ANNUAL RESULTS REPORT 2010 - ReliefWeb
58
Supporting community action on AIDS in developing countries ANNUAL RESULTS REPORT 2010 A SUMMARY OF PROGRESS MADE AGAINST THE STRATEGIC FRAMEWORK TO BE ABLE TO LOOK AFTER MY FAMILY AND BE SELF-SUFFICIENT HAS MADE ME A MUCH HAPPIER PERSON “ ”
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ANNUAL RESULTS REPORT 2010 - ReliefWeb

Supporting community
action on AIDS in developing countries
ANNUAL RESULTS REPORT 2010A SUMMARY OF PROGRESS MADE AGAINST THE STRATEGIC FRAMEWORK
TO BE ABLE TO LOOK AFTER MY FAMILY AND BE SELF-SUFFICIENT HAS MADE ME A MUCH HAPPIER PERSON
“
”

The mission of the International HIV/AIDS Alliance is to support community action to prevent HIV infection, meet the challenges of AIDS, and build healthier communities.
OUR MISSION
OUR VISION
Our strategy:Aim 1 Protect human rightsAim 2 Increase access to health servicesAim 3 Support secure livelihoods
We have four strategic responses in order to achieve these aims:Response 1 Scale up integrated programmingResponse 2 Support well-functioning
community-based organisationsResponse 3 Help form engaged, inclusive
societiesResponse 4 Create a learning Alliance
The vision of the International HIV/AIDS Alliance is a world in which people do not die of AIDS. For us, this means a world in which communities: have brought HIV under control by preventing its transmission; enjoy better health; and can fully exercise their human rights. International HIV/AIDS Alliance
(International Secretariat) Preece House 91-101 Davigdor Road Hove, BN3 1RE UK
Telephone: +44(0)1273 718900 Fax: +44(0)1273 718901 [email protected] www.aidsalliance.org
Registered charity number: 1038860
Published: June 2011
ISBN: 1-905055-89-0
© 2011 International HIV/AIDS Alliance
Design by Red Design
COVER PHOTO CREDITS
Left: Seven year old Juliette Mueswa lost both
her parents to AIDS and was adopted through the
organisation Help a Friend, Mukono, Uganda
© Nell Freeman for the Alliance.
Middle: Men talk on the riverside. Photo taken by Kong
Piseth, a transgender person living in Cambodia
© Kong Piseth/the Alliance/Photovoice.
Right: Peer educator Fabiana Pérez, Ecuador
© Gideon Mendel for the Alliance.
Unless otherwise stated, the appearance of individuals
in this publication gives no indication of either sexuality
or HIV status.The Alliance ‘Partnership Icon’ is a trade mark of the International HIV/AIDS Alliance

ANNUAL RESULTS REPORT 20101
CONTENTS
Message from Alvaro Bermejo 3
Executive Summary 4
Introduction 6
Strategic Responses 7
Strategic Response 1: Scale up integrated programming 7
Strategic Response 2: Support well-functioning community-based organisations 19
Strategic Response 3: Help form engaged, inclusive societies 25
Strategic Response 4: Create a learning Alliance 37
Challenges and Opportunities 47
Building an Effective Alliance 53

2
Abbreviations and Acronyms
AAA Anti-AIDSAssociation,Kyrgyzstan
ABS AllianceBurundaiseContreleSIDA,Burundi
AFRICASO AfricanCouncilofAIDSServiceOrganizations
AIDS AcquiredImmuneDeficiencySyndrome
AMSED AssociationMarocainedeSolidaritéetDéveloppement,Morocco
ANCS AllianceNationaleContreleSIDA,Senegal
ANS-CI L’AllianceNationaleContreleSIDAenCôted’Ivoire
ART Antiretroviraltreatment
CAC CountyAIDSCommissions
CCM CountryCoordinatingMechanism
CHAA CaribbeanHIV/AIDSAlliance
CHAU CommunityHealthAllianceUganda
CiSHAN CivilSocietyforHIV/AIDSinNigeria
CPC ChildProtectionCommittee
DFID DepartmentforInternationalDevelopment
EANNASO EasternAfricaNationalNetworksofAIDSServiceOrganizations
ENDA EnvironmentDevelopmentActionintheThirdWorld
GIPA GreaterinvolvementofpeoplelivingwithHIV
HASAB HIV/AIDSandSTDAllianceBangladeshhttp://www.toplessrobot.com/Thor-Movie-Wallpaper-7-700x525.jpg
HIV HumanImmunodeficiencyVirus
HST HumsafarTrust,India
ICT Informationandcommunicationstechnology
ICW InternationalCommunityofWomenLivingwithHIV/AIDS
INPUD InternationalNetworkofPeoplewhoUseDrugs
IPC InitiativePrivéeetCommunautairedeLutteContreleVIH/SIDAauBurkinaFaso
IRD InternationalReliefandDevelopment
KHANA KhmerHIV/AIDSNGOAlliance
MAC MalaysianAIDSCouncil
MAMTA MAMTAHealthInstituteforMotherandChild
MARP Most-at-riskpopulations
MDG MillenniumDevelopmentGoal
MNCH Maternal,newbornandchildhealth
MONASO MozambiqueNationalAIDSServiceOrganisation
M&E Monitoringandevaluation
NAF NationalAIDSFoundation,Mongolia
NELA NetworkonEthics,Law,HIV/AIDSPrevention,SupportandCare,Nigeria
NGO Non-governmentalorganisation
OAS OrganisationofAmericanStates
OSI OpenSocietyInstitute
OSIWA OpenSocietyInstituteWestAfrica
PEPFAR (US)President’sEmergencyPlanforAIDSRelief
POZ PromoteursObjectifsZerosida,Haiti
PPA ProgrammePartnershipArrangement
PR (GlobalFund)PrincipalRecipient
PWAS PublicWelfareAssistanceScheme
PWDS PalmyrahWorkersDevelopmentSociety
SAC StateAIDSCommission
SAfAIDS SouthernAfricaHIVandAIDSInformationDisseminationService
SASO SocialAwarenessServiceOrganisation
SMOH StateMinistriesofHealth
SMT Substitutionmaintenancetherapy
SRH Sexualandreproductivehealth
SRHR Sexualandreproductivehealthandrights
STI Sexualtransmittedinfection
SUNRISE Scaling-uptheNationalResponsetoHIV/AIDSthroughInformationandServices
TACIT TacklingAIDSandTBthroughCommunicationsandInformationTechnologies
TB Tuberculosis
UNAIDS JointUnitedNationsProgrammeonHIV/AIDS
UNDP UnitedNationsDevelopmentProgramme
UNGASS UnitedNationsGeneralAssemblySpecialSessiononHIV/AIDS
USAID UnitedStatesAgencyforInternationalDevelopment
VCT Voluntarycounsellingandtesting
VMM VasavyaMahilaMandali
WHO WorldHealthOrganization
ZAN ZimbabweAIDSNetwork

ANNUAL RESULTS REPORT 20103
MESSAGE FROM ALVARO BERMEJO
2010 has been another exciting year for the Alliance. In a challenging global environment the Alliance successfully met the targets of our IMPACT 2010 strategy, launched our new strategy HIV and Healthy Communities, established new partnerships and underwent an organisational restructure. I am confident that the Alliance can meet the challenges ahead, and that the model we created of working with communities is even more relevant today than it was when we began in 1993.
As a result of a longer term vision of the AIDS response, and perhaps because there is less money to spend, we have begun to see greater recognition of the role that communities can play. This comes as no surprise to us: we know that a community-based approach is as effective in tackling generalised epidemics as it is in concentrated epidemics.
This report, with its particular focus on Africa proves the point. Our approach to working with communities is the same whether we are building social capital amongst children or sex workers; pregnant mothers or people who use drugs. Alliance programmes are driven by those communities, and as a result, reflect their needs.
Our work with most-at-risk communities stands out for me in 2010. This was the year when our programming for people who use drugs came of age. The Alliance launched its Community Action on Harm Reduction project, which builds on six years of experience of working with people who use drugs in Ukraine. Programming for men who have sex with men had a mixed year. On the one hand, Alliance India launched the largest ever community-driven programme to strengthen HIV prevention among sexual minorities. On the other hand much of our programming with men who have sex with men in Africa suffered from increasing violence and discrimination. Looking to the future, I believe that sex worker programmes must be the next focus, with community-driven programmes taken to scale. There is now widespread recognition that supporting the most vulnerable populations and tackling structural barriers is crucial in dealing with every HIV epidemic.
That’s why we have committed to a much greater role in protecting human rights in our new strategy. Defending human rights is crucial to people affected by HIV; usually the most marginalised in society. I always ask myself when developing a new strategy how it will improve the lives of people I have met, and whose stories haunt me. How will it help the 14 year-old girl struggling to care for younger siblings in Zimbabwe, or the transgender woman in Ecuador for whom the right to be accepted is more important than her positive HIV status? We must understand and respond to the factors that make people vulnerable to HIV. It is clear that unless we address issues of human rights and gender identity within our programmes, we will not effectively tackle HIV.
Of course, there are other organisations that specialise in human rights advocacy and literacy. However, it is clear to me that our role is different. The Alliance is uniquely positioned to make human rights a reality through our programming. This includes interventions which build the capacity of individuals from vulnerable communities to claim their rights, as well as work to hold duty bearers to account, for example by providing or facilitating access to legal advice and representation.
While I am excited about our work in the future, I also want to acknowledge our successes of the past year. I am grateful to all those in the Alliance family who made it possible, to the trustees for agreeing another ambitious strategy, and to our donors whose support helped turn our plans into realities and our hopes into success stories.
Alvaro BermejoExecutive Director

4
In this 2010 report, we have therefore given a special focus to our work with communities in Africa, while highlighting our key achievements from the rest of the world.
The report describes the progress we have made in implementing our new strategy HIV and Healthy Communities. We start by describing the major issues in the global environment that influence and affect the implementation of our new strategy. Significant progress has been made in stabilising the rate of new infections and reducing infection rates in children, but the human tragedy of HIV is still immense. 5,000 people die from AIDS-related illnesses every day. The role of vulnerable populations such as men who have sex with men, sex workers and people who use drugs within generalised epidemics is becoming more visible. They remain the key to tackling some growing epidemics, yet we fear governments under pressure will cut back investments in prevention.
New challenges are emerging. The economic recession is reducing the funds available for the global response to HIV. This is affecting people’s access to treatment now. It also threatens to limit the provision of treatment to all those who need it in the future, with costs expected to rise dramatically.
Alongside the financial shortfall, it is clear that stigma and discrimination are denying most-at-risk populations the prevention, care and support services they need. This is not only dangerous, in terms of allowing the virus to spread, it is a human rights issue for those in society who are already marginalised.
The aids2031 report Future Connect, published in 2010, took a global view of the response so far, and looked at the work still to be done. The report advocates actions that mirror the Alliance’s strategic priorities. Over the years ahead, we must mobilise local responses, build local capacity and enable those most affected by HIV to engage in decisions that affect them. These Alliance priorities are reflected throughout the main part of this Annual Results Report.
The four main sections of this report describe our progress against the strategic responses set out in HIV and Healthy Communities.
EXECUTIVE SUMMARY
2010 has been a busy year for the Alliance: a year of consolidation, reflection and renewed investment. We underwent a comprehensive independent external evaluation commissioned as part of our Programme Partnership Arrangement with the UK government Department for International Development (DFID). One of the recommendations from the evaluation was that we need to articulate better the Alliance response in Africa.

ANNUAL RESULTS REPORT 20105
STRATEGIC RESPONSE 1: Scale up integrated programming
In 2010, we continued our work to scale up the HIV response, with increased focus on Africa. Although we scaled up programmes in 14 countries, overall we reached 5% fewer people this year. Our prevention, care and support services reached 2.9 million people. In this report, we feature programmes that benefited and protected children in Zambia and Burundi. We also describe how communities in Africa have addressed stigma and discrimination, and increased access to services. The Alliance’s approach to addressing stigma is to empower vulnerable communities, a tactic which was praised in an external evaluation of the Alliance’s Africa Regional Programme. In other parts of the world, such as the Caribbean and South Asia, we continued to prioritise prevention interventions for vulnerable populations.
STRATEGIC RESPONSE 2: Support well-functioning community-based organisations
Strategic Response 2 of this report describes our progress in building the capacity of community-based organisations, and improving their performance. Alliance Linking Organisations have an excellent reputation for building the capacity of civil society to respond to HIV. The Alliance Regional Technical Support Hubs played a crucial role in this, responding to a 42% increase in demand for technical support. As programmes expanded, more technical support was needed to help improve management systems and structures.
We use the case study of RedTraSex, the Latin American sex workers network, to illustrate the benefit of the Alliance approach. This example, and others under Strategic Response 3, show how we are building the capacity of organisations to become strategic players influencing programming and policy responses at national and global levels.
STRATEGIC RESPONSE 3: Help form engaged, inclusive societies
In Strategic Response 3 of this report, we describe how we strengthened the capacity of civil society to create enabling environments, defend human rights and engage in national and international decision-making. Throughout 2010, we worked to expose the stigma and discrimination that obstructs the HIV response. In July, we launched a global campaign that exposed barriers to effective prevention, and in November we published a report about discriminatory laws in the Commonwealth. We supported communities in Africa to demand accountability and effective responses to HIV. Linking Organisations in Senegal and Ukraine have been defending the human rights of those most-at-risk, and Ugandan citizens were encouraged to hold leaders to account on their election promises. Across Africa technology was used to support participation of people most affected by HIV. In Latin America, the Alliance supported vulnerable populations to successfully demand their rights to be involved in decisions that affect them.
STRATEGIC RESPONSE 4: Create a learning Alliance
In Strategic Response 4 we talk about joint initiatives that strengthen the Alliance family. Individual Alliance Linking Organisations play a critical role in responses to HIV in their own country, but it is our joint voices and experiences that make the greatest contribution to building healthy communities. In 2010, nine learning exchanges between Linking Organisations built capacity and improved our collective performance. A new internet portal in southern Africa facilitated sharing of best practice and peer reviewed information. 250 citizen journalists continued to get coverage of their experiences of HIV in local and international media. The Alliance family expanded again, with three new Linking Organisations in Africa and three from the rest of the world, bringing the total number in the global partnership to 36. To celebrate and welcome our new members, we include short descriptions of their organisations at the end of this section.
Challenges and opportunities, and building an effective Alliance
In the penultimate section of this report, we reflect on some of the issues that threaten to affect both the HIV response and the role that the Alliance plays within it. In the final section, ‘Building an effective Alliance’, we recognise the need to adjust to the changing environment. The report concludes by describing how we are planning to create efficiencies and save costs at the Secretariat, as well as gain a better understanding of the value of our programmes.

6
1.Over,Mead(2010),SustainingandLeveragingAIDSTreatment,WashingtonDC:CenterforGlobalDevelopment(June).2.UNAIDS2010GlobalReport.3.aids2031Consortium(2010).AIDSTakingaLong-TermView,FTPress,December.
This introduction covers the global environment in which the Alliance operates. By providing the wider context it sets the scene for the Alliance’s work that is covered in the later sections of this report.
The global economic recession continues to cast a shadow over the HIV response. As budgets get tighter there is ever-greater need for non-governmental organisations (NGOs) and international development agencies to demonstrate short-term results, and show that the investments made are delivering sustainable changes.
Against this backdrop, the UNAIDS Global Report for 2009 shows that two decades of investment by the global community is finally beginning to pay off. Fifty-six countries have stabilised or significantly slowed the rate of new HIV infections, including nearly all countries in sub-Saharan Africa.
There has been progress getting treatment to more people. By the end of 2009, 5.2 million people in low and middle-income countries had access to antiretroviral treatment (ART). The cost of the least expensive first-line ART regimen is now less than US$70 per patient, per year, due to competition from generic manufacturers and changes in patent protection for low-income countries. HIV infection rates among children have dropped by almost a quarter (24%) in five years, as a result of progress in prevention of mother-to-child transmission.
However, the flatlining of international funding for HIV treatment is destabilising antiretroviral programmes, with people being turned away from treatment in many African clinics. Coupled with the fact that HIV will eventually develop resistance to first-line treatment, with people needing the more expensive and patent-protected second and third-line regimens, we are facing a treatment time bomb. Some estimates predict that the cost of providing treatment to everyone who needs it by 2030 will increase 17-fold1.
The efforts and hopes of millions of people, supported by sustained investment from major donors, have contributed significantly to the advances. But while the results are promising, and those involved in the response should feel proud, we are acutely aware that future progress rests on a knife-edge. Further advances are threatened by financial constraints. This is not the moment to take the foot off the accelerator. The global community must consolidate and expand progress already made, if we are to achieve the Millennium Development Goals (MDGs) by 2015.
In 2009, 1.8 million people died from HIV-related illnesses. Almost 5,000 men, women and children die every day. Although the rate of new HIV infections has decreased in sub-Saharan Africa, Africa remains at the heart of the struggle against HIV. In 2009, the vast majority of people living with HIV (68%) were Africans. More than five in seven (72%) of the estimated 1.3 million people who died of HIV-related illnesses were from Africa. Three quarters of all adult women living with HIV live in sub-Saharan Africa2. Globally HIV is the leading cause of death of women of reproductive age. As women are still the primary carers this human tragedy adds to the heavy burden faced by families and communities.
The epidemiological data brings home the scale of the suffering and profound consequences for individuals and their families. It also contributes to a greater understanding of changing epidemics, and provides a more robust evidence base from which we can evolve and shape our response.
Stigma, discrimination and human rights abuses are preventing those people most vulnerable to HIV, from seeking treatment and accessing the services they need. Programmes and resources are still not reaching most-at-risk populations in sufficient numbers; particularly those in generalised epidemics. In Africa, recent studies have shown that HIV incidence among men who have sex with men is higher than previously thought. In Kenya, 15% of new infections could be linked to unprotected sex between men.
The aids2031 consortium produced a book3 in 2010 with clear recommendations of the changes the global community needs to make to provide the long-term, sustainable response that the epidemic requires. The recommendations echo the long-held strategy of the Alliance. These include the mobilisation of local responses, building ‘policy space’ to enable targeting of resources to marginalised groups, and building local capacity.
INTRODUCTION

ANNUAL RESULTS REPORT 20107
1. STRATEGIC RESPONSES 2010
In 2010, we reached 2.9 million people with HIV prevention, care and support services.
We began to make our HIV programming more integrated and, as part of our new strategy, we reinforced our focus on Africa.
This section covers our continued efforts to scale up the HIV response, and to begin more integrated HIV programming in the first year of our new strategy. We start by sharing global results for 2010, and then feature some of the communities at the forefront of the response. Particular achievements include our work to address stigma in Africa and an integrated, family-centred approach benefiting children in Zambia. We also feature livelihood interventions for people living with HIV in Africa – an important priority in our new three-year strategy. We finish the section by describing successful prevention programmes working with vulnerable populations in the Caribbean and South Asia.
Alliance reaches 2.9 million people in 2010
In 2010 the Alliance reached 2.9 million people with HIV prevention, care and support services. In spite of the economic downturn 14 countries scaled up their coverage, though overall there was a 5% decline in the number of people reached compared with 2009.
We reached 25% more people in Asia, and more than doubled the number of people reached in Latin America and the Caribbean. The major decline was in Africa where there was a 40% reduction in the number of people reached in 2010. This was mainly due to the close out of a programme with wide coverage, the Uganda Networks project. However, with a new USAID-supported programme to Strengthen the Ugandan National Response for Implementation of Services for Orphans and Vulnerable Children (SUNRISE OVC) the number of people reached in Uganda is set to rise again over the next five years. The US$20 million programme will focus on capacity building of government structures at central, district and community level. So this will ultimately generate sustainable solutions that have the potential to reach many more people.
With the addition of Linking Organisations in Mozambique and Zimbabwe in 2010, we extended our presence to two of the biggest generalised epidemics in the world. The figures from these organisations are not fully represented in our 2010 report, as we have not yet integrated our reporting systems. Following capacity building to help our new Linking Organisations use the Alliance global reporting system, we expect to report significant growth in 2011. In addition, a decision to suspend Civil Society for HIV/AIDS in Nigeria (CiSHAN), our second Linking Organisation in Nigeria, means we are no longer reporting their results (see Strategic Response 4 for more on this).
Strategic Response 1: Scale up integrated programming 1

8
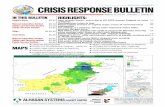
Three African countries, Kenya, Senegal and Côte D’Ivoire, remained in the top ten of Alliance programmes in 2010, with Kenya accounting for the highest proportion (20%) of people reached globally (see figure below). In Africa, over half the people reached (55%) were women.
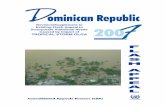
Prevention programming remained a key focus for the Alliance. In Africa, 70% of the people reached were supported with prevention services, up from 59% in 2009. The proportion of those reached with care and support services also increased, from 10% in 2009 to 20% in 2010. The number of people reached with counselling and testing declined from 21% to 8% between 2009 and 2010. This is also accounted for by the close out of the Uganda Networks project.
ALLIANCE GLOBAL – TOP TEN COUNTRIES AS A PROPORTION OF TOTAL REACH 2010
KENYA 20%
INDIA 15%
SENEGAL 8%
CAMBODIA 10%
UKRAINE 14%
BANGLADESH 7%
HAITI 6%
PERU 2%
CÔTE D’IVOIRE 2%
BOLIVIA 2%
OTHER 14%
An estimated 1.2 million people are living with HIV in Zimbabwe. With declining HIV prevalence at 14.3%, Zimbabwe has the fifth highest rate in the world. Mozambique is the only country in southern Africa where HIV incidence is increasing. With HIV prevalence at 11.5%, Mozambique has the eighth highest ratein Africa. There are 1.4 million people living with HIV in Mozambique, the fifth biggest population in the world.

ANNUAL RESULTS REPORT 20109
AFRICA – BREAKDOWN OF TOTAL REACH BY INTERVENTION AREA 2010
PREVENTION 70%
STIGMA & DISCRIMINATION 2%
CARE & SUPPORT 20%
COUNSELLING & TESTING 8%
Communities in Africa respond to the HIV burden
According to UNAIDS, an estimated 22.5 million people live with HIV in sub-Saharan Africa. This means that although this region represents just over 10% of the world’s population, it is home to two thirds of people living with HIV. In 2009, 70% of all new infections occurred in sub-Saharan Africa (1.8 million). Also the vast majority of infections among children occur in sub-Saharan Africa, with 130,000 new infections in 2009.
Average life expectancy in the region is now 52 years. Illness, missed educational opportunities, and death have depleted the workforce, increased food insecurity and led to stagnating economies in many African nations. The infrastructure, systems and staff required to scale up health care are extremely over stretched. Unless the health sector is strengthened and the compounding issues from HIV are addressed rapidly, most African countries will not achieve the health MDGs.
With Alliance support, community-led structures have been developed to respond to the overwhelming burden of HIV on formal health systems and households. An increasing number of indigenous community-based organisations are now providing integrated home-based care to households affected by HIV. They have been equipped to deliver peer-to-peer focused prevention activities, and to help fill gaps in health care provision.
Networks of people living with HIV and other groups across the region are providing a safe place for people most affected by HIV to talk and mobilise. These groups raise awareness about HIV and the issues that affect them. They address stigma and discrimination, and jointly advocate for increased resources for affected communities.

10
Marginalised communities challenge stigma in Africa
The Alliance contributed to reducing stigma and discrimination by working with people living with HIV and other vulnerable groups. We strengthened the involvement of national networks of people living with HIV in policy development and programme implementation.
Funded by the Swedish International Development Cooperation Agency, between 2008 and 2010 the Africa Regional Programme brought together Alliance Linking Organisations and other partner organisations across 20 countries in sub-Saharan Africa.
Using a national trainer of trainers’ model, the stigma programme trained members from networks of people living with HIV, government and policy workers, nurses, clinical officers, and members of the community. These people and organisations integrated the training within their own work, and took responsibility for rolling out the training programmes nationally. This model maximised participation and reach through the multiplier effect of training trainers, and helped improve public services. In 2010, we trained 332 people, who in turn trained over 29,000 more people.
An independent external evaluation of the Africa Regional Programme highlighted the success of the stigma and discrimination component of the programme. “(The) programme has grown organically and been innovative and creative, using participatory training methodologies that can be easily adapted to most contexts and levels, even conservative faith settings.”
As part of the evaluation, we piloted a social return on investment study to develop a better understanding of the value of the stigma programme. The study focused on two sites in Zambia: Mumbwa – a small rural town that hosted Zambia’s first, but now defunct copper mine; and urbanised Mazabuka, surrounded by sugar cane plantations that have contributed to its growing wealth.
In both sites, the study found that there were positive outcomes for people living with HIV. First, there was as an increase in the percentage of people accessing antiretrovirals. Second, adults and children living with HIV remained within the family unit and more of the adults were able to find work. Third, there was greater awareness of the needs of children living with HIV and increased school attendance. There was universal agreement that reduced stigma is important, and that adults and children should be cared for within their family. However, the study also highlighted that the intervention had some negative impacts initially. It created additional pressure on wider families who had to provide for and support adults and children living with HIV. It meant, for example, that already struggling families had increased food bills, additional costs of school uniforms, and more trips to the clinic.
The study highlighted the complexity of addressing stigma and discrimination, and the need to take a holistic view by engaging stakeholders across sectors. The Alliance’s efforts to realise this more integrated approach are described later.
“(The) programme has grown organically and been innovative and creative, using participatory training methodologies that can be easily adapted to most contexts and levels, even conservative faith settings.”

ANNUAL RESULTS REPORT 201011
Paid and transactional sex work is a significant driver of the HIV epidemic in many countries. It is estimated that almost one third (32%) of new HIV infections in Ghana, 14% in Kenya, and 10% in Uganda are linked to sex work4. Sex workers are frequently stigmatised, criminalised and excluded from services. Addressing the gender barriers that make women economically vulnerable and exposed to stigma and violence, is key to reducing risk to HIV. In both concentrated and generalised epidemics throughout Africa, there are insufficient prevention responses that work with sex workers and their clients, beyond the provision and promotion of condoms. There is a need to expand prevention programmes to reach greater numbers of sex workers in ways that address the vulnerabilities faced by women.
Alliance Linking Organisation Alliance Nationale Contre le SIDA (ANCS) works with sex workers as part of its Global Fund-supported programmes in Senegal. In 2010, the consolidation of Global Fund Round 6 and 9 programmes meant the programme could begin expanding its reach from eight to all 14 regions of Senegal. ANCS took on a second sub-recipient, AWA, at the end of 2009 to support this scale up of services to sex workers. Together AWA and Enda Santé, the other sub-recipient, are expanding activities to include informal sex workers, who do not possess health cards.
The programme builds the capacity of female sex workers’ associations so that they can run sensitisation and support activities on HIV and sexually transmitted infections (STIs), for their members. Activities include peer-to-peer education, psychosocial, legal and social support, provision of condoms, and advocacy to mitigate stigma and discrimination.
In 2010, ANCS provided services to nearly 3,800 sex workers, almost 50% up on the previous year. The strategy to devolve activities to sex workers’ associations and mobile clinics, emphasised in the Round 9 programme, contributed to the sharp increase in the number of people reached in 2010.
ANCS also reaches sex workers through its UN Women (formerly UNIFEM) programme, which they jointly manage with the Society for Women and AIDS. In 2010, the programme started an advocacy campaign targeted at Senegalese Members of Parliament (MPs). The MPs are being called on to improve HIV law so that it takes into account the economic and political needs of women living with HIV. Programme beneficiaries are the Senegalese network of women living with HIV/AIDS (ABOYA) and the network of sex workers living with HIV/AIDS (Karlene). Through the programme, sex workers also benefit from small grants to undertake income-generating activities.
NEW DATA SHOWS MARGINALISED COMMUNITIES AT HIGH RISK OF HIV The HIV epidemic has largely been driven by heterosexual transmission in Africa. However, it has become clear, through better surveillance monitoring by governments, that HIV transmission occurs outside heterosexual relationships too. In several countries, groups such as men who have sex with men and people who use drugs have been identified as particularly vulnerable to HIV and a significant source of new infections. For example, unprotected sex between men accounted for 15–20% of new infections in Kenya, Rwanda and Senegal. Injecting drug use is becoming an important driver of HIV infections in urban areas in eastern and southern Africa (including Kenya, Mauritius, Tanzania and South Africa). In Kenya, 4% of new infections resulted from unsafe drug-injecting practices. Responding to the data, the Alliance is helping to address vulnerabilities among marginalised communities. In 2010, the Alliance began a major harm reduction programme to support people who use drugs in Kenya and four countries in Asia (see box below). Below we describe an important regional initiative supporting, and working with, men who have sex with men.
4.ThisincludesHIVinfectionamongsexworkers,theirclients,ortheirothersexualpartners.
NEW GLOBAL HARM REDUCTION PROJECT
In2010,theAlliancesecuredfundingtoleadanambitiousnewharmreductionprojectinfivecountries,includingKenya.Thefour‐yearproject,fundedbytheDutchMinistryofForeignAffairs,willbeimplementedbyarangeofpartnersincludingAllianceLinkingOrganisationsinKenya,China,India,IndonesiaandMalaysia.TheCommunityActiononHarmReductionprojectwillprovideawiderangeofservicestomorethan180,000peoplewhousedrugs,theirpartnersandchildren.ServiceswillincludeHIVprevention,treatmentandcare,andsexualandreproductivehealth.Thefocuswillbeoninnovationsinoutreachandthecreationofdruguserfriendlyhealthservices.
Sex workers receive advice on safer sex and free condoms as they wait at the maternité polyclinique de Rufisque, Senegal © Nell Freeman for Alliance.
Female sex workers support each other and address stigma

12
Men who have sex with men reached through the North Africa Regional Programme
MenwhohavesexwithmenfacehighlevelsofstigmaanddiscriminationthroughoutAfrica.Since2004,theAllianceRegionalProgrammeinNorthAfricaandtheMiddleEastsoughttoaddressthebarriersthatpreventmenwhohavesexwithmenaccessingservices.
TheAllianceworkswithsixnationalandoneregionalpartnertoimplementaprogrammetoprovidehealthservicestomenwhohavesexwithmeninMorocco,Algeria,TunisiaandLebanon.Theprogramme’sobjectivesinclude:
> buildingthecapacityofcivilsocietyorganisationstoprovidesustainableHIVandSTIpreventionservices,whichaddressthevulnerabilitiesofmenwhohavesexwithmen
> scalinguptheHIV/STIservicesofferedtomenwhohavesexwithmen
> facilitatingthesharingofexperiencesandlessonslearntacrosstheregion
> influencingtheinstitutionalandorganisationalenvironmentforastrongerresponsetoHIVatlocal,nationalandregionallevels.
Theprogrammeenjoyedincreasedvisibilityduring2010.Keysuccessesandlessonslearntweresharedatthe2010InternationalAIDSConferenceinVienna,wheretherewasmarkedinterestintheprogramme’sapproachfromdelegatesfromtheMiddleEastandNorthAfrica,aswellasotherregions.AtaUNAIDSregionalworkshopinLebanoninNovember,theprogrammewashighlightedasleadingtheregionalresponseinworkwithmenwhohavesexwithmen.
TheprogrammehasexpandeditsactivitiestonewsitesinMorocco,TunisiaandLebanon,alongsidestrengtheningnewpartnerships.Forexample,followingasuccessfuladvocacycampaignwithlocalhealthservices,AssociationTunisiennedeLutteinTunisiahaspartneredwithahealthauthority.Togethertheywillsupportavoluntarycounsellingandtesting(VCT)centrewheremenwhohavesexwithmencansafelyandanonymouslyaccessVCTservices.ThiscollaborationfacilitatedasimilarpartnershipinTozeur,anewsiteinthesouth.
Inaddition,therehasbeenexpansionofoutreachactivitiestoaddressothervulnerabilityfactorsidentifiedasaprioritybyimplementingpartners.Forexample,inLebanontheapproachofpartneringacounsellorwithapeereducatorduringweeklymobileVCToutingscontinuestoprovesuccessfulintargetinghardtoreachmen,includingpeoplewhousedrugsandsexworkersoutsidecities.ThesemenaregenerallynotableorwillingtoaccesspermanentVCTcentresduetoself-stigmaandtheneedforanonymity.
PartnershavestrengthenedtheirrelationswithlocalVCTservicesandothersocialsupportservices.PartnerOpals/FesinMoroccoorganisedstigmareductiontrainingbringingtogether18doctorsaffiliatedtolocalVCTservices.SoinsInfirmiersetDéveloppementCommunautaireinLebanonorganisedtwoawarenessraisingdaysonVCTservices,with14participantsfromlocalcivilsocietyorganisations,thelocalhospitalandalocalIslamicreligiouscommunityhealthcentre.InAlgeria,AssociationdeProtectioncontreleSIDAscaleduptheirworkwithVCTstaffinuniversitycampusesandhavecontacted42youthcentrestoensuremoreuser-friendlyservicesformenwhohavesexwithmen.
In2010,theregionalprogrammehadtrained105serviceprovidersinHIVprevention,andreached3,000menwhohavesexwithmenwithHIVpreventionactivities.137peoplewerereferredforSTIdiagnosisandtreatmentandover49,000condomsandalmost28,000packetsoflubricantweredistributed.
Social,culturalandpoliticalenvironmentsarecriticalfactorsenablingorganisationstocarryoutprogrammesworkingwithmenwhohavesexwithmen.InStrategicResponse3,wediscusshowhostileenvironmentsinmanyAfricancountriesarepresentingchallengesforeffectivepreventionwiththisgroup.
The programme was highlighted as leading the regional response in work with men who have sex with men.

ANNUAL RESULTS REPORT 201013
At the MDG summit in September 2010, governments, private sector organisations, foundations, international organisations and civil society launched a concerted worldwide effort to accelerate progress on women’s and children’s health. With calls from the global community for greater programme integration and an increased focus on women and children, the Alliance was able to demonstrate progress in these areas.
In Zambia, the Alliance showed how taking a family-centred approach to programming with children can improve children’s school attendance, academic performance and self-esteem. The three-year project (2008-2010) helped six community-based organisations, in the Copperbelt Province, to coordinate and integrate their efforts with the Public Welfare Assistance Scheme (PWAS). The assistance scheme is a social protection initiative of the government, designed to support the poorest communities, particularly those affected by HIV.
“The PWAS uses a decentralised approach which means that the programme is owned by the community,” explains Harriet Lombe Ngosa, district social welfare officer in Ndola. “The community is in charge of selecting and approving
clients that should access assistance. This is because community members are better placed to know the most needy and vulnerable in the community. The successful implementation of PWAS cannot be left to the department alone. Stakeholders at all levels, particularly the community, are crucial.”
Alliance Zambia ran training workshops with partners to strengthen financial management, monitoring and documentation, and to increase understanding of national child policy and the assistance scheme. They helped community-based organisations understand how beneficiaries are selected through the assistance scheme. Equipped with training and support, Community Welfare Assistance Committees and community-based organisations identified and selected households with vulnerable children, and accessed support through the government assistance scheme.
670 households were supported with a comprehensive package of educational, nutritional, livelihoods and psychosocial support. For example, children received books, uniforms and shoes, and their school fees were paid. Households received food parcels and cooking demonstrations to help carers cook nutritious food. Parents and guardians were supported with economic strengthening initiatives such as cash grants, agricultural inputs and small livestock. This helped families to improve food security and their children’s nutrition. The cash grants were used by some households to start small businesses – buying and reselling food items for example. Psychosocial activities included sports, traditional games and art, which enabled children to share their experiences and aspirations. In addition, parents and carers were trained in paediatric HIV treatment adherence to ensure treatment success. A qualitative research study with parents found that children’s sense of self-belief improved, along with their attendance at school and their academic performance.
By taking an integrated, family-centred approach, the individual needs of children were met, along with the needs of their family. This approach makes families healthier and stronger, and better able to care for, protect and support their children. Linking families to existing government welfare support meant the project avoided duplication of effort, making it more sustainable in the long-term. Because the approach drew on existing welfare support it meant greater numbers of families could be reached.
Children’s attendance records, academic performance and self-esteem improved.
Year 4 students at Hillside Basic School attend one of their regular classes, Zambia © Nell Freeman for the Alliance
Vulnerable children benefit from family-centred approach in Zambia

14
CASE STUDY
MaryfromLubuto,inNdola,Zambia,describesthesupportshereceivedfromtheproject.
“I have seven children. We had many problems. We did not have regular meals and I was unable to send my children to school. I found out about the scheme from a Community Welfare Assistant Committee member who works with VOWAS (a community-based organisation supported through this project). They visited my house and interviewed me. Afterwards they told me that I could receive support from the scheme.
“I received a cash grant of ZMK 500,000 (approximately $100) which has enabled me to start up my own business. I now knit jerseys, pouches, tablecloths and so on, which I sell in the community and surrounding townships within Ndola. I have also received food supplements that have assisted me and my children greatly. With the money I make from my business, I can now support my children to attend school and buy food for my family, so we are no longer hungry. To be able to look after my family and be self-sufficient has made me a much happier person.
“To think of the future, I want all my children to finish school. Most children don’t get any support to go to college and it would be good if the project could help them to do that also. And I want my business to grow so I can satisfy my clients and continue to support my family.
“I am very grateful to VOWAS for helping us get support from the scheme.”
This example demonstrates how the Alliance is building partnerships with existing social protection systems to ensure that people living with, and affected by HIV receive a holistic package of care and support. With other initiatives described below, this is an important part of our new strategy.
SUPPORTING MARY’S LIVELIHOOD, ZAMBIA
COMMUNITIES PROTECT CHILDREN IN BURUNDI
Thereareanestimated720,000orphansandvulnerablechildreninBurundi.Yearsofconflicthavecreatedextremelychallengingconditionsformanychildren.Overhalfamillionpeoplehavebeeninternallydisplacedwhichhasdisruptedfamilystructures.Childrenhavelosttheirparentsincombatandgirlshavesufferedgender-basedviolence,suchasrape.Theimpactofthewaronhealthservicesandfacilities(especiallyinthenorth)hasincreasedthevulnerabilityoffamilies,andparticularlychildren.Thisiscompoundedbypoorsystemsforidentifyingandlookingafterorphansandvulnerablechildren,andalackofappropriatefacilitiesforchildren.
InBurundi,AllianceBurundaiseContreleSIDA(ABS)isworkingtodevelopandstrengthencommunitychildprotectionandwelfaresystemsthroughchildprotectioncommittees(CPCs).Byprovidingsocialservicessuchaschildprotectionandalternativecare,community-basedchildprotectiongoesbeyondsocialassistancetofamilies.WithfundingfromGlobalFundRound8(whichbeganinJanuary2010),ABSaimstosupportover3,000CPCsacrossnineofBurundi’s17provinces.
ABSbuildsthecapacityofCPCstoidentifywhichchildrenaremostvulnerable.CPCmembersidentifystresseswithinfamiliessuchaspoverty,illnessandviolence.Theyaretrainedtoprovidecounsellingandtomakereferralsintheabsenceofprofessionalsupport.ABSsupportstheCPCsindevelopingprotocolsforrespondingtochildprotectionviolations,andmonitoringtheirownperformancethroughself-assessment.
Forexample,inacommunityintheBururiprovince,theCPCinvestigatedconcernsaboutasixyear-oldchildwhowasbeingraisedbyhermaternaluncle,asoldierwhoresidedintheBururimilitarycamp.Theuncle’swifesubjectedthechildtoabuseincludingdailybeatingsandphysicallabourbeyondherability.Shewasmadetowashtheclothesofhercousins,cleanthehousedailyandpeelvegetables.Aspunishmentfortasksnotcompletedshewassubjectedtoharshphysicalabuseandmadetogowithoutfoodallday.TeachershadnoticedthegirlcryingduringbreaktimesandreferredhercasetotheCPC.TheCPCinvestigatedtheinjuriesandabuse,andmadeappropriatereferralstothepoliceandjusticebureau.TheCPCalsotookstepstoprotectthechildbyarrangingtemporaryalternativefostercare,whileanappropriatelong-termfamily-basedplacementwasfound.

ANNUAL RESULTS REPORT 201015
Improvements in access to ART and treatment adherence are helping people living with HIV to have longer, healthier lives. They can now take an active role providing for their families. The Alliance aims to partner with organisations that can support the economic well-being of people living with HIV, and their families.
Some Alliance Linking Organisations are already involved in livelihoods work as part of their programmes. For example, in Nigeria the Network on Ethics, Law, HIV/AIDS Prevention, Support and Care (NELA) partnered with METHACRE, a faith-based community organisation which provides a microcredit scheme and skills training to caregivers to strengthen the economic capacity of vulnerable households. In Burundi, in 2010, ABS provided income generating support and training for 76 orphans and vulnerable children through its Global Fund-supported programme. Income generating activities and skills building included agricultural projects, driving lessons, welding and cooking. ABS supported a group of young men who have sex with men to set up and run an internet cafe. This programme will be scaled up in 2011.
The Alliance aims to expand its partnerships to include NGOs providing livelihoods support. For example, in Ethiopia the Alliance is working in a consortium led by PATH (and funded by USAID) on an initiative called Strengthening Communities’ Responses to HIV/AIDS. The initiative builds on governmental and civil society efforts to: improve community access to HIV services; improve the quality of community and home-based services; and mobilise people to seek high-quality, comprehensive, and affordable services. The consortium brings together international partners including International Relief and Development (IRD), WESTAT and International Training and Education Center for Health, with national implementing partners, the Ministry of Health, and the Federal HIV/AIDS Prevention Control Office. A key part of the programme, led by IRD, focuses on economic strengthening. This initiative provides the Alliance with an important opportunity to learn about economic strengthening interventions and to share this learning across the Alliance family.
The Alliance is developing new partnerships to support people living with HIV, now that they are living longer.
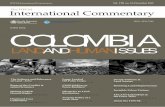
1,600,000
1,400,000
1,200,000
1,000,000
800,000
600,000
400,000
200,000
0
TOTAL REACH BY ALLIANCE REGION AND INTERVENTION 2010
Africa
Prevention
Care & Support
Counselling & Testing
Stigma & Discrimination
Asia and Eastern Europe
Latin America and the
Caribbean
Orphans and children of people living with HIV/AIDS learn new skills, Côte d’Ivoire © Nell Freeman for the Alliance
People living with HIV get livelihoods support

16
Sexual minorities recognised in HIV prevention in India
In October 2010, Alliance India launched the Pehchān programme. This is the first Global Fund grant (Round 9) to support a programme developed and managed by community organisations of men who have sex with men and transgender people.
HIV prevalence among men who have sex with men in India is estimated at over 7%, compared to a national prevalence rate of less than 1%. In Mumbai, National Sentinel Surveillance data estimates HIV prevalence among men who have sex with men to be 10%, and as high as 49% among transgender people. Higher prevalence rates among men who have sex with men are attributed to low awareness levels, unsafe sexual practices, inadequate services and social marginalisation. Because of the much higher prevalence rate among men who have sex with men, transgender people and hijra, national strategies have prioritised their needs, alongside sex workers and people who use drugs.
The Pehchān programme builds on the expertise of Alliance India and six regional civil society partners who have pioneered HIV programming with vulnerable populations. In Urdu the word Pehchān means identity and recognition, powerfully evoking the principle behind the programme. Pehchān will develop and build the programmatic, organisational and institutional capacities of 200 community-based organisations across 17 states. Together they will reach more than 450,000 people with a comprehensive package of HIV prevention services, over a period of five years.
Professor Michel Kazatchkine, Executive Director of the Global Fund, said that, “This work is of great importance, involving civil society working with marginalised groups and linking these populations to government systems.”
Alliance India launched the first Global Fund grant (Round 9) to support a programme developed and managed by community organisations of men who have sex with men and transgender people.
Prioritising prevention for most-at-risk populations
As in Africa, we continued to prioritise prevention activities for most-at-risk populations in other parts of the world (see table on previous page). In September 2010, the successful East Caribbean Community Action Project came to an end. Funded by USAID, the three-year project increased access to prevention services for vulnerable communities, including men who have sex with men and sex workers. The programme was implemented in Antigua and Barbuda, Barbados, St Kitts and Nevis, and St Vincent and the Grenadines by the Caribbean HIV/AIDS Alliance (CHAA). An external evaluation by the Institute of Development Studies highlighted the project’s achievements.
“Access has radically improved for most-at-risk populations in the programme countries covered by (the project) and CHAA has played a unique and pivotal role in developing and enhancing this. Work carried out to date has begun to institutionalise the idea that access for most-at-risk populations must be a key component of national HIV/AIDS strategies. This is notable in each of the countries where CHAA is operating.”
Recognising the fledgling nature of many groups in the Caribbean, the evaluation also highlighted CHAA’s operational approach to civil society strengthening.
“Among both state and non-state stakeholders in all four operational countries, CHAA is highly valued for its engagement and support of communities and organisations – it plays a unique role in this regard – as well as with government structures.”

ANNUAL RESULTS REPORT 201017
CASE STUDY
Since November 2010, Simran Shaikh has worked for Alliance India on the Pehchān programme. She is an important representative of the hijra (transgender) community, and a powerful advocate for their rights.
At the age of 14, Simran discovered that she was an outcast in her own family. Her father referred to her as effeminate in a derogatory way in front of family friends. That night Simran left home with no more than 16 rupees in her pocket. After three nights without shelter or food, Simran was taken in by Rani (named changed), a traditional hijra. Rani helped Simran discover her true identity as a woman, and gave her tips on how to wear a sari and make-up. Rani also helped Simran train to be a dancer and find work in dance bars. By night Simran worked to pay the bills; by day she put herself through school.
After graduating Simran worked voluntarily, and then professionally, for a series of NGOs that promoted the rights of sexual minorities and raised awareness about HIV. She rose quickly through the ranks, becoming programme manager for DAI Welfare Society, and later, communications and training officer for Hindustan Latex Family Planning Promotion Trust.
The source of Simran’s greatest pride is Reshma (name changed) who was three days old when Simran adopted her. Since the tragic death of Reshma’s mother, Simran has taken care of her. As a transgender person, Simran cannot get a voter’s ID so adoption wasn’t straight-forward. This is one of the many ways that hijra are disenfranchised.
Simran explains, “Reshma is growing up now. I am very proud of this. It gives me light in my darkness.” However, Simran’s joy is also tainted with some foreboding. Simran wonders what this carefree and non-judgemental little girl will make of her hijra guardian as she gets older and is exposed to the cruel and unthinking comments of others.
For Simran her greatest challenge is the stigma and discrimination she faces every day. It is the way people stare, move away or make lewd gestures that hurt the most. Simran explains, “People look at me as if I am an alien”. The prejudice faced by Simran and her community is what drives her to change things.
“Gender rights and health issues are the top priority for us (hijras). These are things we have wanted for so many years. For example, it is very difficult for a hijra to have her own property. If I had the money today to buy a property I cannot. I don’t have any legal documents in my name. What is the proof you are speaking to Simran Shaikh? Does she exist on this earth?”
Simran believes the Pehchān project will make a big difference. Supported by the Global Fund, the Pehchān programme will strengthen HIV prevention among men who have sex with men, transgender people and hijra communities, and help them claim their sexual health rights.
“I think the Pehchān project will have a massive impact, especially for the hijra community. We will be reaching around 15% of the hijra population through community-based hijra organisations. We are going to do advocacy to secure legal rights, identity rights”.
THE STORY OF SIMRAN SHAIKHALLIANCE INDIA, PROGRAMME OFFICER WORKING ON THE PEHCHĀN PROJECT
©theAlliance

18
Among other groups, the Alliance is engaging with young people living with HIV, young women, young people who use drugs, and young men who have sex with men and transgender people. Community Action for Sexual and Reproductive Health and Rights Policies in Asia is a regional initiative that brings together Alliance Linking Organisation MAMTA Health Institute for Mother and Child and Social Awareness Service Organisation (SASO) in India, and HIV/AIDS and STD Alliance Bangladesh (HASAB) in Bangladesh.
By the end of 2010, the project partners had supported the establishment of 88 youth groups across Bangladesh (18), and Manipur (30) and Uttar Pradesh (40) in India. The youth groups are providing opportunities for young people, aged between 15 and 24, to access sexual and reproductive health and life skills information. Youth leaders receive training with specifically developed resources to facilitate sessions with their peers. Project partners have developed factsheets on sexual and reproductive health.
In addition to working directly with young people, the project also aims to build capacity among local civil society organisations in the areas of young people’s sexual and reproductive health rights and related advocacy. To do this, project partners developed a training curriculum, which accommodates regional differences, with a focus on young key populations. Training workshops have been run for 62 civil society organisations across the regions. Each workshop resulted in the development of state-level advocacy plans that civil society organisations will be jointly implementing during 2011.
In summary
The Alliance made good progress in the first year of its new strategy HIV and Healthy Communities. In the new strategy we committed to scale up integrated HIV programming, with a renewed focus on Africa. In 2010, we scaled up programmes in 14 countries, and globally we supported 2.9 million people with HIV prevention, care and support services. In 2010, six new organisations, including three in Africa, joined the Alliance family. Two of the organisations in Africa work in the biggest generalised epidemics in the world. This increased presence in Africa will help us to reach more people in 2011.
In our strategy, we set out our commitment to human rights-based programming. An external evaluation of the Alliance’s Africa Regional Programme suggested strong support for the Alliance approach of addressing stigma by empowering vulnerable communities. We have seen in this section how men who have sex with men and sex workers addressed stigma and delivered prevention services in their communities. In addition, the North Africa Regional Programme was highlighted as leading the regional response in work with men who have sex with men.
We also showed how the Alliance built partnerships to deliver more integrated interventions. These included health and welfare services for families and children affected by HIV. We showed how vulnerable children benefited from a family-centred approach in Zambia and how people living with, and affected by, HIV secured support for livelihoods in other parts of Africa. Elsewhere in the world, we continued to prioritise prevention interventions for vulnerable populations in the Caribbean and South Asia.
Young people get sex education in South Asia
In South Asia, we are working with young people to empower them to advocate for their participation in sexual and reproductive health programming and policy processes.
The largest generation of young people in history is approaching adulthood. In Asia, many adolescents are out of school, get married early, work in vulnerable situations, are sexually active, and are exposed to peer pressure. Policies and prevailing social attitudes in much of Asia continue to assume that young people are not, or should not be sexually active. As a result, young people are often denied information and services that could prevent them contracting HIV and other STIs, and from having unwanted pregnancies.
MorethanhalfofallSTIs,otherthanHIV,occuramongyoungpeopleaged15to24(morethan180million,outof340millionannually).Anestimated900,000newHIVinfectionsoccurredamongyoungpeoplein2008.ComprehensiveknowledgeofHIVamongyoungmenandwomenhasincreasedgloballyto34%since2008.However,thisrepresentsbarelyonethirdoftheUNGASStargetof95%(UNAIDS).

ANNUAL RESULTS REPORT 201019
In 2010, the Alliance supported 1,491 non-governmental and community-based organisations to work with communities.
We helped improve the performance of community-based organisations through our Linking Organisations and Regional Technical Support Hubs.
This section covers Alliance work to provide technical and financial support to civil society, helping to strengthen the HIV response. It starts by describing our work in South Sudan to develop the capacity of community-based organisations and the newly formed government. We then highlight increased demand for technical support from our Regional Technical Support Hubs. We feature an innovative and cost-effective initiative to increase the quality of technical support. The online distance learning course exploits new media to reduce costs. Finally, we report on the number of Alliance Linking Organisations now supported by Global Fund grants. This includes two notable Round 10 success stories: that of Initiative Privée et Communautaire de Lutte Contre le VIH/SIDA au Burkina Faso (IPC) who can now increase representation of civil society in the national response, and the Latin American Sex Workers Network (RedTraSex) who can scale up their important work to represent and defend the rights of sex workers.
2Strategic Response 2: Support well-functioning community-based organisations
Mukono Health Centre, Mukono District, Uganda © Nell Freeman for the Alliance

20
Alliance supports the community and government in South Sudan
TheAllianceexiststoprovidecost-effectivefinancialandtechnicalsupporttocommunity-basedorganisationsandsmallNGOs,enablingthemtosupportcommunityactiononHIV.AllianceLinkingOrganisationsplayacrucialroleinbuildingthecapacityofimplementingpartnersintechnicalandorganisationalissues.
Theexternalevaluation,commissionedaspartofourProgrammePartnershipArrangement(PPA)withDFID,recognisedthestrengthoftheAlliancemodel,sayingtheAlliancehas,“anexcellentreputationforbuildingcivilsocietycapacitytorespondtoHIV”.
WhilecommunityactionisattheheartoftheAlliancestrategy,effectivenationalresponsesalsodependongovernments.TomeetthechallengesofHIVandAIDS,governmentsneedboththecapacityandthewilltoworkinpartnership.InSouthSudan,theAlliancemandateistobuildcapacityforanintegratedHIVresponse.Followingthecivilwar,theunderdevelopmentofgovernmentandcivilsocietystructuresleftagapintheHIVresponse.Afterthepeaceagreementwassignedin2005,theAllianceapproachtocommunitysystemsstrengtheninghashelpedfillthegap.SeenasthemostimportantlocalNGOworkingonhealthanddevelopment,AllianceSouthSudansupports90community-basedorganisationsacross18countiesinfourofSouthSudan’stenstates.
AllianceSouthSudandevelopedastrongworkingrelationshipwiththegovernmentofSouthSudan.ThispavedthewayfortheAlliancetoplayapivotalroleinfluencingtheadoptionofappropriatenationalHIVpolicies.In2009,therelationshipwasreinforcedwhenaMemorandumofUnderstandingwassignedwiththeSouthernSudanAIDSCommission.ThisformalisedtheAlliance’sroleasleadagencystrengtheningthecivilsocietyresponsetoHIV,alongsidethegovernment.
In2010,thepartnershipwascementedfurtherwhenAllianceSouthSudansecuredaUS$1.6milliongrantfromtheWorldBank-managedMultiDonorTrustFund.ThefundsaredisbursedthroughtheSouthernSudanHIV/AIDSCommission,forprovisionofHIVprevention,careandtreatmentservicedeliveryinCentralandEasternEquatorialstates.
TheprojectissupportingtheStateAIDSCommissions(SACs)andStateMinistriesofHealth(SMOH)toleadandmanagetheHIVresponseinclosecollaborationwithlocalCountyHealthDepartmentsandtheCountyAIDSCommissions(CACs).Inparallel,appropriatetechnicalandfinancialresourcesarechannelledtoanarrayofprimaryhealthcarecentres,community-basedorganisationsandothergroups,likenetworksofpeoplelivingwithHIV.
First,theprojectaimstostrengthenthekeystewardshipfunctionsofSACsandSMOHHIVdepartments.TheAllianceistransferringexpertiseandimprovingperformancethroughinitialtrainingfollowedbymentoring,on-the-jobskillsreinforcement,provisionofnecessarytoolsandjointsupportsupervisionvisits.Second,itaimstostrengtheninstitutionalandtechnicalcapacityofcommunity-basedorganisationsandnetworksofpeoplelivingwithHIV.ThisenableslocalgovernmentstoplanandmanageimplementationandcoordinationofcomprehensiveHIVandAIDSserviceswiththefullparticipationofthecommunity.
In2010,42participantsfrom15community-basedorganisationsweretrained.Also,twonetworksofpeoplelivingwithHIVandcountyandstateAIDSofficersweretrained.Wewillprovidesub-grantstothe15community-basedorganisationsforthemtodeliverHIVprevention,careandsupportservices,aswellasprovidereferralstoincreaseuptakeofotherservices.Overthe18-monthprogrammeserviceswillbedeliveredto90,000people.
Demand grows for Alliance technical support
IncreasinglytheAlliancebuildsthecapacityofNGOsbyprovidingtechnicalsupportthroughitssevenRegionalTechnicalSupportHubs.In2010,thenumberoftechnicalsupportdaysprovidedbytheseHubsincreasedby42%.TheHubscollectivelyprovided4,091daysoftechnicalsupportcomparedto2,890daysin2009.WhilethePPAevaluationnotedthestrengthoftheAllianceincapacitybuilding,italsoidentifiedqualitycontrolchallengesassociatedwithdecentralisingthetechnicalsupportfunctiontoregionalHubs.Inthiscontext,itunderlinedthecontinuedneedforinvestmentandsupport.
The Alliance has, “an excellent reputation for building civil society capacity to respond to HIV”.

ANNUAL RESULTS REPORT 201021
Whiledemandincreasedoverall,therewasa40%declineinthenumberoftechnicalsupportdaysprovidedbytheUganda-based,East,CentralandSouthernAfricaHub.Thedropindaysfrom2009to2010wasaresultoftheclose-outoftheCOREInitiativeinUganda.TheCOREInitiativepreviouslyaccountedforsignificantin-countrydemandfortheHub.WhiletheHubreduceditssupporttoAllianceprogrammes,itdramaticallyincreaseditsregionalcoveragetonon-Allianceprogrammes,fulfillingoneofitskeyaimsto
strengthencivilsocietyorganisationsoutsidetheAlliance.ThisincreasewaslargelyaresultoftheuptakeofsupportfromGlobalFundprincipalandsub-recipients.In2010,civilsocietyorganisationsinDemocraticRepublicofCongo,Ethiopia,Kenya,Malawi,SouthAfrica,SouthSudan,Uganda,ZambiaandZimbabwerequestedtechnicalsupportfromtheEast,CentralandSouthernAfricaHub.GlobalFundassignmentsfortheHubin2010included:Kenya,SouthSudan,ZambiaandZimbabwe.
1600
1400
1200
1000
800
600
400
200
0
TECHNICAL ASSISTANCE DAYS BY REGIONAL HUB: 2009 AND 2010
Num
ber o
f Day
s
Regional Hub
Caribbean Latin America
Eastern Europe & Central Asia
South AsiaEast, Central & Southern Africa
Southeast Asia & Pacific
West & North Africa
2009 2010
ALLIANCE TECHNICAL SUPPORT FOR GLOBAL FUND SUB-RECIPIENT IN ZIMBABWE
Todate,theZimbabweAIDSNetwork(ZAN)hasbeenasub-recipientofallGlobalFundHIVgrantsinZimbabwe(Rounds1,5,and8).InRound8assub-recipienttotheUnitedNationsDevelopmentProgramme(UNDP),ZANismanagingarapidexpansioningrantsize,geographicalcoverageandresponsibilityformanagingsub-sub-recipients.Theprogrammecovers62districts,athree-foldincreasefrom22inthepreviousround.ZANisalsonowresponsibleformanagingthreebigsub-sub-recipients,whointurnprovidegrantstocommunity-basedorganisations.ManagingGlobalFundgrantsrequiresrobustmonitoring,evaluationandreportingsystemsandcapacitytomanageandinputlargevolumesofdata.ZANrequestedtechnicalsupportfromtheAllianceEast,CentralandSouthernAfrica(ESCA)TechnicalSupportHub.Theyneededhelptodevelopsystemsformanagingandreportingonthegrant.
Thetechnicalsupportconsultantreviewedtheexistingprimarydatacollectiontoolsoftheparticipatingorganisations.Buildingoncurrentsystems,adjustmentswererecommendedtoaligntoolswiththenationalmonitoringandevaluationframework.Recommendationsweremadeandsupportprovidedtoimproveindicatordefinitions.Theconsultantdevelopedadataanalysisplan(identifyingwhatdatatocollectandanalyse,andatwhatlevel)andadataanalysisframeworkforuseatdistrict,provincialandnationallevel.Whenthedataanalysisframeworkwasfinalised,monitoringandevaluationofficersweretrainedsotheywouldknowhowtouseit.
(ZANjoinedtheAlliancefamilyin2010.SeetheirprofileinStrategicResponse4.)

22
New media exploited to improve technical support and reduce costs
ToimprovethequalityoftechnicalsupportprovidedbyregionalHubs,theAlliancedevelopedonlinedistancelearningcoursesin2010.Thisnewapproachhasthepotentialtogreatlyexpandthereach,andconsiderablyreducethecosts,oflearninganddevelopment.TheAllianceinitiallydevelopedtwoonlinecoursesfortechnicalsupportproviders;oneonconsultingskillsandtheotheronGlobalFundprocesses.
Theconsultingskillscoursecoversarangeofsoftandhardskillsincludingorganisationalchange,facilitationskillsandconflictmanagementtechniques.Thecoursebenefitsfromtheinvolvementofafacilitatorforeachcohortofstudents.
Withthematerialandthemethodologyinplace,thecostsofrunningthecourseissignificantlylessthantraditionaltrainingwhichrequiresparticipantsand/ortrainerstotravel.
TheGlobalFundmoduleengagesthelearnersthrougharangeofexercisesbasedontheGlobalFundgrantcycle.Practicalexercisesdrawonrealcountrysituationstohelplearnersapplytheacquiredknowledge.Whilethemoduledevelopsconsultantscapacitytoprovidetechnicalsupporttocivilsociety,ithasbeendesignedtobuildoverallcompetenciesinGlobalFundsystems.Thiswillallowthecoursetobeusedbyconsultantsworkingfordifferenttypesoforganisations.
Afteranevaluationbothcourseswillbefine-tuned.TheywillthenbemadeavailableinFrenchandSpanishtotechnicalsupportprovidersacrosstheworld,withinandbeyondtheAlliancefamily.Thiswillenabletechnicalsupportproviderstoimprovetheirknowledgeandskillsatminimalcost.Furthermore,thelessonslearnedindevelopingthesecourseswillbeusedinsubsequentonlinecourses,providingacost-effectivewayofbuildingcapacityaroundtheworld.
“I have found the (course) useful and informative in terms of professional skills development andimprovement. I suggest it is introduced to otherconsultants in the HIV/AIDS field.”
ParticipantfromECSATechnicalSupportHub
“The course was an eye opener. I benefited somuch from the course, all the topics were important to me. They added value to my work. I am now a confident consultant because of this course.”
ParticipantfromECSATechnicalSupportHub

ANNUAL RESULTS REPORT 201023
Alliance Global Fund portfolio increased globally
TheAlliance’sGlobalFund-supportedprogrammesincreasedglobally,particularlyinAfrica,astheAlliancefamilygrewandexistingLinkingOrganisationssecuredprincipalandsub-recipientgrants.
OurGlobalFundportfoliocontinuedtogrowinAfrica.BothAllianceZambiaandAssociationMarocainedeSolidaritéetDeveloppement(AMSED)wereagainnamedGlobalFundsub-recipients,thistimeinRound10.Inamuch-deservedsignofrecognition,AllianceLinkingOrganisationIPCinBurkinaFasowasnamedco-principalrecipientforRound10.However,withfundingdelayeduntil2012,theprogrammewillnotbeabletoscaleupforanotheryear.ThissuccessistheculminationoftwoyearsofIPC’seffortstostrengthen
ALLIANCE GLOBAL FUND PRINCIPAL RECIPIENTS (7) ALLIANCE GLOBAL FUND SUB-RECIPIENTS (17)
AllianceIndia(HIVRounds6and9)AllianceUkraine(HIVRounds1,6and10)Kimirina,Ecuador(MalariaRound8,HIVRound9)ANCS,Senegal(HIVRound6and9)ANS-CI,Côted’Ivoire(HIVRound9)IPC,BurkinaFaso(HIVRound10)MAC,Malaysia(MARPsRound10)
ViaLibre,PeruPOZ,HaitiAllianceMyanmarKHANA,CambodiaHASAB,BangladeshAllianceUkraineABS,BurundiMONASO,MozambiqueZAN,Zimbabwe
NAF,MongoliaAAA,KyrgyzstanAllianceZambiaAMSED,MoroccoLepra,IndiaPWDS,IndiaMAMTA,IndiaVMM,IndiaHumsafarTrust,India
representationofcivilsocietyinthenationalresponse.DespitehavingmadeasignificantcontributiontoreachingnationaltargetsfororphansandvulnerablechildreninBurkinaFaso,IPCrepeatedlyfailedtosecuresufficientfundingtomaintainprogrammingatthatscale.Thelackoffundingeventuallyresultedinprogrammeclosuresandstafflosses.Nevertheless,IPCstruggledontorepresenttheinterestsofpeoplemostaffectedbyHIV.DuringthepreparationoftheRound8proposal,IPCbecameanactivememberoftheGlobalFund’sCountryCoordinatingMechanism(CCM).HavingledthedevelopmentoftheCivilSocietyPlatform,IPCwasabletorepresentcivilsocietyinthenationalresponse.Thiseventuallyledtotheirsuccessasco-principalrecipientinRound10.ThiswillmeanIPCcanstrengthenthecapacityofcivilsocietyintheHIVresponse.

24
Sex workers become Global Fund recipient
In Latin America, RedTraSex developed a 13-country regional proposal that was approved by the Global Fund in Round 10. This news was particularly significant as RedTraSex is the Latin American network of sex workers, in a region where sex work is criminalised. Social and institutional violence against female sex workers has increased in the region over the last decade. In almost all countries in Latin America sex workers are arbitrarily arrested by police and subjected to abuse and extortion. For the last seven years, the Alliance has worked with RedTraSex to build their organisational capacity so they can address human rights violations, protect themselves, and tackle stigma and discrimination. Last year we reported that RedTraSex was able to ensure active participation of sex workers in 15 Global Fund CCMs in the region. They also received endorsement from 15 CCMs for a Global Fund Round 9 proposal that they developed. That proposal was unsuccessful, however their efforts to represent their constituency finally paid off in 2010.
In summary
Alliance Linking Organisations strengthened the capacity of civil society to respond to HIV. An external evaluation acknowledged our “excellent reputation” in this area.
Training requested from Alliance Regional Technical Support Hubs increased by 42%. The technical support provided has helped civil society organisations strengthen and improve the quality of programming, policy and advocacy. There was ever-greater need for technical support as more Linking Organisations became Global Fund recipients, expanding quickly and needing to improve management systems and structures.
With technical support and funding from the Alliance, organisations have been able to represent their interests, create more enabling environments and contribute to more effective HIV responses. The example of RedTraSex demonstrates the impact of strategic financing and capacity building that goes beyond project implementation. By supporting organisations to do more than just deliver programmes, we are building their capacity to become national, regional and international players, influencing national and global strategies.
CASE STUDY
“In the beginning we were up against a huge level of discrimination, from donors, from agencies, from the United Nations. The people from the Alliance came and placed all their trust in us. They did not come charging in saying, ‘We have an agenda and you must carry it out’ but they came to ask, ‘What is it that you want to do?’
“Becoming part of the Alliance meant not only gaining the funding needed to carry out the activities we wanted to do, but also the money to have a qualified team. We women are the drivers, the administrators, the ones who bring ideas to the project. To have somebody qualified who knows how to capture, how to interpret what we want, that has given great strength to the organisation. I mean, we started with only four organisations and in five years we now have 17 countries with over 60 organisations of sex workers.
“It is true to say that we have demonstrated over these past five years that ‘Yes! We can do it’. We have the knowledge, we make mistakes but we pick ourselves up again. You see, today we can say, ‘We know what we want and we know where we want to get to’.”
Elena Reynaga, Executive Director of RedTraSex
THE VALUE OF WORKING WITH THE ALLIANCE
©theAlliance
ANNUAL RESULTS REPORT 201025
In 25% of countries where the Alliance works, representatives of key populations participate in decision-making bodies on HIV funding.
We strengthened the capacity of civil society to engage in national and international decision-making, create enabling environments, and defend human rights. We also made sure the voices of those most affected by HIV were heard by key decision-makers.
Engaging communities in the response to HIV is particularly challenging in hostile environments. Laws discriminate and persecute marginalised groups, such as sex workers, men who have sex with men, and people who use drugs. Consequently, resources and services are often denied to the people most in need of them. The Alliance’s priority therefore is to strengthen civil society to engage in global and national policy on programming and funding allocation, and to hold governments to account.
In this section we describe our efforts to highlight the stigma and discrimination that continues to hamper the HIV response. This includes the publication of a report that spotlights discriminatory laws in the Commonwealth and a global campaign exposing barriers to effective prevention. We report on advocacy initiatives in 2010 aimed at defending the human rights of those most-at-risk. We feature reports from Senegal, where persecution of men who have sex with men has eased following international pressure, and Ukraine, where the Alliance campaigned on behalf of a doctor arrested for treating people who use drugs.
We support communities in their efforts to demand effective HIV responses and hold their governments to account. During 2010, Ugandan citizens were encouraged to hold leaders to account on their election promises. Across east and southern Africa new technology was used to support meaningful participation of people most affected by HIV. In Latin America, vulnerable populations became more visible to the public and decision-makers, increasing their ability to influence policy.
To inform global HIV policies the Alliance placed community experience centre stage. We feature here our contributions to groups such as the US Government Prevention Steering Committee. We also highlight our efforts to increase and sustain funding for the health MDGs.
3Strategic Response 3: Help form engaged, inclusive societies

26
Human rights of sexual minorities trampled
Persecution of sexual minorities is sometimes fuelled by political leaders. In November 2010, Kenyan Prime Minister Raila Odinga made a speech declaring homosexuality unnatural and called for the arrest of homosexuals. Earlier the same month, sexual orientation was removed from the UN resolution condemning extrajudicial, summary or arbitrary executions, following an amendment by the African Group in the UN and the Organisation of the Islamic Conference. The resolution previously urged states to protect the right to life of all people and called on governments to investigate killings based on discriminatory grounds. For ten years, the resolution included sexual orientation in the list of discriminatory grounds on which killings are based. It is notable that most countries that supported the removal of sexual orientation from the resolution have high HIV prevalence among either their general populations or sexual minorities.
Fortunately, in a later vote the UN General Assembly kept the reference to sexual orientation in the resolution. This time, sense and justice prevailed, but it is of concern that governments conspired to stamp on the rights of their citizens. Such episodes underline why the Alliance believes defending human rights has to be the basis of effective responses to HIV.
Alliance puts spotlight on discriminatory laws in the Commonwealth
Many African countries have regressive and dangerous laws regarding homosexuality and other sexual minorities. 38 countries still have laws inherited from colonial times, which criminalise homosexuality. The ‘crime’ is punishable by the death penalty or harsh jail sentences.
In 2010, the Alliance sought to influence Commonwealth leaders in an effort to challenge discriminatory laws. In collaboration with the Commonwealth Foundation, Commonwealth Secretariat and Commonwealth HIV and AIDS Action Group, the Alliance produced a report entitled Enabling legal environments for effective HIV responses: a leadership challenge for the Commonwealth.
Almost a third (30%) of the world’s population live in Commonwealth countries, yet these countries are home to nearly two thirds (60%) of people living with HIV. Given this, the report aimed to define an agenda for action on HIV and law in Commonwealth states. It sought to inform the work of legislators, officials and diplomats, and to assist civil society organisations to engage with their governments on the legal dimensions of the HIV response.
The report was launched at the first World AIDS Day Commonwealth HIV and Human Rights Lecture in London on 30 November 2010, hosted by Cherie Booth QC. The lecture was given by Chief Justice, Ajit Prakash Shah. The year before Justice Shah had created shockwaves around the world when he overturned a 150-year-old British law banning gay sex between consenting adults in India. At the lecture, Justice Shah said,
“Indian society is very conservative, but from the evidence presented I could see that without changing the legal framework to help men who have sex with men access good health care and HIV prevention services, we would not successfully be able to deal with the epidemic in our country.”
“We reject discrimination in general, and in particular discrimination based on sexual orientation and gender identity. Whenindividuals are attacked, abused or imprisonedbecause of their sexual orientation, we must speak out. We cannot stand by. We cannot be silent. This is all the more true in cases ofviolence. These are not merely assaults onindividuals. They are attacks on all of us.”
BanKiMoon10November2010HumanRightsDay

ANNUAL RESULTS REPORT 201027
Discrimination against men who have sex with men eases in Senegal
Similar to the situation in many Commonwealth countries, the HIV response in Senegal is carried out in the context of underfunding, discrimination and sanctioned violence against minorities. Following a notorious case of persecution, the Alliance has monitored human rights abuses of men who have sex with men in Senegal over the last two years. In 2008 the arrest and detention of nine AIDS activists gained international attention. The activists were members of AIDES Senegal, an implementing partner of Linking Organisation ANCS. Although the environment remains hostile for men who have sex with men in Senegal there were some reasons for hope by the end of 2010. The advocacy efforts aimed at legal representatives, politicians and religious leaders to create greater tolerance started to pay off.
In August 2010, ANCS held a joint workshop with Environment Development Action in the Third World (ENDA) and Open Society Institute West Africa (OSIWA) on HIV, human rights and universal access. ENDA is a sub-recipient of ANCS’s Global Fund grant for interventions aimed at most-at-risk-populations. OSIWA has valuable experience
of integrating human rights in HIV programming. Leaders of organisations of men who have sex with men were given a platform to talk about their rights, and to speak with journalists who were present; a significant step forward given the role of the media in perpetuating violence against them in the past.
While arrests of men are still being made, there has been less physical violence and secrecy as the police are more conscious of the attention this draws. In addition, the media are no longer publishing information about men suspected of having sex with other men, which had previously incited people to violence. In October, Human Rights Watch published a report on the situation in Senegal and to date there appears to have been no public backlash. ANCS continues to work with AIDES Senegal, and on behalf of men who have sex with men.
But there is still much more to do. There is a need for greater involvement of men who have sex with men in advocacy and programming to enable them to voice their concerns, represent themselves and influence decisions that affect them.
Yewu Yeeté, a social and discussion group for MSM in Senegal © Nell Freeman for Alliance

Effective prevention still falling short
The Senegalese case demonstrates the corrosive impact of discrimination and the constraints it places on organisations trying to reach vulnerable communities. In many African countries discrimination is fuelled by the active enforcement of laws that criminalise HIV transmission and sexual minorities. Almost half the countries in sub-Saharan Africa have laws or regulations that create an obstacle to effective HIV prevention.
There is evidence that national HIV responses often neglect key populations. Fewer than half of low and middle-income countries collect data on their most-at-risk populations, for UNGASS indicators. If they do not collect the data, they cannot address the risk factors facing their most vulnerable populations. There is a clear need for stronger prevention activities to help protect men who have sex with men, sex workers, people who use drugs and people living with HIV.
Evidence shows that prevalence rates among men who have sex with men are higher than in the general population. But because of discrimination, programmes to address their needs are frequently not adequately resourced. Funding between 2006 and 2008 illustrates this. During this time UNAIDS estimated Africa would need US$353 million for HIV prevention activities with men who have sex with men. Research for the International Gay and Lesbian Human Rights Commission found the actual amount committed was less than US$2 million.
In 2010, UNAIDS put human rights firmly back on the international HIV agenda by including it as one of three pillars in their new 2011 to 2015 strategy Getting to Zero. In doing so they highlighted the structural drivers of the epidemic – the social and legal frameworks that fail to protect against stigma and discrimination and impede access to HIV programmes.
Alliance calls for human rights approach to prevention
To emphasise the need for a human rights approach to effective prevention efforts, the Alliance developed a global campaign. What’s preventing prevention was launched at the International HIV/AIDS Conference in Vienna in July. The campaign facilitates international advocacy and dialogue to ensure access for key populations to HIV prevention services, and supports national level advocacy efforts.
As part of the campaign, Community Health Alliance Uganda (CHAU) commissioned research (to be published in 2011) to improve understanding of the conditions for most-at-risk populations in Uganda. The research aims to provide robust evidence to inform national advocacy to improve HIV prevention. It is estimated that the proportion of HIV prevention expenditure devoted to programmes for sex workers and their clients, men who have sex with men, and people who use drugs is only 0.2% in Uganda. To effectively tackle the epidemic in Uganda it is critical that prevention programmes for most-at-risk populations are adequately funded.
InararestudyonHIVamongmenwhohavesexwithmeninKenyain2007,asurveyof285meninMombasafoundHIVprevalenceof43%amongmenwhohadsexwithmenexclusively,and12.3%amongmenwhohadsexwithbothmenandwomenagainstanationalHIVprevalencerateof7.4%.

ANNUAL RESULTS REPORT 201029
Like men who have sex with men, the criminalisation of people who use drugs prevents access to health and HIV prevention services. Globally, there are an estimated 3 million people who inject drugs living with HIV – with nearly 13 million more at risk of HIV infection. In Asia, injecting drug use is fuelling new epidemics, with an estimated 16% of people who use drugs living with HIV. In some countries prevalence is even higher. In parts of Indonesia, more than half of people who use drugs are HIV-positive. It is therefore essential to ensure that prevention programmes for people who use drugs are integrated into wider health services, as part of efforts to strengthen health systems.
Social marginalisation and self-stigma of women who use drugs forces them underground and makes them more vulnerable to HIV. Research conducted by Alliance partner SASO in Manipur, India, indicates that most women who inject drugs know about HIV transmission. Therefore their vulnerability is not a result of lack of knowledge, but lack of power and social capital.
The International Harm Reduction Conference, held in the UK in May 2010, provided a platform for the Alliance to put its concerns on a global stage. The Alliance joined forces with other organisations to call for more resources for harm reduction programming. Our joint advocacy was based on recommendations from 3 cents a day is not enough, a report published by the International Harm Reduction Association. Speaking at the opening plenary, Alliance Executive Director Alvaro Bermejo highlighted the substantial threat to resources for targeted HIV-related interventions for people who use drugs. He articulated fears that harm reduction interventions are unlikely to be sustained unless funds have been specifically earmarked for them. Bermejo called for more user-friendly health care and harm reduction programmes to protect people from HIV.
The Alliance has provided financial support to the newly established International Network of People who Use Drugs (INPUD) to enable people who use drugs to participate in global policy. We also supported the nomination of Mat Southwell from INPUD to the UNAIDS Programme Coordinating Board. In addition, we have worked with the Global Fund to expand the list of interventions that define harm reduction to include human rights and community focused interventions such as legal services and family support services.
Alliance fights for rights of people who use drugs in Ukraine
At a national level, the Alliance aims to create an environment in which people who use drugs can get the support they need to protect themselves from HIV. Alliance Ukraine has been at the forefront of this work. In 2010, two leading authorities on health, the World Health Organization (WHO)5 and the Lancet6, acknowledged the value and success of Alliance Ukraine’s harm reduction programme. But even with such prestigious acclaim, some programme activities were hampered by the authorities.
In Ukraine substitution maintenance therapy (SMT) is legal and forms an important part of the national HIV response. Despite this, law enforcement agencies took action against those who use and administer SMT in 2010. Over the year, Alliance Ukraine monitored cases of human rights abuses of patients and medical staff. These included spot checks of medical facilities that implement SMT programmes and the unlawful removal of lists of drug-dependent patients, with personal details. Authorities also conducted unlawful home searches, subjecting patients and medical staff to psychological pressure, and hindered the supply of medication.
In May, 62-year-old physician, Dr Illya Poldolyan was detained by the police and charged with fabricated offences related to drug trafficking. Alliance Ukraine immediately mobilised support for a petition targeting Ukraine’s Prime Minister Mykola Azarov and Prosecutor General Oleksandr Medvedko. The petition called on the government to protect
5.WHOcitedAllianceUkraineasasuccessstoryattheAIDS2010conferenceinVienna.6.http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2810%2961899-5/fulltext
Outreach work with injecting drug users © Malaysian AIDS Council
Prevention programmes threatened for people who use drugs

30
the rights of patients and doctors, and remove barriers to SMT. Alliance Ukraine also organised an impromptu press conference. At the conference organisers called on police to release the doctor and put an end to criminal prosecutions of SMT patients and staff engaged in the programmes. Andriy Klepikov, Executive Director of Alliance Ukraine, raised the issue with the relevant national councils and the Ministries of Health and Internal Affairs. Alliance Ukraine, together with other organisations, lobbied for months and sent open letters to the authorities calling for the release of Podolyan.
Eventually in September, after four months in custody, the Court of Appeal of Odessa ruled that Podolyan should be released as he awaits trial. Since his release Podolyan has been reinstated as a narcologist doctor working at the same clinic as before. The episode clearly hasn‘t deterred the doctor as he continues to administer and advocate for SMT. Invited by Alliance Ukraine, Podolyan was a special speaker in November 2010 at the National AIDS Conference in Kiev organised by the Ministry of Health.
The case highlights the need to be constantly vigilant when it comes to protecting the rights of vulnerable and stigmatised people. Even when the national policy framework is in place, as in this case, it is necessary to monitor the behaviour of officials and departments who can have their own agendas.
This example demonstrates the importance of public accountability of both government and its institutions. The next four items describe the efforts of the Alliance to support communities in making their governments more accountable.
Ugandans supported to demand accountability
InUgandaaninitiativesupportedbytheAllianceishelpingtoincreasegovernmentaccountability.In2010,CommunityHealthAllianceUganda(CHAU)andothercivilsocietypartnersworkedtogethertodevelopa‘Citizens’Manifesto’.Themanifestodocumentedtheelectionpromisesandpoliciesofthecandidatesintherunuptothe2011nationalelections.Candidateswerecalledontosignthemanifestotoacknowledgethattheywillhonourtheirpromisesifelected.ThemanifestowaslaunchedinSeptember2010tosupportapublicdialogueprocessaroundthecountry.Dubbed‘thecitizens’caravan’communitiesaremobilisedtounderstandtheirrightsandengageintheelectionprocess.
In2010,wecarriedoutasurveyofLinkingOrganisationstomapAllianceeffortstoprotectandpromotehumanrights.ThevastmajorityofAllianceLinkingOrganisations(77%)reportedtheyareinvolvedinworkthathelpsrights’holdersclaimtheirrights.
Themanifestowillsetthepolicyagendaforcivilsocietyorganisationsforthenextfiveyears,withaparticularfocusonhealth.Indoingso,itwillbuildastronggrassrootsmonitoringprocess.
“ThroughtheCitizens’Manifesto,”explainsBishopZacNiringye,KampalaDiocese,“ordinaryUgandansaresaying,‘wehaveadreamforapositivefutureforourcountry–weknowwhatoursocio-economic,politicalandotherneedsare,andwecalluponourleaderstolistentothem’.Theirunitedvoicesdemandfarreachingsocial,economicandpoliticalreforms.ThiswillhelptoensureUganda’sdemocraticandsocio-economicgainsareprotectedandconsolidated.”
Technology supports participation for more effective HIV responses
TheNationalPartnershipsPlatforminUgandaisanindependentnationalmechanismforjointcivilsocietyactiononHIV,TBandhealth-relatedpolicy.AnewregionalinitiativeaimstosupporttheUgandanNationalPartnershipPlatformalongwithotherplatformsacrosstheregion.TheinitiativewillfacilitateeffectiveparticipationofpeoplemostaffectedbyHIVinnationalHIVandTBstrategies.
TheprojectTackling AIDS and TB through Communications and Information Technologies (TACIT)aimstostrengthenadvocacycapacitybyharnessingthepowerofinformationandcommunicationstechnology(ICT).TheprojectsupportsNationalPartnershipPlatformsinZambia,Namibia,UgandaandKenya.Itstrengthensthepartnershipplatformasamechanismthroughwhichcommunity-basedorganisationsandNGOscometogethertoanalysenationalresponses,anddefinepriorityadvocacyissues.
TheinitiativebringstogetherregionalpartnersSouthernAfricaHIVandAIDSInformationDisseminationService(SAfAIDS)andtheEastAfricanNationalNetworksofAIDSServiceOrganisations(EANNASO)withAIDSPortaltobuildtworegionalICTplatforms.Theplatformswillenableknowledgesharing,networkingandconsultationwithconstituenciesineasternandsouthernAfrica.ItwillalsodevelopthecapacityofcommunitiesinICT,policyandadvocacy,andindocumentation.Givingcommunitiesthepowertoaccessanduseinformationenablesthemtotakeamoreactiveroleindecisionsthataffecttheirlivesandholdleaderstoaccount.
Communities call on governments to address maternal mortality
WithadditionalfundingreceivedfromUKaid(fromtheDepartmentforInternationalDevelopment)in2010,wewerealsoabletobuildontheICTprogrammetofurtherintegrateHIVandmaternalhealthresponses.TheinitiativewillputpressureongovernmentsinfourAfricancountriestoimprovematernalhealththroughmoreintegratedhealthstrategies.

ANNUAL RESULTS REPORT 201031
ThelinksbetweenmaternalmortalityandHIVarenotwellunderstood.HIV-positivewomenareatbetweenfourandeighttimesgreaterriskofmaternalmortalitythanotherwomen.Inthehigh-prevalencesettingofsouthernAfrica,AIDShasbecometheleadingcauseofmaternaldeath.Thepandemicmakesthegoaltoreducematernalmortalityextremelychallenging.SoitiscrucialthatmaternalhealthandHIVresponsesaredevisedandimplementedjointly,buildingonthestrengthsofthedifferentapproaches.
Toaddressthis,theAllianceissupportingtheNationalPartnershipPlatformsinKenya,UgandaandZambia.TheprojectwillgenerateevidencefromcommunitieswhohaveahighburdenofmaternalmortalityandHIV.Thisevidencewillbeusedtoraiseawarenessandbuildpoliticalmomentumto
shapeeffectivepoliciesatthenationallevel.Theplatformsarecallingongovernmentstointegrateservicestosupportpregnantwomenandmothers.Inaddition,communitymobilisationwillbelinkedtoappropriatereferralandfollowupofHIV-positivepregnantwomen.ThefundinghasalsoenabledustostartanadvocacyplatforminSouthSudan–acountrywhosematernalmortalityratioisamongtheworstintheworld(2,054per100,000livebirths).
“Improvingreproductive,maternalandnewbornhealthinthedevelopingworldisamajorpriorityfortheBritishgovernment,”saysMarkMallalieu,deputyheadofDFIDSudan.“Investinginreproductive,maternalandnewbornhealthishighlycosteffectiveandhasfarreachingreturnsforwomen,families,societies,economiesandtheenvironment.”
CASE STUDY
Here we highlight the poor state of public maternal health services in Zambia and the value of Bwafwano, an Alliance-supported community-based organisation.
Bwafwano provides a package of integrated services for a community of around 50,000 people in the Chabata catchment area, just outside Lusaka in Zambia. Bwafwano, which means ‘helping one another’, began work in 1996 as a home-based care initiative. The organisation has gradually developed into a one-stop shop for community health care.
Bwafwano receives support to develop the maternal and child health part of their programme. They train and recruit prevention-of-mother-to-child-transmission specialists for their antiretroviral clinic. Through community-based caregivers and health advisers they raise awareness among communities of issues relating to maternal, neonatal and child health. Pregnant women living with HIV are also referred to their clinic for treatment, care and support.
“I came to Bwafwano through a friend who knew it,” explains Esther, a beneficiary of the programme. “I felt so ill. I was getting medication through the government clinic, but it wasn’t enough. Sometimes I was too ill to collect it, other times they would tell me to come in a few weeks, and by then I was too ill again. Whenever I went to a government clinic, there were too many people waiting. If you are sick, nobody cares and you can wait all day just waiting to be seen. Bwafwano caregivers came (to my) home to assess me and make sure I was well. They would follow up with me regularly. If I hadn’t taken my medication they would come and make sure I took it. Now I am strong enough to come here for my treatment. People here are nice and so understanding. I have made many friends here. Before coming here, I couldn’t talk about my condition to anybody in my community. Here, I feel better and happier, and I don’t mind talking about HIV. I could be dead by now if it wasn’t for Bwafwano. Here I not only get the treatment I need, but I am also part of the food programme, and they provide me with food support.”
SUPPORTING PREGNANT, HIV-POSITIVE WOMEN

32
Key populations in Latin America empowered to improve governance
The Latin America Programme Partnership Arrangement (LAPPA) with DFID provided critical support for the Alliance’s work in Latin America from 2005 to March 2011. The second phase of the project (2008-2011) supported six national and two regional programmes, and was independently evaluated by the Overseas Development Institute in 2010. The evaluation cited three main outcomes of the programme. These were that national and regional organisations of key populations now have increased capacity and reach. Organisations of vulnerable populations have increased their advocacy capacity to hold governments, state and relevant global institutions to account. The organisations also now have a broader funding base, and an increasing percentage of existing resources to reach key populations.
The multi-country and regional programme successfully supported key populations to advocate for their rights, and to hold governments to account. One activity that contributed to improved governance was a citizen observatory project implemented in Ecuador, Colombia, Bolivia and Peru.
For example, in Peru, Viviendo en Positivo (Living Positively), a community-based organisation comprising key populations (people living with HIV, men who have sex with men, sex workers and transgender people) runs the citizen observatory in Chiclayo city, in the Lambayeque region. The observatory monitors the implementation of the national multi-sectoral HIV/AIDS plan through the documentation of human rights violations and inadequate provision of services for most-at-risk populations. Cases are presented to the ‘personeros’, the government’s official local representative for human rights. Personeros then raise the issues with the relevant authorities. Between 2008 and 2010, Viviendo en Positivo brought to light 827 human rights abuses.
Organisations of vulnerable populations have increased their advocacy capacity to hold governments, state and relevant global institutions to account.
Peer educator Fabiana Pérez, Ecuador © Gideon Mendel for the Alliance

ANNUAL RESULTS REPORT 201033
As a result of the programmes, key populations have made themselves more visible to the public and to national and international policymakers. This has allowed them to influence decision-making processes at national and regional levels. For example, REDLACTRANS, the regional network of transgender people influenced the Organisation of American States (OAS) to include transgender people as a separate group to men who have sex with men. Marcela Romero, the president of REDLACTRANS, spoke at the organisation’s Annual Assembly in 2009. It was the first time that a transgender leader had taken part in a meeting of the OAS. During the Assembly the resolution on Human Rights, Sexual Orientation and Gender Identity was approved. The word ‘trans’ has increasingly become part of public discourse, and transgender people are being identified as distinct from men who have sex with men; a population with their own needs and aspirations. As a result of support from the Latin America PPA, transgender people in the Lambayeque region have become more visible and less fearful of presenting themselves in society.
A major achievement has been the inclusion of representatives from sex worker and transgender groups in the Global Fund CCMs and the increased capacity of REDLACTRANS and RedTraSex (featured in Strategic Response 2). The programme has had a significant impact on the lives of people from key populations. They have improved self-confidence, and now feel part of a wider community. With increased awareness of their rights they are now able to report abuses by the police, claim their rights to health services and, in some countries, continue to work as sex workers with legal protection.
“There has been a change in political media representation,” explains Alfonso Lescano, Project Co-ordinator for Via Libre. “There’s a change in the level of participation, and people becoming involved. There is evidence of having reached beneficiaries, of having achieved things… But the best part of it all is that there is a change in people… and I think that is priceless.”
“There has been a change in political media representation,” explains Alfonso Lescano, Project Co-ordinator for Via Libre. “There’s a change in the level of participation, and people becoming involved. There is evidence of having reached beneficiaries, of having achieved things… But the best part of it all is that there is a change in people… and I think that is priceless.”
CASE STUDY
LIVING POSITIVELY
“Viviendo en Positivo (Living Positively) was born thanks to an invitation from Via Libre, who came from the city of Lima to give a presentation, to propose the idea of raising political awareness among key communities. It was the first time that the Lambayeque region had seen a single organisation uniting transgender people, gays, sex workers and people living with HIV.
“I have HIV. I have lived with HIV for eight years now. For me Living Positively has been like a school, a school where I learned to keep moving forward. It has taught me to stand up and be heard, not only at a local level, but also regionally and nationally.”
Humberto Esteves, President of Viviendo en Positivo
Through these programmes we have demonstrated the importance of situating an HIV programme within the wider context of human rights and universal access to health care. As a result stigma and discrimination and violence against marginalised groups has become part of a broader social and political agenda in Latin America. This approach is critical if we are to change the shape of the epidemic in the region.
©theAlliance

34
Alliance brings voice of communities to global policy
So far in this section of the report we have seen how the Alliance supports communities to build inclusive societies that support human rights and hold governments to account. Apart from work with national and regional partners on initiatives to create enabling environments and increase accountability, the Alliance contributes to and engages with global think tanks, working groups and international policy processes. Our engagement in global policy forums is informed by the experience of our Linking Organisations and their work with communities. The Alliance ensures the voice of those communities informs efforts to enhance the quality and effectiveness of responses to health and HIV.
In 2010, the Alliance continued to contribute to a wide range of international policy and working groups such as: UNAIDS Reference Group on HIV and Human Rights; UNAIDS Prevention Reference Group; the Monitoring and Evaluation Reference Group; Women Deliver; and the Interagency Working Group on Sexual and Reproductive Health and HIV Integration. Here we provide a brief description of our contributions to just three of these global initiatives.
UNAIDS REFERENCE GROUP ON HIV AND HUMAN RIGHTS The Alliance is an active member of the UNAIDS Human Rights Reference Group, providing advisory support to UNAIDS on matters relating to HIV and human rights. In 2010, the group’s contribution ensured that defending human rights was a central pillar to UNAIDS’ 2011 to 2015 strategy.
“The Alliance is a very good organisation that is at the forefront of HIV work, especially lobbying and advocacy. They are prominent in certain platforms… such as with UNAIDS and the Global Fund… The way they link community, regional and global issues is very valuable.” – DFID Programme Partnership Arrangement evaluation.
Members of the people living with HIV Multi-Purpose group, in Nyimbwa, Uganda © Nell Freeman for the Alliance

ANNUAL RESULTS REPORT 201035
The reference group also made a submission to the Global Commission on HIV and the Law. The Global Commission on HIV and the Law was established in 2010 to provide global leadership on legal and human rights related to HIV. It focuses on how laws and law enforcement can support effective HIV responses. The Commission provides a unique opportunity for the Alliance, and other actors, to highlight human rights issues, and make recommendations on how to address them through a process of hearings.
In 2010, the Alliance made its own submission to the Commission, highlighting some of the human rights concerns identified by Linking Organisations. The submission addressed specific issues, like the detainment of people who use drugs in drug detention centres, and the prosecution of people working in HIV, such as methadone doctors and outreach workers.
The Alliance called on the Commission to make specific recommendations for legal reform. These included calls for the decriminalisation of sex work, drug use and sex between men, and the reform of laws that criminalise HIV transmission. In its submission the Alliance called for laws to protect people living with HIV, key populations and women and girls in particular, from discrimination and violence. This was backed up with demands for effective legal instruments and the prosecution of human rights violations by law enforcement agencies.
INFLUENCING THE GLOBAL PREVENTION AGENDA Through our participation in global meetings on prevention the Alliance is influencing and guiding the development of policies to address the needs of communities. In our role as a member of the Prevention Working Group of the Global AIDS Round Table we engaged with the Interagency Prevention Steering Committee of the United States government. This Committee includes representatives from USAID, the Center for Disease Control and the Office of the Global AIDS Coordinator. As part of the working group the Alliance supported the development of guidance on effective HIV prevention programming for US delegations in partner countries.
After the meeting with the US Interagency Prevention Steering Committee, the working group followed up with written recommendations on behavioural, biomedical and prevention interventions, as well as combination prevention. Our recommendations included a list of resources on evidence and programmes including the Alliance guidelines on positive prevention; the Alliance’s Commonwealth law reform report; the Good Practice Guide on Greater Involvement of People Living with HIV; and the community systems strengthening framework. The US government guidance on prevention is expected to be released in spring 2011.
In 2010, we worked with the UNAIDS Prevention Reference Group to develop the concept and guidelines for combination prevention. Through the guidelines we brought greater focus on structural drivers of HIV transmission and set the basis for the ‘prevention revolution’ that UNAIDS is now talking about in its new strategy.
ALLIANCE PROVIDES HIV FOCUS FOR WOMEN DELIVERThe Alliance contributed to the global Women Deliver conference in Washington in June. Working with the International Community of Women Living with HIV/AIDS (ICW), the Alliance co-organised the HIV track, by organising eight thematic panel discussions. This was the first time that the conference included an HIV element. The panels underscored the critical links between HIV and women’s health, rights and development. They explored how we can work across the Millennium Development Goals to strengthen partnerships and action among organisations working on maternal, newborn and child health (MNCH), sexual reproductive and health rights (SRHR) and HIV. Key to addressing the needs of women and girls globally are the provision of comprehensive HIV, SRHR and MNCH services. This will only come about with involvement of and increased support to communities and their organisations in leading, delivering and advocating for such services. In organising the panels, the Alliance and ICW created a space to hear the voices and experiences of women from the global South.
Alliance lobbies for increased financing for the health-related MDGs
And finally, as well as influencing global policy on HIV, the Alliance campaigned to secure sufficient levels of finance for an effective HIV response. Of increasing concern to the Alliance, and other development and health organisations, is the need for sufficient and sustained funding from the global donor community. Having foreseen the impact of the global financial crisis on donor countries, the Alliance was quick to pursue financing mechanisms that would support progress on universal access to treatment, as well as broader health and development commitments.
In 2010, the Alliance continued to play a crucial role in the Robin Hood Tax campaign in the UK and around the world. We worked in partnership with a broad coalition of NGOs, labour unions and social movements in the UK. So far, the UK government has committed to introduce a new levy on banks that will raise over US$4 billion. The campaign is pushing for more progressive taxation to raise an additional US$32 billion, half of which could be used for the global public good, including support to achieve the MDGs and combat climate change.
Through policy engagement with French NGOs, the Alliance supported the launch of the Robin Hood Tax campaign in France. This initiative convinced President Sarkozy to champion a financial transactions’ tax for development during his presidency of the G8 and G20 in 2011. As a result, President Sarkozy has become the greatest advocate among global leaders for a financial transactions’ tax.
In Europe, through the Stop AIDS Alliance, the Alliance worked as part of a cross-European coalition of NGOs advocating for the tax. In August, Stop AIDS Alliance participated in a media stunt during the European Finance Ministers’ meeting, leading to a wide range of radio, television and print coverage. Media coverage across Europe was sympathetic to the aims of the campaign and included images of the stunt and interviews with coalition

36
spokespeople, including Eva Nilsson from Stop AIDS Alliance. In October, Stop AIDS Alliance was invited to the European Commission’s monthly Global Health Policy Forum, where it proposed a financial transaction tax to support spending on global health initiatives.
Prior to 2010, there was little momentum behind the financial transactions’ tax campaign in the US. The Alliance helped mobilise a coalition to support the campaign working with trade unions and HIV, health and broader development NGOs. This resulted in the tabling of a congressional bill (Investing in Our Future Act) in July 2010. The bill proposes a tax on currency transactions with the proceeds being used to provide billions in new funding for domestic and global priorities, including climate change and health. The coalition is now lobbying President Obama to champion the initiative in Congress and at the G8 and G20 meetings in 2011.
In 2011, the Alliance will continue to support the campaign’s efforts to secure G8 and G20 leadership for new levies on the financial sector to raise resources for global health.
In summary
In its 2010 to 2012 strategy HIV and healthy communities, the Alliance committed to help form engaged and inclusive societies. In this section we have shown how, in 2010, the Alliance campaigned to address barriers to effective prevention. In November, the Alliance launched a report to encourage decision-makers in the Commonwealth to work with civil society to change discriminatory laws and respect the rights of key populations. Our global campaign What’s preventing prevention? highlighted the damaging impact of hostile policy environments.
Enabling people to demand their rights and expect government accountability is another core commitment of the new strategy. In 2010, an initiative in Uganda helped to engage citizens to know their health rights, engage in the election process, and monitor the promises of elected representatives. The National Partnership Platforms in Kenya, Namibia, Uganda and Zambia were all strengthened through new media technology. They can now more easily engage communities to take an active role in decisions that affect their lives and hold their leaders to account. In Kenya, Uganda and Zambia another initiative helped communities demand that their governments improve maternal health services.
Alongside these regional and national campaigns, the Alliance has worked to bring the voice of communities to global policies. The Alliance participated in policy forums to improve the quality of HIV responses to health and HIV. Informed by Linking Organisations, the Alliance has drawn on the experience and knowledge of communities working at the frontline of the HIV response. The Alliance also played an important role in a global campaign to generate increased funding for the health MDGs.

ANNUAL RESULTS REPORT 201037
20% of Alliance Linking Organisations have documented programme improvements on the basis of accreditation criteria. Improvements include effectiveness, efficiency and good practice of programmes.
We created platforms for South-to-South learning and knowledge sharing. We strengthened our accreditation system, knowledge sharing and capacity building.
In this section we report on shared learning, the development of our accreditation system and a platform for hearing community voices. A new internet portal in southern Africa provides opportunities for sharing best practice and peer-reviewed information. We feature a South-to-South learning exchange for a new Linking Organisation in Mozambique. We cover the success of our citizen journalists to get the experiences of people and communities affected by HIV covered through local and international media. A key correspondent from Zimbabwe gets an article in a Sunday newspaper highlighting government human rights abuses. Finally we explain how the Alliance family expanded in 2010 with three new Linking Organisations in Africa and three others from the rest of the world. As our accreditation system matures, five existing partners were fully accredited and one was suspended.
New portals set to increase shared learning
Shared learning across countries in southern and eastern Africa was dramatically improved following the launch of the southern Africa web portal www.hivsouthernafrica.info. The dynamic web portal has the potential to be the most useful source of HIV information related to southern Africa. Part of the TACIT project, the site will support and strengthen regional HIV knowledge management.
The site shares prevention information and connects individuals and organisations from the southern Africa region. It provides a platform and voice for local programmes and organisations. The site allows users to access and share peer-reviewed information and best practice. It also provides an opportunity to contribute to national and regional discussion forums. As covered under Strategic Response 3 the site is a key advocacy tool for the Alliance National Partnership Platforms. An equivalent portal will be launched for eastern Africa in 2011. Both sites build on the lessons learned in the development and running of AIDSPortal and PortalSIDA.
4STRATEGIC Response 4: Create a learning Alliance

38
Linking Organisations provide learning exchanges
TheAllianceencouragesandpromoteshorizontallearningexchangesbetweenLinkingOrganisations.Oftheninehorizontallearningexchangesin2010,threetookplaceintheAfricaregion.ThelearningexchangesprovideanimportantopportunityforLinkingOrganisationstoshareexpertiseandprovidepeer-ledcapacitybuildinginprogrammingandorganisationalcapacitybuilding.AsLinkingOrganisationshavebecomelargerandmorefinanciallyrobust,wehaveseenincreaseddemandforsupportintheareasofmonitoringandevaluationandfinancialmanagement.Forexample,inDecember2010twomembersofstafffromMozambiqueNationalAIDSServiceOrganisation(MONASO)visitedZimbabweAIDSNetwork(ZAN)inZimbabwetobetterunderstandsystemsusedtosupportonwardgranting.
Earlierin2010,thenewAlliancepartnershipwithMONASOledtothesuccessfulawardofUS$1.3millionfromanewlycreatedmechanismknownastheRapidResultsFund.Thismechanismwasdevelopedtorespondtotheneedsofcivilsocietyorganisations.TheWorldBank,undertheMulti-SectoralAccelerationProgrammeinconjunctionwiththeGovernmentofMozambique,UNAIDSandUNDP,decidedtoredirectfundspreviouslyallocatedtotheNationalAIDSCouncildirectlytocivilsociety.The12-monthprojectwillsupportcapacitybuildingamongcivilsocietyorganisationsinsixoutof11provincesinMozambique.
MONASOwaschargedwithimplementingarapidresponsefundingmechanismtoprovidegrantsandtechnicalassistancetoaround60civilsocietyorganisationsinfiveprovinces.Tohelpthemdothis,MONASOwantedtolearnfromZANabouttheirpracticalexperiencesofmanaginggrantprocesses.DuringtheexchangeMONASOgainedanewunderstandingoftheimportanceofhavinganinternalauditor,whichcansavemoneyinthelongrun,andagrantsmanagementunit.MONASO’slearningwillhelpthemtobecomemoreaccountable,moreefficient,andmoreeffectiveatworkingwithgrantees.
Key Correspondents get their experiences out to the world
ThroughitsvibrantnetworkofcitizenjournaliststheAlliancegetstheexperiencesofpeopleandcommunitiesairedthroughlocalmediaandonlinenetworks.TheKeyCorrespondentteamismadeupof250citizenjournalistsbasedin50countries.50correspondentswritestoriesandrespondtobriefingsregularly.ManyofthecorrespondentsarepeoplelivingwithHIV.Theyallwriteaboutthehealthanddevelopmentissuesaffectingthemselvesandtheircommunities.
In2010,72newcorrespondentsweretrained.ThenewcorrespondentsaremostlybasedineasternandsouthernAfrica(Zambia,UgandaandNamibia).Asaresultoftheircombinedefforts1,100articleswerepostedonhealthdev.net,awebsitecreatedforthepurpose.Theprolificreportingin2010increasedvisitstothewebsiteby45%.
AmongKeyCorrespondentsarejournalists,researchersandactivistswhogettheirworkpublishedmuchmorewidelythan
healthdev.net.InUganda,correspondentHenryZakumumpahadanarticlepublishedintheDailyMonitor,‘ThousandsriskearlydeathasAIDScarecentresturnawaynewpatients’.ThearticlehighlightedthecriticalimpactoftheflatliningoffundingforHIVtreatmentoncommunities.CorrespondentFungaiMachirorihadherarticlepublishedinTheStandard,aZimbabweannewspaper.‘SilenceonZimrightsabusescondemned’reportedonaspeechmadeattheViennaAIDSconference.ThearticleraisedtheissueofsexualviolenceusedasaweaponbyMugabe’srulingpartyinZimbabwe’spoliticalstruggle.InherarticleMachioricalledontheinternationalcommunitytotakeaction.
ApartfromtheInternationalAIDSConference,KeyCorrespondentsattendedotherconferencesin2010toprovidecommunityperspectivesoninternationaldebates.CorrespondentsattendedWomenDeliverinWashingtonDCinJuneandthe41stUnionWorldConferenceonLungHealthinBerlininNovember.ManyofthearticlesproducedduringthelatterconferenceweredisseminatedviatheStopTBe-forumasaresultofcollaborationbetweentheAlliance,theStopTBPartnershipandtheInternationalUnionagainstTuberculosisandLungDiseases.
The Alliance expanded its presence in Africa
ThreenewAllianceLinkingOrganisationsinAfricaextendedtheglobalpartnershiptoZimbabwe(ZAN),Burundi(ABS)andMozambique(MONASO).HavingworkedinfourprovincesinMozambiqueforsevenyears,theAlliancestrengtheneditscountrystrategyin2010byjoiningforceswithanewpartnerthathasnationalcoverage(seeMONASOprofile).
InotherregionsthreenewpartnersjoinedtheAlliancefromHaiti(POZ),ElSalvador(Atlacatl)andIndia(HumsafarTrust).ThisbringstheglobalpartnershipofAllianceLinkingOrganisationsto36.Profilesofalltheneworganisationsareincludedhere.
Five Linking Organisations fully accredited, and one suspended
TojointheAlliancefamily,organisationsgothroughaninitial‘light’accreditationprocess.Apartfromthesixnewmemberstotheglobalpartnership,theAlliancefullyaccreditedafurtherfiveexistingLinkingOrganisations.Organisationsaccreditedin2010include:LEPRASociety(India),ViaLibre(Peru),CorporaciónKimirina(Ecuador),AssociationMarocainedeSolidaritéetDéveloppement(AMSED)(Morocco)andNetworkonEthics,Law,HIV/AIDSPrevention,SupportandCare(NELA)(Nigeria).
Attheendof2010,adecisionwastakentosuspendCivilSocietyforHIV/AIDSinNigeria(CiSHAN)fromtheAlliancefamily.ChangesinitsorganisationalgovernancestructuremeantthatitwasnolongerabletomeetfundamentalrequirementsoftheAllianceaccreditationsystem.UntilthesituationcanberemedieditwasdecidedthatCiSHANshouldnolongerbelinkedwiththeAlliancebrand.ThisactionfollowedaseriesofmeetingsbetweentheAllianceandCiSHAN.UnfortunatelyCiSHANfailedtomakesufficientprogressagainststepstheAlliancedeemednecessaryfortheorganisationtoremainintheAlliancefamily.

ANNUAL RESULTS REPORT 201039
CASE STUDY
CASE STUDY
L’ALLIANCE BURUNDAISE CONTRE LE SIDA – BURUNDI
MOZAMBIQUE NATIONAL AIDS SERVICE ORGANISATION
ABS works in close partnership with the Burundian network of people living with HIV as well as being a member of key forums to promote more effective integration of civil society in policy and strategy. For example, ABS is a member of the National AIDS Commission, Executive Committee and General Assembly; the UNAIDS technical working group on HIV; the national strategy monitoring and evaluation working group; the national UNGASS committee; EANNASO; and AFRICASO. ABS also sits on the Global Fund’s CCM and is a sub-recipient of a Global Fund grant from Round 8.
“By becoming members of the Alliance we benefit from, and belong to, this community of learning and sharing so that we can achieve the same vision. Now the ABS is connected to different local and national responses throughout the world and can contribute to the global response through sharing diverse resources.”
Patience Kubwumuremyi, National Coordinator of Alliance Burundaise Contre le SIDA
The organisation is represented on key HIV coordination mechanisms like the National AIDS Council, the Global Fund CCM and government technical working groups. MONASO works in close cooperation with several other key stakeholders, including UNAIDS.
MONASO prioritises advocacy, organising the first National Civil Society AIDS Conference attended by community-based organisations, NGOs and government members. MONASO successfully mobilised communities to advocate for a law to protect the rights of people living with HIV. This eventually resulted in a favourable new law in 2009 (Rights and Responsibilities of People Living with HIV & AIDS).
“We’ve joined the Alliance since we aspire to better respond to the needs of our members and of civil society in Mozambique, so they are all engaged in the fight against HIV. We can share our 18 years of experience and learn with the other partners of the Alliance family. To join the Alliance takes MONASO’s action to a global level and increases its credibility and responsibility at national level.”
Gaspar Sitefane, Executive Director of Mozambique NationalAIDS Service Organisation
Burundi’s leading coalition of civil society organisations responding to HIV joined the Alliance in January 2010. L’Alliance Burundaise Contre le SIDA (ABS) represents
over 400 member organisations across all regions of Burundi. Members work in prevention, treatment and care and support of people living with HIV.
Over half its population of 8.5 million are under the age of 18. Burundi recently emerged from a prolonged civil war that devastated its economy, infrastructure and social services. The conflict had a profound impact on the living conditions of the population, significantly increasing its vulnerability to poverty, violence, food insecurity, disease and HIV.
In March 2010, the Mozambique National AIDS Service Organisation (MONASO) joined the Alliance family. Established in 1993, MONASO has offices in every province of Mozambique. Its 1,356 members* include
community-based organisations and NGOs working in 99 of the country’s 128 districts. Highly regarded by government and civil society, MONASO coordinates its work with several other networks and NGOs.
MONASO’s vision is for people living with and affected by HIV, to be free from stigma and discrimination, and have access to prevention, treatment and care. It helps civil society organisations provide an effective response to HIV. MONASO’s six strategic priorities are networking; lobbying and advocacy; training and capacity building; organisational development; institutional capacity development; and onward granting.
*MONASO members represent a wide range of different types of organisations. MONASO is currently reviewing the type and nature of its partnerships to better identify and categorise its members.

40
CASE STUDY
ZIMBABWE AIDS NETWORK
planning, governance, project management, monitoring and evaluation, and financial and human resources’ management. ZAN builds capacity in HIV programming in the areas of prevention, treatment, care and support. For example, it produced materials and provided training on gender and sexuality in relation to HIV prevention. The training explored the dynamics of human sexuality in a gender sensitive manner.
A major activity for ZAN is advocacy to improve the national response to HIV. It works closely with the Parliamentary Portfolio Committee on Health and Child Welfare and other relevant committees. It advocates for universal access to services, TB and HIV co-infection management, protection of human rights in the constitution, and support for most-at-risk populations. Key advocacy successes include improved access to treatment, reduction of user-fees, and supporting the Domestic Violence Bill to become an Act of Parliament.
“One of the Alliance’s core values is that of enabling communities, including the most vulnerable and marginalised people, to actively participate in various responses to health challenges affecting them… For ZAN, membership of the Alliance presents great opportunities to contribute to the empowerment of communities through engaging with a wider network of like-minded organisations.”
Lindiwe Chaza-Jangira, National Director of Zimbabwe AIDS Network
Established in 1991, Zimbabwe AIDS Network (ZAN) is a national network of AIDS service organisations, private sector companies and faith-based organisations contributing to the national HIV response. ZAN has over 200 member organisations* drawn from across all ten provinces of the country. The
organisation has developed a strong national reputation in the HIV field, in the face of unprecedented challenges during the 2007-2008 political and economic crises. Through its head office in Harare and provincial offices it increases the capacity of its members, enabling them to take a lead role in the national response to the AIDS epidemic. Aligned with Alliance principles, ZAN joined the growing global partnership in 2010.
To improve the quality of members’ community HIV services, ZAN provides technical support through volunteer placements, mentoring and training. It facilitates exchange visits and workshops to share information and experience, so that members can learn successful approaches and good practice from each other. As a result members have developed skills in areas such as strategic
*ZAN members represent a wide range of different types of organisations. ZAN is currently reviewing the type and nature of its partnerships to better identify and categorise its members.

ANNUAL RESULTS REPORT 201041
CASE STUDY
HUMSAFAR TRUST – INDIA
Humsafar reaches more than 12,000 clients annually with HIV and health services at three clinics and drop-in centres, as well as through street outreach and other prevention programmes. The 150-strong team of outreach workers and peer educators distribute around 700,000 condoms every year. The organisation has two professional counsellors from sexual minority communities who are personally familiar with many of the clients. The clinical services are supported by seven part-time doctors, a nutritionist, and three laboratory technicians. In 1999, Humsafar was accredited as a voluntary counselling and confidential testing centre for Mumbai, and it has subsequently built its clinical component alongside its prevention and support activities, integrating and strengthening services. For the last eight years, Humsafar has acted as a sentinel surveillance site for the National AIDS Control Organisation.
“Humsafar, as part of expanding its networking and continuing the practice of learning from good models, decided to be part of the Alliance family. It was a decision made by the community governing board that HST should look at models of HIV from across the world. Apart from gaining from the expertise of other Linking Organisations, it can also share its experiences of working with men who have sex with men and transgender communities in India. HST is hoping that by being part of the Alliance family it will strengthen its capacity, both at an organisational, as well programme and staff level, thereby improving the quality of services being offered to its community.”
Vivek Anand, Chief Executive Officer of The Humsafar Trust
The Humsafar Trust (HST) was set up in April 1994 by leading gay activist Ashok Row Kavi. With colleagues, Row Kavi recognised the need to develop a support system for men who have sex with men, rather than accept the marginalised and
criminalised existence imposed on them. Humsafar, which means ‘companions on a journey’, created a safe haven, and provided support for Mumbai’s emerging community of men who have sex with men and transgender people. Humsafar Trust has since built a reputation as a pioneer in HIV-related service provision in Mumbai. Apart from HIV prevention, care and support, Humsafar provides general health care services to sexual minorities in and around Mumbai.
Humsafar Trust also advocates for the rights of sexual minorities. Although some of its advocacy activities are nationally focused, Humsafar has endeavoured to remain community-based, mainly serving Mumbai, India’s most populous city.
To support the growing number of organisations working with men who have sex with men, transgender people and other sexual minorities in India, Humsafar initiated the establishment of the India Network for Sexual Minorities in 2003. The organisation now works with more than 80 groups across the country.

42
CASE STUDY
ASOCIACION ATLACATL VIVO POSITIVO – EL SALVADOR
In April 2010, Atlacatl presented a petition to the state to create a national day for people living with HIV. Members of parliament and legislators united in support of the petition and in May 2010, El Salvador’s Legislative Assembly declared 12 May ‘National Day of Solidarity with People Living with HIV’.
Working with the Alliance, Atlacatl builds the capacity of organisations formed by, and working with, four key populations: men who have sex with men, transgender people, sex workers and people living with HIV. Following the model of the Alliance’s successful Vida Digna (life with dignity) project in Mexico, these vulnerable communities are supported to identify and respond to HIV-related stigma and discrimination in their communities.
Atlacatl runs a weekly, national, hour-long radio programme to provide information and provoke debate about HIV, and leads a media campaign to raise awareness and fight discrimination. The campaign enjoys support from many high profile people, including the vice-president.
“Being part of the Alliance makes our work with people living with HIV more visible, we are able to show the changes we can make within national public policies that benefit thousands of people... Being part of the Alliance is a unique experience that enables us to see the work of each other as one, with a greater impact.”
Odir Miranda, President and Executive Director of Asociacion Atlacatl Vivo Positivo
In November 2010, Asociacion Atlacatl Vivo Positivo (Atlacatl) became a Linking Organisation, having worked with the Alliance since 2008. Established in 1998 by HIV-positive activists, Atacatl set out to defend human rights and secure access to health, education and employment for people living with HIV. Their first action was to take the Salvadorean government to the
Inter-American Court of Human Rights to claim their right to free medication. As a result of their landmark victory, the government now provides free medication to all people living with HIV. The ruling encouraged other Latin American governments to provide treatment, and so avoid legal action. Atlacatl is a significant regional player and is influential in shaping HIV-related policy. It leads the Salvadorean chapter of the Central American Human Rights Network on HIV/AIDS, and currently houses the regional secretariat for the Central American Network of People Living with HIV/AIDS. It is also represented on the National Commission to reform HIV law. Atlacatl led a process to amend El Salvador’s labour code, so that employers can no longer ask candidates to take an HIV test.

ANNUAL RESULTS REPORT 201043
CASE STUDY
PROMOTEURS OBJECTIFS ZEROSIDA – HAITI
In June 2008, POZ began a project funded by the UK’s Big Lottery Fund to increase uptake of HIV prevention, care and treatment services in Cap Haitien, Jacmel and Port-au-Prince. The organisation worked with local leaders, health providers and members of communities to address HIV-related stigma and discrimination. Through one-to-one meetings and group meetings the peer outreach workers and leaders reached members of the public with anti-stigma messages, and over 150 care providers were given anti-stigma training. The project also used mass media to broadcast positive images of people living with HIV speaking openly about HIV. Programmes included radio call-in shows. People living with HIV reported that these activities helped to reduce stigma.
Apart from POZ’s strong expertise in stigma and discrimination, it also has expertise in livelihoods’ initiatives. Since 2005, working with a cooperative in St Marc, POZ has been training people affected by HIV in microcredit and management of small loans.
“POZ has created a strong partnership with the Alliance which has enabled it to strengthen its leadership and diversify its areas of intervention. POZ believes that the Technical Support Hubs offer an important opportunity for strengthening the Alliance/POZ relationship further.”
Marie Mercy Zevallos, Executive Director of Promoteurs Objectifs Zerosida
In 2010, Promoteurs Objectifs Zerosida (POZ) joined the global partnership of Alliance Linking Organisations, after five years of collaboration. Established in 1995, the mission of POZ is to support the response to AIDS through community mobilisation, advocacy and provision of services to reduce the impact of HIV and STIs. POZ
currently supports people living with HIV, and groups of people living with HIV, across seven of the country’s ten departments. Its experience in HIV prevention, care and support programmes led POZ to become a Global Fund sub-recipient. Many organisations now employ POZ-trained people living with HIV in their programmes, and POZ is frequently asked to train staff from other institutions.
Since 2005, POZ has helped to strengthen and raise the profile of the newly formed network of Haitian people living with HIV. POZ helped the network represent its constituents, while encouraging them to participate in HIV programme planning, decision-making and advocacy. A project evaluation in 2008 concluded that, as a result of support from POZ, the network was more strategic and had a better organisational structure. Consequently it was able to mobilise funds and people living with HIV. The number of member associations doubled from six at the beginning of the project to 13 in March 2008.
In the earthquake that destroyed the capital Port au Prince in January 2010, POZ lost two of its three main buildings. However, POZ demonstrated its commitment and stability by continuing its work amidst the devastation. Two weeks after the earthquake, POZ resumed almost all of its activities by providing services to people living with HIV out of tents. In an effort to locate all the people who accessed its services before the earthquake, POZ employed outreach workers, community leaders and a truck that delivered messages to people in shelters and camps. The truck reached approximately 60,000 people in just 30 days. In 2010, POZ reached 183,768 people with HIV services.
Followingthecollapseofit’sofficesintheJanuary2010earthquake,CentreEspoirhascontinueditsworkfromthistent©theAlliance.

44
In summary
Strategic Response 4 committed to create a learning organisation by strengthening Alliance systems and knowledge sharing processes. In 2010, a partnership facilitated shared learning in southern and eastern Africa through new web portals. The portals allowed users to access and share peer-reviewed information and good practice. The Alliance supported Linking Organisations to engage in nine learning exchanges to share expertise and provide peer-led capacity building. 72 citizen journalists were trained to document and share their experiences of HIV in communities.
The global partnership expanded with six new Linking Organisations joining the Alliance family in 2010. Following further development of our accreditation system five existing Linking Organisations were fully accredited, while one member was suspended.

ANNUAL RESULTS REPORT 201045
As we begin to implement our strategy HIV and Healthy Communities, we face emerging challenges, as well as opportunities, for addressing HIV and realising the health MDGs. These challenges include the global economic crisis and its impact on financing the HIV response. In an environment of spending cuts, increased scrutiny of public spending has magnified the need to deliver results and demonstrate value for money. This puts pressure on funding for areas like capacity building, which have less quantifiable short- term outcomes. However, the opportunities ahead include two key events that will help to refocus attention on the critical role that communities play in the HIV response. In this section we expand on these challenges and opportunities.
2011 marks 30 years since the first case of AIDS was identified. Over the last three decades the shape and scale of the epidemic has changed exponentially. The HIV epidemic continues to present the international community with one of the most significant development challenges in history. For communities, HIV presents personal, social and cultural challenges that can only be faced with deep reserves of strength and commitment. The Alliance has worked alongside these communities, in partnership with policymakers, donors and multilateral agencies, to address the social, health and human rights issues related to the epidemic.
The global financial crisis will take its toll on the inhabitants of many countries. It is estimated that one billion people do not have enough to eat. Global unemployment has reached the highest level ever recorded. Rising food prices, stagnating incomes and a lack of employment opportunities are combining to increase vulnerability and insecurity. This is putting national governments under increasing strain and making them less able to deliver on their social and health commitments.
The Alliance will continue to support HIV-affected communities. This means supporting people on treatment, and preventing others from becoming HIV-positive. Effective prevention strategies include outreach to men who have sex with men and sex workers, harm reduction for people who use drugs, sexual health education for young people, and tackling stigma and discrimination. Preventing HIV transmission remains a better option than paying the personal and economic costs of lives on treatment. But as financial resources get tighter, and political imperatives prevail, we fear the prioritisation of treatment over prevention. To effectively respond to HIV it is imperative that we continue to do both.
Within donor countries, we have contributed to building momentum for a financial transaction tax to raise resources for global health and development. However, we fear that domestic pressures for growth and the powerful lobbying of the financial sector may drown out our collective voices.
Donors are increasingly demanding value for money, which means finding more efficient ways of achieving the same, or greater levels of results. In this harsh economic climate, donors themselves are under more pressure to account for the money they spend on development aid. On the one hand we are well prepared, as we have set up cost-efficient systems and our monitoring and evaluation (M&E) systems provide excellent reporting and accountability. On the other hand, we are concerned that strategic long-term programmes, those that strengthen communities and health systems, that have the potential to deliver far-reaching and sustainable results, may lose out to projects that deliver shorter-term results.
The financial modelling conducted by the aids2031 project has provided important information to inform Alliance thinking in the value-for-money debate. Few sectors have been able to analyse the cost of interventions and articulate future financial scenarios to achieve the MDGs. The HIV sector, on the other hand, has a track record in monitoring national expenditure right down to the community level. We therefore have access to information to inform our understanding of the cost of community interventions. But measuring value for money is not that simple.
The challenge in the value-for-money debate is to understand what ‘value’ means from the point of view of communities. For example, the value of a women being empowered to make informed decisions about her sexual health may be well understood, but measuring empowerment is a lot more complex. How do we measure concepts like empowerment, or capacity building? The nature of these processes makes it difficult to demonstrate quantitative results.
Yet as the aids2031 report acknowledged, capacity building is crucial. In Strategic Response 1, we showed how the Alliance’s programmes have become increasingly focused on capacity building in government health systems, such as in South Sudan and in Uganda as part of the SUNRISE OVC project. This is critical to help build sustainable national responses to HIV and other health issues. In the long run, strengthened government institutions are able to reach many more people than individual short-term service delivery projects.
CHALLENGES AND OPPORTUNITIES

46
Another difficulty in measuring value is that local community-based organisations and NGOs often lack capacity in monitoring and evaluation. They may not always be able to document the results that donors need for accountability purposes. Here the Alliance plays an important role. In this report, we have seen that one of the reasons that MONASO and ZAN joined the Alliance was to increase their capacity in M&E (see Strategic Responses 2 and 4). They needed to improve their approach to record keeping, synthesising data across a network and building the M&E capacity of their diverse members. The Alliance is well placed to provide this support, having developed robust systems at the Secretariat and overcome the challenges of reporting results from a network of organisations. However, M&E itself needs further investment, so we can capture the longer-term outcomes of our work. This can only be achieved with strategic funding.
The Alliance model of national Linking Organisations supporting community-based organisations and local NGOs has proved effective for channelling funding and technical support to communities at the centre of the response. This long-term sustainable approach may require significant initial investments and the results may not always be immediately quantifiable in the first couple of years. However, as the Alliance has repeatedly demonstrated, it is always more effective to support communities in their own efforts to respond to HIV.
The Global Fund has had a significant impact on communities’ ability to meet the challenges of HIV. It has provided funding to affected communities to implement programmes. Through the CCM architecture affected communities have secured a voice in decision-making. The progress we have made towards meeting MDG 6 would undoubtedly not have been possible without this. However, at the Global Fund replenishment meeting in October the financial pledges of US$11.7 billion for 2011 to 2013 fell far short of the commitments needed for Round 11. The future for Round 12 also seems uncertain. Shortfalls now would have a significant, adverse impact on countries’ ability to tackle HIV.
But there are two important opportunities on the global stage that will allow the Alliance to shape global policy based on community experience.
2011 will mark ten years since the United Nations General Assembly Special Session on HIV/AIDS. It will be five years since the 2006 High Level Meeting that made a commitment to universal access. UNGASS 2011 will provide an opportunity to showcase the contribution that civil society has made to the HIV response. It will be an opportunity to influence the role of civil society in accelerating efforts to meet MDG 6 on HIV.
The choice of Washington, DC as the site for the XIX International AIDS Conference (AIDS 2012) comes after years of campaigning to end the US entry restrictions on people living with HIV. The decision to drop these restrictions represents a momentous victory for human rights. The conference, in July 2012, provides an important opportunity for people living with HIV to put HIV in the global spotlight once again and put communities at the heart of the debate.

ANNUAL RESULTS REPORT 201047
In this section we describe the measures we have taken over the last year to make the Alliance even more effective. We emphasise the value of strategic funding to the Alliance family, and the role the Secretariat plays in leveraging the greatest value from this funding.
We start by describing our overall financial position for the year and how we have responded to a challenging financial environment and the demands of a new strategy. We then describe the value of strategic funding to the Alliance, and explain how it helps us to:
> buildcapacityofLinkingOrganisationstomanagelargescalegrants
> documentandreportresults,ateachlevelofservicedelivery
> supportthecontinuityofLinkingOrganisations> providevalueformoney.
To conclude the report, we summarise our commitments to achieve our ambitious new strategy, HIV and Healthy Communities.
The summary information provided in this section of the report relates to the audited statutory accounts approved by the Alliance Board of Trustees in April 2011. Full details of the Alliance’s 2010 financial results are provided in a separate Report and Accounts.
BUILDING AN EFFECTIVE ALLIANCE
©NellFreem
anfo
rtheAlliance
“Donors provide strategic funding to theAlliance because this produces results that they could not achieve alone. Areas of the Alliance’s work particularly valued by donors include global and local advocacy, systematic capacity building support to CBOs, reach to key populations and the community level, and linking HIV and SRH.”
EvaluationoftheDFIDPartnershipArrangement,RogerDrew(2010)
Buiilding a new centre for Nyimbwa Multi-Purpose Group for people living with HIV, Uganda

48
Our overall financial position: meeting the challenges
In 2010, the expenditure of the Alliance global partnership7 grew to over US$98.1 million (from US$92.2 million in 2009). This was accounted for by significant increases for KHANA (US$2.9 million ) and ANCS (US$2.2 million), and the addition of new members to the Alliance, such as POZ (US$0.4 million).
Of this total, the Alliance Secretariat received US$11.5 million in strategic income. The UK government continued to be the largest contributor of strategic funding providing US$7.1 million (61%), followed by the Swedish government US$1.9 million (17%), Danish government US$1.7 million (15%), and Norwegian government US$0.5 million (4%).
Overall, our strategic funding decreased slightly from 2009 when we received US$11.7 million. The difference between 2009 and 2010 is accounted for by fluctuations in exchange rates and the end of a strategic funding agreement with the Ford Foundation, worth US$180,000. Additionally, the Canadian government contributions made in 2008 did not continue in 2009 or 2010 – despite their commitment to fund the IMPACT 2010 strategy. In addition to strategic funding, the Secretariat recovered US$2.8 million in indirect costs from restricted grants in 2010. The graph below shows the sources of Alliance strategic funding.
Alliance Secretariat expenditure in 2010 totalled US$41.5 million (compared to US$50.5 million in 2009). Secretariat expenditure in Africa represented US$10.7 million, down from US$15.1 million in 2009. This is largely accounted for by the closure of the Networks project in Uganda and a reduction in funding for Zambia and South Sudan. Total expenditure from the Secretariat to Asia and Eastern Europe fell slightly to US$18.3 million (down from US$21.4 million), due to the shift to direct funding in Alliance Ukraine. Spending in Latin America was also down slightly from US$8.3 million in 2009 to US$7.7 million in 2010. Expenditures for global policy, technical support, planning, analysis and learning totalled $US4.5 million in 2010 (compared to US$5.4 million in 2009).
To meet the challenges of our new strategic framework with decreased funds available through the Secretariat, we took a decision to restructure the organisation in 2010. We reduced staff by 11%, which cut our annual salary costs by US$1.15 million. The full costs of the restructure were met in 2010, so the savings start in 2011. This exercise has positioned the Alliance strongly to meet the challenges of a more dynamic and competitive environment.
Strategic funding is critical to build the capacity of Linking Organisations
In 2010, over half (58%) of Alliance family expenditure went direct to countries. While this reflects a trend among donors to fund national civil society organisations directly, it also demonstrates the increased capacity of Alliance Linking Organisations to access and manage large-scale funding. Strategic funding is critical to build the capacity of Linking Organisations. The Alliance uses strategic funding to support institutional learning systems, monitoring and evaluation systems, horizontal capacity building initiatives, and accreditation. The graph below highlights the trend to in-country funding over the last three years.
7.TheAllianceglobalpartnershipisthenetworkoftheAlliancegroupandtheindependentLinkingOrganisationsthatworktogethertosupportcommunityactiononHIV.TheAlliancegroupconsistsoftheAllianceSecretariatintheUK,subsidiariesinIndia,ZambiaandtheUnitedStates,andbranchesinChina,Myanmar,SouthSudan,UgandaandUkraine.
14
12
10
8
6
4
2
0
TRENDS IN STRATEGIC INCOME SOURCES 2008 TO 2010
$US millions
2008
Other
Canada (CIDA)
Ford Foundation
United Kingdom (UKAID)
Norway (NORAD)
Denmark (DANIDA)
Sweden (SIDA)
2009 2010
GLOBAL ALLIANCE ACCOUNTS
$US millions
2008
Direct in-country funding
Alliance group restricted expenditure
Secretariat strategic income
2009 2010
100
80
60
40
20
0

ANNUAL RESULTS REPORT 201049
While the trend to support programmes in-country is a positive one, it is also important to fund the Secretariat adequately so it can continue to play its role supporting the wider Alliance family.
Strategic funding helps report results at each level of service delivery
Donors, and therefore NGOs, are under increasing pressure to demonstrate quantifiable results. This is the Alliance’s strength, and it is another important element of our work supported by strategic funding.
The Alliance has developed robust systems to measure over 50 indicators, from national to community level. The DFID PPA evaluation found that “the Alliance is perceived to be ‘ahead of the game’ in terms of demonstrating and reporting results”.8 In feedback provided to the evaluation, DFID also noted that, “(the) Alliance has shown itself to be a civil society leader in its monitoring and evaluation work.”
The Alliance’s leadership in M&E was demonstrated again when we developed indicators for HIV and Healthy Communities. This required us to redefine our core indicators to allow us to report against the new strategy. New thematic areas of the strategic framework include the integration between HIV and human rights, sexual and reproductive health, TB, and drug use. The process of developing the new indicators involved consultation between Linking Organisations, the Best Practice unit and the M&E team. The new process indicators will be integrated into the monitoring and reporting system in 2011.
“(the) Alliance has shown itself to be a civil society leader in its monitoring and evaluation work.”
8.Drew,R.(2010),EvaluationoftheProgrammePartnershipArrangement,Brighton:IHAA,p.8.
DEVELOPING HUMAN RIGHTS INDICATORS
Thereisalackofrecognisedindicatorsdesignedtoexplicitlymeasuresupportforhumanrightsinasociety.Forexample,thelatestGlobalFundguidanceincludesonlyonehumanrights-specificindicator,whichisthepercentageofmunicipalitieswithinwhichthereisafunctioninghumanrightsnetwork.
Recognisingthisgap,andtobuildarobustmonitoringfunctionfortheAlliance’snewstrategy,theAlliancedevelopedasetofhumanrightsindicatorsin2010.Theindicatorsareframedaroundasetofindexes.TheseindexeswillenableustogainabetterunderstandingofthenationalhumanrightscontextthroughanassessmentofnationalHIVpolicyandlegislation.Basedonthelearningfromthiswork,wehavemaderecommendationstotheGlobalFundtofurtherdevelopspecifichumanrightsindicatorsforGlobalFund-supportedprogrammes.Therecommendationspaper,whichweco-authoredwiththeOpenSocietyInstituteandUNDP,waspresentedataStrategicConveningontheGlobalFundandHumanRightsinMarch2011.

50
While integrating new indicators we redefined the existing set of core indicators in our monitoring and reporting system. The existing indicators were modified in line with the latest PEPFAR next generation indicators guidance. For instance, all in-service training will now be captured within one overarching indicator.
A new M&E guidance document will be launched in 2011 to support Linking Organisations to integrate the new reporting requirements into their systems. This will be supported by the Secretariat’s Planning, Analysis and Learning team to ensure that data is mapped accurately, and therefore reported at each level of service delivery.
In addition, in 2010 we piloted and began to roll out the toolkit Measuring Up. The training pack was developed to help measure the results of our policy work. In 2010, the toolkit was piloted at a workshop in India, with participants from Alliance India, Alliance Ukraine, Malaysian AIDS Council (MAC) and Kenya AIDS NGO Consortium (KANCO). As a result of the pilot the toolkit was improved with examples of advocacy initiatives with key populations, representing participants’ experience in this area. The final version of the training pack was launched in July 2010.
Measuring Up was used by ANCS in a workshop with partner organisations working with men who have sex with men to help develop their policy work. “Measuring Up is a tool that suits the needs of our organisations very well,” explains Massogui Thiandoum, Programme Manager of ANCS. “It allows us to be very clear on our key messages, the target groups for our advocacy activities, and the outcomes of what we do. It also enables us to plan better and identify allies.
“Another important element (of Measuring Up) is the participatory approach that allows all stakeholders to be involved in all steps of the process. Putting men who have sex with men at the heart of our action is something we do better now. We used to do advocacy for them... now vulnerable groups identify their problems and agree on the best advocacy approach to implement and how best to evaluate it. They felt really empowered by the methodological approach used by ANCS during the workshop.”
Strategic funding supports the continuity of Linking Organisations
We use strategic funding to provide strategic grants and continuity funding to Linking Organisations. Linking Organisations use the strategic grants to support organisational development, programme strengthening and policy work.
For example, a strategic grant given to IPC in Burkina Faso supported their policy and advocacy efforts to develop the Civil Society Platform in Burkina Faso. The creation of the platform facilitated strong coordination among civil society actors and contributed to the success of the Global Fund Round 10 application (see Strategic Response 2).
When necessary, we also use strategic funding to provide bridge financing to cover gaps in project funding. The great majority of funding that Linking Organisations receive in-country is restricted to the delivery of specific projects over a set time period. If continuation or bridge funding is not secured between projects, organisations can experience boom and bust situations, where staff and capacity are lost, undermining project gains and learning. Most importantly, these fluctuations in funding affect the delivery of vital services to communities.
In 2010, we saw this happen in South Sudan and Uganda. In Sudan, the Alliance went ‘out of contract’ while waiting for a delayed, but positive decision from the World Bank. In Uganda, the end of the Networks project left a significant gap in funding before the successful award of the SUNRISE OVC programme in June 2010.
Strategic funding from the Alliance Secretariat played a crucial role in supporting the continuity of organisations through these difficult periods. This type of support is essential for stability and enabling organisations to maintain their commitments to communities.
Strategic funding provides value for money
While strategic funding is essential, it is sometimes less easy to quantify its value. As described already, the global economic climate has brought financing for international development under the spotlight. As people in many donor countries are forced to accept severe public spending cuts, questions have increasingly been raised about the value of aid programmes.
“Putting men who have sex with men at the heart of our action is something we do better now. We used to do advocacy for them... now vulnerable groups identify their problems and agree on the best advocacy approach to implement and how best to evaluate it.”

ANNUAL RESULTS REPORT 201051
In June 2010, the UK’s Secretary of State for International Development, Andrew Mitchell, promised “... a new agenda, one of value for money, accountability, transparency and empowerment”. In the same opening speech9 in Washington, DC, Mitchell explained that, “In these difficult economic times donors have a double duty, a responsibility to achieve maximum value for money: not just results, but results at the lowest possible cost.”
The Alliance has kept abreast of this emerging discourse and has taken steps to define our approach, at an organisational level, and implement value for money practices within our programming. We have undertaken a number of initiatives to support this.
We have continued our rigorous drive towards maximising internal cost efficiency. For example, apart from reducing staff in 2010, we cut travel costs by 28%. In addition we have undertaken an analysis of our overall programmatic cost of reaching individuals with services, at both national and project level.
We partnered with the Futures Institute to implement costing studies of our programmes in Burkina Faso, Senegal and Côte d’Ivoire. While it is important to consider variations in unit costs and methods of service delivery, data from this exercise has generated important information for programme managers to consider.
9.Thetextofthespeechcanbefoundatwww.dfid.gov.uk/Media-Room/Speeches-and-articles/2010/Placing-women-at-the-heart-of-development
Thisresultschainshowshowinputsfeedactivitiesthatgenerateoutputs,whichinturncontributetooutcomesandimpact.Demonstratingvalueformoneymayinvolvemeasurementatalloftheselevels.
INPUTS ACTIVITIES OUTPUTS
COST EFFECTIVENESS
EFFECTIVENESSCOST EFFICIENCY
OUTCOMES IMPACT
FIGURE 1: CONCEPTUAL FRAMEWORK FOR THE VfM PROJECT

52
We have also piloted in-depth, value-for-money studies in India and Zambia (featured under Strategic Response 1) using social return on investment methodologies. These studies measured and assessed the value-for-money of outcomes and impacts, on the right of the results chain (see figure 1). The studies are pioneering in the UK development sector, and have provided rich evidence to measure value for money in programmes to inform future programme planning. For example, the study of the stigma programme in Zambia showed how some beneficiaries initially experienced higher social and economic burdens, as a result of the interventions. The universal benefits of the interventions only accrued after an initial adjustment period. This important learning helps to improve the quality and value of future programmes, while increasing accountability to our ultimate stakeholders.
Recognising the benefit of working together, we organised a seminar in December 2010 to discuss the value-for-money agenda with the UK NGO sector. We co-organised the seminar ‘Measuring and Improving the Value for Money of HIV/AIDS Programming of UK NGOs: Challenges and Opportunities’ with the UK Consortium on AIDS and International Development. The seminar was attended by many UK NGOs as well as representatives from DFID, the New Economics Foundation, and the National Institute for Health and Clinical Excellence.
Through these initiatives, we have developed a firm commitment and greater understanding of how to improve and demonstrate value for money. We have shared our approach and learning with other actors such as the World Bank, Global Fund and UNAIDS to advance dialogue on value-for-money approaches within the AIDS response and wider health community.
We will continue to find new ways to become even more effective with the resources we have, to ensure maximum impact for the beneficiaries of our programmes.

ANNUAL RESULTS REPORT 201053
LOOKING FORWARD
Essential to the success of our new strategy, the Alliance will continue to improve the organisational capacity of Linking Organisations, particularly around governance and good practice programming. We will continue to invest in our Regional Technical Support Hubs, building on the model of South-to-South technical support, with a special emphasis on strategic support for Global Fund grant recipients. We will use our What’s Preventing Prevention? campaign as a focus for advocacy activities to get HIV prevention and human rights high on the agenda.
Over the coming years we will continue to ensure the Alliance applies its learning internally and externally, using evidence from research. For example, the Community Action on Harm Reduction programme offers an important opportunity for cross-organisational learning. The programme will contribute to building a greater body of evidence on community-based harm reduction programming and contribute to a global understanding of good practice.
Individually, each Alliance Linking Organisation plays a critical role in its country’s national response to the HIV epidemic. By sharing our expertise, with others working in maternal and child health and sexual and reproductive health, we aim to create greater efficiencies across sectors. This will also ensure a greater collective contribution to achieving the health-related MDGs.
At the beginning of 2011, with the new structure in place and these new initiatives underway, we will work harder to demonstrate the value of the Alliance (the Secretariat, Linking Organisations and partnerships) in the HIV response.
The combined voices and experiences of the Alliance family, and the leverage this gives us, allows us to make a significant contribution to building healthy communities. But we will only be able to realise our ambitions, and meet the challenges ahead, with continued support from our strategic donors. We end this report by thanking our donors for their continued investment and commitment to our work. We would particularly like to express our gratitude to our strategic donors: the UK government’s Department for International Department, Swedish International Development Cooperation Agency, Danish International Development Agency, and Norwegian Agency for Development Cooperation.

©NellFreem
anfo
rtheAlliance
©GideonMendelfo
rtheAlliance

The Alliance receives support from many contributors and would like particularly to thank the following:
THANK YOU
THE GOVERNMENTS OF:
United States (USAID)
United Kingdom (UKaid from the Department for International Development)
Sweden (Sida)
Netherlands (BUZA)
Norway (Norad)
Denmark (Danida)
Ireland (Irish Aid)
Australia (AusAID)
Switzerland (SDC)
ALSO:
3 Diseases Fund
Big Lottery Fund
Bill and Melinda Gates Foundation
Commonwealth Foundation
Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ)
European Commission
The Global Fund to Fight AIDS, Tuberculosis and Malaria
Levi Strauss Foundation
MAC AIDS Fund
UNAIDS
UNFPA
United Nations Foundation
ViiV Healthcare Positive Action Programme
World Bank
World Health Organisation
TRUSTEES
Teresita Bagasao, Philippines ***
Carmen Barroso, Brazil *
Jan Cedergren, Sweden
Martin Dinham, UK *
Peter Freeman, UK ***
Callisto Madavo, Zimbabwe **
Carole Presern, UK
Prasada Rao, India *
Kevin Ryan, Australia
Nafis Sadik, Pakistan
Steven Sinding, USA – Chair
Fatimata Sy, Senegal – Vice Chair
Jens Van Roey, Belgium
* appointed November 2010
** resigned November 2010
*** retired April 2011

REPO
RT A
ND
ACC
OUN
TS 2
010
56
BangladeshHIV/AIDS & STD Alliance Bangladesh (HASAB)[email protected]
BelgiumStop AIDS Alliance (Brussels)[email protected]
BoliviaInstituto para el Desarrollo Humano (IDH)[email protected]
Botswana**Botswana Network on Ethics, Law and HIV/AIDS (BONELA)[email protected] www.bonela.org
Burkina Faso*Initiative Privée et Communautaire de Lutte Contre le VIH/SIDA au Burkina Faso (IPC)[email protected]
BurundiAlliance Burundaise Contre le SIDA (ABS)[email protected]
Cambodia*[email protected] [email protected]
Caribbean*Caribbean HIV/AIDS Alliance (CHAA)[email protected] www.caribbeanhivaidsalliance.org
ChinaInternational HIV/AIDS Alliance in [email protected]
Côte d’IvoireAlliance Nationale Contre le SIDA en Côte d’Ivoire (ANS-CI)[email protected]
EcuadorCorporación [email protected]
El SalvadorAsociacion Atlacatl Vivo Positivo (Atlacatl)[email protected]
HaitiPromoteurs Objectif Zerosida (POZ)[email protected]
India*International HIV/AIDS Alliance – India Secretariat (New Delhi)[email protected]@allianceindia.orgwww.allianceindia.org
The Humsafar Trust [email protected]
LEPRA Society [email protected]
MAMTA Health Institute for Mother and [email protected]
Palmyrah Workers Development Society (PWDS) [email protected]
Vasavya Mahila Mandali (VMM) [email protected]
IndonesiaRumah Cemara (RC)[email protected]
Kenya*Kenya AIDS NGO Consortium (KANCO)[email protected]
KyrgyzstanAnti-AIDS Association (AAA)[email protected] [email protected]
MalaysiaMalaysian AIDS Council (MAC) [email protected]
MexicoColectivo [email protected] www.colectivosol.org
MongoliaNational AIDS Foundation (NAF)[email protected]
MoroccoAssociation Marocaine de Solidarité et Développement (AMSED)[email protected]@hotmail.comhttp:/amsed.mtds.com
MozambiqueMozambican Network of AIDS Service Organisations (MONASO)[email protected]
MyanmarInternational HIV/AIDS Alliance in [email protected]
NigeriaNetwork on Ethics, Law, HIV/AIDS Prevention, Support and Care (NELA)[email protected]@yahoo.comwww.nelanigeria.org
Peru*Via [email protected]
PhilippinesPhilippines NGO Support Program (PHANSuP)[email protected]
SenegalAlliance Nationale Contre le SIDA (ANCS)[email protected]
South Africa**The AIDS [email protected]
South SudanInternational HIV/AIDS Alliance in South [email protected]
SwitzerlandStop AIDS Alliance (Geneva)[email protected]
UgandaCommunity Health Alliance Uganda (CHAU)[email protected]
Ukraine*International HIV/AIDS Alliance in [email protected]
United KingdomInternational HIV/AIDS Alliance (International Secretariat)[email protected]
USAInternational HIV/AIDS Alliance (Washington)[email protected]
Vietnam**Supporting Community Development Initiatives (SCDI)[email protected]
Zambia The Alliance for Community Action on Health in [email protected]
ZimbabweThe Zimbabwe AIDS Network (ZAN)[email protected]
A global partnership: International HIV/AIDS AllianceSupporting community action on AIDS in developing countries
ARR10 06/11
The Alliance is a global partnership that includes 37 Linking Organisations and Country Offices, seven Technical Support Hubs and an International Secretariat.
For more information please contact [email protected]
List accurate as at June 2011 **Joined in 2011
*Regional Technical Support Hubs hosted here