Antibody Titration Test Method - NSW Health Pathology
17
Antibody Titration Test Method NSWHP_PR_063 Page 1 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library www.pathology.health.nsw.gov.au 1. Purpose This document outlines the Bio-Rad CAT methodology for performing antibody titration testing across NSW Health Pathology Laboratories. 1.1. Principle of Assay Titration studies are semi-quantitative and undertaken to support the prediction and management of Haemolytic Disease of the Fetus and Newborn (HDFN), ABO mismatched organ transplants and Allogeneic Transplant of ABO mismatch Bone Marrow and Peripheral Blood Stem Cell Transplants. A titre is a measure of the strength of an antibody. Titration values can help quantify the relative antibody concentration in the plasma, or the relative strength of antigen expression on red cells. In general, an antibody reacting at a high titre (e.g. 128) will cause greater red cell destruction than an antibody reacting at a low titre (e.g. 2). The titre is obtained by testing serial dilutions of the antibody against appropriate red cells and a titre value assigned based on the highest dilution of the antibody still causing a positive reaction of a particular strength, depending on the antibody being titred. The haemagglutination titre is expressed as the reciprocal of the highest serum dilution in which agglutination is observed as a score of 1. At Royal Prince Alfred Hospital the renal titre end point is 2. Titres have wide application in the Transfusion laboratory: • Monitoring the antibody level in an antenatal patient • Monitoring antibody mediated rejection (ABMR) following ABO mismatched organ transplants. • Anti-A and anti-B titres are performed pre and post-pheresis prior to the infusion of mismatched bone marrow or stem cells for transplant. • Detection of underlying alloantibodies in patients with autoantibodies • Identification and investigation of HTLA antibodies. Antenatal Titres Antibody titres are performed on antenatal patients where potentially clinically significant IAT reactive antibodies are detected to estimate the risk of HDFN. Anti-D, c and K are most commonly associated with HDFN but anti-C, Cw, E, e, k, Fy, Jk, M, S are potentially significant and require titration. An increase in the antibody titre may relate to an increase in the concentration of antibody which could reflect an increase in risk to the fetus. However previous history is not indicative of the severity of disease for anti-K antibodies. After identification and titration, plasma is separated and stored frozen for parallel titration with subsequent samples. This will ensure that any apparent change in titre is not due to technique or reagent variation. Anti-c and immune anti-D are referred to Australian Red Cross Lifeblood (ARCL) reference laboratory for antibody quantitation. ABO Titres The ABO antibody that is titrated in the patient has the specificity of the ABO antigen being transplanted from the donor, e.g. If the patient is Group O and the Donor is Group A, then Anti-A in the patient will be titred. ABO Tires are performed using Bio-Rad ID-Diacell ABO (A1, A2, B Cells) Pooled Red Cells for Reverse Serum Grouping as follows:
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Antibody Titration Test Method - NSW Health Pathology

Antibody Titration Test Method NSWHP_PR_063
Page 1 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
1. Purpose
This document outlines the Bio-Rad CAT methodology for performing antibody titration testing across
NSW Health Pathology Laboratories.
1.1. Principle of Assay
Titration studies are semi-quantitative and undertaken to support the prediction and management of
Haemolytic Disease of the Fetus and Newborn (HDFN), ABO mismatched organ transplants and
Allogeneic Transplant of ABO mismatch Bone Marrow and Peripheral Blood Stem Cell Transplants. A
titre is a measure of the strength of an antibody. Titration values can help quantify the relative antibody
concentration in the plasma, or the relative strength of antigen expression on red cells. In general, an
antibody reacting at a high titre (e.g. 128) will cause greater red cell destruction than an antibody
reacting at a low titre (e.g. 2).
The titre is obtained by testing serial dilutions of the antibody against appropriate red cells and a titre
value assigned based on the highest dilution of the antibody still causing a positive reaction of a
particular strength, depending on the antibody being titred. The haemagglutination titre is expressed as
the reciprocal of the highest serum dilution in which agglutination is observed as a score of 1. At Royal
Prince Alfred Hospital the renal titre end point is 2.
Titres have wide application in the Transfusion laboratory:
• Monitoring the antibody level in an antenatal patient
• Monitoring antibody mediated rejection (ABMR) following ABO mismatched organ transplants.
• Anti-A and anti-B titres are performed pre and post-pheresis prior to the infusion of mismatched bone
marrow or stem cells for transplant.
• Detection of underlying alloantibodies in patients with autoantibodies
• Identification and investigation of HTLA antibodies.
Antenatal Titres
Antibody titres are performed on antenatal patients where potentially clinically significant IAT reactive antibodies are detected to estimate the risk of HDFN. Anti-D, c and K are most commonly associated with HDFN but anti-C, Cw, E, e, k, Fy, Jk, M, S are potentially significant and require titration. An increase in the antibody titre may relate to an increase in the concentration of antibody which could reflect an increase in risk to the fetus. However previous history is not indicative of the severity of disease for anti-K antibodies.
After identification and titration, plasma is separated and stored frozen for parallel titration with
subsequent samples. This will ensure that any apparent change in titre is not due to technique or
reagent variation. Anti-c and immune anti-D are referred to Australian Red Cross Lifeblood (ARCL)
reference laboratory for antibody quantitation.
ABO Titres
The ABO antibody that is titrated in the patient has the specificity of the ABO antigen being transplanted
from the donor, e.g. If the patient is Group O and the Donor is Group A, then Anti-A in the patient will be
titred. ABO Tires are performed using Bio-Rad ID-Diacell ABO (A1, A2, B Cells) Pooled Red Cells for
Reverse Serum Grouping as follows:
Antibody Titration Test Method NSWHP_PR_063
Page 2 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
1. Renal transplant patients having an ABO-incompatible transplant.
Pretransplant workup titre against potential donor, A1, A2 or B cells depending on the blood group or
group A sub-type of the donor.
Peri and Post-transplant titre against A1, A2 or B cells depending on the blood group or the group A
sub-type of the donor.
2. Anti-A titres are performed on all group O and group B pre-liver transplant patients.
3. Haematology Patients undergoing Allogeneic Transplant of ABO Major mismatch Haemopoietic
progenitor cells (HPC). Titre against A1 or B cells as indicated.
Patients undergoing an ABO incompatible renal transplant often require titres to be performed. Titres are
performed pre transplant to monitor the response to treatment and post transplant to aid in the
assessment of the success of the transplant. The titres are performed for Anti-A1, Anti-A2 and Anti-B,
based upon the blood group of the patient and potential donor.
Prior to Allogeneic Transplant of ABO major mismatch HPC donor cells plasmapheresis may be
performed if the ABO titre of the patient is high to reduce or remove the ABO IgM antibodies. This will
minimise the destruction of ABO Major mismatch transplanted cells which may be destroyed if high titres
of ABO antibodies are present. A post plasmapheresis sample, prior to the transplant date may be
received to measure the success of plasmapheresis in the removal of these IgM antibodies. Further
plasma exchanges may occur if the desired ABO titre has not been achieved. Donor ABO Titres (anti-A
and/or anti-B titres) are performed for minor mismatch. If the donor titre is high plasma reduction will be
performed on bone marrow or peripheral blood stem cell collection.
1.2. Scope
This test method applies to all NSW Health Pathology scientific and technical staff involved in
pretransfusion laboratory practice.
1.3. Test Frequency and Expected Turnaround Time
Performed on request during laboratory hours.
Refer to local laboratory procedures for expected turnaround times.
1.4. Definitions
ABOi: Blood group incompatibility
IgM: Immunoglobulin M
IgG: Immunoglobulin G
HDFN: Haemolytic Disease of the Fetus and Newborn
ABMR: Antibody Mediated Rejection
IAT: Indirect Antiglobulin Test
CAT: Column Agglutination Technology
EDTA: Ethylenediaminetetraacetic acid
LIS: Laboratory Information System

Antibody Titration Test Method NSWHP_PR_063
Page 3 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
RCPA QAP: Royal College of Pathologists of Australasia Quality Assurance Program
ARCL: Australian Red Cross Lifeblood
2. Method Specifications
2.1. Potential Sources of Assay Variability
• Bacterial or other contaminations of reagents can cause false positive or false negative results, look
for turbidity. Repeat test with new reagents.
• Fibrin in the plasma or red cell aggregates in the red cell suspension may trap non-agglutinated cells
at the top of the gel while most of the cells are on the bottom of the microtube after centrifugation.
Remove fibrin and repeat test.
• Elevated white cell counts may cause false positive reactions. Consult with laboratory senior.
• Too heavy or too light red cell suspensions may cause discrepant results.
• Correct pipetting technique must be used to avoid contact of the pipette tip with the contents of the
microtubes to prevent carryover.
3. Pre-Analytical
3.1. Primary Specimen Type e.g. blood, urine, tissue
Venous blood collected aseptically.
3.2. Specimen containers including any additives, anticoagulants, buffers, acid
• An anticoagulated EDTA (pink or purple top) specimen tube centrifuged as per local policy prior to
testing.
• Other tube types that may be accepted for testing include citrate (blue top) clotted blood (red top) and
CPD-A centrifuged as per local policy prior to testing.
• Lithium heparin (green top) and serum gel tubes are not acceptable due to the potential for the gel to
absorb antibodies resulting in false negative results.
Note: Throughout the document reference to plasma and serum is interchangeable.
3.3. Assay Validation and Verification
Validation and Verification documentation of the test method is reviewed and signed by the Supervising
Pathologist and retained in the Quality Management System. For further information refer to Verification
Procedure for the Bio-Rad IH 1000, IH 500 and Bio-Rad Saxo Analysers NSWHP_PR_046.
3.4. Sensitivity, Specificity of detection
An anti-D titre using Securacell 1 must be performed daily when a titre is performed. The expected
titration endpoint of Securacell 1 is 32 (+/-1). If this result is not achieved all testing including the
Securacell 1 quality control is repeated.
3.5. Patient preparation e.g. fasting, time after last dose – if applicable

Antibody Titration Test Method NSWHP_PR_063
Page 4 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
Not Applicable
3.6. Specimen Rejection Criteria
A specimen will be rejected for testing if:
• The specimen does not meet the criteria outlined in Labelling Requirements for Pathology and Forensic
Specimens NSWHP_PD_023. It is not necessary that the additional requirements for Transfusion
specimens are met.
• The specimen is insufficiently filled. Refer to local recollection procedures.
• The specimen is grossly haemolysed. Refer to local recollection procedures.
3.7. Specimen Transport Requirements – frozen, room temp, on ice, other
Specimens may be transported at room temperature or 2-8oC.
3.8. Specimen Stability, Storage and Retention
Specimens should be tested within 24 hours of collection wherever possible, and testing completed
within 48 hours when kept at room temperature (18-25ºC) and up to 7 days when stored between 2-8oC.
Specimens stored at 2-8oC are not used for serological testing beyond 7 days from the date of collection.
If specimens are required to be routinely tested after 7 days, they must be separated, and the plasma
stored frozen at -20 ºC for up to 3 months. If parallel testing with a sample older than 3 months is
required, an anti-D titre with Securacell 1 can be performed in parallel as a control. Refer to local
laboratory procedures for specimen retention time.
4. Reagents, Supplies and Equipment
4.1. Required Reagents and Reagent Source
DiaClon ID-Card LISS/Coombs: Indirect and Direct Coombs Test (Product ID 50531)
ID-Diacell (I-II-III) Test cell reagents for antibody screening (Product ID 45184)
ID-DiaPanel (Set of 11 vials) Test cell reagents for antibody identification- IAT (ID 45161)
ID-Diacell ABO (A1, A2, B Cells) Pooled Red Cells for Reverse Serum Grouping (ID 45082)
ID-Diluent 2 modified LISS for red cell suspensions (Product ID 05761)
ID-Titration racks- containing 60 dilution wells for use on the IH-500 (Product ID 05770)
ID-Titration Solution- Bovine Serum Albumin (BSA) based diluent (Product ID 05780)
0.9% Buffered Saline Solution pH 7.1
Securacell
4.2. Reagent Preparation
Not Applicable

Antibody Titration Test Method NSWHP_PR_063
Page 5 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
4.3. Reagent Stability and Storage
• ID-Diacell (I-II-III), ID-DiaPanel and ID-Diacell ABO red cell reagents store at 2-8ºC and do not store
near any heat, air conditioning sources or ventilation outlets. Red cell reagents must be gently
resuspended and at room temperature (18-25 °C) when used for manual testing. Reagents are used
until the expiry date as indicated by the manufacturer. Refrigerated reagents stored onboard the IH-
500 analyser are stable for 7 days.
• ID-Titration Solution store at 2-8ºC and do not store near any heat, air conditioning sources or
ventilation outlets. The Titration Solution is used until the expiry date as indicated by the
manufacturer, once opened the expiry of the vial is 4 weeks.
• DiaClon ID-Cards store at 18-25ºC. Inspect cards before use ensuring that buffer covers the gel and
that there are no bubbles in the gel. DiaClon ID-Cards are used until the expiry date as indicated by
the manufacturer. ID-Cards stored onboard the IH-500 analyser are valid for 21 days.
• Securacell store at 2-8ºC and do not store near any heat, air conditioning sources or ventilation
outlets. Reagents are used until the expiry date as indicated by the manufacturer.
4.4. Laboratory Equipment
Automated Bio-Rad CAT method
Testing is performed on the Bio-Rad IH-500 fully automated system for immunohaematology
diagnostics.
Manual Bio-Rad CAT Method
The Bio-Rad Saxo ID-Reader II is a semi-automated system for immunohaematology diagnostics and
relies heavily on the technician correctly following testing procedures. Manually pipetted gel cards are
incubated, centrifuged, the reactions read by the integrated camera and the results interpreted by the
interpretation software.
• ID-Dispenser (for the ID-Diluent 2)
• Pipette and Pipette tips
• ID-Working table
• Test tubes
• ID-Incubator L
• ID-Centrifuge L (back up centrifuge)
4.5. Quality Control and QC Acceptance Criteria
Pre acceptance testing is performed on all new batches of ID-Diacell (I-II-III), ID-DiaPanel, ID-Diacell
ABO red cell reagents and ID-Cards before being placed into general use. Refer to Pre Acceptance
Testing of Red Cell Reagents NSWHP_PR_051 and Pre Acceptance Testing Transport and Storage of
Bio-Rad ID-Cards and Solutions NSWHP_PR_050 for further information.
Quality control for the Forward/Reverse Cards, Group Check Cards, LISS/Coombs ID-Cards, and ID-
Diacell (I-II-III) are performed daily using QC material. An anti-D titre using Securacell 1 is performed
daily for each technician when performing titres manually and daily for the analyser if testing is
automated. The expected titration endpoint of Securacell 1 is 1:32 (+/-1). QC results will be accepted for

Antibody Titration Test Method NSWHP_PR_063
Page 6 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
validation if the expected titration endpoint is reached. If this result is not achieved, all testing (including
any patients run in parallel with the QC anti-D titre) must be repeated, ensuring the appropriate R2R2
screening cell is selected and that Securacell 1 has not expired. Any discrepancies must be investigated,
report unresolved QC out of range to laboratory senior. Patient antibody titre results will not be accepted
until QC results are acceptable.
4.6. Calibration Procedures
The calibration and preventative maintenance of the Bio-Rad Saxo ID-Reader II, ID-Incubator L and ID-
Centrifuge L is performed annually by qualified Bio-Rad engineers.
The calibration of the IH-500 is performed at 6 monthly preventative maintenance services by qualified
Bio-Rad engineers.
Pipette checks are performed 6 months.
Centrifuge calibrations are performed annually.
4.7. Quality Assurance Programs
NSWHP Laboratories are enrolled in RCPA QAP programmes, laboratories performing antibody titres
are enrolled in the Antibody Titre module. NSWHP Transfusion Laboratories participate in an
interlaboratory sample exchange program for tests in scope not covered by RCPA QAP. Refer to local
Quality Assurance standard operating procedures for further information. All staff must participate in the
quality assurance program and undertake at least two exercises per year to ensure their gradings are
correct and that all positive tests are being detected.
5. Method Detail
5.1. Full Procedure
Automation on the Bio-Rad IH-500 is the preferred method. Results for patient testing performed on
the Bio-Rad Saxo ID-Reader and IH-500 are stored in the IH-Com database along with the patient
details, batch numbers and expiry dates of reagents, cells, ID-Cards and Diluents. All staff are allocated
a unique user ID and password which allows traceability of the user actions performed at all stages of
testing.
Standard Laboratory Procedure
1. Perform routine antibody identification or for ABO titration requests check the history of the patient in the LIS to determine which ABO antibody requires titration. For all titres check the previous titre result (if available).
2. For antenatal testing locate the frozen aliquot of a previous sample (if available), allow to thaw prior to testing in parallel with current sample.
3. Order Antibody Titration in IH-Com for tests not ordered in the LIS.
4. All results are to be printed from IH-Com (Print, Results and Protocols), ensuring the Securacell 1 has been performed and the result is printed with all patient samples.
Refer to:
• Bio-Rad Saxo ID-Reader II NSWHP_PR_057, for instructions on how to assign, centrifuge and read
ID-Cards

Antibody Titration Test Method NSWHP_PR_063
Page 7 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
• Bio-Rad IH-500 Immunohaematology Analyser NSWHP_PR_055 for information on processing
specimens on the analyser.
• Bio-Rad IH-Com Data Management Software NSWHP_PR_054 for instructions on how to order tests
and review results in IH-Com.
5.2. Ordering Anti-D Quality Control – Securacell 1
An anti-D titration of a known endpoint must be performed each day a titre is performed using Securacell
1 on the IH-500. If the antibody titration is being performed manually with the Saxo ID-Reader II
Securacell 1 must be performed manually each day by each technician performing an antibody titration.
In IH-Com, select Work list tab, select ‘Quick Request’.
From the drop down list select the test ‘Anti-D titre’
Scan the barcode on Securacell 1.
Depending on the method of testing, either follow the steps for 5.7 Antibody Titre by manual CAT
method or 5.8 Antibody Titre by automated CAT method.
5.3. Ordering an Antibody Titration in IH-Com
At the Main (Analyser) screen, select ‘Data Management’.
Select the ‘Work List’ tab.
Right Click and select ‘Quick Request’.
Select the test from the dropdown list.
The syntax of the titration test is:
Titration [gel card name], [dilution level], [incubation temperature] x [reagent code]
e.g. Titration LISS/Coombs (5053), 1-6, 37ºC x 0609
The reagent code is the individual cell number associated with each reagent bottle and is the first
4 digits on the barcode of the reagent bottle. This unique reagent code is displayed in IH-Com
when the respective reagent red cells are onboard the IH-500. It is important to take care when
selecting the test as the reagent code identifies the red cells to be titred.
A titration can be ordered on any of the following reagent red cells for a 1:32 or 1:2048 dilution.
a. Individual cells from 0.8% ID-DiaCell I-II-III
b. Individual cells from 0.8% ID-DiaPanel
c. A1, A2 or B cells from 0.8% ID-Diacell ABO
Refer to local laboratory procedure at Royal Prince Alfred Hospital for ABO incompatible renal
transplant workup and procedure to titre donor red cells against the recipients plasma
Scan the sample barcode, IH-Com may identify the patient, A window box will open with ‘The
sample number is already in use for another patient: Surname,Firstname,Dob (Sex)[MRN}’
select ‘Yes’ if this is the correct patient.
Click ‘Order Now’ and ‘Close’.

Antibody Titration Test Method NSWHP_PR_063
Page 8 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
5.4. Ordering an Antibody Titration in IH-Com while reviewing the antibody results:
This procedure cannot be used for ABO titrations
In IH-Com, under the Results tab, review the correct patient’s antibody screen and panel results
in the Result verification screen.
If a titration is possible on the header of the positive well, a small tick box will be present, select
this box for the antibody titration to be performed.
Confirm the request by selecting the ‘Order Titration’ button at the bottom of the
screen.
The selection is displayed with a message for acknowledgement. Confirm the message by
selecting ‘OK’.
5.5. Selection of Test Cells for Antenatal Patients
A constant source of cells, that is a fixed antigen site density, eliminates one major variable which can
influence the results of titration. For anti-D titres R2R2 cells are generally used as they have the strongest
expression of the D antigen the cell of choice is cell II from 0.8% ID-DiaCell I-II-III.

Antibody Titration Test Method NSWHP_PR_063
Page 9 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
If the patient has additional alloantibodies, select R2R2 cells for the Anti-D titre, ensuring it is negative for
the additional alloantibodies present. Ensure selected homozygous cells are reading consistently with
other homozygous cells in the panel.
Rh antibodies
Single Antibody Cells Required Multiple Antibodies Cells Required
Anti-D R2R2 Anti-D and anti-C R1R1 or R2R2
Anti-C R1R1 Anti-D and anti-E R2R2
Anti-E R2R2
Anti-e R1R1
Anti-c R2R2
Other Atypical Antibodies
For other antibodies, use a single homozygous positive cell for the titre being performed
from the 0.8% ID-Panel. Anti-K is an exception where homozygous expression is rare
and not found routinely in panel cells. If the titre has been previously performed using
cells heterozygote for the antigen being titred then it is important to continue with
heterozygous cells.
e.g. for Anti-Fya Fya+b- (homozygous cell)
Antibody Mixtures
For mixtures of antibodies, cells selected to estimate the strength of each antibody may
be used by selecting cells homozygous for one of the antibodies and negative for the
other.
e.g. Where anti-K and anti-Fya is present Titrate against K-, Fya+b- cells and K+, Fya-
cells
5.6. Selection of Test Cells for ABO Titrations
The selection of cells will be depending upon the antibody being titred, using A1, A2 or B cells from 0.8%
ID-Diacell ABO. If the patient has an alloantibody, the cells used for the titre must also be antigen
negative. The antibody being titred is determined by the antibody the recipient has but the donor lacks
which may affect recipient donor compatibility.

Antibody Titration Test Method NSWHP_PR_063
Page 10 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
Titres can be ordered by requesting a 1:2048 titration
Test Code including Individual Cell Number Cell
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0608 I
ID-DiaCell I-II-III 0.8% Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0609 II
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0610 III
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0617 1
ID-Panel 0.8%
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0618 2
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0619 3
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0620 4
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0621 5
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0622 6
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0623 7
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0624 8
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0625 9
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0626 10
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0627 11

Antibody Titration Test Method NSWHP_PR_063
Page 11 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
Titres can be ordered by requesting a 1:32 titration
Please note, the titre endpoint must be followed by two negative wells.
Test Code including Individual Cell Number Cell
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0608 I
ID-DiaCell I-II-III
0.8% Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0609 II
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0610 III
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0617 1
ID-Panel 0.8%
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0618 2
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0619 3
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0620 4
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0621 5
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0622 6
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0623 7
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0624 8
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0625 9
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0626 10
Titration LISS/Coombs (5053) 1-6, 37oC TLIS1_0627 11

Antibody Titration Test Method NSWHP_PR_063
Page 12 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
For patients requiring an ABO titration, select one of the following options.
Test Code including Individual Cell Number Cell
Titration LISS/Coombs (5053) 1-6, 37oC, TLIS1_0601 A1
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0601 A1
Titration LISS/Coombs (5053) 1-6, 37oC, TLIS1_0602 A2
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0602 A2
Titration LISS/Coombs (5053) 1-6, 37oC, TLIS1_0603 B
Titration LISS/Coombs (5053) 1-12, 37oC, TLIS3_0603 B
Titration Coombs Anti-IgG (5053) 1-6, 37oC x 0601 A1
Titration Coombs Anti-IgG (5053) 1-12, 37oC x 0601 A1
Titration Coombs Anti-IgG (5053) 1-6, 37oC x 0601 A2
Titration Coombs Anti-IgG (5053) 1-12, 37oC x 0601 A2
Titration Coombs Anti-IgG (5053) 1-6, 37oC x 0603 B
Titration Coombs Anti-IgG (5053) 1-12, 37oC x 0603 B
5.7. Antibody Titre by manual CAT method
The manual CAT method is performed using the Saxo ID-Reader II, refer to Bio-Rad Saxo ID-Reader II
NSWHP_PR_057 for instructions on how to assign ID-Cards and print a barcode label.
Prepare a twofold serial dilution:
Label a row of test tubes 2 to 12.
Pipette 200 µL of ID-Titration Solution to tubes 2 to 12.
Add 200 µL of patient plasma to tube two and mix thoroughly by aspirating and dispensing the
contents with a fresh pipette tip.
Pipette 200 µl of the dilution from tube two (1:2 dilution) to the tube three (1:4 dilution), change
pipette tips and mix tube three thoroughly.
Continue serial dilution of the patient’s plasma by repeating this procedure through to tube twelve
ensuring each tube is mixed thoroughly with a new pipette tip before transfer to the next tube to
avoid carry over of plasma.
• The titre can be extended if it is expected to exceed 1/2048 (12 tubes).
Antibody Titration Test Method NSWHP_PR_063
Page 13 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
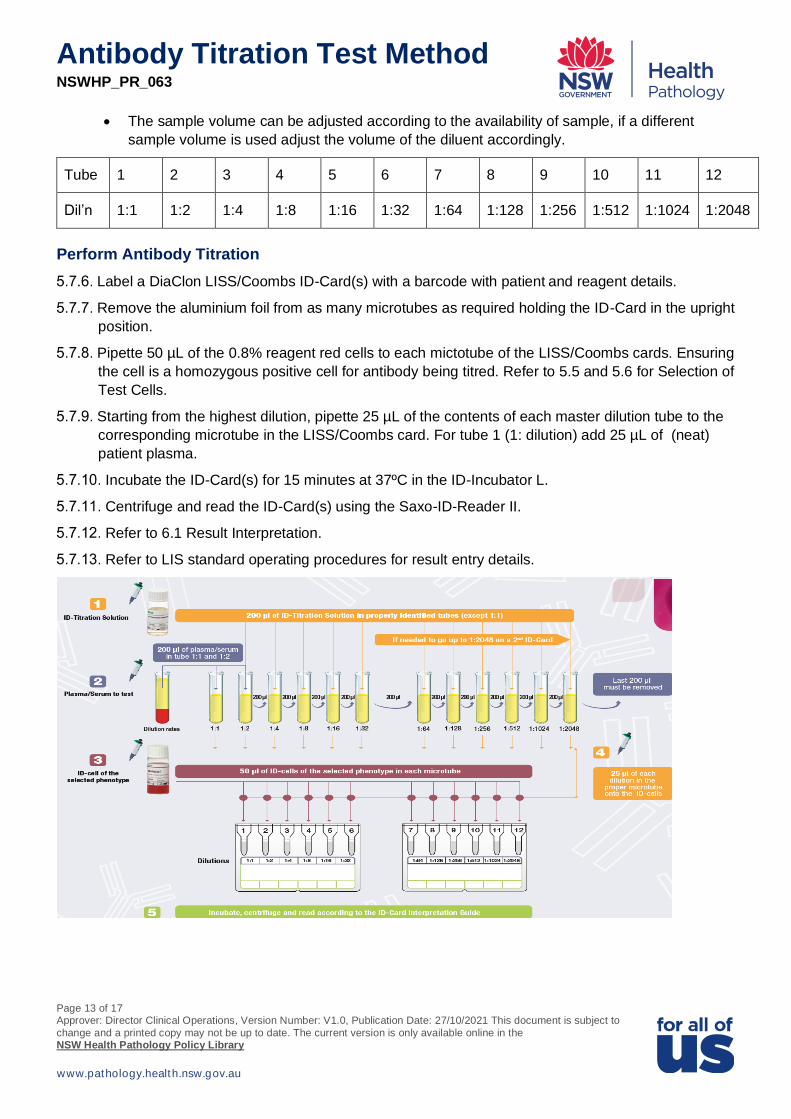
• The sample volume can be adjusted according to the availability of sample, if a different
sample volume is used adjust the volume of the diluent accordingly.
Tube 1 2 3 4 5 6 7 8 9 10 11 12
Dil’n 1:1 1:2 1:4 1:8 1:16 1:32 1:64 1:128 1:256 1:512 1:1024 1:2048
Perform Antibody Titration
Label a DiaClon LISS/Coombs ID-Card(s) with a barcode with patient and reagent details.
Remove the aluminium foil from as many microtubes as required holding the ID-Card in the upright
position.
Pipette 50 µL of the 0.8% reagent red cells to each mictotube of the LISS/Coombs cards. Ensuring
the cell is a homozygous positive cell for antibody being titred. Refer to 5.5 and 5.6 for Selection of
Test Cells.
Starting from the highest dilution, pipette 25 µL of the contents of each master dilution tube to the
corresponding microtube in the LISS/Coombs card. For tube 1 (1: dilution) add 25 µL of (neat)
patient plasma.
Incubate the ID-Card(s) for 15 minutes at 37ºC in the ID-Incubator L.
Centrifuge and read the ID-Card(s) using the Saxo-ID-Reader II.
Refer to 6.1 Result Interpretation.
Refer to LIS standard operating procedures for result entry details.

Antibody Titration Test Method NSWHP_PR_063
Page 14 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
5.8. Antibody Titre by automated CAT method
The test is performed on the Bio-Rad IH-500 using the same volumes and same dilutions as outlined in
5.7 Antibody Titre by manual CAT method. Refer to 5.3 and 5.4 Ordering an Antibody titre in IH-Com for
instructions on how to request a test not ordered in the LIS. Once the testing has been requested in IH-
Com place the patient sample in the sample rack and load onto the Bio-Rad IH-500 analyser. Ensure ID-
Titration solution (at least 2 mL), ID-Titration racks and required test red cells have been loaded on
board the IH-500 via the left drawer, each titre will use 6 or 12 microtubes depending on the test being
requested. All blood groups and antibody testing will have priority over titration requests.
5.9. Result Out-Of-Range / Reflex Testing / Supplementary Testing
Not Applicable
5.10. Calculations
Not Applicable
6. Reporting Result
Refer to LIS standard operating procedures for result entry details.
6.1. Result Interpretation and choice of Coded Comments
Positive: Agglutinated cells forming a red line on the surface of the gel or dispersed in the gel.
Negative: Compact button of cells on the bottom of the microtube.
Reaction Grading for Bio-Rad CAT Testing
The titre is the reciprocal of the highest plasma dilution, which gives a strength of 1+ reaction (the
exception is the renal titre end point at Royal Prince Alfred Hospital which is 2) e.g. a 1+ reaction in the
1:8 well is reported as a titre of 8. If the titration end point exceeds 1:2048, testing must be continued by
manual technique with additional dilutions included. Two negative reactions in subsequent dilutions must
follow the end point.
Where possible each sample should be tested in parallel with the previous sample and the results
compared to identify a significant rise in antibody concentration. A rise of at least 2 dilutions is
considered to be a significant increase in titre.
Anti-K antibodies are clinically significant regardless of titre, or reaction strength. Anti-K is the most likely
to cause HDFN other than anti-D and anti-c. While most antibodies associated with HDFN result is
immune destruction of the red blood cells, Anti-K is of greater clinicial significance in HDFN due to the
suppression of erythropoiesis as well as immune red blood cell destruction.

Antibody Titration Test Method NSWHP_PR_063
Page 15 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
Anti-D and Anti-c titres sample require an aliquot of plasma (minimum of 1 mL of separated plasma) to
be sent to ARCL for an antibody quantitation. If the sample is insufficient for both an antibody titre and
antibody quantitation send the sample for antibody quantition. Refer to local laboratory procedures for
referring samples to ARCL
6.2. Critical Alert Values or Notifications required5,6
If there is a significant increase in the titre end point from the previous titre result the Clinician may be notified refer to local procedure.

Antibody Titration Test Method NSWHP_PR_063
Page 16 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
6.3. In-House IVD class 1-3 or other Disclaimer Required
Not Applicable
6.4. Record Retention
Refer to NPAAC Retention of laboratory records7.
7. Roles and Responsibilities
1. The Supervising Pathologist discharges the supervision responsibilities as set out in the NPAAC
requirements and Supervision Requirements, including documented review of audits, new tests and
equipment, external QAP, internal Quality Control and Quality Assurance9.
2. Laboratory managers are responsible for ensuring staff are trained in the use of this test method and
are deemed competent. Managers are also responsible for ensuring that records are retained
according to NPAAC requirements7.
3. Technical and Scientific staff are responsible for performing the antibody titration test method and
reporting results as outlined in this document.
8. Legal and Policy Framework
1. Saxo ID Reader II User Manual, DiaMed GmbH Version 2- 08/2016, SAP H007416
2. IH-500 User Manual, DiaMed GmbH Version 2.2- 11/2018, DOC H009225
3. IH-Com user Manual, DiaMed GmbH Version 2-04/2019 DOC H009146
4. NPAAC Requirements for Medical Pathology Services, Third Edition 2018 (Tier 2)
https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-npaac-docs-medpathserv-
2018
5. NPAAC Requirements for Transfusion Laboratory Practice, Fourth Edition 2019 (Tier 4)
http://www.health.gov.au/internet/main/publishing.nsf/Content/npaac-pub-transfusion
6. ANZSBT Guidelines for Transfusion and Immunohaematology Laboratory Practice, Australasian
Society of Blood Transfusion Inc 1st Edition, revised January 2020 https://anzsbt.org.au/guidelines-
standards/anzsbt-guidelines/
7. NPAAC, Requirements for the Retention of Laboratory Records and Diagnostic Material, Eighth
Edition 2021 (Tier 3) https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-npaac-
docs-RetLabRecDI-2018
8. NPAAC, Requirements for Supervision in the Clinical Governance of Medical Pathology
Laboratories, Sixth Edition 2021
https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-npaac-docs-supervision.htm
9. NSW Health Pathology Supervision Policy NSWHP_PD_019
8.1. Related Documents
Bio-Rad Saxo ID-Reader II NSWHP_PR_057
Bio-Rad IH-500 Immunohaematology Analyser NSWHP_PR_055

Antibody Titration Test Method NSWHP_PR_063
Page 17 of 17 Approver: Director Clinical Operations, Version Number: V1.0, Publication Date: 27/10/2021 This document is subject to
change and a printed copy may not be up to date. The current version is only available online in the NSW Health Pathology Policy Library
www.pathology.health.nsw.gov.au
Bio-Rad IH-Com Data Management Software NSWHP_PR_054
NSWHP Transfusion Test Methods
9. Review
This procedure will be reviewed by 14/10/2023.
10. Risk
Risk Statement A patient with a high titre antibody can be an indication of HDFN,
or ABMR following an incompatible ABO organ transplant, if
results are not reported accurately, appropriate treatment may not
be given and if this occurs the consequences could result in major
harm to the patient.
Risk Category Clinical Care and Patient Safety
10.1. Key WHS Information
Key WHS Factors and Risks WHS Controls
Reagents and patient
specimens should be treated
as potentially infectious.
Wear PPE while handling or if a spill occurs. Refer to spill clean-
up instructions and product safety data sheets for further details.
11. Further Information
For further information, please contact:
Procedure Contact Officer Position: Chair, Transfusion Clinical Stream
Name: Associate Professor Mark Dean
Telephone: (02) 4320 3894
Email: [email protected]
12. Version History
The approval and amendment history for this document must be listed in the following table.
Version No
Effective Date
Approved By
Approval Date
Procedure Author
Risk Rating Sections Modified
V1.0 27/10/2021 Director Clinical Operations
27/10/2021 Associate Professor Mark Dean
High New Test Procedure