-relevant data is
available somewhere else perhaps in a different format, language or source. These
considerations are ineffective for sensitive domains like healthcare since such data is
usually heavily protected and is available with scrutiny and restrictions. Therefore, the only
logical option left is to use data generation techniques to simulate domain-relevant data.
Data generation techniques vary for each domain and require domain knowledge. In the
NLP domain, synonym replacement [112] is a simple technique that is also the most natural
choice to augment small datasets [113]. In its simplified form, synonym replacement
generates new textual units by replacing words from its synonyms. Most implementations
of this technique use thesaurus like WordNet [114] or thesaurus.com [115] to get the list
of synonyms for replacement. Synonym replacement requires two things for execution:
which words in the text should be replaced, and which synonyms should be used for the
replacement [113]. In synonym replacement, words to replace are identified from the
original dataset, whereas, synonyms are extracted from knowledge sources. Once both:
words and synonyms; are identified, then each word is permuted with its synonyms to
generate new variations of text.
In this work, we generated domain-relevant data based on the synonym replacement
technique. To apply this technique in our domain, we considered synonyms as those
medical concepts that belong to the same semantic classes. We used MeSH [107] as the
knowledge source to extract medical concepts within the healthcare domain. MeSH is a
thesaurus that lists medical concepts in a tree hierarchy. Previous work has also shown to
use MeSH with the same technique for the data simplification task [116]. We used
Metamap [106] to identify medical concepts within our dataset, which is a concept
recognizer that annotates medical concepts within texts. Our data generation method
consists of three steps.

58
• STEP 1: PATTERN EXTRACTION
Each sentence within our dataset can have multiple medical concepts. We observe that
most of the time, these concepts semantically depend on each other, and a replacement can
semantically invalidate the sentence. As an example, in the sentence, “She was prescribed
a course of cephalexin to treat bacterial infection”, there are three medical concepts:
“prescribed”, “cephalexin” and “bacterial infection”. The concepts “cephalexin” and
“bacterial infection” belong to ‘drug’ and ‘disease’ classes respectively and are
semantically dependent upon each other. A replacement of the ‘disease’ concept “bacterial
infection” to another ‘disease’ concept “lung cancer” might semantically invalidate the
sentence. Therefore, we approached for extracting patterns from the sentences, so that a
replacement does not invalidate the semantics. We define that a pattern within a sentence
has exactly one medical concept while having maximum neighboring words that are not
medical concepts. In our given example, patterns are “She was prescribed a course of”, “a
course of cephalexin to treat” and “to treat bacterial infection”. Since our goal is to generate
robust language models, we generated patterns with overlaps to maximize the count of
neighbors around the medical concepts.
Figure 4.1 Steps of Pattern Extraction
Pattern extraction starts by annotating a sentence using MetaMap by restricting it to use
MeSH vocabulary. These annotations are upon the concepts within the sentence. The
number of annotations defines the number of patterns that can be extracted from the
sentence. Each annotation is then used as the starting point of a new pattern. All the words
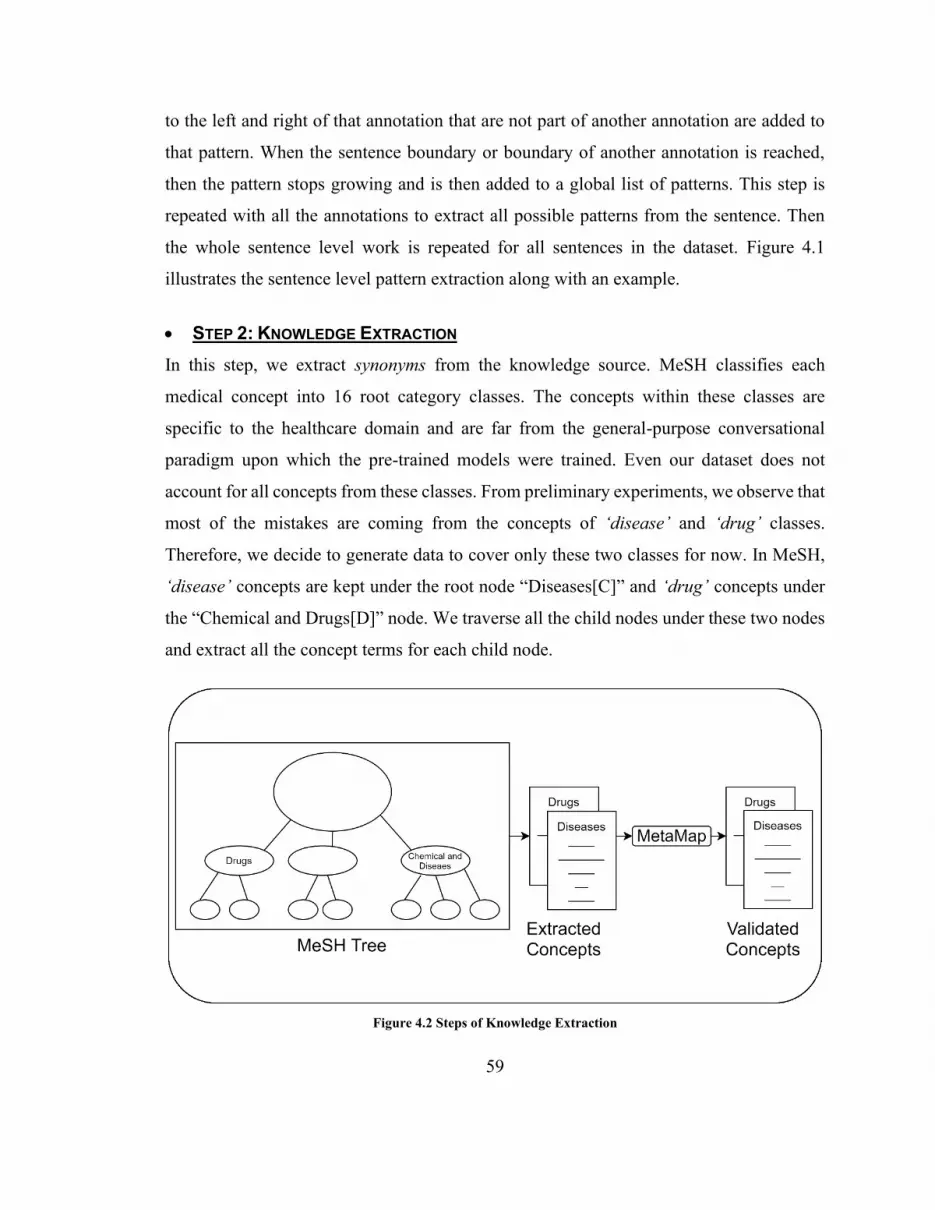
59
to the left and right of that annotation that are not part of another annotation are added to
that pattern. When the sentence boundary or boundary of another annotation is reached,
then the pattern stops growing and is then added to a global list of patterns. This step is
repeated with all the annotations to extract all possible patterns from the sentence. Then
the whole sentence level work is repeated for all sentences in the dataset. Figure 4.1
illustrates the sentence level pattern extraction along with an example.
• STEP 2: KNOWLEDGE EXTRACTION
In this step, we extract synonyms from the knowledge source. MeSH classifies each
medical concept into 16 root category classes. The concepts within these classes are
specific to the healthcare domain and are far from the general-purpose conversational
paradigm upon which the pre-trained models were trained. Even our dataset does not
account for all concepts from these classes. From preliminary experiments, we observe that
most of the mistakes are coming from the concepts of ‘disease’ and ‘drug’ classes.
Therefore, we decide to generate data to cover only these two classes for now. In MeSH,
‘disease’ concepts are kept under the root node “Diseases[C]” and ‘drug’ concepts under
the “Chemical and Drugs[D]” node. We traverse all the child nodes under these two nodes
and extract all the concept terms for each child node.
Figure 4.2 Steps of Knowledge Extraction

60
In MeSH, each medical concept enlists all candidate and qualifier terms, while defining a
separate list for the preferred terms of that concept. Many of these terms are closely related
to the concept but are not strictly synonymous with the terms that are in use by the
physicians. Moreover, root nodes of MeSH include all the concepts that are from all
domains of medical science, while for this work we are only interested in those concepts
that are applicable in the pediatric emergency departments. As an example, the “Chemical
and Drugs[D]” node contains a concept “Propoxur” which is an insecticide. “Propoxur” is
not related to pediatric care and is not applicable in our case. Therefore, it is required to
filter out such terms from our extracted lists to ensure that the terms are semantically
similar to our working domain. To filter the lists, we considered a validation step where
only those terms are validated and kept that are semantically closer to our dataset, and all
other terms were dropped.
To validate the extracted concepts, we passed each concept term to the Metamap and
examined the detected semantic type. If the semantic type matches those that are already
existing in our dataset while the semantic type belongs to the same root node from which
the term is coming, then we consider that term as valid. We collected all the valid terms
for each of the two semantic classes that we extracted. Figure 4.2 depicts the whole process
of knowledge extraction. After the extraction and validation of concepts, we get 24,071
concepts from the ‘disease’ class and 29,935 concepts from the ‘drug’ class.
• STEP 3: AUGMENTATION
In this step, we generate simulated data by using patterns and medical concepts extracted
in previous steps and then augment the simulated data with our original text corpus. Our
strategy in this step is similar to synonym replacement, with a small change that seeks
selection of concept list depending upon the class of concept within each pattern. For this
step, we know that each pattern has exactly one medical concept within it.

61
Figure 4.3 Steps to Generate Augmented Corpus
For each pattern from the patterns list, we check the class of the medical concept. If the
concept belongs to the ‘drug’ class, we select the list of drugs for the augmentation. In case
the concept belongs to the ‘disease’ class, we select the list of diseases. For anything else,
the pattern does not augment. To augment the pattern with the selected list of concepts,
each concept within the list is used to replace the existing concept in the pattern to form a
simulated variation. Each new variation after the replacement is then recorded in the list of
simulated patterns (Figure 4.3). These simulated patterns are then combined with the
original text corpus to form an augmented corpus.
Our data augmentation task enabled us to work with two datasets: original and augmented.
We use both datasets to evaluate our language modeling methods that we define in later
tasks. For the evaluations, we require data augmentation on multiple subsets of our original
dataset. Therefore, we develop a utility program using JAVA to automate the augmentation
process. Our utility program takes lists of concepts (Drugs and Diseases) and a text dataset,
and then it outputs the augmented dataset.
4.5.2 Developing Domain-Specific Language Models
In this task, we develop language models using only the domain-relevant data. For this
purpose, we use both datasets: original and augmented. Augmentation is done using the

62
methods presented in the previous task. Language models are created using the KenLM
toolkit.
KenLM provides methods to develop n-gram based language models in ARPA [117]
format. ARPA is a file format to list down all the calculated probabilities within an n-gram
language model. ARPA formatted models are bulky and not efficient to use for inferences;
hence, for efficient execution, it is required to convert ARPA models into specific data
structures [118]. KenLM also provides functions to convert the ARPA formatted models
into PROBING and TRIE data structure based language models [91]. PROBING data
structure is faster but uses extensive amounts of memory for inferences. In comparison, the
TRIE data structure aims to lower memory consumption. As our compute environment has
a limited stack of memory, we adapt the TRIE data structure to develop our language
models. Project DeepSpeech also supports TRIE structure by providing a native client to
convert the TRIE based language models into efficient binaries that aim speedy execution.
In this task, we use four steps to develop language models. In the first step, we streamline
the dataset by removing all leading and trailing whitespaces from all the sentences and
converting them into lower case. In the second step, the streamlined dataset trains an ARPA
based language model of the 5th order. We use the maximum n-gram order length of 5
because the pre-trained model from DeepSpeech uses the maximum of 5-grams; therefore,
we keep the n-gram order similar for valid comparisons. In the third step, the ARPA model
converts into a TRIE based model. Finally, the TRIE model converts into DeepSpeech
specific binary using its native client.
In this task, we develop language models in two strategies. In the first strategy, we directly
use the original dataset to develop the language models. In the second strategy, we apply
augmentation methods on our original dataset and then use the augmented dataset to
develop the language models.

63
4.5.3 Enhancing Pre-Trained Language Model
In this task, we enhance the pre-trained language model by incorporating information from
our domain-relevant dataset. There are two main reasons to seek this task for the
development of robust language models. The first reason is the insufficiency of our
domain-relevant dataset. We have only 127 kilobytes of text available in the original
dataset. Although after augmenting, we are able to generate about 2 gigabytes of text;
however, the pre-trained DeepSpeech model is trained on about 4 gigabytes of text, which
is still double. Therefore, we hypothesize that developing language models using text from
both data sources can be a better solution. The second reason is due to the preliminary
analysis, where DeepSpeech, with its pre-trained language model, made more critical
mistakes then general mistakes. From the nature of mistakes, we observed that the pre-
trained language model lacks domain-specific vocabulary, evidently due to its training
upon an out-of-domain data source. Therefore, we consider a reduction in critical errors by
introducing domain-relevant vocabulary in the pre-trained model.
Enhancement of the language model entails combining the information from other data
sources (domains) to the existing language model. Language models can be combined by
any of two methods: pooling and interpolation. In the pooling method, the corpus of the
existing language model is pooled with the text from other data sources. The pooled corpus
then trains an enhanced language model. In the interpolation method, a separate language
model is trained using the text from each data source. Afterward, all language models;
existing and newly trained, are merged using weights that are tuned on some validation
text. This validation text is fetched from the target domain.
The interpolation method has some variations [119]. The simplest of all is linear
interpolation, in which all intermediary language models (𝑃𝑖) are combined linearly using
tuned weights (𝜆𝑖) (Equation 3). These weights are tuned over the validation set such that
it maximizes the likelihood operator 𝑃(𝑊|𝐻) for the combined model.

64
Equation 3
𝑃(𝑊|𝐻) = ∑ 𝑃𝑖(𝑊|𝐻)𝜆𝑖
𝑖
KenLM [91] toolkit uses the log-linear interpolation method, which is a slight variation of
the linear interpolation method. In the log-linear interpolation method, individual models
are merged by applying weights as the power and multiplying the powered models
(Equation 4).
Equation 4
𝑃(𝑊|𝐻) = 1
𝑍𝜆(𝐻)∏ 𝑃𝑖(𝑊|𝐻)𝜆𝑖
𝑖
After merging all the models, to complete the interpolation probability, the product is
divided by a normalizing term 𝑍𝜆(𝐻) to ensure that the sum of all probabilities over words
W equals to 1. The normalizing term calculates the product of all words in the vocabulary
of all language models (Equation 5).
Equation 5
𝑍𝜆(𝐻) = ∑ ∏ 𝑃𝑖(𝑊|𝐻)𝜆𝑖
𝑖𝑊
To enhance the pre-trained language model, we experiment with both; pooling and
interpolation; methods. Similar to the previous task, we adopt strategies to use both
datasets; original and augmented. In total, we develop language models in four strategies,
by the combination of methods and datasets. In the first strategy, we use the original dataset
to enhance the pre-trained language model using the pooling method. In the second
strategy, the same dataset is used with the interpolation method. The third and fourth
strategies are similar to the first two, in terms of methods; however, we use augmented
dataset in these strategies.

65
When we use the pooling method, the source corpus of the pre-trained model is pooled
with the domain-specific text of our datasets, and then the pooled text trains new language
models. When we apply the interpolation method, the pre-trained model remains the first
intermediary model, while we train separate models from our datasets and interpolate all
intermediaries. All the models developed in this task are trained using the n-gram order of
5, which denotes the maximum n-gram length in the language model.
4.5.4 Summary
In the language modeling phase, we work on three tasks. In the first task, we focus on the
generation of artificial domain-relevant data using the principles of the synonym
replacement method. We define a three-step method that expects a text corpus to work on,
and in turn, it provides an augmented corpus. In the second and third tasks, we provide
strategies to develop language models by using both datasets; original and augmented. Both
tasks, in combination, develop six strategies to train language models.
1) Training a new language model using the original dataset.
2) Training a new language model using the augmented dataset
3) Enhancing the pre-trained language model using the original dataset using the pooling
method.
4) Enhancing the pre-trained language model using the augmented dataset using the
pooling method.
5) Enhancing the pre-trained language model using the original dataset using the
interpolation method.
6) Enhancing the pre-trained language model using the augmented dataset using the
interpolation method.
All these strategies seek the development of n-gram based language models that are of 5th
order.

66
4.6 Discussion
We consider our solution to be replicable in other domains where noise and domain
robustness is required, and there is insufficient relevant data available. In the acoustic
modeling method, we approached to fine-tune a general-purpose model. As this model is
generic, the same method can be applied in any other domain. However, to replicate our
language modeling methods, particularly the data augmentation, one will need to look for
the domain-specific knowledge sources and concept detection tools for the successful
adaptation of these techniques.
4.7 Conclusion
In this chapter, we present our explored techniques and developed methods to train robust
and domain-specific models. Our methods focused on those acoustically distorted and
sensitive scenarios where there is a shortage of domain-relevant data. We first did the
preliminary analysis using pre-trained models of DeepSpeech. We then developed acoustic
modeling and language modeling methods by taking insights from the analysis. The
acoustic modeling method sought domain adaptation of the pre-built model along with a
fine-tuning operation using our dataset. On the other hand, language modeling focus on the
generation of domain-relevant data. It worked on a three-step method to generate an
augmented dataset, and then it developed six strategies to develop robust language models.

67
Chapter 5. SPEECH RECOGNITION – EVALUATIONS
5.1 Introduction
This chapter provides a detailed evaluation of the methods that we presented in the previous
chapter. Evaluations were done in 2 phases. Figure 5.1 shows the flow of the experiments
that we executed for our evaluations.
Figure 5.1 Flow of experiments
5.2 Setup
5.2.1 Evaluation Phases
Our solution defines methods to enhance both, acoustic and language models within the
speech recognition system, therefore our evaluation strategy consisted of two phases.
1) In the first phase, methods pertaining to each model were evaluated in isolation.
When evaluating the acoustic modeling method (in Section 0), we used the pre-
trained language model for the experiments. Similarly, when evaluating language
modeling methods (in Section 5.4), we used the pre-trained acoustic model. For the
evaluations in this phase, we did experiments with both, training and testing data to

68
analyze the performance when models have seen everything as compared to unseen
environments. We did not use the testing results to tweak the models, therefore we
did not use any separate validation set to test the models in this phase.
2) In the second phase, we evaluated both models in combination. The best performing
models from the first phase were selected to perform evaluations in combination.
We did not evaluate low performing methods in this phase, particularly due to the
fact that the first step of evaluation already gave us such insights. Finally, in this
phase, we used our validation set to present the final validation of our trained
models.
5.2.2 Cross-Validation
We used 10-fold cross-validation throughout the evaluations. Since we used the same
dataset to train both: acoustic and language: models, a conventional method of cross-
validation where the dataset shuffles and split into folds each time before conducting an
experiment can cause problems; specifically in the second phase of evaluations where we
intend to use trained models in combinations. Due to the limited dataset, we also cannot
afford to set aside a testing dataset. Therefore, to ensure reliable and valid evaluations, we
performed the shuffling and splitting task once, and recorded all the folds. Afterward, we
supplied the same folds whenever an experiment used cross-validation.
5.2.3 Interpretation of Results
In the evaluations, we analyze the impact of our methods by examining the difference in
performance and comparing it to baselines. As speech recognition systems are primarily
evaluated on error rates, we will be considering Word Error Rate (WER) along with our
custom metric Critical Error Rate (CER) to measure the performance where a lower error
rate means better performance. However, all the crucial decisions are made on the basis of
CER. There are two ways to examine the difference in performance. One way is to examine
the absolute change in error rates, while the other is to check the relative change with
respect to the error rate of baseline. In our evaluations, we have considered both ways to
examine our results, however, attention is given to the relative performance differences.

69
5.3 Evaluating Acoustic Modeling
This section provides an evaluation of our acoustic modeling method. In this method, we
fine-tuned the pre-trained acoustic model with our dataset. Fine-tuning was done till 8
epochs. We stopped at the 8th epoch due to the continuous increase in testing error rates.
Cross-validation was used to calculate testing error rates. For each of the 10 folds, the pre-
trained model was separately fine-tuned, and the error rates from all folds were averaged.
This process was repeated at each epoch. Error rates for training cases were calculated
directly by using the whole dataset for fine-tuning and using the same data to calculate
errors. Figure 5.2 shows the trend of errors on each epoch (horizontal axis) for both error
rates (vertical axis) and Table 5.1 lists down the values of error rates
Figure 5.2 Error loss in Acoustic Model training

70
Table 5.1 Training and testing error rates for Acoustic Model training
CER WER
Training CV Testing Training CV Testing
nth
Ep
och
1 27.59% 38.09% 26.84% 36.94%
2 19.62% 32.31% 19.43% 32.04%
3 16.47% 29.57% 16.56% 29.77%
4 13.06% 27.42% 13.53% 27.83%
5 12.57% 27.45% 12.94% 28.11%
6 10.84% 27.22% 11.47% 28.01%
7 9.25% 28.17% 9.84% 28.86%
8 9.37% 28.35% 9.75% 29.28%
5.3.1 Analysis
Analysis of error rates in comparison with the number of epochs showed that the model
reached a local minima on our dataset on around 4th to 6th epochs. Our analysis of the error
rates shows that the 6th epoch is the most efficient (CER: 27.22%) on the basis of CER,
while the 4th epoch is the most efficient (WER: 27.83%) on the basis of WER. With the
fine-tuning method, we were able to achieve 22.16% absolute and 44.88% relative
reduction in CER and 18.8% absolute and 40.32% relative reduction in WER (Table 5.2).
As the performance comparison was very close (error difference within a range of 0.2%),
models from the 4th to 6th epoch were selected for further evaluations of the second phase.
Table 5.2 Absolute and relative change in error rates after acoustic modeling
CER WER
Pre-trained AM 49.38% 46.63%
Pre-trained AM + fine-tuning 27.22% 27.83%
└ Absolute change -22.16% -18.80%
└ Relative change -44.88% -40.32%

71
5.4 Evaluating Language Modeling Methods
This section provides an evaluation of our language modeling methods. We provided six
strategies to train domain-relevant language models for improved recognition. In our
evaluations, we combined all those strategies to develop 8 evaluation scenarios that cover
all methods. Table 5.3 provides the details of each evaluation scenario.
Table 5.3 List of scenarios for Language Model evaluations
S.
No. Evaluation Scenario Strategy Details
1 Pre-trained LM Baseline: Performance from the preliminary
experiment is considered.
2 No LM No LM is used in this scenario.
3 New LM
+ Original in-domain corpus
New LM is trained using the text corpus from
the original in-domain dataset.
4 New LM
+ Augmented in-domain corpus
New LM is trained using the text corpus from
the augmented in-domain dataset.
5
Pre-trained LM
+ Original in-domain corpus
+ Pooling Method
Pre-trained LM is enhanced using the text
corpus from the original in-domain dataset
using the pooling method.
6
Pre-trained LM
+ Original in-domain corpus
+ Interpolation Method
Pre-trained LM is enhanced using the text
corpus from the original in-domain dataset
using the interpolation method.
7
Pre-trained LM
+ Augmented in-domain corpus
+ Pooling Method
Pre-trained LM is enhanced using the text
corpus from the augmented in-domain dataset
using the pooling method.
8
Pre-trained LM
+ Augmented in-domain corpus
+ Interpolation Method
Pre-trained LM is enhanced using the text
corpus from the augmented in-domain dataset
using an interpolation method.

72
Scenario 1 was developed to provide a baseline for this evaluation; therefore, we did not
run any experiments in this scenario; instead, the results from preliminary experiments
were considered. Scenario 2 was developed to test the performance of DeepSpeech without
the use of any language model, as it is not a required component in speech recognition. For
the experiments within this scenario, all audio clips from our original dataset were used to
calculate error rates. In all other scenarios, language models were trained and tested using
training and testing datasets. While evaluating the training error rates, language models
were trained using the whole text corpus from the original dataset and all audio clips from
the same dataset were used to test those models. While evaluating testing error rates, we
used 10-fold cross-validation.
5.4.1 Analysis
The analysis of our results shows that DeepSpeech did mistakes for more than half the time
in scenario 2 when no language model was used. Upon comparing the error rates with
baseline, one can see that the average CER increased around 8% and WER increased
around 10% when DeepSpeech did not use any language model. This provides evidence of
the importance of language models in the process of speech recognition. Moreover, when
such language models were used that has already seen the testing data while training, the
recognition performance matched the top of the line cloud-based SR (Google). This is not
a valid comparison to build a conclusion; nevertheless, it highlights the ability of language
models to significantly boost the recognition performance. Table 5.4 shows the error rates
for all scenarios when the training dataset was used to test the models that were trained
using the corpus from the same dataset. The table also shows error rates from the first 2
scenarios to provide a comparison, even though no language model was trained in those
scenarios.

73
Table 5.4 Training error rates from each evaluation scenario
Table 5.5 Cross-validated error rates from each evaluation scenario

74
Cross-validated experiments show that all our methods improved DeepSpeech
performance since we observe lower error rates as compared to the baseline in each
experimented scenario. We note a maximum absolute reduction of 4.81% WER and 9.9%
CER in our experiments, which translates into a 10.31% relative reduction in WER and
20.04% CER. Table 5.5 presents a bar chart plot and values of error rates in each scenario,
while Table 5.6 lists the absolute and relative differences as compared to the baseline.
Table 5.6 Absolute and relative change in error rates compared to baseline
Evaluation
Scenario
Critical
Error
Rate
Absolute
Difference
(CER)
Relative
Difference
(CER)
Word
Error
Rate
Absolute
Difference
(WER)
Relative
Difference
(WER)
Baseline
Pre-Trained LM 49.38% 0.00% 0.00% 46.63% 0.00% 0.00%
New LM
+ Original corpus 39.49% -9.9% -20.04% 41.82% -4.81% -10.31%
New LM
+ Augmented corpus 45.05% -4.33% -8.77% 43.10% -3.53% -7.57%
Pre-trained LM
+ Original corpus
+ Pooled
47.12% -2.26% -4.59% 45.03% -1.6% -3.43%
Pre-trained LM
+ Original corpus
+ Interpolated
42.40% -6.98% -14.13% 43.28% -3.35% -7.18%
Pre-trained LM
+ Augmented corpus
+ Pooled
47.04% -2.35% -4.75% 44.56% -2.07% -4.43%
Pre-trained LM
+ Augmented corpus
+ Interpolated
44.02% -5.36% -10.86% 42.76% -3.87% -8.29%

75
As we presented multiple methods that are applied in combination with each evaluation
scenario, we were interested in analyzing the impact of each individual method on the
performance of DeepSpeech. Therefore, we defined four independent variables based on
our methods, whose values represent results from each experimented scenario. Table 5.7
lists all variables and their values along with the scenarios that are represented by each
value combination. We assigned the value 1 to denote a True or ‘Yes’, meaning that the
respective variable was applied to the scenario, whereas, the value 0 denotes False or ‘No’.
Table 5.7 Variables to analyze each experimented method
Variables → Augmentation
of Original corpus
Development of in-domain
LM
Enhancement of Pre-Trained
LM using Pooling
Enhancement of Pre-Trained
LM using Interpolation
Evaluation Scenario ↓
3 0 1 0 0
4 1 1 0 0
5 0 0 1 0
6 0 0 0 1
7 1 0 1 0
8 1 0 0 1
Based on these variables, we analyzed the contribution of each method in improving the
performance of DeepSpeech. For this analysis, we applied linear regression where the null
hypothesis is that there is no change in performance within the different experimented
scenarios. Our analysis used only three of these variables since we had to drop the use of
variable “Development of in-domain LM” due to its direct correlation with other
enhancement variables (“Enhancement of Pre-Trained LM using Pooling” and
“Enhancement of Pre-Trained LM using Interpolation”). In scenarios 3 and 4, we
experimented with the methods that are based on the dropped variable; however, values
from other variables are still able to represent these scenarios (False for both of
enhancement variables translates into a True for dropped variable). We applied regression
analysis on both error rates individually by keeping them as the dependent variables. Figure
5.3 shows the results summary of regression analysis when WER is taken as the predicted
variable. Figure 5.4 shows the results summary of regression analysis for CER. In total 6

76
scenarios were compared each having 100 observations, therefore the summaries have
shown 600 observation count.
Figure 5.3 Result summary of regression analysis using WER
Figure 5.4 Result summary of regression analysis using CER
The ANOVA results from regression analyses reject the null hypothesis when CER is taken
as the performance factor, which provides the domain-specific error rate. Due to the
importance of critical errors, we argue that some of our methods have a significant impact
on the performance of recognition than others, even when there does not seem to have a
significant difference in general word errors. However, in these analyses, we were not able
to support any single method in providing a significant contribution to error reduction.
Therefore, we investigated more on our results to see the combined effects of our methods.

77
We firstly analyzed the results of those scenarios that applied the augmentation method to
compare with those scenarios that used original datasets. We observe that the augmentation
method increased error rates as compared to those language models that were created only
with our original dataset corpus. However, in those scenarios where we were enhancing
the pre-trained language model, the augmentation method did show some reduction in error
rates. We noted a maximum of 1.19% relative reduction in WER and 0.18% relative
reduction in CER; however, these reductions are not reliable, as we also observe substantial
increase (3.81% relative) in critical errors when enhancement is done using an interpolation
method. Table 5.8 mentions absolute and relative differences between all scenarios using
original and augmented datasets.
Table 5.8 Comparing error rates between original and augmented corpus
CER WER
New
LM
Pre-
Trained
LM
+Pooling
Pre-Trained
LM
+Interpolation
New
LM
Pre-
Trained
LM +
Pooling
Pre-Trained
LM
+Interpolation
Original corpus 39.49% 47.12% 42.40% 41.82% 45.03% 43.28%
Augmented corpus 45.05% 47.04% 44.02% 43.10% 44.56% 42.76%
└Absolute Diff. 5.57% -0.08% 1.62% 1.28% -0.47% -0.52%
└Relative Diff. 14.10% -0.18% 3.81% 3.05% -1.03% -1.19%
Secondly, we analyzed all those scenarios which train new language models to compare
with those scenarios that enhance the pre-trained model using the pooling method as well
as those using the interpolation method. We note that enhancement, in general, is not
effective in reducing error rates; however when interpolation is used to enhance the pre-
trained model, we observed 2.29% relative reduction of CER and 0.78% of WER using the
augmented corpus. From all other scenarios, a new language model using only the original
(un-augmented) corpus gave us the lowest error rates. Table 5.9 and Table 5.10 lists the
absolute and relative differences in error rates when using pooling and interpolation
methods in comparison to the new domain-specific language modeling method.

78
Table 5.9 Comparing error rates between new and enhanced pooled model
CER WER
Using
Original
Corpus
Using
Augmented
Corpus
Using
Original
Corpus
Using
Augmented
Corpus
New LM 39.49% 45.05% 41.82% 43.10%
└Enhanced LM using Pooling 47.12% 47.04% 45.03% 44.56%
└Absolute Difference 7.63% 1.98% 3.21% 1.46%
└Relative Difference 19.33% 4.40% 7.67% 3.40%
Table 5.10 Comparing error rates between new and enhanced interpolated model
CER WER
Using
Original
Corpus
Using
Augmented
Corpus
Using
Original
Corpus
Using
Augmented
Corpus
New LM 39.49% 45.05% 41.82% 43.10%
└Enhanced LM using Interpolation 42.40% 44.02% 43.28% 42.76%
└Absolute Difference 2.92% -1.03% 1.46% -0.33%
└Relative Difference 7.39% -2.29% 3.48% -0.78%
To sum up our analysis, we observe three key performance behaviors of our methods. 1)
The pooling method to enhance the pre-trained model has the least impact on the reduction
of error rates. 2) The application of the augmentation method on our original dataset,
however, did enhance the impact of the pooling method, yet it was not able to surpass the
standalone impact of the interpolation method. 3) Nevertheless, the development of simple
domain-specific language models has the highest impact, although, enhancement of the
pre-trained model seems a more logical option as it provides an opportunity to generate
models that are trained on a larger set of information.
To understand these behaviors, we analyzed the construction of the clinical notes from our
dataset i.e., our target domain. In the notes, we observe many patterns that were recurring

79
in almost the whole dataset. An instance that we observe that usually occur in the start of
every note is, “This is a <age> <weeks/month/year> old <white/black/other ethnicity>
<male/female> …”. Some examples that follow this pattern are; “This is a 2 months old
white male …”, “This is a 4-year-old black female ...”. Due to many of such patterns that
physicians mostly follow while dictating notes, a language model needs to learn them in
order to perform efficient recognition. If there happens to be a glitchy output from the
acoustic side, a language model will only be able to refine that output if it is already aware
of such patterns. The main purpose of language model training is, in fact, to pick the
recurring patterns from the training set. Therefore, when we talk about the pre-trained
model, it implies that this model has already identified patterns from the datasets on which
it was trained. Hence, when we try to enhance the pre-trained model, we try to teach it
some new patterns. The pre-trained model was trained on about 4 gigabytes of text,
whereas the text from our original dataset all combined is not more than 150 kilobytes.
Therefore, we consider that our smaller text corpus was not able to make a significant
impact while enhancing the pre-trained model due to the smaller size. The property of the
pooling method to give equal weight to all data sources also supports this idea. This also
explains the increased impact of error reduction by the use of the augmentation dataset, as
it increases the size of the domain-relevant text corpus.
After analysis, we selected language models from all scenarios for the second phase
experiments, except those scenarios that implement the pooling method. We dropped the
pooling method for further evaluations due to two main reasons. Firstly, it has shown the
least performance gains, as we have mentioned above. Secondly, pooling is one of the two
model enhancement methods that we experimented with; therefore, we only wanted to
continue with one best method of enhancement.

80
5.5 Combined Evaluation
In this section, we provide our second phase of evaluation. In this phase, no new model
was trained, instead, the best performing models; that we selected from previous
evaluations; were analyzed further. We selected multiples of both: acoustic and language;
models and tested all their combinations on our original dataset using the same cross-
validation folds upon which the models were trained. Table 5.11 lists the error rates for all
tested combinations in this evaluation phase.
Table 5.11 Error rates after testing with combined models.
CER WER
Acoustic Model → 4th Epoch 5th Epoch 6th Epoch 4th Epoch 5th Epoch 6th Epoch
Language Model ↓
Pre-trained LM
+ Original Corpus
+ Interpolated
26.55% 26.04% 25.51% 28.30% 28.12% 27.90%
Pre-trained LM
+ Augmented Corpus
+ Interpolated
25.73% 25.89% 25.17% 26.97% 27.41% 26.95%
New LM
+ Original Corpus 24.03% 24.28% 24.05% 27.18% 27.51% 27.35%
New LM
+ Augmented Corpus 26.65% 26.10% 25.74% 27.13% 27.49% 27.23%
5.5.1 Analysis
The combined evaluation showed that we achieved the lowest word error rate (WER:
26.95%) from the combination of the acoustic model of the 6th epoch and the pre-trained
language model that is enhanced using augmented corpus. However, this model
combination was slightly behind with respect to critical error rates. The lowest critical error
rate (CER: 24.03%) was achieved by the 4th epoch acoustic model in combination with a
new language model that was trained using only the original dataset.
The analysis of results shows that the language modeling methods of dataset augmentation
and model interpolation works best in combination to reduce general error rates. In terms

81
of WER, the augmented interpolated language models performed better than standalone
augmented and standalone interpolated models and were also the overall best performing
models.
Table 5.12 Performance comparison of DeepSpeech (before and after) with Google
When analyzing critical errors, we found that the 4th epoch acoustic model did less critical
mistakes when combined with new language models, and the 6th epoch acoustic models
did less critical mistakes with interpolated language models. However, the lowest critical
error rate was achieved by newly trained language models on the original dataset. The
augmented interpolated language models were the second-lowest with about 4.7% relative
difference.

82
In the end, we found that all of our acoustic and language modeling methods, in
combination, were able to significantly improve the performance of DeepSpeech by
reducing error rates from 46.63% to 26.95% WER and from 49.38% to 25.17% CER. This
reduction relatively translates into a 42.2% reduction in WER and 49.02% in CER. This
improvement enables DeepSpeech to deliver performance that is relatively close to the
performance of top-of-the-line cloud-based SR (Google). Table 5.12 shows the error rates
of Google, DeepSpech before applying our methods and DeepSpeech after applying our
acoustic and language modeling methods.
5.6 Working Examples
In this section, we have provided examples of critical and word errors within the
transcribed notes that we observed with the best performing model combinations. In this
section, we present a best-case examining transcribed note with the least critical errors, a
worst-case examining a note with the most critical errors and two random cases. The two
model combinations that we are examining are 1) 4th epoch acoustic model and new
language model with the original corpus, and 2) 6th epoch acoustic model and enhanced
pre-trained language model with the augmented corpus.
5.6.1 Best Case
In all our 100 notes, the best-transcribed note achieved a CER as low as 6.25% with the 1st
model combination where it made only 5 critical mistakes out of 80 total critical concepts.
With the 2nd model combination, it achieved 7.5% CER and made 6 critical mistakes. The
quality of the corresponding speech in the audio note is found to be clear without any
background noise. The dictation is at a normal pace and it appears to be recorded in a closed
room with a relaxed environment. Almost all critical mistakes, in this case, were found to
be homonyms. For example, “enterovirus” was mistaken as “ether is” and “two older” as
“told or”. Table 5.13 lists transcriptions from both model combinations. All the highlighted
and bold words and phrases are the errors. The yellow highlights are general word errors,
while green highlighted and underlined are critical errors.
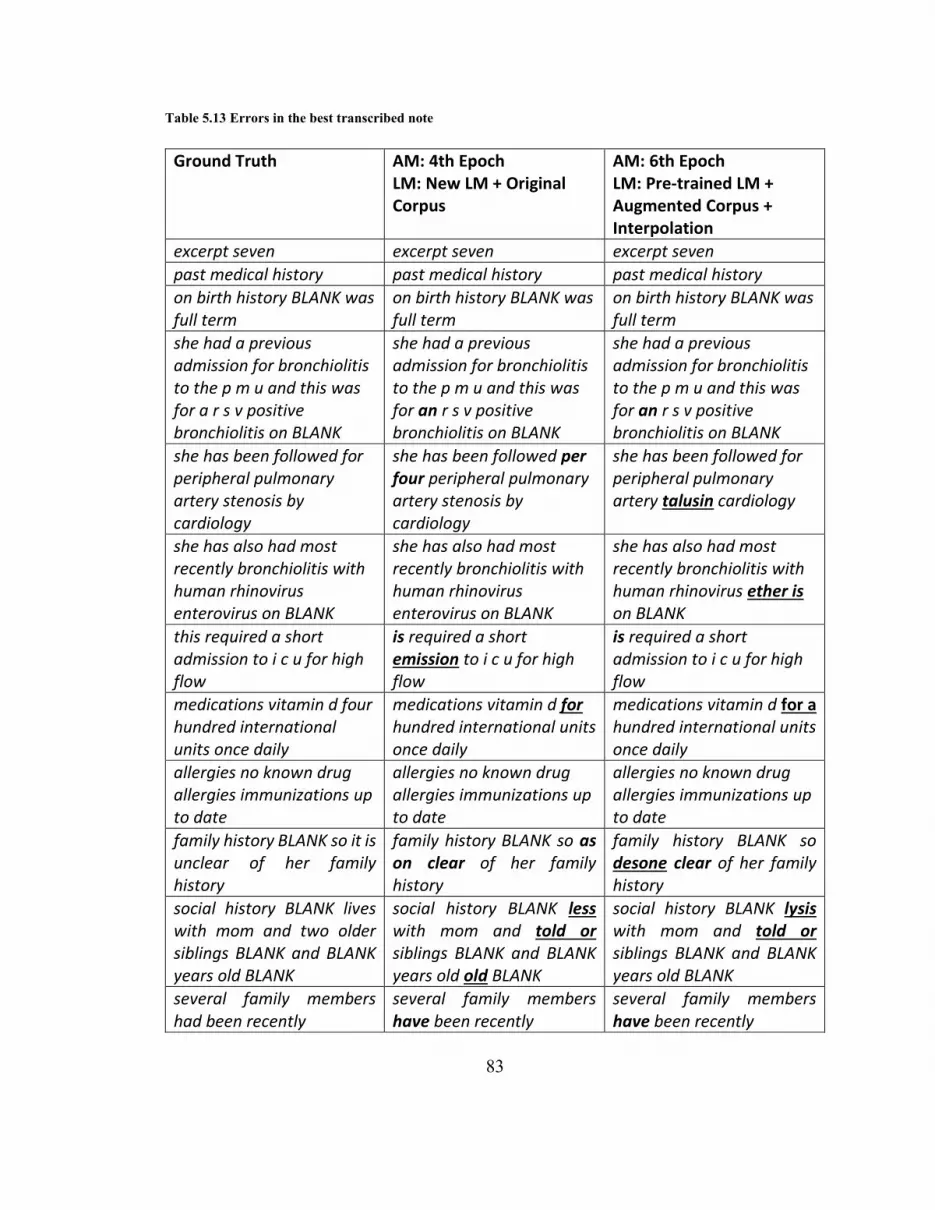
83
Table 5.13 Errors in the best transcribed note
Ground Truth AM: 4th Epoch LM: New LM + Original Corpus
AM: 6th Epoch LM: Pre-trained LM + Augmented Corpus + Interpolation
excerpt seven excerpt seven excerpt seven
past medical history past medical history past medical history
on birth history BLANK was full term
on birth history BLANK was full term
on birth history BLANK was full term
she had a previous admission for bronchiolitis to the p m u and this was for a r s v positive bronchiolitis on BLANK
she had a previous admission for bronchiolitis to the p m u and this was for an r s v positive bronchiolitis on BLANK
she had a previous admission for bronchiolitis to the p m u and this was for an r s v positive bronchiolitis on BLANK
she has been followed for peripheral pulmonary artery stenosis by cardiology
she has been followed per four peripheral pulmonary artery stenosis by cardiology
she has been followed for peripheral pulmonary artery talusin cardiology
she has also had most recently bronchiolitis with human rhinovirus enterovirus on BLANK
she has also had most recently bronchiolitis with human rhinovirus enterovirus on BLANK
she has also had most recently bronchiolitis with human rhinovirus ether is on BLANK
this required a short admission to i c u for high flow
is required a short emission to i c u for high flow
is required a short admission to i c u for high flow
medications vitamin d four hundred international units once daily
medications vitamin d for hundred international units once daily
medications vitamin d for a hundred international units once daily
allergies no known drug allergies immunizations up to date
allergies no known drug allergies immunizations up to date
allergies no known drug allergies immunizations up to date
family history BLANK so it is unclear of her family history
family history BLANK so as on clear of her family history
family history BLANK so desone clear of her family history
social history BLANK lives with mom and two older siblings BLANK and BLANK years old BLANK
social history BLANK less with mom and told or siblings BLANK and BLANK years old old BLANK
social history BLANK lysis with mom and told or siblings BLANK and BLANK years old BLANK
several family members had been recently
several family members have been recently
several family members have been recently

84
5.6.2 Worst Case
In our results, the worst transcription achieved the CER of 59.6% with 2nd model
combination and 54.8% CER with 1st model combination. We observed that the quality of
the corresponding audio note is significantly lower than other notes. We note high echo
and reverberation in the audio while appearing that the speaker is away from the recording
device. This audio note was also filled with a high amount of background noise, especially
the overlapping noise that is corrupting the speech signals. We hear loud baby cries and
parents trying to soothe the baby in the background by talking and playing with the baby.
These interruptions reflect on the mistakes. For example, in one place “abdominal pain” is
mistaken as “a dona panadol”. This transcription is not a homonym for its gold standard.
Another similar example is when “upper respiratory tract infection” transcribes into “offer
reichstein”. These examples show that due to overlapping noise, a lot of speech signal is
lost, resulting in a sloppy transcription. Table 5.14 presents the comparison of
transcriptions for both model combinations. Green highlights show critical mistakes.
Table 5.14 Errors in the worst transcribed note
Ground Truth AM: 4th Epoch LM: New LM + Original Corpus
AM: 6th Epoch LM: Pre-trained LM + Augmented Corpus + Interpolation
this is a four year almost
five year old female with
trisomy twenty one
he is a four year always
five year old female at ten
twenty one
he is a four year as five
year old female as try
twenty one
presenting with two to
three week history of upper
respiratory tract infection
that has lingered
awakening with a cough
and having the cough
during the day and
sometimes at night
is an in a to the three
weeks history as offer
rather infection of lines
waiting with her cough
and having (the) cough
during the day and some
time at night
is anion so to three weeks
history as offer reichstein
of linear waiting with call
and having (the) cough
during the day had some
time (at) tight
ventolin of no benefit
recently
that on no better we that on no batel rashes
she has had no fevers with
this
she (has) had no fevers
with this
(she has) at no fevers with
this

85
possible headache no other
pain
four headache nor her
pain
four endantadine
she has had abdominal
pain and vomiting a week
ago that resolved over
about a day and resulted in
multiple episodes of
vomiting
she has had a do paid
(and) vomiting a week no
that resolved over about a
vein (and) result is well
colitis following
she has had a dona
panadol in a week no the
resolved over about ada in
result as well colicines
following
she has been on p o
steroids for the last five
days as per the parents
usual approach to acute
asthma
she says on p o per i for
(the last) five days her the
parents usual got his used
for as no
she see n p o ser for (the
last) five days her the
parents usual proctocele
for as mopeg
paragraph past medical
history immunizations are
up to date
paragraph past medical
history immunizations are
(up to) date
ph past medical history
immunizations (are) up to
date
she has had a tetralogy of
fallot repaired trisomy
twenty one and she is on
valproic acid and
clobazam for seizure
disorder which is quiescent
for the last two years
ten had also or care
trisomy twenty one and she
(is) on a for acid episode
for (seizure disorder)
which is a two years
on fenoterol some or
paired trisomy twenty one
and she (is) on dolo acidic
anorectics two years
on exam no respiratory
stress normal air entry
with no wheeze airway
breathing and circulation
stable
on exam no respiratory
stress normal artery with
no wheezer we breathing
in certain stable
on exam no respiratory
stress normal reentry with
no leader we breathing and
circulation stable
pink soft belly normal left
ear normal right ear
pain saw a day normal as
ear nor rays
pain sagatal normal last
ear nor river
snotty nose but not
dramatically swollen
tonsils, slightly red, no pus.
not dramatically acute
not of note a iron in last or
or to widened no refused
to one week ago i saw so
so i group is probably a
mild mild being a certain
in wide per were more
operation the in are work
but i do an a b released
nodose but no oestro
intraorbital red neural
perforin was miosis so so
iridoids probably mild
iletin ceresan viper werner
osteoid an a b q resin

86
5.6.3 Random Cases
We chose two random notes, in between the above-presented best and worst cases, to
analyze the mistakes. Upon examining the corresponding audio recordings, we found that
the noise levels remained between the above-defined two example cases. There were no
overlapping noises, however, we could listen to some reverberation. On a few occasions,
the physician’s dictation pace increased dramatically, which directly increased mistakes in
transcriptions. On one of such occasions, the phrase “feet swept out from underneath him”
was mistaken as “feet slept out from under eat him”.
The first random note we examined achieved 11.66% CER with the 1st model combination
and 14.4% CER with 2nd model combination. Table 5.15 mentions the transcription we
received with both model combinations.
Table 5.15 Errors in the first examined note transcription
Ground Truth AM: 4th Epoch LM: New LM + Original Corpus
AM: 6th Epoch LM: Pre-trained LM + Augmented Corpus + Interpolation
this is an eighteen month old black female
this is a ten month old black female
this is a ten month old black female
presenting with a seizure like episode at home
presenting with a seizure like episode at home
presenting with a seizure like episode at home
child was perfectly well until three days ago when sniffles and cough became apparent
child was perfectly well until three days ago when sniffles and cough became apparent
child was perfectly well until three days ago when sniffles and cough became apparent
last evening at about eighteen hundred hours the child experienced a mild fever of thirty eight point five
last evening (at) about eighteen hundred hours the child experience on mild (of) fever thirty eight point five
last evening (at) about eighteen hundred hours the child experience a mild fever (of) thirty eight point five
this morning on rousing her from her bed and she stiffened exhibited five to fifteen seconds of shaking movements suggestive of
this morning on rising her for her bed if she stiffened excited five to fifteen seconds of of shaking movement suggestive of
this morning on the rising her for her bed if she stiffened excited five to fifteen seconds of of shaking movement

87
tonic clonic seizure and then settled into a deep sleep from which she roused fifteen minutes later
tonic clonic seizure and in settled into a deep sleep for which she was fifteen minutes later
suggestive of tonic clonic seizure and intensain to a deep sleep for which she resistin in the later
by the time she arrived at the i w k emergency she was awake and alert and cranky
in time she wrist the i w k emergency is she was awake and alert and cranky
date she arrived at the i w k emergency i she was awake and alert and cranky
parents have never seen similar seizure activity before
parents have never seen similar seizure activity before
parents have never seen similar seizure activity before
past medical history reveals immunizations up to date and normal birth and pregnancy history with no specialist and no regular medications and no known allergies
past medical history revealed immunizations up to date a normal birth and pregnancy history with no specialists and no regular medications and no known allergies
past medical history reveals immunizations up to date a normal birth and pregnancy history with no specialist and no regular medications and no known allergies
family history reveals febrile seizures in dad as a child
family history reveals febrile seizures in dad as a child
family history reveals febrile seizures in dead as a child
physical exam revealed a cranky child who settled with care
physical exam revealed a cranky child who settled with care
physical exam revealed a cranky child who settled with care
ear nose and throat exam revealed a red throat with no exudate suggestive of a viral pharyngitis
ear nose and throat exam revealed a red throat with no x date suggestive of a viral pharyngitis
ear nose and throat exam revealed a red throat with no exo date suggestive of a viral paris
ears were normal lungs were clear
ears were normal lungs were clear
ears were normal lungs were clear
cardiac exam was unremarkable
cardiac exam was unremarkable
cardiac exam was unremarkable
abdominal exam was normal
abdominal exam was normal
abdominal exam was normal
neurological exam revealed a child who following ibuprofen was playful and interactive and no focal finding on
neurological exam revealed a child who following ibuprofen was playful and interim and no focal findings on
neurological exam revealed a child who following ibuprofen was playful and interacting and no focal findings under local exam is cover

88
neurological exam was discovered
neurological exam is descend
new paragraph impression is that this is simple febrile seizure
new paragraph impression is that this is simple febrile seizure
new paragraph impression is that this is simple febrile seizure
parents were counseled and reassured
parents were counseled and reassured
parents were counseled and reassured
instructions were given with regards to the delivery of ibuprofen as needed for pain and fever but the parents were cautioned that this would not reduce the risk of further seizures.
instructions were given with regards to the delivery of ibuprofen as needed for pain and fever by the parents were cousin that this would not reduced the risk of for other seizures
instructions were given with regards to the delivery of i do provided for pain and fever but the parents were cation that this would not reduced the rose of further seizures
we stated the seizure risk at about one or two percent over the rest of this illness
we stayed the seizures (risk) at about one or two percent over the rest of the illness
we state the seizure risk at about one or two percent over the rest of the sinus
but cautioned them that further febrile seizures were likely between now and six years of age
but out on them that further febrile i sure were likely between now and six years of age
but cation them that further febrile tissue (were) likely between no and six years of age
her parents were advised to return to the emergency department with further seizures for further assessment
a parents were advised to return to the emergency department with rather seizures refer her assessment
a parents were advised to return to the emergency department with further seizures refer assessment
diagnosis viral upper respiratory tract infection with febrile seizure
diagnosis for upper respiratory tract infection with febrile seizures
diagnosis boro upper parry tract infection with febrile seizure

89
The second random note we examined achieved 22.41% CER with the 1st model
combination and 24.13% CER with 2nd model combination. Table 5.16 shows the
transcription of the second random note we examined.
Table 5.16 Errors in the second examined note transcription
Ground Truth AM: 4th Epoch LM: New LM + Original Corpus
AM: 6th Epoch LM: Pre-trained LM + Augmented Corpus + Interpolation
excerpt thirty one excerpt thirty one excerpt thirty one
medications at admission medications at admission medications at admission
two hundred and fifty
milligrams of amoxil t i d
for ten days started on
BLANK
to turn fifty milligrams of a
lot p i d for ten days see on
BLANK
to endrin fifty milligrams of
a moban t i d for ten days
are on BLANK
examination at admission examination and admission examination and admission
BLANK was afebrile and
vitally stable
BLANK is a febrile advised
this table
BLANK was a febrile and
vita e table
head and neck exam was
unremarkable cervical
lymph nodes were palpable
and less than one point five
centimeters in diameter
head and neck exam was
unremarkable service
lymph nodes with health
able and less than one point
five centimeters and via
head and neck exam was
unremarkable service
lymph nodes but palpable
and less than one point five
centimeters and dia
cardiac exam was normal cardiac exam was normal carb exam was normal
respiratory exam showed
increased work of
breathing
respiratory exam showed
increased work of everting
respiratory exam showed
increased work of retin
intercostal indrawing on
the right side
intercostal indrawing on
the right side
intercostal in von on vit
side
good air entry bilaterally
and course crackles and
wheezes throughout both
lung fields
a good air entry bilaterally
and course crackles one a
throat business
a good air entry bilaterally
and coarse crackles and
tear out pulseless
her abdominal exam was
unremarkable
her abdominal exam was
unremarkable
her abdominal exam was
unremarkable
allergies none allergies non allergies on
immunization status immunizations status immunizations status

90
After reviewing the individual cases, we observed that DeepSpeech was able to understand
the domain-specific speech for the most part. However, we noted 3 factors that are
prominently linked with the errors.
1) Reverberation
On average our dataset has low levels of reverberation. However, those audio notes
having high reverberation are consistently linked with high numbers of errors.
2) Overlapping Noise
Similar to reverberations, most of the notes in our dataset have moderate noise levels
that do not interfere with the speech. Therefore, such instances skew the performance
of transcriptions to a large extent.
3) Dictation Pace
Within the notes, we observed that the commonly occurring phrases are uttered at a
high pace, while complicated sentences are uttered slowly. However, when the speech
pace is up, transcription starts to show errors mostly by skipping critical words.

91
5.7 Final Validation
In this section, we report the results of our acoustic and language models on a separate
validation dataset. In the process of dataset preparation (Section 3.4.2), we separated a
validation set that we did not use in any of our prior experiments. Therefore, in this final
validation, we used our validation dataset upon all of our selected models, which were
trained from the whole original dataset. Table 5.17 lists the error rates for all model
combinations.
Table 5.17 Error rates on the validation dataset
CER WER
Acoustic Model → 4th Epoch 5th Epoch 6th Epoch 4th Epoch 5th Epoch 6th Epoch
Language Model ↓
Pre-trained LM
+ Original Corpus
+ Interpolated
32.09% 30.52% 30.41% 35.99% 34.39% 34.65%
Pre-trained LM
+ Augmented Corpus
+ Interpolated
33.24% 32.04% 33.30% 35.20% 34.23% 35.02%
New LM
+ Original Corpus 30.98% 29.63% 28.96% 34.99% 34.14% 33.84%
New LM
+ Augmented Corpus 34.30% 33.89% 34.61% 35.70% 35.34% 35.79%
We observed similar behaviors from the results of the final validation. With respect to
WER, the lowest error rates were from the enhanced pre-trained models that use the
augmented dataset and newly trained models on the original dataset. The lowest two error
rates from these language models only had an absolute difference of 0.09%. However, with
respect to CER, we found that newly trained models on the original dataset did a relative
maximum of 5% less critical mistakes then the enhanced pre-trained models.

92
5.8 Discussion
Throughout the evaluations, we observe that newly trained language models on our original
(un-augmented) dataset were performing similar to, or sometimes better than those
language models that apply our augmentation and model enhancement methods,
specifically in regard to critical errors. We consider that this was due to the extremely small
size of our dataset, which impacts the performance in two ways.
1) Language modeling is all about vocabulary and speech patterns. Thus, the small size
of our dataset does not cover both aspects sufficiently to reflect the target domain. We
tried to handle the vocabulary aspect by dataset augmentation method; however, we
were not able to introduce more domain-specific speech patterns.
2) The pre-trained model is trained on a significantly larger dataset than ours. Moreover,
when our small dataset breaks down into folds for cross-validation, it creates many
unseen scenarios for the testing. Thus, all those unseen domain-specific speech patterns
get compensation by the prior knowledge of the pre-trained model, which does not
reflect our target domain.
In addition to these two reasons, our limited implementation of the augmentation method
also hinders the reduction of critical errors. Since our definition of critical errors entails all
the domain-specific vocabulary, yet we only used two domain-specific classes (drugs and
diseases) to augment our augmentation method. Therefore, all the concepts of remaining
domain-specific classes also remain unseen in the experiments with testing folds.
The interpolation method that develops a language model using information from multiple
data sources has the ability to adjust in case the volume of data is not similar across all
sources. As there is a huge size difference in the data source of the pre-trained language
model and our dataset, the interpolation method logically has the means to cope up in this
situation. However, interpolation requires a separate tuning set from the target domain to
calculate weights for each data source. Since our dataset is already limited, fetching a
tuning set from it makes it even smaller. Therefore, we found that in our experiments the

93
interpolation method performed fairly closer to stand-alone models, but they were not able
to surpass the performance. Had we had a slightly larger dataset; we consider that the
interpolation method would have been the best in performance.
5.9 Conclusion
This chapter presents an evaluation of our defined methods. We have shown that by using
the fine-tuning method on the pre-trained deep speech acoustic model, WER relatively
decreased by 40.32% CER by 44.88% on our original dataset. After applying the data
augmentation method to our dataset and using the interpolation method to enhance the pre-
trained language model, we managed to reduce the error rates further relatively by 42.2%
WER and 49.02% CER. In our evaluations, we observed that the pooling method to
enhance the pre-trained language model had the least impact on the reduction of error rates.
Furthermore, when we applied our language modeling methods in isolation, neither of
those methods had a reducing impact on error rates. However, when applied in
combination, we observed lower error rates when the pre-trained language model was
enhanced using the interpolation method and augmented dataset.

94
Chapter 6. CLASSIFICATION OF TRANSCRIPTION INTO
SOAP CATEGORIES
6.1 Introduction
This chapter presents our work to categorize clinical transcriptions as a SOAP structured
clinical report. To achieve our second objective, we have selected an exemplar-based
concept detection algorithm [102] with the motivation to extend it for SOAP classification.
This algorithm was chosen particularly due to its nature of using the word n-gram based
approach that we consider working in our problem. In previous work, Mowery [101] have
used an n-gram based approach as well and showed positive results. However, their work
poses two major limitations. This exemplar-based algorithm takes care of both limitations.
Firstly, it makes use of overlapping word grams that fully exploit the sentence sequences.
Secondly, since it works on exemplar matching, it should not have an impact on class
imbalance.
6.2 Methods
6.2.1 Assigning SOAP categories to Dataset
Our dataset did not provide prior assignments of sentences into SOAP categories; hence
we perform data labeling manually on our dataset. We perform this task before working on
methods to analyze class proportions of our dataset and to make logical decisions. To label
the sentences within our dataset, we referred to the definitions of SOAP categories and
related literature to identify the guiding principles for each category. Learning on those
principles we skimmed over the dataset looking for commonly occurring patterns within
each category. Based on the understanding we developed by these guiding principles and
patterns, we heuristically assigned a SOAP label with each sentence within our dataset.
The heuristics we applied for each of the SOAP category is given below.
1) Subjective
Sentences having narrations of tales happened to patients and are from the patient’s
perspective. Subjective sentences are mostly in the past tense defining a scene
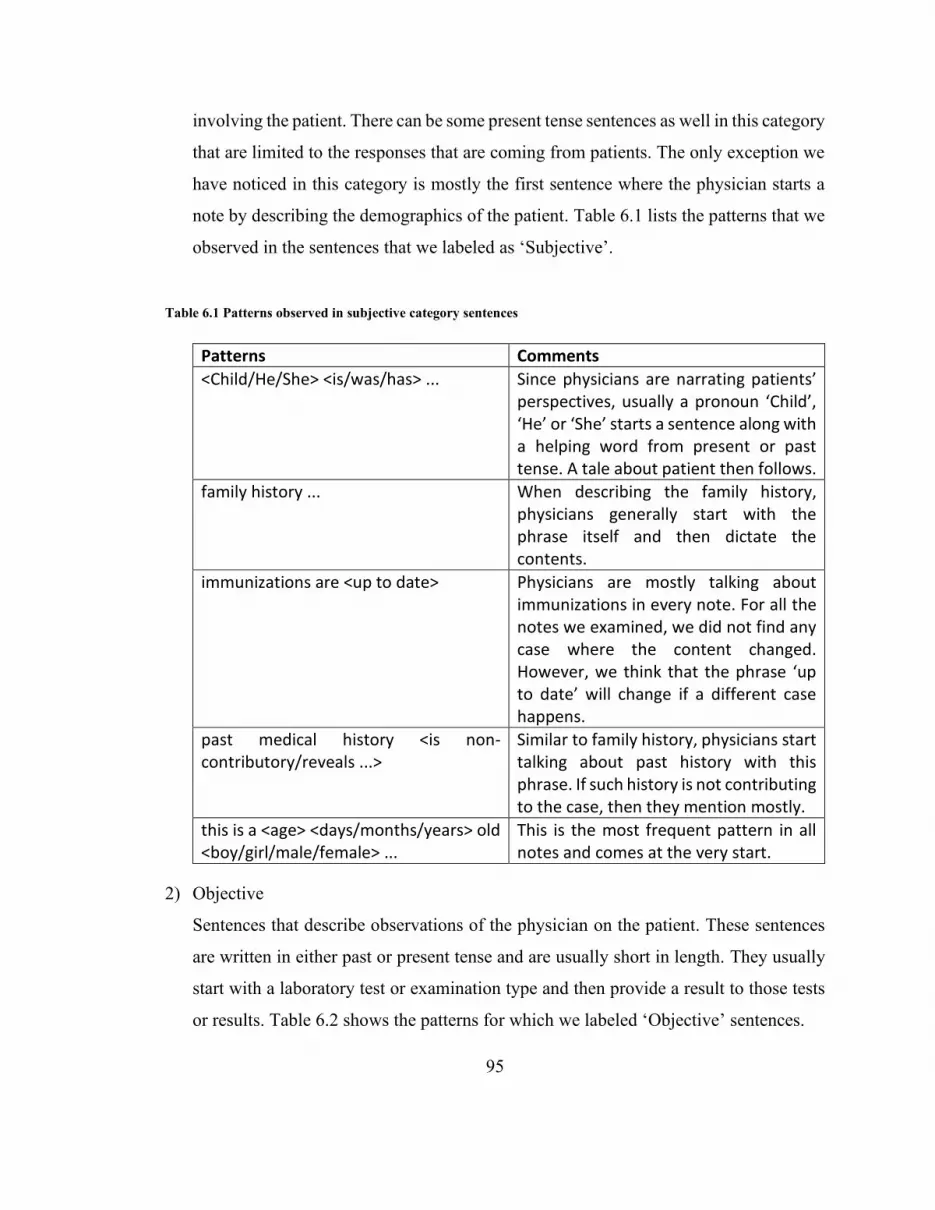
95
involving the patient. There can be some present tense sentences as well in this category
that are limited to the responses that are coming from patients. The only exception we
have noticed in this category is mostly the first sentence where the physician starts a
note by describing the demographics of the patient. Table 6.1 lists the patterns that we
observed in the sentences that we labeled as ‘Subjective’.
Table 6.1 Patterns observed in subjective category sentences
Patterns Comments
<Child/He/She> <is/was/has> ... Since physicians are narrating patients’ perspectives, usually a pronoun ‘Child’, ‘He’ or ‘She’ starts a sentence along with a helping word from present or past tense. A tale about patient then follows.
family history ... When describing the family history, physicians generally start with the phrase itself and then dictate the contents.
immunizations are <up to date> Physicians are mostly talking about immunizations in every note. For all the notes we examined, we did not find any case where the content changed. However, we think that the phrase ‘up to date’ will change if a different case happens.
past medical history <is non-contributory/reveals ...>
Similar to family history, physicians start talking about past history with this phrase. If such history is not contributing to the case, then they mention mostly.
this is a <age> <days/months/years> old <boy/girl/male/female> ...
This is the most frequent pattern in all notes and comes at the very start.
2) Objective
Sentences that describe observations of the physician on the patient. These sentences
are written in either past or present tense and are usually short in length. They usually
start with a laboratory test or examination type and then provide a result to those tests
or results. Table 6.2 shows the patterns for which we labeled ‘Objective’ sentences.

96
Table 6.2 Patterns observed in objective category sentences
Patterns Comments
<EXAM NAME> <is/was> <normal/unremarkable/uncomplicated/...>
Subjective sentences are talking about laboratory and physical exam results. Mostly these exams are good, so physicians are noting that down.
<EXAM NAME> reveals ... In case an exam reveals something, they also mention that.
On exam <child/he/she> <was/has> ... Mostly for physical exams, physicians simply use ‘On exam’.
the rest of exam <was/is> ... This pattern is also fairly visible in the notes.
<BODY PART> <is/are> <normal/clear/...> While defining results of physical exam, physicians note down the state of each body part they examined.
3) Assessment
Sentences that describe the assessment of the physician on the patient. These sentences
usually have the word ‘diagnosis’ in them along with a disease or medical condition.
Table 6.3 mentions some patters for ‘Assessment’ sentences
Table 6.3 Patterns observed in assessment category sentences
Patterns Comments
diagnosis is <DIAGNOSIS> The word ‘diagnosis’ is prominent in assessment category sentences.
<Medicine name and dosage> was prescribed
This is a loose pattern that we don’t find following a general style. In concept, this pattern mentions about the medications and treatments that are prescribed to the patient.
parents were <reassured/instructed> ... This pattern mentions all the instructions and reassurances that the physician has given to the parents of the patient which starts with the phrase ‘parents were instructed …’ and ‘parents were reassured that…’

97
4) Plan
Sentences that describe plans of the physician for the future treatments on the patient.
These sentences are usually written in the future tense. Table 6.4 lists the patterns for
‘Plan’ category sentences.
Table 6.4 Patterns observed in plan category sentences
Patterns Comments
... follow up ... This is a loose pattern that look for sentences with the phrase ‘follow up’. One variation that we observed multiple time is “Follow up as necessary”
<child/parents> <was/were> advised to return if...
This pattern mentions the advice of physician to return if some condition happens.
<Plans for future treatments> This is also a loose pattern. Generally, it looks for future treatment options. Physician does not seem to follow a strict word sequence for this.
All the sentences from our original dataset are extracted, and each sentence is manually
labeled according to the heuristics defined above. The labeled dataset is saved such that
features represent sentences and labels consist of one of the SOAP categories. In this
process, we observe that there is a class imbalance in our dataset. We note around 47%
Subjective, 35.3% Objective, 11% Assessment, and 6.7% Plan sentences in our dataset.
The imbalance property of our dataset matches the way clinical reports are usually written.
The same spread of classes is shown by Mowery [101] which also supports our observation.

98
6.2.2 Exemplar-based Concept Detection
Concept detection is a problem in NLP to extract relevant information from text
collections. Juckett presents an exemplar-based algorithm to link text to semantically
similar classes [102]. It maps each word within the text with probable class assignments.
Figure 6.1 highlights the algorithm. The algorithm is named Fuzzy matching. Juckett then
presents another algorithm Output array creation that takes the output values from Fuzzy
matching to create an array of detected concepts.
Figure 6.1 Exemplar based algorithms proposed by Juckett [102]
The Fuzzy matching algorithm expects to have some relevant text available that are already
categorized by human annotators to train exemplars. Exemplars are defined as the
collection of unique text strings that belong to specific semantic classes. In this algorithm,
exemplars are stored as Bag of Words (BOW) and Bag of Bi-characters (BOB). For each
sentence in the training set, an exemplar pair of BOW and BOB is created. BOW is the set
of all words within the training sentence. BOB is created after removing spaces from the

99
sentence and then extracting all overlapping character bi-grams. All generated exemplar
BOW and BOB are then stored along with the class assignments of training sentences.
To perform concept detection, the query sentence is first filtered for punctuations and
determiners are removed. It then creates overlapping word n-grams to the maximum of 5th
order (1-gram, 2-gram … 5-gram). Each word n-gram is converted into BOW and BOB
and stored. It gives a list of BOW and BOB for all possible word n-grams (till the order 5)
within the query. For each word n-gram, exemplars are selected that are of length between
n and 4n. For each selected exemplar, the Jaccard Index [120] of exemplar and word n-
gram is calculated for both; BOW and BOB, and the larger of these two values is selected.
After having similarity values of word n-gram with each exemplar, top n values are
selected. Word n-gram and exemplar information for the selected values are then stored.
Figure 6.2 Outline of word-class array [102]
After selecting the top n values, the algorithm Output array creation generates a word-by-
class map. Word-by-class map is a two-dimensional array where rows are the words in the
query text, and columns are the classes. Each cell within the array gets the score of word-
class combination. From the stored values in fuzzy matching, all values are selected whose
n-gram has the word, and exemplar belongs to the class. All these values are then added,
and the resultant value is stored as the word-class combination score. Figure 6.2 highlights
a word-class matrix as shown in [102].

100
6.2.3 Exemplar-based Sentence Classification
The second objective of this thesis requires the classification of textual units from
transcriptions into one of the SOAP categories. We consider sentences as a textual unit. To
achieve our objective, we develop an exemplar-based sentence classification algorithm on
the principles of exemplar-based concept detection by extending it to work on whole
sentences and provide confidence scores for each class. We use this algorithm due to its
nature to exploit word sequences. Moreover, since this algorithm work on exemplars, class
imbalance does not make a huge impact. As it selects top n scores for each n-gram, it can
optimally perform as long as there is a minimum of n exemplars available for each class.
Juckett took many assumptions during the development of the concept-detection algorithm
[102]. Since we adapt and extend this algorithm for a different problem and situation, we
identify four key areas that possibly develop an issue. Therefore, we investigate each of
those areas to find an optimal solution. After having a solution, we consider each area as
an independent variable to test the impact of our solution concerning the original
implementation. Details for each identified area are given below.
1) Stop Words
Stop words removal is a widely accepted and effective pre-processing step in various
problems of NLP [121]. However, the concept detection algorithm does not remove
stop words from their processing step. Moreover, in the arguments, Juckett [102] does
not provide any justification for keeping the stop words. Therefore, in this work, we
consider the removal of stop words since it has shown to have significant performance
improvements in text categorization tasks [122]. We apply a step to remove stop words
and make it optional in our classification algorithm by including it as an input
parameter.
2) Maximum word n-gram length limit
In the concept-detection algorithm, the query sentence converts into word-grams of
varying lengths from 1-gram to the maximum of 5-grams. There were two reasons
given for limiting the maximum n-gram length till the 5th order. Frist is that the dataset

101
on which Juckett [102] experimented, had shorter exemplars where 2/3rd of exemplars
were of word length five or less. The second reason is that each increasing word-gram
length increases the computation time exponentially. In our situation, the dataset has
sentences with an average length of 13 words, whereas 2/3rd of sentences are about 17
words or lower. With the same reasoning, we should look at 17-gram exemplars.
However, since the magnitude of the difference is more than double, a limit of 17-
grams can cause the algorithm to run for much more extended periods. Therefore, we
approach not to limit the length of maximum word n-grams in the algorithm; instead,
move the limit as an input parameter. There are two reasons for this approach. First, it
is easier to evaluate with varying maximum lengths. Second, this enables adaptation of
this algorithm to use on a dataset having sentences of different average lengths.
3) Exemplar type
The concept detection algorithm keeps full-text strings in the exemplars. Juckett [102]
does not report the considerations they took while defining exemplars. As we extend
the algorithm in our problem domain, we recognize that keeping full-text strings in
exemplars can cause some problems.
The current approach creates one exemplar per text string from the training text. We
have a small dataset, in which sentence length ranges from 3 words to 49 words. These
text strings come from natural speech and can have larger compound sentences.
Creating one exemplar for these larger text strings limits the opportunity to create
multiple exemplars. Moreover, due to the longer size of such text strings, they will be
skipped in many comparisons with shorter word n-grams, as the algorithm only selects
exemplars of length n to 4n for comparison with any word n-gram.
Size Sentence
A 5 Past medical history is unremarkable
B 5 Immunizations are up to date
C 11 Past medical history shows immunizations are up to date and unremarkable
102
As an example, in the given sentences: A, B and C; sentence C contains semantics of
both A and B. However if sentence C is used as exemplar, and sentence A and B are
used as query, they will get lower scores since there will only be a partial match among
the exemplar and query. Besides, shorter word n-grams from the query text, 1-grams,
and 2-grams specifically, will get 0 scores since the exemplar will not be selected for
comparison as its length is greater than 4 (n=1, 4n=4) and 8 (n=2, 4n=8).
To solve these problems, we consider using word n-gram based exemplars. The text
strings from the training set converts into word n-grams and are stored with the class
assignment as exemplars. This way, each overlapped word n-gram (sub-string) from
the training text string gets an opportunity to have representation. In our algorithm, we
implement both types of exemplars and gave options in the input parameter to choose
the exemplar type.
4) Similarity function
The concept detection algorithm uses the Jaccard Index as the similarity measure,
which does not take word count and sequence for similarity calculations. Cosine
similarity [123], on the other hand, is built upon the idea of tf-idf, which takes the count
of each dimension in the calculations. Both of these similarity measures are extensively
used in the information retrieval domain. However, a comparison of documents
retrieved from Google search shows that cosine similarity is the most relevant metric
to compare text documents [124]. As we deal with natural speech in our dataset, we
hypothesize that cosine similarity will improve the classification performance in
comparison with the Jaccard Index. Therefore, we apply both in our algorithm while
giving an option to use any one of them in the input parameter.
After investigating all four key areas, we extend the concept detection algorithm into a
classifier by applying a two-step process to the word-by-class map output. In the first step,
a single score calculates for each class by adding the scores of all words. In the second
step, scores of all classes are normalized to get confidence scores in the range of 0 and 1.
The pseudocode for the algorithm after the extension is showed in Figure 6.3.

103
Figure 6.3 Pseudocode for Exemplar-based Sentence Classification Algorithm

104
6.2.4 Summary
To achieve our objective, we extend the exemplar-based concept detection algorithm for
SOAP classification. Five changes are done in this regard. The first change is to give an
option in the input parameter to remove stop words. Second, maximum word n-gram length
is made variable by taking a max length as input. Third, a word n-gram based exemplar is
developed, and an option is given as an input parameter to select the exemplar type. Fourth,
an option is given as an input parameter for similarity matric to use either the Jaccard Index
or Cosine Similarity. Fifth, the word-by-class map output is processed using a two-step
process to calculate a single confidence score for each class for the query.

105
6.3 Evaluation
6.3.1 Experimental Setup
We implemented our exemplar-based sentence classifier and then evaluated it on our
dataset using four independent variables that correspond to the four proposed
improvements. These variables are directly derived from the key areas that we identified
and enhanced. One of the independent variables is the maximum word n-gram length limit,
for which we did not specify any length; therefore, we experimented with lengths from 1
to 15. All other independent variables have two conditions each that give us 8 cases for
experiments. All these cases are given a number. Table 6.5 shows all the cases. Each of
these cases is experimented with varying maximum word n-gram length limits, which gave
us 120 total conditions to experiment (8 cases x 15 maximum word n-gram length limits).
Table 6.5 Cases based on Stop Word, Similarity Function and Exemplar type
Cases Stop Word Similarity Function Exemplar Type
1
w/ Stop Words
Cosine Sentence
2 n-gram
3 Jaccard
Sentence
4 n-gram
5
w/o Stop Words
Cosine Sentence
6 n-gram
7 Jaccard
Sentence
8 n-gram
For each condition, experiments are done in a one-vs-rest method, which means for each
SOAP category, a different binary classifier is trained and tested. For instance, when
experimenting with the ‘Subjective’ category, all subjective sentences in the dataset are
given positive labels (1), and all other sentences are given a negative label (0). The same
is repeated for all other categories. Although our classifier can perform multi-class
classification, yet we choose this strategy because SOAP categories have a very thin line
of separation which can impact the classification performance with our imbalanced dataset.
As an example, the sentence “we prescribed him ...” should be an assessment, whereas,
with a subtle change “we will prescribe him …” becomes a plan. However, in our dataset,

106
both of these categories have limited sentences. We also observe Mowery [101] applying
the same evaluation strategy, due to the same problems.
We conducted all experiments with 5x5 cross-validations. Dataset was randomly shuffled,
and 5-fold cross-validation was performed. This process was repeated four more times. For
each SOAP category, 25 results were retrieved, which in total gave us 100 results for each
condition. Ground truth, confidence score, and condition details were stored from all
experiments.
Confidence scores from our classifier show the predicted probability of having a positive
label. In this work, we did not specify any mechanism to select any threshold for binary
prediction (positive or negative). Therefore, to evaluate our classifier and to compare all
the experimental conditions, we used Precision-Recall Curve (PRC), since it provides an
accurate evaluation in case of imbalance dataset as compared to Receiver Operating
Characteristic (ROC) [125].
Area Under PRC (AUPRC) is represented by Average Precision (AP), where higher AP
means better classification performance. In this work, we used AP as the main
performance evaluation measure, which also serves as the dependent variable for all our
independent variables. We used regression testing to analyze the impact of each
independent variable, and based on the results, we selected the most optimal combination
of independent variables. We then thoroughly analyze the classification performance of the
experimental condition that is according to the selected variables. Three of our independent
variables: stop words, similarity function, and exemplar type; are categorical, though has
only two values in each. Therefore, we converted them into numerical variables for
regression testing.
We analyzed results from all SOAP categories separately as well as in combination. To
analyze the overall performance, we took both averages: micro-average and macro-
average. In micro-averaging, we directly calculate precision and recall values from overall

107
results, whereas, in macro-averaging, we calculated precision and recall values first for
individual categories and then averaged them.
Table 6.6 Conversion of categorical variables to numeric
Independent Variable Categorical Value Numeric Value
Maximum word n-gram Length Limit - 1 … 15
Stop Words w/ Stop Words 0
w/o Stop Words 1
Similarity Function Cosine 0
Jaccard 1
Exemplar Type Sentence 0
n-gram 1
In this evaluation, we focus on six main questions.
1. What is the baseline performance of the classifier before improvements?
2. What is the optimal maximum word n-gram length limit for SOAP classification?
3. Does the removal of stop words enhance classification performance?
4. What is the best exemplar type for SOAP classification?
5. What is the best similarity function for SOAP classification?
6. What is the performance of the classifier using optimal conditions?
6.3.2 Results
We experimented with all 120 conditions and analyzed the results to answer the six
questions. In this section, we first analyze the baseline performance of the classifier before
applying any improvement. Then we analyze the impact of each improvement on the
classification performance and select the optimal values for each improvement category.
Finally, we analyze the performance of the classifier on the conditions that correspond to
the optimal values.

108
• BASELINE PERFORMANCE
We consider case 3 using a maximum word n-gram length limit of 5 as the baseline
condition, as this condition equals of classifier without having any improvements. In this
condition, we observed an overall micro-averaged AP score of 0.886, while having AP
scores of 0.932 for ‘Subjective’, 0.911 for ‘Objective’, 0.563 for ‘Assessment’ and 0.765
for ‘Plan’ category. Figure 6.4 shows the AUPRC for the baseline condition.
Figure 6.4 Precision-Recall curve of the baseline condition
We compiled a list of example sentences along with their confidence scores from baseline
condition and actual SOAP category in Table 6.7. We highlight the top confidence scores
while underlined scores show that the highest confidence score is given to the actual SOAP
category. The list shows 3 examples each from the ‘Subjective’ and ‘Objective’ category,
and 2 examples each from ‘Assessment’ and ‘Plan’ categories.

109
Table 6.7 Confidence scores of sentences from the baseline condition
Sentence Confidence Scores Actual
SOAP Category
Subjective Objective Assessment Plan
1
paragraph past medical history immunizations are up to date
0.88791 0.0884 0.04866 0.05589 Subjective
2
immunizations up to date and no significant medical issues
0.83285 0.14976 0.11717 0.11628 Subjective
3
child was already starting to show return to normal function with crying and purposeful movements
0.46867 0.47539 0.41664 0.35019 Subjective
4
ear nose and throat exam revealed a runny nose mildly red throat and normal ears
0.17412 0.8412 0.11327 0.13244 Objective
5
new paragraph family sorry physical exam revealed entirely normal neurological exam with no focal findings
0.29106 0.69507 0.13999 0.14118 Objective
6
blood work was taken four hours after ingestion revealing non toxic acetaminophen levels
0.59756 0.23034 0.41212 0.14035 Objective
7 a diagnosis was croup treatment
0.3143 0.30527 0.71247 0.18112 Assessment
8 i note no allergies 0.66861 0.32717 0.19232 0.07669 Assessment
9 child will follow up with family doctor
0.23159 0.17391 0.12547 0.74356 Plan
10
a throat swab was sent today should it be positive we will call her and start her on antibiotics
0.3523 0.46499 0.41026 0.3531 Plan

110
• ANALYZING THE IMPACT OF IMPROVEMENTS
In all experimented conditions, the overall best performance was achieved by the condition
using case 1 with maximum word n-gram length limit of 5th order. This condition achieved
the highest micro-averaged AP score of 0.897. However, we observed that for individual
SOAP categories, different conditions showed better performance for different categories,
and no one condition was optimal for all SOAP categories. We list down the highest and
lowest AP scores we observed for each SOAP category along with overall combined scores
in Table 6.8. The magnitude of different highlights that our suggested improvements are
having a major impact on performance, especially with assessment and plan categories.
Table 6.8 Highest and Lowest AP scores for SOAP categories
SOAP Category Highest AP Lowest AP Difference
Subjective 0.957 0.881 0.076
Objective 0.919 0.836 0.083
Assessment 0.626 0.396 0.230
Plan 0.820 0.705 0.115
Micro-Averaged 0.897 0.812 0.085
Macro-Averaged 0.808 0.716 0.092
Results from regression tests on all 120 conditions showed that all independent variables
influenced classification performance, except similarity function which is consistently
insignificant for all SOAP categories. Table 6.9 highlights the results of regression testing.
Table 6.9 Summary of regression analysis results
Independent
Variables → Max n-gram Length Stop Words
Similarity
Function Exemplar Type
SOAP Categories ↓ P-value T Stat P-value T Stat P-value T Stat P-value T Stat
Subjective 1.125E-08 6.155 1.554E-19 -10.944 0.512 0.658 0.0725 -1.812
Objective 2.988E-07 5.444 3.503E-10 -6.869 0.189 1.321 2.920E-27 -14.292
Assessment 0.046 -2.019 1.036E-21 -11.874 0.375 -0.891 0.011 -2.584
Plan 0.009 -2.625 0.002 3.215 0.068 -1.841 0.039 -2.090
Micro-Average 3.375E-06 4.885 2.783E-32 -16.585 0.284 1.077 2.596E-11 -7.386
Macro-Average 0.984 -0.020 3.292E-22 -12.087 0.256 -1.141 2.490E-09 -6.469

111
• IMPACT OF MAXIMUM N-GRAM LENGTH LIMIT
Regression analysis showed that changing the maximum n-gram length limit had a
significant change in performance. However, the direction of change varied within SOAP
categories. We observed that sentences from ‘Subjective’ and ‘Objective’ categories were
better classified with higher order of n-grams, whereas, ‘Assessment’ and ‘Plan’ categories
favored shorter n-grams. Figure 6.5 draws the trend line of 6th-degree polynomial after
plotting all AP scores for all cases on ordinate with max n-gram lengths on the abscissa.
Figure 6.5 All AP scores over n-gram max length

112
The trend line validates the regression analysis; however, it highlights diminishing
increment in AP for ‘Subjective’ and ‘Objective’ categories with the increasing n-gram
lengths. For the ‘Assessment’ category, we see continuous declination of performance
along n-gram lengths. ‘Plan’ category, however, shows inconsistency, where performance
rapidly increased for the first few increments in n-gram lengths, then it started to fall,
nevertheless, the fall was not much. These opposite behaviors from SOAP categories
regarding max n-gram length explain the high P-value (0.984) for macro-averaged scores.
All 8 cases mostly followed the same trend; however, we did observe some anomalies. In
the ‘Subjective’ category, we marked 3 cases to have slight differences. In cases 3 and 8,
we saw another spike in scores with the higher values of max n-gram length. In case 5
specifically, we observed that n-gram lengths had no significant impact. We had the same
observation about the ‘Objective’ category in case 5. For the ‘Assessment’ category, cases
5 and 6 seemed to have no impact due to n-gram lengths, and case 8 was observed to be
favoring larger n-grams. We observed the same behavior with the ‘Plan’ category, where
cases 5 and 8 had no impact, whereas, case 6 favored larger n-grams. Overall, case 5
(without stop words, cosine similarity, sentence exemplars) appeared to be immune to the
n-gram lengths. We confirmed this observation by applying a t-test on the AP scores which
gave us a P-value of 0.196. After analyzing scores, we realized that there cannot be a single
selection for max n-gram length; therefore, we picked the best performing max n-gram
length from each case (Table 6.10).
Table 6.10 Best performing values for maximum n-gram length for each case
SOAP Categories ↓ All Cases Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8
Subjective 8 8 9 14 6 11 9 14 15
Objective 11 11 5 11 7 6 7 12 12
Assessment 1 1 3 1 2 15 15 1 15
Plan 6 2 3 2 2 14 8 6 8
Micro-Average 5 5 5 14 7 15 9 10 15
Macro-Average 3 3 3 6 2 15 15 6 15

113
• IMPACT OF STOP WORDS REMOVAL
It is evident from the regression analysis that stop words removal had a significant change
in the classification performance for all categories. However, for all the categories except
‘Plan’, the direction of change is negative (-ve t-stat value). This means that the
performance of only the ‘Plan’ category increased by removing stop words, whereas, all
other categories performed better when we keep stop-words in the sentences. Figure 6.6
shows the box plots for AP scores after categorizing them with and without stop words.
In Figure 6.6, all box plots are placed in the same sequence as shown in the legends on the
left. To be specific, from left to right, the first 2 plots represents the results from all SOAP
categories combined, the second pair represents results only for ‘Subjective’ category, the
third pair represents ‘Objective’ category, the fourth pair represent ‘Assessment’ category
and the fifth pair represent ‘Plan’ category. All the blue shaded plots (left on each pair) are
made from performance scores when stop words were kept in the sentences. On the other
hand, green-shaded plots (right on each pair) are from the scores when stop words were
removed. The x mark within plots shows the mean, and the dots outside plots show outliers.
While analyzing these plots, we can see that although ‘Plan’ sentences were better
classified without stop words, this performance was not very reliable, since the plot spread
is wider along with some outliers.
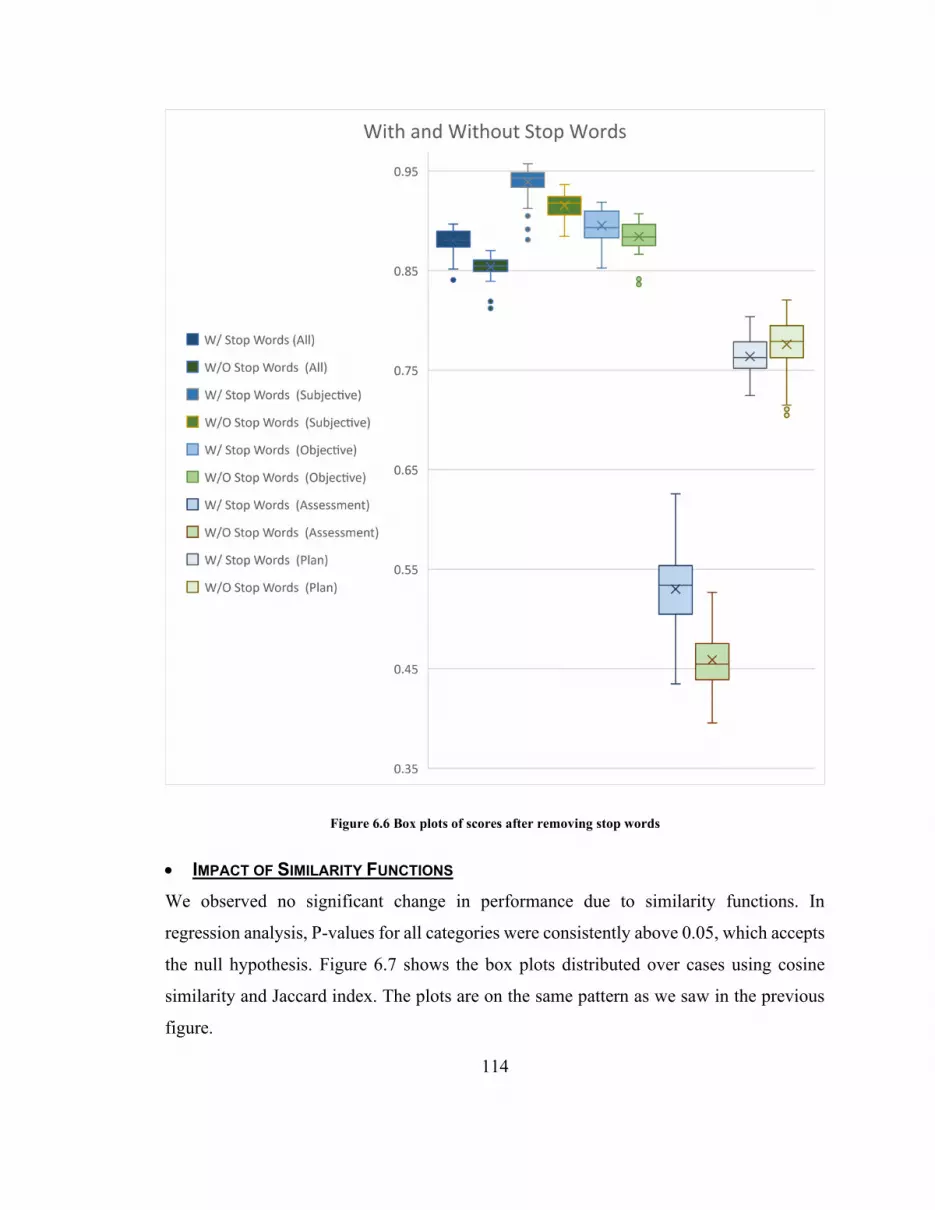
114
Figure 6.6 Box plots of scores after removing stop words
• IMPACT OF SIMILARITY FUNCTIONS
We observed no significant change in performance due to similarity functions. In
regression analysis, P-values for all categories were consistently above 0.05, which accepts
the null hypothesis. Figure 6.7 shows the box plots distributed over cases using cosine
similarity and Jaccard index. The plots are on the same pattern as we saw in the previous
figure.

115
Figure 6.7 Comparing performance based on similarity function (Cosine vs Jaccard)
• IMPACT OF EXEMPLAR TYPES
In our analysis, sentence based exemplars were better than n-gram based exemplars on all
SOAP categories. Figure 6.8 shows the box plots for scores based on exemplar-type. Blue
shaded plots are for sentence based exemplars and green shaded plots are for n-gram
exemplars. These plots validate the results of regression analysis as the mean and median
for each blue shaded plot is higher than the corresponding green-shaded plot.

116
Figure 6.8 Comparing performance based on exemplar type (sentence vs n-gram)
• OPTIMAL PERFORMANCE
Results from regression analysis presented that classification performance varied across
individual SOAP categories. Therefore, we inspected the optimal performance for each
category separately. We select the conditions having the highest AP scores for each
category and analyze the improvements that go within that condition. We also calculate the
F1 scores for the selected conditions using varying threshold levels. The highest F1 scores
are reported with each category. Table 6.11 provides a summary of optimal conditions for

117
each SOAP category along with the magnitude of improvement as compared to baseline
performance.
Table 6.11 Summary of optimal conditions for each SOAP category
SOAP Category
Base AP Score
Max AP Score
AP Improved
Optimal Maximum word n-gram length limit
Best Case
Subjective 0.932 0.957 0.025 8 1
Objective 0.911 0.919 0.008 11 3
Assessment 0.563 0.626 0.063 1 1
Plan 0.765 0.82 0.55 6 7
For the ‘Subjective’ category, we achieved max performance (AP: 0.957) with case 1 using
the maximum word n-gram length limit of the 8th order. This means that when our classifier
is set to break query sentences in word n-grams till 8-grams, use sentence based exemplar
and keep stop words, it will give the best classify ‘Subjective’ category sentences. Since
the similarity function has no significance, we select the condition with cosine similarity
as its score was moderately better. Figure 6.9 shows the AUPRC for this condition, where
we achieved an F1 score of 0.912.
Figure 6.9 Precision-Recall Curve of best performing condition for Subjective

118
We selected some examples and list them in Table 6.12 showing sentences with their actual
SOAP category and confidence scores we obtained using our classifiers with this condition.
The top 6 example shows the behavior of this condition on ‘Subjective’ sentences, while
rest shows behavior on other categories. We highlight the top-scoring category while
underline shows that our classifier predicted the actual category for the given sentence.
Table 6.12 Confidence scores of sentences from case 1 using 8-gram limit
Sentence Confidence Scores Actual SOAP
Category Subjective Objective Assessment Plan
1 no concussive findings
0.80509 0.296 0.25021 0 Subjective
2
immediately afterwards paramedics were called on arrival
0.4717 0.3464 0.50901 0.23972 Subjective
3 no medications 0.75963 0.24037 0.211 0 Subjective
4
past medical history reveals a healthy athletic male with no significant medical issues
0.75253 0.25061 0.22631 0.17429 Subjective
5
by the time she arrived at the IWK emergency she was awake and alert and cranky
0.51804 0.41937 0.33357 0.38002 Subjective
6
family history reveals febrile seizures in dad as a child
0.51926 0.40717 0.30884 0.38605 Subjective
7 tracheal palpation did not elicit pain
0.76971 0.39352 0.15284 0.24594 Objective
8 lungs were clear 0.18333 0.77103 0.24431 0.19585 Objective
9 the likely choice of antibiotics will be amoxicillin
0.36357 0.37519 0.42211 0.57157 Plan
10 diagnosis fracture radius ulna
0 0.55951 0.60422 0 Assessment

119
For the ‘Objective’ category, best scores (AP: 0.919) were achieved by condition using
case 3 and the maximum word n-gram length limit of 11. We achieved an F1 score of 0.846
in this condition. Figure 6.10 illustrates the AUPRC for this condition. Table 6.13 mentions
some examples from this condition, where the top 5 examples show the behavior of this
condition over the ‘Objective’ category. The rest of the examples show the performance
over other SOAP categories.
Table 6.13 Confidence scores of sentences from case 3 using 11-gram limit
Sentence Confidence Scores Actual
SOAP Category
Subjective Objective Assessment Plan
1
ear nose and throat exam revealed a red throat with no exudate suggestive of a viral pharyngitis
0.27987 0.72597 0.18146 0.1777 Objective
2
blood work was taken four hours after ingestion revealing non toxic acetaminophen levels
0.62871 0.20222 0.37966 0.14458 Objective
3 rest of the physical exam was without comment
0.20491 0.83209 0.15358 0.24458 Objective
4
new paragraph family sorry physical exam revealed entirely normal neurological exam with no focal findings
0.28433 0.71114 0.12414 0.12644 Objective
5
his neurovascular status in the effected limb is normal
0 0.67539 0 0 Objective
6
past medical history reveals immunizations up to date and normal
0.76841 0.22902 0.15446 0.13135 Subjective

120
birth and pregnancy history with no specialist and no regular medications and no known allergies
7 diagnosis fracture radius ulna
0 0.49184 0.69675 0 Assessment
8 chest xray revealed a dense left lower consolidation
0.34847 0.69141 0.21597 0.11372 Assessment
9 child will follow up with family doctor
0.29484 0.15295 0.0951 0.7286 Plan
10 parents were counseled and reassured
0.35712 0.33844 0.61333 0.29793 Plan
Figure 6.10 Precision-Recall Curve of best performing condition for Objective

121
For the ‘Assessment’ category, case 1 using maximum word n-gram length limit of 1st
order excelled (AP: 0.626) among all other conditions. This condition managed an F1 score
of 0.63. Figure 6.11 depicts AUPRC for this condition. Table 6.14 lists example sentences
from this condition showing highlighted confidence scores along with the actual SOAP
category. Top 5 examples show the behavior of this condition over ‘Assessment’ category
sentences, while rest show the behavior over other categories.
Table 6.14 Confidence scores of sentences from case 1 using 1-gram limit
Sentence Confidence Scores Actual SOAP
Category Subjective Objective Assessment Plan
1 a diagnosis was croup treatment
0.39702 0.299 0.71162 0.18063 Assessment
2 diagnosis is viral respiratory tract infection
0.41961 0.33547 0.64259 0.10616 Assessment
3 croup instructions were delivered
0.41324 0.5422 0.54945 0.33527 Assessment
4 i note no allergies 0.65644 0.35877 0.31561 0.14695 Assessment
5
diagnosis viral upper respiratory tract infection with febrile seizure
0.44084 0.31599 0.52301 0.18636 Assessment
6
immediately afterwards paramedics were called on arrival
0.4717 0.3464 0.50901 0.23972 Subjective
7
new paragraph impression is that this is simple febrile seizure
0.49094 0.33401 0.5078 0.33077 Objective
8
post reduction film showed good placement of the bones
0.5516 0.49871 0.49488 0.31146 Objective
9 child was hydrated and happy
0.44425 0.55868 0.4596 0.40219 Objective
10 parents were counseled and reassured
0.40641 0.38024 0.54527 0.38648 Plan
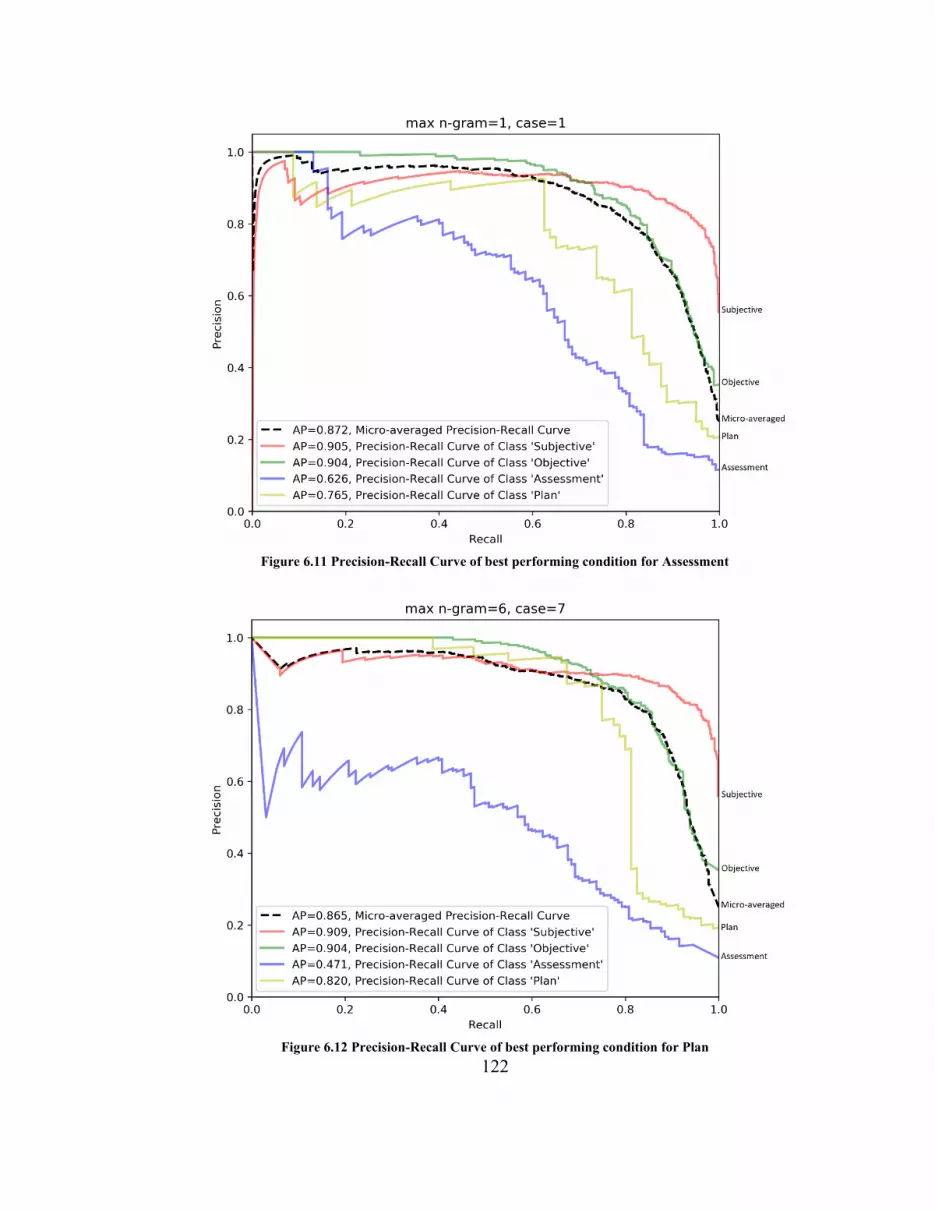
122
Figure 6.11 Precision-Recall Curve of best performing condition for Assessment
Figure 6.12 Precision-Recall Curve of best performing condition for Plan
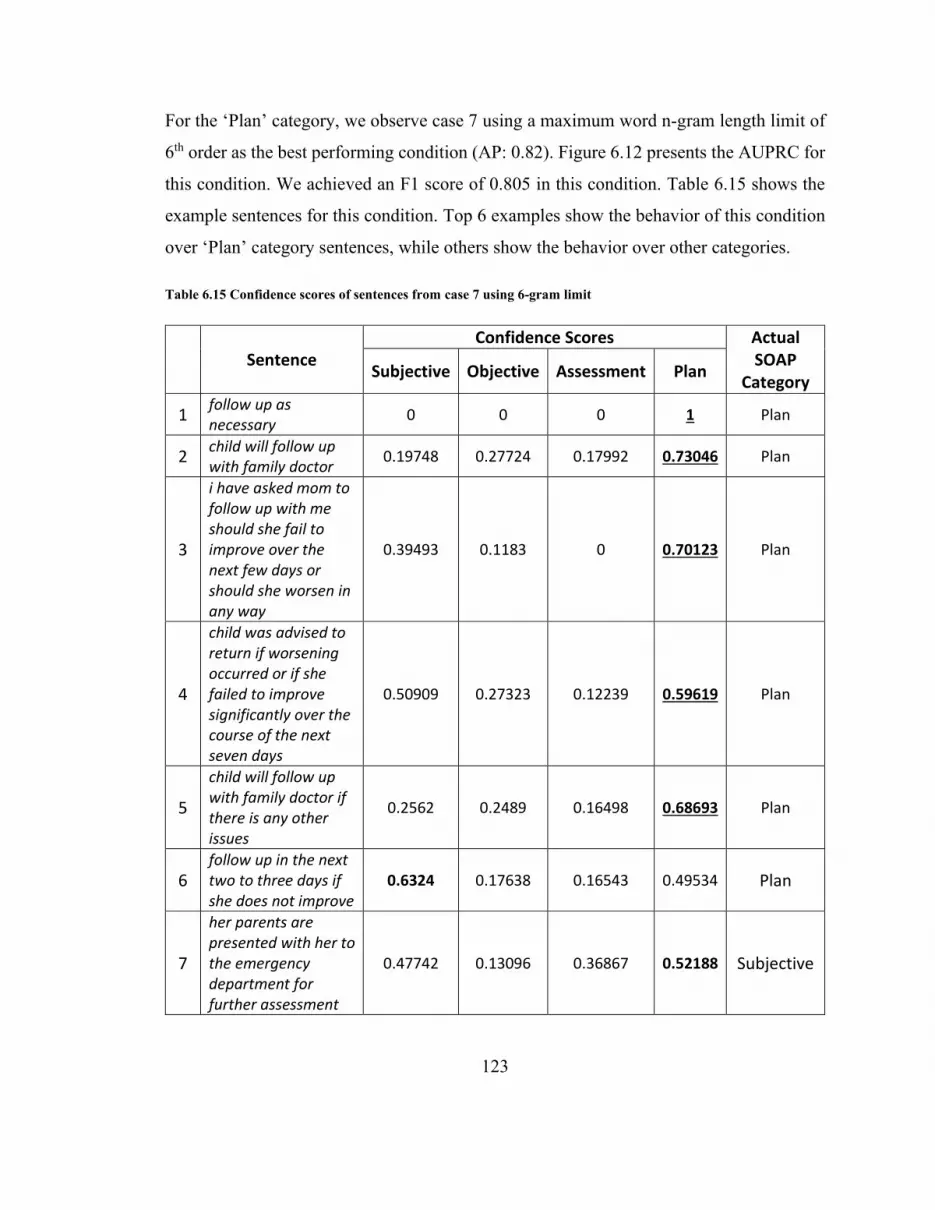
123
For the ‘Plan’ category, we observe case 7 using a maximum word n-gram length limit of
6th order as the best performing condition (AP: 0.82). Figure 6.12 presents the AUPRC for
this condition. We achieved an F1 score of 0.805 in this condition. Table 6.15 shows the
example sentences for this condition. Top 6 examples show the behavior of this condition
over ‘Plan’ category sentences, while others show the behavior over other categories.
Table 6.15 Confidence scores of sentences from case 7 using 6-gram limit
Sentence Confidence Scores Actual
SOAP Category
Subjective Objective Assessment Plan
1 follow up as necessary
0 0 0 1 Plan
2 child will follow up with family doctor
0.19748 0.27724 0.17992 0.73046 Plan
3
i have asked mom to follow up with me should she fail to improve over the next few days or should she worsen in any way
0.39493 0.1183 0 0.70123 Plan
4
child was advised to return if worsening occurred or if she failed to improve significantly over the course of the next seven days
0.50909 0.27323 0.12239 0.59619 Plan
5
child will follow up with family doctor if there is any other issues
0.2562 0.2489 0.16498 0.68693 Plan
6 follow up in the next two to three days if she does not improve
0.6324 0.17638 0.16543 0.49534 Plan
7
her parents are presented with her to the emergency department for further assessment
0.47742 0.13096 0.36867 0.52188 Subjective

124
8
child was already starting to show return to normal function with crying and purposeful movements
0.5657 0.35864 0.31614 0.47694 Subjective
9
she presented to a walk in clinic where she was told that she did not have a concussion
0.53009 0.36812 0.36995 0.54721 Subjective
10
instructions were given with regards to the delivery of ibuprofen as needed for pain and fever but the parents were cautioned that this would not reduce the risk of further seizures
0.43787 0.35454 0.3649 0.44165 Objective
6.4 Discussion
In this evaluation, we used 238 sentences to evaluate our classifier, which is far less than
4130 sentences that Mowery [101] used in their study; however, we achieved comparable
performance in almost all SOAP categories.
The performance of our classifier significantly improved with ‘Plan’ category sentences
when we applied the stop word removal operation. We observe that this change is
specifically due to the nature of ‘Plan’ sentences. Usually, in this category, physicians talk
in the future tense. For example, “Child will follow up …” and “We will perform …”. In
this case, when stop words are removed, the grammatical structure of a sentence becomes
more prominent and highlights those keywords like ‘will’ and ‘shall’ that be the key
identifiers of the future tense.
In our experiments, we also noticed a significant performance change with varying
maximum n-gram lengths, which ranged from the lowest overall AP score of 0.81 to the
highest of 0.89. We also observed that each SOAP category behaves differently with

125
different n-grams. Juckett [102] has implemented the concept-detection algorithm with the
max n-gram length equals to 5 for each class, owing to the small-phrase lengths of their
dataset. Using the same principle, we expected better performance with longer n-grams.
In this work, we also evaluated the use of the Jaccard index as the similarity function in
comparison to the cosine similarity function. We argued that the Jaccard Index only takes
the union of all lexicons for calculations and does not impact with repeated words, and
cosine similarity should work better. However, after experiments, our argument failed to
achieve support from the results, which made it evident that similarity function has no
significant impact on the performance.
6.5 Conclusion
This chapter provides an approach to use an exemplar-based concept detection algorithm
to develop a SOAP classifier. This classifier was implemented and was experimented with
four independent variables having a total of 120 variations where each variation was tested
for each of the SOAP categories separately. These experiments were defined to show a
directional insight into our approach, yet due to the small dataset, it does not provide a
meaningful conclusion. With the provided dataset, we make two suggestions. The first
suggestion is to use the longer n-grams for better classification in ‘Subjective’ and
‘Objective’ categories, whereas shorter n-grams for ‘Assessment’ and ‘Plan’ categories.
However, the drawback of longer n-grams is that for each increasing n-gram, processing
time increases exponentially. The second suggestion is to make separate classifiers for each
of the SOAP categories and remove stop words specifically for Plan category classifiers.

126
Chapter 7. DISCUSSION
7.1 Introduction
This chapter constructs a thorough discussion based on our work for both of our research
objectives. It highlights the observations that we made while performing this research. This
chapter then presents a 3-Layer solution framework that is based upon our observations.
Afterward, it reports the limitations of this work and provides possible and potential
improvements that can be done in the future. Finally, this chapter ends by providing a
conclusion towards this thesis.
7.2 Observations
We demonstrated our work on a 2-layer solution model, with the approach of having an
end-to-end solution. However, when we observe the output of the first layer, we found no
punctuation marks. The reason for this is that SR returns speech in free text format. These
texts bare no lexical entities other than words, such as punctuation marks, paragraph
indentation. On the other hand, Natural Language Processing (NLP) tasks usually work on
text data that are rich with punctuation marks. It means that output from SR systems can
create havoc with NLP methods; therefore, it is highly desired to enrich SR output with
punctuation marks before transmitting it to our final layer.
While working with the dictations, we also observed that some of them were recorded
while patients were still in the room. For our experiments, this created issues because of
the increased level of background noise. As we are working towards an end-to-end
solution, we made a realization that an autonomous report generation solution will allow
providers to record dictations anywhere and anytime. Most of the time, it should be
happening right after the encounter, possibly in front of the patient. For such scenarios, we
believe that patients will be hearing of what is said, hence they will get the chance to
provide clarification for any detail, which will be beneficial in reducing the dictation errors.
Fratzke [51] observed the same pattern when they implemented a voice-assisted
technology.

127
7.3 3-Layer Solution Framework
In this thesis, we observed that the output from the first layer is not fully compatible to be
used as the input of our second layer. Therefore, to develop a true end-to-end solution, we
need to specify a processing layer in between both layers whose purpose should be to
streamline the output of the first layer for the next layer.
Sentence boundaries are marked by using a dot, also known as period. This dot shows
where a sentence has ended in the text. In our final layer, we are using the sentence as the
unit to classify. Therefore, those transcriptions without punctuation marks will certainly
have some issues. A quick review shows that there are various solutions available that deal
with the punctuation prediction task. We found a punctuation predictor based on a
bidirectional recurrent neural network model with attention mechanism [126] that provides
pre-trained models based on Wikipedia text. We tested this solution on our dataset and
analyzed the results visually. We observed a few mistakes, though it generally felt
satisfactory. This simple review of the problem shown us that punctuation prediction is an
established problem in the research domain; hence we should give it a separate focus in
our solution.
Figure 7.1 Design for 3-Layer Solution Framework
With all the observations we made in this work, we present a potential 3-layer solution
framework for the problem of clinical documentation. All of the layers in this framework
are connected as a pipeline. Figure 7.1 represents the design of the 3-layer solution
framework. Each layer of this framework is defined below.

128
1. The first layer of this framework expects physicians recorded audio clips. This layer
processes the input audio into text by using a noise and domain robust speech
recognition system.
2. In the second layer, the transcriptions from the first layers are analyzed for
punctuations. Transcriptions are enriched with predicted punctuations and are given to
the third layer.
3. In the third layer, punctuated transcriptions are then classified for clinical reports.
Sentences from transcriptions are extracted and then classified for various categories
of the report structure.
7.4 Limitations
The size of the dataset possesses the biggest limitation of this work. Due to the small size
of the dataset, we had to tweak our experiments accordingly. While experimenting with
acoustic models, we initially wanted to train standalone models as well to hold a
comparison. However, a few trials with training exhibited the limitations. Therefore, we
skipped that scenario from our experiments. Similarly, during the SOAP classification, we
sensed a lower level of overall classification performance. The algorithm that we extended
and implemented in this layer was tested on a dataset five times in size than ours. Hence,
we believe that a lower dataset has introduced a limitation in our work.
Another limitation of this work is that all of the dataset labeling tasks were done by us,
without the help of any domain specialist. We perceived the need for a specialist at two
points. Firstly, at the time of generating gold standard transcriptions for dictation audios,
and secondly, when we labeled the sentences into SOAP categories. While preparing
transcriptions, we took help from one of the fellow members of our research group, who
has a medical degree. However, we do not consider this fellow a domain specialist since it
never practiced in the domain.

129
7.5 Future Work
This work is primarily experimental; however, it sets a direction for further research. This
thesis presents the solutions in terms of research areas that combine to form a solution
framework. Particularly, the solution depends on three research areas: continuous speech
recognition, punctuation prediction, and sentence classification. Any work that is done in
any of these research areas has the potential to enhance the presented solution framework.
Open-sourced offline SR are improving at a rapid pace. While working on this thesis, a
new open-sourced offline SR Wav2Letter++ [94] was released reporting better
performance then DeepSpeech [76] using similar models and datasets. Wav2Letter++ is
developed to scale and work in real-life environments. At the time of our experimentations,
its pre-trained models were not released, however, they are available at the time of writing
this thesis. Wav2Letter++ is also based on the concept of end-to-end SR, whilst providing
features to use custom acoustic models of different architectures. Therefore, we consider
that using this toolkit can be a perfect next step towards the enhancement of this work.
At the time of selecting methods for our final layer, we did not explore the sentence
classification solutions from other domains. One can argue this as a limitation, but we
consider this as the opportunity to move ahead in a logical manner. Since we were only
able to find one study that addressed the problem of sentence segmentation for SOAP
categories, the next logical step we took was to explore for similar problems within the
same (healthcare) domain. Therefore, we consider that this work provides the basis to
explore solution ideas from a different domain. We expect that examination of supervised
approaches towards text classification for this problem can pose as an appropriate work in
this direction.
In the previous subsections, this chapter presented a 3-layer solution framework. We
consider that this provides the opportunity to research the problem of clinical
documentation in a more systematic way. However, the framework still needs active
research and evaluations. Therefore, as future work, this 3-layer solution framework can
be enhanced.

130
7.6 Conclusion
Clinical documentation is a challenging process that poses multiple problems. Researchers
are experimenting with speech recognition since its inception to develop efficient solutions.
A review suggests that such solutions still lack adoption among healthcare providers. One
reason is the lack of accuracy in domain-specific noisy environments. Another reason is
that providers still need to intervene and perform manual changes. Therefore, this thesis
considers the problem from the end-to-end perspective. It identifies two research objectives
and translates them into individual layers of a solution model.
The first layer seeks efficient transcription of dictations in domain-specific and acoustically
distorted environments. We selected the DeepSpeech speech recognition system and
performed preliminary experiments. We then presented methods to enhance the
performance of both: acoustic and language; models. Evaluations show that all our
modeling methods improve DeepSpeech performance. We show that by adapting and fine-
tuning the pre-trained acoustic model, along with enhancing the pre-trained language
model using the augmented corpus from the domain-specific dataset, DeepSpeech can
achieve performance levels very close to Google Speech API.
The second layer aims to categorize transcriptions into SOAP categories. We select an
exemplar-based concept detection algorithm and extend it to develop a sentence classifier.
We identify four areas to enhance and implement our classifier for SOAP classification.
Evaluations show that each SOAP category requires a separate setting for optimal
performance, and no single set of independent variables will deliver the best performance
for all categories.
In this work, we observe that a two-layer solution could not exhibit as an end-to-end
solution due to the lack of punctuations in the transcriptions. Therefore, this thesis
discusses a 3-layered solution framework that can have the potential to become an end-to-
end solution.

131
REFERENCES
[1] T. K. Colicchio and J. J. Cimino, “Clinicians’ reasoning as reflected in electronic
clinical note-entry and reading/retrieval: a systematic review and qualitative
synthesis,” J. Am. Med. Informatics Assoc., vol. 26, no. 2, pp. 172–184, 2019.
[2] A. Mathioudakis, I. Rousalova, A. A. Gagnat, N. Saad, and G. Hardavella, “How to
keep good clinical records,” Breathe, vol. 12, no. 4, pp. 371–375, Dec. 2016.
[3] B. G. Arndt et al., “Tethered to the EHR: Primary care physician workload
assessment using EHR event log data and time-motion observations,” Ann. Fam.
Med., vol. 15, no. 5, pp. 419–426, 2017.
[4] C. Sinsky et al., “Allocation of physician time in ambulatory practice: A time and
motion study in 4 specialties,” Ann. Intern. Med., vol. 165, no. 11, pp. 753–760,
Dec. 2016.
[5] J. Holbrook and R. Aghababian, “A computerized audit of 15,009 emergency
department records,” Ann. Emerg. Med., vol. 19, no. 2, pp. 139–144, 1990.
[6] T. G. Poder, J. F. Fisette, and V. Déry, “Speech Recognition for Medical Dictation:
Overview in Quebec and Systematic Review,” J. Med. Syst., vol. 42, no. 5, p. 89,
May 2018.
[7] “mozilla/DeepSpeech: A TensorFlow implementation of Baidu’s DeepSpeech
architecture.” [Online]. Available: https://github.com/mozilla/DeepSpeech.
[Accessed: 20-Nov-2019].
[8] M. Amatayakul, “EHR versus EMR: what’s in a name?,” J. Healthc. Financ.
Manag. Assoc., vol. 63, no. 3, p. 24, 2009.
[9] W. Kondro, “CMAJ 2011 election survey: research.,” CMAJ, vol. 183, no. 8, pp.
E463--4, May 2011.

132
[10] J. H. Seo et al., “A pilot study on the evaluation of medical student documentation:
assessment of SOAP notes,” Korean J. Med. Educ., vol. 28, no. 2, pp. 237–241, Jun.
2016.
[11] M. Gardiner, “Clinical documentation.,” Texas dental journal, 2013. [Online].
Available: https://searchhealthit.techtarget.com/definition/clinical-documentation-
healthcare.
[12] D. R. Maines, Social Organization of Medical Work (Book)., vol. 8, no. 4. Chicago,
IL, US, IL, US: University of Chicago Press, 1986.
[13] K. R. Sando, E. Skoy, C. Bradley, J. Frenzel, J. Kirwin, and E. Urteaga, “Assessment
of SOAP note evaluation tools in colleges and schools of pharmacy,” Curr. Pharm.
Teach. Learn., vol. 9, no. 4, pp. 576–584, Jul. 2017.
[14] J. L. Belden, R. J. Koopman, S. J. Patil, N. J. Lowrance, G. F. Petroski, and J. B.
Smith, “Dynamic electronic health record note prototype: Seeing more by showing
less,” Journal of the American Board of Family Medicine, vol. 30, no. 6. American
Board of Family Medicine, pp. 691–700, 01-Nov-2017.
[15] M. R. Andrus et al., “Development and Validation of a Rubric to Evaluate Diabetes
SOAP Note Writing in APPE,” Am. J. Pharm. Educ., vol. 82, no. 9, p. 6725, 2018.
[16] L. A. Lenert, “Toward Medical Documentation That Enhances Situational
Awareness Learning,” AMIA ... Annu. Symp. proceedings. AMIA Symp., vol. 2016,
pp. 763–771, 2016.
[17] K. M. Lisenby et al., “Ambulatory care preceptors’ perceptions on SOAP note
writing in advanced pharmacy practice experiences (APPEs),” Curr. Pharm. Teach.
Learn., vol. 10, no. 12, pp. 1574–1578, Dec. 2018.
[18] P. F. Pearce, L. A. Ferguson, G. S. George, and C. A. Langford, “The essential
SOAP note in an EHR age,” Nurse Pract., vol. 41, no. 2, pp. 29–36, Feb. 2016.

133
[19] C. T. Lin, M. McKenzie, J. Pell, and L. Caplan, “Health care provider satisfaction
with a new electronic progress note format: SOAP vs APSO format,” JAMA Internal
Medicine, vol. 173, no. 2. American Medical Association, pp. 160–162, 28-Jan-
2013.
[20] E. L. Siegler and R. Adelman, “Copy and Paste: A Remediable Hazard of Electronic
Health Records,” American Journal of Medicine, vol. 122, no. 6, pp. 495–496, Jun-
2009.
[21] F. Jelinek, R. L. Mercer, and L. R. Bahl, “25 Continuous speech recognition:
Statistical methods,” in Handbook of Statistics, vol. 2, 1982, pp. 549–573.
[22] J. Li, L. Deng, Y. Gong, and R. Haeb-Umbach, “An overview of noise-robust
automatic speech recognition,” IEEE Trans. Audio, Speech Lang. Process., vol. 22,
no. 4, pp. 745–777, Apr. 2014.
[23] W. Ghai and N. Singh, “Literature Review on Automatic Speech Recognition,” Int.
J. Comput. Appl., vol. 41, no. 8, pp. 42–50, Mar. 2012.
[24] K. Jing and J. Xu, “A Survey on Neural Network Language Models.”
[25] A. J. Nathan and A. Scobell, “How China sees America,” Foreign Aff., vol. 91, no.
5, pp. 391–397, 2012.
[26] K. Saxena, R. Diamond, R. F. Conant, T. H. Mitchell, I. G. Gallopyn, and K. E.
Yakimow, “Provider Adoption of Speech Recognition and its Impact on
Satisfaction, Documentation Quality, Efficiency, and Cost in an Inpatient EHR.,”
AMIA Jt. Summits Transl. Sci. proceedings. AMIA Jt. Summits Transl. Sci., vol.
2017, pp. 186–195, 2018.
[27] F. R. Goss et al., “A clinician survey of using speech recognition for clinical
documentation in the electronic health record,” Int. J. Med. Inform., vol. 130, p.
103938, Oct. 2019.

134
[28] “Home - PubMed - NCBI.” [Online]. Available:
https://www.ncbi.nlm.nih.gov/pubmed/. [Accessed: 25-Nov-2019].
[29] L. Zhou et al., “Analysis of Errors in Dictated Clinical Documents Assisted by
Speech Recognition Software and Professional Transcriptionists,” JAMA Netw.
Open, vol. 1, no. 3, p. e180530, Jul. 2018.
[30] T. Hodgson, F. Magrabi, and E. Coiera, “Evaluating the efficiency and safety of
speech recognition within a commercial electronic health record system: A
replication study,” Appl. Clin. Inform., vol. 9, no. 2, pp. 326–335, 2018.
[31] B. W. Leeming, D. Porter, J. D. Jackson, H. L. Bleich, and M. Simon,
“Computerized radiologic reporting with voice data-entry,” Radiology, vol. 138, no.
5, pp. 585–588, Mar. 1981.
[32] A. H. Robbins et al., “Speech-controlled generation of radiology reports,”
Radiology, vol. 164, no. 2, pp. 569–573, Aug. 1987.
[33] A. Zafar, J. M. Overhage, and C. J. McDonald, “Continuous speech recognition for
clinicians,” J. Am. Med. Informatics Assoc., vol. 6, no. 3, pp. 195–204, 1999.
[34] M. M. Teel, R. Sokolowski, D. Rosenthal, and M. Belge, “Voice-enabled structured
medical reporting,” Conf. Hum. Factors Comput. Syst. - Proc., vol. 13, no. 1, pp.
595–602, 1998.
[35] K. Korn, “Voice recognition software for clinical use.,” J. Am. Acad. Nurse Pract.,
vol. 10, no. 11, pp. 515–517, 1998.
[36] R. Et, “Voice-enabled Reporting Systems Application of Information Technology,”
1997.
[37] O. A. Buch and N. P. Reddy, “Speaker verification for telemedical applications,”
Annu. Int. Conf. IEEE Eng. Med. Biol. - Proc., vol. 2, no. C, pp. 902–903, 1997.

135
[38] T. M. Murray, M. L. Kruse, J. A. Battcher, J. W. Woods, H. L. Edmonds, and M. P.
Palaheimo, “’Hands-off’--Voice activated automated anesthesia recordkeeping and
monitoring system (ARMS),” in Conference Proceedings - IEEE
SOUTHEASTCON, 1990, vol. 3, pp. 822–824.
[39] N. A. Linn, R. M. Rubenstein, A. E. Bowler, and J. L. Dixon, “Improving the quality
of emergency department documentation using the voice-activated word processor:
interim results.,” Proc. Annu. Symp. Comput. Appl. Med. Care, vol. 1992, no. 1, pp.
772–776, 1992.
[40] D. N. Mohr, D. W. Turner, G. R. Pond, J. S. Kamath, C. B. De Vos, and P. C.
Carpenter, “Speech recognition as a transcription aid: A randomized comparison
with standard transcription,” J. Am. Med. Informatics Assoc., vol. 10, no. 1, pp. 85–
93, 2003.
[41] Y. D. Derman, T. Arenovich, and J. Strauss, “Speech recognition software and
electronic psychiatric progress notes: Physicians’ ratings and preferences,” BMC
Med. Inform. Decis. Mak., vol. 10, no. 1, p. 44, Aug. 2010.
[42] G. C. David, A. C. Garcia, A. W. Rawls, and D. Chand, “Listening to what is said -
Transcribing what is heard: The impact of speech recognition technology (SRT) on
the practice of medical transcription (MT),” Sociol. Heal. Illn., vol. 31, no. 6, pp.
924–938, Sep. 2009.
[43] R. M. Issenman and I. H. Jaffer, “Use of voice recognition software in an outpatient
pediatric specialty practice,” Pediatrics, vol. 114, no. 3, pp. e290--e293, 2004.
[44] R. Hoyt and A. Yoshihashi, “Lessons learned from implementation of voice
recognition for documentation in the military electronic health record system.,”
Perspect. Health Inf. Manag., vol. 7, no. Winter, p. 1e, Jan. 2010.
[45] K. Patel and M. Harbord, “Digital dictation and voice transcription software
enhances outpatient clinic letter production: a crossover study,” Frontline
Gastroenterol., vol. 3, no. 3, pp. 162–165, Jul. 2012.

136
[46] T. Marukami, S. Tani, A. Matsuda, K. Takemoto, A. Shindo, and H. Inada, “A basic
study on application of voice recognition input to an electronic nursing record
system-evaluation of the function as an input interface,” J. Med. Syst., vol. 36, no.
3, pp. 1053–1058, Jun. 2012.
[47] M. Johnson et al., “A systematic review of speech recognition technology in health
care,” BMC Med. Inform. Decis. Mak., vol. 14, no. 1, p. 94, Dec. 2014.
[48] H. Suominen, L. Zhou, L. Hanlen, and G. Ferraro, “Benchmarking Clinical Speech
Recognition and Information Extraction: New Data, Methods, and Evaluations,”
JMIR Med. Informatics, vol. 3, no. 2, p. e19, Apr. 2015.
[49] S. Ajami, “Use of speech-to-text technology for documentation by healthcare
providers,” Natl. Med. J. India, vol. 29, no. 3, pp. 148–152, 2016.
[50] J. Fernandes, I. Brunton, G. Strudwick, S. Banik, and J. Strauss, “Physician
experience with speech recognition software in psychiatry: Usage and perspective,”
BMC Research Notes, vol. 11, no. 1. BioMed Central, p. 690, 01-Oct-2018.
[51] J. Fratzke, S. Tucker, H. Shedenhelm, J. Arnold, T. Belda, and M. Petera,
“Enhancing nursing practice by utilizing voice recognition for direct
documentation,” J. Nurs. Adm., vol. 44, no. 2, pp. 79–86, Feb. 2014.
[52] A. H. Abdelaziz, “Comparing Fusion Models for DNN-Based Audiovisual
Continuous Speech Recognition,” IEEE/ACM Trans. Audio Speech Lang. Process.,
vol. 26, no. 3, pp. 475–484, Mar. 2018.
[53] G. Saon, T. Sercu, S. Rennie, and H. K. J. Kuo, “The IBM 2016 English
conversational telephone speech recognition system,” in Proceedings of the Annual
Conference of the International Speech Communication Association,
INTERSPEECH, 2016, vol. 08-12-Sept, pp. 7–11.

137
[54] W. Xiong et al., “The microsoft 2016 conversational speech recognition system,”
ICASSP, IEEE Int. Conf. Acoust. Speech Signal Process. - Proc., pp. 5255–5259,
Sep. 2017.
[55] K. Garg and G. Jain, “A comparative study of noise reduction techniques for
automatic speech recognition systems,” in 2016 International Conference on
Advances in Computing, Communications and Informatics, ICACCI 2016, 2016, pp.
2098–2103.
[56] Y. Gong, “Speech recognition in noisy environments: A survey,” Speech Commun.,
vol. 16, no. 3, pp. 261–291, Apr. 1995.
[57] K. Kinoshita et al., “The reverb challenge: Acommon evaluation framework for
dereverberation and recognition of reverberant speech,” in IEEE Workshop on
Applications of Signal Processing to Audio and Acoustics, 2013, pp. 1–4.
[58] S. Thomas, S. Ganapathy, and H. Hermansky, “Recognition of reverberant speech
using frequency domain linear prediction,” IEEE Signal Process. Lett., vol. 15, pp.
681–684, 2008.
[59] A. Wisler, V. Berisha, A. Spanias, and J. Liss, “Noise robust dysarthric speech
classification using domain adaptation,” in 2016 Digital Media Industry and
Academic Forum, DMIAF 2016 - Proceedings, 2016, pp. 135–138.
[60] L. Deng et al., “Distributed speech processing in MiPad’s multimodal user
interface,” IEEE Trans. Speech Audio Process., vol. 10, no. 8, pp. 605–619, Nov.
2002.
[61] M. L. Seltzer, D. Yu, and Y. Wang, “An investigation of deep neural networks for
noise robust speech recognition,” in ICASSP, IEEE International Conference on
Acoustics, Speech and Signal Processing - Proceedings, 2013, pp. 7398–7402.

138
[62] H. Meutzner, S. Araki, M. Fujimoto, and T. Nakatani, “A generative-discriminative
hybrid approach to multi-channel noise reduction for robust automatic speech
recognition,” in ICASSP, IEEE International Conference on Acoustics, Speech and
Signal Processing - Proceedings, 2016, vol. 2016-May, pp. 5740–5744.
[63] T. Menne, R. Schluter, and H. Ney, “Speaker Adapted Beamforming for Multi-
Channel Automatic Speech Recognition,” 2018 IEEE Spok. Lang. Technol. Work.
SLT 2018 - Proc., pp. 535–541, Jun. 2019.
[64] S. F. Boll, “Suppression of Acoustic Noise in Speech Using Spectral Subtraction,”
IEEE Trans. Acoust., vol. 27, no. 2, pp. 113–120, Apr. 1979.
[65] J. S. Lim and A. V. Oppenheim, “Enhancement and Bandwidth Compression of
Noisy Speech,” Proc. IEEE, vol. 67, no. 12, pp. 1586–1604, 1979.
[66] R. Rehr and T. Gerkmann, “Cepstral noise subtraction for robust automatic speech
recognition,” in ICASSP, IEEE International Conference on Acoustics, Speech and
Signal Processing - Proceedings, 2015, vol. 2015-Augus, pp. 375–378.
[67] S. Park, Y. Jeong, M. S. Kim, and H. S. Kim, “Linear prediction-based
dereverberation with very deep convolutional neural networks for reverberant
speech recognition,” in International Conference on Electronics, Information and
Communication, ICEIC 2018, 2018, vol. 2018-Janua, no. 1, pp. 1–2.
[68] F. Weninger, S. Watanabe, Y. Tachioka, and B. Schuller, “Deep recurrent de-
noising auto-encoder and blind de-reverberation for reverberated speech
recognition,” in ICASSP, IEEE International Conference on Acoustics, Speech and
Signal Processing - Proceedings, 2014, no. 2, pp. 4623–4627.
[69] J. Li, Y. Huang, and Y. Gong, “Improved cepstra minimum-mean-square-error noise
reduction algorithm for robust speech recognition,” in ICASSP, IEEE International
Conference on Acoustics, Speech and Signal Processing - Proceedings, 2017, pp.
4865–4869.

139
[70] A. Narayanan and D. Wang, “Joint noise adaptive training for robust automatic
speech recognition,” in ICASSP, IEEE International Conference on Acoustics,
Speech and Signal Processing - Proceedings, 2014, pp. 2504–2508.
[71] A. Prodeus and K. Kukharicheva, “Training of automatic speech recognition system
on noised speech,” in 2016 IEEE 4th International Conference Methods and Systems
of Navigation and Motion Control, MSNMC 2016 - Proceedings, 2016, pp. 221–
223.
[72] J. Rajnoha, “Multi-Condition Training for Unknown Environment Adaptation in
Robust ASR Under Real Conditions,” Acta Polytech., vol. 49, no. 2, pp. 3–7, Jan.
2009.
[73] M. Fujimoto and H. Kawai, “Comparative evaluations of various factored deep
convolutional rnn architectures for noise robust speech recognition,” in ICASSP,
IEEE International Conference on Acoustics, Speech and Signal Processing -
Proceedings, 2018, vol. 2018-April, pp. 4829–4833.
[74] A. Prodeus and K. Kukharicheva, “Automatic speech recognition performance for
training on noised speech,” in 2nd International Conference on Advanced
Information and Communication Technologies, AICT 2017 - Proceedings, 2017, pp.
71–74.
[75] S. Watanabe et al., “ESPNet: End-to-end speech processing toolkit,” in Proceedings
of the Annual Conference of the International Speech Communication Association,
INTERSPEECH, 2018, vol. 2018-Septe, pp. 2207–2211.
[76] D. Amodei et al., “Deep speech 2: End-to-end speech recognition in English and
Mandarin,” 33rd Int. Conf. Mach. Learn. ICML 2016, vol. 1, pp. 312–321, Dec.
2016.
[77] A. Hannun et al., “Deep Speech: Scaling up end-to-end speech recognition,” Dec.
2014.

140
[78] D. Yu and J. Li, “Recent progresses in deep learning based acoustic models,”
IEEE/CAA J. Autom. Sin., vol. 4, no. 3, pp. 396–409, Jul. 2017.
[79] C. X. Qin, D. Qu, and L. H. Zhang, “Towards end-to-end speech recognition with
transfer learning,” Eurasip J. Audio, Speech, Music Process., vol. 2018, no. 1, p. 18,
Dec. 2018.
[80] Z. You, D. Su, and D. Yu, “Teach an All-rounder with Experts in Different
Domains,” in ICASSP, IEEE International Conference on Acoustics, Speech and
Signal Processing - Proceedings, 2019, vol. 2019-May, pp. 6425–6429.
[81] R. Lyer, M. Ostendorf, and H. Gish, “Using out-of-domain data to improve in-
domain language models,” IEEE Signal Process. Lett., vol. 4, no. 8, pp. 221–223,
Aug. 1997.
[82] D. Janiszek, R. De Mori, and F. Bechet, “Data augmentation and language model
adaptation,” in ICASSP, IEEE International Conference on Acoustics, Speech and
Signal Processing - Proceedings, 2001, vol. 1, pp. 549–552.
[83] M. Creutz, S. Virpioja, and A. Kovaleva, “Web augmentation of language models
for continuous speech recognition of SMS text messages,” in EACL 2009 - 12th
Conference of the European Chapter of the Association for Computational
Linguistics, Proceedings, 2009, pp. 157–165.
[84] H. Cucu, L. Besacier, C. Burileanu, and A. Buzo, “ASR domain adaptation methods
for low-resourced languages: Application to Romanian language,” in European
Signal Processing Conference, 2012, pp. 1648–1652.
[85] A. Sethy, S. Narayanan, and B. Ramabhadran, “Data Driven Approach for Language
Model Adaptation using Stepwise Relative Entropy Minimization,” in 2007 IEEE
International Conference on Acoustics, Speech and Signal Processing - ICASSP ’07,
2007, vol. 4, pp. IV-177-IV–180.

141
[86] A. K. Baughman, S. Hammer, and D. Provan, “Using language models for
improving speech recognition for U.S. Open Tennis Championships,” IBM J. Res.
Dev., vol. 61, no. 4/5, pp. 15:1-15:9, Jul. 2017.
[87] A. Graves and N. Jaitly, “Towards end-to-end speech recognition with recurrent
neural networks,” in 31st International Conference on Machine Learning, ICML
2014, 2014, vol. 5, pp. 3771–3779.
[88] J. J. Godfrey, E. C. Holliman, and J. McDaniel, “SWITCHBOARD: Telephone
speech corpus for research and development,” in ICASSP, IEEE International
Conference on Acoustics, Speech and Signal Processing - Proceedings, 1992, vol.
1, pp. 517–520.
[89] M. Schuster and K. K. Paliwal, “Bidirectional recurrent neural networks,” IEEE
Trans. Signal Process., vol. 45, no. 11, pp. 2673–2681, 1997.
[90] “TensorFlow.” [Online]. Available: https://www.tensorflow.org/. [Accessed: 05-
Nov-2019].
[91] Kenneth Heafield, “KenLM: Faster and Smaller Language Model Queries,” in
Proceedings of the Sixth Workshop on Statistical Machine Translation, 2011, pp.
187--197.
[92] D. Povey et al., “The Kaldi Speech Recognition Toolkit,” in IEEE 2011 Workshop
on Automatic Speech Recognition and Understanding, Hilton Waikoloa Village, Big
Island, Hawaii, US, Cambridge: IEEE Signal Processing Society, 2011.
[93] “PyTorch.” [Online]. Available: https://pytorch.org/. [Accessed: 05-Nov-2019].
[94] V. Pratap et al., “Wav2Letter++: A Fast Open-source Speech Recognition System,”
in ICASSP, IEEE International Conference on Acoustics, Speech and Signal
Processing - Proceedings, 2019, vol. 2019-May, pp. 6460–6464.
[95] A. Hannun, A. Lee, Q. Xu, and R. Collobert, “Sequence-to-Sequence Speech
Recognition with Time-Depth Separable Convolutions.”

142
[96] T. Likhomanenko, G. Synnaeve, and R. Collobert, “WHO NEEDS WORDS?
LEXICON-FREE SPEECH RECOGNITION A PREPRINT,” 2019.
[97] R. Singh, W. Walker, and P. Wolf, “The CMU Sphinx-4 Speech Recognition
System,” Evaluation, pp. 2–5.
[98] V. Këpuska, “Comparing Speech Recognition Systems (Microsoft API, Google API
And CMU Sphinx),” Int. J. Eng. Res. Appl., vol. 07, no. 03, pp. 20–24, Mar. 2017.
[99] A. Lee and T. Kawahara, “Recent development of open-source speech recognition
engine Julius,” APSIPA ASC 2009 - Asia-Pacific Signal Inf. Process. Assoc. 2009
Annu. Summit Conf., pp. 131–137, 2009.
[100] Google Cloud STT, “Cloud Speech-to-Text - Speech Recognition | Cloud Speech-
to-Text API | Google Cloud,” 2018. [Online]. Available:
https://cloud.google.com/speech-to-text/. [Accessed: 05-Nov-2019].
[101] D. Mowery, J. Wiebe, S. Visweswaran, H. Harkema, and W. W. Chapman,
“Building an automated SOAP classifier for emergency department reports,” J.
Biomed. Inform., vol. 45, no. 1, pp. 71–81, Feb. 2012.
[102] D. A. Juckett, E. P. Kasten, F. N. Davis, and M. Gostine, “Concept detection using
text exemplars aligned with a specialized ontology,” Data and Knowledge
Engineering, vol. 119, North-Holland, pp. 22–35, 01-Jan-2019.
[103] C. Cieri, D. Miller, and K. Walker, “The fisher corpus: A resource for the next
generations of speech-to-text,” in Proceedings of the 4th International Conference
on Language Resources and Evaluation, LREC 2004, 2004, pp. 69–71.
[104] V. Panayotov, G. Chen, D. Povey, and S. Khudanpur, “Librispeech: An ASR corpus
based on public domain audio books,” in ICASSP, IEEE International Conference
on Acoustics, Speech and Signal Processing - Proceedings, 2015, vol. 2015-Augus,
pp. 5206–5210.

143
[105] D. E. R. T. U. München and E. Gazetić, “Comparison Between Cloud-based and
Offline Speech Recognition Systems,” DER TECHNISCHEN UNIVERSITÄT
MÜNCHEN, 2018.
[106] A. R. Aronson and F. M. Lang, “An overview of MetaMap: Historical perspective
and recent advances,” J. Am. Med. Informatics Assoc., vol. 17, no. 3, pp. 229–236,
2010.
[107] “MeSH Browser.” [Online]. Available: http. [Accessed: 06-Nov-2019].
[108] “Deep Domain Adaptation In Computer Vision - Towards Data Science.” [Online].
Available: https://towardsdatascience.com/deep-domain-adaptation-in-computer-
vision-8da398d3167f. [Accessed: 16-Nov-2019].
[109] I. Redko, E. Morvant, A. Habrard, M. Sebban, and Y. Bennani, Advances in Domain
Adaptation Theory. ISTE Press - Elsevier, 2019.
[110] S. Ben-David, J. Blitzer, K. Crammer, A. Kulesza, F. Pereira, and J. W. Vaughan,
“A theory of learning from different domains,” Mach. Learn., vol. 79, no. 1–2, pp.
151–175, May 2010.
[111] M. Suzuki, N. Itoh, T. Nagano, G. Kurata, and S. Thomas, “Improvements to N-
gram Language Model Using Text Generated from Neural Language Model,” in
ICASSP, IEEE International Conference on Acoustics, Speech and Signal
Processing - Proceedings, 2019, vol. 2019-May, pp. 7245–7249.
[112] “These are the Easiest Data Augmentation Techniques in Natural Language
Processing you can think of — and they work.” [Online]. Available:
https://towardsdatascience.com/these-are-the-easiest-data-augmentation-
techniques-in-natural-language-processing-you-can-think-of-88e393fd610.
[Accessed: 13-Nov-2019].

144
[113] X. Zhang, J. Zhao, and Y. LeCun, “Character-level Convolutional Networks for
Text Classification,” Adv. Neural Inf. Process. Syst., vol. 2015-Janua, pp. 649–657,
Sep. 2015.
[114] “WordNet | A Lexical Database for English.” [Online]. Available:
https://wordnet.princeton.edu/. [Accessed: 18-Nov-2019].
[115] “Thesaurus.com | Synonyms and Antonyms of Words at Thesaurus.com.” [Online].
Available: https://www.thesaurus.com/. [Accessed: 18-Nov-2019].
[116] E. Abrahamsson, T. Forni, M. Skeppstedt, and M. Kvist, “Medical text
simplification using synonym replacement: Adapting assessment of word difficulty
to a compounding language.”
[117] S. Young Gunnar Evermann Mark Gales Thomas Hain Dan Kershaw Xunying Liu
Gareth Moore Julian Odell Dave Ollason Dan Povey Valtcho Valtchev Phil
Woodland, “The HTK Book,” 1995.
[118] “ARPA Language models – CMUSphinx Open Source Speech Recognition.”
[Online]. Available: https://cmusphinx.github.io/wiki/arpaformat/. [Accessed: 12-
Dec-2019].
[119] D. Klakow, “Log-linear interpolation of language models,” in ICSLP, 1998, no.
January, pp. 1–4.
[120] “Jaccard Index Definition | DeepAI.” [Online]. Available:
https://deepai.org/machine-learning-glossary-and-terms/jaccard-index. [Accessed:
19-Nov-2019].
[121] A. Schofield, M. Magnusson, and D. Mimno, “Pulling Out the Stops: Rethinking
Stopword Removal for Topic Models.”
[122] C. Silva and B. Ribeiro, “The Importance of Stop Word Removal on Recall Values
in Text Categorization,” in Proceedings of the International Joint Conference on
Neural Networks, 2003, vol. 3, pp. 1661–1666.

145
[123] G. Salton and M. J. McGill, Introduction to Modern Information Retrieval - Chapter
6, page 203. New York, NY, USA: McGraw-Hill, Inc., 1986.
[124] V. Thada and V. Jaglan, “Comparison of Jaccard, Dice, Cosine Similarity
Coefficient To Find Best Fitness Value for Web Retrieved Documents Using
Genetic Algorithm.”
[125] T. Saito and M. Rehmsmeier, “The precision-recall plot is more informative than
the ROC plot when evaluating binary classifiers on imbalanced datasets,” PLoS One,
vol. 10, no. 3, p. e0118432, Mar. 2015.
[126] O. Tilk and T. Alumäe, “Bidirectional recurrent neural network with attention
mechanism for punctuation restoration,” Proc. Annu. Conf. Int. Speech Commun.
Assoc. INTERSPEECH, vol. 08-12-Sept, no. September, pp. 3047–3051, 2016.

Appendix A. AP SCORES FOR SOAP CLASSIFICATION
Table A.1 Micro-Averaged AP-Scores of All Classes
Conditions
1 2 3 4 5 6 7 8
max
n-g
ram
len
gth
1 0.87152 0.84058 0.84252 0.85159 0.85459 0.81910 0.85184 0.81206
2 0.88061 0.86977 0.86825 0.87163 0.85796 0.84112 0.84968 0.84737
3 0.89237 0.86801 0.88100 0.87971 0.85346 0.84504 0.86390 0.85155
4 0.88720 0.87295 0.88759 0.87017 0.86087 0.85578 0.84566 0.84874
5 0.89675 0.88257 0.88595 0.87578 0.85288 0.83935 0.86702 0.86095
6 0.88218 0.87506 0.89358 0.87889 0.86509 0.84752 0.86476 0.84768
7 0.89209 0.87731 0.89252 0.88206 0.85856 0.85403 0.85644 0.85793
8 0.89512 0.87937 0.89425 0.88162 0.86106 0.85125 0.86177 0.84217
9 0.89086 0.88086 0.89328 0.87426 0.85684 0.85889 0.86656 0.85883
10 0.88856 0.88010 0.88967 0.87997 0.86259 0.84090 0.87013 0.85468
11 0.89134 0.87508 0.89125 0.87686 0.85885 0.85197 0.85369 0.84510
12 0.88846 0.87587 0.89400 0.88105 0.85362 0.84972 0.86796 0.85585
13 0.88870 0.86693 0.89375 0.87600 0.85575 0.83931 0.85644 0.85642
14 0.87369 0.87150 0.89542 0.87421 0.86041 0.85231 0.86727 0.84845
15 0.88625 0.87110 0.88969 0.87362 0.86681 0.85358 0.85403 0.86945
Table A.2 Macro-Averaged AP-Scores of All Classes
Conditions
1 2 3 4 5 6 7 8
max
n-g
ram
len
gth
1 0.79998 0.75426 0.76915 0.76028 0.76414 0.71638 0.77121 0.72274
2 0.80459 0.77561 0.79090 0.79243 0.75770 0.75826 0.76001 0.75260
3 0.80807 0.78539 0.79045 0.78538 0.76450 0.75281 0.76895 0.76315
4 0.79333 0.78249 0.78759 0.76358 0.76157 0.75335 0.75009 0.75843
5 0.80807 0.78237 0.79266 0.76794 0.75546 0.75181 0.75882 0.77015
6 0.78405 0.77931 0.80132 0.76689 0.76495 0.75031 0.77623 0.75212
7 0.79768 0.77712 0.79728 0.76820 0.76913 0.75521 0.74464 0.76786
8 0.79060 0.77587 0.79075 0.77641 0.76729 0.76235 0.76174 0.75969
9 0.79412 0.77728 0.78958 0.75259 0.76786 0.75242 0.74746 0.76732
10 0.78881 0.77820 0.78910 0.76923 0.76689 0.76032 0.76641 0.75721
11 0.79597 0.77398 0.79302 0.77094 0.76086 0.76354 0.76075 0.73879
12 0.78550 0.77857 0.79082 0.78332 0.74792 0.76637 0.76998 0.76448
13 0.79340 0.76907 0.79065 0.75373 0.75489 0.74406 0.75701 0.75932
14 0.77876 0.77184 0.79121 0.76499 0.76382 0.75211 0.75768 0.76184
15 0.78395 0.76465 0.78830 0.76070 0.77167 0.77614 0.74695 0.77150

147
Table A.3 AP-Scores of Two Classes (Subjective vs All)
Conditions
1 2 3 4 5 6 7 8 m
ax n
-gra
m le
ngt
h
1 0.90501 0.89149 0.88107 0.90806 0.91505 0.89741 0.89351 0.88440
2 0.93336 0.92283 0.91246 0.92152 0.92710 0.89072 0.88780 0.91804
3 0.94239 0.91865 0.92768 0.94003 0.90400 0.90593 0.91811 0.90613
4 0.94333 0.93144 0.94016 0.93299 0.92555 0.92370 0.90864 0.91680
5 0.95273 0.94288 0.93150 0.94842 0.92308 0.89751 0.92782 0.92390
6 0.94767 0.94021 0.94799 0.95153 0.92594 0.90369 0.90920 0.91275
7 0.94967 0.94131 0.94568 0.94773 0.90604 0.92381 0.92287 0.93336
8 0.95740 0.93798 0.94737 0.95101 0.92411 0.91136 0.90881 0.90886
9 0.94873 0.95107 0.94773 0.94274 0.90559 0.93126 0.92834 0.92388
10 0.94585 0.94358 0.94162 0.94536 0.92514 0.90118 0.93022 0.91742
11 0.94941 0.94000 0.93928 0.94745 0.92916 0.91121 0.90954 0.92416
12 0.95327 0.93872 0.94868 0.94808 0.91769 0.90859 0.92494 0.91523
13 0.95026 0.93438 0.95207 0.94390 0.92459 0.90395 0.90351 0.92396
14 0.93729 0.92832 0.95703 0.95128 0.91915 0.91917 0.93349 0.92274
15 0.95010 0.93111 0.94280 0.94444 0.92890 0.90565 0.91919 0.93660
Table A.4 AP-Scores of Two Classes (Objective vs All)
Conditions
1 2 3 4 5 6 7 8
max
n-g
ram
len
gth
1 0.90375 0.85260 0.87347 0.85891 0.87562 0.83632 0.87708 0.84159
2 0.89769 0.88483 0.89230 0.88298 0.88828 0.87137 0.88961 0.87662
3 0.90800 0.87393 0.90164 0.88555 0.89864 0.86943 0.88837 0.87976
4 0.90251 0.88142 0.90932 0.88496 0.89250 0.88372 0.88241 0.88566
5 0.90749 0.89293 0.91095 0.87892 0.87744 0.87557 0.90670 0.87394
6 0.89953 0.87594 0.91214 0.88282 0.90129 0.87362 0.90426 0.87490
7 0.90831 0.88341 0.90971 0.89423 0.89659 0.88469 0.88819 0.87681
8 0.91126 0.89258 0.91615 0.88261 0.88810 0.87390 0.89979 0.86681
9 0.91129 0.88297 0.91712 0.89106 0.90063 0.87826 0.90311 0.87514
10 0.91113 0.88707 0.91147 0.89191 0.89916 0.87251 0.90402 0.87803
11 0.91130 0.89220 0.91876 0.88074 0.88890 0.87459 0.90308 0.87257
12 0.90712 0.88976 0.91710 0.88228 0.89269 0.87452 0.90712 0.88933
13 0.90656 0.87141 0.91521 0.89360 0.89582 0.87049 0.90602 0.88417
14 0.90707 0.88522 0.91463 0.87518 0.89538 0.88458 0.90084 0.86635
15 0.90746 0.88614 0.91403 0.88204 0.89858 0.87836 0.88369 0.88256

148
Table A.5 AP-Scores of Two Classes (Assessment vs All)
Conditions
1 2 3 4 5 6 7 8 m
ax n
-gra
m le
ngt
h
1 0.62572 0.51981 0.58515 0.54963 0.48264 0.42715 0.50811 0.41564
2 0.58350 0.52195 0.56644 0.57512 0.43244 0.49223 0.47429 0.44123
3 0.59137 0.55334 0.55362 0.53872 0.44582 0.47400 0.47320 0.48630
4 0.53987 0.53424 0.54579 0.47043 0.43733 0.45967 0.40620 0.45350
5 0.60639 0.50124 0.56271 0.48171 0.43891 0.45345 0.42155 0.51026
6 0.51899 0.50746 0.56486 0.47294 0.43950 0.46482 0.47102 0.44875
7 0.55083 0.49840 0.57151 0.48657 0.48152 0.46541 0.42106 0.47560
8 0.53778 0.49373 0.55106 0.49727 0.45034 0.46598 0.46191 0.46540
9 0.55811 0.50911 0.53652 0.43471 0.45231 0.46446 0.44352 0.49112
10 0.55279 0.52788 0.53187 0.47275 0.43585 0.47011 0.46762 0.45519
11 0.56682 0.51310 0.55637 0.51224 0.43034 0.49273 0.44681 0.44773
12 0.54444 0.50459 0.54401 0.54557 0.43188 0.50355 0.44888 0.48709
13 0.56513 0.49285 0.53277 0.44201 0.39557 0.44036 0.45409 0.45822
14 0.52844 0.51922 0.53272 0.48407 0.42753 0.42670 0.42524 0.49405
15 0.54566 0.50524 0.53355 0.45283 0.49985 0.52671 0.44175 0.52557
Table A.6 AP-Scores of Two Classes (Plan vs All)
Conditions
1 2 3 4 5 6 7 8
max
n-g
ram
len
gth
1 0.76542 0.75312 0.73690 0.72453 0.78324 0.70465 0.80615 0.74932
2 0.80380 0.77281 0.79240 0.79008 0.78297 0.77872 0.78832 0.77451
3 0.79052 0.79562 0.77884 0.77720 0.80953 0.76187 0.79611 0.78040
4 0.78761 0.78287 0.75510 0.76593 0.79089 0.74632 0.80311 0.77775
5 0.76565 0.79241 0.76548 0.76269 0.78241 0.78070 0.77922 0.77251
6 0.77001 0.79364 0.78029 0.76025 0.79305 0.75910 0.82042 0.77209
7 0.78190 0.78535 0.76220 0.74425 0.79237 0.74693 0.74642 0.78567
8 0.75596 0.77918 0.74840 0.77476 0.80662 0.79814 0.77646 0.79768
9 0.75836 0.76597 0.75696 0.74186 0.81290 0.73569 0.71488 0.77912
10 0.74545 0.75426 0.77144 0.76691 0.80741 0.79749 0.76379 0.77821
11 0.75635 0.75062 0.75767 0.74334 0.79502 0.77564 0.78358 0.71071
12 0.73718 0.78119 0.75350 0.75734 0.74943 0.77882 0.79898 0.76625
13 0.75164 0.77764 0.76255 0.73542 0.80356 0.76144 0.76442 0.77093
14 0.74224 0.75461 0.76046 0.74943 0.81323 0.77798 0.77115 0.76423
15 0.73256 0.73611 0.76280 0.76349 0.75936 0.79384 0.74318 0.74126
Copyright © 2022 FDOKUMEN




















